-
8/7/2019 lecture regulation of resp
1/15
Regulation of respiration
Controls of Ventilation
A). Brain1.Respiratory Center
i). Dorsal Respiratory Groupii). Ventral Respiratory Groupiii)
Pneumotaxic Area of the Pons
2). Hypothalamus:3). Higher Cortical Functions
B). Chemical Signals1). PCO22) H a Rate of breathing
increases3). PO2
-
8/7/2019 lecture regulation of resp
2/15
Respiratory center(RC) is located in the medulla oblongata which
is thelowermost part of the brain stem. RC receives controlling
signals of neural,chemical and hormonal natures and controls the
rate and depth of respiratorymovements of the diaphragm and other
respiratory muscles. Injury to this centermay lead to central
respiratory failure which necessitates mechanical ventilation
but usually the prognosis is grave
The groups of nerve cells in the brain which regulates the
respiration rhythmicallyare collectively known as respiratory
centres. respiratory centre is composed ofseveral widely dispersed
groups of neurons.
Groups: Respiratory centre is divided four major groups.
Respiratorycentres
Location Name of nucleus
Function
1. Inspiratorycentre ( Dorsalrespiratorygroup)
Dorsal portion ofmedullaoblongate
Nucleus ofTractus solitarius
It causes inspirationwhile stimulated.
2. Expiratorycentre ( VentralrespiratoryGroup)
Antero- lateralpart of medulla,about 5 mmanterior andlateral to
dorsalrespiratory group
Nucleusambiguous andnucleus retroambiguous.
1. It causes eitherexpiration or inspirationdepending upon
whichneuron in the group arestimulated. Butgenerally causes
expiration
2. It sends inhibitoryimpulse to theapneustic centre.
3. Pneumotaxiccentre
Upper part ofpons
Nucleusparabrachialis
1.It controls both rateand pattern ofbreathing
2. It sends impulses to
limit inspiration.
http://en.wikipedia.org/wiki/Medulla_oblongatahttp://en.wikipedia.org/wiki/Brain_stemhttp://en.wikipedia.org/w/index.php?title=Central_respiratory_failure&action=edit&redlink=1http://en.wikipedia.org/wiki/Medulla_oblongatahttp://en.wikipedia.org/wiki/Brain_stemhttp://en.wikipedia.org/w/index.php?title=Central_respiratory_failure&action=edit&redlink=1
-
8/7/2019 lecture regulation of resp
3/15
Apneustic centre In the lower partof the pons.
1. It dischargesstimulatory impulse tothe inspiratory
centrecausing inspiration.
2. It receives inhibitoryimpulse frompneumotaxic centre andfrom
stretch receptor oflung.
3. It dischargesinhibitory impulse toexpiratory centre.
(Ref. Guyton & Hall11th P. 515)
-
8/7/2019 lecture regulation of resp
4/15
Apneustic respirationApneustic respiration (apneusis) is an
abnormal pattern of breathingcharacterized by deep, gasping
inspiration with a pause at full inspirationfollowed by a brief,
insufficient release.
Causes
It is caused by damage to the pons or uppermedulla caused by
strokes ortrauma. Specifically, concurrent removal of input from
the vagus nerve and the
pneumotaxic centercauses this pattern of breathing.
It can also be temporarily caused by some drugs, such as
ketamine.
Nervous regulation of respiration/Rhythmic breathingInhaling
& expiring of air at a regular interval of time is rhythmic
breathing.
http://en.wikipedia.org/wiki/Ponshttp://en.wikipedia.org/wiki/Medulla_oblongatahttp://en.wikipedia.org/wiki/Vagus_nervehttp://en.wikipedia.org/wiki/Pneumotaxic_centerhttp://en.wikipedia.org/wiki/Ketaminehttp://en.wikipedia.org/wiki/Ponshttp://en.wikipedia.org/wiki/Medulla_oblongatahttp://en.wikipedia.org/wiki/Vagus_nervehttp://en.wikipedia.org/wiki/Pneumotaxic_centerhttp://en.wikipedia.org/wiki/Ketamine
-
8/7/2019 lecture regulation of resp
5/15
Process
Spontaneous inspiratory rampsignal produced b inspiratory
center. \
Passing through phrenic & intcostal nervesafter 2 sec. ramp
signal switch-off by pneumotaxic center
expiration fakes place by passive way.
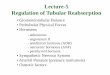
Chemical regulation of respirationThe rhythmic discharge is
regulated by alteration in arterial PO2, PCO2, & [H
+] thischemical control is supported by non-chemical
influences.
A number of chemical factors such as1) Elevated bloodPco2 for
concentration of C02.2) Elevatedblood H+ (i.e. PH) and
3) Decreased blood P02 (or concentration of 02) areinvolved in
chemical controlof respiration.
Effects of C02 on alveolar ventilation:-- C02 itself has little
direct effect in stimulating the respiratory centre.-- Reflex
action:The C02 diffuses through the blood- brain barrier into CSF
and combines withwater to form carbonic acid, which dissociates
into H+ and HCO3
- ions. The H+
then stimulates the central chemoreceptor area.
As a result the rate and depth of respiration is increased.
A maximal increase in CO2 can increase alveolar ventilation
about 10- fold.
Effect of H+ (i.e.pH) on alveolar ventilation:Increased blood H
concentration (i.e. decreased pH increased alveolar ventilation.The
effects of blob H+ concentration on ventilation are thought to be
mediated byway of peripheral chemoreceptors in addition to direct
effects on the respiratorycentre.Central chemoreceptors are
stimulated only slightly by increased, H+
concentration in the blood because the blood- brain barrier is
relatively
impermeable to H+
A maximalincrease in H+
concentration can increase alveolarventilation about 4-fold.
Effect of decreasedO2 on alveolar ventilation:Peripheral
chemoreceptors in the carotid and aortic bodies are stimulated
bydecreased 02 in the arterial blood. But, the arterial P02must
decrease to below60 mm Hg for stimulation to occur.
-
8/7/2019 lecture regulation of resp
6/15
-
8/7/2019 lecture regulation of resp
7/15
-
8/7/2019 lecture regulation of resp
8/15
Exercise on respiration
Effect of exercise on respiration
Para meter Effect
1. O2 Consumption Increase
2. O2 Production and elimination Increase
3. Ventilation Increase
4. Arterial PO2 + PCO2 No overall change
5. Arterial pH No change in moderate exercise
Decreases in strenuous exercise
6. Venous PCO2 Increases
7. Pulmonary blood flow Increases ( which always equals
thecardiac out put)
8. Ventilation perfusion ratio More evenly distributed in
lung
Regulation of respiration during exercise
During exercise, the rate of respiration increases. This
increases in respiration iscontrolled by both neural and chemical
mechanisms.
1. Nervous factor or direct stimulation of respiratory centre
from motorcortex:
a. During exercise the brain transmitting impulses to, the
contracting musclesalso transmit collateral impulses to
therespiratory centre.
b. This stimulation of respiratory centre increases the rate
ofrespiration.\
2. Chemical factors or stimulation caused by chemical
substances:
a. During exercise, the Pco2 increases andO2 decreases due to
excessmetabolism in the cells.
-
8/7/2019 lecture regulation of resp
9/15
b. This then stimulates chemosensitive area of
brainthroughchemoreceptors which then increase the rate of
respiration.
3. . Indirect stimulation from proprioceptors
a. During exercise, the movements of the limbs and body excites
theproprioceptors
b. This then transmits impulse to the respiratory centres
c. This increase rate ofrespiration
4. Hypoxia: During exercise, hypoxia develops in the muscles
that elicitsafferent nerve signal to the respiratory to excite
respiration
How is extra amount of 02 supplied to the tissues during
exercise?
Ans. Extra amount of O2 is supplied to the tissues during
exercise by:1. Breathing: Increase in pulmonary ventilation
introduces large amounts of
fresh air into the lung.2. O2 uptake in the lung: Large amount
of oxygen are taken up from the
lungs by the blood. \3. Supply of oxygen to the tissues: A great
blood supply to the muscle due to
increased cardiac out put and redistribution of blood to the
systemiccirculation.
4. Removal of oxygen by the tissues: This is effected as
follows-
a. Dilatation and increase in the number of patent capillaries
in themuscles slows the rate of the blood how.
b. Low oxygen tension allows oxygen to diffuse more rapidly and
to agreater extent. \
c. High CO2 tension and raised temperature increases the extent
andrate of dissociation of oxyhaemoglobin,
Respiratory insufficiency
It means abnormalities in normal rate & depth of
respiration.Cause:
1.inadequate ventilation.2. Reduce gaseous diffusion through
respiratory membrane.3.Abnormal ventilationperfusion ratio.Eupnea:
Means normal breathing.
-
8/7/2019 lecture regulation of resp
10/15
Tachypnea: Means rapid breathing than normal. Bradypnea: Means
slow breathing than normal.Hypoxia: Means decreased O2 in
tissue.Anoxia: Means total lack of O2Hypoxaemia: Means reduced O2in
blood.
Hypercapnia: Means excess CO2 in blood.Hypocapnia: Means
depressed CO2 in blood.Dyspnoea: Means difficulty in
breathing.Apnoea: Means temporary cessation of breathing.
HYPOXIA
Hypoxia is oxygen (O2) deficiency at the tissue level.
Types with causes:1. Hypoxic hypoxia (anoxic anoxia): PO2 of the
arterial blood is reduced.
When a person exposed to high altitude (e.g. - in the plane
flying above16,000 meters), Hypoxic hypox develops. It is due to a
sudden drop in theinspired Po2 (
-
8/7/2019 lecture regulation of resp
11/15
b. Ventilation-perfusion imbalance.ii. Shunt Venous to arterial
shunt (right to left cardiac shunt).
iii. Pump failure (ventilatory failure)a. Fatigue
b. Mechenical defects
c. Depression of respiratory controller in the brain.
2.Anaemic hypoxia: It occurs due to-
a. Lack of hemoglobin
b. CO poisoningc. Abnormal Hb due to poisoning with nitrates,
nitric oxide and other
metals.
3. Stagnant or ischaemic hypoxia:It occurs due to-a. Decreased
cardiac output due to heart failure.b. Decreased blood flow to the
organ.c. Impaired venous return. haemorrhage and shock.
4. Histotoxic hypoxia: It occurs due to-a. Poisoning with
potassium cyanide which interferes tissue oxidation by
paralysis the enzyme cytocrom oxidase.b. Narcotics also
depressed tissue oxidation by interfere with dehydrogenous
system.
Acclimatization:Acclimatization means the adjustment of the
human body to suit in a new
climate. (E.g.-High altitude)
The five principal means by which acclimatization occur are:1.
Pulmonary ventilation.2. Red blood cell & Hb (about 20 gm/dl)3.
Diffusion capacity of the lungs.4. Vascularity of the tissues.5.
Ability of the cells to utilize 02 despite low P02.
CYANOSISBluish discoloration or skin of mucous membrane due to
presence of largeamount of reduced Hbin subcutaneous vessels.
-
8/7/2019 lecture regulation of resp
12/15
Amount of reduced fib showed the at least 5-7gm/dl.Occurs in
arterial hypoxia of stagnant hypoxia.
Causes:o Formation ofaltered Hbo Polycythemia
oRt of left shunt of heart
Type:Central Cyanosis- Causedby cardiac failure or pulmonary
disorder. eg- Tip ofthe tongue.Peripheral cyanosis- Local vascular
stains, shock, cold, temperature eg- Tip ofthe fingers.
Hypercapnea
Hypercapnea means excess CO2 in the body fluid
Cause
1. Hypoventilation
2. Obstruction in respiratory
3. Respiratory diseases such as asthma
Clinical features:
1. Depression of CNS : confusion
2. Respiratory depression
3. Come & death.
Effects of hypercapnoea:1. PCO2 more than 60 -75 mm Hg causes
severe dyspnoea.2. PCO2 more than 80-100 mm Hg causes a person
lathergic some times evensemicomatoes.3. PCO2 more than 100-150 mm
Hg causes anaesthesia & death.
-
8/7/2019 lecture regulation of resp
13/15
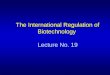
Cheyne stokes breathing
It is characterized by slow waxing & waning respiration
occurring over againevery 40 60 sec.Mechanism:
When the respiration becomes much more rapid & deeper than
usual,the PCO2in pulmonary blood decreases.This decreased PCO2
inhibit respiration by depressing respiratory center.
As a result, the pulmonary blood PCO2 increases.Then this blood
enters into the respiratory center & stimulate respiration
again, thus making the person over breath once again &
initiating a new cycle ofdepressed respiration.
Thecycle thus continue on & on, causing Cheyne-stokes
breathing.
Cheyne-Stokes breathing and its effect on arterial O2
saturation. Cheyne-
Stokes breathing occurs frequently during sleep, especially in
subjects at highaltitude, as in this example. In the presence of
preexisting hypoxemia secondaryto high altitude or other causes,
the periods ofapnea may result in further falls of O2 saturation to
dangerous levels.Falling PO2 and rising PCO2 during the apnea
intervals ultimatelyinduce a response and breathing returns,
reducing thestimuli and leading to a new period of apnea.
-
8/7/2019 lecture regulation of resp
14/15
Ventilation-perfusion ratioAns.D efinition : The ratio of
alveolar ventilation and alveolar blood flow is called
ventilation - perfusion ratio. It isabout 0.8.VA .... Alveolar
ventilation (V)This is expressed as Q ..... Cardiac output (Q)
4.2 L/min5L/min= 0.84
Explanation:1. When VA & Q is normal for a given alveolus,
The VA/Qwill be normal.2. When VA is zero but Q of the alveolus is
normal, then VA/Qwill he zero.3.When VA is normal but Q is
zero,then VA/Q will be infinity.At a ratio of either zero or
infinity, there is no exchange of gases through the
respiratory membrane of the affected alveoli.
Physiologic shuntThe total quantitative amount of shunted blood
per minute is called physiologicshunt. The greater the amount of
physiologic shunt the greater the amount ofblood fails to be
oxygenated as it passes through the lungs.
-
8/7/2019 lecture regulation of resp
15/15
Respiratory exchange ratio
The ratio of carbondioxide outside to oxygenuptake is called the
respiratory
e.\change ratio (R). That is.Rate of carbon dioxide outputR =
Rate of oxygen uptake
The value for R changes under different metabolic conditions.
When a person isusing exclusively carbohydrates for body
metabolism. R rises to 1.00.Conversely, when the person is using
exclusively fats for metabolic energy, the Rlevel falls to as low
as 0.7.