Embed Size (px)
Citation preview

Week beginning14 October 2013
Lecture 19
Vision & Visual Disorders
Lecturer: Dr Lucy [email protected]

Lecture Slides Lundy: Chapter 16 (not much) Tortura or any A&P on special senses
Reading
Lundy-Ekman. Neuroscience: Fundamentals for Rehabilitation, 4th Edition. W.B. Saunders Company, 2013.
Kandel et al. Principles of Neural Science, 5th Edition. McGraw Hill, 2012.
Tortura & Derrickson. Principles of anatomy and physiology, 13th Edition. Wiley. 2012.

The Retina Visual Pathways Accommodation Acquired Visual Disorders (10)
Overview

Learning Objectives
Have an in depth understanding of the anatomy of the retina and visual pathways through the brain
Understand the accommodation reflex neural pathways
Be able to name and describe the ten acquired disorders affecting vision outlined in this lecture
Gain an appreciation for the wonderment of intact visual processing!

Introduction Brain is responsible for organizing incoming
sensory information into something meaningful enough to guide our behaviours
Considering vision alone, the perception of a scene is complicated and involves many different factors◦ Forms, colours, textures, locations, 3-D,
movement◦ PLUS: our own body/eye movement◦ PLUS: knowing/understanding objects etc
We really “see” with our brain

Central retinal artery & central retinal vein

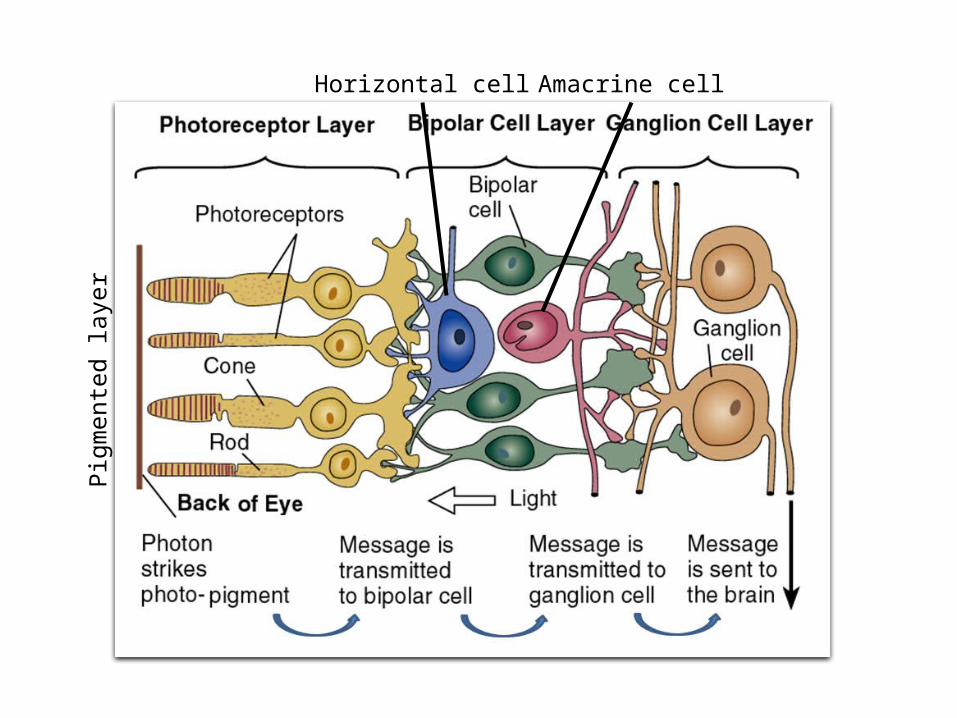
Optic disc (blind spot): site where CN II exits eyeball
Macula lutea: exact centre of retina
Retina
View through an opthalmascope

Pigmented layer and neural layer
Retina
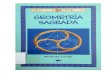
Pigmented layer: sheet of melanin-containing epithelial cells – helps absorb light-rays
Neural layer: outgrowth of brain that processes visual data extensively before transmitting impulses to via optic nerve
Detached retina occurs between these two layers. Fluid accumulates b/t layers and forces retina to billow outward, resulting in distortion or blindness in corresponding field of vision

Neural layer has 3 sub-layers:◦ Photoreceptor layer (rods & cones): process
light rays. Rods allow us to see in dim light, black & white. Cones produce colour vision (blue, green, red) Outer synaptic layer (synapses)
◦ Bipolar layer (bipolar cells, horizontal cells & amacrine cells): direct neural circuits laterally Inner synaptic layer (synapses)
◦ Ganglion cell layer: axons of ganglion cells form optic nerve
Retina
LIGHT
TO BRAIN
Not primary colours!

Outer synaptic layer
Inner synaptic layer
Pigm
ente
d layer
Pigm
ente
d layer
Horizontal cell Amacrine cell
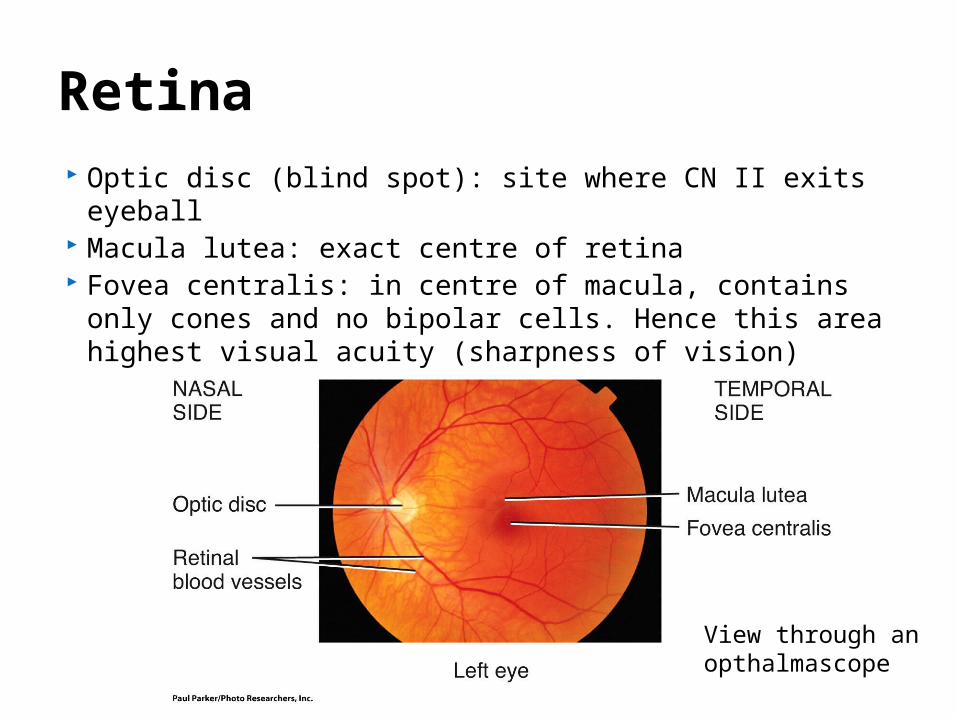
Optic disc (blind spot): site where CN II exits eyeball Macula lutea: exact centre of retina Fovea centralis: in centre of macula, contains only
cones and no bipolar cells. Hence this area highest visual acuity (sharpness of vision)
Retina
View through an opthalmascope

Within retina overall convergence predominates (126m photoreceptors, 1m ganglion cells)
Cells in bipolar layer have jobs in pre-processing vision (lateral inhibition, illumination level, etc) FYI
Most axons forming optic tract terminate in the lateral geniculate nucleus (thalamus) -> neurons forming optic radiation to primary visual cortex
Some fibers from optic tract terminate in superior colliculi – control extrinsic eye muscles/gaze
Some fibers terminate in pretectal nuclei (midbrain) – control pupillary and accommodation reflexes
Perception of vision (at highest level) is processed in 3 systems: shape, colour, and movement/location
Visual Pathway

Optic radiationGeniculocalcarine tract
Projections from the optic tract to the pretectal area, superior colliculi/tectum, and lateral geniculate nuclei and cortex

Flow of visual signals from the retina to the visual cortex, tectum (superior colliculi), and pretectal area. Signals arriving in the visual cortex are analyzed and then sent to other areas of the cerebral cortex, where directions for movement are created and where objects are recognized visually. Signals arriving in the tectum are used for orientation and eye movement control. Signals arriving in the pretectal area produce pupillary reflexes. Blue indicates sensory receptors and perception; pink indicates movement.

“Where” pathway
Parietal LobePerception of the spatial location/movement of objects
“What” pathway
Temporal Lobe3-D perception of size, shape, orientation, and colour

Accommodation is a change in curvature of the lens, contraction of the pupil, and position of the eyes in response to viewing a near object.
Accommodation Reflex

Afferent limb (blue)
The afferent limb is the retino-geniculo-calcarine pathway.
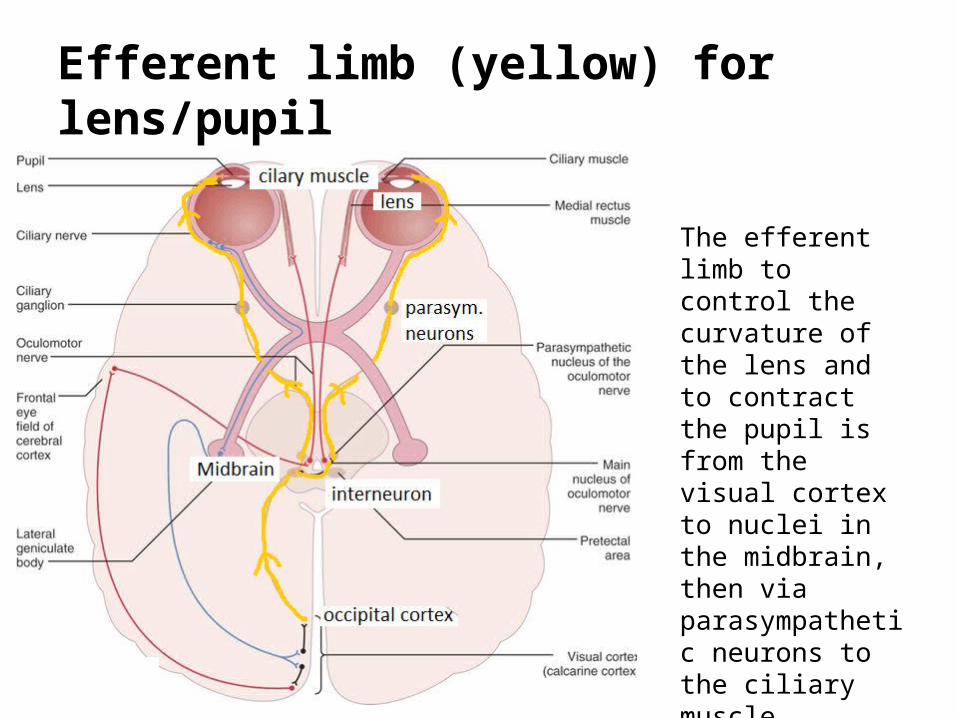
Efferent limb (yellow) for lens/pupil
The efferent limb to control the curvature of the lens and to contract the pupil is from the visual cortex to nuclei in the midbrain, then via parasympathetic neurons to the ciliary muscle.

The efferent limb to move the pupils toward the midline is from the visual cortex to the frontal eye fields, then to the main oculomotor nucleus, then the oculomotor nerve, which controls contraction of the medial rectus muscles.
Efferent limb (red) for pupils to midline

Fractured Minds
By Jenni A. Ogden Compilation of Jenni’s
experiences in her work as a Clinical Neuropsychologist
About $120 at bookstore
Second edition now available
Acquired Visual Disorders
1. Cortical Blindness2. Apperceptive Agnosia3. Object/Visual Agnosia 4. Prosopagnosia 5. Balint’s Syndrome6. Amusia (not solely
visual)7. Achromatopsia 8. Akinetopsia9. Hemineglect10. Split-brain syndrome
Janice, have taken this out

1. Cortical Blindness
Cortical = CortexSo this refers to the brain
Grey matter layer on the outside is the cortex

1. Cortical Blindness Often called
“Blindsight” A impairment to
higher vision caused by bilateral (both sides) damage to the occipital lobes
Patients believe they can not see
Eyes and visual pathways into the brain intact
Problem is here

1. Cortical Blindness Although conscious awareness of any
stimuli is denied, subjects show residual (left over) visual ability
E.g., patients can discriminate (tell the difference in)◦ shape◦ orientation◦ direction of movement◦ colour
above chance levels (not just guessing)

1. Cortical Blindness
Q: What shape is this?A: I can’t see, so I don’t know
Q: If you had to choose between square and circle?
A: Circle
(over many trials, more than 50% correct answers)

1. Cortical Blindness
Q: Which direction is this object moving?A: I can’t see, so I don’t know
Q: If you had to choose between right and left?
A: Right

2. Apperceptive AgnosiaA (without) pperceptive (perception) A (without) gnosia (knowledge)
An inability to “see” or perceive visual stimuli properly
Impairment of basic shape discrimination Low level visual processing is intact (i.e.
retina, optic nerve, etc, etc, colour, depth ok)
Area of damage usually diffuse (big and spread), affecting the occipital lobes and surrounding areas


Copies by Mr S.

Patients with apperceptive agnosia are unable to distinguish the different items in an array such as this.
If started on the hat by researcher, patient unable to continue tracing the hat with a pencil.

3. Object/Visual AgnosiaA (without) gnosia (knowledge)
An inability to recognize objects visually Occurs with bilateral (both sides) damage to the
occipital lobes Not a naming problem (know the names of
things) Objects can be recognized via other modalities,
i.e., semantic (meaning), tactile (touch), olfactory (smell), auditory (hearing), etc.
Patients can “see”/perceive properly (patients with apperceptive agnosia can’t do this)
Can be specific to categories of objects, i.e., vegetables, instruments, tools, etc.

3. Object/Visual Agnosia
• Patients can copy pictures but have no idea what they’re drawing
• Association problem (inability to go from ‘visual form’ to ‘interpretation of meaning’)
• Often called Associative Agnosia

If asked which of the two bottom pictures match the top picture, “A” would be chosen correctly.
A B

If asked which of the two bottom pictures match the top picture, chicken would not be pointed to reliably.
…from Fractured Minds
“When shown an object or a drawing of an object, his strategy is to describe its shape to himself and to guess what the object might be from his verbal description. A yellow feather he called a flower, a safety pin he called a clothes peg, and a vegetable peeler he called a razor. When shown a key, he described it thus: “a circle; there is a long, thin piece off one side; it is smooth on the top but seems to have a jagged edge on the bottom,” but he could not recognize it.”
“When shown a drawing of a cat sitting upright facing the camera, he described it as follows: “Here is a face, and these look like legs; it must be a person!”

…from Fractured Minds
“He can draw in a simplistic fashion, but his drawing of a flower looked more like a palm tree, and he drew a bed as a rectangle with four legs. He would not even attempt more complex or unfamiliar objects, such as a telephone or a broom, because he said he could not think how they might look.”
Unable to visualize, locate visual memories and bring into awareness
Doesn’t dream – lack of ability to generate visual images

Psychology: The Science of Behavior
Visual Agnosia: Lack of Awareness of Visual Perceptions Carlson F 9.10
A system incorporating the motor system might be used to prompt the correct answer.Could also result in prompting an incorrect answer!
The normal way would be for the sight of a pistol registered in the visual system to then relay to a store of knowledge about what an item like that is called.

…from Fractured Minds
“He can draw in a simplistic fashion, but his drawing of a flower looked more like a palm tree, and he drew a bed as a rectangle with four legs. He would not even attempt more complex or unfamiliar objects, such as a telephone or a broom, because he said he could not think how they might look.”
Unable to visualize, locate visual memories and bring into awareness
Doesn’t dream – lack of ability to generate visual images
http://www.youtube.com/watch?v=rwQpaHQ0hYw

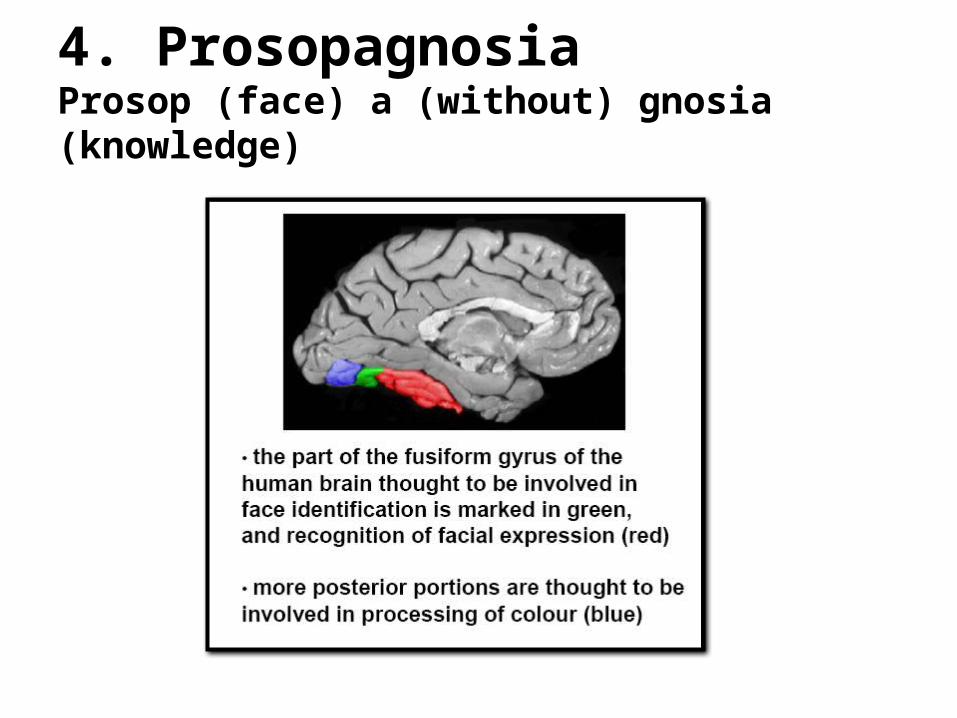
4. ProsopagnosiaProsop (face) a (without) gnosia (knowledge) An inability to recognize any individual’s
face visually Occurs with bilateral damage to the
occipital lobes Faces recognized as faces but not WHOSE
face Do not recognize themselves or loved ones! Loved ones can be recognized by other
modalities, e.g., gait, mole, etc.
4. ProsopagnosiaProsop (face) a (without) gnosia (knowledge)


…from Fractured Minds
“When asked how old a baby in a photograph might be, he said it looked like an old man because it did not have much hair.”
“He was able to identify a face as a face, but he often made errors across species. For example, he identified pictures of the faces of a teddy-bear, cat, and monkey as human faces.”
http://www.youtube.com/watch?v=ZogbIvdgfzQ&feature=related
5. Balint’s Syndrome Named after Rezső Bálint, who discovered
the syndrome in 1909. Disruption in the ability to keep track of
the location of objects in the visual scene An inability to see all of the objects in the
visual field simultaneously Patients can recognise individual objects
when they look directly at them but are unable to see where they are located.
The scene in front of them is a jumble of objects, arranged in no particular order.

5. Balint’s Syndrome
Damage is to the ‘start’ of the “where” pathway
“What” pathway
Parietal LobePerception of the spatial location/movement of objects
Temporal Lobe3-D perception of size, shape, orientation, and colour
Occipito-parietal region

Loss of colour perception
7. Achromatopsia
without colour vision
7. Achromatopsia
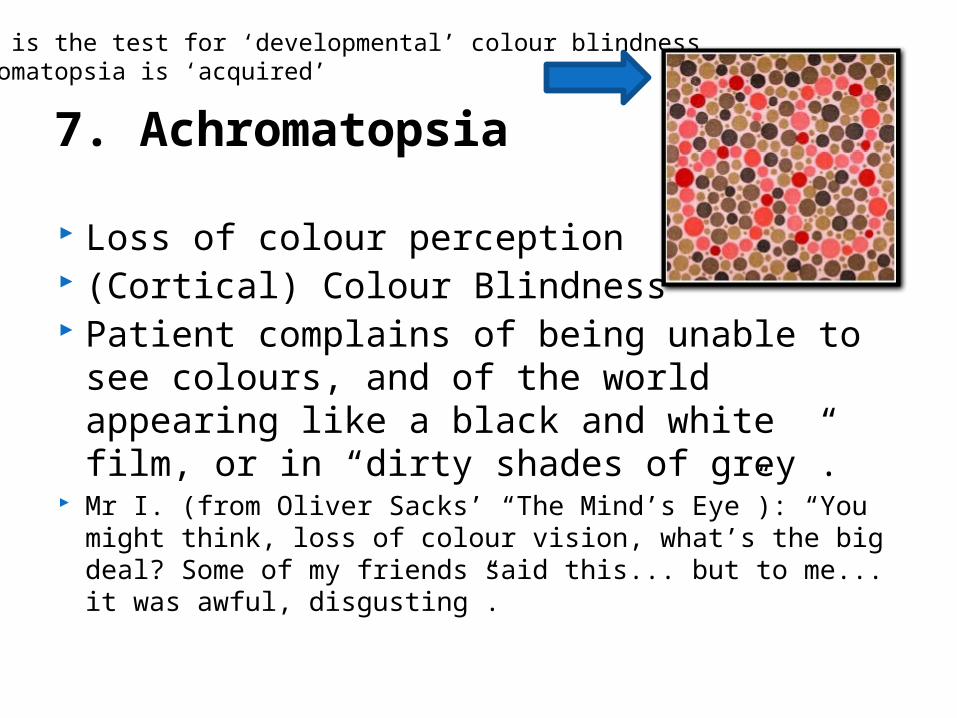
Loss of colour perception (Cortical) Colour Blindness Patient complains of being unable to see
colours, and of the world appearing like a black and white film, or in “dirty shades of grey”.
Mr I. (from Oliver Sacks’ “The Mind’s Eye”): “You might think, loss of colour vision, what’s the big deal? Some of my friends said this... but to me... it was awful, disgusting”.
This is the test for ‘developmental’ colour blindnessAchromatopsia is ‘acquired’
7. Achromatopsia
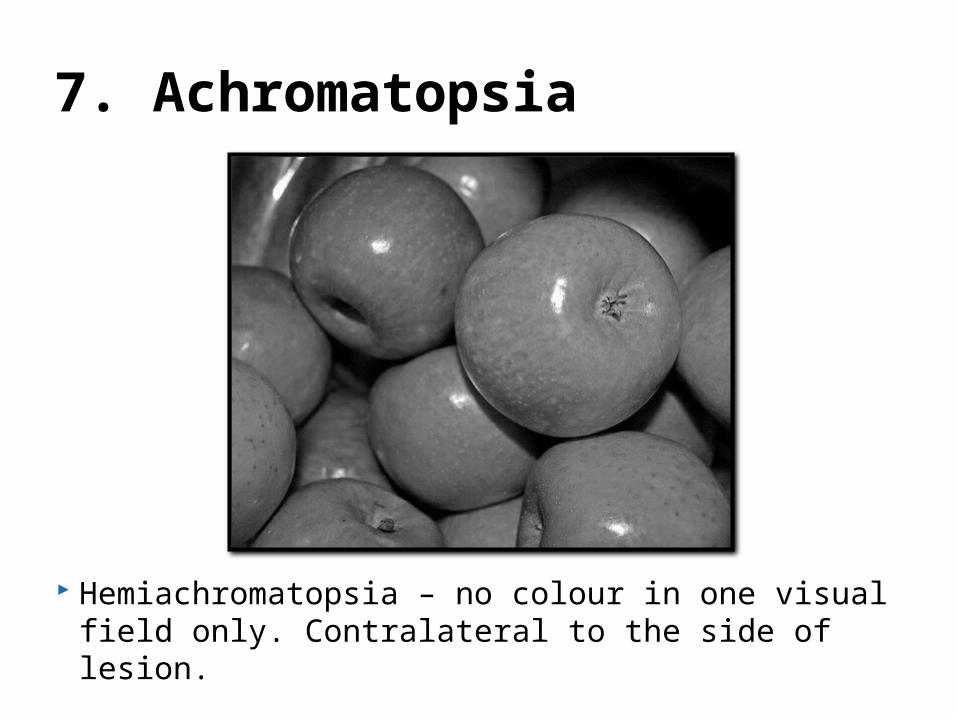
Hemiachromatopsia – no colour in one visual field only. Contralateral to the side of lesion.

8. AkinetopsiaA (without) kine (movement) topsia (vision)
Loss of movement perception Motion Blindness Other senses suggest
movement but vision suggests no movement
Lesions bilaterally (both sides) early on in dorsal/ventral pathways
World appears as a sequence of still images

9. HemineglectHemi (half) neglect (to unwittingly ignore) Impairment of the visual awareness to one
side of space. Usually occurs with damage to the right
parietal lobe (the “where” pathway).◦ Does occur transiently (briefly)
with damage to left parietal lobe.
◦ Possible that damage to right is more long-lasting because this is the dominant hemisphere for visuospatial perception.

9. HemineglectHemi (half) neglect (to unwittingly ignore)
Parietal lobe involved with spatial perception
Can be shown that information in the neglected side is processed to some degree e.g., like in Blindsight (unconscious perception)◦ House burning example (later)

9. Hemineglect
A CT scan of “Janet’s” brain showing a large glioma (tumor) in the right posterior parietal lobe (Ogden, 1996).
Neglect works contralaterally, so left visual field will be neglected due to right hemisphere lesion
9. Hemineglect Symptoms of hemineglect include:
◦ Banging into doorframes on the left side◦ Not dressing left side of body◦ Not acknowledging the arm and leg on left are patient’s
limbs◦ Not reading left side of page/words (e.g., downtown)◦ Not eating left side of plate!◦ Not acknowledging (or cursing!) those who approach
from left side◦ Not drawing the left side of pictures
Method used to curb problematic symptoms◦ Bells put on left wrist (draws attention that way)◦ Plate turned 180°


Left neglect
Right neglect
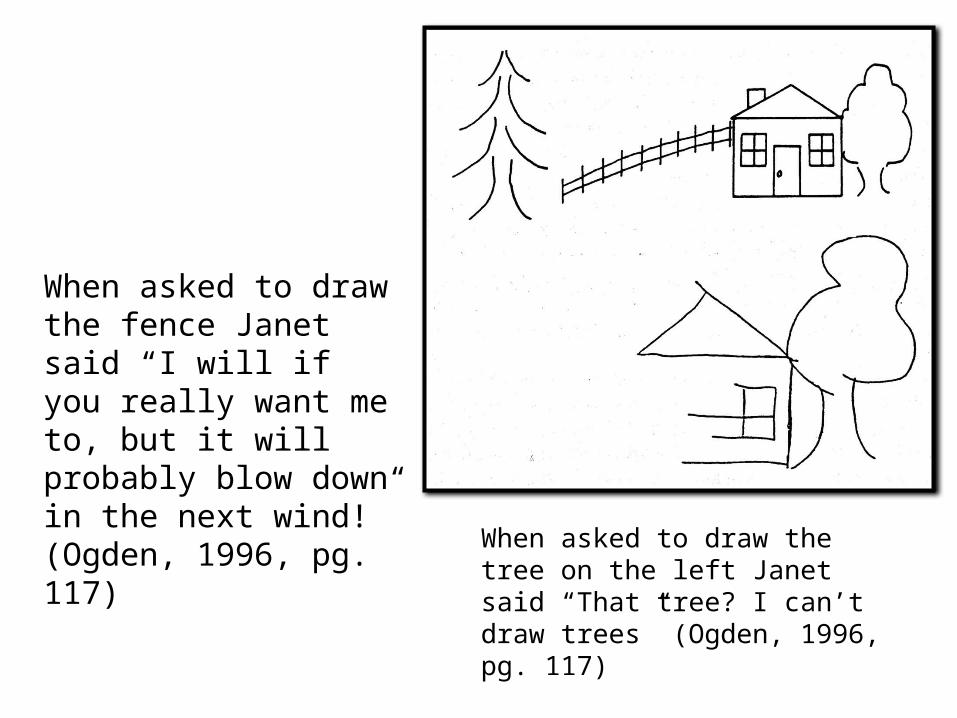
When asked to draw the fence Janet said “I will if you really want me to, but it will probably blow down in the next wind!” (Ogden, 1996, pg. 117) When asked to draw the tree
on the left Janet said “That tree? I can’t draw trees” (Ogden, 1996, pg. 117)

When asked to draw the fence, this patient said “That will blow down before the night is out!” (Ogden, 1996, pg. 117)

Line bisection
Normal controls bisect ~2% to the left (inferring dominance of right hemisphere).
Patients with hemineglect will bisect line WAY over to the right.

9. Hemineglect
This patient has been asked to “cross out” all the lines on the page

9. Hemineglect
This patient has been asked to find all the trees on the page

9. Hemineglect
Patients with hemineglect do not notice that these pictures depict a “chimera” (two things stuck together), they think it’s a picture of the face of one person.

Q: are the images the same or different?
A: the same
Q: if you had to choose one, which house would you prefer to live in?
A: the bottom house
Q: why is that?
A: I don’t know

10. Split-Brain Syndrome
Split-brain surgery: Corpus callosum severed
For people with profound, intractable epilepsy
About 100 split brain patients in the world Laboratory testing reveals separable
abilities of left and right hemispheres Most dramatic is right hemisphere’s
inability to speak◦ Broca’s Area and Wernicke’s Area both in LEFT
HEMISPHERE (96% of dextrals)


The paradigm

APPLE SPOON
Experimenter: What did you see?
Subject: Apple
Experimenter: Anything else?
Subject: No
SPOON APPLE

SPOON APPLE
APPLE SPOON
Experimenter: “Please pick up what you saw”
Apple picked up with right hand
Spoon picked up with left hand

SPOON APPLE
APPLE SPOON
Speak “apple”
OR
Pick up apple with right hand
Left hand can pick up spoon
Subject’s Action: