Embed Size (px)
Citation preview
Dr. Soliman Mohammed Soliman
Lecturer of Infectious Diseases
Dept. of Medicine and Infectious Diseases
Cou
rse
45
3
1. RABIES.
2. FELINE PAN-LEUKOPENIA VIRUS (FPV).
COMMON VIRAL DISEASES OF DOGS & CATS
4. INFECTIOUS CANINE HEPATITIS.
2. CANINE DISTEMPER.
3. CANINE PARVO. 3. FELINE INFECTIOUS PERITONITIS (FIP).
5. FELINE LEUKEMIA.
4. FELINE INFLUENZA.
1. RABIES
Viral Diseases Of Cats
2. FELINE PAN-LEUKOPENIA VIRUS (FPV).
3. FELINE INFECTIOUS PERITONITIS (FIP).
5. FELINE LEUKEMIA.
4. FELINE INFLUENZA.
1. RABIES
FELINE PANLEUKOPENIA
Susceptibility
• All cats are susceptible.
• The disease is seen most frequently in recently weaned kittens and young cats, less than 16 weeks (3 - 5 months) of age especially unvaccinated cats.
Feline Parvovirus Infection, Feline Infectious Enteritis, Feline Distemper.
• Feline panleukopenia, is an acute, highly contagious viral disease of catscharacterized by sudden onset, pyrexia, dehydration, vomition and diarrhea,profound leukopenia with high mortality.
Etiology
A parvovirus DNA, Parvoviridae which is closely related to canine parvovirus type 2but:
• There is no cardiac form
• The virus can infect fetuses causing cerebellar hypoplasia.
Distribution
• Worldwide in distribution.
• Endemic in almost all cat populations.
Mode of Infection/Transmission and Reservoir• The virus is present in all body secretions and excretions of affected animals;
nasal secretions, feces and urine.
• Mode of infection via inhalation or ingestion (fecal-oral).
• Transmitted by direct/indirect contact.
• The fetus is infected transplacentally.
• Recovered animals may shed virus for months as well as the virus remains in environment for years.
• Reservoir: kennels, pet shops and shelters
Pathogenesis• After infection the virus begins with initial replication in tonsils followed by
viraemia which results in infection of tissues.
• The virus required actively divided cells for effective replication as bonemarrow, spleen and intestinal crypts.
• The rapid destruction of these tissues will results in panleukopenia and stunted villi.
Clinical Signs• Incubation period 2-10 days (usually less than 10).
• The presence of signs is quite variable; some cats show none to few. Often manifest as sudden death or acute illness.
1) Subclinical infection
• Usually in older kittens and adults.
• Appear as fever without clinical signs followed by long life immunity.
2) Acute disease
• Severe in kittens between 6-24 weeks of age.
• Characterized by sudden onset of pyrexia, depression and anorexia.
• Vomiting accompanied with diarrhea (1-2 days).
• There is severe dehydration although affected cats appear thirstily.
• The hair becomes rough and the skin losses its elasticity.
• Abdominal palpation may elicit pain.
• Subnormal temp. followed by coma and death.
4) Per-acute cases:
• Sudden onset of severe depression, abdominal pain and hypothermia are followed by death in 24 hours.
• Mortality ranged from 25-90%.
• Infection of kittens in utero causes abortions and fetal brain defects in pregnant cats (feline cerebellar hypoplasia → ataxia).
• Not the same as canine distemper, and not contagious to dogs.
Signs includes:
Sudden onset,
High fever followed by, anorexia, depression, weakness,
Sternal recumbency with splayed legs and head droop (hunchingposture),
Vomiting, diarrhea, dehydration and
Profound leukopenia with high mortality (75% death rate).
Diagnosis
• A presumptive diagnosis of FP is sometimes made on the history of no vaccination, susceptible age, clinical signs, characteristic course and a severe leukopenia.
• A definitive diagnosis is based on laboratory findings.
2. Un-clotted blood for leukocytic count. Leukopenia in most acute cases is due to neutropenia is suggestive.
1. Portions of small intestine, lung, kidney, lymph node and spleen for histopathology. Also fetuses in abortions and if cerebellar hypoplasia is suspected.
Intranuclear inclusions in intestinal epithelial cells are significant. The microscopic changes in the small bowel, which include crypt necrosis, villous loss or shortening and collapse of the lamina propria, are diagnostic. The fetal brain is examined for evidence of cerebellar hypoplasia.
3. Portions of small intestine and spleen for fluorescent antibody (FA) staining. Specific fluorescent antibody staining of small intestine and spleen is reliable.
Differential diagnosis
• Feline infectious peritonitis, feline enteric coronavirus infection, feline leukemia, feline herpesvirus infection, feline calicivirus infection and feline immunodeficiency virus infection should be considered.
4. Feces for electron microscopy: The presence of parvovirus in feces can be determined by electron microscopy.
5. Kits are available to detect feline parvovirus in the feces of cats suspected of having FP.
• Because the virus produces little or no cytopathic changes, virus isolation is not usually carried out.
6. Serological tests as the HI test and virus neutralization test to detect a rising antibody titer.
Treatment
• No treatment after infection except for supportive care.
• Supportive to cope with dehydration and provide nutrients.
• Broad-spectrum antibiotics may be used to cope with secondary bacterial infections.
• Blood transfusions.
• With adequate treatment and care most kittens and cats recover.
• Recovered cats may shed virus for up to six weeks.
Control
• Modified live virus vaccine is usually given at 9 - 14 weeks of age.
• Live vaccines are contraindicated in pregnant queens and in kittens less than 4 weeks of age. Killed vaccines can be used in pregnant and young animals.
• Kitten should be vaccinated first at 8-10 weeks of age, again at 12-14 weeks and then annually.
• Booster vaccination is recommended.
• The virus is very resistant to environmental conditions and some common disinfectants. 1% Sodium hypochlorite solution (Clorox) is very effective.
Feline Enteric Coronavirus
Infection
Distribution
• Infection with FECV is common and occurs worldwide.
• Kittens in the age range of 6 - 12 weeks appear to be most susceptible by ingestion of contaminated food.
• The disease is usually mild and signs may include vomiting and diarrhea which accompanied with blood.
• Feline coronaviruses (Coronaviridae) are divided into two groups: The pathogenic strains that cause feline infectious peritonitis (FIP) and those feline enteric coronaviruses (FECV) that cause a subclinical or mild enteric infection. Viruses of these two categories are closely related.
Treatment
• Supportive and aimed at coping with the dehydration.
Diagnosis
• Supported by demonstrating with electron microscopy the characteristic coronavirus in the feces.
Control
• Impractical given the ubiquity of the virus.
Feline Infectious Peritonitis
(FIP)
• Feline infectious peritonitis (FIP) and pleuritis is a progressive, immune-mediated, debilitating, viral disease manifested in three forms:
1) The "wet" form with peritonitis
2) The "dry" mitted form.
3) The "mixed" form with pyogranuloma
• FIP usually associated with feline leukemia virus and feline infectious anemia virus.
• Probably the most common cause of unexplained fever in cats.
Etiology:
• FIP is caused by highly pathogenic strains of corona virus (Coronaviridae) that are closely related to feline enteric coronaviruses.
• There is the hypothesis that FIP can result from mutation of the feline enteric coronavirus within a carrier cat.
• It is RNA, sporadic virus
• Coronaviruses isolated from kittens with diarrhea and mild enteritis does not cause FIP.
Distribution:
• Probably worldwide.
• The general incidence is estimated to be 1 - 2 %, but can be much higher in some catteries.
Susceptibility:
• The infection occurs in cats and larger felidae of all ages but is most frequent at six months to five years of age.
• Most infections are dormant and clinical disease may not develop for months or years.
• About 5 - 10 % of seropositive cats, develop FIP.
• When the clinical disease develops it is usually fatal in a few weeks.
Mode of Infection/Transmission:
• The disease is contagious.
• The common route of infection is oronasal.
• In utero infections result in stillbirths and infected kittens.
Pathogenesis:
• The forms of the disease depend on the immune responses as follows:
1.Weak cell-mediated responses = persistent viremia and the effusive or "wet" form probably due to immune complexes. There is a vasculitis with leakage of serum and protein.
2.Moderate cell-mediated responses = the "dry", chronic non-effusive form. There is a delayed hypersensitivity which is responsible for the granulomatous lesions.
3.Strong cell-mediated = asymptomatic, persistent carriers or recovery.
Clinical Features:
Depending on the form, clinical signs may include:
Abdominal enlargement, depression, in appetence, fever, emaciation, anemia, neurologic and ocular signs.
Incubation: 2 weeks-2 months.
1. The "wet" form:
• Characterized by a chronic serofibrinous peritonitis or pleuritis, ascites and gradual abdominal enlargement. Adhesions, with septic peritonitis (the wet form mostly affect peritoneum, pericardium and thorax).
• Characteristic of the wet form, but not in all cases, are ascites, pericardial and pleural effusions, dyspnea and jaundice.
2. The "dry", granulomatous, or non-exudative form:
• Usually involves the brain, eye, or abdominal and thoracic viscera.
• The disease affect liver, kidney, eye (Uvitis and blindness) and CNS (paresis, paralysis and convulsions)
3. Intermediate clinical forms also occur.
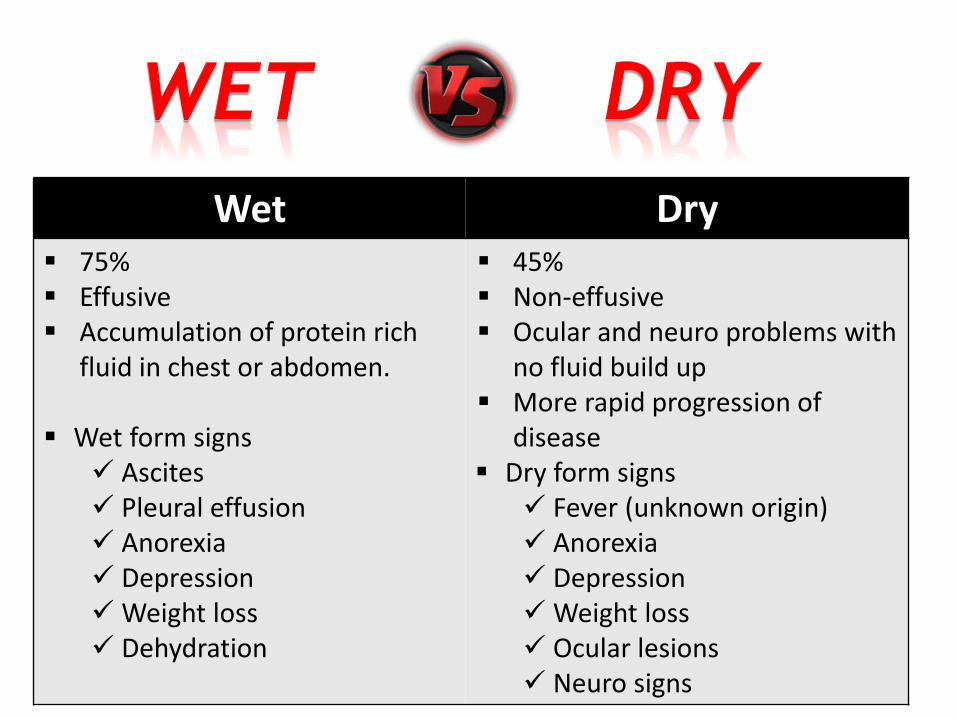
DryWet 45% Non-effusive Ocular and neuro problems with
no fluid build up More rapid progression of
disease Dry form signs
Fever (unknown origin) Anorexia Depression Weight loss Ocular lesions Neuro signs
75% Effusive Accumulation of protein rich
fluid in chest or abdomen.
Wet form signs Ascites Pleural effusion Anorexia Depression Weight loss Dehydration
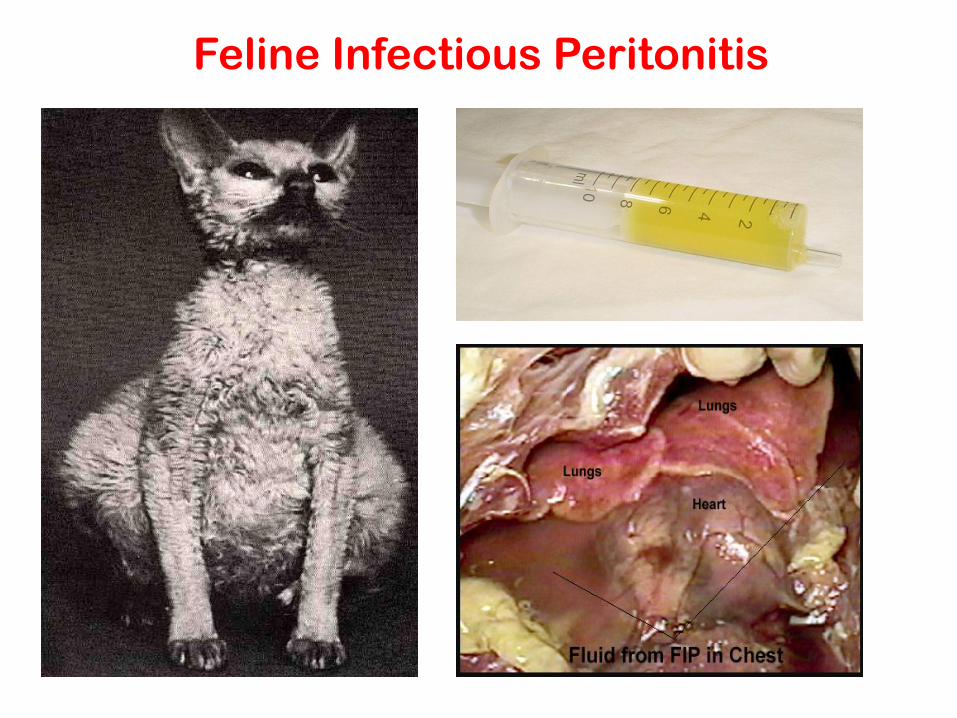
Feline Infectious Peritonitis
Diagnosis
1. Clinical signs:
• The disease is suspected when there is a fever that doesn't respond to antibiotics, along with the presence of fluid exudates in the thoracic and peritoneal cavities without an obvious infectious agent (high protein content of the effusion in the wet form).
2. Virus isolation for various reasons is not practicable.
3. Serological procedures:
• Some diagnostic laboratories do not offer serological testing for FIP because of the difficulty of interpreting results.
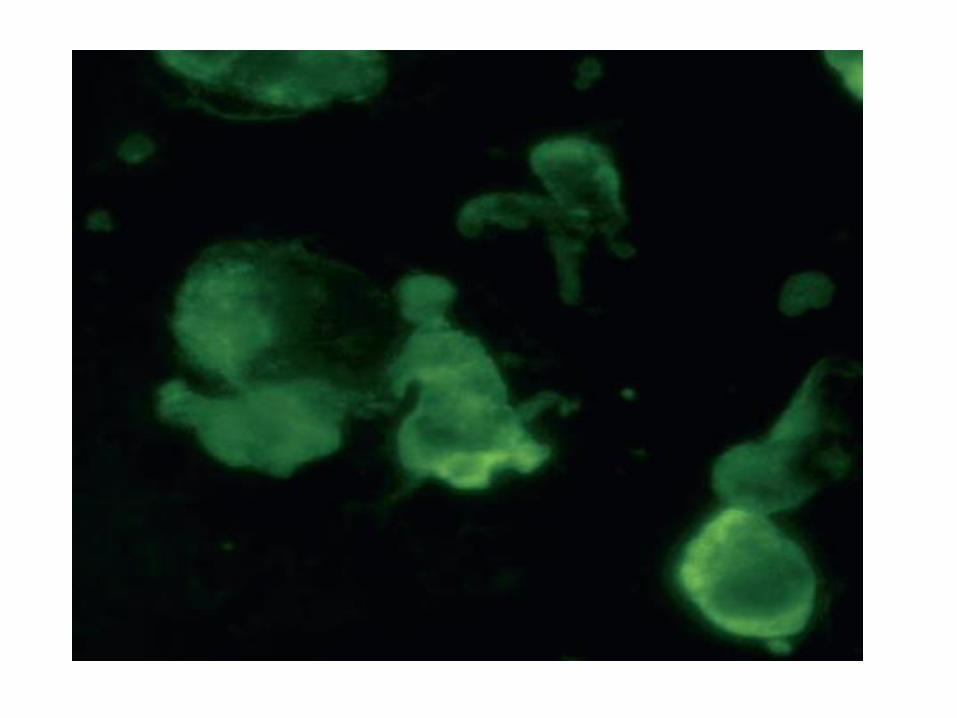
• A positive FIP-indirect immunofluorescence assay (IFA) only means the animal has been exposed to a coronavirus.
• The IFA test for antibody is preferred over the ELISA although both IFA and ELISA detect antibodies for both FIP and feline enteric coronavirus, thus a positive titer does not confirm a diagnosis of FIP.
• A positive FIP-IFA test (titers of 1:50 up to 1:6000), along with clinical signs of FIP, would support a diagnosis of FIP. Although uncommon, some cats with FIP are serologically negative.
• Commercial kits for ELISA and IFA are available to test for antibodies to feline coronavirus but results must be interpreted with caution.
4. Histopathology:
• Biopsy is taken from the affected organ.
5. Moderate to severe anemia, neutrophilia and leukopenia are suggestive of FIP.
Differential diagnosis:
• Cardiac failure, lymphosarcoma and ruptured lymphatic duct, i.e., diseases resulting in thoracic and abdominal cavity effusions, should be considered as well as feline leukemia, feline immunodeficiency virus infection and feline panleukopenia.
Treatment
• No specific treatment; supportive care.
Control
• If feasible, isolate serologically positive cats and strict sanitation.
• Killed and attenuated live vaccines have not been considered effective although efficacy has been claimed for an intranasal, modified live virus vaccine.
Feline Upper Respiratory Disease
Complex
Feline Influenza, Cat Flu
• Feline upper respiratory complex includes diseases characterizedby rhinitis, conjunctivitis, lacrimation, coughing, salivation and oralulceration.
• Those infections are discussed together for practical reasons; theirdifferential diagnosis; laboratory diagnosis; treatment and control arenearly similar, thus making differential diagnosis difficult. Laboratorydiagnosis is recommended for their differentiation.
• The various agents of these respiratory infections are mainly spreadby direct contact, via fomites and by aerosol inhalation and ingestion.Agents may be present in saliva, nasal and ocular discharges.Crowding contributes to spread.
• Infections can be more severe if the immune system is impaired byinfection with FeLV or FIV. Although infections are usually limitedto the upper respiratory tract they may be complicated by bronchialinfection or pneumonia. Generally speaking infections are moresevere in kittens and older cats.
Etiology:
• Feline Herpes virus-1 (50%) {Feline Viral Rhinotracheitis (FVR)}
• Feline Calici virus (40%) {Feline Calicivirus Infection (FCV)}
• Chlamydia psittaci + Mycoplasma + Reoviruses (5-10%)
Susceptibly:
• Most infections occur in kittens around 5-8 weeks of age in FVR while in calicivirus at 2-6 months (8-24 weeks) of age.
• High morbidity low mortality unless there is secondary bacterial infection.
MOI:
• Droplet infection (inhalation).
Transmission:
• Direct and indirect contact.
• FVR Virus shed intermittently, while FCV shed continuously in convalescent cats.
Symptoms: I.P 2-10 days
• Upper respiratory infection caused by a Herpes virus-1.
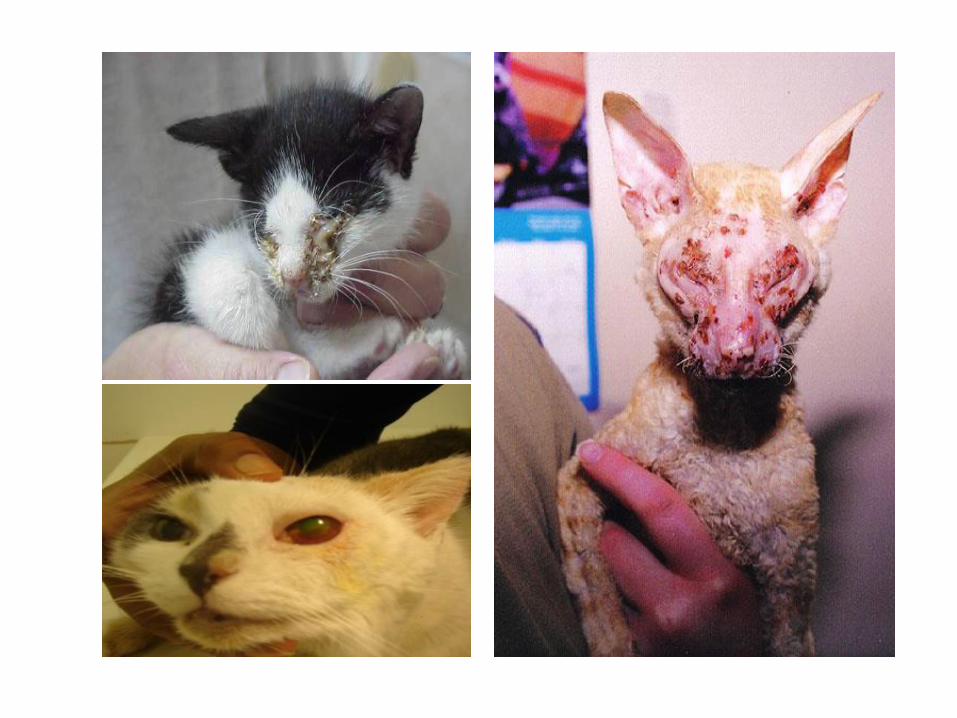
• Characterized by sudden onset of fever (40.5°C), sneezing, coughing, salivation, bilateral copious mucoid nasal discharge (serous then become purulent and may form crusts that close the nostrils) and lacrimation.
• Ocular disease can be severe, with keratitis and conjunctivitis.
• Off food (because it cannot smell the food/ pharyngitis/ ulcerative stomatitis).
• The disease is most severe in kittens when pneumonia occurs and mortality can be high. (complication)
• There may be corneal ulcer (ulcerative keratitis) and a severe panophthalmitis with opacity (neonatal ophthalmia→delayed separation of eyelids).
• Abortion may be seen during the sixth week of gestation in pregnant queens.
Feline Viral Rhinotracheitis (FVR):
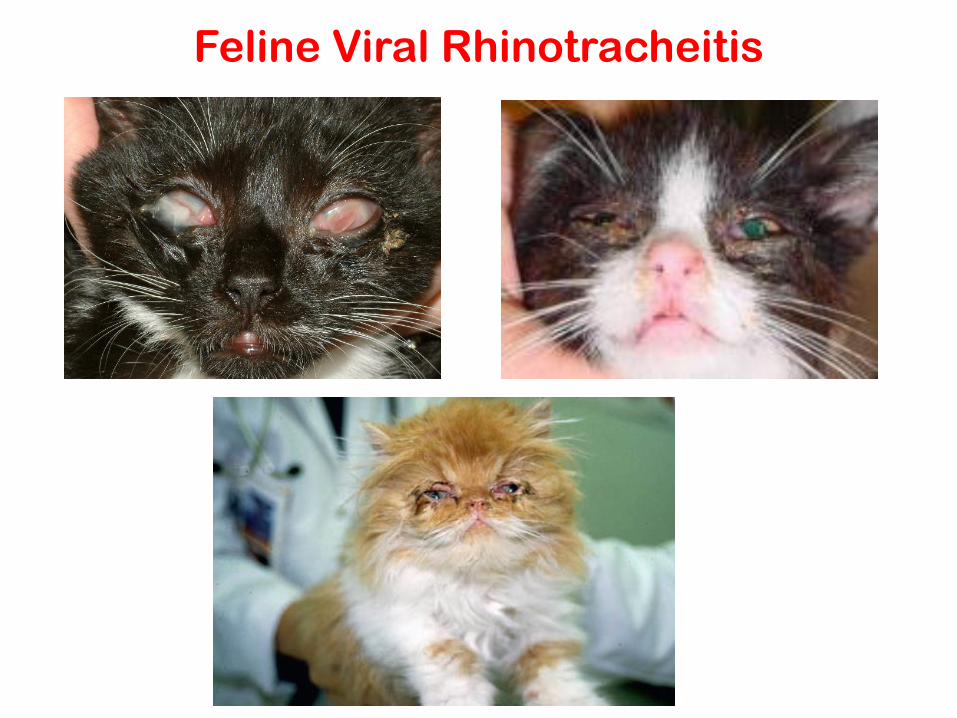
Feline Viral Rhinotracheitis

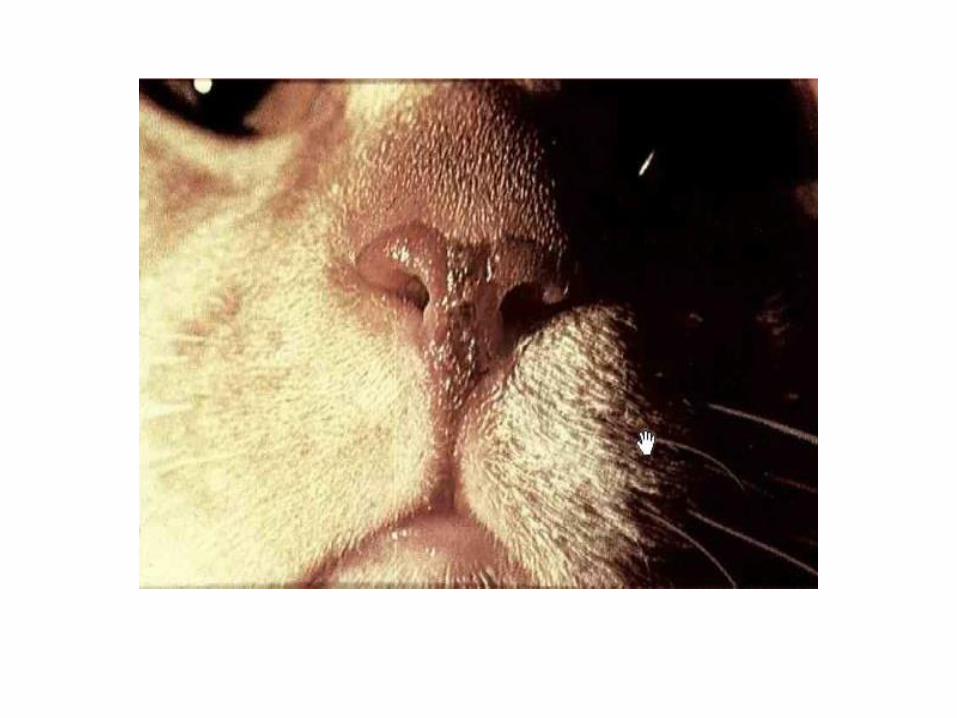
• Upper respiratory disease caused by a vesivirus in the family Caliciviridae.
• Characterized by fever, rhinitis, conjunctivitis with ocular and nasal discharge.
• Nasal and oral ulcers on dorsal surface of tongue and hard palate/ salivation.
• When bronchopneumonia develops, the mortality rate may exceed 30 %.
• Abortion may occur in queens.
• Lameness occurs following infection with some strains of calicivirus.
• Infected cats may become carriers and the virus can be shed continuously from the pharynx and tonsils for months and sometimes for years.
Symptoms: I.P 2-10 days
Feline Calicivirus Infection (FCV):

Feline Calicivirus

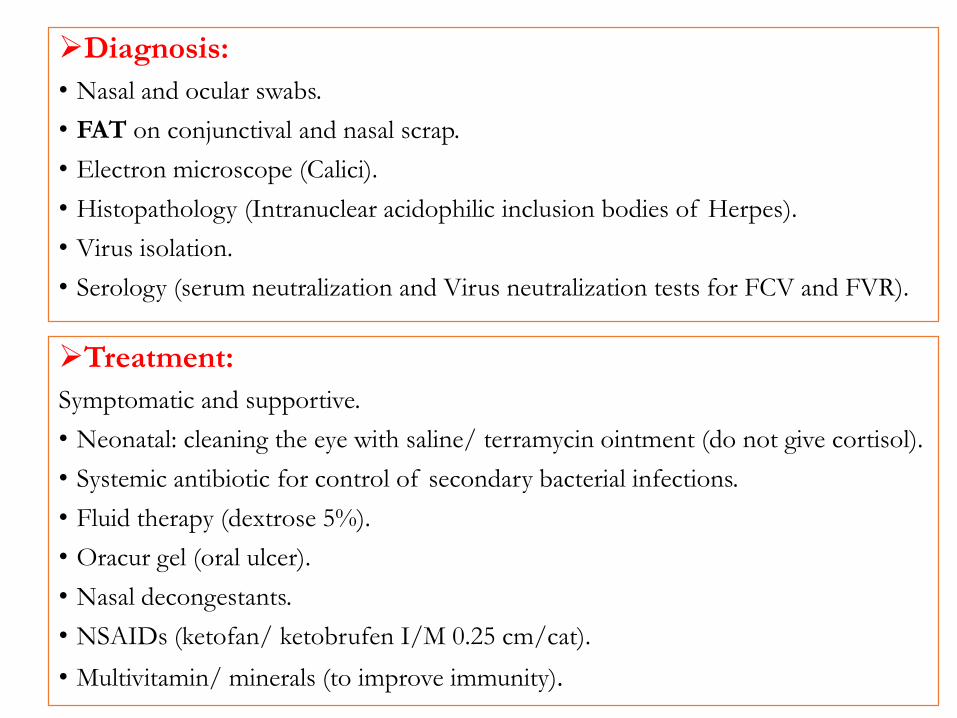
Diagnosis:
• Nasal and ocular swabs.
• FAT on conjunctival and nasal scrap.
• Electron microscope (Calici).
• Histopathology (Intranuclear acidophilic inclusion bodies of Herpes).
• Virus isolation.
• Serology (serum neutralization and Virus neutralization tests for FCV and FVR).
Treatment:
Symptomatic and supportive.
• Neonatal: cleaning the eye with saline/ terramycin ointment (do not give cortisol).
• Systemic antibiotic for control of secondary bacterial infections.
• Fluid therapy (dextrose 5%).
• Oracur gel (oral ulcer).
• Nasal decongestants.
• NSAIDs (ketofan/ ketobrufen I/M 0.25 cm/cat).
• Multivitamin/ minerals (to improve immunity).
Control:
Vaccination:
• Felocell [Herpes + Calici + Chlamydia + Panleukopenia]
• Live attenuated tissue culture vaccine (contraindicated in pregnant because in contains herpes)
• Given at 8 weeks with first booster after 3 weeks and second booster after 3 weeks then repeated annually.
• The 2 boosters to avoid maternal immunity which can neutralize the vaccine.
• If the dam is not immunized we can start the first dose at 6 weeks.
• Pregnant queens should be vaccinated with only killed feline calicivirusvaccine.
• Do not vaccinate feverish, sick, immune-suppressed or hypothermic animals.
Feline Leukemia Virus Infection
(FeLV)
• Feline leukemia virus infection is a Contagious fatal viral disease frequentlyoccurred caused by a retrovirus (feline leukemia virus; FeLV) Attacks anddestroys the immune system and manifested in a variety of clinical andpathologic forms.
• Considered the most serious and common killer of cats.
Etiology:
• A gamma retrovirus (Retroviridae). There are three subtypes, A, B. and C.
Distribution:
• Worldwide; it is estimated that 8 - 12 % of sick cats and 1 - 3 % of asymptomatic cats in the United States are infected.
Mode of Infection:
• Ingestion, transplacental and transmammary transmission possible.
Transmission:
• The virus is present in the saliva, urine, milk and feces. So,transmissioneither direct (e.g., licking, bite wounds) or indirect contact with vertical and horizontal transmission.
Susceptibility:
• FeLV infection is limited to the cat family.
• All domestic breeds, small exotic cats, European wildcats and jungle cats are susceptible.
• Young kittens are more susceptible to FeLV and susceptibility decreasing with age (Adults less often infected).
• Colostrum appears to protect kittens for the first month of life.
• Many cats may harbor the virus and even spread it to other cats before they show symptoms.
• It is estimated that only about 1 in 5 cats exposed at 10 weeks of age will develop persistent infection. Kittens of a persistently infected queen will usually become infected.
• Kittens that become infected may die, become immune, or not show symptoms for years
Pathogenesis:
• The main stages in the progression of FeLV infection are as follows:
2- Extensive involvement of organs
• The bone marrow, stomach, pharynx, esophagus, salivary glands, bladder and respiratory tract are involved that leading to:
Virus elimination, Latent infection or Active infection
With active infection, virus is excreted in saliva, feces, urine and respiratory secretions
Clinical disease is manifested in various forms.
1- Initial infection
• Virus replicating in surrounding lymphatic tissues Primary or transient viremia.
• Replication in systemic lymphatic tissues, bone marrow and other tissues Secondary or persistent viremia
• Incubation period: 2-3 years
• Clinical signs vary with the different forms of the disease and are related to the nature, extent and location of lesions as well as asymptomatic carriers are common.
Clinical Signs and Forms of the Disease
• Generally: Clinical signs are Fever, Anorexia, Weight loss, Anemia, Secondary infections, Vomiting and diarrhea, Abortion, Renal disease and Neuro problems.
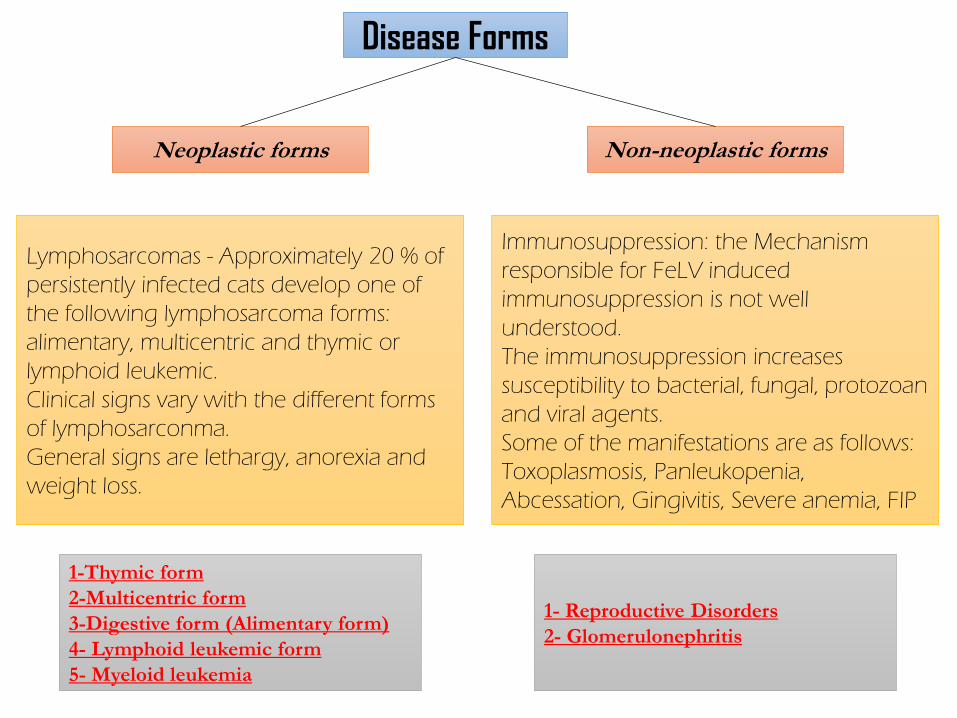
Disease Forms
Neoplastic forms Non-neoplastic forms
Lymphosarcomas - Approximately 20 % of
persistently infected cats develop one of
the following lymphosarcoma forms:
alimentary, multicentric and thymic or
lymphoid leukemic.
Clinical signs vary with the different forms
of lymphosarconma.
General signs are lethargy, anorexia and
weight loss.
Immunosuppression: the Mechanism
responsible for FeLV induced
immunosuppression is not well
understood.
The immunosuppression increases
susceptibility to bacterial, fungal, protozoan
and viral agents.
Some of the manifestations are as follows:
Toxoplasmosis, Panleukopenia,
Abcessation, Gingivitis, Severe anemia, FIP
1-Thymic form
2-Multicentric form
3-Digestive form (Alimentary form)
4- Lymphoid leukemic form
5- Myeloid leukemia
1- Reproductive Disorders
2- Glomerulonephritis
Clinical signs:
A- Neoplastic forms:
• Lymphosarcomas - Approximately 20 % of persistently infected cats develop one of the following lymphosarcoma forms: alimentary, multicentric and thymic or lymphoid leukemic.
• Clinical signs vary with the different forms of lymphosarconma.
• General signs are lethargy, anorexia and weight loss.
3-Digestive form (Alimentary form):
• The cat may display anorexia, vomiting and diarrhea. Abdominal masses involve the small intestine, cecum and colon; associated mesenteric lymph nodes may be affected.
1-Thymic form:
• Mediastainal lesions press on heart, trachea and oesoghagus.
• The heart has no sound (muffling of heart).
• Dysphagia and dyspnea are common signs and cyanosis may be present in advanced cases. Pleural fluid may contain neoplastic cells.
2-Multicentric form:
• Generalized lymphadenopathy, renal lymphosarcoma, splenomegaly and hepatomegaly may be found.
• This form is usually seen in young cats.
• Nodules in all organs include kindey, eye, liver.
4- Lymphoid leukemic form:
• The bone marrow is primarily involved and cancerous lymphocytes circulate in the blood.
• Jaundice, fever, anemia and pale mucous membranes are frequent and lymphadenopathy, splenomegaly and hepatomegaly may be present.
• Varying degrees of fever, anorexia and weakness are evident.
5- Myeloid leukemia:
• The primary lesion of this non-lymphosarcoma form is in the bone marrow with secondary involvement in the liver, spleen and lymph nodes.
• This form of leukemia is named according to which hematopoietic cell line is affected, e.g., myelogenous leukemia, erythroleukemia and lymphoblastic leukemia.
• Signs include progressive anemia, recurring fever and weight loss.
Clinical signs:
B- Non-neoplastic forms• Immunosuppression: the Mechanism responsible for FeLV induced immunosuppression is not well
understood. • The immunosuppression increases susceptibility to bacterial, fungal, protozoan and viral agents. • Some of the manifestations are as follows:
1. Toxoplasmosis.2. Panleukopenia.3. Abcessation.4. Gingivitis.5. Severe anemia.6. FIP
1- Reproductive Disorders:• FeLV infection may result in fetal death (fetal resorption), abortion (late gestation) and infertility. • Fetal death is thought to be due to endometritis and placentitis. It is estimated that about 75 % of
infected queens abort.• Fetuses that survive to term are persistently infected and the resulting kittens are weak and sickly. • FeLV infection is considered a cause of fading kitten syndrome.
2- Glomerulonephritis:• Glomerulonephritis may be present in cats with persistent FeLV infection. • It is thought to be due to the deposition of antigen-antibody complexes in the kidney. • There is evidence that this immune complex-mediated glomerular nephritis is an important cause of
death in FeLV infection.
Diagnosis:
• Test kit ELISA to detect both primary and secondary stages of viremia.
• The test is highly sensitive and can identify cats with very early infections. So, Positive cats (virus is in the body) should be retested in 3-4 months or 60-90 days. If still positive, cat is infected for life.
• IFA which detects the progressive phase of the infection secondary viremia only, and cats with positive results for this test are unlikely to clear the virus. So, the majority of positive-testing cats remain infected for life.
• Histopathologic examination of biopsies, bone marrow examinations and cytology of thoracic and abdominal fluids.
• The cat's blood may reveal certain abnormalities indicative of FeLVinfection, including: Anemia, Lymphopenia and Neutropenia.
Treatment:
• Supportive therapy.
• Chemotherapy and irradiation may prolong life in cats with neoplasia.
• Antiviral agents may delay the onset of clinical signs but are not curative.
• Immuno- mediator interference drugs.
Control
• Isolate infected cats
• No treatment
• Vaccinate infected cats for other diseases
• Reduce stress
• The FeLV is labile and quickly loses its infectivity apart from the host. It is inactivated by commonly used disinfectants.
• There should be an interval of at least 1 month before introducing negative cats to a formerly infected environment.
• Sub-unit and killed virus vaccine are available and administered from nine weeks of age. They do not eliminate preexisting infections.
Feline Leukemia Virus







![Feline Infectious Peritonitis Virus Infection...Feline infectious peritonitis virus (FIPV) is a mutant form (biotype) of FECV ([Pedersen et al 1981b], [Poland et al 1996] and [Vennema](https://img.pdfslide.net/doc/110x75/5f0407097e708231d40bf544/feline-infectious-peritonitis-virus-infection-feline-infectious-peritonitis.jpg)





















