Embed Size (px)
Citation preview
Lee Memorial Health System Governance Board & Full Board of
Directors Meetings Thursday, March 28, 2013
1:00 p.m.
BOARD OF DIRECTORS
OFFICE 239-343-1500
FAX: 239-343-1599
13685 DOCTORS WAY #190
FT MYERS, FLORIDA 33912
CAPE CORAL HOSPITAL
GULF COAST MEDICAL CENTER HEALTHPARK MEDICAL CENTER
LEE MEMORIAL HOSPITAL
THE CHILDREN’S HOSPITAL THE REHABILITATION HOSPITAL
LEE PHYSICIAN GROUP
LEE CONVENIENT CARE
BOARD OF DIRECTORS
DISTRICT ONE
Stephen R. Brown, M.D.
Marilyn Stout
DISTRICT TWO
Richard B. Akin
Nancy M. McGovern, RN, MSM
DISTRICT THREE
Sanford N. Cohen, M.D.
David Collins
DISTRICT FOUR
Diane Champion
Chris Hansen
DISTRICT FIVE
Jessica Carter
Stephanie Meyer, BSN, RN
AGENDA
GOVERNANCE BOARD & FULL BOARD OF DIRECTORS’
MEETINGS March 28, 2013 1:00 p.m.
Gulf Coast Medical Center – Boardroom (Medical Office Building) 13685 Doctors Way, Ft. Myers, FL 33912
032813 GOVERNANCE BOARD & FULL BOARD\AGENDA(FINAL).doc Page 1 of 2
1. CALL TO ORDER (Richard Akin, Board Chairman) Lee Memorial Health System Board of Directors, sitting as the Lee Memorial Health System (LMHS) Board of Directors for Gulf Coast Medical Center & Lee Memorial Hospital/HealthPark Medical Center and the Board of Directors of its subsidiary corporations, including but not limited to Cape Memorial Hospital, Inc. doing business as Cape Coral Hospital; Lee Memorial Medical Management Inc.; Lee Memorial Home Health, Inc.; and HealthPark Care Center, Inc.
2. INVOCATION & PLEDGE OF ALLEGIANCE (Rev. Bill Miller, MDiv, BCC)
3. PUBLIC INPUT – Agenda Items: Any Public Input is limited to three minutes and a “Request to Address the Board of Directors” card must be completed and submitted to the Board Administrator prior to meeting.
4. RETIREMENT RECOGNITIONS: A. Alawayne Cartwright, R.N., 42 Years of Service, Radiology,
Cape Coral Hospital B. Walt E. Ittenbach, C.R.R.N., F.A.C.H.E, Service Years 1984 - 2013
Vice President, Rehabilitation Hospital
5. PRESIDENTS REPORT (Jim Nathan, CEO/President) (Verbal)
6. MEDICAL STAFF BUSINESS: (Approvals) A. Medical Staff Recommendations of 3/27/13 for:
Cape Coral Hospital; Gulf Coast Medical Center; HealthPark Medical Center; Lee Memorial Hospital; Golisano Children’s Hospital of SW Florida
B. Bylaw Revisions to Part I, Section 2.3.2; Part III, Section 2.1.14.2; Part III, Section 4.2.1.4.2 for:
Cape Coral Hospital; Gulf Coast Medical Center; HealthPark Medical Center; Lee Memorial Hospital; Golisano Children’s Hospital of SW Florida
7. FINANCIAL & STATISTICAL REPORTS - FEB 28, 2013 (Acceptance) (Mike German, Chief Financial Officer)
8. LABELLE PHYSICIAN OFFICE LEASE (Approval) (Dr. Avra Bowers, Lee Physician Group System Medical Director & Kris Fay, Lee Physician Group, Chief Administrative Officer)
BOARD OF DIRECTORS
OFFICE 239-343-1500
FAX: 239-343-1599
13685 DOCTORS WAY #190 FT MYERS, FLORIDA 33912
CAPE CORAL HOSPITAL
GULF COAST MEDICAL CENTER
HEALTHPARK MEDICAL CENTER
LEE MEMORIAL HOSPITAL
THE CHILDREN’S HOSPITAL
THE REHABILITATION HOSPITAL
LEE PHYSICIAN GROUP
LEE CONVENIENT CARE
BOARD OF DIRECTORS
DISTRICT ONE
Stephen R. Brown, M.D.
Marilyn Stout
DISTRICT TWO
Richard B. Akin
Nancy M. McGovern, RN, MSM
DISTRICT THREE
Sanford N. Cohen, M.D.
David Collins
DISTRICT FOUR
Diane Champion
Chris Hansen
DISTRICT FIVE
Jessica Carter
Stephanie Meyer, BSN, RN
032813 GOVERNANCE BOARD & FULLBOARD\AGENDA(FINAL).doc Page 2 of 2
GOVERNANCE BOARD LIAISON: DAVID COLLINS
9. CONSENT AGENDA: (All Directors) (Approval) A. Governance Meeting Minutes of October 18, 2012 B. Board Budget, FYTD 2013 C. Updated 2013 Board Community Consultants List D. Board Scorecard Results, October – December 2012
10. THE GOVERNANCE INSTITUTE (Gregg Loughman, Vice President, Governance Institute) A. Board Assessment Results (Acceptance)
11. PRESIDENT & CEO A. Annual Evaluation (Approval)(Jon Cecil, Chief Human Resources Officer) B. 40.09B: Presidents Unplanned Succession Process (Discussion)
(Sanford Cohen, M.D., Board Vice Chairman)
12.
BOARD POLICIES (Cathy Stephens, Board Administrator) REVIEW – NO CHANGES for the following policies:
1) 10.05E: Duties and Responsibility of Board of Directors 2) 10.23B: Certificate of Need Applications 3) 20.06C: Contract (Purchase, Sale, Transfer or Lease) 4) 30.01C: Organized Medical Staff 5) 40.01C: Pay Policy Statement
RETIREMENT of the following policies: 1) 10.18C: Quality and Performance Improvement 2) 10.25B: No Smoking Policy 3) 40.07A: Corrective Action Exemption
ADOPT revisions to the following policies: 1) Motion to Remove from TABLE: 20.14F: Use of Funds for Education,
Travel & Business Meeting/Special Event Expenses Tabled from Jan 24, 2013 Meeting
2) 10.09D: Agenda Item Background Material 3) 10.27F: Reporting and Accreditation 4) 10.43D: Board Member Standards 5) 10.47C: Compliance Program 6) 10.53A: Electronic Tablets 7) 10.54: Grievance Process 8) 30.04: Medical Staff Representation 9) 40.05C: Staffing Reductions
13. OTHER ITEMS A. From 10/18/12 Discussion: Board Event Attendance & Boardroom Modification B. Alzheimer’s Program (Steve Brown, MD, Board Member)
14. Date of the next GOVERNANCE BOARD MEETING Thursday, November 7, 2013 – 1:00 p.m. Gulf Coast Medical Center - Boardroom (Medical Office Building) 13685 Doctors Way, Fort Myers, FL 33912
LMHS SYSTEM BUSINESS - RICHARD AKIN, BOARD CHAIRMAN
15. OLD/NEW BUSINESS
16. BOARD OF DIRECTORS & BOARD ADMINISTRATOR REPORTS
17. Date of the next Regular Meeting: Thursday, April 11, 2013 - 1:00 p.m. QUALITY & SAFETY BOARD & FULL BOARD OF DIRECTORS MEETINGS FOLLOWED BY EDUCATIONAL WORKSHOP Gulf Coast Medical Center – Boardroom (13685 Doctors Way, Ft. Myers, FL 33912)
18. ADJOURN (Richard Akin, Board Chairman)
BOARD OF DIRECTORS
Invocation Prayer &
Pledge of Allegiance
___________________ L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
PUBLIC INPUT – AGENDA ITEMS:
Any public input
pertaining to items on the Agenda is limited to three
minutes and a “Request to Address the Board of Directors”
card must be completed and submitted to
the Board Administrator prior to meeting.
Refer to Board Policy: 10:15E: Public Addressing the Board Non-Agenda Item: Individuals wishing to address the Board on an item NOT on the Agenda, the Board office must be notified of subject matter at least seven (7) days prior to the meeting to allow staff time to prepare and to insure the matter is within the jurisdiction of the Board.
___________________
L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
RECOGNITIONS:
RETIREMENT RECOGNITIONS: Alawayne Cartwright, R.N., 42 years
of Service, Radiology Department, Cape Coral Hospital Walter E. Ittenbach, C.R.R.N.,
F.A.C.H.E, Years of Service: 1984 - 2013, Vice President; Rehabilitation Hospital
Proclamation
______________________________________________________________________________
L E E M E M O R I A L HEALTH SYSTEM BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
MMMaaarrrccchhh 222888,,, 222000111333 would like to recognize with sincere appreciation
Alawayne Cartwright, R.N. in her retirement of 42 dedicated service years
to the Lee Memorial Health System. The entire system wishes you health & happiness,
and all the best in your future endeavors.
BOARD OF DIRECTORS District 1 – Stephen R. Brown, MD • Marilyn Stout
District 2 – Richard B. Akin • Nancy M. McGovern, RN, MSM District 3 – Sanford N. Cohen, M.D. • David F. Collins
District 4 – Diane Champion • Chris Hansen District 5 – Jessica Carter • Stephanie L. Meyer, BSN, RN
Proclamation
______________________________________________________________________________
L E E M E M O R I A L HEALTH SYSTEM BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
MMMaaarrrccchhh 222888,,, 222000111333 would like to recognize with sincere appreciation
Walt E. Ittenbach, C.R.R.N, F.A.C.H.E in his retirement of dedicated service years 1984 - 2013
to the Lee Memorial Health System. The entire system wishes you health & happiness,
and all the best in your future endeavors.
BOARD OF DIRECTORS District 1 – Stephen R. Brown, MD • Marilyn Stout
District 2 – Richard B. Akin • Nancy M. McGovern, RN, MSM District 3 – Sanford N. Cohen, M.D. • David F. Collins
District 4 – Diane Champion • Chris Hansen District 5 – Jessica Carter • Stephanie L. Meyer, BSN, RN
___________________
L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
PRESIDENT’S REPORT
Jim Nathan CEO/President
(Verbal)
___________________
L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
MEDICAL STAFF BUSINESS FOR:
A. Medical Staff Recommendations of 3/27/13 B. Bylaw Revisions to Part I, Section 2.3.2;
Part III, Section 2.1.14.2; Part III, Section 4.2.1.4.2
Cape Coral Hospital Gulf Coast Medical Center HealthPark Medical Center Lee Memorial Hospital Golisano Children’s Hospital of SW Florida
LEE MEMORIAL HEALTH SYSTEM
Lee County, Florida #2
M E M O R A N D U M
To: Board of Directors From: Nancy A. Taylor, CPMSM, CPCS Director, Centralized Credentialing Services Subject: Cape Coral Hospital Medical Staff Recommendations Date: March 27, 2013 The Facility Medical Executive Committee of the Medical Staff recommends the following physicians and allied health practitioners and certifies they have met the requirements set forth in the bylaws:
1. Associate Staff Appointment: a. Michael L. Caselnova, M.D. – Family Medicine b. Denise A. Drago, M.D. - Pediatrics c. Basudev Pudasaini, M.D. – Nephrology d. Sat P. Punyani, M.D. – Emergency Medicine
2. Telemedicine Appointment – Privileges Only:
a. Carl V. Bundschuh, M.D. – Teleradiology b. Steven J. Karidas, M.D. - Teleradiology
3. Intrasystem Application:
a. Moses Shieh, D.O. – General Surgery 4. M.S. and A.H.P. Reappointments – 04-01-13 to 03-31-15 (list attached) 5. Temporary Privileges:
a. Ndidi N. Nwamu, M.D. – Internal Medicine, 03-21-13 – 04-19-13
6. First Year Completion – Active Staff Appointment: a. Sivakumar Raman, M.D. – Infectious Disease
7. First Year Completion – Associate Staff Appointment:
a. Barry K. Butler, M.D. – Internal Medicine b. Jay Wang, M.D. – Oncology/Hematology
6. Leave of Absence:
a. Luz Peguero, M.D. – Internal Medicine, 02-19-13 – 07-08-13 7. Return from Leave of Absence:
a. Michelle Mon, M.D. – General Surgery, 04-01-13 8. Resignations:
a. Shiyama Mudali, M.D. – Pathology, effective 04-06-13 b. Scott Orth, D.O. – Psychiatry, effective 07-16-13
Memorandum to Board of Directors - CCH March 27, 2013 Page 2 of 2 9. Privilege Request:
a. Richard J. Weiss, M.D. – Refer and follow 10. Allied Health Practitioners:
a. Pablo Banderas PA – Dr. Torricelli b. Christie Freese, PA – Inpatients Specialists of SW FL c. Janine Hass, ARNP – Pain Management Consultants of SW FL d. Adam Quarles ARNP – ICU Practitioners
11. Allied Health Practitioners – Additional Sponsor:
a. Michael DePalma, PA – Dr. Chavakula 12. Practitioner–in-Training:
a. April Smith, Nurse Practitioner Student – Dr. James Gostigian and Dr. Eihab Hassanein, 03-18-13 – 06-30-13
Approved by the Board of Directors – March 28, 2013
__________________________________________ Richard B. Akin, Chairman – Board of Directors
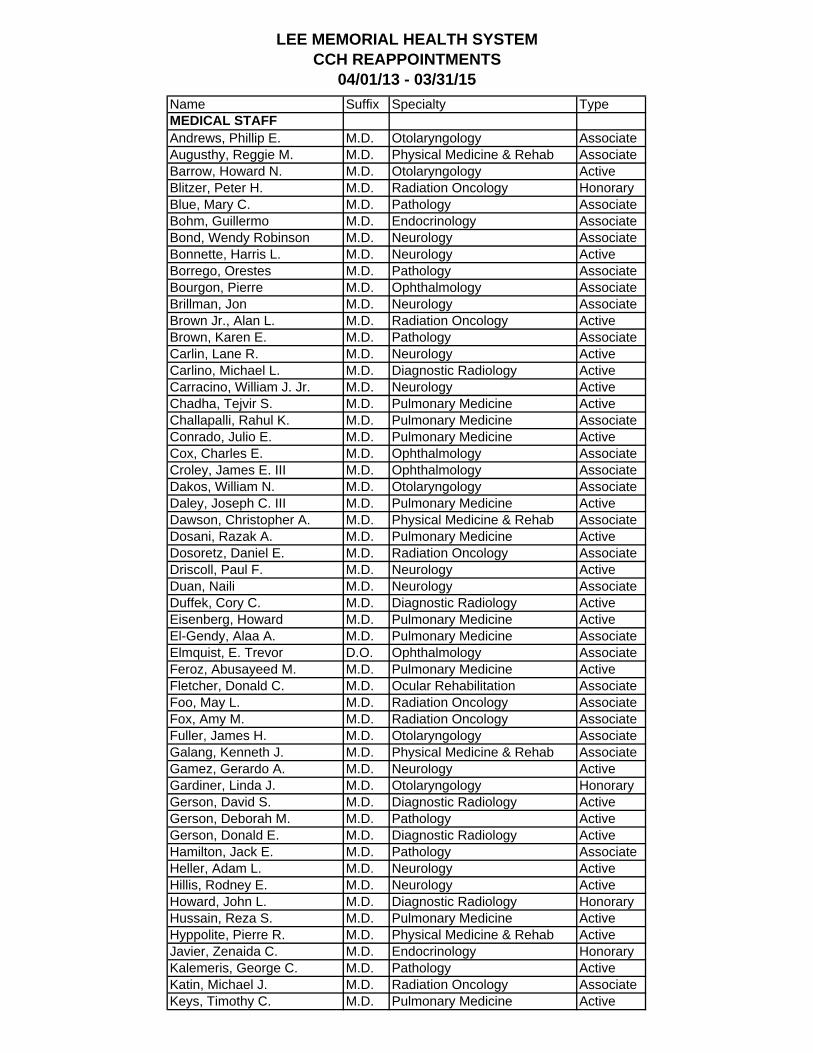
LEE MEMORIAL HEALTH SYSTEMCCH REAPPOINTMENTS
04/01/13 - 03/31/15
Name Suffix Specialty TypeMEDICAL STAFFAndrews, Phillip E. M.D. Otolaryngology AssociateAugusthy, Reggie M. M.D. Physical Medicine & Rehab AssociateBarrow, Howard N. M.D. Otolaryngology ActiveBlitzer, Peter H. M.D. Radiation Oncology HonoraryBlue, Mary C. M.D. Pathology AssociateBohm, Guillermo M.D. Endocrinology AssociateBond, Wendy Robinson M.D. Neurology AssociateBonnette, Harris L. M.D. Neurology ActiveBorrego, Orestes M.D. Pathology AssociateBourgon, Pierre M.D. Ophthalmology AssociateBrillman, Jon M.D. Neurology AssociateBrown Jr., Alan L. M.D. Radiation Oncology ActiveBrown, Karen E. M.D. Pathology AssociateCarlin, Lane R. M.D. Neurology ActiveCarlino, Michael L. M.D. Diagnostic Radiology ActiveCarracino, William J. Jr. M.D. Neurology ActiveChadha, Tejvir S. M.D. Pulmonary Medicine ActiveChallapalli, Rahul K. M.D. Pulmonary Medicine AssociateConrado, Julio E. M.D. Pulmonary Medicine ActiveCox, Charles E. M.D. Ophthalmology AssociateCroley, James E. III M.D. Ophthalmology AssociateDakos, William N. M.D. Otolaryngology AssociateDaley, Joseph C. III M.D. Pulmonary Medicine ActiveDawson, Christopher A. M.D. Physical Medicine & Rehab AssociateDosani, Razak A. M.D. Pulmonary Medicine ActiveDosoretz, Daniel E. M.D. Radiation Oncology AssociateDriscoll, Paul F. M.D. Neurology ActiveDuan, Naili M.D. Neurology AssociateDuffek, Cory C. M.D. Diagnostic Radiology ActiveEisenberg, Howard M.D. Pulmonary Medicine ActiveEl-Gendy, Alaa A. M.D. Pulmonary Medicine AssociateElmquist, E. Trevor D.O. Ophthalmology AssociateFeroz, Abusayeed M. M.D. Pulmonary Medicine ActiveFletcher, Donald C. M.D. Ocular Rehabilitation AssociateFoo, May L. M.D. Radiation Oncology AssociateFox, Amy M. M.D. Radiation Oncology AssociateFuller, James H. M.D. Otolaryngology AssociateGalang, Kenneth J. M.D. Physical Medicine & Rehab AssociateGamez, Gerardo A. M.D. Neurology ActiveGardiner, Linda J. M.D. Otolaryngology HonoraryGerson, David S. M.D. Diagnostic Radiology ActiveGerson, Deborah M. M.D. Pathology ActiveGerson, Donald E. M.D. Diagnostic Radiology ActiveHamilton, Jack E. M.D. Pathology AssociateHeller, Adam L. M.D. Neurology ActiveHillis, Rodney E. M.D. Neurology ActiveHoward, John L. M.D. Diagnostic Radiology HonoraryHussain, Reza S. M.D. Pulmonary Medicine ActiveHyppolite, Pierre R. M.D. Physical Medicine & Rehab ActiveJavier, Zenaida C. M.D. Endocrinology HonoraryKalemeris, George C. M.D. Pathology ActiveKatin, Michael J. M.D. Radiation Oncology AssociateKeys, Timothy C. M.D. Pulmonary Medicine Active
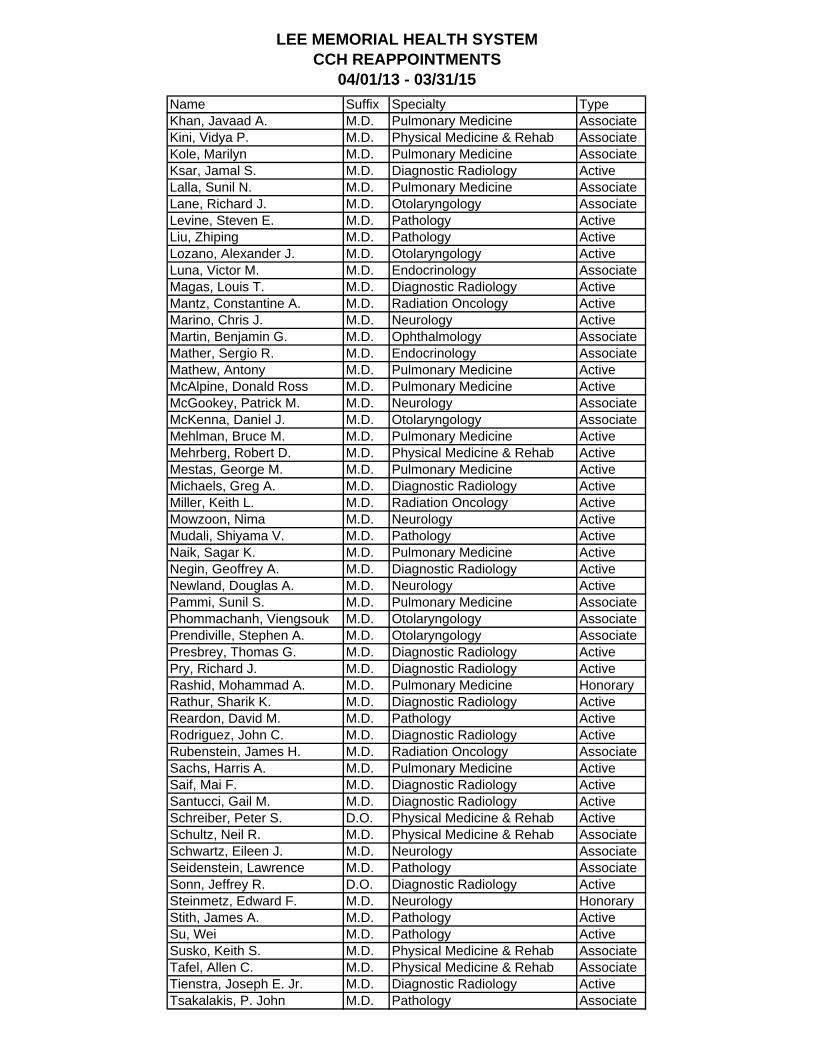
LEE MEMORIAL HEALTH SYSTEMCCH REAPPOINTMENTS
04/01/13 - 03/31/15
Name Suffix Specialty TypeKhan, Javaad A. M.D. Pulmonary Medicine AssociateKini, Vidya P. M.D. Physical Medicine & Rehab AssociateKole, Marilyn M.D. Pulmonary Medicine AssociateKsar, Jamal S. M.D. Diagnostic Radiology ActiveLalla, Sunil N. M.D. Pulmonary Medicine AssociateLane, Richard J. M.D. Otolaryngology AssociateLevine, Steven E. M.D. Pathology ActiveLiu, Zhiping M.D. Pathology ActiveLozano, Alexander J. M.D. Otolaryngology ActiveLuna, Victor M. M.D. Endocrinology AssociateMagas, Louis T. M.D. Diagnostic Radiology ActiveMantz, Constantine A. M.D. Radiation Oncology ActiveMarino, Chris J. M.D. Neurology ActiveMartin, Benjamin G. M.D. Ophthalmology AssociateMather, Sergio R. M.D. Endocrinology AssociateMathew, Antony M.D. Pulmonary Medicine ActiveMcAlpine, Donald Ross M.D. Pulmonary Medicine ActiveMcGookey, Patrick M. M.D. Neurology AssociateMcKenna, Daniel J. M.D. Otolaryngology AssociateMehlman, Bruce M. M.D. Pulmonary Medicine ActiveMehrberg, Robert D. M.D. Physical Medicine & Rehab ActiveMestas, George M. M.D. Pulmonary Medicine ActiveMichaels, Greg A. M.D. Diagnostic Radiology ActiveMiller, Keith L. M.D. Radiation Oncology ActiveMowzoon, Nima M.D. Neurology ActiveMudali, Shiyama V. M.D. Pathology ActiveNaik, Sagar K. M.D. Pulmonary Medicine ActiveNegin, Geoffrey A. M.D. Diagnostic Radiology ActiveNewland, Douglas A. M.D. Neurology ActivePammi, Sunil S. M.D. Pulmonary Medicine AssociatePhommachanh, Viengsouk M.D. Otolaryngology AssociatePrendiville, Stephen A. M.D. Otolaryngology AssociatePresbrey, Thomas G. M.D. Diagnostic Radiology ActivePry, Richard J. M.D. Diagnostic Radiology ActiveRashid, Mohammad A. M.D. Pulmonary Medicine HonoraryRathur, Sharik K. M.D. Diagnostic Radiology ActiveReardon, David M. M.D. Pathology ActiveRodriguez, John C. M.D. Diagnostic Radiology ActiveRubenstein, James H. M.D. Radiation Oncology AssociateSachs, Harris A. M.D. Pulmonary Medicine ActiveSaif, Mai F. M.D. Diagnostic Radiology ActiveSantucci, Gail M. M.D. Diagnostic Radiology ActiveSchreiber, Peter S. D.O. Physical Medicine & Rehab ActiveSchultz, Neil R. M.D. Physical Medicine & Rehab AssociateSchwartz, Eileen J. M.D. Neurology AssociateSeidenstein, Lawrence M.D. Pathology AssociateSonn, Jeffrey R. D.O. Diagnostic Radiology ActiveSteinmetz, Edward F. M.D. Neurology HonoraryStith, James A. M.D. Pathology ActiveSu, Wei M.D. Pathology ActiveSusko, Keith S. M.D. Physical Medicine & Rehab AssociateTafel, Allen C. M.D. Physical Medicine & Rehab AssociateTienstra, Joseph E. Jr. M.D. Diagnostic Radiology ActiveTsakalakis, P. John M.D. Pathology Associate
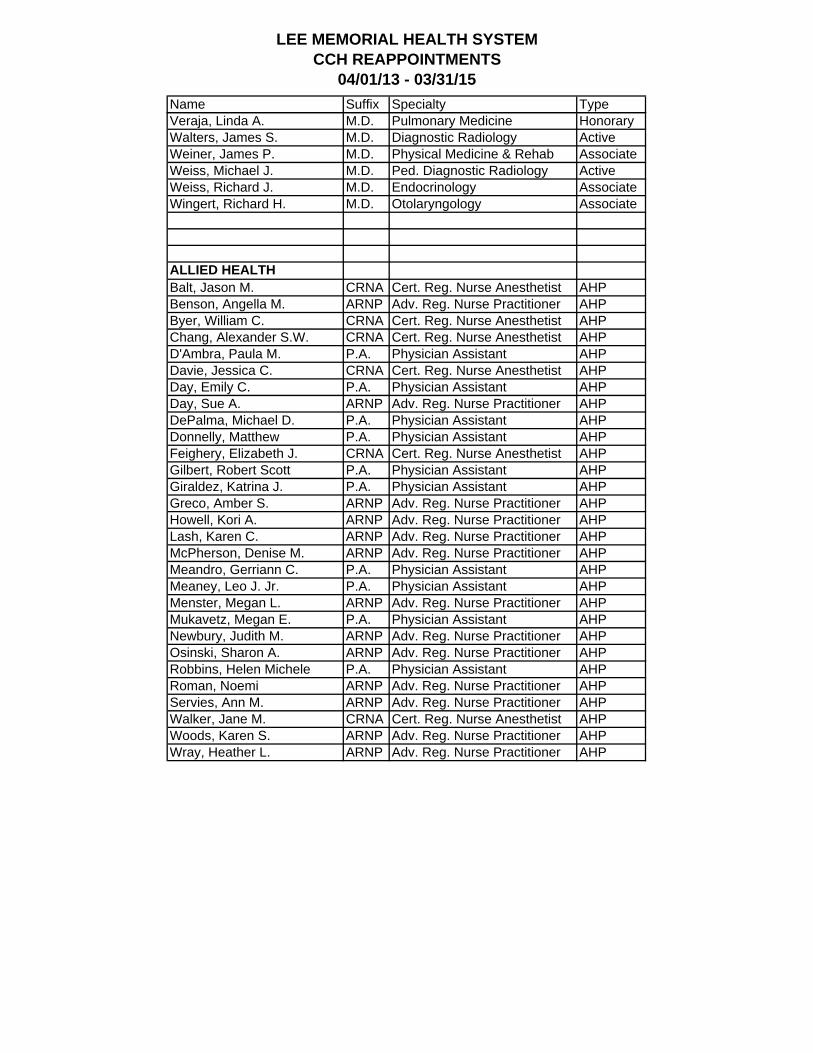
LEE MEMORIAL HEALTH SYSTEMCCH REAPPOINTMENTS
04/01/13 - 03/31/15
Name Suffix Specialty TypeVeraja, Linda A. M.D. Pulmonary Medicine HonoraryWalters, James S. M.D. Diagnostic Radiology ActiveWeiner, James P. M.D. Physical Medicine & Rehab AssociateWeiss, Michael J. M.D. Ped. Diagnostic Radiology ActiveWeiss, Richard J. M.D. Endocrinology AssociateWingert, Richard H. M.D. Otolaryngology Associate
ALLIED HEALTHBalt, Jason M. CRNA Cert. Reg. Nurse Anesthetist AHPBenson, Angella M. ARNP Adv. Reg. Nurse Practitioner AHPByer, William C. CRNA Cert. Reg. Nurse Anesthetist AHPChang, Alexander S.W. CRNA Cert. Reg. Nurse Anesthetist AHPD'Ambra, Paula M. P.A. Physician Assistant AHPDavie, Jessica C. CRNA Cert. Reg. Nurse Anesthetist AHPDay, Emily C. P.A. Physician Assistant AHPDay, Sue A. ARNP Adv. Reg. Nurse Practitioner AHPDePalma, Michael D. P.A. Physician Assistant AHPDonnelly, Matthew P.A. Physician Assistant AHPFeighery, Elizabeth J. CRNA Cert. Reg. Nurse Anesthetist AHPGilbert, Robert Scott P.A. Physician Assistant AHPGiraldez, Katrina J. P.A. Physician Assistant AHPGreco, Amber S. ARNP Adv. Reg. Nurse Practitioner AHPHowell, Kori A. ARNP Adv. Reg. Nurse Practitioner AHPLash, Karen C. ARNP Adv. Reg. Nurse Practitioner AHPMcPherson, Denise M. ARNP Adv. Reg. Nurse Practitioner AHPMeandro, Gerriann C. P.A. Physician Assistant AHPMeaney, Leo J. Jr. P.A. Physician Assistant AHPMenster, Megan L. ARNP Adv. Reg. Nurse Practitioner AHPMukavetz, Megan E. P.A. Physician Assistant AHPNewbury, Judith M. ARNP Adv. Reg. Nurse Practitioner AHPOsinski, Sharon A. ARNP Adv. Reg. Nurse Practitioner AHPRobbins, Helen Michele P.A. Physician Assistant AHPRoman, Noemi ARNP Adv. Reg. Nurse Practitioner AHPServies, Ann M. ARNP Adv. Reg. Nurse Practitioner AHPWalker, Jane M. CRNA Cert. Reg. Nurse Anesthetist AHPWoods, Karen S. ARNP Adv. Reg. Nurse Practitioner AHPWray, Heather L. ARNP Adv. Reg. Nurse Practitioner AHP
LEE MEMORIAL HEALTH SYSTEM Lee County, Florida
#3 M E M O R A N D U M
To: Board of Directors
From: Nancy A. Taylor, CPMSM, CPCS Director, Centralized Credentialing Services
Subject: Gulf Coast Medical Center Medical Staff Recommendations
Date: March 27, 2013
The Facility Medical Executive Committee of the Medical Staff recommends the following physicians and allied health practitioners and certifies they have met the requirements set forth in the bylaws:
1. Associate Staff Appointment: a. Michael L. Caselnova, M.D. – Family Medicine b. Basudev Pudasaini, M.D. – Nephrology c. Lewis M. Satloff, M.D. - Anesthesiology
2. Telemedicine Appointment – Privileges Only:
a. Carl V. Bundschuh, M.D. – Teleradiology b. Steven J. Karidas, M.D. - Teleradiology
3. M.S. and A.H.P. Reappointments – 04-01-13 to 03-31-15 (list attached) 4. Temporary Privileges:
a. Ndidi N. Nwamu, M.D. – Internal Medicine, 03-21-13 – 04-19-13
5. First Year Completion – Active Staff Appointment: a. Sivakumar Raman, M.D. – Infectious Disease
6. First Year Completion – Associate Staff Appointment:
a. Barry K. Butler, M.D. – Internal Medicine b. Ahmed A. Hassan, M.D. – Family Medicine c. Jay Wang, M.D. – Oncology/Hematology
7. Leave of Absence:
a. Luz Peguero, M.D. – Internal Medicine, 02-19-13 – 07-08-13 8. Return from Leave of Absence:
a. Michelle Mon, M.D. – General Surgery, 04-01-13 9. Resignations:
a. Shiyama Mudali, M.D. – Pathology, effective 04-06-13 b. Scott Orth, D.O. – Psychiatry, effective 07-16-13
Memorandum to Board of Directors - GCMC March 27, 2013 Page 2 of 2 10. Privilege Request:
a. Michael Frey, M.D. – Balloon kyphoplasty, percutaneous lumbar discectomy b. Richard J. Weiss, M.D. – Refer and follow c. Basudev Pudasaini, M.D. – Medical management of the kidney transplant patient d. Cecile Saint Paul, M.D. – Laparoscopic ectopic pregnancy treatment, endometrial
ablation 11. Allied Health Practitioners:
a. Pablo Banderas PA – Dr. Torricelli b. Lois Corey, CRNA – Anesthesia & Pain Consultants c. Bernard S. Davis, PA – Orthopedic Center of Florida d. Christie Freese, PA – Inpatients Specialists of SW FL e. Tanya Gallagher, CNM – Family Health Center f. Janine Hass, ARNP – Pain Management Consultants of SW FL g. Adam Quarles ARNP – ICU Practitioners
12. Allied Health Practitioners – Sponsor change:
a. George Baker, PA – Eye Centers of Florida b. Jeffrey Finn, PA – Orthopedic Specialists of SW FL
13. Allied Health Practitioners – Additional Sponsor:
a. Debra Dean, PA – Dr. Moses Shieh b. Michael DePalma, PA – Dr. Chavakula
14. Practitioners–in-Training:
a. Scott Hackman, Medical Student – Dr. Robert Turner, 04-01-13 - 04-12-13 b. April Smith, Nurse Practitioner Student – Dr. James Gostigian and Dr. Eihab
Hassanein, 03-18-13 – 06-30-13 c. Rachel Wenzel, Medical Student – Dr. Shalin Mehta, 03-14-13 - 03-29-13
Approved by the Board of Directors – March 28, 2013
_________________________________________ Richard B. Akin, Chairman, Board of Directors
LEE MEMORIAL HEALTH SYSTEMGCMC REAPPOINTMENTS
04/01/13 - 03/31/15
Name Suffix Specialty TypeMEDICAL STAFFAdi, Ashish M. M.D. Pulmonary Medicine ActiveAhmad, Imtiaz M.D. Pulmonary Medicine ActiveAlexander, Stanley G. M.D. Diagnostic Radiology ActiveAl-Nakeeb, Sadiq J. M.D. Pulmonary Medicine ActiveAnderson III, Cyrus T. M.D. Diagnostic Radiology ActiveAndrews, Phillip E. M.D. Otolaryngology AssociateAouchiche, Rachid M.D. Ophthalmology AssociateAugusthy, Reggie M. M.D. Physical Medicine & Rehab AssociateBanas, Jon M. D.O. Diagnostic Radiology ActiveBarrow, Howard N. M.D. Otolaryngology ActiveBerdick, Kenneth A. M.D. Internal Medicine AssociateBhavnani, Vinod D. M.D. Ophthalmology AssociateBiskup, Darius M.D. Diagnostic Radiology ActiveBlair, Michele M. D.O. Diagnostic Radiology AssociateBlitzer, Peter H. M.D. Radiation Oncology HonoraryBlue, Mary C. M.D. Pathology ActiveBobman, Stuart A M.D. Diagnostic Radiology ActiveBohm, Guillermo M.D. Endocrinology AssociateBond, Wendy Robinson M.D. Neurology AssociateBonnette, Harris L. M.D. Neurology ActiveBorrego, Orestes M.D. Pathology AssociateBourgon, Pierre M.D. Ophthalmology AssociateBravo Jr., Lazaro O. M.D. Pulmonary Medicine ActiveBrillman, Jon M.D. Neurology AssociateBrown Jr., Alan L. M.D. Radiation Oncology ActiveBrown, David C. M.D. Ophthalmology AssociateBrown, Karen E. M.D. Pathology AssociateCarlin, Lane R. M.D. Neurology ActiveCarracino, William J. Jr. M.D. Neurology ActiveCarron, Michael J. M.D. Diagnostic Radiology ActiveChadha, Tejvir S. M.D. Pulmonary Medicine ActiveChallapalli, Rahul K. M.D. Pulmonary Medicine ActiveCollins, Michael J. Jr. M.D. Ophthalmology AssociateConrado, Julio E. M.D. Pulmonary Medicine ActiveCox, Charles E. M.D. Ophthalmology AssociateCrandall, Valerie M.D. Ophthalmology AssociateCroley, James E. III M.D. Ophthalmology AssociateDakos, William N. M.D. Otolaryngology AssociateDaley, Joseph C. III M.D. Pulmonary Medicine ActiveDanehy, Edward J. M.D. Diagnostic Radiology AssociateDavis, Edward L. D.O. Neurology HonoraryDavis, Richard M. M.D. Ophthalmology AssociateDawson, Christopher A. M.D. Physical Medicine & Rehab AssociateDosani, Razak A. M.D. Pulmonary Medicine ActiveDosoretz, Daniel E. M.D. Radiation Oncology AssociateDriscoll, Paul F. M.D. Neurology ActiveDuan, Naili M.D. Neurology ActiveEaton, Alexander M. M.D. Ophthalmology AssociateEisenberg, Howard M.D. Pulmonary Medicine AssociateEl-Gendy, Alaa A. M.D. Pulmonary Medicine AssociateElmquist, E. Trevor D.O. Ophthalmology AssociateFeroz, Abusayeed M. M.D. Pulmonary Medicine AssociateFerreira, Claudio A. M.D. Ophthalmology Associate
LEE MEMORIAL HEALTH SYSTEMGCMC REAPPOINTMENTS
04/01/13 - 03/31/15
Name Suffix Specialty TypeFlaharty, Patrick M. M.D. Ophthalmology AssociateFletcher, Donald C. M.D. Ocular Rehabilitation AssociateFoo, May L. M.D. Radiation Oncology AssociateFox, Amy M. M.D. Radiation Oncology AssociateFrantz, Jonathan M. M.D. Ophthalmology AssociateFrey, Michael E. M.D. Physical Medicine & Rehab ActiveFuller, James H. M.D. Otolaryngology AssociateGalang, Kenneth J. M.D. Physical Medicine & Rehab ActiveGamez, Gerardo A. M.D. Neurology ActiveGeller, Scott L. M.D. Ophthalmology AssociateGerson, Deborah M. M.D. Pathology ActiveGhitis, Joseph M.D. Diagnostic Radiology ActiveGhuman, A. Thomas M.D. Ophthalmology AssociateGinsberg, Barrett R. M.D. Ophthalmology AssociateGoodwich, Ronald B. M.D. Diagnostic Radiology ActiveGoodwin, R. Thad M.D. Ophthalmology AssociateGorovoy, Mark S. M.D. Ophthalmology AssociateGrassi, Frank T. M.D. Pulmonary Medicine ActiveGuterman, Steven M.D. Diagnostic Radiology AssociateHamilton, Jack E. M.D. Pathology AssociateHarig, Bette M. M.D. Diagnostic Radiology ActiveHearn, William B. D.O. Diagnostic Radiology ActiveHeller, Adam L. M.D. Neurology ActiveHillis, Rodney E. M.D. Neurology ActiveHussain, Reza S. M.D. Pulmonary Medicine ActiveHyppolite, Pierre R. M.D. Physical Medicine & Rehab ActiveKalemeris, George C. M.D. Pathology AssociateKatin, Michael J. M.D. Radiation Oncology AssociateKazim, Nadia A. M.D. Ophthalmology AssociateKeys, Timothy C. M.D. Pulmonary Medicine ActiveKhan, Javaad A. M.D. Pulmonary Medicine ActiveKibria, Eshan M. D.O. Neurology AssociateKini, Vidya P. M.D. Physical Medicine & Rehab ActiveKnific, Randolph J. M.D. Diagnostic Radiology ActiveKole, Marilyn M.D. Pulmonary Medicine AssociateKonowal, Alexandra M. D.O. Ophthalmology AssociateKrivisky, Brian A. M.D. Diagnostic Radiology ActiveKushen, Medina C. M.D. Diagnostic Radiology ActiveLalla, Sunil N. M.D. Pulmonary Medicine ActiveLane, Richard J. M.D. Otolaryngology ActiveLaquis, Stephen J. M.D. Ophthalmology ActiveLeigh, Lawrence D. M.D. Diagnostic Radiology ActiveLevine, Steven E. M.D. Pathology AssociateLewis, Michael M. M.D. Ophthalmology AssociateLiu, Zhiping M.D. Pathology ActiveLozano, Alexander J. M.D. Otolaryngology AssociateLuna, Victor M. M.D. Endocrinology AssociateMakhlouf, Paul C. M.D. Diagnostic Radiology AssociateMalkani, Sunil M. M.D. Ophthalmology AssociateMantz, Constantine A. M.D. Radiation Oncology ActiveMarino, Chris J. M.D. Neurology ActiveMartin, Benjamin G. M.D. Ophthalmology AssociateMather, Sergio R. M.D. Endocrinology AssociateMcAlpine, Donald Ross M.D. Pulmonary Medicine Active
LEE MEMORIAL HEALTH SYSTEMGCMC REAPPOINTMENTS
04/01/13 - 03/31/15
Name Suffix Specialty TypeMcKenna, Daniel J. M.D. Otolaryngology AssociateMehlman, Bruce M. M.D. Pulmonary Medicine ActiveMehrberg, Robert D. M.D. Physical Medicine & Rehab ActiveMestas, George M. M.D. Pulmonary Medicine ActiveMiller, Keith L. M.D. Radiation Oncology ActiveMowzoon, Nima M.D. Neurology ActiveMudali, Shiyama V. M.D. Pathology ActiveNaik, Sagar K. M.D. Pulmonary Medicine AssociateNakfoor, Bruce M. M.D. Radiation Oncology AssociateNewland, Douglas A. M.D. Neurology ActivePacheco, Jose Cassini M.D. Diagnostic Radiology ActivePagliara, Richard D. D.O. Diagnostic Radiology ActivePalmon, Florentino E. M.D. Ophthalmology AssociatePammi, Sunil S. M.D. Pulmonary Medicine ActivePatel, Saurabh N. M.D. Ophthalmology AssociatePeterson, Mary Kay M.D. Diagnostic Radiology AssociatePhommachanh, Viengsouk M.D. Otolaryngology ActiveQuigley, Thomas A. III M.D. Ophthalmology AssociateRaju, Krishna Priya M. M.D. Pulmonary Medicine AssociateRashid, Mohammad A. M.D. Pulmonary Medicine HonoraryRaskauskas, Paul A. M.D. Ophthalmology AssociateReardon, David M. M.D. Pathology AssociateRubenstein, James H. M.D. Radiation Oncology AssociateSachs, Harris A. M.D. Pulmonary Medicine ActiveSantiago, Maximo J. M.D. Diagnostic Radiology ActiveSantucci, Raymond D. M.D. Pulmonary Medicine ActiveSchreiber, Peter S. D.O. Physical Medicine & Rehab AssociateSchultz, Neil R. M.D. Physical Medicine & Rehab AssociateSchwartz, Eileen J. M.D. Neurology ActiveScott, Peter L. M.D. Diagnostic Radiology ActiveSeidenstein, Lawrence M.D. Pathology ActiveSharma, Ashish G. M.D. Ophthalmology ActiveShenoy, Parna G. M.D. Ophthalmology AssociateSims, C. Norton M.D. Ophthalmology AssociateSmith, Stephen E. M.D. Ophthalmology AssociateSnead, John W. M.D. Ophthalmology AssociateSteinmetz, Edward F. M.D. Neurology HonoraryStith, James A. M.D. Pathology ActiveSu, Wei M.D. Pathology AssociateSusko, Keith S. M.D. Physical Medicine & Rehab ActiveSwift, John E. M.D. Ophthalmology AssociateTafel, Allen C. M.D. Physical Medicine & Rehab AssociateTaha, Margaret D. M.D. Diagnostic Radiology ActiveTolep, Kenneth A. M.D. Pulmonary Medicine ActiveTsakalakis, P. John M.D. Pathology AssociateTurkel, David H. M.D. Diagnostic Radiology ActiveTyson, Farrell C. II M.D. Ophthalmology AssociateVeraja, Linda A. M.D. Pulmonary Medicine HonoraryWafapoor, Hussein M.D. Ophthalmology ActiveWalker, Joseph P. M.D. Ophthalmology AssociateWeiner, James P. M.D. Physical Medicine & Rehab AssociateWeiss, Richard J. M.D. Endocrinology AssociateWing, Glenn L. M.D. Ophthalmology Associate
LEE MEMORIAL HEALTH SYSTEMGCMC REAPPOINTMENTS
04/01/13 - 03/31/15
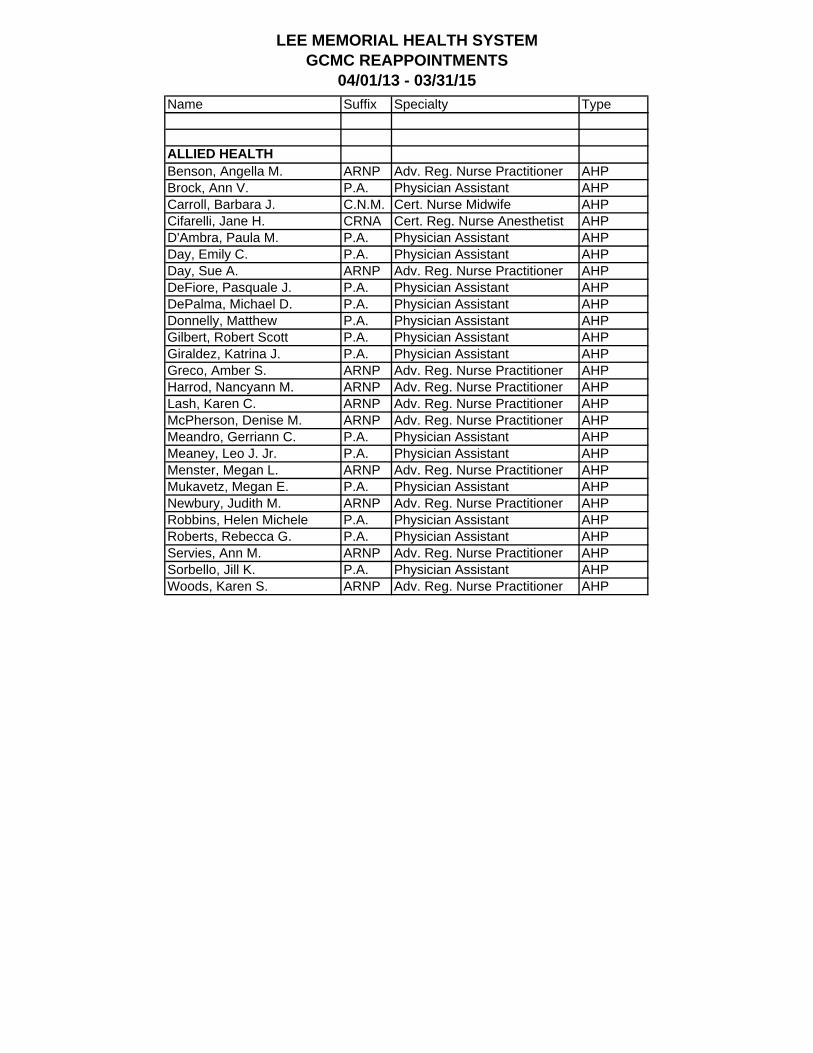
Name Suffix Specialty Type
ALLIED HEALTHBenson, Angella M. ARNP Adv. Reg. Nurse Practitioner AHPBrock, Ann V. P.A. Physician Assistant AHPCarroll, Barbara J. C.N.M. Cert. Nurse Midwife AHPCifarelli, Jane H. CRNA Cert. Reg. Nurse Anesthetist AHPD'Ambra, Paula M. P.A. Physician Assistant AHPDay, Emily C. P.A. Physician Assistant AHPDay, Sue A. ARNP Adv. Reg. Nurse Practitioner AHPDeFiore, Pasquale J. P.A. Physician Assistant AHPDePalma, Michael D. P.A. Physician Assistant AHPDonnelly, Matthew P.A. Physician Assistant AHPGilbert, Robert Scott P.A. Physician Assistant AHPGiraldez, Katrina J. P.A. Physician Assistant AHPGreco, Amber S. ARNP Adv. Reg. Nurse Practitioner AHPHarrod, Nancyann M. ARNP Adv. Reg. Nurse Practitioner AHPLash, Karen C. ARNP Adv. Reg. Nurse Practitioner AHPMcPherson, Denise M. ARNP Adv. Reg. Nurse Practitioner AHPMeandro, Gerriann C. P.A. Physician Assistant AHPMeaney, Leo J. Jr. P.A. Physician Assistant AHPMenster, Megan L. ARNP Adv. Reg. Nurse Practitioner AHPMukavetz, Megan E. P.A. Physician Assistant AHPNewbury, Judith M. ARNP Adv. Reg. Nurse Practitioner AHPRobbins, Helen Michele P.A. Physician Assistant AHPRoberts, Rebecca G. P.A. Physician Assistant AHPServies, Ann M. ARNP Adv. Reg. Nurse Practitioner AHPSorbello, Jill K. P.A. Physician Assistant AHPWoods, Karen S. ARNP Adv. Reg. Nurse Practitioner AHP
LEE MEMORIAL HEALTH SYSTEM Lee County, Florida
#4 M E M O R A N D U M
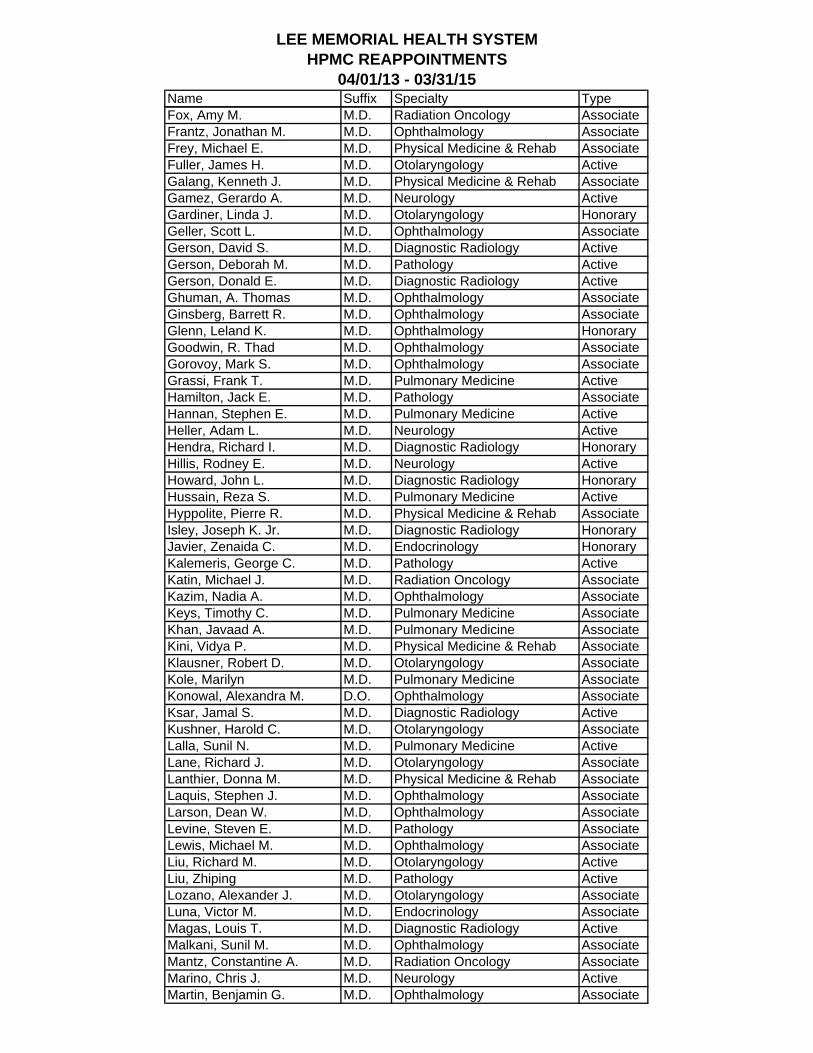
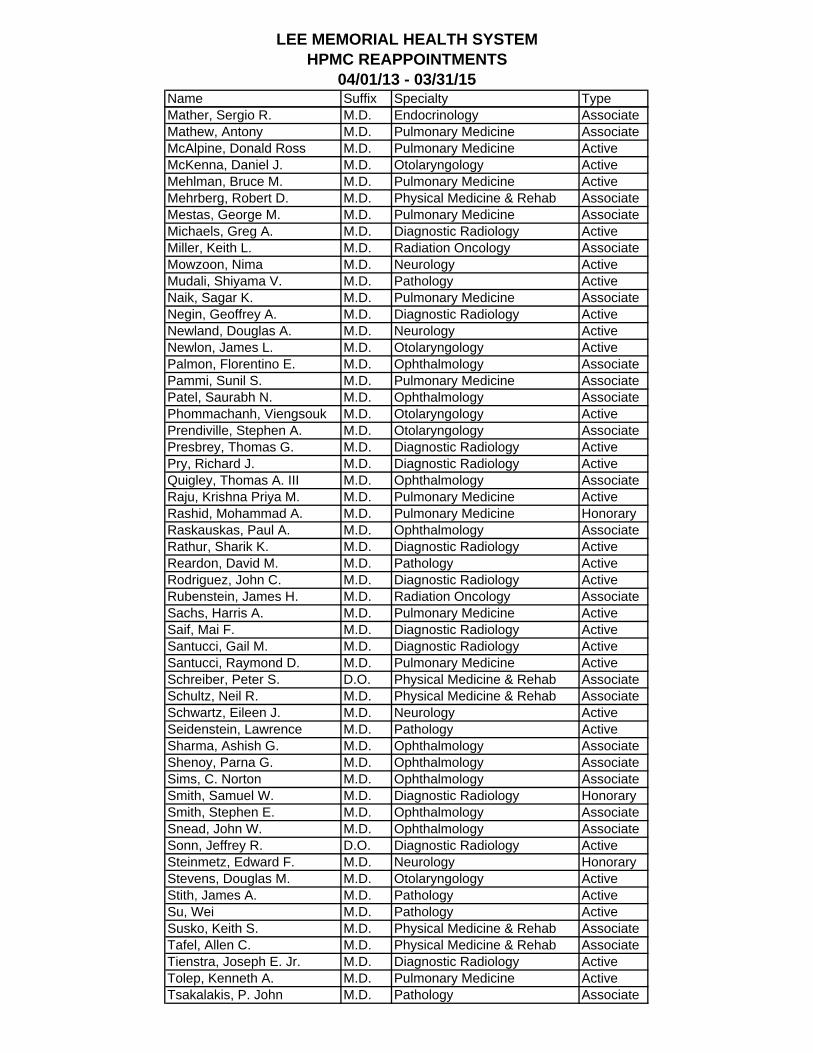
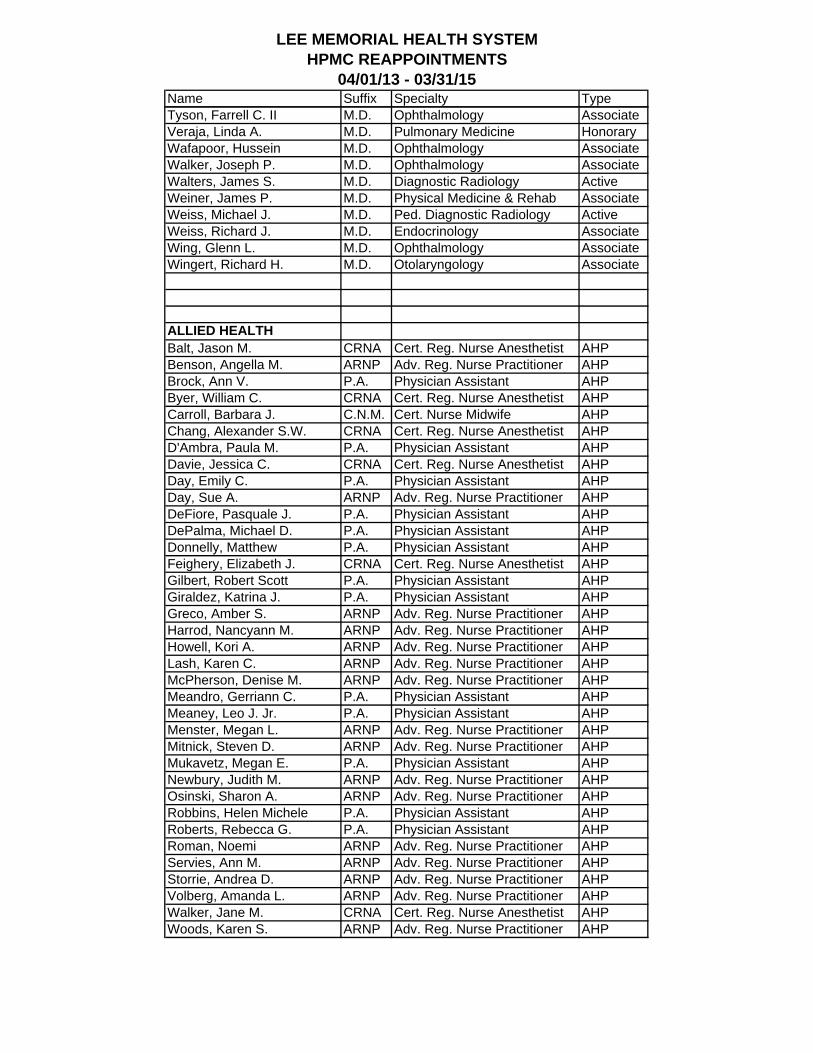
To: Board of Directors From: Nancy A. Taylor, CPMSM, CPCS Director, Centralized Credentialing Services Date: March 27, 2013 Subject: HealthPark Medical Center Medical Staff Recommendations The Facility Medical Executive Committee of the Medical Staff recommends the following physicians and allied health practitioners and certifies they have met the requirements set forth in the bylaws:
1. Associate Staff Appointment: a. Michael L. Caselnova, M.D. – Family Medicine b. Denise A. Drago, M.D. - Pediatrics c. Basudev Pudasaini, M.D. – Nephrology d. Thomas J. Traikoff, D.O. – Family Medicine
2. Telemedicine Appointment – Privileges Only:
a. Carl V. Bundschuh, M.D. – Teleradiology b. Steven J. Karidas, M.D. - Teleradiology
3. M.S. and A.H.P. Reappointments – 04-01-13 to 03-31-15 (list attached) 4. Temporary Privileges:
a. Ndidi N. Nwamu, M.D. – Internal Medicine, 03-21-13 – 04-19-13
5. First Year Completion – Associate Staff Appointment: a. Shawn Chopra, M.D. – Internal Medicine b. Ahmed A. Hassan, M.D. – Family Medicine c. Andrew H. Singh, M.D. – Occupational Medicine d. Jay Wang, M.D. – Oncology/Hematology
6. Leave of Absence:
a. Luz Peguero, M.D. – Internal Medicine, 02-19-13 – 07-08-13 7. Return from Leave of Absence:
a. Michelle Mon, M.D. – General Surgery, 04-01-13 8. Resignations:
a. Pedro Marcucci, M.D. – Urology, effective 02-22-13 b. Shiyama Mudali, M.D. – Pathology, effective 04-06-13 c. Scott Orth, D.O. – Psychiatry, effective 07-16-13
Memorandum to Board of Directors - HPMC March 27, 2013 Page 2 of 2 9. Privilege Request:
a. Peter Denk, M.D. - Robotic assisted surgery b. Michael Frey, M.D. – Balloon kyphoplasty, percutaneous lumbar discectomy c. Richard J. Weiss, M.D. – Refer and follow d. Cecile Saint Paul, M.D. – Laparoscopic ectopic pregnancy treatment, endometrial
ablation 10. Allied Health Practitioners:
a. Pablo Banderas PA – Dr. Torricelli b. Bernard S. Davis, PA – Orthopedic Center of Florida c. Christie Freese, PA – Inpatients Specialists of SW FL d. Tanya Gallagher, CNM – Family Health Center e. Janine Hass, ARNP – Pain Management Consultants of SW FL f. Adam Quarles ARNP – ICU Practitioners g. Laura Walgate, PA – Gulfstream Urology
11. Allied Health Practitioners – Sponsor change:
a. George Baker, PA – Eye Centers of Florida b. Jeffrey Finn, PA – Orthopedic Specialists of SW FL c. Alison Ridgway, PA – LMHS ER Physicians
12. Allied Health Practitioners – Additional Sponsor:
a. Debra Dean, PA – Dr. Moses Shieh b. Michael DePalma, PA – Dr. Chavakula
13. Practitioners–in-Training:
a. Amy Bonanno, Nurse Midwifery Student – Dr. Bipin Shah, 03-14-13 - 06-30-13 b. April Smith, Nurse Practitioner Student – Dr. James Gostigian and Dr. Eihab
Hassanein, 03-18-13 – 06-30-13 c. Rachel Wenzel, Medical Student – Dr. Shalin Mehta, 03-14-13 - 03-29-13
Approved by the Board of Directors – March 28, 2013
__________________________________________ Richard B. Akin, Chairman - Board of Directors
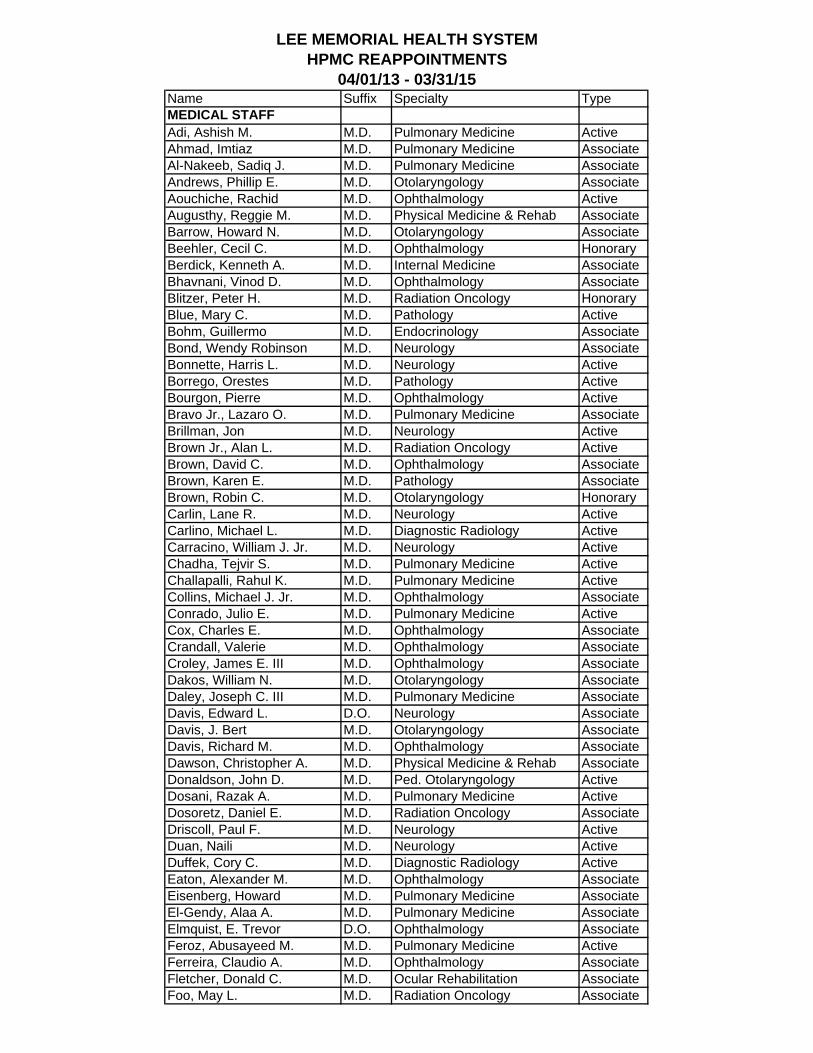
LEE MEMORIAL HEALTH SYSTEMHPMC REAPPOINTMENTS
04/01/13 - 03/31/15Name Suffix Specialty TypeMEDICAL STAFFAdi, Ashish M. M.D. Pulmonary Medicine ActiveAhmad, Imtiaz M.D. Pulmonary Medicine AssociateAl-Nakeeb, Sadiq J. M.D. Pulmonary Medicine AssociateAndrews, Phillip E. M.D. Otolaryngology AssociateAouchiche, Rachid M.D. Ophthalmology ActiveAugusthy, Reggie M. M.D. Physical Medicine & Rehab AssociateBarrow, Howard N. M.D. Otolaryngology AssociateBeehler, Cecil C. M.D. Ophthalmology HonoraryBerdick, Kenneth A. M.D. Internal Medicine AssociateBhavnani, Vinod D. M.D. Ophthalmology AssociateBlitzer, Peter H. M.D. Radiation Oncology HonoraryBlue, Mary C. M.D. Pathology ActiveBohm, Guillermo M.D. Endocrinology AssociateBond, Wendy Robinson M.D. Neurology AssociateBonnette, Harris L. M.D. Neurology ActiveBorrego, Orestes M.D. Pathology ActiveBourgon, Pierre M.D. Ophthalmology ActiveBravo Jr., Lazaro O. M.D. Pulmonary Medicine AssociateBrillman, Jon M.D. Neurology ActiveBrown Jr., Alan L. M.D. Radiation Oncology ActiveBrown, David C. M.D. Ophthalmology AssociateBrown, Karen E. M.D. Pathology AssociateBrown, Robin C. M.D. Otolaryngology HonoraryCarlin, Lane R. M.D. Neurology ActiveCarlino, Michael L. M.D. Diagnostic Radiology ActiveCarracino, William J. Jr. M.D. Neurology ActiveChadha, Tejvir S. M.D. Pulmonary Medicine ActiveChallapalli, Rahul K. M.D. Pulmonary Medicine ActiveCollins, Michael J. Jr. M.D. Ophthalmology AssociateConrado, Julio E. M.D. Pulmonary Medicine ActiveCox, Charles E. M.D. Ophthalmology AssociateCrandall, Valerie M.D. Ophthalmology AssociateCroley, James E. III M.D. Ophthalmology AssociateDakos, William N. M.D. Otolaryngology AssociateDaley, Joseph C. III M.D. Pulmonary Medicine AssociateDavis, Edward L. D.O. Neurology AssociateDavis, J. Bert M.D. Otolaryngology AssociateDavis, Richard M. M.D. Ophthalmology AssociateDawson, Christopher A. M.D. Physical Medicine & Rehab AssociateDonaldson, John D. M.D. Ped. Otolaryngology ActiveDosani, Razak A. M.D. Pulmonary Medicine ActiveDosoretz, Daniel E. M.D. Radiation Oncology AssociateDriscoll, Paul F. M.D. Neurology ActiveDuan, Naili M.D. Neurology ActiveDuffek, Cory C. M.D. Diagnostic Radiology ActiveEaton, Alexander M. M.D. Ophthalmology AssociateEisenberg, Howard M.D. Pulmonary Medicine AssociateEl-Gendy, Alaa A. M.D. Pulmonary Medicine AssociateElmquist, E. Trevor D.O. Ophthalmology AssociateFeroz, Abusayeed M. M.D. Pulmonary Medicine ActiveFerreira, Claudio A. M.D. Ophthalmology AssociateFletcher, Donald C. M.D. Ocular Rehabilitation AssociateFoo, May L. M.D. Radiation Oncology Associate
LEE MEMORIAL HEALTH SYSTEMHPMC REAPPOINTMENTS
04/01/13 - 03/31/15Name Suffix Specialty TypeFox, Amy M. M.D. Radiation Oncology AssociateFrantz, Jonathan M. M.D. Ophthalmology AssociateFrey, Michael E. M.D. Physical Medicine & Rehab AssociateFuller, James H. M.D. Otolaryngology ActiveGalang, Kenneth J. M.D. Physical Medicine & Rehab AssociateGamez, Gerardo A. M.D. Neurology ActiveGardiner, Linda J. M.D. Otolaryngology HonoraryGeller, Scott L. M.D. Ophthalmology AssociateGerson, David S. M.D. Diagnostic Radiology ActiveGerson, Deborah M. M.D. Pathology ActiveGerson, Donald E. M.D. Diagnostic Radiology ActiveGhuman, A. Thomas M.D. Ophthalmology AssociateGinsberg, Barrett R. M.D. Ophthalmology AssociateGlenn, Leland K. M.D. Ophthalmology HonoraryGoodwin, R. Thad M.D. Ophthalmology AssociateGorovoy, Mark S. M.D. Ophthalmology AssociateGrassi, Frank T. M.D. Pulmonary Medicine ActiveHamilton, Jack E. M.D. Pathology AssociateHannan, Stephen E. M.D. Pulmonary Medicine ActiveHeller, Adam L. M.D. Neurology ActiveHendra, Richard I. M.D. Diagnostic Radiology HonoraryHillis, Rodney E. M.D. Neurology ActiveHoward, John L. M.D. Diagnostic Radiology HonoraryHussain, Reza S. M.D. Pulmonary Medicine ActiveHyppolite, Pierre R. M.D. Physical Medicine & Rehab AssociateIsley, Joseph K. Jr. M.D. Diagnostic Radiology HonoraryJavier, Zenaida C. M.D. Endocrinology HonoraryKalemeris, George C. M.D. Pathology ActiveKatin, Michael J. M.D. Radiation Oncology AssociateKazim, Nadia A. M.D. Ophthalmology AssociateKeys, Timothy C. M.D. Pulmonary Medicine AssociateKhan, Javaad A. M.D. Pulmonary Medicine AssociateKini, Vidya P. M.D. Physical Medicine & Rehab AssociateKlausner, Robert D. M.D. Otolaryngology AssociateKole, Marilyn M.D. Pulmonary Medicine AssociateKonowal, Alexandra M. D.O. Ophthalmology AssociateKsar, Jamal S. M.D. Diagnostic Radiology ActiveKushner, Harold C. M.D. Otolaryngology AssociateLalla, Sunil N. M.D. Pulmonary Medicine ActiveLane, Richard J. M.D. Otolaryngology AssociateLanthier, Donna M. M.D. Physical Medicine & Rehab AssociateLaquis, Stephen J. M.D. Ophthalmology AssociateLarson, Dean W. M.D. Ophthalmology AssociateLevine, Steven E. M.D. Pathology AssociateLewis, Michael M. M.D. Ophthalmology AssociateLiu, Richard M. M.D. Otolaryngology ActiveLiu, Zhiping M.D. Pathology ActiveLozano, Alexander J. M.D. Otolaryngology AssociateLuna, Victor M. M.D. Endocrinology AssociateMagas, Louis T. M.D. Diagnostic Radiology ActiveMalkani, Sunil M. M.D. Ophthalmology AssociateMantz, Constantine A. M.D. Radiation Oncology AssociateMarino, Chris J. M.D. Neurology ActiveMartin, Benjamin G. M.D. Ophthalmology Associate
LEE MEMORIAL HEALTH SYSTEMHPMC REAPPOINTMENTS
04/01/13 - 03/31/15Name Suffix Specialty TypeMather, Sergio R. M.D. Endocrinology AssociateMathew, Antony M.D. Pulmonary Medicine AssociateMcAlpine, Donald Ross M.D. Pulmonary Medicine ActiveMcKenna, Daniel J. M.D. Otolaryngology ActiveMehlman, Bruce M. M.D. Pulmonary Medicine ActiveMehrberg, Robert D. M.D. Physical Medicine & Rehab AssociateMestas, George M. M.D. Pulmonary Medicine AssociateMichaels, Greg A. M.D. Diagnostic Radiology ActiveMiller, Keith L. M.D. Radiation Oncology AssociateMowzoon, Nima M.D. Neurology ActiveMudali, Shiyama V. M.D. Pathology ActiveNaik, Sagar K. M.D. Pulmonary Medicine AssociateNegin, Geoffrey A. M.D. Diagnostic Radiology ActiveNewland, Douglas A. M.D. Neurology ActiveNewlon, James L. M.D. Otolaryngology ActivePalmon, Florentino E. M.D. Ophthalmology AssociatePammi, Sunil S. M.D. Pulmonary Medicine AssociatePatel, Saurabh N. M.D. Ophthalmology AssociatePhommachanh, Viengsouk M.D. Otolaryngology ActivePrendiville, Stephen A. M.D. Otolaryngology AssociatePresbrey, Thomas G. M.D. Diagnostic Radiology ActivePry, Richard J. M.D. Diagnostic Radiology ActiveQuigley, Thomas A. III M.D. Ophthalmology AssociateRaju, Krishna Priya M. M.D. Pulmonary Medicine ActiveRashid, Mohammad A. M.D. Pulmonary Medicine HonoraryRaskauskas, Paul A. M.D. Ophthalmology AssociateRathur, Sharik K. M.D. Diagnostic Radiology ActiveReardon, David M. M.D. Pathology ActiveRodriguez, John C. M.D. Diagnostic Radiology ActiveRubenstein, James H. M.D. Radiation Oncology AssociateSachs, Harris A. M.D. Pulmonary Medicine ActiveSaif, Mai F. M.D. Diagnostic Radiology ActiveSantucci, Gail M. M.D. Diagnostic Radiology ActiveSantucci, Raymond D. M.D. Pulmonary Medicine ActiveSchreiber, Peter S. D.O. Physical Medicine & Rehab AssociateSchultz, Neil R. M.D. Physical Medicine & Rehab AssociateSchwartz, Eileen J. M.D. Neurology ActiveSeidenstein, Lawrence M.D. Pathology ActiveSharma, Ashish G. M.D. Ophthalmology AssociateShenoy, Parna G. M.D. Ophthalmology AssociateSims, C. Norton M.D. Ophthalmology AssociateSmith, Samuel W. M.D. Diagnostic Radiology HonorarySmith, Stephen E. M.D. Ophthalmology AssociateSnead, John W. M.D. Ophthalmology AssociateSonn, Jeffrey R. D.O. Diagnostic Radiology ActiveSteinmetz, Edward F. M.D. Neurology HonoraryStevens, Douglas M. M.D. Otolaryngology ActiveStith, James A. M.D. Pathology ActiveSu, Wei M.D. Pathology ActiveSusko, Keith S. M.D. Physical Medicine & Rehab AssociateTafel, Allen C. M.D. Physical Medicine & Rehab AssociateTienstra, Joseph E. Jr. M.D. Diagnostic Radiology ActiveTolep, Kenneth A. M.D. Pulmonary Medicine ActiveTsakalakis, P. John M.D. Pathology Associate
LEE MEMORIAL HEALTH SYSTEMHPMC REAPPOINTMENTS
04/01/13 - 03/31/15Name Suffix Specialty TypeTyson, Farrell C. II M.D. Ophthalmology AssociateVeraja, Linda A. M.D. Pulmonary Medicine HonoraryWafapoor, Hussein M.D. Ophthalmology AssociateWalker, Joseph P. M.D. Ophthalmology AssociateWalters, James S. M.D. Diagnostic Radiology ActiveWeiner, James P. M.D. Physical Medicine & Rehab AssociateWeiss, Michael J. M.D. Ped. Diagnostic Radiology ActiveWeiss, Richard J. M.D. Endocrinology AssociateWing, Glenn L. M.D. Ophthalmology AssociateWingert, Richard H. M.D. Otolaryngology Associate
ALLIED HEALTHBalt, Jason M. CRNA Cert. Reg. Nurse Anesthetist AHPBenson, Angella M. ARNP Adv. Reg. Nurse Practitioner AHPBrock, Ann V. P.A. Physician Assistant AHPByer, William C. CRNA Cert. Reg. Nurse Anesthetist AHPCarroll, Barbara J. C.N.M. Cert. Nurse Midwife AHPChang, Alexander S.W. CRNA Cert. Reg. Nurse Anesthetist AHPD'Ambra, Paula M. P.A. Physician Assistant AHPDavie, Jessica C. CRNA Cert. Reg. Nurse Anesthetist AHPDay, Emily C. P.A. Physician Assistant AHPDay, Sue A. ARNP Adv. Reg. Nurse Practitioner AHPDeFiore, Pasquale J. P.A. Physician Assistant AHPDePalma, Michael D. P.A. Physician Assistant AHPDonnelly, Matthew P.A. Physician Assistant AHPFeighery, Elizabeth J. CRNA Cert. Reg. Nurse Anesthetist AHPGilbert, Robert Scott P.A. Physician Assistant AHPGiraldez, Katrina J. P.A. Physician Assistant AHPGreco, Amber S. ARNP Adv. Reg. Nurse Practitioner AHPHarrod, Nancyann M. ARNP Adv. Reg. Nurse Practitioner AHPHowell, Kori A. ARNP Adv. Reg. Nurse Practitioner AHPLash, Karen C. ARNP Adv. Reg. Nurse Practitioner AHPMcPherson, Denise M. ARNP Adv. Reg. Nurse Practitioner AHPMeandro, Gerriann C. P.A. Physician Assistant AHPMeaney, Leo J. Jr. P.A. Physician Assistant AHPMenster, Megan L. ARNP Adv. Reg. Nurse Practitioner AHPMitnick, Steven D. ARNP Adv. Reg. Nurse Practitioner AHPMukavetz, Megan E. P.A. Physician Assistant AHPNewbury, Judith M. ARNP Adv. Reg. Nurse Practitioner AHPOsinski, Sharon A. ARNP Adv. Reg. Nurse Practitioner AHPRobbins, Helen Michele P.A. Physician Assistant AHPRoberts, Rebecca G. P.A. Physician Assistant AHPRoman, Noemi ARNP Adv. Reg. Nurse Practitioner AHPServies, Ann M. ARNP Adv. Reg. Nurse Practitioner AHPStorrie, Andrea D. ARNP Adv. Reg. Nurse Practitioner AHPVolberg, Amanda L. ARNP Adv. Reg. Nurse Practitioner AHPWalker, Jane M. CRNA Cert. Reg. Nurse Anesthetist AHPWoods, Karen S. ARNP Adv. Reg. Nurse Practitioner AHP
LEE MEMORIAL HEALTH SYSTEM Lee County, Florida
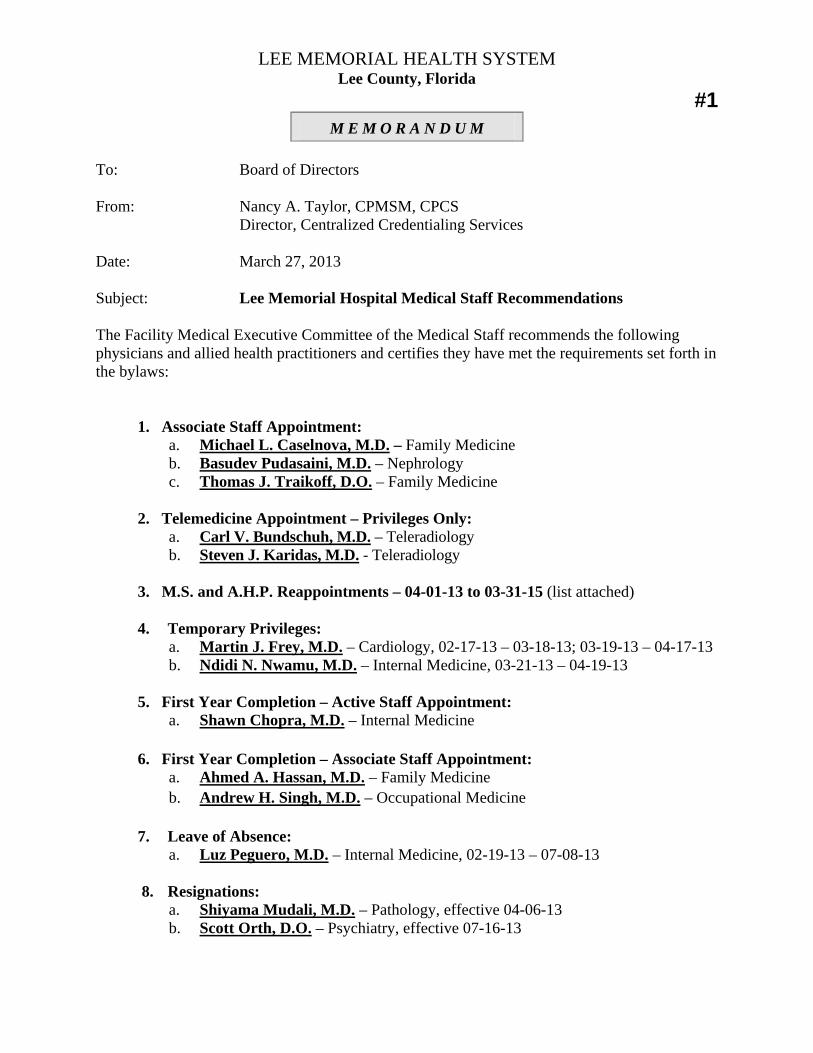
#1 M E M O R A N D U M
To: Board of Directors From: Nancy A. Taylor, CPMSM, CPCS Director, Centralized Credentialing Services Date: March 27, 2013 Subject: Lee Memorial Hospital Medical Staff Recommendations The Facility Medical Executive Committee of the Medical Staff recommends the following physicians and allied health practitioners and certifies they have met the requirements set forth in the bylaws:
1. Associate Staff Appointment: a. Michael L. Caselnova, M.D. – Family Medicine b. Basudev Pudasaini, M.D. – Nephrology c. Thomas J. Traikoff, D.O. – Family Medicine
2. Telemedicine Appointment – Privileges Only:
a. Carl V. Bundschuh, M.D. – Teleradiology b. Steven J. Karidas, M.D. - Teleradiology
3. M.S. and A.H.P. Reappointments – 04-01-13 to 03-31-15 (list attached) 4. Temporary Privileges:
a. Martin J. Frey, M.D. – Cardiology, 02-17-13 – 03-18-13; 03-19-13 – 04-17-13 b. Ndidi N. Nwamu, M.D. – Internal Medicine, 03-21-13 – 04-19-13
5. First Year Completion – Active Staff Appointment:
a. Shawn Chopra, M.D. – Internal Medicine
6. First Year Completion – Associate Staff Appointment: a. Ahmed A. Hassan, M.D. – Family Medicine b. Andrew H. Singh, M.D. – Occupational Medicine
7. Leave of Absence:
a. Luz Peguero, M.D. – Internal Medicine, 02-19-13 – 07-08-13 8. Resignations:
a. Shiyama Mudali, M.D. – Pathology, effective 04-06-13 b. Scott Orth, D.O. – Psychiatry, effective 07-16-13
Memorandum to Board of Directors - LMH March 27, 2013 Page 2 of 2 9. Privilege Request:
a. Michael Frey, M.D. – Balloon kyphoplasty, percutaneous lumbar discectomy b. Richard J. Weiss, M.D. – Refer and follow c. Cecile Saint Paul, M.D. – Laparoscopic ectopic pregnancy treatment, endometrial
ablation 10. Allied Health Practitioners:
a. Pablo Banderas PA – Dr. Torricelli b. Bernard S. Davis, PA – Orthopedic Center of Florida c. Christie Freese, PA – Inpatients Specialists of SW FL d. Tanya Gallagher, CNM – Family Health Center e. Janine Hass, ARNP – Pain Management Consultants of SW FL f. Adam Quarles ARNP – ICU Practitioners
11. Allied Health Practitioners – Sponsor change:
a. George Baker, PA – Eye Centers of Florida b. Jeffrey Finn, PA – Orthopedic Specialists of SW FL c. Alison Ridgway, PA – LMHS ER Physicians
12. Allied Health Practitioners – Additional Sponsor:
a. Debra Dean, PA – Dr. Moses Shieh b. Michael DePalma, PA – Dr. Chavakula
13. Allied Health Practitioners – Privilege Request:
a. Matthew Donnelly, PA – Tube thoracostomy, central venous catheter, percutaneous tracheostomy
b. Wendy Featherstone, PA – Tube thoracostomy, central venous catheter, arterial line, percutaneous tracheostomy
c. Erin Ross, PA – Tube thoracostomy, central venous catheter, arterial line, percutaneous tracheostomy, hemodialysis catheter
d. David Zimmerman, PA – Tube thoracostomy, central venous catheter, arterial line, percutaneous tracheostomy, hemodialysis catheter
14. Practitioners–in-Training:
a. Amy Bonanno, Nurse Midwifery Student – Dr. Bipin Shah, 03-14-13 - 06-30-13 b. April Smith, Nurse Practitioner Student – Dr. James Gostigian and Dr. Eihab
Hassanein, 03-18-13 – 06-30-13 c. Rachel Wenzel, Medical Student – Dr. Shalin Mehta, 03-14-13 - 03-29-13
Approved by the Board of Directors – March 28, 2013
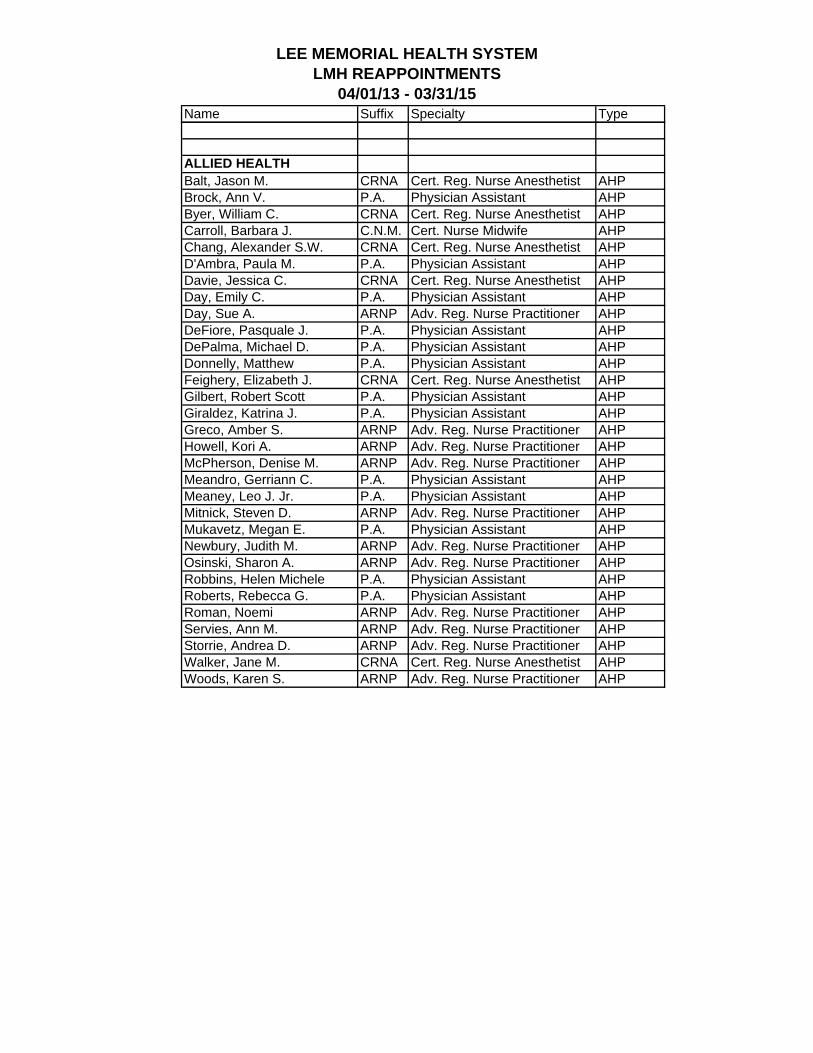
__________________________________________ Richard B. Akin, Chairman - Board of Directors
LEE MEMORIAL HEALTH SYSTEMLMH REAPPOINTMENTS
04/01/13 - 03/31/15Name Suffix Specialty TypeMEDICAL STAFFAhmad, Imtiaz M.D. Pulmonary Medicine AssociateAndrews, Phillip E. M.D. Otolaryngology ActiveAouchiche, Rachid M.D. Ophthalmology AssociateAugusthy, Reggie M. M.D. Physical Medicine & Rehab AssociateBarrow, Howard N. M.D. Otolaryngology AssociateBeehler, Cecil C. M.D. Ophthalmology HonoraryBerdick, Kenneth A. M.D. Internal Medicine AssociateBhavnani, Vinod D. M.D. Ophthalmology AssociateBlitzer, Peter H. M.D. Radiation Oncology HonoraryBlue, Mary C. M.D. Pathology AssociateBohm, Guillermo M.D. Endocrinology AssociateBond, Wendy Robinson M.D. Neurology AssociateBonnette, Harris L. M.D. Neurology ActiveBorrego, Orestes M.D. Pathology AssociateBourgon, Pierre M.D. Ophthalmology AssociateBrillman, Jon M.D. Neurology AssociateBrown Jr., Alan L. M.D. Radiation Oncology ActiveBrown, David C. M.D. Ophthalmology AssociateBrown, Karen E. M.D. Pathology AssociateBrown, Robin C. M.D. Otolaryngology HonoraryCarlin, Lane R. M.D. Neurology ActiveCarlino, Michael L. M.D. Diagnostic Radiology ActiveCarracino, William J. Jr. M.D. Neurology ActiveChadha, Tejvir S. M.D. Pulmonary Medicine ActiveChallapalli, Rahul K. M.D. Pulmonary Medicine AssociateCollins, Michael J. Jr. M.D. Ophthalmology AssociateConrado, Julio E. M.D. Pulmonary Medicine ActiveCox, Charles E. M.D. Ophthalmology AssociateCrandall, Valerie M.D. Ophthalmology AssociateCroley, James E. III M.D. Ophthalmology AssociateDakos, William N. M.D. Otolaryngology AssociateDaley, Joseph C. III M.D. Pulmonary Medicine AssociateDavis, Edward L. D.O. Neurology AssociateDavis, J. Bert M.D. Otolaryngology AssociateDavis, Richard M. M.D. Ophthalmology AssociateDawson, Christopher A. M.D. Physical Medicine & Rehab AssociateDosani, Razak A. M.D. Pulmonary Medicine ActiveDosoretz, Daniel E. M.D. Radiation Oncology AssociateDriscoll, Paul F. M.D. Neurology ActiveDuan, Naili M.D. Neurology AssociateDuffek, Cory C. M.D. Diagnostic Radiology ActiveEaton, Alexander M. M.D. Ophthalmology AssociateEisenberg, Howard M.D. Pulmonary Medicine AssociateEl-Gendy, Alaa A. M.D. Pulmonary Medicine ActiveElmquist, E. Trevor D.O. Ophthalmology AssociateFeroz, Abusayeed M. M.D. Pulmonary Medicine ActiveFerreira, Claudio A. M.D. Ophthalmology AssociateFletcher, Donald C. M.D. Ocular Rehabilitation AssociateFoo, May L. M.D. Radiation Oncology AssociateFox, Amy M. M.D. Radiation Oncology AssociateFrantz, Jonathan M. M.D. Ophthalmology AssociateFrey, Michael E. M.D. Physical Medicine & Rehab Associate
LEE MEMORIAL HEALTH SYSTEMLMH REAPPOINTMENTS
04/01/13 - 03/31/15Name Suffix Specialty TypeFuller, James H. M.D. Otolaryngology ActiveGalang, Kenneth J. M.D. Physical Medicine & Rehab AssociateGamez, Gerardo A. M.D. Neurology ActiveGardiner, Linda J. M.D. Otolaryngology HonoraryGeller, Scott L. M.D. Ophthalmology AssociateGerson, David S. M.D. Diagnostic Radiology ActiveGerson, Deborah M. M.D. Pathology AssociateGerson, Donald E. M.D. Diagnostic Radiology ActiveGhuman, A. Thomas M.D. Ophthalmology AssociateGinsberg, Barrett R. M.D. Ophthalmology AssociateGlenn, Leland K. M.D. Ophthalmology HonoraryGoodwin, R. Thad M.D. Ophthalmology AssociateGorovoy, Mark S. M.D. Ophthalmology AssociateHamilton, Jack E. M.D. Pathology AssociateHeller, Adam L. M.D. Neurology ActiveHendra, Richard I. M.D. Diagnostic Radiology HonoraryHillis, Rodney E. M.D. Neurology ActiveHoward, John L. M.D. Diagnostic Radiology HonoraryHussain, Reza S. M.D. Pulmonary Medicine AssociateHyppolite, Pierre R. M.D. Physical Medicine & Rehab ActiveIsley, Joseph K. Jr. M.D. Diagnostic Radiology HonoraryJavier, Zenaida C. M.D. Endocrinology HonoraryKalemeris, George C. M.D. Pathology ActiveKatin, Michael J. M.D. Radiation Oncology AssociateKazim, Nadia A. M.D. Ophthalmology AssociateKeys, Timothy C. M.D. Pulmonary Medicine AssociateKhan, Javaad A. M.D. Pulmonary Medicine AssociateKini, Vidya P. M.D. Physical Medicine & Rehab ActiveKole, Marilyn M.D. Pulmonary Medicine AssociateKonowal, Alexandra M. D.O. Ophthalmology AssociateKsar, Jamal S. M.D. Diagnostic Radiology ActiveKushner, Harold C. M.D. Otolaryngology AssociateLalla, Sunil N. M.D. Pulmonary Medicine AssociateLane, Richard J. M.D. Otolaryngology ActiveLanthier, Donna M. M.D. Physical Medicine & Rehab AssociateLaquis, Stephen J. M.D. Ophthalmology ActiveLarson, Dean W. M.D. Ophthalmology AssociateLevine, Steven E. M.D. Pathology AssociateLewis, Michael M. M.D. Ophthalmology AssociateLiu, Zhiping M.D. Pathology AssociateLozano, Alexander J. M.D. Otolaryngology AssociateLuna, Victor M. M.D. Endocrinology AssociateMagas, Louis T. M.D. Diagnostic Radiology ActiveMalkani, Sunil M. M.D. Ophthalmology AssociateMantz, Constantine A. M.D. Radiation Oncology ActiveMarino, Chris J. M.D. Neurology ActiveMartin, Benjamin G. M.D. Ophthalmology AssociateMather, Sergio R. M.D. Endocrinology AssociateMathew, Antony M.D. Pulmonary Medicine AssociateMcAlpine, Donald Ross M.D. Pulmonary Medicine AssociateMcKenna, Daniel J. M.D. Otolaryngology ActiveMehlman, Bruce M. M.D. Pulmonary Medicine ActiveMehrberg, Robert D. M.D. Physical Medicine & Rehab Associate
LEE MEMORIAL HEALTH SYSTEMLMH REAPPOINTMENTS
04/01/13 - 03/31/15Name Suffix Specialty TypeMestas, George M. M.D. Pulmonary Medicine AssociateMichaels, Greg A. M.D. Diagnostic Radiology ActiveMiller, Keith L. M.D. Radiation Oncology ActiveMowzoon, Nima M.D. Neurology ActiveMudali, Shiyama V. M.D. Pathology AssociateNaik, Sagar K. M.D. Pulmonary Medicine ActiveNegin, Geoffrey A. M.D. Diagnostic Radiology ActiveNewland, Douglas A. M.D. Neurology ActiveNewlon, James L. M.D. Otolaryngology AssociatePalmon, Florentino E. M.D. Ophthalmology AssociatePammi, Sunil S. M.D. Pulmonary Medicine AssociatePatel, Saurabh N. M.D. Ophthalmology AssociatePhommachanh, Viengsouk M.D. Otolaryngology ActivePrendiville, Stephen A. M.D. Otolaryngology ActivePresbrey, Thomas G. M.D. Diagnostic Radiology ActivePry, Richard J. M.D. Diagnostic Radiology ActiveQuigley, Thomas A. III M.D. Ophthalmology AssociateRashid, Mohammad A. M.D. Pulmonary Medicine HonoraryRathur, Sharik K. M.D. Diagnostic Radiology ActiveReardon, David M. M.D. Pathology AssociateRodriguez, John C. M.D. Diagnostic Radiology ActiveRubenstein, James H. M.D. Radiation Oncology AssociateSachs, Harris A. M.D. Pulmonary Medicine ActiveSaif, Mai F. M.D. Diagnostic Radiology ActiveSantucci, Gail M. M.D. Diagnostic Radiology ActiveSchreiber, Peter S. D.O. Physical Medicine & Rehab ActiveSchultz, Neil R. M.D. Physical Medicine & Rehab AssociateSchwartz, Eileen J. M.D. Neurology ActiveSeidenstein, Lawrence M.D. Pathology AssociateSharma, Ashish G. M.D. Ophthalmology AssociateShenoy, Parna G. M.D. Ophthalmology AssociateSims, C. Norton M.D. Ophthalmology AssociateSmith, Samuel W. M.D. Diagnostic Radiology HonorarySmith, Stephen E. M.D. Ophthalmology AssociateSnead, John W. M.D. Ophthalmology AssociateSonn, Jeffrey R. D.O. Diagnostic Radiology ActiveSteinmetz, Edward F. M.D. Neurology HonoraryStith, James A. M.D. Pathology ActiveSu, Wei M.D. Pathology ActiveSusko, Keith S. M.D. Physical Medicine & Rehab AssociateTafel, Allen C. M.D. Physical Medicine & Rehab ActiveTienstra, Joseph E. Jr. M.D. Diagnostic Radiology ActiveTsakalakis, P. John M.D. Pathology ActiveTyson, Farrell C. II M.D. Ophthalmology AssociateVeraja, Linda A. M.D. Pulmonary Medicine HonoraryWafapoor, Hussein M.D. Ophthalmology AssociateWalker, Joseph P. M.D. Ophthalmology AssociateWalters, James S. M.D. Diagnostic Radiology ActiveWeiner, James P. M.D. Physical Medicine & Rehab AssociateWeiss, Michael J. M.D. Ped. Diagnostic Radiology ActiveWeiss, Richard J. M.D. Endocrinology AssociateWing, Glenn L. M.D. Ophthalmology AssociateWingert, Richard H. M.D. Otolaryngology Associate
LEE MEMORIAL HEALTH SYSTEMLMH REAPPOINTMENTS
04/01/13 - 03/31/15Name Suffix Specialty Type
ALLIED HEALTHBalt, Jason M. CRNA Cert. Reg. Nurse Anesthetist AHPBrock, Ann V. P.A. Physician Assistant AHPByer, William C. CRNA Cert. Reg. Nurse Anesthetist AHPCarroll, Barbara J. C.N.M. Cert. Nurse Midwife AHPChang, Alexander S.W. CRNA Cert. Reg. Nurse Anesthetist AHPD'Ambra, Paula M. P.A. Physician Assistant AHPDavie, Jessica C. CRNA Cert. Reg. Nurse Anesthetist AHPDay, Emily C. P.A. Physician Assistant AHPDay, Sue A. ARNP Adv. Reg. Nurse Practitioner AHPDeFiore, Pasquale J. P.A. Physician Assistant AHPDePalma, Michael D. P.A. Physician Assistant AHPDonnelly, Matthew P.A. Physician Assistant AHPFeighery, Elizabeth J. CRNA Cert. Reg. Nurse Anesthetist AHPGilbert, Robert Scott P.A. Physician Assistant AHPGiraldez, Katrina J. P.A. Physician Assistant AHPGreco, Amber S. ARNP Adv. Reg. Nurse Practitioner AHPHowell, Kori A. ARNP Adv. Reg. Nurse Practitioner AHPMcPherson, Denise M. ARNP Adv. Reg. Nurse Practitioner AHPMeandro, Gerriann C. P.A. Physician Assistant AHPMeaney, Leo J. Jr. P.A. Physician Assistant AHPMitnick, Steven D. ARNP Adv. Reg. Nurse Practitioner AHPMukavetz, Megan E. P.A. Physician Assistant AHPNewbury, Judith M. ARNP Adv. Reg. Nurse Practitioner AHPOsinski, Sharon A. ARNP Adv. Reg. Nurse Practitioner AHPRobbins, Helen Michele P.A. Physician Assistant AHPRoberts, Rebecca G. P.A. Physician Assistant AHPRoman, Noemi ARNP Adv. Reg. Nurse Practitioner AHPServies, Ann M. ARNP Adv. Reg. Nurse Practitioner AHPStorrie, Andrea D. ARNP Adv. Reg. Nurse Practitioner AHPWalker, Jane M. CRNA Cert. Reg. Nurse Anesthetist AHPWoods, Karen S. ARNP Adv. Reg. Nurse Practitioner AHP
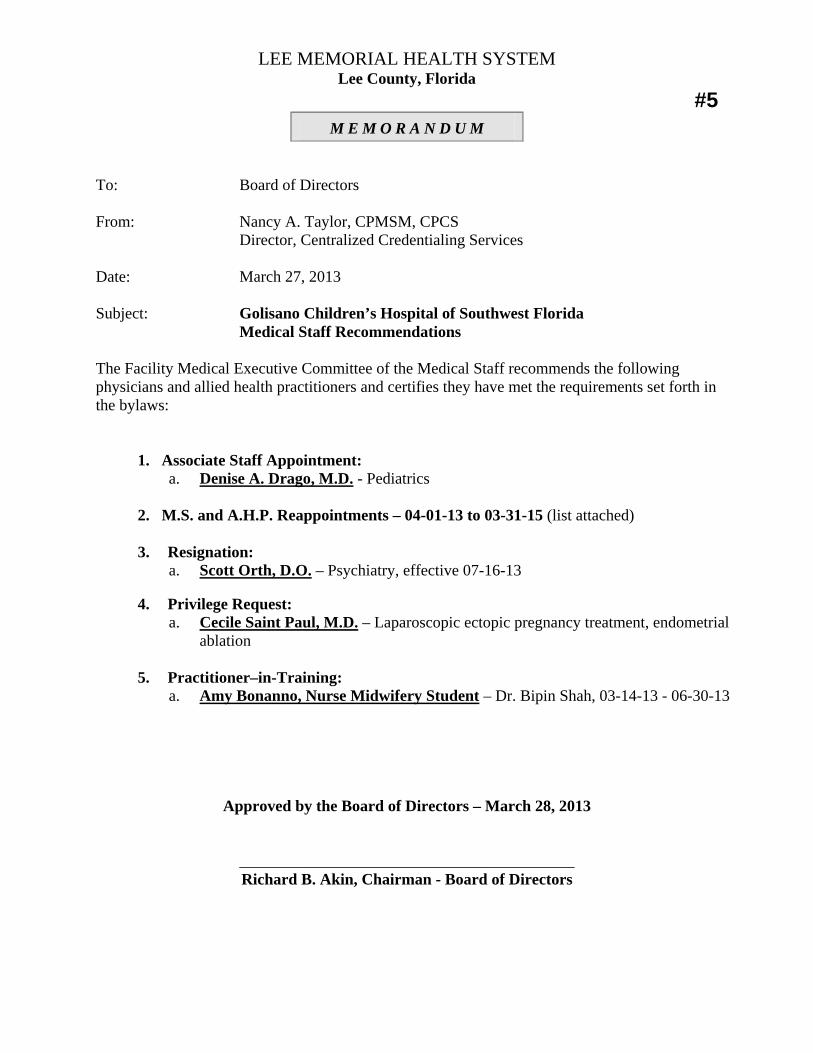
LEE MEMORIAL HEALTH SYSTEM Lee County, Florida
#5 M E M O R A N D U M
To: Board of Directors From: Nancy A. Taylor, CPMSM, CPCS Director, Centralized Credentialing Services Date: March 27, 2013 Subject: Golisano Children’s Hospital of Southwest Florida
Medical Staff Recommendations The Facility Medical Executive Committee of the Medical Staff recommends the following physicians and allied health practitioners and certifies they have met the requirements set forth in the bylaws:
1. Associate Staff Appointment: a. Denise A. Drago, M.D. - Pediatrics
2. M.S. and A.H.P. Reappointments – 04-01-13 to 03-31-15 (list attached) 3. Resignation:
a. Scott Orth, D.O. – Psychiatry, effective 07-16-13 4. Privilege Request:
a. Cecile Saint Paul, M.D. – Laparoscopic ectopic pregnancy treatment, endometrial ablation
5. Practitioner–in-Training:
a. Amy Bonanno, Nurse Midwifery Student – Dr. Bipin Shah, 03-14-13 - 06-30-13
Approved by the Board of Directors – March 28, 2013
__________________________________________ Richard B. Akin, Chairman - Board of Directors
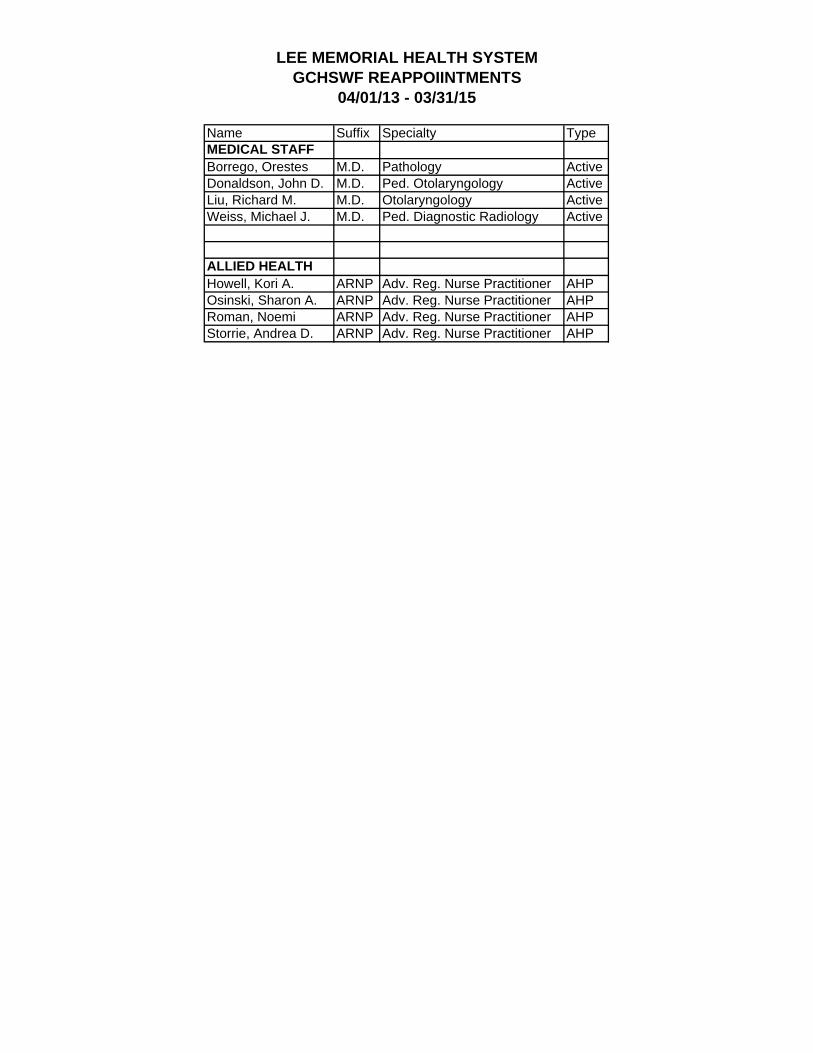
LEE MEMORIAL HEALTH SYSTEMGCHSWF REAPPOIINTMENTS
04/01/13 - 03/31/15
Name Suffix Specialty TypeMEDICAL STAFFBorrego, Orestes M.D. Pathology ActiveDonaldson, John D. M.D. Ped. Otolaryngology ActiveLiu, Richard M. M.D. Otolaryngology ActiveWeiss, Michael J. M.D. Ped. Diagnostic Radiology Active
ALLIED HEALTHHowell, Kori A. ARNP Adv. Reg. Nurse Practitioner AHPOsinski, Sharon A. ARNP Adv. Reg. Nurse Practitioner AHPRoman, Noemi ARNP Adv. Reg. Nurse Practitioner AHPStorrie, Andrea D. ARNP Adv. Reg. Nurse Practitioner AHP
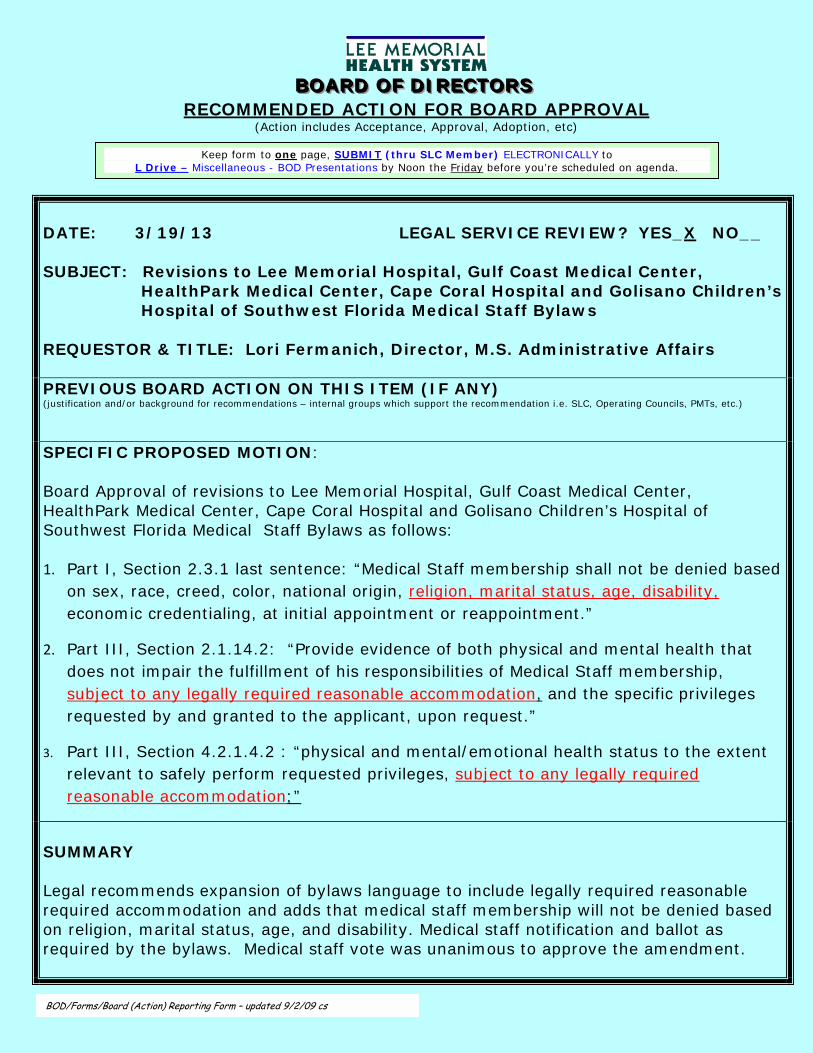
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS RECOMMENDED ACTION FOR BOARD APPROVAL
(Action includes Acceptance, Approval, Adoption, etc)
DATE: 3/19/13 LEGAL SERVICE REVIEW? YES_X NO__ SUBJECT: Revisions to Lee Memorial Hospital, Gulf Coast Medical Center, HealthPark Medical Center, Cape Coral Hospital and Golisano Children’s Hospital of Southwest Florida Medical Staff Bylaws REQUESTOR & TITLE: Lori Fermanich, Director, M.S. Administrative Affairs PREVIOUS BOARD ACTION ON THIS ITEM (IF ANY) (justification and/or background for recommendations – internal groups which support the recommendation i.e. SLC, Operating Councils, PMTs, etc.) SPECIFIC PROPOSED MOTION: Board Approval of revisions to Lee Memorial Hospital, Gulf Coast Medical Center, HealthPark Medical Center, Cape Coral Hospital and Golisano Children’s Hospital of Southwest Florida Medical Staff Bylaws as follows: 1. Part I, Section 2.3.1 last sentence: “Medical Staff membership shall not be denied based
on sex, race, creed, color, national origin, religion, marital status, age, disability, economic credentialing, at initial appointment or reappointment.”
2. Part III, Section 2.1.14.2: “Provide evidence of both physical and mental health that does not impair the fulfillment of his responsibilities of Medical Staff membership, subject to any legally required reasonable accommodation, and the specific privileges requested by and granted to the applicant, upon request.”
3. Part III, Section 4.2.1.4.2 : “physical and mental/emotional health status to the extent relevant to safely perform requested privileges, subject to any legally required reasonable accommodation;”
SUMMARY Legal recommends expansion of bylaws language to include legally required reasonable required accommodation and adds that medical staff membership will not be denied based on religion, marital status, age, and disability. Medical staff notification and ballot as required by the bylaws. Medical staff vote was unanimous to approve the amendment.
BOD/Forms/Board (Action) Reporting Form – updated 9/2/09 cs
Keep form to one page, SUBMIT (thru SLC Member) ELECTRONICALLY to L Drive – Miscellaneous - BOD Presentations by Noon the Friday before you’re scheduled on agenda.
Cape Coral Hospital
Medical Staff
Bylaws
Adopted: May 28, 2009 Revision approved by BOD June 24, 2010
Revision approved by BOD August 26, 2010 Revisions approved by BOD June 16, 2011
Revisions approved by BOD December 6, 2012
1
TABLE OF CONTENTS PART 1: GOVERNANCE 6 SECTION 1 MEDICAL STAFF PURPOSE & AUTHORITY 6 1.1 Purposes 6 1.2 Authority 6 1.3 Medical Staff (Term) 6 SECTION 2 MEDICAL STAFF MEMBERSHIP 7 2.1 Nature of Medical Staff Membership 7 2.2 Qualifications for Membership 7 2.3 Nondiscrimination 7 2.3.1 No Automatic Entitlement 7 2.4 Conditions and Duration of Appointment 7 2.5 Medical Staff Membership and Clinical Privileges 8 2.6 Medical Staff Members’ Responsibilities 8 2.7 Basic Responsibilities of Applicants and Appointees 8 2.8 Member Rights 11 2.9 Medical Staff Dues and Assessments 11 2.10 Conflict of Interest 12 SECTION 3 CONFIDENTIALITY, IMMUNITY AND RELEASES 12 3.1 Confidentiality 12 3.2 Immunity 13 3.3 Releases 14 SECTION 4 CATEGORIES OF THE MEDICAL STAFF 14 4.1 Active Category 14 4.2 Associate Category 15 4.3 Honorary Category 16 SECTION 5 OFFICERS OF THE MEDICAL STAFF 16 5.1 Officers of Medical Staff and FMEC at-Large Members 16 5.2 Qualifications of Officers and FMEC at-Large Members 16 5.3 Election of Officers and FMEC at-Large Members 16 5.4 Terms of Office 17 5.5 Vacancies of Office 17 5.6 Duties of Officers and FMEC at-Large Members 17 5.7 Removal and Resignation of Officer or FMEC at-Large Members 19 SECTION 6 MEDICAL STAFF ORGANIZATION 20 6.1 Departments 20 6.2 Qualifications, Selection, Term, Removal and Responsibility of Department Chair 21 6.3 Assignment to Department 23 SECTION 7 MEDICAL STAFF GOVERNANCE COMMITTEES 23
2
7.1 Designation of the LMHS MS Physician Leadership Council (PLC) 23 7.2 Composition of the LMHS PLC 23 7.3 Staff Functions 25
7.4 Facility Medical Executive Committee (FMEC) (Composition, Selection and Tenure) 25 7.5 Duties and Responsibilities of the FMEC’s 25 7.6 System Medical Staff Committees 27 7.6.1 Purpose 27 7.6.2 Organization to Perform Functions 27 7.6.2.1 System Credentialing/Privileging Committee 27 7.6.2.2 System Medical Staff Quality Committee 27 7.6.2.3 System Practitioner Resource Committee 27 7.6.2.4 System Bylaws Committee 28 7.6.2.5 System Emergency Services Committee 29 7.6.3 Composition & Meetings of System MS Committees 29 7.7 Facility Medical Staff Committees 30 7.7.1 Purpose 30 7.7.2 Standing Facility Medical Staff Committees 30 SECTION 8 MEDICAL STAFF MEETINGS 31 8.1 General Medical Staff Meetings 31 8.2 Departments, Sections and Committee Meetings 31 8.3 Special Meetings of Departments, Sections and Committees 31 8.4 Quorum 31 8.5 Attendance Requirements 32 8.6 Participation by Administration 32 8.7 Robert’s Rules of Order 32 8.8 Notice of Meetings 33 8.9 Action of PLC, FMEC, General Medical Staff, Department, Section or Committee 33 8.10 Rights of Ex Officio Members 33 8.11 Minutes 33 SECTION 9 DECISION MAKING METHODS AND CONFLICT RESOLUTION 33 SECTION 10 REVIEW, REVISION ADOPTION AND AMENDMENT 34 10.1 Medical Staff Responsibility 34 10.2 Methods of Amendment and Adoption to these Bylaws 35 10.3 Methods of Amendment and Adoption to any Medical Staff Rules, Regulations and Policies 35 Appendix A PRINCIPLES OF MEDICAL ETHICS 37 PART II: INVESTIGATIONS, CORRECTIVE ACTION, HEARING AND APPEAL PLAN 39 SECTION 1 ROUTINE CORRECTIVE ACTION & INVESTIGATIONS 39 1.1 Progressive Intervention 39 1.2 Basis for Routine Corrective Action 39 1.3 Requests and Notices 40 1.4 Investigations 40 1.5 FMEC Action 41 1.6 Notice of FMEC Action 42 1.7 Board of Directions Action 42
3
SECTION 2 EMERGENCY CORRECTIVE ACTION/PRECAUTIONARY SUSPENSION OF CLINICAL PRIVILEGES 42 2.1 Basis for Emergency Corrective Action/Precautionary Suspension 42 2.2 Notice of Emergency Corrective Action/Precautionary Suspension 42 2.3 FMEC Procedure 43 2.4 Provision of Patient Care 43 2.5 Recission of Emergency Corrective Action/Precautionary Suspension 43 SECTION 3 AUTOMATIC SUSPENSION AND TERMINATION 43 3.1 Basis for Automatic Suspension and Termination 43 3.1.1 Loss of License 43 3.1.2 Residence or Office Outside Lee County 43 3.1.3 Lack of Active Practice 44 3.1.4 Criminal Conviction 44 3.1.5 Loss or Restriction of DEA Certificate 44 3.1.6 Exclusion From Federal or State Health Care Programs 44 3.1.7 Failure to Pay Fees and Assessments 44 3.1.8 Failure to Provide Requested Information 44 3.1.9 Failure to Request Reappointment or Provide Requested Information Related to Reappointment 45 3.1.10 Failure to Request Reinstatement Following Leave of Absence 45 3.1.11 Failure to Complete Medical Records 45 3.1.12 Failure to Comply with Special Meeting Attendance Requirements 45 3.2 Right to Limited Hearing for Automatic/Voluntary Suspension and Termination 45 SECTION 4 HEARING AND APPEAL PROCEDURES 46 4.1 Grounds for Hearing 46 4.2 Notice of Recommendation 46 4.3 Request for Hearing 47 4.4 Preliminary Interview 47 SECTION 5 FAIR HEARING PROCEDURE 47 5.1 System Representative, Hearing Panel and Hearing Officer 47 5.1.1 System Representative 48 5.1.2 Hearing Panel 48 5.1.3 Hearing Officer – Qualifications & Authority 48 5.2 Challenge to Hearing Panel Members or Hearing Officer 50 SECTION 6 HEARING PROCEDURES 50 6.1 Provision of Relevant Information 50 6.2 Pre-Hearing Conference 51 6.3 Failure to Appear 51 6.4 Record of Hearing 51 6.5 Rights of Both Sides 52 6.6 Admissibility of Evidence 52 6.7 Burden of Presenting Evidence and Proof 52 SECTION 7 HEARING CONCLUSION, DELIBERATIONS AND RECOMMENDATIONS 52 7.1 Deliberations and Recommendation of the Hearing Panel/Hearing Officer 52 7.2 Disposition of Hearing Panel Report 53
4
SECTION 8 APPEAL PROCEDURE 53 8.1 Request & Time for Appeal 53 8.2 Grounds for Appeal 54 8.3 Time, Place and Notice 54 8.4 Nature of Appellate Review 54 8.4.1 Review Panel 55 8.4.2 Position Papers 55 8.4.3 Oral Argument 55 8.4.4 Recommendation 55 SECTION 9 FINAL DECISION OF THE BOARD 55 SECTION 10 RIGHT TO ONE HEARING AND ONE APPEAL ONLY 55 PART III: CREDENTIALING PROCEDURES 56 SECTION 1 SYSTEM CREDENTIALING/PRIVILEGING COMMITTEE 56 1.1 Organizational Structure 56 1.2 Transition Issues 56 1.3 Purpose of the System Credentialing/Privileging Committee 56 1.4 Composition of the System Credentialing/Privileging Committee 57 1.5 Duties and Responsibilities of the System Credentialing/Privileging Committee 57 SECTION 2 QUALIFICATIONS FOR MEMBERSHIP AND PRIVILEGES 58 2.1 Qualifications for MS appointment, reappointment or clinical privileges 58 2.1.15 Exceptions 58 SECTION 3 PRE-APPLICATION PROCESS 60 SECTION 4 INITIAL APPOINTMENT PROCESS 61 4.1 Completion of Application 61 4.2 Applicant’s Attestation, Authorization and Acknowledgement 63 4.3 Application Evaluation 64 4.3.1 Expedited Credentialing 64 4.3.2 Applicant Interview 64 4.3.3 Department Chair Action 64 4.3.4 MS System Credentialing/Privileging Committee Action 65 4.3.5 FMEC Action 66 4.3.6 Applicants Applying to Multiple Facilities 66 4.3.7 Board Action 66 4.3.8 Notice of Final Decision 67 4.3.9 Periods for Processing 67 SECTION 5 FOCUSED PROFESSIONAL PRACTICE EVALUATION (FPPE) 67 SECTION 6 CRITERIA FOR REAPPOINTMENT 68 6.1 Criteria for Reappointment 68 6.3 Evaluation of Application for Reappointment of Membership and/or Privileges 70
5
SECTION 7 CLINICAL PRIVILEGES 70 7.1 Exercise of Privileges 70 7.2 Requests 70 7.3 Basis for Privileges Determination 70 7.4 Special Conditions for Podiatric Privileges 72 7.5 Special Conditions for Residents or Fellows in Training 73 7.6 Special Conditions for the Aging Practitioner 73 7.7 Temporary Privileges 73 7.7.8 Disaster Privileges 75 SECTION 8 PRECEPTORSHIP 76 SECTION 9 REAPPLICATION AFTER MODIFICATIONS OF MEMBERSHIP STATUS OF PRIVILEGES AND EXHAUSTION OF REMEDIES 77 9.1 Reapplication After Adverse Credentials Decision 77 9.2 Request for Modification of Appointment Status or Privileges 77 9.3 Resignation of Staff Appointment or Privileges 77 9.4 Exhaustion of Administrative Remedies 77 9.5 Reporting Requirements 78 SECTION 10 LEAVE OF ABSENCE 78 10.1 Leave Request 78 10.2 Termination of Leave 78 10.3 Failure to Request Reinstatement 78 SECTION 11 PRACTITIONERS PROVIDING CONTRACTED SERVICES 79 11.3 Contract Services/Department or Service Closure 79 11.4 Qualifications 80 11.5 Terms 80 11.6 Effect of Contract or Employment Expiration or Termination 80 SECTION 12 MEDICAL ADMINISTRATIVE OFFICERS 80
6
PART 1: GOVERNANCE
SECTION 1 MEDICAL STAFF PURPOSES & AUTHORITY 1.1 Purposes
The purposes of the Medical Staffs of Lee Memorial Health System are to:
1.1.1 Serve as the formal organizational structure of those practitioners granted the privilege of practicing in the hospitals and other facilities of the System.
1.1.2 Serve as the primary means for accountability to the Board for the professional
performance, the quality of medical care provided to patients, and ethical conduct of its members. The Board shall have the ultimate responsibility for the quality of medical care provided to patients and the ultimate authority to approve the granting of privileges, to make appointments and reappointments to membership on the Medical Staffs, and to approve the adoption of Medical Staff Bylaws and Rules and Regulations. Such authority will be exercised based on the standard set forth in Section 1.2.
1.1.3 Provide a means through which members of the Medical Staffs may address with
the Board those aspects of policy that involve professional practice or may affect the care of patients.
1.2 Authority
The Medical Staffs of Lee Memorial Health System are authorized by the Lee Memorial Health System Board of Directors (“the Board”) to exercise such power as is necessary to discharge its responsibilities under these Bylaws consistent with the Bylaws of Lee Memorial Health System. Lee Memorial Health System (“the System” or “the Health System”) includes acute care facilities known as Cape Coral Hospital, Gulf Coast Medical Center, HealthPark Medical Center, Lee Memorial Hospital, and The Children’s Hospital (individually known as “the hospital” and collectively known as “the hospitals”). The Board recognizes that a well-organized, self-governing Medical Staff that provides oversight of care, treatment, and services provided by practitioners with privileges is in the best interest of patients. When acting with respect to matters of the Medical Staff, the Board shall at all times comply with the Medical Staff Bylaws, the Rules and Regulations of the Medical Staff, and applicable law.
1.3 Medical Staff The term “Medical Staff” as used herein shall mean, on a collective basis, those
practitioners who are authorized by the Board to exercise privileges at one or more of the System’s hospitals, and, on a component basis, those practitioners who are authorized by the Board to exercise privileges at a particular system hospital. The latter may be referred to herein as the “Medical Staff of a facility.” The term “he”, “him”, or “his” means of a male or female gender.
7
SECTION 2 MEDICAL STAFF MEMBERSHIP 2.1 Nature of Medical Staff Membership
Membership on the Medical Staff is a privilege that shall be extended only to professionally competent physicians (M.D. or D.O.), dentists, podiatrists and/or psychologists who continuously meet the qualifications, standards, and requirements set forth in these Bylaws and associated policies of the Medical Staff and the hospitals. Medical Staff membership is a privilege and not a right of any practitioner or other person. Medical Staff membership and the exercise of privileges in connection therewith shall be extended only to practitioners who continuously meet the requirements of these Bylaws. The Board makes decisions regarding Medical Staff matters, based on Medical Staff recommendations, in accordance with these Bylaws. Membership on the Medical Staff shall confer on the Medical Staff member only such rights as set forth in the Bylaws. No person shall admit patients to a System hospital unless he is appointed to the Medical Staff of such hospital. For purposes of these Bylaws, “membership in” is used synonymously with “appointment to” the Medical Staff. Medical Staff members granted membership and privileges at a hospital, which has services and facilities that are provider based to a main provider and are authorized to exercise those privileges at the main provider.
2.2 Qualifications for Membership
2.2.1 The qualifications for Medical Staff membership are delineated in Part III of these Bylaws (Credentials Procedures).
2.3 Nondiscrimination
2.3.1 No Automatic Entitlement
No person shall be automatically entitled to Medical Staff membership or to the exercise of clinical privileges merely because he is licensed to practice, is a member of any professional organization, is certified by any board, or had held (but not currently) Medical Staff membership or clinical privileges at a System hospital or at any other health care facility. The burden shall be on the applicant to establish his qualifications. Acceptance of Medical Staff membership or exercise of clinical privileges shall constitute an agreement to strictly abide by these Bylaws, the applicable Medical Staff Policies, the Rules and Regulations, and the Principles of Medical Ethics set forth in Appendix A hereof and all other appropriate ethical standards governing the practitioner’s practice. No person shall be initially appointed to the Medical Staff or granted clinical privileges if the hospitals are unable to provide adequate facilities and supportive services for the applicant and his patients. Medical Staff membership shall not be denied based on sex, race, creed, color, national origin, religion, marital status, age, disability, or economic credentialing, at initial appointment or reappointment.
2.4 Conditions and Duration of Appointment
2.4.1 The Board shall act on appointment and reappointment only after the Medical Staff has had an opportunity to submit a recommendation from the Facility Medical Executive Committee (FMEC). Appointment and reappointment to the Medical Staff shall be for no more than twenty-four (24) calendar months.
8
2.5 Medical Staff Membership and Clinical Privileges
2.5.1 Requests for Medical Staff membership and/or clinical privileges will be processed only when the potential applicant meets the current minimum qualifying criteria recommended by the System Credentialing/Privileging Committee and FMEC and approved by the Board. Membership and/or privileges will be granted and administered as delineated in Part III (Credentials Procedures) of these Bylaws, including but not limited to, Part III, Sections 3 and 11.3 regarding Contracted practitioners.
2.6 Medical Staff Members’ Responsibilities
2.6.1 Duties of Appointees Appointment to the Medical Staff shall require that each practitioner assume such reasonable duties and responsibilities, as the Medical Staff shall require.
2.7 Basic Responsibilities of Applicants and Appointees The following basic responsibilities and requirements shall be applicable to every applicant
and appointee for Medical Staff appointment or reappointment as a condition of consideration of such application and as a condition of continued Medical Staff appointment if granted:
2.7.1 an obligation to provide for appropriate and timely care and supervision to all
patients in the hospital for whom the individual has responsibility (Standard of Care);
2.7.2 an agreement to abide by all Bylaws, Rules and Regulations and Policies of the Medical Staff and the Hospital, as shall be in force during the time the individual is appointed to the Medical Staff (Conformance to Rules);
2.7.2.1 provide a current cell phone number and email address to be used for
emergency or disaster purposes in accordance with Medical Staff Services Dept. policy.
2.7.3 an agreement to accept committee assignments and such other reasonable duties
and responsibilities as shall be assigned (Committee Assignments);
2.7.4 to not participate in illegal fee splitting or other illegal inducements relating to patient referral;
2.7.5 to promptly notify Medical Staff Services (Notification Requirements);
2.7.5.1 if his professional license in any state is suspended or revoked; 2.7.5.2 of the imposition of any conditions by any state licensing authority on his
continued ability to practice his profession, including probation or limitations on the scope of practice;
2.7.5.3 of the loss or restriction of Medical Staff membership or privileges at any
other health care facility;
9
2.7.5.4 if his Drug Enforcement Agency (DEA) license number is suspended, revoked or voluntarily relinquished;
2.7.5.5 of any change in eligibility for participation in Federal Health Care
Programs including any sanctions imposed or recommended by the Federal Department of Health and Human Services, Florida State Agency for Health Care Administration and/or the receipt of any citation and/or quality denial letter concerning alleged quality problems in patient care;
2.7.5.6 if the practitioner enters, participates in, or against medical advice, leaves
or refuses any program of treatment prescribed or required by the Florida Physicians’ Recovery Network;
2.7.5.7 if the practitioner is admitted for, seeks, or is undergoing treatment for
substance or alcohol abuse or a behavioral health problem. “Substance abuse” shall include but not limited to, use or ingestion of illegal drugs, or use or ingestion of prescription medications not prescribed in the ordinary course of treatment of injury or disease. “Behavioral health problem” shall mean any condition or disease of a psychiatric or psychological nature which, in the opinion of a qualified psychiatrist, adversely affects the practitioner’s ability to care for patients or practice his profession in accordance with the applicable prevailing standard of care; or
2.7.5.8 the conviction of, or pleading of nolo contendere to, a crime constituting a
felony in any jurisdiction. 2.7.6 to abide by generally recognized ethical principles applicable to the applicant’s or
appointee’s profession and by the code of ethics set forth in Appendix A (Ethics);
2.7.7 to respect the confidentiality of all information obtained in connection with his responsibility as a Medical Staff member and comply with the requirements of the Health Insurance Portability and Accountability Act (HIPAA) (Confidentiality);
2.7.8 to provide medical consultation in a timely fashion in accordance with all
applicable Rules & Regulations and Medical Staff Policies (Consultation);
2.7.9 to participate in the monitoring and evaluation activities of Clinical Sections and cooperate with other members of the Medical Staff and the System, in programs designed to improve the quality of care to reduce or eliminate waste in the use of scarce System resources and to reduce the risk of injury to patients and others in the provision of care (Quality Review Participation);
2.7.10 to complete in a timely and legible manner the medical records and other required
records for all patients as required by these Bylaws, applicable Rules and Regulations, and other applicable policies of the hospital (Medical Records);
2.7.11 to pay promptly any applicable Medical Staff assessments and dues (Dues); 2.7.12 to participate in continuing education programs for the benefit of the applicant or
appointee and for the benefit of other professionals and System hospital personnel (CME);
10
2.7.13 to authorize the release of all information necessary for an evaluation of the
individual’s qualifications for initial or continued appointment, reappointment, and/or clinical privileges (Release of Information);
2.7.14 to submit to an evaluation of his physical and/or mental health status by a
physician or physicians acceptable to the FMEC or Board, whenever the FMEC or Board has reason to question the physical and/or mental health status of the practitioner, as a prerequisite to further consideration of his application for appointment or reappointment, the exercise of previously granted privileges or maintenance of his Medical Staff appointment (Physical/Mental Exam);
2.7.15 to recognize the obligations established to fulfill the hospital’s responsibilities
under the Emergency Medical Treatment and Women in Labor Act (EMTALA), the Access to Emergency Services and Care Act and/or other applicable regulations, requirements or standards and to share in the responsibility for providing physician coverage on an emergency basis in the Emergency Department, in accordance with the provisions of the Medical Staff Bylaws and all applicable facility-specific Rules & Regulations and Medical Staff Policies (On Call Coverage);
2.7.16 to provide his professional services to hospitalized or emergency room patients
covered by Medicaid and similar programs of indigent care, or such patients without personal physicians or insurance coverage, in accordance with Medical Staff Rules & Regulations adopted by the FMEC delineating the responsibility to provide services to those patients (Services to Indigent Patient);
2.7.17 provide proof of financial responsibility to pay claims or costs associated with the
rendering of, or failure to render, medical care or services in compliance with Florida law governing the practitioner’s license to practice in the State of Florida. Proof of financial responsibility shall be provided at the time of initial appointment and on reappointment, at the time the practitioner changes the method of meeting his financial responsibility and at any other time on the request of Medical Staff Services (Financial Responsibility);
2.7.18 to behave in a professional and civil manner and conduct himself in a manner
conducive to excellent patient care and to work cooperatively with Medical Staff appointees, and with other health care professionals, and Hospital personnel, so as not to adversely affect patient care. This requirement is not in any way intended to interfere with a practitioner’s right: (1) to express opinions freely and to support positions whether or not they are in dispute with those of other Medical Staff members; (2) to engage in honest differences of opinion with respect to diagnosis and treatment; or (3) to engage in a good faith criticism of others. The following types of behavior, however, which constitute some examples of an inability to interact on a professional basis with others or to behave in a professional and civil manner, are deemed unacceptable for a member of the Medical Staff:
2.7.18.1 conduct that reasonably could be characterized as sexual and/or racial
harassment;
2.7.18.2 threats of physical assault or actual physical assault, harassment, or the placing of others in fear by engaging in threatening behavior;
11
2.7.18.3 the unnecessary, unwarranted and unjustifiable knowing use of loud, profane or abusive language directed toward members of the Medical Staff, patient and others; or
2.7.18.4 written or oral statements that constitute the intentional expression of falsehoods, or constitute deliberately disparaging statements made with reckless disregard for their truth or for the reputation and feelings of others;
2.7.18.5 doing anything of a similar nature that the practitioner has been warned
not to do by the President of the Medical Staff or FMEC Committee (Professional and Civil Behavior);
2.7.19 duty to give notice if the practitioner is not actively engaged in the practice of his
profession in Lee County (Lack of Active Practice);
2.7.20 duty to give notice if practitioner does not maintain a full-time residence and office in Lee County, unless the residence and office requirements have been waived in accordance with these Bylaws (Residence or Office in Lee County).
2.8 Member Rights
The following basic rights shall apply to Medical Staff practitioners: 2.8.1 Each Medical Staff member, in the active category, has the right to a meeting with
the FMEC and/or the Physician Leadership Council (PLC) on matters relevant to the responsibilities of the FMEC and/or the PLC, provided that the practitioner has attempted to resolve a matter of concern after working with his Department Chair or other appropriate hospital and/or Health System Medical Staff leader(s). Upon written notice to the President of the Medical Staff, two (2) weeks in advance of a regular meeting, the active Medical Staff member may meet with the FMEC and/or the PLC to discuss the issue.
2.8.2 Each Medical Staff member, in the active category, has the right to initiate a recall
election of a Medical Staff officer by following the procedure outlined in Section 5.7 of these Bylaws regarding removal and resignation from office.
2.8.3 Each Medical Staff member, in the active category, may request a special meeting
of the Medical Staff, upon presentation of a petition, stating the purpose of the meeting and signed by ten (10) members of the Active Medical Staff. The FMEC shall schedule a special meeting for the specific purposes addressed by the petitioners in accordance with Section ten (10) of these Bylaws. No business other than that detailed in the petition may be transacted.
2.8.4 An applicant or an individual holding a Medical Staff appointment shall be entitled to
request a hearing/appeal pursuant to the conditions and procedures described in Part II of these Bylaws (Investigations, Corrective Action, Hearing and Appeal Plan).
2.8.5 All other rights as specified by these Bylaws.
2.9 Medical Staff Dues and Assessments
2.9.1 Annual Medical Staff dues, if any, shall be determined by the FMEC. Failure of a Medical Staff member to pay dues shall be considered a voluntary resignation from
12
the Medical Staff. The FMEC may pass policies from time to time that exempt certain categories of membership or members holding specified leadership positions from payment of dues. The FMEC shall authorize the use of Medical Staff dues.
2.9.2 Medical Staff System-wide assessments, such as a library assessment, shall be
determined by the PLC, on behalf of the FMECs. Failure of a Medical Staff member to pay any assessment(s) shall be considered a voluntary resignation from the Medical Staff. The PLC, on behalf of the FMECs, may pass policies from time to time that exempt certain categories of membership or members holding specific leadership positions from payment of such assessment(s).
2.9.3 The PLC, on behalf of the FMECs, shall authorize the use of Medical Staff
assessments consistent with the purpose of the assessment. 2.10 Conflict of Interest
2.10.1 In any instance where an officer, committee Chair, or member of any Medical Staff committee has, or reasonably could be perceived to have a conflict of interest, or to be biased in any matter involving another Medical Staff appointee or any other matter that comes before such individual or committee, or in any instance where any such individual brought the complaint against that practitioner, such individual shall not participate in the discussion or voting on the matter and shall be excused from any meeting during that time, although that individual may be asked and may answer, any questions concerning the matter before leaving. As a matter of procedure, the Chair of that committee designated to review the matter shall inquire, prior to any discussion of the matter, whether any member has any conflict of interest or bias. The existence of a potential conflict of interest or bias on the part of any committee member may be called to the attention of the Chair by any committee member with knowledge of the matter.
2.10.2 In any instance where an officer, committee Chair, or member of any Medical Staff
committee has a conflict of interest in any matter that comes before such individual or committee, such individual has the right to abstain or recuse himself from voting on such matter. Such abstention or recusal shall not prohibit such individual from providing factual information or participating in discussion on such matter. If an individual is requested to abstain or recuse himself and refuses to do so, the potential conflict of interest issue will be reviewed and resolved by the next highest authority as outlined in these Bylaws. As a matter of procedure, the Chair of that committee designated to review the matter shall inquire, prior to any discussion of the matter, whether any member has any conflict of interest or bias. The existence of a potential conflict of interest or bias on the part of any committee member may be called to the attention of the Chair by any committee member with knowledge of the matter.
2.10.3 Assurance of a conflict of interest or bias can be determined by a majority vote of
the members of the committee where a quorum is present. SECTION 3 CONFIDENTIALITY, IMMUNITY AND RELEASES 3.1 Confidentiality
Information with respect to any practitioner or regarding any other subject discussed, submitted, collected or prepared by any representative of the Lee Memorial Health System,
13
including officers or members of organized committees of the Health System’s Medical Staffs, or any other healthcare professional, healthcare facility, organization or Medical Staff, for the purpose of achieving and maintaining the quality of care, reducing morbidity or mortality or contributing to clinical research shall, in accordance with Florida law, be confidential and shall not be disseminated or used for any purpose other than the foregoing. Such information shall not be deemed a part of the patient medical record, and shall not be filed therein. Each individual or committee member participating in such activities shall agree to make no disclosures of any such information except as authorized, in writing, by the Chief Executive Officer (CEO) or by legal counsel to the hospitals. Any breach of confidentiality by an individual or committee member may result in a professional review action, and/or may result in appropriate legal action to ensure that confidentiality is preserved, including application to a court of law for injunctive or other relief.
3.2 Immunity 3.2.1 Any Medical Staff officer, Department Chair, Section Chief, committee Chair,
committee member, and individual staff appointee who acts in good faith for and on behalf of any System hospital in discharging duties, functions or responsibilities stated in these Medical Staff Bylaws, applicable Policies, and/or Rules and Regulations shall be afforded protection by the Board of Directors to the fullest extent permitted by law in accordance with written policies adopted by the Board. Individuals and organizations independent of the Medical Staff or any of its members who may be engaged by the Health System to perform the review, analysis and evaluation of the qualification and/or performance of practitioners with membership and/or privileges on the Medical Staff are afforded protection by the Board of Directors in accordance with written policies adopted by the Board, provided such individuals or organizations act in good faith.
3.2.2 To the fullest extent permitted by law, each applicant and appointee to the Medical
Staff releases from any and all liability, and extends absolute immunity to System hospitals and the Board and its individual members, and to the System’s authorized representatives and agents, with respect to any acts, communications or documents, recommendations or disclosures involving the applicant or appointee, concerning the following:
3.2.2.1 applications for appointment or clinical privileges, including temporary
privileges and/or emergency privileges;
3.2.2.2 evaluations concerning reappointment or changes in clinical privileges;
3.2.2.3 proceedings for suspension or reduction of clinical privileges or for revocation of Medical Staff appointment, or any other disciplinary sanction;
3.2.2.4 summary suspension;
3.2.2.5 hearings and appellate reviews; 3.2.2.6 medical/surgical care evaluations; 3.2.2.7 utilization reviews;
3.2.2.8 other activities relating to the quality of patient care or professional
conduct;
14
3.2.2.9 matters of inquiries concerning the applicant’s or appointee’s professional
qualifications, credentials, clinical competence, character, mental or emotional stability, physical condition, ethics or behavior; and/or
3.2.2.10 any other matter that directly or indirectly might relate to the applicants or
appointee’s competence, and/or to patient care.
3.3 Releases
3.3.1 Authorization to Obtain Information
The applicant or appointee specifically authorizes the Medical Staff and its authorized representatives to consult with any third party who may have information bearing on the individual’s professional qualifications, credentials, clinical competence, character, mental or emotional stability, physical condition, ethics, behavior, or any other matter reasonably having a bearing on the applicant’s or appointee’s satisfaction of the criteria for initial and continued appointment to the Medical Staff. This authorization also covers the right to inspect, or obtain all communications, reports, records, statements, documents, recommendations or disclosures of said third parties that may be relevant to such questions. The individual also specifically authorizes said third parties to release said information to the Medical Staff and its authorized representatives upon request.
3.3.2 Legal Effect
The confidentiality provisions and protections described in this Section shall not limit
or supersede any protection or immunity afforded by law. SECTION 4 CATEGORIES OF THE MEDICAL STAFF 4.1 Active Category
4.1.1 Qualifications: Members of this category must have served on the Medical Staff, maintained a residence and office in Lee County (4.1.3.3) for one year, and be involved in twenty-four (24) patient contacts per year (i.e., a patient contact is defined as an inpatient admission, consultation, or an inpatient or outpatient surgical procedure) at the hospital except as expressly waived for practitioners with at least twenty (20) years of service in the active category or for those physicians who document their efforts to support the hospital’s patient care mission to the satisfaction of the FMEC.
In the event that a member of the active category does not meet the qualifications for reappointment to the active category, and if the member is otherwise abiding by all Bylaws, Rules and Regulations, and policies of the Medical Staff and hospital, the member may be appointed to another Medical Staff category if he meets the eligibility requirements for such category.
4.1.2 Prerogatives: Members of this category may:
4.1.2.1 Attend Medical Staff/Department meetings of which he is a member and any Medical Staff or hospital education programs;
15
4.1.2.2 Vote on all matters presented by the Medical Staff, Department, and committee(s) to which the member is assigned;
4.1.2.3 Hold office and sit on or be the Chair of any committee in accordance with
any qualifying criteria set forth elsewhere in the Medical Staff Bylaws or Medical Staff policies.
4.1.3 Responsibilities: Members of this category shall:
4.1.3.1 Contribute to the organizational and administrative affairs of the Medical Staff;
4.1.3.2 Actively participate as requested or required in activities and
functions of the Medical Staff, including quality/performance improvement and peer review, credentialing, risk and utilization management, medical records completion, monitoring activities and in the discharge of other Medical Staff functions as may be required by the FMEC;
4.1.3.3 The one-year residence and office requirement may be explicitly
waived by majority vote of the FMEC, on written request of the practitioner, at the time of appointment, if the practitioner affirmatively demonstrates to the FMEC in writing that the quality of patient care is not likely to be affected by his not living and having an office in Lee County and that the practitioner’s obligation to provide emergency room call and to attend hospitalized patient can be met.
4.1.3.4 Fulfill or comply with any applicable Medical Staff or hospital
policies or procedures as requested by the FMEC. 4.1.3.5 Fulfill basic responsibilities and requirements set forth in Section
2.7 of this Part, including but not limited to, Emergency Department call responsibilities in accordance with facility specific rules and regulations, unless exempted from Emergency Department call responsibilities as defined by their Section (if applicable) or Department and approved by the FMEC. In the event facility specific rules and regulations require physicians to accept emergency department referrals to the physician’s office, Lee Memorial Health System will provide facility support and services for such patients.
4.2 Associate Category 4.2.1 Qualifications: The associate category is reserved for Medical Staff members who
do not meet the eligibility requirements for the active category or choose not to pursue active status. This category includes physicians during their first year on the Medical Staff, as well as low volume/no volume physicians.
4.2.2 Prerogatives: Members of this category may:
4.2.2.1 Attend general Medical Staff Department meetings of which he is a member and any Medical Staff or hospital education programs.
16
4.2.2.2 Members of the associate category may not vote on matters at general Medical Staff, Department meetings or be an officer of the Medical Staff.
4.2.2.3 Members of the associate category may serve on facility and system
Medical Staff committees, other than the FMEC, and may vote on matters that come before such committees.
4.2.3 Responsibilities: Members of this category shall have the same responsibilities as
active category members, as set forth in Section 4.1 and Section 2.7 of this Part.
4.3 Honorary Category 4.3.1 The Honorary category is restricted to those individuals recommended by the FMEC
and approved by the Board. Appointment to this category is entirely discretionary and may be rescinded at any time. Members of the honorary category shall consist of those members who have retired from active hospital practice, who are of outstanding reputation, and have provided distinguished service to the hospital. They may attend general Medical Staff meetings, Department meetings, continuing medical education (CME) activities, and may be appointed to committees. They shall not hold clinical privileges, hold office or be eligible to vote.
SECTION 5 OFFICERS OF THE MEDICAL STAFF 5.1 Officers of the Medical Staff and FMEC at-large Members: Each hospital is
authorized to have the following officers:
5.1.1 Facility President of the Medical Staff 5.1.2 Facility President-Elect of the Medical Staff
5.1.3 Facility Secretary/Treasurer 5.1.4 Facility Past President of the Medical Staff
5.2 Qualifications of Officers and FMEC at-large Members 5.2.1 Officers must be members in good standing of the active category for at least three
(3) years or actively involved in patient care in the community, have previously served in a significant leadership position on a Medical Staff, (i.e. Department Chair, Section Chief or Committee Chair), indicate a willingness and ability to serve, have no pending adverse recommendations concerning Medical Staff appointment or clinical privileges, have a history of attendance at continuing education programs (provided by the System) relating to Medical Staff leadership and/or be willing to do so during their term or office, have demonstrated an ability to work well with others, be in compliance with the professional conduct policies of the Medical Staff, and should have excellent administrative and communication skills.
FMEC at large members must be members in good standing of the active category for at least two (2) years or actively involved in patient care in the community.
5.2.2 Officers and FMEC at-large members must disclose leadership positions on another
hospital Medical Staff. 5.3 Election of Officers and FMEC at-large Members
17
5.3.1 Every year, the FMEC shall appoint a nominations committee Chaired by the
immediate Past Facility President of the Medical Staff and comprised of at least five (5) at large members of the active Medical Staff at least ninety (90) days prior to
the election. Representatives of administration shall not serve on the nominations committee. Nominations will be solicited from the Medical Staff for consideration prior to the committee meeting. The committee shall offer at least one nominee for each office. Nominations must be announced, and the names of the nominees distributed to all members of the active Medical Staff at least forty-five (45) days prior to the election. A petition signed by at least 20% of the members of the active Medical Staff may also make nominations. Such petition must be submitted to the President of the Medical Staff at least twenty (20) days prior to the election for placement on the ballot.
5.3.2 Officers and FMEC at-large members shall be elected, as needed every year at an
election that takes place at least one (1) month prior to the expiration of the term of the current officers. Only members of the active category shall be eligible to vote. The FMEC will determine the mechanisms by which votes may be cast. The mechanisms that may be considered include written mail ballots; electronic voting via computer, fax, or other technology for transmitting the members’ voting choices. No proxy voting will be permissible. The nominee receiving the greatest number of votes will be elected. In the event of a tie vote, the Medical Staff support professional will arrange for a repeat vote(s) until one candidate receives a greater number of votes.
5.3.3 Medical Staff members will be notified of the election date and final slate of
nominees ten (10) days prior to the election. 5.4 Terms of Office 5.4.1 Officers and FMEC at-large members serve terms as follows: 5.4.1.1 Facility President-Elect of the Medical Staff – one (1) year 5.4.1.2 Facility President of the Medical Staff – two (2) years 5.4.1.3 Facility Past President of the Medical Staff – one (1) year 5.4.1.4 Facility Secretary/Treasurer – one (1) year 5.4.1.5 FMEC Members-at-Large – two (2) years 5.4.2 Officers shall take office October 1. Officers may be re-elected to office except that
the Facility President of the Medical Staff may not be re-elected for successive terms.
5.5 Vacancies of Office 5.5.1 The FMEC shall fill vacancies of office during the Medical Staff year, except the
office of the Facility President of the Medical Staff. If there is a vacancy in the office of the Facility President of the Medical Staff, the
Facility President-Elect of the Medical Staff shall serve the remainder of the term. 5.6 Duties of Officers and FMEC At-Large Members 5.6.1 Facility President of the Medical Staff – The Facility President shall represent the
interests of the Medical Staff to the FMEC and the Board. The Facility President will fulfill the duties specified in Section 5.6.2 of these Bylaws, as well as additional
18
duties as reasonably requested by the FMEC in order to implement and/or enforce all provisions of the Bylaws and the interests of the Medical Staff.
5.6.2 Responsibilities of the Facility President of the Medical Staff The Facility President of the Medical Staff is the primary elected officer of the
Medical Staff and is the Medical Staff’s advocate and representative in its relationships to the Board, the Facility Chief Administrative Officer (CAO) and the Health System administration. The Facility President of the Medical Staff, jointly with the FMEC, provides direction to and oversees Medical Staff activities related to assessing and promoting continuous improvement in the quality of clinical services and all other functions of the Medical Staff as outlined in the Medical Staff Bylaws, Rules and Regulations and Policies. Specific responsibilities and authority include:
5.6.2.1 Call and preside at all general and special meetings of the Medical Staff; 5.6.2.2 Serve as Chair of the FMEC, a voting member of the PLC and as ex-officio
member of all other Medical Staff committees without vote, and to participate as invited by the Board and the Facility CAO on hospital or Board committees;
5.6.2.3 Shall not vote at the FMEC, unless their vote is needed to break a tie vote; 5.6.2.4 Enforce Medical Staff Bylaws, Rules and Regulations and Medical
Staff/hospital/System Policies; 5.6.2.5 Except as stated otherwise, appoint committee Chairs and all members of
Medical Staff standing and ad hoc committees; in consultation with hospital administration, appoint Medical Staff members to appropriate hospital committees, in consultation with the Chair of the Board, appoint the Medical Staff members to appropriate Board committees when those are not designated by position or by specific direction of the Board or otherwise prohibited by state law;
5.6.2.6 Support and encourage Medical Staff leadership and participation on
interdisciplinary clinical performance improvement activities; 5.6.2.7 Report to the Board, through the PLC, the FMEC’s recommendations
concerning appointment, reappointment, delineation of clinical privileges or specified services and corrective action with respect to practitioners or allied health practitioners who are applying for appointment or privileges, or who are granted privileges or providing services in the hospital;
5.6.2.8 With the support of the facility Credentials/Privileging Committee and the
System Credentialing/Privileging Committee, evaluate and periodically report to the FMEC, PLC and the Board regarding the effectiveness of the credentialing and privileging processes;
5.6.2.9 Review and enforce compliance with standards of ethical conduct and
professional demeanor among the members of the Medical Staff in their relations with each other, the Board, hospital/System management, other professional and support staff, and the community the hospital serves;
5.6.2.10 Communicate and represent the opinions and concerns of the Medical
Staff and its individual members on organizational and individual matters
19
affecting hospital operations to the Facility CAO, the FMEC, PLC and the Board;
5.6.2.11 attends Board meetings and Board committee meetings as deemed
appropriate by Facility Medical Staff President; 5.6.2.12 ensures that the decisions of the Board are communicated and carried out
within the Medical Staff; 5.6.2.13 performs such other duties, and exercises such authority commensurate
with the office as are set forth in the Medical Staff Bylaws.
5.6.3 Facility President-Elect of the Medical Staff – In the absence of the Facility President, the Facility President-Elect or the Facility Past President shall assume all the duties and have the authority of the Facility President. He shall perform such further duties to assist the Facility President as the Facility President may request from time to time. The Facility President-Elect, upon the end of the term of the Facility President, shall automatically succeed to the office of Facility President.
5.6.4 Facility Secretary/Treasurer – This officer will collaborate with the hospital’s
Medical Staff office, assure maintenance of minutes, attend to correspondence, act as Medical Staff treasurer, and coordinate communication within the Medical Staff. He shall perform such further duties to assist the Facility President as the Facility President may from time to time request.
5.6.5 Facility Past President of the Medical Staff – This officer will serve as a
consultant to the Facility President and the Facility President-Elect as requested by the FMEC and provide feedback to the officers regarding their performance of assigned duties on an annual basis.
He shall perform such further duties to assist the Facility President as the
Facility President may request. He shall serve as a member of the System Credentialing/Privileging Committee.
5.6.6 FMEC at-large members – shall advise and support the Medical Staff officers
and are responsible for representing the needs/interests of the entire Medical Staff and not simply representing the preferences of their own clinical specialty.
5.7 Removal and Resignation of Officer or FMEC At-Large Member 5.7.1 The Medical Staff may remove any facility officer or FMEC at-large member by
petition of 20% of the active Medical Staff members and a subsequent affirmative vote by two-thirds (2/3) of those active Medical Staff members’ casting votes.
5.7.2 Recall of Officers or FMEC at-large members The FMEC may remove any facility Medical Staff officer or FMEC at-large
member for conduct detrimental to the interests of the Medical Staff or if the officer is suffering from a physical or mental infirmity that renders the individual incapable of fulfilling the duties of the office. At least ten (10) days notice prior to the date of the meeting shall be provided, in writing, to the affected officer or FMEC at-large member. The officer or at-large member shall be afforded the opportunity to speak prior to the taking of any vote on such removal. For recall
20
of an officer or at-large member, a two-thirds (2/3) vote of approval is required with three-fourths (3/4) of the FMEC members present and voting. Affected officer or at-large member does not count as quorum and does not vote.
5.7.3 Resignation of Officers or FMEC at-large members Any elected officer or FMEC at-large member may resign at any time by giving
written notice to the FMEC. Such resignation takes effect on the date of receipt, when a successor is elected, or any later time specified therein.
SECTION 6 MEDICAL STAFF ORGANIZATION The organized Medical Staff is actively involved in Medical Staff governance, peer review,
credentialing/privileging and communication. Medical Staff members are accountable to the FMEC.
The Medical Staff facility officers (Section 5), Medical Staff governance committees (PLC, Section 7.1 and FMEC, Section 7.4), Department Chairs (Section 6.1), clinical Section Chiefs (Section 6.1.1), hospital (as appropriate) System Medical Staff committee Chairs, (Section 7.6) and facility Medical Staff committee Chairs (Section 7.7) are responsible for working collaboratively to develop a process for communication of Medical Staff functions. Periodic reports, as appropriate, are given to each FMEC, Medical Staff Departments, Medical Staff committees and the PLC as needed to ensure adherence to regulatory requirements and accreditation standards.
Additionally, Medical Staff officers may appoint, in collaboration with the Facility Medical
Director, designated physician leaders to serve on the following Medical Staff committees to help ensure Medical Staff input and oversight with clinical functions such as System Bylaws, Cancer Care, CME/Medical Library, Ethics, Institutional Review, System Credentialing/Privileging, Critical Care, System Emergency Services, Infection Control, Pharmacy and Therapeutics, System Medical Staff Quality, System Practitioner Resource, Trauma Quality, Vascular Lab, in addition to the Children’s Hospital committees (Cancer Care, Ethics, Neonatal Intensive Care Unit (NICU) Pediatric Intensive Care Unit (PICU) Perinatal and Medical Staff Quality and other such functions as determined by the FMEC and/or the PLC.
6.1 Departments The Medical Staff shall be organized as a Departmentalized staff. The current
Departments authorized by the FMECs are Medicine, Surgery, Pediatrics, Obstetrics and Gynecology, Anesthesiology, Pathology, Radiology and Emergency Medicine. Departments fulfill the duties listed in Section 6.2.4 of these Bylaws within a specific hospital or facility and/or across the Health System as necessary. Departments shall meet as frequently as needed to fulfill assigned duties and when requested by the FMEC.
The Medical Staff may create Clinical Sections (as specified in these Bylaws) within
a Department in order to facilitate Medical Staff activities.
6.1.1 Any FMEC may recognize any group of like American Board of Medical Specialties, (ABMS) approved specialties with at least three (3) Medical Staff members or service lines that wish to organize themselves into a Clinical Section. Any Clinical Section, if organized shall not be required to hold regularly scheduled meetings, keep routine minutes, or require attendance.
21
A written report is required only when the Clinical Section is making a formal report. A Clinical Section shall elect a Clinical Section Chief. The Clinical Section Chief is responsible for fulfilling the activities listed in Section 6.1.1.1 - 6.1.1.7 of these Bylaws. The procedure for removal of a Clinical Section Chief shall be the same as set forth in Section 6.2.3 for Department Chair. When a clinical Section is making a formal report, the report shall be submitted to the FMEC documenting the specific position of the clinical Section. The President of the Medical Staff and the Clinical Section Chief (or designee) will decide if the report/issue is placed on the FMEC agenda and whether the Clinical Section Chief (or designee) will attend the FMEC meeting to present the report/issue to the FMEC on that specific report/issue. Clinical Sections are optional and shall exist to perform any of the following activities within a specific facility and/or across Health System facilities as necessary:
6.1.1.1 continuing education/Grand Rounds/discussion of patient care;
6.1.1.2 formulation of ED on-call and inpatient consultation and coverage recommendations; 6.1.1.3 discussion of policies and procedures; 6.1.1.4 discussion of equipment needs; 6.1.1.5 development of recommendations for the Department Chair(s), the
FMECs or the PLC; 6.1.1.6 participation in the development of criteria for clinical privileges
when requested by the System Credentialing/Privileging Committee or FMEC;
6.1.1.7 discussion of a specific issue at the request of the PLC or the
FMEC. The FMEC, with the concurrence of the PLC, may designate new Medical Staff Departments or Clinical Sections or dissolve current Departments or Clinical Sections as it determines will best meet the Medical Staff needs for promoting performance improvement, patient safety, and effective credentialing and privileging.
6.2 Qualifications, Selection, Term, and Removal of Department Chair 6.2.1 Each Department Chair shall serve a term of two (2) years commencing on
October 1 and may be elected to serve successive terms. All Chairs must be members of the active Medical Staff with relevant clinical
privileges and be certified by an appropriate specialty board or have affirmatively established comparable competence through the credentialing process.
6.2.2 Department Chairs and Vice-Chairs will be elected by majority vote of the
active members of the Department, subject to ratification by the FMEC.
22
Each Department shall establish procedures for identifying and electing candidates and these procedures must be ratified by the FMEC.
6.2.3 Department Chairs may be removed from office by the FMEC upon receipt
of a recommendation of two-thirds (2/3) of the members of the Department or, in the absence of such recommendation, the FMEC may remove a Chair on its own by a two-third (2/3) vote of a majority of members present and voting, if any of the following occurs:
6.2.3.1 The Chair ceases to be a member in good standing of the Medical
Staff; 6.2.3.2 The Chair suffers an involuntary loss or significant limitation of
practice privileges; 6.2.3.3 The Chair fails, in the opinion of the FMEC, to demonstrate to the
satisfaction of the FMEC, PLC or the Board that he is effectively carrying out the responsibilities of the position;
6.2.3.4 If removal is required, a new election will be held according to the
established Departmental procedures. 6.2.4 Department Chairs shall carry out the following responsibilities: 6.2.4.1 to oversee all clinically-related activities of the Department; 6.2.4.2 to oversee all administratively related activities of the Department
otherwise provided for by the Facility; 6.2.4.3 to provide ongoing surveillance of the performance of all individuals
in the Medical Staff Department who have been granted clinical privileges;
6.2.4.4 to recommend to the System Credentialing/Privileging Committee
Medical Staff Department; 6.2.4.5 to recommend clinical privileges for each member of the
Department and other LIPs practicing with privileges within the scope of the Department;
6.2.4.6 to assess and recommend to the FMEC and Facility CAO off-site
sources for needed patient care services not provided by the Medical Staff Department or Facility;
6.2.4.7 to monitor and evaluate the quality and appropriateness of patient
care provided in the Medical Staff Department and to implement action following review and recommendations by the facility Medical Staff peer review/quality committee and/or the FMEC;
6.2.4.8 to integrate the Department into the primary functions of the
hospital; 6.2.4.9 to coordinate and integrate interdepartmental and
intradepartmental services and communication;
23
6.2.4.10 to participate in the administration of the Department through cooperation with nursing services and hospital administration in matters affecting patient care;
6.2.4.11 to develop and implement Medical Staff and hospital policies and
procedures that guide and support the provision of patient care services;
6.2.4.12 to recommend to the Facility CAO the sufficient numbers of
qualified and competent persons to provide patient care and service;
6.2.4.13 to provide input to the Facility CAO regarding the qualifications and
competence of Department or service personnel who are not Licensed Independent Practitioners (LIPs) but provide patient care, treatment, and services;
6.2.4.14 to provide continuous assessment and improvement of the quality
of care, treatment, and services; 6.2.4.15 to maintain quality control programs as appropriate; 6.2.4.16 to orient and continuously educate all persons in the Department; 6.2.4.17 to make recommendations to the FMEC and to the Facility CAO for
space and other resources needed by the Medical Staff Department to provide patient care services.
6.3 Assignment to Department 6.3.1 The FMEC will, after consideration of the recommendation of the Chair of the
appropriate Department, recommend Department assignments for all members in accordance with their qualifications. Each member will be assigned to one primary Department. Clinical privileges are independent of the Department assignment.
SECTION 7 MEDICAL STAFF GOVERNANCE COMMITTEES 7.1 Designation of the Lee Memorial Health System Medical Staff Physician Leadership
Council (PLC)
7.1.1 There shall be a Lee Memorial Health System Medical Staff Physician Leadership Council (PLC) and such other standing and special committees as determined by the PLC.
7.1.2 There shall be a Facility Medical Executive Committee (FMEC) at each hospital and
such other facility standing and special committees as established by the FMEC.
7.2 Composition of the Lee Memorial Health System Medical Staff PLC 7.2.1 Composition: The PLC shall consist of the following voting members: Each Facility President and
each Facility President–Elect or each Facility Immediate Past President and two (2)
24
at-large Medical Staff members elected by each FMEC. All shall serve a 2-year term except the Facility President-Elect and Facility Past President shall serve 1-year term. The Chairs of the System Credentialing/Privileging Committee and System Quality Committee, the system CEO or Designee, the System Chief Medical Officer and the Chair of the Board and up to two (2) other Board consultants, shall serve as ex-officio, non-voting members. The PLC will elect the PLC Chair and a Vice Chair who shall serve a 2-year term.
In the event that the PLC composition does not include one anesthesiologist,
emergency medicine physician, hospitalist or intensivist, radiologist and pathologist, the PLC may appoint an active Medical Staff member from each of these hospital-based specialties to be voting members of the PLC.
7.2.2 Duties: The duties of the Lee Memorial Health System PLC are:
7.2.2.1 to work in a cooperative and professional manner with the FMECs System and Facility Administration and the Board to ensure Medical Staff input into the plans, goals and mission of the Lee Memorial Health System;
7.2.2.2 receive, review, and transmit FMEC recommendations to the
Board; 7.2.2.3 review and attempt to resolve any inconsistency emanating from
the FMEC recommendation(s) and transmit FMEC recommendations to the Board concerning all matters relating to appointments, reappointments, staff category, facility assignments, clinical privileges subject to the conflict resolution process herein, unless due process rights are triggered pursuant to Part II.
The PLC is acting as a duly constituted peer review committee under Florida law when it is reviewing the quality of care or performance of any particular physician.
7.2.2.4 consistent with the hospital and Medical Staff mission and
philosophy, the PLC will participate and encourage participation of the FMECs in identifying community health needs and in setting goals and work with the System administration and the facility CAO(s) to design and implement programs to meet those needs;
7.2.2.5 work with the FMECs to ensure understanding and the consistent
application of Medical Staff Rules and Regulations, Policies and Procedures; and
7.2.2.6 govern the collection of Medical Staff system-wide assessments
and authorize the use of Medical Staff assessments consistent with the purpose of the assessment.
7.2.3 Meetings:
The PLC shall meet as frequently as needed, but at least quarterly, to perform its assigned functions. Records of its proceedings and actions shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
25
7.3 Staff Functions
7.3.1 The PLC exists to promote communication, collaboration and coordination
between physicians, System and facility administration and the Board concerning the work of each FMEC and planning activities of the Lee Memorial Health System that impact members of the Medical Staff.
7.4 Facility Medical Executive Committee (FMEC) Composition Selection and Tenure
7.4.1 Each Medical Staff may determine the number of Medical Staff members
appointed or elected to the FMEC. The composition of the FMEC shall consist of at least the following voting members: Facility President of the Medical Staff, Facility Immediate Past President, Facility President-Elect of the Medical Staff, Facility Secretary/Treasurer, physician representative from the System Credentialing/Privileging Committee, Chair of the Facility Quality Committee, the Department Chairs from Medicine, Surgery, Anesthesiology, Radiology, Pathology, Pediatrics, Obstetrics/Gynecology and Emergency Services, two (2) at-large active members of the Medical Staff appointed by the FMEC and two (2) at-large active members of the Medical Staff elected by the general Medical Staff.
One Board member, the CAO, the facility Vice-President of Nursing, the
facility Medical Director (as appropriate) will serve in a non-voting, ex-officio capacity. The Facility President of the Medical Staff shall serve as the Chair of the FMEC.
7.4.2 Each FMEC composition description shall be listed in the Facility Rules &
Regulations.
7.4.3 FMEC members shall disclose in writing to the Medical Staff, prior to the date of election of appointment, any personal, professional or financial applications or responsibilities with Lee Memorial Health System and any competing hospital, healthcare organization or Health System.
FMEC members shall serve 2-year terms, except Facility Past President and
Facility President-Elect shall serve 1-year terms. The FMEC and the Nominations Committee shall stagger the terms of appointed and elected at-large members to ensure continuity of leadership. Such physicians must be on Active Staff and be a member in good standing at all times.
All FMEC members are expected to participate in orientation and continuing
education activities as related to the operation of the Medical Staff.
7.5 Duties and Responsibilities of the Facility Medical Executive Committees 7.5.1 To represent, to initiate action and act on behalf of the Medical Staff
members with privileges at the Facility in fulfilling the duties of Medical Staff self governance, credentialing/privileging and quality/peer review, after seeking input and recommendations from Sections and/or Departments affected by FMEC action (if applicable).
26
7.5.2 To receive recommendations from the System Credentialing/Privileging
Committee and the Facility Quality/Peer Review Committee and make recommendations to the Board (and for informational purposes only) to the PLC concerning:
7.5.2.1 appointments, reappointments and granting of clinical privileges; 7.5.2.2 necessity for special investigations of issues pertaining to
practitioner competence of behavior; 7.5.2.3 needed performance improvements and peer review results; 7.5.2.4 policies and procedures development and enforcement; 7.5.2.5 facility Medical Staff Department and committee structure; and 7.5.2.6 other matters relevant to the provision of patient care, operation of
the Medical Staff or proposed Bylaws amendments. 7.5.3 Receive or act upon reports and recommendations concerning patient care
quality and appropriateness reviews, evaluation and monitoring functions, and the discharge of their delegated administrative responsibilities;
7.5.4 Recommend to the Board, and for information purposes only to the PLC,
specific programs and systems to perform Medical Staff peer review, quality monitoring, communication, governance, credentialing/privileging and planning functions;
7.5.5 Coordinate the implementation of policies adopted by the Board; 7.5.6 Oversee the facility multi-specialty peer review and quality monitoring
activities in a manner consistent with federal and state law; 7.5.7 Take reasonable steps to encourage professionally ethical conduct and
competent clinical performance of Medical Staff members at the facility including collegial and educational efforts;
7.5.8 Participate in identifying community health needs and in setting facility-
specific goals and implementing programs to meet those needs; 7.5.9 Design and implement facility-specific rules and regulations that will not
conflict with the Medical Staff Bylaws; 7.5.10 Work with Facility and System administration to promote effective, efficient
and safe patient care practice within the facility; 7.5.11 Take reasonable steps to encourage professionally ethical conduct and
competent clinical performance on the part of staff appointees including initiating investigations, and pursuing corrective action, when warranted;
27
7.5.12 Provide oversight concerning the quality and safety of the care provided by residents, interns, students, and ensure that the same act within approved guidelines established by the Medical Staff and the Board.
Reviews and ensure corrective action regarding applicable Residency Review Commission findings and recommendations;
7.5.13 Keep the Medical Staff up to date concerning the licensure and
accreditation status of the System and hospitals; 7.5.14 Request evaluations of practitioners privileged through the Medical Staff
process in instances in which there is question about an applicant or member’s ability to perform privileges requested or currently granted;
7.5.15 Consult with administration on the quality, timeliness, and appropriateness
of aspects of contracts for patient care services provided to the hospital by entities outside the hospital;
7.5.16 Hold Medical Staff leaders, committees, and Departments accountable for
fulfillment of their duties and responsibilities; 7.5.17 Advise and assist the PLC, when and to the extent possible, as requested
by the PLC, the Board and the System or Facility administration; 7.5.18 Grant, deny or rescind exemptions related to ED call responsibility; 7.5.19 Meetings: The FMEC shall meet ten (10) times per year, or more
frequently as needed to perform its assigned functions. Records of its proceedings and actions shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
7.6 System Medical Staff Committees 7.6.1 Purpose. There shall be system Medical Staff committees established by the
Medical Staff to carry out the responsibilities of the Medical Staff with regard to measuring and assessing the performance of the Medical Staff providing medical care within the hospitals and Health System facilities.
7.6.2 Organization to Perform Functions. The PLC with the input and approval of each
FMEC shall establish system Medical Staff committees comprised of members of the Medical Staff and others as may be deemed appropriate or necessary. The delineation of specific duties, committee size, liaison with other committees and Departments, and other matters necessary to the efficient performance of Medical Staff functions shall be set forth in these Bylaws. The only voting members of system Medical Staff committees are members of the Medical Staff unless otherwise determined by the FMEC. System Medical Staff committees consist of the following, shall report to and through the FMECs on matters relating to all FMECs, and shall report to each FMEC on facility specific matters:
7.6.2.1 System Credentialing/Privileging Committee (See Part III, Section 1 of
these Bylaws); 7.6.2.2 System Medical Staff Quality Committee (See Medical Staff Quality
Manual); 7.6.2.3 System Practitioner Resource Committee.
28
Membership: Membership shall be established by the PLC with the input and approval of
each FMEC. The term of office shall be for a period of two (2) years with staggered terms, so as to provide continuity and development of expertise.
Referrals: Concerns that a member of the Medical Staff may be suffering from a
physical or mental impairment that might impact their ability to practice medicine or may be a threat to themselves or others, including but not limited to impairment due to substance abuse, should be communicated to the President of the Medical Staff or to the affected practitioner’s Department Chair. The President of the Medical Staff or Department Chair, after consultation with others, if deemed appropriate, may refer the affected practitioner to the practitioner Resource Committee for review, evaluation and follow-up.
Responsibilities: The committee shall have no authority to take disciplinary action. Nor
does the committee provide treatment. The committee is responsible to: 7.6.2.3.1 Receive and evaluate concerns about practitioner health and
functioning;
7.6.2.3.2 Provide assistance and encourage a practitioner impaired by virtue of physical or psychiatric condition, problems in living, or issues related to alcohol use or drug use to voluntarily accept referral for the evaluation, treatment or assistance;
7.6.2.3.3 Assume an advocacy role on behalf of the affected practitioner;
7.6.2.3.4 Serve as an advisor to the President of the Medical Staff, Department Chair and/or FMEC, including advice relating to alternatives in the event that the practitioner fails to accept referral or fails to adequately recover from treatment;
7.6.2.3.5 Consider referring an affected practitioner to appropriate resources
for treatment and advice on the appropriateness of treatment, rehabilitation planning and monitoring provisions;
7.6.2.3.6 Utilize the Florida Medical Association Physician Resource Network,
Intervention Project for Nurses or other resources, if appropriate;
7.6.2.3.7 Maintain the confidentiality of information regarding matters referred to the committee;
7.6.2.3.8 Refer to the Medical Staff President Department Chair or FMEC
those situations that may require possible corrective actions. 7.6.2.4 System Bylaws Committee
29
Membership: The Bylaws Committee shall be a standing committee of the Medical Staff
and shall be composed of at least five (5) active Medical Staff appointees (including one (1) member from each FMEC appointed by the facility Medical Staff President) and the System Chief Medical Officer (CMO) or his designee (who shall serve as a non-voting member).
Duties: The duties of the Bylaws Committee shall be to:
7.6.2.4.1 Conduct an annual review of the Medical Staff Bylaws, Medical Staff
Rules and Regulations and Policies; and 7.6.2.4.2 Review recommendations for changes in the Medical Staff Bylaws,
Rules and Regulations and Policies made by the Medical Staff committees, Departments, or by the Board.
Meetings, Reports and Recommendations: The Bylaws Committee shall meet at least annually or as necessary to
accomplish its duties, shall maintain a permanent record of its proceedings and actions, and shall report its recommendations to the FMECs.
7.6.2.5 System Emergency Services Committee Membership: The System Emergency Services Committee shall be an ad hoc committee
of the Medical Staff and shall be composed of the Emergency Department Medical Directors, at least three (3) Active Staff members, and other Active Staff members as needed.
Duties: The duties of the System Emergency Services Committee shall be to: 7.6.2.5.1 conduct an annual review of system-wide emergency services; 7.6.2.5.2 ensure emergency call is fair to physicians while providing adequate
coverage to patients of our community; 7.6.2.5.3 review emergency call rules system-wide for recommendation to
FMECs.
Meetings: The System Emergency Services Committee will meet at least once per year or as needed.
7.6.3 Composition and Meetings of System Medical Staff Committees:
30
7.6.3.1 Unless otherwise provided for in these Bylaws, System Medical Staff committees shall be composed of physician members from each facility, as appointed by each FMEC;
7.6.3.2 Each System Medical Staff committee shall elect a physician Chairperson
and physician vice Chairperson for their respective committee;
7.6.3.3 System Medical Staff committee members shall serve terms of 2 years and may be reappointed;
7.6.3.4 System Medical Staff committee members who cease to be members of
the Medical Staff of Lee Memorial Health System shall automatically cease to serve as committee members. Vacancies on committees shall be filled by the appropriate FMEC;
7.6.3.5 System Medical Staff committees shall meet as often as necessary to
discharge the duties of the respective committees in accordance with these Bylaws.
Reasonable notice of meetings shall be provided to committee members
and may include providing a written schedule of meetings on an annual or more frequent basis.
7.7 Facility Medical Staff Committees: 7.7.1 Purpose: There shall be committees to carry out certain essential functions
within each facility as determined by each FMEC. The FMEC may establish such committees from time to time in addition to those set forth in the Bylaws.
7.7.2 Standing Facility Medical Staff Committees: The following facility committees
are approved as standing committees of the FMEC: 7.7.2.1 GCMC Credentialing/Privileging Committee (see Part III, Section 1 of
these Bylaws); 7.7.2.2 LMHS Credentialing/Privileging Committee (see Part III, Section 1 of these
Bylaws); 7.7.2.3 Nominations Committees (See Part 1, Section 5.3 of these Bylaws);
7.7.2.4 Facility Medical Staff Quality Committees (see Medical Staff Quality Manual);
7.7.2.5 Facility Rules and Regulations Committees Composition: The Facility Rules and Regulations Committee shall be a
standing committee of the Medical Staff and shall be composed of at least two (2) active Staff members appointed by the FMEC.
Duties: The duties shall be to review and recommend changes in the
Facility Rules and Regulations and policies to the FMEC. 7.7.2.6 Trauma Quality Management
31
Composition, membership and duties are mandated by the State regulations for designated trauma centers.
SECTION 8 MEDICAL STAFF MEETINGS 8.1 General Medical Staff Meetings 8.1.1 An annual meeting and other general Medical Staff meetings shall be held at a
time determined by the FMEC. Notice of the meeting shall be given to all Medical Staff members via appropriate media and posted conspicuously at least ten (10) days before the meeting.
8.1.2 Except for Bylaws amendments or as otherwise specified in these Bylaws, the
actions of a majority of the members present and voting at a meeting of the Medical Staff is the action of the group.
Action may be taken without a meeting of the Medical Staff by presentation of
the question to each Medical Staff member eligible to vote, in person, via telephone, and/or by mail or internet, and their vote recorded in accordance with procedures approved by the FMEC. Such vote shall be binding so long as the question that is voted on receives a majority of the votes cast.
8.1.3 Special Meetings of the General Medical Staff 8.1.3.1 The President of the Medical Staff may call a special general Medical
Staff meeting at any time. Such request or resolution shall state the purpose of the meeting. The President of the Medical Staff shall designate the time and place of any special general Medical Staff meeting.
8.1.3.2 Written or electronic notice stating the time, place and purposes of
any special general Medical Staff meeting shall be conspicuously posted and shall be sent to each member of the Medical Staff at least three (3) days before the date of such meeting. No business shall be transacted at any special general Medical Staff meeting, except that stated in the notice of such meeting.
8.2 Departments, Sections and Committee Meetings 8.2.1 Regular Meetings of Medical Staff Departments, Sections and Committees
8.2.2 Departments, Sections and Committees may, by resolution, provide the time for holding regular meetings without notice other than such resolution.
8.3 Special Meetings of Departments, Sections and Committees 8.3.1 A special meeting of any Department, Section or Committee may be called by
the Chair thereof or by the President of the Medical Staff. 8.4 Quorum
32
8.4.1 Medical Staff meetings: Unless otherwise specified in these Bylaws, a quorum shall consist of those present or those eligible Medical Staff members voting on an issue.
8.4.2 FMEC, Credentialing/Privileges Committee, Medical Staff Quality/Peer Review
Committee: A quorum will exist when 50% of the members are present. 8.4.3 Departments, Sections or Committees other than those listed in Sections 6 and
7 above or unless otherwise specified in these Bylaws, a quorum shall consist of those present or those eligible Medical Staff members voting on an issue.
8.5 Attendance Requirements 8.5.1 Members of the Medical Staff are encouraged to attend meetings of the Medical
Staff. 8.5.1.1 FMEC, Credentialing/Privileges Committee, and Medical Staff
Quality/Peer Review Committee meetings: Members of these committees are expected to attend at least 75% of the meetings held.
8.5.1.2 Special meeting attendance requirements: Whenever there is
suspected or actual non-compliance with Medical Staff or hospital policies or suspected deviation from standard clinical or professional practice, the President of the Medical Staff or the applicable Department/Section/Committee Chair may require the practitioner to confer with him or with a standing or ad hoc committee that is considering the matter. The practitioner will be given special notice of the meeting, by personal delivery or U.S. Mail certified return receipt requested, at least five (5) days prior to the meeting, including the date, time, place, a statement of the issue involved and that the practitioner’s appearance is mandatory.
Failure of the practitioner to appear at any such meeting after two (2)
notices, unless excused by the FMEC upon showing good cause, will result in an automatic termination of membership pursuant to the Automatic Suspension and Termination provisions of these Bylaws. Such termination will not give rise to a fair hearing, but will automatically be rescinded upon the practitioner’s participation in the previously referenced meeting.
8.5.1.3 Nothing in the foregoing paragraph shall preclude the initiation of
precautionary restriction or suspension of clinical privileges as outlined in Part II of these Bylaws (Investigations, Corrective Action, Hearing and Appeal Plan).
8.6 Participation by Administration
8.6.1 Administration may attend any general, Department, Section or Committee meetings of the Medical Staff, unless otherwise specified or requested by the committee.
8.7 Robert’s Rules of Order
33
8.7.1 Medical Staff Department, Section and Committee meetings shall be run in a manner determined by the individual who is the Chair of the meeting. When parliamentary procedure is needed, as determined by the Chair or evidenced by a majority vote of those attending the meeting, the latest edition of Robert’s Rules of Order shall determine procedure.
8.8 Notice of Meetings 8.8.1 Unless otherwise specified in these Bylaws, written or electronic notice stating
the place, day, and hour of any special meeting or of any regular meeting not held pursuant to resolution shall be delivered or sent to each member of the Department or committee not less than five (5) days before the time of such meeting by the person or persons calling the meeting. The attendance of a member at a meeting shall constitute a waiver of notice of such meeting.
8.9 Action of PLC, FMEC, General Medical Staff, Department, Section or Committee 8.9.1 The recommendation of a majority of its members present at a meeting at which
a quorum is present shall be the action of a Department, Section and Committee, FMEC, PLC or General Medical Staff meeting. Such recommendation will then be forwarded to the FMEC for action.
8.10 Rights of Ex Officio Members 8.10.1 Except as otherwise provided in these Bylaws, persons serving as ex officio
members of a committee shall have all rights and privileges of regular members thereof, (except that they shall not vote or be counted in determining the existence of a quorum).
8.11 Minutes 8.11.1 Minutes of each regular and special meeting of a committee shall be prepared
and shall include a record of the attendance of members and the vote taken on each matter. The presiding Chair shall authenticate the minutes and copies thereof shall be submitted to the FMEC or other designated committee. Minutes shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
SECTION 9 DECISION MAKING METHODS AND CONFLICT RESOLUTION 9.1 FMEC recommendations will be forwarded to the PLC for information and to ensure
communication between all facility Medical Staffs, System and facility administration and Board leaders. Routine FMEC communication and recommendations that are consistent between the FMECs and that are consistent with Medical Staff and hospital policy and procedures will be transmitted to the Board.
9.2 Conflict resolution: If the PLC determines a recommendation of a FMEC may be contrary
to the opinion of the PLC, or if a decision of the Board is contrary to a recommendation of the PLC and/or a FMEC, the PLC shall not make a recommendation to the Board regarding such matter. The PLC will first refer the matter back to the FMEC(s) for further consideration at their next meeting, together with pertinent suggestions and comments of the PLC.
34
9.3 If the FMEC recommendation and the opinion of the PLC remain inconsistent after the next meeting of the FMEC, the matter will be referred to an Initial Joint Conference Committee to be convened within thirty (30) days of that FMEC meeting. Such Initial Joint Conference Committee may be convened at any time sooner by mutual agreement of the FMEC and PLC. The Initial Joint Conference Committee shall be composed of two (2) representatives selected by the PLC, two (2) representatives selected by the FMEC, one (1) administrative representative and one (1) Board member.
9.3.1 The positions established at the Initial Joint Conference Committee will be reported
in full to the FMEC and the PLC. The FMEC will discuss the issue at its next meeting. In the event the FMEC(s)’ recommendation remains contrary to the opinion of the PLC, the recommendation of the FMEC(s) shall be forwarded to the Board, along with pertinent, applicable information.
The PLC, at its discretion, may include a divergent opinion along with pertinent,
applicable information. The Board shall have sixty (60) days to adopt the recommendation of the FMEC(s), or may choose to refer the matter(s) to a Final Joint Conference Committee at any time within the 60-day period.
9.4 A Final Joint Conference Committee will be convened if: 9.4.1 requested by the Board; 9.4.2 requested by the PLC, FMEC(s) or Initial Joint Conference Committee (if the Initial
Joint Conference Committee is unable to resolve conflicts and divergent opinions remain between the PLC, FMEC(s) and/or Initial Joint Conference Committee); or
9.4.3 in the event the Board does not accept or adopt a recommendation by the
FMEC(s) within sixty (60) days of receiving such recommendation(s) as set forth in Section 9.3.1.
The Final Joint Conference Committee will convene within thirty (30) days of such request,
or occurrence. The Final Joint Conference Committee will be composed of two (2) representatives selected by the PLC, two (2) representatives selected by the FMEC and two (2) representatives (which may or may not be Board members) of the Board for review and recommendation to the full Board. The Final Joint Conference Committee will have up to sixty (60) days to report its recommendation(s), and will issue its complete report simultaneously to the FMEC(s), PLC, Initial Joint Conference members and Board. If either the FMEC(s) or PLC continues to have a dissenting opinion/recommendation from that of the Final Joint Conference Committee, both (FMEC and PLC) shall each have the right for a representative of each to report its recommendation/opinion at the same time to the Board. After such report(s), the Board will make a determination, which shall be final.
9.5 The Chair of the Board, PLC or FMEC may call for an Initial Joint Conference as described
above at any time and for any reason in order to seek direct input from the Board, PLC and/or FMEC Medical Staff leaders, clarify any issue, or relay information directly to Medical Staff leaders.
9.6 The provisions of this article are not applicable to matters subject to the provisions of the
Medical Staff Bylaws, Rules and Regulations, or Policies relating to Peer Review, Corrective Action or the Fair Hearing process.
SECTION 10 REVIEW, REVISION, ADOPTION, AND AMENDMENT
35
10.1 Medical Staff Responsibility 10.1.1 The Medical Staff shall have the responsibility to formulate, review at least
biennially, and recommend to the Board any Medical Staff Bylaws, rules, regulations, policies and procedures, and amendments as needed, which shall be effective when approved by the Board.
The Medical Staff can exercise this responsibility through its elected and appointed leaders or through direct vote of its membership.
10.2 Methods of Amendment and Adoption to these Bylaws
10.2.1 Proposed amendments to these Bylaws may be originated by the System Bylaws
Committee for consideration of all FMECs and each general Medical Staff or by a petition signed by twenty-five (25) active staff members.
10.2.1.1 Each active member of the Medical Staff will be eligible to vote on the
proposed amendment to these Bylaws via printed or secure electronic ballot in a manner determined by the FMEC. All active members of the Medical Staff shall receive at least thirty (30) days advance notice of the proposed changes. Proposed amendments must:
10.2.1.1.1 receive a simple majority of the votes cast by those active
Medical Staff members eligible to vote at the initiating FMEC;
10.2.1.1.2 receive a simple majority of the votes cast by the active
Medical Staff members eligible to vote at each FMEC; 10.2.1.1.3 receive a simple majority of the votes cast by the active
Medical Staff members eligible to vote on each facility general Medical Staff.
10.2.1.2 Amendments so adopted shall be effective when approved by the Board.
Neither the Board nor the Medical Staff shall have the power or authority to unilaterally adopt or amend Medical Staff Bylaws.
10.3 Methods of Amendment and Adoption to any Medical Staff Rules, Regulations and
Policies: 10.3.1 The Medical Staff may adopt additional rules, regulations and policies as necessary
to carry out its functions and meet its responsibilities under these Bylaws. A Rules, and Regulations and Policies Manual may be utilized to organize these additional documents. Should a conflict exist between the provisions of the Medical Staff Bylaws and the Rules and Regulations or Medical Staff Policies, the Bylaws will prevail. Should a conflict exist between the provisions of the Rules and Regulations and the Medical Staff Policies, the Rules and Regulations will prevail.
10.3.2 Proposed amendments to the Rules, Regulations and Policy Manual may be
originated by the FMEC. 10.3.3 The Medical Staff itself may recommend directly to the Board an amendment(s) to
any rule, regulation, or policy by submitting a petition signed by twenty-five (25) active Medical Staff members. Upon presentation of such petition, the adoption process outlined in 10.2.1 above will be followed.
36
10.3.4 The FMEC shall vote on the proposed language changes at a regular meeting, or at a special meeting called for such purpose. Following an affirmative vote by the FMEC, any of these documents may be adopted, amended or repealed, in whole or in part and such changes shall be effective when approved by the Board, subject to Section 9 of this Part in the event of a conflict.
10.4 The FMEC may adopt such amendments to these Bylaws, Rules and Regulations, and
policies that are, in the committee’s judgment, technical or legal modifications or clarifications, reorganization or renumbering or those needed due to punctuation, spelling, or other errors of grammar or expression. Such amendments need not be approved by the entire Board but must be approved by the System CEO.
37
Appendix A PRINCIPLES OF MEDICAL ETHICS**
PREAMBLE The medical professions have long subscribed to a body of ethical statements developed primarily for the benefit of the patient. As a member of this profession, a health professional must recognize responsibility to patients first and foremost, as well as to society, to other health professionals and to self. The following Principles are not laws but standards of conduct, which define the essentials of honorable behavior for the health professional. Section 1 A health professional shall be dedicated to providing competent medical care with compassion and respect for human dignity and rights. Section 2 A health professional shall uphold the standards of professionalism, be honest in all professional interactions, and strive to report health professionals deficient in character or competence, or engaging in fraud or deception, to appropriate entities. Section 3 A health professional shall respect the law and also recognize a responsibility to seek changes in those requirements, which are contrary to the best interests of the patient. Section 4 A health professional shall respect the rights of patients, colleagues, and other health professionals and shall safeguard patient confidences and privacy within the constraints of the law. Section 5 A health professional shall continue to study, apply and advance scientific
knowledge, maintain a commitment to medical education, make relevant information available to patients, colleagues and the public, obtain consultation, and use the talents of other health professions when indicated.
38
Section 6 A health professional shall, in the provision of appropriate patient care, except in emergencies be free to choose whom to serve, with whom to associate and the environment in which to provide medical care. Section 7 A health professional shall recognize a responsibility to participate in activities contributing to an improved community and the betterment of pubic health. Section 8 A health professional shall, while caring for a patient, regard responsibility
to the patient as paramount.
Section 9 A health professional shall support access to medical care for all people. **Adapted from the American Medical Association’s “Principles of Medical Ethics” (adopted by the AMA’s
House of Delegates June 17, 2001).
39
PART II: INVESTIGATIONS, CORRECTIVE ACTION, HEARING AND APPEAL PLAN
SECTION 1 ROUTINE CORRECTIVE ACTION & INVESTIGATIONS 1.1 Progressive Intervention These Bylaws encourage the use of progressive steps by Medical Staff leaders and
hospital administration, beginning with collegial and education efforts, to address questions relating to a practitioner’s clinical practice and/or professional conduct. The goal of these efforts is to arrive at voluntary, responsive actions by the practitioner to resolve questions that have been raised. All collegial intervention efforts by Medical Staff leaders and hospital management are part of the hospital’s performance improvement and professional review activities. Collegial intervention efforts are encouraged, but are not mandatory, and shall be within the discretion of the appropriate Medical Staff leaders and hospital administration.
When any observations arise, suggesting opportunities for a practitioner to improve, the matter may be referred in accordance with the performance improvement and professional conduct policies adopted by the Medical Staff and hospital.
Corrective actions and investigations shall be undertaken: 1.1.1 in the reasonable belief that the action is in the furtherance of quality health care; 1.1.2 after a reasonable effort to obtain the facts of the matter,
1.1.3 after adequate notice and hearing procedures are afforded to the practitioner as set forth herein, and
1.1.4 in the reasonable belief that the action is warranted by the facts known after such reasonable effort to obtain the facts.
1.2 Basis for Routine Corrective Action Whenever a concern or question has been raised regarding: 1.2.1 the clinical competence or clinical practice of any appointee; 1.2.2 the care or treatment of a patient or patients or management of a case by any
appointee; 1.2.3 activities or professional conduct that may be detrimental to patient safety; 1.2.4 the known or suspected violation by any Medical Staff appointee of these Bylaws,
the Policies, or the Rules and Regulations of the Medical Staff, System or Department
1.2.5 behavior or conduct on the part of any Medical Staff appointee that is considered lower than the standards of the hospital, disruptive to the hospital or its Medical Staff, including the inability of the appointee to work harmoniously with others; or
1.2.6 impairment, a request for corrective action may be made by any practitioner on the Medical Staff, any
member of the System administration, System or Medical Staff committee, or the Board of
40
Directors, after making sufficient inquiry to satisfy themselves that the concern or question raised is credible.
1.3 Requests and Notices All requests for corrective action shall be made in writing to the President of the Medical
Staff and the Chief Medical Officer, with a copy to the Medical Staff Services Office. The request must be signed by the complainant, clearly state those facts that support the request in sufficient detail to permit an investigation to be pursued, and, if possible, state what corrective action is deemed appropriate by the complainant. The President of the Medical Staff shall notify the FMEC at its next regular meeting that a request for corrective action has been made. The affected practitioner shall be given written notice of the request, and a copy of the same. All notices provided under this Part II shall be hand delivered or sent via certified mail, return receipt requested. All time limits shall begin upon receipt of notice.
1.4 Investigations
1.4.1 When a request for corrective action has been received by the FMEC, the committee shall determine as soon as possible, but no later than at its next regularly scheduled meeting, either to discuss the matter with the appointee concerned, or to begin an investigation. If the concern states sufficient information to warrant action, the FMEC, at its discretion, may initiate an investigation, with or without a personal interview with the practitioner being investigated. The FMEC may seek input from the practitioner’s Department or Section prior to initiating investigation. An investigation shall begin only after a formal resolution of the FMEC to that effect. The affected practitioner shall be given written notice of the initiation of an investigation. If the Board of Directors wishes to begin such an investigation, it shall also formally resolve to do so by mandating the FMEC to begin an investigation.
1.4.2 Upon resolving to initiate an investigation, the Medical Staff President through the
FMEC or President of the Medical Staff shall immediately appoint a member(s) of the Active Medical Staff to conduct an investigation of the matters contained in the request. Investigators shall not include partners, associates or relatives of the practitioner being investigated and should be objective and familiar with the types of issues raised in the request for corrective action.
1.4.3 The investigator(s) may consult with other members of the Medical Staff as
appropriate in order to determine the facts of the case, or to obtain professional opinions relative to the matter under consideration.
1.4.4 The investigator(s) shall have available the full resources of the Medical Staff and
the System, as well as the authority to use outside consultants, if needed. 1.4.5 The investigation should be completed within thirty (30) working days of the
appointment of the investigator(s), unless an extension of not more than thirty (30) additional working days has been granted by the FMEC or President of the Medical Staff.
1.4.6 At the conclusion of the investigation, the investigator(s) shall prepare a written
report of the findings and transmit the same to the President of the Medical Staff and the Chief Medical Officer. In addition to setting forth findings of fact and, if
41
applicable, the clinical opinion of the investigator(s) and other practitioners with whom he may have consulted, the report shall recommend that corrective action be imposed, or that the complaint against the affected practitioner be dismissed.
The investigator may recommend a type or degree of corrective action deemed
appropriate. 1.4.7 The President of the Medical Staff shall review the investigator’s report when it is
received, and if emergency corrective action is indicated, proceed to impose the same pursuant to Section 2 of this part. Otherwise, the President shall submit the investigator’s report to the FMEC for consideration at its next regular meeting.
1.4.8 In cases suggesting practitioner impairment, the President of the Medical Staff shall
confer with a member of the Medical Administrative Staff, designated by the System President and the practitioner’s Department Chair, and if they concur, shall refer the request to the Practitioner Resource Committee for disposition; otherwise, the request shall be referred to the FMEC for consideration at its next regular meeting.
1.5 FMEC Action 1.5.1 If the FMEC determines that there are no reasonable grounds to believe that the
affected practitioner has committed an offense requiring corrective action under these Bylaws, the complaint shall be dismissed. The affected practitioner and complainant shall be given written notification of dismissal.
1.5.2 If the FMEC determines that there are reasonable grounds to believe that the
affected practitioner is subject to corrective action, the Committee may elect to recommend corrective action to the Board, which, at the discretion of the FMEC, may consist of:
1.5.2.1 A written warning that corrective action measures will be taken in the
future if the affected practitioner does not reform his conduct in the manner set forth in the warning;
1.5.2.2 A written reprimand stating the Committee’s displeasure at the affected
practitioner’s behavior, and directing the affected practitioner to cease the same immediately;
1.5.2.3 Mandated education to improve the affected practitioner’s knowledge,
skills and ability in clinical as well as non-clinical subjects;
1.5.2.4 Mandated clinical review or supervision to see that the affected practitioner’s performance attains an acceptable level;
1.5.2.5 Limitation of privileges restricting those procedures that the affected
practitioner may perform at the Facility;
1.5.2.6 Removal of privileges eliminating the affected practitioner’s ability to perform any procedure at the Facility. If the affected practitioner is a member of the Medical Staff, removal of privileges shall also entail revocation of Medical Staff membership. If removal of privileges is recommended at the time of the affected practitioner’s biennial reappointment, this may be accomplished by not recommending the affected practitioner for reappointment;
1.5.2.7 Make such other recommendations, as it deems necessary or appropriate.
42
1.6 Notice of FMEC Action Whenever a recommendation for corrective action has been made by the FMEC, or
corrective action has been taken by the Board on its own initiative, written notice of the same shall be sent to the affected practitioner by certified mail, return receipt requested, or hand delivery with receipt. Such notice shall be consistent with the notice provision set forth in Subsection 1.3. The notice shall set forth the nature of the complaint, the reasons for the corrective action, a description of the corrective action, and a short summary of the affected practitioner’s right to a fair hearing pursuant to these Bylaws, including any time limits within which the affected practitioner must act. The affected practitioner may request a hearing pursuant to the provisions of Section 4.
1.7 Board of Directors Action If the time, during which an affected practitioner may request a hearing pursuant has
expired without a request being made, or such hearing, including appeal to the Board, has been concluded, then at the next regular meeting thereafter of the Board of Directors, the Board shall consider the recommended corrective action. In the event that the Board rejects such recommendation, the Board may remand the recommendation to the FMEC with instructions to reconsider the matter, including the nature and degree of the corrective action. The Board shall consider recommendations of the FMEC following remand in the same manner as other recommendations for corrective action.
SECTION 2 EMERGENCY CORRECTIVE ACTION/PRECAUTIONARY SUSPENSION
OF CLINICAL PRIVILEGES 2.1 Basis for Emergency Corrective Action/Precautionary Suspension The President of the Medical Staff, the Chief Medical Officer (or his designee), or the FMEC
shall have the authority to immediately suspend all or any portion of the clinical privileges of a Medical Staff practitioner or other individual, whenever failure to take such action may result in an imminent danger to the health and/or safety of any individual. Such precautionary suspension shall be deemed an interim precautionary step in the professional review activity related to the ultimate professional review action that may be taken with respect to the suspended individual but is not a complete professional review action in and of itself. It shall not imply any final finding of responsibility for the situation that caused the suspension, nor shall it entitle the practitioner to a fair hearing except as provided under this Section. Those parties with the authority to impose emergency corrective action shall consult with a physician member of the Administration designated by the System President and System legal counsel before imposing any emergency corrective action. This Subsection shall not apply if a clear and present danger exists which requires immediate action and consultation is not feasible.
2.2 Notice of Emergency Corrective Action/Precautionary Suspension
43
Upon imposition of emergency corrective action, the President of the Medical Staff shall immediately give notice to the affected practitioner of such action.
Such notice may be oral, but shall be confirmed in writing as soon as possible, but no later
than the next business day. The written notice shall state the reasons for the emergency corrective action and the nature of corrective action imposed. A copy of the notice shall also be given to the Chief Medical Officer, Department Chair, and FMEC.
2.3 FMEC Procedure When instituted, a precautionary suspension of clinical privileges will automatically expire in
seven (7) days, unless extended by the FMEC, with return of all previous clinical privileges unless the suspension is confirmed by a majority vote of the FMEC in special session. The FMEC shall review the matter resulting in precautionary suspension within a reasonable period not to exceed fourteen (14) days. Unless the FMEC promptly terminates or extends the precautionary suspension prior to or immediately after reviewing the suspension, the practitioner shall be entitled to the procedural rights afforded by the Fair Hearing and Appeal plan once the restrictions or suspension last more than fourteen (14) calendar days. Restrictions or suspensions which last fourteen (14) days or less shall not trigger rights under the Fair Hearing and Appeal Plan.
2.4 Provision of Patient Care Immediately upon the imposition of a precautionary suspension, the appropriate
Department Chair or, if unavailable, the President of the Medical Staff shall assign responsibility for care of the suspended practitioner’s patients still in a System’s facility to another practitioner with appropriate clinical privileges. The assignment shall be effective until the patients are discharged. The wishes of the patient shall be considered in the selection of the assigned practitioner. It shall be the duty of all Medical Staff practitioners to cooperate with the President of the Medical Staff, the Department Chair concerned, the FMEC and the Chief Medical Officer in enforcing all suspensions.
2.5 Recission of Emergency Corrective Action/Precautionary Suspension The person imposing emergency corrective action may, at any time prior to ratification of
such action by the FMEC, rescind the action, and the affected practitioner shall be restored to the status he enjoyed prior to the imposition of emergency correction action. Following ratification of emergency corrective action by the Executive Committee, the person imposing such action may recommend to the FMEC that such action be rescinded. The FMEC shall consider such recommendation at its next regular meeting thereafter. Any pending request for a hearing pursuant to Section 4 shall be made moot and void by such recission.
SECTION 3 AUTOMATIC SUSPENSION AND TERMINATION 3.1 Basis for Automatic Suspension and Termination A practitioner’s clinical privileges shall automatically be revoked, limited or suspended as
appropriate, which action shall be final without a right to due process except as provided in this Section, upon the occurrence of the following circumstances: 3.1.1 Loss of License. The practitioner’s license to practice in the State of Florida is
suspended, limited or terminated.
44
3.1.2 Residence or Office Outside Lee County. The practitioner does not maintain a full-time residence and office in Lee County as
required by these Bylaws, unless such requirements are waived by the FMEC pursuant to said Subsection. Return of United States mail sent by the System Medical Staff Services Office to a practitioner at his Lee County home or office address with “addressee unknown” or similar endorsement shall be prima facie evidence that the practitioner does not comply with these Bylaws. Failure of a practitioner to supply a current residence and office address within 15 working days of a request of the Medical Staff Services Office for the same shall be deemed prima facie evidence that the practitioner does not comply with these Bylaws. This shall not apply to practitioners granted a leave of absence by the FMEC pursuant to these Bylaws.
3.1.3 Lack of Active Practice. The practitioner is not actively engaged in the practice of
his profession in Lee County; that is, he is not seeing, examining, treating or otherwise caring for patients, and has not done so for a period of more than six months, unless the practitioner shall have notified the Medical Staff Services Office prior to beginning such absence, and arranged for suitable coverage during such time period. This shall not apply to practitioners granted a leave of absence by the FMEC pursuant to these Bylaws, or to members of the Honorary Medical Staff.
3.1.4 Criminal Conviction. The practitioner has been, while a practitioner on the Medical
Staff, convicted in any jurisdiction of the United States; of a felony or misdemeanor involving actual or threatened bodily harm, actual or threatened sexual misbehavior or stalking, controlled substance possession or use, or of any felony or misdemeanor described in any Florida law pertaining to governing or regulating the health professions or health facilities. A practitioner whose membership or privileges are automatically terminated pursuant to this Subsection shall not be disqualified from applying for appointment following completion of his sentence, or during a period of time when he is on probation. However, the fact that the practitioner has completed his sentence after criminal conviction, or is on probation, shall not require the Medical Staff to make such appointment, and the FMEC may elect not to do so in its discretion, consistent with its responsibility towards patients, other practitioners, Facility/System employees, and the public in general.
3.1.5 Loss or Restriction of DEA Certificate. The clinical privileges of a practitioner whose
Drug Enforcement Agency (DEA) certification is terminated, revoked, or suspended shall automatically and immediately be modified to revoke the right to prescribe controlled substances. The practitioner shall immediately inform the Medical Staff Services Office regarding the change in status in his DEA certification. The matter shall promptly be referred, for investigation and further action in accordance with the provisions of these Bylaws.
3.1.6 Exclusion From Federal or State Health Care Programs. The Medical Staff
appointment and clinical privileges of a practitioner who becomes an ineligible person with regard to participation in Federal or State Health Care Programs shall automatically and immediately be suspended.
The practitioner shall immediately inform the Medical Staff Services Office regarding
the change of his eligibility status. This triggers the right to due process. The matter shall promptly be referred for investigation and further action in accordance with all the due process provisions of this Part.
45
3.1.7 Failure to Pay Fees and Assessments. The practitioner fails to pay when due any fee or assessment imposed pursuant to these Bylaws or Medical Staff or System policy.
3.1.8 Failure to Provide Requested Information. If at any time a practitioner fails to
provide required information pursuant to a formal request by the System Credentialing/Privileging Committee, Medical Executive Committee or the Medical Staff Services Office, the practitioner’s clinical privileges shall be deemed to be voluntarily relinquished until the required information is provided to the satisfaction of the requesting party. For purposes of this Section, required information shall include but not be limited to: 1. physical or mental examination reports as specified elsewhere in this policy, or 2. information necessary to explain an investigation, professional review action, or resignation from another health care facility or agency.
3.1.9 Failure to Request Reappointment or Provide Requested Information Related to
Reappointment. If a practitioner fails to request reappointment for membership and/or privileges or fails to provide requested information pursuant to Part III, Section 5 of these Bylaws, the practitioner’s membership and privileges shall be deemed voluntarily relinquished.
3.1.10 Failure to Request Reinstatement Following Leave of Absence. Failure to request
reinstatement shall be deemed a voluntary resignation from the Medical Staff and shall result in automatic termination of membership, privileges, and prerogatives. Members whose membership is automatically terminated shall not be entitled to the procedural rights provided in the Medical Staff Bylaws.
3.1.11 Failure to Complete Medical Records. All elective admitting, consulting and clinical
privileges of any practitioner shall be deemed to be voluntarily relinquished for failure to complete medical records in accordance with the provisions of the Medical Staff Rules and Regulations. Such relinquishment shall continue until all the records of the practitioner’s patients are no longer delinquent. Such relinquishment does not exempt the practitioner from fulfilling their on-call responsibilities. Failure to complete the medical records that caused relinquishment of clinical privileges within sixty (60) days from the relinquishment of such privileges shall be grounds for further disciplinary action in accordance with the provisions of these Bylaws.
3.1.12 Failure to Comply with Special Meeting Attendance Requirements. Failure of a
practitioner to attend a special meeting called pursuant to the Bylaws. 3.2 Right to Limited Hearing for Automatic/Voluntary Suspension and Termination A practitioner affected by this Section shall be sent a written notice stating the reasons for
automatic suspension within 24-hours of the same having been imposed, and shall have the right to present evidence to the FMEC in written form, or by appearing personally at a regular meeting of the committee, to demonstrate that the reason that automatic suspension was imposed is untrue.
3.2.1 Such written evidence or a written request to meet with the FMEC shall be
submitted to the President of the Medical Staff within ten (10) working days of the date the notice of automatic suspension was sent. Failure to submit written evidence or a request shall be deemed a waiver of any right to consideration of the same.
46
3.2.2 Evidence presented by the affected practitioner shall be limited to whether or not the grounds for automatic suspension are true. The FMEC shall not consider evidence or argument, which presents mitigating circumstances or excuse.
3.2.3 After receipt of an affected practitioner’s written evidence, and prior to the next
regular meeting of the FMEC, the President of the Medical Staff, with the concurrence of a member of the Medical Administrative Staff designated by the System President, may determine that the evidence so presented demonstrates that
the reasons that automatic suspension was imposed are untrue, and revoke the
suspension, restoring the affected practitioner to the status he previously enjoyed. 3.2.4 The President of the Medical Staff may, at any time, provisionally reinstate a
practitioner suspended pursuant to this Section if the President is satisfied by the available written documentation that the reasons for automatic suspension were untrue. The President shall present the provisional reinstatement for ratification by the FMEC at its next regular meeting.
3.2.5 At its next regular meeting following automatic suspension, the FMEC shall consider
the reasons therefore, together with any evidence or argument presented by the affected practitioner, and if the reasons for automatic suspension are found to be true, recommend to the Board termination of the affected practitioner’s Medical Staff membership and/or privileges. If the FMEC finds that the reasons are untrue or corrected, the suspension shall be revoked, and the affected practitioner restored to the status he previously enjoyed.
SECTION 4 HEARING AND APPEAL PROCEDURES 4.1 Grounds for Hearing An applicant or an individual holding a Medical Staff appointment shall be entitled to
request a hearing whenever the FMEC or the Board of Directors has made one of the following adverse recommendations:
4.1.1 denial of initial Medical Staff appointment; 4.1.2 denial of Medical Staff reappointment; 4.1.3 revocation of Medical Staff appointment; 4.1.4 denial of requested initial clinical privileges; 4.1.5 denial of requested additional clinical privileges; 4.1.6 decrease of clinical privileges;
4.1.7 suspension of clinical privileges (other than emergency corrective action/precautionary suspension);
4.1.8 imposition of mandatory concurring consultation requirement. No other recommendations except those enumerated in this Section shall entitle the practitioner to request a hearing. Neither voluntary relinquishment of clinical privileges, as provided in these Bylaws, nor the imposition of any general consultation requirement, nor the imposition of a requirement for retraining, additional training or continuing education, shall constitute grounds for a hearing, but shall take effect without hearing or appeal. The hearing shall be conducted in as informal a manner as possible, subject to the rules and procedures set forth in these Bylaws.
47
4.2 Notice of Recommendation When a recommendation is made which, according to these Bylaws entitles a practitioner to
a hearing prior to a final decision of the Board, the affected practitioner shall promptly be given notice by the President of the Medical Staff or Chief Medical Officer or his designee, in writing, certified mail, return receipt requested or in person. This notice shall contain:
4.2.1 a statement of the recommendation made, the action which is being taken or which may be taken, and the general reasons for it; 4.2.2 notice that the practitioner has the right to request a hearing on the
recommendation within thirty (30) days of receipt of this notice; and 4.2.3 a copy of this Part outlining the rights in the hearing as provided for in these
Bylaws.
4.3 Request for Hearing A practitioner shall have thirty (30) days following the date of the receipt of such notice
within which to request the hearing. The request shall be in writing to the President of the Medical Staff or Chief Medical Officer with a copy to the Medical Staff Services Office and signed by the affected practitioner making such request. In the event the practitioner does not request a hearing within the time and in the manner required by these Bylaws, the practitioner shall be deemed to have waived the right to the hearing and to have accepted the action involved. That action shall become effective immediately upon final Board action.
4.4 Preliminary Interview The affected practitioner may request, at the time of submitting a request for hearing or
within ten (10) working days thereafter, an informal preliminary interview with the decision making body (FMEC or Board of Directors). The decision making body shall grant all such requests, and the affected practitioner shall be scheduled to appear before it at its next regular meeting. 4.4.1 The purpose of the preliminary interview shall be to permit the affected practitioner
to personally present any argument or evidence showing that the adverse recommendation has been wrongfully imposed, in fact, or in violation of these Bylaws; or to present any mitigating circumstances.
4.4.2 The preliminary interview is informal and not a hearing. It is optional with the
affected practitioner, and accordingly, legal counsel shall be excluded. 4.4.3 The decision making body may impose a limit on the amount of time to be devoted
to a preliminary interview, but not less than thirty minutes. 4.4.4 Failure to request a preliminary interview shall not be considered in any hearing or
deliberation conducted pursuant to these Bylaws, nor shall the affected practitioner’s right to a hearing be affected thereby.
48
4.4.5 Following a preliminary interview, the decision making body shall deliberate, and may elect to withdraw or reduce the severity of the adverse recommendation imposed upon the affected practitioner, or may take no action.
If no action is taken, the adverse recommendation shall continue in effect, and the hearing provided for hereunder shall proceed.
4.4.6 Notice shall be given to the affected practitioner of the decision following a
preliminary interview in the manner provided in Subsection 1.3.
SECTION 5 FAIR HEARING PROCEDURE 5.1 System Representative, Hearing Panel and Hearing Officer 5.1.1 System Representative 5.1.1.1 When the FMEC of the Medical Staff is the decision making body, the
President of the Medical Staff shall appoint a person to represent the interests and position of the Medical Staff in all proceedings provided for in this Section. Such individual shall be in an adversarial role opposed to the affected practitioner. If the affected practitioner is not represented by legal counsel, the Medical Staff representative shall not be an attorney, but shall be a member of the Active Medical Staff.
5.1.1.2 When the Board is the decision making body, as defined herein, the
Chair of the Board shall appoint a person to represent the interests and position of the Board in all proceedings provided for in this Section. Such individual shall be in an adversarial role opposed to the affected practitioner. If the affected practitioner is not represented by legal counsel, the Board representative shall not be an attorney, but shall be a member of the administration.
5.1.1.3 For purposes of these Bylaws, the Medical Staff or Board representative
appointed under this Section shall be called the “System Representative.”
5.1.2 Hearing Panel 5.1.2.1 Unless the FMEC or Board elects to have the matter heard by a Hearing
Officer possessing the qualifications set forth in Subsection 5.1.3, all hearings shall be conducted by a Hearing Panel appointed by the President of the Medical Staff or the Chair of the Board, as applicable,
composed of five (5) members, presided over by a qualified professional selected in accordance with Subsection 5.1.3. The Hearing Panel shall be composed of Active Medical Staff practitioners who shall not have actively participated in the consideration of the matter involved at any previous level. Knowledge of the matter involved shall not preclude any individual from serving as a member of the Hearing Panel.
If the hearing has been requested based on Board action, 3 of the
members of the Hearing Panel shall be members of the Board of Directors. The Hearing Panel will be presided over by a Hearing Officer.
5.1.2.2 The Hearing Panel shall not include any individual who is in direct
economic competition with the affected person or has any other personal interest in the proceeding, financial or otherwise, or any such individual
49
who is professionally associated with or related to the affected practitioner.
5.1.3 Hearing Officer – Qualifications & Authority 5.1.3.1 The FMEC or the Board may elect to have the hearing provided for in
this Section held by a Hearing Officer sitting alone. In such case, the Hearing Officer shall perform all of the functions of the Hearing Panel described herein.
In cases where a panel is appointed, the Hearing Officer will preside over
the proceeding but not participate in the deliberations or vote on the recommendation.
5.1.3.2 The Hearing Officer:
5.1.3.2.1 shall be an attorney licensed in the State of Florida who is
knowledgeable and has experience in health care law, including Medical Staff law; or shall be a non-lawyer who has experience as a Hearing Officer;
5.1.3.2.2 shall not be, or have been, employed or retained by the Lee
Memorial Health System, or any practitioner on the Medical Staff, including the affected practitioner, for any purpose other than to serve as a Hearing Officer in Medical Staff proceedings;
5.1.3.2.3 shall have no personal interest in the proceeding, financial or
otherwise; 5.1.3.2.4 shall be selected by the affected practitioner from a list
provided to the affected practitioner by the General Counsel for the Health System of the names of not less than three (3) persons meeting the requirements of 1-3 above. The affected practitioner shall select the Hearing Officer from the list submitted to him and within forty-eight (48) hours of receiving said list, notify the General Counsel for the Health System in writing of said selection.
Failure of the affected practitioner to select within the
previously mentioned period shall constitute a waiver by the affected practitioner of this Subsection, and the General Counsel for the Health System shall thereafter select the Hearing Officer.
5.1.3.3 The Hearing Officer shall: 5.1.3.3.1 act to insure that all participants in the hearing have a
reasonable opportunity to be heard and to present oral and documentary evidence subject to reasonable limits on the number of witnesses and duration of direct and cross examination, applicable to both sides, as may be necessary to avoid cumulative or irrelevant testimony or to prevent abuse of the hearing process;
50
5.1.3.3.2 prohibit conduct or presentation of evidence that is cumulative, excessive, irrelevant, and abusive or that causes undue delay;
5.1.3.3.3 maintain decorum throughout the hearing; 5.1.3.3.4 determine the order of procedure throughout the hearing; 5.1.3.3.5 have the authority and discretion, in accordance with these
Bylaws, to make rulings on all questions that pertain to matters of procedure and to the admissibility of evidence and qualifications of witnesses;
5.1.3.3.6 act in such a way that the Hearing Panel in formulating its
recommendations considers all information relevant to the continued appointment or clinical privileges of the practitioner requesting the hearing;
5.1.3.3.7 conduct argument by counsel on procedural points outside
the presence of the Hearing Panel unless the Panel wishes to be present;
5.1.3.3.8 grant continuances and postponements as appropriate; and 5.1.3.3.9 take official notice of any matters, either technical or scientific,
relating to the issues under consideration that could have been judicially noticed by the courts of this state, inform the participants of the matters to be officially noticed and provide each party the opportunity to request that a matter be officially noticed or to refute the noticed matter by evidence or by written or oral presentation of authority.
5.2 Challenge to Hearing Panel Members or Hearing Officer
The affected practitioner may challenge the objectivity of any member of the Hearing Panel, or the Hearing Officer, at any time prior to the taking of testimony at the hearing. Such challenge shall be in writing and specify facts demonstrating that a member of the Hearing Panel or the Hearing Officer lacks objectivity or is biased against the affected practitioner. The challenge shall be directed to the President of the Medical Staff or the Chair of the Board, as applicable, who shall consider the challenge and either sustain or overrule it. If the challenge is sustained, the challenged member of the Hearing Panel or the Hearing Officer shall be replaced.
SECTION 6 HEARING PROCEDURES 6.1 Provision of Relevant Information
6.1.1 There is no right to discovery in connection with the hearing. However, the
practitioner requesting the hearing shall be entitled, upon specific request, to the following, subject to a stipulation signed by both parties that such documents shall be maintained as confidential and shall not be disclosed or used for any purpose outside of the hearing:
51
6.1.1.1 copies of, or reasonable access to, all patient medical records referred to in the Statement of Reasons, at the practitioner’s expense;
6.1.1.2 reports of experts relied upon by the FMEC or the Board; 6.1.1.3 redacted copies of relevant committee or Department meeting minutes
(such provision does not constitute a waiver of the state peer review protection statute); and
6.1.1.4 copies of any other documents relied upon by the FMEC or the Board.
6.1.2 Prior to the hearing, on dates set by the Hearing Officer or agreed upon by counsel
for both sides, each party shall provide the other party with a list of proposed exhibits. All objections to documents or witnesses to the extent then reasonably known, shall be submitted in writing in advance of the hearing. The Hearing Officer shall not entertain subsequent objections unless the party offering the objection demonstrates good cause.
6.1.3 Prior to the hearing, on dates set by the Hearing Officer, the practitioner requesting
the hearing shall, upon specific request, provide the FMEC (or the Board of Directors) copies of any expert report or other documents relied upon by the practitioner.
6.1.4 Neither the affected practitioner, nor his attorney, nor any other person on behalf of
the affected practitioner, shall contact members of the hearing committee or the Hearing Officer, or hospital employees appearing on the hospital’s witness list concerning the subject matter of the hearing, unless specifically agreed upon by counsel.
6.2 Pre-Hearing Conference The Hearing Officer may require counsel for the practitioner and for the FMEC (or the
Board) to participate in a pre-hearing conference for purposes of resolving all procedural questions in advance of the hearing. The Hearing Officer may specifically require that:
6.2.1 all documentary evidence to be submitted by the parties be presented at this
conference; any objections to the documents shall be made at that time and the Hearing Officer shall resolve such objections;
6.2.2 evidence unrelated to the reasons for the unfavorable recommendation or unrelated
to the practitioner’s qualifications for appointment or the relevant clinical privileges be excluded;
6.2.3 the names of all witnesses and a brief statement of their anticipated testimony are
submitted, if not previously provided; 6.2.4 the time granted to each witness’ testimony and cross-examination be agreed upon,
or determined by the Hearing Officer, in advance; and 6.2.5 witnesses and documentation not provided and agreed upon in advance of the
hearing may be excluded from the hearing. 6.3 Failure to Appear
52
Failure, without good cause, of the practitioner requesting the hearing to appear and proceed at such a hearing shall be deemed to constitute voluntary acceptance of the pending recommendations or actions, which shall then be forwarded to the Board for final action. The Hearing Officer may impose sanctions upon either party for failure to appear, including the assessment of the costs and attorneys’ fees of the party in attendance against the offending party.
6.4 Record of Hearing A record shall be made at the expense of the Lee Memorial Health System, if any, the pre-
hearing conference and the hearing, using the services of a court reporter. No record of the in camera deliberations of the decision making body or the hearing committee shall be
made. Either party shall be entitled to have a record made of any other proceeding related to the hearing process, at that party’s expense. The expense of transcripts shall be borne by the party requesting them. Oral evidence shall be taken only on oath or affirmation administered by any person designated by such body and entitled to notarize documents in this State.
6.5 Rights of Both Sides At a hearing, both sides shall have the following rights, subject to reasonable limits
determined by the Hearing Officer: 6.5.1 to call and examine witnesses to the extent available; 6.5.2 to introduce exhibits; 6.5.3 to cross-examine any witness on any matter relevant to the issues and to rebut any
evidence; 6.5.4 to be represented by counsel who may call, examine, and cross-examine witnesses
and present the case. (Both sides shall notify the other of the name of that counsel at least ten (10) days prior to the date of the pre-hearing conference and hearing); and
6.5.5 to submit a post-hearing memorandum of points and authorities (The Hearing Panel may request such a memorandum to be filed following the close of the hearing).
Any practitioner requesting a hearing, who does not testify on his own behalf, may be called
and examined as if under cross-examination. The Hearing Panel or Hearing Officer may question the witnesses, call additional witnesses or request additional documentary evidence.
6.6 Admissibility of Evidence The rules of evidence applicable to the courtroom shall not apply, and the Hearing Officer
may admit any evidence that might be relied upon by a reasonable person. Notwithstanding the foregoing, a party shall have the right to object to any evidence on
grounds of hearsay, relevance, or other grounds available under the Florida Evidence Code, and the Hearing Officer shall have the authority to rule on such objections.
6.7 Burden of Presenting Evidence and Proof The burden of going forward with evidence supporting the adverse action or
recommendation is on the FMEC or Board, whichever initially prompted the hearing. Once that burden has been met to the satisfaction of the Hearing Panel/Hearing Officer, the practitioner shall bear the burden of proof, under a preponderance of the evidence, which is a lesser standard than clear and convincing evidence, that the action and penalty taken or
53
proposed against the practitioner was wrongfully or arbitrarily imposed, not in accordance with these Bylaws, or lacks any factual basis.
SECTION 7 HEARING CONCLUSION, DELIBERATIONS AND RECOMMENDATIONS
7.1 Deliberations and Recommendation of the Hearing Panel/Hearing Officer
7.1.1 The recommendation of the Hearing Panel/Hearing Officer shall be based on the evidence produced at the hearing. This evidence may consist of oral testimony of witnesses; memorandum of points and authorities presented in connection with the hearing, any information regarding the practitioner who requested the hearing so long as that information has been admitted into evidence at the hearing and the person who requested the hearing had the opportunity to comment on and, by other evidence, refute it, any and all applications, references, and accompanying documents; other documented evidence, including medical records and any other information presented at the hearing.
7.1.2 Within thirty (30) working days after final adjournment of the hearing, the Hearing
Panel shall conduct its deliberations outside the presence of any other person except the Hearing Officer, and shall prepare a recommended order containing the findings of fact, findings regarding the applicability of these Bylaws, any rules, regulations or policies of the Medical Staff or the Lee Memorial Health System, and the statutory and decisional law of Florida; and a recommendation that adverse action be upheld, modified or withdrawn. If the FMEC or the Board selected a Hearing Officer sitting alone, the Hearing Officer shall prepare a recommended order in the same manner outlined above.
7.1.3 The Hearing Officer shall not participate in the deliberations of the Hearing Panel,
nor be involved in the decision of the Hearing Panel regarding its recommended order.
However, the Hearing Officer may assist the Hearing Panel with regard to the form,
organization and syntax of the recommended order. The recommended order shall be signed by each member of the Hearing Panel or the Hearing Officer, as applicable, and copies provided in person by certified mail, return receipt requested, to the affected practitioner and System Representative.
7.2 Disposition of Hearing Panel Report The Hearing Panel/Hearing Officer shall deliver its report and recommendation to the Chief
Medical Officer or his designee who shall forward it, along with all supporting documentation, to the Board and/or FMEC.
The recommended order shall be considered by the FMEC or Board at its next regular meeting, and may be adopted or rejected by it. If adopted, the recommended order shall become the final decision of the original decision making body (FMEC or Board).
If rejected, the FMEC or Board shall render its own final written decision upholding the
original recommendation, modifying or withdrawing the action. Any action imposed through the final order that requires action by the Board of Directors shall be referred to the Board for final disposition at its next regular meeting.
SECTION 8 APPEAL PROCEDURE
54
8.1 Request & Time for Appeal Within ten (10) working days of receipt of the final written decision following a hearing,
either party may appeal the recommendation. The request shall be in writing, signed by the requesting party and delivered to the Chief Medical Officer either in person or by certified mail, return receipt requested, with a copy to the Medical Staff Services Office. The request shall include a statement of the reasons for appeal and the facts or circumstances that justify further review. If such appellate review is not requested within ten (10) working days as provided herein, both parties shall be deemed to have waived the right to an appeal, and the Hearing Panel or Hearing Officer’s report and recommendation shall be forwarded to the Board for final action.
8.2 Grounds for Appeal The grounds for appeal shall be limited to the following: 8.2.1 there was substantial failure to comply with these Bylaws or hospital policies prior to
the hearing so as to deny a fair hearing; or 8.2.2 the recommendations of the Hearing Panel were made arbitrarily, capriciously or
with prejudice. 8.3 Time, Place and Notice Whenever an appeal is requested as set forth in the preceding Sections, the Chair of the
Board shall, as soon as arrangements can reasonably be made, taking into account the schedules of all participants, schedule and arrange for an appellate review. The affected practitioner shall be given notice of the time, place and date of the appellate review. When a request for appellate review is from a appointee who is under a suspension then in effect, the appellate Review panel shall be convened not more than 14-days from the date of receipt of the request for an appeal unless the practitioner agrees to a longer period. The time for appellate review may be extended by the Chair of the Board for good cause.
8.4 Nature of Appellate Review 8.4.1 Review panel. The Chair of the Board shall appoint a Review panel composed of 5
members, 3 of the panel members shall be members of the Board of Directors and 2 panel members shall be Active members of the Medical Staff. The Board may establish rules of procedure to govern the conduct of appellate hearings under this Section and the Chair of the Board, or his or her designee, shall preside at appellate proceedings.
8.4.2 Position Papers. Each party shall have the right to present a written statement in
support of its position on appeal. Position papers that do not conform to the following requirements may be excluded from consideration in the appeal.
8.4.2.1 The position papers shall set forth a statement of the facts and of the
applicable Bylaws provisions or other authority, as well as any other matters that the parties wish to bring before the appellate body in support of their respective positions.
8.4.2.2 Twelve copies of the affected practitioner’s position paper shall be filed
with Medical Staff Services within (fifteen)15 working days of the filing of
55
the notice of appeal. The System Representative shall also file with Medical Staff Services, 12 copies of his position paper within ten (10) working days of his receipt of a copy of the affected practitioner’s position paper.
8.4.2.3 Position papers shall be limited to no more than thirty (30) pages,
exclusive of exhibits, and shall be on letter-size paper, typewritten, double-spaced and shall be neatly bound or stapled.
8.4.2.4 Each party shall provide a copy of his position paper to the other at the
same time the party’s position paper is filed with Medical Staff Services. 8.4.2.5 Exhibits attached to the position paper shall not duplicate exhibits or
documents contained in the hearing record, and shall be consecutively numbered and attached at the end of the position paper.
8.4.2.6 In referring to the record, position papers shall reference specific pages of
the hearing record and of exhibits that are part of the record. 8.4.3 Oral Argument. The affected practitioner and the System Representative shall be
entitled to present oral argument. Oral argument shall be requested at the time the party submits his position paper. Failure to request oral argument shall constitute a waiver of the right to it. The Board may limit the time for oral argument, but each side shall not have less than thirty (30) minutes. Oral argument shall not include the introduction of evidence and appellate review shall not constitute a hearing de novo.
A record shall be made at the expense of the Lee Memorial Health System of the presentation of oral argument, using the services of a court reporter.
8.4.4 Recommendation. The review panel shall recommend final action to the Board
within thirty (30) working days after the completion of oral argument, or if no oral argument is requested, within forty-five (45) working days after the submission of the position papers of both parties.
SECTION 9 FINAL DECISION OF THE BOARD Within thirty (30) working days after receipt of the Review panel’s recommendation, the Board shall render a final decision in writing, including specific reasons and shall deliver copies thereof to the affected practitioner, the FMEC, and the Medical Staff Services Office, in person or by certified mail, return receipt requested. The decision shall uphold or reverse the final written decision rendered by the decision making body, or may remand the case for reconsideration by the decision making body. If the matter is referred for further action and recommendation, such recommendation shall be promptly made to the Board in accordance with the instructions given by the Board within thirty (30) days. The final decision of the Board following the appeal shall be effective immediately and shall not be subject to further review. SECTION 10 RIGHT TO ONE HEARING AND ONE APPEAL ONLY 10.1 No applicant or Medical Staff practitioner shall be entitled to more than one (1) hearing and
one (1) appeal on any matter that may be the subject of an appeal. A final appellate
56
decision upholding or reversing a final, written decision shall be final and there shall be no right to further hearing on the matter.
10.2 If the Board determines to deny initial Medical Staff appointment or reappointment to an
applicant, or to revoke or terminate the Medical Staff appointment and/or clinical privileges of a current practitioner, that practitioner may not apply for Staff appointment or for those clinical privileges at this hospital for a period of five (5) years unless the Board provides otherwise.
PART III: CREDENTIALING PROCEDURES
SECTION 1 SYSTEM CREDENTIALING/PRIVILEGING COMMITTEE 1.1 Organizational Structure
It is the intention of the Medical Staff Organizations of Lee Memorial Health System (LMHS) to ultimately establish one (1) System Credentialing/Privileging Committee (hereinafter referred to as the Credentialing/Privileging Committee) to act on behalf of all the Medical Staff of LMHS. It has been determined that the two (2) Credentialing/Privileging Committees in effect at the time of the approval of this document may continue for a maximum period of two (2) years. During this transition time, the two (2) Credentialing/Privileging Committees will meet jointly on at least a quarterly basis (the Credentialing/Privileging Committees will not meet separately during the months that the joint meetings occur) and through this process will effect a smooth transition to a single System Credentialing/Privileging Committee. The single System Credentialing/Privileging Committee may decide to merge prior to the end of the two 2-year period.
1.2 Transition Issues
At the time of adoption of PART III, two (2) Credentialing/Privileging Committees exist. Chairs of each of these Credentialing/Privileging Committees have been appointed in accordance to procedures that were in existence prior to the adoption of these Credentials Procedures. During the transition period (moving from two (2) committees to a single System Credentialing/Privileging Committee), these Chairs will continue to serve as the Chairs of the applicable practitioner System Credentialing/Privileging Committee and together will serve as Co-Chairs of the System Credentialing/Privileging Committee (which will meet at least quarterly (see Section 1.1).
The initial composition of the System Credentialing/Privileging Committee will be made up of
the membership of the two (2) separate Credentialing/Privileging Committees, with the current Chairs serving as Co-Chairs. During the first year of the System Credentialing/Privileging Committee, the committee will plan to evolve to the composition of the System Credentialing/Privileging Committee as established in Section 1.4 by the end of twenty-four (24) months.
1.3 Purpose of the System Credentialing/Privileging Committee
The System Credentialing/Privileging Committee exists to oversee all credentialing and privileging activities related to Medical Staff members and privileged Allied Health
57
practitioners on behalf of the Facility Medical Executive Committees (FMECs). These credentialing and privileging activities include processes related to the following:
1.3.1 initial appointment; 1.3.2 focused professional practice evaluation; 1.3.3 reappointment; 1.3.4 delineation of clinical privileges, including temporary privileges; and 1.3.5 development of privilege delineation forms and criteria for all LMHS facilities. Credentialing activities are to be carried out in accordance with specific policies and
procedures developed to ensure current clinical competency of the practitioners who are credentialed and privileged at LMHS. The purpose of the System Credentialing/Privileging
Committee also includes development of implementation of credentialing and privileging policies and procedures designed to ensure compliance with regulatory requirements.
1.4 Composition of the System Credentialing/Privileging Committee The leadership and membership of the System Credentialing/Privileging Committee shall be
as follows: 1.4.1 Consist of not less than 15 members of the active Medical Staff selected on a basis
that will ensure, insofar as feasible, balanced representation of the LMHS sites. 1.4.2 The System Medical Director will serve as a non-voting member. 1.4.3 The Immediate Past President of each FMEC will serve as voting members and will
serve a 2-year term. The FMEC may appoint this practitioner, as a member once the Immediate Past President is no longer in office.
1.4.4 Each FMEC will appoint two (2) additional representatives. 1.4.5 A quorum of 50% is required to conduct a meeting. 1.4.6 Members shall serve for two (2) years and may be reappointed to consecutive terms. 1.4.7 Each member shall be required to attend 75% of the meetings during the Medical
Staff year. Failure to attend 75% of the meetings may result in dismissal of the member from committee service and selection of an alternative member by the affected FMEC.
1.4.8 The committee members from among the committee membership will elect the Co-
Chairs of the System Credentialing/Privileging Committee. One of the Co-Chairs will be from a medical specialty and the other Co-Chair will be from a surgical specialty.
1.5 Duties and Responsibilities of the System Credentialing/Privileging Committee The System Credentialing/Privileging Committee shall: 1.5.1 Meet to evaluate credentialing-related requests (initial appointment, reappointment,
requests for clinical privileges and leave of absence, etc.) on behalf of the FMECs. 1.5.2 Monitor the granting of temporary privileges to assure that temporary privileges are
granted in compliance with approved policies and procedures. (The System Credentialing/Privileging Committee does not evaluate requests for temporary
58
privileges. These requests are handled in accordance with specific policies and procedures that are overseen by the System Credentialing/Privileging Committee).
1.5.3 Oversee the processes related to focused professional performance evaluations and
related proctoring and other mechanisms and tools employed to evaluate competency.
1.5.4 Assure uniformity in both the development and application of privileging criteria
utilized throughout LMHS facilities. 1.5.5 Assure the FMECs and Board that Medical Staff Bylaws Provisions that relate to
credentialing and privileging processes are being fulfilled, as well as credentialing policies and procedures and other credentialing-related Medical Staff documents. Monitor compliance with all credentialing and privileging policies and procedures.
1.5.6 Be responsible for evaluating recommendations made by Department Chairs. The committee is looking for completeness, thoroughness and adherence to
credentialing and privileging policies and criteria. Assure the FMECs that specialty-specific criteria for clinical privileges comply with Medical Staff Bylaws, credentialing policies and procedures, and criteria is applied fairly and uniformly to each practitioner.
1.5.7 Focuses in on the files that are determined to need clarification or additional
information (i.e., time gaps, problems with references, malpractice claims, etc.) and assures that all issues have been appropriately addressed and that there is complete and thorough documentation for the recommendation(s) that have been made to the FMECs.
1.5.8 Be responsible and aware of regulatory requirements related to credentialing activities
and to make the FMECs and Board aware when changes in credentialing policies and procedures need to be made in order to meet requirements.
1.5.9 Commission, receive and analyze the results of compliance audits of credentialing
and privileging processes. The System Credentialing/Privileging Committee makes recommendations to the FMECs and the Board when the System Credentialing/Privileging Committee believes, based on results of reports that improvements can and should be made in credentialing and privileging policies and procedures.
SECTION 2 QUALIFICATIONS FOR MEMBERSHIP AND PRIVLEGES 2.1 The following qualifications must be met by all applicants for Medical Staff
appointment, reappointment or clinical privileges:
2.1.1 Associate and Active Staff shall live and maintain an office in Lee County, unless this requirement is waived by the FMEC;
2.1.2 Demonstrate that he has successfully graduated from an approved school of
medicine (MD or DO), dentistry, podiatry, clinical psychology or applicable recognized course of training in a clinical profession eligible to hold privileges;
59
2.1.3 Have a current unrestricted state or federal license as a physician, dentist, podiatrist or clinical psychologist, applicable to his or her profession, and providing permission to practice within the State of Florida;
2.1.4 Have a record that is free from current Medicare/Medicaid sanctions and not be on
the Office of Inspector General (OIG) or General Services Administration (GSA) List of Excluded practitioners/entities;
2.1.5 Have a record that is free of felony convictions or occurrences that would raise
questions of undesirable conduct, which could injure the reputation of the Medical Staffs, hospital or Health System;
2.1.6 A physician (MD or DO) must have successfully completed an allopathic or
osteopathic residency program, approved by the Accreditation Council for Graduate Medical Education (ACGME) or the American Osteopathic Association (AOA) and be currently board certified or become board certified following the completion of formal training within the timeframes as defined by the appropriate specialty board of the American Board of Medical Specialties or the American Osteopathic Association. If no time limits for certification are specified by a given Board, then the applicant will be required to become Board certified within seven (7) years of completing formal training as defined by the appropriate specialty Board of the American Board of Medical Specialties or the American Osteopathic Association. If an applicant is beyond seven (7) years of completing formal training, current Board certification will be required for consideration of membership and privileges. Once a member of the Medical Staff becomes Board certified, recertification is not a requirement of continued membership and privileges;
2.1.7 Dentists must have graduated from an American Dental Association approved
school of dentistry accredited by the Commission of Dental Accreditation; 2.1.8 Oral and maxillofacial surgeons must have graduated from an American Dental
Association approved school of dentistry accredited by the Commission of Dental Accreditation and successfully completed an American Dental Association approved residency program and be board certified or become board certified within five (5) years of completing formal training as defined by the American Board of Oral and Maxillofacial Surgery;
2.1.9 A podiatric physician (DPM) must have successfully completed a two 2-year
residency program in surgical, orthopedic, or podiatric medicine approved by the Council on Podiatric Medical Education of the American Podiatric Medical Association (APMA), and be board certified or become board certified within five (5) years of completing formal training as determined by the American Board of Podiatric Surgery or the American Board of Podiatric Orthopedics and Primary Podiatric Medicine;
2.1.10 A psychologist, must have earned a doctorate degree, (PhD or Psy.D. in
psychology) from an educational institution accredited by the American Psychological Association and have completed at least two (2) years of clinical experience in an organized healthcare setting, supervised by a licensed psychologist, one 1-year of which must have been post doctorate, and have completed an internship endorsed by the American Psychological Association (APA);
2.1.11 Possess a current, valid, Drug Enforcement Administration (DEA) number if
applicable to the privileges requested;
60
2.1.12 Have appropriate written and verbal communication skills; 2.1.13 Have appropriate personal qualifications, including applicant’s consistent
observance of ethical and professional standards. These standards include, at a minimum:
2.1.13.1 Abstinence from any participation in fee splitting or other illegal payment,
receipt, or remuneration with respect to referral or patient service opportunities;
2.1.13.2 A history of consistently acting in a professional, appropriate and
collegial manner with others in previous clinical and professional settings.
2.1.14 The following qualifications must also be met by all applicants requesting clinical
privileges: 2.1.14.1 Demonstrate his background, experience, training, current competence,
knowledge, judgment and the ability to perform all privileges requested.
2.1.14.2 Provide evidence of both physical and mental health that does not impair the fulfillment of his responsibilities of Medical Staff membership subject to any legally required reasonable accommodation, and the specific privileges requested by and granted to the applicant, upon request.
2.1.14.3 Any practitioner granted privileges that may have occasion to admit an
inpatient must demonstrate the capability to provide continuous and timely care to the satisfaction of the FMEC and Board.
2.1.14.4 Demonstrate recent clinical performance (within the last twelve (12)
months with an active clinical practice in the area in which clinical privileges are sought adequate to meet current clinical competence criteria.
2.1.14.5 The applicant is requesting privileges for a service the Board has
determined appropriate for performance at the hospital. There must also be a need for this service under any Board approved Medical Staff development plan.
2.1.14.6 Provide evidence of financial responsibility consistent with the
requirements set forth in Part I. 2.1.15 Exceptions: All practitioners who are current Medical Staff members and/or hold privileges as of
May 28, 2009 and who have met prior qualifications for membership and/or privileges shall be exempt from Board specialty certification requirements.
SECTION 3 PRE-APPLICATION PROCESS
61
3.1 Only those practitioners that meet the following minimum criteria for appointment to the Medical Staff will be provided applications. Practitioners provided applications would be those: 3.1.1 which are not governed by an exclusive arrangement or who are joining a group
providing services governed by an exclusive arrangement; and
3.1.2 who meet the minimum criteria as developed by the System Credentialing/Privileging Committee and approved by FMECs and the Board.
The purpose for the pre-application screening process shall be to avoid the costly
and time-consuming application process in those circumstances where an applicant fails to meet minimum eligibility criteria. Practitioners who do not meet the minimum eligibility criteria for appointment are not entitled to fair hearing rights.
The System Credentialing/Privileging Committee shall review all requests for
application and determine whether the criteria for issuing an application have been met.
SECTION 4 INITIAL APPOINTMENT PROCESS
4.1 Completion of Application 4.1.1 All requests for application for appointment to the Medical Staff and requests for
clinical privileges will be forwarded to the Medical Staff Services Department. If the applicant successfully completed the pre-application screening process, the Medical Staff Services Department will provide the applicant an application packet, which will include a complete set or overview of the relevant Medical Staff Bylaws or reference to an electronic source for this information. This packet will enumerate the eligibility requirements for Medical Staff membership (for each facility of LMHS) and/or privileges and a list of expectations of performance for practitioners granted Medical Staff membership or privileges (if such expectations have been adopted by each Facility Medical Staff).
A completed application includes, at a minimum: 4.1.1.1 a completed, signed, dated application form; 4.1.1.2 a completed privilege delineation form if requesting privileges; 4.1.1.3 copies of all requested documents and information necessary to confirm
the applicant meets criteria for membership and/or privileges and to establish current competency;
4.1.1.4 all applicable fees; 4.1.1.5 complete reference information; references shall be from peers (same
specialty) knowledgeable about the applicant’s experience, ability and current competence to perform the privileges being requested;
4.1.1.6 relevant practitioner-specific data as compared to aggregate data, when
available
62
4.1.1.7 morbidity and mortality data, when available. Each applicant must indicate the LMHS facility anticipated to be his
primary facility (i.e., the facility where the majority of his clinical activity is performed). It should be noted that this designation is important for credentialing purposes (interviews, implementation of focused professional practice evaluation, etc.) and will be confirmed by LMHS data at periodic intervals and prior to any subsequent reappointments.
An application shall be deemed incomplete if any of the above items are
missing or if the need arises for new, additional or clarifying information in the course of reviewing an application. An incomplete application will not be processed and the applicant will not be entitled to a fair hearing.
Anytime in the credentialing process it becomes apparent that an
applicant does not meet all eligibility criteria for membership or privileges, the credentialing process will be terminated and no further action taken. Applications will not be accepted from practitioners that are not eligible to take the Board certification examination.
4.1.2 The burden is on the applicant to provide all required information. It is the
applicant’s responsibility to ensure that the Medical Staff Services Department receives all required supporting documents verifying information on the application and to provide sufficient evidence, as required in the sole discretion of the Health System that the applicant meets the requirements for the Medical Staff membership and/or the privileges requested. If information is missing from the application or new, additional or clarifying information is required, a letter requesting such information will be sent to the applicant. If the requested information is not returned to the Medical Staff Services Department within thirty (30) calendar days of the receipt of the requested letter, the application will be deemed to have been voluntarily withdrawn.
4.1.3 Upon receipt of a completed application, the System Medical Director will determine
if the requirements of Section 2.1 are met. In the event the requirements of Section 2.1 are not met, the applicant will be notified that he is ineligible to apply for membership or privileges on the Medical Staff, the application will not be processed and the applicant will not be eligible for a fair hearing. If the requirements of Section 2.1 are met, the application will be accepted for further processing.
4.1.4 Practitioners seeking appointment shall have the burden of producing information
deemed adequate by the hospital for a proper evaluation of current competence, character, ethics, other qualifications and of resolving any doubts.
4.1.5 Upon receipt of a completed application, the Medical Staff Services Department will
verify current licensure, education, relevant training and current competence from the primary source whenever feasible in accordance with the Verification Methods and Requirements document.
When it is not possible to obtain information from the primary source, reliable
secondary sources may be used if there has been a documented attempt to contact the primary source.
Note: In the event there is undue delay in obtaining required information, the
Medical Staff Services Department will request assistance from the applicant. During this time, the period for processing, the application will be appropriately
63
modified. Failure of an applicant to respond to a request for assistance adequately after thirty (30) calendar days the application will be deemed to have been voluntarily withdrawn.
4.1.6 When all items identified in the Verification Methods and Requirements document
have been obtained and verified, the application will be considered eligible for evaluation.
4.2 Applicant’s Attestation, Authorization and Acknowledgement 4.2.1 The applicant must complete and sign the application form. By signing this
application the applicant: 4.2.1.1 Attests to the accuracy and completeness of all information on the
application or accompanying documents and agreement that any inaccuracy, omission or misrepresentation, whether intentional or not, may be grounds for termination of the application process without the right to a fair hearing or appeal.
If the inaccuracy, omission or misstatement is discovered after a
practitioner has been granted appointment and/or clinical privileges, the practitioner’s appointment and privileges shall lapse effective immediately upon notification of the practitioner without the right to a fair hearing or appeal.
4.2.1.2 Consents to appear for any requested interviews about his application. 4.2.1.3 Authorizes the applicable hospital and Medical Staff representative to
consult with prior and current associates and others who may have information bearing on his professional competence, character, ability to perform the privileges requested, ethical qualifications, ability to work cooperatively with others and other qualifications for requested membership and/or clinical privileges.
4.2.1.4 Consents to the Health System and Medical Staff representatives’
inspections of all records and documents that may be material to an evaluation of:
4.2.1.4.1 professional qualifications and competence to carry out the
clinical privileges requested;
4.2.1.4.2 physical and mental/emotional health status to the extent relevant to safely perform requested privileges subject to any legally required reasonable accommodation;
4.2.1.4.3 professional and ethical qualifications;
4.2.1.4.4 professional liability actions including currently pending claims involving the applicant;
64
4.2.1.4.5 any other issue relevant to establishing the applicant’s suitability for membership and/or privileges.
4.2.1.5 Releases from liability, promises not to sue and grants immunity to the
Health System, its Medical Staffs and its representatives for acts performed and statements made in good faith in connection with evaluation of the application and his credentials and qualifications fully permitted by the law.
4.2.1.6 Releases from liability and promises not to sue, all practitioners and
organizations who provide information to the Health System or the applicable Medical Staff(s) in good faith, including otherwise privileged or confidential information to the System/hospital representatives concerning his background/experience, competence, professional ethics, character, physical and mental health to the extent relevant to the capacity to fulfill requested privileges, emotional stability, utilization practice patterns, and other qualifications for staff appointment and clinical privileges.
4.2.1.7 Authorizes the Health System, Medical Staff and Administrative
representatives to obtain credentialing and peer review information from other hospitals, medical associations, licensing boards, appropriate government bodies and other health care entities concerned with this provider’s performance and releases representatives of the Health System from liability for so doing.
4.2.1.8 Acknowledges that the applicant has had access to relevant Medical
Staff Bylaws, including all rules, regulations, policies and procedures of the relevant Medical Staffs and agrees to abide by their provisions.
Notwithstanding Section 3.2 of Part II, if a practitioner institutes legal
action and does not prevail, he shall reimburse the Health System and any member of the Medical Staff named in the action for all costs incurred in defending such legal action, including reasonable attorney(s) fees.
4.2.1.9 Agrees to provide accurate answers to all the questions on the
application form, and agrees to immediately notify the System in writing should any of the information regarding these items change during the period of the applicant’s Medical Staff membership and/or privileges.
4.3 Application Evaluation
4.3.1 Expedited Credentialing: 4.3.1.1 An expedited Credentialing/Privileging Committee review and approval
process may be used for initial appointment in accordance with the Expedited Credentialing Policy.
4.3.2 Applicant Interview
4.3.2.1 All applicants for appointment to the Medical Staff and/or the granting of
clinical privileges are required to participate in interviews. The interviews are used to solicit information required to complete the credentials file or
65
clarify information previously provided, e.g., clinical knowledge and judgment, professional behavior, malpractice history, reasons for leaving past healthcare organizations, or other matters bearing on the applicant’s ability to render care at the generally recognized level for the community and in compliance with LMHS privileging criteria. Interviews may also be used to communicate Medical Staff performance expectations.
Applicants for appointment will participate in a minimum of two (2)
interviews. One interview will be conducted by the applicable Department Chair or designated Section Chief of the applicant’s anticipated primary LMHS facility and the second interview will be with a member of the System Credentialing/Privileging Committee. Applicants that are applying for multiple facilities within LMHS may be required to participate in additional Department Chair/Section Chief interviews at the discretion of the Department Chairs of the facility(ies) that are designated as non-primary.
4.3.2.2 Procedure: the applicant will be notified of required interview(s). Failure
of the applicant to appear for a scheduled interview will be deemed a voluntary withdrawal of the application.
4.3.3 Department Chair Action 4.3.3.1 Each Department Chair of an LMHS facility where the applicant has
requested privileges makes a recommendation related to membership and privileges, as applicable.
All completed applications are presented to the appropriate Department
Chair(s) for review and recommendation (which is made by completion of a standardized form provided to the Chair by the Medical Staff Services Department). The Department Chair(s) reviews the application to ensure that it fulfills the established standards for membership and/or clinical privileges. The Department Chair(s) may obtain input if necessary from an appropriate subject matter expert(s).
If a Department Chair believes a conflict of interest exists that, might
preclude his ability to make an unbiased recommendation, he will notify the Medical Staff Services Department and forward the application without comment.
4.3.3.2 The Department Chair(s) forwards to the System
Credentialing/Privileging Committee the following: 4.3.3.2.1 A written recommendation to approve the applicant’s request
for membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges (a summary of the interview conducted by the Department Chair or his designee is included in this written recommendation);
4.3.3.2.2 Written comments supporting his recommendations. The Department Chair of the applicant’s anticipated primary
facility also makes a written recommendation to define those circumstances, which require monitoring and evaluation of
66
clinical performance after the initial granting of clinical privileges (i.e., focused professional practice evaluation).
4.3.4 Medical Staff System Credentialing/Privileging Committee Action 4.3.4.1 The System Credentialing/Privileging Committee reviews the application
and forwards the following to the applicable FMEC(s): 4.3.4.1.1 A recommendation to approve the applicant’s request for
membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges;
4.3.4.1.2 A recommendation to define those circumstances, which
require monitoring, and evaluation of clinical performance after initial granting of clinical privileges (Focused Professional Practice Evaluation) (FPPE);
Comments supporting the above recommendation. 4.3.5 FMEC Action
4.3.5.1 Each FMEC of LMHS where membership and/or privileges have been requested forwards the following to the Board:
4.3.5.1.1 A recommendation to approve the applicant’s request for
membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges;
4.3.5.1.2 Comments supporting the above recommendation.
The FMEC of the applicant’s anticipated primary facility also makes a recommendation to define those circumstances that require monitoring and evaluation of clinical performance after initial granting of clinical privileges (FPPE).
Whenever a FMEC makes an adverse recommendation to the Board, a notice,
stating the reason, will be sent to the applicant who shall then be entitled to the procedural rights provided in the Investigation, Corrective Action, Hearing and Appeal Plan of the Medical Staff Bylaws. When multiple FMECs are making recommendations related to the same applicant, an adverse recommendation is not considered final until after the PLC attempts to facilitate resolution of the issues (this facilitation occurs when there are disparate recommendations – for example, one (1) positive recommendation and one negative recommendation).
4.3.6 Applicants Applying to Multiple Facilities Applicants may simultaneously make application for membership and/or privileges
to multiple facilities within LMHS. The Medical Staff Services Department coordinates this information so that the recommendations from all FMECs come to the Board together. If there are disparate recommendations (defined as conflicting) related to membership and/or requested clinical privileges on the same applicant, the PLC will meet and attempt to reconcile the disparate recommendations prior to forwarding the recommendations to the Board.
67
If the PLC is unable to facilitate resolution of the issues (in accordance with the Medical Staff Bylaws – Part I, Governance – Section 9 Decision Making Methods and Conflict Resolution) the disparate recommendations will go forward to the Board.
4.3.7 Board Action:
4.3.7.1 The Board reviews the recommendation and votes for one (1) of the following actions:
4.3.7.1.1 The Board may adopt or reject in whole or in part a
recommendation of the FMEC(s) or refer the recommendation to the FMEC(s) for further consideration stating the reasons for such referral back and setting a time limit within which a subsequent recommendation must be made.
4.3.7.1.2 If the Board concurs with the applicant’s request for
membership and/or privileges, it will grant the appropriate membership and/or privileges for a period not to exceed 24 months.
4.3.7.1.3 If the Board’s action is adverse to the applicant, a notice,
stating the reason, will be sent to the applicant who shall then be entitled to the procedural rights provided in the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) unless the applicant received procedural rights under Part II, Section 3.2.5.
4.3.7.1.4 The Board shall take final action in the matter as provided in
the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan).
4.3.8 Notice of Final Decision:
4.3.8.1 Notice of the Board’s final decision shall be given through the Medical
Staff Services Department to the applicable FMEC(s) and to the Chair of each Department concerned. The applicant shall receive written notice of appointment and special notice of any adverse final decisions in a timely manner. A decision and notice of appointment includes the staff category(ies) to which the applicant is appointed, the Department(s) to which he is assigned, the clinical privileges he may exercise, notification of orientation and any special conditions attached to the appointment.
4.3.9 Periods for Processing: 4.3.9.1 All practitioners and groups acting on an application for staff
appointment and/or clinical privileges must do so in a timely and good faith manner, and except for good cause, each application will be processed within 180 calendar days. The 180 Calendar days begin on the date that the application is declared complete to begin processing.
68
4.3.9.2 These processing periods are deemed guidelines and do not create
any right to have an application processed within these precise periods. If the provisions of the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) are activated, the time requirements provided therein govern the continued process of the application.
SECTION 5 FOCUSED PROFESSIONAL PRACTICE EVALUATION (FPPE) 5.1 CRITERIA FOR FPPE 5.1.1 The Department Chair (or designated Section Chief) of the applicant’s anticipated
primary facility will define circumstances that require monitoring and evaluation of the clinical performance of each practitioner following his or her initial granting of clinical privileges.
Such monitoring may utilize a range of techniques, including but not limited to: chart
review, the tracking of performance monitors/indicators, proctoring, external peer review, simulations, morbidity/mortality reviews, and discussion with other healthcare practitioners involved in the care of each patient. The FPPE plan is created as part of the initial recommendation for appointment and privileges and is forwarded to the System Credentialing/Privileging Committee and to the FMEC(s).
The System Credentialing/Privileging Committee will establish via policy the
anticipated duration for FPPE. The Physician Quality Committee will establish the triggers that indicate the need for
performance monitoring after the initial granting of privileges. SECTION 6 CRITERIA FOR REAPPOINTMENT 6.1 Criteria for Reappointment 6.1.1 It is the policy of the Health System to approve for reappointment and/or renewal of
privileges only those practitioners who meet the criteria for initial appointment as identified in Section 2, Part 1. The practitioner must also be determined by each applicable FMEC to be a provider of effective care that is consistent with the Health System standards of ongoing quality and the hospital performance improvement program and provide the information enumerated in Section 5.1.1.
All reappointments and renewals of clinical privileges are for a period not to exceed
24 months. The granting of new clinical privileges to existing Medical Staff members will follow the steps described in Section 4 concerning the initial granting of new clinical privileges and Section 5 concerning FPPE. A suitable peer shall substitute for the Department Chair in the evaluation of current competency of the
69
Department Chair, and recommend appropriate action to the System Credentialing/Privileging Committee.
In the event a practitioner finds no need to utilize the facilities or resources of LMHS
for purposes of patient care through either admission, performance of a procedure, consultation, or referral, during a two-year period he may not be eligible for reappointment or continued privileges. Such practitioner may apply as a new applicant at any time subsequent to the expiration of the current appointment or privileges. This provision applies to practitioners who have been granted a leave of absence, moved their practice location, established a relationship with another institution or otherwise find no need to utilize the clinical resources of LMHS. Exceptions to this provision may be made by the Board upon recommendation of the applicable FMEC(s).
As long as a practitioner has adequate clinical activity to maintain privileges at one
LMHS facility (and is recommended for continuation of privileges at his primary LMHS facility) the practitioner may maintain the applicable clinical privileges and staff category (potentially Associate if there is no or minimal clinical activity) at other LMHS facility(ies).
6.2.1 Information, Collection and Verification 6.2.1.1 From practitioner: On or before 4 months prior to the date of expiration of
a Medical Staff appointment or granting of privileges, a representative from the Medical Staff Services Department notifies the practitioner of the date of expiration and supplies him with an application for reappointment for membership and/or privileges. At least sixty (60) calendar days prior to this date, the practitioner must return the following to the Medical Staff Services Department:
6.2.1.1.1 A completed reapplication form, which includes complete
information to update his file on items listed in his original application, any required new, additional, or clarifying information, and any required fees or dues;
6.2.1.1.2 Information concerning continuing training and education
internal and external to the hospital during the preceding period;
6.2.1.1.3 By signing the reapplication form, the practitioner agrees to
the same terms as identified in Section 4.2. 6.2.2 From internal and/or external sources: The Medical Staff Services Department
collects and verifies information regarding each staff practitioner’s professional and collegial activities to include those items listed in Section 2.1.
6.2.3 The following information is also collected and verified:
6.2.3.1 A summary of clinical activity at each LMHS facility for each practitioner due for reappointment.
6.2.3.2 Performance and conduct in each LMHS facility and other healthcare
organizations in which the practitioner has provided substantial clinical care since the last reappointment, including patient care, medical/clinical
70
knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism and system-based practice.
6.2.3.3 Documentation of CME activity; 6.2.3.4 Service on Medical Staff, Department and hospital committees; 6.2.3.5 Timely and accurate completion of medical records; 6.2.3.6 Compliance with all applicable Bylaws, policies, rules, regulations, and
procedures of the System and the Medical Staff(s); 6.2.3.7 Any significant gaps in employment or practice since the previous
appointment or reappointment; and 6.2.3.8 Additional items as identified in the Verification Methods and
Requirements document.
6.2.4 Failure, without good cause, to provide any requested information, at least forty-five (45) calendar days prior to the expiration of appointment will result in a cessation of processing of the application and automatic expiration of appointment when the appointment period is concluded. Once the information is received, the Medical Staff Services Department verifies this additional information and notifies the staff practitioner of any additional information that may be needed to resolve any doubts about performance or material in the credentials file.
6.3 Evaluation of Application for Reappointment of Membership and/or Privileges
6.3.1 The reappointment application will be reviewed and acted upon as described in Sections 4.3.3 through 4.3.8. For the purpose of reappointment, an “adverse recommendation” by the Board as used in Section 4.3 means a recommendation or action to deny reappointment, or to deny or restrict requested clinical privileges or any action that would entitle the applicant to a Fair Hearing under the Medical Staff Bylaws. The terms “applicant” and “appointment” as used in these Sections shall be read respectively, as “staff practitioner” and “reappointment”.
SECTION 7 CLINICAL PRIVILEGES 7.1 Exercise of Privileges
A practitioner providing clinical services at a LMHS facility may exercise only those privileges granted to him by the Board or emergency and disaster privileges as described herein. Privileges may be granted by the Board upon recommendation of the FMEC(s) to practitioners who are not members of the Medical Staff. Such practitioners may include Advanced Registered Nurse Practitioners (ARNPs), Physician Assistants (PAs), practitioners serving short locum tenens positions, telemedicine physicians or others deemed appropriate by the FMEC(s) and Board.
7.2 Requests
When applicable, each application for appointment or reappointment to the Medical Staff must contain a request for the specific clinical privileges desired by the applicant. Specific
71
requests must also be submitted for temporary privileges and for modifications of privileges in the interim between reappointments and/or granting of privileges.
7.3 Basis for Privileges Determination 7.3.1 Requests for clinical privileges will be considered only when accompanied by
evidence of education, training, experience, and demonstrated current competence as specified by the System in its Board approved criteria for clinical privileges.
7.3.2 Privileges for which no criteria have been established: 7.3.2.1 In the event a request for a privilege is submitted for a new technology, a
procedure new to the System, an existing procedure used in a significantly different manner, or involving a cross-specialty privilege for which no criteria have been established, the request will be tabled for a reasonable period of time, usually not to exceed sixty (60) calendar days. During this time, the System Credentialing/Privileging Committee may refer the request for review by a task force appointed to review the request.
Task forces formed for purposes of establishment of evaluation of new
privileges and potential determination of criteria will be appointed by the Chairs of the System Credentialing/Privileging Committee, and will include the System Medical Director of Clinical Effectiveness and the Director of Supply Chain Management. The task force will:
7.3.2.1.1 Review the community, patient and System need for the
privilege and reach agreement with management and the Board that the privilege is approved to be exercised at the hospital;
7.3.2.1.2 Review with appropriate individuals/groups
the efficacy and clinical viability of the requested privilege and confirm that this privilege is approved for use in the setting-specific area of the hospital by appropriate regulatory agencies (FDA, OSHA, etc.);
7.3.2.1.3 Meet with management to ensure that the new privilege is
consistent with the Health System’s mission, values, strategic, operating, capital, information and staffing plans;
7.3.2.1.4 Work with management to ensure that any/all exclusive
contract issues, if applicable are resolved in such a way to allow the new or cross-specialty privileges in question to be provided without violating the existing contract. Upon recommendation from the System Credentialing/Privileging Committee and appropriate clinical services/specialty or subject matter experts (as determined by the System Credentialing/Privileging Committee), the criteria will be recommended to each FMEC and then to the Board. Once objective criteria have been established, the original request will be processed as described herein.
7.3.2.2 For the development of criteria, the Medical Staff Services Department (or
designee) will compile information relevant to the privileges requested which may include, but need not be limited to, position and opinion papers
72
from specialty organization, position and opinion statements from interested individuals or groups and documentation from other hospitals in the region as appropriate.
7.3.2.3 Criteria to be established for the privilege(s) in question include education,
training, board status or certification (if applicable), experience and evidence of current competence. Proctoring requirements, if any, will be addressed including who may serve as proctor and how many proctored cases will be required.
Hospital related issues such as exclusive contracts, equipment, clinical
support staff and management would be referred to the appropriate hospital administrator and/or Department Director.
7.3.2.4 If the privileges requested overlap two (2) or more specialty disciplines, an
ad hoc committee may be appointed by the System Credentialing/Privileging Committee to recommend criteria for the privilege(s) in question. This ad hoc committee will consist of at least one (1) but no more than two (2) members from each involved discipline. The Chair of the ad hoc committee will be a member of the System Credentialing/Privileging Committee who has no vested interest in the issue (see Medical Staff Privilege Dispute Resolution Policy).
7.3.3 Requests for clinical privileges will be consistently evaluated on the basis of prior
and continuing education, training, experience, utilization practice patterns, current ability to perform the privileges requested and demonstrated current competence,
ability, and judgment. Additional factors that may be used in determining privileges are patient care needs and the System’s capability to support the type of privileges being requested and the availability of qualified coverage in the applicant’s absence. The basis for privileges determination to be made in connection with periodic reappointment or a requested change in privileges must include documented clinical performance and results of the staff’s performance improvement program activities.
Privilege determinations will also be based on pertinent information from other
sources, such as peers and/or faculty from other institutions and healthcare settings where the practitioner exercises clinical privileges.
7.3.4 The procedure by which requests for clinical privileges are processed are as outlined in Section 4.
7.3.5 Special Conditions for Dental Privileges
Requests for clinical privileges for dentists are processed in the same manner as all other privilege requests. Privileges for surgical procedures performed by dentists and/or oral and maxillofacial surgeons will require that all dental patients receive a basic medical evaluation (history and physical) by a physician member of the Medical Staff with privileges to perform such an evaluation, which will be recorded in the medical record. Oral and maxillofacial surgeons may be granted the privilege of performing a history and physical on their own patients upon submission of documentation of completion of an accredited postgraduate residency in oral and maxillofacial surgery and demonstrated current competence.
7.3.6 Special Conditions for practitioners not Qualified for Medical Staff Appointment but Practicing Pursuant to Clinical Privileges per System Policy.
73
Requests for privileges, from such practitioners, are processed in the same manner as requests for clinical privileges by providers eligible for Medical Staff membership, with the exception that such practitioners are not eligible for membership on a Medical Staff and do not have the rights and privileges of such membership (all rights and responsibilities are defined in the Allied Health Practitioner (AHP) Privileging Policy and Procedure). Only those categories of practitioners approved by the Board for providing services at the hospital are eligible to apply for privileges. AHP(s) in this category may, subject to any licensure requirements or other limitations, exercise independent judgment only within the areas of their professional competence and participate directly in the medical management of patients under the supervision of a physician who has been accorded privileges to provide such care.
7.4 Special Conditions for Podiatric Privileges Requests for clinical privileges for podiatrists are processed in the same manner as all other privilege requests.
Practitioners granted podiatric privileges may perform and shall record in the medical
record a basic medical evaluation history and physical for the practitioner’s podiatric patients if consistent with the privileges granted to the practitioner, state law governing the practitioner’s practice and federal law.
7.5 Special Conditions for Residents or Fellows in Training
Residents or Fellows in Training in the Health System shall not normally hold membership on the Medical Staff and shall not normally be granted specific clinical privileges. Rather, they shall be permitted to function clinically only in accordance with the written training protocols developed by the Professional Graduate Education Committee in conjunction with the Residency Training Program. The protocols must delineate the roles, responsibilities, and patient care activities of residents and fellows including which types of residents may write patient care orders, under what circumstances why they may do so, and what entries a supervising physician must countersign. The protocol must also describe the mechanisms through which resident directors and supervisors make decisions about a resident’s progressive involvement and independence in delivering patient care and how these decisions will be communicated to appropriate Medical Staff and hospital leaders.
The Post-Graduate Education Program Director or Committee must communicate
periodically with each applicable FMEC and the Board about the performance of its residents, patient safety issues and quality of patient care and must work with the FMEC to assure that all supervising physicians possess clinical privileges commensurate with their supervising activities.
7.6 Special Conditions for the Aging Practitioner
At the age of 70, practitioners shall complete an annual examination that addresses both the physical and mental capacity for the privileges requested. The annual physical and mental exams are to be conducted by an independent Medical examiner acceptable to the System Credentialing/Privileging Committee, documented on the approved form and submitted to the System Credentialing/Privileging Committee by the
74
date requested. The physical exam is a “fitness to work” evaluation and must indicate that the practitioner has no physical or mental problem that may interfere with the safe and effective provision of care permitted under the privileges granted. In addition to the physical exam, a practitioner may be required to undergo proctoring of his clinical performance as part of the assessment of his capacity to perform the requested privileges. Such proctoring may be required in the absence of any previous performance concerns. The scope and duration of the proctoring shall be determined by the FMEC upon recommendation of the Department Chair of the practitioner’s primary facility and System Credentialing/Privileging Committee. The practitioner shall pay the cost of the physical and mental exam.
7.7 Temporary Privileges 7.7.1 Temporary privileges may be granted by the CEO, or designee, acting on behalf of
the Board and based on the recommendation of the President of the Medical Staff or designee to be approved at the next FMEC meeting, provided there is verification of current licensure and current competence. Temporary privileges may be granted only in two (2) circumstances: 1) to fulfill an important patient care, treatment or service need, or 2) when an initial applicant with a complete application that raises no concerns is awaiting review and approval of the FMEC and the Board. Applications pending completion of the initial appointment process must always be reviewed and a recommendation made by the System Credentialing/Privileging Committee prior to the granting of temporary privileges.
7.7.2 Important Patient Care, Treatment or Service Need: Temporary privileges may be
granted on a case-by-case basis when an important patient care, treatment or service need exists that mandates an immediate authorization to practice, for a limited time, not to exceed 30 calendar days (from date privileges are granted). Temporary privileges may be extended for two separate 30-day intervals upon approval of the Board of Directors. For the purposes of granting temporary privileges, an important patient care, treatment or service need is defined as including the following:
7.7.2.1 a circumstance in which one or more individual patients will experience
care that does not adequately meet their clinical needs if the temporary privileges under consideration are not granted, (i.e., a patient scheduled for urgent surgery who would not be able to undergo the surgery in a timely manner);
7.7.2.2 a circumstance in which the institution will be placed at risk of not
adequately meeting the needs of patients who seek care, treatment or service from the institution if the temporary privileges under consideration are not granted (i.e., the institution will not be able to provide adequate emergency room coverage in the providers specialty, or the Board has granted privileges involving new technology to a physician on the staff provided the physician is precepted for a specific number of initial cases and the precepting physician, who is not seeking Medical Staff membership, requires temporary privileges to serve as a preceptor);
7.7.2.3 a circumstance in which a group of patients in the community will be
placed at risk if not receiving patient care that meets their clinical needs if the temporary privileges under consideration are not granted (i.e. a
75
physician who has a large practice in the community for which adequate coverage of hospital care for those patients cannot be arranged).
7.7.3 Clean Application (Expedited) Awaiting Approval: Temporary privileges may be
granted for up to 30 calendar days (from date privileges are issued) approved by the Executive Committee with two 30-day extensions approved by the Board (see the policy and procedure on Expedited Credentialing) when the new applicant for Medical Staff membership and/or privileges is waiting for review and recommendation by the FMEC and approval by the Board.
7.7.4 Special requirements of consultation and reporting may be imposed as part of the
granting of temporary privileges. Except in unusual circumstances, temporary privileges will not be granted unless the practitioner has agreed in writing to abide by the Bylaws, rules, and regulations and policies of the Medical Staff and hospital in all matters relating to his temporary privileges. Whether or not such written agreement is obtained, these Bylaws, rules, regulations and policies control all matters relating to the exercise of clinical privileges.
7.7.5 Termination of temporary privileges: The CEO, acting on behalf of the Board and
after consultation with the President of the Medical Staff, may terminate any or all of the practitioner’s privileges based upon the discovery of any information or the occurrence of any event of a nature, which raises questions about a practitioner’s privileges.
Where the life or well-being of a patient is determined to be endangered, any person
entitled to impose precautionary suspension under the Medical Staff Bylaws may effect the termination. In the event of any such termination, the CEO or his designee then will assign the practitioner’s patients to another practitioner. The wishes of the patient shall be considered when feasible, in choosing a substitute practitioner.
7.7.6 Rights of the practitioner with temporary privileges: A practitioner is not entitled to
the procedural rights afforded in the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) because his request for temporary privileges is refused or because all or any part of his temporary privileges are terminated or suspended unless based on a determination of clinical incompetence or unprofessional conduct.
7.7.7 Emergency Privileges: In the case of a medical emergency, any practitioner is
authorized to do everything possible to save the patient’s life or to save the patient from serious harm, to the degree permitted by the practitioner’s license, regardless of facility affiliation, staff category, or level of privileges. A practitioner exercising emergency privileges is obligated to summon all consultative assistance deemed necessary and to arrange appropriate follow-up.
7.7.8 Disaster Privileges 7.7.8.1 If the System’s Disaster Plan has been activated and the organization is
unable to meet immediate patient needs, the CEO and such other individuals as identified in the System’s Disaster Plan with such authority, may, on a case by case basis consistent with medical licensing and other relevant state statutes, grant disaster privileges to provide patient care to selected Licensing Independent Practitioners (LIP’s), who must at a minimum present a valid governmental-issued photo identification issued
76
by a state or federal agency (e.g. driver’s license or passport) and at least one of the following:
7.7.8.1.1 a current picture hospital ID card that clearly identifies
professional designation; 7.7.8.1.2 a current license to practice; 7.7.8.1.3 primary source verification of the license;
7.7.8.1.4 identification indicating that the practitioner is a member of a
Disaster Medical Assistance Team (DMAT), or Medical Reserve Corps (MRC), Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VHP), or other recognized state or federal organizations or groups;
7.7.8.1.5 identification indicating that the practitioner has been
granted authority to render patient care, treatment, and services in disaster circumstances (such authority having been granted by a federal, state, or municipal entity);
7.7.8.1.6 identification by a current hospital or Medical Staff
member(s) who possesses personal knowledge regarding the volunteer’s ability to act as a LIP during a disaster.
7.7.8.2 The Medical Staff oversees the professional performance of
volunteer practitioners who have been granted disaster privileges by direct observation, mentoring or clinical record review.
The organization makes a decision (based on information obtained regarding the professional practice of the volunteer) within 72 hours related to the continuation of the disaster privileges initially granted.
7.7.8.3 Primary source verification of licensure begins as soon as the
immediate situation is under control, and is completed within 72 hours from the time the volunteer practitioner presents to the organization.
7.7.8.4 Once the immediate situation has passed and such determination
has been made consistent with the institution’s Disaster Plan, the practitioner’s disaster privileges will terminate immediately.
7.7.8.5 Any individual identified in the institution’s Disaster Plan with the
authority to grant disaster privileges shall also have the authority to terminate disaster privileges. Such authority may be exercised at the sole discretion of the hospital and will not give rise to a right to a fair hearing or an appeal.
SECTION 8 PRECEPTORSHIP
8.1 A practitioner who has not provided acute inpatient care within the past 24 months who requests clinical privileges at the hospital must arrange for a preceptorship either with a
77
current member in good standing of the Medical Staff who practices in the same specialty or with an academic training program or other equivalently competent physician practicing outside of the hospital. The practitioner must assume responsibility for any financial costs required to fulfill the requirements of Sections 8.1 and 8.2.
8.2 A description of the preceptorship program, including details of monitoring and consultation
must be written and submitted for approval to the applicable Department Chair, System Credentialing/Privileging Committee and FMEC. At a minimum, the preceptorship program description must include the following: 8.2.1 The scope and intensity of required preceptorship activities; 8.2.2 The requirement for submission of a written report from the preceptor prior to
termination of the preceptorship period assessing, at a minimum, the applicant’s demonstrated clinical competence related to the privileges requested, ability to get along with others, the quality and timeliness of medical records documentation, ability to perform the privileges requested, and professional ethics and conduct.
SECTION 9 REAPPLICATION AFTER MODIFCATIONS OF MEMBERSHIP STATUS OF PRIVILEGES AND EXHAUSTION OF REMEDIES
9.1 Reapplication After Adverse Credentials Decision
9.1.1 Except as otherwise determined by the Board, a practitioner who has received a
final adverse decision or who has resigned or withdrawn an application for appointment, reappointment or clinical privileges while under investigation or to avoid an investigation is not eligible to reapply to the Medical Staff for a period of five (5) years from the date of the notice of the final adverse decision or the effective date of the resignation or application withdrawal. Any such application is processed in accordance with the procedures then in force. As part of the reapplication, the practitioner must submit such additional information as the Medical Staff and/or Board requires, demonstrating that the basis of the earlier adverse action no longer exists. If such information is not provided, the reapplication will be considered incomplete and voluntarily withdrawn and will not be processed any further.
9.2 Request for Modification of Appointment Status or Privileges
9.2.1 A staff member, either in connection with reappointment or at any other time, may
request modification of staff category, Department assignment, or clinical privileges by submitting a written request to the Medical Staff Services Department. A modification request must be on the prescribed form and must contain all pertinent information supportive of the request. All requests for additional clinical privileges must be accompanied by information demonstrating additional education, training, and current clinical competence in the specific privileges requested. A modification application is processed in the same manner as a reappointment, which is outlined in Section 6 of this manual. A practitioner who determines that he no longer exercises, or wishes to restrict or limit the exercise of, particular privileges that he has been granted shall send written notice, through the Medical Staff Services Department to the System Credentialing/Privileging Committee, and FMEC. A copy of this notice shall be included in the practitioner’s credentials file.
9.3 Resignation of Staff Appointment or Privileges
78
9.3.1 A practitioner who wishes to resign his staff appointment and/or clinical privileges must provide written notice to the appropriate Department Chair or President of the Medical Staff. The resignation shall specify the reason for the resignation and the effective date. A practitioner who resigns his staff appointment and/or clinical privileges is obligated to accurately complete all portions of all medical records for which he is responsible prior to the effective date of resignation. Failure to do so shall result in an entry in the practitioner’s credentials file acknowledging the resignation and indicating that it became effective under unfavorable circumstances.
9.4 Exhaustion of Administrative Remedies
9.4.1 Every practitioner agrees that he will exhaust all the administrative remedies
afforded in the various Sections of Part I: Governance, Part II: Investigations, Corrective Action, Hearing and Appeal Plan and Part III: Credentialing Procedures before initiating legal action against the System or its agents.
9.5 Reporting Requirements
9.5.1 The CMO or his designee shall be responsible for assuring that the hospital satisfies
its obligations under the Health Care Quality Improvement Act of 1986 and its successor statutes. Actions that must be reported include any negative professional review action against a physician or dentist related to clinical incompetence or misconduct that leads to a denial of appointment and/or reappointment, reduction in clinical privileges for greater that thirty (30) calendar days; resignation, surrender of privileges, or acceptance of privilege reduction either during an investigation or to avoid an investigation.
SECTION 10 LEAVE OF ABSENCE
10.1 Leave Request
10.1.1 A leave of absence is a matter of courtesy, not of right. In the event that it is
determined that a practitioner has not demonstrated good cause for a leave, or where a request for extension is not granted, the determination shall be final, with no recourse to a hearing and appeal. A leave of absence must be requested for any absence from the Medical Staff and/or patient care responsibilities longer than thirty (30) days if such absence is related to the practitioner’s physical or mental health or to the ability to care for patients safely and competently. A practitioner who wishes to obtain a voluntary leave of absence must provide written notice to the President of the Medical Staff stating the reasons for the leave and approximate period of the leave, which may not exceed one 1-year except for military service or express permission by the Board. Requests for leave must be forwarded, with a recommendation from the FMEC, and affirmed by the Board. While on leave of absence, the practitioner may not exercise clinical privileges or prerogatives and has no obligation to fulfill Medical Staff responsibilities.
10.2 Termination of Leave
10.2.1 At least thirty (30) calendar days prior to the termination of the leave, or at any
earlier time, the practitioner may request reinstatement by sending a written notice to the President of the Medical Staff. The practitioner must submit a written summary of relevant activities during the leave if the FMEC or Board so requests.
79
A practitioner returning from a leave of absence for health reasons must provide a report from his physician that answers any questions that the FMEC or Board may have as part of considering the request for reinstatement. The FMEC makes a recommendation to the Board concerning reinstatement, and the applicable procedures concerning the granting of privileges are followed. If the practitioner’s current grant of membership and for privileges is due to expire during the leave of absence, the practitioner must apply for reappointment or his appointment and/or clinical privileges shall lapse at the end of the appointment period.
10.3 Failure to Request Reinstatement 10.3.1 Failure, without good cause, to request reinstatement shall be deemed a voluntary
resignation from the Medical Staff and shall result in automatic termination of membership, privileges, and prerogatives. A practitioner whose membership is automatically terminated shall not be entitled to the procedural rights provided in the Medical Staff Bylaws. A request for Medical Staff membership subsequently received from a member so terminated shall be submitted and processed in the manner specified for applications for initial appointments.
SECTION 11 PRACTITIONERS PROVIDING CONTRACTED SERVICES 11.1.1 When the System or hospital contracts for patient care services with LIPs who
provide official readings of images, tracings or specimens through a telemedicine mechanism, and these practitioner’s services are under the control of a Joint Commission accredited organization, the hospital will:
11.1.1.1 specify in a contract that the entity providing these services by contract
(the contracting entity) will ensure that all services provided under this contract by individuals who are LIPs will be within the scope of those practitioner’s privileges at the contracting entity; or
11.1.1.2 verify that all individuals who are LIPs and providing services under the
contract have privileges that include the services provided under the contract.
11.2 When the System/hospital contracts for care services with LIPs, who provide official
readings of images, tracings or specimens through a telemedicine mechanism, and these practitioner’s services are not under the control of a Joint Commission accredited organization, all LIPs who will be providing services under this contract will be permitted to do so only after being granted privileges at the hospital through the mechanisms established in this manual.
11.3 Contract Services/Department or Service Closure
11.3.1 The membership and privileges on the Medical Staff of any practitioner who has a
contractual relationship with the System or with an entity that has a contractual relationship with the System to provide professional services to patients shall be subject to those provisions contained in said contract with regard to the termination of Medical Staff membership and privileges upon the expiration, lapse, cancellation or termination of the contract. If the contract so provides, the affected practitioner shall have no right to a hearing regarding termination of Medical Staff membership or privileges.

80
11.3.2 In the event a hospital Department is closed, discontinued or provided through an exclusive contract, such establishment shall not adversely impact the ability of any physician to continue to maintain clinical membership and exercise privileges in existence at the time of such closure, discontinuance or exclusive contract. Initial applications for Medical Staff membership and privileges will not be extended, provided, accepted, processed or approved to or from physicians unless they are joining groups who are actively contracted for exclusively contracted services.
11.3.3 In the event the Board determines that a patient care service shall be closed,
discontinued, or provided through an exclusive contract, such action shall require approval by the affected FMEC.
Both parties agree that any Department or service closure shall occur solely so that
the health and wellbeing of the patients and the best interests of the hospital under these Bylaws may be served at all times. Notwithstanding any other provision in the Bylaws, if the Board and the affected FMEC are unable to agree upon the closure of a Department or service, the matter shall undergo the conflict resolution process set forth in Part I, Section 9 of these Bylaws.
If the parties are still in disagreement regarding the closure of a Department or
service upon completion of the conflict resolution process, the parties shall engage in mediation in accordance with the procedures set forth by the American Health Lawyers Association’s Alternative Dispute Resolution Service or another independent mediation service mutually agreeable to the parties. In the event the Board and FMEC are at impasse at mediation and conflict remains, the Board and the FMEC retain the right to seek a resolution through litigation. Further, the Board shall not close a Department or service for a period of three months following impasse at mediation.
11.4 Qualifications
11.4.1 A practitioner who is or will be providing specified professional services pursuant to
a contract or a letter of agreement with the Health System must meet the same qualifications, must be processed in the same manner, and must fulfill all the obligations of his appointment category as any other applicant or staff practitioner.
11.5 The terms of the Medical Staff Bylaws will govern disciplinary action taken by or
recommended by the FMEC.
11.6 Effect of Contract or Employment Expiration or Termination
11.6.1 The effect of expiration or other termination of a contract upon a practitioner’s staff appointment and clinical privileges will be governed solely by the terms of the practitioner’s contract with the System. If the contract or the employment agreement is silent on the matter, then contract expiration or other termination alone will not affect the practitioner’s staff appointment status or clinical privileges.
SECTION 12 MEDICAL ADMINISTRATIVE OFFICERS
12.1 A Medical Administrative Officer is a practitioner engaged full or part- time by the hospital in an administratively responsible capacity, whose activities may also include clinical responsibilities such as direct patient care, teaching, or supervision of the patient care activities of other practitioners under the officer’s direction.
81
12.2 Each Medical Administrative Officer must achieve and maintain Medical Staff appointment
and clinical privileges appropriate to his clinical responsibilities and discharge staff obligations appropriate to his staff category in the same manner applicable to all other staff members.
12.3 Effect of removal from office or adverse change in appointment status or clinical privileges:
12.3.1 Where a contract exists between the officer and the Health System, its terms
govern the effect of removal from the Medical Administrative Office on the officer’s staff appointment and privileges and the effect an adverse change in the officer’s staff appointment or clinical privileges has on his remaining in office.
12.3.2 In the absence of a contract or where the contract is silent on the matter, removal
from office has no effect on appointment status or clinical privileges. The effect of an adverse change in appointment status or clinical privileges on continuance in office will be determined by the Board.
12.3.3 A Medical Administrative Officer has the same procedural rights as all other staff
members in the event of an adverse change in appointment status or clinical privileges unless the change is, by contract a consequence of removal from office.
82
83
Gulf Coast Medical Center
Medical Staff
Bylaws
Adopted: May 28, 2009 Revision approved by BOD June 24, 2010
Revision approved by BOD August 26, 2010 Revisions approved by BOD June 16, 2011
Revision approved by BOD December 6, 2012
1
TABLE OF CONTENTS PART 1: GOVERNANCE 6 SECTION 1 MEDICAL STAFF PURPOSE & AUTHORITY 6 1.1 Purposes 6 1.2 Authority 6 1.3 Medical Staff (Term) 6 SECTION 2 MEDICAL STAFF MEMBERSHIP 7 2.1 Nature of Medical Staff Membership 7 2.2 Qualifications for Membership 7 2.3 Nondiscrimination 7 2.3.1 No Automatic Entitlement 7 2.4 Conditions and Duration of Appointment 7 2.5 Medical Staff Membership and Clinical Privileges 8 2.6 Medical Staff Members’ Responsibilities 8 2.7 Basic Responsibilities of Applicants and Appointees 8 2.8 Member Rights 11 2.9 Medical Staff Dues and Assessments 11 2.10 Conflict of Interest 12 SECTION 3 CONFIDENTIALITY, IMMUNITY AND RELEASES 12
3.1 Confidentiality 12 3.2 Immunity 13 3.3 Releases 14 SECTION 4 CATEGORIES OF THE MEDICAL STAFF 14 4.1 Active Category 14 4.2 Associate Category 15 4.3 Honorary Category 16 SECTION 5 OFFICERS OF THE MEDICAL STAFF 16 5.1 Officers of Medical Staff and FMEC at-Large Members 16 5.2 Qualifications of Officers and FMEC at-Large Members 16 5.3 Election of Officers and FMEC at-Large Members 16 5.4 Terms of Office 17 5.5 Vacancies of Office 17 5.6 Duties of Officers and FMEC at-Large Members 17 5.7 Removal and Resignation of Officer or FMEC at-Large Members 19 SECTION 6 MEDICAL STAFF ORGANIZATION 20 6.1 Departments 20 6.2 Qualifications, Selection, Term, Removal and Responsibility of Department Chair 21 6.3 Assignment to Department 23 SECTION 7 MEDICAL STAFF GOVERNANCE COMMITTEES 23
2
7.1 Designation of the LMHS MS Physician Leadership Council (PLC) 23 7.2 Composition of the LMHS PLC 23 7.3 Staff Functions 25
7.4 Facility Medical Executive Committee (FMEC) (Composition, Selection and Tenure) 25 7.5 Duties and Responsibilities of the FMEC’s 25 7.6 System Medical Staff Committees 27 7.6.1 Purpose 27 7.6.2 Organization to Perform Functions 27 7.6.2.1 System Credentialing/Privileging Committee 27 7.6.2.2 System Medical Staff Quality Committee 27 7.6.2.3 System Practitioner Resource Committee 27 7.6.2.4 System Bylaws Committee 28 7.6.2.5 System Emergency Services Committee 29 7.6.3 Composition & Meetings of System MS Committees 29 7.7 Facility Medical Staff Committees 30 7.7.1 Purpose 30 7.7.2 Standing Facility Medical Staff Committees 30 SECTION 8 MEDICAL STAFF MEETINGS 31 8.1 General Medical Staff Meetings 31 8.2 Departments, Sections and Committee Meetings 31 8.3 Special Meetings of Departments, Sections and Committees 31 8.4 Quorum 31 8.5 Attendance Requirements 32 8.6 Participation by Administration 32 8.7 Robert’s Rules of Order 32 8.8 Notice of Meetings 33 8.9 Action of PLC, FMEC, General Medical Staff, Department, Section or Committee 33 8.10 Rights of Ex Officio Members 33 8.11 Minutes 33 SECTION 9 DECISION MAKING METHODS AND CONFLICT RESOLUTION 33 SECTION 10 REVIEW, REVISION ADOPTION AND AMENDMENT 34 10.1 Medical Staff Responsibility 34 10.2 Methods of Amendment and Adoption to these Bylaws 35 10.3 Methods of Amendment and Adoption to any Medical Staff Rules, Regulations and Policies 35 Appendix A PRINCIPLES OF MEDICAL ETHICS 37 PART II: INVESTIGATIONS, CORRECTIVE ACTION, HEARING AND APPEAL PLAN 39 SECTION 1 ROUTINE CORRECTIVE ACTION & INVESTIGATIONS 39 1.1 Progressive Intervention 39 1.2 Basis for Routine Corrective Action 39 1.3 Requests and Notices 40 1.4 Investigations 40 1.5 FMEC Action 41 1.6 Notice of FMEC Action 42 1.7 Board of Directions Action 42
3
SECTION 2 EMERGENCY CORRECTIVE ACTION/PRECAUTIONARY SUSPENSION OF CLINICAL PRIVILEGES 42 2.1 Basis for Emergency Corrective Action/Precautionary Suspension 42 2.2 Notice of Emergency Corrective Action/Precautionary Suspension 42 2.3 FMEC Procedure 43 2.4 Provision of Patient Care 43 2.5 Recission of Emergency Corrective Action/Precautionary Suspension 43 SECTION 3 AUTOMATIC SUSPENSION AND TERMINATION 43 3.1 Basis for Automatic Suspension and Termination 43 3.1.1 Loss of License 43 3.1.2 Residence or Office Outside Lee County 43 3.1.3 Lack of Active Practice 44 3.1.4 Criminal Conviction 44 3.1.5 Loss or Restriction of DEA Certificate 44 3.1.6 Exclusion From Federal or State Health Care Programs 44 3.1.7 Failure to Pay Fees and Assessments 44 3.1.8 Failure to Provide Requested Information 44 3.1.9 Failure to Request Reappointment or Provide Requested Information Related to Reappointment 45 3.1.10 Failure to Request Reinstatement Following Leave of Absence 45 3.1.11 Failure to Complete Medical Records 45 3.1.12 Failure to Comply with Special Meeting Attendance Requirements 45 3.2 Right to Limited Hearing for Automatic/Voluntary Suspension and Termination 45 SECTION 4 HEARING AND APPEAL PROCEDURES 46 4.1 Grounds for Hearing 46 4.2 Notice of Recommendation 46 4.3 Request for Hearing 47 4.4 Preliminary Interview 47 SECTION 5 FAIR HEARING PROCEDURE 47 5.1 System Representative, Hearing Panel and Hearing Officer 47 5.1.1 System Representative 48 5.1.2 Hearing Panel 48 5.1.3 Hearing Officer – Qualifications & Authority 48 5.2 Challenge to Hearing Panel Members or Hearing Officer 50 SECTION 6 HEARING PROCEDURES 50 6.1 Provision of Relevant Information 50 6.2 Pre-Hearing Conference 51 6.3 Failure to Appear 51 6.4 Record of Hearing 51 6.5 Rights of Both Sides 52 6.6 Admissibility of Evidence 52 6.7 Burden of Presenting Evidence and Proof 52 SECTION 7 HEARING CONCLUSION, DELIBERATIONS AND RECOMMENDATIONS 52 7.1 Deliberations and Recommendation of the Hearing Panel/Hearing Officer 52 7.2 Disposition of Hearing Panel Report 53
4
SECTION 8 APPEAL PROCEDURE 53 8.1 Request & Time for Appeal 53 8.2 Grounds for Appeal 54 8.3 Time, Place and Notice 54 8.4 Nature of Appellate Review 54 8.4.1 Review Panel 55 8.4.2 Position Papers 55 8.4.3 Oral Argument 55 8.4.4 Recommendation 55 SECTION 9 FINAL DECISION OF THE BOARD 55 SECTION 10 RIGHT TO ONE HEARING AND ONE APPEAL ONLY 55 PART III: CREDENTIALING PROCEDURES 56 SECTION 1 SYSTEM CREDENTIALING/PRIVILEGING COMMITTEE 56 1.1 Organizational Structure 56 1.2 Transition Issues 56 1.3 Purpose of the System Credentialing/Privileging Committee 56 1.4 Composition of the System Credentialing/Privileging Committee 57 1.5 Duties and Responsibilities of the System Credentialing/Privileging Committee 57 SECTION 2 QUALIFICATIONS FOR MEMBERSHIP AND PRIVILEGES 58 2.1 Qualifications for MS appointment, reappointment or clinical privileges 58 2.1.15 Exceptions 58 SECTION 3 PRE-APPLICATION PROCESS 60 SECTION 4 INITIAL APPOINTMENT PROCESS 61 4.1 Completion of Application 61 4.2 Applicant’s Attestation, Authorization and Acknowledgement 63 4.3 Application Evaluation 64 4.3.1 Expedited Credentialing 64 4.3.2 Applicant Interview 64 4.3.3 Department Chair Action 64 4.3.4 MS System Credentialing/Privileging Committee Action 65 4.3.5 FMEC Action 66 4.3.6 Applicants Applying to Multiple Facilities 66 4.3.7 Board Action 66 4.3.8 Notice of Final Decision 67 4.3.9 Periods for Processing 67 SECTION 5 FOCUSED PROFESSIONAL PRACTICE EVALUATION (FPPE) 67 SECTION 6 CRITERIA FOR REAPPOINTMENT 68 6.1 Criteria for Reappointment 68 6.3 Evaluation of Application for Reappointment of Membership and/or Privileges 70
5
SECTION 7 CLINICAL PRIVILEGES 70 7.1 Exercise of Privileges 70 7.2 Requests 70 7.3 Basis for Privileges Determination 70 7.4 Special Conditions for Podiatric Privileges 72 7.5 Special Conditions for Residents or Fellows in Training 73 7.6 Special Conditions for the Aging Practitioner 73 7.7 Temporary Privileges 73 7.7.8 Disaster Privileges 75 SECTION 8 PRECEPTORSHIP 76 SECTION 9 REAPPLICATION AFTER MODIFICATIONS OF MEMBERSHIP STATUS OF PRIVILEGES AND EXHAUSTION OF REMEDIES 77 9.1 Reapplication After Adverse Credentials Decision 77 9.2 Request for Modification of Appointment Status or Privileges 77 9.3 Resignation of Staff Appointment or Privileges 77 9.4 Exhaustion of Administrative Remedies 77 9.5 Reporting Requirements 78 SECTION 10 LEAVE OF ABSENCE 78 10.1 Leave Request 78 10.2 Termination of Leave 78 10.3 Failure to Request Reinstatement 78 SECTION 11 PRACTITIONERS PROVIDING CONTRACTED SERVICES 79 11.3 Contract Services/Department or Service Closure 79 11.4 Qualifications 80 11.5 Terms 80 11.6 Effect of Contract or Employment Expiration or Termination 80 SECTION 12 MEDICAL ADMINISTRATIVE OFFICERS 80
6
PART 1: GOVERNANCE
SECTION 1 MEDICAL STAFF PURPOSES & AUTHORITY 1.1 Purposes
The purposes of the Medical Staffs of Lee Memorial Health System are to:
1.1.1 Serve as the formal organizational structure of those practitioners granted the privilege of practicing in the hospitals and other facilities of the System.
1.1.2 Serve as the primary means for accountability to the Board for the professional
performance, the quality of medical care provided to patients, and ethical conduct of its members. The Board shall have the ultimate responsibility for the quality of medical care provided to patients and the ultimate authority to approve the granting of privileges, to make appointments and reappointments to membership on the Medical Staffs, and to approve the adoption of Medical Staff Bylaws and Rules and Regulations. Such authority will be exercised based on the standard set forth in Section 1.2.
1.1.3 Provide a means through which members of the Medical Staffs may address with
the Board those aspects of policy that involve professional practice or may affect the care of patients.
1.2 Authority
The Medical Staffs of Lee Memorial Health System are authorized by the Lee Memorial Health System Board of Directors (“the Board”) to exercise such power as is necessary to discharge its responsibilities under these Bylaws consistent with the Bylaws of Lee Memorial Health System. Lee Memorial Health System (“the System” or “the Health System”) includes acute care facilities known as Cape Coral Hospital, Gulf Coast Medical Center, HealthPark Medical Center, Lee Memorial Hospital, and The Children’s Hospital (individually known as “the hospital” and collectively known as “the hospitals”). The Board recognizes that a well-organized, self-governing Medical Staff that provides oversight of care, treatment, and services provided by practitioners with privileges is in the best interest of patients. When acting with respect to matters of the Medical Staff, the Board shall at all times comply with the Medical Staff Bylaws, the Rules and Regulations of the Medical Staff, and applicable law.
1.3 Medical Staff The term “Medical Staff” as used herein shall mean, on a collective basis, those
practitioners who are authorized by the Board to exercise privileges at one or more of the System’s hospitals, and, on a component basis, those practitioners who are authorized by the Board to exercise privileges at a particular system hospital. The latter may be referred to herein as the “Medical Staff of a facility.” The term “he”, “him”, or “his” means of a male or female gender.
7
SECTION 2 MEDICAL STAFF MEMBERSHIP 2.1 Nature of Medical Staff Membership
Membership on the Medical Staff is a privilege that shall be extended only to professionally competent physicians (M.D. or D.O.), dentists, podiatrists and/or psychologists who continuously meet the qualifications, standards, and requirements set forth in these Bylaws and associated policies of the Medical Staff and the hospitals. Medical Staff membership is a privilege and not a right of any practitioner or other person. Medical Staff membership and the exercise of privileges in connection therewith shall be extended only to practitioners who continuously meet the requirements of these Bylaws. The Board makes decisions regarding Medical Staff matters, based on Medical Staff recommendations, in accordance with these Bylaws. Membership on the Medical Staff shall confer on the Medical Staff member only such rights as set forth in the Bylaws. No person shall admit patients to a System hospital unless he is appointed to the Medical Staff of such hospital. For purposes of these Bylaws, “membership in” is used synonymously with “appointment to” the Medical Staff. Medical Staff members granted membership and privileges at a hospital, which has services and facilities that are provider based to a main provider and are authorized to exercise those privileges at the main provider.
2.2 Qualifications for Membership
2.2.1 The qualifications for Medical Staff membership are delineated in Part III of these Bylaws (Credentials Procedures).
2.3 Nondiscrimination
2.3.1 No Automatic Entitlement
No person shall be automatically entitled to Medical Staff membership or to the exercise of clinical privileges merely because he is licensed to practice, is a member of any professional organization, is certified by any board, or had held (but not currently) Medical Staff membership or clinical privileges at a System hospital or at any other health care facility. The burden shall be on the applicant to establish his qualifications. Acceptance of Medical Staff membership or exercise of clinical privileges shall constitute an agreement to strictly abide by these Bylaws, the applicable Medical Staff Policies, the Rules and Regulations, and the Principles of Medical Ethics set forth in Appendix A hereof and all other appropriate ethical standards governing the practitioner’s practice. No person shall be initially appointed to the Medical Staff or granted clinical privileges if the hospitals are unable to provide adequate facilities and supportive services for the applicant and his patients. Medical Staff membership shall not be denied based on sex, race, creed, color, national origin, religion, marital status, age, disability, or economic credentialing, at initial appointment or reappointment.
2.4 Conditions and Duration of Appointment
2.4.1 The Board shall act on appointment and reappointment only after the Medical Staff has had an opportunity to submit a recommendation from the Facility Medical Executive Committee (FMEC). Appointment and reappointment to the Medical Staff shall be for no more than twenty-four (24) calendar months.
8
2.5 Medical Staff Membership and Clinical Privileges
2.5.1 Requests for Medical Staff membership and/or clinical privileges will be processed only when the potential applicant meets the current minimum qualifying criteria recommended by the System Credentialing/Privileging Committee and FMEC and approved by the Board. Membership and/or privileges will be granted and administered as delineated in Part III (Credentials Procedures) of these Bylaws, including but not limited to, Part III, Sections 3 and 11.3 regarding Contracted practitioners.
2.6 Medical Staff Members’ Responsibilities
2.6.1 Duties of Appointees Appointment to the Medical Staff shall require that each practitioner assume such reasonable duties and responsibilities, as the Medical Staff shall require.
2.7 Basic Responsibilities of Applicants and Appointees The following basic responsibilities and requirements shall be applicable to every applicant
and appointee for Medical Staff appointment or reappointment as a condition of consideration of such application and as a condition of continued Medical Staff appointment if granted:
2.7.1 an obligation to provide for appropriate and timely care and supervision to all
patients in the hospital for whom the individual has responsibility (Standard of Care);
2.7.2 an agreement to abide by all Bylaws, Rules and Regulations and Policies of the Medical Staff and the Hospital, as shall be in force during the time the individual is appointed to the Medical Staff (Conformance to Rules);
2.7.2.1 provide a current cell phone number and email address to be used for
emergency or disaster purposes in accordance with Medical Staff Services Dept. policy.
2.7.3 an agreement to accept committee assignments and such other reasonable duties
and responsibilities as shall be assigned (Committee Assignments);
2.7.4 to not participate in illegal fee splitting or other illegal inducements relating to patient referral;
2.7.5 to promptly notify Medical Staff Services (Notification Requirements);
2.7.5.1 if his professional license in any state is suspended or revoked; 2.7.5.2 of the imposition of any conditions by any state licensing authority on his
continued ability to practice his profession, including probation or limitations on the scope of practice;
2.7.5.3 of the loss or restriction of Medical Staff membership or privileges at any
other health care facility;
2.7.5.4 if his Drug Enforcement Agency (DEA) license number is suspended, revoked or voluntarily relinquished;
9
2.7.5.5 of any change in eligibility for participation in Federal Health Care
Programs including any sanctions imposed or recommended by the Federal Department of Health and Human Services, Florida State Agency for Health Care Administration and/or the receipt of any citation and/or quality denial letter concerning alleged quality problems in patient care;
2.7.5.6 if the practitioner enters, participates in, or against medical advice, leaves
or refuses any program of treatment prescribed or required by the Florida Physicians’ Recovery Network;
2.7.5.7 if the practitioner is admitted for, seeks, or is undergoing treatment for
substance or alcohol abuse or a behavioral health problem. “Substance abuse” shall include but not limited to, use or ingestion of illegal drugs, or use or ingestion of prescription medications not prescribed in the ordinary course of treatment of injury or disease. “Behavioral health problem” shall mean any condition or disease of a psychiatric or psychological nature which, in the opinion of a qualified psychiatrist, adversely affects the practitioner’s ability to care for patients or practice his profession in accordance with the applicable prevailing standard of care; or
2.7.5.8 the conviction of, or pleading of nolo contendere to, a crime constituting a
felony in any jurisdiction. 2.7.6 to abide by generally recognized ethical principles applicable to the applicant’s or
appointee’s profession and by the code of ethics set forth in Appendix A (Ethics);
2.7.7 to respect the confidentiality of all information obtained in connection with his responsibility as a Medical Staff member and comply with the requirements of the Health Insurance Portability and Accountability Act (HIPAA) (Confidentiality);
2.7.8 to provide medical consultation in a timely fashion in accordance with all
applicable Rules & Regulations and Medical Staff Policies (Consultation);
2.7.9 to participate in the monitoring and evaluation activities of Clinical Sections and cooperate with other members of the Medical Staff and the System, in programs designed to improve the quality of care to reduce or eliminate waste in the use of scarce System resources and to reduce the risk of injury to patients and others in the provision of care (Quality Review Participation);
2.7.10 to complete in a timely and legible manner the medical records and other required
records for all patients as required by these Bylaws, applicable Rules and Regulations, and other applicable policies of the hospital (Medical Records);
2.7.11 to pay promptly any applicable Medical Staff assessments and dues (Dues); 2.7.12 to participate in continuing education programs for the benefit of the applicant or
appointee and for the benefit of other professionals and System hospital personnel (CME);
10
2.7.13 to authorize the release of all information necessary for an evaluation of the individual’s qualifications for initial or continued appointment, reappointment, and/or clinical privileges (Release of Information);
2.7.14 to submit to an evaluation of his physical and/or mental health status by a
physician or physicians acceptable to the FMEC or Board, whenever the FMEC or Board has reason to question the physical and/or mental health status of the practitioner, as a prerequisite to further consideration of his application for appointment or reappointment, the exercise of previously granted privileges or maintenance of his Medical Staff appointment (Physical/Mental Exam);
2.7.15 to recognize the obligations established to fulfill the hospital’s responsibilities
under the Emergency Medical Treatment and Women in Labor Act (EMTALA), the Access to Emergency Services and Care Act and/or other applicable regulations, requirements or standards and to share in the responsibility for providing physician coverage on an emergency basis in the Emergency Department, in accordance with the provisions of the Medical Staff Bylaws and all applicable facility-specific Rules & Regulations and Medical Staff Policies (On Call Coverage);
2.7.16 to provide his professional services to hospitalized or emergency room patients
covered by Medicaid and similar programs of indigent care, or such patients without personal physicians or insurance coverage, in accordance with Medical Staff Rules & Regulations adopted by the FMEC delineating the responsibility to provide services to those patients (Services to Indigent Patient);
2.7.17 provide proof of financial responsibility to pay claims or costs associated with the
rendering of, or failure to render, medical care or services in compliance with Florida law governing the practitioner’s license to practice in the State of Florida. Proof of financial responsibility shall be provided at the time of initial appointment and on reappointment, at the time the practitioner changes the method of meeting his financial responsibility and at any other time on the request of Medical Staff Services (Financial Responsibility);
2.7.18 to behave in a professional and civil manner and conduct himself in a manner
conducive to excellent patient care and to work cooperatively with Medical Staff appointees, and with other health care professionals, and Hospital personnel, so as not to adversely affect patient care. This requirement is not in any way intended to interfere with a practitioner’s right: (1) to express opinions freely and to support positions whether or not they are in dispute with those of other Medical Staff members; (2) to engage in honest differences of opinion with respect to diagnosis and treatment; or (3) to engage in a good faith criticism of others. The following types of behavior, however, which constitute some examples of an inability to interact on a professional basis with others or to behave in a professional and civil manner, are deemed unacceptable for a member of the Medical Staff:
2.7.18.1 conduct that reasonably could be characterized as sexual and/or racial
harassment;
2.7.18.2 threats of physical assault or actual physical assault, harassment, or the placing of others in fear by engaging in threatening behavior;
11
2.7.18.3 the unnecessary, unwarranted and unjustifiable knowing use of loud, profane or abusive language directed toward members of the Medical Staff, patient and others; or
2.7.18.4 written or oral statements that constitute the intentional expression of falsehoods, or constitute deliberately disparaging statements made with reckless disregard for their truth or for the reputation and feelings of others;
2.7.18.5 doing anything of a similar nature that the practitioner has been warned
not to do by the President of the Medical Staff or FMEC Committee (Professional and Civil Behavior);
2.7.19 duty to give notice if the practitioner is not actively engaged in the practice of his
profession in Lee County (Lack of Active Practice);
2.7.20 duty to give notice if practitioner does not maintain a full-time residence and office in Lee County, unless the residence and office requirements have been waived in accordance with these Bylaws (Residence or Office in Lee County).
2.8 Member Rights
The following basic rights shall apply to Medical Staff practitioners: 2.8.1 Each Medical Staff member, in the active category, has the right to a meeting with
the FMEC and/or the Physician Leadership Council (PLC) on matters relevant to the responsibilities of the FMEC and/or the PLC, provided that the practitioner has attempted to resolve a matter of concern after working with his Department Chair or other appropriate hospital and/or Health System Medical Staff leader(s). Upon written notice to the President of the Medical Staff, two (2) weeks in advance of a regular meeting, the active Medical Staff member may meet with the FMEC and/or the PLC to discuss the issue.
2.8.2 Each Medical Staff member, in the active category, has the right to initiate a recall
election of a Medical Staff officer by following the procedure outlined in Section 5.7 of these Bylaws regarding removal and resignation from office.
2.8.3 Each Medical Staff member, in the active category, may request a special meeting
of the Medical Staff, upon presentation of a petition, stating the purpose of the meeting and signed by ten (10) members of the Active Medical Staff. The FMEC shall schedule a special meeting for the specific purposes addressed by the petitioners in accordance with Section ten (10) of these Bylaws. No business other than that detailed in the petition may be transacted.
2.8.4 An applicant or an individual holding a Medical Staff appointment shall be entitled to
request a hearing/appeal pursuant to the conditions and procedures described in Part II of these Bylaws (Investigations, Corrective Action, Hearing and Appeal Plan).
2.8.5 All other rights as specified by these Bylaws.
2.9 Medical Staff Dues and Assessments
2.9.1 Annual Medical Staff dues, if any, shall be determined by the FMEC. Failure of a Medical Staff member to pay dues shall be considered a voluntary resignation from
12
the Medical Staff. The FMEC may pass policies from time to time that exempt certain categories of membership or members holding specified leadership positions from payment of dues. The FMEC shall authorize the use of Medical Staff dues.
2.9.2 Medical Staff System-wide assessments, such as a library assessment, shall be
determined by the PLC, on behalf of the FMECs. Failure of a Medical Staff member to pay any assessment(s) shall be considered a voluntary resignation from the Medical Staff. The PLC, on behalf of the FMECs, may pass policies from time to time that exempt certain categories of membership or members holding specific leadership positions from payment of such assessment(s).
2.9.3 The PLC, on behalf of the FMECs, shall authorize the use of Medical Staff
assessments consistent with the purpose of the assessment. 2.10 Conflict of Interest
2.10.1 In any instance where an officer, committee Chair, or member of any Medical Staff committee has, or reasonably could be perceived to have a conflict of interest, or to be biased in any matter involving another Medical Staff appointee or any other matter that comes before such individual or committee, or in any instance where any such individual brought the complaint against that practitioner, such individual shall not participate in the discussion or voting on the matter and shall be excused from any meeting during that time, although that individual may be asked and may answer, any questions concerning the matter before leaving. As a matter of procedure, the Chair of that committee designated to review the matter shall inquire, prior to any discussion of the matter, whether any member has any conflict of interest or bias. The existence of a potential conflict of interest or bias on the part of any committee member may be called to the attention of the Chair by any committee member with knowledge of the matter.
2.10.2 In any instance where an officer, committee Chair, or member of any Medical Staff
committee has a conflict of interest in any matter that comes before such individual or committee, such individual has the right to abstain or recuse himself from voting on such matter. Such abstention or recusal shall not prohibit such individual from providing factual information or participating in discussion on such matter. If an individual is requested to abstain or recuse himself and refuses to do so, the potential conflict of interest issue will be reviewed and resolved by the next highest authority as outlined in these Bylaws. As a matter of procedure, the Chair of that committee designated to review the matter shall inquire, prior to any discussion of the matter, whether any member has any conflict of interest or bias. The existence of a potential conflict of interest or bias on the part of any committee member may be called to the attention of the Chair by any committee member with knowledge of the matter.
2.10.3 Assurance of a conflict of interest or bias can be determined by a majority vote of
the members of the committee where a quorum is present. SECTION 3 CONFIDENTIALITY, IMMUNITY AND RELEASES 3.1 Confidentiality
Information with respect to any practitioner or regarding any other subject discussed, submitted, collected or prepared by any representative of the Lee Memorial Health System,
13
including officers or members of organized committees of the Health System’s Medical Staffs, or any other healthcare professional, healthcare facility, organization or Medical Staff, for the purpose of achieving and maintaining the quality of care, reducing morbidity or mortality or contributing to clinical research shall, in accordance with Florida law, be confidential and shall not be disseminated or used for any purpose other than the foregoing. Such information shall not be deemed a part of the patient medical record, and shall not be filed therein. Each individual or committee member participating in such activities shall agree to make no disclosures of any such information except as authorized, in writing, by the Chief Executive Officer (CEO) or by legal counsel to the hospitals. Any breach of confidentiality by an individual or committee member may result in a professional review action, and/or may result in appropriate legal action to ensure that confidentiality is preserved, including application to a court of law for injunctive or other relief.
3.2 Immunity 3.2.1 Any Medical Staff officer, Department Chair, Section Chief, committee Chair,
committee member, and individual staff appointee who acts in good faith for and on behalf of any System hospital in discharging duties, functions or responsibilities stated in these Medical Staff Bylaws, applicable Policies, and/or Rules and Regulations shall be afforded protection by the Board of Directors to the fullest extent permitted by law in accordance with written policies adopted by the Board. Individuals and organizations independent of the Medical Staff or any of its members who may be engaged by the Health System to perform the review, analysis and evaluation of the qualification and/or performance of practitioners with membership and/or privileges on the Medical Staff are afforded protection by the Board of Directors in accordance with written policies adopted by the Board, provided such individuals or organizations act in good faith.
3.2.2 To the fullest extent permitted by law, each applicant and appointee to the Medical
Staff releases from any and all liability, and extends absolute immunity to System hospitals and the Board and its individual members, and to the System’s authorized representatives and agents, with respect to any acts, communications or documents, recommendations or disclosures involving the applicant or appointee, concerning the following:
3.2.2.1 applications for appointment or clinical privileges, including temporary
privileges and/or emergency privileges;
3.2.2.2 evaluations concerning reappointment or changes in clinical privileges;
3.2.2.3 proceedings for suspension or reduction of clinical privileges or for revocation of Medical Staff appointment, or any other disciplinary sanction;
3.2.2.4 summary suspension;
3.2.2.5 hearings and appellate reviews; 3.2.2.6 medical/surgical care evaluations; 3.2.2.7 utilization reviews;
3.2.2.8 other activities relating to the quality of patient care or professional
conduct;
14
3.2.2.9 matters of inquiries concerning the applicant’s or appointee’s professional
qualifications, credentials, clinical competence, character, mental or emotional stability, physical condition, ethics or behavior; and/or
3.2.2.10 any other matter that directly or indirectly might relate to the applicants or
appointee’s competence, and/or to patient care.
3.3 Releases
3.3.1 Authorization to Obtain Information
The applicant or appointee specifically authorizes the Medical Staff and its authorized representatives to consult with any third party who may have information bearing on the individual’s professional qualifications, credentials, clinical competence, character, mental or emotional stability, physical condition, ethics, behavior, or any other matter reasonably having a bearing on the applicant’s or appointee’s satisfaction of the criteria for initial and continued appointment to the Medical Staff. This authorization also covers the right to inspect, or obtain all communications, reports, records, statements, documents, recommendations or disclosures of said third parties that may be relevant to such questions. The individual also specifically authorizes said third parties to release said information to the Medical Staff and its authorized representatives upon request.
3.3.2 Legal Effect
The confidentiality provisions and protections described in this Section shall not limit
or supersede any protection or immunity afforded by law. SECTION 4 CATEGORIES OF THE MEDICAL STAFF 4.1 Active Category
4.1.1 Qualifications: Members of this category must have served on the Medical Staff, maintained a residence and office in Lee County (4.1.3.3) for one year, and be involved in twenty-four (24) patient contacts per year (i.e., a patient contact is defined as an inpatient admission, consultation, or an inpatient or outpatient surgical procedure) at the hospital except as expressly waived for practitioners with at least twenty (20) years of service in the active category or for those physicians who document their efforts to support the hospital’s patient care mission to the satisfaction of the FMEC.
In the event that a member of the active category does not meet the qualifications for reappointment to the active category, and if the member is otherwise abiding by all Bylaws, Rules and Regulations, and policies of the Medical Staff and hospital, the member may be appointed to another Medical Staff category if he meets the eligibility requirements for such category.
4.1.2 Prerogatives: Members of this category may:
4.1.2.1 Attend Medical Staff/Department meetings of which he is a member and any Medical Staff or hospital education programs;
15
4.1.2.2 Vote on all matters presented by the Medical Staff, Department, and committee(s) to which the member is assigned;
4.1.2.3 Hold office and sit on or be the Chair of any committee in accordance with
any qualifying criteria set forth elsewhere in the Medical Staff Bylaws or Medical Staff policies.
4.1.3 Responsibilities: Members of this category shall:
4.1.3.1 Contribute to the organizational and administrative affairs of the Medical Staff;
4.1.3.2 Actively participate as requested or required in activities and
functions of the Medical Staff, including quality/performance improvement and peer review, credentialing, risk and utilization management, medical records completion, monitoring activities and in the discharge of other Medical Staff functions as may be required by the FMEC;
4.1.3.3 The one-year residence and office requirement may be explicitly
waived by majority vote of the FMEC, on written request of the practitioner, at the time of appointment, if the practitioner affirmatively demonstrates to the FMEC in writing that the quality of patient care is not likely to be affected by his not living and having an office in Lee County and that the practitioner’s obligation to provide emergency room call and to attend hospitalized patient can be met.
4.1.3.4 Fulfill or comply with any applicable Medical Staff or hospital
policies or procedures as requested by the FMEC. 4.1.3.5 Fulfill basic responsibilities and requirements set forth in Section
2.7 of this Part, including but not limited to, Emergency Department call responsibilities in accordance with facility specific rules and regulations, unless exempted from Emergency Department call responsibilities as defined by their Section (if applicable) or Department and approved by the FMEC. In the event facility specific rules and regulations require physicians to accept emergency department referrals to the physician’s office, Lee Memorial Health System will provide facility support and services for such patients.
4.2 Associate Category 4.2.1 Qualifications: The associate category is reserved for Medical Staff members who
do not meet the eligibility requirements for the active category or choose not to pursue active status. This category includes physicians during their first year on the Medical Staff, as well as low volume/no volume physicians.
4.2.2 Prerogatives: Members of this category may:
4.2.2.1 Attend general Medical Staff Department meetings of which he is a member and any Medical Staff or hospital education programs.
16
4.2.2.2 Members of the associate category may not vote on matters at general Medical Staff, Department meetings or be an officer of the Medical Staff.
4.2.2.3 Members of the associate category may serve on facility and system
Medical Staff committees, other than the FMEC, and may vote on matters that come before such committees.
4.2.3 Responsibilities: Members of this category shall have the same responsibilities as
active category members, as set forth in Section 4.1 and Section 2.7 of this Part.
4.3 Honorary Category 4.3.1 The Honorary category is restricted to those individuals recommended by the FMEC
and approved by the Board. Appointment to this category is entirely discretionary and may be rescinded at any time. Members of the honorary category shall consist of those members who have retired from active hospital practice, who are of outstanding reputation, and have provided distinguished service to the hospital. They may attend general Medical Staff meetings, Department meetings, continuing medical education (CME) activities, and may be appointed to committees. They shall not hold clinical privileges, hold office or be eligible to vote.
SECTION 5 OFFICERS OF THE MEDICAL STAFF 5.1 Officers of the Medical Staff and FMEC at-large Members: Each hospital is
authorized to have the following officers:
5.1.1 Facility President of the Medical Staff 5.1.2 Facility President-Elect of the Medical Staff
5.1.3 Facility Secretary/Treasurer 5.1.4 Facility Past President of the Medical Staff
5.2 Qualifications of Officers and FMEC at-large Members 5.2.1 Officers must be members in good standing of the active category for at least three
(3) years or actively involved in patient care in the community, have previously served in a significant leadership position on a Medical Staff, (i.e. Department Chair, Section Chief or Committee Chair), indicate a willingness and ability to serve, have no pending adverse recommendations concerning Medical Staff appointment or clinical privileges, have a history of attendance at continuing education programs (provided by the System) relating to Medical Staff leadership and/or be willing to do so during their term or office, have demonstrated an ability to work well with others, be in compliance with the professional conduct policies of the Medical Staff, and should have excellent administrative and communication skills.
FMEC at large members must be members in good standing of the active category for at least two (2) years or actively involved in patient care in the community.
5.2.2 Officers and FMEC at-large members must disclose leadership positions on another
hospital Medical Staff. 5.3 Election of Officers and FMEC at-large Members
17
5.3.1 Every year, the FMEC shall appoint a nominations committee Chaired by the
immediate Past Facility President of the Medical Staff and comprised of at least five (5) at large members of the active Medical Staff at least ninety (90) days prior to
the election. Representatives of administration shall not serve on the nominations committee. Nominations will be solicited from the Medical Staff for consideration prior to the committee meeting. The committee shall offer at least one nominee for each office. Nominations must be announced, and the names of the nominees distributed to all members of the active Medical Staff at least forty-five (45) days prior to the election. A petition signed by at least 20% of the members of the active Medical Staff may also make nominations. Such petition must be submitted to the President of the Medical Staff at least twenty (20) days prior to the election for placement on the ballot.
5.3.2 Officers and FMEC at-large members shall be elected, as needed every year at an
election that takes place at least one (1) month prior to the expiration of the term of the current officers. Only members of the active category shall be eligible to vote. The FMEC will determine the mechanisms by which votes may be cast. The mechanisms that may be considered include written mail ballots; electronic voting via computer, fax, or other technology for transmitting the members’ voting choices. No proxy voting will be permissible. The nominee receiving the greatest number of votes will be elected. In the event of a tie vote, the Medical Staff support professional will arrange for a repeat vote(s) until one candidate receives a greater number of votes.
5.3.3 Medical Staff members will be notified of the election date and final slate of
nominees ten (10) days prior to the election. 5.4 Terms of Office 5.4.1 Officers and FMEC at-large members serve terms as follows: 5.4.1.1 Facility President-Elect of the Medical Staff – one (1) year 5.4.1.2 Facility President of the Medical Staff – two (2) years 5.4.1.3 Facility Past President of the Medical Staff – one (1) year 5.4.1.4 Facility Secretary/Treasurer – one (1) year 5.4.1.5 FMEC Members-at-Large – two (2) years 5.4.2 Officers shall take office October 1. Officers may be re-elected to office except that
the Facility President of the Medical Staff may not be re-elected for successive terms.
5.5 Vacancies of Office 5.5.1 The FMEC shall fill vacancies of office during the Medical Staff year, except the
office of the Facility President of the Medical Staff. If there is a vacancy in the office of the Facility President of the Medical Staff, the
Facility President-Elect of the Medical Staff shall serve the remainder of the term. 5.6 Duties of Officers and FMEC At-Large Members 5.6.1 Facility President of the Medical Staff – The Facility President shall represent the
interests of the Medical Staff to the FMEC and the Board. The Facility President will fulfill the duties specified in Section 5.6.2 of these Bylaws, as well as additional
18
duties as reasonably requested by the FMEC in order to implement and/or enforce all provisions of the Bylaws and the interests of the Medical Staff.
5.6.2 Responsibilities of the Facility President of the Medical Staff The Facility President of the Medical Staff is the primary elected officer of the
Medical Staff and is the Medical Staff’s advocate and representative in its relationships to the Board, the Facility Chief Administrative Officer (CAO) and the Health System administration. The Facility President of the Medical Staff, jointly with the FMEC, provides direction to and oversees Medical Staff activities related to assessing and promoting continuous improvement in the quality of clinical services and all other functions of the Medical Staff as outlined in the Medical Staff Bylaws, Rules and Regulations and Policies. Specific responsibilities and authority include:
5.6.2.1 Call and preside at all general and special meetings of the Medical Staff; 5.6.2.2 Serve as Chair of the FMEC, a voting member of the PLC and as ex-officio
member of all other Medical Staff committees without vote, and to participate as invited by the Board and the Facility CAO on hospital or Board committees;
5.6.2.3 Shall not vote at the FMEC, unless their vote is needed to break a tie vote; 5.6.2.4 Enforce Medical Staff Bylaws, Rules and Regulations and Medical
Staff/hospital/System Policies; 5.6.2.5 Except as stated otherwise, appoint committee Chairs and all members of
Medical Staff standing and ad hoc committees; in consultation with hospital administration, appoint Medical Staff members to appropriate hospital committees, in consultation with the Chair of the Board, appoint the Medical Staff members to appropriate Board committees when those are not designated by position or by specific direction of the Board or otherwise prohibited by state law;
5.6.2.6 Support and encourage Medical Staff leadership and participation on
interdisciplinary clinical performance improvement activities; 5.6.2.7 Report to the Board, through the PLC, the FMEC’s recommendations
concerning appointment, reappointment, delineation of clinical privileges or specified services and corrective action with respect to practitioners or allied health practitioners who are applying for appointment or privileges, or who are granted privileges or providing services in the hospital;
5.6.2.8 With the support of the facility Credentials/Privileging Committee and the
System Credentialing/Privileging Committee, evaluate and periodically report to the FMEC, PLC and the Board regarding the effectiveness of the credentialing and privileging processes;
5.6.2.9 Review and enforce compliance with standards of ethical conduct and
professional demeanor among the members of the Medical Staff in their relations with each other, the Board, hospital/System management, other professional and support staff, and the community the hospital serves;
5.6.2.10 Communicate and represent the opinions and concerns of the Medical
Staff and its individual members on organizational and individual matters
19
affecting hospital operations to the Facility CAO, the FMEC, PLC and the Board;
5.6.2.11 attends Board meetings and Board committee meetings as deemed
appropriate by Facility Medical Staff President; 5.6.2.12 ensures that the decisions of the Board are communicated and carried out
within the Medical Staff; 5.6.2.13 performs such other duties, and exercises such authority commensurate
with the office as are set forth in the Medical Staff Bylaws.
5.6.3 Facility President-Elect of the Medical Staff – In the absence of the Facility President, the Facility President-Elect or the Facility Past President shall assume all the duties and have the authority of the Facility President. He shall perform such further duties to assist the Facility President as the Facility President may request from time to time. The Facility President-Elect, upon the end of the term of the Facility President, shall automatically succeed to the office of Facility President.
5.6.4 Facility Secretary/Treasurer – This officer will collaborate with the hospital’s
Medical Staff office, assure maintenance of minutes, attend to correspondence, act as Medical Staff treasurer, and coordinate communication within the Medical Staff. He shall perform such further duties to assist the Facility President as the Facility President may from time to time request.
5.6.5 Facility Past President of the Medical Staff – This officer will serve as a
consultant to the Facility President and the Facility President-Elect as requested by the FMEC and provide feedback to the officers regarding their performance of assigned duties on an annual basis.
He shall perform such further duties to assist the Facility President as the
Facility President may request. He shall serve as a member of the System Credentialing/Privileging Committee.
5.6.6 FMEC at-large members – shall advise and support the Medical Staff officers
and are responsible for representing the needs/interests of the entire Medical Staff and not simply representing the preferences of their own clinical specialty.
5.7 Removal and Resignation of Officer or FMEC At-Large Member 5.7.1 The Medical Staff may remove any facility officer or FMEC at-large member by
petition of 20% of the active Medical Staff members and a subsequent affirmative vote by two-thirds (2/3) of those active Medical Staff members’ casting votes.
5.7.2 Recall of Officers or FMEC at-large members The FMEC may remove any facility Medical Staff officer or FMEC at-large
member for conduct detrimental to the interests of the Medical Staff or if the officer is suffering from a physical or mental infirmity that renders the individual incapable of fulfilling the duties of the office. At least ten (10) days notice prior to the date of the meeting shall be provided, in writing, to the affected officer or FMEC at-large member. The officer or at-large member shall be afforded the opportunity to speak prior to the taking of any vote on such removal. For recall
20
of an officer or at-large member, a two-thirds (2/3) vote of approval is required with three-fourths (3/4) of the FMEC members present and voting. Affected officer or at-large member does not count as quorum and does not vote.
5.7.3 Resignation of Officers or FMEC at-large members Any elected officer or FMEC at-large member may resign at any time by giving
written notice to the FMEC. Such resignation takes effect on the date of receipt, when a successor is elected, or any later time specified therein.
SECTION 6 MEDICAL STAFF ORGANIZATION The organized Medical Staff is actively involved in Medical Staff governance, peer review,
credentialing/privileging and communication. Medical Staff members are accountable to the FMEC.
The Medical Staff facility officers (Section 5), Medical Staff governance committees (PLC, Section 7.1 and FMEC, Section 7.4), Department Chairs (Section 6.1), clinical Section Chiefs (Section 6.1.1), hospital (as appropriate) System Medical Staff committee Chairs, (Section 7.6) and facility Medical Staff committee Chairs (Section 7.7) are responsible for working collaboratively to develop a process for communication of Medical Staff functions. Periodic reports, as appropriate, are given to each FMEC, Medical Staff Departments, Medical Staff committees and the PLC as needed to ensure adherence to regulatory requirements and accreditation standards.
Additionally, Medical Staff officers may appoint, in collaboration with the Facility Medical
Director, designated physician leaders to serve on the following Medical Staff committees to help ensure Medical Staff input and oversight with clinical functions such as System Bylaws, Cancer Care, CME/Medical Library, Ethics, Institutional Review, System Credentialing/Privileging, Critical Care, System Emergency Services, Infection Control, Pharmacy and Therapeutics, System Medical Staff Quality, System Practitioner Resource, Trauma Quality, Vascular Lab, in addition to the Children’s Hospital committees (Cancer Care, Ethics, Neonatal Intensive Care Unit (NICU) Pediatric Intensive Care Unit (PICU) Perinatal and Medical Staff Quality and other such functions as determined by the FMEC and/or the PLC.
6.1 Departments The Medical Staff shall be organized as a Departmentalized staff. The current
Departments authorized by the FMECs are Medicine, Surgery, Pediatrics, Obstetrics and Gynecology, Anesthesiology, Pathology, Radiology and Emergency Medicine. Departments fulfill the duties listed in Section 6.2.4 of these Bylaws within a specific hospital or facility and/or across the Health System as necessary. Departments shall meet as frequently as needed to fulfill assigned duties and when requested by the FMEC.
The Medical Staff may create Clinical Sections (as specified in these Bylaws) within
a Department in order to facilitate Medical Staff activities.
6.1.1 Any FMEC may recognize any group of like American Board of Medical Specialties, (ABMS) approved specialties with at least three (3) Medical Staff members or service lines that wish to organize themselves into a Clinical Section. Any Clinical Section, if organized shall not be required to hold regularly scheduled meetings, keep routine minutes, or require attendance.
21
A written report is required only when the Clinical Section is making a formal report. A Clinical Section shall elect a Clinical Section Chief. The Clinical Section Chief is responsible for fulfilling the activities listed in Section 6.1.1.1 - 6.1.1.7 of these Bylaws. The procedure for removal of a Clinical Section Chief shall be the same as set forth in Section 6.2.3 for Department Chair. When a clinical Section is making a formal report, the report shall be submitted to the FMEC documenting the specific position of the clinical Section. The President of the Medical Staff and the Clinical Section Chief (or designee) will decide if the report/issue is placed on the FMEC agenda and whether the Clinical Section Chief (or designee) will attend the FMEC meeting to present the report/issue to the FMEC on that specific report/issue. Clinical Sections are optional and shall exist to perform any of the following activities within a specific facility and/or across Health System facilities as necessary:
6.1.1.1 continuing education/Grand Rounds/discussion of patient care;
6.1.1.2 formulation of ED on-call and inpatient consultation and coverage recommendations; 6.1.1.3 discussion of policies and procedures; 6.1.1.4 discussion of equipment needs; 6.1.1.5 development of recommendations for the Department Chair(s), the
FMECs or the PLC; 6.1.1.6 participation in the development of criteria for clinical privileges
when requested by the System Credentialing/Privileging Committee or FMEC;
6.1.1.7 discussion of a specific issue at the request of the PLC or the
FMEC. The FMEC, with the concurrence of the PLC, may designate new Medical Staff Departments or Clinical Sections or dissolve current Departments or Clinical Sections as it determines will best meet the Medical Staff needs for promoting performance improvement, patient safety, and effective credentialing and privileging.
6.2 Qualifications, Selection, Term, and Removal of Department Chair 6.2.1 Each Department Chair shall serve a term of two (2) years commencing on
October 1 and may be elected to serve successive terms. All Chairs must be members of the active Medical Staff with relevant clinical
privileges and be certified by an appropriate specialty board or have affirmatively established comparable competence through the credentialing process.
6.2.2 Department Chairs and Vice-Chairs will be elected by majority vote of the
active members of the Department, subject to ratification by the FMEC.
22
Each Department shall establish procedures for identifying and electing candidates and these procedures must be ratified by the FMEC.
6.2.3 Department Chairs may be removed from office by the FMEC upon receipt
of a recommendation of two-thirds (2/3) of the members of the Department or, in the absence of such recommendation, the FMEC may remove a Chair on its own by a two-third (2/3) vote of a majority of members present and voting, if any of the following occurs:
6.2.3.1 The Chair ceases to be a member in good standing of the Medical
Staff; 6.2.3.2 The Chair suffers an involuntary loss or significant limitation of
practice privileges; 6.2.3.3 The Chair fails, in the opinion of the FMEC, to demonstrate to the
satisfaction of the FMEC, PLC or the Board that he is effectively carrying out the responsibilities of the position;
6.2.3.4 If removal is required, a new election will be held according to the
established Departmental procedures. 6.2.4 Department Chairs shall carry out the following responsibilities: 6.2.4.1 to oversee all clinically-related activities of the Department; 6.2.4.2 to oversee all administratively related activities of the Department
otherwise provided for by the Facility; 6.2.4.3 to provide ongoing surveillance of the performance of all individuals
in the Medical Staff Department who have been granted clinical privileges;
6.2.4.4 to recommend to the System Credentialing/Privileging Committee
Medical Staff Department; 6.2.4.5 to recommend clinical privileges for each member of the
Department and other LIPs practicing with privileges within the scope of the Department;
6.2.4.6 to assess and recommend to the FMEC and Facility CAO off-site
sources for needed patient care services not provided by the Medical Staff Department or Facility;
6.2.4.7 to monitor and evaluate the quality and appropriateness of patient
care provided in the Medical Staff Department and to implement action following review and recommendations by the facility Medical Staff peer review/quality committee and/or the FMEC;
6.2.4.8 to integrate the Department into the primary functions of the
hospital; 6.2.4.9 to coordinate and integrate interdepartmental and
intradepartmental services and communication;
23
6.2.4.10 to participate in the administration of the Department through cooperation with nursing services and hospital administration in matters affecting patient care;
6.2.4.11 to develop and implement Medical Staff and hospital policies and
procedures that guide and support the provision of patient care services;
6.2.4.12 to recommend to the Facility CAO the sufficient numbers of
qualified and competent persons to provide patient care and service;
6.2.4.13 to provide input to the Facility CAO regarding the qualifications and
competence of Department or service personnel who are not Licensed Independent Practitioners (LIPs) but provide patient care, treatment, and services;
6.2.4.14 to provide continuous assessment and improvement of the quality
of care, treatment, and services; 6.2.4.15 to maintain quality control programs as appropriate; 6.2.4.16 to orient and continuously educate all persons in the Department; 6.2.4.17 to make recommendations to the FMEC and to the Facility CAO for
space and other resources needed by the Medical Staff Department to provide patient care services.
6.3 Assignment to Department 6.3.1 The FMEC will, after consideration of the recommendation of the Chair of the
appropriate Department, recommend Department assignments for all members in accordance with their qualifications. Each member will be assigned to one primary Department. Clinical privileges are independent of the Department assignment.
SECTION 7 MEDICAL STAFF GOVERNANCE COMMITTEES 7.1 Designation of the Lee Memorial Health System Medical Staff Physician Leadership
Council (PLC)
7.1.1 There shall be a Lee Memorial Health System Medical Staff Physician Leadership Council (PLC) and such other standing and special committees as determined by the PLC.
7.1.2 There shall be a Facility Medical Executive Committee (FMEC) at each hospital and
such other facility standing and special committees as established by the FMEC.
7.2 Composition of the Lee Memorial Health System Medical Staff PLC 7.2.1 Composition: The PLC shall consist of the following voting members: Each Facility President and
each Facility President–Elect or each Facility Immediate Past President and two (2)
24
at-large Medical Staff members elected by each FMEC. All shall serve a 2-year term except the Facility President-Elect and Facility Past President shall serve 1-year term. The Chairs of the System Credentialing/Privileging Committee and System Quality Committee, the system CEO or Designee, the System Chief Medical Officer and the Chair of the Board and up to two (2) other Board consultants, shall serve as ex-officio, non-voting members. The PLC will elect the PLC Chair and Vice Chair who shall serve a 2-year term.
In the event that the PLC composition does not include one anesthesiologist,
emergency medicine physician, hospitalist or intensivist, radiologist and pathologist, the PLC may appoint an active Medical Staff member from each of these hospital-based specialties to be voting members of the PLC.
7.2.2 Duties: The duties of the Lee Memorial Health System PLC are:
7.2.2.1 to work in a cooperative and professional manner with the FMECs System and Facility Administration and the Board to ensure Medical Staff input into the plans, goals and mission of the Lee Memorial Health System;
7.2.2.2 receive, review, and transmit FMEC recommendations to the
Board; 7.2.2.3 review and attempt to resolve any inconsistency emanating from
the FMEC recommendation(s) and transmit FMEC recommendations to the Board concerning all matters relating to appointments, reappointments, staff category, facility assignments, clinical privileges subject to the conflict resolution process herein, unless due process rights are triggered pursuant to Part II.
The PLC is acting as a duly constituted peer review committee under Florida law when it is reviewing the quality of care or performance of any particular physician.
7.2.2.4 consistent with the hospital and Medical Staff mission and
philosophy, the PLC will participate and encourage participation of the FMECs in identifying community health needs and in setting goals and work with the System administration and the facility CAO(s) to design and implement programs to meet those needs;
7.2.2.5 work with the FMECs to ensure understanding and the consistent
application of Medical Staff Rules and Regulations, Policies and Procedures; and
7.2.2.6 govern the collection of Medical Staff system-wide assessments
and authorize the use of Medical Staff assessments consistent with the purpose of the assessment.
7.2.3 Meetings:
The PLC shall meet as frequently as needed, but at least quarterly, to perform its assigned functions. Records of its proceedings and actions shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
25
7.3 Staff Functions
7.3.1 The PLC exists to promote communication, collaboration and coordination
between physicians, System and facility administration and the Board concerning the work of each FMEC and planning activities of the Lee Memorial Health System that impact members of the Medical Staff.
7.4 Facility Medical Executive Committee (FMEC) Composition Selection and Tenure
7.4.1 Each Medical Staff may determine the number of Medical Staff members
appointed or elected to the FMEC. The composition of the FMEC shall consist of at least the following voting members: Facility President of the Medical Staff, Facility Immediate Past President, Facility President-Elect of the Medical Staff, Facility Secretary/Treasurer, physician representative from the System Credentialing/Privileging Committee, Chair of the Facility Quality Committee, the Department Chairs from Medicine, Surgery, Anesthesiology, Radiology, Pathology, Pediatrics, Obstetrics/Gynecology and Emergency Services, two (2) at-large active members of the Medical Staff appointed by the FMEC and two (2) at-large active members of the Medical Staff elected by the general Medical Staff.
One Board member, the CAO, the facility Vice-President of Nursing, the
facility Medical Director (as appropriate) will serve in a non-voting, ex-officio capacity. The Facility President of the Medical Staff shall serve as the Chair of the FMEC.
7.4.2 Each FMEC composition description shall be listed in the Facility Rules &
Regulations.
7.4.3 FMEC members shall disclose in writing to the Medical Staff, prior to the date of election of appointment, any personal, professional or financial applications or responsibilities with Lee Memorial Health System and any competing hospital, healthcare organization or Health System.
FMEC members shall serve 2-year terms, except Facility Past President and
Facility President-Elect shall serve 1-year terms. The FMEC and the Nominations Committee shall stagger the terms of appointed and elected at-large members to ensure continuity of leadership. Such physicians must be on Active Staff and be a member in good standing at all times.
All FMEC members are expected to participate in orientation and continuing
education activities as related to the operation of the Medical Staff.
7.5 Duties and Responsibilities of the Facility Medical Executive Committees 7.5.1 To represent, to initiate action and act on behalf of the Medical Staff
members with privileges at the Facility in fulfilling the duties of Medical Staff self governance, credentialing/privileging and quality/peer review, after seeking input and recommendations from Sections and/or Departments affected by FMEC action (if applicable).
26
7.5.2 To receive recommendations from the System Credentialing/Privileging
Committee and the Facility Quality/Peer Review Committee and make recommendations to the Board (and for informational purposes only) to the PLC concerning:
7.5.2.1 appointments, reappointments and granting of clinical privileges; 7.5.2.2 necessity for special investigations of issues pertaining to
practitioner competence of behavior; 7.5.2.3 needed performance improvements and peer review results; 7.5.2.4 policies and procedures development and enforcement; 7.5.2.5 facility Medical Staff Department and committee structure; and 7.5.2.6 other matters relevant to the provision of patient care, operation of
the Medical Staff or proposed Bylaws amendments. 7.5.3 Receive or act upon reports and recommendations concerning patient care
quality and appropriateness reviews, evaluation and monitoring functions, and the discharge of their delegated administrative responsibilities;
7.5.4 Recommend to the Board, and for information purposes only to the PLC,
specific programs and systems to perform Medical Staff peer review, quality monitoring, communication, governance, credentialing/privileging and planning functions;
7.5.5 Coordinate the implementation of policies adopted by the Board; 7.5.6 Oversee the facility multi-specialty peer review and quality monitoring
activities in a manner consistent with federal and state law; 7.5.7 Take reasonable steps to encourage professionally ethical conduct and
competent clinical performance of Medical Staff members at the facility including collegial and educational efforts;
7.5.8 Participate in identifying community health needs and in setting facility-
specific goals and implementing programs to meet those needs; 7.5.9 Design and implement facility-specific rules and regulations that will not
conflict with the Medical Staff Bylaws; 7.5.10 Work with Facility and System administration to promote effective, efficient
and safe patient care practice within the facility; 7.5.11 Take reasonable steps to encourage professionally ethical conduct and
competent clinical performance on the part of staff appointees including initiating investigations, and pursuing corrective action, when warranted;
27
7.5.12 Provide oversight concerning the quality and safety of the care provided by residents, interns, students, and ensure that the same act within approved guidelines established by the Medical Staff and the Board.
Reviews and ensure corrective action regarding applicable Residency Review Commission findings and recommendations;
7.5.13 Keep the Medical Staff up to date concerning the licensure and
accreditation status of the System and hospitals; 7.5.14 Request evaluations of practitioners privileged through the Medical Staff
process in instances in which there is question about an applicant or member’s ability to perform privileges requested or currently granted;
7.5.15 Consult with administration on the quality, timeliness, and appropriateness
of aspects of contracts for patient care services provided to the hospital by entities outside the hospital;
7.5.16 Hold Medical Staff leaders, committees, and Departments accountable for
fulfillment of their duties and responsibilities; 7.5.17 Advise and assist the PLC, when and to the extent possible, as requested
by the PLC, the Board and the System or Facility administration; 7.5.18 Grant, deny or rescind exemptions related to ED call responsibility; 7.5.19 Meetings: The FMEC shall meet ten (10) times per year, or more
frequently as needed to perform its assigned functions. Records of its proceedings and actions shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
7.6 System Medical Staff Committees 7.6.1 Purpose. There shall be system Medical Staff committees established by the
Medical Staff to carry out the responsibilities of the Medical Staff with regard to measuring and assessing the performance of the Medical Staff providing medical care within the hospitals and Health System facilities.
7.6.2 Organization to Perform Functions. The PLC with the input and approval of each
FMEC shall establish system Medical Staff committees comprised of members of the Medical Staff and others as may be deemed appropriate or necessary. The delineation of specific duties, committee size, liaison with other committees and Departments, and other matters necessary to the efficient performance of Medical Staff functions shall be set forth in these Bylaws. The only voting members of system Medical Staff committees are members of the Medical Staff unless otherwise determined by the FMEC. System Medical Staff committees consist of the following, shall report to and through the FMECs on matters relating to all FMECs, and shall report to each FMEC on facility specific matters:
7.6.2.1 System Credentialing/Privileging Committee (See Part III, Section 1 of
these Bylaws); 7.6.2.2 System Medical Staff Quality Committee (See Medical Staff Quality
Manual); 7.6.2.3 System Practitioner Resource Committee.
28
Membership: Membership shall be established by the PLC with the input and approval of
each FMEC. The term of office shall be for a period of two (2) years with staggered terms, so as to provide continuity and development of expertise.
Referrals: Concerns that a member of the Medical Staff may be suffering from a
physical or mental impairment that might impact their ability to practice medicine or may be a threat to themselves or others, including but not limited to impairment due to substance abuse, should be communicated to the President of the Medical Staff or to the affected practitioner’s Department Chair. The President of the Medical Staff or Department Chair, after consultation with others, if deemed appropriate, may refer the affected practitioner to the practitioner Resource Committee for review, evaluation and follow-up.
Responsibilities: The committee shall have no authority to take disciplinary action. Nor
does the committee provide treatment. The committee is responsible to: 7.6.2.3.1 Receive and evaluate concerns about practitioner health and
functioning;
7.6.2.3.2 Provide assistance and encourage a practitioner impaired by virtue of physical or psychiatric condition, problems in living, or issues related to alcohol use or drug use to voluntarily accept referral for the evaluation, treatment or assistance;
7.6.2.3.3 Assume an advocacy role on behalf of the affected practitioner;
7.6.2.3.4 Serve as an advisor to the President of the Medical Staff, Department Chair and/or FMEC, including advice relating to alternatives in the event that the practitioner fails to accept referral or fails to adequately recover from treatment;
7.6.2.3.5 Consider referring an affected practitioner to appropriate resources
for treatment and advice on the appropriateness of treatment, rehabilitation planning and monitoring provisions;
7.6.2.3.6 Utilize the Florida Medical Association Physician Resource Network,
Intervention Project for Nurses or other resources, if appropriate;
7.6.2.3.7 Maintain the confidentiality of information regarding matters referred to the committee;
7.6.2.3.8 Refer to the Medical Staff President Department Chair or FMEC
those situations that may require possible corrective actions. 7.6.2.4 System Bylaws Committee
29
Membership: The Bylaws Committee shall be a standing committee of the Medical Staff
and shall be composed of at least five (5) active Medical Staff appointees (including one (1) member from each FMEC appointed by the facility Medical Staff President) and the System Chief Medical Officer (CMO) or his designee (who shall serve as a non-voting member).
Duties: The duties of the Bylaws Committee shall be to:
7.6.2.4.1 Conduct an annual review of the Medical Staff Bylaws, Medical Staff
Rules and Regulations and Policies; and 7.6.2.4.2 Review recommendations for changes in the Medical Staff Bylaws,
Rules and Regulations and Policies made by the Medical Staff committees, Departments, or by the Board.
Meetings, Reports and Recommendations: The Bylaws Committee shall meet at least annually or as necessary to
accomplish its duties, shall maintain a permanent record of its proceedings and actions, and shall report its recommendations to the FMECs.
7.6.2.5 System Emergency Services Committee Membership: The System Emergency Services Committee shall be an ad hoc committee
of the Medical Staff and shall be composed of the Emergency Department Medical Directors, at least three (3) Active Staff members, and other Active Staff members as needed.
Duties: The duties of the System Emergency Services Committee shall be to: 7.6.2.5.1 conduct an annual review of system-wide emergency services; 7.6.2.5.2 ensure emergency call is fair to physicians while providing adequate
coverage to patients of our community; 7.6.2.5.3 review emergency call rules system-wide for recommendation to
FMECs.
Meetings: The System Emergency Services Committee will meet at least once per year or as needed.
7.6.3 Composition and Meetings of System Medical Staff Committees:
30
7.6.3.1 Unless otherwise provided for in these Bylaws, System Medical Staff committees shall be composed of physician members from each facility, as appointed by each FMEC;
7.6.3.2 Each System Medical Staff committee shall elect a physician Chairperson
and physician vice Chairperson for their respective committee;
7.6.3.3 System Medical Staff committee members shall serve terms of 2 years and may be reappointed;
7.6.3.4 System Medical Staff committee members who cease to be members of
the Medical Staff of Lee Memorial Health System shall automatically cease to serve as committee members. Vacancies on committees shall be filled by the appropriate FMEC;
7.6.3.5 System Medical Staff committees shall meet as often as necessary to
discharge the duties of the respective committees in accordance with these Bylaws.
Reasonable notice of meetings shall be provided to committee members
and may include providing a written schedule of meetings on an annual or more frequent basis.
7.7 Facility Medical Staff Committees: 7.7.1 Purpose: There shall be committees to carry out certain essential functions
within each facility as determined by each FMEC. The FMEC may establish such committees from time to time in addition to those set forth in the Bylaws.
7.7.2 Standing Facility Medical Staff Committees: The following facility committees
are approved as standing committees of the FMEC: 7.7.2.1 GCMC Credentialing/Privileging Committee (see Part III, Section 1 of
these Bylaws); 7.7.2.2 LMHS Credentialing/Privileging Committee (see Part III, Section 1 of these
Bylaws); 7.7.2.3 Nominations Committees (See Part 1, Section 5.3 of these Bylaws);
7.7.2.4 Facility Medical Staff Quality Committees (see Medical Staff Quality Manual);
7.7.2.5 Facility Rules and Regulations Committees Composition: The Facility Rules and Regulations Committee shall be a
standing committee of the Medical Staff and shall be composed of at least two (2) active Staff members appointed by the FMEC.
Duties: The duties shall be to review and recommend changes in the
Facility Rules and Regulations and policies to the FMEC. 7.7.2.6 Trauma Quality Management
31
Composition, membership and duties are mandated by the State regulations for designated trauma centers.
SECTION 8 MEDICAL STAFF MEETINGS 8.1 General Medical Staff Meetings 8.1.1 An annual meeting and other general Medical Staff meetings shall be held at a
time determined by the FMEC. Notice of the meeting shall be given to all Medical Staff members via appropriate media and posted conspicuously at least ten (10) days before the meeting.
8.1.2 Except for Bylaws amendments or as otherwise specified in these Bylaws, the
actions of a majority of the members present and voting at a meeting of the Medical Staff is the action of the group.
Action may be taken without a meeting of the Medical Staff by presentation of
the question to each Medical Staff member eligible to vote, in person, via telephone, and/or by mail or internet, and their vote recorded in accordance with procedures approved by the FMEC. Such vote shall be binding so long as the question that is voted on receives a majority of the votes cast.
8.1.3 Special Meetings of the General Medical Staff 8.1.3.1 The President of the Medical Staff may call a special general Medical
Staff meeting at any time. Such request or resolution shall state the purpose of the meeting. The President of the Medical Staff shall designate the time and place of any special general Medical Staff meeting.
8.1.3.2 Written or electronic notice stating the time, place and purposes of
any special general Medical Staff meeting shall be conspicuously posted and shall be sent to each member of the Medical Staff at least three (3) days before the date of such meeting. No business shall be transacted at any special general Medical Staff meeting, except that stated in the notice of such meeting.
8.2 Departments, Sections and Committee Meetings 8.2.1 Regular Meetings of Medical Staff Departments, Sections and Committees
8.2.2 Departments, Sections and Committees may, by resolution, provide the time for holding regular meetings without notice other than such resolution.
8.3 Special Meetings of Departments, Sections and Committees 8.3.1 A special meeting of any Department, Section or Committee may be called by
the Chair thereof or by the President of the Medical Staff. 8.4 Quorum
32
8.4.1 Medical Staff meetings: Unless otherwise specified in these Bylaws, a quorum shall consist of those present or those eligible Medical Staff members voting on an issue.
8.4.2 FMEC, Credentialing/Privileges Committee, Medical Staff Quality/Peer Review
Committee: A quorum will exist when 50% of the members are present. 8.4.3 Departments, Sections or Committees other than those listed in Sections 6 and
7 above or unless otherwise specified in these Bylaws, a quorum shall consist of those present or those eligible Medical Staff members voting on an issue.
8.5 Attendance Requirements 8.5.1 Members of the Medical Staff are encouraged to attend meetings of the Medical
Staff. 8.5.1.1 FMEC, Credentialing/Privileges Committee, and Medical Staff
Quality/Peer Review Committee meetings: Members of these committees are expected to attend at least 75% of the meetings held.
8.5.1.2 Special meeting attendance requirements: Whenever there is
suspected or actual non-compliance with Medical Staff or hospital policies or suspected deviation from standard clinical or professional practice, the President of the Medical Staff or the applicable Department/Section/Committee Chair may require the practitioner to confer with him or with a standing or ad hoc committee that is considering the matter. The practitioner will be given special notice of the meeting, by personal delivery or U.S. Mail certified return receipt requested, at least five (5) days prior to the meeting, including the date, time, place, a statement of the issue involved and that the practitioner’s appearance is mandatory.
Failure of the practitioner to appear at any such meeting after two (2)
notices, unless excused by the FMEC upon showing good cause, will result in an automatic termination of membership pursuant to the Automatic Suspension and Termination provisions of these Bylaws. Such termination will not give rise to a fair hearing, but will automatically be rescinded upon the practitioner’s participation in the previously referenced meeting.
8.5.1.3 Nothing in the foregoing paragraph shall preclude the initiation of
precautionary restriction or suspension of clinical privileges as outlined in Part II of these Bylaws (Investigations, Corrective Action, Hearing and Appeal Plan).
8.6 Participation by Administration
8.6.1 Administration may attend any general, Department, Section or Committee meetings of the Medical Staff, unless otherwise specified or requested by the committee.
8.7 Robert’s Rules of Order
33
8.7.1 Medical Staff Department, Section and Committee meetings shall be run in a manner determined by the individual who is the Chair of the meeting. When parliamentary procedure is needed, as determined by the Chair or evidenced by a majority vote of those attending the meeting, the latest edition of Robert’s Rules of Order shall determine procedure.
8.8 Notice of Meetings 8.8.1 Unless otherwise specified in these Bylaws, written or electronic notice stating
the place, day, and hour of any special meeting or of any regular meeting not held pursuant to resolution shall be delivered or sent to each member of the Department or committee not less than five (5) days before the time of such meeting by the person or persons calling the meeting. The attendance of a member at a meeting shall constitute a waiver of notice of such meeting.
8.9 Action of PLC, FMEC, General Medical Staff, Department, Section or Committee 8.9.1 The recommendation of a majority of its members present at a meeting at which
a quorum is present shall be the action of a Department, Section and Committee, FMEC, PLC or General Medical Staff meeting. Such recommendation will then be forwarded to the FMEC for action.
8.10 Rights of Ex Officio Members 8.10.1 Except as otherwise provided in these Bylaws, persons serving as ex officio
members of a committee shall have all rights and privileges of regular members thereof, (except that they shall not vote or be counted in determining the existence of a quorum).
8.11 Minutes 8.11.1 Minutes of each regular and special meeting of a committee shall be prepared
and shall include a record of the attendance of members and the vote taken on each matter. The presiding Chair shall authenticate the minutes and copies thereof shall be submitted to the FMEC or other designated committee. Minutes shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
SECTION 9 DECISION MAKING METHODS AND CONFLICT RESOLUTION 9.1 FMEC recommendations will be forwarded to the PLC for information and to ensure
communication between all facility Medical Staffs, System and facility administration and Board leaders. Routine FMEC communication and recommendations that are consistent between the FMECs and that are consistent with Medical Staff and hospital policy and procedures will be transmitted to the Board.
9.2 Conflict resolution: If the PLC determines a recommendation of a FMEC may be contrary
to the opinion of the PLC, or if a decision of the Board is contrary to a recommendation of the PLC and/or a FMEC, the PLC shall not make a recommendation to the Board regarding such matter. The PLC will first refer the matter back to the FMEC(s) for further consideration at their next meeting, together with pertinent suggestions and comments of the PLC.
34
9.3 If the FMEC recommendation and the opinion of the PLC remain inconsistent after the next meeting of the FMEC, the matter will be referred to an Initial Joint Conference Committee to be convened within thirty (30) days of that FMEC meeting. Such Initial Joint Conference Committee may be convened at any time sooner by mutual agreement of the FMEC and PLC. The Initial Joint Conference Committee shall be composed of two (2) representatives selected by the PLC, two (2) representatives selected by the FMEC, one (1) administrative representative and one (1) Board member.
9.3.1 The positions established at the Initial Joint Conference Committee will be reported
in full to the FMEC and the PLC. The FMEC will discuss the issue at its next meeting. In the event the FMEC(s)’ recommendation remains contrary to the opinion of the PLC, the recommendation of the FMEC(s) shall be forwarded to the Board, along with pertinent, applicable information.
The PLC, at its discretion, may include a divergent opinion along with pertinent,
applicable information. The Board shall have sixty (60) days to adopt the recommendation of the FMEC(s), or may choose to refer the matter(s) to a Final Joint Conference Committee at any time within the 60-day period.
9.4 A Final Joint Conference Committee will be convened if: 9.4.1 requested by the Board; 9.4.2 requested by the PLC, FMEC(s) or Initial Joint Conference Committee (if the Initial
Joint Conference Committee is unable to resolve conflicts and divergent opinions remain between the PLC, FMEC(s) and/or Initial Joint Conference Committee); or
9.4.3 in the event the Board does not accept or adopt a recommendation by the
FMEC(s) within sixty (60) days of receiving such recommendation(s) as set forth in Section 9.3.1.
The Final Joint Conference Committee will convene within thirty (30) days of such request,
or occurrence. The Final Joint Conference Committee will be composed of two (2) representatives selected by the PLC, two (2) representatives selected by the FMEC and two (2) representatives (which may or may not be Board members) of the Board for review and recommendation to the full Board. The Final Joint Conference Committee will have up to sixty (60) days to report its recommendation(s), and will issue its complete report simultaneously to the FMEC(s), PLC, Initial Joint Conference members and Board. If either the FMEC(s) or PLC continues to have a dissenting opinion/recommendation from that of the Final Joint Conference Committee, both (FMEC and PLC) shall each have the right for a representative of each to report its recommendation/opinion at the same time to the Board. After such report(s), the Board will make a determination, which shall be final.
9.5 The Chair of the Board, PLC or FMEC may call for an Initial Joint Conference as described
above at any time and for any reason in order to seek direct input from the Board, PLC and/or FMEC Medical Staff leaders, clarify any issue, or relay information directly to Medical Staff leaders.
9.6 The provisions of this article are not applicable to matters subject to the provisions of the
Medical Staff Bylaws, Rules and Regulations, or Policies relating to Peer Review, Corrective Action or the Fair Hearing process.
SECTION 10 REVIEW, REVISION, ADOPTION, AND AMENDMENT
35
10.1 Medical Staff Responsibility 10.1.1 The Medical Staff shall have the responsibility to formulate, review at least
biennially, and recommend to the Board any Medical Staff Bylaws, rules, regulations, policies and procedures, and amendments as needed, which shall be effective when approved by the Board.
The Medical Staff can exercise this responsibility through its elected and appointed leaders or through direct vote of its membership.
10.2 Methods of Amendment and Adoption to these Bylaws
10.2.1 Proposed amendments to these Bylaws may be originated by the System Bylaws
Committee for consideration of all FMECs and each general Medical Staff or by a petition signed by twenty-five (25) active staff members.
10.2.1.1 Each active member of the Medical Staff will be eligible to vote on the
proposed amendment to these Bylaws via printed or secure electronic ballot in a manner determined by the FMEC. All active members of the Medical Staff shall receive at least thirty (30) days advance notice of the proposed changes. Proposed amendments must:
10.2.1.1.1 receive a simple majority of the votes cast by those active
Medical Staff members eligible to vote at the initiating FMEC;
10.2.1.1.2 receive a simple majority of the votes cast by the active
Medical Staff members eligible to vote at each FMEC; 10.2.1.1.3 receive a simple majority of the votes cast by the active
Medical Staff members eligible to vote on each facility general Medical Staff.
10.2.1.2 Amendments so adopted shall be effective when approved by the Board.
Neither the Board nor the Medical Staff shall have the power or authority to unilaterally adopt or amend Medical Staff Bylaws.
10.3 Methods of Amendment and Adoption to any Medical Staff Rules, Regulations and
Policies: 10.3.1 The Medical Staff may adopt additional rules, regulations and policies as necessary
to carry out its functions and meet its responsibilities under these Bylaws. A Rules, and Regulations and Policies Manual may be utilized to organize these additional documents. Should a conflict exist between the provisions of the Medical Staff Bylaws and the Rules and Regulations or Medical Staff Policies, the Bylaws will prevail. Should a conflict exist between the provisions of the Rules and Regulations and the Medical Staff Policies, the Rules and Regulations will prevail.
10.3.2 Proposed amendments to the Rules, Regulations and Policy Manual may be
originated by the FMEC. 10.3.3 The Medical Staff itself may recommend directly to the Board an amendment(s) to
any rule, regulation, or policy by submitting a petition signed by twenty-five (25) active Medical Staff members. Upon presentation of such petition, the adoption process outlined in 10.2.1 above will be followed.
36
10.3.4 The FMEC shall vote on the proposed language changes at a regular meeting, or at a special meeting called for such purpose. Following an affirmative vote by the FMEC, any of these documents may be adopted, amended or repealed, in whole or in part and such changes shall be effective when approved by the Board, subject to Section 9 of this Part in the event of a conflict.
10.4 The FMEC may adopt such amendments to these Bylaws, Rules and Regulations, and
policies that are, in the committee’s judgment, technical or legal modifications or clarifications, reorganization or renumbering or those needed due to punctuation, spelling, or other errors of grammar or expression. Such amendments need not be approved by the entire Board but must be approved by the System CEO.
37
Appendix A PRINCIPLES OF MEDICAL ETHICS**
PREAMBLE The medical professions have long subscribed to a body of ethical statements developed primarily for the benefit of the patient. As a member of this profession, a health professional must recognize responsibility to patients first and foremost, as well as to society, to other health professionals and to self. The following Principles are not laws but standards of conduct, which define the essentials of honorable behavior for the health professional. Section 1 A health professional shall be dedicated to providing competent medical care with compassion and respect for human dignity and rights. Section 2 A health professional shall uphold the standards of professionalism, be honest in all professional interactions, and strive to report health professionals deficient in character or competence, or engaging in fraud or deception, to appropriate entities. Section 3 A health professional shall respect the law and also recognize a responsibility to seek changes in those requirements, which are contrary to the best interests of the patient. Section 4 A health professional shall respect the rights of patients, colleagues, and other health professionals and shall safeguard patient confidences and privacy within the constraints of the law. Section 5 A health professional shall continue to study, apply and advance scientific
knowledge, maintain a commitment to medical education, make relevant information available to patients, colleagues and the public, obtain consultation, and use the talents of other health professions when indicated.
38
Section 6 A health professional shall, in the provision of appropriate patient care, except in emergencies be free to choose whom to serve, with whom to associate and the environment in which to provide medical care. Section 7 A health professional shall recognize a responsibility to participate in activities contributing to an improved community and the betterment of pubic health. Section 8 A health professional shall, while caring for a patient, regard responsibility
to the patient as paramount.
Section 9 A health professional shall support access to medical care for all people. **Adapted from the American Medical Association’s “Principles of Medical Ethics” (adopted by the AMA’s
House of Delegates June 17, 2001).
39
PART II: INVESTIGATIONS, CORRECTIVE ACTION, HEARING AND APPEAL PLAN
SECTION 1 ROUTINE CORRECTIVE ACTION & INVESTIGATIONS 1.1 Progressive Intervention These Bylaws encourage the use of progressive steps by Medical Staff leaders and
hospital administration, beginning with collegial and education efforts, to address questions relating to a practitioner’s clinical practice and/or professional conduct. The goal of these efforts is to arrive at voluntary, responsive actions by the practitioner to resolve questions that have been raised. All collegial intervention efforts by Medical Staff leaders and hospital management are part of the hospital’s performance improvement and professional review activities. Collegial intervention efforts are encouraged, but are not mandatory, and shall be within the discretion of the appropriate Medical Staff leaders and hospital administration.
When any observations arise, suggesting opportunities for a practitioner to improve, the matter may be referred in accordance with the performance improvement and professional conduct policies adopted by the Medical Staff and hospital.
Corrective actions and investigations shall be undertaken: 1.1.1 in the reasonable belief that the action is in the furtherance of quality health care; 1.1.2 after a reasonable effort to obtain the facts of the matter,
1.1.3 after adequate notice and hearing procedures are afforded to the practitioner as set forth herein, and
1.1.4 in the reasonable belief that the action is warranted by the facts known after such reasonable effort to obtain the facts.
1.2 Basis for Routine Corrective Action Whenever a concern or question has been raised regarding: 1.2.1 the clinical competence or clinical practice of any appointee; 1.2.2 the care or treatment of a patient or patients or management of a case by any
appointee; 1.2.3 activities or professional conduct that may be detrimental to patient safety; 1.2.4 the known or suspected violation by any Medical Staff appointee of these Bylaws,
the Policies, or the Rules and Regulations of the Medical Staff, System or Department
1.2.5 behavior or conduct on the part of any Medical Staff appointee that is considered lower than the standards of the hospital, disruptive to the hospital or its Medical Staff, including the inability of the appointee to work harmoniously with others; or
1.2.6 impairment, a request for corrective action may be made by any practitioner on the Medical Staff, any
member of the System administration, System or Medical Staff committee, or the Board of
40
Directors, after making sufficient inquiry to satisfy themselves that the concern or question raised is credible.
1.3 Requests and Notices All requests for corrective action shall be made in writing to the President of the Medical
Staff and the Chief Medical Officer, with a copy to the Medical Staff Services Office. The request must be signed by the complainant, clearly state those facts that support the request in sufficient detail to permit an investigation to be pursued, and, if possible, state what corrective action is deemed appropriate by the complainant. The President of the Medical Staff shall notify the FMEC at its next regular meeting that a request for corrective action has been made. The affected practitioner shall be given written notice of the request, and a copy of the same. All notices provided under this Part II shall be hand delivered or sent via certified mail, return receipt requested. All time limits shall begin upon receipt of notice.
1.4 Investigations
1.4.1 When a request for corrective action has been received by the FMEC, the committee shall determine as soon as possible, but no later than at its next regularly scheduled meeting, either to discuss the matter with the appointee concerned, or to begin an investigation. If the concern states sufficient information to warrant action, the FMEC, at its discretion, may initiate an investigation, with or without a personal interview with the practitioner being investigated. The FMEC may seek input from the practitioner’s Department or Section prior to initiating investigation. An investigation shall begin only after a formal resolution of the FMEC to that effect. The affected practitioner shall be given written notice of the initiation of an investigation. If the Board of Directors wishes to begin such an investigation, it shall also formally resolve to do so by mandating the FMEC to begin an investigation.
1.4.2 Upon resolving to initiate an investigation, the Medical Staff President through the
FMEC or President of the Medical Staff shall immediately appoint a member(s) of the Active Medical Staff to conduct an investigation of the matters contained in the request. Investigators shall not include partners, associates or relatives of the practitioner being investigated and should be objective and familiar with the types of issues raised in the request for corrective action.
1.4.3 The investigator(s) may consult with other members of the Medical Staff as
appropriate in order to determine the facts of the case, or to obtain professional opinions relative to the matter under consideration.
1.4.4 The investigator(s) shall have available the full resources of the Medical Staff and
the System, as well as the authority to use outside consultants, if needed. 1.4.5 The investigation should be completed within thirty (30) working days of the
appointment of the investigator(s), unless an extension of not more than thirty (30) additional working days has been granted by the FMEC or President of the Medical Staff.
1.4.6 At the conclusion of the investigation, the investigator(s) shall prepare a written
report of the findings and transmit the same to the President of the Medical Staff and the Chief Medical Officer. In addition to setting forth findings of fact and, if
41
applicable, the clinical opinion of the investigator(s) and other practitioners with whom he may have consulted, the report shall recommend that corrective action be imposed, or that the complaint against the affected practitioner be dismissed.
The investigator may recommend a type or degree of corrective action deemed
appropriate. 1.4.7 The President of the Medical Staff shall review the investigator’s report when it is
received, and if emergency corrective action is indicated, proceed to impose the same pursuant to Section 2 of this part. Otherwise, the President shall submit the investigator’s report to the FMEC for consideration at its next regular meeting.
1.4.8 In cases suggesting practitioner impairment, the President of the Medical Staff shall
confer with a member of the Medical Administrative Staff, designated by the System President and the practitioner’s Department Chair, and if they concur, shall refer the request to the Practitioner Resource Committee for disposition; otherwise, the request shall be referred to the FMEC for consideration at its next regular meeting.
1.5 FMEC Action 1.5.1 If the FMEC determines that there are no reasonable grounds to believe that the
affected practitioner has committed an offense requiring corrective action under these Bylaws, the complaint shall be dismissed. The affected practitioner and complainant shall be given written notification of dismissal.
1.5.2 If the FMEC determines that there are reasonable grounds to believe that the
affected practitioner is subject to corrective action, the Committee may elect to recommend corrective action to the Board, which, at the discretion of the FMEC, may consist of:
1.5.2.1 A written warning that corrective action measures will be taken in the
future if the affected practitioner does not reform his conduct in the manner set forth in the warning;
1.5.2.2 A written reprimand stating the Committee’s displeasure at the affected
practitioner’s behavior, and directing the affected practitioner to cease the same immediately;
1.5.2.3 Mandated education to improve the affected practitioner’s knowledge,
skills and ability in clinical as well as non-clinical subjects;
1.5.2.4 Mandated clinical review or supervision to see that the affected practitioner’s performance attains an acceptable level;
1.5.2.5 Limitation of privileges restricting those procedures that the affected
practitioner may perform at the Facility;
1.5.2.6 Removal of privileges eliminating the affected practitioner’s ability to perform any procedure at the Facility. If the affected practitioner is a member of the Medical Staff, removal of privileges shall also entail revocation of Medical Staff membership. If removal of privileges is recommended at the time of the affected practitioner’s biennial reappointment, this may be accomplished by not recommending the affected practitioner for reappointment;
1.5.2.7 Make such other recommendations, as it deems necessary or appropriate.
42
1.6 Notice of FMEC Action Whenever a recommendation for corrective action has been made by the FMEC, or
corrective action has been taken by the Board on its own initiative, written notice of the same shall be sent to the affected practitioner by certified mail, return receipt requested, or hand delivery with receipt. Such notice shall be consistent with the notice provision set forth in Subsection 1.3. The notice shall set forth the nature of the complaint, the reasons for the corrective action, a description of the corrective action, and a short summary of the affected practitioner’s right to a fair hearing pursuant to these Bylaws, including any time limits within which the affected practitioner must act. The affected practitioner may request a hearing pursuant to the provisions of Section 4.
1.7 Board of Directors Action If the time, during which an affected practitioner may request a hearing pursuant has
expired without a request being made, or such hearing, including appeal to the Board, has been concluded, then at the next regular meeting thereafter of the Board of Directors, the Board shall consider the recommended corrective action. In the event that the Board rejects such recommendation, the Board may remand the recommendation to the FMEC with instructions to reconsider the matter, including the nature and degree of the corrective action. The Board shall consider recommendations of the FMEC following remand in the same manner as other recommendations for corrective action.
SECTION 2 EMERGENCY CORRECTIVE ACTION/PRECAUTIONARY SUSPENSION
OF CLINICAL PRIVILEGES 2.1 Basis for Emergency Corrective Action/Precautionary Suspension The President of the Medical Staff, the Chief Medical Officer (or his designee), or the FMEC
shall have the authority to immediately suspend all or any portion of the clinical privileges of a Medical Staff practitioner or other individual, whenever failure to take such action may result in an imminent danger to the health and/or safety of any individual. Such precautionary suspension shall be deemed an interim precautionary step in the professional review activity related to the ultimate professional review action that may be taken with respect to the suspended individual but is not a complete professional review action in and of itself. It shall not imply any final finding of responsibility for the situation that caused the suspension, nor shall it entitle the practitioner to a fair hearing except as provided under this Section. Those parties with the authority to impose emergency corrective action shall consult with a physician member of the Administration designated by the System President and System legal counsel before imposing any emergency corrective action. This Subsection shall not apply if a clear and present danger exists which requires immediate action and consultation is not feasible.
2.2 Notice of Emergency Corrective Action/Precautionary Suspension
43
Upon imposition of emergency corrective action, the President of the Medical Staff shall immediately give notice to the affected practitioner of such action.
Such notice may be oral, but shall be confirmed in writing as soon as possible, but no later
than the next business day. The written notice shall state the reasons for the emergency corrective action and the nature of corrective action imposed. A copy of the notice shall also be given to the Chief Medical Officer, Department Chair, and FMEC.
2.3 FMEC Procedure When instituted, a precautionary suspension of clinical privileges will automatically expire in
seven (7) days, unless extended by the FMEC, with return of all previous clinical privileges unless the suspension is confirmed by a majority vote of the FMEC in special session. The FMEC shall review the matter resulting in precautionary suspension within a reasonable period not to exceed fourteen (14) days. Unless the FMEC promptly terminates or extends the precautionary suspension prior to or immediately after reviewing the suspension, the practitioner shall be entitled to the procedural rights afforded by the Fair Hearing and Appeal plan once the restrictions or suspension last more than fourteen (14) calendar days. Restrictions or suspensions which last fourteen (14) days or less shall not trigger rights under the Fair Hearing and Appeal Plan.
2.4 Provision of Patient Care Immediately upon the imposition of a precautionary suspension, the appropriate
Department Chair or, if unavailable, the President of the Medical Staff shall assign responsibility for care of the suspended practitioner’s patients still in a System’s facility to another practitioner with appropriate clinical privileges. The assignment shall be effective until the patients are discharged. The wishes of the patient shall be considered in the selection of the assigned practitioner. It shall be the duty of all Medical Staff practitioners to cooperate with the President of the Medical Staff, the Department Chair concerned, the FMEC and the Chief Medical Officer in enforcing all suspensions.
2.5 Recission of Emergency Corrective Action/Precautionary Suspension The person imposing emergency corrective action may, at any time prior to ratification of
such action by the FMEC, rescind the action, and the affected practitioner shall be restored to the status he enjoyed prior to the imposition of emergency correction action. Following ratification of emergency corrective action by the Executive Committee, the person imposing such action may recommend to the FMEC that such action be rescinded. The FMEC shall consider such recommendation at its next regular meeting thereafter. Any pending request for a hearing pursuant to Section 4 shall be made moot and void by such recission.
SECTION 3 AUTOMATIC SUSPENSION AND TERMINATION 3.1 Basis for Automatic Suspension and Termination A practitioner’s clinical privileges shall automatically be revoked, limited or suspended as
appropriate, which action shall be final without a right to due process except as provided in this Section, upon the occurrence of the following circumstances: 3.1.1 Loss of License. The practitioner’s license to practice in the State of Florida is
suspended, limited or terminated.
44
3.1.2 Residence or Office Outside Lee County. The practitioner does not maintain a full-time residence and office in Lee County as
required by these Bylaws, unless such requirements are waived by the FMEC pursuant to said Subsection. Return of United States mail sent by the System Medical Staff Services Office to a practitioner at his Lee County home or office address with “addressee unknown” or similar endorsement shall be prima facie evidence that the practitioner does not comply with these Bylaws. Failure of a practitioner to supply a current residence and office address within 15 working days of a request of the Medical Staff Services Office for the same shall be deemed prima facie evidence that the practitioner does not comply with these Bylaws. This shall not apply to practitioners granted a leave of absence by the FMEC pursuant to these Bylaws.
3.1.3 Lack of Active Practice. The practitioner is not actively engaged in the practice of
his profession in Lee County; that is, he is not seeing, examining, treating or otherwise caring for patients, and has not done so for a period of more than six months, unless the practitioner shall have notified the Medical Staff Services Office prior to beginning such absence, and arranged for suitable coverage during such time period. This shall not apply to practitioners granted a leave of absence by the FMEC pursuant to these Bylaws, or to members of the Honorary Medical Staff.
3.1.4 Criminal Conviction. The practitioner has been, while a practitioner on the Medical
Staff, convicted in any jurisdiction of the United States; of a felony or misdemeanor involving actual or threatened bodily harm, actual or threatened sexual misbehavior or stalking, controlled substance possession or use, or of any felony or misdemeanor described in any Florida law pertaining to governing or regulating the health professions or health facilities. A practitioner whose membership or privileges are automatically terminated pursuant to this Subsection shall not be disqualified from applying for appointment following completion of his sentence, or during a period of time when he is on probation. However, the fact that the practitioner has completed his sentence after criminal conviction, or is on probation, shall not require the Medical Staff to make such appointment, and the FMEC may elect not to do so in its discretion, consistent with its responsibility towards patients, other practitioners, Facility/System employees, and the public in general.
3.1.5 Loss or Restriction of DEA Certificate. The clinical privileges of a practitioner whose
Drug Enforcement Agency (DEA) certification is terminated, revoked, or suspended shall automatically and immediately be modified to revoke the right to prescribe controlled substances. The practitioner shall immediately inform the Medical Staff Services Office regarding the change in status in his DEA certification. The matter shall promptly be referred, for investigation and further action in accordance with the provisions of these Bylaws.
3.1.6 Exclusion From Federal or State Health Care Programs. The Medical Staff
appointment and clinical privileges of a practitioner who becomes an ineligible person with regard to participation in Federal or State Health Care Programs shall automatically and immediately be suspended.
The practitioner shall immediately inform the Medical Staff Services Office regarding
the change of his eligibility status. This triggers the right to due process. The matter shall promptly be referred for investigation and further action in accordance with all the due process provisions of this Part.
45
3.1.7 Failure to Pay Fees and Assessments. The practitioner fails to pay when due any fee or assessment imposed pursuant to these Bylaws or Medical Staff or System policy.
3.1.8 Failure to Provide Requested Information. If at any time a practitioner fails to
provide required information pursuant to a formal request by the System Credentialing/Privileging Committee, Medical Executive Committee or the Medical Staff Services Office, the practitioner’s clinical privileges shall be deemed to be voluntarily relinquished until the required information is provided to the satisfaction of the requesting party. For purposes of this Section, required information shall include but not be limited to: 1. physical or mental examination reports as specified elsewhere in this policy, or 2. information necessary to explain an investigation, professional review action, or resignation from another health care facility or agency.
3.1.9 Failure to Request Reappointment or Provide Requested Information Related to
Reappointment. If a practitioner fails to request reappointment for membership and/or privileges or fails to provide requested information pursuant to Part III, Section 5 of these Bylaws, the practitioner’s membership and privileges shall be deemed voluntarily relinquished.
3.1.10 Failure to Request Reinstatement Following Leave of Absence. Failure to request
reinstatement shall be deemed a voluntary resignation from the Medical Staff and shall result in automatic termination of membership, privileges, and prerogatives. Members whose membership is automatically terminated shall not be entitled to the procedural rights provided in the Medical Staff Bylaws.
3.1.11 Failure to Complete Medical Records. All elective admitting, consulting and clinical
privileges of any practitioner shall be deemed to be voluntarily relinquished for failure to complete medical records in accordance with the provisions of the Medical Staff Rules and Regulations. Such relinquishment shall continue until all the records of the practitioner’s patients are no longer delinquent. Such relinquishment does not exempt the practitioner from fulfilling their on-call responsibilities. Failure to complete the medical records that caused relinquishment of clinical privileges within sixty (60) days from the relinquishment of such privileges shall be grounds for further disciplinary action in accordance with the provisions of these Bylaws.
3.1.12 Failure to Comply with Special Meeting Attendance Requirements. Failure of a
practitioner to attend a special meeting called pursuant to the Bylaws. 3.2 Right to Limited Hearing for Automatic/Voluntary Suspension and Termination A practitioner affected by this Section shall be sent a written notice stating the reasons for
automatic suspension within 24-hours of the same having been imposed, and shall have the right to present evidence to the FMEC in written form, or by appearing personally at a regular meeting of the committee, to demonstrate that the reason that automatic suspension was imposed is untrue.
3.2.1 Such written evidence or a written request to meet with the FMEC shall be
submitted to the President of the Medical Staff within ten (10) working days of the date the notice of automatic suspension was sent. Failure to submit written evidence or a request shall be deemed a waiver of any right to consideration of the same.
46
3.2.2 Evidence presented by the affected practitioner shall be limited to whether or not the grounds for automatic suspension are true. The FMEC shall not consider evidence or argument, which presents mitigating circumstances or excuse.
3.2.3 After receipt of an affected practitioner’s written evidence, and prior to the next
regular meeting of the FMEC, the President of the Medical Staff, with the concurrence of a member of the Medical Administrative Staff designated by the System President, may determine that the evidence so presented demonstrates that
the reasons that automatic suspension was imposed are untrue, and revoke the
suspension, restoring the affected practitioner to the status he previously enjoyed. 3.2.4 The President of the Medical Staff may, at any time, provisionally reinstate a
practitioner suspended pursuant to this Section if the President is satisfied by the available written documentation that the reasons for automatic suspension were untrue. The President shall present the provisional reinstatement for ratification by the FMEC at its next regular meeting.
3.2.5 At its next regular meeting following automatic suspension, the FMEC shall consider
the reasons therefore, together with any evidence or argument presented by the affected practitioner, and if the reasons for automatic suspension are found to be true, recommend to the Board termination of the affected practitioner’s Medical Staff membership and/or privileges. If the FMEC finds that the reasons are untrue or corrected, the suspension shall be revoked, and the affected practitioner restored to the status he previously enjoyed.
SECTION 4 HEARING AND APPEAL PROCEDURES 4.1 Grounds for Hearing An applicant or an individual holding a Medical Staff appointment shall be entitled to
request a hearing whenever the FMEC or the Board of Directors has made one of the following adverse recommendations:
4.1.1 denial of initial Medical Staff appointment; 4.1.2 denial of Medical Staff reappointment; 4.1.3 revocation of Medical Staff appointment; 4.1.4 denial of requested initial clinical privileges; 4.1.5 denial of requested additional clinical privileges; 4.1.6 decrease of clinical privileges;
4.1.7 suspension of clinical privileges (other than emergency corrective action/precautionary suspension);
4.1.8 imposition of mandatory concurring consultation requirement. No other recommendations except those enumerated in this Section shall entitle the practitioner to request a hearing. Neither voluntary relinquishment of clinical privileges, as provided in these Bylaws, nor the imposition of any general consultation requirement, nor the imposition of a requirement for retraining, additional training or continuing education, shall constitute grounds for a hearing, but shall take effect without hearing or appeal. The hearing shall be conducted in as informal a manner as possible, subject to the rules and procedures set forth in these Bylaws.
47
4.2 Notice of Recommendation When a recommendation is made which, according to these Bylaws entitles a practitioner to
a hearing prior to a final decision of the Board, the affected practitioner shall promptly be given notice by the President of the Medical Staff or Chief Medical Officer or his designee, in writing, certified mail, return receipt requested or in person. This notice shall contain:
4.2.1 a statement of the recommendation made, the action which is being taken or which may be taken, and the general reasons for it; 4.2.2 notice that the practitioner has the right to request a hearing on the
recommendation within thirty (30) days of receipt of this notice; and 4.2.3 a copy of this Part outlining the rights in the hearing as provided for in these
Bylaws.
4.3 Request for Hearing A practitioner shall have thirty (30) days following the date of the receipt of such notice
within which to request the hearing. The request shall be in writing to the President of the Medical Staff or Chief Medical Officer with a copy to the Medical Staff Services Office and signed by the affected practitioner making such request. In the event the practitioner does not request a hearing within the time and in the manner required by these Bylaws, the practitioner shall be deemed to have waived the right to the hearing and to have accepted the action involved. That action shall become effective immediately upon final Board action.
4.4 Preliminary Interview The affected practitioner may request, at the time of submitting a request for hearing or
within ten (10) working days thereafter, an informal preliminary interview with the decision making body (FMEC or Board of Directors). The decision making body shall grant all such requests, and the affected practitioner shall be scheduled to appear before it at its next regular meeting. 4.4.1 The purpose of the preliminary interview shall be to permit the affected practitioner
to personally present any argument or evidence showing that the adverse recommendation has been wrongfully imposed, in fact, or in violation of these Bylaws; or to present any mitigating circumstances.
4.4.2 The preliminary interview is informal and not a hearing. It is optional with the
affected practitioner, and accordingly, legal counsel shall be excluded. 4.4.3 The decision making body may impose a limit on the amount of time to be devoted
to a preliminary interview, but not less than thirty minutes. 4.4.4 Failure to request a preliminary interview shall not be considered in any hearing or
deliberation conducted pursuant to these Bylaws, nor shall the affected practitioner’s right to a hearing be affected thereby.
48
4.4.5 Following a preliminary interview, the decision making body shall deliberate, and may elect to withdraw or reduce the severity of the adverse recommendation imposed upon the affected practitioner, or may take no action.
If no action is taken, the adverse recommendation shall continue in effect, and the hearing provided for hereunder shall proceed.
4.4.6 Notice shall be given to the affected practitioner of the decision following a
preliminary interview in the manner provided in Subsection 1.3.
SECTION 5 FAIR HEARING PROCEDURE 5.1 System Representative, Hearing Panel and Hearing Officer 5.1.1 System Representative 5.1.1.1 When the FMEC of the Medical Staff is the decision making body, the
President of the Medical Staff shall appoint a person to represent the interests and position of the Medical Staff in all proceedings provided for in this Section. Such individual shall be in an adversarial role opposed to the affected practitioner. If the affected practitioner is not represented by legal counsel, the Medical Staff representative shall not be an attorney, but shall be a member of the Active Medical Staff.
5.1.1.2 When the Board is the decision making body, as defined herein, the
Chair of the Board shall appoint a person to represent the interests and position of the Board in all proceedings provided for in this Section. Such individual shall be in an adversarial role opposed to the affected practitioner. If the affected practitioner is not represented by legal counsel, the Board representative shall not be an attorney, but shall be a member of the administration.
5.1.1.3 For purposes of these Bylaws, the Medical Staff or Board representative
appointed under this Section shall be called the “System Representative.”
5.1.2 Hearing Panel 5.1.2.1 Unless the FMEC or Board elects to have the matter heard by a Hearing
Officer possessing the qualifications set forth in Subsection 5.1.3, all hearings shall be conducted by a Hearing Panel appointed by the President of the Medical Staff or the Chair of the Board, as applicable,
composed of five (5) members, presided over by a qualified professional selected in accordance with Subsection 5.1.3. The Hearing Panel shall be composed of Active Medical Staff practitioners who shall not have actively participated in the consideration of the matter involved at any previous level. Knowledge of the matter involved shall not preclude any individual from serving as a member of the Hearing Panel.
If the hearing has been requested based on Board action, 3 of the
members of the Hearing Panel shall be members of the Board of Directors. The Hearing Panel will be presided over by a Hearing Officer.
5.1.2.2 The Hearing Panel shall not include any individual who is in direct
economic competition with the affected person or has any other personal interest in the proceeding, financial or otherwise, or any such individual
49
who is professionally associated with or related to the affected practitioner.
5.1.3 Hearing Officer – Qualifications & Authority 5.1.3.1 The FMEC or the Board may elect to have the hearing provided for in
this Section held by a Hearing Officer sitting alone. In such case, the Hearing Officer shall perform all of the functions of the Hearing Panel described herein.
In cases where a panel is appointed, the Hearing Officer will preside over
the proceeding but not participate in the deliberations or vote on the recommendation.
5.1.3.2 The Hearing Officer:
5.1.3.2.1 shall be an attorney licensed in the State of Florida who is
knowledgeable and has experience in health care law, including Medical Staff law; or shall be a non-lawyer who has experience as a Hearing Officer;
5.1.3.2.2 shall not be, or have been, employed or retained by the Lee
Memorial Health System, or any practitioner on the Medical Staff, including the affected practitioner, for any purpose other than to serve as a Hearing Officer in Medical Staff proceedings;
5.1.3.2.3 shall have no personal interest in the proceeding, financial or
otherwise; 5.1.3.2.4 shall be selected by the affected practitioner from a list
provided to the affected practitioner by the General Counsel for the Health System of the names of not less than three (3) persons meeting the requirements of 1-3 above. The affected practitioner shall select the Hearing Officer from the list submitted to him and within forty-eight (48) hours of receiving said list, notify the General Counsel for the Health System in writing of said selection.
Failure of the affected practitioner to select within the
previously mentioned period shall constitute a waiver by the affected practitioner of this Subsection, and the General Counsel for the Health System shall thereafter select the Hearing Officer.
5.1.3.3 The Hearing Officer shall: 5.1.3.3.1 act to insure that all participants in the hearing have a
reasonable opportunity to be heard and to present oral and documentary evidence subject to reasonable limits on the number of witnesses and duration of direct and cross examination, applicable to both sides, as may be necessary to avoid cumulative or irrelevant testimony or to prevent abuse of the hearing process;
50
5.1.3.3.2 prohibit conduct or presentation of evidence that is cumulative, excessive, irrelevant, and abusive or that causes undue delay;
5.1.3.3.3 maintain decorum throughout the hearing; 5.1.3.3.4 determine the order of procedure throughout the hearing; 5.1.3.3.5 have the authority and discretion, in accordance with these
Bylaws, to make rulings on all questions that pertain to matters of procedure and to the admissibility of evidence and qualifications of witnesses;
5.1.3.3.6 act in such a way that the Hearing Panel in formulating its
recommendations considers all information relevant to the continued appointment or clinical privileges of the practitioner requesting the hearing;
5.1.3.3.7 conduct argument by counsel on procedural points outside
the presence of the Hearing Panel unless the Panel wishes to be present;
5.1.3.3.8 grant continuances and postponements as appropriate; and 5.1.3.3.9 take official notice of any matters, either technical or scientific,
relating to the issues under consideration that could have been judicially noticed by the courts of this state, inform the participants of the matters to be officially noticed and provide each party the opportunity to request that a matter be officially noticed or to refute the noticed matter by evidence or by written or oral presentation of authority.
5.2 Challenge to Hearing Panel Members or Hearing Officer
The affected practitioner may challenge the objectivity of any member of the Hearing Panel, or the Hearing Officer, at any time prior to the taking of testimony at the hearing. Such challenge shall be in writing and specify facts demonstrating that a member of the Hearing Panel or the Hearing Officer lacks objectivity or is biased against the affected practitioner. The challenge shall be directed to the President of the Medical Staff or the Chair of the Board, as applicable, who shall consider the challenge and either sustain or overrule it. If the challenge is sustained, the challenged member of the Hearing Panel or the Hearing Officer shall be replaced.
SECTION 6 HEARING PROCEDURES 6.1 Provision of Relevant Information
6.1.1 There is no right to discovery in connection with the hearing. However, the
practitioner requesting the hearing shall be entitled, upon specific request, to the following, subject to a stipulation signed by both parties that such documents shall be maintained as confidential and shall not be disclosed or used for any purpose outside of the hearing:
51
6.1.1.1 copies of, or reasonable access to, all patient medical records referred to in the Statement of Reasons, at the practitioner’s expense;
6.1.1.2 reports of experts relied upon by the FMEC or the Board; 6.1.1.3 redacted copies of relevant committee or Department meeting minutes
(such provision does not constitute a waiver of the state peer review protection statute); and
6.1.1.4 copies of any other documents relied upon by the FMEC or the Board.
6.1.2 Prior to the hearing, on dates set by the Hearing Officer or agreed upon by counsel
for both sides, each party shall provide the other party with a list of proposed exhibits. All objections to documents or witnesses to the extent then reasonably known, shall be submitted in writing in advance of the hearing. The Hearing Officer shall not entertain subsequent objections unless the party offering the objection demonstrates good cause.
6.1.3 Prior to the hearing, on dates set by the Hearing Officer, the practitioner requesting
the hearing shall, upon specific request, provide the FMEC (or the Board of Directors) copies of any expert report or other documents relied upon by the practitioner.
6.1.4 Neither the affected practitioner, nor his attorney, nor any other person on behalf of
the affected practitioner, shall contact members of the hearing committee or the Hearing Officer, or hospital employees appearing on the hospital’s witness list concerning the subject matter of the hearing, unless specifically agreed upon by counsel.
6.2 Pre-Hearing Conference The Hearing Officer may require counsel for the practitioner and for the FMEC (or the
Board) to participate in a pre-hearing conference for purposes of resolving all procedural questions in advance of the hearing. The Hearing Officer may specifically require that:
6.2.1 all documentary evidence to be submitted by the parties be presented at this
conference; any objections to the documents shall be made at that time and the Hearing Officer shall resolve such objections;
6.2.2 evidence unrelated to the reasons for the unfavorable recommendation or unrelated
to the practitioner’s qualifications for appointment or the relevant clinical privileges be excluded;
6.2.3 the names of all witnesses and a brief statement of their anticipated testimony are
submitted, if not previously provided; 6.2.4 the time granted to each witness’ testimony and cross-examination be agreed upon,
or determined by the Hearing Officer, in advance; and 6.2.5 witnesses and documentation not provided and agreed upon in advance of the
hearing may be excluded from the hearing. 6.3 Failure to Appear
52
Failure, without good cause, of the practitioner requesting the hearing to appear and proceed at such a hearing shall be deemed to constitute voluntary acceptance of the pending recommendations or actions, which shall then be forwarded to the Board for final action. The Hearing Officer may impose sanctions upon either party for failure to appear, including the assessment of the costs and attorneys’ fees of the party in attendance against the offending party.
6.4 Record of Hearing A record shall be made at the expense of the Lee Memorial Health System, if any, the pre-
hearing conference and the hearing, using the services of a court reporter. No record of the in camera deliberations of the decision making body or the hearing committee shall be
made. Either party shall be entitled to have a record made of any other proceeding related to the hearing process, at that party’s expense. The expense of transcripts shall be borne by the party requesting them. Oral evidence shall be taken only on oath or affirmation administered by any person designated by such body and entitled to notarize documents in this State.
6.5 Rights of Both Sides At a hearing, both sides shall have the following rights, subject to reasonable limits
determined by the Hearing Officer: 6.5.1 to call and examine witnesses to the extent available; 6.5.2 to introduce exhibits; 6.5.3 to cross-examine any witness on any matter relevant to the issues and to rebut any
evidence; 6.5.4 to be represented by counsel who may call, examine, and cross-examine witnesses
and present the case. (Both sides shall notify the other of the name of that counsel at least ten (10) days prior to the date of the pre-hearing conference and hearing); and
6.5.5 to submit a post-hearing memorandum of points and authorities (The Hearing Panel may request such a memorandum to be filed following the close of the hearing).
Any practitioner requesting a hearing, who does not testify on his own behalf, may be called
and examined as if under cross-examination. The Hearing Panel or Hearing Officer may question the witnesses, call additional witnesses or request additional documentary evidence.
6.6 Admissibility of Evidence The rules of evidence applicable to the courtroom shall not apply, and the Hearing Officer
may admit any evidence that might be relied upon by a reasonable person. Notwithstanding the foregoing, a party shall have the right to object to any evidence on
grounds of hearsay, relevance, or other grounds available under the Florida Evidence Code, and the Hearing Officer shall have the authority to rule on such objections.
6.7 Burden of Presenting Evidence and Proof The burden of going forward with evidence supporting the adverse action or
recommendation is on the FMEC or Board, whichever initially prompted the hearing. Once that burden has been met to the satisfaction of the Hearing Panel/Hearing Officer, the practitioner shall bear the burden of proof, under a preponderance of the evidence, which is a lesser standard than clear and convincing evidence, that the action and penalty taken or
53
proposed against the practitioner was wrongfully or arbitrarily imposed, not in accordance with these Bylaws, or lacks any factual basis.
SECTION 7 HEARING CONCLUSION, DELIBERATIONS AND RECOMMENDATIONS
7.1 Deliberations and Recommendation of the Hearing Panel/Hearing Officer
7.1.1 The recommendation of the Hearing Panel/Hearing Officer shall be based on the evidence produced at the hearing. This evidence may consist of oral testimony of witnesses; memorandum of points and authorities presented in connection with the hearing, any information regarding the practitioner who requested the hearing so long as that information has been admitted into evidence at the hearing and the person who requested the hearing had the opportunity to comment on and, by other evidence, refute it, any and all applications, references, and accompanying documents; other documented evidence, including medical records and any other information presented at the hearing.
7.1.2 Within thirty (30) working days after final adjournment of the hearing, the Hearing
Panel shall conduct its deliberations outside the presence of any other person except the Hearing Officer, and shall prepare a recommended order containing the findings of fact, findings regarding the applicability of these Bylaws, any rules, regulations or policies of the Medical Staff or the Lee Memorial Health System, and the statutory and decisional law of Florida; and a recommendation that adverse action be upheld, modified or withdrawn. If the FMEC or the Board selected a Hearing Officer sitting alone, the Hearing Officer shall prepare a recommended order in the same manner outlined above.
7.1.3 The Hearing Officer shall not participate in the deliberations of the Hearing Panel,
nor be involved in the decision of the Hearing Panel regarding its recommended order.
However, the Hearing Officer may assist the Hearing Panel with regard to the form,
organization and syntax of the recommended order. The recommended order shall be signed by each member of the Hearing Panel or the Hearing Officer, as applicable, and copies provided in person by certified mail, return receipt requested, to the affected practitioner and System Representative.
7.2 Disposition of Hearing Panel Report The Hearing Panel/Hearing Officer shall deliver its report and recommendation to the Chief
Medical Officer or his designee who shall forward it, along with all supporting documentation, to the Board and/or FMEC.
The recommended order shall be considered by the FMEC or Board at its next regular meeting, and may be adopted or rejected by it. If adopted, the recommended order shall become the final decision of the original decision making body (FMEC or Board).
If rejected, the FMEC or Board shall render its own final written decision upholding the
original recommendation, modifying or withdrawing the action. Any action imposed through the final order that requires action by the Board of Directors shall be referred to the Board for final disposition at its next regular meeting.
SECTION 8 APPEAL PROCEDURE
54
8.1 Request & Time for Appeal Within ten (10) working days of receipt of the final written decision following a hearing,
either party may appeal the recommendation. The request shall be in writing, signed by the requesting party and delivered to the Chief Medical Officer either in person or by certified mail, return receipt requested, with a copy to the Medical Staff Services Office. The request shall include a statement of the reasons for appeal and the facts or circumstances that justify further review. If such appellate review is not requested within ten (10) working days as provided herein, both parties shall be deemed to have waived the right to an appeal, and the Hearing Panel or Hearing Officer’s report and recommendation shall be forwarded to the Board for final action.
8.2 Grounds for Appeal The grounds for appeal shall be limited to the following: 8.2.1 there was substantial failure to comply with these Bylaws or hospital policies prior to
the hearing so as to deny a fair hearing; or 8.2.2 the recommendations of the Hearing Panel were made arbitrarily, capriciously or
with prejudice. 8.3 Time, Place and Notice Whenever an appeal is requested as set forth in the preceding Sections, the Chair of the
Board shall, as soon as arrangements can reasonably be made, taking into account the schedules of all participants, schedule and arrange for an appellate review. The affected practitioner shall be given notice of the time, place and date of the appellate review. When a request for appellate review is from a appointee who is under a suspension then in effect, the appellate Review panel shall be convened not more than 14-days from the date of receipt of the request for an appeal unless the practitioner agrees to a longer period. The time for appellate review may be extended by the Chair of the Board for good cause.
8.4 Nature of Appellate Review 8.4.1 Review panel. The Chair of the Board shall appoint a Review panel composed of 5
members, 3 of the panel members shall be members of the Board of Directors and 2 panel members shall be Active members of the Medical Staff. The Board may establish rules of procedure to govern the conduct of appellate hearings under this Section and the Chair of the Board, or his or her designee, shall preside at appellate proceedings.
8.4.2 Position Papers. Each party shall have the right to present a written statement in
support of its position on appeal. Position papers that do not conform to the following requirements may be excluded from consideration in the appeal.
8.4.2.1 The position papers shall set forth a statement of the facts and of the
applicable Bylaws provisions or other authority, as well as any other matters that the parties wish to bring before the appellate body in support of their respective positions.
8.4.2.2 Twelve copies of the affected practitioner’s position paper shall be filed
with Medical Staff Services within (fifteen)15 working days of the filing of
55
the notice of appeal. The System Representative shall also file with Medical Staff Services, 12 copies of his position paper within ten (10) working days of his receipt of a copy of the affected practitioner’s position paper.
8.4.2.3 Position papers shall be limited to no more than thirty (30) pages,
exclusive of exhibits, and shall be on letter-size paper, typewritten, double-spaced and shall be neatly bound or stapled.
8.4.2.4 Each party shall provide a copy of his position paper to the other at the
same time the party’s position paper is filed with Medical Staff Services. 8.4.2.5 Exhibits attached to the position paper shall not duplicate exhibits or
documents contained in the hearing record, and shall be consecutively numbered and attached at the end of the position paper.
8.4.2.6 In referring to the record, position papers shall reference specific pages of
the hearing record and of exhibits that are part of the record. 8.4.3 Oral Argument. The affected practitioner and the System Representative shall be
entitled to present oral argument. Oral argument shall be requested at the time the party submits his position paper. Failure to request oral argument shall constitute a waiver of the right to it. The Board may limit the time for oral argument, but each side shall not have less than thirty (30) minutes. Oral argument shall not include the introduction of evidence and appellate review shall not constitute a hearing de novo.
A record shall be made at the expense of the Lee Memorial Health System of the presentation of oral argument, using the services of a court reporter.
8.4.4 Recommendation. The review panel shall recommend final action to the Board
within thirty (30) working days after the completion of oral argument, or if no oral argument is requested, within forty-five (45) working days after the submission of the position papers of both parties.
SECTION 9 FINAL DECISION OF THE BOARD Within thirty (30) working days after receipt of the Review panel’s recommendation, the Board shall render a final decision in writing, including specific reasons and shall deliver copies thereof to the affected practitioner, the FMEC, and the Medical Staff Services Office, in person or by certified mail, return receipt requested. The decision shall uphold or reverse the final written decision rendered by the decision making body, or may remand the case for reconsideration by the decision making body. If the matter is referred for further action and recommendation, such recommendation shall be promptly made to the Board in accordance with the instructions given by the Board within thirty (30) days. The final decision of the Board following the appeal shall be effective immediately and shall not be subject to further review. SECTION 10 RIGHT TO ONE HEARING AND ONE APPEAL ONLY 10.1 No applicant or Medical Staff practitioner shall be entitled to more than one (1) hearing and
one (1) appeal on any matter that may be the subject of an appeal. A final appellate
56
decision upholding or reversing a final, written decision shall be final and there shall be no right to further hearing on the matter.
10.2 If the Board determines to deny initial Medical Staff appointment or reappointment to an
applicant, or to revoke or terminate the Medical Staff appointment and/or clinical privileges of a current practitioner, that practitioner may not apply for Staff appointment or for those clinical privileges at this hospital for a period of five (5) years unless the Board provides otherwise.
PART III: CREDENTIALING PROCEDURES
SECTION 1 SYSTEM CREDENTIALING/PRIVILEGING COMMITTEE 1.1 Organizational Structure
It is the intention of the Medical Staff Organizations of Lee Memorial Health System (LMHS) to ultimately establish one (1) System Credentialing/Privileging Committee (hereinafter referred to as the Credentialing/Privileging Committee) to act on behalf of all the Medical Staff of LMHS. It has been determined that the two (2) Credentialing/Privileging Committees in effect at the time of the approval of this document may continue for a maximum period of two (2) years. During this transition time, the two (2) Credentialing/Privileging Committees will meet jointly on at least a quarterly basis (the Credentialing/Privileging Committees will not meet separately during the months that the joint meetings occur) and through this process will effect a smooth transition to a single System Credentialing/Privileging Committee. The single System Credentialing/Privileging Committee may decide to merge prior to the end of the two 2-year period.
1.2 Transition Issues
At the time of adoption of PART III, two (2) Credentialing/Privileging Committees exist. Chairs of each of these Credentialing/Privileging Committees have been appointed in accordance to procedures that were in existence prior to the adoption of these Credentials Procedures. During the transition period (moving from two (2) committees to a single System Credentialing/Privileging Committee), these Chairs will continue to serve as the Chairs of the applicable practitioner System Credentialing/Privileging Committee and together will serve as Co-Chairs of the System Credentialing/Privileging Committee (which will meet at least quarterly (see Section 1.1).
The initial composition of the System Credentialing/Privileging Committee will be made up of
the membership of the two (2) separate Credentialing/Privileging Committees, with the current Chairs serving as Co-Chairs. During the first year of the System Credentialing/Privileging Committee, the committee will plan to evolve to the composition of the System Credentialing/Privileging Committee as established in Section 1.4 by the end of twenty-four (24) months.
1.3 Purpose of the System Credentialing/Privileging Committee
The System Credentialing/Privileging Committee exists to oversee all credentialing and privileging activities related to Medical Staff members and privileged Allied Health
57
practitioners on behalf of the Facility Medical Executive Committees (FMECs). These credentialing and privileging activities include processes related to the following:
1.3.1 initial appointment; 1.3.2 focused professional practice evaluation; 1.3.3 reappointment; 1.3.4 delineation of clinical privileges, including temporary privileges; and 1.3.5 development of privilege delineation forms and criteria for all LMHS facilities. Credentialing activities are to be carried out in accordance with specific policies and
procedures developed to ensure current clinical competency of the practitioners who are credentialed and privileged at LMHS. The purpose of the System Credentialing/Privileging
Committee also includes development of implementation of credentialing and privileging policies and procedures designed to ensure compliance with regulatory requirements.
1.4 Composition of the System Credentialing/Privileging Committee The leadership and membership of the System Credentialing/Privileging Committee shall be
as follows: 1.4.1 Consist of not less than 15 members of the active Medical Staff selected on a basis
that will ensure, insofar as feasible, balanced representation of the LMHS sites. 1.4.2 The System Medical Director will serve as a non-voting member. 1.4.3 The Immediate Past President of each FMEC will serve as voting members and will
serve a 2-year term. The FMEC may appoint this practitioner, as a member once the Immediate Past President is no longer in office.
1.4.4 Each FMEC will appoint two (2) additional representatives. 1.4.5 A quorum of 50% is required to conduct a meeting. 1.4.6 Members shall serve for two (2) years and may be reappointed to consecutive terms. 1.4.7 Each member shall be required to attend 75% of the meetings during the Medical
Staff year. Failure to attend 75% of the meetings may result in dismissal of the member from committee service and selection of an alternative member by the affected FMEC.
1.4.8 The committee members from among the committee membership will elect the Co-
Chairs of the System Credentialing/Privileging Committee. One of the Co-Chairs will be from a medical specialty and the other Co-Chair will be from a surgical specialty.
1.5 Duties and Responsibilities of the System Credentialing/Privileging Committee The System Credentialing/Privileging Committee shall: 1.5.1 Meet to evaluate credentialing-related requests (initial appointment, reappointment,
requests for clinical privileges and leave of absence, etc.) on behalf of the FMECs. 1.5.2 Monitor the granting of temporary privileges to assure that temporary privileges are
granted in compliance with approved policies and procedures. (The System Credentialing/Privileging Committee does not evaluate requests for temporary
58
privileges. These requests are handled in accordance with specific policies and procedures that are overseen by the System Credentialing/Privileging Committee).
1.5.3 Oversee the processes related to focused professional performance evaluations and
related proctoring and other mechanisms and tools employed to evaluate competency.
1.5.4 Assure uniformity in both the development and application of privileging criteria
utilized throughout LMHS facilities. 1.5.5 Assure the FMECs and Board that Medical Staff Bylaws Provisions that relate to
credentialing and privileging processes are being fulfilled, as well as credentialing policies and procedures and other credentialing-related Medical Staff documents. Monitor compliance with all credentialing and privileging policies and procedures.
1.5.6 Be responsible for evaluating recommendations made by Department Chairs. The committee is looking for completeness, thoroughness and adherence to
credentialing and privileging policies and criteria. Assure the FMECs that specialty-specific criteria for clinical privileges comply with Medical Staff Bylaws, credentialing policies and procedures, and criteria is applied fairly and uniformly to each practitioner.
1.5.7 Focuses in on the files that are determined to need clarification or additional
information (i.e., time gaps, problems with references, malpractice claims, etc.) and assures that all issues have been appropriately addressed and that there is complete and thorough documentation for the recommendation(s) that have been made to the FMECs.
1.5.8 Be responsible and aware of regulatory requirements related to credentialing activities
and to make the FMECs and Board aware when changes in credentialing policies and procedures need to be made in order to meet requirements.
1.5.9 Commission, receive and analyze the results of compliance audits of credentialing
and privileging processes. The System Credentialing/Privileging Committee makes recommendations to the FMECs and the Board when the System Credentialing/Privileging Committee believes, based on results of reports that improvements can and should be made in credentialing and privileging policies and procedures.
SECTION 2 QUALIFICATIONS FOR MEMBERSHIP AND PRIVLEGES 2.1 The following qualifications must be met by all applicants for Medical Staff
appointment, reappointment or clinical privileges:
2.1.1 Associate and Active Staff shall live and maintain an office in Lee County, unless this requirement is waived by the FMEC;
2.1.2 Demonstrate that he has successfully graduated from an approved school of
medicine (MD or DO), dentistry, podiatry, clinical psychology or applicable recognized course of training in a clinical profession eligible to hold privileges;
59
2.1.3 Have a current unrestricted state or federal license as a physician, dentist, podiatrist or clinical psychologist, applicable to his or her profession, and providing permission to practice within the State of Florida;
2.1.4 Have a record that is free from current Medicare/Medicaid sanctions and not be on
the Office of Inspector General (OIG) or General Services Administration (GSA) List of Excluded practitioners/entities;
2.1.5 Have a record that is free of felony convictions or occurrences that would raise
questions of undesirable conduct, which could injure the reputation of the Medical Staffs, hospital or Health System;
2.1.6 A physician (MD or DO) must have successfully completed an allopathic or
osteopathic residency program, approved by the Accreditation Council for Graduate Medical Education (ACGME) or the American Osteopathic Association (AOA) and be currently board certified or become board certified following the completion of formal training within the timeframes as defined by the appropriate specialty board of the American Board of Medical Specialties or the American Osteopathic Association. If no time limits for certification are specified by a given Board, then the applicant will be required to become Board certified within seven (7) years of completing formal training as defined by the appropriate specialty Board of the American Board of Medical Specialties or the American Osteopathic Association. If an applicant is beyond seven (7) years of completing formal training, current Board certification will be required for consideration of membership and privileges. Once a member of the Medical Staff becomes Board certified, recertification is not a requirement of continued membership and privileges;
2.1.7 Dentists must have graduated from an American Dental Association approved
school of dentistry accredited by the Commission of Dental Accreditation; 2.1.8 Oral and maxillofacial surgeons must have graduated from an American Dental
Association approved school of dentistry accredited by the Commission of Dental Accreditation and successfully completed an American Dental Association approved residency program and be board certified or become board certified within five (5) years of completing formal training as defined by the American Board of Oral and Maxillofacial Surgery;
2.1.9 A podiatric physician (DPM) must have successfully completed a two 2-year
residency program in surgical, orthopedic, or podiatric medicine approved by the Council on Podiatric Medical Education of the American Podiatric Medical Association (APMA), and be board certified or become board certified within five (5) years of completing formal training as determined by the American Board of Podiatric Surgery or the American Board of Podiatric Orthopedics and Primary Podiatric Medicine;
2.1.10 A psychologist, must have earned a doctorate degree, (PhD or Psy.D. in
psychology) from an educational institution accredited by the American Psychological Association and have completed at least two (2) years of clinical experience in an organized healthcare setting, supervised by a licensed psychologist, one 1-year of which must have been post doctorate, and have completed an internship endorsed by the American Psychological Association (APA);
2.1.11 Possess a current, valid, Drug Enforcement Administration (DEA) number if
applicable to the privileges requested;
60
2.1.12 Have appropriate written and verbal communication skills; 2.1.13 Have appropriate personal qualifications, including applicant’s consistent
observance of ethical and professional standards. These standards include, at a minimum:
2.1.13.1 Abstinence from any participation in fee splitting or other illegal payment,
receipt, or remuneration with respect to referral or patient service opportunities;
2.1.13.2 A history of consistently acting in a professional, appropriate and
collegial manner with others in previous clinical and professional settings.
2.1.14 The following qualifications must also be met by all applicants requesting clinical
privileges: 2.1.14.1 Demonstrate his background, experience, training, current competence,
knowledge, judgment and the ability to perform all privileges requested. 2.1.14.2 Provide evidence of both physical and mental health that does not impair
the fulfillment of his responsibilities of Medical Staff membership subject to any legally required reasonable accommodation, and the specific privileges requested by and granted to the applicant, upon request.
2.1.14.3 Any practitioner granted privileges that may have occasion to admit an
inpatient must demonstrate the capability to provide continuous and timely care to the satisfaction of the FMEC and Board.
2.1.14.4 Demonstrate recent clinical performance (within the last twelve (12)
months with an active clinical practice in the area in which clinical privileges are sought adequate to meet current clinical competence criteria.
2.1.14.5 The applicant is requesting privileges for a service the Board has
determined appropriate for performance at the hospital. There must also be a need for this service under any Board approved Medical Staff development plan.
2.1.14.6 Provide evidence of financial responsibility consistent with the
requirements set forth in Part I. 2.1.15 Exceptions: All practitioners who are current Medical Staff members and/or hold privileges as of
May 28, 2009 and who have met prior qualifications for membership and/or privileges shall be exempt from Board specialty certification requirements.
SECTION 3 PRE-APPLICATION PROCESS
61
3.1 Only those practitioners that meet the following minimum criteria for appointment to the Medical Staff will be provided applications. Practitioners provided applications would be those: 3.1.1 which are not governed by an exclusive arrangement or who are joining a group
providing services governed by an exclusive arrangement; and
3.1.2 who meet the minimum criteria as developed by the System Credentialing/Privileging Committee and approved by FMECs and the Board.
The purpose for the pre-application screening process shall be to avoid the costly
and time-consuming application process in those circumstances where an applicant fails to meet minimum eligibility criteria. Practitioners who do not meet the minimum eligibility criteria for appointment are not entitled to fair hearing rights.
The System Credentialing/Privileging Committee shall review all requests for
application and determine whether the criteria for issuing an application have been met.
SECTION 4 INITIAL APPOINTMENT PROCESS
4.1 Completion of Application 4.1.1 All requests for application for appointment to the Medical Staff and requests for
clinical privileges will be forwarded to the Medical Staff Services Department. If the applicant successfully completed the pre-application screening process, the Medical Staff Services Department will provide the applicant an application packet, which will include a complete set or overview of the relevant Medical Staff Bylaws or reference to an electronic source for this information. This packet will enumerate the eligibility requirements for Medical Staff membership (for each facility of LMHS) and/or privileges and a list of expectations of performance for practitioners granted Medical Staff membership or privileges (if such expectations have been adopted by each Facility Medical Staff).
A completed application includes, at a minimum: 4.1.1.1 a completed, signed, dated application form; 4.1.1.2 a completed privilege delineation form if requesting privileges; 4.1.1.3 copies of all requested documents and information necessary to confirm
the applicant meets criteria for membership and/or privileges and to establish current competency;
4.1.1.4 all applicable fees; 4.1.1.5 complete reference information; references shall be from peers (same
specialty) knowledgeable about the applicant’s experience, ability and current competence to perform the privileges being requested;
4.1.1.6 relevant practitioner-specific data as compared to aggregate data, when
available
62
4.1.1.7 morbidity and mortality data, when available. Each applicant must indicate the LMHS facility anticipated to be his
primary facility (i.e., the facility where the majority of his clinical activity is performed). It should be noted that this designation is important for credentialing purposes (interviews, implementation of focused professional practice evaluation, etc.) and will be confirmed by LMHS data at periodic intervals and prior to any subsequent reappointments.
An application shall be deemed incomplete if any of the above items are
missing or if the need arises for new, additional or clarifying information in the course of reviewing an application. An incomplete application will not be processed and the applicant will not be entitled to a fair hearing.
Anytime in the credentialing process it becomes apparent that an
applicant does not meet all eligibility criteria for membership or privileges, the credentialing process will be terminated and no further action taken. Applications will not be accepted from practitioners that are not eligible to take the Board certification examination.
4.1.2 The burden is on the applicant to provide all required information. It is the
applicant’s responsibility to ensure that the Medical Staff Services Department receives all required supporting documents verifying information on the application and to provide sufficient evidence, as required in the sole discretion of the Health System that the applicant meets the requirements for the Medical Staff membership and/or the privileges requested. If information is missing from the application or new, additional or clarifying information is required, a letter requesting such information will be sent to the applicant. If the requested information is not returned to the Medical Staff Services Department within thirty (30) calendar days of the receipt of the requested letter, the application will be deemed to have been voluntarily withdrawn.
4.1.3 Upon receipt of a completed application, the System Medical Director will determine
if the requirements of Section 2.1 are met. In the event the requirements of Section 2.1 are not met, the applicant will be notified that he is ineligible to apply for membership or privileges on the Medical Staff, the application will not be processed and the applicant will not be eligible for a fair hearing. If the requirements of Section 2.1 are met, the application will be accepted for further processing.
4.1.4 Practitioners seeking appointment shall have the burden of producing information
deemed adequate by the hospital for a proper evaluation of current competence, character, ethics, other qualifications and of resolving any doubts.
4.1.5 Upon receipt of a completed application, the Medical Staff Services Department will
verify current licensure, education, relevant training and current competence from the primary source whenever feasible in accordance with the Verification Methods and Requirements document.
When it is not possible to obtain information from the primary source, reliable
secondary sources may be used if there has been a documented attempt to contact the primary source.
Note: In the event there is undue delay in obtaining required information, the
Medical Staff Services Department will request assistance from the applicant. During this time, the period for processing, the application will be appropriately
63
modified. Failure of an applicant to respond to a request for assistance adequately after thirty (30) calendar days the application will be deemed to have been voluntarily withdrawn.
4.1.6 When all items identified in the Verification Methods and Requirements document
have been obtained and verified, the application will be considered eligible for evaluation.
4.2 Applicant’s Attestation, Authorization and Acknowledgement 4.2.1 The applicant must complete and sign the application form. By signing this
application the applicant: 4.2.1.1 Attests to the accuracy and completeness of all information on the
application or accompanying documents and agreement that any inaccuracy, omission or misrepresentation, whether intentional or not, may be grounds for termination of the application process without the right to a fair hearing or appeal.
If the inaccuracy, omission or misstatement is discovered after a
practitioner has been granted appointment and/or clinical privileges, the practitioner’s appointment and privileges shall lapse effective immediately upon notification of the practitioner without the right to a fair hearing or appeal.
4.2.1.2 Consents to appear for any requested interviews about his application. 4.2.1.3 Authorizes the applicable hospital and Medical Staff representative to
consult with prior and current associates and others who may have information bearing on his professional competence, character, ability to perform the privileges requested, ethical qualifications, ability to work cooperatively with others and other qualifications for requested membership and/or clinical privileges.
4.2.1.4 Consents to the Health System and Medical Staff representatives’
inspections of all records and documents that may be material to an evaluation of:
4.2.1.4.1 professional qualifications and competence to carry out the
clinical privileges requested;
4.2.1.4.2 physical and mental/emotional health status to the extent relevant to safely perform requested privileges subject to any legally required reasonable accommodation;
4.2.1.4.3 professional and ethical qualifications;
4.2.1.4.4 professional liability actions including currently pending claims involving the applicant;
64
4.2.1.4.5 any other issue relevant to establishing the applicant’s suitability for membership and/or privileges.
4.2.1.5 Releases from liability, promises not to sue and grants immunity to the
Health System, its Medical Staffs and its representatives for acts performed and statements made in good faith in connection with evaluation of the application and his credentials and qualifications fully permitted by the law.
4.2.1.6 Releases from liability and promises not to sue, all practitioners and
organizations who provide information to the Health System or the applicable Medical Staff(s) in good faith, including otherwise privileged or confidential information to the System/hospital representatives concerning his background/experience, competence, professional ethics, character, physical and mental health to the extent relevant to the capacity to fulfill requested privileges, emotional stability, utilization practice patterns, and other qualifications for staff appointment and clinical privileges.
4.2.1.7 Authorizes the Health System, Medical Staff and Administrative
representatives to obtain credentialing and peer review information from other hospitals, medical associations, licensing boards, appropriate government bodies and other health care entities concerned with this provider’s performance and releases representatives of the Health System from liability for so doing.
4.2.1.8 Acknowledges that the applicant has had access to relevant Medical
Staff Bylaws, including all rules, regulations, policies and procedures of the relevant Medical Staffs and agrees to abide by their provisions.
Notwithstanding Section 3.2 of Part II, if a practitioner institutes legal
action and does not prevail, he shall reimburse the Health System and any member of the Medical Staff named in the action for all costs incurred in defending such legal action, including reasonable attorney(s) fees.
4.2.1.9 Agrees to provide accurate answers to all the questions on the
application form, and agrees to immediately notify the System in writing should any of the information regarding these items change during the period of the applicant’s Medical Staff membership and/or privileges.
4.3 Application Evaluation
4.3.1 Expedited Credentialing: 4.3.1.1 An expedited Credentialing/Privileging Committee review and approval
process may be used for initial appointment in accordance with the Expedited Credentialing Policy.
4.3.2 Applicant Interview
4.3.2.1 All applicants for appointment to the Medical Staff and/or the granting of
clinical privileges are required to participate in interviews. The interviews are used to solicit information required to complete the credentials file or
65
clarify information previously provided, e.g., clinical knowledge and judgment, professional behavior, malpractice history, reasons for leaving past healthcare organizations, or other matters bearing on the applicant’s ability to render care at the generally recognized level for the community and in compliance with LMHS privileging criteria. Interviews may also be used to communicate Medical Staff performance expectations.
Applicants for appointment will participate in a minimum of two (2)
interviews. One interview will be conducted by the applicable Department Chair or designated Section Chief of the applicant’s anticipated primary LMHS facility and the second interview will be with a member of the System Credentialing/Privileging Committee. Applicants that are applying for multiple facilities within LMHS may be required to participate in additional Department Chair/Section Chief interviews at the discretion of the Department Chairs of the facility(ies) that are designated as non-primary.
4.3.2.2 Procedure: the applicant will be notified of required interview(s). Failure
of the applicant to appear for a scheduled interview will be deemed a voluntary withdrawal of the application.
4.3.3 Department Chair Action 4.3.3.1 Each Department Chair of an LMHS facility where the applicant has
requested privileges makes a recommendation related to membership and privileges, as applicable.
All completed applications are presented to the appropriate Department
Chair(s) for review and recommendation (which is made by completion of a standardized form provided to the Chair by the Medical Staff Services Department). The Department Chair(s) reviews the application to ensure that it fulfills the established standards for membership and/or clinical privileges. The Department Chair(s) may obtain input if necessary from an appropriate subject matter expert(s).
If a Department Chair believes a conflict of interest exists that, might
preclude his ability to make an unbiased recommendation, he will notify the Medical Staff Services Department and forward the application without comment.
4.3.3.2 The Department Chair(s) forwards to the System
Credentialing/Privileging Committee the following: 4.3.3.2.1 A written recommendation to approve the applicant’s request
for membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges (a summary of the interview conducted by the Department Chair or his designee is included in this written recommendation);
4.3.3.2.2 Written comments supporting his recommendations. The Department Chair of the applicant’s anticipated primary
facility also makes a written recommendation to define those circumstances, which require monitoring and evaluation of
66
clinical performance after the initial granting of clinical privileges (i.e., focused professional practice evaluation).
4.3.4 Medical Staff System Credentialing/Privileging Committee Action 4.3.4.1 The System Credentialing/Privileging Committee reviews the application
and forwards the following to the applicable FMEC(s): 4.3.4.1.1 A recommendation to approve the applicant’s request for
membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges;
4.3.4.1.2 A recommendation to define those circumstances, which
require monitoring, and evaluation of clinical performance after initial granting of clinical privileges (Focused Professional Practice Evaluation) (FPPE);
Comments supporting the above recommendation. 4.3.5 FMEC Action
4.3.5.1 Each FMEC of LMHS where membership and/or privileges have been requested forwards the following to the Board:
4.3.5.1.1 A recommendation to approve the applicant’s request for
membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges;
4.3.5.1.2 Comments supporting the above recommendation.
The FMEC of the applicant’s anticipated primary facility also makes a recommendation to define those circumstances that require monitoring and evaluation of clinical performance after initial granting of clinical privileges (FPPE).
Whenever a FMEC makes an adverse recommendation to the Board, a notice,
stating the reason, will be sent to the applicant who shall then be entitled to the procedural rights provided in the Investigation, Corrective Action, Hearing and Appeal Plan of the Medical Staff Bylaws. When multiple FMECs are making recommendations related to the same applicant, an adverse recommendation is not considered final until after the PLC attempts to facilitate resolution of the issues (this facilitation occurs when there are disparate recommendations – for example, one (1) positive recommendation and one negative recommendation).
4.3.6 Applicants Applying to Multiple Facilities Applicants may simultaneously make application for membership and/or privileges
to multiple facilities within LMHS. The Medical Staff Services Department coordinates this information so that the recommendations from all FMECs come to the Board together. If there are disparate recommendations (defined as conflicting) related to membership and/or requested clinical privileges on the same applicant, the PLC will meet and attempt to reconcile the disparate recommendations prior to forwarding the recommendations to the Board.
67
If the PLC is unable to facilitate resolution of the issues (in accordance with the Medical Staff Bylaws – Part I, Governance – Section 9 Decision Making Methods and Conflict Resolution) the disparate recommendations will go forward to the Board.
4.3.7 Board Action:
4.3.7.1 The Board reviews the recommendation and votes for one (1) of the following actions: 4.3.7.1.1 The Board may adopt or reject in whole or in part a
recommendation of the FMEC(s) or refer the recommendation to the FMEC(s) for further consideration stating the reasons for such referral back and setting a time limit within which a subsequent recommendation must be made.
4.3.7.1.2 If the Board concurs with the applicant’s request for
membership and/or privileges, it will grant the appropriate membership and/or privileges for a period not to exceed 24 months.
4.3.7.1.3 If the Board’s action is adverse to the applicant, a notice,
stating the reason, will be sent to the applicant who shall then be entitled to the procedural rights provided in the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) unless the applicant received procedural rights under Part II, Section 3.2.5.
4.3.7.1.4 The Board shall take final action in the matter as provided in
the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan).
4.3.8 Notice of Final Decision:
4.3.8.1 Notice of the Board’s final decision shall be given through the Medical
Staff Services Department to the applicable FMEC(s) and to the Chair of each Department concerned. The applicant shall receive written notice of appointment and special notice of any adverse final decisions in a timely manner. A decision and notice of appointment includes the staff category(ies) to which the applicant is appointed, the Department(s) to which he is assigned, the clinical privileges he may exercise, notification of orientation and any special conditions attached to the appointment.
4.3.9 Periods for Processing: 4.3.9.1 All practitioners and groups acting on an application for staff
appointment and/or clinical privileges must do so in a timely and good faith manner, and except for good cause, each application will be processed within 180 calendar days. The 180 Calendar days begin on the date that the application is declared complete to begin processing.
4.3.9.2 These processing periods are deemed guidelines and do not create
any right to have an application processed within these precise periods. If the provisions of the Medical Staff Bylaws (Investigation,
68
Corrective Action, Hearing and Appeal Plan) are activated, the time requirements provided therein govern the continued process of the application.
SECTION 5 FOCUSED PROFESSIONAL PRACTICE EVALUATION (FPPE) 5.1 CRITERIA FOR FPPE 5.1.1 The Department Chair (or designated Section Chief) of the applicant’s anticipated
primary facility will define circumstances that require monitoring and evaluation of the clinical performance of each practitioner following his or her initial granting of clinical privileges.
Such monitoring may utilize a range of techniques, including but not limited to: chart
review, the tracking of performance monitors/indicators, proctoring, external peer review, simulations, morbidity/mortality reviews, and discussion with other healthcare practitioners involved in the care of each patient. The FPPE plan is created as part of the initial recommendation for appointment and privileges and is forwarded to the System Credentialing/Privileging Committee and to the FMEC(s).
The System Credentialing/Privileging Committee will establish via policy the
anticipated duration for FPPE. The Physician Quality Committee will establish the triggers that indicate the need for
performance monitoring after the initial granting of privileges. SECTION 6 CRITERIA FOR REAPPOINTMENT 6.1 Criteria for Reappointment 6.1.1 It is the policy of the Health System to approve for reappointment and/or renewal of
privileges only those practitioners who meet the criteria for initial appointment as identified in Section 2, Part 1. The practitioner must also be determined by each applicable FMEC to be a provider of effective care that is consistent with the Health System standards of ongoing quality and the hospital performance improvement program and provide the information enumerated in Section 5.1.1.
All reappointments and renewals of clinical privileges are for a period not to exceed
24 months. The granting of new clinical privileges to existing Medical Staff members will follow the steps described in Section 4 concerning the initial granting of new clinical privileges and Section 5 concerning FPPE. A suitable peer shall substitute for the Department Chair in the evaluation of current competency of the Department Chair, and recommend appropriate action to the System Credentialing/Privileging Committee.
In the event a practitioner finds no need to utilize the facilities or resources of LMHS
for purposes of patient care through either admission, performance of a procedure, consultation, or referral, during a two-year period he may not be eligible for reappointment or continued privileges. Such practitioner may apply as a new applicant at any time subsequent to the expiration of the current appointment or privileges. This provision applies to practitioners who have been granted a leave of absence, moved their practice location, established a relationship with another institution or otherwise find no need to utilize the clinical resources of LMHS.
69
Exceptions to this provision may be made by the Board upon recommendation of the applicable FMEC(s).
As long as a practitioner has adequate clinical activity to maintain privileges at one
LMHS facility (and is recommended for continuation of privileges at his primary LMHS facility) the practitioner may maintain the applicable clinical privileges and staff category (potentially Associate if there is no or minimal clinical activity) at other LMHS facility(ies).
6.2.1 Information, Collection and Verification 6.2.1.1 From practitioner: On or before 4 months prior to the date of expiration of
a Medical Staff appointment or granting of privileges, a representative from the Medical Staff Services Department notifies the practitioner of the date of expiration and supplies him with an application for reappointment for membership and/or privileges. At least sixty (60) calendar days prior to this date, the practitioner must return the following to the Medical Staff Services Department:
6.2.1.1.1 A completed reapplication form, which includes complete
information to update his file on items listed in his original application, any required new, additional, or clarifying information, and any required fees or dues;
6.2.1.1.2 Information concerning continuing training and education
internal and external to the hospital during the preceding period;
6.2.1.1.3 By signing the reapplication form, the practitioner agrees to
the same terms as identified in Section 4.2. 6.2.2 From internal and/or external sources: The Medical Staff Services Department
collects and verifies information regarding each staff practitioner’s professional and collegial activities to include those items listed in Section 2.1.
6.2.3 The following information is also collected and verified:
6.2.3.1 A summary of clinical activity at each LMHS facility for each practitioner due for reappointment.
6.2.3.2 Performance and conduct in each LMHS facility and other healthcare
organizations in which the practitioner has provided substantial clinical care since the last reappointment, including patient care, medical/clinical knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism and system-based practice.
6.2.3.3 Documentation of CME activity; 6.2.3.4 Service on Medical Staff, Department and hospital committees; 6.2.3.5 Timely and accurate completion of medical records; 6.2.3.6 Compliance with all applicable Bylaws, policies, rules, regulations, and
procedures of the System and the Medical Staff(s);
70
6.2.3.7 Any significant gaps in employment or practice since the previous appointment or reappointment; and
6.2.3.8 Additional items as identified in the Verification Methods and
Requirements document.
6.2.4 Failure, without good cause, to provide any requested information, at least forty-five (45) calendar days prior to the expiration of appointment will result in a cessation of processing of the application and automatic expiration of appointment when the appointment period is concluded. Once the information is received, the Medical Staff Services Department verifies this additional information and notifies the staff practitioner of any additional information that may be needed to resolve any doubts about performance or material in the credentials file.
6.3 Evaluation of Application for Reappointment of Membership and/or Privileges
6.3.1 The reappointment application will be reviewed and acted upon as described in Sections 4.3.3 through 4.3.8. For the purpose of reappointment, an “adverse recommendation” by the Board as used in Section 4.3 means a recommendation or action to deny reappointment, or to deny or restrict requested clinical privileges or any action that would entitle the applicant to a Fair Hearing under the Medical Staff Bylaws. The terms “applicant” and “appointment” as used in these Sections shall be read respectively, as “staff practitioner” and “reappointment”.
SECTION 7 CLINICAL PRIVILEGES 7.1 Exercise of Privileges
A practitioner providing clinical services at a LMHS facility may exercise only those privileges granted to him by the Board or emergency and disaster privileges as described herein. Privileges may be granted by the Board upon recommendation of the FMEC(s) to practitioners who are not members of the Medical Staff. Such practitioners may include Advanced Registered Nurse Practitioners (ARNPs), Physician Assistants (PAs), practitioners serving short locum tenens positions, telemedicine physicians or others deemed appropriate by the FMEC(s) and Board.
7.2 Requests
When applicable, each application for appointment or reappointment to the Medical Staff must contain a request for the specific clinical privileges desired by the applicant. Specific requests must also be submitted for temporary privileges and for modifications of privileges in the interim between reappointments and/or granting of privileges.
7.3 Basis for Privileges Determination 7.3.1 Requests for clinical privileges will be considered only when accompanied by
evidence of education, training, experience, and demonstrated current competence as specified by the System in its Board approved criteria for clinical privileges.
7.3.2 Privileges for which no criteria have been established: 7.3.2.1 In the event a request for a privilege is submitted for a new technology, a
procedure new to the System, an existing procedure used in a significantly
71
different manner, or involving a cross-specialty privilege for which no criteria have been established, the request will be tabled for a reasonable period of time, usually not to exceed sixty (60) calendar days. During this time, the System Credentialing/Privileging Committee may refer the request for review by a task force appointed to review the request.
Task forces formed for purposes of establishment of evaluation of new
privileges and potential determination of criteria will be appointed by the Chairs of the System Credentialing/Privileging Committee, and will include the System Medical Director of Clinical Effectiveness and the Director of Supply Chain Management. The task force will:
7.3.2.1.1 Review the community, patient and System need for the
privilege and reach agreement with management and the Board that the privilege is approved to be exercised at the hospital;
7.3.2.1.2 Review with appropriate individuals/groups
the efficacy and clinical viability of the requested privilege and confirm that this privilege is approved for use in the setting-specific area of the hospital by appropriate regulatory agencies (FDA, OSHA, etc.);
7.3.2.1.3 Meet with management to ensure that the new privilege is
consistent with the Health System’s mission, values, strategic, operating, capital, information and staffing plans;
7.3.2.1.4 Work with management to ensure that any/all exclusive
contract issues, if applicable are resolved in such a way to allow the new or cross-specialty privileges in question to be provided without violating the existing contract. Upon recommendation from the System Credentialing/Privileging Committee and appropriate clinical services/specialty or subject matter experts (as determined by the System Credentialing/Privileging Committee), the criteria will be recommended to each FMEC and then to the Board. Once objective criteria have been established, the original request will be processed as described herein.
7.3.2.2 For the development of criteria, the Medical Staff Services Department (or
designee) will compile information relevant to the privileges requested which may include, but need not be limited to, position and opinion papers from specialty organization, position and opinion statements from interested individuals or groups and documentation from other hospitals in the region as appropriate.
7.3.2.3 Criteria to be established for the privilege(s) in question include education,
training, board status or certification (if applicable), experience and evidence of current competence. Proctoring requirements, if any, will be addressed including who may serve as proctor and how many proctored cases will be required.
Hospital related issues such as exclusive contracts, equipment, clinical
support staff and management would be referred to the appropriate hospital administrator and/or Department Director.
72
7.3.2.4 If the privileges requested overlap two (2) or more specialty disciplines, an
ad hoc committee may be appointed by the System Credentialing/Privileging Committee to recommend criteria for the privilege(s) in question. This ad hoc committee will consist of at least one (1) but no more than two (2) members from each involved discipline. The Chair of the ad hoc committee will be a member of the System Credentialing/Privileging Committee who has no vested interest in the issue (see Medical Staff Privilege Dispute Resolution Policy).
7.3.3 Requests for clinical privileges will be consistently evaluated on the basis of prior
and continuing education, training, experience, utilization practice patterns, current ability to perform the privileges requested and demonstrated current competence,
ability, and judgment. Additional factors that may be used in determining privileges are patient care needs and the System’s capability to support the type of privileges being requested and the availability of qualified coverage in the applicant’s absence. The basis for privileges determination to be made in connection with periodic reappointment or a requested change in privileges must include documented clinical performance and results of the staff’s performance improvement program activities.
Privilege determinations will also be based on pertinent information from other
sources, such as peers and/or faculty from other institutions and healthcare settings where the practitioner exercises clinical privileges.
7.3.4 The procedure by which requests for clinical privileges are processed are as outlined in Section 4.
7.3.5 Special Conditions for Dental Privileges
Requests for clinical privileges for dentists are processed in the same manner as all other privilege requests. Privileges for surgical procedures performed by dentists and/or oral and maxillofacial surgeons will require that all dental patients receive a basic medical evaluation (history and physical) by a physician member of the Medical Staff with privileges to perform such an evaluation, which will be recorded in the medical record. Oral and maxillofacial surgeons may be granted the privilege of performing a history and physical on their own patients upon submission of documentation of completion of an accredited postgraduate residency in oral and maxillofacial surgery and demonstrated current competence.
7.3.6 Special Conditions for practitioners not Qualified for Medical Staff Appointment but Practicing Pursuant to Clinical Privileges per System Policy. Requests for privileges, from such practitioners, are processed in the same manner as requests for clinical privileges by providers eligible for Medical Staff membership, with the exception that such practitioners are not eligible for membership on a Medical Staff and do not have the rights and privileges of such membership (all rights and responsibilities are defined in the Allied Health Practitioner (AHP) Privileging Policy and Procedure). Only those categories of practitioners approved by the Board for providing services at the hospital are eligible to apply for privileges. AHP(s) in this category may, subject to any licensure requirements or other limitations, exercise independent judgment only within the areas of their professional competence and participate directly in the medical management of patients under
73
the supervision of a physician who has been accorded privileges to provide such care.
7.4 Special Conditions for Podiatric Privileges Requests for clinical privileges for podiatrists are processed in the same manner as all other privilege requests.
Practitioners granted podiatric privileges may perform and shall record in the medical
record a basic medical evaluation history and physical for the practitioner’s podiatric patients if consistent with the privileges granted to the practitioner, state law governing the practitioner’s practice and federal law.
7.5 Special Conditions for Residents or Fellows in Training
Residents or Fellows in Training in the Health System shall not normally hold membership on the Medical Staff and shall not normally be granted specific clinical privileges. Rather, they shall be permitted to function clinically only in accordance with the written training protocols developed by the Professional Graduate Education Committee in conjunction with the Residency Training Program. The protocols must delineate the roles, responsibilities, and patient care activities of residents and fellows including which types of residents may write patient care orders, under what circumstances why they may do so, and what entries a supervising physician must countersign. The protocol must also describe the mechanisms through which resident directors and supervisors make decisions about a resident’s progressive involvement and independence in delivering patient care and how these decisions will be communicated to appropriate Medical Staff and hospital leaders.
The Post-Graduate Education Program Director or Committee must communicate
periodically with each applicable FMEC and the Board about the performance of its residents, patient safety issues and quality of patient care and must work with the FMEC to assure that all supervising physicians possess clinical privileges commensurate with their supervising activities.
7.6 Special Conditions for the Aging Practitioner
At the age of 70, practitioners shall complete an annual examination that addresses both the physical and mental capacity for the privileges requested. The annual physical and mental exams are to be conducted by an independent Medical examiner acceptable to the System Credentialing/Privileging Committee, documented on the approved form and submitted to the System Credentialing/Privileging Committee by the date requested. The physical exam is a “fitness to work” evaluation and must indicate that the practitioner has no physical or mental problem that may interfere with the safe and effective provision of care permitted under the privileges granted. In addition to the physical exam, a practitioner may be required to undergo proctoring of his clinical performance as part of the assessment of his capacity to perform the requested privileges. Such proctoring may be required in the absence of any previous performance concerns. The scope and duration of the proctoring shall be determined by the FMEC upon recommendation of the Department Chair of the practitioner’s primary facility and System Credentialing/Privileging Committee. The practitioner shall pay the cost of the physical and mental exam.
74
7.7 Temporary Privileges 7.7.1 Temporary privileges may be granted by the CEO, or designee, acting on behalf of
the Board and based on the recommendation of the President of the Medical Staff or designee to be approved at the next FMEC meeting, provided there is verification of current licensure and current competence. Temporary privileges may be granted only in two (2) circumstances: 1) to fulfill an important patient care, treatment or service need, or 2) when an initial applicant with a complete application that raises no concerns is awaiting review and approval of the FMEC and the Board. Applications pending completion of the initial appointment process must always be reviewed and a recommendation made by the System Credentialing/Privileging Committee prior to the granting of temporary privileges.
7.7.2 Important Patient Care, Treatment or Service Need: Temporary privileges may be
granted on a case-by-case basis when an important patient care, treatment or service need exists that mandates an immediate authorization to practice, for a limited time, not to exceed 30 calendar days (from date privileges are granted). Temporary privileges may be extended for two separate 30-day intervals upon approval of the Board of Directors. For the purposes of granting temporary privileges, an important patient care, treatment or service need is defined as including the following:
7.7.2.1 a circumstance in which one or more individual patients will experience
care that does not adequately meet their clinical needs if the temporary privileges under consideration are not granted, (i.e., a patient scheduled for urgent surgery who would not be able to undergo the surgery in a timely manner);
7.7.2.2 a circumstance in which the institution will be placed at risk of not
adequately meeting the needs of patients who seek care, treatment or service from the institution if the temporary privileges under consideration are not granted (i.e., the institution will not be able to provide adequate emergency room coverage in the providers specialty, or the Board has granted privileges involving new technology to a physician on the staff provided the physician is precepted for a specific number of initial cases and the precepting physician, who is not seeking Medical Staff membership, requires temporary privileges to serve as a preceptor);
7.7.2.3 a circumstance in which a group of patients in the community will be
placed at risk if not receiving patient care that meets their clinical needs if the temporary privileges under consideration are not granted (i.e. a physician who has a large practice in the community for which adequate coverage of hospital care for those patients cannot be arranged).
7.7.3 Clean Application (Expedited) Awaiting Approval: Temporary privileges may be
granted for up to 30 calendar days (from date privileges are issued) approved by the Executive Committee with two 30-day extensions approved by the Board (see the policy and procedure on Expedited Credentialing) when the new applicant for Medical Staff membership and/or privileges is waiting for review and recommendation by the FMEC and approval by the Board.
7.7.4 Special requirements of consultation and reporting may be imposed as part of the
granting of temporary privileges. Except in unusual circumstances, temporary privileges will not be granted unless the practitioner has agreed in writing to abide by the Bylaws, rules, and regulations and policies of the Medical Staff and hospital
75
in all matters relating to his temporary privileges. Whether or not such written agreement is obtained, these Bylaws, rules, regulations and policies control all matters relating to the exercise of clinical privileges.
7.7.5 Termination of temporary privileges: The CEO, acting on behalf of the Board and
after consultation with the President of the Medical Staff, may terminate any or all of the practitioner’s privileges based upon the discovery of any information or the occurrence of any event of a nature, which raises questions about a practitioner’s privileges.
Where the life or well-being of a patient is determined to be endangered, any person
entitled to impose precautionary suspension under the Medical Staff Bylaws may effect the termination. In the event of any such termination, the CEO or his designee then will assign the practitioner’s patients to another practitioner. The wishes of the patient shall be considered when feasible, in choosing a substitute practitioner.
7.7.6 Rights of the practitioner with temporary privileges: A practitioner is not entitled to
the procedural rights afforded in the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) because his request for temporary privileges is refused or because all or any part of his temporary privileges are terminated or suspended unless based on a determination of clinical incompetence or unprofessional conduct.
7.7.7 Emergency Privileges: In the case of a medical emergency, any practitioner is
authorized to do everything possible to save the patient’s life or to save the patient from serious harm, to the degree permitted by the practitioner’s license, regardless of facility affiliation, staff category, or level of privileges. A practitioner exercising emergency privileges is obligated to summon all consultative assistance deemed necessary and to arrange appropriate follow-up.
7.7.8 Disaster Privileges 7.7.8.1 If the System’s Disaster Plan has been activated and the organization is
unable to meet immediate patient needs, the CEO and such other individuals as identified in the System’s Disaster Plan with such authority, may, on a case by case basis consistent with medical licensing and other relevant state statutes, grant disaster privileges to provide patient care to selected Licensing Independent Practitioners (LIP’s), who must at a minimum present a valid governmental-issued photo identification issued by a state or federal agency (e.g. driver’s license or passport) and at least one of the following:
7.7.8.1.1 a current picture hospital ID card that clearly identifies
professional designation; 7.7.8.1.2 a current license to practice; 7.7.8.1.3 primary source verification of the license;
7.7.8.1.4 identification indicating that the practitioner is a member of a
Disaster Medical Assistance Team (DMAT), or Medical Reserve Corps (MRC), Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VHP), or other recognized state or federal organizations or groups;
76
7.7.8.1.5 identification indicating that the practitioner has been
granted authority to render patient care, treatment, and services in disaster circumstances (such authority having been granted by a federal, state, or municipal entity);
7.7.8.1.6 identification by a current hospital or Medical Staff
member(s) who possesses personal knowledge regarding the volunteer’s ability to act as a LIP during a disaster.
7.7.8.2 The Medical Staff oversees the professional performance of
volunteer practitioners who have been granted disaster privileges by direct observation, mentoring or clinical record review.
The organization makes a decision (based on information obtained regarding the professional practice of the volunteer) within 72 hours related to the continuation of the disaster privileges initially granted.
7.7.8.3 Primary source verification of licensure begins as soon as the
immediate situation is under control, and is completed within 72 hours from the time the volunteer practitioner presents to the organization.
7.7.8.4 Once the immediate situation has passed and such determination
has been made consistent with the institution’s Disaster Plan, the practitioner’s disaster privileges will terminate immediately.
7.7.8.5 Any individual identified in the institution’s Disaster Plan with the
authority to grant disaster privileges shall also have the authority to terminate disaster privileges. Such authority may be exercised at the sole discretion of the hospital and will not give rise to a right to a fair hearing or an appeal.
SECTION 8 PRECEPTORSHIP
8.1 A practitioner who has not provided acute inpatient care within the past 24 months who requests clinical privileges at the hospital must arrange for a preceptorship either with a current member in good standing of the Medical Staff who practices in the same specialty or with an academic training program or other equivalently competent physician practicing outside of the hospital. The practitioner must assume responsibility for any financial costs required to fulfill the requirements of Sections 8.1 and 8.2.
8.2 A description of the preceptorship program, including details of monitoring and consultation
must be written and submitted for approval to the applicable Department Chair, System Credentialing/Privileging Committee and FMEC. At a minimum, the preceptorship program description must include the following: 8.2.1 The scope and intensity of required preceptorship activities; 8.2.2 The requirement for submission of a written report from the preceptor prior to
termination of the preceptorship period assessing, at a minimum, the applicant’s demonstrated clinical competence related to the privileges requested, ability to get
77
along with others, the quality and timeliness of medical records documentation, ability to perform the privileges requested, and professional ethics and conduct.
SECTION 9 REAPPLICATION AFTER MODIFCATIONS OF MEMBERSHIP STATUS OF PRIVILEGES AND EXHAUSTION OF REMEDIES
9.1 Reapplication After Adverse Credentials Decision
9.1.1 Except as otherwise determined by the Board, a practitioner who has received a
final adverse decision or who has resigned or withdrawn an application for appointment, reappointment or clinical privileges while under investigation or to avoid an investigation is not eligible to reapply to the Medical Staff for a period of five (5) years from the date of the notice of the final adverse decision or the effective date of the resignation or application withdrawal. Any such application is processed in accordance with the procedures then in force. As part of the reapplication, the practitioner must submit such additional information as the Medical Staff and/or Board requires, demonstrating that the basis of the earlier adverse action no longer exists. If such information is not provided, the reapplication will be considered incomplete and voluntarily withdrawn and will not be processed any further.
9.2 Request for Modification of Appointment Status or Privileges
9.2.1 A staff member, either in connection with reappointment or at any other time, may
request modification of staff category, Department assignment, or clinical privileges by submitting a written request to the Medical Staff Services Department. A modification request must be on the prescribed form and must contain all pertinent information supportive of the request. All requests for additional clinical privileges must be accompanied by information demonstrating additional education, training, and current clinical competence in the specific privileges requested. A modification application is processed in the same manner as a reappointment, which is outlined in Section 6 of this manual. A practitioner who determines that he no longer exercises, or wishes to restrict or limit the exercise of, particular privileges that he has been granted shall send written notice, through the Medical Staff Services Department to the System Credentialing/Privileging Committee, and FMEC. A copy of this notice shall be included in the practitioner’s credentials file.
9.3 Resignation of Staff Appointment or Privileges
9.3.1 A practitioner who wishes to resign his staff appointment and/or clinical privileges
must provide written notice to the appropriate Department Chair or President of the Medical Staff. The resignation shall specify the reason for the resignation and the effective date. A practitioner who resigns his staff appointment and/or clinical privileges is obligated to accurately complete all portions of all medical records for which he is responsible prior to the effective date of resignation. Failure to do so shall result in an entry in the practitioner’s credentials file acknowledging the resignation and indicating that it became effective under unfavorable circumstances.
9.4 Exhaustion of Administrative Remedies
9.4.1 Every practitioner agrees that he will exhaust all the administrative remedies
afforded in the various Sections of Part I: Governance, Part II: Investigations, Corrective Action, Hearing and Appeal Plan and Part III: Credentialing Procedures before initiating legal action against the System or its agents.
78
9.5 Reporting Requirements
9.5.1 The CMO or his designee shall be responsible for assuring that the hospital satisfies
its obligations under the Health Care Quality Improvement Act of 1986 and its successor statutes. Actions that must be reported include any negative professional review action against a physician or dentist related to clinical incompetence or misconduct that leads to a denial of appointment and/or reappointment, reduction in clinical privileges for greater that thirty (30) calendar days; resignation, surrender of privileges, or acceptance of privilege reduction either during an investigation or to avoid an investigation.
SECTION 10 LEAVE OF ABSENCE
10.1 Leave Request
10.1.1 A leave of absence is a matter of courtesy, not of right. In the event that it is
determined that a practitioner has not demonstrated good cause for a leave, or where a request for extension is not granted, the determination shall be final, with no recourse to a hearing and appeal. A leave of absence must be requested for any absence from the Medical Staff and/or patient care responsibilities longer than thirty (30) days if such absence is related to the practitioner’s physical or mental health or to the ability to care for patients safely and competently. A practitioner who wishes to obtain a voluntary leave of absence must provide written notice to the President of the Medical Staff stating the reasons for the leave and approximate period of the leave, which may not exceed one 1-year except for military service or express permission by the Board. Requests for leave must be forwarded, with a recommendation from the FMEC, and affirmed by the Board. While on leave of absence, the practitioner may not exercise clinical privileges or prerogatives and has no obligation to fulfill Medical Staff responsibilities.
10.2 Termination of Leave
10.2.1 At least thirty (30) calendar days prior to the termination of the leave, or at any
earlier time, the practitioner may request reinstatement by sending a written notice to the President of the Medical Staff. The practitioner must submit a written summary of relevant activities during the leave if the FMEC or Board so requests.
A practitioner returning from a leave of absence for health reasons must provide a
report from his physician that answers any questions that the FMEC or Board may have as part of considering the request for reinstatement. The FMEC makes a recommendation to the Board concerning reinstatement, and the applicable procedures concerning the granting of privileges are followed. If the practitioner’s current grant of membership and for privileges is due to expire during the leave of absence, the practitioner must apply for reappointment or his appointment and/or clinical privileges shall lapse at the end of the appointment period.
10.3 Failure to Request Reinstatement
10.3.1 Failure, without good cause, to request reinstatement shall be deemed a voluntary resignation from the Medical Staff and shall result in automatic termination of membership, privileges, and prerogatives. A practitioner whose membership is automatically terminated shall not be entitled to the procedural rights provided in the
79
Medical Staff Bylaws. A request for Medical Staff membership subsequently received from a member so terminated shall be submitted and processed in the manner specified for applications for initial appointments.
SECTION 11 PRACTITIONERS PROVIDING CONTRACTED SERVICES 11.1.1 When the System or hospital contracts for patient care services with LIPs who
provide official readings of images, tracings or specimens through a telemedicine mechanism, and these practitioner’s services are under the control of a Joint Commission accredited organization, the hospital will:
11.1.1.1 specify in a contract that the entity providing these services by contract
(the contracting entity) will ensure that all services provided under this contract by individuals who are LIPs will be within the scope of those practitioner’s privileges at the contracting entity; or
11.1.1.2 verify that all individuals who are LIPs and providing services under the
contract have privileges that include the services provided under the contract.
11.2 When the System/hospital contracts for care services with LIPs, who provide official
readings of images, tracings or specimens through a telemedicine mechanism, and these practitioner’s services are not under the control of a Joint Commission accredited organization, all LIPs who will be providing services under this contract will be permitted to do so only after being granted privileges at the hospital through the mechanisms established in this manual.
11.3 Contract Services/Department or Service Closure
11.3.1 The membership and privileges on the Medical Staff of any practitioner who has a
contractual relationship with the System or with an entity that has a contractual relationship with the System to provide professional services to patients shall be subject to those provisions contained in said contract with regard to the termination of Medical Staff membership and privileges upon the expiration, lapse, cancellation or termination of the contract. If the contract so provides, the affected practitioner shall have no right to a hearing regarding termination of Medical Staff membership or privileges.
11.3.2 In the event a hospital Department is closed, discontinued or provided through an
exclusive contract, such establishment shall not adversely impact the ability of any physician to continue to maintain clinical membership and exercise privileges in existence at the time of such closure, discontinuance or exclusive contract. Initial applications for Medical Staff membership and privileges will not be extended, provided, accepted, processed or approved to or from physicians unless they are joining groups who are actively contracted for exclusively contracted services.
11.3.3 In the event the Board determines that a patient care service shall be closed,
discontinued, or provided through an exclusive contract, such action shall require approval by the affected FMEC.
80
Both parties agree that any Department or service closure shall occur solely so that the health and wellbeing of the patients and the best interests of the hospital under these Bylaws may be served at all times. Notwithstanding any other provision in the Bylaws, if the Board and the affected FMEC are unable to agree upon the closure of a Department or service, the matter shall undergo the conflict resolution process set forth in Part I, Section 9 of these Bylaws.
If the parties are still in disagreement regarding the closure of a Department or
service upon completion of the conflict resolution process, the parties shall engage in mediation in accordance with the procedures set forth by the American Health Lawyers Association’s Alternative Dispute Resolution Service or another independent mediation service mutually agreeable to the parties. In the event the Board and FMEC are at impasse at mediation and conflict remains, the Board and the FMEC retain the right to seek a resolution through litigation. Further, the Board shall not close a Department or service for a period of three months following impasse at mediation.
11.4 Qualifications
11.4.1 A practitioner who is or will be providing specified professional services pursuant to
a contract or a letter of agreement with the Health System must meet the same qualifications, must be processed in the same manner, and must fulfill all the obligations of his appointment category as any other applicant or staff practitioner.
11.5 The terms of the Medical Staff Bylaws will govern disciplinary action taken by or
recommended by the FMEC.
11.6 Effect of Contract or Employment Expiration or Termination
11.6.1 The effect of expiration or other termination of a contract upon a practitioner’s staff appointment and clinical privileges will be governed solely by the terms of the practitioner’s contract with the System. If the contract or the employment agreement is silent on the matter, then contract expiration or other termination alone will not affect the practitioner’s staff appointment status or clinical privileges.
SECTION 12 MEDICAL ADMINISTRATIVE OFFICERS
12.1 A Medical Administrative Officer is a practitioner engaged full or part- time by the hospital in an administratively responsible capacity, whose activities may also include clinical responsibilities such as direct patient care, teaching, or supervision of the patient care activities of other practitioners under the officer’s direction.
12.2 Each Medical Administrative Officer must achieve and maintain Medical Staff appointment
and clinical privileges appropriate to his clinical responsibilities and discharge staff obligations appropriate to his staff category in the same manner applicable to all other staff members.
12.3 Effect of removal from office or adverse change in appointment status or clinical privileges:
12.3.1 Where a contract exists between the officer and the Health System, its terms
govern the effect of removal from the Medical Administrative Office on the officer’s staff appointment and privileges and the effect an adverse change in the officer’s staff appointment or clinical privileges has on his remaining in office.
81
12.3.2 In the absence of a contract or where the contract is silent on the matter, removal
from office has no effect on appointment status or clinical privileges. The effect of an adverse change in appointment status or clinical privileges on continuance in office will be determined by the Board.
12.3.3 A Medical Administrative Officer has the same procedural rights as all other staff
members in the event of an adverse change in appointment status or clinical privileges unless the change is, by contract a consequence of removal from office.
82
83
HealthPark Medical Center
Medical Staff
Bylaws
Adopted: May 28, 2009 Revision approved by BOD June 24, 2010 Revision approved by BOD August 26, 2010 Revisions approved by BOD June 16, 2011
Revision approved by BOD December 6, 2012
1
TABLE OF CONTENTS PART 1: GOVERNANCE 6 SECTION 1 MEDICAL STAFF PURPOSE & AUTHORITY 6 1.1 Purposes 6 1.2 Authority 6 1.3 Medical Staff (Term) 6 SECTION 2 MEDICAL STAFF MEMBERSHIP 7 2.1 Nature of Medical Staff Membership 7 2.2 Qualifications for Membership 7 2.3 Nondiscrimination 7 2.3.1 No Automatic Entitlement 7 2.4 Conditions and Duration of Appointment 7 2.5 Medical Staff Membership and Clinical Privileges 8 2.6 Medical Staff Members’ Responsibilities 8 2.7 Basic Responsibilities of Applicants and Appointees 8 2.8 Member Rights 11 2.9 Medical Staff Dues and Assessments 11 2.10 Conflict of Interest 12 SECTION 3 CONFIDENTIALITY, IMMUNITY AND RELEASES 12 3.1 Confidentiality 12 3.2 Immunity 13 3.3 Releases 14 SECTION 4 CATEGORIES OF THE MEDICAL STAFF 14 4.1 Active Category 14 4.2 Associate Category 15 4.3 Honorary Category 16 SECTION 5 OFFICERS OF THE MEDICAL STAFF 16 5.1 Officers of Medical Staff and FMEC at-Large Members 16 5.2 Qualifications of Officers and FMEC at-Large Members 16 5.3 Election of Officers and FMEC at-Large Members 16 5.4 Terms of Office 17 5.5 Vacancies of Office 17 5.6 Duties of Officers and FMEC at-Large Members 17 5.7 Removal and Resignation of Officer or FMEC at-Large Members 19 SECTION 6 MEDICAL STAFF ORGANIZATION 20 6.1 Departments 20 6.2 Qualifications, Selection, Term, Removal and Responsibility of Department Chair 21 6.3 Assignment to Department 23 SECTION 7 MEDICAL STAFF GOVERNANCE COMMITTEES 23 7.1 Designation of the LMHS MS Physician Leadership Council (PLC) 23
2
7.2 Composition of the LMHS PLC 23
7.3 Staff Functions 25 7.4 Facility Medical Executive Committee (FMEC)
(Composition, Selection and Tenure) 25 7.5 Duties and Responsibilities of the FMEC’s 25 7.6 System Medical Staff Committees 27 7.6.1 Purpose 27 7.6.2 Organization to Perform Functions 27 7.6.2.1 System Credentialing/Privileging Committee 27 7.6.2.2 System Medical Staff Quality Committee 27 7.6.2.3 System Practitioner Resource Committee 27 7.6.2.4 System Bylaws Committee 28 7.6.2.5 System Emergency Services Committee 29 7.6.3 Composition & Meetings of System MS Committees 29 7.7 Facility Medical Staff Committees 30 7.7.1 Purpose 30 7.7.2 Standing Facility Medical Staff Committees 30 SECTION 8 MEDICAL STAFF MEETINGS 31 8.1 General Medical Staff Meetings 31 8.2 Departments, Sections and Committee Meetings 31 8.3 Special Meetings of Departments, Sections and Committees 31 8.4 Quorum 31 8.5 Attendance Requirements 32 8.6 Participation by Administration 32 8.7 Robert’s Rules of Order 32 8.8 Notice of Meetings 33 8.9 Action of PLC, FMEC, General Medical Staff, Department, Section or Committee 33 8.10 Rights of Ex Officio Members 33 8.11 Minutes 33 SECTION 9 DECISION MAKING METHODS AND CONFLICT RESOLUTION 33 SECTION 10 REVIEW, REVISION ADOPTION AND AMENDMENT 34 10.1 Medical Staff Responsibility 34 10.2 Methods of Amendment and Adoption to these Bylaws 35 10.3 Methods of Amendment and Adoption to any Medical Staff Rules, Regulations and Policies 35 Appendix A PRINCIPLES OF MEDICAL ETHICS 37 PART II: INVESTIGATIONS, CORRECTIVE ACTION, HEARING AND APPEAL PLAN 39 SECTION 1 ROUTINE CORRECTIVE ACTION & INVESTIGATIONS 39 1.1 Progressive Intervention 39 1.2 Basis for Routine Corrective Action 39 1.3 Requests and Notices 40 1.4 Investigations 40 1.5 FMEC Action 41 1.6 Notice of FMEC Action 42 1.7 Board of Directions Action 42
3
SECTION 2 EMERGENCY CORRECTIVE ACTION/PRECAUTIONARY SUSPENSION OF CLINICAL PRIVILEGES 42 2.1 Basis for Emergency Corrective Action/Precautionary Suspension 42 2.2 Notice of Emergency Corrective Action/Precautionary Suspension 42 2.3 FMEC Procedure 43 2.4 Provision of Patient Care 43 2.5 Recission of Emergency Corrective Action/Precautionary Suspension 43 SECTION 3 AUTOMATIC SUSPENSION AND TERMINATION 43 3.1 Basis for Automatic Suspension and Termination 43 3.1.1 Loss of License 43 3.1.2 Residence or Office Outside Lee County 43 3.1.3 Lack of Active Practice 44 3.1.4 Criminal Conviction 44 3.1.5 Loss or Restriction of DEA Certificate 44 3.1.6 Exclusion From Federal or State Health Care Programs 44 3.1.7 Failure to Pay Fees and Assessments 44 3.1.8 Failure to Provide Requested Information 44 3.1.9 Failure to Request Reappointment or Provide Requested Information Related to Reappointment 45 3.1.10 Failure to Request Reinstatement Following Leave of Absence 45 3.1.11 Failure to Complete Medical Records 45 3.1.12 Failure to Comply with Special Meeting Attendance Requirements 45 3.2 Right to Limited Hearing for Automatic/Voluntary Suspension and Termination 45 SECTION 4 HEARING AND APPEAL PROCEDURES 46 4.1 Grounds for Hearing 46 4.2 Notice of Recommendation 46 4.3 Request for Hearing 47 4.4 Preliminary Interview 47 SECTION 5 FAIR HEARING PROCEDURE 47 5.1 System Representative, Hearing Panel and Hearing Officer 47 5.1.1 System Representative 48 5.1.2 Hearing Panel 48 5.1.3 Hearing Officer – Qualifications & Authority 48 5.2 Challenge to Hearing Panel Members or Hearing Officer 50 SECTION 6 HEARING PROCEDURES 50 6.1 Provision of Relevant Information 50 6.2 Pre-Hearing Conference 51 6.3 Failure to Appear 51 6.4 Record of Hearing 51 6.5 Rights of Both Sides 52 6.6 Admissibility of Evidence 52 6.7 Burden of Presenting Evidence and Proof 52 SECTION 7 HEARING CONCLUSION, DELIBERATIONS AND RECOMMENDATIONS 52 7.1 Deliberations and Recommendation of the Hearing Panel/Hearing Officer 52 7.2 Disposition of Hearing Panel Report 53
4
SECTION 8 APPEAL PROCEDURE 53 8.1 Request & Time for Appeal 53 8.2 Grounds for Appeal 54 8.3 Time, Place and Notice 54 8.4 Nature of Appellate Review 54 8.4.1 Review Panel 55 8.4.2 Position Papers 55 8.4.3 Oral Argument 55 8.4.4 Recommendation 55 SECTION 9 FINAL DECISION OF THE BOARD 55 SECTION 10 RIGHT TO ONE HEARING AND ONE APPEAL ONLY 55 PART III: CREDENTIALING PROCEDURES 56 SECTION 1 SYSTEM CREDENTIALING/PRIVILEGING COMMITTEE 56 1.1 Organizational Structure 56 1.2 Transition Issues 56 1.3 Purpose of the System Credentialing/Privileging Committee 56 1.4 Composition of the System Credentialing/Privileging Committee 57 1.5 Duties and Responsibilities of the System Credentialing/Privileging Committee 57 SECTION 2 QUALIFICATIONS FOR MEMBERSHIP AND PRIVILEGES 58 2.1 Qualifications for MS appointment, reappointment or clinical privileges 58 2.1.15 Exceptions 58 SECTION 3 PRE-APPLICATION PROCESS 60 SECTION 4 INITIAL APPOINTMENT PROCESS 61 4.1 Completion of Application 61 4.2 Applicant’s Attestation, Authorization and Acknowledgement 63 4.3 Application Evaluation 64 4.3.1 Expedited Credentialing 64 4.3.2 Applicant Interview 64 4.3.3 Department Chair Action 64 4.3.4 MS System Credentialing/Privileging Committee Action 65 4.3.5 FMEC Action 66 4.3.6 Applicants Applying to Multiple Facilities 66 4.3.7 Board Action 66 4.3.8 Notice of Final Decision 67 4.3.9 Periods for Processing 67 SECTION 5 FOCUSED PROFESSIONAL PRACTICE EVALUATION (FPPE) 67 SECTION 6 CRITERIA FOR REAPPOINTMENT 68 6.1 Criteria for Reappointment 68 6.3 Evaluation of Application for Reappointment of Membership and/or Privileges 70
5
SECTION 7 CLINICAL PRIVILEGES 70 7.1 Exercise of Privileges 70 7.2 Requests 70 7.3 Basis for Privileges Determination 70 7.4 Special Conditions for Podiatric Privileges 72 7.5 Special Conditions for Residents or Fellows in Training 73 7.6 Special Conditions for the Aging Practitioner 73 7.7 Temporary Privileges 73 7.7.8 Disaster Privileges 75 SECTION 8 PRECEPTORSHIP 76 SECTION 9 REAPPLICATION AFTER MODIFICATIONS OF MEMBERSHIP STATUS OF PRIVILEGES AND EXHAUSTION OF REMEDIES 77 9.1 Reapplication After Adverse Credentials Decision 77 9.2 Request for Modification of Appointment Status or Privileges 77 9.3 Resignation of Staff Appointment or Privileges 77 9.4 Exhaustion of Administrative Remedies 77 9.5 Reporting Requirements 78 SECTION 10 LEAVE OF ABSENCE 78 10.1 Leave Request 78 10.2 Termination of Leave 78 10.3 Failure to Request Reinstatement 78 SECTION 11 PRACTITIONERS PROVIDING CONTRACTED SERVICES 79 11.3 Contract Services/Department or Service Closure 79 11.4 Qualifications 80 11.5 Terms 80 11.6 Effect of Contract or Employment Expiration or Termination 80 SECTION 12 MEDICAL ADMINISTRATIVE OFFICERS 80
6
PART 1: GOVERNANCE
SECTION 1 MEDICAL STAFF PURPOSES & AUTHORITY 1.1 Purposes
The purposes of the Medical Staffs of Lee Memorial Health System are to:
1.1.1 Serve as the formal organizational structure of those practitioners granted the privilege of practicing in the hospitals and other facilities of the System.
1.1.2 Serve as the primary means for accountability to the Board for the professional
performance, the quality of medical care provided to patients, and ethical conduct of its members. The Board shall have the ultimate responsibility for the quality of medical care provided to patients and the ultimate authority to approve the granting of privileges, to make appointments and reappointments to membership on the Medical Staffs, and to approve the adoption of Medical Staff Bylaws and Rules and Regulations. Such authority will be exercised based on the standard set forth in Section 1.2.
1.1.3 Provide a means through which members of the Medical Staffs may address with
the Board those aspects of policy that involve professional practice or may affect the care of patients.
1.2 Authority
The Medical Staffs of Lee Memorial Health System are authorized by the Lee Memorial Health System Board of Directors (“the Board”) to exercise such power as is necessary to discharge its responsibilities under these Bylaws consistent with the Bylaws of Lee Memorial Health System. Lee Memorial Health System (“the System” or “the Health System”) includes acute care facilities known as Cape Coral Hospital, Gulf Coast Medical Center, HealthPark Medical Center, Lee Memorial Hospital, and The Children’s Hospital (individually known as “the hospital” and collectively known as “the hospitals”). The Board recognizes that a well-organized, self-governing Medical Staff that provides oversight of care, treatment, and services provided by practitioners with privileges is in the best interest of patients. When acting with respect to matters of the Medical Staff, the Board shall at all times comply with the Medical Staff Bylaws, the Rules and Regulations of the Medical Staff, and applicable law.
1.3 Medical Staff The term “Medical Staff” as used herein shall mean, on a collective basis, those
practitioners who are authorized by the Board to exercise privileges at one or more of the System’s hospitals, and, on a component basis, those practitioners who are authorized by the Board to exercise privileges at a particular system hospital. The latter may be referred to herein as the “Medical Staff of a facility.” The term “he”, “him”, or “his” means of a male or female gender.
7
SECTION 2 MEDICAL STAFF MEMBERSHIP 2.1 Nature of Medical Staff Membership
Membership on the Medical Staff is a privilege that shall be extended only to professionally competent physicians (M.D. or D.O.), dentists, podiatrists and/or psychologists who continuously meet the qualifications, standards, and requirements set forth in these Bylaws and associated policies of the Medical Staff and the hospitals. Medical Staff membership is a privilege and not a right of any practitioner or other person. Medical Staff membership and the exercise of privileges in connection therewith shall be extended only to practitioners who continuously meet the requirements of these Bylaws. The Board makes decisions regarding Medical Staff matters, based on Medical Staff recommendations, in accordance with these Bylaws. Membership on the Medical Staff shall confer on the Medical Staff member only such rights as set forth in the Bylaws. No person shall admit patients to a System hospital unless he is appointed to the Medical Staff of such hospital. For purposes of these Bylaws, “membership in” is used synonymously with “appointment to” the Medical Staff. Medical Staff members granted membership and privileges at a hospital, which has services and facilities that are provider based to a main provider and are authorized to exercise those privileges at the main provider.
2.2 Qualifications for Membership
2.2.1 The qualifications for Medical Staff membership are delineated in Part III of these Bylaws (Credentials Procedures).
2.3 Nondiscrimination
2.3.1 No Automatic Entitlement
No person shall be automatically entitled to Medical Staff membership or to the exercise of clinical privileges merely because he is licensed to practice, is a member of any professional organization, is certified by any board, or had held (but not currently) Medical Staff membership or clinical privileges at a System hospital or at any other health care facility. The burden shall be on the applicant to establish his qualifications. Acceptance of Medical Staff membership or exercise of clinical privileges shall constitute an agreement to strictly abide by these Bylaws, the applicable Medical Staff Policies, the Rules and Regulations, and the Principles of Medical Ethics set forth in Appendix A hereof and all other appropriate ethical standards governing the practitioner’s practice. No person shall be initially appointed to the Medical Staff or granted clinical privileges if the hospitals are unable to provide adequate facilities and supportive services for the applicant and his patients. Medical Staff membership shall not be denied based on sex, race, creed, color, national origin, religion, marital status, age, disability, or economic credentialing, at initial appointment or reappointment.
2.4 Conditions and Duration of Appointment
2.4.1 The Board shall act on appointment and reappointment only after the Medical Staff has had an opportunity to submit a recommendation from the Facility Medical Executive Committee (FMEC). Appointment and reappointment to the Medical Staff shall be for no more than twenty-four (24) calendar months.
8
2.5 Medical Staff Membership and Clinical Privileges
2.5.1 Requests for Medical Staff membership and/or clinical privileges will be processed only when the potential applicant meets the current minimum qualifying criteria recommended by the System Credentialing/Privileging Committee and FMEC and approved by the Board. Membership and/or privileges will be granted and administered as delineated in Part III (Credentials Procedures) of these Bylaws, including but not limited to, Part III, Sections 3 and 11.3 regarding Contracted practitioners.
2.6 Medical Staff Members’ Responsibilities
2.6.1 Duties of Appointees Appointment to the Medical Staff shall require that each practitioner assume such reasonable duties and responsibilities, as the Medical Staff shall require.
2.7 Basic Responsibilities of Applicants and Appointees The following basic responsibilities and requirements shall be applicable to every applicant
and appointee for Medical Staff appointment or reappointment as a condition of consideration of such application and as a condition of continued Medical Staff appointment if granted:
2.7.1 an obligation to provide for appropriate and timely care and supervision to all
patients in the hospital for whom the individual has responsibility (Standard of Care);
2.7.2 an agreement to abide by all Bylaws, Rules and Regulations and Policies of the Medical Staff and the Hospital, as shall be in force during the time the individual is appointed to the Medical Staff (Conformance to Rules);
2.7.2.1 provide a current cell phone number and email address to be used for
emergency or disaster purposes in accordance with Medical Staff Services Dept. policy.
2.7.3 an agreement to accept committee assignments and such other reasonable duties
and responsibilities as shall be assigned (Committee Assignments);
2.7.4 to not participate in illegal fee splitting or other illegal inducements relating to patient referral;
2.7.5 to promptly notify Medical Staff Services (Notification Requirements);
2.7.5.1 if his professional license in any state is suspended or revoked; 2.7.5.2 of the imposition of any conditions by any state licensing authority on his
continued ability to practice his profession, including probation or limitations on the scope of practice;
2.7.5.3 of the loss or restriction of Medical Staff membership or privileges at any
other health care facility;
2.7.5.4 if his Drug Enforcement Agency (DEA) license number is suspended, revoked or voluntarily relinquished;
9
2.7.5.5 of any change in eligibility for participation in Federal Health Care
Programs including any sanctions imposed or recommended by the Federal Department of Health and Human Services, Florida State Agency for Health Care Administration and/or the receipt of any citation and/or quality denial letter concerning alleged quality problems in patient care;
2.7.5.6 if the practitioner enters, participates in, or against medical advice, leaves
or refuses any program of treatment prescribed or required by the Florida Physicians’ Recovery Network;
2.7.5.7 if the practitioner is admitted for, seeks, or is undergoing treatment for
substance or alcohol abuse or a behavioral health problem. “Substance abuse” shall include but not limited to, use or ingestion of illegal drugs, or use or ingestion of prescription medications not prescribed in the ordinary course of treatment of injury or disease. “Behavioral health problem” shall mean any condition or disease of a psychiatric or psychological nature which, in the opinion of a qualified psychiatrist, adversely affects the practitioner’s ability to care for patients or practice his profession in accordance with the applicable prevailing standard of care; or
2.7.5.8 the conviction of, or pleading of nolo contendere to, a crime constituting a
felony in any jurisdiction. 2.7.6 to abide by generally recognized ethical principles applicable to the applicant’s or
appointee’s profession and by the code of ethics set forth in Appendix A (Ethics);
2.7.7 to respect the confidentiality of all information obtained in connection with his responsibility as a Medical Staff member and comply with the requirements of the Health Insurance Portability and Accountability Act (HIPAA) (Confidentiality);
2.7.8 to provide medical consultation in a timely fashion in accordance with all
applicable Rules & Regulations and Medical Staff Policies (Consultation);
2.7.9 to participate in the monitoring and evaluation activities of Clinical Sections and cooperate with other members of the Medical Staff and the System, in programs designed to improve the quality of care to reduce or eliminate waste in the use of scarce System resources and to reduce the risk of injury to patients and others in the provision of care (Quality Review Participation);
2.7.10 to complete in a timely and legible manner the medical records and other required
records for all patients as required by these Bylaws, applicable Rules and Regulations, and other applicable policies of the hospital (Medical Records);
2.7.11 to pay promptly any applicable Medical Staff assessments and dues (Dues); 2.7.12 to participate in continuing education programs for the benefit of the applicant or
appointee and for the benefit of other professionals and System hospital personnel (CME);
10
2.7.13 to authorize the release of all information necessary for an evaluation of the individual’s qualifications for initial or continued appointment, reappointment, and/or clinical privileges (Release of Information);
2.7.14 to submit to an evaluation of his physical and/or mental health status by a
physician or physicians acceptable to the FMEC or Board, whenever the FMEC or Board has reason to question the physical and/or mental health status of the practitioner, as a prerequisite to further consideration of his application for appointment or reappointment, the exercise of previously granted privileges or maintenance of his Medical Staff appointment (Physical/Mental Exam);
2.7.15 to recognize the obligations established to fulfill the hospital’s responsibilities
under the Emergency Medical Treatment and Women in Labor Act (EMTALA), the Access to Emergency Services and Care Act and/or other applicable regulations, requirements or standards and to share in the responsibility for providing physician coverage on an emergency basis in the Emergency Department, in accordance with the provisions of the Medical Staff Bylaws and all applicable facility-specific Rules & Regulations and Medical Staff Policies (On Call Coverage);
2.7.16 to provide his professional services to hospitalized or emergency room patients
covered by Medicaid and similar programs of indigent care, or such patients without personal physicians or insurance coverage, in accordance with Medical Staff Rules & Regulations adopted by the FMEC delineating the responsibility to provide services to those patients (Services to Indigent Patient);
2.7.17 provide proof of financial responsibility to pay claims or costs associated with the
rendering of, or failure to render, medical care or services in compliance with Florida law governing the practitioner’s license to practice in the State of Florida. Proof of financial responsibility shall be provided at the time of initial appointment and on reappointment, at the time the practitioner changes the method of meeting his financial responsibility and at any other time on the request of Medical Staff Services (Financial Responsibility);
2.7.18 to behave in a professional and civil manner and conduct himself in a manner
conducive to excellent patient care and to work cooperatively with Medical Staff appointees, and with other health care professionals, and Hospital personnel, so as not to adversely affect patient care. This requirement is not in any way intended to interfere with a practitioner’s right: (1) to express opinions freely and to support positions whether or not they are in dispute with those of other Medical Staff members; (2) to engage in honest differences of opinion with respect to diagnosis and treatment; or (3) to engage in a good faith criticism of others. The following types of behavior, however, which constitute some examples of an inability to interact on a professional basis with others or to behave in a professional and civil manner, are deemed unacceptable for a member of the Medical Staff:
2.7.18.1 conduct that reasonably could be characterized as sexual and/or racial
harassment;
2.7.18.2 threats of physical assault or actual physical assault, harassment, or the placing of others in fear by engaging in threatening behavior;
11
2.7.18.3 the unnecessary, unwarranted and unjustifiable knowing use of loud, profane or abusive language directed toward members of the Medical Staff, patient and others; or
2.7.18.4 written or oral statements that constitute the intentional expression of falsehoods, or constitute deliberately disparaging statements made with reckless disregard for their truth or for the reputation and feelings of others;
2.7.18.5 doing anything of a similar nature that the practitioner has been warned
not to do by the President of the Medical Staff or FMEC Committee (Professional and Civil Behavior);
2.7.19 duty to give notice if the practitioner is not actively engaged in the practice of his
profession in Lee County (Lack of Active Practice);
2.7.20 duty to give notice if practitioner does not maintain a full-time residence and office in Lee County, unless the residence and office requirements have been waived in accordance with these Bylaws (Residence or Office in Lee County).
2.8 Member Rights
The following basic rights shall apply to Medical Staff practitioners: 2.8.1 Each Medical Staff member, in the active category, has the right to a meeting with
the FMEC and/or the Physician Leadership Council (PLC) on matters relevant to the responsibilities of the FMEC and/or the PLC, provided that the practitioner has attempted to resolve a matter of concern after working with his Department Chair or other appropriate hospital and/or Health System Medical Staff leader(s). Upon written notice to the President of the Medical Staff, two (2) weeks in advance of a regular meeting, the active Medical Staff member may meet with the FMEC and/or the PLC to discuss the issue.
2.8.2 Each Medical Staff member, in the active category, has the right to initiate a recall
election of a Medical Staff officer by following the procedure outlined in Section 5.7 of these Bylaws regarding removal and resignation from office.
2.8.3 Each Medical Staff member, in the active category, may request a special meeting
of the Medical Staff, upon presentation of a petition, stating the purpose of the meeting and signed by ten (10) members of the Active Medical Staff. The FMEC shall schedule a special meeting for the specific purposes addressed by the petitioners in accordance with Section ten (10) of these Bylaws. No business other than that detailed in the petition may be transacted.
2.8.4 An applicant or an individual holding a Medical Staff appointment shall be entitled to
request a hearing/appeal pursuant to the conditions and procedures described in Part II of these Bylaws (Investigations, Corrective Action, Hearing and Appeal Plan).
2.8.5 All other rights as specified by these Bylaws.
2.9 Medical Staff Dues and Assessments
2.9.1 Annual Medical Staff dues, if any, shall be determined by the FMEC. Failure of a Medical Staff member to pay dues shall be considered a voluntary resignation from
12
the Medical Staff. The FMEC may pass policies from time to time that exempt certain categories of membership or members holding specified leadership positions from payment of dues. The FMEC shall authorize the use of Medical Staff dues.
2.9.2 Medical Staff System-wide assessments, such as a library assessment, shall be
determined by the PLC, on behalf of the FMECs. Failure of a Medical Staff member to pay any assessment(s) shall be considered a voluntary resignation from the Medical Staff. The PLC, on behalf of the FMECs, may pass policies from time to time that exempt certain categories of membership or members holding specific leadership positions from payment of such assessment(s).
2.9.3 The PLC, on behalf of the FMECs, shall authorize the use of Medical Staff
assessments consistent with the purpose of the assessment. 2.10 Conflict of Interest
2.10.1 In any instance where an officer, committee Chair, or member of any Medical Staff committee has, or reasonably could be perceived to have a conflict of interest, or to be biased in any matter involving another Medical Staff appointee or any other matter that comes before such individual or committee, or in any instance where any such individual brought the complaint against that practitioner, such individual shall not participate in the discussion or voting on the matter and shall be excused from any meeting during that time, although that individual may be asked and may answer, any questions concerning the matter before leaving. As a matter of procedure, the Chair of that committee designated to review the matter shall inquire, prior to any discussion of the matter, whether any member has any conflict of interest or bias. The existence of a potential conflict of interest or bias on the part of any committee member may be called to the attention of the Chair by any committee member with knowledge of the matter.
2.10.2 In any instance where an officer, committee Chair, or member of any Medical Staff
committee has a conflict of interest in any matter that comes before such individual or committee, such individual has the right to abstain or recuse himself from voting on such matter. Such abstention or recusal shall not prohibit such individual from providing factual information or participating in discussion on such matter. If an individual is requested to abstain or recuse himself and refuses to do so, the potential conflict of interest issue will be reviewed and resolved by the next highest authority as outlined in these Bylaws. As a matter of procedure, the Chair of that committee designated to review the matter shall inquire, prior to any discussion of the matter, whether any member has any conflict of interest or bias. The existence of a potential conflict of interest or bias on the part of any committee member may be called to the attention of the Chair by any committee member with knowledge of the matter.
2.10.3 Assurance of a conflict of interest or bias can be determined by a majority vote of
the members of the committee where a quorum is present. SECTION 3 CONFIDENTIALITY, IMMUNITY AND RELEASES 3.1 Confidentiality
Information with respect to any practitioner or regarding any other subject discussed, submitted, collected or prepared by any representative of the Lee Memorial Health System,
13
including officers or members of organized committees of the Health System’s Medical Staffs, or any other healthcare professional, healthcare facility, organization or Medical Staff, for the purpose of achieving and maintaining the quality of care, reducing morbidity or mortality or contributing to clinical research shall, in accordance with Florida law, be confidential and shall not be disseminated or used for any purpose other than the foregoing. Such information shall not be deemed a part of the patient medical record, and shall not be filed therein. Each individual or committee member participating in such activities shall agree to make no disclosures of any such information except as authorized, in writing, by the Chief Executive Officer (CEO) or by legal counsel to the hospitals. Any breach of confidentiality by an individual or committee member may result in a professional review action, and/or may result in appropriate legal action to ensure that confidentiality is preserved, including application to a court of law for injunctive or other relief.
3.2 Immunity 3.2.1 Any Medical Staff officer, Department Chair, Section Chief, committee Chair,
committee member, and individual staff appointee who acts in good faith for and on behalf of any System hospital in discharging duties, functions or responsibilities stated in these Medical Staff Bylaws, applicable Policies, and/or Rules and Regulations shall be afforded protection by the Board of Directors to the fullest extent permitted by law in accordance with written policies adopted by the Board. Individuals and organizations independent of the Medical Staff or any of its members who may be engaged by the Health System to perform the review, analysis and evaluation of the qualification and/or performance of practitioners with membership and/or privileges on the Medical Staff are afforded protection by the Board of Directors in accordance with written policies adopted by the Board, provided such individuals or organizations act in good faith.
3.2.2 To the fullest extent permitted by law, each applicant and appointee to the Medical
Staff releases from any and all liability, and extends absolute immunity to System hospitals and the Board and its individual members, and to the System’s authorized representatives and agents, with respect to any acts, communications or documents, recommendations or disclosures involving the applicant or appointee, concerning the following:
3.2.2.1 applications for appointment or clinical privileges, including temporary
privileges and/or emergency privileges;
3.2.2.2 evaluations concerning reappointment or changes in clinical privileges;
3.2.2.3 proceedings for suspension or reduction of clinical privileges or for revocation of Medical Staff appointment, or any other disciplinary sanction;
3.2.2.4 summary suspension;
3.2.2.5 hearings and appellate reviews; 3.2.2.6 medical/surgical care evaluations; 3.2.2.7 utilization reviews;
3.2.2.8 other activities relating to the quality of patient care or professional
conduct;
14
3.2.2.9 matters of inquiries concerning the applicant’s or appointee’s professional
qualifications, credentials, clinical competence, character, mental or emotional stability, physical condition, ethics or behavior; and/or
3.2.2.10 any other matter that directly or indirectly might relate to the applicants or
appointee’s competence, and/or to patient care.
3.3 Releases
3.3.1 Authorization to Obtain Information
The applicant or appointee specifically authorizes the Medical Staff and its authorized representatives to consult with any third party who may have information bearing on the individual’s professional qualifications, credentials, clinical competence, character, mental or emotional stability, physical condition, ethics, behavior, or any other matter reasonably having a bearing on the applicant’s or appointee’s satisfaction of the criteria for initial and continued appointment to the Medical Staff. This authorization also covers the right to inspect, or obtain all communications, reports, records, statements, documents, recommendations or disclosures of said third parties that may be relevant to such questions. The individual also specifically authorizes said third parties to release said information to the Medical Staff and its authorized representatives upon request.
3.3.2 Legal Effect
The confidentiality provisions and protections described in this Section shall not limit
or supersede any protection or immunity afforded by law. SECTION 4 CATEGORIES OF THE MEDICAL STAFF 4.1 Active Category
4.1.1 Qualifications: Members of this category must have served on the Medical Staff, maintained a residence and office in Lee County (4.1.3.3) for one year, and be involved in twenty-four (24) patient contacts per year (i.e., a patient contact is defined as an inpatient admission, consultation, or an inpatient or outpatient surgical procedure) at the hospital except as expressly waived for practitioners with at least twenty (20) years of service in the active category or for those physicians who document their efforts to support the hospital’s patient care mission to the satisfaction of the FMEC.
In the event that a member of the active category does not meet the qualifications for reappointment to the active category, and if the member is otherwise abiding by all Bylaws, Rules and Regulations, and policies of the Medical Staff and hospital, the member may be appointed to another Medical Staff category if he meets the eligibility requirements for such category.
4.1.2 Prerogatives: Members of this category may:
4.1.2.1 Attend Medical Staff/Department meetings of which he is a member and any Medical Staff or hospital education programs;
15
4.1.2.2 Vote on all matters presented by the Medical Staff, Department, and committee(s) to which the member is assigned;
4.1.2.3 Hold office and sit on or be the Chair of any committee in accordance with
any qualifying criteria set forth elsewhere in the Medical Staff Bylaws or Medical Staff policies.
4.1.3 Responsibilities: Members of this category shall:
4.1.3.1 Contribute to the organizational and administrative affairs of the Medical Staff;
4.1.3.2 Actively participate as requested or required in activities and
functions of the Medical Staff, including quality/performance improvement and peer review, credentialing, risk and utilization management, medical records completion, monitoring activities and in the discharge of other Medical Staff functions as may be required by the FMEC;
4.1.3.3 The one-year residence and office requirement may be explicitly
waived by majority vote of the FMEC, on written request of the practitioner, at the time of appointment, if the practitioner affirmatively demonstrates to the FMEC in writing that the quality of patient care is not likely to be affected by his not living and having an office in Lee County and that the practitioner’s obligation to provide emergency room call and to attend hospitalized patient can be met.
4.1.3.4 Fulfill or comply with any applicable Medical Staff or hospital
policies or procedures as requested by the FMEC. 4.1.3.5 Fulfill basic responsibilities and requirements set forth in Section
2.7 of this Part, including but not limited to, Emergency Department call responsibilities in accordance with facility specific rules and regulations, unless exempted from Emergency Department call responsibilities as defined by their Section (if applicable) or Department and approved by the FMEC. In the event facility specific rules and regulations require physicians to accept emergency department referrals to the physician’s office, Lee Memorial Health System will provide facility support and services for such patients.
4.2 Associate Category 4.2.1 Qualifications: The associate category is reserved for Medical Staff members who
do not meet the eligibility requirements for the active category or choose not to pursue active status. This category includes physicians during their first year on the Medical Staff, as well as low volume/no volume physicians.
4.2.2 Prerogatives: Members of this category may:
4.2.2.1 Attend general Medical Staff Department meetings of which he is a member and any Medical Staff or hospital education programs.
16
4.2.2.2 Members of the associate category may not vote on matters at general Medical Staff, Department meetings or be an officer of the Medical Staff.
4.2.2.3 Members of the associate category may serve on facility and system
Medical Staff committees, other than the FMEC, and may vote on matters that come before such committees.
4.2.3 Responsibilities: Members of this category shall have the same responsibilities as
active category members, as set forth in Section 4.1 and Section 2.7 of this Part.
4.3 Honorary Category 4.3.1 The Honorary category is restricted to those individuals recommended by the FMEC
and approved by the Board. Appointment to this category is entirely discretionary and may be rescinded at any time. Members of the honorary category shall consist of those members who have retired from active hospital practice, who are of outstanding reputation, and have provided distinguished service to the hospital. They may attend general Medical Staff meetings, Department meetings, continuing medical education (CME) activities, and may be appointed to committees. They shall not hold clinical privileges, hold office or be eligible to vote.
SECTION 5 OFFICERS OF THE MEDICAL STAFF 5.1 Officers of the Medical Staff and FMEC at-large Members: Each hospital is
authorized to have the following officers:
5.1.1 Facility President of the Medical Staff 5.1.2 Facility President-Elect of the Medical Staff
5.1.3 Facility Secretary/Treasurer 5.1.4 Facility Past President of the Medical Staff
5.2 Qualifications of Officers and FMEC at-large Members 5.2.1 Officers must be members in good standing of the active category for at least three
(3) years or actively involved in patient care in the community, have previously served in a significant leadership position on a Medical Staff, (i.e. Department Chair, Section Chief or Committee Chair), indicate a willingness and ability to serve, have no pending adverse recommendations concerning Medical Staff appointment or clinical privileges, have a history of attendance at continuing education programs (provided by the System) relating to Medical Staff leadership and/or be willing to do so during their term or office, have demonstrated an ability to work well with others, be in compliance with the professional conduct policies of the Medical Staff, and should have excellent administrative and communication skills.
FMEC at large members must be members in good standing of the active category for at least two (2) years or actively involved in patient care in the community.
5.2.2 Officers and FMEC at-large members must disclose leadership positions on another
hospital Medical Staff. 5.3 Election of Officers and FMEC at-large Members
17
5.3.1 Every year, the FMEC shall appoint a nominations committee Chaired by the
immediate Past Facility President of the Medical Staff and comprised of at least five (5) at large members of the active Medical Staff at least ninety (90) days prior to
the election. Representatives of administration shall not serve on the nominations committee. Nominations will be solicited from the Medical Staff for consideration prior to the committee meeting. The committee shall offer at least one nominee for each office. Nominations must be announced, and the names of the nominees distributed to all members of the active Medical Staff at least forty-five (45) days prior to the election. A petition signed by at least 20% of the members of the active Medical Staff may also make nominations. Such petition must be submitted to the President of the Medical Staff at least twenty (20) days prior to the election for placement on the ballot.
5.3.2 Officers and FMEC at-large members shall be elected, as needed every year at an
election that takes place at least one (1) month prior to the expiration of the term of the current officers. Only members of the active category shall be eligible to vote. The FMEC will determine the mechanisms by which votes may be cast. The mechanisms that may be considered include written mail ballots; electronic voting via computer, fax, or other technology for transmitting the members’ voting choices. No proxy voting will be permissible. The nominee receiving the greatest number of votes will be elected. In the event of a tie vote, the Medical Staff support professional will arrange for a repeat vote(s) until one candidate receives a greater number of votes.
5.3.3 Medical Staff members will be notified of the election date and final slate of
nominees ten (10) days prior to the election. 5.4 Terms of Office 5.4.1 Officers and FMEC at-large members serve terms as follows: 5.4.1.1 Facility President-Elect of the Medical Staff – one (1) year 5.4.1.2 Facility President of the Medical Staff – two (2) years 5.4.1.3 Facility Past President of the Medical Staff – one (1) year 5.4.1.4 Facility Secretary/Treasurer – one (1) year 5.4.1.5 FMEC Members-at-Large – two (2) years 5.4.2 Officers shall take office October 1. Officers may be re-elected to office except that
the Facility President of the Medical Staff may not be re-elected for successive terms.
5.5 Vacancies of Office 5.5.1 The FMEC shall fill vacancies of office during the Medical Staff year, except the
office of the Facility President of the Medical Staff. If there is a vacancy in the office of the Facility President of the Medical Staff, the
Facility President-Elect of the Medical Staff shall serve the remainder of the term. 5.6 Duties of Officers and FMEC At-Large Members 5.6.1 Facility President of the Medical Staff – The Facility President shall represent the
interests of the Medical Staff to the FMEC and the Board. The Facility President will fulfill the duties specified in Section 5.6.2 of these Bylaws, as well as additional
18
duties as reasonably requested by the FMEC in order to implement and/or enforce all provisions of the Bylaws and the interests of the Medical Staff.
5.6.2 Responsibilities of the Facility President of the Medical Staff The Facility President of the Medical Staff is the primary elected officer of the
Medical Staff and is the Medical Staff’s advocate and representative in its relationships to the Board, the Facility Chief Administrative Officer (CAO) and the Health System administration. The Facility President of the Medical Staff, jointly with the FMEC, provides direction to and oversees Medical Staff activities related to assessing and promoting continuous improvement in the quality of clinical services and all other functions of the Medical Staff as outlined in the Medical Staff Bylaws, Rules and Regulations and Policies. Specific responsibilities and authority include:
5.6.2.1 Call and preside at all general and special meetings of the Medical Staff; 5.6.2.2 Serve as Chair of the FMEC, a voting member of the PLC and as ex-officio
member of all other Medical Staff committees without vote, and to participate as invited by the Board and the Facility CAO on hospital or Board committees;
5.6.2.3 Shall not vote at the FMEC, unless their vote is needed to break a tie vote; 5.6.2.4 Enforce Medical Staff Bylaws, Rules and Regulations and Medical
Staff/hospital/System Policies; 5.6.2.5 Except as stated otherwise, appoint committee Chairs and all members of
Medical Staff standing and ad hoc committees; in consultation with hospital administration, appoint Medical Staff members to appropriate hospital committees, in consultation with the Chair of the Board, appoint the Medical Staff members to appropriate Board committees when those are not designated by position or by specific direction of the Board or otherwise prohibited by state law;
5.6.2.6 Support and encourage Medical Staff leadership and participation on
interdisciplinary clinical performance improvement activities; 5.6.2.7 Report to the Board, through the PLC, the FMEC’s recommendations
concerning appointment, reappointment, delineation of clinical privileges or specified services and corrective action with respect to practitioners or allied health practitioners who are applying for appointment or privileges, or who are granted privileges or providing services in the hospital;
5.6.2.8 With the support of the facility Credentials/Privileging Committee and the
System Credentialing/Privileging Committee, evaluate and periodically report to the FMEC, PLC and the Board regarding the effectiveness of the credentialing and privileging processes;
5.6.2.9 Review and enforce compliance with standards of ethical conduct and
professional demeanor among the members of the Medical Staff in their relations with each other, the Board, hospital/System management, other professional and support staff, and the community the hospital serves;
5.6.2.10 Communicate and represent the opinions and concerns of the Medical
Staff and its individual members on organizational and individual matters
19
affecting hospital operations to the Facility CAO, the FMEC, PLC and the Board;
5.6.2.11 attends Board meetings and Board committee meetings as deemed
appropriate by Facility Medical Staff President; 5.6.2.12 ensures that the decisions of the Board are communicated and carried out
within the Medical Staff; 5.6.2.13 performs such other duties, and exercises such authority commensurate
with the office as are set forth in the Medical Staff Bylaws.
5.6.3 Facility President-Elect of the Medical Staff – In the absence of the Facility President, the Facility President-Elect or the Facility Past President shall assume all the duties and have the authority of the Facility President. He shall perform such further duties to assist the Facility President as the Facility President may request from time to time. The Facility President-Elect, upon the end of the term of the Facility President, shall automatically succeed to the office of Facility President.
5.6.4 Facility Secretary/Treasurer – This officer will collaborate with the hospital’s
Medical Staff office, assure maintenance of minutes, attend to correspondence, act as Medical Staff treasurer, and coordinate communication within the Medical Staff. He shall perform such further duties to assist the Facility President as the Facility President may from time to time request.
5.6.5 Facility Past President of the Medical Staff – This officer will serve as a
consultant to the Facility President and the Facility President-Elect as requested by the FMEC and provide feedback to the officers regarding their performance of assigned duties on an annual basis.
He shall perform such further duties to assist the Facility President as the
Facility President may request. He shall serve as a member of the System Credentialing/Privileging Committee.
5.6.6 FMEC at-large members – shall advise and support the Medical Staff officers
and are responsible for representing the needs/interests of the entire Medical Staff and not simply representing the preferences of their own clinical specialty.
5.7 Removal and Resignation of Officer or FMEC At-Large Member 5.7.1 The Medical Staff may remove any facility officer or FMEC at-large member by
petition of 20% of the active Medical Staff members and a subsequent affirmative vote by two-thirds (2/3) of those active Medical Staff members’ casting votes.
5.7.2 Recall of Officers or FMEC at-large members The FMEC may remove any facility Medical Staff officer or FMEC at-large
member for conduct detrimental to the interests of the Medical Staff or if the officer is suffering from a physical or mental infirmity that renders the individual incapable of fulfilling the duties of the office. At least ten (10) days notice prior to the date of the meeting shall be provided, in writing, to the affected officer or FMEC at-large member. The officer or at-large member shall be afforded the opportunity to speak prior to the taking of any vote on such removal. For recall
20
of an officer or at-large member, a two-thirds (2/3) vote of approval is required with three-fourths (3/4) of the FMEC members present and voting. Affected officer or at-large member does not count as quorum and does not vote.
5.7.3 Resignation of Officers or FMEC at-large members Any elected officer or FMEC at-large member may resign at any time by giving
written notice to the FMEC. Such resignation takes effect on the date of receipt, when a successor is elected, or any later time specified therein.
SECTION 6 MEDICAL STAFF ORGANIZATION The organized Medical Staff is actively involved in Medical Staff governance, peer review,
credentialing/privileging and communication. Medical Staff members are accountable to the FMEC.
The Medical Staff facility officers (Section 5), Medical Staff governance committees (PLC, Section 7.1 and FMEC, Section 7.4), Department Chairs (Section 6.1), clinical Section Chiefs (Section 6.1.1), hospital (as appropriate) System Medical Staff committee Chairs, (Section 7.6) and facility Medical Staff committee Chairs (Section 7.7) are responsible for working collaboratively to develop a process for communication of Medical Staff functions. Periodic reports, as appropriate, are given to each FMEC, Medical Staff Departments, Medical Staff committees and the PLC as needed to ensure adherence to regulatory requirements and accreditation standards.
Additionally, Medical Staff officers may appoint, in collaboration with the Facility Medical
Director, designated physician leaders to serve on the following Medical Staff committees to help ensure Medical Staff input and oversight with clinical functions such as System Bylaws, Cancer Care, CME/Medical Library, Ethics, Institutional Review, System Credentialing/Privileging, Critical Care, System Emergency Services, Infection Control, Pharmacy and Therapeutics, System Medical Staff Quality, System Practitioner Resource, Trauma Quality, Vascular Lab, in addition to the Children’s Hospital committees (Cancer Care, Ethics, Neonatal Intensive Care Unit (NICU) Pediatric Intensive Care Unit (PICU) Perinatal and Medical Staff Quality and other such functions as determined by the FMEC and/or the PLC.
6.1 Departments The Medical Staff shall be organized as a Departmentalized staff. The current
Departments authorized by the FMECs are Medicine, Surgery, Pediatrics, Obstetrics and Gynecology, Anesthesiology, Pathology, Radiology and Emergency Medicine. Departments fulfill the duties listed in Section 6.2.4 of these Bylaws within a specific hospital or facility and/or across the Health System as necessary. Departments shall meet as frequently as needed to fulfill assigned duties and when requested by the FMEC.
The Medical Staff may create Clinical Sections (as specified in these Bylaws) within
a Department in order to facilitate Medical Staff activities.
6.1.1 Any FMEC may recognize any group of like American Board of Medical Specialties, (ABMS) approved specialties with at least three (3) Medical Staff members or service lines that wish to organize themselves into a Clinical Section. Any Clinical Section, if organized shall not be required to hold regularly scheduled meetings, keep routine minutes, or require attendance.
21
A written report is required only when the Clinical Section is making a formal report. A Clinical Section shall elect a Clinical Section Chief. The Clinical Section Chief is responsible for fulfilling the activities listed in Section 6.1.1.1 - 6.1.1.7 of these Bylaws. The procedure for removal of a Clinical Section Chief shall be the same as set forth in Section 6.2.3 for Department Chair. When a clinical Section is making a formal report, the report shall be submitted to the FMEC documenting the specific position of the clinical Section. The President of the Medical Staff and the Clinical Section Chief (or designee) will decide if the report/issue is placed on the FMEC agenda and whether the Clinical Section Chief (or designee) will attend the FMEC meeting to present the report/issue to the FMEC on that specific report/issue. Clinical Sections are optional and shall exist to perform any of the following activities within a specific facility and/or across Health System facilities as necessary:
6.1.1.1 continuing education/Grand Rounds/discussion of patient care;
6.1.1.2 formulation of ED on-call and inpatient consultation and coverage recommendations; 6.1.1.3 discussion of policies and procedures; 6.1.1.4 discussion of equipment needs; 6.1.1.5 development of recommendations for the Department Chair(s), the
FMECs or the PLC; 6.1.1.6 participation in the development of criteria for clinical privileges
when requested by the System Credentialing/Privileging Committee or FMEC;
6.1.1.7 discussion of a specific issue at the request of the PLC or the
FMEC. The FMEC, with the concurrence of the PLC, may designate new Medical Staff Departments or Clinical Sections or dissolve current Departments or Clinical Sections as it determines will best meet the Medical Staff needs for promoting performance improvement, patient safety, and effective credentialing and privileging.
6.2 Qualifications, Selection, Term, and Removal of Department Chair 6.2.1 Each Department Chair shall serve a term of two (2) years commencing on
October 1 and may be elected to serve successive terms. All Chairs must be members of the active Medical Staff with relevant clinical
privileges and be certified by an appropriate specialty board or have affirmatively established comparable competence through the credentialing process.
6.2.2 Department Chairs and Vice-Chairs will be elected by majority vote of the
active members of the Department, subject to ratification by the FMEC.
22
Each Department shall establish procedures for identifying and electing candidates and these procedures must be ratified by the FMEC.
6.2.3 Department Chairs may be removed from office by the FMEC upon receipt
of a recommendation of two-thirds (2/3) of the members of the Department or, in the absence of such recommendation, the FMEC may remove a Chair on its own by a two-third (2/3) vote of a majority of members present and voting, if any of the following occurs:
6.2.3.1 The Chair ceases to be a member in good standing of the Medical
Staff; 6.2.3.2 The Chair suffers an involuntary loss or significant limitation of
practice privileges; 6.2.3.3 The Chair fails, in the opinion of the FMEC, to demonstrate to the
satisfaction of the FMEC, PLC or the Board that he is effectively carrying out the responsibilities of the position;
6.2.3.4 If removal is required, a new election will be held according to the
established Departmental procedures. 6.2.4 Department Chairs shall carry out the following responsibilities: 6.2.4.1 to oversee all clinically-related activities of the Department; 6.2.4.2 to oversee all administratively related activities of the Department
otherwise provided for by the Facility; 6.2.4.3 to provide ongoing surveillance of the performance of all individuals
in the Medical Staff Department who have been granted clinical privileges;
6.2.4.4 to recommend to the System Credentialing/Privileging Committee
Medical Staff Department; 6.2.4.5 to recommend clinical privileges for each member of the
Department and other LIPs practicing with privileges within the scope of the Department;
6.2.4.6 to assess and recommend to the FMEC and Facility CAO off-site
sources for needed patient care services not provided by the Medical Staff Department or Facility;
6.2.4.7 to monitor and evaluate the quality and appropriateness of patient
care provided in the Medical Staff Department and to implement action following review and recommendations by the facility Medical Staff peer review/quality committee and/or the FMEC;
6.2.4.8 to integrate the Department into the primary functions of the
hospital; 6.2.4.9 to coordinate and integrate interdepartmental and
intradepartmental services and communication;
23
6.2.4.10 to participate in the administration of the Department through cooperation with nursing services and hospital administration in matters affecting patient care;
6.2.4.11 to develop and implement Medical Staff and hospital policies and
procedures that guide and support the provision of patient care services;
6.2.4.12 to recommend to the Facility CAO the sufficient numbers of
qualified and competent persons to provide patient care and service;
6.2.4.13 to provide input to the Facility CAO regarding the qualifications and
competence of Department or service personnel who are not Licensed Independent Practitioners (LIPs) but provide patient care, treatment, and services;
6.2.4.14 to provide continuous assessment and improvement of the quality
of care, treatment, and services; 6.2.4.15 to maintain quality control programs as appropriate; 6.2.4.16 to orient and continuously educate all persons in the Department; 6.2.4.17 to make recommendations to the FMEC and to the Facility CAO for
space and other resources needed by the Medical Staff Department to provide patient care services.
6.3 Assignment to Department 6.3.1 The FMEC will, after consideration of the recommendation of the Chair of the
appropriate Department, recommend Department assignments for all members in accordance with their qualifications. Each member will be assigned to one primary Department. Clinical privileges are independent of the Department assignment.
SECTION 7 MEDICAL STAFF GOVERNANCE COMMITTEES 7.1 Designation of the Lee Memorial Health System Medical Staff Physician Leadership
Council (PLC)
7.1.1 There shall be a Lee Memorial Health System Medical Staff Physician Leadership Council (PLC) and such other standing and special committees as determined by the PLC.
7.1.2 There shall be a Facility Medical Executive Committee (FMEC) at each hospital and
such other facility standing and special committees as established by the FMEC.
7.2 Composition of the Lee Memorial Health System Medical Staff PLC 7.2.1 Composition: The PLC shall consist of the following voting members: Each Facility President and
each Facility President–Elect or each Facility Immediate Past President and two (2)
24
at-large Medical Staff members elected by each FMEC. All shall serve a 2-year term except the Facility President-Elect and Facility Past President shall serve 1-year term. The Chairs of the System Credentialing/Privileging Committee and System Quality Committee, the system CEO or Designee, the System Chief Medical Officer and the Chair of the Board and up to two (2) other Board consultants, shall serve as ex-officio, non-voting members. The PLC will elect the PLC Chair and Vice Chair who shall serve a 2-year term.
In the event that the PLC composition does not include one anesthesiologist,
emergency medicine physician, hospitalist or intensivist, radiologist and pathologist, the PLC may appoint an active Medical Staff member from each of these hospital-based specialties to be voting members of the PLC.
7.2.2 Duties: The duties of the Lee Memorial Health System PLC are:
7.2.2.1 to work in a cooperative and professional manner with the FMECs System and Facility Administration and the Board to ensure Medical Staff input into the plans, goals and mission of the Lee Memorial Health System;
7.2.2.2 receive, review, and transmit FMEC recommendations to the
Board; 7.2.2.3 review and attempt to resolve any inconsistency emanating from
the FMEC recommendation(s) and transmit FMEC recommendations to the Board concerning all matters relating to appointments, reappointments, staff category, facility assignments, clinical privileges subject to the conflict resolution process herein, unless due process rights are triggered pursuant to Part II.
The PLC is acting as a duly constituted peer review committee under Florida law when it is reviewing the quality of care or performance of any particular physician.
7.2.2.4 consistent with the hospital and Medical Staff mission and
philosophy, the PLC will participate and encourage participation of the FMECs in identifying community health needs and in setting goals and work with the System administration and the facility CAO(s) to design and implement programs to meet those needs;
7.2.2.5 work with the FMECs to ensure understanding and the consistent
application of Medical Staff Rules and Regulations, Policies and Procedures; and
7.2.2.6 govern the collection of Medical Staff system-wide assessments
and authorize the use of Medical Staff assessments consistent with the purpose of the assessment.
7.2.3 Meetings:
The PLC shall meet as frequently as needed, but at least quarterly, to perform its assigned functions. Records of its proceedings and actions shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
25
7.3 Staff Functions
7.3.1 The PLC exists to promote communication, collaboration and coordination
between physicians, System and facility administration and the Board concerning the work of each FMEC and planning activities of the Lee Memorial Health System that impact members of the Medical Staff.
7.4 Facility Medical Executive Committee (FMEC) Composition Selection and Tenure
7.4.1 Each Medical Staff may determine the number of Medical Staff members
appointed or elected to the FMEC. The composition of the FMEC shall consist of at least the following voting members: Facility President of the Medical Staff, Facility Immediate Past President, Facility President-Elect of the Medical Staff, Facility Secretary/Treasurer, physician representative from the System Credentialing/Privileging Committee, Chair of the Facility Quality Committee, the Department Chairs from Medicine, Surgery, Anesthesiology, Radiology, Pathology, Pediatrics, Obstetrics/Gynecology and Emergency Services, two (2) at-large active members of the Medical Staff appointed by the FMEC and two (2) at-large active members of the Medical Staff elected by the general Medical Staff.
One Board member, the CAO, the facility Vice-President of Nursing, the
facility Medical Director (as appropriate) will serve in a non-voting, ex-officio capacity. The Facility President of the Medical Staff shall serve as the Chair of the FMEC.
7.4.2 Each FMEC composition description shall be listed in the Facility Rules &
Regulations.
7.4.3 FMEC members shall disclose in writing to the Medical Staff, prior to the date of election of appointment, any personal, professional or financial applications or responsibilities with Lee Memorial Health System and any competing hospital, healthcare organization or Health System.
FMEC members shall serve 2-year terms, except Facility Past President and
Facility President-Elect shall serve 1-year terms. The FMEC and the Nominations Committee shall stagger the terms of appointed and elected at-large members to ensure continuity of leadership. Such physicians must be on Active Staff and be a member in good standing at all times.
All FMEC members are expected to participate in orientation and continuing
education activities as related to the operation of the Medical Staff.
7.5 Duties and Responsibilities of the Facility Medical Executive Committees 7.5.1 To represent, to initiate action and act on behalf of the Medical Staff
members with privileges at the Facility in fulfilling the duties of Medical Staff self governance, credentialing/privileging and quality/peer review, after seeking input and recommendations from Sections and/or Departments affected by FMEC action (if applicable).
26
7.5.2 To receive recommendations from the System Credentialing/Privileging
Committee and the Facility Quality/Peer Review Committee and make recommendations to the Board (and for informational purposes only) to the PLC concerning:
7.5.2.1 appointments, reappointments and granting of clinical privileges; 7.5.2.2 necessity for special investigations of issues pertaining to
practitioner competence of behavior; 7.5.2.3 needed performance improvements and peer review results; 7.5.2.4 policies and procedures development and enforcement; 7.5.2.5 facility Medical Staff Department and committee structure; and 7.5.2.6 other matters relevant to the provision of patient care, operation of
the Medical Staff or proposed Bylaws amendments. 7.5.3 Receive or act upon reports and recommendations concerning patient care
quality and appropriateness reviews, evaluation and monitoring functions, and the discharge of their delegated administrative responsibilities;
7.5.4 Recommend to the Board, and for information purposes only to the PLC,
specific programs and systems to perform Medical Staff peer review, quality monitoring, communication, governance, credentialing/privileging and planning functions;
7.5.5 Coordinate the implementation of policies adopted by the Board; 7.5.6 Oversee the facility multi-specialty peer review and quality monitoring
activities in a manner consistent with federal and state law; 7.5.7 Take reasonable steps to encourage professionally ethical conduct and
competent clinical performance of Medical Staff members at the facility including collegial and educational efforts;
7.5.8 Participate in identifying community health needs and in setting facility-
specific goals and implementing programs to meet those needs; 7.5.9 Design and implement facility-specific rules and regulations that will not
conflict with the Medical Staff Bylaws; 7.5.10 Work with Facility and System administration to promote effective, efficient
and safe patient care practice within the facility; 7.5.11 Take reasonable steps to encourage professionally ethical conduct and
competent clinical performance on the part of staff appointees including initiating investigations, and pursuing corrective action, when warranted;
27
7.5.12 Provide oversight concerning the quality and safety of the care provided by residents, interns, students, and ensure that the same act within approved guidelines established by the Medical Staff and the Board.
Reviews and ensure corrective action regarding applicable Residency Review Commission findings and recommendations;
7.5.13 Keep the Medical Staff up to date concerning the licensure and
accreditation status of the System and hospitals; 7.5.14 Request evaluations of practitioners privileged through the Medical Staff
process in instances in which there is question about an applicant or member’s ability to perform privileges requested or currently granted;
7.5.15 Consult with administration on the quality, timeliness, and appropriateness
of aspects of contracts for patient care services provided to the hospital by entities outside the hospital;
7.5.16 Hold Medical Staff leaders, committees, and Departments accountable for
fulfillment of their duties and responsibilities; 7.5.17 Advise and assist the PLC, when and to the extent possible, as requested
by the PLC, the Board and the System or Facility administration; 7.5.18 Grant, deny or rescind exemptions related to ED call responsibility; 7.5.19 Meetings: The FMEC shall meet ten (10) times per year, or more
frequently as needed to perform its assigned functions. Records of its proceedings and actions shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
7.6 System Medical Staff Committees 7.6.1 Purpose. There shall be system Medical Staff committees established by the
Medical Staff to carry out the responsibilities of the Medical Staff with regard to measuring and assessing the performance of the Medical Staff providing medical care within the hospitals and Health System facilities.
7.6.2 Organization to Perform Functions. The PLC with the input and approval of each
FMEC shall establish system Medical Staff committees comprised of members of the Medical Staff and others as may be deemed appropriate or necessary. The delineation of specific duties, committee size, liaison with other committees and Departments, and other matters necessary to the efficient performance of Medical Staff functions shall be set forth in these Bylaws. The only voting members of system Medical Staff committees are members of the Medical Staff unless otherwise determined by the FMEC. System Medical Staff committees consist of the following, shall report to and through the FMECs on matters relating to all FMECs, and shall report to each FMEC on facility specific matters:
7.6.2.1 System Credentialing/Privileging Committee (See Part III, Section 1 of
these Bylaws); 7.6.2.2 System Medical Staff Quality Committee (See Medical Staff Quality
Manual); 7.6.2.3 System Practitioner Resource Committee.
28
Membership: Membership shall be established by the PLC with the input and approval of
each FMEC. The term of office shall be for a period of two (2) years with staggered terms, so as to provide continuity and development of expertise.
Referrals: Concerns that a member of the Medical Staff may be suffering from a
physical or mental impairment that might impact their ability to practice medicine or may be a threat to themselves or others, including but not limited to impairment due to substance abuse, should be communicated to the President of the Medical Staff or to the affected practitioner’s Department Chair. The President of the Medical Staff or Department Chair, after consultation with others, if deemed appropriate, may refer the affected practitioner to the practitioner Resource Committee for review, evaluation and follow-up.
Responsibilities: The committee shall have no authority to take disciplinary action. Nor
does the committee provide treatment. The committee is responsible to: 7.6.2.3.1 Receive and evaluate concerns about practitioner health and
functioning;
7.6.2.3.2 Provide assistance and encourage a practitioner impaired by virtue of physical or psychiatric condition, problems in living, or issues related to alcohol use or drug use to voluntarily accept referral for the evaluation, treatment or assistance;
7.6.2.3.3 Assume an advocacy role on behalf of the affected practitioner;
7.6.2.3.4 Serve as an advisor to the President of the Medical Staff, Department Chair and/or FMEC, including advice relating to alternatives in the event that the practitioner fails to accept referral or fails to adequately recover from treatment;
7.6.2.3.5 Consider referring an affected practitioner to appropriate resources
for treatment and advice on the appropriateness of treatment, rehabilitation planning and monitoring provisions;
7.6.2.3.6 Utilize the Florida Medical Association Physician Resource Network,
Intervention Project for Nurses or other resources, if appropriate;
7.6.2.3.7 Maintain the confidentiality of information regarding matters referred to the committee;
7.6.2.3.8 Refer to the Medical Staff President Department Chair or FMEC
those situations that may require possible corrective actions. 7.6.2.4 System Bylaws Committee
29
Membership: The Bylaws Committee shall be a standing committee of the Medical Staff
and shall be composed of at least five (5) active Medical Staff appointees (including one (1) member from each FMEC appointed by the facility Medical Staff President) and the System Chief Medical Officer (CMO) or his designee (who shall serve as a non-voting member).
Duties: The duties of the Bylaws Committee shall be to:
7.6.2.4.1 Conduct an annual review of the Medical Staff Bylaws, Medical Staff
Rules and Regulations and Policies; and 7.6.2.4.2 Review recommendations for changes in the Medical Staff Bylaws,
Rules and Regulations and Policies made by the Medical Staff committees, Departments, or by the Board.
Meetings, Reports and Recommendations: The Bylaws Committee shall meet at least annually or as necessary to
accomplish its duties, shall maintain a permanent record of its proceedings and actions, and shall report its recommendations to the FMECs.
7.6.2.5 System Emergency Services Committee Membership: The System Emergency Services Committee shall be an ad hoc committee
of the Medical Staff and shall be composed of the Emergency Department Medical Directors, at least three (3) Active Staff members, and other Active Staff members as needed.
Duties: The duties of the System Emergency Services Committee shall be to: 7.6.2.5.1 conduct an annual review of system-wide emergency services; 7.6.2.5.2 ensure emergency call is fair to physicians while providing adequate
coverage to patients of our community; 7.6.2.5.3 review emergency call rules system-wide for recommendation to
FMECs.
Meetings: The System Emergency Services Committee will meet at least once per year or as needed.
7.6.3 Composition and Meetings of System Medical Staff Committees:
30
7.6.3.1 Unless otherwise provided for in these Bylaws, System Medical Staff committees shall be composed of physician members from each facility, as appointed by each FMEC;
7.6.3.2 Each System Medical Staff committee shall elect a physician Chairperson
and physician vice Chairperson for their respective committee;
7.6.3.3 System Medical Staff committee members shall serve terms of 2 years and may be reappointed;
7.6.3.4 System Medical Staff committee members who cease to be members of
the Medical Staff of Lee Memorial Health System shall automatically cease to serve as committee members. Vacancies on committees shall be filled by the appropriate FMEC;
7.6.3.5 System Medical Staff committees shall meet as often as necessary to
discharge the duties of the respective committees in accordance with these Bylaws.
Reasonable notice of meetings shall be provided to committee members
and may include providing a written schedule of meetings on an annual or more frequent basis.
7.7 Facility Medical Staff Committees: 7.7.1 Purpose: There shall be committees to carry out certain essential functions
within each facility as determined by each FMEC. The FMEC may establish such committees from time to time in addition to those set forth in the Bylaws.
7.7.2 Standing Facility Medical Staff Committees: The following facility committees
are approved as standing committees of the FMEC: 7.7.2.1 GCMC Credentialing/Privileging Committee (see Part III, Section 1 of
these Bylaws); 7.7.2.2 LMHS Credentialing/Privileging Committee (see Part III, Section 1 of these
Bylaws); 7.7.2.3 Nominations Committees (See Part 1, Section 5.3 of these Bylaws);
7.7.2.4 Facility Medical Staff Quality Committees (see Medical Staff Quality Manual);
7.7.2.5 Facility Rules and Regulations Committees Composition: The Facility Rules and Regulations Committee shall be a
standing committee of the Medical Staff and shall be composed of at least two (2) active Staff members appointed by the FMEC.
Duties: The duties shall be to review and recommend changes in the
Facility Rules and Regulations and policies to the FMEC. 7.7.2.6 Trauma Quality Management
31
Composition, membership and duties are mandated by the State regulations for designated trauma centers.
SECTION 8 MEDICAL STAFF MEETINGS 8.1 General Medical Staff Meetings 8.1.1 An annual meeting and other general Medical Staff meetings shall be held at a
time determined by the FMEC. Notice of the meeting shall be given to all Medical Staff members via appropriate media and posted conspicuously at least ten (10) days before the meeting.
8.1.2 Except for Bylaws amendments or as otherwise specified in these Bylaws, the
actions of a majority of the members present and voting at a meeting of the Medical Staff is the action of the group.
Action may be taken without a meeting of the Medical Staff by presentation of
the question to each Medical Staff member eligible to vote, in person, via telephone, and/or by mail or internet, and their vote recorded in accordance with procedures approved by the FMEC. Such vote shall be binding so long as the question that is voted on receives a majority of the votes cast.
8.1.3 Special Meetings of the General Medical Staff 8.1.3.1 The President of the Medical Staff may call a special general Medical
Staff meeting at any time. Such request or resolution shall state the purpose of the meeting. The President of the Medical Staff shall designate the time and place of any special general Medical Staff meeting.
8.1.3.2 Written or electronic notice stating the time, place and purposes of
any special general Medical Staff meeting shall be conspicuously posted and shall be sent to each member of the Medical Staff at least three (3) days before the date of such meeting. No business shall be transacted at any special general Medical Staff meeting, except that stated in the notice of such meeting.
8.2 Departments, Sections and Committee Meetings 8.2.1 Regular Meetings of Medical Staff Departments, Sections and Committees
8.2.2 Departments, Sections and Committees may, by resolution, provide the time for holding regular meetings without notice other than such resolution.
8.3 Special Meetings of Departments, Sections and Committees 8.3.1 A special meeting of any Department, Section or Committee may be called by
the Chair thereof or by the President of the Medical Staff. 8.4 Quorum
32
8.4.1 Medical Staff meetings: Unless otherwise specified in these Bylaws, a quorum shall consist of those present or those eligible Medical Staff members voting on an issue.
8.4.2 FMEC, Credentialing/Privileges Committee, Medical Staff Quality/Peer Review
Committee: A quorum will exist when 50% of the members are present. 8.4.3 Departments, Sections or Committees other than those listed in Sections 6 and
7 above or unless otherwise specified in these Bylaws, a quorum shall consist of those present or those eligible Medical Staff members voting on an issue.
8.5 Attendance Requirements 8.5.1 Members of the Medical Staff are encouraged to attend meetings of the Medical
Staff. 8.5.1.1 FMEC, Credentialing/Privileges Committee, and Medical Staff
Quality/Peer Review Committee meetings: Members of these committees are expected to attend at least 75% of the meetings held.
8.5.1.2 Special meeting attendance requirements: Whenever there is
suspected or actual non-compliance with Medical Staff or hospital policies or suspected deviation from standard clinical or professional practice, the President of the Medical Staff or the applicable Department/Section/Committee Chair may require the practitioner to confer with him or with a standing or ad hoc committee that is considering the matter. The practitioner will be given special notice of the meeting, by personal delivery or U.S. Mail certified return receipt requested, at least five (5) days prior to the meeting, including the date, time, place, a statement of the issue involved and that the practitioner’s appearance is mandatory.
Failure of the practitioner to appear at any such meeting after two (2)
notices, unless excused by the FMEC upon showing good cause, will result in an automatic termination of membership pursuant to the Automatic Suspension and Termination provisions of these Bylaws. Such termination will not give rise to a fair hearing, but will automatically be rescinded upon the practitioner’s participation in the previously referenced meeting.
8.5.1.3 Nothing in the foregoing paragraph shall preclude the initiation of
precautionary restriction or suspension of clinical privileges as outlined in Part II of these Bylaws (Investigations, Corrective Action, Hearing and Appeal Plan).
8.6 Participation by Administration
8.6.1 Administration may attend any general, Department, Section or Committee meetings of the Medical Staff, unless otherwise specified or requested by the committee.
8.7 Robert’s Rules of Order
33
8.7.1 Medical Staff Department, Section and Committee meetings shall be run in a manner determined by the individual who is the Chair of the meeting. When parliamentary procedure is needed, as determined by the Chair or evidenced by a majority vote of those attending the meeting, the latest edition of Robert’s Rules of Order shall determine procedure.
8.8 Notice of Meetings 8.8.1 Unless otherwise specified in these Bylaws, written or electronic notice stating
the place, day, and hour of any special meeting or of any regular meeting not held pursuant to resolution shall be delivered or sent to each member of the Department or committee not less than five (5) days before the time of such meeting by the person or persons calling the meeting. The attendance of a member at a meeting shall constitute a waiver of notice of such meeting.
8.9 Action of PLC, FMEC, General Medical Staff, Department, Section or Committee 8.9.1 The recommendation of a majority of its members present at a meeting at which
a quorum is present shall be the action of a Department, Section and Committee, FMEC, PLC or General Medical Staff meeting. Such recommendation will then be forwarded to the FMEC for action.
8.10 Rights of Ex Officio Members 8.10.1 Except as otherwise provided in these Bylaws, persons serving as ex officio
members of a committee shall have all rights and privileges of regular members thereof, (except that they shall not vote or be counted in determining the existence of a quorum).
8.11 Minutes 8.11.1 Minutes of each regular and special meeting of a committee shall be prepared
and shall include a record of the attendance of members and the vote taken on each matter. The presiding Chair shall authenticate the minutes and copies thereof shall be submitted to the FMEC or other designated committee. Minutes shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
SECTION 9 DECISION MAKING METHODS AND CONFLICT RESOLUTION 9.1 FMEC recommendations will be forwarded to the PLC for information and to ensure
communication between all facility Medical Staffs, System and facility administration and Board leaders. Routine FMEC communication and recommendations that are consistent between the FMECs and that are consistent with Medical Staff and hospital policy and procedures will be transmitted to the Board.
9.2 Conflict resolution: If the PLC determines a recommendation of a FMEC may be contrary
to the opinion of the PLC, or if a decision of the Board is contrary to a recommendation of the PLC and/or a FMEC, the PLC shall not make a recommendation to the Board regarding such matter. The PLC will first refer the matter back to the FMEC(s) for further consideration at their next meeting, together with pertinent suggestions and comments of the PLC.
34
9.3 If the FMEC recommendation and the opinion of the PLC remain inconsistent after the next meeting of the FMEC, the matter will be referred to an Initial Joint Conference Committee to be convened within thirty (30) days of that FMEC meeting. Such Initial Joint Conference Committee may be convened at any time sooner by mutual agreement of the FMEC and PLC. The Initial Joint Conference Committee shall be composed of two (2) representatives selected by the PLC, two (2) representatives selected by the FMEC, one (1) administrative representative and one (1) Board member.
9.3.1 The positions established at the Initial Joint Conference Committee will be reported
in full to the FMEC and the PLC. The FMEC will discuss the issue at its next meeting. In the event the FMEC(s)’ recommendation remains contrary to the opinion of the PLC, the recommendation of the FMEC(s) shall be forwarded to the Board, along with pertinent, applicable information.
The PLC, at its discretion, may include a divergent opinion along with pertinent,
applicable information. The Board shall have sixty (60) days to adopt the recommendation of the FMEC(s), or may choose to refer the matter(s) to a Final Joint Conference Committee at any time within the 60-day period.
9.4 A Final Joint Conference Committee will be convened if: 9.4.1 requested by the Board; 9.4.2 requested by the PLC, FMEC(s) or Initial Joint Conference Committee (if the Initial
Joint Conference Committee is unable to resolve conflicts and divergent opinions remain between the PLC, FMEC(s) and/or Initial Joint Conference Committee); or
9.4.3 in the event the Board does not accept or adopt a recommendation by the
FMEC(s) within sixty (60) days of receiving such recommendation(s) as set forth in Section 9.3.1.
The Final Joint Conference Committee will convene within thirty (30) days of such request,
or occurrence. The Final Joint Conference Committee will be composed of two (2) representatives selected by the PLC, two (2) representatives selected by the FMEC and two (2) representatives (which may or may not be Board members) of the Board for review and recommendation to the full Board. The Final Joint Conference Committee will have up to sixty (60) days to report its recommendation(s), and will issue its complete report simultaneously to the FMEC(s), PLC, Initial Joint Conference members and Board. If either the FMEC(s) or PLC continues to have a dissenting opinion/recommendation from that of the Final Joint Conference Committee, both (FMEC and PLC) shall each have the right for a representative of each to report its recommendation/opinion at the same time to the Board. After such report(s), the Board will make a determination, which shall be final.
9.5 The Chair of the Board, PLC or FMEC may call for an Initial Joint Conference as described
above at any time and for any reason in order to seek direct input from the Board, PLC and/or FMEC Medical Staff leaders, clarify any issue, or relay information directly to Medical Staff leaders.
9.6 The provisions of this article are not applicable to matters subject to the provisions of the
Medical Staff Bylaws, Rules and Regulations, or Policies relating to Peer Review, Corrective Action or the Fair Hearing process.
SECTION 10 REVIEW, REVISION, ADOPTION, AND AMENDMENT
35
10.1 Medical Staff Responsibility 10.1.1 The Medical Staff shall have the responsibility to formulate, review at least
biennially, and recommend to the Board any Medical Staff Bylaws, rules, regulations, policies and procedures, and amendments as needed, which shall be effective when approved by the Board.
The Medical Staff can exercise this responsibility through its elected and appointed leaders or through direct vote of its membership.
10.2 Methods of Amendment and Adoption to these Bylaws
10.2.1 Proposed amendments to these Bylaws may be originated by the System Bylaws
Committee for consideration of all FMECs and each general Medical Staff or by a petition signed by twenty-five (25) active staff members.
10.2.1.1 Each active member of the Medical Staff will be eligible to vote on the
proposed amendment to these Bylaws via printed or secure electronic ballot in a manner determined by the FMEC. All active members of the Medical Staff shall receive at least thirty (30) days advance notice of the proposed changes. Proposed amendments must:
10.2.1.1.1 receive a simple majority of the votes cast by those active
Medical Staff members eligible to vote at the initiating FMEC;
10.2.1.1.2 receive a simple majority of the votes cast by the active
Medical Staff members eligible to vote at each FMEC; 10.2.1.1.3 receive a simple majority of the votes cast by the active
Medical Staff members eligible to vote on each facility general Medical Staff.
10.2.1.2 Amendments so adopted shall be effective when approved by the Board.
Neither the Board nor the Medical Staff shall have the power or authority to unilaterally adopt or amend Medical Staff Bylaws.
10.3 Methods of Amendment and Adoption to any Medical Staff Rules, Regulations and
Policies: 10.3.1 The Medical Staff may adopt additional rules, regulations and policies as necessary
to carry out its functions and meet its responsibilities under these Bylaws. A Rules, and Regulations and Policies Manual may be utilized to organize these additional documents. Should a conflict exist between the provisions of the Medical Staff Bylaws and the Rules and Regulations or Medical Staff Policies, the Bylaws will prevail. Should a conflict exist between the provisions of the Rules and Regulations and the Medical Staff Policies, the Rules and Regulations will prevail.
10.3.2 Proposed amendments to the Rules, Regulations and Policy Manual may be
originated by the FMEC. 10.3.3 The Medical Staff itself may recommend directly to the Board an amendment(s) to
any rule, regulation, or policy by submitting a petition signed by twenty-five (25) active Medical Staff members. Upon presentation of such petition, the adoption process outlined in 10.2.1 above will be followed.
36
10.3.4 The FMEC shall vote on the proposed language changes at a regular meeting, or at a special meeting called for such purpose. Following an affirmative vote by the FMEC, any of these documents may be adopted, amended or repealed, in whole or in part and such changes shall be effective when approved by the Board, subject to Section 9 of this Part in the event of a conflict.
10.4 The FMEC may adopt such amendments to these Bylaws, Rules and Regulations, and
policies that are, in the committee’s judgment, technical or legal modifications or clarifications, reorganization or renumbering or those needed due to punctuation, spelling, or other errors of grammar or expression. Such amendments need not be approved by the entire Board but must be approved by the System CEO.
37
Appendix A PRINCIPLES OF MEDICAL ETHICS**
PREAMBLE The medical professions have long subscribed to a body of ethical statements developed primarily for the benefit of the patient. As a member of this profession, a health professional must recognize responsibility to patients first and foremost, as well as to society, to other health professionals and to self. The following Principles are not laws but standards of conduct, which define the essentials of honorable behavior for the health professional. Section 1 A health professional shall be dedicated to providing competent medical care with compassion and respect for human dignity and rights. Section 2 A health professional shall uphold the standards of professionalism, be honest in all professional interactions, and strive to report health professionals deficient in character or competence, or engaging in fraud or deception, to appropriate entities. Section 3 A health professional shall respect the law and also recognize a responsibility to seek changes in those requirements, which are contrary to the best interests of the patient. Section 4 A health professional shall respect the rights of patients, colleagues, and other health professionals and shall safeguard patient confidences and privacy within the constraints of the law. Section 5 A health professional shall continue to study, apply and advance scientific
knowledge, maintain a commitment to medical education, make relevant information available to patients, colleagues and the public, obtain consultation, and use the talents of other health professions when indicated.
38
Section 6 A health professional shall, in the provision of appropriate patient care, except in emergencies be free to choose whom to serve, with whom to associate and the environment in which to provide medical care. Section 7 A health professional shall recognize a responsibility to participate in activities contributing to an improved community and the betterment of pubic health. Section 8 A health professional shall, while caring for a patient, regard responsibility
to the patient as paramount.
Section 9 A health professional shall support access to medical care for all people. **Adapted from the American Medical Association’s “Principles of Medical Ethics” (adopted by the AMA’s
House of Delegates June 17, 2001).
39
PART II: INVESTIGATIONS, CORRECTIVE ACTION, HEARING AND APPEAL PLAN
SECTION 1 ROUTINE CORRECTIVE ACTION & INVESTIGATIONS 1.1 Progressive Intervention These Bylaws encourage the use of progressive steps by Medical Staff leaders and
hospital administration, beginning with collegial and education efforts, to address questions relating to a practitioner’s clinical practice and/or professional conduct. The goal of these efforts is to arrive at voluntary, responsive actions by the practitioner to resolve questions that have been raised. All collegial intervention efforts by Medical Staff leaders and hospital management are part of the hospital’s performance improvement and professional review activities. Collegial intervention efforts are encouraged, but are not mandatory, and shall be within the discretion of the appropriate Medical Staff leaders and hospital administration.
When any observations arise, suggesting opportunities for a practitioner to improve, the matter may be referred in accordance with the performance improvement and professional conduct policies adopted by the Medical Staff and hospital.
Corrective actions and investigations shall be undertaken: 1.1.1 in the reasonable belief that the action is in the furtherance of quality health care; 1.1.2 after a reasonable effort to obtain the facts of the matter,
1.1.3 after adequate notice and hearing procedures are afforded to the practitioner as set forth herein, and
1.1.4 in the reasonable belief that the action is warranted by the facts known after such reasonable effort to obtain the facts.
1.2 Basis for Routine Corrective Action Whenever a concern or question has been raised regarding: 1.2.1 the clinical competence or clinical practice of any appointee; 1.2.2 the care or treatment of a patient or patients or management of a case by any
appointee; 1.2.3 activities or professional conduct that may be detrimental to patient safety; 1.2.4 the known or suspected violation by any Medical Staff appointee of these Bylaws,
the Policies, or the Rules and Regulations of the Medical Staff, System or Department
1.2.5 behavior or conduct on the part of any Medical Staff appointee that is considered lower than the standards of the hospital, disruptive to the hospital or its Medical Staff, including the inability of the appointee to work harmoniously with others; or
1.2.6 impairment, a request for corrective action may be made by any practitioner on the Medical Staff, any
member of the System administration, System or Medical Staff committee, or the Board of
40
Directors, after making sufficient inquiry to satisfy themselves that the concern or question raised is credible.
1.3 Requests and Notices All requests for corrective action shall be made in writing to the President of the Medical
Staff and the Chief Medical Officer, with a copy to the Medical Staff Services Office. The request must be signed by the complainant, clearly state those facts that support the request in sufficient detail to permit an investigation to be pursued, and, if possible, state what corrective action is deemed appropriate by the complainant. The President of the Medical Staff shall notify the FMEC at its next regular meeting that a request for corrective action has been made. The affected practitioner shall be given written notice of the request, and a copy of the same. All notices provided under this Part II shall be hand delivered or sent via certified mail, return receipt requested. All time limits shall begin upon receipt of notice.
1.4 Investigations
1.4.1 When a request for corrective action has been received by the FMEC, the committee shall determine as soon as possible, but no later than at its next regularly scheduled meeting, either to discuss the matter with the appointee concerned, or to begin an investigation. If the concern states sufficient information to warrant action, the FMEC, at its discretion, may initiate an investigation, with or without a personal interview with the practitioner being investigated. The FMEC may seek input from the practitioner’s Department or Section prior to initiating investigation. An investigation shall begin only after a formal resolution of the FMEC to that effect. The affected practitioner shall be given written notice of the initiation of an investigation. If the Board of Directors wishes to begin such an investigation, it shall also formally resolve to do so by mandating the FMEC to begin an investigation.
1.4.2 Upon resolving to initiate an investigation, the Medical Staff President through the
FMEC or President of the Medical Staff shall immediately appoint a member(s) of the Active Medical Staff to conduct an investigation of the matters contained in the request. Investigators shall not include partners, associates or relatives of the practitioner being investigated and should be objective and familiar with the types of issues raised in the request for corrective action.
1.4.3 The investigator(s) may consult with other members of the Medical Staff as
appropriate in order to determine the facts of the case, or to obtain professional opinions relative to the matter under consideration.
1.4.4 The investigator(s) shall have available the full resources of the Medical Staff and
the System, as well as the authority to use outside consultants, if needed. 1.4.5 The investigation should be completed within thirty (30) working days of the
appointment of the investigator(s), unless an extension of not more than thirty (30) additional working days has been granted by the FMEC or President of the Medical Staff.
1.4.6 At the conclusion of the investigation, the investigator(s) shall prepare a written
report of the findings and transmit the same to the President of the Medical Staff and the Chief Medical Officer. In addition to setting forth findings of fact and, if
41
applicable, the clinical opinion of the investigator(s) and other practitioners with whom he may have consulted, the report shall recommend that corrective action be imposed, or that the complaint against the affected practitioner be dismissed.
The investigator may recommend a type or degree of corrective action deemed
appropriate. 1.4.7 The President of the Medical Staff shall review the investigator’s report when it is
received, and if emergency corrective action is indicated, proceed to impose the same pursuant to Section 2 of this part. Otherwise, the President shall submit the investigator’s report to the FMEC for consideration at its next regular meeting.
1.4.8 In cases suggesting practitioner impairment, the President of the Medical Staff shall
confer with a member of the Medical Administrative Staff, designated by the System President and the practitioner’s Department Chair, and if they concur, shall refer the request to the Practitioner Resource Committee for disposition; otherwise, the request shall be referred to the FMEC for consideration at its next regular meeting.
1.5 FMEC Action 1.5.1 If the FMEC determines that there are no reasonable grounds to believe that the
affected practitioner has committed an offense requiring corrective action under these Bylaws, the complaint shall be dismissed. The affected practitioner and complainant shall be given written notification of dismissal.
1.5.2 If the FMEC determines that there are reasonable grounds to believe that the
affected practitioner is subject to corrective action, the Committee may elect to recommend corrective action to the Board, which, at the discretion of the FMEC, may consist of:
1.5.2.1 A written warning that corrective action measures will be taken in the
future if the affected practitioner does not reform his conduct in the manner set forth in the warning;
1.5.2.2 A written reprimand stating the Committee’s displeasure at the affected
practitioner’s behavior, and directing the affected practitioner to cease the same immediately;
1.5.2.3 Mandated education to improve the affected practitioner’s knowledge,
skills and ability in clinical as well as non-clinical subjects;
1.5.2.4 Mandated clinical review or supervision to see that the affected practitioner’s performance attains an acceptable level;
1.5.2.5 Limitation of privileges restricting those procedures that the affected
practitioner may perform at the Facility;
1.5.2.6 Removal of privileges eliminating the affected practitioner’s ability to perform any procedure at the Facility. If the affected practitioner is a member of the Medical Staff, removal of privileges shall also entail revocation of Medical Staff membership. If removal of privileges is recommended at the time of the affected practitioner’s biennial reappointment, this may be accomplished by not recommending the affected practitioner for reappointment;
1.5.2.7 Make such other recommendations, as it deems necessary or appropriate.
42
1.6 Notice of FMEC Action Whenever a recommendation for corrective action has been made by the FMEC, or
corrective action has been taken by the Board on its own initiative, written notice of the same shall be sent to the affected practitioner by certified mail, return receipt requested, or hand delivery with receipt. Such notice shall be consistent with the notice provision set forth in Subsection 1.3. The notice shall set forth the nature of the complaint, the reasons for the corrective action, a description of the corrective action, and a short summary of the affected practitioner’s right to a fair hearing pursuant to these Bylaws, including any time limits within which the affected practitioner must act. The affected practitioner may request a hearing pursuant to the provisions of Section 4.
1.7 Board of Directors Action If the time, during which an affected practitioner may request a hearing pursuant has
expired without a request being made, or such hearing, including appeal to the Board, has been concluded, then at the next regular meeting thereafter of the Board of Directors, the Board shall consider the recommended corrective action. In the event that the Board rejects such recommendation, the Board may remand the recommendation to the FMEC with instructions to reconsider the matter, including the nature and degree of the corrective action. The Board shall consider recommendations of the FMEC following remand in the same manner as other recommendations for corrective action.
SECTION 2 EMERGENCY CORRECTIVE ACTION/PRECAUTIONARY SUSPENSION
OF CLINICAL PRIVILEGES 2.1 Basis for Emergency Corrective Action/Precautionary Suspension The President of the Medical Staff, the Chief Medical Officer (or his designee), or the FMEC
shall have the authority to immediately suspend all or any portion of the clinical privileges of a Medical Staff practitioner or other individual, whenever failure to take such action may result in an imminent danger to the health and/or safety of any individual. Such precautionary suspension shall be deemed an interim precautionary step in the professional review activity related to the ultimate professional review action that may be taken with respect to the suspended individual but is not a complete professional review action in and of itself. It shall not imply any final finding of responsibility for the situation that caused the suspension, nor shall it entitle the practitioner to a fair hearing except as provided under this Section. Those parties with the authority to impose emergency corrective action shall consult with a physician member of the Administration designated by the System President and System legal counsel before imposing any emergency corrective action. This Subsection shall not apply if a clear and present danger exists which requires immediate action and consultation is not feasible.
2.2 Notice of Emergency Corrective Action/Precautionary Suspension
43
Upon imposition of emergency corrective action, the President of the Medical Staff shall immediately give notice to the affected practitioner of such action.
Such notice may be oral, but shall be confirmed in writing as soon as possible, but no later
than the next business day. The written notice shall state the reasons for the emergency corrective action and the nature of corrective action imposed. A copy of the notice shall also be given to the Chief Medical Officer, Department Chair, and FMEC.
2.3 FMEC Procedure When instituted, a precautionary suspension of clinical privileges will automatically expire in
seven (7) days, unless extended by the FMEC, with return of all previous clinical privileges unless the suspension is confirmed by a majority vote of the FMEC in special session. The FMEC shall review the matter resulting in precautionary suspension within a reasonable period not to exceed fourteen (14) days. Unless the FMEC promptly terminates or extends the precautionary suspension prior to or immediately after reviewing the suspension, the practitioner shall be entitled to the procedural rights afforded by the Fair Hearing and Appeal plan once the restrictions or suspension last more than fourteen (14) calendar days. Restrictions or suspensions which last fourteen (14) days or less shall not trigger rights under the Fair Hearing and Appeal Plan.
2.4 Provision of Patient Care Immediately upon the imposition of a precautionary suspension, the appropriate
Department Chair or, if unavailable, the President of the Medical Staff shall assign responsibility for care of the suspended practitioner’s patients still in a System’s facility to another practitioner with appropriate clinical privileges. The assignment shall be effective until the patients are discharged. The wishes of the patient shall be considered in the selection of the assigned practitioner. It shall be the duty of all Medical Staff practitioners to cooperate with the President of the Medical Staff, the Department Chair concerned, the FMEC and the Chief Medical Officer in enforcing all suspensions.
2.5 Recission of Emergency Corrective Action/Precautionary Suspension The person imposing emergency corrective action may, at any time prior to ratification of
such action by the FMEC, rescind the action, and the affected practitioner shall be restored to the status he enjoyed prior to the imposition of emergency correction action. Following ratification of emergency corrective action by the Executive Committee, the person imposing such action may recommend to the FMEC that such action be rescinded. The FMEC shall consider such recommendation at its next regular meeting thereafter. Any pending request for a hearing pursuant to Section 4 shall be made moot and void by such recission.
SECTION 3 AUTOMATIC SUSPENSION AND TERMINATION 3.1 Basis for Automatic Suspension and Termination A practitioner’s clinical privileges shall automatically be revoked, limited or suspended as
appropriate, which action shall be final without a right to due process except as provided in this Section, upon the occurrence of the following circumstances: 3.1.1 Loss of License. The practitioner’s license to practice in the State of Florida is
suspended, limited or terminated.
44
3.1.2 Residence or Office Outside Lee County. The practitioner does not maintain a full-time residence and office in Lee County as
required by these Bylaws, unless such requirements are waived by the FMEC pursuant to said Subsection. Return of United States mail sent by the System Medical Staff Services Office to a practitioner at his Lee County home or office address with “addressee unknown” or similar endorsement shall be prima facie evidence that the practitioner does not comply with these Bylaws. Failure of a practitioner to supply a current residence and office address within 15 working days of a request of the Medical Staff Services Office for the same shall be deemed prima facie evidence that the practitioner does not comply with these Bylaws. This shall not apply to practitioners granted a leave of absence by the FMEC pursuant to these Bylaws.
3.1.3 Lack of Active Practice. The practitioner is not actively engaged in the practice of
his profession in Lee County; that is, he is not seeing, examining, treating or otherwise caring for patients, and has not done so for a period of more than six months, unless the practitioner shall have notified the Medical Staff Services Office prior to beginning such absence, and arranged for suitable coverage during such time period. This shall not apply to practitioners granted a leave of absence by the FMEC pursuant to these Bylaws, or to members of the Honorary Medical Staff.
3.1.4 Criminal Conviction. The practitioner has been, while a practitioner on the Medical
Staff, convicted in any jurisdiction of the United States; of a felony or misdemeanor involving actual or threatened bodily harm, actual or threatened sexual misbehavior or stalking, controlled substance possession or use, or of any felony or misdemeanor described in any Florida law pertaining to governing or regulating the health professions or health facilities. A practitioner whose membership or privileges are automatically terminated pursuant to this Subsection shall not be disqualified from applying for appointment following completion of his sentence, or during a period of time when he is on probation. However, the fact that the practitioner has completed his sentence after criminal conviction, or is on probation, shall not require the Medical Staff to make such appointment, and the FMEC may elect not to do so in its discretion, consistent with its responsibility towards patients, other practitioners, Facility/System employees, and the public in general.
3.1.5 Loss or Restriction of DEA Certificate. The clinical privileges of a practitioner whose
Drug Enforcement Agency (DEA) certification is terminated, revoked, or suspended shall automatically and immediately be modified to revoke the right to prescribe controlled substances. The practitioner shall immediately inform the Medical Staff Services Office regarding the change in status in his DEA certification. The matter shall promptly be referred, for investigation and further action in accordance with the provisions of these Bylaws.
3.1.6 Exclusion From Federal or State Health Care Programs. The Medical Staff
appointment and clinical privileges of a practitioner who becomes an ineligible person with regard to participation in Federal or State Health Care Programs shall automatically and immediately be suspended.
The practitioner shall immediately inform the Medical Staff Services Office regarding
the change of his eligibility status. This triggers the right to due process. The matter shall promptly be referred for investigation and further action in accordance with all the due process provisions of this Part.
45
3.1.7 Failure to Pay Fees and Assessments. The practitioner fails to pay when due any fee or assessment imposed pursuant to these Bylaws or Medical Staff or System policy.
3.1.8 Failure to Provide Requested Information. If at any time a practitioner fails to
provide required information pursuant to a formal request by the System Credentialing/Privileging Committee, Medical Executive Committee or the Medical Staff Services Office, the practitioner’s clinical privileges shall be deemed to be voluntarily relinquished until the required information is provided to the satisfaction of the requesting party. For purposes of this Section, required information shall include but not be limited to: 1. physical or mental examination reports as specified elsewhere in this policy, or 2. information necessary to explain an investigation, professional review action, or resignation from another health care facility or agency.
3.1.9 Failure to Request Reappointment or Provide Requested Information Related to
Reappointment. If a practitioner fails to request reappointment for membership and/or privileges or fails to provide requested information pursuant to Part III, Section 5 of these Bylaws, the practitioner’s membership and privileges shall be deemed voluntarily relinquished.
3.1.10 Failure to Request Reinstatement Following Leave of Absence. Failure to request
reinstatement shall be deemed a voluntary resignation from the Medical Staff and shall result in automatic termination of membership, privileges, and prerogatives. Members whose membership is automatically terminated shall not be entitled to the procedural rights provided in the Medical Staff Bylaws.
3.1.11 Failure to Complete Medical Records. All elective admitting, consulting and clinical
privileges of any practitioner shall be deemed to be voluntarily relinquished for failure to complete medical records in accordance with the provisions of the Medical Staff Rules and Regulations. Such relinquishment shall continue until all the records of the practitioner’s patients are no longer delinquent. Such relinquishment does not exempt the practitioner from fulfilling their on-call responsibilities. Failure to complete the medical records that caused relinquishment of clinical privileges within sixty (60) days from the relinquishment of such privileges shall be grounds for further disciplinary action in accordance with the provisions of these Bylaws.
3.1.12 Failure to Comply with Special Meeting Attendance Requirements. Failure of a
practitioner to attend a special meeting called pursuant to the Bylaws. 3.2 Right to Limited Hearing for Automatic/Voluntary Suspension and Termination A practitioner affected by this Section shall be sent a written notice stating the reasons for
automatic suspension within 24-hours of the same having been imposed, and shall have the right to present evidence to the FMEC in written form, or by appearing personally at a regular meeting of the committee, to demonstrate that the reason that automatic suspension was imposed is untrue.
3.2.1 Such written evidence or a written request to meet with the FMEC shall be
submitted to the President of the Medical Staff within ten (10) working days of the date the notice of automatic suspension was sent. Failure to submit written evidence or a request shall be deemed a waiver of any right to consideration of the same.
46
3.2.2 Evidence presented by the affected practitioner shall be limited to whether or not the grounds for automatic suspension are true. The FMEC shall not consider evidence or argument, which presents mitigating circumstances or excuse.
3.2.3 After receipt of an affected practitioner’s written evidence, and prior to the next
regular meeting of the FMEC, the President of the Medical Staff, with the concurrence of a member of the Medical Administrative Staff designated by the System President, may determine that the evidence so presented demonstrates that
the reasons that automatic suspension was imposed are untrue, and revoke the
suspension, restoring the affected practitioner to the status he previously enjoyed. 3.2.4 The President of the Medical Staff may, at any time, provisionally reinstate a
practitioner suspended pursuant to this Section if the President is satisfied by the available written documentation that the reasons for automatic suspension were untrue. The President shall present the provisional reinstatement for ratification by the FMEC at its next regular meeting.
3.2.5 At its next regular meeting following automatic suspension, the FMEC shall consider
the reasons therefore, together with any evidence or argument presented by the affected practitioner, and if the reasons for automatic suspension are found to be true, recommend to the Board termination of the affected practitioner’s Medical Staff membership and/or privileges. If the FMEC finds that the reasons are untrue or corrected, the suspension shall be revoked, and the affected practitioner restored to the status he previously enjoyed.
SECTION 4 HEARING AND APPEAL PROCEDURES 4.1 Grounds for Hearing An applicant or an individual holding a Medical Staff appointment shall be entitled to
request a hearing whenever the FMEC or the Board of Directors has made one of the following adverse recommendations:
4.1.1 denial of initial Medical Staff appointment; 4.1.2 denial of Medical Staff reappointment; 4.1.3 revocation of Medical Staff appointment; 4.1.4 denial of requested initial clinical privileges; 4.1.5 denial of requested additional clinical privileges; 4.1.6 decrease of clinical privileges;
4.1.7 suspension of clinical privileges (other than emergency corrective action/precautionary suspension);
4.1.8 imposition of mandatory concurring consultation requirement. No other recommendations except those enumerated in this Section shall entitle the practitioner to request a hearing. Neither voluntary relinquishment of clinical privileges, as provided in these Bylaws, nor the imposition of any general consultation requirement, nor the imposition of a requirement for retraining, additional training or continuing education, shall constitute grounds for a hearing, but shall take effect without hearing or appeal. The hearing shall be conducted in as informal a manner as possible, subject to the rules and procedures set forth in these Bylaws.
47
4.2 Notice of Recommendation When a recommendation is made which, according to these Bylaws entitles a practitioner to
a hearing prior to a final decision of the Board, the affected practitioner shall promptly be given notice by the President of the Medical Staff or Chief Medical Officer or his designee, in writing, certified mail, return receipt requested or in person. This notice shall contain:
4.2.1 a statement of the recommendation made, the action which is being taken or which may be taken, and the general reasons for it; 4.2.2 notice that the practitioner has the right to request a hearing on the
recommendation within thirty (30) days of receipt of this notice; and 4.2.3 a copy of this Part outlining the rights in the hearing as provided for in these
Bylaws.
4.3 Request for Hearing A practitioner shall have thirty (30) days following the date of the receipt of such notice
within which to request the hearing. The request shall be in writing to the President of the Medical Staff or Chief Medical Officer with a copy to the Medical Staff Services Office and signed by the affected practitioner making such request. In the event the practitioner does not request a hearing within the time and in the manner required by these Bylaws, the practitioner shall be deemed to have waived the right to the hearing and to have accepted the action involved. That action shall become effective immediately upon final Board action.
4.4 Preliminary Interview The affected practitioner may request, at the time of submitting a request for hearing or
within ten (10) working days thereafter, an informal preliminary interview with the decision making body (FMEC or Board of Directors). The decision making body shall grant all such requests, and the affected practitioner shall be scheduled to appear before it at its next regular meeting. 4.4.1 The purpose of the preliminary interview shall be to permit the affected practitioner
to personally present any argument or evidence showing that the adverse recommendation has been wrongfully imposed, in fact, or in violation of these Bylaws; or to present any mitigating circumstances.
4.4.2 The preliminary interview is informal and not a hearing. It is optional with the
affected practitioner, and accordingly, legal counsel shall be excluded. 4.4.3 The decision making body may impose a limit on the amount of time to be devoted
to a preliminary interview, but not less than thirty minutes. 4.4.4 Failure to request a preliminary interview shall not be considered in any hearing or
deliberation conducted pursuant to these Bylaws, nor shall the affected practitioner’s right to a hearing be affected thereby.
48
4.4.5 Following a preliminary interview, the decision making body shall deliberate, and may elect to withdraw or reduce the severity of the adverse recommendation imposed upon the affected practitioner, or may take no action.
If no action is taken, the adverse recommendation shall continue in effect, and the hearing provided for hereunder shall proceed.
4.4.6 Notice shall be given to the affected practitioner of the decision following a
preliminary interview in the manner provided in Subsection 1.3.
SECTION 5 FAIR HEARING PROCEDURE 5.1 System Representative, Hearing Panel and Hearing Officer 5.1.1 System Representative 5.1.1.1 When the FMEC of the Medical Staff is the decision making body, the
President of the Medical Staff shall appoint a person to represent the interests and position of the Medical Staff in all proceedings provided for in this Section. Such individual shall be in an adversarial role opposed to the affected practitioner. If the affected practitioner is not represented by legal counsel, the Medical Staff representative shall not be an attorney, but shall be a member of the Active Medical Staff.
5.1.1.2 When the Board is the decision making body, as defined herein, the
Chair of the Board shall appoint a person to represent the interests and position of the Board in all proceedings provided for in this Section. Such individual shall be in an adversarial role opposed to the affected practitioner. If the affected practitioner is not represented by legal counsel, the Board representative shall not be an attorney, but shall be a member of the administration.
5.1.1.3 For purposes of these Bylaws, the Medical Staff or Board representative
appointed under this Section shall be called the “System Representative.”
5.1.2 Hearing Panel 5.1.2.1 Unless the FMEC or Board elects to have the matter heard by a Hearing
Officer possessing the qualifications set forth in Subsection 5.1.3, all hearings shall be conducted by a Hearing Panel appointed by the President of the Medical Staff or the Chair of the Board, as applicable,
composed of five (5) members, presided over by a qualified professional selected in accordance with Subsection 5.1.3. The Hearing Panel shall be composed of Active Medical Staff practitioners who shall not have actively participated in the consideration of the matter involved at any previous level. Knowledge of the matter involved shall not preclude any individual from serving as a member of the Hearing Panel.
If the hearing has been requested based on Board action, 3 of the
members of the Hearing Panel shall be members of the Board of Directors. The Hearing Panel will be presided over by a Hearing Officer.
5.1.2.2 The Hearing Panel shall not include any individual who is in direct
economic competition with the affected person or has any other personal interest in the proceeding, financial or otherwise, or any such individual
49
who is professionally associated with or related to the affected practitioner.
5.1.3 Hearing Officer – Qualifications & Authority 5.1.3.1 The FMEC or the Board may elect to have the hearing provided for in
this Section held by a Hearing Officer sitting alone. In such case, the Hearing Officer shall perform all of the functions of the Hearing Panel described herein.
In cases where a panel is appointed, the Hearing Officer will preside over
the proceeding but not participate in the deliberations or vote on the recommendation.
5.1.3.2 The Hearing Officer:
5.1.3.2.1 shall be an attorney licensed in the State of Florida who is
knowledgeable and has experience in health care law, including Medical Staff law; or shall be a non-lawyer who has experience as a Hearing Officer;
5.1.3.2.2 shall not be, or have been, employed or retained by the Lee
Memorial Health System, or any practitioner on the Medical Staff, including the affected practitioner, for any purpose other than to serve as a Hearing Officer in Medical Staff proceedings;
5.1.3.2.3 shall have no personal interest in the proceeding, financial or
otherwise; 5.1.3.2.4 shall be selected by the affected practitioner from a list
provided to the affected practitioner by the General Counsel for the Health System of the names of not less than three (3) persons meeting the requirements of 1-3 above. The affected practitioner shall select the Hearing Officer from the list submitted to him and within forty-eight (48) hours of receiving said list, notify the General Counsel for the Health System in writing of said selection.
Failure of the affected practitioner to select within the
previously mentioned period shall constitute a waiver by the affected practitioner of this Subsection, and the General Counsel for the Health System shall thereafter select the Hearing Officer.
5.1.3.3 The Hearing Officer shall: 5.1.3.3.1 act to insure that all participants in the hearing have a
reasonable opportunity to be heard and to present oral and documentary evidence subject to reasonable limits on the number of witnesses and duration of direct and cross examination, applicable to both sides, as may be necessary to avoid cumulative or irrelevant testimony or to prevent abuse of the hearing process;
50
5.1.3.3.2 prohibit conduct or presentation of evidence that is cumulative, excessive, irrelevant, and abusive or that causes undue delay;
5.1.3.3.3 maintain decorum throughout the hearing; 5.1.3.3.4 determine the order of procedure throughout the hearing; 5.1.3.3.5 have the authority and discretion, in accordance with these
Bylaws, to make rulings on all questions that pertain to matters of procedure and to the admissibility of evidence and qualifications of witnesses;
5.1.3.3.6 act in such a way that the Hearing Panel in formulating its
recommendations considers all information relevant to the continued appointment or clinical privileges of the practitioner requesting the hearing;
5.1.3.3.7 conduct argument by counsel on procedural points outside
the presence of the Hearing Panel unless the Panel wishes to be present;
5.1.3.3.8 grant continuances and postponements as appropriate; and 5.1.3.3.9 take official notice of any matters, either technical or scientific,
relating to the issues under consideration that could have been judicially noticed by the courts of this state, inform the participants of the matters to be officially noticed and provide each party the opportunity to request that a matter be officially noticed or to refute the noticed matter by evidence or by written or oral presentation of authority.
5.2 Challenge to Hearing Panel Members or Hearing Officer
The affected practitioner may challenge the objectivity of any member of the Hearing Panel, or the Hearing Officer, at any time prior to the taking of testimony at the hearing. Such challenge shall be in writing and specify facts demonstrating that a member of the Hearing Panel or the Hearing Officer lacks objectivity or is biased against the affected practitioner. The challenge shall be directed to the President of the Medical Staff or the Chair of the Board, as applicable, who shall consider the challenge and either sustain or overrule it. If the challenge is sustained, the challenged member of the Hearing Panel or the Hearing Officer shall be replaced.
SECTION 6 HEARING PROCEDURES 6.1 Provision of Relevant Information
6.1.1 There is no right to discovery in connection with the hearing. However, the
practitioner requesting the hearing shall be entitled, upon specific request, to the following, subject to a stipulation signed by both parties that such documents shall be maintained as confidential and shall not be disclosed or used for any purpose outside of the hearing:
51
6.1.1.1 copies of, or reasonable access to, all patient medical records referred to in the Statement of Reasons, at the practitioner’s expense;
6.1.1.2 reports of experts relied upon by the FMEC or the Board; 6.1.1.3 redacted copies of relevant committee or Department meeting minutes
(such provision does not constitute a waiver of the state peer review protection statute); and
6.1.1.4 copies of any other documents relied upon by the FMEC or the Board.
6.1.2 Prior to the hearing, on dates set by the Hearing Officer or agreed upon by counsel
for both sides, each party shall provide the other party with a list of proposed exhibits. All objections to documents or witnesses to the extent then reasonably known, shall be submitted in writing in advance of the hearing. The Hearing Officer shall not entertain subsequent objections unless the party offering the objection demonstrates good cause.
6.1.3 Prior to the hearing, on dates set by the Hearing Officer, the practitioner requesting
the hearing shall, upon specific request, provide the FMEC (or the Board of Directors) copies of any expert report or other documents relied upon by the practitioner.
6.1.4 Neither the affected practitioner, nor his attorney, nor any other person on behalf of
the affected practitioner, shall contact members of the hearing committee or the Hearing Officer, or hospital employees appearing on the hospital’s witness list concerning the subject matter of the hearing, unless specifically agreed upon by counsel.
6.2 Pre-Hearing Conference The Hearing Officer may require counsel for the practitioner and for the FMEC (or the
Board) to participate in a pre-hearing conference for purposes of resolving all procedural questions in advance of the hearing. The Hearing Officer may specifically require that:
6.2.1 all documentary evidence to be submitted by the parties be presented at this
conference; any objections to the documents shall be made at that time and the Hearing Officer shall resolve such objections;
6.2.2 evidence unrelated to the reasons for the unfavorable recommendation or unrelated
to the practitioner’s qualifications for appointment or the relevant clinical privileges be excluded;
6.2.3 the names of all witnesses and a brief statement of their anticipated testimony are
submitted, if not previously provided; 6.2.4 the time granted to each witness’ testimony and cross-examination be agreed upon,
or determined by the Hearing Officer, in advance; and 6.2.5 witnesses and documentation not provided and agreed upon in advance of the
hearing may be excluded from the hearing. 6.3 Failure to Appear
52
Failure, without good cause, of the practitioner requesting the hearing to appear and proceed at such a hearing shall be deemed to constitute voluntary acceptance of the pending recommendations or actions, which shall then be forwarded to the Board for final action. The Hearing Officer may impose sanctions upon either party for failure to appear, including the assessment of the costs and attorneys’ fees of the party in attendance against the offending party.
6.4 Record of Hearing A record shall be made at the expense of the Lee Memorial Health System, if any, the pre-
hearing conference and the hearing, using the services of a court reporter. No record of the in camera deliberations of the decision making body or the hearing committee shall be
made. Either party shall be entitled to have a record made of any other proceeding related to the hearing process, at that party’s expense. The expense of transcripts shall be borne by the party requesting them. Oral evidence shall be taken only on oath or affirmation administered by any person designated by such body and entitled to notarize documents in this State.
6.5 Rights of Both Sides At a hearing, both sides shall have the following rights, subject to reasonable limits
determined by the Hearing Officer: 6.5.1 to call and examine witnesses to the extent available; 6.5.2 to introduce exhibits; 6.5.3 to cross-examine any witness on any matter relevant to the issues and to rebut any
evidence; 6.5.4 to be represented by counsel who may call, examine, and cross-examine witnesses
and present the case. (Both sides shall notify the other of the name of that counsel at least ten (10) days prior to the date of the pre-hearing conference and hearing); and
6.5.5 to submit a post-hearing memorandum of points and authorities (The Hearing Panel may request such a memorandum to be filed following the close of the hearing).
Any practitioner requesting a hearing, who does not testify on his own behalf, may be called
and examined as if under cross-examination. The Hearing Panel or Hearing Officer may question the witnesses, call additional witnesses or request additional documentary evidence.
6.6 Admissibility of Evidence The rules of evidence applicable to the courtroom shall not apply, and the Hearing Officer
may admit any evidence that might be relied upon by a reasonable person. Notwithstanding the foregoing, a party shall have the right to object to any evidence on
grounds of hearsay, relevance, or other grounds available under the Florida Evidence Code, and the Hearing Officer shall have the authority to rule on such objections.
6.7 Burden of Presenting Evidence and Proof The burden of going forward with evidence supporting the adverse action or
recommendation is on the FMEC or Board, whichever initially prompted the hearing. Once that burden has been met to the satisfaction of the Hearing Panel/Hearing Officer, the practitioner shall bear the burden of proof, under a preponderance of the evidence, which is a lesser standard than clear and convincing evidence, that the action and penalty taken or
53
proposed against the practitioner was wrongfully or arbitrarily imposed, not in accordance with these Bylaws, or lacks any factual basis.
SECTION 7 HEARING CONCLUSION, DELIBERATIONS AND RECOMMENDATIONS
7.1 Deliberations and Recommendation of the Hearing Panel/Hearing Officer
7.1.1 The recommendation of the Hearing Panel/Hearing Officer shall be based on the evidence produced at the hearing. This evidence may consist of oral testimony of witnesses; memorandum of points and authorities presented in connection with the hearing, any information regarding the practitioner who requested the hearing so long as that information has been admitted into evidence at the hearing and the person who requested the hearing had the opportunity to comment on and, by other evidence, refute it, any and all applications, references, and accompanying documents; other documented evidence, including medical records and any other information presented at the hearing.
7.1.2 Within thirty (30) working days after final adjournment of the hearing, the Hearing
Panel shall conduct its deliberations outside the presence of any other person except the Hearing Officer, and shall prepare a recommended order containing the findings of fact, findings regarding the applicability of these Bylaws, any rules, regulations or policies of the Medical Staff or the Lee Memorial Health System, and the statutory and decisional law of Florida; and a recommendation that adverse action be upheld, modified or withdrawn. If the FMEC or the Board selected a Hearing Officer sitting alone, the Hearing Officer shall prepare a recommended order in the same manner outlined above.
7.1.3 The Hearing Officer shall not participate in the deliberations of the Hearing Panel,
nor be involved in the decision of the Hearing Panel regarding its recommended order.
However, the Hearing Officer may assist the Hearing Panel with regard to the form,
organization and syntax of the recommended order. The recommended order shall be signed by each member of the Hearing Panel or the Hearing Officer, as applicable, and copies provided in person by certified mail, return receipt requested, to the affected practitioner and System Representative.
7.2 Disposition of Hearing Panel Report The Hearing Panel/Hearing Officer shall deliver its report and recommendation to the Chief
Medical Officer or his designee who shall forward it, along with all supporting documentation, to the Board and/or FMEC.
The recommended order shall be considered by the FMEC or Board at its next regular meeting, and may be adopted or rejected by it. If adopted, the recommended order shall become the final decision of the original decision making body (FMEC or Board).
If rejected, the FMEC or Board shall render its own final written decision upholding the
original recommendation, modifying or withdrawing the action. Any action imposed through the final order that requires action by the Board of Directors shall be referred to the Board for final disposition at its next regular meeting.
SECTION 8 APPEAL PROCEDURE
54
8.1 Request & Time for Appeal Within ten (10) working days of receipt of the final written decision following a hearing,
either party may appeal the recommendation. The request shall be in writing, signed by the requesting party and delivered to the Chief Medical Officer either in person or by certified mail, return receipt requested, with a copy to the Medical Staff Services Office. The request shall include a statement of the reasons for appeal and the facts or circumstances that justify further review. If such appellate review is not requested within ten (10) working days as provided herein, both parties shall be deemed to have waived the right to an appeal, and the Hearing Panel or Hearing Officer’s report and recommendation shall be forwarded to the Board for final action.
8.2 Grounds for Appeal The grounds for appeal shall be limited to the following: 8.2.1 there was substantial failure to comply with these Bylaws or hospital policies prior to
the hearing so as to deny a fair hearing; or 8.2.2 the recommendations of the Hearing Panel were made arbitrarily, capriciously or
with prejudice. 8.3 Time, Place and Notice Whenever an appeal is requested as set forth in the preceding Sections, the Chair of the
Board shall, as soon as arrangements can reasonably be made, taking into account the schedules of all participants, schedule and arrange for an appellate review. The affected practitioner shall be given notice of the time, place and date of the appellate review. When a request for appellate review is from a appointee who is under a suspension then in effect, the appellate Review panel shall be convened not more than 14-days from the date of receipt of the request for an appeal unless the practitioner agrees to a longer period. The time for appellate review may be extended by the Chair of the Board for good cause.
8.4 Nature of Appellate Review 8.4.1 Review panel. The Chair of the Board shall appoint a Review panel composed of 5
members, 3 of the panel members shall be members of the Board of Directors and 2 panel members shall be Active members of the Medical Staff. The Board may establish rules of procedure to govern the conduct of appellate hearings under this Section and the Chair of the Board, or his or her designee, shall preside at appellate proceedings.
8.4.2 Position Papers. Each party shall have the right to present a written statement in
support of its position on appeal. Position papers that do not conform to the following requirements may be excluded from consideration in the appeal.
8.4.2.1 The position papers shall set forth a statement of the facts and of the
applicable Bylaws provisions or other authority, as well as any other matters that the parties wish to bring before the appellate body in support of their respective positions.
8.4.2.2 Twelve copies of the affected practitioner’s position paper shall be filed
with Medical Staff Services within (fifteen)15 working days of the filing of

55
the notice of appeal. The System Representative shall also file with Medical Staff Services, 12 copies of his position paper within ten (10) working days of his receipt of a copy of the affected practitioner’s position paper.
8.4.2.3 Position papers shall be limited to no more than thirty (30) pages,
exclusive of exhibits, and shall be on letter-size paper, typewritten, double-spaced and shall be neatly bound or stapled.
8.4.2.4 Each party shall provide a copy of his position paper to the other at the
same time the party’s position paper is filed with Medical Staff Services. 8.4.2.5 Exhibits attached to the position paper shall not duplicate exhibits or
documents contained in the hearing record, and shall be consecutively numbered and attached at the end of the position paper.
8.4.2.6 In referring to the record, position papers shall reference specific pages of
the hearing record and of exhibits that are part of the record. 8.4.3 Oral Argument. The affected practitioner and the System Representative shall be
entitled to present oral argument. Oral argument shall be requested at the time the party submits his position paper. Failure to request oral argument shall constitute a waiver of the right to it. The Board may limit the time for oral argument, but each side shall not have less than thirty (30) minutes. Oral argument shall not include the introduction of evidence and appellate review shall not constitute a hearing de novo.
A record shall be made at the expense of the Lee Memorial Health System of the presentation of oral argument, using the services of a court reporter.
8.4.4 Recommendation. The review panel shall recommend final action to the Board
within thirty (30) working days after the completion of oral argument, or if no oral argument is requested, within forty-five (45) working days after the submission of the position papers of both parties.
SECTION 9 FINAL DECISION OF THE BOARD Within thirty (30) working days after receipt of the Review panel’s recommendation, the Board shall render a final decision in writing, including specific reasons and shall deliver copies thereof to the affected practitioner, the FMEC, and the Medical Staff Services Office, in person or by certified mail, return receipt requested. The decision shall uphold or reverse the final written decision rendered by the decision making body, or may remand the case for reconsideration by the decision making body. If the matter is referred for further action and recommendation, such recommendation shall be promptly made to the Board in accordance with the instructions given by the Board within thirty (30) days. The final decision of the Board following the appeal shall be effective immediately and shall not be subject to further review. SECTION 10 RIGHT TO ONE HEARING AND ONE APPEAL ONLY 10.1 No applicant or Medical Staff practitioner shall be entitled to more than one (1) hearing and
one (1) appeal on any matter that may be the subject of an appeal. A final appellate
56
decision upholding or reversing a final, written decision shall be final and there shall be no right to further hearing on the matter.
10.2 If the Board determines to deny initial Medical Staff appointment or reappointment to an
applicant, or to revoke or terminate the Medical Staff appointment and/or clinical privileges of a current practitioner, that practitioner may not apply for Staff appointment or for those clinical privileges at this hospital for a period of five (5) years unless the Board provides otherwise.
PART III: CREDENTIALING PROCEDURES
SECTION 1 SYSTEM CREDENTIALING/PRIVILEGING COMMITTEE 1.1 Organizational Structure
It is the intention of the Medical Staff Organizations of Lee Memorial Health System (LMHS) to ultimately establish one (1) System Credentialing/Privileging Committee (hereinafter referred to as the Credentialing/Privileging Committee) to act on behalf of all the Medical Staff of LMHS. It has been determined that the two (2) Credentialing/Privileging Committees in effect at the time of the approval of this document may continue for a maximum period of two (2) years. During this transition time, the two (2) Credentialing/Privileging Committees will meet jointly on at least a quarterly basis (the Credentialing/Privileging Committees will not meet separately during the months that the joint meetings occur) and through this process will effect a smooth transition to a single System Credentialing/Privileging Committee. The single System Credentialing/Privileging Committee may decide to merge prior to the end of the two 2-year period.
1.2 Transition Issues
At the time of adoption of PART III, two (2) Credentialing/Privileging Committees exist. Chairs of each of these Credentialing/Privileging Committees have been appointed in accordance to procedures that were in existence prior to the adoption of these Credentials Procedures. During the transition period (moving from two (2) committees to a single System Credentialing/Privileging Committee), these Chairs will continue to serve as the Chairs of the applicable practitioner System Credentialing/Privileging Committee and together will serve as Co-Chairs of the System Credentialing/Privileging Committee (which will meet at least quarterly (see Section 1.1).
The initial composition of the System Credentialing/Privileging Committee will be made up of
the membership of the two (2) separate Credentialing/Privileging Committees, with the current Chairs serving as Co-Chairs. During the first year of the System Credentialing/Privileging Committee, the committee will plan to evolve to the composition of the System Credentialing/Privileging Committee as established in Section 1.4 by the end of twenty-four (24) months.
1.3 Purpose of the System Credentialing/Privileging Committee
The System Credentialing/Privileging Committee exists to oversee all credentialing and privileging activities related to Medical Staff members and privileged Allied Health
57
practitioners on behalf of the Facility Medical Executive Committees (FMECs). These credentialing and privileging activities include processes related to the following:
1.3.1 initial appointment; 1.3.2 focused professional practice evaluation; 1.3.3 reappointment; 1.3.4 delineation of clinical privileges, including temporary privileges; and 1.3.5 development of privilege delineation forms and criteria for all LMHS facilities. Credentialing activities are to be carried out in accordance with specific policies and
procedures developed to ensure current clinical competency of the practitioners who are credentialed and privileged at LMHS. The purpose of the System Credentialing/Privileging
Committee also includes development of implementation of credentialing and privileging policies and procedures designed to ensure compliance with regulatory requirements.
1.4 Composition of the System Credentialing/Privileging Committee The leadership and membership of the System Credentialing/Privileging Committee shall be
as follows: 1.4.1 Consist of not less than 15 members of the active Medical Staff selected on a basis
that will ensure, insofar as feasible, balanced representation of the LMHS sites. 1.4.2 The System Medical Director will serve as a non-voting member. 1.4.3 The Immediate Past President of each FMEC will serve as voting members and will
serve a 2-year term. The FMEC may appoint this practitioner, as a member once the Immediate Past President is no longer in office.
1.4.4 Each FMEC will appoint two (2) additional representatives. 1.4.5 A quorum of 50% is required to conduct a meeting. 1.4.6 Members shall serve for two (2) years and may be reappointed to consecutive terms. 1.4.7 Each member shall be required to attend 75% of the meetings during the Medical
Staff year. Failure to attend 75% of the meetings may result in dismissal of the member from committee service and selection of an alternative member by the affected FMEC.
1.4.8 The committee members from among the committee membership will elect the Co-
Chairs of the System Credentialing/Privileging Committee. One of the Co-Chairs will be from a medical specialty and the other Co-Chair will be from a surgical specialty.
1.5 Duties and Responsibilities of the System Credentialing/Privileging Committee The System Credentialing/Privileging Committee shall: 1.5.1 Meet to evaluate credentialing-related requests (initial appointment, reappointment,
requests for clinical privileges and leave of absence, etc.) on behalf of the FMECs. 1.5.2 Monitor the granting of temporary privileges to assure that temporary privileges are
granted in compliance with approved policies and procedures. (The System Credentialing/Privileging Committee does not evaluate requests for temporary
58
privileges. These requests are handled in accordance with specific policies and procedures that are overseen by the System Credentialing/Privileging Committee).
1.5.3 Oversee the processes related to focused professional performance evaluations and
related proctoring and other mechanisms and tools employed to evaluate competency.
1.5.4 Assure uniformity in both the development and application of privileging criteria
utilized throughout LMHS facilities. 1.5.5 Assure the FMECs and Board that Medical Staff Bylaws Provisions that relate to
credentialing and privileging processes are being fulfilled, as well as credentialing policies and procedures and other credentialing-related Medical Staff documents. Monitor compliance with all credentialing and privileging policies and procedures.
1.5.6 Be responsible for evaluating recommendations made by Department Chairs. The committee is looking for completeness, thoroughness and adherence to
credentialing and privileging policies and criteria. Assure the FMECs that specialty-specific criteria for clinical privileges comply with Medical Staff Bylaws, credentialing policies and procedures, and criteria is applied fairly and uniformly to each practitioner.
1.5.7 Focuses in on the files that are determined to need clarification or additional
information (i.e., time gaps, problems with references, malpractice claims, etc.) and assures that all issues have been appropriately addressed and that there is complete and thorough documentation for the recommendation(s) that have been made to the FMECs.
1.5.8 Be responsible and aware of regulatory requirements related to credentialing activities
and to make the FMECs and Board aware when changes in credentialing policies and procedures need to be made in order to meet requirements.
1.5.9 Commission, receive and analyze the results of compliance audits of credentialing
and privileging processes. The System Credentialing/Privileging Committee makes recommendations to the FMECs and the Board when the System Credentialing/Privileging Committee believes, based on results of reports that improvements can and should be made in credentialing and privileging policies and procedures.
SECTION 2 QUALIFICATIONS FOR MEMBERSHIP AND PRIVLEGES 2.1 The following qualifications must be met by all applicants for Medical Staff
appointment, reappointment or clinical privileges:
2.1.1 Associate and Active Staff shall live and maintain an office in Lee County, unless this requirement is waived by the FMEC;
2.1.2 Demonstrate that he has successfully graduated from an approved school of
medicine (MD or DO), dentistry, podiatry, clinical psychology or applicable recognized course of training in a clinical profession eligible to hold privileges;
59
2.1.3 Have a current unrestricted state or federal license as a physician, dentist, podiatrist or clinical psychologist, applicable to his or her profession, and providing permission to practice within the State of Florida;
2.1.4 Have a record that is free from current Medicare/Medicaid sanctions and not be on
the Office of Inspector General (OIG) or General Services Administration (GSA) List of Excluded practitioners/entities;
2.1.5 Have a record that is free of felony convictions or occurrences that would raise
questions of undesirable conduct, which could injure the reputation of the Medical Staffs, hospital or Health System;
2.1.6 A physician (MD or DO) must have successfully completed an allopathic or
osteopathic residency program, approved by the Accreditation Council for Graduate Medical Education (ACGME) or the American Osteopathic Association (AOA) and be currently board certified or become board certified following the completion of formal training within the timeframes as defined by the appropriate specialty board of the American Board of Medical Specialties or the American Osteopathic Association. If no time limits for certification are specified by a given Board, then the applicant will be required to become Board certified within seven (7) years of completing formal training as defined by the appropriate specialty Board of the American Board of Medical Specialties or the American Osteopathic Association. If an applicant is beyond seven (7) years of completing formal training, current Boad certification will be required for consideration of membership and privileges. Once a member of the Medical Staff becomes Board certified, recertification is not a requirement of continued membership and privileges;
2.1.7 Dentists must have graduated from an American Dental Association approved
school of dentistry accredited by the Commission of Dental Accreditation; 2.1.8 Oral and maxillofacial surgeons must have graduated from an American Dental
Association approved school of dentistry accredited by the Commission of Dental Accreditation and successfully completed an American Dental Association approved residency program and be board certified or become board certified within five (5) years of completing formal training as defined by the American Board of Oral and Maxillofacial Surgery;
2.1.9 A podiatric physician (DPM) must have successfully completed a two 2-year
residency program in surgical, orthopedic, or podiatric medicine approved by the Council on Podiatric Medical Education of the American Podiatric Medical Association (APMA), and be board certified or become board certified within five (5) years of completing formal training as determined by the American Board of Podiatric Surgery or the American Board of Podiatric Orthopedics and Primary Podiatric Medicine;
2.1.10 A psychologist, must have earned a doctorate degree, (PhD or Psy.D. in
psychology) from an educational institution accredited by the American Psychological Association and have completed at least two (2) years of clinical experience in an organized healthcare setting, supervised by a licensed psychologist, one 1-year of which must have been post doctorate, and have completed an internship endorsed by the American Psychological Association (APA);
2.1.11 Possess a current, valid, Drug Enforcement Administration (DEA) number if
applicable to the privileges requested;
60
2.1.12 Have appropriate written and verbal communication skills; 2.1.13 Have appropriate personal qualifications, including applicant’s consistent
observance of ethical and professional standards. These standards include, at a minimum:
2.1.13.1 Abstinence from any participation in fee splitting or other illegal payment,
receipt, or remuneration with respect to referral or patient service opportunities;
2.1.13.2 A history of consistently acting in a professional, appropriate and
collegial manner with others in previous clinical and professional settings.
2.1.14 The following qualifications must also be met by all applicants requesting clinical
privileges: 2.1.14.1 Demonstrate his background, experience, training, current competence,
knowledge, judgment and the ability to perform all privileges requested. 2.1.14.2 Provide evidence of both physical and mental health that does not impair
the fulfillment of his responsibilities of Medical Staff membership subject to any legally required reasonable accommodation, and the specific privileges requested by and granted to the applicant, upon request.
2.1.14.3 Any practitioner granted privileges that may have occasion to admit an
inpatient must demonstrate the capability to provide continuous and timely care to the satisfaction of the FMEC and Board.
2.1.14.4 Demonstrate recent clinical performance (within the last twelve (12)
months with an active clinical practice in the area in which clinical privileges are sought adequate to meet current clinical competence criteria.
2.1.14.5 The applicant is requesting privileges for a service the Board has
determined appropriate for performance at the hospital. There must also be a need for this service under any Board approved Medical Staff development plan.
2.1.14.6 Provide evidence of financial responsibility consistent with the
requirements set forth in Part I. 2.1.15 Exceptions: All practitioners who are current Medical Staff members and/or hold privileges as of
May 28, 2009 and who have met prior qualifications for membership and/or privileges shall be exempt from Board specialty certification requirements.
SECTION 3 PRE-APPLICATION PROCESS
61
3.1 Only those practitioners that meet the following minimum criteria for appointment to the Medical Staff will be provided applications. Practitioners provided applications would be those: 3.1.1 which are not governed by an exclusive arrangement or who are joining a group
providing services governed by an exclusive arrangement; and
3.1.2 who meet the minimum criteria as developed by the System Credentialing/Privileging Committee and approved by FMECs and the Board.
The purpose for the pre-application screening process shall be to avoid the costly
and time-consuming application process in those circumstances where an applicant fails to meet minimum eligibility criteria. Practitioners who do not meet the minimum eligibility criteria for appointment are not entitled to fair hearing rights.
The System Credentialing/Privileging Committee shall review all requests for
application and determine whether the criteria for issuing an application have been met.
SECTION 4 INITIAL APPOINTMENT PROCESS
4.1 Completion of Application 4.1.1 All requests for application for appointment to the Medical Staff and requests for
clinical privileges will be forwarded to the Medical Staff Services Department. If the applicant successfully completed the pre-application screening process, the Medical Staff Services Department will provide the applicant an application packet, which will include a complete set or overview of the relevant Medical Staff Bylaws or reference to an electronic source for this information. This packet will enumerate the eligibility requirements for Medical Staff membership (for each facility of LMHS) and/or privileges and a list of expectations of performance for practitioners granted Medical Staff membership or privileges (if such expectations have been adopted by each Facility Medical Staff).
A completed application includes, at a minimum: 4.1.1.1 a completed, signed, dated application form; 4.1.1.2 a completed privilege delineation form if requesting privileges; 4.1.1.3 copies of all requested documents and information necessary to confirm
the applicant meets criteria for membership and/or privileges and to establish current competency;
4.1.1.4 all applicable fees; 4.1.1.5 complete reference information; references shall be from peers (same
specialty) knowledgeable about the applicant’s experience, ability and current competence to perform the privileges being requested;
4.1.1.6 relevant practitioner-specific data as compared to aggregate data, when
available
62
4.1.1.7 morbidity and mortality data, when available. Each applicant must indicate the LMHS facility anticipated to be his
primary facility (i.e., the facility where the majority of his clinical activity is performed). It should be noted that this designation is important for credentialing purposes (interviews, implementation of focused professional practice evaluation, etc.) and will be confirmed by LMHS data at periodic intervals and prior to any subsequent reappointments.
An application shall be deemed incomplete if any of the above items are
missing or if the need arises for new, additional or clarifying information in the course of reviewing an application. An incomplete application will not be processed and the applicant will not be entitled to a fair hearing.
Anytime in the credentialing process it becomes apparent that an
applicant does not meet all eligibility criteria for membership or privileges, the credentialing process will be terminated and no further action taken. Applications will not be accepted from practitioners that are not eligible to take the Board certification examination.
4.1.2 The burden is on the applicant to provide all required information. It is the
applicant’s responsibility to ensure that the Medical Staff Services Department receives all required supporting documents verifying information on the application and to provide sufficient evidence, as required in the sole discretion of the Health System that the applicant meets the requirements for the Medical Staff membership and/or the privileges requested. If information is missing from the application or new, additional or clarifying information is required, a letter requesting such information will be sent to the applicant. If the requested information is not returned to the Medical Staff Services Department within thirty (30) calendar days of the receipt of the requested letter, the application will be deemed to have been voluntarily withdrawn.
4.1.3 Upon receipt of a completed application, the System Medical Director will determine
if the requirements of Section 2.1 are met. In the event the requirements of Section 2.1 are not met, the applicant will be notified that he is ineligible to apply for membership or privileges on the Medical Staff, the application will not be processed and the applicant will not be eligible for a fair hearing. If the requirements of Section 2.1 are met, the application will be accepted for further processing.
4.1.4 Practitioners seeking appointment shall have the burden of producing information
deemed adequate by the hospital for a proper evaluation of current competence, character, ethics, other qualifications and of resolving any doubts.
4.1.5 Upon receipt of a completed application, the Medical Staff Services Department will
verify current licensure, education, relevant training and current competence from the primary source whenever feasible in accordance with the Verification Methods and Requirements document.
When it is not possible to obtain information from the primary source, reliable
secondary sources may be used if there has been a documented attempt to contact the primary source.
Note: In the event there is undue delay in obtaining required information, the
Medical Staff Services Department will request assistance from the applicant. During this time, the period for processing, the application will be appropriately
63
modified. Failure of an applicant to respond to a request for assistance adequately after thirty (30) calendar days the application will be deemed to have been voluntarily withdrawn.
4.1.6 When all items identified in the Verification Methods and Requirements document
have been obtained and verified, the application will be considered eligible for evaluation.
4.2 Applicant’s Attestation, Authorization and Acknowledgement 4.2.1 The applicant must complete and sign the application form. By signing this
application the applicant: 4.2.1.1 Attests to the accuracy and completeness of all information on the
application or accompanying documents and agreement that any inaccuracy, omission or misrepresentation, whether intentional or not, may be grounds for termination of the application process without the right to a fair hearing or appeal.
If the inaccuracy, omission or misstatement is discovered after a
practitioner has been granted appointment and/or clinical privileges, the practitioner’s appointment and privileges shall lapse effective immediately upon notification of the practitioner without the right to a fair hearing or appeal.
4.2.1.2 Consents to appear for any requested interviews about his application. 4.2.1.3 Authorizes the applicable hospital and Medical Staff representative to
consult with prior and current associates and others who may have information bearing on his professional competence, character, ability to perform the privileges requested, ethical qualifications, ability to work cooperatively with others and other qualifications for requested membership and/or clinical privileges.
4.2.1.4 Consents to the Health System and Medical Staff representatives’
inspections of all records and documents that may be material to an evaluation of:
4.2.1.4.1 professional qualifications and competence to carry out the
clinical privileges requested;
4.2.1.4.2 physical and mental/emotional health status to the extent relevant to safely perform requested privileges subject to any legally required reasonable accommodation;
4.2.1.4.3 professional and ethical qualifications;
4.2.1.4.4 professional liability actions including currently pending claims involving the applicant;
64
4.2.1.4.5 any other issue relevant to establishing the applicant’s suitability for membership and/or privileges.
4.2.1.5 Releases from liability, promises not to sue and grants immunity to the
Health System, its Medical Staffs and its representatives for acts performed and statements made in good faith in connection with evaluation of the application and his credentials and qualifications fully permitted by the law.
4.2.1.6 Releases from liability and promises not to sue, all practitioners and
organizations who provide information to the Health System or the applicable Medical Staff(s) in good faith, including otherwise privileged or confidential information to the System/hospital representatives concerning his background/experience, competence, professional ethics, character, physical and mental health to the extent relevant to the capacity to fulfill requested privileges, emotional stability, utilization practice patterns, and other qualifications for staff appointment and clinical privileges.
4.2.1.7 Authorizes the Health System, Medical Staff and Administrative
representatives to obtain credentialing and peer review information from other hospitals, medical associations, licensing boards, appropriate government bodies and other health care entities concerned with this provider’s performance and releases representatives of the Health System from liability for so doing.
4.2.1.8 Acknowledges that the applicant has had access to relevant Medical
Staff Bylaws, including all rules, regulations, policies and procedures of the relevant Medical Staffs and agrees to abide by their provisions.
Notwithstanding Section 3.2 of Part II, if a practitioner institutes legal
action and does not prevail, he shall reimburse the Health System and any member of the Medical Staff named in the action for all costs incurred in defending such legal action, including reasonable attorney(s) fees.
4.2.1.9 Agrees to provide accurate answers to all the questions on the
application form, and agrees to immediately notify the System in writing should any of the information regarding these items change during the period of the applicant’s Medical Staff membership and/or privileges.
4.3 Application Evaluation
4.3.1 Expedited Credentialing: 4.3.1.1 An expedited Credentialing/Privileging Committee review and approval
process may be used for initial appointment in accordance with the Expedited Credentialing Policy.
4.3.2 Applicant Interview
4.3.2.1 All applicants for appointment to the Medical Staff and/or the granting of
clinical privileges are required to participate in interviews. The interviews are used to solicit information required to complete the credentials file or
65
clarify information previously provided, e.g., clinical knowledge and judgment, professional behavior, malpractice history, reasons for leaving past healthcare organizations, or other matters bearing on the applicant’s ability to render care at the generally recognized level for the community and in compliance with LMHS privileging criteria. Interviews may also be used to communicate Medical Staff performance expectations.
Applicants for appointment will participate in a minimum of two (2)
interviews. One interview will be conducted by the applicable Department Chair or designated Section Chief of the applicant’s anticipated primary LMHS facility and the second interview will be with a member of the System Credentialing/Privileging Committee. Applicants that are applying for multiple facilities within LMHS may be required to participate in additional Department Chair/Section Chief interviews at the discretion of the Department Chairs of the facility(ies) that are designated as non-primary.
4.3.2.2 Procedure: the applicant will be notified of required interview(s). Failure
of the applicant to appear for a scheduled interview will be deemed a voluntary withdrawal of the application.
4.3.3 Department Chair Action 4.3.3.1 Each Department Chair of an LMHS facility where the applicant has
requested privileges makes a recommendation related to membership and privileges, as applicable.
All completed applications are presented to the appropriate Department
Chair(s) for review and recommendation (which is made by completion of a standardized form provided to the Chair by the Medical Staff Services Department). The Department Chair(s) reviews the application to ensure that it fulfills the established standards for membership and/or clinical privileges. The Department Chair(s) may obtain input if necessary from an appropriate subject matter expert(s).
If a Department Chair believes a conflict of interest exists that, might
preclude his ability to make an unbiased recommendation, he will notify the Medical Staff Services Department and forward the application without comment.
4.3.3.2 The Department Chair(s) forwards to the System
Credentialing/Privileging Committee the following: 4.3.3.2.1 A written recommendation to approve the applicant’s request
for membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges (a summary of the interview conducted by the Department Chair or his designee is included in this written recommendation);
4.3.3.2.2 Written comments supporting his recommendations. The Department Chair of the applicant’s anticipated primary
facility also makes a written recommendation to define those circumstances, which require monitoring and evaluation of
66
clinical performance after the initial granting of clinical privileges (i.e., focused professional practice evaluation).
4.3.4 Medical Staff System Credentialing/Privileging Committee Action 4.3.4.1 The System Credentialing/Privileging Committee reviews the application
and forwards the following to the applicable FMEC(s): 4.3.4.1.1 A recommendation to approve the applicant’s request for
membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges;
4.3.4.1.2 A recommendation to define those circumstances, which
require monitoring, and evaluation of clinical performance after initial granting of clinical privileges (Focused Professional Practice Evaluation) (FPPE);
Comments supporting the above recommendation. 4.3.5 FMEC Action
4.3.5.1 Each FMEC of LMHS where membership and/or privileges have been requested forwards the following to the Board:
4.3.5.1.1 A recommendation to approve the applicant’s request for
membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges;
4.3.5.1.2 Comments supporting the above recommendation.
The FMEC of the applicant’s anticipated primary facility also makes a recommendation to define those circumstances that require monitoring and evaluation of clinical performance after initial granting of clinical privileges (FPPE).
Whenever a FMEC makes an adverse recommendation to the Board, a notice,
stating the reason, will be sent to the applicant who shall then be entitled to the procedural rights provided in the Investigation, Corrective Action, Hearing and Appeal Plan of the Medical Staff Bylaws. When multiple FMECs are making recommendations related to the same applicant, an adverse recommendation is not considered final until after the PLC attempts to facilitate resolution of the issues (this facilitation occurs when there are disparate recommendations – for example, one (1) positive recommendation and one negative recommendation).
4.3.6 Applicants Applying to Multiple Facilities Applicants may simultaneously make application for membership and/or privileges
to multiple facilities within LMHS. The Medical Staff Services Department coordinates this information so that the recommendations from all FMECs come to the Board together. If there are disparate recommendations (defined as conflicting) related to membership and/or requested clinical privileges on the same applicant, the PLC will meet and attempt to reconcile the disparate recommendations prior to forwarding the recommendations to the Board.
67
If the PLC is unable to facilitate resolution of the issues (in accordance with the Medical Staff Bylaws – Part I, Governance – Section 9 Decision Making Methods and Conflict Resolution) the disparate recommendations will go forward to the Board.
4.3.7 Board Action:
4.3.7.1 The Board reviews the recommendation and votes for one (1) of the following actions: 4.3.7.1.1 The Board may adopt or reject in whole or in part a
recommendation of the FMEC(s) or refer the recommendation to the FMEC(s) for further consideration stating the reasons for such referral back and setting a time limit within which a subsequent recommendation must be made.
4.3.7.1.2 If the Board concurs with the applicant’s request for membership and/or privileges, it will grant the appropriate membership and/or privileges for a period not to exceed 24 months.
4.3.7.1.3 If the Board’s action is adverse to the applicant, a notice,
stating the reason, will be sent to the applicant who shall then be entitled to the procedural rights provided in the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) unless the applicant received procedural rights under Part II, Section 3.2.5.
4.3.7.1.4 The Board shall take final action in the matter as provided in
the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan).
4.3.8 Notice of Final Decision:
4.3.8.1 Notice of the Board’s final decision shall be given through the Medical
Staff Services Department to the applicable FMEC(s) and to the Chair of each Department concerned. The applicant shall receive written notice of appointment and special notice of any adverse final decisions in a timely manner. A decision and notice of appointment includes the staff category(ies) to which the applicant is appointed, the Department(s) to which he is assigned, the clinical privileges he may exercise, notification of orientation and any special conditions attached to the appointment.
4.3.9 Periods for Processing: 4.3.9.1 All practitioners and groups acting on an application for staff
appointment and/or clinical privileges must do so in a timely and good faith manner, and except for good cause, each application will be processed within 180 calendar days. The 180 Calendar days begin on the date that the application is declared complete to begin processing.
68
4.3.9.2 These processing periods are deemed guidelines and do not create any right to have an application processed within these precise periods. If the provisions of the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) are activated, the time requirements provided therein govern the continued process of the application.
SECTION 5 FOCUSED PROFESSIONAL PRACTICE EVALUATION (FPPE) 5.1 CRITERIA FOR FPPE 5.1.1 The Department Chair (or designated Section Chief) of the applicant’s anticipated
primary facility will define circumstances that require monitoring and evaluation of the clinical performance of each practitioner following his or her initial granting of clinical privileges.
Such monitoring may utilize a range of techniques, including but not limited to: chart
review, the tracking of performance monitors/indicators, proctoring, external peer review, simulations, morbidity/mortality reviews, and discussion with other healthcare practitioners involved in the care of each patient. The FPPE plan is created as part of the initial recommendation for appointment and privileges and is forwarded to the System Credentialing/Privileging Committee and to the FMEC(s).
The System Credentialing/Privileging Committee will establish via policy the
anticipated duration for FPPE. The Physician Quality Committee will establish the triggers that indicate the need for
performance monitoring after the initial granting of privileges. SECTION 6 CRITERIA FOR REAPPOINTMENT 6.1 Criteria for Reappointment 6.1.1 It is the policy of the Health System to approve for reappointment and/or renewal of
privileges only those practitioners who meet the criteria for initial appointment as identified in Section 2, Part 1. The practitioner must also be determined by each applicable FMEC to be a provider of effective care that is consistent with the Health System standards of ongoing quality and the hospital performance improvement program and provide the information enumerated in Section 5.1.1.
All reappointments and renewals of clinical privileges are for a period not to exceed
24 months. The granting of new clinical privileges to existing Medical Staff members will follow the steps described in Section 4 concerning the initial granting of new clinical privileges and Section 5 concerning FPPE. A suitable peer shall substitute for the Department Chair in the evaluation of current competency of the Department Chair, and recommend appropriate action to the System Credentialing/Privileging Committee.
69
In the event a practitioner finds no need to utilize the facilities or resources of LMHS
for purposes of patient care through either admission, performance of a procedure, consultation, or referral, during a two-year period he may not be eligible for reappointment or continued privileges. Such practitioner may apply as a new applicant at any time subsequent to the expiration of the current appointment or privileges. This provision applies to practitioners who have been granted a leave of absence, moved their practice location, established a relationship with another institution or otherwise find no need to utilize the clinical resources of LMHS. Exceptions to this provision may be made by the Board upon recommendation of the applicable FMEC(s).
As long as a practitioner has adequate clinical activity to maintain privileges at one
LMHS facility (and is recommended for continuation of privileges at his primary LMHS facility) the practitioner may maintain the applicable clinical privileges and staff category (potentially Associate if there is no or minimal clinical activity) at other LMHS facility(ies).
6.2.1 Information, Collection and Verification 6.2.1.1 From practitioner: On or before 4 months prior to the date of expiration of
a Medical Staff appointment or granting of privileges, a representative from the Medical Staff Services Department notifies the practitioner of the date of expiration and supplies him with an application for reappointment for membership and/or privileges. At least sixty (60) calendar days prior to this date, the practitioner must return the following to the Medical Staff Services Department:
6.2.1.1.1 A completed reapplication form, which includes complete
information to update his file on items listed in his original application, any required new, additional, or clarifying information, and any required fees or dues;
6.2.1.1.2 Information concerning continuing training and education
internal and external to the hospital during the preceding period;
6.2.1.1.3 By signing the reapplication form, the practitioner agrees to
the same terms as identified in Section 4.2. 6.2.2 From internal and/or external sources: The Medical Staff Services Department
collects and verifies information regarding each staff practitioner’s professional and collegial activities to include those items listed in Section 2.1.
6.2.3 The following information is also collected and verified:
6.2.3.1 A summary of clinical activity at each LMHS facility for each practitioner due for reappointment.
6.2.3.2 Performance and conduct in each LMHS facility and other healthcare
organizations in which the practitioner has provided substantial clinical care since the last reappointment, including patient care, medical/clinical knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism and system-based practice.
70
6.2.3.3 Documentation of CME activity; 6.2.3.4 Service on Medical Staff, Department and hospital committees; 6.2.3.5 Timely and accurate completion of medical records; 6.2.3.6 Compliance with all applicable Bylaws, policies, rules, regulations, and
procedures of the System and the Medical Staff(s); 6.2.3.7 Any significant gaps in employment or practice since the previous
appointment or reappointment; and 6.2.3.8 Additional items as identified in the Verification Methods and
Requirements document.
6.2.4 Failure, without good cause, to provide any requested information, at least forty-five (45) calendar days prior to the expiration of appointment will result in a cessation of processing of the application and automatic expiration of appointment when the appointment period is concluded. Once the information is received, the Medical Staff Services Department verifies this additional information and notifies the staff practitioner of any additional information that may be needed to resolve any doubts about performance or material in the credentials file.
6.3 Evaluation of Application for Reappointment of Membership and/or Privileges
6.3.1 The reappointment application will be reviewed and acted upon as described in Sections 4.3.3 through 4.3.8. For the purpose of reappointment, an “adverse recommendation” by the Board as used in Section 4.3 means a recommendation or action to deny reappointment, or to deny or restrict requested clinical privileges or any action that would entitle the applicant to a Fair Hearing under the Medical Staff Bylaws. The terms “applicant” and “appointment” as used in these Sections shall be read respectively, as “staff practitioner” and “reappointment”.
SECTION 7 CLINICAL PRIVILEGES 7.1 Exercise of Privileges
A practitioner providing clinical services at a LMHS facility may exercise only those privileges granted to him by the Board or emergency and disaster privileges as described herein. Privileges may be granted by the Board upon recommendation of the FMEC(s) to practitioners who are not members of the Medical Staff. Such practitioners may include Advanced Registered Nurse Practitioners (ARNPs), Physician Assistants (PAs), practitioners serving short locum tenens positions, telemedicine physicians or others deemed appropriate by the FMEC(s) and Board.
7.2 Requests
When applicable, each application for appointment or reappointment to the Medical Staff must contain a request for the specific clinical privileges desired by the applicant. Specific requests must also be submitted for temporary privileges and for modifications of privileges in the interim between reappointments and/or granting of privileges.
7.3 Basis for Privileges Determination
71
7.3.1 Requests for clinical privileges will be considered only when accompanied by
evidence of education, training, experience, and demonstrated current competence as specified by the System in its Board approved criteria for clinical privileges.
7.3.2 Privileges for which no criteria have been established: 7.3.2.1 In the event a request for a privilege is submitted for a new technology, a
procedure new to the System, an existing procedure used in a significantly different manner, or involving a cross-specialty privilege for which no criteria have been established, the request will be tabled for a reasonable period of time, usually not to exceed sixty (60) calendar days. During this time, the System Credentialing/Privileging Committee may refer the request for review by a task force appointed to review the request.
Task forces formed for purposes of establishment of evaluation of new
privileges and potential determination of criteria will be appointed by the Chairs of the System Credentialing/Privileging Committee, and will include the System Medical Director of Clinical Effectiveness and the Director of Supply Chain Management. The task force will:
7.3.2.1.1 Review the community, patient and System need for the
privilege and reach agreement with management and the Board that the privilege is approved to be exercised at the hospital;
7.3.2.1.2 Review with appropriate individuals/groups
the efficacy and clinical viability of the requested privilege and confirm that this privilege is approved for use in the setting-specific area of the hospital by appropriate regulatory agencies (FDA, OSHA, etc.);
7.3.2.1.3 Meet with management to ensure that the new privilege is
consistent with the Health System’s mission, values, strategic, operating, capital, information and staffing plans;
7.3.2.1.4 Work with management to ensure that any/all exclusive
contract issues, if applicable are resolved in such a way to allow the new or cross-specialty privileges in question to be provided without violating the existing contract. Upon recommendation from the System Credentialing/Privileging Committee and appropriate clinical services/specialty or subject matter experts (as determined by the System Credentialing/Privileging Committee), the criteria will be recommended to each FMEC and then to the Board. Once objective criteria have been established, the original request will be processed as described herein.
7.3.2.2 For the development of criteria, the Medical Staff Services Department (or
designee) will compile information relevant to the privileges requested which may include, but need not be limited to, position and opinion papers from specialty organization, position and opinion statements from interested individuals or groups and documentation from other hospitals in the region as appropriate.
72
7.3.2.3 Criteria to be established for the privilege(s) in question include education, training, board status or certification (if applicable), experience and evidence of current competence. Proctoring requirements, if any, will be addressed including who may serve as proctor and how many proctored cases will be required.
Hospital related issues such as exclusive contracts, equipment, clinical
support staff and management would be referred to the appropriate hospital administrator and/or Department Director.
7.3.2.4 If the privileges requested overlap two (2) or more specialty disciplines, an
ad hoc committee may be appointed by the System Credentialing/Privileging Committee to recommend criteria for the privilege(s) in question. This ad hoc committee will consist of at least one (1) but no more than two (2) members from each involved discipline. The Chair of the ad hoc committee will be a member of the System Credentialing/Privileging Committee who has no vested interest in the issue (see Medical Staff Privilege Dispute Resolution Policy).
7.3.3 Requests for clinical privileges will be consistently evaluated on the basis of prior
and continuing education, training, experience, utilization practice patterns, current ability to perform the privileges requested and demonstrated current competence,
ability, and judgment. Additional factors that may be used in determining privileges are patient care needs and the System’s capability to support the type of privileges being requested and the availability of qualified coverage in the applicant’s absence. The basis for privileges determination to be made in connection with periodic reappointment or a requested change in privileges must include documented clinical performance and results of the staff’s performance improvement program activities.
Privilege determinations will also be based on pertinent information from other
sources, such as peers and/or faculty from other institutions and healthcare settings where the practitioner exercises clinical privileges.
7.3.4 The procedure by which requests for clinical privileges are processed are as outlined in Section 4.
7.3.5 Special Conditions for Dental Privileges
Requests for clinical privileges for dentists are processed in the same manner as all other privilege requests. Privileges for surgical procedures performed by dentists and/or oral and maxillofacial surgeons will require that all dental patients receive a basic medical evaluation (history and physical) by a physician member of the Medical Staff with privileges to perform such an evaluation, which will be recorded in the medical record. Oral and maxillofacial surgeons may be granted the privilege of performing a history and physical on their own patients upon submission of documentation of completion of an accredited postgraduate residency in oral and maxillofacial surgery and demonstrated current competence.
7.3.6 Special Conditions for practitioners not Qualified for Medical Staff Appointment but Practicing Pursuant to Clinical Privileges per System Policy. Requests for privileges, from such practitioners, are processed in the same manner as requests for clinical privileges by providers eligible for Medical Staff membership, with the exception that such practitioners are not eligible for membership on a Medical Staff and do not have the rights and privileges of such membership (all
73
rights and responsibilities are defined in the Allied Health Practitioner (AHP) Privileging Policy and Procedure). Only those categories of practitioners approved by the Board for providing services at the hospital are eligible to apply for privileges. AHP(s) in this category may, subject to any licensure requirements or other limitations, exercise independent judgment only within the areas of their professional competence and participate directly in the medical management of patients under the supervision of a physician who has been accorded privileges to provide such care.
7.4 Special Conditions for Podiatric Privileges Requests for clinical privileges for podiatrists are processed in the same manner as all other privilege requests.
Practitioners granted podiatric privileges may perform and shall record in the medical
record a basic medical evaluation history and physical for the practitioner’s podiatric patients if consistent with the privileges granted to the practitioner, state law governing the practitioner’s practice and federal law.
7.5 Special Conditions for Residents or Fellows in Training
Residents or Fellows in Training in the Health System shall not normally hold membership on the Medical Staff and shall not normally be granted specific clinical privileges. Rather, they shall be permitted to function clinically only in accordance with the written training protocols developed by the Professional Graduate Education Committee in conjunction with the Residency Training Program. The protocols must delineate the roles, responsibilities, and patient care activities of residents and fellows including which types of residents may write patient care orders, under what circumstances why they may do so, and what entries a supervising physician must countersign. The protocol must also describe the mechanisms through which resident directors and supervisors make decisions about a resident’s progressive involvement and independence in delivering patient care and how these decisions will be communicated to appropriate Medical Staff and hospital leaders.
The Post-Graduate Education Program Director or Committee must communicate
periodically with each applicable FMEC and the Board about the performance of its residents, patient safety issues and quality of patient care and must work with the FMEC to assure that all supervising physicians possess clinical privileges commensurate with their supervising activities.
7.6 Special Conditions for the Aging Practitioner
At the age of 70, practitioners shall complete an annual examination that addresses both the physical and mental capacity for the privileges requested. The annual physical and mental exams are to be conducted by an independent Medical examiner acceptable to the System Credentialing/Privileging Committee, documented on the approved form and submitted to the System Credentialing/Privileging Committee by the date requested. The physical exam is a “fitness to work” evaluation and must indicate that the practitioner has no physical or mental problem that may interfere with the safe and
74
effective provision of care permitted under the privileges granted. In addition to the physical exam, a practitioner may be required to undergo proctoring of his clinical performance as part of the assessment of his capacity to perform the requested privileges. Such proctoring may be required in the absence of any previous performance concerns. The scope and duration of the proctoring shall be determined by the FMEC upon recommendation of the Department Chair of the practitioner’s primary facility and System Credentialing/Privileging Committee. The practitioner shall pay the cost of the physical and mental exam.
7.7 Temporary Privileges 7.7.1 Temporary privileges may be granted by the CEO, or designee, acting on behalf of
the Board and based on the recommendation of the President of the Medical Staff or designee to be approved at the next FMEC meeting, provided there is verification of current licensure and current competence. Temporary privileges may be granted only in two (2) circumstances: 1) to fulfill an important patient care, treatment or service need, or 2) when an initial applicant with a complete application that raises no concerns is awaiting review and approval of the FMEC and the Board. Applications pending completion of the initial appointment process must always be reviewed and a recommendation made by the System Credentialing/Privileging Committee prior to the granting of temporary privileges.
7.7.2 Important Patient Care, Treatment or Service Need: Temporary privileges may be
granted on a case-by-case basis when an important patient care, treatment or service need exists that mandates an immediate authorization to practice, for a limited time, not to exceed 30 calendar days (from date privileges are granted). Temporary privileges may be extended for two separate 30-day intervals upon approval of the Board of Directors. For the purposes of granting temporary privileges, an important patient care, treatment or service need is defined as including the following:
7.7.2.1 a circumstance in which one or more individual patients will experience
care that does not adequately meet their clinical needs if the temporary privileges under consideration are not granted, (i.e., a patient scheduled for urgent surgery who would not be able to undergo the surgery in a timely manner);
7.7.2.2 a circumstance in which the institution will be placed at risk of not
adequately meeting the needs of patients who seek care, treatment or service from the institution if the temporary privileges under consideration are not granted (i.e., the institution will not be able to provide adequate emergency room coverage in the providers specialty, or the Board has granted privileges involving new technology to a physician on the staff provided the physician is precepted for a specific number of initial cases and the precepting physician, who is not seeking Medical Staff membership, requires temporary privileges to serve as a preceptor);
7.7.2.3 a circumstance in which a group of patients in the community will be
placed at risk if not receiving patient care that meets their clinical needs if the temporary privileges under consideration are not granted (i.e. a
75
physician who has a large practice in the community for which adequate coverage of hospital care for those patients cannot be arranged).
7.7.3 Clean Application (Expedited) Awaiting Approval: Temporary privileges may be
granted for up to 30 calendar days (from date privileges are issued) approved by the Executive Committee with two 30-day extensions approved by the Board (see the policy and procedure on Expedited Credentialing) when the new applicant for Medical Staff membership and/or privileges is waiting for review and recommendation by the FMEC and approval by the Board.
7.7.4 Special requirements of consultation and reporting may be imposed as part of the
granting of temporary privileges. Except in unusual circumstances, temporary privileges will not be granted unless the practitioner has agreed in writing to abide by the Bylaws, rules, and regulations and policies of the Medical Staff and hospital in all matters relating to his temporary privileges. Whether or not such written agreement is obtained, these Bylaws, rules, regulations and policies control all matters relating to the exercise of clinical privileges.
7.7.5 Termination of temporary privileges: The CEO, acting on behalf of the Board and
after consultation with the President of the Medical Staff, may terminate any or all of the practitioner’s privileges based upon the discovery of any information or the occurrence of any event of a nature, which raises questions about a practitioner’s privileges.
Where the life or well-being of a patient is determined to be endangered, any person
entitled to impose precautionary suspension under the Medical Staff Bylaws may effect the termination. In the event of any such termination, the CEO or his designee then will assign the practitioner’s patients to another practitioner. The wishes of the patient shall be considered when feasible, in choosing a substitute practitioner.
7.7.6 Rights of the practitioner with temporary privileges: A practitioner is not entitled to
the procedural rights afforded in the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) because his request for temporary privileges is refused or because all or any part of his temporary privileges are terminated or suspended unless based on a determination of clinical incompetence or unprofessional conduct.
7.7.7 Emergency Privileges: In the case of a medical emergency, any practitioner is
authorized to do everything possible to save the patient’s life or to save the patient from serious harm, to the degree permitted by the practitioner’s license, regardless of facility affiliation, staff category, or level of privileges. A practitioner exercising emergency privileges is obligated to summon all consultative assistance deemed necessary and to arrange appropriate follow-up.
7.7.8 Disaster Privileges 7.7.8.1 If the System’s Disaster Plan has been activated and the organization is
unable to meet immediate patient needs, the CEO and such other individuals as identified in the System’s Disaster Plan with such authority, may, on a case by case basis consistent with medical licensing and other relevant state statutes, grant disaster privileges to provide patient care to selected Licensing Independent Practitioners (LIP’s), who must at a minimum present a valid governmental-issued photo identification issued
76
by a state or federal agency (e.g. driver’s license or passport) and at least one of the following:
7.7.8.1.1 a current picture hospital ID card that clearly identifies
professional designation; 7.7.8.1.2 a current license to practice; 7.7.8.1.3 primary source verification of the license;
7.7.8.1.4 identification indicating that the practitioner is a member of a
Disaster Medical Assistance Team (DMAT), or Medical Reserve Corps (MRC), Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VHP), or other recognized state or federal organizations or groups;
7.7.8.1.5 identification indicating that the practitioner has been
granted authority to render patient care, treatment, and services in disaster circumstances (such authority having been granted by a federal, state, or municipal entity);
7.7.8.1.6 identification by a current hospital or Medical Staff
member(s) who possesses personal knowledge regarding the volunteer’s ability to act as a LIP during a disaster.
7.7.8.2 The Medical Staff oversees the professional performance of
volunteer practitioners who have been granted disaster privileges by direct observation, mentoring or clinical record review.
The organization makes a decision (based on information obtained regarding the professional practice of the volunteer) within 72 hours related to the continuation of the disaster privileges initially granted.
7.7.8.3 Primary source verification of licensure begins as soon as the
immediate situation is under control, and is completed within 72 hours from the time the volunteer practitioner presents to the organization.
7.7.8.4 Once the immediate situation has passed and such determination
has been made consistent with the institution’s Disaster Plan, the practitioner’s disaster privileges will terminate immediately.
7.7.8.5 Any individual identified in the institution’s Disaster Plan with the
authority to grant disaster privileges shall also have the authority to terminate disaster privileges. Such authority may be exercised at the sole discretion of the hospital and will not give rise to a right to a fair hearing or an appeal.
SECTION 8 PRECEPTORSHIP
8.1 A practitioner who has not provided acute inpatient care within the past 24 months who requests clinical privileges at the hospital must arrange for a preceptorship either with a
77
current member in good standing of the Medical Staff who practices in the same specialty or with an academic training program or other equivalently competent physician practicing outside of the hospital. The practitioner must assume responsibility for any financial costs required to fulfill the requirements of Sections 8.1 and 8.2.
8.2 A description of the preceptorship program, including details of monitoring and consultation
must be written and submitted for approval to the applicable Department Chair, System Credentialing/Privileging Committee and FMEC. At a minimum, the preceptorship program description must include the following: 8.2.1 The scope and intensity of required preceptorship activities; 8.2.2 The requirement for submission of a written report from the preceptor prior to
termination of the preceptorship period assessing, at a minimum, the applicant’s demonstrated clinical competence related to the privileges requested, ability to get along with others, the quality and timeliness of medical records documentation, ability to perform the privileges requested, and professional ethics and conduct.
SECTION 9 REAPPLICATION AFTER MODIFCATIONS OF MEMBERSHIP STATUS OF PRIVILEGES AND EXHAUSTION OF REMEDIES
9.1 Reapplication After Adverse Credentials Decision
9.1.1 Except as otherwise determined by the Board, a practitioner who has received a
final adverse decision or who has resigned or withdrawn an application for appointment, reappointment or clinical privileges while under investigation or to avoid an investigation is not eligible to reapply to the Medical Staff for a period of five (5) years from the date of the notice of the final adverse decision or the effective date of the resignation or application withdrawal. Any such application is processed in accordance with the procedures then in force. As part of the reapplication, the practitioner must submit such additional information as the Medical Staff and/or Board requires, demonstrating that the basis of the earlier adverse action no longer exists. If such information is not provided, the reapplication will be considered incomplete and voluntarily withdrawn and will not be processed any further.
9.2 Request for Modification of Appointment Status or Privileges
9.2.1 A staff member, either in connection with reappointment or at any other time, may
request modification of staff category, Department assignment, or clinical privileges by submitting a written request to the Medical Staff Services Department. A modification request must be on the prescribed form and must contain all pertinent information supportive of the request. All requests for additional clinical privileges must be accompanied by information demonstrating additional education, training, and current clinical competence in the specific privileges requested. A modification application is processed in the same manner as a reappointment, which is outlined in Section 6 of this manual. A practitioner who determines that he no longer exercises, or wishes to restrict or limit the exercise of, particular privileges that he has been granted shall send written notice, through the Medical Staff Services Department to the System Credentialing/Privileging Committee, and FMEC. A copy of this notice shall be included in the practitioner’s credentials file.
9.3 Resignation of Staff Appointment or Privileges
78
9.3.1 A practitioner who wishes to resign his staff appointment and/or clinical privileges must provide written notice to the appropriate Department Chair or President of the Medical Staff. The resignation shall specify the reason for the resignation and the effective date. A practitioner who resigns his staff appointment and/or clinical privileges is obligated to accurately complete all portions of all medical records for which he is responsible prior to the effective date of resignation. Failure to do so shall result in an entry in the practitioner’s credentials file acknowledging the resignation and indicating that it became effective under unfavorable circumstances.
9.4 Exhaustion of Administrative Remedies
9.4.1 Every practitioner agrees that he will exhaust all the administrative remedies
afforded in the various Sections of Part I: Governance, Part II: Investigations, Corrective Action, Hearing and Appeal Plan and Part III: Credentialing Procedures before initiating legal action against the System or its agents.
9.5 Reporting Requirements
9.5.1 The CMO or his designee shall be responsible for assuring that the hospital satisfies
its obligations under the Health Care Quality Improvement Act of 1986 and its successor statutes. Actions that must be reported include any negative professional review action against a physician or dentist related to clinical incompetence or misconduct that leads to a denial of appointment and/or reappointment, reduction in clinical privileges for greater that thirty (30) calendar days; resignation, surrender of privileges, or acceptance of privilege reduction either during an investigation or to avoid an investigation.
SECTION 10 LEAVE OF ABSENCE
10.1 Leave Request
10.1.1 A leave of absence is a matter of courtesy, not of right. In the event that it is
determined that a practitioner has not demonstrated good cause for a leave, or where a request for extension is not granted, the determination shall be final, with no recourse to a hearing and appeal. A leave of absence must be requested for any absence from the Medical Staff and/or patient care responsibilities longer than thirty (30) days if such absence is related to the practitioner’s physical or mental health or to the ability to care for patients safely and competently. A practitioner who wishes to obtain a voluntary leave of absence must provide written notice to the President of the Medical Staff stating the reasons for the leave and approximate period of the leave, which may not exceed one 1-year except for military service or express permission by the Board. Requests for leave must be forwarded, with a recommendation from the FMEC, and affirmed by the Board. While on leave of absence, the practitioner may not exercise clinical privileges or prerogatives and has no obligation to fulfill Medical Staff responsibilities.
10.2 Termination of Leave
10.2.1 At least thirty (30) calendar days prior to the termination of the leave, or at any
earlier time, the practitioner may request reinstatement by sending a written notice to the President of the Medical Staff. The practitioner must submit a written summary of relevant activities during the leave if the FMEC or Board so requests.
79
A practitioner returning from a leave of absence for health reasons must provide a report from his physician that answers any questions that the FMEC or Board may have as part of considering the request for reinstatement. The FMEC makes a recommendation to the Board concerning reinstatement, and the applicable procedures concerning the granting of privileges are followed. If the practitioner’s current grant of membership and for privileges is due to expire during the leave of absence, the practitioner must apply for reappointment or his appointment and/or clinical privileges shall lapse at the end of the appointment period.
10.3 Failure to Request Reinstatement 10.3.1 Failure, without good cause, to request reinstatement shall be deemed a voluntary
resignation from the Medical Staff and shall result in automatic termination of membership, privileges, and prerogatives. A practitioner whose membership is automatically terminated shall not be entitled to the procedural rights provided in the Medical Staff Bylaws. A request for Medical Staff membership subsequently received from a member so terminated shall be submitted and processed in the manner specified for applications for initial appointments.
SECTION 11 PRACTITIONERS PROVIDING CONTRACTED SERVICES 11.1.1 When the System or hospital contracts for patient care services with LIPs who
provide official readings of images, tracings or specimens through a telemedicine mechanism, and these practitioner’s services are under the control of a Joint Commission accredited organization, the hospital will:
11.1.1.1 specify in a contract that the entity providing these services by contract
(the contracting entity) will ensure that all services provided under this contract by individuals who are LIPs will be within the scope of those practitioner’s privileges at the contracting entity; or
11.1.1.2 verify that all individuals who are LIPs and providing services under the
contract have privileges that include the services provided under the contract.
11.2 When the System/hospital contracts for care services with LIPs, who provide official
readings of images, tracings or specimens through a telemedicine mechanism, and these practitioner’s services are not under the control of a Joint Commission accredited organization, all LIPs who will be providing services under this contract will be permitted to do so only after being granted privileges at the hospital through the mechanisms established in this manual.
11.3 Contract Services/Department or Service Closure
11.3.1 The membership and privileges on the Medical Staff of any practitioner who has a
contractual relationship with the System or with an entity that has a contractual relationship with the System to provide professional services to patients shall be subject to those provisions contained in said contract with regard to the termination of Medical Staff membership and privileges upon the expiration, lapse, cancellation or termination of the contract. If the contract so provides, the affected practitioner shall have no right to a hearing regarding termination of Medical Staff membership or privileges.
80
11.3.2 In the event a hospital Department is closed, discontinued or provided through an exclusive contract, such establishment shall not adversely impact the ability of any physician to continue to maintain clinical membership and exercise privileges in existence at the time of such closure, discontinuance or exclusive contract. Initial applications for Medical Staff membership and privileges will not be extended, provided, accepted, processed or approved to or from physicians unless they are joining groups who are actively contracted for exclusively contracted services.
11.3.3 In the event the Board determines that a patient care service shall be closed,
discontinued, or provided through an exclusive contract, such action shall require approval by the affected FMEC.
Both parties agree that any Department or service closure shall occur solely so that
the health and wellbeing of the patients and the best interests of the hospital under these Bylaws may be served at all times. Notwithstanding any other provision in the Bylaws, if the Board and the affected FMEC are unable to agree upon the closure of a Department or service, the matter shall undergo the conflict resolution process set forth in Part I, Section 9 of these Bylaws.
If the parties are still in disagreement regarding the closure of a Department or
service upon completion of the conflict resolution process, the parties shall engage in mediation in accordance with the procedures set forth by the American Health Lawyers Association’s Alternative Dispute Resolution Service or another independent mediation service mutually agreeable to the parties. In the event the Board and FMEC are at impasse at mediation and conflict remains, the Board and the FMEC retain the right to seek a resolution through litigation. Further, the Board shall not close a Department or service for a period of three months following impasse at mediation.
11.4 Qualifications
11.4.1 A practitioner who is or will be providing specified professional services pursuant to
a contract or a letter of agreement with the Health System must meet the same qualifications, must be processed in the same manner, and must fulfill all the obligations of his appointment category as any other applicant or staff practitioner.
11.5 The terms of the Medical Staff Bylaws will govern disciplinary action taken by or
recommended by the FMEC.
11.6 Effect of Contract or Employment Expiration or Termination
11.6.1 The effect of expiration or other termination of a contract upon a practitioner’s staff appointment and clinical privileges will be governed solely by the terms of the practitioner’s contract with the System. If the contract or the employment agreement is silent on the matter, then contract expiration or other termination alone will not affect the practitioner’s staff appointment status or clinical privileges.
SECTION 12 MEDICAL ADMINISTRATIVE OFFICERS
12.1 A Medical Administrative Officer is a practitioner engaged full or part- time by the hospital in an administratively responsible capacity, whose activities may also include clinical responsibilities such as direct patient care, teaching, or supervision of the patient care activities of other practitioners under the officer’s direction.
81
12.2 Each Medical Administrative Officer must achieve and maintain Medical Staff appointment
and clinical privileges appropriate to his clinical responsibilities and discharge staff obligations appropriate to his staff category in the same manner applicable to all other staff members.
12.3 Effect of removal from office or adverse change in appointment status or clinical privileges:
12.3.1 Where a contract exists between the officer and the Health System, its terms
govern the effect of removal from the Medical Administrative Office on the officer’s staff appointment and privileges and the effect an adverse change in the officer’s staff appointment or clinical privileges has on his remaining in office.
12.3.2 In the absence of a contract or where the contract is silent on the matter, removal
from office has no effect on appointment status or clinical privileges. The effect of an adverse change in appointment status or clinical privileges on continuance in office will be determined by the Board.
12.3.3 A Medical Administrative Officer has the same procedural rights as all other staff
members in the event of an adverse change in appointment status or clinical privileges unless the change is, by contract a consequence of removal from office.
82
83
Lee Memorial Hospital
Medical Staff
Bylaws
Adopted: May 28, 2009 Revision approved by BOD June 24, 2010
Revision approved by BOD August 26, 2010 Revisions approved by BOD June 16, 2011
Revisions approved by BOD December 6, 2012
1
TABLE OF CONTENTS PART 1: GOVERNANCE 6 SECTION 1 MEDICAL STAFF PURPOSE & AUTHORITY 6 1.1 Purposes 6 1.2 Authority 6 1.3 Medical Staff (Term) 6 SECTION 2 MEDICAL STAFF MEMBERSHIP 7 2.1 Nature of Medical Staff Membership 7 2.2 Qualifications for Membership 7 2.3 Nondiscrimination 7 2.3.1 No Automatic Entitlement 7 2.4 Conditions and Duration of Appointment 7 2.5 Medical Staff Membership and Clinical Privileges 8 2.6 Medical Staff Members’ Responsibilities 8 2.7 Basic Responsibilities of Applicants and Appointees 8 2.8 Member Rights 11 2.9 Medical Staff Dues and Assessments 11 2.10 Conflict of Interest 12 SECTION 3 CONFIDENTIALITY, IMMUNITY AND RELEASES 12 3.1 Confidentiality 12 3.2 Immunity 13 3.3 Releases 14 SECTION 4 CATEGORIES OF THE MEDICAL STAFF 14 4.1 Active Category 14 4.2 Associate Category 15 4.3 Honorary Category 16 SECTION 5 OFFICERS OF THE MEDICAL STAFF 16 5.1 Officers of Medical Staff and FMEC at-Large Members 16 5.2 Qualifications of Officers and FMEC at-Large Members 16 5.3 Election of Officers and FMEC at-Large Members 16 5.4 Terms of Office 17 5.5 Vacancies of Office 17 5.6 Duties of Officers and FMEC at-Large Members 17 5.7 Removal and Resignation of Officer or FMEC at-Large Members 19 SECTION 6 MEDICAL STAFF ORGANIZATION 20 6.1 Departments 20 6.2 Qualifications, Selection, Term, Removal and Responsibility of Department Chair 21 6.3 Assignment to Department 23 SECTION 7 MEDICAL STAFF GOVERNANCE COMMITTEES 23
2
7.1 Designation of the LMHS MS Physician Leadership Council (PLC) 23 7.2 Composition of the LMHS PLC 23 7.3 Staff Functions 25 7.4 Facility Medical Executive Committee (FMEC) (Composition, Selection and Tenure) 25 7.5 Duties and Responsibilities of the FMEC’s 25 7.6 System Medical Staff Committees 27 7.6.1 Purpose 27 7.6.2 Organization to Perform Functions 27 7.6.2.1 System Credentialing/Privileging Committee 27 7.6.2.2 System Medical Staff Quality Committee 27 7.6.2.3 System Practitioner Resource Committee 27 7.6.2.4 System Bylaws Committee 28 7.6.2.5 System Emergency Services Committee 29 7.6.3 Composition & Meetings of System MS Committees 29 7.7 Facility Medical Staff Committees 30 7.7.1 Purpose 30 7.7.2 Standing Facility Medical Staff Committees 30 SECTION 8 MEDICAL STAFF MEETINGS 31 8.1 General Medical Staff Meetings 31 8.2 Departments, Sections and Committee Meetings 31 8.3 Special Meetings of Departments, Sections and Committees 31 8.4 Quorum 31 8.5 Attendance Requirements 32 8.6 Participation by Administration 32 8.7 Robert’s Rules of Order 32 8.8 Notice of Meetings 33 8.9 Action of PLC, FMEC, General Medical Staff, Department, Section or Committee 33 8.10 Rights of Ex Officio Members 33 8.11 Minutes 33 SECTION 9 DECISION MAKING METHODS AND CONFLICT RESOLUTION 33 SECTION 10 REVIEW, REVISION ADOPTION AND AMENDMENT 34 10.1 Medical Staff Responsibility 34 10.2 Methods of Amendment and Adoption to these Bylaws 35 10.3 Methods of Amendment and Adoption to any Medical Staff Rules, Regulations and Policies 35 Appendix A PRINCIPLES OF MEDICAL ETHICS 37 PART II: INVESTIGATIONS, CORRECTIVE ACTION, HEARING AND APPEAL PLAN 39 SECTION 1 ROUTINE CORRECTIVE ACTION & INVESTIGATIONS 39 1.1 Progressive Intervention 39 1.2 Basis for Routine Corrective Action 39 1.3 Requests and Notices 40 1.4 Investigations 40 1.5 FMEC Action 41 1.6 Notice of FMEC Action 42 1.7 Board of Directions Action 42
3
SECTION 2 EMERGENCY CORRECTIVE ACTION/PRECAUTIONARY SUSPENSION OF CLINICAL PRIVILEGES 42 2.1 Basis for Emergency Corrective Action/Precautionary Suspension 42 2.2 Notice of Emergency Corrective Action/Precautionary Suspension 42 2.3 FMEC Procedure 43 2.4 Provision of Patient Care 43 2.5 Recission of Emergency Corrective Action/Precautionary Suspension 43 SECTION 3 AUTOMATIC SUSPENSION AND TERMINATION 43 3.1 Basis for Automatic Suspension and Termination 43 3.1.1 Loss of License 43 3.1.2 Residence or Office Outside Lee County 43 3.1.3 Lack of Active Practice 44 3.1.4 Criminal Conviction 44 3.1.5 Loss or Restriction of DEA Certificate 44 3.1.6 Exclusion From Federal or State Health Care Programs 44 3.1.7 Failure to Pay Fees and Assessments 44 3.1.8 Failure to Provide Requested Information 44 3.1.9 Failure to Request Reappointment or Provide Requested Information Related to Reappointment 45 3.1.10 Failure to Request Reinstatement Following Leave of Absence 45 3.1.11 Failure to Complete Medical Records 45 3.1.12 Failure to Comply with Special Meeting Attendance Requirements 45 3.2 Right to Limited Hearing for Automatic/Voluntary Suspension and Termination 45 SECTION 4 HEARING AND APPEAL PROCEDURES 46 4.1 Grounds for Hearing 46 4.2 Notice of Recommendation 46 4.3 Request for Hearing 47 4.4 Preliminary Interview 47 SECTION 5 FAIR HEARING PROCEDURE 47 5.1 System Representative, Hearing Panel and Hearing Officer 47 5.1.1 System Representative 48 5.1.2 Hearing Panel 48 5.1.3 Hearing Officer – Qualifications & Authority 48 5.2 Challenge to Hearing Panel Members or Hearing Officer 50 SECTION 6 HEARING PROCEDURES 50 6.1 Provision of Relevant Information 50 6.2 Pre-Hearing Conference 51 6.3 Failure to Appear 51 6.4 Record of Hearing 51 6.5 Rights of Both Sides 52 6.6 Admissibility of Evidence 52 6.7 Burden of Presenting Evidence and Proof 52 SECTION 7 HEARING CONCLUSION, DELIBERATIONS AND RECOMMENDATIONS 52 7.1 Deliberations and Recommendation of the Hearing Panel/Hearing Officer 52 7.2 Disposition of Hearing Panel Report 53
4
SECTION 8 APPEAL PROCEDURE 53 8.1 Request & Time for Appeal 53 8.2 Grounds for Appeal 54 8.3 Time, Place and Notice 54 8.4 Nature of Appellate Review 54 8.4.1 Review Panel 55 8.4.2 Position Papers 55 8.4.3 Oral Argument 55 8.4.4 Recommendation 55 SECTION 9 FINAL DECISION OF THE BOARD 55 SECTION 10 RIGHT TO ONE HEARING AND ONE APPEAL ONLY 55 PART III: CREDENTIALING PROCEDURES 56 SECTION 1 SYSTEM CREDENTIALING/PRIVILEGING COMMITTEE 56 1.1 Organizational Structure 56 1.2 Transition Issues 56 1.3 Purpose of the System Credentialing/Privileging Committee 56 1.4 Composition of the System Credentialing/Privileging Committee 57 1.5 Duties and Responsibilities of the System Credentialing/Privileging Committee 57 SECTION 2 QUALIFICATIONS FOR MEMBERSHIP AND PRIVILEGES 58 2.1 Qualifications for MS appointment, reappointment or clinical privileges 58 2.1.15 Exceptions 58 SECTION 3 PRE-APPLICATION PROCESS 60 SECTION 4 INITIAL APPOINTMENT PROCESS 61 4.1 Completion of Application 61 4.2 Applicant’s Attestation, Authorization and Acknowledgement 63 4.3 Application Evaluation 64 4.3.1 Expedited Credentialing 64 4.3.2 Applicant Interview 64 4.3.3 Department Chair Action 64 4.3.4 MS System Credentialing/Privileging Committee Action 65 4.3.5 FMEC Action 66 4.3.6 Applicants Applying to Multiple Facilities 66 4.3.7 Board Action 66 4.3.8 Notice of Final Decision 67 4.3.9 Periods for Processing 67 SECTION 5 FOCUSED PROFESSIONAL PRACTICE EVALUATION (FPPE) 67 SECTION 6 CRITERIA FOR REAPPOINTMENT 68 6.1 Criteria for Reappointment 68 6.3 Evaluation of Application for Reappointment of Membership and/or Privileges 70
5
SECTION 7 CLINICAL PRIVILEGES 70 7.1 Exercise of Privileges 70 7.2 Requests 70 7.3 Basis for Privileges Determination 70 7.4 Special Conditions for Podiatric Privileges 72 7.5 Special Conditions for Residents or Fellows in Training 73 7.6 Special Conditions for the Aging Practitioner 73 7.7 Temporary Privileges 73 7.7.8 Disaster Privileges 75 SECTION 8 PRECEPTORSHIP 76 SECTION 9 REAPPLICATION AFTER MODIFICATIONS OF MEMBERSHIP STATUS OF PRIVILEGES AND EXHAUSTION OF REMEDIES 77 9.1 Reapplication After Adverse Credentials Decision 77 9.2 Request for Modification of Appointment Status or Privileges 77 9.3 Resignation of Staff Appointment or Privileges 77 9.4 Exhaustion of Administrative Remedies 77 9.5 Reporting Requirements 78 SECTION 10 LEAVE OF ABSENCE 78 10.1 Leave Request 78 10.2 Termination of Leave 78 10.3 Failure to Request Reinstatement 78 SECTION 11 PRACTITIONERS PROVIDING CONTRACTED SERVICES 79 11.3 Contract Services/Department or Service Closure 79 11.4 Qualifications 80 11.5 Terms 80 11.6 Effect of Contract or Employment Expiration or Termination 80 SECTION 12 MEDICAL ADMINISTRATIVE OFFICERS 80
6
PART 1: GOVERNANCE
SECTION 1 MEDICAL STAFF PURPOSES & AUTHORITY 1.1 Purposes
The purposes of the Medical Staffs of Lee Memorial Health System are to:
1.1.1 Serve as the formal organizational structure of those practitioners granted the privilege of practicing in the hospitals and other facilities of the System.
1.1.2 Serve as the primary means for accountability to the Board for the professional
performance, the quality of medical care provided to patients, and ethical conduct of its members. The Board shall have the ultimate responsibility for the quality of medical care provided to patients and the ultimate authority to approve the granting of privileges, to make appointments and reappointments to membership on the Medical Staffs, and to approve the adoption of Medical Staff Bylaws and Rules and Regulations. Such authority will be exercised based on the standard set forth in Section 1.2.
1.1.3 Provide a means through which members of the Medical Staffs may address with
the Board those aspects of policy that involve professional practice or may affect the care of patients.
1.2 Authority
The Medical Staffs of Lee Memorial Health System are authorized by the Lee Memorial Health System Board of Directors (“the Board”) to exercise such power as is necessary to discharge its responsibilities under these Bylaws consistent with the Bylaws of Lee Memorial Health System. Lee Memorial Health System (“the System” or “the Health System”) includes acute care facilities known as Cape Coral Hospital, Gulf Coast Medical Center, HealthPark Medical Center, Lee Memorial Hospital, and The Children’s Hospital (individually known as “the hospital” and collectively known as “the hospitals”). The Board recognizes that a well-organized, self-governing Medical Staff that provides oversight of care, treatment, and services provided by practitioners with privileges is in the best interest of patients. When acting with respect to matters of the Medical Staff, the Board shall at all times comply with the Medical Staff Bylaws, the Rules and Regulations of the Medical Staff, and applicable law.
1.3 Medical Staff The term “Medical Staff” as used herein shall mean, on a collective basis, those
practitioners who are authorized by the Board to exercise privileges at one or more of the System’s hospitals, and, on a component basis, those practitioners who are authorized by the Board to exercise privileges at a particular system hospital. The latter may be referred to herein as the “Medical Staff of a facility.” The term “he”, “him”, or “his” means of a male or female gender.
7
SECTION 2 MEDICAL STAFF MEMBERSHIP 2.1 Nature of Medical Staff Membership
Membership on the Medical Staff is a privilege that shall be extended only to professionally competent physicians (M.D. or D.O.), dentists, podiatrists and/or psychologists who continuously meet the qualifications, standards, and requirements set forth in these Bylaws and associated policies of the Medical Staff and the hospitals. Medical Staff membership is a privilege and not a right of any practitioner or other person. Medical Staff membership and the exercise of privileges in connection therewith shall be extended only to practitioners who continuously meet the requirements of these Bylaws. The Board makes decisions regarding Medical Staff matters, based on Medical Staff recommendations, in accordance with these Bylaws. Membership on the Medical Staff shall confer on the Medical Staff member only such rights as set forth in the Bylaws. No person shall admit patients to a System hospital unless he is appointed to the Medical Staff of such hospital. For purposes of these Bylaws, “membership in” is used synonymously with “appointment to” the Medical Staff. Medical Staff members granted membership and privileges at a hospital, which has services and facilities that are provider based to a main provider and are authorized to exercise those privileges at the main provider.
2.2 Qualifications for Membership
2.2.1 The qualifications for Medical Staff membership are delineated in Part III of these Bylaws (Credentials Procedures).
2.3 Nondiscrimination
2.3.1 No Automatic Entitlement
No person shall be automatically entitled to Medical Staff membership or to the exercise of clinical privileges merely because he is licensed to practice, is a member of any professional organization, is certified by any board, or had held (but not currently) Medical Staff membership or clinical privileges at a System hospital or at any other health care facility. The burden shall be on the applicant to establish his qualifications. Acceptance of Medical Staff membership or exercise of clinical privileges shall constitute an agreement to strictly abide by these Bylaws, the applicable Medical Staff Policies, the Rules and Regulations, and the Principles of Medical Ethics set forth in Appendix A hereof and all other appropriate ethical standards governing the practitioner’s practice. No person shall be initially appointed to the Medical Staff or granted clinical privileges if the hospitals are unable to provide adequate facilities and supportive services for the applicant and his patients. Medical Staff membership shall not be denied based on sex, race, creed, color, national origin, religion, marital status, age, disability, or economic credentialing, at initial appointment or reappointment.
2.4 Conditions and Duration of Appointment
2.4.1 The Board shall act on appointment and reappointment only after the Medical Staff has had an opportunity to submit a recommendation from the Facility Medical Executive Committee (FMEC). Appointment and reappointment to the Medical Staff shall be for no more than twenty-four (24) calendar months.
8
2.5 Medical Staff Membership and Clinical Privileges
2.5.1 Requests for Medical Staff membership and/or clinical privileges will be processed only when the potential applicant meets the current minimum qualifying criteria recommended by the System Credentialing/Privileging Committee and FMEC and approved by the Board. Membership and/or privileges will be granted and administered as delineated in Part III (Credentials Procedures) of these Bylaws, including but not limited to, Part III, Sections 3 and 11.3 regarding Contracted practitioners.
2.6 Medical Staff Members’ Responsibilities
2.6.1 Duties of Appointees Appointment to the Medical Staff shall require that each practitioner assume such reasonable duties and responsibilities, as the Medical Staff shall require.
2.7 Basic Responsibilities of Applicants and Appointees The following basic responsibilities and requirements shall be applicable to every applicant
and appointee for Medical Staff appointment or reappointment as a condition of consideration of such application and as a condition of continued Medical Staff appointment if granted:
2.7.1 an obligation to provide for appropriate and timely care and supervision to all
patients in the hospital for whom the individual has responsibility (Standard of Care);
2.7.2 an agreement to abide by all Bylaws, Rules and Regulations and Policies of the Medical Staff and the Hospital, as shall be in force during the time the individual is appointed to the Medical Staff (Conformance to Rules);
2.7.2.1 provide a current cell phone number and email address to be used for
emergency or disaster purposes in accordance with Medical Staff Services Dept. policy.
2.7.3 an agreement to accept committee assignments and such other reasonable duties
and responsibilities as shall be assigned (Committee Assignments);
2.7.4 to not participate in illegal fee splitting or other illegal inducements relating to patient referral;
2.7.5 to promptly notify Medical Staff Services (Notification Requirements);
2.7.5.1 if his professional license in any state is suspended or revoked; 2.7.5.2 of the imposition of any conditions by any state licensing authority on his
continued ability to practice his profession, including probation or limitations on the scope of practice;
2.7.5.3 of the loss or restriction of Medical Staff membership or privileges at any
other health care facility;
2.7.5.4 if his Drug Enforcement Agency (DEA) license number is suspended, revoked or voluntarily relinquished;
9
2.7.5.5 of any change in eligibility for participation in Federal Health Care Programs including any sanctions imposed or recommended by the Federal Department of Health and Human Services, Florida State Agency for Health Care Administration and/or the receipt of any citation and/or quality denial letter concerning alleged quality problems in patient care;
2.7.5.6 if the practitioner enters, participates in, or against medical advice, leaves
or refuses any program of treatment prescribed or required by the Florida Physicians’ Recovery Network;
2.7.5.7 if the practitioner is admitted for, seeks, or is undergoing treatment for
substance or alcohol abuse or a behavioral health problem. “Substance abuse” shall include but not limited to, use or ingestion of illegal drugs, or use or ingestion of prescription medications not prescribed in the ordinary course of treatment of injury or disease. “Behavioral health problem” shall mean any condition or disease of a psychiatric or psychological nature which, in the opinion of a qualified psychiatrist, adversely affects the practitioner’s ability to care for patients or practice his profession in accordance with the applicable prevailing standard of care; or
2.7.5.8 the conviction of, or pleading of nolo contendere to, a crime constituting a
felony in any jurisdiction. 2.7.6 to abide by generally recognized ethical principles applicable to the applicant’s or
appointee’s profession and by the code of ethics set forth in Appendix A (Ethics);
2.7.7 to respect the confidentiality of all information obtained in connection with his responsibility as a Medical Staff member and comply with the requirements of the Health Insurance Portability and Accountability Act (HIPAA) (Confidentiality);
2.7.8 to provide medical consultation in a timely fashion in accordance with all
applicable Rules & Regulations and Medical Staff Policies (Consultation);
2.7.9 to participate in the monitoring and evaluation activities of Clinical Sections and cooperate with other members of the Medical Staff and the System, in programs designed to improve the quality of care to reduce or eliminate waste in the use of scarce System resources and to reduce the risk of injury to patients and others in the provision of care (Quality Review Participation);
2.7.10 to complete in a timely and legible manner the medical records and other required
records for all patients as required by these Bylaws, applicable Rules and Regulations, and other applicable policies of the hospital (Medical Records);
2.7.11 to pay promptly any applicable Medical Staff assessments and dues (Dues); 2.7.12 to participate in continuing education programs for the benefit of the applicant or
appointee and for the benefit of other professionals and System hospital personnel (CME);
2.7.13 to authorize the release of all information necessary for an evaluation of the
individual’s qualifications for initial or continued appointment, reappointment, and/or clinical privileges (Release of Information);
10
2.7.14 to submit to an evaluation of his physical and/or mental health status by a
physician or physicians acceptable to the FMEC or Board, whenever the FMEC or Board has reason to question the physical and/or mental health status of the practitioner, as a prerequisite to further consideration of his application for appointment or reappointment, the exercise of previously granted privileges or maintenance of his Medical Staff appointment (Physical/Mental Exam);
2.7.15 to recognize the obligations established to fulfill the hospital’s responsibilities
under the Emergency Medical Treatment and Women in Labor Act (EMTALA), the Access to Emergency Services and Care Act and/or other applicable regulations, requirements or standards and to share in the responsibility for providing physician coverage on an emergency basis in the Emergency Department, in accordance with the provisions of the Medical Staff Bylaws and all applicable facility-specific Rules & Regulations and Medical Staff Policies (On Call Coverage);
2.7.16 to provide his professional services to hospitalized or emergency room patients
covered by Medicaid and similar programs of indigent care, or such patients without personal physicians or insurance coverage, in accordance with Medical Staff Rules & Regulations adopted by the FMEC delineating the responsibility to provide services to those patients (Services to Indigent Patient);
2.7.17 provide proof of financial responsibility to pay claims or costs associated with the
rendering of, or failure to render, medical care or services in compliance with Florida law governing the practitioner’s license to practice in the State of Florida. Proof of financial responsibility shall be provided at the time of initial appointment and on reappointment, at the time the practitioner changes the method of meeting his financial responsibility and at any other time on the request of Medical Staff Services (Financial Responsibility);
2.7.18 to behave in a professional and civil manner and conduct himself in a manner
conducive to excellent patient care and to work cooperatively with Medical Staff appointees, and with other health care professionals, and Hospital personnel, so as not to adversely affect patient care. This requirement is not in any way intended to interfere with a practitioner’s right: (1) to express opinions freely and to support positions whether or not they are in dispute with those of other Medical Staff members; (2) to engage in honest differences of opinion with respect to diagnosis and treatment; or (3) to engage in a good faith criticism of others. The following types of behavior, however, which constitute some examples of an inability to interact on a professional basis with others or to behave in a professional and civil manner, are deemed unacceptable for a member of the Medical Staff:
2.7.18.1 conduct that reasonably could be characterized as sexual and/or racial
harassment;
2.7.18.2 threats of physical assault or actual physical assault, harassment, or the placing of others in fear by engaging in threatening behavior;
2.7.18.3 the unnecessary, unwarranted and unjustifiable knowing use of loud,
profane or abusive language directed toward members of the Medical Staff, patient and others; or
11
2.7.18.4 written or oral statements that constitute the intentional expression of
falsehoods, or constitute deliberately disparaging statements made with reckless disregard for their truth or for the reputation and feelings of others;
2.7.18.5 doing anything of a similar nature that the practitioner has been warned
not to do by the President of the Medical Staff or FMEC Committee (Professional and Civil Behavior);
2.7.19 duty to give notice if the practitioner is not actively engaged in the practice of his
profession in Lee County (Lack of Active Practice);
2.7.20 duty to give notice if practitioner does not maintain a full-time residence and office in Lee County, unless the residence and office requirements have been waived in accordance with these Bylaws (Residence or Office in Lee County).
2.8 Member Rights
The following basic rights shall apply to Medical Staff practitioners: 2.8.1 Each Medical Staff member, in the active category, has the right to a meeting with
the FMEC and/or the Physician Leadership Council (PLC) on matters relevant to the responsibilities of the FMEC and/or the PLC, provided that the practitioner has attempted to resolve a matter of concern after working with his Department Chair or other appropriate hospital and/or Health System Medical Staff leader(s). Upon written notice to the President of the Medical Staff, two (2) weeks in advance of a regular meeting, the active Medical Staff member may meet with the FMEC and/or the PLC to discuss the issue.
2.8.2 Each Medical Staff member, in the active category, has the right to initiate a recall
election of a Medical Staff officer by following the procedure outlined in Section 5.7 of these Bylaws regarding removal and resignation from office.
2.8.3 Each Medical Staff member, in the active category, may request a special meeting
of the Medical Staff, upon presentation of a petition, stating the purpose of the meeting and signed by ten (10) members of the Active Medical Staff. The FMEC shall schedule a special meeting for the specific purposes addressed by the petitioners in accordance with Section ten (10) of these Bylaws. No business other than that detailed in the petition may be transacted.
2.8.4 An applicant or an individual holding a Medical Staff appointment shall be entitled to
request a hearing/appeal pursuant to the conditions and procedures described in Part II of these Bylaws (Investigations, Corrective Action, Hearing and Appeal Plan).
2.8.5 All other rights as specified by these Bylaws.
2.9 Medical Staff Dues and Assessments
2.9.1 Annual Medical Staff dues, if any, shall be determined by the FMEC. Failure of a Medical Staff member to pay dues shall be considered a voluntary resignation from the Medical Staff. The FMEC may pass policies from time to time that exempt certain categories of membership or members holding specified leadership positions from payment of dues. The FMEC shall authorize the use of Medical Staff dues.
12
2.9.2 Medical Staff System-wide assessments, such as a library assessment, shall be determined by the PLC, on behalf of the FMECs. Failure of a Medical Staff member to pay any assessment(s) shall be considered a voluntary resignation from the Medical Staff. The PLC, on behalf of the FMECs, may pass policies from time to time that exempt certain categories of membership or members holding specific leadership positions from payment of such assessment(s).
2.9.3 The PLC, on behalf of the FMECs, shall authorize the use of Medical Staff
assessments consistent with the purpose of the assessment. 2.10 Conflict of Interest
2.10.1 In any instance where an officer, committee Chair, or member of any Medical Staff committee has, or reasonably could be perceived to have a conflict of interest, or to be biased in any matter involving another Medical Staff appointee or any other matter that comes before such individual or committee, or in any instance where any such individual brought the complaint against that practitioner, such individual shall not participate in the discussion or voting on the matter and shall be excused from any meeting during that time, although that individual may be asked and may answer, any questions concerning the matter before leaving. As a matter of procedure, the Chair of that committee designated to review the matter shall inquire, prior to any discussion of the matter, whether any member has any conflict of interest or bias. The existence of a potential conflict of interest or bias on the part of any committee member may be called to the attention of the Chair by any committee member with knowledge of the matter.
2.10.2 In any instance where an officer, committee Chair, or member of any Medical Staff
committee has a conflict of interest in any matter that comes before such individual or committee, such individual has the right to abstain or recuse himself from voting on such matter. Such abstention or recusal shall not prohibit such individual from providing factual information or participating in discussion on such matter. If an individual is requested to abstain or recuse himself and refuses to do so, the potential conflict of interest issue will be reviewed and resolved by the next highest authority as outlined in these Bylaws. As a matter of procedure, the Chair of that committee designated to review the matter shall inquire, prior to any discussion of the matter, whether any member has any conflict of interest or bias. The existence of a potential conflict of interest or bias on the part of any committee member may be called to the attention of the Chair by any committee member with knowledge of the matter.
2.10.3 Assurance of a conflict of interest or bias can be determined by a majority vote of
the members of the committee where a quorum is present. SECTION 3 CONFIDENTIALITY, IMMUNITY AND RELEASES 3.1 Confidentiality
Information with respect to any practitioner or regarding any other subject discussed, submitted, collected or prepared by any representative of the Lee Memorial Health System, including officers or members of organized committees of the Health System’s Medical Staffs, or any other healthcare professional, healthcare facility, organization or Medical Staff, for the purpose of achieving and maintaining the quality of care, reducing morbidity or mortality or contributing to clinical research shall, in accordance with Florida law,
13
be confidential and shall not be disseminated or used for any purpose other than the foregoing. Such information shall not be deemed a part of the patient medical record, and shall not be filed therein. Each individual or committee member participating in such activities shall agree to make no disclosures of any such information except as authorized, in writing, by the Chief Executive Officer (CEO) or by legal counsel to the hospitals. Any breach of confidentiality by an individual or committee member may result in a professional review action, and/or may result in appropriate legal action to ensure that confidentiality is preserved, including application to a court of law for injunctive or other relief.
3.2 Immunity 3.2.1 Any Medical Staff officer, Department Chair, Section Chief, committee Chair,
committee member, and individual staff appointee who acts in good faith for and on behalf of any System hospital in discharging duties, functions or responsibilities stated in these Medical Staff Bylaws, applicable Policies, and/or Rules and Regulations shall be afforded protection by the Board of Directors to the fullest extent permitted by law in accordance with written policies adopted by the Board. Individuals and organizations independent of the Medical Staff or any of its members who may be engaged by the Health System to perform the review, analysis and evaluation of the qualification and/or performance of practitioners with membership and/or privileges on the Medical Staff are afforded protection by the Board of Directors in accordance with written policies adopted by the Board, provided such individuals or organizations act in good faith.
3.2.2 To the fullest extent permitted by law, each applicant and appointee to the Medical
Staff releases from any and all liability, and extends absolute immunity to System hospitals and the Board and its individual members, and to the System’s authorized representatives and agents, with respect to any acts, communications or documents, recommendations or disclosures involving the applicant or appointee, concerning the following:
3.2.2.1 applications for appointment or clinical privileges, including temporary
privileges and/or emergency privileges;
3.2.2.2 evaluations concerning reappointment or changes in clinical privileges;
3.2.2.3 proceedings for suspension or reduction of clinical privileges or for revocation of Medical Staff appointment, or any other disciplinary sanction;
3.2.2.4 summary suspension;
3.2.2.5 hearings and appellate reviews; 3.2.2.6 medical/surgical care evaluations; 3.2.2.7 utilization reviews;
3.2.2.8 other activities relating to the quality of patient care or professional
conduct;
3.2.2.9 matters of inquiries concerning the applicant’s or appointee’s professional qualifications, credentials, clinical competence, character, mental or emotional stability, physical condition, ethics or behavior; and/or
14
3.2.2.10 any other matter that directly or indirectly might relate to the applicants or
appointee’s competence, and/or to patient care.
3.3 Releases
3.3.1 Authorization to Obtain Information
The applicant or appointee specifically authorizes the Medical Staff and its authorized representatives to consult with any third party who may have information bearing on the individual’s professional qualifications, credentials, clinical competence, character, mental or emotional stability, physical condition, ethics, behavior, or any other matter reasonably having a bearing on the applicant’s or appointee’s satisfaction of the criteria for initial and continued appointment to the Medical Staff. This authorization also covers the right to inspect, or obtain all communications, reports, records, statements, documents, recommendations or disclosures of said third parties that may be relevant to such questions. The individual also specifically authorizes said third parties to release said information to the Medical Staff and its authorized representatives upon request.
3.3.2 Legal Effect
The confidentiality provisions and protections described in this Section shall not limit
or supersede any protection or immunity afforded by law. SECTION 4 CATEGORIES OF THE MEDICAL STAFF 4.1 Active Category
4.1.1 Qualifications: Members of this category must have served on the Medical Staff, maintained a residence and office in Lee County (4.1.3.3) for one year, and be involved in twenty-four (24) patient contacts per year (i.e., a patient contact is defined as an inpatient admission, consultation, or an inpatient or outpatient surgical procedure) at the hospital except as expressly waived for practitioners with at least twenty (20) years of service in the active category or for those physicians who document their efforts to support the hospital’s patient care mission to the satisfaction of the FMEC.
In the event that a member of the active category does not meet the qualifications for reappointment to the active category, and if the member is otherwise abiding by all Bylaws, Rules and Regulations, and policies of the Medical Staff and hospital, the member may be appointed to another Medical Staff category if he meets the eligibility requirements for such category.
4.1.2 Prerogatives: Members of this category may:
4.1.2.1 Attend Medical Staff/Department meetings of which he is a member and any Medical Staff or hospital education programs;
4.1.2.2 Vote on all matters presented by the Medical Staff, Department, and
committee(s) to which the member is assigned;
15
4.1.2.3 Hold office and sit on or be the Chair of any committee in accordance with any qualifying criteria set forth elsewhere in the Medical Staff Bylaws or Medical Staff policies.
4.1.3 Responsibilities: Members of this category shall:
4.1.3.1 Contribute to the organizational and administrative affairs of the Medical Staff;
4.1.3.2 Actively participate as requested or required in activities and
functions of the Medical Staff, including quality/performance improvement and peer review, credentialing, risk and utilization management, medical records completion, monitoring activities and in the discharge of other Medical Staff functions as may be required by the FMEC;
4.1.3.3 The one-year residence and office requirement may be explicitly
waived by majority vote of the FMEC, on written request of the practitioner, at the time of appointment, if the practitioner affirmatively demonstrates to the FMEC in writing that the quality of patient care is not likely to be affected by his not living and having an office in Lee County and that the practitioner’s obligation to provide emergency room call and to attend hospitalized patient can be met.
4.1.3.4 Fulfill or comply with any applicable Medical Staff or hospital
policies or procedures as requested by the FMEC. 4.1.3.5 Fulfill basic responsibilities and requirements set forth in Section
2.7 of this Part, including but not limited to, Emergency Department call responsibilities in accordance with facility specific rules and regulations, unless exempted from Emergency Department call responsibilities as defined by their Section (if applicable) or Department and approved by the FMEC. In the event facility specific rules and regulations require physicians to accept emergency department referrals to the physician’s office, Lee Memorial Health System will provide facility support and services for such patients.
4.2 Associate Category 4.2.1 Qualifications: The associate category is reserved for Medical Staff members who
do not meet the eligibility requirements for the active category or choose not to pursue active status. This category includes physicians during their first year on the Medical Staff, as well as low volume/no volume physicians.
4.2.2 Prerogatives: Members of this category may:
4.2.2.1 Attend general Medical Staff Department meetings of which he is a member and any Medical Staff or hospital education programs.
4.2.2.2 Members of the associate category may not vote on matters at general
Medical Staff, Department meetings or be an officer of the Medical Staff.

16
4.2.2.3 Members of the associate category may serve on facility and system Medical Staff committees, other than the FMEC, and may vote on matters that come before such committees.
4.2.3 Responsibilities: Members of this category shall have the same responsibilities as
active category members, as set forth in Section 4.1 and Section 2.7 of this Part.
4.3 Honorary Category 4.3.1 The Honorary category is restricted to those individuals recommended by the FMEC
and approved by the Board. Appointment to this category is entirely discretionary and may be rescinded at any time. Members of the honorary category shall consist of those members who have retired from active hospital practice, who are of outstanding reputation, and have provided distinguished service to the hospital. They may attend general Medical Staff meetings, Department meetings, continuing medical education (CME) activities, and may be appointed to committees. They shall not hold clinical privileges, hold office or be eligible to vote.
SECTION 5 OFFICERS OF THE MEDICAL STAFF 5.1 Officers of the Medical Staff and FMEC at-large Members: Each hospital is
authorized to have the following officers:
5.1.1 Facility President of the Medical Staff 5.1.2 Facility President-Elect of the Medical Staff
5.1.3 Facility Secretary/Treasurer 5.1.4 Facility Past President of the Medical Staff
5.2 Qualifications of Officers and FMEC at-large Members 5.2.1 Officers must be members in good standing of the active category for at least three
(3) years or actively involved in patient care in the community, have previously served in a significant leadership position on a Medical Staff, (i.e. Department Chair, Section Chief or Committee Chair), indicate a willingness and ability to serve, have no pending adverse recommendations concerning Medical Staff appointment or clinical privileges, have a history of attendance at continuing education programs (provided by the System) relating to Medical Staff leadership and/or be willing to do so during their term or office, have demonstrated an ability to work well with others, be in compliance with the professional conduct policies of the Medical Staff, and should have excellent administrative and communication skills.
FMEC at large members must be members in good standing of the active category for at least two (2) years or actively involved in patient care in the community.
5.2.2 Officers and FMEC at-large members must disclose leadership positions on another
hospital Medical Staff. 5.3 Election of Officers and FMEC at-large Members 5.3.1 Every year, the FMEC shall appoint a nominations committee chaired by the
immediate Past Facility President of the Medical Staff and comprised of at least
17
five (5) at large members of the active Medical Staff at least ninety (90) days prior to the election. Representatives of administration shall not serve on the nominations committee. Nominations will be solicited from the Medical Staff for consideration prior to the committee meeting. The committee shall offer at least one nominee for each office. Nominations must be announced, and the names of the nominees distributed to all members of the active Medical Staff at least forty-five (45) days prior to the election. A petition signed by at least 20% of the members of the active Medical Staff may also make nominations. Such petition must be submitted to the President of the Medical Staff at least twenty (20) days prior to the election for placement on the ballot.
5.3.2 Officers and FMEC at-large members shall be elected, as needed every year at an
election that takes place at least one (1) month prior to the expiration of the term of the current officers. Only members of the active category shall be eligible to vote. The FMEC will determine the mechanisms by which votes may be cast. The mechanisms that may be considered include written mail ballots; electronic voting via computer, fax, or other technology for transmitting the members’ voting choices. No proxy voting will be permissible. The nominee receiving the greatest number of votes will be elected. In the event of a tie vote, the Medical Staff support professional will arrange for a repeat vote(s) until one candidate receives a greater number of votes.
5.3.3 Medical Staff members will be notified of the election date and final slate of
nominees ten (10) days prior to the election. 5.4 Terms of Office 5.4.1 Officers and FMEC at-large members serve terms as follows: 5.4.1.1 Facility President-Elect of the Medical Staff – one (1) year 5.4.1.2 Facility President of the Medical Staff – two (2) years 5.4.1.3 Facility Past President of the Medical Staff – one (1) year 5.4.1.4 Facility Secretary/Treasurer – one (1) year 5.4.1.5 FMEC Members-at-Large – two (2) years 5.4.2 Officers shall take office October 1. Officers may be re-elected to office except that
the Facility President of the Medical Staff may not be re-elected for successive terms.
5.5 Vacancies of Office 5.5.1 The FMEC shall fill vacancies of office during the Medical Staff year, except the
office of the Facility President of the Medical Staff. If there is a vacancy in the office of the Facility President of the Medical Staff, the
Facility President-Elect of the Medical Staff shall serve the remainder of the term. 5.6 Duties of Officers and FMEC At-Large Members 5.6.1 Facility President of the Medical Staff – The Facility President shall represent the
interests of the Medical Staff to the FMEC and the Board. The Facility President will fulfill the duties specified in Section 5.6.2 of these Bylaws, as well as additional duties as reasonably requested by the FMEC in order to implement and/or enforce all provisions of the Bylaws and the interests of the Medical Staff.
5.6.2 Responsibilities of the Facility President of the Medical Staff
18
The Facility President of the Medical Staff is the primary elected officer of the
Medical Staff and is the Medical Staff’s advocate and representative in its relationships to the Board, the Facility Chief Administrative Officer (CAO) and the Health System administration. The Facility President of the Medical Staff, jointly with the FMEC, provides direction to and oversees Medical Staff activities related to assessing and promoting continuous improvement in the quality of clinical services and all other functions of the Medical Staff as outlined in the Medical Staff Bylaws, Rules and Regulations and Policies. Specific responsibilities and authority include:
5.6.2.1 Call and preside at all general and special meetings of the Medical Staff; 5.6.2.2 Serve as Chair of the FMEC, a voting member of the PLC and as ex-officio
member of all other Medical Staff committees without vote, and to participate as invited by the Board and the Facility CAO on hospital or Board committees;
5.6.2.3 Shall not vote at the FMEC, unless their vote is needed to break a tie vote; 5.6.2.4 Enforce Medical Staff Bylaws, Rules and Regulations and Medical
Staff/hospital/System Policies; 5.6.2.5 Except as stated otherwise, appoint committee Chairs and all members of
Medical Staff standing and ad hoc committees; in consultation with hospital administration, appoint Medical Staff members to appropriate hospital committees, in consultation with the Chair of the Board, appoint the Medical Staff members to appropriate Board committees when those are not designated by position or by specific direction of the Board or otherwise prohibited by state law;
5.6.2.6 Support and encourage Medical Staff leadership and participation on
interdisciplinary clinical performance improvement activities; 5.6.2.7 Report to the Board, through the PLC, the FMEC’s recommendations
concerning appointment, reappointment, delineation of clinical privileges or specified services and corrective action with respect to practitioners or allied health practitioners who are applying for appointment or privileges, or who are granted privileges or providing services in the hospital;
5.6.2.8 With the support of the facility Credentials/Privileging Committee and the
System Credentialing/Privileging Committee, evaluate and periodically report to the FMEC, PLC and the Board regarding the effectiveness of the credentialing and privileging processes;
5.6.2.9 Review and enforce compliance with standards of ethical conduct and
professional demeanor among the members of the Medical Staff in their relations with each other, the Board, hospital/System management, other professional and support staff, and the community the hospital serves;
5.6.2.10 Communicate and represent the opinions and concerns of the Medical
Staff and its individual members on organizational and individual matters affecting hospital operations to the Facility CAO, the FMEC, PLC and the Board;
19
5.6.2.11 attends Board meetings and Board committee meetings as deemed appropriate by Facility Medical Staff President;
5.6.2.12 ensures that the decisions of the Board are communicated and carried out
within the Medical Staff; 5.6.2.13 performs such other duties, and exercises such authority commensurate
with the office as are set forth in the Medical Staff Bylaws.
5.6.3 Facility President-Elect of the Medical Staff – In the absence of the Facility President, the Facility President-Elect or the Facility Past President shall assume all the duties and have the authority of the Facility President. He shall perform such further duties to assist the Facility President as the Facility President may request from time to time. The Facility President-Elect, upon the end of the term of the Facility President, shall automatically succeed to the office of Facility President.
5.6.4 Facility Secretary/Treasurer – This officer will collaborate with the hospital’s
Medical Staff office, assure maintenance of minutes, attend to correspondence, act as Medical Staff treasurer, and coordinate communication within the Medical Staff. He shall perform such further duties to assist the Facility President as the Facility President may from time to time request.
5.6.5 Facility Past President of the Medical Staff – This officer will serve as a
consultant to the Facility President and the Facility President-Elect as requested by the FMEC and provide feedback to the officers regarding their performance of assigned duties on an annual basis.
He shall perform such further duties to assist the Facility President as the
Facility President may request. He shall serve as a member of the System Credentialing/Privileging Committee.
5.6.6 FMEC at-large members – shall advise and support the Medical Staff officers
and are responsible for representing the needs/interests of the entire Medical Staff and not simply representing the preferences of their own clinical specialty.
5.7 Removal and Resignation of Officer or FMEC At-Large Member 5.7.1 The Medical Staff may remove any facility officer or FMEC at-large member by
petition of 20% of the active Medical Staff members and a subsequent affirmative vote by two-thirds (2/3) of those active Medical Staff members’ casting votes.
5.7.2 Recall of Officers or FMEC at-large members The FMEC may remove any facility Medical Staff officer or FMEC at-large
member for conduct detrimental to the interests of the Medical Staff or if the officer is suffering from a physical or mental infirmity that renders the individual incapable of fulfilling the duties of the office. At least ten (10) days notice prior to the date of the meeting shall be provided, in writing, to the affected officer or FMEC at-large member. The officer or at-large member shall be afforded the opportunity to speak prior to the taking of any vote on such removal. For recall of an officer or at-large member, a two-thirds (2/3) vote of approval is required with three-fourths (3/4) of the FMEC members present and voting. Affected officer or at-large member does not count as quorum and does not vote.
20
5.7.3 Resignation of Officers or FMEC at-large members Any elected officer or FMEC at-large member may resign at any time by giving
written notice to the FMEC. Such resignation takes effect on the date of receipt, when a successor is elected, or any later time specified therein.
SECTION 6 MEDICAL STAFF ORGANIZATION The organized Medical Staff is actively involved in Medical Staff governance, peer review,
credentialing/privileging and communication. Medical Staff members are accountable to the FMEC.
The Medical Staff facility officers (Section 5), Medical Staff governance committees (PLC, Section 7.1 and FMEC, Section 7.4), Department Chairs (Section 6.1), clinical Section Chiefs (Section 6.1.1), hospital (as appropriate) System Medical Staff committee Chairs, (Section 7.6) and facility Medical Staff committee Chairs (Section 7.7) are responsible for working collaboratively to develop a process for communication of Medical Staff functions. Periodic reports, as appropriate, are given to each FMEC, Medical Staff Departments, Medical Staff committees and the PLC as needed to ensure adherence to regulatory requirements and accreditation standards.
Additionally, Medical Staff officers may appoint, in collaboration with the Facility Medical
Director, designated physician leaders to serve on the following Medical Staff committees to help ensure Medical Staff input and oversight with clinical functions such as System Bylaws, Cancer Care, CME/Medical Library, Ethics, Institutional Review, System Credentialing/Privileging, Critical Care, System Emergency Services, Infection Control, Pharmacy and Therapeutics, System Medical Staff Quality, System Practitioner Resource, Trauma Quality, Vascular Lab, in addition to the Children’s Hospital committees (Cancer Care, Ethics, Neonatal Intensive Care Unit (NICU) Pediatric Intensive Care Unit (PICU) Perinatal and Medical Staff Quality and other such functions as determined by the FMEC and/or the PLC.
6.1 Departments The Medical Staff shall be organized as a Departmentalized staff. The current
Departments authorized by the FMECs are Medicine, Surgery, Pediatrics, Obstetrics and Gynecology, Anesthesiology, Pathology, Radiology and Emergency Medicine. Departments fulfill the duties listed in Section 6.2.4 of these Bylaws within a specific hospital or facility and/or across the Health System as necessary. Departments shall meet as frequently as needed to fulfill assigned duties and when requested by the FMEC.
The Medical Staff may create Clinical Sections (as specified in these Bylaws) within
a Department in order to facilitate Medical Staff activities.
6.1.1 Any FMEC may recognize any group of like American Board of Medical Specialties, (ABMS) approved specialties with at least three (3) Medical Staff members or service lines that wish to organize themselves into a Clinical Section. Any Clinical Section, if organized shall not be required to hold regularly scheduled meetings, keep routine minutes, or require attendance. A written report is required only when the Clinical Section is making a formal report. A Clinical Section shall elect a Clinical Section Chief.
21
The Clinical Section Chief is responsible for fulfilling the activities listed in Section 6.1.1.1 - 6.1.1.7 of these Bylaws. The procedure for removal of a Clinical Section Chief shall be the same as set forth in Section 6.2.3 for Department Chair. When a clinical Section is making a formal report, the report shall be submitted to the FMEC documenting the specific position of the clinical Section. The President of the Medical Staff and the Clinical Section Chief (or designee) will decide if the report/issue is placed on the FMEC agenda and whether the Clinical Section Chief (or designee) will attend the FMEC meeting to present the report/issue to the FMEC on that specific report/issue. Clinical Sections are optional and shall exist to perform any of the following activities within a specific facility and/or across Health System facilities as necessary:
6.1.1.1 continuing education/Grand Rounds/discussion of patient care;
6.1.1.2 formulation of ED on-call and inpatient consultation and coverage recommendations; 6.1.1.3 discussion of policies and procedures; 6.1.1.4 discussion of equipment needs; 6.1.1.5 development of recommendations for the Department Chair(s), the
FMECs or the PLC; 6.1.1.6 participation in the development of criteria for clinical privileges
when requested by the System Credentialing/Privileging Committee or FMEC;
6.1.1.7 discussion of a specific issue at the request of the PLC or the
FMEC. The FMEC, with the concurrence of the PLC, may designate new Medical Staff Departments or Clinical Sections or dissolve current Departments or Clinical Sections as it determines will best meet the Medical Staff needs for promoting performance improvement, patient safety, and effective credentialing and privileging.
6.2 Qualifications, Selection, Term, and Removal of Department Chair 6.2.1 Each Department Chair shall serve a term of two (2) years commencing on
October 1 and may be elected to serve successive terms. All Chairs must be members of the active Medical Staff with relevant clinical
privileges and be certified by an appropriate specialty board or have affirmatively established comparable competence through the credentialing process.
6.2.2 Department Chairs and Vice-Chairs will be elected by majority vote of the
active members of the Department, subject to ratification by the FMEC. Each Department shall establish procedures for identifying and electing candidates and these procedures must be ratified by the FMEC.
22
6.2.3 Department Chairs may be removed from office by the FMEC upon receipt of a recommendation of two-thirds (2/3) of the members of the Department or, in the absence of such recommendation, the FMEC may remove a Chair on its own by a two-third (2/3) vote of a majority of members present and voting, if any of the following occurs:
6.2.3.1 The Chair ceases to be a member in good standing of the Medical
Staff; 6.2.3.2 The Chair suffers an involuntary loss or significant limitation of
practice privileges; 6.2.3.3 The Chair fails, in the opinion of the FMEC, to demonstrate to the
satisfaction of the FMEC, PLC or the Board that he is effectively carrying out the responsibilities of the position;
6.2.3.4 If removal is required, a new election will be held according to the
established Departmental procedures. 6.2.4 Department Chairs shall carry out the following responsibilities: 6.2.4.1 to oversee all clinically-related activities of the Department; 6.2.4.2 to oversee all administratively related activities of the Department
otherwise provided for by the Facility; 6.2.4.3 to provide ongoing surveillance of the performance of all individuals
in the Medical Staff Department who have been granted clinical privileges;
6.2.4.4 to recommend to the System Credentialing/Privileging Committee
Medical Staff Department; 6.2.4.5 to recommend clinical privileges for each member of the
Department and other LIPs practicing with privileges within the scope of the Department;
6.2.4.6 to assess and recommend to the FMEC and Facility CAO off-site
sources for needed patient care services not provided by the Medical Staff Department or Facility;
6.2.4.7 to monitor and evaluate the quality and appropriateness of patient
care provided in the Medical Staff Department and to implement action following review and recommendations by the facility Medical Staff peer review/quality committee and/or the FMEC;
6.2.4.8 to integrate the Department into the primary functions of the
hospital; 6.2.4.9 to coordinate and integrate interdepartmental and
intradepartmental services and communication;
6.2.4.10 to participate in the administration of the Department through cooperation with nursing services and hospital administration in matters affecting patient care;
23
6.2.4.11 to develop and implement Medical Staff and hospital policies and
procedures that guide and support the provision of patient care services;
6.2.4.12 to recommend to the Facility CAO the sufficient numbers of
qualified and competent persons to provide patient care and service;
6.2.4.13 to provide input to the Facility CAO regarding the qualifications and
competence of Department or service personnel who are not Licensed Independent Practitioners (LIPs) but provide patient care, treatment, and services;
6.2.4.14 to provide continuous assessment and improvement of the quality
of care, treatment, and services; 6.2.4.15 to maintain quality control programs as appropriate; 6.2.4.16 to orient and continuously educate all persons in the Department; 6.2.4.17 to make recommendations to the FMEC and to the Facility CAO for
space and other resources needed by the Medical Staff Department to provide patient care services.
6.3 Assignment to Department 6.3.1 The FMEC will, after consideration of the recommendation of the Chair of the
appropriate Department, recommend Department assignments for all members in accordance with their qualifications. Each member will be assigned to one primary Department. Clinical privileges are independent of the Department assignment.
SECTION 7 MEDICAL STAFF GOVERNANCE COMMITTEES 7.1 Designation of the Lee Memorial Health System Medical Staff Physician Leadership
Council (PLC)
7.1.1 There shall be a Lee Memorial Health System Medical Staff Physician Leadership Council (PLC) and such other standing and special committees as determined by the PLC.
7.1.2 There shall be a Facility Medical Executive Committee (FMEC) at each hospital and
such other facility standing and special committees as established by the FMEC.
7.2 Composition of the Lee Memorial Health System Medical Staff PLC 7.2.1 Composition: The PLC shall consist of the following voting members: Each Facility President and
each Facility President–Elect or each Facility Immediate Past President and two (2) at-large Medical Staff members elected by each FMEC. All shall serve a 2-year term except the Facility President-Elect and Facility Past President shall serve 1-year term. The Chairs of the System Credentialing/Privileging Committee and
24
System Quality Committee, the system CEO or Designee, the System Chief Medical Officer and the Chair of the Board and up to two (2) other Board consultants, shall serve as ex-officio, non-voting members. The PLC will elect the PLC Chair and Vice Chair who shall serve a 2-year term.
In the event that the PLC composition does not include one anesthesiologist,
emergency medicine physician, hospitalist or intensivist, radiologist and pathologist, the PLC may appoint an active Medical Staff member from each of these hospital-based specialties to be voting members of the PLC.
7.2.2 Duties: The duties of the Lee Memorial Health System PLC are:
7.2.2.1 to work in a cooperative and professional manner with the FMECs System and Facility Administration and the Board to ensure Medical Staff input into the plans, goals and mission of the Lee Memorial Health System;
7.2.2.2 receive, review, and transmit FMEC recommendations to the
Board; 7.2.2.3 review and attempt to resolve any inconsistency emanating from
the FMEC recommendation(s) and transmit FMEC recommendations to the Board concerning all matters relating to appointments, reappointments, staff category, facility assignments, clinical privileges subject to the conflict resolution process herein, unless due process rights are triggered pursuant to Part II.
The PLC is acting as a duly constituted peer review committee under Florida law when it is reviewing the quality of care or performance of any particular physician.
7.2.2.4 consistent with the hospital and Medical Staff mission and
philosophy, the PLC will participate and encourage participation of the FMECs in identifying community health needs and in setting goals and work with the System administration and the facility CAO(s) to design and implement programs to meet those needs;
7.2.2.5 work with the FMECs to ensure understanding and the consistent
application of Medical Staff Rules and Regulations, Policies and Procedures; and
7.2.2.6 govern the collection of Medical Staff system-wide assessments
and authorize the use of Medical Staff assessments consistent with the purpose of the assessment.
7.2.3 Meetings:
The PLC shall meet as frequently as needed, but at least quarterly, to perform its assigned functions. Records of its proceedings and actions shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
25
7.3 Staff Functions
7.3.1 The PLC exists to promote communication, collaboration and coordination
between physicians, System and facility administration and the Board concerning the work of each FMEC and planning activities of the Lee Memorial Health System that impact members of the Medical Staff.
7.4 Facility Medical Executive Committee (FMEC) Composition Selection and Tenure
7.4.1 Each Medical Staff may determine the number of Medical Staff members
appointed or elected to the FMEC. The composition of the FMEC shall consist of at least the following voting members: Facility President of the Medical Staff, Facility Immediate Past President, Facility President-Elect of the Medical Staff, Facility Secretary/Treasurer, physician representative from the System Credentialing/Privileging Committee, Chair of the Facility Quality Committee, the Department Chairs from Medicine, Surgery, Anesthesiology, Radiology, Pathology, Pediatrics, Obstetrics/Gynecology and Emergency Services, two (2) at-large active members of the Medical Staff appointed by the FMEC and two (2) at-large active members of the Medical Staff elected by the general Medical Staff.
One Board member, the CAO, the facility Vice-President of Nursing, the
facility Medical Director (as appropriate) will serve in a non-voting, ex-officio capacity. The Facility President of the Medical Staff shall serve as the Chair of the FMEC.
7.4.2 Each FMEC composition description shall be listed in the Facility Rules &
Regulations.
7.4.3 FMEC members shall disclose in writing to the Medical Staff, prior to the date of election of appointment, any personal, professional or financial applications or responsibilities with Lee Memorial Health System and any competing hospital, healthcare organization or Health System.
FMEC members shall serve 2-year terms, except Facility Past President and
Facility President-Elect shall serve 1-year terms. The FMEC and the Nominations Committee shall stagger the terms of appointed and elected at-large members to ensure continuity of leadership. Such physicians must be on Active Staff and be a member in good standing at all times.
All FMEC members are expected to participate in orientation and continuing
education activities as related to the operation of the Medical Staff.
7.5 Duties and Responsibilities of the Facility Medical Executive Committees 7.5.1 To represent, to initiate action and act on behalf of the Medical Staff
members with privileges at the Facility in fulfilling the duties of Medical Staff self governance, credentialing/privileging and quality/peer review, after seeking input and recommendations from Sections and/or Departments affected by FMEC action (if applicable).
26
7.5.2 To receive recommendations from the System Credentialing/Privileging
Committee and the Facility Quality/Peer Review Committee and make recommendations to the Board (and for informational purposes only) to the PLC concerning:
7.5.2.1 appointments, reappointments and granting of clinical privileges; 7.5.2.2 necessity for special investigations of issues pertaining to
practitioner competence of behavior; 7.5.2.3 needed performance improvements and peer review results; 7.5.2.4 policies and procedures development and enforcement; 7.5.2.5 facility Medical Staff Department and committee structure; and 7.5.2.6 other matters relevant to the provision of patient care, operation of
the Medical Staff or proposed Bylaws amendments. 7.5.3 Receive or act upon reports and recommendations concerning patient care
quality and appropriateness reviews, evaluation and monitoring functions, and the discharge of their delegated administrative responsibilities;
7.5.4 Recommend to the Board, and for information purposes only to the PLC,
specific programs and systems to perform Medical Staff peer review, quality monitoring, communication, governance, credentialing/privileging and planning functions;
7.5.5 Coordinate the implementation of policies adopted by the Board; 7.5.6 Oversee the facility multi-specialty peer review and quality monitoring
activities in a manner consistent with federal and state law; 7.5.7 Take reasonable steps to encourage professionally ethical conduct and
competent clinical performance of Medical Staff members at the facility including collegial and educational efforts;
7.5.8 Participate in identifying community health needs and in setting facility-
specific goals and implementing programs to meet those needs; 7.5.9 Design and implement facility-specific rules and regulations that will not
conflict with the Medical Staff Bylaws; 7.5.10 Work with Facility and System administration to promote effective, efficient
and safe patient care practice within the facility; 7.5.11 Take reasonable steps to encourage professionally ethical conduct and
competent clinical performance on the part of staff appointees including initiating investigations, and pursuing corrective action, when warranted;
7.5.12 Provide oversight concerning the quality and safety of the care provided by
residents, interns, students, and ensure that the same act within approved guidelines established by the Medical Staff and the Board.
27
Reviews and ensure corrective action regarding applicable Residency Review Commission findings and recommendations;
7.5.13 Keep the Medical Staff up to date concerning the licensure and
accreditation status of the System and hospitals; 7.5.14 Request evaluations of practitioners privileged through the Medical Staff
process in instances in which there is question about an applicant or member’s ability to perform privileges requested or currently granted;
7.5.15 Consult with administration on the quality, timeliness, and appropriateness
of aspects of contracts for patient care services provided to the hospital by entities outside the hospital;
7.5.16 Hold Medical Staff leaders, committees, and Departments accountable for
fulfillment of their duties and responsibilities; 7.5.17 Advise and assist the PLC, when and to the extent possible, as requested
by the PLC, the Board and the System or Facility administration; 7.5.18 Grant, deny or rescind exemptions related to ED call responsibility; 7.5.19 Meetings: The FMEC shall meet ten (10) times per year, or more
frequently as needed to perform its assigned functions. Records of its proceedings and actions shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
7.6 System Medical Staff Committees 7.6.1 Purpose. There shall be system Medical Staff committees established by the
Medical Staff to carry out the responsibilities of the Medical Staff with regard to measuring and assessing the performance of the Medical Staff providing medical care within the hospitals and Health System facilities.
7.6.2 Organization to Perform Functions. The PLC with the input and approval of each
FMEC shall establish system Medical Staff committees comprised of members of the Medical Staff and others as may be deemed appropriate or necessary. The delineation of specific duties, committee size, liaison with other committees and Departments, and other matters necessary to the efficient performance of Medical Staff functions shall be set forth in these Bylaws. The only voting members of system Medical Staff committees are members of the Medical Staff unless otherwise determined by the FMEC. System Medical Staff committees consist of the following, shall report to and through the FMECs on matters relating to all FMECs, and shall report to each FMEC on facility specific matters:
7.6.2.1 System Credentialing/Privileging Committee (See Part III, Section 1 of
these Bylaws); 7.6.2.2 System Medical Staff Quality Committee (See Medical Staff Quality
Manual); 7.6.2.3 System Practitioner Resource Committee. Membership:
28
Membership shall be established by the PLC with the input and approval of each FMEC. The term of office shall be for a period of two (2) years with staggered terms, so as to provide continuity and development of expertise.
Referrals: Concerns that a member of the Medical Staff may be suffering from a
physical or mental impairment that might impact their ability to practice medicine or may be a threat to themselves or others, including but not limited to impairment due to substance abuse, should be communicated to the President of the Medical Staff or to the affected practitioner’s Department Chair. The President of the Medical Staff or Department Chair, after consultation with others, if deemed appropriate, may refer the affected practitioner to the practitioner Resource Committee for review, evaluation and follow-up.
Responsibilities: The committee shall have no authority to take disciplinary action. Nor
does the committee provide treatment. The committee is responsible to: 7.6.2.3.1 Receive and evaluate concerns about practitioner health and
functioning;
7.6.2.3.2 Provide assistance and encourage a practitioner impaired by virtue of physical or psychiatric condition, problems in living, or issues related to alcohol use or drug use to voluntarily accept referral for the evaluation, treatment or assistance;
7.6.2.3.3 Assume an advocacy role on behalf of the affected practitioner;
7.6.2.3.4 Serve as an advisor to the President of the Medical Staff, Department Chair and/or FMEC, including advice relating to alternatives in the event that the practitioner fails to accept referral or fails to adequately recover from treatment;
7.6.2.3.5 Consider referring an affected practitioner to appropriate resources
for treatment and advice on the appropriateness of treatment, rehabilitation planning and monitoring provisions;
7.6.2.3.6 Utilize the Florida Medical Association Physician Resource Network,
Intervention Project for Nurses or other resources, if appropriate;
7.6.2.3.7 Maintain the confidentiality of information regarding matters referred to the committee;
7.6.2.3.8 Refer to the Medical Staff President Department Chair or FMEC
those situations that may require possible corrective actions. 7.6.2.4 System Bylaws Committee Membership:
29
The Bylaws Committee shall be a standing committee of the Medical Staff and shall be composed of at least five (5) active Medical Staff appointees (including one (1) member from each FMEC appointed by the facility Medical Staff President) and the System Chief Medical Officer (CMO) or his designee (who shall serve as a non-voting member).
Duties: The duties of the Bylaws Committee shall be to:
7.6.2.4.1 Conduct an annual review of the Medical Staff Bylaws, Medical Staff
Rules and Regulations and Policies; and 7.6.2.4.2 Review recommendations for changes in the Medical Staff Bylaws,
Rules and Regulations and Policies made by the Medical Staff committees, Departments, or by the Board.
Meetings, Reports and Recommendations: The Bylaws Committee shall meet at least annually or as necessary to
accomplish its duties, shall maintain a permanent record of its proceedings and actions, and shall report its recommendations to the FMECs.
7.6.2.5 System Emergency Services Committee Membership: The System Emergency Services Committee shall be an ad hoc committee
of the Medical Staff and shall be composed of the Emergency Department Medical Directors, at least three (3) Active Staff members, and other Active Staff members as needed.
Duties: The duties of the System Emergency Services Committee shall be to: 7.6.2.5.1 conduct an annual review of system-wide emergency services; 7.6.2.5.2 ensure emergency call is fair to physicians while providing adequate
coverage to patients of our community;
7.6.2.5.3 review emergency call rules system-wide for recommendation to FMECs.
Meetings: The System Emergency Services Committee will meet at least once per year or as needed.
7.6.3 Composition and Meetings of System Medical Staff Committees:
7.6.3.1 Unless otherwise provided for in these Bylaws, System Medical Staff committees shall be composed of physician members from each facility, as appointed by each FMEC;
30
7.6.3.2 Each System Medical Staff committee shall elect a physician Chairperson
and physician vice Chairperson for their respective committee;
7.6.3.3 System Medical Staff committee members shall serve terms of 2 years and may be reappointed;
7.6.3.4 System Medical Staff committee members who cease to be members of
the Medical Staff of Lee Memorial Health System shall automatically cease to serve as committee members. Vacancies on committees shall be filled by the appropriate FMEC;
7.6.3.5 System Medical Staff committees shall meet as often as necessary to
discharge the duties of the respective committees in accordance with these Bylaws.
Reasonable notice of meetings shall be provided to committee members
and may include providing a written schedule of meetings on an annual or more frequent basis.
7.7 Facility Medical Staff Committees: 7.7.1 Purpose: There shall be committees to carry out certain essential functions
within each facility as determined by each FMEC. The FMEC may establish such committees from time to time in addition to those set forth in the Bylaws.
7.7.2 Standing Facility Medical Staff Committees: The following facility committees
are approved as standing committees of the FMEC: 7.7.2.1 GCMC Credentialing/Privileging Committee (see Part III, Section 1 of
these Bylaws); 7.7.2.2 LMHS Credentialing/Privileging Committee (see Part III, Section 1 of these
Bylaws); 7.7.2.3 Nominations Committees (See Part 1, Section 5.3 of these Bylaws);
7.7.2.4 Facility Medical Staff Quality Committees (see Medical Staff Quality Manual);
7.7.2.5 Facility Rules and Regulations Committees Composition: The Facility Rules and Regulations Committee shall be a
standing committee of the Medical Staff and shall be composed of at least two (2) active Staff members appointed by the FMEC.
Duties: The duties shall be to review and recommend changes in the
Facility Rules and Regulations and policies to the FMEC. 7.7.2.6 Trauma Quality Management Composition, membership and duties are mandated by the State
regulations for designated trauma centers.
31
SECTION 8 MEDICAL STAFF MEETINGS 8.1 General Medical Staff Meetings 8.1.1 An annual meeting and other general Medical Staff meetings shall be held at a
time determined by the FMEC. Notice of the meeting shall be given to all Medical Staff members via appropriate media and posted conspicuously at least ten (10) days before the meeting.
8.1.2 Except for Bylaws amendments or as otherwise specified in these Bylaws, the
actions of a majority of the members present and voting at a meeting of the Medical Staff is the action of the group.
Action may be taken without a meeting of the Medical Staff by presentation of
the question to each Medical Staff member eligible to vote, in person, via telephone, and/or by mail or internet, and their vote recorded in accordance with procedures approved by the FMEC. Such vote shall be binding so long as the question that is voted on receives a majority of the votes cast.
8.1.3 Special Meetings of the General Medical Staff 8.1.3.1 The President of the Medical Staff may call a special general Medical
Staff meeting at any time. Such request or resolution shall state the purpose of the meeting. The President of the Medical Staff shall designate the time and place of any special general Medical Staff meeting.
8.1.3.2 Written or electronic notice stating the time, place and purposes of
any special general Medical Staff meeting shall be conspicuously posted and shall be sent to each member of the Medical Staff at least three (3) days before the date of such meeting. No business shall be transacted at any special general Medical Staff meeting, except that stated in the notice of such meeting.
8.2 Departments, Sections and Committee Meetings 8.2.1 Regular Meetings of Medical Staff Departments, Sections and Committees
8.2.2 Departments, Sections and Committees may, by resolution, provide the time for holding regular meetings without notice other than such resolution.
8.3 Special Meetings of Departments, Sections and Committees 8.3.1 A special meeting of any Department, Section or Committee may be called by
the Chair thereof or by the President of the Medical Staff. 8.4 Quorum 8.4.1 Medical Staff meetings: Unless otherwise specified in these Bylaws, a quorum
shall consist of those present or those eligible Medical Staff members voting on an issue.
32
8.4.2 FMEC, Credentialing/Privileges Committee, Medical Staff Quality/Peer Review Committee: A quorum will exist when 50% of the members are present.
8.4.3 Departments, Sections or Committees other than those listed in Sections 6 and
7 above or unless otherwise specified in these Bylaws, a quorum shall consist of those present or those eligible Medical Staff members voting on an issue.
8.5 Attendance Requirements 8.5.1 Members of the Medical Staff are encouraged to attend meetings of the Medical
Staff. 8.5.1.1 FMEC, Credentialing/Privileges Committee, and Medical Staff
Quality/Peer Review Committee meetings: Members of these committees are expected to attend at least 75% of the meetings held.
8.5.1.2 Special meeting attendance requirements: Whenever there is
suspected or actual non-compliance with Medical Staff or hospital policies or suspected deviation from standard clinical or professional practice, the President of the Medical Staff or the applicable Department/Section/Committee Chair may require the practitioner to confer with him or with a standing or ad hoc committee that is considering the matter. The practitioner will be given special notice of the meeting, by personal delivery or U.S. Mail certified return receipt requested, at least five (5) days prior to the meeting, including the date, time, place, a statement of the issue involved and that the practitioner’s appearance is mandatory.
Failure of the practitioner to appear at any such meeting after two (2)
notices, unless excused by the FMEC upon showing good cause, will result in an automatic termination of membership pursuant to the Automatic Suspension and Termination provisions of these Bylaws. Such termination will not give rise to a fair hearing, but will automatically be rescinded upon the practitioner’s participation in the previously referenced meeting.
8.5.1.3 Nothing in the foregoing paragraph shall preclude the initiation of
precautionary restriction or suspension of clinical privileges as outlined in Part II of these Bylaws (Investigations, Corrective Action, Hearing and Appeal Plan).
8.6 Participation by Administration
8.6.1 Administration may attend any general, Department, Section or Committee meetings of the Medical Staff, unless otherwise specified or requested by the committee.
8.7 Robert’s Rules of Order 8.7.1 Medical Staff Department, Section and Committee meetings shall be run in a
manner determined by the individual who is the Chair of the meeting. When parliamentary procedure is needed, as determined by the Chair or evidenced by a majority vote of those attending the meeting, the latest edition of Robert’s Rules of Order shall determine procedure.
33
8.8 Notice of Meetings 8.8.1 Unless otherwise specified in these Bylaws, written or electronic notice stating
the place, day, and hour of any special meeting or of any regular meeting not held pursuant to resolution shall be delivered or sent to each member of the Department or committee not less than five (5) days before the time of such meeting by the person or persons calling the meeting. The attendance of a member at a meeting shall constitute a waiver of notice of such meeting.
8.9 Action of PLC, FMEC, General Medical Staff, Department, Section or Committee 8.9.1 The recommendation of a majority of its members present at a meeting at which
a quorum is present shall be the action of a Department, Section and Committee, FMEC, PLC or General Medical Staff meeting. Such recommendation will then be forwarded to the FMEC for action.
8.10 Rights of Ex Officio Members 8.10.1 Except as otherwise provided in these Bylaws, persons serving as ex officio
members of a committee shall have all rights and privileges of regular members thereof, (except that they shall not vote or be counted in determining the existence of a quorum).
8.11 Minutes 8.11.1 Minutes of each regular and special meeting of a committee shall be prepared
and shall include a record of the attendance of members and the vote taken on each matter. The presiding Chair shall authenticate the minutes and copies thereof shall be submitted to the FMEC or other designated committee. Minutes shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
SECTION 9 DECISION MAKING METHODS AND CONFLICT RESOLUTION 9.1 FMEC recommendations will be forwarded to the PLC for information and to ensure
communication between all facility Medical Staffs, System and facility administration and Board leaders. Routine FMEC communication and recommendations that are consistent between the FMECs and that are consistent with Medical Staff and hospital policy and procedures will be transmitted to the Board.
9.2 Conflict resolution: If the PLC determines a recommendation of a FMEC may be contrary
to the opinion of the PLC, or if a decision of the Board is contrary to a recommendation of the PLC and/or a FMEC, the PLC shall not make a recommendation to the Board regarding such matter. The PLC will first refer the matter back to the FMEC(s) for further consideration at their next meeting, together with pertinent suggestions and comments of the PLC.
9.3 If the FMEC recommendation and the opinion of the PLC remain inconsistent after the next
meeting of the FMEC, the matter will be referred to an Initial Joint Conference Committee to be convened within thirty (30) days of that FMEC meeting. Such Initial Joint Conference Committee may be convened at any time sooner by mutual agreement of the FMEC and PLC. The Initial Joint Conference Committee shall be composed of two (2) representatives selected by the PLC, two (2) representatives selected by the FMEC, one (1) administrative representative and one (1) Board member.
34
9.3.1 The positions established at the Initial Joint Conference Committee will be reported
in full to the FMEC and the PLC. The FMEC will discuss the issue at its next meeting. In the event the FMEC(s)’ recommendation remains contrary to the opinion of the PLC, the recommendation of the FMEC(s) shall be forwarded to the Board, along with pertinent, applicable information.
The PLC, at its discretion, may include a divergent opinion along with pertinent,
applicable information. The Board shall have sixty (60) days to adopt the recommendation of the FMEC(s), or may choose to refer the matter(s) to a Final Joint Conference Committee at any time within the 60-day period.
9.4 A Final Joint Conference Committee will be convened if: 9.4.1 requested by the Board; 9.4.2 requested by the PLC, FMEC(s) or Initial Joint Conference Committee (if the Initial
Joint Conference Committee is unable to resolve conflicts and divergent opinions remain between the PLC, FMEC(s) and/or Initial Joint Conference Committee); or
9.4.3 in the event the Board does not accept or adopt a recommendation by the
FMEC(s) within sixty (60) days of receiving such recommendation(s) as set forth in Section 9.3.1.
The Final Joint Conference Committee will convene within thirty (30) days of such request,
or occurrence. The Final Joint Conference Committee will be composed of two (2) representatives selected by the PLC, two (2) representatives selected by the FMEC and two (2) representatives (which may or may not be Board members) of the Board for review and recommendation to the full Board. The Final Joint Conference Committee will have up to sixty (60) days to report its recommendation(s), and will issue its complete report simultaneously to the FMEC(s), PLC, Initial Joint Conference members and Board. If either the FMEC(s) or PLC continues to have a dissenting opinion/recommendation from that of the Final Joint Conference Committee, both (FMEC and PLC) shall each have the right for a representative of each to report its recommendation/opinion at the same time to the Board. After such report(s), the Board will make a determination, which shall be final.
9.5 The Chair of the Board, PLC or FMEC may call for an Initial Joint Conference as described
above at any time and for any reason in order to seek direct input from the Board, PLC and/or FMEC Medical Staff leaders, clarify any issue, or relay information directly to Medical Staff leaders.
9.6 The provisions of this article are not applicable to matters subject to the provisions of the
Medical Staff Bylaws, Rules and Regulations, or Policies relating to Peer Review, Corrective Action or the Fair Hearing process.
SECTION 10 REVIEW, REVISION, ADOPTION, AND AMENDMENT 10.1 Medical Staff Responsibility
10.1.1 The Medical Staff shall have the responsibility to formulate, review at least
biennially, and recommend to the Board any Medical Staff Bylaws, rules, regulations, policies and procedures, and amendments as needed, which shall be effective when approved by the Board.
35
The Medical Staff can exercise this responsibility through its elected and appointed leaders or through direct vote of its membership.
10.2 Methods of Amendment and Adoption to these Bylaws
10.2.1 Proposed amendments to these Bylaws may be originated by the System Bylaws
Committee for consideration of all FMECs and each general Medical Staff or by a petition signed by twenty-five (25) active staff members.
10.2.1.1 Each active member of the Medical Staff will be eligible to vote on the
proposed amendment to these Bylaws via printed or secure electronic ballot in a manner determined by the FMEC. All active members of the Medical Staff shall receive at least thirty (30) days advance notice of the proposed changes. Proposed amendments must:
10.2.1.1.1 receive a simple majority of the votes cast by those active
Medical Staff members eligible to vote at the initiating FMEC;
10.2.1.1.2 receive a simple majority of the votes cast by the active
Medical Staff members eligible to vote at each FMEC; 10.2.1.1.3 receive a simple majority of the votes cast by the active
Medical Staff members eligible to vote on each facility general Medical Staff.
10.2.1.2 Amendments so adopted shall be effective when approved by the Board.
Neither the Board nor the Medical Staff shall have the power or authority to unilaterally adopt or amend Medical Staff Bylaws.
10.3 Methods of Amendment and Adoption to any Medical Staff Rules, Regulations and
Policies: 10.3.1 The Medical Staff may adopt additional rules, regulations and policies as necessary
to carry out its functions and meet its responsibilities under these Bylaws. A Rules, and Regulations and Policies Manual may be utilized to organize these additional documents. Should a conflict exist between the provisions of the Medical Staff Bylaws and the Rules and Regulations or Medical Staff Policies, the Bylaws will prevail. Should a conflict exist between the provisions of the Rules and Regulations and the Medical Staff Policies, the Rules and Regulations will prevail.
10.3.2 Proposed amendments to the Rules, Regulations and Policy Manual may be
originated by the FMEC. 10.3.3 The Medical Staff itself may recommend directly to the Board an amendment(s) to
any rule, regulation, or policy by submitting a petition signed by twenty-five (25) active Medical Staff members. Upon presentation of such petition, the adoption process outlined in 10.2.1 above will be followed.
10.3.4 The FMEC shall vote on the proposed language changes at a regular meeting, or at
a special meeting called for such purpose. Following an affirmative vote by the FMEC, any of these documents may be adopted, amended or repealed, in whole or in part and such changes shall be effective when approved by the Board, subject to Section 9 of this Part in the event of a conflict.

36
10.4 The FMEC may adopt such amendments to these Bylaws, Rules and Regulations, and
policies that are, in the committee’s judgment, technical or legal modifications or clarifications, reorganization or renumbering or those needed due to punctuation, spelling, or other errors of grammar or expression. Such amendments need not be approved by the entire Board but must be approved by the System CEO.
37
Appendix A
PRINCIPLES OF MEDICAL ETHICS**
PREAMBLE The medical professions have long subscribed to a body of ethical statements developed primarily for the benefit of the patient. As a member of this profession, a health professional must recognize responsibility to patients first and foremost, as well as to society, to other health professionals and to self. The following Principles are not laws but standards of conduct, which define the essentials of honorable behavior for the health professional. Section 1 A health professional shall be dedicated to providing competent medical care with compassion and respect for human dignity and rights. Section 2 A health professional shall uphold the standards of professionalism, be honest in all professional interactions, and strive to report health professionals deficient in character or competence, or engaging in fraud or deception, to appropriate entities. Section 3 A health professional shall respect the law and also recognize a responsibility to seek changes in those requirements, which are contrary to the best interests of the patient. Section 4 A health professional shall respect the rights of patients, colleagues, and other health professionals and shall safeguard patient confidences and privacy within the constraints of the law. Section 5 A health professional shall continue to study, apply and advance scientific
knowledge, maintain a commitment to medical education, make relevant information available to patients, colleagues and the public, obtain consultation, and use the talents of other health professions when indicated.
Section 6 A health professional shall, in the provision of appropriate patient care, except in emergencies be free to choose whom to serve, with whom to associate and the environment in which to provide medical care.
38
Section 7 A health professional shall recognize a responsibility to participate in activities contributing to an improved community and the betterment of pubic health. Section 8 A health professional shall, while caring for a patient, regard responsibility
to the patient as paramount.
Section 9 A health professional shall support access to medical care for all people. **Adapted from the American Medical Association’s “Principles of Medical Ethics” (adopted by the AMA’s
House of Delegates June 17, 2001).
39
PART II: INVESTIGATIONS, CORRECTIVE ACTION, HEARING AND APPEAL PLAN
SECTION 1 ROUTINE CORRECTIVE ACTION & INVESTIGATIONS 1.1 Progressive Intervention These Bylaws encourage the use of progressive steps by Medical Staff leaders and
hospital administration, beginning with collegial and education efforts, to address questions relating to a practitioner’s clinical practice and/or professional conduct. The goal of these efforts is to arrive at voluntary, responsive actions by the practitioner to resolve questions that have been raised. All collegial intervention efforts by Medical Staff leaders and hospital management are part of the hospital’s performance improvement and professional review activities. Collegial intervention efforts are encouraged, but are not mandatory, and shall be within the discretion of the appropriate Medical Staff leaders and hospital administration.
When any observations arise, suggesting opportunities for a practitioner to improve, the matter may be referred in accordance with the performance improvement and professional conduct policies adopted by the Medical Staff and hospital.
Corrective actions and investigations shall be undertaken: 1.1.1 in the reasonable belief that the action is in the furtherance of quality health care; 1.1.2 after a reasonable effort to obtain the facts of the matter,
1.1.3 after adequate notice and hearing procedures are afforded to the practitioner as set forth herein, and
1.1.4 in the reasonable belief that the action is warranted by the facts known after such reasonable effort to obtain the facts.
1.2 Basis for Routine Corrective Action Whenever a concern or question has been raised regarding: 1.2.1 the clinical competence or clinical practice of any appointee; 1.2.2 the care or treatment of a patient or patients or management of a case by any
appointee; 1.2.3 activities or professional conduct that may be detrimental to patient safety; 1.2.4 the known or suspected violation by any Medical Staff appointee of these Bylaws,
the Policies, or the Rules and Regulations of the Medical Staff, System or Department
1.2.5 behavior or conduct on the part of any Medical Staff appointee that is considered lower than the standards of the hospital, disruptive to the hospital or its Medical Staff, including the inability of the appointee to work harmoniously with others; or
1.2.6 impairment, a request for corrective action may be made by any practitioner on the Medical Staff, any
member of the System administration, System or Medical Staff committee, or the Board of Directors, after making sufficient inquiry to satisfy themselves that the concern or question raised is credible.
40
1.3 Requests and Notices All requests for corrective action shall be made in writing to the President of the Medical
Staff and the Chief Medical Officer, with a copy to the Medical Staff Services Office. The request must be signed by the complainant, clearly state those facts that support the request in sufficient detail to permit an investigation to be pursued, and, if possible, state what corrective action is deemed appropriate by the complainant. The President of the Medical Staff shall notify the FMEC at its next regular meeting that a request for corrective action has been made. The affected practitioner shall be given written notice of the request, and a copy of the same. All notices provided under this Part II shall be hand delivered or sent via certified mail, return receipt requested. All time limits shall begin upon receipt of notice.
1.4 Investigations
1.4.1 When a request for corrective action has been received by the FMEC, the committee shall determine as soon as possible, but no later than at its next regularly scheduled meeting, either to discuss the matter with the appointee concerned, or to begin an investigation. If the concern states sufficient information to warrant action, the FMEC, at its discretion, may initiate an investigation, with or without a personal interview with the practitioner being investigated. The FMEC may seek input from the practitioner’s Department or Section prior to initiating investigation. An investigation shall begin only after a formal resolution of the FMEC to that effect. The affected practitioner shall be given written notice of the initiation of an investigation. If the Board of Directors wishes to begin such an investigation, it shall also formally resolve to do so by mandating the FMEC to begin an investigation.
1.4.2 Upon resolving to initiate an investigation, the Medical Staff President through the
FMEC or President of the Medical Staff shall immediately appoint a member(s) of the Active Medical Staff to conduct an investigation of the matters contained in the request. Investigators shall not include partners, associates or relatives of the practitioner being investigated and should be objective and familiar with the types of issues raised in the request for corrective action.
1.4.3 The investigator(s) may consult with other members of the Medical Staff as
appropriate in order to determine the facts of the case, or to obtain professional opinions relative to the matter under consideration.
1.4.4 The investigator(s) shall have available the full resources of the Medical Staff and
the System, as well as the authority to use outside consultants, if needed. 1.4.5 The investigation should be completed within thirty (30) working days of the
appointment of the investigator(s), unless an extension of not more than thirty (30) additional working days has been granted by the FMEC or President of the Medical Staff.
1.4.6 At the conclusion of the investigation, the investigator(s) shall prepare a written
report of the findings and transmit the same to the President of the Medical Staff and the Chief Medical Officer. In addition to setting forth findings of fact and, if applicable, the clinical opinion of the investigator(s) and other practitioners with whom he may have consulted, the report shall recommend that corrective action be imposed, or that the complaint against the affected practitioner be dismissed.
The investigator may recommend a type or degree of corrective action deemed
appropriate.
41
1.4.7 The President of the Medical Staff shall review the investigator’s report when it is received, and if emergency corrective action is indicated, proceed to impose the same pursuant to Section 2 of this part. Otherwise, the President shall submit the investigator’s report to the FMEC for consideration at its next regular meeting.
1.4.8 In cases suggesting practitioner impairment, the President of the Medical Staff shall
confer with a member of the Medical Administrative Staff, designated by the System President and the practitioner’s Department Chair, and if they concur, shall refer the request to the Practitioner Resource Committee for disposition; otherwise, the request shall be referred to the FMEC for consideration at its next regular meeting.
1.5 FMEC Action 1.5.1 If the FMEC determines that there are no reasonable grounds to believe that the
affected practitioner has committed an offense requiring corrective action under these Bylaws, the complaint shall be dismissed. The affected practitioner and complainant shall be given written notification of dismissal.
1.5.2 If the FMEC determines that there are reasonable grounds to believe that the
affected practitioner is subject to corrective action, the Committee may elect to recommend corrective action to the Board, which, at the discretion of the FMEC, may consist of:
1.5.2.1 A written warning that corrective action measures will be taken in the
future if the affected practitioner does not reform his conduct in the manner set forth in the warning;
1.5.2.2 A written reprimand stating the Committee’s displeasure at the affected
practitioner’s behavior, and directing the affected practitioner to cease the same immediately;
1.5.2.3 Mandated education to improve the affected practitioner’s knowledge,
skills and ability in clinical as well as non-clinical subjects;
1.5.2.4 Mandated clinical review or supervision to see that the affected practitioner’s performance attains an acceptable level;
1.5.2.5 Limitation of privileges restricting those procedures that the affected
practitioner may perform at the Facility;
1.5.2.6 Removal of privileges eliminating the affected practitioner’s ability to perform any procedure at the Facility. If the affected practitioner is a member of the Medical Staff, removal of privileges shall also entail revocation of Medical Staff membership. If removal of privileges is recommended at the time of the affected practitioner’s biennial reappointment, this may be accomplished by not recommending the affected practitioner for reappointment;
1.5.2.7 Make such other recommendations, as it deems necessary or appropriate.
42
1.6 Notice of FMEC Action Whenever a recommendation for corrective action has been made by the FMEC, or
corrective action has been taken by the Board on its own initiative, written notice of the same shall be sent to the affected practitioner by certified mail, return receipt requested, or hand delivery with receipt. Such notice shall be consistent with the notice provision set forth in Subsection 1.3. The notice shall set forth the nature of the complaint, the reasons for the corrective action, a description of the corrective action, and a short summary of the affected practitioner’s right to a fair hearing pursuant to these Bylaws, including any time limits within which the affected practitioner must act. The affected practitioner may request a hearing pursuant to the provisions of Section 4.
1.7 Board of Directors Action If the time, during which an affected practitioner may request a hearing pursuant has
expired without a request being made, or such hearing, including appeal to the Board, has been concluded, then at the next regular meeting thereafter of the Board of Directors, the Board shall consider the recommended corrective action. In the event that the Board rejects such recommendation, the Board may remand the recommendation to the FMEC with instructions to reconsider the matter, including the nature and degree of the corrective action. The Board shall consider recommendations of the FMEC following remand in the same manner as other recommendations for corrective action.
SECTION 2 EMERGENCY CORRECTIVE ACTION/PRECAUTIONARY SUSPENSION
OF CLINICAL PRIVILEGES 2.1 Basis for Emergency Corrective Action/Precautionary Suspension The President of the Medical Staff, the Chief Medical Officer (or his designee), or the FMEC
shall have the authority to immediately suspend all or any portion of the clinical privileges of a Medical Staff practitioner or other individual, whenever failure to take such action may result in an imminent danger to the health and/or safety of any individual. Such precautionary suspension shall be deemed an interim precautionary step in the professional review activity related to the ultimate professional review action that may be taken with respect to the suspended individual but is not a complete professional review action in and of itself. It shall not imply any final finding of responsibility for the situation that caused the suspension, nor shall it entitle the practitioner to a fair hearing except as provided under this Section. Those parties with the authority to impose emergency corrective action shall consult with a physician member of the Administration designated by the System President and System legal counsel before imposing any emergency corrective action. This Subsection shall not apply if a clear and present danger exists which requires immediate action and consultation is not feasible.
2.2 Notice of Emergency Corrective Action/Precautionary Suspension Upon imposition of emergency corrective action, the President of the Medical Staff shall
immediately give notice to the affected practitioner of such action. Such notice may be oral, but shall be confirmed in writing as soon as possible, but no later
than the next business day. The written notice shall state the reasons for the emergency corrective action and the nature of corrective action imposed. A copy of the notice shall also be given to the Chief Medical Officer, Department Chair, and FMEC.
43
2.3 FMEC Procedure When instituted, a precautionary suspension of clinical privileges will automatically expire in
seven (7) days, unless extended by the FMEC, with return of all previous clinical privileges unless the suspension is confirmed by a majority vote of the FMEC in special session. The FMEC shall review the matter resulting in precautionary suspension within a reasonable period not to exceed fourteen (14) days. Unless the FMEC promptly terminates or extends the precautionary suspension prior to or immediately after reviewing the suspension, the practitioner shall be entitled to the procedural rights afforded by the Fair Hearing and Appeal plan once the restrictions or suspension last more than fourteen (14) calendar days. Restrictions or suspensions which last fourteen (14) days or less shall not trigger rights under the Fair Hearing and Appeal Plan.
2.4 Provision of Patient Care Immediately upon the imposition of a precautionary suspension, the appropriate
Department Chair or, if unavailable, the President of the Medical Staff shall assign responsibility for care of the suspended practitioner’s patients still in a System’s facility to another practitioner with appropriate clinical privileges. The assignment shall be effective until the patients are discharged. The wishes of the patient shall be considered in the selection of the assigned practitioner. It shall be the duty of all Medical Staff practitioners to cooperate with the President of the Medical Staff, the Department Chair concerned, the FMEC and the Chief Medical Officer in enforcing all suspensions.
2.5 Recission of Emergency Corrective Action/Precautionary Suspension The person imposing emergency corrective action may, at any time prior to ratification of
such action by the FMEC, rescind the action, and the affected practitioner shall be restored to the status he enjoyed prior to the imposition of emergency correction action. Following ratification of emergency corrective action by the Executive Committee, the person imposing such action may recommend to the FMEC that such action be rescinded. The FMEC shall consider such recommendation at its next regular meeting thereafter. Any pending request for a hearing pursuant to Section 4 shall be made moot and void by such recission.
SECTION 3 AUTOMATIC SUSPENSION AND TERMINATION 3.1 Basis for Automatic Suspension and Termination A practitioner’s clinical privileges shall automatically be revoked, limited or suspended as
appropriate, which action shall be final without a right to due process except as provided in this Section, upon the occurrence of the following circumstances: 3.1.1 Loss of License. The practitioner’s license to practice in the State of Florida is
suspended, limited or terminated. 3.1.2 Residence or Office Outside Lee County. The practitioner does not maintain a full-time residence and office in Lee County as
required by these Bylaws, unless such requirements are waived by the FMEC pursuant to said Subsection. Return of United States mail sent by the System Medical Staff Services Office to a practitioner at his Lee County home or office address with “addressee unknown” or similar endorsement shall be prima facie
44
evidence that the practitioner does not comply with these Bylaws. Failure of a practitioner to supply a current residence and office address within 15 working days of a request of the Medical Staff Services Office for the same shall be deemed prima facie evidence that the practitioner does not comply with these Bylaws. This shall not apply to practitioners granted a leave of absence by the FMEC pursuant to these Bylaws.
3.1.3 Lack of Active Practice. The practitioner is not actively engaged in the practice of
his profession in Lee County; that is, he is not seeing, examining, treating or otherwise caring for patients, and has not done so for a period of more than six months, unless the practitioner shall have notified the Medical Staff Services Office prior to beginning such absence, and arranged for suitable coverage during such time period. This shall not apply to practitioners granted a leave of absence by the FMEC pursuant to these Bylaws, or to members of the Honorary Medical Staff.
3.1.4 Criminal Conviction. The practitioner has been, while a practitioner on the Medical
Staff, convicted in any jurisdiction of the United States; of a felony or misdemeanor involving actual or threatened bodily harm, actual or threatened sexual misbehavior or stalking, controlled substance possession or use, or of any felony or misdemeanor described in any Florida law pertaining to governing or regulating the health professions or health facilities. A practitioner whose membership or privileges are automatically terminated pursuant to this Subsection shall not be disqualified from applying for appointment following completion of his sentence, or during a period of time when he is on probation. However, the fact that the practitioner has completed his sentence after criminal conviction, or is on probation, shall not require the Medical Staff to make such appointment, and the FMEC may elect not to do so in its discretion, consistent with its responsibility towards patients, other practitioners, Facility/System employees, and the public in general.
3.1.5 Loss or Restriction of DEA Certificate. The clinical privileges of a practitioner whose
Drug Enforcement Agency (DEA) certification is terminated, revoked, or suspended shall automatically and immediately be modified to revoke the right to prescribe controlled substances. The practitioner shall immediately inform the Medical Staff Services Office regarding the change in status in his DEA certification. The matter shall promptly be referred, for investigation and further action in accordance with the provisions of these Bylaws.
3.1.6 Exclusion From Federal or State Health Care Programs. The Medical Staff
appointment and clinical privileges of a practitioner who becomes an ineligible person with regard to participation in Federal or State Health Care Programs shall automatically and immediately be suspended.
The practitioner shall immediately inform the Medical Staff Services Office regarding
the change of his eligibility status. This triggers the right to due process. The matter shall promptly be referred for investigation and further action in accordance with all the due process provisions of this Part.
3.1.7 Failure to Pay Fees and Assessments. The practitioner fails to pay when due any
fee or assessment imposed pursuant to these Bylaws or Medical Staff or System policy.
3.1.8 Failure to Provide Requested Information. If at any time a practitioner fails to
provide required information pursuant to a formal request by the System Credentialing/Privileging Committee, Medical Executive Committee or the Medical Staff Services Office, the practitioner’s clinical privileges shall be deemed to be
45
voluntarily relinquished until the required information is provided to the satisfaction of the requesting party. For purposes of this Section, required information shall include but not be limited to: 1. physical or mental examination reports as specified elsewhere in this policy, or 2. information necessary to explain an investigation, professional review action, or resignation from another health care facility or agency.
3.1.9 Failure to Request Reappointment or Provide Requested Information Related to
Reappointment. If a practitioner fails to request reappointment for membership and/or privileges or fails to provide requested information pursuant to Part III, Section 5 of these Bylaws, the practitioner’s membership and privileges shall be deemed voluntarily relinquished.
3.1.10 Failure to Request Reinstatement Following Leave of Absence. Failure to request
reinstatement shall be deemed a voluntary resignation from the Medical Staff and shall result in automatic termination of membership, privileges, and prerogatives. Members whose membership is automatically terminated shall not be entitled to the procedural rights provided in the Medical Staff Bylaws.
3.1.11 Failure to Complete Medical Records. All elective admitting, consulting and clinical
privileges of any practitioner shall be deemed to be voluntarily relinquished for failure to complete medical records in accordance with the provisions of the Medical Staff Rules and Regulations. Such relinquishment shall continue until all the records of the practitioner’s patients are no longer delinquent. Such relinquishment does not exempt the practitioner from fulfilling their on-call responsibilities. Failure to complete the medical records that caused relinquishment of clinical privileges within sixty (60) days from the relinquishment of such privileges shall be grounds for further disciplinary action in accordance with the provisions of these Bylaws.
3.1.12 Failure to Comply with Special Meeting Attendance Requirements. Failure of a
practitioner to attend a special meeting called pursuant to the Bylaws. 3.2 Right to Limited Hearing for Automatic/Voluntary Suspension and Termination A practitioner affected by this Section shall be sent a written notice stating the reasons for
automatic suspension within 24-hours of the same having been imposed, and shall have the right to present evidence to the FMEC in written form, or by appearing personally at a regular meeting of the committee, to demonstrate that the reason that automatic suspension was imposed is untrue.
3.2.1 Such written evidence or a written request to meet with the FMEC shall be
submitted to the President of the Medical Staff within ten (10) working days of the date the notice of automatic suspension was sent. Failure to submit written evidence or a request shall be deemed a waiver of any right to consideration of the same.
3.2.2 Evidence presented by the affected practitioner shall be limited to whether or not the
grounds for automatic suspension are true. The FMEC shall not consider evidence or argument, which presents mitigating circumstances or excuse.
3.2.3 After receipt of an affected practitioner’s written evidence, and prior to the next
regular meeting of the FMEC, the President of the Medical Staff, with the concurrence of a member of the Medical Administrative Staff designated by the System President, may determine that the evidence so presented demonstrates that
46
the reasons that automatic suspension was imposed are untrue, and revoke the suspension, restoring the affected practitioner to the status he previously enjoyed.
3.2.4 The President of the Medical Staff may, at any time, provisionally reinstate a
practitioner suspended pursuant to this Section if the President is satisfied by the available written documentation that the reasons for automatic suspension were untrue. The President shall present the provisional reinstatement for ratification by the FMEC at its next regular meeting.
3.2.5 At its next regular meeting following automatic suspension, the FMEC shall consider
the reasons therefore, together with any evidence or argument presented by the affected practitioner, and if the reasons for automatic suspension are found to be true, recommend to the Board termination of the affected practitioner’s Medical Staff membership and/or privileges. If the FMEC finds that the reasons are untrue or corrected, the suspension shall be revoked, and the affected practitioner restored to the status he previously enjoyed.
SECTION 4 HEARING AND APPEAL PROCEDURES 4.1 Grounds for Hearing An applicant or an individual holding a Medical Staff appointment shall be entitled to
request a hearing whenever the FMEC or the Board of Directors has made one of the following adverse recommendations:
4.1.1 denial of initial Medical Staff appointment; 4.1.2 denial of Medical Staff reappointment; 4.1.3 revocation of Medical Staff appointment; 4.1.4 denial of requested initial clinical privileges; 4.1.5 denial of requested additional clinical privileges; 4.1.6 decrease of clinical privileges;
4.1.7 suspension of clinical privileges (other than emergency corrective action/precautionary suspension);
4.1.8 imposition of mandatory concurring consultation requirement. No other recommendations except those enumerated in this Section shall entitle the practitioner to request a hearing. Neither voluntary relinquishment of clinical privileges, as provided in these Bylaws, nor the imposition of any general consultation requirement, nor the imposition of a requirement for retraining, additional training or continuing education, shall constitute grounds for a hearing, but shall take effect without hearing or appeal. The hearing shall be conducted in as informal a manner as possible, subject to the rules and procedures set forth in these Bylaws.
4.2 Notice of Recommendation When a recommendation is made which, according to these Bylaws entitles a practitioner to
a hearing prior to a final decision of the Board, the affected practitioner shall promptly be given notice by the President of the Medical Staff or Chief Medical Officer or his designee, in writing, certified mail, return receipt requested or in person. This notice shall contain:
47
4.2.1 a statement of the recommendation made, the action which is being taken or which may be taken, and the general reasons for it; 4.2.2 notice that the practitioner has the right to request a hearing on the
recommendation within thirty (30) days of receipt of this notice; and 4.2.3 a copy of this Part outlining the rights in the hearing as provided for in these
Bylaws.
4.3 Request for Hearing A practitioner shall have thirty (30) days following the date of the receipt of such notice
within which to request the hearing. The request shall be in writing to the President of the Medical Staff or Chief Medical Officer with a copy to the Medical Staff Services Office and signed by the affected practitioner making such request. In the event the practitioner does not request a hearing within the time and in the manner required by these Bylaws, the practitioner shall be deemed to have waived the right to the hearing and to have accepted the action involved. That action shall become effective immediately upon final Board action.
4.4 Preliminary Interview The affected practitioner may request, at the time of submitting a request for hearing or
within ten (10) working days thereafter, an informal preliminary interview with the decision making body (FMEC or Board of Directors). The decision making body shall grant all such requests, and the affected practitioner shall be scheduled to appear before it at its next regular meeting. 4.4.1 The purpose of the preliminary interview shall be to permit the affected practitioner
to personally present any argument or evidence showing that the adverse recommendation has been wrongfully imposed, in fact, or in violation of these Bylaws; or to present any mitigating circumstances.
4.4.2 The preliminary interview is informal and not a hearing. It is optional with the
affected practitioner, and accordingly, legal counsel shall be excluded. 4.4.3 The decision making body may impose a limit on the amount of time to be devoted
to a preliminary interview, but not less than thirty minutes. 4.4.4 Failure to request a preliminary interview shall not be considered in any hearing or
deliberation conducted pursuant to these Bylaws, nor shall the affected practitioner’s right to a hearing be affected thereby.
4.4.5 Following a preliminary interview, the decision making body shall deliberate, and
may elect to withdraw or reduce the severity of the adverse recommendation imposed upon the affected practitioner, or may take no action.
If no action is taken, the adverse recommendation shall continue in effect, and the hearing provided for hereunder shall proceed.
4.4.6 Notice shall be given to the affected practitioner of the decision following a
preliminary interview in the manner provided in Subsection 1.3.
SECTION 5 FAIR HEARING PROCEDURE 5.1 System Representative, Hearing Panel and Hearing Officer
48
5.1.1 System Representative 5.1.1.1 When the FMEC of the Medical Staff is the decision making body, the
President of the Medical Staff shall appoint a person to represent the interests and position of the Medical Staff in all proceedings provided for in this Section. Such individual shall be in an adversarial role opposed to the affected practitioner. If the affected practitioner is not represented by legal counsel, the Medical Staff representative shall not be an attorney, but shall be a member of the Active Medical Staff.
5.1.1.2 When the Board is the decision making body, as defined herein, the
Chair of the Board shall appoint a person to represent the interests and position of the Board in all proceedings provided for in this Section. Such individual shall be in an adversarial role opposed to the affected practitioner. If the affected practitioner is not represented by legal counsel, the Board representative shall not be an attorney, but shall be a member of the administration.
5.1.1.3 For purposes of these Bylaws, the Medical Staff or Board representative
appointed under this Section shall be called the “System Representative.”
5.1.2 Hearing Panel 5.1.2.1 Unless the FMEC or Board elects to have the matter heard by a Hearing
Officer possessing the qualifications set forth in Subsection 5.1.3, all hearings shall be conducted by a Hearing Panel appointed by the President of the Medical Staff or the Chair of the Board, as applicable,
composed of five (5) members, presided over by a qualified professional selected in accordance with Subsection 5.1.3. The Hearing Panel shall be composed of Active Medical Staff practitioners who shall not have actively participated in the consideration of the matter involved at any previous level. Knowledge of the matter involved shall not preclude any individual from serving as a member of the Hearing Panel.
If the hearing has been requested based on Board action, 3 of the
members of the Hearing Panel shall be members of the Board of Directors. The Hearing Panel will be presided over by a Hearing Officer.
5.1.2.2 The Hearing Panel shall not include any individual who is in direct
economic competition with the affected person or has any other personal interest in the proceeding, financial or otherwise, or any such individual who is professionally associated with or related to the affected practitioner.
5.1.3 Hearing Officer – Qualifications & Authority 5.1.3.1 The FMEC or the Board may elect to have the hearing provided for in
this Section held by a Hearing Officer sitting alone. In such case, the Hearing Officer shall perform all of the functions of the Hearing Panel described herein.
49
In cases where a panel is appointed, the Hearing Officer will preside over the proceeding but not participate in the deliberations or vote on the recommendation.
5.1.3.2 The Hearing Officer:
5.1.3.2.1 shall be an attorney licensed in the State of Florida who is
knowledgeable and has experience in health care law, including Medical Staff law; or shall be a non-lawyer who has experience as a Hearing Officer;
5.1.3.2.2 shall not be, or have been, employed or retained by the Lee
Memorial Health System, or any practitioner on the Medical Staff, including the affected practitioner, for any purpose other than to serve as a Hearing Officer in Medical Staff proceedings;
5.1.3.2.3 shall have no personal interest in the proceeding, financial or
otherwise; 5.1.3.2.4 shall be selected by the affected practitioner from a list
provided to the affected practitioner by the General Counsel for the Health System of the names of not less than three (3) persons meeting the requirements of 1-3 above. The affected practitioner shall select the Hearing Officer from the list submitted to him and within forty-eight (48) hours of receiving said list, notify the General Counsel for the Health System in writing of said selection.
Failure of the affected practitioner to select within the
previously mentioned period shall constitute a waiver by the affected practitioner of this Subsection, and the General Counsel for the Health System shall thereafter select the Hearing Officer.
5.1.3.3 The Hearing Officer shall: 5.1.3.3.1 act to insure that all participants in the hearing have a
reasonable opportunity to be heard and to present oral and documentary evidence subject to reasonable limits on the number of witnesses and duration of direct and cross examination, applicable to both sides, as may be necessary to avoid cumulative or irrelevant testimony or to prevent abuse of the hearing process;
5.1.3.3.2 prohibit conduct or presentation of evidence that is
cumulative, excessive, irrelevant, and abusive or that causes undue delay;
5.1.3.3.3 maintain decorum throughout the hearing; 5.1.3.3.4 determine the order of procedure throughout the hearing; 5.1.3.3.5 have the authority and discretion, in accordance with these
Bylaws, to make rulings on all questions that pertain to
50
matters of procedure and to the admissibility of evidence and qualifications of witnesses;
5.1.3.3.6 act in such a way that the Hearing Panel in formulating its
recommendations considers all information relevant to the continued appointment or clinical privileges of the practitioner requesting the hearing;
5.1.3.3.7 conduct argument by counsel on procedural points outside
the presence of the Hearing Panel unless the Panel wishes to be present;
5.1.3.3.8 grant continuances and postponements as appropriate; and 5.1.3.3.9 take official notice of any matters, either technical or scientific,
relating to the issues under consideration that could have been judicially noticed by the courts of this state, inform the participants of the matters to be officially noticed and provide each party the opportunity to request that a matter be officially noticed or to refute the noticed matter by evidence or by written or oral presentation of authority.
5.2 Challenge to Hearing Panel Members or Hearing Officer
The affected practitioner may challenge the objectivity of any member of the Hearing Panel, or the Hearing Officer, at any time prior to the taking of testimony at the hearing. Such challenge shall be in writing and specify facts demonstrating that a member of the Hearing Panel or the Hearing Officer lacks objectivity or is biased against the affected practitioner. The challenge shall be directed to the President of the Medical Staff or the Chair of the Board, as applicable, who shall consider the challenge and either sustain or overrule it. If the challenge is sustained, the challenged member of the Hearing Panel or the Hearing Officer shall be replaced.
SECTION 6 HEARING PROCEDURES 6.1 Provision of Relevant Information
6.1.1 There is no right to discovery in connection with the hearing. However, the
practitioner requesting the hearing shall be entitled, upon specific request, to the following, subject to a stipulation signed by both parties that such documents shall be maintained as confidential and shall not be disclosed or used for any purpose outside of the hearing:
6.1.1.1 copies of, or reasonable access to, all patient medical records referred to
in the Statement of Reasons, at the practitioner’s expense; 6.1.1.2 reports of experts relied upon by the FMEC or the Board; 6.1.1.3 redacted copies of relevant committee or Department meeting minutes
(such provision does not constitute a waiver of the state peer review protection statute); and
6.1.1.4 copies of any other documents relied upon by the FMEC or the Board.
51
6.1.2 Prior to the hearing, on dates set by the Hearing Officer or agreed upon by counsel
for both sides, each party shall provide the other party with a list of proposed exhibits. All objections to documents or witnesses to the extent then reasonably known, shall be submitted in writing in advance of the hearing. The Hearing Officer shall not entertain subsequent objections unless the party offering the objection demonstrates good cause.
6.1.3 Prior to the hearing, on dates set by the Hearing Officer, the practitioner requesting
the hearing shall, upon specific request, provide the FMEC (or the Board of Directors) copies of any expert report or other documents relied upon by the practitioner.
6.1.4 Neither the affected practitioner, nor his attorney, nor any other person on behalf of
the affected practitioner, shall contact members of the hearing committee or the Hearing Officer, or hospital employees appearing on the hospital’s witness list concerning the subject matter of the hearing, unless specifically agreed upon by counsel.
6.2 Pre-Hearing Conference The Hearing Officer may require counsel for the practitioner and for the FMEC (or the
Board) to participate in a pre-hearing conference for purposes of resolving all procedural questions in advance of the hearing. The Hearing Officer may specifically require that:
6.2.1 all documentary evidence to be submitted by the parties be presented at this
conference; any objections to the documents shall be made at that time and the Hearing Officer shall resolve such objections;
6.2.2 evidence unrelated to the reasons for the unfavorable recommendation or unrelated
to the practitioner’s qualifications for appointment or the relevant clinical privileges be excluded;
6.2.3 the names of all witnesses and a brief statement of their anticipated testimony are
submitted, if not previously provided; 6.2.4 the time granted to each witness’ testimony and cross-examination be agreed upon,
or determined by the Hearing Officer, in advance; and 6.2.5 witnesses and documentation not provided and agreed upon in advance of the
hearing may be excluded from the hearing. 6.3 Failure to Appear Failure, without good cause, of the practitioner requesting the hearing to appear and
proceed at such a hearing shall be deemed to constitute voluntary acceptance of the pending recommendations or actions, which shall then be forwarded to the Board for final action. The Hearing Officer may impose sanctions upon either party for failure to appear, including the assessment of the costs and attorneys’ fees of the party in attendance against the offending party.
6.4 Record of Hearing
52
A record shall be made at the expense of the Lee Memorial Health System, if any, the pre-hearing conference and the hearing, using the services of a court reporter. No record of the in camera deliberations of the decision making body or the hearing committee shall be
made. Either party shall be entitled to have a record made of any other proceeding related to the hearing process, at that party’s expense. The expense of transcripts shall be borne by the party requesting them. Oral evidence shall be taken only on oath or affirmation administered by any person designated by such body and entitled to notarize documents in this State.
6.5 Rights of Both Sides At a hearing, both sides shall have the following rights, subject to reasonable limits
determined by the Hearing Officer: 6.5.1 to call and examine witnesses to the extent available; 6.5.2 to introduce exhibits; 6.5.3 to cross-examine any witness on any matter relevant to the issues and to rebut any
evidence; 6.5.4 to be represented by counsel who may call, examine, and cross-examine witnesses
and present the case. (Both sides shall notify the other of the name of that counsel at least ten (10) days prior to the date of the pre-hearing conference and hearing); and
6.5.5 to submit a post-hearing memorandum of points and authorities (The Hearing Panel may request such a memorandum to be filed following the close of the hearing).
Any practitioner requesting a hearing, who does not testify on his own behalf, may be called
and examined as if under cross-examination. The Hearing Panel or Hearing Officer may question the witnesses, call additional witnesses or request additional documentary evidence.
6.6 Admissibility of Evidence The rules of evidence applicable to the courtroom shall not apply, and the Hearing Officer
may admit any evidence that might be relied upon by a reasonable person. Notwithstanding the foregoing, a party shall have the right to object to any evidence on
grounds of hearsay, relevance, or other grounds available under the Florida Evidence Code, and the Hearing Officer shall have the authority to rule on such objections.
6.7 Burden of Presenting Evidence and Proof The burden of going forward with evidence supporting the adverse action or
recommendation is on the FMEC or Board, whichever initially prompted the hearing. Once that burden has been met to the satisfaction of the Hearing Panel/Hearing Officer, the practitioner shall bear the burden of proof, under a preponderance of the evidence, which is a lesser standard than clear and convincing evidence, that the action and penalty taken or proposed against the practitioner was wrongfully or arbitrarily imposed, not in accordance with these Bylaws, or lacks any factual basis.
SECTION 7 HEARING CONCLUSION, DELIBERATIONS AND RECOMMENDATIONS
7.1 Deliberations and Recommendation of the Hearing Panel/Hearing Officer
53
7.1.1 The recommendation of the Hearing Panel/Hearing Officer shall be based on the evidence produced at the hearing. This evidence may consist of oral testimony of witnesses; memorandum of points and authorities presented in connection with the hearing, any information regarding the practitioner who requested the hearing so long as that information has been admitted into evidence at the hearing and the person who requested the hearing had the opportunity to comment on and, by other evidence, refute it, any and all applications, references, and accompanying documents; other documented evidence, including medical records and any other information presented at the hearing.
7.1.2 Within thirty (30) working days after final adjournment of the hearing, the Hearing
Panel shall conduct its deliberations outside the presence of any other person except the Hearing Officer, and shall prepare a recommended order containing the findings of fact, findings regarding the applicability of these Bylaws, any rules, regulations or policies of the Medical Staff or the Lee Memorial Health System, and the statutory and decisional law of Florida; and a recommendation that adverse action be upheld, modified or withdrawn. If the FMEC or the Board selected a Hearing Officer sitting alone, the Hearing Officer shall prepare a recommended order in the same manner outlined above.
7.1.3 The Hearing Officer shall not participate in the deliberations of the Hearing Panel,
nor be involved in the decision of the Hearing Panel regarding its recommended order.
However, the Hearing Officer may assist the Hearing Panel with regard to the form,
organization and syntax of the recommended order. The recommended order shall be signed by each member of the Hearing Panel or the Hearing Officer, as applicable, and copies provided in person by certified mail, return receipt requested, to the affected practitioner and System Representative.
7.2 Disposition of Hearing Panel Report The Hearing Panel/Hearing Officer shall deliver its report and recommendation to the Chief
Medical Officer or his designee who shall forward it, along with all supporting documentation, to the Board and/or FMEC.
The recommended order shall be considered by the FMEC or Board at its next regular meeting, and may be adopted or rejected by it. If adopted, the recommended order shall become the final decision of the original decision making body (FMEC or Board).
If rejected, the FMEC or Board shall render its own final written decision upholding the
original recommendation, modifying or withdrawing the action. Any action imposed through the final order that requires action by the Board of Directors shall be referred to the Board for final disposition at its next regular meeting.
SECTION 8 APPEAL PROCEDURE 8.1 Request & Time for Appeal Within ten (10) working days of receipt of the final written decision following a hearing,
either party may appeal the recommendation. The request shall be in writing, signed by the requesting party and delivered to the Chief Medical Officer either in person or by certified mail, return receipt requested, with a copy to the Medical Staff Services Office. The request shall include a statement of the reasons for appeal and the facts or circumstances that justify further review. If such appellate review is not requested within ten (10) working days
54
as provided herein, both parties shall be deemed to have waived the right to an appeal, and the Hearing Panel or Hearing Officer’s report and recommendation shall be forwarded to the Board for final action.
8.2 Grounds for Appeal The grounds for appeal shall be limited to the following: 8.2.1 there was substantial failure to comply with these Bylaws or hospital policies prior to
the hearing so as to deny a fair hearing; or 8.2.2 the recommendations of the Hearing Panel were made arbitrarily, capriciously or
with prejudice. 8.3 Time, Place and Notice Whenever an appeal is requested as set forth in the preceding Sections, the Chair of the
Board shall, as soon as arrangements can reasonably be made, taking into account the schedules of all participants, schedule and arrange for an appellate review. The affected practitioner shall be given notice of the time, place and date of the appellate review. When a request for appellate review is from a appointee who is under a suspension then in effect, the appellate Review panel shall be convened not more than 14-days from the date of receipt of the request for an appeal unless the practitioner agrees to a longer period. The time for appellate review may be extended by the Chair of the Board for good cause.
8.4 Nature of Appellate Review 8.4.1 Review panel. The Chair of the Board shall appoint a Review panel composed of 5
members, 3 of the panel members shall be members of the Board of Directors and 2 panel members shall be Active members of the Medical Staff. The Board may establish rules of procedure to govern the conduct of appellate hearings under this Section and the Chair of the Board, or his or her designee, shall preside at appellate proceedings.
8.4.2 Position Papers. Each party shall have the right to present a written statement in
support of its position on appeal. Position papers that do not conform to the following requirements may be excluded from consideration in the appeal.
8.4.2.1 The position papers shall set forth a statement of the facts and of the
applicable Bylaws provisions or other authority, as well as any other matters that the parties wish to bring before the appellate body in support of their respective positions.
8.4.2.2 Twelve copies of the affected practitioner’s position paper shall be filed
with Medical Staff Services within (fifteen)15 working days of the filing of the notice of appeal. The System Representative shall also file with Medical Staff Services, 12 copies of his position paper within ten (10) working days of his receipt of a copy of the affected practitioner’s position paper.
8.4.2.3 Position papers shall be limited to no more than thirty (30) pages,
exclusive of exhibits, and shall be on letter-size paper, typewritten, double-spaced and shall be neatly bound or stapled.
55
8.4.2.4 Each party shall provide a copy of his position paper to the other at the same time the party’s position paper is filed with Medical Staff Services.
8.4.2.5 Exhibits attached to the position paper shall not duplicate exhibits or
documents contained in the hearing record, and shall be consecutively numbered and attached at the end of the position paper.
8.4.2.6 In referring to the record, position papers shall reference specific pages of
the hearing record and of exhibits that are part of the record. 8.4.3 Oral Argument. The affected practitioner and the System Representative shall be
entitled to present oral argument. Oral argument shall be requested at the time the party submits his position paper. Failure to request oral argument shall constitute a waiver of the right to it. The Board may limit the time for oral argument, but each side shall not have less than thirty (30) minutes. Oral argument shall not include the introduction of evidence and appellate review shall not constitute a hearing de novo.
A record shall be made at the expense of the Lee Memorial Health System of the presentation of oral argument, using the services of a court reporter.
8.4.4 Recommendation. The review panel shall recommend final action to the Board
within thirty (30) working days after the completion of oral argument, or if no oral argument is requested, within forty-five (45) working days after the submission of the position papers of both parties.
SECTION 9 FINAL DECISION OF THE BOARD Within thirty (30) working days after receipt of the Review panel’s recommendation, the Board shall render a final decision in writing, including specific reasons and shall deliver copies thereof to the affected practitioner, the FMEC, and the Medical Staff Services Office, in person or by certified mail, return receipt requested. The decision shall uphold or reverse the final written decision rendered by the decision making body, or may remand the case for reconsideration by the decision making body. If the matter is referred for further action and recommendation, such recommendation shall be promptly made to the Board in accordance with the instructions given by the Board within thirty (30) days. The final decision of the Board following the appeal shall be effective immediately and shall not be subject to further review. SECTION 10 RIGHT TO ONE HEARING AND ONE APPEAL ONLY 10.1 No applicant or Medical Staff practitioner shall be entitled to more than one (1) hearing and
one (1) appeal on any matter that may be the subject of an appeal. A final appellate decision upholding or reversing a final, written decision shall be final and there shall be no right to further hearing on the matter.
10.2 If the Board determines to deny initial Medical Staff appointment or reappointment to an
applicant, or to revoke or terminate the Medical Staff appointment and/or clinical privileges of a current practitioner, that practitioner may not apply for Staff appointment or for those clinical privileges at this hospital for a period of five (5) years unless the Board provides otherwise.
56
PART III: CREDENTIALING PROCEDURES
SECTION 1 SYSTEM CREDENTIALING/PRIVILEGING COMMITTEE 1.1 Organizational Structure
It is the intention of the Medical Staff Organizations of Lee Memorial Health System (LMHS) to ultimately establish one (1) System Credentialing/Privileging Committee (hereinafter referred to as the Credentialing/Privileging Committee) to act on behalf of all the Medical Staff of LMHS. It has been determined that the two (2) Credentialing/Privileging Committees in effect at the time of the approval of this document may continue for a maximum period of two (2) years. During this transition time, the two (2) Credentialing/Privileging Committees will meet jointly on at least a quarterly basis (the Credentialing/Privileging Committees will not meet separately during the months that the joint meetings occur) and through this process will effect a smooth transition to a single System Credentialing/Privileging Committee. The single System Credentialing/Privileging Committee may decide to merge prior to the end of the two 2-year period.
1.2 Transition Issues
At the time of adoption of PART III, two (2) Credentialing/Privileging Committees exist. Chairs of each of these Credentialing/Privileging Committees have been appointed in accordance to procedures that were in existence prior to the adoption of these Credentials Procedures. During the transition period (moving from two (2) committees to a single System Credentialing/Privileging Committee), these Chairs will continue to serve as the Chairs of the applicable practitioner System Credentialing/Privileging Committee and together will serve as Co-Chairs of the System Credentialing/Privileging Committee (which will meet at least quarterly (see Section 1.1).
The initial composition of the System Credentialing/Privileging Committee will be made up of
the membership of the two (2) separate Credentialing/Privileging Committees, with the current Chairs serving as Co-Chairs. During the first year of the System Credentialing/Privileging Committee, the committee will plan to evolve to the composition of the System Credentialing/Privileging Committee as established in Section 1.4 by the end of twenty-four (24) months.
1.3 Purpose of the System Credentialing/Privileging Committee
The System Credentialing/Privileging Committee exists to oversee all credentialing and privileging activities related to Medical Staff members and privileged Allied Health practitioners on behalf of the Facility Medical Executive Committees (FMECs). These credentialing and privileging activities include processes related to the following:
1.3.1 initial appointment; 1.3.2 focused professional practice evaluation; 1.3.3 reappointment; 1.3.4 delineation of clinical privileges, including temporary privileges; and 1.3.5 development of privilege delineation forms and criteria for all LMHS facilities.
57
Credentialing activities are to be carried out in accordance with specific policies and procedures developed to ensure current clinical competency of the practitioners who are credentialed and privileged at LMHS. The purpose of the System Credentialing/Privileging
Committee also includes development of implementation of credentialing and privileging policies and procedures designed to ensure compliance with regulatory requirements.
1.4 Composition of the System Credentialing/Privileging Committee The leadership and membership of the System Credentialing/Privileging Committee shall be
as follows: 1.4.1 Consist of not less than 15 members of the active Medical Staff selected on a basis
that will ensure, insofar as feasible, balanced representation of the LMHS sites. 1.4.2 The System Medical Director will serve as a non-voting member. 1.4.3 The Immediate Past President of each FMEC will serve as voting members and will
serve a 2-year term. The FMEC may appoint this practitioner, as a member once the Immediate Past President is no longer in office.
1.4.4 Each FMEC will appoint two (2) additional representatives. 1.4.5 A quorum of 50% is required to conduct a meeting. 1.4.6 Members shall serve for two (2) years and may be reappointed to consecutive terms. 1.4.7 Each member shall be required to attend 75% of the meetings during the Medical
Staff year. Failure to attend 75% of the meetings may result in dismissal of the member from committee service and selection of an alternative member by the affected FMEC.
1.4.8 The committee members from among the committee membership will elect the Co-
Chairs of the System Credentialing/Privileging Committee. One of the Co-Chairs will be from a medical specialty and the other Co-Chair will be from a surgical specialty.
1.5 Duties and Responsibilities of the System Credentialing/Privileging Committee The System Credentialing/Privileging Committee shall: 1.5.1 Meet to evaluate credentialing-related requests (initial appointment, reappointment,
requests for clinical privileges and leave of absence, etc.) on behalf of the FMECs. 1.5.2 Monitor the granting of temporary privileges to assure that temporary privileges are
granted in compliance with approved policies and procedures. (The System Credentialing/Privileging Committee does not evaluate requests for temporary privileges. These requests are handled in accordance with specific policies and procedures that are overseen by the System Credentialing/Privileging Committee).
1.5.3 Oversee the processes related to focused professional performance evaluations and
related proctoring and other mechanisms and tools employed to evaluate competency.
1.5.4 Assure uniformity in both the development and application of privileging criteria
utilized throughout LMHS facilities.
58
1.5.5 Assure the FMECs and Board that Medical Staff Bylaws Provisions that relate to credentialing and privileging processes are being fulfilled, as well as credentialing policies and procedures and other credentialing-related Medical Staff documents. Monitor compliance with all credentialing and privileging policies and procedures.
1.5.6 Be responsible for evaluating recommendations made by Department Chairs. The committee is looking for completeness, thoroughness and adherence to
credentialing and privileging policies and criteria. Assure the FMECs that specialty-specific criteria for clinical privileges comply with Medical Staff Bylaws, credentialing policies and procedures, and criteria is applied fairly and uniformly to each practitioner.
1.5.7 Focuses in on the files that are determined to need clarification or additional
information (i.e., time gaps, problems with references, malpractice claims, etc.) and assures that all issues have been appropriately addressed and that there is complete and thorough documentation for the recommendation(s) that have been made to the FMECs.
1.5.8 Be responsible and aware of regulatory requirements related to credentialing activities
and to make the FMECs and Board aware when changes in credentialing policies and procedures need to be made in order to meet requirements.
1.5.9 Commission, receive and analyze the results of compliance audits of credentialing
and privileging processes. The System Credentialing/Privileging Committee makes recommendations to the FMECs and the Board when the System Credentialing/Privileging Committee believes, based on results of reports that improvements can and should be made in credentialing and privileging policies and procedures.
SECTION 2 QUALIFICATIONS FOR MEMBERSHIP AND PRIVLEGES 2.1 The following qualifications must be met by all applicants for Medical Staff
appointment, reappointment or clinical privileges:
2.1.1 Associate and Active Staff shall live and maintain an office in Lee County, unless this requirement is waived by the FMEC;
2.1.2 Demonstrate that he has successfully graduated from an approved school of
medicine (MD or DO), dentistry, podiatry, clinical psychology or applicable recognized course of training in a clinical profession eligible to hold privileges;
2.1.3 Have a current unrestricted state or federal license as a physician, dentist, podiatrist
or clinical psychologist, applicable to his or her profession, and providing permission to practice within the State of Florida;
2.1.4 Have a record that is free from current Medicare/Medicaid sanctions and not be on
the Office of Inspector General (OIG) or General Services Administration (GSA) List of Excluded practitioners/entities;
2.1.5 Have a record that is free of felony convictions or occurrences that would raise
questions of undesirable conduct, which could injure the reputation of the Medical Staffs, hospital or Health System;
59
2.1.6 A physician (MD or DO) must have successfully completed an allopathic or osteopathic residency program, approved by the Accreditation Council for Graduate Medical Education (ACGME) or the American Osteopathic Association (AOA) and be currently board certified or become board certified following the completion of formal training within the timeframes as defined by the appropriate specialty board of the American Board of Medical Specialties or the American Osteopathic Association. If no time limits for certification are specified by a given Board, then the applicant will be required to become Board certified within seven (7) years of completing formal training as defined by the appropriate specialty Board of the American Board of Medical Specialties or the American Osteopathic Association. If an applicant is beyond seven (7) years of completing formal training, current Board certification will be required for consideration of membership and privileges. Once a member of the Medical Staff becomes Board certified, recertification is not a requirement of continued membership and privileges;
2.1.7 Dentists must have graduated from an American Dental Association approved
school of dentistry accredited by the Commission of Dental Accreditation; 2.1.8 Oral and maxillofacial surgeons must have graduated from an American Dental
Association approved school of dentistry accredited by the Commission of Dental Accreditation and successfully completed an American Dental Association approved residency program and be board certified or become board certified within five (5) years of completing formal training as defined by the American Board of Oral and Maxillofacial Surgery;
2.1.9 A podiatric physician (DPM) must have successfully completed a two 2-year
residency program in surgical, orthopedic, or podiatric medicine approved by the Council on Podiatric Medical Education of the American Podiatric Medical Association (APMA), and be board certified or become board certified within five (5) years of completing formal training as determined by the American Board of Podiatric Surgery or the American Board of Podiatric Orthopedics and Primary Podiatric Medicine;
2.1.10 A psychologist, must have earned a doctorate degree, (PhD or Psy.D. in
psychology) from an educational institution accredited by the American Psychological Association and have completed at least two (2) years of clinical experience in an organized healthcare setting, supervised by a licensed psychologist, one 1-year of which must have been post doctorate, and have completed an internship endorsed by the American Psychological Association (APA);
2.1.11 Possess a current, valid, Drug Enforcement Administration (DEA) number if
applicable to the privileges requested; 2.1.12 Have appropriate written and verbal communication skills; 2.1.13 Have appropriate personal qualifications, including applicant’s consistent
observance of ethical and professional standards. These standards include, at a minimum:
2.1.13.1 Abstinence from any participation in fee splitting or other illegal payment,
receipt, or remuneration with respect to referral or patient service opportunities;
60
2.1.13.2 A history of consistently acting in a professional, appropriate and collegial manner with others in previous clinical and professional settings.
2.1.14 The following qualifications must also be met by all applicants requesting clinical
privileges: 2.1.14.1 Demonstrate his background, experience, training, current competence,
knowledge, judgment and the ability to perform all privileges requested. 2.1.14.2 Provide evidence of both physical and mental health that does not impair
the fulfillment of his responsibilities of Medical Staff membership subject to any legally required reasonable accommodation, and the specific privileges requested by and granted to the applicant, upon request.
2.1.14.3 Any practitioner granted privileges that may have occasion to admit an
inpatient must demonstrate the capability to provide continuous and timely care to the satisfaction of the FMEC and Board.
2.1.14.4 Demonstrate recent clinical performance (within the last twelve (12)
months with an active clinical practice in the area in which clinical privileges are sought adequate to meet current clinical competence criteria.
2.1.14.5 The applicant is requesting privileges for a service the Board has
determined appropriate for performance at the hospital. There must also be a need for this service under any Board approved Medical Staff development plan.
2.1.14.6 Provide evidence of financial responsibility consistent with the
requirements set forth in Part I. 2.1.15 Exceptions: All practitioners who are current Medical Staff members and/or hold privileges as of
May 28, 2009 and who have met prior qualifications for membership and/or privileges shall be exempt from Board specialty certification requirements.
SECTION 3 PRE-APPLICATION PROCESS
3.1 Only those practitioners that meet the following minimum criteria for appointment to the
Medical Staff will be provided applications. Practitioners provided applications would be those: 3.1.1 which are not governed by an exclusive arrangement or who are joining a group
providing services governed by an exclusive arrangement; and
3.1.2 who meet the minimum criteria as developed by the System Credentialing/Privileging Committee and approved by FMECs and the Board.
The purpose for the pre-application screening process shall be to avoid the costly
and time-consuming application process in those circumstances where an applicant

61
fails to meet minimum eligibility criteria. Practitioners who do not meet the minimum eligibility criteria for appointment are not entitled to fair hearing rights.
The System Credentialing/Privileging Committee shall review all requests for
application and determine whether the criteria for issuing an application have been met.
SECTION 4 INITIAL APPOINTMENT PROCESS
4.1 Completion of Application 4.1.1 All requests for application for appointment to the Medical Staff and requests for
clinical privileges will be forwarded to the Medical Staff Services Department. If the applicant successfully completed the pre-application screening process, the Medical Staff Services Department will provide the applicant an application packet, which will include a complete set or overview of the relevant Medical Staff Bylaws or reference to an electronic source for this information. This packet will enumerate the eligibility requirements for Medical Staff membership (for each facility of LMHS) and/or privileges and a list of expectations of performance for practitioners granted Medical Staff membership or privileges (if such expectations have been adopted by each Facility Medical Staff).
A completed application includes, at a minimum: 4.1.1.1 a completed, signed, dated application form; 4.1.1.2 a completed privilege delineation form if requesting privileges; 4.1.1.3 copies of all requested documents and information necessary to confirm
the applicant meets criteria for membership and/or privileges and to establish current competency;
4.1.1.4 all applicable fees; 4.1.1.5 complete reference information; references shall be from peers (same
specialty) knowledgeable about the applicant’s experience, ability and current competence to perform the privileges being requested;
4.1.1.6 relevant practitioner-specific data as compared to aggregate data, when
available 4.1.1.7 morbidity and mortality data, when available. Each applicant must indicate the LMHS facility anticipated to be his
primary facility (i.e., the facility where the majority of his clinical activity is performed). It should be noted that this designation is important for credentialing purposes (interviews, implementation of focused professional practice evaluation, etc.) and will be confirmed by LMHS data at periodic intervals and prior to any subsequent reappointments.
An application shall be deemed incomplete if any of the above items are
missing or if the need arises for new, additional or clarifying information
62
in the course of reviewing an application. An incomplete application will not be processed and the applicant will not be entitled to a fair hearing.
Anytime in the credentialing process it becomes apparent that an
applicant does not meet all eligibility criteria for membership or privileges, the credentialing process will be terminated and no further action taken. Applications will not be accepted from practitioners that are not eligible to take the Board certification examination.
4.1.2 The burden is on the applicant to provide all required information. It is the
applicant’s responsibility to ensure that the Medical Staff Services Department receives all required supporting documents verifying information on the application and to provide sufficient evidence, as required in the sole discretion of the Health System that the applicant meets the requirements for the Medical Staff membership and/or the privileges requested. If information is missing from the application or new, additional or clarifying information is required, a letter requesting such information will be sent to the applicant. If the requested information is not returned to the Medical Staff Services Department within thirty (30) calendar days of the receipt of the requested letter, the application will be deemed to have been voluntarily withdrawn.
4.1.3 Upon receipt of a completed application, the System Medical Director will determine
if the requirements of Section 2.1 are met. In the event the requirements of Section 2.1 are not met, the applicant will be notified that he is ineligible to apply for membership or privileges on the Medical Staff, the application will not be processed and the applicant will not be eligible for a fair hearing. If the requirements of Section 2.1 are met, the application will be accepted for further processing.
4.1.4 Practitioners seeking appointment shall have the burden of producing information
deemed adequate by the hospital for a proper evaluation of current competence, character, ethics, other qualifications and of resolving any doubts.
4.1.5 Upon receipt of a completed application, the Medical Staff Services Department will
verify current licensure, education, relevant training and current competence from the primary source whenever feasible in accordance with the Verification Methods and Requirements document.
When it is not possible to obtain information from the primary source, reliable
secondary sources may be used if there has been a documented attempt to contact the primary source.
Note: In the event there is undue delay in obtaining required information, the
Medical Staff Services Department will request assistance from the applicant. During this time, the period for processing, the application will be appropriately modified. Failure of an applicant to respond to a request for assistance adequately after thirty (30) calendar days the application will be deemed to have been voluntarily withdrawn.
4.1.6 When all items identified in the Verification Methods and Requirements document
have been obtained and verified, the application will be considered eligible for evaluation.
63
4.2 Applicant’s Attestation, Authorization and Acknowledgement 4.2.1 The applicant must complete and sign the application form. By signing this
application the applicant: 4.2.1.1 Attests to the accuracy and completeness of all information on the
application or accompanying documents and agreement that any inaccuracy, omission or misrepresentation, whether intentional or not, may be grounds for termination of the application process without the right to a fair hearing or appeal.
If the inaccuracy, omission or misstatement is discovered after a
practitioner has been granted appointment and/or clinical privileges, the practitioner’s appointment and privileges shall lapse effective immediately upon notification of the practitioner without the right to a fair hearing or appeal.
4.2.1.2 Consents to appear for any requested interviews about his application. 4.2.1.3 Authorizes the applicable hospital and Medical Staff representative to
consult with prior and current associates and others who may have information bearing on his professional competence, character, ability to perform the privileges requested, ethical qualifications, ability to work cooperatively with others and other qualifications for requested membership and/or clinical privileges.
4.2.1.4 Consents to the Health System and Medical Staff representatives’
inspections of all records and documents that may be material to an evaluation of:
4.2.1.4.1 professional qualifications and competence to carry out the
clinical privileges requested;
4.2.1.4.2 physical and mental/emotional health status to the extent relevant to safely perform requested privileges subject to any legally required reasonable accommodation;
4.2.1.4.3 professional and ethical qualifications;
4.2.1.4.4 professional liability actions including currently pending claims involving the applicant;
4.2.1.4.5 any other issue relevant to establishing the applicant’s
suitability for membership and/or privileges.
4.2.1.5 Releases from liability, promises not to sue and grants immunity to the
Health System, its Medical Staffs and its representatives for acts performed and statements made in good faith in connection with evaluation of the application and his credentials and qualifications fully permitted by the law.
4.2.1.6 Releases from liability and promises not to sue, all practitioners and
organizations who provide information to the Health System or the applicable Medical Staff(s) in good faith, including otherwise privileged or
64
confidential information to the System/hospital representatives concerning his background/experience, competence, professional ethics, character, physical and mental health to the extent relevant to the capacity to fulfill requested privileges, emotional stability, utilization practice patterns, and other qualifications for staff appointment and clinical privileges.
4.2.1.7 Authorizes the Health System, Medical Staff and Administrative
representatives to obtain credentialing and peer review information from other hospitals, medical associations, licensing boards, appropriate government bodies and other health care entities concerned with this provider’s performance and releases representatives of the Health System from liability for so doing.
4.2.1.8 Acknowledges that the applicant has had access to relevant Medical
Staff Bylaws, including all rules, regulations, policies and procedures of the relevant Medical Staffs and agrees to abide by their provisions.
Notwithstanding Section 3.2 of Part II, if a practitioner institutes legal
action and does not prevail, he shall reimburse the Health System and any member of the Medical Staff named in the action for all costs incurred in defending such legal action, including reasonable attorney(s) fees.
4.2.1.9 Agrees to provide accurate answers to all the questions on the
application form, and agrees to immediately notify the System in writing should any of the information regarding these items change during the period of the applicant’s Medical Staff membership and/or privileges.
4.3 Application Evaluation
4.3.1 Expedited Credentialing: 4.3.1.1 An expedited Credentialing/Privileging Committee review and approval
process may be used for initial appointment in accordance with the Expedited Credentialing Policy.
4.3.2 Applicant Interview
4.3.2.1 All applicants for appointment to the Medical Staff and/or the granting of
clinical privileges are required to participate in interviews. The interviews are used to solicit information required to complete the credentials file or clarify information previously provided, e.g., clinical knowledge and judgment, professional behavior, malpractice history, reasons for leaving past healthcare organizations, or other matters bearing on the applicant’s ability to render care at the generally recognized level for the community and in compliance with LMHS privileging criteria. Interviews may also be used to communicate Medical Staff performance expectations.
Applicants for appointment will participate in a minimum of two (2)
interviews. One interview will be conducted by the applicable Department Chair or designated Section Chief of the applicant’s anticipated primary LMHS facility and the second interview will be with a member of the System Credentialing/Privileging Committee. Applicants that are applying for multiple facilities within LMHS may be required to
65
participate in additional Department Chair/Section Chief interviews at the discretion of the Department Chairs of the facility(ies) that are designated as non-primary.
4.3.2.2 Procedure: the applicant will be notified of required interview(s). Failure
of the applicant to appear for a scheduled interview will be deemed a voluntary withdrawal of the application.
4.3.3 Department Chair Action 4.3.3.1 Each Department Chair of an LMHS facility where the applicant has
requested privileges makes a recommendation related to membership and privileges, as applicable.
All completed applications are presented to the appropriate Department
Chair(s) for review and recommendation (which is made by completion of a standardized form provided to the Chair by the Medical Staff Services Department). The Department Chair(s) reviews the application to ensure that it fulfills the established standards for membership and/or clinical privileges. The Department Chair(s) may obtain input if necessary from an appropriate subject matter expert(s).
If a Department Chair believes a conflict of interest exists that, might
preclude his ability to make an unbiased recommendation, he will notify the Medical Staff Services Department and forward the application without comment.
4.3.3.2 The Department Chair(s) forwards to the System
Credentialing/Privileging Committee the following: 4.3.3.2.1 A written recommendation to approve the applicant’s request
for membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges (a summary of the interview conducted by the Department Chair or his designee is included in this written recommendation);
4.3.3.2.2 Written comments supporting his recommendations. The Department Chair of the applicant’s anticipated primary
facility also makes a written recommendation to define those circumstances, which require monitoring and evaluation of clinical performance after the initial granting of clinical privileges (i.e., focused professional practice evaluation).
4.3.4 Medical Staff System Credentialing/Privileging Committee Action 4.3.4.1 The System Credentialing/Privileging Committee reviews the application
and forwards the following to the applicable FMEC(s): 4.3.4.1.1 A recommendation to approve the applicant’s request for
membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges;
66
4.3.4.1.2 A recommendation to define those circumstances, which require monitoring, and evaluation of clinical performance after initial granting of clinical privileges (Focused Professional Practice Evaluation) (FPPE);
Comments supporting the above recommendation. 4.3.5 FMEC Action
4.3.5.1 Each FMEC of LMHS where membership and/or privileges have been requested forwards the following to the Board:
4.3.5.1.1 A recommendation to approve the applicant’s request for
membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges;
4.3.5.1.2 Comments supporting the above recommendation.
The FMEC of the applicant’s anticipated primary facility also makes a recommendation to define those circumstances that require monitoring and evaluation of clinical performance after initial granting of clinical privileges (FPPE).
Whenever a FMEC makes an adverse recommendation to the Board, a notice,
stating the reason, will be sent to the applicant who shall then be entitled to the procedural rights provided in the Investigation, Corrective Action, Hearing and Appeal Plan of the Medical Staff Bylaws. When multiple FMECs are making recommendations related to the same applicant, an adverse recommendation is not considered final until after the PLC attempts to facilitate resolution of the issues (this facilitation occurs when there are disparate recommendations – for example, one (1) positive recommendation and one negative recommendation).
4.3.6 Applicants Applying to Multiple Facilities Applicants may simultaneously make application for membership and/or privileges
to multiple facilities within LMHS. The Medical Staff Services Department coordinates this information so that the recommendations from all FMECs come to the Board together. If there are disparate recommendations (defined as conflicting) related to membership and/or requested clinical privileges on the same applicant, the PLC will meet and attempt to reconcile the disparate recommendations prior to forwarding the recommendations to the Board.
If the PLC is unable to facilitate resolution of the issues (in accordance with the
Medical Staff Bylaws – Part I, Governance – Section 9 Decision Making Methods and Conflict Resolution) the disparate recommendations will go forward to the Board.
4.3.7 Board Action:
4.3.7.1 The Board reviews the recommendation and votes for one (1) of the following actions: 4.3.7.1.1 The Board may adopt or reject in whole or in part a
recommendation of the FMEC(s) or refer the recommendation to the FMEC(s) for further consideration stating the reasons
67
for such referral back and setting a time limit within which a subsequent recommendation must be made.
4.3.7.1.2 If the Board concurs with the applicant’s request for
membership and/or privileges, it will grant the appropriate membership and/or privileges for a period not to exceed 24 months.
4.3.7.1.3 If the Board’s action is adverse to the applicant, a notice,
stating the reason, will be sent to the applicant who shall then be entitled to the procedural rights provided in the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) unless the applicant received procedural rights under Part II, Section 3.2.5.
4.3.7.1.4 The Board shall take final action in the matter as provided in
the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan).
4.3.8 Notice of Final Decision:
4.3.8.1 Notice of the Board’s final decision shall be given through the Medical
Staff Services Department to the applicable FMEC(s) and to the Chair of each Department concerned. The applicant shall receive written notice of appointment and special notice of any adverse final decisions in a timely manner. A decision and notice of appointment includes the staff category(ies) to which the applicant is appointed, the Department(s) to which he is assigned, the clinical privileges he may exercise, notification of orientation and any special conditions attached to the appointment.
4.3.9 Periods for Processing: 4.3.9.1 All practitioners and groups acting on an application for staff
appointment and/or clinical privileges must do so in a timely and good faith manner, and except for good cause, each application will be processed within 180 calendar days. The 180 Calendar days begin on the date that the application is declared complete to begin processing.
4.3.9.2 These processing periods are deemed guidelines and do not create
any right to have an application processed within these precise periods. If the provisions of the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) are activated, the time requirements provided therein govern the continued process of the application.
SECTION 5 FOCUSED PROFESSIONAL PRACTICE EVALUATION (FPPE) 5.1 CRITERIA FOR FPPE 5.1.1 The Department Chair (or designated Section Chief) of the applicant’s anticipated
primary facility will define circumstances that require monitoring and evaluation of
68
the clinical performance of each practitioner following his or her initial granting of clinical privileges.
Such monitoring may utilize a range of techniques, including but not limited to: chart
review, the tracking of performance monitors/indicators, proctoring, external peer review, simulations, morbidity/mortality reviews, and discussion with other healthcare practitioners involved in the care of each patient. The FPPE plan is created as part of the initial recommendation for appointment and privileges and is forwarded to the System Credentialing/Privileging Committee and to the FMEC(s).
The System Credentialing/Privileging Committee will establish via policy the
anticipated duration for FPPE. The Physician Quality Committee will establish the triggers that indicate the need for
performance monitoring after the initial granting of privileges. SECTION 6 CRITERIA FOR REAPPOINTMENT 6.1 Criteria for Reappointment 6.1.1 It is the policy of the Health System to approve for reappointment and/or renewal of
privileges only those practitioners who meet the criteria for initial appointment as identified in Section 2, Part 1. The practitioner must also be determined by each applicable FMEC to be a provider of effective care that is consistent with the Health System standards of ongoing quality and the hospital performance improvement program and provide the information enumerated in Section 5.1.1.
All reappointments and renewals of clinical privileges are for a period not to exceed
24 months. The granting of new clinical privileges to existing Medical Staff members will follow the steps described in Section 4 concerning the initial granting of new clinical privileges and Section 5 concerning FPPE. A suitable peer shall substitute for the Department Chair in the evaluation of current competency of the Department Chair, and recommend appropriate action to the System Credentialing/Privileging Committee.
In the event a practitioner finds no need to utilize the facilities or resources of LMHS
for purposes of patient care through either admission, performance of a procedure, consultation, or referral, during a two-year period he may not be eligible for reappointment or continued privileges. Such practitioner may apply as a new applicant at any time subsequent to the expiration of the current appointment or privileges. This provision applies to practitioners who have been granted a leave of absence, moved their practice location, established a relationship with another institution or otherwise find no need to utilize the clinical resources of LMHS. Exceptions to this provision may be made by the Board upon recommendation of the applicable FMEC(s).
As long as a practitioner has adequate clinical activity to maintain privileges at one
LMHS facility (and is recommended for continuation of privileges at his primary LMHS facility) the practitioner may maintain the applicable clinical privileges and staff category (potentially Associate if there is no or minimal clinical activity) at other LMHS facility(ies).
6.2.1 Information, Collection and Verification
69
6.2.1.1 From practitioner: On or before 4 months prior to the date of expiration of a Medical Staff appointment or granting of privileges, a representative from the Medical Staff Services Department notifies the practitioner of the date of expiration and supplies him with an application for reappointment for membership and/or privileges. At least sixty (60) calendar days prior to this date, the practitioner must return the following to the Medical Staff Services Department:
6.2.1.1.1 A completed reapplication form, which includes complete
information to update his file on items listed in his original application, any required new, additional, or clarifying information, and any required fees or dues;
6.2.1.1.2 Information concerning continuing training and education
internal and external to the hospital during the preceding period;
6.2.1.1.3 By signing the reapplication form, the practitioner agrees to
the same terms as identified in Section 4.2. 6.2.2 From internal and/or external sources: The Medical Staff Services Department
collects and verifies information regarding each staff practitioner’s professional and collegial activities to include those items listed in Section 2.1.
6.2.3 The following information is also collected and verified:
6.2.3.1 A summary of clinical activity at each LMHS facility for each practitioner due for reappointment.
6.2.3.2 Performance and conduct in each LMHS facility and other healthcare
organizations in which the practitioner has provided substantial clinical care since the last reappointment, including patient care, medical/clinical knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism and system-based practice.
6.2.3.3 Documentation of CME activity; 6.2.3.4 Service on Medical Staff, Department and hospital committees; 6.2.3.5 Timely and accurate completion of medical records; 6.2.3.6 Compliance with all applicable Bylaws, policies, rules, regulations, and
procedures of the System and the Medical Staff(s); 6.2.3.7 Any significant gaps in employment or practice since the previous
appointment or reappointment; and 6.2.3.8 Additional items as identified in the Verification Methods and
Requirements document.
6.2.4 Failure, without good cause, to provide any requested information, at least forty-five (45) calendar days prior to the expiration of appointment will result in a cessation of processing of the application and automatic expiration of appointment when the appointment period is concluded. Once the information is received, the Medical Staff Services Department verifies this additional information and notifies the staff
70
practitioner of any additional information that may be needed to resolve any doubts about performance or material in the credentials file.
6.3 Evaluation of Application for Reappointment of Membership and/or Privileges
6.3.1 The reappointment application will be reviewed and acted upon as described in Sections 4.3.3 through 4.3.8. For the purpose of reappointment, an “adverse recommendation” by the Board as used in Section 4.3 means a recommendation or action to deny reappointment, or to deny or restrict requested clinical privileges or any action that would entitle the applicant to a Fair Hearing under the Medical Staff Bylaws. The terms “applicant” and “appointment” as used in these Sections shall be read respectively, as “staff practitioner” and “reappointment”.
SECTION 7 CLINICAL PRIVILEGES 7.1 Exercise of Privileges
A practitioner providing clinical services at a LMHS facility may exercise only those privileges granted to him by the Board or emergency and disaster privileges as described herein. Privileges may be granted by the Board upon recommendation of the FMEC(s) to practitioners who are not members of the Medical Staff. Such practitioners may include Advanced Registered Nurse Practitioners (ARNPs), Physician Assistants (PAs), practitioners serving short locum tenens positions, telemedicine physicians or others deemed appropriate by the FMEC(s) and Board.
7.2 Requests
When applicable, each application for appointment or reappointment to the Medical Staff must contain a request for the specific clinical privileges desired by the applicant. Specific requests must also be submitted for temporary privileges and for modifications of privileges in the interim between reappointments and/or granting of privileges.
7.3 Basis for Privileges Determination 7.3.1 Requests for clinical privileges will be considered only when accompanied by
evidence of education, training, experience, and demonstrated current competence as specified by the System in its Board approved criteria for clinical privileges.
7.3.2 Privileges for which no criteria have been established: 7.3.2.1 In the event a request for a privilege is submitted for a new technology, a
procedure new to the System, an existing procedure used in a significantly different manner, or involving a cross-specialty privilege for which no criteria have been established, the request will be tabled for a reasonable period of time, usually not to exceed sixty (60) calendar days. During this time, the System Credentialing/Privileging Committee may refer the request for review by a task force appointed to review the request.
Task forces formed for purposes of establishment of evaluation of new
privileges and potential determination of criteria will be appointed by the Chairs of the System Credentialing/Privileging Committee, and will include the System Medical Director of Clinical Effectiveness and the Director of Supply Chain Management. The task force will:
71
7.3.2.1.1 Review the community, patient and System need for the
privilege and reach agreement with management and the Board that the privilege is approved to be exercised at the hospital;
7.3.2.1.2 Review with appropriate individuals/groups
the efficacy and clinical viability of the requested privilege and confirm that this privilege is approved for use in the setting-specific area of the hospital by appropriate regulatory agencies (FDA, OSHA, etc.);
7.3.2.1.3 Meet with management to ensure that the new privilege is
consistent with the Health System’s mission, values, strategic, operating, capital, information and staffing plans;
7.3.2.1.4 Work with management to ensure that any/all exclusive
contract issues, if applicable are resolved in such a way to allow the new or cross-specialty privileges in question to be provided without violating the existing contract. Upon recommendation from the System Credentialing/Privileging Committee and appropriate clinical services/specialty or subject matter experts (as determined by the System Credentialing/Privileging Committee), the criteria will be recommended to each FMEC and then to the Board. Once objective criteria have been established, the original request will be processed as described herein.
7.3.2.2 For the development of criteria, the Medical Staff Services Department (or
designee) will compile information relevant to the privileges requested which may include, but need not be limited to, position and opinion papers from specialty organization, position and opinion statements from interested individuals or groups and documentation from other hospitals in the region as appropriate.
7.3.2.3 Criteria to be established for the privilege(s) in question include education,
training, board status or certification (if applicable), experience and evidence of current competence. Proctoring requirements, if any, will be addressed including who may serve as proctor and how many proctored cases will be required.
Hospital related issues such as exclusive contracts, equipment, clinical
support staff and management would be referred to the appropriate hospital administrator and/or Department Director.
7.3.2.4 If the privileges requested overlap two (2) or more specialty disciplines, an
ad hoc committee may be appointed by the System Credentialing/Privileging Committee to recommend criteria for the privilege(s) in question. This ad hoc committee will consist of at least one (1) but no more than two (2) members from each involved discipline. The Chair of the ad hoc committee will be a member of the System Credentialing/Privileging Committee who has no vested interest in the issue (see Medical Staff Privilege Dispute Resolution Policy).
72
7.3.3 Requests for clinical privileges will be consistently evaluated on the basis of prior and continuing education, training, experience, utilization practice patterns, current ability to perform the privileges requested and demonstrated current competence,
ability, and judgment. Additional factors that may be used in determining privileges are patient care needs and the System’s capability to support the type of privileges being requested and the availability of qualified coverage in the applicant’s absence. The basis for privileges determination to be made in connection with periodic reappointment or a requested change in privileges must include documented clinical performance and results of the staff’s performance improvement program activities.
Privilege determinations will also be based on pertinent information from other
sources, such as peers and/or faculty from other institutions and healthcare settings where the practitioner exercises clinical privileges.
7.3.4 The procedure by which requests for clinical privileges are processed are as outlined in Section 4.
7.3.5 Special Conditions for Dental Privileges
Requests for clinical privileges for dentists are processed in the same manner as all other privilege requests. Privileges for surgical procedures performed by dentists and/or oral and maxillofacial surgeons will require that all dental patients receive a basic medical evaluation (history and physical) by a physician member of the Medical Staff with privileges to perform such an evaluation, which will be recorded in the medical record. Oral and maxillofacial surgeons may be granted the privilege of performing a history and physical on their own patients upon submission of documentation of completion of an accredited postgraduate residency in oral and maxillofacial surgery and demonstrated current competence.
7.3.6 Special Conditions for practitioners not Qualified for Medical Staff Appointment but Practicing Pursuant to Clinical Privileges per System Policy. Requests for privileges, from such practitioners, are processed in the same manner as requests for clinical privileges by providers eligible for Medical Staff membership, with the exception that such practitioners are not eligible for membership on a Medical Staff and do not have the rights and privileges of such membership (all rights and responsibilities are defined in the Allied Health Practitioner (AHP) Privileging Policy and Procedure). Only those categories of practitioners approved by the Board for providing services at the hospital are eligible to apply for privileges. AHP(s) in this category may, subject to any licensure requirements or other limitations, exercise independent judgment only within the areas of their professional competence and participate directly in the medical management of patients under the supervision of a physician who has been accorded privileges to provide such care.
7.4 Special Conditions for Podiatric Privileges Requests for clinical privileges for podiatrists are processed in the same manner as all other privilege requests.
Practitioners granted podiatric privileges may perform and shall record in the medical
record a basic medical evaluation history and physical for the practitioner’s podiatric
73
patients if consistent with the privileges granted to the practitioner, state law governing the practitioner’s practice and federal law.
7.5 Special Conditions for Residents or Fellows in Training
Residents or Fellows in Training in the Health System shall not normally hold membership on the Medical Staff and shall not normally be granted specific clinical privileges. Rather, they shall be permitted to function clinically only in accordance with the written training protocols developed by the Professional Graduate Education Committee in conjunction with the Residency Training Program. The protocols must delineate the roles, responsibilities, and patient care activities of residents and fellows including which types of residents may write patient care orders, under what circumstances why they may do so, and what entries a supervising physician must countersign. The protocol must also describe the mechanisms through which resident directors and supervisors make decisions about a resident’s progressive involvement and independence in delivering patient care and how these decisions will be communicated to appropriate Medical Staff and hospital leaders.
The Post-Graduate Education Program Director or Committee must communicate
periodically with each applicable FMEC and the Board about the performance of its residents, patient safety issues and quality of patient care and must work with the FMEC to assure that all supervising physicians possess clinical privileges commensurate with their supervising activities.
7.6 Special Conditions for the Aging Practitioner
At the age of 70, practitioners shall complete an annual examination that addresses both the physical and mental capacity for the privileges requested. The annual physical and mental exams are to be conducted by an independent Medical examiner acceptable to the System Credentialing/Privileging Committee, documented on the approved form and submitted to the System Credentialing/Privileging Committee by the date requested. The physical exam is a “fitness to work” evaluation and must indicate that the practitioner has no physical or mental problem that may interfere with the safe and effective provision of care permitted under the privileges granted. In addition to the physical exam, a practitioner may be required to undergo proctoring of his clinical performance as part of the assessment of his capacity to perform the requested privileges. Such proctoring may be required in the absence of any previous performance concerns. The scope and duration of the proctoring shall be determined by the FMEC upon recommendation of the Department Chair of the practitioner’s primary facility and System Credentialing/Privileging Committee. The practitioner shall pay the cost of the physical and mental exam.
7.7 Temporary Privileges 7.7.1 Temporary privileges may be granted by the CEO, or designee, acting on behalf of
the Board and based on the recommendation of the President of the Medical Staff or designee to be approved at the next FMEC meeting, provided there is verification of current licensure and current competence. Temporary privileges may be granted only in two (2) circumstances: 1) to fulfill an important patient care, treatment or service need, or 2) when an initial applicant with a complete application that raises no concerns is awaiting review and approval of the FMEC and the Board. Applications pending completion of the initial appointment process must always be
74
reviewed and a recommendation made by the System Credentialing/Privileging Committee prior to the granting of temporary privileges.
7.7.2 Important Patient Care, Treatment or Service Need: Temporary privileges may be
granted on a case-by-case basis when an important patient care, treatment or service need exists that mandates an immediate authorization to practice, for a limited time, not to exceed 30 calendar days (from date privileges are granted). Temporary privileges may be extended for two separate 30-day intervals upon approval of the Board of Directors. For the purposes of granting temporary privileges, an important patient care, treatment or service need is defined as including the following:
7.7.2.1 a circumstance in which one or more individual patients will experience
care that does not adequately meet their clinical needs if the temporary privileges under consideration are not granted, (i.e., a patient scheduled for urgent surgery who would not be able to undergo the surgery in a timely manner);
7.7.2.2 a circumstance in which the institution will be placed at risk of not
adequately meeting the needs of patients who seek care, treatment or service from the institution if the temporary privileges under consideration are not granted (i.e., the institution will not be able to provide adequate emergency room coverage in the providers specialty, or the Board has granted privileges involving new technology to a physician on the staff provided the physician is precepted for a specific number of initial cases and the precepting physician, who is not seeking Medical Staff membership, requires temporary privileges to serve as a preceptor);
7.7.2.3 a circumstance in which a group of patients in the community will be
placed at risk if not receiving patient care that meets their clinical needs if the temporary privileges under consideration are not granted (i.e. a physician who has a large practice in the community for which adequate coverage of hospital care for those patients cannot be arranged).
7.7.3 Clean Application (Expedited) Awaiting Approval: Temporary privileges may be
granted for up to 30 calendar days (from date privileges are issued) approved by the Executive Committee with two 30-day extensions approved by the Board (see the policy and procedure on Expedited Credentialing) when the new applicant for Medical Staff membership and/or privileges is waiting for review and recommendation by the FMEC and approval by the Board.
7.7.4 Special requirements of consultation and reporting may be imposed as part of the
granting of temporary privileges. Except in unusual circumstances, temporary privileges will not be granted unless the practitioner has agreed in writing to abide by the Bylaws, rules, and regulations and policies of the Medical Staff and hospital in all matters relating to his temporary privileges. Whether or not such written agreement is obtained, these Bylaws, rules, regulations and policies control all matters relating to the exercise of clinical privileges.
7.7.5 Termination of temporary privileges: The CEO, acting on behalf of the Board and
after consultation with the President of the Medical Staff, may terminate any or all of the practitioner’s privileges based upon the discovery of any information or the occurrence of any event of a nature, which raises questions about a practitioner’s privileges.
75
Where the life or well-being of a patient is determined to be endangered, any person entitled to impose precautionary suspension under the Medical Staff Bylaws may effect the termination. In the event of any such termination, the CEO or his designee then will assign the practitioner’s patients to another practitioner. The wishes of the patient shall be considered when feasible, in choosing a substitute practitioner.
7.7.6 Rights of the practitioner with temporary privileges: A practitioner is not entitled to
the procedural rights afforded in the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) because his request for temporary privileges is refused or because all or any part of his temporary privileges are terminated or suspended unless based on a determination of clinical incompetence or unprofessional conduct.
7.7.7 Emergency Privileges: In the case of a medical emergency, any practitioner is
authorized to do everything possible to save the patient’s life or to save the patient from serious harm, to the degree permitted by the practitioner’s license, regardless of facility affiliation, staff category, or level of privileges. A practitioner exercising emergency privileges is obligated to summon all consultative assistance deemed necessary and to arrange appropriate follow-up.
7.7.8 Disaster Privileges 7.7.8.1 If the System’s Disaster Plan has been activated and the organization is
unable to meet immediate patient needs, the CEO and such other individuals as identified in the System’s Disaster Plan with such authority, may, on a case by case basis consistent with medical licensing and other relevant state statutes, grant disaster privileges to provide patient care to selected Licensing Independent Practitioners (LIP’s), who must at a minimum present a valid governmental-issued photo identification issued by a state or federal agency (e.g. driver’s license or passport) and at least one of the following:
7.7.8.1.1 a current picture hospital ID card that clearly identifies
professional designation; 7.7.8.1.2 a current license to practice; 7.7.8.1.3 primary source verification of the license;
7.7.8.1.4 identification indicating that the practitioner is a member of a
Disaster Medical Assistance Team (DMAT), or Medical Reserve Corps (MRC), Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VHP), or other recognized state or federal organizations or groups;
7.7.8.1.5 identification indicating that the practitioner has been
granted authority to render patient care, treatment, and services in disaster circumstances (such authority having been granted by a federal, state, or municipal entity);
7.7.8.1.6 identification by a current hospital or Medical Staff
member(s) who possesses personal knowledge
76
regarding the volunteer’s ability to act as a LIP during a disaster.
7.7.8.2 The Medical Staff oversees the professional performance of
volunteer practitioners who have been granted disaster privileges by direct observation, mentoring or clinical record review.
The organization makes a decision (based on information obtained regarding the professional practice of the volunteer) within 72 hours related to the continuation of the disaster privileges initially granted.
7.7.8.3 Primary source verification of licensure begins as soon as the
immediate situation is under control, and is completed within 72 hours from the time the volunteer practitioner presents to the organization.
7.7.8.4 Once the immediate situation has passed and such determination
has been made consistent with the institution’s Disaster Plan, the practitioner’s disaster privileges will terminate immediately.
7.7.8.5 Any individual identified in the institution’s Disaster Plan with the
authority to grant disaster privileges shall also have the authority to terminate disaster privileges. Such authority may be exercised at the sole discretion of the hospital and will not give rise to a right to a fair hearing or an appeal.
SECTION 8 PRECEPTORSHIP
8.1 A practitioner who has not provided acute inpatient care within the past 24 months who requests clinical privileges at the hospital must arrange for a preceptorship either with a current member in good standing of the Medical Staff who practices in the same specialty or with an academic training program or other equivalently competent physician practicing outside of the hospital. The practitioner must assume responsibility for any financial costs required to fulfill the requirements of Sections 8.1 and 8.2.
8.2 A description of the preceptorship program, including details of monitoring and consultation
must be written and submitted for approval to the applicable Department Chair, System Credentialing/Privileging Committee and FMEC. At a minimum, the preceptorship program description must include the following: 8.2.1 The scope and intensity of required preceptorship activities; 8.2.2 The requirement for submission of a written report from the preceptor prior to
termination of the preceptorship period assessing, at a minimum, the applicant’s demonstrated clinical competence related to the privileges requested, ability to get along with others, the quality and timeliness of medical records documentation, ability to perform the privileges requested, and professional ethics and conduct.
SECTION 9 REAPPLICATION AFTER MODIFCATIONS OF MEMBERSHIP STATUS OF PRIVILEGES AND EXHAUSTION OF REMEDIES
77
9.1 Reapplication After Adverse Credentials Decision
9.1.1 Except as otherwise determined by the Board, a practitioner who has received a
final adverse decision or who has resigned or withdrawn an application for appointment, reappointment or clinical privileges while under investigation or to avoid an investigation is not eligible to reapply to the Medical Staff for a period of five (5) years from the date of the notice of the final adverse decision or the effective date of the resignation or application withdrawal. Any such application is processed in accordance with the procedures then in force. As part of the reapplication, the practitioner must submit such additional information as the Medical Staff and/or Board requires, demonstrating that the basis of the earlier adverse action no longer exists. If such information is not provided, the reapplication will be considered incomplete and voluntarily withdrawn and will not be processed any further.
9.2 Request for Modification of Appointment Status or Privileges
9.2.1 A staff member, either in connection with reappointment or at any other time, may
request modification of staff category, Department assignment, or clinical privileges by submitting a written request to the Medical Staff Services Department. A modification request must be on the prescribed form and must contain all pertinent information supportive of the request. All requests for additional clinical privileges must be accompanied by information demonstrating additional education, training, and current clinical competence in the specific privileges requested. A modification application is processed in the same manner as a reappointment, which is outlined in Section 6 of this manual. A practitioner who determines that he no longer exercises, or wishes to restrict or limit the exercise of, particular privileges that he has been granted shall send written notice, through the Medical Staff Services Department to the System Credentialing/Privileging Committee, and FMEC. A copy of this notice shall be included in the practitioner’s credentials file.
9.3 Resignation of Staff Appointment or Privileges
9.3.1 A practitioner who wishes to resign his staff appointment and/or clinical privileges
must provide written notice to the appropriate Department Chair or President of the Medical Staff. The resignation shall specify the reason for the resignation and the effective date. A practitioner who resigns his staff appointment and/or clinical privileges is obligated to accurately complete all portions of all medical records for which he is responsible prior to the effective date of resignation. Failure to do so shall result in an entry in the practitioner’s credentials file acknowledging the resignation and indicating that it became effective under unfavorable circumstances.
9.4 Exhaustion of Administrative Remedies
9.4.1 Every practitioner agrees that he will exhaust all the administrative remedies
afforded in the various Sections of Part I: Governance, Part II: Investigations, Corrective Action, Hearing and Appeal Plan and Part III: Credentialing Procedures before initiating legal action against the System or its agents.
9.5 Reporting Requirements
78
9.5.1 The CMO or his designee shall be responsible for assuring that the hospital satisfies its obligations under the Health Care Quality Improvement Act of 1986 and its successor statutes. Actions that must be reported include any negative professional review action against a physician or dentist related to clinical incompetence or misconduct that leads to a denial of appointment and/or reappointment, reduction in clinical privileges for greater that thirty (30) calendar days; resignation, surrender of privileges, or acceptance of privilege reduction either during an investigation or to avoid an investigation.
SECTION 10 LEAVE OF ABSENCE
10.1 Leave Request
10.1.1 A leave of absence is a matter of courtesy, not of right. In the event that it is
determined that a practitioner has not demonstrated good cause for a leave, or where a request for extension is not granted, the determination shall be final, with no recourse to a hearing and appeal. A leave of absence must be requested for any absence from the Medical Staff and/or patient care responsibilities longer than thirty (30) days if such absence is related to the practitioner’s physical or mental health or to the ability to care for patients safely and competently. A practitioner who wishes to obtain a voluntary leave of absence must provide written notice to the President of the Medical Staff stating the reasons for the leave and approximate period of the leave, which may not exceed one 1-year except for military service or express permission by the Board. Requests for leave must be forwarded, with a recommendation from the FMEC, and affirmed by the Board. While on leave of absence, the practitioner may not exercise clinical privileges or prerogatives and has no obligation to fulfill Medical Staff responsibilities.
10.2 Termination of Leave
10.2.1 At least thirty (30) calendar days prior to the termination of the leave, or at any
earlier time, the practitioner may request reinstatement by sending a written notice to the President of the Medical Staff. The practitioner must submit a written summary of relevant activities during the leave if the FMEC or Board so requests.
A practitioner returning from a leave of absence for health reasons must provide a
report from his physician that answers any questions that the FMEC or Board may have as part of considering the request for reinstatement. The FMEC makes a recommendation to the Board concerning reinstatement, and the applicable procedures concerning the granting of privileges are followed. If the practitioner’s current grant of membership and for privileges is due to expire during the leave of absence, the practitioner must apply for reappointment or his appointment and/or clinical privileges shall lapse at the end of the appointment period.
10.3 Failure to Request Reinstatement 10.3.1 Failure, without good cause, to request reinstatement shall be deemed a voluntary
resignation from the Medical Staff and shall result in automatic termination of membership, privileges, and prerogatives. A practitioner whose membership is automatically terminated shall not be entitled to the procedural rights provided in the Medical Staff Bylaws. A request for Medical Staff membership subsequently received from a member so terminated shall be submitted and processed in the manner specified for applications for initial appointments.
79
SECTION 11 PRACTITIONERS PROVIDING CONTRACTED SERVICES 11.1.1 When the System or hospital contracts for patient care services with LIPs who
provide official readings of images, tracings or specimens through a telemedicine mechanism, and these practitioner’s services are under the control of a Joint Commission accredited organization, the hospital will:
11.1.1.1 specify in a contract that the entity providing these services by contract
(the contracting entity) will ensure that all services provided under this contract by individuals who are LIPs will be within the scope of those practitioner’s privileges at the contracting entity; or
11.1.1.2 verify that all individuals who are LIPs and providing services under the
contract have privileges that include the services provided under the contract.
11.2 When the System/hospital contracts for care services with LIPs, who provide official
readings of images, tracings or specimens through a telemedicine mechanism, and these practitioner’s services are not under the control of a Joint Commission accredited organization, all LIPs who will be providing services under this contract will be permitted to do so only after being granted privileges at the hospital through the mechanisms established in this manual.
11.3 Contract Services/Department or Service Closure
11.3.1 The membership and privileges on the Medical Staff of any practitioner who has a
contractual relationship with the System or with an entity that has a contractual relationship with the System to provide professional services to patients shall be subject to those provisions contained in said contract with regard to the termination of Medical Staff membership and privileges upon the expiration, lapse, cancellation or termination of the contract. If the contract so provides, the affected practitioner shall have no right to a hearing regarding termination of Medical Staff membership or privileges.
11.3.2 In the event a hospital Department is closed, discontinued or provided through an
exclusive contract, such establishment shall not adversely impact the ability of any physician to continue to maintain clinical membership and exercise privileges in existence at the time of such closure, discontinuance or exclusive contract. Initial applications for Medical Staff membership and privileges will not be extended, provided, accepted, processed or approved to or from physicians unless they are joining groups who are actively contracted for exclusively contracted services.
11.3.3 In the event the Board determines that a patient care service shall be closed,
discontinued, or provided through an exclusive contract, such action shall require approval by the affected FMEC.
Both parties agree that any Department or service closure shall occur solely so that
the health and wellbeing of the patients and the best interests of the hospital under these Bylaws may be served at all times. Notwithstanding any other provision in the Bylaws, if the Board and the affected FMEC are unable to agree upon the closure of a Department or service, the matter shall undergo the conflict resolution process set forth in Part I, Section 9 of these Bylaws.
80
If the parties are still in disagreement regarding the closure of a Department or
service upon completion of the conflict resolution process, the parties shall engage in mediation in accordance with the procedures set forth by the American Health Lawyers Association’s Alternative Dispute Resolution Service or another independent mediation service mutually agreeable to the parties. In the event the Board and FMEC are at impasse at mediation and conflict remains, the Board and the FMEC retain the right to seek a resolution through litigation. Further, the Board shall not close a Department or service for a period of three months following impasse at mediation.
11.4 Qualifications
11.4.1 A practitioner who is or will be providing specified professional services pursuant to
a contract or a letter of agreement with the Health System must meet the same qualifications, must be processed in the same manner, and must fulfill all the obligations of his appointment category as any other applicant or staff practitioner.
11.5 The terms of the Medical Staff Bylaws will govern disciplinary action taken by or
recommended by the FMEC.
11.6 Effect of Contract or Employment Expiration or Termination
11.6.1 The effect of expiration or other termination of a contract upon a practitioner’s staff appointment and clinical privileges will be governed solely by the terms of the practitioner’s contract with the System. If the contract or the employment agreement is silent on the matter, then contract expiration or other termination alone will not affect the practitioner’s staff appointment status or clinical privileges.
SECTION 12 MEDICAL ADMINISTRATIVE OFFICERS
12.1 A Medical Administrative Officer is a practitioner engaged full or part- time by the hospital in an administratively responsible capacity, whose activities may also include clinical responsibilities such as direct patient care, teaching, or supervision of the patient care activities of other practitioners under the officer’s direction.
12.2 Each Medical Administrative Officer must achieve and maintain Medical Staff appointment
and clinical privileges appropriate to his clinical responsibilities and discharge staff obligations appropriate to his staff category in the same manner applicable to all other staff members.
12.3 Effect of removal from office or adverse change in appointment status or clinical privileges:
12.3.1 Where a contract exists between the officer and the Health System, its terms
govern the effect of removal from the Medical Administrative Office on the officer’s staff appointment and privileges and the effect an adverse change in the officer’s staff appointment or clinical privileges has on his remaining in office.
12.3.2 In the absence of a contract or where the contract is silent on the matter, removal
from office has no effect on appointment status or clinical privileges. The effect of an adverse change in appointment status or clinical privileges on continuance in office will be determined by the Board.

81
12.3.3 A Medical Administrative Officer has the same procedural rights as all other staff members in the event of an adverse change in appointment status or clinical privileges unless the change is, by contract a consequence of removal from office.
82
83
The Children’s Hospital
Medical Staff
Bylaws
Adopted: May 28, 2009 Revision approved by BOD June 24, 2010
Revision approved by BOD August 26, 2010 Revision approved by BOD August 25, 2011
Revision approved by BOD December 6, 2012
1
TABLE OF CONTENTS PART 1: GOVERNANCE 6 SECTION 1 MEDICAL STAFF PURPOSE & AUTHORITY 6 1.1 Purposes 6 1.2 Authority 6 1.3 Medical Staff (Term) 6 SECTION 2 MEDICAL STAFF MEMBERSHIP 7 2.1 Nature of Medical Staff Membership 7 2.2 Qualifications for Membership 7 2.3 Nondiscrimination 7 2.3.1 No Automatic Entitlement 7 2.4 Conditions and Duration of Appointment 7 2.5 Medical Staff Membership and Clinical Privileges 8 2.6 Medical Staff Members’ Responsibilities 8 2.7 Basic Responsibilities of Applicants and Appointees 8 2.8 Member Rights 11 2.9 Medical Staff Dues and Assessments 11 2.10 Conflict of Interest 12 SECTION 3 CONFIDENTIALITY, IMMUNITY AND RELEASES 12 SECTION 4 CATEGORIES OF THE MEDICAL STAFF 14 4.1 Active Category 14 4.2 Associate Category 15 4.3 Honorary Category 16 SECTION 5 OFFICERS OF THE MEDICAL STAFF 16 5.1 Officers of Medical Staff and FMEC at-Large Members 16 5.2 Qualifications of Officers and FMEC at-Large Members 16 5.3 Election of Officers and FMEC at-Large Members 16 5.4 Terms of Office 17 5.5 Vacancies of Office 17 5.6 Duties of Officers and FMEC at-Large Members 17 5.7 Removal and Resignation of Officer or FMEC at-Large Members 19 SECTION 6 MEDICAL STAFF ORGANIZATION 20 6.1 Departments 20 6.2 Qualifications, Selection, Term, Removal and Responsibility of Department Chair 21 6.3 Assignment to Department 23 SECTION 7 MEDICAL STAFF GOVERNANCE COMMITTEES 23 7.1 Designation of the LMHS MS Physician Leadership Council (PLC) 23 7.2 Composition of the LMHS PLC 23 7.3 Staff Functions 25
2
7.4 Facility Medical Executive Committee (FMEC) (Composition, Selection and Tenure) 25 7.5 Duties and Responsibilities of the FMEC’s 25 7.6 System Medical Staff Committees 27 7.6.1 Purpose 27 7.6.2 Organization to Perform Functions 27 7.6.2.1 System Credentialing/Privileging Committee 27 7.6.2.2 System Medical Staff Quality Committee 27 7.6.2.3 System Practitioner Resource Committee 27 7.6.2.4 System Bylaws Committee 28 7.6.2.5 System Emergency Services Committee 29 7.6.3 Composition & Meetings of System MS Committees 29 7.7 Facility Medical Staff Committees 30 7.7.1 Purpose 30 7.7.2 Standing Facility Medical Staff Committees 30 SECTION 8 MEDICAL STAFF MEETINGS 31 8.1 General Medical Staff Meetings 31 8.2 Departments, Sections and Committee Meetings 31 8.3 Special Meetings of Departments, Sections and Committees 31 8.4 Quorum 31 8.5 Attendance Requirements 32 8.6 Participation by Administration 32 8.7 Robert’s Rules of Order 32 8.8 Notice of Meetings 33 8.9 Action of PLC, FMEC, General Medical Staff, Department, Section or Committee 33 8.10 Rights of Ex Officio Members 33 8.11 Minutes 33 SECTION 9 DECISION MAKING METHODS AND CONFLICT RESOLUTION 33 SECTION 10 REVIEW, REVISION ADOPTION AND AMENDMENT 34 10.1 Medical Staff Responsibility 34 10.2 Methods of Amendment and Adoption to these Bylaws 35 10.3 Methods of Amendment and Adoption to any Medical Staff Rules, Regulations and Policies 35 Appendix A PRINCIPLES OF MEDICAL ETHICS 37 PART II: INVESTIGATIONS, CORRECTIVE ACTION, HEARING AND APPEAL PLAN 39 SECTION 1 ROUTINE CORRECTIVE ACTION & INVESTIGATIONS 39 1.1 Progressive Intervention 39 1.2 Basis for Routine Corrective Action 39 1.3 Requests and Notices 40 1.4 Investigations 40 1.5 FMEC Action 41 1.6 Notice of FMEC Action 42 1.7 Board of Directions Action 42
3
SECTION 2 EMERGENCY CORRECTIVE ACTION/PRECAUTIONARY SUSPENSION OF CLINICAL PRIVILEGES 42 2.1 Basis for Emergency Corrective Action/Precautionary Suspension 42 2.2 Notice of Emergency Corrective Action/Precautionary Suspension 42 2.3 FMEC Procedure 43 2.4 Provision of Patient Care 43 2.5 Recission of Emergency Corrective Action/Precautionary Suspension 43 SECTION 3 AUTOMATIC SUSPENSION AND TERMINATION 43 3.1 Basis for Automatic Suspension and Termination 43 3.1.1 Loss of License 43 3.1.2 Residence or Office Outside Lee County 43 3.1.3 Lack of Active Practice 44 3.1.4 Criminal Conviction 44 3.1.5 Loss or Restriction of DEA Certificate 44 3.1.6 Exclusion From Federal or State Health Care Programs 44 3.1.7 Failure to Pay Fees and Assessments 44 3.1.8 Failure to Provide Requested Information 44 3.1.9 Failure to Request Reappointment or Provide Requested Information Related to Reappointment 45 3.1.10 Failure to Request Reinstatement Following Leave of Absence 45 3.1.11 Failure to Complete Medical Records 45 3.1.12 Failure to Comply with Special Meeting Attendance Requirements 45 3.2 Right to Limited Hearing for Automatic/Voluntary Suspension and Termination 45 SECTION 4 HEARING AND APPEAL PROCEDURES 46 4.1 Grounds for Hearing 46 4.2 Notice of Recommendation 46 4.3 Request for Hearing 47 4.4 Preliminary Interview 47 SECTION 5 FAIR HEARING PROCEDURE 47 5.1 System Representative, Hearing Panel and Hearing Officer 47 5.1.1 System Representative 48 5.1.2 Hearing Panel 48 5.1.3 Hearing Officer – Qualifications & Authority 48 5.2 Challenge to Hearing Panel Members or Hearing Officer 50 SECTION 6 HEARING PROCEDURES 50 6.1 Provision of Relevant Information 50 6.2 Pre-Hearing Conference 51 6.3 Failure to Appear 51 6.4 Record of Hearing 51 6.5 Rights of Both Sides 52 6.6 Admissibility of Evidence 52 6.7 Burden of Presenting Evidence and Proof 52 SECTION 7 HEARING CONCLUSION, DELIBERATIONS AND RECOMMENDATIONS 52 7.1 Deliberations and Recommendation of the Hearing Panel/Hearing Officer 52 7.2 Disposition of Hearing Panel Report 53
4
SECTION 8 APPEAL PROCEDURE 53 8.1 Request & Time for Appeal 53 8.2 Grounds for Appeal 54 8.3 Time, Place and Notice 54 8.4 Nature of Appellate Review 54 8.4.1 Review Panel 55 8.4.2 Position Papers 55 8.4.3 Oral Argument 55 8.4.4 Recommendation 55 SECTION 9 FINAL DECISION OF THE BOARD 55 SECTION 10 RIGHT TO ONE HEARING AND ONE APPEAL ONLY 55 PART III: CREDENTIALING PROCEDURES 56 SECTION 1 SYSTEM CREDENTIALING/PRIVILEGING COMMITTEE 56 1.1 Organizational Structure 56 1.2 Transition Issues 56 1.3 Purpose of the System Credentialing/Privileging Committee 56 1.4 Composition of the System Credentialing/Privileging Committee 57 1.5 Duties and Responsibilities of the System Credentialing/Privileging Committee 57 SECTION 2 QUALIFICATIONS FOR MEMBERSHIP AND PRIVILEGES 58 2.1 Qualifications for MS appointment, reappointment or clinical privileges 58 2.1.15 Exceptions 58 SECTION 3 PRE-APPLICATION PROCESS 60 SECTION 4 INITIAL APPOINTMENT PROCESS 61 4.1 Completion of Application 61 4.2 Applicant’s Attestation, Authorization and Acknowledgement 62 4.3 Application Evaluation 64 4.3.1 Expedited Credentialing 64 4.3.2 Applicant Interview 64 4.3.3 Department Chair Action 64 4.3.4 MS System Credentialing/Privileging Committee Action 65 4.3.5 FMEC Action 66 4.3.6 Applicants Applying to Multiple Facilities 66 4.3.7 Board Action 66 4.3.8 Notice of Final Decision 67 4.3.9 Periods for Processing 67 SECTION 5 FOCUSED PROFESSIONAL PRACTICE EVALUATION (FPPE) 67 SECTION 6 CRITERIA FOR REAPPOINTMENT 68 6.1 Criteria for Reappointment 68 6.3 Evaluation of Application for Reappointment of Membership and/or Privileges 70
5
SECTION 7 CLINICAL PRIVILEGES 70 7.1 Exercise of Privileges 70 7.2 Requests 70 7.3 Basis for Privileges Determination 70 7.4 Special Conditions for Podiatric Privileges 72 7.5 Special Conditions for Residents or Fellows in Training 73 7.6 Special Conditions for the Aging Practitioner 73 7.7 Temporary Privileges 73 7.7.8 Disaster Privileges 75 SECTION 8 PRECEPTORSHIP 76 SECTION 9 REAPPLICATION AFTER MODIFICATIONS OF MEMBERSHIP STATUS OF PRIVILEGES AND EXHAUSTION OF REMEDIES 76 9.1 Reapplication After Adverse Credentials Decision 77 9.2 Request for Modification of Appointment Status or Privileges 77 9.3 Resignation of Staff Appointment or Privileges 77 9.4 Exhaustion of Administrative Remedies 77 9.5 Reporting Requirements 77 SECTION 10 LEAVE OF ABSENCE 78 10.1 Leave Request 78 10.2 Termination of Leave 78 10.3 Failure to Request Reinstatement 78 SECTION 11 PRACTITIONERS PROVIDING CONTRACTED SERVICES 78 11.3 Contract Services/Department or Service Closure 79 11.4 Qualifications 80 11.5 Terms 80 11.6 Effect of Contract or Employment Expiration or Termination 80 SECTION 12 MEDICAL ADMINISTRATIVE OFFICERS 80
6
PART 1: GOVERNANCE
SECTION 1 MEDICAL STAFF PURPOSES & AUTHORITY 1.1 Purposes
The purposes of the Medical Staffs of Lee Memorial Health System are to:
1.1.1 Serve as the formal organizational structure of those practitioners granted the privilege of practicing in the hospitals and other facilities of the System.
1.1.2 Serve as the primary means for accountability to the Board for the professional
performance, the quality of medical care provided to patients, and ethical conduct of its members. The Board shall have the ultimate responsibility for the quality of medical care provided to patients and the ultimate authority to approve the granting of privileges, to make appointments and reappointments to membership on the Medical Staffs, and to approve the adoption of Medical Staff Bylaws and Rules and Regulations. Such authority will be exercised based on the standard set forth in Section 1.2.
1.1.3 Provide a means through which members of the Medical Staffs may address with
the Board those aspects of policy that involve professional practice or may affect the care of patients.
1.2 Authority
The Medical Staffs of Lee Memorial Health System are authorized by the Lee Memorial Health System Board of Directors (“the Board”) to exercise such power as is necessary to discharge its responsibilities under these Bylaws consistent with the Bylaws of Lee Memorial Health System. Lee Memorial Health System (“the System” or “the Health System”) includes acute care facilities known as Cape Coral Hospital, Gulf Coast Medical Center, HealthPark Medical Center, Lee Memorial Hospital, and The Children’s Hospital (individually known as “the hospital” and collectively known as “the hospitals”). The Board recognizes that a well-organized, self-governing Medical Staff that provides oversight of care, treatment, and services provided by practitioners with privileges is in the best interest of patients. When acting with respect to matters of the Medical Staff, the Board shall at all times comply with the Medical Staff Bylaws, the Rules and Regulations of the Medical Staff, and applicable law.
1.3 Medical Staff The term “Medical Staff” as used herein shall mean, on a collective basis, those
practitioners who are authorized by the Board to exercise privileges at one or more of the System’s hospitals, and, on a component basis, those practitioners who are authorized by the Board to exercise privileges at a particular system hospital. The latter may be referred to herein as the “Medical Staff of a facility.” The term “he”, “him”, or “his” means of a male or female gender.
7
SECTION 2 MEDICAL STAFF MEMBERSHIP 2.1 Nature of Medical Staff Membership
Membership on the Medical Staff is a privilege that shall be extended only to professionally competent physicians (M.D. or D.O.), dentists, podiatrists and/or psychologists who continuously meet the qualifications, standards, and requirements set forth in these Bylaws and associated policies of the Medical Staff and the hospitals. Medical Staff membership is a privilege and not a right of any practitioner or other person. Medical Staff membership and the exercise of privileges in connection therewith shall be extended only to practitioners who continuously meet the requirements of these Bylaws. The Board makes decisions regarding Medical Staff matters, based on Medical Staff recommendations, in accordance with these Bylaws. Membership on the Medical Staff shall confer on the Medical Staff member only such rights as set forth in the Bylaws. No person shall admit patients to a System hospital unless he is appointed to the Medical Staff of such hospital. For purposes of these Bylaws, “membership in” is used synonymously with “appointment to” the Medical Staff. Medical Staff members granted membership and privileges at a hospital, which has services and facilities that are provider based to a main provider and are authorized to exercise those privileges at the main provider.
2.2 Qualifications for Membership
2.2.1 The qualifications for Medical Staff membership are delineated in Part III of these Bylaws (Credentials Procedures).
2.3 Nondiscrimination
2.3.1 No Automatic Entitlement
No person shall be automatically entitled to Medical Staff membership or to the exercise of clinical privileges merely because he is licensed to practice, is a member of any professional organization, is certified by any board, or had held (but not currently) Medical Staff membership or clinical privileges at a System hospital or at any other health care facility. The burden shall be on the applicant to establish his qualifications. Acceptance of Medical Staff membership or exercise of clinical privileges shall constitute an agreement to strictly abide by these Bylaws, the applicable Medical Staff Policies, the Rules and Regulations, and the Principles of Medical Ethics set forth in Appendix A hereof and all other appropriate ethical standards governing the practitioner’s practice. No person shall be initially appointed to the Medical Staff or granted clinical privileges if the hospitals are unable to provide adequate facilities and supportive services for the applicant and his patients. Medical Staff membership shall not be denied based on sex, race, creed, color, national origin, religion, marital status, age, disability, or economic credentialing, at initial appointment or reappointment.
2.4 Conditions and Duration of Appointment
2.4.1 The Board shall act on appointment and reappointment only after the Medical Staff has had an opportunity to submit a recommendation from the Facility Medical Executive Committee (FMEC). Appointment and reappointment to the Medical Staff shall be for no more than twenty-four (24) calendar months.
8
2.5 Medical Staff Membership and Clinical Privileges
2.5.1 Requests for Medical Staff membership and/or clinical privileges will be processed only when the potential applicant meets the current minimum qualifying criteria recommended by the System Credentialing/Privileging Committee and FMEC and approved by the Board. Membership and/or privileges will be granted and administered as delineated in Part III (Credentials Procedures) of these Bylaws, including but not limited to, Part III, Sections 3 and 11.3 regarding Contracted practitioners.
2.6 Medical Staff Members’ Responsibilities
2.6.1 Duties of Appointees Appointment to the Medical Staff shall require that each practitioner assume such reasonable duties and responsibilities, as the Medical Staff shall require.
2.7 Basic Responsibilities of Applicants and Appointees The following basic responsibilities and requirements shall be applicable to every applicant
and appointee for Medical Staff appointment or reappointment as a condition of consideration of such application and as a condition of continued Medical Staff appointment if granted:
2.7.1 an obligation to provide for appropriate and timely care and supervision to all
patients in the hospital for whom the individual has responsibility (Standard of Care);
2.7.2 an agreement to abide by all Bylaws, Rules and Regulations and Policies of the Medical Staff and the Hospital, as shall be in force during the time the individual is appointed to the Medical Staff (Conformance to Rules);
2.7.2.1 provide a current cell phone number and email address to be used for
emergency or disaster purposes in accordance with Medical Staff Services Dept. policy.
2.7.3 an agreement to accept committee assignments and such other reasonable duties
and responsibilities as shall be assigned (Committee Assignments);
2.7.4 to not participate in illegal fee splitting or other illegal inducements relating to patient referral;
2.7.5 to promptly notify Medical Staff Services (Notification Requirements);
2.7.5.1 if his professional license in any state is suspended or revoked; 2.7.5.2 of the imposition of any conditions by any state licensing authority on his
continued ability to practice his profession, including probation or limitations on the scope of practice;
2.7.5.3 of the loss or restriction of Medical Staff membership or privileges at any
other health care facility;
2.7.5.4 if his Drug Enforcement Agency (DEA) license number is suspended, revoked or voluntarily relinquished;
9
2.7.5.5 of any change in eligibility for participation in Federal Health Care Programs including any sanctions imposed or recommended by the Federal Department of Health and Human Services, Florida State Agency for Health Care Administration and/or the receipt of any citation and/or quality denial letter concerning alleged quality problems in patient care;
2.7.5.6 if the practitioner enters, participates in, or against medical advice, leaves
or refuses any program of treatment prescribed or required by the Florida Physicians’ Recovery Network;
2.7.5.7 if the practitioner is admitted for, seeks, or is undergoing treatment for
substance or alcohol abuse or a behavioral health problem. “Substance abuse” shall include but not limited to, use or ingestion of illegal drugs, or use or ingestion of prescription medications not prescribed in the ordinary course of treatment of injury or disease. “Behavioral health problem” shall mean any condition or disease of a psychiatric or psychological nature which, in the opinion of a qualified psychiatrist, adversely affects the practitioner’s ability to care for patients or practice his profession in accordance with the applicable prevailing standard of care; or
2.7.5.8 the conviction of, or pleading of nolo contendere to, a crime constituting a
felony in any jurisdiction. 2.7.6 to abide by generally recognized ethical principles applicable to the applicant’s or
appointee’s profession and by the code of ethics set forth in Appendix A (Ethics);
2.7.7 to respect the confidentiality of all information obtained in connection with his responsibility as a Medical Staff member and comply with the requirements of the Health Insurance Portability and Accountability Act (HIPAA) (Confidentiality);
2.7.8 to provide medical consultation in a timely fashion in accordance with all
applicable Rules & Regulations and Medical Staff Policies (Consultation);
2.7.9 to participate in the monitoring and evaluation activities of Clinical Sections and cooperate with other members of the Medical Staff and the System, in programs designed to improve the quality of care to reduce or eliminate waste in the use of scarce System resources and to reduce the risk of injury to patients and others in the provision of care (Quality Review Participation);
2.7.10 to complete in a timely and legible manner the medical records and other required
records for all patients as required by these Bylaws, applicable Rules and Regulations, and other applicable policies of the hospital (Medical Records);
2.7.11 to pay promptly any applicable Medical Staff assessments and dues (Dues); 2.7.12 to participate in continuing education programs for the benefit of the applicant or
appointee and for the benefit of other professionals and System hospital personnel (CME);
2.7.13 to authorize the release of all information necessary for an evaluation of the
individual’s qualifications for initial or continued appointment, reappointment, and/or clinical privileges (Release of Information);
10
2.7.14 to submit to an evaluation of his physical and/or mental health status by a
physician or physicians acceptable to the FMEC or Board, whenever the FMEC or Board has reason to question the physical and/or mental health status of the practitioner, as a prerequisite to further consideration of his application for appointment or reappointment, the exercise of previously granted privileges or maintenance of his Medical Staff appointment (Physical/Mental Exam);
2.7.15 to recognize the obligations established to fulfill the hospital’s responsibilities
under the Emergency Medical Treatment and Women in Labor Act (EMTALA), the Access to Emergency Services and Care Act and/or other applicable regulations, requirements or standards and to share in the responsibility for providing physician coverage on an emergency basis in the Emergency Department, in accordance with the provisions of the Medical Staff Bylaws and all applicable facility-specific Rules & Regulations and Medical Staff Policies (On Call Coverage);
2.7.16 to provide his professional services to hospitalized or emergency room patients
covered by Medicaid and similar programs of indigent care, or such patients without personal physicians or insurance coverage, in accordance with Medical Staff Rules & Regulations adopted by the FMEC delineating the responsibility to provide services to those patients (Services to Indigent Patient);
2.7.17 provide proof of financial responsibility to pay claims or costs associated with the
rendering of, or failure to render, medical care or services in compliance with Florida law governing the practitioner’s license to practice in the State of Florida. Proof of financial responsibility shall be provided at the time of initial appointment and on reappointment, at the time the practitioner changes the method of meeting his financial responsibility and at any other time on the request of Medical Staff Services (Financial Responsibility);
2.7.18 to behave in a professional and civil manner and conduct himself in a manner
conducive to excellent patient care and to work cooperatively with Medical Staff appointees, and with other health care professionals, and Hospital personnel, so as not to adversely affect patient care. This requirement is not in any way intended to interfere with a practitioner’s right: (1) to express opinions freely and to support positions whether or not they are in dispute with those of other Medical Staff members; (2) to engage in honest differences of opinion with respect to diagnosis and treatment; or (3) to engage in a good faith criticism of others. The following types of behavior, however, which constitute some examples of an inability to interact on a professional basis with others or to behave in a professional and civil manner, are deemed unacceptable for a member of the Medical Staff:
2.7.18.1 conduct that reasonably could be characterized as sexual and/or racial
harassment;
2.7.18.2 threats of physical assault or actual physical assault, harassment, or the placing of others in fear by engaging in threatening behavior;
2.7.18.3 the unnecessary, unwarranted and unjustifiable knowing use of loud,
profane or abusive language directed toward members of the Medical Staff, patient and others; or
11
2.7.18.4 written or oral statements that constitute the intentional expression of
falsehoods, or constitute deliberately disparaging statements made with reckless disregard for their truth or for the reputation and feelings of others;
2.7.18.5 doing anything of a similar nature that the practitioner has been warned
not to do by the President of the Medical Staff or FMEC Committee (Professional and Civil Behavior);
2.7.19 duty to give notice if the practitioner is not actively engaged in the practice of his
profession in Lee County (Lack of Active Practice);
2.7.20 duty to give notice if practitioner does not maintain a full-time residence and office in Lee County, unless the residence and office requirements have been waived in accordance with these Bylaws (Residence or Office in Lee County).
2.8 Member Rights
The following basic rights shall apply to Medical Staff practitioners: 2.8.1 Each Medical Staff member, in the active category, has the right to a meeting with
the FMEC and/or the Physician Leadership Council (PLC) on matters relevant to the responsibilities of the FMEC and/or the PLC, provided that the practitioner has attempted to resolve a matter of concern after working with his Department Chair or other appropriate hospital and/or Health System Medical Staff leader(s). Upon written notice to the President of the Medical Staff, two (2) weeks in advance of a regular meeting, the active Medical Staff member may meet with the FMEC and/or the PLC to discuss the issue.
2.8.2 Each Medical Staff member, in the active category, has the right to initiate a recall
election of a Medical Staff officer by following the procedure outlined in Section 5.7 of these Bylaws regarding removal and resignation from office.
2.8.3 Each Medical Staff member, in the active category, may request a special meeting
of the Medical Staff, upon presentation of a petition, stating the purpose of the meeting and signed by ten (10) members of the Active Medical Staff. The FMEC shall schedule a special meeting for the specific purposes addressed by the petitioners in accordance with Section ten (10) of these Bylaws. No business other than that detailed in the petition may be transacted.
2.8.4 An applicant or an individual holding a Medical Staff appointment shall be entitled to
request a hearing/appeal pursuant to the conditions and procedures described in Part II of these Bylaws (Investigations, Corrective Action, Hearing and Appeal Plan).
2.8.5 All other rights as specified by these Bylaws.
2.9 Medical Staff Dues and Assessments
2.9.1 Annual Medical Staff dues, if any, shall be determined by the FMEC. Failure of a Medical Staff member to pay dues shall be considered a voluntary resignation from the Medical Staff. The FMEC may pass policies from time to time that exempt certain categories of membership or members holding specified leadership positions from payment of dues. The FMEC shall authorize the use of Medical Staff dues.
12
2.9.2 Medical Staff System-wide assessments, such as a library assessment, shall be determined by the PLC, on behalf of the FMECs. Failure of a Medical Staff member to pay any assessment(s) shall be considered a voluntary resignation from the Medical Staff. The PLC, on behalf of the FMECs, may pass policies from time to time that exempt certain categories of membership or members holding specific leadership positions from payment of such assessment(s).
2.9.3 The PLC, on behalf of the FMECs, shall authorize the use of Medical Staff
assessments consistent with the purpose of the assessment. 2.10 Conflict of Interest
2.10.1 In any instance where an officer, committee Chair, or member of any Medical Staff committee has, or reasonably could be perceived to have a conflict of interest, or to be biased in any matter involving another Medical Staff appointee or any other matter that comes before such individual or committee, or in any instance where any such individual brought the complaint against that practitioner, such individual shall not participate in the discussion or voting on the matter and shall be excused from any meeting during that time, although that individual may be asked and may answer, any questions concerning the matter before leaving. As a matter of procedure, the Chair of that committee designated to review the matter shall inquire, prior to any discussion of the matter, whether any member has any conflict of interest or bias. The existence of a potential conflict of interest or bias on the part of any committee member may be called to the attention of the Chair by any committee member with knowledge of the matter.
2.10.2 In any instance where an officer, committee Chair, or member of any Medical Staff
committee has a conflict of interest in any matter that comes before such individual or committee, such individual has the right to abstain or recuse himself from voting on such matter. Such abstention or recusal shall not prohibit such individual from providing factual information or participating in discussion on such matter. If an individual is requested to abstain or recuse himself and refuses to do so, the potential conflict of interest issue will be reviewed and resolved by the next highest authority as outlined in these Bylaws. As a matter of procedure, the Chair of that committee designated to review the matter shall inquire, prior to any discussion of the matter, whether any member has any conflict of interest or bias. The existence of a potential conflict of interest or bias on the part of any committee member may be called to the attention of the Chair by any committee member with knowledge of the matter.
2.10.3 Assurance of a conflict of interest or bias can be determined by a majority vote of
the members of the committee where a quorum is present. SECTION 3 CONFIDENTIALITY, IMMUNITY AND RELEASES 3.1 Confidentiality
Information with respect to any practitioner or regarding any other subject discussed, submitted, collected or prepared by any representative of the Lee Memorial Health System, including officers or members of organized committees of the Health System’s Medical Staffs, or any other healthcare professional, healthcare facility, organization or Medical Staff, for the purpose of achieving and maintaining the quality of care, reducing morbidity or mortality or contributing to clinical research shall, in accordance with Florida law,
13
be confidential and shall not be disseminated or used for any purpose other than the foregoing. Such information shall not be deemed a part of the patient medical record, and shall not be filed therein. Each individual or committee member participating in such activities shall agree to make no disclosures of any such information except as authorized, in writing, by the Chief Executive Officer (CEO) or by legal counsel to the hospitals. Any breach of confidentiality by an individual or committee member may result in a professional review action, and/or may result in appropriate legal action to ensure that confidentiality is preserved, including application to a court of law for injunctive or other relief.
3.2 Immunity 3.2.1 Any Medical Staff officer, Department Chair, Section Chief, committee Chair,
committee member, and individual staff appointee who acts in good faith for and on behalf of any System hospital in discharging duties, functions or responsibilities stated in these Medical Staff Bylaws, applicable Policies, and/or Rules and Regulations shall be afforded protection by the Board of Directors to the fullest extent permitted by law in accordance with written policies adopted by the Board. Individuals and organizations independent of the Medical Staff or any of its members who may be engaged by the Health System to perform the review, analysis and evaluation of the qualification and/or performance of practitioners with membership and/or privileges on the Medical Staff are afforded protection by the Board of Directors in accordance with written policies adopted by the Board, provided such individuals or organizations act in good faith.
3.2.2 To the fullest extent permitted by law, each applicant and appointee to the Medical
Staff releases from any and all liability, and extends absolute immunity to System hospitals and the Board and its individual members, and to the System’s authorized representatives and agents, with respect to any acts, communications or documents, recommendations or disclosures involving the applicant or appointee, concerning the following:
3.2.2.1 applications for appointment or clinical privileges, including temporary
privileges and/or emergency privileges;
3.2.2.2 evaluations concerning reappointment or changes in clinical privileges;
3.2.2.3 proceedings for suspension or reduction of clinical privileges or for revocation of Medical Staff appointment, or any other disciplinary sanction;
3.2.2.4 summary suspension;
3.2.2.5 hearings and appellate reviews; 3.2.2.6 medical/surgical care evaluations; 3.2.2.7 utilization reviews;
3.2.2.8 other activities relating to the quality of patient care or professional
conduct;
3.2.2.9 matters of inquiries concerning the applicant’s or appointee’s professional qualifications, credentials, clinical competence, character, mental or emotional stability, physical condition, ethics or behavior; and/or
14
3.2.2.10 any other matter that directly or indirectly might relate to the applicants or
appointee’s competence, and/or to patient care.
3.3 Releases
3.3.1 Authorization to Obtain Information
The applicant or appointee specifically authorizes the Medical Staff and its authorized representatives to consult with any third party who may have information bearing on the individual’s professional qualifications, credentials, clinical competence, character, mental or emotional stability, physical condition, ethics, behavior, or any other matter reasonably having a bearing on the applicant’s or appointee’s satisfaction of the criteria for initial and continued appointment to the Medical Staff. This authorization also covers the right to inspect, or obtain all communications, reports, records, statements, documents, recommendations or disclosures of said third parties that may be relevant to such questions. The individual also specifically authorizes said third parties to release said information to the Medical Staff and its authorized representatives upon request.
3.3.2 Legal Effect
The confidentiality provisions and protections described in this Section shall not limit
or supersede any protection or immunity afforded by law. SECTION 4 CATEGORIES OF THE MEDICAL STAFF 4.1 Active Category
4.1.1 Qualifications: Members of this category must have served on the Medical Staff, maintained a residence and office in Lee County (4.1.3.3) for one year, and be involved in twenty-four (24) patient contacts per year (i.e., a patient contact is defined as an inpatient admission, consultation, or an inpatient or outpatient surgical procedure) at the hospital except as expressly waived for practitioners with at least twenty (20) years of service in the active category or for those physicians who document their efforts to support the hospital’s patient care mission to the satisfaction of the FMEC.
In the event that a member of the active category does not meet the qualifications for reappointment to the active category, and if the member is otherwise abiding by all Bylaws, Rules and Regulations, and policies of the Medical Staff and hospital, the member may be appointed to another Medical Staff category if he meets the eligibility requirements for such category.
4.1.2 Prerogatives: Members of this category may:
4.1.2.1 Attend Medical Staff/Department meetings of which he is a member and any Medical Staff or hospital education programs;
4.1.2.2 Vote on all matters presented by the Medical Staff, Department, and
committee(s) to which the member is assigned;
15
4.1.2.3 Hold office and sit on or be the Chair of any committee in accordance with any qualifying criteria set forth elsewhere in the Medical Staff Bylaws or Medical Staff policies.
4.1.3 Responsibilities: Members of this category shall:
4.1.3.1 Contribute to the organizational and administrative affairs of the Medical Staff;
4.1.3.2 Actively participate as requested or required in activities and
functions of the Medical Staff, including quality/performance improvement and peer review, credentialing, risk and utilization management, medical records completion, monitoring activities and in the discharge of other Medical Staff functions as may be required by the FMEC;
4.1.3.3 The one-year residence and office requirement may be explicitly
waived by majority vote of the FMEC, on written request of the practitioner, at the time of appointment, if the practitioner affirmatively demonstrates to the FMEC in writing that the quality of patient care is not likely to be affected by his not living and having an office in Lee County and that the practitioner’s obligation to provide emergency room call and to attend hospitalized patient can be met.
4.1.3.4 Fulfill or comply with any applicable Medical Staff or hospital
policies or procedures as requested by the FMEC. 4.1.3.5 Fulfill basic responsibilities and requirements set forth in Section
2.7 of this Part, including but not limited to, Emergency Department call responsibilities in accordance with facility specific rules and regulations, unless exempted from Emergency Department call responsibilities as defined by their Section (if applicable) or Department and approved by the FMEC. In the event facility specific rules and regulations require physicians to accept emergency department referrals to the physician’s office, Lee Memorial Health System will provide facility support and services for such patients.
4.2 Associate Category 4.2.1 Qualifications: The associate category is reserved for Medical Staff members who
do not meet the eligibility requirements for the active category or choose not to pursue active status. This category includes physicians during their first year on the Medical Staff, as well as low volume/no volume physicians.
4.2.2 Prerogatives: Members of this category may:
4.2.2.1 Attend general Medical Staff Department meetings of which he is a member and any Medical Staff or hospital education programs.
4.2.2.2 Members of the associate category may not vote on matters at general
Medical Staff, Department meetings or be an officer of the Medical Staff.
16
4.2.2.3 Members of the associate category may serve on facility and system Medical Staff committees, other than the FMEC, and may vote on matters that come before such committees.
4.2.3 Responsibilities: Members of this category shall have the same responsibilities as
active category members, as set forth in Section 4.1 and Section 2.7 of this Part.
4.3 Honorary Category 4.3.1 The Honorary category is restricted to those individuals recommended by the FMEC
and approved by the Board. Appointment to this category is entirely discretionary and may be rescinded at any time. Members of the honorary category shall consist of those members who have retired from active hospital practice, who are of outstanding reputation, and have provided distinguished service to the hospital. They may attend general Medical Staff meetings, Department meetings, continuing medical education (CME) activities, and may be appointed to committees. They shall not hold clinical privileges, hold office or be eligible to vote.
SECTION 5 OFFICERS OF THE MEDICAL STAFF 5.1 Officers of the Medical Staff and FMEC at-large Members: Each hospital is
authorized to have the following officers:
5.1.1 Facility President of the Medical Staff 5.1.2 Facility President-Elect of the Medical Staff
5.1.3 Facility Secretary/Treasurer 5.1.4 Facility Past President of the Medical Staff
5.2 Qualifications of Officers and FMEC at-large Members 5.2.1 Officers must be members in good standing of the active category for at least three
(3) years or actively involved in patient care in the community, have previously served in a significant leadership position on a Medical Staff, (i.e. Department Chair, Section Chief or Committee Chair), indicate a willingness and ability to serve, have no pending adverse recommendations concerning Medical Staff appointment or clinical privileges, have a history of attendance at continuing education programs (provided by the System) relating to Medical Staff leadership and/or be willing to do so during their term or office, have demonstrated an ability to work well with others, be in compliance with the professional conduct policies of the Medical Staff, and should have excellent administrative and communication skills.
FMEC at large members must be members in good standing of the active category for at least two (2) years or actively involved in patient care in the community.
5.2.2 Officers and FMEC at-large members must disclose leadership positions on another
hospital Medical Staff. 5.3 Election of Officers and FMEC at-large Members 5.3.1 Every year, the FMEC shall appoint a nominations committee Chaired by the
immediate Past Facility President of the Medical Staff and comprised of at least
17
five (5) at large members of the active Medical Staff at least ninety (90) days prior to the election. Representatives of administration shall not serve on the nominations committee. Nominations will be solicited from the Medical Staff for consideration prior to the committee meeting. The committee shall offer at least one nominee for each office. Nominations must be announced, and the names of the nominees distributed to all members of the active Medical Staff at least forty-five (45) days prior to the election. A petition signed by at least 20% of the members of the active Medical Staff may also make nominations. Such petition must be submitted to the President of the Medical Staff at least twenty (20) days prior to the election for placement on the ballot.
5.3.2 Officers and FMEC at-large members shall be elected, as needed every year at an
election that takes place at least one (1) month prior to the expiration of the term of the current officers. Only members of the active category shall be eligible to vote. The FMEC will determine the mechanisms by which votes may be cast. The mechanisms that may be considered include written mail ballots; electronic voting via computer, fax, or other technology for transmitting the members’ voting choices. No proxy voting will be permissible. The nominee receiving the greatest number of votes will be elected. In the event of a tie vote, the Medical Staff support professional will arrange for a repeat vote(s) until one candidate receives a greater number of votes.
5.3.3 Medical Staff members will be notified of the election date and final slate of
nominees ten (10) days prior to the election. 5.4 Terms of Office 5.4.1 Officers and FMEC at-large members serve terms as follows: 5.4.1.1 Facility President-Elect of the Medical Staff – one (1) year 5.4.1.2 Facility President of the Medical Staff – two (2) years 5.4.1.3 Facility Past President of the Medical Staff – one (1) year 5.4.1.4 Facility Secretary/Treasurer – one (1) year 5.4.1.5 FMEC Members-at-Large – two (2) years 5.4.2 Officers shall take office October 1. Officers may be re-elected to office except that
the Facility President of the Medical Staff may not be re-elected for successive terms.
5.5 Vacancies of Office 5.5.1 The FMEC shall fill vacancies of office during the Medical Staff year, except the
office of the Facility President of the Medical Staff. If there is a vacancy in the office of the Facility President of the Medical Staff, the
Facility President-Elect of the Medical Staff shall serve the remainder of the term. 5.6 Duties of Officers and FMEC At-Large Members 5.6.1 Facility President of the Medical Staff – The Facility President shall represent the
interests of the Medical Staff to the FMEC and the Board. The Facility President will fulfill the duties specified in Section 5.6.2 of these Bylaws, as well as additional duties as reasonably requested by the FMEC in order to implement and/or enforce all provisions of the Bylaws and the interests of the Medical Staff.
5.6.2 Responsibilities of the Facility President of the Medical Staff
18
The Facility President of the Medical Staff is the primary elected officer of the
Medical Staff and is the Medical Staff’s advocate and representative in its relationships to the Board, the Facility Chief Administrative Officer (CAO) and the Health System administration. The Facility President of the Medical Staff, jointly with the FMEC, provides direction to and oversees Medical Staff activities related to assessing and promoting continuous improvement in the quality of clinical services and all other functions of the Medical Staff as outlined in the Medical Staff Bylaws, Rules and Regulations and Policies. Specific responsibilities and authority include:
5.6.2.1 Call and preside at all general and special meetings of the Medical Staff; 5.6.2.2 Serve as Chair of the FMEC, a voting member of the PLC and as ex-officio
member of all other Medical Staff committees without vote, and to participate as invited by the Board and the Facility CAO on hospital or Board committees;
5.6.2.3 Shall not vote at the FMEC, unless their vote is needed to break a tie vote; 5.6.2.4 Enforce Medical Staff Bylaws, Rules and Regulations and Medical
Staff/hospital/System Policies; 5.6.2.5 Except as stated otherwise, appoint committee Chairs and all members of
Medical Staff standing and ad hoc committees; in consultation with hospital administration, appoint Medical Staff members to appropriate hospital committees, in consultation with the Chair of the Board, appoint the Medical Staff members to appropriate Board committees when those are not designated by position or by specific direction of the Board or otherwise prohibited by state law;
5.6.2.6 Support and encourage Medical Staff leadership and participation on
interdisciplinary clinical performance improvement activities; 5.6.2.7 Report to the Board, through the PLC, the FMEC’s recommendations
concerning appointment, reappointment, delineation of clinical privileges or specified services and corrective action with respect to practitioners or allied health practitioners who are applying for appointment or privileges, or who are granted privileges or providing services in the hospital;
5.6.2.8 With the support of the facility Credentials/Privileging Committee and the
System Credentialing/Privileging Committee, evaluate and periodically report to the FMEC, PLC and the Board regarding the effectiveness of the credentialing and privileging processes;
5.6.2.9 Review and enforce compliance with standards of ethical conduct and
professional demeanor among the members of the Medical Staff in their relations with each other, the Board, hospital/System management, other professional and support staff, and the community the hospital serves;
5.6.2.10 Communicate and represent the opinions and concerns of the Medical
Staff and its individual members on organizational and individual matters affecting hospital operations to the Facility CAO, the FMEC, PLC and the Board;
19
5.6.2.11 attends Board meetings and Board committee meetings as deemed appropriate by Facility Medical Staff President;
5.6.2.12 ensures that the decisions of the Board are communicated and carried out
within the Medical Staff; 5.6.2.13 performs such other duties, and exercises such authority commensurate
with the office as are set forth in the Medical Staff Bylaws.
5.6.3 Facility President-Elect of the Medical Staff – In the absence of the Facility President, the Facility President-Elect or the Facility Past President shall assume all the duties and have the authority of the Facility President. He shall perform such further duties to assist the Facility President as the Facility President may request from time to time. The Facility President-Elect, upon the end of the term of the Facility President, shall automatically succeed to the office of Facility President.
5.6.4 Facility Secretary/Treasurer – This officer will collaborate with the hospital’s
Medical Staff office, assure maintenance of minutes, attend to correspondence, act as Medical Staff treasurer, and coordinate communication within the Medical Staff. He shall perform such further duties to assist the Facility President as the Facility President may from time to time request.
5.6.5 Facility Past President of the Medical Staff – This officer will serve as a
consultant to the Facility President and the Facility President-Elect as requested by the FMEC and provide feedback to the officers regarding their performance of assigned duties on an annual basis.
He shall perform such further duties to assist the Facility President as the
Facility President may request. He shall serve as a member of the System Credentialing/Privileging Committee.
5.6.6 FMEC at-large members – shall advise and support the Medical Staff officers
and are responsible for representing the needs/interests of the entire Medical Staff and not simply representing the preferences of their own clinical specialty.
5.7 Removal and Resignation of Officer or FMEC At-Large Member 5.7.1 The Medical Staff may remove any facility officer or FMEC at-large member by
petition of 20% of the active Medical Staff members and a subsequent affirmative vote by two-thirds (2/3) of those active Medical Staff members’ casting votes.
5.7.2 Recall of Officers or FMEC at-large members The FMEC may remove any facility Medical Staff officer or FMEC at-large
member for conduct detrimental to the interests of the Medical Staff or if the officer is suffering from a physical or mental infirmity that renders the individual incapable of fulfilling the duties of the office. At least ten (10) days notice prior to the date of the meeting shall be provided, in writing, to the affected officer or FMEC at-large member. The officer or at-large member shall be afforded the opportunity to speak prior to the taking of any vote on such removal. For recall of an officer or at-large member, a two-thirds (2/3) vote of approval is required with three-fourths (3/4) of the FMEC members present and voting. Affected officer or at-large member does not count as quorum and does not vote.
20
5.7.3 Resignation of Officers or FMEC at-large members Any elected officer or FMEC at-large member may resign at any time by giving
written notice to the FMEC. Such resignation takes effect on the date of receipt, when a successor is elected, or any later time specified therein.
SECTION 6 MEDICAL STAFF ORGANIZATION The organized Medical Staff is actively involved in Medical Staff governance, peer review,
credentialing/privileging and communication. Medical Staff members are accountable to the FMEC.
The Medical Staff facility officers (Section 5), Medical Staff governance committees (PLC, Section 7.1 and FMEC, Section 7.4), Department Chairs (Section 6.1), clinical Section Chiefs (Section 6.1.1), hospital (as appropriate) System Medical Staff committee Chairs, (Section 7.6) and facility Medical Staff committee Chairs (Section 7.7) are responsible for working collaboratively to develop a process for communication of Medical Staff functions. Periodic reports, as appropriate, are given to each FMEC, Medical Staff Departments, Medical Staff committees and the PLC as needed to ensure adherence to regulatory requirements and accreditation standards.
Additionally, Medical Staff officers may appoint, in collaboration with the Facility Medical
Director, designated physician leaders to serve on the following Medical Staff committees to help ensure Medical Staff input and oversight with clinical functions such as System Bylaws, Cancer Care, CME/Medical Library, Ethics, Institutional Review, System Credentialing/Privileging, Critical Care, System Emergency Services, Infection Control, Pharmacy and Therapeutics, System Medical Staff Quality, System Practitioner Resource, Trauma Quality, Vascular Lab, in addition to the Children’s Hospital committees (Cancer Care, Ethics, Neonatal Intensive Care Unit (NICU) Pediatric Intensive Care Unit (PICU) Perinatal and Medical Staff Quality and other such functions as determined by the FMEC and/or the PLC.
6.1 Departments The Medical Staff shall be organized as a Departmentalized staff. The current
Departments authorized by the FMECs are Medicine, Surgery, Pediatrics, Obstetrics and Gynecology, Anesthesiology, Pathology, Radiology and Emergency Medicine. Departments fulfill the duties listed in Section 6.2.4 of these Bylaws within a specific hospital or facility and/or across the Health System as necessary. Departments shall meet as frequently as needed to fulfill assigned duties and when requested by the FMEC.
The Medical Staff may create Clinical Sections (as specified in these Bylaws) within
a Department in order to facilitate Medical Staff activities.
6.1.1 Any FMEC may recognize any group of like American Board of Medical Specialties, (ABMS) approved specialties with at least three (3) Medical Staff members or service lines that wish to organize themselves into a Clinical Section. Any Clinical Section, if organized shall not be required to hold regularly scheduled meetings, keep routine minutes, or require attendance. A written report is required only when the Clinical Section is making a formal report. A Clinical Section shall elect a Clinical Section Chief.
21
The Clinical Section Chief is responsible for fulfilling the activities listed in Section 6.1.1.1 - 6.1.1.7 of these Bylaws. The procedure for removal of a Clinical Section Chief shall be the same as set forth in Section 6.2.3 for Department Chair. When a clinical Section is making a formal report, the report shall be submitted to the FMEC documenting the specific position of the clinical Section. The President of the Medical Staff and the Clinical Section Chief (or designee) will decide if the report/issue is placed on the FMEC agenda and whether the Clinical Section Chief (or designee) will attend the FMEC meeting to present the report/issue to the FMEC on that specific report/issue. Clinical Sections are optional and shall exist to perform any of the following activities within a specific facility and/or across Health System facilities as necessary:
6.1.1.1 continuing education/Grand Rounds/discussion of patient care;
6.1.1.2 formulation of ED on-call and inpatient consultation and coverage recommendations; 6.1.1.3 discussion of policies and procedures; 6.1.1.4 discussion of equipment needs; 6.1.1.5 development of recommendations for the Department Chair(s), the
FMECs or the PLC; 6.1.1.6 participation in the development of criteria for clinical privileges
when requested by the System Credentialing/Privileging Committee or FMEC;
6.1.1.7 discussion of a specific issue at the request of the PLC or the
FMEC. The FMEC, with the concurrence of the PLC, may designate new Medical Staff Departments or Clinical Sections or dissolve current Departments or Clinical Sections as it determines will best meet the Medical Staff needs for promoting performance improvement, patient safety, and effective credentialing and privileging.
6.2 Qualifications, Selection, Term, and Removal of Department Chair 6.2.1 Each Department Chair shall serve a term of two (2) years commencing on
October 1 and may be elected to serve successive terms. All Chairs must be members of the active Medical Staff with relevant clinical
privileges and be certified by an appropriate specialty board or have affirmatively established comparable competence through the credentialing process.
6.2.2 Department Chairs and Vice-Chairs will be elected by majority vote of the
active members of the Department, subject to ratification by the FMEC. Each Department shall establish procedures for identifying and electing candidates and these procedures must be ratified by the FMEC.
22
6.2.3 Department Chairs may be removed from office by the FMEC upon receipt of a recommendation of two-thirds (2/3) of the members of the Department or, in the absence of such recommendation, the FMEC may remove a Chair on its own by a two-third (2/3) vote of a majority of members present and voting, if any of the following occurs:
6.2.3.1 The Chair ceases to be a member in good standing of the Medical
Staff; 6.2.3.2 The Chair suffers an involuntary loss or significant limitation of
practice privileges; 6.2.3.3 The Chair fails, in the opinion of the FMEC, to demonstrate to the
satisfaction of the FMEC, PLC or the Board that he is effectively carrying out the responsibilities of the position;
6.2.3.4 If removal is required, a new election will be held according to the
established Departmental procedures. 6.2.4 Department Chairs shall carry out the following responsibilities: 6.2.4.1 to oversee all clinically-related activities of the Department; 6.2.4.2 to oversee all administratively related activities of the Department
otherwise provided for by the Facility; 6.2.4.3 to provide ongoing surveillance of the performance of all individuals
in the Medical Staff Department who have been granted clinical privileges;
6.2.4.4 to recommend to the System Credentialing/Privileging Committee
Medical Staff Department; 6.2.4.5 to recommend clinical privileges for each member of the
Department and other LIPs practicing with privileges within the scope of the Department;
6.2.4.6 to assess and recommend to the FMEC and Facility CAO off-site
sources for needed patient care services not provided by the Medical Staff Department or Facility;
6.2.4.7 to monitor and evaluate the quality and appropriateness of patient
care provided in the Medical Staff Department and to implement action following review and recommendations by the facility Medical Staff peer review/quality committee and/or the FMEC;
6.2.4.8 to integrate the Department into the primary functions of the
hospital; 6.2.4.9 to coordinate and integrate interdepartmental and
intradepartmental services and communication;
6.2.4.10 to participate in the administration of the Department through cooperation with nursing services and hospital administration in matters affecting patient care;
23
6.2.4.11 to develop and implement Medical Staff and hospital policies and
procedures that guide and support the provision of patient care services;
6.2.4.12 to recommend to the Facility CAO the sufficient numbers of
qualified and competent persons to provide patient care and service;
6.2.4.13 to provide input to the Facility CAO regarding the qualifications and
competence of Department or service personnel who are not Licensed Independent Practitioners (LIPs) but provide patient care, treatment, and services;
6.2.4.14 to provide continuous assessment and improvement of the quality
of care, treatment, and services; 6.2.4.15 to maintain quality control programs as appropriate; 6.2.4.16 to orient and continuously educate all persons in the Department; 6.2.4.17 to make recommendations to the FMEC and to the Facility CAO for
space and other resources needed by the Medical Staff Department to provide patient care services.
6.3 Assignment to Department 6.3.1 The FMEC will, after consideration of the recommendation of the Chair of the
appropriate Department, recommend Department assignments for all members in accordance with their qualifications. Each member will be assigned to one primary Department. Clinical privileges are independent of the Department assignment.
SECTION 7 MEDICAL STAFF GOVERNANCE COMMITTEES 7.1 Designation of the Lee Memorial Health System Medical Staff Physician Leadership
Council (PLC)
7.1.1 There shall be a Lee Memorial Health System Medical Staff Physician Leadership Council (PLC) and such other standing and special committees as determined by the PLC.
7.1.2 There shall be a Facility Medical Executive Committee (FMEC) at each hospital and
such other facility standing and special committees as established by the FMEC.
7.2 Composition of the Lee Memorial Health System Medical Staff PLC 7.2.1 Composition: The PLC shall consist of the following voting members: Each Facility President and
each Facility President–Elect or each Facility Immediate Past President and two (2) at-large Medical Staff members elected by each FMEC. All shall serve a 2-year term except the Facility President-Elect and Facility Past President shall serve 1-year term. The Chairs of the System Credentialing/Privileging Committee and
24
System Quality Committee, the system CEO or Designee, the System Chief Medical Officer and the Chair of the Board and up to two (2) other Board consultants, shall serve as ex-officio, non-voting members. The PLC will elect the PLC Chair who shall serve a 2-year term.
In the event that the PLC composition does not include one anesthesiologist,
emergency medicine physician, hospitalist or intensivist, radiologist and pathologist, the PLC may appoint an active Medical Staff member from each of these hospital-based specialties to be voting members of the PLC.
7.2.2 Duties: The duties of the Lee Memorial Health System PLC are:
7.2.2.1 to work in a cooperative and professional manner with the FMECs System and Facility Administration and the Board to ensure Medical Staff input into the plans, goals and mission of the Lee Memorial Health System;
7.2.2.2 receive, review, and transmit FMEC recommendations to the
Board; 7.2.2.3 review and attempt to resolve any inconsistency emanating from
the FMEC recommendation(s) and transmit FMEC recommendations to the Board concerning all matters relating to appointments, reappointments, staff category, facility assignments, clinical privileges subject to the conflict resolution process herein, unless due process rights are triggered pursuant to Part II.
The PLC is acting as a duly constituted peer review committee under Florida law when it is reviewing the quality of care or performance of any particular physician.
7.2.2.4 consistent with the hospital and Medical Staff mission and
philosophy, the PLC will participate and encourage participation of the FMECs in identifying community health needs and in setting goals and work with the System administration and the facility CAO(s) to design and implement programs to meet those needs;
7.2.2.5 work with the FMECs to ensure understanding and the consistent
application of Medical Staff Rules and Regulations, Policies and Procedures; and
7.2.2.6 govern the collection of Medical Staff system-wide assessments
and authorize the use of Medical Staff assessments consistent with the purpose of the assessment.
7.2.3 Meetings:
The PLC shall meet ten (10) times per year, or more frequently as needed to perform its assigned functions. Records of its proceedings and actions shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
25
7.3 Staff Functions
7.3.1 The PLC exists to promote communication, collaboration and coordination
between physicians, System and facility administration and the Board concerning the work of each FMEC and planning activities of the Lee Memorial Health System that impact members of the Medical Staff.
7.4 Facility Medical Executive Committee (FMEC) Composition Selection and Tenure
7.4.1 Each Medical Staff may determine the number of Medical Staff members
appointed or elected to the FMEC. The composition of the FMEC shall consist of at least the following voting members: Facility President of the Medical Staff, Facility Immediate Past President, Facility President-Elect of the Medical Staff, Facility Secretary/Treasurer, physician representative from the System Credentialing/Privileging Committee, Chair of the Facility Quality Committee, the Department Chairs from Medicine, Surgery, Anesthesiology, Radiology, Pathology, Pediatrics, Obstetrics/Gynecology and Emergency Services, two (2) at-large active members of the Medical Staff appointed by the FMEC and two (2) at-large active members of the Medical Staff elected by the general Medical Staff.
One Board member, the CAO, the facility Vice-President of Nursing, the
facility Medical Director (as appropriate) will serve in a non-voting, ex-officio capacity. The Facility President of the Medical Staff shall serve as the Chair of the FMEC.
7.4.2 Each FMEC composition description shall be listed in the Facility Rules &
Regulations.
7.4.3 FMEC members shall disclose in writing to the Medical Staff, prior to the date of election of appointment, any personal, professional or financial applications or responsibilities with Lee Memorial Health System and any competing hospital, healthcare organization or Health System.
FMEC members shall serve 2-year terms, except Facility Past President and
Facility President-Elect shall serve 1-year terms. The FMEC and the Nominations Committee shall stagger the terms of appointed and elected at-large members to ensure continuity of leadership. Such physicians must be on Active Staff and be a member in good standing at all times.
All FMEC members are expected to participate in orientation and continuing
education activities as related to the operation of the Medical Staff.
7.5 Duties and Responsibilities of the Facility Medical Executive Committees 7.5.1 To represent, to initiate action and act on behalf of the Medical Staff
members with privileges at the Facility in fulfilling the duties of Medical Staff self governance, credentialing/privileging and quality/peer review, after seeking input and recommendations from Sections and/or Departments affected by FMEC action (if applicable).
26
7.5.2 To receive recommendations from the System Credentialing/Privileging
Committee and the Facility Quality/Peer Review Committee and make recommendations to the Board (and for informational purposes only) to the PLC concerning:
7.5.2.1 appointments, reappointments and granting of clinical privileges; 7.5.2.2 necessity for special investigations of issues pertaining to
practitioner competence of behavior; 7.5.2.3 needed performance improvements and peer review results; 7.5.2.4 policies and procedures development and enforcement; 7.5.2.5 facility Medical Staff Department and committee structure; and 7.5.2.6 other matters relevant to the provision of patient care, operation of
the Medical Staff or proposed Bylaws amendments. 7.5.3 Receive or act upon reports and recommendations concerning patient care
quality and appropriateness reviews, evaluation and monitoring functions, and the discharge of their delegated administrative responsibilities;
7.5.4 Recommend to the Board, and for information purposes only to the PLC,
specific programs and systems to perform Medical Staff peer review, quality monitoring, communication, governance, credentialing/privileging and planning functions;
7.5.5 Coordinate the implementation of policies adopted by the Board; 7.5.6 Oversee the facility multi-specialty peer review and quality monitoring
activities in a manner consistent with federal and state law; 7.5.7 Take reasonable steps to encourage professionally ethical conduct and
competent clinical performance of Medical Staff members at the facility including collegial and educational efforts;
7.5.8 Participate in identifying community health needs and in setting facility-
specific goals and implementing programs to meet those needs; 7.5.9 Design and implement facility-specific rules and regulations that will not
conflict with the Medical Staff Bylaws; 7.5.10 Work with Facility and System administration to promote effective, efficient
and safe patient care practice within the facility; 7.5.11 Take reasonable steps to encourage professionally ethical conduct and
competent clinical performance on the part of staff appointees including initiating investigations, and pursuing corrective action, when warranted;
7.5.12 Provide oversight concerning the quality and safety of the care provided by
residents, interns, students, and ensure that the same act within approved guidelines established by the Medical Staff and the Board.
27
Reviews and ensure corrective action regarding applicable Residency Review Commission findings and recommendations;
7.5.13 Keep the Medical Staff up to date concerning the licensure and
accreditation status of the System and hospitals; 7.5.14 Request evaluations of practitioners privileged through the Medical Staff
process in instances in which there is question about an applicant or member’s ability to perform privileges requested or currently granted;
7.5.15 Consult with administration on the quality, timeliness, and appropriateness
of aspects of contracts for patient care services provided to the hospital by entities outside the hospital;
7.5.16 Hold Medical Staff leaders, committees, and Departments accountable for
fulfillment of their duties and responsibilities; 7.5.17 Advise and assist the PLC, when and to the extent possible, as requested
by the PLC, the Board and the System or Facility administration; 7.5.18 Grant, deny or rescind exemptions related to ED call responsibility; 7.5.19 Meetings: The FMEC shall meet ten (10) times per year, or more
frequently as needed to perform its assigned functions. Records of its proceedings and actions shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
7.6 System Medical Staff Committees 7.6.1 Purpose. There shall be system Medical Staff committees established by the
Medical Staff to carry out the responsibilities of the Medical Staff with regard to measuring and assessing the performance of the Medical Staff providing medical care within the hospitals and Health System facilities.
7.6.2 Organization to Perform Functions. The PLC with the input and approval of each
FMEC shall establish system Medical Staff committees comprised of members of the Medical Staff and others as may be deemed appropriate or necessary. The delineation of specific duties, committee size, liaison with other committees and Departments, and other matters necessary to the efficient performance of Medical Staff functions shall be set forth in these Bylaws. The only voting members of system Medical Staff committees are members of the Medical Staff unless otherwise determined by the FMEC. System Medical Staff committees consist of the following, shall report to and through the FMECs on matters relating to all FMECs, and shall report to each FMEC on facility specific matters:
7.6.2.1 System Credentialing/Privileging Committee (See Part III, Section 1 of
these Bylaws); 7.6.2.2 System Medical Staff Quality Committee (See Medical Staff Quality
Manual); 7.6.2.3 System Practitioner Resource Committee. Membership:
28
Membership shall be established by the PLC with the input and approval of each FMEC. The term of office shall be for a period of two (2) years with staggered terms, so as to provide continuity and development of expertise.
Referrals: Concerns that a member of the Medical Staff may be suffering from a
physical or mental impairment that might impact their ability to practice medicine or may be a threat to themselves or others, including but not limited to impairment due to substance abuse, should be communicated to the President of the Medical Staff or to the affected practitioner’s Department Chair. The President of the Medical Staff or Department Chair, after consultation with others, if deemed appropriate, may refer the affected practitioner to the practitioner Resource Committee for review, evaluation and follow-up.
Responsibilities: The committee shall have no authority to take disciplinary action. Nor
does the committee provide treatment. The committee is responsible to: 7.6.2.3.1 Receive and evaluate concerns about practitioner health and
functioning;
7.6.2.3.2 Provide assistance and encourage a practitioner impaired by virtue of physical or psychiatric condition, problems in living, or issues related to alcohol use or drug use to voluntarily accept referral for the evaluation, treatment or assistance;
7.6.2.3.3 Assume an advocacy role on behalf of the affected practitioner;
7.6.2.3.4 Serve as an advisor to the President of the Medical Staff, Department Chair and/or FMEC, including advice relating to alternatives in the event that the practitioner fails to accept referral or fails to adequately recover from treatment;
7.6.2.3.5 Consider referring an affected practitioner to appropriate resources
for treatment and advice on the appropriateness of treatment, rehabilitation planning and monitoring provisions;
7.6.2.3.6 Utilize the Florida Medical Association Physician Resource Network,
Intervention Project for Nurses or other resources, if appropriate;
7.6.2.3.7 Maintain the confidentiality of information regarding matters referred to the committee;
7.6.2.3.8 Refer to the Medical Staff President Department Chair or FMEC
those situations that may require possible corrective actions. 7.6.2.4 System Bylaws Committee Membership:
29
The Bylaws Committee shall be a standing committee of the Medical Staff and shall be composed of at least five (5) active Medical Staff appointees (including one (1) member from each FMEC appointed by the facility Medical Staff President) and the System Chief Medical Officer (CMO) or his designee (who shall serve as a non-voting member).
Duties: The duties of the Bylaws Committee shall be to:
7.6.2.4.1 Conduct an annual review of the Medical Staff Bylaws, Medical Staff
Rules and Regulations and Policies; and 7.6.2.4.2 Review recommendations for changes in the Medical Staff Bylaws,
Rules and Regulations and Policies made by the Medical Staff committees, Departments, or by the Board.
Meetings, Reports and Recommendations: The Bylaws Committee shall meet at least annually or as necessary to
accomplish its duties, shall maintain a permanent record of its proceedings and actions, and shall report its recommendations to the FMECs.
7.6.2.5 System Emergency Services Committee Membership: The System Emergency Services Committee shall be an ad hoc committee
of the Medical Staff and shall be composed of the Emergency Department Medical Directors, at least three (3) Active Staff members, and other Active Staff members as needed.
Duties: The duties of the System Emergency Services Committee shall be to: 7.6.2.5.1 conduct an annual review of system-wide emergency services; 7.6.2.5.2 ensure emergency call is fair to physicians while providing adequate
coverage to patients of our community; 7.6.2.5.3 review emergency call rules system-wide for recommendation to
FMECs.
Meetings: The System Emergency Services Committee will meet at least once per year or as needed.
7.6.3 Composition and Meetings of System Medical Staff Committees:
7.6.3.1 Unless otherwise provided for in these Bylaws, System Medical Staff committees shall be composed of physician members from each facility, as appointed by each FMEC;
30
7.6.3.2 Each System Medical Staff committee shall elect a physician Chairperson
and physician vice Chairperson for their respective committee;
7.6.3.3 System Medical Staff committee members shall serve terms of 2 years and may be reappointed;
7.6.3.4 System Medical Staff committee members who cease to be members of
the Medical Staff of Lee Memorial Health System shall automatically cease to serve as committee members. Vacancies on committees shall be filled by the appropriate FMEC;
7.6.3.5 System Medical Staff committees shall meet as often as necessary to
discharge the duties of the respective committees in accordance with these Bylaws.
Reasonable notice of meetings shall be provided to committee members
and may include providing a written schedule of meetings on an annual or more frequent basis.
7.7 Facility Medical Staff Committees: 7.7.1 Purpose: There shall be committees to carry out certain essential functions
within each facility as determined by each FMEC. The FMEC may establish such committees from time to time in addition to those set forth in the Bylaws.
7.7.2 Standing Facility Medical Staff Committees: The following facility committees
are approved as standing committees of the FMEC: 7.7.2.1 GCMC Credentialing/Privileging Committee (see Part III, Section 1 of
these Bylaws); 7.7.2.2 LMHS Credentialing/Privileging Committee (see Part III, Section 1 of these
Bylaws); 7.7.2.3 Nominations Committees (See Part 1, Section 5.3 of these Bylaws);
7.7.2.4 Facility Medical Staff Quality Committees (see Medical Staff Quality Manual);
7.7.2.5 Facility Rules and Regulations Committees Composition: The Facility Rules and Regulations Committee shall be a
standing committee of the Medical Staff and shall be composed of at least two (2) active Staff members appointed by the FMEC.
Duties: The duties shall be to review and recommend changes in the
Facility Rules and Regulations and policies to the FMEC. 7.7.2.6 Trauma Quality Management Composition, membership and duties are mandated by the State
regulations for designated trauma centers.
31
SECTION 8 MEDICAL STAFF MEETINGS 8.1 General Medical Staff Meetings 8.1.1 An annual meeting and other general Medical Staff meetings shall be held at a
time determined by the FMEC. Notice of the meeting shall be given to all Medical Staff members via appropriate media and posted conspicuously at least ten (10) days before the meeting.
8.1.2 Except for Bylaws amendments or as otherwise specified in these Bylaws, the
actions of a majority of the members present and voting at a meeting of the Medical Staff is the action of the group.
Action may be taken without a meeting of the Medical Staff by presentation of
the question to each Medical Staff member eligible to vote, in person, via telephone, and/or by mail or internet, and their vote recorded in accordance with procedures approved by the FMEC. Such vote shall be binding so long as the question that is voted on receives a majority of the votes cast.
8.1.3 Special Meetings of the General Medical Staff 8.1.3.1 The President of the Medical Staff may call a special general Medical
Staff meeting at any time. Such request or resolution shall state the purpose of the meeting. The President of the Medical Staff shall designate the time and place of any special general Medical Staff meeting.
8.1.3.2 Written or electronic notice stating the time, place and purposes of
any special general Medical Staff meeting shall be conspicuously posted and shall be sent to each member of the Medical Staff at least three (3) days before the date of such meeting. No business shall be transacted at any special general Medical Staff meeting, except that stated in the notice of such meeting.
8.2 Departments, Sections and Committee Meetings 8.2.1 Regular Meetings of Medical Staff Departments, Sections and Committees
8.2.2 Departments, Sections and Committees may, by resolution, provide the time for holding regular meetings without notice other than such resolution.
8.3 Special Meetings of Departments, Sections and Committees 8.3.1 A special meeting of any Department, Section or Committee may be called by
the Chair thereof or by the President of the Medical Staff. 8.4 Quorum 8.4.1 Medical Staff meetings: Unless otherwise specified in these Bylaws, a quorum
shall consist of those present or those eligible Medical Staff members voting on an issue.
32
8.4.2 FMEC, Credentialing/Privileges Committee, Medical Staff Quality/Peer Review Committee: A quorum will exist when 50% of the members are present.
8.4.3 Departments, Sections or Committees other than those listed in Sections 6 and
7 above or unless otherwise specified in these Bylaws, a quorum shall consist of those present or those eligible Medical Staff members voting on an issue.
8.5 Attendance Requirements 8.5.1 Members of the Medical Staff are encouraged to attend meetings of the Medical
Staff. 8.5.1.1 FMEC, Credentialing/Privileges Committee, and Medical Staff
Quality/Peer Review Committee meetings: Members of these committees are expected to attend at least 75% of the meetings held.
8.5.1.2 Special meeting attendance requirements: Whenever there is
suspected or actual non-compliance with Medical Staff or hospital policies or suspected deviation from standard clinical or professional practice, the President of the Medical Staff or the applicable Department/Section/Committee Chair may require the practitioner to confer with him or with a standing or ad hoc committee that is considering the matter. The practitioner will be given special notice of the meeting, by personal delivery or U.S. Mail certified return receipt requested, at least five (5) days prior to the meeting, including the date, time, place, a statement of the issue involved and that the practitioner’s appearance is mandatory.
Failure of the practitioner to appear at any such meeting after two (2)
notices, unless excused by the FMEC upon showing good cause, will result in an automatic termination of membership pursuant to the Automatic Suspension and Termination provisions of these Bylaws. Such termination will not give rise to a fair hearing, but will automatically be rescinded upon the practitioner’s participation in the previously referenced meeting.
8.5.1.3 Nothing in the foregoing paragraph shall preclude the initiation of
precautionary restriction or suspension of clinical privileges as outlined in Part II of these Bylaws (Investigations, Corrective Action, Hearing and Appeal Plan).
8.6 Participation by Administration
8.6.1 Administration may attend any general, Department, Section or Committee meetings of the Medical Staff, unless otherwise specified or requested by the committee.
8.7 Robert’s Rules of Order 8.7.1 Medical Staff Department, Section and Committee meetings shall be run in a
manner determined by the individual who is the Chair of the meeting. When parliamentary procedure is needed, as determined by the Chair or evidenced by a majority vote of those attending the meeting, the latest edition of Robert’s Rules of Order shall determine procedure.
33
8.8 Notice of Meetings 8.8.1 Unless otherwise specified in these Bylaws, written or electronic notice stating
the place, day, and hour of any special meeting or of any regular meeting not held pursuant to resolution shall be delivered or sent to each member of the Department or committee not less than five (5) days before the time of such meeting by the person or persons calling the meeting. The attendance of a member at a meeting shall constitute a waiver of notice of such meeting.
8.9 Action of PLC, FMEC, General Medical Staff, Department, Section or Committee 8.9.1 The recommendation of a majority of its members present at a meeting at which
a quorum is present shall be the action of a Department, Section and Committee, FMEC, PLC or General Medical Staff meeting. Such recommendation will then be forwarded to the FMEC for action.
8.10 Rights of Ex Officio Members 8.10.1 Except as otherwise provided in these Bylaws, persons serving as ex officio
members of a committee shall have all rights and privileges of regular members thereof, (except that they shall not vote or be counted in determining the existence of a quorum).
8.11 Minutes 8.11.1 Minutes of each regular and special meeting of a committee shall be prepared
and shall include a record of the attendance of members and the vote taken on each matter. The presiding Chair shall authenticate the minutes and copies thereof shall be submitted to the FMEC or other designated committee. Minutes shall be maintained in accordance with the System’s Records Retention and Disposition Policy.
SECTION 9 DECISION MAKING METHODS AND CONFLICT RESOLUTION 9.1 FMEC recommendations will be forwarded to the PLC for information and to ensure
communication between all facility Medical Staffs, System and facility administration and Board leaders. Routine FMEC communication and recommendations that are consistent between the FMECs and that are consistent with Medical Staff and hospital policy and procedures will be transmitted to the Board.
9.2 Conflict resolution: If the PLC determines a recommendation of a FMEC may be contrary
to the opinion of the PLC, or if a decision of the Board is contrary to a recommendation of the PLC and/or a FMEC, the PLC shall not make a recommendation to the Board regarding such matter. The PLC will first refer the matter back to the FMEC(s) for further consideration at their next meeting, together with pertinent suggestions and comments of the PLC.
9.3 If the FMEC recommendation and the opinion of the PLC remain inconsistent after the next
meeting of the FMEC, the matter will be referred to an Initial Joint Conference Committee to be convened within thirty (30) days of that FMEC meeting. Such Initial Joint Conference Committee may be convened at any time sooner by mutual agreement of the FMEC and PLC. The Initial Joint Conference Committee shall be composed of two (2) representatives selected by the PLC, two (2) representatives selected by the FMEC, one (1) administrative representative and one (1) Board member.
34
9.3.1 The positions established at the Initial Joint Conference Committee will be reported
in full to the FMEC and the PLC. The FMEC will discuss the issue at its next meeting. In the event the FMEC(s)’ recommendation remains contrary to the opinion of the PLC, the recommendation of the FMEC(s) shall be forwarded to the Board, along with pertinent, applicable information.
The PLC, at its discretion, may include a divergent opinion along with pertinent,
applicable information. The Board shall have sixty (60) days to adopt the recommendation of the FMEC(s), or may choose to refer the matter(s) to a Final Joint Conference Committee at any time within the 60-day period.
9.4 A Final Joint Conference Committee will be convened if: 9.4.1 requested by the Board; 9.4.2 requested by the PLC, FMEC(s) or Initial Joint Conference Committee (if the Initial
Joint Conference Committee is unable to resolve conflicts and divergent opinions remain between the PLC, FMEC(s) and/or Initial Joint Conference Committee); or
9.4.3 in the event the Board does not accept or adopt a recommendation by the
FMEC(s) within sixty (60) days of receiving such recommendation(s) as set forth in Section 9.3.1.
The Final Joint Conference Committee will convene within thirty (30) days of such request,
or occurrence. The Final Joint Conference Committee will be composed of two (2) representatives selected by the PLC, two (2) representatives selected by the FMEC and two (2) representatives (which may or may not be Board members) of the Board for review and recommendation to the full Board. The Final Joint Conference Committee will have up to sixty (60) days to report its recommendation(s), and will issue its complete report simultaneously to the FMEC(s), PLC, Initial Joint Conference members and Board. If either the FMEC(s) or PLC continues to have a dissenting opinion/recommendation from that of the Final Joint Conference Committee, both (FMEC and PLC) shall each have the right for a representative of each to report its recommendation/opinion at the same time to the Board. After such report(s), the Board will make a determination, which shall be final.
9.5 The Chair of the Board, PLC or FMEC may call for an Initial Joint Conference as described
above at any time and for any reason in order to seek direct input from the Board, PLC and/or FMEC Medical Staff leaders, clarify any issue, or relay information directly to Medical Staff leaders.
9.6 The provisions of this article are not applicable to matters subject to the provisions of the
Medical Staff Bylaws, Rules and Regulations, or Policies relating to Peer Review, Corrective Action or the Fair Hearing process.
SECTION 10 REVIEW, REVISION, ADOPTION, AND AMENDMENT 10.1 Medical Staff Responsibility
10.1.1 The Medical Staff shall have the responsibility to formulate, review at least
biennially, and recommend to the Board any Medical Staff Bylaws, rules, regulations, policies and procedures, and amendments as needed, which shall be effective when approved by the Board.
35
The Medical Staff can exercise this responsibility through its elected and appointed leaders or through direct vote of its membership.
10.2 Methods of Amendment and Adoption to these Bylaws
10.2.1 Proposed amendments to these Bylaws may be originated by the System Bylaws
Committee for consideration of all FMECs and each general Medical Staff or by a petition signed by twenty-five (25) active staff members.
10.2.1.1 Each active member of the Medical Staff will be eligible to vote on the
proposed amendment to these Bylaws via printed or secure electronic ballot in a manner determined by the FMEC. All active members of the Medical Staff shall receive at least thirty (30) days advance notice of the proposed changes. Proposed amendments must:
10.2.1.1.1 receive a simple majority of the votes cast by those active
Medical Staff members eligible to vote at the initiating FMEC;
10.2.1.1.2 receive a simple majority of the votes cast by the active
Medical Staff members eligible to vote at each FMEC; 10.2.1.1.3 receive a simple majority of the votes cast by the active
Medical Staff members eligible to vote on each facility general Medical Staff.
10.2.1.2 Amendments so adopted shall be effective when approved by the Board.
Neither the Board nor the Medical Staff shall have the power or authority to unilaterally adopt or amend Medical Staff Bylaws.
10.3 Methods of Amendment and Adoption to any Medical Staff Rules, Regulations and
Policies: 10.3.1 The Medical Staff may adopt additional rules, regulations and policies as necessary
to carry out its functions and meet its responsibilities under these Bylaws. A Rules, and Regulations and Policies Manual may be utilized to organize these additional documents. Should a conflict exist between the provisions of the Medical Staff Bylaws and the Rules and Regulations or Medical Staff Policies, the Bylaws will prevail. Should a conflict exist between the provisions of the Rules and Regulations and the Medical Staff Policies, the Rules and Regulations will prevail.
10.3.2 Proposed amendments to the Rules, Regulations and Policy Manual may be
originated by the FMEC. 10.3.3 The Medical Staff itself may recommend directly to the Board an amendment(s) to
any rule, regulation, or policy by submitting a petition signed by twenty-five (25) active Medical Staff members. Upon presentation of such petition, the adoption process outlined in 10.2.1 above will be followed.
10.3.4 The FMEC shall vote on the proposed language changes at a regular meeting, or at
a special meeting called for such purpose. Following an affirmative vote by the FMEC, any of these documents may be adopted, amended or repealed, in whole or in part and such changes shall be effective when approved by the Board, subject to Section 9 of this Part in the event of a conflict.

36
10.4 The FMEC may adopt such amendments to these Bylaws, Rules and Regulations, and
policies that are, in the committee’s judgment, technical or legal modifications or clarifications, reorganization or renumbering or those needed due to punctuation, spelling, or other errors of grammar or expression. Such amendments need not be approved by the entire Board but must be approved by the System CEO.
37
Appendix A
PRINCIPLES OF MEDICAL ETHICS**
PREAMBLE The medical professions have long subscribed to a body of ethical statements developed primarily for the benefit of the patient. As a member of this profession, a health professional must recognize responsibility to patients first and foremost, as well as to society, to other health professionals and to self. The following Principles are not laws but standards of conduct, which define the essentials of honorable behavior for the health professional. Section 1 A health professional shall be dedicated to providing competent medical care with compassion and respect for human dignity and rights. Section 2 A health professional shall uphold the standards of professionalism, be honest in all professional interactions, and strive to report health professionals deficient in character or competence, or engaging in fraud or deception, to appropriate entities. Section 3 A health professional shall respect the law and also recognize a responsibility to seek changes in those requirements, which are contrary to the best interests of the patient. Section 4 A health professional shall respect the rights of patients, colleagues, and other health professionals and shall safeguard patient confidences and privacy within the constraints of the law. Section 5 A health professional shall continue to study, apply and advance scientific
knowledge, maintain a commitment to medical education, make relevant information available to patients, colleagues and the public, obtain consultation, and use the talents of other health professions when indicated.
Section 6 A health professional shall, in the provision of appropriate patient care, except in emergencies be free to choose whom to serve, with whom to associate and the environment in which to provide medical care.
38
Section 7 A health professional shall recognize a responsibility to participate in activities contributing to an improved community and the betterment of pubic health. Section 8 A health professional shall, while caring for a patient, regard responsibility
to the patient as paramount.
Section 9 A health professional shall support access to medical care for all people. **Adapted from the American Medical Association’s “Principles of Medical Ethics” (adopted by the AMA’s
House of Delegates June 17, 2001).
39
PART II: INVESTIGATIONS, CORRECTIVE ACTION, HEARING AND APPEAL PLAN
SECTION 1 ROUTINE CORRECTIVE ACTION & INVESTIGATIONS 1.1 Progressive Intervention These Bylaws encourage the use of progressive steps by Medical Staff leaders and
hospital administration, beginning with collegial and education efforts, to address questions relating to a practitioner’s clinical practice and/or professional conduct. The goal of these efforts is to arrive at voluntary, responsive actions by the practitioner to resolve questions that have been raised. All collegial intervention efforts by Medical Staff leaders and hospital management are part of the hospital’s performance improvement and professional review activities. Collegial intervention efforts are encouraged, but are not mandatory, and shall be within the discretion of the appropriate Medical Staff leaders and hospital administration.
When any observations arise, suggesting opportunities for a practitioner to improve, the matter may be referred in accordance with the performance improvement and professional conduct policies adopted by the Medical Staff and hospital.
Corrective actions and investigations shall be undertaken: 1.1.1 in the reasonable belief that the action is in the furtherance of quality health care; 1.1.2 after a reasonable effort to obtain the facts of the matter,
1.1.3 after adequate notice and hearing procedures are afforded to the practitioner as set forth herein, and
1.1.4 in the reasonable belief that the action is warranted by the facts known after such reasonable effort to obtain the facts.
1.2 Basis for Routine Corrective Action Whenever a concern or question has been raised regarding: 1.2.1 the clinical competence or clinical practice of any appointee; 1.2.2 the care or treatment of a patient or patients or management of a case by any
appointee; 1.2.3 activities or professional conduct that may be detrimental to patient safety; 1.2.4 the known or suspected violation by any Medical Staff appointee of these Bylaws,
the Policies, or the Rules and Regulations of the Medical Staff, System or Department
1.2.5 behavior or conduct on the part of any Medical Staff appointee that is considered lower than the standards of the hospital, disruptive to the hospital or its Medical Staff, including the inability of the appointee to work harmoniously with others; or
1.2.6 impairment, a request for corrective action may be made by any practitioner on the Medical Staff, any
member of the System administration, System or Medical Staff committee, or the Board of Directors, after making sufficient inquiry to satisfy themselves that the concern or question raised is credible.
40
1.3 Requests and Notices All requests for corrective action shall be made in writing to the President of the Medical
Staff and the Chief Medical Officer, with a copy to the Medical Staff Services Office. The request must be signed by the complainant, clearly state those facts that support the request in sufficient detail to permit an investigation to be pursued, and, if possible, state what corrective action is deemed appropriate by the complainant. The President of the Medical Staff shall notify the FMEC at its next regular meeting that a request for corrective action has been made. The affected practitioner shall be given written notice of the request, and a copy of the same. All notices provided under this Part II shall be hand delivered or sent via certified mail, return receipt requested. All time limits shall begin upon receipt of notice.
1.4 Investigations
1.4.1 When a request for corrective action has been received by the FMEC, the committee shall determine as soon as possible, but no later than at its next regularly scheduled meeting, either to discuss the matter with the appointee concerned, or to begin an investigation. If the concern states sufficient information to warrant action, the FMEC, at its discretion, may initiate an investigation, with or without a personal interview with the practitioner being investigated. The FMEC may seek input from the practitioner’s Department or Section prior to initiating investigation. An investigation shall begin only after a formal resolution of the FMEC to that effect. The affected practitioner shall be given written notice of the initiation of an investigation. If the Board of Directors wishes to begin such an investigation, it shall also formally resolve to do so by mandating the FMEC to begin an investigation.
1.4.2 Upon resolving to initiate an investigation, the Medical Staff President through the
FMEC or President of the Medical Staff shall immediately appoint a member(s) of the Active Medical Staff to conduct an investigation of the matters contained in the request. Investigators shall not include partners, associates or relatives of the practitioner being investigated and should be objective and familiar with the types of issues raised in the request for corrective action.
1.4.3 The investigator(s) may consult with other members of the Medical Staff as
appropriate in order to determine the facts of the case, or to obtain professional opinions relative to the matter under consideration.
1.4.4 The investigator(s) shall have available the full resources of the Medical Staff and
the System, as well as the authority to use outside consultants, if needed. 1.4.5 The investigation should be completed within thirty (30) working days of the
appointment of the investigator(s), unless an extension of not more than thirty (30) additional working days has been granted by the FMEC or President of the Medical Staff.
1.4.6 At the conclusion of the investigation, the investigator(s) shall prepare a written
report of the findings and transmit the same to the President of the Medical Staff and the Chief Medical Officer. In addition to setting forth findings of fact and, if applicable, the clinical opinion of the investigator(s) and other practitioners with whom he may have consulted, the report shall recommend that corrective action be imposed, or that the complaint against the affected practitioner be dismissed.
The investigator may recommend a type or degree of corrective action deemed
appropriate.
41
1.4.7 The President of the Medical Staff shall review the investigator’s report when it is received, and if emergency corrective action is indicated, proceed to impose the same pursuant to Section 2 of this part. Otherwise, the President shall submit the investigator’s report to the FMEC for consideration at its next regular meeting.
1.4.8 In cases suggesting practitioner impairment, the President of the Medical Staff shall
confer with a member of the Medical Administrative Staff, designated by the System President and the practitioner’s Department Chair, and if they concur, shall refer the request to the Practitioner Resource Committee for disposition; otherwise, the request shall be referred to the FMEC for consideration at its next regular meeting.
1.5 FMEC Action 1.5.1 If the FMEC determines that there are no reasonable grounds to believe that the
affected practitioner has committed an offense requiring corrective action under these Bylaws, the complaint shall be dismissed. The affected practitioner and complainant shall be given written notification of dismissal.
1.5.2 If the FMEC determines that there are reasonable grounds to believe that the
affected practitioner is subject to corrective action, the Committee may elect to recommend corrective action to the Board, which, at the discretion of the FMEC, may consist of:
1.5.2.1 A written warning that corrective action measures will be taken in the
future if the affected practitioner does not reform his conduct in the manner set forth in the warning;
1.5.2.2 A written reprimand stating the Committee’s displeasure at the affected
practitioner’s behavior, and directing the affected practitioner to cease the same immediately;
1.5.2.3 Mandated education to improve the affected practitioner’s knowledge,
skills and ability in clinical as well as non-clinical subjects;
1.5.2.4 Mandated clinical review or supervision to see that the affected practitioner’s performance attains an acceptable level;
1.5.2.5 Limitation of privileges restricting those procedures that the affected
practitioner may perform at the Facility;
1.5.2.6 Removal of privileges eliminating the affected practitioner’s ability to perform any procedure at the Facility. If the affected practitioner is a member of the Medical Staff, removal of privileges shall also entail revocation of Medical Staff membership. If removal of privileges is recommended at the time of the affected practitioner’s biennial reappointment, this may be accomplished by not recommending the affected practitioner for reappointment;
1.5.2.7 Make such other recommendations, as it deems necessary or appropriate.
42
1.6 Notice of FMEC Action Whenever a recommendation for corrective action has been made by the FMEC, or
corrective action has been taken by the Board on its own initiative, written notice of the same shall be sent to the affected practitioner by certified mail, return receipt requested, or hand delivery with receipt. Such notice shall be consistent with the notice provision set forth in Subsection 1.3. The notice shall set forth the nature of the complaint, the reasons for the corrective action, a description of the corrective action, and a short summary of the affected practitioner’s right to a fair hearing pursuant to these Bylaws, including any time limits within which the affected practitioner must act. The affected practitioner may request a hearing pursuant to the provisions of Section 4.
1.7 Board of Directors Action If the time, during which an affected practitioner may request a hearing pursuant has
expired without a request being made, or such hearing, including appeal to the Board, has been concluded, then at the next regular meeting thereafter of the Board of Directors, the Board shall consider the recommended corrective action. In the event that the Board rejects such recommendation, the Board may remand the recommendation to the FMEC with instructions to reconsider the matter, including the nature and degree of the corrective action. The Board shall consider recommendations of the FMEC following remand in the same manner as other recommendations for corrective action.
SECTION 2 EMERGENCY CORRECTIVE ACTION/PRECAUTIONARY SUSPENSION
OF CLINICAL PRIVILEGES 2.1 Basis for Emergency Corrective Action/Precautionary Suspension The President of the Medical Staff, the Chief Medical Officer (or his designee), or the FMEC
shall have the authority to immediately suspend all or any portion of the clinical privileges of a Medical Staff practitioner or other individual, whenever failure to take such action may result in an imminent danger to the health and/or safety of any individual. Such precautionary suspension shall be deemed an interim precautionary step in the professional review activity related to the ultimate professional review action that may be taken with respect to the suspended individual but is not a complete professional review action in and of itself. It shall not imply any final finding of responsibility for the situation that caused the suspension, nor shall it entitle the practitioner to a fair hearing except as provided under this Section. Those parties with the authority to impose emergency corrective action shall consult with a physician member of the Administration designated by the System President and System legal counsel before imposing any emergency corrective action. This Subsection shall not apply if a clear and present danger exists which requires immediate action and consultation is not feasible.
2.2 Notice of Emergency Corrective Action/Precautionary Suspension Upon imposition of emergency corrective action, the President of the Medical Staff shall
immediately give notice to the affected practitioner of such action. Such notice may be oral, but shall be confirmed in writing as soon as possible, but no later
than the next business day. The written notice shall state the reasons for the emergency corrective action and the nature of corrective action imposed. A copy of the notice shall also be given to the Chief Medical Officer, Department Chair, and FMEC.
43
2.3 FMEC Procedure When instituted, a precautionary suspension of clinical privileges will automatically expire in
seven (7) days, unless extended by the FMEC, with return of all previous clinical privileges unless the suspension is confirmed by a majority vote of the FMEC in special session. The FMEC shall review the matter resulting in precautionary suspension within a reasonable period not to exceed fourteen (14) days. Unless the FMEC promptly terminates or extends the precautionary suspension prior to or immediately after reviewing the suspension, the practitioner shall be entitled to the procedural rights afforded by the Fair Hearing and Appeal plan once the restrictions or suspension last more than fourteen (14) calendar days. Restrictions or suspensions which last fourteen (14) days or less shall not trigger rights under the Fair Hearing and Appeal Plan.
2.4 Provision of Patient Care Immediately upon the imposition of a precautionary suspension, the appropriate
Department Chair or, if unavailable, the President of the Medical Staff shall assign responsibility for care of the suspended practitioner’s patients still in a System’s facility to another practitioner with appropriate clinical privileges. The assignment shall be effective until the patients are discharged. The wishes of the patient shall be considered in the selection of the assigned practitioner. It shall be the duty of all Medical Staff practitioners to cooperate with the President of the Medical Staff, the Department Chair concerned, the FMEC and the Chief Medical Officer in enforcing all suspensions.
2.5 Recission of Emergency Corrective Action/Precautionary Suspension The person imposing emergency corrective action may, at any time prior to ratification of
such action by the FMEC, rescind the action, and the affected practitioner shall be restored to the status he enjoyed prior to the imposition of emergency correction action. Following ratification of emergency corrective action by the Executive Committee, the person imposing such action may recommend to the FMEC that such action be rescinded. The FMEC shall consider such recommendation at its next regular meeting thereafter. Any pending request for a hearing pursuant to Section 4 shall be made moot and void by such recission.
SECTION 3 AUTOMATIC SUSPENSION AND TERMINATION 3.1 Basis for Automatic Suspension and Termination A practitioner’s clinical privileges shall automatically be revoked, limited or suspended as
appropriate, which action shall be final without a right to due process except as provided in this Section, upon the occurrence of the following circumstances: 3.1.1 Loss of License. The practitioner’s license to practice in the State of Florida is
suspended, limited or terminated. 3.1.2 Residence or Office Outside Lee County. The practitioner does not maintain a full-time residence and office in Lee County as
required by these Bylaws, unless such requirements are waived by the FMEC pursuant to said Subsection. Return of United States mail sent by the System Medical Staff Services Office to a practitioner at his Lee County home or office address with “addressee unknown” or similar endorsement shall be prima facie
44
evidence that the practitioner does not comply with these Bylaws. Failure of a practitioner to supply a current residence and office address within 15 working days of a request of the Medical Staff Services Office for the same shall be deemed prima facie evidence that the practitioner does not comply with these Bylaws. This shall not apply to practitioners granted a leave of absence by the FMEC pursuant to these Bylaws.
3.1.3 Lack of Active Practice. The practitioner is not actively engaged in the practice of
his profession in Lee County; that is, he is not seeing, examining, treating or otherwise caring for patients, and has not done so for a period of more than six months, unless the practitioner shall have notified the Medical Staff Services Office prior to beginning such absence, and arranged for suitable coverage during such time period. This shall not apply to practitioners granted a leave of absence by the FMEC pursuant to these Bylaws, or to members of the Honorary Medical Staff.
3.1.4 Criminal Conviction. The practitioner has been, while a practitioner on the Medical
Staff, convicted in any jurisdiction of the United States; of a felony or misdemeanor involving actual or threatened bodily harm, actual or threatened sexual misbehavior or stalking, controlled substance possession or use, or of any felony or misdemeanor described in any Florida law pertaining to governing or regulating the health professions or health facilities. A practitioner whose membership or privileges are automatically terminated pursuant to this Subsection shall not be disqualified from applying for appointment following completion of his sentence, or during a period of time when he is on probation. However, the fact that the practitioner has completed his sentence after criminal conviction, or is on probation, shall not require the Medical Staff to make such appointment, and the FMEC may elect not to do so in its discretion, consistent with its responsibility towards patients, other practitioners, Facility/System employees, and the public in general.
3.1.5 Loss or Restriction of DEA Certificate. The clinical privileges of a practitioner whose
Drug Enforcement Agency (DEA) certification is terminated, revoked, or suspended shall automatically and immediately be modified to revoke the right to prescribe controlled substances. The practitioner shall immediately inform the Medical Staff Services Office regarding the change in status in his DEA certification. The matter shall promptly be referred, for investigation and further action in accordance with the provisions of these Bylaws.
3.1.6 Exclusion From Federal or State Health Care Programs. The Medical Staff
appointment and clinical privileges of a practitioner who becomes an ineligible person with regard to participation in Federal or State Health Care Programs shall automatically and immediately be suspended.
The practitioner shall immediately inform the Medical Staff Services Office regarding
the change of his eligibility status. This triggers the right to due process. The matter shall promptly be referred for investigation and further action in accordance with all the due process provisions of this Part.
3.1.7 Failure to Pay Fees and Assessments. The practitioner fails to pay when due any
fee or assessment imposed pursuant to these Bylaws or Medical Staff or System policy.
3.1.8 Failure to Provide Requested Information. If at any time a practitioner fails to
provide required information pursuant to a formal request by the System Credentialing/Privileging Committee, Medical Executive Committee or the Medical Staff Services Office, the practitioner’s clinical privileges shall be deemed to be
45
voluntarily relinquished until the required information is provided to the satisfaction of the requesting party. For purposes of this Section, required information shall include but not be limited to: 1. physical or mental examination reports as specified elsewhere in this policy, or 2. information necessary to explain an investigation, professional review action, or resignation from another health care facility or agency.
3.1.9 Failure to Request Reappointment or Provide Requested Information Related to
Reappointment. If a practitioner fails to request reappointment for membership and/or privileges or fails to provide requested information pursuant to Part III, Section 5 of these Bylaws, the practitioner’s membership and privileges shall be deemed voluntarily relinquished.
3.1.10 Failure to Request Reinstatement Following Leave of Absence. Failure to request
reinstatement shall be deemed a voluntary resignation from the Medical Staff and shall result in automatic termination of membership, privileges, and prerogatives. Members whose membership is automatically terminated shall not be entitled to the procedural rights provided in the Medical Staff Bylaws.
3.1.11 Failure to Complete Medical Records. All elective admitting, consulting and clinical
privileges of any practitioner shall be deemed to be voluntarily relinquished for failure to complete medical records in accordance with the provisions of the Medical Staff Rules and Regulations. Such relinquishment shall continue until all the records of the practitioner’s patients are no longer delinquent. Such relinquishment does not exempt the practitioner from fulfilling their on-call responsibilities. Failure to complete the medical records that caused relinquishment of clinical privileges within sixty (60) days from the relinquishment of such privileges shall be grounds for further disciplinary action in accordance with the provisions of these Bylaws.
3.1.12 Failure to Comply with Special Meeting Attendance Requirements. Failure of a
practitioner to attend a special meeting called pursuant to the Bylaws. 3.2 Right to Limited Hearing for Automatic/Voluntary Suspension and Termination A practitioner affected by this Section shall be sent a written notice stating the reasons for
automatic suspension within 24-hours of the same having been imposed, and shall have the right to present evidence to the FMEC in written form, or by appearing personally at a regular meeting of the committee, to demonstrate that the reason that automatic suspension was imposed is untrue.
3.2.1 Such written evidence or a written request to meet with the FMEC shall be
submitted to the President of the Medical Staff within ten (10) working days of the date the notice of automatic suspension was sent. Failure to submit written evidence or a request shall be deemed a waiver of any right to consideration of the same.
3.2.2 Evidence presented by the affected practitioner shall be limited to whether or not the
grounds for automatic suspension are true. The FMEC shall not consider evidence or argument, which presents mitigating circumstances or excuse.
3.2.3 After receipt of an affected practitioner’s written evidence, and prior to the next
regular meeting of the FMEC, the President of the Medical Staff, with the concurrence of a member of the Medical Administrative Staff designated by the System President, may determine that the evidence so presented demonstrates that
46
the reasons that automatic suspension was imposed are untrue, and revoke the suspension, restoring the affected practitioner to the status he previously enjoyed.
3.2.4 The President of the Medical Staff may, at any time, provisionally reinstate a
practitioner suspended pursuant to this Section if the President is satisfied by the available written documentation that the reasons for automatic suspension were untrue. The President shall present the provisional reinstatement for ratification by the FMEC at its next regular meeting.
3.2.5 At its next regular meeting following automatic suspension, the FMEC shall consider
the reasons therefore, together with any evidence or argument presented by the affected practitioner, and if the reasons for automatic suspension are found to be true, recommend to the Board termination of the affected practitioner’s Medical Staff membership and/or privileges. If the FMEC finds that the reasons are untrue or corrected, the suspension shall be revoked, and the affected practitioner restored to the status he previously enjoyed.
SECTION 4 HEARING AND APPEAL PROCEDURES 4.1 Grounds for Hearing An applicant or an individual holding a Medical Staff appointment shall be entitled to
request a hearing whenever the FMEC or the Board of Directors has made one of the following adverse recommendations:
4.1.1 denial of initial Medical Staff appointment; 4.1.2 denial of Medical Staff reappointment; 4.1.3 revocation of Medical Staff appointment; 4.1.4 denial of requested initial clinical privileges; 4.1.5 denial of requested additional clinical privileges; 4.1.6 decrease of clinical privileges;
4.1.7 suspension of clinical privileges (other than emergency corrective action/precautionary suspension);
4.1.8 imposition of mandatory concurring consultation requirement. No other recommendations except those enumerated in this Section shall entitle the practitioner to request a hearing. Neither voluntary relinquishment of clinical privileges, as provided in these Bylaws, nor the imposition of any general consultation requirement, nor the imposition of a requirement for retraining, additional training or continuing education, shall constitute grounds for a hearing, but shall take effect without hearing or appeal. The hearing shall be conducted in as informal a manner as possible, subject to the rules and procedures set forth in these Bylaws.
4.2 Notice of Recommendation When a recommendation is made which, according to these Bylaws entitles a practitioner to
a hearing prior to a final decision of the Board, the affected practitioner shall promptly be given notice by the President of the Medical Staff or Chief Medical Officer or his designee, in writing, certified mail, return receipt requested or in person. This notice shall contain:
47
4.2.1 a statement of the recommendation made, the action which is being taken or which may be taken, and the general reasons for it; 4.2.2 notice that the practitioner has the right to request a hearing on the
recommendation within thirty (30) days of receipt of this notice; and 4.2.3 a copy of this Part outlining the rights in the hearing as provided for in these
Bylaws.
4.3 Request for Hearing A practitioner shall have thirty (30) days following the date of the receipt of such notice
within which to request the hearing. The request shall be in writing to the President of the Medical Staff or Chief Medical Officer with a copy to the Medical Staff Services Office and signed by the affected practitioner making such request. In the event the practitioner does not request a hearing within the time and in the manner required by these Bylaws, the practitioner shall be deemed to have waived the right to the hearing and to have accepted the action involved. That action shall become effective immediately upon final Board action.
4.4 Preliminary Interview The affected practitioner may request, at the time of submitting a request for hearing or
within ten (10) working days thereafter, an informal preliminary interview with the decision making body (FMEC or Board of Directors). The decision making body shall grant all such requests, and the affected practitioner shall be scheduled to appear before it at its next regular meeting. 4.4.1 The purpose of the preliminary interview shall be to permit the affected practitioner
to personally present any argument or evidence showing that the adverse recommendation has been wrongfully imposed, in fact, or in violation of these Bylaws; or to present any mitigating circumstances.
4.4.2 The preliminary interview is informal and not a hearing. It is optional with the
affected practitioner, and accordingly, legal counsel shall be excluded. 4.4.3 The decision making body may impose a limit on the amount of time to be devoted
to a preliminary interview, but not less than thirty minutes. 4.4.4 Failure to request a preliminary interview shall not be considered in any hearing or
deliberation conducted pursuant to these Bylaws, nor shall the affected practitioner’s right to a hearing be affected thereby.
4.4.5 Following a preliminary interview, the decision making body shall deliberate, and
may elect to withdraw or reduce the severity of the adverse recommendation imposed upon the affected practitioner, or may take no action.
If no action is taken, the adverse recommendation shall continue in effect, and the hearing provided for hereunder shall proceed.
4.4.6 Notice shall be given to the affected practitioner of the decision following a
preliminary interview in the manner provided in Subsection 1.3.
SECTION 5 FAIR HEARING PROCEDURE 5.1 System Representative, Hearing Panel and Hearing Officer
48
5.1.1 System Representative 5.1.1.1 When the FMEC of the Medical Staff is the decision making body, the
President of the Medical Staff shall appoint a person to represent the interests and position of the Medical Staff in all proceedings provided for in this Section. Such individual shall be in an adversarial role opposed to the affected practitioner. If the affected practitioner is not represented by legal counsel, the Medical Staff representative shall not be an attorney, but shall be a member of the Active Medical Staff.
5.1.1.2 When the Board is the decision making body, as defined herein, the
Chair of the Board shall appoint a person to represent the interests and position of the Board in all proceedings provided for in this Section. Such individual shall be in an adversarial role opposed to the affected practitioner. If the affected practitioner is not represented by legal counsel, the Board representative shall not be an attorney, but shall be a member of the administration.
5.1.1.3 For purposes of these Bylaws, the Medical Staff or Board representative
appointed under this Section shall be called the “System Representative.”
5.1.2 Hearing Panel 5.1.2.1 Unless the FMEC or Board elects to have the matter heard by a Hearing
Officer possessing the qualifications set forth in Subsection 5.1.3, all hearings shall be conducted by a Hearing Panel appointed by the President of the Medical Staff or the Chair of the Board, as applicable,
composed of five (5) members, presided over by a qualified professional selected in accordance with Subsection 5.1.3. The Hearing Panel shall be composed of Active Medical Staff practitioners who shall not have actively participated in the consideration of the matter involved at any previous level. Knowledge of the matter involved shall not preclude any individual from serving as a member of the Hearing Panel.
If the hearing has been requested based on Board action, 3 of the
members of the Hearing Panel shall be members of the Board of Directors. The Hearing Panel will be presided over by a Hearing Officer.
5.1.2.2 The Hearing Panel shall not include any individual who is in direct
economic competition with the affected person or has any other personal interest in the proceeding, financial or otherwise, or any such individual who is professionally associated with or related to the affected practitioner.
5.1.3 Hearing Officer – Qualifications & Authority 5.1.3.1 The FMEC or the Board may elect to have the hearing provided for in
this Section held by a Hearing Officer sitting alone. In such case, the Hearing Officer shall perform all of the functions of the Hearing Panel described herein.
49
In cases where a panel is appointed, the Hearing Officer will preside over the proceeding but not participate in the deliberations or vote on the recommendation.
5.1.3.2 The Hearing Officer:
5.1.3.2.1 shall be an attorney licensed in the State of Florida who is
knowledgeable and has experience in health care law, including Medical Staff law; or shall be a non-lawyer who has experience as a Hearing Officer;
5.1.3.2.2 shall not be, or have been, employed or retained by the Lee
Memorial Health System, or any practitioner on the Medical Staff, including the affected practitioner, for any purpose other than to serve as a Hearing Officer in Medical Staff proceedings;
5.1.3.2.3 shall have no personal interest in the proceeding, financial or
otherwise; 5.1.3.2.4 shall be selected by the affected practitioner from a list
provided to the affected practitioner by the General Counsel for the Health System of the names of not less than three (3) persons meeting the requirements of 1-3 above. The affected practitioner shall select the Hearing Officer from the list submitted to him and within forty-eight (48) hours of receiving said list, notify the General Counsel for the Health System in writing of said selection.
Failure of the affected practitioner to select within the
previously mentioned period shall constitute a waiver by the affected practitioner of this Subsection, and the General Counsel for the Health System shall thereafter select the Hearing Officer.
5.1.3.3 The Hearing Officer shall: 5.1.3.3.1 act to insure that all participants in the hearing have a
reasonable opportunity to be heard and to present oral and documentary evidence subject to reasonable limits on the number of witnesses and duration of direct and cross examination, applicable to both sides, as may be necessary to avoid cumulative or irrelevant testimony or to prevent abuse of the hearing process;
5.1.3.3.2 prohibit conduct or presentation of evidence that is
cumulative, excessive, irrelevant, and abusive or that causes undue delay;
5.1.3.3.3 maintain decorum throughout the hearing; 5.1.3.3.4 determine the order of procedure throughout the hearing; 5.1.3.3.5 have the authority and discretion, in accordance with these
Bylaws, to make rulings on all questions that pertain to
50
matters of procedure and to the admissibility of evidence and qualifications of witnesses;
5.1.3.3.6 act in such a way that the Hearing Panel in formulating its
recommendations considers all information relevant to the continued appointment or clinical privileges of the practitioner requesting the hearing;
5.1.3.3.7 conduct argument by counsel on procedural points outside
the presence of the Hearing Panel unless the Panel wishes to be present;
5.1.3.3.8 grant continuances and postponements as appropriate; and 5.1.3.3.9 take official notice of any matters, either technical or scientific,
relating to the issues under consideration that could have been judicially noticed by the courts of this state, inform the participants of the matters to be officially noticed and provide each party the opportunity to request that a matter be officially noticed or to refute the noticed matter by evidence or by written or oral presentation of authority.
5.2 Challenge to Hearing Panel Members or Hearing Officer
The affected practitioner may challenge the objectivity of any member of the Hearing Panel, or the Hearing Officer, at any time prior to the taking of testimony at the hearing. Such challenge shall be in writing and specify facts demonstrating that a member of the Hearing Panel or the Hearing Officer lacks objectivity or is biased against the affected practitioner. The challenge shall be directed to the President of the Medical Staff or the Chair of the Board, as applicable, who shall consider the challenge and either sustain or overrule it. If the challenge is sustained, the challenged member of the Hearing Panel or the Hearing Officer shall be replaced.
SECTION 6 HEARING PROCEDURES 6.1 Provision of Relevant Information
6.1.1 There is no right to discovery in connection with the hearing. However, the
practitioner requesting the hearing shall be entitled, upon specific request, to the following, subject to a stipulation signed by both parties that such documents shall be maintained as confidential and shall not be disclosed or used for any purpose outside of the hearing:
6.1.1.1 copies of, or reasonable access to, all patient medical records referred to
in the Statement of Reasons, at the practitioner’s expense; 6.1.1.2 reports of experts relied upon by the FMEC or the Board; 6.1.1.3 redacted copies of relevant committee or Department meeting minutes
(such provision does not constitute a waiver of the state peer review protection statute); and
6.1.1.4 copies of any other documents relied upon by the FMEC or the Board.
51
6.1.2 Prior to the hearing, on dates set by the Hearing Officer or agreed upon by counsel
for both sides, each party shall provide the other party with a list of proposed exhibits. All objections to documents or witnesses to the extent then reasonably known, shall be submitted in writing in advance of the hearing. The Hearing Officer shall not entertain subsequent objections unless the party offering the objection demonstrates good cause.
6.1.3 Prior to the hearing, on dates set by the Hearing Officer, the practitioner requesting
the hearing shall, upon specific request, provide the FMEC (or the Board of Directors) copies of any expert report or other documents relied upon by the practitioner.
6.1.4 Neither the affected practitioner, nor his attorney, nor any other person on behalf of
the affected practitioner, shall contact members of the hearing committee or the Hearing Officer, or hospital employees appearing on the hospital’s witness list concerning the subject matter of the hearing, unless specifically agreed upon by counsel.
6.2 Pre-Hearing Conference The Hearing Officer may require counsel for the practitioner and for the FMEC (or the
Board) to participate in a pre-hearing conference for purposes of resolving all procedural questions in advance of the hearing. The Hearing Officer may specifically require that:
6.2.1 all documentary evidence to be submitted by the parties be presented at this
conference; any objections to the documents shall be made at that time and the Hearing Officer shall resolve such objections;
6.2.2 evidence unrelated to the reasons for the unfavorable recommendation or unrelated
to the practitioner’s qualifications for appointment or the relevant clinical privileges be excluded;
6.2.3 the names of all witnesses and a brief statement of their anticipated testimony are
submitted, if not previously provided; 6.2.4 the time granted to each witness’ testimony and cross-examination be agreed upon,
or determined by the Hearing Officer, in advance; and 6.2.5 witnesses and documentation not provided and agreed upon in advance of the
hearing may be excluded from the hearing. 6.3 Failure to Appear Failure, without good cause, of the practitioner requesting the hearing to appear and
proceed at such a hearing shall be deemed to constitute voluntary acceptance of the pending recommendations or actions, which shall then be forwarded to the Board for final action. The Hearing Officer may impose sanctions upon either party for failure to appear, including the assessment of the costs and attorneys’ fees of the party in attendance against the offending party.
6.4 Record of Hearing
52
A record shall be made at the expense of the Lee Memorial Health System, if any, the pre-hearing conference and the hearing, using the services of a court reporter. No record of the in camera deliberations of the decision making body or the hearing committee shall be
made. Either party shall be entitled to have a record made of any other proceeding related to the hearing process, at that party’s expense. The expense of transcripts shall be borne by the party requesting them. Oral evidence shall be taken only on oath or affirmation administered by any person designated by such body and entitled to notarize documents in this State.
6.5 Rights of Both Sides At a hearing, both sides shall have the following rights, subject to reasonable limits
determined by the Hearing Officer: 6.5.1 to call and examine witnesses to the extent available; 6.5.2 to introduce exhibits; 6.5.3 to cross-examine any witness on any matter relevant to the issues and to rebut any
evidence; 6.5.4 to be represented by counsel who may call, examine, and cross-examine witnesses
and present the case. (Both sides shall notify the other of the name of that counsel at least ten (10) days prior to the date of the pre-hearing conference and hearing); and
6.5.5 to submit a post-hearing memorandum of points and authorities (The Hearing Panel may request such a memorandum to be filed following the close of the hearing).
Any practitioner requesting a hearing, who does not testify on his own behalf, may be called
and examined as if under cross-examination. The Hearing Panel or Hearing Officer may question the witnesses, call additional witnesses or request additional documentary evidence.
6.6 Admissibility of Evidence The rules of evidence applicable to the courtroom shall not apply, and the Hearing Officer
may admit any evidence that might be relied upon by a reasonable person. Notwithstanding the foregoing, a party shall have the right to object to any evidence on
grounds of hearsay, relevance, or other grounds available under the Florida Evidence Code, and the Hearing Officer shall have the authority to rule on such objections.
6.7 Burden of Presenting Evidence and Proof The burden of going forward with evidence supporting the adverse action or
recommendation is on the FMEC or Board, whichever initially prompted the hearing. Once that burden has been met to the satisfaction of the Hearing Panel/Hearing Officer, the practitioner shall bear the burden of proof, under a preponderance of the evidence, which is a lesser standard than clear and convincing evidence, that the action and penalty taken or proposed against the practitioner was wrongfully or arbitrarily imposed, not in accordance with these Bylaws, or lacks any factual basis.
SECTION 7 HEARING CONCLUSION, DELIBERATIONS AND RECOMMENDATIONS
7.1 Deliberations and Recommendation of the Hearing Panel/Hearing Officer
53
7.1.1 The recommendation of the Hearing Panel/Hearing Officer shall be based on the evidence produced at the hearing. This evidence may consist of oral testimony of witnesses; memorandum of points and authorities presented in connection with the hearing, any information regarding the practitioner who requested the hearing so long as that information has been admitted into evidence at the hearing and the person who requested the hearing had the opportunity to comment on and, by other evidence, refute it, any and all applications, references, and accompanying documents; other documented evidence, including medical records and any other information presented at the hearing.
7.1.2 Within thirty (30) working days after final adjournment of the hearing, the Hearing
Panel shall conduct its deliberations outside the presence of any other person except the Hearing Officer, and shall prepare a recommended order containing the findings of fact, findings regarding the applicability of these Bylaws, any rules, regulations or policies of the Medical Staff or the Lee Memorial Health System, and the statutory and decisional law of Florida; and a recommendation that adverse action be upheld, modified or withdrawn. If the FMEC or the Board selected a Hearing Officer sitting alone, the Hearing Officer shall prepare a recommended order in the same manner outlined above.
7.1.3 The Hearing Officer shall not participate in the deliberations of the Hearing Panel,
nor be involved in the decision of the Hearing Panel regarding its recommended order.
However, the Hearing Officer may assist the Hearing Panel with regard to the form,
organization and syntax of the recommended order. The recommended order shall be signed by each member of the Hearing Panel or the Hearing Officer, as applicable, and copies provided in person by certified mail, return receipt requested, to the affected practitioner and System Representative.
7.2 Disposition of Hearing Panel Report The Hearing Panel/Hearing Officer shall deliver its report and recommendation to the Chief
Medical Officer or his designee who shall forward it, along with all supporting documentation, to the Board and/or FMEC.
The recommended order shall be considered by the FMEC or Board at its next regular meeting, and may be adopted or rejected by it. If adopted, the recommended order shall become the final decision of the original decision making body (FMEC or Board).
If rejected, the FMEC or Board shall render its own final written decision upholding the
original recommendation, modifying or withdrawing the action. Any action imposed through the final order that requires action by the Board of Directors shall be referred to the Board for final disposition at its next regular meeting.
SECTION 8 APPEAL PROCEDURE 8.1 Request & Time for Appeal Within ten (10) working days of receipt of the final written decision following a hearing,
either party may appeal the recommendation. The request shall be in writing, signed by the requesting party and delivered to the Chief Medical Officer either in person or by certified mail, return receipt requested, with a copy to the Medical Staff Services Office. The request shall include a statement of the reasons for appeal and the facts or circumstances that justify further review. If such appellate review is not requested within ten (10) working days
54
as provided herein, both parties shall be deemed to have waived the right to an appeal, and the Hearing Panel or Hearing Officer’s report and recommendation shall be forwarded to the Board for final action.
8.2 Grounds for Appeal The grounds for appeal shall be limited to the following: 8.2.1 there was substantial failure to comply with these Bylaws or hospital policies prior to
the hearing so as to deny a fair hearing; or 8.2.2 the recommendations of the Hearing Panel were made arbitrarily, capriciously or
with prejudice. 8.3 Time, Place and Notice Whenever an appeal is requested as set forth in the preceding Sections, the Chair of the
Board shall, as soon as arrangements can reasonably be made, taking into account the schedules of all participants, schedule and arrange for an appellate review. The affected practitioner shall be given notice of the time, place and date of the appellate review. When a request for appellate review is from a appointee who is under a suspension then in effect, the appellate Review panel shall be convened not more than 14-days from the date of receipt of the request for an appeal unless the practitioner agrees to a longer period. The time for appellate review may be extended by the Chair of the Board for good cause.
8.4 Nature of Appellate Review 8.4.1 Review panel. The Chair of the Board shall appoint a Review panel composed of 5
members, 3 of the panel members shall be members of the Board of Directors and 2 panel members shall be Active members of the Medical Staff. The Board may establish rules of procedure to govern the conduct of appellate hearings under this Section and the Chair of the Board, or his or her designee, shall preside at appellate proceedings.
8.4.2 Position Papers. Each party shall have the right to present a written statement in
support of its position on appeal. Position papers that do not conform to the following requirements may be excluded from consideration in the appeal.
8.4.2.1 The position papers shall set forth a statement of the facts and of the
applicable Bylaws provisions or other authority, as well as any other matters that the parties wish to bring before the appellate body in support of their respective positions.
8.4.2.2 Twelve copies of the affected practitioner’s position paper shall be filed
with Medical Staff Services within (fifteen)15 working days of the filing of the notice of appeal. The System Representative shall also file with Medical Staff Services, 12 copies of his position paper within ten (10) working days of his receipt of a copy of the affected practitioner’s position paper.
8.4.2.3 Position papers shall be limited to no more than thirty (30) pages,
exclusive of exhibits, and shall be on letter-size paper, typewritten, double-spaced and shall be neatly bound or stapled.
55
8.4.2.4 Each party shall provide a copy of his position paper to the other at the same time the party’s position paper is filed with Medical Staff Services.
8.4.2.5 Exhibits attached to the position paper shall not duplicate exhibits or
documents contained in the hearing record, and shall be consecutively numbered and attached at the end of the position paper.
8.4.2.6 In referring to the record, position papers shall reference specific pages of
the hearing record and of exhibits that are part of the record. 8.4.3 Oral Argument. The affected practitioner and the System Representative shall be
entitled to present oral argument. Oral argument shall be requested at the time the party submits his position paper. Failure to request oral argument shall constitute a waiver of the right to it. The Board may limit the time for oral argument, but each side shall not have less than thirty (30) minutes. Oral argument shall not include the introduction of evidence and appellate review shall not constitute a hearing de novo.
A record shall be made at the expense of the Lee Memorial Health System of the presentation of oral argument, using the services of a court reporter.
8.4.4 Recommendation. The review panel shall recommend final action to the Board
within thirty (30) working days after the completion of oral argument, or if no oral argument is requested, within forty-five (45) working days after the submission of the position papers of both parties.
SECTION 9 FINAL DECISION OF THE BOARD Within thirty (30) working days after receipt of the Review panel’s recommendation, the Board shall render a final decision in writing, including specific reasons and shall deliver copies thereof to the affected practitioner, the FMEC, and the Medical Staff Services Office, in person or by certified mail, return receipt requested. The decision shall uphold or reverse the final written decision rendered by the decision making body, or may remand the case for reconsideration by the decision making body. If the matter is referred for further action and recommendation, such recommendation shall be promptly made to the Board in accordance with the instructions given by the Board within thirty (30) days. The final decision of the Board following the appeal shall be effective immediately and shall not be subject to further review. SECTION 10 RIGHT TO ONE HEARING AND ONE APPEAL ONLY 10.1 No applicant or Medical Staff practitioner shall be entitled to more than one (1) hearing and
one (1) appeal on any matter that may be the subject of an appeal. A final appellate decision upholding or reversing a final, written decision shall be final and there shall be no right to further hearing on the matter.
10.2 If the Board determines to deny initial Medical Staff appointment or reappointment to an
applicant, or to revoke or terminate the Medical Staff appointment and/or clinical privileges of a current practitioner, that practitioner may not apply for Staff appointment or for those clinical privileges at this hospital for a period of five (5) years unless the Board provides otherwise.
56
PART III: CREDENTIALING PROCEDURES
SECTION 1 SYSTEM CREDENTIALING/PRIVILEGING COMMITTEE 1.1 Organizational Structure
It is the intention of the Medical Staff Organizations of Lee Memorial Health System (LMHS) to ultimately establish one (1) System Credentialing/Privileging Committee (hereinafter referred to as the Credentialing/Privileging Committee) to act on behalf of all the Medical Staff of LMHS. It has been determined that the two (2) Credentialing/Privileging Committees in effect at the time of the approval of this document may continue for a maximum period of two (2) years. During this transition time, the two (2) Credentialing/Privileging Committees will meet jointly on at least a quarterly basis (the Credentialing/Privileging Committees will not meet separately during the months that the joint meetings occur) and through this process will effect a smooth transition to a single System Credentialing/Privileging Committee. The single System Credentialing/Privileging Committee may decide to merge prior to the end of the two 2-year period.
1.2 Transition Issues
At the time of adoption of PART III, two (2) Credentialing/Privileging Committees exist. Chairs of each of these Credentialing/Privileging Committees have been appointed in accordance to procedures that were in existence prior to the adoption of these Credentials Procedures. During the transition period (moving from two (2) committees to a single System Credentialing/Privileging Committee), these Chairs will continue to serve as the Chairs of the applicable practitioner System Credentialing/Privileging Committee and together will serve as Co-Chairs of the System Credentialing/Privileging Committee (which will meet at least quarterly (see Section 1.1).
The initial composition of the System Credentialing/Privileging Committee will be made up of
the membership of the two (2) separate Credentialing/Privileging Committees, with the current Chairs serving as Co-Chairs. During the first year of the System Credentialing/Privileging Committee, the committee will plan to evolve to the composition of the System Credentialing/Privileging Committee as established in Section 1.4 by the end of twenty-four (24) months.
1.3 Purpose of the System Credentialing/Privileging Committee
The System Credentialing/Privileging Committee exists to oversee all credentialing and privileging activities related to Medical Staff members and privileged Allied Health practitioners on behalf of the Facility Medical Executive Committees (FMECs). These credentialing and privileging activities include processes related to the following:
1.3.1 initial appointment; 1.3.2 focused professional practice evaluation; 1.3.3 reappointment; 1.3.4 delineation of clinical privileges, including temporary privileges; and 1.3.5 development of privilege delineation forms and criteria for all LMHS facilities.
57
Credentialing activities are to be carried out in accordance with specific policies and procedures developed to ensure current clinical competency of the practitioners who are credentialed and privileged at LMHS. The purpose of the System Credentialing/Privileging
Committee also includes development of implementation of credentialing and privileging policies and procedures designed to ensure compliance with regulatory requirements.
1.4 Composition of the System Credentialing/Privileging Committee The leadership and membership of the System Credentialing/Privileging Committee shall be
as follows: 1.4.1 Consist of not less than 15 members of the active Medical Staff selected on a basis
that will ensure, insofar as feasible, balanced representation of the LMHS sites. 1.4.2 The System Medical Director will serve as a non-voting member. 1.4.3 The Immediate Past President of each FMEC will serve as voting members and will
serve a 2-year term. The FMEC may appoint this practitioner, as a member once the Immediate Past President is no longer in office.
1.4.4 Each FMEC will appoint two (2) additional representatives. 1.4.5 A quorum of 50% is required to conduct a meeting. 1.4.6 Members shall serve for two (2) years and may be reappointed to consecutive terms. 1.4.7 Each member shall be required to attend 75% of the meetings during the Medical
Staff year. Failure to attend 75% of the meetings may result in dismissal of the member from committee service and selection of an alternative member by the affected FMEC.
1.4.8 The committee members from among the committee membership will elect the Co-
Chairs of the System Credentialing/Privileging Committee. One of the Co-Chairs will be from a medical specialty and the other Co-Chair will be from a surgical specialty.
1.5 Duties and Responsibilities of the System Credentialing/Privileging Committee The System Credentialing/Privileging Committee shall: 1.5.1 Meet to evaluate credentialing-related requests (initial appointment, reappointment,
requests for clinical privileges and leave of absence, etc.) on behalf of the FMECs. 1.5.2 Monitor the granting of temporary privileges to assure that temporary privileges are
granted in compliance with approved policies and procedures. (The System Credentialing/Privileging Committee does not evaluate requests for temporary privileges. These requests are handled in accordance with specific policies and procedures that are overseen by the System Credentialing/Privileging Committee).
1.5.3 Oversee the processes related to focused professional performance evaluations and
related proctoring and other mechanisms and tools employed to evaluate competency.
1.5.4 Assure uniformity in both the development and application of privileging criteria
utilized throughout LMHS facilities.
58
1.5.5 Assure the FMECs and Board that Medical Staff Bylaws Provisions that relate to credentialing and privileging processes are being fulfilled, as well as credentialing policies and procedures and other credentialing-related Medical Staff documents. Monitor compliance with all credentialing and privileging policies and procedures.
1.5.6 Be responsible for evaluating recommendations made by Department Chairs. The committee is looking for completeness, thoroughness and adherence to
credentialing and privileging policies and criteria. Assure the FMECs that specialty-specific criteria for clinical privileges comply with Medical Staff Bylaws, credentialing policies and procedures, and criteria is applied fairly and uniformly to each practitioner.
1.5.7 Focuses in on the files that are determined to need clarification or additional
information (i.e., time gaps, problems with references, malpractice claims, etc.) and assures that all issues have been appropriately addressed and that there is complete and thorough documentation for the recommendation(s) that have been made to the FMECs.
1.5.8 Be responsible and aware of regulatory requirements related to credentialing activities
and to make the FMECs and Board aware when changes in credentialing policies and procedures need to be made in order to meet requirements.
1.5.9 Commission, receive and analyze the results of compliance audits of credentialing
and privileging processes. The System Credentialing/Privileging Committee makes recommendations to the FMECs and the Board when the System Credentialing/Privileging Committee believes, based on results of reports that improvements can and should be made in credentialing and privileging policies and procedures.
SECTION 2 QUALIFICATIONS FOR MEMBERSHIP AND PRIVLEGES 2.1 The following qualifications must be met by all applicants for Medical Staff
appointment, reappointment or clinical privileges:
2.1.1 Associate and Active Staff shall live and maintain an office in Lee County, unless this requirement is waived by the FMEC;
2.1.2 Demonstrate that he has successfully graduated from an approved school of
medicine (MD or DO), dentistry, podiatry, clinical psychology or applicable recognized course of training in a clinical profession eligible to hold privileges;
2.1.3 Have a current unrestricted state or federal license as a physician, dentist, podiatrist
or clinical psychologist, applicable to his or her profession, and providing permission to practice within the State of Florida;
2.1.4 Have a record that is free from current Medicare/Medicaid sanctions and not be on
the Office of Inspector General (OIG) or General Services Administration (GSA) List of Excluded practitioners/entities;
2.1.5 Have a record that is free of felony convictions or occurrences that would raise
questions of undesirable conduct, which could injure the reputation of the Medical Staffs, hospital or Health System;
59
2.1.6 A physician (MD or DO) must have successfully completed an allopathic or osteopathic residency program, approved by the Accreditation Council for Graduate Medical Education (ACGME) or the American Osteopathic Association (AOA) and be currently board certified or become board certified following the completion of formal training within the timeframes as defined by the appropriate specialty board of the American Board of Medical Specialties or the American Osteopathic Association. If no time limits for certification are specified by a given Board, then the applicant will be required to become Board certified within seven (7) years of completing formal training as defined by the appropriate specialty Board of the American Board of Medical Specialties or the American Osteopathic Association. Once a member of the Medical Staff becomes Board certified, recertification is not a requirement of continued membership and privileges. The requirements of this subsection may be waived in accordance with Medical Staff Policies and Procedures governing such waivers;
2.1.7 Dentists must have graduated from an American Dental Association approved
school of dentistry accredited by the Commission of Dental Accreditation; 2.1.8 Oral and maxillofacial surgeons must have graduated from an American Dental
Association approved school of dentistry accredited by the Commission of Dental Accreditation and successfully completed an American Dental Association approved residency program and be board certified or become board certified within five (5) years of completing formal training as defined by the American Board of Oral and Maxillofacial Surgery;
2.1.9 A podiatric physician (DPM) must have successfully completed a two 2-year
residency program in surgical, orthopedic, or podiatric medicine approved by the Council on Podiatric Medical Education of the American Podiatric Medical Association (APMA), and be board certified or become board certified within five (5) years of completing formal training as determined by the American Board of Podiatric Surgery or the American Board of Podiatric Orthopedics and Primary Podiatric Medicine;
2.1.10 A psychologist, must have earned a doctorate degree, (PhD or Psy.D. in
psychology) from an educational institution accredited by the American Psychological Association and have completed at least two (2) years of clinical experience in an organized healthcare setting, supervised by a licensed psychologist, one 1-year of which must have been post doctorate, and have completed an internship endorsed by the American Psychological Association (APA);
2.1.11 Possess a current, valid, Drug Enforcement Administration (DEA) number if
applicable to the privileges requested; 2.1.12 Have appropriate written and verbal communication skills; 2.1.13 Have appropriate personal qualifications, including applicant’s consistent
observance of ethical and professional standards. These standards include, at a minimum:
2.1.13.1 Abstinence from any participation in fee splitting or other illegal payment,
receipt, or remuneration with respect to referral or patient service opportunities;
60
2.1.13.2 A history of consistently acting in a professional, appropriate and collegial manner with others in previous clinical and professional settings.
2.1.14 The following qualifications must also be met by all applicants requesting clinical
privileges: 2.1.14.1 Demonstrate his background, experience, training, current competence,
knowledge, judgment and the ability to perform all privileges requested. 2.1.14.2 Provide evidence of both physical and mental health that does not impair
the fulfillment of his responsibilities of Medical Staff membership subject to any legally required reasonable accommodation and the specific privileges requested by and granted to the applicant, upon request.
2.1.14.3 Any practitioner granted privileges that may have occasion to admit an
inpatient must demonstrate the capability to provide continuous and timely care to the satisfaction of the FMEC and Board.
2.1.14.4 Demonstrate recent clinical performance (within the last twelve (12)
months with an active clinical practice in the area in which clinical privileges are sought adequate to meet current clinical competence criteria.
2.1.14.5 The applicant is requesting privileges for a service the Board has
determined appropriate for performance at the hospital. There must also be a need for this service under any Board approved Medical Staff development plan.
2.1.14.6 Provide evidence of financial responsibility consistent with the
requirements set forth in Part I. 2.1.15 Exceptions: All practitioners who are current Medical Staff members and/or hold privileges as of
May 28, 2009 and who have met prior qualifications for membership and/or privileges shall be exempt from Board specialty certification requirements.
SECTION 3 PRE-APPLICATION PROCESS
3.1 Only those practitioners that meet the following minimum criteria for appointment to the
Medical Staff will be provided applications. Practitioners provided applications would be those: 3.1.1 which are not governed by an exclusive arrangement or who are joining a group
providing services governed by an exclusive arrangement; and
3.1.2 who meet the minimum criteria as developed by the System Credentialing/Privileging Committee and approved by FMECs and the Board.
The purpose for the pre-application screening process shall be to avoid the costly
and time-consuming application process in those circumstances where an applicant
61
fails to meet minimum eligibility criteria. Practitioners who do not meet the minimum eligibility criteria for appointment are not entitled to fair hearing rights.
The System Credentialing/Privileging Committee shall review all requests for
application and determine whether the criteria for issuing an application have been met.
SECTION 4 INITIAL APPOINTMENT PROCESS
4.1 Completion of Application 4.1.1 All requests for application for appointment to the Medical Staff and requests for
clinical privileges will be forwarded to the Medical Staff Services Department. If the applicant successfully completed the pre-application screening process, the Medical Staff Services Department will provide the applicant an application packet, which will include a complete set or overview of the relevant Medical Staff Bylaws or reference to an electronic source for this information. This packet will enumerate the eligibility requirements for Medical Staff membership (for each facility of LMHS) and/or privileges and a list of expectations of performance for practitioners granted Medical Staff membership or privileges (if such expectations have been adopted by each Facility Medical Staff).
A completed application includes, at a minimum: 4.1.1.1 a completed, signed, dated application form; 4.1.1.2 a completed privilege delineation form if requesting privileges; 4.1.1.3 copies of all requested documents and information necessary to confirm
the applicant meets criteria for membership and/or privileges and to establish current competency;
4.1.1.4 all applicable fees; 4.1.1.5 complete reference information; references shall be from peers (same
specialty) knowledgeable about the applicant’s experience, ability and current competence to perform the privileges being requested;
4.1.1.6 relevant practitioner-specific data as compared to aggregate data, when
available 4.1.1.7 morbidity and mortality data, when available. Each applicant must indicate the LMHS facility anticipated to be his
primary facility (i.e., the facility where the majority of his clinical activity is performed). It should be noted that this designation is important for credentialing purposes (interviews, implementation of focused professional practice evaluation, etc.) and will be confirmed by LMHS data at periodic intervals and prior to any subsequent reappointments.
An application shall be deemed incomplete if any of the above items are
missing or if the need arises for new, additional or clarifying information
62
in the course of reviewing an application. An incomplete application will not be processed and the applicant will not be entitled to a fair hearing.
Anytime in the credentialing process it becomes apparent that an
applicant does not meet all eligibility criteria for membership or privileges, the credentialing process will be terminated and no further action taken. Applications will not be accepted from practitioners that are not eligible to take the Board certification examination.
4.1.2 The burden is on the applicant to provide all required information. It is the
applicant’s responsibility to ensure that the Medical Staff Services Department receives all required supporting documents verifying information on the application and to provide sufficient evidence, as required in the sole discretion of the Health System that the applicant meets the requirements for the Medical Staff membership and/or the privileges requested. If information is missing from the application or new, additional or clarifying information is required, a letter requesting such information will be sent to the applicant. If the requested information is not returned to the Medical Staff Services Department within thirty (30) calendar days of the receipt of the requested letter, the application will be deemed to have been voluntarily withdrawn.
4.1.3 Upon receipt of a completed application, the System Medical Director will determine
if the requirements of Section 2.1 are met. In the event the requirements of Section 2.1 are not met, the applicant will be notified that he is ineligible to apply for membership or privileges on the Medical Staff, the application will not be processed and the applicant will not be eligible for a fair hearing. If the requirements of Section 2.1 are met, the application will be accepted for further processing.
4.1.4 Practitioners seeking appointment shall have the burden of producing information
deemed adequate by the hospital for a proper evaluation of current competence, character, ethics, other qualifications and of resolving any doubts.
4.1.5 Upon receipt of a completed application, the Medical Staff Services Department will
verify current licensure, education, relevant training and current competence from the primary source whenever feasible in accordance with the Verification Methods and Requirements document.
When it is not possible to obtain information from the primary source, reliable
secondary sources may be used if there has been a documented attempt to contact the primary source.
Note: In the event there is undue delay in obtaining required information, the
Medical Staff Services Department will request assistance from the applicant. During this time, the period for processing, the application will be appropriately modified. Failure of an applicant to respond to a request for assistance adequately after thirty (30) calendar days the application will be deemed to have been voluntarily withdrawn.
4.1.6 When all items identified in the Verification Methods and Requirements document
have been obtained and verified, the application will be considered eligible for evaluation.
4.2 Applicant’s Attestation, Authorization and Acknowledgement
63
4.2.1 The applicant must complete and sign the application form. By signing this application the applicant:
4.2.1.1 Attests to the accuracy and completeness of all information on the
application or accompanying documents and agreement that any inaccuracy, omission or misrepresentation, whether intentional or not, may be grounds for termination of the application process without the right to a fair hearing or appeal.
If the inaccuracy, omission or misstatement is discovered after a
practitioner has been granted appointment and/or clinical privileges, the practitioner’s appointment and privileges shall lapse effective immediately upon notification of the practitioner without the right to a fair hearing or appeal.
4.2.1.2 Consents to appear for any requested interviews about his application. 4.2.1.3 Authorizes the applicable hospital and Medical Staff representative to
consult with prior and current associates and others who may have information bearing on his professional competence, character, ability to perform the privileges requested, ethical qualifications, ability to work cooperatively with others and other qualifications for requested membership and/or clinical privileges.
4.2.1.4 Consents to the Health System and Medical Staff representatives’
inspections of all records and documents that may be material to an evaluation of:
4.2.1.4.1 professional qualifications and competence to carry out the
clinical privileges requested;
4.2.1.4.2 physical and mental/emotional health status to the extent relevant to safely perform requested privileges subject to any legally required reasonable accommodation;
4.2.1.4.3 professional and ethical qualifications;
4.2.1.4.4 professional liability actions including currently pending claims involving the applicant;
4.2.1.4.5 any other issue relevant to establishing the applicant’s
suitability for membership and/or privileges.
4.2.1.5 Releases from liability, promises not to sue and grants immunity to the
Health System, its Medical Staffs and its representatives for acts performed and statements made in good faith in connection with evaluation of the application and his credentials and qualifications fully permitted by the law.
4.2.1.6 Releases from liability and promises not to sue, all practitioners and
organizations who provide information to the Health System or the applicable Medical Staff(s) in good faith, including otherwise privileged or confidential information to the System/hospital representatives
64
concerning his background/experience, competence, professional ethics, character, physical and mental health to the extent relevant to the capacity to fulfill requested privileges, emotional stability, utilization practice patterns, and other qualifications for staff appointment and clinical privileges.
4.2.1.7 Authorizes the Health System, Medical Staff and Administrative
representatives to obtain credentialing and peer review information from other hospitals, medical associations, licensing boards, appropriate government bodies and other health care entities concerned with this provider’s performance and releases representatives of the Health System from liability for so doing.
4.2.1.8 Acknowledges that the applicant has had access to relevant Medical
Staff Bylaws, including all rules, regulations, policies and procedures of the relevant Medical Staffs and agrees to abide by their provisions.
Notwithstanding Section 3.2 of Part II, if a practitioner institutes legal
action and does not prevail, he shall reimburse the Health System and any member of the Medical Staff named in the action for all costs incurred in defending such legal action, including reasonable attorney(s) fees.
4.2.1.9 Agrees to provide accurate answers to all the questions on the
application form, and agrees to immediately notify the System in writing should any of the information regarding these items change during the period of the applicant’s Medical Staff membership and/or privileges.
4.3 Application Evaluation
4.3.1 Expedited Credentialing: 4.3.1.1 An expedited Credentialing/Privileging Committee review and approval
process may be used for initial appointment in accordance with the Expedited Credentialing Policy.
4.3.2 Applicant Interview
4.3.2.1 All applicants for appointment to the Medical Staff and/or the granting of
clinical privileges are required to participate in interviews. The interviews are used to solicit information required to complete the credentials file or clarify information previously provided, e.g., clinical knowledge and judgment, professional behavior, malpractice history, reasons for leaving past healthcare organizations, or other matters bearing on the applicant’s ability to render care at the generally recognized level for the community and in compliance with LMHS privileging criteria. Interviews may also be used to communicate Medical Staff performance expectations.
Applicants for appointment will participate in a minimum of two (2)
interviews. One interview will be conducted by the applicable Department Chair or designated Section Chief of the applicant’s anticipated primary LMHS facility and the second interview will be with a member of the System Credentialing/Privileging Committee. Applicants that are applying for multiple facilities within LMHS may be required to participate in additional Department Chair/Section Chief interviews at the
65
discretion of the Department Chairs of the facility(ies) that are designated as non-primary.
4.3.2.2 Procedure: the applicant will be notified of required interview(s). Failure
of the applicant to appear for a scheduled interview will be deemed a voluntary withdrawal of the application.
4.3.3 Department Chair Action 4.3.3.1 Each Department Chair of an LMHS facility where the applicant has
requested privileges makes a recommendation related to membership and privileges, as applicable.
All completed applications are presented to the appropriate Department
Chair(s) for review and recommendation (which is made by completion of a standardized form provided to the Chair by the Medical Staff Services Department). The Department Chair(s) reviews the application to ensure that it fulfills the established standards for membership and/or clinical privileges. The Department Chair(s) may obtain input if necessary from an appropriate subject matter expert(s).
If a Department Chair believes a conflict of interest exists that, might
preclude his ability to make an unbiased recommendation, he will notify the Medical Staff Services Department and forward the application without comment.
4.3.3.2 The Department Chair(s) forwards to the System
Credentialing/Privileging Committee the following: 4.3.3.2.1 A written recommendation to approve the applicant’s request
for membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges (a summary of the interview conducted by the Department Chair or his designee is included in this written recommendation);
4.3.3.2.2 Written comments supporting his recommendations. The Department Chair of the applicant’s anticipated primary
facility also makes a written recommendation to define those circumstances, which require monitoring and evaluation of clinical performance after the initial granting of clinical privileges (i.e., focused professional practice evaluation).
4.3.4 Medical Staff System Credentialing/Privileging Committee Action 4.3.4.1 The System Credentialing/Privileging Committee reviews the application
and forwards the following to the applicable FMEC(s): 4.3.4.1.1 A recommendation to approve the applicant’s request for
membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges;
66
4.3.4.1.2 A recommendation to define those circumstances, which require monitoring, and evaluation of clinical performance after initial granting of clinical privileges (Focused Professional Practice Evaluation) (FPPE);
Comments supporting the above recommendation. 4.3.5 FMEC Action
4.3.5.1 Each FMEC of LMHS where membership and/or privileges have been requested forwards the following to the Board:
4.3.5.1.1 A recommendation to approve the applicant’s request for
membership and/or privileges; to approve membership but modify the requested privileges; or deny membership and/or privileges;
4.3.5.1.2 Comments supporting the above recommendation.
The FMEC of the applicant’s anticipated primary facility also makes a recommendation to define those circumstances that require monitoring and evaluation of clinical performance after initial granting of clinical privileges (FPPE).
Whenever a FMEC makes an adverse recommendation to the Board, a notice,
stating the reason, will be sent to the applicant who shall then be entitled to the procedural rights provided in the Investigation, Corrective Action, Hearing and Appeal Plan of the Medical Staff Bylaws. When multiple FMECs are making recommendations related to the same applicant, an adverse recommendation is not considered final until after the PLC attempts to facilitate resolution of the issues (this facilitation occurs when there are disparate recommendations – for example, one (1) positive recommendation and one negative recommendation).
4.3.6 Applicants Applying to Multiple Facilities Applicants may simultaneously make application for membership and/or privileges
to multiple facilities within LMHS. The Medical Staff Services Department coordinates this information so that the recommendations from all FMECs come to the Board together. If there are disparate recommendations (defined as conflicting) related to membership and/or requested clinical privileges on the same applicant, the PLC will meet and attempt to reconcile the disparate recommendations prior to forwarding the recommendations to the Board.
If the PLC is unable to facilitate resolution of the issues (in accordance with the
Medical Staff Bylaws – Part I, Governance – Section 9 Decision Making Methods and Conflict Resolution) the disparate recommendations will go forward to the Board.
4.3.7 Board Action:
4.3.7.1 The Board reviews the recommendation and votes for one (1) of the following actions:
67
4.3.7.1.1 The Board may adopt or reject in whole or in part a
recommendation of the FMEC(s) or refer the recommendation to the FMEC(s) for further consideration stating the reasons for such referral back and setting a time limit within which a subsequent recommendation must be made.
4.3.7.1.2 If the Board concurs with the applicant’s request for membership and/or privileges, it will grant the appropriate membership and/or privileges for a period not to exceed 24 months.
4.3.7.1.3 If the Board’s action is adverse to the applicant, a notice,
stating the reason, will be sent to the applicant who shall then be entitled to the procedural rights provided in the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) unless the applicant received procedural rights under Part II, Section 3.2.5.
4.3.7.1.4 The Board shall take final action in the matter as provided in
the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan).
4.3.8 Notice of Final Decision:
4.3.8.1 Notice of the Board’s final decision shall be given through the Medical
Staff Services Department to the applicable FMEC(s) and to the Chair of each Department concerned. The applicant shall receive written notice of appointment and special notice of any adverse final decisions in a timely manner. A decision and notice of appointment includes the staff category(ies) to which the applicant is appointed, the Department(s) to which he is assigned, the clinical privileges he may exercise, notification of orientation and any special conditions attached to the appointment.
4.3.9 Periods for Processing: 4.3.9.1 All practitioners and groups acting on an application for staff
appointment and/or clinical privileges must do so in a timely and good faith manner, and except for good cause, each application will be processed within 180 calendar days. The 180 Calendar days begin on the date that the application is declared complete to begin processing.
4.3.9.2 These processing periods are deemed guidelines and do not create
any right to have an application processed within these precise periods. If the provisions of the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) are activated, the time requirements provided therein govern the continued process of the application.
SECTION 5 FOCUSED PROFESSIONAL PRACTICE EVALUATION (FPPE)
68
5.1 CRITERIA FOR FPPE 5.1.1 The Department Chair (or designated Section Chief) of the applicant’s anticipated
primary facility will define circumstances that require monitoring and evaluation of the clinical performance of each practitioner following his or her initial granting of clinical privileges.
Such monitoring may utilize a range of techniques, including but not limited to: chart
review, the tracking of performance monitors/indicators, proctoring, external peer review, simulations, morbidity/mortality reviews, and discussion with other healthcare practitioners involved in the care of each patient. The FPPE plan is created as part of the initial recommendation for appointment and privileges and is forwarded to the System Credentialing/Privileging Committee and to the FMEC(s).
The System Credentialing/Privileging Committee will establish via policy the
anticipated duration for FPPE. The Physician Quality Committee will establish the triggers that indicate the need for
performance monitoring after the initial granting of privileges. SECTION 6 CRITERIA FOR REAPPOINTMENT 6.1 Criteria for Reappointment 6.1.1 It is the policy of the Health System to approve for reappointment and/or renewal of
privileges only those practitioners who meet the criteria for initial appointment as identified in Section 2, Part 1. The practitioner must also be determined by each applicable FMEC to be a provider of effective care that is consistent with the Health System standards of ongoing quality and the hospital performance improvement program and provide the information enumerated in Section 5.1.1.
All reappointments and renewals of clinical privileges are for a period not to exceed
24 months. The granting of new clinical privileges to existing Medical Staff members will follow the steps described in Section 4 concerning the initial granting of new clinical privileges and Section 5 concerning FPPE. A suitable peer shall substitute for the Department Chair in the evaluation of current competency of the Department Chair, and recommend appropriate action to the System Credentialing/Privileging Committee.
In the event a practitioner finds no need to utilize the facilities or resources of LMHS
for purposes of patient care through either admission, performance of a procedure, consultation, or referral, during a two-year period he may not be eligible for reappointment or continued privileges. Such practitioner may apply as a new applicant at any time subsequent to the expiration of the current appointment or privileges. This provision applies to practitioners who have been granted a leave of absence, moved their practice location, established a relationship with another institution or otherwise find no need to utilize the clinical resources of LMHS. Exceptions to this provision may be made by the Board upon recommendation of the applicable FMEC(s).
As long as a practitioner has adequate clinical activity to maintain privileges at one
LMHS facility (and is recommended for continuation of privileges at his primary
69
LMHS facility) the practitioner may maintain the applicable clinical privileges and staff category (potentially Associate if there is no or minimal clinical activity) at other LMHS facility(ies).
6.2.1 Information, Collection and Verification 6.2.1.1 From practitioner: On or before 4 months prior to the date of expiration of
a Medical Staff appointment or granting of privileges, a representative from the Medical Staff Services Department notifies the practitioner of the date of expiration and supplies him with an application for reappointment for membership and/or privileges. At least sixty (60) calendar days prior to this date, the practitioner must return the following to the Medical Staff Services Department:
6.2.1.1.1 A completed reapplication form, which includes complete
information to update his file on items listed in his original application, any required new, additional, or clarifying information, and any required fees or dues;
6.2.1.1.2 Information concerning continuing training and education
internal and external to the hospital during the preceding period;
6.2.1.1.3 By signing the reapplication form, the practitioner agrees to
the same terms as identified in Section 4.2. 6.2.2 From internal and/or external sources: The Medical Staff Services Department
collects and verifies information regarding each staff practitioner’s professional and collegial activities to include those items listed in Section 2.1.
6.2.3 The following information is also collected and verified:
6.2.3.1 A summary of clinical activity at each LMHS facility for each practitioner due for reappointment.
6.2.3.2 Performance and conduct in each LMHS facility and other healthcare
organizations in which the practitioner has provided substantial clinical care since the last reappointment, including patient care, medical/clinical knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism and system-based practice.
6.2.3.3 Documentation of CME activity; 6.2.3.4 Service on Medical Staff, Department and hospital committees; 6.2.3.5 Timely and accurate completion of medical records; 6.2.3.6 Compliance with all applicable Bylaws, policies, rules, regulations, and
procedures of the System and the Medical Staff(s); 6.2.3.7 Any significant gaps in employment or practice since the previous
appointment or reappointment; and 6.2.3.8 Additional items as identified in the Verification Methods and
Requirements document.
70
6.2.4 Failure, without good cause, to provide any requested information, at least forty-five
(45) calendar days prior to the expiration of appointment will result in a cessation of processing of the application and automatic expiration of appointment when the appointment period is concluded. Once the information is received, the Medical Staff Services Department verifies this additional information and notifies the staff practitioner of any additional information that may be needed to resolve any doubts about performance or material in the credentials file.
6.3 Evaluation of Application for Reappointment of Membership and/or Privileges
6.3.1 The reappointment application will be reviewed and acted upon as described in Sections 4.3.3 through 4.3.8. For the purpose of reappointment, an “adverse recommendation” by the Board as used in Section 4.3 means a recommendation or action to deny reappointment, or to deny or restrict requested clinical privileges or any action that would entitle the applicant to a Fair Hearing under the Medical Staff Bylaws. The terms “applicant” and “appointment” as used in these Sections shall be read respectively, as “staff practitioner” and “reappointment”.
SECTION 7 CLINICAL PRIVILEGES 7.1 Exercise of Privileges
A practitioner providing clinical services at a LMHS facility may exercise only those privileges granted to him by the Board or emergency and disaster privileges as described herein. Privileges may be granted by the Board upon recommendation of the FMEC(s) to practitioners who are not members of the Medical Staff. Such practitioners may include Advanced Registered Nurse Practitioners (ARNPs), Physician Assistants (PAs), practitioners serving short locum tenens positions, telemedicine physicians or others deemed appropriate by the FMEC(s) and Board.
7.2 Requests
When applicable, each application for appointment or reappointment to the Medical Staff must contain a request for the specific clinical privileges desired by the applicant. Specific requests must also be submitted for temporary privileges and for modifications of privileges in the interim between reappointments and/or granting of privileges.
7.3 Basis for Privileges Determination 7.3.1 Requests for clinical privileges will be considered only when accompanied by
evidence of education, training, experience, and demonstrated current competence as specified by the System in its Board approved criteria for clinical privileges.
7.3.2 Privileges for which no criteria have been established: 7.3.2.1 In the event a request for a privilege is submitted for a new technology, a
procedure new to the System, an existing procedure used in a significantly different manner, or involving a cross-specialty privilege for which no criteria have been established, the request will be tabled for a reasonable period of time, usually not to exceed sixty (60) calendar days. During this time, the System Credentialing/Privileging Committee may refer the request for review by a task force appointed to review the request.
71
Task forces formed for purposes of establishment of evaluation of new
privileges and potential determination of criteria will be appointed by the Chairs of the System Credentialing/Privileging Committee, and will include the System Medical Director of Clinical Effectiveness and the Director of Supply Chain Management. The task force will:
7.3.2.1.1 Review the community, patient and System need for the
privilege and reach agreement with management and the Board that the privilege is approved to be exercised at the hospital;
7.3.2.1.2 Review with appropriate individuals/groups
the efficacy and clinical viability of the requested privilege and confirm that this privilege is approved for use in the setting-specific area of the hospital by appropriate regulatory agencies (FDA, OSHA, etc.);
7.3.2.1.3 Meet with management to ensure that the new privilege is
consistent with the Health System’s mission, values, strategic, operating, capital, information and staffing plans;
7.3.2.1.4 Work with management to ensure that any/all exclusive
contract issues, if applicable are resolved in such a way to allow the new or cross-specialty privileges in question to be provided without violating the existing contract. Upon recommendation from the System Credentialing/Privileging Committee and appropriate clinical services/specialty or subject matter experts (as determined by the System Credentialing/Privileging Committee), the criteria will be recommended to each FMEC and then to the Board. Once objective criteria have been established, the original request will be processed as described herein.
7.3.2.2 For the development of criteria, the Medical Staff Services Department (or
designee) will compile information relevant to the privileges requested which may include, but need not be limited to, position and opinion papers from specialty organization, position and opinion statements from interested individuals or groups and documentation from other hospitals in the region as appropriate.
7.3.2.3 Criteria to be established for the privilege(s) in question include education,
training, board status or certification (if applicable), experience and evidence of current competence. Proctoring requirements, if any, will be addressed including who may serve as proctor and how many proctored cases will be required.
Hospital related issues such as exclusive contracts, equipment, clinical
support staff and management would be referred to the appropriate hospital administrator and/or Department Director.
7.3.2.4 If the privileges requested overlap two (2) or more specialty disciplines, an
ad hoc committee may be appointed by the System Credentialing/Privileging Committee to recommend criteria for the privilege(s) in question. This ad hoc committee will consist of at least one
72
(1) but no more than two (2) members from each involved discipline. The Chair of the ad hoc committee will be a member of the System Credentialing/Privileging Committee who has no vested interest in the issue (see Medical Staff Privilege Dispute Resolution Policy).
7.3.3 Requests for clinical privileges will be consistently evaluated on the basis of prior
and continuing education, training, experience, utilization practice patterns, current ability to perform the privileges requested and demonstrated current competence,
ability, and judgment. Additional factors that may be used in determining privileges are patient care needs and the System’s capability to support the type of privileges being requested and the availability of qualified coverage in the applicant’s absence. The basis for privileges determination to be made in connection with periodic reappointment or a requested change in privileges must include documented clinical performance and results of the staff’s performance improvement program activities.
Privilege determinations will also be based on pertinent information from other
sources, such as peers and/or faculty from other institutions and healthcare settings where the practitioner exercises clinical privileges.
7.3.4 The procedure by which requests for clinical privileges are processed are as outlined in Section 4.
7.3.5 Special Conditions for Dental Privileges
Requests for clinical privileges for dentists are processed in the same manner as all other privilege requests. Privileges for surgical procedures performed by dentists and/or oral and maxillofacial surgeons will require that all dental patients receive a basic medical evaluation (history and physical) by a physician member of the Medical Staff with privileges to perform such an evaluation, which will be recorded in the medical record. Oral and maxillofacial surgeons may be granted the privilege of performing a history and physical on their own patients upon submission of documentation of completion of an accredited postgraduate residency in oral and maxillofacial surgery and demonstrated current competence.
7.3.6 Special Conditions for practitioners not Qualified for Medical Staff Appointment but Practicing Pursuant to Clinical Privileges per System Policy. Requests for privileges, from such practitioners, are processed in the same manner as requests for clinical privileges by providers eligible for Medical Staff membership, with the exception that such practitioners are not eligible for membership on a Medical Staff and do not have the rights and privileges of such membership (all rights and responsibilities are defined in the Allied Health Practitioner (AHP) Privileging Policy and Procedure). Only those categories of practitioners approved by the Board for providing services at the hospital are eligible to apply for privileges. AHP(s) in this category may, subject to any licensure requirements or other limitations, exercise independent judgment only within the areas of their professional competence and participate directly in the medical management of patients under the supervision of a physician who has been accorded privileges to provide such care.
7.4 Special Conditions for Podiatric Privileges
73
Requests for clinical privileges for podiatrists are processed in the same manner as all other privilege requests.
Practitioners granted podiatric privileges may perform and shall record in the medical
record a basic medical evaluation history and physical for the practitioner’s podiatric patients if consistent with the privileges granted to the practitioner, state law governing the practitioner’s practice and federal law.
7.5 Special Conditions for Residents or Fellows in Training
Residents or Fellows in Training in the Health System shall not normally hold membership on the Medical Staff and shall not normally be granted specific clinical privileges. Rather, they shall be permitted to function clinically only in accordance with the written training protocols developed by the Professional Graduate Education Committee in conjunction with the Residency Training Program. The protocols must delineate the roles, responsibilities, and patient care activities of residents and fellows including which types of residents may write patient care orders, under what circumstances why they may do so, and what entries a supervising physician must countersign. The protocol must also describe the mechanisms through which resident directors and supervisors make decisions about a resident’s progressive involvement and independence in delivering patient care and how these decisions will be communicated to appropriate Medical Staff and hospital leaders.
The Post-Graduate Education Program Director or Committee must communicate
periodically with each applicable FMEC and the Board about the performance of its residents, patient safety issues and quality of patient care and must work with the FMEC to assure that all supervising physicians possess clinical privileges commensurate with their supervising activities.
7.6 Special Conditions for the Aging Practitioner
At the age of 70, practitioners shall complete an annual examination that addresses both the physical and mental capacity for the privileges requested. The annual physical and mental exams are to be conducted by an independent Medical examiner acceptable to the System Credentialing/Privileging Committee, documented on the approved form and submitted to the System Credentialing/Privileging Committee by the date requested. The physical exam is a “fitness to work” evaluation and must indicate that the practitioner has no physical or mental problem that may interfere with the safe and effective provision of care permitted under the privileges granted. In addition to the physical exam, a practitioner may be required to undergo proctoring of his clinical performance as part of the assessment of his capacity to perform the requested privileges. Such proctoring may be required in the absence of any previous performance concerns. The scope and duration of the proctoring shall be determined by the FMEC upon recommendation of the Department Chair of the practitioner’s primary facility and System Credentialing/Privileging Committee. The practitioner shall pay the cost of the physical and mental exam.
7.7 Temporary Privileges 7.7.1 Temporary privileges may be granted by the CEO, or designee, acting on behalf of
the Board and based on the recommendation of the President of the Medical Staff or designee to be approved at the next FMEC meeting, provided there is verification
74
of current licensure and current competence. Temporary privileges may be granted only in two (2) circumstances: 1) to fulfill an important patient care, treatment or service need, or 2) when an initial applicant with a complete application that raises no concerns is awaiting review and approval of the FMEC and the Board. Applications pending completion of the initial appointment process must always be reviewed and a recommendation made by the System Credentialing/Privileging Committee prior to the granting of temporary privileges.
7.7.2 Important Patient Care, Treatment or Service Need: Temporary privileges may be
granted on a case-by-case basis when an important patient care, treatment or service need exists that mandates an immediate authorization to practice, for a limited time, not to exceed 30 calendar days (from date privileges are granted). Temporary privileges may be extended for two separate 30-day intervals upon approval of the Board of Directors. For the purposes of granting temporary privileges, an important patient care, treatment or service need is defined as including the following:
7.7.2.1 a circumstance in which one or more individual patients will experience
care that does not adequately meet their clinical needs if the temporary privileges under consideration are not granted, (i.e., a patient scheduled for urgent surgery who would not be able to undergo the surgery in a timely manner);
7.7.2.2 a circumstance in which the institution will be placed at risk of not
adequately meeting the needs of patients who seek care, treatment or service from the institution if the temporary privileges under consideration are not granted (i.e., the institution will not be able to provide adequate emergency room coverage in the providers specialty, or the Board has granted privileges involving new technology to a physician on the staff provided the physician is precepted for a specific number of initial cases and the precepting physician, who is not seeking Medical Staff membership, requires temporary privileges to serve as a preceptor);
7.7.2.3 a circumstance in which a group of patients in the community will be
placed at risk if not receiving patient care that meets their clinical needs if the temporary privileges under consideration are not granted (i.e. a physician who has a large practice in the community for which adequate coverage of hospital care for those patients cannot be arranged).
7.7.3 Clean Application (Expedited) Awaiting Approval: Temporary privileges may be
granted for up to 30 calendar days (from date privileges are issued) approved by the Executive Committee with two 30-day extensions approved by the Board (see the policy and procedure on Expedited Credentialing) when the new applicant for Medical Staff membership and/or privileges is waiting for review and recommendation by the FMEC and approval by the Board.
7.7.4 Special requirements of consultation and reporting may be imposed as part of the
granting of temporary privileges. Except in unusual circumstances, temporary privileges will not be granted unless the practitioner has agreed in writing to abide by the Bylaws, rules, and regulations and policies of the Medical Staff and hospital in all matters relating to his temporary privileges. Whether or not such written agreement is obtained, these Bylaws, rules, regulations and policies control all matters relating to the exercise of clinical privileges.
75
7.7.5 Termination of temporary privileges: The CEO, acting on behalf of the Board and after consultation with the President of the Medical Staff, may terminate any or all of the practitioner’s privileges based upon the discovery of any information or the occurrence of any event of a nature, which raises questions about a practitioner’s privileges.
Where the life or well-being of a patient is determined to be endangered, any person
entitled to impose precautionary suspension under the Medical Staff Bylaws may effect the termination. In the event of any such termination, the CEO or his designee then will assign the practitioner’s patients to another practitioner. The wishes of the patient shall be considered when feasible, in choosing a substitute practitioner.
7.7.6 Rights of the practitioner with temporary privileges: A practitioner is not entitled to
the procedural rights afforded in the Medical Staff Bylaws (Investigation, Corrective Action, Hearing and Appeal Plan) because his request for temporary privileges is refused or because all or any part of his temporary privileges are terminated or suspended unless based on a determination of clinical incompetence or unprofessional conduct.
7.7.7 Emergency Privileges: In the case of a medical emergency, any practitioner is
authorized to do everything possible to save the patient’s life or to save the patient from serious harm, to the degree permitted by the practitioner’s license, regardless of facility affiliation, staff category, or level of privileges. A practitioner exercising emergency privileges is obligated to summon all consultative assistance deemed necessary and to arrange appropriate follow-up.
7.7.8 Disaster Privileges 7.7.8.1 If the System’s Disaster Plan has been activated and the organization is
unable to meet immediate patient needs, the CEO and such other individuals as identified in the System’s Disaster Plan with such authority, may, on a case by case basis consistent with medical licensing and other relevant state statutes, grant disaster privileges to provide patient care to selected Licensing Independent Practitioners (LIP’s), who must at a minimum present a valid governmental-issued photo identification issued by a state or federal agency (e.g. driver’s license or passport) and at least one of the following:
7.7.8.1.1 a current picture hospital ID card that clearly identifies
professional designation; 7.7.8.1.2 a current license to practice; 7.7.8.1.3 primary source verification of the license;
7.7.8.1.4 identification indicating that the practitioner is a member of a
Disaster Medical Assistance Team (DMAT), or Medical Reserve Corps (MRC), Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VHP), or other recognized state or federal organizations or groups;
7.7.8.1.5 identification indicating that the practitioner has been
granted authority to render patient care, treatment, and services in disaster circumstances (such
76
authority having been granted by a federal, state, or municipal entity);
7.7.8.1.6 identification by a current hospital or Medical Staff
member(s) who possesses personal knowledge regarding the volunteer’s ability to act as a LIP during a disaster.
7.7.8.2 The Medical Staff oversees the professional performance of
volunteer practitioners who have been granted disaster privileges by direct observation, mentoring or clinical record review.
The organization makes a decision (based on information obtained regarding the professional practice of the volunteer) within 72 hours related to the continuation of the disaster privileges initially granted.
7.7.8.3 Primary source verification of licensure begins as soon as the
immediate situation is under control, and is completed within 72 hours from the time the volunteer practitioner presents to the organization.
7.7.8.4 Once the immediate situation has passed and such determination
has been made consistent with the institution’s Disaster Plan, the practitioner’s disaster privileges will terminate immediately.
7.7.8.5 Any individual identified in the institution’s Disaster Plan with the
authority to grant disaster privileges shall also have the authority to terminate disaster privileges. Such authority may be exercised at the sole discretion of the hospital and will not give rise to a right to a fair hearing or an appeal.
SECTION 8 PRECEPTORSHIP
8.1 A practitioner who has not provided acute inpatient care within the past 24 months who requests clinical privileges at the hospital must arrange for a preceptorship either with a current member in good standing of the Medical Staff who practices in the same specialty or with an academic training program or other equivalently competent physician practicing outside of the hospital. The practitioner must assume responsibility for any financial costs required to fulfill the requirements of Sections 8.1 and 8.2.
8.2 A description of the preceptorship program, including details of monitoring and consultation
must be written and submitted for approval to the applicable Department Chair, System Credentialing/Privileging Committee and FMEC. At a minimum, the preceptorship program description must include the following: 8.2.1 The scope and intensity of required preceptorship activities; 8.2.2 The requirement for submission of a written report from the preceptor prior to
termination of the preceptorship period assessing, at a minimum, the applicant’s demonstrated clinical competence related to the privileges requested, ability to get along with others, the quality and timeliness of medical records documentation, ability to perform the privileges requested, and professional ethics and conduct.
77
SECTION 9 REAPPLICATION AFTER MODIFCATIONS OF MEMBERSHIP STATUS OF PRIVILEGES AND EXHAUSTION OF REMEDIES
9.1 Reapplication After Adverse Credentials Decision
9.1.1 Except as otherwise determined by the Board, a practitioner who has received a
final adverse decision or who has resigned or withdrawn an application for appointment, reappointment or clinical privileges while under investigation or to avoid an investigation is not eligible to reapply to the Medical Staff for a period of five (5) years from the date of the notice of the final adverse decision or the effective date of the resignation or application withdrawal. Any such application is processed in accordance with the procedures then in force. As part of the reapplication, the practitioner must submit such additional information as the Medical Staff and/or Board requires, demonstrating that the basis of the earlier adverse action no longer exists. If such information is not provided, the reapplication will be considered incomplete and voluntarily withdrawn and will not be processed any further.
9.2 Request for Modification of Appointment Status or Privileges
9.2.1 A staff member, either in connection with reappointment or at any other time, may
request modification of staff category, Department assignment, or clinical privileges by submitting a written request to the Medical Staff Services Department. A modification request must be on the prescribed form and must contain all pertinent information supportive of the request. All requests for additional clinical privileges must be accompanied by information demonstrating additional education, training, and current clinical competence in the specific privileges requested. A modification application is processed in the same manner as a reappointment, which is outlined in Section 6 of this manual. A practitioner who determines that he no longer exercises, or wishes to restrict or limit the exercise of, particular privileges that he has been granted shall send written notice, through the Medical Staff Services Department to the System Credentialing/Privileging Committee, and FMEC. A copy of this notice shall be included in the practitioner’s credentials file.
9.3 Resignation of Staff Appointment or Privileges
9.3.1 A practitioner who wishes to resign his staff appointment and/or clinical privileges
must provide written notice to the appropriate Department Chair or President of the Medical Staff. The resignation shall specify the reason for the resignation and the effective date. A practitioner who resigns his staff appointment and/or clinical privileges is obligated to accurately complete all portions of all medical records for which he is responsible prior to the effective date of resignation. Failure to do so shall result in an entry in the practitioner’s credentials file acknowledging the resignation and indicating that it became effective under unfavorable circumstances.
9.4 Exhaustion of Administrative Remedies
9.4.1 Every practitioner agrees that he will exhaust all the administrative remedies
afforded in the various Sections of Part I: Governance, Part II: Investigations, Corrective Action, Hearing and Appeal Plan and Part III: Credentialing Procedures before initiating legal action against the System or its agents.
9.5 Reporting Requirements
78
9.5.1 The CMO or his designee shall be responsible for assuring that the hospital satisfies its obligations under the Health Care Quality Improvement Act of 1986 and its successor statutes. Actions that must be reported include any negative professional review action against a physician or dentist related to clinical incompetence or misconduct that leads to a denial of appointment and/or reappointment, reduction in clinical privileges for greater that thirty (30) calendar days; resignation, surrender of privileges, or acceptance of privilege reduction either during an investigation or to avoid an investigation.
SECTION 10 LEAVE OF ABSENCE
10.1 Leave Request
10.1.1 A leave of absence is a matter of courtesy, not of right. In the event that it is
determined that a practitioner has not demonstrated good cause for a leave, or where a request for extension is not granted, the determination shall be final, with no recourse to a hearing and appeal. A leave of absence must be requested for any absence from the Medical Staff and/or patient care responsibilities longer than thirty (30) days if such absence is related to the practitioner’s physical or mental health or to the ability to care for patients safely and competently. A practitioner who wishes to obtain a voluntary leave of absence must provide written notice to the President of the Medical Staff stating the reasons for the leave and approximate period of the leave, which may not exceed one 1-year except for military service or express permission by the Board. Requests for leave must be forwarded, with a recommendation from the FMEC, and affirmed by the Board. While on leave of absence, the practitioner may not exercise clinical privileges or prerogatives and has no obligation to fulfill Medical Staff responsibilities.
10.2 Termination of Leave
10.2.1 At least thirty (30) calendar days prior to the termination of the leave, or at any
earlier time, the practitioner may request reinstatement by sending a written notice to the President of the Medical Staff. The practitioner must submit a written summary of relevant activities during the leave if the FMEC or Board so requests.
A practitioner returning from a leave of absence for health reasons must provide a
report from his physician that answers any questions that the FMEC or Board may have as part of considering the request for reinstatement. The FMEC makes a recommendation to the Board concerning reinstatement, and the applicable procedures concerning the granting of privileges are followed. If the practitioner’s current grant of membership and for privileges is due to expire during the leave of absence, the practitioner must apply for reappointment or his appointment and/or clinical privileges shall lapse at the end of the appointment period.
10.3 Failure to Request Reinstatement 10.3.1 Failure, without good cause, to request reinstatement shall be deemed a voluntary
resignation from the Medical Staff and shall result in automatic termination of membership, privileges, and prerogatives. A practitioner whose membership is automatically terminated shall not be entitled to the procedural rights provided in the Medical Staff Bylaws. A request for Medical Staff membership subsequently
79
received from a member so terminated shall be submitted and processed in the manner specified for applications for initial appointments.
SECTION 11 PRACTITIONERS PROVIDING CONTRACTED SERVICES 11.1.1 When the System or hospital contracts for patient care services with LIPs who
provide official readings of images, tracings or specimens through a telemedicine mechanism, and these practitioner’s services are under the control of a Joint Commission accredited organization, the hospital will:
11.1.1.1 specify in a contract that the entity providing these services by contract
(the contracting entity) will ensure that all services provided under this contract by individuals who are LIPs will be within the scope of those practitioner’s privileges at the contracting entity; or
11.1.1.2 verify that all individuals who are LIPs and providing services under the
contract have privileges that include the services provided under the contract.
11.2 When the System/hospital contracts for care services with LIPs, who provide official
readings of images, tracings or specimens through a telemedicine mechanism, and these practitioner’s services are not under the control of a Joint Commission accredited organization, all LIPs who will be providing services under this contract will be permitted to do so only after being granted privileges at the hospital through the mechanisms established in this manual.
11.3 Contract Services/Department or Service Closure
11.3.1 The membership and privileges on the Medical Staff of any practitioner who has a
contractual relationship with the System or with an entity that has a contractual relationship with the System to provide professional services to patients shall be subject to those provisions contained in said contract with regard to the termination of Medical Staff membership and privileges upon the expiration, lapse, cancellation or termination of the contract. If the contract so provides, the affected practitioner shall have no right to a hearing regarding termination of Medical Staff membership or privileges.
11.3.2 In the event a hospital Department is closed, discontinued or provided through an
exclusive contract, such establishment shall not adversely impact the ability of any physician to continue to maintain clinical membership and exercise privileges in existence at the time of such closure, discontinuance or exclusive contract. Initial applications for Medical Staff membership and privileges will not be extended, provided, accepted, processed or approved to or from physicians unless they are joining groups who are actively contracted for exclusively contracted services.
11.3.3 In the event the Board determines that a patient care service shall be closed,
discontinued, or provided through an exclusive contract, such action shall require approval by the affected FMEC.
Both parties agree that any Department or service closure shall occur solely so that
the health and wellbeing of the patients and the best interests of the hospital under these Bylaws may be served at all times. Notwithstanding any other provision in the Bylaws, if the Board and the affected FMEC are unable to agree upon the closure of
80
a Department or service, the matter shall undergo the conflict resolution process set forth in Part I, Section 9 of these Bylaws.
If the parties are still in disagreement regarding the closure of a Department or
service upon completion of the conflict resolution process, the parties shall engage in mediation in accordance with the procedures set forth by the American Health Lawyers Association’s Alternative Dispute Resolution Service or another independent mediation service mutually agreeable to the parties. In the event the Board and FMEC are at impasse at mediation and conflict remains, the Board and the FMEC retain the right to seek a resolution through litigation. Further, the Board shall not close a Department or service for a period of three months following impasse at mediation.
11.4 Qualifications
11.4.1 A practitioner who is or will be providing specified professional services pursuant to
a contract or a letter of agreement with the Health System must meet the same qualifications, must be processed in the same manner, and must fulfill all the obligations of his appointment category as any other applicant or staff practitioner.
11.5 The terms of the Medical Staff Bylaws will govern disciplinary action taken by or
recommended by the FMEC.
11.6 Effect of Contract or Employment Expiration or Termination
11.6.1 The effect of expiration or other termination of a contract upon a practitioner’s staff appointment and clinical privileges will be governed solely by the terms of the practitioner’s contract with the System. If the contract or the employment agreement is silent on the matter, then contract expiration or other termination alone will not affect the practitioner’s staff appointment status or clinical privileges.
SECTION 12 MEDICAL ADMINISTRATIVE OFFICERS
12.1 A Medical Administrative Officer is a practitioner engaged full or part- time by the hospital in an administratively responsible capacity, whose activities may also include clinical responsibilities such as direct patient care, teaching, or supervision of the patient care activities of other practitioners under the officer’s direction.
12.2 Each Medical Administrative Officer must achieve and maintain Medical Staff appointment
and clinical privileges appropriate to his clinical responsibilities and discharge staff obligations appropriate to his staff category in the same manner applicable to all other staff members.
12.3 Effect of removal from office or adverse change in appointment status or clinical privileges:
12.3.1 Where a contract exists between the officer and the Health System, its terms
govern the effect of removal from the Medical Administrative Office on the officer’s staff appointment and privileges and the effect an adverse change in the officer’s staff appointment or clinical privileges has on his remaining in office.
12.3.2 In the absence of a contract or where the contract is silent on the matter, removal
from office has no effect on appointment status or clinical privileges. The effect of

81
an adverse change in appointment status or clinical privileges on continuance in office will be determined by the Board.
12.3.3 A Medical Administrative Officer has the same procedural rights as all other staff
members in the event of an adverse change in appointment status or clinical privileges unless the change is, by contract a consequence of removal from office.

82
83
84
Lee Memorial Health SystemBoard of Directors
Financial Update
For Month Ending 02/28/13
Presented 03/28/13
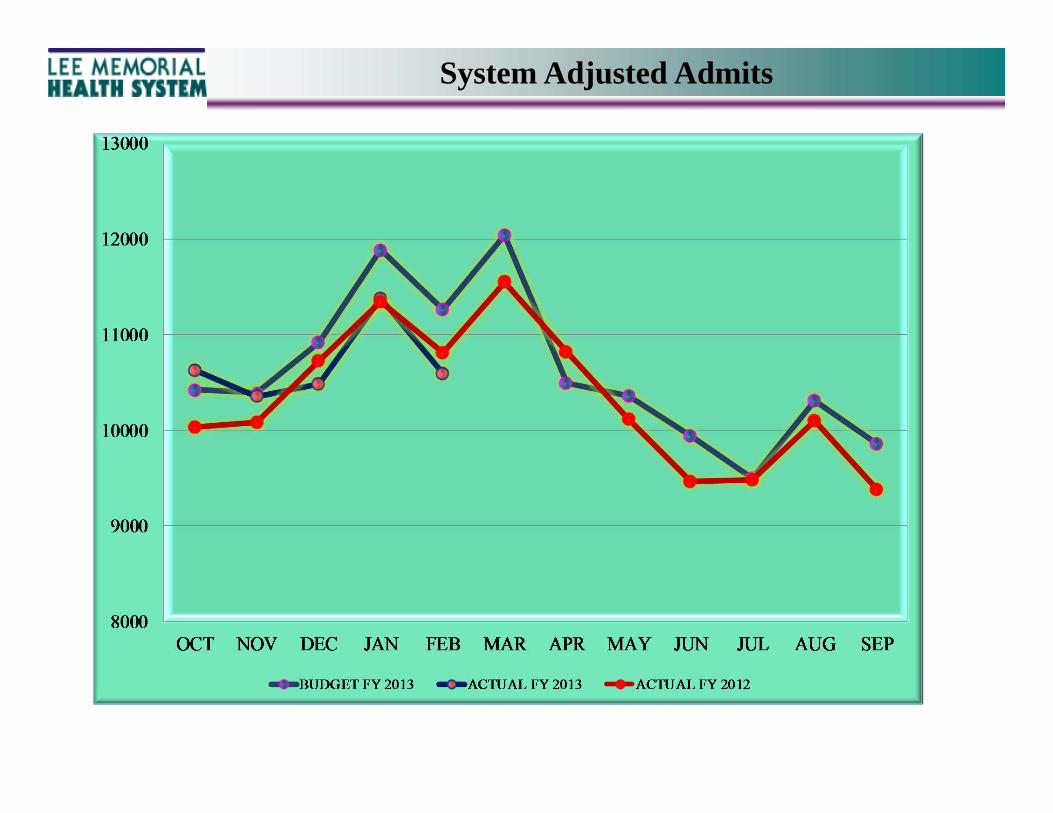
System Adjusted Admits
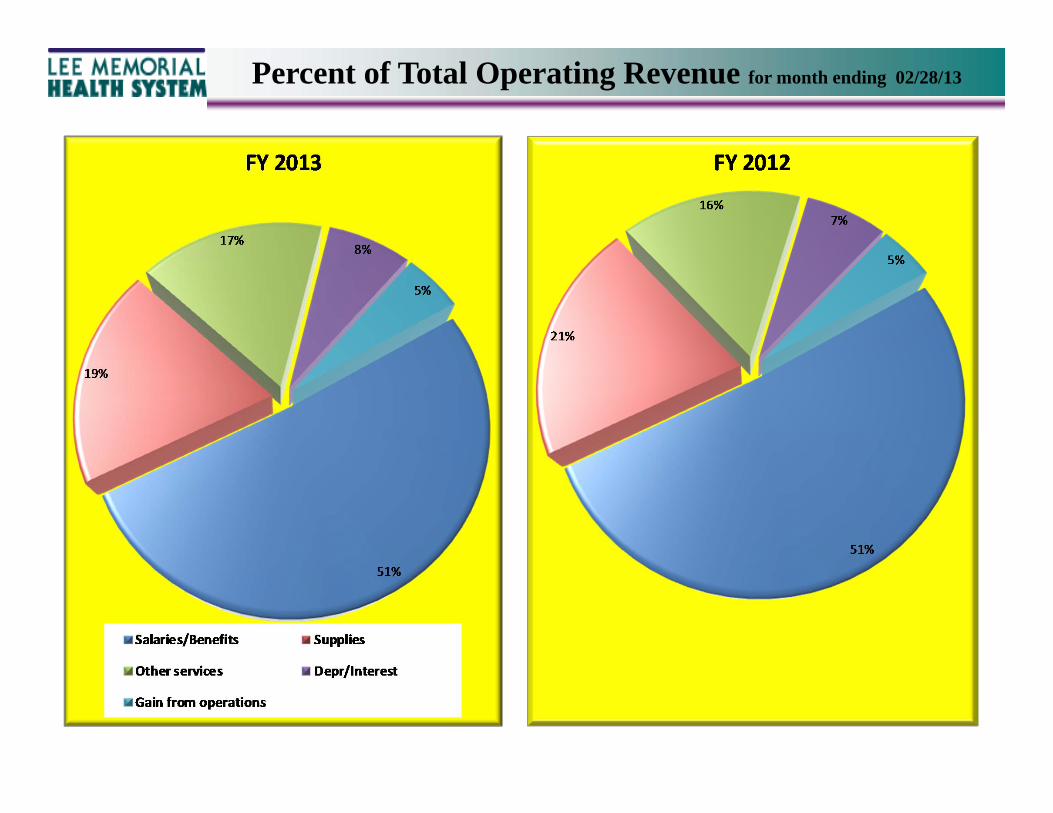
Percent of Total Operating Revenue for month ending 02/28/13
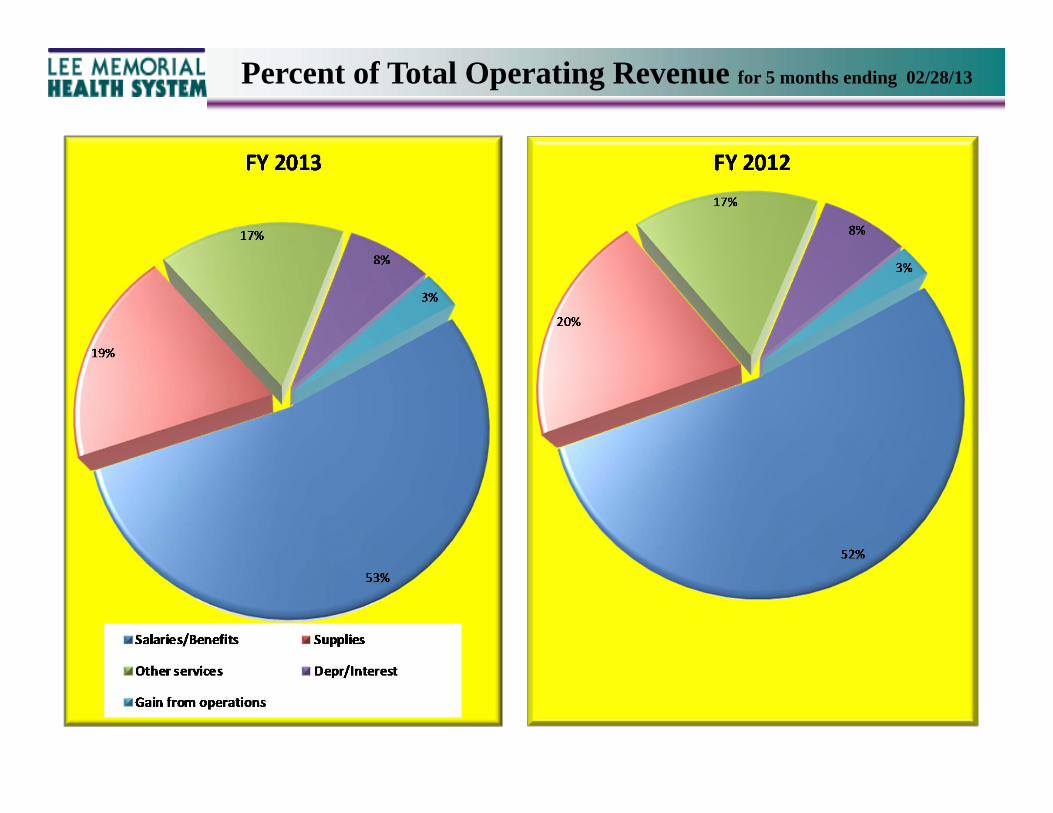
Percent of Total Operating Revenue for 5 months ending 02/28/13
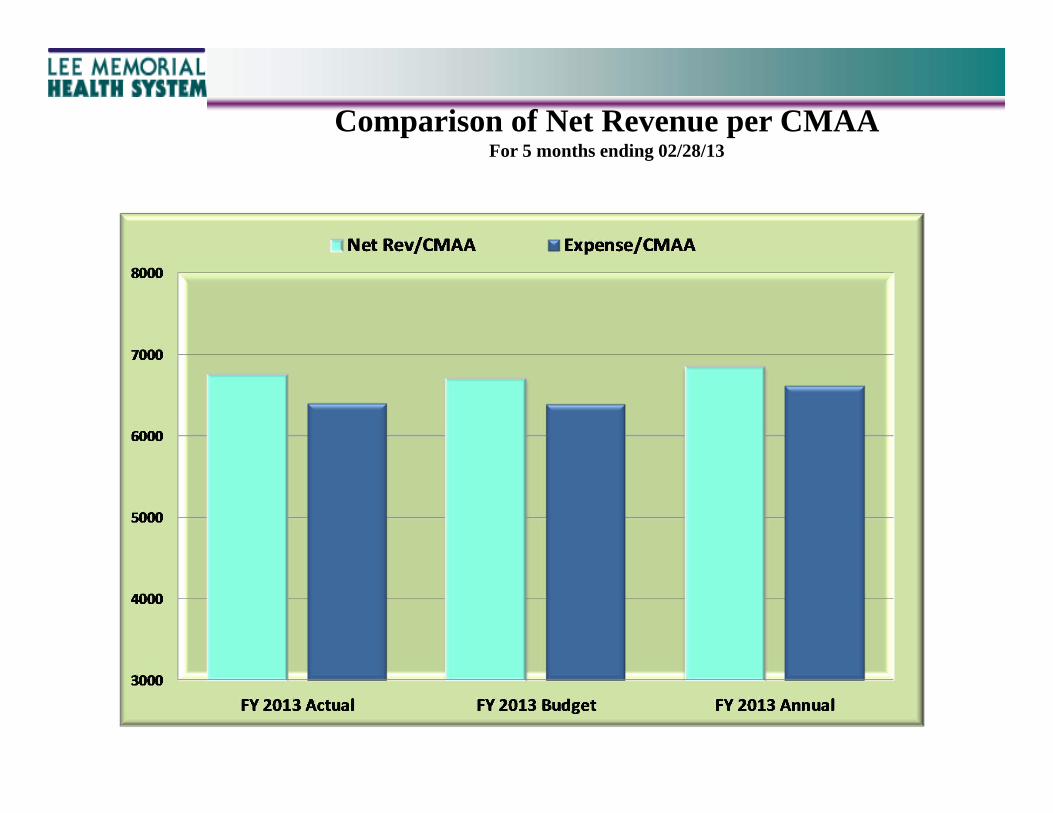
Comparison of Net Revenue per CMAAFor 5 months ending 02/28/13
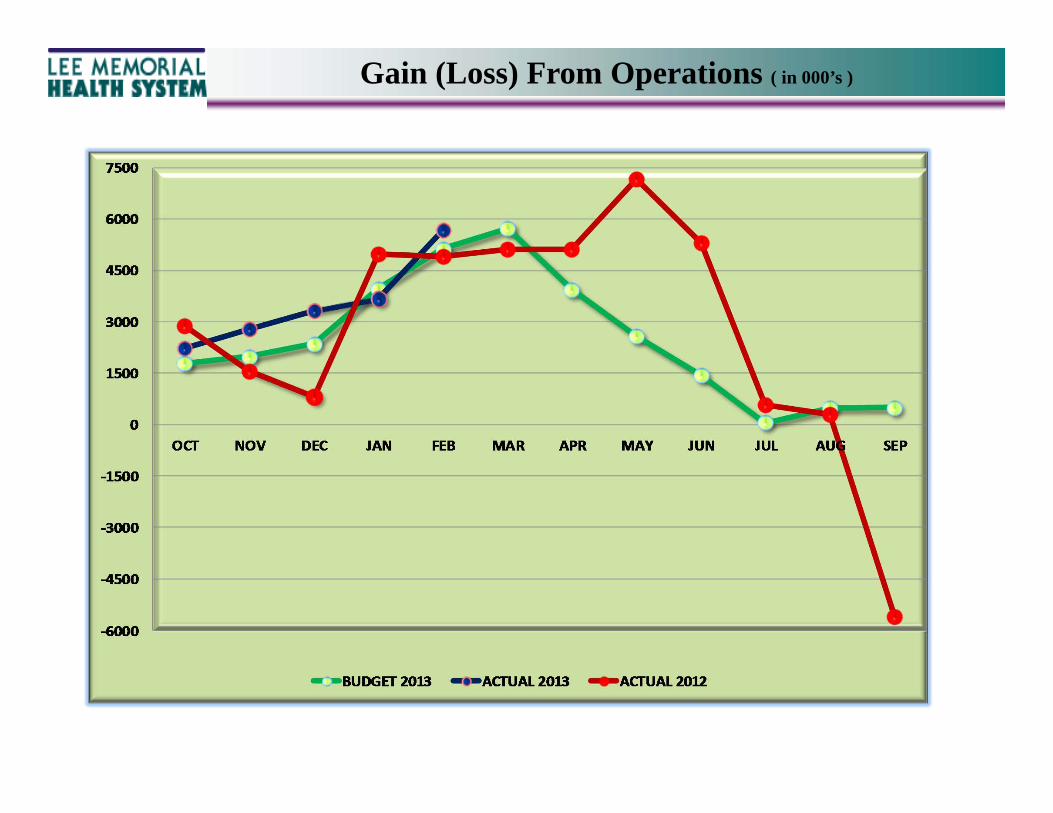
Gain (Loss) From Operations ( in 000’s )
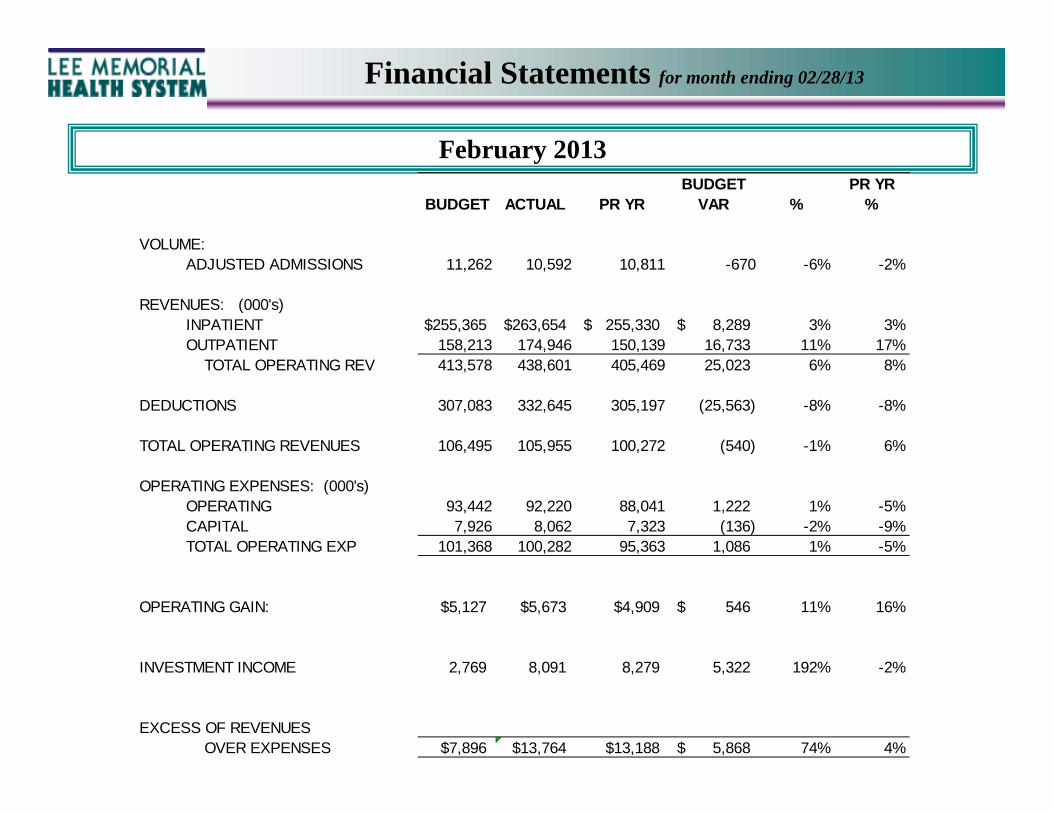
Financial Statements for month ending 02/28/13
February 2013BUDGET PR YR
BUDGET ACTUAL PR YR VAR % %
VOLUME:ADJUSTED ADMISSIONS 11,262 10,592 10,811 -670 -6% -2%
REVENUES: (000's)INPATIENT $255,365 263,654$ 255,330$ 8,289$ 3% 3%OUTPATIENT 158,213 174,946 150,139 16,733 11% 17% TOTAL OPERATING REV 413,578 438,601 405,469 25,023 6% 8%
DEDUCTIONS 307,083 332,645 305,197 (25,563) -8% -8%
TOTAL OPERATING REVENUES 106,495 105,955 100,272 (540) -1% 6%
OPERATING EXPENSES: (000's)OPERATING 93,442 92,220 88,041 1,222 1% -5%CAPITAL 7,926 8,062 7,323 (136) -2% -9%TOTAL OPERATING EXP 101,368 100,282 95,363 1,086 1% -5%
OPERATING GAIN: $5,127 $5,673 $4,909 546$ 11% 16%
INVESTMENT INCOME 2,769 8,091 8,279 5,322 192% -2%
EXCESS OF REVENUES OVER EXPENSES $7,896 $13,764 $13,188 5,868$ 74% 4%
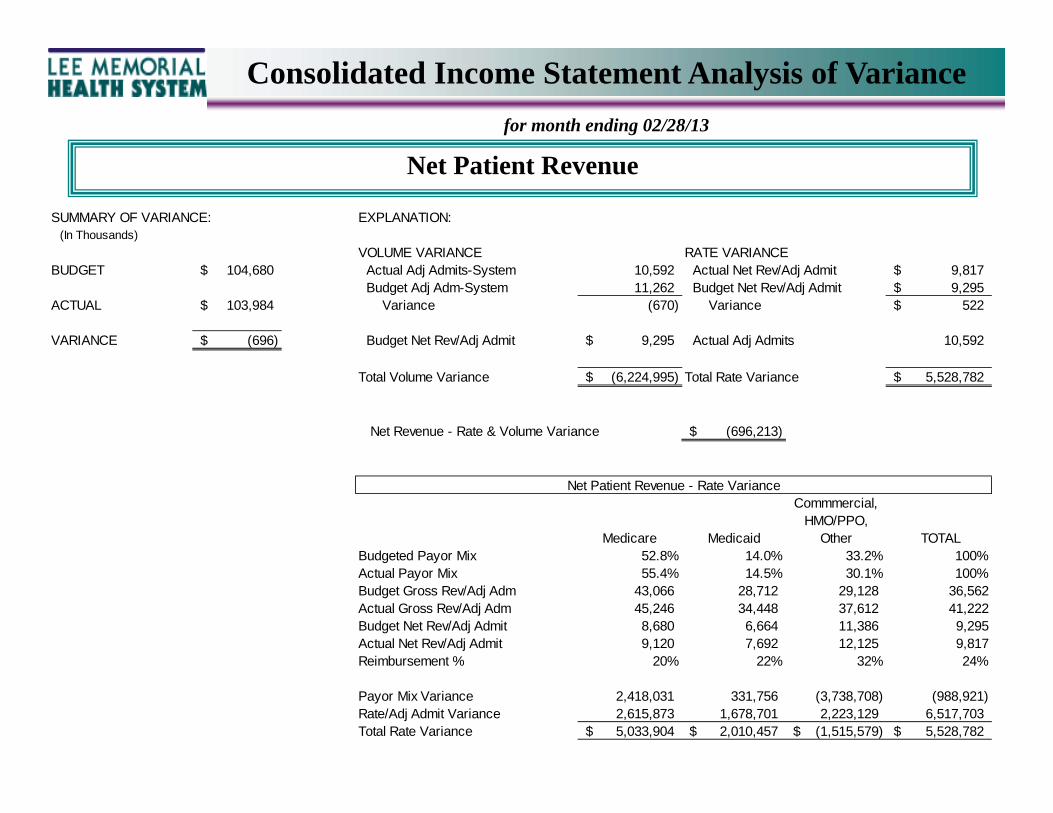
Net Patient Revenue
Consolidated Income Statement Analysis of Variance
for month ending 02/28/13
SUMMARY OF VARIANCE: EXPLANATION: (In Thousands)
VOLUME VARIANCE RATE VARIANCEBUDGET 104,680$ Actual Adj Admits-System 10,592 Actual Net Rev/Adj Admit 9,817$
Budget Adj Adm-System 11,262 Budget Net Rev/Adj Admit 9,295$ ACTUAL 103,984$ Variance (670) Variance 522$
VARIANCE (696)$ Budget Net Rev/Adj Admit 9,295$ Actual Adj Admits 10,592
Total Volume Variance (6,224,995)$ Total Rate Variance 5,528,782$
Net Revenue - Rate & Volume Variance (696,213)$
Medicare Medicaid
Commmercial, HMO/PPO,
Other TOTAL Budgeted Payor Mix 52.8% 14.0% 33.2% 100%Actual Payor Mix 55.4% 14.5% 30.1% 100%Budget Gross Rev/Adj Adm 43,066 28,712 29,128 36,562Actual Gross Rev/Adj Adm 45,246 34,448 37,612 41,222Budget Net Rev/Adj Admit 8,680 6,664 11,386 9,295Actual Net Rev/Adj Admit 9,120 7,692 12,125 9,817Reimbursement % 20% 22% 32% 24%
Payor Mix Variance 2,418,031 331,756 (3,738,708) (988,921) Rate/Adj Admit Variance 2,615,873 1,678,701 2,223,129 6,517,703 Total Rate Variance 5,033,904$ 2,010,457$ (1,515,579)$ 5,528,782$
Net Patient Revenue - Rate Variance
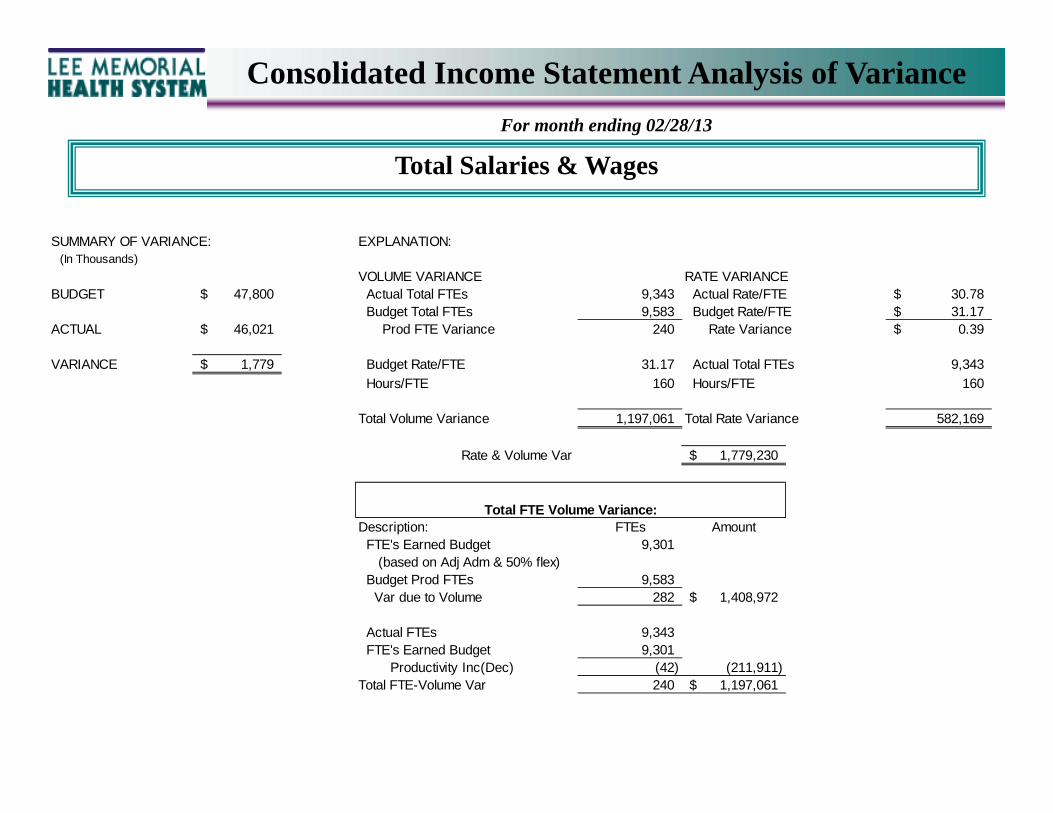
Total Salaries & Wages
Consolidated Income Statement Analysis of Variance
For month ending 02/28/13
SUMMARY OF VARIANCE: EXPLANATION: (In Thousands)
VOLUME VARIANCE RATE VARIANCEBUDGET 47,800$ Actual Total FTEs 9,343 Actual Rate/FTE 30.78$
Budget Total FTEs 9,583 Budget Rate/FTE 31.17$ ACTUAL 46,021$ Prod FTE Variance 240 Rate Variance 0.39$
VARIANCE 1,779$ Budget Rate/FTE 31.17 Actual Total FTEs 9,343
Hours/FTE 160 Hours/FTE 160
Total Volume Variance 1,197,061 Total Rate Variance 582,169
Rate & Volume Var 1,779,230$
Description: FTEs Amount FTE's Earned Budget 9,301 (based on Adj Adm & 50% flex) Budget Prod FTEs 9,583 Var due to Volume 282 1,408,972$
Actual FTEs 9,343 FTE's Earned Budget 9,301 Productivity Inc(Dec) (42) (211,911) Total FTE-Volume Var 240 1,197,061$
Total FTE Volume Variance:
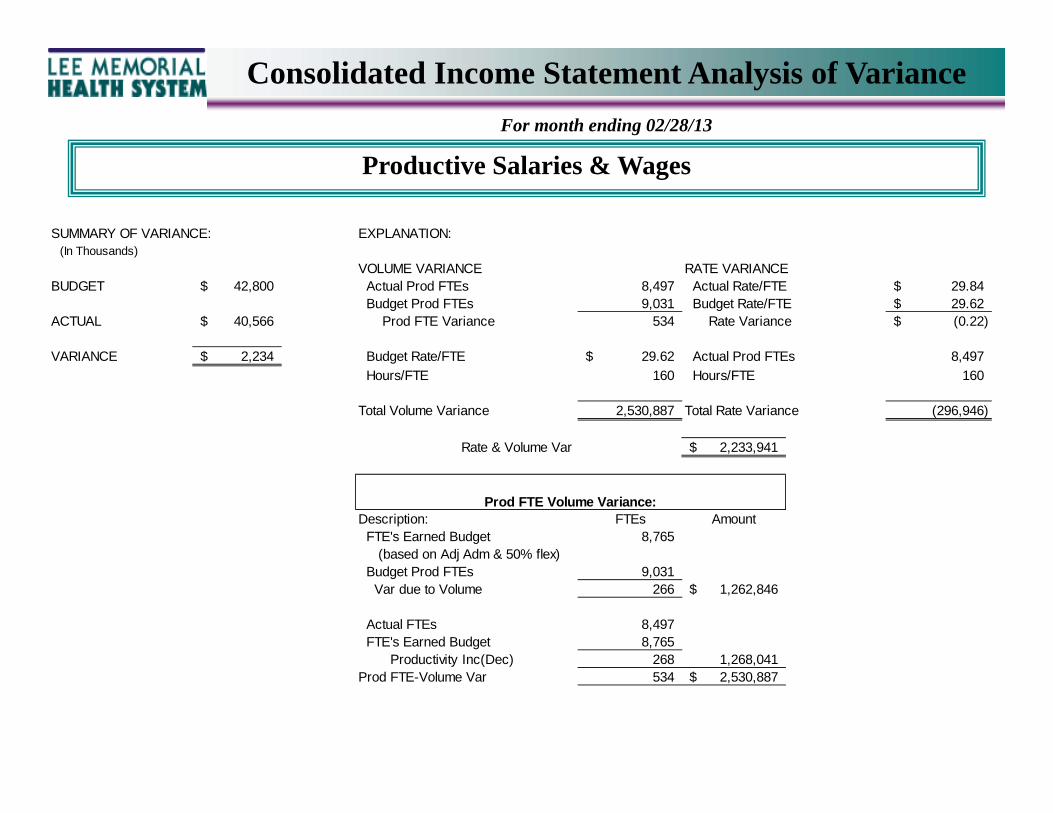
Consolidated Income Statement Analysis of Variance
For month ending 02/28/13
Productive Salaries & Wages
SUMMARY OF VARIANCE: EXPLANATION: (In Thousands)
VOLUME VARIANCE RATE VARIANCEBUDGET 42,800$ Actual Prod FTEs 8,497 Actual Rate/FTE 29.84$
Budget Prod FTEs 9,031 Budget Rate/FTE 29.62$ ACTUAL 40,566$ Prod FTE Variance 534 Rate Variance (0.22)$
VARIANCE 2,234$ Budget Rate/FTE 29.62$ Actual Prod FTEs 8,497
Hours/FTE 160 Hours/FTE 160
Total Volume Variance 2,530,887 Total Rate Variance (296,946)
Rate & Volume Var 2,233,941$
Description: FTEs Amount FTE's Earned Budget 8,765 (based on Adj Adm & 50% flex) Budget Prod FTEs 9,031 Var due to Volume 266 1,262,846$
Actual FTEs 8,497 FTE's Earned Budget 8,765 Productivity Inc(Dec) 268 1,268,041 Prod FTE-Volume Var 534 2,530,887$
Prod FTE Volume Variance:
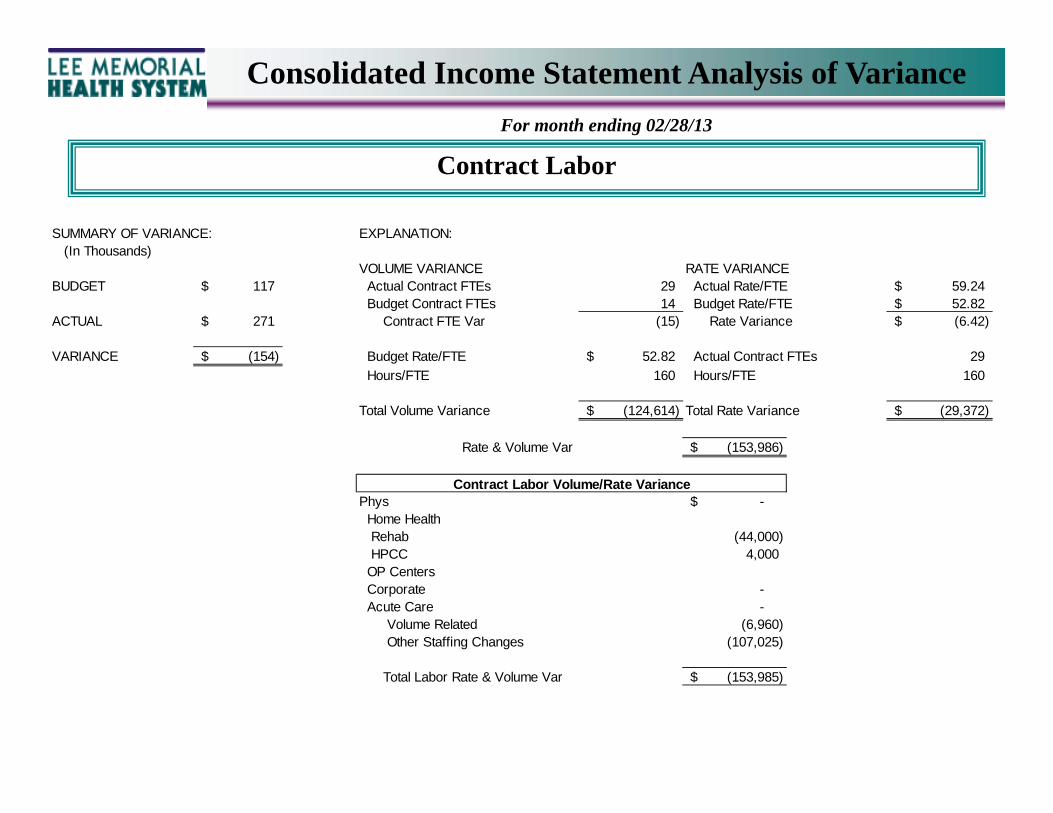
Consolidated Income Statement Analysis of Variance
For month ending 02/28/13
Contract Labor
SUMMARY OF VARIANCE: EXPLANATION: (In Thousands)
VOLUME VARIANCE RATE VARIANCEBUDGET 117$ Actual Contract FTEs 29 Actual Rate/FTE 59.24$
Budget Contract FTEs 14 Budget Rate/FTE 52.82$ ACTUAL 271$ Contract FTE Var (15) Rate Variance (6.42)$
VARIANCE (154)$ Budget Rate/FTE 52.82$ Actual Contract FTEs 29
Hours/FTE 160 Hours/FTE 160
Total Volume Variance (124,614)$ Total Rate Variance (29,372)$
Rate & Volume Var (153,986)$
Phys -$ Home Health Rehab (44,000) HPCC 4,000 OP Centers Corporate - Acute Care - Volume Related (6,960) Other Staffing Changes (107,025)
Total Labor Rate & Volume Var (153,985)$
Contract Labor Volume/Rate Variance
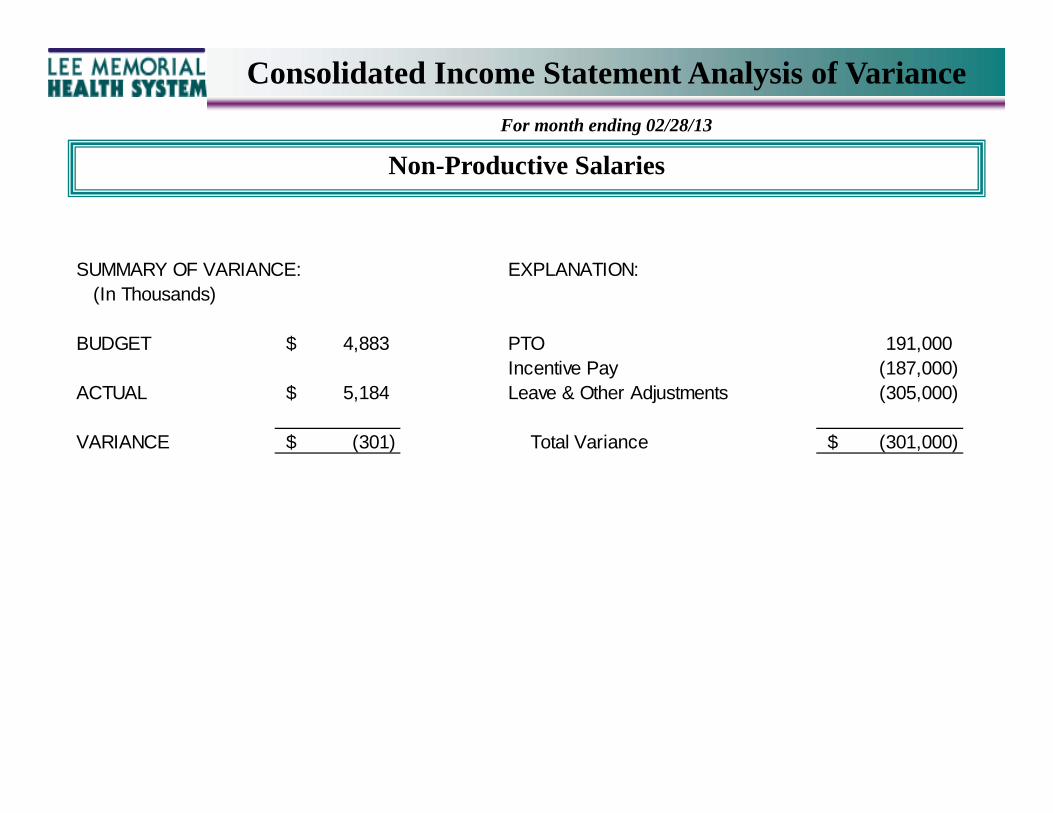
Consolidated Income Statement Analysis of Variance
For month ending 02/28/13
Non-Productive Salaries
SUMMARY OF VARIANCE: EXPLANATION: (In Thousands)
BUDGET 4,883$ PTO 191,000 Incentive Pay (187,000)
ACTUAL 5,184$ Leave & Other Adjustments (305,000)
VARIANCE (301)$ Total Variance (301,000)$

Consolidated Income Statement Analysis of Variance
For month ending 02/28/13
Other Supplies
SUMMARY OF VARIANCE: EXPLANATION: (In Thousands)
VOLUME VARIANCE RATE VARIANCEBUDGET 20,306$ Actual Adj Admissions 10,592 Actual Supplies/Adj Adm 1,919$
Budget Adj Admissions 11,262 Budget Supplies/Adj Adm 1,803$ ACTUAL 20,329 Variance 670 Rate Variance (116)$
VARIANCE (23)$ Budget Supplies/Adj Adm 1,803$ Actual Adj Admissions 10,592
Total Volume Variance 1,207,564 Total Rate Variance (1,230,546)
Rate & Volume Var (22,983)$
Budget/AA Actual/AA Variance
(Inc) Dec in Drug Expense 443$ 461$ (191,311)$ (Inc) Dec in Implant Costs 541$ 580$ (418,087) (Inc) Dec in Med/Surg Supplies 590$ 598$ (79,988) (Inc) Dec in Other Supplies (541,160)
Total Variance 984 1,041 (1,230,546)
Rate Variance
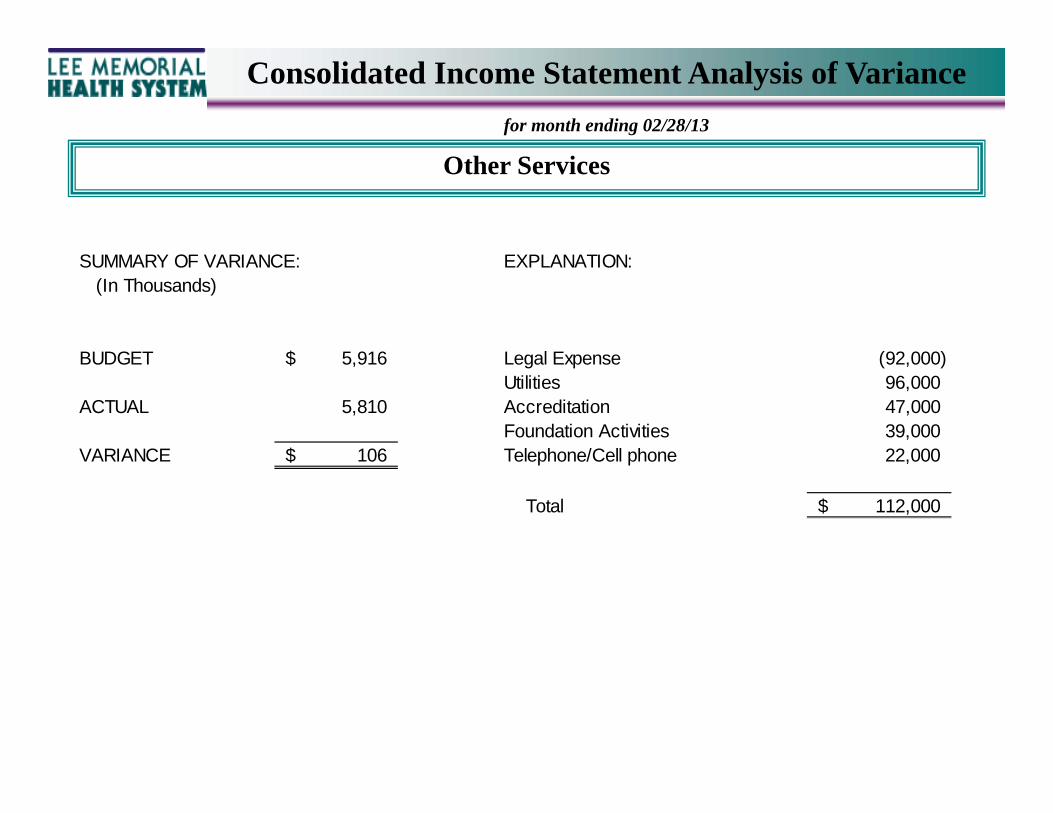
Consolidated Income Statement Analysis of Variance
for month ending 02/28/13
Other Services
SUMMARY OF VARIANCE: EXPLANATION: (In Thousands)
BUDGET 5,916$ Legal Expense (92,000) Utilities 96,000
ACTUAL 5,810 Accreditation 47,000 Foundation Activities 39,000
VARIANCE 106$ Telephone/Cell phone 22,000
Total 112,000$
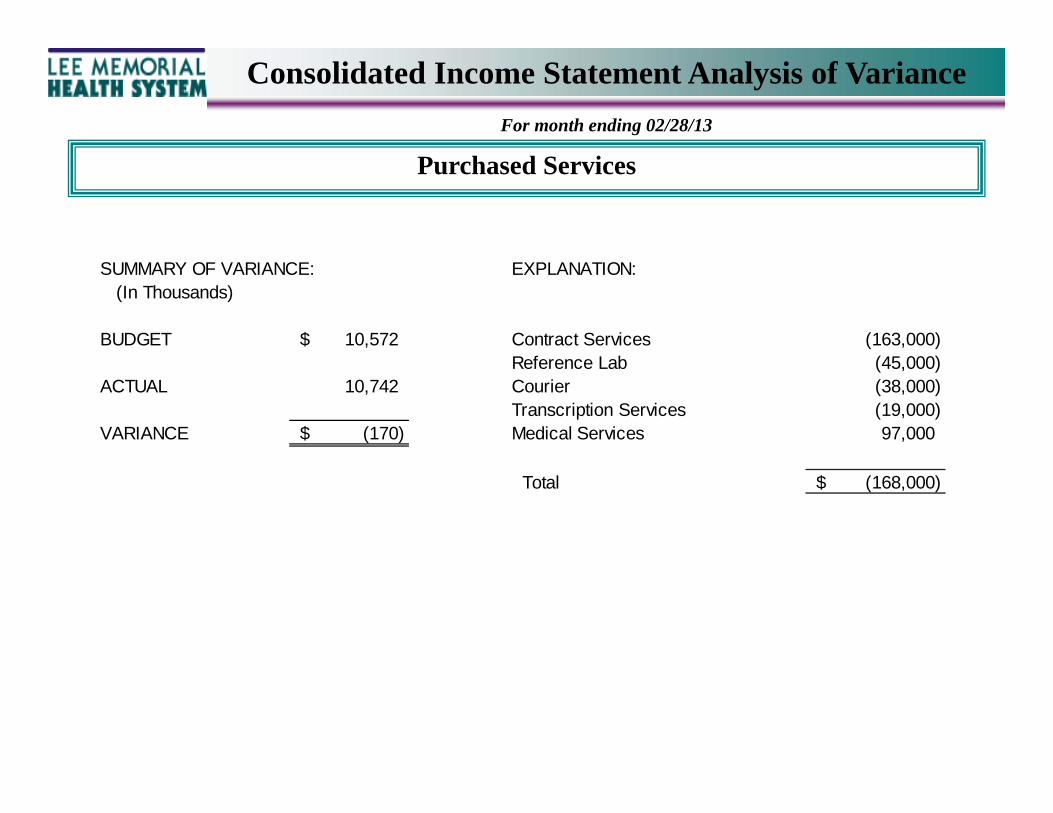
Consolidated Income Statement Analysis of Variance
For month ending 02/28/13
Purchased Services
SUMMARY OF VARIANCE: EXPLANATION: (In Thousands)
BUDGET 10,572$ Contract Services (163,000) Reference Lab (45,000)
ACTUAL 10,742 Courier (38,000) Transcription Services (19,000)
VARIANCE (170)$ Medical Services 97,000
Total (168,000)$
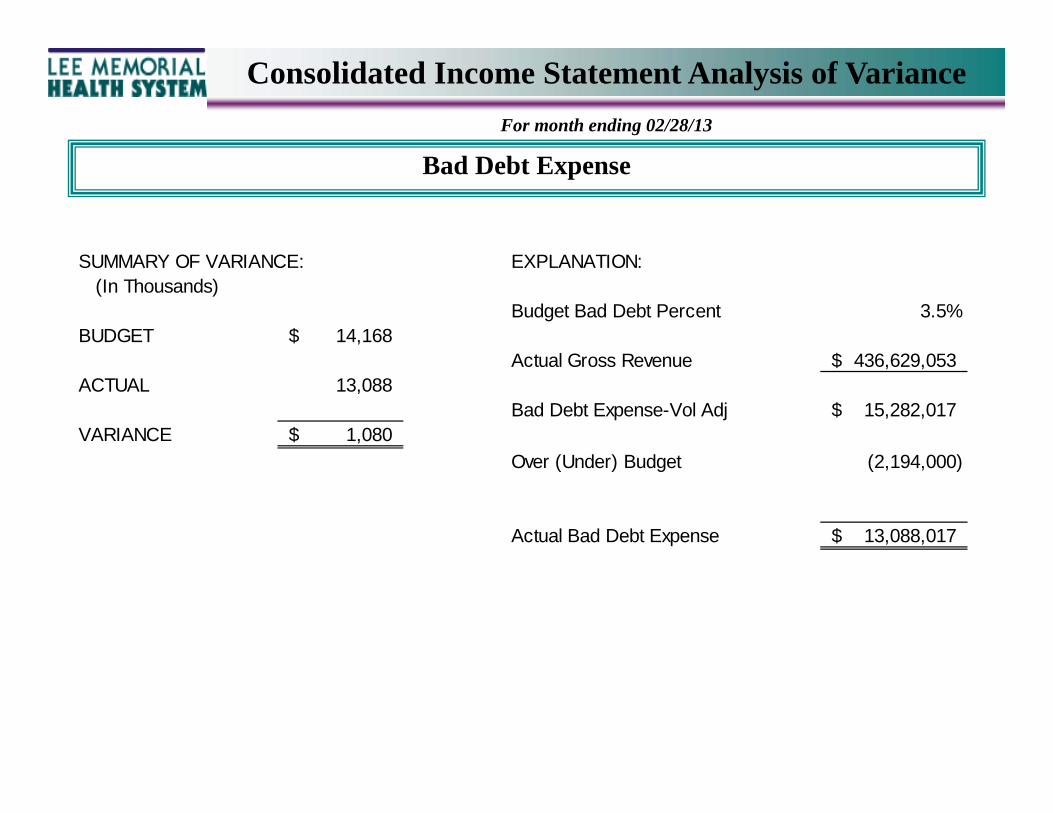
Consolidated Income Statement Analysis of Variance
For month ending 02/28/13
Bad Debt Expense
SUMMARY OF VARIANCE: EXPLANATION: (In Thousands)
Budget Bad Debt Percent 3.5%BUDGET 14,168$
Actual Gross Revenue 436,629,053$ ACTUAL 13,088
Bad Debt Expense-Vol Adj 15,282,017$ VARIANCE 1,080$
Over (Under) Budget (2,194,000)
Actual Bad Debt Expense 13,088,017$
LEE MEMORIAL HEALTH SYSTEM
LEE COUNTY, FLORIDA CONSOLIDATED FINANCIAL STATEMENTS AND STATISTICAL REPORTS
FEBRUARY 28, 2013
LEE MEMORIAL HEALTH SYSTEM CONSOLIDATED FINANCIAL STATEMENTS & STATISTICAL REPORTS TABLE OF CONTENTS SECTION A PAGE CONSOLIDATED SCHEDULES HIGHLIGHTS A.1 CONSOLIDATED STATISTICAL REPORT A.3 CONSOLIDATED INCOME STATEMENT A.4 SOURCES & APPLICATIONS OF FUNDS A.6 CONSOLIDATED BALANCE SHEET A.7 CONSOLIDATED FINANCIAL RATIOS A.8 CONSOLIDATED PAYOR MIX A.10 CAPITAL STATUS REPORT A.11 INVESTMENT PERFORMANCE SUMMARY A.12
Lee Memorial Health System Operating Highlights
For the month ended February 28, 2013 Actual adjusted admits (overall inpatient & outpatient volume indicator) for the month ended February 28, 2013 are 10,592 which is 5.9% less than budget. Actual inpatient admits for the month are 6,396 or 8.4% less than budget and actual patient days are 33,011 or 5.5% less than budget which resulted in a 5.2 day length of stay. Emergency room visits are 1.9% greater than budget while outpatient surgeries are 1.3% greater than budget. Net patient revenue for February 2013 reflects a $0.7 million or a 0.7% unfavorable variance to budget. This unfavorable variance in net patient revenue is the net result of the 5.9% decrease in adjusted admits offset by a 5.2% increase in reimbursement. Total operating expenses before depreciation and interest expense are $1.2 million less than budget. Favorable variances are reflected is salaries/wages and other services. Actual total operating costs per case mix adjusted admit is .2% greater than budget (6,397 act; 6,384 bud). Productivity as measured by FTEs/AOB decreased by .4% (4.79 actual, 4.77 budget) during February 2013. For February 2013, the gain from operations is $5.7 million versus a budgeted gain of $5.1 million. Excess revenue over expenses is a gain of $13.7 million versus a budgeted gain of $7.9 million. Other Non-Operating Revenue was budgeted at $2.7 million while the actual income was $8.0 million. Investments were budgeted to return $2.2 million for the month but the actual investment return was $4.6 million along with restricted donations of $3.3 million.
Page A.1
Lee Memorial Health System Operating Highlights
For the month ended February 28, 2013 For the month, Cash & Investments increased by $15.9 million to $529.7 million. Operations increased cash by $19.4 million while working capital increased cash by $0.9 million. Cash was reduced by $3.1 million for routine equipment replacement along with $0.2 million principal payment on bonds & notes payable. Days in Accounts Receivable decreased to 60.5 days and resulted in a $1.2 million decrease in cash. Total Notes & Bonds payable on February 28, 2013 is $673.8 million resulting in a Cash to Debt ratio of 78.6%. Net Patient Revenue per adjusted admit CMI for the month ended February 28, 2013 is $6,759 while the Operating Expense per adjusted admit CMI is $6,397. The difference which represents the gain from operations per adjusted admit is $362.00 while the budgeted gain from operations is $323.00. Wages & Benefits as a percent of Net Operating Revenue is 51.0% for February 2013 versus a budget of 52.0%. The actual hourly pay rate is $30.78 which is 39 cents less than budget. Post Acute entities provided the following YTD contributions to Acute Care by allowing charity care patients into their respective programs: Lee Memorial Home Health $421,000; HealthPark Care Center $172,984; The Rehabilitation Hospital $228,347. The Lee Physician Group YTD loss per physician is $28,929. This includes practice revenue and expenses along with ancillary revenue referred to LMHS. The YTD loss is $5,229 per physician better than budget due to the following main contributing factors: higher collections per visit, lower operating cost than budgeted, and the additional collection of the “EMR Meaningful Use funds”.
Page A.2
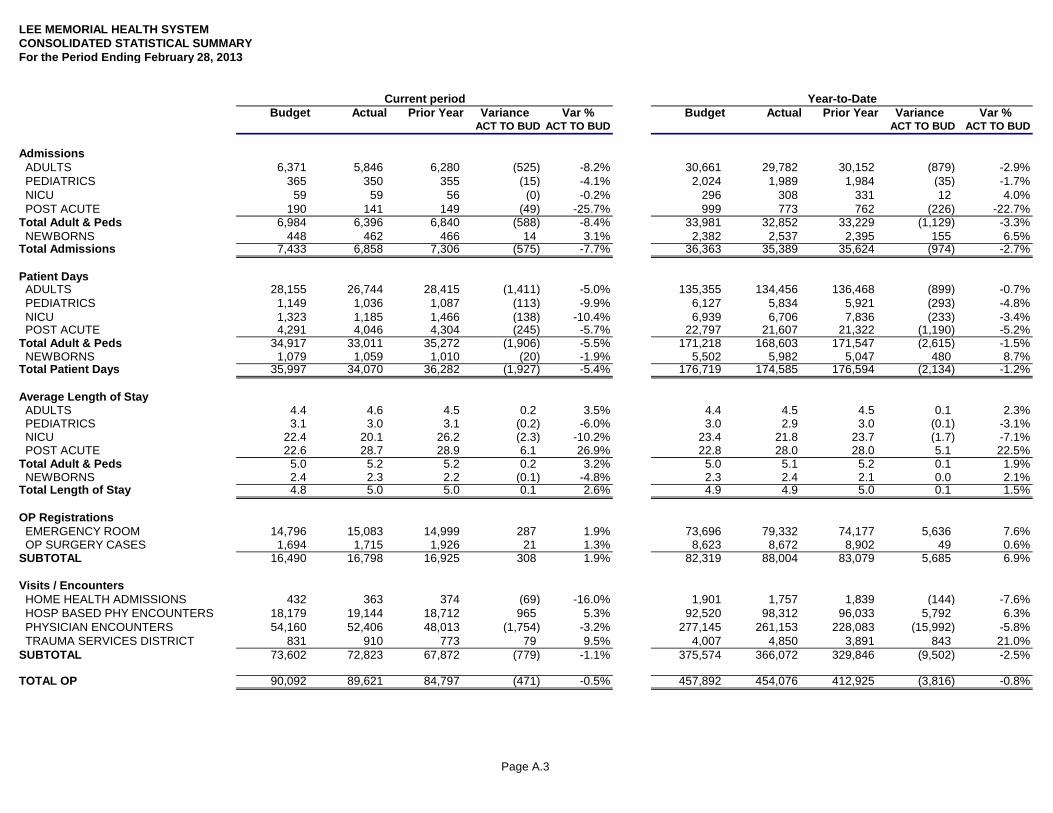
Page A.3
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATED STATISTICAL SUMMARYFor the Period Ending February 28, 2013
Current period Year-to-DateBudget Actual Prior Year Variance Var % Budget Actual Prior Year Variance Var %
ACT TO BUD ACT TO BUD ACT TO BUD ACT TO BUD
Admissions ADULTS 6,371 5,846 6,280 (525) -8.2% 30,661 29,782 30,152 (879) -2.9% PEDIATRICS 365 350 355 (15) -4.1% 2,024 1,989 1,984 (35) -1.7% NICU 59 59 56 (0) -0.2% 296 308 331 12 4.0% POST ACUTE 190 141 149 (49) -25.7% 999 773 762 (226) -22.7%Total Adult & Peds 6,984 6,396 6,840 (588) -8.4% 33,981 32,852 33,229 (1,129) -3.3% NEWBORNS 448 462 466 14 3.1% 2,382 2,537 2,395 155 6.5%Total Admissions 7,433 6,858 7,306 (575) -7.7% 36,363 35,389 35,624 (974) -2.7%
Patient Days ADULTS 28,155 26,744 28,415 (1,411) -5.0% 135,355 134,456 136,468 (899) -0.7% PEDIATRICS 1,149 1,036 1,087 (113) -9.9% 6,127 5,834 5,921 (293) -4.8% NICU 1,323 1,185 1,466 (138) -10.4% 6,939 6,706 7,836 (233) -3.4% POST ACUTE 4,291 4,046 4,304 (245) -5.7% 22,797 21,607 21,322 (1,190) -5.2%Total Adult & Peds 34,917 33,011 35,272 (1,906) -5.5% 171,218 168,603 171,547 (2,615) -1.5% NEWBORNS 1,079 1,059 1,010 (20) -1.9% 5,502 5,982 5,047 480 8.7%Total Patient Days 35,997 34,070 36,282 (1,927) -5.4% 176,719 174,585 176,594 (2,134) -1.2%
Average Length of Stay ADULTS 4.4 4.6 4.5 0.2 3.5% 4.4 4.5 4.5 0.1 2.3% PEDIATRICS 3.1 3.0 3.1 (0.2) -6.0% 3.0 2.9 3.0 (0.1) -3.1% NICU 22.4 20.1 26.2 (2.3) -10.2% 23.4 21.8 23.7 (1.7) -7.1% POST ACUTE 22.6 28.7 28.9 6.1 26.9% 22.8 28.0 28.0 5.1 22.5%Total Adult & Peds 5.0 5.2 5.2 0.2 3.2% 5.0 5.1 5.2 0.1 1.9% NEWBORNS 2.4 2.3 2.2 (0.1) -4.8% 2.3 2.4 2.1 0.0 2.1%Total Length of Stay 4.8 5.0 5.0 0.1 2.6% 4.9 4.9 5.0 0.1 1.5%
OP Registrations EMERGENCY ROOM 14,796 15,083 14,999 287 1.9% 73,696 79,332 74,177 5,636 7.6% OP SURGERY CASES 1,694 1,715 1,926 21 1.3% 8,623 8,672 8,902 49 0.6%SUBTOTAL 16,490 16,798 16,925 308 1.9% 82,319 88,004 83,079 5,685 6.9%
Visits / Encounters HOME HEALTH ADMISSIONS 432 363 374 (69) -16.0% 1,901 1,757 1,839 (144) -7.6% HOSP BASED PHY ENCOUNTERS 18,179 19,144 18,712 965 5.3% 92,520 98,312 96,033 5,792 6.3% PHYSICIAN ENCOUNTERS 54,160 52,406 48,013 (1,754) -3.2% 277,145 261,153 228,083 (15,992) -5.8% TRAUMA SERVICES DISTRICT 831 910 773 79 9.5% 4,007 4,850 3,891 843 21.0%SUBTOTAL 73,602 72,823 67,872 (779) -1.1% 375,574 366,072 329,846 (9,502) -2.5%
TOTAL OP 90,092 89,621 84,797 (471) -0.5% 457,892 454,076 412,925 (3,816) -0.8%
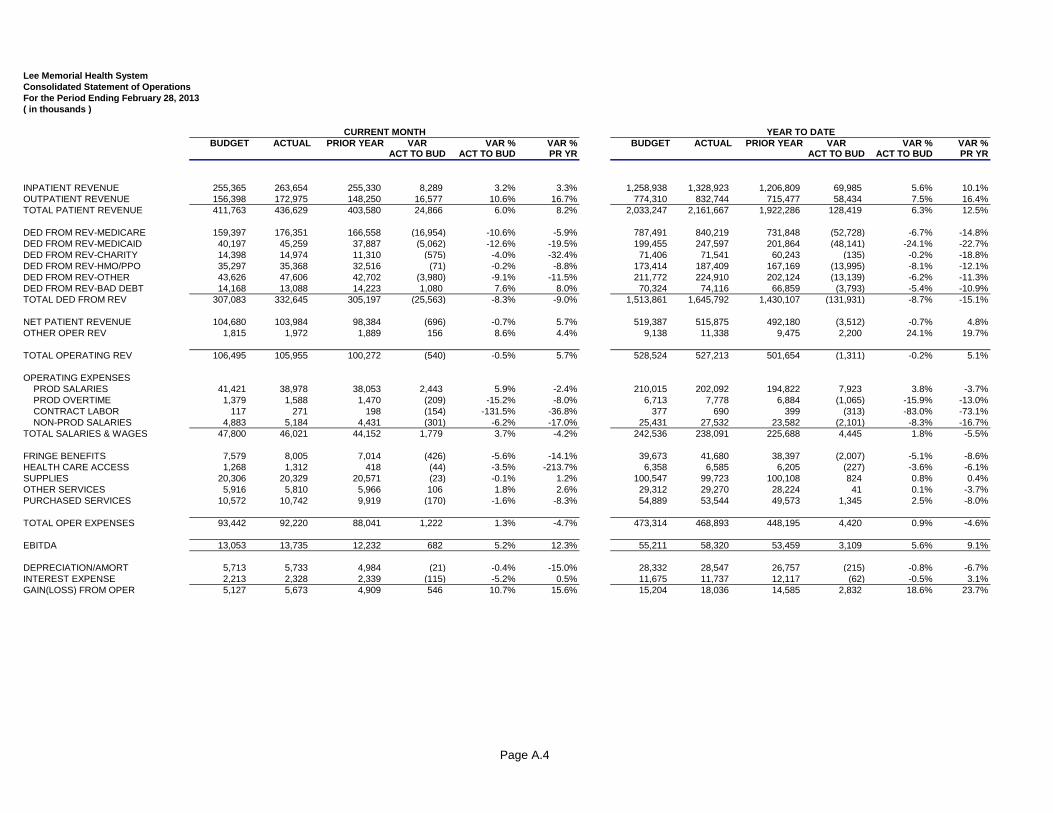
Page A.4
Lee Memorial Health SystemConsolidated Statement of OperationsFor the Period Ending February 28, 2013( in thousands )
BUDGET ACTUAL PRIOR YEAR VAR VAR % VAR % BUDGET ACTUAL PRIOR YEAR VAR VAR % VAR %ACT TO BUD ACT TO BUD PR YR ACT TO BUD ACT TO BUD PR YR
INPATIENT REVENUE 255,365 263,654 255,330 8,289 3.2% 3.3% 1,258,938 1,328,923 1,206,809 69,985 5.6% 10.1%OUTPATIENT REVENUE 156,398 172,975 148,250 16,577 10.6% 16.7% 774,310 832,744 715,477 58,434 7.5% 16.4%TOTAL PATIENT REVENUE 411,763 436,629 403,580 24,866 6.0% 8.2% 2,033,247 2,161,667 1,922,286 128,419 6.3% 12.5%
DED FROM REV-MEDICARE 159,397 176,351 166,558 (16,954) -10.6% -5.9% 787,491 840,219 731,848 (52,728) -6.7% -14.8%DED FROM REV-MEDICAID 40,197 45,259 37,887 (5,062) -12.6% -19.5% 199,455 247,597 201,864 (48,141) -24.1% -22.7%DED FROM REV-CHARITY 14,398 14,974 11,310 (575) -4.0% -32.4% 71,406 71,541 60,243 (135) -0.2% -18.8%DED FROM REV-HMO/PPO 35,297 35,368 32,516 (71) -0.2% -8.8% 173,414 187,409 167,169 (13,995) -8.1% -12.1%DED FROM REV-OTHER 43,626 47,606 42,702 (3,980) -9.1% -11.5% 211,772 224,910 202,124 (13,139) -6.2% -11.3%DED FROM REV-BAD DEBT 14,168 13,088 14,223 1,080 7.6% 8.0% 70,324 74,116 66,859 (3,793) -5.4% -10.9%TOTAL DED FROM REV 307,083 332,645 305,197 (25,563) -8.3% -9.0% 1,513,861 1,645,792 1,430,107 (131,931) -8.7% -15.1%
NET PATIENT REVENUE 104,680 103,984 98,384 (696) -0.7% 5.7% 519,387 515,875 492,180 (3,512) -0.7% 4.8%OTHER OPER REV 1,815 1,972 1,889 156 8.6% 4.4% 9,138 11,338 9,475 2,200 24.1% 19.7%
TOTAL OPERATING REV 106,495 105,955 100,272 (540) -0.5% 5.7% 528,524 527,213 501,654 (1,311) -0.2% 5.1%
OPERATING EXPENSES PROD SALARIES 41,421 38,978 38,053 2,443 5.9% -2.4% 210,015 202,092 194,822 7,923 3.8% -3.7% PROD OVERTIME 1,379 1,588 1,470 (209) -15.2% -8.0% 6,713 7,778 6,884 (1,065) -15.9% -13.0% CONTRACT LABOR 117 271 198 (154) -131.5% -36.8% 377 690 399 (313) -83.0% -73.1% NON-PROD SALARIES 4,883 5,184 4,431 (301) -6.2% -17.0% 25,431 27,532 23,582 (2,101) -8.3% -16.7%TOTAL SALARIES & WAGES 47,800 46,021 44,152 1,779 3.7% -4.2% 242,536 238,091 225,688 4,445 1.8% -5.5%
FRINGE BENEFITS 7,579 8,005 7,014 (426) -5.6% -14.1% 39,673 41,680 38,397 (2,007) -5.1% -8.6%HEALTH CARE ACCESS 1,268 1,312 418 (44) -3.5% -213.7% 6,358 6,585 6,205 (227) -3.6% -6.1%SUPPLIES 20,306 20,329 20,571 (23) -0.1% 1.2% 100,547 99,723 100,108 824 0.8% 0.4%OTHER SERVICES 5,916 5,810 5,966 106 1.8% 2.6% 29,312 29,270 28,224 41 0.1% -3.7%PURCHASED SERVICES 10,572 10,742 9,919 (170) -1.6% -8.3% 54,889 53,544 49,573 1,345 2.5% -8.0%
TOTAL OPER EXPENSES 93,442 92,220 88,041 1,222 1.3% -4.7% 473,314 468,893 448,195 4,420 0.9% -4.6%
EBITDA 13,053 13,735 12,232 682 5.2% 12.3% 55,211 58,320 53,459 3,109 5.6% 9.1%
DEPRECIATION/AMORT 5,713 5,733 4,984 (21) -0.4% -15.0% 28,332 28,547 26,757 (215) -0.8% -6.7%INTEREST EXPENSE 2,213 2,328 2,339 (115) -5.2% 0.5% 11,675 11,737 12,117 (62) -0.5% 3.1%GAIN(LOSS) FROM OPER 5,127 5,673 4,909 546 10.7% 15.6% 15,204 18,036 14,585 2,832 18.6% 23.7%
CURRENT MONTH YEAR TO DATE
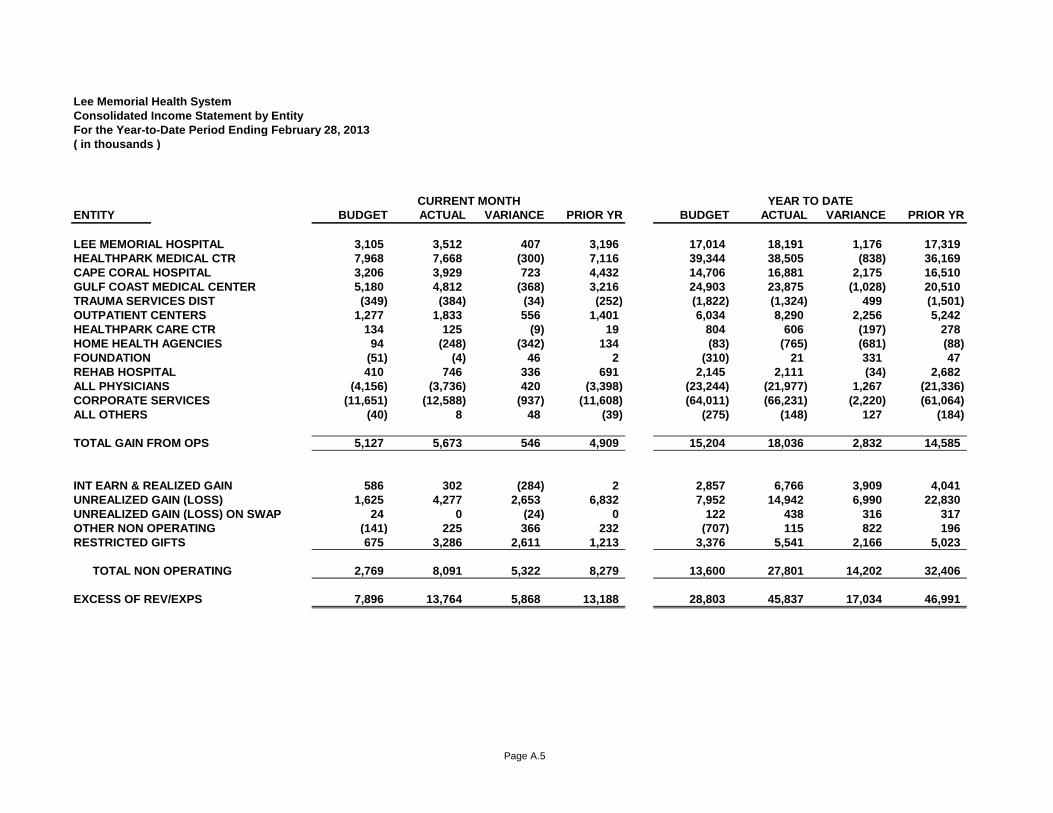
Page A.5
Lee Memorial Health SystemConsolidated Income Statement by EntityFor the Year-to-Date Period Ending February 28, 2013( in thousands )
ENTITY BUDGET ACTUAL VARIANCE PRIOR YR BUDGET ACTUAL VARIANCE PRIOR YR
LEE MEMORIAL HOSPITAL 3,105 3,512 407 3,196 17,014 18,191 1,176 17,319HEALTHPARK MEDICAL CTR 7,968 7,668 (300) 7,116 39,344 38,505 (838) 36,169CAPE CORAL HOSPITAL 3,206 3,929 723 4,432 14,706 16,881 2,175 16,510GULF COAST MEDICAL CENTER 5,180 4,812 (368) 3,216 24,903 23,875 (1,028) 20,510TRAUMA SERVICES DIST (349) (384) (34) (252) (1,822) (1,324) 499 (1,501)OUTPATIENT CENTERS 1,277 1,833 556 1,401 6,034 8,290 2,256 5,242HEALTHPARK CARE CTR 134 125 (9) 19 804 606 (197) 278HOME HEALTH AGENCIES 94 (248) (342) 134 (83) (765) (681) (88)FOUNDATION (51) (4) 46 2 (310) 21 331 47REHAB HOSPITAL 410 746 336 691 2,145 2,111 (34) 2,682ALL PHYSICIANS (4,156) (3,736) 420 (3,398) (23,244) (21,977) 1,267 (21,336)CORPORATE SERVICES (11,651) (12,588) (937) (11,608) (64,011) (66,231) (2,220) (61,064)ALL OTHERS (40) 8 48 (39) (275) (148) 127 (184)
TOTAL GAIN FROM OPS 5,127 5,673 546 4,909 15,204 18,036 2,832 14,585
INT EARN & REALIZED GAIN 586 302 (284) 2 2,857 6,766 3,909 4,041UNREALIZED GAIN (LOSS) 1,625 4,277 2,653 6,832 7,952 14,942 6,990 22,830UNREALIZED GAIN (LOSS) ON SWAP 24 0 (24) 0 122 438 316 317OTHER NON OPERATING (141) 225 366 232 (707) 115 822 196RESTRICTED GIFTS 675 3,286 2,611 1,213 3,376 5,541 2,166 5,023
TOTAL NON OPERATING 2,769 8,091 5,322 8,279 13,600 27,801 14,202 32,406
EXCESS OF REV/EXPS 7,896 13,764 5,868 13,188 28,803 45,837 17,034 46,991
CURRENT MONTH YEAR TO DATE
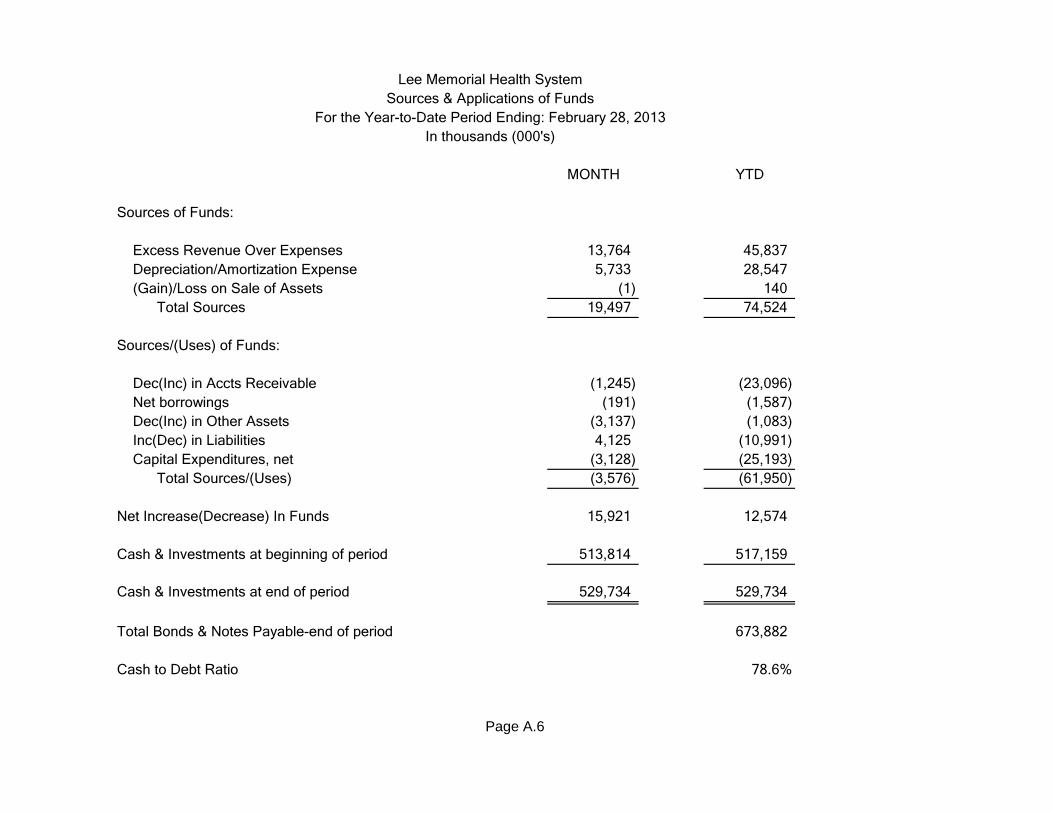
MONTH YTD
Sources of Funds:
Excess Revenue Over Expenses 13,764 45,837 Depreciation/Amortization Expense 5,733 28,547 (Gain)/Loss on Sale of Assets (1) 140 Total Sources 19,497 74,524
Sources/(Uses) of Funds:
Dec(Inc) in Accts Receivable (1,245) (23,096) Net borrowings (191) (1,587) Dec(Inc) in Other Assets (3,137) (1,083) Inc(Dec) in Liabilities 4,125 (10,991) Capital Expenditures, net (3,128) (25,193) Total Sources/(Uses) (3,576) (61,950)
Net Increase(Decrease) In Funds 15,921 12,574
Cash & Investments at beginning of period 513,814 517,159
Cash & Investments at end of period 529,734 529,734
Total Bonds & Notes Payable-end of period 673,882
Cash to Debt Ratio 78.6%
Page A.6
Lee Memorial Health SystemSources & Applications of Funds
For the Year-to-Date Period Ending: February 28, 2013In thousands (000's)
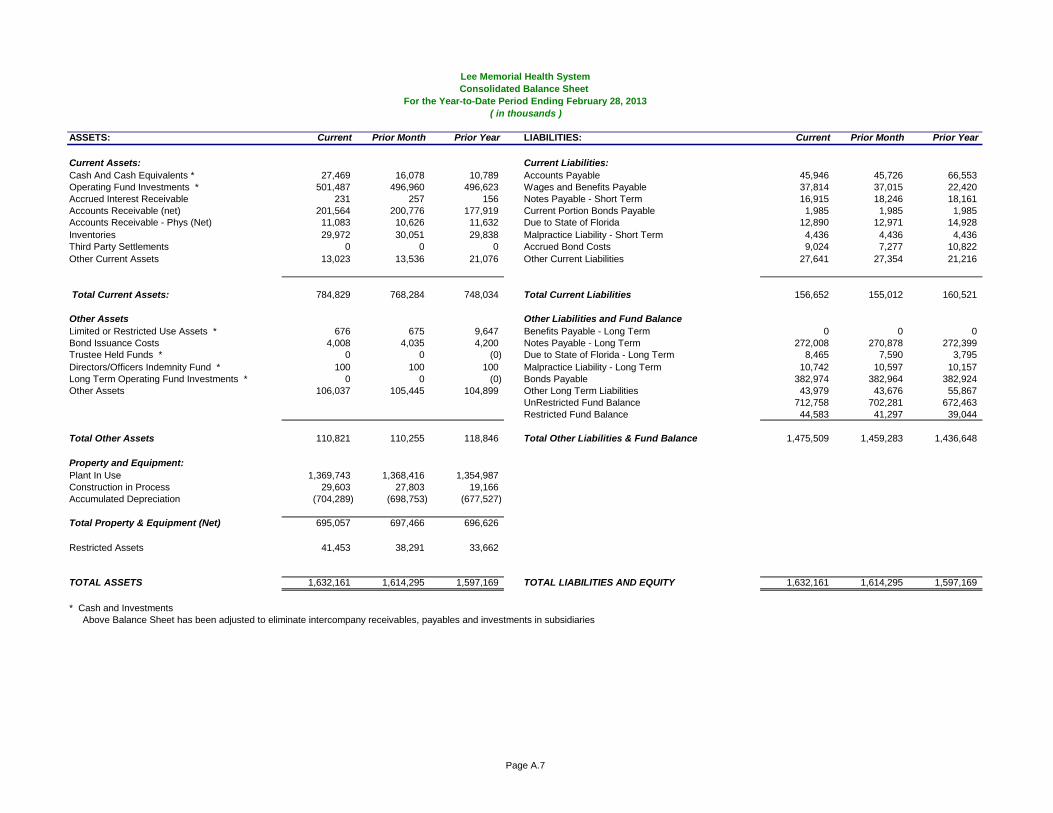
Page A.7
Lee Memorial Health SystemConsolidated Balance Sheet
For the Year-to-Date Period Ending February 28, 2013 ( in thousands )
ASSETS: Current Prior Month Prior Year LIABILITIES: Current Prior Month Prior Year
Current Assets: Current Liabilities:Cash And Cash Equivalents * 27,469 16,078 10,789 Accounts Payable 45,946 45,726 66,553Operating Fund Investments * 501,487 496,960 496,623 Wages and Benefits Payable 37,814 37,015 22,420Accrued Interest Receivable 231 257 156 Notes Payable - Short Term 16,915 18,246 18,161Accounts Receivable (net) 201,564 200,776 177,919 Current Portion Bonds Payable 1,985 1,985 1,985Accounts Receivable - Phys (Net) 11,083 10,626 11,632 Due to State of Florida 12,890 12,971 14,928Inventories 29,972 30,051 29,838 Malpractice Liability - Short Term 4,436 4,436 4,436Third Party Settlements 0 0 0 Accrued Bond Costs 9,024 7,277 10,822Other Current Assets 13,023 13,536 21,076 Other Current Liabilities 27,641 27,354 21,216
Total Current Assets: 784,829 768,284 748,034 Total Current Liabilities 156,652 155,012 160,521
Other Assets Other Liabilities and Fund BalanceLimited or Restricted Use Assets * 676 675 9,647 Benefits Payable - Long Term 0 0 0Bond Issuance Costs 4,008 4,035 4,200 Notes Payable - Long Term 272,008 270,878 272,399Trustee Held Funds * 0 0 (0) Due to State of Florida - Long Term 8,465 7,590 3,795Directors/Officers Indemnity Fund * 100 100 100 Malpractice Liability - Long Term 10,742 10,597 10,157Long Term Operating Fund Investments * 0 0 (0) Bonds Payable 382,974 382,964 382,924Other Assets 106,037 105,445 104,899 Other Long Term Liabilities 43,979 43,676 55,867
UnRestricted Fund Balance 712,758 702,281 672,463Restricted Fund Balance 44,583 41,297 39,044
Total Other Assets 110,821 110,255 118,846 Total Other Liabilities & Fund Balance 1,475,509 1,459,283 1,436,648
Property and Equipment:Plant In Use 1,369,743 1,368,416 1,354,987Construction in Process 29,603 27,803 19,166Accumulated Depreciation (704,289) (698,753) (677,527)
Total Property & Equipment (Net) 695,057 697,466 696,626
Restricted Assets 41,453 38,291 33,662
TOTAL ASSETS 1,632,161 1,614,295 1,597,169 TOTAL LIABILITIES AND EQUITY 1,632,161 1,614,295 1,597,169
* Cash and InvestmentsAbove Balance Sheet has been adjusted to eliminate intercompany receivables, payables and investments in subsidiaries
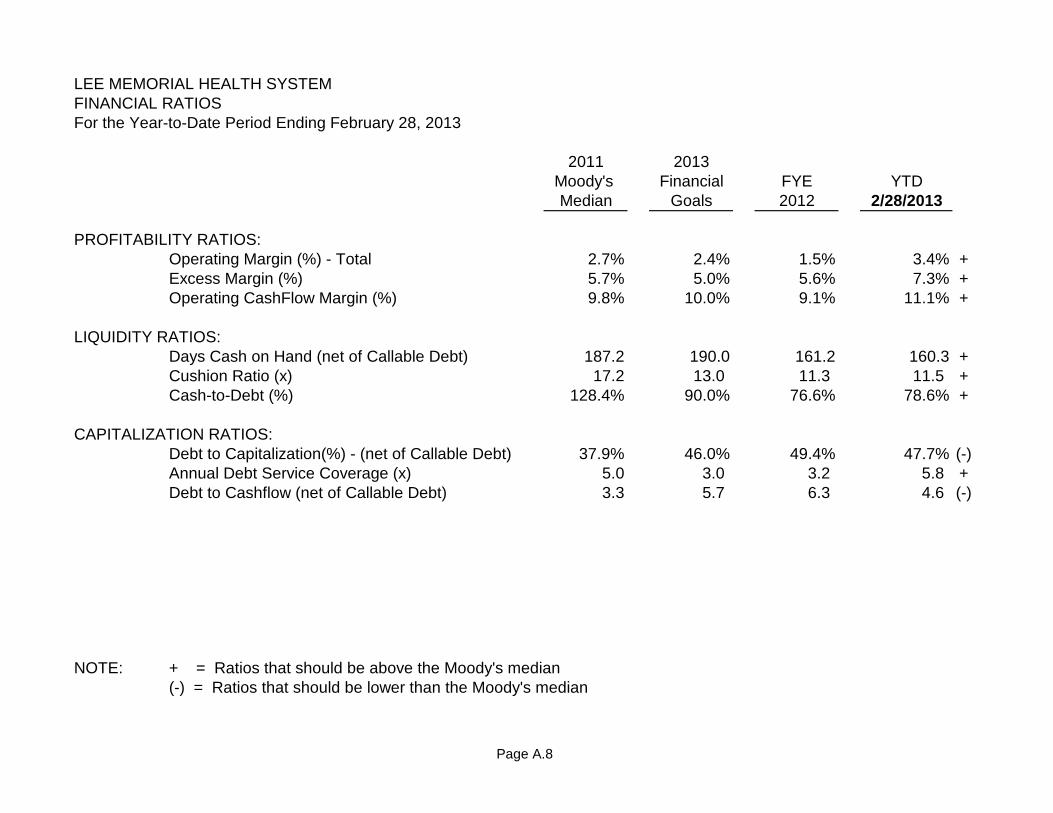
Page A.8
LEE MEMORIAL HEALTH SYSTEMFINANCIAL RATIOSFor the Year-to-Date Period Ending February 28, 2013
2011 2013Moody's Financial FYE YTDMedian Goals 2012 2/28/2013
PROFITABILITY RATIOS:Operating Margin (%) - Total 2.7% 2.4% 1.5% 3.4% +Excess Margin (%) 5.7% 5.0% 5.6% 7.3% +Operating CashFlow Margin (%) 9.8% 10.0% 9.1% 11.1% +
LIQUIDITY RATIOS:Days Cash on Hand (net of Callable Debt) 187.2 190.0 161.2 160.3 +Cushion Ratio (x) 17.2 13.0 11.3 11.5 +Cash-to-Debt (%) 128.4% 90.0% 76.6% 78.6% +
CAPITALIZATION RATIOS:Debt to Capitalization(%) - (net of Callable Debt) 37.9% 46.0% 49.4% 47.7% (-)Annual Debt Service Coverage (x) 5.0 3.0 3.2 5.8 +Debt to Cashflow (net of Callable Debt) 3.3 5.7 6.3 4.6 (-)
NOTE: + = Ratios that should be above the Moody's median(-) = Ratios that should be lower than the Moody's median
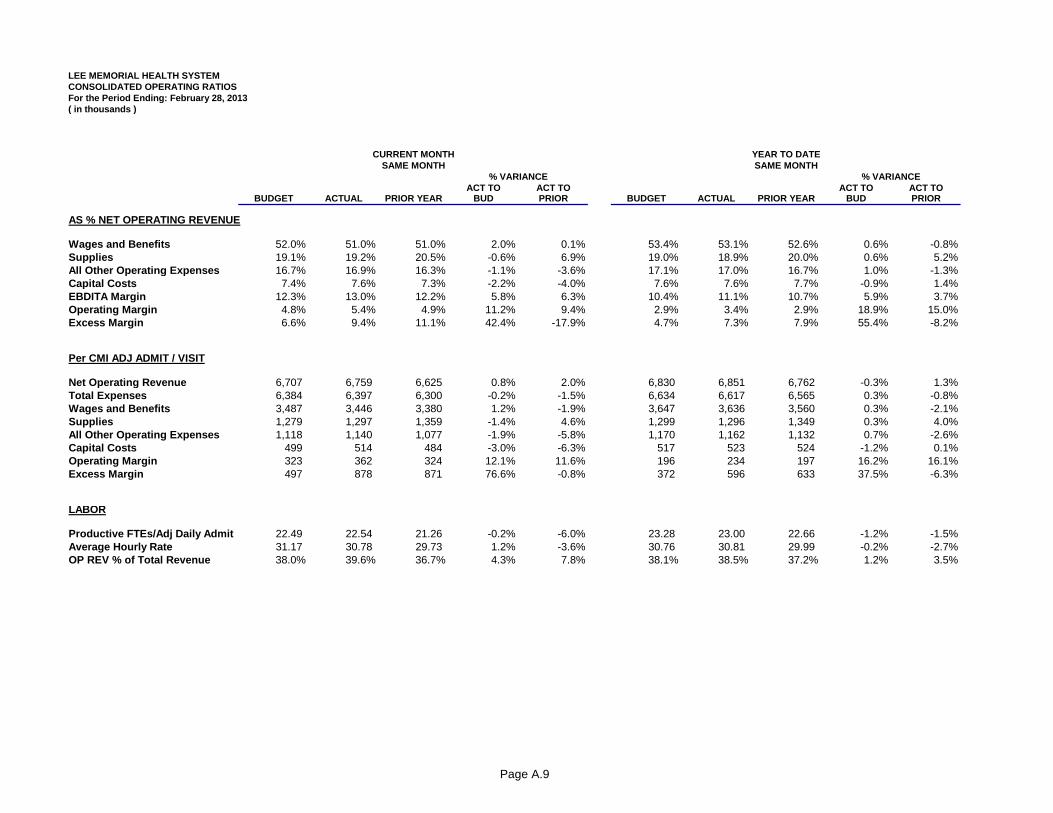
Page A.9
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATED OPERATING RATIOSFor the Period Ending: February 28, 2013( in thousands )
ACT TO ACT TO ACT TO ACT TOBUDGET ACTUAL PRIOR YEAR BUD PRIOR BUDGET ACTUAL PRIOR YEAR BUD PRIOR
AS % NET OPERATING REVENUE
Wages and Benefits 52.0% 51.0% 51.0% 2.0% 0.1% 53.4% 53.1% 52.6% 0.6% -0.8%Supplies 19.1% 19.2% 20.5% -0.6% 6.9% 19.0% 18.9% 20.0% 0.6% 5.2%All Other Operating Expenses 16.7% 16.9% 16.3% -1.1% -3.6% 17.1% 17.0% 16.7% 1.0% -1.3%Capital Costs 7.4% 7.6% 7.3% -2.2% -4.0% 7.6% 7.6% 7.7% -0.9% 1.4%EBDITA Margin 12.3% 13.0% 12.2% 5.8% 6.3% 10.4% 11.1% 10.7% 5.9% 3.7%Operating Margin 4.8% 5.4% 4.9% 11.2% 9.4% 2.9% 3.4% 2.9% 18.9% 15.0%Excess Margin 6.6% 9.4% 11.1% 42.4% -17.9% 4.7% 7.3% 7.9% 55.4% -8.2%
Per CMI ADJ ADMIT / VISIT
Net Operating Revenue 6,707 6,759 6,625 0.8% 2.0% 6,830 6,851 6,762 -0.3% 1.3%Total Expenses 6,384 6,397 6,300 -0.2% -1.5% 6,634 6,617 6,565 0.3% -0.8%Wages and Benefits 3,487 3,446 3,380 1.2% -1.9% 3,647 3,636 3,560 0.3% -2.1%Supplies 1,279 1,297 1,359 -1.4% 4.6% 1,299 1,296 1,349 0.3% 4.0%All Other Operating Expenses 1,118 1,140 1,077 -1.9% -5.8% 1,170 1,162 1,132 0.7% -2.6%Capital Costs 499 514 484 -3.0% -6.3% 517 523 524 -1.2% 0.1%Operating Margin 323 362 324 12.1% 11.6% 196 234 197 16.2% 16.1%Excess Margin 497 878 871 76.6% -0.8% 372 596 633 37.5% -6.3%
LABOR
Productive FTEs/Adj Daily Admit 22.49 22.54 21.26 -0.2% -6.0% 23.28 23.00 22.66 -1.2% -1.5%Average Hourly Rate 31.17 30.78 29.73 1.2% -3.6% 30.76 30.81 29.99 -0.2% -2.7%OP REV % of Total Revenue 38.0% 39.6% 36.7% 4.3% 7.8% 38.1% 38.5% 37.2% 1.2% 3.5%
CURRENT MONTH YEAR TO DATESAME MONTH SAME MONTH
% VARIANCE % VARIANCE
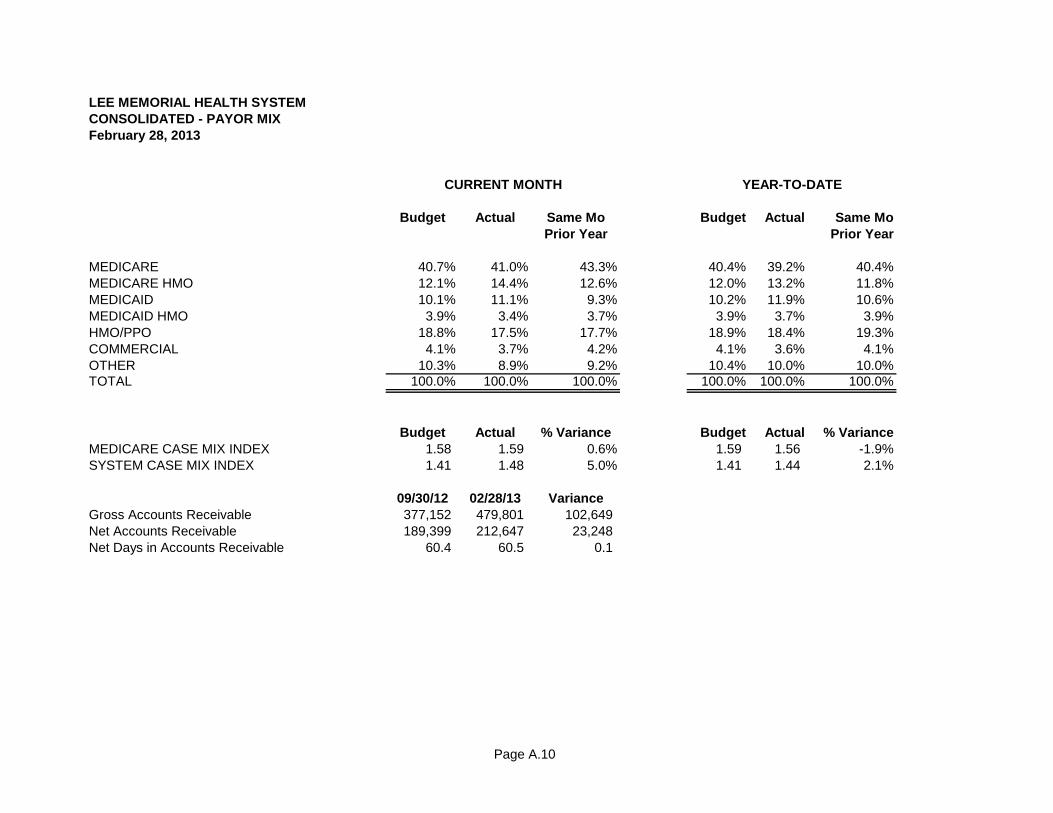
Page A.10
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATED - PAYOR MIXFebruary 28, 2013
Budget Actual Same Mo Budget Actual Same MoPrior Year Prior Year
MEDICARE 40.7% 41.0% 43.3% 40.4% 39.2% 40.4%MEDICARE HMO 12.1% 14.4% 12.6% 12.0% 13.2% 11.8%MEDICAID 10.1% 11.1% 9.3% 10.2% 11.9% 10.6%MEDICAID HMO 3.9% 3.4% 3.7% 3.9% 3.7% 3.9%HMO/PPO 18.8% 17.5% 17.7% 18.9% 18.4% 19.3%COMMERCIAL 4.1% 3.7% 4.2% 4.1% 3.6% 4.1%OTHER 10.3% 8.9% 9.2% 10.4% 10.0% 10.0%TOTAL 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
Budget Actual % Variance Budget Actual % VarianceMEDICARE CASE MIX INDEX 1.58 1.59 0.6% 1.59 1.56 -1.9%SYSTEM CASE MIX INDEX 1.41 1.48 5.0% 1.41 1.44 2.1%
09/30/12 02/28/13 VarianceGross Accounts Receivable 377,152 479,801 102,649 Net Accounts Receivable 189,399 212,647 23,248 Net Days in Accounts Receivable 60.4 60.5 0.1
CURRENT MONTH YEAR-TO-DATE
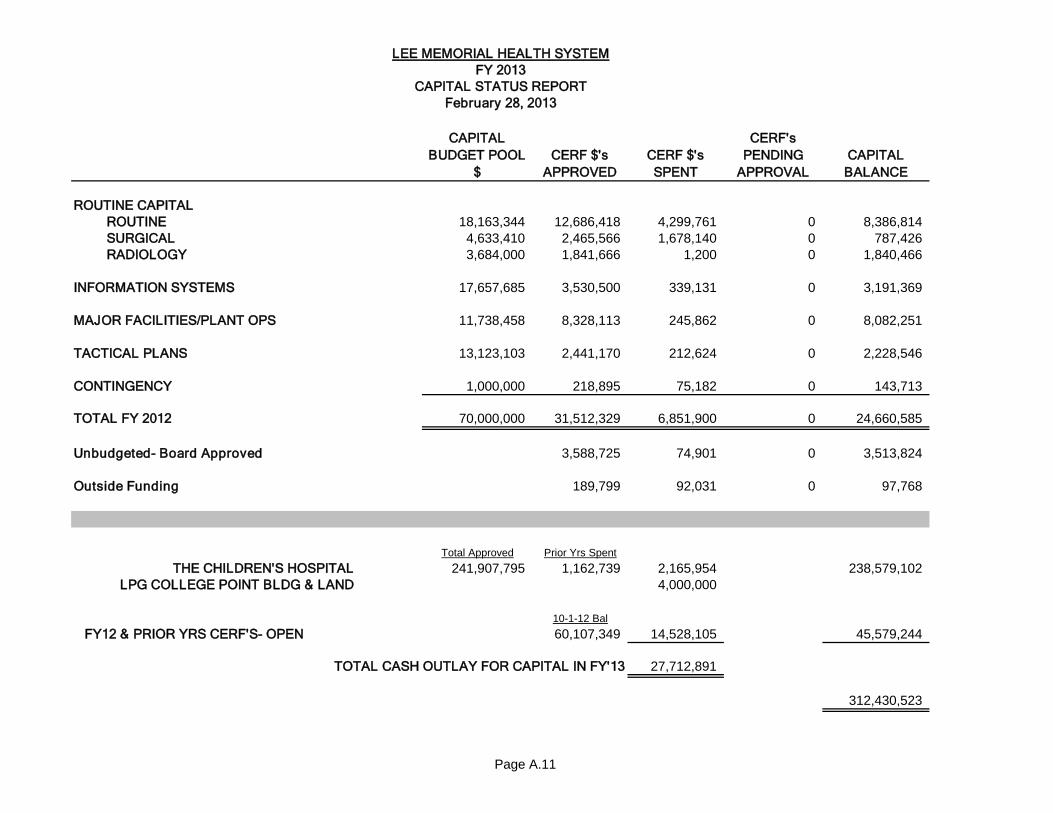
Page A.11
CAPITAL BUDGET POOL
$ CERF $'s
APPROVEDCERF $'s SPENT
CERF's PENDING
APPROVALCAPITAL
BALANCE
ROUTINE CAPITALROUTINE 18,163,344 12,686,418 4,299,761 0 8,386,814SURGICAL 4,633,410 2,465,566 1,678,140 0 787,426RADIOLOGY 3,684,000 1,841,666 1,200 0 1,840,466
INFORMATION SYSTEMS 17,657,685 3,530,500 339,131 0 3,191,369
MAJOR FACILITIES/PLANT OPS 11,738,458 8,328,113 245,862 0 8,082,251
TACTICAL PLANS 13,123,103 2,441,170 212,624 0 2,228,546
CONTINGENCY 1,000,000 218,895 75,182 0 143,713
TOTAL FY 2012 70,000,000 31,512,329 6,851,900 0 24,660,585
Unbudgeted- Board Approved 3,588,725 74,901 0 3,513,824
Outside Funding 189,799 92,031 0 97,768
Total Approved Prior Yrs Spent
THE CHILDREN'S HOSPITAL 241,907,795 1,162,739 2,165,954 238,579,102LPG COLLEGE POINT BLDG & LAND 4,000,000
10-1-12 Bal
FY12 & PRIOR YRS CERF'S- OPEN 60,107,349 14,528,105 45,579,244
27,712,891
312,430,523
TOTAL CASH OUTLAY FOR CAPITAL IN FY'13
LEE MEMORIAL HEALTH SYSTEMFY 2013
CAPITAL STATUS REPORTFebruary 28, 2013
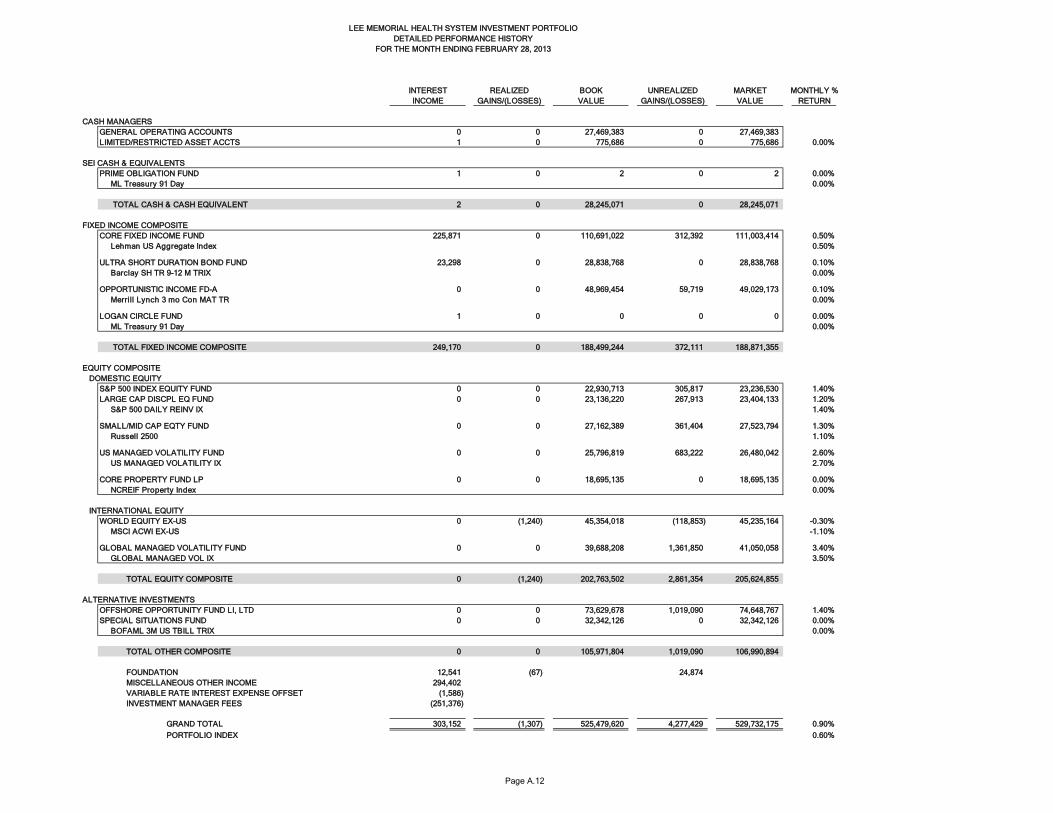
Page A.12
INTEREST REALIZED BOOK UNREALIZED MARKET MONTHLY %INCOME GAINS/(LOSSES) VALUE GAINS/(LOSSES) VALUE RETURN
CASH MANAGERSGENERAL OPERATING ACCOUNTS 0 0 27,469,383 0 27,469,383LIMITED/RESTRICTED ASSET ACCTS 1 0 775,686 0 775,686 0.00%
SEI CASH & EQUIVALENTSPRIME OBLIGATION FUND 1 0 2 0 2 0.00% ML Treasury 91 Day 0.00%
TOTAL CASH & CASH EQUIVALENT 2 0 28,245,071 0 28,245,071
FIXED INCOME COMPOSITECORE FIXED INCOME FUND 0.353 225,871 0 110,691,022 312,392 111,003,414 0.50% Lehman US Aggregate Index 0.50%
ULTRA SHORT DURATION BOND FUND 0.093 23,298 0 28,838,768 0 28,838,768 0.10% Barclay SH TR 9-12 M TRIX 0.00%
OPPORTUNISTIC INCOME FD-A 0.257 0 0 48,969,454 59,719 49,029,173 0.10% Merrill Lynch 3 mo Con MAT TR 0.00%
LOGAN CIRCLE FUND 0.257 1 0 0 0 0 0.00% ML Treasury 91 Day 0.00%
TOTAL FIXED INCOME COMPOSITE 249,170 0 188,499,244 372,111 188,871,355
EQUITY COMPOSITE DOMESTIC EQUITY
S&P 500 INDEX EQUITY FUND 0 0 22,930,713 305,817 23,236,530 1.40%LARGE CAP DISCPL EQ FUND 23.4% 0 0 23,136,220 267,913 23,404,133 1.20% S&P 500 DAILY REINV IX 1.40%
SMALL/MID CAP EQTY FUND 6.5% 0 0 27,162,389 361,404 27,523,794 1.30% Russell 2500 1.10%
US MANAGED VOLATILITY FUND 0 0 25,796,819 683,222 26,480,042 2.60% US MANAGED VOLATILITY IX 2.70%
CORE PROPERTY FUND LP 0 0 18,695,135 0 18,695,135 0.00% NCREIF Property Index 0.00%
INTERNATIONAL EQUITYWORLD EQUITY EX-US 0 (1,240) 45,354,018 (118,853) 45,235,164 -0.30% MSCI ACWI EX-US -1.10%
GLOBAL MANAGED VOLATILITY FUND 0 0 39,688,208 1,361,850 41,050,058 3.40% GLOBAL MANAGED VOL IX 3.50%
TOTAL EQUITY COMPOSITE 0 (1,240) 202,763,502 2,861,354 205,624,855
ALTERNATIVE INVESTMENTSOFFSHORE OPPORTUNITY FUND LI, LTD 0 0 73,629,678 1,019,090 74,648,767 1.40%SPECIAL SITUATIONS FUND 0 0 32,342,126 0 32,342,126 0.00% BOFAML 3M US TBILL TRIX 0.00%
TOTAL OTHER COMPOSITE 0 0 105,971,804 1,019,090 106,990,894
FOUNDATION 12,541 (67) 24,874 MISCELLANEOUS OTHER INCOME 294,402 VARIABLE RATE INTEREST EXPENSE OFFSET (1,586) INVESTMENT MANAGER FEES (251,376)
GRAND TOTAL 303,152 (1,307) 525,479,620 4,277,429 529,732,175 0.90%PORTFOLIO INDEX 0.60%
LEE MEMORIAL HEALTH SYSTEM INVESTMENT PORTFOLIODETAILED PERFORMANCE HISTORY
FOR THE MONTH ENDING FEBRUARY 28, 2013
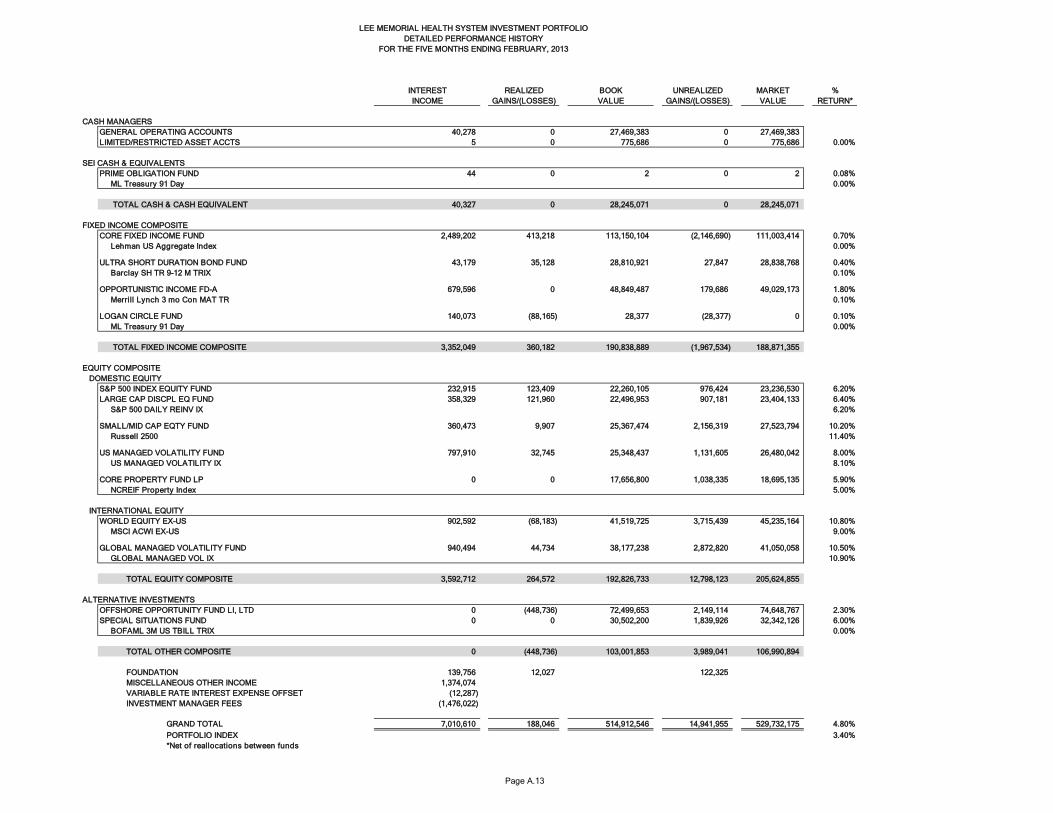
Page A.13
INTEREST REALIZED BOOK UNREALIZED MARKET %INCOME GAINS/(LOSSES) VALUE GAINS/(LOSSES) VALUE RETURN*
CASH MANAGERSGENERAL OPERATING ACCOUNTS 40,278 0 27,469,383 0 27,469,383LIMITED/RESTRICTED ASSET ACCTS 5 0 775,686 0 775,686 0.00%
SEI CASH & EQUIVALENTSPRIME OBLIGATION FUND 44 0 2 0 2 0.08% ML Treasury 91 Day 0.00%
TOTAL CASH & CASH EQUIVALENT 40,327 0 28,245,071 0 28,245,071
FIXED INCOME COMPOSITECORE FIXED INCOME FUND 2,489,202 413,218 113,150,104 (2,146,690) 111,003,414 0.70% Lehman US Aggregate Index 0.00%
ULTRA SHORT DURATION BOND FUND 43,179 35,128 28,810,921 27,847 28,838,768 0.40% Barclay SH TR 9-12 M TRIX 0.10%
OPPORTUNISTIC INCOME FD-A 679,596 0 48,849,487 179,686 49,029,173 1.80% Merrill Lynch 3 mo Con MAT TR 0.10%
LOGAN CIRCLE FUND 140,073 (88,165) 28,377 (28,377) 0 0.10% ML Treasury 91 Day 0.00%
TOTAL FIXED INCOME COMPOSITE 3,352,049 360,182 190,838,889 (1,967,534) 188,871,355
EQUITY COMPOSITE DOMESTIC EQUITY
S&P 500 INDEX EQUITY FUND 232,915 123,409 22,260,105 976,424 23,236,530 6.20%LARGE CAP DISCPL EQ FUND 358,329 121,960 22,496,953 907,181 23,404,133 6.40% S&P 500 DAILY REINV IX 6.20%
SMALL/MID CAP EQTY FUND 360,473 9,907 25,367,474 2,156,319 27,523,794 10.20% Russell 2500 11.40%
US MANAGED VOLATILITY FUND 797,910 32,745 25,348,437 1,131,605 26,480,042 8.00% US MANAGED VOLATILITY IX 8.10%
CORE PROPERTY FUND LP 0 0 17,656,800 1,038,335 18,695,135 5.90% NCREIF Property Index 5.00%
INTERNATIONAL EQUITYWORLD EQUITY EX-US 902,592 (68,183) 41,519,725 3,715,439 45,235,164 10.80% MSCI ACWI EX-US 9.00%
GLOBAL MANAGED VOLATILITY FUND 940,494 44,734 38,177,238 2,872,820 41,050,058 10.50% GLOBAL MANAGED VOL IX 10.90%
TOTAL EQUITY COMPOSITE 3,592,712 264,572 192,826,733 12,798,123 205,624,855
ALTERNATIVE INVESTMENTSOFFSHORE OPPORTUNITY FUND LI, LTD 0 (448,736) 72,499,653 2,149,114 74,648,767 2.30%SPECIAL SITUATIONS FUND 0 0 30,502,200 1,839,926 32,342,126 6.00% BOFAML 3M US TBILL TRIX 0.00%
TOTAL OTHER COMPOSITE 0 (448,736) 103,001,853 3,989,041 106,990,894
FOUNDATION 139,756 12,027 122,325 MISCELLANEOUS OTHER INCOME 1,374,074 VARIABLE RATE INTEREST EXPENSE OFFSET (12,287) INVESTMENT MANAGER FEES (1,476,022)
GRAND TOTAL 7,010,610 188,046 514,912,546 14,941,955 529,732,175 4.80%PORTFOLIO INDEX 3.40%*Net of reallocations between funds
LEE MEMORIAL HEALTH SYSTEM INVESTMENT PORTFOLIODETAILED PERFORMANCE HISTORY
FOR THE FIVE MONTHS ENDING FEBRUARY, 2013
LEE MEMORIAL HEALTH SYSTEM CONSOLIDATED FINANCIAL STATEMENTS & STATISTICAL REPORTS TABLE OF CONTENTS SECTION B PAGE CONSOLIDATING SCHEDULES CONSOLIDATING STATISTICAL REPORT B.1 CONSOLIDATING INCOME STATEMENT – MONTH B.7 YTD B.10 CONSOLIDATING FINANCIAL RATIOS B.13 STAFFING SUMMARY B.17 SUMMARY OF ACCOUNTS RECEIVABLE B.18
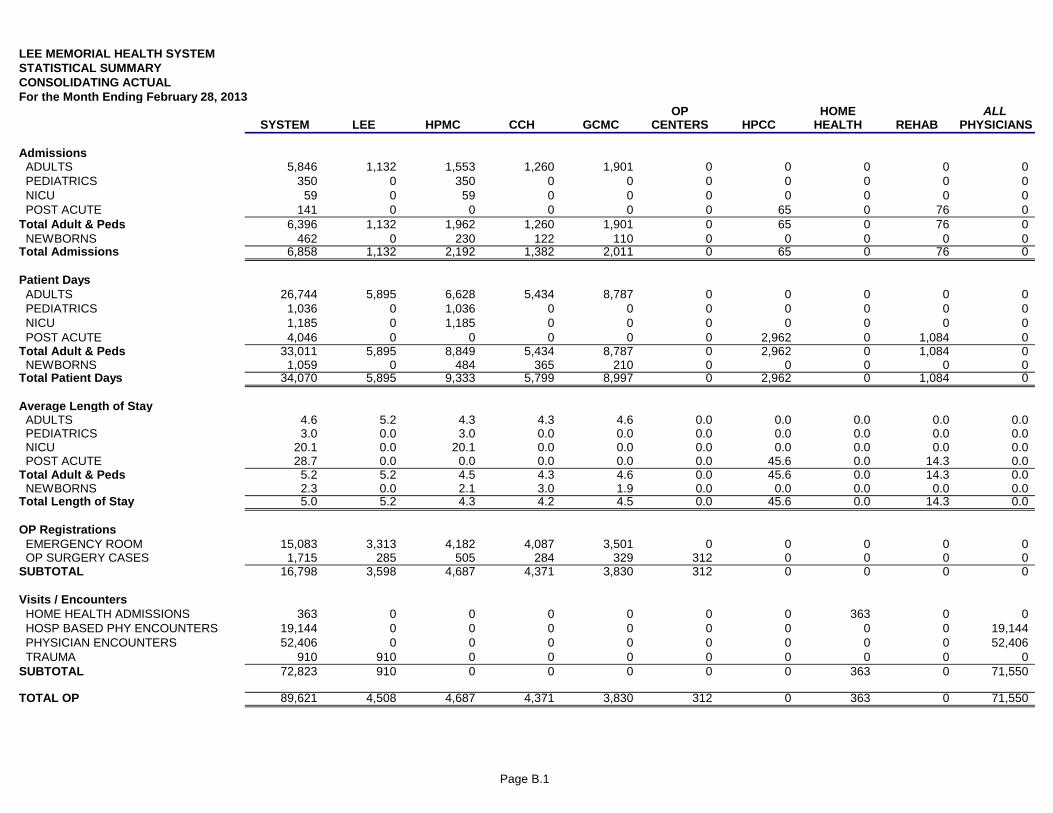
Page B.1
LEE MEMORIAL HEALTH SYSTEMSTATISTICAL SUMMARYCONSOLIDATING ACTUALFor the Month Ending February 28, 2013
OP HOME ALLSYSTEM LEE HPMC CCH GCMC CENTERS HPCC HEALTH REHAB PHYSICIANS
Admissions ADULTS 5,846 1,132 1,553 1,260 1,901 0 0 0 0 0 PEDIATRICS 350 0 350 0 0 0 0 0 0 0 NICU 59 0 59 0 0 0 0 0 0 0 POST ACUTE 141 0 0 0 0 0 65 0 76 0Total Adult & Peds 6,396 1,132 1,962 1,260 1,901 0 65 0 76 0 NEWBORNS 462 0 230 122 110 0 0 0 0 0Total Admissions 6,858 1,132 2,192 1,382 2,011 0 65 0 76 0
Patient Days ADULTS 26,744 5,895 6,628 5,434 8,787 0 0 0 0 0 PEDIATRICS 1,036 0 1,036 0 0 0 0 0 0 0 NICU 1,185 0 1,185 0 0 0 0 0 0 0 POST ACUTE 4,046 0 0 0 0 0 2,962 0 1,084 0Total Adult & Peds 33,011 5,895 8,849 5,434 8,787 0 2,962 0 1,084 0 NEWBORNS 1,059 0 484 365 210 0 0 0 0 0Total Patient Days 34,070 5,895 9,333 5,799 8,997 0 2,962 0 1,084 0
Average Length of Stay ADULTS 4.6 5.2 4.3 4.3 4.6 0.0 0.0 0.0 0.0 0.0 PEDIATRICS 3.0 0.0 3.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 NICU 20.1 0.0 20.1 0.0 0.0 0.0 0.0 0.0 0.0 0.0 POST ACUTE 28.7 0.0 0.0 0.0 0.0 0.0 45.6 0.0 14.3 0.0Total Adult & Peds 5.2 5.2 4.5 4.3 4.6 0.0 45.6 0.0 14.3 0.0 NEWBORNS 2.3 0.0 2.1 3.0 1.9 0.0 0.0 0.0 0.0 0.0Total Length of Stay 5.0 5.2 4.3 4.2 4.5 0.0 45.6 0.0 14.3 0.0
OP Registrations EMERGENCY ROOM 15,083 3,313 4,182 4,087 3,501 0 0 0 0 0 OP SURGERY CASES 1,715 285 505 284 329 312 0 0 0 0SUBTOTAL 16,798 3,598 4,687 4,371 3,830 312 0 0 0 0
Visits / Encounters HOME HEALTH ADMISSIONS 363 0 0 0 0 0 0 363 0 0 HOSP BASED PHY ENCOUNTERS 19,144 0 0 0 0 0 0 0 0 19,144 PHYSICIAN ENCOUNTERS 52,406 0 0 0 0 0 0 0 0 52,406 TRAUMA 910 910 0 0 0 0 0 0 0 0SUBTOTAL 72,823 910 0 0 0 0 0 363 0 71,550
TOTAL OP 89,621 4,508 4,687 4,371 3,830 312 0 363 0 71,550
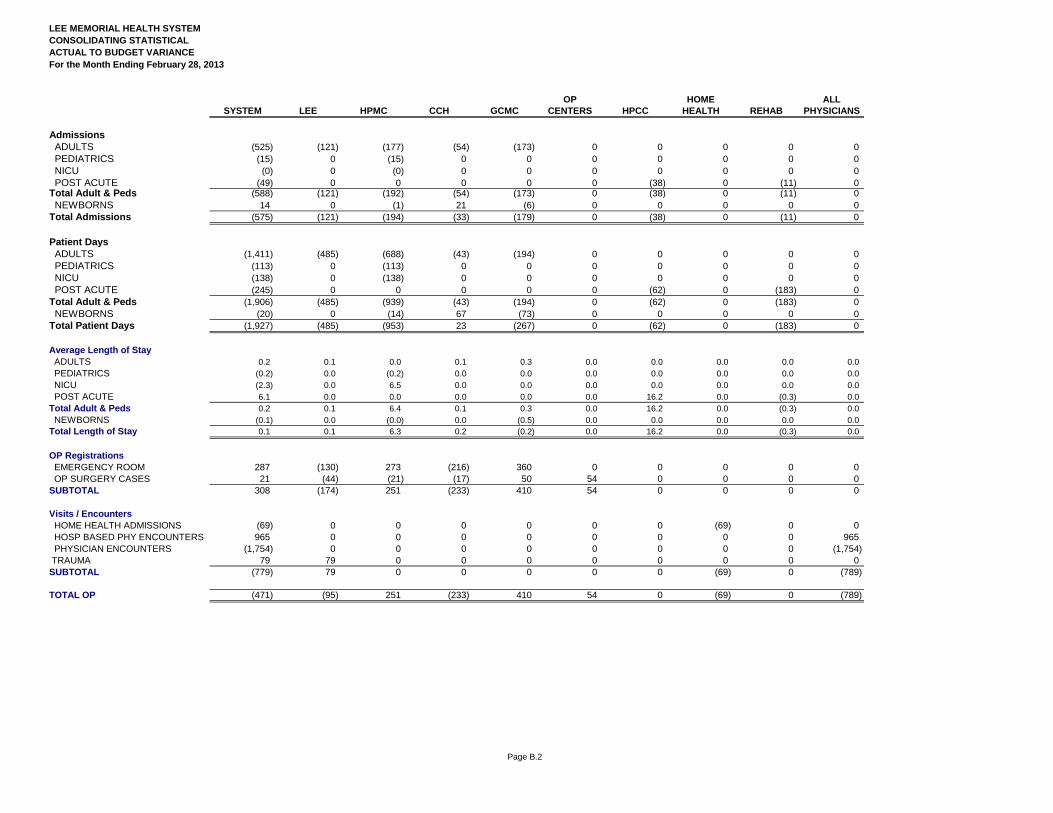
Page B.2
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATING STATISTICALACTUAL TO BUDGET VARIANCEFor the Month Ending February 28, 2013
OP HOME ALLSYSTEM LEE HPMC CCH GCMC CENTERS HPCC HEALTH REHAB PHYSICIANS
Admissions ADULTS (525) (121) (177) (54) (173) 0 0 0 0 0 PEDIATRICS (15) 0 (15) 0 0 0 0 0 0 0 NICU (0) 0 (0) 0 0 0 0 0 0 0 POST ACUTE (49) 0 0 0 0 0 (38) 0 (11) 0Total Adult & Peds (588) (121) (192) (54) (173) 0 (38) 0 (11) 0 NEWBORNS 14 0 (1) 21 (6) 0 0 0 0 0Total Admissions (575) (121) (194) (33) (179) 0 (38) 0 (11) 0
Patient Days ADULTS (1,411) (485) (688) (43) (194) 0 0 0 0 0 PEDIATRICS (113) 0 (113) 0 0 0 0 0 0 0 NICU (138) 0 (138) 0 0 0 0 0 0 0 POST ACUTE (245) 0 0 0 0 0 (62) 0 (183) 0Total Adult & Peds (1,906) (485) (939) (43) (194) 0 (62) 0 (183) 0 NEWBORNS (20) 0 (14) 67 (73) 0 0 0 0 0Total Patient Days (1,927) (485) (953) 23 (267) 0 (62) 0 (183) 0
Average Length of Stay ADULTS 0.2 0.1 0.0 0.1 0.3 0.0 0.0 0.0 0.0 0.0 PEDIATRICS (0.2) 0.0 (0.2) 0.0 0.0 0.0 0.0 0.0 0.0 0.0 NICU (2.3) 0.0 6.5 0.0 0.0 0.0 0.0 0.0 0.0 0.0 POST ACUTE 6.1 0.0 0.0 0.0 0.0 0.0 16.2 0.0 (0.3) 0.0Total Adult & Peds 0.2 0.1 6.4 0.1 0.3 0.0 16.2 0.0 (0.3) 0.0 NEWBORNS (0.1) 0.0 (0.0) 0.0 (0.5) 0.0 0.0 0.0 0.0 0.0Total Length of Stay 0.1 0.1 6.3 0.2 (0.2) 0.0 16.2 0.0 (0.3) 0.0
OP Registrations EMERGENCY ROOM 287 (130) 273 (216) 360 0 0 0 0 0 OP SURGERY CASES 21 (44) (21) (17) 50 54 0 0 0 0SUBTOTAL 308 (174) 251 (233) 410 54 0 0 0 0
Visits / Encounters HOME HEALTH ADMISSIONS (69) 0 0 0 0 0 0 (69) 0 0 HOSP BASED PHY ENCOUNTERS 965 0 0 0 0 0 0 0 0 965 PHYSICIAN ENCOUNTERS (1,754) 0 0 0 0 0 0 0 0 (1,754) TRAUMA 79 79 0 0 0 0 0 0 0 0SUBTOTAL (779) 79 0 0 0 0 0 (69) 0 (789)
TOTAL OP (471) (95) 251 (233) 410 54 0 (69) 0 (789)
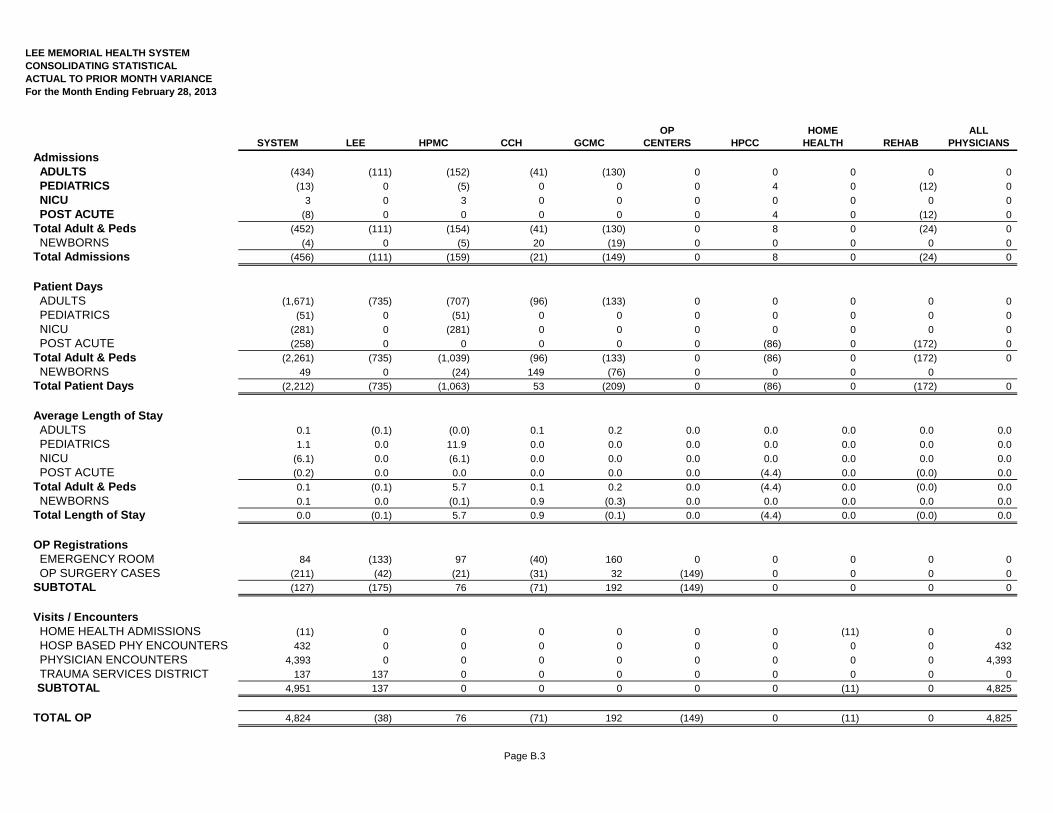
Page B.3
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATING STATISTICALACTUAL TO PRIOR MONTH VARIANCEFor the Month Ending February 28, 2013
OP HOME ALLSYSTEM LEE HPMC CCH GCMC CENTERS HPCC HEALTH REHAB PHYSICIANS
Admissions ADULTS (434) (111) (152) (41) (130) 0 0 0 0 0
PEDIATRICS (13) 0 (5) 0 0 0 4 0 (12) 0
NICU 3 0 3 0 0 0 0 0 0 0
POST ACUTE (8) 0 0 0 0 0 4 0 (12) 0
Total Adult & Peds (452) (111) (154) (41) (130) 0 8 0 (24) 0
NEWBORNS (4) 0 (5) 20 (19) 0 0 0 0 0
Total Admissions (456) (111) (159) (21) (149) 0 8 0 (24) 0
Patient Days ADULTS (1,671) (735) (707) (96) (133) 0 0 0 0 0
PEDIATRICS (51) 0 (51) 0 0 0 0 0 0 0
NICU (281) 0 (281) 0 0 0 0 0 0 0
POST ACUTE (258) 0 0 0 0 0 (86) 0 (172) 0
Total Adult & Peds (2,261) (735) (1,039) (96) (133) 0 (86) 0 (172) 0
NEWBORNS 49 0 (24) 149 (76) 0 0 0 0
Total Patient Days (2,212) (735) (1,063) 53 (209) 0 (86) 0 (172) 0
Average Length of Stay ADULTS 0.1 (0.1) (0.0) 0.1 0.2 0.0 0.0 0.0 0.0 0.0
PEDIATRICS 1.1 0.0 11.9 0.0 0.0 0.0 0.0 0.0 0.0 0.0
NICU (6.1) 0.0 (6.1) 0.0 0.0 0.0 0.0 0.0 0.0 0.0
POST ACUTE (0.2) 0.0 0.0 0.0 0.0 0.0 (4.4) 0.0 (0.0) 0.0
Total Adult & Peds 0.1 (0.1) 5.7 0.1 0.2 0.0 (4.4) 0.0 (0.0) 0.0
NEWBORNS 0.1 0.0 (0.1) 0.9 (0.3) 0.0 0.0 0.0 0.0 0.0
Total Length of Stay 0.0 (0.1) 5.7 0.9 (0.1) 0.0 (4.4) 0.0 (0.0) 0.0
OP Registrations EMERGENCY ROOM 84 (133) 97 (40) 160 0 0 0 0 0
OP SURGERY CASES (211) (42) (21) (31) 32 (149) 0 0 0 0
SUBTOTAL (127) (175) 76 (71) 192 (149) 0 0 0 0
Visits / Encounters HOME HEALTH ADMISSIONS (11) 0 0 0 0 0 0 (11) 0 0
HOSP BASED PHY ENCOUNTERS 432 0 0 0 0 0 0 0 0 432
PHYSICIAN ENCOUNTERS 4,393 0 0 0 0 0 0 0 0 4,393
TRAUMA SERVICES DISTRICT 137 137 0 0 0 0 0 0 0 0
SUBTOTAL 4,951 137 0 0 0 0 0 (11) 0 4,825
TOTAL OP 4,824 (38) 76 (71) 192 (149) 0 (11) 0 4,825
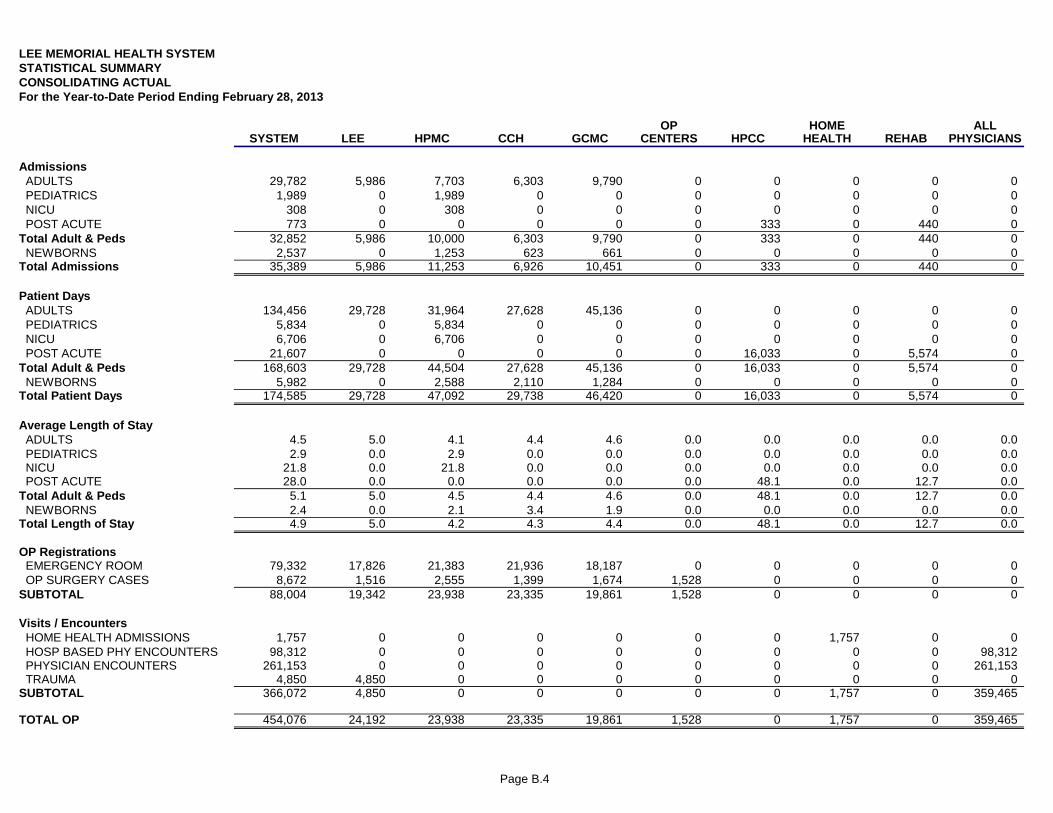
Page B.4
LEE MEMORIAL HEALTH SYSTEMSTATISTICAL SUMMARYCONSOLIDATING ACTUALFor the Year-to-Date Period Ending February 28, 2013
OP HOME ALLSYSTEM LEE HPMC CCH GCMC CENTERS HPCC HEALTH REHAB PHYSICIANS
Admissions ADULTS 29,782 5,986 7,703 6,303 9,790 0 0 0 0 0 PEDIATRICS 1,989 0 1,989 0 0 0 0 0 0 0 NICU 308 0 308 0 0 0 0 0 0 0 POST ACUTE 773 0 0 0 0 0 333 0 440 0Total Adult & Peds 32,852 5,986 10,000 6,303 9,790 0 333 0 440 0 NEWBORNS 2,537 0 1,253 623 661 0 0 0 0 0Total Admissions 35,389 5,986 11,253 6,926 10,451 0 333 0 440 0
Patient Days ADULTS 134,456 29,728 31,964 27,628 45,136 0 0 0 0 0 PEDIATRICS 5,834 0 5,834 0 0 0 0 0 0 0 NICU 6,706 0 6,706 0 0 0 0 0 0 0 POST ACUTE 21,607 0 0 0 0 0 16,033 0 5,574 0Total Adult & Peds 168,603 29,728 44,504 27,628 45,136 0 16,033 0 5,574 0 NEWBORNS 5,982 0 2,588 2,110 1,284 0 0 0 0 0Total Patient Days 174,585 29,728 47,092 29,738 46,420 0 16,033 0 5,574 0
Average Length of Stay ADULTS 4.5 5.0 4.1 4.4 4.6 0.0 0.0 0.0 0.0 0.0 PEDIATRICS 2.9 0.0 2.9 0.0 0.0 0.0 0.0 0.0 0.0 0.0 NICU 21.8 0.0 21.8 0.0 0.0 0.0 0.0 0.0 0.0 0.0 POST ACUTE 28.0 0.0 0.0 0.0 0.0 0.0 48.1 0.0 12.7 0.0Total Adult & Peds 5.1 5.0 4.5 4.4 4.6 0.0 48.1 0.0 12.7 0.0 NEWBORNS 2.4 0.0 2.1 3.4 1.9 0.0 0.0 0.0 0.0 0.0Total Length of Stay 4.9 5.0 4.2 4.3 4.4 0.0 48.1 0.0 12.7 0.0
OP Registrations EMERGENCY ROOM 79,332 17,826 21,383 21,936 18,187 0 0 0 0 0 OP SURGERY CASES 8,672 1,516 2,555 1,399 1,674 1,528 0 0 0 0SUBTOTAL 88,004 19,342 23,938 23,335 19,861 1,528 0 0 0 0
Visits / Encounters HOME HEALTH ADMISSIONS 1,757 0 0 0 0 0 0 1,757 0 0 HOSP BASED PHY ENCOUNTERS 98,312 0 0 0 0 0 0 0 0 98,312 PHYSICIAN ENCOUNTERS 261,153 0 0 0 0 0 0 0 0 261,153 TRAUMA 4,850 4,850 0 0 0 0 0 0 0 0SUBTOTAL 366,072 4,850 0 0 0 0 0 1,757 0 359,465
TOTAL OP 454,076 24,192 23,938 23,335 19,861 1,528 0 1,757 0 359,465
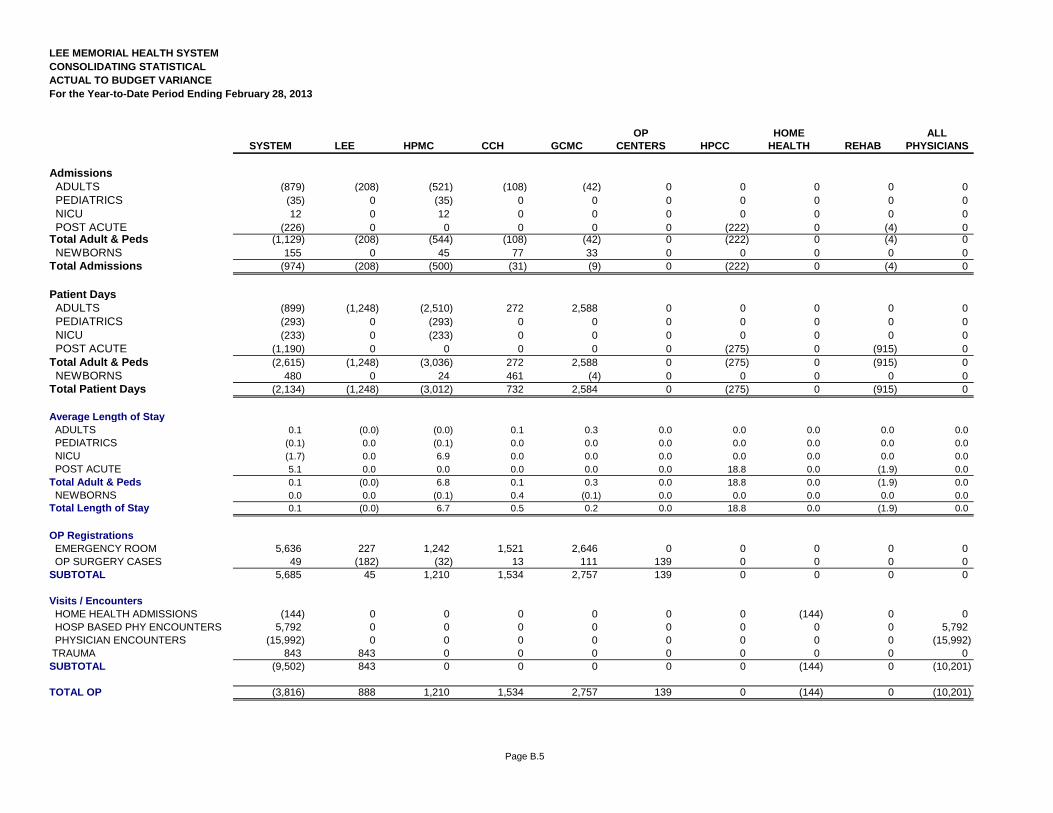
Page B.5
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATING STATISTICALACTUAL TO BUDGET VARIANCEFor the Year-to-Date Period Ending February 28, 2013
OP HOME ALLSYSTEM LEE HPMC CCH GCMC CENTERS HPCC HEALTH REHAB PHYSICIANS
Admissions ADULTS (879) (208) (521) (108) (42) 0 0 0 0 0 PEDIATRICS (35) 0 (35) 0 0 0 0 0 0 0 NICU 12 0 12 0 0 0 0 0 0 0 POST ACUTE (226) 0 0 0 0 0 (222) 0 (4) 0Total Adult & Peds (1,129) (208) (544) (108) (42) 0 (222) 0 (4) 0 NEWBORNS 155 0 45 77 33 0 0 0 0 0Total Admissions (974) (208) (500) (31) (9) 0 (222) 0 (4) 0
Patient Days ADULTS (899) (1,248) (2,510) 272 2,588 0 0 0 0 0 PEDIATRICS (293) 0 (293) 0 0 0 0 0 0 0 NICU (233) 0 (233) 0 0 0 0 0 0 0 POST ACUTE (1,190) 0 0 0 0 0 (275) 0 (915) 0Total Adult & Peds (2,615) (1,248) (3,036) 272 2,588 0 (275) 0 (915) 0 NEWBORNS 480 0 24 461 (4) 0 0 0 0 0Total Patient Days (2,134) (1,248) (3,012) 732 2,584 0 (275) 0 (915) 0
Average Length of Stay ADULTS 0.1 (0.0) (0.0) 0.1 0.3 0.0 0.0 0.0 0.0 0.0 PEDIATRICS (0.1) 0.0 (0.1) 0.0 0.0 0.0 0.0 0.0 0.0 0.0 NICU (1.7) 0.0 6.9 0.0 0.0 0.0 0.0 0.0 0.0 0.0 POST ACUTE 5.1 0.0 0.0 0.0 0.0 0.0 18.8 0.0 (1.9) 0.0Total Adult & Peds 0.1 (0.0) 6.8 0.1 0.3 0.0 18.8 0.0 (1.9) 0.0 NEWBORNS 0.0 0.0 (0.1) 0.4 (0.1) 0.0 0.0 0.0 0.0 0.0Total Length of Stay 0.1 (0.0) 6.7 0.5 0.2 0.0 18.8 0.0 (1.9) 0.0
OP Registrations EMERGENCY ROOM 5,636 227 1,242 1,521 2,646 0 0 0 0 0 OP SURGERY CASES 49 (182) (32) 13 111 139 0 0 0 0SUBTOTAL 5,685 45 1,210 1,534 2,757 139 0 0 0 0
Visits / Encounters HOME HEALTH ADMISSIONS (144) 0 0 0 0 0 0 (144) 0 0 HOSP BASED PHY ENCOUNTERS 5,792 0 0 0 0 0 0 0 0 5,792 PHYSICIAN ENCOUNTERS (15,992) 0 0 0 0 0 0 0 0 (15,992) TRAUMA 843 843 0 0 0 0 0 0 0 0SUBTOTAL (9,502) 843 0 0 0 0 0 (144) 0 (10,201)
TOTAL OP (3,816) 888 1,210 1,534 2,757 139 0 (144) 0 (10,201)
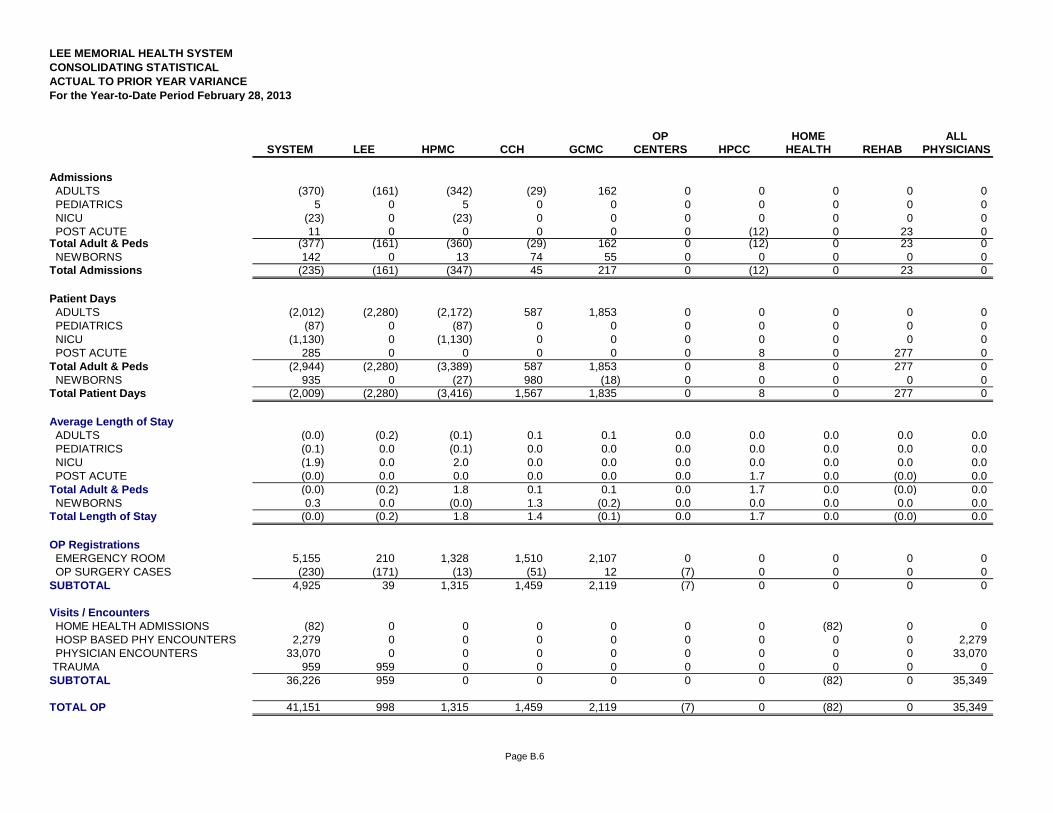
Page B.6
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATING STATISTICALACTUAL TO PRIOR YEAR VARIANCEFor the Year-to-Date Period February 28, 2013
OP HOME ALLSYSTEM LEE HPMC CCH GCMC CENTERS HPCC HEALTH REHAB PHYSICIANS
Admissions ADULTS (370) (161) (342) (29) 162 0 0 0 0 0 PEDIATRICS 5 0 5 0 0 0 0 0 0 0 NICU (23) 0 (23) 0 0 0 0 0 0 0 POST ACUTE 11 0 0 0 0 0 (12) 0 23 0Total Adult & Peds (377) (161) (360) (29) 162 0 (12) 0 23 0 NEWBORNS 142 0 13 74 55 0 0 0 0 0Total Admissions (235) (161) (347) 45 217 0 (12) 0 23 0
Patient Days ADULTS (2,012) (2,280) (2,172) 587 1,853 0 0 0 0 0 PEDIATRICS (87) 0 (87) 0 0 0 0 0 0 0 NICU (1,130) 0 (1,130) 0 0 0 0 0 0 0 POST ACUTE 285 0 0 0 0 0 8 0 277 0Total Adult & Peds (2,944) (2,280) (3,389) 587 1,853 0 8 0 277 0 NEWBORNS 935 0 (27) 980 (18) 0 0 0 0 0Total Patient Days (2,009) (2,280) (3,416) 1,567 1,835 0 8 0 277 0
Average Length of Stay ADULTS (0.0) (0.2) (0.1) 0.1 0.1 0.0 0.0 0.0 0.0 0.0 PEDIATRICS (0.1) 0.0 (0.1) 0.0 0.0 0.0 0.0 0.0 0.0 0.0 NICU (1.9) 0.0 2.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 POST ACUTE (0.0) 0.0 0.0 0.0 0.0 0.0 1.7 0.0 (0.0) 0.0Total Adult & Peds (0.0) (0.2) 1.8 0.1 0.1 0.0 1.7 0.0 (0.0) 0.0 NEWBORNS 0.3 0.0 (0.0) 1.3 (0.2) 0.0 0.0 0.0 0.0 0.0Total Length of Stay (0.0) (0.2) 1.8 1.4 (0.1) 0.0 1.7 0.0 (0.0) 0.0
OP Registrations EMERGENCY ROOM 5,155 210 1,328 1,510 2,107 0 0 0 0 0 OP SURGERY CASES (230) (171) (13) (51) 12 (7) 0 0 0 0SUBTOTAL 4,925 39 1,315 1,459 2,119 (7) 0 0 0 0
Visits / Encounters HOME HEALTH ADMISSIONS (82) 0 0 0 0 0 0 (82) 0 0 HOSP BASED PHY ENCOUNTERS 2,279 0 0 0 0 0 0 0 0 2,279 PHYSICIAN ENCOUNTERS 33,070 0 0 0 0 0 0 0 0 33,070 TRAUMA 959 959 0 0 0 0 0 0 0 0SUBTOTAL 36,226 959 0 0 0 0 0 (82) 0 35,349
TOTAL OP 41,151 998 1,315 1,459 2,119 (7) 0 (82) 0 35,349
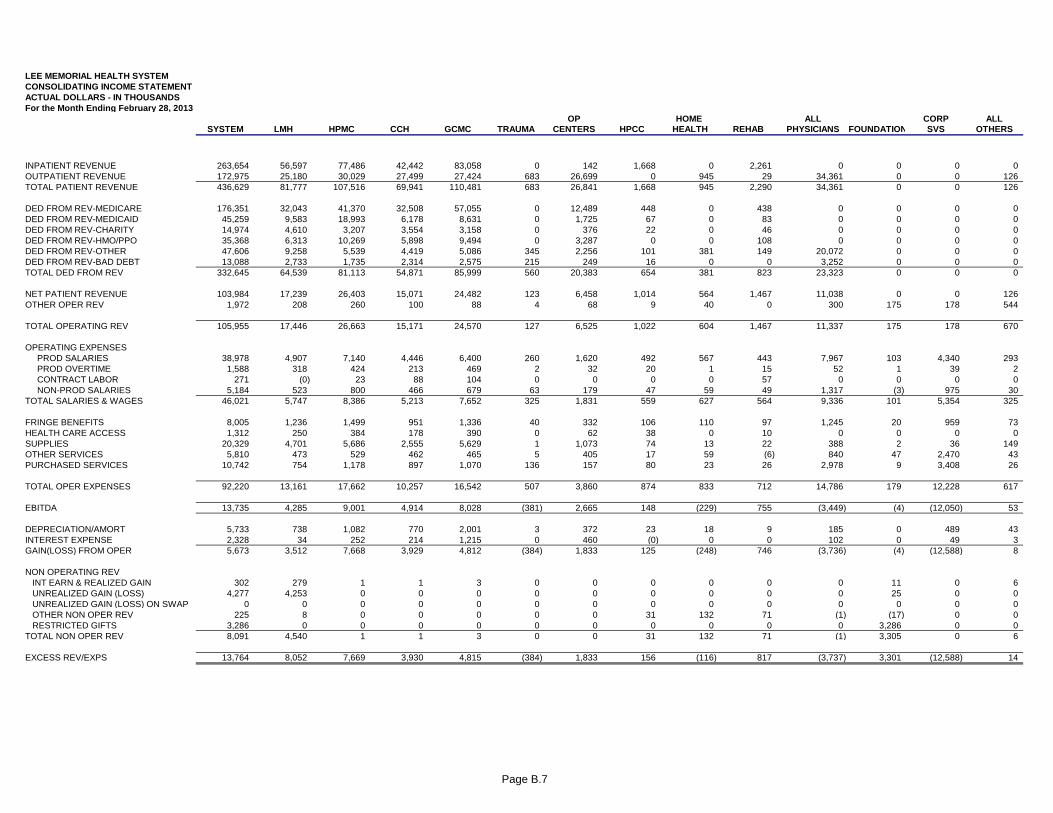
Page B.7
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATING INCOME STATEMENTACTUAL DOLLARS - IN THOUSANDSFor the Month Ending February 28, 2013
OP HOME ALL CORP ALLSYSTEM LMH HPMC CCH GCMC TRAUMA CENTERS HPCC HEALTH REHAB PHYSICIANS FOUNDATION SVS OTHERS
INPATIENT REVENUE 263,654 56,597 77,486 42,442 83,058 0 142 1,668 0 2,261 0 0 0 0OUTPATIENT REVENUE 172,975 25,180 30,029 27,499 27,424 683 26,699 0 945 29 34,361 0 0 126TOTAL PATIENT REVENUE 436,629 81,777 107,516 69,941 110,481 683 26,841 1,668 945 2,290 34,361 0 0 126
DED FROM REV-MEDICARE 176,351 32,043 41,370 32,508 57,055 0 12,489 448 0 438 0 0 0 0DED FROM REV-MEDICAID 45,259 9,583 18,993 6,178 8,631 0 1,725 67 0 83 0 0 0 0DED FROM REV-CHARITY 14,974 4,610 3,207 3,554 3,158 0 376 22 0 46 0 0 0 0DED FROM REV-HMO/PPO 35,368 6,313 10,269 5,898 9,494 0 3,287 0 0 108 0 0 0 0DED FROM REV-OTHER 47,606 9,258 5,539 4,419 5,086 345 2,256 101 381 149 20,072 0 0 0DED FROM REV-BAD DEBT 13,088 2,733 1,735 2,314 2,575 215 249 16 0 0 3,252 0 0 0TOTAL DED FROM REV 332,645 64,539 81,113 54,871 85,999 560 20,383 654 381 823 23,323 0 0 0
NET PATIENT REVENUE 103,984 17,239 26,403 15,071 24,482 123 6,458 1,014 564 1,467 11,038 0 0 126OTHER OPER REV 1,972 208 260 100 88 4 68 9 40 0 300 175 178 544
TOTAL OPERATING REV 105,955 17,446 26,663 15,171 24,570 127 6,525 1,022 604 1,467 11,337 175 178 670
OPERATING EXPENSES PROD SALARIES 38,978 4,907 7,140 4,446 6,400 260 1,620 492 567 443 7,967 103 4,340 293 PROD OVERTIME 1,588 318 424 213 469 2 32 20 1 15 52 1 39 2 CONTRACT LABOR 271 (0) 23 88 104 0 0 0 0 57 0 0 0 0 NON-PROD SALARIES 5,184 523 800 466 679 63 179 47 59 49 1,317 (3) 975 30TOTAL SALARIES & WAGES 46,021 5,747 8,386 5,213 7,652 325 1,831 559 627 564 9,336 101 5,354 325
FRINGE BENEFITS 8,005 1,236 1,499 951 1,336 40 332 106 110 97 1,245 20 959 73HEALTH CARE ACCESS 1,312 250 384 178 390 0 62 38 0 10 0 0 0 0SUPPLIES 20,329 4,701 5,686 2,555 5,629 1 1,073 74 13 22 388 2 36 149OTHER SERVICES 5,810 473 529 462 465 5 405 17 59 (6) 840 47 2,470 43PURCHASED SERVICES 10,742 754 1,178 897 1,070 136 157 80 23 26 2,978 9 3,408 26
TOTAL OPER EXPENSES 92,220 13,161 17,662 10,257 16,542 507 3,860 874 833 712 14,786 179 12,228 617
EBITDA 13,735 4,285 9,001 4,914 8,028 (381) 2,665 148 (229) 755 (3,449) (4) (12,050) 53
DEPRECIATION/AMORT 5,733 738 1,082 770 2,001 3 372 23 18 9 185 0 489 43INTEREST EXPENSE 2,328 34 252 214 1,215 0 460 (0) 0 0 102 0 49 3GAIN(LOSS) FROM OPER 5,673 3,512 7,668 3,929 4,812 (384) 1,833 125 (248) 746 (3,736) (4) (12,588) 8
NON OPERATING REV INT EARN & REALIZED GAIN 302 279 1 1 3 0 0 0 0 0 0 11 0 6 UNREALIZED GAIN (LOSS) 4,277 4,253 0 0 0 0 0 0 0 0 0 25 0 0 UNREALIZED GAIN (LOSS) ON SWAP 0 0 0 0 0 0 0 0 0 0 0 0 0 0 OTHER NON OPER REV 225 8 0 0 0 0 0 31 132 71 (1) (17) 0 0 RESTRICTED GIFTS 3,286 0 0 0 0 0 0 0 0 0 0 3,286 0 0TOTAL NON OPER REV 8,091 4,540 1 1 3 0 0 31 132 71 (1) 3,305 0 6
EXCESS REV/EXPS 13,764 8,052 7,669 3,930 4,815 (384) 1,833 156 (116) 817 (3,737) 3,301 (12,588) 14
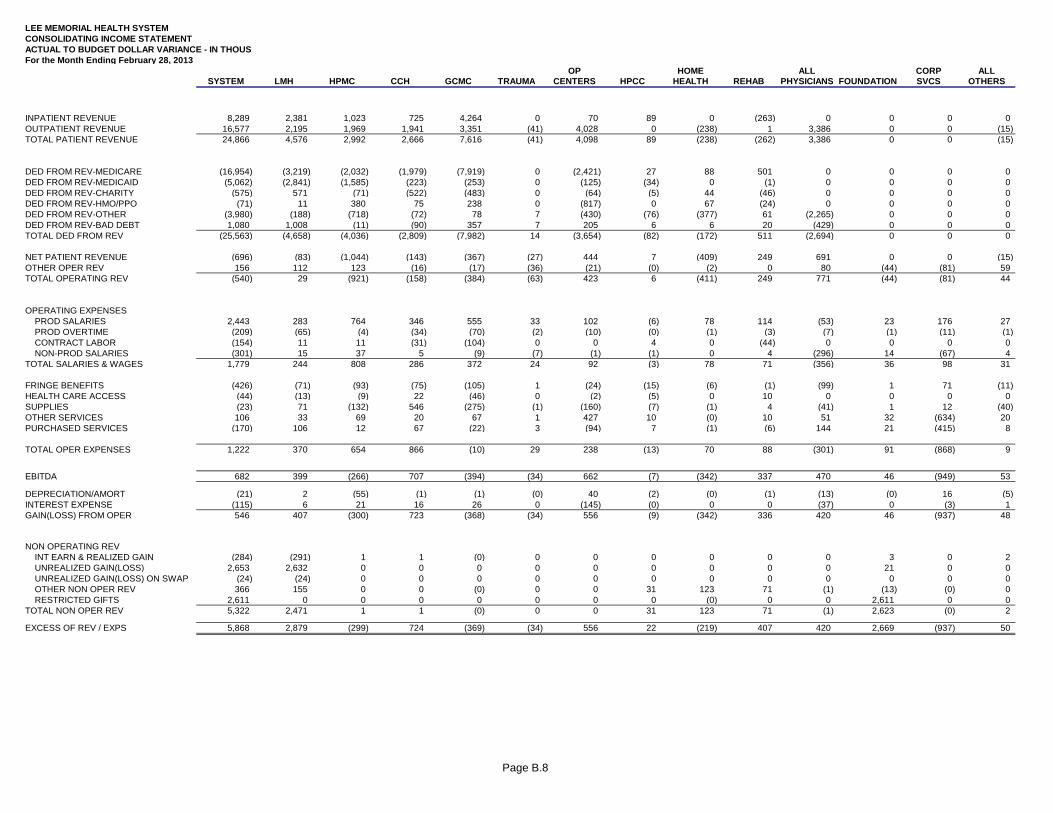
Page B.8
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATING INCOME STATEMENTACTUAL TO BUDGET DOLLAR VARIANCE - IN THOUSFor the Month Ending February 28, 2013
OP HOME ALL CORP ALLSYSTEM LMH HPMC CCH GCMC TRAUMA CENTERS HPCC HEALTH REHAB PHYSICIANS FOUNDATION SVCS OTHERS
INPATIENT REVENUE 8,289 2,381 1,023 725 4,264 0 70 89 0 (263) 0 0 0 0OUTPATIENT REVENUE 16,577 2,195 1,969 1,941 3,351 (41) 4,028 0 (238) 1 3,386 0 0 (15)TOTAL PATIENT REVENUE 24,866 4,576 2,992 2,666 7,616 (41) 4,098 89 (238) (262) 3,386 0 0 (15)
DED FROM REV-MEDICARE (16,954) (3,219) (2,032) (1,979) (7,919) 0 (2,421) 27 88 501 0 0 0 0DED FROM REV-MEDICAID (5,062) (2,841) (1,585) (223) (253) 0 (125) (34) 0 (1) 0 0 0 0DED FROM REV-CHARITY (575) 571 (71) (522) (483) 0 (64) (5) 44 (46) 0 0 0 0DED FROM REV-HMO/PPO (71) 11 380 75 238 0 (817) 0 67 (24) 0 0 0 0DED FROM REV-OTHER (3,980) (188) (718) (72) 78 7 (430) (76) (377) 61 (2,265) 0 0 0DED FROM REV-BAD DEBT 1,080 1,008 (11) (90) 357 7 205 6 6 20 (429) 0 0 0TOTAL DED FROM REV (25,563) (4,658) (4,036) (2,809) (7,982) 14 (3,654) (82) (172) 511 (2,694) 0 0 0
NET PATIENT REVENUE (696) (83) (1,044) (143) (367) (27) 444 7 (409) 249 691 0 0 (15)OTHER OPER REV 156 112 123 (16) (17) (36) (21) (0) (2) 0 80 (44) (81) 59TOTAL OPERATING REV (540) 29 (921) (158) (384) (63) 423 6 (411) 249 771 (44) (81) 44
OPERATING EXPENSES PROD SALARIES 2,443 283 764 346 555 33 102 (6) 78 114 (53) 23 176 27 PROD OVERTIME (209) (65) (4) (34) (70) (2) (10) (0) (1) (3) (7) (1) (11) (1) CONTRACT LABOR (154) 11 11 (31) (104) 0 0 4 0 (44) 0 0 0 0 NON-PROD SALARIES (301) 15 37 5 (9) (7) (1) (1) 0 4 (296) 14 (67) 4TOTAL SALARIES & WAGES 1,779 244 808 286 372 24 92 (3) 78 71 (356) 36 98 31
FRINGE BENEFITS (426) (71) (93) (75) (105) 1 (24) (15) (6) (1) (99) 1 71 (11)HEALTH CARE ACCESS (44) (13) (9) 22 (46) 0 (2) (5) 0 10 0 0 0 0SUPPLIES (23) 71 (132) 546 (275) (1) (160) (7) (1) 4 (41) 1 12 (40)OTHER SERVICES 106 33 69 20 67 1 427 10 (0) 10 51 32 (634) 20PURCHASED SERVICES (170) 106 12 67 (22) 3 (94) 7 (1) (6) 144 21 (415) 8
TOTAL OPER EXPENSES 1,222 370 654 866 (10) 29 238 (13) 70 88 (301) 91 (868) 9
EBITDA 682 399 (266) 707 (394) (34) 662 (7) (342) 337 470 46 (949) 53
DEPRECIATION/AMORT (21) 2 (55) (1) (1) (0) 40 (2) (0) (1) (13) (0) 16 (5)INTEREST EXPENSE (115) 6 21 16 26 0 (145) (0) 0 0 (37) 0 (3) 1GAIN(LOSS) FROM OPER 546 407 (300) 723 (368) (34) 556 (9) (342) 336 420 46 (937) 48
NON OPERATING REV INT EARN & REALIZED GAIN (284) (291) 1 1 (0) 0 0 0 0 0 0 3 0 2 UNREALIZED GAIN(LOSS) 2,653 2,632 0 0 0 0 0 0 0 0 0 21 0 0 UNREALIZED GAIN(LOSS) ON SWAP (24) (24) 0 0 0 0 0 0 0 0 0 0 0 0 OTHER NON OPER REV 366 155 0 0 (0) 0 0 31 123 71 (1) (13) (0) 0 RESTRICTED GIFTS 2,611 0 0 0 0 0 0 0 (0) 0 0 2,611 0 0TOTAL NON OPER REV 5,322 2,471 1 1 (0) 0 0 31 123 71 (1) 2,623 (0) 2
EXCESS OF REV / EXPS 5,868 2,879 (299) 724 (369) (34) 556 22 (219) 407 420 2,669 (937) 50
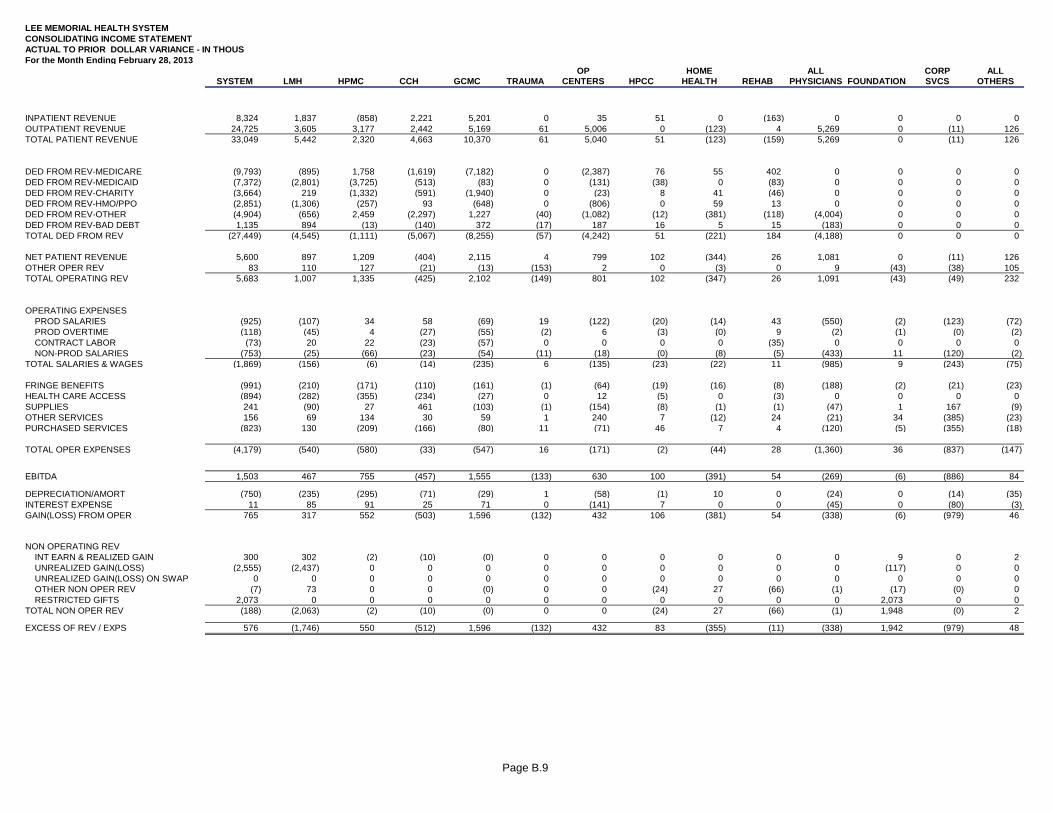
Page B.9
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATING INCOME STATEMENTACTUAL TO PRIOR DOLLAR VARIANCE - IN THOUSFor the Month Ending February 28, 2013
OP HOME ALL CORP ALLSYSTEM LMH HPMC CCH GCMC TRAUMA CENTERS HPCC HEALTH REHAB PHYSICIANS FOUNDATION SVCS OTHERS
INPATIENT REVENUE 8,324 1,837 (858) 2,221 5,201 0 35 51 0 (163) 0 0 0 0OUTPATIENT REVENUE 24,725 3,605 3,177 2,442 5,169 61 5,006 0 (123) 4 5,269 0 (11) 126TOTAL PATIENT REVENUE 33,049 5,442 2,320 4,663 10,370 61 5,040 51 (123) (159) 5,269 0 (11) 126
DED FROM REV-MEDICARE (9,793) (895) 1,758 (1,619) (7,182) 0 (2,387) 76 55 402 0 0 0 0DED FROM REV-MEDICAID (7,372) (2,801) (3,725) (513) (83) 0 (131) (38) 0 (83) 0 0 0 0DED FROM REV-CHARITY (3,664) 219 (1,332) (591) (1,940) 0 (23) 8 41 (46) 0 0 0 0DED FROM REV-HMO/PPO (2,851) (1,306) (257) 93 (648) 0 (806) 0 59 13 0 0 0 0DED FROM REV-OTHER (4,904) (656) 2,459 (2,297) 1,227 (40) (1,082) (12) (381) (118) (4,004) 0 0 0DED FROM REV-BAD DEBT 1,135 894 (13) (140) 372 (17) 187 16 5 15 (183) 0 0 0TOTAL DED FROM REV (27,449) (4,545) (1,111) (5,067) (8,255) (57) (4,242) 51 (221) 184 (4,188) 0 0 0
NET PATIENT REVENUE 5,600 897 1,209 (404) 2,115 4 799 102 (344) 26 1,081 0 (11) 126OTHER OPER REV 83 110 127 (21) (13) (153) 2 0 (3) 0 9 (43) (38) 105TOTAL OPERATING REV 5,683 1,007 1,335 (425) 2,102 (149) 801 102 (347) 26 1,091 (43) (49) 232
OPERATING EXPENSES PROD SALARIES (925) (107) 34 58 (69) 19 (122) (20) (14) 43 (550) (2) (123) (72) PROD OVERTIME (118) (45) 4 (27) (55) (2) 6 (3) (0) 9 (2) (1) (0) (2) CONTRACT LABOR (73) 20 22 (23) (57) 0 0 0 0 (35) 0 0 0 0 NON-PROD SALARIES (753) (25) (66) (23) (54) (11) (18) (0) (8) (5) (433) 11 (120) (2)TOTAL SALARIES & WAGES (1,869) (156) (6) (14) (235) 6 (135) (23) (22) 11 (985) 9 (243) (75)
FRINGE BENEFITS (991) (210) (171) (110) (161) (1) (64) (19) (16) (8) (188) (2) (21) (23)HEALTH CARE ACCESS (894) (282) (355) (234) (27) 0 12 (5) 0 (3) 0 0 0 0SUPPLIES 241 (90) 27 461 (103) (1) (154) (8) (1) (1) (47) 1 167 (9)OTHER SERVICES 156 69 134 30 59 1 240 7 (12) 24 (21) 34 (385) (23)PURCHASED SERVICES (823) 130 (209) (166) (80) 11 (71) 46 7 4 (120) (5) (355) (18)
TOTAL OPER EXPENSES (4,179) (540) (580) (33) (547) 16 (171) (2) (44) 28 (1,360) 36 (837) (147)
EBITDA 1,503 467 755 (457) 1,555 (133) 630 100 (391) 54 (269) (6) (886) 84
DEPRECIATION/AMORT (750) (235) (295) (71) (29) 1 (58) (1) 10 0 (24) 0 (14) (35)INTEREST EXPENSE 11 85 91 25 71 0 (141) 7 0 0 (45) 0 (80) (3)GAIN(LOSS) FROM OPER 765 317 552 (503) 1,596 (132) 432 106 (381) 54 (338) (6) (979) 46
NON OPERATING REV INT EARN & REALIZED GAIN 300 302 (2) (10) (0) 0 0 0 0 0 0 9 0 2 UNREALIZED GAIN(LOSS) (2,555) (2,437) 0 0 0 0 0 0 0 0 0 (117) 0 0 UNREALIZED GAIN(LOSS) ON SWAP 0 0 0 0 0 0 0 0 0 0 0 0 0 0 OTHER NON OPER REV (7) 73 0 0 (0) 0 0 (24) 27 (66) (1) (17) (0) 0 RESTRICTED GIFTS 2,073 0 0 0 0 0 0 0 0 0 0 2,073 0 0TOTAL NON OPER REV (188) (2,063) (2) (10) (0) 0 0 (24) 27 (66) (1) 1,948 (0) 2
EXCESS OF REV / EXPS 576 (1,746) 550 (512) 1,596 (132) 432 83 (355) (11) (338) 1,942 (979) 48
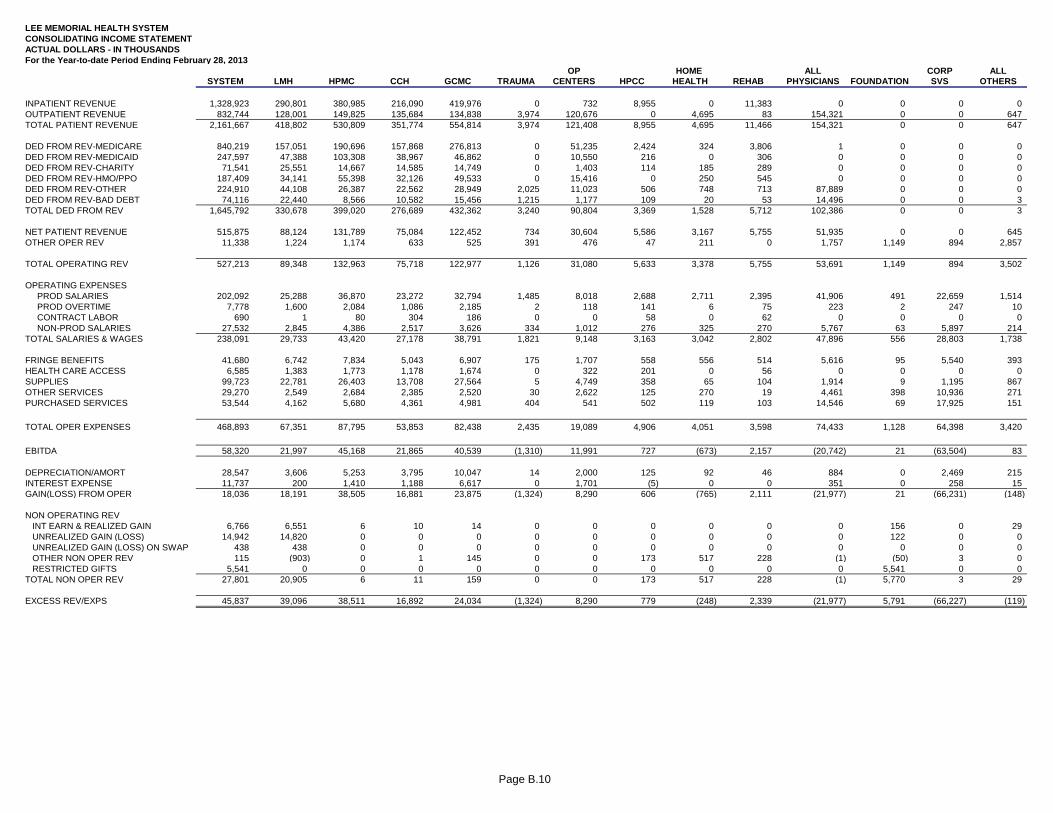
Page B.10
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATING INCOME STATEMENTACTUAL DOLLARS - IN THOUSANDSFor the Year-to-date Period Ending February 28, 2013
OP HOME ALL CORP ALLSYSTEM LMH HPMC CCH GCMC TRAUMA CENTERS HPCC HEALTH REHAB PHYSICIANS FOUNDATION SVS OTHERS
INPATIENT REVENUE 1,328,923 290,801 380,985 216,090 419,976 0 732 8,955 0 11,383 0 0 0 0OUTPATIENT REVENUE 832,744 128,001 149,825 135,684 134,838 3,974 120,676 0 4,695 83 154,321 0 0 647TOTAL PATIENT REVENUE 2,161,667 418,802 530,809 351,774 554,814 3,974 121,408 8,955 4,695 11,466 154,321 0 0 647
DED FROM REV-MEDICARE 840,219 157,051 190,696 157,868 276,813 0 51,235 2,424 324 3,806 1 0 0 0DED FROM REV-MEDICAID 247,597 47,388 103,308 38,967 46,862 0 10,550 216 0 306 0 0 0 0DED FROM REV-CHARITY 71,541 25,551 14,667 14,585 14,749 0 1,403 114 185 289 0 0 0 0DED FROM REV-HMO/PPO 187,409 34,141 55,398 32,126 49,533 0 15,416 0 250 545 0 0 0 0DED FROM REV-OTHER 224,910 44,108 26,387 22,562 28,949 2,025 11,023 506 748 713 87,889 0 0 0DED FROM REV-BAD DEBT 74,116 22,440 8,566 10,582 15,456 1,215 1,177 109 20 53 14,496 0 0 3TOTAL DED FROM REV 1,645,792 330,678 399,020 276,689 432,362 3,240 90,804 3,369 1,528 5,712 102,386 0 0 3
NET PATIENT REVENUE 515,875 88,124 131,789 75,084 122,452 734 30,604 5,586 3,167 5,755 51,935 0 0 645OTHER OPER REV 11,338 1,224 1,174 633 525 391 476 47 211 0 1,757 1,149 894 2,857
TOTAL OPERATING REV 527,213 89,348 132,963 75,718 122,977 1,126 31,080 5,633 3,378 5,755 53,691 1,149 894 3,502
OPERATING EXPENSES PROD SALARIES 202,092 25,288 36,870 23,272 32,794 1,485 8,018 2,688 2,711 2,395 41,906 491 22,659 1,514 PROD OVERTIME 7,778 1,600 2,084 1,086 2,185 2 118 141 6 75 223 2 247 10 CONTRACT LABOR 690 1 80 304 186 0 0 58 0 62 0 0 0 0 NON-PROD SALARIES 27,532 2,845 4,386 2,517 3,626 334 1,012 276 325 270 5,767 63 5,897 214TOTAL SALARIES & WAGES 238,091 29,733 43,420 27,178 38,791 1,821 9,148 3,163 3,042 2,802 47,896 556 28,803 1,738
FRINGE BENEFITS 41,680 6,742 7,834 5,043 6,907 175 1,707 558 556 514 5,616 95 5,540 393HEALTH CARE ACCESS 6,585 1,383 1,773 1,178 1,674 0 322 201 0 56 0 0 0 0SUPPLIES 99,723 22,781 26,403 13,708 27,564 5 4,749 358 65 104 1,914 9 1,195 867OTHER SERVICES 29,270 2,549 2,684 2,385 2,520 30 2,622 125 270 19 4,461 398 10,936 271PURCHASED SERVICES 53,544 4,162 5,680 4,361 4,981 404 541 502 119 103 14,546 69 17,925 151
TOTAL OPER EXPENSES 468,893 67,351 87,795 53,853 82,438 2,435 19,089 4,906 4,051 3,598 74,433 1,128 64,398 3,420
EBITDA 58,320 21,997 45,168 21,865 40,539 (1,310) 11,991 727 (673) 2,157 (20,742) 21 (63,504) 83
DEPRECIATION/AMORT 28,547 3,606 5,253 3,795 10,047 14 2,000 125 92 46 884 0 2,469 215INTEREST EXPENSE 11,737 200 1,410 1,188 6,617 0 1,701 (5) 0 0 351 0 258 15GAIN(LOSS) FROM OPER 18,036 18,191 38,505 16,881 23,875 (1,324) 8,290 606 (765) 2,111 (21,977) 21 (66,231) (148)
NON OPERATING REV INT EARN & REALIZED GAIN 6,766 6,551 6 10 14 0 0 0 0 0 0 156 0 29 UNREALIZED GAIN (LOSS) 14,942 14,820 0 0 0 0 0 0 0 0 0 122 0 0 UNREALIZED GAIN (LOSS) ON SWAP 438 438 0 0 0 0 0 0 0 0 0 0 0 0 OTHER NON OPER REV 115 (903) 0 1 145 0 0 173 517 228 (1) (50) 3 0 RESTRICTED GIFTS 5,541 0 0 0 0 0 0 0 0 0 0 5,541 0 0TOTAL NON OPER REV 27,801 20,905 6 11 159 0 0 173 517 228 (1) 5,770 3 29
EXCESS REV/EXPS 45,837 39,096 38,511 16,892 24,034 (1,324) 8,290 779 (248) 2,339 (21,977) 5,791 (66,227) (119)
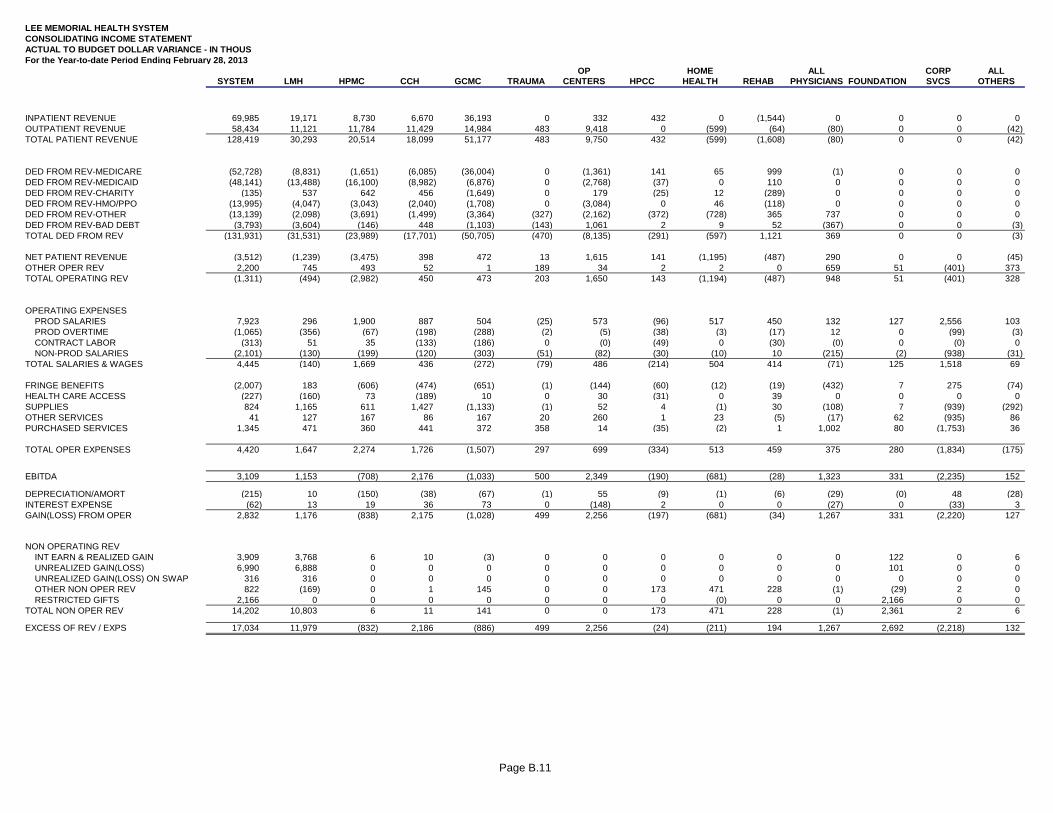
Page B.11
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATING INCOME STATEMENTACTUAL TO BUDGET DOLLAR VARIANCE - IN THOUSFor the Year-to-date Period Ending February 28, 2013
OP HOME ALL CORP ALLSYSTEM LMH HPMC CCH GCMC TRAUMA CENTERS HPCC HEALTH REHAB PHYSICIANS FOUNDATION SVCS OTHERS
INPATIENT REVENUE 69,985 19,171 8,730 6,670 36,193 0 332 432 0 (1,544) 0 0 0 0OUTPATIENT REVENUE 58,434 11,121 11,784 11,429 14,984 483 9,418 0 (599) (64) (80) 0 0 (42)TOTAL PATIENT REVENUE 128,419 30,293 20,514 18,099 51,177 483 9,750 432 (599) (1,608) (80) 0 0 (42)
DED FROM REV-MEDICARE (52,728) (8,831) (1,651) (6,085) (36,004) 0 (1,361) 141 65 999 (1) 0 0 0DED FROM REV-MEDICAID (48,141) (13,488) (16,100) (8,982) (6,876) 0 (2,768) (37) 0 110 0 0 0 0DED FROM REV-CHARITY (135) 537 642 456 (1,649) 0 179 (25) 12 (289) 0 0 0 0DED FROM REV-HMO/PPO (13,995) (4,047) (3,043) (2,040) (1,708) 0 (3,084) 0 46 (118) 0 0 0 0DED FROM REV-OTHER (13,139) (2,098) (3,691) (1,499) (3,364) (327) (2,162) (372) (728) 365 737 0 0 0DED FROM REV-BAD DEBT (3,793) (3,604) (146) 448 (1,103) (143) 1,061 2 9 52 (367) 0 0 (3)TOTAL DED FROM REV (131,931) (31,531) (23,989) (17,701) (50,705) (470) (8,135) (291) (597) 1,121 369 0 0 (3)
NET PATIENT REVENUE (3,512) (1,239) (3,475) 398 472 13 1,615 141 (1,195) (487) 290 0 0 (45)OTHER OPER REV 2,200 745 493 52 1 189 34 2 2 0 659 51 (401) 373TOTAL OPERATING REV (1,311) (494) (2,982) 450 473 203 1,650 143 (1,194) (487) 948 51 (401) 328
OPERATING EXPENSES PROD SALARIES 7,923 296 1,900 887 504 (25) 573 (96) 517 450 132 127 2,556 103 PROD OVERTIME (1,065) (356) (67) (198) (288) (2) (5) (38) (3) (17) 12 0 (99) (3) CONTRACT LABOR (313) 51 35 (133) (186) 0 (0) (49) 0 (30) (0) 0 (0) 0 NON-PROD SALARIES (2,101) (130) (199) (120) (303) (51) (82) (30) (10) 10 (215) (2) (938) (31)TOTAL SALARIES & WAGES 4,445 (140) 1,669 436 (272) (79) 486 (214) 504 414 (71) 125 1,518 69
FRINGE BENEFITS (2,007) 183 (606) (474) (651) (1) (144) (60) (12) (19) (432) 7 275 (74)HEALTH CARE ACCESS (227) (160) 73 (189) 10 0 30 (31) 0 39 0 0 0 0SUPPLIES 824 1,165 611 1,427 (1,133) (1) 52 4 (1) 30 (108) 7 (939) (292)OTHER SERVICES 41 127 167 86 167 20 260 1 23 (5) (17) 62 (935) 86PURCHASED SERVICES 1,345 471 360 441 372 358 14 (35) (2) 1 1,002 80 (1,753) 36
TOTAL OPER EXPENSES 4,420 1,647 2,274 1,726 (1,507) 297 699 (334) 513 459 375 280 (1,834) (175)
EBITDA 3,109 1,153 (708) 2,176 (1,033) 500 2,349 (190) (681) (28) 1,323 331 (2,235) 152
DEPRECIATION/AMORT (215) 10 (150) (38) (67) (1) 55 (9) (1) (6) (29) (0) 48 (28)INTEREST EXPENSE (62) 13 19 36 73 0 (148) 2 0 0 (27) 0 (33) 3GAIN(LOSS) FROM OPER 2,832 1,176 (838) 2,175 (1,028) 499 2,256 (197) (681) (34) 1,267 331 (2,220) 127
NON OPERATING REV INT EARN & REALIZED GAIN 3,909 3,768 6 10 (3) 0 0 0 0 0 0 122 0 6 UNREALIZED GAIN(LOSS) 6,990 6,888 0 0 0 0 0 0 0 0 0 101 0 0 UNREALIZED GAIN(LOSS) ON SWAP 316 316 0 0 0 0 0 0 0 0 0 0 0 0 OTHER NON OPER REV 822 (169) 0 1 145 0 0 173 471 228 (1) (29) 2 0 RESTRICTED GIFTS 2,166 0 0 0 0 0 0 0 (0) 0 0 2,166 0 0TOTAL NON OPER REV 14,202 10,803 6 11 141 0 0 173 471 228 (1) 2,361 2 6
EXCESS OF REV / EXPS 17,034 11,979 (832) 2,186 (886) 499 2,256 (24) (211) 194 1,267 2,692 (2,218) 132
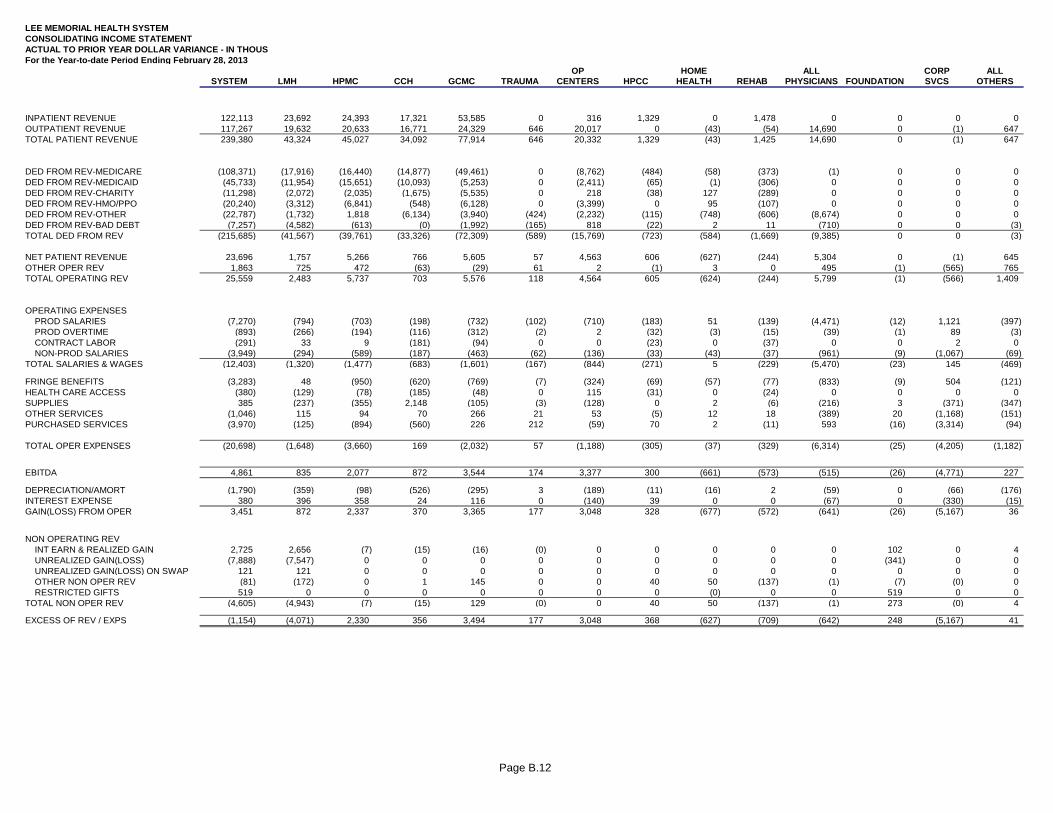
Page B.12
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATING INCOME STATEMENTACTUAL TO PRIOR YEAR DOLLAR VARIANCE - IN THOUSFor the Year-to-date Period Ending February 28, 2013
OP HOME ALL CORP ALLSYSTEM LMH HPMC CCH GCMC TRAUMA CENTERS HPCC HEALTH REHAB PHYSICIANS FOUNDATION SVCS OTHERS
INPATIENT REVENUE 122,113 23,692 24,393 17,321 53,585 0 316 1,329 0 1,478 0 0 0 0OUTPATIENT REVENUE 117,267 19,632 20,633 16,771 24,329 646 20,017 0 (43) (54) 14,690 0 (1) 647TOTAL PATIENT REVENUE 239,380 43,324 45,027 34,092 77,914 646 20,332 1,329 (43) 1,425 14,690 0 (1) 647
DED FROM REV-MEDICARE (108,371) (17,916) (16,440) (14,877) (49,461) 0 (8,762) (484) (58) (373) (1) 0 0 0DED FROM REV-MEDICAID (45,733) (11,954) (15,651) (10,093) (5,253) 0 (2,411) (65) (1) (306) 0 0 0 0DED FROM REV-CHARITY (11,298) (2,072) (2,035) (1,675) (5,535) 0 218 (38) 127 (289) 0 0 0 0DED FROM REV-HMO/PPO (20,240) (3,312) (6,841) (548) (6,128) 0 (3,399) 0 95 (107) 0 0 0 0DED FROM REV-OTHER (22,787) (1,732) 1,818 (6,134) (3,940) (424) (2,232) (115) (748) (606) (8,674) 0 0 0DED FROM REV-BAD DEBT (7,257) (4,582) (613) (0) (1,992) (165) 818 (22) 2 11 (710) 0 0 (3)TOTAL DED FROM REV (215,685) (41,567) (39,761) (33,326) (72,309) (589) (15,769) (723) (584) (1,669) (9,385) 0 0 (3)
NET PATIENT REVENUE 23,696 1,757 5,266 766 5,605 57 4,563 606 (627) (244) 5,304 0 (1) 645OTHER OPER REV 1,863 725 472 (63) (29) 61 2 (1) 3 0 495 (1) (565) 765TOTAL OPERATING REV 25,559 2,483 5,737 703 5,576 118 4,564 605 (624) (244) 5,799 (1) (566) 1,409
OPERATING EXPENSES PROD SALARIES (7,270) (794) (703) (198) (732) (102) (710) (183) 51 (139) (4,471) (12) 1,121 (397) PROD OVERTIME (893) (266) (194) (116) (312) (2) 2 (32) (3) (15) (39) (1) 89 (3) CONTRACT LABOR (291) 33 9 (181) (94) 0 0 (23) 0 (37) 0 0 2 0 NON-PROD SALARIES (3,949) (294) (589) (187) (463) (62) (136) (33) (43) (37) (961) (9) (1,067) (69)TOTAL SALARIES & WAGES (12,403) (1,320) (1,477) (683) (1,601) (167) (844) (271) 5 (229) (5,470) (23) 145 (469)
FRINGE BENEFITS (3,283) 48 (950) (620) (769) (7) (324) (69) (57) (77) (833) (9) 504 (121)HEALTH CARE ACCESS (380) (129) (78) (185) (48) 0 115 (31) 0 (24) 0 0 0 0SUPPLIES 385 (237) (355) 2,148 (105) (3) (128) 0 2 (6) (216) 3 (371) (347)OTHER SERVICES (1,046) 115 94 70 266 21 53 (5) 12 18 (389) 20 (1,168) (151)PURCHASED SERVICES (3,970) (125) (894) (560) 226 212 (59) 70 2 (11) 593 (16) (3,314) (94)
TOTAL OPER EXPENSES (20,698) (1,648) (3,660) 169 (2,032) 57 (1,188) (305) (37) (329) (6,314) (25) (4,205) (1,182)
EBITDA 4,861 835 2,077 872 3,544 174 3,377 300 (661) (573) (515) (26) (4,771) 227
DEPRECIATION/AMORT (1,790) (359) (98) (526) (295) 3 (189) (11) (16) 2 (59) 0 (66) (176)INTEREST EXPENSE 380 396 358 24 116 0 (140) 39 0 0 (67) 0 (330) (15)GAIN(LOSS) FROM OPER 3,451 872 2,337 370 3,365 177 3,048 328 (677) (572) (641) (26) (5,167) 36
NON OPERATING REV INT EARN & REALIZED GAIN 2,725 2,656 (7) (15) (16) (0) 0 0 0 0 0 102 0 4 UNREALIZED GAIN(LOSS) (7,888) (7,547) 0 0 0 0 0 0 0 0 0 (341) 0 0 UNREALIZED GAIN(LOSS) ON SWAP 121 121 0 0 0 0 0 0 0 0 0 0 0 0 OTHER NON OPER REV (81) (172) 0 1 145 0 0 40 50 (137) (1) (7) (0) 0 RESTRICTED GIFTS 519 0 0 0 0 0 0 0 (0) 0 0 519 0 0TOTAL NON OPER REV (4,605) (4,943) (7) (15) 129 (0) 0 40 50 (137) (1) 273 (0) 4
EXCESS OF REV / EXPS (1,154) (4,071) 2,330 356 3,494 177 3,048 368 (627) (709) (642) 248 (5,167) 41
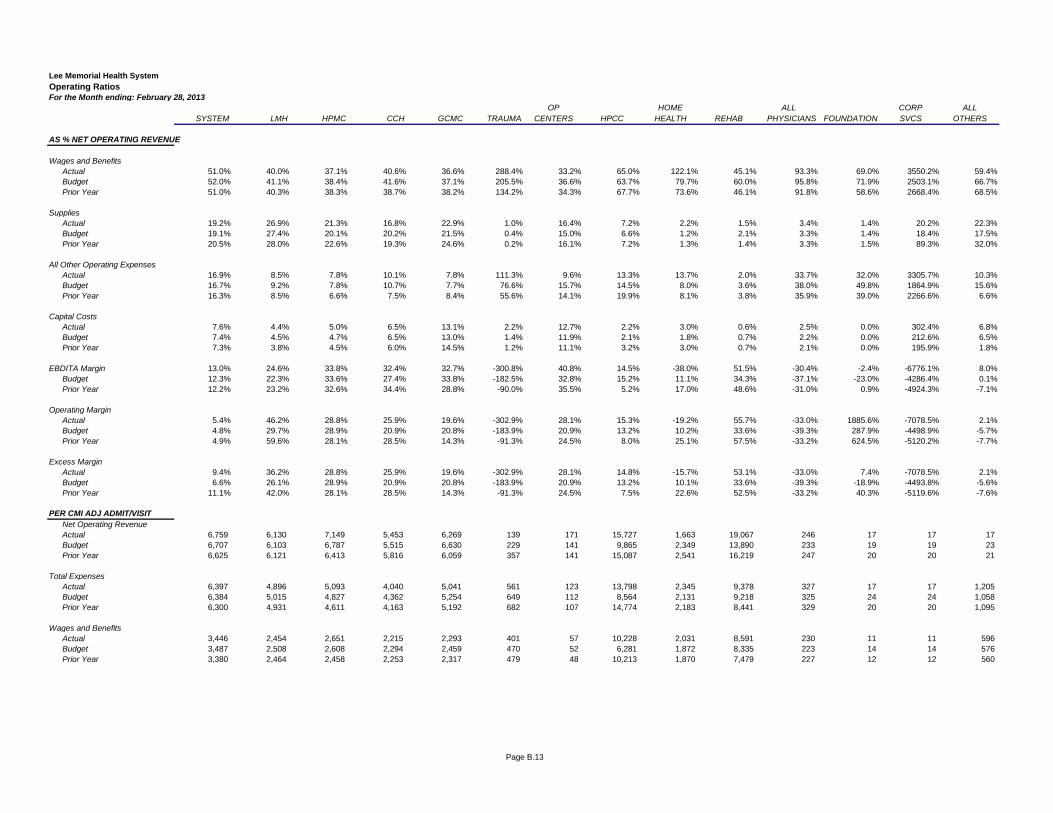
Page B.13
Lee Memorial Health SystemOperating RatiosFor the Month ending: February 28, 2013
OP HOME ALL CORP ALLSYSTEM LMH HPMC CCH GCMC TRAUMA CENTERS HPCC HEALTH REHAB PHYSICIANS FOUNDATION SVCS OTHERS
AS % NET OPERATING REVENUE
Wages and BenefitsActual 51.0% 40.0% 37.1% 40.6% 36.6% 288.4% 33.2% 65.0% 122.1% 45.1% 93.3% 69.0% 3550.2% 59.4%Budget 52.0% 41.1% 38.4% 41.6% 37.1% 205.5% 36.6% 63.7% 79.7% 60.0% 95.8% 71.9% 2503.1% 66.7%Prior Year 51.0% 40.3% 38.3% 38.7% 38.2% 134.2% 34.3% 67.7% 73.6% 46.1% 91.8% 58.6% 2668.4% 68.5%
SuppliesActual 19.2% 26.9% 21.3% 16.8% 22.9% 1.0% 16.4% 7.2% 2.2% 1.5% 3.4% 1.4% 20.2% 22.3%Budget 19.1% 27.4% 20.1% 20.2% 21.5% 0.4% 15.0% 6.6% 1.2% 2.1% 3.3% 1.4% 18.4% 17.5%Prior Year 20.5% 28.0% 22.6% 19.3% 24.6% 0.2% 16.1% 7.2% 1.3% 1.4% 3.3% 1.5% 89.3% 32.0%
All Other Operating ExpensesActual 16.9% 8.5% 7.8% 10.1% 7.8% 111.3% 9.6% 13.3% 13.7% 2.0% 33.7% 32.0% 3305.7% 10.3%Budget 16.7% 9.2% 7.8% 10.7% 7.7% 76.6% 15.7% 14.5% 8.0% 3.6% 38.0% 49.8% 1864.9% 15.6%Prior Year 16.3% 8.5% 6.6% 7.5% 8.4% 55.6% 14.1% 19.9% 8.1% 3.8% 35.9% 39.0% 2266.6% 6.6%
Capital CostsActual 7.6% 4.4% 5.0% 6.5% 13.1% 2.2% 12.7% 2.2% 3.0% 0.6% 2.5% 0.0% 302.4% 6.8%Budget 7.4% 4.5% 4.7% 6.5% 13.0% 1.4% 11.9% 2.1% 1.8% 0.7% 2.2% 0.0% 212.6% 6.5%Prior Year 7.3% 3.8% 4.5% 6.0% 14.5% 1.2% 11.1% 3.2% 3.0% 0.7% 2.1% 0.0% 195.9% 1.8%
EBDITA Margin 13.0% 24.6% 33.8% 32.4% 32.7% -300.8% 40.8% 14.5% -38.0% 51.5% -30.4% -2.4% -6776.1% 8.0%Budget 12.3% 22.3% 33.6% 27.4% 33.8% -182.5% 32.8% 15.2% 11.1% 34.3% -37.1% -23.0% -4286.4% 0.1%Prior Year 12.2% 23.2% 32.6% 34.4% 28.8% -90.0% 35.5% 5.2% 17.0% 48.6% -31.0% 0.9% -4924.3% -7.1%
Operating MarginActual 5.4% 46.2% 28.8% 25.9% 19.6% -302.9% 28.1% 15.3% -19.2% 55.7% -33.0% 1885.6% -7078.5% 2.1%Budget 4.8% 29.7% 28.9% 20.9% 20.8% -183.9% 20.9% 13.2% 10.2% 33.6% -39.3% 287.9% -4498.9% -5.7%Prior Year 4.9% 59.6% 28.1% 28.5% 14.3% -91.3% 24.5% 8.0% 25.1% 57.5% -33.2% 624.5% -5120.2% -7.7%
Excess MarginActual 9.4% 36.2% 28.8% 25.9% 19.6% -302.9% 28.1% 14.8% -15.7% 53.1% -33.0% 7.4% -7078.5% 2.1%Budget 6.6% 26.1% 28.9% 20.9% 20.8% -183.9% 20.9% 13.2% 10.1% 33.6% -39.3% -18.9% -4493.8% -5.6%Prior Year 11.1% 42.0% 28.1% 28.5% 14.3% -91.3% 24.5% 7.5% 22.6% 52.5% -33.2% 40.3% -5119.6% -7.6%
PER CMI ADJ ADMIT/VISITNet Operating RevenueActual 6,759 6,130 7,149 5,453 6,269 139 171 15,727 1,663 19,067 246 17 17 17Budget 6,707 6,103 6,787 5,515 6,630 229 141 9,865 2,349 13,890 233 19 19 23Prior Year 6,625 6,121 6,413 5,816 6,059 357 141 15,087 2,541 16,219 247 20 20 21
Total ExpensesActual 6,397 4,896 5,093 4,040 5,041 561 123 13,798 2,345 9,378 327 17 17 1,205Budget 6,384 5,015 4,827 4,362 5,254 649 112 8,564 2,131 9,218 325 24 24 1,058Prior Year 6,300 4,931 4,611 4,163 5,192 682 107 14,774 2,183 8,441 329 20 20 1,095
Wages and BenefitsActual 3,446 2,454 2,651 2,215 2,293 401 57 10,228 2,031 8,591 230 11 11 596Budget 3,487 2,508 2,608 2,294 2,459 470 52 6,281 1,872 8,335 223 14 14 576Prior Year 3,380 2,464 2,458 2,253 2,317 479 48 10,213 1,870 7,479 227 12 12 560
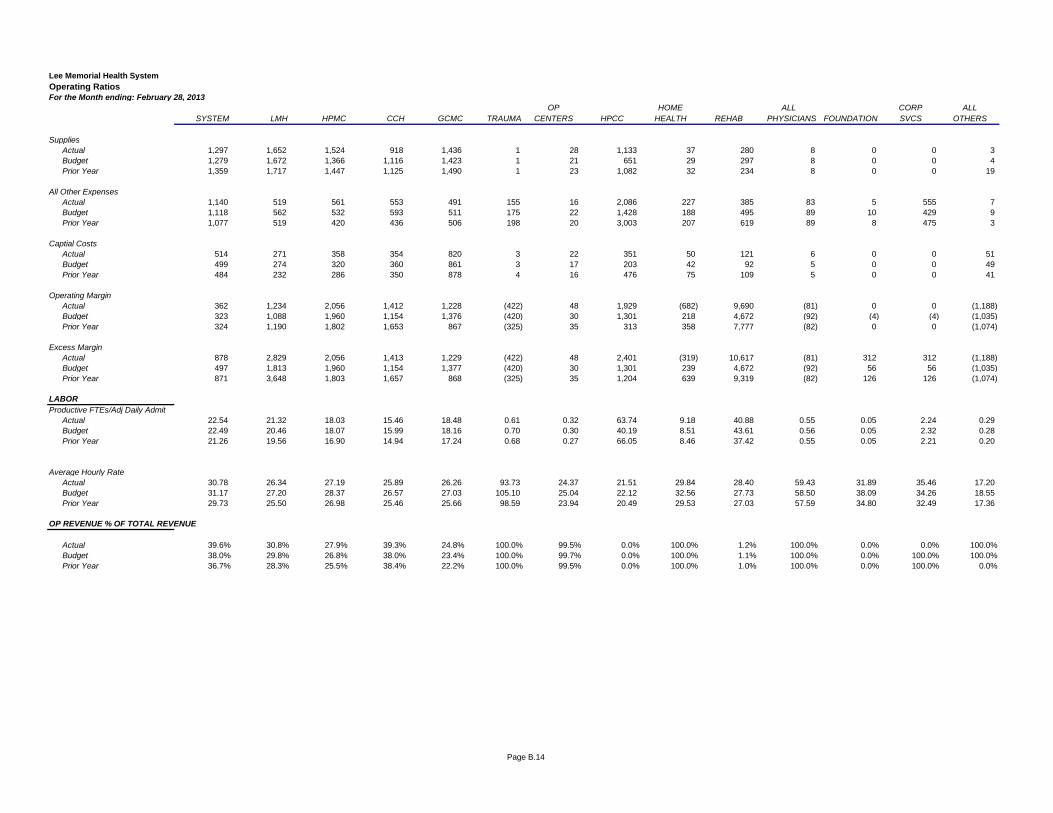
Page B.14
Lee Memorial Health SystemOperating RatiosFor the Month ending: February 28, 2013
OP HOME ALL CORP ALLSYSTEM LMH HPMC CCH GCMC TRAUMA CENTERS HPCC HEALTH REHAB PHYSICIANS FOUNDATION SVCS OTHERS
SuppliesActual 1,297 1,652 1,524 918 1,436 1 28 1,133 37 280 8 0 0 3Budget 1,279 1,672 1,366 1,116 1,423 1 21 651 29 297 8 0 0 4Prior Year 1,359 1,717 1,447 1,125 1,490 1 23 1,082 32 234 8 0 0 19
All Other ExpensesActual 1,140 519 561 553 491 155 16 2,086 227 385 83 5 555 7Budget 1,118 562 532 593 511 175 22 1,428 188 495 89 10 429 9Prior Year 1,077 519 420 436 506 198 20 3,003 207 619 89 8 475 3
Captial CostsActual 514 271 358 354 820 3 22 351 50 121 6 0 0 51Budget 499 274 320 360 861 3 17 203 42 92 5 0 0 49Prior Year 484 232 286 350 878 4 16 476 75 109 5 0 0 41
Operating MarginActual 362 1,234 2,056 1,412 1,228 (422) 48 1,929 (682) 9,690 (81) 0 0 (1,188)Budget 323 1,088 1,960 1,154 1,376 (420) 30 1,301 218 4,672 (92) (4) (4) (1,035)Prior Year 324 1,190 1,802 1,653 867 (325) 35 313 358 7,777 (82) 0 0 (1,074)
Excess MarginActual 878 2,829 2,056 1,413 1,229 (422) 48 2,401 (319) 10,617 (81) 312 312 (1,188)Budget 497 1,813 1,960 1,154 1,377 (420) 30 1,301 239 4,672 (92) 56 56 (1,035)Prior Year 871 3,648 1,803 1,657 868 (325) 35 1,204 639 9,319 (82) 126 126 (1,074)
LABORProductive FTEs/Adj Daily Admit
Actual 22.54 21.32 18.03 15.46 18.48 0.61 0.32 63.74 9.18 40.88 0.55 0.05 2.24 0.29Budget 22.49 20.46 18.07 15.99 18.16 0.70 0.30 40.19 8.51 43.61 0.56 0.05 2.32 0.28Prior Year 21.26 19.56 16.90 14.94 17.24 0.68 0.27 66.05 8.46 37.42 0.55 0.05 2.21 0.20
Average Hourly RateActual 30.78 26.34 27.19 25.89 26.26 93.73 24.37 21.51 29.84 28.40 59.43 31.89 35.46 17.20 Budget 31.17 27.20 28.37 26.57 27.03 105.10 25.04 22.12 32.56 27.73 58.50 38.09 34.26 18.55 Prior Year 29.73 25.50 26.98 25.46 25.66 98.59 23.94 20.49 29.53 27.03 57.59 34.80 32.49 17.36
OP REVENUE % OF TOTAL REVENUE
Actual 39.6% 30.8% 27.9% 39.3% 24.8% 100.0% 99.5% 0.0% 100.0% 1.2% 100.0% 0.0% 0.0% 100.0%Budget 38.0% 29.8% 26.8% 38.0% 23.4% 100.0% 99.7% 0.0% 100.0% 1.1% 100.0% 0.0% 100.0% 100.0%Prior Year 36.7% 28.3% 25.5% 38.4% 22.2% 100.0% 99.5% 0.0% 100.0% 1.0% 100.0% 0.0% 100.0% 0.0%
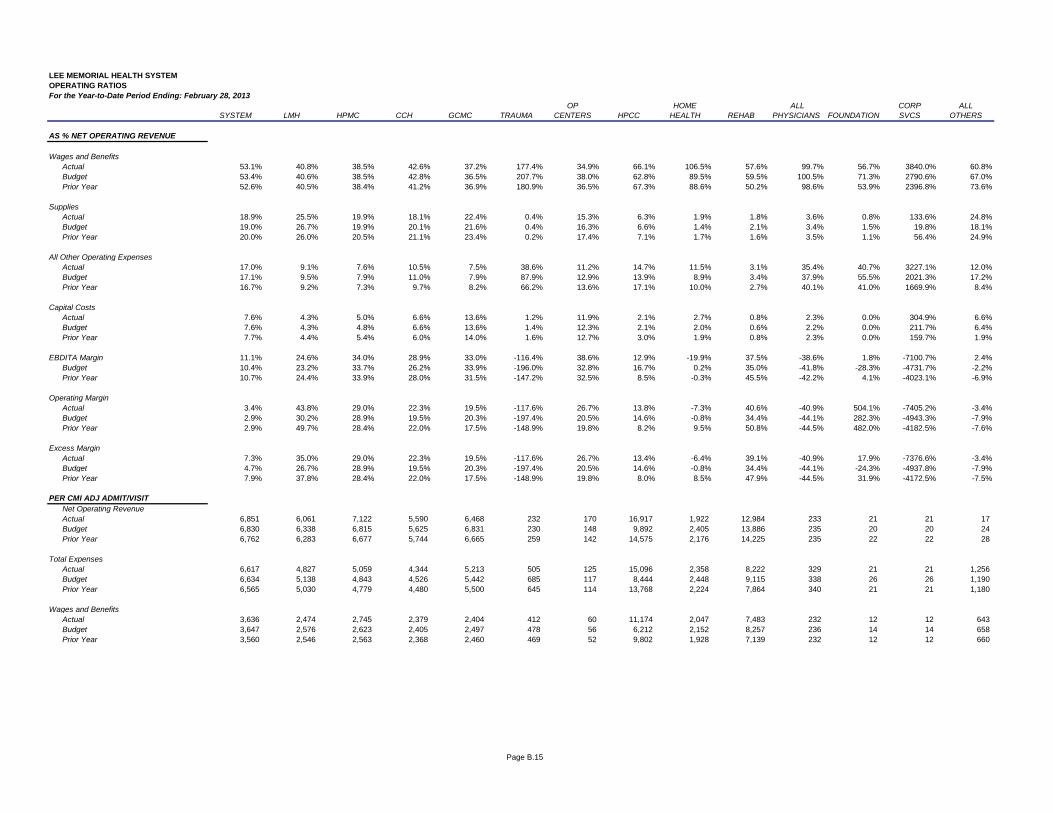
Page B.15
LEE MEMORIAL HEALTH SYSTEMOPERATING RATIOSFor the Year-to-Date Period Ending: February 28, 2013
OP HOME ALL CORP ALLSYSTEM LMH HPMC CCH GCMC TRAUMA CENTERS HPCC HEALTH REHAB PHYSICIANS FOUNDATION SVCS OTHERS
AS % NET OPERATING REVENUE
Wages and BenefitsActual 53.1% 40.8% 38.5% 42.6% 37.2% 177.4% 34.9% 66.1% 106.5% 57.6% 99.7% 56.7% 3840.0% 60.8%Budget 53.4% 40.6% 38.5% 42.8% 36.5% 207.7% 38.0% 62.8% 89.5% 59.5% 100.5% 71.3% 2790.6% 67.0%Prior Year 52.6% 40.5% 38.4% 41.2% 36.9% 180.9% 36.5% 67.3% 88.6% 50.2% 98.6% 53.9% 2396.8% 73.6%
SuppliesActual 18.9% 25.5% 19.9% 18.1% 22.4% 0.4% 15.3% 6.3% 1.9% 1.8% 3.6% 0.8% 133.6% 24.8%Budget 19.0% 26.7% 19.9% 20.1% 21.6% 0.4% 16.3% 6.6% 1.4% 2.1% 3.4% 1.5% 19.8% 18.1%Prior Year 20.0% 26.0% 20.5% 21.1% 23.4% 0.2% 17.4% 7.1% 1.7% 1.6% 3.5% 1.1% 56.4% 24.9%
All Other Operating ExpensesActual 17.0% 9.1% 7.6% 10.5% 7.5% 38.6% 11.2% 14.7% 11.5% 3.1% 35.4% 40.7% 3227.1% 12.0%Budget 17.1% 9.5% 7.9% 11.0% 7.9% 87.9% 12.9% 13.9% 8.9% 3.4% 37.9% 55.5% 2021.3% 17.2%Prior Year 16.7% 9.2% 7.3% 9.7% 8.2% 66.2% 13.6% 17.1% 10.0% 2.7% 40.1% 41.0% 1669.9% 8.4%
Capital CostsActual 7.6% 4.3% 5.0% 6.6% 13.6% 1.2% 11.9% 2.1% 2.7% 0.8% 2.3% 0.0% 304.9% 6.6%Budget 7.6% 4.3% 4.8% 6.6% 13.6% 1.4% 12.3% 2.1% 2.0% 0.6% 2.2% 0.0% 211.7% 6.4%Prior Year 7.7% 4.4% 5.4% 6.0% 14.0% 1.6% 12.7% 3.0% 1.9% 0.8% 2.3% 0.0% 159.7% 1.9%
EBDITA Margin 11.1% 24.6% 34.0% 28.9% 33.0% -116.4% 38.6% 12.9% -19.9% 37.5% -38.6% 1.8% -7100.7% 2.4%Budget 10.4% 23.2% 33.7% 26.2% 33.9% -196.0% 32.8% 16.7% 0.2% 35.0% -41.8% -28.3% -4731.7% -2.2%Prior Year 10.7% 24.4% 33.9% 28.0% 31.5% -147.2% 32.5% 8.5% -0.3% 45.5% -42.2% 4.1% -4023.1% -6.9%
Operating MarginActual 3.4% 43.8% 29.0% 22.3% 19.5% -117.6% 26.7% 13.8% -7.3% 40.6% -40.9% 504.1% -7405.2% -3.4%Budget 2.9% 30.2% 28.9% 19.5% 20.3% -197.4% 20.5% 14.6% -0.8% 34.4% -44.1% 282.3% -4943.3% -7.9%Prior Year 2.9% 49.7% 28.4% 22.0% 17.5% -148.9% 19.8% 8.2% 9.5% 50.8% -44.5% 482.0% -4182.5% -7.6%
Excess MarginActual 7.3% 35.0% 29.0% 22.3% 19.5% -117.6% 26.7% 13.4% -6.4% 39.1% -40.9% 17.9% -7376.6% -3.4%Budget 4.7% 26.7% 28.9% 19.5% 20.3% -197.4% 20.5% 14.6% -0.8% 34.4% -44.1% -24.3% -4937.8% -7.9%Prior Year 7.9% 37.8% 28.4% 22.0% 17.5% -148.9% 19.8% 8.0% 8.5% 47.9% -44.5% 31.9% -4172.5% -7.5%
PER CMI ADJ ADMIT/VISITNet Operating RevenueActual 6,851 6,061 7,122 5,590 6,468 232 170 16,917 1,922 12,984 233 21 21 17Budget 6,830 6,338 6,815 5,625 6,831 230 148 9,892 2,405 13,886 235 20 20 24Prior Year 6,762 6,283 6,677 5,744 6,665 259 142 14,575 2,176 14,225 235 22 22 28
Total ExpensesActual 6,617 4,827 5,059 4,344 5,213 505 125 15,096 2,358 8,222 329 21 21 1,256Budget 6,634 5,138 4,843 4,526 5,442 685 117 8,444 2,448 9,115 338 26 26 1,190Prior Year 6,565 5,030 4,779 4,480 5,500 645 114 13,768 2,224 7,864 340 21 21 1,180
Wages and BenefitsActual 3,636 2,474 2,745 2,379 2,404 412 60 11,174 2,047 7,483 232 12 12 643Budget 3,647 2,576 2,623 2,405 2,497 478 56 6,212 2,152 8,257 236 14 14 658Prior Year 3,560 2,546 2,563 2,368 2,460 469 52 9,802 1,928 7,139 232 12 12 660
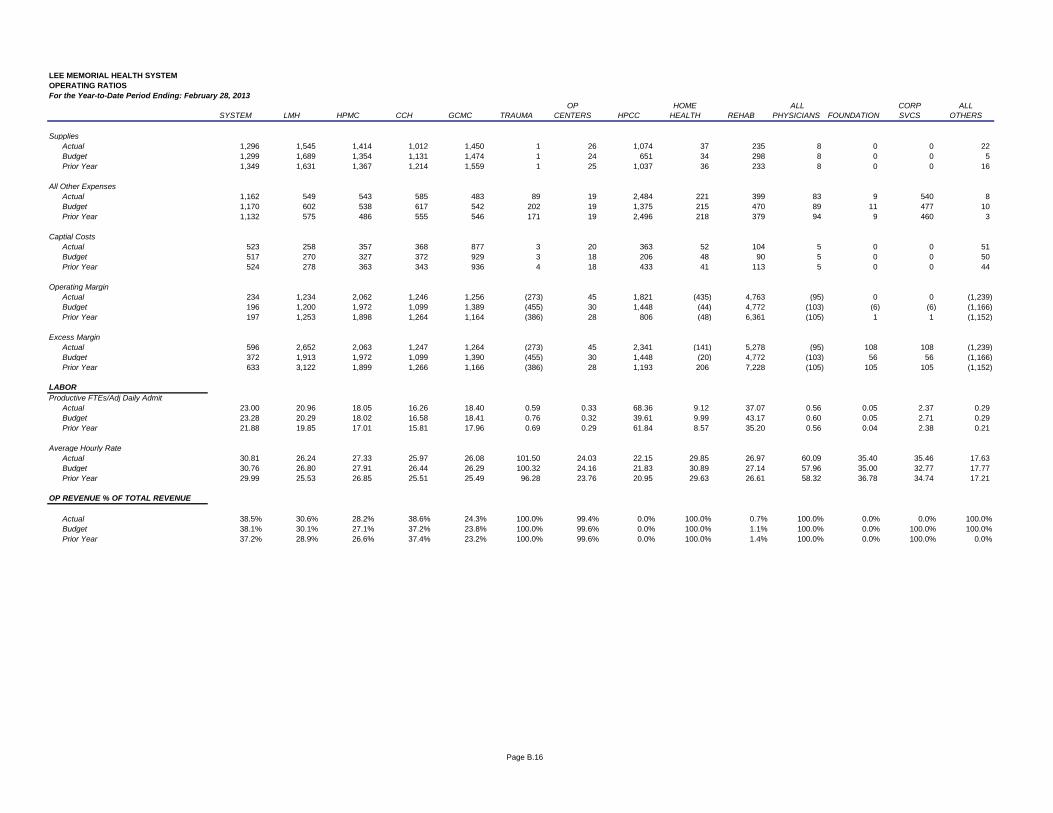
Page B.16
LEE MEMORIAL HEALTH SYSTEMOPERATING RATIOSFor the Year-to-Date Period Ending: February 28, 2013
OP HOME ALL CORP ALLSYSTEM LMH HPMC CCH GCMC TRAUMA CENTERS HPCC HEALTH REHAB PHYSICIANS FOUNDATION SVCS OTHERS
SuppliesActual 1,296 1,545 1,414 1,012 1,450 1 26 1,074 37 235 8 0 0 22Budget 1,299 1,689 1,354 1,131 1,474 1 24 651 34 298 8 0 0 5Prior Year 1,349 1,631 1,367 1,214 1,559 1 25 1,037 36 233 8 0 0 16
All Other ExpensesActual 1,162 549 543 585 483 89 19 2,484 221 399 83 9 540 8Budget 1,170 602 538 617 542 202 19 1,375 215 470 89 11 477 10Prior Year 1,132 575 486 555 546 171 19 2,496 218 379 94 9 460 3
Captial CostsActual 523 258 357 368 877 3 20 363 52 104 5 0 0 51Budget 517 270 327 372 929 3 18 206 48 90 5 0 0 50Prior Year 524 278 363 343 936 4 18 433 41 113 5 0 0 44
Operating MarginActual 234 1,234 2,062 1,246 1,256 (273) 45 1,821 (435) 4,763 (95) 0 0 (1,239)Budget 196 1,200 1,972 1,099 1,389 (455) 30 1,448 (44) 4,772 (103) (6) (6) (1,166)Prior Year 197 1,253 1,898 1,264 1,164 (386) 28 806 (48) 6,361 (105) 1 1 (1,152)
Excess MarginActual 596 2,652 2,063 1,247 1,264 (273) 45 2,341 (141) 5,278 (95) 108 108 (1,239)Budget 372 1,913 1,972 1,099 1,390 (455) 30 1,448 (20) 4,772 (103) 56 56 (1,166)Prior Year 633 3,122 1,899 1,266 1,166 (386) 28 1,193 206 7,228 (105) 105 105 (1,152)
LABORProductive FTEs/Adj Daily Admit
Actual 23.00 20.96 18.05 16.26 18.40 0.59 0.33 68.36 9.12 37.07 0.56 0.05 2.37 0.29Budget 23.28 20.29 18.02 16.58 18.41 0.76 0.32 39.61 9.99 43.17 0.60 0.05 2.71 0.29Prior Year 21.88 19.85 17.01 15.81 17.96 0.69 0.29 61.84 8.57 35.20 0.56 0.04 2.38 0.21
Average Hourly RateActual 30.81 26.24 27.33 25.97 26.08 101.50 24.03 22.15 29.85 26.97 60.09 35.40 35.46 17.63 Budget 30.76 26.80 27.91 26.44 26.29 100.32 24.16 21.83 30.89 27.14 57.96 35.00 32.77 17.77 Prior Year 29.99 25.53 26.85 25.51 25.49 96.28 23.76 20.95 29.63 26.61 58.32 36.78 34.74 17.21
OP REVENUE % OF TOTAL REVENUE
Actual 38.5% 30.6% 28.2% 38.6% 24.3% 100.0% 99.4% 0.0% 100.0% 0.7% 100.0% 0.0% 0.0% 100.0%Budget 38.1% 30.1% 27.1% 37.2% 23.8% 100.0% 99.6% 0.0% 100.0% 1.1% 100.0% 0.0% 100.0% 100.0%Prior Year 37.2% 28.9% 26.6% 37.4% 23.2% 100.0% 99.6% 0.0% 100.0% 1.4% 100.0% 0.0% 100.0% 0.0%
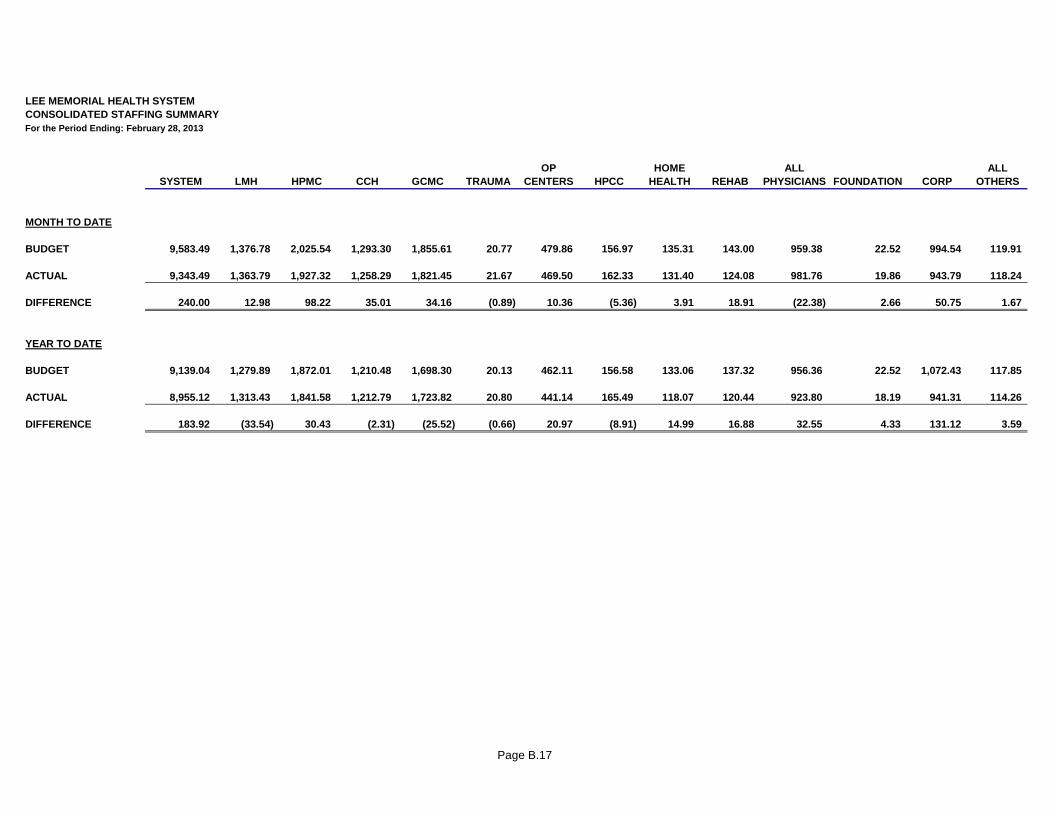
Page B.17
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATED STAFFING SUMMARYFor the Period Ending: February 28, 2013
OP HOME ALL ALLSYSTEM LMH HPMC CCH GCMC TRAUMA CENTERS HPCC HEALTH REHAB PHYSICIANS FOUNDATION CORP OTHERS
MONTH TO DATE
BUDGET 9,583.49 1,376.78 2,025.54 1,293.30 1,855.61 20.77 479.86 156.97 135.31 143.00 959.38 22.52 994.54 119.91
ACTUAL 9,343.49 1,363.79 1,927.32 1,258.29 1,821.45 21.67 469.50 162.33 131.40 124.08 981.76 19.86 943.79 118.24
DIFFERENCE 240.00 12.98 98.22 35.01 34.16 (0.89) 10.36 (5.36) 3.91 18.91 (22.38) 2.66 50.75 1.67
YEAR TO DATE
BUDGET 9,139.04 1,279.89 1,872.01 1,210.48 1,698.30 20.13 462.11 156.58 133.06 137.32 956.36 22.52 1,072.43 117.85
ACTUAL 8,955.12 1,313.43 1,841.58 1,212.79 1,723.82 20.80 441.14 165.49 118.07 120.44 923.80 18.19 941.31 114.26
DIFFERENCE 183.92 (33.54) 30.43 (2.31) (25.52) (0.66) 20.97 (8.91) 14.99 16.88 32.55 4.33 131.12 3.59
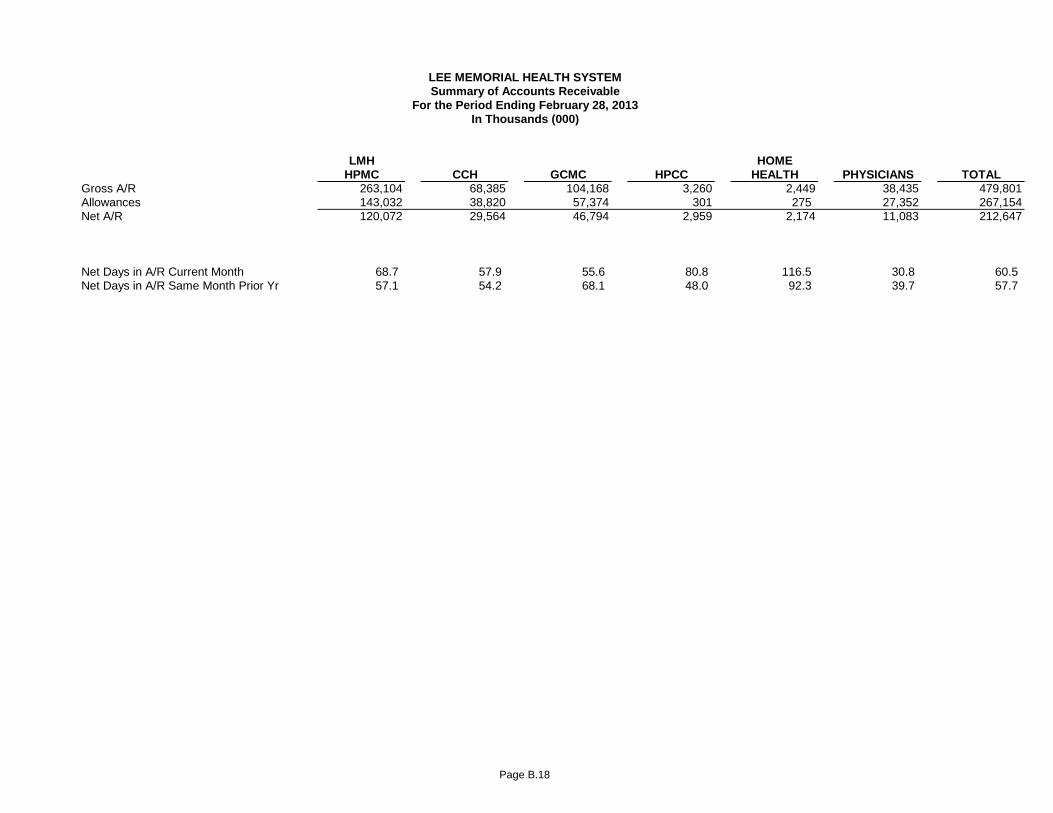
Page B.18
LMH HOMEHPMC CCH GCMC HPCC HEALTH PHYSICIANS TOTAL
Gross A/R 263,104 68,385 104,168 3,260 2,449 38,435 479,801Allowances 143,032 38,820 57,374 301 275 27,352 267,154Net A/R 120,072 29,564 46,794 2,959 2,174 11,083 212,647
Net Revenue Per Day 1,749 511 841 37 19 360 3,516
Net Days in A/R Current Month 68.7 57.9 55.6 80.8 116.5 30.8 60.5 Net Days in A/R Same Month Prior Yr 57.1 54.2 68.1 48.0 92.3 39.7 57.7 % Change
In Thousands (000)For the Period Ending February 28, 2013
Summary of Accounts ReceivableLEE MEMORIAL HEALTH SYSTEM
LEE MEMORIAL HEALTH SYSTEM
LEE COUNTY, FLORIDA
UNCONSOLIDATED
FINANCIAL STATEMENTS AND
STATISTICAL REPORTS
FEBRUARY 28, 2013

LEE MEMORIAL HEALTH SYSTEM
UNCONSOLIDATED
TABLE OF CONTENTS
SECTION C
PAGE LEESAR REGIONAL SERVICE CENTER C.1 ACCESS MEDICAL SOUTH, LC C.2 BONITA COMMUNITY HEALTH CENTER, INC. C.3
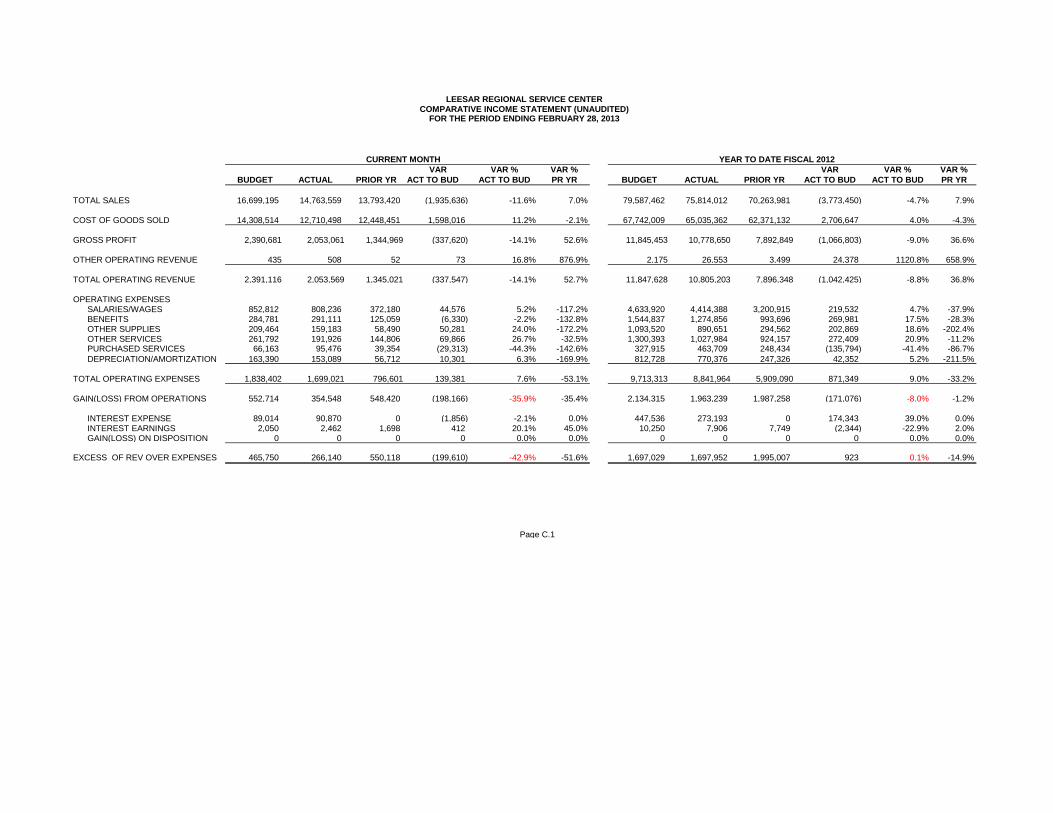
VAR VAR % VAR % VAR VAR % VAR %BUDGET ACTUAL PRIOR YR ACT TO BUD ACT TO BUD PR YR BUDGET ACTUAL PRIOR YR ACT TO BUD ACT TO BUD PR YR
TOTAL SALES 16,699,195 14,763,559 13,793,420 (1,935,636) -11.6% 7.0% 79,587,462 75,814,012 70,263,981 (3,773,450) -4.7% 7.9%
COST OF GOODS SOLD 14,308,514 12,710,498 12,448,451 1,598,016 11.2% -2.1% 67,742,009 65,035,362 62,371,132 2,706,647 4.0% -4.3% GROSS PROFIT 2,390,681 2,053,061 1,344,969 (337,620) -14.1% 52.6% 11,845,453 10,778,650 7,892,849 (1,066,803) -9.0% 36.6%
OTHER OPERATING REVENUE 435 508 52 73 16.8% 876.9% 2,175 26,553 3,499 24,378 1120.8% 658.9%
TOTAL OPERATING REVENUE 2,391,116 2,053,569 1,345,021 (337,547) -14.1% 52.7% 11,847,628 10,805,203 7,896,348 (1,042,425) -8.8% 36.8%
OPERATING EXPENSES SALARIES/WAGES 852,812 808,236 372,180 44,576 5.2% -117.2% 4,633,920 4,414,388 3,200,915 219,532 4.7% -37.9% BENEFITS 284,781 291,111 125,059 (6,330) -2.2% -132.8% 1,544,837 1,274,856 993,696 269,981 17.5% -28.3% OTHER SUPPLIES 209,464 159,183 58,490 50,281 24.0% -172.2% 1,093,520 890,651 294,562 202,869 18.6% -202.4% OTHER SERVICES 261,792 191,926 144,806 69,866 26.7% -32.5% 1,300,393 1,027,984 924,157 272,409 20.9% -11.2% PURCHASED SERVICES 66,163 95,476 39,354 (29,313) -44.3% -142.6% 327,915 463,709 248,434 (135,794) -41.4% -86.7% DEPRECIATION/AMORTIZATION 163,390 153,089 56,712 10,301 6.3% -169.9% 812,728 770,376 247,326 42,352 5.2% -211.5%
TOTAL OPERATING EXPENSES 1,838,402 1,699,021 796,601 139,381 7.6% -53.1% 9,713,313 8,841,964 5,909,090 871,349 9.0% -33.2%
GAIN(LOSS) FROM OPERATIONS 552,714 354,548 548,420 (198,166) -35.9% -35.4% 2,134,315 1,963,239 1,987,258 (171,076) -8.0% -1.2%
INTEREST EXPENSE 89,014 90,870 0 (1,856) -2.1% 0.0% 447,536 273,193 0 174,343 39.0% 0.0% INTEREST EARNINGS 2,050 2,462 1,698 412 20.1% 45.0% 10,250 7,906 7,749 (2,344) -22.9% 2.0% GAIN(LOSS) ON DISPOSITION 0 0 0 0 0.0% 0.0% 0 0 0 0 0.0% 0.0%
EXCESS OF REV OVER EXPENSES 465,750 266,140 550,118 (199,610) -42.9% -51.6% 1,697,029 1,697,952 1,995,007 923 0.1% -14.9%
Page C.1
LEESAR REGIONAL SERVICE CENTERCOMPARATIVE INCOME STATEMENT (UNAUDITED)
FOR THE PERIOD ENDING FEBRUARY 28, 2013
CURRENT MONTH YEAR TO DATE FISCAL 2012
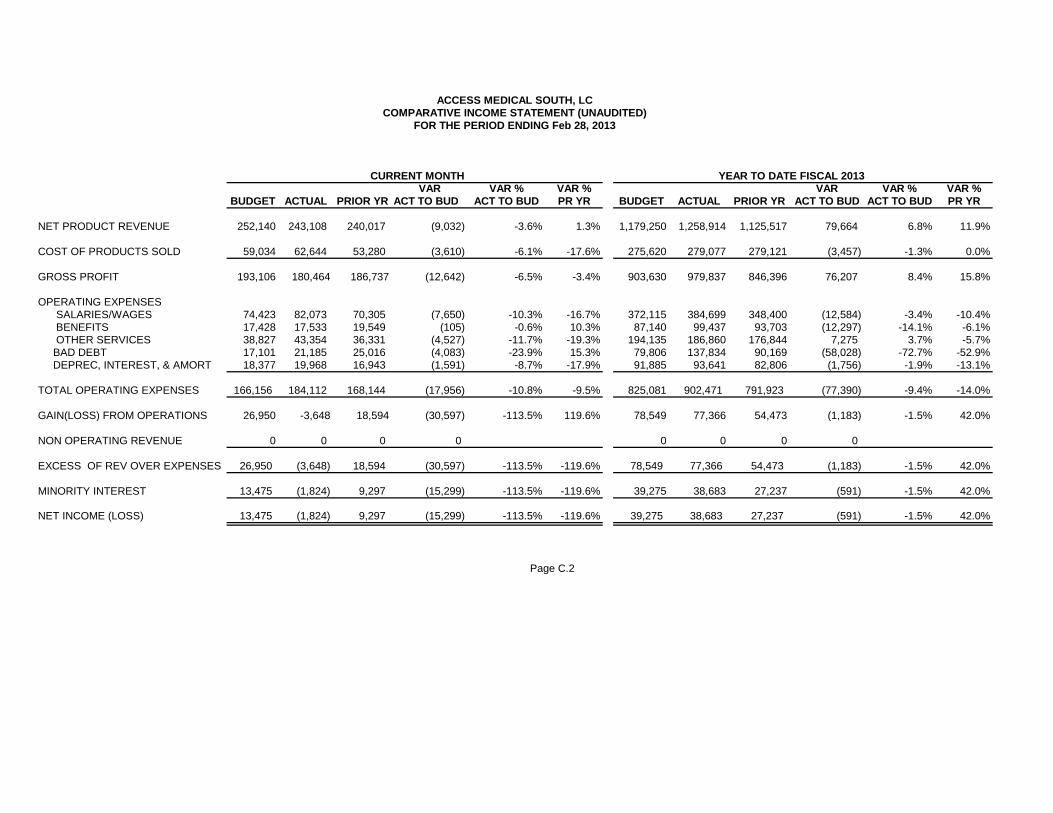
VAR VAR % VAR % VAR VAR % VAR %BUDGET ACTUAL PRIOR YR ACT TO BUD ACT TO BUD PR YR BUDGET ACTUAL PRIOR YR ACT TO BUD ACT TO BUD PR YR
NET PRODUCT REVENUE 252,140 243,108 240,017 (9,032) -3.6% 1.3% 1,179,250 1,258,914 1,125,517 79,664 6.8% 11.9%
COST OF PRODUCTS SOLD 59,034 62,644 53,280 (3,610) -6.1% -17.6% 275,620 279,077 279,121 (3,457) -1.3% 0.0%
GROSS PROFIT 193,106 180,464 186,737 (12,642) -6.5% -3.4% 903,630 979,837 846,396 76,207 8.4% 15.8%
OPERATING EXPENSES SALARIES/WAGES 74,423 82,073 70,305 (7,650) -10.3% -16.7% 372,115 384,699 348,400 (12,584) -3.4% -10.4% BENEFITS 17,428 17,533 19,549 (105) -0.6% 10.3% 87,140 99,437 93,703 (12,297) -14.1% -6.1% OTHER SERVICES 38,827 43,354 36,331 (4,527) -11.7% -19.3% 194,135 186,860 176,844 7,275 3.7% -5.7% BAD DEBT 17,101 21,185 25,016 (4,083) -23.9% 15.3% 79,806 137,834 90,169 (58,028) -72.7% -52.9% DEPREC, INTEREST, & AMORT 18,377 19,968 16,943 (1,591) -8.7% -17.9% 91,885 93,641 82,806 (1,756) -1.9% -13.1%
TOTAL OPERATING EXPENSES 166,156 184,112 168,144 (17,956) -10.8% -9.5% 825,081 902,471 791,923 (77,390) -9.4% -14.0%
GAIN(LOSS) FROM OPERATIONS 26,950 -3,648 18,594 (30,597) -113.5% 119.6% 78,549 77,366 54,473 (1,183) -1.5% 42.0%
NON OPERATING REVENUE 0 0 0 0 0 0 0 0
EXCESS OF REV OVER EXPENSES 26,950 (3,648) 18,594 (30,597) -113.5% -119.6% 78,549 77,366 54,473 (1,183) -1.5% 42.0%
MINORITY INTEREST 13,475 (1,824) 9,297 (15,299) -113.5% -119.6% 39,275 38,683 27,237 (591) -1.5% 42.0% NET INCOME (LOSS) 13,475 (1,824) 9,297 (15,299) -113.5% -119.6% 39,275 38,683 27,237 (591) -1.5% 42.0%
Page C.2
ACCESS MEDICAL SOUTH, LCCOMPARATIVE INCOME STATEMENT (UNAUDITED)
FOR THE PERIOD ENDING Feb 28, 2013
CURRENT MONTH YEAR TO DATE FISCAL 2013
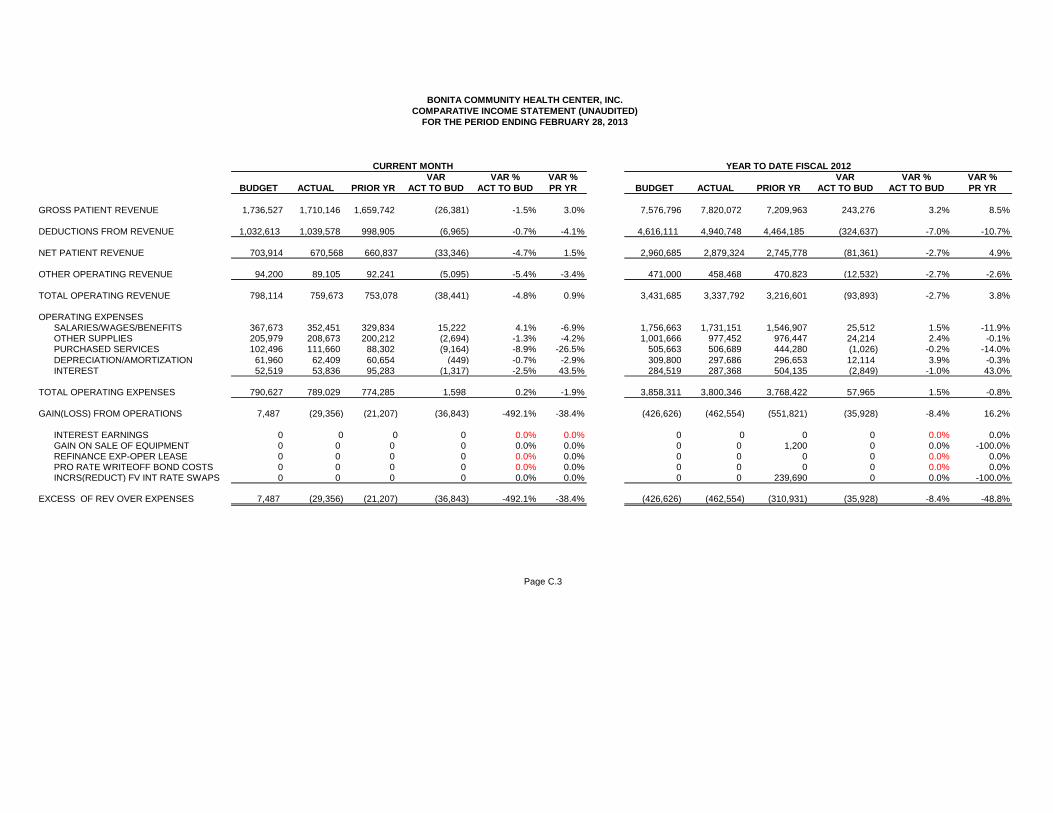
VAR VAR % VAR % VAR VAR % VAR %BUDGET ACTUAL PRIOR YR ACT TO BUD ACT TO BUD PR YR BUDGET ACTUAL PRIOR YR ACT TO BUD ACT TO BUD PR YR
GROSS PATIENT REVENUE 1,736,527 1,710,146 1,659,742 (26,381) -1.5% 3.0% 7,576,796 7,820,072 7,209,963 243,276 3.2% 8.5%
DEDUCTIONS FROM REVENUE 1,032,613 1,039,578 998,905 (6,965) -0.7% -4.1% 4,616,111 4,940,748 4,464,185 (324,637) -7.0% -10.7% NET PATIENT REVENUE 703,914 670,568 660,837 (33,346) -4.7% 1.5% 2,960,685 2,879,324 2,745,778 (81,361) -2.7% 4.9%
OTHER OPERATING REVENUE 94,200 89,105 92,241 (5,095) -5.4% -3.4% 471,000 458,468 470,823 (12,532) -2.7% -2.6%
TOTAL OPERATING REVENUE 798,114 759,673 753,078 (38,441) -4.8% 0.9% 3,431,685 3,337,792 3,216,601 (93,893) -2.7% 3.8%
OPERATING EXPENSES SALARIES/WAGES/BENEFITS 367,673 352,451 329,834 15,222 4.1% -6.9% 1,756,663 1,731,151 1,546,907 25,512 1.5% -11.9% OTHER SUPPLIES 205,979 208,673 200,212 (2,694) -1.3% -4.2% 1,001,666 977,452 976,447 24,214 2.4% -0.1% PURCHASED SERVICES 102,496 111,660 88,302 (9,164) -8.9% -26.5% 505,663 506,689 444,280 (1,026) -0.2% -14.0% DEPRECIATION/AMORTIZATION 61,960 62,409 60,654 (449) -0.7% -2.9% 309,800 297,686 296,653 12,114 3.9% -0.3% INTEREST 52,519 53,836 95,283 (1,317) -2.5% 43.5% 284,519 287,368 504,135 (2,849) -1.0% 43.0%
TOTAL OPERATING EXPENSES 790,627 789,029 774,285 1,598 0.2% -1.9% 3,858,311 3,800,346 3,768,422 57,965 1.5% -0.8%
GAIN(LOSS) FROM OPERATIONS 7,487 (29,356) (21,207) (36,843) -492.1% -38.4% (426,626) (462,554) (551,821) (35,928) -8.4% 16.2%
INTEREST EARNINGS 0 0 0 0 0.0% 0.0% 0 0 0 0 0.0% 0.0% GAIN ON SALE OF EQUIPMENT 0 0 0 0 0.0% 0.0% 0 0 1,200 0 0.0% -100.0% REFINANCE EXP-OPER LEASE 0 0 0 0 0.0% 0.0% 0 0 0 0 0.0% 0.0% PRO RATE WRITEOFF BOND COSTS 0 0 0 0 0.0% 0.0% 0 0 0 0 0.0% 0.0% INCRS(REDUCT) FV INT RATE SWAPS 0 0 0 0 0.0% 0.0% 0 0 239,690 0 0.0% -100.0%
EXCESS OF REV OVER EXPENSES 7,487 (29,356) (21,207) (36,843) -492.1% -38.4% (426,626) (462,554) (310,931) (35,928) -8.4% -48.8%
Page C.3
BONITA COMMUNITY HEALTH CENTER, INC.COMPARATIVE INCOME STATEMENT (UNAUDITED)
FOR THE PERIOD ENDING FEBRUARY 28, 2013
CURRENT MONTH YEAR TO DATE FISCAL 2012
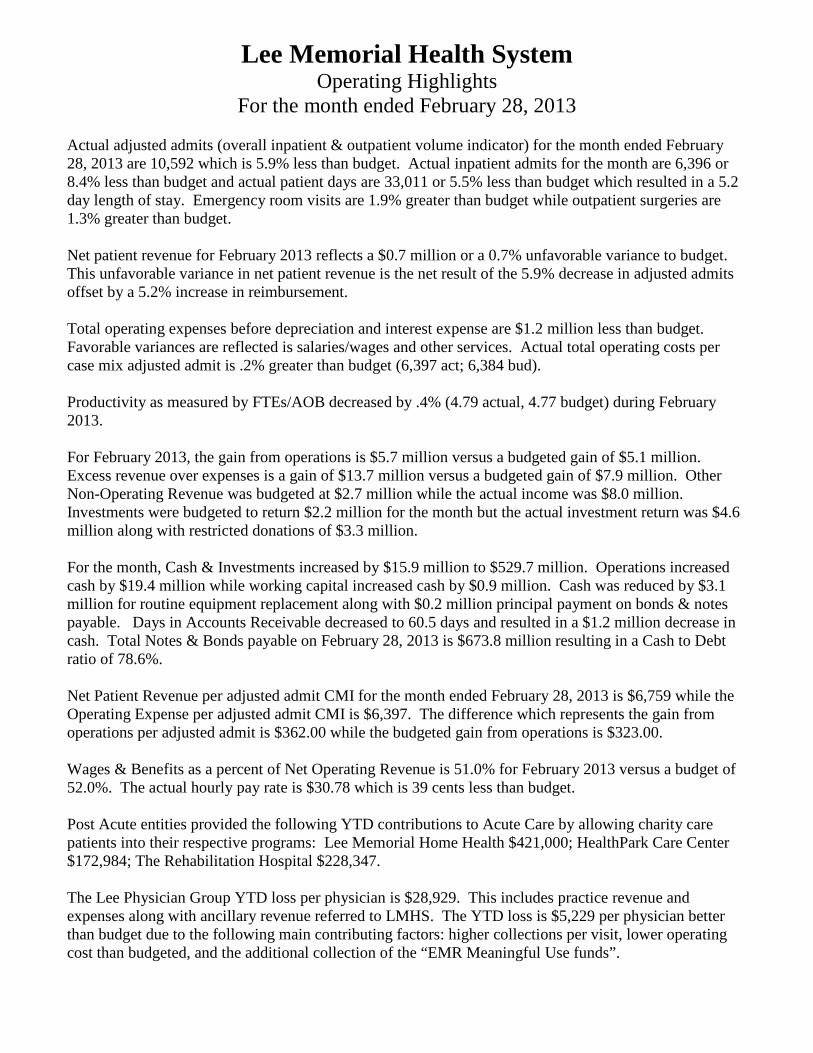
Lee Memorial Health System Operating Highlights
For the month ended February 28, 2013 Actual adjusted admits (overall inpatient & outpatient volume indicator) for the month ended February 28, 2013 are 10,592 which is 5.9% less than budget. Actual inpatient admits for the month are 6,396 or 8.4% less than budget and actual patient days are 33,011 or 5.5% less than budget which resulted in a 5.2 day length of stay. Emergency room visits are 1.9% greater than budget while outpatient surgeries are 1.3% greater than budget. Net patient revenue for February 2013 reflects a $0.7 million or a 0.7% unfavorable variance to budget. This unfavorable variance in net patient revenue is the net result of the 5.9% decrease in adjusted admits offset by a 5.2% increase in reimbursement. Total operating expenses before depreciation and interest expense are $1.2 million less than budget. Favorable variances are reflected is salaries/wages and other services. Actual total operating costs per case mix adjusted admit is .2% greater than budget (6,397 act; 6,384 bud). Productivity as measured by FTEs/AOB decreased by .4% (4.79 actual, 4.77 budget) during February 2013. For February 2013, the gain from operations is $5.7 million versus a budgeted gain of $5.1 million. Excess revenue over expenses is a gain of $13.7 million versus a budgeted gain of $7.9 million. Other Non-Operating Revenue was budgeted at $2.7 million while the actual income was $8.0 million. Investments were budgeted to return $2.2 million for the month but the actual investment return was $4.6 million along with restricted donations of $3.3 million. For the month, Cash & Investments increased by $15.9 million to $529.7 million. Operations increased cash by $19.4 million while working capital increased cash by $0.9 million. Cash was reduced by $3.1 million for routine equipment replacement along with $0.2 million principal payment on bonds & notes payable. Days in Accounts Receivable decreased to 60.5 days and resulted in a $1.2 million decrease in cash. Total Notes & Bonds payable on February 28, 2013 is $673.8 million resulting in a Cash to Debt ratio of 78.6%. Net Patient Revenue per adjusted admit CMI for the month ended February 28, 2013 is $6,759 while the Operating Expense per adjusted admit CMI is $6,397. The difference which represents the gain from operations per adjusted admit is $362.00 while the budgeted gain from operations is $323.00. Wages & Benefits as a percent of Net Operating Revenue is 51.0% for February 2013 versus a budget of 52.0%. The actual hourly pay rate is $30.78 which is 39 cents less than budget. Post Acute entities provided the following YTD contributions to Acute Care by allowing charity care patients into their respective programs: Lee Memorial Home Health $421,000; HealthPark Care Center $172,984; The Rehabilitation Hospital $228,347. The Lee Physician Group YTD loss per physician is $28,929. This includes practice revenue and expenses along with ancillary revenue referred to LMHS. The YTD loss is $5,229 per physician better than budget due to the following main contributing factors: higher collections per visit, lower operating cost than budgeted, and the additional collection of the “EMR Meaningful Use funds”.
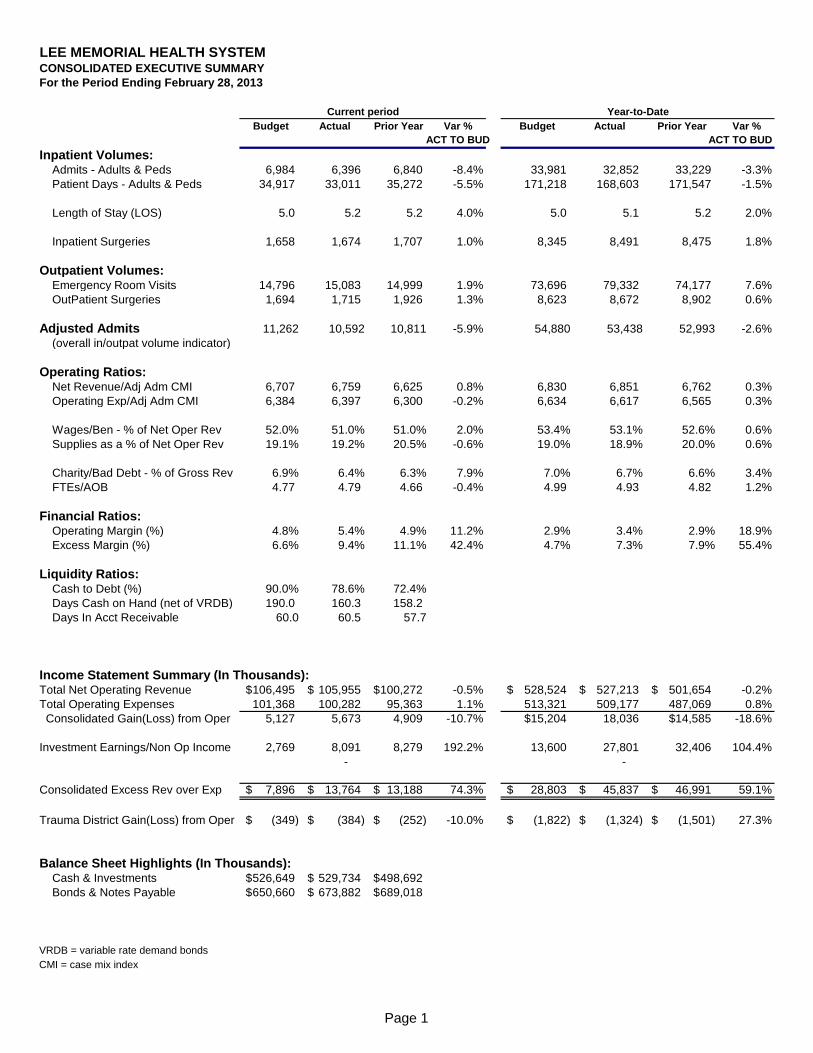
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATED EXECUTIVE SUMMARY
For the Period Ending February 28, 2013
Current period Year-to-Date
Budget Actual Prior Year Var % Budget Actual Prior Year Var %
ACT TO BUD ACT TO BUD
Inpatient Volumes: Admits - Adults & Peds 6,984 6,396 6,840 -8.4% 33,981 32,852 33,229 -3.3%
Patient Days - Adults & Peds 34,917 33,011 35,272 -5.5% 171,218 168,603 171,547 -1.5%
Length of Stay (LOS) 5.0 5.2 5.2 4.0% 5.0 5.1 5.2 2.0%
Inpatient Surgeries 1,658 1,674 1,707 1.0% 8,345 8,491 8,475 1.8%
Outpatient Volumes: Emergency Room Visits 14,796 15,083 14,999 1.9% 73,696 79,332 74,177 7.6%
OutPatient Surgeries 1,694 1,715 1,926 1.3% 8,623 8,672 8,902 0.6%
Adjusted Admits 11,262 10,592 10,811 -5.9% 54,880 53,438 52,993 -2.6%
(overall in/outpat volume indicator)
Operating Ratios: Net Revenue/Adj Adm CMI 6,707 6,759 6,625 0.8% 6,830 6,851 6,762 0.3%
Operating Exp/Adj Adm CMI 6,384 6,397 6,300 -0.2% 6,634 6,617 6,565 0.3%
Wages/Ben - % of Net Oper Rev 52.0% 51.0% 51.0% 2.0% 53.4% 53.1% 52.6% 0.6%
Supplies as a % of Net Oper Rev 19.1% 19.2% 20.5% -0.6% 19.0% 18.9% 20.0% 0.6%
Charity/Bad Debt - % of Gross Rev 6.9% 6.4% 6.3% 7.9% 7.0% 6.7% 6.6% 3.4%
FTEs/AOB 4.77 4.79 4.66 -0.4% 4.99 4.93 4.82 1.2%
Financial Ratios: Operating Margin (%) 4.8% 5.4% 4.9% 11.2% 2.9% 3.4% 2.9% 18.9%
Excess Margin (%) 6.6% 9.4% 11.1% 42.4% 4.7% 7.3% 7.9% 55.4%
Liquidity Ratios: Cash to Debt (%) 90.0% 78.6% 72.4%
Days Cash on Hand (net of VRDB) 190.0 160.3 158.2
Days In Acct Receivable 60.0 60.5 57.7
Income Statement Summary (In Thousands):Total Net Operating Revenue 106,495$ 105,955$ 100,272$ -0.5% 528,524$ 527,213$ 501,654$ -0.2%
Total Operating Expenses 101,368 100,282 95,363 1.1% 513,321 509,177 487,069 0.8%
Consolidated Gain(Loss) from Oper 5,127 5,673 4,909 -10.7% $15,204 18,036 $14,585 -18.6%
Investment Earnings/Non Op Income 2,769 8,091 8,279 192.2% 13,600 27,801 32,406 104.4%
- -
Consolidated Excess Rev over Exp 7,896$ 13,764$ 13,188$ 74.3% 28,803$ 45,837$ 46,991$ 59.1%
Trauma District Gain(Loss) from Oper (349)$ (384)$ (252)$ -10.0% (1,822)$ (1,324)$ (1,501)$ 27.3%
Balance Sheet Highlights (In Thousands): Cash & Investments 526,649$ 529,734$ 498,692$
Bonds & Notes Payable 650,660$ 673,882$ 689,018$
VRDB = variable rate demand bonds
CMI = case mix index
Page 1
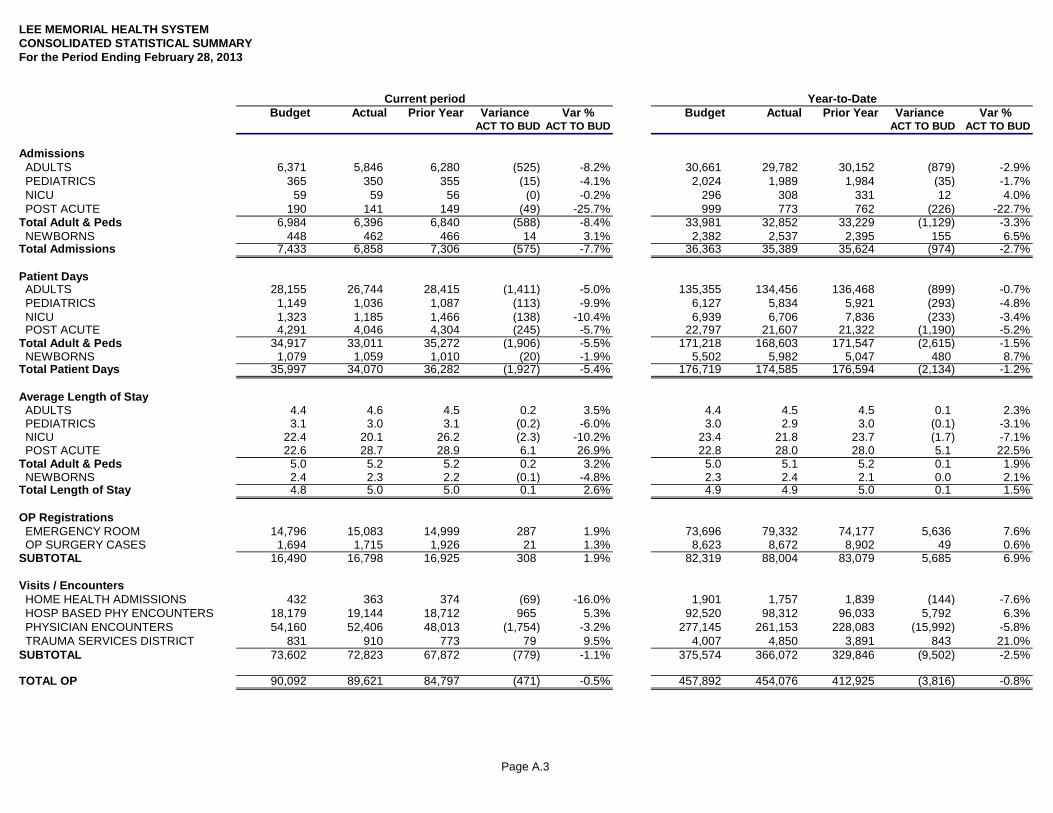
Page A.3
LEE MEMORIAL HEALTH SYSTEMCONSOLIDATED STATISTICAL SUMMARYFor the Period Ending February 28, 2013
Current period Year-to-DateBudget Actual Prior Year Variance Var % Budget Actual Prior Year Variance Var %
ACT TO BUD ACT TO BUD ACT TO BUD ACT TO BUD
Admissions ADULTS 6,371 5,846 6,280 (525) -8.2% 30,661 29,782 30,152 (879) -2.9% PEDIATRICS 365 350 355 (15) -4.1% 2,024 1,989 1,984 (35) -1.7% NICU 59 59 56 (0) -0.2% 296 308 331 12 4.0% POST ACUTE 190 141 149 (49) -25.7% 999 773 762 (226) -22.7%Total Adult & Peds 6,984 6,396 6,840 (588) -8.4% 33,981 32,852 33,229 (1,129) -3.3% NEWBORNS 448 462 466 14 3.1% 2,382 2,537 2,395 155 6.5%Total Admissions 7,433 6,858 7,306 (575) -7.7% 36,363 35,389 35,624 (974) -2.7%
Patient Days ADULTS 28,155 26,744 28,415 (1,411) -5.0% 135,355 134,456 136,468 (899) -0.7% PEDIATRICS 1,149 1,036 1,087 (113) -9.9% 6,127 5,834 5,921 (293) -4.8% NICU 1,323 1,185 1,466 (138) -10.4% 6,939 6,706 7,836 (233) -3.4% POST ACUTE 4,291 4,046 4,304 (245) -5.7% 22,797 21,607 21,322 (1,190) -5.2%Total Adult & Peds 34,917 33,011 35,272 (1,906) -5.5% 171,218 168,603 171,547 (2,615) -1.5% NEWBORNS 1,079 1,059 1,010 (20) -1.9% 5,502 5,982 5,047 480 8.7%Total Patient Days 35,997 34,070 36,282 (1,927) -5.4% 176,719 174,585 176,594 (2,134) -1.2%
Average Length of Stay ADULTS 4.4 4.6 4.5 0.2 3.5% 4.4 4.5 4.5 0.1 2.3% PEDIATRICS 3.1 3.0 3.1 (0.2) -6.0% 3.0 2.9 3.0 (0.1) -3.1% NICU 22.4 20.1 26.2 (2.3) -10.2% 23.4 21.8 23.7 (1.7) -7.1% POST ACUTE 22.6 28.7 28.9 6.1 26.9% 22.8 28.0 28.0 5.1 22.5%Total Adult & Peds 5.0 5.2 5.2 0.2 3.2% 5.0 5.1 5.2 0.1 1.9% NEWBORNS 2.4 2.3 2.2 (0.1) -4.8% 2.3 2.4 2.1 0.0 2.1%Total Length of Stay 4.8 5.0 5.0 0.1 2.6% 4.9 4.9 5.0 0.1 1.5%
OP Registrations EMERGENCY ROOM 14,796 15,083 14,999 287 1.9% 73,696 79,332 74,177 5,636 7.6% OP SURGERY CASES 1,694 1,715 1,926 21 1.3% 8,623 8,672 8,902 49 0.6%SUBTOTAL 16,490 16,798 16,925 308 1.9% 82,319 88,004 83,079 5,685 6.9%
Visits / Encounters HOME HEALTH ADMISSIONS 432 363 374 (69) -16.0% 1,901 1,757 1,839 (144) -7.6% HOSP BASED PHY ENCOUNTERS 18,179 19,144 18,712 965 5.3% 92,520 98,312 96,033 5,792 6.3% PHYSICIAN ENCOUNTERS 54,160 52,406 48,013 (1,754) -3.2% 277,145 261,153 228,083 (15,992) -5.8% TRAUMA SERVICES DISTRICT 831 910 773 79 9.5% 4,007 4,850 3,891 843 21.0%SUBTOTAL 73,602 72,823 67,872 (779) -1.1% 375,574 366,072 329,846 (9,502) -2.5%
TOTAL OP 90,092 89,621 84,797 (471) -0.5% 457,892 454,076 412,925 (3,816) -0.8%
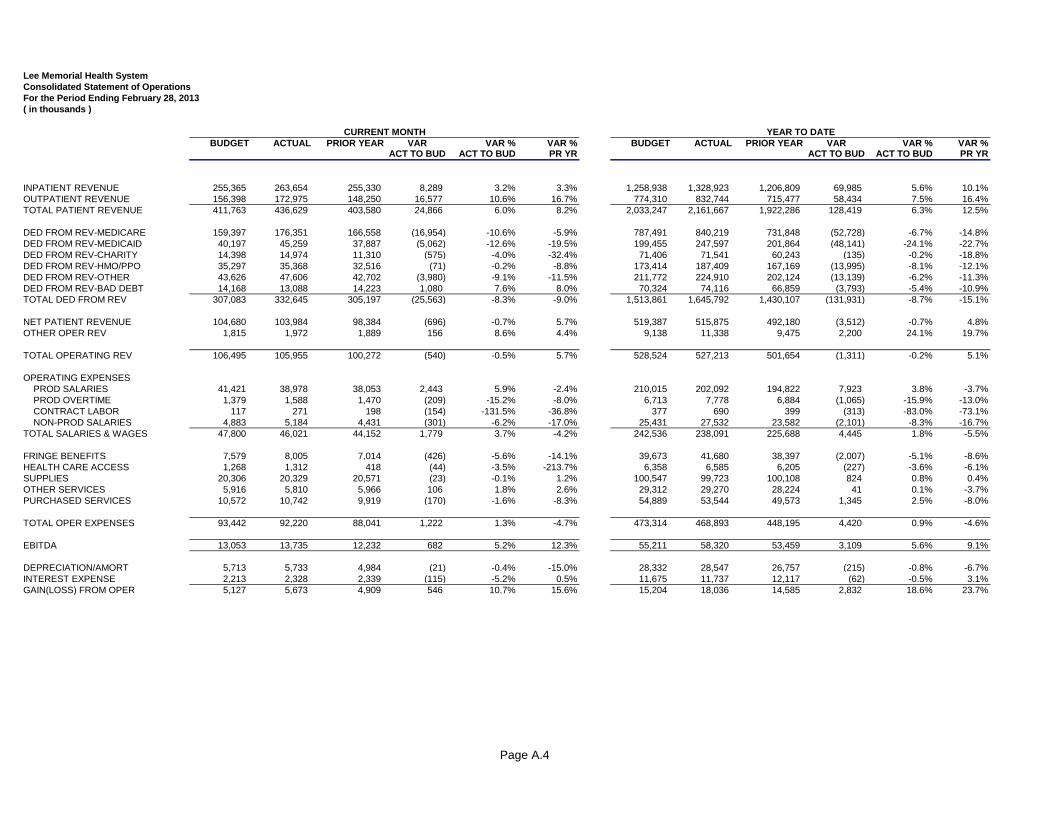
Page A.4
Lee Memorial Health SystemConsolidated Statement of OperationsFor the Period Ending February 28, 2013( in thousands )
BUDGET ACTUAL PRIOR YEAR VAR VAR % VAR % BUDGET ACTUAL PRIOR YEAR VAR VAR % VAR %ACT TO BUD ACT TO BUD PR YR ACT TO BUD ACT TO BUD PR YR
INPATIENT REVENUE 255,365 263,654 255,330 8,289 3.2% 3.3% 1,258,938 1,328,923 1,206,809 69,985 5.6% 10.1%OUTPATIENT REVENUE 156,398 172,975 148,250 16,577 10.6% 16.7% 774,310 832,744 715,477 58,434 7.5% 16.4%TOTAL PATIENT REVENUE 411,763 436,629 403,580 24,866 6.0% 8.2% 2,033,247 2,161,667 1,922,286 128,419 6.3% 12.5%
DED FROM REV-MEDICARE 159,397 176,351 166,558 (16,954) -10.6% -5.9% 787,491 840,219 731,848 (52,728) -6.7% -14.8%DED FROM REV-MEDICAID 40,197 45,259 37,887 (5,062) -12.6% -19.5% 199,455 247,597 201,864 (48,141) -24.1% -22.7%DED FROM REV-CHARITY 14,398 14,974 11,310 (575) -4.0% -32.4% 71,406 71,541 60,243 (135) -0.2% -18.8%DED FROM REV-HMO/PPO 35,297 35,368 32,516 (71) -0.2% -8.8% 173,414 187,409 167,169 (13,995) -8.1% -12.1%DED FROM REV-OTHER 43,626 47,606 42,702 (3,980) -9.1% -11.5% 211,772 224,910 202,124 (13,139) -6.2% -11.3%DED FROM REV-BAD DEBT 14,168 13,088 14,223 1,080 7.6% 8.0% 70,324 74,116 66,859 (3,793) -5.4% -10.9%TOTAL DED FROM REV 307,083 332,645 305,197 (25,563) -8.3% -9.0% 1,513,861 1,645,792 1,430,107 (131,931) -8.7% -15.1%
NET PATIENT REVENUE 104,680 103,984 98,384 (696) -0.7% 5.7% 519,387 515,875 492,180 (3,512) -0.7% 4.8%OTHER OPER REV 1,815 1,972 1,889 156 8.6% 4.4% 9,138 11,338 9,475 2,200 24.1% 19.7%
TOTAL OPERATING REV 106,495 105,955 100,272 (540) -0.5% 5.7% 528,524 527,213 501,654 (1,311) -0.2% 5.1%
OPERATING EXPENSES PROD SALARIES 41,421 38,978 38,053 2,443 5.9% -2.4% 210,015 202,092 194,822 7,923 3.8% -3.7% PROD OVERTIME 1,379 1,588 1,470 (209) -15.2% -8.0% 6,713 7,778 6,884 (1,065) -15.9% -13.0% CONTRACT LABOR 117 271 198 (154) -131.5% -36.8% 377 690 399 (313) -83.0% -73.1% NON-PROD SALARIES 4,883 5,184 4,431 (301) -6.2% -17.0% 25,431 27,532 23,582 (2,101) -8.3% -16.7%TOTAL SALARIES & WAGES 47,800 46,021 44,152 1,779 3.7% -4.2% 242,536 238,091 225,688 4,445 1.8% -5.5%
FRINGE BENEFITS 7,579 8,005 7,014 (426) -5.6% -14.1% 39,673 41,680 38,397 (2,007) -5.1% -8.6%HEALTH CARE ACCESS 1,268 1,312 418 (44) -3.5% -213.7% 6,358 6,585 6,205 (227) -3.6% -6.1%SUPPLIES 20,306 20,329 20,571 (23) -0.1% 1.2% 100,547 99,723 100,108 824 0.8% 0.4%OTHER SERVICES 5,916 5,810 5,966 106 1.8% 2.6% 29,312 29,270 28,224 41 0.1% -3.7%PURCHASED SERVICES 10,572 10,742 9,919 (170) -1.6% -8.3% 54,889 53,544 49,573 1,345 2.5% -8.0%
TOTAL OPER EXPENSES 93,442 92,220 88,041 1,222 1.3% -4.7% 473,314 468,893 448,195 4,420 0.9% -4.6%
EBITDA 13,053 13,735 12,232 682 5.2% 12.3% 55,211 58,320 53,459 3,109 5.6% 9.1%
DEPRECIATION/AMORT 5,713 5,733 4,984 (21) -0.4% -15.0% 28,332 28,547 26,757 (215) -0.8% -6.7%INTEREST EXPENSE 2,213 2,328 2,339 (115) -5.2% 0.5% 11,675 11,737 12,117 (62) -0.5% 3.1%GAIN(LOSS) FROM OPER 5,127 5,673 4,909 546 10.7% 15.6% 15,204 18,036 14,585 2,832 18.6% 23.7%
CURRENT MONTH YEAR TO DATE
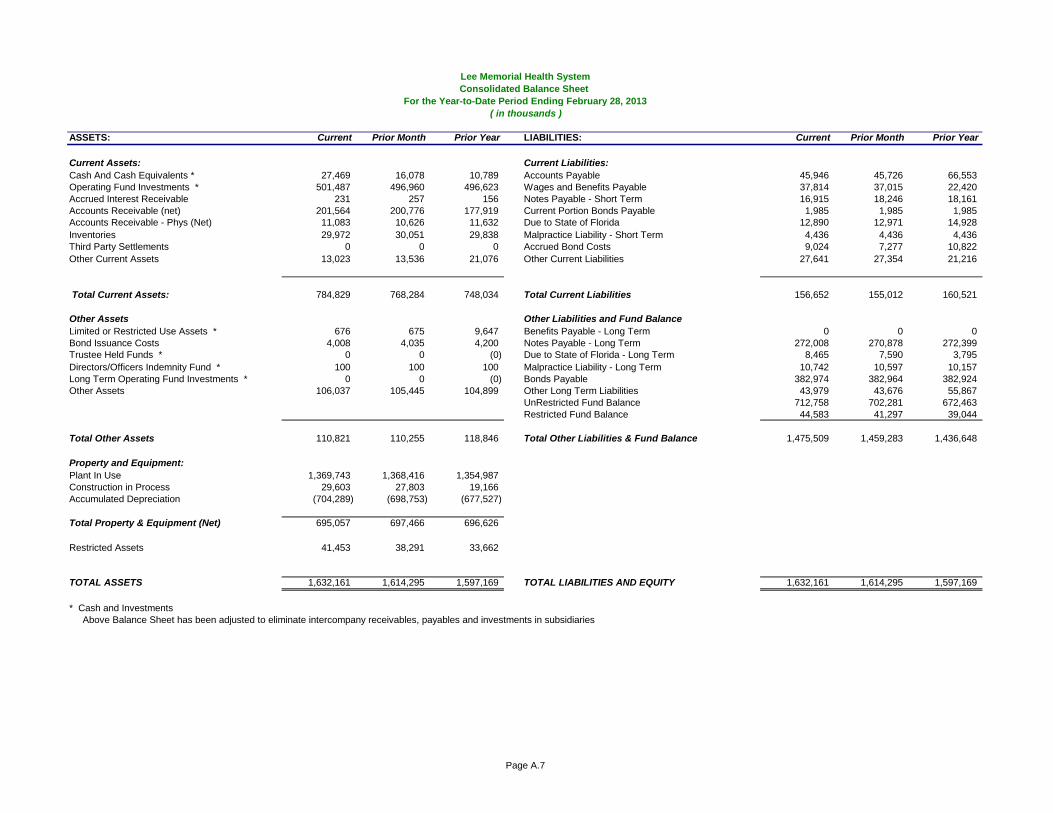
Page A.7
Lee Memorial Health SystemConsolidated Balance Sheet
For the Year-to-Date Period Ending February 28, 2013 ( in thousands )
ASSETS: Current Prior Month Prior Year LIABILITIES: Current Prior Month Prior Year
Current Assets: Current Liabilities:Cash And Cash Equivalents * 27,469 16,078 10,789 Accounts Payable 45,946 45,726 66,553Operating Fund Investments * 501,487 496,960 496,623 Wages and Benefits Payable 37,814 37,015 22,420Accrued Interest Receivable 231 257 156 Notes Payable - Short Term 16,915 18,246 18,161Accounts Receivable (net) 201,564 200,776 177,919 Current Portion Bonds Payable 1,985 1,985 1,985Accounts Receivable - Phys (Net) 11,083 10,626 11,632 Due to State of Florida 12,890 12,971 14,928Inventories 29,972 30,051 29,838 Malpractice Liability - Short Term 4,436 4,436 4,436Third Party Settlements 0 0 0 Accrued Bond Costs 9,024 7,277 10,822Other Current Assets 13,023 13,536 21,076 Other Current Liabilities 27,641 27,354 21,216
Total Current Assets: 784,829 768,284 748,034 Total Current Liabilities 156,652 155,012 160,521
Other Assets Other Liabilities and Fund BalanceLimited or Restricted Use Assets * 676 675 9,647 Benefits Payable - Long Term 0 0 0Bond Issuance Costs 4,008 4,035 4,200 Notes Payable - Long Term 272,008 270,878 272,399Trustee Held Funds * 0 0 (0) Due to State of Florida - Long Term 8,465 7,590 3,795Directors/Officers Indemnity Fund * 100 100 100 Malpractice Liability - Long Term 10,742 10,597 10,157Long Term Operating Fund Investments * 0 0 (0) Bonds Payable 382,974 382,964 382,924Other Assets 106,037 105,445 104,899 Other Long Term Liabilities 43,979 43,676 55,867
UnRestricted Fund Balance 712,758 702,281 672,463Restricted Fund Balance 44,583 41,297 39,044
Total Other Assets 110,821 110,255 118,846 Total Other Liabilities & Fund Balance 1,475,509 1,459,283 1,436,648
Property and Equipment:Plant In Use 1,369,743 1,368,416 1,354,987Construction in Process 29,603 27,803 19,166Accumulated Depreciation (704,289) (698,753) (677,527)
Total Property & Equipment (Net) 695,057 697,466 696,626
Restricted Assets 41,453 38,291 33,662
TOTAL ASSETS 1,632,161 1,614,295 1,597,169 TOTAL LIABILITIES AND EQUITY 1,632,161 1,614,295 1,597,169
* Cash and InvestmentsAbove Balance Sheet has been adjusted to eliminate intercompany receivables, payables and investments in subsidiaries
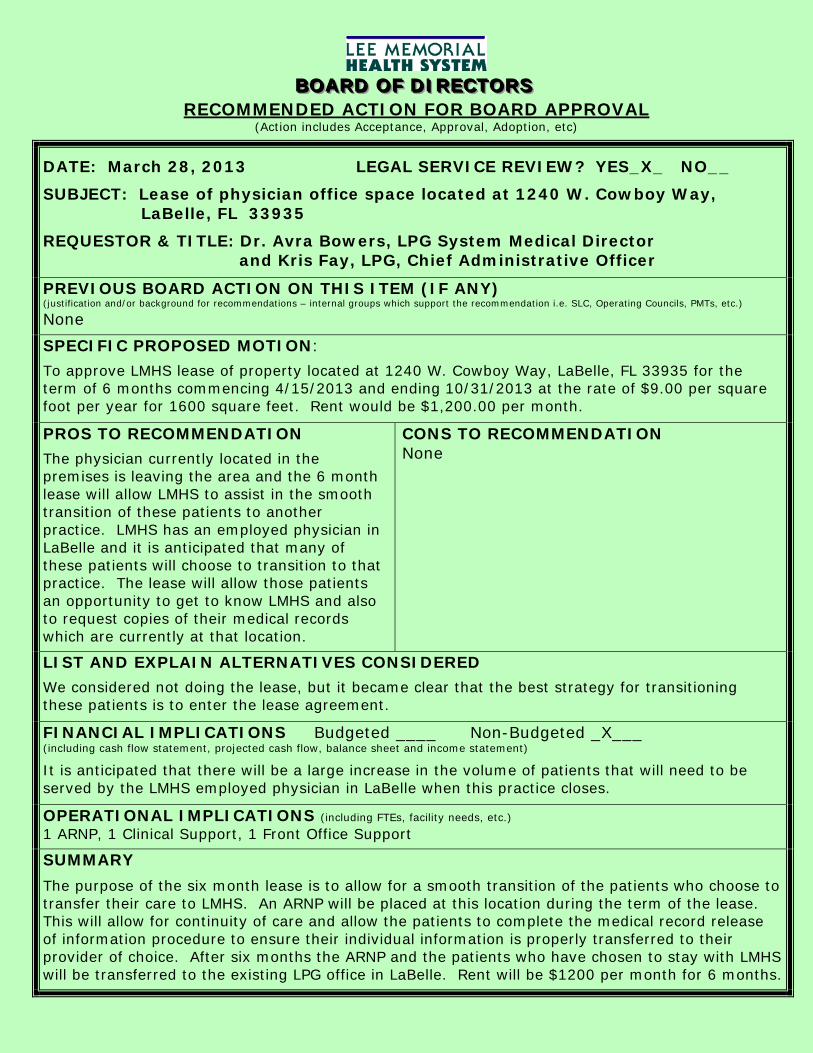
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS RECOMMENDED ACTION FOR BOARD APPROVAL
(Action includes Acceptance, Approval, Adoption, etc)
DATE: March 28, 2013 LEGAL SERVICE REVIEW? YES_X_ NO__
SUBJECT: Lease of physician office space located at 1240 W. Cowboy Way, LaBelle, FL 33935
REQUESTOR & TITLE: Dr. Avra Bowers, LPG System Medical Director and Kris Fay, LPG, Chief Administrative Officer
PREVIOUS BOARD ACTION ON THIS ITEM (IF ANY) (justification and/or background for recommendations – internal groups which support the recommendation i.e. SLC, Operating Councils, PMTs, etc.)
None
SPECIFIC PROPOSED MOTION:
To approve LMHS lease of property located at 1240 W. Cowboy Way, LaBelle, FL 33935 for the term of 6 months commencing 4/15/2013 and ending 10/31/2013 at the rate of $9.00 per square foot per year for 1600 square feet. Rent would be $1,200.00 per month.
PROS TO RECOMMENDATION
The physician currently located in the premises is leaving the area and the 6 month lease will allow LMHS to assist in the smooth transition of these patients to another practice. LMHS has an employed physician in LaBelle and it is anticipated that many of these patients will choose to transition to that practice. The lease will allow those patients an opportunity to get to know LMHS and also to request copies of their medical records which are currently at that location.
CONS TO RECOMMENDATION None
LIST AND EXPLAIN ALTERNATIVES CONSIDERED
We considered not doing the lease, but it became clear that the best strategy for transitioning these patients is to enter the lease agreement.
FINANCIAL IMPLICATIONS Budgeted ____ Non-Budgeted _X___ (including cash flow statement, projected cash flow, balance sheet and income statement)
It is anticipated that there will be a large increase in the volume of patients that will need to be served by the LMHS employed physician in LaBelle when this practice closes.
OPERATIONAL IMPLICATIONS (including FTEs, facility needs, etc.) 1 ARNP, 1 Clinical Support, 1 Front Office Support
SUMMARY
The purpose of the six month lease is to allow for a smooth transition of the patients who choose to transfer their care to LMHS. An ARNP will be placed at this location during the term of the lease. This will allow for continuity of care and allow the patients to complete the medical record release of information procedure to ensure their individual information is properly transferred to their provider of choice. After six months the ARNP and the patients who have chosen to stay with LMHS will be transferred to the existing LPG office in LaBelle. Rent will be $1200 per month for 6 months.
Page 1 of 14
LEASE
LANDLORD
Grace M. Guadiz, M.D.
And
TENANT
Lee Memorial Health System
For Premises Described As:
1240 W. Cowboy Way LaBelle, FL 33935
Lease Commencement Date: April 15, 2013
Lease End Date: Oct 31, 2013
Lee Memorial Health System Property Management Department
Page 2 of 14
LEASE AGREEMENT THIS LEASE is made and entered into between Grace M. Guadiz, M.D. (hereinafter “Landlord”) and Lee Memorial Health System (hereinafter “Tenant”), who agree and covenant as follows: 1. Description of Premises. That Landlord in consideration of the covenants and agreements to be performed by Tenant and upon the terms and conditions stated herein does hereby lease unto Tenant the space (hereinafter referred to as “the Premises") and generally known as: The Building Located at 1240 W. Cowboy Way, LaBelle, FL 33935 Consisting of approximately 1600 square feet of rentable space. The Premises are described the parcel located in R-1-07-43-29-040-0000-017.0 L V HULLS S/D N 200 FT OF S 218 FT OF E 200 FT OFLOT 19 0.92 AC. 2. Use of Premises. Tenant intends to use the Premises for the purpose of conducting physician medical office practices and medical outpatient services, but shall be allowed to use the Premises for other uses allowed by law, and approved by Landlord.
3. Lease Term.
a. The commencement date of the term of this Lease shall be April 15, 2013. This Lease shall be for a term of six (6) calendar months, plus the remaining portion of any month in which the commencement date occurs if the commencement date does not occur on the first day of a month, commencing on the "commencement date" and ending on the expiration of number of months stated above, unless sooner terminated as herein provided.
b. Notwithstanding any provision set forth in Paragraph 3.a. above, Landlord may terminate this lease at any time for any reason upon giving Tenant a sixty (60) day notice of such termination. 4. Renewal Options. This Lease shall have no renewal options. 5. Rent.
a. Tenant agrees to pay Landlord rent, without deduction, set off, or demand, for the premises at the rate of $1,200.00 per month ("Basic Rent).
b. The Basic Rent is based upon annual rent of $9.00 per square foot of leaseable space, which shall be defined as the total area of the demised premises measured from the outside line of the exterior walls.
c. The Basic Rent shall be due and payable by Tenant to Landlord on or before the
Page 3 of 14
first day of each calendar month during the term of this Lease. Rent for any portion of a month shall be prorated and shall, if occurring at the beginning of this Lease, be due and payable on occupancy, and if at the end of this Lease, at the time the premises are vacated. 6. Common Area Maintenance Charges. Landlord shall be responsible for the maintenance of the Premises and shall pay all costs associated with such maintenance including but not limited to: all maintenance charges; housekeeping charges; security charges; utility charges; real estate taxes; all taxes and special assessments on the premises; roof and building maintenance of the interior and exterior of the building; property management fees; all utility costs of the building and common areas, such as water, sewage disposal, garbage removal and electricity; any and all assessments of any property owners associations, all maintenance costs of the common areas, including, but not limited to, lighting, heating, air conditioning, painting, cleaning, policing, security, landscaping maintenance, repairs, replacement of personality or fixtures, paving, lighting, striping and re-paving the parking lot, elevator maintenance, fire control and the cost of hazard, public liability and other insurance costs. 7. Delinquency in Paying Rent. In the event that any installment of the Basic Rent, or any other sums which are owed by Tenant to Landlord under the provisions of this Lease are not received within twenty (20) days after the due date thereof (without in any way implying Landlord's consent to such late payment), Tenant shall pay, in addition to said installment of the Basic Rent or such other sums owed, a late payment charge equal to five percent (5%) of any amount so unpaid. It is understood and agreed by Tenant that said late payment charge shall be for the purpose of reimbursing Landlord for the additional cost and expense in the handling and processing of late payments, and is in addition to and exclusive of, any interest charged on overdue payments of rent or other charges. 8. Landlord's Obligations.
a. Any obligation of the Landlord hereunder to make available utility services shall be subject to the rules and regulations of the supplier of such service and of any governmental authority regulating the business of providing such utility service.
b. Landlord shall not in any way be liable to Tenant for any loss or damage or
expense which Tenant may sustain or incur if either the quantity or character of any utility is changed or is no longer available or is no longer suitable for Tenant's requirements.
c. Any utility service outage or interruption that is due to circumstances beyond
Landlord's control, or that occurs because of Landlord’s compliance with any requirement established by any governmental agency, board or bureau shall not render Landlord liable in any respect for damages to Tenant or any other person, property or business, or be construed as an eviction of Tenant.
d. Landlord shall be responsible for the installation, repair of and payment for all
Page 4 of 14
telephone equipment in the Premises. In the event any installation charges are billed to Tenant, Landlord shall reimburse Tenant for such charges immediately upon receipt of a statement from Landlord. Tenant will be responsible for 75% of monthly phone charges.
e. Landlord shall be responsible for the payment of utility company charges for usual and customary usage in the Premises.
f. Landlord shall be responsible for keeping the landlord share of premises clean. Landlord will also be responsible to keep the total premise vermin free and shall pay any charges or costs associated with landlord proportionate share cleaning services and pest control of the total premises. 9. Tenant's Obligations Regarding Premises.
a. Tenant shall throughout the term of this Lease take good care of the Premises and keep them free from waste and nuisance of any kind.
b. Tenant will reimburse the landlord seventy five percent (75%) of the actual utility expenses per month. Utilities will include cleaning services, electricity, water, sewer and garbage. Tenant will be responsible for cleaning the leased portion of the premises at tenant cost.
c. Tenant shall not in any manner deface or damage the building, and will pay the
cost of repairing any damage or removing any defacement done to the building or any part thereof by Tenant or Tenant's agents, employees or invitees. If Tenant fails to commence to make such repairs within 15 days after the occurrence of the damage or injury, Landlord may at its option make such repairs, and Tenant shall, upon demand therefore, pay Landlord for the cost thereof.
d. At the termination of this Lease, Tenant shall deliver up the Premises with all
improvements located thereon (except as otherwise herein provided) in good repair and condition, reasonable wear and tear excepted, and shall deliver to Landlord all keys to the Premises. All furniture, medical or dental equipment purchased at the onset of this lease from Dr. Patrick Guadiz, and all movable trade fixtures installed by Tenant may be removed by Tenant at the termination of this Lease. All such removal and restoration shall be accomplished in a good workmanlike manner so as not to damage the primary structure or structural qualities of the building or the plumbing, electrical lines or other utilities. 10. Assignment and Subletting. Tenant shall not assign or in any manner transfer this Lease or any estate or interest therein without the prior written consent of Landlord, which shall not be unreasonably denied or delayed. Consent by Landlord to one or more assignments shall not operate as a waiver of Landlord's rights as to any subsequent assignments. Tenant intends to sublease the entire Premises to Lee Memorial Health System under the same terms and conditions of the Lease Agreement and Landlord specifically consents to such subletting.
Page 5 of 14
11. Use and Compliance with Laws. Tenant shall not occupy or use, or permit any portion of the Premises to be occupied or used for any business or purpose other than that described in Section 2 hereof, or for any use or purpose which is unlawful in part or in whole or is deemed by Landlord to be disreputable in any manner. Tenant shall maintain the Premises in a clean, healthful and safe condition; and will comply with all laws, ordinances, orders, rules and regulations of state, federal, municipal and other agencies or authorities with reference to the use, condition, or occupancy of the demised premises, including those related to protection of the environment, and those providing for access by those persons having a physical disability. 12. Hazardous Uses Prohibited. Tenant shall not use or permit the use of the Premises in any manner that creates an unusual hazard on account of fire, explosion, escape of toxic liquids, fumes or other substances or other hazard. Nor shall Tenant permit anything to be done that will in any way increase the rate of fire or other casualty insurance on the building or its contents, and in event that, by reasons of acts of Tenant, there shall be any increase in the rate of insurance on the building or its contents created by Tenant's acts or conduct of business, then Tenant hereby agrees to pay such increase. 13. Subordination of Lease.
a. Tenant accepts this Lease subject to any future ground leases and to any mortgages which might constitute a lien upon the building, the land upon which it is situated or upon Landlord's leasehold estate or easements and other conditions of record, and to zoning ordinances and other building and fire ordinances and governmental regulations relating to the use of the property. Tenant shall at any time hereafter on demand, execute any instruments, releases or other documents that may be required by any mortgagee for the purpose of subjecting and subordinating this Lease to the lien of any such mortgage.
b. In the event that any mortgagee, ground lessor, or other person acquires title to or rights of possession in the building pursuant to the exercise of any remedy provided for in a mortgage or ground Lease, the Lease shall continue in full force as a direct Lease between Tenant and such new landlord upon all the terms, covenants, conditions and agreements set forth herein. Provided Tenant is not in default under the Lease, Landlord shall require that the new landlord or the holder of the mortgage to which this Lease is or becomes subject, execute and deliver to Tenant non-disturbance agreements in a form acceptable to Tenant.
c. In the event that any mortgagee, ground lessor or other person acquires any title or right of possession in the building pursuant to the exercise of any remedy provided for in the mortgage or ground Lease, Tenant agrees that it shall not terminate this Lease and hereby waives any right that it may have to do so, subject to Landlord’s acknowledgement of Tenant’s foregoing rights under this lease.
Page 6 of 14
d. With regard to any non-disturbance agreement issued pursuant to Subsection 16b above, Landlord shall require that the non-disturbance agreement provide that so long as Tenant is not in default under the Lease, that Tenant's leasehold interest shall continue notwithstanding any default by Landlord under such ground Lease or mortgage. 14. Right of Entry. Landlord or its officers, agents and employees shall have the right, upon reasonable advance notice to enter into and upon any and all parts of the Premises, at all reasonable hours, or, to inspect, to clean, or to make repairs, alterations or additions as Landlord may deem necessary, or to show the Premises to prospective tenants, purchasers or lenders. In the event of an emergency wherein an immediate threat to person or property exists, Landlord shall have the right to enter into and upon all parts of the Premises only for the purpose of responding to such emergency. Tenant shall not be entitled to any abatement or reduction of rent by reason of Landlord’s entry onto the Premises in accordance with this Section 16, nor shall such be deemed to be an actual or constructive eviction. Exercise of this right of entry shall not be construed as requiring Landlord to make any repairs, alterations or additions to the Premises, except as expressly provided for herein.
15. Nuisance. Tenant will conduct his business and control his officers, agents, employees and invitees in such a manner as not to create any nuisance, nor interfere with Landlord in management of building. 16. Condemnation. If the Premises, or any part thereof, or the building or any portion of the building, shall be taken or condemned in whole or in part for public purposes, or sold in lieu of condemnation, leaving the remainder of the building unsuitable for use comparable to its use on the commencement date of this Lease, or for its intended use if prior to the commencement date of this Lease, then this Lease shall forthwith cease and terminate. All compensation awarded for any taking or sale proceeds in lieu thereof awarded to compensate Landlord for the loss of the building or portion thereof shall be the property of Landlord, and Tenant shall have no claim thereto, the same being hereby expressly waived by Tenant. Tenant shall have the right to pursue recovery against the authority exercising its right of condemnation of the Premises, of any losses it may suffer as a result of such taking, including but not limited to, value of lost business opportunity, expense of removal and/or diminution in value of personal property on the Premises, and the value of any improvements to the Premises made at Tenant’s expense. 17. Fire or Other Casualty.
a. In the event that the building should be totally destroyed by fire, tornado, or other casualty, or should be so damaged that rebuilding or repairs cannot be completed within sixty (60) days after the date of such damage, either party may at its option terminate this Lease, in which event the rent shall not be due for the unexpired portion of the term of this Lease, effective with the date of such damage.
b. However, Landlord may elect to proceed to rebuild and repair the building and so
Page 7 of 14
notify Tenant of such election in writing, upon which, Tenant may elect to not terminate this Lease and remain a tenant following reconstruction. If Landlord elects to rebuild and repair, Landlord shall within thirty (30) days after the date of such damage retain an architect to design, permit and rebuild or repair the building and shall proceed with reasonable diligence to restore the building to substantially the same condition in which it was immediately prior to the happening of the casualty, except that Landlord shall not be required to rebuild, repair or replace any part of the partitions, fixtures, and other improvements which may have been placed by Tenant. No rent shall be due during the period of time required for rebuilding or repair, but Tenant’s obligation to pay rent shall recommence on the date that the Premises are suitable for occupancy.
c. In the event the building should be damaged by fire, tornado or other casualty covered by Landlord's insurance, but only to such extent that rebuilding or repairs can be completed within sixty (60) days after the date of such damage, or if the damage should be more serious but Landlord does not elect to terminate the Lease, in either such event Landlord shall allow Tenant a fair diminution of rent during the time the demised premises are unfit for occupancy. In the event any mortgagee under a mortgage on the building should require that the insurance proceeds be used to retire the mortgage debt, Landlord shall have no obligation to rebuild or repair, but if Landlord does not rebuild or repair, this Lease shall terminate, in which event the rent shall be abated during the unexpired portion of this Lease effective with the date of such damage. Any insurance which may be carried by Landlord or Tenant against loss or damage to the building or to the demised premises shall be for the sole benefit of the party carrying such insurance and under its sole control. 18. Holding Over. Should Tenant, or any of its successors in interest, hold over the Premises, or any part thereof, after the expiration of the term of this Lease, unless otherwise agreed in writing, such holding over shall constitute and be construed as tenancy from month to month only, at rent equal to the rent payable for the last month of the term of this Lease. 19. Sales and Other Taxes. Landlord shall pay all sales taxes and similar assessments and governmental charges, as well as ad valorem property taxes, if any; that may be levied or assessed against the rent, or other sum or any portion thereof, that Tenant may be required to pay to Landlord pursuant to this Lease. 20. Rent Increases. There shall be no rent increases during the term of this Lease. 21. Default. The following events shall be deemed to be events of default by Tenant under this Lease:
a. Failure of Tenant to comply with any term, provision, or covenant of this Lease which is not cured within sixty (60) days after Landlord has provided written notice thereof to Tenant, or if the matter is of such a nature as to not be curable within said time period, then failure of Tenant to initiate action to effect such cure within such time period and
Page 8 of 14
diligently pursue such action to completion.
b. Tenant shall make an assignment for the benefit of creditors.
c. Any petition shall be filed that is not removed or stayed within 90 days of filing by or against Tenant or any guarantor of Tenant's obligations hereunder, under any section or chapter of the National Bankruptcy Act, as amended, or under any similar law or statute of the United States or any State thereof; or Tenant or any guarantor of Tenant's obligations hereunder shall be adjudged bankrupt or insolvent in proceedings filed thereunder and such adjudication shall not be vacated or set aside or stayed within the time permitted by law.
d. A receiver or Trustee shall be appointed for all or substantially all of the assets of Tenant and such receivership shall not be terminated or stayed within the time permitted by law. 22. Landlord’s Remedies On Default. Upon the occurrence of any of those events of default set forth in Section 23, Landlord shall to the fullest extent allowed by law, have the option to pursue any one or more of the following remedies without any notice or demand whatsoever:
a. Terminate this Lease in which event Tenant shall immediately surrender the Premises to Landlord, and if Tenant fails to do so, Landlord may, without prejudice to any other remedy which it may have for possession or to sue for delinquent rent, enter upon and take possession and expel or remove Tenant and any other person who may be occupying the Premises or any part thereof, by force if necessary, without being liable for prosecution or any claim of damages therefore; and Tenant agrees to pay to Landlord on demand the amount of all loss and damages which Landlord may suffer by reason of such termination, whether through inability to re-let the Premises on terms at least as favorable as those in this Lease, or otherwise.
b. Enter upon and take possession of the Premises and expel or remove Tenant and any other person who may be occupying the Premises or any part thereof, by force, if necessary, without being liable for prosecution or any claim of damages therefore, and if Landlord so elects, re-let the Premises on such terms as Landlord shall deem advisable and receive the rent therefore; and Tenant agrees to pay to Landlord on demand any deficiency between the rent so received and the Basic Rent.
c. Enter upon the Premises by force, if necessary, without being liable for prosecution or any claim of damages therefore, and do whatever Tenant is obligated to do under the provisions of this Lease; and Tenant agrees to reimburse Landlord on demand for any expenses which Landlord may incur in thus effecting compliance with Tenant's obligations under this Lease, and Tenant further agrees that Landlord shall not be liable for any damages resulting to the Tenant from such action.
Page 9 of 14
d. No re-entry or taking possession of the Premises by Landlord shall be construed
as an election on its part to terminate this Lease, unless a written notice of such intention is given to Tenant. Notwithstanding any such re-letting or re-entry or taking possession, Landlord may at any time thereafter elect to terminate this Lease for a previous default. Pursuit of any of the foregoing remedies shall not preclude pursuit of any of the other remedies herein provided or any other remedies provided by law, nor shall pursuit of any remedy provided for herein constitute a forfeiture or waiver of any rent due to Landlord hereunder or of any damages accruing to Landlord by reason of the violation of any of the terms, provisions and covenants herein contained. No waiver by Landlord of any violation or breach of any of the terms, provisions, and covenants herein contained shall be deemed or construed to constitute a waiver of any other violation or breach of any of the terms, provisions, and covenants herein contained. Forbearance by Landlord to enforce one or more of the remedies herein provided upon an event of default shall not be deemed or construed to constitute a waiver of such default. The loss or damage that Landlord may suffer by reason of termination of this Lease or the deficiency from any re-letting as provided for above shall include the expense of repossession and any repairs or remodeling undertaken by Landlord following repossession. Should Landlord at any time terminate this Lease for any default, in addition to any other remedy Landlord may have, Landlord may recover from Tenant all damages Landlord may incur by reason of such default, including the cost of recovering the Premises and the loss of rent for the remainder of the Lease term. 23. Waiver of Breach. No act or omission of Landlord or its officers, agents or employees during the term of this Lease shall be construed as an acceptance of a surrender of the Premises; and no agreement to accept a surrender of the Premises shall be valid unless in writing and signed by Landlord. The receipt by Landlord of rent with knowledge of the breach of any covenant in this Lease shall not be deemed a waiver of such breach. No provision of this Lease shall be deemed to have been waived by the Landlord unless such waiver is in writing and signed by the Landlord. 24. Attorneys Fees and Costs. Should it be necessary for either party to retain the services of an attorney or attorneys to bring any action under this Lease, or to consult with, or to place said Lease with, or to seek enforcement of any of their respective rights hereunder; the parties agree in such case that the prevailing party in such action shall be entitled to a reasonable attorney's fee, together with the costs of any legal action or other expense incurred in retaining said attorney or attorneys, or enforcing the prevailing party’s rights hereunder, or collecting any sum due the prevailing party from the other party. 25. Mechanic's Liens. Tenant will not permit any mechanic's lien or liens to be placed upon the Premises or the building or any improvement thereon during the term hereof, and in case of the filing of any such lien, Tenant will promptly secure the release of same. If default in securing release thereof shall continue for twenty (20) days after written notice thereof from Landlord to Tenant, the Landlord shall have the right and privilege at Landlord's option of securing release of the same or any portion thereof without inquiry as
Page 10 of 14
to the validity thereof, and any amounts paid to secure such release, including expenses and interest, shall be so much additional indebtedness hereunder due from Tenant to Landlord and shall be repaid to Landlord immediately on rendition of bill therefore, together with interest at the highest rate permitted by law. Landlord reserves the right to record a Notice on the Public Records of Lee County in compliance with section 713.10, Florida Statutes, placing persons who may have the right to impose liens on the Premises on notice that they may not impose a lien on the Premises for work ordered by the Tenant or any sub-tenant. 26. Delivery of Notices and Payments. All requirements with regard to the sending, mailing or delivery of any notice; or the payment of rent or other sums due to Landlord by Tenant, shall be deemed to be complied with if the following steps are taken:
a. All rent and other payments required to be made by Tenant to Landlord hereunder shall be payable to Landlord in Lee County, Florida at the address set forth below, or at such other address as Landlord may designate from time to time by written notice delivered to Tenant as provided in this Section.
b. Any notice or document required to be delivered hereunder shall be deemed to be delivered when deposited in the United States mail, postage prepaid, certified or registered mail (with or without return receipt requested) addressed to the respective addresses set out below, or at such other address as they have designated by written notice delivered in accordance with this Section: Landlord: Grace M. Guadiz, M.D.
PO Box 625 LaBelle, FL 33975-0625
Tenant: Lee Memorial Health System Attn Property Management 636 Del Prado Blvd. South
Cape Coral, FL 33990 27. Computation of Time.
a. Whenever any specific period of time is required for the performance of any act under this Lease, the day upon which performance shall be calculated to be due, if it should fall on a Saturday, Sunday or legal holiday, shall be due on the first business day following such Saturday, Sunday or legal holiday. b. Whenever a period of time is required under this Lease for action to be taken by either party, the party so obligated shall not be liable or responsible for and there shall be
Page 11 of 14
excluded from the computation of any such period of time, any delay due to strikes, riots, acts of God, shortages of labor or materials, war, or governmental laws, regulations, or restrictions if such delay is beyond the control of the obligated party.
28. Invalid Provisions. If any clause or provision of this Lease is found to be illegal, invalid or unenforceable under those laws effective during the term of this Lease, it is the intent of the parties that the remainder of this Lease shall not be affected thereby, and this Lease shall continue in full force and effect as regards the remaining portions of this Lease. It is also the intent of the parties that any clause or provision of this Lease that is found to be illegal, invalid or unenforceable shall be construed in a manner which, to the extent possible, will render it legal, valid and enforceable. 29. Entire Agreement and Amendment. This instrument constitutes the entire agreement between the parties, and this Lease shall not be amended except by an instrument in writing signed by both parties. No provision of this Lease shall be deemed to have been waived by Landlord unless such waiver be in writing signed by Landlord, nor shall any custom or practice which may evolve between the parties in the administration of the terms hereof be construed to waive the right of Landlord to insist upon strict performance by Tenant of the terms hereof. 30. Interpretation. Words of any gender used in this Lease shall construed to include the other gender, and words in the singular number shall be held to include the plural, unless the context otherwise requires. Paragraph captions, wherever used, are for convenience only and shall not be used or deemed to construe, limit, enlarge or otherwise affect any provision of this Lease. Each and every covenant and agreement contained in this Lease is, and shall be construed to be, a separate and independent covenant and agreement. Time is of the essence, and the performance of all duties at those times set forth in this Lease shall be strictly adhered to without delay. 31. Insurance.
a. The Tenant covenants and agrees to protect and save harmless the Landlord against all liability arising during the term of this Lease for any loss, injury or damage resulting to any person, persons or property, sustained on or about the leased Premises or any appurtenances thereto, including loss, injuries and damage to Tenant, its employees and its property, and from any liability arising from the operation of Tenant's business resulting from any cause whatsoever, and should any party or parties institute an action at law or otherwise against said Landlord for any such loss, injury or damage, then and in that event, it shall be obligatory upon the Tenant to defend said action at Tenant's own expense and indemnify and save harmless Landlord from any loss, expense, cost or damage for or on account of such action. In furtherance of the above, Tenant shall maintain at all times during the lease term, at Tenant's cost, a comprehensive public liability insurance policy with insurance companies authorized to do business in Florida and satisfactory to Landlord. Such policy or policies shall protect Landlord against all claims or demands that may arise or be claimed on account of Tenant's use of the Premises, in an amount of at least

Page 12 of 14
$500,000 for injuries to persons in one accident, $300,000 for injuries to any one person. In addition, Tenant shall maintain fire and casualty insurance with respect to its personal property, including inventory, in an amount equal to the greater of $100,000 or the full insurable value of personal property within the Leased Premises, as determined from time to time. In addition, throughout the lease term, Tenant shall maintain any workman’s Compensation coverage in full force and effect required under Florida law, as well as wind and flood coverage. Landlord is to be named as an additional insured on each insurance policy required in this lease.
b. Landlord may, throughout the term of this Lease, procure and maintain a policy or policies of insurance, at its sole cost and expense, insuring Landlord against all claims, demands or actions arising out of or in connection with Landlord’s use of the leased premises, or in connection with the condition of the leased premises. The limits of such policy or policies shall be in such amounts as Landlord may from time to time determine. Such insurance shall be written by insurance companies qualified to do business in the State of Florida.
c. Landlord and Tenant hereby waive as against the other any and all claims and demands of whatsoever nature for damages, loss or injury to the other's property in, upon or about the leased premises or the building, when such damages, loss or injury is covered by valid and collectible insurance, to the extent of such insurance coverage. Said mutual waiver shall be in addition to, and not in limitation or degradation of any other waiver or release contained in this Lease with respect to any such damages, loss or injury to the property of the parties hereto. Each party hereto agrees that it will request its insurance carrier to endorse all applicable policies waiving the carrier's right of recovery under subrogation or otherwise against the other party. 32. Estoppel Certificates. Tenant agrees to furnish from time to time when requested by Landlord, the holder of any deed of trust or mortgage or the lessor under any ground Lease covering all or any part of the building or the improvements therein or the Premises or any interest of Landlord therein, a certificate signed by Tenant confirming and containing such factual certifications and representations deemed appropriate by Landlord, the holder of any deed of trust or mortgage or the lessor under any ground Lease covering all or any part of the building or the improvements therein or the demised premises or any interest of Landlord therein, and Tenant shall, within ten days following receipt of said proposed certificate from Landlord, return a fully executed copy of the same to Landlord. In the event Tenant shall fail to return a fully executed copy of such certificate to Landlord within the foregoing ten-day period, then Tenant shall be deemed to have approved and confirmed all of the terms, certifications and representations contained in such certificate. 33. Notice to Lender. If the Premises or the building or any part thereof is at any time subject to a first mortgage or a first deed of trust or other similar instrument and this Lease or the rentals due hereunder are assigned to such mortgagee, trustee or beneficiary and the Tenant is given written notice thereof, then the Tenant shall not terminate this Lease or
Page 13 of 14
abate rent for any default on the part of the Landlord without first giving written notice by certified or registered mail, return receipt requested, to such assignee, specifying the default in reasonable detail, and affording such assignee a reasonable opportunity to make performance, at its election, for and on behalf of the Landlord. 34. Radon Gas. Radon gas is a naturally occurring radioactive gas that, when it has accumulated in a building in sufficient quantities, may present health risks to persons who are exposed to it over time. Levels of radon that exceed federal and state guidelines have been found in buildings in Florida. Additional information regarding radon and radon testing may be obtained from your county health department. 35. Successors and Assigns. Subject to the terms and provisions of Section 11 above, this Lease shall apply to and bind the respective heirs, successors, personal representatives, and assigns of the parties hereto. The terms "Landlord" and "Tenant" shall include the successors and assigns of either such party, whether immediate or remote. 36. Jurisdiction and Venue. This Lease shall be construed in accordance with the laws of the State of Florida, and venue for any legal proceeding hereunder shall be in Lee County, Florida. This Lease shall not be recorded upon the Public Records of Lee County, Florida, or any other county within the State of Florida.
WHEREFORE the parties have executed this Lease, by and through their authorized representatives, on the date(s) shown.
{Signatures on following page}
Page 14 of 14
WITNESS As to Tenant: (Witness Signature) (Witness Printed Name) (Witness Signature) (Witness Printed Name)
TENANT: Lee Memorial Health System By:
(Signature)
Name: Title: Board Chairman Date:
WITNESS As to Landlord: (Witness Signature) (Witness Printed Name) (Witness Signature) (Witness Printed Name)
LANDLORD: Grace M. Guadiz, M.D. By:
(Signature)
Name: Grace M. Guadiz, M.D. Title: Landlord Date:
CHAIRMAN TO GOVERNANCE BOARD LIAISON:
GOVERNANCE BOARD OF DIRECTORS
MEETING Thursday, March 28, 2013
1:00pm
GOVERNANCE BOARD LIAISON:
David Collins
___________________
L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
CONSENT AGENDA (Approval)
A. Governance Meeting Minutes of October 18, 2012
B. Board Budget FYTD 2013
C. Updated 2013 Board Community Consultants List
D. Board Scorecard Results October – December 2012
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS GOVERNANCE BOARD & FULL BOARD OF DIRECTORS MEETING MINUTES
Thursday, October 18, 2012 LOCATION: Gulf Coast Medical Center Boardroom, 13685 Doctors Way, Fort Myers, FL 33912 MEMBERS PRESENT: Richard Akin, Board Chairman; Steve Brown, M.D., Board Vice Chairman; Marilyn Stout, Board Treasurer; Nancy McGovern, RN, MSM, Board Secretary; Chris Hansen, Director; Donald
Brown, Director; Jason Moon, Director; Diane Champion, Director; James Green, Director MEMBERS ABSENT: Linda Brown, MSN, ARNP, Director (Excused) STAFF PRESENT: Jim Nathan, President/CEO; Cathy Stephens, Board Administrator; Jim Humphrey, Board Counsel; Mary McGillicuddy, Chief Legal Officer; Larry Antonucci, M.D., Chief Operating Officer; Jon
Cecil, Chief Human Resources Officer; Chuck Krivenko, Chief Medical Officer/Clinical & Quality Services; Lisa Sgarlata, R.N., Chief Administrative Officer/Lee Memorial Hospital; Scott Kashman, Chief Administrative Officer/Cape Coral Hospital; John Armitstead, System Director/Pharmacy; Mary Briggs, System Director/Media Relations; Bill Silverman, M.D., Quality Community Representative; David Berger, M.D., Quality Community Representative; Rev. Bill Miller, MDiv, Chaplain; Donna Davis, Human Resources/Information Systems Analyst; Kathleen Welch, Media Relations Specialist; Tamra Ellsworth, Executive Secretary/Board of Directors Staff; Laurie Gretten, Executive Secretary/Board of Directors Staff
GUESTS: Jeff Dektas, Lee County Sheriff’s Department; Frank Gluck, Newspress; Nicasio David, M.D.; Cora Deemer; Jessica Carter, Board Candidate; David Collins, Board Candidate; Bob Smith, Board Candidate; Frank Antos, Board Candidate
NOTE: Documents referred to in these minutes are on file by reference to this meeting date in the Office of the Board of Directors and on the Board of Directors website at www.leememorial.org/Boardofdirectors, for public inspection.
SUBJECT DISCUSSION ACTION FOLLOW-UP MEETING
CALLED TO ORDER The GOVERNANCE BOARD & FULL BOARD OF DIRECTORS
MEETINGS were CALLED TO ORDER at 2:06 p.m. by Richard Akin, Board Chairman.
INVOCATION AND
PLEDGE OF ALLEGIANCE
The Invocation was given by Reverend Bill Miller and was followed by the Pledge of Allegiance.
PUBLIC INPUT None at this time.
RECOGNITIONS
RETIREMENT:
CORA DEEMER
RETIREMENT: NICASIO DAVID, M.D.
Donna Davis spoke of Cora Deemer’s employment. Jim Nathan presented a retirement certificate (Exhibit 1) and crystal to Cora Deemer for 29 years of service to Lee Memorial Health System. Cathy Stephens added she was nominated this year for the Doc Coggins Award. Jim Nathan presented a retirement certificate (Exhibit 2) and crystal to Nicasio David, M.D. for 36 years of service to Lee Memorial Health System. Chris Hansen thanked Dr. David for all his service and kindness.
CHAIRMAN CHANGE At 2:17 p.m. Governance Chairman, Donald Brown, CONVENED
the Governance portion of the meeting
CONSENT AGENDA Don Brown asked for a motion to approve the Consent Agenda consisting of:
A. Governance Meeting Minutes of February 23, 2012 B. FY 2013 Board Budget (Exhibit 3) C. Board Counsel Annual Evaluation (Exhibit 4)
Donald Brown pulled the 2013 Board Budget (Exhibit 3). He inquired how the two percent increase adds up. Cathy Stephens indicated food increases, security, the Doc Coggins Award increases, the travel and education budget increases, adding business meeting and expenses have gone down. He is concerned the Board Budget should set the example for the System and the overall is making rules for the hospital and not playing by those rules. Jim Nathan stated that we have growth issues. There are certain growth aspects to deal with, and there are some
A motion was made by Marilyn Stout to approve the balance of the Consent Agenda consisting of:
A. Governance Meeting Minutes of February 23, 2012 B. Item Pulled by Donald Brown. C. Board Counsel Annual Evaluation (Exhibit 4)
The motion was seconded by Chris Hansen and it carried with no opposition.
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS GOVERNANCE BOARD & FULL BOARD OF DIRECTORS MEETING MINUTES
Thursday, October 18, 2012 Page 2 of 5
SUBJECT DISCUSSION ACTION FOLLOW-UP items that have not been captured in the budget. Steve Brown indicated that he has several questions. He wants particular details, and will come back to the Board after he reviews it. He is concerned about the Education we do in this organization. He is disappointed about the membership in Governance Institute; they have a lot of good education. He wants several figures. He wants it tabled to the next meeting.
A motion was made by Steve Brown to Table Item B. FY 2013 Board Budget (Exhibit 3) to the October 25, 2012 Board of Directors meeting. The motion was seconded by Chris Hansen and it carried with no opposition.
B. FY 2013 Board Budget (Exhibit 3) Tabled to October 25, 2012 Board Meeting
PRESIDENTS 2012
EVALUATION RESULTS/GOALS
Jon Cecil presented the Presidents 2012 Evaluation results and goals (Exhibit 5). Marilyn Stout stated that she is someone who rates on the high side where others may not rate. She has never been disappointed in what Jim has done or how he has presented the LMHS system. She said he needs to be in the 90%, she is going to support his salary increase. Jason Moon stated that Jim is a great CEO, and he thinks he is great and he couldn’t imagine anyone else to run this system and there is always room for improvement. Discussion ensued regarding the packet materials, requesting them electronically (no legal issue per Board Counsel since it’s a public document), and problems with gathering data this early in October, requested next year go to November 7th,
time requirements to complete evaluation. Jim Nathan wanted to thank everyone for their support. From his perceptive is that he works as hard as he can, every day and every night he follows his gut.
A motion was made by Richard Akin to accept the annual performance review of the President/CEO pursuant to Board Policy No. 40.02G and Section 4 of the “Employment Agreement” and renewal of employment agreement dated February 26, 2009 for James R. Nathan. The motion was seconded by Nancy McGovern and it carried with no opposition. A motion was made by Richard Akin to recommend revision of packet material for President’s evaluation. The motion was seconded by Diane Champion and carried with no opposition.
Revisions to evaluation documents, including electronic handling.
OTHER ITEMS
2013 BOARD MEETING
SCHEDULE
BOARD SCORECARD
BOARD OFFICER TERM LIMITS
Cathy Stephens presented the 2013 Board Meeting Schedule (Exhibit 6) with the switching of the October 24, 2013 Governance Meeting to November 7, 2013. Steve Brown stated that more of the staff will be here with new time. Jim Nathan stated that staff can’t come late due to working; later afternoon time has created conflict. The Board Scorecard (Exhibit 7) was presented to the Board by Chris Hansen. Discussion ensued. Nancy McGovern proposed that there be Board Officer Term Limits. She believes that any office position should rotate and we all should have a chance. She would like to see service in the officer position for two years, no more. You can run for another officer position but not the same one. Jim Humphrey said the enabling act provides there shall be an annual meeting and it sets the precedence for that meeting. You could set a policy. If one of the members has served four or five years and the majority of the Board wants him to serve again, you could set the policy aside. The election must take place, which is a requirement. It is easy to not adhere to it. Richard Akin stated that in every case we would want to elect the best person to do that job. Every year you have that consideration. If you’re not the best choice then you don’t get put in the job. Discussion ensued regarding
A motion was made by Chris Hansen to approve the 2013 Board of Directors Meeting Schedule (Exhibit 6) with the switching of the Governance meeting October 24, 2013 with November 7, 2013. The motion was seconded by Diane Champion and carried with no opposition. A motion was made by Chris Hansen to approve the Board Scorecard (Exhibit 7). The motion was seconded by Nancy McGovern and carried with no opposition.
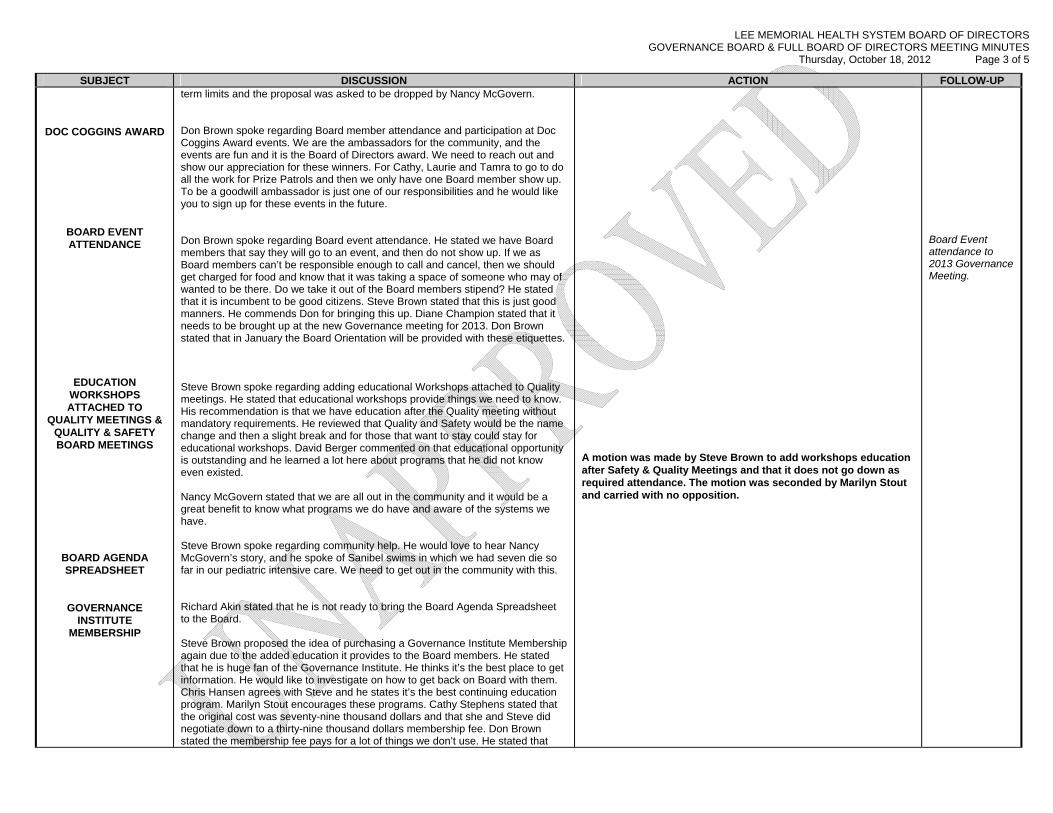
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS GOVERNANCE BOARD & FULL BOARD OF DIRECTORS MEETING MINUTES
Thursday, October 18, 2012 Page 3 of 5
SUBJECT DISCUSSION ACTION FOLLOW-UP
DOC COGGINS AWARD
BOARD EVENT ATTENDANCE
EDUCATION WORKSHOPS ATTACHED TO
QUALITY MEETINGS & QUALITY & SAFETY BOARD MEETINGS
BOARD AGENDA SPREADSHEET
GOVERNANCE INSTITUTE
MEMBERSHIP
term limits and the proposal was asked to be dropped by Nancy McGovern. Don Brown spoke regarding Board member attendance and participation at Doc Coggins Award events. We are the ambassadors for the community, and the events are fun and it is the Board of Directors award. We need to reach out and show our appreciation for these winners. For Cathy, Laurie and Tamra to go to do all the work for Prize Patrols and then we only have one Board member show up. To be a goodwill ambassador is just one of our responsibilities and he would like you to sign up for these events in the future. Don Brown spoke regarding Board event attendance. He stated we have Board members that say they will go to an event, and then do not show up. If we as Board members can’t be responsible enough to call and cancel, then we should get charged for food and know that it was taking a space of someone who may of wanted to be there. Do we take it out of the Board members stipend? He stated that it is incumbent to be good citizens. Steve Brown stated that this is just good manners. He commends Don for bringing this up. Diane Champion stated that it needs to be brought up at the new Governance meeting for 2013. Don Brown stated that in January the Board Orientation will be provided with these etiquettes. Steve Brown spoke regarding adding educational Workshops attached to Quality meetings. He stated that educational workshops provide things we need to know. His recommendation is that we have education after the Quality meeting without mandatory requirements. He reviewed that Quality and Safety would be the name change and then a slight break and for those that want to stay could stay for educational workshops. David Berger commented on that educational opportunity is outstanding and he learned a lot here about programs that he did not know even existed. Nancy McGovern stated that we are all out in the community and it would be a great benefit to know what programs we do have and aware of the systems we have. Steve Brown spoke regarding community help. He would love to hear Nancy McGovern’s story, and he spoke of Sanibel swims in which we had seven die so far in our pediatric intensive care. We need to get out in the community with this. Richard Akin stated that he is not ready to bring the Board Agenda Spreadsheet to the Board. Steve Brown proposed the idea of purchasing a Governance Institute Membership again due to the added education it provides to the Board members. He stated that he is huge fan of the Governance Institute. He thinks it’s the best place to get information. He would like to investigate on how to get back on Board with them. Chris Hansen agrees with Steve and he states it’s the best continuing education program. Marilyn Stout encourages these programs. Cathy Stephens stated that the original cost was seventy-nine thousand dollars and that she and Steve did negotiate down to a thirty-nine thousand dollars membership fee. Don Brown stated the membership fee pays for a lot of things we don’t use. He stated that
A motion was made by Steve Brown to add workshops education after Safety & Quality Meetings and that it does not go down as required attendance. The motion was seconded by Marilyn Stout and carried with no opposition.
Board Event attendance to 2013 Governance Meeting.
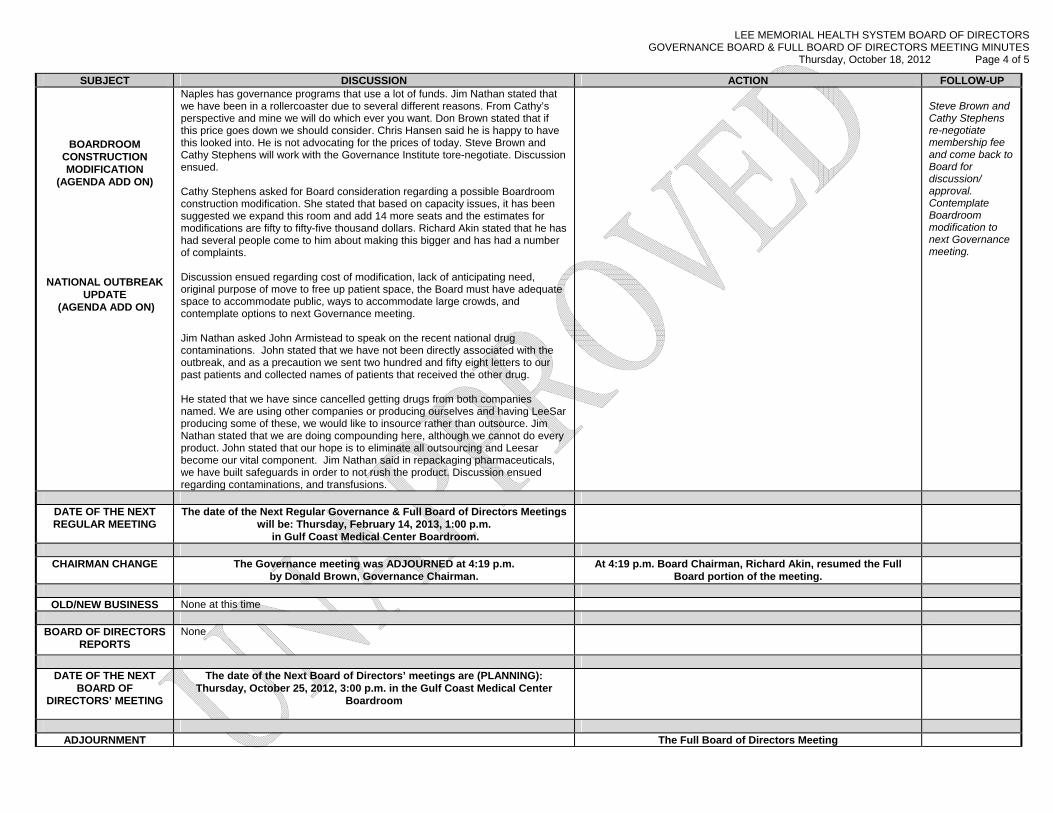
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS GOVERNANCE BOARD & FULL BOARD OF DIRECTORS MEETING MINUTES
Thursday, October 18, 2012 Page 4 of 5
SUBJECT DISCUSSION ACTION FOLLOW-UP
BOARDROOM CONSTRUCTION MODIFICATION
(AGENDA ADD ON)
NATIONAL OUTBREAK UPDATE
(AGENDA ADD ON)
Naples has governance programs that use a lot of funds. Jim Nathan stated that we have been in a rollercoaster due to several different reasons. From Cathy’s perspective and mine we will do which ever you want. Don Brown stated that if this price goes down we should consider. Chris Hansen said he is happy to have this looked into. He is not advocating for the prices of today. Steve Brown and Cathy Stephens will work with the Governance Institute tore-negotiate. Discussion ensued. Cathy Stephens asked for Board consideration regarding a possible Boardroom construction modification. She stated that based on capacity issues, it has been suggested we expand this room and add 14 more seats and the estimates for modifications are fifty to fifty-five thousand dollars. Richard Akin stated that he has had several people come to him about making this bigger and has had a number of complaints. Discussion ensued regarding cost of modification, lack of anticipating need, original purpose of move to free up patient space, the Board must have adequate space to accommodate public, ways to accommodate large crowds, and contemplate options to next Governance meeting. Jim Nathan asked John Armistead to speak on the recent national drug contaminations. John stated that we have not been directly associated with the outbreak, and as a precaution we sent two hundred and fifty eight letters to our past patients and collected names of patients that received the other drug. He stated that we have since cancelled getting drugs from both companies named. We are using other companies or producing ourselves and having LeeSar producing some of these, we would like to insource rather than outsource. Jim Nathan stated that we are doing compounding here, although we cannot do every product. John stated that our hope is to eliminate all outsourcing and Leesar become our vital component. Jim Nathan said in repackaging pharmaceuticals, we have built safeguards in order to not rush the product. Discussion ensued regarding contaminations, and transfusions.
Steve Brown and Cathy Stephens re-negotiate membership fee and come back to Board for discussion/ approval. Contemplate Boardroom modification to next Governance meeting.
DATE OF THE NEXT REGULAR MEETING
The date of the Next Regular Governance & Full Board of Directors Meetings will be: Thursday, February 14, 2013, 1:00 p.m.
in Gulf Coast Medical Center Boardroom.
CHAIRMAN CHANGE The Governance meeting was ADJOURNED at 4:19 p.m.
by Donald Brown, Governance Chairman. At 4:19 p.m. Board Chairman, Richard Akin, resumed the Full
Board portion of the meeting.
OLD/NEW BUSINESS None at this time
BOARD OF DIRECTORS
REPORTS None
DATE OF THE NEXT
BOARD OF DIRECTORS’ MEETING
The date of the Next Board of Directors’ meetings are (PLANNING): Thursday, October 25, 2012, 3:00 p.m. in the Gulf Coast Medical Center
Boardroom
ADJOURNMENT The Full Board of Directors Meeting
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS GOVERNANCE BOARD & FULL BOARD OF DIRECTORS MEETING MINUTES
Thursday, October 18, 2012 Page 5 of 5
SUBJECT DISCUSSION ACTION FOLLOW-UP was ADJOURNED at 4:24 p.m.
by Richard Akin, Board Chairman. Minutes were recorded by Laurie Gretten, Executive Secretary/Board of Directors Office
Diane Champion Board Secretary
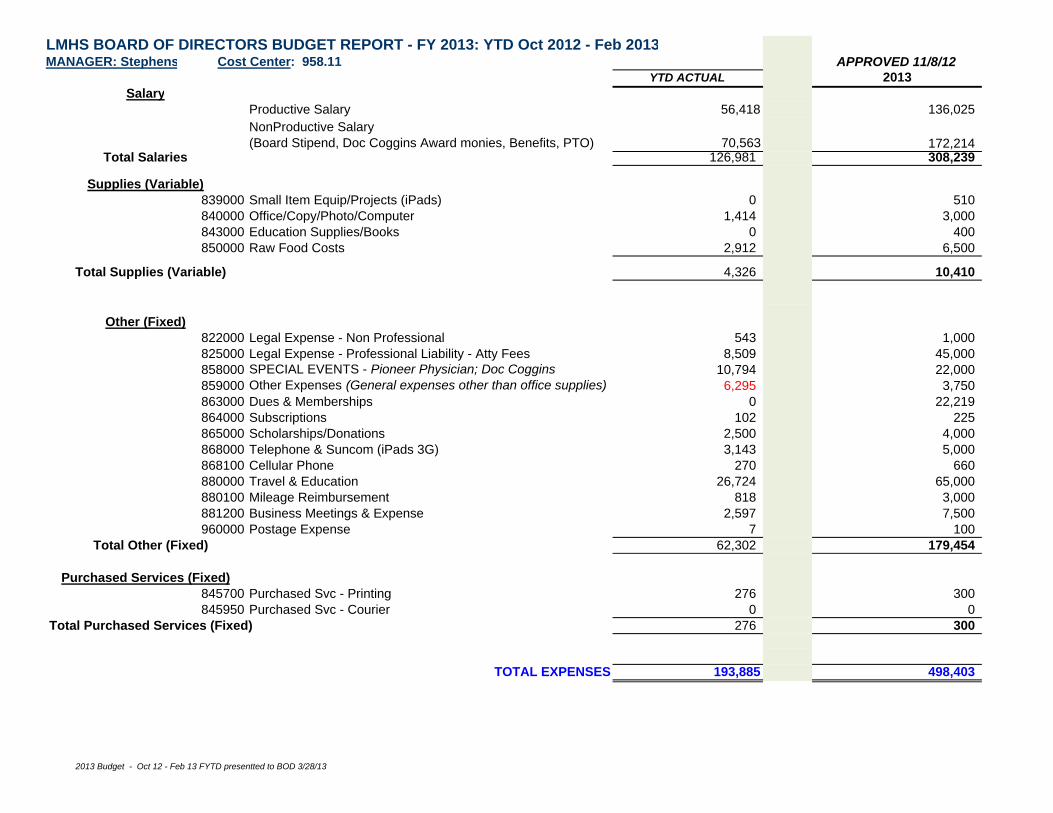
LMHS BOARD OF DIRECTORS BUDGET REPORT - FY 2013: YTD Oct 2012 - Feb 2013MANAGER: Stephens Cost Center: 958.11 APPROVED 11/8/12
YTD ACTUAL 2013Salary
Productive Salary 56,418 136,025NonProductive Salary (Board Stipend, Doc Coggins Award monies, Benefits, PTO) 70,563 172,214
Total Salaries 126,981 308,239
Supplies (Variable)839000 Small Item Equip/Projects (iPads) 0 510840000 Office/Copy/Photo/Computer 1,414 3,000843000 Education Supplies/Books 0 400850000 Raw Food Costs 2,912 6,500
Total Supplies (Variable) 4,326 10,410
Other (Fixed)822000 Legal Expense - Non Professional 543 1,000825000 Legal Expense - Professional Liability - Atty Fees 8,509 45,000858000 SPECIAL EVENTS - Pioneer Physician; Doc Coggins 10,794 22,000859000 Other Expenses (General expenses other than office supplies) 6,295 3,750863000 Dues & Memberships 0 22,219864000 Subscriptions 102 225865000 Scholarships/Donations 2,500 4,000868000 Telephone & Suncom (iPads 3G) 3,143 5,000868100 Cellular Phone 270 660880000 Travel & Education 26,724 65,000880100 Mileage Reimbursement 818 3,000881200 Business Meetings & Expense 2,597 7,500960000 Postage Expense 7 100
Total Other (Fixed) 62,302 179,454
Purchased Services (Fixed)845700 Purchased Svc - Printing 276 300845950 Purchased Svc - Courier 0 0
Total Purchased Services (Fixed) 276 300
TOTAL EXPENSES 193,885 498,403
2013 Budget - Oct 12 - Feb 13 FYTD presentted to BOD 3/28/13
Revised 32813 - 2013 Appointed Community Consultants
___________________ L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
M E M O R A N D U M
TO: LMHS Board of Directors FROM: Richard Akin, Board Chairman & Jim Nathan, CEO/President DATE: March 28, 2013 SUBJECT: Updated 2013 Board Community Consultants
Below is the updated list of the 2013 Community Consultant Appointments to the LMHS Board of Directors.
The members have been selected in accordance to Board Policy 10.52E: Community Consultants Appointments, and are appointed to serve a one calendar year term. QUALITY & SAFETY: PLC Appointment: Don Brown
1. David Berger, MD 2. Bill Silverman, MD 3. Mitchell Cordova, PhD
PLANNING: PLC Appointment: Marliese Mooney, RN, MS
1. Al Hanser 2. Ed Morton 3. Rev. Israel Suarez
FINANCE:
1. Jack Eikenberg 2. Bob Fischer 3. Don Brown
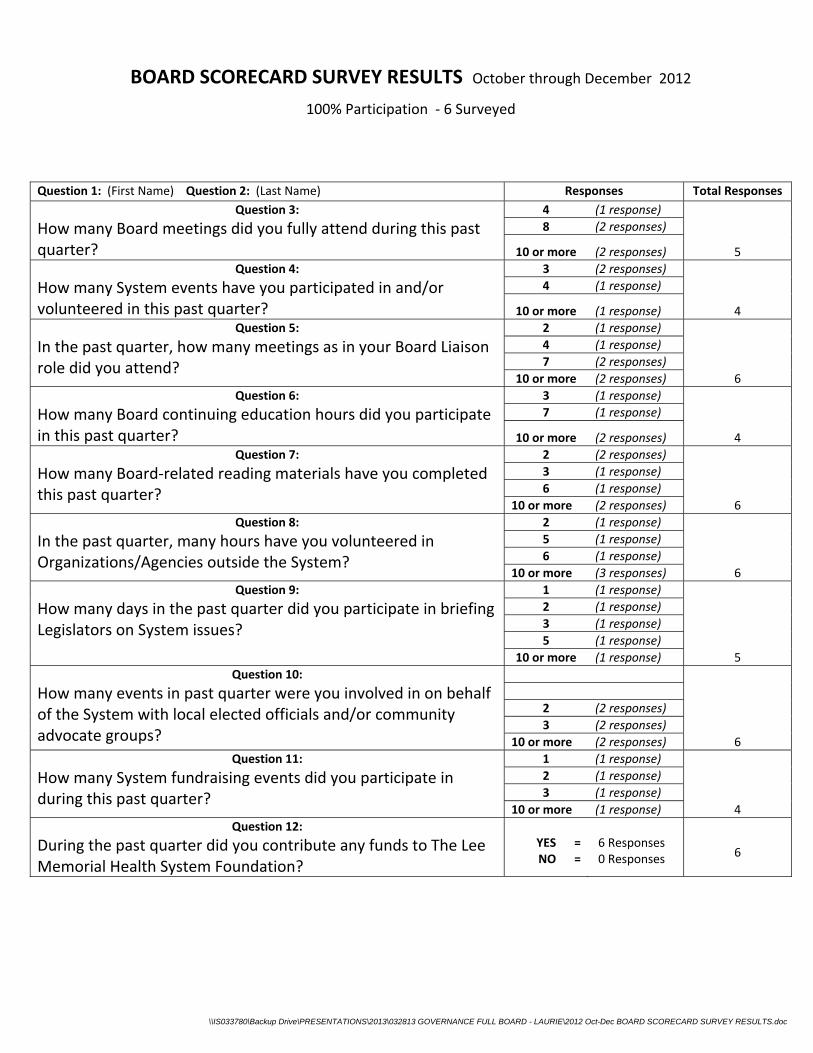
\\IS033780\Backup Drive\PRESENTATIONS\2013\032813 GOVERNANCE FULL BOARD - LAURIE\2012 Oct-Dec BOARD SCORECARD SURVEY RESULTS.doc
BOARD SCORECARD SURVEY RESULTS October through December 2012
100% Participation ‐ 6 Surveyed
Question 1: (First Name) Question 2: (Last Name) Responses Total Responses
Question 3:
How many Board meetings did you fully attend during this past quarter?
4 (1 response)
8 (2 responses)
10 or more (2 responses) 5
Question 4:
How many System events have you participated in and/or volunteered in this past quarter?
3 (2 responses)
4 (1 response)
10 or more (1 response) 4
Question 5:
In the past quarter, how many meetings as in your Board Liaison role did you attend?
2 (1 response)
4 (1 response)
7 (2 responses)
10 or more (2 responses) 6
Question 6:
How many Board continuing education hours did you participate in this past quarter?
3 (1 response)
7 (1 response)
10 or more (2 responses) 4
Question 7:
How many Board‐related reading materials have you completed this past quarter?
2 (2 responses)
3 (1 response)
6 (1 response)
10 or more (2 responses) 6
Question 8:
In the past quarter, many hours have you volunteered in Organizations/Agencies outside the System?
2 (1 response)
5 (1 response)
6 (1 response)
10 or more (3 responses) 6
Question 9:
How many days in the past quarter did you participate in briefing Legislators on System issues?
1 (1 response)
2 (1 response)
3 (1 response)
5 (1 response)
10 or more (1 response) 5
Question 10:
How many events in past quarter were you involved in on behalf of the System with local elected officials and/or community advocate groups?
2 (2 responses)
3 (2 responses)
10 or more (2 responses) 6
Question 11:
How many System fundraising events did you participate in during this past quarter?
1 (1 response)
2 (1 response)
3 (1 response)
10 or more (1 response) 4
Question 12:
During the past quarter did you contribute any funds to The Lee Memorial Health System Foundation?
YES = NO =
6 Responses 0 Responses
6
Lee Memorial Health System
The Governance Institute's
System Board Self-Assessment Report
2013
Lee Memorial Health SystemIntroduction
By completing The Governance Institute’s System Board Self-Assessment, you have committed to a thoughtful review
of your performance as the system board. This report presents the assessment survey findings, highlights areas of
excellence, and recommends areas for improvement.
The results measure your board’s performance against recommended governance practices. One or more of the
recommended practices may not be applicable to your organization—depending on your board culture, the way you
prefer to do business, and the way you prefer to do your board work. You will want to discuss these results as a board
and determine what should or should not apply to your organization.
How This Report is Organized
This report is organized into 10 sections:
· Fiduciary Duty of Care
· Fiduciary Duty of Loyalty
· Fiduciary Duty of Obedience
· Financial Oversight
· Quality Oversight
· Setting Strategic Direction
· Board Self-Assessment & Development
· Management Oversight
· Philanthropy
· Board Member Performance
Data Description & Overview
All of the exhibits show the percent of your board members who responded in a particular way to each of the survey
questions, beginning with the responses to questions showing optimal results/performance.
· Overall and Top-2 Ratings Overall ratings are calculated by combining the overall “top-2” responses for
each category. The overall and subsequent top-2 ratings graphs show the combined response of percentages of your
board responded in the two most positive responses possible in each survey scale (e.g., if the scale is "always," "most of
the time," "sometimes," "rarely," "never," or "don't know," the responses "always" and "most of the time" are the top-2,
most positive possible responses).
· Detail of Results: Detail of your responses for each question in the survey; that is, for each question, the full
range of responses appear, including the percent of respondents who answered “don’t know” to each question and the
number of “no responses” for each question.
Finally, areas of excellence are noted, as well as areas for improvement. The report and a discussion of the results
should encourage you to further assess how effectively your board carries out and/or observes these recommended
practices.
Response RateYour board’s response rate is a key consideration when reviewing the results of your board’s self-assessment. Response
rates may fluctuate from organization to organization and year to year due to a variety of issues/constraints. However, an
80% response rate or higher is considered to be a representative sample that allows for reliable analysis and an accurate
measure of the board’s performance as a whole.
Ten of 10 board members responded to your board’s self-assessment, resulting in a response rate of 100%.
The Governance Institute’s
System Board Self-Assessment
Page 1
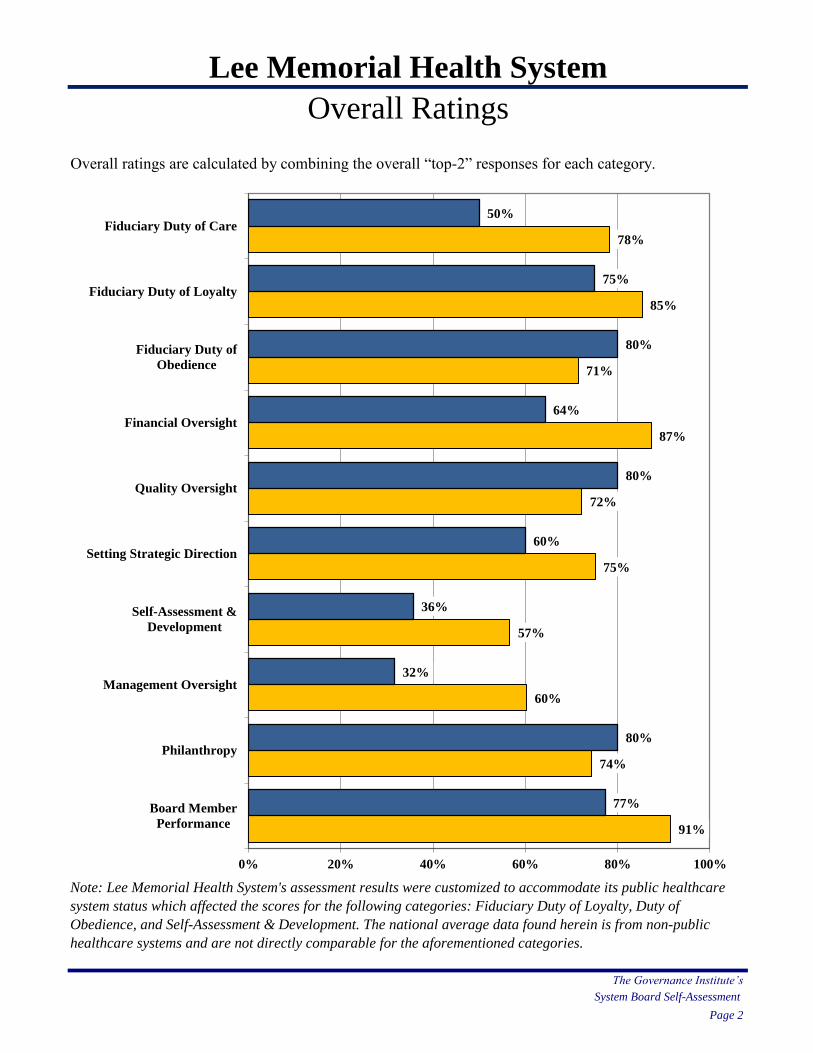
Lee Memorial Health System
Overall Ratings
Overall ratings are calculated by combining the overall “top-2” responses for each category.
Note: Lee Memorial Health System's assessment results were customized to accommodate its public healthcare
system status which affected the scores for the following categories: Fiduciary Duty of Loyalty, Duty of
Obedience, and Self-Assessment & Development. The national average data found herein is from non-public
healthcare systems and are not directly comparable for the aforementioned categories.
The Governance Institute’s
System Board Self-Assessment
Page 2
77%
80%
32%
36%
60%
80%
64%
80%
75%
50%
91%
74%
60%
57%
75%
72%
87%
71%
85%
78%
0% 20% 40% 60% 80% 100%
Board Member
Performance
Philanthropy
Management Oversight
Self-Assessment &
Development
Setting Strategic Direction
Quality Oversight
Financial Oversight
Fiduciary Duty of
Obedience
Fiduciary Duty of Loyalty
Fiduciary Duty of Care
Page
Fiduciary Duty of Care: Exhibit 1 4
Fiduciary Duty of Loyalty: Exhibit 2 5
Fiduciary Duty of Obedience: Exhibit 3 6
Financial Oversight: Exhibit 4 7
Quality Oversight: Exhibit 5 8
Setting Strategic Direction: Exhibit 6 9
Self-Assessment & Development: Exhibit 7 10
Management Oversight: Exhibit 8 11
Philanthropy: Exhibit 9 12
Board Member Performance: Exhibit 10 13
System Board Self-Assessment
Page 3
Lee Memorial Health System
Top-2 Ratings
The first set of exhibits in the report focuses on your organization’s top-2 rating for each question. Top-2
ratings are calculated by combining the “top-2” responses for individual questions in each category.
The Governance Institute’s
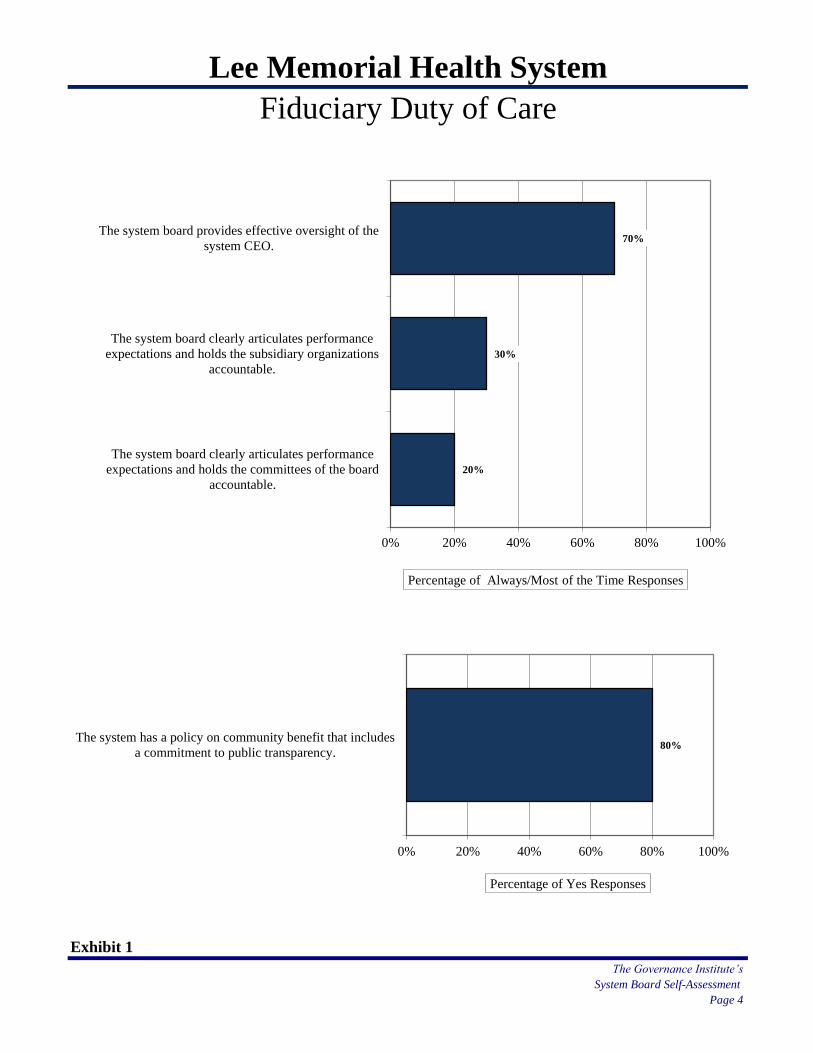
Lee Memorial Health System
Fiduciary Duty of Care
Exhibit 1
The Governance Institute’s
System Board Self-Assessment
Page 4
80%
0% 20% 40% 60% 80% 100%
The system has a policy on community benefit that includes
a commitment to public transparency.
Percentage of Yes Responses
20%
30%
70%
0% 20% 40% 60% 80% 100%
The system board clearly articulates performance
expectations and holds the committees of the board
accountable.
The system board clearly articulates performance
expectations and holds the subsidiary organizations
accountable.
The system board provides effective oversight of the
system CEO.
Percentage of Always/Most of the Time Responses
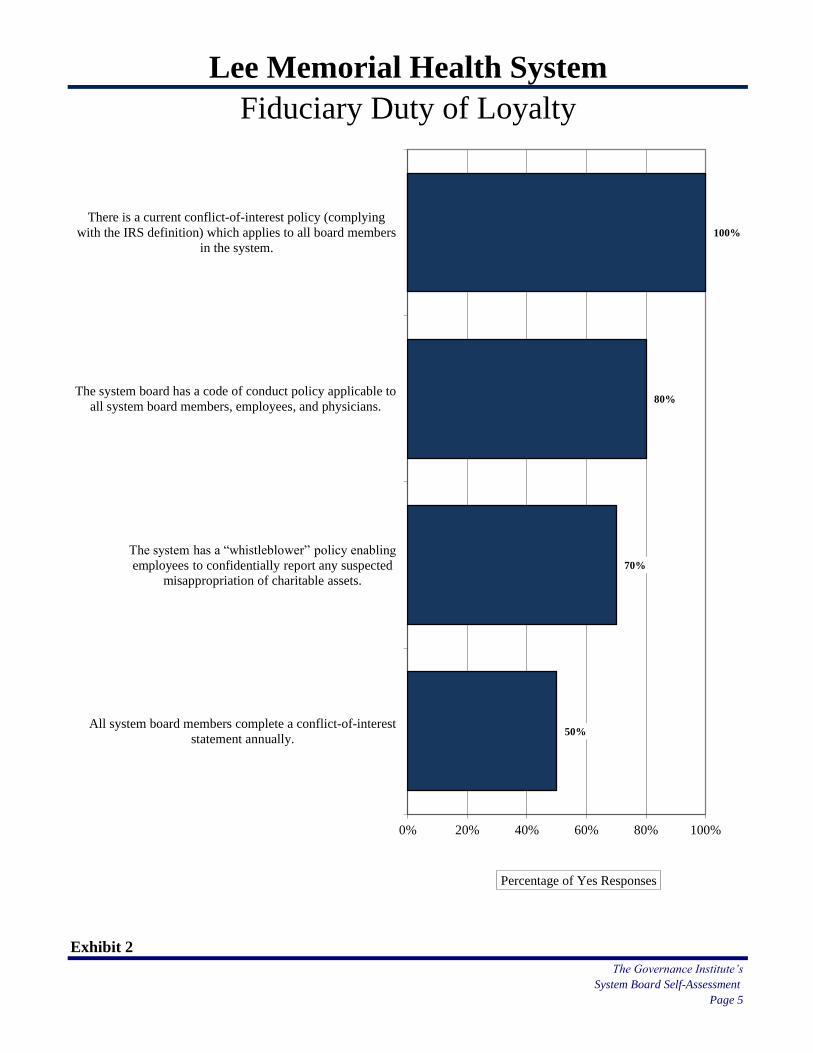
Lee Memorial Health System
Fiduciary Duty of Loyalty
Exhibit 2
The Governance Institute’s
System Board Self-Assessment
Page 5
50%
70%
80%
100%
0% 20% 40% 60% 80% 100%
All system board members complete a conflict-of-interest
statement annually.
The system has a “whistleblower” policy enabling
employees to confidentially report any suspected
misappropriation of charitable assets.
The system board has a code of conduct policy applicable to
all system board members, employees, and physicians.
There is a current conflict-of-interest policy (complying
with the IRS definition) which applies to all board members
in the system.
Percentage of Yes Responses
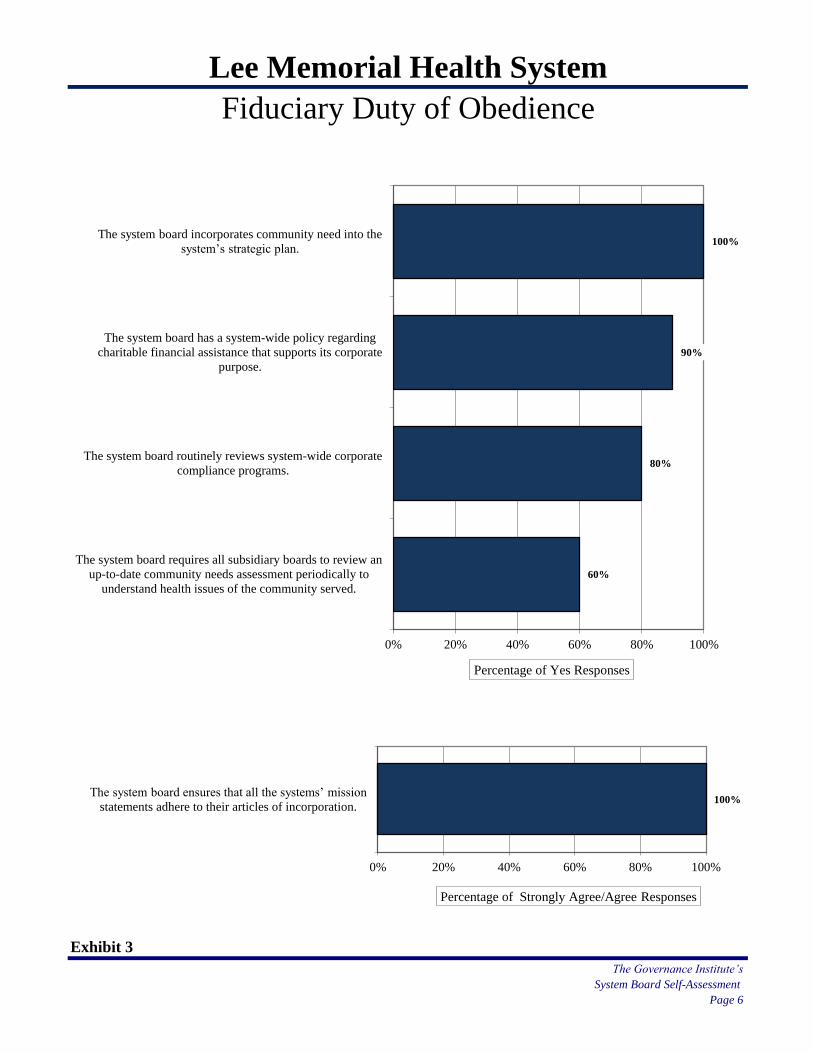
Lee Memorial Health System
Fiduciary Duty of Obedience
Exhibit 3
The Governance Institute’s
System Board Self-Assessment
Page 6
60%
80%
90%
100%
0% 20% 40% 60% 80% 100%
The system board requires all subsidiary boards to review an
up-to-date community needs assessment periodically to
understand health issues of the community served.
The system board routinely reviews system-wide corporate
compliance programs.
The system board has a system-wide policy regarding
charitable financial assistance that supports its corporate
purpose.
The system board incorporates community need into the
system’s strategic plan.
Percentage of Yes Responses
100%
0% 20% 40% 60% 80% 100%
The system board ensures that all the systems’ mission
statements adhere to their articles of incorporation.
Percentage of Strongly Agree/Agree Responses
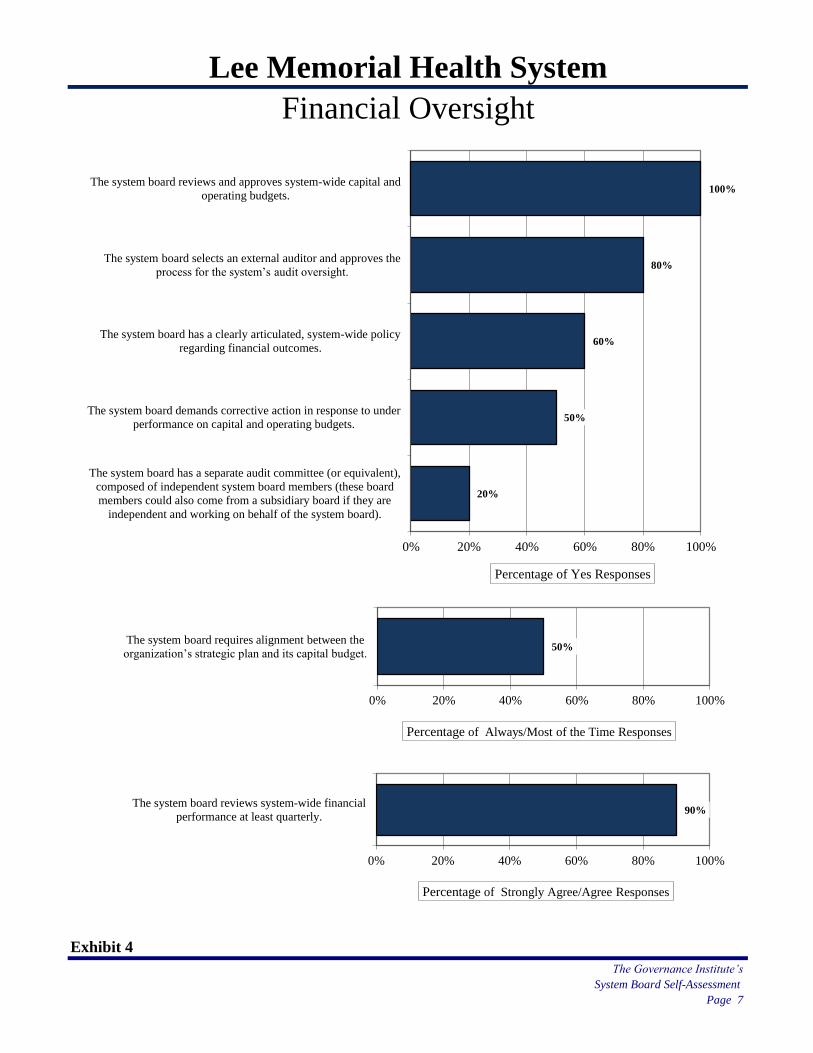
Lee Memorial Health System
Financial Oversight
Exhibit 4
The Governance Institute’s
System Board Self-Assessment
Page 7
20%
50%
60%
80%
100%
0% 20% 40% 60% 80% 100%
The system board has a separate audit committee (or equivalent),
composed of independent system board members (these board
members could also come from a subsidiary board if they are
independent and working on behalf of the system board).
The system board demands corrective action in response to under
performance on capital and operating budgets.
The system board has a clearly articulated, system-wide policy
regarding financial outcomes.
The system board selects an external auditor and approves the
process for the system’s audit oversight.
The system board reviews and approves system-wide capital and
operating budgets.
Percentage of Yes Responses
50%
0% 20% 40% 60% 80% 100%
The system board requires alignment between the
organization’s strategic plan and its capital budget.
Percentage of Always/Most of the Time Responses
90%
0% 20% 40% 60% 80% 100%
The system board reviews system-wide financial
performance at least quarterly.
Percentage of Strongly Agree/Agree Responses
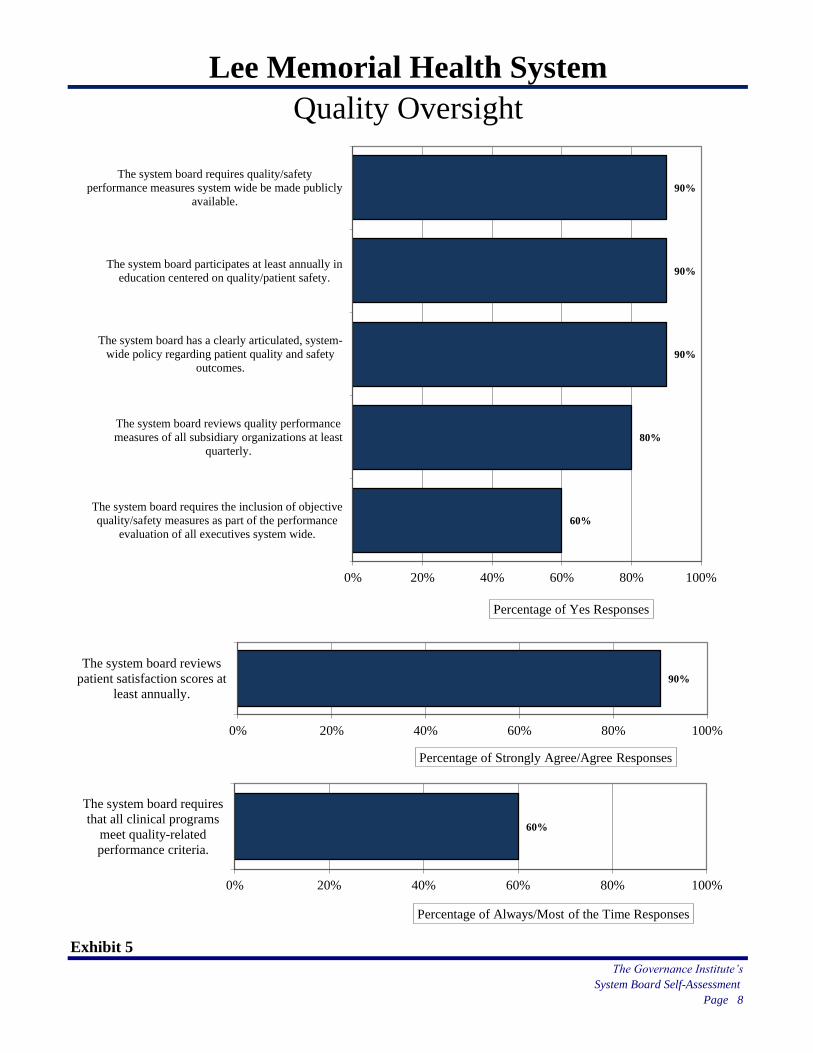
Lee Memorial Health System
Quality Oversight
Exhibit 5
The Governance Institute’s
System Board Self-Assessment
Page 8
60%
80%
90%
90%
90%
0% 20% 40% 60% 80% 100%
The system board requires the inclusion of objective
quality/safety measures as part of the performance
evaluation of all executives system wide.
The system board reviews quality performance
measures of all subsidiary organizations at least
quarterly.
The system board has a clearly articulated, system-
wide policy regarding patient quality and safety
outcomes.
The system board participates at least annually in
education centered on quality/patient safety.
The system board requires quality/safety
performance measures system wide be made publicly
available.
Percentage of Yes Responses
90%
0% 20% 40% 60% 80% 100%
The system board reviews
patient satisfaction scores at
least annually.
Percentage of Strongly Agree/Agree Responses
60%
0% 20% 40% 60% 80% 100%
The system board requires
that all clinical programs
meet quality-related
performance criteria.
Percentage of Always/Most of the Time Responses
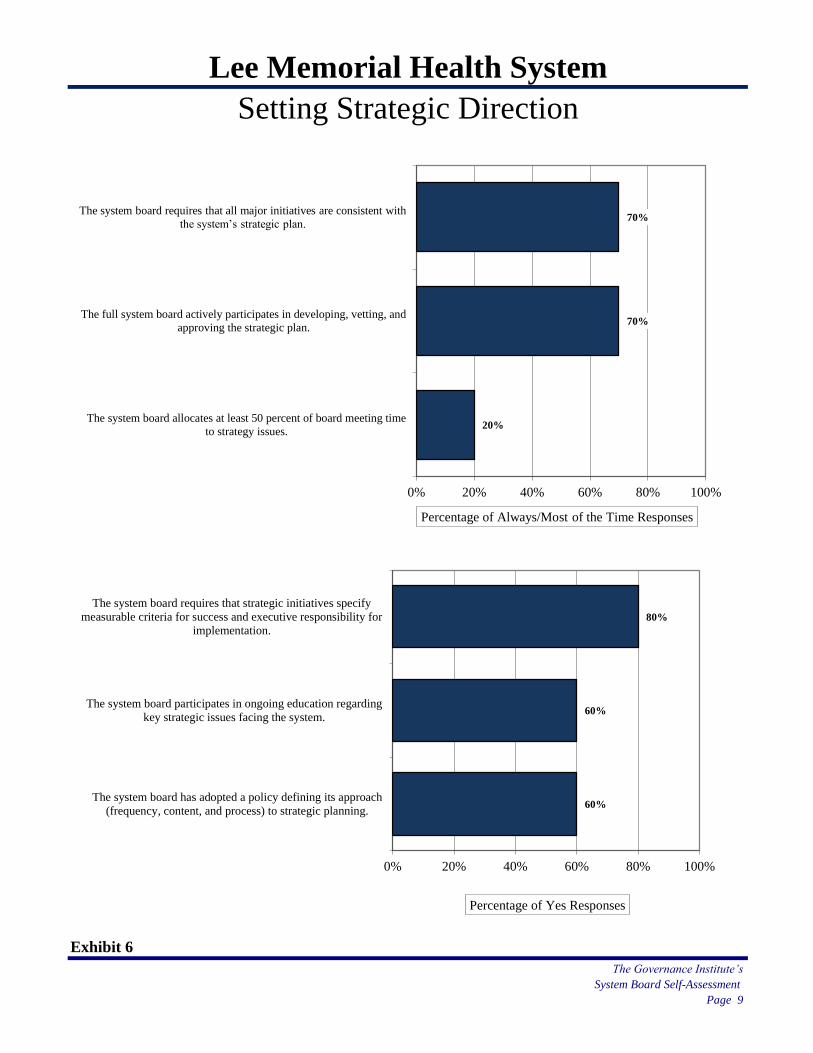
Lee Memorial Health System
Setting Strategic Direction
Exhibit 6
The Governance Institute’s
System Board Self-Assessment
Page 9
20%
70%
70%
0% 20% 40% 60% 80% 100%
The system board allocates at least 50 percent of board meeting time
to strategy issues.
The full system board actively participates in developing, vetting, and
approving the strategic plan.
The system board requires that all major initiatives are consistent with
the system’s strategic plan.
Percentage of Always/Most of the Time Responses
60%
60%
80%
0% 20% 40% 60% 80% 100%
The system board has adopted a policy defining its approach
(frequency, content, and process) to strategic planning.
The system board participates in ongoing education regarding
key strategic issues facing the system.
The system board requires that strategic initiatives specify
measurable criteria for success and executive responsibility for
implementation.
Percentage of Yes Responses
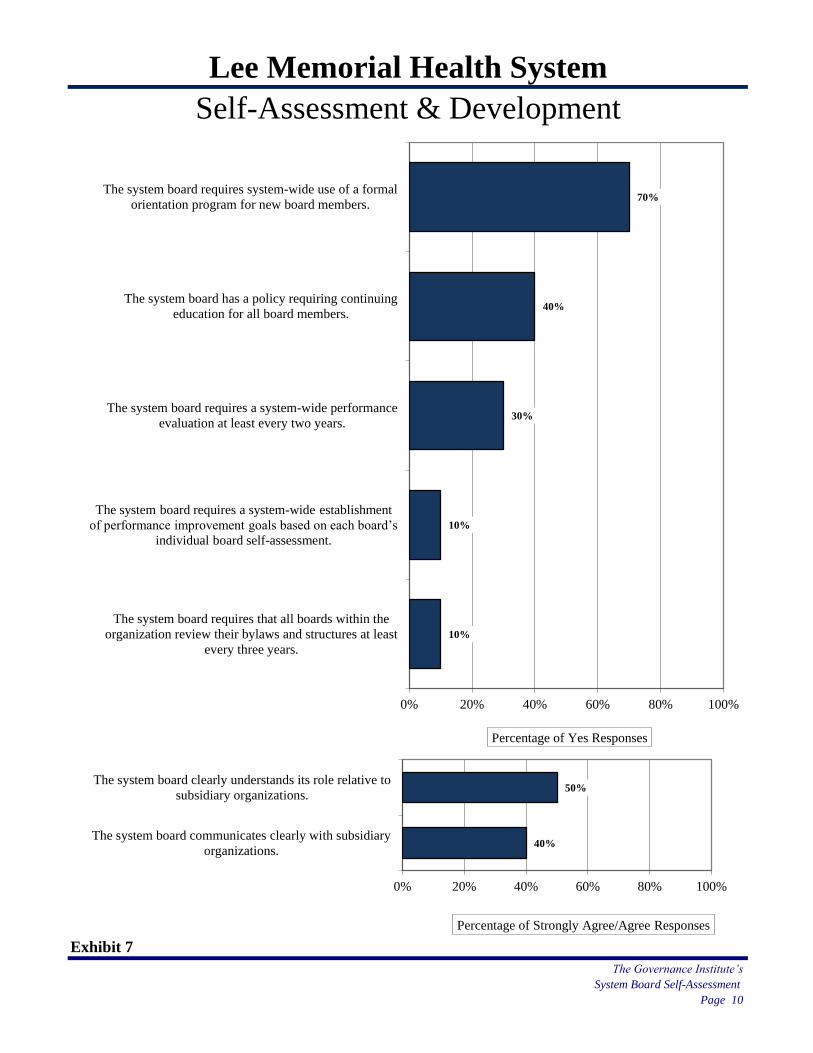
Lee Memorial Health System
Self-Assessment & Development
Exhibit 7
The Governance Institute’s
System Board Self-Assessment
Page 10
10%
10%
30%
40%
70%
0% 20% 40% 60% 80% 100%
The system board requires that all boards within the
organization review their bylaws and structures at least
every three years.
The system board requires a system-wide establishment
of performance improvement goals based on each board’s
individual board self-assessment.
The system board requires a system-wide performance
evaluation at least every two years.
The system board has a policy requiring continuing
education for all board members.
The system board requires system-wide use of a formal
orientation program for new board members.
Percentage of Yes Responses
40%
50%
0% 20% 40% 60% 80% 100%
The system board communicates clearly with subsidiary
organizations.
The system board clearly understands its role relative to
subsidiary organizations.
Percentage of Strongly Agree/Agree Responses
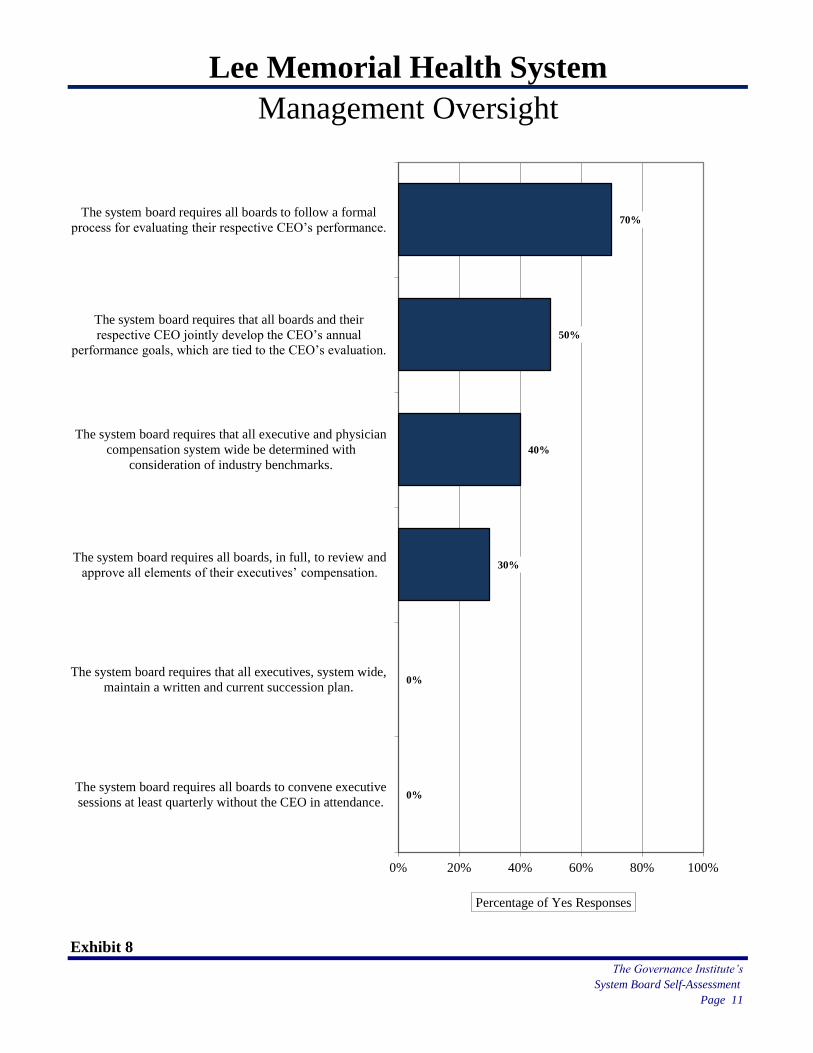
Lee Memorial Health System
Management Oversight
Exhibit 8
The Governance Institute’s
System Board Self-Assessment
Page 11
0%
0%
30%
40%
50%
70%
0% 20% 40% 60% 80% 100%
The system board requires all boards to convene executive
sessions at least quarterly without the CEO in attendance.
The system board requires that all executives, system wide,
maintain a written and current succession plan.
The system board requires all boards, in full, to review and
approve all elements of their executives’ compensation.
The system board requires that all executive and physician
compensation system wide be determined with
consideration of industry benchmarks.
The system board requires that all boards and their
respective CEO jointly develop the CEO’s annual
performance goals, which are tied to the CEO’s evaluation.
The system board requires all boards to follow a formal
process for evaluating their respective CEO’s performance.
Percentage of Yes Responses
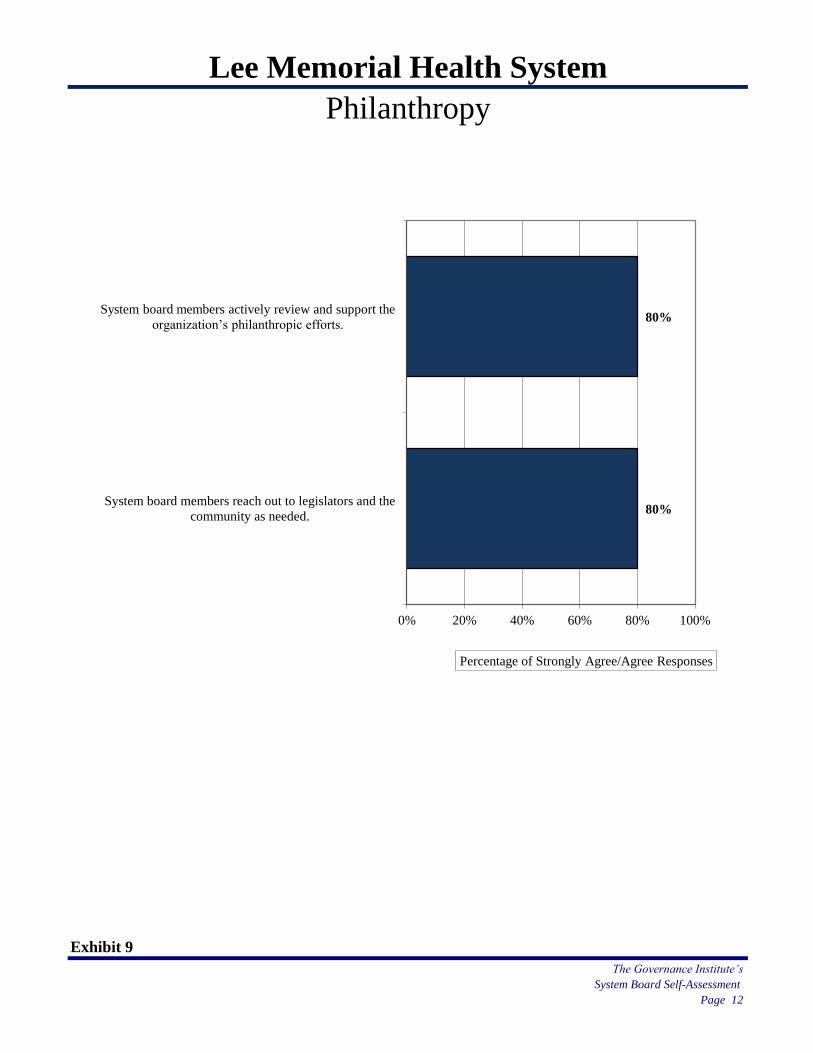
Lee Memorial Health System
Philanthropy
Exhibit 9
The Governance Institute’s
System Board Self-Assessment
Page 12
80%
80%
0% 20% 40% 60% 80% 100%
System board members reach out to legislators and the
community as needed.
System board members actively review and support the
organization’s philanthropic efforts.
Percentage of Strongly Agree/Agree Responses
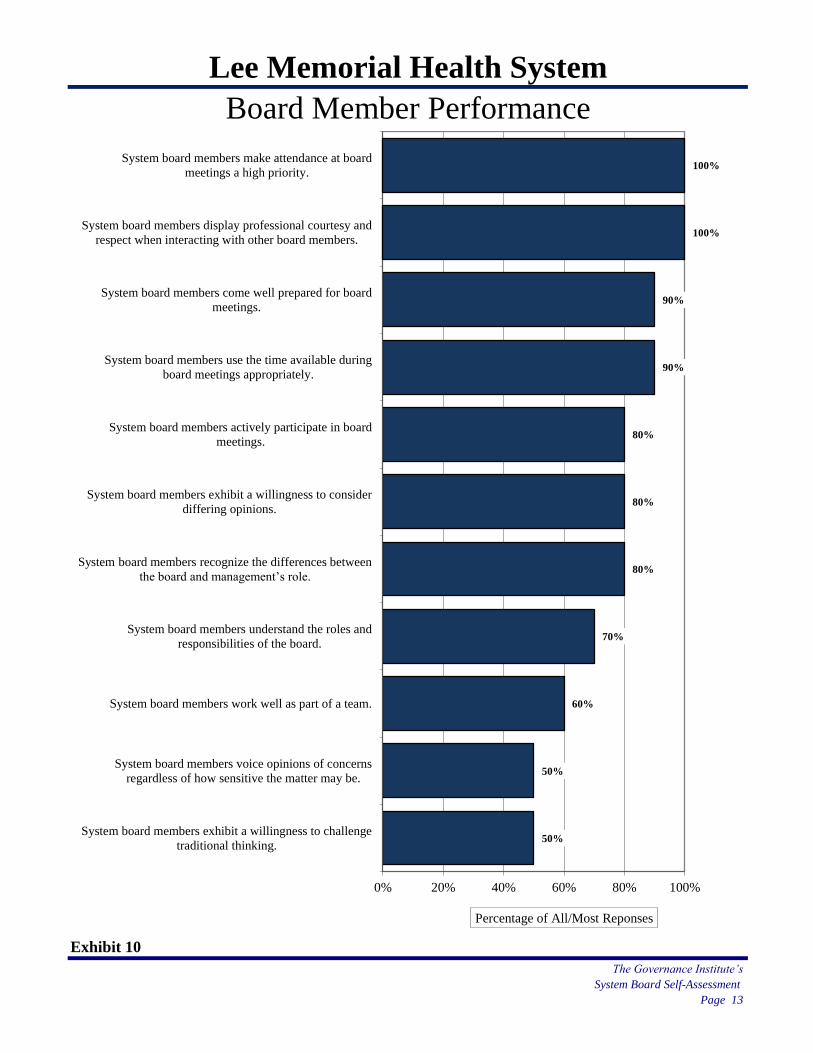
Lee Memorial Health System
Board Member Performance
Exhibit 10
The Governance Institute’s
System Board Self-Assessment
Page 13
50%
50%
60%
70%
80%
80%
80%
90%
90%
100%
100%
0% 20% 40% 60% 80% 100%
System board members exhibit a willingness to challenge
traditional thinking.
System board members voice opinions of concerns
regardless of how sensitive the matter may be.
System board members work well as part of a team.
System board members understand the roles and
responsibilities of the board.
System board members recognize the differences between
the board and management’s role.
System board members exhibit a willingness to consider
differing opinions.
System board members actively participate in board
meetings.
System board members use the time available during
board meetings appropriately.
System board members come well prepared for board
meetings.
System board members display professional courtesy and
respect when interacting with other board members.
System board members make attendance at board
meetings a high priority.
Percentage of All/Most Reponses
Page
Fiduciary Duty of Care: Exhibit 11 15
Fiduciary Duty of Loyalty: Exhibit 12 16
Fiduciary Duty of Obedience: Exhibit 13 17
Financial Oversight: Exhibit 14 18
Quality Oversight: Exhibit 15 19
Setting Strategic Direction: Exhibit 16 20
Self-Assessment & Development: Exhibit 17 21
Management Oversight: Exhibit 18 22
Philanthropy: Exhibit 19 23
Board Member Performance: Exhibit 20 24
Areas of Excellence 25
Areas for Discussion 27
System Board Self-Assessment
Page 14
Lee Memorial Health System
Detail of Results
The second set of exhibits in this report provide the detail of your responses for each question in the
survey; that is, for each question, the full range of responses appear, including the percent of respondents
who answered “don’t know” to each question and the number of “no responses” for each question.
The Governance Institute’s
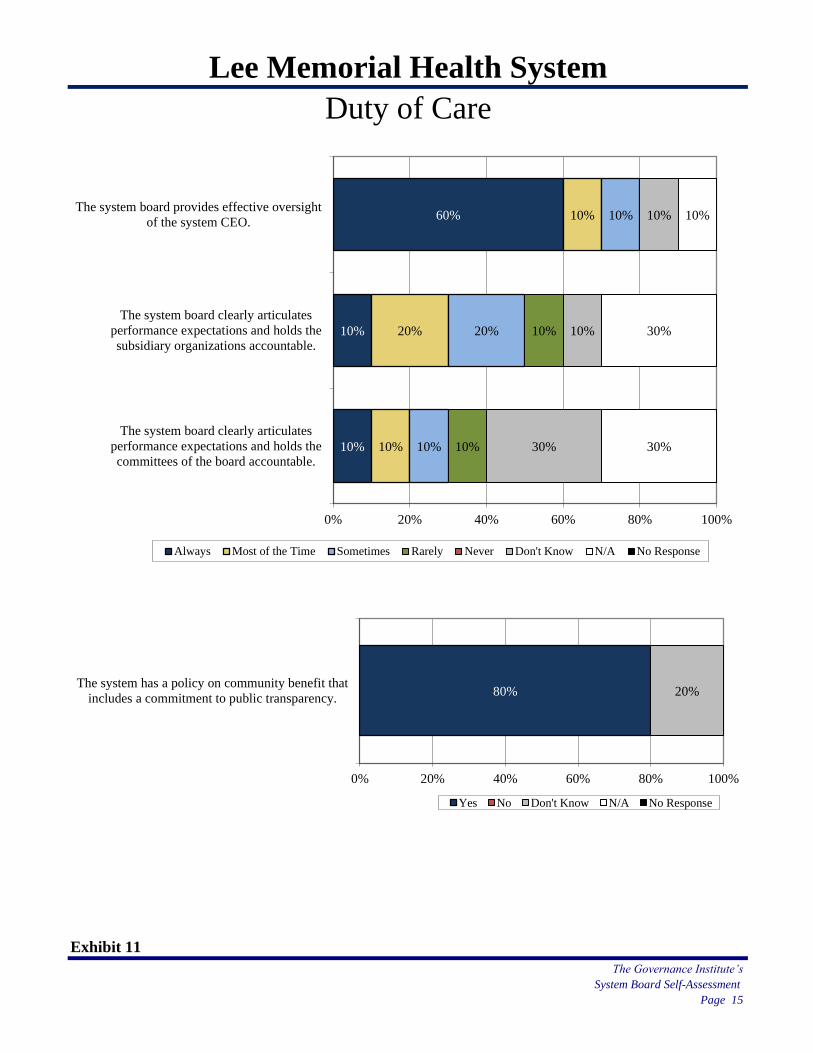
Lee Memorial Health System
Duty of Care
Exhibit 11
The Governance Institute’s
System Board Self-Assessment
Page 15
10%
10%
60%
10%
20%
10%
10%
20%
10%
10%
10%
30%
10%
10%
30%
30%
10%
0% 20% 40% 60% 80% 100%
The system board clearly articulates
performance expectations and holds the
committees of the board accountable.
The system board clearly articulates
performance expectations and holds the
subsidiary organizations accountable.
The system board provides effective oversight
of the system CEO.
Always Most of the Time Sometimes Rarely Never Don't Know N/A No Response
80% 20%
0% 20% 40% 60% 80% 100%
The system has a policy on community benefit that
includes a commitment to public transparency.
Yes No Don't Know N/A No Response
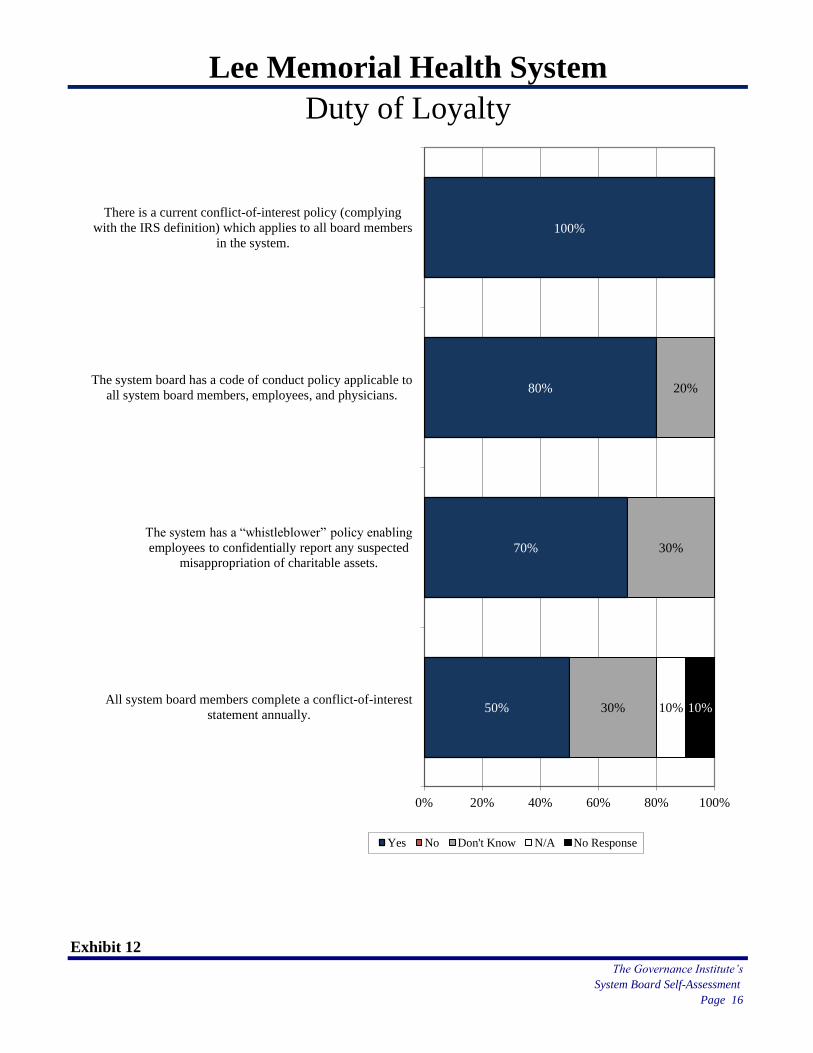
Lee Memorial Health System
Duty of Loyalty
Exhibit 12
The Governance Institute’s
System Board Self-Assessment
Page 16
50%
70%
80%
100%
30%
30%
20%
10% 10%
0% 20% 40% 60% 80% 100%
All system board members complete a conflict-of-interest
statement annually.
The system has a “whistleblower” policy enabling
employees to confidentially report any suspected
misappropriation of charitable assets.
The system board has a code of conduct policy applicable to
all system board members, employees, and physicians.
There is a current conflict-of-interest policy (complying
with the IRS definition) which applies to all board members
in the system.
Yes No Don't Know N/A No Response
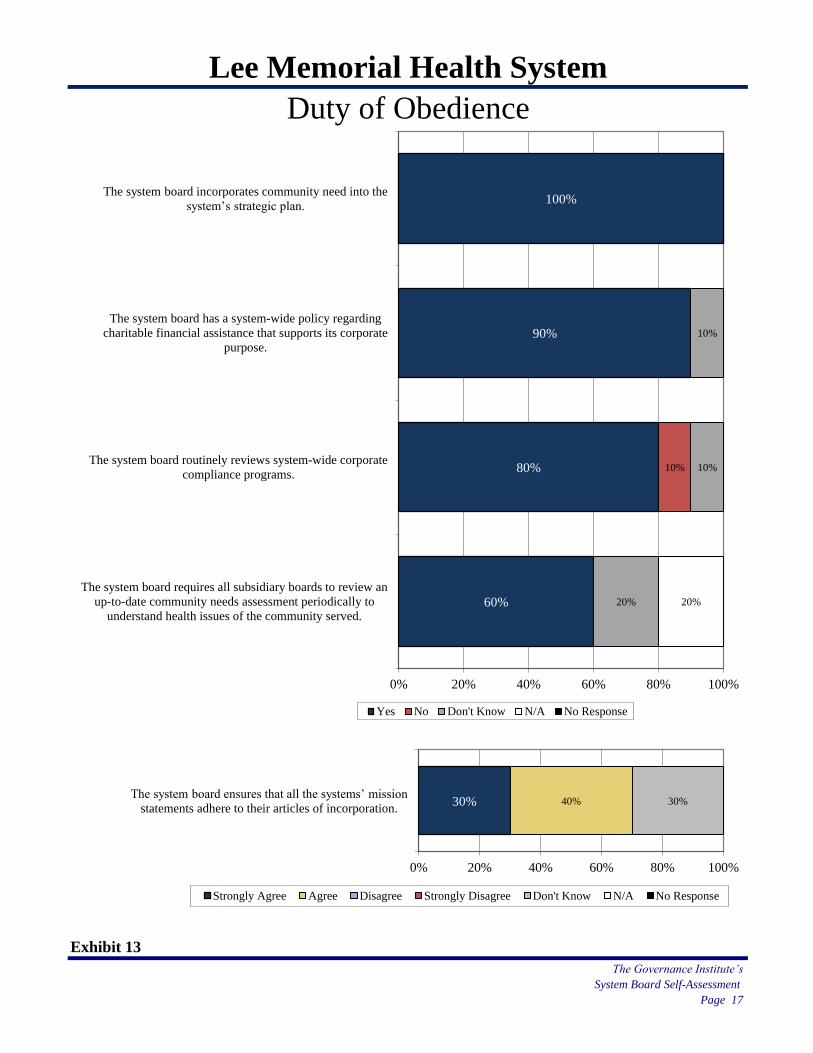
Lee Memorial Health System
Duty of Obedience
Exhibit 13
The Governance Institute’s
System Board Self-Assessment
Page 17
60%
80%
90%
100%
10%
20%
10%
10%
20%
0% 20% 40% 60% 80% 100%
The system board requires all subsidiary boards to review an
up-to-date community needs assessment periodically to
understand health issues of the community served.
The system board routinely reviews system-wide corporate
compliance programs.
The system board has a system-wide policy regarding
charitable financial assistance that supports its corporate
purpose.
The system board incorporates community need into the
system’s strategic plan.
Yes No Don't Know N/A No Response
30% 40% 30%
0% 20% 40% 60% 80% 100%
The system board ensures that all the systems’ mission
statements adhere to their articles of incorporation.
Strongly Agree Agree Disagree Strongly Disagree Don't Know N/A No Response
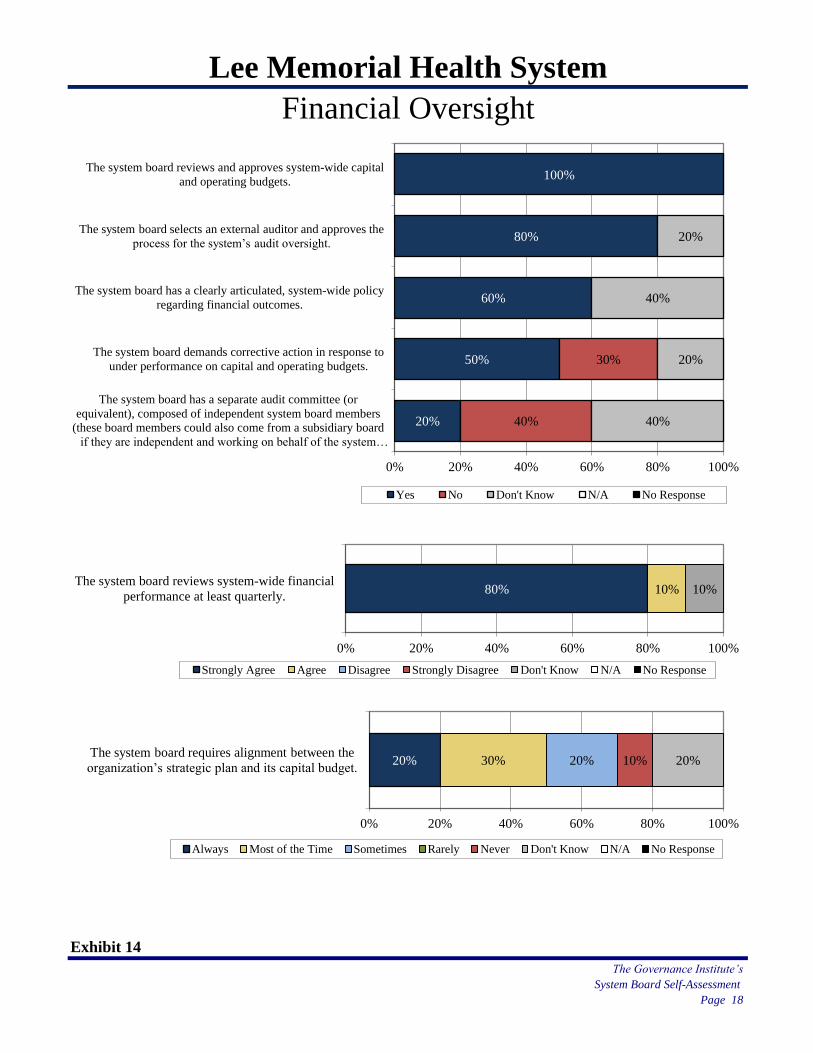
Lee Memorial Health System
Financial Oversight
Exhibit 14
The Governance Institute’s
System Board Self-Assessment
Page 18
20%
50%
60%
80%
100%
40%
30%
40%
20%
40%
20%
0% 20% 40% 60% 80% 100%
The system board has a separate audit committee (or
equivalent), composed of independent system board members
(these board members could also come from a subsidiary board
if they are independent and working on behalf of the system…
The system board demands corrective action in response to
under performance on capital and operating budgets.
The system board has a clearly articulated, system-wide policy
regarding financial outcomes.
The system board selects an external auditor and approves the
process for the system’s audit oversight.
The system board reviews and approves system-wide capital
and operating budgets.
Yes No Don't Know N/A No Response
20% 30% 20% 10% 20%
0% 20% 40% 60% 80% 100%
The system board requires alignment between the
organization’s strategic plan and its capital budget.
Always Most of the Time Sometimes Rarely Never Don't Know N/A No Response
80% 10% 10%
0% 20% 40% 60% 80% 100%
The system board reviews system-wide financial
performance at least quarterly.
Strongly Agree Agree Disagree Strongly Disagree Don't Know N/A No Response
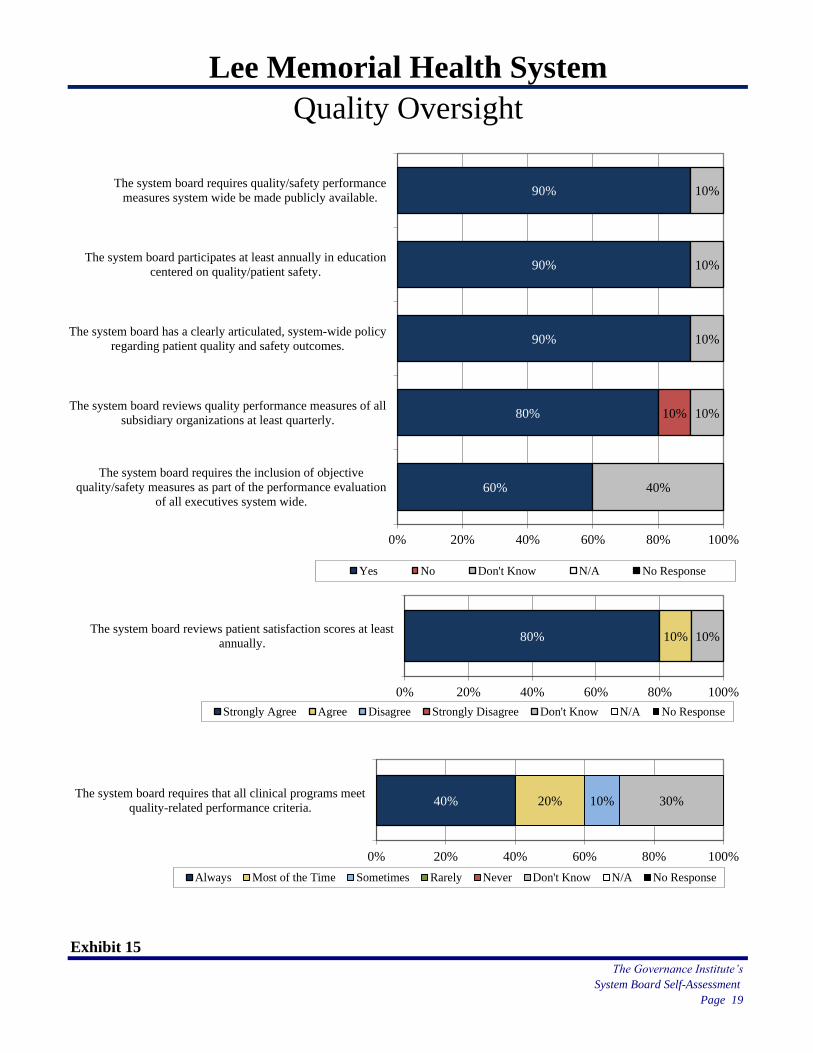
Lee Memorial Health System
Quality Oversight
Exhibit 15
The Governance Institute’s
System Board Self-Assessment
Page 19
60%
80%
90%
90%
90%
10%
40%
10%
10%
10%
10%
0% 20% 40% 60% 80% 100%
The system board requires the inclusion of objective
quality/safety measures as part of the performance evaluation
of all executives system wide.
The system board reviews quality performance measures of all
subsidiary organizations at least quarterly.
The system board has a clearly articulated, system-wide policy
regarding patient quality and safety outcomes.
The system board participates at least annually in education
centered on quality/patient safety.
The system board requires quality/safety performance
measures system wide be made publicly available.
Yes No Don't Know N/A No Response
80% 10% 10%
0% 20% 40% 60% 80% 100%
The system board reviews patient satisfaction scores at least
annually.
Strongly Agree Agree Disagree Strongly Disagree Don't Know N/A No Response
40% 20% 10% 30%
0% 20% 40% 60% 80% 100%
The system board requires that all clinical programs meet
quality-related performance criteria.
Always Most of the Time Sometimes Rarely Never Don't Know N/A No Response
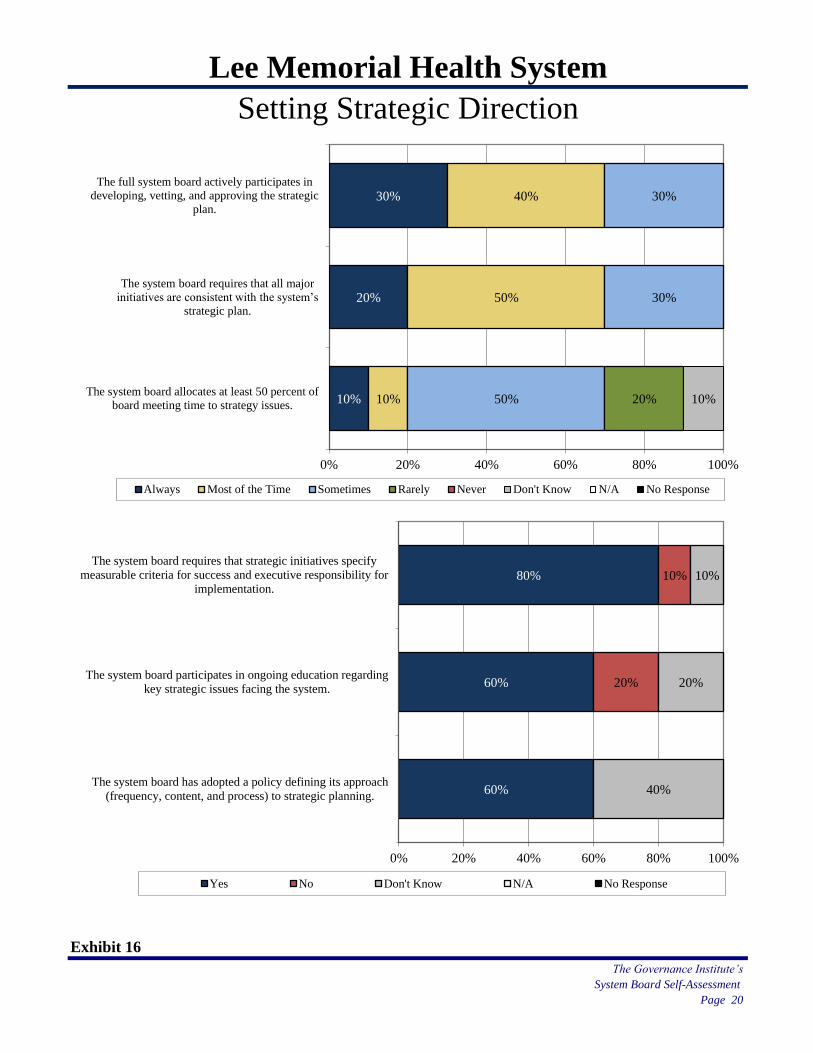
Lee Memorial Health System
Setting Strategic Direction
Exhibit 16
The Governance Institute’s
System Board Self-Assessment
Page 20
10%
20%
30%
10%
50%
40%
50%
30%
30%
20% 10%
0% 20% 40% 60% 80% 100%
The system board allocates at least 50 percent of
board meeting time to strategy issues.
The system board requires that all major
initiatives are consistent with the system’s
strategic plan.
The full system board actively participates in
developing, vetting, and approving the strategic
plan.
Always Most of the Time Sometimes Rarely Never Don't Know N/A No Response
60%
60%
80%
20%
10%
40%
20%
10%
0% 20% 40% 60% 80% 100%
The system board has adopted a policy defining its approach
(frequency, content, and process) to strategic planning.
The system board participates in ongoing education regarding
key strategic issues facing the system.
The system board requires that strategic initiatives specify
measurable criteria for success and executive responsibility for
implementation.
Yes No Don't Know N/A No Response
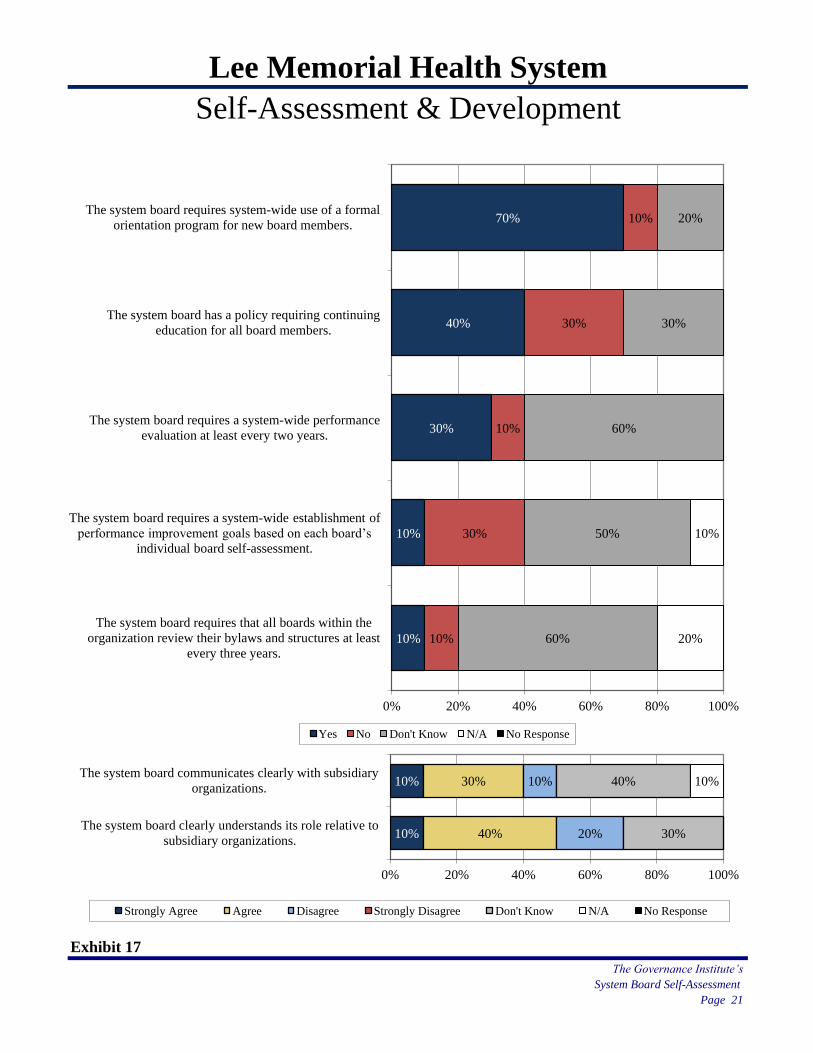
Lee Memorial Health System
Self-Assessment & Development
Exhibit 17
The Governance Institute’s
System Board Self-Assessment
Page 21
10%
10%
30%
40%
70%
10%
30%
10%
30%
10%
60%
50%
60%
30%
20%
20%
10%
0% 20% 40% 60% 80% 100%
The system board requires that all boards within the
organization review their bylaws and structures at least
every three years.
The system board requires a system-wide establishment of
performance improvement goals based on each board’s
individual board self-assessment.
The system board requires a system-wide performance
evaluation at least every two years.
The system board has a policy requiring continuing
education for all board members.
The system board requires system-wide use of a formal
orientation program for new board members.
Yes No Don't Know N/A No Response
10%
10%
40%
30%
20%
10%
30%
40% 10%
0% 20% 40% 60% 80% 100%
The system board clearly understands its role relative to
subsidiary organizations.
The system board communicates clearly with subsidiary
organizations.
Strongly Agree Agree Disagree Strongly Disagree Don't Know N/A No Response
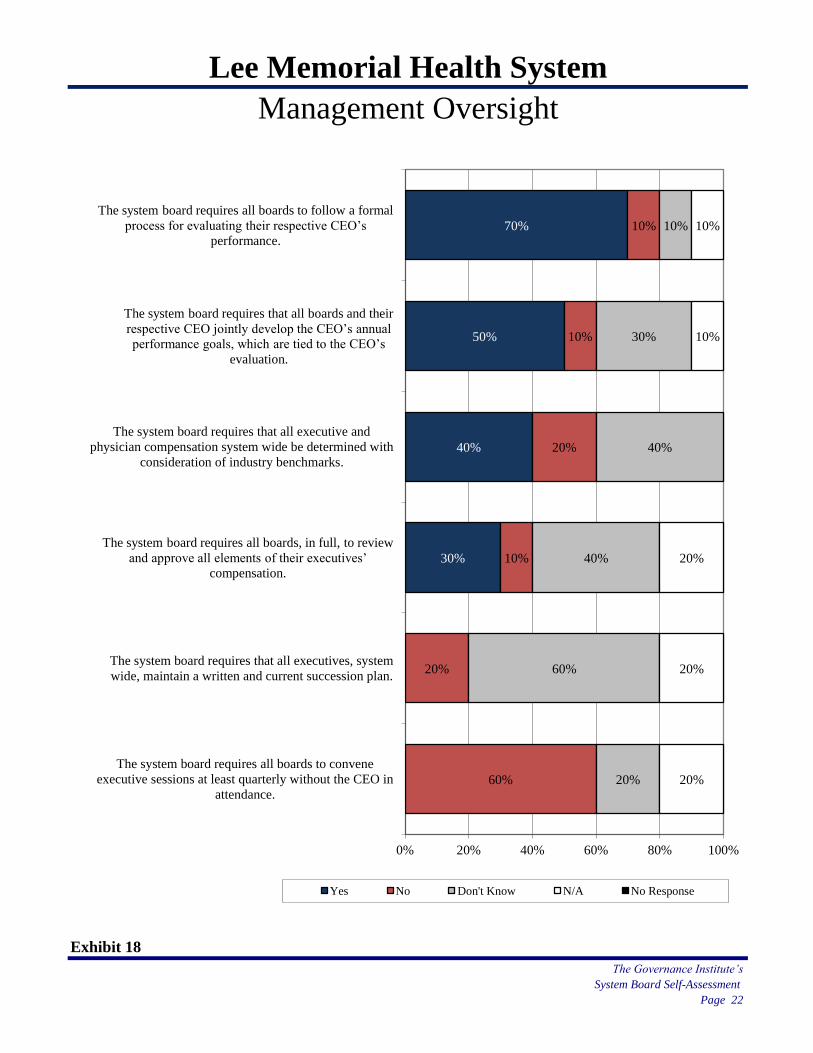
Lee Memorial Health System
Management Oversight
Exhibit 18
The Governance Institute’s
System Board Self-Assessment
Page 22
30%
40%
50%
70%
60%
20%
10%
20%
10%
10%
20%
60%
40%
40%
30%
10%
20%
20%
20%
10%
10%
0% 20% 40% 60% 80% 100%
The system board requires all boards to convene
executive sessions at least quarterly without the CEO in
attendance.
The system board requires that all executives, system
wide, maintain a written and current succession plan.
The system board requires all boards, in full, to review
and approve all elements of their executives’
compensation.
The system board requires that all executive and
physician compensation system wide be determined with
consideration of industry benchmarks.
The system board requires that all boards and their
respective CEO jointly develop the CEO’s annual
performance goals, which are tied to the CEO’s
evaluation.
The system board requires all boards to follow a formal
process for evaluating their respective CEO’s
performance.
Yes No Don't Know N/A No Response
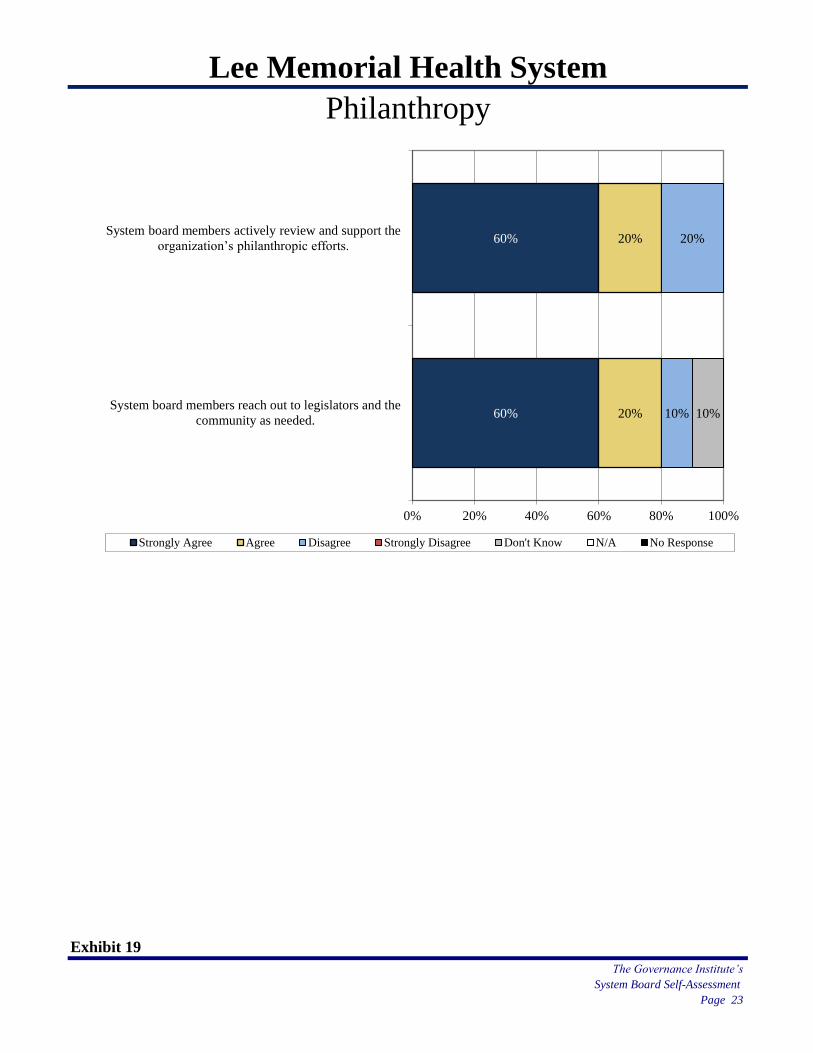
Lee Memorial Health System
Philanthropy
Exhibit 19
The Governance Institute’s
System Board Self-Assessment
Page 23
60%
60%
20%
20%
10%
20%
10%
0% 20% 40% 60% 80% 100%
System board members reach out to legislators and the
community as needed.
System board members actively review and support the
organization’s philanthropic efforts.
Strongly Agree Agree Disagree Strongly Disagree Don't Know N/A No Response
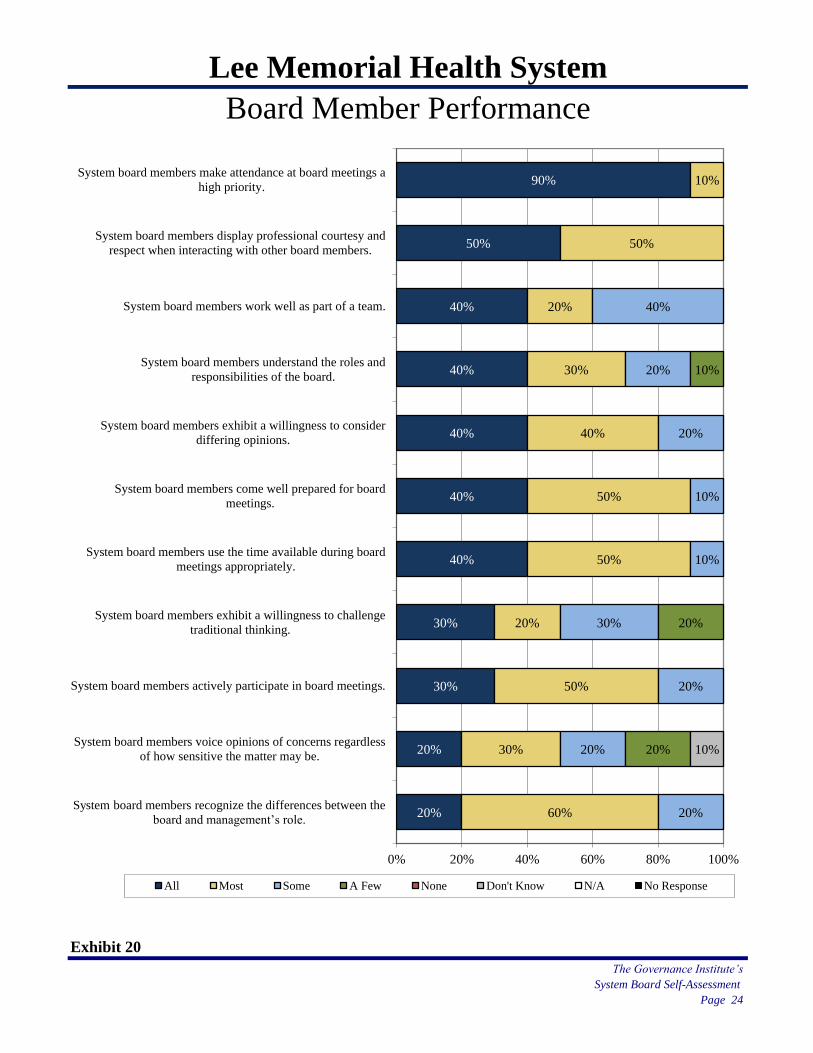
Lee Memorial Health System
Board Member Performance
Exhibit 20
The Governance Institute’s
System Board Self-Assessment
Page 24
20%
20%
30%
30%
40%
40%
40%
40%
40%
50%
90%
60%
30%
50%
20%
50%
50%
40%
30%
20%
50%
10%
20%
20%
20%
30%
10%
10%
20%
20%
40%
20%
20%
10%
10%
0% 20% 40% 60% 80% 100%
System board members recognize the differences between the
board and management’s role.
System board members voice opinions of concerns regardless
of how sensitive the matter may be.
System board members actively participate in board meetings.
System board members exhibit a willingness to challenge
traditional thinking.
System board members use the time available during board
meetings appropriately.
System board members come well prepared for board
meetings.
System board members exhibit a willingness to consider
differing opinions.
System board members understand the roles and
responsibilities of the board.
System board members work well as part of a team.
System board members display professional courtesy and
respect when interacting with other board members.
System board members make attendance at board meetings a
high priority.
All Most Some A Few None Don't Know N/A No Response
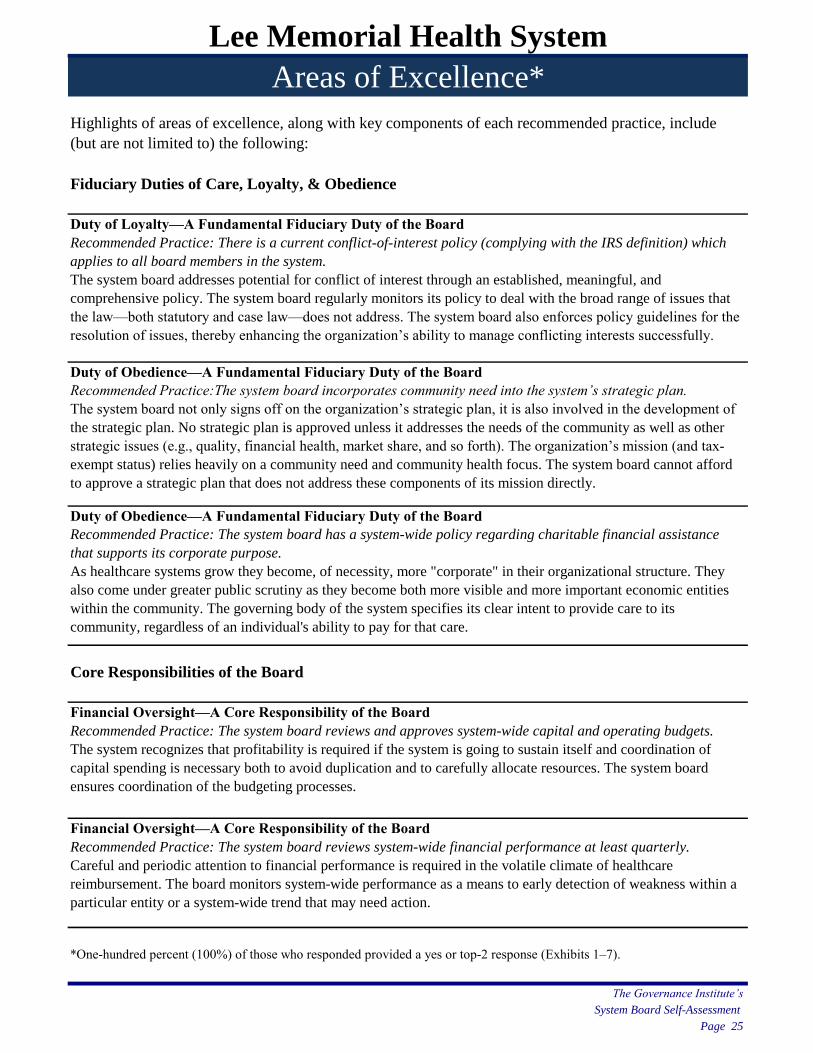
Lee Memorial Health System
Areas of Excellence*
Highlights of areas of excellence, along with key components of each recommended practice, include
(but are not limited to) the following:
Fiduciary Duties of Care, Loyalty, & Obedience
Duty of Loyalty—A Fundamental Fiduciary Duty of the Board
Recommended Practice: There is a current conflict-of-interest policy (complying with the IRS definition) which
applies to all board members in the system.
The system board addresses potential for conflict of interest through an established, meaningful, and
comprehensive policy. The system board regularly monitors its policy to deal with the broad range of issues that
the law—both statutory and case law—does not address. The system board also enforces policy guidelines for the
resolution of issues, thereby enhancing the organization’s ability to manage conflicting interests successfully.
Duty of Obedience—A Fundamental Fiduciary Duty of the Board
Recommended Practice:The system board incorporates community need into the system’s strategic plan.
The system board not only signs off on the organization’s strategic plan, it is also involved in the development of
the strategic plan. No strategic plan is approved unless it addresses the needs of the community as well as other
strategic issues (e.g., quality, financial health, market share, and so forth). The organization’s mission (and tax-
exempt status) relies heavily on a community need and community health focus. The system board cannot afford
to approve a strategic plan that does not address these components of its mission directly.
Duty of Obedience—A Fundamental Fiduciary Duty of the Board
Recommended Practice: The system board has a system-wide policy regarding charitable financial assistance
that supports its corporate purpose.
As healthcare systems grow they become, of necessity, more "corporate" in their organizational structure. They
also come under greater public scrutiny as they become both more visible and more important economic entities
within the community. The governing body of the system specifies its clear intent to provide care to its
community, regardless of an individual's ability to pay for that care.
Core Responsibilities of the Board
Financial Oversight—A Core Responsibility of the Board
Recommended Practice: The system board reviews and approves system-wide capital and operating budgets.
The system recognizes that profitability is required if the system is going to sustain itself and coordination of
capital spending is necessary both to avoid duplication and to carefully allocate resources. The system board
ensures coordination of the budgeting processes.
Financial Oversight—A Core Responsibility of the Board
Recommended Practice: The system board reviews system-wide financial performance at least quarterly.
Careful and periodic attention to financial performance is required in the volatile climate of healthcare
reimbursement. The board monitors system-wide performance as a means to early detection of weakness within a
particular entity or a system-wide trend that may need action.
*One-hundred percent (100%) of those who responded provided a yes or top-2 response (Exhibits 1–7).
The Governance Institute’s
System Board Self-Assessment
Page 25

Lee Memorial Health System
Areas of Excellence* (continued)
Core Responsibilities of the Board
Quality Oversight—A Core Responsibility of the Board
Recommended Practice:The system board participates at least annually in education centered on quality/patient
safety.
The system board keeps up to date on current and emerging issues related to quality of care and recommended
practices for oversight of quality and patient safety.
Quality Oversight—A Core Responsibility of the Board
Recommended Practice: The system board reviews patient satisfaction scores at least annually.
The system board reviews the results of the patient experience on an annual basis and compares them to prior
periods.
Quality Oversight—A Core Responsibility of the Board
Recommended Practice: The system board has a clearly articulated, system-wide policy regarding patient quality
and safety outcomes.
The system board is sets the bar high in the areas of quality and patient safety outcomes ensuring that processes
remain a priority.
Quality Oversight—A Core Responsibility of the Board
Recommended Practice: The system board requires quality/safety performance measures system wide be made
publicly available.
As charitable corporations, the system and its subsidiaries fulfill their obligation to educate and inform their
communities about their quality/safety performance outcomes. Transparency is imperative for the system to be
trusted and respected.
*One-hundred percent (100%) of those who responded provided a yes or top-2 response (Exhibits 1–7).
The Governance Institute’s
System Board Self-Assessment
Page 26
Lee Memorial Health System
Areas of Discussion*
This board can improve its performance in certain key areas; specifically:
Fiduciary Duties of Care, Loyalty, & Obedience
Duty of Care—A Fundamental Fiduciary Duty of the Board
Recommended Practice: The system board clearly articulates performance expectations and holds the committees
of the board accountable.
Committees do not set their own agendas; they take on responsibilities that have been delegated to them by the
full board. The system board must be clear about its expectations.
Duty of Care—A Fundamental Fiduciary Duty of the Board
Recommended Practice: The system board clearly articulates performance expectations and holds the subsidiary
organizations accountable.
Unless otherwise specified by statute, subsidiaries do not set their own agendas; they take on responsibilities that
have been delegated to them by the full system board. The system board must be clear about its expectations.
Duty of Loyalty—A Fundamental Fiduciary Duty of the Board
Recommended Practice: All system board members complete a conflict-of-interest statement annually.
The system board should enforce its policies on conflict of interest and confidentiality consistently and across all
members of the board. Decisions should be made about whether conflicted board members can participate in
board discussion, whether they can be present during a vote, whether they should excuse themselves during
discussion and/or during a vote, etc. The board should avoid making exceptions for specific board members
(whether they be board officers, physicians, legal counsel, for example).
Core Responsibilities of the Board
Financial Oversight—A Core Responsibility of the Board
Recommended Practice: The system board demands corrective action in response to under performance on
capital and operating budgets.
The system board should routinely review the organization’s performance against critical quality indicators. These
indicators should highlight significant trends and variances from performance targets. The board should require
quick and effective action to correct variances.
Financial Oversight—A Core Responsibility of the Board
Recommended Practice: The system board has a separate audit committee (or equivalent), composed of
independent system board members (these board members could also come from a subsidiary board if they are
independent and working on behalf of the system board).
Audit committee should be composed of directors who meet the system board’s guidelines for independence (i.e.,
no material economic or other relationship with the organization).
Financial Oversight—A Core Responsibility of the Board
Recommended Practice: The system board requires alignment between the organization’s strategic plan and its
capital budget.
Articulating strategy without the resources for implementation is a waste of time and, conversely, allocating
capital to a project that doesn't support the system’s future vision is foolhardy. The system must ensure that capital
and strategy are aligned.
*Fifty percent (50%) or less of those who responded provided a yes or top-2 response (Exhibits 1–7).
The Governance Institute’s
System Board Self-Assessment
Page 27
Lee Memorial Health System
Areas of Discussion* (continued)
Core Responsibilities of the Board (continued)
Setting Strategic Direction—A Core Responsibility of the Board
Recommended Practice: The system board allocates at least 50 percent of board meeting time to strategy issues.
Board meetings should focus on discussion and decisions surrounding organizational strategy and policy, not
hearing reports from staff. Such reports should be included in background materials for review by board members
before the meetings. The board chair and/or the CEO should structure the board meeting agenda to devote at least
half of the meeting time to discussion and decision making on issues of strategy (experts recommend 60 to 80%).
“The regularly scheduled board meeting is, perhaps, the most obvious vehicle for engaging the board in strategic-
level discussions on a consistent basis...[high-performing] boards devote approximately 60% of their board
meeting time to strategic-level conversations.” [Setting Strategic Direction , The Governance Institute (white
paper)]
Self-Assessment and Development—A Core Responsibility of the Board
Recommended Practice: The system board requires that all boards within the organization review their bylaws
and structures at least every three years.
The system board or a committee of the system board should review the organization’s bylaws at least every three
years to ensure applicability in the current legal, regulatory, and organizational environment. This also presents a
good opportunity for the board to review its governance structure and practices (e.g., number/type of committees,
term limits, retirement age, meeting frequency, and so forth).
Self-Assessment and Development—A Core Responsibility of the Board
Recommended Practice: The system board requires a system-wide performance evaluation at least every two
years.
It's not always true that "what gets measured, gets done," but measurement should at least provide a scorecard for
evaluating past performance and developing future priorities. The system board is responsible for ensuring this
takes place.
Self-Assessment and Development—A Core Responsibility of the Board
Recommended Practice: The system board requires a system-wide establishment of performance improvement
goals based on each board’s individual board self-assessment.
The purpose of a board self-assessment should be twofold: acknowledgment of achievements and identification of
opportunities for improvement. The system board, itself, should continuously strive to improve on its own
performance and it should expect subsidiary corporations to do the same.
Self-Assessment and Development—A Core Responsibility of the Board
Recommended Practice:The system board clearly understands its role relative to subsidiary organizations.
Governance of a hospital system is complex work taken on largely by groups of individual volunteers; there is a
great deal of room for confusion and misunderstanding. The system board should assume responsibility for
understanding and articulating its role vis-à-vis its subsidiary entities.
Self-Assessment and Development—A Core Responsibility of the Board
Recommended Practice: The system board communicates clearly with subsidiary organizations.
Large healthcare systems may be the most complex organizations known to humankind. Communication is the
lifeblood of managing this complexity and it is the system board’s responsibility to provide leadership by
example.
*Fifty percent (50%) or less of those who responded provided a yes or top-2 response (Exhibits 1–7).
The Governance Institute’s
System Board Self-Assessment
Page 28
Lee Memorial Health System
Areas of Discussion* (continued)Core Responsibilities of the Board
Self-Assessment and Development—A Core Responsibility of the Board
Recommended Practice: The system board has a policy requiring continuing education for all board members.
Healthcare is a dynamic industry driven by public policy, clinical innovation, economic, human resource,
antitrust, and other issues; in other words, governance is not for the faint of heart. Participation in the governance
of a system/subsidiary board is more demanding (and presumably more rewarding) than most other community
endeavors. Effective board members are not just committed to the welfare of their communities; they welcome the
intellectual challenge to stay current. The system board should reflect the necessity of this by carefully developing
a continuing education policy that recognizes the financial limitations of the system and the time demands on its
volunteer trustees.
Management Oversight—A Core Responsibility of the Board
Recommended Practice: The system board requires all boards, in full, to review and approve all elements of their
executives’ compensation.
Only independent board members should determine executive compensation. However, all board members should
be assured that compensation falls within comparable industry corridors.
Management Oversight—A Core Responsibility of the Board
Recommended Practice: The system board requires all boards to convene executive sessions at least quarterly
without the CEO in attendance.
Always a sensitive issue, recommended practice stipulates that the board meets periodically, unencumbered by
any relationship to the CEO. The board chair should be expected to communicate immediately with the CEO
regarding any conclusions reached in executive session.
Management Oversight—A Core Responsibility of the Board
Recommended Practice: The system board requires that all executives, system wide, maintain a written and
current succession plan.
The system board should ensure continuity of leadership by requiring the CEO to have a current, written
succession plan and by engaging in the leadership transition planning process.The most important—and
difficult—decision a hospital or health system board of directors can make involves choosing the next CEO.
Planning for a change in leadership involves usually two, even three years’ effort, and includes a candidate search
and selection process; creating a deliberate, well-communicated and well-understood transition plan; and
delivering a positive message about the organization’s future direction. Last-minute efforts to find a successor
result in lost opportunities for an organization to demonstrate its vigilance in safeguarding the organization’s
current and future successes. (Elements of Governance®: CEO Succession Planning , The Governance Institute)
Management Oversight—A Core Responsibility of the Board
Recommended Practice: The system board requires that all boards and their respective CEO jointly develop the
CEO’s annual performance goals, which are tied to the CEO’s evaluation.
To further emphasize the organization’s commitment to quality and patient safety, the system board should
include quality-related goals in the CEO’s annual performance goals and annual performance evaluation. The
CEO should include similar goals when evaluating his or her senior staff.
Management Oversight—A Core Responsibility of the Board
Recommended Practice: The system board requires that all executive and physician compensation system wide be
determined with consideration of industry benchmarks.
The full system board should approve a compensation policy or philosophy statement and an overall
compensation and incentive plan, and knows and approves compensation at the top.
*Fifty percent (50%) or less of those who responded provided a yes or top-2 response (Exhibits 1–7).
The Governance Institute’s
System Board Self-Assessment
Page 29
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS RECOMMENDED ACTION FOR BOARD APPROVAL
(Action includes Acceptance, Approval, Adoption, etc)
DATE: March 28, 2013 LEGAL SERVICE REVIEW? YES X NO___ SUBJECT: Proposed CEO Evaluation Form REQUESTOR & TITLE: Jon C. Cecil, Chief Human Resources Officer PREVIOUS BOARD ACTION ON THIS ITEM (IF ANY) The October 18, 2012 Board of Directors meeting requested that President & CEO, Jim Nathan’s Annual Evaluation be revised. SPECIFIC PROPOSED MOTION: Acceptance of revised FY 2013 President & CEO evaluation form PROS TO RECOMMENDATION
CONS TO RECOMMENDATION
LIST AND EXPLAIN ALTERNATIVES CONSIDERED N/A FINANCIAL IMPLICATIONS Budgeted ____ Non-Budgeted ____ (including cash flow statement, projected cash flow, balance sheet and income statement)
N/A OPERATIONAL IMPLICATIONS (including FTEs, facility needs, etc.) SUMMARY
BOD/Forms/Board (Action) Reporting Form – updated 9/2/09 cs
Keep form to one page, SUBMIT (thru SLC Member) ELECTRONICALLY to L Drive – Miscellaneous - BOD Presentations by Noon the Friday before you’re scheduled on agenda.
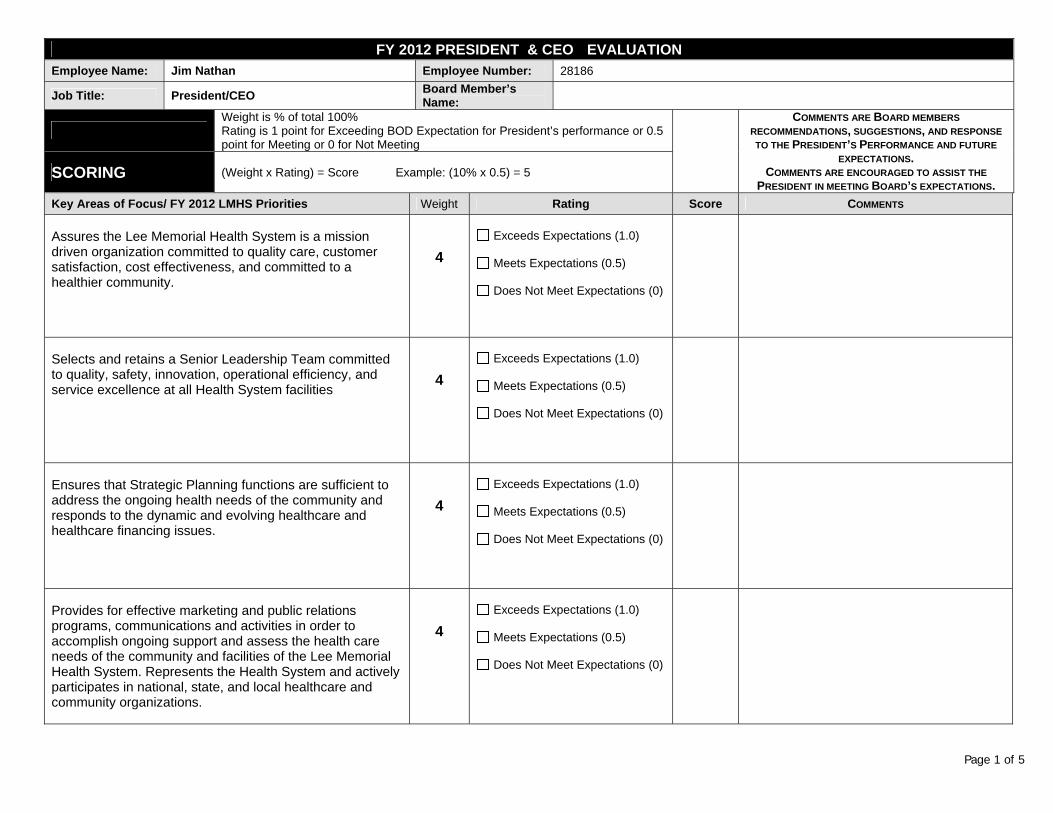
Page 1 of 5
FY 2012 PRESIDENT & CEO EVALUATION Employee Name: Jim Nathan Employee Number: 28186
Job Title: President/CEO Board Member’sName:
Weight is % of total 100% Rating is 1 point for Exceeding BOD Expectation for President’s performance or 0.5 point for Meeting or 0 for Not Meeting
COMMENTS ARE BOARD MEMBERS
RECOMMENDATIONS, SUGGESTIONS, AND RESPONSE
TO THE PRESIDENT’S PERFORMANCE AND FUTURE
EXPECTATIONS. COMMENTS ARE ENCOURAGED TO ASSIST THE
PRESIDENT IN MEETING BOARD’S EXPECTATIONS. SCORING (Weight x Rating) = Score Example: (10% x 0.5) = 5
Key Areas of Focus/ FY 2012 LMHS Priorities Weight Rating Score COMMENTS
Assures the Lee Memorial Health System is a mission driven organization committed to quality care, customer satisfaction, cost effectiveness, and committed to a healthier community.
4
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
Selects and retains a Senior Leadership Team committed to quality, safety, innovation, operational efficiency, and service excellence at all Health System facilities
4
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
Ensures that Strategic Planning functions are sufficient to address the ongoing health needs of the community and responds to the dynamic and evolving healthcare and healthcare financing issues.
4
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
Provides for effective marketing and public relations programs, communications and activities in order to accomplish ongoing support and assess the health care needs of the community and facilities of the Lee Memorial Health System. Represents the Health System and actively participates in national, state, and local healthcare and community organizations.
4
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
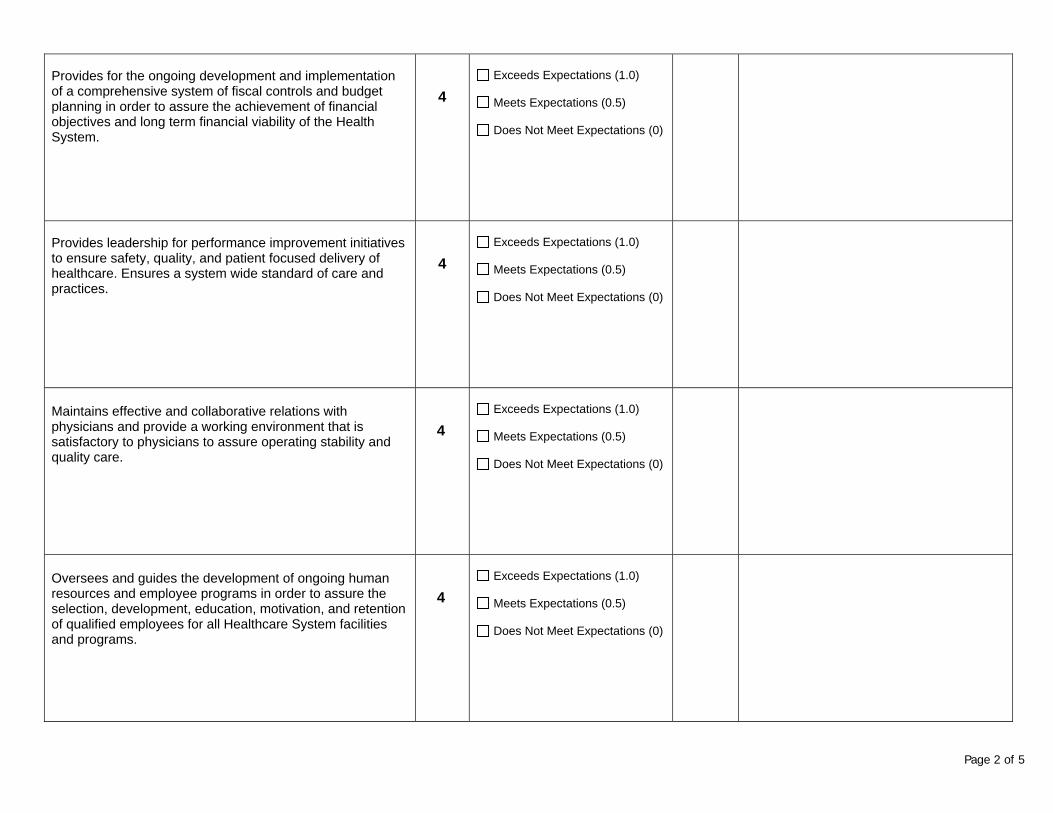
Page 2 of 5
Provides for the ongoing development and implementation of a comprehensive system of fiscal controls and budget planning in order to assure the achievement of financial objectives and long term financial viability of the Health System.
4
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
Provides leadership for performance improvement initiatives to ensure safety, quality, and patient focused delivery of healthcare. Ensures a system wide standard of care and practices.
4
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
Maintains effective and collaborative relations with physicians and provide a working environment that is satisfactory to physicians to assure operating stability and quality care.
4
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
Oversees and guides the development of ongoing human resources and employee programs in order to assure the selection, development, education, motivation, and retention of qualified employees for all Healthcare System facilities and programs.
4
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
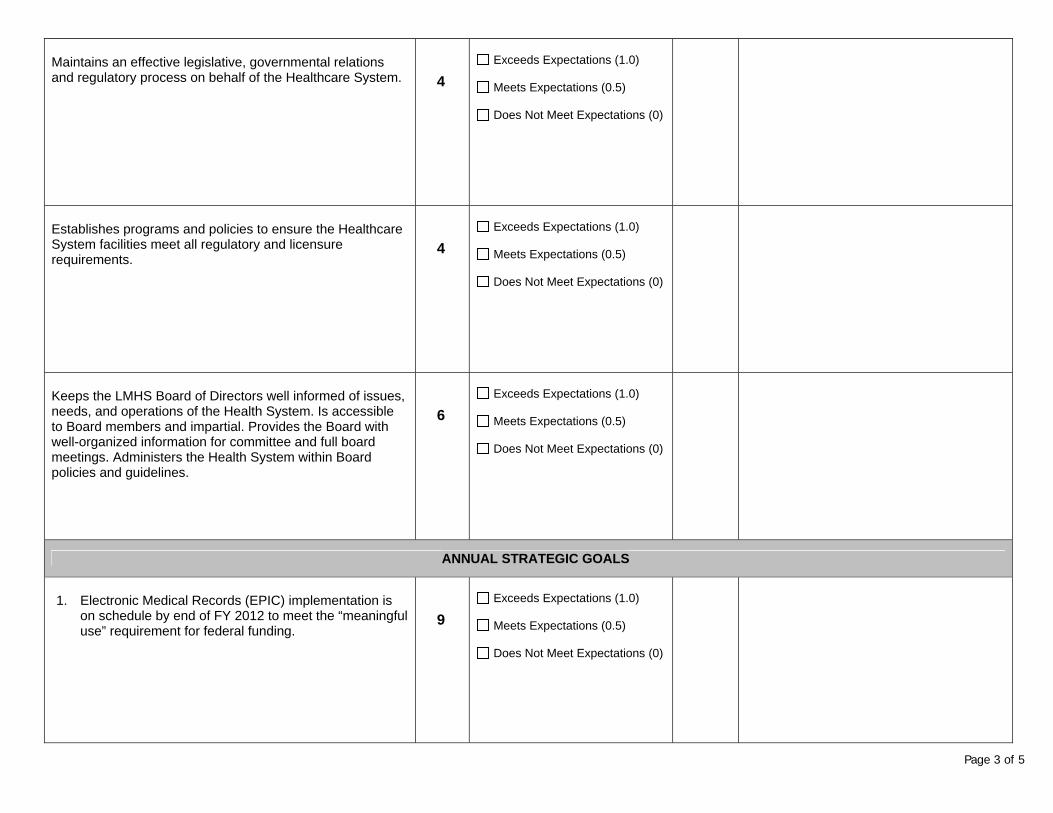
Page 3 of 5
Maintains an effective legislative, governmental relations and regulatory process on behalf of the Healthcare System.
4
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
Establishes programs and policies to ensure the Healthcare System facilities meet all regulatory and licensure requirements.
4
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
Keeps the LMHS Board of Directors well informed of issues, needs, and operations of the Health System. Is accessible to Board members and impartial. Provides the Board with well-organized information for committee and full board meetings. Administers the Health System within Board policies and guidelines.
6
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
ANNUAL STRATEGIC GOALS
1. Electronic Medical Records (EPIC) implementation is
on schedule by end of FY 2012 to meet the “meaningful use” requirement for federal funding.
9
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
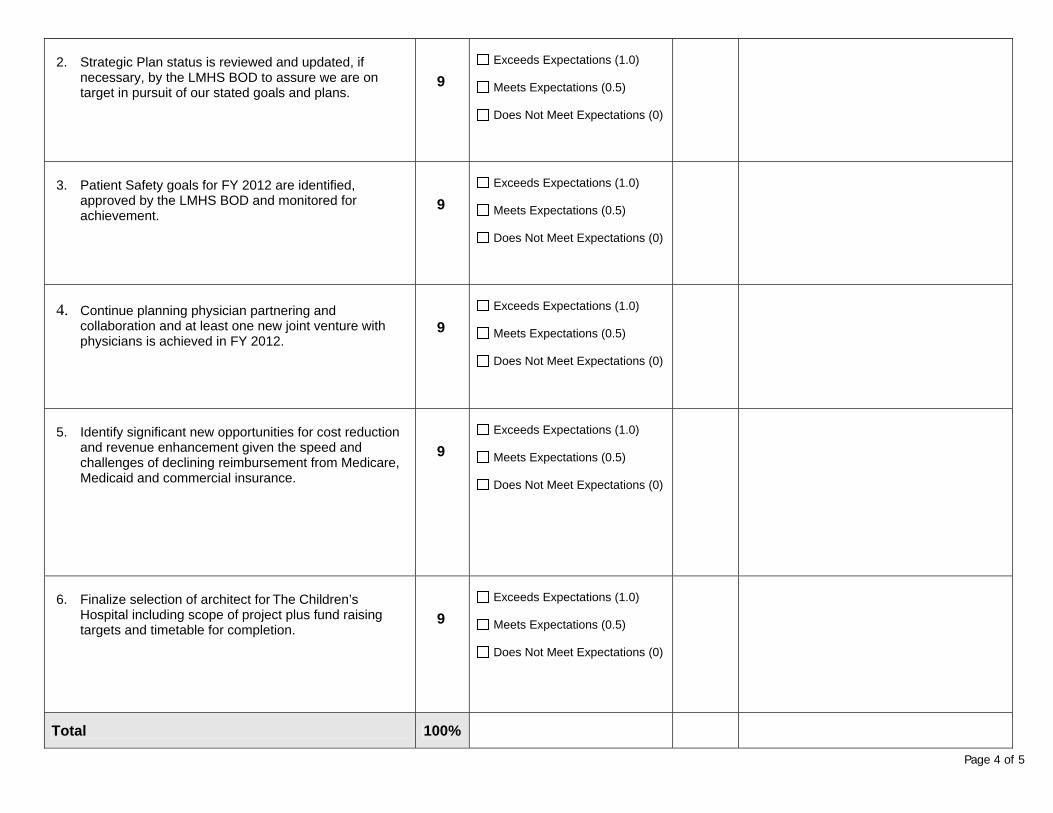
Page 4 of 5
2. Strategic Plan status is reviewed and updated, if
necessary, by the LMHS BOD to assure we are on target in pursuit of our stated goals and plans.
9
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
3. Patient Safety goals for FY 2012 are identified,
approved by the LMHS BOD and monitored for achievement.
9
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
4. Continue planning physician partnering and
collaboration and at least one new joint venture with physicians is achieved in FY 2012.
9
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
5. Identify significant new opportunities for cost reduction
and revenue enhancement given the speed and challenges of declining reimbursement from Medicare, Medicaid and commercial insurance.
9
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
6. Finalize selection of architect for The Children’s
Hospital including scope of project plus fund raising targets and timetable for completion.
9
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
Total 100%
Page 5 of 5
Additional Comments:
Board Member Signature: _______________________________________________ Date: ____________________________
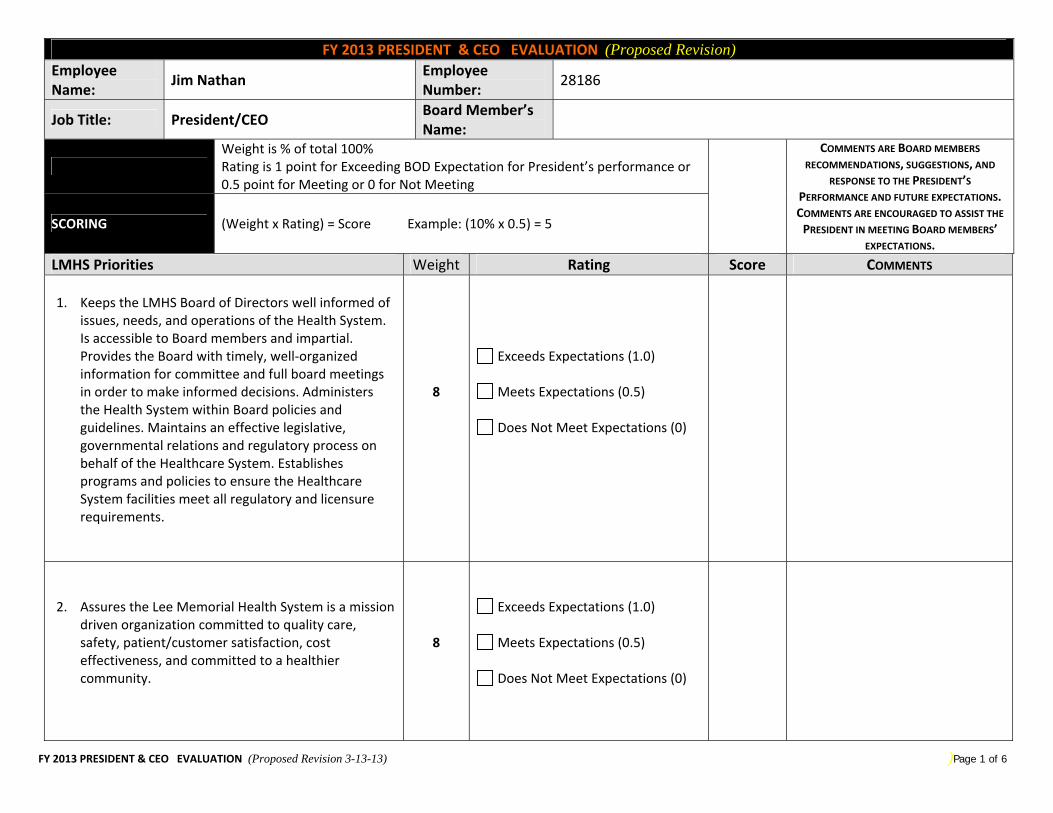
FY 2013 PRESIDENT & CEO EVALUATION (Proposed Revision 3-13-13) )Page 1 of 6
FY 2013 PRESIDENT & CEO EVALUATION (Proposed Revision) Employee Name:
Jim Nathan Employee Number:
28186
Job Title: President/CEO Board Member’s Name:
Weight is % of total 100% Rating is 1 point for Exceeding BOD Expectation for President’s performance or 0.5 point for Meeting or 0 for Not Meeting
COMMENTS ARE BOARD MEMBERS
RECOMMENDATIONS, SUGGESTIONS, AND RESPONSE TO THE PRESIDENT’S
PERFORMANCE AND FUTURE EXPECTATIONS. COMMENTS ARE ENCOURAGED TO ASSIST THE
PRESIDENT IN MEETING BOARD MEMBERS’ EXPECTATIONS.
SCORING (Weight x Rating) = Score Example: (10% x 0.5) = 5
LMHS Priorities Weight Rating Score COMMENTS 1. Keeps the LMHS Board of Directors well informed of
issues, needs, and operations of the Health System. Is accessible to Board members and impartial. Provides the Board with timely, well‐organized information for committee and full board meetings in order to make informed decisions. Administers the Health System within Board policies and guidelines. Maintains an effective legislative, governmental relations and regulatory process on behalf of the Healthcare System. Establishes programs and policies to ensure the Healthcare System facilities meet all regulatory and licensure requirements.
8
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
2. Assures the Lee Memorial Health System is a mission
driven organization committed to quality care, safety, patient/customer satisfaction, cost effectiveness, and committed to a healthier community.
8
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
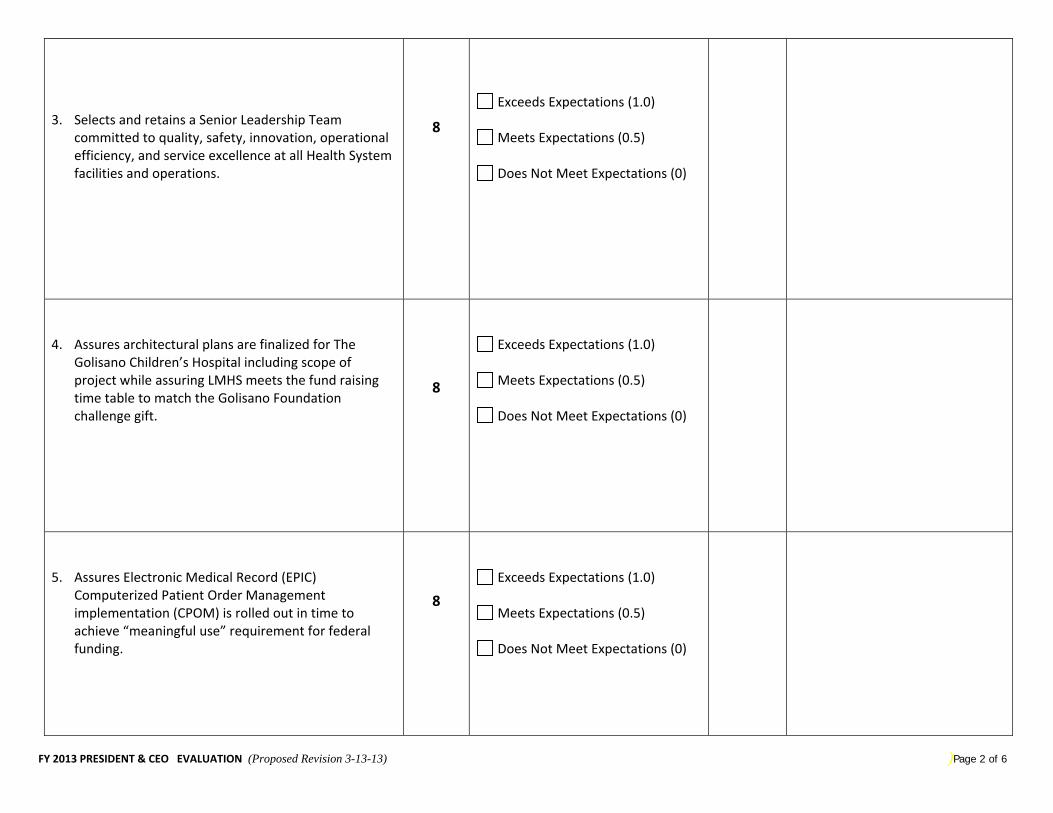
FY 2013 PRESIDENT & CEO EVALUATION (Proposed Revision 3-13-13) )Page 2 of 6
3. Selects and retains a Senior Leadership Team committed to quality, safety, innovation, operational efficiency, and service excellence at all Health System facilities and operations.
8
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
4. Assures architectural plans are finalized for The Golisano Children’s Hospital including scope of project while assuring LMHS meets the fund raising time table to match the Golisano Foundation challenge gift.
8
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
5. Assures Electronic Medical Record (EPIC) Computerized Patient Order Management implementation (CPOM) is rolled out in time to achieve “meaningful use” requirement for federal funding.
8
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
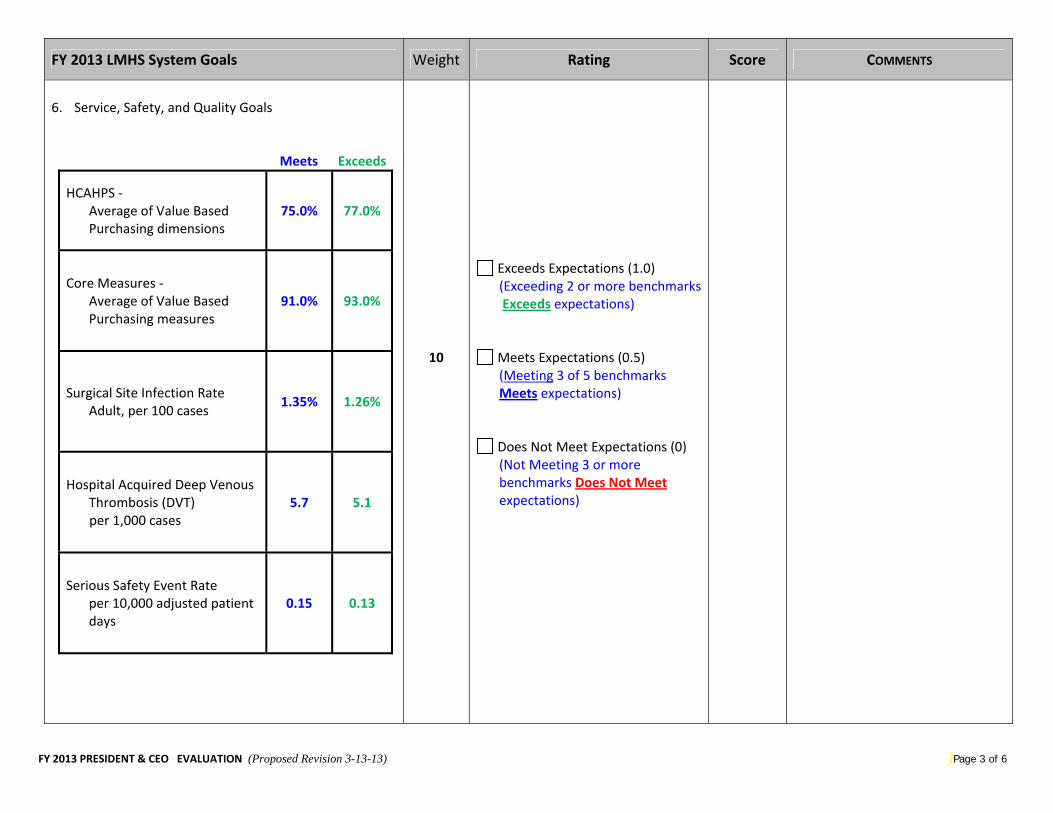
FY 2013 PRESIDENT & CEO EVALUATION (Proposed Revision 3-13-13) )Page 3 of 6
FY 2013 LMHS System Goals Weight Rating Score COMMENTS
6. Service, Safety, and Quality Goals
Meets Exceeds
HCAHPS ‐ Average of Value Based Purchasing dimensions
75.0% 77.0%
Core Measures ‐ Average of Value Based Purchasing measures
91.0% 93.0%
Surgical Site Infection Rate Adult, per 100 cases
1.35% 1.26%
Hospital Acquired Deep Venous Thrombosis (DVT)
per 1,000 cases 5.7 5.1
Serious Safety Event Rate per 10,000 adjusted patient days
0.15 0.13
10
Exceeds Expectations (1.0) (Exceeding 2 or more benchmarks Exceeds expectations)
Meets Expectations (0.5) (Meeting 3 of 5 benchmarks Meets expectations)
Does Not Meet Expectations (0) (Not Meeting 3 or more benchmarks Does Not Meet expectations)
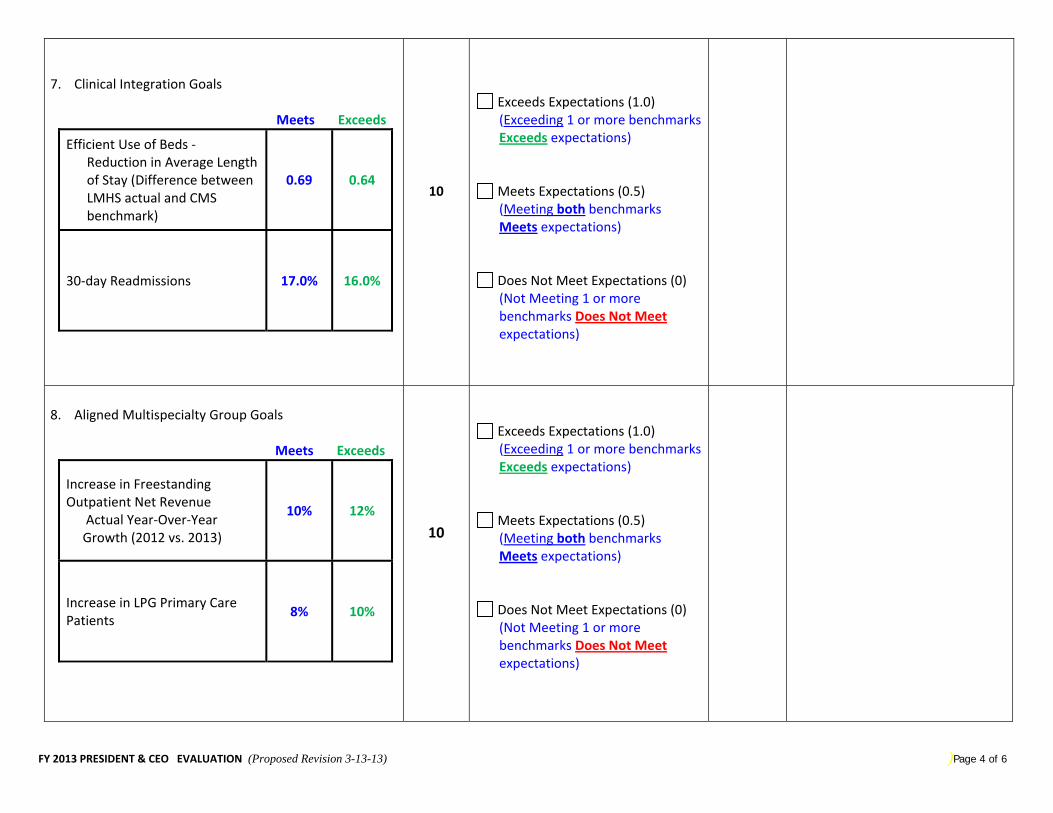
FY 2013 PRESIDENT & CEO EVALUATION (Proposed Revision 3-13-13) )Page 4 of 6
7. Clinical Integration Goals
Meets Exceeds
Efficient Use of Beds ‐ Reduction in Average Length of Stay (Difference between LMHS actual and CMS benchmark)
0.69 0.64
30‐day Readmissions 17.0% 16.0%
10
Exceeds Expectations (1.0) (Exceeding 1 or more benchmarks Exceeds expectations)
Meets Expectations (0.5) (Meeting both benchmarks Meets expectations)
Does Not Meet Expectations (0) (Not Meeting 1 or more benchmarks Does Not Meet expectations)
8. Aligned Multispecialty Group Goals
Meets Exceeds
Increase in Freestanding Outpatient Net Revenue Actual Year‐Over‐Year Growth (2012 vs. 2013)
10% 12%
Increase in LPG Primary Care Patients
8% 10%
10
Exceeds Expectations (1.0) (Exceeding 1 or more benchmarks Exceeds expectations)
Meets Expectations (0.5) (Meeting both benchmarks Meets expectations)
Does Not Meet Expectations (0) (Not Meeting 1 or more benchmarks Does Not Meet expectations)
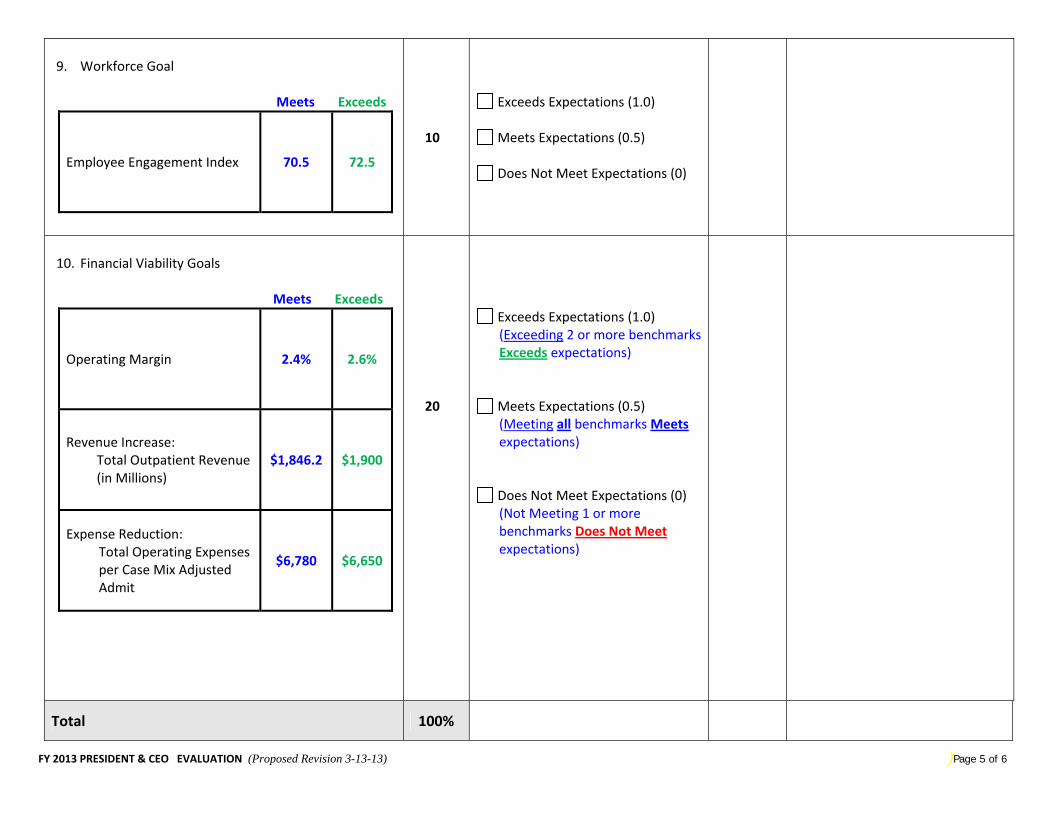
FY 2013 PRESIDENT & CEO EVALUATION (Proposed Revision 3-13-13) )Page 5 of 6
9. Workforce Goal
Meets Exceeds
Employee Engagement Index 70.5 72.5
10
Exceeds Expectations (1.0)
Meets Expectations (0.5)
Does Not Meet Expectations (0)
10. Financial Viability Goals
Meets Exceeds
Operating Margin 2.4% 2.6%
Revenue Increase: Total Outpatient Revenue (in Millions)
$1,846.2 $1,900
Expense Reduction: Total Operating Expenses per Case Mix Adjusted Admit
$6,780 $6,650
20
Exceeds Expectations (1.0) (Exceeding 2 or more benchmarks Exceeds expectations)
Meets Expectations (0.5) (Meeting all benchmarks Meets expectations)
Does Not Meet Expectations (0) (Not Meeting 1 or more benchmarks Does Not Meet expectations)
Total 100%
FY 2013 PRESIDENT & CEO EVALUATION (Proposed Revision 3-13-13) )Page 6 of 6
Additional Comments:
Board Member Signature: _______________________________________________ Date: ____________________________
V:\Board POLICY Manual\40.09B - President Unplanned Succession Process - Approved 102711.doc Page 1 of 2
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL no. 40.09B supersedes no. 40.09A ---------------------------------------------------------------------------------------------------------------------------------
category: Employee Relations
title: President and Chief Executive Officer (CEO) Unplanned Succession Process ---------------------------------------------------------------------------------------------------------------------------------
original adoption: 11/22/02 review date: 3/28/13
revision date: 11/18/2010, 10/27/11 ---------------------------------------------------------------------------------------------------------------------------------
PURPOSE:
To provide the Board of Directors of Lee Memorial Health System guidance for an unplanned departure, death, unexpected retirement, or emergency absence of the President and CEO, separation of employment, and a selection process for replacement of the position -------------------------------------------------------------------------------------------------------------------------------
POLICY: In the short-term absence of the President and CEO, the Chief Operating Officer shall be in charge of the health system’s operations and report to the Board of Directors, as needed.. In the event the President and CEO resigns, retires, dies, becomes incapacitated and can not return to work, or separates employment for any reason, the Chief Operating Officer shall be in charge of the health system’s operations and report to the Board of Directors, until the Board of Directors temporarily appoints an interim President and CEO. The interim President and CEO shall serve until a replacement is appointed by the Board of Directors. If the Board of Directors determines that there is one or more qualified internal candidates, the Board may appoint a replacement for the President and CEO from within the System. If the Board of Directors determines that there are insufficient qualified internal candidates, a Search Committee may be appointed to conduct a statewide or national search.
1. The final selection of the President and CEO shall be by majority vote of the total membership of the Board of Directors.
PROCEDURE: 1. If the President and CEO is unavailable for more than 72 hours, or if an emergency arises and
the President is not accessible, the Chief Operating Officer will be responsible for health system operations until the return of the President. The President will notify the Chairperson of the Board Directors for absences of more than 72 hours.
2. Should the President and CEO resign, retire, become incapacitated and cannot return to work, or separates employment, the Chairperson of the Board of Directors shall call a Special meeting of the Board to begin the selection and replacement process. The Chief Operating Officer shall serve as temporary President and CEO, until the Special Board meeting is convened to formally appoint an interim President and appoint a Search Committee.
V:\Board POLICY Manual\40.09B - President Unplanned Succession Process - Approved 102711.doc Page 2 of 2
3. The Search Committee consists of three Board members, the Board Attorney, the Chief Human Resources Officer, and other community representatives. The community representatives should include members of the Lee Memorial Health System Medical Staff, as well as business leaders and other key community leaders. The Board shall approve the final participants on the Search committee.
4. The Chief Human Resources Officer is responsible for organizing the search process and providing and sending out Request-for-Proposals to search consultant firms. The Chief Human Resources Officer will present a minimum of three search consultant firms to the Search Committee. The Search Committee will interview and select one firm and recommend to the Board of Directors for approval.
5. The Chief Human Resources Officer, working with the Search Consultant, will be responsible for communicating, posting, and advertising as needed for the President and CEO position to assure qualified internal and external candidates are sourced and notified.
6. The Chief Human Resources Officer is responsible for keeping the Board of Directors and the Search Committee informed of the process and timetable of the search, as well as providing any background or market information necessary to assist the Search Committee. The Board Attorney and the Chief Human Resources Officer shall draft an employment agreement and present to the Search Committee. The agreement will include total compensation, benefits, and relocation payment.
7. The Search Committee will recommend the employment agreement to the Board of Directors at a Called or Special Board meeting for their approval.
8. The Chief Human Resources Officer and the Search Consultant are responsible for meeting with the Search Committee, as needed, for informing the committee of the progress of the search process, and presenting to the Search Committee a minimum of three qualified candidates. The Chief Human Resources Officer and Search Consultant are responsible to share total compensation, benefits, and relocation agreements with qualified candidates. All references and information pertinent to the qualifications of the candidates for the President and CEO position will be presented to the Search Committee.
9. The Search Committee, after interviewing qualified candidates, shall recommend to the full Board of Directors two or more candidates to interview with the full Board. The Chief Human Resources Officer, working with the Board Office, shall be responsible for scheduling individual board member interviews with President and CEO candidates, as requested.
10. Upon completion of individual interviews, the Board Chairman shall notice a Special Board Meeting(s) for selection of a candidate. Final candidates shall be present for an interview with the Board of Directors at this meeting.
11. The Board of Directors, at a called or Special Board meeting, shall select a candidate for the President and CEO position.
12. The candidate will either accept the terms of the employment agreement, or request additional terms for consideration. These requests will be considered by the Board of Directors at a Called or Special Meeting and modified and/or approved. The Board Attorney and Chief Human Resources Officer will modify the terms of the agreement as appropriate. The Chairperson of the Board Directors shall be authorized to execute the employment agreement and notify the candidate of the approval of the employment agreement.
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS RECOMMENDED ACTION FOR BOARD APPROVAL
(Action includes Acceptance, Approval, Adoption, etc)
DATE: 3/28/13 LEGAL SERVICE REVIEW? YES__ NO__
SUBJECT: Various Board Policies for Review, Retirement or Adoption
REQUESTOR & TITLE: Cathy Stephens, Board Administrator
SPECIFIC PROPOSED MOTION:
1. Confirm REVIEW – NO CHANGES for the following policies:
A. 10.05E: Duties and Responsibility of Board of Directors B. 10.23B: Certificate of Need Applications C. 20.06C: Contract (Purchase, Sale, Transfer or Lease) D. 30.01C: Organized Medical Staff E. 40.01C: Pay Policy Statement
2. Approve RETIREMENT of the following policies:
A. 10.18C: Quality and Performance Improvement B. 10.25B: No Smoking Policy C. 40.07A: Corrective Action Exemption
3. ADOPT revisions to the following policies:
A. Motion to Remove from TABLE: 20.14F: Use of Funds for Education, Travel & Business Meeting/Special Event Expenses Tabled from Jan 24, 2013 Meeting B. 10.09D: Agenda Item Background Material C. 10.27F: Reporting and Accreditation D. 10.43D: Board Member Standards E. 10.47C: Compliance Program F. 10.53A: Electronic Tablets G. 10.54: Grievance Process H. 30.04: Medical Staff Representation I. 40.05C: Staffing Reductions
SUMMARY In order to be Accreditation compliant, several policies were needing to be either shown as reviewed – no changes, or adopted with changes, or approved to be retired.
Several revisions were made to bring the policies current or maintain consistency with the current System policies, and/or are being proposed for retirement due to duplication/conflict with System policies.
___________________
L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
BOARD POLICIES
Review/No Changes
1. 10.05E: Duties and Responsibility of Board of Directors 2. 10.23B: Certificate of Need Applications 3. 20.06C: Contract (Purchase, Sale, Transfer or
Lease)
4. 30.01C: Organized Medical Staff 5. 40.01C: Pay Policy Statement
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
10.05E-Duties Responsibility of Board of Directors ADOPTED 22510 REVIEW -No Changes 032813.doc REVIEW ONLY-No Changes 032813 Page 1 of 2
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL no. 10.05E Supersedes no. 10.05D
--------------------------------------------------------------------------------------------------------------------------------------------
category: General Operations
title: Duties and Responsibility of Board of Directors --------------------------------------------------------------------------------------------------------------------------------------------
original adoption: 1/08/91 review date: 3/28/13 – No Changes
revision date: 7/31/98, 9/29/00, 7/26/02, 10/31/03, 2/25/10 --------------------------------------------------------------------------------------------------------------------------------------------
PURPOSE:
To provide a comprehensive description of the duties and responsibilities assumed by a Board member elected by the citizens of Lee County or appointed by the Governor of the State of Florida. --------------------------------------------------------------------------------------------------------------------------------------------
POLICY: The duties, responsibilities and expectations of Board members shall be: PARTICIPATION AND PERSONAL DEVELOPMENT 1. Prepare for, attend and actively participate in meetings of the Board and its committees. 2. Make reasonable efforts to be informed on matters affecting the Lee Memorial Health System
and participate in continuing education opportunities and programs. PLANNING OVERSIGHT 1. Adopt a Mission Statement for the Health System. Review the same annually and revise if
appropriate. 2. Adopt a Strategic Plan for the Health System. Review the same annually and revise if
appropriate. QUALITY OVERSIGHT 1. Support the System’s program of continuous quality improvement. 2. Possess a general understanding of standards regarding quality of care imposed by outside
agencies, both governmental and private; and provide direction and support regarding compliance with such standards.
3. Review opinion surveys of patients, employees and practitioners on the medical staffs, and provide direction to System management regarding responses to the same, if appropriate.
COMMUNITY RELATIONS 1. Serve as a representative of the community regarding the scope of and manner of delivery of
services by the Health System. 2. Serve as a representative of the System to the public and government. 3. Adopt policies of non-discrimination in the delivery of care to patients, and in personnel and
medical staff matters.
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
10.05E-Duties Responsibility of Board of Directors ADOPTED 22510 REVIEW -No Changes 032813.doc REVIEW ONLY-No Changes 032813 Page 2 of 2
FINANCIAL OVERSIGHT 1. Adopt an annual budget and a capital expenditure plan for the Health System in accordance with
Board Financial Policy. 2. Require the preparation and review of financial and statistical reports from System management. 3. Adopt a long-term financial plan. Review the same at least annually and revise as necessary.
MANAGEMENT OVERSIGHT 1. Continually respect the difference between the role of the Board in establishing System policy and
direction, and that of management in carrying out daily operations. 2. Hire, evaluate and set the compensation of the System President, the Board Administrator, and
the Board Attorney. 3. Provide a means by which the System President shall report routinely on matters necessary for
the Board of Directors to fulfill its duties and responsibilities. 4. Periodically review and provide recommendations regarding the Health System’s Table of
Organization. 5. Provide recommendations to management regarding operational matters which do not further
Board policy. 6. Act on recommendations of the Corporate Compliance Officer, as required.
MEDICAL STAFF OVERSIGHT 1. Act on recommendations of the System medical staffs regarding appointments and
reappointments to the medical staffs, disciplinary actions, medical staff bylaws adoption and amendment, medical staff rules and regulations adoption and amendment, and other matters submitted by the medical staffs for consideration.
2. Provide a means by which the Presidents of the System medical staffs may routinely report medical staff issues to the Board.
3. In appropriate circumstances, consider institutional needs in the appointment and reappointment of the medical staff members, and the granting of privileges to practitioners.
4. Routinely communicate with the Medical Staff through meetings and/or written communications.
SUBSIDIARIES, SUBAGENCIES AND JOINT VENTURES 1. Create subsidiary corporations and approve articles of incorporation and bylaws for the same. If
the bylaws of such subsidiary corporations so require, appoint directors and officers. Dissolve subsidiary corporations as deemed appropriate.
2. Create and dissolve subagencies by resolution, as deemed appropriate. Resolutions establishing subagencies shall provide for their purpose, their management and their control by Lee Memorial Health System.
3. Approve the form and conditions under which the Health System shall participate with other persons or organizations in business ventures and other cooperative or joint efforts, consistent with the System’s mission.
4. Provide for the financial support of subsidiaries, subagencies and participation in businesses with other persons or organizations.
5. Provide for appropriate oversight of all subsidiaries, subagencies and business ventures with other persons or organizations.
6. Require all System employees serving as System representatives on subsidiary boards of directors, in subagency management, or in business ventures with other persons or organizations, before taking any action in such capacity, to obtain Board approval for such action, if such action in any other context would require the approval of the Board of Directors.
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
10.23B – Certificate Of Need – APPROVED 072602 – Review only – no changes 032813 Page 1 of 1
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL no. 10.23B supersedes no. 10.23A
--------------------------------------------------------------------------------------------------------------------------------
category: General Operations
title: Certificate of Need Applications --------------------------------------------------------------------------------------------------------------------------------
original adoption: 1/08/91 review date: 3/28/13 – No Changes
revision date: 7/31/98, 7/26/02 --------------------------------------------------------------------------------------------------------------------------------
PURPOSE: To comply with Certificate of Need requirements. --------------------------------------------------------------------------------------------------------------------------------
POLICY: The Board of Directors shall authorize the filing of Certificate of Need applications by means of formal resolutions in a format consistent with the Florida Agency for Health Care Administration requirements.
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
20 06C- Contracts Purchase Sale Transfer or Lease Appr 5-28-09 Page 1 of 2
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS POLICY MANUAL no. 20.06 C
supersedes no. 20.06b (combined with retired 20.07b)
-----------------------------------------------------------------------------------------------------------------------------------
category: Financial Operations
title: Contracts (Purchase, Sale, Transfer or Lease) -----------------------------------------------------------------------------------------------------------------------------------
original adoption: 01/08/91 review date:3/28/13 No Changes
revision date: 4/05/91, 7/31/98, 5/28/09 -----------------------------------------------------------------------------------------------------------------------------------
PURPOSE: To provide guidelines for the approval of formal written contracts (purchase, sale, transfer or lease). -----------------------------------------------------------------------------------------------------------------------------------
POLICY:
1. All contracts shall be styled using the legal name: “Lee Memorial Health System”. All contracting involving subsidiaries of Lee Memorial Health System shall indicate in the styling of the contract that it is a subsidiary of the System.
2. All written contracts, except those prepared by or reviewed by the Board’s Attorney, shall be
reviewed for legal sufficiency by an attorney in the health system’s Legal Services Department, consistent with the health system’s administrative policy.
3. Contracts for purchase, sale, transfer or lease of real property (land and/or buildings) shall
be approved by the Board of Directors.
4. All unbudgeted equipment leases in which the annual lease payments are $100,000 or more must be approved by the Board of Directors.
5. Contracts for the construction or improvement of real property that require the awarding of a
professional services contract must abide by Policy 20.15 – Design-Build Contracts.
6. A summary of all new or revised contracts related to the provision of employee benefits shall be reported to the Board of Directors. Formal advance approval of the same by the Board of Directors shall not be required.
7. All other contracts may be approved by the President/CEO or designee without being
referred to the Board of Directors.
8. Once a contract has been approved as required herein, it shall be signed in accordance with health system administrative policy.
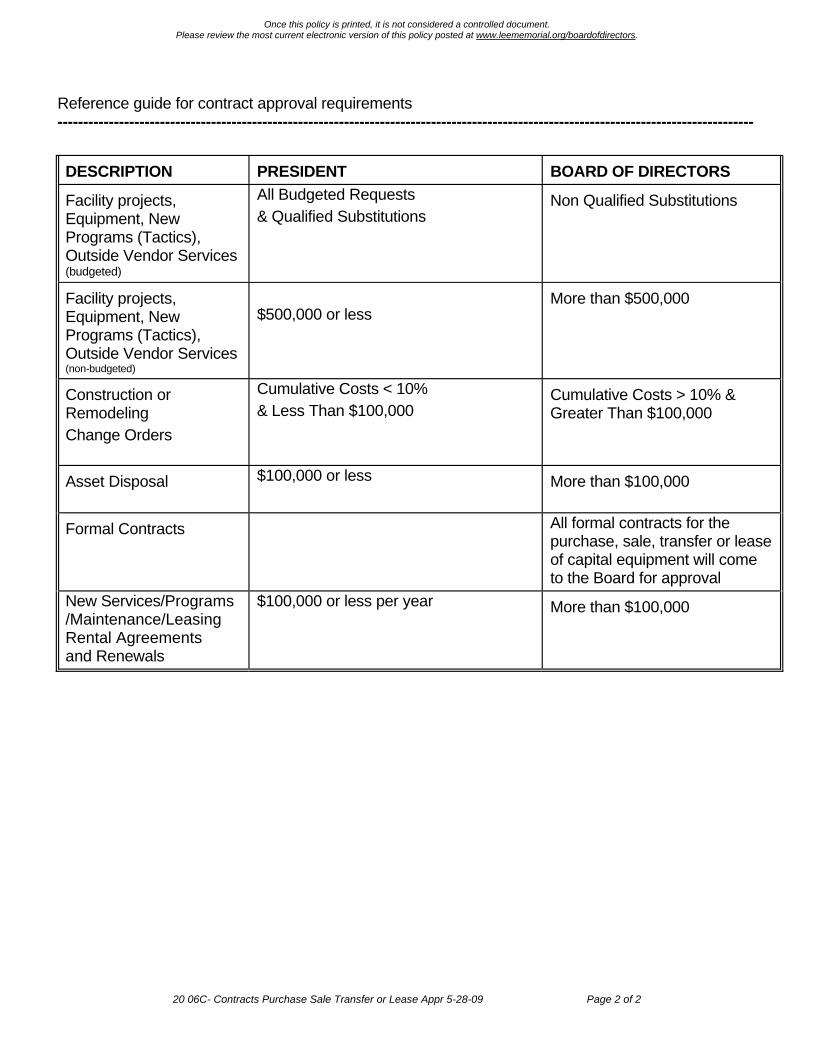
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
20 06C- Contracts Purchase Sale Transfer or Lease Appr 5-28-09 Page 2 of 2
Reference guide for contract approval requirements ----------------------------------------------------------------------------------------------------------------------------------------
DESCRIPTION PRESIDENT BOARD OF DIRECTORS
Facility projects, Equipment, New Programs (Tactics), Outside Vendor Services (budgeted)
All Budgeted Requests & Qualified Substitutions
Non Qualified Substitutions
Facility projects, Equipment, New Programs (Tactics), Outside Vendor Services (non-budgeted)
$500,000 or less
More than $500,000
Construction or Remodeling Change Orders
Cumulative Costs < 10% & Less Than $100,000
Cumulative Costs > 10% & Greater Than $100,000
Asset Disposal $100,000 or less
More than $100,000
Formal Contracts All formal contracts for the purchase, sale, transfer or lease of capital equipment will come to the Board for approval
New Services/Programs /Maintenance/Leasing Rental Agreements and Renewals
$100,000 or less per year More than $100,000
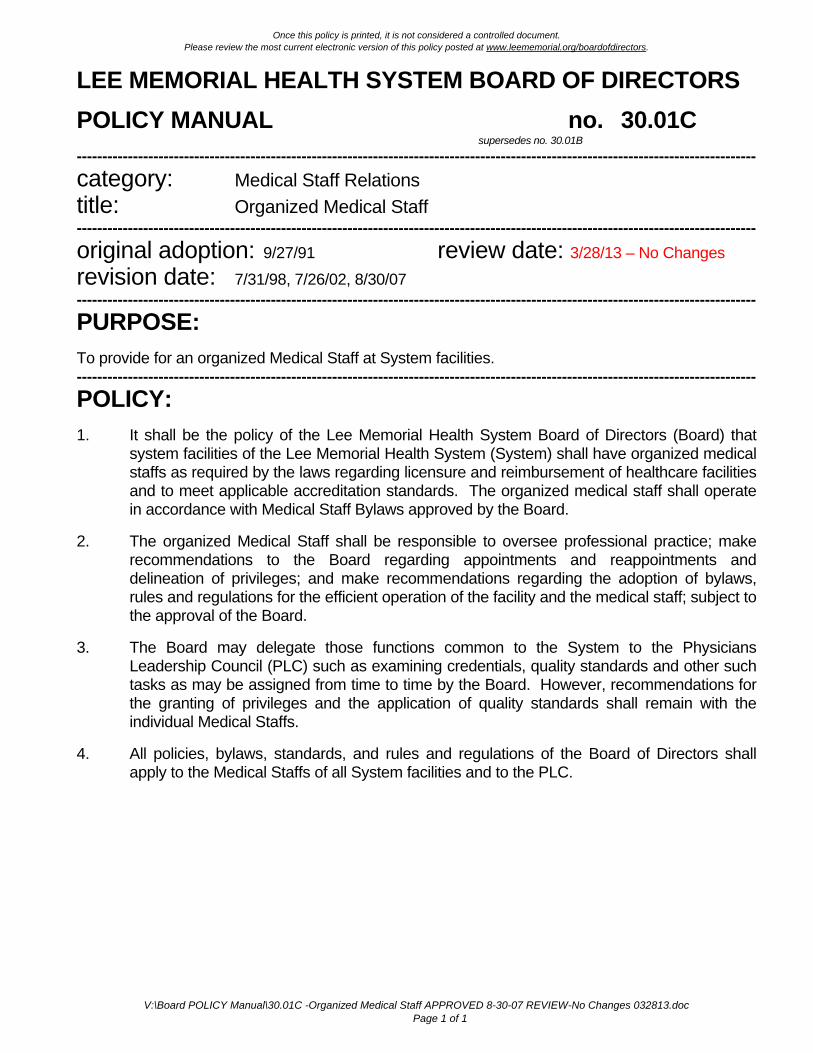
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
V:\Board POLICY Manual\30.01C -Organized Medical Staff APPROVED 8-30-07 REVIEW-No Changes 032813.doc Page 1 of 1
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL no. 30.01C supersedes no. 30.01B
-------------------------------------------------------------------------------------------------------------------------------------
category: Medical Staff Relations
title: Organized Medical Staff -------------------------------------------------------------------------------------------------------------------------------------
original adoption: 9/27/91 review date: 3/28/13 – No Changes
revision date: 7/31/98, 7/26/02, 8/30/07 -------------------------------------------------------------------------------------------------------------------------------------
PURPOSE:
To provide for an organized Medical Staff at System facilities. -------------------------------------------------------------------------------------------------------------------------------------
POLICY:
1. It shall be the policy of the Lee Memorial Health System Board of Directors (Board) that system facilities of the Lee Memorial Health System (System) shall have organized medical staffs as required by the laws regarding licensure and reimbursement of healthcare facilities and to meet applicable accreditation standards. The organized medical staff shall operate in accordance with Medical Staff Bylaws approved by the Board.
2. The organized Medical Staff shall be responsible to oversee professional practice; make recommendations to the Board regarding appointments and reappointments and delineation of privileges; and make recommendations regarding the adoption of bylaws, rules and regulations for the efficient operation of the facility and the medical staff; subject to the approval of the Board.
3. The Board may delegate those functions common to the System to the Physicians Leadership Council (PLC) such as examining credentials, quality standards and other such tasks as may be assigned from time to time by the Board. However, recommendations for the granting of privileges and the application of quality standards shall remain with the individual Medical Staffs.
4. All policies, bylaws, standards, and rules and regulations of the Board of Directors shall apply to the Medical Staffs of all System facilities and to the PLC.
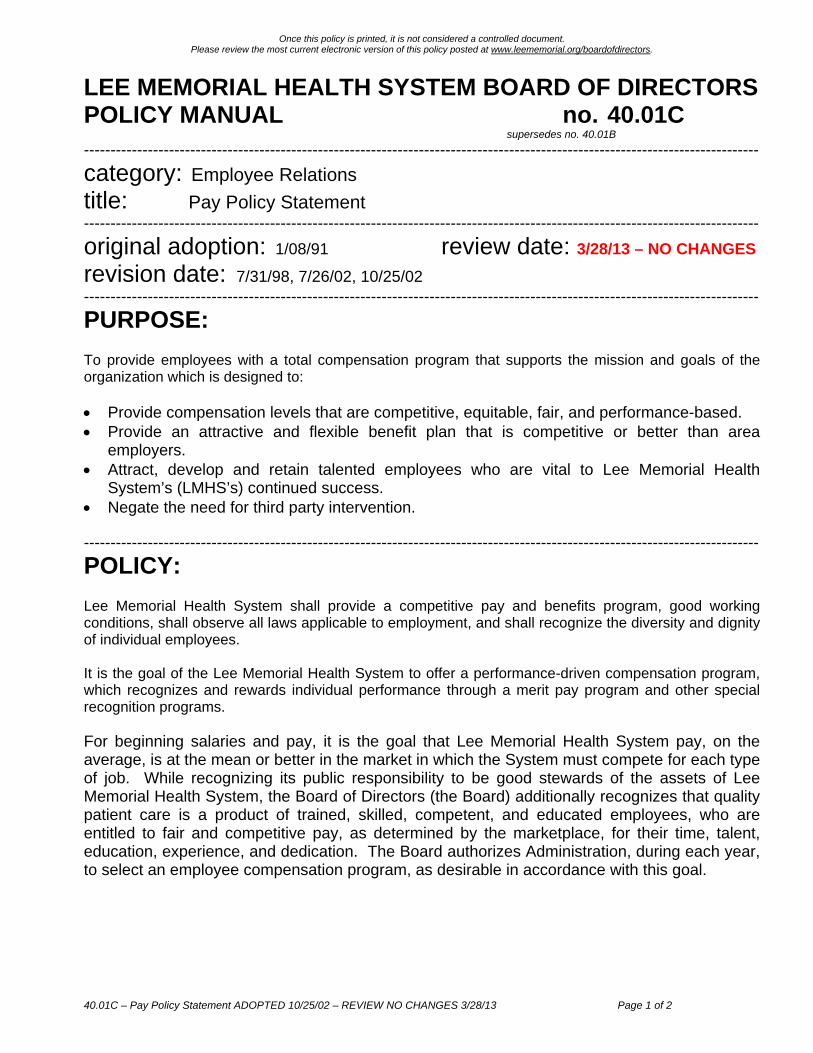
40.01C – Pay Policy Statement ADOPTED 10/25/02 – REVIEW NO CHANGES 3/28/13 Page 1 of 2
Once this policy is printed, it is not considered a controlled document.
Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS POLICY MANUAL no. 40.01C
supersedes no. 40.01B
-------------------------------------------------------------------------------------------------------------------------------
category: Employee Relations
title: Pay Policy Statement -------------------------------------------------------------------------------------------------------------------------------
original adoption: 1/08/91 review date: 3/28/13 – NO CHANGES
revision date: 7/31/98, 7/26/02, 10/25/02 -------------------------------------------------------------------------------------------------------------------------------
PURPOSE: To provide employees with a total compensation program that supports the mission and goals of the organization which is designed to: Provide compensation levels that are competitive, equitable, fair, and performance-based. Provide an attractive and flexible benefit plan that is competitive or better than area
employers. Attract, develop and retain talented employees who are vital to Lee Memorial Health
System’s (LMHS’s) continued success. Negate the need for third party intervention. -------------------------------------------------------------------------------------------------------------------------------
POLICY: Lee Memorial Health System shall provide a competitive pay and benefits program, good working conditions, shall observe all laws applicable to employment, and shall recognize the diversity and dignity of individual employees. It is the goal of the Lee Memorial Health System to offer a performance-driven compensation program, which recognizes and rewards individual performance through a merit pay program and other special recognition programs. For beginning salaries and pay, it is the goal that Lee Memorial Health System pay, on the average, is at the mean or better in the market in which the System must compete for each type of job. While recognizing its public responsibility to be good stewards of the assets of Lee Memorial Health System, the Board of Directors (the Board) additionally recognizes that quality patient care is a product of trained, skilled, competent, and educated employees, who are entitled to fair and competitive pay, as determined by the marketplace, for their time, talent, education, experience, and dedication. The Board authorizes Administration, during each year, to select an employee compensation program, as desirable in accordance with this goal.
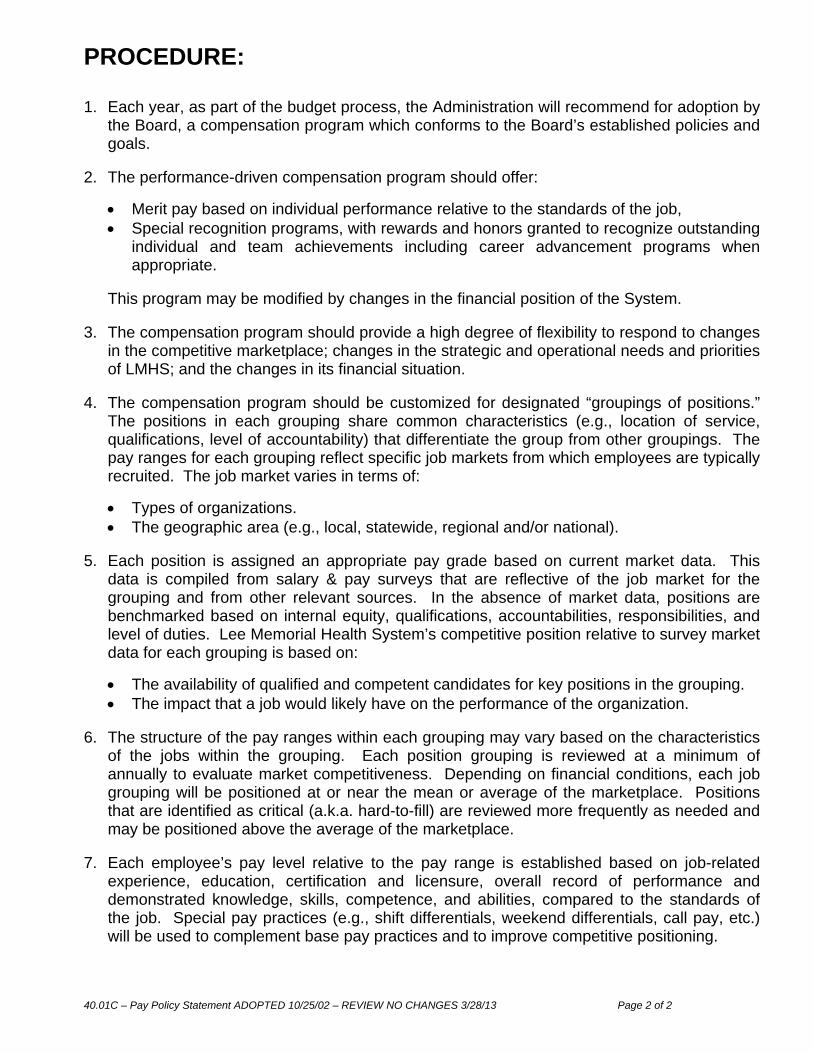
40.01C – Pay Policy Statement ADOPTED 10/25/02 – REVIEW NO CHANGES 3/28/13 Page 2 of 2
PROCEDURE: 1. Each year, as part of the budget process, the Administration will recommend for adoption by
the Board, a compensation program which conforms to the Board’s established policies and goals.
2. The performance-driven compensation program should offer:
Merit pay based on individual performance relative to the standards of the job, Special recognition programs, with rewards and honors granted to recognize outstanding
individual and team achievements including career advancement programs when appropriate.
This program may be modified by changes in the financial position of the System.
3. The compensation program should provide a high degree of flexibility to respond to changes
in the competitive marketplace; changes in the strategic and operational needs and priorities of LMHS; and the changes in its financial situation.
4. The compensation program should be customized for designated “groupings of positions.”
The positions in each grouping share common characteristics (e.g., location of service, qualifications, level of accountability) that differentiate the group from other groupings. The pay ranges for each grouping reflect specific job markets from which employees are typically recruited. The job market varies in terms of:
Types of organizations. The geographic area (e.g., local, statewide, regional and/or national).
5. Each position is assigned an appropriate pay grade based on current market data. This
data is compiled from salary & pay surveys that are reflective of the job market for the grouping and from other relevant sources. In the absence of market data, positions are benchmarked based on internal equity, qualifications, accountabilities, responsibilities, and level of duties. Lee Memorial Health System’s competitive position relative to survey market data for each grouping is based on:
The availability of qualified and competent candidates for key positions in the grouping. The impact that a job would likely have on the performance of the organization.
6. The structure of the pay ranges within each grouping may vary based on the characteristics
of the jobs within the grouping. Each position grouping is reviewed at a minimum of annually to evaluate market competitiveness. Depending on financial conditions, each job grouping will be positioned at or near the mean or average of the marketplace. Positions that are identified as critical (a.k.a. hard-to-fill) are reviewed more frequently as needed and may be positioned above the average of the marketplace.
7. Each employee’s pay level relative to the pay range is established based on job-related experience, education, certification and licensure, overall record of performance and demonstrated knowledge, skills, competence, and abilities, compared to the standards of the job. Special pay practices (e.g., shift differentials, weekend differentials, call pay, etc.) will be used to complement base pay practices and to improve competitive positioning.
___________________
L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
BOARD POLICIES
Retire (Action)
1. 10.18C: Quality and Performance Improvement 2. 10.25B: No Smoking Policy 3. 40.07A: Corrective Action Exemption
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
10.18C: Quality and Performance Improvement PROPOSED TO RETIRE 032813 Page 1 of 1
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL no. 10.18 C supersedes no. 10.18 B ---------------------------------------------------------------------------------------------------------------------------------
category: General Operations
title: Quality and Performance Improvement ---------------------------------------------------------------------------------------------------------------------------------
original adoption: 2/27/98 review date: 3/28/13
revision date: 7/31/98, 7/26/02, 4/29/10, 3/28/13 Proposed to Retire ---------------------------------------------------------------------------------------------------------------------------------
PURPOSE: To provide a comprehensive system of managing organizational and patient service processes to ensure continual improvement in the effectiveness and efficiency of patient centered care within the Lee Memorial Health System. ---------------------------------------------------------------------------------------------------------------------------------
POLICY: Care will be provided in the most appropriate setting, within resources available while consistently achieving optimal patient outcome. The Lee Memorial Health System’s Performance Improvement Process will be founded on the principles of Total Quality Management. Lee Memorial Health System will establish a Performance Improvement Process that supports the System’s Mission, Vision, and Values and provides implementation guidance for the Goals, Objectives and Strategies of the System’s Strategic Plan. Performance of the System will be measured on a continual basis; information used will be reported to the Board and integrated as appropriate to manage System performance. Performance in high volume, high cost, high risk and problem prone areas will receive special attention. Performance against the System Strategic Plan will be evaluated at least annually, in order to better formulate the next fiscal year’s implementation plan. The Senior Leadership Council and the Board of Directors will review the System’s Performance quarterly and make changes as needed in keeping with Board Policy 10.39A “Elements of a System Performance Indicator”; Board Policy 10.40A “Procedure for Additions, Deletions & Retirement of System Performance Indicators” and Board Policy 10.41 A “Governance and Reporting of System Performance Indicators”.
Proposed to Retire due to duplication and/or conflict of language with System policy S06 00 751.
�� ������������������ ���������������������������������������� ��!������"���#����!!#���"�$��!��%�� ���%$��&�%�������%�'�������(��"���������������%����"���(��!����""������(���)�*���������"�$��!��%�� ������%������"���"������+�"�!��� ������������%$��&��(����������� ������� �%�����"���"� ��(����,��!���$�������'���-./0123��4������������������$��&�"�������!��%�)��,�!�����������(� �����$�����"#������%��� #���(���+�����5)�"���$$��� ������%$��&��(���(���+��������$��!��%�� �'������������������������ �����"�)���� ��$��������$���!��%�6�����%������7������8����%�96�78:'������%���������)��������(���+����������"�!�� �������$�� ���������;�����"����������&��)���"��&����������!�$������� ������"���$$�������&� ��'��������� ��������;���"������ ���������� � ����!�$������(#�"���(���(#�%�������(#���������(���"��%$��&��('��6�78�����&�����)��"���� �������)�� ��$��%�����$���������!������"���(��*��������!� ���������(���� �������"�$��!��%�� ���%$��&�%����$�� ���'�����������������������6�78�"�!���������������������(�%����8����%���"���������(���� �%$����������������)�6�78����$��&�"�� �������������&� ���������$�������#������ �������������!� �������"� ������������%$��&������$��!��%�� �'��<�����!!�������� �����������$��%������ ��������!�$���������!���#�6�78������$��&�"���%�%;����!���"� ���=����>�&��)�>����� ��#�66?�9�=>>:���!�"������5�����"�$���������!������(���+������9=84:�)��������@(�� ��!���7����� ����>����� ����"���������9@7>�:#���"�&�������!�����A�$���%�����!�7��������"�7�%���8��&� ���9A778:'��6�78���� �%%����"���� �%$����(�)��������=�������8�!������"���������B%$��&�%����@ ���!�CDDE�9=8�B@:���"�����������(�����$��&���(����"� ��!�"���������������!�����$���������!����)��,�$��"� ��9=8<=:'����� �%$���)��������=8�B@#�6�78�����"�&���$�"���$���������!�����&��������������%��������"�6�����%������7������8����%�=�������8�!����F&���������8����%�96=8F8:�!���$��$�����!� ���� ���(#������+��(#���"���$�����(�=8<=��������=84'������=84�$���� ������$$������������6�78��%$������#�&���������#����"����#�%�"� ������!!�%�%;���#���"��������)��,��(����;����!��!�6�78'��@���=8<=�)������6=8F8�%����;�� ���� ��"������"#������+�"���"���$����"��������=84����� ��"�� ��)����6�78�$��� ���'���GHCIHJIHCKG�� � � � � � � � � � ?�� ,�L��&��,�#��A#�?���!���"� ���4!!� ���A@�F�� � � � � � � � � � � � =46B?M�@A�BNB8�>@�4>�� � � � � �� � �� � � � � � � � �>�&��)�"I>�&���"O��HCIHC�� H��
������������������������� ��� ������������������������������������������� !�"���� !�# $�%&'#&()�*�+�#,���������������������������������������������������������������������������� -����������%*�.(�# $�/0*,1��� �222222222222222222222222���������3'�*($1'(��� �&4(�51#,�&6��# #)(7( &�%6�&(722222222222222�����"����3'��'�&�8� )�51#,�&6�9:;(*&�<(�222222222222222222222���"�����51#,�&6�# $�3#&�( &�%#=(&6�%&'#&()�*�3,# 22222222222222222���"�����+�<(' # *(��=�3('=�'7# *(��7.'�<(7( &�>*&�<�&�(�222�222222222�����?�#'$��=�@�'(*&�'�22222222222222222222222222�����%6�&(7�51#,�&6�%#=(&6��# #)(7( &�A�1 *�,2222222222222222����%6�&(7�51#,�&6�# $�A� =�'7# *(�A�77�&&((2222222222222�22����1,&�$��*�.,� #'6�3('=�'7# *(��7.'�<(7( &�B(#7�2222222222222���C#*�,�&6�51#,�&6�A�77�&&((�2222222222222222222222������($�*#,�%&#==�51#,�&6�A�77�&&((�2222222222222222222�������������3#&�( &�A#'(�%('<�*(�2222222222222222222222222����������9')# �8#&�� ��=�3('=�'7# *(��7.'�<(7( &�D�&4� �3#&�( &�A#'(�%('<�*(�22222���������%( ��'�E1'�� )�F(#$('�4�.�A�1 *�,2222222222222222222���������������9.('#&�� ��A�1 *�,�2222222222222222222222222���"������(#�1'(7( &2222222222222222222222222222����%6�&(7�%&'#&()�*�+�#,�222222222222222222222222����%6�&(7�?�#'$�G(.�'&2222222222222222222222222����# #)(7( &�G(<�(D2222222222222222222222222���� &(' #,�51#,�&6�>1$�&�22222222222222222222222����H �&�F(<(,�� $�*#&�'�2222222222222222222222222���������@(.#'&7( &�F(<(,�� $�*#&�'�222222222222222222222222��"�����3('=�'7# *(��7.'�<(7( &��(&4�$�,�)�(�222222222222222���+,���#'62222222222222222222222222222222����>..( $�0�>I��%9�JKKL�� &('#*&�� ��#&'�022222222222222222��2��>..( $�0�?I��E�>M9N�� &('#*&�� ��#&'�022222222222222222���>..( $�0�AI�F�M%�3'�*(���� &('#*&�� �%(O1( *(��#.2222222222222�����P������P��������Q��������Q��������Q��������R�����R�����S�����S�����S�����S���LK���LK���LK���LK���LK����LL���LL���L-���L-���L-���LP���LP����LP����LT����LQ����LR����LS���
� ��� ���������������� ����������������������� ������ �������������� ����� ������������� �!���"���#�$�%&'(�)�'(!��*+,!�$�&,�!��-�.!&./��!��$��!�!�����'(!�-'%��.��0,�'.0�&$1%�2��!�����'(!��,!'!/,�� �!���1��1(��� �*�/!�3�,!�4(�%&0'5��6&!��'02'.-�,�&.�!�-�.�(�7+8���'(!�-'%��&,�-�.!&./�/,(+�-�'.7&.75��9:�.!&./&.7�!��$��!�!�����'(!�-'%��.��0,;�� �!���-�$$/.&!+�$�'.,�3��$/,!�-�.!&./��!��-�'.7�5����'!<,�3�'!�=�% �%$'.-��>$1%�2�$�.!�&,�'((�'?�/!5������@������� �!���"���#�$�%&'(�)�'(!��*+,!�$�&,�!��?��!���?�,!�1'!&�.!A-�.!�%�0���'(!�-'%��0�(&2�%+�,+,!�$�&.�!���*!'!��� �4(�%&0'8�?+�?'('.-&.7�B/'(&!+8�'--�,,�'.0�-�,!5����&,�?'('.-��&,� /.0'$�.!'(�!��'-�&�2&.7��/%�#&,,&�.5��C+�-�.!&./�/,(+�&$1%�2&.7�!���B/'(&!+�� ��/%�1%�-�,,�,�'.0��/!-�$�,8�1%�2&0&.7�-�.2�.&�.!�,�%2&-�,8�'.0�$'&.!'&.&.7��/%� &.'.-&'(�,!'?&(&!+8�3��3&((�'-�&�2���/%�2&,&�.�� �?�&.7�!���?�,!�&.�4(�%&0'�D�'.0�'�(�'0�%�&.�!���.'!&�.5��:�.!&./�/,�&$1%�2�$�.!�&,�-%&!&-'(�!��!�'!�,/--�,,5������EFGHFIJ�KLM�HN��� �"���#�$�%&'(�)�'(!��*+,!�$�'%��!��,��� �'-�&�2&.7��O-�((�.-�P�QRS/'(&!+�D�TO-�((�.!�1'!&�.!��/!-�$�,�QR:�$$/.&!+�D�TO-�((�.!�-�$$/.&!+���'(!��,+,!�$�QR*�%2&-��D�TO-�((�.!�1'!&�.!��O1�%&�.-��QR=��1(��D�TO-�((�.!���'(!��-'%���$1(�+�%�QR4&.'.-��D�4&.'.-&'(��O-�((�.-�������C�'%0�� �U&%�-!�%,8�#�0&-'(�*!' 8�V0$&.&,!%'!&�.�'.0�"�'0�%,�&1�� �"���#�$�%&'(��'2��-��1�%'!&2�(+�0�2�(�1�0�!���#&,,&�.8�W&,&�.�'.0�*!%'!�7&-�X�'(,�� �!����%7'.&Y'!&�.8�'.0�'(&7.$�.!�� ��?Z�-!&2�,8�$�',/%�$�.!,�'.0�'--�/.!'?&(&!&�,�'!��2�%+�(�2�(�!��,/11�%!�!���,�'%�0�-�$$&!$�.!�!��B/'(&!+�'.0�1�% �%$'.-��&$1%�2�$�.!5������[\]_a�b[cdef\e� X��7%'1�&-'((+�(�-'!�0�&.�,�/!�3�,!�4(�%&0'8�"#)*�,�%2�,�'�2&!'(�%�(��&.�!���-�$$/.&!+�',�'�1%�2&0�%�� �1%&$'%+8�,�-�.0'%+8�'.0�!�%!&'%+���'(!��-'%��,�%2&-�,5��#�0&-'(�'.0�,/%7&-'(�-�.!&.//$�� �,�%2&-�,�&,�1%�2&0�0� �%�'((�'7�,5��"#)*�1%�2&0�,�!�����'(!��-'%��.��0,�� �!���-&!&Y�.,�� �"���:�/.!+�3&!��!���ghih�1�1/('!&�.�� �jik8lmn5��V,�'�1/?(&-8�.�!A �%A1%� &!�,1�-&'(�/.&!�� �7�2�%.$�.!8�"���#�$�%&'(�)�'(!��*+,!�$�&,�.�!�7�2�%.�0�?+�o*)V�%�7/('!&�.,5��>.�'--�%0'.-��3&!�� �0�%'(�'.0�,!'!��%�7/('!&�.,8�1%� �,,&�.'(�1%'-!&-��,!'.0'%0,�'.0�-�0�,8�"#)*�1%�2&0�,�!���-�$$/.&!+�'.0�,/%%�/.0&.7�-�$$/.&!&�,�3&!��'� /((�%'.7��� �,�%2&-�,�&.-(/0&.78�?/!�.�!�(&$&!�0�!�P�� QR:(&.&-'(�:'%��*�%2&-�,�QRU&'7.�,!&-p�%�'!$�.!�'.0�6�((.�,,�*�%2&-�,�QR:(&.&-'(�*/11�%!�*�%2&-�,�QRq�.A:(&.&-'(�*/11�%!�*�%2&-�,�C�(�3�'%��!���,-�1��'.0��O-(/,&�.,�� �!���"#)*���,1&!'(,�',�,�1'%'!�0�?+�!���:#*�::q�0�,&7.'!&�.P� �_]�\r_c�\e]fs_ct���ufe_vwxyza{_[fcfs|��r}f[ef[cda~QRX�.�%'(�#�0&-&.��QRX�.�%'(�*/%7�%+�
� ��� ������������������� ��� ����������������� �������� ��������������� ������������ ������� �������������������������� ������� �������������������������������������������������� � !"#$%&'�()*+�,,-�./$�012134%'10�/'�1 !"#$%&'�53&4�2.1�316#%3141'2$�015%'10�7%2.%'�89:;<<=�,"/#$1�()*�5&3�>3&0#!2�?1$%@'�/'0�?1A1"&B41'2�C/$10�#B&'�,,-�#$%'@�&'"D�B3&A1'�412.&0$E�231/241'2$E�16#%B41'2E�/'0�410%!/2%&'$)��,/B1�,&3/"�-&$B%2/"�0&1$�'&2�B/32%!%B/21�%'�01A1"&B%'@�'17�412.&0$E�231/241'2$�&3�410%!/2%&'$)���F11�G14&3%/"�-&$B%2/"�HFG-I�%$�/�*JJKC10�5/!%"%2DE�$13A%!1$�%'!"#01+����LM�����N������������O��������� �P����������Q��� ����������������������R����������� �����������S�������T��������U�����������V�W��RR�X���T����������������������������������������� Y.1�Z1./C%"%2/2%&'�-&$B%2/"�HYZ-I�%$�/�[<�C10�.&$B%2/"�"&!/210�7%2.%'�F11�G14&3%/"�-&$B%2/")�913A%!1$�%'!"#01+������������ �������� ���������X������\������ ��X��������������� �]V����������������X��������� �� ��������-1/"2.�>/3_�G10%!/"�,1'213�H->G,I�%$�/�*[�C10�5/!%"%2D)�913A%!1$�%'!"#01+���������W�� �������W� ����������� ����������������R����W��������������������������Q��� �������������������������������� �a� ��������������a���W�� ����������������������������������
� ��� �������������� ��������������������� ��������������������� !�"#!$�%&��'��"(�#)�*+,-��!�&�./�0���1������� !��#!$�%&���#1&%���2�%����"�&�%��3&�4�5���1&�����%��6�*��7�1�!���1�8��9����:���;�<�����= �������>� ������:����?��@�:�A�������=���������B���������>���=�C�=���D���BD���� �����>� ���E�=�������C������ �F���G=�����=���H�����������:I@��J�KA������ ����H������C������ �L�����;�>�������E�=�������M���C������ ���M���C������ �K =�=��N��D��=�=�����@���=���C�������������>��������������OP1�8!�#��Q6R9�-5"S�"35�S��T"S���"��&!���%��U�����&���P1�8!�#��)�#U�%�����V8���U��%!���)�����2�%����W*X.YYZ���&8!��Q6R�)#��3�#�81%�[�!�\��&���[�7��#$U��%�0&!���8$#��-5"S�"35�S��T"S���"�8!��\�#��]�$�#7���U�%�#�!S�%��&%U��%!S��V8�$U��%S�&���U���1&%�#�!6��-5"S�"35�S��T"�&�����"��#��#%�$&�%�1�$&%�����%�����7��#$U��%�#)���2�U�%�#�!S�%��&%U��%!�#��U���1&%�#�!6���OP1�8!�#��Q66Z9��T"��#1&%���2�%����-5"�1&U$8!��!�&11����%���0]�%����#UU�!!�#��#��_11����%&%�#��#)�T��&0���%&%�#��,&1���%��!�'�_T,(6�������)#��S�W_"X�!%&��&��!�2����0����U�%���%#���7��2�%���3�]!�1&��O�7��#�U��%�&���-�)��*&)�%]���V8���U��%!6���a8�)��#&!%�5���1&�����%���'a�5�(��!�&�Rb.�0���)&1���%]6�*��7�1�!���1�8��9�������>���=�������=�=���������� �����������c����F���G������=���K��:=G�� �����������E���=��������d��G������������������<���C��D�������=J�����������KA������ ����H�� =�=�� ����������H����������� ���������������H������e�� ���� OP1�8!�#��Q6R9�a�5���&!���%��U�����&���P1�8!�#��)�#U�%�����V8���U��%!���)�����2�%����W*X.YYZ�Q6R�)#��3�#�81%�[�!�\��&���[�7��#$U��%�0&!���8$#��a�5��8!��\�#��]�$�#7���U�%�#�!S�%��&%U��%!S��V8�$U��%S�&���U���1&%�#�!6�a�5���#�!��#%�$&�%�1�$&%�������7��#$U��%�#)���2�U�%�#�!S�%��&%U��%S�&���U���1&%�#�!6�����
� ����������������� ��������� ���������������������� ������������� ��������� ���!"��""�#$#�%&'()*+,�-&+,.&/�!"��""�011�2*'&.3�-&+,.&/�!"��""�45$��+,*.+6/�7(6/8,9�:(38,;�!"��""�#<5�-&+,.&/�&=�>&+'&+=&.)8+?��.&3(',�!"��""�#<<�-&..*',8@*�:',8&+�&=�>&+'&+=&.)8,8*;� ���ABBC�DEFEFG��� HI���J�HI���K�JL���M�L�N�O ��H������M�P�GL� L��FBCCQ� R"��""�0<4��.*@*+,8@*�:',8&+�&=��&,*+,86/�>&+'&+=&.)8,8*;��+,*?.6,*3�R*.@8'*�!6+(6/�&=��.&'*3(.*;�!"��""�$4$�R,.&S*��*.=&.)6+'*��)T.&@*)*+,��/6+�U&6.3��&/8'9�6+3�U9/6V;�!*38'6/�R,6==�U9/6V;�� ��� ��������N� R'&T*W;X�&=�R*.@8'*�Y.?6+8Z6,8&+6/�-[6.,W;X���\�L� R,6+36.3;�=&.�U/&&3�U6+S;�6+3�].6+;=(;8&+�R*.@8'*;��������J� �� � _ ������ ���� a��� b����� �*.=&.)6+'*��)T.&@*)*+,�&TT&.,(+8,8*;�6.*�83*+,8=8*3�8+�;*@*.6/�V69;c�de2*@8*V�&=�T*.=&.)6+'*�8+38'6,&.;�def**3g6'S�=.&)�T6,8*+,h�T[9;8'86+�6+3�*)T/&9**�;6,8;=6',8&+�;(.@*9;h�8+'/(38+?�'(;,&)*.�'&))*+,;�de-&)T6.8;&+;�,&�8+3(;,.9�,.*+3;�dei@83*+'*�g6;*3�T.6',8'*�dei@6/(6,8&+�&=�;*.8&(;�;6=*,9�6+3�T.*'(.;&.�;6=*,9�*@*+,;��-.8,*.86�(;*3�8+�T.8&.8,8Z8+?�T.&j*',;�8+'/(3*�de�)T6',�&.�T&,*+,86/�8)T6',�&+�T6,8*+,�6+3�;,6==�;6=*,9�de�3*+,8=8'6,8&+�&=�[8?[�.8;Sh�[8?[�@&/()*�6+3�T.&g/*)�T.&+*�T.&'*;;*;�de�*.=&.)6+'*�6?68+;,�;,.6,*?8'�?&6/;��� �.&j*',;�6.*�T.8&.8,8Z*3�6,�,[*�6TT.&T.86,*�/*@*/�&=�,[*�&.?6+8Z6,8&+���f&.�8+;,6+'*h�,[*�U&6.3�&=�%8.*',&.;h�&.�7(6/8,9�6+3�R6=*,9�!6+6?*)*+,�-&(+'8/�)69�T.8&.8,8Z*�T.&j*',;�&=�;9;,*)�V83*�8)T6',���][*�(+8,�7(6/8,9�-&(+'8/�&.�/*63*.;[8T�,*6)�)69�T.8&.8,8Z*�T.&j*',;�6,�6�(+8,�/*@*/���bE����� ������J�� ������P����������� ��J����� :;�T6.,�&=�,[*�7(6/8,9�R,.6,*?8'�k&6/h�l!mR�[6;�3*@*/&T*3�,[*�7(6/8,9�6+3��6,8*+,�R6=*,9�R,.6,*?8'��/6+���][*�T(.T&;*�&=�,[*�T/6+�8;�,&�*+;(.*�,[*�[*6/,[�6+3�;6=*,9�&=�&(.�T6,8*+,;�g9�;*,,8+?�,[*�[8?[*;,�;,6+36.3;�&=�;6=*,9h�n(6/8,9�6+3�&(,'&)*;���][*�)8;;8&+�&=�,[*�T/6+�8;�,&�8)T.&@*�T6,8*+,�&(,'&)*;�g9c�� de�)T.&@8+?�!*38'6,8&+�R6=*,9�de�)T/*)*+,8+?��+=&.)6,8&+�R9;,*);�,&��)T.&@*�R6=*,9�de�+;,8,(,8+?�-/8+8'6/�R6=*,9��.&'*;;*;�dei3('6,8+?�&+�R6=*,9�de%*@*/&T8+?�!*,[&3;�,&�!&+8,&.�6+3�:;;(.*�R6=*,9�de�.&@838+?�6�R6=*�i+@8.&+)*+,��
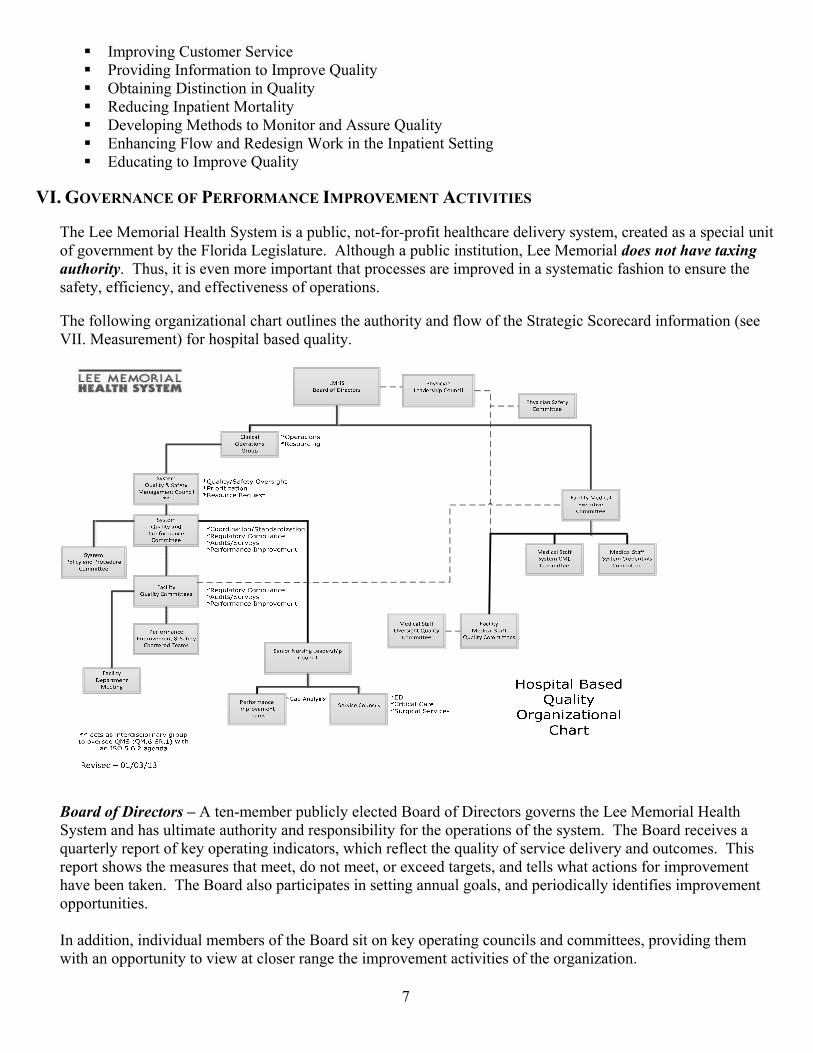
������������ �������������������������������������������� ���������������������� ���������� �������������������������������������������������� �� ���� �������!�����"��#�����������$��%���������������������!� ����������������� ������&'()*+&,-./.0,)+1)2,-1+-3/.0,)'32-+&,3,.4)/04'&'4',5)� 6���7�����������8������������������ ���9���:���:�������������������������������9��������������������� ���������������������"������7������ ��;�� ���� ������ ������� ��9�7�����������<=>?@A=B@CDE>@BDFGAH@DIBC=JGBK;��6� �9������������������������������������������������������������������������� �������������9��������9���������������������������;�� 6��������#������L������������� ���������� �������������#�����������������������������������M������N��;����� �����O�������������������P ����;�� �� Q�� ���R=DJ<@=S@TGJ>UB=J?@V@ @��:�������� ��������������W����������������������������7�����������8�������������������� �������� ���������������������������������������������������;��6���W���������������P ������������������%������������������9�#����������������P ��������������������������� ������;��6�������������#���������� �������������9�����������9�����X������������9����������#�����������������������������������%�;��6���W����������������������������� ��������9�������������������������������������� ���;���������9���� ������������������W����������%������������� ����������������9�������������#����������� ��������#�������������������������������������������������L���;��
� ��� ����������� ����� ����� � ������������������������������� �!"�#""!$%�&�'���(�")*%"!+!,!'-�+-�'���.�/��0*#(&�*1�2!(�3'*("�'*��%"4(��'�#'�'���*($#%!5#'!*%�!6),�6�%'"�#%&�6#!%'#!%"�#%��11�3'!7��84#,!'-�6#%#$�6�%'�"-"'�69�:'�!%"4(�"�'�#'�3*((�3'!7��#%&�)(�7�%'!7��#3'!*%"�'#;�%�+-�'���*($#%!5#'!*%�#(��!6),�6�%'�&<�6�#"4(�&�#%&�6*%!'*(�&9���*�6��'�'�!"�(�")*%"!+!,!'-<�'������� �!%'�$(#'�"<�#%#,-5�"�#%&�(�7!�="�84#,!'-�#%&�"#1�'-�!%1*(6#'!*%�1*(�*($#%!5#'!*%�&�3!"!*%>6#;!%$�#%&�)�(1*(6#%3��!6)(*7�6�%'9�����������!%1*(6#'!*%�!%3,4&�"�'���4%&�("'#%&!%$�*1�)#'!�%'�!%&!3#'*("�*1�"�(7!3��#%&�84#,!'-<�*)�(#'!*%#,�)�(1*(6#%3�<�"#1�'-<�*($#%!5#'!*%#,�3#)#+!,!'!�"<�#%&�+�%3�6#(;�!%1*(6#'!*%9��������� �#&7!"�"�'���0*#(&<���&!3#,��'#11<�#%&� ,!%!3#,�?)�(#'!*%"�@(*4)�*%�*))*('4%!'!�"�1*(�!6)(*7�6�%'<�3*%"!"'�%'�=!'��+4"!%�""�%��&"�#%&�)(!*(!'!�"�*1�'���*($#%!5#'!*%9��:'�&�,�$#'�"�'���3�#('�(!%$�*1�"-"'�6>=!&��)�(1*(6#%3��!6)(*7�6�%'�'�#6"�#%&�!"�(�")*%"!+,��1*(�*7�("!$�'�*1�'�*"��'�#6"�'�(*4$����%!*(�A4("��.�#&�("�!)� *4%3!,9������!%'�(&!"3!),!%#(-�$(*4)�'�#'�*7�("��"�'����4#,!'-��#%#$�6�%'��-"'�6�3*%"!"'"�*1�(�)(�"�%'#'!*%�1(*6�B�1*(�C&6!%!"'(#'!*%<�A4("!%$<�D�#(6#3-���(7!3�"<�C%3!,,#(-���(7!3�"<�:%1*(6#'!*%��#%#$�6�%'<�E!";�B��#1�'-��#%#$�6�%'<��4#,!'-�F#3!,!'#'*(�B��#%#$�6�%'�E�)(�"�%'#'!7��#%&���&!3#,��'#11�6�6+�("�=�*�64"'�+��&*3'*("�*1�6�&!3!%��*(�*"'�*)#'�-9���������� �3*6),�'�"�'���6#%#$�6�%'�(�7!�=�*1�!%)4'"�!%�#33*(&#%3��'���:�?�GHHI�J9K9L�3,#4"��#%&�A:C/?�"'#%&#(&���9K��E9I�(�$#(&!%$�'����11�3'!7�%�""�*1�'����4#,!'-��#%#$�6�%'��-"'�69������!%)4'�'*�6#%#$�6�%'�!%3,4&�"�(�"4,'"�*1�#4&!'"�M!%'�(%#,<��N'�(%#,�#%&�(�$4,#'*(-O�34"'*6�(�1��&+#3;<�)�(1*(6#%3��#%&�"�(7!3��3*%1*(6!'-<�"'#'4"�*1�)(�7�%'#'!7��#%&�3*((�3'!7��#3'!*%"<�1*,,*=>4)�1(*6�)(�7!*4"�6#%#$�6�%'�(�7!�="<�"4)),!�(�&#'#�#%&�(�3*66�%&#'!*%"�1*(�!6)(*7!%$�'���84#,!'-�6#%#$�6�%'�"-"'�69����6+�("�*1�'������� �!%3,4&��0?2�.!#!"*%P� *664%!'-�E�)(�"�%'#'!7�<� �!�1���&!3#,�2!(�3'*(B ,!%!3#,�Q��4#,!'-���(7!3�"P� �!�1�D#'!�%'��#1�'-�?11!3�(<� �!�1�D#'!�%'� #(��?11!3�(P� �!�1�.�$#,�?11!3�(P�� �!�1�?)�(#'!%$�?11!3�(<� �!�1�:%1*(6#'!*%�?11!3�(<� *()*(#'�� *6),!#%3��?11!3�(<�R!3��D(�"!&�%'�*1��4#,!'-P��-"'�6���&!3#,�2!(�3'*("<��-"'�6�2!(�3'*(�*1�D�#(6#3-<��-"'�6�2!(�3'*(�*1� #(���#%#$�6�%'<��-"'�6�2!(�3'*(�*1���&!3#,��'#11��4#,!'-P��-"'�6�2!(�3'*(�*1�2�3!"!*%��4))*('<��-"'�6�2!(�3'*(�*1�S%7!(*%6�%'#,��#1�'-��#%&�E!";��#%#$�6�%'9������1*,,*=!%$�$(*4)"�(�)*('�'*�'����-"'�6��4#,!'-��#1�'-�#%&��#%#$�6�%'� *4%3!,T�� UV������� ���� �W������X ���������������YZ[Z������ �!"�#""!$%�&�(�")*%"!+!,!'-�1*(�3*%'!%4*4"�(�7!�=�!%�#�"�,1>#""�""6�%'�)�(")�3'!7��'*�&�'�(6!%��'����4#,!'-��#%#$�6�%'��-"'�6��#"�+��%��11�3'!7�,-�!6),�6�%'�&�#%&�6#!%'#!%�&9���!"�3*66!''���!"�(�")*%"!+,��1*(��7#,4#'!%$�A:C/?�"'#%&#(&"<�:�?GHHI�3,#4"�"<� ���#%&�*'��(�(�$4,#'!*%"�7#,!&#'!%$�3*%1*(6#%3��'�(*4$���N!"'!%$�6*%!'*("�*(�!%!'!#'!*%�*1�6*%!'*("�=��(��34((�%'�3*%1*(6#%3��!"�4%;%*=%�*(�%*'�(�3�%',-�&*346�%'�&9��*�#""4(��'��������#"�+��%��11�3'!7�,-�!6),�6�%'�&�#%&�6#!%'#!%�&�+-�#""�""!%$�#33(�&!'#'!*%�"4(7�-�(�#&!%�""<�3*%1*(6#%3��'*�(�$4,#'*(-�"'#%&#(&"<�3*((�3'!*%"�#%&�3*((�3'!7��#3'!*%�),#%"<�)(�7�%'#'!7��#3'!*%"�"43��#"�/RC<�F#!,4(���*&��S11�3'"�C%#,-"!"<�:�?�!%'�(%#,�"4(7�-"<�)�(1*(6#%3��!6)(*7�6�%'�'�#6"�#%&�!%!'!#'!7�"<�(�$4,#'*(-�3*6),#!%'"�#%&�3*6),#!%'�!%7�"'!$#'!*%"9�� ��6+�("�!%3,4&�"�R!3��D(�"!&�%'"�*1�D#'!�%'� #(�<�R!3��D(�"!&�%'�*1��4#,!'-<�F4%3'!*%#,�.�#&�("�1(*6��)!(!'4#,���(7!3�"<� #(���#%#$�6�%'<� ,!%!3#,�.�#(%!%$<�2�3!"!*%��4))*('<�:%1�3'!*%� *%'(*,<�?($#%!5#'!*%#,�S11�3'!7�%�""<�S%7!(*%6�%'#,��#1�'-<�2!�'#(-<�/:�<���&!3#,��'#11��4#,!'-<�E#&!*,*$-<�E�")!(#'*(-� #(�<�.#+*(#'*(-P�E!";��#%#$�6�%'P�.���D�-"!3!#%���(7!3�"P��'#11�2�7�,*)6�%'P� ,!%!3#,�:%1*(6#'!*%��-"'�6"P�/46#%�E�"*4(3�"P�0?2P�D�#(6#3-�#%&�'��\D(*$(#6��#%#$�("�1*(��'#%&#(&"�#%&��4#,!'-9�UV����W����]��� X��]X�_������ ��������� �1*(6"�#%&�3�#('�("�64,'!&!"3!),!%#(-�!6)(*7�6�%'�'�#6"�#"�%��&�&9����6+�("�!)�"�*4,&�!%3,4&��,�#&�("�#%&�"'#11�=�*�#(��3,*"�"'�#%&�6*"'�#=#(��*1�'���)(*3�""�!%�84�"'!*%<�#%&�'���%��&"�#""*3!#'�&�=!'��'���)#'!�%'9�D:�'�#6"�6#-+��(�$!"'�(�&�!%�'���D:�D(*a�3'�2#'#�0#"��'*�!6)(*7��3*664%!3#'!*%�#%&�!%'�$(#'!*%�*1�D:�)(*a�3'"9��
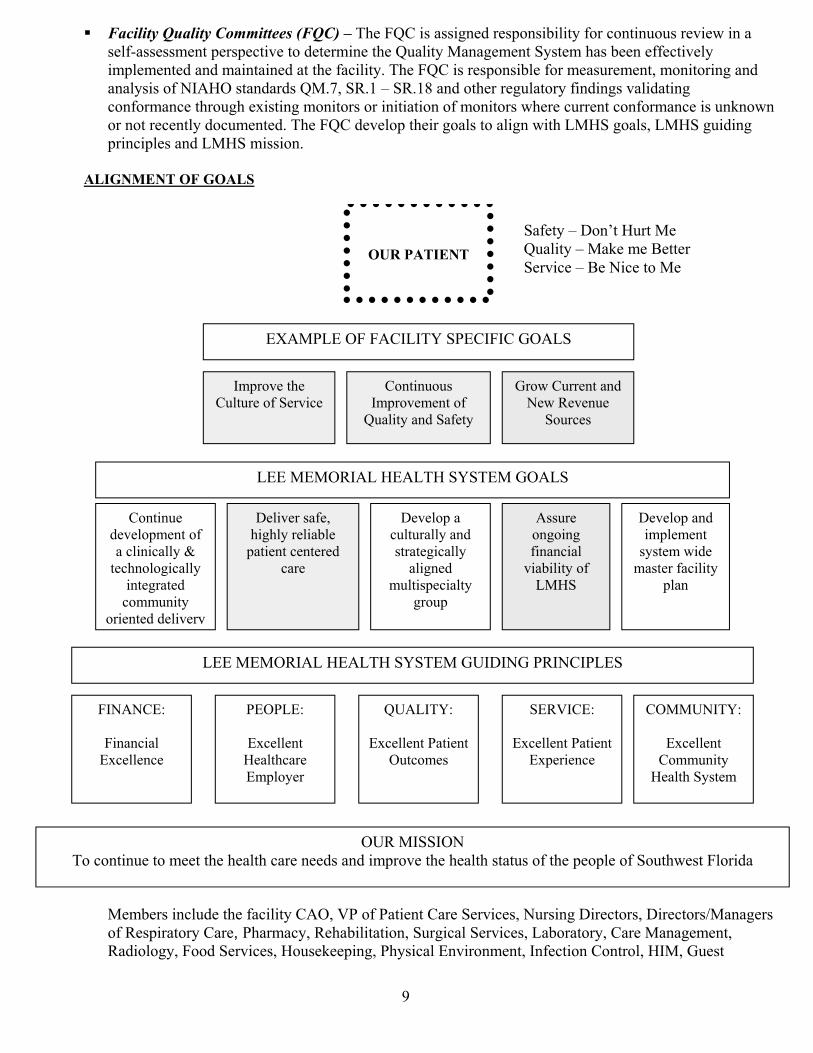
����������������� ������������������������������� �!��"#���$�%�&'�(#!�)#�&��*#*��!�+��,��������%(-������.��&�"�!�"�)&�+��&#� �&�!.����&����*�%�&'�/�����.��&�0'�&�.�����$�����((�)&�+�%'��."%�.��&� ��� �.���&���� ��&�&���(�)�%�&'1������������!��"#���$%��(#!�.���*!�.��&2�.#��&#!������ ����%'����#(�34567��&�� �! ���/182�091:�;�091:<��� �#&��!�!��*%�&#!'�(�� �����+�%� �&����)#�(#!.��)��&�!#*����=��&����.#��&#!��#!����&��&�#��#(�.#��&#!��,��!��)*!!��&�)#�(#!.��)�����*�>�#,��#!��#&�!�)��&%'� #)*.��&� 1��������� �+�%#"�&���!��#�%��&#��%����,�&��?/60��#�%�2�?/60��*� ����"!��)�"%����� �?/60�.����#�1�@ABCDEFGEH@IJ@DIABK@ @?LL�/L/7945?�6L5?�6�0M0�L/�N75?0��� 4."!#+��&����*%&*!��#(�0�!+�)��� N!#,��*!!��&��� �3�,�9�+��*��0#*!)����#�&��*#*��4."!#+�.��&�#(��*�%�&'��� �0�(�&'�LO5/P?L�7���5�4?4�M�0PL�4�4��N75?0� Q�+�%#"��� ��."%�.��&��'�&�.�,� ��.��&�!�(�)�%�&'�"%�����#�&��*�� �+�%#".��&�#(���)%���)�%%'�R�&�)��#%#��)�%%'���&��!�&� �)#..*��&'�#!���&� � �%�+�!'� Q�%�+�!���(�2�����%'�!�%��$%��"�&���&�)��&�!� �)�!���� Q�+�%#"���)*%&*!�%%'��� ��&!�&���)�%%'��%���� �.*%&��"�)��%&'��!#*"� 5��*!��#��#����(����)��%�+��$�%�&'�#(�?/60����IST@UAHCGEH@�?LL�/L/7945?�6L5?�6�0M0�L/�NV4Q43N�P943�4P?L0��4353�LW�������)��%�L=)�%%��)��� �V5?4�MW��L=)�%%��&�P�&���&�7*&)#.���� 0L9X4�LW��L=)�%%��&�P�&���&�L="�!���)��� �7//V34�MW��L=)�%%��&��#..*��&'�6��%&��0'�&�.�PL7P?LW��L=)�%%��&�6��%&�)�!��L."%#'�!� 7V9�/400473��#�)#�&��*��&#�.��&�&������%&��)�!����� ���� ��."!#+��&������%&���&�&*��#(�&���"�#"%��#(�0#*&�,��&��%#!� ��0�(�&'�;�Q#�Y&�6*!&�/���*�%�&'�;�/�>��.��Z�&&�!�0�!+�)��;�Z��3�)��&#�/��� /�.$�!����)%* ��&���(�)�%�&'��572�XP�#(�P�&���&���!��0�!+�)��2�3*!�����Q�!�)&#!�2�Q�!�)&#!�[/�����!��#(�9��"�!�&#!'���!�\�P��!.�)'2�9���$�%�&�&�#�2�0*!��)�%�0�!+�)��2�?�$#!�&#!'2���!��/�����.��&2�9� �#%#�'2��## �0�!+�)��2�6#*��>��"���2�P�'��)�%�L�+�!#�.��&2�4�(�)&�#���#�&!#%2�64/2�N*��&�� ]��
� ���� ����������� �������� ���������������� ������������������� ����� ������������������������������� �������������� ����������������� ���� �� ��������� ������ �������!�� ����"�#��������������� ���������������������� ������������� �������������������������������������������������� ��$���� �������������!���� %�&'()*+,-./+00-12+,)/3-4566)//''7-8��������� ������������ ������������� ����������������������������� �������������������������������9��������������������������������!��:��������������������������������������������#�������������������$�;���<���������������� ��������� ����� ����������� ���� �����=>?@A��� ����!��?���������� �����������B����$�A ��� ���� ����� ��� ��? ����!����������������������������������� ������������ ����� ����� ��� ��������� ��������������������� �� ���������������� ��������������������� !�?��������� ���������������������������������������#��������������� ������������ ��������$��;���������� ������������������C������������@�����������D������ ����������������� ������� ������������������ ���� ���� ����!��� %�E+/)'F/-4+G'-.'GH)*'7-8��������� ������������� ��#������������������ ��������������������� �� ���������������C������������@�����������!��������������������������� ��������� ����� ���������� ��������� ������������������ ����;�����I������������������ ���������<��������������������������������������� ���!����������� ��#������������J��� �������������������������� ��������� ������������������� ��������������"������!���������� �$�������������������������������� ���� ���� ��� ������K"�������:I����� ��L�$������������ ��� �� ���� �� �������������� ���������� ���������������� �$��������������������������������������!�� ������������������� ���>�������� ����� ������ ��#���������������������������$��;�������������������� �������������������� � ���� ����������� ���� ������� ������������������������ ����������� �!����������������������������������%�A�M������������������ ����� ��� ����������� ��������� �������%�>�� ��������� ����������� ��������������������������%����������������������� ��� ������ �� ������������ ��������� ��������������� ����������� ��� ����� � ���� ��������������������������������I����� ��!���� NGO+F)P+/)5F-50-E'G05G6+F*'-Q6RG5H'6'F/-S)/T)F-E+/)'F/-4+G'-.'GH)*'7��������� � ���� ���������������������� ����������������� ������������ ��� ����������� ���>�������� ����� U������ ��#������������V��W����X�XY!�-%�.'F)5G-Z2G7)FO-['+('G7T)R-452F*),\]\������ ����=��� ��C���������#�� ����������������������������������������� �������� ���������������������� ����� ��� ��� �����������������������������!�������� ����������������������� ������ � ��� ���������� ������������ ������������������ ������������ ������� ��$��������������� ���������������������� �������������������� ��� �����������������������������- %� F)/-12+,)/3-452F*),7�_��>������������������� ������������������� �������������� �����������#�� �������������������� ��$������������ ����������� ����>�B����� ������!�� ���������������� ������������������ ��������� ������������� �������������#�� ����� ��� �� �������������� �!���- %�aT'-Z2G7)FO-b'7'+G*T-452F*),-c�:I�������������������������� <��������� �� ��� ��������������������� �������������������������� � ������� ���� �������������� ��� ����������� ������� ����������������!�����������$����������������� ��� ������������ ������� ����������� ��� ������������������� ���� ���������������$���������������� � ���� ����������� ��!����������� �����������B���������=����#�� �����=��������������#�� �����:��������=��� ��C������9����� ���������>Bd�C���� ��� ����=��� ��C������� ��������� ���������������!���
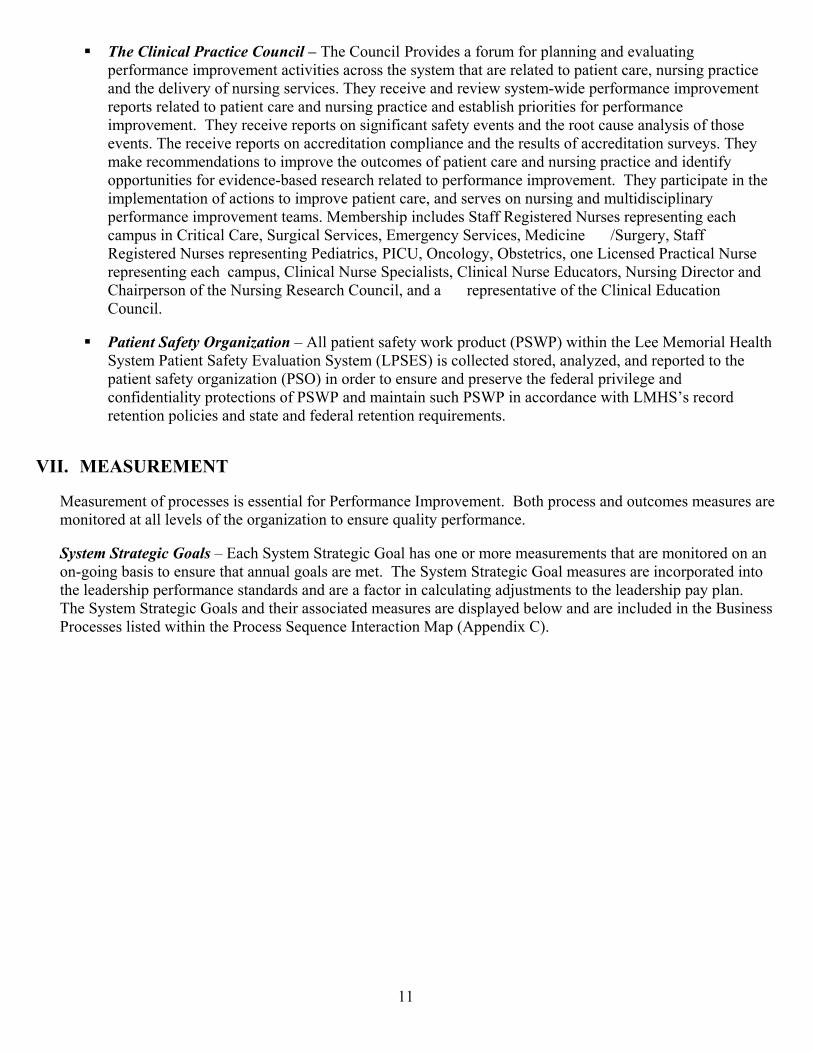
� ����� ��������� ��� ���������������������������� �!�"�#�$���%�$���&�#����'�#�!�� #��#(��'�&��$��%#�����%&�� �%��(�#�(� �(��"�#���""�(���")"(�%�(�#(�#������#(�!�(��&#(���(��#��*����"��'�&�#�(����#�!�(���!��� ��)��$����"��'�"�� ���"+����)������ ��#�!��� ��,�")"(�%-,�!��&��$��%#�����%&�� �%��(���&��("����#(�!�(��&#(���(��#���#�!����"��'�&�#�(����#�!��"(#.��"��&�����(��"�$���&��$��%#�����%&�� �%��(+�����)������ ����&��("����"�'��$��#�(�"#$�()�� ��("�#�!�(������(��#�"��#�#�)"�"��$�(��"��� ��("+���������� ����&��("����#����!�(#(������%&��#����#�!�(�����"��("��$�#����!�(#(����"�� �)"+����)�%#/������%%��!#(���"�(���%&�� ��(�����(��%�"��$�&#(���(��#���#�!����"��'�&�#�(����#�!��!��(�$)��&&��(���(��"�$���� �!����-.#"�!���"�#�������#(�!�(��&��$��%#�����%&�� �%��(+�����)�&#�(���&#(�����(����%&��%��(#(�����$�#�(���"�(���%&�� ��&#(���(��#��*�#�!�"�� �"�������"��'�#�!�%��(�!�"��&���#�)�&��$��%#�����%&�� �%��(�(�#%"+�0�%.��"��&������!�"�1(#$$�2�'�"(���!�3��"�"���&��"��(��'��#����#%&�"�������(��#���#��*�1��'��#��1�� ���"*�4%��'���)�1�� ���"*�0�!������� 51��'��)*�1(#$$�2�'�"(���!�3��"�"���&��"��(��'���!�#(���"*��6�7*�8�����')*�8."(�(���"*�����9����"�!���#�(��#��3��"����&��"��(��'��#�����#%&�"*�������#��3��"��1&���#��"("*�������#��3��"��4!��#(��"*�3��"��'�:����(���#�!���#��&��"����$�(���3��"��'�2�"�#�����������*�#�!�#�� ��&��"��(#(� ���$�(���������#��4!��#(�����������+��� ��� �����; <��=�>�? �@ ����A�B���&#(���(�"#$�()�,��/�&��!��(�C�1D�E�,�(����(���9���0�%���#��F�#�(��1)"(�%��#(���(�1#$�()�4 #��#(����1)"(�%�C9�141E��"�������(�!�"(���!*�#�#�)G�!*�#�!���&��(�!�(��(���&#(���(�"#$�()���'#��G#(����C�18E������!���(����"����#�!�&��"�� ��(���$�!��#��&�� ���'��#�!����$�!��(�#��()�&��(��(���"��$��1D��#�!�%#��(#���"�����1D�����#����!#����,�(��90F1H"������!���(��(����&������"�#�!�"(#(��#�!�$�!��#����(��(������I����%��("+���JKKLMMMNOPQRSONOTUM� 0�#"���%��(��$�&����""�"��"��""��(�#��$������$��%#����6%&�� �%��(+��V�(��&����""�#�!���(��%�"�%�#"���"�#���%���(���!�#(�#����� ��"��$�(�����'#��G#(����(����"����I�#��()�&��$��%#���+��;=W��X�;�� ��?��Y� W�A�4#���1)"(�%�1(�#(�'���Z�#���#"��������%����%�#"���%��("�(�#(�#���%���(���!����#����-'���'�.#"�"�(����"����(�#(�#���#��'�#�"�#���%�(+������1)"(�%�1(�#(�'���Z�#��%�#"���"�#��������&��#(�!���(��(�����#!��"��&�&��$��%#����"(#�!#�!"�#�!�#���#�$#�(�������#����#(��'�#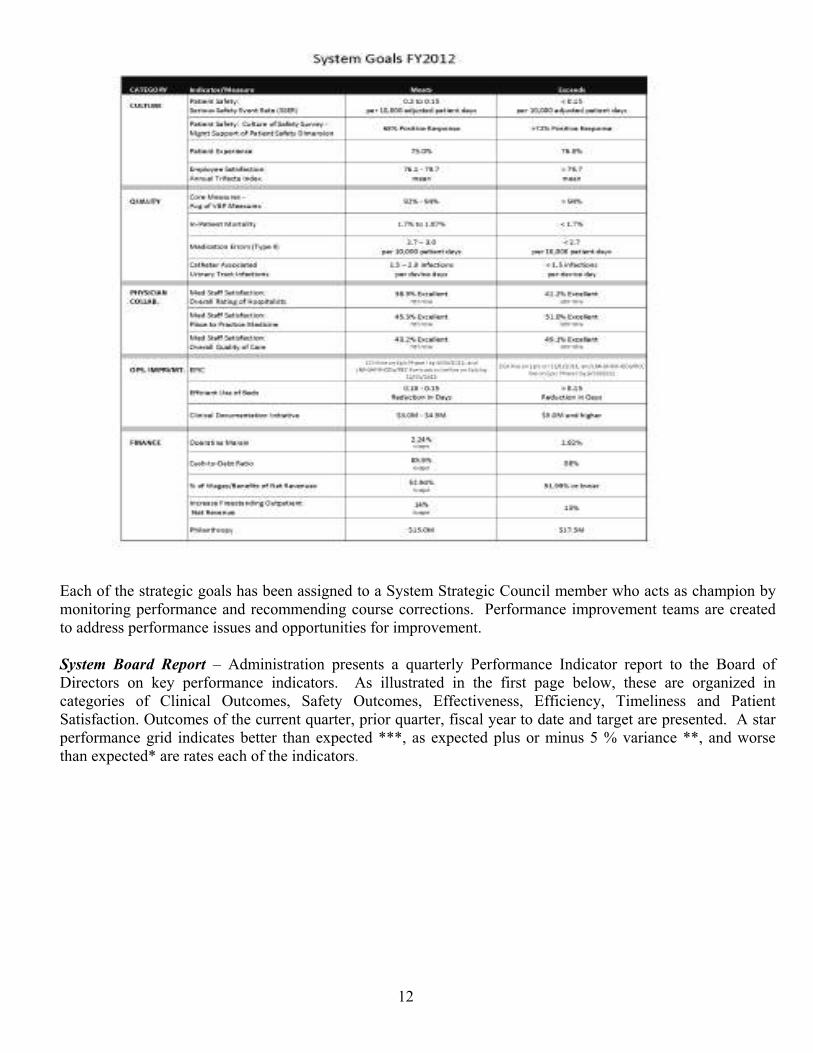
�� ������������������������� ������������������������������������������ ��������������������������������������������������������������������������������������������������������������������������������������������������������������������������� ����� !"#$%&!'�(#%��)�*��������������������+���� ������������,��������������������-�������.���������/������������������������*�� ������������������������� ��0��������������1������������������� ����� �2������0��������2������0������������0�����������0�3��� �����������������������������2��������������������+����0�����+����0����� ������������������������������������*���������������������������������������4�������5550����4�������� ���������6�7���������550���������������4������5�������������������������������������������� 89�� �
�������������� ��� ��������������������� ������ ���� ��������� ������ ��� ���!������ ����"#$%&�� �� � � ���'�������� ������ ���(��)��* � ��+� �����,�������� �����,�� ��� ��-.//�01���$����-.//2 ��� ( ��� �� �� ������������� ���������� ��������)��*����3������� ������ ���4��(��������������������������5� ��6� � �7������� ���� ���������������)��*�������� ����� ����8������6�������������������������5� ���3���� � ���� ����� ������� ��3���� ���*�����*������ *4�!����)��������)��* � ������ ����� �����������3�������������������� 7������ ��� ����� ��(�� �������������� ���������� ����������������)���� ���*�� �� ���������*� ����*����4��9:;:<=>=;?@A=BC=DEFE!�7�� �� ����6���)� ��� 7�������$ ��)��*��7�������)����57�������� ��G �������� ���������57�������� ��G ����4��H���������3� ��5������� ���� �������7���*��� ���7� ������)��* � ����**��������������������I�������J� ������������ ��4�!������� ��� ���� ��������������� ����� ������� ���3����5�������*����6� ������� ����� �*�����4��H������ �*��� ��������� ����)�����+ � ��*����K����3� ���3����5�����)��*��� ������� �������� ��� �������7���*��� ���7�� )��7�+ � ��*�������� ��� ��� �� �*���*�*��)��� �� ��� ��74�� L;?=M;:N@OP:NC?Q@RPSC?T@U@J+V��W����� ���� ���7�!�������� �������*������ ��������� ����)�����57�����W�X�Y../��� �� ���0����J+V��W����� ���� ���7�!�����(��� 7��.Z�..�[-\24��H���������7�� ��7������ �� *���������� �������� ��8� ���7� ������5������� ���� ���� ������ ������ �*���������)�����W�X�Y../��� �� ��4�� ������� /]��
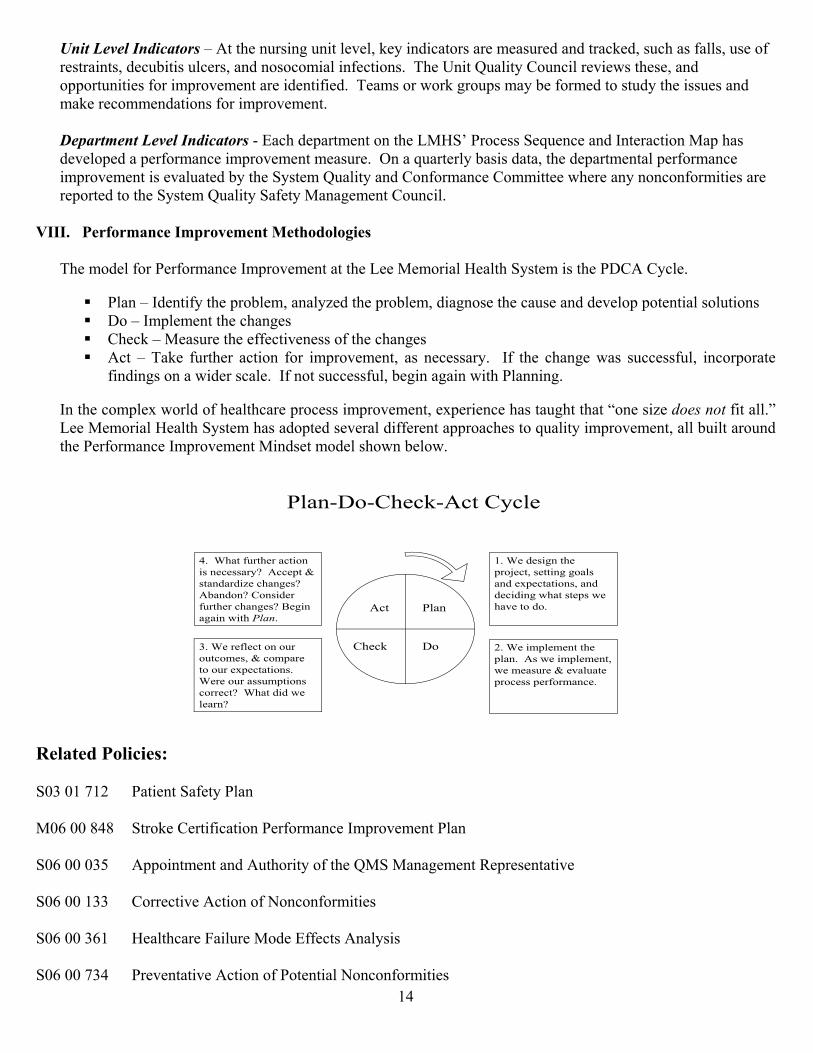
��������������� ������������������������������������ ���!�"#�$���#���%�#����!�#�!���#"��!����"��#��&#���������$&������#������!�"�'�������"�����#�!��$�$"$%�#����&�"��$��(��)���*����+�#��� �,$��"��������-���������#�!�$..$����������&$���%.�$��%����#����!����&��!(��)�#%��$��-$�����$�.��%# �'��&$�%�!��$����! ������������#�!�%#�����"$%%��!#��$���&$���%.�$��%���(��/�0 ��1������������� �����2�3#"��!�.#��%����$������45678�9�$"����7�:���"��#�!�;����#"��$��5#.��#��!����$.�!�#�.��&$�%#�"���%.�$��%����%�#����(��<��#�:�#����� �'#����!#�#������!�.#��%���#��.��&$�%#�"���%.�$��%���������#��#��!�' �����7 ���%�+�#��� �#�!�,$�&$�%#�"��,$%%������-�����#� ��$�"$�&$�%������#�����.$���!��$�����7 ���%�+�#��� �7#&�� �5#�#��%����,$��"��(�=>???@===ABCDECFGHIB=?FJCEKBFBHL=MBLNEOEPEQRBS== )���%$!���&$��9��&$�%#�"��;%.�$��%����#������4���5�%$��#��6�#����7 ���%��������9T,��, "��(�� UV9�#����;!����& �����.�$'��%��#�#� W�!�����.�$'��%��!�#��$�������"#����#�!�!����$.�.$�����#���$����$���UVT$���;%.��%��������"�#�����UV,��"����5�#����������&&�"���������$&�����"�#�����UV�"����)#���&�������#"��$��&$���%.�$��%�����#����"���#� (��;&�����"�#����-#����""���&������"$�.$�#���&��!�����$��#�-�!����"#��(��;&��$����""���&����'�����#�#���-����9�#�����(��;������"$%.��X�-$��!�$&���#���"#���.�$"�����%.�$��%������X.�����"���#���#�������#��Y$�����W��Z[\]_[�&���#��(a��4���5�%$��#��6�#����7 ���%��#��#!$.��!������#��!�&&������#..�$#"�����$�:�#��� ��%.�$��%�����#���'�����#�$��!�����9��&$�%#�"��;%.�$��%����5��!����%$!�����$-��'��$-(�9�#�2T$2,��"�2�"��, "��b(�c���%.��%��������.�#�(�����-���%.��%�����-��%�#�����d���#��#���.�$"����.��&$�%#�"�(��9�#�T$,��"��"� e(�c��!����������.�$f�"������������$#���#�!��X.�"�#��$����#�!�!�"�!����-�#�����.��-���#����$�!$(�g(�c����&��"��$��$���$��"$%����d�"$%.#����$�$����X.�"�#��$��(��c����$���#���%.��$���"$���"�h��c�#��!�!�-����#��hi(��c�#��&�������#"��$�������"���#� h���""�.��d���#�!#�!�W��"�#����h���'#�!$�h�,$���!���&�������"�#����h�j�����#�#���-����klm_( �nBPGLBO=AEPRIRBSo===7pg�pe�qeb��9#������7#&�� �9�#���5pr�pp�sis�7��$���,����&�"#��$��9��&$�%#�"��;%.�$��%����9�#���7pr�pp�pgt���..$���%����#�!�����$��� �$&�����+57�5#�#��%����u�.������#������7pr�pp�egg� ,$���"������"��$��$&�v$�"$�&$�%�������7pr�pp�gre��6�#���"#���w#������5$!��3&&�"�����#� �����7pr�pp�qgi� 9������#������"��$��$&�9$�����#��v$�"$�&$�%������� ei��
� ������������������� ���� �� ������������������� � ������ ���������� ���� �� ������������������ ����������������������������������������������������������������������� ���� ������������ �����!"#"$"%&"'()))*�� ��������+������,����� ��� �����-����������.�+�� /�� ������������0�1�����.������,��� ����*�� �������������02�� �������+�������������3�42 ���������1515��678''9$:)8#);"$<'(),-30�=�,+��������-����������3������������02�� ���,>.��=�,����+��>��+����������,3�=�,��2����3��� ��?����@.��=�@������� �������,.�=�� ���,�� � ����� ���.�� ����-�=���������-�� ����*�=��� �������*2�?������,,�=������ A�����A�����,�B2�����,�� �� �����=�������������� ����C��� �� ������ ������=��� � ��������� � ��� ���--��=��������������-����������-2�������� ����D� �D���+����������������D.�=�D�� �������������E0�=�E�� � ���02�� ����� �����F��=�F2���������� ����������-,-���=�-�� ������2����,������������-������������� �����������������-���=�-������������� ������+������-���=�-���������G���� ����������-H,�=�-�/����H2�����? � ���,����� ����=������� ��������I�=������� �������I� ����.�=��������� ������������ /�� ��.�+�� /�� ���3@ ����� �2� ����3�� �J�@����>�-�=�>������� ���-�� ����
� ������������������� ���� �������������������������� ���� ����������� ������� ������� �� ���������������������� ��������������������������� ���� ��� ������!� ������������ ��������� ���� ��� �! ��" ����� #�$� %��������� ��$� ��& ������ ������ ���& ��� ��� ����� ����� ������������ �����'(������ �)�')�(���*�+��������������� �����&���������(,������� ���������������( ���,������ ���� ������� ����� �! ��" ������-����� ������� �����-�*��������.����.� ������ � !�����.�����.� ������ � !������������/�$��� � ����+������ �� ���+�����.((���������.� ����� ���(��� ����(�������.��(���������.� ������ ������ � !�����(������������� �� �����0��������1(����1���(�������2����&�� ��1���$�1������ %���� ������&�� ��3����3�������������
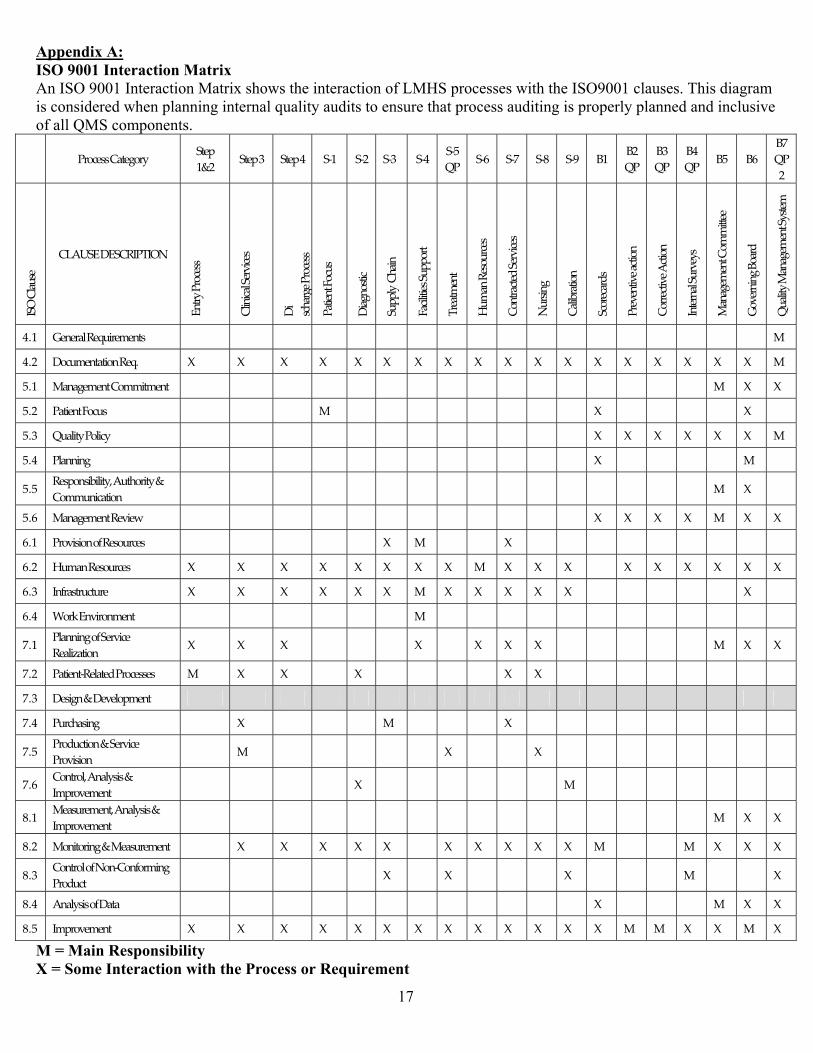
� ��������������� ������������������������������������ !"#�$%��&"�!$'�()%*(��) �$�� !"#�$%��%+�,&-��.!%# (( (�*$�)��) ���������#/"0( (1�2)$(�3$"4!"5�$(�#%�($3 ! 3�*) ��./"��$�4�$�� !�"/�60"/$�7�"03$�(��%� �(0! ��)"��.!%# ((�"03$�$�4�$(�.!%. !/7�./"�� 3�"�3�$�#/0($8 �%+�"//�9&��#%5.%� ��(1�: ;<=>?@@:ABC?D=<E: FC?G:HIJ: FC?G:K: FC?G:L: FMH: FMJ:FMK: FML: FMN:O;: FMP: FMQ: FMR: FMS: TH: TJ:O;: TK:O;: TL:O;: TN: TP: TQ:O;J:UFV:AWBX@?: AYZ[F\:]\FAU;_UV : \aC<E:;<=>?@@: AWbab>BW:F?<cb>?@: ]b: @>dB<D?:;<=>?@@: ;BCb?aC:e=>X@: ]bBDa=@Cb>: FXGGWE::AdBba: eB>bWbCb?@:FXGG=<C: _<?BCf?aC: gXfBa:?@=X<>?@: A=aC<B>C?h:F?<cb>?@: X<@baD: ABWbi<BCb=a: F>=<?>B<h@: ;<?c?aCbc?:B>Cb=a: A=<<?>Cbc?:Z>Cb=a: UaC?<aBW:FX<c?E@: jBaBD?f?aC:A=ffbCC??: k=c?<abaD:T=B<h: OXBWbCE:jBaBD?f?aC:FE@C?f:LlH:k?a?<BW:?mXb<?f?aC@: : : : : : : : : : : : : : : : : : : j:LlJ:]=>Xf?aCBCb=a:?ml: n: n: n: n: n: n: n: n: n: n: n: n: n: n: n: n: n: n: j:NlH:jBaBD?f?aC:A=ffbCf?aC: : : : : : : : : : : : : : : : : j: n: n:NlJ:;BCb?aC:e=>X@: : : : j: : : : : : : : : n: : : : : n: :NlK:OXBWbCE:;=Wb>E: : : : : : : : : : : : : n: n: n: n: n: n: j:NlL:;WBaabaD: : : : : : : : : : : : : n: : : : : j: :NlN: ?@G=a@bibWbCEo:ZXCd=<bCE:I:A=ffXab>BCb=a: : : : : : : : : : : : : : : : : j: n: :NlP:jBaBD?f?aC:?cb?p: : : : : : : : : : : : : n: n: n: n: j: n: n:PlH:;<=cb@b=a:=q:?@=X<>?@: : : : : : n: j: : : n: : : : : : : : : :PlJ:gXfBa:?@=X<>?@: n: n: n: n: n: n: n: n: j: n: n: n: : n: n: n: n: n: n:PlK:Uaq<B@C<X>CX<?: n: n: n: n: n: n: j: n: n: n: n: n: : : : : : n: :PlL:r=<s:\acb<=af?aC: : : : : : : j: : : : : : : : : : : : :QlH:;WBaabaD:=q:F?<cb>?:?BWbtBCb=a: n: n: n: : : : n: : n: n: n: : : : : : j: n: n:QlJ:;BCb?aCM?WBC?h:;<=>?@@?@: j: n: n: : n: : : : : n: n: : : : : : : : :QlK:]?@bDa:I:]?c?W=Gf?aC: : : : : : : : : : : : : : : : : : : :QlL:;X<>dB@baD: : n: : : : j: : : : n: : : : : : : : : :QlN:;<=hX>Cb=a:I:F?<cb>?:;<=cb@b=a: : j: : : : : : n: : : n: : : : : : : : :QlP:A=aC<=Wo:ZaBWE@b@:I:UfG<=c?f?aC: : : : : n: : : : : : : j: : : : : : : :RlH:j?B@X<?f?aCo:ZaBWE@b@:I:UfG<=c?f?aC: : : : : : : : : : : : : : : : : j: n: n:RlJ:j=abC=<baD:I:j?B@X<?f?aC: : n: n: n: n: n: : n: n: n: n: n: j: : : j: n: n: n:RlK:A=aC<=W:=q:=aMA=aq=<fbaD:;<=hX>C: : : : : : n: : n: : : : n: : : : j: : : n:RlL:ZaBWE@b@:=q:]BCB: : : : : : : : : : : : : n: : : : j: n: n:RlN:UfG<=c?f?aC: n: n: n: n: n: n: n: n: n: n: n: n: n: j: j: n: n: j: n:�u����v�w���w�x�y��z{u �|������������}��~�~������ww��v������|���
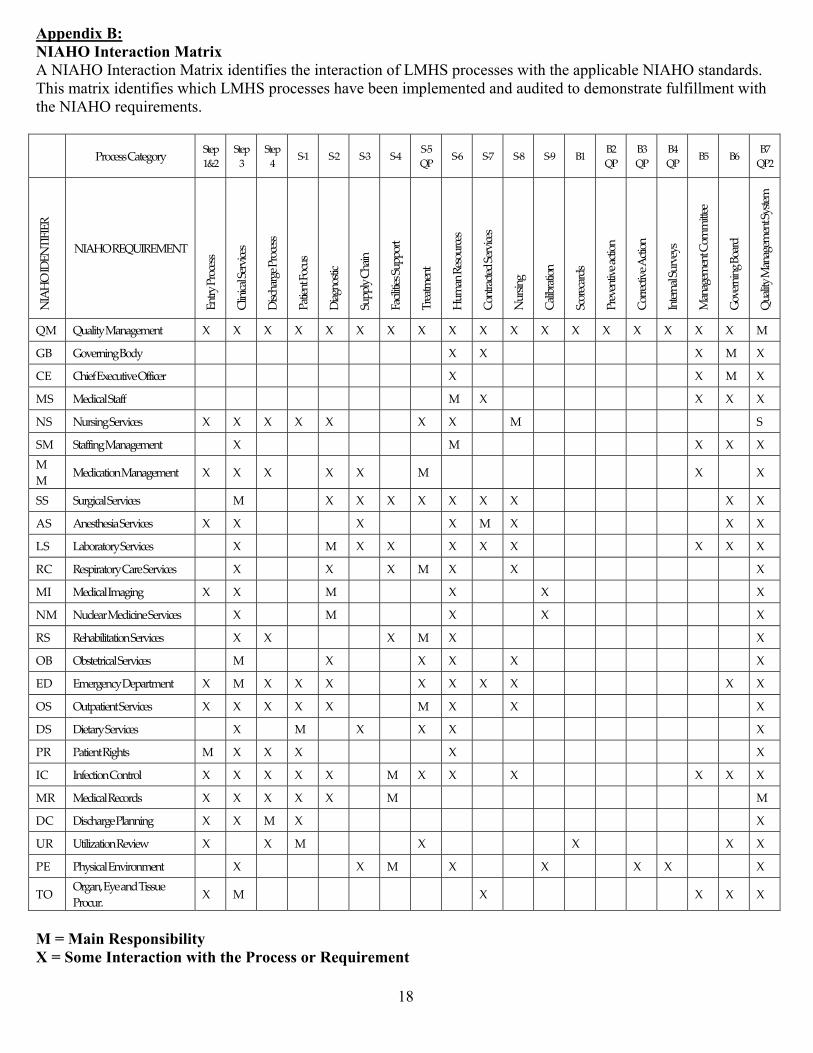
� ������������� ��������������������������������� !�"#��$ ��"%�"&���"'"�(��)��"���� !�"#��#'�*$�+�,�#!�((�(�-"�)��)�� ,,."! /.��������(� �& �&(0��1)"(�2 ��"%�"&���"'"�(�-)"!)�*$�+�,�#!�((�(�) 3��/����"2,.�2����&� �&� 4&"��&��#�&�2#�(�� ���'4.'"..2����-"�)��)����������54"��2���(0�67 89:;<==7>?@<A:9B7 C@<D7EFG7 C@<D7H7 C@<D7I7 CJE7 CJG7 CJH7 CJI7 CJK7L87 CJM7 CJN7 CJO7 CJP7 QE7 QG7L87 QH7L87 QI7L87 QK7 QM7 QN7L8G7RSTUV7SWXRYSZSX[7 RSTUV7[XL\S[X]XRY7 X@9B789:;<==7 >_;?_7C<9a;<=7 W=;b?9A<789:;<==7 8?@<@7Z:;c=7 W?A:=@;7 CcDD_B7>b?7 Z?;_@<=7CcDD:9@7 Y9<?@d<@7 Ucd?7[<=:c9;<=7 >:@9?;@<e7C<9a;<=7 Rc9=A7 >?_f9?@:7 C;:9<;?9e=7 89<a<@a<7?;@:7 >:99<;@a<7T;@:7 S@<9?_7Cc9a<B=7 ]??A<d<@7>:dd@@<<7 g:a<9A7Q:?9e7 Lc?_@B7]??A<d<@7CB=@<d7L]7 Lc?_@B7]??A<d<@7 h7 h7 h7 h7 h7 h7 h7 h7 h7 h7 h7 h7 h7 h7 h7 h7 h7 h7 ]7gQ7 g:a<9 A7Q:eB7 7 7 7 7 7 7 7 7 h7 h7 7 7 7 7 7 7 h7 ]7 h7>X7 >b<i7Xj<;c@a<7Vii;<97 7 7 7 7 7 7 7 7 h7 7 7 7 7 7 7 7 h7 ]7 h7]C7 ]<e;?_7C@?ii7 7 7 7 7 7 7 7 7 ]7 h7 7 7 7 7 7 7 h7 h7 h7RC7 Rc9=A7C<9a;<=7 h7 h7 h7 h7 h7 7 7 h7 h7 7 ]7 7 7 7 7 7 7 7 C7C]7 C@?iiA7]??A<d<@7 7 h7 7 7 7 7 7 7 ]7 7 7 7 7 7 7 7 h7 h7 h7]]7 ]<e;?@:7]??A<d<@7 h7 h7 h7 7 h7 h7 7 ]7 7 7 7 7 7 7 7 7 h7 7 h7CC7 Cc9A;?_7C<9a;<=7 7 ]7 7 7 h7 h7 h7 h7 h7 h7 h7 7 7 7 7 7 7 h7 h7TC7 T<=@b<=?7C<9a;<=7 h7 h7 7 7 7 h7 7 7 h7 ]7 h7 7 7 7 7 7 7 h7 h7kC7 k?f:9?@:9B7C<9a;<=7 7 h7 7 7 ]7 h7 h7 7 h7 h7 h7 7 7 7 7 7 h7 h7 h7[>7 [<=D9?@:9B7>?9<7C<9a;<=7 7 h7 7 7 h7 7 h7 ]7 h7 7 h7 7 7 7 7 7 7 7 h7]S7 ]<e;?_7Sd?AA7 h7 h7 7 7 ]7 7 7 7 h7 7 7 h7 7 7 7 7 7 7 h7R]7 Rc;_<?97]<e;<7C<9a;<=7 7 h7 7 7 ]7 7 7 7 h7 7 7 h7 7 7 7 7 7 7 h7[C7 [<b?f_@?@:7C<9a;<=7 7 h7 h7 7 7 7 h7 ]7 h7 7 7 7 7 7 7 7 7 7 h7VQ7 Vf=@<@9;?_7C<9a;<=7 7 ]7 7 7 h7 7 7 h7 h7 7 h7 7 7 7 7 7 7 7 h7XW7 Xd<9A<;B7W<D?9@d<@7 h7 ]7 h7 h7 h7 7 7 h7 h7 h7 h7 7 7 7 7 7 7 h7 h7VC7 Vc@D?@<@7C<9a;<=7 h7 h7 h7 h7 h7 7 7 ]7 h7 7 h7 7 7 7 7 7 7 7 h7WC7 W<@?9B7C<9a;<=7 7 h7 7 ]7 7 h7 7 h7 h7 7 7 7 7 7 7 7 7 7 h78[7 8?@<@7[Ab@=7 ]7 h7 h7 h7 7 7 7 7 h7 7 7 7 7 7 7 7 7 7 h7S>7 Si<;@:7>:@9:_7 h7 h7 h7 h7 h7 7 ]7 h7 h7 7 h7 7 7 7 7 7 h7 h7 h7][7 ]<e;?_7[<;:9e=7 h7 h7 h7 h7 h7 7 ]7 7 7 7 7 7 7 7 7 7 7 7 ]7W>7 W=;b?9A<78_?^A7 h7 h7 ]7 h7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 h7\[7 \@_l?@:7[<a<m7 h7 7 h7 ]7 7 7 7 h7 7 7 7 7 h7 7 7 7 7 h7 h78X7 8bB=;?_7Xa9:d<@7 7 h7 7 7 7 h7 ]7 7 h7 7 7 h7 7 7 h7 h7 7 7 h7YV7 V9A?n7XB<7?e7Y==c<789:;c9o7 h7 ]7 7 7 7 7 7 7 7 h7 7 7 7 7 7 7 h7 h7 h76�p����q�r���r�s�t��uvpw�x������������y��z�z�{����rr��q�|}���x���
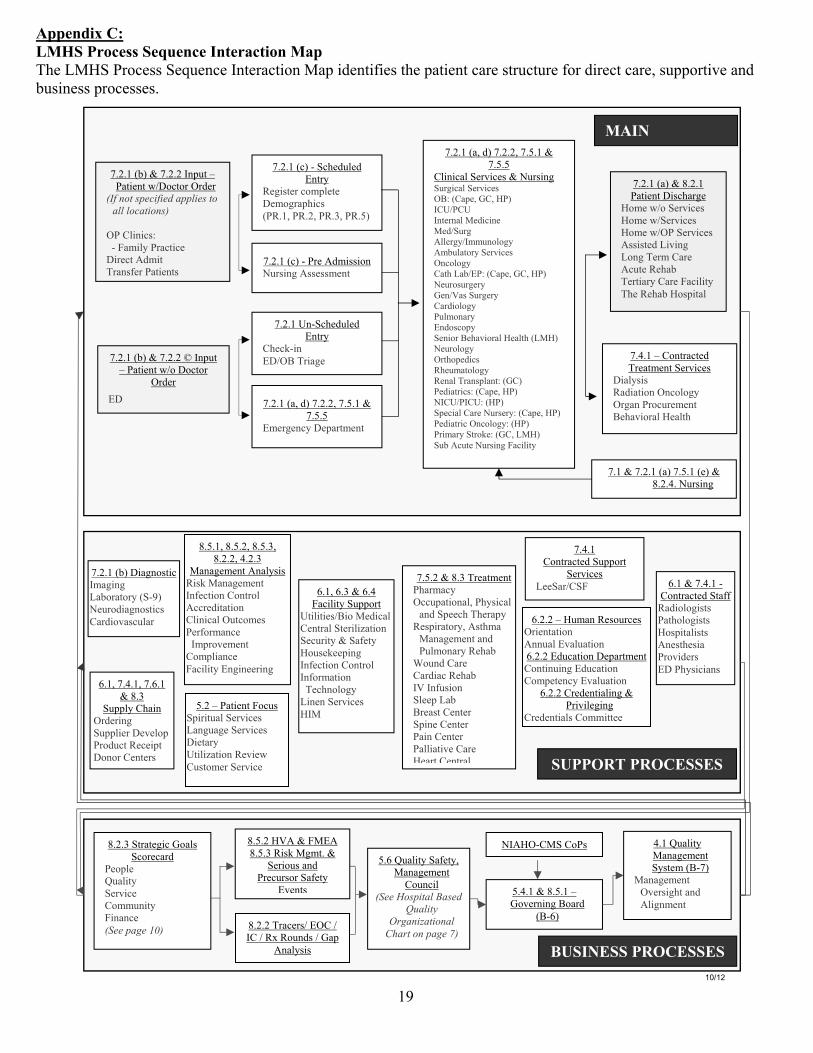
�������������� ��������� ��������������������������������� !"#�$$���%&�'#��(')�!*#)+"'��*,�+-�')+.+�$�)���,*)+�')�#*!��$)!&#)&!��."!�-+!�#)�#*!�/�$&,,"!)+0��*'-�1&$+'�$$�,!"#�$$�$2�� 3 ���4�52627�8*/�-9�52626/�52:27�;�52:2:� 7<�� 52627�819�;�52626�(',&)�=� *)+�')�>?@"#)"!�A!-�!�BCDEFGHEIJKLMDMKNEOJJPMKIEHGEOPPEPGLOHMGFIQE�A �RS+'+#$T���U�V*W+SX� !*#)+#��@+!�#)�Y-W+)��!*'$.�!� *)+�')$� 52627�8#9�U��#��-&S�-� �RS+'+#*S���!0+#�$�;�Z&!$+'[\')!X�]�[+$)�!�#"W,S�)��@�W"[!*,�+#$�8 ]27/� ]26/� ]2/� ]2:9�352627�8#9�U� !��Y-W+$$+"'�Z&!$+'[�Y$$�$$W�')��52627�_'U�#��-&S�-�\')!X�R��#U+'�\@?Aa��!+*[���52627�8*/�-9�52626/�52:27�;�52:2:�\W�![�'#X�@�,*!)W�')�� ��&![+#*S���!0+#�$�AaT�8R*,�/�bR/�� 9�(R_? R_�(')�!'*S���-+#+'����-?�&![�YSS�![X?(WW&'"S"[X�YW1&S*)"!X���!0+#�$�A'#"S"[X�R*)���*1?\ T�8R*,�/�bR/�� 9�Z�&!"$&![�!X�b�'?c*$��&![�!X�R*!-+"S"[X� &SW"'*!X�\'-"$#",X���'+"!�a��*0+"!*S���*S)��8���9�Z�&!"S"[X�A!)�",�-+#$�]��&W*)"S"[X�]�'*S��!*'$,S*')T�8bR9� �-+*)!+#$T�8R*,�/�� 9�Z(R_? (R_T�8� 9��,�#+*S�R*!��Z&!$�!XT�8R*,�/�� 9� �-+*)!+#�A'#"S"[XT�8� 9� !+W*!X��)!"�T�8bR/����9��&1�Y#&)��Z&!$+'[�V*#+S+)X� 52627�8*9�;�d2627� *)+�')�@+$#�*![���"W��>?"���!0+#�$��"W��>?��!0+#�$��"W��>?A ���!0+#�$�Y$$+$)�-��+0+'[��"'[���!W�R*!��Y#&)��]��*1���!)+*!X�R*!��V*#+S+)X�����]��*1��"$,+)*S�52e27�=�R"')!*#)�-�52627�819�;�52626�f�(',&)� �!�*)W�')���!0+#�$�@+*SX$+$�]*-+*)+"'�A'#"S"[X�A![*'� !"#&!�W�')�a��*0+"!*S���*S)���=� *)+�')�>?"�@"#)"!�A!-�!���\@� 527�;�52627�8*9�52:27�8�9�;�d262e2�Z&!$+'[��d2:27/�d2:26/�d2:2/� 52e27:26�=� *)+�')�V"#&$��,+!+)&*S���!0+#�$��*'[&*[����!0+#�$�@+�)*!X�_)+S+g*)+"'�]�0+�>�R&$)"W�!���!0+#��52627�819�@+*['"$)+#�(W*[+'[��*1"!*)"!X�8�U<9�Z�&!"-+*['"$)+#$�R*!-+"0*$#&S*!�h27/�52e27/�52h27�;�d2��&,,SX�R�*+'�A!-�!+'[��&,,S+�!�@�0�S",� !"-&#)�]�#�+,)�@"'"!�R�')�!$� h27/�h2�;�h2e�V*#+S+)X��&,,"!)�_)+S+)+�$?a+"���-+#*SR�')!*S��)�!+S+g*)+"'���#&!+)X�;��*.�)X��"&$���,+'[�('.�#)+"'�R"')!"S��('."!W*)+"'������#�'"S"[X��+'�'���!0+#�$��(�� 52:26�;�d2��!�*)W�') �*!W*#X�A##&,*)+"'*S/� �X$+#*S�*'-��,��#�����!*,X�]�$,+!*)"!X/�Y$)�W*��*'*[�W�')�*'-� &SW"'*!X�]��*1�i"&'-�R*!�����R*!-+*#�]��*1�(c�('.&$+"'����������� ��S��,��*1��a!�*$)�R�')�!��,+'��R�')�!� *+'�R�')�!� *SS+*)+0��R*!����*!)R�')!*S h2626�=��&W*'�]�$"&!#�$�A!+�')*)+"'�Y''&*S�\0*S&*)+"'�h2626�\-&#*)+"'�@�,*!)W�')�R"')+'&+'[�\-&#*)+"'�R"W,�)�'#X�\0*S&*)+"'�h2626�R!�-�')+*S+'[�;� !+0+S�[+'[�R!�-�')+*S$�R"WW+))��� h27�;�52e27�U�R"')!*#)�-��)*..]*-+"S"[+$)$� *)�"S"[+$)$��"$,+)*S+$)$�Y'�$)��$+*� !"0+-�!$�\@� �X$+#+*'$��R"')!*#)�-��&,,"!)�d2626/�e262��*'*[�W�')�Y'*SX$+$ ��!0+#�$�����*!?R�V��]+$��*'*[�W�')�('.�#)+"'�R"')!"S�Y##!�-+)*)+"'�RS+'+#*S�A&)#"W�$� �!."!W*'#�������(W,!"0�W�')�R"W,S+*'#��V*#+S+)X�\'[+'��!+'[� j��klm��lk�n n �d2:26��cY�;�V�\Yd262��)!*)�[+#�b"*S$��#"!�#*!-� �",S��o&*S+)X���!0+#��R"WW&'+)X�V+'*'#��BpKKEJOqKErsQE �d2:2�]+$��[W)2�;� e27�o&*S+)X�Z(Y�AUR���R" $��!+"&$�*'-� !�#&!$"!��*.�)X�\0�')$d2626��!*#�!$?�\AR�?�(R�?�]t�]"&'-$�?�b*,�Y'*SX$+$� :2h�o&*S+)X��*.�)X/��*'*[�W�')�R"&'#+S�BpKKEuGIJMHOPEvOIKNEwxOPMHyEz{qOFM|OHMGFOPE}~O{HEGFEJOqKE�QE � �*'*[�W�')��X$)�W�8aU59��*'*[�W�')�A0�!$+[�)�*'-�YS+['W�')�:2e27�;�d2:27�=�b"0�!'+'[�a"*!-�8aUh9��j �4n ��lk�n n ������3
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
10.25B – No Smoking Policy for RETIREMENT 032813 Page 1 of 1
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL no. 10.25B supersedes no. 10.25A
-------------------------------------------------------------------------------------------------------------------------------
category: General Operations
title: No Smoking Policy -------------------------------------------------------------------------------------------------------------------------------
original adoption: 01/08/91 review date: 3/28/13
revision date: 07/31/98, 07/26/02, 3/28/13 Proposed to Retire --------------------------------------------------------------------------------------------------------------------------------
PURPOSE: To promote a healthful environment by limitation of smoking in the Health System. --------------------------------------------------------------------------------------------------------------------------------
POLICY: The Board of Directors of Lee Memorial Health System directs there be no smoking in any System facility As a healthcare institution, Lee Memorial Health System has a responsibility to encourage good health practices, to protect the lives and well-being of its patients and to respect the rights of non-smokers to breathe smoke-free air. Policy: - Smoking is prohibited indoors in all Health System facilities. - Smoking is permitted only in designated areas outside of Health System facilities.
Smoking is prohibited in all other exterior areas. - An employee who smokes in an unauthorized area, but not an unsafe or hazardous
area, is subject to the progressive corrective action process. - Smoking is prohibited in any room, ward or compartment where oxygen, flammable
liquids, or combustible gases are used or cylinders (E) stored, and in any other hazardous location. An employee who smokes in a hazardous area is subject to immediate termination, since this is deemed to be outrageous conduct.
This policy is adopted and in conjunction with and does not replace the general smoking policies of the Health System.
Proposed to Retire due to duplication and/or conflict of language with System policy S08 05 876.
������������������ ���������������������� �������� ��������������������� ����������� ������ ����������������� ����������� ����������������������� !!�"#$% �#&!#'�������������������������������������������������������������������������(�)!�*��+�,������������������������������������ � � ��������*-.*-/011/21234560/716087/9:9812/;305<:/=/;43<1>?41/26@?60/83A6<<3/B411/1@C543@21@8// 03<6834/@?2A14///8/:/;/1/ / ///9DEFGHIJKLG/I�M�+� &�N�O'�'!&!#'��+�$�NP!OQ�%#'!#'O�RS�N%�TUQ��#V�!WS!�'�'%�#O���������RS ��!VP !U�'X�'��SSN%!O�'��!$! T�!&SN�T!!�'X �P)X�P'�'X!�YTO'!&Z��������///2[\FKLKE]K\K_aD/b�M�+� &�N�O'�'!&!#'��+�$�NP!OQ�%#'!#'O�RS�N%�TUQ��#V�!WS!�'�'%�#O���������RS ��!VP !U�'X�'��SSN%!O�'��&� !�'X�#��#!�V%O�%SN%#!��#V�%O�POP�NNT��+����N%#%��N�����������#�'P !Z��<cG]d/eG\fJ/\\/aGE/Ff/JcK]c/FcKE/ \KGEg/////// �//>G aFHG_F\/I/M�+� &�N�O'�'!&!#'��+�$�NP!OQ�%#'!#'O�RS�N%�TUQ��#V�!WS!�'�'%�#O��������RS ��!VP !U�!W�NPO%$!�'����S� '%�PN� �V!S� '&!#'�� �) �PS��+�S!�SN!�h%'X%#����������������������V!S� '&!#'��'��#!�� �&PN'%SN!�N���'%�#O�'X�'�V�!O�#�'�%&S��'��#T��'X! �� !�Z�������� <76;814i/ 9jk/////////86Ai// /jl/////////;305<:/mi/ kno//////>KE]K\K_GE/p/\f]FKf_E/Ff/JcK]c/FcKE/H[\FKLKE]K\K_aD/f\K]D/ \KGEi/� �q!�N'X�r#+� &�'%�#�s�#�)!&!#'� �(X� &��T� �M�P'!�t� !�q�OS%'�N�uP O%#)��q�PO!v!!S%#)� �(N�#'�wS! �'%�#O� �M&�PN�'� T�Y! $%�!O��r#+� &�'%�#�YTO'!&O� �x�V%�N�)T� �q�&!�q!�N'X��y��� �'� T� �x!X��%N%'�'%�#�Y! $%�!O� �q(tt��y!)�N�Y! $%�!O� �x!OS% �'� T� �(XTO%�%�#�w++%�!O��uP' %'%�#� �Y!�P %'T� �x!X���q�OS%'�N��w'X///////////! � � �> FG/3aKzK_FGLi//kpk{/ 4G|KGJGL/p/@f/4G|KEKf_i/}pkk~/kpkk~/npk�~/�jp�j~/�{p�}~/lp�l~/kp�k~/�{pjj~/{pj�~/�pjn~/�p�{/ > FGE/4G|KEGLi/}pj�~/{pjl~/�pjo~/�jpj�~/{p�j~/�{p�{// @G�F/4G|KGJ/> FGi//�{p��/6[Fcfa�E�i///�G_LD/;KE]Kd~/29@~/4@~/<<4@~/@16IA<~/B6<71/4G|KGJGL/eD/i//<\K_K]\/;a]FK]G/<f[_]K\i/ //////////////////////// > FGi/ ///<\K_K]\/1L[]FKf_/<f[_]K\///////////////1L[]FKf_/4G�[KaGLi/////////////////////////////////////////////////////////////////////1L[]FKf_/<fH \GFGLi/:GE//@fi////////////////////////////////////////////////////////////////////////////// /////////// > FGi//> FGi/ //6 af|GL/eDi///////////////////////////////////////////////////////;f\K]D/6LHK_KEFaFfai// ///////> |G/�KEFG\~/C;/f�/B]K\KFKGE/=/9[ faF/9Ga|K]GE/ //> FGi///�pj}p{j�}//6E/@GGLGLi/2GLK]\/>KaG]Ffai/ / > FGi/ /AfaL/f�/>KaG]FfaEi/ / > FGi/ ///;?4;391i������ !��)#%�!�'X!�X!�N'XQ�O�+!'T��#V��!#!+%'O��+�O&�v!b+ !!��% ��#V��O���X!�N'X��� !�S �$%V! Q�'X!�OS!�%�N� !OS�#O%�%N%'T�'X�'�y!!�s!&� %�N�q!�N'X�YTO'!&�RysqYU�X�O�%#�!O'��N%OX%#)Q�S �&�'%#)��#V�&�%#'�%#%#)���X!�N'XT��#V�O�+!�!#$% �#&!#'�+� ��P ���&&P#%'TZ��MNN�ysqY���&SPO!OQ�S !&%O!OQ�+��%N%'%!O��#V�!&SN�T! ��h#!V�� �N!�O!V�$!X%�N!O�� !�'�������+ !!��
������������������ ���������������������� �������� ��������������������� ����������� ������ ����������������� ����������� ����������������������� !!�"#$% �#&!#'�������������������������������������������������������������������������(�)!�*��+�,������������������������������������ � � ��������-*.-*/!#$% �#&!#'0�12! !�'2!�30!��+�'�������4 �53�'0��+��#6�'64!7�%#�835%#)��3'�#�'�8%&%'!5�'�7��%)� !''!07��%)� 07�4%4!07�0&�9!8!00�'������7��2!17�0#3++7��#5�5%4�%0�0' %�'86�4 �2%�%'!5:��2!���������30!��+�'2!�!8!�' �#%���%)� !''!��#5.� ��'2! �&!�#0��+�;$�4%#)<�� !��80��4 �2%�%'!5:�/=>?@ABC���D0���2!�8'2��� !�%#0'%'3'%�#7�EFGH�2�0��� !04�#0%�%8%'6�'��!#��3 �)!�)��5�2!�8'2�4 ��'%�!07�'��4 �'!�'�'2!�8%$!0��#5�1!88��!%#)��+�%'0�4�'%!#'07�$%0%'� 07�!&48�6!!0��#5�$�83#'!! 0��#5�'�� !04!�'�'2!� %)2'0��+�#�#I0&�9! 0�'��� !�'2!�0&�9!I+ !!��% :���2!��55%�'%$!�#�'3 !��+�'�������4 �53�'0�%0�+3886� !��)#%J!5��6�EFGH��#5�0344� '�'���88�!&48�6!!0�1%88��!��++! !5�'���00%0'�%#��!�0%#)�'2!�!&48�6!!K0�30�)!��+�'�������4 �53�'0:���� &0��+�0344� '�1%88��!�4 �$%5!5�'2 �3)2�"&48�6!!�G!�8'27��#5�'2!�"&48�6!!�D00%0'�#�!�( �) �&7��#5�1%88�%#�835!�'�������30!��!00�'%�#�4 �) �&07�!53��'%�#7��#5�0344� '��#5��!00�'%�#��%50�03�2��0�&!5%��'%�#07�#%��'%#!�4�'�2!07�!'�:��D44 �4 %�'!�0%)#�)!�1%88��!�4�0'!5�%#���#04%�3�30�� !�0��'��88�EFGH�4 !&%0!0�%#�� 5! �'��#�'%+6�'2!�43�8%���+�EFGHK�'�������+ !!�!#$% �#&!#'�0'�'30:�/D:� L0!��+�'�������4 �53�'0��+��#6�+� &�%0�4 �2%�%'!5�%#0%5!��#5��3'0%5!��+��88�EFGH�4 !&%0!07��3%85%#)07�) �3#507�4� 9%#)�8�'0��#5�1%'2%#��#6�4! 0�#�886��1#!5�$!2%�8!0�12!#�8���'!5��#��#6�EFGH�4 !&%0!0��#5.� ��'��#6�'%&!�1%'2%#�$!2%�8!0��1#!57�8!�0!5�� ��4! �'!5��6�EFGH:��M:� �2%0�4�8%�6��448%!0�'���88�%#5%$%53�80�%#�� �� �3#5��#6�EFGH�4 !&%0!0�%#�835%#)7��3'�#�'�8%&%'!5�'��4�'%!#'07�+�&%86�&!&�! 07�$%0%'� 07�!&48�6!!07�4260%�%�#07�4260%�%�#0�4! 0�##!87�$�83#'!! 07�$!#5� 0��#5���#' ��'� 0:��� N:� EFGH�!&48�6!!0�&�6�#�'�30!�'�������4 �53�'0�53 %#)�1� 9%#)�'%&!7�%#�835%#)��#6�4�%5�� !�90:��"&48�6!!0�&�6�30!�'�������4 �53�'0�53 %#)�'2!% �3#4�%5�&!�8�� !�9O0P�4 �$%5!5�03�2�30!�%0�#�'��#��#6��+�'2!�4 !&%0!0�5!0� %�!5����$!�� �%#�$%!1��+��8%!#'07�4�'%!#'07�� �$%0%'� 0:�� Q:� D#�!&48�6!!�12��+�%80�'����&486�1%'2�'2%0�4�8%�6��#5�30!0�'�������4 �53�'0�%#�� �� �3#5��#6�EFGH�4 !&%0!0�&�6��!�03�R!�'�'���� !�'%$!���'%�#�34�'���#5�%#�835%#)�'! &%#�'%�#�%#����� 5�#�!�1%'2�EFGH�N� !�'%$!�D�'%�#�( ��!00�4�8%�6�HST�SU�-VS:����� "WN"(�XYZ[��\!0%5!#'0��+�G!�8'2(� 9�N� !��#5�\!2��%8%'�'%�#�N!#'! �12��1! !��5&%''!5�'��'2!�+��%8%'6�4 %� �'��Z�$!&�! �-T7�*SST7�12��2�$!�4! &%''!5�0&�9%#)��0�4� '��+�'2!% �48�#��+��� !�1%88��!�4! &%''!5�'����#'%#3!�'��0&�9!��+'! �Z�$!&�! �-T7�*SST:��\!0%5!#'0��5&%''!5��+'! �Z�$!&�! �-T7�*SST�� ��5&%''!5��+'! ��!%#)�%#+� &!5��+�'2!���������� !!�"#$% �#&!#'�4�8%�67�1%88�#�'��!�4! &%''!5�'��0&�9!�%#���&48%�#�!�1%'2�'2%0�4�8%�6:��=]>A _ ] C///D:// abcdeffg/h/idcjklffmg//-:� Q!4� '&!#'�5% !�'� 0��#5�&�#�)! 0�� !� !04�#0%�8!�'��%#+� &�'2!% �!&48�6!!0�.�$�83#'!! 0��+�'2!�'�������+ !!�!#$% �#&!#'�4�8%�%!0:�����
������������������ ���������������������� �������� ��������������������� ����������� ������ ����������������� ����������� ����������������������� !!�"#$% �#&!#'�������������������������������������������������������������������������(�)!�*��+�,������������������������������������ � � ��������-./-.0.1� 2�#3"4!&5'�!&56�7!!8�6!�$%#)���&598�+� �':!% �9#5�%;�&!�6�� !�<�&98'��6��<�%#��� �#;��9'�%#����� ;�#�!�=%':�':!��%&!<!!5%#)�5�6%�7�>?@�?A�BC.1��2���;;%'%�#�6�� !�<�5! %�;8�� !��66�=!;�+� ��#7�!&56�7!!�D!4!&5'�� �#�#3!4!&5'E�+� �59 5�8!8��+�9'%6%F%#)�'�������5 �;9�'81�� *1� "&56�7!!8�&�7�#�'�98!�'�������5 �;9�'8��#�8%;!=�6<8G�8' !!'8��#;�#!%):�� %#)�5 �5! '%!8�=:! !�':!7�&�7��!�$%!=!;��7�5�'%!#'8��#;�$%8%'� 81���A1� H'�%8�':!�9#%'�I!�;! J8� !85�#8%�%6%'7�'���;; !88��#7�$%�6�'%�#��+�IKL>���������� !!�"#$% �#&!#'�5�6%�7�%#����� ;�#�!�=%':�IKL>��� !�'%$!�M�'%�#�5 ��!88�5�6%�7�>?@�?N�-A?1����O1� PQRSTURV0W0XSVSRYZV00-1� (�'%!#'8��#;�$%8%'� 8�=%66��!�#�'%+%!;��+�':%8�5�6%�7�95�#�� %$�6��#;��!+� !��!%#)��;&%''!;�'��IKL>1���:!�'�������+ !!�!#$% �#&!#'�%#+� &�'%�#�=%66��!�&�;!��$�%6��6!�'���66�5�'%!#'8��#;�$%8%'� 8��#;�=%66��!��9'6%#!;�%#�':!�5�'%!#'�:�#;���<�':�'�%8�)%$!#�=%':�':!��;&%88%�#�<%'�+� ��66�5�'%!#'8��#;�#!=�5�'%!#'�!#��9#'! 81���:!�'�������+ !!�!#$% �#&!#'�%#+� &�'%�#�=%66��68���!��$�%6��6!�%#��66��9'5�'%!#'�+��%6%'%!81�� .1� M66�!&56�7!!8�=%66��!� !85�#8%�6!�+� �5�6%'!67��8<%#)�D#�'%+7%#)E�5�'%!#'8��#;�$%8%'� 8�'����&567�=%':�':!�5�6%�71�� *1� ��[6%#%��6�8'�++� !85�#8%�%6%'%!8�+� �&�#�)!&!#'��+�%#5�'%!#'8\�� �1� H#5�'%!#'8�=%66��!�%#+� &!;�':�'�6!�$%#)�':!�:�85%'�6�) �9#;8�'��98!�'�������5 �;9�'8�%8�5 �:%�%'!;1�����1� (:78%�%�#8\��:!��''!#;%#)�5:78%�%�#�8:�96;��88!88��#;�;%8�988�':!�#!!;�+� �2%��'%#!�]!56��!&!#'��:! �57�D2]�E�=%':�':!�5�'%!#'1��:!#���5�'%!#'�%8��;&%''!;�+� �!6!�'%$!�89 )! 7�� ���5 ��!;9 !G�':!��''!#;%#)�5:78%�%�#�8:�96;�;%8�988�':!���������� !!�"#$% �#&!#'�(�6%�7��!+� !�:�85%'�6%F�'%�#1�� _ abc�M�5:78%�%�#J8�� ;! �'���66�=���5�'%!#'�'��8&�<!�=%66�#�'��!�:�#� !;1�� �1� 29 8%#)\��d5�#��;&%88%�#G�':!�]2�=%66��8<�!��:�5�'%!#'�%+�':!7��9 !#'67�98!�'��������#;�;��9&!#'�':!� !85�#8!�%#�':!�5�'%!#'�;�'���8!1���� �':�8!�':�'� !85�#;��++% &�'%$!67�':!�]2�=%66�5 �$%;!��#;�;��9&!#'�':!��55 �$!;�5�'%!#'�!;9��'%�#�6�&�'! %�68��#;��#�!456�#�'%�#��+�':!�IKL>���������� !!�"#$% �#&!#'�(�6%�71��;1� ]!)%8' �'%�#�/�( !3M;&%88%�#��!8'%#)\��M'�':!�'%&!��+�5 !3 !)%8'! %#)�/�5 !3�;&%88%�#�'!8'%#)���5�'%!#'�+� �89 )! 7�� ���5 ��!;9 !G�':!� !)%8' � �=%66��;$%8!�':!�5�'%!#'�':�'�':!7�=%66��!��� !;�+� �%#���'������3+ !!�!#$% �#&!#'��#;��;$%8!�':!�5�'%!#'�'��;%8�988�':!% �#!!;8�;9 %#)�:�85%'�6%F�'%�#�=%':�':!% �5:78%�%�#��#;�5 �$%;!��#�!456�#�'%�#��+�':!�IKL>���������� !!�"#$% �#&!#'�(�6%�71��
������������������ ���������������������� �������� ��������������������� ����������� ������ ����������������� ����������� ����������������������� !!�"#$% �#&!#'�������������������������������������������������������������������������(�)!�*��+�,������������������������������������ � � ��������-./-.0!1� 2+��+'! ��33�!45��'%�#�3��''!&6'7�8�$!��!!#�&�4!���6�'%!#'�7'%33�9%78!7�'��3!�$!�'8!% � ��&�'��5'%3%:!�'�������6 �45�'7�'8!;�9%33��!�%#+� &!4�'8�'�'8!;�� !��8��7%#)�'��4��7���)�%#7'�&!4%��3��4$%�!��'�'8!% ��9#� %7<��#4�'8!;�9%33�#�'��!���3!�'�� !&�%#��7���8�76%'�3%:!4�6�'%!#'1���8%7�9%33��!�4��5&!#'!4�%#�'8!�&!4%��3� !�� 41��� +1� �8!�#5 7!�&57'�%#+� &�'8!�6�'%!#'����5'�'8!�%&63%��'%�#7��+�75�8����8�%�!��#4�4��5&!#'�'8�'�!45��'%�#1�� )1� �8!�6�'%!#'�%7�'��7%)#�'8!�='�'!&!#'��+�(�'%!#'�>!�$%#)�?)�%#7'�@!4%��3�?4$%�!�A�@�B�CCCDE�� 81� �8!��''!#4%#)�68;7%�%�#�%7�'���!�#�'%+%!4��+�'8!�6�'%!#'F7�4!�%7%�#�'��3!�$!�?@?G��#4�4��5&!#'!4�%#�'8!�&!4%��3� !�� 41�� %1� ?33�2HF7��#4��� 4%���&�#%'� %#)�� !�'���!�4%7��#'%#5!4�6 %� �'��'8!�6�'%!#'F7�3!�$%#)1��*1� I5'6�'%!#'�='�++�J!76�#7%�%3%'%!7K�� �1� (8;7%�%�#7K��=8�534��77!77��#4�4%7�577�'8!�#!!4�+� �L%��'%#!�J!63��!&!#'��8! �6;�9%'8�'8!�6�'%!#'�98!#��663%���3!1���1� "45��'%�#�3�&�'! %�37�9%33��!��$�%3��3!�'���33�6�'%!#'7��#4�$%7%'� 7�56�#� !M5!7'1��,1� H%7%'� 7K�N �1� 2#+� &�'%�#��� 47�� !��$�%3��3!�+� ��33�7'�++�'��)%$!�'��$%7%'� 7�98��� !���7! $!4�57%#)�'�������6 �45�'7��#�>@O=�6 �6! ';1�����1� L%��'%#!�J!63��!&!#'��8! �6;�ALJ�E�%7��$�%3��3!�+� �$%7%'� 7�56�#� !M5!7'��'�76!�%+%��4%7' %�5'%�#�3���'%�#71��?#�%#+� &�'%�#�3�3!�+3!'�9%33��!�)%$!#�'��'8!�$%7%'� ��3�#)�9%'8�'8!�LJ�1�� P1� 2+�7'�++�8�$!� !�7�#��3!���7%7�'���!3%!$!�'8�'���6�'%!#'�%7�5'%3%:%#)�'�������6 �45�'7�%#�8%7�/�8! � ��&�%#�$%�3�'%�#��+�'8!���������� !!�"#$% �#&!#'�(�3%�;G�'8!;�9%33K���1� Q��5&!#'�'8%7�%#�'8!�#5 7%#)�#�'!71���1� (�3%'!3;�%#+� &�'8!�6�'%!#'�A�#4��#;�$%7%'� 7�98��� !�7576!�'!4��+�� %#)%#)�'�������6 �45�'7�'��'8!�6�'%!#'E�'8�'�57!��+�'�������6 �45�'7�%#�'8!� ��&�%7�6 �8%�%'!4��;�>@O=�6�3%�;1��J!M5!7'�'8!�6�'%!#'�7'�6�'8!�57!��+�'�������6 �45�'7��#4�7!#4�8�&!�� � !&�$!�'�������6 �45�'71���1� 2+�'8!�6�'%!#'�6! 7%7'7�%#�5'%3%:%#)�'�������6 �45�'7G�� �7'�'!7�'8�'�'8!�57!��+�'�������6 �45�'7�9%33���#'%#5!� !)� 43!77��+�6�3%�;G�6�3%'!3;�%#+� &�'8!�6�'%!#'�A�#4�$%7%'� 7E�'8�'�'8!�8�76%'�3�8�7�'8!� %)8'�'��!#+� �!�'8!�57!��+�'�������6 �45�'7���#1������
������������������ ���������������������� �������� ��������������������� ����������� ������ ����������������� ����������� ����������������������� !!�"#$% �#&!#'�������������������������������������������������������������������������(�)!�*��+�*������������������������������������ � � ��������,-.,-/01� �2!�3�'%!#'45�3265%�%�#7�'2!�#8 5%#)�0% !�'� �.�&�#�)! 7��#0�.�� ��0&%#%5' �'%$!�583! $%5� 7��#0�'2!�3�'%!#'� !3 !5!#'�'%$!5�9%::��!��0$%5!0��+�'2!�%558!�%+�%'��33!� 5�'2�'���#!!0�+� ���5!� �2��#0�5!%;8 !�%5�3 ����:!1��!1� <+�'2!�85!��+�'�������3 �08�'5���#'%#8!5��#0�'2!�3�'%!#'��!��&!5��)) !55%$!7�'2!�=!�8 %'6�>!3� '&!#'�9%::��!���#'��'!07��#0�'2!�#8 5!�%#��2� )!��#0���=!�8 %'6�?++%�! �9%::��''!&3'�'��'�:@�'2!�3�'%!#'�%#'����#+� &%#)�'��'2!�3�:%�6��#0�$�:8#'� %:6�'8 #%#)��$! �'�������3 �08�'51��<+�'2%5�+�%:57�'2!�3265%�%�#�9%::��!���#'��'!0� !)� 0%#)�3�'!#'%�:�#!!0�'��0%5�2� )!�'2!�3�'%!#'�+� �#�#A��&3:%�#�!�9%'2�&!0%��:��� !�3:�#1��+1� B#�%#�%0!#'� !3� '�0!'�%:%#)�'2!�!$!#'�9%::��!���&3:!'!0��#0�+� 9� 0!0�'��C!)�:�=! $%�!5��)1� (�'%!#'5�92��0��85!�'�������3 �08�'5�� !��++! !0�!08��'%�#7�%#�:80%#)�%#+� &�'%�#����8'�5&�@%#)��!55�'%�#1��DEFGHEI/JKFLMLENO//PQR�QS�SQT��(�'%!#'�C!�$%#)�B)�%#5'�P!0%��:�B0$%�!�UBPBV�=QS�Q-�*W*��P�'� �X!2%�:!5��#0�B8'2� %;!0�> %$! 5�=QW�Q*�TYY��?Z6)!#�[�;� 05�=QW�Q*�W,*��=�+!'6�P�#�)!&!#'�=65'!&�(:�#�=QW�QT�-WS���% !�=�+!'6�P�#�)!&!#'�(:�#�=QW�QT�W,S��=! $%�!�\�&3�#6�.�\�#' ��'� �]!8% !&!#'5�=QW�QT�W,W��=! $%�!�\�&3�#6�.�\�#' ��'� �]!8% !&!#'5�?++5%'!��=QW�QS�-WS���� !#5%��='�++�? %!#'�'%�#�=QW�QS�WQY��=!�8 %'6�P�#�)!&!#'�( �) �&�]%5@�B55!55&!#'�=QY�Q_�WS-���%&!@!!3%#)��#0�(�6 �::�"Z�!3'%�#5�=QY�QT�,_Q��\� !�'%$!�B�'%�#�( ��!55�=QY�QT�,W-��> !55�\�0!�P,*�QQ�S,S�(! +� &�#�!�<&3 �$!&!#'�(:�#�A�(�'%!#'�\� !�=! $%�!5�,Q1-*��CP[=��� 0��+�>% !�'� 5�(�:%�6�P�#8�:�/
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
40.07A – Corrective Action Exemption PROPOSED FOR RETIREMENT 032813 Page 1 of 1
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL no. 40.07A supersedes no. 40.07 ------------------------------------------------------------------------------------------------------------------------------------
category: Employee Relations
title: Corrective Action Exemption ------------------------------------------------------------------------------------------------------------------------------------
date adopted: 10/27/00 review date: 3/28/13 revision date: 10/27/00, 7/26/02, 3/28/13 Proposed to Retire ------------------------------------------------------------------------------------------------------------------------------------
PURPOSE: To provide for a corrective action process for a performance score below 300 unless the failure to meet expected outcomes comes from non-individual performance or accountability. ------------------------------------------------------------------------------------------------------------------------------------
POLICY: Non-individual performance statistics may be utilized for purposes of evaluating employee performance and in determining compensation. However, non-individual statistics shall be excluded in determining the competence of all employees, and in determining whether the Corrective Action Process established in the system is to be initiated for an employee.
Proposed to Retire due to duplication and/or conflict of language with System policy S09 02 135.
������������������ ���������������������� �������� ��������������������� ����������� ������ ����������������� ����������� ���������������������� !"#$$�$$����"%&�'&(�""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""%('�")"�*"+" " """""""""""""""""""""" """"""""""""""""),-),./00.1012345/.605/76.898701.:2/4;9.5<=.:32;0=>30.15<>5/..;21:070<;9.58808810<7.:32?351... /2;5723.<>[email protected].:.0. . ...8ABCDEFGHID.F"#"*�&�(J"$�(������"�*"K(JL�$M"N�����$"O��JN !PM"(�Q"�R�� �(�N��$"""""""""O�&� �QL&�P"�S(�"(��JN�$"��"�K�&!"���J�!��"�S&�L'S�L�"�S�"T!$���U""""""""...1VWCHIHBXHYWHZ[\A.]"#"*�&�(J"$�(������"�*"K(JL�$M"N�����$"O��JN !PM"(�Q"�R�� �(�N��$"""""""""O�&� �QL&�P"�S(�"(��JN�$"��"��&�"�S(�"���"QN$ N�JN��"(�Q"N$"L$L(JJ!"�*"(" JN�N (J"""""""""""�(�L&�U""; DX_.DWaG.[WW.[\D[B.Ca.G HX.CHB.[YYWHDBb....... "..=DY[\CEDZC[W.F.#"*�&�(J"$�(������"�*"K(JL�$M"N�����$"O��JN !PM"(�Q"�R�� �(�N��$""""""""O�&� �QL&�P"�R JL$NK�"��"("�(&�N LJ(&"Q��(&�����"�&"'&�L�"�*"����J�"cN�SN�"(""""""""""""""""""""Q��(&�����"(�"���"�&"�LJ�N�J�"J� (�N��$"�S(�"Q��$"���"N��( �"(�!"��S�&"(&�(U"""""""" ;65:703d. 8ef.........75@d.. .eg....:2/4;9.hd. ijk.=HBXHYWHZDB.l.WaX[CHaZB.Ca.G HX.CHB.EVWCHIHBXHYWHZ[\A.YaWHXA.[YYWHDBd.� "m�(J�S"n�*�&�(�N��"o(�('�����" "%S(&�( !" "# L��"�(&�"m�$�N�(J"pL&$N�'""m�L$�q���N�'" "%J(��"r��&(�N��$" "#�sLJ(��&!"T�&KN �$""n�*�&�(�N��"T!$���$" "t(QN�J�'!" "m���"m�(J�S""u(s�&(��&!" "t�S(sNJN�(�N��"T�&KN �$" "m%��""u�'(J"T�&KN �$" "t�$�N&(��&!" "%S!$N N(�"r**N �$""pL�&N�N��" "T� L&N�!" "t�S(s"m�$�N�(J""r�S�&" " "...........=[CD.2\HvHZ[CDId..jlfk. 3DwHDGDId.kleex.ielejx.ilii.. =[CDB.3DwHBDId.jleix.ielejx.jleyx.zleyx.iele{x.igle{x.klezx.|liix.jligx.zligx.iglig. <D}C.3DwHDG.=[CDd...igliy.5VCa\~B�d...5WHBaZ.7V\[Vx.8ABCDE.=H\DXCa\.;aEYDZB[CHaZ.l.@DZD�HCB.3DwHDGDI.Ad.................................................................................................;WHZHX[W.:\[XCHXD.;aVZXHWd. . =[CDd. .;WHZHX[W.0IVX[CHaZ.;aVZXHW.........0IVX[CHaZ.:W[Z.3D�VH\DId....................................................................0IVX[CHaZ.;aEYWDCDId.9DB..<ad.............................................................................. . =[CDd..=[CDd. ..5YY\awDI.Ad.......................................................:aWHXA.5IEHZHBC\[Ca\d.. ...........................�aZ.;b.;DXHWx.;632. ..=[CDd...igliglig..5B.<DDIDId.1DIHX[W.=H\DXCa\d. .. =[CDd. .@a[\I.a�.=H\DXCa\Bd. . =[CDd. ...:>3:280d....��"�$�(sJN$S"("�&� �$$"�S(�"S�J�$"��$L&�"���J�!��$"c�&qN�'"*�&"�S�"u��"o���&N(J"m�(J�S"T!$���"OuomTP"(&�" ��������"��"��&*�&�"�S�N&"��s$U"
������������������ ���������������������� �������� ��������������������� ����������� ������ ����������������� ����������� ���������������������� !"#$$�$$����"%&�'&(�""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""%('�")"�*"+" " """""""""""""""""""""" """""""""""""""",)-,)./012345..,6" 789:";($"�$�(<=>$;�?"(" ������� !"($$�$$����"�&� �$$"��";�=�"��$@&�"�;(�"�;�$�">�?>A>?@(=$";>&�?"<!"�;�":!$���"(&�" ��������"��"��&*�&�"�;�"B�<"*@� �>��$"*�&"C;> ;"�;�!"(&�";>&�?"(�?"�;(�" ������� !">$"�(>��(>��?"(�?">��&�A�?"��"(�"��'�>�'"<($>$6"")6" D��(&�����"7�(?�&$"(&�"&�$���$><=�"*�&" &�(�>�'"("C�&E"��A>&������"�;(�";�=�$"$�(**"&�(=>F�"C;(�"�;�!"���?"��"=�(&�"(�?"($$>$�"�;��G"($"(��&��&>(��G">�"( H@>&>�'"��C"E��C=�?'�"(�?"$E>==$6""0IJKLMNMJOL5."#=="��C"���=�!��$"C>=="�(&�> >�(��">�"P�QR�(&?>�'"�&>���(�>��-�?@ (�>��"�&�'&(�$"�;(�"C>==";�=�"��$@&�"�;�!"(&�"*@==!"�H@>���?"��"��&*�&�"�;�>&"B�<$6""S;�$�"�&�'&(�$" ��$>$�"�*"(�"=�($�"�;�"*�==�C>�'T"",6" :!$���QC>?�"P�QR�(&?>�'"P&>���(�>��6""U�&"��&�"?��(>=�?">�*�&�(�>��"&�*�&"��"�;�"%�=> !"(�?"%&� �?@&�"8(�@(=G"%�=> !":VW"V,"XYW6""")6" Z@&$>�'"P&>���(�>��"["*�&"(=="�(�>���" (&�"$�&A> �$"$�(**6""\6" D��(&�����"P&>���(�>��"]$��"%�=> !"(�?"%&� �?@&�"8(�@(=G"%�=> !":VW"V,",,_6""Y6" P�Q�;�QB�<"�&(>�>�'"��"�&�A>?�"$�� >*> ">�*�&�(�>��"&�=(��?"��"�;�"B�<6"""2LJMJN.3OabKMKLcd.effKffaKLM5.",6" D@&>�'"?��(&�����"�&>���(�>��"(=="��C"���=�!��$"C>=="<�"'>A��"(" ��!"�*"�;�>&"B�<"?�$ &>��>��G" ������� !"&�H@>&�����$">� =@?>�'"���@=(�>��"$�&A�?" ������� >�$G" ������� !"���="*�&�$G"(�?"��&*�&�(� �"$�(�?(&?$"-"�g�� �(�>��$6"U�&"%(�>���"�(&�":�&A> �$":�(**G"$��"%�=> !"8,h"VV"+hV"Z@&$>�'":�&A> �$":�(**"�������� �6"")6" D@&>�'"�;�">��&�?@ ��&!"]�&>���(�>��_"��&>�?G"�;�"���=�!��i$" ������� �G"$E>=="(�?"��&*�&�(� �"$;(=="<�"($$�$$�?6""j*"(�"���=�!��">$"@�(<=�"��"����"(=="�*"�;�"$E>==$"C>�;>�""""""""�;�"?�$>'�(��?"�>��"��&>�?G"�&">*"��&*�&�(� �"(�?" ������� !"?��$"���"����"$�(�?(&?$G"���=�!����"�(!"<�"��&�>�(��?6""j*G";�C�A�&G"�;�"?>&� ��&"�&"$@��&A>$�&"?���&�>��$"�;(�"(??>�>��(="�>��"$;�@=?"<�"'>A��"*�&"�A(=@(�>��"�@&��$�$G"�;�">�>�>(=">��&�?@ ��&!"��&>�?"�(!"<�"�g���?�?"�� �"@�"��"\VQWV"?(!$6""\6" k&>����"�g(�$"�(!"<�"(?�>�>$��&�?"($"("���;�?"�*"($$�$$>�'"E��C=�?'�"( H@>$>�>��"*�&"("'>A��" ������� !6"S;�"�($$>�'"$ �&�"*�&"$�� >*> " ������� >�$"C>=="<�"?���&�>��?"<!"�;�"A(=>?(�>��"�*"�;�"�=>�> (="7�(&�>�'"D��(&�����6""j*"(�"���=�!��"*(>=$"("C&>����"�g(�G"�;�"?>&� ��&"(�?-�&"�?@ (��&"C>=="($$�$$"�;�"E��C=�?'�"?�*> >�G"?�A�=��"("&���?>(�>��"�=(�G"(�?"?���&�>��"�;�"<�$�"���;�?"�*"&�($$�$$>�'"�;�"E��C=�?'�"( H@>$>�>��"�*"�;(�" ������� !6"""Y6" #"H@(=>*>�?"�<$�&A�&"C>=="?���&�>��"$(�>$*( ��&!"��&*�&�(� �"<($�?"��"�;�"C&>����"�&� �?@&�"�&"?�$ &>��>A�"?� @����6""S;>$"��&*�&�(� �">$">�?> (��?"��"�;�">�?>A>?@(=" ������� !"?� @����$6""j*"��&*�&�(� �">$"@�$(�>$*( ��&!G"�;�"�<$�&A�&"C>=="���>*!"�;�":@��&A>$�&"-"D>&� ��&6""
������������������ ���������������������� �������� ��������������������� ����������� ������ ����������������� ����������� ���������������������� !"#$$�$$����"%&�'&(�""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""%('�")"�*"+" " """""""""""""""""""""" """""""""""""""",-.,-/01" 2�&"*(345&�"��"����"$6344$"�&" ������� 3�$"�7(�"8�"���"7(9�"��":�"8����$�&(��8"5��34"(*��&""�7�"���4�!��"7($"$5 �$$*544!" ���4���8"�7�"3��&�85 ��&!"��&3�8;"31�1<"*�&" ������� 3�$""�7(�"7(9�"("$3=>����7"�&"���>!�(&"�3��"��&3�8"*�&"8����$�&(�3��<"�7�"���4�!��"�(!":�"��&�3�(��8"?3�7�5�"3�9�63�'"(44"�*"�7�"*�&�(4"$���$"�*"�7�"��&&� �39�"# �3��"�&� �$$1""@7�"��4!"&�A53&�8"$���"3$"("*�&�(4"$� ��8"?&3����"&��3�8�&"3�*�&�3�'"�7�"���4�!��"�7(�"��&�3�(�3��"?344"&�$54�"3*"�7�"$6344"�&" ������� !" (����":�"8����$�&(��8":!"(" �&�(3�"8(��1""@73$"$� ��8"?&3����"&��3�8�&"$7(44":�"8� 5�����8"��"(�"B��4�!��"���*�&�� �"2�&�"C,,DD1""#"%�&*�&�(� �"E��&�9�����"%4(�"F%E%"*�&�"CDGHIJ"$7�548":�"8�9�4���8"?3�7"�7�"���4�!��"�&3�&"��"�7�"$3=>����7"�&"���>!�(&"�3��"��&3�8"(�8":�*�&�"3�3�3(�3�'"�7�"$� ��8"?&3����"&��3�8�&1"""" 2&��"�3��"��"�3��"��?" ������� 3�$"�&"$6344$"�(!":�"8�9�4���8":� (5$�"�*"��?"�A53�����<"�&� �85&�$<"�&"6�!":5$3��$$"���8$"&�*�&"��"K(�8(��&!"B85 (�3��"(�8"@&(3�3�'"%�43 !"LDM"D,"00+1""E�"3$"�7�"���4�!��N$"&�$���$3:343�!"��"5�343O�"&�$�5& �$"�&�938�8":!"�7�"L!$���"(�8"8����$�&(��$"�7�"$6344$"�&" ������� 3�$"3�"�73$"��?"(&�(1""#�"���4�!��"?7�"*(34$"��"8�"�73$"�(!":�"��&�3�(��8"?3�7�5�"'�3�'"�7&�5'7"(44"�*"�7�"*�&�(4"$���$"�*"�7�" �&&� �39�"( �3��"�&� �$$1""@7�"��4!"&�A53&�8"$���"3$"("*�&�(4"$� ��8"?&3����"&��3�8�&"3�*�&�3�'"�7�"���4�!��"�7(�"��&�3�(�3��"?344"&�$54�"3*"�7�" ������� !" (����":�"8����$�&(��8":!"(" �&�(3�"8(��1""@7�"$� ��8"?&3����"&��3�8�&"$7(44":�"8� 5�����8"��"(�"B��4�!��"���*�&�� �"2�&�"C,,DD1""#"%�&*�&�(� �"E��&�9�����"%4(�"F%E%"*�&�"CDGHIJ"$7�548":�"8�9�4���8"?3�7"�7�"���4�!��"(�8"$7�548"�&� �8�"�7�"$� ��8"?&3����"&��3�8�&1"""""+1" E*"(�"(�!"�3��"("$5��&93$�&"8�5:�$"(�"���4�!��N$" ������� �"�&"$6344"3�"("�(&�3 54(&"(&�(<"�7�"$5��&93$�&"�(!"($6"(�"���4�!��"��"8����$�&(��"�7(�" ������� !1""#�"���4�!��N$"&�*5$(4"��"8����$�&(��" ������� !"�(!"4�(8"��"��&�3�(�3��"�*"���4�!����1""G1" #�"���4�!��"��&�3�(��8"*�&"*(345&�"��"8����$�&(��"("&�A53&�8" ������� !"�&"$6344"�(!"���":�"(:4�"��"5�343O�"�7�"L!$���N$"*�&�(4"'&3�9(� �"�&� �85&�1""P�?�9�&<"3*"�7�"���4�!��"83$('&��$"?3�7"�7�"8� 3$3��"��"��&�3�(��<"7�.$7�"�(!"5�343O�"�7�" 7(3�"�*" ���(�8"(�8"(���(4"��"�7�"(��&��&3(��"(8�3�3$�&(�39�"&��&�$���(�39�"F�7(3�"�*"����(�8"%�43 !"LDM"D+"-G-J1""H1" #44"���>�5&$3�'"(**343(��"*( 54�!"���:�&$"�5$�"(����8"$!$���"�&3���(�3��"�&" ���4���"�7�"$!$���"�&3���(�3��"��854�"�&3�&"��"�7�"�4( �����"�*"$�58���$"3�"�7�"?�&6"$���3�'1""Q5&$3�'"(**343(��"*( 54�!"���:�&$"?344"(����8"�5&$3�'"�&3���(�3��"�&3�&"��"�4( �����"�*"$�58���$"3�"�7�" 43�3 (4"$���3�'1""@7�"Q5&$3�'"R&3���(�3��"���&83�(��&"?344" ��&83�(��"�7�"�&3���(�3��"*�&"(44"(**343(��"*( 54�!"���:�&$"(�8"?344"�&�938�"5�8(��$"��"��?" 43�3 (4" ������� 3�$<"��43 3�$"(�8"�&� �85&�$"($"���8�8<"?3�7"�7�"$5���&�"�*"�7�"�43�3 (4"S�(&�3�'"T��(&�����1""UVWXYWZ[\]V/_[a[bcY\/UWYdW[Ze/"SKPL"&�A53&�$"(44"���4�!��$":�"�9(45(��8"(*��&"��"�&":�*�&�"�7�3&"MD"8(!$"�*"���4�!����"(�8"(��5(44!"�7�&�(*��&1""@7�"��&*�&�(� �"�9(45(�3��"�&� �$$"3� 458�$"�7�"*�44�?3�'f"",1" �������� !"($$�$$����f"(�"($$�$$����"�*"?7��7�&"(�"���4�!��"7($"�7�" (�( 3�!"��"��&*�&�"73$.7�&"g�:"*5� �3��$"?7��7�&<"3�"*( �<"7�.$7�"7($"�7�"6��?4�8'�<"$6344$<"(:343�3�$"(�8" ���3�����"�� �$$(&!"��"*5� �3��"?�44"3�"("�(&�3 54(&"$3�5(�3��1"�������� !"($$�$$����"�5$�":�"9(438(��8":!"(�"3�839385(4"�7(�"7($"�($��&�8"�&"3$"�&�*3 3���"3�"�7�"$6344":�3�'"�9(45(��81""B( 7"4�(8�&"3$"&�$���$3:4�"*�&"�7�" ������� !"9(438(�3��"�&� �$$"5�343O�8"3�"�7�3&"(&�($"�*"&�$���$3:343�!"(�8"�5$�"$�4� �"�7�$�"�=��&�$"?7�" (�"9(438(��"$�� 3*3 ""
������������������ ���������������������� �������� ��������������������� ����������� ������ ����������������� ����������� ���������������������� !"#$$�$$����"%&�'&(�""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""%('�")"�*"+" " """""""""""""""""""""" """""""""""""""",-.,-/ ������� 0�$"."$1022$"&�340&�5"*�&"(22"6�7" 2($$0*0 (�0��$"0�"�8�0&"5��(&�����"."4�0�9"":��8�5$"(�5"�&� �$$�$"*�&" ������� !"($$�$$����";(205(�0��"0� 245�"50&� �"�7$�&;(�0��<"���&"&�;0�=<"5� 4����"&�;0�=<"=&0����.;�&7(2"��$�"(�5"34(20�!"���&0 $9"" >�'�0�'"�&"(��4(2" ������� 0�$"�(!"7�"5�;�2���59""?�"0$"�8�"���2�!��@$"&�$���$07020�!"��"4�020A�"&�$�4& �$"�&�;05�5"7!"�8�"B!$���"(�5"5����$�&(��$"�8�"$1022$"�&" ������� 0�$"0�"�80$"��="(&�(9""#�"���2�!��"=8�"*(02$"��"5�"�80$"�(!"7�"��&�0�(��5"=0�8�4�"'�0�'"�8&�4'8"(22"�*"�8�"*�&�(2"$���$"�*"�8�" �&&� �0;�"( �0��"�&� �$$9""C8�"��2!"&�340&�5"$���"0$"("*�&�(2"$� ��5"=&0����"&��0�5�&"0�*�&�0�'"�8�"���2�!��"�8(�"��&�0�(�0��"=022"&�$42�"0*"�8�" ������� !" (����"7�"5����$�&(��5"7!"(" �&�(0�"5(��9""C8�"$� ��5"=&0����"&��0�5�&"$8(22"7�"5� 4�����5"��"(�"D��2�!��"���*�&�� �"E�&�"F,,GG9""#"%�&*�&�(� �"?��&�;�����"%2(�"H%?%"*�&�"FGIJ)K"$8�425"7�"5�;�2���5"=0�8"�8�"���2�!��"&�'(&50�'" ������� 0�$"(�5"$8�425"�&� �5�"�8�"$� ��5"=&0����"&��0�5�&9""""-9" %�&*�&�(� �"L�;0�="0$"�8�"��($4&�����"�*"(�"���2�!��@$"( �4(2"��&*�&�(� �"0�"("�(&�0 42(&"$0�4(�0��9""?�"5�$ &07�$"8�="=�22"�8�"���2�!��"0���'&(��$"80$.8�&"1��=2�5'�<"(��0�45�$<"$1022$<"(�5"7�8(;0�&$"0�"��&*�&�0�'"�8�"6�7"( �&50�'"��"�M�� �(�0��$9""E�&"(&�($"�*"5�*0 0�� !<"("��&*�&�(� �"0��&�;�����"�2(�"0$"5�;�2���5"(�5"���0��&�5"4��02"��&*�&�(� �"0$"7&�4'8�"4�"��"$�(�5(&5$9""NOPQRSTUOV/WXYZX[/\O]PXTXVUX_/�%��42(�0��"B�&;�5" ������� !"($$�$$����"0$"("&�340&�����"*�&"�;�&!"a��":���&0(2"b�(2�8"B!$���"���2�!��"�8(�"&�'42(&2!"0���&( �$"=0�8"�(�0���$"�&"=8�$�"0�5����5���"645'����<"7($�5"��"���42(�0��"$�&;�5" ��$05�&(�0��"�(!"0��( �"�(�0���"$(*��!<" ���4�0 (�0��"�&"�4� ���$9"""""NOPQRSTUOV/_XYZX[/U_/[XcUVX[/S_/#'�<" 42�4&�"(�5"$�0&0�4(2"7�20�*$"(&�"0���&�(��"�2�����$"0�"8�(2�8" (&�9""C8�"0���&=�;��"&�2(�0��$80�$"7��=���"�8�$�"84�(�"($�� �$"0��( �"8�=" (&�"0$"5�20;�&�5"."�&�;05�59"C8�"*�22�=0�'"�2�����$"(&�"0� 245�5"0�"�8�"5�*0�0�0��d"('�"$�� 0*0 "���5$<" 42�4&(2"."$�0&0�4(2";(24�$<"50$�($�"�&� �$$"�&"50('��$0$<" �'�0�0;�"." ���4�0 (�0��"0��(0&����<"*4� �0��(2"$�(�4$"(�5"=(&"!�(&$"$0� �"$���"�&(4�($"&�2(��"��"50**�&���"�020�(&!" ��*20 �$9""%(�0���$"(&�"'&�4��5"0���"�8�"*�22�=0�'"20*�"$�('�$d""" B�('�","e"f���(��"" " g0&�8"h"-J"5(!$"B�('�",7"e"?�*(��" " " -i"5(!$"h",I"����8$"//////////////////////B�('�"-"e"C�552�&"" " ,J"����8$"h"j"!�(&$"B�('�"j"e"%&�$ 8��2�&" " j"h"+"!�(&$"B�('�")"e"B 8��2"('�" " +"h",-"!�(&$"B�('�"k"h"#5�2�$ ���"" " ,-"e,J"!�(&$"B�('�"+"h"l�4�'"#542�" " ,i"h")G"!�(&$"B�('�"I"e"#542�" " """"""""""")G"e"+k"!�(&$"B�('�"J"e":(�4&�"#542�"" " +km"!�(&$""""
������������������ ���������������������� �������� ��������������������� ����������� ������ ����������������� ����������� ���������������������� !"#$$�$$����"%&�'&(�""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""%('�")"�*"+" " """""""""""""""""""""" """""""""""""""",-.,-/"#��01 (20�"3�2"4�$ &1��1��$"14���1*!"�5�"$�� 1*1 "���60(�1��7$8"$�&9�4":1�5":51 5"�5�"���0�!��"1���&( �$;""""#��01 (20�"3�2"4�$ &1��1��$":100"5(9�"(" ������� !"($$�$$����"(44��46�<":51 5":100"14���1*!"�5�"$�� 1*1 " ������� 1�$"�5(�"�6$�"2�"4����$�&(��4"2!"�5�"���0�!��;""""=��0�!��$":100"&� �19�"�46 (�1��"��"���60(�1��"$�&9�4" (&�"($"���4�4<"�&"($"4���&�1��4"2!"�5�">1&� ��&"."?6��&91$�&"."=46 (��&;"@���" ���0��1��"�*"�5�"�46 (�1��(0" ��������<"�5�"���0�!��A$" ������� !":100"2�"($$�$$�4"6$1�'"("3�2"$�� 1*1 "%��60(�1��"?�&9�4"�������� !"#44��46�;""B5�"4��(&�����"41&� ��&.$6��&91$�&.�46 (��&":100"($$�$$"�( 5"���0�!��A$"���4"*�&"�5�"�46 (�1��(0"��460�<"2($�4"��"01 ��$6&�<"�C��&1�� �<"(�4" 6&&���"�&( �1 �;"""=46 (�1��(0"&�$�6& �$"�&�914�4"2!"�5�"�01�1 (0"D�(&�1�'">��(&�����"1� 064�"("$�0*E$�64!"��460�":1�5":&1����"��$�<"(�4"�E0�(&�1�'"��460�$;"">��(&�����"41&� ��&$"�(!"(0$�"4�9�0��"�5�1&"�:�"4��(&�����"$�� 1*1 "�46 (�1��"�&�'&(�"��"����"�5�"$�� 1*1 "�46 (�1��(0"���4$"�*"�5�"4��(&�����"(�4"�5�"(��&��&1(��"���60(�1��7$8"$�&9�4"2!"�5�"&�$�� �19�"���0�!��$;"""D1 ��$�4"$�(**"4��$"���"���4"��" ���0���"�5�"�46 (�1��(0"��460�"6�0�$$"�5�"4��(&�����"41&� ��&"."$6��&91$�&"."�46 (��&"($$�$$"�5�"���4"*�&"F��:0�4'�"( G61$1�1��"7��:"$�(**":5�"5(9�"2���"�6�"�*" 6&&���"�&( �1 �<"�&":5�"(&�"����&1�'"("��:"$�� 1(0�!"(&�(8;""@�01 ��$�4"$�(**":100" ���0���"�5�"('�"��&�1��"�*"�5�"�46 (�1��(0"&�$�6& �$"�&�914�4;"""B5�"���60(�1��"$�&9�4"(44��46�":100"2�"�(1��(1��4"1�"�5�"���0�!��A$"*10�"1�"�5�"4��(&�����;""B5�"���0�!��":100"(0$�"4� 6����" ���0��1��"�*"���60(�1��"$�&9�4" ������� 1�$"��"�5�1&"H�1�1(0"=46 (�1��"I� �&4"(�4"#��6(0"=46 (�1��"I� �&4;""B5�"H�1�1(0"(�4"."�&"#��6(0"=46 (�1��"I� �&4"1$"(��( 5�4":1�5"�5�"(��01 (20�"��&*�&�(� �"�9(06(�1��"7JK"4(!$"L"H�1�1(0"�&"#��6(0"L"#��6(0"=9(06(�1��8"(�4"(0$�"*10�4"1�"�5�"4��(&�����(0"���0�!��"*10�;""����10(�1��"�*">(�("I�'(&41�'"?�(**"�������� �"%(���&�$"",;" M�"(�"��'�1�'"2($1$"($"�(���&�$"(�4"�&��4$"(&�"14���1*1�4"&�'(&41�'"$�(**" ������� �<"�5�"4��(&�����"$5�604"&�$���4"��"$�(**"0�(&�1�'"���4$":1�5"(��&��&1(��"1�E$�&91 �"�46 (�1��"�&�'&(�$;""-;" B5�&�"1$"("�� 5(�1$�"1�"�0( �"*�&"4��(&�����$"��"�&�914�"*��42( F"��"�&(1�1�'"���4$"��"�01�1 (0"D�(&�1�'"$�"�5(�"�&'(�1N(�1��(0"�&(1�1�'"���4$"�(!"2�"(44&�$$�4;""O;" B5&�6'5"�5�"��&*�&�(� �"1��&�9�����"�&� �$$<"�&'(�1N(�1��(0"�46 (�1��"���4$"14���1*1�4"2!"*6� �1��(0"(�(0!$1$":100"(0$�"2�"$5(&�4":1�5"�01�1 (0"D�(&�1�';""P;" �01�1 (0"D�(&�1�'"(�(0!N�$"3�2"��&*�&�(� �"(��&(1$(0"$ �&�$"(��6(00!"��"14���1*!"����&�6�1�1�$"*�&"1��&�9�����;""//QRSTUVWRUX//,;" B5�"Y6�(�"I�$�6& �$">��(&�����" ��&41�(��$"�5�"9�&1*1 (�1��"�*"�&�E���0�!����"G6(01*1 (�1��$"1�"( �&4(� �":1�5"�5�"I� &61�����"(�4"=��0�!����"%�01 !"?KJ"K)"Z)K<"1�"�5�"%�01 !"(�4"%&� �46&�"[(�6(0;"""
������������������ ���������������������� �������� ��������������������� ����������� ������ ����������������� ����������� ���������������������� !"#$$�$$����"%&�'&(�""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""%('�")"�*")" " """""""""""""""""""""" """"""""""""""""+,-+,.,/" 0�(1�&$23�"4355"��$6&�"�2(�"(55"��4"���5�!��$"(&�"$ 2�165�1"*�&"$!$���7431�"�&3���(�3��"3�"( �&1(� �"43�2"�2�"8�79�(&13�'"%�53 !":;<";+"=><?"3�"�2�"%�53 !"(�1"%&� �16&�"@(�6(5/""A/" B��(&�����"5�(1�&$23�"4355"��$6&�"�2(�"(55"��4"(�1"�&(�$*�&&�1"���5�!��$"(&�"�&3����1"��"�2�3&"1��(&�����"(�1"�2(�"�2�!"&� �3C�"(1�D6(��"��7�2�7E�F"�&(3�3�'"��"��$6&�"�2(�"�2�!"2(C�"(55"�2�"&�$�6& �$"(�1"3�*�&�(�3��"�2�!"���1"��"��&*�&�"�2�3&"E�F$/"">/" B��(&�����"5�(1�&$23�"4355"��$6&�"�2(�"(55"���5�!��$"(&�"�C(56(��1"�&3�&"��"�2�"��1"�*"�2�3&"3�3�3(5"<;71(!"3��&�16 ��&!"G�&3���(�3��H"��&3�1/""I2(�"�C(56(�3��"3� 561�$"F��2"(" ������� !"($$�$$����"(�1"("��&*�&�(� �"(��&(3$(5?"(�1"("1�C�5������"�5(�"�2(�"(11&�$$�$"5�(&�3�'"���1$/""I2�"5�(&�3�'"���1$"(&�"31���3*3�1"F!"��(�$"�*"13$ 6$$3��"F��4���"�2�"���5�!��"(�1"3���13(��"$6��&C3$�&/""""J/" B��(&�����"5�(1�&$23�"4355"��$6&�"�2(�"(*��&"�2�"$6 �$$*65" ���5��3��"�*"3�3�3(5"3��&�16 ��&!"��&3�1"�&"<;71(!"&�C3�4"��&3�1?"(55"���5�!��$"(&�"�C(56(��1"(��6(55!?"('(3�"3�"( �&1(� �"43�2"�2�"KLMNOPQRSTUVTWOXYSQOXZQ[VW\S]SXYPQS_SaQ"%�53 !":;<";)";;,"(�1"bXXcOdQRSTUVTWOXYSQOXZQ[VW\S]SXYPQS_SaQ"%�53 !":;<";)";,)?"3�"�2�"%�53 !"(�1"%&� �16&�"@(�6(5/"")/" 8&'(�3e(�3��(5"�&(3�3�'"���1$"31���3*3�1"�2&�6'2"�2�"��&*�&�(� �"3��&�C�����"�&� �$$"4355"F�"$2(&�1"43�2"�2�"�53�3 (5"0�(&�3�'/""f/" %�&*�&�(� �"&�C3�4"$ �&�$"(&�"(�(5!e�1"(��6(55!/""#�"(��6(5" ������� !"&���&�"3$"*�&4(&1�1"��"�2�"9�(&1"�*"B3&� ��&$"*�&"&�C3�4"(�1"(��&�C(5/""ghijkhl.mniopohqr.:;<";+"JJ)""@(�1(��&!"s16 (�3��"(�1"I&(3�3�'":;<";>"f))""t�7���&!"�*"s��5�!��$"*&��"0�(C�"�*"#F$�� �"@;<";J"f=;"tu"t� �C�&!"%&�'&(�":;<";J"=))""I����&(&!":�(**3�'"t�D6�$�$":;<";)";;,""<;7B(!"%�&*�&�(� �"(�1"�������� !"t�C3�4":;<";)";,)""#��6(5"%�&*�&�(� �"(�1"�������� !"t�C3�4":;<";)"AAJ""v&3�C(� �"u��7@(�('�����":;<";)">A>""w��&�16 ��&!"%�&3�1"7"u�4"s��5�!��"@+J";;")J;""u6&$3�'":�&C3 �$":�(**"�������� �"@+J";;"=A>"":�(**3�'"t�$�6& �"�����&"
___________________
L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
BOARD POLICIES
Adoption (Action)
1) Motion to Remove from TABLE: 20.14F: Use of
Funds for Education, Travel & Business
Meeting/Special Event Expenses Tabled from
Jan 24, 2013 Meeting
2) 10.09D: Agenda Item Background Material
3) 10.27F: Reporting and Accreditation
4) 10.43D: Board Member Standards
5) 10.47C: Compliance Program
6) 10.53A: Electronic Tablets
7) 10.54: Grievance Process
8) 30.04: Medical Staff Representation
TABLED from 1/24/13 TO MARCH GOVERNANCE MEETING Once this policy is printed, it is not considered a controlled document.
Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
20.14F - DRAFT -Use of Funds for Education, Travel and Business Meeting-Special Event Expenses 112912 Page 1 of 2
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL no. 20.14 F E supersedes no. 20.14E D ----------------------------------------------------------------------------------------------------------------------------------------
category: Financial Operations
title: Use of Funds for Education, Travel and Business Meeting/Special Event Expenses ----------------------------------------------------------------------------------------------------------------------------------------
original adoption: 12/13/91 TABLED 11/29/12 & 1/24/13 review date: 3/28/13
revision date: 07/26/02, 07/31/98, 07/27/01, 09/29/05, 05/31/07, 3/28/13 ----------------------------------------------------------------------------------------------------------------------------------------
PURPOSE: To govern the expenditure of funds budgeted by Lee Memorial Health System Board of Directors
(Board) for Board Member Director & Assistant to the Board Administrator education, travel, business meetings and special event expenses.
----------------------------------------------------------------------------------------------------------------------------------------
POLICY: 1. The Board recognizes that travel and related business expenses are an integral and
necessary component of the operation of the Health System. The Board also recognizes the constructive value of professional conferences, seminars, meetings and training in providing ongoing education and vital information relevant to effective policy setting. In recognition of these needs and benefits, the Board provides funding for such activities through the annual budget adoption process. Budgets for travel and related business expenses are intended to reimburse all necessary and reasonable expenses incurred in connection with such activities, subject to compliance with the policies adopted by the Board governing reimbursement of expenses related to such activities.
2. The Office of the Board of Directors shall budget an amount in each Fiscal Year deemed
appropriate to cover the expenses for education, travel, and other System-related business activities/special events of the Board. The funds budgeted shall be divided equally among the ten publicly elected Directors and the Assistant to the Board Administrator. The budget shall further subdivide into Fund A – Group Education and Development & Fund B - Individual Expenses. DiThe budget allocation of an individual Board Member Director should not be transferred or used by another Board Member Director without approval by the Board. Any portion of the budget allocation not expended in any fiscal year shall not be carried over to the next fiscal year.
3. Travel reimbursement shall be governed by the provisions of Section 112.061, Florida Statutes,
as the same may be in effect at the time reimbursement is sought. In accordance with Florida law, all travel must be authorized and approved by the Board Chairman or Vice Chairman if Chairman unavailable.
TABLED from 1/24/13 TO MARCH GOVERNANCE MEETING Once this policy is printed, it is not considered a controlled document.
Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
20.14F - DRAFT -Use of Funds for Education, Travel and Business Meeting-Special Event Expenses 112912 Page 2 of 2
4. The budgeted amount shall be available for the following purposes: a) Fund A: Group Education & Development: Expenses of System-related business, when
such business has been authorized by the Board. This shall be referred to as “Group” to include the business of the Health System or Board or Trauma District such as trips to Tallahassee, AHA, VHA & FHA meetings. To encourage participation, seventy-five percent (75%) Twenty-five percent (25%) of the budget shall be allocated for “Group”.
b) Fund B: Individual Expense: Expenses, other than “Group”, related to individual educational opportunities that are intended to maintain or improve the individual’s ability to perform the duties of the office. This includes travel expenses, seminar tuition, books and periodicals, and audio and video materials. Twenty-five percent (25%) Seventy-five percent (75%) of the budget shall be allocated and divided equally by the eleven. Up to 10% of the “Individual” fund may be used for LMHS related business/special events for ticket purchase for the individual.
5. Assuming there are sufficient funds remaining in the budget, individuals may seek Board pre-
approval for expenditures which would take the individual over his or her designated budgeted allocation.
6. The LMHS Board of Directors has placed s membership with the Governance Institute, which includes conference registration fee, however, any travel & lodging expense would be deducted from Board members’ individual fund. agencies and as such, the Board receives a number of passes annually to their conferences. After our the passes have been utilized, the registration fee for each individual will be divided equally by all the individuals who utilized such passes, and only count that portion as part of the allotted expense.
7. All expenses will be submitted to the Assistant to the Board Administrator for verification & reimbursement on System Form #0878 (Attachment 2).
PROCEDURE:
1) Fund A “Group” expenses are covered by the 75% 25% allocation. Fund B Individual expenses must be pre-authorized by Board Chairman or Vice Chairman if Chairman is unavailable and are covered by the 25% 75% allocation. Reimbursement is made to the individual upon processing the travel claim.
2) Individuals are expected to avoid any last minute cancellations which result in the Health System paying for unused expenditures. All educational expenses, including seminar registration costs, mileage, airline tickets, lodging, car rentals, meals and other miscellaneous expenses shall be submitted in accordance with System Administrative Policy 07 062 on System Form #0878 (Attachment 2).
3) Individuals shall submit requests and verification for payment of expenses to the Assistant to the Board Administrator for processing. Approval of allowable reimbursement shall be the responsibility of the Board Chairman or the Board Chairman may delegate authority to another Director, the Assistant to the Board Administrator or the System President.
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
10.09D-DRAFT Agenda Item Background Material for ADOPTION 032812.doc Page 1 of 1
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL no. 10.09D C supersedes no. 10.09C B
----------------------------------------------------------------------------------------------------------------------------
category: General Operations
title: Agenda Item Background Material ---------------------------------------------------------------------------------------------------------------------------
original adoption: 1/08/91 review date: 3/28/13
revision date: 7/31/98 , 7/26/02, 10/31/03, 3/28/13 --------------------------------------------------------------------------------------------------------------------------------
PURPOSE: To ensure that each member has adequate time to review the necessary material prior to meetings of the Board. and the Committee of the Whole. --------------------------------------------------------------------------------------------------------------------------------
POLICY: All Board packet materials background material for any agenda items requiring Board action shall be electronically distributed to the Board members in the hands of members not less than one week the Friday prior to Thursday’s meeting (except for financial statements if not available due to Board’s meeting
schedule) at which action is to be taken unless the Chairman shall determine that a situation exists including emergency meetings requiring Board action on a non-agenda’ed item, in which case, background material may be distributed as soon as available, including at the meeting where action is to be taken.
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
10.27F - DRAFT Reporting and Accreditation of System Entities FOR ADOPTION 032813.doc Page 1 of 1
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL no. 10.27 F E supersedes no.10.27 E D
----------------------------------------------------------------------------------------------------------------------------------------
category: General Operations
title: Reporting and Accreditation of System Entities ----------------------------------------------------------------------------------------------------------------------------------------
original adoption: 1/08/91 review date: 3/28/13
revision date: 7/31/98, 7/26/02, 2/26/04, 2/26/09, 8/27/09, 3/28/13 ----------------------------------------------------------------------------------------------------------------------------------------
PURPOSE:
To provide a mechanism for reporting of various System entities, operations, collaborations, and support organizations and to provide for certain their accreditation. ----------------------------------------------------------------------------------------------------------------------------------------
POLICY: The Board of Directors shall periodically review and accept a report regarding the following: operation and accreditation of the following entities:
Subsidiaries (Board reporting as required in Bylaws): Subsidiary entities such as Cape Memorial Hospital, Inc. d/b/a Cape Coral Hospital; HealthPark Care Center, Inc.; Lee Memorial Home Health, Inc.; Lee Memorial Medical Management, Inc. will report in accordance with the applicable entity bylaws or as requested by the health system Board of Directors.
Supporting Organizations: Agencies Auxiliaries – (reports annually at Board meetings) Lee Healthcare Resources (report annually) Lee Memorial Health System Foundation – (Board Policy requires *semi-annual report per Board Policy 10.24) to Board)
Subagencies, Service Lines, Operating Collaborations and Acute Care Operations: Areas to report are outlined in the CURRENT Strategic Plan Model, as Key Strategy Areas &/or Core Clinical Services. Reports are to be submitted on the Entity Reporting Executive Summary annually. Subagencies (such as Auxiliaries), service lines (such as neurosciences) and operational collaborations (such as Graduate Medical Education (GME) Program) will report as requested by the health system Board of Directors. Acute care operations will report to the Board on a regular basis consistent with the Board’s meeting calendar.
LMHS Joint Ventures – (report annually) Joint with Naples Community Hospital-Bonita Community Health Center (Naples Community Hospital) Joint with Sarasota Memorial - LeeSar Purchasing Cooperative (Sarasota Memorial) Joint with Sarasota Memorial - Cooperative Services of Florida (CSF) (Sarasota Memorial) Joint with Morton Plant Hospital Association, Inc. - Access Medical South (Morton Plant Hospital
Association) Joint with ProHealth Medical, Inc - Access Infusion Partners
Accreditation for System acute care hospitals and post-acute services (such as home health and rehabilitation) subsidiaries and sub-agencies shall will be obtained and maintained from an accreditation at least one nationally or regionally recognized organization with deemed status from Centers for Medicare & Medicaid Services (CMS) as approved by the Board of Directors. and related to the major work of the unit when such an accreditation program exist.
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
10.43D-Board Member Standards for ADOPTION 032813.doc Page 1 of 1
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS POLICY MANUAL no. 10.43 D C supersedes no. 10.43 BC
---------------------------------------------------------------------------------------------------------------------------------------
category: General Operations
title: Board Member Director Standards ---------------------------------------------------------------------------------------------------------------------------------------
original adoption: 9/29/00 review date: 3/28/13
revision date: 1/2601, 7/26/02, 11/29/07, 3/28/13 ---------------------------------------------------------------------------------------------------------------------------------------
PURPOSE: Lee Memorial Health System is a public safety-net health system and as such believes in a standard of excellence. ---------------------------------------------------------------------------------------------------------------------------------------
POLICY: To promote good governance practices, Board members Directors of the Lee Memorial Health System establish the following guidelines:
1. Maintain a commitment to the mission, values, and objectives of the System while recognizing that the mission, strategy, and objectives are long-term and might extend beyond any Board member’s Director’s term of office.
2. Present the Health System in a positive light while respecting the differences between management and the Board.
3. Exercise due diligence by attendance at all board and committee meetings; and community and educational events when possible, in order that the Board member Director will be reasonably informed about Health System business and make decisions the Board member Director believes is in the Health System’s best interest.
4. Recognize that differences of opinion are healthy and should not lead to conflict. Respecting that right of difference leads to respect for one another whether dealing with each other, administration, the medical staff, or the public at large.
5. Conduct meetings of the Health System Board at which official acts are to be taken or at which public business is to be transacted or discussed in accordance with the Florida Sunshine law.
6. Protect information considered confidential by federal and state law, including health information of patients.
7. Recognize that it is essential to the proper conduct and operation of the Health System that Board members Directors be independent and impartial and that their office not be used for private gain. In the performance of public duties, Board members Directors will observe the standards of ethics and code of conduct consistent with Florida law governing public officers.
8. Act as stewards of Health System resources through responsible oversight of Health System finances and annual budget approval in order to avoid waste and promote cost-effective patient care.
9. Promote transparency through publicly available information about the Health System’s mission, activities, finances and community benefit reporting.
10. Support and monitor Health System fundraising activities to ensure compliance with the law.
11. Support Health System standards for effective document integrity, retention and destruction.
12. Support a culture of compliance through the establishment of an effective Health System compliance program and standards of conduct which provide guidance to Health System employees, medical staff, and volunteers to assist them in carrying out duties and responsibilities.
RECOMMENDED ACTION FOR BOARD APPROVAL (Action includes Acceptance, Approval, Adoption, etc)
DATE: March 28, 2013 LEGAL SERVICE REVIEW? YES_X_ NO__ SUBJECT: Board Policy 10.47C: Compliance Program REQUESTOR & TITLE: Catherine Kahle, Interim Chief Compliance and Internal Audit Officer PREVIOUS BOARD ACTION ON THIS ITEM (IF ANY) (justification and/or background for recommendations – internal groups which support the recommendation i.e. SLC, Operating Councils, PMTs, etc.)
The Compliance Program Board Policy 10.47B (previously modified and adopted by the Board on 10/25/12) has been revised due to requirements in the Patient Protection and Affordable Care Act. SPECIFIC PROPOSED MOTION: Adoption of Board Policy 10.47C: Compliance Program, as revised. PROS TO RECOMMENDATION
CONS TO RECOMMENDATION
LIST AND EXPLAIN ALTERNATIVES CONSIDERED N/A FINANCIAL IMPLICATIONS Budgeted ____ Non-Budgeted ____ (including cash flow statement, projected cash flow, balance sheet and income statement)
N/A OPERATIONAL IMPLICATIONS (including FTEs, facility needs, etc.) N/A SUMMARY The Compliance Program Board Policy 10.47B has been revised to define the scope of entities covered by the LMHS Compliance program.
BOD/Forms/Board (Action) Reporting Form
Keep form to one page, SUBMIT (thru SLC Member) ELECTRONICALLY to L Drive – Miscellaneous - BOD Presentations by Noon the Friday before you’re scheduled on agenda.
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
10.47C - DRAFT UNAPPROVED Compliance Program for ADOPTION 032813 Page 1 of 1
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL no. 10.47 C B supersedes no. 10.47 B A
------------------------------------------------------------------------------------------------------------------------------------------
category: General Operations
title: Compliance Program ------------------------------------------------------------------------------------------------------------------------------------------
original adoption date adopted: 9/27/02 review date: 3/28/13
revision effective date: 9/27/02, 11/29/07, 10/25/12, 3/28/13 ------------------------------------------------------------------------------------------------------------------------------------------
PURPOSE:
To establish and define the general scope of a Compliance Program for Lee Memorial Health System (LMHS). ------------------------------------------------------------------------------------------------------------------------------------------
POLICY:
LMHS is dedicated to being legally and ethically correct in all of its actions. Therefore, it is LMHS policy that all employees, agents, medical staff, volunteers, and individuals doing business with or performing functions or services at LMHS comply with Federal and State statutes and regulations and provisions of private health care programs. LMHS voluntarily established a Compliance Program to assist in maintaining an ethical climate and provide a mechanism to prevent, detect, and correct compliance violations. The program is intended to complement, not replace, other LMHS policies. The Board has general overall oversight responsibility for the Compliance Program and activities. The Chief Compliance Officer will be vested with responsibility of day-to-day operations, to develop and implement the compliance program, which will encompass all adult and pediatric acute care and rehab hospital facilities, outpatient treatment and diagnostic centers, skilled nursing facility, home health agencies, and employed physician practices. The Chief Compliance Officer will provide the The System President and the Board with quarterly updates summarizing the activities of the compliance department. appoint a Chief Compliance Officer, who is responsible for implementing the LMHS Compliance Program. The Chief Compliance Officer reports directly to the System President and to the Board. The System President is responsible for providing executive oversight and authority for allocating appropriate resources to effectively implement the Compliance Program. The Board designates a Liaison to receive periodic updates from the Chief Compliance Officer. Apparent violations estimated to have a material effect on the financial status of the System, involve serious criminal matters or serious contract violations, or appear likely to result in adverse news media coverage are to be reported immediately to the System President and the Board. If situations occur where the System President is involved in unethical matters or is unwilling to take appropriate action when serious regulatory or statutory violations are brought forward by the Chief Compliance Officer, the Chief Compliance Officer will report the matters directly to the Board. The System President will not prevent the Chief Compliance Officer from reporting serious violations to the Board. The Compliance Program is based on guidelines issued by the Department of Health and Human Services, Office of Inspector General. The Chief Compliance Officer provides the Board with quarterly updates summarizing Compliance activities and strives to ensure that all covered by this policy are kept informed of the Standards of Conduct and the Compliance Program.
10.53A-DRAFT-Electronic Tablets for ADOPTION 032813.doc Page 1 of 3
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS POLICY MANUAL no. 10.53A supersedes no. 10.53
----------------------------------------------------------------------------------------------------------------------------------------
category: General Operations
title: Electronic Tablets for Board Members, Board Community Consultants Representatives & Physician Leadership Council (PLC) Consultants to the Board ----------------------------------------------------------------------------------------------------------------------------------------
original adoption: 9/8/2011 review date: 3/28/13
revision date: 3/28/13 ----------------------------------------------------------------------------------------------------------------------------------------
PURPOSE: To provide for the issuance to and use of electronic tablet devices by the Board of Directors, Board Community Consultants Representatives & Physician Leadership Council (PLC) Consultants to the Board. ----------------------------------------------------------------------------------------------------------------------------------------
POLICY: In order to provide the Board of Directors, Board Community Consultants Representatives and Physician Leadership Council (PLC) Consultants to the Board (collectively, the “Users”) with cost efficient, timely, thorough, convenient, and updated information for matters related to the Health System, including without limitation, the Board agenda packets, meeting materials, and emails, it is in the best interest of the Health System to issue each Board Member, Board Community Consultant Representative and Physician Leadership Council (PLC) Consultant to the Board an electronic tablet device. The electronic tablet shall be the property of the Health System and is to be used only by the User and primarily for Health System business. The Users shall be responsible for obtaining all material necessary to prepare for and attend Health System meetings through the electronic tablets or the Health System website. Paper packets will not be available to Users during Health System meetings. ---------------------------------------------------------------------------------------------------------------------------------------
PROCEDURE:
1. Upon User’s execution of the Receipt and Acknowledgement of Responsibility form, the User shall be issued an electronic tablet, identified by serial and model number. The electronic tablet will have a minimum of 16GB of internal storage capacity, Wi-Fi connection capabilities and cellular connection capabilities. The Health System shall provide a 2 GB data plan for cellular connection of the electronic tablets (the “Standard Plan”). The User shall be responsible for any usage costs or fees that exceed the Standard Plan. The Standard Plan does not allow for international cellular connections. This is specifically turned off. When out of the country, use the Wi-Fi connection.
10.53A-DRAFT-Electronic Tablets for ADOPTION 032813.doc Page 2 of 3
2. The electronic tablet shall be password protected and in the event it is lost or stolen, the
User must immediately report the same to the Board Office so that the electronic tablet can be disabled remotely. The tablet will not only be disabled (locked via iCloud), a remote wipe (removal of all data on the tablet) will be performed. If the tablet is offline, the data will be erased the next time it’s online.
3. Each User shall use due care to maintain his or her electronic tablet in good condition and protect it from loss or theft. The Health System shall purchase a two year protection plan to extend service coverage for each electronic tablet and shall provide each User with a standard electronic tablet cover. However, if If the electronic tablet is lost, stolen or damaged, and repair or replacement is not covered under the protection plan, the User must reimburse the Health System for the full cost of a new electronic tablet within thirty days.
4. The Health System may install applications on the electronic tablets and may require the Users to establish certain accounts to access System information or applications. The Health System may provide technological support and training to the Users with respect to their use of the electronic tablets for System business. The Users are requested to reference the user manual and contact the Board Administrator with questions regarding the use of the tablet for System business.
5. The electronic tablets are to be used primarily for Health System business. The information and correspondence related to Health System business contained, viewed, sent or received on or through the electronic tablet may be subject to the public records law and the Users should refer to Policy 10.49. The Users may use the electronic tablet for personal use, however, the Users shall use discretion and shall not download applications or view websites that may be inappropriate or in violation of any Health System policy related to computers, electronic tablets or similar technology. Furthermore, the User shall not allow personal use and applications to interfere with or hinder the use of the electronic tablet for official Health System business. The User shall be responsible for any costs incurred by or through the use of the electronic tablet for any application, hardware, software, service plan, data plan, or other options not provided by the Health System in conjunction with Health System business.
6. Given the constant change in technology and the life span of electronic tablet devices, as
long as a Director has served a minimum of two consecutive years on the Board, at the end of his or her last term or upon resignation from the Board, the electronic tablet shall become the personal property of the Director. If a Board Member resigns prior to serving two years or is removed from the Board for any reason, the Board Member shall immediately return his/her electronic tablet to the Board Office.
7. Board Community Consultants Representatives and Physician Leadership Council (PLC) Consultants to the Board shall return the electronic tablet to the Board Office on or before the last day of his or her final term.
10.53A-DRAFT-Electronic Tablets for ADOPTION 032813.doc Page 3 of 3
Electronic Tablet
Receipt and Acknowledgement of Responsibility Form
Name of User: ______________________________
Electronic Tablet distributed to: (check one)
o Board Member
o Board Community Consultant Representative
o Physician Leadership Council (PLC)
Consultant to the Board
Name of Equipment: _________________________
Serial Number: ______________________________
Model Number: ______________________________
I (please print) ________________________ agree to receipt of an
electronic tablet on this date __________.
I agree to ALL terms and conditions as stated in Board policy
10.53A.
Signed___________________ Date ____________
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS RECOMMENDED ACTION FOR BOARD APPROVAL
(Action includes Acceptance, Approval, Adoption, etc)
DATE: March 28, 2013 LEGAL SERVICE REVIEW? YES_X_ NO__
SUBJECT: Board Policy 10.54: Grievance Process
REQUESTOR & TITLE: Chris Crawford, Standards & Quality and Mary Lorah, Legal Services / Risk Management
PREVIOUS BOARD ACTION ON THIS ITEM (IF ANY) (justification and/or background for recommendations – internal groups which support the recommendation i.e. SLC, Operating Councils, PMTs, etc.)
Since the proposed policy is a new Board policy, no previous board action has occurred.
SPECIFIC PROPOSED MOTION:
Board to Adopt new Board Policy 10.54: Grievance Process.
PROS TO RECOMMENDATION
Compliance with CMS Conditions of Participation for Hospitals
CONS TO RECOMMENDATION None identified
LIST AND EXPLAIN ALTERNATIVES CONSIDERED No alternatives which are consistent with the CMS regulations governing hospitals were identified.
FINANCIAL IMPLICATIONS Budgeted ____ Non-Budgeted ____ (including cash flow statement, projected cash flow, balance sheet and income statement)
None identified OPERATIONAL IMPLICATIONS (including FTEs, facility needs, etc.) None identified
SUMMARY Centers for Medicaid & Medicare Services (CMS) Conditions of Participation for Hospitals require the health system hospitals to ensure that patients or their representative have a mechanism to file a grievance and to make sure that there is a prompt resolution to the grievance. The Board of Directors, as the governing body, must approve and be responsible for the effective operation of the grievance process and must review and resolve grievances unless it delegates the responsibility in writing to a grievance committee.
The proposed policy sets forth the responsibility of the health system hospitals’ Grievance Committees to ensure that there is an effective grievance process, including the review and resolution of grievances received from patients or their representatives in a manner consistent with the CMS Conditions of Participation for Hospitals. The administrative policy is also attached for your review.
BOD/Forms/Board (Action) Reporting Form – updated 9/2/09 cs
Keep form to one page, SUBMIT (thru SLC Member) ELECTRONICALLY to L Drive – Miscellaneous - BOD Presentations by Noon the Friday before you’re scheduled on agenda.
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
10.54 – Board Policy - Grievance Process for ADOPTION 032813 Page 1 of 1
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL DRAFT UNAPPROVED no. 10.54 supersedes no.
----------------------------------------------------------------------------------------------------------------------------
category: General Operations
title: Grievance Process ----------------------------------------------------------------------------------------------------------------------------
original adoption: 3/28/2013 review date: 3/28/13
revision date: ---------------------------------------------------------------------------------------------------------------------------
PURPOSE: To set forth the responsibility of health system hospitals’ Grievance Committees for an effective grievance process, including the review and resolution of grievances received from patients or their representatives in a manner consistent with hospital administrative policy and in accordance the CMS Conditions of Participation for Hospitals. ----------------------------------------------------------------------------------------------------------------------------
POLICY: The health system hospitals have a responsibility to ensure that patients or their representatives have a mechanism to file a grievance and to make sure that there is a prompt resolution to the grievance as set forth in hospital administrative policy and procedure. The Board of Directors delegates the responsibility for the effective operation of the grievance process and for ensuring a process consistent with CMS Conditions of Participation for Hospitals to the Grievance Committee at each hospital. Committee members will include representatives from Administration, Department Directors (which includes clinical representation), Guest Services, Risk Management, Quality and Human Resources. Notice of whom to contact to file a grievance will be given to the patient or their representative in the Patient Guide (or similar communication), in the Florida Patient’s Bill of Rights and on the Lee Memorial website. Grievances regarding quality of care or premature discharge are referred as appropriate to the Quality or Utilization Review Departments.
Once this policy is printed, it is not considered a controlled document. Please review electronic version of this policy for the most current document.
Patient Complaint Grievance Service Recovery Page 1 of 6 8/12
LEE MEMORIAL HEALTH SYSTEM
POLICY & PROCEDURE MANUAL
PATIENT COMPLAINT / GRIEVANCE - SERVICE RECOVERY LOCATOR NUMBER
T Y P E
System-wide - A formal statement of values, intents (policy), and expectations (procedure) that applies to every employee throughout the System.
Multidisciplinary - A formal statement of values, intents (policy), and expectations (procedure) that applies to more than one discipline and is usually of a clinical nature. Check below all areas to which this applies.
Departmental - A formal statement of values, intents (policy), and expectations (procedure) exclusive to a particular department or group of people within a department at one or multiple locations that does not impact any other area.
CHAPTER: S03 TAB: 01
POLICY #: 703
Disciplines / locations to which this multidisciplinary policy applies:
Health Information Management Pharmacy Acute Care Hospital Nursing
Housekeeping Plant Operations Ambulatory Services
Information Systems Radiology Home Health
Laboratory Rehabilitation Services HPCC
Legal Services Respiratory Physician Offices
Nutrition Security Rehab Hospital
Other
Date Originated: 3/95 Reviewed / No Revision:8/99
Dates Revised: 5/95, 5/98, 7/98, 8/99, 4/01, 6/01, 3/04, 7/06. 12/08, 1/09, 10/09, 11/09, 5/10, 8/12
Next Review Date: 8/14
Author(s): Mary Lorah, RN, BA, LHCRM; Jennifer James-Bass, Guest Services Coordinator
Reviewed by: Clinical Practice Council: Date:
Clinical Education Council Education Required:
Education Completed: Yes No:
Date: Date:
Approved by: Policy Administrator: Donna Giannuzzi, RN, MBA, NEA-BC, CPCO Date: 8/2012
As Needed:
Medical Director: Date:
Board of Directors: Date:
PURPOSE: The Lee Memorial Health System (LMHS) Patient Complaint / Grievance-Service Recovery policy has been established to set forth the requirements for prompt resolution of complaints /grievances and for the responsibility of the Grievance Committee.
Once this policy is printed, it is not considered a controlled document. Please review electronic version of this policy for the most current document.
Patient Complaint Grievance Service Recovery Page 2 of 6 8/12
DEFINITION: CMS defines a “patient grievance” as a formal or informal written or verbal complaint that is made to the hospital by a patient, or the patient’s representative, when a patient issue cannot be resolved promptly by staff present. If a complaint cannot be resolved promptly by staff present, it is to be considered a grievance. If a patient or their representative is unable to resolve their concern during their stay or they did not wish to address their issue during their stay and they contact the hospital after their stay this would be considered a grievance. If the patient or their representative requests that their complaint be handled as a formal complaint or grievance or they request a response from the hospital, then the complaint is a grievance. If the patient or the patient’s representative who is in the hospital calls the Guest Service Representative first and has not tried to resolve the issue with the involved department or unit this could be considered a grievance. However, if a Guest Services representative is able to contact the Unit or Department and the patient care staff is able to resolve this issue at that time then it would not be considered a grievance. If the Guest Services representative is a staff member of a particular Unit or Department (i.e. ED), the complaint or concern is addressed with them directly, and they are able to resolve the issue at the time, then it would not be considered a grievance. If the Guest Services representative is asked by a staff member to visit a patient and the representative is able to resolve a complaint/concern at the time then it would not be considered a grievance. If the Guest Services representative is visiting a patient as part of their rounds and they are able to resolve a complaint/concern at the time then it would not be considered a grievance. Any communication in which the person does not identify themselves will not be considered a grievance. Billing issues are not considered grievances unless they contain elements addressing patient services or care issues. POLICY: Lee Memorial Health System has a responsibility to increase patient satisfaction by empowering employees to promptly resolve dissatisfaction issues in a timely, reasonable, and consistent manner. The Lee Memorial Health System Board of Directors (Board of Directors) is responsible for the effectiveness of the grievance process and has delegated the responsibility for review and for resolving grievances to the Grievance Committee established at each acute care facility. Patient concerns involving non-acute care services will be referred to such areas for follow-up.
Once this policy is printed, it is not considered a controlled document. Please review electronic version of this policy for the most current document.
Patient Complaint Grievance Service Recovery Page 3 of 6 8/12
Each department at Lee Memorial Health System is responsible for providing a great patient experience. LMHS employees will participate in an organized approach to resolve patient / customer concerns quickly, fairly, and in a manner that the concerned patient / customer feels satisfied with the experience. LMHS employees will have 24-hour access, seven days a week, to service recovery options.
1. Guest Service Representative at each acute care campus will monitor and coordinate the complaint management system.
2. The Billing Office will handle billing concerns. 3. Lee Physician Group will handle concerns related to treatment provided by Lee
Physician Group and Lee Convenient Care and the MSO will handle concerns related to treatment provided by the MSO.
4. Post Acute Care concerns will be directed to the appropriate manager / director. 5. If a complaint involves a physician who is not employed by LMHS, it may be
necessary to refer a complaint / grievance to the Practice Administrator of the non-employed Physician. This referral may be made at the direction of Risk Management or by one of the Medical Directors. The Guest Services Coordinator will coordinate with the Practice Administrator to ensure that a response is sent to the patient or family as appropriate.
PROCEDURE: A. Hospital staff receiving a direct complaint, concern, or unmet expectation from a patient /
Representative will follow the appropriate steps at the point of contact to resolve the situation. Following these steps should resolve most patient complaints.
1. Listen to what the patient /representative is saying. If the patient /representative
approves, take notes of the concerns so you can appropriately address all issues.
2. Ask open-ended questions to obtain information. Repeat concerns back to patient/representative to ensure you understand all concerns expressed.
3. Determine if you can resolve the problem or if another department should be a part of the resolution process.
4. Genuinely empathize to validate the patient / family feelings or concerns.
5. Clarify the patient / representative’s expectations and possible resolutions.
6. Apologize without blaming anyone.
7. Explain actions that will be taken.
8. If applicable, agree on who the next person will be to contact the patient / representative.
9. Thank the patient / representative for their comments
Once this policy is printed, it is not considered a controlled document. Please review electronic version of this policy for the most current document.
Patient Complaint Grievance Service Recovery Page 4 of 6 8/12
10. Seek assistance from supervisor or manager when necessary.
11. Follow up with patient / Representative on resolution by the end of the shift.
12. Assess and communicate service failures to the appropriate manager / director.
B. Complaints, concerns, or unmet expectations that are received via Board of Directors,
administration, survey, letter, phone, after-hours administrative supervisors, or walk-ins, will be coordinated through the Guest Service Representative at each campus with assistance from affected departments. If a complaint meets the guidelines provided by the CMS Conditions of Participation for a grievance, the procedure listed below will be followed. Steps to accomplish resolution of patient grievances, concerns or unmet expectations will include:
1. Guest Service Representative receives complaint, concern, or unmet
expectations and enters it into the database within 7 business days of receipt of the concern.
2. Guest Service Representative obtains factual information, including source of
complaint, date of service, name, address, phone, complete description of the concerns and expected outcome.
3. Grievances about situations that endanger the patient, such as neglect or abuse,
and concerns involving harm, potential harm or potential liability issues shall be referred immediately to Risk Management for direction.
4. The Guest Service Representative from affected area / department documents
the compliment / complaint in the Customer Compliment / Complaint Management System.
5. Resolution process may include collecting information from staff observations,
Risk Management, review of medical records, review of patient bills and policies / procedures relevant to the issues.
6. If a grievance is not complicated and does not require extensive review, Guest
Service Representatives will attempt to seek resolution within 7 business days. A grievance may be considered complicated when there is more than one issue or department involved, or the medical care is extensive or it is necessary to interview more than one staff member or director. If the grievance is not complicated, the Guest Services Representative will be responsible for ensuring that a response letter is sent to the patient within 7 business days.
7. If the grievance cannot be resolved within 7 business days, or if the review is not
completed, or if the corrective action is still being evaluated, the Guest Services Representative will send a letter to the patient or their representative indicating that the hospital is still working to resolve their concern and that there will be written follow-up as soon as the review is completed. Dependent upon the circumstances every effort will be made to complete the review in 30 days if possible.
Once this policy is printed, it is not considered a controlled document. Please review electronic version of this policy for the most current document.
Patient Complaint Grievance Service Recovery Page 5 of 6 8/12
a. If the grievance was referred to Risk Management for review, the Risk Manager will coordinate with the Guest Services Coordinator to provide direction in regards to length of time it will take to review and who will be responding to the patient in writing. If the Risk Manager determines that care and treatment was appropriate they will advise the Guest Services Representative who will provide the written response to the patient.
b. If the Risk Manager determines that it is not appropriate, the Risk Manager
will be responsible for responding to the patient. The Risk Manager may refer certain quality of care issues to departments such as Care Management, Utilization Review, Quality Management, and / or Infection Prevention for review as appropriate.
c. A written response will include the name of the Guest Service
Representative, Risk Manager or other contact person, the steps taken on behalf of the patient to investigate the grievance, the results of the grievance process and the date of completion.
8. Guest Service Representatives and / or department designee update the
Customer Compliment / Complaint Management System with outcome and resolution.
a. Complaints / grievances are analyzed by department(s) and Guest Service
Representatives and, when indicated, appropriate corrective action is taken to prevent reoccurrence.
C. When, in the judgment of the employee, doing more is necessary, the employee is
empowered to utilize service recovery measures to provide patient satisfaction. This may include purchasing material items or replacing lost or damaged patient property. The following list provides some guidelines and boundaries. If service recovery measures are utilized, the Service Recovery Action component of the Customer Compliment / Complaint Management System must be completed. This tracking mechanism enables LMHS to meet regulatory requirements. 1. Employees may spend up to $10 per occurrence with a maximum of $50 per year
for the same patient for service recovery. (Additional amounts require manager / supervisor approval).
2. Lost items may be replaced at the discretion of the Guest Service
Representatives, Vice Presidents of Patient Care Services, and Chief Administrative Officers at each acute care campus at a cost not to exceed the purchase price of the lost item.
3. “Courtesy Cash” may be redeemed for meals or gift shop purchases. They
should be offered to the patient / family / visitor as a way to perform service recovery.
D. Department manager may use Service Recovery Forms (FM #0063 - Order through
Forms Management / Print-As-Needed menu on Millennium / GEAC on IntraLee) to document cost of service recovery associated with addressing any compliment or concern. The form should be kept in a central location that is available to department
Once this policy is printed, it is not considered a controlled document. Please review electronic version of this policy for the most current document.
Patient Complaint Grievance Service Recovery Page 6 of 6 8/12
employees 24 hours a day, seven days a week. Copy of Service Recovery Form is to be sent to Customer Service for monthly review.
E. Any complaints or areas of dissatisfaction noted on returned surveys are followed up
using Step # B above if the person identifies themselves. F. Campus Administration receives service recovery report on a periodic basis.
G. Notice of whom to contact to file a grievance shall be given to patients in the Patient
Guide, Summary of the Florida Patient’s Bill of Rights and Responsibilities or the Patient Representative section of our external website.
H. As delegated by the Board of Directors the hospital will have a Grievance Committee
that will have oversight responsibility for the Grievance process. Committee members will include Administration, Department Directors (which includes clinical representation) Guest Services Representative, Risk Management, Quality and Human Resources Representatives.
Guest Services will provide the Committee with monthly trending reports for grievances
and will include actions taken to address the grievances and follow up. Committee members will determine if the trends need to be addressed through the performance improvement process and refer such trends to the appropriate Department/area for review, action and reporting back to the Committee.
RELATED POLICIES: S01 01 711 Patient Rights and Responsibilities S06 00 133 Corrective Action of Nonconformities S06 00 734 Preventative Action of Potential Nonconformities REFERENCES: Centers of Medicare / Medicaid Condition of Participation Guidelines- 42 CFR 482.13
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
30.04 formerly 10.14D: Medical Staff Representation for ADOPTON 032813 Page 1 of 1
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL no. 30.04 supersedes no. 10.14D
-------------------------------------------------------------------------------------------------------------------------------------
category: Medical Staff Relations General Operations
title: Medical Staff Representation -------------------------------------------------------------------------------------------------------------------------------
original adoption: 10.14: 1/08/91 30.04: 3/28/13 review date: 3/28/13
revision date: 3/27/92, 7/31/98, 7/26/02, 8/30/07, 3/28/13 -------------------------------------------------------------------------------------------------------------------------------
PURPOSE: To provide an effective mechanism for communication between members of the Board of Directors (Board) and representatives of the Medical Staff. -------------------------------------------------------------------------------------------------------------------------------
POLICY: A standing invitation shall be extended to the Medical Staff to attend meetings of the Board. The Presidents of each Medical Staff, Chairman of the Board or the Board by its action can request a special meeting of the Board with the Medical Staff leadership when appropriate. Physician input is welcomed and encouraged through Board meetings committees. The Board shall schedule regular meetings with the Medical Staff. The Board Chairman will may appoint members of the Board, to each any Medical Staff organization, as a liaison of the Board. The liaison member will communicate pertinent information from the organized Medical Staff to the Board and may assist the Medical Staff organization in interpreting and executing policies of the Board.
Once this policy is printed, it is not considered a controlled document. Please review the most current electronic version of this policy posted at www.leememorial.org/boardofdirectors.
40.05C-DRAFT-Staffing Reductions for ADOPTION 032813 Page 1 of 1
LEE MEMORIAL HEALTH SYSTEM BOARD OF DIRECTORS
POLICY MANUAL no. 40.05 C B supersedes no. 40.05A
------------------------------------------------------------------------------------------------------------------------------------
category: Employee Relations
title: Staffing Reductions ------------------------------------------------------------------------------------------------------------------------------------
original adoption: 7/25/97 review date: 3/28/13
revision date: 7/31/98, 7/26/02, 3/28/13 ------------------------------------------------------------------------------------------------------------------------------------
PURPOSE: To provide for procedure for staff reduction. ------------------------------------------------------------------------------------------------------------------------------------
BACKGROUND: To provide quality patient care, the Lee Memorial Health System (LMHS) must adequately staff its operating units with a qualified, motivated, trained and skilled workforce. Adequate staffing is influenced by economic conditions and by the need to operate in a competitive environment. Due to changes in economic conditions, natural or other disasters, fluctuations in patient census or volumes, restructuring, reorganization, reengineering of health care delivery services or other reasons, LMHS may need to reduce its workforce staffing at one or more of its operating entities, departments or facilities units, i.e., hospitals, outpatient businesses, physician offices and other related businesses.
POLICY: Prior to instituting significant workforce reductions, senior leadership layoffs, management will explore a variety of options as an alternative to a permanent reduction in force. These alternatives include, but are not in priority or limited to:
Reducing staff through attrition Rigorous review and control of hiring for new or replacement staff, including
hiring freezes Discontinuing use of temporary staff or contracted personnel Reducing or eliminating planned overtime Reassigning staff within the System
If other alternatives are unsuccessful or insufficient, After approval by the Board of Directors, the LMHS President has the authority to initiate a significant permanent and temporary reduction in workforce based on System Administrative Policies and Procedures with approval by the Board of Directors. Affected employees may be eligible for severance pay benefits separation and outplacement services consideration based on prevailing economic conditions at the time of a reduction in force to the extent determined by the LMHS President.
___________________
L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
OTHER ITEMS
A. Board Event Attendance (from 10/18/12 discussion)
B. Boardroom Modification (from 10/18/12 discussion)
C. Alzheimer’s Program (Steve Brown, M.D., Board Member)
ADJOURNMENT __________________
L E E M E M O R I A L HEALTH SYSTEM BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
DATE OF THE NEXT SCHEDULED
GOVERNANCE BOARD MEETING
GOVERNANCE FULL BOARD MEETING
Thursday, November 7 2013 at 1:00p.m.
Gulf Coast Medical Center- Boardroom
Medical Office Building 13685 Doctors Way Ft. Myers, FL 33912
GOVERNANCE BOARD LIAISON TO CHAIRMAN:
Lee Memorial Health System FULL BOARD OF
DIRECTORS MEETING Thursday, March 28, 2013
BOARD CHAIRMAN: Richard Akin
___________________
L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
OLD BUSINESS

___________________
L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
NEW BUSINESS
___________________
L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
BOARD OF
DIRECTORS’ REPORTS
___________________
L E E M E M O R I A L HEALTH SYSTEM
BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
BOARD ADMINISTRATOR
REPORT
(Cathy Stephens)
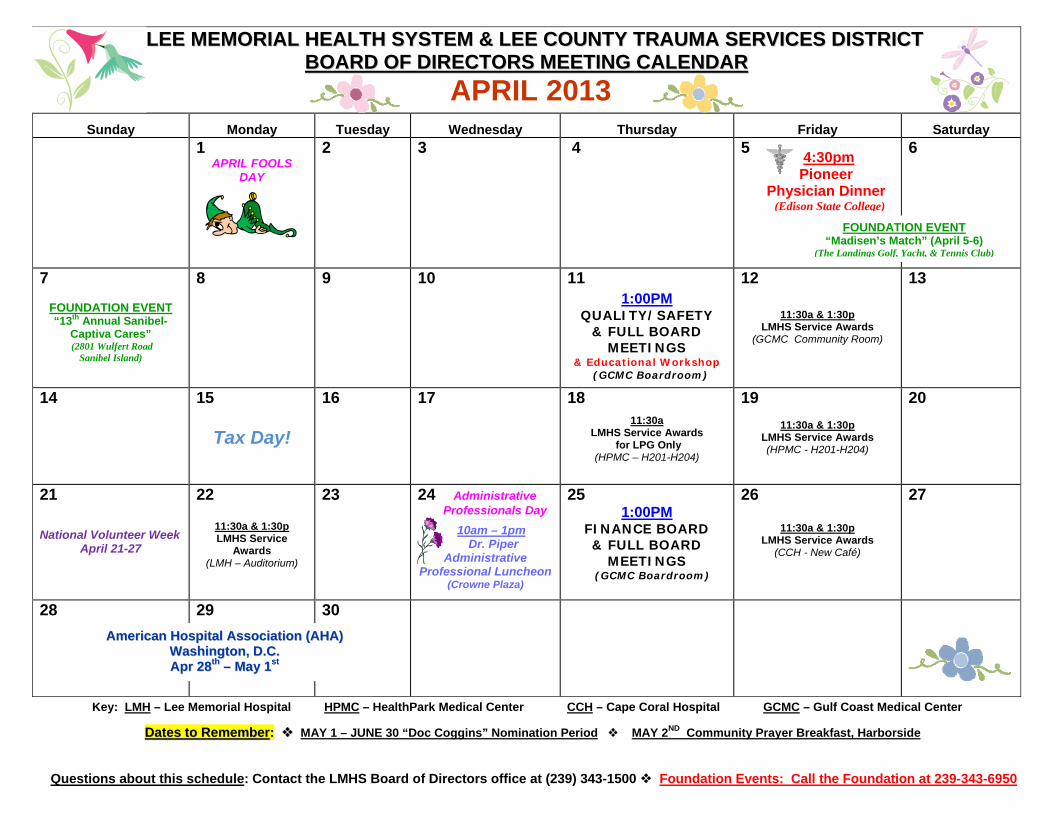
Questions about this schedule: Contact the LMHS Board of Directors office at (239) 343-1500 Foundation Events: Call the Foundation at 239-343-6950
LLEEEE MMEEMMOORRIIAALL HHEEAALLTTHH SSYYSSTTEEMM && LLEEEE CCOOUUNNTTYY TTRRAAUUMMAA SSEERRVVIICCEESS DDIISSTTRRIICCTT BBOOAARRDD OOFF DDIIRREECCTTOORRSS MMEEEETTIINNGG CCAALLEENNDDAARR
APRIL 2013
Sunday Monday Tuesday Wednesday Thursday Friday Saturday
1 APRIL FOOLS
DAY
2
3
4
5
6
7
FOUNDATION EVENT “13th Annual Sanibel-
Captiva Cares” (2801 Wulfert Road
Sanibel Island)
8
9 10
11
1:00PM QUALITY/SAFETY
& FULL BOARD MEETINGS
& Educational Workshop (GCMC Boardroom)
12
11:30a & 1:30p
LMHS Service Awards (GCMC Community Room)
13
14
15
Tax Day!
16
17
18
11:30a LMHS Service Awards
for LPG Only (HPMC – H201-H204)
19
11:30a & 1:30p LMHS Service Awards (HPMC - H201-H204)
20
21
National Volunteer Week April 21-27
22
11:30a & 1:30p LMHS Service
Awards (LMH – Auditorium)
23
24 Administrative Professionals Day
_______________________________
10am – 1pm Dr. Piper
Administrative Professional Luncheon (Crowne Plaza)
25 1:00PM
FINANCE BOARD & FULL BOARD
MEETINGS (GCMC Boardroom)
26
11:30a & 1:30p
LMHS Service Awards (CCH - New Café)
27
28 29
30
Key: LMH – Lee Memorial Hospital HPMC – HealthPark Medical Center CCH – Cape Coral Hospital GCMC – Gulf Coast Medical Center
DDaatteess ttoo RReemmeemmbbeerr:: MAY 1 – JUNE 30 “Doc Coggins” Nomination Period MAY 2ND Community Prayer Breakfast, Harborside
FOUNDATION EVENT“Madisen’s Match” (April 5-6)
(The Landings Golf, Yacht, & Tennis Club)
AAmmeerriiccaann HHoossppiittaall AAssssoocciiaattiioonn ((AAHHAA)) WWaasshhiinnggttoonn,, DD..CC.. AApprr 2288tthh –– MMaayy 11sstt
4:30pm Pioneer Physician Dinner (Edison State College)
ADJOURNMENT ___________________
L E E M E M O R I A L HEALTH SYSTEM BBBOOOAAARRRDDD OOOFFF DDDIIIRRREEECCCTTTOOORRRSSS
DATE OF THE NEXT REGULARLY SCHEDULED
MEETING:
Quality & Safety Board & Full Board of Directors
Meeting & Board Educational Workshop
Thursday, April 11, 2013
1:00pm
Gulf Coast Medical Center Boardroom 13685 Doctors Way, Ft. Myers, FL 33912





























