Embed Size (px)
Citation preview
The Role of Advice Servicesin Health OutcomesEvidence Review and Mapping Study
June 2015
The R
ole
of A
dvic
e S
ervic
es in
Health
Outc
om
es
Published by LAG Education and Service Trust Ltd© Legal Action Group 2015
All rights reserved. No part of this publication may be reproduced, stored in aretrieval system or transmitted in any form or by any means, without priorpermission from the publisher.
Legal Action GroupThe purpose of the Legal Action Group is to promote equal access to justice forall members of society who are socially, economically or otherwisedisadvantaged. To this end, it seeks to improve law and practice, theadministration of justice and legal services.
This report was commissioned from, researched and written byConsilium Research & Consultancy
Printed in the UK by Hobbs the Printers Ltd, Totton, Hampshire SO40 3WX
www.lowcommission.org.ukwww.asauk.org.uk
Ad
vice Services A
lliance and T
he Low
Co
mm
ission
HealthOutcomesReport_Cover 17/06/2015 11:37 Page 1

The Role of Advice Services in Health
Contents Acknowledgements ............................................................................................................................... 2
List of Tables, Figures and Diagrams ...................................................................................................... 3
Glossary of acronyms and terminology ................................................................................................. 4
Foreword by Sir Michael Marmot .......................................................................................................... 7
Executive summary ................................................................................................................................ 9
1 Introduction .................................................................................................................................. 13
2 Policy context ................................................................................................................................ 14
Tackling health inequalities .................................................................................................... 14
Welfare reform ....................................................................................................................... 17
Advice sector funding ............................................................................................................. 17
3 Methodology ................................................................................................................................. 22
Rapid Evidence Assessment .................................................................................................... 22
Mapping exercise .................................................................................................................... 27
4 Evidence review results ................................................................................................................. 28
Debt and mental health .......................................................................................................... 28
Primary care ............................................................................................................................ 33
Secondary or tertiary care ...................................................................................................... 44
5 Mapping of current work joining up health and advice services .................................................. 57
6 Evaluation and monitoring ......................................................................................................... 66
7 Gaps in the evidence base ........................................................................................................... 69
8 Conclusions ................................................................................................................................... 71
9 Bibliography .................................................................................................................................. 76
Appendix 1: Rapid Evidence Assessment approach ............................................................................ 85
Appendix 2: Conceptual framework .................................................................................................... 89
Appendix 3: Membership of the Advice and Health Steering Group .................................................. 94
Appendix 4 Advice and health services ............................................................................................... 95
This study was commissioned by the Advice Services Alliance in partnership with The Low Commission and its results analysed and written up by Andy Parkinson and Jamie Buttrick from Consilium Research & Consultancy. The Project was funded by the Legal Education Foundation through the Future Advice Funders Group.
2
The Role of Advice Services in Health
Acknowledgements
The Low Commission and the Advice Services Alliance wish to thank the following people for their contribution to this report:
Chair of the Advisory Group, Amanda Finlay CBE.
All members of the Advisory Group were drawn from various health and advice sector charities and backgrounds, see Appendix 3.
Research report by Andy Parkinson and Jamie Buttrick of Consilium.
Executive summary by Olivia Butler.
We would like to thank all the advice organisations across the country who so willingly and quickly responded to our request for information about their work. While we only hope to describe the world, advice practitioners are actually changing it. In particular we would like to thank the case study areas for allowing us to highlight their work.
We would particularly like to thank the funders who made this work possible; the Project was funded by the Legal Education Foundation through the Future Advice Funders Group.
The Low Commission is an independent Commission chaired by Lord Colin Low of Dalston on the future of advice and legal support in the social welfare issues (http://www.lowcommission.org.uk/).
The Advice Services Alliance is the umbrella group for the voluntary, free legal advice sector. Our membership includes Advice UK, Age UK, Citizens Advice, Law Centres Network, Scope, Shelter, Shelter Cymru and Youth Access (www.asauk.org.uk).
The report can be found online at: www. asauk.org.uk/policy/healthandadvice
Lindsey Poole, Director, Advice Services Alliance
James Sandbach, Research Manager Low Commission
3
The Role of Advice Services in Health
List of Tables, Figures and Diagrams
Table 3.1 – Research type 24
Table 3.2 – Type of Service 25
Table 3.3 – Wider social determinants 25
Table 3.4 – Setting 25
Diagram 2.1– Commissioning model 18
Diagram 2.2 – Potential links between advice interventions and health outcomes 21
Diagram 4.1 – The Biopsychosocial model of health 38
4
The Role of Advice Services in Health
Glossary of acronyms and terminology
Advice Services
ASTF
Services that diagnose the client’s social welfare/legal problems and any related legal matters; identify relevant legislation and decide how it applies to a client’s particular circumstances, including identifying the implications and consequences of such action and grounds for taking action; providing information on matters relevant to the problem, such as advising on next steps; and identifying dates by which action must be taken in order to secure a client’s rights.
The Big Lottery Fund set up the Advice Services Transition Fund to enable local not-‐for-‐profit providers of advice services in England to continue to give vital help to people and communities.
CAB Citizens Advice Bureau – referring to individual local bureaux.
CCGs Clinical commissioning groups are NHS organisations established under the Health and Social Care Act 2012 to organise delivery of NHS services in England.
CSJS
English and Welsh Civil and Social Justice Survey
DLA
Disability Living Allowance
GHQ-‐12 The General Health Questionnaire is a screening device for identifying minor psychiatric disorders in the general population and within community or non-‐psychiatric clinical settings such as primary care or general medical out-‐patients.
GP General Practitioner
HADS Hospital Anxiety and Depression Scale (HADS), Commonly used by doctors to determine the levels of anxiety and depression that a patient is experiencing.
HAQ Health Assessment Questionnaire
Health and Wellbeing Boards
The Health and Social Care Act 2012 established health and wellbeing boards as a forum where key leaders from the health and care system work together to improve the health and wellbeing of their local population and to reduce health inequalities.
5
The Role of Advice Services in Health
HealthWatch HealthWatch is a new independent consumer champion that gathers and represents the views of the public about health and social care services in England.
IAPT Improving Access to Psychological Therapies
JSNA
Joint Strategic Needs Assessment
LASPO Legal Aid, Sentencing and Punishment of Offenders Act 2012
NEET Not in Education, Employment or Training
NICE National Institute for Health and Care Excellence
Nottingham Health Profile
PHQ-‐9
The Nottingham Health Profile is a general patient reported outcome measure which seeks to measure subjective health status.
Patient Health Questionnaire that is used to monitor the severity of depression and response to treatment.
PIP Personal Independence Payments
Primary care Primary care is the day-‐to-‐day healthcare given by a healthcare provider. Typically this provider acts as the first contact and principal point of continuing care for patients within a healthcare system, and coordinates other specialist care that the patient may need.
QALYS Quality Adjusted Life Years
RCT Randomised Controlled Trial
REA Rapid Evidence Assessment
RCGP
RSL
Royal College of General Practitioners
Registered Social Landlord
Secondary care Secondary care refers to services provided by medical specialists who generally do not have the first contact with a patient, for instance a neurologist or a rehabilitation consultant.

6
The Role of Advice Services in Health
SF-‐ 36 health questionnaire
Short Form 36 is a multi-‐purpose health survey with only 36 questions. It yields an 8-‐scale profile of functional health and wellbeing scores as well as psychometrically-‐based physical and mental health summary measures and a preference-‐based health utility index. It is a generic measure, as opposed to one that targets a specific age, disease, or treatment group.
Social welfare law
Those categories of law which govern entitlement to state benefits and housing; the management of personal and business debt; an employee’s rights at work and access to redress for unfair treatment; and access to appropriate care and support for people with particular health problems.
Specialist debt advice
Advice linked to financial difficulties resulting from a range of reasons including financial shocks, low incomes, poor money management and creditor behaviour.
Specialist employment
advice
Advice covering individuals’ rights at work including leave, flexible working and problems at work and health and safety issues. Within the wider scope of employment advice, the phrase also includes support for those seeking employment or facing redundancy.
Specialist welfare benefits
advice Advice linked to the understanding, access and entitlement to welfare benefits.
Tertiary care Tertiary care is specialised consultative healthcare, usually for inpatients and on referral from a primary or secondary health professional in a facility that has personnel and facilities for advanced medical investigation and treatment.
WEMWEBS The Warwick–Edinburgh Mental Wellbeing Scale is a scale of 14 positively worded items, with five response categories, for assessing a client’s/patient´s mental wellbeing.

7
The Role of Advice Services in Health
Foreword by Sir Michael Marmot
When I started working with the World Health Organisation in setting up the Commission on Social Determinants of Health I posed the question, rhetorically: what good does it do to treat people and send them back to the conditions that made them sick? The ‘conditions that made them sick’, the social determinants of health, were the focus of my review of health inequalities in England, the Marmot Review. We need universal access to high quality medical care, of course, but we also need action at the social level – long term and strategic about the nature of society and how its benefits are shared equitably.
In the meantime there is a vitally important practical concern: how people obtain access to social services and benefits that are currently available. Some enlightened general practitioners have called it social prescribing. This report is a welcome contribution to the discussion about how we can tackle the underlying causes of ill health in the short to medium term It provides us with a wealth of research and a very useful mapping of current initiatives designed to help people to deal with the practical issues that underlie or are associated with so much ill health.
This report reminds us that the patients who are seen in clinical settings may well have problems in their everyday lives that may be causing or exacerbating their mental and physical ill health or may be getting in the way of their recovery. If we do not tackle these everyday “practical health” issues then we are fighting the clinical fight with one hand tied behind our back.
In my review we summarised the evidence on social inequalities in health, and what could be done, under six headings: early child development, education and life long learning, employment and working conditions, having sufficient income for a healthy life, quality and sustainable dwellings and neighbourhoods, and a social determinants approach to prevention. All of these impact on people’s physical and mental health. How many GPs hear people asking for help in sleeping at night when they are understandably lying awake worrying that they are about to lose their job, their home, and maybe their family. We know from Macmillan that cancer sufferers often say “It’s not the cancer that keeps me awake at night; it’s worrying how I will pay the bills”.
For many years enlightened providers of health services have recognised that if they want to improve the health of their patients they need to look after all of their needs: physical health, mental health and what one might term “practical health”-‐ the everyday background of people’s lives: the things that have a real impact on whether they have enough money to live on and not too many difficult things to worry about.
Clinicians cannot do this on their own and indeed it would be a waste of their medical skills and clinical expertise to expect them to master the intricacies of welfare benefits, housing and employment law. They need help from those who are expert in addressing the problems caused by low and unstable income and inadequate access to welfare benefits.
The people who can help with these problems are social welfare law advisors and for many years that help was funded by civil legal aid, by local authorities and by forward thinking health commissioners, either as part of a deliberate public health strategy or through more local arrangements based in GPs surgeries, in mental health settings and in cancer treatment centres.
8
The Role of Advice Services in Health
But massive reductions in local authority funding and drastic cuts in legal aid have decimated the advice provision that used to exist. The Low Commission Report published in January 2014 and the follow up Report in January 2015 set out the huge impact this has had on providing help to the most vulnerable.
This report provides us with a detailed overview of the research evidence available on these initiatives. Because of the cuts in funding some of this report looks back at initiatives that are no longer there. But it also looks at ongoing initiatives which are continuing and, most encouragingly, looks at new initiatives. It provides a mapping of existing services and a rapid assessment of the evidence on the difference that such initiatives have made.
It is clear that there have always been health professionals who could see the difference that the provision of social welfare advice made to their patients, in terms of income maximisation, less anxiety and more autonomy – an essential element of better health. It also makes a difference to the health professional, significantly reducing the estimated 15 % of their time that GPS spend on benefits issues, reducing prescription costs and – by reducing repeat appointments – freeing up time for more patients.
It is encouraging to know that new Clinical Commissioning Groups, such as the Wirral (p60), and Liverpool (p64) are commissioning advice services and that local authorities such as Bradford (p62) are using a combination of Adult Social Care and Public Health funding to commission advice services. What is disappointing is that even when these services are commissioned it is still difficult to persuade those health professionals who do not “get it” that it is worth thinking about how to provide this holistic health care – physical , mental and practical, and to work in partnership with those who are expert in providing these services.
This report helps to tackle that by providing a wealth of examples of where this has worked and the benefits it has delivered, some of it in statistically sound data, much of it in qualitative assessments and some in truly inspiring stories.
The report is frank about the difficulties in evaluating the impact of advice services on health outcomes and the need to develop appropriate measurement systems that capture the benefit provided to the individual who receives the help and to the clinical setting in which they are being looked after.
It is a real contribution to how we need to broaden our thinking in the future if we are really to put patients and their whole experience and needs at the heart of everything we do.
Michael Marmot
Director UCL Institute of Health Equity

9
The Role of Advice Services in Health
Executive summary
This report shows how the right welfare advice in the right place produces real benefits for patient health, especially where advice services work directly with the NHS and care providers. It presents clear evidence that early and effective welfare advice provision reduces demand on the NHS.
The report is an evidence review undertaken through a joint project between the Low Commission and the Advice Services Alliance. It outlines key findings from 140 research studies in the field, and gives an overview of 58 integrated health and welfare advice services. A clear message comes from these wide-‐ranging sources that welfare advice provided in health care settings results in better individual health and well-‐being and lower demand for health services. The report compiles the mounting evidence of both the adverse health impact of social welfare law problems and the beneficial health impact of receiving good welfare advice. It makes recommendations to relevant health and advice bodies.
Key findings
The provision of good welfare advice leads to a variety of positive health outcomes and in addition addresses health inequalities highlighted in the Marmot Review 2010. The effects of welfare advice on patient health are significant and include: lower stress and anxiety, better sleeping patterns, more effective use of medication, smoking cessation, and improved diet and physical activity. These findings are important in the context of addressing the wider social determinants of health and suggest that stronger collaborative working across a range of sectors is required. In particular, there is demonstrable evidence that when advice and health sectors work more closely and strategically to meet advice needs this contributes to reducing health inequalities. Direct commissioning of welfare advice services within specific health settings is most effective as it targets the most vulnerable within settings which they trust and where their specific health needs are understood.
Primary care
Welfare advice provision in primary health settings can reduce by an estimated 15% the time GPs spend on benefits issues, and leads to fewer repeat appointments and fewer prescriptions. Health commissioners in some parts of the country have acted on this intelligence. People who receive welfare advice experience lower anxiety, better general health, better relationships and housing stability. The right advice at the right time helps people manage their own lives, and promotes better physical and mental health. See the following case studies.

10
The Role of Advice Services in Health
• Liverpool CCG has commissioned Liverpool CAB to deliver an Advice on Prescription service through 95 GP practices over three years.
• Croydon Family Navigators advises families with health and care needs on how to improve their resilience to problems and to cope better. It is based in GP surgeries and is provided by Croydon Voluntary Action.
• Transition Project South Tyneside – Age UK South Tyneside: This pilot is being delivered in three GP surgeries in South Tyneside with plans to extend into a further 18 (75% of surgeries in the borough). It provides referrals to advisors from one of three agencies able to offer advice on a wide range of issues including debt, benefits, housing and fuel poverty.
• Wirral CCG has invested in primary care so that all GP practices now have Citizens Advice services, including the Primary Care Advice Liaison service, which gives welfare advice to patients with mental health and long-‐term conditions. Outcomes include: patients report lower anxiety and depression, fewer referrals to specialist services and fewer repeat GP appointments.
Mental heath
Mental ill health is the largest single cause of disability in the UK and there is a significant correlation between debt and mental health. Debt advice can prevent people facing debt from requiring mental health treatment and can improve health outcomes for existing patients. This has been recognised by, for example, health and social care commissioners in Sheffield.
Welfare advice to people using secondary mental health services can reduce in-‐patient stays, prevent homelessness and reduce the chances of relapse. See the following case studies.
• Advice Sheffield is a specialist CAB, supporting adults with mental health difficulties to get the benefits and services they are entitled to. They prioritise people in hospital and people with enduring mental health problems in the community, and are funded by Sheffield City Council, NHS Sheffield CCG and Sheffield Health and Social Care NHS Foundation Trust.
• Heathlands CAB – Rushmoor Citizens Advice Bureau project: delivered in partnership with Surrey and Borders Partnership Trust, includes sessions on the acute psychiatric ward, with Community Mental Health Recovery Services and the Home Treatment Team. This project provides services to clients with severe and enduring mental health issues and to their carers.
Secondary and tertiary care
The provision of welfare advice in secondary and tertiary care settings can both release hospital staff from dealing with patients’ welfare needs and facilitate the planning of hospital discharges. For example

11
The Role of Advice Services in Health
• Camden CAB runs a welfare advice service in Great Ormond Street Hospital for parents and carers, which addresses the unmet needs of sick and disabled children arising from poverty. Outcomes include: family debts written off, reduced stress levels and improved wellbeing, increased numbers of hospital discharges and savings on hospital staff time.
• Clatterbridge Cancer Centre has run a Macmillan Benefits Advice Service for the past 13 years. The service is part of the hospital’s cancer rehabilitation and Support Team (CReST) and provides cancer specific welfare benefits and debt advice to people receiving curative or palliative treatment and care, freeing up staff to spend more time on clinical work.
Improved commissioning
The provision of welfare advice is vital to the health and wellbeing of many service users and there are already a number of innovative and successful health and welfare advice partnerships. Assisted by the Health and Social Care Act 2012 and the Care Act 2014, a number of integrated advice projects have progressed from short-‐term grants to mainstream funding. However some advice providers struggle to meet tight commissioning criteria, suggesting that more needs to be done to support the sector in developing business cases which include the health benefits to advice recipients and the benefits to the health service. In particular, there is a need to develop in partnership with health providers a range of agreed outcome and evaluation measures. This report signposts ways for the NHS, local authorities and the advice sector to commission, evaluate and deliver effective welfare advice in ways that will improve health outcomes, address health inequalities and reduce demand on the NHS.
Conclusions
The pressures on the NHS are increasing, with demand growing rapidly as the population ages, and long-‐term conditions as well as widening health inequalities becoming more common. Welfare advice interventions can deliver a range of health-‐related benefits, such as lower anxiety, better general health and more stable relationships and housing. These are all in addition to people having debt written off, not losing their home and greater annual income – the primary outcomes of advice. Further research would help to address the gaps in the evidence outlined in this report. In particular it would be helpful to have outcome measures and evaluation tools agreed jointly by health services and advice services. These would provide ongoing evidence of the cost and efficiency savings that can be delivered through advice services working in health settings. This evidence would be useful when arguing the case to include advice in health and wellbeing strategies and delivery plans.
Recommendations
This report on the role of welfare Advice Services in health encourages NHS Trusts, Clinical Commissioning Groups, Adult Social Care commissioners, and Health and Wellbeing Boards to use welfare advice services to improve health outcomes, address health inequalities and reduce demand on the NHS, with the following specific recommendations:

12
The Role of Advice Services in Health
For NHS and Local Authority Commissioners, and Health and Wellbeing Boards:
• Health and Social Care Commissioners should include provision for social welfare advice and legal support in their strategic plans in order to address the social determinants of ill-‐health.
• NHS and LA Commissioners should commission social welfare law advice in health-‐specific contexts in order to meet the needs of the most vulnerable, in places they ordinarily go to already, and where their needs are understood.
• NHS and LA Commissioners should include a measurement of health and wellbeing outcomes in the commissioning of any advice service provision
For the Advice Sector:
• Advice Services Alliance and the Low Commission should raise awareness at strategic level in the NHS, local government and the advice sector, including hosting a conference demonstrating the impact of social welfare law provision on health outcomes both in existing initiatives and in the research findings.
• Advice Services Alliance should build capacity in the advice sector, showcasing best practice and identifying key factors in successful partnership working.
• Advice umbrella organisations and others working with Advice Services Alliance should produce and distribute the guidance of welfare advice providers on how to measure the impact of services on clients' health and wellbeing.
• Advice Services Alliance should produce guidance for advice providers on working with Health and Wellbeing Boards, to facilitate advice sector engagement with local strategic plans, and membership of local boards.
13
The Role of Advice Services in Health
1 Introduction
1.1 Consilium Research and Consultancy (Consilium) was commissioned by the Advice Services Alliance (ASA) and The Low Commission in December 2014 to deliver a research project on the role of advice services in health. The main objectives of the research project were to build upon the work which has already been conducted in this area and inform the next steps for the advice sector in engaging and working with health services. Specifically the research aimed to contribute to the following longer-‐term goals:
• to improve access to advice for people who are vulnerable and/or who have health related problems;
• to identify and strengthen the position of advice services in relation to the delivery of health outcomes;
• to identify a range of possible approaches and service models for delivery of advice within a health context, with possible options for piloting or further promotion;
• to develop a strategic advice sector-‐wide approach to promoting the role of advice in partnership within health; and
• to diversify the funding base of advice services through identifying relevant health funding and engaging with NHS and social care commissioners.
1.2 There is mounting evidence of both the adverse health impact of social welfare legal problems and the beneficial health impact of receiving good advice. Many people presenting to health services are key target client groups for advice services and yet given the nature of their problems, it is clear from the evidence base that they have not accessed any advice services. There are many advice and legal support services across the country who have recognised this issue and who are currently working in partnership with health services and/or operating in health settings, such as in GP surgeries and hospitals.
1.3 This narrative report provides a summary of the evidence collated on health outcomes and advice, presenting an overall picture of the effectiveness of advice work in health settings for clients/patients. It also presents the results of a mapping exercise that aimed to identifying current or recent advice work in health settings.
1.4 This report is structured into the following six sections:
Policy context
Methodology
Evidence review results
Mapping of current work joining up health and advice services
Evaluation and Monitoring
Gaps in the evidence base.
14
The Role of Advice Services in Health
2 Policy context
Tackling health inequalities
2.1 There has been a long history of interest in and efforts to tackle health inequalities in society. In 1997, the Independent Inquiry into Inequalities in Health led by Sir Donald Acheson (the ‘Acheson Inquiry’) was commissioned to review the latest information on inequalities in health and to identify priority areas for future policy development to reduce health inequalities. The report also provided the context for the public health strategy in England: Saving lives: Our healthier nation.1
2.2 Resulting policies primarily focused on areas (mainly geographical zones) and on individual employment (through welfare-‐to-‐work strategies) and involved some income redistribution (through tax and benefit reform). Most of the recommendations in the Acheson Inquiry report sought to tackle the wider determinants of ill-‐health across the entire lifespan of the population. A research report published by the Joseph Rowntree Foundation (JRF) in 20032 highlighted that measuring progress of policies tackling health inequalities was difficult for a number of reasons because: the link between policy and health outcomes is uncertain; it is difficult to attribute observed impacts to a particular policy; the most suitable or effective balance of measures across and within policy programmes is unknown; and unintended consequences of policies (such as widening health inequalities) may yet appear. They suggested that better measures of progress were required and that these should: It suggested that better measures of progress were required and that these should:
• incorporate the wider determinants of health; • support a joined-‐up approach across government; • not simply be disease-‐oriented; • not be dominated by healthcare or the NHS; • combine long-‐term/outcome and shorter-‐term/process measures; and • leave scope for local priorities within national policies.
2.3 In 2008 one of the authors of the JRF report, Professor Sir Michael Marmot, was asked by the Secretary of State for Health to chair an independent review to propose the most effective evidence-‐based strategies for reducing health inequalities in England from 2010. The review report (Marmot 2010) places great emphasis on reducing health inequalities as a matter of fairness and social justice, recognising that people experiencing differences in health, wellbeing and longevity merely because of their differing social circumstances is, quite simply, unfair. Taking action to reduce inequalities in health, Marmot argues, does not require a separate health agenda but rather action across the whole of society.
1 https://www.gov.uk/government/publications/saving-‐lives-‐our-‐healthier-‐nation 2 Exworthy, M. Stuart, M. Blane, D. & M. Marmot (2003) -‐ ‘Tackling Health Inequalities since the Acheson Inquiry’. Joseph Rowntree Foundation. March 2003.

15
The Role of Advice Services in Health
2.4 The report argues that social inequalities in health arise because of inequalities in the conditions of daily life and the fundamental drivers that give rise to them: inequities in power, money and resources.3 These social and economic inequalities underpin the determinants of health and the range of interacting factors that shape health and wellbeing. These include: material circumstances, the social environment, psychosocial factors, behaviours and biological factors. In turn, these factors are influenced by social position, itself shaped by education, occupation, income, gender, ethnicity and race. All these influences are affected by the socio-‐political and cultural and social contexts in which they sit.
2.5 One of the priority objectives included in Marmot’s 2010 report relates to prioritising prevention and early detection of those conditions most strongly related to health inequalities. Key risk factors outlined in the report include:
Employment
• Insecure and poor quality employment is associated with an increased deterioration in physical and/or mental health;
• the relationship between employment and health is close, enduring and multi-‐dimensional; and
• unemployment has short-‐term and long-‐term effects on health.
Fuel Poverty
• Cold housing is a health risk. Being able to afford to keep a warm home is clearly a key factor; and
• fuel poverty rates fluctuate with the price of fuel.
Income
• The relationship between low income and poor health is well established;
• particular social groups are at greater risk of having a low income;
• increase in income leads to an increase in psychological wellbeing and a decrease in anxiety and depression; and
• The more debts people have, the more likely they are to have a mental disorder; and
• The welfare system is difficult to access for several disadvantaged groups and take-‐up can be low, for reasons including lack of information and awareness of the system.
Housing
• Poor housing conditions – including homelessness, temporary accommodation, overcrowding, insecurity, and housing in poor condition – constitute a risk to health;
3 Commission on Social Determinants of Health (2008) CSDH Final Report: Closing the gap in a generation: Health equity through action on the social determinants of health. Geneva: World Health Organization.

16
The Role of Advice Services in Health
• reduced supply has led to a ‘residualisation’ effect in the make-‐up of social housing tenants, with higher rates of unemployment, ill health and disability than the rest of the population; and
• children living in bad housing conditions are more likely to have mental health problems, suffer long-‐term ill health and disability, experience slow physical growth and delayed cognitive development.
2.6 It is evident from both the Acheson Report and Marmot Review that successful and sustainable approaches to reducing health inequalities are dependent upon action and support from outside the NHS. Addressing the wider social determinants of health requires stronger collaborative working across a range of sectors.
2.7 Pressures on the NHS are increasing with demand growing rapidly as the population ages, long-‐term conditions are becoming more common and more sophisticated and expensive treatment options are becoming available. The cost of medicines is growing by over £600m per year. In response to this challenge the Health and Social Care Act 20124 places clinicians at the centre of commissioning, aims to free up providers to innovate, while also empowering patients and giving a new focus to public health. For the first time the Act placed a duty on the Secretary of State, NHS England and clinical commissioning groups to give due regard to the reduction of inequalities.
2.8 Since April 2013 all upper tier local authorities have taken over responsibility for improving the health of their local population as part of the implementation of the Health and Social Care Act. They now have a key role in working in partnership with Clinical Commissioning Groups (CCGs), and others, through health and wellbeing boards in their localities. Health and wellbeing boards have been established by local authorities in partnership with NHS clinical commissioning groups and others with responsibilities for preparing comprehensive joint strategic needs assessments (JSNA) and joint health and wellbeing strategies. They also have a role in commissioning plans to take those assessments and strategies properly into account.
2.9 Under the Care Act 2014 local authorities have also taken on new duties and responsibilities to improve people’s independence and wellbeing by providing or arranging services that prevent people developing needs for care and support or prevent their deterioration such that they would need ongoing care and support. Early intervention, prevention and effective commissioning to meet identified local needs are common themes across both the Health and Social Care Act 2012 and the Care Act 2014. The latter also requires local authorities to develop and implement a plan regarding their information and advice services that is integrated into local joint health and wellbeing strategies.
2.10 This stronger focus on prevention, early intervention and coordinated planning around information and advice services should provide new opportunities for health and advice sectors to work more closely to tackle health inequalities and improve health and care outcomes. This may involve exploring solutions for improving the health and wellbeing of
4 http://www.legislation.gov.uk/ukpga/2012/7/contents/enacted
17
The Role of Advice Services in Health
people from marginalised and disadvantaged groups that place greater emphasis on preventative interventions such as social prescribing.
2.11 Social prescribing is about linking people up to non-‐medical sources of support and activities in the community that they might benefit from. There is increasing evidence to support the use of social interventions for people experiencing a range of common mental health problems and it has been shown to be particularly applicable for vulnerable and at-‐risk groups, people with mild to moderate depression and anxiety and people who are frequent attendees in primary care.5
Welfare reform
2.12 The Welfare Reform Act 2012 introduced a wide range of reforms to make the benefits and tax credit system fairer and simpler by creating the right incentives to get more people into work, thus protecting the most vulnerable in our society and delivering fairness to those claiming benefits and to the taxpayer. The government’s welfare changes have been taking place progressively since 2011 starting with the reassessment of incapacity benefit and transfer to Employment and Support Allowance (ESA), followed by transition from Disability Living Allowance (DLA) to Personal Independent Payments (PIPs) and a review of housing benefits. In addition, Universal Credit was scheduled to be introduced from October 2013, adding to the cumulative impact of the preceding welfare benefit changes. In the same period, legal aid for welfare benefit cases going to appeal has been squeezed significantly.
2.13 As outlined in The Low Commission’s (2014) report, with significant and often more restrictive changes to entitlement criteria, the importance of ‘right first time’ in decision making and advice and information to claimants could not be more important. An online survey of Welfare Rights Advisers conducted by The Low Commission between October and December 2014 pointed to a greater need for independent advice to support the best ‘getting it right’ outcomes for claimants. The absence of sufficient capacity and expertise within the independent advice sector raises concerns around the consequences of ‘getting it wrong’ outcomes for claimants, in particular with regards to worsening the conditions most strongly related to health inequalities.
Advice sector funding
2.14 Advice services face a double squeeze. The recession has led to an increase in demand for services with more people being made redundant, more people falling into debt and more people at risk of losing their home. At the same time sources of funding for advice are changing in structure or drying up completely. Whilst advice agencies contribute to a range of outcomes for local and national government they are not a statutory service. This leaves them particularly vulnerable to cuts. An unpublished online survey of Advice UK members in 2010 revealed that 41% had already experienced cuts, 58% were anticipating cuts to their
5 Nesta (2013) ‘More than medicine: New services for people powered health’.
18
The Role of Advice Services in Health
funding in 2011–2012 and 71% were the subject of either voluntary sector or advice service funding reviews.6
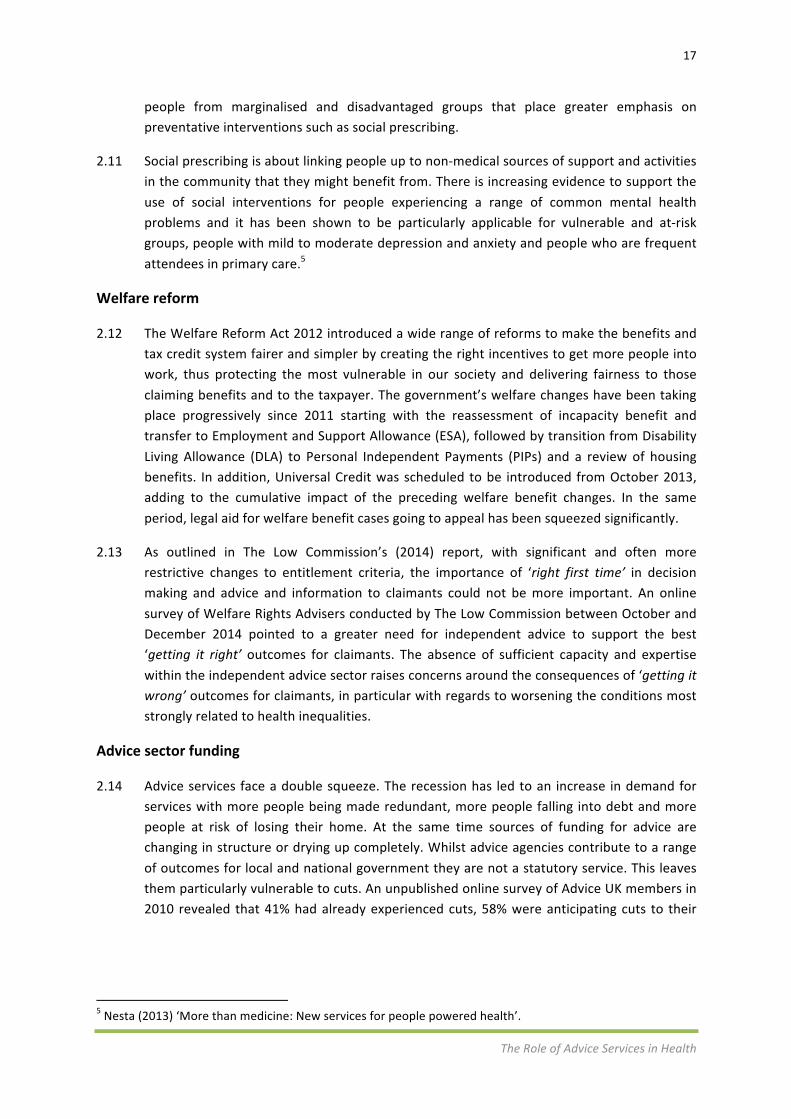
2.15 Recent years have seen a move from local authority grant funding of voluntary organisations towards greater service commissioning. Often this has been reduced to the introduction of competitive procurement, rather than the application of the full commissioning cycle that involves voluntary sector providers in strategic planning, service design and performance review (see Figure 1).
Figure 2.1– Commissioning model7
2.16 Funding for advice services is increasingly under pressure as it is considered a ‘preventative service’ with fewer tangible outcomes than others. Furthermore, provision is discretionary for local councils. This challenge of measuring and demonstrating impact in this area hits both providers (in proving their own case), and funders and councils (who must prioritise the use of the available funds considering where it will be put to most effective use).8
2.17 More specifically for advice services, reforms to Legal Aid funding have been underpinned by market principles. This has brought about changes in the landscape of provision, with some community services disappearing and new entrants to the market. It has also led to a shift in focus towards a target-‐driven, price-‐based, transactional approach, which has affected the purpose and delivery of advice. The Legal Aid, Sentencing and Punishment of Offenders (LASPO) Act 2012 has resulted in a reduction of £89m pa in legal aid on social welfare law, as well as reductions in local authority funding of advice and legal support, estimated to be at
6 Johnson, S. & S. Steed (2011) ‘Advice Services: What Next? Reflections from the BOLD project’. A joint publication from Advice UK and the new economics foundation. 7 Taken from the NHS Information Centre for health and social care; www.ic.nhs.uk/commissioning 8 http://www.sibgroup.org.uk/category/blog/changes-‐to-‐funding-‐of-‐the-‐advice-‐sector/

19
The Role of Advice Services in Health
least £40 million pa by 2015.9 These cutbacks have destabilised and reduced the advice and legal support sector at a time of increased need. As a result, instead of saving money, the cutbacks may end up costing more elsewhere in the system.
2.18 What is clear is that the current approach to the funding of advice is unsustainable, with many advice services being cut in the face of unprecedented demand. Reducing financial support places pressure on services, reduces the number of advice agencies and their capacity to proactively respond to people's issues over the longer term. The Low Commission Report (2014) outlines some key principles underpinning a fresh approach to tackling this advice deficit:
• early intervention and action rather than allowing problems to escalate;
• investment in prevention to avoid wasted costs generated by the failure of public services;
• simplifying the legal system;
• developing different service offerings to meet different types of need;
• investing in a basic level of provision of information and advice; and
• embedding advice in settings where people regularly go, such as GP surgeries and community centres.
2.19 Providing a greater focus on early intervention and prevention is wholly consistent with the recommendations made in The Marmot Review. It also reinforces the message that successful approaches to tackling health inequalities are not solely disease-‐orientated, but should also look to address the wider social determinants of health. In this regard the advice and legal support sector offers considerable expertise, experience and potential.
2.20 The Advice Service Transition Fund (ASTF), set up by the Big Lottery Fund in October 2012, has provided an investment of around £68 million to help the not-‐for-‐profit advice sector to adapt to a new funding environment. Funding has been provided to 228 ASTF partnerships to support the development of new service models, reduce service duplication, more effectively measure the difference advice services make to people’s lives and bring providers together to be more efficient and effective. Many of these partnerships have actively engaged the health sector to explore how new models of collaboration can both address the advice needs of clients/patients whilst also delivering measurable health and wellbeing outcomes.
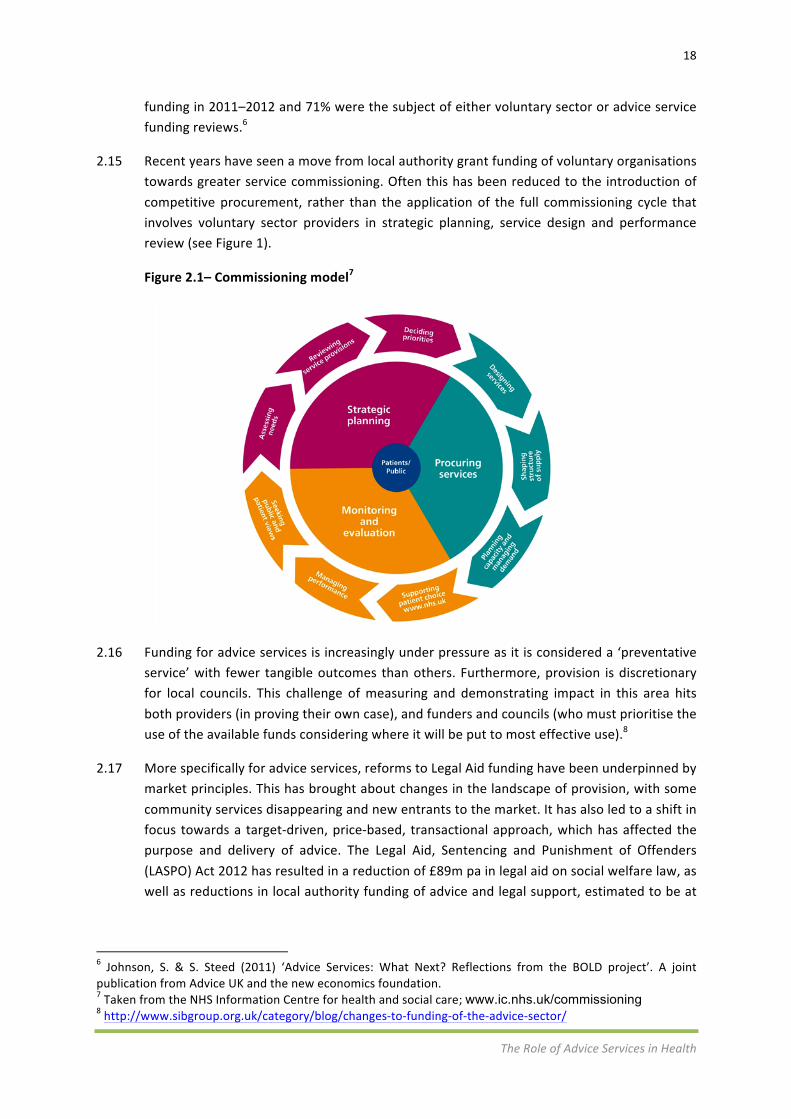
2.21 Although the advice sector has a long track record of contributing to the achievement of better health outcomes, the evidence base in relation to clear health gains is characterised by gaps and variable research quality. Allmark et al. (2013) have established a helpful logic model which outlines the potential links between advice interventions and health outcomes and demonstrates the varying levels of evidence based on an analysis of 87 research documents (see Figure 2.2). They acknowledge that previous systematic reviews have been unable to demonstrate evidence of clear health gain and suggest that one explanation may
9 The Low Commission (2014) ‘Tackling the Advice Deficit: A strategy for access to advice and legal support on social welfare law in England and Wales’. January 2014.

20
The Role of Advice Services in Health
be that the research thus far has been of limited quality. However the logic model serves to illuminate the complexity of elements at all phases of a causal pathway from advice interventions to long-‐term impacts on health and wellbeing.
Summary
• Prioritising prevention and early detection of those conditions most strongly related to health inequalities was one of the priority objectives included in The Marmot Review.
• Successful and sustainable approaches to reducing health inequalities needs action and support from outwith the NHS. Addressing the wider social determinants of health requires stronger collaborative working across a range of sectors.
• The Health and Social Care Act 2012 for the first time places a duty on the Secretary of State, NHS England and CCGs to give due regard to the reduction of inequalities.
• This stronger focus on prevention, early intervention and coordinated planning around information and advice services should provide new opportunities for health and advice sectors to work more closely to tackle health inequalities and improve health and care outcomes.
• The current approach to the funding of advice is unsustainable with many advice services being cut in the face of unprecedented demand. Reducing financial support places pressure on services, reduces the number of advice agencies and their capacity to proactively respond to people’s issues over the longer term.
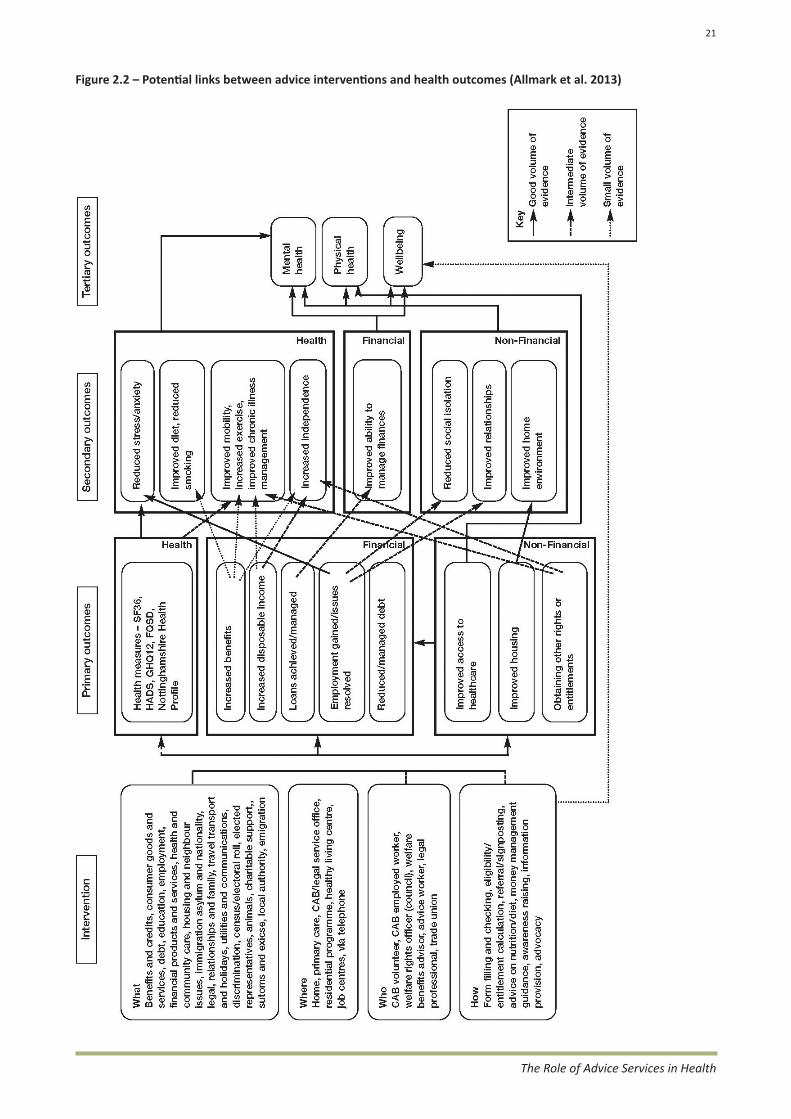
Figure 2.2 – Potential links between advice interventions and health outcomes (Allmark et al. 2013)
21
The Role of Advice Services in Health

22
The Role of Advice Services in Health
3 Methodology
3.1 This research project has incorporated two key elements: first, the completion of a Rapid Evidence Assessment (REA) focused on collating the existing evidence base on health outcomes and advice; and second, a mapping exercise aimed at identifying current or recent advice work in health settings and mapping this against the various health settings.
Rapid Evidence Assessment
3.2 The approach to completing this evidence review has followed established good practice (see Appendix 1) including the formulation of review questions and the development of a conceptual framework (Appendix 2). Inclusion and exclusion criteria were agreed with ASA and The Low Commission. The evidence review was implemented between 5 December 2014 and 28 February 2015.
Search strategy
3.3 The search strategy incorporated a number of approaches to identify research that would assist in answering the key review questions. Searches were undertaken of a range of web-‐based knowledge management systems including the British Library Public Catalogue, Google Scholar, The Cochrane Library, Joseph Rowntree Foundation, Wiley Online Library, Ingenta Connect, Third Sector Knowledge Portal, Online Information Review, The King’s Fund and Taylor & Francis Online.
3.4 The research team was kindly assisted by a number of membership-‐based organisations who cascaded information about the research to their respective networks. This has been particularly valuable in identifying grey literature that is difficult to trace via conventional routes such as published journals, either because it has not been published commercially or is not widely accessible.
3.5 Generating a ‘call for evidence’ across a range of organisations has enabled the evidence review to draw on original and recently published reports. The ‘call for evidence’ was cascaded through members of the Advice and Health Steering Group (see Appendix 3 for membership) and also through a wider network of organisations such as the National Association of Welfare Rights Advisors (NAWRA), the Royal College of General Practitioners (RCGP) and the Association of Directors of Public Health (ADPH).
3.6 Finally, as part of the review and screening process, the research team sourced relevant publications referenced in studies collated as part of the evidence review. All studies identified in the evidence review process have been referenced within a bespoke database to provide a resource that can underpin future research and development.

23
The Role of Advice Services in Health
Screening
3.7 Each document was screened and compared against the final agreed inclusion and exclusion criteria. The initial inclusion and exclusion criteria were modified following discussion with members of the Advice and Health Steering Group to include new research from Australia and the USA.
Inclusion criteria
• studies in England, Wales, Scotland, Northern Ireland, Australia and the United States of America
• studies that focus on the delivery of information, advice and guidance in health settings
• studies that can evidence clearly defined outcomes for healthcare users
• studies that provide evidence of the effectiveness of information, advice and guidance in addressing wider social determinants of health
• formal research (i.e. subject to a clear research process)
• informal published material (i.e. grey literature) with reference to the ‘impact’ of advice within health settings
• studies that report on the delivery of advice in the following areas (as defined above):
• generalist advice services • social welfare law information services • social welfare law advice services • specialist debt advice • specialist welfare benefits advice • specialist housing advice • specialist employment advice • specialist consumer advice • specialist discrimination advice
• guidance and policy related to health which includes access to advice as an integral part.
Exclusion criteria
• studies based outside of the UK with the exception of Australia and the USA
• studies that report on practice that doesn’t have a clearly stated purpose or include clearly defined outcomes
• soft evidence (i.e. primary commentary, anecdotal evidence or interview data)
• studies that report solely on evidence of satisfaction derived from the delivery of information, advice and guidance as opposed to the achievement of clear outcomes
• studies that relate to advice provided in non-‐health settings
• studies published before 1990
24
The Role of Advice Services in Health
• studies not published in English.
Quality assessment
3.8 Given the timescales and limited resources available for the REA the study team screened studies in line with inclusion and exclusion criteria on an ongoing basis, establishing a draft REA database comprising 141 studies. Following this initial screening process the research team reviewed the quality of the studies again and assessed their potential to answer the key research questions. The screening process had to overcome challenges in categorising studies by the type of advice service, health setting and patient/client group and resulted in one study being omitted from the final analysis of 140 documents.
3.9 Many of the studies present evidence of practice in the form of individual case studies. These vary in the strength of their evidence base with a number offering greater value as advocacy or awareness-‐raising publications, rather than robust evidence and insight regarding the health and wellbeing outcomes delivered through targeted advice services in health settings. However, these publications do still retain value in building a picture of the extent of current and recent advice work in health settings. Where the research team considers publications to have value, but to be methodologically weak, this has been denoted with appropriate caveats.
3.10 A breakdown of the research evidence reviewed across a range of variables is provided below:
3.11 Of the 140 studies included, 42 (30%) were based on primary research, 47 (34%) on secondary research and 51 (36%) on a combination of primary and secondary research (Table 3.1).
Table 3.1 – Research type
Number % Mixed 51 36.4 Secondary 47 33.6 Primary 42 30.0 Total 140 100.0
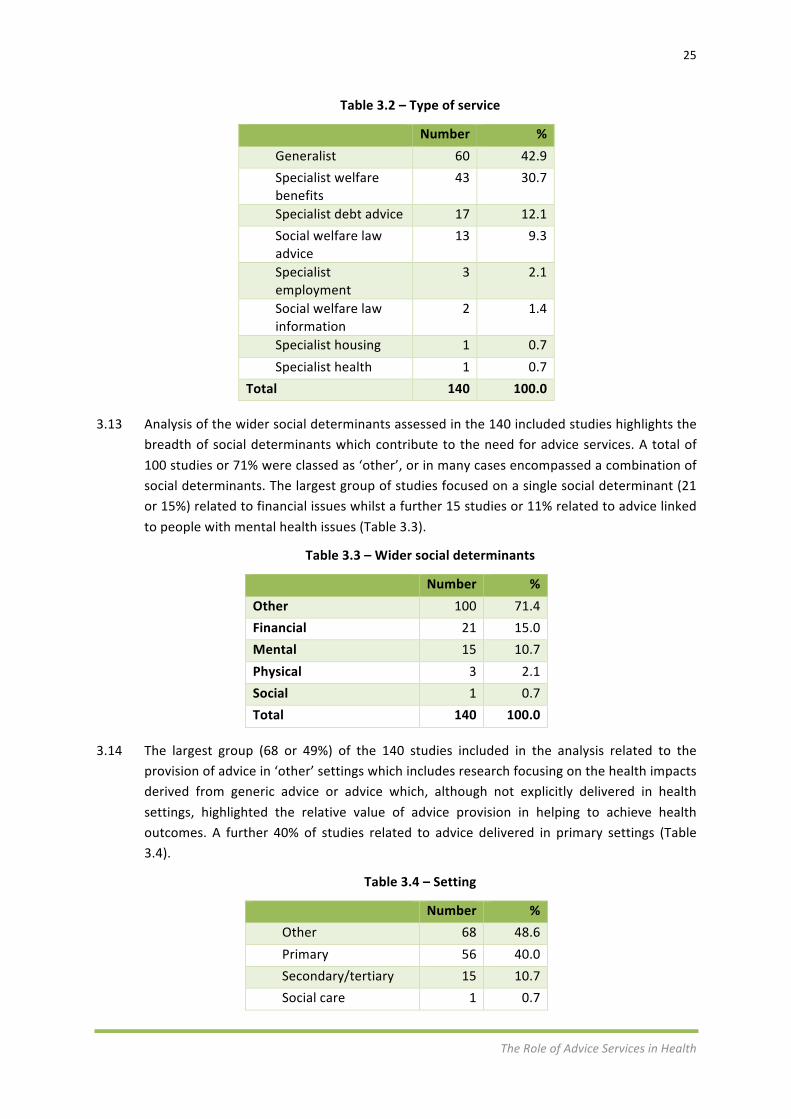
3.12 The largest group (60 or 43%) of the 140 studies included in the analysis related to the provision of generalist advice, whilst 31% of studies related to specialist welfare benefits (Table 3.2).
25
The Role of Advice Services in Health
Table 3.2 – Type of service
Number % Generalist 60 42.9 Specialist welfare benefits
43 30.7
Specialist debt advice 17 12.1 Social welfare law advice
13 9.3
Specialist employment
3 2.1
Social welfare law information
2 1.4
Specialist housing 1 0.7 Specialist health 1 0.7
Total 140 100.0
3.13 Analysis of the wider social determinants assessed in the 140 included studies highlights the breadth of social determinants which contribute to the need for advice services. A total of 100 studies or 71% were classed as ‘other’, or in many cases encompassed a combination of social determinants. The largest group of studies focused on a single social determinant (21 or 15%) related to financial issues whilst a further 15 studies or 11% related to advice linked to people with mental health issues (Table 3.3).
Table 3.3 – Wider social determinants
Number % Other 100 71.4 Financial 21 15.0 Mental 15 10.7 Physical 3 2.1 Social 1 0.7 Total 140 100.0
3.14 The largest group (68 or 49%) of the 140 studies included in the analysis related to the provision of advice in ‘other’ settings which includes research focusing on the health impacts derived from generic advice or advice which, although not explicitly delivered in health settings, highlighted the relative value of advice provision in helping to achieve health outcomes. A further 40% of studies related to advice delivered in primary settings (Table 3.4).
Table 3.4 – Setting
Number % Other 68 48.6 Primary 56 40.0 Secondary/tertiary 15 10.7 Social care 1 0.7

26
The Role of Advice Services in Health
Total 140 100.0
Limitations of the evidence review
3.15 This evidence review has been conducted over a period of 12 weeks which incorporated the research design, the search for evidence, analysis and reporting. Given the benefits of the call for evidence approach in generating research evidence, and in particular grey material, more time might have enabled additional relevant evidence to be identified and reviewed – in particular from partners unable to respond within the short timeframe available.
3.16 The research reports identified in the evidence review vary in quality and rigor. Examples range from research studies based on a randomised control trial (RCT) to small-‐scale pilot studies that present qualitative evidence from a handful of advice service users using a case study format. The wide variance in the definitions of a positive health and wellbeing outcome makes any overall analysis problematic.
3.17 There is also lack of consistency across the research reports regarding the measurement tools used to assess the impact of different advice services working across various health settings. A number of the studies highlight the need for follow-‐up research, in particular longitudinal assessments and studies focusing on cost-‐savings for health services as a result of early intervention and prevention.
3.18 The limitations of the evidence base identified through the REA process highlight both a necessary feature of the process itself (in terms of being driven by tight inclusion and exclusion criteria and the availability of published evidence to form the subsequent analysis and its reporting). Good practice can involve the use of REAs as part of a larger research process which, for example, creates a baseline from which value can be added through further dialogue involving the advice and health sectors.
3.19 The design of the REA Framework and specifically the inclusion and exclusion criteria agreed against the research brief for this study is also restrictive. For example, by focusing on the impact of advice delivered in health settings, the research has failed to capture and explore the existence of comparative evidence from social care. Given the move towards health and social care integration, this represents a valid area for further/wider analysis which could offer examples of good practice and gaps in the existing knowledge base. Moreover, the variety of commissioners and grant funding organisations potentially looking to support the provision of advice in health and/or social care settings highlights the importance of providing as complete an evidence base as possible to support and inform future interventions.

27
The Role of Advice Services in Health
Mapping exercise
3.20 Health and advice projects were identified primarily in conjunction with the REA and the call for evidence in particular. This approach ensured that duplicate requests to the same stakeholders/partnerships were minimised, whilst maximising the knowledge and wider contacts accessible through the Advice and Health Steering Group and wider networks. In addition, the mapping exercise was underpinned by a combination of the following:
• reviews of ASA’s existing databases (including ASTF partnerships); • exploiting the practice knowledge of project advisory group members; • practice knowledge from advice networks; • review of the REA material; • ‘snowball sampling’ from identified health and advice projects; • promotion using social media, websites and mailing across the advice sector; and • internet searches.
3.21 The 58 projects and services identified through the mapping exercise were recorded using a bespoke database. The data fields/project typologies within the database were agreed in advance with the Director of the ASA with the final database capturing basic project information but also informing a synopsis of the context in which the services are offered and the extent to which they are seen to support the model of integrated health and care provision.
3.22 Outline information provided to/sourced by the study team was supplemented by a series of 24 telephone interviews with relevant projects/service staff in order to add depth to mapping analysis and ensure consistency of core data collection across all identified and logged projects. Where relevant, brief descriptions of projects have been utilised to highlight good practice, showcase delivery/funding models and explore approaches to assessing health impacts utilised by a range of partners.
28
The Role of Advice Services in Health
4 Evidence review results
4.1 This section of the report provides a synthesis of the evidence captured through the review process. It presents evidence on the strength of the relationship between advice and health outcomes across a range of health settings and for different population and/or patient groups. Key learning points are summarised at the end of each subsection.
Debt and mental health
4.2 The relationship between indebtedness and poor mental health is explored in a wide range of studies. Jenkins et al. (2008) present an analysis of mental disorder in people with debt in the general population. They report that around half of people with debts in the general population have a mental disorder, compared with 14% of the general population with no debts, and 15% of the general population. People in debt have two to three times the rate of neurosis, three times the rate of psychosis, over twice the rate of alcohol dependence and four times the rate of drug dependence as compared with people with no debt.
4.3 They conclude that debt, disconnected utilities, trying to reduce consumption of utilities and borrowing from informal sources are all predictors of markedly raised rates of all kinds of mental disorder. Having had to face issues like a disconnected utility (e.g. gas, electricity or water), being forced to cut down on utility use and/or to borrow money from informal sources – appears to directly link to increased likelihood of occurrence of mental health problems (when compared with a sample of the population which has not had to face such issues), at rates of 3–4 times, twice, and 2–3 times respectively.
4.4 Whether the association is causal, an outcome of mental illness or reciprocal, their findings demonstrate the mental health aspects and the significant public health impact of debt in the general population and has implications for debt policy, debt counselling agencies and for companies managing loans, repayments and pursuing debt recovery (Jenkins et al. 2008).
4.5 The Low Commission’s (2015) follow up report on tackling the advice deficit states that mental ill health is the largest single cause of disability in the UK, contributing almost 23% of the overall burden of disease (compared, for example to about 16% each for cancer and cardiovascular disease). The economic and social costs of mental health problems in England are estimated at around £105 billion each year.
4.6 In their paper examining the social and demographic predictors of debt problems, Balmer et al. (2008) found that being in receipt of benefits and long-‐term illness or disability were the strongest predictors of debt, with long-‐term ill or disabled respondents also being more susceptible to long-‐term debt. The authors highlight the importance of advice interventions that recognise the link between civil justice problems and health, illness or disability.
4.7 Fitch et al. (2011) also explore the relationship between indebtedness and poor mental health. Based on a systematic review which examined 50 papers, the authors acknowledge that it is difficult to demonstrate definitively whether indebtedness causes, or temporally
29
The Role of Advice Services in Health
precedes, poorer mental health (due to methodological limitations of existing longitudinal studies).
4.8 They conclude that plausible quantitative data exists which indicates that indebtedness may contribute to the development of mental health problems, as well as mediate accepted relationships between poverty and mental disorder. In addition, qualitative data also highlights the lived experience of coping with concurrent financial and mental health problems.
4.9 Earlier research by Skapinakis et al. (2006) demonstrated that individuals who initially have no mental health problems, but find themselves sinking into unmanageable debts, show within a 12-‐month period a 33% higher risk of developing depression and anxiety-‐related problems compared to the general population who do not experience financial problems. This highlights the importance of early identification and intervention to prevent people struggling with debt to access appropriate advice and guidance from requiring mental health treatment.
4.10 A number of evaluation reports covering advice services (not restricted to those in health settings) demonstrate the success of advice professionals in securing financial benefits for clients. Wiggan & Talbot (2006) state that it is important not to underestimate the important contribution that welfare rights advice provides to improving the psychological status among those benefiting from increased incomes.
4.11 In their literature review on the health benefits of financial inclusion, Dobbie & Gillespie (2010) conclude that, based on their assessment of the research to date, there is little need to conduct additional work to determine whether welfare rights advice has a financial effect. They state that future research should be directed at exploring the relationship between debt and mental health and the wider effects of addressing stress and anxiety associated with debt and low income. They also suggest that although the NHS has long recognised the value of improving access to welfare benefits and income maximisation in tackling health inequalities, initiatives that tackle the broader issues relating to financial exclusion (including awareness of financial capability), are relatively recent.
4.12 Pleasence et al. (2007) provide a thorough insight into the impact of debt advice on people’s lives. Their findings, based on four separate studies, confirm the variety of causes of debt problems, with the most common being changing circumstances such as ill-‐health, relationship breakdown and loss of employment. Their research, commissioned by the Department for Constitutional Affairs, also confirms that debt problems can bring about ill health, relationship breakdown and loss of employment. Although the evidence they present is not conclusive, it does nevertheless indicate that people’s levels of anxiety, general health, relationships and housing stability benefited from advice.
4.13 Further evidence is provided by the Improvement Service (2014) in their research into partnership working between the advice and health sectors in Scotland. They suggest that the likelihood of mental ill health increases with the number of debts people have, and while both low income and debt are linked to mental ill health, the effect of income appears to be
30
The Role of Advice Services in Health
mediated to a large extent by debt (i.e. the more debts people had the more likely they were to have mental health issues regardless of income).
4.14 Their earlier report on money advice services across Scotland’s local authorities (Improvement Service 2013) warns that the majority of service providers and funders of money advice services were expecting a significant increase in demand as a result of welfare reform changes. In response to the Scottish Government’s Welfare Reform, a Health Impact Delivery Group (HIDG) and representatives from NHS boards have worked in partnership to develop an outcome-‐focussed plan to mitigate the impact of the UK Government’s welfare reform programme on health and on health services in Scotland.10
4.15 The evaluation of the Money Advice Outreach pilots by Smith & Patel (2008) points to research that shows that people in receipt of advice experienced benefits including lower anxiety, better general health, relationships and housing stability. These were in addition to the cumulative impact of the primary outcomes of advice, such as having debt written off, avoiding losing a home and increasing annual income. They conclude that money advice outreach work can therefore be expected to generate a range of additional benefits for clients and, in turn, save associated public expenditure including the demands on the health service caused by physical or stress-‐related ill health.
4.16 Research undertaken by Wolverhampton CAB (2012) provides further evidence of the positive impact on health of good advice. The report concludes that advice services, including financial and debt relief services, housing advice and benefits advice, are cost-‐effective ways to increase incomes in low-‐income households which can lead to increased standards of living. The report argues that low income, poorly insulated housing and expensive, inadequate heating systems contribute to fuel poverty, which in turn contributes to excess winter mortality and morbidity, in particular among older and disabled people.
4.17 Simkins (2001) provides a useful overview of the challenges of evidencing the wider impacts of advice on health and social wellbeing over and above financial gains. Reporting on an investigation into the health improvements effected by a CAB advice worker seconded for one year to two Health Action Zone wards in the Carlisle area, the research found it challenging to deliver conclusive findings from using the SF-‐36 questionnaire, namely due to small sample sizes. The research was able to present anecdotal evidence of improvements in mental health but was not able to provide statistically significant conclusions based on data gathered from the questionnaires. Similar challenges have been reported through other studies.
4.18 The Baring Foundation (2015) report provides interim findings from a three-‐year project exploring the potential for legal rights advice to deliver positive mental health outcomes. The research used the short, seven-‐question Warwick–Edinburgh Mental Wellbeing Scale (WEMWEBS) prior to assessing young people presenting with social welfare issues. The results, based on the first 100 young people to complete a before and after questionnaire over a nine-‐month period, reveal statistically significant changes in the WEMWEBS score indicating that the legal rights intervention had a large positive impact on mental health. The
10 http://www.gov.scot/Resource/0044/00448578.pdf
31
The Role of Advice Services in Health
research also demonstrates that the intervention is very cost effective, with an estimated cost of £70 per intervention delivering improvements to long-‐term conditions such as depression and anxiety.
4.19 Research by Noble (2012) looking at the Medical–Legal Partnership model in Australia and the United States concludes that providing legal services in partnership with healthcare providers can have a significant impact on the health of disadvantaged people and also help change policies which impact on poor health as well as reducing readmission rates. In other words, the insight gained through a stronger partnership between advice services (in this case legal assistance) and healthcare partners has the potential to affect system change in order to challenge and change policies that are exacerbating health inequalities in society.
4.20 Drawing on insights from legal services that are engaging in multi-‐disciplinary work in the USA, UK and Canada, Gyorki (2014) outlines some of the practical and ethical barriers of integrating legal assistance into healthcare settings and provides guidance on overcoming them. Supporting the findings of Noble (2012), the report argues that integrating legal services into healthcare settings not only provides a direct referral pathway for health professionals who treat patients with legal needs to refer those patients to onsite legal services, but can also bolster patients’ attainment of better health outcomes.
4.21 The evidence review has identified examples of multi-‐agency, area-‐based responses to address the issue of indebtedness and associated health impacts. For example, the London Health Forum (2009) initiated a project to help ameliorate the health burden arising from the recession through early debt advice and other preventive measures. Its project aimed to encourage the NHS to work more closely with London’s boroughs to support the early use of debt advice. The report presents a number of key recommendations:
• councils and Primary Care Trusts to adopt a concerted approach in encouraging local people to seek debt advice as soon as they have worries;
• the NHS to take steps to communicate to healthcare professionals the importance of debt advice in preventing ill health;
• greater use to be made of NHS channels to inform people about the various providers of free debt advice;
• online debt advice to be promoted where appropriate to alleviate the burden on telephone and face-‐to-‐face advice services;
• funding for all types of debt advice to be maintained during what promises to be a protracted period of high unemployment and reduces incomes;
• better links to be introduced between helplines for debt and for mental health; and
• the NHS to support the development of a specialist service for those with debt and mental health problems.

32
The Role of Advice Services in Health
Summary
• Mental ill health is the largest single cause of disability in the UK, contributing almost 23% of the overall burden of disease. Around half of people with debts in the general population have a mental disorder, compared with 14% of the general population with no debts and 15% of the general population.
• The most common causes of debt problems are changing circumstances such as ill-‐health, relationship breakdown and loss of employment.
• It is difficult to demonstrate definitively whether indebtedness causes, or temporally precedes, poorer mental health. However, people receiving advice experienced benefits including lower anxiety, better general health, relationships and housing stability. These were in addition to the cumulative impact of the primary outcomes of advice, such as having debt written off, avoiding home loss and increasing annual income.
• Early identification and intervention are important to prevent people struggling with debt to access appropriate advice and guidance from requiring mental health treatment.
• Specialist welfare advice for people using secondary mental health services can deliver cost savings by reducing inpatient lengths of stay, preventing homelessness and preventing relapse for severe mental illness.
• There is little need to conduct additional work to determine whether welfare rights advice has a financial effect. Future research should be directed at exploring the relationship between debt and mental health and the wider effects of addressing stress and anxiety associated with debt and low income.

33
The Role of Advice Services in Health
Primary care
4.22 General practitioners and other community-‐based health staff are well placed to detect the wider factors affecting the health of a population who might not otherwise access advice services (Waterhouse 2002). With approximately 11,000 GP surgeries serving local communities across the UK (Low Commission 2015) there is considerable potential for strengthening the links between advice services and the primary care sector to better identify clients with advice needs and refer them to available support. The key advantages outlined in the research evidence point to a number of advantages of advice services working in partnership with primary care settings, namely:
• increasing income for clients;
• delivering improvements in health and quality of life by addressing the wider social determinants of health;
• contributing to a reduction in the use of NHS resources through early intervention and effective advice provision;
• providing a resource for health workers to enable GP surgeries to offer a more holistic approach; and
• more effectively meeting the needs of patients.
4.23 As part of The Low Commission’s research in conjunction with the Legal Action Group to quantify the impact of the Legal Aid, Sentencing and Punishment of Offenders Act 2012 (LASPO) and other cuts in social welfare law services, an opinion poll of GPs was commissioned in order to seek their views on whether the incidence of patients who needed advice was increasing, and whether not being able to obtain advice would negatively impact on their health.
4.24 The research was conducted in October 2014 and involved a sample of 1,001 GPs representing the UK regions as part of the GP Omnibus Survey. The findings of the survey demonstrated that most GPs are aware of the problems their patients are facing in the area of social benefits. Headline findings from the survey indicated:
• 67% of GPs believed the number of their patients that would have benefited from legal or specialist advice about benefits had increased in the last year;
• 65% of GPs believed there had been an increase in patients who would have benefited from legal advice in this area since last year;
• 54% of GPs reported the numbers of patients who would have benefited from legal advice on housing problems had increased and 55% said the same regarding community care; and
• 88% of the GPs questioned believed that patients not being able to access legal or specialist advice about their problems would have a negative impact on their health either to a great extent (48%) or to some extent (40%).
34
The Role of Advice Services in Health
4.25 More recently, Citizens Advice have published a similar quantitative survey of GPs.11 This found that 80 per cent of GPs reported that dealing with ‘non-‐health issues’ such as housing, employment and relationship problems, and this meant they had less time for other patients’ health needs. If non-‐health demands could be met in other ways, this could free up GP time to focus on patient healthcare, but most GPs could not respond to non-‐health issues in an integrated way.
4.26 There is a considerable body of evidence presenting examples of partnership working between advice services and the primary care sector. The Low Commission (2015) states that local Citizen’s Advice Bureaux now operate 640 advice surgeries at GP surgeries with overall advice outreach services or projects in 904 health settings.
4.27 This evidence review has identified 56 documents which present analysis and evidence of advice projects working in primary care settings. These cover a diverse range of pilots and service models involving a range of advice service providers. The outcomes described in the evidence base can broadly be placed into three main categories:
1. those that address the wider social determinants of health;
2. those that deliver improvements in health (physical and mental); and
3. those that bring about (or have the potential to bring about) benefits to health settings through efficiency savings, reduced demand and more effective diagnosis and treatment.
4.28 In 2012 Citizens Advice produced an overview of the possible links between advice and health. The information was produced as part of a wider programme funded by the Department of Health focused on enabling Health and Wellbeing boards and new commissioning bodies to make use of evidence from voluntary sector advice agencies. Their research covers a broad range of studies but acknowledges that they did not always find the presented health impact to be statistically significant and includes studies that have not been published in peer reviewed journals (Citizens Advice 2012).
Addressing the social determinants of health
4.29 Improving the financial, material and social circumstances of people presenting to primary care can underpin sustainable improvements in health. In his paper on the provision of welfare benefits advice in primary care, Abbott (2002) suggests that the alleviation of individual poverty can be seen as a health intervention, either as a treatment or health promotion, a position also supported by Moffatt et al. (1999) and Emanuel (2002).
4.30 In their research on the provision of welfare rights through primary care, Sherr et al. (2002) conclude that GPs can contribute to efforts to tackle poverty by increasing welfare benefits take up and tackling other problems with financial causes/remedies. They suggest that an effective welfare rights advice service within GP surgeries can also ameliorate or remedy
11 Capper K and Plunkett J (2015) ‘A very general practice. How much time do GPs spend on issues other than health? Citizens Advice.

35
The Role of Advice Services in Health
other problems associated with poor health which should lead to improvements in physical and mental health.
4.31 An evaluation report on CAB outreach services by Aberdeen University Department of Management Studies (2001) noted that “Many problems presenting themselves to primary care are wholly or partly social in nature. Addressing the social issues relieves demand on health services both directly and indirectly”. In other words, failing to adequately address the wider social determinants of health outlined by Marmot (2010) will do little to alleviate the pressures facing GPs.
4.32 Recent research by Kite (2014) investigates how delivering advice in a GP setting contributes towards the accessibility of advice and also how the advice provided contributes towards the ‘empowerment’ of clients. Her research was conducted in ten CABx from three regions in England and Wales with findings based on responses from 412 clients. Of the clients accessing the advice services, 57% of respondents had a long-‐term health problem or disability, 37% were unable to work because of long-‐term health problems or disability, and 66% felt cut-‐off or alone.
4.33 In the research 65% of clients gave a score of 7 or more for the impact of the advice problem on their health (where 0 was not at all and 10 a great deal) and 24% provided a score of 10. Some 68% said they had spent all or most of their time worrying about their advice problem. This mirrors the findings from similar studies that demonstrate the adverse impact that advice problems can have an on individual’s health and wellbeing (see Citizens Advice 2012 for a useful summary).
4.34 The research further reports that 49% of GP-‐based advice clients said they would be unlikely to visit a high street-‐based advice service for a variety of reasons including concern that they would be seen visiting their local CAB. As such, the location of the advice service in GP surgeries was effective in providing support to clients who would otherwise be unlikely to access advice through other routes (Kite 2014). Clients reported a range of positive outcomes from the advice including:
• feeling in control of the problem (80%);
• knowing about the law and their rights (75%);
• feeling able to enforce their rights (66%);
• feeling able to have a say in the decisions that affect them (65%);
• feeling able to deal with similar problems in the future (64%);
• feeling they have control over their life to live the way they want to (59%); and
• feeling able to influence officials/people in authority (38%).
4.35 Several studies emphasise the value of delivering advice within GP surgeries on the basis of improving access for clients with advice needs. Greasley & Small (2005) state that welfare advice services located in general practice facilitate access to welfare benefits for patients and are particularly effective in identifying health-‐related welfare benefits (e.g. disability benefits) which often go unclaimed due to a lack of awareness of eligibility. As such, they conclude, welfare advice services function to address inequalities in health relating to
36
The Role of Advice Services in Health
poverty and deprivation, providing a means by which primary care organisations can address the social, economic and environmental influences on the health of their population. These, they stress, were priorities outlined in The NHS Plan.12
4.36 A number of other research reports also emphasise the same point: namely that we see benefits for clients of co-‐locating advice services with primary care (Abbott & Hobby 1999; Galvin et al. 2001; Marshall 2013; Toeg et al. 2003; Widdowfield & Rickard 1996) – with many patients accessing welfare advice services at their GP having not previously benefited from welfare advice.
4.37 As outlined by Cawston (2010) in his research into general practice in deprived communities in Glasgow, social needs are far more acute in areas of socio-‐economic disadvantage. As a consequence, GPs working in these areas are very likely to identify a variety of social needs in medical encounters and to receive a high volume of requests for help with these needs. In the words of Cawston, ‘GP practices in deprived areas routinely face the choice of appearing disinterested in their patients’ social problems and becoming swamped by these to the detriment of being able to provide effective primary medical services’.
4.38 Hoskins & Carter (2000) also argue that community nurses have a role to play in tackling income inequality which leads to social isolation and chronic stress, chiefly through ensuring that clients claim their full quote of welfare entitlement.
4.39 The London Health Inequalities Network’s (2013) business case for welfare benefits advice through GPs cites the duty that CCGs have to tackle health inequality, and reports that the provision of specialist support is an appropriate and effective intervention, since welfare affects both physical and mental health. The business case presents a rationale for the provision of welfare services through general practice, including:
• GP surgeries regularly come into contact with vulnerable individuals, for example, people with long-‐term conditions who face serious difficulties in coping with financial insecurity;
• a growing body of studies suggest that welfare benefits advice, through improving take-‐up of entitlements, has a positive impact on mental and physical health;
• the recent report by UCL Institute of Health Equity (2012) recommended improved links between health and social protection systems;
• there is an expectation from patients that GPs and other health professionals will give advice on welfare benefits;
• current welfare reform is increasing the demand on GPs and other health professionals to support patients’ claim for reassessment and transition;
• the stress of dealing with these changes may lead to an increased demand on primary care for mental health support; and
• the loss of access to legal aid in the case of appeal after reassessment is likely to increase the demand for support from GPs and welfare benefit advisers.
12 Department of Health (2000) -‐ ‘The NHS Plan: A plan for investment a plan for reform’. July 2000.
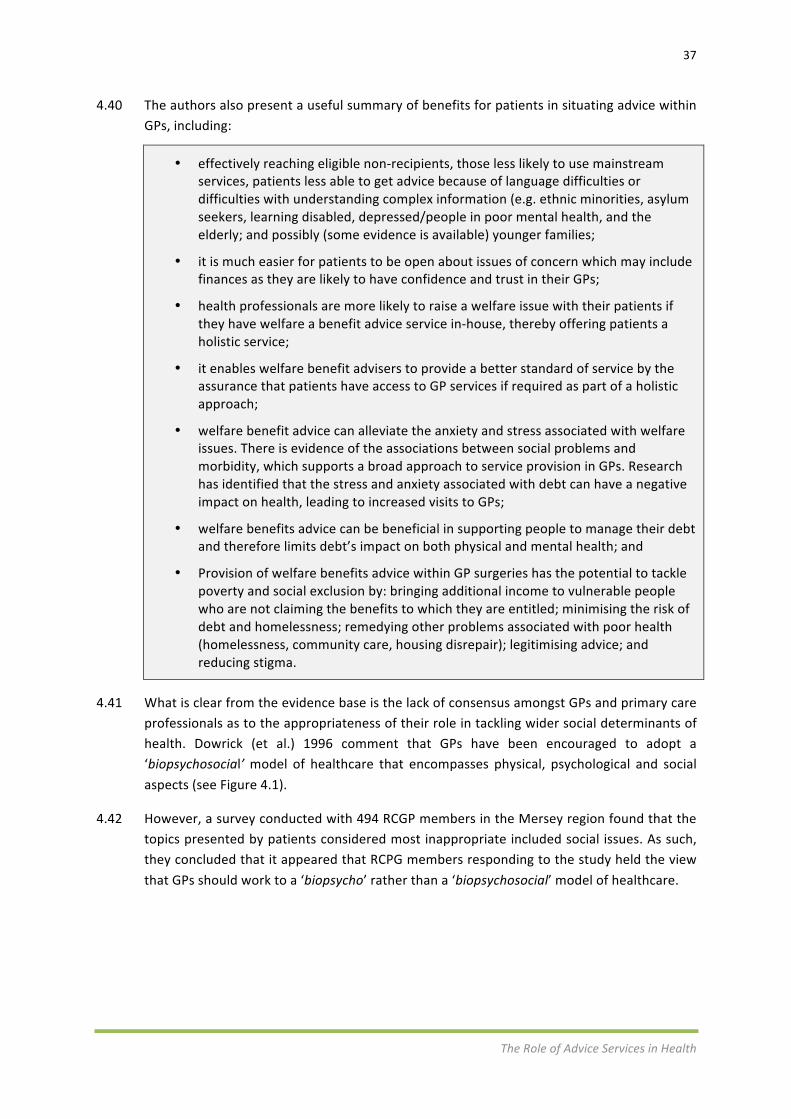
37
The Role of Advice Services in Health
4.40 The authors also present a useful summary of benefits for patients in situating advice within GPs, including:
• effectively reaching eligible non-‐recipients, those less likely to use mainstream services, patients less able to get advice because of language difficulties or difficulties with understanding complex information (e.g. ethnic minorities, asylum seekers, learning disabled, depressed/people in poor mental health, and the elderly; and possibly (some evidence is available) younger families;
• it is much easier for patients to be open about issues of concern which may include finances as they are likely to have confidence and trust in their GPs;
• health professionals are more likely to raise a welfare issue with their patients if they have welfare a benefit advice service in-‐house, thereby offering patients a holistic service;
• it enables welfare benefit advisers to provide a better standard of service by the assurance that patients have access to GP services if required as part of a holistic approach;
• welfare benefit advice can alleviate the anxiety and stress associated with welfare issues. There is evidence of the associations between social problems and morbidity, which supports a broad approach to service provision in GPs. Research has identified that the stress and anxiety associated with debt can have a negative impact on health, leading to increased visits to GPs;
• welfare benefits advice can be beneficial in supporting people to manage their debt and therefore limits debt’s impact on both physical and mental health; and
• Provision of welfare benefits advice within GP surgeries has the potential to tackle poverty and social exclusion by: bringing additional income to vulnerable people who are not claiming the benefits to which they are entitled; minimising the risk of debt and homelessness; remedying other problems associated with poor health (homelessness, community care, housing disrepair); legitimising advice; and reducing stigma.
4.41 What is clear from the evidence base is the lack of consensus amongst GPs and primary care professionals as to the appropriateness of their role in tackling wider social determinants of health. Dowrick (et al.) 1996 comment that GPs have been encouraged to adopt a ‘biopsychosocial’ model of healthcare that encompasses physical, psychological and social aspects (see Figure 4.1).
4.42 However, a survey conducted with 494 RCGP members in the Mersey region found that the topics presented by patients considered most inappropriate included social issues. As such, they concluded that it appeared that RCPG members responding to the study held the view that GPs should work to a ‘biopsycho’ rather than a ‘biopsychosocial’ model of healthcare.

38
The Role of Advice Services in Health
Figure 4.1 – BiopsychoSocial model of health13
4.43 This appears incongruous with the model examples for tackling health inequalities presented by the Marmot Review, a key feature of which includes health centres that have established close links between GPs and patient welfare and benefits advice. It is also contrary to guidance provided to GPs for addressing health inequalities published by RCPG (Ali et al. 2008).
4.44 Marmot (2010) helpfully summarises that the link between social conditions and health is not a footnote to the ‘real’ concerns with health, but should become the main focus. His report outlines that health inequalities result from social inequalities, and as such, action on health inequalities requires action across all the social determinants of health.
4.45 The Royal College of General Practitioners estimates that the average number of consultations carried out by each GP in England per year is currently 10,714 and has increased by approximately 16% since 2008.14 The increasing pressure facing general practice due to rising demand for consultations highlights the importance of addressing one of the key policy objectives recommended by Marmot (2010), namely to strengthen the role and impact of ill health prevention. The evidence base around addressing the wider social determinants of health presents a compelling case for advice services working collaboratively with primary care to ensure early identification and intervention of clients whose advice problems are likely to impact on their immediate and future health and wellbeing.
13 Taken from http://www.physio-‐pedia.com/Biopsychosocial_Model 14http://www.rcgp.org.uk/news/2014/february/34m-‐patients-‐will-‐fail-‐to-‐get-‐appointment-‐with-‐a-‐gp-‐in-‐2014.aspx

39
The Role of Advice Services in Health
Health improvement
4.46 As outlined earlier in this report, the greatest amount of empirical evidence collected to date has focused on the relationship between indebtedness and poor mental health. Consistent with the overview provided by Citizens Advice (2012), there is however an absence of high quality studies demonstrating statistically significant impacts on health as a result of advice services.
4.47 A systematic review of the health, social and financial impacts of welfare rights advice delivered in healthcare settings conducted by Adams et al. (2006) identified 55 studies that reported on health, social and economic impacts. However they report that the majority of these studies were grey literature (i.e. not published in peer-‐reviewed journals), and were of limited scientific quality, in particular with less than 10% of studies using a control or comparison group to assess the impact of the advice. Studies that did include control or comparison groups tended to use non-‐specific measures of general health (e.g. SF-‐36, Nottingham Health Profile and Hospital Anxiety Depression Scale) and found few statistically significant differences between intervention and control or comparison groups. However the review states that sample sizes were often small and follow-‐up limited to a maximum of 12 months, which they suggest is likely to be too short a period to detect changes in health following changes in financial circumstances.
4.48 In response to the relative absence of robust evidence demonstrating the impact of welfare benefits take-‐up on health, Bateman (2008) suggests that this may be because the damage to health may have already occurred before the person with health problems is seen by an adviser linked to a healthcare service. In this regard the health benefits of increased welfare benefits may be temporary or simply be offset by ongoing, irreversible health deterioration.
4.49 Abbott (2002) makes a similar observation, stating that the longer-‐term effects of welfare benefits advice on individuals’ health operate most powerfully on younger clients, whereas in reality, users [presenting to primary care] tend to be older (see later section of this report [paras 4.104 -‐ 4.112?] on advice service interventions targeting young people).
4.50 Greasley & Small (2005) suggest that small improvements in individuals’ health may not be apparent to primary healthcare staff as the instruments used in [research] studies, such as the Nottingham Health Profile, SF-‐36 and the Hospital Anxiety Depression Scale, are not routinely used in primary care. Nor, they argue, is welfare benefits advice in primary care likely to significantly reduce noticeably the work load of primary care. Burrows et al. (2012) also highlight the challenge of demonstrating measureable health improvement and wellbeing in addition to the financial benefits delivered for patients from welfare advice in primary care.
4.51 Moffatt et al. (2006) provide a helpful overview of the use of different research methodologies to evidence the impact of welfare rights advice. Using a qualitative approach to assess the impact of welfare rights advice targeted at people aged 60 years or over and
40
The Role of Advice Services in Health
accessed via primary care, they found that this had a positive impact on quality of life and resulted in increased social participation.
4.52 However, they also acknowledge a divergence of qualitative and quantitative findings. Although the effects of the intervention were wide-‐ranging and positively regarded by participants across a range of physical, psychological and social outcomes, the pilot RCT found little or no differences between intervention and control groups, or between those who did and did not receive additional resources, suggesting that the intervention had no impact on these outcome measures.
4.53 The authors outline that it is not uncommon for qualitative and quantitative studies to produce divergent findings and it is likely that each method, with its different epistemological underpinnings, captured different aspects of phenomena under investigation. The qualitative approach enabled participants to give an account of the various ways in which the intervention impacted on their lives, such as increased independence and improved quality of life, which were not explicitly measured in the pilot RCT and are challenging to capture quantitatively (Moffatt et al. 2006). This raises a wider question as to what evidence standards health commissioners are seeking when commissioning health interventions and the extent to which advice services can (or should be expected to) meet these standards when looking to secure investment.
4.54 A number of studies do present evidence of the impact of advice services in improving health. Abbott et al. (2006) present their findings of research to assess the impact on the health of individuals accessing welfare benefits advice in GP settings. They recruited 345 people to take part in the study which used the SF-‐36 health questionnaire. The study found that better health was associated with increased income, with statistically significant improvements in vitality and mental health at six months for those whose income has increased when compared to those whose income had not increased. The authors concluded that there may be considerable disadvantage to health if benefit entitlements are delayed.
4.55 In their qualitative study exploring the impact of welfare advice in primary care, Moffatt et al. (2004) state that participants reported positive effects on their health, in particular reduced stress and anxiety, better sleeping patterns, reversal of weight loss, changes in medication, reduced contact with the primary care team, reduction or cessation of smoking, improved diet and physical activity.
Service efficiencies
4.56 Less evidence is apparent which clearly demonstrates actual cost or efficiency savings delivered through advice services working in primary care. Where these are included within studies they have largely tended to infer or assume that such savings will be delivered as opposed to actually putting in place appropriate systems to measure these. Key challenges reflected in the evidence relate to the ability to establish causality between the advice services and to demonstrable efficiency improvements within primary care, including for example reducing demand for consultations or issuing fewer prescriptions. However it is unclear to what extent health commissioners and/or individual GPs view this as the most
41
The Role of Advice Services in Health
important gap in the evidence base when assessing the relative merits of funding or working more closely with advice services.
4.57 Abbott (2002) concludes that the provision of welfare advice services in primary care locations appears to add value to services, not only saving the primary health team time, but reaching people with particular needs. However, he reports that while many health professionals are glad to be able to refer their patients to relevant non-‐medical services with easy access, such GPs are a minority, and indeed some explicitly oppose the idea that they have a major responsibility to improve access to such services in this way.
4.58 In their evaluation of the impact of a CAB health outreach service on GP surgeries, Palmer et al. (2010) report that the service was beneficial to patients and did not produce any adverse impact on any other services provided by the six participating practices. Furthermore their study found statistically significant reductions in the number of GP appointments and prescriptions for hypnotics and anxiolytics; as well as non-‐significant reductions in nurse appointments and prescriptions for antidepressants. The number of GP appointments reduced by an average of 0.63 appointments per patient, equating to a total of 93 fewer appointments for the 148 patients. The number of nurse appointments also reduced, but by a smaller proportion.
4.59 As part of a pilot project that aimed to alleviate the burden on primary care in deprived urban areas, Abbott & Davidson (2000) found that visits to the GP by users accessing the service for general advice and signposting did reduce by two a year, although they acknowledge that such reductions by a small number of patients are unlikely to be noticed by GPs. Atherton (2011) and Emaneul & Begum (2000) also report reductions in GP consultation time as a consequence of welfare advice services, albeit these were not reported as statistically significant for the latter.
4.60 While concerns have been raised on the expansion of the remit of health services and the ‘clinical gaze’ into income and welfare rights (see Chaggar 1993 and Abbott 2002), Greasley & Small (2005) challenge the view that additional services may be a burden on GPs. They suggest that advice workers should be seen as a resource to relieve the burden upon primary health teams dealing with patients’ social and economic welfare rights issues.
4.61 A range of other studies concur with this position including the research conducted by ComRes 2014 on GPs and social welfare law, which found that many GPs reported that the number of their patients who would have benefitted from legal or specialist advice on social welfare issues has increased over the past year. The research found that almost half of GPs (48%) recognise that a patient not having access to legal or specialist advice on social welfare issues can have a negative effect on their health to a great extent.
4.62 Borland & Owen’s (2004) research on the Better Advice, Better Health project in Wales found that a random sample of GPs involved in the project showed overwhelming support for the introduction of welfare advice in primary care settings. The GPs reported that the project had extended their practice, removed the stigma from patients seeking advice, enabled more people to access healthcare, reduced health inequalities and enabled patients to access a service that would otherwise be unavailable.

42
The Role of Advice Services in Health
4.63 The evidence base provides other examples of GPs providing positive feedback from closer working with advice services. In their study evaluating the impact of specialist welfare rights advice on general practices in inner London, Harding et al. (2002) found that of the 79 surgeries that participated, those with welfare rights advisers (42) were significantly more likely to report that the current provision was adequate (ie, it was easier for staff to access advise on their patients’ behalf and the process of advice provision ran smoothly). The welfare rights service enabled GPs to ensure that relevant advice is provided without the need for welfare knowledge themselves.
4.64 The business case for the provision of welfare benefits advice through general practice compiled by the London Health Inequalities Network (2013) outlines a range of benefits for GPs, including:
• health professionals becoming more aware of the link between health and welfare as a result of interactions with the welfare rights adviser;
• saving GPs’ time -‐ one study estimated that 15% of GPs’ consultation involved welfare rights issues;
• resulting in reduced costs associated with GP drug prescriptions and reducing the number of patient visits to their GP on an already stretched service; and
• providing an effective tool for GPs to promote health holistically and thereby support income maximisation for the patient.
4.65 In their research on placing employment advisers from Job Centre Plus in GP surgeries as part of a Pathways Advisory Service pilot, Sainsbury et al. (2008) found that it was important that the advisers were based on the surgery premises. This enabled easier referral procedures, which could sometimes be immediate and could avoid the need for formal, written referrals. They also noted that the adviser’s presence in the surgery aided the fostering of good relationships with practice staff. Overall, they found that GPs were enthusiastic and positive about the pilot.
4.66 The value derived from co-‐location of services does however raise a broader issue around the availability of appropriate (i.e. private, confidential) space within general practices and the willingness of GPs to allocate this space for an advice service professional.
4.67 Few studies have attempted to calculate cost-‐savings achieved as a result of locating advice services in GP practices. One such example is provided by Marshall (2013) in her social value assessment of a CAB outreach service provided delivered in the west end of Newcastle upon Tyne. Marshall (2013) estimates cost-‐savings to the NHS relating to reduced GP consultations and prescriptions amounting to £7,500 for the first year following the service and £2,700 for the following six months – nearly double the £5,500 invested in the service by commissioners. This is in addition to the £123,000 additional income secured for clients as a result of the advice they received.

43
The Role of Advice Services in Health
Summary
Addressing the social determinants of health
• Improving the financial, material and social circumstances of people presenting at primary care can underpin sustainable improvements in health. Advice services function to address inequalities in health relating to poverty and deprivation, providing a means by which primary care organisations can address the social, economic and environmental influences on the health of their population.
• Early identification and intervention for those at risk of developing health problems can be cost effective in reducing demand for health services over the longer-‐term.
• GPs and other community-‐based health staff are well placed to detect the wider factors affecting the health of a population, who might not otherwise access advice services.
• The majority of GPs believe that patients not being able to access legal or specialist advice about their problems would have a negative impact on their health. However, there is the lack of consensus amongst GPs and primary care professionals as to the appropriateness of their role in tackling wider social determinants of health.
• The average number of consultations carried out by each GP in England per year is currently 10,714 and has increased by approximately 16% since 2008.
Health improvement
• We lack any high quality studies that can demonstrate statistically significant impacts on health as a result of advice services. This raises a wider question as to what evidence standards health commissioners are seeking when commissioning health interventions and the extent to which advice services can (or should be expected to) meet these standards when looking to secure funding.
• A number of studies do present evidence of the positive impact of advice services in improving health including reduced stress and anxiety, better sleeping patterns, reversal of weight loss, changes in medication, reduced contact with the primary care team, reduction or cessation of smoking, improved diet and physical activity.
Service efficiencies
• Stronger partnership between advice services and healthcare partners has the potential to affect system change in order to challenge and change policies that are exacerbating health inequalities in society and creating demand for health provision.
• Less evidence is available which clearly demonstrates actual cost or efficiency savings delivered through advice services working in primary care. Where these are included within studies they have largely tended to infer or assume that such
44
The Role of Advice Services in Health
savings will be delivered as opposed to actually putting in place appropriate systems to measure these.
Secondary or tertiary care
4.68 The review identified 15 documents which present analysis and evidence of advice projects working in secondary or tertiary care settings. The evidence base includes examples of projects designed to support patients attending cancer units, rheumatology, specialist children’s services and, in particular, mental health services.
4.69 In his article advocating the role of Citizens Advice Bureaux in supporting healthcare, Hall (2004) explains that people affected by severe injury or sudden illness often need advice on issues such as sickness and disability benefits, how to manage debt and mortgages if they are no longer working, and employment rights. It is seldom a single issue that patients have concerns about but often several issues including statutory sick pay, housing costs, employment rights and carers’ allowance. Without effective support, he argues, many people find benefit rules governing hospital stays extremely complex. As such, appropriate advice intervention can support individuals accessing secondary or tertiary care services to mitigate the impact of their health episode on their longer-‐term health and wellbeing.
Rheumatology
4.70 Fruin and Pitt’s (2008) study assesses the effectiveness of using a Health Assessment Questionnaire (HAQ) with patients with arthritis as a tool for identifying patients that may be eligible for benefits and to assist those identified in claiming benefits with the help of a CAB benefits advisor. The service, delivered within a district general hospital rheumatology centre, sent HAQ forms to all patients attending the centre and those with a score indicating moderate to severe disability were contacted initially by telephone by the CAB advisor. Those considered eligible were invited to attend the rheumatology centre to determine their suitability to apply for benefit. Of the 86 patients contacted by the CAB advisor, 8 were advised to have their benefits reviewed and 38 were not in receipt of any benefits. As a result of the service, 29 (63%) were awarded benefits.
4.71 The study concludes that the HAQ was found to be a useful tool for identifying patients with arthritis who may be entitled to welfare benefits and that the CAB advisor was central to the identification and application process for eligible patients. This may suggest that routine screening and assessment of patients accessing specialist hospital services may prove effective in uncovering advice needs and making a positive impact on their financial and social situation.
Children’s services
4.72 A further example of a partnership between the advice sector and a hospital setting is presented by Great Ormond Street Hospital and CAB Camden (2013) and Harris (2013). The establishment of an onsite social welfare law advice service for parents and carers of children attending the hospital was established to address what the authors report as “the
45
The Role of Advice Services in Health
overwhelming evidence linking poverty to poor health and wellbeing and following identification of unmet need by existing family support services”.
4.73 The report outlines the financial reality for families with a sick or disabled child, citing recent research which showed:
• 1 in 6 (17%) going without food;
• more than 1 in 5 (21%) going without heating;
• a quarter (26%) going without specialist equipment or adaptations;
• 86% have gone without leisure and days out;
• almost a third (29%) having taken out a loan – 39% for food and heating;
• a quarter of loans are from quick cash schemes or loan sharks; and
• 1 in 5 (21%) have been threatened with court action for failing to keep up with payments – the majority for missing utility bill payments (46%).
4.74 The report demonstrates the positive impact of the service both for families with children at the hospital but also for existing family support workers integrated as part of existing services. The authors stated that the service ‘proved to be in the right place and at the right time to help families with sick and disabled children’. Using a post-‐advice questionnaire to assess the impact of the service, the report suggests that for 79% of respondents it was the first time they had sought or received independent welfare rights advice.
4.75 Furthermore respondents outlined a range of positive impacts on their health, wellbeing and personal circumstances, including:
• in total £800,000 was gained for families with nearly £100,000 of debts written off or managed – a return of over £8 for every £1 spent;
• families’ high satisfaction ratings for both accessibility and advice – at over 90%;
• reported increases in families wellbeing following advice – 73% reported being less worried/stressed after advice and 54% reporting an improved quality of life;
• five cases of patients being prevented from discharge due to unsuitable housing conditions were resolved; and
• staff time saved by the CAB carrying out work others would have needed to do was estimated at £8,690 per annum.
Cancer units
4.76 Macmillan Cancer Support (2012) present an evidence review of the local benefits of advice services for people affected by cancer. The report outlines the financial pressures facing people following a cancer diagnosis as a result of their change in circumstances, including a loss of income, reducing savings, short or long term unemployment and costs associated with cancer treatment. Indeed their review found that 91% of cancer patients’ households suffer loss of income and/or increased costs as a direct result of cancer and although nurses,
46
The Role of Advice Services in Health
doctors and other patients sometimes offer valuable guidance, many people affected by cancer do not receive it at the right, best or most effective time.
4.77 The review also found that debt can be a major problem during illness, causing deteriorating mental and physical health and in particular having a substantial effect on carers. People affected by cancer often struggle to access generic benefits advice provision. The symptoms of cancer and side effects of treatment can make it difficult for people to access advice via conventional channels. Where people affected by cancer are able to access advice through these conventional channels they often find that the advisers have a lack of understanding of cancer and its treatments meaning that some of the available financial help is missed. The review concludes that cancer-‐specific benefits advice services leading to increased income can be associated with improvements in psycho-‐social aspects of health such as levels of energy and tiredness and improved mental health (Macmillan 2012).
4.78 This is consistent with the conclusions of Moffat et al. (2012) in their evaluation of a welfare rights advice intervention designed to address the financial consequences of cancer. They conclude that “the intervention proved feasible, effectively increased income for cancer patients and was highly valued. Addressing the financial sequelae of cancer can have positive social and psychological consequences that could significantly enhance effective clinical management”. They call for suitable services to be made routinely available.
4.79 Williamson Consulting (2009) presents an evaluation of welfare rights services provided by Macmillan Cancer Support over a three year period in the Altnagelvin hospital in Northern Ireland. Most of the beneficiaries consulted as part of the evaluation indicated that without the service they would not have been aware that they were entitled to support, or how to go about accessing it. Both hospital staff and clients at the hospital stated that is was appropriate that a welfare rights service be based in the hospital setting in order to effectively target people with cancer, particularly within the cancer units where people attend for diagnosis and treatment.
4.80 The welfare rights service was found to complement the medical support provided at the cancer unit in the hospital and the model was recognised through a HPSS Quality Award. The evaluation found that the service provided strong financial gains for patients and also freed up hospital and social work staff from having to meet this advice need (which as the report acknowledges they are not in a position to do given that the provision of benefits advice is not their primary function).
4.81 An evaluation of a Macmillan Welfare Rights Advice Service conducted by Noble et al. (2011) provides detail on the main financial, psychological and social impacts for clients (see over page). The research also found that health service staff became more ‘benefit aware’ and over time became more likely to advise their patients to seek help with benefits. Benefit-‐related workload was also reduced for health service staff, enabling them to concentrate on their clinical work.

47
The Role of Advice Services in Health
Beneficial impact of welfare rights advice for families affected by cancer
Financial and material consequences
• increased ability to afford the additional costs associated with cancer
• lessened impact of loss of earnings associated with absence from work
• increased ability to afford necessities
• reduced need to draw on savings and/or increased ability to save for the unexpected
• ongoing advice and support.
Psychological and social impacts
• reduced stress and anxiety
• increased ability to maintain independence
• greater capacity to engage in ‘normal’ social activities and routines, which impacted positively on wellbeing .
4.82 Scottish Borders Council (2013) provides an overview of the Borders Macmillan Welfare Partnership funded between 2009 and 2013. The partnership was focused on increasing the income of those affected by cancer in the Scottish Borders and also improving access for people affected by cancer to other linked, useful services such as money, housing and energy advice. The report outlines that the service exceeded its first objective, achieving annualised income gains of £5.99 million which was significantly over the target of £2.4 million set. Feedback collated from clients revealed that 80% felt that the help had made a positive difference to their life.
4.83 Clients were also asked if the service had assisted in making changes which has improved their wellbeing. Responses included:
• 80% felt that the help provided had made a positive difference in their life;
• 60% felt less stressed;
• 18% said they felt healthier;
• 12% felt they had fewer visits to health professionals;
• 12% felt they had other changes; and
• 5% felt there was no change.
4.84 The difference that timely and sensitively delivered advice can provide is perhaps best encapsulated in a quote from service user that was supported through Borders Macmillan Welfare Partnership:
48
The Role of Advice Services in Health
“It made things less stressful financially and so benefited me in a healthy way in that I was able to concentrate on getting better”.
4.85 In their response to the Welsh Government’s Advice Services Review (Welsh Government, 2013) Macmillan confirm that people affected by cancer often struggle to access generic benefits advice provision. Macmillan states that whilst there are access issues linked to the symptoms of cancer and side effects of treatment, there are also skills gaps amongst advisers linked to a lack of understanding of cancer and its treatments that affects the quality of advice provided in terms of missed opportunities to access financial help. As such partnership approaches such as those evidenced by Scottish Borders Council (2013) enable specialist advice workers to access clients within cancer care settings and ensure that the advice provided is bespoke, timely and sensitively delivered in order to make a real difference to their care management and recovery.
4.86 Moffatt et al. (2010) concur with the access issues identified by Macmillan. In their paper on the provision of welfare rights advice for people with cancer, they state that the financial strain resulting from a cancer diagnosis is compounded by a lack of easy access to information about benefit entitlements and assistance to claim. Furthermore they argue that proactive welfare rights advice services, working closely with health and social care professionals, can assist with the practical demands that arise from dealing with the illness and should be considered an important part of a holistic approach to cancer treatment. This, they suggest, would enable professionals to concentrate on their core business whilst ensuring that patients obtain the advice and assistance that they require in financial matters.
4.87 The authors reference the UK National Institute for Clinical Excellence (NICE) Guidance on Cancer Services which recommends that ‘patients and carers should be offered assistance to obtain benefits for which they are potentially eligible by professionals who are informed and knowledgeable about the benefits system’ and recognises that some needs of cancer patients can only be met by individuals or agencies outside the NHS.
Mental health services
4.88 Recent estimates suggest that the cost of mental health problems in England increased from £77.4 billion in 2002/03 to £105.2billion in 2009/10 in terms of health and social care costs, output losses in the economy and an imputed monetary valuation of the human cost of mental illness. The London School of Economics calculated that the total loss of output due to depression and chronic anxiety is some £12 billion a year, equating to 1% of our total national income. Of this, the cost to the taxpayer is some £7 billion including incapacity benefits and lost tax receipts (Office for Public Management 2008).
4.89 As with general morbidity, psychiatric morbidity has been linked to an array of social problems. A study conducted by Pleasence & Balmer (2009) found significant associations between rights problems and mental illness, both when experienced in isolation and in

49
The Role of Advice Services in Health
combination with physical illness. Drawing on data from surveys of 2,628 adults in England and Wales and 7,200 people aged ≥15 in New Zealand, their research found that rights problems were reported to have led, on occasion, to stress-‐related illness. The authors conclude that effective coordination of mental health and legal services is likely to improve both health and justice outcomes.
4.90 Shape & Bostock (2002) report on their consultations with psychological therapists to assess what they considered the debt issues were for the people who used their services. The most common types of debt that therapists reported for service users were rent arrears, payments owed to catalogues, loans and credit cards – and the most common causes of debt were thought to be associated with poverty and illness. They described the impact of debt problems on physical and mental health, but also on people’s circumstances (e.g. relationships, housing and leisure).
4.91 Drawing on data from a needs assessment census across Northumberland Locality Mental Health Services their research confirmed that a substantial number of people in different situations and with different diagnoses have financial difficulties, most notably people who have drug and alcohol problems, a diagnosis of personality disorder, or who are unemployed. The research found that although the psychological therapists helped service users deal with debts either by referring them to outside agencies and other team members, or by encouraging them to help themselves, a number of gaps and barriers in services were identified, such as: lack of access to advice; staff and service users’ lack of awareness of services; difficulties accessing welfare benefits; and limited support and information for staff.
4.92 Referencing findings from the wider literature, Shape & Bostock (2002) also highlight that community services are not always accessible to mental health service users and barriers that inhibit the general public from getting help with debts associated with stigma and fear are exacerbated for people who have mental health problems (for example, they may not be able to cope with crowds in a waiting room, or may be terrified of going outside). They conclude that ensuring service users have adequate access to welfare benefits advice to maximise their income, and taking into account issues of poverty when considering psychological interventions, is therefore very important.
4.93 Findings from the first year of a welfare rights project in an in-‐patient hospital unit commissioned by South West Yorkshire Mental Health NHS Trust (Direct Impact Research Group & Minogue 2006) found that a considerable amount of time was spent by nursing staff on welfare benefits prior to the introduction of a specialist welfare rights worker. The welfare rights project was successful in freeing up staff time, reducing patient anxiety about benefits and related problems, and helping patients obtain extra benefit entitlement.
4.94 The report suggests that people who have mental health problems requiring in-‐patient treatment are frequently in a state of crisis when they become in-‐patients or may be in an acute stage of their illness. Having to go in to hospital for unplanned inpatient treatment can mean that people do not have time to organise their finances, welfare benefits, rent or mortgage payments, or discuss any employment issues with employers. Through the project the welfare rights worker gained additional benefits or allowances for nearly 50% of the
50
The Role of Advice Services in Health
clients and helped carers and families. The support provided by the worker helped to reduce anxiety for two-‐thirds of the people advised. In terms of service design the research found that patients in particular valued the ongoing help received after discharge and the fact that contact did not end on leaving the inpatient unit.
4.95 The Centre for Mental Health’s report on welfare advice for people who use mental health services (Parsonage 2013) highlights the contribution that specialist welfare advice can provide in cutting the cost of healthcare. The report cites the potential of specialist welfare advice for people using secondary mental health services to deliver cost savings by reducing inpatient lengths of stay, preventing homelessness and preventing relapse for severe mental illness.
4.96 The research shows that the average cost of an inpatient stay is £330 per day nationally and that specialist advice located in a mental health service can help patients resolve complex problems. These include issues around housing such as eviction or repossession, which may enable them to be discharged from hospital more quickly than would otherwise be possible. This also means that the risk of homelessness can be diminished, as those with severe mental illness are at much higher risk of homelessness than average. Homelessness costs the public sector, including the NHS, up to £30,000 a year as well as causing great distress to the person affected (Parsonage 2013). Welfare advice can also help to prevent relapse of mental illness. For example, a relapse of schizophrenia costs the NHS over £18,000. Specialist welfare advice can act directly on an immediate cause of acute stress which threatens to trigger relapse.
4.97 The report makes a number of recommendations including a call for the National Institute for Health Research and other funders to commission research to establish the effectiveness and cost-‐effectiveness of welfare advice for people with mental health problems and to identify the best models of service delivery.
4.98 The positive link between employment and mental health is firmly established in a range of studies. Research demonstrates that work is good for people and being unemployed is damaging to physical and mental health. The proportion of unemployed people in need of psychological treatment is more than double that of those who are employed (Paul & Moser 2009). There is also a strong correlation between unemployment and higher mortality, higher medical consultation, higher healthcare consumption and higher hospital admission rates (Waddell & Burton 2006). After an individual has been absent from work for six months, there is only a 50% likelihood of the employee returning to work; this falls to 25% after a 12-‐month absence and after two years it is virtually nil (British Society of Rehabilitation Medicine 2001).
4.99 A number of advice projects are currently integrated into NHS IAPT services across England.15 Research by the Office for Public Management (2011) looking at the roll-‐out of integrated clinical and employment support services as part of London’s IAPT programme (the Working for Wellness Employment Support Service) estimates that every £1 spent by
15 ITalk Hampshire, Dorset Mental Health Forum, Isle of Wight IAPT, Talking Change (Portsmouth), Working for Wellness (London) and Twining Enterprise (Hounslow).
51
The Role of Advice Services in Health
the state on IAPT employment services generates £2.79 of benefits, of which £0.84 benefits the individual and £1.95 the state.
“Embedding employment support and advice in healthcare services for individuals experiencing mental health problems is a key element in the recovery process. Whilst health interventions alone can make a contribution to beneficial employment outcomes, there is a growing body of evidence that indicates targeted health and work-‐ related support achieves greater impact. This is true for reducing the incidence of job loss and for promoting people’s return to work”. (Office for Public Management 2011)
4.100 A recent report by Jamieson (2014) explores the links between mental health and financial wellbeing as part of an Advice Services Transition Fund project in South Tyneside. The report aims to inform local approaches for integrating advice services into local health provision and presents compelling evidence on the high costs borne by the NHS as a result of increasing dependency on anti-‐depressants. The research points to the fact that prescribing is the most common patient-‐level intervention in the NHS and is the second highest area of spending in the NHS after staffing costs.
4.101 Specifically for the North East, the report by Jamieson (2014) draws on data released in April 2014 which shows that the region is becoming increasingly dependent on anti-‐depressants as doctors prescribed nearly one million more prescriptions for the drug than in 2010, an increase of 25%. More prescriptions for anti-‐depressants are given out in the North East than anywhere else in the country with more than 4.4m prescriptions being signed off. The region takes up six of the top 10 places in England for the use of anti-‐depressants which has increased the cost up for the NHS to £20.7m for 2013 alone.
4.102 The report makes the case for the development of a social prescribing model, which provides a referral system with improved access to advice agencies in order to improve the mental health and financial wellbeing of the local population and address both economic and health inequalities. Key envisaged improvements proposed in the report by Jamieson (2014) are provided in the following Summary.
4.103 Research by the Mental Health Foundation (2005) found that 78% of GPs had prescribed an antidepressant in the previous three years, despite believing that an alternative treatment might have been more appropriate. It also found that, of the whole sample, 66% had done so because a suitable alternative was not available, 62% because there was a waiting list for the suitable alternative and 33%, because the patient requested antidepressants. Of the GPs surveyed, 60% said they would prescribe antidepressants less frequently if other options were available to them. Specialist debt advice has a clear role to play in supporting people in debt to address their financial difficulties and prevent the development of further mental health problems.

52
The Role of Advice Services in Health
Summary of health and economic benefits of advice
Health
• Cost savings to health services in both time and with prescriptions.
• Help to deliver public health outcomes such as increased life expectancy and reducing differences in life expectancy between communities, particularly in disadvantaged areas.
• Providing alternative and more appropriate support and contact points for frequent attenders (frequent attenders are defined as those who consult their GP more than 30 times in two years. In primary care the top 3% of face-‐to-‐face attendances with a GP account for 15% of all consultations and are more likely to have depressive and anxiety disorders.
Economic
• Clients are financially more secure if they have benefitted from an initial benefit check with an advisor.
• Secure incomes for families to assist with better financial planning in the long term.
• Impact on the borough in terms of increased disposable income and spending on local services and amenities.
• Effective local partnership working between the public and voluntary sector to address local issues (recent publication of NHS England’s Five Year Review highlights the need for stronger partnerships with charitable and voluntary sector organisations).
Personal
• Help to decrease the negative impact on people’s health of recent welfare reforms and the potential to provide increased support in future to people who will be in receipt of Universal Credit.
• Early intervention to ensure issues don’t deteriorate to the point where clients end up in such significant financial difficulties such as fuel poverty, relying on food parcels or being homeless.
• Supporting clients to be better able to deal with problems themselves through improved confidence and awareness of implications (eg, addressing the core aim of Pioneer status in South Tyneside of promoting and advocating self-‐care).
• Preventing mild mental health conditions progressing into more significant emotional wellbeing issues.
• Reduction of impact on physical health/long-‐term conditions .
• Developing an ability to manage money better, plan for the future and to better cope with financial distress if it occurs.
• Improved personal financial situation whereby clients are more in control and able to experience a better standard of living.

53
The Role of Advice Services in Health
4.104 A range of studies focus on the impact of unresolved social welfare problems on young people’s lives. Mental health problems are common among young people. At any one time, around one in six 16–24 year olds meet thresholds for clinical diagnoses of problems such as anxiety and depression (Sefton 2010). When problems such as post-‐traumatic stress, attempted suicide, eating disorders and alcohol and drug dependence are added in, the proportion affected rises to almost a third.
4.105 Mental health problems are also common in the 11–16 age group, with around one in eight meeting thresholds for clinical diagnoses at any one time. Sefton’s (2010) research highlights that mental health problems are much more common among certain groups of young people, such as those looked after by local authorities, and in custody. Evidence from the CSJS suggests that both mental health problems, and social welfare and wider civil law problems, are more common among 18–24 year olds who are Not in Education, Employment or Training (NEET) than those who are working or studying. Stress-‐related illness, loss of confidence and worry, as a result of civil law problems generally, are also more common among those who are NEET.
“Social welfare law and civil law problems can lead to and/or exacerbate stress and depression in particular, and can also have wider impacts on mental health, such as causing worry and loss of confidence. Notwithstanding the difficulties in establishing cause and effect, it seems clear that social welfare law advice should have a role to play in improving mental health, and in thus reducing the social and economic costs associated with mental ill-‐health”.
(Sefton 2010)
4.106 Several studies have sought to demonstrate the impacts of advice quantitatively, using recognised measures of health. Some of these have compared mental health scores before and after advice. Some have also compared changes in mental health scores between clients who received advice and gained as a result, and those who did not. A small number of statistically significant improvements in mental health scores following advice have been noted, as have a small number of significantly greater improvements among those who gained as a result of advice, compared to those who did not. Other quantitative studies, including two randomised controlled trials, did not generate statistically significant findings. This however appears due to methodological limitations as much as anything else (Sefton 2010).
4.107 Kendrick (2009) highlights that social welfare problems relating to issues such as housing, homelessness, debt, welfare benefits, education and employment can lead to a range of adverse consequences for young people, most commonly involving young people becoming ill, losing income or losing confidence. He references the substantial evidence of the adverse impact of social welfare problems on young people’s mental and emotional health, with around a quarter of young adults experiencing stress-‐related illness, of whom around a third go on to use NHS services. However, 70% of young people self-‐reported that their levels of stress improved as a result of getting advice from a youth advice agency. The report also outlines that around one in ten young people also experience physical ill health as a result of

54
The Role of Advice Services in Health
their social welfare problems, with around half of these young people visiting a GP, hospital or other healthcare worker at an average cost to the NHS of around £650 per case.
4.108 Research conducted by Balmer & Pleasence (2012) found exceptionally high levels of mental illness among clients of youth advice users. The research used the General Health Questionnaire (GHQ-‐12) to survey 188 young people presenting for social welfare advice in youth advice settings across 16 sites operated by 14 different agencies throughout England and Wales. All eligible clients presenting for advice during the short survey period were surveyed and the research results revealed:
• 45% of clients reported their health suffering as a result of their social welfare problems;
• 26% of clients visited a doctor or counsellor, equating to a knock-‐on cost to the health service of £181,068 for every 1,000 clients of youth advice agencies;
• 40% of clients became homeless, with knock-‐on costs to public services of £1,438,904 per 1,000 young clients;
• 12% of clients had contact with social services, equating to knock-‐on costs of £1,016,028 per 1,000 young clients;
• 70% of clients felt that advice resulted in improvements in stress (64%) and/or their health in general (34%);
• 42% reported improvements in their housing situation; and
• estimated savings for the NHS from reduced GP visits alone exceeded the average cost of advice provision.
4.109 The research calculated the cost-‐effectiveness of advice on mental health grounds by converting GHQ-‐12 scores from the survey to Quality Adjusted Life Years (QALYS) and concluded that even assuming only modest changes in mental health among those young people reporting improvements, the advice was found to be clearly cost-‐effective on mental health grounds alone (disregarding any other benefits of advice) in a range of scenarios.
4.110 A report on the operation and impact of the Primary Care Advice Liaison (PCAL) service funded by Wirral PCT and delivered by Wirral Citizens Advice Bureau and Advocacy in Wirral provides evidence of the impact of the service on clients and the benefits accruing for GPs (Centre for Labour Market Development 2012). CAB advisers provided generalist advice to 2,163 clients between 1 April 2010 and 31 March 2011 at 62 GP surgeries and within BME communities across the Wirral on issues such as welfare rights, debt and housing. A total of 532 clients were referred to Advocacy in Wirral for longer term mental health support and access to talking therapies. Key impacts highlighted in the report include:
• a decrease in referrals to other specialist mental health services;
• reduced medication for patients;
• reduced levels of anxiety and depression for patients (76% clients reported reduced levels of anxiety and depression as a result of the service); and
• fewer repeat GP appointments.
55
The Role of Advice Services in Health
4.111 The report also provides details on responses from GPs participating in the PCAL service, namely:
• 8% of GPs confirmed that they had reduced the amount of medication for their patients as a result of PCAL interventions;
• 43% of GPs reported a reduction in GP appointments for clients who had been assisted by the PCAL service;
• 85% of GPs noticed a decrease in referrals to other specialist mental health services as a result of referring patients to the PCAL service;
• 100% of GPs indicated they were satisfied with the PCAL service, of which 79% were very satisfied;
• 85% of all GPs agreed that patient access to advice and information would be reduced if the PCAL service was no longer available in their practice; and
• 99% of GPs considered the PCAL service to be informative.
4.112 The Direct Impact Research Group and Minogue (2006) report that the process of receiving some initial support from an adviser can also prove effective in addressing anxiety and associated mental health difficulties and in turn can enable and empower clients to take control of their problems and use self-‐help materials to achieve a more sustainable solution to their problems.
4.113 Face-‐to-‐face contact is important in building trust and enabling the adviser to spend sufficient time to give the clients the level of support and help they need. Providing an overview of CAB research on mental health and social exclusion, Cullen (2004) emphasises the importance of face-‐to-‐face advice which can stop clients’ difficulties mounting to a point where they become so stressful they might suffer serious negative health consequences.
4.114 Consilium Research & Consultancy (2013) provide a useful overview of the effectiveness of the different delivery mechanisms service providers use to provide information, advice and guidance (IAG) to members of the public.
Summary
• People affected by severe injury or sudden illness often need advice on issues such as sickness and disability benefits, how to manage debt and mortgages if they are no longer working, and employment rights. It is seldom a single issue that patients have concerns about and without effective support many people find benefit rules governing hospital stays extremely complex.
• Routine screening and assessment of patients accessing specialist hospital services may prove effective in uncovering advice needs and making a positive impact on their financial and social situation.
• Proactive advice services, working closely with health and social care professionals, can assist with the practical demands that arise from dealing with an illness and

56
The Role of Advice Services in Health
should be considered an important part of a holistic approach to treatment.
• Evidence from advice services working as part of cancer treatment or mental health services demonstrates the range of benefits including improvements in psycho-‐social aspects of health such as levels of energy and tiredness and improved mental health.
• Embedding advice services within secondary or tertiary care settings can free-‐up hospital and social work staff from having to meet this advice need, which they are not in a position to provide given that welfare rights advice is not their primary function. It can also help resolve issues that may prevent scheduled discharge such as, for example, unsuitable housing conditions.
• Community services are not always accessible to mental health service users and barriers that inhibit the general public from getting help with debts associated with stigma and fear are exacerbated for people who have mental health problems. As such, the effective coordination of mental health and legal services is likely to improve both health and justice outcomes.

57
The Role of Advice Services in Health
5 Mapping of current work joining up health and advice services
5.1 The call for examples of existing or recent projects generated 58 examples of advice services working in health settings. Whilst never intended to represent a ‘census’ of all such activity, the selection provides a cross-‐section of projects and reflects the scale, scope and diversity of services, with examples of different approaches and models used across a range of settings, supported by a range of funding mechanisms and with objectives to support a variety of client groups. In many cases (e.g. Macmillan benefits advisors or CAB provision in GP surgeries) the projects will be replicated in other areas using identical models based on established practice.
5.2 Whilst difficult to ascertain funding sources in all cases without detailed consultation, most projects are either commissioned (e.g. through CCGs, public health or adult social care) or supported through one or more grants, with several examples developed as part of the work of the ASTF partnerships. It is apparent that many of the examples have been delivered in some form for several years and have to some extent been reshaped to fit within the parameters and criteria of changing funding arrangements. A number of the projects have progressed from receiving funding from short-‐term grants to now being funded as part of mainstream provision.
Advice services based in primary care settings
5.3 Just over half of the mapped examples are based in or work predominantly in primary care settings.
Advice services based in GP surgeries
5.4 The most common service mapped is the provision of advice services located within GP surgeries. Whilst the parameters of scope of such services varies considerably from small-‐scale pilots in small clusters of surgeries to borough-‐wide initiatives, providers including Citizens Advice Bureaux report the benefits of being able to engage with clients accessing a trusted service/location.
5.5 The mapping exercise highlighted a range of different approaches that advice services are using to engage with clients with advice needs, administer referrals/appointments and ultimately deliver advice to clients who are typically accessing health services through their GP. Variations in the mapped services are summarised next:
• The majority of projects utilise pre-‐booked appointments, mainly in the GP surgery, although there is a small element of drop-‐in provision.
• A small proportion of projects host pre-‐booked sessions in another location (e.g. advice provider premises near to the GP) having obtained a referral from a project/individual based in the GP surgery.
• Appointments and referrals are made by a range of individuals including GP
58
The Role of Advice Services in Health
receptionists, centrally via the advice provider or through an umbrella organisation or website.
5.6 Projects seeking to host, co-‐locate or operate advice services in GP surgeries highlight a number of barriers which have hindered progress in a number of cases. These include:
• A lack of available space in which to undertake confidential discussions in GP surgeries, especially given the range of additional services delivered from these locations.
• Difficulties in engaging GP surgeries to discuss the potential to introduce advice sessions including a lack of top-‐down support from, for example, CCGs, to encourage partnership working and issues with actually contacting GPs given their administrative workload, prioritisation of medical paperwork and lack of local infrastructure to market projects.
• GPs, practice managers and receptionists not recognising the potential value of advice services to their practice and clients.
5.7 Examples of projects operating in primary care settings include:
Transition Project South Tyneside – Age UK South Tyneside
This pilot stage is being delivered in three GP surgeries in South Tyneside with plans to extend into a further 18 (75% of surgeries in the borough) and provides a referral to an advisor from one of three agencies able to offer advice on a wide range of issues including debt, benefits, housing, fuel poverty etc. The project seeks to deliver three main outcomes:
• access for clients to a more efficient, effective and collaborative advice service across the borough;
• access through social prescribing to advice provision via health professionals leading to early intervention and prevention of deeper health and social problems; and
• greater choice of accessibility points and channels of delivery for advice and information needs.
Primary Care Advice, Liaison and Advocacy Service – Wirral Citizens Advice Bureaux
Wirral Citizens Advice Bureaux deliver a generalist advice service for patients referred by their GP with common mental health needs and other long-‐term conditions, providing a telephone gateway and appointment booking service for face-‐to-‐face advice. Clients in need of advocacy services are referred to the Bureau's commissioned partner, Advocacy in Wirral Health. The service has gradually grown to serve all of the 60+ GPs surgeries and medical centres in the area and is now commissioned by the CCG. It has been recognised as an example of good commissioning by NHS clinical commissioners in the ‘Taking the lead' report.
59
The Role of Advice Services in Health
Projects based in secondary/tertiary care settings
5.8 Around 15% of the mapped examples were based in secondary or tertiary care settings (e.g. healthcare provided by a specialist or facility following referral by a primary care physician). The majority of these projects focus on either people affected by cancer and other long-‐term conditions or people with mental health problems. Examples include:
Heathlands CAB – Rushmoor Citizens Advice Bureau
Delivered in partnership with Surrey and Borders Partnership Trust, including sessions on the acute psychiatric ward, Community Mental Health Recovery Services, Home Treatment Team etc., this project provides full CAB casework services to clients with severe and enduring mental health issues and their carers.
Projects supporting people affected by cancer
5.9 Examples of advice services provided to support people affected by cancer are dominated by the work of the Macmillan Welfare Benefits Service which is replicated in many hospital settings around the UK. Two examples taken from the mapping exercise include:
Macmillan Welfare Benefits Service – Scottish Borders Council
This advice service has been fully integrated into the Borders Macmillan Centre at Borders General Hospital in Melrose since August 2009 with staff co-‐located with designated work stations within the centre. Since 2013, the service has been jointly funded by Macmillan Cancer Support and Scottish Borders Council.
Clatterbridge Cancer Centre NHS Foundation Trust (Liverpool)
There has been a Macmillan Benefits Advice Service at Clatterbridge Cancer Centre for the past 13 years. It was initially funded by Macmillan but now the service is funded by the Trust. The service is part of the hospital’s Cancer Rehabilitation and Support Team (CReST) which is a multidisciplinary team including social workers, occupational therapists, physiotherapists, chaplains, specialists in palliative Care, psychological medicine and teenagers and young adults etc.
This project provides cancer-‐specific benefits advice to patients attending for radiotherapy or chemotherapy treatments, or who are admitted as in-‐patients due to treatment for side effects or progressive disease. It also provides advice to people receiving curative treatment as well as those with an incurable disease or nearing end of life. The service can help with simple debt matters but will refer on for complex debt issues.
60
The Role of Advice Services in Health
Projects supporting people with mental health problems
5.10 A small number of projects are focused on clients with mental health problems with objectives to complement health-‐related support with advice and guidance across a range of areas including welfare, employment and housing.
Steps to Wellbeing – Dorset HealthCare
The Steps to Wellbeing Service is a free, confidential NHS service for people aged 18 and over who are experiencing mild to moderate depression and anxiety disorders and are registered at either a Dorset or Southampton GP surgery.
The programme is commissioned by Southampton CCG will run for five years (commencing in 2014). They have a range of KPIs but the ultimate goal is moving people into employment/back into employment and maintaining their employment. Following assessment by a clinical worker the clients received either a quick IA support or longer-‐term invention which may involve the worker liaising with unions or employers on their behalf.
An Employment Service Coordinator is embedded as part of the clinician team and so has access to clinical records of people receiving clinical treatment for mental health issues (through NHS IAPT services treating conditions such as depression and anxiety).
A team of psychological wellbeing practitioners (PWPs) provide most of the assessments in the service and provide a range of different support options including face-‐to-‐face and telephone guided self-‐help, groups and computerised Cognitive Behavioural Therapy (cCBT) programmes. The key role of the PWP is to support people to better understand the difficulties they are experiencing and to develop the skills and resources to manage or overcome them. This could include signposting people to other agencies and services that may be able to them.
Other health settings
5.11 Around a third of mapped examples are based in other settings (e.g. outreach provision in community venues) but maintain strong links with health services (mainly as a source of referral).
5.12 The mapping exercise identified a range of complementary or underlying services and initiatives which operate from or through health settings in order to strengthen the quality of referrals and advice provision overall. There are several examples of projects which are complemented by the development of common referral systems and training for advisers in order to increase the efficiency and quality of referral mechanisms and ultimately the effectiveness of the advice.
Wigan Borough Clinical Commissioning Group started a pilot Community Connector project with two GP clusters in January 2015. The project has aims to support patients in connecting to appropriate non-‐medical support with a strong emphasis on voluntary and community sector services including advice and information services. The project combines

61
The Role of Advice Services in Health
development of a common referral system with training and establishing a Skype service in community venues.
5.13 A number of projects highlight the use of staff (e.g. key workers) employed to link advice services with a range of health settings and professionals. The role is usually centred on establishing relationships with services supporting people with a range of advice needs and encouraging the efficient signposting and referral of cases. Examples include:
The ASTF-‐funded project, Transforming Advice, in Hertsmere, is working in conjunction with the new role of Community Navigator, who in turn works directly with hospital discharge teams. Two of the partners are mental health charities offering drop-‐in provision on Thursday mornings alongside another charity supporting carers whilst other partners have contact with clinical commissioning groups and carers’ champions enabling outreach provision to be available every day in the borough with three venues increasing to nine.
Croydon Voluntary Action employs ‘family navigators’ as part of its Croydon Family Power project based part-‐time in GP surgeries to work with families and take a key worker role in referring families to other services. Family navigators will each work with 50 families, playing an advocacy role and helping families to navigate the raft of services and support, enabling them to cope better and improve their resilience. The Family Navigators enable parents to make independent choices that are good for them and their families, accessing intensive support where needed. Family navigators work closely with the local early intervention and family support service including the family resilience service, children centres, extended school clusters and commissioned service and voluntary sector service providers.
Manchester Advice Alliance, Manchester Citizens Advice Bureaux
The Manchester Advice Alliance is a network of advice agencies working together to improve advice and information services for the residents of Manchester. The Alliance has been developed in order to sustain and transform existing advice provision through partnership working (e.g. shared funding bids) and with an emphasis on increasing the influence of advice providers to work more effectively with commissioners and stakeholders (e.g. RSLs and GPs). It also aims to embed advice within a range of services including health in addition to upskilling information and advice workers to support effective signposting.
A range of projects are ongoing in the Manchester area with the support of Manchester Advice Alliance partners including an ongoing contract to deliver outreach advice services in GP surgeries in one of the three CCG areas covering Manchester; Shelter working in partnership to support troubled families in hospital/urban village settings; and work just beginning through Age UK to place staff/volunteers in the A&E department in Manchester Royal Infirmary.
62
The Role of Advice Services in Health
Bradford Community Advice Network
The Community Advice Network (CAN) is a federation of local advice charities working across Bradford District. It provides free and quality assured advice to local people in the areas of social welfare legal rights, assisting people with issues from debt and benefits to housing, homelessness, employment rights, immigration, community care and health.
‘Full’ members of CAN have been awarded the national Advice Quality Standard (AQS) or the Specialist Quality Mark (SQM). A registered charity, the elected Trustee Board is made up of 15 ‘full member’ representatives from local advice charities.
The Network aims to improve the knowledge and skills base of members of independent advice centres, the legal, social work and community work professions, public authorities and interested members of the public generally by:
• increasing knowledge of social welfare law and policies as they affect people suffering financial hardship or discrimination within the Bradford district; and
• developing the quantity, quality and efficiency of independent legal advice services for people experiencing financial hardship or discrimination within the Bradford district.
This is achieved by supporting advice workers in places where people already go or where they are more likely to have an advice need to prevent problems escalating in both complexity and cost. Support is available in almost all GP surgeries/primary healthcare centres in the district whilst key community mental health centres also host advice sessions.
Services are funded by Bradford Council, using a combination of adult social care and public health funding. Promotion of advice sessions takes place at the GP surgeries, health centres and mental health centres with most targeted at ‘registered patients/service users only’ and booked at the health centre. Sessions can also be booked via the CAN website or through the main offices of the delivery agencies where reception staff can check if the client is registered with a GP and contact the surgery to check for the next available appointment.
Approaches to monitoring and evaluation
5.14 Generally advice services tend to collect simple output information as standard – such as the number of advice sessions delivered and the number and characteristics of clients (age, gender, advice areas covered etc.). Where impact evidence is collected this focuses on the wider social determinants of health such as increased income rather than the health outcomes resulting from the advice. Where evidence of health outcomes are gathered this is largely characterised by anecdotal evidence and qualitative case studies.
5.15 It is evident from a number of the mapped services that advice providers are not being required to gather evidence of health outcomes or service efficiencies to report back to funders. The reasons for this are unclear and merit further exploration with commissioners to determine what level of evidence of impact they are looking for to have confidence that the commissioned service is meeting local health and advice needs.
5.16 Based on consultations with a sample of advice services the provision of stronger guidance and support from commissioners would greatly assist the process of establishing appropriate monitoring and measurement systems to gather health impact evidence.
63
The Role of Advice Services in Health
5.17 In many cases additional resources and support are likely to be required to ensure that the approach to measuring impact is robust, credible and suitably aligned to meet the advice and health needs outlined in the local health and wellbeing strategy.
5.18 Where systems for capturing health outcomes are in use, evidence from the mapped services suggests that this is generally undertaken using a before and after assessment with clients, most commonly using the Warwick–Edinburgh Mental Wellbeing Scale (WEMWBS). However, there are few examples of published impact data based on this approach with the majority of services relying on anecdotal feedback from clients. Whilst qualitative feedback provides a useful source of data to support an assessment of impact this may fall short of the evidence standards that commissioners may be looking for to clearly demonstrate the impact of advice on alleviating pressure on health services and contributing to sustainable improvement in the health of the local population. Examples of the approaches used by mapped services to evaluate health impacts are provided below.
Mental ill-‐Health and Benefits project – Money Advice Unit, Hertfordshire County Council
Funded through mainstream budgets from April 2014, the Mental ill-‐Health and Benefits project supports three community-‐based advisers to work alongside multi-‐disciplinary mental health staff to resolve the many benefit and money problems that impact on mental health – fitness for work assessments, PIP and DLA claims, benefit sanctions, anxiety caused by high-‐cost loans and debt etc. The project has aims to both improve individuals’ financial position and their mental health and wellbeing with a view to benefiting the NHS in terms of reduced hospital admissions, fewer GP visits, reduced medications and other interventions.
Service users complete a ‘before and after’ wellbeing survey (WEMWBS) to gauge if the intervention has made any difference to them, albeit with limited results to date because of the time required to action benefit assessments and decisions.
The staff are managed by the Money Advice Unit, but mainly community-‐based within mental health teams supplying advice, support, training and expertise as well as taking on casework. Referrals can be made by any health or social care professional from GPs through to support workers and psychiatrists although the majority of referrals come from health professionals within mental health teams.
Scarborough and District Citizens Advice Bureau
ASTF funding has supported a two year project targeted at people with mental health problems and/or physical/sensory impairment. Managed by Scarborough and District CAB in partnership with MIND and two local disability charities, the project receives referrals from any health organisation for a fast-‐track appointment with CAB to assess advice needs and if required a further referral to MIND or the disability charities for long-‐term support offering a sustainable outcome. Approximately 20% of the 700 people supported by the project are referred directly through health settings/professionals, with the remainder engaged indirectly through project promotion.
The project has developed its own assessment tool, the 'Wheel', to assess progress in terms of health and wellbeing. Clients are asked how they feel against key criteria on entry to the service, asked where they'd like to reach on scale of 1–10 and asked again at the end of a three-‐month period.

64
The Role of Advice Services in Health
The ‘Wheel’ was developed by MIND locally along with an evaluation of the impact and validity of the tool by a funded PhD researcher from Leeds University. The local CCG will also be analysing data from 50 clients supported through the project in order to assess cost savings to health attributable to the project.
Common themes
5.19 A number of common themes have emerged in the process of collating information of current or recent advice projects active in health settings. One of these relates to the considerable variation across commissioners on their approach to engaging the advice sector or requirements when commissioning services. At one end of the spectrum there are examples of commissioning partners making considerable investments in advice services to address deprivation and health inequalities. For example Liverpool CCG has commissioned Liverpool Citizens Advice Bureaux to deliver a £1 million Advice on Prescription service across 95 GP practices over three years. At the other end of the spectrum advice service providers are struggling to engage key commissioners and services are being decommissioned due to financial pressures. Anecdotally a number of advice service providers report struggling to fit existing services within rigid commissioning criteria and losing funding as a consequence.
5.20 Another common theme relates to challenges of securing buy-‐in and participation from GPs. A number of the services have struggled to secure buy-‐in even though the service has been directly commissioned through the CCG or public health team. Whilst financial support through health commissioners can help achieve better buy-‐in. This is by no means guaranteed: suggesting that stronger messaging and direction from central government, Public Health England and professional membership bodies such as the Royal College of GPs is needed to pave the way for more fruitful partnership working at the local level.
5.21 Consultation with a sample of advice organisations and services may also suggest that further work is needed to ensure that the advice sector is more clearly represented within the new health and wellbeing boards. Given the evidence base highlighting the important contribution that advice services can make to tackling the wider social determinants of health, it is essential that the advice sector has a stronger voice in the local structures used to enable health and care partners to work collaboratively to improve the health and wellbeing of their local population and reduce health inequalities.
5.22 The advice sector is also well placed to contribute to the process of compiling the local JSNA and ultimately the health and wellbeing strategies. Indeed given that local authorities now have a duty under the Care Act 2014 to develop and implement a plan for information and advice services that are integrated into the local joint health and wellbeing strategies, commissioners should actively engage advice service providers to support the development of a strategic approach to addressing the advice needs of the population.

65
The Role of Advice Services in Health
Summary
• The mapping has identified examples of different approaches and models of advice services working across a range of health settings, supported by a range of funding mechanisms and with objectives to support a variety of client/patient groups.
• Many of the advice services have been delivered in some form for several years and have been reshaped to fit within the parameters and criteria of changing funding arrangements. A number of the projects have progressed from receiving funding from short-‐term grants to now being funded as part of mainstream provision.
• Where impact evidence is collected this focuses on the wider social determinants of health such as increased income rather than the health outcomes resulting from the advice. In many cases advice providers are not required to gather evidence of health outcomes or service efficiencies to report back to funders.
• There is evidence of considerable variation across commissioners as to their approach to engaging the advice sector or their requirements when commissioning services. A number of advice service providers report that they are struggling to fit existing services within rigid commissioning criteria and have lost funding as a consequence.
66
The Role of Advice Services in Health
6 Evaluation and monitoring
6.1 The importance of robust, appropriate and credible approaches to measuring the impact of advice services work is a common theme running through both the evidence review and the mapping work. Indeed the stronger focus on outcomes-‐based commissioning reinforces the need for advice providers to ensure that they have sufficient capacity, skills and expertise to measure their success in meeting their commissioned outcome targets.
6.2 However, advice projects face real challenges in establishing appropriate measurement systems that can report statistically significant differences between the health outcomes achieved for people accessing advice services and those with advice problems that do not. Designing and delivering robust evaluative studies also requires suitable support from health partners, in particular facilitating access to personal health records and data which can be used alongside self-‐reported data from clients gathered using questionnaire-‐based measurement systems.
6.3 The lack of studies with long-‐term follow-‐up of clients is important as physical health benefits might take time to emerge following an advice intervention. Equally improvements in mental wellbeing may be temporary and as such it is pertinent to understand the extent to which the advice is effective in empowering clients and building their resilience (see Consilium Research & Consultancy 2013 for further detail). As outlined by Allmark et al. (2013) the demonstration of significant positive effects using standard baseline and outcome measures presents considerable challenges.
6.4 Given these challenges and the lack of clear guidance from commissioners about what health outcomes they would like to see advice services contributing to, it is unsurprising that many have focused on evidencing non-‐health outcomes. The question this raises is whether being able to provide evidence of progress in achieving the ‘primary outcomes’ outlined in the logic model produced by Allmark et al. (2013) is sufficient for commissioners given the strong evidence base linking these social determinants to improvements in health and wellbeing.
6.5 The evidence review and existing advice services suggest than a number of health measurement tools have and are being used to demonstrate the health and wellbeing improvements achieved as a consequence of an effective advice intervention. Examples of tools which have been used successfully include:
• General Health questionnaire (GHQ-‐12) • Hospital Anxiety and Depression Scale • Health Assessment questionnaire • Nottingham Health Profile • Patient Health questionnaire 9 (PHQ-‐9) • SF-‐36 health questionnaire
67
The Role of Advice Services in Health
• Warwick–Edinburgh Mental Wellbeing Scale (WEMWEBS).
6.6 However, the evidence review also illustrates that qualitative and quantitative approaches can produce divergent findings when applied to the same intervention. Each method may capture different aspects of the service.
6.7 A qualitative approach can enable participants to give an account of the various ways in which the advice intervention impacted on their lives which are not explicitly measured in an RCT approach and are challenging to capture quantitatively (Moffatt et al. 2006).
6.8 Many of the research reports reviewed in part 4 identify a need for further research to improve the level of understanding of the complex links between advice and health. Dialogue between the advice sector and commissioners could help identify those priority areas where the evidence base needs to be strengthened through further research. This process can help to better position the advice sector to compete for opportunities through local commissioning arrangements and to make a stronger case for the role of advice in supporting local health and wellbeing priorities.
6.9 The intended outcomes of advice services can be mapped onto the outcome frameworks used by adult social care,16 the NHS17 and Public Health England18 within which self-‐reported wellbeing and quality of life feature prominently. The NHS Outcomes Framework specifically focusses on helping people recover from episodes of ill health or injury, in a process , as the evidence review highlights, advice services can play a central role. Gaining a better understanding of the frameworks of health and social care outcomes and of the language of commissioning will be an important step to prevent the existing evidence base in the most relevant and compelling way.
16 https://www.gov.uk/government/publications/adult-‐social-‐care-‐outcomes-‐framework-‐ascof-‐2015-‐to-‐2016 17 https://www.gov.uk/government/publications/nhs-‐outcomes-‐framework-‐2015-‐to-‐2016 18 https://www.gov.uk/government/statistics/public-‐health-‐outcomes-‐framework-‐february-‐2015-‐data-‐update

68
The Role of Advice Services in Health
Summary
• The stronger focus on outcomes-‐based commissioning reinforces the need for advice providers to have sufficient capacity, skills and expertise to measure their success in meeting their commissioned outcome targets.
• Advice services face real challenges in establishing appropriate measurement systems that can report statistically significant differences between the health outcomes achieved for people accessing advice and those with advice problems that are not accessing advice.
• There is a wider question as to what evidence standards commissioners expect and what is realistic given the context of clients accessing support through advice services, and the methodological and ethical issues presented by longitudinal tracking.
69
The Role of Advice Services in Health
7 Gaps in the evidence base
7.1 This evidence review acknowledges the relative absence of robust evidence, quantifying the health outcomes derived from locating advice services in health settings – in particular where the advice helps to address the wider social determinants of health.
7.2 The main gap in the evidence base is empirical work proving the outcomes and impacts of advice services in health settings, especially evidence produced as a result of controlled or longitudinal studies. Inescapably, the longer term benefits of advice provision can take many years to fully emerge and in some cases interventions may require many levels of support for clients over a period of time. As such, analysis undertaken as part of time-‐limited evaluations will inevitably fail to capture longer-‐term outcomes and may struggle to disaggregate or identify the catalysts for improving health outcomes.
7.3 Much of the research base also fails to provide a robust analysis of the actual cost-‐benefits and efficiencies delivered for health services (i.e. the degree to which the provision of advice in health settings can be attributed to reduced clinical pressures, earlier hospital discharge, prevention of relapse and reduced readmission rates). Crucially, the strength of causality between advice and health-‐related outcomes is entirely significant when analysing the effectiveness and added value provided by different approaches and delivery models.
7.4 An analysis of the evidence base reveals a lack of studies focusing on specific advice areas or exploring solutions to issues resulting from a specific social determinant (e.g. financial problems or a physical disability). With relevance to the multi-‐faceted nature of advice problems which contribute to ill health, many projects and studies offer a generalist service with the offer of signposting or referral to specialist services where required.
7.5 There is also a relative absence in the evidence base of studies providing learning and insight from the delivery of advice to specific groups including migrants and asylum seekers. Many studies, especially those based in primary health settings, provide analysis across a range of client groups (i.e. a universal service). Moreover, the evidence base offers little in terms of demonstrating positive physical health outcomes which can be attributed to advice provision. Indeed, most studies, where health outcomes are assessed to varying degrees, focus on wellbeing or generic outcome indicators.
7.6 The nature of the REA Framework agreed for this study has maintained a focus on the impact of advice delivered in health settings (e.g. GPs, hospitals and specialist health services). With the move towards health and social care integration, a wider range and a greater number of settings could also be incorporated into the REA process. Indeed, it is highly likely that some advice providers will be active in a range of social care settings (e.g. residential care, day care or domiciliary care), complementing the advice delivered in health settings and supporting the aggregation of overall health outcomes.
70
The Role of Advice Services in Health
7.7 This point is of particular importance given the existence of multiple commissioners and range of grant funding available to support relevant interventions, with a need for advice partners to engage not only with CCGs and public health commissioners, but also adult social care commissioners and children’s services commissioners.
7.8 Acknowledging the limitations of the REA process, the gaps in evidence are reflected in the following calls for future research:
• Studies to assess the health impacts of advice delivered in social care settings and/or where health and social care providers work in partnership.
• More research is needed looking into the longer-‐term health impacts of advice delivered in health settings through longitudinal assessments and/or studies revisiting clients accessing services in the past to analyse impact.
• Efforts to gain a greater understanding of actual and perceived barriers that exist amongst primary care professionals (and indeed funders and commissioning bodies) which can be used to promote greater partnership working with advice providers in the future. And
• Future research exploring the impacts of advice projects offering services to specific client groups or concentrating on specific service areas in order to explore the relative strengths and impacts of the component elements of many ‘multi-‐faceted support packages’.
71
The Role of Advice Services in Health
8 Conclusions
8.1 This report provides a summary of the evidence collated on health outcomes and advice and presents an overall picture of the effectiveness of work with clients/patients. It also presents the results of a mapping exercise aimed at identifying current or recent advice work in health settings.
8.2 Pressures on the NHS are increasing all the time; demand is growing rapidly with the aging population and with long-‐term conditions becoming more common. More sophisticated and expensive treatment options are also becoming available, further increasing the workload of health care professionals and demands on the system. Both the Acheson Report and The Marmot Review highlight that a successful and sustainable approach to reducing health inequalities will require action and support from outside of the NHS. Addressing the wider social determinants of health demands stronger collaborative working across a range of sectors.
8.3 The Health and Social Care Act 2012 for the first time placed a duty on the Secretary of State, NHS England and clinical commissioning groups to give due regard to the reduction of inequalities. Local authorities have taken on new duties around public health and are also required to develop and implement a plan regarding their information and advice services under the Care Act 2014. A stronger focus on prevention, early intervention and coordinated planning around information and advice services should provide new opportunities for health and advice sectors to work more closely to tackle health inequalities and improve health and care outcomes.
8.4 What is apparent is that the current approach to the funding of advice is unsustainable with people in need of support finding it increasingly difficult to access services due to funding cuts. The reduction of financial support is placing pressure on advice services, with fewer advice agencies and diminished capacity among those that survive to proactively respond to people's issues over the longer term. There is considerable scope for the advice and health sectors to work more closely and strategically to meet advice needs and contribute to reducing health inequalities by addressing the wider social determinants of health.
Evidence review
8.5 There is considerable variation in the quality and rigor of the research reports identified in the evidence review. Examples range from research studies based on a randomised control trial to small-‐scale pilot studies that present qualitative evidence from a handful of advice service users using a case study format. The evidence also provides wide variance in the definition of a positive health and wellbeing outcome which makes any overall analysis problematic.

72
The Role of Advice Services in Health
8.6 There is also a lack of consistency in the research reports regarding the measurement tools used to assess the impact of different advice services working across various health settings. A number of studies point to the need for follow-‐up research, in particular longitudinal assessments and studies focusing on the potential for cost-‐savings for health services of early intervention and prevention.
8.7 The relationship between indebtedness and poor mental health is explored in a wide range of studies. The evidence demonstrates that people getting advice experience a range of benefits in terms of lower anxiety, better general health and relationships, and housing stability. These are in addition to the cumulative impact of the primary outcomes of advice, such as having debt written off, home loss avoided and increase in annual income.
8.8 Early identification and intervention are important to prevent people struggling with debt to access appropriate advice and guidance from requiring mental health treatment. Specialist welfare advice for people using secondary mental health services can deliver cost savings by reducing inpatient lengths of stay, preventing homelessness and preventing relapse for severe mental illness.
8.9 Improving the financial, material and social circumstances of people presenting at primary care can underpin sustainable improvements in health. Advice services function to address inequalities in health relating to poverty and deprivation, providing a means by which primary care organisations can address the social, economic and environmental influences on the health of the population. Stronger partnerships between advice services and healthcare partners have the potential to affect system change in order to challenge and change policies that are exacerbating health inequalities in society and creating demand for health provision.
8.10 GPs and other community-‐based health staff are well placed to detect the wider factors affecting the health of a population, who might not otherwise access advice services. Although the majority of GPs believe that patients not being able to access legal or specialist advice about their problems would have a negative impact on their health, there is a lack of consensus amongst GPs and primary care professionals as to the appropriateness of their role in tackling wider social determinants of health.
8.11 There is also an absence of high quality studies demonstrating statistically significant impacts on health of advice services. This raises a wider question as to what evidence standards health commissioners are seeking when commissioning health interventions and the extent to which advice services can (or should be expected to) meet these standards when looking to secure investment. A number of studies do present evidence of positive impact of advice services in improving health including reduced stress and anxiety, better sleeping patterns, reversal of weight loss, changes in medication, reduced contact with the primary care team, reduction or cessation of smoking, and improved diet and physical activity.
8.12 Less evidence is available which clearly demonstrates actual cost or efficiency savings delivered through advice services working in primary care. Where these are included within studies they have largely tended to infer or assume that such savings will be delivered (as

73
The Role of Advice Services in Health
opposed to offering concrete suggestions as to how to establish appropriate systems to measure these savings).
8.13 People affected by severe injury or sudden illness often need advice on issues such as sickness and disability benefits, how to manage debt and mortgages if no longer working, and employment rights. Patients are rarely concerned about a single issue, and without effective support many people find benefit rules governing hospital stays extremely complex.
8.14 The evidence base suggests that routine screening and assessment of patients accessing specialist hospital services may prove effective in uncovering advice needs and making a positive impact on their financial and social situation. Proactive advice services, working closely with health and social care professionals, can assist with the practical demands that arise from dealing with an illness and should be considered an important part of a holistic approach to treatment.
8.15 Embedding advice services within secondary or tertiary care settings can free-‐up hospital and social work staff from having to meet identified advice need, which they are not in a position to provide given that welfare rights advice is not their primary function. The evidence also demonstrates that it can help to resolve issues that may prevent scheduled discharge such as, for example, unsuitable housing conditions.
Mapping
8.16 The mapping exercise has identified examples of different approaches and models of advice services working across a range of health settings, supported by a range of funding mechanisms and with objectives to support a variety of client/patient groups. Many of these advice services have been delivered in some form for several years and have been reshaped to fit within the parameters and criteria of changing funding arrangements. A number of the projects have progressed from receiving funding from short-‐term grants to being funded as part of mainstream provision.
8.17 Where impact evidence is collected this focuses on the wider social determinants of health such as increased income rather than health outcomes resulting from the advice. In many cases advice providers are not required to gather evidence of health outcomes or service efficiencies to report back to funders. There is evidence of considerable variation across commissioners as to their approach to engaging the advice sector or their requirements when commissioning services. A number of advice service providers report to be struggling to fit existing services within rigid commissioning criteria and have lost funding as a consequence.
8.18 A common theme from the evidence review and mapping exercise relates to the challenge of securing buy-‐in and participation from GPs. A number of the advice services identified in the mapping report to have struggled to secure buy-‐in even though the service has been directly commissioned through the CCG or public health team. Whilst financial support through health commissioners can help to achieve better buy-‐in it is by no means a guarantee, suggesting that stronger messaging and direction from central government and

74
The Role of Advice Services in Health
professional membership bodies such as the Royal College of General Practitioners is needed to pave the way for more fruitful partnership working at local levels.
8.19 Consultation with a sample of advice organisations and services also suggests that further work is needed to ensure that the advice sector is more clearly represented within the new health and wellbeing boards. It is essential that the advice sector has a stronger voice in the local structures used to enable health and care partners work collaboratively to improve health and wellbeing in their local communities and reduce health inequalities.
8.20 The advice sector is also well placed to contribute to the process of compiling the local JSNA and ultimately the health and wellbeing strategies. Given that local authorities now have a duty under the Care Act 2014 to develop and implement a plan for information and advice services that are integrated into the local joint health and wellbeing strategies, commissioners should actively engage advice service providers to support the development of a strategic approach to addressing the advice needs of the population.
Evaluation and monitoring
8.21 The stronger focus on outcomes-‐based commissioning reinforces the need for advice providers to have sufficient capacity, skills and expertise to measure their success in meeting their commissioned outcome targets. Advice service face real challenges in establishing appropriate measurement systems that can effectively report statistically significant differences between the health outcomes achieved for people accessing advice and those with advice problems that are not accessing help.
8.22 This raises a wider question as to what evidence standards commissioners expect and what is realistic given the context of clients/patients accessing support through advice services and the methodological and ethical issues presented by longitudinal tracking.
Gaps in the evidence base
8.23 The major gap in the evidence base is empirical work depicting the outcomes and impacts of advice services in health settings and especially evidence produced as a result of controlled or longitudinal studies. Inescapably, the longer term benefits of advice provision can take many years to fully emerge and in some cases interventions may require many levels of support for clients over a period of time. As such, analysis undertaken as part of time-‐limited evaluations will inevitably fail to capture longer-‐term outcomes and may struggle to disaggregate or identify the catalysts for improving health outcomes.
8.24 Much of the research base also fails to provide a robust analysis of the actual cost-‐benefits and efficiencies delivered for health services (i.e. the degree to which the provision of advice in health settings can be attributed to reduced clinical pressures, earlier hospital discharge, the prevention of relapse and reduced readmissions). Crucially, the strength of causality between advice and health-‐related outcomes is significant when analysing the effectiveness and added value provided by different approaches and delivery models.
75
The Role of Advice Services in Health
Recommendations
8.25 The recent follow-‐up report on tackling the advice deficit published by The Low Commission (2015) incorporates a series of recommendations supported by this evidence review and mapping exercise.19 Key amongst these are:
Health and social care commissioners should always ensure that their plans include social welfare advice and legal support provision.
Every mental health service should secure specialist welfare advice to help to support recovery and to intervene early when difficulties emerge.
Government should consider including welfare advice in its outcomes frameworks for the NHS, social care and public health.
8.26 The following recommendations are also provided and reflect the key themes identified in this report:
1. The Project Advisory Steering Group should convene a workshop involving advice sector representatives and health and social care commissioners to explore the key themes from this report and in particular seek guidance from commissioners on what evidence standards they require when commissioning services to meet local health and care needs.
2. Guidance is needed for commissioners on how to engage and involve the advice sector to support the local JSNA process, and health and wellbeing strategies should also be developed.
3. Clear guidance is also needed for the advice sector on how to use measurement tools and approaches to evidence the impact of advice on clients’ health and wellbeing.
4. Research should be commissioned to address the gaps in the evidence base, most notably research capable of demonstrating actual cost or efficiency savings that could be delivered through advice services working in health settings and proving the longer-‐term health benefits for supported clients.
5. Current health and wellbeing strategies and emerging information and advice plans produced as a statutory requirement of the Care Act 2014 should be reviewed.
6. A project collating evidence of advice services working in social care settings should be commissioned.
19 http://www.lowcommission.org.uk

76
The Role of Advice Services in Health
9 Bibliography
Abbott, S. (2002) ‘Prescribing welfare benefits advice in primary care: is it a health intervention, and if so, what sort?’ Journal of Public Health Medicine 24(4)307–12.
Abbott, S. & L. Davidson (2000) ‘Easing the burden in primary care in deprived urban areas: a service model’ Primary Care Res Dev I. 201–06.
Abbott, S. & L. Hobby (1999) ‘An evaluation of the health and advice project: Its impact on the health of those using the service’. The Health and Community Care Research Unit, University of Liverpool Report. 99/63.
––––– (2000) ‘Welfare benefits advice in primary care: evidence of improvements in health’. Public Health 114(5)324–7.
––––– (2003) ‘Who uses welfare benefits advice services in primary care?’ Health and Social Care in the Community (2003) 11(2)168–74.
––––– (2005) ‘Poverty and health: Primary care patients living at the interface’. Health Education Journal December 2005 64(4)363–71.
Abbott, S., L. Hobby & S. Cotter (2006) ‘What is the impact on individual health of services in general practice settings which offer welfare benefits advice?’ Health Soc Care Community. 14(1)1–8. January 2006.
Aberdeen University Department of Management Studies (2001) ‘CAB Outreach Services: Report on Evaluation of Citizens Advice Bureau Outreach Services at Aberdeen Royal Infirmary and Banff & Buchan’. Aberdeen: AUDMS.
Adams, J. et al. (2006) ‘A systematic review of the health, social and financial impacts of welfare rights advice delivered in healthcare settings’. BMC Public Health 2006(6)81.
Advice Services Alliance (2003) ‘The Impact of Advice’. Advice Services Alliance.
Advice UK (2008) ‘The impact of debt advice on health and wellbeing’. Advice UK .
Ali, A. Wright, N. & M. Rae (2008) ‘Addressing Health Inequalities: A Guide for General Practitioners’. London, UK: RCGP.
Allmark, P. et al.(2013) ‘Assessing the health benefits of advice services: using research evidence and logic model methods to explore complex pathways’. Health and Social Care in the Community (2013) 21(1)59–68.
Atherton, J. (2011) ‘Solid Foundations: Building for the Future’. NHS Sefton.
Balmer, N. & P. Pleasence (2012) ‘The Legal Problems and Mental Health Needs of Youth Advice Service Users: The Case for Advice’. Youth Access.
77
The Role of Advice Services in Health
Balmer, N. Pleasence, P. Buck, A. & H. C. Walker (2006) ‘Worried Sick: The Experience of Debt Problems and their Relationship with Health, Illness and Disability’. Social Policy and Society. 5(1)39–51.
The Baring Foundation (2015) ‘Health Outcomes from Advice: Interim Report’. The Baring Foundation.
Bateman, N. (2008) ‘Just what the doctor ordered: Welfare benefits advice and healthcare’. Age Concern.
Benzeval, M. et al. (2014) ‘How does money influence health?’ Joseph Rowntree Foundation.
Borland, J. (2004) ‘Better Advice, Better Health Final Evaluation Report’. University of Wales.
Borland, J. & D. Owens (2004) ‘Welfare Advice in General Practice – The Better Advice, Better Health Project in Wales’. University of Wales.
British Society of Rehabilitation Medicine (2001) ‘Vocational rehabilitation: the way forward’. London: BSRM.
Brown, I. (2004) ‘The role of the Citizens Advice Bureau in supporting healthcare’. NT Clinical. 7 September 2004, 100(36).
Buck, D. & F. Frosini (2012) ‘Clustering of unhealthy behaviours over time: Implications for policy and practice’. The Kings Fund.
Buck, D. & J. Jabbal (2014) ‘Tackling poverty: Making more of the NHS in England’. The Kings Fund.
Burrows, J. et al. (2011) ‘Citizens advice in primary care: a qualitative study of the views and experiences of service users and staff. Public Health. 2011 Oct. 125(10)704–10.
Burrows, J. et al. (2012) ‘Welfare advice in primary care: A qualitative study of service user and staff perceptions’. School of Health and Related Research, University of Sheffield.
Caiels, J. & M. Thurson (2005) ‘Evaluation of Warrington District CAB GP Outreach Project’.
Cawston, P. (2010) ‘Deep End Report 8: Social prescribing’. Royal College of General Practitioners (Scotland).
The Centre for Labour Market Development, University of Chester (2012) ‘Report into the added value of Wirral CAB’. Wirral CAB .
Chalmers, T. & L. Jones (2005) ‘Final report of the Evaluation of 3 different benefits advice services for people affected by cancer’. Scottish Centre for Social Research.
Citizens Advice (2012) ‘An overview of possible links between advice and health’. Citizens Advice
Collaborations for Leadership in Applied Health Research and Care (2012) ‘The health effects of welfare rights advice and welfare benefits: a critical review’. National Institute for Health Research.
78
The Role of Advice Services in Health
ComRes (2014) ‘GPs and social welfare law’. ComRes.
Consilium Research and Consultancy (2013) ‘Rapid Evidence Assessment: The Effective Delivery of Information Advice and Guidance’. Welsh Government 70/2013.
Cookson, G. & F. Mold (2014) ‘The business case for social welfare advice services: An evidence review – lay summary’. Legal Action.
Cooper, K. & K. Stewart (2013) ‘Does money effect children's outcomes? A systematic review’. Joseph Rowntree Foundation.
Coppel, D.H., C. J. Packham & M. A. Varnam (1999) ‘Providing welfare rights advice in primary care. Public Health 113(3)131–5.
Derbyshire County PCT (2013) ‘Citizen's Advice Bureaux in General Practice’. Derbyshire County PCT.
Direct Impact Research Group & Minogue, V. (2006) ‘Evaluation of a Citizens Advice Bureau (CAB) Mental Health Welfare Rights Project’. Mental Health and Learning Disabilities Research and Practice.
Dobbie, L. & M. Gillespie (2010) ‘The Health Benefits of Financial Inclusion: A Literature Review’. Scottish Poverty Information Unit, Glasgow Caledonian University.
Dowrick, C. May, C. Richardson, M. & P. Bundred (1996) ‘The biopsychosocial model of general practice: rhetoric or reality?’ British Journal of General Practice. 46. 105–7
Dunning, A. (2005) ‘Information, advice and advocacy for older people’. Joseph Rowntree Foundation.
Emanuel, J. & S. Begum (2000) ‘What do you advise, doc? A Citizen's Advice Bureau in primary care in the West Midlands’. Manchester Monographs 40. Centre for Higher and Adult Education, Faculty of Education, University of Manchester.
Ennals, S., J. A. G. Paris & D. Player (1993) ‘Citizens' advice in general practice: A burden GPs could do without’. British Medical Journal.307. 24 July 1993.
Farr, M. et al. (2014) ‘Proving the value of advice: A study of the impact of Citizens’ Advice Bureau Services’. University of Bath.
Finn, D. & J. Goodship (2014) ‘Take-‐up of benefits and poverty: an evidence and policy review’. Centre for Economic and Social Inclusion.
Fitch, C. et al.(2011) ‘The relationship between personal debt and mental health: a systematic review’. Mental Health Review Journal, 16(4)153––66.
Fitch, C et al. (2009) ‘ Debt and mental health’. Royal College of Psychiatrists.

79
The Role of Advice Services in Health
Fitch, C. et al. (2007) ‘Mental Health and debt: challenges for knowledge, practice and identity’. Journal of Psychiatric and Mental Health Nursing 14 128–33. Fleming, B. & L. Golding (1997) ‘Evaluation of a CAT funded citizens' advice bureaux units’. Soundings Research.
Fruin, C. & P. Pitt (2008) ‘Welfare benefit promotion within a district general hospital rheumatology centre: A joint project with the local Citizens Advice Bureau, Musculoskeletal Care. 6(4)211–20.
Galvin, K. Sharples, A. & D. Jackson (2001) ‘Citizens Advice Bureaux in general practice: an illuminative evaluation’. Health and Social Care in the Community. 8(4)441–53.
Girach, M., H. Hardisty & A. Massey (2012) ‘A Clinical Commissioner’s Guide to the Voluntary Sector’. ACEVO.
Glennerster, H. et al. (2009) ‘Reducing the risks to health: the role of social protection’. Report of the social protection task group for the strategic review of health inequalities in England post-‐010. Centre for Analysis of Social Exclusion, London School of Economics.
Greasley, P. (2003) ‘The Health Plus Project: Advice Workers in Primary Care in Inner City Bradford: Evaluation Report’. Department of Community and Primary Care, School of Health Studies, University of Bradford.
––––– (2006) ‘Filming Patient Interviews to Demonstrate the Value of Welfare Advice in General Practice: A Strategy for the Dissemination of Project Outcomes’. Int. J. Social Research Methodology. 9(3) 245–53. July 2006.
Greasley, P. & N. Small (2002) ‘Welfare Advice in Primary Care’. School of Health Studies, University of Bradford.
–––––(2002) ‘Welfare Advice in Primary Care: A Review of the Literature’. Leeds: Nuffield Institute for Health Portfolio Program.
––––– (2005) ‘Providing welfare advice in general practice: referrals, issues and outcomes’. Health Soc Care Community. 13(3):249–58.
––––– (2005) ‘Establishing a welfare advice service in family practices: views of advice workers and primary care staff’. Family Practice 17 June 2005.
Great Ormond Street Hospital & CAB Camden (2013) ‘Providing advice in the right place at the right time’. Citizens Advice.
––––– (2014) ‘Providing advice in the right place at the right time’. Annual report 2013/14.
Gyorki, L. (2014) ‘Breaking down the silos: Overcoming the Practical and Ethical Barriers of Integrating Legal Assistance into a Healthcare Setting’. Churchill Trust.
Haighton, C. et al. (2012) ‘The Do-‐Well study: protocol for a randomised controlled trial, economic and qualitative process evaluations of domiciliary welfare rights advice for socioeconomically disadvantaged older people recruited via primary healthcare’. BMC Public Health. 2012(12)382.

80
The Role of Advice Services in Health
Harding, R. et al. (2002) ‘Welfare rights advice in primary care: prevalence processes and specialist provision’. Family Practice. 20(1)48–53.
––––– (2002) ‘Evaluation of welfare rights advice in primary care: the general practice perspective’. Health and Social Care in the Community (2002). 10(6)417–22.
Harris, H. (2013) ‘Delivering welfare rights advice in the acute hospital setting’. Health Protection Agency.
Harrop, A. & C. Potter (2009) ‘British Medical Association consultation: Developing general practice, listening to patients’. Age Concern & Help the Aged.
Hobby, L. & J. Emanuel (1998) ‘Citizen's Advice Bureaux in primary care in England and Wales: A review of available information’.
Hoskins, R. & L. Smith (2002) ‘Nurse-‐led welfare benefits screening in a general practice located in a deprived area’. Public Health. 116. 214–20.
Hoskins, R. & D. Cater (2000) ‘Welfare benefits screening and referral: a new direction for community nurses’. Health Social Care Community. 8. 390–97.
Hoskins, R. et al. (2005) ‘Roll-‐out of a nurse-‐led welfare benefits screening service throughout the largest Local Healthcare Co-‐operative in Glasgow: an evaluation study’. Public Health.119(10)853–61. October 2005.
Hunt, P. & S. Gilmour (2010) ‘Tackling inequalities in general practice’. The Kings Fund.
Improvement Service (2013) ‘Money advice services across Scotland’s local authorities’. Improvement Service.
––––– (2014) ‘Learning Point: Referrals and Partnership Working between Advice and the Health Sector in Scotland’. Improvement Service.
Institute of Health Equity (2012) ‘The impact of the economic downturn and policy changes on health inequalities in London’. UCL. Institute of Health Equity.
Jacoby, M. (2002) ‘Does indebtedness influence health? A preliminary inquiry’. Journal of Law, Medicine & Ethics. 30(4)560–71.
Jamieson, J. (2014) ‘Report on Links to Mental Health & Financial Wellbeing: Integrating Advice Services into Local Health Provision’. Age UK South Tyneside.
Jenkins, R. et al. (2008) ‘Mental Disorder in People with Debt in the General Population’. Psychological Medicine. 38. 1485–93.
Jones, K. (2009) ‘Outcomes of a Longitudinal Study of Citizens Advice Service Clients in Wales’. Bangor University & Citizens Advice Cymru.
81
The Role of Advice Services in Health
Joseph Rowntree Foundation (2014) ‘Reducing Poverty in the UK: A collection of evidence reviews’. Joseph Rowntree Foundation.
Kemp, M. (2005) ‘Prescribing advice Improving health through CAB advice services’. Citizens Advice.
Kenrick, J. (2009) ‘Young people’s access to advice: the evidence’. Youth Access.
––––– (2011) ‘The outcomes & impact of youth advice – the evidence’. Youth Access.
––––– (2012) ‘Youth Advice: a mental health intervention?’. Youth Access.
Kite, A. (2014) ‘Citizens Advice in GP Surgeries: an investigation’. Bristol University PhD
KPMG (2010) ‘Review and Evaluation of the Macmillan CAB Welfare Benefits Advice Service for Belfast Hospital Trust’. KPMG.
Lawton, E & Tobin Tyler, E (2013) ‘Optimizing the Health Impacts of Civil Legal Aid Interventions’. The Public Health Framework of Medical-‐Legal Partnerships, Rhode Island Medical Journal.
Leeds City Council (2011) ‘Improving Public Health Through Income Maximisation’. Leeds City Council. April.
Legal Services Research Centre (2009) ‘Young People, Advice & Mental Health: A Data Digest’. Legal Services Research Centre.
––––– Factsheet No 1 (2009) ‘Civil Law, Social Problems and Mental Health’. Legal Services Research Centre.
Levy, J. & M. Payne (2006) ‘Welfare Rights Advocacy in a Specialist Health and Social Care Setting: A Service Audit’. British Journal of Social Work. . 36(2) 323–31. February 2006.
The London Health Forum (2009) ‘London: Capital of Debt-‐Reducing the Health Consequences of Personal Debt’. The London Health Forum.
London Health Inequalities Network (2013) ‘Welfare Benefits Advice through General Practices: A Business case’. London Health Inequalities Network.
Low Commission (2014) ‘Tackling the Advice Deficit: A strategy for access to advice and legal support on social welfare law in England and Wales’. Low Commission.
Macmillan Cancer Support (2012) Local benefits advice services: An evidence review’. Macmillan Cancer Support. May.
Marshall, E. (2013) ‘Westgate General Practice: CAB Outreach A Social Value Assessment’. South East Staffordshire CAB.
Mind (2008) ‘In the Red: Debt and Mental Health’. Mind.
Mobbs, D. (2014) ‘The Link Between Social Welfare Advice and Health’. MAP.

82
The Role of Advice Services in Health
Moffatt, S. et al. (2006) ‘The acceptability and impact of a randomised controlled trial of welfare rights advice accessed via primary healthcare: qualitative study’. BMC Public Health. 2006(6)163.
Moffatt, S., E. Noble & C. Exley (2010) ‘ “Done more for me in a fortnight than anybody done in all me life”: How welfare rights advice can help people with cancer’. BMC Health Services Research. 2010(10)259.
Moffatt, S., E. Noble & M. White (2012) ‘Addressing the Financial Consequences of Cancer: Qualitative Evaluation of a Welfare Rights Advice Service’. Plos One 2012, 7(8)e42979.
Moffatt, S. et al. (2004) ‘The impact of welfare advice in primary care: a qualitative study’. Critical Public Health.
Morris, M. (2013)‘ Primary Care Welfare Advice Hubs in the London Borough of Haringey’. London Borough of Haringey.
Noble, E., S. Moffatt & M. White (2011) ‘The impact of a dedicated welfare rights advice service for people affected by cancer’. Newcastle University.
Noble, P. (2012) ‘Advocacy Health Alliances – Better Health through Legal Partnerships’. Advocacy Health Alliances.
Office for Public Management (2011) ‘IAPT Employment Support Services in London: Assessment of the Economic Impact’. Office for Public Management.
Palmer, S. et al. (2010) ‘Evaluation of the impact on GP surgeries of the Citizen’s Advice Bureau Health Outreach service’. NHS Sefton.
Paris, J. A. G. & D. Player (1993) ‘Citizens' advice in general practice’. British Medical Journal. 306, 5 June 1993.
Parsonage, M. (2013) ‘Welfare advice for people who use mental health services: Developing the business case’. Centre for Mental Health.
Paul, K. & K. Moser (2009) ‘Unemployment impairs mental health: Meta-‐analyses’. Journal of Vocational Behaviour. 264–82.
Pethcy, R. & Y. Carter (2006) ‘Evaluation of the BIG Living with Cancer Initiative’. Big Lottery Fund.
Pleasence, P., N. J. Balmer (2007) ‘Mental health and the experience of housing problems involving rights’. People, Place & Policy Online. 2007(2/1) 4–16.
––––– (2009) ‘Mental Health and the Experience of Social Problems Involving Rights: Findings from the United Kingdom and New Zealand’. Psychiatry, Psychology and Law. 16(1).
Pleasence, P. N. J. Balmer & A. Buck (2007) ‘Health Professionals as Rights Advisers: Rights Advice and Primary Healthcare Services’. Legal Services Research Centre.
83
The Role of Advice Services in Health
––––– (2008) ‘The Health Cost of Civil-‐Law Problems: Further Evidence of Links Between Civil Law Problems and Morbidity, and the Consequential Use of Health Services’. Journal of Empirical Legal Studies.5(2).
Pleasence, P. et al. (2004)‘Civil Law Problems and Morbidity’. Journal of Epidemiology and Community Health. 57(7).
–––––(2007) ‘A Helping Hand: The Impact of Debt Advice on People’s Lives’. Legal Services Research Centre.
––––– (2007) ‘Mounting Problems: Further Evidence of the Social, Economic and Health Consequences of Civil Justice Problems’. In Pleasance, P. A. Buck, A. & N. J. Balmer (Eds) Transforming Lives: Law and Social Process. Norwich. TSO.
Porter, H. (1998) ‘Prescribing citizen's advice’. The Health Summary (The Fundholding Summary) xv(2)9–10.
Reading, R., S. Steel & S. Reynolds (2002) ‘Citizens advice in primary care for families with young children’. Child: Care, Health and Development. 28(1)39–45.
Richardson, C. (2014) ‘Welfare rights: a key driver to improving mental health and wellbeing’. Durham County Council .
Sainsbury, R. et al. (2008) ‘The Pathways Advisory Service: Placing employment advisers in GP surgeries’. Department for Work and Pensions.
Scottish Borders Council (2013) ‘Borders Macmillan Welfare Benefits Partnership’. Scottish Borders Council.
Sefton, M. (2010) ‘With rights in mind: Is there a role for social welfare law advice in improving young people’s mental health?’ Youth Access.
Shape, J. & J. Bostock (2002) ‘Supporting People with Debt and Mental Health Problems: Research with Psychological Therapists in Northumberland’. Northumberland Health Action Zone.
Sheffield Mental Health CAB (2014) ‘Review of Sheffield Mental Health CAB and Advocacy Service 1976 to October 2013’. Sheffield Mental Health CAB.
Sherr, L. et al.(2002) ‘A stitch in time: Accessing and funding welfare rights through Health Service Primary Care’. University College London .
Sherratt, M. Jones, K. & P. Middleton (2000) ‘A citizens advice service in primary care: improving patient access to benefits’. Primary Care Res Dev. I. 139–46.
Simkins, H. (2001) ‘Welfare Benefits Advice in Primary Care Settings in North Cumbria’. Carlisle & District Citizens Advice Bureau.

84
The Role of Advice Services in Health
Skapinakis, P. et al. (2006) ‘Socio-‐economic position and common mental disorders’. Longitudinal study in the general population in the UK. British Journal of Psychiatry. 189:109–17.
Smith, M. & A. Patel (2008) ‘Money Advice Outreach Evaluation: Cost and Effectiveness of the Outreach Pilots’. Legal Services Research Centre.
Taylor, M. (2011) ‘The long term impacts of financial capability: Evidence from the BHPS’. The Consumer Financial Education Body.
Taylor, M., S. Jenkins & A. Sacker (2009) ‘Financial capability and wellbeing: Evidence from the BHPS. Financial Services Authority.
Toeg, D. et al. (2003) ‘Proactive, targeted benefits advice for older people in general practice: a feasibility study’. Health and Social Care in the Community. (2003(11)124–8.
Torjesen, I. (2010) ‘Recession Medicine’. British Medical Journal. 340. 26 June 2010.
Veitch, D. (1995) ‘Prescribing citizen's advice: An evaluation of the social work of CAB with Health and Social Services in Birmingham’. Birmingham CAB
Veitch, T. & A. Terry (1993) ‘Citizen's advice in general practice: Patients benefit from advice’. BMJ. 307. 262.
Waddell, G. & K. Burton (2006) ‘Is Work Good for your Health and Wellbeing?’. Norwich: TSO.
Waterhouse, P. (2002) ‘Health Links Advice Project: Taking Advice into the Community’. Hackney Health Links Advice Project.
Welsh Government (2013) Advice Services Review: Final Research Report. Welsh Government.
Widdowfield, H. & P. Rickard (1996) ‘Health centre advice service report’. Sunderland: Wear Valley Citizens' Advice Bureau.
Wiggan, J. & C. Talbot (2006) ‘The benefits of welfare rights advice: a review of the literature’. National Association of Welfare Rights Advisors.
Williams, C. (2009) ‘Transforming adult social care: access to information, advice and advocacy’. I&DeA.
Williamson Consulting (2009) ‘Macmillan Welfare Advice Project – Altnagelvin’. Macmillan Cancer Support . April.
Winder, R. et al. (2008) ‘Receiving specialist welfare benefit advice with Social Services: a qualitative interview study of older people and their carers’. Research Policy and Planning. 26(1)33–43.
Wolverhampton CAB (2012) ‘The Health Impact of Good Advice’. Wolverhampton CAB.
Youth Access (2012) ‘Youth Advice: a mental health intervention? Summary of a research study on the mental health benefits and cost-‐effectiveness of youth advice services’. Youth Access.
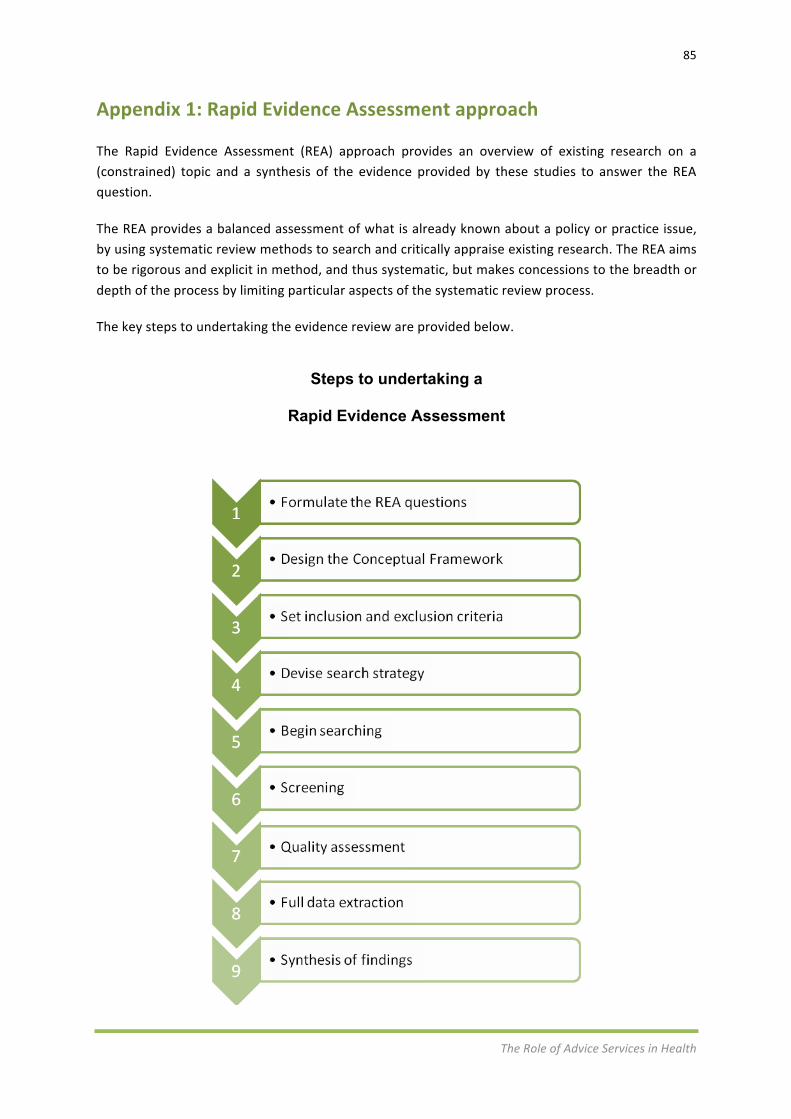
85
The Role of Advice Services in Health
Appendix 1: Rapid Evidence Assessment approach
The Rapid Evidence Assessment (REA) approach provides an overview of existing research on a (constrained) topic and a synthesis of the evidence provided by these studies to answer the REA question.
The REA provides a balanced assessment of what is already known about a policy or practice issue, by using systematic review methods to search and critically appraise existing research. The REA aims to be rigorous and explicit in method, and thus systematic, but makes concessions to the breadth or depth of the process by limiting particular aspects of the systematic review process.
The key steps to undertaking the evidence review are provided below.
Steps to undertaking a
Rapid Evidence Assessment

86
The Role of Advice Services in Health
Formulate REA questions
This leads the direction of the review and therefore the conclusions that follow. It is important to make clear any assumptions associated with for example, the conceptual framework for the review. It is important that any REA question:
• drives the process.
• is a statement that can be investigated not a subject area of interest.
• is clear and answerable. • requires an answer worth asking.
Two main types of questions used: 1. What works (impact)? 2. What do you need to make it work? (non-‐impact: e.g. what do
people need or want, attitudes, what do people think? etc.)
Conceptual framework
A conceptual framework is a type of intermediate theory that can connect to all aspects of an inquiry. In the context of this REA the framework clarified the parameters of the evidence review, introduced the key concepts (e.g. effectiveness of different delivery methods, types and levels of service), explained the definitions used and highlighted any underlying assumptions associated with the research. The production of the framework assisted the research team in clarifying the REA parameters when engaging with key organisations and individuals that may be able to provide relevant secondary source data.
Set inclusion and exclusion criteria
The process of setting inclusion and exclusion criteria was included in the development of the conceptual framework and helped to guide the development of the search strategy for the REA. In the context of this research the criteria included the following: • Geographical parameters (e.g. UK only, international). • Date of publication (e.g. 10 years). • Subsections of service types. • Scale of service / delivery organisation. • Definition of client types (e.g. age, health status or advice needs). • Language.
Devise search strategy
The search strategy is governed by the inclusion and exclusion criteria and designed against the following areas: Identification of key organisations and networks Based on our knowledge of the IAG sector and the guidance and support of the Steering Group, key organisations and networks were identified that could be approached as part of a ‘call for evidence’.

87
The Role of Advice Services in Health
We approached each organisation/network in a standard email to seek relevant research material and evidence that may not be publicly available (i.e. grey literature) or historical reports/publications which are no longer held on organisation websites. Identification of key publications In addition to the publications provided as part of the ‘call for evidence’ our team also searched key academic, government and sector publications (e.g. peer-‐reviewed journal articles, government research) in order to identify relevant content. The conceptual framework helped to focus the search of the key publications/documents which would be identified using an appropriate online bibliographic service, online search engines and reference lists. Example academic journals and information management systems which were searched and reviewed included: • Applied Social Sciences Index and Abstracts (ASSIA). • British Library Public Catalogue. • Cochrane Library. • Google Scholar. • Ingenta Connect. • Social Care Online. • Taylor & Francis Online. • Wiley Online Library.
Begin searching Using pre-‐determined databases, websites and contacts, begin searching using search terms and combinations. Articles identified in this initial search are recorded in a bespoke database. Included articles based on inclusion and exclusion criteria.
Screening (abstract)
All identified and received material should be screened by a member of the research team to compare against the agreed inclusion and exclusion criteria. All received material should be logged in a bespoke REA database which recorded whether the material had been accepted to the next stage of the review or, if rejected, the reason for the exclusion. Our database is available for the Steering Group to use as a future resource. The collation of the material within a database will enable the team to produce a robust bibliography as part of the process of providing the narrative report. The database fields are : • document Number • title • author • publisher • year

88
The Role of Advice Services in Health
• month • source type • geographical scope • research type • methodological summary • content summary • web link url • downloaded/available electronically (y/n) • entry made by • included (y) or excluded (n) • reason for exclusion • funding • service provider • type of service • wider social determinants • setting • client group
Quality assessment Once the research team screened the abstracts and selected the material considered in more detail, each publication was reviewed in order to draw out the evidence that will contribute to answering the agreed research question(s). A secondary screening process would be undertaken to exclude material that, following in-‐depth review, is considered too weak to be included. Where our research team considers that the report has some value but is methodologically weak, it would be included with appropriate caveats.
Full data extraction Once a study has been assessed for relevance and quality, full data extraction for inclusion in the narrative report can take place.
Synthesis of findings
This will vary depending on research questions but requires consideration of all evidence extracted using narrative or thematic synthesis. Consideration needs to be given to integrating qualitative and quantitative studies into the evidence synthesis to ‘tell the story’ from the findings.

89
The Role of Advice Services in Health
Appendix 2: Conceptual framework
Rapid Evidence Assessment key questions
The formulation of the key research questions forms an important step in guiding the subsequent Rapid Evidence Assessment (REA). Based on our experience of conducing similar reviews it is helpful to maintain a focus on the key questions to manage in the REA process. However, the process can also be supported by a series of additional questions which sit underneath the key research questions.
For the purposes of this study, the REA questions have been split into ‘impact’ and ‘non-‐impact’ questions. This REA can address more than one type of question, particularly in combining impact questions (what works) with implementation (what is required to make it work).
Building on the discussion at the inception meeting on 1 December 2014 the following key questions are proposed:
Impact questions • What evidence is there of advice services engaging with health services on a strategic basis?
• What evidence is there of the impact of effective advice services delivered in health settings on the efficiency of health service delivery?
• What evidence is there of the impact of effective advice services delivered in health settings on the wider social determinants of health?
• What is the effectiveness of the different delivery mechanisms used by service providers to provide information, advice and guidance to members of the public?
• Which delivery mechanisms are known to ensure positive outcomes for and changes in the behaviour of service users?
Non-‐impact questions
• What have we learned about the links between health and advice?
• What are the challenges and barriers in integrating advice within health?
• What are the opportunities for stronger integration of advice and health services?
• What are the models of delivery involving advice within health settings and how prevalent are they?
90
The Role of Advice Services in Health
Key concepts and assumptions
Developing a shared understanding of key terminology and concepts linked to the delivery of information, advice and guidance in health settings will be crucial in informing the development and population of the REA database and the subsequent analysis of the evidence.
This REA process does not seek to impose a set of definitions but merely to clarify the key concepts and definitions that apply to this research. This will aid communication of the research objectives and parameters to organisations engaged through the search strategy. It will also facilitate the identification of research evidence relevant to the objectives of the research and associated key research questions.
Key concepts
Definitions of the key concepts likely to be used in the REA process are outlined below. The key concept definitions mirror those utilised in the Welsh Government’s Advice Services Review published in March 2013.20
Types of service provision
Generalist advice – The IAG service provided is deemed to be ‘generalist advice’ when it does not meet the definition of ‘specialist advice’ and either the adviser makes an emergency intervention for the client at the first contact; or the adviser carries out all of the following:
• conducts one or more one-‐to-‐one interviews with the client, collecting appropriate information from the client as a basis for advice;
• establishes client expectations and explains what the service can and cannot provide;
• furthers the diagnosis made at triage about the issue(s) presented by the client and identifies other related issues;
• explains relevant options, consequences and limitations applicable to the particular circumstances of that client
• recommends a course of action to the client, giving an objective assessment of the likely most successful remedy if one is available
• provides information relevant to the person and their particular situation, including any entitlement calculations.
A generalist advice session may also involve the adviser doing the following:
• assisting the client through: completing forms, making telephone calls, drafting and writing letters, negotiating on behalf of the client;
• referring the client to a caseworker ;
• making referrals to other agencies where the service cannot provide the necessary advice
20 http://wales.gov.uk/topics/housingandcommunity/research/community/advice-‐services-‐review-‐final-‐research-‐report/?lang=en
91
The Role of Advice Services in Health
Social welfare law – refers to those categories of law which govern entitlement to state benefits and housing; the management of personal and business debt; an employee’s rights at work and access to redress for unfair treatment; and access to appropriate care and support for people with particular health problems.
Within the not-‐for-‐profit advice sector, advice is often given to members of the public on the following types or ‘categories’ of social welfare law:
-‐ welfare benefit -‐ debt -‐ housing -‐ employment -‐ community care.
Some advice services also give advice in issues such as education, family, consumer and general contract. Immigration and asylum law may also be considered as social welfare law.
Specialist debt advice – linked to financial difficulties resulting from a range of reasons including financial shocks, low income, poor money management and creditor behaviour.
Specialist welfare benefits advice – linked to the understanding, access and entitlement to welfare benefits.
Specialist housing advice – including issues linked to homelessness, housing standards, energy efficiency, and adaptations and in relation to tenancy issues.
Specialist employment advice – covers individuals’ rights at work including leave, flexible working, problems at work and health and safety issues. Within the wider scope of employment advice also includes support for those seeking employment or facing redundancy.
Specialist consumer advice – relates to the purchase or use of goods and services, and can range from information and advice on financial services and products, to considering the impact of rising fuel costs on people living in poverty, through to miss-‐selling and aggressive sales tactics.
Specialist discrimination advice — relates to equality legislation and ensuring those within protected characteristic groups are not discriminated against within society, as well as ensuring the safeguarding of human rights.
Settings
Primary — relates to the day-‐to-‐day healthcare given by a healthcare provider. Typically this provider acts as the first contact and principal point of continuing care for patients within a healthcare system, and coordinates other specialist care that the patient may need. Such a professional can be a primary care physician (general practitioner or family physician), a nurse practitioner (adult-‐gerontology nurse practitioner, family nurse practitioner, or paediatric nurse practitioner), a behavioural care provider, a pharmacist, an occupational therapist, a physical therapist, a physician assistant or a registered nurse.
Secondary — relates to the healthcare services provided by medical specialists and other health professionals who generally do not have first contact with patients, for example, cardiologists, urologists and dermatologists. It includes acute care: necessary treatment for a short period of time for a brief but serious illness, injury or other health condition, such as in a hospital A&E department.
92
The Role of Advice Services in Health
Tertiary — relates to specialised consultative healthcare, usually for inpatients and on referral from a primary or secondary health professional. Examples of tertiary care services are cancer management, neurosurgery, cardiac surgery, plastic surgery, treatment for severe burns, advanced neonatology services, palliative and other complex medical and surgical interventions.
Social care — relates to the provision of social work, personal care, protection or social support services to children or adults in need or at risk, or adults with needs arising from illness, disability, old age or poverty.
Assumptions
The following underlying assumptions underpin the REA process.
• It will be possible to distinguish between the health setting and/or service from where the advice service is provided.
• It will be possible to identify the contribution of the advice provision in addressing wider social determinants of health.
• It will be possible to identify the profile of the healthcare users accessing advice.
• The delivery of information, advice and guidance will be clearly defined.
• It will be possible to distinguish the quality of the research evidence.
Inclusion and exclusion criteria
Based on the key research questions, key concepts and underlying assumptions, the following inclusion and exclusion criteria will be applied to the REA process to establish parameters for the search strategy.
Inclusion criteria
• Studies in England, Wales, Scotland, Northern Ireland, Australia and the United States of America.
• Studies that focus on the delivery of information, advice and guidance in health settings.
• Studies that can evidence clearly defined outcomes for healthcare users.
• Studies that provide evidence of the effectiveness of information, advice and guidance in addressing wider social determinants of health.
• Formal research (i.e. subject to a clear research process).
• Informal published material (i.e. grey literature) with reference to the ‘impact’ of advice within health settings.
• Studies that report on the delivery of advice in the following areas (as defined above):
• Generalist advice services • Social welfare law information services • Social welfare law advice services • Specialist debt advice • Specialist welfare benefits advice • Specialist housing advice
93
The Role of Advice Services in Health
• Specialist employment advice • Specialist consumer advice • Specialist discrimination advice.
• Guidance and policy related to health which includes access to advice as an integral part
Exclusion criteria
• Studies based outside of the UK with the exception of Australia and the United States of America.
• Studies that report on practice that doesn’t have a clearly stated purpose or include clearly defined outcomes.
• Soft evidence (i.e. primary commentary, anecdotal evidence or interview data).
• Studies that report solely on evidence of satisfaction derived from the delivery of information, advice and guidance as opposed to the achievement of clear outcomes.
• Studies that relate to advice provided in non-‐health settings.
• Studies published before 1990.
• Studies not published in English.

94
The Role of Advice Services in Health
Appendix 3: Membership of the Advice and Health Steering Group
• Amanda Finlay (Chair), Low Commission
• Alison Ingram, Age UK
• Andy Kempster, Mind
• Chris Fitch, Royal College of Psychiatrists
• Dan Mobbs, MAP, Norfolk
• Emma Cross, Macmillan
• Enrique Saenz, Advice UK
• Gerard Crofton-‐Martin, Healthwatch
• Helen Paris, Citizens Advice
• James Kenrick, Youth Access
• James Sandbach, Low Commission
• Lindsey Poole, Advice Services Alliance
• Mark Gamsu , Leeds Beckett University
• Matthew Smerdon, Future Advice Funders Group
• Nimrod Ben Cnaan, Law Centres Federation
• Rachel Billet, Future Advice Funders Group
• Richard Humphries, The Kings Fund
• Sean Duggan, Centre for Mental Health
• Tamsin Shulker, Citizens Advice
• Simon Bottery (Independent Age), Care and Support Alliance.

95
The Role of Advice Services in Health
Appendix 4 Advice and health services
Advice in GP Surgeries, Derbyshire and Districts Citizens Advice Bureaux
Advice in GP Surgeries, Advice Leeds
Advice in GP Surgeries, Family Action Bradford
Advice in GP Surgeries, Age UK Newcastle
Advice on Prescription, South Liverpool Citizens Advice Bureau
Advice Project, Halton CAB
Advice Service Transition Fund, CAB Oxford
Anchor Centre advice surgery, Coventry Law Centre
Benefit and Debt Advice Services, South Bradford Advice
Benefits for Better Mental Health, Oxfordshire Mind
Bradford Community Advice Network, Bradford Community Advice Network
Broughton Health Project Salford City Council
Camden Futures, Elfrida Rathbone Camden
Citizens Advice Bureau in General Practice, Derbyshire County Council
Clatterbridge Cancer Centre NHS Foundation Trust, Clatterbridge Cancer Centre NHS Foundation Trust
Community Navigator, Hertsmere CAB
Croydon Family Power, Croydon Voluntary Action
Dorset Mental Health Advocacy Service, Dorset Mental Health Forum
Dundee Early Intervention Team, Dundee Early Intervention Team
Edinburgh Community Health Partnership, Edinburgh Community Health Partnership, NHS Lothian
Employment Support Service, Twining Enterprise
Generalist GP outreach Project Citizens Advice & Law Centre, Derby
Generalist Advice Service, Thetford & District Citizens Advice Bureau
Generalist Advice Service, Scarborough and District CAB
GP Care Advisor Service, Colchester Borough Council
GP Care Advisors, Anglian Community Enterprise (ACE) Community Interest Company
GP Surgery Outreach, Merton Advice
Havering A2A Project (Access to Advice), Havering Citizens Advice Bureau
Heathlands CAB , Rushmoor Citizens Advice Bureau
ITalk Hampshire, Solent Mind & Southern Health NHS Foundation Trust
Ladywell GP Outreach Services, Citizens Advice Edinburgh

96
The Role of Advice Services in Health
Live Well, Spend Well Project, Halton CAB
Macmillan Welfare Benefits Service, Scottish Borders Council
Manchester Advice Alliance, Manchester CAB
Mental Health Support Service, Gateshead Advice Centre
Mental ill-‐Health and Benefits Project, Hertfordshire County Council
Middlesbrough & Stockton MIND Community Advice Sessions, Middlesbrough Advice Partnership
Prescribing Advice, South East Staffordshire Citizens Advice Bureau
Primary Care Advice, Liaison and Advocacy Service, Wirral Citizens Advice Bureaux
Primary Care Mental Health Team, Isle of Wight NHS Trust
Robin Hood Cluster Welfare Rights in GP Surgeries, Nottingham Law Centre
Royds Advice Service, Royds Community Association
Saffron Group Practice, Community Advice and Law Service
Sheffield Mental Health CAB Project, Sheffield Citizens Advice
Social Prescriber Project , Bromley by Bow Health Centre
South London and Maudsley Mental Health Foundation Trust Welfare service, South London and Maudsley NHS Foundation Trust
South Yorkshire Partnership NHS Foundation Trust – ‘Right Conversation at the Right Time, Altogether Better’
Springfield Law Centre, Springfield Law Centre
Steps to Wellbeing, Dorset Health NHS Trust
Stockton Welfare Advice Network (SWAN), Stockton and District Advice and Information Service
Talking Change, Portsmouth, Solent NHS Trust
Transition Project South Tyneside, Age UK South Tyneside
Wigan Advice Network Development Project, Wigan Citizens Advice Bureau
Working for Wellness, London Health Programmes.