Embed Size (px)
Citation preview
7/03/2017
1
Imaging of Benign and MalignantBone tumors
F.M. Vanhoenacker
Outline
• Introduction
• Benign tumors
• Pseudotumors/ tumor-like lesions
• Malignant tumors
• Conclusion
Where science meets medicine for the benefit of the patient
Introduction
Where science meets medicine for the benefit of the patient
Case 1: 12-y-o female with low back pain
A. Benign tumor
B. Malignant tumor
C. Tumor-like
D. Pseudotumor
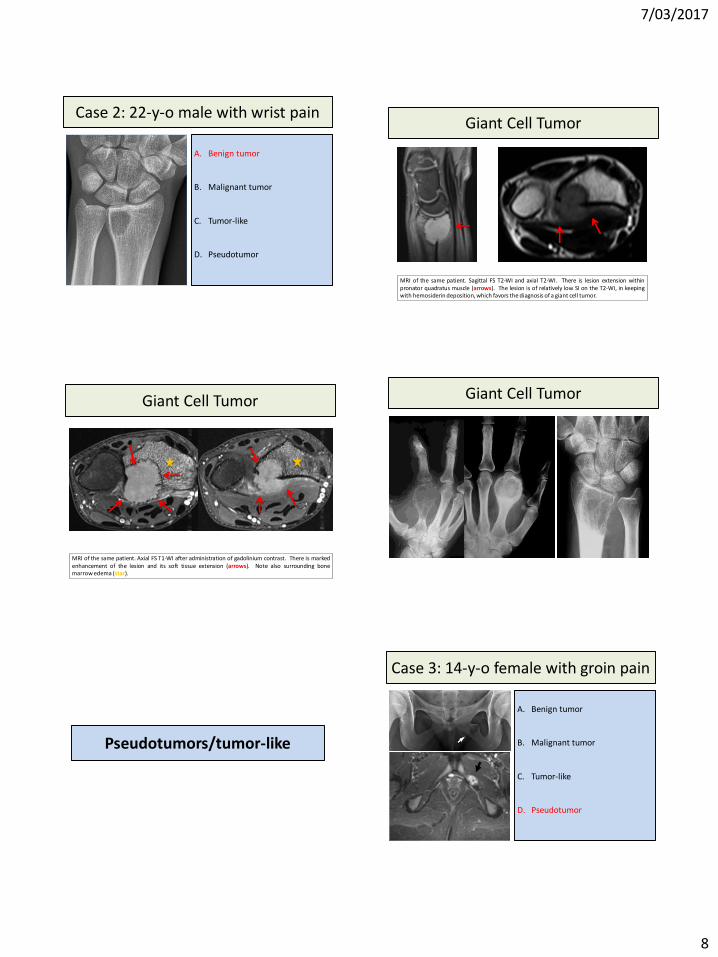
Case 2: 22-y-o male with wrist pain
A. Benign tumor
B. Malignant tumor
C. Tumor-like
D. Pseudotumor
Case 3: 14-y-o female with groin pain
A. Benign tumor
B. Malignant tumor
C. Tumor-like
D. Pseudotumor
7/03/2017
2
Benign tumors
Where science meets medicine for the benefit of the patient
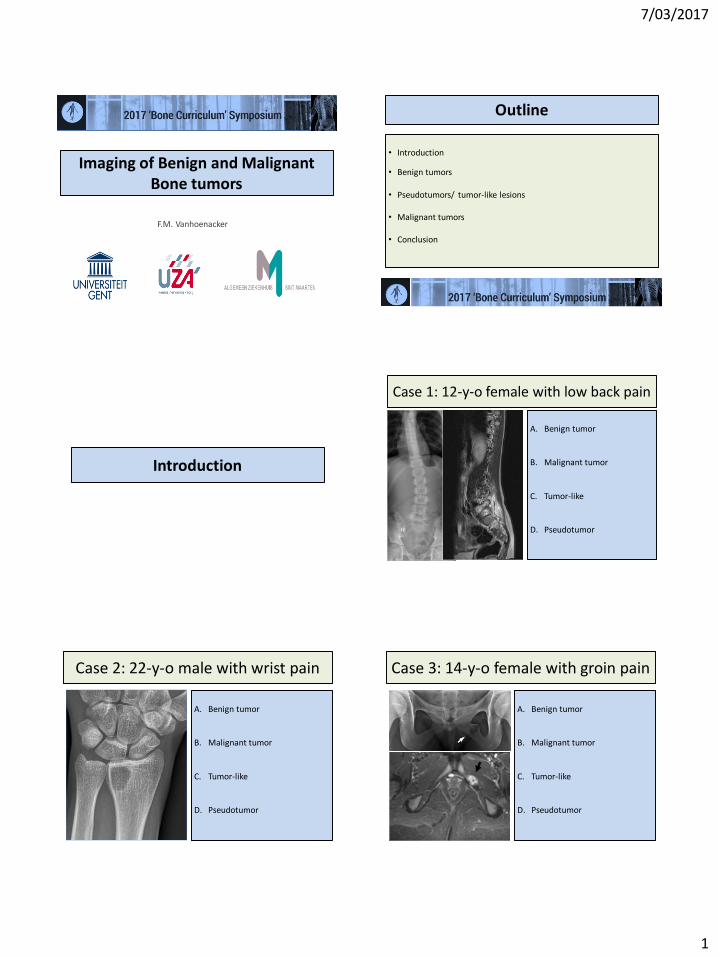
Dense bone island
XR: spicular margins; CT high density (HU); MRI low SI on all pulse sequences
Dense bone island
XR: spicular margins; CT high density; MRI low SI on all pulse sequences
Osteoid Osteoma
MRI shows BME; CT is the preferred technique for demonstration of nidus
Case 1: 12-yo female with low back pain
A. Benign tumor: O.O.
B. Malignant tumor
C. Tumor-like
D. Pseudotumor
7/03/2017
3
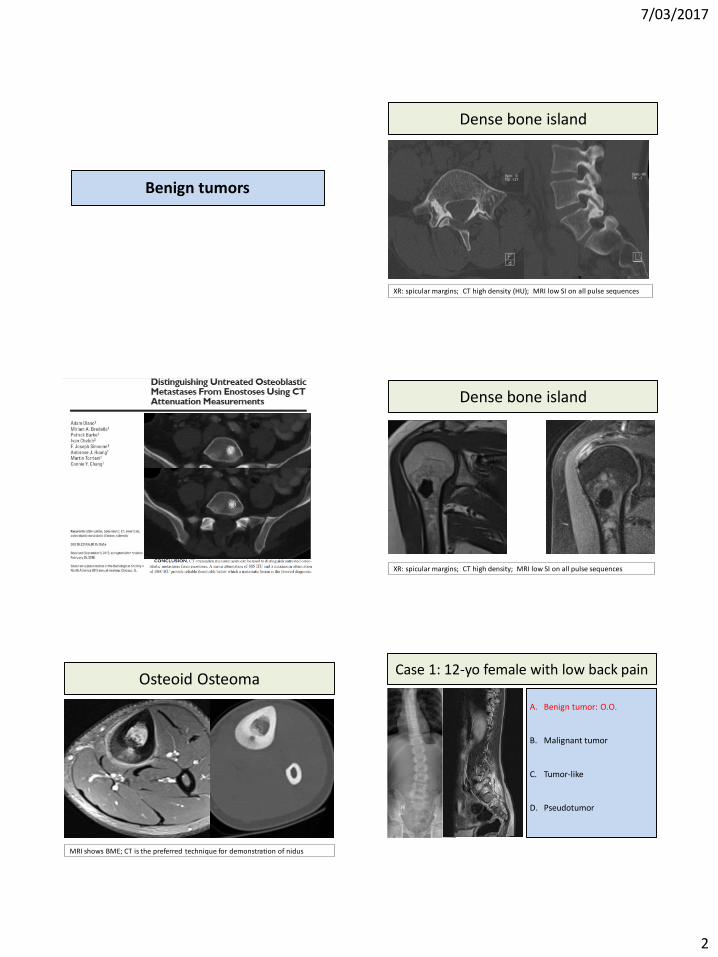
Osteoid Osteoma
MRI shows BME; CT for demonstration of nidus; spine posterior
Osteoblastoma
Larger nidus ≥ 1,5 cm, less typical clinical symptoms
Osteoblastoma Non Ossifying Fibroma (NOF)
XR: well defined, progressive sclerosis; MRI variable SI, no soft tissue mass
Non Ossifying Fibroma (NOF)
XR: well defined, progressive sclerosis; MRI variable SI, no soft tissue mass
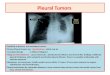
Adamantinoma
Young age XR: anterior tibia cortex;lytic-sclerotic; MRI, 2/3 extension axial images
7/03/2017
4
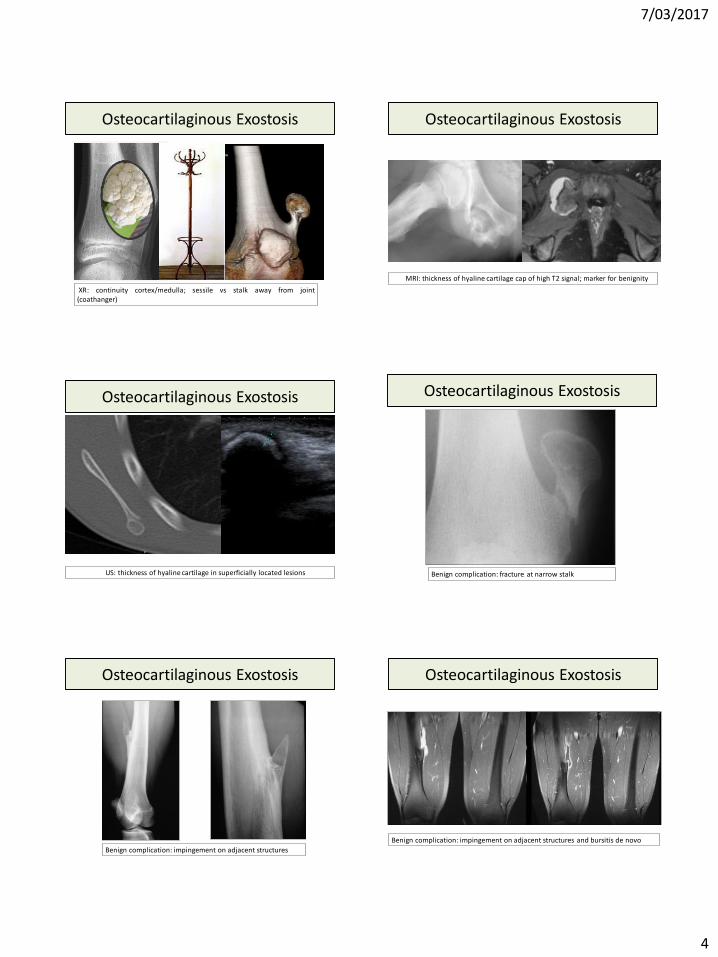
Osteocartilaginous Exostosis
XR: continuity cortex/medulla; sessile vs stalk away from joint(coathanger)
Osteocartilaginous Exostosis
MRI: thickness of hyaline cartilage cap of high T2 signal; marker for benignity
Osteocartilaginous Exostosis
US: thickness of hyaline cartilage in superficially located lesions Benign complication: fracture at narrow stalk
Osteocartilaginous Exostosis
Osteocartilaginous Exostosis
Benign complication: impingement on adjacent structures
Benign complication: impingement on adjacent structures and bursitis de novo
Osteocartilaginous Exostosis
7/03/2017
5
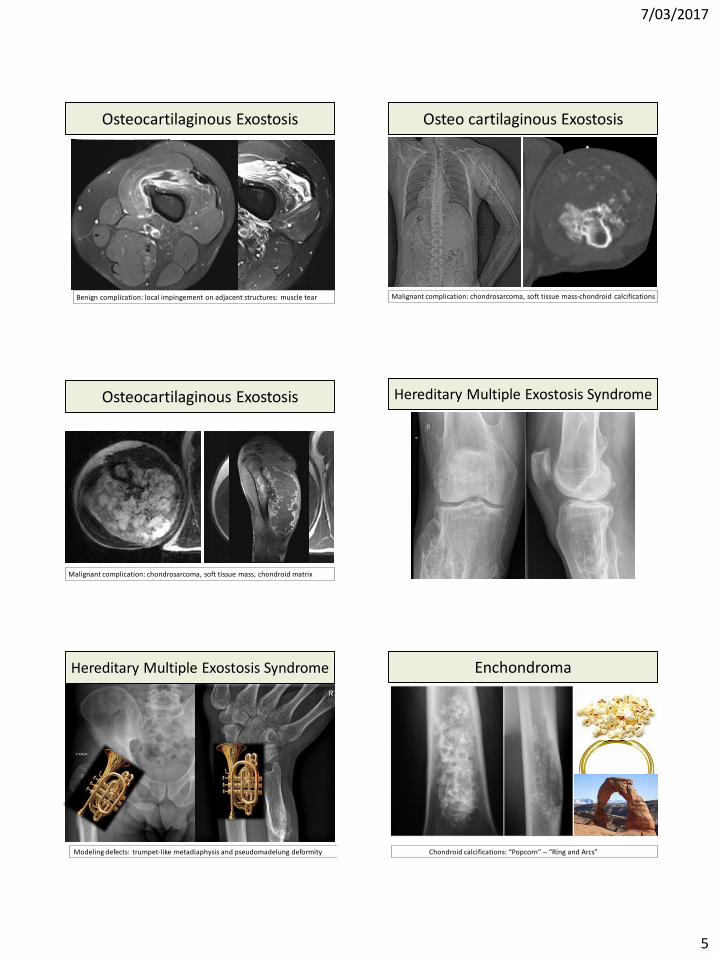
Osteocartilaginous Exostosis
Benign complication: local impingement on adjacent structures: muscle tear
Osteo cartilaginous Exostosis
Malignant complication: chondrosarcoma, soft tissue mass-chondroid calcifications
Osteocartilaginous Exostosis
Malignant complication: chondrosarcoma, soft tissue mass, chondroid matrix
Hereditary Multiple Exostosis Syndrome
Hereditary Multiple Exostosis Syndrome
Modeling defects: trumpet-like metadiaphysis and pseudomadelung deformity
Enchondroma
Chondroid calcifications: “Popcorn” – “Ring and Arcs”
7/03/2017
6
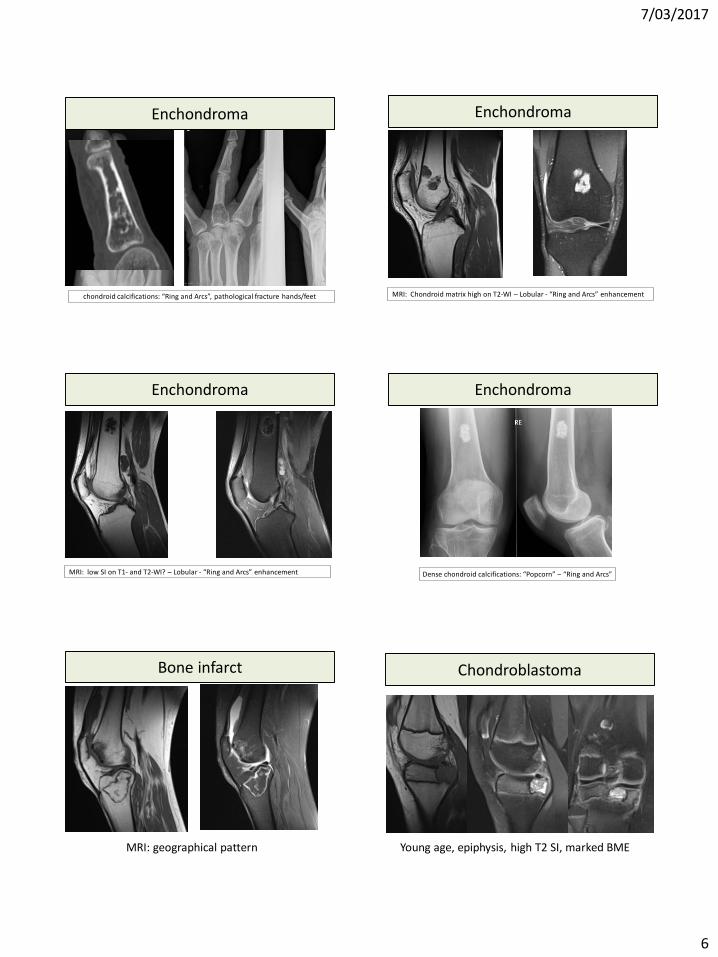
Enchondroma
chondroid calcifications: “Ring and Arcs”, pathological fracture hands/feet
Enchondroma
MRI: Chondroid matrix high on T2-WI – Lobular - “Ring and Arcs” enhancement
Enchondroma
MRI: low SI on T1- and T2-WI? – Lobular - “Ring and Arcs” enhancement
Enchondroma
Dense chondroid calcifications: “Popcorn” – “Ring and Arcs”
MRI: geographical pattern
Bone infarct Chondroblastoma
Young age, epiphysis, high T2 SI, marked BME
7/03/2017
7
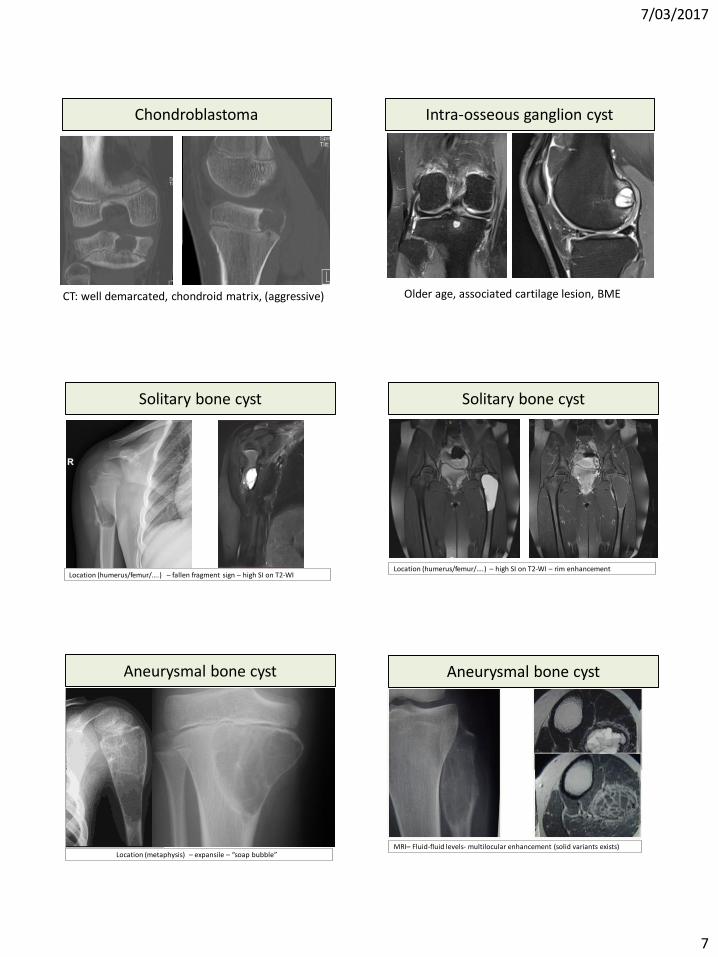
Chondroblastoma
CT: well demarcated, chondroid matrix, (aggressive)
Intra-osseous ganglion cyst
Older age, associated cartilage lesion, BME
Solitary bone cyst
Location (humerus/femur/….) – fallen fragment sign – high SI on T2-WI
Solitary bone cyst
Location (humerus/femur/….) – high SI on T2-WI – rim enhancement
Aneurysmal bone cyst
Location (metaphysis) – expansile – “soap bubble”
Aneurysmal bone cyst
MRI– Fluid-fluid levels- multilocular enhancement (solid variants exists)
7/03/2017
8
Case 2: 22-y-o male with wrist pain
A. Benign tumor
B. Malignant tumor
C. Tumor-like
D. Pseudotumor
MRI of the same patient. Sagittal FS T2-WI and axial T2-WI. There is lesion extension withinpronator quadratus muscle (arrows). The lesion is of relatively low SI on the T2-WI, in keepingwith hemosiderin deposition, which favors the diagnosis of a giant cell tumor.
Giant Cell Tumor
MRI of the same patient. Axial FS T1-WI after administration of gadolinium contrast. There is markedenhancement of the lesion and its soft tissue extension (arrows). Note also surrounding bonemarrow edema (star).
Giant Cell Tumor Giant Cell Tumor
Pseudotumors/tumor-like
Where science meets medicine for the benefit of the patient
Case 3: 14-y-o female with groin pain
A. Benign tumor
B. Malignant tumor
C. Tumor-like
D. Pseudotumor
7/03/2017
9
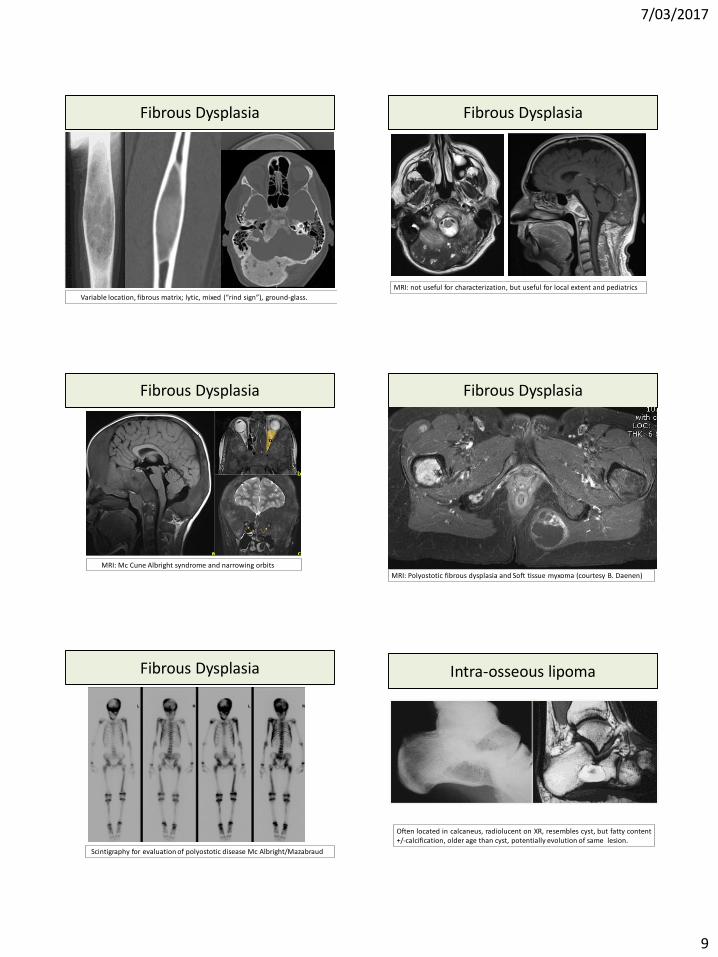
Fibrous Dysplasia
Variable location, fibrous matrix; lytic, mixed (“rind sign”), ground-glass.
Fibrous Dysplasia
MRI: not useful for characterization, but useful for local extent and pediatrics
Fibrous Dysplasia
MRI: Mc Cune Albright syndrome and narrowing orbits
Fibrous Dysplasia
MRI: Polyostotic fibrous dysplasia and Soft tissue myxoma (courtesy B. Daenen)
Fibrous Dysplasia
Scintigraphy for evaluation of polyostotic disease Mc Albright/Mazabraud
Intra-osseous lipoma
Often located in calcaneus, radiolucent on XR, resembles cyst, but fatty content+/-calcification, older age than cyst, potentially evolution of same lesion.
7/03/2017
10
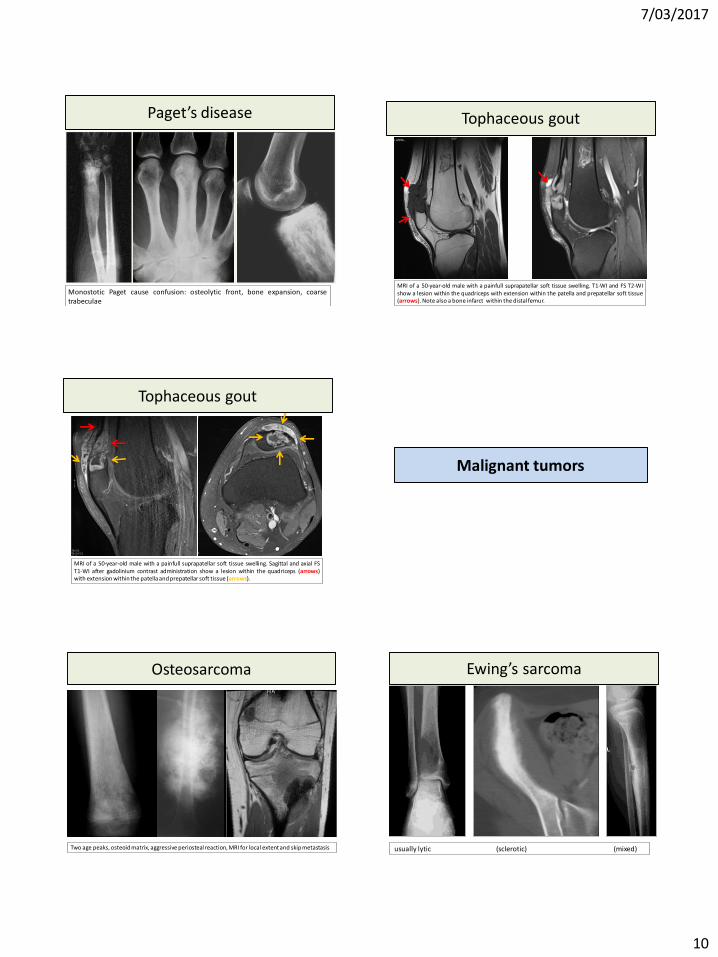
Paget’s disease
Monostotic Paget cause confusion: osteolytic front, bone expansion, coarsetrabeculae
MRI of a 50-year-old male with a painfull suprapatellar soft tissue swelling. T1-WI and FS T2-WIshow a lesion within the quadriceps with extension within the patella and prepatellar soft tissue(arrows). Note also a bone infarct within the distal femur.
Tophaceous gout
MRI of a 50-year-old male with a painfull suprapatellar soft tissue swelling. Sagittal and axial FST1-WI after gadolinium contrast administration show a lesion within the quadriceps (arrows)with extension within the patella and prepatellar soft tissue (arrows).
Tophaceous gout
Malignant tumors
Where science meets medicine for the benefit of the patient
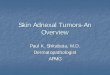
Osteosarcoma
Two age peaks, osteoid matrix, aggressive periosteal reaction, MRI for local extent and skip metastasis
Ewing’s sarcoma
usually lytic (sclerotic) (mixed)
7/03/2017
11
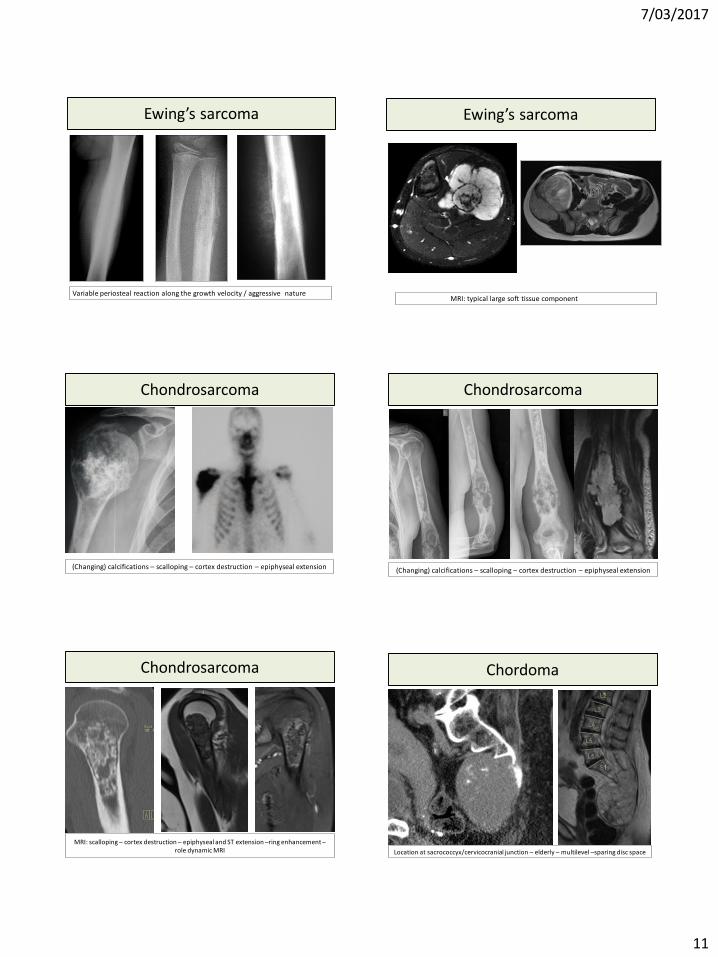
Ewing’s sarcoma
Variable periosteal reaction along the growth velocity / aggressive nature
Ewing’s sarcoma
MRI: typical large soft tissue component
(Changing) calcifications – scalloping – cortex destruction – epiphyseal extension
Chondrosarcoma Chondrosarcoma
(Changing) calcifications – scalloping – cortex destruction – epiphyseal extension
Chondrosarcoma
MRI: scalloping – cortex destruction – epiphyseal and ST extension –ring enhancement –role dynamic MRI
Chordoma
Location at sacrococcyx/cervicocranial junction – elderly – multilevel –sparing disc space
7/03/2017
12
ConclusionBasic principles in diagnosis
Age
Location
Multiplicity
Imaging parameters
Conclusion
• Plain films are the mainstay– Detection– Characterization– CT: complex anatomical regions
• MRI– Local staging– (Characterization)– Follow-up after treatment
Conclusion