Embed Size (px)
Citation preview

Otolaryngol Clin N Am
40 (2007) 479–519
Lesions of the Petrous Apex: Diagnosisand Management
Brandon Isaacson, MD*, J. Walter Kutz, MD,Peter S. Roland, MD
Department of Otolaryngology–Head and Neck Surgery,
The University of Texas–Southwestern Medical Center,
5323 Harry Hines Blvd., Dallas, TX 75390-9035, USA
Anatomy
The petrous apex is a pyramid-shaped structure that is the most medialaspect of the temporal bone. The base of the pyramid is the otic capsule,semi-canal of the tensor tympani and the petrous carotid artery. The superiorsurfacedor meatal planedextends from the arcuate eminence to the pre-cavernous carotid artery and Meckel’s cave. The posterior surface faces thecerebellopontine angle and begins laterally at the common crus/vestibularaqueduct and ends medially at Dorello’s canal and petroclinoid ligament.The jugular fossa and inferior petrosal sinus are located at the inferior aspectof the petrous apex. The internal carotid artery enters the petrous apex alongthe inferior surface via the carotid canal. The internal auditory canal begins atthe porus acousticus on the posterior face of the petrous apex and ends at thefundus. When viewed from above, the petrous apex may be divided intoanterior and posterior segments by drawing a parallel line through the in-ternal auditory canal. The cochlear aqueduct enters the petrous apex alongits inferior surface just medial to the jugular fossa. The petrous apex isprimarily composed of bone marrow or dense bone, with only 9% to 30%of subjects showing some pneumatization. Pneumatization of the petrousapex is variable and often differs among sides in the same subject [1].
Presentation
Petrous apex lesions can present with various symptoms and signs, de-pending on the size, location, and nature of the pathologic process. Muckle
* Corresponding author.
E-mail address: [email protected] (B. Isaacson).
0030-6665/07/$ - see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.otc.2007.03.003 oto.theclinics.com

480 ISAACSON et al
and colleagues [2] reported hearing loss as the most common symptomfollowed by vestibular dysfunction, headache, tinnitus, facial spasm, diplo-pia, facial paralysis, and otorrhea. Symptoms often present months or yearsbefore diagnosis, and incidental discovery is not uncommon.
Imaging
CT
CT of the temporal bone enables a detailed evaluation of the osseousarchitecture of the petrous apex. Lesions within or involving the petrousapex may be further characterized based with CT by evaluating for differentpatterns of bone erosion or invasion. A distinct advantage of CT is the abil-ity to determine the proximity of a petrous apex lesiondwith submillimeteraccuracydto critical structures, such as the internal auditory canal, oticcapsule, and carotid artery. CT is often complementary to MRI in evaluat-ing petrous apex pathology [4,5].
MRI
Before the introduction of MRI, evaluation of petrous apex pathologywas limited to evaluating changes in the temporal bone with plain films,tomography, and early CT. In most cases, MRI with the history and phys-ical examination allows the clinician to make a diagnosis without obtainingtissue for pathologic examination. Most of the reported petrous apex lesionshave unique MRI characteristics that allow for definitive diagnosis (Table 1)[4,5].
Angiography: conventional, magnetic resonance angiography,magnetic resonance venography, computed tomographyangiography/venography
Petrous apex lesions may compress, invade, or abut the carotid artery,jugular bulb, and inferior and superior petrosal sinuses. Angiographic studiesprovide detailed information about these vascular structures and may helpthe surgeon to select an appropriate surgical approach. Conventional angiog-raphy via femoral artery or vein catheterization provides an opportunity toassess a lesion’s vascularity and its relationship to other vascular structures[6]. This technique also provides an opportunity to devascularize lesionsand extensive feeding vessels to decrease intraoperative blood loss [7–9].The primary disadvantage of conventional angiography is its risk of hema-toma, stroke, pseudoaneurysm formation, and risk of cranial nerve palsies[6]. The introduction of magnetic resonance angiography and venographyhas provided a low-risk technique of assessing the skull base vasculature.Although the resolution of these studies is good, the primary disadvantageof magnetic resonance angiography/venography is the inability to perform

481LESIONS OF THE PETROUS APEX
interventional measures [10]. CT angiography and venography allow for an-other detailed means of assessing petrous apex lesions and vessels. This tech-nique uses ultra-thin slices with timed administration of contrast andprovides incredible detailed information. An additional advantage of tempo-ral bone CT angiography compared with its counterparts is the ability todefine the vascular structures and their relationship with the lesion and otherstructures in or adjacent to the petrous apex [11].
Management
Surgical approaches
Nonhearing preservationInfracochlear. Traditionally, the most common approach to cystic lesions ofthe petrous apex in patients with serviceable hearing was the infralabyrin-thine approach. This approach is limited in patients with a high jugularbulb, however. The alternative in these patients is the infracochlear ap-proach to the petrous apex [12,13]. There are several advantages to the in-fracochlear approach, including dependent drainage in a well-aeratedmiddle space adjacent to the eustachian tube, adequate access to the petrousapex despite a high jugular bulb, simple revision if required, and preserva-tion of the normal middle ear mechanisms [14].
Continuous intraoperative facial nerve monitoring is recommended. Astandard postauricular incision is made. An incision is made in the mastoidperiosteum along the linea temporalis and is extended inferiorly to themastoid tip. The periosteum is elevated anteriorly until the osseous externalauditory canal is exposed. The external auditory canal is transected throughthe cartilaginous portion. Canal incisions are made at 2 and 10 o’clock, anda tympanomeatal flap is elevated. The tympanic membrane remains atta-ched to the umbo and superior canal wall. Removing an adequate amountof anterior and inferior tympanic bone within the external auditory canal isa critical step to expose the hypotympanum. Once exposure is adequate, thechorda tympani nerve can be traced posteriorly and inferiorly to identify thefacial nerve. Next the jugular bulb and petrous carotid artery are identified.Once these structures have been identified, medial dissection continues withdiamond burs and curettes. The boundaries of the dissection include thecarotid artery anteriorly, the jugular bulb inferiorly, the facial nerve poste-riorly, and the basal turn of the cochlea superiorly. Jacobson’s nerve can befollowed inferiorly and leads to the bone between the carotid artery and jug-ular bulb. Confining the exposure inferior to the round window prevents in-advertent injury to the basal turn of the cochlea during dissection. The cystis entered and the loose contents are removed using suction and irrigation.Apiece of Silastic tubing is placed in the surgical defect. The bony defect of theinferior bony annulus is repaired with bone pate. The tympanomeatal flap is
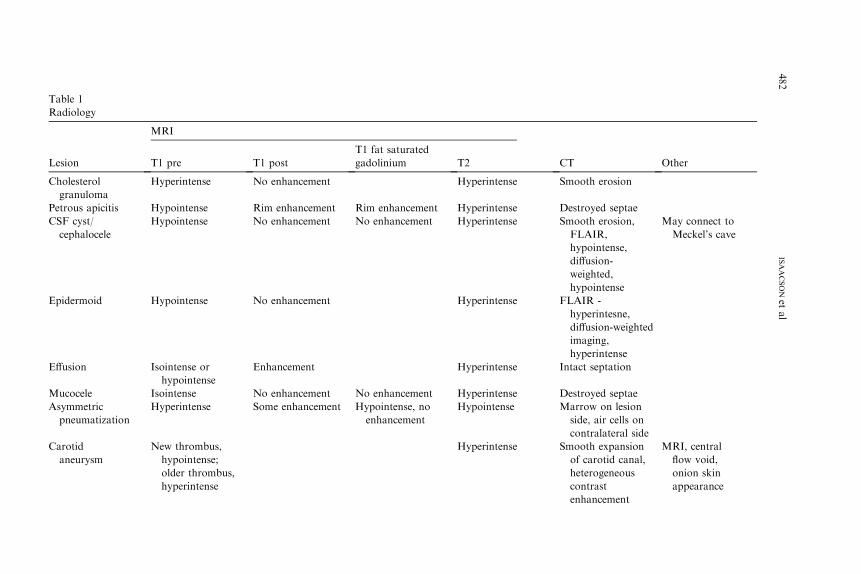
Tabl
Radi
Lesio CT Other
Chol
gra
Smooth erosion
Petro Destroyed septae
CSF
cep
Smooth erosion,
FLAIR,
hypointense,
diffusion-
weighted,
hypointense
May connect to
Meckel’s cave
Epid FLAIR -
hyperintesne,
diffusion-weighted
imaging,
hyperintense
Effus Intact septation
Muc Destroyed septae
Asym
pn
Marrow on lesion
side, air cells on
contralateral side
Caro
an
Smooth expansion
of carotid canal,
heterogeneous
contrast
enhancement
MRI, central
flow void,
onion skin
appearance
482
ISAACSONet
al
e 1
ology
MRI
n T1 pre T1 post
T1 fat saturated
gadolinium T2
esterol
nuloma
Hyperintense No enhancement Hyperintense
us apicitis Hypointense Rim enhancement Rim enhancement Hyperintense
cyst/
halocele
Hypointense No enhancement No enhancement Hyperintense
ermoid Hypointense No enhancement Hyperintense
ion Isointense or
hypointense
Enhancement Hyperintense
ocele Isointense No enhancement No enhancement Hyperintense
metric
eumatization
Hyperintense Some enhancement Hypointense, no
enhancement
Hypointense
tid
eurysm
New thrombus,
hypointense;
older thrombus,
hyperintense
Hyperintense

Chordoma Hypointense/ Enhancement less Enhancement Hyperintense Lobulated, bone
destruction with
residual bone
fragments
Centrally located
in clivus with
lateral spread
to petrous apex
C Hyperintense,
heterogeneous
Infiltrative,
remnants of
eroded bone
Centered in petrous
apex in region
of foramen
lacerum,
calcified areas
may show as
signal voids
M Depends
on primary
Bone erosion Depends on
primary tumor
P Hyperintense Opacified and
destroyed
air cells
Flow voids, blush
on angio, salt
and pepper
M Isointense/
hyperintense
Hyperostosis,
isointense or
hyperdense,
calcification
Dural tails, sessile,
eccentric
S Hyperintense or
hypointense
May show dilation
of internal
auditory canal
Centered in
internal
auditory canal
483
LESIO
NSOFTHEPETROUSAPEX
isointense intense than
chondrosarcoma
hondrosarcoma Hypointense/
isointense,
homogeneous
Enhance Enhancement
etastasis Depends on
primary
Enhancement Enhancement
araganglioma Isointense Enhancement Enhancement
eningioma Isointense/
hyperintense
Enhancement Enhancement
chwannoma Isointense Enhancement Enhancement
Data from References [3,4,69,75,84,89].

484 ISAACSON et al
returned to its normal position. The external auditory canal is packed withGelfoam, and the postauricular incision is closed [12,13].
Brackmann and Toh [14] reported a recurrence rate of 16.7% in choles-terol granulomas treated with the infracochlear approach. Fibrous occlusionof the drainage tract was responsible for all failures. The use of Silastic tub-ing decreases the rate of recurrence in infralabyrinthine and infracochlearapproaches [14,15]. Because recurrence can occur years after the initial sur-gery, long-term radiographic follow-up is necessary. Preoperative symptomsof hearing loss, vertigo, and cranial nerve deficits often improve or resolveafter treatment [2]. Complications are rare; however, inadvertent injury tothe carotid artery is a potentially devastating injury. The infracochlear ap-proach to the petrous apex should be performed by a surgeon with an inti-mate knowledge of the anatomy.
Subtemporal approaches
The subtemporal approaches provide varying degrees of exposure to thepetrous apex, clivus, ventral brainstem, and anterior cerebellopontine angle[3]. The standard and extended middle fossa approaches provide excellentexposure of the internal auditory canal from the porus acousticus to thefundus [16]. The extended approach requires more extensive bone removalanterior and posterior to the internal auditory canal. This additional boneremoval, which exenterates a significant portion of the anterior and poste-rior petrous apex, provides additional exposure to the cerebellopontineangle. The anterior limit of dissection is the lateral wall of Meckel’s cave,whereas the posterior limit is the blue-lined superior semicircular canal[17]. The Kawase approach is a further elaboration of the extended middlefossa approach that requires downfracturing of the zygoma [18,19]. Thisapproach provides access to the ventral pons by removing the anteriorpetrous apex down to the level of the horizontal petrous carotid artery.The primary disadvantage of the subtemporal approaches is an increasedrisk of facial nerve injury because of its anterior superior location in theinternal auditory canal; however, several studies have demonstrated nolong-term difference [20,21]. Temporal lobe injury from prolonged retrac-tion or injury to the vein of Labbe is also an important considerationwhen using these approaches [22]. The subtemporal approaches do notpermit visualization of the inferior cerebellopontine angle. The subtemporalapproaches may be combined with the pre- and postsigmoid approaches toaddress lesions that extend into multiple intracranial compartments [23].
Various skin incisions may be used for the subtemporal approaches. Oncethe skin and subcutaneous tissues are elevated, the temporalis muscle is cutjust proximal to its origin from the temporal line to provide a site of attach-ment during closure. The temporalis muscle is elevated anteriorly andinferiorly and is secured with retractors or hooks. Identification of thezygoma and the osseous external auditory canal provides landmarks for

485LESIONS OF THE PETROUS APEX
the craniotomy bone flap. A 4 cm � 5 cm craniotomy bone flap that iscentered 1.5 cm anteriorly to the root of zygoma is elevated. Occasionally,additional squamous temporal bone cortex must be removed so that thecraniotomy is flush with the middle fossa floor. Once the craniotomybone flap has been elevated, the dura is elevated off the floor of the middlefossa from posterior to anterior to prevent avulsion of the greater superficialpetrosal nerve. The dura is elevated from the petrous ridge posteriorly to thedura of Meckel’s cave anteriorly. Cauterization or clipping of the middlemeningeal is often necessary. The greater superficial petrosal nerve, arcuateeminence, petrous ridge, middle meningeal artery, and foramen ovale allserve as landmarks to guide the surgeon. House [24], Fisch [25], and Jackler[26] each described three separate techniques to identify the internal audi-tory canal. A lateral to medial technique, described by Fisch, begins byblue-lining the superior semicircular canal and then identifying the internalauditory canal at a 60� degree angle. William House [27] identified the fun-dus of the internal auditory canal by tracing the greater superficial petrosalnerve to the geniculate ganglion. Jackler and Gladstone [26] described a me-dial to lateral technique that begins with drilling at the petrous ridge andidentifying the internal auditory canal at the porous acousticus and follow-ing it laterally to the fundus. Once tumor removal is complete, air cells arewaxed and muscle or fat is used to obliterate the defect.
Infralabyrinthine approachDuring the preantibiotic era, the infralabyrinthine approach was most
commonly used to drain petrous apex abscesses [28,29]. With the adventof antibiotics, petrous apex infections are rare; however, the sameapproaches can be used to drain cystic lesions of the petrous apex. Theadvantages of the infralabyrinthine approach to the petrous apex includean anatomy familiar to most otologists, direct route to most cysts of thepetrous apex, and avoidance of entering the middle ear. A high-riding jug-ular bulb may necessitate the use of the infracochlear approach as opposedto the infralabyrinthine approach.
The surgical procedure begins with a simple mastoidectomy. The middlefossa plate, sigmoid sinus, and facial nerve are identified. The posteriorportion of the lateral semicircular canal and the posterior semicircular canalare skeletonized, with care taken not to create a fistula in the semicircularcanals. Next, the sigmoid sinus is followed inferiorly until the jugular bulbis identified. The boundaries of the approach include the posterior semicir-cular canal, facial nerve, jugular bulb, and the posterior fossa dura. Medialdissection continues with diamond burs and curettes until the cyst is entered.The loose contents of the cyst are removed with suction and irrigation.A piece of Silastic tubing is placed through the surgical tract to preventrestenosis of the surgical drainage tract.
Complications reported as a result of the infralabyrinthine approachinclude sensorineural hearing loss and facial nerve paresis [15,30].

486 ISAACSON et al
Preoperative deficits, including hearing loss, imbalance, and cranial nerveneuropathies, may resolve after surgery, depending on the lesion. Long-term radiographic follow-up is necessary because recurrences can occuryears after drainage. Importantly, the lack of aeration alone postoperativelyshould not be considered a failure; however, increased size of the lesion orreturn of symptoms is a sign of recurrence and may require re-exploration.
Subarcuate and sinodural angle approachesThe subarcuate and sinodural angle approaches are mainly used in
suppurative processes of the petrous apex. These approaches are rarelyused because of the limited access provided. A standard mastoidectomy isused in both approaches. In the subarcuate approach all three semicircularcanals are skeletonized. A small diamond bur is used to open the area infe-rior to the superior semicircular canal and superior to the vestibule thatfollows the path of the subarcuate artery. In cases of suppuration of the pos-terior petrous apex, fistulous tracts may be found in this pathway and can befollowed to the petrous apex. The sinodural angle is another avenue that canbe followed to the posterior petrous apex, where air cells of the sinoduralangle are followed to the posterior petrous apex [1].
Supracochlear approachThe supracochlear approach allows for drainage or biopsy of lesions
located on the anterior superior aspect of the petrous apex. This approachbegins with a standard mastoidectomy followed by an extended antrotomythat exposes the zygomatic root cells. In some cases the incus body andoccasionally the malleus head must be removed. Drilling with a 2- to 3-mmdiamond bur begins anterior to the superior semicircular canal, between thetegmen tympani and the tympanic facial nerve. In the series by Telischi andcolleagues [31] of 20 temporal bones, removal of the incus was required inmany of the specimens to access the supracochlear air cell tract. Telischifound that the mean dimensions of the supracochlear triangle are 7.0 �5.3 � 4.8 mm. The advantage of this approach, which provides access tothe anterior superior petrous apex, is preservation of the external auditorycanal and labyrinth. Unfavorable aspects of this approach include a signifi-cant risk to the labyrinthine facial nerve and the potential need for removalof the malleus head and incus. Intraoperative facial nerve monitoring is rec-ommended with this approach because of the proximity of the tympanic andlabyrinthine facial nerve.
Retrosigmoid approachThe retrosigmoid approach gives excellent access for tumors that arise in
the cerebellopontine angle and involve the posterior cranial fossa. Thisapproach is limited when tumors extend into the middle fossa and involveMeckel’s cave, however. In 1995, Cheung and colleagues [32] described anapproach combining a retrosigmoid craniotomy with opening of Meckel’s

487LESIONS OF THE PETROUS APEX
cave by removing bone anterior to the internal auditory canal. Samii andcolleagues [33] later reported a series of 12 petroclival meningiomas ap-proached through a similar approach called the retrosigmoid intraduralsuprameatal approach. The suprameatal extension of the retrosigmoidapproach allows improved access to the petrous bone anterior to the inter-nal auditory canal and allows better visualization of the prepontine cistern,clivus, oculomotor nerve, and the posterior cerebral arteries.
Seoane and Rhoton [34] studied the anatomic relationships concerning thesuprameatal approach to Meckel’s cave. The suprameatal tubercle is a bonyprominence superior to the internal auditory canal and blocks access toMeckel’s cave, the prepontine cistern, and clivus from a posterior approach.Removal of this bone allows approximately 1 cm additional exposure of theposterior root of the trigeminal nerve and an additional 1.3 cm of anterior ex-tension to the retrosigmoid approach. This approach is most ideal for petro-clival meningiomas or posterior fossa trigeminal schwannomas with a limitedamount of middle fossa involvement. Disadvantages include drilling in a tightspace with adjacent critical neurovascular structures, poor access to thecavernous sinus, and further working distance to the petrous apex whencompared with other approaches [35].
Combined approachesThe combined approaches provide exposure for lesions that extend in the
middle and posterior fossa. These approaches typically use a transtemporalapproach (retrolabyrinthine, translabyrinthine, and transcochlear) in addi-tion to a middle fossa craniotomy. The technical details of this approachalready have been described except for several critical steps. The superior pe-trosal sinusmust be divided after cauterization or placement of clips. After thetranstemporal and middle fossa craniotomies are completed, the tentorium isdivided being careful not to injure the trochlear nerve, Dandy vein, superiorcerebellar artery, and vein of Labbe [23]. Prolonged retraction of the temporallobe dura poses a risk of injury or thrombosis of the vein of Labbe. Intermit-tent release of the retractor or division of the sigmoid sinusmay prevent injuryto the vein of Labbe [22]. The primary advantages of these combined ap-proaches are decreased brain retraction,which eliminates the need for a stagedapproach, improved exposure, which allows for a more complete excision,and the possibility of hearing preservation (retrolabyrinthine). The primarydisadvantage to the combined craniotomy is sacrifice of hearing if either thetranslabyrinthine or the transcochlear approach is used [3].
Infratemporal approach
The preauricular infratemporal approach and its modifications providegenerous access to the petrous apex and clivus. Various incisions havebeen used and described for the infratemporal approach, including a Yincision, a large postauricular C-shaped incision, and a pretragal incision

488 ISAACSON et al
[36–38]. The skin flaps are elevated over the temporalis fascia until the tem-poral fat pad is identified. An incision is made in the superficial layer of thedeep temporal fascia and dissection proceeds just lateral to the temporal fatdown to the level of the zygoma. The periosteum of the zygoma is transectedalong its superior-medial surface and elevated to preserve the frontal branchof the facial nerve. Identifying the main trunk of the extratemporal facialnerve at the stylomastoid foramen allows for more generous inferior expo-sure of the infratemporal fossa. The zygoma is exposed from the root to theorbital rim. Miniplate drill holes are placed before performing the zygomaticosteotomy for later reconstruction. The zygoma is then transposed inferiorlywith the attached masseter muscle.
The temporalis muscle is cut along its origin, taking care to preservea cuff of muscle for later reattachment if necessary. The temporalis is care-fully reflected inferiorly toward its insertion on the coronoid process so asnot to interrupt the vascular supply. The mandibular condyle is displacedout of the glenoid fossa with a retractor or can be resected to providemore generous exposure. A high-speed otologic drill is then used to removethe glenoid fossa and expose the petrous carotid artery. The eustachian tubeserves as a useful landmark for the carotid artery and must be obliterated.Division and cauterization of the mandibular division of the trigeminalnerve and middle meningeal artery permits exposure of the precavernouspetrous carotid artery and the anterior clivus. Once the petrous carotidartery has been skeletonized, generous exposure of the anterior petrousapex and clivus is afforded. Inferior mobilization of the carotid artery pro-vides improved visualization of the petrous apex and clivus but is associatedwith an additional risk of inadvertent injury or vasospasm. If a large defectis present, the temporalis muscle may be rotated into the defect. Lesions thatextend into the middle ear may require additional exposure [36,37].
Transnasal endoscopic approachEndoscopic-assisted pituitary surgery has become the favored technique
in many centers, with resulting decreased hospital stay, decreased recoverytimes, and better visualization for tumor excision [39,40]. More recently,several centers have pushed the envelope by performing transnasal endo-scopic approaches to posterior, middle, and anterior cranial base lesions.Kassam and Jho [41,42] recently reported on a modular approach to access-ing posterior fossa lesions, including the petrous apex and jugular foramen,via a transnasal endoscopic approach. These techniques require intimateknowledge of the complex skull base anatomy. Petrous apex cholesterolgranulomas and epidermoids occasionally can be drained into the sphenoidsinus if the carotid artery is not in the drainage pathway [43,44]. Kassamand colleagues [41] also described an endoscopic technique that mobilizesthe petrous carotid artery to access the petrous apex. These endoscopic skullbase techniques hold the same potential promise that endoscopic pituitaryapproaches provide but require advanced knowledge and training.

489LESIONS OF THE PETROUS APEX
Translabyrinthine approachThe translabyrinthine approach was reintroduced by Drs. Hitselberger
and House [45], and with the introduction of the operating microscope, ini-tiated the era of modern skull base surgery. This approach is often used inthe surgical management of petrous apex lesions when hearing is poor or thetumor is large [3].
A postauricular incision is made to expose the mastoid periosteum. Themastoid periosteum is divided carefully so as not to overlap the cutaneousincision from the periosteal incision. Once the periosteum is dissectedfrom the cortex, an extensive mastoidectomy is performed carefully so asto identify the mastoid tegmen, posterior fossa plate, sigmoid sinus, andexternal auditory canal. The antrum is opened and the lateral semicircularcanal is identified along with the previously mentioned structures. A labyrin-thectomy is performed, leaving the ampullated end of the superior semicir-cular canal as a landmark. The internal auditory canal is then identified, anda thin layer of bone is left over its surface. Removing bone inferior andsuperior to the internal auditory canal often exposes air cells or pathologyinvolving the anterior petrous apex. This approach gives wide exposure tothe posterior petrous apex and adequate exposure to the anterior petrousapex. The primary disadvantages of this approach are the loss of any resid-ual hearing, worsening balance function, and vertigo that occurs immedi-ately after the surgery. There is also a significant risk of a cerebrospinalfluid (CSF) leak if the dura is violated. An abdominal fat graft is oftenharvested and later used to obliterate the cavity once the resection hasbeen completed [3].
Transotic and transcochlear approachesThe transotic and transcochlear approaches, described by Fisch and
House [46,47], respectively, were introduced to provide more anterior cere-bellopontine angle exposure. These approaches and their variations allowfor substantial exposure of the prepontine cistern and its contents, includingthe pons, medulla, basilar artery, vertebrobasilar junction, cranial nerves Vthrough XI, and the clivus [48]. The transcochlear approach is an extensionof the translabyrinthine approach but includes removal of the entire oticcapsule and posterior rerouting of the facial nerve from the porous acousti-cus to the stylomastoid foramen. The originally described transcochlearapproach preserves the middle ear and external auditory canal, whereasthe extended version requires removal of these structures with obliterationof the eustachian tube and over closure of the external auditory meatus[46,48]. The transotic approach was introduced to remove small cerebello-pontine angle tumors and decrease the risk of CSF leak. This approach pre-serves the bone overlying the sigmoid sinus and requires removal of theexternal auditory canal with obliteration of the eustachian tube. The facialnerve is left in situ, and the external auditory meatus is overclosured to pro-vide a water-tight seal [47]. The primary disadvantages of these approaches

490 ISAACSON et al
are hearing sacrifice and the potential for permanent facial nerve weaknessin cases in which the nerve is mobilized. For complete facial nerve mobiliza-tion, additional morbidity includes sectioning of chorda tympani andgreater superficial petrosal nerves [3].
Lesions of the petrous apex
Inflammatory/cystic
Cholesterol granulomaCholesterol granuloma is the most common abnormality found within the
petrous apex. It is a cystic lesion that was first recognized as a distinct clinicalentity in the early 1980s [49]. Together with mucocele and cholesteatoma,cholesterol granuloma accounts for more than 90% of the lesions of thepetrous apex. Cholesterol granuloma is an intraosseous cyst filled withdark, viscous, chocolate brown fluid and granulation tissue. Birefringentcholesterol crystals can be seen on microscopy. The cyst is often containedwithin a fairly thick fibrous capsule but has no true epithelial lining. (Conse-quently, complete surgical excision is not required.) Lo and colleagues [50]estimated that cholesterol granulomas of petrous apex occur in approxi-mately 0.6 per 1 million individuals. Cholesterol granulomas have beenrecognized in the middle ear and mastoid for many decades and havetraditionally been described as ‘‘blue dome eardrum’’ or ‘‘blue dome cyst.’’They are seen occasionally in individuals with chronic middle ear or mastoiddisease. They can occur anywhere within the pneumatized temporal bone[51,52].
Traditional pathophysiology proposes that the cysts form in response toanaerobic catabolism of blood and blood products. Specifically, these cystsare believed to arise as an inflammatory reaction to cholesterol crystalsreleased from blood breakdown products. Several histopathologic studieshave verified that blood breakdown products can incite an inflammatoryresponse [53–57].
The traditionally accepted hypothesis is that blood enters the mucosa-lined pneumatic air cell tracts of the temporal bone as a result of negativepressure, which arises either as a consequence of eustachian tube dysfunc-tion or because mucosal edema has obstructed the passage of air throughthe air cell system. Negative pressure within these mucosa-lined air cellsthen results in transudative hemorrhage. Anaerobic breakdown of the tran-sudated red blood cells frees cholesterol crystals. A foreign body giant cellreaction and cyst formation then develops in response to irritation producedby these cholesterol crystals.
Jackler and Cho [58] raised cogent objections to this conventional hy-pothesis and noted the following points:
1. Transudative hemorrhage rarely follows as a result of long-term eusta-chian tube dysfunction. Negative pressure generated as a consequence

491LESIONS OF THE PETROUS APEX
of obstruction of air flow through the mastoid air cell tract system doesnot seem to be sufficient to produce hemorrhage and bleeding, evenwhen it is sufficient (over time) to produce significant tympanicmembraneretraction.
2. Cholesterol granuloma occurs only in well-pneumatized temporalbones. Extensive pneumatization is usually associated with a patent eu-stachian tube and unrestricted movement of air through the air cellstracts. Extensively pneumatized temporal bones are only uncommonlyassociated with chronic middle ear or mastoid disease.
3. Once air cells have been filled with effusion (bloody or otherwise), thepressure should be equalized. The process should then stop. No addi-tional bleeding should occur. Jackler and Cho [55] stated several argu-ments that a single episode of bleeding would be insufficient to producean expanding cholesterol granuloma.
Jackler and Cho [58] proposed an alternative mechanism. They suggestedthat cholesterol granuloma results as a consequence of dehiscence of thebony partition between the petrous apex air cell system and bone marrowin the anterior temporal bone or clivus. Exposed marrow is a potentialsource for repeated hemorrhage. Their argument is supported by a radio-logic investigation that demonstrates dehiscence between bone marrow inthe petrous air cell system contralateral to a cholesterol granuloma in 6 of13 patients. No control patients with highly pneumatized petrous apicesdbut without cholesterol granuloma formationdhad such dehiscences.
Extensive pneumatization of the petrous apex is variously reported asoccurring in somewhere between 10%and 30%of patients; thus only a limitedsegment of the population is potentially vulnerable to development ofa petrous apex cholesterol granuloma [59,60].
Brackmann and Toh [14] listed the signs and symptoms present in individ-uals at the time they seek help for cholesterol granulomas: 65% of patientshad hearing loss or one of its associated symptoms (tinnitus, aural fullness).More than 50% of individuals reported dizziness. Headache occurred in onethird of patients. One of five patients had either facial twitching or facialnumbness. Facial weakness and diplopia were uncommon.
Unfortunately, Brackmann and Toh [14] do not indicate the reasonfor which individuals sought care or accepted surgery for the removal oftheir cholesterol granulomas. Given the frequency of hearing loss in thepopulation, it is likely that hearing loss was present incidentally and notas a consequence of the petrous apex abnormality in at least somesubjects.
Hughes and colleagues [49] indicated that most patients seeking inter-vention for petrous apex cholesterol granuloma do so because of headache.The pathognomonic headache for petrous apex cholesterol granuloma isretro-orbital, although generalized temporoparietal headache may occur asa consequence of irritation of the petrous apex.

492 ISAACSON et al
Care should be taken to establish the petrous apex lesion as the cause ofthe headache. Headaches are common, and an effort should be made to de-termine whether the headache is related to the petrous apex cholesterolgranuloma. A neurology consultation or migraine management is oftenhelpful in determining the relationship of the lesion to the symptom.
Facial twitching is much more common than facial weakness and occursin one fifth of patients with cholesterol granuloma of the petrous apex.Facial numbness and paresthesia (usually in the distribution of V3) alsooccurs in approximately one out of five patients and is easier to link tothe pathologic process [14]. It is often difficult to determine whether the cys-tic petrous apex lesion is causing the patient’s symptoms. If the symptomsare consistent with the anatomic location of the lesion, however (ie, neuro-sensory hearing loss is present and the lesion clearly encroaches on the oticcapsule or internal auditory canal), then treatment should be initiated.Conversely, if the patient complains of facial paresthesia but the cholesterolgranuloma is restricted to the interior/posterior petrous air cells, it is prob-ably prudent to observe the lesion.
Diagnosis depends on imaging. Cholesterol granulomas are relativelyunique in that they show a hyperintense signal on T1 and T2 images onMRI (Figs. 1 and 2). Most of the other lesions confused with cholesterolgranuloma (eg, cholesteatoma, fluid, mucocele, neoplasia) demonstrateonly low or medium signal intensity on T1 images. The exception isasymmetric pneumatization of the petrous apex [14,49]. Bone marrow inthe nonpneumatized apex may suggest the presence of a lesion. Bone mar-row can have a high signal intensity on T1- and T2-weighted images, but
Fig. 1. Cholesterol granuloma. Axial T1-weighted magnetic resonance fat-saturated image with
gadolinium demonstrates a heterogeneous, hyperintense lesion in the right petrous apex.

493LESIONS OF THE PETROUS APEX
it is usually lower on T2-weighted images, which is sufficient to distinguish itfrom a granuloma on MRI [61]. Cholesterol granulomas do not enhancewith contrast, and contrast enhancement suggests a neoplasm.
The decision to operate on cholesterol granulomas of the petrous apex isoften made only after determining that the lesion shows evidence of boneerosion or expansion or both. Consequently, fine-cut CT of the temporalbone is usually more useful in assessing and following these lesions thanis MRI.
The first thing one should look for on a CT is the presence of normalseptation of the air cell system in the petrous apex. If the lesion is not erod-ing and destroying these thin delicate septae, it is unlikely that it is growingor expanding. The presence of intact septation suggests that the lesion is notcausing symptoms and can be ‘‘left alone.’’ Lesions that show normalseptation rarely require intervention. There are some exceptions, however,as discussed in the section on petrous effusion.
Signs of erosion and expansion include scalloping and notching of thelesion into the clivus and posterior expansion into the labyrinth or internalauditory canal. Large cholesterol granulomas frequently bulge medially intothe posterior fossa. They usually carry with them a rim of sclerotic bone thatis often thin but detectable on CT. Cholesterol granulomas do not generallyenhance with intravenous contrast, although some rim enhancement isconsistent with a cholesterol granuloma.
If it is decided that intervention is necessary, several surgical approachesare available to remove lesions of the petrous apex (Box 1). If serviceablehearing is present, every attempt should be made to conserve it; severalsurgical procedures can do so. The infralabyrinthine approach has been
Fig. 2. Cholesterol granuloma. Axial T2-weighted MRI demonstrates a heterogeneous, hyper-
intense lesion in the right petrous apex.

494 ISAACSON et al
widely used as a hearing conservation technique. It is relatively quick andeasy to perform and can provide dependent drainage to the cyst. Anatomicstudies have shown that as much as 11 mm of space may be available usingthis approach, although on average approximately 5 mm is available [62,63].If the jugular bulb is high, however, access through this approach is notpossible, which seems to be the case in approximately 40% to 50% ofpatients [62].
Surgical approaches to the petrous apex. First five approaches can allpreserve hearing, the last two cannot.
The infracochlear approach has been championed by Brackmann andToh. An infracochlear channel into the petrous apex cyst seems to havethe highest likelihood of staying open. The approach is nondestructiveand relatively straightforward. As noted by Brackmann and Toh [14], theinfracochlear approach permits a fairly straightforward revision surgery.
The middle fossa approach permits wider exposure than the infracochlearand infralabyrinthine approach, except for the most inferior/posterior aircells. Cholesterol granulomas are often fairly extensively loculated, and itcan be difficult or even impossible to break up these loculations and drainthe entire cyst through the small openings afforded by the infracochlearor infralabyrinthine approaches.
The biggest disadvantage to the middle fossa approach is the lack of de-pendent drainage. At UT Southwestern we have used a small piece of shunttubing placed from the petrous apex over the internal auditory canal intothe mastoid air cell system to encourage aeration. Long-term postoperativeaeration of the involved petrous apex has been the exception rather than therule, however.
The endoscopic transsphenoidal approach is appealing for lesions thatexpand anteriorly into the sphenoid sinus itself. In such circumstances, theendoscopic transsphenoidal approach can be used successfully to drainthe cyst. Brackmann and Presutti [14,64], however, indicated that long-term aeration is uncommon after endoscopic transsphenoidal procedures.If there is significant bone between the anterior margins of the petrous
Box 1. Surgical procedures
1. Infracochlear2. Infralabyrinthine3. Middle fossa4. Transsphenoidal5. Transtemporal, preauricular6. Translabyrinthine7. Transcochlear

495LESIONS OF THE PETROUS APEX
apex cyst and the sphenoid sinus itself, it is a difficult and potentially dan-gerous operation.
Neurosurgeons sometimes use the transtemporal, preauricular approachso as to completely remove cholesterol granulomas of the petrous apex butsave hearing. Although such approaches seem to be successful, they seemunnecessarily invasive compared with the infracochlear and infralabyrin-thine approaches [65].
In individuals who have lost all hearing (usually as a result of disease),translabyrinthine and transcochlear approaches provide generous accessto the petrous apex and a high likelihood of persistent postoperative aera-tion. An experienced otologic surgeon can perform these procedures safelyand relatively rapidly. Complete loss of residual hearing is inherent in theseapproaches. Most patients recover well from the associated loss of balancefunction, but these operations should be used with caution in individualswho have contralateral labyrinthine hypofunction.
Classical literature suggests that pneumatization is required to preventrecurrence. The extent to which this is true is unclear. Simple opacificationof the cyst with an effusion does not necessarily indicate recurrence of thelesion; that is, nonopacified petrous apex cholesterol granulomas mayremain asymptomatic indefinitely. The fact that the cystic area has filledwith fluid does not necessarily mean it has become expansive or erosive.In Brackmann and Toh’s [14] series of 21 patients who received postopera-tive imaging, only lesions were aerated. All lesions that were aerated hadundergone infracochlear approaches. Of the 15 nonaerated lesions, only 1had increased in size and only 5 have required revision surgery.
Epidermoid/cholesteatomaPetrous apex epidermoid or cholesteatoma is a rare entity that comprises
4% to 9% of all petrous apex lesions [66,67]. These lesions are classified asacquired or congenital, with the former being referred to as cholesteatomaand the latter referred to as epidermoid [68]. Cholesteatoma that involvesthe petrous apex originates from disease in the middle ear or mastoid thatgains access to the petrous apex via several preformed pathways. Epithelialcell remnants from an anomalous developing first branchial cleft or frommultipotential embryonic cells or displaced otic capsule cells are thoughtto be the mechanism for epidermoid formation. Despite their different ori-gins, cholesteatoma and epidermoid have an identical appearance on path-ologic examination [68]. An anatomic classification system reported bySanna [69] includes five categories: supralabyrinthine, infralabyrinthine,massive labyrinthine, infralabyrinthine-apical, and apical. Presenting symp-toms include hearing loss, facial paresis/paralysis, dizziness, otorrhea,trigeminal paresthesia, and diplopia. In Kaylie’s [70] series, cranial nervesV, VII, and VIII were most commonly involved. Cranial nerve deficits arethought to arise from encasement with resultant ischemia. CT often demon-strates a low-density mass that does not enhance but demonstrates smooth

496 ISAACSON et al
bone erosion. The T1- and T2-weighted MRI characteristics of petrous apexcholesteatomas are the same as CSF and arachnoid cysts (Figs. 3 and 4).Unlike CSF and arachnoid cysts, fast fluid-attenuated inversion-recovery(FLAIR) and diffusion-weighted imaging reveal a hyperintense lesion withpetrous cholesteatomas (Figs. 5 and 6) [71,72]. The presence of gadoliniumenhancement should raise the suspicion of carcinoma within the lesion. Thepresence of a focus of squamous cell carcinoma despite a complete excisionportends a poor prognosis [3].
Surgical excision or exteriorization is the treatment of choice dependingon the location of the lesion and the presenting symptoms. Various surgicalapproaches have been described, including the middle fossa, translaby-rinthine, transotic, transcochlear, and infratemporal approaches. The appr-oach selected depends on the extent and location of the disease and thehearing status [68,70,73]. The geniculate facial nerve is the most commonsite of involvement in patients who present with facial weakness from petro-sal cholesteatomas. The nerve may have undergone extensive fibrosis, and asa result, decompression and rerouting have little chance of improving func-tion. Axon [68,69] recommended excision of the ischemic, fibrotic segmentwith the adherent matrix and primary anastomosis to maximize chancesof recovery in patients with complete paralysis. Chemical meningitis as a re-sult of spillage of keratin debris in the subarachnoid space is another possi-ble complication. Yasargil and colleagues [74] and Yamakawa andcolleagues [75] demonstrated a reduction in the rate of chemical meningitiswith the administration of perioperative steroids. Recurrence is another
Fig. 3. Epidermoid. Axial T1-weighted MRI with fat saturation and gadolinium demonstrates
a hypointense signal in the clivus and right petrous apex. Notice there is no enhancement.
497LESIONS OF THE PETROUS APEX
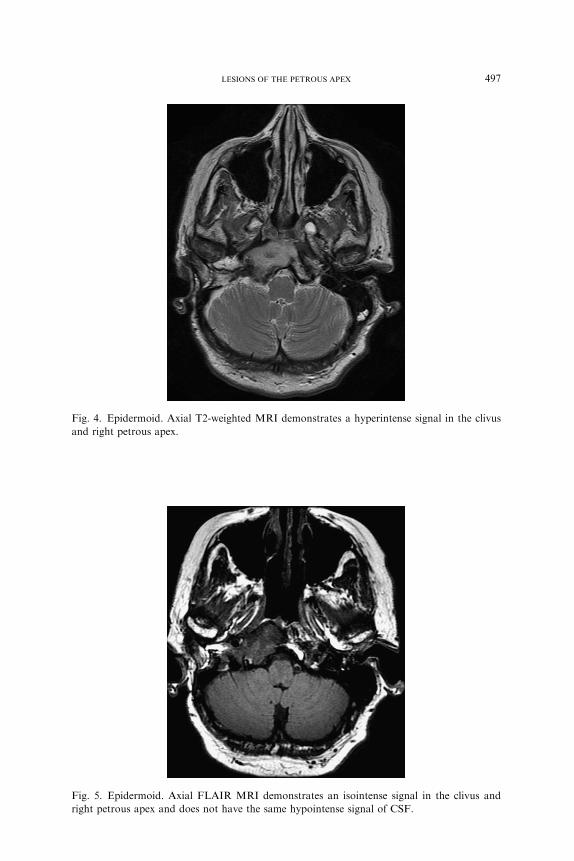
Fig. 4. Epidermoid. Axial T2-weighted MRI demonstrates a hyperintense signal in the clivus
and right petrous apex.
Fig. 5. Epidermoid. Axial FLAIR MRI demonstrates an isointense signal in the clivus and
right petrous apex and does not have the same hypointense signal of CSF.

498 ISAACSON et al
significant consideration when managing petrosal cholesteatomas, with themost common location for recurrence being the petrous carotid artery.
Adherence of matrix to critical and delicate structures, such as the carotidartery, jugular bulb, facial nerve, and dura, makes complete excision chal-lenging even in the most experienced hands. Generous exposure with variousapproaches decreases recurrence by allowing direct visualization of the dis-ease. Visualization also may be improved with the use of rigid straight andangled endoscopes [68]. Exteriorization of the disease may result in a largecavity that may be difficult to maintain. Obliteration with blind-sac closureof the external auditory canal to decrease problematic cavity maintenancewas described recently. MRI provides an excellent means to follow subjectswith obliterated cavities because different imaging techniques allow for differ-entiation of recurrence from obliteration materials (ie, fat and muscle) [3].
Effusion
Petrous apex effusion, also known as ‘‘retained’’ or ‘‘trapped’’ fluid, ismostcommonly discovered as an incidental finding on routine imaging studies. Theincidence of this lesion is 1% of all cranial MRI studies and is thought to beone of the most common petrous apex imaging findings, according to
Fig. 6. Epidermoid. Axial diffusion-weighted MRI demonstrates an isointense signal in the
clivus and right petrous apex and does not have the same hyperintense signal of CSF.
499LESIONS OF THE PETROUS APEX
Harnsberger [76]. Effusions can be found only in a pneumatized petrous apex,which occurs in approximately one third of patients. Effusions are thought toarise as a result of infection in themiddle ear ormastoid with subsequent trap-ping of residual fluid in the petrous apex from mucosal edema [77].
Presenting symptoms may include hearing loss, positional vertigo, head-ache, aural pressure, pain, and facial spasm. Petrous apex effusions appearhyperintense on T2-weighted images and hypo- or isointense on T1-weightedimages, with no enhancement with gadolinium. CT demonstrates opacifica-tion of the petrous apex air cells with no evidence of coalescence [77].
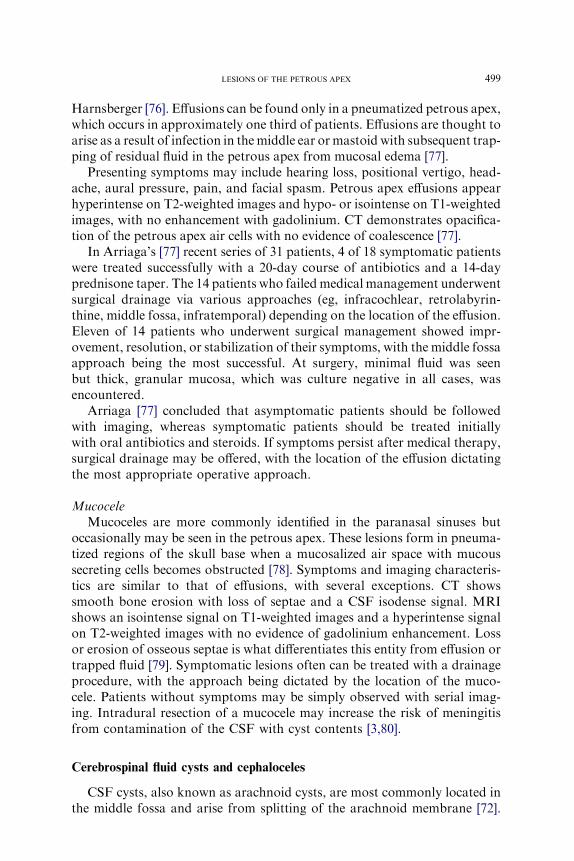
In Arriaga’s [77] recent series of 31 patients, 4 of 18 symptomatic patientswere treated successfully with a 20-day course of antibiotics and a 14-dayprednisone taper. The 14 patients who failedmedical management underwentsurgical drainage via various approaches (eg, infracochlear, retrolabyrin-thine, middle fossa, infratemporal) depending on the location of the effusion.Eleven of 14 patients who underwent surgical management showed impr-ovement, resolution, or stabilization of their symptoms, with the middle fossaapproach being the most successful. At surgery, minimal fluid was seenbut thick, granular mucosa, which was culture negative in all cases, wasencountered.
Arriaga [77] concluded that asymptomatic patients should be followedwith imaging, whereas symptomatic patients should be treated initiallywith oral antibiotics and steroids. If symptoms persist after medical therapy,surgical drainage may be offered, with the location of the effusion dictatingthe most appropriate operative approach.
MucoceleMucoceles are more commonly identified in the paranasal sinuses but
occasionally may be seen in the petrous apex. These lesions form in pneuma-tized regions of the skull base when a mucosalized air space with mucoussecreting cells becomes obstructed [78]. Symptoms and imaging characteris-tics are similar to that of effusions, with several exceptions. CT showssmooth bone erosion with loss of septae and a CSF isodense signal. MRIshows an isointense signal on T1-weighted images and a hyperintense signalon T2-weighted images with no evidence of gadolinium enhancement. Lossor erosion of osseous septae is what differentiates this entity from effusion ortrapped fluid [79]. Symptomatic lesions often can be treated with a drainageprocedure, with the approach being dictated by the location of the muco-cele. Patients without symptoms may be simply observed with serial imag-ing. Intradural resection of a mucocele may increase the risk of meningitisfrom contamination of the CSF with cyst contents [3,80].
Cerebrospinal fluid cysts and cephaloceles
CSF cysts, also known as arachnoid cysts, are most commonly located inthe middle fossa and arise from splitting of the arachnoid membrane [72].

500 ISAACSON et al
CSF cysts located in the cerebellopontine anglemay erode the posterior aspectof the petrous apex [71]. These lesions are often incidentally discovered but oc-casionally produce symptoms of hearing loss, vertigo, tinnitus, headaches,and dysequilibrium [71]. Symptoms are thought to arise from several possiblemechanisms, includingdirect compression of cranial nerves, brainstem, or cer-ebellum and obstruction of the normal flow of CSF [81,82]. Incidentally dis-covered lesions that are asymptomatic may be followed with serial imaging[71]. Not surprisingly, these lesions have the exact MRI characteristics asCSF.Diffusion-weighted imaging andFLAIR sequences allow differentiationfrom epidermoids [71]. There have been occasional reports of cyst wall en-hancement, but this is an exception. In most cases, CT shows smooth orslightly scalloped bone erosion involving the posterior petrous apex [83]. Pa-tientswhose symptoms canbe attributed to the cyst because of neural or brain-stem compression may warrant surgical intervention via shunting proceduresor retrosigmoid craniotomy with wide marsupialization [71].
CSF cephaloceles, also known as Meckel’s cave diverticulum, are thoughtto arise from the protrusion of arachnoid or dura from Meckel’s cave [84].Increased intracranial pressure may be an initiating factor that causes pro-gressive cephalocele enlargement. These lesions are typically located in theanterior petrous apex and may erode into the otic capsule or internal audi-tory canal. Patients may present with cranial nerve findings, headaches, andCSF otorhinorrhea [71]. These lesions have the same MRI characteristics asCSF cysts except they are centered in the anterior petrous apex and are oftencontinuous with Meckel’s cave (Fig. 7). CT may show extensive erosion ofthe petrous apex with either a smooth or scalloped border (Fig. 8) [84]. Anextradural middle fossa approach with obliteration of the cyst cavity withfat or muscle is the recommended approach for symptomatic lesions. Serialimaging is used for patients with asymptomatic lesions or patients whosymptoms cannot be attributed to the location of the lesion. An infraco-chlear or infralabyrinthine approach is not recommended because thesecysts often communicate with the subarachnoid space [71].
Petrous apicitis/abscess
Petrous apicitis is a rarely encountered entity since the introduction of an-tibiotics, with an incidence of 2 in 100,000 patients with acute otitis media [85].These infectionswere often associatedwith highmorbidity andmortality ratesin the preantibiotic era,when surgicalmanagementwas the only treatment op-tion available [86]. The pathophysiology of petrous apicitis results fromspread of infection to the petrous apex through preformed air-cell tracts inthe temporal bone [59]. The most common offending organisms are thesame as those that cause acute otitis media: Haemophilus influenzae, Strepto-coccus pneumoniae, and B-hemolytic streptococcus species. Staphylococcusand Pseudomonasmay be identified in individuals with skull base osteomyeli-tis or chronic otitis media [3,59,85,86].

501LESIONS OF THE PETROUS APEX
It is the exception rather than the norm that a patient present with thecomplete picture of Gradenigo’s syndrome, which includes retro-orbitalpain, otorrhea, and lateral gaze palsy from abducens nerve inflammation.Intracranial extension of the infection may result in meningitis, epidural,subdural, or intraparenchymal abscess, and dural venous sinus thrombosis[87].
Fig. 7. MRI of a petrous apex cephalocele. (A) Axial T2-weighted image shows a hyperintense
lesion (arrow). (B) Axial fluid inversion recovery image (FLAIR) shows the same lesion (arrow),
which is hypointense. (C) Axial T1-weighted image without gadolinium or fat saturation shows
a hypointense lesion (arrow) abutting the petrous carotid artery. (D) Coronal T1-weighted
image without fat saturation with contrast demonstrates a hypointense lesion (arrow) centered
in the right petrous apex.

502 ISAACSON et al
CT scans often demonstrate opacification and destruction of the petrousapex air cell system (Fig. 9). MRI may show a hypointense lesion with rimenhancement on T1-weighted images and a hyperintense signal on T2-weighted images (Figs. 10 and 11) [86]. Fortunately, petrous apicitis is often
Fig. 8. Axial CT scan of a petrous apex cephalocele using a bone window algorithm. (A) An
expansile lesion (large arrow) with smooth margins is noted in the right petrous apex at the level
of the cochlear aqueduct (small arrow). (B) At the level of the internal auditory canal (small
arrow), the lesion (large arrow) demonstrates significant erosion of the otic capsule bone and
encroaches on the internal auditory canal.
Fig. 9. Petrous apicits. Axial temporal bone CT scan demonstrates destruction of the left
petrous apex air cells septae and adjacent cortex. Note the opacification of the middle ear
and mastoid air cells.

503LESIONS OF THE PETROUS APEX
treated successfully with intravenous antibiotics and myringotomy withaspiration and culture of the middle ear [87]. Patients who fail to improveor develop progressive symptoms despite medical management may requiresurgical treatment. Approaches that can be used to treat petrous apicitisinclude subarcuate, supralabyrinthine, infralabyrinthine, infracochlear, mid-dle fossa, and circumferential petrousectomy in patients with intact hearing.The translabyrinthine approach offers wide exposure of the petrous apex inpatients with no functional hearing [86].
Petrous carotid aneurysm
Petrous carotid artery aneurysm is a rare entity that is often discoveredas an incidental finding on imaging studies [87–90]. The petrous carotidartery begins at the skull base at the carotid canal and consists of a 1-cmvertical segment, the genu, and a 2-cm horizontal segment. The petrouscarotid artery is in close proximity to multiple structures, including thecochlea (posterior-superior), eustachian tube (lateral), tensor tympani(lateral), and greater and lesser superficial petrosal nerves (superior-lateral)[91,92].
Petrous carotid aneurysms are thought to originate from weak areas in thearterial wall at the origin of several embryonic vessels, including the vidian,caroticotympanic, pterygoid, and stapedial arteries. Three main mechanismsfor aneurysm formation include traumatic, congenital, and mycotic. True an-eurysms of the petrous carotid artery are most commonly fusiform and havewalls that are continuouswith the normal vessel. Pseudoaneurysms lack a truewall, may expand rapidly if they communicate with the vessel lumen, and
Fig. 10. Petrous apicitis. Axial T1-weighted MRI with fat saturation and gadolinium demon-
strates an enhancing lesion centered in the left petrous apex abutting the precavernous carotid
artery.

504 ISAACSON et al
originate from injuries of all layers of the arterial wall. These lesions may beasymptomatic or can present with various symptoms, including headache,hearing loss, dizziness, pulsatile tinnitus, and cranial nerve palsies. Aneurysmrupture results in massive hemorrhage either from the nose or ear with no re-ports of intracranial bleeding because of the vessels’ extradural location [91].
Imaging characteristics of petrous carotid aneurysms include smoothbone erosion of the petrous apex that is centered in the carotid canal.MRI often shows a central flow void if the vessel is patent and a character-istic onionskin appearance. Once a petrous carotid aneurysm is suspected,conventional angiography with possible balloon test occlusion is needed iftreatment becomes necessary [3].
A detailed discussion of management options for petrous carotid aneu-rysms is beyond the scope of this article, but options include observationwith serial imaging, balloon occlusion, endovascular coil or stent placement,and aneurysm exclusion with bypass revascularization [91].
Asymmetric pneumatization
The petrous apex contains air cells in 10% to 30% of temporal bones [1].Asymmetric pneumatization is defined as the presence of unilateral petrousapex air cells occurring concurrently with a marrow-filled petrous apex in
Fig. 11. Petrous apicitis. Axial T2-weighted MRI demonstrates a hyperintense lesion centered
in the left petrous apex. Notice a similar signal intensity in the mastoid and middle ear.

505LESIONS OF THE PETROUS APEX
the contralateral temporal bone in one individual. Asymmetric pneumatiza-tion of the petrous apex occurs in 5% to 10% of individuals. Bone marrow,depending on its fat content, can produce a hyperintense signal on T1- andT2-weighted MRI. Although it is reasonable to assume that bone marrow inthe petrous apex should have the same signal intensity as bone marrow inthe clivus, this is not always the case. Consequently, it is possible fora hyperintense signal to be generated on T1-weighted MRI in one petrousapex that is meaningfully different than the image generated in eitherthe contralateral pneumatized petrous apex or the clivus. The nonpneuma-tized petrous apex can be confused with a cholesterol granuloma, althoughsignal intensity typically is iso- or hypointense on T2-weighted images,especially with longer echo time. This slight dimunition of signal intensityon T2-weighted images compared with T1-weighted images can distinguishnormal bone marrow from cholesterol granulomas and mucoceles [61].
In cases in which the significance of such asymmetric signal intensity isunclear, an unenhanced fine-cut CT of the temporal bone is almost alwaysdiagnostic. Asymmetric petrous apex pneumatization is clearly an unusualvariant of normal anatomy that requires no treatment [4].
Neoplasms
Chondrosarcoma
Chondrosarcomas are rare malignancies that arise from embryologiccartilage rests along the sphenopetroclival fissure. They account for 0.15%of all intracranial tumors and 6% of skull base neoplasms [93]. Chondrosar-comas are more common in patients with Ollier’s disease, Maffucci syndrome(enchondroma with multiple angiomas), Paget’s disease, and osteochon-droma, although most chondrosarcomas arise de novo.
Because of the slow growth and insidious nature of chondrosarcomas,diagnosis is not uncommonly delayed. Diplopia, headache, and hoarsenessare the most common presenting symptoms; however, a wide variety ofpresenting signs and symptoms can be found, including hearing loss, dizzi-ness, aural fullness, dysphagia, facial paresthesias or paralysis, and visualimpairment [94,95].
The differential diagnosis for solid lesions of the petrous apex is broadbut can be narrowed with radiographic evaluation. CT provides excellentbony detail and is useful for determining the location of origin of skullbase neoplasms. Chondrosarcomas generally arise from the sphenopetro-clival synchondrosis, although 28% may originate from the clivus [96].CT often demonstrates areas of calcification, giving a characteristic ‘‘pop-corn’’ pattern [97]. Chondrosarcomas are generally hypo- to isointensewith T1-weighted MRI, hyperintense on T2-weighted MRI, and demon-strate heterogeneous enhancement with gadolinium enhancement [98].

506 ISAACSON et al
Chondrosarcomas are classified into five different histologic subtypes:conventional, clear cell, myxoid, mesenchymal, and dedifferentiated. Prog-nosis depends on the histologic grade, which is divided into grades I (welldifferentiated) to grade III (poorly differentiated). Evans and colleagues[99] reported 5-year survival rates for grade I, II, and III to be 90%,81%, and 43%, respectively. Immunohistochemical staining is importantto differentiate chondrosarcoma from chondroid chondroma; however,unlike chordomas, chondrosarcomas do not stain for epithelial membraneantigen or cytokeratin [96].
Themainstay of treatment for chondrosarcoma of the skull base is surgery.Gross tumor removal often can be achieved with contemporary skull basetechniques [100,101]. Surgical approach should be selected based on tumorlocation and surgeon’s preference and experience. Multiple surgical ap-proaches have been described, including translabyrinthine, transcochlear,type B infratemporal fossa, extended middle fossa, subtemporal-infratempo-ral, fronto-orbitozygomatic, transmaxillary, and endoscopic transnasaltranssphenoidal approaches. The petrous carotid artery and cavernous sinusare often involved with tumor, and there is considerable debate as to howaggressive the surgeon should be in attempting gross tumor removal. Becausethey are generally slow-growing tumors with a low incidence of metastasis,preservation of vital structures despite less than total tumor removal is a viableoption. Some authors recommend resection and grafting of the petrouscarotid artery when involved and collateral arterial flow is confirmed withangiography [102].
Tzortzidis and colleagues [102] also demonstrated decreased disease-freesurvival in patients who require multiple operations. Radiation therapy isan important adjunctive therapy in themanagement of chondrosarcomas. Be-cause most series include chordomas and chondrosarcomas together, resultsof radiotherapy for chondrosarcomas are difficult to interpret. Radiosurgeryhas shown better control rates for chondrosarcoma than chordoma and isuseful to treat small residual tumors after incomplete resection [103,104].Fractionated proton beam therapy also has shown promise in the treatmentof residual chondrosarcoma and achieves better control rates than chordo-mas [105,106]. Oghalai and colleagues [100] demonstrated a decreased inci-dence of recurrence in patients who underwent postoperative radiotherapy.
Chondrosarcomas of the skull base are rare neoplasms that present a for-midable challenge to the skull base surgeon. Surgical management is themainstay of therapy; however, adjuvant radiation therapy is often neededto control residual tumor. Stereotactic radiosurgery and fractionated protonbeam therapy seem to offer the best control for residual disease.
Chordoma
Chordomas are rare tumors that originate from embryologic remnants ofthe notochord that forms the nucleus pulposus of the intervertebral disks in

507LESIONS OF THE PETROUS APEX
normal patients. They are midline lesions that occur anywhere from theclivus to the sacrum, with approximately one third involving the clivus[107]. Chordomas are rare, with an incidence of 0.08 cases per 100,000[108]. Chordomas are more common in male patients and rarely presentin patients older than age 40. Female patients and younger patients aremore likely to present with a chordoma located in the skull base [108].
Because chordomas are slow growing and have an insidious course, mosttumors are large at the time diagnosis. In a large series by Tzortzidis andcolleagues [109], 81% of tumors were larger than 2 cm at presentation,with 37.8% larger than 4 cm. The most common presenting symptoms arediplopia, headache, and lower cranial nerve deficits [110,111]. Skull basechordomas are typically more aggressive in the pediatric population, witha wider range of presentation, atypical morphology, and greater incidenceof metastasis [112].
Radiographic evaluation is essential not only for diagnosis but also fortreatment planning. CT demonstrates a locally destructive lesion centeredat the clivus (Fig. 12). Bony trabeculae may be seen and true calcificationsmay occur in the chondroid chordoma variant. There is moderate to markedenhancement with contrast, and low signal areas may be present and repre-sent areas of gelatinous material. MRI allows determination of the extent ofdisease and reveals the presence of intracranial or cavernous sinus involve-ment. With T1-weighted MRI, chordomas are hypointense and contrastwell against the hyperintense fat in the clival bone marrow. Chordomasappear hyperintense on T2-weighted MRI and contrast well against adja-cent neural structures (Fig. 13). With T1-weighted MRI enhanced with
Fig. 12. Chordoma. Axial temporal bone CT scan demonstrates a lytic lesion centered in the
clivus. This lesion extends into the right petrous apex posterior to the vertical petrous carotid
artery.

508 ISAACSON et al
gadolinium, chordomas have variable enhancement and may have a charac-teristic ‘‘honeycomb’’ pattern (Fig. 14) [113].
Grossly, chordomas are grayish, semitransparent, andmultiloculated. His-tology reveals the characteristic physaliphorous cell, which has a vacuolated
Fig. 13. Chordoma. Axial T2-weighted MRI demonstrates a hyperintense lesion centered in the
right petrous apex and clivus.
Fig. 14. Chordoma. Axial T1-weighted MRI with fat saturation and gadolinium demonstrates
an enhancing lesion centered in the right petrous apex and clivus.

509LESIONS OF THE PETROUS APEX
cytoplasm and a ‘‘soap bubble’’ appearance. Immunohistochemical stainingis important to differentiate chordoma from chondrosarcoma because the his-tologic appearance may be similar and prognosis much different. Chordomasstain positive for S-100, epithelial membrane antigen, and cytokeratin. Chon-drosarcomas do not stain positive for cytokeratin or epithelial membrane an-tigen [114]. Chondroid chordoma is a variant with cartilaginous componentsfound in the matrix [115].
Because of the extensive nature of chordomas and the surrounding vitalstructures, a combination of surgery and radiation therapy is generallyrequired. The location of the lesion and surgeon’s preferences dictates thesurgical approach, with combined approaches sometimes necessary. Tumorslocated on the upper clivus and limited to the midline may be treated witha transbasal craniotomy. Tumors that involve the middle and upper clivuswithmore lateral extension beyond the cavernous sinus are better approachedwith a fronto-orbitozygomatic craniotomy. Tumors that are centered at themidclivus or are paramedian may be approached with a subtemporal-infratemporal approach with transpetrosal extension if the posterior petrousapex is involved. Tumors that involve the nasopharynx or craniocervicaljunction can be managed with a transmaxillary approach or extreme lateraltranscondylar approaches. Endoscopic transnasal transsphenoidal approa-ches to the skull base recently were described for resection of clival chordomas[42,116,117].
Despite advances and decreased morbidity with contemporary skull basetechniques, gross total resection is achieved less than half the time[110,118]. Surgical seeding also has been reported [119,120]. As a resultof these various factors, recurrences are common and long-term radio-graphic surveillance is necessary. Options for recurrence include reopera-tion, external beam radiation therapy, radiosurgery, and proton beamtherapy. Patients who require reoperation have a lower recurrence-free sur-vival rate compared with patients who require only primary treatment[109]. Chordomas are relatively radioresistant. Treatment with externalbeam radiotherapy has produced poor tumor control rates [121–123]. Ste-reotactic radiosurgery has produced superior results to external beam radi-ation therapy. Krishnan and colleagues [103] reported a 72% control ratefor chordomas treated with a median tumor margin dose of 15 Gy. Debusand colleagues [104] also had good tumor control rates of 82% at 2-yearfollow-up using fractionated radiosurgery; however, the control rate fellto 50% at 5 years. Better control rates have been achieved with a combina-tion of photon and proton beam therapy. In a large series of 132 patientsthat combined photon and proton beam radiation therapy, Terahara andcolleagues [124] achieved actuarial local control rates of 59% and 44%at 5 and 10 years, respectively. For unclear reasons, female patients treatedwith proton therapy for skull base chordomas have an increased incidenceof recurrence [105,124]. Carbon ion radiotherapy has been used for treat-ment of skull base chordomas with encouraging results; however, longer

510 ISAACSON et al
follow-up is needed to demonstrate superior efficacy to already establishedtherapies [125].
Chordomas present a unique challenge to the skull base surgeon because oftheir location, surrounding vital structures, and propensity for recurrence.Surgical therapy is the mainstay of treatment; however, recurrences are com-mon and adjunctive therapies are often required. There is no consensus for theoptimal treatment for skull base chordomas; however, fractionated protonbeam radiosurgery likely will continue to evolve as an important componentof treatment.
Meningioma
In 1922, Cushing [126] introduced the term ‘‘meningioma’’ to describea tumor that was initially described by Felix Plater in 1614. Meningiomascomprise 13% to 26% of all intracranial tumors and are more commonlydiscovered in middle-aged and elderly women. It seems that the incidenceof meningiomas increases with age and has increased with time. This tumoris rarely found in children and is typically more aggressive or even malignantin this population. Aside from female gender, radiation exposure is the onlyknown factor that increases the risk of developing a meningioma. Mostmeningiomas are sporadic, with only 2% being related to syndromes,including neurofibromatosis type 2 [3,127]. Arachnoidal cap cells from theexternal layer of the arachnoid membrane are the cells of origin for menin-giomas. These tumors are typically have a broad-based attachment to thedura and may be associated with hyperostosis of the underlying calvariumor skull base [3]. Meningiomas are classified into three separate WorldHealth Organization grades according histologic subtype and likelihoodof recurrence. The grade I lesions are the most common and include themeningothelial, fibrous, transitional, microcystic, secretory, lymphoplasma-cyte-rich, metaplastic, psammomatous, and angiomatous histologic types.These grade I lesions are associated with a low risk of recurrence withcomplete excision. Grade II lesions consist of the atypical, chordoid, andclear cell histologic subtypes. Grade II lesions are typically more aggressiveand have a higher incidence of recurrence when compared with grade Itumors. Grade III tumors have the highest rates of recurrence and consistof the anaplastic, papillary, and rhabdoid histologic subtypes. In additionto these subtypes, any meningioma with a high proliferation index (O20mitoses per high powered field) with or without brain invasion is classifiedas grade III [3,127,128]. A 2.4-mm per year mean growth rate was reportedin 60 patients with asymptomatic meningiomas [129].
MRI with gadolinium is the procedure of choice when evaluating menin-giomas, and it may detect lesions as small as 3 mm. Meningiomas appear assessile, extra-axial mass with accompanying dural tails. These lesions aremost commonly isointense or have a slight hypointensity on T1-weightedimages and enhance with gadolinium (Fig. 15). On T2-weighted images,

511LESIONS OF THE PETROUS APEX
meningiomas most commonly have an isointense to hyperintense signal[130]. Petroclival meningiomas may present with myriad symptoms, includ-ing headache, facial pain, decreased hearing, balance disturbance, and vom-iting, with gait disturbance being the most common [131–133]. Cranial nervedeficits are present in a large majority of patients, with nerves V, VII, andVIII being the most commonly affected [131].
The management of a petroclival meningioma is predicated on multiplefactors, including a patient’s age, medical comorbidities, presenting symp-toms, and the location and size of the lesion. Treatment options include ob-servation, microsurgical excision, external beam radiation, and stereotacticradiosurgery alone or in combination. Resection of these lesions is compli-cated because of their location and frequent involvement of the dural venoussinuses, brainstem, cranial nerves, petrous carotid artery, and vertobrobasi-lar arterial system [134,135]. Extension to the internal auditory canal, Meck-el’s cave, foramen magnum, and middle cranial fossa is not unusual. Theretrosigmoid, combined, frontotemporal approaches, and many other ap-proaches have been reported for excision of petroclival meningiomas [3].These tumors were previously considered inoperable because of the highmorbidity and mortality (50%) associated with attempted excision [136].More recent series have demonstrated a significant decline in morbidityand mortality (!10%). A recent meta-analysis by Selesnick and colleagues[137] demonstrated that complete excision of these tumors is achieved in68% of cases. Reasons for incomplete excision include brainstem adherence,adhesions to cranial nerves, encasement of vessels, and hypervascularity.
Fig. 15. Meningioma. An axial T1-weighted MRI with fat saturation and gadolinium demon-
strates an enhancing sessile, eccentric left petrous lesion.

512 ISAACSON et al
Incomplete excision with observation or adjunctive radiation is a reasonablemanagement strategy in patients with large tumors or significant neurovas-cular involvement [138].
Conventional fractionated radiation and stereotactic radiosurgery areacceptable and sometimes preferred treatment options in patients whohave petrous apex meningiomas. Conventional external beam radiationhas not traditionally been used as a primary treatment modality andtypically has been used as adjuvant therapy for incompletely excised tumors.A combination of surgery and radiation has favorable tumor control resultsin comparison to incomplete excision alone. Several centers using stereo-tactic radiosurgery have demonstrated favorable tumor control rates(86.7%–100%) with limited follow-up. Radiosurgery is not an option inpatients with larger tumors (O3 cm). Complications of radiosurgery includecranial nerve deficits, hydrocephalus, radiation necrosis, and rarely, malig-nant transformation [138,139]. In certain circumstances, observation maybe prudent, especially in elderly patients, patients with multiple medicalcomorbidities, and patients with small asymptomatic tumors [131].
Metastasis
Most metastatic neoplasms are identified in patients between the ages of50 and 70 years old. Metastatic petrous apex lesions are most commonlyidentified in the same age group [140,141]. The petrous apex is the mostcommonly involved site in the temporal bone (82.9%), with it being thesole site of involvement in 31.6% of cases in a series of 212 patients. Themost commonly reported symptom is hearing loss; in one study, however,36.2% of patients had no neurotologic symptoms [141]. Other studieshave demonstrated that most temporal bone metastatic disease is asymp-tomatic [142,143]. Vertigo, dizziness, facial weakness, tinnitus, otalgia,otorrhea, external auditory canal mass, and nystagmus have been reportedin patients with metastasis. In the series by Gloria-Cruz and colleagues[141], 14 of 212 patients had facial canal involvement, with only 6 showingsigns of facial nerve weakness. All 6 patients with facial weakness had tumorinvasion of the facial nerve epineurium.
The mechanisms for metastatic tumor involvement include hematogenousspread from distant tumors or leukemia/lymphoma, direct extension via anextra or intracranial neoplasm, and leptomeningeal extension from a distantor intracranial primary neoplasm. Hematogenous spread is thought to occurbecause of slow blood flow through the petrous apex marrow, which allowsfiltering and deposition of tumor cells [141,144]. In the series by Gloria-Cruz and colleagues [141] that discussed 415 temporal bones from 212patients with nondisseminatedmalignant tumors, 76 (18.3%) temporal bonesand 47 (22.2%) patients were found to have temporal bone involvement.Twenty different tumor cell types were identified, with breast carcinomabeing the most commonly encountered metastatic temporal bone neoplasm,

513LESIONS OF THE PETROUS APEX
followed by lung, prostate, melanoma, and kidney. Adenocarcinoma was themost common cell type identified in the petrous apex. Seventy-five percent oftumors were found to spread by a hematogenous route. Otic capsule involve-ment was rare, and when invasion was identified, no patient had vestibularmanifestations. No cases were reported in which the temporal bone was theonly site of hematogenous spread, with the lung and gastrointestinal tractbeing the most common concurrent sites. Twelve patients were found tohave an occult neoplasm discovered at autopsy; only 1was found to have tem-poral bone involvement in the petrous apex. The imaging characteristics ofpetrous apex metastasis depend largely on the primary tumor but oftenshow significant bone destruction and enhance with the administration ofcontrast. Surgical management of petrous apex metastasis is unwarranted,and treatment often consists of palliative therapy.
Uncommon lesions
Schwannomas, paragangliomas, and endolymphatic sac tumors occasion-ally involve the petrous apex. Petrous apex schwannomas may originate fromcranial nerves IV, V, VI, VII, or VIII. Petrous apex involvement usuallyresults from direct extension and typically does not arise within the petrousapex. Paragangliomas also may invade the petrous apex via preformed aircell tracts from their site of origin in the jugular foramen or middle ear.Endolymphatic sac tumors arise from the proximal rugose portion of theendolymphatic sac located halfway between the internal auditory canal andjugular foramen along the posterior aspect of the temporal bone [145]. Thesetumors typically extend into the mastoid from the inner ear and may invadethe petrous apex [146].
Summary
Advances in diagnostic imaging, microsurgical techniques, and the intro-duction of stereotactic radiosurgery have made the management of petrousapex pathology less daunting for modern skull base surgeons. Decreasingpatient morbidity and mortality and improving outcomes are the ultimategoal for surgeons treating petrous apex pathology. Unfortunately, meaning-ful prospective outcome studies are lacking and not likely to occur becauseof the rarity of these lesions.
References
[1] Chole RA. Petrous apicitis: surgical anatomy. Ann Otol Rhinol Laryngol 1985;94:251–7.
[2] Muckle RP, De la Cruz A, Lo WM. Petrous apex lesions. Am J Otol 1998;19:219–25.
[3] Jackler RK, Brackmann DE. Neurotology. Philadelphia: Elsevier Mosby; 2005.
[4] Moore KR, Harnsberger HR, Shelton C, et al. ‘‘Leave me alone’’ lesions of the petrous
apex. AJNR Am J Neuroradiol 1998;19:733–8.

514 ISAACSON et al
[5] Chang P, Fagan PA, Atlas MD, et al. Imaging destructive lesions of the petrous apex.
Laryngoscope 1998;108:599–604.
[6] Lasjaunias P, Berenstein A. Endovascular treatment of craniofacial lesions. In: Surgical
neuroangiography. Berlin: Springer-Verlag; 1987.
[7] ValavanisA. Preoperative embolization of the head and neck: indications, patient selection,
goals, and precautions. AJNR Am J Neuroradiol 1986;7:943–52.
[8] Schick PM, Hieshima GB, White RA, et al. Arterial catheter embolization followed by
surgery for large chemodectoma. Surgery 1980;87:459–64.
[9] Murphy TP, Brackmann DE. Effects of preoperative embolization on glomus jugulare
tumors. Laryngoscope 1989;99:1244–7.
[10] Stewart K, Kountakis SE, Chang CY, et al. Magnetic resonance angiography in the
evaluation of glomus tympanicum tumors. Am J Otolaryngol 1997;18:116–20.
[11] Cristobal R,Metts B, MichelMA, et al. Three dimensional computed tomography angiog-
raphy in imaging jugular foramen lesions. Otol Neurotol 2006, in press.
[12] Ghorayeb BY, Jahrsdoerfer RA. Subcochlear approach for cholesterol granulomas of the
inferior petrous apex. Otolaryngol Head Neck Surg 1990;103:60–5.
[13] Giddings NA, Brackmann DE, Kwartler JA. Transcanal infracochlear approach to the
petrous apex. Otolaryngol Head Neck Surg 1991;104:29–36.
[14] Brackmann DE, Toh EH. Surgical management of petrous apex cholesterol granulomas.
Otol Neurotol 2002;23:529–33.
[15] Mosnier I, Cyna-Gorse F, Grayeli AB, et al. Management of cholesterol granulomas of the
petrous apex based on clinical and radiologic evaluation. Otol Neurotol 2002;23:522–8.
[16] Brackmann DE, House JR 3rd, Hitselberger WE. Technical modifications to the middle
fossa craniotomy approach in removal of acoustic neuromas. Am J Otol 1994;15:614–9.
[17] Wigand ME, Haid T, Berg M. The enlarged middle cranial fossa approach for surgery of
the temporal bone and of the cerebellopontine angle. Arch Otorhinolaryngol 1989;246:
299–302.
[18] KawaseT, ShiobaraR, Toya S.Anterior transpetrosal-transtentorial approach for spheno-
petroclival meningiomas: surgical method and results in 10 patients. Neurosurgery 1991;28:
869–75 [discussion: 75–6].
[19] Kawase T, Toya S, Shiobara R, et al. Transpetrosal approach for aneurysms of the lower
basilar artery. J Neurosurg 1985;63:857–61.
[20] Isaacson B, Telian SA, El-Kashlan HK. Facial nerve outcomes in middle cranial fossa vs
translabyrinthine approaches. Otolaryngol Head Neck Surg 2005;133:906–10.
[21] Satar B, Jackler RK, Oghalai J, et al. Risk-benefit analysis of using the middle fossa
approach for acoustic neuromas with O10 mm cerebellopontine angle component.
Laryngoscope 2002;112:1500–6.
[22] Lustig LR, Jackler RK. The vulnerability of the vein of Labbe’ during combined craniot-
omies of the posterior and middle fossae. Skull Base Surgery 1998;8:1–9.
[23] Oghalai JS, Jackler RK. Anatomy of the combined retrolabyrinthine-middle fossa craniot-
omy. Neurosurg Focus 2003;14:e8.
[24] Fisch U. Transtemporal surgery of the internal auditory canal. Report of 92 cases, tech-
nique, indications and results. Adv Otorhinolaryngol 1970;17:203–40.
[25] House WF. Surgical exposure of the internal auditory canal and its contents through the
middle cranial fossa. Laryngoscope 1961;71:1363–85.
[26] Jackler RK, Gladstone HB. Locating the internal auditory canal during the middle fossa
approach: an alternative technique. Skull Base Surgery 1995;5:63–7.
[27] House WF. Surgical exposure of the internal auditory canal and its contents through the
middle cranial fossa. Laryngoscope 1961;71:1363–85.
[28] Dearmin R. A logical survival approach to the tip cells of the petrous pyramid. Arch
Otolaryngol 1937;26:321–6.
[29] Farrior JB. The supralabyrinthine exenteration of the petrous apex. Ann Otol Rhinol
Laryngol 1942;51:1007–16.

515LESIONS OF THE PETROUS APEX
[30] Goldofsky E, Hoffman RA, Holliday RA, et al. Cholesterol cysts of the temporal bone:
diagnosis and treatment. Ann Otol Rhinol Laryngol 1991;100:181–7.
[31] Telischi FF, Luntz M, Whiteman ML. Supracochlear approach to the petrous apex: case
report and anatomic study. Am J Otol 1999;20:500–4.
[32] Cheung SW, Jackler RK, Pitts LH, et al. Interconnecting the posterior and middle cranial
fossae for tumors that traverse Meckel’s cave. Am J Otol 1995;16:200–8.
[33] Samii M, Tatagiba M, Carvalho GA. Retrosigmoid intradural suprameatal approach to
Meckel’s cave and the middle fossa: surgical technique and outcome. J Neurosurg 2000;
92:235–41.
[34] Seoane E, Rhoton AL Jr. Suprameatal extension of the retrosigmoid approach: microsur-
gical anatomy. Neurosurgery 1999;44:553–60.
[35] Chanda A, Nanda A. Retrosigmoid intradural suprameatal approach: advantages and
disadvantages from an anatomical perspective. Neurosurgery 2006;59:ONS1–6 [discussion:
ONS1-S6].
[36] FischU, Fagan P, Valavanis A. The infratemporal fossa approach for the lateral skull base.
Otolaryngol Clin North Am 1984;17:513–52.
[37] Fisch U, Pillsbury HC. Infratemporal fossa approach to lesions in the temporal bone and
base of the skull. Arch Otolaryngol 1979;105:99–107.
[38] VilelaMD,RostomilyRC.Temporomandibular joint-preservingpreauricular subtemporal-
infratemporal fossa approach: surgical technique and clinical application. Neurosurgery
2004;55:143–53 [discussion: 53–4].
[39] White DR, Sonnenburg RE, Ewend MG, et al. Safety of minimally invasive pitu-
itary surgery (MIPS) compared with a traditional approach. Laryngoscope 2004;114:
1945–8.
[40] Carrau RL, Kassam AB, Snyderman CH. Pituitary surgery. Otolaryngol Clin North Am
2001;34:1143–55, ix.
[41] Kassam AB, Gardner P, Snyderman C, et al. Expanded endonasal approach: fully endo-
scopic, completely transnasal approach to the middle third of the clivus, petrous bone,
middle cranial fossa, and infratemporal fossa. Neurosurg Focus 2005;19:E6.
[42] Jho HD, Carrau RL, McLaughlin ML, et al. Endoscopic transsphenoidal resection of
a large chordoma in the posterior fossa: case report. Neurosurg Focus 1996;1:e3 [discus-
sion: 1p, e3].
[43] Griffith AJ, Terrell JE. Transsphenoid endoscopicmanagement of petrous apex cholesterol
granuloma. Otolaryngol Head Neck Surg 1996;114:91–4.
[44] Esposito F, Becker DP, Villablanca JP, et al. Endonasal transsphenoidal transclival
removal of prepontine epidermoid tumors: technical note. Neurosurgery 2005;56:E443
[discussion: E].
[45] Hitselberger WE, House WF. Transtemporal bone microsurgical removal of acoustic
neuromas: tumors of the cerebellopontine angle. Arch Otolaryngol 1964;80:720–31.
[46] House WF, Hitselberger WE. The transcochlear approach to the skull base. Arch Otolar-
yngol 1976;102:334–42.
[47] Browne JD, Fisch U. Transotic approach to the cerebellopontine angle. Otolaryngol Clin
North Am 1992;25:331–46.
[48] Angeli SI, De la Cruz A, Hitselberger W. The transcochlear approach revisited. Otol
Neurotol 2001;22:690–5.
[49] Hughes GB, Lee J, Ruggeieri PM. Surgery for cystic lesions of the petrous apex. In: Glass-
cock ME , Gulya AJ, editors. Surgery of the ear. Ontario (Canada): BC Decker; 2003.
p. 689–711.
[50] Lo WW, Solti-Bohman LG, Brackmann DE, et al. Cholesterol granuloma of the petrous
apex: CT diagnosis. Radiology 1984;153:705–11.
[51] Bodo G. Blue ear drum due to cholesterin granuloma. Acta Otolaryngol 1956;56:11–6.
[52] Paparella MM, Lim DJ. Pathogenesis and pathology of the ‘‘idiopathic’’ blue ear drum.
Arch Otolaryngol 1967;85:249–58.

516 ISAACSON et al
[53] Goycoolea MV, Paparella MM, Juhn SK, et al. Otitis media with perforation of the
tympanic membrane: a longitudinal experimental study. Laryngoscope 1980;90:
2037–45.
[54] Rosenberg RA, Hammerschlag PE, Cohen NL, et al. Cholesteatoma vs. cholesterol gran-
uloma of the petrous apex. Otolaryngol Head Neck Surg 1986;94:322–7.
[55] Sakamoto T. Electron microscopic studies on the origin of cholesterin crystal in (the)
cholesterin granuloma (in human ears). Nippon Jibiinkoka Gakkai Kaiho 1967;70:
1926–31.
[56] Friedmann I, GrahamMD. The ultrastructure of cholesterol granuloma of the middle ear:
an electron microscope study. J Laryngol Otol 1979;93:433–42.
[57] Paparella MM, Hiraide F, Juhn SK, et al. Cellular events involved in middle ear fluid
production. Ann Otol Rhinol Laryngol 1970;79:766–79.
[58] Jackler RK, Cho M. A new theory to explain the genesis of petrous apex cholesterol
granuloma. Otol Neurotol 2003;24:96–106.
[59] Chole RA, Donald PJ. Petrous apicitis: clinical considerations. Ann Otol Rhinol Laryngol
1983;92:544–51.
[60] MyersonMC,Rubin J,Gilbert JG.Anatomic studies of the petrous portion of the temporal
bone. Arch Otolaryngol 1934;20:195–210.
[61] Roland PS, Meyerhoff WL, Judge LO, et al. Asymmetric pneumatization of the petrous
apex. Otolaryngol Head Neck Surg 1990;103:80–8.
[62] Jacob CE, Rupa V. Infralabyrinthine approach to the petrous apex. Clin Anat 2005;18:
423–7.
[63] Haberkamp TJ. Surgical anatomy of the transtemporal approaches to the petrous apex.
Am J Otol 1997;18:501–6.
[64] Presutti L, Villari D, Marchioni D. Petrous apex cholesterol granuloma: transsphenoid
endoscopic approach. J Laryngol Otol 2006;120:e20.
[65] Bockmuhl U, Khalil HS, Draf W. Clinicoradiological and surgical considerations in the
treatment of cholesterol granuloma of the petrous pyramid. Skull Base 2005;15:263–7
[discussion: 7–8].
[66] King TT, Benjamin JC, Morrison AW. Epidermoid and cholesterol cysts in the apex of the
petrous bone. Br J Neurosurg 1989;3:451–61.
[67] de Souza CE, Sperling NM, da Costa SS, et al. Congenital cholesteatomas of the cerebel-
lopontine angle. Am J Otol 1989;10:358–63.
[68] Axon PR, Fergie N, Saeed SR, et al. Petrosal cholesteatoma: management considerations
for minimizing morbidity. Am J Otol 1999;20:505–10.
[69] SannaM, Zini C, Gamoletti R, et al. Petrous bone cholesteatoma. Skull Base Surgery 1993;
3:201–13.
[70] Kaylie DM, Warren FM 3rd, Haynes DS, et al. Neurotologic management of intracranial
epidermoid tumors. Laryngoscope 2005;115:1082–6.
[71] Isaacson B, Coker NJ, Vrabec JT, et al. Invasive cerebrospinal fluid cysts and cephaloceles
of the petrous apex. Otol Neurotol 2006;27(8):1131–41.
[72] Dutt SN,Mirza S, Chavda SV, et al. Radiologic differentiation of intracranial epidermoids
from arachnoid cysts. Otol Neurotol 2002;23:84–92.
[73] Atlas MD,Moffat DA, Hardy DG. Petrous apex cholesteatoma: diagnostic and treatment
dilemmas. Laryngoscope 1992;102:1363–8.
[74] Yasargil MG, Abernathey CD, Sarioglu AC.Microneurosurgical treatment of intracranial
dermoid and epidermoid tumors. Neurosurgery 1989;24:561–7.
[75] Yamakawa K, Shitara N, Genka S, et al. Clinical course and surgical prognosis of 33 cases
of intracranial epidermoid tumors. Neurosurgery 1989;24:568–73.
[76] Harnsberger HR. Trapped fluid, petrous apex. In: Harnsberger HR, Wiggins RH, Hudg-
ins PA, editors. Diagnostic imaging: head and neck. Oxford (UK): Elsevier; 2004.
p. 162–5.
[77] Arriaga MA. Petrous apex effusion: a clinical disorder. Laryngoscope 2006;116:1349–56.

517LESIONS OF THE PETROUS APEX
[78] Close LG,O’ConnerWE. Sphenoethmoidal mucoceles with intracranial extension. Otolar-
yngol Head Neck Surg 1983;91:350–7.
[79] Larson TL,WongML. Primarymucocele of the petrous apex:MR appearance. AJNRAm
J Neuroradiol 1992;13:203–4.
[80] Nugent GR, Sprinkle P, Bloor BM. Sphenoid sinus mucoceles. J Neurosurg 1970;32:
443–51.
[81] Jallo GI, WooHH,Meshki C, et al. Arachnoid cysts of the cerebellopontine angle: diagno-
sis and surgery. Neurosurgery 1997;40:31–7 [discussion: 7–8].
[82] Buongiorno G, Ricca G. Supratentorial arachnoid cyst mimicking a Meniere’s disease
attack. J Laryngol Otol 2003;117:728–30.
[83] BatraA, TripathiRP, SinghAK, et al. Petrous apex arachnoid cyst extending intoMeckel’s
cave. Australas Radiol 2002;46:295–8.
[84] Moore KR, Fischbein NJ, Harnsberger HR, et al. Petrous apex cephaloceles. AJNR Am
J Neuroradiol 2001;22:1867–71.
[85] Goldstein NA, Casselbrant ML, Bluestone CD, et al. Intratemporal complications of
acute otitis media in infants and children. Otolaryngol Head Neck Surg 1998;119:
444–54.
[86] VisoskyAM, IsaacsonB,Oghalai JS. Circumferential petrosectomy for petrous apicitis and
cranial base osteomyelitis. Otol Neurotol 2006;27:1003–13.
[87] Minotti AM, Kountakis SE. Management of abducens palsy in patients with petrositis.
Ann Otol Rhinol Laryngol 1999;108:897–902.
[88] AndersonRD,LiebeskindA, SchechterMM, et al. Aneurysms of the internal carotid artery
in the carotid canal of the petrous temporal bone. Radiology 1972;102:639–42.
[89] Frank E, Brown BM,WilsonDF. Asymptomatic fusiform aneurysm of the petrous carotid
artery in a patient with von Recklinghausen’s neurofibromatosis. Surg Neurol 1989;32:
75–8.
[90] Halbach VV, Higashida RT, Hieshima GB, et al. Aneurysms of the petrous portion of the
internal carotid artery: results of treatment with endovascular or surgical occlusion. AJNR
Am J Neuroradiol 1990;11:253–7.
[91] Liu JK, Gottfried ON, Amini A, et al. Aneurysms of the petrous internal carotid artery:
anatomy, origins, and treatment. Neurosurg Focus 2004;17:E13.
[92] Bouthillier A, van Loveren HR, Keller JT. Segments of the internal carotid artery: a new
classification. Neurosurgery 1996;38:425–32 [discussion 32–3].
[93] Cianfriglia F, Pompili A, Occhipinti E. Intracranial malignant cartilaginous tumours:
report of two cases and review of literature. Acta Neurochir (Wien) 1978;45:163–75.
[94] Korten AG, ter Berg HJ, Spincemaille GH, et al. Intracranial chondrosarcoma: review of
the literature and report of 15 cases. J Neurol Neurosurg Psychiatry 1998;65:88–92.
[95] Seidman MD, Nichols RD, Raju UB, et al. Extracranial skull base chondrosarcoma. Ear
Nose Throat J 1989;68:626–32 35.
[96] Rosenberg AE, Nielsen GP, Keel SB, et al. Chondrosarcoma of the base of the skull:
a clinicopathologic study of 200 cases with emphasis on its distinction from chordoma.
Am J Surg Pathol 1999;23:1370–8.
[97] Grossman RI, Davis KR. Cranial computed tomographic appearance of chondrosarcoma
of the base of the skull. Radiology 1981;141:403–8.
[98] Meyers SP, Hirsch WL Jr, Curtin HD, et al. Chondrosarcomas of the skull base: MR
imaging features. Radiology 1992;184:103–8.
[99] Evans HL, Ayala AG, Romsdahl MM. Prognostic factors in chondrosarcoma of bone:
a clinicopathologic analysis with emphasis on histologic grading. Cancer 1977;40:
818–31.
[100] Oghalai JS, Buxbaum JL, Jackler RK, et al. Skull base chondrosarcoma originating from
the petroclival junction. Otol Neurotol 2005;26:1052–60.
[101] BrackmannDE, TeufertKB. Chondrosarcoma of the skull base: long-term follow-up. Otol
Neurotol 2006;27:981–91.

518 ISAACSON et al
[102] Tzortzidis F, Elahi F, Wright DC, et al. Patient outcome at long-term follow-up after
aggressive microsurgical resection of cranial base chondrosarcomas. Neurosurgery 2006;
58:1090–8 [discussion: -8].
[103] Krishnan S, Foote RL, Brown PD, et al. Radiosurgery for cranial base chordomas and
chondrosarcomas. Neurosurgery 2005;56:777–84 [discussion: -84].
[104] Debus J, Schulz-Ertner D, Schad L, et al. Stereotactic fractionated radiotherapy for
chordomas and chondrosarcomas of the skull base. Int J Radiat Oncol Biol Phys 2000;
47:591–6.
[105] Hug EB, Loredo LN, Slater JD, et al. Proton radiation therapy for chordomas and
chondrosarcomas of the skull base. J Neurosurg 1999;91:432–9.
[106] NoelG,Habrand JL,MammarH, et al. Combination of photon and proton radiation ther-
apy for chordomas and chondrosarcomas of the skull base: the Centre de Protontherapie
D’Orsay experience. Int J Radiat Oncol Biol Phys 2001;51:392–8.
[107] Brown RV, Sage MR, Brophy BP. CT andMR findings in patients with chordomas of the
petrous apex. AJNR Am J Neuroradiol 1990;11:121–4.
[108] McMaster ML, Goldstein AM, Bromley CM, et al. Chordoma: incidence and survival
patterns in the United States, 1973–1995. Cancer Causes Control 2001;12:1–11.
[109] Tzortzidis F, Elahi F,Wright D, et al. Patient outcome at long-term follow-up after aggres-
sive microsurgical resection of cranial base chordomas. Neurosurgery 2006;59:230–7 [dis-
cussion: -7].
[110] al-Mefty O, Borba LA. Skull base chordomas: a management challenge. J Neurosurg 1997;
86:182–9.
[111] Heffelfinger MJ, Dahlin DC, MacCarty CS, et al. Chordomas and cartilaginous tumors at
the skull base. Cancer 1973;32:410–20.
[112] Borba LA, Al-Mefty O, Mrak RE, et al. Cranial chordomas in children and adolescents.
J Neurosurg 1996;84:584–91.
[113] Erdem E, Angtuaco EC, Van Hemert R, et al. Comprehensive review of intracranial chor-
doma. Radiographics 2003;23:995–1009.
[114] Colli BO, Al-Mefty O. Chordomas of the skull base: follow-up review and prognostic
factors. Neurosurg Focus 2001;10:E1.
[115] Volpe NJ, Liebsch NJ, Munzenrider JE, et al. Neuro-ophthalmologic findings in
chordoma and chondrosarcoma of the skull base. Am J Ophthalmol 1993;115:
97–104.
[116] Solares CA, Fakhri S, Batra PS, et al. Transnasal endoscopic resection of lesions of the
clivus: a preliminary report. Laryngoscope 2005;115:1917–22.
[117] Frank G, Sciarretta V, Calbucci F, et al. The endoscopic transnasal transsphenoidal
approach for the treatment of cranial base chordomas and chondrosarcomas. Neurosur-
gery 2006;59:ONS50–7 [discussion: ONS-7].
[118] Gay E, Sekhar LN, Rubinstein E, et al. Chordomas and chondrosarcomas of the cra-
nial base: results and follow-up of 60 patients. Neurosurgery 1995;36:887–96 [discus-
sion: 96–7].
[119] Arnautovic KI, Al-Mefty O. Surgical seeding of chordomas. Neurosurg Focus 2001;10:E7.
[120] Asano S, Kawahara N, Kirino T. Intradural spinal seeding of a clival chordoma. Acta
Neurochir (Wien) 2003;145:599–603.
[121] Fuller DB, Bloom JG. Radiotherapy for chordoma. Int J Radiat Oncol Biol Phys 1988;15:
331–9.
[122] Catton C, O’Sullivan B, Bell R, et al. Chordoma: long-term follow-up after radical photon
irradiation. Radiother Oncol 1996;41:67–72.
[123] Romero J, CardenesH, la TorreA, et al. Chordoma: results of radiation therapy in eighteen
patients. Radiother Oncol 1993;29:27–32.
[124] Terahara A, Niemierko A, Goitein M, et al. Analysis of the relationship between tumor
dose inhomogeneity and local control in patients with skull base chordoma. Int J Radiat
Oncol Biol Phys 1999;45:351–8.

519LESIONS OF THE PETROUS APEX
[125] Schulz-Ertner D, Haberer T, Jakel O, et al. Radiotherapy for chordomas and low-grade
chondrosarcomas of the skull base with carbon ions. Int J Radiat Oncol Biol Phys 2002;
53:36–42.
[126] Cushing H. The meningiomas (dural endotheliomas): their source, and favored seats of
origin. Brain 1922;45:282–316.
[127] LouisDN, Scheithauer BW,BudkaH.Meningiomas. In:Kleihues P, CaveneeWK, editors.
Pathology and genetics of tumors of the nervous system. Lyon (France): IARC Press; 2000.
p. 314.
[128] Maier H, Ofner D, Hittmair A, et al. Classic, atypical, and anaplastic meningioma: three
histopathological subtypes of clinical relevance. J Neurosurg 1992;77:616–23.
[129] OliveroWC, Lister JR, Elwood PW. The natural history and growth rate of asymptomatic
meningiomas: a review of 60 patients. J Neurosurg 1995;83:222–4.
[130] EngelhardHH. Progress in the diagnosis and treatment of patients withmeningiomas. Part
I: diagnostic imaging, preoperative embolization. Surg Neurol 2001;55:89–101.
[131] Hakuba A, Nishimura S, Tanaka K, et al. Clivus meningioma: six cases of total removal.
Neurol Med Chir (Tokyo) 1977;17:63–77.
[132] Samii M, Ammirati M, Mahran A, et al. Surgery of petroclival meningiomas: report of
24 cases. Neurosurgery 1989;24:12–7.
[133] Mayberg MR, Symon L. Meningiomas of the clivus and apical petrous bone: report of
35 cases. J Neurosurg 1986;65:160–7.
[134] Sekhar LN, Swamy NK, Jaiswal V, et al. Surgical excision of meningiomas involving the
clivus: preoperative and intraoperative features as predictors of postoperative functional
deterioration. J Neurosurg 1994;81:860–8.
[135] Sekhar LN, Wright DC, Richardson R, et al. Petroclival and foramen magnum meningio-
mas: surgical approaches and pitfalls. J Neurooncol 1996;29:249–59.
[136] Castellano F, Ruggerio G. Meningiomas of the posterior fossa. Acta Radiol (Suppl) 1953;
104:1–177.
[137] Selesnick SH, Nguyen TD, Gutin PH, et al. Posterior petrous face meningiomas. Otolar-
yngol Head Neck Surg 2001;124:408–13.
[138] Park CK, Jung HW, Kim JE, et al. The selection of the optimal therapeutic strategy for
petroclival meningiomas. Surg Neurol 2006;66:160–5 [discussion: 5–6].
[139] Subach BR, Lunsford LD, Kondziolka D, et al. Management of petroclival meningiomas
by stereotactic radiosurgery. Neurosurgery 1998;42:437–43 [discussion: 43–5].
[140] MaddoxHE 3rd.Metastatic tumors of the temporal bone.AnnOtolRhinol Laryngol 1967;
76:149–65.
[141] Gloria-Cruz TI, Schachern PA, Paparella MM, et al. Metastases to temporal bones from
primary nonsystemic malignant neoplasms. Arch Otolaryngol Head Neck Surg 2000;126:
209–14.
[142] JahnAF, Farkashidy J, Berman JM.Metastatic tumors in the temporal bone: a pathophys-
iologic study. J Otolaryngol 1979;8:85–95.
[143] Nelson EG, Hinojosa R. Histopathology of metastatic temporal bone tumors. Arch
Otolaryngol Head Neck Surg 1991;117:189–93.
[144] Berlinger NT,Koutroupas S, AdamsG, et al. Patterns of involvement of the temporal bone
in metastatic and systemic malignancy. Laryngoscope 1980;90:619–27.
[145] Poe DS, Tarlov EC, Thomas CB, et al. Aggressive papillary tumors of temporal bone.
Otolaryngol Head Neck Surg 1993;108:80–6.
[146] Mukherji SK, Albernaz VS, Lo WW, et al. Papillary endolymphatic sac tumors: CT, MR
imaging, and angiographic findings in 20 patients. Radiology 1997;202:801–8.