Embed Size (px)
Citation preview

Lessons learned from the National Coal Workers Autopsy Study (NCWAS) and opportunities
for the future
Francis H.Y. Green, MD Cummings School of Medicine, University of Calgary, Alberta, Canada

Disclosure
• No commercial conflict of interest• Expenses for travel paid for by Alpha Foundation
Grant• Opinions are my own and not those of NIOSH

Value of Pathology
• To enable compensation for miners and their families• Improve accuracy of death certification• Improve accuracy in diagnosis of the disease of interest• Testing regulatory standards• Can be used to identify exposures and new diseases• Ability to correlate exposure and disease at the tissue level• Ability to explore pathogenesis using molecular markers and
other techniques• To enable compensation miners and their families

Overview
• History of the NCWAS• Overview of the program
• Compensation• Disaster support• Research
• Research• Major contributions
• Testing the efficacy of dust standards
• Forensic investigation of mine disasters
• Silicosis• Emphysema• Interstitial fibrosis• Lung cancer• X-ray – pathology correlations
• Major contributions cont.• Pulmonary vascular abnormalities• Techniques for dust analysis• Free radical biology• Accuracy of death certification• Comparison with other databases• Cor Pulmonale (right heart
disease)• Ongoing Studies
• Rapidly Progressive CWP• Pathology of PMF• Pathology of interstitial fibrosis
• Future Potential• Genetic studies• Molecular biology• Role of Ultrafine particles

Overview
• History of the NCWAS• Overview of the program
• Compensation• Disaster support• Research
• Research• Major contributions
• Testing the efficacy of dust standards
• Forensic investigation of mine disasters
• Silicosis• Emphysema• Interstitial fibrosis• Lung cancer• X-ray – pathology correlations
• Major contributions cont.• Pulmonary vascular abnormalities• Techniques for dust analysis• Free radical biology• Accuracy of death certification• Comparison with other databases• Cor Pulmonale (right heart
disease)• Ongoing Studies
• Rapidly Progressive CWP• Pathology of PMF• Pathology of interstitial fibrosis
• Future Potential• Genetic studies• Molecular biology• Role of Ultrafine particles

History of the NCWAS
• Initiated in 1969 under Title 42 of Federal Coal mine Health and Safety Act
• Primary purpose to provide evidence for Black Lung claims for next of kin. Pathology reviews for Black Lung claims by NIOSH pathologists are done on request of the family
• Research: intended to be used as repository of materials for study of the natural history and pathogenesis of coal workers lung and heart diseases
• Disaster Investigation support

History of the NCWAS
• Conducted by independent pathologists• Minimum requirements are:
• Clinical summary• Copy of autopsy report (age, diagnosis etc.)• Weights of lungs and heart• Minimum of 3 blocks and H & E stained slides of lungs• Consent, release and history form signed by next of kin

History of the NCWAS
The consent, release and history form has information on:
• Years of underground and surface mining• Last job title• Principle mining occupation• Name and location of last mine worked • Smoking history
• Years smoked• Number of cigarettes• If ex-smoker, years quit smoking

Research using NCWAS data and tissues (selected Studies)
Analysis of cases submitted in the first 25 years (1971 – 1996) to determine if the 2mg/m3 dust standard had
reduced the prevalence and severity of CWP
• All 6990 cases reviewed independently by three pathologists (VV, JK, FG) using NIOSH/CAP diagnostic criteria
• Cases randomized and pathologists blinded to all information on the case
• Lesions of simple CWP and silicosis identified and graded into absent, mild, moderate and severe
• PMF documented as present/absent• Statistical analyses, including logistic regression models
Research

Classic Simple CWP
Macules Nodules

Classic Simple CWPCoal dust macule with emphysema Coal Dust Nodule
Silicotic NodulesEmphysema

Classic Features of CWPPMF

Data Analysis
• Descriptive statistics
• Prevalence and severity of specific CWP lesions by underground mining tenure
• Prevalence of specific pneumoconiosis lesions and working before or after 1970 dust regulations

Characteristics of autopsy population
(NCWAS) 1971–1996)Total number of cases 6103
Age at death, mean ± SD
(min–max)
63.7 ± 11.5
(20 – 98)
Mining tenure, mean ± SD
(min–max)
27.2 ± 12.9
(1 – 73)
Ever smoker (%) 75.7
Number of states from which autopsies received 29

Pneumoconiosis LesionsDisease
SeverityFrequency (%) Mining Tenure
(mean years ± SD)
p-values†
Coal Macules
absentmild
moderatesevere
22.033.131.113.7
21.0 ± 13.024.0 ± 13.328.2 ± 12.731.7 ± 11.4
< 0.0001
Coal Nodules
absentmild
moderatesevere
59.819.011.59.7
22.5 ± 12.928.5 ± 12.630.8 ± 12.234.0 ± 10.9
< 0.001
Silicotic Nodules
absentmild
moderatesevere
76.313.35.94.5
24.1 ± 13.129.8 ± 12.431.9 ± 11.733.6 ± 11.9
< 0.001
Progressive Massive Fibrosis (PMF)absentpresent
92.97.1
25.2 ± 13.233.3 ± 11.4
< 0.01
Prevalence and severity of specific CWP lesions by underground mining tenure
The longer the miner worked the more severe was the CWP; validates data base and pathology

PneumoconiosisLesion Category Total (N) Prevalence
(%) Odds Ratio‡95%
Confidence Interval
p-values
Coal Macules
Old regulations 2217 82.6 1.0 - -
New regulations 662 58.8 0.44 0.32–0.60 < 0.001
Coal Nodules
Old regulations 2216 46.3 1.0 - -
New regulations 662 15.0 0.23 0.17–0.32 < 0.001
Silicosis
Old regulations 2214 28.2 1.0 - -
New regulations 661 8.0 0.22 0.15–0.32 < 0.001
PMF
Old regulations 2213 10.3 1.0 - -
New regulations 662 1.2 0.11 0.05–0.24 < 0.001
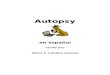
Prevalence of specific pneumoconiosis lesions and working before or after 1970 dust regulations
All types of pneumoconiosis greatly reduced under the lower dust standard, PMF showed ten-
fold reduction up to end of 1996

0102030405060708090
100
>1940 1941-49 1950-59 1960-69 1970 <
MACNODSILPMF
Prevalence and type of pneumoconiosis by decade of initial employment

Prevalence of specific CWP lesions by state of mining employment (NCWAS), 1971–1996
State N Coal Macules (%) Coal Nodules (%) Silicosis (%)PMF
(%)
Kentucky 476 72.1 24.4 9.7 1.9
Pennsylvania 2480 81.1 47.1 30.0 9.7
West Virginia 1863 76.6 39.4 23.1 7.0
Western States† 105 70.5 34.3 23.8 6.7
Other States† 1131 74.0 32.4 16.4 3.9
All Cases 6055 77.9 40.2 23.7 7.1

Research on Emphysema in US Coal Miners
• 615 autopsied underground miners and 108 non-miners from S. West Virginia
• Information on years of mining, jobs worked, smoking and medical histories
• Chest x-rays (N=466) and FEV1 data (N=115) were available for some cases
• Estimates of airborne dust exposure
• Full autopsies with whole lung sections for estimates of type and severity of pneumoconiosis and emphysema
• For a subgroup of 131 miners, retained lung dust was available

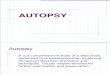
Cumulative Coal Mine Dust Exposure and Predicted Emphysema Index
Cumulative Coal Dust Exposure
Emph
ysem
a Sc
ore
0 50 100 150 200 250 300
020
040
060
080
010
00
Non-white Smoker
Non-white Non-smoker
White SmokerWhite
Non-Smoker
FEV1 65%
Kuempel ED, Vallyathan V, Green FHY. Emphysema and pulmonary impairment in coal miners: quantitative relationship with dust exposure and cigarette smoking. J Physics: Conference Series 151:108, 2009.

Emphysema Study Results
Significant positive relationships were seen between emphysema score and:
Years of underground mining Estimated cumulative dust exposure Retained lung dust (p<0.0001) Radiographic category of pneumoconiosis (p<0.0001) Pathologic type and severity of pneumoconiosis FEV1 (p<0.001) Cigarette smoking (p<0.006) Race Age The models indicate that exposure at the 1mg/m3 level would
contribute equally to 1 pk/day smoking to the emphysema.

Ongoing StudiesRapidly Progressive Pneumoconiosis (RPP)
• Defined radiologically, progression of one ILO radiographic category or more over a 5 year period or development of PMF in miner who has worked under current dust standards
• Recognized post 2000, increasing incidence of disease• Associated with small mines in southern Appalachia• Associated with face work using newer cutting machines that
produce large amounts of rock• Cause not known but excessive rock dust (silica and silicates), small
fractured particles and poor dust control implicated• On going (Alpha) project to study dust from miners with RPP with
dust from miners with classic CWP• Initial results show a pathologically unique type of pneumoconiosis
with massive amounts of rock dust in the miners lungs with RPP

RPP Explanted Lung
Progressive Massive Fibrosis
Immature silicotic nodules
Interstitial fibrosis

Case 2 RPP Immature Silicotic Nodules

Features of acute silicosis
RPP explanted lung
To next slide

Case 2
Alveolar proteinosis(acute silicosis)
Large numbers of birefringent rock dust particles
RPP explanted lung

RPP inflammation and dust in explanted lung
High power view of fibrosis and inflammation viewed with regular light.
Some black particles can be seen.
Same area of lung but now viewed with polarized light to show large numbers of
silica and silicate (rock) crystals

Coal Mine Dust and Inflammation in the RPP Lung compared to classic CWP
• Black to golden brown in color (bituminous coal)• Minimal Fibrosis (scar tissue)• No Inflammation
RPP lungClassic Features
• less black (coal) dust• Much scar tissue (pink areas)• Intense inflammation (small round blue cells)

Other pathologic Features in RPP• Lymphoid Hyperplasia
Case 1
Macrophage death

Interstitial fibrosisresembling UIP
(IPF)

UIP type interstitial fibrosis

Massive fibrotic lesion
Plaque-like pleural fibrosis(Resembles asbestos plaque)
Fibrous silicates
RPP pleural fibrosis

Mineral dust small airway disease
• Areas of relatively normal lung
• Minimal emphysema• No classic lesions of coal
workers pneumoconiosis
RPP Interstitial fibrosis

RPP mineral dust small airway disease
RPP Small Airway Disease compared to normal small airway and classic CWP
Normal respiratory bronchiole
Classic coal macule with centri-acinar emphysema

Case of RPP from Dr Jerry Abraham
• 28 year old male with progressive exertional dyspnea over a year. underground coal miner for 6 years before joining the military
• Worked mostly at the face of coal mines in WV and KY

RPP case analysis results

Evolution of the lesions of silicosis

Often very severe
Classic CWP
Immature silicotic nodules
Inflammation (lymphocytes)
Acute silicosis
Lots of fibroblasts
YES
Immature collagen (scar tissue)
Silica / silicate dust load
Interstitial fibrosis
Rapidly Progressive CWP
Very rare
NO
NO
YES
NO
NO
Moderate
Yes but usually mild
YES
YES
YES
YES
NO
YES
YES
Differentiating classic CWP from RPP
16OV-01
Lots of coal dust
Pathologic feature Comments
NOSmall airway disease
Often very prominent
in RPP
Very High in RPP
YES

Classic CWP
Coal macules
Emphysema
Coal nodules
RPP
YES
YES
YES
NO
Modified nodules
Rare
Differentiating classic CWP from RPP
16OV-02
Comments
Replaced by mineral dustsmall airway disease in RPP
Immature silicotic
Bottom line: Pathologically RPP is an entirely different disease from classical CWP
• More rock dust, less coal dust than traditionally seen• Very different pathology• Large inflammatory component may be very important
observation

Is this the resurgence of an old disease?Accelerated Silicosis: Hawks Nest, West Virginia
• 1927 – Construction began• 700 – 1,000 deaths among 3,000 workers• Most deaths occurred within a few years of exposure• Pathology showed accelerated silicosis

• More silica and silicates–Smaller particles–Fractured particles–Fragmented silicates with irregular and sometimes fibrous
morphology–Surface free radicals
• Metals–Hard metals (tungsten and cobalt)?–Other titanium, vanadium, cadmium etc?
Pathogenesis of RPPChanges in mining technology/practice may be affecting exposures

RPP Pathogenesis
Mustafa, Shelan. (2010). Chapter 4 Size–dependent structure parameter for silicon nanowires and nanoparticles 4.1. Introduction. 10 13140/RG 2 2 13743 94889
The surface area to volume ratio of a respirable dust particle increases exponentially as the particle gets smaller

Metal ions O2 −OH
SiOH Silanol groups
Si Surface radicalsFe2+
Jim Clark (2012) Giant Covalent Structures http://www.chemguide.co.uk/atoms/structures/giantcov.htmlModified from Borm et al. Critical Reviews in Toxicology 41(2011)756-770
••
Silicon AtomOxygen Atom
−SiO(s)• + H2O →−SiOH(s) + HO•−

Silica
Silanol groups
Surface radicals
Lysosome
Nucleus
Free radicals: O2−
HO (H2O2)ONO−
Phagocytosis

PhagocytosisCathepsin
D
Proteolytic enzymes
Lysosome
Nucleus
Free radicals: O2−
HO (H2O2)ONO−
Fibrogeniccytokines:IL-1βTNF-αMIP-1/MIP2 MCP-1IL-8

Free radicals: O2−
HO (H2O2)ONO−
Apoptosis(Programmed Cell Death)
Lysosome
Nucleus
CathepsinD
Proteolytic enzymes
Fibrogeniccytokines:IL-1βTNF-αMIP-1/MIP2 MCP-1IL-8

Pathogenesis of RPP
• The dust is triggering an abnormal immune response– Some metals can initiate abnormal responses (eg Beryllium)– Silica can initiate auto immune disease
• Classic example in coal miners is Caplans disease (rheumatoid pneumoconiosis)
• Silica is associated with Autoimmune Vasculitis, Scleroderma, Lupus, Renal disease. Also so called Idiopathic Pulmonary Fibrosis
– We have no data on the pathologic effects of fibrous or plate like silicates
• The finding of dense fibrosis of the pleura in some cases of RPP is suggestive of a role
Pathogenesis of RPPHas the biologic response to coal mine dust changed?

• Understanding Rapidly Progressive CWP– Selecting historic controls for cases of RPP– Review recent (post 1996) cases accessioned into the program for
cases of RPP
• Is PMF a single disease or does it have different manifestations (types)
• Determine Prevalence and Types of Interstitial Fibrosis in Coal Miners
• Understanding Rapidly Progressive CWP– Selecting historic controls for cases of RPP– Review recent (post 1996) cases accessioned into the
program for cases of RPP
• Is PMF a single disease or does it have different manifestations (types)
• Determine Prevalence and Types of Interstitial Fibrosis in Coal Miners
Future work

Conclusions
• The NCWAS has accessioned approximately 7,000 cases since 1970
• It represents a unique resource for studying diseases of the heart and lung in coal workers
• To date it has been used in 16 published studies (see appendix)• Data from NCWAS, like the Living Miner Data shows that
pneumoconiosis prevalence declined in the first 25 years since enactment of the 2 mg/m3 standard
• It has contributed to our understanding of the prevalence of different types of pneumoconiosis and the role of coal mine dust in causing emphysema, among others. Currently it is a critical resource for studying the causes of Rapidly Progressive CWP
• Going forward it will provide a better understanding of PMF and interstitial fibrosis and will serve as a unique biobank for molecular and genetic studies

AcknowledgementsNational Institute for
Occupational Safety and Health• David Weissman• Ann Hubbs• Marlene Orandle• Mike Attfield• Eileen Kuempel• Anita Wolfe• Kathy Boyce• Val Vallyathan
Miners Health Study Group
• University of Illinois: Robert Cohen, Leonard Go, Kirsten Almberg
• National Jewish Health, Denver: Cecile Rose, Lauren Zell-Baran
• SUNY Syracuse: Jerrold Abraham, Soma Sanyal.
• West Virginia University: Lee Petsonk• University of Calgary: Francis H.Y.
Green, Angela Franko• NIOH – South Africa: Jill Murray,
Naseema Vorajee• Virginia Tech: Emily Sarver• USGS: Heather Lowers, Geoffrey
Plumlee
Thank youQuestions?

Appendix:Publications based on the NCWAS program
• Kleinerman J, Green FHY, et al. Pathology standards for coal workers' pneumoconiosis. (A report of the Pneumoconiosis Committee of the college of American Pathologists). Arch Path and Lab Med (Special Issue) 101:375-431, 1979.
• LeFevre ME, Green FHY, Joel DD, Laqueur W. Frequency of black pigment in liver and spleen of coal workers: Correlation with pulmonary pathology and occupational information. Human Pathol 13:1121-1126, 1982.
• Vallyathan V, Green FHY, Rodman NF, Boyd CB, Althouse R. Lung carcinoma by histologic type in coal workers. Arch Pathol Lab Med 109:419-423, 1985.
• Green FHY, Althouse R, Frost JL, Wheeler RW, Shores SK. Forensic investigation of coal mine fatalities. In: Wheeler RW (ed), Proceedings International Conference on the Health of Miners. Am Conf Gov Indust Hyg 117 124, 1986.
• Vallyathan V, Althouse R, Green FHY, Boyd E, Rodman N. Are coal miners at increased risk for scar cancer? Chest 915:25-35, 1987.
• McConnochie K, Green FHY, Vallyathan V, Wagner JC, Seal RME, Lyons JP. Interstitial fibrosis in coal workers - experience in Wales and West Virginia. Ann Occup Hyg 32: 553-560, Supplement 1, 1988.
• Green FHY, Althouse R, Weber KC. Prevalence of silicosis at death in underground coal miners. Am J Indust Med 16:605-615, 1989.
• Hu, SN, Vallyathan V, Green FHY, Weber KC, Laqueur W. Pulmonary arteriolar muscularization in coal workers pneumoconiosis and its correlation with right ventricular hypertrophy. Arch Pathol Lab Med 114:1063-1070, 1990.

Publications based on the NCWAS program
• Dalal NS, Jafari B, Peterson M, Green FHY, Vallyathan V. Presence of stable coal radicals in autopsied coal miners lungs and their possible correlation to coal workers pneumoconiosis. Arch Environ Health 46:366-372, 1991.
• Attfield M, Vallyathan V, Green FHY. Radiographic appearances of small opacities and their correlation with pathology grading of macules, nodules and dust burden in the lungs. Ann Occup Hyg 38:783-790, 1994.
• .Vallyathan V, Brower PS, Green FHY, Attfield MD. Radiographic and pathologic correlation of coal workers pneumoconiosis. Am J Resp Crit Care Med 154: 741-748, 1996.
• Naidoo RN, Robins TG, Murray J, Green FH, Vallyathan V. Validation of autopsy data for epidemiologic studies of coal miners. American journal of industrial medicine. 2005 Jan;47(1):83-90.
• Kuempel E, Wheeler M, Smith RJ, Vallyathan V, Green FHY. Contributions of dust exposure and cigarette smoking to emphysema severity in U.S. coal miners in the United States. American Journal of Respiratory and Critical Care Medicine 180(3):257-264, August 2009 [PMID: 19423717].
• Kuempel ED, Vallyathan V, Green FHY. Emphysema and pulmonary impairment in coal miners: quantitative relationship with dust exposure and cigarette smoking. J Physics: Conference Series 151:108, 2009.
• Saxena RK, McClure ME, Hays MD, Green FHY, McPhee LJ, Vallyathan V, Gilmour MI. Quantitative assessment of elemental carbon in the lungs of never smokers, cigarette smokers and coal miners. J Toxicology & Environmental Health 74(11):706-715, 2011 [PMID: 21480045].
• Vallyathan V, Landsittel D, Petsonk E, Jeffery K, Parker J, Tofflemire Osiowy K, Green FHY. The influence of dust standards on the prevalence and severity of coal workers’ pneumoconiosis at autopsy in the United States of America, Archives of Pathology & Laboratory Medicine 135(12):1550-1556, December 2011 [PMID: 22120182].

Spare Slides

313291
628
369376345
320322314
255235
310
259249231220184191190179192
168133117
188
118110
6140 29 39 27150
100200300400500600700
1972
1975
1978
1981
1984
1987
1990
1993
1996
1999
2002
National Coal Workers’ Autopsy Study
Autopsy Count

The National Study of Coal Workers Pneumoconiosis
12.711.2
3.03.9 3.5
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
1969-71 1972-75 1977-81 1985-88 2002Prev
alen
ce o
f sm
all r
ound
ed o
paci
ties
cat 1
or g
reat
er

0102030405060708090
Macules Nodules Silicosis PMF
Perc
ent
Non-SmokersSmokers
Prevalence of Pneumoconiosis by smoking status

Case 1