Embed Size (px)
Citation preview

Lessons Learned through Research: Do Hospitals and Ambulatory Centers Follow Guideline Recommended
Care
Nancy Albert, PhD, RN, CCNS, CCRN, NE-BC, FAHA, FCCM
Senior Director Nursing Research and Innovation;CNS, Kaufman Center for Heart Failure
May 2012

2
Presenter Disclosure InformationNancy M. Albert PhD, CCNS, CHFN, CCEN, FAHA, FCCMLessons Learned through Research: Do Hospitals and AmbulatoryCenters Follow Guideline Recommended Care
2
FINANCIAL DISCLOSURE:No relevant financial relationship exists

National Trends in Readmission Rates after HF Hospitalization
Ross JS, et al. Circ Heart Fail 2010;3:97-103.
RSRR, Risk-standardized 30 D all-cause readmission rate
2004 2005 2006
RS
RR
0.15
0.2
0.25
0.3

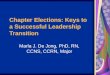
All Cause Mortality After Each Subsequent Hospitalization for HF
Setoguchi et al. Am Heart J. 2007;154:260-6.
Time Since Admission
0.0
0.2
Ka
pla
n-M
eie
r C
un
. Mo
rta
lity
0.8
1.0CHF1st Admission (n = 14,374)2nd Admission (n = 3,358)3rd admission (n = 1,123)4th Admission (n = 417)
1st hospitalization: 30 d mortality = 12%; 1 yr = 34%
0.6
0.4
0.0 0.5 1.0 1.5 2.0

Risk-Treatment Mismatch in HF: Canadian EFFECT Study
Use rates in absence of contraindications. For all drug classes, P < .001 for trend.
EFFECT, Enhanced Feedback for Effective Cardiac Treatment. Lee D. JAMA. 2005;294:1240-1247.
At Hospital Discharge 90-Day Follow-Up 1-Year Follow-Up
010
20
30
40
50
60
70
80
90
Low Risk Average Risk High Risk
ACEI ACEI or ARB
-Blocker
1-Year Mortality Rate
Pat
ien
ts, %
ACEI ACEI or ARB
-Blocker

ACADEMIC DETAILING
734 physicians surveyed
• Guidelines helped a moderate (47%) or great amount (23%) in clinical decision making
–21% respondents reported ACE-I are contraindicated if s cr. > 2.0 mg/dL
–27% thought intermittent inotropic therapy is reasonable practice per guidelines
–33.9% underestimated HF prevalence in US
–75.2% underestimated 1-year mortality for Medicare patients
Hauptman PJ, et al. Am J Medicine. 2008;121;127-135.

Timeline from Concept to Clinical Adoption of Neurohormonal Treatments in Heart Failure
1970 1980 1990 2000 2012
ACE Inhibitors
-Blockers
Concept 1st Data Definitive Approval 50% use
Adapted from M Konstam, HFSA 2000.
Aldosterone Antagonists
X

PACE of Improvement
• From 1998-1999 to 2000-2001 performance on the typical CMS inpatient/outpatient measures improved from 69.5% to 73.4%, a 12.8% relative improvement
• At this rate, by 2024, we will have 95% performance on the measures that were current in 2002

ADHERE: Variation in ACEI Use
ADHERE: Dec 2002, 206 Hospitals; 23,193 patients (subset with LVEF < .40)
ORYX Core Measure: HF 3 - LVEF < 40% prescribed ACEI at discharge
Rat
e (%
)0
2040
6080
100
ADHERE Hospitals

ADHERE: Variation in Beta Blocker Use
ADHERE: Dec 2002, 206 Hospitals (Subset with LVEF < 0.40)
ADHERE Hospitals
Rat
e (%
)0
2040
6080
100
Use of Beta blocker at Discharge for Patients with LVEF <= 40%

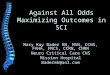
GWTG-HF- Aldosterone AntagonistsHospitals' use of Aldosterone Antagonist
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1 6 11 16 21 26 31 36 41 46 51 56 61 66 71 76 81 86 91 96 101 106 111 116 121 126 131 136 141
Hospital ID
Rate
of
Ald
oste
ron
e A
nta
go
nis
t U
se
• 34% of patients received Tx by end of 2007
Albert NM, et al JAMA; 2009;302:1658.
• In 140 hospitals w 10/more patients meeting criteria, use was highly variable: median, 28.3%

Albert NM, et al. JAMA 2009; 302:1658
GWTG-HF Aldosterone Ant. Tx
0%
20%
40%
60%
80%
100%
2005, Q 1-2 2005, Q 3-4 2006, Q 1-2 2006, Q 3-4 2007, Q 1-2 2007, Q 3-4
Use over time, N = 12,565; P = 0.0005
28.0%34.5%

GWTG-HF Aldosterone Antagonist Tx- Trends in Adherence Over Time
Albert NM, et al. JAMA 2009; 302:1658
Aldosterone Ant. Users (n / N)
Jan-Jun 05
%
Jul-Dec 05
%
Jan-Jun 06
%
Jul-Dec 06
%
Jan-Jun 07
%
Jul-Dec 07
%P
value*
Inappropriate use overall (n= 640; 7.43%)
7.61 8.25 7.05 7.61 7.91 6.31 0.49
Serum K+ >5.5 & <6.0 mEq/L (n=18; 0.21%)
0.18 0.09 0.07 0.44 0.29 0.48 0.09
Serum Cr. ≥2.5 & < 3.0 mg/dL (n= 233; 2.71%)
3.61 3.53 2.57 2.64 3.63 1.45 0.66
EF >40% and without HTN (n= 396; 4.60%)
4.60 5.51 5.16 5.07 4.92 4.88 0.75

Albert NM, et al. JAMA 2009; 302:1658
GWTG-HF Aldosterone Ant. Tx
50
60
70
80
90
100
DischargeInstructions
LV Function ACE-I/ARB in LVSD Beta-blocker inLVSD
Warfarin in AF
Yes, Aldosterone AntNo, Aldosterone Ant.
%,
Per
form
ance
Mea
sure
Co
nfo
rmit
y

GWTG-HF: Warfarin at Hospital Discharge Among Pts Admitted for HF w Atrial Fibrillation• 72,534 pts from 01/2005 – 03/2008
–255 hospitals
• Results:
–20.5%, atrial fib on admission (n=14,901)
–13.7%, prior Hx atrial fib but SR at adm. (n=9,918)
–Contraindications to warfarin Tx were documented in 9.2%
–Median prevalence of warfarin Tx, 64.9%Piccini JP et al. JACC 2009;54:1280-1289

Warfarin at Hospital Discharge Among Pts Admitted for HF w AF
• Median prevalence of warfarin Tx, 64.9%• Trend over time, P = 0.146
Piccini JP et al. JACC 2009;54:1280-1289
0%
20%
40%
60%
80%
100%
2005 2006 2007 2008, 1st QTR
Warfarin Use Over Time

Piccini JP et al. JACC 2009;54:1280-1289
GWTG-HF: Warfarin at Hospital Discharge Among Pts Admitted for HF w Atrial Fib
Site1 8 15
War
fari
n D
isch
arg
e (%
)
0
20
40
60
80
100
22 29 36 43 50 57 64 71 78 85 92 99 106 113 120 127 134 141 148 155 162 169 176

GWTG-HF: Warfarin at Hospital Discharge Among Pts Admitted for HF w Atrial Fib
Piccini JP et al. JACC 2009;54:1280-1289
CHADS2 score: CHF, HTN, age > 75, DM, prior stroke/TIA
War
fari
n D
isch
arg
e (%
)
01
20
40
60
80
100
2 3 4 5 6Chads2 Score
70.966.5 63.6 64.3 65.8
59.5
P<.0001 for trend
Are hospitals delivering
optimal evidence-based
recommendations?

Hernandez, A. F. et al. JAMA 2007;298:1525-1532.
GWTG-HF: Race and Gender Disparities in ICD Use at Discharge Among Eligible Patients With HF
Black female
White female
Black male
0 0.4 0.80.2 0.6 1.0
43.633.4 29.8 28.2
0102030405060708090
100
White Male
Black Male
WhiteFemale
BlackFemale
N= 13,034 pts

GWTG-HF: Hospital Variation and Characteristics of ICD Use
• January 2005 – June 2007
• New or Discharge prescription for ICD Tx in patients with EF ≤ 30% without documented contraindication
–54,750 pts from 234 hospitals
–Of 12,693 pts, 2545 had prior ICD (20% use)
–Of 10,148 (134 hospitals):
–Overall Use/Planned implementation = 20%
Shah B, et al. JACC 2009;53:416-22.

Hospital Variation in ICD Use
Patient Factors
High Use
N=48
Med. Use
N=42
Low Use
N=44
P Value
Female 34% 38% 36% <0.03
Race-AA 22% 33% 32% <0.001
High Chol 38% 32% 30% <0.001
Hx MI 15% 9% 11% <0.001
Hx HTN 63% 66% 64% 0.004
Shah B, et al. JACC 2009;53:416-22.
Are disparities in care present
by patient features?

New or Planned ICD Use-GWTG-HF
Shah B, et al. JACC 2009;53:416-22.
GWTG - HF Hospital Site
1 11 21 31 41 51 61 71 81 91 101 111 121 131
Ho
spit
al I
CD
rat
e (%
)
0
20
40
60
80
100

Hospital ICD Use Associations with Hospital Characteristics
Shah B, et al. JACC 2009;53:416-22.
Aca
dem
ic
Adj
uste
d IC
D r
ate
(%)
0
20
40
60
80
100N
on-a
cade
mic
Hea
rt tra
nspl
ants
No
hear
t tra
nspl
ants
PC
I cap
able
No
PC
IC
AB
G c
apab
leN
o C
AB
GN
orth
east
Mid
wes
tS
outh
Wes
tB
eds
<100
Bed
s 10
0-19
9B
eds
200-
299
Bed
s 30
0-39
9B
eds
400-
499
>50
0 B
eds
Are disparities in care present
by hospital features?

Median, 49.1Mean, 50.7
IMPROVE-HF: Variation in OPD HF Care
Fonarow GC, et al. Circ Heart Fail. 2008;1:98–106.

ADHERE-HF: Rates of Conformity by Practice Setting and Differences in Hospital Level Outcomes; > 80,000 Hosp. Admissions
Fonarow GC, et al. Arch Intern Med 2005; 165:1469–1477

Median, 33.3Mean, 35.0
IMPROVE-HF: Variation in OPD HF Care
Fonarow GC, et al. Circ Heart Fail. 2008;1:98–106.

Median, 33.3Mean, 37.3
IMPROVE-HF: Variation in OPD HF Care
Fonarow GC, et al. Circ Heart Fail. 2008;1:98–106.

Median, 60.7Mean, 59.8
IMPROVE-HF: Variation in OPD HF Care
Fonarow GC, et al. Circ Heart Fail. 2008;1:98–106.
Are cardiologist practices
delivering optimal
evidence-based
recommendations?

IMPROVE-HF: Improvement in Quality Measures at 24 Months (Pt. Level Analysis)
80%
86%
34%
69%
38%
49%
62%
84%
93%
51%
69%
58%
71%69%
87%
94%
62%
69% 69%
79%
71%
0%
20%
40%
60%
80%
100%
Baseline 12 months 24 months
ACEI/ARB ß-blocker Aldosterone Antagonist
Anticoagulant for AF
CRT ICD HF Education
*
*
*
*
*
**
*
*
*
**
Eli
gib
le P
atie
nts
Tre
ate
dE
lig
ible
Pat
ien
ts T
rea
ted
Fonarow GC, et al. Circulation. 2010;122:585-96.
P-values are for relative change; *, P <0.001 vs. baselineBaseline N= 15,177; 24 Mo. N= 11,621; 167 practices

IMPROVE-HF: Baseline Measure Conformity: Alive vs. Dead at 24-Months
The baseline process measure conformity was significantly lower among patients who died compared with those who survived for 5 of 7 individual measures.
The baseline process measure conformity was significantly lower among patients who died compared with those who survived for 5 of 7 individual measures.
Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.

IMPROVE-HF Nested Case-Control Analysis: Baseline Use of Guideline Recommended Therapies in Cases (N=1376; Dead) and Controls (N= 2752; Alive) at 24-months (matched at 1:2 ratio)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
ACEi/ARB
B-Block
ers
Aldo. Antag
onist
Anticoag fo
r AF
ICD/CRT-D
CRT-P/C
RT-D
HF Educa
tion
CasesControls
P<0.0001
P=0.4046
P=0.0094
P<0.0001
P=0.0019
P<0.0001
P<0.0001
Fonarow GC, et al. J Am Heart Assoc 2012;1:16-26.

IMPROVE-HF Nested Case-Control Analysis: Mortality Reduction Based on Number of Guideline-Recommended Therapies at Baseline
24 Month MortalityAdjusted Odds Ratios (95% CI)
24 Month MortalityAdjusted Odds Ratios (95% CI)
Number of Therapies (vs. 0 or 1 therapy)
2 therapies
3 therapies
4 therapies
5, 6, or 7 therapies
Odds Ratio(95% confidence interval)
0.63 (0.47-0.85)(P =0.0026)
0.38 (0.29-0.51)(P <0.0001)
0.30 (0.23-0.41)(P <0.0001)
0.31 (0.23-0.42)(P <0.0001)
0 0.5 1 1.5 2
Fonarow GC, et al. J Am Heart Assoc 2012;1:16-26.

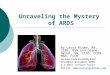
IMPROVE-HF: Incremental Benefits with HF Therapies(Cumulative % Reduction in Odds of Death at 24 Months)
-39%
-63%
-76%-81% -83% -81%
-100%
-90%
-80%
-70%
-60%
-50%
-40%
-30%
-20%
-10%
0%Beta Blocker
Beta Blocker +ACEI/ARB
Beta Blocker +ACEI/ARB + ICD
Beta Blocker +ACEI/ARB + ICD + HF
Education
Beta Blocker +ACEI/ARB + ICD + HF
Education +anticoagulants for AF
Beta Blocker +ACEIARB + ICD + HF
Education +Anticoagulant for AF
+ CRT
-28% to -49%P<0.0001
-54% to -71%P<0.0001
-68% to -81%P<0.0001
-75% to -86%P<0.0001
-77% to -88%P<0.0001
-72% to -87%P<0.0001
Fonarow GC, et al. J Am Heart Assoc 2012;1:16-26.

IMPROVE-HF: Incremental Benefit with HF Therapies(Cumulative % Reduction in Odds of Death at 24 Months Associated with Sequential Treatments)
-38%
-77%-90%
-100%
-90%
-80%
-70%
-60%
-50%
-40%
-30%
-20%
-10%
0%ACEI/ARB ACEI/ARB + BB ACEI/ARB + BB + CRT + ICD
+20% to -68%P=0.1566
-43% to -91%P<0.0001
-70% to -96%P<0.0001
Fonarow GC, et al. J Am Heart Assoc 2012;1:16-26.

Hospitalization for HF : CV / Medical Conditions
Klapholz, et al. JACC 2004;43:1423-8.
Reasons for Clinical Decompensation were Identified in only ½ of Patients
Syst. BP >200 mmHg
Non-Compliance
MR / AR >3+
ACS
Renal Insuff.
Afib / Flutter / SVT
Sev. COPD / Asthma
Pneumonia
AS / MS <1.0 cm2
Sepsis
Patients (%)0 3 6 9 12 15
Did we assess patient
knowledge, psychosocial,
behavioral, economic
needs/issues?

Primary endpoint was:Mortality or Readmission for heart failure
COACH Study: Self-Care Compliance

COACH study: Self-Care ComplianceCOACH study: Self-Care Compliance
Van der Wal MH, et al. Eur Heart J 2010;31:1486-1493Van der Wal MH, et al. Eur Heart J 2010;31:1486-1493
Compliance = scoring “mostly” or “always” in following 3 recommendations: 1) Sodium-restricted diet2) Fluid restriction3) Exercise
Compliance = daily weight monitoring three times per week to daily
Compliance measured 1 month after hospital discharge & followed for 18 months
48% (N=830 patients)
Cu
m s
urv
ival
Time to primary endpoint
0 100 200 300 400 500 6000.0
0.2
0.4
0.6
0.8
1.0
Overall non-compliantOverall compliantHR 1.40 (1.08-182); P=0.01

Van der Wal MH, et al. Eur Heart J 2010;31:1486-1493
Compliance with advice on weight monitoring, low sodium diet, fluid restriction and exercise
*, P< 0.01; **P<0.05
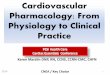
COACH study: Self-Care ComplianceCOACH study: Self-Care Compliance
0
20
40
60
% p
rim
ary
end
po
int
Total compliance score (0-4)
4 3 2 1 or 0
25%
38% 36%
45%*
**
*

Non-compliance adjusted HR (95% CI)Primary endpoint: 1.48 (1.15-1.91) P=0.002Time to:-- HF readmission: 1.55 (1.13-2.13) P=0.007-- Death: 1.24 (0.89-1.72) P=0.20
Non-compliance adjusted HR (95% CI)Primary endpoint: 1.20 (0.87-1.65) P=0.27Time to:-- HF readmission: .93 (0.60-1.44) P=0.76-- Death: 1.58 (1.08-2.27) P=0.02
Van der Wal MH, et al. Eur Heart J 2010;31:1486-1493
COACH study: Self-Care ComplianceCOACH study: Self-Care ComplianceC
um
su
rviv
al
Time to primary endpoint0 100 200 300 400 500 600
0.0
0.2
0.4
0.6
0.8
1.0
Non-compliant exerciseCompliant exercise
Time to primary endpoint0 100 200 300 400 500 600
Non-compliant weighingCompliant weighing
Compliant with exercise Compliant with daily weighing
0.0
0.2
0.4
0.6
0.8
1.0

COACH study: Self-Care ComplianceCOACH study: Self-Care Compliance
Conclusion: Advice and compliance in all 4 self-care behaviors are important
Time to primary endpoint0 100 200 300 400 500 600
Non-compliant exerciseCompliant exercise
Time to primary endpoint0 100 200 300 400 500 600
Non-compliant fluidCompliant fluid
Compliant with diet
Cu
m s
urv
ival
0.0
0.2
0.4
0.6
0.8
1.0
0.0
0.2
0.4
0.6
0.8
1.0
Compliant with fluid restriction
Van der Wal MH, et al. Eur Heart J 2010;31:1486-1493
Do we assess patient’s
adherence to self-care and
learn reasons for
non-adherence?

Performance Measures & Quality
• Based on nationally established guidelines• Include outcomes and processes of care
known to positively influence overall outcomes of care–Institution and system level
–Hospital–Healthcare practitioners/care providers
–Incorporate risk-adjustment methodology to account for significant differences in patient populations among institutions

Performance Measures & Quality• Often, we question the reliability of
performance measures in specific settings–Documentation of patient education
–Checking a box does not reflect delivery of quality care
1. Koelling TM, et al. Circulation 2005;111:179-185.2. Krumholz HM et al. JACC 2002;39:83-89.
• 1:1 RN-delivered comprehensive HF education during a 1-hour hospital session decreased 6-month days hospitalized or days dead1
• RN delivered, 1 hour, comprehensive hospital education + ongoing 1 year telephone-based support decreased 1-year hospital readmission rate and hospital costs2

Performance Measures & Quality• Public release of performance data in changing
the behavior of healthcare consumers, professionals or organizations –> 35,000 consumers & 1560 hospitals
• Conclusions: –“The small body of evidence available
provides no consistent evidence that the public release of performance data changes consumer behavior or improves care.
–Evidence that the public release of performance data may have an impact on the behavior of healthcare professionals or organizations is lacking.”
Ketelaar NA, et al. Cochrane Database Syst Rev. 2011;11:CD004538.

PROGRAMS Developed to Improve Performance Measures• Usually designed to enhance quality of patient care
that promotes adoption of evidence-based, guideline-recommended therapies
–Force a deeper look into actions and practices
–Requires:
–Leadership
–Evidence-based clinical decision support (algorithms; pocket cards, customizable order sets...)
–Patient education resources
–Regular review of data; benchmarking
–Process improvement model of change