Embed Size (px)
Citation preview

Levers for Change1st May Taunton Racecourse
Event Evaluation

Contents
This document is designed to be read on screen
Programme for the day slide 3What you thought of the presentations slide 4What you said about the day slide 5What you said were the best things about the day slides 6
& 7What you didn’t like about the day slide 8The outcomes you would like to see as a result of the day slides 9,
10 & 11Locality discussions slides 12 - 23

Programme for the day
9.30 Registration and Refreshments• 10.00 Welcome • Judy Walker, Director of Operations, Stroke Association• 10.15 World Class Commissioning, Dr Steve Feast, Department of Health
10.30 Doing your local leadership differently Professor Steve Onyett, South West Development Centre
11.15 Refreshment break11.30 Putting People First, Pam Richards, South West Personalisation Coordinator11.50 Doing commissioning locally, Jan Evans, Commissioning Manager, Wiltshire 12.15 The ‘Richard and Judy’ ShowThe views of service users and carers, South West Alliance of Neurological Organisations1.00 Locality Discussion
1.15 Lunch and exhibition2.00 A model for a network, Lynne Barr, North East Long Term Conditions Team2.30 Locality discussion
3.00 Final Comments and Close

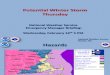
What you thought of the presentations
0
5
10
15
20
25
30
Steve Feast Steve Onyett Pam Richards J an Evans Richard and J udy Lynne Barr
poor
fair
good
very good
excellent

What you said about the dayHas today helped you with what you need or want to do as part of your work or involvement?
0
2
4
6
8
10
12
14
16
18
not at all a little moderately quite a bit extremely

What you said were the best things about the day
Hearing the views of service users and carers in the ‘Richard and Judy’ show, invaluable information and great to get their perspective (x22)
Service user and carer involvement in the day (x2) Willingness to challenge current thinking Local leadership presentation, Inspirational leadership talk (x3) Good programme, varied speakers, good venue Time out to focus on these issues Very inspiring lectures Network model (x3) Inspiring to think that one can get a successful network running with no funding
initially Networking (x5) Information on the exhibition stands Meeting people, meeting people from other organisations in the SW Sitting at a ‘Wiltshire’ table so that we could apply the bigger picture to our own
patch

What you said were the best things about the day
Well structured with useful consistency of themes Good balance, wide ranging A thoughtful overview of key issues Gaining ideas about how to change service at all levels Good relationships Opportunity to meet with other care providers from different backgrounds,
carers and associations Awareness of who is doing what, or not Great mix of people on the tables Opportunity to dedicate physical and head time to considering
commissioning- how in my job I influence and am affected by it Good venue, lunch directions etc. Chocolates! Lunch!

What you didn’t like about the day Prof Onyett’s talk was too short ! (x4) Too much PowerPoint, you can not listen and read at the same time The leadership stuff – ego fuelled and lacked structure, all theory , no practical
application Speakers rushed as the timescales were too tight, this ate into the time for
networking too (x2) The partnership talk didn’t add anything to the info I already had Network discussion too late in the day, no time for questions Network discussion was tricky to hold on tables with very small geographical
representation, might have been better to hold a plenary discussion Presented network model doesn’t reflect the local situation (x2) The DVD – should have been there in person, patronising and too long and
didn’t work properly, too much jargon, needed examples to explain the ideas (x3)
Some sheets of blank paper for notes would have been useful (x2) Too much sat listening, other delivery styles needed, chance to move around
and get to know who else was there needs to be built in to the day Got very cold with excessive air con in the morning, later resolved Venues should have accessible dedicated disabled parking bays Buildings should be completely compliant with DDA I.e. provision of WCs for
disabled

The outcomes you would like to see as a result of the day
This process is a whole system change – I hope it moves forward involving every agency
People just to get on with it and not be tokenistic or waste money Further NSF implementation, more focus on neurological conditions(x2) and
reporting information back to delegates Joined up thinking resulting in across-the-board communication and
coordination (x2) More productive partnership working, closer working between health and
social care locally (x3) Implementation of key points made, such as health professional responding to
the need to improve communication and coordination Investment in delivering services for people living with long term neurological
conditions in the community Feedback from services users experiences of personalisation More time to discuss future proposed plans A cradle-to-grave pathway for cerebral palsy within a general neurology
pathway

The outcomes you would like to see as a result of the day
Further events giving examples of good practice Follow up groups – assessment staff to be included especially in further
events Time to work on the big picture as well as meeting clinical needs Valuing the work of frontline clinicians to a greater degree leading to
cascading of leadership roles and empowering individuals More services, improvement in access to services Better publicity and information about different conditions Services developing in Wiltshire Engagement of patients in developing stroke services in Gloucestershire Return to patient centred care Promotion of appropriate service provision Increased connections between professionals across health and social care More volunteers supported to engage in co-production Improved commissioning of services that allows frontline staff to really meet the
needs of service users and not be restricted by protocols and funding Patient related outcomes that are measurable and real and make real
changes for people and their carers Patient reported outcome measures for each specific neurological
condition

The outcomes you would like to see as a result of the day
A regional neuro network for commissioners The creation of a sub regional or regional network (x2) A network for Wiltshire that we define for ourselves Beginning of the process of networking to aid our development of the
coordination of these new developments for patient input Network developed in Plymouth and Cornwall A network that works! Development of a Devon network A good network of neuro colleagues across health, social care and voluntary
sector so we can share best practice Action!

Locality discussions each table was asked to think about the following questions
Who are your local leaders?• Is there a local vision for future services?• Is there a local plan for achieving this vision? • Are the voluntary sector, service users and carers involved in
developing and implementing this plan? E.g. via surveys, consultations, as board members, in references groups, as service providers
• Do you need help to engage with the voluntary sector, service users and carers?
Network - Good idea or not?• If yes, should the network be regional, sub regional or local?• Where will the leadership come from?• Where will the funding come from?• Who should be involved?• Would YOU like to be involved? If yes, your name please• Suggest a name for the network

Locality discussions: Table 1
Who are the local leaders? Medical and social, including clinicians, physiotherapists, OTs, professionals and others
with special interests, GPs, pharmacists, mobility professionals, social care staff and family counselling services.
Some of the above will be non-professional, third sector and the group felt that there would need to be nomination of network leads and effective communication channels in all directions.
Local vision It was felt that there was ‘vision impairment’ and that it was not whole, with patchy levels of
service. It was agreed that small, local hospitals offer good valueLocal plan Planning is at varying stages of development, mostly at the ‘early’. The group felt that there
was a lack of things being joined up and that baseline assessments would be helpful in determining a starting point.
Voluntary sector, service user involvement etc Not always the case with specialist services and levels of support for personalisation
insufficient to enable people to make informed choices - and considered patchy. There are good examples but not for neurology as a whole. A participant who had a long term condition noted that he was involved in training some professionals, which was good for him and for those being trained. Fifty-percent of the consultants with whom he had worked had not seen PD patients during training.
Help needed engaging with voluntary sector, service users and carers?
• Yes!

Locality discussions: Table 1
Network discussion: Networks are a good idea. Networks should be at regional, sub regional and local level Leadership should come from within ‘from each according to their
abilities’ Should be a ‘doing’ network and not a steering group, involved in:
Development, Dialogue, Sharing, Supporting Emphasising excellence through sharing Everyone needs to recognise that mistakes can be made and learned
from There are various possibilities for funding, which does not always have
to be new Expenses and accommodation need to be covered Identify needs and then seek to identify potential sources

Locality discussions: Table 2Local leaders names given Very new local vision, Neuro Specialist Team set up in N Somerset Pathways being slowly formulated Voluntary sector, service users and carers involved in acute service, and
BNSSG (?) Evaluations being done Headway are good, but not good in S Glos, loss of partnership board in S Glos MS centre Nailsea and Warminster Vassal Centre Spinal injury centre in Salisbury but services not readily available on
discharge Consultation with all conditions not good, tokenism and box ticking PCTs and Acute Trust do not work together in BNSSG Problem with sharing the community work – money Works well in BaNES Friction in N Somerset Lack of patient choice on discharge – hospitals are making the decisions Carers are the unsung heroes Fire-fighting all the time which blocks the good ideas Lack of money and resources How creative can you be? Giving time means NBRS (?) not achieved

Locality discussions: Table 2
Network is a good idea, should be sub regional Leadership should come from the PCT with the support of the SHA Funding should come from the SHA All groups should be included, plus local forum MDTs/clinical groups should be local forum otherwise network is too
big University and SWMPO (?) Suggested name: Neurosouthwest

Locality discussions: Table 3
Local Leadership Via the SHA Frontline service staff need to be more engaged in leadership – as
collaborators rather than followers South Petherton Hospital and Bridgewater Health Campus
developments achieved via leadership through an inclusive approach NSF Implementation Plan Role for vol orgs re hard to reach groups but must be credible as
gateway/conduit to service users/carers LINks role needs developing re LTNC groups/focus Specialist Nurses much valued by service users and as well as direct
service providers also act as a point of leadership for their specialist area
Regional Network We thought it would be a good thing and were for it! Who would initiate – SHA?/Specialised Commissioning?/SWANO?

Locality discussions: Table 4
Local leaders: named The LIT is a big group that meets quarterly and includes service users, carers, there is managerial representation, neuro services clinicians, Headway, MS, MND, PSP, Huntingdons, PD, CP etc. There are also disease specific sub groups. They are looking to restructure as the group is too big
The local vision for future service:There is a recognition that neuro is under resourced, a cinderella serviceThere is a realisation they need to involve the local authority and personalisationThe third sector has been vital in keeping everything goingAs the plan is pan Dorset there have to be different models of delivery as some is rural and some urban
The plan:Looking at different models as the LIT too big - may be senior strategic commissioning managers feeding in to relevant sub Groups that feed into LIT. Chairs of the sub Groups = the LIT. Each sub group to be condition specific to see where they are with the NSF. Will be firming up TORs to ensure all groups are the same. There are programme leads, one of which is LTC. They are 'bunching up' groups of conditions with groups involving contract managers, local authority etc to look at commonalities and tie into the NSF.

Locality discussions: Table 4
Is the VCS involved: They are actively engaging with everyone to write a service specification. Patients are to be involved in the writing of the commissioning spec. They are feeding in what they want so they feel involved and valued!! They feel the are working well with the VCS etc but there is always room for improvement!
Network:When we discussed the Network idea we did not get very far as Dorset feels it really does not fit in the region very easily and they work closely with Hampshire in the South East. Their commissioners feed in to Southampton, there is no specialist unit in the county so they work with them.They feel any network should be local as any bigger gets too big and cumbersome.

Locality discussions: Table 5
Local leaders are health and social care teams in each locality. Names given
No local vision yet – meeting being held on 15/05/09 Voluntary sector and services users and carers are involved, but also
need well-publicised contact at Wiltshire Council Do not need any help to engage with the voluntary sector
Networks are a good idea, but capacity is a big issue. We all have existing networks
Within Wilts/Swindon, a neuro sub-group is being considered This would bring health and social care planning together and would
look at the big picture Could SWANO be developed into a network? Or could it support a
Wiltshire network?

Locality discussions: Table 6 Leadership Lack of link with people working on the frontline and commissioners No integrated records between health, intermediate car Review by PCT but did not involve frontline staff, public invited, but no
feedback Lack of coordination between acute and primary Care Services Improvement
Partnership no sharing of information so communication is difficult MND coordination driven by MND association Review of stroke services involved service users and carers and voluntary
organisation Need to avoid tokenism Changes recently introduced need to bed down before further action is
taken
Network good idea, either at PCT level, or north and south of the region, regionally to influence future commissioning
Network would give the opportunity for local bottom up approach – there has been a user engagement event for a neurological review, but need to include clinicians perspective. We are all leaders but needs coordination
PCTS/PCOs will be future commissioners so align in some way for future funding

Locality discussions: Table 7
Ensure region meet specialist needs Joint transition group in Torbay Only professionals working in joint services know their leaders (or providers) But external organisations find it difficult to find out who to approach, have to enquire and
may get passed around Difficulty with cross PCT work There is some vision and there are some plans Larger representative groups have specialist commissioning but the commissioning is the
difficult part of planning and providing services Torbay has projects in attempt to join up planning Devon is still subject to reorganisation/ vacant posts/ funding problems etc. Finance battles between health and social services are less in Torbay No involvement of services users and carers yet. Parkinson’s, service users involved in the
recruitment of specialist nurses Devon: re establishing itself to involve service users again after a review, now on the
agenda Concern about voluntary organisations creating specialist posts which are time limited.
PCTs have to have commitment to continue funding posts, no guarantees in place. People need training and devlopment to be consulted/ engaged, to make views valid to the
process. There are ‘professional’ users who are consulted too regularly. PCTs go to clinicians for people to approach – may not have necessary experiences about services that are, or should be, available
What needs to be commissioned nationally and those locally is an issue. Both should exist

Locality discussions: Table 7
Network is a problem – current groups exist, not covering all south west, or only certain conditions, needs to be all inclusive
Lots of good work overlaps, perhaps needs to be local, feeding into sub regional then regional
Local people should be used with regional representatives at regional level
Time is limited, problem with time being allocated Education and connexions need to be included People should be nominated by their organisation to demonstrate
commitment . People should identify key players in the region otherwise it will be the
usual professionals. May need core membership, but bring in others as planning needs arise
Suggested name SW Neuro-alliance Network (SW NAN)