Embed Size (px)
Citation preview

Volume 356 — April 12, 2007 — Number 15 ( pp. 1493-1596 )
Article Summaries
Tobacco Tightrope — Balancing Disease Prevention and Economic Development in China
A. A. Wright and I. T. Katz
Making Smoking History Worldwide
H. K. Koh, L. X. Joossens, and G. N. Connolly
Focus on Research: Diabetes Treatment — Bridging the Divide
K. I. Rother
Optimal Medical Therapy with or without PCI for Stable Coronary Disease
W. E. Boden and Others
Interleukin-1–Receptor Antagonist in Type 2 Diabetes Mellitus
C. M. Larsen and Others
Radiotherapy for Glioblastoma in the Elderly
F. Keime-Guibert and Others
Randomized, Placebo-Controlled Trial of Inactivated Poliovirus Vaccine in Cuba
The Cuba IPV Study Collaborative Group
Medical Progress: Strategies for Safer Liver Surgery and Partial Liver Transplantation
P.-A. Clavien, H. Petrowsky, M. L. DeOliveira, and R. Graf

Liver Transplantation for Polycystic Liver Disease
W. J. Wall
Gravid Uterus in an Incisional Hernia
C. Chanana and N. Malhotra
Case 11-2007 — A 59-Year-Old Man with Neck Pain, Weakness in the Arms, and Cranial-Nerve Palsies
D. M. Greer and Others
Does Preventive PCI Work?
J. S. Hochman and P. G. Steg Extract | Full Text | PDF
Clinical Trials in the Elderly — A Concept Comes of Age
L. L. Siu
Retinal Progenitor Cells — Timing Is Everything
J. Bennett
Sunitinib and Hypothyroidism
Trial Registration
Five-Gene Signature in Non–Small-Cell Lung Cancer
Childhood Progression of Hereditary Medullary Thyroid Cancer
Autoimmune Pancreatitis
Primary Percutaneous Coronary Intervention
Effects of Dietary Nitrate on Blood Pressure
Fatal Reactivation of Hepatitis B with Temozolomide

The Ghost Map: The Story of London's Most Terrifying Epidemic — And How It Changed Science, Cities, and the Modern World The Strange Case of the Broad Street Pump: John Snow and the Mystery of Cholera
Pioneers in Surgical Gastroenterology
Journey into the Heart: A Tale of Pioneering Doctors and Their Race to Transform Cardiovascular Medicine

Perspective
The NEW ENGLAND JOURNAL of MEDICINE
april 12, 2007
n engl j med 356;15 www.nejm.org april 12, 2007 1493
live in China — more than in the United States and all European countries combined. The World Health Organization (WHO) pre-dicts that 70% of the deaths from smoking-related illnesses will oc-cur in low- and middle-income countries by 2020. Smoking is likely to have a particularly dev-astating effect on China, where the annual death toll from smok-ing-related diseases already ex-ceeds 1 million — 2.5 times that in the United States — and is ex-pected to double by 2025 if smok-ing rates are not reduced.1 The ripple effects are painfully visible: because China has no national health care system and little pri-vate health insurance, many Chi-
nese people go bankrupt taking care of sick family members. “With other health problems,” says Kath-ryn Mulvey, executive director of the nonprofit organization Corpo-rate Accountability International, “you’ve got rats or mosquitoes, but in this case the tobacco industry is the vector of disease.”
The Chinese tobacco epidemic will soon encounter some new re-sistance — oddly enough, from the owner of the largest cigarette monopoly in the world: the Chi-nese government. In 2005, China ratified the WHO Framework Con-vention on Tobacco Control. To date, 145 countries, representing more than 80% of the world’s pop-ulation, have ratified this first in-
ternational public health treaty, which took effect in February 2005 (see map). The treaty aims to reg-ulate tobacco companies’ actions, using proven strategies: raising taxes on tobacco products, lim-iting smoking in public, requiring new health warnings on ciga-rette packages, and regulating the firms’ manufacturing and market-ing efforts.
China’s surprising decision to ratify the treaty has won it influ-ential friends in the global to-bacco-control community. One in-ternational program that will be investing heavily in China is the new $125 million Bloomberg Global Initiative to Reduce Tobac-co Use, funded by New York City Mayor Michael Bloomberg. Bloom-berg has tapped Judith Mackay, a Hong Kong–based physician and senior policy advisor to the WHO, to help coordinate his efforts. Mackay’s longtime leadership in
Tobacco Tightrope — Balancing Disease Prevention and Economic Development in ChinaAlexi A. Wright, M.D., and Ingrid T. Katz, M.D., M.H.S.
During the past 20 years, as smoking rates have fallen in high-income countries, the tobacco
industry has found new and bigger markets in the developing world. One third of current smokers

PERSPECTIVE
n engl j med 356;15 www.nejm.org april 12, 20071494
the fight against transnational tobacco companies has earned her the fear of such major players as British American Tobacco, which once named her one of the three most dangerous people in the world. She was instrumental in crafting the WHO treaty, and she will now be able to help Asian countries implement it. Because the Bloomberg initiative has doubled the available funding for tobacco control in low- and middle-income countries at this critical moment, many people see it as a crucial catalyst for translating international law into action.
Although sobering statistics have turned many low- and mid-dle-income countries into advo-cates of strict regulation, some wealthier countries, such as the United States, have remained am-bivalent. Throughout the 4 years
of negotiations preceding the World Health Assembly’s unani-mous adoption of the treaty in 2005, U.S. objections were often closely aligned with the interests of the tobacco industry. “In the third round of negotiations, Philip Morris prepared a wish list for the treaty, and the Bush administra-tion took 10 out of 11 of their positions,” said Mulvey. “The Unit-ed States fought tooth and nail against a ban on tobacco adver-tising and sponsorship. It was re-ally clear that a few wealthy na-tions with close ties to the tobacco industry were holding back coun-tries that wanted to embrace strong policies.”
Other observers, including Derek Yach, former head of the WHO’s tobacco-control initiative, argue that the position of the Unit-ed States is much more complex. It’s easy to blame the conservative
Bush administration, “but the United States has always been wary of international treaties,” Yach explains. During negotia-tions, “there was a constant ten-sion between the State Department, which wanted less engagement, and the Health Department, which wanted more.”
In 2004, Secretary of Health and Human Services Tommy Thompson announced that the United States had adopted the treaty without reservation, but Congress has yet to ratify it. Some say the State Department has pre-vented congressional debate on the treaty by holding it hostage “un-der review”: approval by two thirds of the Senate is required for rat-ification, but the Bush adminis-tration hasn’t sent the treaty to the Senate for a vote. Matt Myers, president of the Campaign for Tobacco-Free Kids, an advocacy
Tobacco Tightrope — Balancing Disease Prevention and Economic Development in China
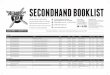
Countries That Are Party to the WHO’s Framework Convention on Tobacco Control.
Data are from the WHO.

n engl j med 356;15 www.nejm.org april 12, 2007
PERSPECTIVE
1495
organization and partner in the Bloomberg initiative, argues that special interests have intervened: “A majority of members of both the House and Senate are support-ive of tobacco-control efforts. That leaves the unmistakable impres-sion that the Bush administration is simply giving in to pressure from tobacco companies.”
Ironically, many poorer coun-tries that, like China, rely on to-bacco for economic growth have ratified the treaty. When China joined the World Trade Organiza-tion in 2001, it obtained a special exemption to maintain its monop-oly, China National Tobacco, which produces 1.8 trillion cigarettes an-nually.2 Although China agreed, in principle, to phase out quotas on imports, it also began a radi-cal restructuring of its industry, centralizing manufacturing, lim-iting the number of brands in an effort to build brand loyalty, and quietly expanding its sales abroad.3 As international pressure to cut tobacco use mounts, the Chinese
government struggles to balance advancing the country’s econo-my with maintaining the health of its society and garnering global support.
In 2005, cigarette sales gener-ated $32.5 billion in taxes and profits in China, approximately 7.6% of the government’s total revenue. In contrast, the govern-ment spent $31,000 on tobacco control. Tobacco remains a pillar of the Chinese economy: consum-ers spend more on cigarettes than on alcohol or personal care prod-ucts. Moreover, tobacco is seen as key to economic growth in the more remote, poorer sections of the country, such as Yunnan prov-ince, whose government depends on tobacco sales for more than 50% of its revenues.
The health effects of smoking are commonly downplayed in Chi-na, even by those in key political positions. Half of all male Chi-nese doctors smoke, as do some politicians. Even a few Chinese tobacco-control advocates express
mixed feelings about promoting the use of graphic warning labels on cigarette packages, recognizing that ugly pictures would mar the packs traditionally given as pres-ents to wedding guests.
At the same time, tobacco-control experts fear that Chinese women and children will begin to smoke if transnational tobacco manufacturers gain a foothold in the country. Currently, only 3% of women and 10% of middle-school children smoke, but international manufacturers are already target-ing these populations. Mulvey of Corporate Accountability Interna-tional argues that tobacco com-panies are manipulating Western images of independence to seduce teenagers and increasingly liber-ated women in developing coun-tries. Such marketing can be frighteningly effective: when South Korea opened its markets to Amer-ican cigarettes, the rate of smok-ing among teenage girls quintu-pled in 1 year, and the rate among adolescent boys doubled.4 Billions of foreign cigarettes are already smuggled into China each year, but recently, candy-flavored cig-arettes have become one of the most popular illegal imports. Pub-lic health experts describe these as “starter cigarettes” aimed at children. As a competing manu-facturer, China has already re-sponded by producing its own fruit-f lavored cigarettes.
Western tobacco companies have been eager to make further inroads into China’s market. In 2005, Philip Morris joined forces with China National Tobacco to market Marlboro cigarettes in the country. Other brands, such as Camel, Lucky Strike, and Kool, have also been sold. Although for-eign brands have garnered only 3% of the Chinese market, that
Tobacco Tightrope — Balancing Disease Prevention and Economic Development in China
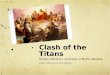
Packs of Chinese Cigarettes Made for Export to Australia, which Requires Graphic Warnings (Left), and for Sale in China, which Currently Does Not (Right).
Dam
on M
ogle
n, C
ampa
ign
for
Toba
cco-
Free
Kid
s.

PERSPECTIVE
n engl j med 356;15 www.nejm.org april 12, 20071496
amounts to 51 billion cigarettes per year.
By signing on to the WHO’s mandate, China agreed that by 2008, clear health warnings would occupy more than 30% of the sur-face of every cigarette pack sold. It is already technically illegal in China to promote tobacco on bill-boards or in magazines, and all forms of advertising will be banned by 2010. There are also plans for a “smoke-free Olympics” in 2008, and some tobacco-control advo-cates hope that the cities hosting the Olympics will become smoke-free forever. Hong Kong has al-ready outlawed smoking in pub-lic places, as of January 2007.
Some skeptics fear that it may be too late to quell the tobacco epidemic in many developing countries. Even the most optimis-tic observers recognize that it will take at least a generation of hard work to see real change. In the meantime, millions more people will lose their lives to tobacco-related diseases, and low-income countries will need to come to grips with the devastation that tobacco can wreak.
An interview with Dr. Steven Schro-eder, director of the Smoking Cessa-tion Leadership Center at the Univer-sity of California, San Francisco, can be heard at www.nejm.org.
Dr. Wright is a fellow in hematology–oncol-ogy at the Dana–Farber Cancer Institute, Boston, and Dr. Katz is a fellow in infectious disease at the Beth Israel Deaconess Medi-cal Center, Boston.
Hu T-W, Mao Z, Ong M, et al. China at the crossroads: the economics of tobacco and health. Tob Control 2006;15:Suppl 1:i37-i41.
Mackay J, Eriksen M, Shafey O. The to-bacco atlas. 2nd ed. Atlanta: American Can-cer Society, 2006.
Fell J, Khoo E, Adelman D. Tobacco indus-try overview: China: the final frontier. New York: Morgan Stanley Equity Research, July 26, 2005.
Taylor A, Chaloupka F, Guindon E, et al. The impact of trade liberalization on tobacco consumption. In: Jha P, Chaloupka FJ, eds. Tobacco control in developing countries. Ox-ford, England: Oxford University Press, 2000: 343-64.Copyright © 2007 Massachusetts Medical Society.
1.
2.
3.
4.
Tobacco Tightrope — Balancing Disease Prevention and Economic Development in China
Making Smoking History WorldwideHoward K. Koh, M.D., M.P.H., Luk X. Joossens, M.A., and Gregory N. Connolly, D.M.D., M.P.H.
It seemed impossible at first. But in 2004, Ireland made his-
tory as the first country to im-plement a comprehensive smoking ban in indoor workplaces, includ-ing restaurants and bars. Defying dire predictions, Ireland’s policy has proved to be both popular and enforceable, with ready compli-ance,1 no decline in business, and improved health outcomes for hos-pitality workers. Overwhelming public support for the ban has come from smokers and nonsmok-ers alike, dispelling the belief that restaurants and bars should rep-resent bastions of smoking and socialization. For a country tra-ditionally known for its smoke-filled pubs, the new societal stan-dard represents a breathtaking (or breath-enhancing) revolution.
Historians may someday view Ireland’s bold move as a tipping point for global public health.
Previous actions worldwide had stemmed from mounting scien-tific evidence, summarized most recently in the 2006 U.S. Surgeon General’s report,2 confirming that exposure to secondhand smoke leads to premature death and dis-ease, including lung cancer and ischemic heart disease. For exam-ple, in 1998, California became the first U.S. state to adopt smoke-free policies for all restaurants and bars. South Africa passed national laws in 2000 making public places smoke-free, although exemptions for bars and restaurants were al-lowed. Most recently, the Bloom-berg Global Initiative to Reduce Tobacco Use has been funded by New York City Mayor Michael Bloomberg with the aim of re-ducing tobacco use in low- and middle-income countries.
When Ireland enacted its smoke-free policy, startled observ-
ers wondered whether other coun-tries would follow suit. The answer came within months, when New Zealand successfully implemented a comprehensive ban. Global mo-mentum has since accelerated, with a host of additional countries enacting policies within a few years (see map). Most smoke-free countries are in Europe (although a number of these countries allow for the possibility of a designat-ed, enclosed, ventilated smoking room). But other continents have seen activity as well: Australia and Canada are poised to join the group, and a growing number of countries are considering legis-lation. Though the United States lacks a federal policy, 17 states and dozens of municipalities are rec-ognized as having smoke-free pub-lic places.
Furthermore, the 2003 World Health Organization Framework

n engl j med 356;15 www.nejm.org april 12, 2007
PERSPECTIVE
1497
Convention on Tobacco Control (FCTC) has galvanized commit-ment. This first international pub-lic health treaty calls for countries to adopt clean-air policies, as well as initiatives such as price and tax increases, advertising bans, and warning labels for tobacco pack-ages. (However, since the FCTC’s language regarding smoke-free places leaves room for partial re-strictions that may not protect public health, Ireland’s compre-hensive approach should serve as a model.) To date, 145 countries have ratified this treaty, but the United States is not among them.
Policies requiring clean indoor air have already improved public health. Studies in the United States, Scotland, Norway, and New Zea-land, like those in Ireland, dem-
onstrate benefits such as improve-ments in the respiratory health of hospitality workers. Overall, in-door smoking bans have been as-sociated with a 3.8% reduction in the prevalence of smoking.3 Pop-ular support for smoke-free bars and restaurants increases after such legislation passes, because clean-air environments become viewed as those most conducive to leisure-time enjoyment.
In short, the world has begun to reclaim clean air as the social norm. For too long, the tobacco industry has spent billions to nor-malize, market, and glamorize a behavior that is now recognized as a tragic drug addiction. Indus-try marketing has fueled global consumption exceeding 5 trillion cigarettes annually, leading to
100 million deaths in the 20th century and a billion deaths pro-jected for the century ahead.4 Fur-thermore, evidence points to sys-tematic increases in nicotine yields from cigarettes marketed in the United States in recent years. Fun-damental to industry success is the portrayal of smoking as a desir-able way of staying “alive with pleasure.” Now, however, entire countries have begun to deglam-orize and denormalize this ad-diction.
Fundamental shifts in social norms never come easily, however. These gains have materialized only after decades of committed lead-ership in public health practice bridging the worlds of science, government, politics, advocacy, and other arenas. Examination of
Making Smoking History Worldwide
Countries, States, and Provinces That Have Banned Smoking in Indoor Workplaces and Other Indoor Public Places.
Legislation in some countries and regions (shown in green) allows for the possibility of a designated, enclosed, ventilated smoking room. Full bans are also in force in Rhode Island, Hawaii, Puerto Rico, Washington, DC, Bermuda, the British Virgin Islands, Bhutan, and the Australian Capital Territory; legislation allowing for designated smoking rooms is in force in Malta. Full bans will go into effect in Quebec in 2008 and in Montana, Utah, and Hong Kong in 2009; a law allowing for the possibility of designated smoking rooms will go into effect in Finland in 2009.

PERSPECTIVE
n engl j med 356;15 www.nejm.org april 12, 20071498
the inner workings of successful initiatives reveals some critical lessons. In Ireland, the ban suc-ceeded with support from govern-ment and opposition parties, health care organizations, trade unions, public health advocates, and oth-ers. In New Zealand, the forces of science, public health advocacy, and public education also con-verged to advance legislation. In Bhutan, Buddhism was the cul-tural backdrop for a smoke-free policy that includes the world’s only national ban on the sale of tobacco. In Uruguay, a national smoking ban was strongly sup-ported by the president, an on-cologist. In many countries, pri-vate businesses, including hotel chains, have instituted smoke-free environments for customers and employees alike.
Changing social norms requires perseverance. Some countries have passed partial smoking bans as part of a strategy for transition-ing toward comprehensive bans. France, after partially restricting smoking in bars and restaurants in 1991 but not enforcing the law, is currently phasing in a ban to be completed in 2008, backed up by a social marketing campaign, an enormous cadre of agents for enforcement, and fines for non-compliance. Change also entails confronting unfounded econom-ic arguments: although critics reg-ularly assail smoking bans for hurting business, more than 20 high-quality studies have shown no negative economic effect of smoke-free policies on restaurants and bars.5
Such fundamental social chang-es threaten the tobacco industry, which has a record of nimbly re-sponding to market pressures. Over time, manufacturers have carefully cultivated market share by targeting children, members of minority groups, women, and in-creasingly, new customers in the developing world. To curry con-sumer acceptance, they not only have added chemicals to mask smoke’s odor but also have in-stituted myriad design changes involving filters, ventilation sys-tems, “light” and “low-tar” ciga-rettes, and “potential reduced-exposure products.” In addition, they are now actively marketing smokeless tobacco products, no doubt partly in response to the in-creasing number of smoke-free en-vironments. And all products are marketed in the complete absence of product regulation.
Given these developments, the world’s nearly 1.3 billion smokers deserve heightened support. Stud-ies indicate that most smokers want to quit but are unable to do so. Smoke-free policies remove the social stimuli that promote re-lapse, motivating smokers to de-crease consumption and quit. But battling this addiction also re-quires better systems of care, in-cluding behavioral modification, counseling, pharmacologic inter-ventions, telephone “quit lines,” and other services. Providing ac-cess to such resources, a challenge in high-income countries, is even more daunting in the developing world. Furthermore, since the ad-diction disproportionately burdens
those of lower socioeconomic sta-tus, tobacco control must rank as a prime focus of global efforts to eliminate health disparities.
The first few years of the 21st century have made possible what was once considered impossible. In the face of an escalating pan-demic, a global haze may be start-ing to lift. We are witnessing a public health evolution in which the once-extraordinary is rapidly becoming the social norm. Mak-ing smoking history moves us closer to reaffirming the right to the highest standard of human health for all.
Dr. Koh is a professor of the practice of pub-lic health and an associate dean, and Dr. Connolly is a professor of the practice of public health, at the Harvard School of Pub-lic Health, Boston. Mr. Joossens is an offi-cer of the Association of European Cancer Leagues, Brussels.
Fong GT, Hyland A, Borland R, et al. Re-ductions in tobacco smoke pollution and in-creases in support for smoke-free public places following the implementation of com-prehensive smoke-free workplace legislation in the Republic of Ireland: findings from the ITC Ireland/UK Survey. Tob Control 2006;15:Suppl 3:iii51-iii58.
The health consequences of involuntary exposure to tobacco smoke: a report of the Surgeon General — executive summary. Rockville, MD: Department of Health and Human Services, 2006.
Fichtenberg CM, Glantz SA. Effect of smoke-free workplaces on smoking behav-iour: systematic review. BMJ 2002;325:188.
Mackay J, Eriksen M, Shafey O. The to-bacco atlas. 2nd ed. Atlanta: American Can-cer Society, 2006.
Scollo M, Lal A, Hyland A, Glantz S. Re-view of the quality of studies on the econom-ic effects of smoke-free policies on the hos-pitality industry. Tob Control 2003;12:13-20.Copyright © 2007 Massachusetts Medical Society.
1.
2.
3.
4.
5.
Making Smoking History Worldwide

n engl j med 356;15 www.nejm.org april 12, 2007
PERSPECTIVE
1499
In the simplest terms, diabetes mellitus results when pancreat-
ic beta cells are unable to main-tain adequate insulin secretion to prevent hyperglycemia. A combi-nation of genetic and environmen-tal factors causes the underlying beta-cell failure. In type 1 diabe-tes, a T-cell–mediated autoimmune response against beta cells appears to be the main disease mecha-nism, whereas insulin resistance is the key metabolic abnormality in type 2 diabetes. Yet the way in which insulin resistance triggers beta-cell failure remains obscure. The report by Larsen et al. in this issue of the Journal (pages 1517–1526) provides insight into a shared mechanism of beta-cell dysfunction in type 1 diabetes and type 2 diabetes and suggests a new therapeutic approach to type 2 dia-betes. The authors report that anakinra, a receptor antagonist of the inflammatory cytokine inter-leukin-1, which has long been im-plicated in beta-cell damage in type 1 diabetes, improved blood glucose control and insulin secre-tion in patients with type 2 diabe-tes. This agent also reduced mark-ers of systemic inflammation.
For many years, attempts to distinguish different types of di-abetes have been associated with changing definitions that reflect the state of our knowledge. Terms have changed from juvenile and adult diabetes to insulin-dependent and non-insulin-dependent diabe-tes and finally to type 1 and type 2 diabetes. In addition, there are several intermediate forms, such
as latent autoimmune diabetes in adults, or “type 1.5.” The genetic determinants of the two main forms of diabetes are distinct. Type 1 diabetes is strongly asso-ciated with certain HLA haplo-types, a link that supports the notion that this condition is pri-marily an autoimmune disease. In type 2 diabetes, examples of candidate genes are KCNJ11 (po-tassium inwardly rectifying chan-nel, subfamily J, member 11), which encodes the islet ATP-sensitive potassium channel Kir6.2, and TCF7L2 (transcription factor 7–like 2), which regulates proglucagon gene expression and thus the production of glucagon-like pep-tide 1.
It has become clear that the effectors of beta-cell failure are similar in the two main types of diabetes, regardless of the incit-ing event (see illustration). Glu-cotoxicity and lipotoxicity induce oxidative stress and up-regulate inflammatory cytokines, thereby leading to cellular damage and promoting apoptosis in all beta cells, regardless of the type of diabetes. Recently, abnormal islet innervation has been described as another common contributing el-ement in animal models of type 1 and type 2 diabetes. Thus, al-leviating beta-cell stress opens the door to therapeutic approaches that would probably be useful in all types of diabetes.
An example is treatment with anakinra, a recombinant version of the naturally occurring human interleukin-1–receptor antagonist
that blocks the effects of inter-leukin-1α and β.1 Both forms of interleukin-1, which are produced by many cells (e.g., lymphocytes, endothelial cells, adipocytes, and beta cells), play important roles in host defense but also can induce fever, anorexia, hypotension, car-tilage destruction, and beta-cell apoptosis. Treatment with inter-leukin-1–receptor antagonist was approved by the Food and Drug Administration for rheumatoid ar-thritis in 2001. The drug has also been shown to alleviate symptoms in neonatal-onset multisystem inflammatory disease. Generally, few side effects have been ob-served, but one death from car-diac causes was recently reported in a patient with Still’s disease (systemic-onset juvenile rheuma-toid arthritis) shortly after the ini-tiation of anakinra therapy.2
The value of the observations reported by Larsen et al. goes be-yond the specific role of the in-terleukin-receptor antagonist. An important consideration is that although the role of “smoldering” inflammation in the pathogenesis of insulin resistance is well es-tablished, its relevance to mech-anisms of beta-cell dysfunction and death is poorly understood.3 In this respect, the study by Lars-en et al. raises an interesting point. The authors report a modest im-provement in insulin secretion, along with a sharp drop in the levels of C-reactive protein and in-terleukin-6. Although the authors do not favor this interpretation, the response to anakinra might
Diabetes Treatment — Bridging the Divide
FOCUS ON RESEARCH
Diabetes Treatment — Bridging the DivideKristina I. Rother, M.D.
Related article, page 1517

PERSPECTIVE
n engl j med 356;15 www.nejm.org april 12, 20071500
also be attributable to mildly im-proved insulin sensitivity resulting from reduced systemic inflamma-tion. Such a conclusion is consis-tent with the demonstration that certain cytokines impair insulin
signaling and supports the con-cept that treating the underlying inflammation improves diabetes control, which is probably an as-pect of the beneficial effects of statins and glitazones.
Anakinra is not alone in bridg-ing the divide between disease mechanisms and appropriate treat-ments for the different types of diabetes. For example, some oral agents that are administered to improve insulin sensitivity in type 2 diabetes are also antiapoptotic (metformin) or have immune-modulatory effects (glitazones). Thus, these or similar drugs may find a place in the treatment of type 1 diabetes. There is growing interest in developing therapies that not only improve beta-cell function in the short term (con-trolling postprandial hyperglyce-mia, for example) but also pre-serve beta-cell mass or promote beta-cell regeneration. Two re-cently approved drugs (exenatide and sitagliptin) not only are in-sulinotropic but also promote beta-cell proliferation in rodents. It remains to be seen whether these effects occur in humans with diabetes as well. The basis of these new therapeutic approach-es is the identification of various molecular mechanisms of beta-cell failure and the recognition that beta cells have an innate abil-ity to replicate, albeit very slowly.4
A note of caution, however: anakinra treatment led to a mod-est improvement in the control of glycemia, with a maximal ef-fect at 4 weeks but with an up-ward trend in the glycated hemo-globin level at 13 weeks. Since the patients varied with respect to baseline blood-glucose control and type of concomitant treatment, it is difficult to deduce the effec-tiveness of anakinra therapy in various stages of disease. More-over, none of the currently avail-able medications (including the aforementioned oral agents) are successful as long-term mono-
Diabetes Treatment — Bridging the Divide
03/26/07
AUTHOR PLEASE NOTE:Figure has been redrawn and type has been reset
Please check carefully
Author
Fig #Title
ME
DEArtist
Issue date
COLOR FIGURE
Version 6Rother1
LAM
4/12/07
Diabetes
JRIMP
Pancreas
Diseased beta cell with decreased insulin secretion
Healthy but genetically susceptible beta cells
Interleukin-1– receptor antagonist
With no intervention,impaired self-repair and induction of apoptosis
Improved insulin secretion
Adipokines, viral infection, and other insults
Glucotoxicity, oxidative stress, proinflammatory cytokines (e.g., interleukin-1)
Adipokines, viral infection, and other insults
Glucotoxicity, oxidative stress, proinflammatory cytokines (e.g., interleukin-1)
Development of Diabetes.
In the upper part of the diagram, a beta cell receives a primary insult. It is not known whether this insult is identical in type 1 diabetes and type 2 diabetes but leads to dif-ferent responses because of variations in genetic susceptibility. The currently accepted view is that an immune-mediated insult leads to the primary beta-cell dysfunction in type 1 diabetes, whereas a different, unknown insult causes type 2 diabetes. Once injured, beta cells have a similar fate in the two types of diabetes. Glucotoxicity, oxida-tive stress, and cytotoxic cytokines lead to further damage, which eventually results in beta-cell death if the process is not countered by effective self-repair and therapeutic interventions.

n engl j med 356;15 www.nejm.org april 12, 2007
PERSPECTIVE
1501
therapy, and none of them have effectively halted the continuous decline in beta-cell mass. Although the findings regarding anakinra break new ground by demonstrat-ing that inhibition of cytokine function can restore insulin se-cretion, the ultimate goal is the improvement of blood-glucose control without the need for tri-ple- and quadruple-combination therapies, as well as the preven-tion of beta-cell death.
In the first century b.c., Pub-lilius Syrus declared, “Better use medicines at the outset than at the last moment.” His recommenda-tion may serve as a motto for our continued search for an optimal remedy for diabetes.
Dr. Rother is an attending physician and principal investigator in the Clinical Endo-crinology Branch, National Institute of Dia-betes and Digestive and Kidney Diseases, Bethesda, MD.
Perrier S, Darakhshan F, Hajduch E. IL-1 1.
receptor antagonist in metabolic diseases: Dr Jekyll or Mr Hyde? FEBS Lett 2006;580: 6289-94.
Ruiz PJ, Masliah E, Doherty TA, Quach A, Firestein GS. Cardiac death in a patient with adult-onset Still’s disease treated with the interleukin 1 receptor inhibitor anakinra. Ann Rheum Dis 2007;66:422-3.
Hotamisligil GS. Inflammation and meta-bolic disorders. Nature 2006;444:860-7.
Meier JJ, Bhushan A, Butler AE, Rizza RA, Butler PC. Sustained beta cell apoptosis in patients with long-standing type 1 diabetes: indirect evidence for islet regeneration? Dia-betologia 2005;48:2221-8.Copyright © 2007 Massachusetts Medical Society.
2.
3.
4.
Diabetes Treatment — Bridging the Divide

n engl j med 356;15 www.nejm.org april 12, 20071502
original article
Optimal Medical Therapy with or without PCI for Stable Coronary Disease
In a randomized trial, 2287 patients with coronary ar-tery disease and evidence of ischemia were assigned to receive optimal medical therapy with or without percu-taneous coronary intervention (PCI). At a median of 4.6 years, the rates of death and myocardial infarction were 19.0% in the PCI group and 18.5% in the medical-therapy group. The PCI group had lower rates of angina and repeat revascularization.
See p. 1503; Editorial, P. 1572; CME, P. 1599
Original Article
Interleukin-1–Receptor Antagonist in Type 2 Diabetes Mellitus
The expression of interleukin-1–receptor antagonist is reduced in pancreatic islets in type 2 diabetes, and high glucose concentrations induce interleukin-1β pro-duction in human pancreatic beta cells, suggesting that the interleukin-1 pathway may be a treatment tar-get. This randomized trial showed that the interleu-kin-1–receptor antagonist anakinra (100 mg) improved glycemia and beta-cell secretory function and reduced markers of systemic inflammation, as compared with placebo.
See P. 1517; Perspective, P. 1499
Original Article
Radiotherapy for Glioblastoma in the Elderly
This trial compared radiotherapy plus supportive care with supportive care alone in patients with glioblastoma who were 70 years of age or older. As compared with supportive care alone, radiotherapy improved survival by about 3 months and did not impair quality of life or cognition. The trial also showed that, despite some chal-lenges, elderly patients can participate in a random-ized, controlled clinical trial.
See P. 1527; Editorial, P. 1575
Original Article
Inactivated Poliovirus Vaccine in Cuba
Limited data exist on the immunogenicity of inacti-vated poliovirus vaccine (IPV) in tropical developing countries. As the use of the oral poliovirus vaccine di-minishes, data demonstrating that IPV is effective in this setting are needed. This randomized, controlled trial of IPV in Cuba shows that IPV is immunogenic and diminishes the excretion of oral poliovirus in the stool after challenge with oral poliovirus vaccine.
See P. 1536
Medical Progress
Safer Liver Surgery and Partial Liver Transplantation
The liver possesses the unique ability to regenerate within a short period of time, a feature that has led to the development of innovative strategies in liver sur-gery and transplantation. This review presents both established and novel methods for manipulating liver volume to attain improved liver surgery and transplan-tation.
See P. 1545; CME, P. 1597
CASE RECORDS OF THE MASSACHUSETTS GENERAL HOSPITAL
A 59-Year-Old Man with Neck Pain, Weakness in the Arms, and Cranial-Nerve Palsies
A 59-year-old man was admitted to this hospital with fever and the subacute onset of progressive neuro-logic symptoms that included multiple cranial-nerve palsies. Magnetic resonance imaging of the brain and spine showed leptomeningeal enhancement. Analy-sis of the cerebrospinal fluid disclosed a lymphocytic pleocytosis and elevated protein and glucose levels. Respiratory failure developed, requiring intubation and mechanical ventilation. The result of a diagnostic test was received.
See P. 1561; CME, P. 1598
Clinical Implications of Basic Research
Repairing the Retina
Permitting progenitor photoreceptor cells from donors to differentiate before transplanting them is key to their successful integration into the retina.
See P. 1577

n engl j med 356;15 www.nejm.org april 12, 2007 1503
The new england journal of medicineestablished in 1812 april 12, 2007 vol. 356 no. 15
Optimal Medical Therapy with or without PCI for Stable Coronary Disease
William E. Boden, M.D., Robert A. O’Rourke, M.D., Koon K. Teo, M.B., B.Ch., Ph.D., Pamela M. Hartigan, Ph.D., David J. Maron, M.D., William J. Kostuk, M.D., Merril Knudtson, M.D., Marcin Dada, M.D., Paul Casperson, Ph.D.,
Crystal L. Harris, Pharm.D., Bernard R. Chaitman, M.D., Leslee Shaw, Ph.D., Gilbert Gosselin, M.D., Shah Nawaz, M.D., Lawrence M. Title, M.D., Gerald Gau, M.D., Alvin S. Blaustein, M.D., David C. Booth, M.D.,
Eric R. Bates, M.D., John A. Spertus, M.D., M.P.H., Daniel S. Berman, M.D., G.B. John Mancini, M.D., and William S. Weintraub, M.D., for the COURAGE Trial Research Group*
A BS TR AC T
Affiliations for all authors are listed in the Appendix. Address reprint requests to Dr. Boden at the Division of Cardiology, Buffalo General Hospital, 100 High St., Buffalo, NY 14203, or at [email protected].
*Members of the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial are listed in the Appendix and in the Supplementary Appendix, available with the full text of this article at www.nejm.org.
This article (10.1056/NEJMoa070829) was published at www.nejm.org on March 26, 2007.
N Engl J Med 2007;356:150316.Copyright © 2007 Massachusetts Medical Society.
Background
In patients with stable coronary artery disease, it remains unclear whether an initial management strategy of percutaneous coronary intervention (PCI) with intensive pharmacologic therapy and lifestyle intervention (optimal medical therapy) is superior to optimal medical therapy alone in reducing the risk of cardiovascular events.
Methods
We conducted a randomized trial involving 2287 patients who had objective evidence of myocardial ischemia and significant coronary artery disease at 50 U.S. and Cana-dian centers. Between 1999 and 2004, we assigned 1149 patients to undergo PCI with optimal medical therapy (PCI group) and 1138 to receive optimal medical therapy alone (medical-therapy group). The primary outcome was death from any cause and non-fatal myocardial infarction during a follow-up period of 2.5 to 7.0 years (median, 4.6).
Results
There were 211 primary events in the PCI group and 202 events in the medical-therapy group. The 4.6-year cumulative primary-event rates were 19.0% in the PCI group and 18.5% in the medical-therapy group (hazard ratio for the PCI group, 1.05; 95% confidence interval [CI], 0.87 to 1.27; P = 0.62). There were no significant differences between the PCI group and the medical-therapy group in the composite of death, myocardial infarction, and stroke (20.0% vs. 19.5%; hazard ratio, 1.05; 95% CI, 0.87 to 1.27; P = 0.62); hospitalization for acute coronary syndrome (12.4% vs. 11.8%; hazard ratio, 1.07; 95% CI, 0.84 to 1.37; P = 0.56); or myocardial infarction (13.2% vs. 12.3%; hazard ratio, 1.13; 95% CI, 0.89 to 1.43; P = 0.33).
Conclusions
As an initial management strategy in patients with stable coronary artery disease, PCI did not reduce the risk of death, myocardial infarction, or other major cardio-vascular events when added to optimal medical therapy. (ClinicalTrials.gov number, NCT00007657.)

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071504
During the past 30 years, the use of percutaneous coronary intervention (PCI) has become common in the initial man-
agement strategy for patients with stable coronary artery disease in North America, even though treat-ment guidelines advocate an initial approach with intensive medical therapy, a reduction of risk fac-tors, and lifestyle intervention (known as optimal medical therapy).1,2 In 2004, more than 1 million coronary stent procedures were performed in the United States,3 and recent registry data indicate that approximately 85% of all PCI procedures are undertaken electively in patients with stable cor-onary artery disease.4 PCI reduces the incidence of death and myocardial infarction in patients who present with acute coronary syndromes,5-10 but similar benefit has not been shown in patients with stable coronary artery disease.11-15 This issue has been studied in fewer than 3000 patients,16 many of whom were treated before the widespread use of intracoronary stents and current standards of medical management.17-28
Although successful PCI of flow-limiting ste-noses might be expected to reduce the rate of death, myocardial infarction, and hospitalization for acute coronary syndromes, previous studies have shown only that PCI decreases the frequency of angina and improves short-term exercise per-formance.11,12,15 Thus, the long-term prognostic effect of PCI on cardiovascular events in patients with stable coronary artery disease remains un-certain. Our study, the Clinical Outcomes Utiliz-ing Revascularization and Aggressive Drug Evalu-ation (COURAGE) trial, was designed to determine whether PCI coupled with optimal medical ther-apy reduces the risk of death and nonfatal myo-cardial infarction in patients with stable coro-nary artery disease, as compared with optimal medical therapy alone.
Me thods
Study Design
The methods we used in the trial have been de-scribed previously.29,30 Sponsorship and oversight of the trial were provided by the Department of Veterans Affairs Cooperative Studies Program. Additional funding was provided by the Canadian Institutes of Health Research. Supplemental cor-porate support from several pharmaceutical com-panies included funding and in-kind support. All
support from the pharmaceutical industry con-sisted of unrestricted research grants payable to the Department of Veterans Affairs.
The study protocol was approved by the hu-man rights committee at the coordinating center and by the local institutional review board at each participating center. An independent data and safety monitoring board oversaw the conduct, safe-ty, and efficacy of the trial. Data management and statistical analyses were performed solely by the data coordinating center with oversight by the trial executive committee, whose members, after un-blinding, had full access to the data and vouch for the accuracy and completeness of the data and the analyses. The companies that provided finan-cial support, products, or both had no role in the design, analysis, or interpretation of the study.
Study Population
Patients with stable coronary artery disease and those in whom initial Canadian Cardiovascular Society (CCS) class IV angina subsequently stabi-lized medically were included in the study. Entry criteria included stenosis of at least 70% in at least one proximal epicardial coronary artery and ob-jective evidence of myocardial ischemia (substan-tial changes in ST-segment depression or T-wave inversion on the resting electrocardiogram or in-ducible ischemia with either exercise or pharma-cologic vasodilator stress) or at least one coronary stenosis of at least 80% and classic angina with-out provocative testing. Exclusion criteria included persistent CCS class IV angina, a markedly posi-tive stress test (substantial ST-segment depression or hypotensive response during stage 1 of the Bruce protocol), refractory heart failure or cardio-genic shock, an ejection fraction of less than 30%, revascularization within the previous 6 months, and coronary anatomy not suitable for PCI. A de-tailed description of the inclusion and exclusion criteria is included in the Supplementary Appen-dix (available with the full text of this article at www.nejm.org). Patients who were eligible for the study underwent randomization after providing written informed consent.
Treatment
Patients were randomly assigned to undergo PCI and optimal medical therapy (PCI group) or opti-mal medical therapy alone (medical-therapy group). A permuted-block design was used to generate

Optimal Medical Ther apy with or without PCI for Stable Coronary Disease
n engl j med 356;15 www.nejm.org april 12, 2007 1505
random assignments within each study site along with previous coronary-artery bypass grafting (CABG) as a stratifying variable. All patients re-ceived antiplatelet therapy with aspirin at a dose of 81 to 325 mg per day or 75 mg of clopidogrel per day, if aspirin intolerance was present. Patients undergoing PCI received aspirin and clopidogrel, in accordance with accepted treatment guidelines and established practice standards. Medical anti-ischemic therapy in both groups included long-acting metoprolol, amlodipine, and isosorbide mononitrate, alone or in combination, along with either lisinopril or losartan as standard second-ary prevention. All patients received aggressive therapy to lower low-density lipoprotein (LDL) cholesterol levels (simvastatin alone or in combi-nation with ezetimibe) with a target level of 60 to 85 mg per deciliter (1.55 to 2.20 mmol per liter). After the LDL cholesterol target was achieved, an attempt was made to raise the level of high-den-sity lipoprotein (HDL) cholesterol to a level above 40 mg per deciliter (1.03 mmol per liter) and lower triglyceride to a level below 150 mg per deciliter (1.69 mmol per liter) with exercise, extended-release niacin, or fibrates, alone or in combination.
In patients undergoing PCI, target-lesion revas-cularization was always attempted, and complete revascularization was performed as clinically ap-propriate. Success after PCI as seen on angiogra-phy was defined as normal coronary-artery flow and less than 50% stenosis in the luminal diam-eter after balloon angioplasty and less than 20% after coronary stent implantation, as assessed by visual estimation of the angiograms before and after the procedure. Clinical success was defined as angiographic success plus the absence of in-hospital myocardial infarction, emergency CABG, or death. Drug-eluting stents were not approved for clinical use until the final 6 months of the study, so few patients received these intracoronary devices.
Clinical Outcome
Clinical outcome was adjudicated by an indepen-dent committee whose members were unaware of treatment assignments. The primary outcome mea-sure was a composite of death from any cause and nonfatal myocardial infarction. Secondary out-comes included a composite of death, myocardial infarction, and stroke and hospitalization for un-stable angina with negative biomarkers. The an-
gina status of patients was assessed according to the CCS classification during each visit. Further analyses of other secondary outcomes — includ-ing quality of life, the use of resources, and cost-effectiveness — are being conducted but have not yet been completed.
The prespecified definition of myocardial in-farction (whether periprocedural or spontaneous) required a clinical presentation consistent with an acute coronary syndrome and either new ab-normal Q waves in two or more electrocardio-graphic leads or positive results in cardiac bio-markers. Silent myocardial infarction, as detected by abnormal Q waves, was confirmed by a core laboratory and was also included as an outcome of myocardial infarction.
Statistical Analysis
We projected composite 3-year event rates of 21.0% in the medical-therapy group and 16.4% in the PCI group (relative difference, 22%) during a follow-up period of 2.5 to 7.0 years. We also incorporated assumptions about crossover between study groups and loss to follow-up.31 We estimated that the en-rollment of 2270 patients would provide a power of 85% to detect the anticipated difference in the primary outcome at the 5% two-sided level of significance. A detailed description of the sam-ple-size calculation is included in the Supplemen-tary Appendix.
Estimates of the cumulative event rate were calculated by the Kaplan–Meier method,32 and the primary efficacy of PCI, as compared with optimal medical therapy, was assessed by the stratified log-rank statistic.33 The treatment ef-fect, as measured by the hazard ratio and its associated 95% confidence interval (CI), was esti-mated with the use of the Cox proportional-haz-ards model.34 Data for patients who were lost to follow-up were censored at the time of the last contact. Analyses were performed according to the intention-to-treat principle. Categorical variables were compared by use of the chi-square test or the Wilcoxon rank-sum test, and continuous vari-ables were compared by use of the Student t-test. Adjusted analysis of the primary outcome was performed with the use of a Cox proportional-hazards regression model with eight preidentified covariates of interest — age, sex, race, previous myocardial infarction, extent or distribution of angiographic coronary artery disease, ejection frac-

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071506
tion, presence or absence of diabetes, and health care system (Veterans Affairs or non–Veterans Affairs facility in the United States, or a Canadian facility) — as well as the stratifying variable of previous CABG. All other comparisons were un-adjusted. A level of significance of less than 0.01 was used for all subgroup analyses and interac-tions.
R esult s
Baseline Characteristics and Angiographic Data
Between June 1999 and January 2004, a total of 2287 patients were enrolled in the trial at 50 U.S. and Canadian centers (Fig. 1). Of these patients, 1149 were randomly assigned to the PCI group and 1138 to the medical-therapy group. The base-line characteristics of the patients were recently published35 and were similar in the two groups (Table 1). The median time from the first episode of angina before randomization was 5 months (median, three episodes per week, with exertion or at rest), and 58% of patients had CCS class II or III angina. A total of 2168 patients (95%) had ob-jective evidence of myocardial ischemia, whereas the remaining 119 patients with classic angina (CCS class III) and severe coronary stenoses did not undergo ischemia testing (56 in the PCI group and 63 in the medical-therapy group). Among pa-tients who underwent myocardial perfusion im-aging at baseline, 90% had either single (23%) or multiple (67%) reversible defects for inducible is-chemia. Two thirds of the patients had multivessel coronary artery disease.
Of the 1149 patients in the PCI group, 46 never underwent a procedure because the patient either declined treatment or had coronary anatomy un-suitable for PCI, as determined on clinical reas-sessment. In 27 patients (2%), the operator was unable to cross any lesions. PCI was attempted for 1688 lesions in 1077 patients, of whom 1006 (94%) received at least one stent. In the stent group, 590 patients (59%) received one stent and 416 (41%) more than one stent. Drug-eluting stents were used in 31 patients. On average, stenosis in the luminal diameter, as evaluated on visual assessment of angiograms, was reduced from a mean (±SD) of 83±14% to 31±34% in the 244 lesions not treated with stents and from 82±12% to 1.9±8% in the 1444 lesions treated with stents.
After PCI, successful treatment as seen on angi-ography was achieved in 1576 of 1688 lesions (93%), and clinical success (i.e., all lesions success-fully dilated and no in-hospital complications) was achieved in 958 of 1077 patients (89%).
Medication and Treatment Targets
Patients had a high rate of receiving multiple, evidence-based therapies after randomization and during follow-up, with similar rates in both study groups (Table 2). At the 5-year follow-up visit, 70% of subjects had an LDL cholesterol level of less than 85 mg per deciliter (2.20 mmol per liter) (median, 71±1.3 mg per deciliter [1.84±0.03 mmol per liter]); 65% and 94% had systolic and diastolic blood pressure targets of less than 130 mm Hg and 85 mm Hg, respectively; and 45% of patients with diabetes had a glycated hemoglobin level of no more than 7.0% (Table 2). Patients had high rates of adherence to the regimen of diet, regular exercise, and smoking cessation as recommended by clinical practice guidelines,1,2 although the mean body-mass index did not decrease.
Follow-up Period
The median follow-up period was 4.6 years (inter-quartile range, 3.3 to 5.7) and was similar in the two study groups, with a total of 120,895 patient-months at risk. Only 9% of patients were lost to follow-up in the two groups (107 in the PCI group and 97 in the medical-therapy group, P = 0.51) be-fore the occurrence of a primary outcome or the end of follow-up. Vital status was not ascertained in 194 patients (99 in the PCI group and 95 in the medical-therapy group, P = 0.81).
Primary Outcome
The primary outcome (a composite of death from any cause and nonfatal myocardial infarction) oc-curred in 211 patients in the PCI group and 202 patients in the medical-therapy group (Table 3). The estimated 4.6-year cumulative primary event rates were 19.0% in the PCI group and 18.5% in the medical-therapy group (unadjusted hazard ra-tio for the PCI group, 1.05; 95% CI, 0.87 to 1.27; P = 0.62) (Fig. 2).
Secondary Outcomes
For the prespecified composite outcome of death, nonfatal myocardial infarction, and stroke, the event rate was 20.0% in the PCI group and 19.5%

Optimal Medical Ther apy with or without PCI for Stable Coronary Disease
n engl j med 356;15 www.nejm.org april 12, 2007 1507
33p9
3071 Met eligibility criteria
2287 Consented to participate(74% of patients with protocol eligibility)
35,539 Patients underwent assessment
32,468 Were excluded8677 Did not meet inclusion criteria
5155 Had undocumented ischemia3961 Did not meet protocol for vessels
6554 Were excluded for logistic reasons18,360 Had one or more exclusions
4513 Had undergone recent (<6 mo) revascu-larization
4939 Had an inadequate ejection fraction2987 Had a contraindication to PCI2542 Had a serious coexisting illness1285 Had concomitant valvular disease1203 Had class IV angina1071 Had a failure of medical therapy947 Had left main coronary artery stenosis
>50%722 Had only PCI restenosis (no new lesions)528 Had complications after myocardial
infarction
784 Did not provide consent450 Did not receive physician’s
approval237 Declined to give permission97 Had an unknown reason
1149 Were assigned to PCI group46 Did not undergo PCI27 Had a lesion that could not be dilated
1006 Received at least one stent
107 Were lost to follow-up
1138 Were assigned to medical-therapy group
97 Were lost to follow-up
1149 Were included in the primary analysis 1138 Were included in the primary analysis
AUTHOR:
FIGURE:
JOB: ISSUE:
4-CH/T
RETAKE
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
Enon
1st2nd3rd
Boden
1 of 3
04-12-07
ARTIST: ts
35615
Figure 1. Enrollment and Outcomes.
Of 35,539 patients who were assessed for eligibility in the trial, 32,468 were excluded for a variety of reasons (patients could have more than one reason for exclusion). A total of 3071 patients met all inclusion criteria. Of these, 2287 (74%) consented to participate in the study (932 in Canada, 968 in U.S. Veterans Affairs facilities, and 387 in U.S. facilities other than Veterans Affairs hospitals). Of these patients, 1149 were randomly assigned to the PCI group and 1138 to the medicaltherapy group. The median followup was 4.6 years for both study groups.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071508
Table 1. Baseline Clinical and Angiographic Characteristics.*
CharacteristicPCI Group (N = 1149)
Medical-Therapy Group (N = 1138) P Value
Demographic
Age — yr 61.5±10.1 61.8±9.7 0.54
Sex — no. (%) 0.95
Male 979 (85) 968 (85)
Female 169 (15) 169 (15)
Race or ethnic group — no. (%)† 0.64
White 988 (86) 975 (86)
Black 57 (5) 57 (5)
Hispanic 68 (6) 58 (5)
Other 35 (3) 47 (4)
Clinical
Angina (CCS class) — no. (%) 0.24
0 135 (12) 148 (13)
I 340 (30) 341 (30)
II 409 (36) 425 (37)
III 261 (23) 221 (19)
Missing data 3 (<1) 2 (<1)
Duration of angina — mo 0.53
Median 5 5
Interquartile range 1–15 1–15
Episodes/wk with exertion or at rest within last mo 0.83
Median 3 3
Interquartile range 1–6 1–6
History — no. (%)
Diabetes 367 (32) 399 (35) 0.12
Hypertension 757 (66) 764 (67) 0.53
Congestive heart failure 57 (5) 51 (4) 0.59
Cerebrovascular disease 100 (9) 102 (9) 0.83
Myocardial infarction 437 (38) 439 (39) 0.80
Previous PCI 174 (15) 185 (16) 0.49
CABG 124 (11) 124 (11) 0.94
Stress test‡
Total patients — no. (%) 972 (85) 977 (86) 0.84
Treadmill test — no. (%) 555 (57) 553 (57)
Duration of treadmill test — min 7.0±2.7 6.9±2.3 0.43
Pharmacologic stress — no. (%) 417 (43) 424 (43)
Echocardiography — no. (%) 63 (6) 54 (6)
Nuclear imaging — no. (%) 685 (70) 708 (72) 0.59
Single reversible defect§ 154 (22) 161 (23) 0.09
Multiple reversible defects§ 444 (65) 483 (68) 0.09

Optimal Medical Ther apy with or without PCI for Stable Coronary Disease
n engl j med 356;15 www.nejm.org april 12, 2007 1509
in the medical-therapy group (hazard ratio, 1.05; 95% CI, 0.87 to 1.27; P = 0.62) (Table 3 and Fig. 2). The rates of hospitalization for acute coronary syn-dromes were 12.4% in the PCI group and 11.8% in the medical-therapy group (hazard ratio, 1.07; 95% CI, 0.84 to 1.37; P = 0.56), and adjudicated rates of myocardial infarction were 13.2% and 12.3%, respectively (hazard ratio, 1.13; 95% CI, 0.89 to 1.43; P = 0.33). For death alone, the rates were 7.6% and 8.3%, respectively (hazard ratio, 0.87; 95% CI, 0.65 to 1.16); the mortality curves for the two groups were virtually identical during the initial 4.6 years of the study. For stroke alone, the rate was 2.1% in the PCI group and 1.8% in the medical-therapy group (hazard ratio, 1.56; 95% CI, 0.80 to 3.04; P = 0.19). When the primary end point was calculated with the exclusion of periproce-dural myocardial infarction, the event rates were 16.2% and 17.9% (hazard ratio, 0.90; 95% CI, 0.73 to 1.10; P = 0.29).
At a median follow-up of 4.6 years, 21.1% of patients in the PCI group had additional revascu-larization, as compared with 32.6% of those in the medical-therapy group (hazard ratio, 0.60; 95% CI, 0.51 to 0.71; P<0.001). In the PCI group, 77 patients subsequently underwent CABG, as com-pared with 81 patients in the medical-therapy group. Revascularization was performed for an-gina that was unresponsive to maximal medical therapy or when there was objective evidence of worsening ischemia on noninvasive testing, at the
discretion of the patient’s physician. The median time to subsequent revascularization was 10.0 months (interquartile range, 4.5 to 28.0) in the PCI group and 10.8 months (interquartile range, 3.2 to 30.7) in the medical-therapy group.
There was a substantial reduction in the preva-lence of angina in both groups during follow-up. There was a statistically significant difference in the rates of freedom from angina throughout most of the follow-up period, in favor of the PCI group (Table 2). At 5 years, 74% of patients in the PCI group and 72% of those in the medical-therapy group were free of angina (P = 0.35).
Subgroup Analyses
There was no significant interaction (P<0.01) be-tween treatment effect and any predefined sub-group variable (Fig. 3). Of note, among patients with multivessel coronary artery disease, previous myocardial infarction, and diabetes, the rate of the primary end point was similar for both groups. When subgroup variables were included in a multi-variate analysis, the hazard ratio for treatment was essentially unchanged (1.09; 95% CI, 0.90 to 1.33; P = 0.77).
Discussion
As an initial management strategy, PCI added to optimal medical therapy did not reduce the pri-mary composite end point of death and nonfatal
Table 1. (Continued.)
CharacteristicPCI Group (N = 1149)
Medical-Therapy Group (N = 1138) P Value
Angiographic
Vessels with disease — no. (%) 0.72
1 361 (31) 343 (30)
2 446 (39) 439 (39)
3 341 (30) 355 (31)
Disease in graft¶ 77 (62) 85 (69) 0.36
Proximal LAD disease 360 (31) 417 (37) 0.01
Ejection fraction 60.8±11.2 60.9±10.3 0.86
* Plus–minus values are means ±SD. Baseline data were missing for one patient in each study group. CCS denotes Canadian Cardiovascular Society, CABG coronaryartery bypass grafting, and LAD left anterior descending artery.
† Race or ethnicity was reported by the patient at enrollment.‡ Nuclear imaging could have been performed after either an exercise treadmill test or pharmacologic stress.§ The percentage in this category is the proportion of patients who underwent imaging.¶ The percentage in this category is the proportion of patients who had undergone previous CABG.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071510
Table 2. Clinical Status, Risk and Lifestyle Factors, and Use of Medication.*
Variable PCI Group (N = 1149) Medical-Therapy Group (N = 1138)
Baseline 1 Yr 3 Yr 5 Yr Baseline 1 Yr 3 Yr 5 Yr
median ±SE
Clinical status
No. evaluated 1148 1031 820 423 1137 1010 824 406
Blood pressure — mm Hg
Systolic 131±0.77 126±0.64 125±0.68 124±0.81 130±0.66 124±0.73 123±0.78 122±0.92
Diastolic 74±0.33 72±0.35 70±0.52 70±0.81 74±0.33 70±0.43 70±0.52 70±0.65
Cholesterol — mg/dl
Total 172±1.37 156±1.17 148±1.13 143±1.74 177±1.41 150±1.10 145±1.30 140±1.64
HDL 39±0.39 42±0.39 43±0.47 41±0.67 39±0.37 41±0.42 42±0.49 41±0.75
LDL 100±1.17 84±0.97 76±0.85 71±1.33 102±1.22 81±0.86 74±0.92 72±1.21
Triglycerides — mg/dl 143±2.96 129±2.74 124±2.79 123±4.13 149±3.03 133±2.90 126±2.84 131±4.70
Bodymass index 28.7±0.18 28.5±0.19 29.0±0.21 29.0±0.34 28.9±0.17 29.0±0.19 29.3±0.21 29.5±0.31
Anginafree — no. (%)† 135 (12) 680 (66) 602 (72) 316 (74) 148 (13) 595 (58) 558 (67) 296 (72)
Risk or lifestyle factor
Current smoker — no. (%) 260 (23) 206 (20) 156 (19) 74 (17) 259 (23) 206 (20) 160 (19) 80 (20)
AHA Step 2 diet — no. (%) 626 (55) 803 (78) 631 (77) 326 (77) 613 (54) 800 (79) 660 (80) 312 (77)
Moderate activity — no. (%)‡ 290 (25) 473 (46) 351 (42) 179 (42) 279 (25) 433 (43) 330 (40) 146 (36)
Glycated hemoglobin in patients with diabetes
No. evaluated 319 239 197 97 336 286 233 123
Level — % 6.9±0.1 7.1±0.1 7.1±0.1 7.1±0.1 7.1±0.1 7.0±0.1 7.1±0.1 7.1±0.1
Medication
No. evaluated 1147 1044 837 428 1138 1028 838 417
ACE inhibitor — no. (%) 669 (58) 668 (64) 536 (64) 284 (66) 680 (60) 633 (62) 522 (62) 260 (62)
ARB — no. (%) 48 (4) 93 (9) 104 (12) 49 (11) 54 (5) 99 (10) 108 (13) 67 (16)
Statin — no. (%) 992 (86) 972 (93) 780 (93) 398 (93) 1014 (89) 972 (95) 769 (92) 386 (93)
Other antilipid — no. (%) 89 (8) 236 (23) 324 (39) 211 (49) 94 (8) 253 (25) 321 (38) 224 (54)
Aspirin — no. (%) 1097 (96) 995 (95) 792 (95) 408 (95) 1077 (95) 977 (95) 796 (95) 391 (94)
Betablocker — no. (%) 975 (85) 887 (85) 705 (84) 363 (85) 1008 (89) 916 (89) 724 (86) 357 (86)
Calciumchannel blocker — no. (%)§ 459 (40) 415 (40) 360 (43) 180 (42) 488 (43) 501 (49) 418 (50) 217 (52)
Nitrates — no. (%)¶ 714 (62) 553 (53) 396 (47) 173 (40) 825 (72) 690 (67) 511 (61) 237 (57)
* Plus–minus values are medians ±SE, with the SE calculated with the use of the interquartile range. To convert cholesterol values to millimoles per liter, multiply by 0.02586. To convert triglyceride values to millimoles per liter, multiply by 0.01129. ACE denotes angiotensin converting enzyme, and ARB angiotensinreceptor blocker.
† The comparison between the PCI group and the medicaltherapy group was significant at 1 year (P<0.001) and 3 years (P = 0.02) but not at baseline or at 5 years.
‡ This category includes at least 30 to 45 minutes of moderate activity five times per week or vigorous activity three times per week.§ The comparison between the PCI group and the medicaltherapy group was significant at 1 year (P<0.001), 3 years (P = 0.005), and 5 years
(P = 0.003).¶ The comparison between the PCI group and the medicaltherapy group was significant at all time points (P<0.001).

Optimal Medical Ther apy with or without PCI for Stable Coronary Disease
n engl j med 356;15 www.nejm.org april 12, 2007 1511
myocardial infarction or reduce major cardiovas-cular events, as compared with optimal medical therapy alone, during follow-up of 2.5 to 7.0 years, despite a high baseline prevalence of clinical co-existing illnesses, objective evidence of ischemia, and extensive coronary artery disease as seen on angiography. Although the degree of angina re-lief was significantly higher in the PCI group than in the medical-therapy group, there was also substantial improvement in the medical-therapy
group. All secondary outcomes and individual com-ponents of the primary outcome showed no sig-nificant differences between the study groups, nor was there a significant interaction between treatment effect and any prespecified subgroup variable. For the primary outcome, the 95% CI excludes a relative benefit of more than 13% in the PCI group. Thus, it is highly unlikely that we missed a prognostically important treatment ben-efit in favor of the initial PCI strategy.
Table 3. Primary and Secondary Outcomes.*
Outcome Number of Events Hazard Ratio (95% CI)† P Value† Cumulative Rate at 4.6 Years
PCI GroupMedicalTherapy
Group PCI GroupMedicalTherapy
Group
%
Death and nonfatal myocardial infarction‡
211 202 1.05 (0.87–1.27) 0.62 19.0 18.5
Death§ 68 74
Periprocedural myocardial infarction
35 9
Spontaneous myocardial infarction 108 119
Death, myocardial infarction, and stroke
222 213 1.05 (0.87–1.27) 0.62 20.0 19.5
Hospitalization for ACS 135 125 1.07 (0.84–1.37) 0.56 12.4 11.8
Death§ 85 95 0.87 (0.65–1.16) 0.38 7.6 8.3
Cardiac 23 25
Other 45 51
Unknown 17 19
Total nonfatal myocardial infarction 143 128 1.13 (0.89–1.43) 0.33 13.2 12.3
Periprocedural myocardial infarction
35 9
Spontaneous myocardial infarction 108 119
Death, myocardial infarction, and ACS 294 288 1.05 (0.90–1.24) 0.52 27.6 27.0
Stroke 22 14 1.56 (0.80–3.04) 0.19 2.1 1.8
Revascularization (PCI or CABG)¶ 228 348 0.60 (0.51–0.71) <0.001 21.1 32.6
* ACS denotes acute coronary syndrome, PCI percutaneous coronary intervention, and CABG coronaryartery bypass grafting.† The hazard ratio is for the PCI group as compared with the medicaltherapy group, and P values were calculated by the logrank test and are
unadjusted for multiple variables. ‡ The definition of myocardial infarction was the finding of new Q waves at any time; a spontaneous creatine kinase MB fraction of at least
1.5 times the upper limit of normal or a troponin T or I level of at least 2.0 times the upper limit of normal; during a PCI procedure, a creatine kinase MB fraction of at least 3 times the upper limit of normal or a troponin T or I level of at least 5.0 times the upper limit of normal, associated with new ischemic symptoms; and after CABG, a creatine kinase MB fraction or a troponin T or I level of at least 10.0 times the upper limit of normal. If periprocedural myocardial infarction is excluded from the primary outcome, the hazard ratio is 0.90 (95% CI, 0.73 to 1.10; P = 0.29).
§ Some patients had a nonfatal myocardial infarction before their subsequent death so that the number of deaths overall is greater than the number of deaths in the primary outcome analysis, which includes the time until the first event.
¶ Values exclude the initial PCI procedure in patients who were originally assigned to the PCI group.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071512
Our findings may be explained, in part, by dif-ferences in atherosclerotic plaque morphology and vascular remodeling associated with acute coro-nary syndromes, as compared with stable coronary artery disease. Vulnerable plaques (precursors of acute coronary syndromes) tend to have thin fibrous caps, large lipid cores, fewer smooth-muscle cells, more macrophages, and less colla-gen, as compared with stable plaques, and are associated with outward (expansive) remodeling of the coronary-artery wall, causing less stenosis of the coronary lumen.36 As a result, vulnerable plaques do not usually cause significant stenosis before rupture and the precipitation of an acute coronary syndrome.36 By contrast, stable plaques tend to have thick fibrous caps, small lipid cores,
more smooth-muscle cells, fewer macrophages, and more collagen and are ultimately associated with inward (constrictive) remodeling that nar-rows the coronary lumen. These lesions produce ischemia and anginal symptoms and are easily detected by coronary angiography but are less like-ly to result in an acute coronary syndrome.37,38
Thus, unstable coronary lesions that lead to myocardial infarction are not necessarily severely stenotic, and severely stenotic lesions are not nec-essarily unstable. Focal management of even severely stenotic coronary lesions with PCI in our study did not reduce the rate of death and myo-cardial infarction, presumably because the treated stenoses were not likely to trigger an acute coro-nary event. Furthermore, our lower-than-projected
AUTHOR:
FIGURE:
JOB: ISSUE:
4-CH/T
RETAKE
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE:Figure has been redrawn and type has been reset.
Please check carefully.
REG F
Enon
1st2nd
3rd
Boden
2 of 3
04-12-07
ARTIST: ts
35615
39p6
No. at RiskMedical therapyPCI
3035
192200
408417
638637
834833
959952
10171013
11381149
Surv
ival
Fre
e of
Dea
th fr
omA
ny C
ause
and
Myo
card
ial
Infa
rctio
n1.0
0.9
0.7
0.6
0.5
0.8
00 1 2 3 4 75 6
Years
Medical therapy
Medical therapy
Medical therapy Medical therapy
PCI
PCI
Hazard ratio, 1.05; 95% CI (0.87–1.27); P=0.62
PCI
Hazard ratio, 0.87; 95% CI (0.65–1.16); P=0.38
Hazard ratio, 1.07; 95% CI (0.84–1.37); P=0.56
PCI
Hazard ratio, 1.13; 95% CI (0.89–1.43); P=0.33
A B
C D
No. at RiskMedical therapyPCI
3844
302312
468488
717733
917929
10291051
10731094
11381149
Ove
rall
Surv
ival
1.0
0.9
0.7
0.6
0.5
0.8
00 1 2 3 4 75 6
Years
No. at RiskMedical therapyPCI
127134
236246
418431
662667
833835
956957
10251027
11381149
Surv
ival
Fre
e of
AC
S
1.0
0.9
0.7
0.6
0.5
0.8
00 1 2 3 4 75 6
Years
No. at RiskMedical therapyPCI
120134
192200
409418
638637
834833
962954
10191015
11381149
Surv
ival
Fre
e of
Myo
card
ial
Infa
rctio
n
1.0
0.9
0.7
0.6
0.5
0.8
00 1 2 3 4 75 6
Years
Figure 2. Kaplan–Meier Survival Curves.
In Panel A, the estimated 4.6year rate of the composite primary outcome of death from any cause and nonfatal myocardial infarction was 19.0% in the PCI group and 18.5% in the medicaltherapy group. In Panel B, the estimated 4.6year rate of death from any cause was 7.6% in the PCI group and 8.3% in the medicaltherapy group. In Panel C, the estimated 4.6year rate of hospitalization for acute coronary syndrome (ACS) was 12.4% in the PCI group and 11.8% in the medicaltherapy group. In Panel D, the estimated 4.6year rate of acute myocardial infarction was 13.2% in the PCI group and 12.3% in the medicaltherapy group.

Optimal Medical Ther apy with or without PCI for Stable Coronary Disease
n engl j med 356;15 www.nejm.org april 12, 2007 1513
event rate in the medical-therapy group may be explained by systemic therapy that reduced plaque vulnerability through aggressive intervention for multiple risk factors and evidence-based use of medication.
Rates of angina were consistently lower in the PCI group than in the medical-therapy group dur-
ing follow-up, and rates of subsequent revascu-larization were likewise lower. However, there was a substantial increase in freedom from an-gina in patients in the medical-therapy group as well, most of which had taken place at 1 year but with a further improvement at 5 years. To what extent this finding reflects a benefit of specific
39p6
0.25 0.50 1.00 2.001.751.50
Medical TherapyBetter
PCI Better
Overall
Sex
Male
Female
Myocardial infarction
Yes
No
Extent of CAD
Multivessel disease
Single-vessel disease
Smoking
Current
Not current
Diabetes
Yes
No
CCS angina class
0 or I
II or III
Ejection fraction
≤50%
>50%
Age
>65 yr
≤65 yr
Previous CABG
No
Yes
Race
White
Nonwhite
Health care system
Canadian
U.S. non-VA
U.S. VA
No. ofPatients Hazard Ratio (95% CI)
Medical Therapy
Event Rate for the Primary OutcomeBaseline Characteristics
0.19
0.18
0.26
0.25
0.14
0.21
0.12
0.21
0.18
0.24
0.15
0.20
0.18
0.26
0.16
0.22
0.16
0.17
0.29
0.18
0.24
0.14
0.21
0.22
1.15 (0.93–1.42)
1.05 (0.87–1.27)
0.87 (0.54–1.42)
1.27 (0.90–1.78)
0.71 (0.44–1.14)1.06 (0.80–1.38)
1.08 (0.87–1.34)
0.98 (0.52–1.82)
1.04 (0.84–1.29)
1.00 (0.77–1.32)
1.10 (0.83–1.46)
1.05 (0.84–1.32)
1.14 (0.77–1.70)
1.09 (0.85–1.40)
1.01 (0.75–1.38)
1.20 (0.92–1.56)
0.99 (0.73–1.32)
1.08 (0.86–1.36)
1.00 (0.71–1.41)
1.17 (0.76–1.80)
1.04 (0.84–1.30)
1.22 (0.93–1.60)
0.91 (0.69–1.21)
0.65 (0.40–1.06)
P Value
0.19
0.19
0.18
0.23
0.17
0.21
0.15
0.20
0.19
0.25
0.17
0.17
0.20
0.28
0.17
0.24
0.16
0.17
0.34
0.19
0.19
0.17
0.15
0.22
PCI
2287
1947
338
876
1371
1581
700
653
1631
766
1468
964
1371
406
1848
904
1381
2039
248
1963
322
932
387
968
0.03
0.15
0.65
0.71
0.33
0.73
0.72
0.62
0.81
0.43
0.17
AUTHOR:
FIGURE:
JOB: ISSUE:
4-CH/T
RETAKE
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE:Figure has been redrawn and type has been reset.
Please check carefully.
REG F
Enon
1st2nd
3rd
Boden
3 of 3
04-12-07
ARTIST: ts
35615
Figure 3. Subgroup Analyses.
The chart shows hazard ratios (black squares, sized in proportion to the number of subjects in a group), 95% CIs (horizontal lines), cumulative 4.6year event rates for the composite primary outcome (death from any cause and nonfatal myocardial infarction) for the PCI group versus the medicaltherapy group for the specified subgroups, and P values for the interaction between the treatment effects and subgroup variables. P values were calculated with the use of the Wald statistic. There was no significant interaction between treatment and subgroup variables as defined according to the prespecified value for interaction (P<0.01), although there was a trend for interaction with respect to sex (P = 0.03). PCI denotes percutaneous coronary intervention, CAD coronary artery disease, CCS Canadian Cardiovascular Society, CABG coronaryartery bypass grafting, and VA Veterans Affairs.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071514
antianginal medications (e.g., nitrates and beta-blockers) or a favorable effect of therapies such as statins on endothelial function and atheroscle-rosis is unclear.
Our findings parallel those reported in recent trials,39,40 in which observed clinical-event rates that were associated with optimal medical ther-apy were lower than projected in the trial design. These results are also concordant with a meta-analysis of all previous trials involving PCI ver-sus medical management.16 In the aggregate, these studies, including our own, include out-come data on more than 5000 patients and show that PCI has no effect in reducing major cardio-vascular events.
The preponderance of male patients (85%) is a limitation of our study, as is the lack of ethnic diversity (14% of the patients were nonwhite). We used bare-metal stents, since drug-eluting stents were not available until late during accrual. Al-though the latter factor may be perceived as a limitation, published data indicate no benefit (either short-term or long-term) with respect to death and myocardial infarction in patients with stable coronary artery disease who receive drug-eluting stents, as compared with those who re-ceive bare-metal stents.41-46
Our findings reinforce existing clinical prac-tice guidelines, which state that PCI can be safely deferred in patients with stable coronary artery disease, even in those with extensive, multivessel involvement and inducible ischemia, provided that intensive, multifaceted medical therapy is institut-ed and maintained.1,2 As an initial management approach, optimal medical therapy without rou-tine PCI can be implemented safely in the major-ity of patients with stable coronary artery disease. However, approximately one third of these pa-tients may subsequently require revascularization
for symptom control or for subsequent develop-ment of an acute coronary syndrome.
In summary, our trial compared optimal med-ical therapy alone or in combination with PCI as an initial management strategy in patients with stable coronary artery disease. Although the ad-dition of PCI to optimal medical therapy reduced the prevalence of angina, it did not reduce long-term rates of death, nonfatal myocardial infarc-tion, and hospitalization for acute coronary syn-dromes.
Supported by the Cooperative Studies Program of the U.S. De-partment of Veterans Affairs Office of Research and Development, in collaboration with the Canadian Institutes of Health Research; and by unrestricted research grants from Merck, Pfizer, Bristol-Myers Squibb, Fujisawa, Kos Pharmaceuticals, Datascope, Astra-Zeneca, Key Pharmaceutical, Sanofi-Aventis, First Horizon, and GE Healthcare. All industrial funding in support of the trial was directed through the U.S. Department of Veterans Affairs.
Dr. Boden reports receiving consulting fees and lecture fees from Kos Pharmaceuticals, PDL BioPharma, Pfizer, CV Thera-peutics, and Sanofi-Aventis, and grant support from Merck and Abbott Laboratories; Dr. O’Rourke, consulting fees from King Pharmaceuticals, Lilly, and CV Therapeutics; Dr. Teo, grant sup-port from Boehringer Ingelheim; Dr. Knudtson, lecture fees from Medtronic and Lilly; Dr. Harris, having equity ownership in Amgen; Dr. Chaitman, receiving consulting fees from CV Thera-peutics, Merck, and Bayer, lecture fees from Pfizer, AstraZeneca, and CV Therapeutics, and grant support from Pfizer, CV Thera-peutics, and Sanofi-Aventis; Dr. Shaw, grant support from Bristol-Myers Squibb and Astellas Healthcare; Dr. Booth, grant support from Actelion; Dr. Bates, consulting fees from Sanofi-Aventis and AstraZeneca and lecture fees from Sanofi-Aventis; Dr. Sper-tus, consulting fees from Amgen and United Healthcare and grant support from Amgen, Roche Diagnostics, and Lilly (and in the past, consulting fees and grant support from CV Therapeu-tics and owning the copyright for the Seattle Angina Question-naire, the Peripheral Artery Questionnaire, and the Kansas City Cardiomyopathy Questionnaire); Dr. Berman, consulting fees and lecture fees from Bristol-Myers Squibb, Astellas, Tyco, and Siemens and grant support from Bristol-Myers Squibb and As-tellas; Dr. Mancini, consulting and lecture fees from Pfizer, Abbott, and GlaxoSmithKline, lecture fees from Merck and Sanofi-Aventis, and grant support from Cordis and GlaxoSmith-Kline; and Dr. Weintraub, consulting fees from Sanofi-Aventis and Bristol-Myers Squibb and grant support from Sanofi-Aventis. No other potential conflict of interest relevant to this article was reported.
AppendixThe authors’ affiliations are as follows: Western New York Veterans Affairs (VA) Healthcare Network and Buffalo General Hospital–SUNY, Buffalo, NY (W.E.B.); South Texas Veterans Health Care System–Audie Murphy Campus, San Antonio, TX (R.A.O., P.C.); Mc-Master University Medical Center, Hamilton, ON, Canada (K.K.T.); VA Cooperative Studies Program Coordinating Center, VA Con-necticut Healthcare System, West Haven, CT (P.M.H); Vanderbilt University Medical Center, Nashville (D.J.M); London Health Sciences Centre, London, ON, Canada (W.J.K.); Foothills Hospital, Calgary, AB, Canada (M.K.); Hartford Hospital, Hartford, CT (M.D.); VA Cooperative Studies Program Clinical Research Pharmacy Coordinating Center, Albuquerque, NM (C.L.H.); Saint Louis University, St. Louis (B.R.C.); Cedars–Sinai Medical Center, Los Angeles (L.S., D.S.B.); Montreal Heart Institute, Montreal (G. Gosselin); Sudbury Regional Hospital, Sudbury, ON, Canada (S.N.); Queen Elizabeth Health Sciences Centre, Halifax, NS, Canada (L.M.T.); Mayo Clinic, Rochester, MN (G. Gau); Houston VA Medical Center, Houston (A.S.B.); Lexington VA Medical Center, Lexington, KY (D.C.B.); Uni-versity of Michigan Medical Center, Ann Arbor (E.R.B.); Mid America Heart Institute, Kansas City, MO (J.A.S.); Vancouver Hospital and Health Sciences Centre, Vancouver, BC, Canada (G.B.J.M.); and Christiana Care Health System, Newark, DE (W.S.W.).
The members of the COURAGE trial were as follows: Writing Committee: W. Boden (study cochair), R. O’Rourke (study cochair) K. Teo (study cochair), P. Hartigan. W. Weintraub, D. Maron, J. Mancini; Executive Committee: W. Weintraub (chair), W. Boden, R. O’Rourke, K. Teo, P. Hartigan, M. Knudtson, D. Maron, E. Bates, A. Blaustein, D. Booth, R. Carere, S. Ellis, G. Gosselin, G. Gau, A. Jacobs,

Optimal Medical Ther apy with or without PCI for Stable Coronary Disease
n engl j med 356;15 www.nejm.org april 12, 2007 1515
S. King, III, W. Kostuk, C. Harris, J. Spertus; P. Peduzzi (ex officio); Data and Safety Monitoring Board: T. Ryan (chair), B. Turnbull, T. Feldman, R. Bonow, W. Haskell, P. Diehr, P. Lachenbruch, D. Waters, D. Johnstone; Adjudication Committee: L. Cohen (chair), B. Cantin, W. Hager, F. Samaha, J. Januzzi, J. Arrighi, B. Chaitman; Economics Committee: W. Weintraub (chair), P. Hartigan, R. O’Rourke, W. Boden, P. Barnett, J. Spertus, R. Goeree; Optimal Medical Therapy Committee: D. Maron (chair), W. Boden, R. O’Rourke, K. Teo, W. Weintraub.
The following members assisted in coordination of the study: VA Cooperative Studies Program Coordinating Center, VA Connecticut Healthcare System, West Haven, CT — P. Peduzzi (director); M. Antonelli, (associate director of operations); J. Smith (project manager); R. Kilstrom, B. Hunter (coordinators); L. Durant (quality assurance officer); S. O’Neil (end points coordinator); T. Economou, J. Nabors (programmers); A. Kossack (data clerk); VA Cooperative Studies Program Clinical Research Pharmacy Coordinating Center, Albuquer-que, NM — M. Sather (director), C. Harris (assistant director), W. Gagne (project manager), C. Fye (pharmacist); VA Cooperative Stud-ies Human Rights Committee, West Haven, CT — R. Marottoli (chair), H. Allore, D. Beckwith, W. Farrell, R. Feldman, R. Mehta, J. Neiderman, E. Perry, S. Kasl, M. Zeman; VA Office of Research and Development, Clinical Science Research and Development, Wash-ington, DC — T. O’Leary (acting director), G. Huang (deputy director, Cooperative Studies Program); Study Chairs Offices — Western New York VA Healthcare Network and Buffalo General Hospital–SUNY, Buffalo, NY — W. Boden (study cochair), M. Dada, K. Potter (national coordinators), T. Rivera (program assistant); South Texas Veterans Health Care System, San Antonio, TX — R. O’Rourke (study cochair), P. Casperson (national coordinator), A. O’Shea (program assistant); McMaster University Medical Center, Hamilton, ON, Canada — K. Teo (study cochair), G. Woodcock (coordinator); Laboratories: Christiana Care Center for Outcomes Research, Newark, DE, and Emory University, Atlanta — W. Weintraub; Health Economics Research Center, Menlo Park, CA — P. Barnett; Pro-gram for Assessment of Technology in Health, Hamilton, ON, Canada — R. Goeree, B. O’Brien; Vancouver Hospital, Cardiovascular Imaging Research Core Laboratory, Vancouver, BC, Canada — G.B.J. Mancini, E. Yeoh; Washington University Central Lipid Core Laboratory, St. Louis — J. Ladenson, V. Thompson; Saint Louis University ECG Core Laboratory, St. Louis — B. Chaitman, T. Bertran; Cedars–Sinai Medical Center Nuclear Core Laboratory, Los Angeles — D. Berman, J. Gerlach, R. Littman, L. Shaw; San Diego State University PACE Program, San Diego, CA — K. Calfas, J. Sallis.
The following investigators are listed according to their clinical study sites: VA: South Texas Veterans Health Care System, San Antonio, TX — R. O’Rourke, P. Baker, J. Bolton; VA Medical Center, Houston — A. Blaustein, C. Rowe; VA Medical Center, Durham, NC — K. Morris, S. Hoffman; VA Health Care System, New York — S. Sedlis, M. Keary; VA Health Care System, Ann Arbor, MI — C. Duvernoy, C. Majors; VA Medical Center, Lexington, KY — Booth, M. Shockey; James A. Haley Veterans Hospital, Tampa, FL — R. Zoble, I. Fernandez; VA Health Care System, Puget Sound, WA — K. Lehmann, A. Sorley, M. Abel; VA Health Care System, Albuquerque, NM — M. Sheldon, K. Wagoner; Portland VA Medical Center, Portland, OR — E. Murphy, K. Avalos; Iowa City VA Medical Center, Iowa City — J. Rossen, K. Schneider; Central Arkansas Veterans Health Care System, Little Rock, AR — B. Molavi, L. Garza, P. Barton; VA Medical Center, Atlanta — K. Mavromatis, Z. Forghani; Tennessee Valley Health Care System, Nashville — R. Smith, C. Mitchell; VA Medical Center, Memphis, TN — K. Ramanathan, T. Touchstone. Canada: London Health Sciences Centre, London, ON — W. Kostuk, K. Sridhar, S. Carr, D. Wiseman; Sudbury Regional Hospital, Sudbury, ON — S. Nawaz, C. Dion; Montreal Heart Institute, Montreal — G. Gosselin, J. Theberge, M. Cuso; Queen Elizabeth II Health Care Center, Halifax, NS — L. Title, P. Simon, L. Carroll, K. Courtney-Cox; Sunnybrook Health Care Centre, Toronto — E. Cohen, E. Hsu; University Health Network–Toronto Hospital, Toronto — V. Dzavik, J. Lan; Foothills Hospital, Calgary, AB — M. Knudtson, D. Lundberg; Hamilton General Hospital–McMaster Clinic, Hamilton, ON — M. Natarajan, G. Cappelli; St. Michael’s Hospital, Toronto — M. Kutryk, A. DiMarco, B. Strauss; Vancouver Hospital, Vancouver, BC — A. Fung, J. Chow; Saint John Regional Hospital, Saint John, NB — D. Marr, F. Fitzgerald; St. Paul’s Hospital, Vancouver, BC — R. Carere, T. Nacario; University of Alberta Hospital, Edmonton — W. Tymchak, L. Harris; Trillium Health Care, Newmarket, ON — C. Lazzam, A. Carter; Hôpital du Sacre Coeur de Montreal, Montreal — D. Palisaitis, C. Mercure. U.S. Non-VA: Mayo Clinic, Rochester, MN — M. Bell, M. Peterson; MIMA Century Research Associates, Melbourne, FL — R. Vicari, M. Carroll; University of Michigan Medical Center, Ann Arbor — E. Bates, A. Luciano; Southern California Kaiser Permanente Medical Group, CA — P. Mahrer; S. Reyes; University of Oklahoma, Oklahoma City — J. Saucedo, D. vanWieren; Mid America Heart Institute, St. Louis — J. O’Keefe, P. Kennedy; Boston Medical Center, Boston — A. Jacobs. C. Berger, S. Mayo; Emory University Hospital, Atlanta — J. Miller, T. Arnold; Hartford Hospital, Hartford, CT — F. Kiernan, D. Murphy; Henry Ford Health System, Detroit — A. Kugelmass, R. Pangilinan; University of Rochester Medical Center, Rochester, NY — R. Schwartz, L. Caufield; Vanderbilt University Hospital, Nash-ville — D. Hansen, C. Mitchell; SUNY University Hospital, Syracuse, NY — R. Carhart, A. Pennella; Cleveland Clinic, Cleveland — S. Ellis, C. Stevenson; Barnes–Jewish Hospital, St. Louis — R. Krone, J. Humphrey; Mayo Clinic, Scottsdale, AZ — C. Appleton, J. Wisbey; Christiana Care Health Systems, Wilmington, DE — M. Stillabower, A. DiSabatino; Rush–Presbyterian–St. Luke’s Medical Center, Chicago — M. Davidson, J. Mathien.
References
Gibbons RJ, Abrams J, Chatterjee K, et al. ACC/AHA 2002 guideline update for the management of patients with chronic stable angina — summary article: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on the Management of Patients with Chronic Sta-ble Angina). J Am Coll Cardiol 2003;41: 159-68.
Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 guide-line update for percutaneous coronary in-tervention — summary article: a report of the American College of Cardiology/Amer-ican Heart Association Task Force on Prac-tice Guidelines (ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines
1.
2.
for Percutaneous Coronary Intervention). Circulation 2006;113:156-75.
Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics — 2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Cir-culation 2007;115(5):e69-e171.
Feldman DN, Gade CL, Slotwiner AJ, et al. Comparison of outcomes of percuta-neous coronary interventions in patients of three age groups (<60, 60 to 80, and >80 years) (from the New York State Angio-plasty Registry). Am J Cardiol 2006;98: 1334-9.
Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the man-agement of patients with ST-elevation myo-
3.
4.
5.
cardial infarction — executive summary: a report of the American College of Cardi-ology/American Heart Association Task Force on Practice Guidelines (Writing Com-mittee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). Circulation 2004; 110:588-636. [Erratum, Circulation 2005; 111:2013.]
Keeley EC, Boura JA, Grines CL. Prima-ry angioplasty versus intravenous throm-bolytic therapy for acute myocardial infarc-tion: a quantitative review of 23 randomised trials. Lancet 2003;361:13-20.
Fragmin and Fast Revascularisation during InStability in Coronary artery dis-ease Investigators. Invasive compared with non-invasive treatment in unstable coro-
6.
7.

n engl j med 356;15 www.nejm.org april 12, 20071516
Optimal Medical Ther apy with or without PCI for Stable Coronary Disease
nary-artery disease: FRISC II prospective randomised multicentre study. Lancet 1999; 354:708-15.
Cannon CP, Weintraub WS, Demopou-los LA, et al. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofi-ban. N Engl J Med 2001;344:1879-87.
Fox KA, Poole-Wilson PA, Henderson RA, et al. Interventional versus conserva-tive treatment for patients with unstable angina or non-ST-elevation myocardial infarction: the British Heart Foundation RITA 3 randomised trial: Randomized In-tervention Trial of unstable Angina. Lancet 2002;360:743-51.
Mehta SR, Cannon CP, Fox KA, et al. Routine vs selective invasive strategies in patients with acute coronary syndromes: a collaborative meta-analysis of random-ized trials. JAMA 2005;293:2908-17.
Parisi AF, Folland ED, Hartigan P. A comparison of angioplasty with medi-cal therapy in the treatment of single-ves-sel coronary artery disease. N Engl J Med 1992;326:10-6.
Coronary angioplasty versus medical therapy for angina: the second Randomised Intervention Treatment of Angina (RITA-2) trial. Lancet 1997;350:461-8.
Pitt B, Waters D, Brown WV, et al. Ag-gressive lipid-lowering therapy compared with angioplasty in stable coronary artery disease. N Engl J Med 1999;341:70-6.
Hueb W, Soares PR, Gersh BJ, et al. The Medicine, Angioplasty, or Surgery Study (MASS-II): a randomized, controlled clinical trial of three therapeutic strate-gies for multivessel coronary artery dis-ease: one-year results. J Am Coll Cardiol 2004;43:1743-51.
Henderson RA, Pocock SJ, Clayton TC, et al. Seven-year outcome in the RITA-2 trial: coronary angioplasty versus medical therapy. J Am Coll Cardiol 2003;42:1161-70.
Katritsis DG, Ioannidis JP. Percutane-ous coronary intervention versus conser-vative therapy in nonacute coronary artery disease: a meta-analysis. Circulation 2005; 111:2906-12.
Yusuf S, Wittes J, Friedman L. Overview of results of randomized clinical trials in heart disease. I. Treatments following myo-cardial infarction. JAMA 1988;260:2088-93.
A randomized trial of propranolol in patients with acute myocardial infarction. I. Mortality results. JAMA 1982;247:1707-14.
Pfeffer MA, Braunwald E, Moyé LA, et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction: results of the Survival and Ventricular En-largement trial. N Engl J Med 1992;327: 669-77.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
The SOLVD Investigators. Effect of enalapril on survival in patients with re-duced left ventricular ejection fractions and congestive heart failure. N Engl J Med 1991;325:293-302.
The Heart Outcomes Prevention Eval-uation Study Investigators. Effects of an angiotensin-converting–enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med 2000;342:145-53. [Errata, N Engl J Med 2000;342:748, 1376.]
Fox KM. Efficacy of perindopril in re-duction of cardiovascular events among patients with stable coronary artery dis-ease: randomised, double-blind, placebo-controlled, multicentre trial (the EUROPA study). Lancet 2003;362:782-8.
Randomised trial of cholesterol low-ering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Sur-vival Study (4S). Lancet 1994;344:1383-9.
Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a ran-domised placebo-controlled trial. Lancet 2002;360:7-22.
LaRosa JC, Grundy SM, Waters DD, et al. Intensive lipid lowering with atorvas-tatin in patients with stable coronary dis-ease. N Engl J Med 2005;352:1425-35.
The Clopidogrel in Unstable Angina to Prevent Events Trial Investigators. Ef-fects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med 2001;345:494-502. [Errata, N Engl J Med 2001;345:1506, 1716.]
de Lorgeril M, Salen P, Martin JL, Monjaud I, Delaye J, Mamelle N. Mediter-ranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: final report of the Lyon Diet Heart Study. Circulation 1999;99:779-85.
O’Connor GT, Buring JE, Yusuf S, et al. An overview of randomized trials of reha-bilitation with exercise after myocardial infarction. Circulation 1989;80:234-44.
Boden WE, O’Rourke RA, Teo KK, et al. Design and rationale of the Clinical Out-comes Utilizing Revascularization and Ag-gressive DruG Evaluation (COURAGE) trial Veterans Affairs Cooperative Studies Pro-gram no. 424. Am Heart J 2006;151:1173-9.
Weintraub WS, Barnett P, Chen S, et al. Economics methods in the Clinical Out-comes Utilizing percutaneous coronary Revascularization and Aggressive Guide-line-driven drug Evaluation (COURAGE) trial. Am Heart J 2006;151:1180-5.
Shih JH. Sample size calculation for complex clinical trials with survival end-points. Control Clin Trials 1995;16:395-407.
Kaplan EL, Meier P. Nonparametric es-
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
timation from incomplete observations. J Am Stat Assoc 1958;53:457-81.
Schoenfeld DA, Tsiatis AA. A modified log rank test for highly stratified data. Biometrika 1987;74:167-75.
Cox DR. Regression models and life-tables. J R Stat Soc [B] 1972;34:187-220.
Boden WE, O’Rourke RA, Teo KK, et al. The evolving pattern of symptomatic coronary artery disease in the United States and Canada: baseline characteristics of the Clinical Outcomes Utilizing Revascular-ization and Aggressive DruG Evaluation (COURAGE) trial. Am J Cardiol 2007;99: 208-12.
Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assess-ment strategies. Circulation 2003;108:1664-72.
Ambrose JA, Tannenbaum MA, Alexo-poulos D, et al. Angiographic progression of coronary artery disease and the devel-opment of myocardial infarction. J Am Coll Cardiol 1988;12:56-62.
Little WC, Constantinescu M, Apple-gate RJ, et al. Can coronary angiography predict the site of a subsequent myocar-dial infarction in patients with mild-to-moderate coronary artery disease? Circu-lation 1988;78:1157-66.
Hochman JS, Lamas GA, Buller CE, et al. Coronary intervention for persistent occlusion after myocardial infarction. N Engl J Med 2006;355:2395-407.
de Winter RJ, Windhausen F, Cornel JH, et al. Early invasive versus selectively invasive management for acute coronary syndromes. N Engl J Med 2005;353:1095-104.
Curfman GD, Morrissey S, Jarcho JA, Drazen JM. Drug-eluting coronary stents: promise and uncertainty. N Engl J Med 2007;356:1059-60.
Spaulding C, Daemen J, Boersma E, Cutlip DE, Serruys PW. A pooled analysis of data comparing sirolimus-eluting stents with bare-metal stents. N Engl J Med 2007; 356:989-97.
Stone GW, Moses JW, Ellis SG, et al. Safety and efficacy of sirolimus- and pacli-taxel-eluting coronary stents. N Engl J Med 2007;356:998-1008.
Kastrati A, Mehilli J, Pache J, et al. Analysis of 14 trials comparing sirolimus-eluting stents with bare-metal stents. N Engl J Med 2007;356:1030-9.
Lagerqvist B, James SK, Stenestrand U, Lindbäck J, Nilsson T, Wallentin L. Long-term outcomes with drug-eluting stents versus bare-metal stents in Sweden. N Engl J Med 2007;356:1009-19.
Mauri L, Hsieh W, Massaro JM, Ho KKL, D’Agostino R, Cutlip DE. Stent throm-bosis in randomized clinical trials of drug-eluting stents. N Engl J Med 2007;356:1020-9.Copyright © 2007 Massachusetts Medical Society.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 2007 1517
original article
Interleukin-1–Receptor Antagonist in Type 2 Diabetes Mellitus
Claus M. Larsen, M.D., Mirjam Faulenbach, M.D., Allan Vaag, M.D., Ph.D., Aage Vølund, M.Sc., Jan A. Ehses, Ph.D., Burkhardt Seifert, Ph.D., Thomas Mandrup-Poulsen, M.D., Ph.D., and Marc Y. Donath, M.D.
From the Steno Diabetes Center, Gentofte (C.M.L., A. Vaag, T.M.-P.), and Biostatis-tics, Novo Nordisk, Bagsvaerd (A. Vølund) — both in Denmark; the Clinic for Endo-crinology and Diabetes, University Hos-pital Zurich and Center for Integrative Hu-man Physiology (M.F., J.A.E., M.Y.D.), and the Department of Biostatistics, Univer-sity of Zurich (B.S.) — both in Zurich; and the University of Lund, Lund (A. Vaag), and the Karolinska Institute, Stockholm (T.M.-P.) — both in Sweden. Address re-print requests to Dr. Donath at the Di- vision of Endocrinology and Diabetes, University Hospital, CH-8091 Zurich, Swit-zerland, or at [email protected].
Drs. Larsen, Faulenbach, Mandrup-Poulsen, and Donath contributed equally to this article.
N Engl J Med 2007;356:1517-26.Copyright © 2007 Massachusetts Medical Society.
A BS TR AC T
Background
The expression of interleukin-1–receptor antagonist is reduced in pancreatic islets of patients with type 2 diabetes mellitus, and high glucose concentrations induce the production of interleukin-1β in human pancreatic beta cells, leading to impaired insulin secretion, decreased cell proliferation, and apoptosis.
Methods
In this double-blind, parallel-group trial involving 70 patients with type 2 diabetes, we randomly assigned 34 patients to receive 100 mg of anakinra (a recombinant human interleukin-1–receptor antagonist) subcutaneously once daily for 13 weeks and 36 patients to receive placebo. At baseline and at 13 weeks, all patients under-went an oral glucose-tolerance test, followed by an intravenous bolus of 0.3 g of glucose per kilogram of body weight, 0.5 mg of glucagon, and 5 g of arginine. In addition, 35 patients underwent a hyperinsulinemic–euglycemic clamp study. The primary end point was a change in the level of glycated hemoglobin, and secondary end points were changes in beta-cell function, insulin sensitivity, and inflammatory markers.
Results
At 13 weeks, in the anakinra group, the glycated hemoglobin level was 0.46 per-centage point lower than in the placebo group (P = 0.03); C-peptide secretion was enhanced (P = 0.05), and there were reductions in the ratio of proinsulin to insulin (P = 0.005) and in levels of interleukin-6 (P<0.001) and C-reactive protein (P = 0.002). Insulin resistance, insulin-regulated gene expression in skeletal muscle, serum adipokine levels, and the body-mass index were similar in the two study groups. Symptomatic hypoglycemia was not observed, and there were no apparent drug-related serious adverse events.
Conclusions
The blockade of interleukin-1 with anakinra improved glycemia and beta-cell secre-tory function and reduced markers of systemic inflammation. (ClinicalTrials.gov number, NCT00303394.)

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071518
T ype 2 diabetes mellitus occurs when beta-cell function fails to compensate for insulin resistance.1,2 Beta-cell function pro-
gressively deteriorates with an increasing dura-tion of diabetes,3 partly because of beta-cell demise through apoptosis.4-6
Interleukin-1β, a proinflammatory cytokine7 implicated as an effector molecule of inflam-matory beta-cell destruction leading to type 1 dia-betes,8 inhibits the function and promotes the apoptosis of beta cells.9 Beta cells producing inter-leukin-1β have been observed in pancreatic sec-tions obtained from patients with type 2 diabe-tes.10 Depending on culture conditions, high glucose levels increase beta-cell production and the release of interleukin-1β, followed by func-tional impairment and apoptosis.10-13 These find-ings suggest that intra-islet production of inflam-matory mediators has a role in the pathogenesis of type 2 diabetes and that interleukin-1β is a potential therapeutic target for preserving beta-cell mass and function in patients with this con-dition.
Interleukin-1–receptor antagonist, a naturally occurring competitive inhibitor of interleukin-1 binding to the type I receptor,7,14 protects human beta cells from glucose-induced functional im-pairment and apoptosis.10 Interleukin-1–receptor antagonist is reported to have no agonistic activ-ity.7,15 The expression of interleukin-1–receptor antagonist is decreased in beta cells obtained from patients with type 2 diabetes.16 Given these observations, we hypothesized that intervening in the islet balance between interleukin-1–receptor antagonist and interleukin-1β might improve beta-cell function and glycemic control in patients with type 2 diabetes.
Me thods
Study Design
This placebo-controlled, double-blind, parallel-group study involved 70 patients with type 2 dia-betes at two centers (31 patients in Denmark and 39 patients in Switzerland) who were recruited from January 2004 to March 2005. Patients re-ceived either once-daily recombinant human inter-leukin-1–receptor antagonist (100 mg of anakinra [Kineret] donated by Amgen) or placebo by sub-cutaneous self-administration in the morning for 13 weeks. Patients continued their baseline anti-diabetic therapy, dietary habits, and other lifestyle habits.
The County Pharmacy of Zurich was responsi-ble for the blinding and randomization procedure; the latter was performed with the use of permut-ed blocks within the recruiting center. The au-thors designed the study, gathered and analyzed the data, wrote the manuscript, and vouch for the accuracy and completeness of the data and the analysis. There was no confidentiality agreement between the authors or their institutions and Amgen, which provided the study drugs.
Patients
We conducted the study in accordance with the ethical guidelines of the Declaration of Helsinki II; the study design was approved by regional and institutional review boards. Written informed con-sent was obtained from all patients before ran-domization.
The inclusion criteria were an age of 20 years or more, type 2 diabetes diagnosed according to American Diabetes Association criteria17 with a duration of more than 3 months, a body-mass index (BMI, the weight in kilograms divided by the square of the height in meters) of more than 27, and a glycated hemoglobin level of more than 7.5% (upper limit of the normal range, 6.4%). Eligible patients had had no changes in either types or doses of medications during the 3-month period preceding the study.
The exclusion criteria were the presence of autoantibodies to glutamic acid decarboxylase 65 or islet-cell autoantibody-2; a glycated hemoglobin level of more than 12%; a fasting C-peptide level of less than 400 pmol per liter; current treatment with antiinflammatory drugs, including cortico-steroids and nonsteroidal antiinflammatory drugs (100 mg or less of aspirin per day was allowed); signs of current infection, including a C-reactive protein level of more than 30 mg per liter, fever, current treatment with antibiotics, chronic gran-ulomatous infections (e.g., a previous diagnosis of tuberculosis or a current diagnosis based on chest radiography or a Mantoux test); a history of recurrent infection or a predisposition to infec-tion; neutropenia (a leukocyte count of less than 2000 per cubic millimeter) or anemia (a hemo-globin level of less than 11 g per deciliter for men and less than 10 g per deciliter for women); pregnancy or breast-feeding (contraception for at least 3 months before inclusion was required for fertile women); liver or renal disease (a level of aspartate aminotransferase or alanine amino-transferase of more than three times the upper

Interleukin-1–Receptor Antagonist in Type 2 Diabetes
n engl j med 356;15 www.nejm.org april 12, 2007 1519
limit of the normal range and a serum creati-nine level of more than 130 μmol per liter); on-going or previous cancer; the use of any other investigational drug within 30 days before en-rollment or within five half-lives of the medica-tion used in the other study, whichever was the longer period; and immunosuppressive treatment or immunodeficiency.
Study Procedures
At baseline and 13 weeks, a 2-hour oral glucose-tolerance test was performed with 75 g of glucose, followed by measurements of plasma glucose, pro-insulin, insulin, and C-peptide 10 minutes before and during the test and measurements of plasma glucose, insulin, and C-peptide 30, 60, 90, and 120 minutes after the test. Immediately after the end of the oral glucose-tolerance test, an intrave-nous injection of 0.3 g of glucose per kilogram of body weight, 0.5 mg of glucagon, and 5 g of argi-nine was administered. Blood was then sampled at 0, 3, 6, 9, and 12 minutes. The patients were asked to forgo their antidiabetic medication and to fast for 8 to 9 hours before the test.
At baseline and 13 weeks, euglycemic–hyper-insulinemic clamp studies18 and muscle biopsies were performed. All patients were asked to par-ticipate in the clamp and muscle-biopsy studies, although participation in these studies was not a requirement for remaining in the overall study. The patients were required to forgo antidiabetic treatment for 8 to 9 hours and to avoid strenuous physical exercise for 24 hours before the clamp study. The clamp procedure was performed 2 to 7 days after the oral glucose-tolerance test. Indi-rect calorimetry was performed during the insu-lin-stimulated 30-minute steady-state period. The insulin-sensitivity index during the clamp proce-dure was calculated by dividing the M value (the glucose infusion rate during the steady-state period divided by the total body weight) by the steady-state plasma insulin level.
Biopsy specimens were obtained from the vas-tus lateralis muscle immediately after the ad-ministration of the intravenous bolus at the end of the oral glucose-tolerance test. Messenger RNA (mRNA) from glucose transporter 4 (GLUT4) and peroxisome-proliferator–activated receptor γ co-activator 1α (PGC-1α)19,20 was quantified as de-scribed in the Supplementary Appendix (avail-able with the full text of this article at www.nejm.org).
Levels of C peptide, insulin, and proinsulin
were determined centrally at the Steno Diabetes Center. Insulin and proinsulin were assessed by enzyme-linked immunosorbent assays,21,22 and C-peptide levels were determined by a time-resolved fluoroimmunoassay.23 Measurements of glycated hemoglobin levels and routine clinical laboratory tests were performed in the central laboratory units of the two participating centers. For glycat-ed hemoglobin, 22 coded samples from patients were tested at both laboratories. Regression analy-sis showed an r2 value of 0.97 for agreement be-tween the test results (P<0.001). Serum adipo-kines were assayed with the use of Luminex technology (Millipore) according to the manufac-turer’s instructions.
A physical examination and blood tests were performed at baseline and at 4 and 13 weeks. Fasting plasma glucose levels were measured weekly at home by the patients. At baseline and 13 weeks, funduscopy was performed, and uri-nary albumin excretion, creatinine clearance, and (in women) human chorionic gonadotropin were measured.
Study End Points
The predefined primary end point was the change in the glycated hemoglobin level between baseline and 13 weeks. Predefined secondary end points included a change by week 13 in the area under the concentration–time curve (AUC) for stimulat-ed C-peptide during an oral glucose-tolerance test and after intravenous stimulation, a change in the ratio of fasting proinsulin to insulin, a change in the insulin-sensitivity index derived from the oral glucose-tolerance test,24 a change in serum adipo-kine levels, a change in insulin sensitivity as as-sessed by a euglycemic–hyperinsulinemic clamp study (in the 35 patients who provided consent for this procedure), a change in insulin-regulated genes in biopsy specimens obtained from skele-tal muscle, and changes in levels of fasting plasma glucose, interleukin-6, and C-reactive protein as markers of systemic inflammation.
Statistical Analysis
No interim analyses were carried out in this study. Data from all patients were analyzed. Values are expressed as means (±SD) unless otherwise spec-ified. Differences were tested with the use of an unpaired t-test and with a Wilcoxon rank-sum test in the case of non-normal distribution. For cate-gorical end points, Pearson’s chi-square test was used. Correlations were performed by regression

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071520
analysis. To analyze the effect of baseline charac-teristics on the primary end point, bivariate re-gression analyses including the treatment effect were performed. A P value of less than 0.05 was considered to indicate statistical significance. All reported P values are two-sided and have not been adjusted for multiple testing.
R esult s
Baseline Characteristics and Adherence
Seventy of the 124 subjects who underwent initial screening were randomly assigned to receive ei-ther anakinra or placebo (Fig. 1). In the placebo group, a late positive Mantoux reaction developed in one patient, suggesting a reactivation of tuber-culosis, and the patient was excluded before start-ing study medication. Table 1 shows the baseline characteristics of the two study groups after ran-domization.
All 34 patients receiving anakinra completed the study, as did 33 of 35 patients receiving pla-cebo. In the placebo group, a phlegmonous foot infection developed in one patient after 4 weeks, and one patient identified his study-group assign-ment by performing a biochemical analysis of the study drug after 5 weeks. Two patients in the anakinra group and one in the placebo group re-duced the dose of their antidiabetic medication during the intervention because of improvement in glycemia but were not excluded from the study, according to the intention-to-treat principle. The remaining patients did not change their antidia-betic therapy during the 13-week study period, as reflected by recorded types and doses of antidia-betic medication at baseline and at 4 and 13 weeks (data not shown). Thirty-five subjects (16 in the anakinra group and 19 in the placebo group) gave informed consent to participate in the clamp and muscle-biopsy studies. The patients who provided consent did not differ in their baseline character-istics from those who declined (data not shown). The peak serum levels of interleukin-1–receptor antagonist, measured 1 to 2 hours after the last injection of anakinra or placebo at 13 weeks, were 1256±958 μg per liter in the anakinra group and 0.6±0.4 μg per liter in the placebo group (P< 0.001).
Primary End Point
The average absolute difference in glycated hemo-globin levels between baseline and 13 weeks was a reduction of 0.33 percentage point (from 8.69±0.17 to 8.37±0.21) in the anakinra group and an in-crease of 0.13 percentage point (from 8.23±0.28 to 8.37±0.46) in the placebo group, yielding a be-tween-group difference of 0.46 percentage point (95% confidence interval [CI], 0.01 to 0.90; P = 0.03) (Fig. 2A). The number of patients who had any reduction in glycated hemoglobin levels
22p3
124 Were screened
70 Underwent randomization
34 Were assignedto anakinra
35 Were assignedto placebo
312 Patients were recruited
188 Did not respond,were not interested,or were not eligible
33 Completed the study34 Completed the study
54 Were not eligible
1 Was excluded from placebogroup because of a late
positive Mantoux reaction
2 Withdrew1 Had a phlegmonous
foot infection 1 Became aware of his
study-group assign-ment
AUTHOR:
FIGURE:
JOB: ISSUE:
4-CH/T
RETAKE
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
Enon
1st
2nd3rd
Larsen (Donath)
1 of 4
04-12-07
ARTIST: ts
35615
Figure 1. Enrollment and Outcomes.
A total of 312 patients with type 2 diabetes mellitus were recruited either in the outpatient clinics of the two participating centers or through newspaper advertisements. Of those, 188 patients did not respond, were not interest-ed, or were not eligible on the basis of their medical history. Of the 124 pa-tients who underwent physical and biochemical screening, 54 were found to be ineligible according to entry criteria, in most cases because they had either a glycated hemoglobin level of less than 7.5% or a fasting C-peptide level of less than 400 pmol per liter. Seventy patients were randomly assigned to receive either anakinra or placebo. In the placebo group, one patient was excluded before starting study medication and two patients withdrew after 4 and 5 weeks of treatment. A total of 67 patients completed the 13-week treatment and evaluation of study end points.

Interleukin-1–Receptor Antagonist in Type 2 Diabetes
n engl j med 356;15 www.nejm.org april 12, 2007 1521
at 13 weeks was 21 of 34 patients in the anakinra group, as compared with 10 of 33 patients in the placebo group (P<0.001). Glycated hemoglobin levels were significantly lower in the anakinra group after 4 weeks than in the placebo group (an absolute reduction of 0.36%; 95% CI, 0.11 to 0.60; P = 0.004) (Fig. 2A). When the patients were stratified into three equal groups according to body-surface area as a surrogate for drug distri-bution volume, the difference in glycated hemo-globin levels in the anakinra group was a reduc-tion of 0.84% in the lowest third (<2.00 m2), a reduction of 0.30% in the intermediate group
(2.00 to 2.24 m2), and an increase of 0.11% in the highest third (>2.24 m2) (P = 0.02 for all compari-sons) (Fig. 2C). Accordingly, body-surface area cor-related with the changes in glycated hemoglobin levels in the anakinra group (r2 = 0.22, P = 0.007) but not in the placebo group (r2 = 0.001, P = 0.87).
Secondary End PointsGlycemiaFasting plasma glucose levels that were measured by the patients at home once weekly were consis-tently lower in the anakinra group than in the placebo group (Fig. 2B). At 13 weeks, plasma glu-
Table 1. Baseline Characteristics of the Patients.*
Characteristic Anakinra (N = 34) Placebo (N = 35) P Value
Age (yr) 60.6±8.7 60.3±8.6 0.89
Sex (no.)
Male 23 27
Female 11 8 0.39
Body-mass index 31.5±5.2 31.8±4.4 0.82
Weight (kg) 94.5±16.7 97.0±9.0 0.43
Glycated hemoglobin (%) 8.7±1.0 8.2±0.9 0.05
Fasting plasma glucose (mmol/liter) 10.8±2.7 10.0±3.1 0.24
Fasting C-peptide (pmol/liter) 958±312 907±508 0.62
Diabetes duration (yr) 10.6±6.2 11.0±7.3 0.82
Smoking status (%)
Current 15 17
Former 41 33 0.79
Cholesterol (mmol/liter)
Total 4.65±1.12 4.86±1.42 0.50
HDL 1.35±1.27 1.09±0.33 0.25
Creatinine (μmol/liter) 91.5±21.5 94.3±21.9 0.60
Blood pressure (mm Hg)
Systolic 145.8±15.9 146.4±18.7 0.89
Diastolic 83.4±7.9 82.7±8.2 0.75
Use of antihypertensive medication (%) 71 74 0.73
History of cardiovascular disease (%) 47 23 0.04
Albumin excretion rate >30 mg/liter/24 hr (%) 33 32 0.93
Retinopathy (%) 21 31 0.31
Antidiabetic treatment (%) 0.53
Diet 9 6
Oral drug 53 43
Insulin (alone or with oral drug) 38 51
* Plus–minus values are means ±SD. The body-mass index is the weight in kilograms divided by the square of the height in meters. To convert cholesterol values to milligrams per deciliter, divide by 0.02586. To convert creatinine values to milligrams per deciliter, divide by 88.4. HDL denotes high-density lipoprotein.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071522
cose levels at the beginning and end of a 2-hour oral glucose-tolerance test were reduced by 0.6 mM (95% CI, 0.05 to 1.60; P = 0.29) and 1.3 mM (95% CI, 0.00 to 2.6; P = 0.05), respectively, in the ana-kinra group, as compared with the placebo group.
Beta-Cell Secretory FunctionAt 13 weeks, beta-cell function increased in the anakinra group and decreased in the placebo group (Fig. 3). In particular, the ratio of proinsulin to in-sulin was markedly lower in the anakinra group (P = 0.005). The changes in beta-cell function as-sessed on the basis of the AUC from the oral glucose-tolerance test and intravenous tests were
significantly correlated (P<0.001) (data not shown). The change in beta-cell function was correlated with changes in glycated hemoglobin levels in pa-tients in the anakinra group but not in the placebo group. The correlation between the change in gly-cated hemoglobin levels and the AUC for stimu-lated C-peptide during the oral glucose-tolerance test was r2 = 0.13 (P = 0.04) in the anakinra group and r2 = 0.04 (P = 0.76) in the placebo group; the cor-relation for intravenous stimulation was r2 = 0.32 (P<0.001) in the anakinra group and r2 = 0.03 (P = 0.29) in the placebo group; and the correlation for the two tests combined was r2 = 0.18 (P = 0.02) in the anakinra group and r2 = 0.01 (P = 0.59) in
AUTHOR:
FIGURE:
JOB: ISSUE:
4-CH/T
RETAKE
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE:Figure has been redrawn and type has been reset.
Please check carefully.
REG F
Enon
1st2nd3rd
Larsen (Donath)
2 of 4
04-12-07
ARTIST: ts
35615
33p9
Gly
cate
d H
emog
lobi
n (%
)0.1
0.2
0.0
−0.1
−0.3
−0.4
−0.2
−0.5
−0.64 13
Week
0.3
P=0.004P=0.03
Fast
ing
Plas
ma
Glu
cose
(mm
ol/l
iter)
0.5
0.0
−0.5
−1.0
−2.0
−1.5
1 2 3 4 5 6 7 8 9 10 11 120 13
Week
1.0
P<0.05P<0.0
5P<0.01
P<0.01
Gly
cate
d H
emog
lobi
n (%
)
0.0
−0.4
−0.8
−1.2<2.00 2.00–2.24 >2.24 <2.13 2.13–2.23 >2.23
Body-Surface Area (m2)
Anakinra Placebo
0.4P=0.02
Gly
cate
d H
emog
lobi
n (%
)
0.0
−0.4
−0.8
−1.2
Body-Surface Area (m2)
0.4
A B
C D
Placebo
Placebo
Anakinra
Anakinra
Figure 2. Changes in Glycated Hemoglobin and Fasting Plasma Glucose Levels during the 13-Week Study Period.
Panel A shows the average absolute difference in glycated hemoglobin levels between baseline and 4 and 13 weeks in each study group. Panel B shows the average absolute differences in fasting plasma glucose levels between the baseline value and weekly measurements performed by the patients at home during the 13-week study period. Pan-els C and D show the average absolute differences in glycated hemoglobin levels at 13 weeks in each study group stratified into thirds according to body-surface area. In the placebo group, the analysis included 35 patients at week 4, 34 at week 5, and 33 at week 13. In the anakinra group, the analysis included 34 patients at each weekly measure. The I bars indicate standard errors.

Interleukin-1–Receptor Antagonist in Type 2 Diabetes
n engl j med 356;15 www.nejm.org april 12, 2007 1523
the placebo group. Baseline glycated hemoglobin values did not correlate with the beta-cell secre-tion tests in patients in the anakinra group. The correlation between the starting glycated hemo-globin level and the AUC for stimulated C-pep-tide during the oral glucose-tolerance test was r2 = 0.05 (P = 0.22), the correlation for intravenous stimulation was r2 = 0.09 (P = 0.10), and the cor-relation for both tests combined was r2 = 0.06 (P = 0.17).
Insulin SensitivityWith the dose of anakinra used in this study, no differences in insulin sensitivity were found at 13 weeks. The M value divided by the plasma insulin level during the steady-state period in the euglyce-mic–hyperinsulinemic clamp study was reduced by 0.13±1.76 μg of glucose per kilogram of body weight per picomole of insulin per minute in the anakinra group and by 0.56±2.52 μg of glucose per kilogram of body weight per picomole of insu-lin per minute in the placebo group (P = 0.58). The insulin-sensitivity index, as calculated by the ho-meostasis model assessment (HOMA) on the basis of the oral glucose-tolerance test in all patients, increased by 0.003±0.179 square liter per milliunit of insulin per millimole of glucose in the anakinra group and by 0.029±0.228 square liter per milliunit of insulin per millimole of glucose in the placebo group (P = 0.60). The insulin-sensitivity index on the basis of data from the oral glucose-tolerance test strongly correlated with the clamp data (r2 = 0.53, P<0.001). There was no correlation be-tween insulin sensitivity as determined by the clamp method and the primary end point at 13 weeks (r2 = 0.005, P = 0.60) and no change in oxida-tion rates of glucose, with an increase of 0.02±0.7 mg of oxidized glucose per kilogram per minute in the anakinra group and a decrease of 0.15±0.37 mg per kilogram per minute in the placebo group (P = 0.44) or of fat, with a decrease of 0.05±0.26 mg per kilogram per minute in the anakinra group and an increase of 0.03±0.2 mg per kilogram per minute in the placebo group (P = 0.36).
Markers of Systemic InflammationLevels of C-reactive protein were significantly lower after 4 and 13 weeks in the anakinra group than in the placebo group (P = 0.02 after 4 weeks and P = 0.002 after 13 weeks) (Fig. 4A). Similar declines in interleukin-6 levels were observed
(P<0.001 after both 4 and 13 weeks) (Fig. 4B). Neither baseline values nor changes in levels of C-reactive protein or interleukin-6 were signifi-cantly correlated with changes in glycated hemo-globin in the anakinra group: r2<0.001 (P = 0.89) for baseline C-reactive protein levels, r2<0.001 (P = 0.95) for changes in C-reactive protein, r2 = 0.005 (P = 0.70) for baseline interleukin-6, and r2 = 0.001 (P = 0.86) for changes in interleukin-6. As previously ob-served,25 neutrophil and platelet counts were slight-ly and reversibly decreased during anakinra ther-apy. Neutrophil counts decreased by 1200±1400
22p3
Placebo Anakinra Placebo Anakinra
Placebo Anakinra Placebo Anakinra
AUTHOR:
FIGURE:
JOB: ISSUE:
4-CH/T
RETAKE
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE:Figure has been redrawn and type has been reset.
Please check carefully.
REG F
Enon
1st2nd
3rd
Larsen (Donath)
3 of 4
04-12-07
ARTIST: ts
35615
Cha
nge
from
Bas
elin
e
0.0
−0.1
−0.2
0.1
P=0.005
P=0.05
Cha
nge
from
Bas
elin
e (n
mol
/lite
r ×m
in)
10
0
−10
−20
20
Cha
nge
from
Bas
elin
e (n
mol
/lite
r ×m
in)
0
1
2
−1
−2
−4
−3
3
P=0.08P=0.05
Cha
nge
from
Bas
elin
e (n
mol
/lite
r ×m
in)
0
10
5
15
20
−10
−5
−15
−20
25
A Ratio of Proinsulin to Insulin B AUC for C-Peptide after Oral Glucose
C AUC for C-Peptide after IV Glucose D AUC for C-Peptide after Oral and IV Glucose Combined
Figure 3. Beta-Cell Secretory Function.
Beta-cell secretory function was assessed by analysis of the ratio of pro-insulin to insulin and by a 2-hour oral glucose-tolerance test, followed by intravenous stimulation with 0.3 g of glucose per kilogram of body weight, 0.5 mg of glucagon, and 5 g of arginine. Average absolute differences be-tween baseline and 13 weeks in each study group are shown, including the change in the ratio of proinsulin to insulin (Panel A), the change in the area under the concentration–time curve (AUC) for C-peptide in response to a 2-hour oral glucose-tolerance test (Panel B), the change in the AUC for C-peptide in response to an intravenous (IV) stimulation test (Panel C), and the change in the AUC for the combination of oral and intravenous stimulation (Panel D). The analysis included 33 patients in the placebo group and 34 in the anakinra group. The I bars indicate standard errors.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071524
per cubic millimeter in the anakinra group and by 100±1300 per cubic millimeter in the placebo group; platelet counts decreased by 16,000±25,400 per cubic millimeter in the anakinra group and increased by 3000±23,000 per cubic millimeter in the placebo group (P<0.001).
Insulin-Regulated Gene ExpressionTreatment with anakinra for 13 weeks did not significantly change the mRNA expression levels of the insulin-regulated genes GLUT4 (P = 0.81) and PGC-1α (P = 0.26) in biopsy specimens of skeletal muscle, with decreases of 0.23±1.43 for the rela-tive expression levels of GLUT4 and 0.12±0.87 for PGC-1α normalized to the housekeeping gene cyclophilin A in the anakinra group, as compared with decreases of 0.34±0.72 in the expression lev-els of GLUT4 and 0.52±0.79 for PGC-1α in the placebo group.
Serum AdipokinesLevels of serum adipokines were not significantly changed at 13 weeks in either the anakinra group or the placebo group. The levels changed as fol-lows for the comparison between the study groups: leptin, a decrease of 0.40±6.86 ng per milliliter in the anakinra group and an increase of 2.81±10.98 ng per milliliter in the placebo group (P = 0.16); adiponectin, an increase of 3.69±11.36 μg per milliliter in the anakinra group and a decrease of 1.00±8.59 μg per milliliter in the placebo group
(P = 0.07); resistin, a decrease of 2.80±8.56 ng per milliliter in the anakinra group and an increase of 0.27±7.65 ng per milliliter in the placebo group (P = 0.14); tumor necrosis factor α, a decrease of 0.13±1.44 pg per milliliter in the anakinra group and an increase of 0.11±1.56 pg per milliliter in the placebo group (P = 0.52); monocyte chemotac-tic factor 1, an increase of 9.2±50.8 pg per milli-liter in the anakinra group and a decrease of 3.3±93.0 pg per milliliter in the placebo group (P = 0.50); and interleukin-8, a decrease of 0.81±4.55 pg per milliliter in the anakinra group and a de-crease of 0.08±1.17 pg per milliliter in the placebo group (P = 0.40).
Other Outcomes
The baseline body weight and BMI were signif-icantly correlated with changes in glycated he-moglobin levels (covariate effect, P = 0.003 and P = 0.004, respectively; treatment effect, P = 0.08 and P = 0.05, respectively; and combined effect, P = 0.001 and P = 0.002, respectively). This corre-lation was not observed for the other baseline variables.
Adverse Events
There were no significant changes in BMI in either group from baseline to 13 weeks, with levels chang-ing from 31.5±5.2 to 31.8±5.6 in the anakinra group (P = 0.82) and 31.8±4.4 to 32.0±4.4 in the placebo group (P = 0.85) (P = 0.38 for the compari-son between study groups). No patient withdrew from the study because of drug-related adverse events. In particular, symptomatic hypoglycemia was not observed, even in patients with a marked improvement in glycated hemoglobin levels. All reported adverse events are listed in Table 2. In the anakinra group, the improvement in glycated hemoglobin levels did not differ between patients who had injection-site reactions and those who did not. There was a decrease of 0.24±0.18% in the glycated hemoglobin level in patients with injec-tion-site reactions and a decrease of 0.64±0.32% in those without injection-site reactions (P = 0.54). No changes were observed in blood pressure or heart rate or in levels of serum sodium, potassium, aspartate aminotransferase, alanine aminotrans-ferase, lipids (including free fatty acids, total cho-lesterol, high-density lipoprotein, low-density lipo-protein, and triglycerides), cystatin C, or creatinine or in creatinine clearance, 24-hour urinary albu-min excretion, or retinal fundus. Total hemoglo-
22p3
AUTHOR:
FIGURE:
JOB: ISSUE:
4-CH/T
RETAKE
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE:Figure has been redrawn and type has been reset.
Please check carefully.
REG F
Enon
1st2nd3rd
Larsen (Donath)
4 of 4
04-12-07
ARTIST: ts
35615
Cha
nge
from
Bas
elin
e (m
g/lit
er)
0
−1
−2
−3
−4
−5
−6
Week
1 P=0.002P=0.02 P<0.001P<0.001
Cha
nge
from
Bas
elin
e (n
g/lit
er)
0
−1
−3
−2
Week
1
A C-Reactive Protein B Interleukin-6
4 13 4 13
Placebo Anakinra Placebo Anakinra
Figure 4. Markers of Systemic Inflammation.
The average absolute differences between baseline and 4 and 13 weeks in each study group are shown for levels of circulating C-reactive protein (Panel A) and interleukin-6 (Panel B). In the placebo group, the analysis included 35 patients at week 4 and 33 at week 13. In the anakinra group, the analysis in-cluded 34 patients at weeks 4 and 13. The I bars indicate standard errors.

Interleukin-1–Receptor Antagonist in Type 2 Diabetes
n engl j med 356;15 www.nejm.org april 12, 2007 1525
bin was unchanged, a finding that made changes in erythrocyte turnover unlikely as a confounder.
Discussion
Our study shows that antagonism of interleukin-1 signaling with anakinra improved glycemic con-trol in patients with type 2 diabetes, most likely through enhanced beta-cell secretory function. In-deed, improved glycemia in patients who received anakinra correlated with improved measures of beta-cell secretory capacity. There were no altera-tions in insulin sensitivity on the basis of insulin clamp studies, insulin sensitivity indexes modeled on the oral glucose-tolerance test, insulin-regu-lated gene expression in skeletal muscle, or serum adipokine levels. Finally, the BMIs of patients re-mained stable, thus excluding an anorexigenic effect of anakinra. However, we cannot exclude the possibility that higher doses of anakinra might improve insulin sensitivity.
Neither baseline levels of C-reactive protein or interleukin-6 nor changes in the levels correlated with changes in glycated hemoglobin levels, sug-gesting that reduced systemic inflammation did not play an important part in improved insulin secretion. Genetic ablation of systemic interleu-kin-1 action causes obesity.26,27 It has therefore been proposed that interleukin-1 regulates body composition and fat distribution, mainly through the regulation of feeding behavior, satiety regula-tion, and energy metabolism, including thermo-genesis. The integral physiological measure of these actions is body weight. In our study, the in-hibition of the action of interleukin-1 by anakinra did not increase body weight.
Limitations of our study include its short dura-tion and the lack of dose finding. Considering the short half-life of anakinra (6 to 8 hours), it is pos-sible that higher doses or longer-lasting antago-nism of interleukin-1 might improve the outcome.28 The association between body weight or body-surface area at baseline and the glycemic outcome suggests that the anakinra dose might be increased according to the drug-distribution volume.
Apart from self-limited local reactions at the injection site, we observed no clear difference in the frequency of adverse events between the ana-kinra group and the placebo group. No patient stopped treatment because of adverse reactions. Symptomatic hypoglycemia was not reported by any patient. A potential concern with the use of
interleukin-1 blockade is the inhibition of innate immunity and the occurrence of infection. How-ever, in more than 100,000 patients with rheuma-toid arthritis who underwent long-term treatment with anakinra, there was no significant increase in the incidence of infectious disease, despite con-comitant immunosuppression.28
In summary, our study suggests that antago-nism of interleukin-1 has possible therapeutic potential in the treatment of type 2 diabetes. Fur-ther studies are needed to test higher doses of anakinra, to evaluate its long-term use, and to test interleukin-1 antagonists that have a pro-longed half-life, with the aim of preventing beta-cell destruction and promoting beta-cell regener-ation in type 2 diabetes.
Supported by the Bonizzi-Theler and Hartmann-Müller Foun-dations, the Center of Clinical Studies at the University of Zurich, the Swiss National Science Foundation, the European Union, and Novo Nordisk. Amgen provided the study drugs at no cost.
Dr. Donath is listed as the inventor on a patent (WO6709) filed in 2003 for the use of an interleukin-1–receptor antagonist for the treatment of or prophylaxis against type 2 diabetes. The patent is owned by the University of Zurich, and Dr. Donath has no financial interest in the patent. Dr. Vølund reports being an employee of Novo Nordisk. Drs. Larsen, Vaag, Vølund, and Man-drup-Poulsen report having an equity interest in Novo Nordisk. Drs. Vaag and Mandrup-Poulsen report receiving grant support from Novo Nordisk. No other potential conflict of interest rele-vant to this article was reported.
We thank Erol Cerasi and Steven Kahn for their advice and critical reading of the manuscript; study nurses Erika Wettstein and Regula Messmer; laboratory technicians Hanne Foght, Helle Niebling, Charlotte Leth, Marianne Modest, and Margaretha Siegfried-Kellenberger; and study administrators Karen Kruse and Michèle Rothfuchs.
Table 2. Adverse Events.
Event Anakinra (N = 34)
Placebo (N = 35)
no. of patients
Transient injection-site reactions* 17 0
Minor injection-site hematoma 1 0
Mild nausea 1 0
Transient peripheral facial-nerve palsy (day 40) 1 0
Urinary tract infection (days 26–28) 1 0
Upper respiratory tract infection (days 41–45) 1 0
Transient mild elevation of aspartate amino-transferase (day 87) 1 0
Dry cough 0 1
Peroneal-nerve palsy 0 1
Calf pain 0 1
Phlegmonous foot infection 0 1
* The reactions were first seen between days 6 and 14 and disappeared between days 19 and 38.

n engl j med 356;15 www.nejm.org april 12, 20071526
Interleukin-1–Receptor Antagonist in Type 2 Diabetes
References
full text of all journal articles on the world wide web
Access to the complete text of the Journal on the Internet is free to all subscribers. To use this Web site, subscribers should go to the Journal’s home page (www.nejm.org) and register by entering their names and subscriber numbers as they appear on their mailing labels. After this one-time registration, subscribers can use their passwords to log on for electronic access to the entire Journal from any computer that is connected to the Internet. Features include a library of all issues since January 1993 and abstracts since January 1975, a full-text search capacity, and a personal archive for saving articles and search results of interest. All articles can be printed in a format that is virtually identical to that of the typeset pages. Beginning 6 months after publication, the full text of all Original Articles and Special Articles is available free to nonsubscribers who have completed a brief registration.
Cerasi E, Luft R. Insulin response to glucose infusion in diabetic and non-dia-betic monozygotic twin pairs: genetic con-trol of insulin response? Acta Endocrinol (Copenh) 1967;55:330-45.
DeFronzo RA. Lilly Lecture 1987. The triumvirate: beta-cell, muscle, liver — a collusion responsible for NIDDM. Dia-betes 1988;37:667-87.
U.K. Prospective Diabetes Study Group. U.K. Prospective Diabetes Study 16 — overview of 6 years’ therapy of type II diabetes: a progressive disease. Diabetes 1995;44:1249-58. [Erratum, Diabetes 1996; 45:1655.]
Butler AE, Janson J, Bonner-Weir S, Ritzel R, Rizza RA, Butler PC. Beta-cell deficit and increased beta-cell apoptosis in humans with type 2 diabetes. Diabetes 2003;52:102-10.
Hellerstrom C. The life story of the pancreatic B cell. Diabetologia 1984;26: 393-400.
Donath MY, Halban PA. Decreased beta-cell mass in diabetes: significance, mechanisms and therapeutic implications. Diabetologia 2004;47:581-9.
Dinarello CA. Biologic basis for inter-leukin-1 in disease. Blood 1996;87:2095-147.
Mandrup-Poulsen T. The role of inter-leukin-1 in the pathogenesis of IDDM. Diabetologia 1996;39:1005-29.
Bendtzen K, Mandrup-Poulsen T, Nerup J, Nielsen JH, Dinarello CA, Sven-son M. Cytotoxicity of human pI 7 inter-leukin-1 for pancreatic islets of Langer-hans. Science 1986;232:1545-7.
Maedler K, Sergeev P, Ris F, et al. Glucose-induced beta-cell production of IL-1beta contributes to glucotoxicity in human pancreatic islets. J Clin Invest 2002;110:851-60.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Maedler K, Spinas GA, Lehmann R, et al. Glucose induces beta-cell apoptosis via upregulation of the Fas-receptor in human islets. Diabetes 2001;50:1683-90.
Maedler K, Storling J, Sturis J, et al. Glucose- and interleukin-1beta-induced beta-cell apoptosis requires Ca2+ influx and extracellular signal-regulated kinase (ERK) 1/2 activation and is prevented by a sulfonylurea receptor 1/inwardly rectify-ing K+ channel 6.2 (SUR/Kir6.2) selective potassium channel opener in human islets. Diabetes 2004;53:1706-13.
Welsh N, Cnop M, Kharroubi I, et al. Is there a role for locally produced inter-leukin-1 in the deleterious effects of high glucose or the type 2 diabetes milieu to human pancreatic islets? Diabetes 2005;54: 3238-44.
Dinarello CA. The role of the interleu-kin-1–receptor antagonist in blocking in-f lammation mediated by interleukin-1. N Engl J Med 2000;343:732-4.
Zumsteg U, Reimers JI, Pociot F, et al. Differential interleukin-1 receptor antag-onism on pancreatic beta and alpha cells: studies in rodent and human islets and in normal rats. Diabetologia 1993;36:759-66.
Maedler K, Sergeev P, Ehses JA, et al. Leptin modulates beta cell expression of IL-1 receptor antagonist and release of IL-1beta in human islets. Proc Natl Acad Sci U S A 2004;101:8138-43.
American Diabetes Association. Diag-nosis and classification of diabetes melli-tus. Diabetes Care 2006;29:Suppl 1:S43-S48.
Vaag A, Alford F, Henriksen FL, Chris-topher M, Beck-Nielsen H. Multiple de-fects of both hepatic and peripheral intra-cellular glucose processing contribute to the hyperglycaemia of NIDDM. Diabeto-logia 1995;38:326-36.
11.
12.
13.
14.
15.
16.
17.
18.
Mootha VK, Lindgren CM, Eriksson KF, et al. PGC-1alpha-responsive genes involved in oxidative phosphorylation are coordinately downregulated in human dia-betes. Nat Genet 2003;34:267-73.
Ling C, Poulsen P, Carlsson E, et al. Multiple environmental and genetic fac-tors influence skeletal muscle PGC-1alpha and PGC-1beta gene expression in twins. J Clin Invest 2004;114:1518-26.
Andersen L, Dinesen B, Jorgensen PN, Poulsen F, Roder ME. Enzyme immunoas-say for intact human insulin in serum or plasma. Clin Chem 1993;39:578-82.
Hartling SG, Dinesen B, Kappelgard AM, Faber OK, Binder C. ELISA for hu-man proinsulin. Clin Chim Acta 1986;156: 289-97.
Heding LG. Radioimmunological de-termination of human C-peptide in serum. Diabetologia 1975;11:541-8.
Wallace TM, Levy JC, Matthews DR. Use and abuse of HOMA modeling. Dia-betes Care 2004;27:1487-95.
Goldbach-Mansky R, Dailey NJ, Canna SW, et al. Neonatal-onset multisystem in-flammatory disease responsive to inter-leukin-1β inhibition. N Engl J Med 2006; 355:581-92.
Garcia MC, Wernstedt I, Berndtsson A, et al. Mature-onset obesity in interleu-kin-1 receptor I knockout mice. Diabetes 2006;55:1205-13.
Chida D, Osaka T, Hashimoto O, Iwakura Y. Combined interleukin-6 and interleukin-1 deficiency causes obesity in young mice. Diabetes 2006;55:971-7.
Dinarello CA. The many worlds of reducing interleukin-1. Arthritis Rheum 2005;52:1960-7.Copyright © 2007 Massachusetts Medical Society.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 2007 1527
original article
Radiotherapy for Glioblastoma in the ElderlyFlorence Keime-Guibert, M.D., Olivier Chinot, M.D., Luc Taillandier, M.D.,
Stéphanie Cartalat-Carel, M.D., Marc Frenay, M.D., Guy Kantor, M.D., Jean-Sébastien Guillamo, M.D., Eric Jadaud, M.D., Philippe Colin, M.D.,
Pierre-Yves Bondiau, M.D., Philippe Meneï, M.D., Hugues Loiseau, M.D., Valérie Bernier, M.D., Jérôme Honnorat, M.D., Maryline Barrié, M.D.,
Karima Mokhtari, M.D., Jean-Jacques Mazeron, M.D., Anne Bissery, M.D., and Jean-Yves Delattre, M.D., for the Association of French-Speaking
Neuro-Oncologists*
From Groupe Hospitalier Pitié–Salpêtrière, Assistance Publique–Hôpitaux de Paris; INSERM Unité 711; and Université Pierre et Marie Curie, Paris (F.K.-G., K.M., J.-J.M., A.B., J.-Y.D.); Hôpital de la Timone, Mar-seille, France (O.C., M.B.); Hôpital Saint-Julien, Nancy, France (L.T., V.B.); Univer-sité Claude Bernard Lyon 1, INSERM Unité 842, and Hospices Civils de Lyon, Lyon, France (S.C.-C., J.H.); Centre Antoine Lacassagne, Nice, France (M.F., P.-Y.B.); Institut Bergonie, Bordeaux, France (G.K.); Centre Hospitalo-Universitaire Côte de Nacre, Caen, France ( J.-S.G.); Centre Paul Papin, Angers, France (E.J.); Polyclinique de Courlancy, Reims, France (P.C.); Cen-tre Hospitalo-Universitaire, Angers, France (P.M.); and Centre Hospitalo-Universi-taire, Bordeaux, France (H.L.). Address reprint requests to Dr. Delattre at Service de Neurologie Mazarin, Hôpital de la Salpêtrière, 47 Blvd. de l’Hôpital, 75013, Paris, France, or at [email protected].
*Participants in the Association of French-Speaking Neuro-Oncologists Radiother-apy for Glioblastoma in the Elderly Study are listed in the Appendix.
N Engl J Med 2007;356:1527-35.Copyright © 2007 Massachusetts Medical Society.
A BS TR AC T
Background
There is no community standard for the treatment of glioblastoma in patients 70 years of age or older. We conducted a randomized trial that compared radiotherapy and supportive care with supportive care alone in such patients.
Methods
Patients 70 years of age or older with a newly diagnosed anaplastic astrocytoma or glioblastoma and a Karnofsky performance score of 70 or higher were randomly assigned to receive supportive care only or supportive care plus radiotherapy (focal radiation in daily fractions of 1.8 Gy given 5 days per week, for a total dose of 50 Gy). The primary end point was overall survival; secondary end points were progression-free survival, tolerance of radiotherapy, health-related quality of life, and cognition.
Results
We randomly assigned 85 patients from 10 centers to receive either radiotherapy and supportive care or supportive care alone. The trial was discontinued at the first interim analysis, which showed that with a preset boundary of efficacy, radiotherapy and supportive care were superior to supportive care alone. A final analysis was carried out for the 81 patients with glioblastoma (median age, 73 years; range, 70 to 85). At a median follow-up of 21 weeks, the median survival for the 39 patients who received radiotherapy plus supportive care was 29.1 weeks, as compared with 16.9 weeks for the 42 patients who received supportive care alone. The hazard ratio for death in the radiotherapy group was 0.47 (95% confidence interval, 0.29 to 0.76; P = 0.002). There were no severe adverse events related to radiotherapy. The results of quality-of-life and cognitive evaluations over time did not differ significantly between the treatment groups.
Conclusions
Radiotherapy results in a modest improvement in survival, without reducing the quality of life or cognition, in elderly patients with glioblastoma. (ClinicalTrials.gov number, NCT00430911.)

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071528
The incidence of malignant glioma is increasing among elderly patients,1-3 whose advanced age has been associated
not only with a poor prognosis but also with a reduced tolerance of treatment and a decreased efficacy of therapy.4-6 Since the optimal manage-ment of malignant glioma in patients who are in their eighth or ninth decade of life has not been determined, we evaluated the efficacy of radio-therapy in this population.
Me thods
Patients
Patients 70 years of age or older were eligible to participate in the study if they had histologically proven, newly diagnosed glioblastoma multiforme or anaplastic astrocytoma on the basis of the World Health Organization (WHO) classification and a Karnofsky performance score of 70 or more. Written informed consent was obtained from all patients, and the study was approved by the ethics committee of the Salpêtrière Hospital in Paris.
Treatment
After undergoing surgery, patients were random-ly assigned to receive supportive care alone (the supportive care group) or supportive care in combi-nation with radiotherapy (the radiotherapy group). Randomization was performed at the data center of the Delegation for Clinical Research of the As-sistance Publique–Hôpitaux de Paris, and patients were stratified according to the treatment center. Randomization and initiation of assigned treat-ments were required within 4 weeks after surgery. Supportive care consisted of treatment with corti-costeroids and anticonvulsant agents, physical and psychological support, and management by a palliative care team. Radiotherapy, delivered by means of linear accelerators with a nominal energy of 6 mV or more, consisted of fractionated focal irradiation, at a dose of 1.8 Gy per fraction, given once daily 5 days per week, for a total dose of 50 Gy. The dose was defined according to the guidelines of the International Commission on Radiation Units and Measurements. The clinical target vol-ume included the area of contrast enhancement on magnetic resonance imaging (MRI) and a tumor margin of 2 cm.
Surveillance and Follow-Up
The baseline examination included computed to-mographic (CT) or MRI studies; complete blood
counts and blood chemical tests; neurologic ex-amination; assessment of the Karnofsky perfor-mance status; evaluation of the health-related qual-ity of life with the use of a questionnaire developed by the European Organization for Research and Treatment of Cancer (EORTC QLQ-C30, version 2.0), which has a specific module for brain can-cer (QLQ-BN20); and a neuropsychological eval-uation that included the Mini–Mental State Exam-ination (MMSE), the Mattis Dementia Rating Scale (MDRS), and the Neuropsychiatric Inventory. Pa-tients were assessed every month during the first 3 months and then every 6 weeks by means of CT or MRI, neurologic examination, MMSE, and the health-related EORTC questionnaire (QLQ-C30). The MDRS and Neuropsychiatric Inventory were administered at days 60 and 135 and then every 3 months.
Tumor progression was defined as an increase in tumor size by 25% or more or the appearance of new lesions on CT or MRI. Patients with tumor progression received supportive care. Toxic effects were graded according to the National Cancer Institute Common Toxicity Criteria, version 2.
Assessment of Health-Related Quality of Life
The QLQ-C30 questionnaire7 comprises five scales that measure functioning (physical, role [work and household activities], emotional, cognitive, and social), three symptom scales (fatigue, vomit-ing, and pain), and six single-item scales (dyspnea, insomnia, anorexia, constipation, diarrhea, and financial difficulties). The QLQ-BN20 question-naire8 includes 20 items covering functional def-icits, symptoms, toxic effects of treatment, and uncertainty about the future. The two question-naires were scored according to the EORTC scor-ing manual.9 For both questionnaires, scores can range from 0 to 100, with higher scores on the global health status and functioning scales and lower scores on the symptom scales and single-item measures indicating better performance.
Neuropsychological Evaluation
The MMSE was used as a measure of general cog-nitive status. Higher scores on this 30-point scale indicate better cognitive function. The Neuropsy-chiatric Inventory is a 12-item rating instrument that covers a range of psychological and behav-ioral symptoms (delusions, hallucinations, agita-tion or aggression, depression or dysphoria, anxi-ety, euphoria or elation, apathy or indifference, dysinhibition, irritability or lability, aberrant motor

R adiother apy for Glioblastoma
n engl j med 356;15 www.nejm.org april 12, 2007 1529
behavior, and problems with sleeping or appe-tite).10 The scores range from 0 to 144 for the pa-tient’s rating (obtained from the caregivers), with 0 indicating the optimal rating. The MDRS ex-amines attention, memory, initiation and mainte-nance of verbal and motor responses, and concep-tualization and construction (design copying).11 Scores range from 0 to 144, with higher scores indicating better cognitive function.
Statistical Analysis
The primary end point was survival; the secondary end points were progression-free survival, tolerance of treatment, health-related quality of life, and cog-nitive functioning. Comparisons between the two groups were made on an intention-to-treat basis.
The trial was initially designed to have 80% statistical power to detect a 100% increase in the median overall survival from 16 to 32 weeks (haz-ard ratio for death, 0.5) in the radiotherapy group as compared with the supportive care group, with a two-sided significance level of 0.05. Seventy-four patients with a minimum follow-up of 1 year were required for this analysis. However, after the inclusion of the 72nd patient, an amendment to the protocol was made to permit an interim analy-sis. This was done because the investigators, who had no access to any part of the outcome data at that point, were concerned about the possibility of a premature, inconclusive termination of the study.
A procedure of sequential planning, associated with the continuation of recruitment, was insti-tuted with a triangular sequential design for two-sided alternatives. This sequential design permit-ted discontinuation of the trial according to preset boundaries (Fig. 1) if radiotherapy was found to be significantly superior to supportive care (the upper boundary) or if there was no significant difference between the two groups (the lower boundary). After termination of the trial, we per-formed a final analysis, using the sequential method, of the data from all the patients who had undergone randomization by the time the efficacy boundary was crossed.
Secondary analyses were performed with the use of the Cox proportional-hazards regression model, with adjustments for relevant covariates. Survival curves were based on Kaplan–Meier esti-mates. The absolute health-related quality of life scores and all the cognitive scores were analyzed by means of a mixed-effects model for repeated measures; the method of empirical variances was
used to estimate the standard error, with a first-order autoregressive covariance structure. A gen-eralized estimating equation fitting the propor-tional-odds model for correlated ordinal data was used to analyze changes in the Karnofsky perfor-mance status over time.
Monitoring of the trial and data collection were performed by the Delegation for Clinical Research of the Assistance Publique–Hôpitaux de Paris. Site visits were performed at all centers. All histologic specimens were subject to a central review.
R esult s
Patients
From February 2001 to January 2005, a total of 85 patients from 10 institutions were randomly as-signed to receive supportive care (the supportive care group) or supportive care plus radiotherapy (the radiotherapy group). The first interim analy-sis was carried out after inclusion of the 85th pa-
22p3
Log-
Ran
k St
atis
tic (Z
)
10
12
8
6
2
0
−6
4
−4
−2
−850 10 15 20 25 30
Variance of Log-Rank Statistic (V)
Efficacy boundaryfor radiotherapy
Inefficacy boundary for radiotherapy
Boundary for no differencebetween groups
14Analysis, Nov. 2005
(P<0.005)
AUTHOR:
FIGURE:
JOB: ISSUE:
4-CH/T
RETAKE
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE:Figure has been redrawn and type has been reset.
Please check carefully.
REG F
Enon
1st2nd
3rd
Keime-Guibert (Delattre)
1 of 3
04-12-07
ARTIST: ts
35615
Termination of trial,Jan. 4, 2005
Figure 1. Design of the Triangular Test and Results of the Analysis.
The log-rank statistic (Z) summarizes the difference in survival between the group of patients who received radiotherapy plus supportive care and the group of patients who received supportive care only. The variance of the log-rank statistic (V) represents the quantity of information accumulated since the beginning of the trial, and it is closely related to the number of deaths. For each analysis, the two statistics Z and V were calculated and defined by a point shown on the graph. Three boundaries are shown: one indicating the inefficacy of radiotherapy plus supportive care as compared with sup-portive care alone (dotted line), one indicating no difference between the groups (dashed line), and one indicating the superiority of radiotherapy plus supportive care (the efficacy boundary for radiotherapy, solid line). The trial was discontinued at the first interim analysis, on January 4, 2005, after the upper boundary, indicating the superiority of radiotherapy, had been crossed. The analysis (in November 2005) incorporated the data from pa-tients who had already been recruited when the trial was discontinued, and was continued for the specified length of time.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071530
Table 1. Baseline Characteristics of the Patients Who Underwent Randomization.
CharacteristicSupportive Care
(N = 42)
Supportive Care plus Radiotherapy
(N = 39)
Age — yr
Median 73 75
Range 70–85 70–84
Sex — no.
Male 28 23
Female 14 16
Karnofsky performance score — no.*
70 23 20
80 14 15
90 3 4
100 2 0
Extent of surgery — no.
Biopsy 22 20
Partial resection 7 7
Complete resection 13 12
Corticosteroid therapy — no. (%)
Yes 36 (86) 32 (82)
No 6 (14) 7 (18)
* Higher Karnofsky performance scores indicate better performance.
Table 2. Outcomes in the Radiotherapy Group.
Variable Patients (N = 39)
Never started radiotherapy — no. (%) 1 (3)
Received ≤90% of planned dose — no. (%) 6 (15)
Dose — Gy
Median 50
Range 10–52
Fraction size — Gy
Median 1.8
Range 1.6–2.0
No. of fractions
Median 28
Range 5–31
Duration of radiotherapy
Median 5.9
Range 1.0–8.4
Time from diagnosis to radiotherapy — wk
Median 5.3
Range 2.6–10.0
Interruption or delay in radiotherapy — no. (%) 11 (28)
tient (in January 2005). In this analysis, the log-rank statistic for the difference in survival between the two groups crossed the upper boundary for efficacy (Fig. 1), and the trial was discontinued because of the superiority of radiotherapy over supportive care.
Histologic slides were submitted for 84 of the 85 patients (99%), and a central pathological review confirmed the diagnosis of malignant astrocytoma in 83 of these patients (99%). The tumors included glioblastoma in 81 of the 84 patients (96%) and anaplastic astrocytoma in 2 pa-tients (2%). On central review, one patient was found to have had a stroke. Owing to the very small number of anaplastic astrocytomas, this analysis focuses solely on the 81 patients with glioblastoma. The characteristics of the two groups of patients with glioblastoma were similar at base-line (Table 1). The median age in the supportive care group was 73 years and the median age in the supportive care plus radiotherapy group was 75, and 39 of the 81 patients (48%) had under-gone debulking surgery.
Treatment
The median time from diagnosis to the start of radiotherapy was 5.3 weeks (range, 2.6 to 10.0) — about 1 week more than was expected. Table 2 summarizes the details of treatment. One patient who was assigned to the radiotherapy group did not receive radiation because another tumor (duo-denal cancer) developed before the start of radio-therapy; this patient received supportive care only. Six patients received 90% or less of the planned radiation dose because of tumor progression (in five patients) and sudden death related to a pul-monary embolus (in one patient).
Survival and Progression
At a median follow-up of 21 weeks, 73 patients (90%) had died. The hazard ratio for death in the radiotherapy group was 0.47 (95% confidence in-terval [CI], 0.29 to 0.76; P = 0.002 by the log-rank test), indicating a 53% relative reduction in the risk of death for patients who received radiother-apy plus supportive care as compared with those who received only supportive care. The median survival benefit was 12.2 weeks; the median sur-vival was 29.1 weeks (95% CI, 25.4 to 34.9) with radiotherapy plus supportive care and 16.9 weeks (95% CI, 13.4 to 21.4) with supportive care alone (Fig. 2). The median progression-free survival was

R adiother apy for Glioblastoma
n engl j med 356;15 www.nejm.org april 12, 2007 1531
14.9 weeks (95% CI, 10.9 to 22.1) with radiother-apy plus supportive care and 5.4 weeks (95% CI, 4.4 to 7.6) with supportive care alone (Fig. 3). The hazard ratio for disease progression in the radio-therapy group was 0.28 (95% CI, 0.17 to 0.47; P<0.001 by the log-rank test).
We used Cox proportional-hazard models to adjust the hazard ratio for death. In addition to the stratification factor (the treatment center to which the patient was assigned), other possible confound-ing factors — age, the extent of surgery, and per-formance status — were included. The adjusted hazard ratio for death in the radiotherapy group was 0.42 (95% CI, 0.25 to 0.68). The extent of surgery, according to the surgeon’s report (com-plete resection vs. partial resection or biopsy), was associated with survival (hazard ratio for death among patients who underwent complete resection, 0.49; 95% CI, 0.29 to 0.81; P = 0.005). The survival benefit of radiotherapy was indepen-dent of the extent of surgery.
Performance Status and Quality of Life
The Karnofsky performance status declined over time, but there were no significant differences be-tween the two groups (P = 0.22). The rate of com-pliance with the health-related quality-of-life as-sessment decreased over time in both the group that received supportive care alone and the group that received radiotherapy plus supportive care, from 93% and 90% at baseline to 60% and 67% at day 135, respectively (see Tables 1 and 2 of the Supplementary Appendix, available with the full text of this article at www.nejm.org). Few patients were alive after the first four follow-up evaluations (up to day 135). For this reason, analyses of health-related quality of life were restricted to evaluations at days 1, 30, 60, 90, and 135. Table 3 shows chang-es in the mean health-related quality-of-life scores over time. In both groups, scores were significant-ly worse over time on the physical (P<0.001), cog-nitive (P = 0.01), social (P = 0.02), fatigue (P = 0.008), and motor dysfunction (P = 0.001) scales, whereas scores on the other scales, particularly the global score for health-related quality of life, did not change significantly (Fig. 1 of the Supplementary Appendix). Global assessments of deterioration over time also did not differ significantly between the two groups. Only the scale that assessed un-certainty about the future showed a different pat-tern of scores over time in the two groups, but no pattern exhibited a clear trend.
Neuropsychological Evaluation
The MMSE scores declined over time in both groups (P = 0.007), with no significant differences be-tween the two groups (P = 0.13). Analyses of the Neuropsychiatric Inventory and MDRS scores were
AUTHOR:
FIGURE:
JOB: ISSUE:
4-CH/T
RETAKE
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE:Figure has been redrawn and type has been reset.
Please check carefully.
REG F
Enon
1st
2nd3rd
Keime-Guibert (Delattre)
2 of 3
04-12-07
ARTIST: ts
35615
Supportive carealone
Radiotherapy plus supportive care
22p3
1.00
Prob
abili
ty o
f Sur
viva
l
0.75
0.25
0.50
0.000 20 6040 80 100
Weeks
No. at RiskSupportive care
aloneRadiotherapy plus
supportive care
0
1
0
3
3
8
17
24
42
39
Figure 2. Kaplan–Meier Estimates of Overall Survival According to Treatment Group.
The hazard ratio for death among patients who received radiotherapy plus supportive care as compared with those who received supportive care alone was 0.47 (95% CI, 0.29 to 0.76; P = 0.002).
AUTHOR:
FIGURE:
JOB: ISSUE:
4-CH/T
RETAKE
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE:Figure has been redrawn and type has been reset.
Please check carefully.
REG F
Enon
1st2nd3rd
Keime-Guibert (Delattre)
3 of 3
04-12-07
ARTIST: ts
35615
Supportive care alone
Radiotherapy plus supportive care
22p3
1.00
Prob
abili
ty o
f Pro
gres
sion
-free
Surv
ival
0.75
0.25
0.50
0.000 2010 4030 50 60
Weeks
No. at RiskSupportive care
aloneRadiotherapy plus
supportive care
0
4
2
15
42
39
Figure 3. Kaplan–Meier Estimates of Progression-free Survival According to Treatment Group.
The hazard ratio for disease progression among patients who received radio-therapy plus supportive care as compared with those who received supportive care alone was 0.28 (95% CI, 0.17 to 0.47; P<0.001).

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071532
also restricted to 135 days of follow-up (Table 3 of the Supplementary Appendix). The global scores on the Neuropsychiatric Inventory did not change significantly over time (P = 0.18), and there were no significant differences in these scores between the two groups (P = 0.84). The MDRS score did not change significantly over time, except for pro-gressive deterioration on the initiation (P = 0.03) and construction (P = 0.05) subscales in both groups (Table 4 of the Supplementary Appendix).
Safety
All patients in the radiotherapy group tolerated the treatment. One patient had transient early de-layed somnolence (abnormal sleepiness) shortly af-ter the completion of radiotherapy. Complications of corticosteroid treatment included diabetes in seven patients in the supportive care group and in two patients in the radiotherapy group and myop-athy in three patients in the supportive care group and in six patients in the radiotherapy group.
Table 3. Scores for Health-Related Quality of Life over Time.*
Measure Score P Value
Baseline Day 30 Day 60 Day 90 Day 135Treatment
EffectTime Effect
Interaction Effect
QLQ-C30
Global 0.79 0.17 0.12
Supportive care 62.7±4.1 61.8±4.7 60.3±5.0 56.7±6.3 48.1±6.7
Supportive care plus radiotherapy 62.9±3.4 57.6±3.5 55.6±3.9 49.1±4.0 58.8±4.47
Functioning
Physical 0.57 <0.001 0.97
Supportive care 75.4±4.6 64.9±6.3 53.8±7.6 51.9±7.9 37.2±15.9
Supportive care plus radiotherapy 70.3±6.3 58.8±5.5 51.9±7.3 44.1±7.4 36.8±8.0
Role (work and household activities) 0.29 0.07 0.90
Supportive care 66.3±5.7 59.1±6.8 61.8±8.5 56.6±7.8 45.1±14.5
Supportive care plus radiotherapy 63.1±6.4 56.1±6.4 50.0±7.4 43.5±6.9 39.0±9.3
Emotional 0.92 0.95 0.71
Supportive care 71.7±4.4 75.6±4.8 70.5±5.5 71.6±5.2 70.6±7.8
Supportive care plus radiotherapy 75.6±4.3 70.5±5.0 70.5±5.2 69.7±5.2 71.1±5.7
Cognitive 0.21 0.01 0.13
Supportive care 68.7±5.0 60.0±6.1 63.0±5.6 63.8±6.2 56.8±7.8
Supportive care plus radiotherapy 66.8±4.7 59.6±4.9 57.4±6.7 42.8±7.1 43.8±6.7
Social 0.49 0.02 0.83
Supportive care 73.7±6.1 66.1±6.0 63.8±7.3 67.8±8.2 43.6±16.2
Supportive care plus radiotherapy 73.3±5.3 58.0±6.4 52.7±7.3 56.8±7.0 50.2±8.2
Symptoms
Fatigue 0.49 0.008 0.57
Supportive care 36.7±5.4 37.4±5.2 40.3±6.8 41.1±5.8 57.4±10.8
Supportive care plus radiotherapy 33.0±4.0 39.5±4.9 48.9±6.3 52.8±5.0 57.9±5.3
Nausea and vomiting 0.49 0.32 0.42
Supportive care 0.9±0.7 0.5±0.7 5.7±4.9 5.7±3.9 2.2±1.9
Supportive care plus radiotherapy 3.3±1.3 4.3±2.7 5.1±2.7 10.7±5.5 0.9±1.0
Insomnia 0.19 0.14 0.80
Supportive care 17.4±4.9 21.8±6.1 13.0±4.7 6.4±3.2 14.4±8.2
Supportive care plus radiotherapy 25.9±5.4 24.4±5.2 15.9±5.1 18.9±5.6 21.3±6.2

R adiother apy for Glioblastoma
n engl j med 356;15 www.nejm.org april 12, 2007 1533
Treatment after Disease Progression
After disease progression, supportive care was given, with a few exceptions. Two patients in the radiotherapy group and one patient in the suppor-tive care group received temozolomide. One pa-tient in the supportive care group underwent re-operation.
Discussion
This study shows that the addition of radiotherapy to supportive care prolongs survival and does not reduce the health-related quality of life or cogni-tive function of patients with newly diagnosed glioblastoma who are 70 years of age or older. The 16.9-week median survival of patients in our study who received only supportive care is consistent with the median survival reported more than two decades ago for younger patients treated with sup-portive care alone.12,13 Conversely, the 12.2-week survival benefit with radiotherapy in the older patients in our study is about half the survival gain reported in the two earlier studies (22 and 24 weeks), which compared conventional radio-
therapy (a total dose of 45 to 60 Gy, given in frac-tions of 1.7 to 2.0 Gy) with supportive care in a younger population.12,13
We selected a conventional 50-Gy schedule to minimize the age-related risk of radiation-induced neurotoxicity.5 With this schedule, there were no cases of delayed neurotoxicity,14 but the short sur-vival of the patients in our study may have pre-cluded the development of late toxicity. The opti-mal dose of radiotherapy in elderly patients remains undetermined. It is unclear whether a total dose of 60 Gy would increase the survival benefit of radiotherapy in older patients, as it does in young-er patients.15,16 In our trial, the 29.1-week median survival and 15% rate of discontinuation of radio-therapy compare favorably with the 22.1-week survival and 26% rate of discontinuation reported in a prospective study in which a dose of 60 Gy was delivered in 30 fractions over a period of 6 weeks in older patients.17 In that study, an abbre-viated course of radiotherapy (40 Gy in 15 frac-tions over a period of 3 weeks), as compared with the 60-Gy schedule, resulted in a similar median survival (24.3 weeks vs. 22.1 weeks), but
Table 3. (Continued.)
Measure Score P Value
Baseline Day 30 Day 60 Day 90 Day 135Treatment
EffectTime Effect
Interaction Effect
QLQ-BN20 (symptoms)
Future uncertainty 0.85 0.67 0.002
Supportive care 33.3±4.7 31.3±4.5 36.4±6.0 28.6±5.5 32.5±8.0
Supportive care plus radiotherapy 28.7±4.6 34.0±5.1 32.3±5.1 41.6±4.5 30.3±4.0
Visual disorder 0.88 0.29 0.98
Supportive care 19.8±2.9 22.1±3.2 25.2±4.0 27.3±5.7 28.7±6.4
Supportive care plus radiotherapy 21.9±2.7 22.2±2.8 26.1±3.9 27.1±3.3 28.8±2.8
Motor dysfunction 0.50 0.001 0.46
Supportive care 20.2±4.1 23.6±5.8 27.6±7.2 29.6±6.8 54.0±16.4
Supportive care plus radiotherapy 19.4±4.8 34.3±5.4 40.9±6.4 38.6±4.7 43.6±5.9
Communication deficit 0.24 0.12 0.44
Supportive care 26.9±5.2 25.6±5.1 25.7±6.0 29.9±7.2 36.2±8.9
Supportive care plus radiotherapy 27.9±5.5 39.6±6.6 36.6±7.0 41.1±7.0 44.8±8.0
Bothered by hair loss 0.06 0.09 0.16
Supportive care 4.6±2.1 3.1±1.6 3.7±2.3 14.2±5.9 10.9±8.2
Supportive care plus radiotherapy 7.9±4.1 16.5±6.0 22.6±5.9 26.2±7.7 16.2±6.5
* Plus–minus values are means ±SD. Scores on both the QLQ-C30 and the QLQ-BN20 questionnaires can range from 0 to 100, with higher scores on the global health status and functioning scales and lower scores on the symptom scales and single-item measures indicating better per-formance.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071534
a lower rate of premature discontinuation of ra-diotherapy (10% vs. 26%).17
Since the goal of the treatment of glioblas-toma in older patients is palliation, the quality of life is relevant. The evaluation of health-related quality of life in patients with malignant glioma is notoriously difficult.18-20 The main limitation is that severely ill patients with a rapidly progres-sive, fatal disease are not always compliant with such evaluations. To our knowledge, only one pro-spective study in the elderly attempted to evalu-ate health-related quality of life sequentially in patients with glioblastoma, but the data could not be analyzed because the compliance rate was too low (15 to 21% immediately after radiotherapy).17 In our study, the rate of compliance with the questionnaires was similar to that in the few re-ported studies of patients with glioblastoma.19-21 We were able to conduct a meaningful analysis of the data obtained from the first four follow-up evaluations (135 days of follow-up). Thereafter, the number of patients was too small for a reli-able analysis.
At baseline, scores for the health-related qual-ity of life did not differ significantly between the two groups and were similar to scores reported previously.20 During and after treatment, scores on several evaluation scales (physical, cognitive, social, fatigue, and motor dysfunction) progres-sively declined in both groups, although the global score for health-related quality of life did not change significantly over time in either group. We did not observe the mild-to-moderate im-provement on several scales that was reported in younger patients after radiotherapy, with or with-out chemotherapy.20
The evaluation of neuropsychiatric symptoms and cognitive function is associated with the same compliance limitation as the health-related
quality-of-life analysis. The Neuropsychiatric In-ventory did not show a time or treatment effect, particularly in the case of depression. In contrast, the cognitive evaluation (the MMSE and the ini-tiation subscale of the MDRS) showed signifi-cant deterioration over time in both groups. How-ever, as compared with supportive care alone, radiotherapy plus supportive care did not have a detrimental effect on cognitive function.
The population of elderly patients with cancer is underrepresented in clinical trials.22,23 Likely causes of this underrepresentation are study-imposed restrictions, coexisting conditions, con-cern about the toxic effects of treatment, patient and family preferences, and the reluctance of phy-sicians to enroll elderly patients in clinical trials.24 Nevertheless, our study shows that these barriers may be overcome,25 even in trials that involve a rapidly progressive, fatal disease, such as glioblas-toma, and a palliative-care comparison group.
In conclusion, radiotherapy increases the me-dian survival of elderly patients with glioblastoma who have a good performance status at the start of treatment. As compared with supportive care, radiotherapy in such patients does not cause fur-ther deterioration in the Karnofsky performance status, health-related quality of life, or cognitive functions, but the survival benefit is modest.
Supported by a grant (PHRC AOM 98071, P000502) from the Programme Hospitalier de Recherche Clinique.
No potential conflict of interest relevant to this article was reported.
This article is dedicated to each patient in this trial and to their families who went through the informed-consent process and agreed to participate in a study with a palliative care group. Knowing the situation, they chose to participate in solidarity with future patients.
We thank Lucette Lacomblez and Michele Levy-Soussan for assistance with the design of the study (cognitive evaluation and supportive care program); Alain Mallet, Jacques Medioni, and Philippe Broet for their help with the statistical design of the study; and the neuropsychologists and supportive care team members who participated in the study.
APPENDIXIn addition to the authors, the following investigators participated in the Radiotherapy for Glioblastoma in the Elderly Study: Groupe Hospitalier Pitié–Salpêtrière, Paris — L. Lacomblez, M. Levy-Soussan, A. Mallet, C. Houssard, D. Delgadillo, M. Poitou, K. Hoang-Xuan, M. Sanson, A.F. Carpentier, F. Laigle-Donadey, S. Taillibert, P. Cornu, A. Omuro, L. Capelle, A.-L. Boch, H. Duffau, J.-M. Simon; Hôpital Européen Georges Pompidou, Paris — J. Medioni; Hôpital Paul Brousse, Villejuif — P. Broet; Hôpital de la Timone, Marseille, France — A. Schmitt; Hôpital Saint-Julien, Nancy, France — E. Garat, P. Mathieu; Institut Fédératif des Neurosciences, Hospices Civils de Lyon, Lyon, France — N. Camille, J.-P. Collin; Centre Antoine Lacassagne, Nice, France — B. Bailet, C. Ciais, F. Fauchon, C. Lebrun; Institut Bergonie, Bordeaux, France — G. Gues-dan, N. Stadelmaier, I. Lombard; Centre Hospitalo-Universitaire Côte de Nacre, Caen, France — P. Delassus, C. Lalevec; Centre Hospitalo-Universi-taire, Angers, France — G. Aubin, D. Fournier, and G. Hayek.
References
Fleury A, Menegoz F, Grosclaude P, et al. Descriptive epidemiology of cerebral gliomas in France. Cancer 1997;79:1195-202.
Chakrabarti I, Cockburn M, Cozen W,
1.
2.
et al. A population-based description of glioblastoma multiforme in Los Angeles County, 1974-1999. Cancer 2005;104:2798-806.
Elia-Pasquet S, Provost D, Jaffre A, et 3.
al. Incidence of central nervous system tu-mors in Gironde, France. Neuroepidemiol-ogy 2004;23:110-7.
Curran WJ Jr, Scott CB, Horton J, et al. Recursive partitioning analysis of prog-4.

R adiother apy for Glioblastoma
n engl j med 356;15 www.nejm.org april 12, 2007 1535
nostic factors in three Radiation Therapy Oncology Group malignant glioma trials. J Natl Cancer Inst 1993;85:704-10.
Asai A, Matsutani M, Kohno T, et al. Subacute brain atrophy after radiation ther-apy for malignant brain tumor. Cancer 1989;63:1962-74.
Grant R, Liang BC, Page MA, Crane DL, Greenberg HS, Junck L. Age influences chemotherapy response in astrocytomas. Neurology 1995;45:929-33.
Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993;85:365-76.
Osoba D, Aaronson NK, Muller M, et al. The development and psychometric vali-dation of a brain cancer quality-of-life questionnaire for use in combination with general cancer-specific questionnaires. Qual Life Res 1996;5:139-50.
Fayers PM, Aaronson NK, Bjordal K, Groenvold M, Curren D, Bottomley A. The EORTC QLQ-C30 scoring manual. 3rd ed. Brussels: European Organization for Re-search and Treatment of Cancer, 2001.
Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gorn-bein J. The Neuropsychiatric Inventory: comprehensive assessment of psychopa-thology in dementia. Neurology 1994;44: 2308-14.
Mattis S. Dementia Rating Scale: pro-fessional manual. Odessa, FL: Psychologi-cal Assessment Resources, 1988.
5.
6.
7.
8.
9.
10.
11.
Walker MD, Green SB, Byar DP, et al. Randomized comparisons of radiotherapy and nitrosoureas for the treatment of ma-lignant glioma after surgery. N Engl J Med 1980;303:1323-9.
Kristiansen K, Hagen S, Kollevold T, et al. Combined modality therapy of oper-ated astrocytomas grade III and IV: con-firmation of the value of postoperative irradiation and lack of potentiation of bleomycin on survival time — prospective multicenter trial of the Scandinavian Glio-blastoma Study Group. Cancer 1981;47: 649-52.
Sheline GE, Wara WM, Smith V. Ther-apeutic irradiation and brain injury. Int J Radiat Oncol Biol Phys 1980;6:1215-28.
Walker MD, Strike TA, Sheline GE. An analysis of dose-effect relationship in the radiotherapy of malignant gliomas. Int J Radiat Oncol Biol Phys 1979;5:1725-31.
Bleehen NM, Stenning SP. A Medical Research Council trial of two radiotherapy doses in the treatment of grades 3 and 4 astrocytoma. Br J Cancer 1991;64:769-74.
Roa W, Brasher PMA, Bauman G, et al. Abbreviated course of radiation therapy in older patients with glioblastoma multi-forme: a prospective randomized clinical trial. J Clin Oncol 2004;22:1583-8.
Efficace F, Bottomley A. Health relat-ed quality of life assessment methodology and reported outcomes in randomised controlled trials of primary brain cancer patients. Eur J Cancer 2002;38:1824-31.
Walker M, Brown J, Brown K, Gregor
12.
13.
14.
15.
16.
17.
18.
19.
A, Whittle IR, Grant R. Practical problems with the collection and interpretation of serial quality of life assessments in pa-tients with malignant glioma. J Neuro-oncol 2003;63:179-86.
Taphhoorn MJ, Stupp R, Coens C, et al. Health-related quality of life in patients with glioblastoma: a randomised con-trolled trial. Lancet Oncol 2005;6:937-44.
Osoba D, Brada M, Yung WK, Prados M. Health-related quality of life in patients treated with temozolomide versus procar-bazine for recurrent glioblastoma multi-forme. J Clin Oncol 2000;18:1481-91.
Hutchins LF, Unger JM, Crowley JJ, Coltman CA Jr, Albain KS. Underrepre-sentation of patients 65 years of age or older in cancer-treatment trials. N Engl J Med 1999;341:2061-7.
Gross CP, Herrin J, Wong N, Krumholz HM. Enrolling older persons in cancer trials: the effect of socio-demographic, protocol, and recruitment center charac-teristics. J Clin Oncol 2005;23:4755-63.
Yee KW, Pater JL, Pho L, Zee B, Siu LL. Enrollment of older patients in cancer treatment trials in Canada: why age is a barrier? J Clin Oncol 2003;21:1618-23.
Unger JM, Coltman CA Jr, Crowley JJ, et al. Impact of the year 2000 Medicare policy change on older patient enrollment to cancer clinical trials. J Clin Oncol 2006; 24:141-4.Copyright © 2007 Massachusetts Medical Society.
20.
21.
22.
23.
24.
25.
clinical trial registration
The Journal requires investigators to register their clinical trials in a public trials registry. The members of the International Committee
of Medical Journal Editors (ICMJE) will consider most clinical trials for publication only if they have been registered (see N Engl J Med 2004;351:1250-1).
Current information on requirements and appropriate registries is available at www.icmje.org/faq.pdf.

original article
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071536
Randomized, Placebo-Controlled Trial of Inactivated Poliovirus Vaccine in Cuba
The Cuba IPV Study Collaborative Group
The institutions of the Cuba IPV Study Collaborative Group and their representa-tives (Miguel Galindo, M.D., Cuban Min-istry of Public Health, Havana; Pedro Más Lago, M.D., Ph.D., Pedro Kourí Institute for Tropical Medicine, Havana; Victor Cáceres, M.D., M.P.H., Centers for Disease Control and Prevention, Atlanta; Mauricio Landaverde, M.D., Pan American Health Organization, Washington, DC; and Roland Sutter, M.D., M.P.H.&T.M., World Health Organization, Geneva) assume re-sponsibility for the overall content and integrity of the article. Address reprint re-quests to Dr. Cáceres at the Centers for Disease Control and Prevention, Coordi-nating Office for Global Health, Division of Epidemiology and Surveillance Capac-ity Development, Mailstop E-93, 1600 Clifton Rd., Atlanta, GA 30333.
N Engl J Med 2007;356:1536-44.Copyright © 2007 Massachusetts Medical Society.
A bs tr ac t
Background
After poliomyelitis has been eradicated, access to live polioviruses will be highly restricted and the use of oral poliovirus vaccine (OPV) will probably be discontin-ued. Countries using OPV must decide whether to switch to inactivated poliovirus vaccine (IPV) or stop polio vaccination. Because data on the immunogenicity of IPV in tropical developing countries are limited, we conducted a randomized, controlled trial of IPV in Cuba.
Methods
The study population consisted of healthy infants born in Havana. A total of 166 infants were randomly assigned to two groups. Group A received a combination of the diphtheria–pertussis–tetanus (DPT) vaccine, the Haemophilus inf luenzae type b (Hib) vaccine, and IPV (DPT-Hib-IPV) at 6, 10, and 14 weeks of age. Group B, the control group, received a combination of the DPT vaccine and the Hib vaccine at 6, 10, and 14 weeks of age. Another group (group C, 100 infants), which did not undergo randomization at the same time as groups A and B, received the DPT-Hib-IPV com-bination at 8 and 16 weeks of age. Serum samples were collected before vaccination and at least 4 weeks after the last dose. Stool samples were obtained before and 7 days after challenge with OPV.
Results
The seroconversion rates in group A were 94%, 83%, and 100% for types 1, 2, and 3 poliovirus, respectively. There were no seroconversions in group B. The serocon-version rates in group C were 90%, 89%, and 90% for poliovirus types 1, 2, and 3, respectively. For groups A, B, and C, the virus isolation rates after challenge with OPV were 94%, 91%, and 97%, respectively, and the mean log10 viral titers of any serotype were 3.46, 3.89, and 3.37, respectively. There was one major adverse event, an episode of hypotonia.
Conclusions
Vaccination with two or three doses of IPV resulted in a rate of seroconversion of at least 90%, except for seroconversion against type 2. The viral titer of OPV shed in the stool after OPV challenge was reduced in both groups receiving IPV. (ClinicalTrials.gov number, NCT00260312.)

Inactivated Poliovirus Vaccine in Cuba
n engl j med 356;15 www.nejm.org april 12, 2007 1537
A t the time that interruption of wild poliovirus transmission is achieved, the world will probably discontinue the
use of oral poliovirus vaccine (OPV)1,2 because of the potential for the vaccine virus to acquire the neurovirulence and transmission characteristics of wild poliovirus. Acquisition of these character-istics could then lead to endemic and epidemic transmission, as was documented during the past 6 years in Hispaniola, the Philippines, Madagascar, and China, and earlier in Egypt.3-6
Inactivated poliovirus vaccine (IPV) will be the only vaccine available for routine immunization if the use of OPV is discontinued.7,8 Whereas in-dustrialized countries may continue vaccinating against poliomyelitis with a combination vaccine that includes IPV, many developing countries may decide to stop polio vaccination and divert scarce resources to other health priorities. Important considerations include how and when to discon-tinue the use of OPV and whether to expand the use of IPV into developing countries.
Data on the immunogenicity of IPV in develop-ing countries are limited, and the interpretation of the available data remains complicated by the potential secondary exposure of participants in studies of IPV to circulating OPV viruses or wild polioviruses.9-11 This phenomenon may have led to an overestimate of the rates of IPV-induced humoral and mucosal immunity. To minimize this concern, IPV trials should be conducted in settings free of live polioviruses, where no OPV is used and there is no circulating wild poliovirus. Cuba has been free of polio since 1963, and OPV is administered only during annual national mass campaigns (typically during February and April), with documented absence of Sabin-vaccine virus-es from each July to the following January.12-14 Most developing countries routinely administer diphtheria and tetanus toxoids and pertussis vac-cine (i.e., the DPT vaccine) to children at 6, 10, and 14 weeks of age; however, countries in the Western Hemisphere use a schedule of 8, 16, and 24 weeks of age. Because there is limited infor-mation on the extent to which maternal antibod-ies interfere with seroconversion when vaccine is administered early in life, it is critical that addi-tional data be generated on IPV administered ac-cording to the accelerated schedule.15 We per-formed a randomized, placebo-controlled trial in Cuba to evaluate the immunogenicity of IPV in combination with the DPT and Haemophilus inf lu-
enzae type b (Hib) vaccines (DPT-Hib-IPV) admin-istered at 6, 10, and 14 weeks and at 8 and 16 weeks of age.
Me thods
Study Design
The study population consisted of infants born in the four principal maternity hospitals in Havana from July 10 through November 10, 2001. Infants were eligible for inclusion if they were healthy, were born at full term (after at least 37 weeks of gestation), weighed at least 2.5 kg at birth, and had 1- and 5-minute Apgar scores of at least 7. Infants not meeting these criteria and those re-quiring hospitalization during the study were ex-cluded.
After the infants had been selected from a list of consecutive births and their eligibility had been determined, their parents or guardians were in-vited to participate and written informed consent was obtained. The infants were then randomly assigned to one of two groups by the Cuban Ministry of Public Health Epidemiology Division with the use of Epidat 2.1 software. Group A re-ceived a combination pentavalent vaccine (DPT-Hib-IPV). Group B, the control group, received a tetravalent vaccine containing the DPT and Hib vaccines (DPT-Hib). Both groups received the vac-cine at 6, 10, and 14 weeks of age.
A third group (group C) was included to assess a schedule of two doses of DPT-Hib-IPV given at 8 and 16 weeks of age. Unfortunately, the interval that was free of Sabin-vaccine virus in Cuba was too short to allow the assessment of a group re-ceiving a full three-dose schedule (at 8, 16, and 24 weeks of age); nevertheless, we believed that in-clusion of the group receiving a two-dose sched-ule could yield programmatically useful data. The infants in group C did not undergo randomiza-tion with the infants in the other two groups be-cause they had to start receiving vaccine earlier than the infants in groups A and B in order to receive the challenge OPV dose on time (i.e., dur-ing the national OPV campaign on March 12 and 13, 2002).
Minor adverse events, such as injection-site discomfort, were monitored for 7 days after vac-cination. Other adverse events were recorded with the use of a protocol established by the national surveillance system for vaccine-associated adverse events in Cuba.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071538
The study was approved by the institutional review boards of the Pedro Kourí Institute in Ha-vana and the Centers for Disease Control and Pre-vention in Atlanta. The Cuban Ministry of Public Health was responsible for operational aspects of the study, and the Pedro Kourí Institute con-ducted laboratory analyses. The institutions of the Cuba IPV Study Collaborative Group and their representatives take responsibility for the overall content and integrity of this article.
Statistical Analysis
Our target sample size (100 per group) allowed for attrition and was based on the lowest predicted seroconversion rate for the group receiving IPV at 6, 10, and 14 weeks (60%) according to data from Thailand.10 To achieve a probability of 0.85 that the estimate from this study was in error by 10% or less, we needed to enroll at least 50 infants in each group receiving IPV. This calculation was based on the normal approximation to the bino-mial distribution. The proportions of subjects shedding virus after challenge in the control and intervention groups were compared with the use of a two-tailed Fisher’s exact test. Assuming a predicted rate of excretion after challenge in the IPV and control groups of 60% and 85%, respec-tively, we calculated a minimum sample size of 55 infants for each group, so that we would have a power of 90% to detect a significant difference at the 0.05 level.
Vaccines
PENTAct-HIB is a combination vaccine produced by Sanofi Pasteur containing H. inf luenzae type b vaccine, DPT vaccine, and IPV. It is an injectable suspension formed by reconstituting lyophilized polyribosylribitol phosphate–tetanus-toxoid conju-gated vaccine (PRP-T) (Act-HIB, Sanofi Pasteur) with a syringe filled with a DPT–IPV liquid com-bination (Tetracoq). TETRAct-HIB is a combina-tion vaccine produced by Sanofi Pasteur contain-ing H. inf luenzae type b vaccine and DPT. It is an injectable suspension formed by reconstituting lyophilized PRP-T (Act-HIB) with a syringe or am-pule (0.5 ml) of DPT (DTCoq). The vaccines were masked for groups A and B (but not C). The study vaccines were donated by the manufacturer, which did not participate in study implementation, data analyses, or the preparation of the manuscript. The OPV in the national campaign was a live at-tenuated vaccine containing at least 106, 105, and
105.8 median tissue-culture infective doses (TCID50 ) to poliovirus types 1, 2, and 3, respectively.
Sample collection
Serologic specimens were taken from infants im-mediately before administration of the first vac-cine dose and approximately 4 weeks after the last dose of study vaccine (preceding the national OPV campaign on March 12 and 13, 2002). Serologic specimens were stored at −20°C at the Pedro Kourí Institute and tested collectively to determine anti-body titers for poliovirus types 1, 2, and 3. To eval-uate the effect of IPV on intestinal excretion of poliovirus after challenge, a stool specimen was obtained from each study infant 2 or 3 days before administration of the OPV challenge and 7 days afterward. The initial stool specimen was collected to verify our assumption that no child was excret-ing poliovirus before receiving the challenge dose.
Determination of neutralizing antibodies
Neutralizing antibodies were determined by the method recommended by the World Health Orga-nization (WHO).16 Microneutralization was per-formed on microtiter plates with the use of serial dilutions, by a factor of two, of serum beginning at 1:8. At each dilution, 25 µl of serum was mixed with 25 µl of Eagle’s medium containing 100 TCID50 (range, 32 to 320) of Sabin poliovirus type 1, 2, or 3. The virus–serum mixture was incubated for 4 hours at 37°C in an atmosphere of 5% car-bon dioxide. One hundred microliters of HEp-2 (Cincinnati subline) cell suspension (200,000 cells per milliliter) was added and incubated as before for 5 days. Each serum sample was tested in trip-licate. Each test batch was accompanied by a cell control, a “serum toxicity” control (for the pos-sible cytopathic effect of the serum alone), and virus dose and titration controls with the use of an in-house reference serum validated against the international standard.
Seroconversion was defined as an increase by a factor of four in antibody titer from prevaccina-tion to postvaccination values, with correction for maternal antibody decay at an estimated half-life of 30 days. If the predicted end-point titer for maternal antibody decay was 7 or less (the cutoff value for detection), a second serum titer of 14 or more would indicate seroconversion. The asso-ciation between prevaccination and postvaccina-tion antibody titers was assessed by a two-tailed Spearman rank-order correlation coefficient test.

Inactivated Poliovirus Vaccine in Cuba
n engl j med 356;15 www.nejm.org april 12, 2007 1539
Isolation and identification of poliovirus in stool
Isolation of the virus was performed by WHO-recommended methods, with the following modi-fications.16 A 20% suspension was made of each stool sample in phosphate-buffered saline with antibiotics. The samples were clarified by centri-fugation at 10,000 rpm. The supernatant was stored at −20°C until 0.2 ml of supernatant was inoculated onto rhabdomyosarcoma and L20B cell lines. The tubes were incubated at 37°C and exam-ined 24 hours later. Those showing cytopathic effect were frozen and thawed for passage to new cell tubes. A sample was observed for up to 12 days before it was determined to be negative. In those tubes in which a cytopathic effect appeared in the L20B cells, identification was made by neu-tralization with poliovirus hyperimmune serum samples. Samples showing cytopathic effect only in rhabdomyosarcoma cells were passed to L20B cells. If the cytopathic effect persisted, identifica-tion proceeded as described above. Isolates posi-tive for poliovirus were titrated by a micromethod in four replicates with log10 dilutions from 1 to 6, with the use of L20B cells concentrated at 100,000 per milliliter.
R esult s
Enrollment
Two hundred sixty-six of 1062 screened infants (25.0%) were enrolled in the trial (Fig. 1). By the end of the study, 88 infants had not received one or more vaccinations: 30 in group A, 30 in group B, and 28 in group C. The reasons for withdrawal are summarized in Figure 1. The decision to with-draw consent for further vaccinations was mainly due to one major adverse event, a transient epi-sode of hypotonia in an infant after the first dose, which was attributed to the pertussis-antigen com-ponent. In addition, there were five episodes of persistent crying. The percentages of males in groups A, B, and C were 52%, 63%, and 54%, re-spectively, at the end of the study, as compared with 53%, 68%, and 43% at initial enrollment. The 178 infants completing all study vaccinations resided in neighborhoods widely spread through-out and representative of Havana.
Of the 300 IPV doses administered, 34 (11%) were given to infants more than 7 days before or after the date they were due to be given the dose. Eliminating the data from these children did not
affect the results, and therefore they were in-cluded in the analyses. The median ages at which each dose was given are summarized in Table 1.
Seroconversion
Group A (which received DPT-Hib-IPV at 6, 10, and 14 weeks of age) had seroconversion rates of 49 of 52 recipients (94%), 43 of 52 (83%), and 52 of 52 (100%) for poliovirus types 1, 2, and 3, re-spectively (Table 2). As anticipated, there were no seroconversions in group B (which received DPT-Hib at 6, 10, and 14 weeks), a result consistent with the absence of circulating polioviruses in the population. Group C (which received DPT-Hib-IPV at 8 and 16 weeks) had seroconversion rates of 65 of 72 recipients (90%), 64 of 72 (89%), and 65 of 72 (90%) for poliovirus types 1, 2, and 3, respec-tively.
Interference of maternal antibody
The potential interference of preexisting maternal antibody was assessed by plotting pre- and post-vaccination log2 titers for poliovirus types 1 and 2 in intervention groups A and C (data not shown). Poliovirus type 2 was the only type for which pre- and postvaccination antibodies had a significant inverse correlation (for group A, Spearman’s cor-relation coefficient, −0.49; P<0.001; for group C, Spearman’s correlation coefficient, −0.54; P<0.001); this result implies interference with maternal antibody.
Isolation of poliovirus in stools
Table 3 summarizes the results from stool speci-mens taken 7 days after the national OPV cam-paign. No polioviruses were isolated in initial stool specimens, before the campaign, from infants in any of the groups. In the second stool specimen, after OPV administration, the rates of isolation of any type of poliovirus were 49 of 52 infants (94%), 49 of 54 (91%), and 70 of 72 (97%) in groups A, B, and C, respectively. The excretion rates did not differ according to group when each IPV inter-vention group (A and C) was compared separately with group B. Among those shedding poliovirus, the mean log10 titers in groups A, B, and C were 3.46, 3.89, and 3.37, respectively. Both IPV groups had lower mean viral titers than the control group (P = 0.06 for group A and P = 0.005 for group C), with the reduction in group C reaching statistical significance based on a two-tailed Mann–Whit-ney test.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071540
Discussion
These data assess the immunogenicity of IPV in a tropical developing country where study partici-pants were not exposed secondarily to circulat-ing wild-type or OPV viruses. Despite the absence of secondary exposure, our study documented high levels of seroconversion for poliovirus types 1 and 3 after the administration of three doses of IPV at the ages of 6, 10, and 14 weeks, with a somewhat lower rate of seroconversion for type 2. Two IPV doses, administered at the ages of 8 and 16 weeks, resulted in moderately lower overall seroconversion rates. Similar proportions of in-fants in each study group excreted virus after OPV challenge; however, both groups receiving IPV had lower viral titers than the control group.
IPV immunogenicity is directly related to the prevalence and titer of maternally derived anti-body.8-10,18,19 Indirectly, IPV-induced immunoge-nicity levels can be inferred by the administration schedule (i.e., number of doses, age at first dose, and interval between doses).9 Therefore, the WHO-recommended immunization schedule for devel-oping countries, with doses administered at the ages of 6, 10, and 14 weeks, provides a substan-tial challenge to IPV performance. Nevertheless, in Cuba, administration of three doses resulted in rates of seroconversion to poliovirus types 1 and 3 of at least 90%. Maternally derived antibody inter-fered with type 2 seroconversion, resulting in some-what lower rates of seroconversion to type 2. Type 2 seroconversion could be boosted by an ad-ditional dose given at 9 months of age (with mea-sles vaccine), although the costs and benefits of this added dose would need to be considered.
Although these results are encouraging, they must be viewed in the context of Cuba, where there are generally good standards of public health and hygiene. Mothers born after 1962 in Cuba have only vaccine-induced immunity against polio.14 Whether these results can be generalized to settings with more recent circulation of wild polioviruses remains uncertain. A WHO evalua-tion demonstrated interference of maternally de-rived antibody with types 1 and 2 seroconversion in Thailand, a country with more recent circula-tion of wild poliovirus.10
Two doses of IPV administered at 8 and 16 weeks of age produced only moderately lower rates of seroconversion than three doses given at 6, 10, and 14 weeks of age, a result suggesting that
administering doses at 2, 4, and 6 months of age would result in higher rates of seroconversion to IPV in Cuba. Since the 2-, 4-, and 6-month schedule is used extensively in the Western Hemi-sphere, such countries could expect high IPV im-munogenicity if they added IPV to the currently used combination vaccines. Tropical developing countries considering adding IPV to a 6-, 10-, and 14-week schedule, however, should consider add-ing an additional IPV dose at 9 months (with measles vaccine) or in the second year of life (with DPT), to ensure high seroconversion rates.20 If OPV vaccination is phased out, then high sero-conversion after IPV will be essential, since there will be no catch-up indirect immunization by secondary spread from OPV.
Data on IPV performance from developing countries are limited.1,3,21-24 These data demon-strate that the seroconversion or seroprevalence levels achieved by IPV may be inflated by second-ary exposure to OPV, which is used in routine programs or mass campaigns in most tropical de-veloping countries. More important, the reported decreases in viral excretion after challenge vac-cine doses (with trivalent or monovalent OPV) in these studies appear to be due almost exclusive-ly to mucosal immunity gained from secondary
Figure 1 (facing page). Enrollment of Study Participants and Completion of the Vaccine Trial.
Group A received a combination of diphtheria–pertussis–tetanus vaccine, Haemophilus influenzae type b vaccine, and inactivated poliovirus vaccine (DPT-Hib-IPV) at 6, 10, and 14 weeks of age. Group B, the control group, received a combination of DPT vaccine and Hib vaccine at 6, 10, and 14 weeks. Group C received the DPT-Hib-IPV combination at 8 and 16 weeks. The study was conducted between September 2001 and March 2002. OPV denotes oral poliovirus vaccine. Infants withdrawn from the study were referred back to the routine Cuban vaccination pro-gram. Any illnesses were typical (non–life-threatening) pediatric illnesses that were present at the time of the next scheduled dose and resulted in postponement of vaccination. Hypotonia is a transient, shocklike state occurring within 24 hours after vaccination, from which our patient completely recovered. It was attributed to the pertussis component of the vaccine. The rate of occurrence in our study was 1 in 573 doses (0.17%). A rate of 0.06% is cited in the literature.17 Persistent crying was defined as acute, uncontrollable crying last-ing at least 3 hours and occurring within 48 hours after vaccination. It was attributed to the pertussis compo-nent of the vaccine. The rate of occurrence in our study was 5 in 573 doses (0.87%). A rate of 3.50% is cited in the literature.17

Inactivated Poliovirus Vaccine in Cuba
n engl j med 356;15 www.nejm.org april 12, 2007 1541
39p6
266 Enrolled in study
166 Underwent randomization
82 Were assigned to group A 84 Were assigned to group B 100 Were assigned to group C
82 Received vaccine dose 1 andgave serum sample 1
84 Received vaccine dose 1 andgave serum sample 1
100 Received vaccine dose 1 andgave serum sample 1
23 Withdrew2 Illness2 Persistent cry
19 Consent withdrawn
23 Withdrew1 Illness1 Persistent cry
19 Consent withdrawn2 Lost to follow-up
24 Withdrew2 Illness1 Hypotonia
20 Consent withdrawn1 Lost to follow-up
5 Withdrew1 Illness2 Consent withdrawn2 Lost to follow-up
4 Withdrew3 Consent withdrawn1 Lost to follow-up
4 Withdrew2 Persistent cry2 Consent withdrawn
3 Withdrew1 Insufficient serum
sample1 Consent withdrawn1 Lost follow-up
2 Withdrew1 Insufficient serum
sample1 Consent withdrawn
58 Received vaccine dose 2 61 Received vaccine dose 2 77 Received vaccine dose 2
54 Received vaccine dose 3 57 Received vaccine dose 3
52 Gave serum sample 2and stool sample 1
52 Received challenge OPV 54 Received challenge OPV 72 Received challenge OPV
54 Gave stool sample 2 andcompleted the study
72 Gave stool sample 2 andcompleted the study
AUTHOR:
FIGURE:
JOB: ISSUE:
4-CH/T
RETAKE
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
Enon
1st
2nd3rd
Galindo (Caceres)
1 of 1
04-12 -07
ARTIST: ts
35615
54 Gave serum sample 2and stool sample 1
72 Gave serum sample 2and stool sample 1
52 Gave stool sample 2 andcompleted the study
OPV exposure. For example, in an evaluation con-ducted in Oman, 13% of subjects in a four-dose OPV group, 10% of those in a three-dose IPV group, and 11% of those in a combined four-dose OPV and three-dose IPV group excreted poliovirus type 1 one week after challenge with monovalent
OPV type 1.10 If one does not account for the secondary OPV “contamination effect,” the Oman excretion data would suggest that IPV conferred substantial mucosal resistance that was similar to that in the two groups receiving OPV. This finding is in direct conflict with our data from

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071542
Cuba and earlier data from industrialized coun-tries.25-27
In our study, the prevalence of excretion after receiving trivalent OPV was high (more than 90% for any poliovirus) and was similar among all three groups, including the control group, but viral titers were lower in both IPV groups, sug-gesting an effect of IPV vaccination on replica-tion of polioviruses. These data from stool titers are consistent with a body of literature suggest-ing that previous vaccination with IPV can reduce the prevalence, duration, and titers of poliovirus in the stool.25-27
Table 2. Prevaccination and Postvaccination Antibody Titers and Seroconversion Rates According to Study Group and Poliovirus Type.*
Poliovirus Type Group A (N = 52) Group B (N = 54) Group C (N = 72)
Type 1
Median titer — value (95% CI)
Before vaccination 33 (11–45) 27 (13–45) 22 (13–27)
After vaccination 304 (180–428) Not detectable 304 (177–428)
Seroconversion
No. of infants 49 0 65
Rate — % (95% CI)† 94 (84–99) 0 (0–5) 90 (81–96)
Type 2
Median titer — value (95% CI)
Before vaccination 22 (9–38) 21 (9–27) 11 (8–66)
After vaccination 304 (98–536) Not detectable 197 (84–428)
Seroconversion
No. of infants 43 0 64
Rate — % (95% CI)† 83 (70–92) 0 (0–5) 89 (79–95)
Type 3
Median titer — value (95% CI)
Before vaccination Not detectable Not detectable Not detectable
After vaccination 858 (500–1216) Not detectable 723 (332–916)
Seroconversion
No. of infants 52 0 65
Rate — % (95% CI)† 100 (94–100) 0 (0–5) 90 (81–96)
* Group A received a combination of diphtheria–pertussis–tetanus vaccine, Haemophilus influenzae type b vaccine, and inactivated poliovirus vaccine (DPT-Hib-IPV) at 6, 10, and 14 weeks of age. Group B, the control group, received a combination of DPT vaccine and Hib vaccine at 6, 10, and 14 weeks. Group C received the DPT-Hib-IPV combination at 8 and 16 weeks. Antibody titers were the reciprocals of antiserum di-lution that neutralized 50% of wells.
† Exact confidence intervals are based on the binomial distribution.
Table 1. Ages at Which Infants Received Doses of Vaccine.*
Dose Group A Group B Group C
median days of age (range)
1 43 (27–54) 43 (29–51) 58 (30–68)
2 72 (64–76) 71 (65–85) 114 (92–116)
3 100 (91–108) 99 (95–114) —
* Group A received a combination of diphtheria–pertussis–tetanus vaccine, Haemophilus influenzae type b vaccine, and inactivated poliovirus vaccine (DPT-Hib-IPV) at 6, 10, and 14 weeks of age. Group B, the control group, re-ceived a combination of DPT vaccine and Hib vaccine at 6, 10, and 14 weeks. Group C received the DPT-Hib-IPV combination at 8 and 16 weeks. The dash denotes not applicable.

Inactivated Poliovirus Vaccine in Cuba
n engl j med 356;15 www.nejm.org april 12, 2007 1543
Our study has limitations, and the results should be interpreted with caution. Maternally derived antibodies in Cuba were vaccine induced and have not been boosted by circulating wild polioviruses. To assess mucosal immunity, we examined a single stool sample for shedding of OPV administered during the national immuniza-tion campaign. Finally, our study was affected by substantial attrition due primarily to one major adverse event.
As more countries, including middle-income countries, switch to the use of IPV, there will be increasing opportunities to study the natural his-tory of Sabin viruses in an IPV environment. The WHO is implementing demonstration projects that introduce IPV into large areas within tropical developing countries. It will also be important to evaluate the effect of increasing demand for IPV
on its affordability in developing countries. These demonstration projects and other studies will provide additional, critical information to the WHO and its member countries as they determine the role of IPV in routine immunization programs to safely protect children from all three polio-virus types and to respond to reemergent polio-viruses.
Supported by a grant from the World Health Organization. Aventis Pasteur (now Sanofi Pasteur) contributed the vaccines PENTAct-HIB and TETRAct-HIB.
No potential conflict of interest relevant to this article was reported.
We thank the Cuban Ministry of Public Health for its valuable support; the Directorate of the Provincial Center for Health in Havana for providing more than 1000 of its dedicated staff to implement the study; the Pedro Kourí Institute for laboratory and technical support; the study coordinators, doctors, and nurses in each of the municipalities selected; the children and parents who volunteered for the study; and Drs. Mark Pallansch, Walter Dowdle, and David Wood for reviewing the manuscript.
Table 3. Isolation of Poliovirus in Stool Samples 1 Week after Oral Poliovirus Vaccine Challenge According to Study Group and Poliovirus Type.*
Group†No. ofInfants Type 1 Type 2 Type 3 Any Type of Poliovirus
No. % (95% CI) No. % (95% CI) No. % (95% CI) No. % (95% CI)Mean Log10 Titer in
Fecal Sample (95% CI)‡
A 52 10 19 (10–33) 45 87 (74–94) 5 10 (3–21) 49 94 (84–99) 3.46 (3.17–3.75)
B 54 9 17 (8–29) 48 89 (77–96) 3 6 (1–15) 49 91 (80–97) 3.89 (3.64–4.14)
C 72 13 18 (10–29) 67 93 (85–98) 10 14 (7–24) 70 97 (90–100) 3.37 (3.14–3.60)
* All stool samples taken from study participants just before the challenge dose were negative for poliovirus. Exact confidence intervals (CIs) are based on the binomial distribution.
† Group A received a combination of diphtheria–pertussis–tetanus vaccine, Haemophilus influenzae type b vaccine, and inactivated poliovirus vaccine (DPT-Hib-IPV) at 6, 10, and 14 weeks of age. Group B, the control group, received a combination of DPT vaccine and Hib vaccine at 6, 10, and 14 weeks. Group C received the DPT-Hib-IPV combination at 8 and 16 weeks.
‡ Mean values are given for excretors of poliovirus.
References
Progress towards global poliomyelitis eradication: preparation for the oral polio-virus vaccine cessation era. Wkly Epide-miol Rec 2004;79:349-55.
Conclusions and recommendations of the Ad Hoc Advisory Committee on Polio-myelitis Eradication, Geneva, 21-22 Sep-tember 2004. Wkly Epidemiol Rec 2004; 79:401-7.
Kew O, Morris-Glasgow V, Landaverde M, et al. Outbreak of poliomyelitis in His-paniola associated with circulating type 1 vaccine-derived poliovirus. Science 2002; 296:356-9.
Shimizu H, Thorley B, Paladin FJ, et al. Circulation of type 1 vaccine-derived po-liovirus in the Philippines in 2001. J Virol 2004;78:13512-21.
Rousset D, Rakato-Andrianarivelo M,
1.
2.
3.
4.
5.
Razafindratsimandresy R, et al. Recom-binant vaccine-derived poliovirus in Mad-agascar. Emerg Infect Dis 2003;9:885-7.
Yang CF, Naguib T, Yang SJ, et al. Circu-lation of endemic type 2 vaccine-derived poliovirus in Egypt from 1983 to 1993. J Virol 2003;77:8366-77.
Aylward RB, Sutter RW, Heymann DL. OPV cessation — the final step to a “polio-free” world. Science 2005;310:625-6.
Sutter RW, Cáceres VM, Más Lago P. The role of routine polio immunization in the post-certification era. Bull World Health Organ 2004;82:31-3.
Introduction of inactivated poliovirus vaccine into oral poliovirus vaccine-using countries. Wkly Epidemiol Rec 2003;78: 241-52.
WHO Collaborative Study Group on
6.
7.
8.
9.
10.
Oral and Inactivated Poliovirus Vaccines. Combined immunization of infants with oral and inactivated poliovirus vaccines: results of a randomized trial in the Gam-bia, Oman, and Thailand. Bull World Health Organ 1996;74:253-68.
Ramsay ME, Begg NT, Gandhi J, Brown D. Antibody response and viral ex-cretion after live polio vaccine or a com-bined schedule of live and inactivated po-lio vaccines. Pediatr Infect Dis J 1994;13: 1117-21.
Más Lago P, Cáceres VM, Galindo MA, et al. Persistence of vaccine-derived polio-virus following a mass vaccination cam-paign in Cuba: implications for stopping polio vaccination after global eradication. Int J Epidemiol 2001;30:1029-34.
Más Lago P, Gary HE Jr, Perez LS, et al.
11.
12.
13.

n engl j med 356;15 www.nejm.org april 12, 20071544
Inactivated Poliovirus Vaccine in Cuba
Poliovirus detection in wastewater and stools following an immunization cam-paign in Havana, Cuba. Int J Epidemiol 2003;32:772-7.
Más Lago P. Eradication of poliomy-elitis in Cuba: a historical perspective. Bull World Health Organ 1999;77:681-7.
Dayan GH, Thorley M, Yamamura Y, et al. Serologic response to inactivated poliovirus vaccine: a randomized clinical trial comparing 2 vaccination schedules in Puerto Rico. J Infect Dis 2007;195:12-20.
WHO Department of Immunization, Vaccines and Biologicals. Polio laboratory manual. 4th ed. Geneva: World Health Organization, 2004. (WHO/IVB/04.10.)
Cody CL, Baraff LJ, Cherry JD, Marcy SM, Manclark CR. Nature and rates of ad-verse reactions associated with DPT and DT immunizations in infants and chil-dren. Pediatrics 1981;68:650-60.
Parent du Chatelet I, Merchant AT, Fisher-Hoch S, et al. Serological response
14.
15.
16.
17.
18.
and poliovirus excretion following differ-ent combined oral and inactivated polio-virus vaccines immunization schedules. Vaccine 2003;21:1710-8.
Kok PW, Leeuwenburg P, Tukei P, et al. Serological and virological assessment of oral and inactivated poliovirus vaccines in a rural population in Kenya. Bull World Health Organ 1992;70:93-103.
Sutter RW, Suleiman AJM, Malankar P, et al. Trial of a supplemental dose of four poliovirus vaccines. N Engl J Med 2000;343:767-73.
Vidor E, Caudrelier P, Plotkin SA. The place of DTP/eIPV vaccine in routine pae-diatric vaccination. Rev Med Virol 1994;4: 261-77.
Murdin AD, Barreto L, Plotkin S. In-activated poliovirus vaccine: past and pres-ent experience. Vaccine 1996;14:735-46.
Krishnan R, Jadhav M, John TJ. Efficacy of inactivated poliovirus vaccine in India. Bull World Health Organ 1983;61:689-92.
19.
20.
21.
22.
23.
Simoes EA, Padmini B, Steinhoff MC, Jadhav M, John TJ. Antibody response of infants to two doses of inactivated polio-virus vaccine of enhanced potency. Am J Dis Child 1985;139:977-80.
Ghendon YUZ, Sanakoyeva II. Com-parison of resistance of the intestinal tract to poliomyelitis vaccine (Sabin’s strains) in persons after naturally and experimen-tally acquired immunity. Acta Virol 1961;5: 265-73.
Henry JL, Jaikaran ES, Davies JR, et al. A study of poliovaccination in infancy: ex-cretion following challenge with live virus by children given killed or living poliovac-cine. J Hyg (Lond) 1966;64:105-20.
Marine WM, Chin TD, Gravelle CR. Limitation of fecal and pharyngeal polio-virus excretion in Salk-vaccinated children: a family study during a type 1 poliomy-elitis epidemic. Am J Hyg 1962;76:173-95.Copyright © 2007 Massachusetts Medical Society.
24.
25.
26.
27.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 2007 1545
review article
medical progress
Strategies for Safer Liver Surgery and Partial Liver TransplantationPierre-Alain Clavien, M.D., Ph.D., Henrik Petrowsky, M.D.,
Michelle L. DeOliveira, M.D., and Rolf Graf, Ph.D.
From the Swiss Hepato-Pancreatico-Bili-ary (HPB) Center, Department of Visceral and Transplantation Surgery, University Hospital Zurich, Zurich, Switzerland. Ad-dress reprint requests to Dr. Clavien at the Department of Visceral and Transplanta-tion Surgery, University Hospital Zurich, Rämistr. 100, CH-8091 Zurich, Switzer-land, or at [email protected].
N Engl J Med 2007;356:1545-59.Copyright © 2007 Massachusetts Medical Society.
The liver possesses the unique ability to regenerate within a short period.1-3 This feature has led to the development of innovative strate-gies in liver surgery and transplantation. The anatomy of the liver is paramount
in considering advances in hepatic surgery. The liver is divided into eight segments (Fig. 1). In healthy adults, the liver weighs about 1.5 kg (3.3 lb).4 The blood supply of the liver is carried through two major vessels, the hepatic artery and the portal vein. The portal vein carries a large volume of venous blood to the liver from the gut, pancreas, and spleen, permitting hepatic processing of ingested and absorbed nutrients, among many other functions of the liver. The hepatic veins empty into the inferior vena cava.
l i v er r esec tion a nd l i v er tr a nspl a n tation
Resection of hepatic tumors is being performed with increasing frequency world-wide, because it is now possible to select patients with a tumor load restricted to the liver, or with limited extrahepatic disease, thanks to the availability of imaging techniques such as the combination of positron-emission tomography and com-puted tomography (CT)5-7 and improved intraoperative and postoperative manage-ment.8-10 This ability to resect hepatic tumors currently offers the only curative op-tion for many patients with primary or secondary liver tumors.8-10 Liver resection is limited, however, by the need to preserve a sufficient amount of functional liver, because excessive resection leads to liver failure and death within a few days after surgery. Strategies have been developed to increase the volume and function of the potential liver remnant before resection of the diseased part, with the intention of making surgery safer and expanding indications for liver resection.
Liver transplantation has also progressed during the past decade. One of the landmark advances in liver transplantation is the ability to use partial liver grafts obtained from either a deceased donor (a single liver thus obtained can be split and used for two recipients, usually an adult and a child) or a living donor. The minimal amount of functional liver necessary for successful transplantation has been a major concern. For reasons that are unclear, a larger allograft volume is needed for trans-plantation than might be expected on the basis of experience with liver resection.11 The possibility of using a small amount of liver tissue (e.g., segments II and III, which are used in transplantation in children with a body weight of ≤15 kg [33 lb]12) might solve the worldwide problem of a shortage of liver grafts: two adults could benefit from one graft from a single deceased donor, and living donation might gain wider acceptance than is now the case, because a bisegmentectomy (segments II and III) in a healthy donor is associated with a lower relative risk — similar to that of kidney donation — than is a right hemihepatectomy (segments V through

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071546
A
E
Normal anatomy B Occlusion of right portal vein
D Occlusion of right portal vein withtumorectomies in left hemiliver
VIII IV
Right portalvein
Portal vein
Left medial branch
Left portal vein
Atrophy Hypertrophy
VVI
VII
II
III
VIII IV
VVI
VII
II
III
Hypertrophy of the left hemiliver andtumor shrinkage after chemotherapy F Right hemihepatectomy
C Multiple liver tumors
Tumor
03/22/07
AUTHOR PLEASE NOTE:Figure has been redrawn and type has been reset
Please check carefully
Author
Fig #Title
ME
DEArtist
Issue date
COLOR FIGURE
Rev7Dr. Clavien
Ingelfinger
04/12/2007
1
Daniel Muller
Figure 1. Normal Liver Anatomy and the Principle of Portal-Vein Occlusion with and without Concomitant Chemotherapy.
Panel A shows normal liver anatomy, with segments II through VIII shown. Segment I, which lies posteriorly, next to the vena cava, is not shown. The portal vein is shown, with the right portal vein, the left portal vein, and the left medial branch to segment IV. Panel B shows occlusion of the right portal vein, which results in ipsilateral atrophy of the right hemiliver (segments V through VIII) and contralateral compensatory hypertrophy of the left hemiliver seg-ments I through IV. Panel C shows metastases throughout the liver. Panels D, E, and F show a two-stage procedure. In the first stage, small tumorectomies in the potential left remnant hemiliver and occlusion of the right portal vein by means of portal-vein embolization or ligation are performed (Panel D) with concomitant local intraarterial or sys-temic chemotherapy, resulting in the shrinkage of residual tumors and the right hemiliver, with compensatory hyper-trophy of the contralateral hemiliver (Panel E). In the second stage, a curative liver resection (right hemihepatectomy, segments V through VIII, or extended right hemihepatectomy, including segment IV) is performed (Panel F).

Medical Progress
n engl j med 356;15 www.nejm.org april 12, 2007 1547
VIII) (Fig. 1). The current mortality rate for a right hemihepatectomy in a living donor, which is the resection used for transplantation in an adult recipient, is about 0.2 to 0.5%, with a rate of complications of 15 to 30%.11,13,14
This review presents both established and new methods for manipulating liver volume to improve liver surgery and transplantation. We first discuss the process of liver regeneration, then assessment of the minimal liver volume necessary for a given patient and prediction of hepatic function after surgery. Current practice is discussed, along with promising strategies to maximize liver regener-ation.
L i v er R egener at ion
response to major tissue loss
The human body responds to partial hepatectomy not by regenerating lost segments but by induc-ing hyperplasia in the liver remnant.1-3 The ana-tomical structures of a liver that has undergone partial hepatectomy are therefore distinctly differ-ent from those of the original liver.
The process of restoration of liver volume in humans is initiated by the replication of various types of intrahepatic cells, followed by an increase in cell size. The onset and peak of hepatocyte rep-lication vary among species. In humans, replication of hepatocytes generally starts within 1 day after a major resection. Nonparenchymal cells, such as endothelial cells, Kupffer cells (macrophages res-ident in the liver), and biliary-duct cells, replicate in a delayed fashion. After replication has been completed, growth consisting of an increase in cell size occurs over several additional days.
The initiation and synchronization of replica-tion in different types of hepatic cells depend on the extent of the resection, tissue damage, or both. Low-grade tissue damage (e.g., toxic or ischemic injury) or a relatively small resection (removal of less than 30% of the liver) substantially reduces the replication rate, which also appears to be less syn-chronized than after a large resection (removal of 70% of the liver).1,3,15 After a massive resection, up to 90% of the hepatocytes appear to replicate.1
molecular basis of liver regeneration
Liver regeneration has been studied in rodent mod-els, an approach that permits the determination of cellular events and the analysis of the molecu-lar triggers governing regeneration.1-3 Briefly, the
process of liver regeneration involves mediators similar to those found in acute inflammation. Nor-mally, hepatocytes are in the quiescent G0 phase. After resection, the remaining hepatocytes enter the G1 phase. Cytokines derived predominantly from Kupffer cells prime hepatocytes; tumor ne-crosis factor α (TNF-α) and, subsequently, inter-leukin-6 are released, contributing to the initia-tion of the cell cycle (Fig. 2).16,17 Mitogenic factors are required for the regenerative process to enter the S phase, primarily growth factors such as epi-dermal growth factor, hepatocyte growth factor, and transforming growth factor α (TGF-α).18,19 Integration of these signals induces full and syn-chronized regeneration. Failure to activate this signal cascade can result in a delay in the onset of regeneration, inadequate recovery of liver vol-ume, and eventually clinical signs of liver failure.20 Termination of the regenerative process appears to be controlled by the action of transforming growth factor β (TGF-β) and other members of the activin family.21
Two recent reports shed further light on the mechanisms of regeneration. In one report from our group, platelets (thrombocytes) were shown to be critically involved in regeneration.22 Sero-tonin, a neurotransmitter transported within the peripheral circulation by platelets, appears to be a co-mitogen that is essential for hepatic regenera-tion. Mice deficient in tryptophan hydroxylase 1, which lack peripheral serotonin, have dimin-ished hepatocyte proliferation after partial hepa-tectomy.22
According to another recent report, bile acids also appear to influence regeneration.23 In experi-ments in animals in which bile-acid pools were high, regeneration was complete, whereas low bile flow was associated with reduced hepatocyte rep-lication. The signal responsible for this feedback mechanism of regeneration is a nuclear bile recep-tor, the farnesoid X receptor. This mechanism may be important in integrating the metabolic load of the liver and may have a direct effect on regenera-tion.23 The integration of all these signals is neces-sary for full and synchronized regeneration.
l i v er volume
Minimal volume for the Surgically Created Liver Remnant or Allograft
Below a certain threshold volume, a liver rem-nant cannot sustain metabolic, synthetic, and

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071548
detoxifying functions. In this situation, the post-operative course evolves with signs of liver failure, primarily jaundice, coagulopathy, encephalopathy, and ascites, as well as renal and pulmonary fail-ure, all of which may become apparent only 3 to 5 days after surgery. Together, these signs have been termed the “small-for-size syndrome.”24,25 Studies in mice suggest that the failure of a par-tial liver to regenerate is the most important con-tributing factor in the small-for-size-syndrome.20
Although the removal of up to 75% of the total liver volume is feasible in a young patient (≤40 years of age) with normal hepatic parenchy-ma, resection must be more conservative in the presence of underlying liver diseases or in elderly patients (e.g., ≥70 years of age) (Table 1).
Cirrhosis
The best-studied underlying liver disease in persons undergoing resection is cirrhosis, which is associated with the development of hepatocel-lular carcinoma. The cirrhotic liver tolerates acute tissue loss poorly, given its impaired function and decreased ability to regenerate.26 In addition, por-tal hypertension, if present, is associated with a poor outcome because of compromised portal f low and the risk of postoperative upper gastro-intestinal bleeding.27 These features are critical in selecting patients with cirrhosis for surgery.27 For example, a right hemihepatectomy is associated with a low risk of liver failure or death in patients with cirrhosis who have normal serum bilirubin levels and prothrombin times and do not have
Platelets
Vascular endothelialgrowth factor
Serotonin
Lipopoly-saccharides
Leukocyte
Bile acids
Stellate cell
Sinusoidalendothelial cell
Interleukin-6
Inactive hepatocytegrowth factor
Matrixmetalloproteases
Extracellularproteases
Hepatocytegrowth factor
Nucleus
Farnesoid Xreceptor
Tumornecrosisfactor α
Transforminggrowth factor β
Inhibition
Transforminggrowth factor α
Release
Hepatocyte
Kupffer cell
Epidermalgrowth factor
G0 or G1
phase
G1 phase
S phase
03/26/07
AUTHOR PLEASE NOTE:Figure has been redrawn and type has been reset
Please check carefully
Author
Fig #Title
ME
DEArtist
Issue date
COLOR FIGURE
Rev 6Dr. Clavien
IngelfingerES
04/12/2007
2
Daniel Muller
Figure 2. Pathways of Liver Regeneration Initiated by Major Hepatectomy.
After hepatectomy, nonparenchymal cells, such as stellate cells, Kupffer cells, leukocytes, and platelets, are activated by soluble factors, such as vascular endothelial growth factor and lipopolysaccharide. Interaction between activated vascular components, including platelets, leukocytes, sinusoidal endothelial cells, and Kupffer cells, results in the release of tumor necrosis factor α, interleukin-6, and serotonin. The cytokines cause a priming of the remnant hepatocytes, and concurrently, extracellular proteases such as urokinase-type plasminogen ac-tivator convert inactive hepatocyte growth factor to its active form. Inactive hepatocyte growth factor, which is secreted by stellate cells, is a mitogen that induces hepatocyte proliferation. Matrix metalloproteases convert membrane-bound transforming growth factor α into the soluble form. In an autocrine loop, transforming growth factor α, along with endothelial growth factor, signals through the endothelial growth factor receptor. The cytokines and the growth factors act in concert to initiate the reentry of quiescent hepatocytes (in the G0 phase) into the cell cycle from the G1 phase to the S phase, resulting in DNA synthesis and hepatocyte proliferation. To signal the end of proliferation, transforming growth factor β blocks further replication. The metabolic load resulting from the loss of hepatocytes is indi-cated by the accumulation of bile acids in the blood. The bile acids enter the hepatocytes and drive bile acid receptors such as the farne-soid X receptor, resulting in increased protein and DNA synthesis.

Medical Progress
n engl j med 356;15 www.nejm.org april 12, 2007 1549
any signs of portal hypertension. In contrast, even a limited wedge (localized) resection may result in liver failure and death in patients with poor liver function and portal hypertension.
fatty liver
Liver steatosis is another common condition and is usually related to obesity, the presence of met-abolic disorders, or the intake of alcohol or drugs; hepatic steatosis increases the risk of liver resection, according to most large studies.8,28,29 Experimental data indicate that macrosteatosis (the presence of a single large droplet of fat, dis-placing the nucleus, in hepatocytes) increases this risk more than does microsteatosis (the presence of small, multiple fat deposits in hepatocytes).30 How to adjust the extent of liver resection in pa-tients with steatosis is unclear, but most experi-enced surgeons consider that mild steatosis (up to 30% of hepatocytes containing fat) represents a minimal additional risk or none, whereas patients with severe steatosis (more than 60% of hepato-cytes containing fat) should undergo only limited resection (e.g., one or two segments). In patients with moderate steatosis (30 to 60% of hepato-cytes containing fat), caution is necessary, par-ticularly if macrosteatosis is present, and con-servative resection should be favored over major resection.29 Steatosis can often be treated success-fully within a few weeks if the patient is placed on a strict low-fat, high-protein diet (initially, 1400 calories per day, with a rapid reduction to 1200 and then to 1000 calories).31 Liver biopsies should be performed in patients with suspected moderate-to-severe steatosis to document improve-ment with such a diet. The association between inflammation (marked by leukocyte infiltration), hepatocellular ballooning, and steatosis, termed nonalcoholic steatohepatitis, constitutes an addi-tional operative risk.32-34
liver after chemotherapy
An increasing number of patients with tumors undergo extensive chemotherapy with multiple drugs before surgery. Drugs such as irinotecan (Campto, Pfizer) and, to a lesser degree, oxaliplatin (Eloxatin, Sanofi Aventis) have been associated with the development of steatohepatitis,33,34 and among patients receiving these drugs, the rates of complications and death after major liver resec-tion are likely to be increased, as compared with the rates among patients not receiving these drugs.33,34 We and others avoid major resection in
such patients.33 In addition, severe hepatic sinu-soidal obstruction, occasionally associated with nodular regenerative hyperplasia, has been ascribed to oxaliplatin-based chemotherapy.35-37 These vascular obstructions result in a bluish appearance of the liver, known as the blue liver syndrome.36 Patients with this histologic feature are at higher risk for intraoperative blood loss and postopera-tive complications than are patients without this feature. Bevacizumab (Avastin, Hoffmann–La Roche), a monoclonal antibody targeting vascular endothelial growth factor (VEGF) in combination with cytotoxic chemotherapy, appears to improve survival in patients with metastatic colorectal can-cer.38 Because VEGF influences liver regeneration through its regulation of angiogenesis and the release of growth factors, and because bevacizu-mab therapy impairs wound healing,39 the effect of bevacizumab may be deleterious.40 However, when there is a window of 6 to 8 weeks between the administration of bevacizumab and the sur-gery, the risk of perioperative complications after liver resection may not be increased.41 Although most experienced clinicians favor wedge, rather than major, resection in patients exposed to ex-tensive chemotherapy, there is currently no con-sensus for managing the care of such patients, and the optimal window between the completion of chemotherapy and surgery remains uncertain.
remnant donor liver and partial graft
Particular caution is indicated when subjecting healthy living donors to the major liver surgery that donation necessitates. Zero mortality and low morbidity are the goals, and surgery should not be considered if the liver remnant of a poten-tial donor would be below 35% of its initial vol-ume.11,42 Furthermore, although potential donors with up to 15% steatosis are generally accepted
Table 1. Risk Factors for Postoperative Liver Failure.
Older age (e.g., ≥70 yr)
Cirrhosis
Fibrosis
Hepatitis
Intraoperative blood loss
Ischemia
Obstructive cholestasis
Preoperative chemotherapy
Steatosis

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071550
by most transplantation centers, those with high-er liver-fat content are usually not accepted or are placed in a weight-loss program.
An important concept in the growing field of partial liver transplantation is that of minimal viable graft volume. An allograft mass that is 35 to 40% of a normal liver, often expressed as a ratio of the graft to the total body weight of the recipient (0.8 to 1%), must be obtained to ensure successful and viable transplantation.43 On the basis of such a measure, a transplant recipient with a body weight of 75 kg (165 lb) should receive a graft weighing 600 to 750 g (1.3 to 1.7 lb), which is usually obtained only by a right hemi-hepatectomy. Recipients with more severe disease require a higher graft volume.42 Also, surgical technique, such as reconstruction of the hepatic veins to make optimal outflow possible, is cru-cial to ensure early postoperative function and regeneration of the graft.44
pr eoper ati v e e va luation
clinical and biochemical tests
Assessment of the volume of the potential liver remnant or allograft as well as measurement of preoperative liver function are essential. Routine liver biochemical measurements (i.e., bilirubin, aspartate aminotransferase, alanine aminotrans-
ferase, and alkaline phosphatase levels), a coagu-lation profile, and a platelet count, combined with the proper assessment of the predicted volume of the liver remnant on CT or magnetic resonance imaging (MRI), generally suffice for an assess-ment of a candidate with normal liver parenchy-ma for major liver surgery. The situation is more complicated in a candidate with preexisting liver dysfunction. In a patient with cirrhosis, the evalu-ation most often used relies on the Child–Turcotte–Pugh classification, which is based on a score that includes bilirubin and albumin levels, pro-thrombin time, and the presence or absence of ascites and encephalopathy (Table 2).46,47 Many clinicians add upper gastrointestinal endoscopy to rule out esophagogastric varices, a sign of portal hypertension. A low platelet count (<100,000 per cubic millimeter) or the presence of large varices on preoperative imaging (CT or MRI) rules out patients with cirrhosis as candidates for major liver resection.48 Other practitioners recommend direct measurement of the actual hepatic venous pressure gradient in order to select patients with cirrhosis who might be candidates for liver resec-tion.27
dynamic liver tests
Other quantitative liver-function tests are most often used in Asia, where the majority of patients
Table 2. Child–Turcotte–Pugh Classification.*
Biochemical and Clinical Criteria Points
1 2 3
Albumin (g/dl) >3.5 2.8–3.5 <2.8
Bilirubin (mg/dl) >2.0 2.0–3.0 <3.0
Prothrombin time
Seconds <4 4–6 >6.0
International normalized ratio <1.7 1.7–2.3 >2.3
Ascites None Moderate (or suppressed with medication)
Tense (or refractory to medication)
Encephalopathy None Grades I–II (or suppressed with medication)
Grades III–IV (or refractory to medication)
* Most authors divide the cumulative score of the Child–Turcotte–Pugh classification into grade A (5–6 points, indicating well-compensated disease), grade B (7–9 points, significant functional compromise), and grade C (10–15 points, decom-pensated disease). Encephalopathy is graded according to the West Haven criteria of altered mental state in hepatic encephalopathy,45 as follows: grade I, lack of awareness, shortened attention, euphoria, or anxiety; grade II, lethargy or apathy and minimal disorientation; grade III, somnolence to semistupor with gross disorientation; grade IV, coma with unresponsiveness to verbal or noxious stimuli. Asterixis (“flapping tremor”) is often observed in patients with grade I altered mental state and is always present in patients with grades II and III. To convert values for bilirubin to micro-moles per liter, multiply by 17.1.

Medical Progress
n engl j med 356;15 www.nejm.org april 12, 2007 1551
undergoing liver surgery have hepatocellular car-cinoma related to hepatitis B or C cirrhosis. Met-abolic tests (Table 3) target different aspects of hepatic physiology.49-51 The most commonly used test is intravenous injection of indocyanine green (0.5 mg per kilogram), a dark bluish-green tricarbo-cyanine dye that rapidly binds to plasma β-lipo-protein and is completely and exclusively removed by hepatocytes. Indocyanine green is excreted into bile in unmodified form and does not enter the enterohepatic recirculation.52 The rate of retention of indocyanine green determined at 15 minutes after injection must be interpreted in the context of other factors.50,52 For example, patients with a favorable Child–Turcotte–Pugh score of A (Ta-ble 2) and a retention rate of indocyanine green at 15 minutes of less than 14% generally tolerate major hepatectomy well, whereas those with a retention rate greater than 20% should be ex-cluded from major liver resection. Patients with retention rates between 14 and 20% should un-dergo surgery only after an assessment of liver volume with possible preoperative portal-vein embolization (Fig. 3A).48,53
s a fer l i v er r esec tion a nd pa rti a l l i v er tr a nspl a n tation
Strategies for Manipulating Liver volume
Experiments performed almost a century ago sug-gested that selective occlusion of the portal branch
causes atrophy of the ipsilateral liver lobe and hypertrophy of the contralateral lobe.54 Induced atrophy of the occluded hemiliver is triggered by increased apoptotic activity, whereas hypertrophy of the nonoccluded lobe appears to be linked to increased cellular proliferation.55 In the late 1980s, Makuuchi and colleagues first used the selective-occlusion strategy in patients to extend the limits of liver resection (Fig. 1).56 Selective interruption of the portal flow to a portion of the liver can be achieved by means of portal-vein embolization or ligation. Although portal-vein ligation requires a surgical (open or laparoscopic) approach, portal-vein embolization can be performed percutaneous-ly, usually by means of a transhepatic approach using embolic materials such as gelatin sponge, cyanoacrylate with ethiodized oil, alcohol, fibrin glue, particles, or coils.57 Both embolization and ligation of the portal vein are usually performed at the right portal vein in preparation for a right hemihepatectomy (removal of segments V through VIII) or an extended right hemihepatectomy (re-moval also of segment IV) in instances when the potential liver remnant would otherwise be too small.56,58-61 When an extended right hemihepa-tectomy is to be performed, the volume of the liver remnant is optimized by the addition of oc-clusion of the left medial branch (segment IV) (Fig. 1).62 Portal-vein embolization or ligation has recently been integrated into and is considered es-sential to a strategy for two-stage hepatectomy
Table 3. Dynamic Tests to Assess Liver Function Preoperatively.
Function Measured Test Principle of Test
Microsomal hepatic function
Breath tests (C-labeled aminopyrine, methacetin, caffeine)
Breath tests are used to probe hepatic microsomal P450 enzyme activity and investigate hepatocellular function by assessing liver oxidation. The exhaled labeled CO2 is measured.
Clearance tests (antipyrine, caffeine, lidocaine)
Clearance tests probe the hepatic microsomal P450 enzyme activity and measure either the metabolic elimination of the test compound or the appearance of metabolites in the blood that are primarily dependent on the hepatic metabolic capacity.
Cytosolic hepatic function
Elimination capacity test (galactose) The capacity for elimination of galactose is estimated by serial measurements of serum galactose levels after administration of an intravenous bolus of galactose; galactose is metabolized by the cytosolic enzyme galactokinase.
Liver perfusion and biliary excretion
Clearance test (indocyanine green) Indocyanine green is distributed in the serum, removed by the liver, and excret-ed unchanged into bile without entering the enterohepatic circulation.
Liver perfusion Clearance tests (low-dose galactose, sorbitol)
The high rate of hepatic extraction of low-dose galactose and sorbitol by the sinusoidal membrane of hepatocytes implies a hepatic plasma flow– dependent mechanism.
Hepatocyte mass Uptake test (technetium-99m– galactosyl human serum albumin labeling)
Technetium-99m–galactosyl human serum albumin accumulates only in the liver by ligand–receptor binding and is visualized on scintigraphy.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071552
for initially unresectable, multiple liver tumors (Fig. 1).63-65 Currently, portal-vein ligation is used only during an open procedure — for example, insertion of a device for selective intraarterial de-livery of chemotherapy or limited hepatectomy for planned two-stage procedures.65
indications for portal-vein occlusion
Portal-vein embolization is indicated only if the volume of the potential liver remnant would be below the threshold associated with a high risk of inadequate liver volume after surgery.66,67 Most surgeons consider a major resection 2 to 4 weeks after portal-vein occlusion, when the maximal changes in volume have been reached.68 Portal-vein embolization is also increasingly used as a dynamic preoperative test to identify patients in whom liver regeneration will be impaired, who for that reason should not undergo the surgery.66 This approach is especially relevant for patients with chronic liver diseases, cholestasis, and a history of chemotherapy.66,69 It is supported by a study in patients with cirrhosis in whom the failure of re-generation after portal-vein embolization predict-ed a poor outcome after surgery.67 Although there are no universally accepted guidelines, two algo-rithms for the treatment of patients with normal livers (Fig. 3A) or cirrhotic livers (Fig. 3B) sum-marize what we consider a reasonable approach to major resection.
portal-vein occlusion with chemotherapy
New strategies have focused on combining selec-tive portal-vein obstruction with the concomitant administration of systemic59,64,69,70 or selective intraarterial hepatic65 chemotherapy before liver resection, with the aim of achieving both a reduc-tion in the tumor size and a change in liver vol-ume (Fig. 1 and Fig. 4). These strategies have been applied mainly in patients with a nonresectable, advanced tumor load and a liver remnant that was predicted to be too small for resection. The regimen and the timing of systemic chemother-apy and portal-vein embolization have been vari-able, but fluorouracil-based chemotherapy with or without oxaliplatin, irinotecan, or bevacizumab is the regimen most often used.59,64,70 In a pilot study, continuous delivery of selective intraarte-rial chemotherapy with floxuridine (FUDR, Hoff-mann–La Roche) and right portal-vein ligation in 11 patients with multiple nonresectable metasta-ses of colorectal origin were associated with a
significant decrease in tumor volume and a sig-nificant increase in the volume of the contralat-eral left hemiliver (Fig. 4).65 About one third of the patients receiving this treatment underwent cu-rative liver resection 3 months after the start of treatment. Impairment of the hypertrophy induced by portal-vein obstruction that results from con-comitant continuous chemotherapy, although a concern, has not been observed to date.71 When liver resection is not performed after portal-vein embolization or ligation, the use of further sys-temic or regional chemotherapy remains possi-ble. The main complication of selective hepatic delivery of floxuridine appears to be the develop-ment of intrahepatic and extrahepatic biliary stric-tures.72,73
portal-vein embolization with chemoembolization
Another strategy in patients with hepatocellular carcinoma is the sequential use of transarterial chemoembolization, portal-vein embolization, and then major liver resection.67,74 Transarterial chemo-embolization is directed both to the tumor treat-ment and to embolization of arterioportal shunts, which are frequently present in cirrhosis. Trans-arterial chemoembolization may prevent tumor progression during the period of portal-vein em-bolization and the planned surgery.75 This ap-proach, as compared with portal-vein emboliza-tion alone, has been associated with more efficient hypertrophy and improved tumor control before major hepatectomy.67
portal-vein embolization with biliary drainage
Patients with hilar cholangiocarcinomas often re-quire complex liver resection. Since segment I is also removed during such resection because of a high incidence of recurrence at this location, the
Figure 3 (facing page). Proposed Decision Tree for Major Hepatectomy in Patients with Normal Liver Parenchyma and Those with Cirrhosis.
The cutoff points of 30% volume (Panel A) and 50% volume (Panel B) for the potential liver remnant are based on our current practice and available data. For cirrhotic livers with a rate of retention of indocyanine green (ICG) that is less than 14% at 15 minutes (Panel B) and livers with underlying noncirrhotic diseases such as steatosis or fibrosis, we apply the algorithm for nor-mal liver parenchyma with a higher cutoff point (35 to 40%) for the volume of the potential liver remnant.

Medical Progress
n engl j med 356;15 www.nejm.org april 12, 2007 155333p9
Potential liver remnant>30% volume
Normal liver
Patients with a Normal Liver
Patients with Cirrhosis
Yes
Yes
Resection No resection
No
NoYes
Portal-vein embolization
Potential liver remnant>30% volume
Cirrhotic liver
Child–Turcotte–Pughscore of A
Child–Turcotte–Pughscore of B or C
YesNo
No resectionResection
AUTHOR:
FIGURE:
JOB: ISSUE:
4-CH/T
RETAKE
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
Enon
1st
2nd3rd
Clavien
3 of 3
04-12-06
ARTIST: ts
35615
A
B
Portal hypertension
No
Retention of ICG at 15 minutes
14–20%<14% >20%
Yes No
Portal-vein embolization
Potential liver remnant>50% volume
Potential liver remnant>50% volume

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071554
16p6
AUTHOR Clavien
FIGURE 4a&b of 4
JOB: ISSUE:
4-CH/T
RETAKE 1st2nd
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
4-12-07
mst
35615
A
B
Figure 4. CT Images of the Effects of Portal-Vein Ligation and Selective Administration of Intraarterial Chemotherapy.
A 58-year-old patient with multifocal colorectal liver metastases underwent ligation of the right portal vein (segments V through VIII) and the medial portal vein (segment IV) to induce compensatory hypertrophy of segments II and III (red, before ligation) and the implan-tation of a pump to selectively deliver chemotherapy in the gastroduodenal artery (Panel A). After administra-tion of continuous intraarterial chemotherapy with floxu-ridin, the colorectal liver metastases were significantly reduced (by about 60%), and significant hypertrophy (100%) (green, after ligation) developed in the left liver 3 months later (Panel B). Adapted from Selzner et al.,65 with the permission of the publisher.
liver remnant typically consists only of segments II and III and the upper part of segment IV.76,77 These patients frequently present with severe cho-lestasis and impaired liver function due to ob-struction of the bile duct. A preoperative strategy of biliary drainage of the potential liver remnant followed by portal-vein embolization of the area
of the planned resection has been reported to re-verse cholestasis and increase the size of the po-tential liver remnant before surgery.77-79 Although the optimal timing of these interventions has not been determined, we, and others,80 now perform portal-vein embolization within 1 to 3 weeks after biliary drainage and consider surgery after the cholestasis resolves (usually when the bili-rubin level is less than 50 μmol per liter [2.9 mg per deciliter]) and there is an adequate regenera-tive response (Fig. 3). With the use of this strat-egy, several studies of extensive liver resections for hilar cholangiocarcinomas without perioperative deaths have been reported.61,77,78
effect on tumor growth
A legitimate concern is whether the stimulus for liver regeneration induced by portal-vein occlusion might enhance tumor growth. Although there have been few reports of an influence of portal-vein occlusion on tumor growth,70,81-83 most other studies of colorectal liver metastases have failed to show any negative effect of portal-vein occlu-sion on tumor growth or reduced patient survival after surgery.59,65,84,85 One study reported a lower rate of recurrence of hepatic cancer after portal-vein embolization that was followed by surgery, as compared with resection alone.85 However, the in-tuitive concern that metastases in the nonembo-lized hemiliver might grow more rapidly after right portal-vein embolization has led to the pro-posal of a two-stage procedure. In the first stage, all visible metastases in the left hemiliver are cleared in association with right portal-vein em-bolization64 or ligation,65 and in the second stage, about 4 weeks later, a right or extended right hemihepatectomy is performed. When concomi-tant chemotherapy is used, definitive liver resec-tion is usually performed 3 or more months after the start of treatment (Fig. 1).
small liver graft
In liver transplantation, only a few clinically appli-cable strategies are available to ensure sufficient function of undersize grafts obtained from living or deceased donors. Prolonged cold ischemia dur-ing organ procurement has a negative effect on liver regeneration86 and the clinical outcome after transplantation.87 Therefore, efforts should be made to keep the ischemia time as short as pos-sible. Recipients who are in poor general condi-tion and have low hepatic reserve are at increased

Medical Progress
n engl j med 356;15 www.nejm.org april 12, 2007 1555
risk for complications after partial liver trans-plantation.42 Such patients should be considered candidates only for the transplantation of a whole cadaveric organ.
Injury to small grafts is associated with portal hyperperfusion, caused by the combination of a low liver volume and preexisting portal hyper-tension.25 Although enhanced liver regeneration might have been anticipated on the basis of in-creased portal f low, portal hyperperfusion is currently seen by many as the cause of failure in small grafts. One explanation is that changes in portal flow induce reciprocal effects on hepatic arterial flow, implying that post-transplantation portal hyperperfusion results in a compensatory decrease in arterial flow.88 A reduction in the por-tal venous flow by means of portal banding, splenic-artery ligation, or a hemiportocaval shunt may prevent postoperative liver failure, resulting in improved survival of the graft and the patient after transplantation of a partial liver graft.25,89 For split-liver transplantation of a cadaveric graft, only optimal grafts are used, and grafts from older donors (>50 years of age), steatotic organs, and organs with a low ratio of the graft weight to the total body weight of the recipient should be avoided.90,91
Hepat opro tec ti v e S tr ategies
pharmacologic approaches
Efforts to develop pharmacologic means of pro-tecting the liver from damage during regeneration have identified a few molecular targets. Our group has recently shown that pentoxifylline (Trental, Hoechst–Roussel), an inhibitor of TNF-α synthe-sis in Kupffer cells that has other properties such as vasodilatation and induction of the inter-leukin-6 pathway, reduces the likelihood of inad-equate liver function in the liver remnant in a murine model of partial liver transplantation.20 Pretreatment of a small graft (30% of the total liver volume) and of the recipient with pentoxifyl-line prevents lethal outcomes and fully restores regeneration.16
Acetylcysteine, a precursor of glutathione, has been widely studied as a protective molecule. Clini-cal trials of its use in the perioperative treatment of patients undergoing liver transplantation showed reduced levels of circulating selectins92 and a reduction in the severity of rejection in pediatric patients undergoing liver transplantation,93 but
neither study showed an overt benefit for the patient.
Other molecules, such as cardiotrophin-1, a member of the interleukin-6 cytokine family, have shown a hepatoprotective potential in rescu-ing regeneration and in animal survival after 90% hepatectomy in rats.94 Drugs associated with a reduction in portal pressure, such as somatostat-in,95 fingolimod (FTY720, Novartis Pharma),96 or the low-dose nitric oxide donor FK 409,97 provid-ed significant protection in rat models of small-graft transplantation. These drugs have additional effects that might contribute to protection, such as down-regulation of endothelin-1, up-regulation of heme oxygenase-195,97 or interleukin-10,97 and activation of Akt signaling, which has been shown to be related to cell survival.96 An immunosup-pressive agent, sirolimus (Rapamune, Wyeth–Ayerst), has also been shown to minimize injury and improve survival — effects that may be re-lated to suppression of the activation of hepatic stellate cells — in a model of partial graft trans-plantation in cirrhotic rats.98 Although these strategies have been successful in animal models, their usefulness in humans remains to be dem-onstrated in clinical trials.
surgical approaches
Occlusion of the portal triad (the Pringle maneu-ver) and total vascular exclusion (concomitant clamping of the infrahepatic and suprahepatic vena cava and the portal triad) are techniques used to minimize blood loss and the need for blood transfusions during liver surgery.8,99 Both techniques, however, cause inevitable ischemic injury that may impair liver regeneration after major hepatectomy.100 Intermittent clamping of the portal triad and ischemic preconditioning (a brief period of ischemia followed by a short interval of reperfusion) are established nonphar-macologic strategies to protect the liver from pro-longed ischemic injury.101-103 The underlying pro-tective principle of ischemic preconditioning is that cells are exposed to a limited stress that trig-gers natural defense mechanisms against subse-quent ischemic injury.104-106 Intermittent clamp-ing and ischemic preconditioning are highly and equally effective in minimizing postoperative injury to the liver, but intermittent clamping ap-pears to be superior for long periods of ischemia (≥75 minutes).103,107,108 (For detailed insights into hepatoprotective strategies, see Selzner et al.109)

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071556
Conclusions
There has been substantial progress in both liver surgery and liver transplantation owing to im-proved preoperative diagnosis and intraoperative and postoperative care. Factors that limit the achievement of curative tumor resection are the high morbidity and mortality rates associated with insufficient volume of the liver remnant. Many tumors that were previously considered to be unresectable are now amenable to complete re-section through innovative strategies that make manipulation of the liver volume possible. Portal-vein embolization or ligation causes atrophy of the ipsilateral hemiliver and hypertrophy of the contralateral side. Portal-vein embolization ap-pears to be particularly valuable in patients who have underlying liver disease. The concomitant administration of chemotherapy may further de-crease both the tumor load and postoperative re-currences.
The use of partial liver transplantation is also rapidly increasing, as transplantation surgeons and hepatologists attempt to overcome the world-wide shortage of organs available for transplan-tation. Unfortunately, there is still a need for a substantial graft volume to support life, which places healthy donors at substantial risk. In the future, the use of new drugs based on innova-tive experimental models, together with a better understanding of the pathways leading to liver regeneration, may permit a very small liver rem-nant to regenerate, resulting in safer surgery for living donors and for patients with large tumors.
Supported by grants from the National Institutes of Health (DK54048-01A1) and the Swiss National Science Foundation (SNF3200-061411) to Dr. Clavien.
Dr. Petrowsky reports receiving the Novartis fellowship in Hepato-Pancreato-Biliary (HPB) Surgery and Liver Transplanta-tion at the Swiss HPB Center, University of Zurich, Zurich, Swit-zerland. No other potential conflict of interest relevant to this article was reported.
References
Taub R. Liver regeneration: from myth to mechanism. Nat Rev Mol Cell Biol 2004; 5:836-47.
Michalopoulos GK, DeFrances M. Liver regeneration. Adv Biochem Eng Biotechnol 2005;93:101-34.
Fausto N, Campbell JS, Riehle KJ. Liver regeneration. Hepatology 2006;43:Suppl 1:S45-S53.
de la Grandmaison GL, Clairand I, Durigon M. Organ weight in 684 adult au-topsies: new tables for a Caucasoid popu-lation. Forensic Sci Int 2001;119:149-54.
Selzner M, Hany TF, Wildbrett P, Mc-Cormack L, Kadry Z, Clavien PA. Does the novel PET/CT imaging modality impact on the treatment of patients with meta-static colorectal cancer of the liver? Ann Surg 2004;240:1027-34.
Petrowsky H, Wildbrett P, Husarik DB, et al. Impact of integrated positron emis-sion tomography and computed tomogra-phy on staging and management of gall-bladder cancer and cholangiocarcinoma. J Hepatol 2006;45:43-50.
Juweid ME, Cheson BD. Positron-emission tomography and assessment of cancer therapy. N Engl J Med 2006;354: 496-507.
Belghiti J, Hiramatsu K, Benoist S, Massault P, Sauvanet A, Farges O. Seven hundred forty-seven hepatectomies in the 1990s: an update to evaluate the actual risk of liver resection. J Am Coll Surg 2000;191:38-46.
Jarnagin WR, Gonen M, Fong Y, et al. Improvement in perioperative outcome after hepatic resection: analysis of 1,803
1.
2.
3.
4.
5.
6.
7.
8.
9.
consecutive cases over the past decade. Ann Surg 2002;236:397-406.
Poon RT, Fan ST, Lo CM, et al. Im-proving perioperative outcome expands the role of hepatectomy in management of benign and malignant hepatobiliary diseases: analysis of 1222 consecutive pa-tients from a prospective database. Ann Surg 2004;240:698-708.
Tanaka K, Yamada T. Living donor liver transplantation in Japan and Kyoto University: what can we learn? J Hepatol 2005;42:25-8.
Broelsch CE, Whitington PF, Emond JC, et al. Liver transplantation in children from living related donors: surgical tech-niques and results. Ann Surg 1991;214: 428-37.
Middleton PF, Duffield M, Lynch SV, et al. Living donor liver transplantation — adult donor outcomes: a systematic re-view. Liver Transpl 2006;12:24-30.
Trotter JF, Adam R, Lo CM, Kenison J. Documented deaths of hepatic lobe donors for living donor liver transplantation. Liver Transpl 2006;12:1485-8.
Nocito A, Georgiev P, Dahm F, et al. Platelets and platelet-derived serotonin promote tissue repair after normothermic hepatic ischemia in mice. Hepatology 2007; 45:369-76.
Cressman DE, Greenbaum LE, DeAn-gelis RA, et al. Liver failure and defective hepatocyte regeneration in interleukin-6-deficient mice. Science 1996;274:1379-83.
Yamada Y, Kirillova I, Peschon JJ, Fausto N. Initiation of liver growth by tumor necrosis factor: deficient liver re-
10.
11.
12.
13.
14.
15.
16.
17.
generation in mice lacking type I tumor necrosis factor receptor. Proc Natl Acad Sci U S A 1997;94:1441-6.
Mead JE, Fausto N. Transforming growth factor alpha may be a physiological regulator of liver regeneration by means of an autocrine mechanism. Proc Natl Acad Sci U S A 1989;86:1558-62.
Pediaditakis P, Lopez-Talavera JC, Pe-tersen B, Monga SP, Michalopoulos GK. The processing and utilization of hepato-cyte growth factor/scatter factor following partial hepatectomy in the rat. Hepatology 2001;34:688-93.
Tian Y, Jochum W, Georgiev P, Moritz W, Graf R, Clavien PA. Kupffer cell-depen-dent TNF-alpha signaling mediates injury in the arterialized small-for-size liver transplantation in the mouse. Proc Natl Acad Sci U S A 2006;103:4598-603.
Strain AJ, Frazer A, Hill DJ, Milner RD. Transforming growth factor beta inhibits DNA synthesis in hepatocytes isolated from normal and regenerating rat liver. Biochem Biophys Res Commun 1987;145: 436-42.
Lesurtel M, Graf R, Aleil B, et al. Platelet-derived serotonin mediates liver regeneration. Science 2006;312:104-7.
Huang W, Ma K, Zhang J, et al. Nuclear receptor-dependent bile acid signaling is required for normal liver regeneration. Science 2006;312:233-6.
Kam I, Lynch S, Svanas G, et al. Evi-dence that host size determines liver size: studies in dogs receiving orthotopic liver transplants. Hepatology 1987;7:362-6.
Dahm F, Georgiev P, Clavien PA. Small-
18.
19.
20.
21.
22.
23.
24.
25.

Medical Progress
n engl j med 356;15 www.nejm.org april 12, 2007 1557
for-size syndrome after partial liver trans-plantation: definition, mechanisms of disease and clinical implications. Am J Transplant 2005;5:2605-10.
Nagasue N, Yukaya H, Ogawa Y, Kohno H, Nakamura T. Human liver regenera-tion after major hepatic resection: a study of normal liver and livers with chronic hepatitis and cirrhosis. Ann Surg 1987;206: 30-9.
Bruix J, Castells A, Bosch J, et al. Sur-gical resection of hepatocellular carcinoma in cirrhotic patients: prognostic value of preoperative portal pressure. Gastroenter-ology 1996;111:1018-22.
Kooby DA, Fong Y, Suriawinata A, et al. Impact of steatosis on perioperative out-come following hepatic resection. J Gastro-intest Surg 2003;7:1034-44.
McCormack L, Petrowsky H, Jochum C, Furrer K, Clavien PA. Hepatic steatosis is a risk factor for postoperative complica-tions after major hepatectomy: a case-matched control study. Ann Surg (in press).
Selzner N, Selzner M, Jochum W, Amann-Vesti B, Graf R, Clavien PA. Mouse livers with macrosteatosis are more sus-ceptible to normothermic ischemic injury than those with microsteatosis. J Hepatol 2006;44:694-701.
Nakamuta M, Morizono S, Soejima Y, et al. Short-term intensive treatment for donors with hepatic steatosis in living-donor liver transplantation. Transplanta-tion 2005;80:608-12.
Ekstedt M, Franzen LE, Mathiesen UL, et al. Long-term follow-up of patients with NAFLD and elevated liver enzymes. Hepatology 2006;44:865-73.
Fernandez FG, Ritter J, Goodwin JW, Linehan DC, Hawkins WG, Strasberg SM. Effect of steatohepatitis associated with irinotecan or oxaliplatin pretreatment on resectability of hepatic colorectal metas-tases. J Am Coll Surg 2005;200:845-53.
Vauthey JN, Pawlik TM, Ribero D, et al. Chemotherapy regimen predicts steato-hepatitis and an increase in 90-day mor-tality after surgery for hepatic colorectal metastases. J Clin Oncol 2006;24:2065-72.
Rubbia-Brandt L, Audard V, Sartoretti P, et al. Severe hepatic sinusoidal obstruc-tion associated with oxaliplatin-based che-motherapy in patients with metastatic colorectal cancer. Ann Oncol 2004;15: 460-6.
Bilchik AJ, Poston G, Curley SA, et al. Neoadjuvant chemotherapy for metastatic colon cancer: a cautionary note. J Clin On-col 2005;23:9073-8. [Erratum, J Clin Oncol 2006;24:1648.]
Aloia T, Sebagh M, Plasse M, et al. Liver histology and surgical outcomes af-ter preoperative chemotherapy with fluo-rouracil plus oxaliplatin in colorectal can-cer liver metastases. J Clin Oncol 2006;24: 4983-90.
Hurwitz H, Fehrenbacher L, Novotny
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 2004;350: 2335-42.
Scappaticci FA, Fehrenbacher L, Cart-wright T, et al. Surgical wound healing complications in metastatic colorectal can-cer patients treated with bevacizumab. J Surg Oncol 2005;91:173-80.
Ellis LM, Curley SA, Grothey A. Surgi-cal resection after downsizing of colorec-tal liver metastasis in the era of bevaci-zumab. J Clin Oncol 2005;23:4853-5.
D’Angelica M, Kornprat P, Gonen M, et al. Lack of evidence for increased opera-tive morbidity after hepatectomy with peri-operative use of bevacizumab: a matched case-control study. Ann Surg Oncol 2007; 14:759-65.
Tan HP, Patel-Tom K, Marcos A. Adult living donor liver transplantation: who is the ideal donor and recipient? J Hepatol 2005;43:13-7.
Trotter JF, Wachs M, Everson GT, Kam I. Adult-to-adult transplantation of the right hepatic lobe from a living donor. N Engl J Med 2002;346:1074-82.
Malago M, Testa G, Frilling A, et al. Right living donor liver transplantation: an option for adult patients: single institu-tion experience with 74 patients. Ann Surg 2003;238:853-62.
Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg 1973;60:646-9.
Ferenci P, Lockwood A, Mullen K, Tarter R, Weissenborn K, Blei AT. Hepatic encephalopathy — definition, nomencla-ture, diagnosis, and quantification: final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology 2002;35:716-21.
Child CG, Turcotte JG. Surgery and portal hypertension. In: Child CG, ed. The liver and portal hypertension. Philadelphia: Saunders, 1964:50-62.
Poon RT, Fan ST. Assessment of he-patic reserve for indication of hepatic re-section: how I do it. J Hepatobiliary Pan-creat Surg 2005;12:31-7.
Armuzzi A, Candelli M, Zocco MA, et al. Breath testing for human liver func-tion assessment. Aliment Pharmacol Ther 2002;16:1977-96.
Imamura H, Sano K, Sugawara Y, Kokudo N, Makuuchi M. Assessment of hepatic reserve for indication of hepatic resection: decision tree incorporating in-docyanine green test. J Hepatobiliary Pan-creat Surg 2005;12:16-22.
Kokudo N, Vera DR, Makuuchi M. Clinical application of TcGSA. Nucl Med Biol 2003;30:845-9.
Mullin EJ, Metcalfe MS, Maddern GJ. How much liver resection is too much? Am J Surg 2005;190:87-97.
Fan ST, Lo CM, Liu CL, et al. Hepatec-tomy for hepatocellular carcinoma: toward
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
zero hospital deaths. Ann Surg 1999;229: 322-30.
Rous P, Larimore LD. Relation of the portal blood to liver maintenance. J Exp Med 1920;31:609-32.
Harada H, Imamura H, Miyagawa S, Kawasaki S. Fate of the human liver after hemihepatic portal vein embolization: cell kinetic and morphometric study. Hepatol-ogy 1997;26:1162-70.
Makuuchi M, Thai BL, Takayasu K, et al. Preoperative portal embolization to increase safety of major hepatectomy for hilar bile duct carcinoma: a preliminary report. Surgery 1990;107:521-7.
Madoff DC, Abdalla EK, Vauthey JN. Portal vein embolization in preparation for major hepatic resection: evolution of a new standard of care. J Vasc Interv Radiol 2005;16:779-90.
Imamura H, Shimada R, Kubota M, et al. Preoperative portal vein embolization: an audit of 84 patients. Hepatology 1999; 29:1099-105.
Azoulay D, Castaing D, Smail A, et al. Resection of nonresectable liver metasta-ses from colorectal cancer after percuta-neous portal vein embolization. Ann Surg 2000;231:480-6.
Broering DC, Hillert C, Krupski G, et al. Portal vein embolization vs. portal vein ligation for induction of hypertrophy of the future liver remnant. J Gastrointest Surg 2002;6:905-13.
Nagino M, Kamiya J, Nishio H, Ebata T, Arai T, Nimura Y. Two hundred forty consecutive portal vein embolizations be-fore extended hepatectomy for biliary can-cer: surgical outcome and long-term fol-low-up. Ann Surg 2006;243:364-72.
Nagino M, Kamiya J, Kanai M, et al. Right trisegment portal vein embolization for biliary tract carcinoma: technique and clinical utility. Surgery 2000;127:155-60.
Kianmanesh R, Farges O, Abdalla EK, Sauvanet A, Ruszniewski P, Belghiti J. Right portal vein ligation: a new planned two-step all-surgical approach for com-plete resection of primary gastrointestinal tumors with multiple bilateral liver me-tastases. J Am Coll Surg 2003;197:164-70.
Jaeck D, Oussoultzoglou E, Rosso E, Greget M, Weber JC, Bachellier P. A two-stage hepatectomy procedure combined with portal vein embolization to achieve curative resection for initially unresect-able multiple and bilobar colorectal liver metastases. Ann Surg 2004;240:1037-49.
Selzner N, Pestalozzi BC, Kadry Z, Selzner M, Wildermuth S, Clavien PA. Downstaging colorectal liver metastases by concomitant unilateral portal vein liga-tion and selective intra-arterial chemother-apy. Br J Surg 2006;93:587-92.
Farges O, Belghiti J, Kianmanesh R, et al. Portal vein embolization before right hepatectomy: prospective clinical trial. Ann Surg 2003;237:208-17.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071558
Ogata S, Belghiti J, Farges O, Varma D, Sibert A, Vilgrain V. Sequential arterial and portal vein embolizations before right hepatectomy in patients with cirrhosis and hepatocellular carcinoma. Br J Surg 2006; 93:1091-8.
Abdalla EK, Hicks ME, Vauthey JN. Portal vein embolization: rationale, tech-nique and future prospects. Br J Surg 2001; 88:165-75.
Adam R, Delvart V, Pascal G, et al. Rescue surgery for unresectable colorec-tal liver metastases downstaged by chemo-therapy: a model to predict long-term survival. Ann Surg 2004;240:644-57.
Elias D, Ouellet JF, De Baere T, Lasser P, Roche A. Preoperative selective portal vein embolization before hepatectomy for liver metastases: long-term results and im-pact on survival. Surgery 2002;131:294-9.
Goere D, Farges O, Leporrier J, Sau-vanet A, Vilgrain V, Belghiti J. Chemo-therapy does not impair hypertrophy of the left liver after right portal vein obstruc-tion. J Gastrointest Surg 2006;10:365-70.
Clavien PA, Selzner N, Morse M, Selz-ner M, Paulson E. Downstaging of hepa-tocellular carcinoma and liver metastases from colorectal cancer by selective intra-arterial chemotherapy. Surgery 2002;131: 433-42.
Kemeny NE, Niedzwiecki D, Hollis DR, et al. Hepatic arterial infusion versus systemic therapy for hepatic metastases from colorectal cancer: a randomized trial of efficacy, quality of life, and molecular markers (CALGB 9481). J Clin Oncol 2006; 24:1395-403.
Aoki T, Imamura H, Hasegawa K, et al. Sequential preoperative arterial and portal venous embolizations in patients with hepatocellular carcinoma. Arch Surg 2004;139:766-74.
Kokudo N, Makuuchi M. Current role of portal vein embolization/hepatic artery chemoembolization. Surg Clin North Am 2004;84:643-57.
Neuhaus P, Jonas S, Bechstein WO, et al. Extended resections for hilar cholangio-carcinoma. Ann Surg 1999;230:808-18.
Seyama Y, Kubota K, Sano K, et al. Long-term outcome of extended hemi-hepatectomy for hilar bile duct cancer with no mortality and high survival rate. Ann Surg 2003;238:73-83.
Kawasaki S, Imamura H, Kobayashi A, Noike T, Miwa S, Miyagawa S. Results of surgical resection for patients with hilar bile duct cancer: application of extended hepatectomy after biliary drainage and hemihepatic portal vein embolization. Ann Surg 2003;238:84-92.
Takahashi T, Togo S, Tanaka K, Endo I, Fujii Y, Shimada H. Safe and permissible limits of hepatectomy in obstructive jaun-dice patients. World J Surg 2004;28:475-81.
Ishizawa T, Hasegawa K, Sano K, Imamura H, Kokudo N, Makuuchi M. Se-
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
lective versus total biliary drainage for ob-structive jaundice caused by a hepatobil-iary malignancy. Am J Surg 2007;193: 149-54.
Barbaro B, Di Stasi C, Nuzzo G, Vellone M, Giuliante F, Marano P. Preoperative right portal vein embolization in patients with metastatic liver disease: metastatic liver volumes after RPVE. Acta Radiol 2003;44:98-102.
Kokudo N, Tada K, Seki M, et al. Pro-liferative activity of intrahepatic colorec-tal metastases after preoperative hemihe-patic portal vein embolization. Hepatology 2001;34:267-72.
Heinrich S, Jochum W, Graf R, Cla-vien PA. Portal vein ligation and partial hepatectomy differentially influence growth of intrahepatic metastasis and liver re-generation in mice. J Hepatol 2006;45:35-42.
Wakabayashi H, Ishimura K, Okano K, et al. Is preoperative portal vein emboliza-tion effective in improving prognosis after major hepatic resection in patients with advanced-stage hepatocellular carcinoma? Cancer 2001;92:2384-90.
Oussoultzoglou E, Bachellier P, Rosso E, et al. Right portal vein embolization before right hepatectomy for unilobar colorectal liver metastases reduces the in-trahepatic recurrence rate. Ann Surg 2006; 244:71-9.
Selzner N, Selzner M, Tian Y, Kadry Z, Clavien PA. Cold ischemia decreases liver regeneration after partial liver transplanta-tion in the rat: a TNF-alpha/IL-6-dependent mechanism. Hepatology 2002;36:812-8.
Cameron AM, Ghobrial RM, Yersiz H, et al. Optimal utilization of donor grafts with extended criteria: a single-center ex-perience in over 1000 liver transplants. Ann Surg 2006;243:748-53.
Bolognesi M, Sacerdoti D, Bombonato G, et al. Change in portal f low after liver transplantation: effect on hepatic arterial resistance indices and role of spleen size. Hepatology 2002;35:601-8.
Troisi R, Ricciardi S, Smeets P, et al. Effects of hemi-portocaval shunts for inf low modulation on the outcome of small-for-size grafts in living donor liver transplantation. Am J Transplant 2005;5: 1397-404.
Azoulay D, Castaing D, Adam R, et al. Split-liver transplantation for two adult recipients: feasibility and long-term out-comes. Ann Surg 2001;233:565-74.
Yersiz H, Renz JF, Farmer DG, Hisa-take GM, McDiarmid SV, Busuttil RW. One hundred in situ split-liver transplan-tations: a single-center experience. Ann Surg 2003;238:496-505.
Weigand MA, Plachky J, Thies JC, et al. N-acetylcysteine attenuates the increase in alpha-glutathione S-transferase and cir-culating ICAM-1 and VCAM-1 after reper-fusion in humans undergoing liver trans-
81.
82.
83.
84.
85.
86.
87.
88.
89.
90.
91.
92.
plantation. Transplantation 2001;72:694- 8.
Bucuvalas JC, Ryckman FC, Krug S, Alonso MH, Balistreri WF, Kotagal U. Ef-fect of treatment with prostaglandin E1 and N-acetylcysteine on pediatric liver transplant recipients: a single-center study. Pediatr Transplant 2001;5:274-8.
Bustos M, Beraza N, Lasarte JJ, et al. Protection against liver damage by cardio-trophin-1: a hepatocyte survival factor up-regulated in the regenerating liver in rats. Gastroenterology 2003;125:192-201.
Xu X, Man K, Zheng SS, et al. Attenu-ation of acute phase shear stress by soma-tostatin improves small-for-size liver graft survival. Liver Transpl 2006;12:621-7.
Zhao Y, Man K, Lo CM, et al. Attenua-tion of small-for-size liver graft injury by FTY720: significance of cell-survival Akt signaling pathway. Am J Transplant 2004; 4:1399-407.
Man K, Lee TK, Liang TB, et al. FK 409 ameliorates small-for-size liver graft injury by attenuation of portal hyperten-sion and down-regulation of Egr-1 path-way. Ann Surg 2004;240:159-68.
Man K, Su M, Ng KT, et al. Rapamycin attenuates liver graft injury in cirrhotic recipient — the significance of down-regulation of Rho-ROCK-VEGF pathway. Am J Transplant 2006;6:697-704.
Kooby DA, Stockman J, Ben-Porat L, et al. Influence of transfusions on periop-erative and long-term outcome in patients following hepatic resection for colorectal metastases. Ann Surg 2003;237:860-9.
Selzner M, Camargo CA, Clavien PA. Ischemia impairs liver regeneration after major tissue loss in rodents: protective effects of interleukin-6. Hepatology 1999; 30:469-75.
Belghiti J, Noun R, Malafosse R, et al. Continuous versus intermittent portal triad clamping for liver resection: a con-trolled study. Ann Surg 1999;229:369-75.
Clavien PA, Selzner M, Rudiger HA, et al. A prospective randomized study in 100 consecutive patients undergoing ma-jor liver resection with versus without ischemic preconditioning. Ann Surg 2003; 238:843-50.
Petrowsky H, McCormack L, Trujillo M, Selzner M, Jochum W, Clavien PA. A prospective randomized controlled trial comparing intermittent portal triad clamp-ing versus ischemic preconditioning with continuous clamping for major liver resec-tion. Ann Surg 2006;244:921-30.
Rudiger HA, Graf R, Clavien PA. Sub-lethal oxidative stress triggers the protec-tive effects of ischemic preconditioning in the mouse liver. J Hepatol 2003;39:972-7.
Peralta C, Bulbena O, Xaus C, et al. Ischemic preconditioning: a defense mech-anism against the reactive oxygen species generated after hepatic ischemia reperfu-sion. Transplantation 2002;73:1203-11.
93.
94.
95.
96.
97.
98.
99.
100.
101.
102.
103.
104.
105.

Medical Progress
n engl j med 356;15 www.nejm.org april 12, 2007 1559
Peralta C, Prats N, Xaus C, Gelpi E, Rosello-Catafau J. Protective effect of liver ischemic preconditioning on liver and lung injury induced by hepatic ischemia-reperfu-sion in the rat. Hepatology 1999;30:1481-9.
Rudiger HA, Kang KJ, Sindram D, Riehle HM, Clavien PA. Comparison of is-
106.
107.
chemic preconditioning and intermittent and continuous inf low occlusion in the murine liver. Ann Surg 2002;235:400-7.
Vajdova K, Heinrich S, Tian Y, Graf R, Clavien PA. Ischemic preconditioning and intermittent clamping improve murine hepatic microcirculation and Kupffer cell
108.
function after ischemic injury. Liver Transpl 2004;10:520-8.
Selzner N, Rudiger H, Graf R, Cla-vien PA. Protective strategies against is-chemic injury of the liver. Gastroenterol-ogy 2003;125:917-36.Copyright © 2007 Massachusetts Medical Society.
109.

images in clinical medicine
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071560
A 51-year-old woman with polycystic liver and kidney disease had undergone renal transplantation 21 years before presentation. She had no evidence of cerebrovascular malformations. Both her father and aunt also
had polycystic kidney disease. After the renal transplantation, her liver had become progressively diseased and enlarged through cystic changes. Early satiety, malnutri-tion, and abdominal pain necessitated a liver transplantation. The recipient’s weight at transplantation was 59 kg. A 9.1-kg liver (white arrow) was removed and replaced with a whole graft that was one tenth the weight of the diseased liver (black arrow-head). A large cyst at the dome of the native liver had to be decompressed (white arrowhead) to allow for access to the recipient’s suprahepatic vena cava. She made an excellent recovery and had normal kidney and liver function at 4 years of follow-up.Copyright © 2007 Massachusetts Medical Society.
Liver Transplantation for Polycystic Liver Disease
William J. Wall, M.D.
London Health Sciences Centre London, ON N6A 5A5, Canada [email protected]
39p6
AUTHOR
FIGURE
JOB: ISSUE:
4-CH/T
RETAKE 1st2nd
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
Wall
A
4-12-07
mleahy
35615

case records of the massachusetts general hospital
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 2007 1561
Founded by Richard C. Cabot Nancy Lee Harris, m.d., Editor Eric S. Rosenberg, m.d., Associate EditorJo-Anne O. Shepard, m.d., Associate Editor Alice M. Cort, m.d., Associate EditorSally H. Ebeling, Assistant Editor Christine C. Peters, Assistant Editor
From the Departments of Neurology (D.M.G., S.R.P.), Radiology (P.W.S.), and Pathology (R.P.H.), and the Division of Rheumatology, Allergy and Immunology (A.C.S.), Massachusetts General Hospi-tal; and the Departments of Neurology (D.M.G., S.R.P.), Radiology (P.W.S.), Pa-thology (R.P.H.), and Medicine (A.C.S.), Harvard Medical School.
N Engl J Med 2007;356:1561-70.Copyright © 2007 Massachusetts Medical Society.
Pr esen tation of C a se
A 59-year-old man was admitted to this hospital in late summer because of back pain, weakness in the right arm, and cranial-nerve palsies.
The patient was in his usual state of health until the first week in July, 5 weeks before admission, when fevers led to body temperatures up to 39.4°C and neck stiffness developed. He saw his primary care physician, who noted thrombocyto-penia; a viral illness was diagnosed, and antibiotics were administered. The fevers resolved within 5 days after they started, and the platelet count returned to normal within 2 weeks. However, the discomfort in his neck gradually worsened. One week before admission, numbness of the right hand developed, followed by weak-ness of the right hand and neck during the next 3 days.
Four days before admission, the patient was evaluated by an orthopedist. Mag-netic resonance imaging (MRI) of the neck 2 days later revealed degenerative changes of the spine at multiple levels from C3 to T2, with a broad-based central herniation at the C3–C4 level and mild protrusions at other cervical levels. An electrocardiogram was normal. Ibuprofen, methocarbamol, and oxycodone–acet-aminophen were administered. The right arm became weaker, and the patient reported that the neck pain became sharp and more severe (9 on a scale of 1 to 10, with 1 being the least severe), radiating down the spine.
The day before admission, left ptosis and diplopia developed. On the day of admission, the patient was seen at another hospital. He did not have fever, headache, nausea, vomiting, or a skin rash. The blood pressure was 156/85 mm Hg, the pulse 101 beats per minute, the respiration 20 breaths per minute, and the temperature 36.1°C. The oxygen saturation was 95% while the patient was breathing ambient air. Gaze was directed to the right, and strength in the right hand was decreased. Hydromorphone was administered intravenously for pain control. Computed tomo-graphic (CT) scanning of the head showed no abnormalities suggestive of acute disease. He was transferred to the emergency department of this hospital.
Diabetes mellitus had been diagnosed 1 year earlier and was managed with glipizide (5 mg daily). A lumbar laminectomy had been performed in the past. He
Case 11-2007: A 59-Year-Old Man with Neck Pain, Weakness in the Arms,
and Cranial-Nerve PalsiesDavid M. Greer, M.D., M.A., Pamela W. Schaefer, M.D., Scott R. Plotkin, M.D., Ph.D.,
Robert P. Hasserjian, M.D., and Allen C. Steere, M.D.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071562
had a 30-pack-year smoking history and a chronic nonproductive cough; he did not drink alcohol or use illicit drugs. He had no allergies to medica-tions. He was married, worked as a land surveyor, lived in a wooded area north of Boston, owned two dogs, and played golf frequently. He had had many tick bites in the past but none recently, and the bites had not been followed by rashes. His maternal grandmother had lived to be more than 100 years of age and had had breast cancer, and another grandparent also had had cancer. His parents and children were in good health.
On examination, the patient appeared alert and uncomfortable, and he had pain in the neck, back, and left eye. The blood pressure was 163/89 mm Hg; the other vital signs were normal. There was tenderness on palpation of the left orbit and globe; the pupils were 3 mm in diame-ter, round, and reactive to light. The visual fields and visual acuity were normal, and the optic disks were sharp. Left ptosis was present, and the pa-tient kept the right eyelid shut because of diplopia. He was unable to adduct, fully elevate, or depress his left eye; intorsion of the eye was possible, and there was no nystagmus. There was incomplete closure of both eyes against resistance. Corneal and sneeze reflexes were present and symmetrical. The jaw-jerk reflex was 1, with normal strength in the pterygoid, masseter, and temporalis mus-cles. The left nasolabial fold was flattened, and the smile was asymmetric. There was minor
weakness of the shoulder shrug bilaterally but not of the sternocleidomastoid muscles. Muscle strength was reduced in both arms and was 3/5 in the right wrist f lexors, wrist extensors, and interosseous muscles; it was normal (5/5) in the other muscle groups. Muscle bulk and tone were normal. The sensations of light touch, pinprick, and temperature in the right hand and forearm were decreased. The biceps and triceps reflexes were 2 on the left and absent on the right, patellar reflexes were 3 bilaterally, and both ankle reflexes were 1; a Babinski reflex was present on the left. On index-finger-to-nose testing, there was marked dysmetria bilaterally, and the gait was unsteady. The remainder of the physical examination was normal.
The patient was admitted to the hospital. The pulmonary vital capacity was between 3.0 and 3.7 liters. The levels of serum electrolytes, calci-um, phosphorus, protein, albumin, and globulin; tests of renal and hepatic function; and a com-plete blood count were normal. The glucose level was 210 mg per deciliter (11.7 mmol per liter), and the sodium 134 mmol per liter. A lumbar puncture revealed an opening pressure of 266 mm H2O; results of tests on the cerebrospinal fluid are shown in Tables 1 and 2. Gram’s stain-ing showed mononuclear cells and no organisms. MRI scanning of the brain was degraded by mo-tion artifact but showed enhancement of the bi-lateral fifth and bilateral third cranial nerves and
Table 1. Results of Cerebrospinal Fluid Tests.
VariableReference Range,
Adults*Hospital Day 1,
Tube 1Hospital Day 1,
Tube 4Hospital Day 7,
Tube 1 Hospital Day 7,
Tube 4
Red cells (per mm3) None 42 10
White cells (per mm3) 0–5 453 383 169 430
Neutrophils (%) 40–70 2 0 2 0
Lymphocytes (%) 22–44 77 77 90 73
Monocytes (%) 4–11 19 22 7 7
Eosinophils (%) 0–8 0 0 0 2
Nonhematic cells (%) None 2 1 1 0
Unidentified cells (%) None 0 0 0 18
Glucose (mg/dl)† 50–75 88
Total protein (mg/dl) 5–55 379
* Reference values are affected by many variables, including the patient population and the laboratory methods used. The ranges used at Massachusetts General Hospital are for adults who are not pregnant and do not have medical conditions that could affect the results. The ranges may therefore not be appropriate for all patients.
† To convert the values for glucose to millimoles per liter, multiply by 0.05551.

case records of the massachusetts gener al hospital
n engl j med 356;15 www.nejm.org april 12, 2007 1563
evidence of microangiopathic disease. Narcotic analgesia was continued for pain. The next day, muscle strength was decreased to 3/5 in both arms and 4/5 in both legs. The erythrocyte sedi-mentation rate was 3 mm per hour. MRI scan-ning of the spine after the administration of gadolinium revealed leptomeningeal enhancement that extended from the lower thoracic portion of the spinal cord to the conus medullaris and in-volved the roots of the cauda equina.
On the third hospital day, a repeated lumbar puncture showed an opening pressure of 24 mm H2O. Analysis of the cerebrospinal f luid showed an elevated lymphocyte count and atypi-cal cells of uncertain origin; f low-cytometric analysis revealed large CD19+ and CD20− cells that lacked demonstrable surface light-chain ex-pression, CD4+ and CD8+ T cells, and polyclonal CD20+ B cells (with cytoplasmic kappa and lambda light-chain expression).
On the fourth hospital day, dyspnea and dys-arthria developed. The vital capacity was 2.8 liters. Radiographs of the chest showed low lung vol-umes and bibasilar parenchymal opacities, consis-tent with atelectasis. The level of carcinoembryonic antigen was normal. Transthoracic echocardiog-raphy revealed a dilated left ventricle, an ejection fraction of 60 percent, and pseudodyskinesis, with-out a source of infection or emboli. The next day, intravenous administration of ceftriaxone (2 g twice daily) was begun.
On the sixth hospital day, the patient was un-able to lift his head independently, the gag reflex was diminished, and dyspnea increased. The vital capacity was 2.6 liters. The oxygen saturation de-creased to 91% while the patient was breathing ambient air; it increased to 97% with the admin-istration of 2 liters of oxygen by nasal cannula. Serum testing for cytomegalovirus antigen was negative, the C-reactive protein was 53.1 mg per liter, and the lipid levels were normal. CT scan-ning revealed opacification of the left lower lobe of the lung and atelectasis in the right lung base, a cyst in the right kidney that was 3 cm in diam-eter, and multiple, small, low-density lesions in the liver suggestive of cysts. Scrotal ultrasonogra-phy was normal.
The next day, respiratory failure developed; the oxygen saturation was 84% while the patient was breathing ambient air and increased to 93% while the patient was breathing supplemental oxygen by nasal cannula; albuterol treatment was given by
means of a nebulizer, and naloxone was admin-istered. The vital capacity was 1.0 liter, and the partial pressure of carbon dioxide was 64 mm Hg. The trachea was intubated, and mechanical venti-lation and sedation with propofol were begun. The patient was transferred to the intensive care unit.
Tests for antineutrophil cytoplasmic antibody (ANCA) and rheumatoid factor were negative; a test for antinuclear antibody was positive at a dilution of 1:160, with a speckled pattern. A re-peated lumbar puncture was performed; cytologic examination of the cerebrospinal fluid revealed atypical lymphocytes that were suspicious for a lymphoproliferative disorder; Gram’s staining showed mononuclear cells and no organisms. A Venereal Disease Research Laboratory test for syphilis was negative; other results are shown in Tables 1 and 2. Metronidazole was given for 1 day and discontinued. Doxycycline and acyclovir were begun. A polymerase-chain-reaction (PCR) assay, performed on the first sample of cerebrospinal
Table 2. Results of Microbiologic Tests.*
Test Result
Blood or serum
Brucella agglutination Negative (titer, <1:20)
Cytomegalovirus antigenemia assay Negative
Epstein–Barr virus anti-VCA IgG 1:80
Epstein–Barr virus anti-VCA IgM <1:20
Epstein–Barr virus early antigen 1:80
Epstein–Barr virus antinuclear antigen 1:320
Herpes simplex virus type 1 antibody IgG Positive
Herpes simplex virus type 2 antibody IgG Negative
Lyme antibody Positive
Rocky Mountain spotted fever antibody <1:32
Cerebrospinal fluid
Acid-fast smear No bacilli seen
Cryptococcal antigen Negative
Fungal wet preparation No fungi seen
Fungal culture No growth
Herpes simplex virus DNA amplification Negative for type 1 and type 2
Mycobacterial culture No growth
Venereal Disease Research Laboratory test for syphilis
Nonreactive
West Nile virus IgM Negative
* VCA denotes viral capsid antigen.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071564
f luid, revealed a single, discrete rearrangement of the immunoglobulin heavy-chain gene, suspici-ous for the presence of a clonal B-cell population.
During the next 3 days, the patient’s maximum body temperature was 37.9°C. The neurologic deficits persisted. Additional laboratory-test re-sults were pending. On the 11th hospital day, the results of a diagnostic test were received.
Differ en ti a l Di agnosis
Dr. David M. Greer: May we see the imaging studies?Dr. Pamela W. Schaefer: Gadolinium-enhanced
T1-weighted images of the spine show leptomen-ingeal enhancement in the region of the lower thoracic cord, conus medullaris, and cauda equi-na (Fig. 1A). Gadolinium-enhanced T1-weighted images of the brain show enhancement of the third and fifth cranial nerves bilaterally (Fig. 1B through 1E). Fluid-attenuated inversion recovery (FLAIR) images of the brain show scattered, non-specific, hyperintense foci in the white matter. The differential diagnosis for leptomeningeal dis-ease and cranial-nerve enhancement includes metastatic disease, as well as inflammatory and infectious processes.
Dr. Greer: This 59-year-old man presented with a febrile illness accompanied by transient thrombo-cytopenia, followed by the subacute onset of pro-gressive neurologic symptoms that included multi-ple cranial-nerve palsies (left third, bilateral seventh, and possibly left sixth), motor weakness and hy-perreflexia in all extremities, and respiratory fail-ure. MRI showed leptomeningeal enhancement of the thoracic and lumbar cord and roots and pos-sibly of several cranial nerves, and examination of the cerebrospinal fluid showed a lymphocytic pleocytosis, with elevated protein and glucose levels (although the serum glucose level was not checked concomitantly in this patient who had diabetes). At the time this patient was admitted, our differential diagnosis included autoimmune, inflammatory, neoplastic, and infectious pro-cesses (Table 3).
Autoimmune Disorders
There are two autoimmune disorders to consider in this patient: acute inflammatory demyelinating polyradiculoneuropathy (the Guillain–Barré syn-drome) and myasthenia gravis. Acute inflamma-tory demyelinating polyradiculoneuropathy com-monly presents with rapidly developing weakness
during a period of days to weeks, as seen in this patient. The weakness is often ascending, but the arms and face may be affected first. Oropharyn-geal weakness can develop, as can diaphragmatic weakness, sometimes leading to respiratory fail-ure. The disease is typically preceded by a viral ill-ness, and this patient had such a prodrome. How-ever, the cerebrospinal fluid is most often acellular, the protein level is typically highly elevated, and neuroimaging is most often normal or shows only subtle enhancement of nerve roots.
Myasthenia gravis would also be a considera-tion in this patient, since it presents with pro-gressive or fluctuating weakness, and the extra-ocular and other cranial muscles are commonly affected. Respiratory failure can occur. Facial and neck weakness are common. However, myasthe-nia gravis is typically painless, and this patient had severe neck and back pain. In addition, patients with myasthenia gravis typically have normal cerebrospinal fluid and neuroimaging stu-dies, but both were abnormal in this patient.
Inflammatory Disorders
Inflammatory disorders to consider in this case include Wegener’s granulomatosis and neurosar-coidosis. Wegener’s granulomatosis is a systemic vasculitis that commonly affects the central ner-vous system. The orbits are affected in approxi-mately 50% of cases, often leading to proptosis; this patient had pain and tenderness in his left eye and orbit. Cranial-nerve palsies can occur (most commonly affecting the second, sixth, and seventh nerves), as in this patient, and pachymen-ingitis can develop, producing changes like those seen on this patient’s MRI.1 However, this patient did not have involvement of other commonly af-fected organ systems; also, this patient had throm-bocytopenia, whereas Wegener’s granulomatosis may cause thrombocytosis. In addition, ANCA testing was negative.
Neurologic manifestations occur in up to 5% of patients with sarcoidosis. Facial-nerve palsies oc-cur in up to 50% of such patients and are often bilateral.2 This patient had two findings sugges-tive of neurosarcoidosis: leptomeningeal enhance-ment and a mononuclear pleocytosis of the cere-brospinal f luid. However, this patient did not have other systemic manifestations of sarcoido-sis, and the normal levels of angiotensin-convert-ing enzyme in the serum and cerebrospinal fluid make this diagnosis unlikely.

case records of the massachusetts gener al hospital
n engl j med 356;15 www.nejm.org april 12, 2007 156533p9
AUTHOR
FIGURE
JOB: ISSUE:
4-CH/T
RETAKE 1st
2nd
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
Greer
1a-e of 2
4-12-07
mst
35615
A B
E
DC
Figure 1. MRI of the Brain and Spinal Cord.
Gadolinium-enhanced sagittal T1-weighted images of the lumbar spine (Panel A) demonstrate smooth leptomeningeal enhancement surrounding the conus medullaris and along the cauda equina. Fat-saturated, gadolinium-enhanced T1-weighted images through the brain stem show enhancement of the bilateral fifth cranial nerves (Panels B and C, arrows) and of the bilateral third cranial nerves (Panels D and E, arrows).

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071566
Infectious Disorders
Potential infectious causes of this patient’s syn-drome include neurosyphilis, brucellosis, crypto-coccal meningitis, and neuroborreliosis. Syphilit-ic meningitis typically occurs approximately 12 months after the primary infection. Headache, meningeal signs, and cranial-nerve palsies are common. Pachymeningitis can affect the brain or spinal cord, and with vascular involvement can cause ischemic strokes.3 Although the findings on MRI and cerebrospinal fluid analysis were con-sistent with this diagnosis, serologic testing in the patient was negative for syphilis.
Brucellosis can cause an acute, subacute, or chronic granulomatous process with a broad range of neurologic manifestations. Although we con-sidered brucellosis, serologic testing for brucella agglutination was negative in this patient, and he had no known risk factors for this infection. Cryptococcal meningitis was also considered, but the patient had no known predisposing factors for cryptococcal disease; this diagnosis was quick-ly ruled out with a negative cerebrospinal f luid test for cryptococcal antigen.
Many features of this patient’s clinical presen-tation were compatible with neuroborreliosis, or Lyme disease. Neurologic involvement develops in approximately 15% of patients with Lyme dis-ease. The three cardinal findings are lymphocytic meningitis, cranial neuropathies (the seventh nerve being most commonly affected, often bilaterally), and a painful radiculitis.4 Peripheral neuropathies can occur, presenting as radiculopathy, plexopa-thy, or a diffuse polyneuropathy, often mimicking acute inflammatory demyelinating polyradiculo-neuropathy. MRI scanning with gadolinium may reveal enhancement of the nerve root, focal brain, or spinal cord. Examination of the cerebrospinal fluid reveals a lymphocytic pleocytosis, often up
to several hundred cells. The protein level may be slightly increased or normal, and the glucose level slightly decreased or normal.
This patient’s overall clinical picture and the presence of Lyme antibodies in the serum con-firming previous exposure to ticks are strongly suggestive of Lyme disease. However, respiratory failure and neck weakness are very unusual for Lyme disease; these findings led us to consider alternative diagnoses, even though respiratory failure caused by diaphragmatic paralysis has been reported in patients with Lyme disease.5
Neoplastic Disorders
Leptomeningeal metastases from a malignant tu-mor, particularly lymphoma, are an important consideration in this case and became a particular concern when the abnormal lymphocytes were seen in the cerebrospinal fluid. Clinical symptoms typically develop during a period of days to weeks and include cranial-nerve dysfunction as well as symptoms related to involvement of the spinal cord or roots.6 Leptomeningeal enhancement is common. The cerebrospinal fluid is abnormal, and flow cytometry can be helpful in revealing an abnormal population of T or B lymphoid cells. In this case, the presence of cranial-nerve, spinal-cord, and nerve-root involvement and leptomen-ingeal enhancement on MRI were consistent with the invasion of the meninges by a neoplastic pro-cess, and flow cytometry and molecular genetic analysis both raised suspicion for B-cell lympho-ma. Therefore, we requested consultation from the neuro-oncology service.
Dr. Scott R. Plotkin: The neuro-oncology service was asked to consider whether this patient could have had lymphoma. There were two possible diagnoses: primary central nervous system lym-phoma and leptomeningeal involvement by a sys-temic lymphoma. Primary central nervous system lymphoma is a rare form of extranodal non-Hodgkin’s lymphoma involving the brain, eyes, and meninges; it is usually of the diffuse large-B-cell type. Leptomeningeal involvement occurs in up to 40% of patients with primary central nervous system lymphoma and is the sole mani-festation of disease at the time of diagnosis in about 8% of those patients.7,8 Central nervous system involvement at presentation occurs in about 2% of patients with systemic non-Hodgkin’s lym-phoma.9
The diagnosis of leptomeningeal involvement by systemic lymphoma or by primary lymphoma
Table 3. Differential Diagnosis.
Autoimmune disorderAcute inflammatory demyelinating polyradiculo-
neuropathy (Guillain–Barré syndrome)Myasthenia gravis
InflammationWegener’s granulomatosisNeurosarcoidosis
NeoplasmLeptomeningeal metastases
InfectionsNeurosyphilisBrucellosisNeuroborreliosis

case records of the massachusetts gener al hospital
n engl j med 356;15 www.nejm.org april 12, 2007 1567
of the central nervous system is usually made by cytologic analysis of the cerebrospinal fluid. How-ever, up to 40% of patients with systemic lym-phoma and a negative cytologic examination have leptomeningeal lymphoma that is confirmed path-ologically on autopsy.10 In patients with a negative cytologic examination, the diagnosis is based on the presence of compatible imaging findings or neurologic deficits in a patient with a known lym-phoma. This patient had atypical cells in his cere-brospinal fluid but had no evidence of primary lymphoma of the central nervous system or sys-temic lymphoma on imaging studies, including testicular ultrasound examination.
An important part of our evaluation of this patient was review of the cerebrospinal fluid find-ings with a pathologist. This consultation oc-curred urgently on a Friday afternoon in the summer.
Pathol o gic a l Discussion
Dr. Robert P. Hasserjian: The cell counts of the cere-brospinal fluid samples are shown in Table 2. On morphologic examination, the lymphocytes had a spectrum of cell sizes and included many large, atypical forms and cells with plasmacytoid fea-tures (Fig. 2). Flow cytometry showed a mixture of CD4+ and CD8+ T cells, B cells, and plasma cells (see Fig. 1 of the Supplementary Appendix, available with the full text of this article at www.nejm.org). The B cells lacked demonstrable sur-face light-chain expression, but analysis of per-meabilized cells showed the presence of polytypic kappa and lambda light chains, a finding typical of plasma cells. Surprisingly, a PCR study revealed the presence of a clonal rearrangement of the immunoglobulin heavy-chain gene (see Fig. 2 of the Supplementary Appendix), indicating a clonal B-cell population.
The diagnosis of lymphomas typically requires the integration of morphology, immunopheno-type, genetic features, and clinical information. In this case, the morphology was markedly atypi-cal and raised the possibility of lymphoma. How-ever, leptomeningeal disease without lymphade-nopathy or an extranodal mass would be highly unusual for a primary presentation of lympho-ma.11 Flow cytometry greatly enhances the as-sessment of fluids for the presence of lymphoma, and in this case the demonstration of polytypic cytoplasmic immunoglobulin favored a non-neo-plastic process.12
PCR amplification of antigen-receptor genes is a highly sensitive technique for detecting small clonal populations of lymphoid cells and is very useful in disclosing minimal amounts of disease after therapy for lymphomas.13 However, in a pa-tient with no history of lymphoma, PCR results must be interpreted with caution. Clonal expan-sions of B cells, such as were identified in this patient, can occur in inflammatory processes and have been reported in patients with multiple scle-rosis and in those with Lyme disease.14,15 In addi-tion, in cases of acute neuroborreliosis, the cere-brospinal f luid typically shows a lymphocytic pleocytosis (median, 160 per mm3) and can show markedly atypical lymphocyte morphology and plasmacytosis mimicking lymphoma.16-18
Dr. Plotkin: After this joint review of the patho-logical and clinical findings, we concluded that a diagnosis of lymphoma was not warranted.
Dr. Greer: Although we had been very concerned about the possibility of lymphoma, we were re-assured by this consultation. At this point, our leading diagnosis was neuroborreliosis, and we requested consultation from the infectious dis-ease service.
Dr. Nancy Lee Harris (Pathology): Although Dr. Steere is a rheumatologist, not an infectious dis-ease consultant, I have asked him to discuss the manifestations of neuroborreliosis as they relate to this patient and to tell us about the diagnostic testing in this case.
16p6
AUTHOR
FIGURE
JOB: ISSUE:
4-CH/T
RETAKE 1st
2nd
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
Greer
2 of 2
4-12-07
mst
35615
Figure 2. Specimen of Cerebrospinal Fluid Obtained on Admission.
Lymphocytic pleocytosis encompasses a spectrum of small, medium, and large atypical forms with irregular nuclei. Frequent plasmacytoid forms with eccentric, basophilic cytoplasm (inset, arrows) were also present (Wright–Giemsa stain of cytocentrifuge preparation of cerebrospinal fluid).

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071568
Manifestations of neuroborreliosis
Dr. Allen C. Steere: This 59-year-old man initially had fever, neck stiffness, and thrombocytopenia. Is that enough to arouse suspicion of the diagnosis of Lyme disease or other tick-borne infection? He lived in a wooded area of New England, and the onset of symptoms in the first week of July would be within the peak period of onset for tickborne infection in New England.19
Most patients with Lyme disease present with an expanding skin lesion, erythema migrans, which occurs at the site of the tick bite. This pa-tient had neither of these findings.20 However, the next most common presentation is with sys-temic, influenza-like symptoms (fever, myalgias, headache, and malaise), without erythema mi-grans.21 As in this case, such patients may ini-tially have fever and chills for several days and pain and stiffness in the back of the neck and head.22 On physical examination, neck stiffness is usually subtle. In addition, vague or migratory
arthralgias are common, but they were lacking in this patient.
Thrombocytopenia was noted on the patient’s initial examination. This finding should raise the possibility of infection with one of the two other infectious agents that are occasionally transmit-ted by nymphal Ixodes scapularis.23,24 Anaplasma phagocytophilum (previously referred to as the agent of human granulocytic ehrlichiosis), which in-fects neutrophils, may cause leukopenia; Babesia microti, which parasitizes red cells, may cause hemolytic anemia; and both agents may cause thrombocytopenia. In contrast, infection with Borrelia burgdorferi is not usually associated with hematologic abnormalities. In this patient, throm-bocytopenia did not persist.
Within several weeks, the patient had menin-gitis, cranial neuritis, and radiculoneuritis, the classic triad of neurologic abnormalities in Lyme disease. However, dysarthrias and respiratory com-promise, which developed in this patient, are very unusual in cases of Lyme disease. Phrenic-nerve paralysis in patients with Lyme disease may cause shortness of breath25 but not dysarthria, and the chest film did not show an elevated diaphragm. There is one case report in which a patient with early Lyme disease died from acute respiratory distress syndrome,26 but this was not the clinical picture in this case. In Europe, where Borrelia garinii is the most common cause of neurobor-reliosis, several cases have been reported of pa-tients with cerebrovascular occlusive events, often involving the vertebrobasilar system, resulting in thalamic infarcts and dysarthria.27 However, this patient’s MRI of the brain did not show cerebral infarcts. In this case, severe cervical radiculopa-thy, unrecognized weakness of pharyngeal mus-cles, or both may have led to aspiration pneumo-nia and respiratory compromise.
Cl inic a l Di agnosis
Neuroborreliosis.
Pathol o gic a l Discussion
Dr. Steere: In clinical practice, antibody testing is used for the confirmation of Lyme neuroborreli-osis. The Centers for Disease Control and Preven-tion recommends two-tier serologic testing by enzyme-linked immunosorbent assay (ELISA) and Western blotting.28 On the 11th hospital day, the
Table 4. Results of Diagnostic Tests for Lyme Neuroborreliosis.
Test Results
PCR assay for B. burgdorferi DNA in cerebrospinal fluid Positive
Antibody to B. burgdorferi in serum by two-test approach
ELISA
IgM (U) 400
IgG (U) 400
Western blotting
IgM (kD) Positive bands: 23, 41
IgG (kD) Positive bands: 23, 39, 41
Antibody to B. burgdorferi by antibody-capture immunoassay*
Serum
IgM (OD ratio) >16.7
IgG (OD ratio) 1.4
IgA (OD ratio) 3
Cerebrospinal fluid
IgM (OD ratio) >16.7
IgG (OD ratio) 8.1
IgA (OD ratio) >6.1
* The value is the ratio of the optical density (OD) of the well containing the pa-tient’s serum or cerebrospinal fluid divided by the OD of the control well. An OD ratio greater than 1 was defined as a positive response. For IgG and IgA antibody isotypes, the OD ratio was greater in cerebrospinal fluid, which indi-cates intrathecal antibody production. IgM values in serum and cerebrospinal fluid were both above the measured range, and therefore, the ratio cannot be determined. However, since IgM antibody does not cross the blood-brain bar-rier easily, the high levels of specific IgM antibody in cerebrospinal fluid are suggestive of intrathecal IgM antibody production.

case records of the massachusetts gener al hospital
n engl j med 356;15 www.nejm.org april 12, 2007 1569
results of cerebrospinal fluid tests for B. burgdor-feri antibody and nucleic acid were reported (Ta-ble 4). The positive PCR result for B. burgdorferi DNA in cerebrospinal fluid suggests that relatively large numbers of organisms were present in the meninges. In addition, a positive IgM antibody response and an indeterminate IgG antibody re-sponse were seen in serum by the standard two-test approach of ELISA and Western blotting, con-sistent with infection of several weeks’ duration. Finally, this patient had evidence of intrathecal IgM, IgG, and IgA antibody production in the cerebrospinal fluid. This combination of test re-sults is diagnostic of Lyme neuroborreliosis.29-31
How does one explain the presence of large B cells in the cerebrospinal fluid, which raised the possibility of B-cell lymphoma? Both B cells and plasma cells have been noted in the cerebro-spinal fluid of patients with neuroborreliosis.32,33 In a recent analysis, the B-lymphocyte chemoat-tractant CXCL13 was found in the cerebrospinal fluid of patients with Lyme neuroborreliosis but not in those with other infectious diseases or inflammatory conditions of the nervous system, possibly explaining this finding in this case.34
Discussion of M a nagemen t
Dr. Steere: The Infectious Diseases Society of Amer-ica recommends the intravenous administration of ceftriaxone (2 g daily) for 2 to 4 weeks for the
treatment of Lyme neuroborreliosis,35 and this patient received this therapy for 6 weeks. Neuro-pathic pain usually begins to improve within days, but weeks may be required for the resolu-tion of pleocytosis in the cerebrospinal fluid, and months may be necessary for total or nearly complete resolution of sensory or motor neurop-athies. Because of the slow resolution of signs and symptoms, it can be difficult to assess wheth-er the duration of therapy is adequate for spiro-chetal eradication. However, relapse is rare after 2 to 4 weeks of intravenous antibiotic therapy, and within the following months, most patients have complete or nearly complete recovery of neurologic function.
Dr. Greer: The patient was discharged after 30 days in this hospital and then spent 3 more weeks at a rehabilitation hospital. He is now living at home and is independent. He has resid-ual weakness and decreased dexterity of the hands and continues to have pain in his neck and shoulder.
A nat omic a l Di agnosis
Lyme disease of the nervous system (neurobor-reliosis).
Dr. Greer reports receiving lecture fees from Boehringer Ingel-heim. Dr. Steere reports receiving an honorarium from Novartis. No other potential conflict of interest relevant to this article was reported.
ReferencesNewman NJ, Slamovits TL, Friedland
S, Wilson WB. Neuro-ophthalmic mani-festations of meningocerebral inflamma-tion from the limited form of Wegener’s granulomatosis. Am J Ophthalmol 1995; 120:613-21.
Colover J. Sarcoidosis with involvement of the nervous system. Brain 1948;71:451-75.
Luxon L, Lees AJ, Greenwood RJ. Neu-rosyphilis today. Lancet 1979;1:90-3.
Reik L, Steere AC, Bartenhagen NH, Shope RE, Malawista SE. Neurologic ab-normalities of Lyme disease. Medicine (Baltimore) 1979;58:281-94.
Abbott RA, Hammans S, Margarson M, Aji BM. Diaphragmatic paralysis and respiratory failure as a complication of Lyme disease. J Neurol Neurosurg Psychia-try 2005;76:1306-7.
Leptomeningeal metastases. In: Pos-ner JB. Neurologic complications of can-cer. Philadelphia: F.A. Davis, 1995:143-71.
CBTRUS. Statistical report: primary brain tumors in the United States, 1998-
1.
2.
3.
4.
5.
6.
7.
2002. Hinsdale, IL: Central Brain Tumor Registry of the United States, 2005. (Ac-cessed March 19, 2007, at http://www.cbtrus.org/reports//2005-2006/2006report.pdf.)
Lachance DH, O’Neill BP, Macdonald DR, et al. Primary leptomeningeal lym-phoma: report of 9 cases, diagnosis with immunocytochemical analysis, and review of the literature. Neurology 1991;41:95-100.
Bollen EL, Brouwer RE, Hamers S, et al. Central nervous system relapse in non-Hodgkin lymphoma: a single-center study of 532 patients. Arch Neurol 1997;54: 854-9.
Glass JP, Melamed M, Chernik NL, Posner JB. Malignant cells in cerebrospi-nal f luid (CSF): the meaning of a positive CSF cytology. Neurology 1979;29:1369-75.
Shenkier TN. Unusual variants of pri-mary central nervous system lymphoma. Hematol Oncol Clin North Am 2005;19: 651-64.
8.
9.
10.
11.
Roma AA, Garcia A, Avagnina A, Res-cia C, Elsner B. Lymphoid and myeloid neoplasms involving cerebrospinal fluid: comparison of morphologic examination and immunophenotyping by flow cytom-etry. Diagn Cytopathol 2002;27:271-5.
van der Velden VH, Hochhaus A, Caz-zaniga G, Szczepanski T, Gabert J, van Dongen JJ. Detection of minimal residual disease in hematologic malignancies by real-time quantitative PCR: principles, ap-proaches, and laboratory aspects. Leuke-mia 2003;17:1013-34.
Jacobsen M, Zhou D, Cepok S, et al. Clonal accumulation of activated CD8+ T cells in the central nervous system dur-ing the early phase of neuroborreliosis. J Infect Dis 2003;187:963-73.
Owens GP, Ritchie AM, Burgoon MP, Williamson RA, Corboy JR, Gilden DH. Single-cell repertoire analysis demonstrates that clonal expansion is a prominent fea-ture of the B cell response in multiple sclerosis cerebrospinal fluid. J Immunol 2003;171:2725-33.
12.
13.
14.
15.

n engl j med 356;15 www.nejm.org april 12, 20071570
case records of the massachusetts gener al hospital
Lakos A. CSF findings in Lyme men-ingitis. J Infect 1992;25:155-61.
Walther EU, Seelos K, Bise K, Mayer M, Straube A. Lyme neuroborreliosis mimick-ing primary CNS lymphoma. Eur Neurol 2004;51:43-5.
Kieslich M, Fiedler A, Driever PH, Weis R, Schwabe D, Jacobi G. Lyme bor-reliosis mimicking central nervous system malignancy: the diagnostic pitfall of cere-brospinal fluid cytology. Brain Dev 2000; 22:403-6.
Steere AC, Coburn J, Glickstein L. The emergence of Lyme disease. J Clin Invest 2004;113:1093-101.
Smith RP, Schoen RT, Rahn DW, et al. Clinical characteristics and treatment out-come of early Lyme disease in patients with microbiologically confirmed erythe-ma migrans. Ann Intern Med 2002;136: 421-8.
Steere AC, Sikand VK. The presenting manifestations of Lyme disease and the outcomes of treatment. N Engl J Med 2003; 348:2472-4.
Steere AC, Dhar A, Hernandez J, et al. Systemic symptoms without erythema migrans as the presenting picture of early Lyme disease. Am J Med 2003;114:58-62.
Krause PJ, Telford SR III, Spielman A,
16.
17.
18.
19.
20.
21.
22.
23.
et al. Concurrent Lyme disease and babe-siosis: evidence for increased severity and duration of illness. JAMA 1996;275:1657-60.
Krause PJ, McKay K, Thompson CA, et al. Disease-specific diagnosis of coinfect-ing tickborne zoonoses: babesiosis, hu-man granulocytic ehrlichiosis, and Lyme disease. Clin Infect Dis 2002;34:1184-91.
Ishaq S, Quinet R, Saba J. Phrenic nerve paralysis secondary to Lyme neu-roborreliosis. Neurology 2002;59:1810-1.
Kirsch M, Ruben FL, Steere AC, Duray PH, Norden CW, Winkelstein A. Fatal adult respiratory distress syndrome in a patient with Lyme disease. JAMA 1988;259: 2737-9.
Reik L Jr. Stroke due to Lyme disease. Neurology 1993;43:2705-7.
Recommendations for test perfor-mance and interpretation from the Second International Conference on Serologic Diagnosis of Lyme Disease. MMWR Morb Mortal Wkly Rep 1995;44:590-1.
Dressler F, Whalen JA, Reinhardt BN, Steere AC. Western blotting in the sero-diagnosis of Lyme disease. J Infect Dis 1993;167:392-400.
Steere AC, Berardi VP, Weeks KE, Logi-gian EL, Ackermann R. Evaluation of the
24.
25.
26.
27.
28.
29.
30.
intrathecal antibody response to Borrelia burgdorferi as a diagnostic test for Lyme neuroborreliosis. J Infect Dis 1990;161: 1203-9.
Wilske B, Schierz G, Preac-Mursic V, et al. Intrathecal production of specific antibodies against Borrelia burgdorferi in patients with lymphocytic meningoradic-ulitis (Bannwarth’s syndrome). J Infect Dis 1986;153:304-14.
Case Records of the Massachusetts General Hospital (Case 29-1984). N Engl J Med 1984;311:172-81.
Baig S, Olsson T, Link H. Predomi-nance of Borrelia burgdorferi specific B cells in cerebrospinal fluid in neuroborrelio-sis. Lancet 1989;2:71-4.
Rupprecht TA, Pfister HW, Angele B, Kastenbauer S, Wilske B, Koedel U. The chemokine CXCL13 (BLC): a putative diag-nostic marker for neuroborreliosis. Neu-rology 2005;65:448-50.
Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treat-ment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of Ameri-ca. Clin Infect Dis 2006;43:1089-134.Copyright © 2007 Massachusetts Medical Society.
31.
32.
33.
34.
35.
Lantern Slides Updated: Complete PowerPoint Slide Sets from the Clinicopathological Conferences
Any reader of the Journal who uses the Case Records of the Massachusetts General Hospital as a teaching exercise or reference material is now eligible to receive a complete set of PowerPoint slides, including digital images, with identifying legends, shown at the live Clinicopathological Conference (CPC) that is the basis of the Case Record. This slide set contains all of the images from the CPC, not only those published in the Journal. Radiographic, neurologic, and cardiac studies, gross specimens, and photomicrographs, as well as unpublished text slides, tables, and diagrams, are included. Every year 40 sets are produced, averaging 50-60 slides per set. Each set is supplied on a compact disc and is mailed to coincide with the publication of the Case Record.
The cost of an annual subscription is $600, or individual sets may be purchased for $50 each. Application forms for the current subscription year, which began in January, may be obtained from the Lantern Slides Service, Department of Pathology, Massachusetts General Hospital, Boston, MA 02114 (telephone 617-726-2974) or e-mail [email protected].

e d i t o r i a l s
n engl j med 356;15 www.nejm.org april 12, 20071572
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
Does Preventive PCI Work?Judith S. Hochman, M.D., and P. Gabriel Steg, M.D.
Treatments are designed to make people feel bet-ter or live longer. Percutaneous coronary interven-tion (PCI) is effective at reducing angina in pa-tients with symptomatic coronary artery disease and at reducing mortality in patients who have acute myocardial infarction with ST-segment ele-vation and in those who have high-risk acute cor-onary syndromes without ST-segment elevation.1 Such successes have often been extrapolated in support of more widespread use of PCI in patients with stable coronary artery disease in hopes of reducing subsequent cardiac events.
With the increasing availability of noninvasive imaging of coronary artery disease, asymptomatic patients are often referred for PCI. But preventive intervention presupposes a threat that can be averted at an acceptable cost. In the case of stable coronary artery disease, the threat is subsequent myocardial infarction and death. The questions are How likely is this threat? And does PCI pro-vide an appropriate answer to it? In this issue of the Journal, in a report on the Clinical Out-comes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE, NCT00007657) trial, Boden et al.2 provide some answers to these ques-tions. They report that for a large population with stable coronary artery disease, the 4.6-year cumu-lative rates of myocardial infarction and death were 19.0% in patients who underwent PCI in ad-dition to receiving optimal medical therapy (PCI group) and 18.5% in those who received medical therapy alone (medical-therapy group); the rates of death were approximately 8% in both study groups.
Can these findings be generalized? The large number of patients who were screened for eligi-bility, as compared with those who were enrolled,
raises concern, but the population seems to be representative of patients with stable coronary ar-tery disease who undergo PCI. Most of the patients had preserved ventricular function, and a large majority had angina and multivessel coronary ar-tery disease. Patients whose condition was stable after myocardial infarction were enrolled (38%), and spontaneous or inducible ischemia was re-quired, but patients with severe ventricular dys-function, clinical instability, or very early ST-seg-ment depression or hypotension on stress testing were excluded. Although the trial had slightly less power than anticipated, the 95% confidence intervals indicate that the chance that PCI yield-ed a reduction of more than 13% or an increase of more than 27% in myocardial infarction and death is small.
Patients who were enrolled in the COURAGE trial were quite successful at achieving goals for both lipid levels and blood pressure; they had less success in meeting the more difficult objectives of weight loss, smoking cessation, and increased exercise. The use of antiplatelet agents, statins, angiotensin-converting–enzyme (ACE) inhibitors, and beta-blockers was appropriately high in both groups. The nearly 33% of patients who crossed over from medical therapy to revascularization during the 4.6-year period was higher than antici-pated, but this does not detract from the finding that initial PCI failed to prevent myocardial in-farction and death in this population. Against a backdrop of optimal medical therapy, the trial tested selective PCI for patients with angina that had failed medical management, as compared with preventive PCI for all. The proportion of angina-free patients was modestly but significant-ly higher at 1 and 3 years in the PCI group (with

editorials
n engl j med 356;15 www.nejm.org april 12, 2007 1573
lower use of antianginal medications), but not at 5 years. The substantial increase in the proportion of angina-free patients in the medical-therapy group cannot be ascribed solely to the perfor-mance of revascularization during follow-up but appears to derive mostly from intensive control of risk factors (leading to better endothelial function) and antianginal medication. Although quality-of-life data are not yet available, this study confirms previous observations that PCI is effec-tive at relieving symptoms.
Why did PCI fail to reduce events beyond in-tensive medical therapy? This result was not due to the fact that the COURAGE trial enrolled a low-risk population (the annualized rate of myocardial infarction and death was >4%). In this stable pop-ulation, the proportion of deaths from cardiac causes was relatively low, but there are pitfalls in the classification of death. The 2.8% of patients who had periprocedural myocardial infarction (clinical events with an increase in levels of bio-chemical markers by a factor of more than 3 for the creatine kinase MB fraction and more than 5 for troponin) is within the reported range,3 but some observers may consider the rate high for a population with stable angina. However, this cat-egory includes patients with repeat PCI events, and often multiple lesions were dilated. Also, 38% of patients had had a previous myocardial infarction (in an unknown percentage, the myo-cardial infarction was recent) and therefore were at higher risk for early events. During the study period, there was a change in clinical practice to more aggressive clopidogrel regimens before and after PCI procedures, and the effect of this change on the frequency of myocardial infarction is unknown. There was an excess of only 26 peri-procedural myocardial infarctions in the PCI group, and exclusion of all periprocedural myo-cardial infarctions (an unrealistic clinical scenar-io) still reveals no significant benefit for PCI.
Despite the widespread belief that PCI may re-duce the incidence of cardiac events, the findings of this study are understandable. Tight stenoses, responsible for stable angina, are a marker for many more nonobstructive, lipid-laden lesions,4 which are also at risk for inflammation and rup-ture and therefore have a cumulatively higher like-lihood of triggering an acute coronary syndrome and sudden death.5,6 Since the risk of coronary occlusion is not proportional to the previous se-
verity of stenosis,7 it is not surprising that treat-ing one or more stable, tight lesions did not re-duce rates of subsequent myocardial infarction and death. The effectiveness of intensive modi-fication of risk factors that was observed in the COURAGE trial is consistent with the secondary prevention observed with aggressive lipid-lowering therapy in coronary artery disease.8,9 Lipid-lower-ing therapy has been shown to be more success-ful at reducing cardiac events than at reducing the severity of stenosis,10 presumably through im-proved endothelial function and plaque stabili-zation.
The findings of the COURAGE trial are con-sistent with those of previous smaller studies involving patients with stable coronary artery dis-ease, which reported no reduction in myocardial infarction and death with PCI but a reduction in angina.11 The COURAGE trial was the first to use stents routinely along with what has now become optimal medical therapy. Although drug-eluting stents reduce the need for repeat revasculariza-tion, they have not been shown to reduce myocar-dial infarction and death, as compared with bare-metal stents, and there is concern about late stent thrombosis.12 However, the rate of repeat revascu-larization is consistently lower with drug-eluting stents. Hence, their use in the COURAGE trial would probably have translated into a rate of repeat revascularization that was lower than the reported 21%, and possibly less angina.
Despite the lack of significant interaction be-tween subgroups of patients and the effect of PCI on myocardial infarction and death, there will be a temptation to overinterpret data from subgroups in search of one in which benefit from PCI is sug-gested (on the basis of sex, type of hospital, or a combination of high-risk variables). Unfortunate-ly, the proportion of women and nonwhite patients was small in this study. But the pitfalls of sub-group analyses (multiplicity, smaller size, and con-founding) are well known.13 Although there were only 406 patients with an ejection fraction be-tween 30 and 50%, there was no suggestion of treatment interaction. Additional data are needed in patients with depressed ventricular function and in women.
Would surgical revascularization have fared better than PCI? The trials comparing medical therapy with surgery are old and relatively small. As for PCI versus surgery, guidelines3,14 summa-

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071574
rize the trial evidence as suggesting that for most patients either procedure is an effective option for the treatment of symptoms, and both are asso-ciated with similar long-term outcomes. Some high-risk patients, however, may do better with surgery.
The COURAGE trial adds to the still limited body of evidence for strategy selection in coronary artery disease. Trials involving patients with dia-betes and those with heart failure and severe ven-tricular dysfunction are ongoing. The recent Oc-cluded Artery Trial (OAT, NCT00004562), which showed no benefit for PCI, provided information on patients whose condition is stable after myo-cardial infarction with persistent occlusion of the infarct artery.15
The COURAGE trial should lead to changes in the treatment of patients with stable coronary ar-tery disease, with expected substantial health care savings. PCI has an established place in treating angina but is not superior to intensive medical therapy to prevent myocardial infarction and death in symptomatic or asymptomatic patients such as those in this study. Secondary prevention has proved its worth, with lipid-modulating therapy, lifestyle modification, and the use of aspirin, beta-blockers, and ACE inhibitors. Patients whose con-dition is clinically unstable, who have left main coronary artery disease, or in whom medical ther-apy has failed to control symptoms remain can-didates for revascularization, but PCI should not play a major role as part of a secondary prevention strategy.
Dr. Hochman reports receiving consulting fees from Eli Lilly, Bristol-Myers Squibb, Johnson & Johnson, GlaxoSmithKline, CV Therapeutics, and Sanofi-Aventis; speaking fees from the Network for Continuing Medical Education (supported by Bristol-Myers Squibb and Sanofi-Aventis); and grant support to her institution from Eli Lilly. Dr. Steg reports receiving consulting fees from AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Merck, GlaxoSmithKline, Sanofi-Aventis, Pfizer, Servier, and Takeda; lecture fees from Boehringer Ingelheim, Bristol-Myers Squibb, GlaxoSmithKline, Merck, Novartis, Nycomed, Sanofi-Aventis, Sankyo, Servier, and ZLB Behring; and grant support from Sanofi-Aventis. No other potential conflict of interest relevant to this article was reported.
This article (10.1056/NEJMe078036) was published at www.nejm.org on March 26, 2007.
From the Cardiovascular Clinical Research Center, Leon Char-ney Division of Cardiology, New York University School of Med-icine, New York ( J.S.H.); and Centre Hospitalier Bichat–Claude Bernard, Université Paris VII–Denis Diderot, Paris (P.G.S.).
Mehta SR, Cannon CP, Fox KA, et al. Routine vs selective invasive strategies in patients with acute coronary syndromes: a collaborative meta-analysis of randomized trials. JAMA 2005; 293:2908-17.
Boden WE, O’Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med 2007;356:1503-16.
Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 guideline update for percutaneous coronary interven-tion — summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention). J Am Coll Cardiol 2006;47:216-35.
Nakagomi A, Celermajer DS, Lumley T, Freedman SB. An-giographic severity of coronary narrowing is a surrogate marker for the extent of coronary atherosclerosis. Am J Cardiol 1996; 78:516-9.
Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assess-ment strategies. Circulation 2003;108:1664-72.
Waxman S, Ishibashi F, Muller JE. Detection and treatment of vulnerable plaques and vulnerable patients: novel approaches to prevention of coronary events. Circulation 2006;114:2390-411.
Ambrose JA, Fuster V. The risk of coronary occlusion is not proportional to the prior severity of coronary stenoses. Heart 1998;79:3-4.
Cannon CP, Braunwald E, McCabe CH, et al. Intensive versus moderate lipid lowering with statins after acute coronary syn-dromes. N Engl J Med 2004;350:1495-504.
Pitt B, Waters D, Brown W, et al. Aggressive lipid-lowering therapy compared with angioplasty in stable coronary artery disease. N Engl J Med 1999;341:70-6.
Sdringola S, Loghin C, Boccalandro F, Gould KL. Mecha-nisms of progression and regression of coronary artery disease by PET related to treatment intensity and clinical events at long-term follow-up. J Nucl Med 2006;47:59-67.
Katritsis DG, Ioannidis JP. Percutaneous coronary interven-tion versus conservative therapy in nonacute coronary artery disease: a meta-analysis. Circulation 2005;111:2906-12.
Stone GW, Moses JW, Ellis SG, et al. Safety and efficacy of sirolimus- and paclitaxel-eluting coronary stents. N Engl J Med 2007;356:998-1008.
Lagakos SW. The challenge of subgroup analyses — report-ing without distorting. N Engl J Med 2006;354:1667-9.
Fox K, Garcia MA, Ardissino D, et al. Guidelines on the man-agement of stable angina pectoris: executive summary: the Task Force on the Management of Stable Angina Pectoris of the Euro-pean Society of Cardiology. Eur Heart J 2006;27:1341-81.
Hochman JS, Lamas GA, Buller CE, et al. Coronary interven-tion for persistent occlusion after myocardial infarction. N Engl J Med 2006;355:2395-407.Copyright © 2007 Massachusetts Medical Society.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.

editorials
n engl j med 356;15 www.nejm.org april 12, 2007 1575
Clinical Trials in the Elderly — A Concept Comes of AgeLillian L. Siu, M.D.
A well-conducted, randomized, controlled trial provides a high level of evidence to guide clinical management. Although this tenet is accepted in all fields of medicine, including oncology, con-siderable challenges are associated with conduct-ing randomized, controlled trials successfully in special patient populations such as the elderly. In this issue of the Journal, Keime-Guibert et al.1 describe their multi-institutional trial of radio-therapy for newly diagnosed glioblastoma in pa-tients 70 years of age or older.
Over a period of 4 years, Keime-Guibert and colleagues randomly assigned 85 elderly patients from 10 centers to receive radiotherapy plus sup-portive care or supportive care alone. The trial was discontinued at the first interim analysis be-cause the difference in survival between the two treatment groups surpassed the preset upper boundary of efficacy. At a median follow-up of 21 weeks, the median survival time for the 39 patients who received radiotherapy plus support-ive care was 29.1 weeks, as compared with 16.9 weeks for the 42 patients who received support-ive care alone. There were no deleterious effects on health-related quality of life and cognitive function with the delivery of radiotherapy. These results are applicable only to older patients with sufficient performance status (that is, those who are at least capable of self-care), since it is unreal-istic to expect any meaningful gain in quantity or quality of life in patients with rapidly declin-ing functional status. In terms of the manage-ment of a uniformly fatal disease, radiotherapy was shown to have a modest survival benefit balanced with acceptable toxic effects. Thus, ra-diotherapy may provide a standard of care for glioblastoma in the elderly.
The successful completion of this study by Keime-Guibert and colleagues conveys another important message — in oncology research, age is a barrier that can be overcome. Older patients are underrepresented in clinical trials for the treatment of cancer. Data from large coopera-tive groups have shown that only 22 to 36% of patients 65 years of age or older participate in trials for cancer therapy, even though they repre-sent nearly 60% of the population with cancer.2-5
Barriers related to the trial design, physician, pa-tient, and logistic and financial factors are po-tential deterrents to the recruitment of older patients for clinical trials.6 During the design of a trial, the imposition of restrictions on pro-tocol eligibility that extend beyond safety and scientific concerns should be justified.4 Chrono-logic age per se is not a valid criterion for exclu-sion, and for this reason, most clinical trials run by cooperative groups for cancer therapy in adults do not set an upper age limit. The Food and Drug Administration has also issued guidelines that provide support for the adequate represen-tation of the geriatric population in clinical tri-als.7 However, some physicians are reluctant to enroll older patients in trials for cancer treat-ment, citing concerns about coexisting condi-tions, the toxic effects of treatment, ineligibility, poor compliance, and lack of social support.3,8 The paucity of data from primary research to val-idate or quell these concerns leads to a vicious cycle of care that is not evidence-based; this un-derscores the need to generate knowledge by in-volving older patients in clinical trials.
When approached, many elderly patients are willing to participate in clinical research, but they may be unaware of opportunities other than those offered by their own physicians.9 Logistic and financial barriers may further impede the recruitment of older adults for clinical trials. Ready access to information concerning ongoing studies, the development of an appropriate infra-structure to streamline procedures for clinical trials, a reduction in the number of extraneous protocol investigations, and the reimbursement of patients for costs incurred during clinical trials are practical strategies to optimize the number of older patients who participate in them.
Ageism is probably the greatest impediment to the enrollment of older patients in trials for cancer therapy. Many physicians and patients have an innate bias that associates older age with inferior outcomes. The management of dis-eases in the elderly can be complicated by physi-ological changes in organ functions, coexisting illnesses, and the prevalence of polypharmacy. The concerns that older patients are at risk for

editorials
n engl j med 356;15 www.nejm.org april 12, 20071576
a reduced efficacy and more toxic effects of can-cer therapy may be legitimate, but unless these concerns are substantiated by rigorous data, they do not advance science in any way that enhances patient care.
The performance of clinical trials that have proportionate representation of the elderly would permit the translation of the results to older pa-tients and allow for direct comparisons of re-sults for younger and older patients who have been treated in similar ways. This approach is reasonable for interventions that have favorable therapeutic indexes or if there is preliminary evi-dence suggesting that the tolerability associated with these interventions is independent of the patient’s age. For instance, many molecularly targeted anticancer agents have toxicity profiles that are acceptable in patients in all age ranges, provided that the patient has adequate organ function and sufficient performance status.10 In a randomized, controlled trial of an epidermal growth factor receptor inhibitor in patients with advanced non–small-cell lung cancer, more than half of the total accrual included patients 60 years of age or older.11 There was no difference in the response rate or survival benefit according to age, and the toxic effects of treatment were manage-able overall. The findings from this study can be useful in guiding the treatment of older patients with advanced non–small-cell lung cancer. Clin-ical trials focusing exclusively on the geriatric population, such as the study conducted by Keime-Guibert and colleagues, evaluate therapeutic regi-mens tailored to meet the specific needs of the older patient. These studies, especially in the randomized, phase 3 setting, can be difficult to conduct and complete, even though the ques-tions being addressed are fundamental and of-ten lead to changes in practice. In the cancer lit-erature, examples of trials that have fulfilled these goals are few and far between.12,13
From the societal perspective, the graying of the population has substantial implications for the consumption of drugs and health care. The costs of therapies for cancer, especially in the cur-rent era of molecular targeting, are high and escalating. The evaluation of drugs or other inter-ventions should involve patients with demograph-ic characteristics that are representative of other patients with the disease. The prescription of ther-apies to the elderly on the basis of trial informa-
tion obtained primarily from younger, more fit patients does not constitute good clinical practice. The collection of evidence-based data ensures that therapies are prescribed to the older patient when they may offer a meaningful gain in sur-vival, quality of life, or both, and avoided in situ-ations in which they may not be beneficial. The conduct of randomized, controlled trials for the treatment of cancer in older patients is no longer a theoretical concept — it is a reality that has come of age.
No potential conflict of interest relevant to this article was re-ported.
From the Division of Medical Oncology and Hematology, Prin-cess Margaret Hospital, University Health Network, and the De-partment of Medicine, University of Toronto — both in Toronto.
Keime-Guibert F, Chinot O, Taillandier L, et al. Radiotherapy for glioblastoma in the elderly. N Engl J Med 2007;356:1527-35.
Hutchins LF, Unger JM, Crowley JJ, Coltman CA Jr, Albain KS. Underrepresentation of patients 65 years of age or older in cancer-treatment trials. N Engl J Med 1999;341:2061-7.
Yee KWL, Pater JL, Pho L, Zee B, Siu LL. Enrollment of older patients in cancer treatment trials in Canada: why is age a barrier? J Clin Oncol 2003;21:1618-23.
Lewis JH, Kilgore ML, Goldman DP, et al. Participation of patients 65 years of age or older in cancer clinical trials. J Clin Oncol 2003;21:1383-9.
Kimmick GG, Peterson BL, Kornblith AB, et al. Improving accrual of older patients to cancer treatment trials: a random-ized trial comparing an educational intervention with standard information: CALGB360001. J Clin Oncol 2005;23:2201-7.
Townsley CA, Selby R, Siu LL. Systematic review of barriers to the recruitment of older patients with cancer onto clinical trials. J Clin Oncol 2005;23:3112-24.
Food and Drug Administration. November 1989 guideline for the study of drugs likely to be used in the elderly. Fed Regist 1994;59(102):39398-400. (Accessed March 15, 2007, at http://www.fda.gov/cder/guidance/iche7.pdf.)
Kornblith AB, Kemeny M, Peterson BL, et al. Survey of on-cologists’ perceptions of barriers to accrual of older patients with breast carcinoma to clinical trials. Cancer 2002;95:989-96.
Townsley CA, Chan KK, Pond GR, Marquez C, Siu LL, Straus SE. Understanding the attitudes of the elderly towards enrol-ment into cancer clinical trials. BMC Cancer 2006;6:34.
Townsley CA, Pond GR, Oza AM, et al. Evaluation of adverse events experienced by older patients participating in studies of molecularly targeted agents alone or in combination. Clin Can-cer Res 2006;12:2141-9.
Shepherd FA, Rodrigues Pereira J, Ciuleanu T, et al. Erlotinib in previously treated non–small-cell lung cancer. N Engl J Med 2005;353:123-32.
Sonneveld P, de Ridder M, van der Lelie H, et al. Comparison of doxorubicin and mitoxantrone in the treatment of elderly pa-tients with advanced diffuse non-Hodgkin’s lymphoma using CHOP versus CNOP chemotherapy. J Clin Oncol 1995;13:2530-9.
Gridelli C, Perrone F, Gallo C, et al. Chemotherapy for el-derly patients with advanced non-small-cell lung cancer: the Multicenter Italian Lung Cancer in the Elderly Study (MILES) phase III randomized trial. J Natl Cancer Inst 2003;95:362-72.
Copyright © 2007 Massachusetts Medical Society.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.

n engl j med 356;15 www.nejm.org april 12, 2007 1577
clinical implications of basic research
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
Retinal Progenitor Cells — Timing Is EverythingJean Bennett, M.D., Ph.D.
More than 10 million people in the United States are blind or visually impaired, and 50,000 more will become blind each year. The results of a survey conducted by the American Foundation for the Blind indicate that people with diabetes fear blindness even more than premature death.1 Retinal repair by means of the transplantation of photoreceptor precursors, recently described by MacLaren and colleagues,2 thus holds hope for many people.
Blindness is often caused by degenerative con-ditions in which the sensory cells in the retina deteriorate and die. Such conditions include ret-initis pigmentosa and age-related macular degen-eration. Photoreceptors do not divide after birth, and so previously it was thought that they could not be replaced. However, for decades, research-ers have tested the efficacy of retinal transplan-tation for the treatment of end-stage retinal dis-ease. Transplants of retinas, retinal sheets, and clumps of retinal neurons have been and con-tinue to be performed in mice and humans with retinitis pigmentosa and age-related macular de-generation. These transplants have not caused harm, but there is no evidence that the cells of the transplanted tissue mingle with or develop synaptic connections with host cells.
The key, according to MacLaren et al.,2 is timing — the timing of the harvest of the donor cells. As long as these cells are at the correct stage — a stage at which they have exited the cell cycle and have taken the first steps toward becoming mature photoreceptors — they can be integrated into neonatal, adult, or even diseased retinas. If these cells are isolated just a couple of days too early or too late, they will not inte-grate. When MacLaren and colleagues introduced cells at the correct stage into the retinas of two different animal models of retinitis pigmentosa (Fig. 1), not only did the cells develop into ma-ture rod photoreceptors but the treated eyes also
showed improved pupillary light reflexes. These findings suggested that the transplanted cells were responsive to light and had been integrated into the circuitry connecting the retinal cells to the cells of the central nervous system. The pupillary light response is one of many outcome measures of retinal and visual function; presumably others will be tested as the treatment is improved. The mice with better light responses did not appear to have benefited from the treatment in practical terms — for example, they did not have an im-proved ability to navigate or to track a moving ob-ject. That said, the results of the study by Mac-Laren et al. naturally lead to speculation about the application of these findings to the treatment of blindness in humans.
What would be the best source of donor cells for the treatment of human blindness? If human fetal retinas were used as donor cells, the opti-mal time to obtain the cells would probably be between 11 and 15 weeks of gestation. During this period, the mitosis of neuronal cells ceases, and the cells begin to mature into photorecep-tors.3 It is a common misconception that fetal tissue cannot be used for such a purpose. It can, but the use of this tissue must comply with bans on federal funding and a host of issues and reg-ulations, including those pertaining to informed consent, confidentiality, and the approval of the institution or institutions where the tissue is harvested and the transplant takes place. In fact, trials of transplantation with the use of fe-tal retinal tissue are under way.4
To avoid the bureaucratic hassle, the unpre-dictability of tissue availability, and the un-known factors involved in purifying fetal human progenitor cells, Lamba et al.5 have suggested an alternative. They incubated human embryon-ic stem cells in a complex cocktail that coaxed the cells to become photoreceptor progenitors. These progenitors, like the in vivo–derived pro-

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071578
genitors described by MacLaren et al., were able to integrate into isolated mouse retinas. Thus, it may be possible to prepare unlimited numbers of progenitor cells that are suitable for transplan-tation.
Regardless of whether donor progenitor cells are isolated from human tissue or from human embryonic stem cells that have been coaxed along the appropriate developmental pathway, how can one ensure sufficient numbers of stem cells for
an effective graft? MacLaren et al. showed that it is not necessary to integrate each precursor cell with each secondary neuron to achieve a thera-peutic effect. Also, it may not be important to treat the entire retina; treatment of the macula alone may suffice. A considerable challenge, how-ever, is the efficiency of progenitor integration. MacLaren and colleagues observed that only 0.03 to 0.1% of the transplanted cells were integrated into the retina and made synaptic connections
Figure 1. Wiring the Retina.
Schematic pictures of sections of retinas from a wild-type mouse (left) and two mutant mice with retinal degeneration (right) are shown. Arrows indicate the corresponding layers in the retinas of the rho–/– (mutant 1) and rd (mutant 2) mice. Photoreceptor degenera-tion results in the thinning of the outer nuclear and outer segment layers (which together comprise photoreceptors); this causes the entire retina to become thinner. MacLaren et al.2 injected purified retinal progenitor cells from wild-type mice (red) into the subretinal space in wild-type and mutant mice. Three weeks after the injection, MacLaren and colleagues observed that a small portion of the progenitor cells had migrated into the retina and established synaptic contacts with cells in the inner nuclear layer in the wild-type and mutant 1 mice. The mutant 1 mice have a comparatively slow rate of retinal degeneration, and the transplantation took place at an early stage of the disease, resulting in improved visual function. In contrast, most of the progenitor cells injected into the mutant 2 mice, which had more severe retinal degeneration, did not migrate into the retina.

n engl j med 356;15 www.nejm.org april 12, 2007 1579
with host cells. The remaining cells completed differentiation in the subretinal space. The effect on the restoration of visual function would prob-ably have been much greater if a larger propor-tion of these cells had been integrated. Perhaps integration can be increased by additional pro-genitor-cell manipulations or by coaxing human embryonic stem cells to express particular sets of genes that promote differentiation and inte-gration.
Could transplants of retinal precursors be used to treat humans with profound blindness? Mac-Laren et al. showed that the transplants effec-tively integrated into the retinas in two mouse models of retinitis pigmentosa. The investigators had limited success, however, with a third mouse model — probably because the model involved rapid retinal degeneration and a resultant lack of scaffolding for the transplanted cells. Further studies evaluating the potential effects of the stage of the host tissue at transplantation are war-ranted in this model, and the results may help determine whether humans at analogous stages of retinal degeneration would be likely to benefit from this approach.
Can this technique be used to repopulate other cells in the eye and other organ systems? The findings of MacLaren et al.2 and Lamba et al.5 challenge the theory that the undifferentiated cell is ideal for transplantation. Theoretically, progen-itor cells for other differentiated cell types could be isolated or generated to populate a recipient tissue. For example, it should be possible to iso-
late retinal precursor cells that will become cone photoreceptors instead of rod photoreceptors. Cone photoreceptors mediate color vision and fine visual discrimination, unlike rod photore-ceptors, which mediate vision in dim light. In the industrialized world, where dim lighting is rare, it may be more important to replace cone photo-receptors than rod photoreceptors. Similarly, one could devise experiments to determine whether “differentiated” progenitors, analogous to those described by MacLaren et al.2 and Lamba et al.,5 might have a therapeutic effect in models of Parkinson’s disease or other neurodegenerative conditions.
No potential conflict of interest relevant to this article was re-ported.
From Scheie Eye Institute, University of Pennsylvania, Phila-delphia.
U.S. adults with diabetes fear blindness or vision loss more than premature death: many respondents in international diabe-tes survey worried about quality of life. News release of the Lions Clubs International Foundation, Oak Brook, IL, December 2006. (Accessed March 22, 2007, at http://www.lionsclubs.org/EN/ content/news_news_release58.shtml.)
MacLaren RE, Pearson RA, MacNeil A, et al. Retinal repair by transplantation of photoreceptor precursors. Nature 2006; 444:203-7.
O’Brien KM, Schulte D, Hendrickson AE. Expression of photo-receptor-associated molecules during human fetal eye develop-ment. Mol Vis 2003;9:401-9.
Humayun MS, de Juan E Jr, del Cerro M, et al. Human neu-ral retinal transplantation. Invest Ophthalmol Vis Sci 2000;41: 3100-6.
Lamba DA, Karl MO, Ware CB, Reh TA. Efficient generation of retinal progenitor cells from human embryonic stem cells. Proc Natl Acad Sci U S A 2006;103:12769-74.Copyright © 2007 Massachusetts Medical Society.
1.
2.
3.
4.
5.
clinical implications of basic research
collections of articles on the journal’s web site
The Journal’s Web site (www.nejm.org) sorts published articles into more than 50 distinct clinical collections, which can be used as convenient
entry points to clinical content. In each collection, articles are cited in reverse chronologic order, with the most recent first.

n engl j med 356;15 www.nejm.org april 12, 20071580
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
c o r r e s p o n d e n c e
Sunitinib and Hypothyroidism
To the Editor: In their study of sunitinib versus interferon alfa in the treatment of metastatic renal-cell carcinoma, Motzer et al. (Jan. 11 issue)1 re-port that a high proportion of patients in both study groups had grade 3 or 4 fatigue. We wonder whether hypothyroidism could be a possible ex-planation and whether thyroid function was eval-uated. Interferon can cause thyroid dysfunction,2 and there is growing evidence that sunitinib also causes abnormalities in thyroid function.3-5 In our group of 65 patients who were treated with suni-tinib for renal-cell carcinoma or gastrointestinal stromal tumors, the incidence of laboratory evi-dence of thyroid dysfunction was 60 to 70%. Treat-ment of hypothyroidism was required in 15% of the patients. We recommend monitoring of thy-roid dysfunction in patients receiving sunitinib or similar compounds.
Pascal Wolter, M.D. Herlinde Dumez, M.D., Ph.D. Patrick Schöffski, M.D., M.P.H.University Hospital Gasthuisberg 3000 Leuven, Belgium [email protected]
Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med 2007;356:115-24.
Kabbaj N, Guedira MM, El Atmani H, et al. Thyroid disor-ders during interferon alpha therapy in 625 patients with chron-ic hepatitis C: a prospective cohort study. Ann Endocrinol (Paris) 2006;67:343-7.
Desai J, Yassa L, Marqusee E, et al. Hypothyroidism after sunitinib treatment for patients with gastrointestinal stromal tumors. Ann Intern Med 2006;145:660-4.
Rini BI, Tamaskar I, Shaheen P, et al. Hypothyroidism in patients with metastatic renal cell carcinoma treated with suni-tinib. J Natl Cancer Inst 2007;99:81-3.
Schöffski P, Wolter P, Himpe U, et al. Sunitinib-related thy-roid dysfunction: a single center retrospective and prospective evaluation. J Clin Oncol 2006;24:Suppl:3092. abstract.
The author replies: Although the possibility of hypothyroidism is described in the U.S. package insert for sunitinib, the incidence of clinical hypo-thyroidism was thought to be less than that given in the recent reports cited by Wolter et al. These reports highlight the need for routine monitor-ing of thyroid function and assessment of patients for signs and symptoms associated with hypothy-roidism. The fatigue in some sunitinib-treated pa-tients warrants elucidation. Hypothyroidism may be the cause in some patients, but there is likely to be another mechanism as well. We did not sys-tematically evaluate thyroid function in our trial. However, there was no apparent association be-tween treatment-related grade 3 or 4 fatigue and reports of hypothyroidism by the investigators. Of the 27 patients who had sunitinib-related grade 3 or 4 fatigue (7%), none had concurrent hypothyroidism, and of the 7 patients in whom hypothyroidism developed (2%), none had concur-
1.
2.
3.
4.
5.
this week’s letters
1580 SunitinibandHypothyroidism
1581 TrialRegistration
1581 Five-GeneSignatureinNon–Small-CellLungCancer
1583 ChildhoodProgressionofHereditaryMedullaryThyroidCancer
1586 AutoimmunePancreatitis
1588 PrimaryPCI
1590 EffectsofDietaryNitrateonBloodPressure
1591 FatalReactivationofHepatitisBwithTemozolomide

correspondence
n engl j med 356;15 www.nejm.org april 12, 2007 1581
rent grade 3 or 4 fatigue. Prospective studies in-corporating thyroid-function testing are under way to further define the incidence of sunitinib-induced hypothyroidism and its potential relationship to fatigue as reported by patients.
Robert J. Motzer, M.D.Memorial Sloan-Kettering Cancer Center New York, NY 10021 [email protected]
Trial Registration
To the Editor: In their editorial, Drazen and Zarin (Jan. 11 issue)1 express optimism about the registration of commercially sponsored clinical trials. Citing the ClinicalTrials.gov database, they report that 8% of pharmaceutical-industry regis-trations between January 1, 2006, and Decem-ber 1, 2006, were missing information on out-come measures (down from 26% of registrations before January 1, 2006).
Unfortunately, little is known about the trial-registration policies and practices of major phar-maceutical companies.2 For example, although the registration standards advocated by the Interna-tional Committee of Medical Journal Editors3 are steps in the right direction, they only encourage, rather than guarantee, complete trial registration. In the absence of legal mandates for registration of all clinical trials, including phase 1 and phase 2 studies as well as trial results, no examination of today’s voluntary registries can definitively in-dicate whether transparency in clinical research has truly improved, since unregistered trials nec-essarily remain unaccounted for in any analysis.
Currently, the Fair Access to Clinical Trials Act promises this legal mandate4 yet continues to lie dormant in U.S. congressional committees.5 En-actment of this legislation, should it come to pass, will be true cause for cheer.Jason P. Lott, M.A.University of Pennsylvania Philadelphia, PA 19104 [email protected]
Drazen JM, Zarin DA. Salvation by registration. N Engl J Med 2007;356:184-5.
Lott JP, Katz KA. Pharmaceutical companies’ policies and practices regarding prospective registration of dermatology-related clinical trials. Br J Dermatol 2006;155:635-8.
De Angelis C, Drazen JM, Frizelle FA, et al. Clinical trial registration: a statement from the International Committee of Medical Journal Editors. N Engl J Med 2004;351:1250-1.
Steinbrook R. Registration of clinical trials — voluntary or mandatory? N Engl J Med 2004;351:1820-2.
Henderson JK, Cassady Q. Drug deals 2006: cutting edge legal and regulatory issues in the pharmaceutical industry. Ann Health Law 2006;15:107-49.
The Editor Replies: I concur with Mr. Lott that we would be better served if data on all clinical trials were available in public databases; legisla-tion is one way to achieve this goal. In addition to the Fair Access to Clinical Trials Act, the Ken-nedy–Enzi bill1 was recently introduced, with many of the same broad goals of the Fair Access to Clinical Trials Act.
In the absence of legislation, investigators must be vigilant. It was not my goal to suggest that Dr. Motzer should have personally registered his clinical trial on the treatment of renal-cell carci-noma. Instead, I urge all investigators participat-ing in a clinical trial to check the registration to be sure it is fair, accurate, and fully informative.
Jeffrey M. Drazen, M.D.
Kennedy-Enzi bill, S.484. (Accessed March 22, 2007, at http://thomas.loc.gov/cgi-bin/bdquery/D?d110:464:./list/bss/d110SN.lst::|TOM:/bss/110search.html|.)
1.
2.
3.
4.
5.
1.
Five-Gene Signature in Non–Small-Cell Lung CancerTo the Editor: Chen et al. (Jan. 4 issue)1 state that their five-gene prognostic signature in non–small-cell lung cancer (NSCLC) was validated three times. However, validations 1 and 3 changed the measurement method that was used to define
the signature under validation. Correct validation of a signature requires a new series of patients, a consistent statistical method to define the sig-nature, and the same measurement technique.2 Validation 1 reused the original cohort and

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071582
changed the statistical method. Further doubts arise from the investigators’ use of a decision tree for this analysis.
Stefan Michiels, M.Sc. Catherine Hill, Ph.D.Institut Gustave Roussy 94805 Villejuif, France [email protected]
Chen H-Y, Yu S-L, Chen C-H, et al. A five-gene signature and clinical outcome in non–small-cell lung cancer. N Engl J Med 2007;356:11-20.
Michiels S, Koscielny S, Hill C. Interpretation of microarray data in cancer. Br J Cancer (in press).
To the Editor: Chen et al. report that a five-gene quantitative polymerase-chain-reaction (PCR) as-say stratified patients with early-stage lung cancer into low-risk and high-risk groups with a 5-year survival of approximately 65% and 35%, respec-tively. However, it is unclear whether the model de-scribed by Chen et al. predicts survival indepen-dently of tumor size and whether it is any better than the maximum standardized uptake value (SUV) on positron-emission tomography (PET).
Dan J. Raz, M.D. David M. Jablons, M.D.University of California, San Francisco San Francisco, CA 94143 [email protected]
To the Editor: In Figure 1 of the article by Chen et al., the Kaplan–Meier curves are biased because all the data were first used to identify the infor-mative genes and then reused when the classifier was applied to each individual sample. This type of reuse of data has been shown to constitute a potentially substantial bias1,2 that obscures the true performance of the predictor. Moreover, near-ly unbiased Kaplan–Meier curves could have been constructed without difficulty — for example, by means of a leave-one-out cross-validation that in-cluded the gene selection step.
Kevin K. Dobbin, Ph.D.National Cancer Institute Rockville, MD 20852
Ambroise C, McLachlan GJ. Selection bias in gene extraction on the basis of microarray gene-expression data. Proc Natl Acad Sci U S A 2002;99:6562-6.
Simon R, Radmacher MD, Dobbin K, McShane LM. Pitfalls in the use of DNA microarray data for diagnostic and prognostic classification. J Natl Cancer Inst 2003;95:14-8.
1.
2.
1.
2.
To the Editor: The article by Chen et al. illus-trates how far we still have to go to achieve ac-curate prediction of outcomes in lung cancer. Relapse after surgery is a binary outcome (patients have a relapse or do not). Ideally, relapse-free sur-vival should approach 100% for low-risk patients and should approach 0%, given enough time, for high-risk patients. This is far from what Chen et al. found for the five-gene signature. At 30 months, relapse-free survival was only about 45% in the low-risk group and 18% in the high-risk group. Therefore, since 40% of unselected patients with a low-risk signature will have a relapse, the model may identify a subgroup with worse-than-average prognosis, but for identifying low-risk patients, the model is no better than flipping a coin. The conclusion of Chen et al. that low-risk patients could be spared from unnecessary adju-vant treatment is unwarranted.Ioannis Gounaris, M.D.Plymouth Hospitals National Health Service Trust Plymouth PL6 8DH, United Kingdom [email protected]
To the Editor: We believe that the design of the study by Chen et al. is fundamentally flawed. The reported signature was generated from 125 pa-tients with NSCLC after the analysis of only 672 genes that were previously reported by the authors to be associated with invasive activity.1 In contrast to the approach used in previous studies,2,3 this limited set of genes was derived not from clinical samples but from a poorly differentiated human lung adenocarcinoma cell line (CL1).4 CL1 has been maintained in vitro for more than 60 genera-tions to derive highly metastatic subclones with intrinsic genetic instability.4 The high correlation between gene-expression profiles and the histo-logic type and grade of differentiation of NSCLC2 may hamper the application of this restricted gene set to a heterogeneous population with stage I, II, or III disease. When tested prospectively in nonadenocarcinoma NSCLC, this signature may not necessarily reflect the behavior of the tumor and may therefore not render independent or con-sistently predictive results.Alfonso Quintás-Cardama, M.D. Don L. Gibbons, M.D., Ph.D.M.D. Anderson Cancer Center Houston, TX 77030 [email protected]

correspondence
n engl j med 356;15 www.nejm.org april 12, 2007 1583
Chen JJ, Peck K, Hong TM, et al. Global analysis of gene expression in invasion by a lung cancer model. Cancer Res 2001; 61:5223-30.
Beer DG, Kardia SL, Huang CC, et al. Gene-expression pro-files predict survival of patients with lung adenocarcinoma. Nat Med 2002;8:816-24.
Potti A, Mukherjee S, Petersen R, et al. A genomic strategy to refine prognosis in early-stage non–small-cell lung cancer. N Engl J Med 2006;355:570-80. [Erratum, N Engl J Med 2007; 356:201-2.]
Chu YW, Yang PC, Yang SC, et al. Selection of invasive and metastatic subpopulations from a human lung adenocarcinoma cell line. Am J Respir Cell Mol Biol 1997;17:353-60.
The authors reply: Michiels and Hill state that validation sets 1 and 3 changed the measurement technique used to define the signature under validation, but this may be unavoidable, since we derived the initial gene signature (16 genes) us-ing microarrays and then refined the signature to 5 genes using real-time reverse-transcriptase PCR (RT-PCR) and validated it. The 60 patients (vali-dation 2) who were used to validate the five-gene signature constitute a completely different group from the set of 101 patients in the original cohort. In validation set 3, which involved the use of mi-croarray data from the public domain to validate our RT-PCR signature, certain adjustments, such as using the expression level of the same gene as the reference level, were needed. We used a recursive-partitioning decision-tree model and a variable that can be used repeatedly in different nodes.
With regard to the comments of Raz and Jab-lons: we did not evaluate whether the five-gene signature predicts survival independently of tu-mor size or whether it is better than maximum tumor SUV on PET. These evaluations were not objectives of our study. Tumor stage may be more relevant than tumor size for predicting the out-come in lung cancer, and we did evaluate stage in the multivariate analysis in our study.
Dobbin remarks that there may be bias be-cause all the data were first used to identify the informative genes and then reused when the clas-sifier was applied to each individual sample. We identified the 16-gene signature from a training
1.
2.
3.
4.
cohort of 63 patients and then applied the linear predictor to a separate testing cohort of 62 pa-tients without estimating the coefficients. For both cohorts, there was no reuse of data in the con-struction of the Kaplan–Meier curves.
With regard to the comments of Gounaris, we suggest that low-risk patients could be spared from unnecessary adjuvant treatment. We showed that the 50-month rate of overall survival among patients with a low-risk gene signature was 85% among patients with stage I or stage II disease, 65% in an independent cohort of Chinese pa-tients, and almost 90% in an independent set of published microarray data from patients in West-ern countries.
Quintás-Cardama and Gibbons state that our gene signature was derived not from clinical sam-ples but from a poorly differentiated human lung adenocarcinoma cell line, and they suggest that this approach may be flawed. The truth of the matter lies in validation of the gene signature with the use of independent cohorts of patients with NSCLC and revalidation. Cell lines can be used to derive novel invasion-suppressor genes in patients with NSCLC.1 Drug-sensitivity data based on cell lines, coupled with microarray data, can be used to yield gene-expression signatures that predict the sensitivity of a tumor to chemothera-peutic drugs in patients.2
Hsuan-Yu Chen, Ph.D.Institute of Statistical Science Taipei 115, Taiwan
Wei J. Chen, M.D., Sc.D.National Taiwan University College of Public Health Taipei 100, Taiwan
Pan-Chyr Yang, M.D., Ph.D.National Taiwan University Hospital Taipei 100, Taiwan [email protected]
Shih JY, Yang SC, Hong TM, et al. Collapsin response media-tor protein-1 and the invasion and metastasis of cancer cells. J Natl Cancer Inst 2001;93:1392-400.
Potti A, Dressman HK, Bild A, et al. Genomic signatures to guide the use of chemotherapeutics. Nat Med 2006;12:1294-300.
1.
2.
Childhood Progression of Hereditary Medullary Thyroid CancerTo the Editor: Machens et al. (Oct. 16, 2003, issue)1 confirmed that medullary thyroid carci-noma develops very early in children carrying
a germ-line mutation of the rearranged during transfection (RET) gene. However, an error in Figure 1 of their article may alter the message of

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071584
this important article. According to Figure 1, the risk of medullary thyroid carcinoma for a child with a codon 634 RET mutation is approximately 10% at 5 years of age. This finding seems to be inconsistent with the data provided by Machens et al.: that 75% of children with a codon 634 RET mutation (12 of 16) who underwent prophylactic thyroidectomy before the age of 5 years had med-ullary thyroid carcinoma.
It appears to us that the cumulative risks pre-sented in Figure 1 have been incorrectly calculat-ed by dividing, at each age interval, the number of children with medullary thyroid carcinoma by the total number of children (130), rather than by the number who underwent surgery at each age interval (12 divided by 130 is nearly 10%).
An international consensus established in 1999 and published in 2001 stated that all children with a codon 634 RET mutation should undergo thyroidectomy before 5 years of age.2 Although feasible, this guideline is rarely implemented.3 Correction of Figure 1 might help the medical community understand the reasons behind the guidelines.
Olivier Chabre, M.D., Ph.D. Christian Piolat, M.D. Jean-Francois Dyon, M.D.University Hospital of Grenoble 38043 Grenoble, France [email protected]
Machens A, Niccoli-Sire P, Hoegel J, et al. Early malignant progression of hereditary medullary thyroid cancer. N Engl J Med 2003;349:1517-25.
Brandi ML, Gagel RF, Angeli A, et al. Guidelines for diagno-sis and therapy of MEN type 1 and type 2. J Clin Endocrinol Metab 2001;86:5658-71.
Piolat C, Dyon J-F, Sturm N, et al. Very early prophylactic thyroid surgery for infants with a mutation of the RET proto-oncogene at codon 634: evaluation of the implementation of in-ternational guidelines for MEN type 2 in a single centre. Clin Endocrinol (Oxf) 2006;65:118-24.
The Authors Reply: We welcome the opportu-nity to illustrate the rationale behind the recom-mendation to perform total thyroidectomy in car-riers of codon 634 RET mutations before the age of 5 years.1 In our article on the multicenter Euro-
1.
2.
3.
pean Multiple Endocrine Neoplasia (EUROMEN) study, we presented the cumulative probability of detecting medullary thyroid carcinomas before a certain age among the 130 carriers of codon 634 mutations. As noted by Chabre and colleagues, the Kaplan–Meier curve in Figure 1 cannot be construed as reflecting an age-specific malignant progression of medullary thyroid carcinoma, since this would lead to an underestimation of the risk of cancer at younger ages.
We have reanalyzed our data in order to cor-rect the errors in our original figure (Fig. 1A), using logistic-regression analysis to enforce mono-tonicity of the curve2 and smoothing the esti-mates of cancer rates by modeling the log-preva-lence odds as a linear function of age. The resultant age-related malignant progression of medullary thyroid carcinoma is shown in the corrected fig-ure (Fig. 1B). The model-based estimate of the prevalence of cancer was 52 to 66% before the age of 5 years for asymptomatic carriers of codon 634 mutations in the EUROMEN study. The cor-rected curve supports the need for early prophy-lactic thyroidectomy in asymptomatic carriers of RET gene mutations.
We would like to join Chabre and colleagues in their plea for widespread adoption of early thy-roidectomy before the age of 5 years in carriers of high-risk RET mutations, including those in codon 634, to accomplish complete translation of DNA-based information from the bench to the bedside.Andreas Machens, M.D.Martin-Luther-Universität Halle-Wittenberg 06097 Halle (Saale), Germany [email protected]
Josef Hoegel, Ph.D.Universität Ulm 89081 Ulm, Germany
Henning Dralle, M.D.Martin-Luther-Universität Halle-Wittenberg 06097 Halle (Saale), Germany
Brandi ML, Gagel RF, Angeli A, et al. Guidelines for diagno-sis and therapy of MEN type 1 and type 2. J Clin Endocrinol Metab 2001;86:5658-71.
Dinse GE, Lagakos SW. Regression analysis of tumor-preva-lence data. J R Stat Soc [C] 1983;32:236-48.
1.
2.

correspondence
n engl j med 356;15 www.nejm.org april 12, 2007 1585
33p9
AUTHOR
FIGURE
JOB: ISSUE:
4-CH/T
RETAKE 1st2nd
SIZE
ICM
CASEEMail Line
H/TCombo
Revised
AUTHOR, PLEASE NOTE:Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
Machens
1 of 1
04-12-07
ts
35615
Cum
ulat
ive
Ris
k of
Med
ulla
ry T
hyro
id C
arci
nom
a
Age (yr)
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00 10987654321 11 12 13 201914 15 16 17 18
With or without nodal metastases
With nodal metastases
A
B
Original Curves
Cum
ulat
ive
Ris
k of
Med
ulla
ry T
hyro
id C
arci
nom
a
Age (yr)
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.00 10987654321 11 12 13 201914 15 16 17 18
With or without nodal metastases
With nodal metastases
Corrected Curves
Figure 1. Original Curves (Panel A) and Corrected Curves (Panel B) for the Cumulative Risk of Medullary Thyroid Carcinoma among Carriers of Codon 634 Germ-Line RET Mutations, According to the Presence or Absence of Nodal Metastases and Age.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071586
To the Editor: Finkelberg et al. (Dec. 21 issue)1 review the pathogenesis, diagnosis, and manage-ment of autoimmune pancreatitis. We treated a 67-year-old man with a diagnosis of autoimmune pancreatitis made on the basis of computed to-mography (CT), endoscopic ultrasonography and biopsy, and elevated IgG levels (including IgG4). The patient had worsening fatigue and general-ized weakness. Laboratory studies revealed low levels of thyroid-stimulating hormone, free thy-roxine, corticotropin, cortisol, follicle-stimulat-ing hormone, luteinizing hormone, growth hor-mone, insulin-like growth factor 1, and free testosterone, with a normal prolactin level. Mag-netic resonance imaging (MRI) of the pituitary, performed because of the patient’s panhypopitu-itarism, revealed thickening and masslike enlarge-ment of the infundibulum, consistent with lym-phocytic hypophysitis (Fig. 1). Prednisone (40 mg daily) was initiated, with a dramatic improvement in symptoms. Later, levothyroxine and desmo-pressin were started for diabetes insipidus. Al-though repeat MRI of the pituitary and CT of the pancreas showed marked improvement, the pa-tient continues to require low levels of hormone replacement.
Lymphyocytic hypophysitis, characterized by lymphocytic infiltration of the pituitary gland, is rare but can occur with other autoimmune dis-eases.2-4 Finkelberg et al. mention the involve-ment of extrapancreatic organs in autoimmune pancreatitis. This case shows that pituitary-gland involvement also occurs.Sonia Ralli, M.D. Jeannie Lin, M.D. James Farrell, M.D.David Geffen School of Medicine at UCLA Los Angeles, CA 90095 [email protected]
Finkelberg DL, Sahani D, Deshpande V, Brugge WR. Auto-immune pancreatitis. N Engl J Med 2006;355:2670-6.
Bellastella A, Bizzarro A, Coronella C, Bellastella G, Sinisi AA, De Bellis A. Lymphocytic hypophysitis: a rare or underesti-mated disease? Eur J Endocrinol 2003;149:363-76.
Buxton N, Robertson I. Lymphocytic and granulocytic hypo-physitis: a single centre experience. Br J Neurosurg 2001;15: 242-6.
Thodou E, Asa SL, Kontogeorgos G, Kovacs K, Horvath E, Ezzat S. Clinical case seminar: lymphocytic hypophysitis: clini-copathological findings. J Clin Endocrinol Metab 1995;80:2302-11.
To the Editor: In response to the review of auto-immune pancreatitis by Finkelberg et al., we re-port on a 64-year-old man who presented with rapid-onset jaundice and weight loss without pain. Abdominal MRI and endoscopic retrograde cho-langiopancreatography showed a hilar bile-duct stricture with wall thickening. Hilar cholangio-carcinoma was strongly suspected, and the pa-tient underwent hilar resection with excision of the caudate lobe. During surgery, the pancreatic segment of bile duct was seen to be sheathed in a pancreatic heterogeneous mass, and a cephalic duodenopancreatectomy was performed. Patho-logical analysis of the pancreatic and bile ducts did not show neoplastic lesions but did reveal periductal lymphoplasmacytic infiltration, with diffuse fibrosis suggestive of autoimmune pan-creatitis. The serum IgG4 level was greatly ele-vated.
Stenosis of the bile duct frequently occurs with autoimmune pancreatitis. The stenotic portion is usually the lower bile duct; however, strictures of the hilar bile duct or intrahepatic areas are some-times found.1 Both the bile-duct lesions and pan-creatic lesions can improve after corticosteroid therapy.2 When the presentation is indistinguish-
1.
2.
3.
4.
16p6
AUTHOR Ralli
FIGURE 1 of 1
JOB: ISSUE:
4-CH/T
RETAKE 1st
2nd
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
4-12-07
mst
35615
Figure 1. T1-Weighted MRI Scan of the Pituitary.
Thickening and masslike enlargement of the pituitary stalk are evident. The pituitary gland is mildly enlarged and hyperintense as compared with the brain paren-chyma (arrow), a finding suggestive of lymphocytic hy-pophysitis.
Autoimmune Pancreatitis

correspondence
n engl j med 356;15 www.nejm.org april 12, 2007 1587
able from a cancer, a trial of corticosteroids may make it possible to avoid unnecessary surgery.Philippe Leclercq, M.D. Nicolas Meurisse, M.D. Pierre Honore, M.D., Ph.D.University Hospital of Liege 4000 Liege, Belgium
Kamisawa T, Tu Y, Egawa N, Nakajima H, Tsuruta K, Oka-moto A. Involvement of pancreatic and bile ducts in autoimmune pancreatitis. World J Gastroenterol 2006;12:612-4.
Czako L, Hegykozi E, Palinkas A, Lonovics J. Autoimmune pancreatitis: functional and morphological recovery after steroid therapy. World J Gastroenterol 2006;12:1810-2.
To the Editor: Readers of the review of autoim-mune pancreatitis by Finkelberg et al. may be un-der the impression that 11% of patients with chronic pancreatitis in the United States have auto-immune pancreatitis, which is an overestimation of the disease’s prevalence. The statistic was based on the examination of pancreatic resections for benign disease at the Mayo Clinic,1 rather than on typical clinical cases of chronic pancrea-titis. All 245 cases were forms of chronic pancrea-titis, and 27 cases (11%) represented autoimmune pancreatitis with a “tumefactive” presentation. Al-though some pancreatic resections for suspected cancer are found on histologic analysis to be be-nign cases of chronic pancreatitis, most patients with typical chronic pancreatitis do not undergo surgery. Conversely, autoimmune pancreatitis may present without tumefaction, so not all patients with autoimmune pancreatitis would be represent-ed in this study. Thus, the actual prevalence of autoimmune pancreatitis in the United States is unknown. In Japan, South Korea, and Italy, prev-alences of autoimmune pancreatitis among pa-tients with chronic pancreatitis range from 4.6 to 8.4%.2 The prevalence of autoimmune pancreati-tis in our own experience is even lower.Amit Raina, M.D. Dhiraj Yadav, M.D. Alyssa M. Krasinskas, M.D.University of Pittsburgh Pittsburgh, PA 15213-2546 [email protected]
Yadav D, Notahara K, Smyrk TC, et al. Idiopathic tumefac-tive chronic pancreatitis: clinical profile, histology, and natural history after resection. Clin Gastroenterol Hepatol 2003;1:129-35.
Kamisawa T, Okamoto A. Autoimmune pancreatitis: pro-posal of IgG4-related sclerosing disease. J Gastroenterol 2006; 41:613-25.
1.
2.
1.
2.
The Author Replies: Ralli et al. remark on the extrapancreatic manifestations of autoimmune pancreatitis. Autoimmune pancreatitis is likely to be a systemic autoimmune disease associated with tissue infiltration by IgG4-positive plasma cells. Although renal, pulmonary, hepatic, and gastro-duodenal lesions have been reported, I was not aware of the possibility of infiltration of the cen-tral nervous system. The clinical features of the patient described by Ralli et al. are nearly diag-nostic of autoimmune pancreatitis because of the findings on MRI in combination with the elevated serum IgG4 level. The patient’s response to corti-costeroids is also consistent with autoimmune pancreatitis. Therefore, I agree that the clinical picture is most consistent with autoimmune pan-creatitis with involvement of the hypophysis.
Leclercq et al. comment on bile-duct stenosis as a result of autoimmune pancreatitis. Bile-duct stenosis and its clinical manifestations, such as jaundice and pruritus, are relatively common pre-sentations of autoimmune pancreatitis. Leclercq et al. note one type of stenosis, resulting from extrinsic compression by the involved pancreas. In addition, one must be aware of the possibility of lymphocytic sclerosing cholangitis, which may include diffuse involvement of the bile duct, in contrast to the distal bile-duct stenosis described in their patient. These manifestations are impor-tant to recognize because of their responsiveness to corticosteroid therapy.
Raina et al. address the question of the true prevalence of autoimmune pancreatitis. Certainly, the review of surgical pathological specimens in one center is not an ideal method for determin-ing the prevalence of a disease. Nevertheless, the prevalence figures at the Mayo Clinic do not dif-fer substantially from the estimates in Europe and Asia. The prevalence of autoimmune pancreatitis in association with other clinical findings — such as obstructive jaundice, focal pancreatic strictures, and recurrent pancreatitis — varies tremendously. The importance of autoimmune pancreatitis lies not in its modest prevalence but in its excellent prognosis and responsiveness to therapy.
William R. Brugge, M.D.Massachusetts General Hospital Boston, MA 02114 [email protected]

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071588
To the Editor: In their review of primary percu-taneous coronary intervention (PCI) for myocar-dial infarction with ST-segment elevation, Keeley and Hillis (Jan. 4 issue)1 cite the guidelines of the American College of Cardiology and American Heart Association (ACC–AHA): “Primary PCI is preferred if a . . . catheterization laboratory with surgical backup [is] available and if the pro-cedure can be performed within 90 minutes after initial medical contact. . . .”2 Nationally, for 55% of patients who have myocardial infarction with ST-segment elevation, the door-to-balloon time is less than 90 minutes.3 Between January 2006 and July 2006, the hospital with the highest percentage of patients with myocardial infarction with ST-segment elevation meeting this criterion was a rural hospital that did not have surgical backup: 100% of the patients had door-to-bal-loon times of less than 90 minutes, and the aver-age time was 55 minutes. Among these patients, there was no increase in complications.
Some rural areas have sufficient population to support a program in interventional cardiology but not a program in cardiac surgery. In rural communities, traffic congestion is rarely a prob-lem, so that an interventional team could get to the hospital quickly. Primary PCI can be per-formed safely with superior results in rural set-tings without surgical backup.4 The ACC–AHA guidelines might compromise the care provided to patients with myocardial infarction with ST-seg-ment elevation who live in rural communities.Daniel C. Brown, M.D.St. Luke’s Magic Valley Regional Medical Center Twin Falls, ID 83301 [email protected]
Keeley EC, Hillis LD. Primary PCI for myocardial infarction with ST-segment elevation. N Engl J Med 2007;356:47-54.
Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guide-lines for the management of patients with ST-elevation myocar-dial infarction — executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocar-dial Infarction). J Am Coll Cardiol 2004;44:671-719. [Erratum, J Am Coll Cardiol 2005;45:1376.]
CathPCI Registry. American College of Cardiology, National Cardiovascular Data Registry (ACC–NCDR), 2007. (Accessed March 22, 2007, at http://www.accncdr.com/webncdr/DefaultCathPCI.aspx.)
Brown DC, Mogelson S, Harris R, Kemp D, Massey M. Percu-taneous coronary interventions in a rural hospital without surgi-cal backup: report of one year of experience. Clin Cardiol 2006; 29:337-40.
1.
2.
3.
4.
To the Editor: In their article on primary PCI for patients who have myocardial infarction with ST-segment elevation, Keeley and Hillis describe the management of this potentially fatal coronary event, including medical treatment and mechan-ical therapy with primary PCI. However, some ad-ditional points should be addressed. The authors state that clopidogrel should be administered after it has been determined that emergency bypass surgery is not required. Recent study data indi-cate that the administration of clopidogrel before PCI significantly reduces the incidence of death from cardiovascular causes or from ischemic com-plications without a significant increase in bleed-ing.1,2 Furthermore, the addition of the selective aldosterone blocker eplerenone to optimal medi-cal therapy has been shown to reduce morbidity and mortality among patients with acute myocar-dial infarction complicated by left ventricular dys-function and heart failure and thus should have been mentioned in this article.3 Finally, because of possible adverse effects on the clinical outcome, the risk of thrombocytopenia induced by treat-ment with heparin or glycoprotein IIb/IIIa inhib-itors should also be noted.Sebastian Szabo, M.D. Thomas Oikonomopoulos, M.D. Hans Martin Hoffmeister, M.D.Städtisches Klinikum Solingen 42653 Solingen, Germany [email protected]
Sabatine MS, Cannon CP, Gibson CM, et al. Effect of clopid-ogrel pretreatment before percutaneous coronary intervention in patients with ST-elevation myocardial infarction treated with fibrinolytics: the PCI-CLARITY study. JAMA 2005;294:1224-32.
Chen ZM, Jiang LX, Chen YP, et al. Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction: ran-domised placebo-controlled trial. Lancet 2005;366:1607-21.
Pitt B, Remme W, Zannad F, et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med 2003;348:1309-21. [Erratum, N Engl J Med 2003;348:2271.]
To the Editor: Keeley and Hillis ignore athero-embolic renovascular disease as a cause of ne-phropathy in patients who have undergone PCI. Atheroembolic disease accounts for approximately 5 to 10% of cases of acute renal failure1 and is an increasingly common cause of renal insufficiency in the elderly. A review of 372 autopsies identi-fied cholesterol emboli in 2.4% of renal-tissue samples. Inciting events, including vascular sur-gery, arteriography, angioplasty, anticoagulation
1.
2.
3.
Primary Percutaneous Coronary Intervention

correspondence
n engl j med 356;15 www.nejm.org april 12, 2007 1589
with heparin, and thrombolytic therapy, can be identified in 50% of cases of cholesterol emboli-zation. Arteriographic procedures are the most common cause of cholesterol embolization.2 Show-ers of cholesterol emboli occur in about 50% of PCIs when a guiding catheter is passed through the aorta.3,4 Most of these showers are clinically silent. In approximately 1% of high-risk patients, an acute cholesterol emboli syndrome develops, which is manifested as acute renal failure, mesen-teric ischemia, decreased microcirculation to the extremities, and, in some cases, embolic stroke.3 Since most cases of atheroembolic kidney disease are triggered by angiography, radiocontrast-induced nephropathy is easily invoked as an alternative diagnosis.1
Ajit Singh Kashyap, M.D.Command Hospital (Central Command) Lucknow 226 002, India [email protected]
Shekhar Kashyap, M.D.Dhanvantri Hospital Meerut 250 001, India
Kuldip Parkash Anand, M.D.Command Hospital (Eastern Command) Kolkata 700 027, India
Polu KR, Wolf M. Needle in a haystack. N Engl J Med 2006; 354:68-73.
Badr KF, Brenner BM. Vascular injury to the kidney. In: Kasper DL, Braunwald E, Fauci AS, et al., eds. Harrison’s prin-ciples of internal medicine. 16th ed. New York: McGraw-Hill, 2005:1706-10.
McCullough PA. Interface between renal disease and cardio-vascular disease. In: Zipes DP, Libby P, Bonow RO, Braunwald E, eds. Braunwald’s heart disease: a textbook of cardiovascular medicine. 7th ed. Philadelphia: W.B. Saunders, 2003:2161-72.
Meyrier A. Cholesterol crystal embolism: diagnosis and treatment. Kidney Int 2006;69:1308-12.
The authors reply: We congratulate Brown et al.1 on their excellent outcomes with the use of primary PCI at a rural hospital without surgical backup, but we disagree that this procedure can be performed consistently in this setting and under these circumstances “safely with superior results.” The favorable results of primary PCI re-ported in selected community hospitals that do not have surgical backup, such as the data report-ed by Brown et al.,1 may not be achieved reliably at other facilities. Although urgent coronary-artery bypass grafting (CABG) is not commonly required for patients undergoing primary PCI, it is, in fact, necessary for an occasional patient, and the need often cannot be predicted. When CABG is re-quired, the resultant delay incurred by the trans-fer of the patient to another facility can result in
1.
2.
3.
4.
high morbidity and mortality.2 Primary PCI has been clearly shown to be safe and effective at high-volume centers with surgical backup, with supporting data from 23 randomized, controlled trials.3 In contrast, only one randomized trial comparing primary PCI and fibrinolytic therapy at community hospitals without surgical backup has been reported.4 As a result, according to the ACC–AHA guidelines,5 primary PCI without sur-gical backup is a class IIb indication.
As noted above, an occasional patient under-going primary PCI requires urgent CABG. In such a patient, previous administration of clopidogrel substantially increases the risk of perioperative bleeding. For this reason, clopidogrel should not be given in the setting of primary PCI until it is clear that bypass surgery is not required. In some patients undergoing PCI, thrombocytopenia may develop after the administration of a combina-tion of a platelet glycoprotein IIb/IIIa inhibitor and heparin; the risk is similar among those undergoing primary PCI for myocardial infarc-tion with ST-segment elevation and those under-going elective PCI. Currently, administration of the selective aldosterone blocker eplerenone is not considered a standard of care for patients who have myocardial infarction with ST-segment ele-vation.
Although an occasional patient undergoing an arteriographic procedure may have cholesterol embolization, most cholesterol emboli, as noted by Kashyap et al., are clinically silent. Only rarely do cholesterol emboli cause acute renal failure.Ellen C. Keeley, M.D.University of Virginia School of Medicine Charlottesville, VA 22908
L. David Hillis, M.D.University of Texas Southwestern Medical Center Dallas, TX 75390
Brown DC, Mogelson S, Harris R, Kemp D, Massey M. Per-cutaneous coronary interventions in a rural hospital without surgical backup: report of one year of experience. Clin Cardiol 2006;29:337-40.
Lotfi M, Mackie K, Dzavik V, Seidelin PH. Impact of delays to cardiac surgery after failed angioplasty and stenting. J Am Coll Cardiol 2004;43:337-42.
Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarc-tion: a quantitative review of 23 randomised trials. Lancet 2003; 361:13-20.
Aversano T, Aversano LT, Passamani E, et al. Thrombolytic therapy vs primary percutaneous coronary intervention for myo-cardial infarction in patients presenting to hospitals without on-site cardiac surgery: a randomized controlled trial. JAMA 2002;287:1943-51. [Erratum, JAMA 2002;287:3212.]
Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation
1.
2.
3.
4.
5.

T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 20071590
Effects of Dietary Nitrate on Blood Pressure
To the Editor: Larsen and colleagues (Dec. 28 issue)1 report that oral nitrate (NO3
-) can lower mean arterial blood pressure and is associated with an elevation in blood levels of nitrite (NO2
-). They point out that nitrate is reduced by oral bac-teria to nitrite, which can be converted into nitric oxide or absorbed, and they suggest that the mechanism involved in the blood-pressure–lower-ing effect needs to be clarified.
In studies conducted over the past 5 years, we have shown that nitrite is an intrinsic vasodila-tor.2,3 Within the vasculature, nitrite is reduced to nitric oxide by reaction with deoxygenating hemo-globin and possibly other heme proteins.4,5 These studies show that nitrite levels are higher in the arteries than in the veins in humans, indicating metabolism across the peripheral circulation, and that when nitrite is infused into the brachial ar-tery, it causes vasodilatation. We recently com-pleted a study evaluating the effect of low-dose nitrite infusion in 15 healthy volunteers and found that levels as low as 350 nM resulted in measur-able vasodilatation in the forearm; mean (±SE) values of blood flow ranged from 3.0±0.3 to 3.4±0.3 ml per minute per 100 ml of forearm tis-sue (P = 0.04). We are therefore not surprised that increases in nitrite levels from 138 nM to 219 nM caused by increased dietary intake of nitrate are associated with decreases in blood pressure.André Dejam, M.D., Ph.D. Christian J. Hunter, M.D., Ph.D.Brigham and Women’s Hospital Boston, MA 02115
Mark T. Gladwin, M.D.National Institutes of Health Bethesda, MD 20892 [email protected]
Larsen FJ, Ekblom B, Sahlin K, Lundberg JO, Weitzberg E. Effects of dietary nitrate on blood pressure in healthy volun-teers. N Engl J Med 2006;355:2792-3.
Gladwin MT, Shelhamer JH, Schechter AN, et al. Role of circulating nitrite and S-nitrosohemoglobin in the regulation of regional blood flow in humans. Proc Natl Acad Sci U S A 2000; 97:11482-7.
Cosby K, Partovi KS, Crawford JH, et al. Nitrite reduction to nitric oxide by deoxyhemoglobin vasodilates the human circula-tion. Nat Med 2003;9:1498-505.
Huang Z, Shiva S, Kim-Shapiro DB, et al. Enzymatic func-
1.
2.
3.
4.
tion of hemoglobin as a nitrite reductase that produces NO under allosteric control. J Clin Invest 2005;115:2099-107.
Gladwin MT, Schechter AN, Kim-Shapiro DB, et al. The emerging biology of the nitrite anion. Nat Chem Biol 2005;1:308-14. [Erratum, Nat Chem Biol 2006;2:110.]
The authors reply: We agree that nitrite reduc-tion to nitric oxide is a likely explanation of the hypotensive effects of nitrite, as reported in our letter. We were also not very surprised, since we had previously shown that the administration of oral nitrate leads to increased levels of circulat-ing nitrite1 and that near-physiologic levels of nitrite induce cyclic guanosine monophosphate–dependent vasodilatation in vitro.2 Multiple path-ways for systemic nitrite conversion to nitric oxide have now been described,3,4 but the letter format did not allow a detailed discussion. Dejam and colleagues report vasodilatation at very low plasma levels of nitrite, which supports our findings, al-though a local infusion of nitrite into the fore-arm is not directly comparable to oral nitrate supplementation. Dietary nitrate gives sustained delivery of low-dose nitrite to the circulation, and oral commensal bacteria are essential, since mam-malian enzymes cannot effectively metabolize this anion. Circulating nitrate is greatly enriched in sa-liva, and nitrite is then formed by bacterial nitrate reductases.4 An astonishing overall conclusion from this finding is that, in fact, symbiotic bac-teria are involved in the regulation of cardiovas-cular function in humans.Jon O. Lundberg, M.D., Ph.D. Eddie Weitzberg, M.D., Ph.D.Karolinska Institutet S-171 77 Stockholm, Sweden [email protected]
Lundberg JO, Govoni M. Inorganic nitrate is a possible source for systemic generation of nitric oxide. Free Radic Biol Med 2004;37:395-400.
Modin A, Bjorne H, Herulf M, Alving K, Weitzberg E, Lund-berg JO. Nitrite-derived nitric oxide: a possible mediator of ‘acidic-metabolic’ vasodilation. Acta Physiol Scand 2001;171:9-16.
Lundberg JO, Weitzberg E. NO generation from nitrite and its role in vascular control. Arterioscler Thromb Vasc Biol 2005;25:915-22.
Lundberg JO, Weitzberg E, Cole JA, Benjamin N. Nitrate, bacteria and human health. Nat Rev Microbiol 2004;2:593-602. [Erratum, Nat Rev Microbiol 2004;2:681.]
5.
1.
2.
3.
4.
myocardial infarction — executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise
the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). Circulation 2004;110:588-636. [Erratum, Circulation 2005;111:2013.]

correspondence
n engl j med 356;15 www.nejm.org april 12, 2007 1591
Fatal Reactivation of Hepatitis B with TemozolomideTo the Editor: Encouraging results have led to the use of temozolomide as a first-line therapy for glioblastoma.1 We report on a case of temo-zolomide-associated reactivation of hepatitis B, a complication that may warrant the use of pro-phylactic antiviral agents during treatment with this chemotherapy.2
A 65-year-old Chinese woman with a remote history of hepatitis B underwent total surgical resection of an enhancing mass in the left tem-poral lobe, which was diagnosed as glioblastoma. She received radiation therapy with concurrent daily temozolomide (at a dose of 75 mg per square meter of body-surface area), followed by three cycles of adjuvant temozolomide (200 mg per square meter on days 1 through 5 of a 28-day cycle). She was taking valproic acid for seizure prophylaxis, reported no use of alcohol or herbal remedies, and was otherwise healthy. Dexameth-asone was tapered and eventually stopped dur-ing a 1-week period after surgery. She did not undergo hepatitis studies before starting treat-ment. Her liver enzyme levels were normal at baseline and before her first two cycles of adju-vant chemotherapy (Table 1). Although there was a mild, asymptomatic elevation of the alanine aminotransferase level before the third cycle of temozolomide, the chemotherapy was adminis-tered as planned.
On day 27 of her third cycle of treatment, the
patient was hospitalized because of rapidly pro-gressing encephalopathy. The results of labora-tory studies were consistent with acute liver failure, and valproic acid was discontinued. A hepatitis panel was negative for hepatitis C but positive for hepatitis B core antigen and hepatitis B sur-face antigen (HBsAg). The viral load was more than 500 million particles. Although the patient was treated with entecavir (1 mg daily), her liver function continued to deteriorate, and she died 2 weeks after admission. There was no evidence of tumor recurrence on magnetic resonance imaging after surgery. We attribute her death to hepatitis B reactivation resulting from the use of temozolomide, although hepatotoxic ef-fects of valproic acid or of temozolomide itself cannot be completely ruled out.
It is estimated that more than 1.5 million HBsAg carriers reside in the United States.2 Treat-ment of hematologic cancers with chemotherapy and corticosteroids imparts a high risk of hepa-titis B reactivation (>60%). Reactivation is also associated with pregnancy and liver transplanta-tion and may occur spontaneously. In addition to morbidity from hepatitis, viral reactivation may disrupt cancer treatment, resulting in decreased overall survival. Because of the increasing use of temozolomide in the treatment of brain tumors and systemic cancers,3 prescribing clinicians should be aware of this potentially severe adverse
Table 1. Selected Laboratory Values during Temozolomide Treatment of the Patient.*
Variable BaselineBefore Cycle 1
Before Cycle 2
Before Cycle 3
Day 27 of Cycle 3
2 Weeks after Admission
Total bilirubin (mg/dl) <0.2 0.3 0.3 0.4 2.8 25.9
Alkaline phosphatase (IU/liter) 73 58 45 58 107 75
Alanine aminotransferase (IU/liter)
32 15 16 85 1338 72
Aspartate aminotransferase (IU/liter)
30 30 35 105 2195 78
Ammonia (μmol/liter) — — — — 68 153
International normalized ratio 0.88 — — — 3.65 6.98
Serum valproic acid (μg/ml) 92 93 77 90 132 —
Total neutrophils (per mm3) 7910 2280 1690 1680 1250 5000
Total lymphocytes (per mm3) 890 540 600 530 450 410
* The patient was treated with adjuvant temozolomide (at a dose of 200 mg per square meter of body-surface area) on days 1 through 5 of a 28-day cycle. On day 27 of the third cycle, she was hospitalized because of hepatic encephalopathy. Despite receiving daily treatment with 1 mg of entecavir, she died 2 weeks later.

n engl j med 356;15 www.nejm.org april 12, 20071592
correspondence
event. Data support the use of antiviral agents for HBsAg carriers during chemotherapy.2 We recommend that hepatitis screening and viral prophylaxis be considered when they are clinically appropriate in patients receiving temozolomide.Jai Grewal, M.D. Caryl A. Dellinger, M.D. W.K.A. Yung, M.D.M.D. Anderson Cancer Center Houston, TX 77030 [email protected]
Dr. Yung reports serving on an advisory board for and receiving grant and research support and honoraria from Schering-Plough.
Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005;352:987-96.
Kohrt HE, Ouyang DL, Keeffe EB. Systematic review: lamivu-dine prophylaxis for chemotherapy-induced reactivation of chron-ic hepatitis B virus infection. Aliment Pharmacol Ther 2006;24: 1003-16.
Mutter N, Stupp R. Temozolomide: a milestone in neuro-oncology and beyond? Expert Rev Anticancer Ther 2006;6:1187-204.Correspondence Copyright © 2007 Massachusetts Medical Society.
1.
2.
3.
instructions for letters to the editor
Letters to the Editor are considered for publication, subject to editing and abridgment, provided they do not contain material that has been submitted or published elsewhere. Please note the following: •Letters in reference to a Journal article must not exceed 175 words (excluding references) and must be received within 3 weeks after publication of the article. Letters not related to a Journal article must not exceed 400 words. All letters must be submitted over the Internet at http://authors.nejm.org. •A letter can have no more than five references and one figure or table. •A letter can be signed by no more than three authors. •Financial associations or other possible conflicts of interest must be disclosed. (Such disclosures will be published with the letters. For authors of Journal articles who are responding to letters, this information appears in the published articles.) •Include your full mailing address, telephone number, fax number, and e-mail address with your letter.
Our Web site: http://authors.nejm.org
We cannot acknowledge receipt of your letter, but we will notify you when we have made a decision about publication. Letters that do not adhere to these instructions will not be considered. Rejected letters and figures will not be returned. We are unable to provide prepublication proofs. Submission of a letter constitutes permission for the Massachusetts Medical Society, its licensees, and its assignees to use it in the Journal’s various print and electronic publications and in collections, revisions, and any other form or medium.

n engl j med 356;15 www.nejm.org april 12, 2007 1593
b o ok r e v ie w s
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
The Ghost Map: The Story of London’s Most Terrifying
Epidemic — And How It Changed Science, Cities, and the Modern World
By Steven Johnson. 299 pp., illustrated. New York, Riverhead Books, 2006. $26.95. ISBN 978-1-59448-925-9.
The Strange Case of the Broad Street Pump: John Snow
and the Mystery of Cholera
By Sandra Hempel. 321 pp., illustrated. Berkeley, University of California Press, 2007. $24.95. ISBN 978-0-520-25049-9.
London in 1854 was a virtual sea of hu-man and animal waste, and it stank. Two and
a half million people were crammed into a 30-mile circumference with no means of safe sewage dis-posal. Historically, cholera, which had been en-demic in India for millennia, was spread by peo-ple in caravans, military operations, pilgrimages, and sailing ships to cause seven great pandemics. The disease reached England for the first time during the second pandemic, in June 1831, and again during the third pandemic, in 1853 and 1854. The causative agent, Vibrio cholerae, was un-known until it was isolated in pure culture by Robert Koch in Egypt in 1883. Until John Snow, the subject of the two books under review, con-ducted his experiment, the miasma, or “bad air,” theory of the cause of cholera prevailed over the contagion theory, whose believers held that the disease was somehow transmitted from person to person, but not by water.
Snow (1813–1858) was the founding father of boots-on-the-ground epidemiology. A vegetarian and teetotaler, Snow received his apothecary and surgeon’s licenses at age 25 from the Hunterian School of Medicine and established a general practice in London. He was a witness to one of the first uses of ether in London — for a dental extraction in 1846 — and this started his highly successful career as a researcher and practitioner in anesthesiology. In 1853, he administered
chloroform to Queen Victoria for the birth of her eighth child.
Snow’s interest in cholera began when he saw patients as a physician’s apprentice during the epidemic of 1831 and 1832 in England, which killed 32,000, and was rekindled during the out-break of 1848 and 1849, which killed 52,000. A series of cases and other observations led Snow to hypothesize that the disease was spread from person to person by the oral route and most like-ly through water, in contrast to the prevailing view that it was caused by the stench arising from open sewers, kitchen sinks, and rubbish piles. His 1849 publication describing his conclusions was ignored by the medical establishment. He needed an experimentum crucis, which would be-come known as “Snow’s grand experiment,” to show that water, conveyed to a distant locality where cholera had been hitherto unknown, pro-duced the disease in those who consumed it, whereas those who did not consume it escaped.
This trial came in the summer of 1854, when cases of cholera began occurring mainly among people living along the Thames River, and Snow conceived his perfect experiment. In 1849, both water suppliers — the Lambeth Water Company and the Southwark and Vauxhall Water Company — drew their water from the most polluted part of the river, but in 1852 Lambeth moved its sup-plies north, beyond the city’s outpouring of sewage into the Thames. Snow compared the incidence of cholera in 300,000 people whose circumstanc-es were similar except that one group was sup-plied with water containing the sewage of Lon-don and the other was supplied with water free from the sewage. This involved Snow’s “shoe leather epidemiology” technique of going from house to house to determine which company sup-plied each household’s water. In the first 7 weeks, there were 1263 deaths from cholera in the 40,046 houses with water supplied by Southwark and Vauxhall, a rate of 315 per 10,000 houses. There were 98 deaths from cholera in the 26,107 houses with water supplied by Lambeth, or 37 per 10,000 houses. These figures would be hard for the med-ical community to ignore. But the signal event

The new england journal of medicine
n engl j med 356;15 www.nejm.org april 12, 20071594
was about to occur right in Snow’s neighborhood near Golden Square in Soho, where cholera was out of control — 197 residents had died within 3 days.
Snow again marked the houses where the deaths had occurred and drew “The Ghost Map” showing their distribution. The result: 61 of the 83 people who died had obtained their water from the pump on Broad Street. This evidence convinced the skeptical members of the Board of Governors of St. James Parish to close down the pump by removing its handle on September 8, a week after the outbreak had begun. It is gener-ally acknowledged that the removal of the pump handle had little or no effect on the outbreak, which had already peaked and was in decline — many of the “susceptibles” having fled the area — but it did perhaps prevent a second outbreak. (Curiously, none of the 70 employees of the Lion Brewery a few yards from the pump got cholera. Why? Having free access to malt liquor, they rare-ly, if ever, drank water.)
Snow died of a stroke at age 45, before the impact of his work was fully appreciated. His brief obituary in the Lancet cited his research on anesthetics but did not mention his epic cholera studies. However, his story and the contributions that led to his legacy — the recognition of the importance of clean water — changed the world. Countless millions of lives have been spared as a consequence. The result of his research was cer-tainly equivalent to that of Robert Koch, Louis Pasteur, Alexander Fleming, Albert Sabin, and Jonas Salk.
The two books read like novels. They describe in detail the events and the environs that enabled (and still enable) cholera epidemics, and they de-scribe and discuss the players — the disease itself, patients, officials, and Snow’s other contempo-raries — and their interactions. Florence Night-ingale, a miasmatist, is included, as are Charles Dickens, Friedrich Engels, Karl Marx, and others. Neither of the authors is a scientist, but each has done a creditable job of reporting the science. If forced to choose between the two books, I would lean toward Johnson’s because it is more focused; I found myself somewhat bewildered by the de-tails of Hempel’s book. Both authors certainly presented more than I needed to know about John Snow. Interested readers wanting to learn more may wish to examine the Web site about Snow that is maintained by the Department of Epide-
miology at the University of California, Los An-geles, located at www.ph.ucla.edu/epi/snow.html.Richard A. Finkelstein, Ph.D.University of Missouri School of Medicine Columbia, MO 65212 [email protected]
Pioneers in Surgical Gastroenterology
Edited by Walford Gillison and Henry Buchwald. 336 pp., illustrated. Harley, England, TFM Publishing, 2007. $85.
ISBN 978-1-903378-35-9.
In 1931, Harvey Cushing was an honored guest at the first International Neurological
Congress in Berne, Switzerland. During an inter-mission in the proceedings, Cushing led a coterie, in the rain, on a pilgrimage to the local cemetery, which was the final resting place of Theodor Kocher, Hans Adolf Krebs, and Hugo Kronecker. At the grave of Kocher, who had been Cushing’s mentor, Cushing laid a wreath and uttered these memorable words: “What has been accomplished does not die, but too often, alas, the personality of those who have handed the torch from one generation to another soon fades into oblivion.” Kudos are due to the editors of Pioneers in Surgical Gastroenterology for responding to Cushing’s im-plied plea for remembrance.
In 16 chapters, the book delineates the evolu-tion of surgical gastroenterology. And although many of its 21 contributors represent clinical and academic centers in the United Kingdom, cover-age of the topic is not geographically biased. Fair space is given to achievers in continental Europe, Asia, and the Americas. The stories are informa-tive not only to surgeons but to a wide range of workers concerned with afflictions of the diges-tive system. The trials and triumphs of the pio-neers in surgical gastroenterology are similar to those encountered today, and they offer solace and guidance to those who currently labor in the field.
Attached to selected chapters are detailed bi-ographies of prime movers — among them Joseph Lister, Rudolf Nissen, Theodor Billroth, Owen Wangensteen, and Mark Ravitch — which are supplemented by a comprehensive series of short-er biographical sketches at the end of the book. The text is liberally illustrated with portraits of

book reviews
n engl j med 356;15 www.nejm.org april 12, 2007 1595
surgical pioneers, the instruments they used, and diagrams of their operations. Regrettably, the lack of an index hampers the reader’s search for a particular topic.
Still, the book’s f laws are few. A future edi-tion will benefit from more careful editing and fact-checking. Queen Victoria could not possibly have granted a charter to the Royal College of Surgeons in 1800 (the credit goes to George III); the Cleveland Clinic is not located in Columbus, Ohio; and in the biographical sketches, some of the information about the Mayo family is inaccur-ate. In addition, the binding of the book is not as sturdy as it should be. But these are all mere cavils.
What can be said of the future of surgical gas-troenterology? Will there be momentous shifts in therapy, as there have been over the years in the management of peptic ulcer disease — from medical to surgical, then back to mainly medical? What is the future of surgical research? The pio-neers who are cited in this book worked mainly alone and with meager resources. Now, meaning-ful research requires large teams at mounting costs. In the current era of managed care, surgi-cal centers derive greater revenue from the perfor-mance of operations than from speculative re-
search. Hence, academic surgeons may be impelled to spend more time in the operating room and less in the laboratory. Will this trend impede sur-gical advances? Time will tell.William S. Haubrich, M.D.Scripps Clinic La Jolla, CA 92037 [email protected]
Journey into the Heart: A Tale of Pioneering Doctors and Their Race to Transform
Cardiovascular Medicine
By David Monagan, with David O. Williams. 386 pp., illustrated. New York, Gotham Books, 2007. $27.50.
ISBN 978-1-592-40265-6.
Coronary artery disease, the leading cause of death in the United States, occurs
when the blood vessels that supply the heart be-come blocked, in part, with fatty deposits. One of the procedures used to reopen these conduits is balloon angioplasty, which involves inserting a balloon-tipped catheter into a blocked coro-nary artery. The balloon is inflated, the fatty de-posits are compressed, and normal blood flow is restored to the heart muscle.
Behind the development of this seemingly simple procedure is one of the most fascinating stories in the history of cardiology. Journey into the Heart is an excellent account of the successes and failures that the pioneers of cardiac catheteriza-tion and balloon angioplasty encountered along the way. In the first few chapters, the authors pay tribute to daring investigators — Werner Forss-mann, André Cournand, Dickinson Richards, Frank Mason Sones, and Charles Dotter — and chronicle the establishment of cardiac catheter-ization in clinical medicine. The rest of the book is devoted to the life, accomplishments, and un-timely death of Andreas Roland Gruentzig, the architect of balloon angioplasty for the treatment of coronary artery disease.
I was pleased to find that this book not only contains biographical information but also ex-plores the human characteristics of Gruentzig and other pioneers in the field. The book delineates Gruentzig’s vision, passion, and unrelenting de-sire to succeed, despite the doubts of his peers, while also exploring his disappointments, uncer-
Joseph Lister, circa 1895.
Nat
iona
l Lib
rary
of M
edic
ine.

n engl j med 356;15 www.nejm.org april 12, 20071596
notices
tainties, and weaknesses. Ultimately, the reader is witness to Gruentzig’s achievement of his final goal with the clinical application of balloon an-gioplasty.
The information included in the book was obtained from various publications and, perhaps more important, from interviews with people who were part of Gruentzig’s personal life and medical career. What I most enjoyed about this book was the depth of the character analysis. Against the backdrop of a rather technical story about the development of a medical procedure, a much more intriguing drama emerges as the authors show the key players dealing with their own ambitions, envy, competitiveness, tempers, insecurities, and desire for wealth. The result is a compelling narrative written in familiar language, understandable by any reader, that also happens to be a first-rate source of information regarding cardiac catheterization and interventional coro-nary procedures.
The varied coronary interventions that are per-formed all over the world today exist primarily because of a single catalyst: Andreas Gruentzig. Journey into the Heart pays tribute to this maverick who succeeded despite considerable opposition and explains how he did it. Gruentzig, like other great pioneers in cardiology and other fields, does not appear to have entertained the possibility of failure.Hector O. Ventura, M.D.Ochsner Medical Center New Orleans, LA 70121 [email protected]
Book Reviews Copyright © 2007 Massachusetts Medical Society.
notices
Notices submitted for publication should contain a mailing address and telephone number of a contact person or depart-ment. We regret that we are unable to publish all notices received. Notices also appear on the Journal’s Web site (www.nejm.org/meetings). The listings can be viewed in their entirety or searched by location, month, or key word.
INTERNATIONAL ACADEMY OF CARDIOLOGY ANNUAL SCIENTIFIC SESSIONS 2007
The “13th World Congress on Heart Disease” will be held in Vancouver, BC, Canada, July 28–31.
Contact Dr. Asher Kimchi, International Academy of Cardi-ology, P.O. Box 17659, Beverly Hills, CA 90209; or call (310) 657-8777; or fax (310) 659-4781; or e-mail [email protected]; or see http://www.cardiologyonline.com.
NETHERLANDS INSTITUTE FOR HEALTH SCIENCESThe following courses will be offered in the Netherlands:
“Clinical Trials and Drug Risk Assessment/CE04” (Utrecht, April 23–27); “Health Services: Research and Practice/HS15” (Utrecht, April 23 and 24, May 2); “Planning and Evaluation of Screening/HS05” (Rotterdam, May 7–11); and “Cancer Epide-miology/EP13” (Amsterdam, May 21–25).
Contact the Netherlands Institute for Health Sciences, P.O. Box 2040, 3000 CA Rotterdam, the Netherlands; or call (31) 10 463 8450; or e-mail [email protected]; or see http://www.nihes.nl.
CLEVELAND CLINICThe following courses will be offered in Cleveland, unless
otherwise indicated: “Gamma Knife Radiosurgery Training” (June 4–8, Aug. 20–24, Oct. 22–26, Dec. 3–7) and “Cleveland Spine Review — Hands-On Course” (July 18–24).
Contact The Cleveland Clinic Foundation, 9500 Euclid Ave., Cleveland, OH 44195; or call (800) 223-2273, extension 53449; or fax (216) 445-9999; or e-mail [email protected]; or see http://www.clevelandclinic.org/neuroscience/professionals/cme.
AMERICAN HEADACHE SOCIETYThe following meetings will be held: “49th Annual Scien-
tific Meeting” (Chicago, June 7–10) and “Scottsdale Headache Symposium” (Scottsdale, Ariz., Nov. 1–3).
Contact American Headache Society, 19 Mantua Rd., Mount Royal, NJ 08061; or call (856) 423-0043; or fax (856) 423-0082; or e-mail [email protected]; or see http://www.ahsnet.org.
ROOSEVELT ISLAND HISTORICAL SOCIETYThe Roosevelt Island Historical Society is seeking physicians
who worked on the New York City island as students, interns, and residents to learn about their experiences. The island was known as Welfare Island until 1973.
Contact Judith Berdy, Roosevelt Island Historical Society, 531 Main St., Roosevelt Island, NY 10044; or call (212) 688-4836; or e-mail [email protected].
UNIVERSITY OF CALIFORNIA GENETICS OF ABSOLUTE PITCH STUDY
The University of California is recruiting volunteer partici-pants in a study to identify genes responsible for absolute pitch ability. See http://perfectpitch.ucsf.edu; or call (888) TUNEDIN (886-3346); or e-mail [email protected].
5TH INTERNATIONAL MEETING ON INTENSIVE CARDIAC CARE
The meeting will be held in Tel Aviv, Israel, Oct. 14–16.Contact the Secretariat, 5th International Meeting on Inten-
sive Cardiac Care, P.O. Box 574, Jerusalem 91004, Israel; or call (972) 2-6520574; or fax (972) 2-6520558; or e-mail [email protected]; or see http://www.isas.co.il/cardiac-care2007.
ALLERGY AND ASTHMA RESOURCE FOR CHOOSING BEST HEALTH PLANS
The American College of Asthma, Allergy and Immunology has developed “A Consumer Checklist for Allergy and Asthma Benefits” to advise consumers about the features to look for when they enroll in a managed care or insurance program.
The checklist is available online at http://www.acaai.org; or by calling the American College of Asthma, Allergy and Im-munology at (800) 842-7777.
the journal’s web and e-mail addresses:
For letters to the Editor: authors.nejm.orgFor information about the status of a submitted manuscript:
authors.nejm.orgTo submit a meeting notice: [email protected]
The Journal’s Web pages: www.nejm.org

images in clinical medicine
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 356;15 www.nejm.org april 12, 2007 e13
A 32-year-old healthy woman, gravida 6 with two living children, presented at our clinic for the termination of pregnancy at 18 weeks of gesta-tion. Her only previous abdominal surgeries had been two cesarean sections.
The physical examination showed a gravid uterus; the rectus sheath was deficient in the midline infraumbilical area, a finding consistent with an incisional hernia. This defect had been present since the patient’s last cesarean section 2 years earlier. A medical termination of the pregnancy was performed with the use of a 0.1% solu-tion of ethacridine lactate, which was instilled extraamniotically through a Foley catheter. The termination was uneventful, and the patient was discharged in good condition. An incisional hernia repair was subsequently performed.Copyright © 2007 Massachusetts Medical Society.
Gravid Uterus in an Incisional Hernia
Charu Chanana, M.D. Neena Malhotra, M.D
All India Institute of Medical Sciences New Delhi 110029, India [email protected]
39p6
AUTHOR
FIGURE
JOB: ISSUE:
4-CH/T
RETAKE 1st
2nd
SIZE
ICM
CASE
EMail LineH/TCombo
Revised
AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset.
Please check carefully.
REG F
FILL
TITLE3rd
Enon ARTIST:
Chanana
1
4-12-07
mleahy
35615