Embed Size (px)
Citation preview

Light and Specular Microscopy of the Cornea
Katerina Jirsova

Light and Specular Microscopy of the Cornea

Katerina Jirsova
Light and SpecularMicroscopy of the Cornea
123

Katerina JirsovaLaboratory of the Biology and Pathologyof the Eye, Charles University
Institute of Biology and Medical Genetics,First Faculty of Medicine
PragueCzech Republic
ISBN 978-3-319-48843-1 ISBN 978-3-319-48845-5 (eBook)DOI 10.1007/978-3-319-48845-5
Library of Congress Control Number: 2016955913
© Springer International Publishing AG 2017This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or partof the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations,recitation, broadcasting, reproduction on microfilms or in any other physical way, and transmissionor information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilarmethodology now known or hereafter developed.The use of general descriptive names, registered names, trademarks, service marks, etc. in thispublication does not imply, even in the absence of a specific statement, that such names are exempt fromthe relevant protective laws and regulations and therefore free for general use.The publisher, the authors and the editors are safe to assume that the advice and information in thisbook are believed to be true and accurate at the date of publication. Neither the publisher nor theauthors or the editors give a warranty, express or implied, with respect to the material contained herein orfor any errors or omissions that may have been made.
Printed on acid-free paper
This Springer imprint is published by Springer NatureThe registered company is Springer International Publishing AGThe registered company address is: Gewerbestrasse 11, 6330 Cham, Switzerland

Foreword
Corneal transplant surgery in developed countries is the most widely performedtransplant surgery today. However, there is still an estimated number of 4.9 millionbilaterally corneal blind persons worldwide, making corneal the third commonestcause of blindness. Unlike the leading cause of blindness (cataract), cornealblindness affects equally young and elderly, and it is much more difficult to solve bysurgery. Namely, if well-trained surgeons, modern operating rooms, reliable eyebank facilities and good postoperative follow-up are not available, corneal graftingwill ultimately fail. Unfortunately, most patients affected by corneal diseases areliving in developing countries with inappropriate medical care and insufficientnumber of eye banks providing good quality donor corneal tissues. In order to setup new eye banks and increase corneal distribution, it is crucial to be educated onproper donor corneal assessment. This book-atlas will provide great theoretic andpractical help to every new eye banker, and hopefully help them to increase thenumber of collected and properly selected donor corneas worldwide.
For the success of corneal transplantation and recipient’s safety, it is of outmostimportance to set mandatory standards for processing, storage and microscopicassessment of corneas issued for grafting. This book-atlas places special emphasison the light and specular microscopy of the cornea. Hundreds of photographs ofhealthy and pathological human corneas, as seen in the everyday eye bankingpractice, are extremely valuable contribution to the existing pool of knowledge ineye banking procedures.
Nowadays, with increasing number of corneal grafts performed as lamellarsurgery (in which only diseased part of the cornea is replaced by donor tissue), partof the surgery itself has shifted to the eye bank. In case of endothelial grafts, theadvantage of eye bank prepared lamellar tissue is the ability to assess endotheliumboth prior and after lamellar cut, adding to the safety of surgery itself. This bookwill help also eye bankers, which are just starting with corneal lamellar preparationin their eye banks, to safely evaluate quality of donor endothelium after lamellar
v

preparation. Assessment of the corneal endothelium, so generously presented in thisbook, has always been of greatest interest for eye bankers, since cornealendothelium does not have the ability to regenerate, and without a critical numberof endothelial cells every cornea loses its transparency. The importance ofendothelium may be even more understandable from a quote comparing it with ahuman life: endothelium is like respect—once lost, it is lost forever.
Zagreb, Croatia Iva DekarisPresident of the European Eye Bank Association
vi Foreword

Preface
The cornea is small and, due to its transparency, not commonly noticed, but it is afascinating part of the human body. Its structure and functional endothelial cellsallow the passage of light to the inner parts of the eye, thus enabling the miracle ofvision. Many diseases of the cornea lead to a loss of its function, to opacification,and to the need to replace the cornea, either completely or partially with healthytissue. This atlas primarily describes the preparation and assessment of corneas forgrafting and depicts these processes using images and photographs.
Basic information is presented concerning the anatomy and physiology of thecornea, the storage of corneas in organ culture and under hypothermic conditions,and the related assessment of the cornea using light and specular microscopy. Theatlas may serve as a guide for eye bankers along the path from tissue retrieval to thedistribution of a cornea for grafting. All of the important steps on this path,including retrieval, donor and tissue examinations, and the preparation and storageof corneas, are extensively described. The two basic approaches to corneal storage,organ culture, and hypothermia are presented and the differences between themcharacterized. This book is focused on a critical step in the preparation of thecornea, its microscopic assessment, targeted particularly on the corneal endothe-lium, and the results of which finally indicate whether or not the tissue is suitablefor grafting.
The atlas presents more than 200 photographs of normal and pathological humancorneas as they are observed in daily eye-bank practice. The main causes forexcluding a particular cornea from grafting, such as the presence of dead cells,polymegethism, pleomorphism, cornea guttata, or stromal scars, are illustrated. Thechanges occurring in corneas or corneal lamellae stored in organ culture or underhypothermic conditions are shown with the aim of assessing the suitability of thetissue for grafting. Also included are photographs of pathological corneal explants(Fuchs corneal endothelial dystrophy, posterior polymorphous corneal dystrophy,iridocorneal syndrome, keratolysis, for example) taken using light microscopy and
vii

of the diseased corneas of patients observed using specular microscopy. Theillustrative photographs combined with the educational text help readers differen-tiate between healthy and pathological corneas, assess the suitability of individualcorneas for grafting, and establish a precise corneal, particularly endothelial,diagnosis.
Prague, Czech Republic Katerina Jirsova
viii Preface

Acknowledgement
My thanks go to all my colleagues and friends who participated directly or indirectlyin the preparation of this book. My greatest debts are especially to those colleaguesfrom our eye bank who provided photographs included in the atlas section of thebook, especially to Klara Kopecka, Jaroslava Kortusova, Ivana Rybickova, DenisaNemetova and Viera Vesela. Special thanks go to Jan Bednar for preparing theimages presented throughout the book, and also to James Dutt for his invaluablelanguage supervision and critical comments. I would like to express my sinceregratitude to my colleagues from EEBA, particularly to Elisabeth Pels, who intro-duced me to the techniques needed to culture and assess corneas for grafting.
Finally, I would like to thank Karolinum Press for issuing my book Thepreparation of the cornea for grafting: History, present, and future (2013, inCzech) that became a basis of this publication.
The preparation of this book was partially supported by the Norwegian FinancialMechanism 2009–2014 and the Ministry of Education, Youth and Sports of theCzech Republic under the Project Contract No. MSMT-28477/2014, the 7F14156Project.
Katerina Jirsova
ix

Contents
1 The Cornea, Anatomy and Function . . . . . . . . . . . . . . . . . . . . . . . . . . 1Katerina Jirsova1.1 Cornea . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21.2 Corneal Epithelium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31.3 Basement Membrane of the Epithelium . . . . . . . . . . . . . . . . . . . . . 41.4 Bowman Layer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41.5 Stroma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61.6 Descemet Membrane . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71.7 Endothelium. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
1.7.1 Proliferation, Endothelial Cell Density, and StemCells of the Corneal Endothelium. . . . . . . . . . . . . . . . . . . . 9
1.8 Corneal Transparency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 111.9 Nutrient and Oxygen Supply, the Aqueous Humor . . . . . . . . . . . . 121.10 Blood and Lymphatic Vessels, Immune Privilege, Antigen
Presenting Cells of the Cornea. . . . . . . . . . . . . . . . . . . . . . . . . . . . 121.11 Innervation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
2 Processing Corneas for Grafting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Katerina Jirsova, Patricia Dahl and Jesper Hjortdal2.1 Eye Tissue Donation, Criteria, and Contraindications . . . . . . . . . . 242.2 Donor Screening, the Risk of Disease Transmission,
Tissue Typing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 252.3 Tissue Retrieval and Transport to the Eye Bank . . . . . . . . . . . . . . 282.4 Macroscopic Examination of the Donor Eye . . . . . . . . . . . . . . . . . 292.5 Donor Eye Decontamination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 312.6 Corneoscleral Disc Preparation . . . . . . . . . . . . . . . . . . . . . . . . . . . 322.7 Corneal Lamellae Preparation . . . . . . . . . . . . . . . . . . . . . . . . . . . . 332.8 Corneal Storage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
xi

3 Corneal Storage, Hypothermia, and Organ Culture . . . . . . . . . . . . . 41Katerina Jirsova, Patricia Dahl and W. John Armitage3.1 History. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
3.1.1 Hypothermic Storage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 423.1.2 Organ Culture. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
3.2 Storage Conditions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 433.2.1 Hypothermic Storage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 433.2.2 Organ Culture. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
3.3 Behavior of Corneal Cells During Storage. . . . . . . . . . . . . . . . . . . 473.3.1 Hypothermic Storage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 473.3.2 Organ Culture. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
3.4 Preparation of the Cornea Before Grafting. . . . . . . . . . . . . . . . . . . 483.4.1 Hypothermic Storage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 483.4.2 Organ Culture. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
3.5 Microbiologic Testing of the Cornea . . . . . . . . . . . . . . . . . . . . . . . 493.5.1 Hypothermic Storage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 493.5.2 Organ Culture. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
3.6 Releasing Tissue for Grafting, Graft Survival . . . . . . . . . . . . . . . . 513.6.1 Hypothermic Storage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 513.6.2 Organ Culture. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
3.7 Advantages and Disadvantages of Each Storage Method . . . . . . . . 52References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
4 Various Approaches to the Microscopic Assessmentof the Cornea, Visualization and Image Analysisof the Corneal Endothelium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59Katerina Jirsova, Jameson Clover, Christopher G. Stoegerand Gilles Thuret4.1 Slit Lamp Microscopy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 604.2 Transmitted Light Microscopy . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
4.2.1 Visualization of the Corneal Endothelium . . . . . . . . . . . . . 634.2.2 Imaging of the Endothelium. . . . . . . . . . . . . . . . . . . . . . . . 66
4.3 Specular Microscopy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 674.3.1 Imaging of the Endothelium. . . . . . . . . . . . . . . . . . . . . . . . 68
4.4 Approaches to Assessing the Corneal Endothelium . . . . . . . . . . . . 69References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
5 Light and Specular Microscopy Assessment of the Corneafor Grafting. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75Katerina Jirsova, Jameson Clover, Christopher G. Stoegerand W. John Armitage5.1 Assessment of the Corneal Endothelium . . . . . . . . . . . . . . . . . . . . 76
5.1.1 Endothelial Cell Density (ECD) . . . . . . . . . . . . . . . . . . . . . 775.1.2 Endothelial Cell Vitality and the Presence
of Dead Cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79
xii Contents

5.1.3 Dilatation of the Intercellular Spaces betweenEndothelial Cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
5.1.4 Polymegethism and Pleomorphism . . . . . . . . . . . . . . . . . . . 825.1.5 Descemet Membrane Folds . . . . . . . . . . . . . . . . . . . . . . . . 835.1.6 Cornea Guttata and Other Pathologic Changes . . . . . . . . . . 845.1.7 Intracellular Changes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 865.1.8 Presence of Vessels, Foreign Bodies, and Precipitates . . . . 87
5.2 Assessment of the Corneal Epithelium. . . . . . . . . . . . . . . . . . . . . . 885.3 Assessment of the Corneal Stroma. . . . . . . . . . . . . . . . . . . . . . . . . 895.4 Changes of the Cornea Occurring During Storage . . . . . . . . . . . . . 89
5.4.1 Light Microscopy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 895.4.2 Specular Microscopy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91
5.5 The Preparation and Assessment of Endothelial Lamellae . . . . . . . 915.6 The Changes Characterizing Corneal Pathologies Observed
in Corneal Explants and Patients . . . . . . . . . . . . . . . . . . . . . . . . . . 93References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94
6 Atlas of Light and Specular Microscopy of the Cornea. . . . . . . . . . . 101Katerina Jirsova6.1 Light Microscopy of the Normal Cornea and Limbus . . . . . . . . . . 1036.2 Light Microscopy of Donor Corneas . . . . . . . . . . . . . . . . . . . . . . . 111
6.2.1 Corneas Before Storage in Organ Culture . . . . . . . . . . . . . 1116.2.2 Corneas Before and After Storage in Organ Culture:
A Comparison . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1456.2.3 Corneas Before and After Lamellae Preparation . . . . . . . . . 165
6.3 Donor Corneas Assessed by Specular Microscopy. . . . . . . . . . . . . 1736.4 Pathological Corneal Explants (Light Microscopy)
and Patients’ Corneas (Specular Microscopy) . . . . . . . . . . . . . . . . 195Image Contributors. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 217
Contents xiii

Contributors
Prof. W. John Armitage, Ph.D. Bristol Eye Bank, NHS Blood and Transplant,and School of Clinical Sciences, Bristol Eye Hospital, University of Bristol, Bristol,UK
Jameson Clover, B.S., CEBT Lions VisionGift, Portland, OR, USA
Patricia Dahl, B.S., CEBT The Eye-Bank for Sight Restoration, Inc., New York,NY, USA
Jesper Hjortdal, MD, Ph.D. Department of Ophthalmology, Aarhus UniversityHospital, Denmark, The Netherlands
Assoc. Prof. Katerina Jirsova, Ph.D. Laboratory of the Biology and Pathologyof the Eye, Institute of Biology and Medical Genetics, First Faculty of Medicine,Charles University, Prague, Czech Republic
Christopher G. Stoeger, MBA, CEBT Lions VisionGift, Portland, OR, USA
Prof. Gilles Thuret, MD, Ph.D. Corneal Graft Biology, Engineering, and ImagingLaboratory, Faculty of Medicine, Jean Monnet University, Saint-Etienne, France
xv

Image Contributors
Katerina Jirsova, Charles University, Prague, Czech Republic.If not otherwise indicated, figures in Chaps. 1–5 and parts 6.1, 6.2, and 6.4. Mostphotographs in Chap. 6 were taken in the Ocular Tissue Bank, General UniversityHospital in Prague, between 2000 and 2011.
Sophie Acquart, Eye Bank, French Blood Center, Saint-Etienne, France.Figures 6.87–6.89.
Jameson Clover and Christopher G. Stoeger, Lions VisionGift, Portland, USA.Figures 2.1b, c, 3.1a, and if not otherwise indicated, part 6.3.
Courtesy of Danish Eye Bank, University Hospital, Aarhus, Denmark.Figure 2.3.
Andrea Gareiss-Lok, Hornhautbank, Munich, Germany.Figures 4.1b, 4.2, 4.3, 4.10c.
Jesper Hjortdal, University Hospital, Aarhus, Denmark.Figure 3.2b.
Mozhgan Rezaei Kanavi, Ocular Tissue Engineering Research Center, ShahidBeheshti, University of Medical Sciences, Tehran, Iran.Figure 6.156.
Petra Liskova, General University Hospital in Prague, Prague, Czech Republic.Figures 6.201–6.214.
V. Vinod Mootha, University of Texas Southwestern Medical Center, Dallas, TX,USA.Figure 6.161.
Kim Nielsen and Jesper Hjortdal, Danish Cornea Bank, Aarhus, Denmark.Figure 4.4a.
xvii

Agate Noer, Oslo University Hospital, Norway.Figures 1.5a, 3.2c.
Mohit Parekh, Alessandro Ruzza, and Davide Camposampiero, Veneto Eye BankFoundation, Venice, Italy.Figures 6.116, 6.120, 6.125–6.128.
Ivana Rybickova, Charles University, Prague, Czech Republic.Figures 6.129, 6.130.
Sabine Salla, Martin Hermel, and Wolfgang Plum, RWTH Aachen University,Germany.Figures 3.2d, 6.117, 6.118, 6.121–6.124.
Pavel Studeny, Kralovske Vinohrady, University Hospital, Prague, Czech Republic.Figures 6.129, 6.130.
Gilles Thuret and Zhiguo He, Biology, Engineering and Imaging of Corneal Grafts,Jean Monnet University, St-Etienne, France.Figures 1.5e, 1.7, 4.5, 4.6, 4.10b, 6.8, 6.193, 6.194.
xviii Image Contributors

Chapter 1The Cornea, Anatomy and Function
Katerina Jirsova
Abstract This chapter introduces the structure and anatomy of the cornea in orderto show the most important corneal features from an eye banker’s point of view.The aim is to describe all the corneal characteristics that may be important, par-ticularly in assessing corneal quality for grafting. The cornea is a transparentavascular tissue responsible for more than two thirds of the total refractive power ofthe eye. It is organized into three cellular layers, the epithelium, the stroma, and theendothelium, and three interfaces, the basement membrane of the epithelium,Bowman layer, and Descemet membrane. The epithelium keeps the corneal surfacesmooth and provides a barrier against external biologic agents and chemicaldamage. The stroma provides structural strength, shape, and stability. It has anatural tendency to absorb fluid from the anterior chamber, which can potentiallylead to corneal edema and decreased corneal transparency. The innermost layer ofthe cornea is the endothelium, a monolayer of hexagonal cells. Through ionicpumps and cotransporters, endothelial cells drain excess fluid out of the stroma intothe anterior chamber, thus maintaining corneal transparency. The endothelium doesnot proliferate and therefore, given the importance of its function, its damage ispotentially more serious than that to the other corneal layers. It is the mostimportant layer for maintaining corneal transparency as well as for the long-termsurvival of corneal grafts. This is the corneal layer on which eye bankers have tofocus during the preparation of a cornea for transplantation.
Keywords Cornea � Corneal structure and function � Endothelium � Cornealtransparency
K. Jirsova (&)Laboratory of the Biology and Pathology of the Eye,Institute of Biology and Medical Genetics, First Faculty of Medicine,Charles University, Prague, Czech Republice-mail: [email protected]
© Springer International Publishing AG 2017K. Jirsova, Light and Specular Microscopy of the Cornea,DOI 10.1007/978-3-319-48845-5_1
1

1.1 Cornea
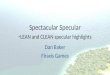
Most information about the outside world is obtained by healthy humans by meansof their visual function. The cornea serves as the gateway for light beams. Whenpassing through the cornea and lens, the light beams bend (refraction). Uponstriking the retina, their energy is converted into electrical and chemical energy, andthe resulting signals are transmitted via the optic nerve to the brain, where they areanalyzed and processed as an image. The cornea overlies the iris, pupil, and anteriorchamber. The structures that compose the anterior chamber are surrounded by thewhite opaque sclera. The cornea is an avascular, transparent, dome-shaped tissuethat refracts light through the pupil to the lens and provides a protective, imper-meable barrier against mechanical damage and infectious agents (Fig. 1.1).
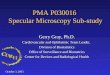
The cornea has about +43 dioptres and is the strongest lens of the eye. Its mainfunction is to allow light to pass into the inner part of the eye. The average size ofthe human cornea is 11–12 mm horizontally and 9–11 mm vertically. It isapproximately 0.5 mm thick, and the thickness increases gradually toward theperiphery. The cornea is composed of six layers: the epithelium and its basementmembrane, Bowman layer, the stroma, Descemet membrane, and the endothelium(Fig. 1.2) [1, 2]. Besides three main cell types, epithelial cells, stromal keratocytes,and endothelial cells, the cornea is endowed with a heterogeneous population ofaccessory cells involved in its homeostasis [3].
Fig. 1.1 Schematic cross-section of the human eye. Drawing by I. Helekal
2 K. Jirsova

1.2 Corneal Epithelium
The nonkeratinized, stratified squamous corneal epithelium is approximately 50 µmthick and consists of five to six layers of cells. Under two to three rows of flatpolygonal cells (see Fig. 6.1) and two to three rows of wing cells, a monolayer ofcolumnar basal cells (see Fig. 6.2) adheres to the basement membrane. Theepithelium arises from the superficial layer of the optical cup, the ectoderm [4]. Theepithelium maintains a barrier function as it protects the ocular surface againstmechanical damage and against infectious agents entering the inner parts of the eye.The epithelium is covered by a tear film that protects the ocular surface fromdehydration, provides smoothness, helps supply the cornea with oxygen andnutrients, and serves as a biodefense system. Only basal cells possess a proliferativecapacity; they differentiate into wing cells, which further migrate to the ocularsurface and differentiate into superficial flat cells [2, 5, 6]. The epithelium turns overapproximately every seven days by sloughing the outer surface cells into the tearfilm [7]. The corneal epithelium is preferentially renewed based on the XYZ theory,
Fig. 1.2 Transverse section of the human cornea. The cornea is composed of six layers: theepithelium, the basement membrane, Bowman layer, the stroma with keratocytes whose density ishigher in the anterior part of the cornea compared to the posterior part, Descemet membrane, andthe endothelium. Drawing by I. Helekal
1 The Cornea, Anatomy and Function 3

where X represents the proliferation and stratification of limbal basal cells, Y is thecentripetal migration of basal cells, and Z is the desquamation of superficial cornealcells [8]; in part, the corneal epithelium may be maintained by the proliferation ofits own basal cells [5]. Limbal stem cells are present in radial fibrovascular ridgescalled the palisades of Vogt, located in the limbus, an interface between the corneaand the sclera (see Figs. 6.10, 6.11 and 6.12). Limbal stem cells divide and give riseto transient amplifying cells that move centripetally to the center of the cornea in thebasal layer of the corneal epithelium. Then, differentiated daughter cells moveanteriorly to replenish cells in the overlying layers [9, 10].
1.3 Basement Membrane of the Epithelium
The basement membrane of the epithelium (BME) is about 40–60 nm thick andconsists of two distinct layers discernible by electron microscopy: a pale layer (thelamina lucida) and a dense layer (the lamina densa) (Fig. 1.3).
BME components are produced by the epithelial cells. The major components ofthe BME are type IV collagen (chains a1–a6) and laminins 1 and 5, but otherstructural compounds crucial for stability, including collagens VII, XII and XVIII,fibronectin, fibrin, and nidogen, are also present [11–14]. Collagen IV is a structuralprotein, while fibrillar collagen VII is involved in anchoring the epithelial cells tothe basement membrane. Collagens IV and XII, occurring in the BME but absent inthe basement membrane of the limbus, provide an interface between the cornea andconjunctiva [11, 12]. Fibronectin is important for healing after acute injury of thecorneal epithelium. The BME influences adhesion, migration, differentiation, andsignal transduction, maintains the polarity of the epithelial cells, and serves as areservoir of growth factors [15]. After damage, if epithelial cells are preserved, theBME regenerates.
1.4 Bowman Layer
Bowman layer is an acellular membrane-like zone about eight to twelve µm thickpositioned between the BME and the anterior stroma. It is produced by stromalkeratocytes and it consists of extracellular matrix (ECM), mostly proteoglycans andcollagens I, III, V, and VII, which are randomly dispersed throughout an amorphousmatrix (Fig. 1.3). Bowman layer is penetrated by unmyelinated nerve axons, andsome authors consider it to be the anterior portion of the corneal stroma [2, 16–20].
The functional role of Bowman layer is not completely known, but it is believedto serve as a barrier that protects the corneal stroma from traumatic injury. It isinvolved in the separation of the epithelium and stroma and may be formed as aresult of cytokine-mediated interactions occurring between epithelial cells andkeratocytes [20]. It has been shown that it facilitates rapid stromal wound healing
4 K. Jirsova

and the restoration of epithelial innervation after photorefractive keratectomy [21].Bowman layer becomes thinner with age, which can be explained by naturallyoccurring gradual cross-linking of collagens or by collagen degradation [22].Stromal collagen fibrils penetrating into Bowman layer increase its strength andstabilize the shape of the outer part of the cornea [23]. It does not regenerate afterinjury but may be substituted very slowly and become structurally different fromthe original structure [2, 20].
Fig. 1.3 Cross-sectional anatomy of the human cornea: photograph of a human cornea (left) andthe corresponding acellular structures of the extracellular matrix, schematic (right). Theconnections between the basement membrane of the epithelium and the underlying Bowmanlayer, the lamellar arrangement of the stroma, and the structure of Descemet membrane are shown.The collagen present in particular layers is indicated by roman numerals. Drawing by I. Helekal
1 The Cornea, Anatomy and Function 5

1.5 Stroma
The stroma is the strongest layer of the cornea, occupying about 90 % of itsthickness. It consists primarily of ECM; up to 15 % of its volume is occupied bystromal cells, keratocytes. The density of keratocytes is highest in the anteriorstroma, reaching about 42,500/mm3; the density then decreases significantly toabout 24,000/mm3 in the posterior part of the stroma [24, 25]. The main function ofthe stroma is the maintenance of corneal shape, physiologic hydration, and thustransparency [25–27]. The most important structural components of the stroma (seeFig. 6.4) are collagens, which constitute 71 % of the dry weight of the cornea [28].
The most abundant of these collagens are collagen I, which gives the tissuetensile strength; collagen V, which through its interaction with collagen I affects thethickness of the fibrils; and collagen III, the amount of which increases with age,healing, and inflammation [17, 29]. Collagen molecules self-assemble into fibrilsand subsequently into collagen fibrils, which are highly uniform in diameter,ranging between 23 and 33 nm. This relatively small diameter and the regulardistance between the collagen fibrils (20–41 nm) are major determinants of cornealtransparency (the diameter of the fibrils in the opaque sclera is between 25 and300 nm) [30–33]. Collagen VI produces corneal microfilamentar structures and bybinding to collagen fibrils may contribute to stabilization and the maintenance of aconstant distance between them [34]. The collagen fibrils of the stroma form about300 lamellae oriented parallel to the ocular surface. Fibrils in adjacent lamellae lieat an angle of 0–90° (Fig. 1.3). Some lamellae extend from the stroma to Bowmanlayer and contribute to the stabilization of the anterior part of the cornea [35].
The spacing and orientation of the collagen fibrils in the stroma are regulated bytheir noncovalent binding to another component of the ECM: proteoglycans.Corneal proteoglycans consist of core proteins to which polysaccharide chainscomposed of disaccharide units are attached; these polysaccharides are termedglycosaminoglycans (GAGs). The main stromal proteoglycans include lumican,keratocan, and mimecan, which have keratan sulfate GAGs attached to theirrespective protein cores, and decorin and biglycan, which have dermatan sulfate andchondroitin sulfate GAGs [36, 37]. GAGs are negatively charged and have theability to absorb and retain large amounts of water and thus maintain physiologicdistances between collagen fibrils as well as corneal hydration [32, 38]. The turnoverof stromal collagens is very slow; their degradation is ensured enzymatically bymatrix metalloproteinases, particularly by collagenases and gelatinases [39].
Keratocytes have a compact cell body and are interconnected in a three-dimensional network with numerous cytoplasmic lamellapodia (see Fig. 6.5). Theyproduce individual components of the ECM and under physiologic conditions arerenewed very slowly. In response to damage, stromal keratocytes are activated, andtheir phenotype (CD34 transmembrane sialomucin and 3G5 ganglioside expres-sion) (Fig. 1.4) is transformed into the phenotype of contractile myofibroblasts(a-SMA smooth muscle actin, homeobox gene visual system VSX1 expression),which significantly contributes to the healing of the stroma [40, 41].
6 K. Jirsova

1.6 Descemet Membrane
Descemet membrane (DM) is a basement membrane of the corneal endothelium. Itis stratified into two morphologically distinct parts: an approximately 3 µm thickanterior banded layer, which is formed during fetal development, and a homoge-neous posterior nonbanded layer that is produced throughout life and whosethickness ranges up to eight to ten µm [42–45].
The anterior banded zone is a highly organized structure composed mostly ofcollagen VIII [46]. This layer is arranged in bands (in cross-section), and when it iscut tangentially a hexagonal grid is apparent (Fig. 1.3) [45, 47]. It is possible thatthis hexagonal network provides structural support against the pressure of theaqueous humor. Other essential components, mainly collagen IV, fibronectin, andlaminin as well as collagens V, VI, XVIII and thrombospondin, are presentthroughout DM [11, 14, 18, 28, 48]. DM is resistant to matrix metalloproteinasesbut is sensitive to mechanical damage [49]; it does not regenerate.
Hassall-Henle bodies (warts) are 30–80 µm long protrusions of DM into theendothelial layer and are present at the periphery of the cornea, depending on age[50]. At the corneal periphery DM is bordered by the Schwalbe line, which indi-cates the interface between the endothelium and the trabecular meshwork [51].
Fig. 1.4 Corneal stroma. Keratocytes are visualized by the detection of CD34 transmembranesialomucin using indirect fluorescent immunohistochemistry (green fluorescent signal; the DNA isvisualized by propidium iodide) and by enzymatic immunohistochemistry (counterstained withhematoxylin). Scale bar = 10 lm
1 The Cornea, Anatomy and Function 7

1.7 Endothelium
The corneal endothelium is composed of a monolayer of polygonal, mostlyhexagonal cells that lie on DM (see Figs. 6.6, 6.7 and 6.8), and their apical side isbathed by the aqueous humor. The endothelium can be visualized by confocal orspecular microscopy, by phase contrast light microscopy, histologically, orimmunohistochemically (Fig. 1.5).
The average size of endothelial cells (ECs) is about 20 µm, their surface arearanges from 100 to 250 lm2, and their thickness from five to six µm. The humancornea contains about 400,000 ECs [50, 52].
The development of the endothelium occurs around the fourth week ofintrauterine embryonic development [53], and endothelial progenitor cells originatefrom the neural crest with the participation of mesenchymal cells of the mesoderm[54, 55]. For the development of the endothelium, the presence of a wide range oftranscription factors, such as FOXC1, Pitx2, and PAX6, is necessary [56, 57].
The ECs are interconnected at their apical side by tight junctions (characterizedby the expression of the integral membrane protein occludin and tight junctionprotein ZO-1) and in their basal side by focal tight joints (macula occludens) andgap junctions (connexin 43). Adhesive junctions contain corneal neuronal-specificcadherin (N-cadherin), epithelial cadherin (E-cadherin), vascular endothelial cad-herin (VE-cadherin), and b- and p120-catenin. The contact between adjacent ECs isnot as occlusive as in the epithelium, and the cell junctions are leaky, thus allowingfluid passage [58–60].
Endothelial cells exhibit large circular nuclei, their cytoplasm is rich in orga-nelles, particularly mitochondria, and their cell membrane contains numerouspinocytary vesicles. Microvilli, located particularly in peripheral ECs, increase thearea exposed to the aqueous humor. Almost no microvilli have been detected in thecentral endothelium [50, 52]. ECs constitutively express various genes involved in
Fig. 1.5 The human corneal endothelium visualized using different techniques. Polygonal cellshape seen using a confocal microscopy, b specular microscopy, c phase contrast lightmicroscopy, d histology: trypan blue and alizarin staining, e immunohistochemistry (ZO-1 protein,green signal, DNA visualized by Hoechst 33342, blue color). Scale bar = 10 lm. (a Courtesy ofAgate Noer, Oslo University Hospital, Norway; e Courtesy of Gilles Thuret and Zhiguo He, JeanMonnet University, St-Etienne, France)
8 K. Jirsova

maintaining stromal dehydration, corneal transparency, metabolic activity, andsignal transduction; 34 % of the transcripts exhibit specificity for the endothelium.The most abundantly expressed molecules are prostaglandin D2 synthase,lactate-dehydrogenase-A, cytochrome c oxidase subunit II, adenosine triphosphatesynthase F0 subunit 6, and carbonic anhydrase XII [61, 62]. Among surfaceadhesion molecules, neural cell adhesion molecule (NCAM) and intercellularadhesion molecule-1 (ICAM-1) are present under physiologic conditions [63].
The main function of the endothelium is to maintain adequate hydration of thecornea, thus ensuring its transparency [64]. The corneal endothelium is themetabolically most active layer of the cornea but also the most sensitive to potentialdamage.
The relatively complex development of the mammalian endothelium may bereflected in the relatively prominent phenotypic heterogeneity of these cells. Theterm endothelium is a misnomer [65], probably based on the similarities betweenthe posterior layer of the cornea and the vascular lining. Fine and colleaguespointed out that the localization of the corneal endothelium is similar to that of themesothelium lining the pleura, the peritoneum, and the pericardium [66].
The influence of neuronal cells on the development of the endothelium isreflected by the expression of neuron-specific enolase, S100 protein, neurofila-ments, and NCAM [63, 67]. The endothelium also expresses markers typical ofepithelial cells, keratins 8 and 18 [68, 69]. In addition, the corneal endotheliumexpresses vimentin [70] and some proteins typical of mesothelial cells [71]. Thetransformation of corneal ECs into other cell types, mostly mesenchymal [72] orepithelial [73, 74], is quite often induced by various pathologic conditions,including posterior polymorphous corneal dystrophy, Fuchs endothelial cornealdystrophy, or congenital hereditary endothelial dystrophy [75].
1.7.1 Proliferation, Endothelial Cell Density, and Stem Cellsof the Corneal Endothelium
Generally, after birth the human corneal endothelium does not proliferate. Mitoticfigures or the incorporation of tritiated thymidine indicating a previous S phase ofthe cell cycle has been observed only during the prenatal period or during the repairof the adult endothelium [76, 77].
The corneal endothelium does possess a proliferative capacity, but ECs areblocked in the G1 phase of the cell cycle [78]. This is mediated by the presence oftransforming growth factor beta (TGF-b) in the aqueous humor and particularly bycell contact inhibition based on the high expression of cyclin-dependent kinaseinhibitors (e.g., p27kip1) that prevent the cells from entering the S phase of the cellcycle [79–82]. The nearly absent replication activity of ECs corresponds with thelength of their telomeres [83]. The proliferative capacity of the endothelium can berestored under certain conditions, e.g., by the loss of contact inhibition during
1 The Cornea, Anatomy and Function 9

cultivation [80]. Generally, higher proliferative activity can be seen in youngerindividuals [84–86].
The mean endothelial cell density (ECD) is about 6000/mm2, but shortly afterbirth the ECD decreases significantly to 4000/mm2 [87, 88]. The timing of thisendothelial loss correlates with a two-year period during which the cornea increasesto its final size, i.e., to an average of 11.75 mm in diameter [89]. At the age of four tofive, the average ECD is about 3500 cells/mm2 [90]. Subsequently, the number ofECs declines by about 0.6 % per year [89, 91]. At age 85 the endothelium has onaverage 2300 cells/mm2 [92], while the mean ECD commonly acceptable for pen-etrating keratoplasty (the entire cornea is replaced) is 2000–2500 cells/mm2 [93, 94].
The ECD at the corneal periphery is higher compared to the central and pericentralparts of the cornea [95]. The percentage of polyploid or multinucleated giant cellsarising by cell fusion increases with damage to the endothelium andwith age [96–98].
The endothelium regenerates only minimally and is renewed by repair. An areawithout cells is restored by the shifting of adjacent cells to fill the denuded DM andby cell spreading (expanding and thinning) (Fig. 1.6) [99–101]. Endothelial cellsdie through necrosis or apoptosis, which can be induced by various pathologicconditions [102].
Endothelial stem cells have been proposed to be located in the transition zonebetween the outer edge of the corneal endothelium and the trabecular meshwork[103, 104]. It was found that the cells just beneath the Schwalbe line (i.e., thetransition zone between the endothelium and the trabecular meshwork) form adiscontinuous cord oriented circumferentially. This area, called the insert, wassuggested to be the putative location for both endothelial and trabecular meshworkstem cells [105, 106]. Recently, clusters of human corneal ECs expressing stem celland proliferative markers (nestin, telomerase, Ki67) were found at the “veryperiphery” of the cornea, closely adjacent to Hassall-Henle bodies, (see Fig. 6.8).These cells exhibit more features of precursor cells than of progenitor cells [107].Moreover, based on a sphere-forming assay, endothelial cell precursors have beenisolated and even used for the replacement of ECs in a rabbit model [108, 109].
Fig. 1.6 The repair of the corneal endothelium in organ culture. Phase contrast micrographs of theendothelium before and after the induction of a lesion in the central part of the cornea: a beforelesioning, b dead cells present immediately after lesion induction, c 7 days postlesion with no deadcells but cell debris is present, d the endothelium is completely repaired 14 days after induction ofthe lesion. Dead cells are stained by trypan blue. Scale bar = 50 lm
10 K. Jirsova

1.8 Corneal Transparency
Corneal transparency is determined by the balance between the two fundamentalmechanisms maintaining the volume of water in the cornea. The passive transportof water and solutes into the stroma is determined by the size and regulararrangement of collagen fibrils and particularly by the presence of negativelycharged GAGs, which absorb water [110]. Water flow into the cornea is controlledby the pump of ECs that ejects water back into the aqueous humor. The physiologichydration of the cornea is 78 %. If the endothelial pump function is decreased orlost, the corneal stroma swells (a larger amount of water binds to the GAGs). Withincreased hydration, stromal edema develops (the increased distance between col-lagen fibrils leads to a deterioration in their arrangement), and the cornea loses itstransparency (Fig. 1.7), resulting in the eventual loss of visual acuity [1, 26].
The tight arrangement of the hexagonal cells of the endothelial mosaic acts as apassive permeable membrane and counteracts the passive entry of water into thestroma. The entry of water into the stroma is maintained particularly by Na+/K+-ATPase but also by bicarbonate-dependent Mg2+-ATPase, both of which are pre-sent mainly on the basolateral part of plasma membranes [64, 111–113]. Theendothelium primarily pumps water from the stroma, and the cells actively transportions, including sodium and bicarbonate, into the fluid chamber. In the outflow ofwater, the selective water channel aquaporin 1 is also involved [114]. If extensiveendothelial damage occurs or if the ECD decreases under 250–500 cells/mm2,corneal decompensation occurs [94, 115, 116]. This can be explained by a decreaseof “pump sites” caused by the decrease of the ECD itself as well as the enlargementof the ECs or the thinning of the endothelial layer between the cells.
Light scattering in the cornea is reduced by the presence within the epithelialcells and keratocytes of crystalline proteins (water-soluble structural proteins thatmatch the refractive index of the cells to that of their surroundings, thus minimizinglight scatter) [117, 118].
Fig. 1.7 Human corneas expressing various degrees of transparency: a a clear, fully transparentcornea, b a cloudy cornea with posterior folds and arcus senillis, c a cornea with central opacity(Courtesy of Gilles Thuret and Zhiguo He, Jean Monnet University, St-Etienne, France)
1 The Cornea, Anatomy and Function 11

1.9 Nutrient and Oxygen Supply, the Aqueous Humor
The highly metabolically active endothelial and epithelial cells are supplied withglucose by diffusion from the aqueous humor. In the absence of blood vessels in thecornea, this supply is a key factor for corneal nutrition [119]. Under aerobic con-ditions, glucose is metabolized by glycolysis to generate adenosine triphosphate.
Most oxygen diffuses into the cornea from the air through the tear film and allcorneal layers up to the endothelium. A small amount of oxygen is transported intothe cornea from the limbal circulation and from the aqueous humor [120]. Thedisruption of the oxygen supply to the cornea can lead to hypoxia and stromaledema. During sleep, when the eyelids are closed, the oxygen supply to the corneais greatly reduced and corneal metabolism is thereby shifted from aerobic toanaerobic. At this point glucose metabolizes to lactate, which can accumulateduring sleep [1, 121].
The corneal endothelium is bathed from inside the eye by the aqueous humor,which is secreted by the ciliary body. The main function of the aqueous humor is tosupply nutrients to the cornea and to remove metabolic wastes. It contributes to themaintenance of intraocular pressure and thus to maintaining the convex shape of thecornea. It is also responsible for the maintenance of the optical properties of the eye.It contains nearly 700 proteins, including structural, immunomodulatory, andantioxidant proteins [122, 123]. The osmolality of the aqueous humor is304 mOsm/kg, while the pH is 7.38 [124].
1.10 Blood and Lymphatic Vessels, Immune Privilege,Antigen Presenting Cells of the Cornea
Blood vessels supplying the cornea with oxygen and nutrients arise from the ciliaryarteries, branches of the ophthalmic artery. They subsequently divide and terminatein the pericorneal plexus of the limbus (see Fig. 6.9). Similarly, the cornea iscircumferentially surrounded by lymphatic vessels located in the limbus. Thismeans that the healthy cornea is devoid of lymphatic and blood vessels, thussuppressing both the afferent (lymphatic) and efferent (vascular) arms of theimmune response and contributing to its immune privilege, which leads to thelonger survival of a corneal graft compared to that of grafts transplanted outside ofthis privileged site [125–128]. Another key factor in maintaining immune privilegeis anterior chamber–associated immune deviation (ACAID), which is characterizedby the antigen-specific down-regulation of delayed-type hypersensitivity responses.The other factors involved in maintaining immune privilege are the expression ofthe Fas ligand and programmed death ligand 1 by corneal cells, which induce theapoptosis of activated T cells at the graft–host interface, the presence of TGF-b andother immunomodulatory agents in the aqueous humor, and the activation of reg-ulatory T cells, which prevent the induction of an immune response [129–132].
12 K. Jirsova

Immunocompetent cells present in the normal cornea include antigen-presentingcells (APCs), Langerhans cells (members of the dendritic cell family) in theepithelium, and dendritic cells and macrophages in the stroma [133–135]. CornealAPCs derived from the myeloid lineage, are present at different stages of maturationwith immature cells prevailing in the central part of the cornea, and express aspecific phenotype based on their functional plasticity in immune regulation [133,134, 136, 137]. The number of APCs increases from the center to the periphery ofthe cornea (Fig. 1.8). During inflammation and after corneal transplantation, amajority of resident APCs undergo maturation, and their number also increasesowing to newly recruited host APCs [138, 139]. The number of donor APCs maybe influenced by the targeted preparation of corneal grafts; for example, prolongedcultivation leads to a decrease in the number of APCs [140–142]. It has alreadybeen shown that the prolonged storage of corneas in organ culture decreases theincidence of endothelial immune reactions and extends graft survival [143, 144].
The rejection of corneal allografts is predominantly mediated by allospecificCD4+ T cells that are activated through the indirect pathway of antigen presenta-tion by host APCs; however, controversy exists about the involvement of the directpathway of antigen presentation and the participation of CD8+ T cells, especially inhigh-risk corneal graft recipients characterized by corneal neovascularization and/orprevious graft rejection [145, 146]. The survival rate of corneal grafts differsconsiderably in low-risk and high-risk settings, since high-risk recipients lose theadvantage of immune privilege [131, 146].
Fig. 1.8 The increase in the number of antigen-presenting cells from the central cornea (Cc)toward the pericentral cornea (Cpc), peripheral cornea (Cp), limbus (Lim), and conjunctiva (Conj).APCs are visualized by anti-HLA-DR antibody, nuclei are counterstained by propidium iodide.Scale bar = 10 lm
1 The Cornea, Anatomy and Function 13

1.11 Innervation
The cornea is primarily innervated by sensory nerve fibers via the ophthalmicdivision of the trigeminal nerve by way of long and short ciliary nerves and bysympathetic autonomic nerve fibers in a minority.
Nerve fibers enter the cornea radially from the periphery of the anterior stroma andpenetrate through Bowman layer and the BME into the epithelium, where they form aterminal subepithelial plexus and terminate in the wing cell level (see Fig. 6.3) [19].Besides light microscopy, the corneal nerves are detectable by slit lamp and confocalmicroscopy aswell as immunohistochemically (Fig. 1.9). The density of nerves in thesub-basal epithelium is about 7000–10,500 lm/mm2 [24, 147], which is 300–400times higher than that in the skin. Epithelial lesionsmay result in the exposure of nerveendings and severe ocular pain. The main neurotransmitters involved in cornealinnervation are neurokinin, substance P, calcitonin gene-related peptide, vasoactivepeptide, catecholamines, and acetylcholine [148, 149].
Acknowledgments The author thanks Professor Thomas Fuchsluger, University HospitalErlangen, Germany, and Professor Keith Meek, Cardiff University, UK, for their critical reading ofthis chapter.
References
1. Mishima S. Clinical investigations on the corneal endothelium-XXXVIII Edward JacksonMemorial Lecture. Am J Ophthalmol. 1982;93:1–29.
2. Nishida T, Saika S. Cornea. In: Krachmer JH, Mannis MJ, Holland EJ, editors. Cornea. 3rded. St. Louis, MO: Elsevier Mosby; 2011. p. 3–24.
3. Shimmura S, Kawakita T. Accessory cell populations in the cornea. Ocul Surf. 2006;4:74–80.
Fig. 1.9 Corneal nerve fibers. Visualization using anti-NCAM antibody. Flat mount of theanterior lamellae showing a the subepithelial area, b the deeper anterior part of the stroma. Scalebar = 10 lm
14 K. Jirsova

4. Barishak YR. Embryology of the eye and its adnexae. Dev Ophthalmol. 1992;24:1–142.5. Chang CY, Green CR, McGhee CN, Sherwin T. Acute wound healing in the human central
corneal epithelium appears to be independent of limbal stem cell influence. InvestOphthalmol Vis Sci. 2008;49:5279–86.
6. Dua HS, Miri A, Alomar T, Yeung AM, Said DG. The role of limbal stem cells in cornealepithelial maintenance: testing the dogma. Ophthalmology. 2009;116:856–63.
7. Hanna C, Bicknell DS, O’Brien JE. Cell turnover in the adult human eye. Arch Ophthalmol.1961;65:695–8.
8. Thoft RA, Friend J. The X, Y, Z hypothesis of corneal epithelial maintenance. InvestOphthalmol Vis Sci. 1983;24:1442–3.
9. Davanger M, Evensen A. Role of the pericorneal papillary structure in renewal of cornealepithelium. Nature. 1971;229:560-1.
10. Lehrer MS, Sun TT, Lavker RM. Strategies of epithelial repair: modulation of stem cell andtransit amplifying cell proliferation. J Cell Sci. 1998;111(Pt 19):2867–75.
11. Ljubimov AV, Burgeson RE, Butkowski RJ, Michael AF, Sun TT, Kenney MC. Humancorneal basement membrane heterogeneity: topographical differences in the expression oftype IV collagen and laminin isoforms. Lab Invest. 1995;72:461–73.
12. Wessel H, Anderson S, Fite D, Halvas E, Hempel J, SundarRaj N. Type XII collagencontributes to diversities in human corneal and limbal extracellular matrices. InvestOphthalmol Vis Sci. 1997;38:2408–22.
13. Lin HC, Chang JH, Jain S, Gabison EE, Kure T, Kato T, et al. Matrilysin cleavage of cornealcollagen type XVIII NC1 domain and generation of a 28-kDa fragment. Invest OphthalmolVis Sci. 2001;42:2517–24.
14. Maatta M, Heljasvaara R, Sormunen R, Pihlajaniemi T, Autio-Harmainen H, Tervo T.Differential expression of collagen types XVIII/endostatin and XV in normal, keratoconus,and scarred human corneas. Cornea. 2006;25:341–9.
15. LeBleu VS, Macdonald B, Kalluri R. Structure and function of basement membranes. ExpBiol Med (Maywood). 2007;232:1121–9.
16. Komai Y, Ushiki T. The three-dimensional organization of collagen fibrils in the humancornea and sclera. Invest Ophthalmol Vis Sci. 2007;32:2244–58.
17. Marshall GE, Konstas AG, Lee WR. Immunogold fine structural localization of extracellularmatrix components in aged human cornea. I. Types I-IV collagen and laminin. Graefes ArchClin Exp Ophthalmol. 1991;229:157–63.
18. Marshall GE, Konstas AG, Lee WR. Immunogold fine structural localization of extracellularmatrix components in aged human cornea. II. Collagen types V and VI. Graefes Arch ClinExp Ophthalmol. 1991;229:164–71.
19. Beuerman RW, Pedroza L. Ultrastructure of the human cornea. Microsc Res Tech.1996;33:320–35.
20. Wilson SE, Hong JW. Bowman’s layer structure and function: critical or dispensable tocorneal function? A hypothesis. Cornea. 2000;19:417–20.
21. Lagali N, Germundsson J, Fagerholm P. The role of Bowman’s layer in corneal regenerationafter phototherapeutic keratectomy: a prospective study using in vivo confocal microscopy.Invest Ophthalmol Vis Sci. 2009;50:4192– 8.
22. Germundsson J, Karanis G, Fagerholm P, Lagali N. Age-related thinning of Bowman’s layerin the human cornea in vivo. Invest Ophthalmol Vis Sci. 2013;54:6143–9.
23. Kobayashi A, Yokogawa H, Sugiyama K. In vivo laser confocal microscopy of Bowman’slayer of the cornea. Ophthalmology. 2006;113:2203–8.
24. Patel SV, Erie JC, McLaren JW, Bourne WM. Keratocyte density and recovery of subbasalnerves after penetrating keratoplasty and in late endothelial failure. Arch Ophthalmol.2007;125:1693–8.
25. Meek KM, Knupp C. Corneal structure and transparency. Prog Retin Eye Res. 2015;49:1–16.
26. Maurice DM. The structure and transparency of the cornea. J Physiol. 1957;136:263–86.
1 The Cornea, Anatomy and Function 15

27. Meek KM, Leonard DW, Connon CJ, Dennis S, Khan S. Transparency, swelling andscarring in the corneal stroma. Eye (Lond). 2003;17:927–36.
28. Newsome DA, Foidart JM, Hassell JR, Krachmer JH, Rodrigues MM, Katz SI. Detection ofspecific collagen types in normal and keratoconus corneas. Invest Ophthalmol Vis Sci.1981;20:738–50.
29. Newsome DA, Gross J, Hassell JR. Human corneal stroma contains three distinct collagens.Invest Ophthalmol Vis Sci. 1982;22:376–81.
30. Meek KM, Fullwood NJ. Corneal and scleral collagens–a microscopist’s perspective.Micron. 2001;32:261–72.
31. Han M, Zickler L, Giese G, Walter M, Loesel FH, Bille JF. Second-harmonic imaging ofcornea after intrastromal femtosecond laser ablation. J Biomed Opt. 2004;9:760–6.
32. Muller LJ, Pels E, Schurmans LR, Vrensen GF. A new three-dimensional model of theorganization of proteoglycans and collagen fibrils in the human corneal stroma. Exp EyeRes. 2004;78:493–501.
33. Watson PG, Young RD. Scleral structure, organisation and disease. A review. Exp Eye Res.2004;78:609–23.
34. Hirano K, Kobayashi M, Kobayashi K, Hoshino T, Awaya S. Experimental formation of100 nm periodic fibrils in the mouse corneal stroma and trabecular meshwork. InvestOphthalmol Vis Sci. 1989;30:869–74.
35. Bron AJ.The architecture of the corneal stroma. Br J Ophthalmol. 2001;85:379–81.36. Funderburgh JL, Hevelone ND, Roth MR, Funderburgh ML, Rodrigues MR, Nirankari VS,
Conrad GW. Decorin and biglycan of normal and pathologic human corneas. InvestOphthalmol Vis Sci. 1998;39:1957–64.
37. Soriano ES, Campos MS, Michelacci YM. Effect of epithelial debridement on glycosamino-glycan synthesis by human corneal explants. Clin Chim Acta. 2000;295;41–62.
38. Scott JE. How rational histochemistry produced order out of chaos in the “amorphousground substance” (with a little help from biochemistry, biophysics etc.). Eur J Histochem.1998;42 Spec No:29–34.
39. Sivak JM, Fini ME. MMPs in the eye: emerging roles for matrix metalloproteinases in ocularphysiology. Prog Retin Eye Res. 2002;21:1–14.
40. Stramer BM, Kwok MG, Farthing-Nayak PJ, Jung JC, Fini ME, Nayak RC. Monoclonalantibody (3G5)-defined ganglioside: cell surface marker of corneal keratocytes. InvestOphthalmol Vis Sci. 2004;45:807–12.
41. Barbaro V, Di Iorio E, Ferrari S, Bisceglia L, Ruzza A, De Luca M, Pellegrini G. Expressionof VSX1 in human corneal keratocytes during differentiation into myofibroblasts in responseto wound healing. Invest Ophthalmol Vis Sci. 2006;47:5243–50.
42. Jakus MA. Studies on the cornea. II. The fine structure of Descement’s membrane. J BiophysBiochem Cytol. 1956;2(4 Suppl):243–52.
43. Wulle KG. Electron microscopy of the fetal development of the corneal endothelium andDescemet’s membrane of the human eye. Invest Ophthalmol. 1972;11:897–904.
44. Waring GO, Laibson PR, Rodrigues M. Clinical and pathologic alterations of Descemet’smembrane: with emphasis on endothelial metaplasia. Surv Ophthalmol. 1974;18:325–68.
45. Murphy C, Alvarado J, Juster R. Prenatal and postnatal growth of the human Descemet’smembrane. Invest Ophthalmol Vis Sci. 1984;25:1402–15.
46. Kenney MC, Nesburn AB, Burgeson RE, Butkowski RJ, Ljubimov AV. Abnormalities ofthe extracellular matrix in keratoconus corneas. Cornea. 1997;16:345–51.
47. Sawada H, Konomi H, Hirosawa K. Characterization of the collagen in the hexagonal latticeof Descemet’s membrane: its relation to type VIII collagen. J Cell Biol. 1990;110:219–27.
48. Tamura Y, Konomi H, Sawada H, Takashima S, Nakajima A. Tissue distribution of typeVIII collagen in human adult and fetal eyes. Invest Ophthalmol Vis Sci. 1991;32:2636–44.
49. Sawada H. The fine structure of the bovine Descemet’s membrane with special reference tobiochemical nature. Cell Tissue Res. 1982;226:241–55.
50. Svedbergh B, Bill A. Scanning electron microscopic studies of the corneal endothelium inman and monkeys. Acta Ophthalmol (Copenh). 1972;50:321–36.
16 K. Jirsova

51. Klintworth GK, Cummings TJ. Normal eye and ocular adnexa. In: Cummings TJ, Mills SE,editors. Histology for pathologists. 3rd ed. Philadelphia: Lippincott Williams & Wilkins;2007. p 349–52.
52. Waring GO 3rd, Bourne WM, Edelhauser HF, Kenyon KR. The corneal endothelium.Normal and pathologic structure and function. Ophthalmology. 1982;89:531–90.
53. Hay ED. Development of the vertebrate cornea. Int Rev Cytol. 1980;63:263–322.54. Gage PJ, Rhoades W, Prucka SK, Hjalt T. Fate maps of neural crest and mesoderm in the
mammalian eye. Invest Ophthalmol Vis Sci. 2005;46:4200–8.55. Sowden JC. Molecular and developmental mechanisms of anterior segment dysgenesis. Eye
(Lond). 2007;21:1310–18.56. Cvekl A, Tamm ER. Anterior eye development and ocular mesenchyme: new insights from
mouse models and human diseases. Bioessays. 2004;26:374–86.57. Gage PJ, Qian M, Wu D, Rosenberg KI. The canonical Wnt signaling antagonist DKK2 is
an essential effector of PITX2 function during normal eye development. Dev Biol.2008;317:310–24.
58. Petroll WM, Hsu JK, Bean J, Cavanagh HD, Jester JV. The spatial organization of apicaljunctional complex-associated proteins in feline and human corneal endothelium. Curr EyeRes. 1999;18:10–19.
59. Valtink M, Gruschwitz R, Funk RH, Engelmann K. Two clonal cell lines of immortalizedhuman corneal endothelial cells show either differentiated or precursor cell characteristics.Cells Tissues Organs. 2008;187:286–94.
60. Zhu YT, Hayashida Y, Kheirkhah A, He H, Chen SY, Tseng SC. Characterization andcomparison of intercellular adherent junctions expressed by human corneal endothelial cellsin vivo and in vitro. Invest Ophthalmol Vis Sci. 2008;49:3879–86.
61. Sakai R, Kinouchi T, Kawamoto S, Dana MR, Hamamoto T, Tsuru T, et al. Construction ofhuman corneal endothelial cDNA library and identification of novel active genes. InvestOphthalmol Vis Sci. 2002;43:1749–56.
62. Gottsch JD, Seitzman GD, Margulies EH, Bowers AL, Michels AJ, Saha S, et al. Geneexpression in donor corneal endothelium. Arch Ophthalmol. 2003;121:252–8.
63. Foets BJ, van denOord JJ, Volpes R,Missotten L. In situ immunohistochemical analysis of celladhesion molecules on human corneal endothelial cells. Br J Ophthalmol. 1992;76:205–9.
64. Maurice DM. The location of the fluid pump in the cornea. J Physiol. 1972;221:43–54.65. Shamsuddin AK, Nirankari VS, Purnell DM, Chang SH. Is the corneal posterior cell layer
truly endothelial? Ophthalmology. 1986;93:1298–1303.66. Fine S, Myron B, Yanoff MD. Ocular histology: a text and atlas. New York: Harper & Row;
1972.67. Hayashi K, Sueishi K, Tanaka K, Inomata H. Immunohistochemical evidence of the origin
of human corneal endothelial cells and keratocytes. Graefes Arch Clin Exp Ophthalmol.1986;224:452–6.
68. Krachmer JH. Posterior polymorphous corneal dystrophy: a disease characterized byepithelial-like endothelial cells which influence management and prognosis. Trans AmOphthalmol Soc. 1985;83:413–75.
69. Merjava S, Neuwirth A, Mandys V, Jirsova K. Cytokeratins 8 and 18 in adult human cornealendothelium. Exp Eye Res. 2009;89:426–31.
70. Zhang XY, Pettengell R, Nasiri N, Kalia V, Dalgleish AG, Barton DP. Characteristics andgrowth patterns of human peritoneal mesothelial cells: comparison between advancedepithelial ovarian cancer and non-ovarian cancer sources. J Soc Gynecol Investig. 1999;6:333–40.
71. Jirsova K, Neuwirth A, Kalasova S, Vesela V, Merjava S. Mesothelial proteins are expressedin the human cornea. Exp Eye Res. 2012;91:623–9.
72. Lee JG, Kay EP. FGF-2-mediated signal transduction during endothelial mesenchymaltransformation in corneal endothelial cells. Exp Eye Res. 2006;83:1309–16.
1 The Cornea, Anatomy and Function 17

73. Tetsumoto K, Kubota T, Rummelt V, Holbach LM, Naumann GO. Epithelial transformationof the corneal endothelium in forceps birth-injury-associated keratopathy. Cornea.1993;12:65–71.
74. Hidayat AA, Cockerham GC. Epithelial metaplasia of the corneal endothelium in Fuchsendothelial dystrophy. Cornea. 2006;25:956–9.
75. Klintworth GK. Corneal dystrophies. Orphanet J Rare Dis. 2009;4:7.76. Treffers WF. Human corneal endothelial wound repair. In vitro and in vivo. Ophthalmology.
1982;89:605–13.77. Laing RA, Neubauer L, Oak SS, Kayne HL, Leibowitz HM. Evidence for mitosis in the
adult corneal endothelium. Ophthalmology, 1984;91:1129–34.78. Joyce NC. Proliferative capacity of the corneal endothelium. Prog Retin Eye Res.
2003;22:359–89.79. Chen KH, Harris DL, Joyce NC. TGF-beta2 in aqueous humor suppresses S-phase entry in
cultured corneal endothelial cells. Invest Ophthalmol Vis Sci. 1999;40:2513–19.80. Chen KH, Azar D, Joyce NC. Transplantation of adult human corneal endothelium ex vivo:
a morphologic study. Cornea. 2001;20:731–7.81. Joyce NC, Harris DL, Mello DM. Mechanisms of mitotic inhibition in corneal endothelium:
contact inhibition and TGF-beta2. Invest Ophthalmol Vis Sci. 2002;43:2152–9.82. Enomoto K, Mimura T, Harris DL, Joyce NC. Age differences in cyclin-dependent kinase
inhibitor expression and rb hyperphosphorylation in human corneal endothelial cells. InvestOphthalmol Vis Sci. 2006;47:4330–40.
83. Egan CA, Savre-Train I, Shay JW, Wilson SE, Bourne WM. Analysis of telomere lengths inhuman corneal endothelial cells from donors of different ages. Invest Ophthalmol Vis Sci.1998;39:648–53.
84. Joyce NC, Zhu CC. Human corneal endothelial cell proliferation: potential for use inregenerative medicine. Cornea. 2004;23 (8 Suppl):S8–S19.
85. Zhu C, Joyce NC. Proliferative response of corneal endothelial cells from young and olderdonors. Invest Ophthalmol Vis Sci. 2004;45:1743–51.
86. Joyce NC. Cell cycle status in human corneal endothelium. Exp Eye Res. 2005;81:629–38.87. Bahn CF, Falls HF, Varley GA, Meyer RF, Edelhauser HF, Bourne WM. Classification of
corneal endothelial disorders based on neural crest origin. Ophthalmology. 1984;91:558–63.88. Bahn CF, Glassman RM, MacCallum DK, Lillie JH, Meyer RF, Robinson BJ, Rich NM.
Postnatal development of corneal endothelium. Invest Ophthalmol Vis Sci. 1986;27:44–51.89. Murphy C, Alvarado J, Juster R, Maglio M. Prenatal and postnatal cellularity of the human
corneal endothelium. A quantitative histologic study. Invest Ophthalmol Vis Sci.1984;25:312–22.
90. Nucci P, Brancato R, Mets MB, Shevell SK. Normal endothelial cell density range inchildhood. Arch Ophthalmol. 1990;108:247–8.
91. Bourne WM, Nelson LR, Hodge DO. Central corneal endothelial cell changes over aten-year period. Invest Ophthalmol Vis Sci. 1997;38:779–82.
92. Yee RW, Matsuda M, Schultz RO, Edelhauser HF. Changes in the normal cornealendothelial cellular pattern as a function of age. Curr Eye Res. 1985;4:671–8.
93. Pels E, Schuchard Y. Tissue storage. E: Organ culture and endothelial evaluation as apreservation method for human corneas. In: Brightbill FS, editor. Corneal surgery. Theory,technique, and tissue. St. Louis: CV Mosby; 1986. pp. 93–102.
94. Armitage WJ, Dick AD, Bourne WM. Predicting endothelial cell loss and long-term cornealgraft survival. Invest Ophthalmol Vis Sci. 2003;44:3326–31.
95. Amann J, Holley GP, Lee SB, Edelhauser HF. Increased endothelial cell density in theparacentral and peripheral regions of the human cornea. Am J Ophthalmol. 2003;135:584–90.
96. Kaufman HE, Capella JA, Robbins JE. The human corneal endothelium. Am J Ophthalmol.1966;61:835–41.
18 K. Jirsova

97. Neubauer L, Baratz RS, Laing RA, Oak SS, Leibowitz HM. Coalescence of endothelial cellsin the traumatized cornea. III. Correlation between specular and scanning electronmicroscopy. Arch Ophthalmol. 1984;102:921–2.
98. Ikebe H, Takamatsu T, Itoi M, Fujita S. Age-dependent changes in nuclear DNA content andcell size of presumably normal human corneal endothelium. Exp Eye Res.1986;43:251–8.
99. Doughman DJ, Van Horn D, Rodman WP, Byrnes P, Lindstrom RL. (1976) Human cornealendothelial layer repair during organ culture. Arch Ophthalmol. 1976;4:1791–6.
100. Hoppenreijs VP, Pels E, Vrensen GF, Treffers WF. Corneal endothelium and growth factors.Surv Ophthalmol. 1996;41:155–64.
101. Nejepinska J, Juklova K, Jirsova K. Organ culture, but not hypothermic storage, facilitatesthe repair of the corneal endothelium following mechanical damage. Acta Ophthalmol.2010;88:413–19.
102. Cho KS, Lee EH, Choi JS, Joo CK. Reactive oxygen species-induced apoptosis and necrosisin bovine corneal endothelial cells. Invest Ophthalmol Vis Sci. 1999;40:911–19.
103. Whikehart DR, Parikh CH, Vaughn AV, Mishler K, Edelhauser HF. Evidence suggesting theexistence of stem cells for the human corneal endothelium. Mol Vis. 2005;11:816–24.
104. McGowan SL, Edelhauser HF, Pfister RR, Whikehart DR. Stem cell markers in the humanposterior limbus and corneal endothelium of unwounded and wounded corneas. Mol Vis.2007;13:1984–2000.
105. Kelley MJ, Rose AY, Keller KE, Hessle H, Samples JR, Acott TS. Stem cells in thetrabecular meshwork: present and future promises. Exp Eye Res. 2009;88:747–51.
106. Yu WY, Sheridan C, Grierson I, Mason S, Kearns V, Lo AC, Wong D. Progenitors for thecorneal endothelium and trabecular meshwork: a potential source for personalized stem celltherapy in corneal endothelial diseases and glaucoma. J Biomed Biotechnol.2011;2011:412743.
107. He Z, Campolmi N, Gain P, Ha Thi BM, Dumollard JM, Duband S, et al. Revisitedmicroanatomy of the corneal endothelial periphery: new evidence for continuous centripetalmigration of endothelial cells in humans. Stem Cells 2012;30:2523–34.
108. Mimura T, Yamagami S, Yokoo S, Usui T, Amano S. Selective isolation of young cells fromhuman corneal endothelium by the sphere-forming assay. Tissue Eng Part C Methods.2010;16:803–12.
109. Yokoo S, Yamagami S, Yanagi Y, Uchida S, Mimura T, Usui T, Amano S. Human cornealendothelial cell precursors isolated by sphere-forming assay. Invest Ophthalmol Vis Sci.2005;46:1626–31.
110. Scott JE, Bosworth TR. A comparative biochemical and ultrastructural study ofproteoglycan-collagen interactions in corneal stroma. Functional and metabolic implications.Biochem J. 1990;270:491–7.
111. Barfort P, Maurice D. Electrical potential and fluid transport across the corneal endothelium.Exp Eye Res. 1974;19:11–19.
112. Tervo T, Palkama A. Histochemical findings on sodium-potassium activated adenosinetriphosphatase (NaK-ATPase) activity in the cornea. Acta Ophthalmol Suppl. 1974;123:88–93.
113. Mergler S, Pleyer U. The human corneal endothelium: new insights into electrophysiologyand ion channels. Prog Retin Eye Res. 2007;26:359–78.
114. Hamann S, Zeuthen T, La Cour M, Nagelhus EA, Ottersen OP, Agre P, Nielsen S.Aquaporins in complex tissues: distribution of aquaporins 1-5 in human and rat eye. Am JPhysiol. 1990;274:C1332–45.
115. Ing JJ, Ing HH, Nelson LR, Hodge DO, Bourne WM. Ten-year postoperative results ofpenetrating keratoplasty. Ophthalmology. 1998;105:1855–65.
116. Thuret G, Chiquet C, Bernal F, Acquart S, Romanet JP, Mouillon M, et al. Prospective,randomized clinical and endothelial evaluation of 2 storage times for cornea donor tissue inorgan culture at 31 degrees C. Arch Ophthalmol. 2003;121:442–50.
117. Jester JV. Corneal crystallins and the development of cellular transparency. Semin Cell DevBiol. 2008;19:82–93.
1 The Cornea, Anatomy and Function 19

118. Gardner SJ, White N, Albon J, Knupp C, Kamma-Lorger CS, Meek KM. Measuring therefractive index of bovine corneal stromal cells using quantitative phase imaging.Biophys J. 2015;109:1592–9.
119. Beebe DC. Maintaining transparency: a review of the developmental physiology andpathophysiology of two avascular tissues. Semin Cell Dev Biol. 2008;19:125–33.
120. Shui YB, Fu JJ, Garcia C, Dattilo LK, Rajagopal R, McMillan S, et al. Oxygen distributionin the rabbit eye and oxygen consumption by the lens. Invest Ophthalmol Vis Sci.2006;47:1571–80.
121. Chhabra M, Prausnitz JM, Radke CJ. Modeling corneal metabolism and oxygen transportduring contact lens wear. Optom Vis Sci. 2009;86:454–66.
122. Richardson MR, Price MO, Price FW, Pardo JC, Grandin JC, You J, et al. Proteomicanalysis of human aqueous humor using multidimensional protein identification technology.Mol Vis. 2009;15:2740–50.
123. Chowdhury UR, Madden BJ, Charlesworth MC, Fautsch MP. Proteome analysis of humanaqueous humor. Invest Ophthalmol Vis Sci. 2010;51:4921–31.
124. Glasser DB, Matsuda M, Ellis JG, Edelhauser HF. Effects of intraocular irrigating solutionson the corneal endothelium after in vivo anterior chamber irrigation. Am J Ophthalmol.1985;99:321–8.
125. Niederkorn JY. The immune privilege of corneal allografts. Transplantation. 1999;67:1503–8.126. Chang JH, Gabison EE, Kato T, Azar DT. Corneal neovascularization. Curr Opin
Ophthalmol. 2001;12:242–9.127. Cursiefen C, Chen L, Dana MR, Streilein JW. Corneal lymphangiogenesis: evidence,
mechanisms, and implications for corneal transplant immunology. Cornea. 2003;22:273–81.128. Chauhan SK, Dohlman TH, Dana R. Corneal lymphatics: role in ocular inflammation as
inducer and responder of adaptive immunity. J Clin Cell Immunol. 2014;5:1000256.129. Niederkorn JY. Immune mechanisms of corneal allograft rejection. Curr Eye Res.
2007;32:1005–16.130. Chauhan SK, Saban DR, Lee HK, Dana R. Levels of Foxp3 in regulatory T cells reflect their
functional status in transplantation. J Immunol. 2009;182:148–53.131. Niederkorn JY. High-risk corneal allografts and why they lose their immune privilege. Curr
Opin Allergy Clin Immunol. 2010;10:493–7.132. Yamada Y, Sugita S, Horie S, Yamagami S, Mochizuki M. Mechanisms of immune
suppression for CD8+ T cells by human corneal endothelial cells via membrane-boundTGFbeta. Invest Ophthalmol Vis Sci. 2010;51:2548–57.
133. Hamrah P, Huq SO, Liu Y, Zhang Q, Dana MR. Corneal immunity is mediated byheterogeneous population of antigen-presenting cells. J Leukoc Biol. 2003;74:172–8.
134. Yamagami S, Yokoo S, Usui T, Yamagami H, Amano S, Ebihara N. Distinct populations ofdendritic cells in the normal human donor corneal epithelium. Invest Ophthalmol Vis Sci.2005;46:4489–94.
135. Knickelbein JE, Watkins SC, McMenamin PG, Hendricks RL. Stratification ofantigen-presenting cells within the normal cornea. Ophthalmol Eye Dis. 2009;1:45–54.
136. Hamrah P, Dana MR. Corneal antigen-presenting cells. Chem Immunol Allergy.2007;92:58–70.
137. Mayer WJ, Irschick UM, Moser P, Wurm M, Huemer HP, Romani N, Irschick EUCharacterization of antigen-presenting cells in fresh and cultured human corneas using noveldendritic cell markers. Invest Ophthalmol Vis Sci. 2007;48:4459–67.
138. Hamrah P, Liu Y, Zhang Q, Dana MR. Alterations in corneal stromal dendritic cellphenotype and distribution in inflammation. Arch Ophthalmol. 2003;121:1132–40.
139. Narumi M, Kashiwagi Y, Namba H, Ohe R, Yamakawa M, Yamashita H. Contribution ofcorneal neovascularization to dendritic cell migration into the central area during humancorneal infection. PLoS One. 2014;9:e109859.
140. Pels E, van der Gaag R. HLA-A,B,C, and HLA-DR antigens and dendritic cells in fresh andorgan culture preserved corneas. Cornea. 1984;3:231–9.
20 K. Jirsova

141. Ardjomand N, Berghold A, Reich ME. Loss of corneal Langerhans cells during storage inorgan culture medium, Optisol and McCarey-Kaufman medium. Eye (Lond). 1998;12(Pt1):134–8.
142. Al-Fakih A, Faltus V, Jirsova K. A decrease in the density of HLA-DR-positive cells occursfaster in corneas stored in organ culture than under hypothermic conditions. Ophthalmic Res.2012;47:39–46.
143. Simon M, Fellner P, El-Shabrawi Y, Ardjomand N. Influence of donor storage time oncorneal allograft survival. Ophthalmology. 111:1534–8.
144. Maier P, Heinzelmann S, Bohringer D, Reinhard T. Prolonged organ culture reduces theincidence of endothelial immune reactions. Eye (Lond). 2016;30:127–32.
145. Qazi Y, Hamrah P. Corneal allograft rejection: immunopathogenesis to therapeutics. J ClinCell Immunol. 2013;(Suppl 9): pii: 006.
146. Yu T, Rajendran V, Griffith M, Forrester JV, Kuffova L. (2016) High-risk corneal allografts:A therapeutic challenge. World J Transplant. 2016;6:10–27.
147. Erie EA, McLaren JW, Kittleson KM, Patel SV, Erie JC, Bourne WM. Corneal subbasalnerve density: a comparison of two confocal microscopes. Eye Contact Lens. 2008;34:322–5.
148. Osborne NN. Neuromediators and their receptors (adrenergic and endothelin types) in theeye. Therapie. 1993;48:549–58.
149. Schmid E, Leierer J, Doblinger A, Laslop A, Fischer-Colbrie R, Humpel C, et al. Neurokinina is a main constituent of sensory neurons innervating the anterior segment of the eye. InvestOphthalmol Vis Sci. 2005;46:268–74.
1 The Cornea, Anatomy and Function 21

Chapter 2Processing Corneas for Grafting
Katerina Jirsova, Patricia Dahl and Jesper Hjortdal
Abstract This chapter describes all of the important steps between the procure-ment and storage of corneal tissue intended for grafting, that is, the criteria andcontraindications for tissue donation, donor screening, tissue retrieval, macroscopicexamination of the donor eye, tissue decontamination, and the preparation of cor-neoscleral discs or corneal lamellae for subsequent storage. Corneal transplantation(keratoplasty) is, with respect to the risk of disease transmission, a very safe pro-cedure. Today, detailed screening of donor tissue is obligatory, and standards fordonor evaluation and testing are typically defined by national legislation.Contraindications to ocular tissue transplantation encompass major communicablediseases such as AIDS, hepatitis B, hepatitis C, degenerative disorders of the brain,and specific malignancies (i.e., lymphoma, leukemia). Whole eye enucleation andin situ excision are the two main approaches to corneal tissue retrieval. The surfaceof any ocular tissue intended for transplantation must be decontaminated at leastonce before tissue storage, such as before in situ excision or after enucleation,generally using a polyvinylpyrrolidone-iodine solution. Similarly, a macroscopicassessment of the whole eye has to be performed with the aim of excludingunsuitable tissue from transplantation. While in situ cornea excision is closelyassociated with hypothermic storage, enucleation often precedes the storage of acornea in organ culture. Corneoscleral discs for penetrating keratoplasty or varioustypes of lamellae, particularly for posterior lamellar keratoplasties, may be routinelyprocessed in eye banks.
K. Jirsova (&)Laboratory of the Biology and Pathology of the Eye, Institute of Biology and MedicalGenetics, First Faculty of Medicine, Charles University, Prague, Czech Republice-mail: [email protected]
P. DahlThe Eye-Bank for Sight Restoration, Inc., 120 Wall Street, New York, NY 10005, USAe-mail: [email protected]
J. HjortdalDepartment of Ophthalmology, Aarhus University Hospital, Norrebrogade 44, 8000 AarhusC, Denmarke-mail: [email protected]
© Springer International Publishing AG 2017K. Jirsova, Light and Specular Microscopy of the Cornea,DOI 10.1007/978-3-319-48845-5_2
23

Keywords Cornea retrieval � Donor screening � Whole eye enucleation � In situexcision � Decontamination � Corneoscleral disc � Corneal lamella � Eye banking
2.1 Eye Tissue Donation, Criteria, and Contraindications
Currently, corneas for transplantation are obtained almost exclusively from deceaseddonors. In most European countries (Denmark, France, Germany, Italy, Sweden,Switzerland, United Kingdom) and the United States, only those who have givenexplicit consent may become donors (opting-in system). Tissue retrieval in thesecountries is conducted on the basis of consent obtained during the life of the personconcerned (first person consent) or the consent of relatives obtained after the death ofa potential donor. A minority of European countries (Austria, Belgium, CzechRepublic, Finland, Hungary, Poland, Russia, Slovakia) assume automatic approvalof tissue retrieval (opting-out system). In this case, those who do not want to donatetissue for grafting must be registered in the relevant databases. In some countries (theNetherlands, Spain) donor recruitment is a mixture of the opting-out and opting-insystems [1]. In the U.S., all 50 states have online electronic donor registries, whicheye banks can access after being notified that a hospital death has occurred. Fifty-twopercent of eye donors in the U.S. are obtained through first-person consent [2].
Donors of eye tissue must be carefully selected and screened according tonational legislation. Detailed information concerning donor eligibility is presentedin the medical standards of professional societies such as the European Eye BankAssociation (EEBA), the Eye Bank Association of America (EBAA), and the EyeBank Association of Australia and New Zealand. The medical standards arereviewed each year, and they do not differ significantly from one another [3–5]. Thelegal reference for donor selection in the European Union is described inCommission Directive 2006/17/EC of [6], while in the U.S. it is stated in the U.S.Food and Drug Administration 21 CFR 1271: Human Cells, Tissues and Cellularand Tissue-Based Products [7].
The medical standards include the information required for donor risk assess-ment, the relevant source of information, microbiologic testing of donors, andcontraindications to ocular tissue transplantation [5]. Besides the donor’s identityand age, basic data concerning his or her death must be known and recorded. Thelist of contraindications must be checked, and particularly the tissue of donorssuffering from neurodegenerative diseases (including those of unknown etiology),malignancies (retinoblastoma, hematologic neoplasms, malignant tumors of theanterior segment of the eye), or eye diseases must be excluded from grafting. Moredetailed information is given in the specific lists of contraindications [4–7].
It has been shown that the causes of donor death (other than those contraindi-cated), including infection, respiratory diseases, and cancer, do not affect the sur-vival of grafts [8]. On the other hand, a decrease of endothelial cell density isassociated with severe long-term diseases such as cancer, leading to cachexia andcatabolism [9]. Similarly, a decline in the number of endothelial cells is often
24 K. Jirsova et al.

associated with donors who died as a consequence of head trauma or multitrauma.In these cases, the reduced endothelial cell density may negatively influence thequality of the cornea [10].
A relative contraindication to corneal donation is the donor’s age. Althoughmany banks have established an upper limit of donor age, numerous studies haveshown that age does not significantly influence graft survival [11, 12], upper limitsare set for donor age in the EEBA (EBAA) medical standards [4, 5]. Most Europeaneye banks fix the upper limit between 65 and 90 years of age. The typical age ofdonors providing corneas for subsequent hypothermic storage is generally slightlylower [13].
In the U.S., the maximum age of the donor is established by the eye bank’smedical director, and most set an upper age limit of 60–65 years [4, 14]. As a result,84 % of donors there are 70 years old or younger [2]. It has been shown that thefive-year graft failure rate is similar using corneas from donors younger than 66 anddonors from 66 to 75 years of age if the corneas are comparable in quality (morethan 2300 endothelial cells/mm2) [15]. This result, together with the increasingdemand for corneas for transplantation and detailed assessment of the cornealendothelium, may indicate that the upper age limit of corneas intended forhypothermic storage, which is the standard storage method used in the U.S., may beincreased in the future [16].
The post-transplant outcome of organ cultured corneas obtained from donorsover 85 years of age, if they have an adequate endothelial cell density, is compa-rable to that of corneas from younger donors [12]. Moreover, cultured corneas fromolder donors are more stable than those from young donors and are associated withbetter graft survival [17, 18]. Finally, it has been shown that corneas with a tissueage of more than 100 years can still function well [19]. These findings indicate thatthe upper age limit is not as important as previously believed and that the onlydecisive factor for the release of a cornea for transplantation is a sufficient numberof viable endothelial cells.
Another relative contraindication to eye tissue retrieval is the interval betweendeath and tissue recovery. According to European Union legislation, the retrievalshould be carried out as soon as possible after the death of the donor, but no timelimit is set. However, a maximum time limit for retrieval may be specified bynational laws. In the U.S., the maximum cornea retrieval time is set by each eyebank’s medical director and may include retrievals up to 20 h after death [4].
2.2 Donor Screening, the Risk of Disease Transmission,Tissue Typing
The obligatory testing performed by eye banks around the world prevents thetransmission of major communicable diseases such as AIDS, viral hepatitis, andsyphilis. Based on European legislation, the donors of ocular tissue are screened forthe presence of AIDS (detection of anti-HIV-1 and anti-HIV-2 antibodies), hepatitis
2 Processing Corneas for Grafting 25

B (detection of hepatitis B core antibodies, anti-HBc, and the surface antigenHBsAg). When anti-HBc testing is positive and HBsAg testing is negative, furtherinvestigation is necessary along with risk assessment to determine the tissue’seligibility for clinical use. In hepatitis C, testing involves detection of anti-HCVantibodies; syphilis testing consists of detection of anti-Treponema pallidum anti-bodies. Blood sampling for serologic screening must be done within 24 h after thedonor’s death, and the testing must be carried out by an accredited laboratory.Any positive result from HIV, hepatitis, or syphilis testing excludes the use of thetissue for transplantation [5, 6]. All nonrequired positive infectious disease resultsmust be shared with the transplant surgeon prior to distribution [4]. Examples ofnonrequired serologic results include human T-cell lymphotropic virus, cytome-galovirus, Epstein-Barr virus, toxoplasmosis, and West Nile virus, which are oftenidentified when a donor is shared as a multiorgan donor.
The transmission of viral and prion diseases via corneal grafts has beenreported, although in the history of corneal transplantation no cases of HIV, hep-atitis C, or syphilis transmission via a corneal graft have been published [20, 21].Several cases of keratoplasties that were performed using tissue from HIV-positivepatients have been described, mostly from the period when standard HIV testing ofcornea donors was not performed. However, no disease was reported to havedeveloped even more than ten years after the grafting of the infected tissue [22–24].Transmission of hepatitis B was observed after the transplantation of grafts fromtwo donors whose sera were stored and subsequently found to be infectious [25].The relatively very low risk of transmission of these diseases via a corneal graft ascompared to via musculoskeletal grafts is in large part the result of the morphologicand physiologic properties of the cornea, in particular the absence of blood vesselsin healthy corneas (for details, see Sect. 1.10) [21].
Nearly ten cases of the recipient’s death after the grafting of corneas infected byrabies have been described [26–28]. Only two recipients of infected corneas fromone donor whose corneas and organs were used for multiple transplantations did notdevelop symptoms, probably because of a low viral concentration in the tissue andthe relatively quick removal of the infected tissue after grafting [29]. Testing for thepresence of the rabies virus is not routinely performed.
The transmission of herpes simplex virus is relatively frequent. This can lead to alack of graft re-epithelization or graft failure. Moreover, postoperative herpetickeratitis has been observed [30–32]. However, in the case of postkeratoplastyherpetic infections, it is still difficult to ascertain whether the virus was transmittedvia the graft, reactivated in the recipient by the surgical procedure, or the recipientwas infected de novo after transplantation [33]. It was found that the presence of thevirus in organ cultured corneas can be indicated by a significantly increased numberof dead cells during or after cultivation [34, 35]. On the other hand, no correlationhas been found between the presence of herpes simplex virus 1 DNA in samples ofculture solutions and cytopathic changes or the loss of endothelial cells [36].
Screening for the presence of pathogenic prions responsible for spreadingtransmissible spongiform encephalopathies is not routinely performed in organ ortissue donors. However, after the recognition of the first cluster of ten cases of the
26 K. Jirsova et al.

human variant form of Creutzfeld-Jakob disease (CJD) in the United Kingdom in1996, many nations implemented policies to reduce the hypothetical risk of thetransmission of prion diseases [37]. Another four possible cases and one probablecase of iatrogenic CJD in corneal graft recipients, with incubation periods rangingfrom 15 months to 30 years, were described later [38–40]. Tullo and colleaguesreported the transplantation of both corneas and scleras to three patients from a donorin whom sporadic CJD was subsequently detected. No signs of CJD in the recipientswere present nine years after surgery, and no prions were detected immunohisto-chemically in tissue removed from the recipients several months after grafting [41].Interestingly, another four cases of CJD in the recipients of corneal transplants havebeen described, but the authors’ opinion is that an occasional case of sporadic CJD ismore likely to appear in recipients than real transmission via a corneal graft [42].
Although the transmission of CJD is lethal for the recipient, no donor screening forthe presence of pathologic prions is performed around the world. The only exceptionis in the Czech Republic, where since 2007 legislation requires the testing of a brainsample (frontal lobe) from every ocular tissue donor for the presence of pathogenicprions. The expected number of CJD cases caused by corneal transplantation is0.00132 per year; therefore, the calculated risk of transmission via a transplantedcornea is very low, on the order of once in more than 750 years. In addition, althoughthe safety of donor eye tissue is presumably increased by such mandatory testing, thescreening is unable to identify all donors with a subclinical form of the disease and,moreover, the testing is associated with a great deal of organizational difficulties,delays in releasing tissue for grafting, and finally with a 10.5 % increase in the totalcost of a cornea [43]. The calculated risk of a prion-infected corneal donor in the U.S.ranges from0.00005 to 0.0005 %, taking into account that CJD increaseswith age andthat more than 90 % of CJD patients are older than 60 years [44]. This risk is muchhigher in countries with a high incidence of the new variant CJD, such as the UnitedKingdom [45]. Besides Creutzfeldt-Jakob disease, no other prion diseases(e.g., Gerstmann-Sträussler-Scheinker syndrome, fatal familial insomnia, or kuru)have been demonstrated to be transmitted via a corneal graft.
The transmission of bacterial and mycotic diseases via a corneal graft has beendescribed repeatedly; the risk of such transmission can be reduced by storing tissuein organ culture, where the propagation of infectious agents can be found macro-scopically and confirmed by microbiology testing of the culture medium (fordetails, see Sect. 3.5.2). On the other hand, no cases of tuberculosis, active leprosy,or typhoid fever being transmitted via a corneal graft have been reported [3].Similarly, no cases of syphilis transmission via a corneal graft have been published,and the possibility of disease transmission is considered to be largely theoreticalbased on experiments using a mammalian model [20, 21].
The screening of the donor to determine blood type is not routinely performed.Since a transplanted graft is generally between 7.25 and 7.75 mm in diameter, a sizein which there is no blood or lymph supply in the healthy tissue, a general consensusexists that testing to determine a donor’s blood type is not necessary. Moreover, itwas shown that ABO donor-recipient incompatibility is not associated with graftfailure caused by rejection or with the occurrence of a rejection episode [46].
2 Processing Corneas for Grafting 27

HLA, human leukocyte antigens, are the molecules responsible for the majorhistocompatibility of tissues and play a major role in graft rejection. In terms ofcorneal transplantation, particularly important are HLA class II proteins: HLA-DR,DP, and DQ. Between 2010 and 2014 in Europe, 7.3 % of the corneas intended forgrafting were HLA II typed and 1.4 % of corneal grafts were HLA II matched [1].The compatibility of these proteins between donor and recipient can positivelyaffect the length of graft survival, especially in risky patients such as those withcorneal vascularization or repeated graft failures [47, 48]. No EBAA data areavailable concerning the number of HLA-typed corneas. HLA-matched corneas aretypically available only if the donor is also a multiorgan donor.
2.3 Tissue Retrieval and Transport to the Eye Bank
Donor eye tissue is usually contaminated [49]; therefore before tissue retrieval, thedonor eye must be decontaminated. Generally, a 5 % solution ofpolyvinylpyrrolidone-iodine (povidone-iodine, PVP-I) is used because of its broadantimicrobial spectrum, which includes most gram-positive and gram-negativebacteria, fungi, yeasts, viruses, and protozoa [50]. It has been shown that even 1 %PVP-I, if applied for 2 min to the conjunctival sac, is equally effective as 5 % PVP-Isolution in decontaminating the native flora of the eye, including coagulase-negativestaphylococci, Corynebacterium, and streptococcal species, gram-negative bacilli,Staphylococcus aureus, anaerobes, and yeast [51]. The EBAA requires its accreditedmembers to include PVP-I in the retrieval process of ocular tissue that is intended fortransplantation. The concentration of the solution and the duration of its applicationare decided by the eye bank’s medical director [4].
Two main approaches are used to obtain the cornea after ocular surfacedecontamination: either enucleation, during which the entire globe is removed, orin situ excision, during which a corneoscleral disc (usually 11–17 mm in diameter)is trephined. The type of retrieval may influence the risk of subsequent tissuecontamination; it is significantly higher after excision compared to enucleation [17].The endothelial cell densities of excised corneas and corneas obtained from enu-cleated globes are comparable or slightly higher in the corneas obtained fromenucleated globes [52, 53]. Enucleation has to be performed if conjunctival orscleral tissue is needed in addition to the cornea.
An enucleated donor eye (Fig. 2.1a) is placed in a moist chamber (a closablesterile container with gauze moistened by a sterile aqueous solution) and kept at anappropriate temperature (2–8 °C) for subsequent graft preparation. A corneoscleraldisc (Fig. 2.1b, c) should be immediately placed in sterile, generally commerciallyavailable medium and then transported to the eye bank, where it is assessed andstored until grafting. Corneas in hypothermic storage solution should be packagedusing a method designed to maintain cool conditions and prevent freezing. Packingshould be done so that the tissue label and the documentation accompanying thetissue do not become wet.
28 K. Jirsova et al.

The two basic approaches to tissue retrieval therefore influence the followingprocesses associated with subsequent preparation and tissue storage:
1. Corneas excised in situ can be placed in a hypothermic storage solution andassessed by slit lamp and specular microscopy. Alternatively, these corneas maybe stored in organ culture and evaluated using slit lamp and light microscopy;the use of specular microscopy is also possible (see Chap. 4).
2. Corneas removed from an enucleated eye under the aseptic conditions of abiosafety cabinet and assessed by light microscopy are usually subsequentlystored in organ culture. Alternatively, these corneas may be removed and storedin hypothermic solution and again assessed by slit lamp microscopy, followedby specular and/or light microscopy.
Basic procedural differences between hypothermic storage and organ culture areshown in Fig. 2.2.
2.4 Macroscopic Examination of the Donor Eye
During the macroscopic examination of the whole eye, the color of the conjunctivaand sclera (yellowing indicates the possible presence of hepatitis), the presence offoreign bodies, and signs of pathology are monitored. The diameter of the cornea isusually measured; corneas of abnormal size (microcornea <11 mm, megalo-cornea >13 mm) [54] and corneas with signs of infection or pterygium should not be
Fig. 2.1 Retrieved eye tissue. a Enucleated donor eye in a sterile moist chamber. b Excisedcorneoscleral disc in a viewing chamber. c The same cornea (viewed from above) (b andc Courtesy of Jameson Clover, Lions VisionGift, Portland, OR, USA)
2 Processing Corneas for Grafting 29

used for grafting. Corneas exhibiting other changes such as arcus senilis, scars in theoptic center, or previous surgery (Fig. 2.3) should be considered based on the resultsof other detailed evaluations (biomicroscopic examination using a slit lamp, lightmicroscopy) and their intended use (penetrating or lamellar keratoplasty).
Besides pathologic signs, the eye should be checked for signs of corneal damageor the presence of ocular hypotonia. The extent of hypotonia can be assessed inseveral degrees: (1) hypotonia is not present; (2) mild hypotonia: a significantreduction of tonus (the sclera is sunken, the shape of the cornea is normal);
Fig. 2.2 Themaindifferences incornealpreparationandstorageunderhypothermicconditionsandinorgan culture (OC): hypothermic storage (green arrow); OC (blue arrow). Corneas intended forhypothermic storage are generally obtained by excision, then placed in a commercially preparedsolution inwhichmicroscopicexamination (slit lamp, specularmicroscopy) isperformed, followedbypreservation at 2–8 °C. Corneas intended for OC are most frequently obtained after enucleation,followed by slit lamp examination, decontamination, and preparation. The corneas are usuallyassessedbylightmicroscopyaftervisualizationof theendothelial cellborders (hypotonic solution)andvital staining (trypan blue). Storage at 31–37 °C allows for appropriate microbiologic examination
30 K. Jirsova et al.

(3) central hypotonia: clearly visible prolapse of the cornea; and (4) significanthypotonia: the complete prolapse of the cornea and surrounding tissue (the cornea isin contact with the iris).
In particular, grades 3 and 4 may indicate the presence of dead endothelial cellsas a result of their contact with the iris. If a whole eye with severe hypotonia is usedfor further evaluation, the presence of dead endothelial cells should be quantifiedmicroscopically.
2.5 Donor Eye Decontamination
First, the enucleated eye is rinsed with a stream of sterile water or sterile saline (1L/min) to remove mechanical debris [55, 56]. Rinsing shock should be consideredif the bulbus is hypotonic and if the stream of water may lead to contact between theiris and the endothelium, as this may result in significant death of endothelial cells[57]. For decontamination, PVP-I is often used at a concentration of 0.5–5 % for2 min. After immersion, PVP-I remains on the outside surface of the eye, andwithout proper rinsing it may injure the endothelium during the preparation of the
Fig. 2.3 The macroscopic examination of whole eyes. a A whole eye showing normal hypotony.b A collapsed eye caused by significant hypotonia. c An eye showing the presence of mechanicaldebris (traffic accident). d A yellow donor eye indicating the presence of jaundice (arcus senilis isalso present). e An eye with marked arcus senilis. f An eye with a cornea exhibiting signs ofprevious surgery (penetrating keratoplasty) (a Courtesy of Erik Blumentritt, General UniversityHospital in Prague, Prague, Czech Republic, b-f Courtesy of Danish Eye Bank, UniversityHospital, Aarhus, Denmark)
2 Processing Corneas for Grafting 31

corneoscleral disc. Some toxic effects of PVP-I have been described for the cornealepithelium and keratocytes using concentrations higher than 25 mg/mL andimmersion periods over 4 min. A sodium thiosulfate solution (usually 2 % solutionfor 1 min) may be used to rinse and reduce the activity of free iodine (Fig. 2.4) [55,56, 58]. Moreover, it was shown that sodium thiosulfate itself may inhibit bacterialgrowth [59]. The decontamination procedure can only be beneficial if aseptichandling is used for subsequent tissue manipulation [58].
Recently, it has been shown that the combined use of 0.5 % PVP-I and 0.02 %chlorhexidine may allow the decontamination of donor globes to a level at whichthe risk of tissue contamination is minimized, while corneal viability is preserved[60]. Alternatively, PVP-I, together with antibiotics or less often antibiotic solutionitself, is used for whole eye decontamination [1]. After decontamination, the eye isplaced in a sterile aqueous solution, usually a phosphate buffer. At this point the eyeis ready for the preparation of a corneoscleral disc.
2.6 Corneoscleral Disc Preparation
The time between tissue retrieval and the preparation of a corneoscleral disc shouldbe as short as possible. In a moist chamber, particularly under hypothermic con-ditions, tissue quality is gradually lost [61].
The corneoscleral disc should be prepared under aseptic conditions, often in aclass A biosafety cabinet. The whole eye is wrapped in sterile gauze, and the
Fig. 2.4 Whole eye decontamination using PVP-I. The eye is immersed in PVP-I, then in athiosulfate solution, followed by immersion in sterile water
32 K. Jirsova et al.

desired size of the corneoscleral disc is trephined. Usually just part of the disc isseparated by trephination; the remaining part of the tissue is prepared using scissors.The corneoscleral disc is carefully separated from the rest of the eye by tweezers(Fig. 2.5) and placed in a sterile vial or Petri dish for subsequent assessment.
A trephine of 12–14 mm in diameter is normally used if the tissue is intended forpenetrating keratoplasty. Corneoscleral discs are prepared somewhat larger than isnecessary for transplantation because the scleral tissue surrounding the cornea ismuch tougher than the cornea itself and thus allows much easier manipulation of thetissue. A cornea of the dimensions required for grafting (usually between 7.5 and7.75 mm) is punched just before surgery in the operating room. For the preparationof various types of corneal lamellae, a larger corneoscleral disc, usually 16–17 mmin diameter, is trephined.
2.7 Corneal Lamellae Preparation
As a result of improved and innovative surgical techniques together with new toolsand advanced equipment (microkeratomes, femtosecond lasers), corneal trans-plantation has undergone profound changes that have led to the gradual replacementof traditional full- thickness corneal transplantation by new techniques for lamellarkeratoplasties, which in 2014 represented 45 and 47 % of corneal transplantsurgeries in the U.S. and Europe, respectively [1, 62]. Revolutionary advances inthe preparation of corneal lamellae include the introduction of the big-bubbletechnique for separating Descemet membrane along with the endothelial layer fromthe stroma and the selective replacement of the posterior part of the cornea viaendothelial keratoplasty [63, 64]. Corneal lamellar grafts (corneal lamellae, len-ticules) use healthy parts of the tissue to selectively replace diseased layers in therecipient’s cornea while leaving the healthy parts intact.
Anterior lamellar keratoplasty (ALK) or deep ALK (DALK) involves the partialor near-total removal of the corneal stroma (and its subsequent replacement) fromthe underlying Descemet membrane. These techniques preserve the host endotheliallayer, thus providing long-term protection from immune-mediated endothelial
Fig. 2.5 The preparation of a corneoscleral disc under aseptic conditions
2 Processing Corneas for Grafting 33

rejection. As long as the patient has a functioning endothelium, anterior lamellaeare used to treat pathologies of the anterior cornea, particularly stromal dystrophies,scars, or keratoconus. In eye banks, anterior lamellae can be prepared using amicrokeratome, a femtosecond laser, or by pneumatic dissection (e.g., thebig-bubble technique) [65–67].
In posterior lamellar keratoplasty (PLK) or endothelial keratoplasty (EK), only aportion of the recipient’s posterior cornea is replaced by healthy tissue. Varioustechniques for the dissection of lamellae for EK have established it as the method ofchoice for treating endothelial dysfunction, particularly endothelial dystrophies andbullous keratopathy. The advantages of EK include quick and efficient surgery withreduced manipulation, low surgical risk, few or no sutures, short recovery time, andimproved visual outcome [68]. A detailed description of the various techniques isbeyond the scope of this chapter, but they have been extensively reviewed [67, 69].Briefly, lamellae for Descemet stripping endothelial keratoplasty (DSEK) orDescemet stripping automated endothelial keratoplasty (DSAEK), prepared with anautomated microkeratome or femtosecond laser involve a thin layer of the stroma inaddition to the endothelium and Descemet membrane. These lamellae are com-monly 100–200 µm thick [69]. Although it has been shown that tissues prepared bya femtosecond laser display greater irregularity of the posterior corneal surface aswell as greater variability in the thickness of the lamellae, no differences were notedin endothelial cell density or viability [69–71]. Current techniques to achieve thinendothelial grafts (mostly � 100 lm) may include the use of two microkeratomepasses with a motorized microkeratome (ultrathin DSAEK, UT DSAEK) [72, 73].
Lamellae for Descemet membrane endothelial keratoplasty (DMEK) consist ofthe endothelium and the membrane. There are several approaches employed for themechanical dissection of donor tissue, most utilizing a pneumatic dissection usingan air bubble or liquid and/or the mechanical peeling or stripping of the membrane,along with the endothelium, from the stroma [68, 74–79]. The main advantage ofDMEK over DSAEK is that DMEK results in better visual acuity; on the otherhand, its use is limited by its surgical complexity, the technically demandingpreparation and handling of the graft that is required, and a reported higher graftdetachment rate [80].
Several techniques for the preparation of hybrid lamellae (Descemet membraneand endothelium in the central part and an additional layer of posterior stroma in theperipheral part) have been developed with the goal of maintaining the features ofthin lamellae while adding the structural support of the stromal tissue [81–83].Additionally, techniques for the dissection of two lamellae (for DALK and DMEKor both for DMEK) from one donor cornea have been introduced [77, 84].
Initially, lamellae for EK were dissected manually by the surgeon in the oper-ating room, but recently eye banks have developed methodologies for supplyinglamellar grafts with comparable results. Over time, and with the increased experi-ence of eye bankers, better standardization and increased tissue quality provided forgrafting have been achieved. The preparation of lamellae in an eye bank (precutlamellae) has several advantages: standardized methodology, storage, and qualitycontrol as well as reduction of the potential for errors occurring in the operating
34 K. Jirsova et al.

room that can result in cancelled surgeries or the necessity for spending timepreparing additional lamellae [69, 85, 86]. In the bank, lamellae dissection is per-formed under aseptic conditions, followed by appropriate storage in hypothermia ororgan culture and quality assessment. The preparation of lamellae for DMEK [68,75, 78], DSAEK [87], and hybrid lamellae [88] has been standardized and validatedby the long-term outcomes of their use (for details, see Sect. 5.5).
2.8 Corneal Storage
There are two main approaches to the storage of corneas for transplantation:hypothermia and organ culture (see Chap. 3). The main aim of both methods ispreserving tissue vitality while maintaining a sufficient number of endothelial cells,both of which are decisive for functionality and graft survival [89]. The compo-sition of the storage solution is formulated so that it meets the requirements of theendothelium. While hypothermic storage is widely used around the world (in theU.S., 98 % of corneas are retrieved by in situ corneoscleral disc excision and storedin hypothermic solution), organ culture is preferred in Europe, where 82 % ofprocessed corneas are stored this way [1, 62].
References
1. EEBA Directory. European Eye Bank Association, Directory, 24th ed. Copenhagen: Aarhus;2016.
2. EBAA Statistical Report (2015). Washington DC: EBBA; 2016.3. Borderie VM. Donor selection, retrieval and preparation of donor tissue. Donor selection. Dev
Ophthalmol. 2009;43:22–30.4. EBAA Medical Standards. Washington DC: EBAA; 2015. www.restoresight.org.5. EEBA Minimum Medical Standards (2015). http://www.europeaneyebanksorg/downloads/
EEBA%20Minimum%20Medical%20Standards%20Rev%202%20-%202015Finalpdf6. Commission Directive 2006/17/EC (2006). http://eur-lex.europa.eu/LexUriServ/LexUriServ.
do?uri=OJ:L:2006:038:0040:0052:EN:PDF.7. US FDA 21 CFR 1271 (2009). http://www.ecfr.gov/cgi-bin/text-idx?SID=876fde511f3990
88164c5cae89899e41&mc=true&node=pt21.8.1271&rgn=div58. Armitage WJ, Jones MN, Zambrano I, Carley F, Tole DM, Group NOTA, Contributing
Ophthalmologists OAS. The suitability of corneas stored by organ culture for penetratingkeratoplasty and influence of donor and recipient factors on 5-year graft survival. InvestOphthalmol Vis Sci. 2014;55:784–91.
9. Krohn J, Hovding G. The influence of donor age and cause of death on corneal endothelialcell density. Acta Ophthalmol Scand. 2005;83:746–50.
10. Grabska-Liberek I, Szaflik J, Brix-Warzecha M. The importance of various factors relating tothe morphological quality of corneas used for PKP by the Warsaw Eye Bank from 1996 to2002. Ann Transplant. 2003;8:26–31.
11. Wakefield MJ, Armitage WJ, Jones MN, Kaye SB, Larkin DF, Tole D, et al. The impact ofdonor age and endothelial cell density on graft survival following penetrating keratoplasty.
2 Processing Corneas for Grafting 35

Br J Ophthalmol. 2015 Nov 13. pii: bjophthalmol-2015-306871. doi:10.1136/bjophthalmol-2015-306871. [Epub ahead of print]
12. Gain P, Thuret G, Chiquet C, Rizzi P, Pugniet JL, Acquart S, et al. Cornea procurement fromvery old donors: post organ culture cornea outcome and recipient graft outcome. Br JOphthalmol. 2002;86:404–11.
13. EEBA Directory. European Eye Bank Association, Directory. 23rd ed. Venice, Italy;2005.14. Armitage WJ. Preservation of human cornea. Transfus Med Hemother. 2001;38:143–7.15. Cornea Donor Study Investigator G, Gal RL, Dontchev M, Beck RW, Mannis MJ,
Holland EJ, et al. The effect of donor age on corneal transplantation outcome results of thecornea donor study. Ophthalmology. 2008;115:620–6.
16. Sugar A, Montoya MM, Beck R, Cowden JW, Dontchev M, Gal RL, et al. Impact of thecornea donor study on acceptance of corneas from older donors. Cornea. 2012;31:1441–5.
17. Borderie VM, Laroche L. Microbiologic study of organ-cultured donor corneas.Transplantation. 1998;66:120–3.
18. Armitage WJ, Easty DL. Factors influencing the suitability of organ-cultured corneas fortransplantation. Invest Ophthalmol Vis Sci. 1997;38:16–24.
19. Visby E, Hjortdal J, Nielsen K. Evaluation of grafted patients with donor corneas that todayare more than 100 years old. Acta Ophthalmol. 2014;92:478–81.
20. Gandhi SS, Lamberts DW, Perry HD. Donor to host transmission of disease via cornealtransplantation. Surv Ophthalmol. 1981;25:306–11.
21. Pruss A, Caspari G, Kruger DH, Blumel J, Nubling CM, Gurtler L, Gerlich WH. Tissuedonation and virus safety: more nucleic acid amplification testing is needed. Transpl InfectDis. 2010;12:375–86.
22. Pepose JS, MacRae S, Quinn TC, Ward JW. Serologic markers after the transplantation ofcorneas from donors infected with human immunodeficiency virus. Am J Ophthalmol.1987;103:798–801.
23. Schwartz JS, Kinosian BP, Pierskalla WP, Lee H. Strategies for screening blood for humanimmunodeficiency virus antibody. Use of a decision support system. JAMA. 1990;264:1704–10.
24. Eastlund T. Infectious disease transmission through cell, tissue, and organ transplantation:reducing the risk through donor selection. Cell Transplant. 1995;4:455–77.
25. Hoft RH, Pflugfelder SC, Forster RK, Ullman S, Polack FM, Schiff ER. Clinical evidence forhepatitis B transmission resulting from corneal transplantation. Cornea. 1997;16:132–7.
26. Houff SA, Burton RC, Wilson RW, Henson TE, London WT, Baer GM, et al.Human-to-human transmission of rabies virus by corneal transplant. N Engl J Med.1979;300:603–4.
27. Gode GR, Bhide NK. Two rabies deaths after corneal grafts from one donor. Lancet.1988;2:791.
28. Javadi MA, Fayaz A, Mirdehghan SA, Ainollahi B. Transmission of rabies by corneal graft.Cornea. 1996;15:431–3.
29. Maier T, Schwarting A, Mauer D, Ross RS, Martens A, Kliem V, et al. Management andoutcomes after multiple corneal and solid organ transplantations from a donor infected withrabies virus. Clin Infect Dis. 2010;50:1112–19.
30. Biswas S, Suresh P, Bonshek RE, Corbitt G, Tullo AB, Ridgway AE. Graft failure in humandonor corneas due to transmission of herpes simplex virus. Br J Ophthalmol. 2000;84:701–5.
31. Cockerham GC, Bijwaard K, Sheng ZM, Hidayat AA, Font RL, McLean IW. Primary graftfailure: a clinicopathologic and molecular analysis. Ophthalmology. 2000;107:2083–90;discussion 2090–1.
32. Remeijer L, Maertzdorf J, Doornenbal P, Verjans GM, Osterhaus AD. Herpes simplex virus 1transmission through corneal transplantation. Lancet. 2001;357:442.
33. Borderie VM, Meritet JF, Chaumeil C, Rozenberg F, Baudrimont M, Touzeau O, et al.Culture-proven herpetic keratitis after penetrating keratoplasty in patients with no previoushistory of herpes disease. Cornea. 2004;23:118–24.
36 K. Jirsova et al.

34. Sengler U, Reinhard T, Adams O, Krempe C, Sundmacher R. Herpes simplex virus infectionin the media of donor corneas during organ culture: frequency and consequences. Eye (Lond).2001;15(Pt 5):644–7.
35. Hermel M, Salla S, Hamsley N, Steinfeld A, Walter P. Detection of contamination duringorgan culture of the human cornea. Graefes Arch Clin Exp Ophthalmol. 2010;248:117–26.
36. Garweg JG, Boehnke M. Low rate shedding of HSV-1 DNA, but not of infectious virus fromhuman donor corneae into culture media. J Med Virol. 1997;52:320–5.
37. Will RG, Ironside JW, Zeidler M, Cousens SN, Estibeiro K, Alperovitch A, et al. A newvariant of Creutzfeldt-Jakob disease in the UK. Lancet. 1996;347:921–5.
38. Chazot G, Broussolle E, Lapras C, Blattler T, Aguzzi A, Kopp N. New variant ofCreutzfeldt-Jakob disease in a 26-year-old French man. Lancet. 1996;347:1181.
39. Heckmann M, Pirthauer M, Plewig G. Adhesion of leukocytes to dermal endothelial cells isinduced after single-dose, but reduced after repeated doses of UVA. J Invest Dermatol.1997;109:710–15.
40. Hammersmith KM, Cohen EJ, Rapuano CJ, Laibson PR. Creutzfeldt-Jakob disease followingcorneal transplantation. Cornea. 2004;23:406–8.
41. Tullo AB, Buckley RJ, Kelly T, Head MW, Bennett P, Armitage WJ, Ironside JW.Transplantation of ocular tissue from a donor with sporadic Creutzfeldt-Jakob disease. ClinExperiment Ophthalmol. 2006;34:645–9.
42. Maddox RA, Belay ED, Curns AT, Zou WQ, Nowicki S, Lembach RG, et al.Creutzfeldt-Jakob disease in recipients of corneal transplants. Cornea. 2008;27:851–4.
43. Jirsova K, Krabcova I, Novakova J, Hnathova I, Koukolik F, Kubesova B, et al. Theassessment of pathogenic prions in the brains of eye tissue donors: 2-years experience in theCzech Republic. Cornea. 2010;29:996–9.
44. Hogan RN, Brown P, Heck E, Cavanagh HD. Risk of prion disease transmission from oculardonor tissue transplantation. Cornea. 1999;18:2–11.
45. Ironside JW, Knight RS, Will RG, Smith PG, Cousens SN. New variant Creutzfeldt-Jakobdisease is more common in Britain than elsewhere. BMJ. 1998;317:352.
46. Dunn SP, Stark WJ, Stulting RD, Lass JH, Sugar A, Pavilack MA, et al. The effect of ABOblood incompatibility on corneal transplant failure in conditions with low-risk of graftrejection. Am J Ophthalmol. 2009;147:432–8.
47. Khaireddin R, Wachtlin J, Hopfenmuller W, Hoffmann F. HLA-A, HLA-B and HLA-DRmatching reduces the rate of corneal allograft rejection. Graefes Arch Clin Exp Ophthalmol2003;241:1020–8.
48. Volker-Dieben HJ, Schreuder GM, Claas FH, Doxiadis, II, Schipper RF, Pels E, et al.Histocompatibility and corneal transplantation. Dev Ophthalmol. 2003;36:22–41.
49. Pardos GJ, Gallagher MA. Microbial contamination of donor eyes. A retrospective study.Arch Ophthalmol. 1982;100:1611–13.
50. Zamora JL. Chemical and microbiologic characteristics and toxicity of povidone-iodinesolutions. Am J Surg. 1986;151:400–6.
51. Lindquist TD, Maxwell AJ, Miller TD, Win ET, Novicki T, Fritsche TR, et al. Preparation ofcorneal donor eyes comparing 1 % versus 5 % povidone-iodine. Cornea. 2011;30:333–7.
52. Jhanji V, Tandon R, Sharma N, Titiyal JS, Satpathy G, Vajpayee RB. Whole globeenucleation versus in situ excision for donor corneal retrieval–a prospective comparativestudy. Cornea. 2008;27:1103–8.
53. Kim JH, Kim MJ, Stoeger C, Clover J, Kim JY, Tchah H. Comparison of in situ excision andwhole-globe recovery of corneal tissue in a large, single eye bank series. Am J Ophthalmol.2010;150:427–33.
54. Yanoff MD, Sassani JW. Ocular pathology. 6th ed. Philadelphia: Mosby Elsevier; 2009.55. Sperling S, Sorensen IG. Decontamination of cadaver corneas. Acta Ophthalmol (Copenh).
1981;59:126–33.56. Pels E, Beekhuis WH, Völker-Dieben HJ. Long-term tissue storage for keratoplasty. In:
Brightbill FS, editor. Corneal surgery: theory, technique, and tissue. 3rd ed. St. Louis: MosbyCo; 1999. pp 897–906.
2 Processing Corneas for Grafting 37

57. Nartey IN, Sherrard ES, Steele AD. Manipulative damage to the endothelium of infant andadult donor corneas. Br J Ophthalmol. 1990;74:261–4.
58. Pels E, Vrensen GF. Microbial decontamination of human donor eyes with povidone-iodine:penetration, toxicity, and effectiveness. Br J Ophthalmol. 1999;83:1019–26.
59. Gross A, Cofone L, Huff MB. Iodine inactivating agent in surgical scrub testing. Arch Surg.1973;106:175–8.
60. van Luijk CM, Bruinsma M, van der Wees J, Lie JT, Ham L, Melles GR. Combinedchlorhexidine and PVP-I decontamination of human donor eyes prior to corneal preservation.Cell Tissue Bank. 2012;13:333–9.
61. Matsuda M, Yee RW, Glasser DB, Geroski DH, Edelhauser HF. Specular microscopicevaluation of donor corneal endothelium. Arch Ophthalmol. 1986;104:259–62.
62. EBAA Statistical Report. (2014). 1015,18th Street, N.W. Suite 1010, Washington, DC 20036,USA. EBAA 2016. http://www.restoresight.org/wpcontent/uploads/2015/03/2014_Statistical_Report-FINAL.pdf
63. Melles GR, Eggink FA, Lander F, Pels E, Rietveld FJ, Beekhuis WH, Binder PS. A surgicaltechnique for posterior lamellar keratoplasty. Cornea. 1998;17:618–26.
64. Anwar M, Teichmann KD. Big-bubble technique to bare Descemet’s membrane in anteriorlamellar keratoplasty. J Cataract Refract Surg. 2002;28:398–403.
65. Melles GR, Lander F, Rietveld FJ, Remeijer L, Beekhuis WH, Binder PS. A new surgicaltechnique for deep stromal, anterior lamellar keratoplasty. Br J Ophthalmol. 1999;83 :327–33.
66. Suwan-Apichon O, Reyes JM, Griffin NB, Barker J, Gore P, Chuck RS. Microkeratomeversus femtosecond laser predissection of corneal grafts for anterior and posterior lamellarkeratoplasty. Cornea. 2006;25:966–8.
67. Parekh M, Ferrari S, Ponzin D. Eye Banking: Changing Face of Corneal Transplantation.2015, Nova Science Publishers, Inc (US) Hauppauge NY
68. Parekh M, Salvalaio G, Ruzza A, Camposampiero D, Griffoni C, Zampini A, Ponzin D,Ferrari S. Posterior lamellar graft preparation: a prospective review from an eye bank oncurrent and future aspects. J Ophthalmol. 2013;2013:769860. doi: 10.1155/2013/769860.Epub 2013 May 30. PubMed PMID: 23819041; PubMed Central PMCID: PMC3683473.
69. Boynton GE, Woodward MA. Eye-bank preparation of endothelial tissue. Curr OpinOphthalmol. 2014;25:319–24.
70. Mootha VV, Heck E, Verity SM, Petroll WM, Lakshman N, Muftuoglu O, et al. Comparativestudy of descemet stripping automated endothelial keratoplasty donor preparation by MoriaCBm microkeratome, horizon microkeratome, and Intralase FS60. Cornea. 2011;30:320–3.
71. Hjortdal J, Nielsen E, Vestergaard A, Sondergaard A. Inverse cutting of posterior lamellarcorneal grafts by a femtosecond laser. Open Ophthalmol J. 2012;6:19–22.
72. Busin M, Patel AK, Scorcia V, Ponzin D. Microkeratome-assisted preparation of ultrathingrafts for descemet stripping automated endothelial keratoplasty. Invest Ophthalmol Vis Sci.2012;53:521–4.
73. Thomas PB, Mukherjee AN, O’Donovan D, Rajan MS. Preconditioned donor cornealthickness for microthin endothelial keratoplasty. Cornea. 2013;32:e173–8.
74. Melles GR, Wijdh RH, Nieuwendaal CP. A technique to excise the descemet membrane froma recipient cornea (descemetorhexis). Cornea. 2004;23:286–88.
75. Lie JT, Birbal R, Ham L, van der Wees J, Melles GR. Donor tissue preparation for Descemetmembrane endothelial keratoplasty. J Cataract Refract Surg. 2008;34:1578–83.
76. Price MO, Giebel AW, Fairchild KM, Price FW Jr. Descemet’s membrane endothelialkeratoplasty: prospective multicenter study of visual and refractive outcomes and endothelialsurvival. Ophthalmology. 2009;116:2361–8.
77. Groeneveld-van Beek EA, Lie JT, van der Wees J, Bruinsma M, Melles GR. Standardized‘no-touch’ donor tissue preparation for DALK and DMEK: harvesting undamaged anteriorand posterior transplants from the same donor cornea. Acta Ophthalmol. 2013;91:145–50.
78. Muraine M, Gueudry J, He Z, Piselli S, Lefevre S, Toubeau D. Novel technique for thepreparation of corneal grafts for descemet membrane endothelial keratoplasty. Am JOphthalmol. 2013;156:851–59.
38 K. Jirsova et al.

79. Ruzza A, Parekh M, Salvalaio G, Ferrari S, Camposampiero D, Amoureux MC, et al. Bubbletechnique for Descemet membrane endothelial keratoplasty tissue preparation in an eye bank:air or liquid? Acta Ophthalmol. 2015;93:e129–34.
80. Price MO, Price FW Jr. Descemet’s membrane endothelial keratoplasty surgery: update on theevidence and hurdles to acceptance. Curr Opin Ophthalmol. 2013;24:329–35.
81. McCauley MB, Price FW Jr, Price MO. Descemet membrane automated endothelialkeratoplasty: hybrid technique combining DSAEK stability with DMEK visual results.J Cataract Refract Surg. 2009;35:1659–64.
82. Busin M, Patel AK, Scorcia V, Galan A, Ponzin D. Stromal support for Descemet’smembrane endothelial keratoplasty. Ophthalmology. 2010;117:2273–7.
83. Studeny P, Farkas A, Vokrojova M, Liskova P, Jirsova K. Descemet membrane endothelialkeratoplasty with a stromal rim (DMEK-S). Br J Ophthalmol. 2010;94:909–14.
84. Lie JT, Lam FC, Groeneveld-van Beek EA, van der Wees J, Melles GR. Graft preparation forhemi-Descemet membrane endothelial keratoplasty (hemi-DMEK). Br J Ophthalmol.2016;100:420–4.
85. Terry MA. Endothelial keratoplasty: a comparison of complication rates and endothelialsurvival between precut tissue and surgeon-cut tissue by a single DSAEK surgeon. Trans AmOphthalmol Soc. 2009;107:184–91
86. Ragunathan S, Ivarsen A, Nielsen K, Hjortdal J. Comparison of organ cultured precut corneasversus surgeon-cut corneas for Descemet’s stripping automated endothelial keratoplasty. CellTissue Bank. 2014;15:573–8.
87. Chen ES, Terry MA, Shamie N, Hoar KL, Friend DJ. Precut tissue in Descemet’s strippingautomated endothelial keratoplasty donor characteristics and early postoperative complica-tions. Ophthalmology. 2008;115:497–502.
88. Krabcova I, Studeny P, Jirsova K. Endothelial quality of pre-cut posterior corneal lamellae forDescemet membrane endothelial keratoplasty with a stromal rim (DMEK-S): two-yearoutcome of manual preparation in an ocular tissue bank. Cell Tissue Bank. 2013;14:325–31.
89. Jeng BH. Preserving the cornea: corneal storage media. Curr Opin Ophthalmol. 2006;17:332–7.
2 Processing Corneas for Grafting 39

Chapter 3Corneal Storage, Hypothermia,and Organ Culture
Katerina Jirsova, Patricia Dahl and W. John Armitage
Abstract This chapter provides information about hypothermia and organ culture,the two basic approaches to storing corneas for grafting. Procedural simplicity andthe immediate availability of tissue for transplantation make hypothermia the mostwidely used method. The recommended maximum storage time under hypothermicconditions (2–8 °C) is 14 days. Corneas placed in either vials or viewing chamberscontaining a commercially available storage solution and protected by atamper-proof seal may be evaluated by slit lamp and specular microscopy prior tografting. The main goal of hypothermic storage is to use low temperatures tosuppress metabolic activity, inhibit cellular processes, and reduce energy demand inthe tissue and thus maintain the original condition of the cornea. Macromolecules,such as dextran or chondroitin sulfate, are present in the medium control stromalhydration and prevent swelling of the cornea. Organ culture storage is used in about65 % of European eye banks because of the possibility of performing a detailedassessment of the corneal endothelium and extending storage time up to 4–5 weeks.The corneas are generally maintained at 30–37 °C in media based on a minimalessential medium supplemented with fetal bovine serum, thus allowing the corneato metabolize, that is, the endothelium can be repaired and the morphometricparameters improved. Similarly, the epithelium can be renewed from the limbus.Organ culture permits the detailed control of corneal quality, including theassessment of dead endothelial cells using light microscopy. However, during organculture, the stroma typically becomes edematous, and the cornea increases in
K. Jirsova (&)Laboratory of the Biology and Pathology of the Eye, Institute of Biology and MedicalGenetics, First Faculty of Medicine, Charles University, Prague, Czech Republice-mail: [email protected]
P. DahlThe Eye-Bank for Sight Restoration, Inc., 120 Wall Street, New York, NY 10005, USAe-mail: [email protected]
W. J. ArmitageBristol Eye Bank, NHS Blood and Transplant, and School of Clinical Sciences, University ofBristol, Bristol Eye Hospital, Lower Maudlin Street, Bristol BS1 2LX, UKe-mail: [email protected]
© Springer International Publishing AG 2017K. Jirsova, Light and Specular Microscopy of the Cornea,DOI 10.1007/978-3-319-48845-5_3
41

thickness. Shortly before the planned transplant, the cornea is therefore transferredto a medium containing macromolecular substances in which tissue dehydrationand thinning occur. Microbiologic testing of the culture media ensures thatmicroorganisms can be detected throughout the entire storage procedure. It appearsthat both storage methods result in similar graft survival.
Keywords Eye banking � Hypothermic storage � Organ culture � Microbiologictesting � Graft survival
3.1 History
3.1.1 Hypothermic Storage
The hypothermic storage of corneas was introduced by McCarey and Kaufman,who prepared M-K medium (tissue culture medium 199 with the addition ofDextran 40 as a deturgescent agent) in which corneoscleral discs could be stored forup to four days at 4 °C [1]. The method was improved by replacing the dextran withchondroitin sulfate; the resulting media, K-Sol and Dexol, permitted extendedstorage for up to one or two weeks [2, 3]. The current storage medium of choice,Optisol-GS, contains both chondroitin sulfate and dextran [4].
3.1.2 Organ Culture
Organ culture (OC) was first used for the preservation of mammalian and chickencorneas by Summerlin [5]. Together with Summerlin, the storage of corneas in aneye bank was standardized and the quality of the stored tissue was evaluated byDoughman [6]. Before grafting, the corneas were stored for 4–5 weeks in a minimalessential medium [6, 7]. Sperling prevented osmotically-driven tissue swellingduring cultivation by adding the macromolecule dextran T500 [8]. Later studiesshowed that dextran, depending on its osmolality, concentration, and the length ofstorage, penetrates endothelial and epithelial cells as well as keratocytes by endo-cytosis, leading to their vacuolization. It has been shown that the long-term effect ofdextran on corneal tissue is toxic [9, 10]. Therefore, the OC method was changed sothat the cornea is first stored in a medium without dextran, and then before graftingit is transferred to a deswelling medium with dextran, which reverses the cornealedema that occurs during cultivation [11].
Of major importance was the introduction into eye bank practice of the use oftrypan blue for staining dead cells and a hypotonic solution for the subsequentvisualization of the cell borders and the endothelial cellular mosaic [12–14].
42 K. Jirsova et al.

At present, the OC method is still used with only minor differences among eyebanks, typically in the choice of medium composition as well as minor technicaldifferences [15].
3.2 Storage Conditions
3.2.1 Hypothermic Storage
Hypothermia is the method of choice for corneal preservation in North America;moreover, it is used in about 30 % of member banks of the European Eye BankAssociation (EEBA) as well as in eye banks in Asia, Australia, and South America[16–19]. Technically, hypothermic storage is relatively simple, and besides equip-ment for microscopy and refrigeration, it does not require further expensive facilities.
Currently, Optisol-GS (Bausch and Lomb, Rochester, NY) is the most exten-sively used commercially available medium for hypothermic storage in the UnitedStates; in Europe, Eusol-C (Alchimia, Srl, Padova, Italy) is the preferred choice(Fig. 3.1) [19, 20]. In the U.S., in addition to Optisol and Optisol-GS, LIFE4°Cmedium (Duraent Biologicals Ltd., Hyderabad, India) is used [21].
Fig. 3.1 Corneas stored under hypothermic conditions. a Cornea stored in Optisol-GS. b Corneastored in Eusol-C. (a Courtesy of Jameson Clover, Lions VisionGift, Portland, OR)
3 Corneal Storage, Hypothermia, and Organ Culture 43

For hypothermic storage, the cornea is usually placed in 20 mL of media in thestorage container and subsequently assessed by slit lamp and specular microscopy,then kept at a controlled temperature until transplantation. Reduced temperature (2–8 °C) slows cellular processes and energy demand in the tissue.
Optisol-GS is based on medium 199 with the addition of HEPES buffer, 2.5 %chondroitin sulfate, 1 % dextran, ATP precursors, iron, cholesterol,L-hydroxyproline, vitamins, and the antibiotics gentamicin and streptomycin [4, 17,22, 23]. Eusol-C contains amino acids, mineral salts, and vitamins as nutrients,gentamicin sulfate as an antibiotic, dextran as an osmotic agent, sodium pyruvateand glucose as energy sources, HEPES and sodium bicarbonate as buffers, andphenol red as a pH indicator (Eusol-C leaflet). The nutrients enhance cell survival,and deturgescence agents (chondroitin sulfate, dextran) prevent the hydration andsubsequent swelling of the cornea [2, 24]. Chondroitin sulfate may also protect cellssubjected to oxidative stress [25]. Cholesterol stabilizes cell membranes, whilehydroxyproline plays a key role in collagen stability. ATP inhibits the formationand accumulation of lactate, which the cornea cannot metabolize and whoseaccumulation is associated with the loss of endothelial cells [26–28].
The osmolality of the medium for hypothermic storage is usually somewhathigher than the physiologic osmolality of the aqueous humor (Optisol-GS 351–370 mOsm/kg; Eusol-C 255–345 mOsm/kg; see Sect. 1.9).
Corneas should be stored under hypothermic conditions for a relatively shortperiod, up to 14 days. However, it has been shown that storage time longer thanseven days may increase the risk of primary failure; thus most ophthalmologistsprefer to use corneas stored for no longer than this period [29, 30]. In eye bankpractice, the average length of storage is even shorter: 4.5 and 5.4 days in the U.S.and Europe [17–19, 29]. Under experimental conditions, the impending expirationof corneas stored under hypothermic conditions was extended by transferring thecorneas from hypothermic to OC storage [31, 32], but such a procedure is not usedroutinely in eye banking practice.
The key process to judge if the tissue is suitable for grafting, the microscopicassessment of the cornea, is primarily focused on the corneal endothelium. In brief,before corneal tissue is released for penetrating keratoplasty, specular microscopy isusually performed once and slit lamp examination twice (at the beginning and endof storage) to check if the corneal/endothelial quality is consistent with that requiredfor transplantation (see Chap. 5). If the tissue is precut for the preparation oflamellar grafts, it is evaluated again by specular and slit lamp microscopy toconfirm that it was not adversely affected by the procedure (see Sect. 5.5) [33].
3.2.2 Organ Culture
OC storage is used for 82 % of corneas processed in EEBA banks, particularlybecause it allows the possibility of performing a detailed assessment of the cornealendothelium and of extending storage time up to four to five weeks [19]. Organ
44 K. Jirsova et al.

culture storage is time-consuming and technically demanding. Corneal preparationand assessment require establishing and maintaining aseptic conditions, which,besides basic equipment such as biosafety cabinets, incubators, refrigerators, andmicroscopes, is expensive.
Corneas are cultured in a biologic incubator at 30–37 °C, the majority of banksusing a temperature of 31 °C [15, 19]. The wide range of storage temperatures usedindicates that in terms of corneal storage, temperature is not a key variable, onlythat it should not be too low or too high [34].
Themost commonly used storagemedia are based onminimal essential medium orEagle minimal essential medium with Earl salts (E-MEM) supplemented with fetalbovine serum, antibiotics, and antimycotics [18, 35]. Among commercially availablemedia, particularly Tissue-C (Alchimia) and CorneaMax (Eurobio, Les Ulis, France)are used inmember banks of the EEBA. In other eye banks the medium is prepared bythe eye bank staff or by hospital pharmacies. Fetal bovine or bovine serum obtainedfrom animals bred in prion disease-free locations is usually used at concentrations of2–8 %. Penicillin, streptomycin, and gentamicin are the most often used antibiotics,and amphotericin B is the most frequently used antimycotic [19]. The presence ofvarious growth factors, hormones, cytokines, or other biologically active additives(epidermal growth factor, fibroblast growth factor, platelet-derived growth factor,insulin-like growth factor, pentoxifylline) in the culture medium positively influencesthe quality of the corneal endothelium, but these additives are mostly used experi-mentally and are omitted in common eye banking practice [36–38]. The storagemedium in which a cornea is maintained may be changed periodically because thecornea needs sufficient nutrients (such as glucose) and because of the necessity toavoidwaste product accumulation. If changed, themedium is typically renewed every5–7 days, but longer intervals may be used [18, 19]. Before transplantation, thecornea is transferred from a storage medium to a deswelling medium.
The cornea may lie loosely on the bottom of its storage container with theendothelial side uppermost or may be held afloat on a sterile suture or simplesuspension device or fastened to an eyelet connected to the culture vessel, thuskeeping it in a vertical position so that it does not touch the walls or bottom of theculture vessel (Fig. 3.2) [39]. Corneas suspended in the medium have uniformaccess to all nutrients. Compared to a cornea lying on the bottom of a vial, thisapproach is more beneficial because there is no contact between the sensitiveendothelial cells (ECs) and the peeling epithelial cells and cell debris that aredeposited on the bottom of the container. A cornea lying on the bottom is moresusceptible to contact with cellular debris, which may potentially contaminate theendothelium, as can happen when the tissue is moved within the storage bottle.Manipulating the cornea (during macroscopic inspection of the color of the mediumor light microscopy assessment) while keeping the cornea secured on its holder(suture, plastic device) is, however, technically demanding and also more vulner-able to eventual contamination or mechanical damage [35].
To maintain the vitality of cultured corneas, it is also important to ensure theappropriate pH (7.2–7.4) and osmolality (320–350 mOsm/kg) of the medium. Thecorneal endothelium has a relatively high tolerance for pH changes; to maintain an
3 Corneal Storage, Hypothermia, and Organ Culture 45

adequate pH, sodium bicarbonate and HEPES are sufficient. Standard culture mediacontaining phenol red as the pH indicator generally indicate a decrease of pH (as aconsequence of metabolic activity or contamination) by a color change fromred-orange to orange-yellow. The decrease in pH occurs slowly; during theseven-day storage period commonly used, the pH decreases from 7.4 to 7.0 [34].
For corneal cultivation, a system in which no gas exchange between the culturevessel and its surroundings is typically used. The container with the tissue is storedunder normal atmospheric conditions. In most eye banks, corneas are maintained inabout 50–80 mL of media in a glass or plastic 100-mL bottle in order to provide asufficient volume of air above the level of the media. A lack of oxygen in acultivation vessel full of media could lead to an increased lactate concentration, areduced pH, and consequently to corneal edema [40]. The relatively large volumeof storage solution also allows the dilution of toxic metabolites and prevents theiradverse influence on corneal cells [26]. The technical details of storage, such as thecomposition of the basal medium, serum concentration, the concentration and typeof antibiotics and antimycotics, media exchange intervals, maximum storage tem-perature, and pH range vary among individual eye banks [18, 19].
The use of synthetic media that contain no serum or other animal-derivedadditives has become an important trend in the preparation of tissues and cells forgrafting. The use of these media minimizes the possibility of transmitting infectiousagents to the graft recipient [28, 41–43], but currently these media are used more orless only experimentally and not for the routine organ culture of corneas.
Although slit lamp and specular microscopy can be used for examining thecornea, transmitted light microscopy is the method of choice because of its com-patibility with the vital staining used for the visualization of the endothelium. Thevisualization of the intercellular borders is induced by a hypotonic solution, and
Fig. 3.2 The storage of corneas in organ culture. a Cornea lying loosely on the bottom with theendothelial side up. Cornea floating in culture medium suspended on a suture (b) or plastic device(c). d Cornea fastened to a plastic holder. (b Courtesy of Jesper Hjortdal, University Hospital,Aarhus, Denmark; c Agate Noer, Oslo University, Norway; d Martin Hermel and Sabine Salla,RWTH Aachen University, Germany)
46 K. Jirsova et al.

dead cells can be observed after trypan blue staining (for details, see Sect. 4.2.1).The particular endothelial parameters that are assessed to determine the overallquality of the endothelium are described in Chap. 5.
3.3 Behavior of Corneal Cells During Storage
3.3.1 Hypothermic Storage
The main principle of hypothermic storage is that reduced temperature decreasesthe rates of chemical reactions and thus cellular processes and energy demand in thecornea. On the other hand, low temperature also has deleterious effects on all typesof cells present in various corneal layers and therefore reduces the maximumstorage time. Although the viability of the corneal endothelium is far moreimportant in terms of graft survival, the integrity of the epithelium is a prerequisitefor successful grafting in cases of severe disturbances of the ocular surface.
During hypothermia, the loss of both endothelial and epithelial cells increases withthe length of storage [44–47]. Rates of endothelial cell death reaching up to 20 %werefound in 90 % of corneas stored for 14 days in Optisol-GS [44]. A high percentage ofdead cells was found in corneas with a relatively low original ECD stored in Eusol-C,reaching 25 % dead cells after eight days of storage [47]. No differences in thesurvival of ECs inOptisol-GS versus Eusol-Cwere found in a study performed on 180corneas [48]. Besides cell death, the deterioration of tight junctions and theendothelial cytoskeleton was observed after 2–8 days in hypothermia [49].
Some separation of the surface epithelial cells occurs during corneal storage inOptisol-GS for up to six days, with the percentage of dead cells reaching 20–25 %.At the end of the recommended storage period for Optisol-GS (14 days), significantsloughing of the epithelial cells and the disruption of epithelial junctions occur, and50 % of the remaining epithelial cells are dead [45]. In studies evaluating thesurvival of the corneal epithelium in Optisol-GS and Dexsol or Optisol-GS andLIFE4 °C, it was found that the epithelial cells (except for the basal cells) slough offwithin four days of storage [21, 45, 46]. No endothelial repair or epithelial cellrenewal has been observed under hypothermic conditions.
3.3.2 Organ Culture
Although the composition of the medium and the storage temperature ensure therelatively long-term survival of ECs, a gradual but significant decrease in theirnumber, mainly due to apoptosis, occurs under both storage conditions. It has beenshown that apoptosis may be an important factor in the loss of ECs and thatantiapoptotic gene therapy prolongs their survival during storage [50–52].However, it has also been reported that few apoptotic ECs are evident up to
3 Corneal Storage, Hypothermia, and Organ Culture 47

four weeks of storage [53]. Dead ECs are released into the medium, and the nakedDescemet membrane is covered by the spreading and enlargement of cellsmigrating from the surrounding area [54, 55]. It has been shown that after one weekin OC, about 5 % of the ECs are lost [11], while after three weeks an 11–20 % lossof ECs occurs, depending on the concentration of fetal bovine serum in the medium(2–8 %, respectively) [28]. OC simulates physiologic conditions and therefore alsoallows the repair of larger endothelial lesions [36, 56]. In contrast to fresh tissue, theproliferation of ECs has been observed in OC corneas [57].
During OC the number of epithelial layers decreases from six to seven layers totwo to four [11, 58], but the integrity of the tight junctions and the actincytoskeleton in both epithelial and endothelial cells are maintained for up to28 days [53]. It was shown that epithelial cells are less resistant to apoptosis in OCstorage compared to ECs. The release of epithelial cells is compensated for by theirrenewal. The reticular bundles of the newly formed epithelial layer are clearlyvisible using light microscopy (see Figs. 6.113 and 6.114), and limbal stem cellssurvive even after 30 days of cultivation [59].
It was shown that OC storage leads to a gradual decrease in the number ofantigen-presenting cells (APCs), which are normally located primarily at theperiphery of the cornea; extent of their decrease is dependent on the length ofstorage time [60, 61]. The decreased number of APCs may reduce the immuno-genicity of the tissue without compromising its vitality [11, 62]. The fact that theprolonged storage in OC leads to a lower incidence of endothelial immune reactionsand positively influences allograft survival, particularly in high-risk recipients, wasalso demonstrated in clinical studies [63, 64]. On the other hand, it is necessary tokeep in mind that during OC, the number of ECs decreases; thus the balancebetween the positive effect of APCs losses and the negative effect of ECs lossesshould be considered. Keratocytes, which under physiologic conditions are renewedvery slowly, remain viable up to four weeks when maintained in OC. Thus viablestroma can be grafted within this period [65].
3.4 Preparation of the Cornea Before Grafting
3.4.1 Hypothermic Storage
Before corneal tissue is released for transplantation (assuming that donor selectioncriteria are consistent with the use of the tissue), a slit lamp examination must beperformed to look for epithelial or stromal pathology as well as endothelial disease.Additionally, the ECD must be determined using specular microscopy [33]. Thekey advantage of hypothermic storage is that the cornea, after performing the finalmicroscopic control of tissue quality, is immediately available for transport andsubsequent transplantation. Transporting corneas in hypothermic storage mediarequires wet ice added to an insulated container that has been validated to maintaina temperature of 2–8 °C for the specified length of time (from eye bank to trans-plant facility).
48 K. Jirsova et al.

3.4.2 Organ Culture
During culturing, the cornea spontaneously swells to about twice its normalthickness. This increased thickness should be reversed to normal values beforetransplantation. The grafting of an abnormally thickened cornea needs more carecompared to a cornea of physiologic thickness and may potentially lead to theloosening of the sutures after the transplanted cornea returns to normal thickness(approximately 550 µm). Depending on the degree of corneal hydration, themicroscopic reassessment of the tissue before its release for grafting often cannot beperformed in detail. This means that OC corneas are not always available forimmediate grafting or that they are not ready for use at every time point duringstorage.
Before a planned surgery, the cornea is placed into a deswelling (dehydrating ortransport) medium containing deturgescent macromolecules, usually 4–8 % dex-tran T500. Water is removed from the stroma, thus deswelling the cornea tophysiologic or nearly physiologic thickness, depending on the dextran concentra-tion [66]. For the standard preparation of corneas for grafting, higher concentrationsof dextran are not recommended because of its toxic effect. Ideally, storage in adextran-containing medium should not exceed two days [67]. In most eye banks,corneas are maintained in a deswelling medium for 1–7 days at 20–35 °C [18, 19].The total time that the cornea spends in both media (i.e., storage and deswelling)usually does not exceed four to five weeks, which provides enough time forscreening, microbiologic testing, HLA typing and matching when necessary, andtissue allocation [11, 15, 68]. However, it is possible to maintain the cornea evenlonger, up to 48 days [69]. The average length of storage in EEBA banks is 19 daysin storage medium and another two days in deswelling medium [18, 19, 70].
3.5 Microbiologic Testing of the Cornea
3.5.1 Hypothermic Storage
The activity of antibiotics is much weaker at reduced temperatures; moreover, lowtemperatures inhibit the proliferation of most infectious etiologic agents. Therefore,it is necessary to leave the cornea in storage media at room temperature forthree hours prior to refrigeration. Similarly, warming the tissue at room temperaturebefore planned surgery may enhance the effect of antibiotics [15, 71, 72]. The loweractivity and effectiveness of antibiotics and the reduced capability of most infec-tious agents to proliferate at low temperatures indicate that microbiologic testingcannot be adequately performed during storage under hypothermic conditions.
Corneoscleral rims obtained from corneas prepared for grafting showed thepresence of bacteria or fungi in 10–19 % of cases [73, 74]. More positive cultureswere found with corneas stored in Optisol (20 %) than in Optisol-GS (11 %) [73].
3 Corneal Storage, Hypothermia, and Organ Culture 49

Positive cultures were also more frequently seen in corneas excised in situ (22 %)than for those that were enucleated (13 %) [73, 74], although some studies havereported no differences [75] or even opposite findings [76]. The prognostic role ofdonor corneoscleral rim cultures in predicting the incidence of endophthalmitis aftercorneal grafting was shown in a study that found that bacterial and particularlyfungal endophthalmitis developed more often among recipients of a culture-positivedonor cornea [77].
3.5.2 Organ Culture
The temperature and composition of the culture media allow the growth ofmicroorganisms, and thus microbiologic testing of the storage and deswellingmedia is routinely performed [68, 74]. If the presence of antibiotics and antimy-cotics in OC media does not suppress the infection, microorganism overgrowth willresult in visible changes, such as the loss of transparency of the medium, turbidity,changes in its color, or the presence of structures typical for the growth of yeasts orfilamentous fungi (Fig. 3.3). The macroscopic inspection of the color and trans-parency of the media should be performed regularly during OC [78].
Microbiologic examination of the storage solution can be performed at any timeduring storage, but generally a sample of the storage medium is taken when it isrenewed or when the tissue is transferred into deswelling medium. It is crucial thatmicrobiologic testing be done before the tissue is released for grafting during theperiod that allows the tissue to be excluded from transplantation if contamination isfound. The detection of bacterial or fungal contamination during storage therebyreduces the risk of potentially grafting infected tissue [19, 68]. Although basicmicrobiologic testing can be performed in an eye bank, detailed microbiologictesting is normally performed in specialized departments. It was shown that because
Fig. 3.3 Bacterial and fungal contamination of cultured corneas. a Bacterial contamination ischaracterized by the loss of transparency of the medium, turbidity, and changes in its color.b Fungal contamination is characterized by the presence of fungal structures (arrow)
50 K. Jirsova et al.

of contamination or suspected contamination, about 3 % of corneas are excludedfrom grafting [18, 19]. Other studies have reported that of all contaminated corneas,70 % show bacterial contamination while the remaining 30 % exhibit fungalcontamination [74, 79]. The percentage of positive microbiology results is similarfor OC corneoscleral discs excised from either enucleated or nonenucleated eyes[73, 80].
Fewer positive rim cultures were found postoperatively for corneas stored in OCprior to grafting, with a contamination rate of 1.3 % compared to 9.8 % for corneasstored in hypothermia prior to transplantation [74]; another study reported evenmore pronounced differences [79].
3.6 Releasing Tissue for Grafting, Graft Survival
3.6.1 Hypothermic Storage
Although no contamination threatens during preservation in a closed system and theanti-infectious properties of the recipient’s anterior chamber are relatively powerful,an infection from the donor cornea may be transmitted. Acute endophthalmitis(occurring within 6 weeks of surgery) appears after about 0.3–0.5 % of kerato-plasties performed using corneas stored in hypothermia [73, 81].
In a retrospective study of more than 17,000 corneal grafts stored underhypothermic conditions, it was found that endophthalmitis developed in about1.3 % of patients receiving corneas with a positive microbiologic result of thecorneoscleral rims [77]. Experimentally, it has been demonstrated that the additionof amphotericin B to Optisol-GS may significantly improve its antifungal activity,particularly against contamination with Candida species, which is the primarycause of fungal infection after grafting [82].
After penetrating keratoplasty or after anterior lamellar keratoplasty, the cornealepithelium is renewed primarily based on the differentiation and migration of therecipient’s limbal stem cells; thus the presence of donor epithelial cells is notessential for graft survival. On the other hand, the grafting of corneas with an intactepithelium is particularly important for recipients whose ocular surface is signifi-cantly impaired, especially for patients with Stevens-Johnson syndrome, ocularpemphigoid, scars, severe dry eye syndrome, or limbal stem cell deficiency. Whenre-epithelialization does not occur, post-transplant epithelial defects may increasethe risk of infection, scarring, thinning of the stroma, and corneal perforation, whichfinally may lead to graft failure [17]. Cornea storage in hypothermia for longer thanseven days leads to postoperative epithelial erosion and an increased number ofpersistent epithelial defects [30]. One day after surgery, 31–35 % of patients werefound to have an epithelial defect [83, 84]. Graft re-epithelialization of corneaspreviously stored in hypothermia usually does not take more than seven days, atwhich time confluency reaches 75–91 % [4, 85, 86].
3 Corneal Storage, Hypothermia, and Organ Culture 51

3.6.2 Organ Culture
Insufficient tissue quality, positive serologic results, microbiologic contamination,and donor medical history are the main causes of excluding corneas from grafting[19]. The total amount of discarded tissue using OC reaches 33–43 % for proce-dures based on the microscopic assessment of dead cells [50, 68, 87]. This per-centage is higher than for corneas stored in hypothermia, in part because of therelatively high percentage of OC corneas discarded as a result of positive micro-biologic results (about 3 %) that cannot be adequately checked under hypothermiaand in addition because of inadequate corneal parameters (about 18 %) whosedeterioration is better detected using light microscopy [18, 19]. Fortunately, corneasexcluded from grafting because of the presence of stromal scars or poor endothelialquality may be successfully used for the preparation of lamellar grafts [88, 89].
Complete re-epithelialization of grafted corneas previously stored in OC wasobserved in one day in 29 % of patients, in three days in 66 %, and in seven daysin 94 %. Chronic postoperative epithelial defects occurred in 3 % of patients andhealed within 3–30 weeks after surgery [90]. The incidence of endophthalmitisafter the grafting of OC corneas is relatively rare, occurring in about 0.7 % of graftrecipients, and the incidence of endophthalmitis appearing within six weeks ofsurgery (i.e., as a possible consequence of the storage conditions) is even lower,only 0.16 % [91].
3.7 Advantages and Disadvantages of Each StorageMethod
Considering all aspects of both storage methods, the main relative advantages anddisadvantages of hypothermia and OC are the following:
Hypothermic storage:
+ This method is relatively simple and less expensive.
+ Corneas are available for grafting immediately after obtaining a negative sero-logic result and throughout the whole storage procedure.
+ Manipulation with a closed container is easier, and no contamination threatensduring storage.
− Reduced temperature allows the cornea to be stored for only a relatively shorttime.
− The quality of the endothelium cannot be inspected in detail over the wholeendothelial surface, and an accurate assessment of the presence of dead cellscannot be performed.
− Endothelial repair and epithelial renewal do not occur.− Adequate microbiologic control cannot be done.
52 K. Jirsova et al.

Organ culture:
+ The quality of the endothelium can be inspected over the whole endothelialsurface both before and after storage, and the counting of dead cells can beperformed to determine the true ECD.
+ The repair of the corneal endothelium as well as re-epithelialization occur.+ Interim microbiologic testing minimizes the risk of grafting contaminated tissue.+ Long-term cultivation may lead to a decrease in the number of APCs.− This relatively complicated technique requires well-trained and experienced
personnel.− The corneas are not immediately available for grafting.− The manipulation of the tissue (although working under aseptic conditions) mayincrease the risk of contamination.
References
1. McCarey BE, Kaufman HE. Improved corneal storage. Invest Ophthalmol. 1974;13:165–73.2. Kaufman HE, Varnell ED, Kaufman S, Beuerman RW, Barron BA. K-Sol corneal
preservation. Am J Ophthalmol. 1985;100:299–304.3. Wilson SE, Bourne WM. Corneal preservation. Surv Ophthalmol. 1989;33:237–59.4. Lindstrom RL, Kaufman HE, Skelnik DL, Laing RA, Lass JH, Musch DC, et al. Optisol
corneal storage medium. Am J Ophthalmol. 1992;114:345–56.5. Summerlin WT, Miller GE, Harris JE, Good RA. The organ-cultured cornea: an in vitro
study. Invest Ophthalmol. 1973;12:176–80.6. Doughman DJ, Van Horn D, Harris JE, Miller GE, Lindstrom R, Summerlin W, Good RA.
Endothelium of the human organ cultured cornea: an electron microscopic study. Trans AmOphthalmol Soc. 1973;71:304–24; discussion 325–28.
7. Doughman DJ, Harris JE, Schmitt MK. Penetrating keratoplasty using 37 C organ culturedcornea. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol. 1976;81:778–93.
8. Sperling S. Human corneal endothelium in organ culture. The influence of temperature andmedium of incubation. Acta Ophthalmol (Copenh). 1979;57:269–76.
9. van der Want HJ, Pels E, Schuchard Y, Olesen B, Sperling S. Electron microscopy of culturedhuman corneas. Osmotic hydration and the use of a dextran fraction (dextran T 500) in organculture. Arch Ophthalmol. 1983;101:1920–6.
10. Redbrake C, Salla S, Nilius R, Becker J, Reim M. A histochemical study of the distribution ofdextran 500 in human corneas during organ culture. Curr Eye Res. 1997;16:405–11.
11. Pels E, Schuchard Y. Organ-culture preservation of human corneas. Doc Ophthalmol.1983;56:147–53.
12. Stocker FW, King EH, Lucas DO, Georgiade N. A comparison of two different stainingmethods for evaluating corneal endothelial viability. Arch Ophthalmol. 1996;76:833–5.
13. Kirk AH, Hassard DT. Supravital staining of the corneal endothelium and evidence for amembrane on its surface. Can J Ophthalmol. 1969;4:405–15.
14. Sperling S. Evaluation of the endothelium of human donor corneas by induced dilation ofintercellular spaces and trypan blue. Graefes Arch Clin Exp Ophthalmol. 1986;224:428–34.
15. Pels E, Beele H, Claerhout I. Eye bank issues: II. Preservation techniques: warm versus coldstorage. Int Ophthalmol. 2008;28:155–63.
16. Patel HY, Brookes NH, Moffatt L, Sherwin T, Ormonde S, Clover GM, McGhee CN. TheNew Zealand National Eye Bank study 1991-2003: a review of the source and management ofcorneal tissue. Cornea. 2005;24:576–82.
3 Corneal Storage, Hypothermia, and Organ Culture 53

17. Jeng BH. Preserving the cornea: corneal storagemedia. Curr Opin Ophthalmol. 2006;17:332–7.18. EEBA Directory. European Eye Bank Association, Directory, 23rd ed. Venice, Italy: 2015.19. EEBA Directory. European Eye Bank Association, Directory, 24th ed. Aarhus, Denmark;
2016.20. Armitage WJ. Preservation of human cornea. Transfus Med Hemother. 2011;38:143–7.21. Soni NG, Hoover CK, Da Silva H, Jeng BH. Preservation of the corneal epithelium in
different corneal storage media. Cornea. 2015;34:1400–3.22. Sobottka Ventura AC, Rodokanak-von Schrenk A, Hollstein K, Hagenah M, Böhnke M,
Engelmann K. Endothelial cell death in organ-cultured donor corneae: the influence oftraumatic versus nontraumatic cause of death. Graefes Arch Clin Exp Ophthalmol.1997;235:230–3.
23. Yap C, Wong AM, Naor J, Rootman DS. Corneal temperature reversal after storage in Chenmedium compared with Optisol GS. Cornea. 2001;20:501–4.
24. Kaufman HE, Beuerman RW, Steinemann TL, Thompson HW, Varnell ED. Optisol cornealstorage medium. Arch Ophthalmol. 1991;109:864–8.
25. Canas N, Valero T, Villarroya M, Montell E, Verges J, Garcia AG, Lopez MG. Chondroitinsulfate protects SH-SY5Y cells from oxidative stress by inducing heme oxygenase-1 viaphosphatidylinositol 3-kinase Akt. J Pharmacol Exp Ther. 2007;323:946–53.
26. Ayoubi MG, Armitage WJ, Easty DL. Corneal organ culture: effects of serum and a stabilisedform of L-glutamine. Br J Ophthalmol. 1996;80:740–4.
27. Chen CH, Rama P, Chen AH, Franch A, Sulewski M, Orlin S, et al. Efficacy of mediaenriched with nonlactate-generating substrate for organ preservation: in vitro and clinicalstudies using the cornea model. Transplantation. 1999;67:800–8.
28. Moller-Pedersen T, Hartmann U, Moller HJ, Ehlers N, Engelmann K. Evaluation of potentialorgan culture media for eye banking using human donor corneas. Br J Ophthalmol.2001;85:1075–9.
29. Wilhelmus KR, Stulting RD, Sugar J, Khan MM. Primary corneal graft failure. A nationalreporting system. Medical Advisory Board of the Eye Bank Association of America. ArchOphthalmol. 1995;113:1497–1502.
30. Wagoner MD, Gonnah el S. Corneal graft survival after prolonged storage in Optisol-GS.Cornea. 2005;24:976–9.
31. Camposampiero D, Tiso R, Zanetti E, Ruzza A, Bruni A, Ponzin D. Improvement of humancorneal endothelium in culture after prolonged hypothermic storage. Eur J Ophthalmol.2003;13:745–51.
32. Haug K, Azqueta A, Johnsen-Soriano S, Shahdadfar A, Drolsum LK, Moe MC, et al. Donorcornea transfer from Optisol GS to organ culture storage: a two-step procedure to increasedonor tissue lifespan. Acta Ophthalmol. 2013;91:219–25.
33. EBAA Medical Standards, Washington, D.C.: EBAA; 2015. www.restoresight.org34. Pels E, Schuchard Y. Organ culture in Netherlands. In: Brightbill FS, editor. Corneal surgery:
theory, technique, and tissue. 2nd ed. St. Louis: Mosby Co; 1993. pp 622–32.35. Pels E, Beekhuis WH, Völker-Dieben HJ. Long-term tissue storage for keratoplasty. In:
Brightbill FS, editor. Corneal surgery: theory, technique, and tissue. 3rd ed. St. Louis: MosbyCo; 1999. pp 897–906.
36. Hoppenreijs VP, Pels E, Vrensen GF, Treffers WF. Corneal endothelium and growth factors.Surv Ophthalmol. 1996;41:155–64.
37. Barisani-Asenbauer T, Kaminski S, Schuster E, Dietrich A, Biowski R, Lukas J,Gosch-Baumgartner I. Impact of growth factors on morphometric corneal endothelial cellparameters and cell density in culture-preserved human corneas. Cornea. 1997;16:537–40.
38. Ventura AC, Bohnke M. Pentoxifylline influences the autocrine function of organ cultureddonor corneas and enhances endothelial cell survival. Br J Ophthalmol. 2001;85:1110–14.
39. Lie JT, Lock FM, Mulder PG, van der Wees J, Melles GR. Floating device for donor corneasin organ culture. Br J Ophthalmol. 2008;92:1676–8.
40. Polse KA, Brand RJ, Cohen SR, Guillon M. Hypoxic effects on corneal morphology andfunction. Invest Ophthalmol Vis Sci. 1990;31:1542–54.
54 K. Jirsova et al.

41. Thuret G, Manissolle C, Campos-Guyotat L, Guyotat D, Gain P. Animal compound-freemedium and poloxamer for human corneal organ culture and deswelling. Invest OphthalmolVis Sci. 2005;46:816–22.
42. Zhao XC, Nakamura H, Subramanyam S, Stock LE, Gillette TE, Yoshikawa S, et al.Spontaneous and inheritable R555Q mutation in the TGFBI/BIGH3 gene in two unrelatedfamilies exhibiting Bowman’s layer corneal dystrophy. Ophthalmology. 2007;114:e39–46.
43. Smith VA, Johnson T. Evaluation of Megacell MEM as a storage medium for corneasdestined for transplantation. Ophthalmic Res. 2010;43:18–25.
44. Means TL, Geroski DH, Hadley A, Lynn MJ, Edelhauser HF. Viability of human cornealendothelium following Optisol-GS storage. Arch Ophthalmol. 1995;113:805–9.
45. Means TL, Geroski DH, L’Hernault N, Grossniklaus HE, Kim T, Edelhauser HF. The cornealepithelium after optisol-GS storage. Cornea. 1966;15:599–605.
46. Greenbaum A, Hasany SM, Rootman D. Optisol vs Dexsol as storage media for preservationof human corneal epithelium. Eye (Lond). 2004;18:519–24.
47. Yuksel B, Uzunel UD, Kusbeci T. Endothelial cell viability of donor corneas preserved inEusol-C corneal storage medium. Exp Clin Transplant. 2015; doi:10.6002/ect.2014.0295[Epub ahead of print].
48. Kanavi MR, Javadi MA, Chamani T, Fahim P, Javadi F. Comparing quantitative andqualitative indices of the donated corneas maintained in Optisol-GS with those kept inEusol-C. Cell Tissue Bank. 2015;16:243–7.
49. Hsu JK, Cavanagh HD, Jester JV, Ma L, Petroll WM. Changes in corneal endothelial apicaljunctional protein organization after corneal cold storage. Cornea. 1999;18:712–20.
50. Albon J, Tullo AB, Aktar S, Boulton ME. Apoptosis in the endothelium of human corneas fortransplantation. Invest Ophthalmol Vis Sci. 2000;41:2887–93.
51. Gain P, Thuret G, Chiquet C, Dumollard JM, Mosnier JF, Burillon C, et al. Value of twomortality assessment techniques for organ cultured corneal endothelium: trypan blue versusTUNEL technique. Br J Ophthalmol. 2002;86:306–10.
52. Fuchsluger TA, Jurkunas U, Kazlauskas A, Dana R. Anti-apoptotic gene therapy prolongssurvival of corneal endothelial cells during storage. Gene Ther. 2011;18:778–87.
53. Crewe JM, Armitage WJ. Integrity of epithelium and endothelium in organ-cultured humancorneas. Invest Ophthalmol Vis Sci. 2001;42:1757–61.
54. Doughman DJ, Van Horn D, Rodman WP, Byrnes P, Lindstrom RL. Human cornealendothelial layer repair during organ culture. Arch Ophthalmol. 1976;94:1791–96.
55. Sperling S. Early morphological changes in organ cultured human corneal endothelium. ActaOphthalmol (Copenh). 1978;56:785–92.
56. Nejepinska J, Juklova K, Jirsova K. Organ culture, but not hypothermic storage, facilitates therepair of the corneal endothelium following mechanical damage. ActaOphthalmol.2010;88:413–19.
57. Gan L, Fagerholm P, Ekenbark S. Expression of proliferating cell nuclear antigen in corneaskept in long term culture. Acta Ophthalmol Scand. 1998;76:308–13.
58. Armitage WJ, Crewe JM, Tullo AB. Corneal transplantation: how successful are we? Br JOphthalmol. 2001;85:122.
59. Shanmuganathan VA, Rotchford AP, Tullo AB, Joseph A, Zambrano I, Dua HS. Epithelialproliferative potential of organ cultured corneoscleral rims; implications for allo-limbaltransplantation and eye banking. Br J Ophthalmol. 2006;90:55–8.
60. Ardjomand N, Berghold A, Reich ME. Loss of corneal Langerhans cells during storage inorgan culture medium, Optisol and McCarey-Kaufman medium. Eye (Lond). 1998;12 (Pt1):134–8.
61. Al-Fakih A, Faltus V, Jirsova K. A decrease in the density of HLA-DR-positive cells occursfaster in corneas stored in organ culture than under hypothermic conditions. Ophthalmic Res.2012;47:39–46.
62. Mayer WJ, Irschick UM, Moser P, Wurm M, Huemer HP, Romani N, Irschick EU.Characterization of antigen-presenting cells in fresh and cultured human corneas using noveldendritic cell markers. Invest Ophthalmol Vis Sci. 2007;48:4459–67.
3 Corneal Storage, Hypothermia, and Organ Culture 55

63. Simon M, Fellner P, El-Shabrawi Y, Ardjomand N. Influence of donor storage time oncorneal allograft survival. Ophthalmology. 2004;111:1534–38.
64. Maier P, Heinzelmann S, Bohringer D, Reinhard T. Prolonged organ culture reduces theincidence of endothelial immune reactions. Eye (Lond). 2016;30:127–32.
65. Moller-Pedersen T, Moller HJ. Viability of human corneal keratocytes during organ culture.Acta Ophthalmol Scand. 1996;4:449–55.
66. Pels E, Schuchard Y. The effects of high molecular weight dextran on the preservation ofhuman corneas. Cornea. 1984;3:219–27.
67. Borderie VM, Baudrimont M, Lopez M, Carvajal S, Laroche L. Evaluation of the deswellingperiod in dextran-containing medium after corneal organ culture. Cornea. 1997;16:215–23.
68. Armitage WJ, Easty DL. Factors influencing the suitability of organ-cultured corneas fortransplantation. Invest Ophthalmol Vis Sci. 1997;38:16–24.
69. Frueh BE, Bohnke M. Corneal grafting of donor tissue preserved for longer than 4 weeks inorgan-culture medium. Cornea. 1955;14:463–66.
70. EEBA Directory. European Eye Bank Association Directory, 22nd ed. Lausanne,Switzerland: 2014.
71. Hwang DG, Nakamura T, Trousdale MD, Smith TM. Combination antibiotic supplementationof corneal storage medium. Am J Ophthalmol. 1993;115:299–308.
72. Lass JH, Gordon JF, Sugar A, Norden RA, Reinhart WJ, Meyer RF, Soong HK. Optisolcontaining streptomycin. Am J Ophthalmol. 1993;116:503–4.
73. Wiffen SJ, Weston BC, Maguire LJ, Bourne WM. The value of routine donor corneal rimcultures in penetrating keratoplasty. Arch Ophthalmol. 1997;115:719–24.
74. Fontana L, Errani PG, Zerbinati A, Musacchi Y, Di Pede B, Tassinari G. Frequency ofpositive donor rim cultures after penetrating keratoplasty using hypothermic andorgan-cultured donor corneas. Cornea. 2007;26:552–6.
75. Jhanji V, Tandon R, Sharma N, Titiyal JS, Satpathy G, Vajpayee RB. Whole globeenucleation versus in situ excision for donor corneal retrieval–a prospective comparativestudy. Cornea. 2008;27:1103–8.
76. Gomes JA, Dana MR, Dua HS, Goren MB, Laibson PR, Cohen EJ. Positive donor rim culturein penetrating keratoplasty. Cornea. 1995;14:457–62.
77. Wilhelmus KR, Hassan SS. The prognostic role of donor corneoscleral rim cultures in cornealtransplantation. Ophthalmology. 2007;114:440–5.
78. Pels E, Schuchard Y. Tissue storage. E: Organ culture and endothelial evaluation as apreservation method for human corneas. In: Brightbill FS, editor. Corneal surgery. Theory,technique, and tissue. St. Louis: CV Mosby; 1986. pp 93–102.
79. Borderie VM, Laroche L. Microbiologic study of organ-cultured donor corneas.Transplantation. 1998;66:120–3.
80. Schroeter J, Wilkemeyer I, Herrlinger F, Pruss A. Comparison of in situ corneoscleral discexcision versus whole globe enucleation in cornea donors regarding microbial contaminationin organ culture medium - a prospective monocentric study over 9 years. Transfus MedHemother. 2012;39:391–4.
81. Kloess PM, Stulting RD, Waring GO 3rd, Wilson LA. Bacterial and fungal endophthalmitisafter penetrating keratoplasty. Am J Ophthalmol. 1993;115:309–16.
82. Layer N, Cevallos V, Maxwell AJ, Hoover C, Keenan JD, Jeng BH. Efficacy and safety ofantifungal additives in Optisol-GS corneal storage medium. JAMA Ophthalmol. 2014;132:832–7.
83. Machado RA, Mannis MJ, Mandel HA, Feiz V, Schwab IR, Wang W, Wang JL. Therelationship between first postoperative day epithelial status and eventual health of the ocularsurface in penetrating keratoplasty. Cornea. 2002;21:574–7.
84. Chou L, Cohen EJ, Laibson PR, Rapuano CJ. Factors associated with epithelial defects afterpenetrating keratoplasty. Ophthalmic Surg. 1994;25:700–3.
85. Lass JH, Musch DC, Gordon JF, Laing RA. Epidermal growth factor and insulin use incorneal preservation. Results of a multi-center trial. The Corneal Preservation StudyGroup. Ophthalmology. 1994;101:352–9.
56 K. Jirsova et al.

86. Naor J, Slomovic AR, Chipman M, Rootman DS. A randomized, double-masked clinical trialof Optisol-GS vs Chen medium for human corneal storage. Arch Ophthalmol.2002;120:1280–5.
87. Gavrilov JC, Borderie VM, Laroche L, Delbosc B. Influencing factors on the suitability oforgan-cultured corneas. Eye (Lond). 2010;24:1227–33.
88. Phillips PM, Terry MA, Shamie N, Chen ES, Hoar KL, Stoeger C, et al. Descemet’s strippingautomated endothelial keratoplasty (DSAEK) using corneal donor tissue not acceptable foruse in penetrating keratoplasty as a result of anterior stromal scars, pterygia, and previouscorneal refractive surgical procedures. Cornea. 2009;28:871–6.
89. Parekh M, Salvalaio G, Ruzza A, Camposampiero D, Griffoni C, Zampini A, et al. Posteriorlamellar graft preparation: a prospective review from an eye bank on current and futureaspects. J Ophthalmol. 2013;769860.
90. Borderie VM, Touzeau O, Bourcier T, Allouch C, Laroche L. Graft reepithelialization afterpenetrating keratoplasty using organ-cultured donor tissue. Ophthalmology. 2006;113:2181–6.
91. Chen JY, Jones MN, Srinivasan S, Neal TJ, Armitage WJ, Kaye SB, Group NOTA,Contributing O. Endophthalmitis after penetrating keratoplasty. Ophthalmology. 2015;122:25–30.
3 Corneal Storage, Hypothermia, and Organ Culture 57

Chapter 4Various Approaches to the MicroscopicAssessment of the Cornea, Visualizationand Image Analysis of the CornealEndothelium
Katerina Jirsova, Jameson Clover, Christopher G. Stoegerand Gilles Thuret
Abstract This chapter describes the three main microscopic approaches used toassess corneal quality prior to grafting: slit lamp microscopy, transmitted lightmicroscopy, and specular (i.e., reflection) microscopy. Slit lamp microscopy ispreferably used to evaluate the cornea and the surrounding parts of the eye soon afterenucleation or to assess a cornea placed in a viewing chamber during hypothermicstorage. This approach allows signs of previous surgery, stromal opacities, epithelialdefects, foreign bodies, or an abnormal corneal shape to be detected. Transmittedlight microscopy is typically used to assess corneas during organ culture storage,while specular microscopy is generally used to evaluate corneas stored inhypothermic media. When an eye bank distributes corneas for different types ofsurgery (penetrating or lamellar keratoplasty), a careful examination helps to matchthe available tissue with the requirements of different surgical techniques and thus tooptimize the utilization of a limited resource. Although all of the corneal layers,including the epithelium and the stroma, need to be evaluated if the cornea isintended for penetrating keratoplasty, the assessment is primarily focused on thecorneal endothelium. The open system of organ culture allows the visualization of
K. Jirsova (&)Laboratory of the Biology and Pathology of the Eye, Institute of Biology and MedicalGenetics, First Faculty of Medicine, Charles University, Ke Karlovu 2, 128 08 Prague 2,Czech Republice-mail: [email protected]
J. Clover � C.G. StoegerLions VisionGift, 2201 SE 11th Ave., 97214 Portland, OR, USAe-mail: [email protected]
C.G. Stoegere-mail: [email protected]
G. ThuretCorneal Graft Biology, Engineering, and Imaging Laboratory, Jean Monnet University,10, rue de la Marandière, 42055 Saint-Etienne, Francee-mail: [email protected]
© Springer International Publishing AG 2017K. Jirsova, Light and Specular Microscopy of the Cornea,DOI 10.1007/978-3-319-48845-5_4
59

dead endothelial cells using trypan blue vital staining and of the cell borders usinghypotonic solution. Recent technical progress allows the endothelium to be evalu-ated by various image analysis systems connected to user-friendly software pro-grams that employ semiautomatic or fully automatic algorithms for cell assessment.
Keywords Cornea � Eye bank � Slit lamp microscopy � Specular microscopy �Transmitted light microscopy � Corneal endothelium visualization � Border andcenter methods
4.1 Slit Lamp Microscopy
Slit lamp microscopy is a standard approach for evaluating whole eyes or corneasmaintained in storage solutions, and each prepared cornea that could potentially besuitable for grafting should be examined using a slit lamp. Usually an enucleatedeye is first assessed by slit lamp microscopy and then is used to prepare a cor-neoscleral disc for storage in organ culture (OC). Excised corneas stored underhypothermic conditions are evaluated using a slit lamp after procurement andpreservation. For the examination, a whole eye is fixed in a holder, while an alreadyprepared corneoscleral disc is evaluated in a storage chamber or vial (Fig. 4.1) [1].
A projected light provides illumination that can be adjusted from a large, circulararea of light down to a narrow, slitlike beam. The examination is usually done fromthe peripheral to the central part of the cornea. First, the scleral rim should beinspected for any damage such as the presence of scars or sutures and otherpathologic signs. Diseases affecting the sclera are fortunately rare and include
Fig. 4.1 Assessment of the cornea using a slit lamp. a A whole eye and b corneoscleral disc in aviewing chamber (hypothermic storage) (b Courtesy of Andrea Gareiss-Lok, Hornhautbank,Munich, Germany)
60 K. Jirsova et al.

scleral extension of choroid melanoma, which presents as a dark brown pigmen-tation perforating the sclera. In addition, the diameter and regularity of the scleralrim can be measured to verify its compatibility with the artificial anterior chambersnecessary during lamellar graft preparation.
The slit lamp examination can detect an abnormal corneal shape (keratoconus,keratoglobus, micro- or megalocornea), an abnormally thin cornea (keratoconus orectasia following refractive surgery), the presence of arcus senilis (also known ascorneal arcus or gerontoxon), stromal opacities (scars, neovascularization, linear, ormacular opacities of hereditary dystrophies), evidence of prior surgery in theanterior segment (glaucoma, cataract extraction, radial keratotomy), the presence ofiridocorneal synechiae, exposure and band keratopathy, epithelial erosions ordefects, and the presence of infiltrates or foreign bodies [2, 3].
Signs of modern refractive surgery, such as photorefractive keratectomy orlaser-assisted in situ keratomileusis-flap (LASIK), remain very difficult to detect.Because slit lamps are routinely used in clinical practice and comprehensive atlasesof corneal pathologies have already been published [4, 5], here we only showseveral examples of the evaluation of a donor cornea in eye bank practice (Fig. 4.2).
The presence of some abnormalities does not necessarily mean that the tissuemust be excluded from the donor pool, as this could result in the loss of potentiallyusable material. Rather, it is necessary to consider which type of graft the examinedcornea could be used for. For example, corneas with prominent arcus senilis thatsignificantly reduces the clear corneal diameter (usually under 6 mm) should beexcluded from penetrating keratoplasty (PK), but the tissue can be used forendothelial keratoplasty (EK), depending on its endothelial quality.
Fig. 4.2 The examination of donor eyes by slit lamp microscopy. a A cornea exhibiting signs ofexposure keratopathy. b Band exposure keratopathy. c A more detailed view of band exposurekeratopathy. d A corneal opacity, stromal scar. e A cornea showing the presence of foreign bodies(metal particles). f A cornea with a pterygium (Courtesy of Andrea Gareiss-Lok, Hornhautbank,Munich, Germany)
4 Various Approaches to the Microscopic Assessment … 61

For complete corneal evaluation using a slit lamp microscopy, both the angle ofthe light and the width of the slit beam must be adjusted to produce particular typesof illumination that are utilized to examine different layers of the cornea and to scanfor possible pathologies. Examples of different types of illumination include but arenot limited to direct illumination and retroillumination. Direct illumination revealsgross pathologies, while retroillumination may show subtle optical changes such asvascularization, small peripheral incisions due to intraocular lens implantation orLASIK, and endothelial abnormalities such as guttae [2, 6, 7].
Using high magnification, endothelial cell mosaic or marked endothelial changessuch as Descemet membrane (DM) folds, endothelial precipitates, or cornea guttata(round DM excrescents) may be observed (Fig. 4.3).
4.2 Transmitted Light Microscopy
Transmitted light microscopy (shortened to light microscopy in the following text)is predominantly used to assess corneas stored in OC; both upright and invertedlight microscopes can be used for this purpose. Organ culture is an open system, asystem in which corneas are removed from the storage solution to be evaluated orare transferred from one storage solution to another. Sterile conditions must bemaintained during the assessment. The microscope can be placed directly in thesterile environment of a biosafety cabinet or laminar flow hood where the cornea isprepared or outside if the cornea is protected from contamination during theassessment by being placed in a closed vessel such as an airtight Petri dish. Themicroscope is preferably equipped with a digital camera connected to dedicatedimage analysis software (Fig. 4.4).
Fig. 4.3 A donor corneal endothelium visualized using slit lamp biomicroscopy. a and b Theendothelial mosaic (original magnification, 40�) appears regular. c Folds of Descemet membraneare present (caused by hypotonia and stromal swelling occurring soon after death or a traumaticretrieval procedure) (Courtesy of Andrea Gareiss-Lok, Hornhautbank, Munich, Germany)
62 K. Jirsova et al.

4.2.1 Visualization of the Corneal Endothelium
The aim of the corneal evaluation is to determine the overall condition of the tissue,particularly of the endothelial cells (ECs). The assessment is normally carried out intransparent tissue culture plates or dishes of various diameters (3.5 to 6 cm) [8, 9],and the cornea is usually placed epithelial side down on a drop of sterile solution.
The open system of OC allows observing large areas of the endothelium, but itrequires specific preparation in order to render the endothelial cell borders visibleby light microscopy. In addition, in contrast to the closed hypothermic storagesystem, trypan blue can be used to stain dead endothelial cells (DECs). Trypan blueis a vital stain that is actively excluded by viable cells and accumulates in the nuclei
Fig. 4.4 Assessment of the cornea using transmitted light microscopy. a An upright lightmicroscope, the assessed cornea, and the corneal endothelium in a bright field. b An inverted lightmicroscope, the assessed cornea, and the corneal endothelium in phase contrast (a Courtesy ofKim Nielsen and Jesper Hjortdal, Danish Cornea Bank, Aarhus, Denmark)
4 Various Approaches to the Microscopic Assessment … 63

of cells with severely impaired plasma membranes. DECs appear with a bluenucleus (often a faint staining requiring careful observation), while viable cellsremain unstained. The number of DECs cells can thus be calculated. Besides deadcells, denuded DM is slightly stained (see Fig. 6.18). Commercially produced andcertified trypan blue solutions for use in medicine (Council Directive 93/42/EEC,medical devices) are available [10].
First, a 0.1–0.5 % solution of trypan blue in an aqueous solution such as Ringersolution, saline, or phosphate-buffered saline is applied to the endothelial surface for90–120 s [9, 11, 12]. Because of the toxicity of trypan blue at higher concentrations,it is necessary to always use the lowest effective concentration and the shortestpossible application time [13]. As soon as the dye is rinsed off the tissue with a sterileaqueous solution, the endothelium is briefly (1–4 min) exposed to an iso- orhypotonic solution, which triggers a dilatation of the intercellular spaces and allowsvisualizing the ECs borders. The most commonly used solutions are sodium chloride(0.9 or 0.45 %) or sucrose (0.9 or 1.8 %) in a balanced salt solution, which is themost common fluid used during eye surgery worldwide [10, 14, 15]. The cornea,covered by hypotonic solution to protect the endothelium from drying out, is placedunder the microscope and assessed (Fig. 4.4). It has been suggested that theendothelium should not be exposed to a hypotonic solution for longer than 5 min [8].
With light microscopy, the entire area of the endothelium is scanned for thepresence of any prominent damage incompatible with the intended grafting (PK orEK). The endothelial cell density (ECD) is the crucial parameter determining thequality of the graft and its survival [16, 17]. Scanning the endothelial surface canreveal whether the central and peripheral parts of the endothelium differ markedly.In order to avoid overestimating the ECD, the assessment has to be performed in thecenter of the cornea in the area corresponding to the future graft and the part of theendothelial surface where the ECD is the lowest [18]. The central ECD wasreported to be 9 % lower than the paracentral and 17 % lower than the peripheralECD using specular microscopy [19]. An even greater difference was found whenthe endothelium was stained with alizarin red S, with the central ECD being 24 %lower than the peripheral ECD (Fig. 4.5) [18].
More details of the endothelium can be observed after staining with alizarin redS; however, this stain is toxic in contrast to trypan blue. As such, alizarin red Scannot be used to stain corneas intended for grafting, but it can be useful for thecontinuing education of eye bank technicians such as for confirming findings fromlight microscopy. Alizarin red S is used to visualize the EC borders, where it bindsto calcium located in the intercellular tight junctions or for the localization ofdenuded DM [20]. In combination with trypan blue, alizarin red S staining isessential for visualizing the morphology of ECs and has considerable importance inexperimental work (Fig. 4.6a) [9, 21, 22]. For distinguishing between live and deadcells in order to accurately assess the endothelium, calcein acetoxymethyl ester andethidium homodimer-1 or triple endothelial labelling with Hoechst 33342, ethidiumhomodimere, and calcein acetoxymethyl can be employed (Fig. 4.6b) [23, 24]. Thismethod is toxic to ECs and cannot be used during routine eye banking.
64 K. Jirsova et al.

Fig. 4.6 Visualization of the corneal endothelium using toxic staining incompatible with the useof the tissue for grafting. a Staining with trypan blue and alizarin red. b Triple staining withHoechst 33342, ethidium homodimer-1, and calcein-AM, showing dead cells in a fold ofDescemet membrane (Courtesy of Gilles Thuret and Zhiguo He, Jean Monnet University,St-Etienne, France). Scale bar = 100 lm
Fig. 4.5 Endothelial organization and endothelial cell density differ between the center andperiphery. a The central cornea has the lowest endothelial cell density (ECD), with the cellsdisplaying a regular hexagonal shape. b A higher ECD in the peripheral cornea with the cellsorganized in centripetal rows (arrows). c The extreme periphery of the cornea showing the highestECD and the organization of cell clusters around Hassel-Henle bodies (asterisks). Flat mountedhuman cornea, fluorescence microscopy, nuclei counterstained with Hoechst 33342 (upper panel),alizarin red + nuclei counterstained with Hoechst 33342 (lower panel) (Courtesy of Gilles Thuretand Zhiguo He, Jean Monnet University, St-Etienne, France). Scale bar = 10 lm
4 Various Approaches to the Microscopic Assessment … 65

4.2.2 Imaging of the Endothelium
Images of the endothelium are taken at various magnifications, usually 100 to 400�,while a quick scan of the cornea, particularly of the integrity of the endothelialmosaic, can be performed at magnifications of 40 to 100�. Larger structures such ascorneal scars, opacities, or DM folds as well as the presence of DECs are clearlyvisible at magnifications of 100 to 200�. For the assessment of cellular morphology,it is better to use higher magnifications of 200 to 400�. If 200� magnification isused, the visible area extends to approximately 0.3 mm2. Although phase contrastmicroscopy enables very high-contrast imaging of cellular and intracellularmorphology, bright field microscopy is preferred for assessing the number of DECsstained by trypan blue (Fig. 4.7) [8, 9, 15].
The various approaches for determining the endothelial parameters utilize thesame principle: first, the endothelium is visualized and imaged, then the original ordigitalized image is processed and assessed. The evaluation of the endothelium isgenerally performed from several photographs that are taken when the microscopicassessment is completed and the cornea has been stored under appropriate conditions.An accurate assessment of the endothelium primarily depends on the quality of theimages taken. In turn, their quality is directly influenced by two factors: the quality ofthe cornea/endothelium itself and the standardization of the imaging process. It shouldbe noted that even a perfect system for assessing endothelial quality is unable toproperly evaluate an endothelium that is not clearly visible owing to cloudiness oredema for example, since under these circumstances precise focusing is impossible.
Fig. 4.7 The corneal endothelium viewed by transmitted light microscopy. a Without hypotonictreatment the endothelial mosaic is almost indiscernible. b After treatment with hypotonic solution,the endothelial mosaic is visible using bright field microscopy, while trypan blue staining indicatesthe presence of dead cells. c Both endothelial cell morphology as well as dead endothelial cells areclearly discernible using phase contrast microscopy. Scale bar = 10 µm
66 K. Jirsova et al.

The corneal thickness, which depends on its hydration, is the main parameter interms of the image quality. If the image is taken using an inverted light microscope,the light beam must go through the entire cornea to reach the endothelial layer. Tofocus on the entire endothelial surface is difficult or even impossible in the case ofan edematous cornea. Similarly, in corneas exhibiting exposure keratopathy (dryingof the epithelium), it is difficult, at least if the cornea is assessed using inverted lightmicroscopy, to visualize the endothelial layer because of the reflection of theepithelial cells (Fig. 4.4b). This problem may be partially solved by turning thecornea upside down, that is by placing the endothelial layer down. However, thisassessment provides only basic information about endothelial quality, and thecornea must be assessed again.
The corneal endothelium may be evaluated manually directly from the capturedimages or more often semiautomatically using software programs for endothelialanalysis, several of which are commercially available [9, 17, 25].
Whatever the method used, it must be validated by the eye bank in order toensure reproducibility among technicians. The absence of standardization can leadto potential variability in determining the ECD with a consequent risk of validatinga cornea that is actually unsuitable for grafting or, conversely, discarding a corneathat has a healthy endothelium [26].
4.3 Specular Microscopy
Specularmicroscopy is a noninvasive technique to assess themorphology and densityof the corneal endothelium. There are twomain types of specularmicroscopes: contactand noncontact; both types can be used clinically to examine patients. In eye bankpractice, noncontact specular microscopy is the standard technique used. Clinicalspecular microscopes were created based on a laboratory microscope designed byMaurice to provide a high magnification view of specular reflected light from thecorneal endothelium [27, 28]. The specular reflex occurs at a regular smooth-surfacedinterface of two refractive indices with the light from the subject having an angle ofincidence equal to the angle of reflection to the observer. Endothelial cells can beimaged because their refractive index is greater than that of the aqueous humor orother storage solutions such as Optisol-GS, thus reflecting a portion of the projectedlight [28, 29]. As a result, specular microscopy, as opposed to transmitted lightmicroscopy, does not require osmotic stimulation in order to visualize the ECs.
Special eye bank specular microscopes enable the evaluation of a cornea placedin a closed vial or viewing chamber with storage solution, which protects the tissueagainst potential contamination [30]. This protection is one major advantage ofspecular microscopy as compared to light microscopy; in the latter an open systemis used for corneal assessment and more tissue manipulation is required. There areseveral companies that produce specular microscopes for eye banking, each cap-turing the images at different magnifications and utilizing different calibrationmethods and software (Fig. 4.8) [28].
4 Various Approaches to the Microscopic Assessment … 67

4.3.1 Imaging of the Endothelium
Specular microscopy usually combines imaging the basic morphology of the cor-neal endothelium with a semiautomatic system for its assessment. The resultingimage is black and white, and if the cornea is not too swollen, the borders betweenthe cells, which outline their shape, are clearly visible (Fig. 4.9). Images of theendothelium are usually taken at magnifications of 40 to 200�.
The main disadvantage of specular microscopy is that the method examines onlya relatively small central part of the corneal endothelium; thus this approach doesnot allow scanning the entire surface of the examined area. This limitation resultsfrom the mechanism used to hold the tissue in place for viewing [8, 31]. Ideally, the
Fig. 4.8 Specular microscopy of the corneal endothelium in a closed system as used in eyebanking practice. a A specular microscope is connected to a computer with software for assessingthe quality of a cornea. b View from above showing a cornea in a viewing chamber mounted onthe specular microscope for assessment
Fig. 4.9 Specular microscopy of donor corneas. a Healthy endothelium with a high endothelialcell density. b Pathologic endothelium showing cornea guttata
68 K. Jirsova et al.

specular microscope allows the user to capture multiple images from different areasof the central endothelium to reduce sampling bias. Each image is individuallyanalyzed and then averaged for an overall determination of ECD and other mor-phometric parameters. Normally at least 50–100 cells are analyzed [28, 32].
The use of specular microscopy is not confined to the corneal endothelial mosaicbut may be used at any level through the corneal stroma to the posterior endothelialsurface. Although some stromal pathologies may be observed, such as crystallinedeposits or irregularly rounded deposits of corneal dystrophies [33], in practice, eyebanks do not routinely evaluate changes in the corneal stroma or epithelial defectsby specular microscopy. Besides endothelial parameters, the corneal thickness canbe measured by focusing on the anterior and posterior parts of the cornea [19].Nevertheless, many eye banks in the U.S. now utilize optical coherence tomogra-phy to measure the thickness of the cornea (before and after processing), not aspecular microscope.
Precisely assessing the number of DECs by specular microscopy is very difficult,and thus an overall microscopic assessment is done in combination with a slit lampexamination. One source of difficulty is related to the closed system, which does notallow for vital staining. To compensate for this limitation, apparent DECs areexcluded from the specular analysis. At times it can be difficult to determine if darkzones in the area of specular reflection represent DECs or other findings (for details,see Sect. 5.1.2.2). The degree of DECs may be estimated by a slit lamp exami-nation, during which a more comprehensive evaluation of the entire endotheliumcan be performed without the limitation of viewing only the central endothelium.
It is important to consider both the ECD and the slit lamp evaluation of themonolayer together. If DECs cells are identified as live cells, the ECD could beoverestimated, leading to a lower actual ECD than reported for corneas intended fortransplantation. This may result in a perception of more rapid postoperative cell lossor an earlier onset of corneal decompensation or both [34].
4.4 Approaches to Assessing the Corneal Endothelium
The first software programs for determining the ECD using specular or lightmicroscopy date back to the 1980s [35, 36]. Recent technical progress allowsevaluation of the endothelium by various image analysis systems connected touser-friendly software programs that employ semiautomatic or fully automaticalgorithms for cell assessment [8, 37, 38]. Evaluating the ECD from images cap-tured using either light or specular microscopy utilizes the same principles [32].
The simplest method for assessing the ECD by light microscopy is to use aneyepiece with a counting grid [26]. More often, the ECD is calculated from pho-tographs or images taken of the endothelium.Manual evaluation is time-consumingand exhibits relatively high interobserver variability [37, 39]. To assess theendothelium, a rectangular grid with a size calibrated according to the microscope’smagnification is used. The grid, created on a transparent material (plastic, glass), is
4 Various Approaches to the Microscopic Assessment … 69

placed on a photograph of the endothelial surface, and the ECs present inside the gridas well as the cells located on two adjacent borders are counted; cells lying on theremaining two opposite borders are not counted. This method, in which cells arecounted within a single or multiple grid pattern of known area, is called the fixedframe or L method. The ECD is calculated as the number of cells within the grid andon two borders � 1 mm2/frame size in mm2 [40]. The fixed frame method is alsoavailable in some image analysis systems, although it has been replaced in recentyears by more accurate approaches. The variable frame method employs a similarapproach to calculating the ECD as does the fixed frame method; however, thevariable frame method requires the user to define the area of analysis by outlining acluster of cells. Individual cells are then identified within the defined area. Byincluding all the cells within the frame in the calculation, this method reduces thesubjectivity of deciding which cells to include and which to exclude as in the fixedframe method. Inside the frame (or region of interest), the endothelial cells can beidentified using various methods, generally the border or center method [8, 38, 40].
The border method is based on the manual or computer-assisted identification ofthe borders between the cells. The software recognizes and identifies the cellboundaries based on the contrast differences between the cell borders and the intra-cellular spaces [41, 42]. It then calculates the area of each EC contained in a region ofinterest that has a free form (variable frame method). In contrast to the fixed framemethod, there is no approximation in the ECD calculation because the exact area ofthe frame is the sum of all of the individual cell areas. Some image analysis systemsalso allow for the manual correction of the generated cell borders [42]. This method ismost often used for assessing endothelial images captured by light microscopy andrequires high quality images for accuracy. The ECD and exact cell morphometry(variation in cell size, polymegethism and variation in cell shape, pleomorphism; fordetails, see Sect. 5.1.4) are automatically calculated (Fig. 4.10) [17].
The center (dot) method is semiautomatic (cell selection is manual, calculation isautomatic); the examiner has to manually mark the centers of 50–300 adjacent cellsand then the image is processed and basic quantitative and qualitative parameterssuch as ECD, mean cell area, polymegethism, and pleomorphism are automaticallycalculated by a computer algorithm based on the distance between each markedcenter. The outer ring of counted cells defines the area, but those cells are excludedfrom the analysis. It has been demonstrated that off-center marking has aninsignificant impact on the ECD, but it can affect the assessment of pleomorphism.This approach is commonly used to assess endothelial images from both light andspecular microscopy [28].
A study comparing the border and center methods for evaluating light micro-scopy images found that there were no significant differences between the ECDcalculated by the two methods or their reproducibility. Pleomorphism measure-ments were acceptable using both approaches, but polymegethism was reliablyanalyzed only by the border method because the center method intrinsically tends tominimize variations in cell size. Using the center method, a significant underesti-mation of polymegethism can be slightly improved by accurate marking of the cellcenters. It has been noted that at least 300 cells must be analyzed to provide anaccurate and reproducible ECD [25].
70 K. Jirsova et al.

Clinically, morphometry systems using the border or center method to analyzeimages taken by specular microscopy are more or less comparable in assessing theECD and morphometric parameters [43–45]. Appropriate internal calibration (bymeasuring an external certified scale) has been shown to be a prerequisite forobtaining reliable data [46].
Finally, besides errors inherent in the device or image analysis system used,observer errors resulting from intra- or interobserver variability should be mini-mized. Rigorous training using saved images or specific tools such as micromosaicsmimicking the corneal endothelium on a glass slide [47] can help achieve a highdegree of reliability among eye bank technicians when evaluating the endothelium.
References
1. Kanavi MR, Javadi MA, Chamani T, Fahim P, Javadi F. Comparing quantitative andqualitative indices of the donated corneas maintained in Optisol-GS with those kept inEusol-C. Cell Tissue Bank. 2015;16:243–7.
2. Mootha VV, Dawson D, Kumar A, Gleiser J, Qualls C, Albert DM. Slitlamp, specular, andlight microscopic findings of human donor corneas after laser-assisted in situ keratomileusis.Arch Ophthalmol. 2004;122:686–92.
Fig. 4.10 The assessment of endothelial images captured by light and specular microscopy.a Semiautomatic assessment of the main endothelial parameters. The centers of individual cells aremanually identified; then the cell borders are delineated and morphometric measurementsperformed using a computer (Lucie image analysis system, Laboratory of Imaging, CzechRepublic). b Assessment using the border method (Sambacornea, Tribvn, Chatillon, France)allows the cell edges (green lines) to be automatically delineated in manually selected areas (blackline). The cell density, the total number of counted cells, the maximum and minimum cell size(yellow), and the percentage of hexagonal cells are calculated. c Assessment using the centermethod. After manual identification of the centers of at least 50 adjacent cells, quantitative andqualitative endothelial parameters are automatically calculated (Eye Bank Specular MicroscopeKeratoAnalyzer EKA-10 with software KSS-EB10, Konan Medical Inc., Irvine, CA, US)(b Courtesy of Gilles Thuret and Zhiguo He, Jean Monnet University, St-Etienne, France;c Andrea Gareiss-Lok, Hornhautbank, Munich, Germany)
4 Various Approaches to the Microscopic Assessment … 71

3. EEBA technical guidelines for ocular tissue (2015). http://www.europeaneyebanks.org/files/Technical_Guidelines_Rev7_Jan2015Final.pdf.
4. Krachmer JH, Palay DA. Cornea atlas. 3rd ed. St. Louis: Mosby Elsevier; 2013.5. Gellrich MM. The slit lamp applications for biomicroscopy and videography. Berlin,
Heidelberg: Springer; 2014.6. Hirst LW, Stark WJ. Donor corneal endothelium: slit-lamp examination of buttons in storage
medium. Ophthalmic Surg. 1979;9:51–3.7. Kanavi MR, Javadi MA, Chamani T. Specular microscopic features of corneal endothelial
vacuolation. J Ophthalmic Vis Res. 2011;6:5–7.8. Schroeter J, Rieck P. Endothelial evaluation in the cornea bank. Dev Ophthalmol.
2009;43:47–62.9. Nejepinska J, Juklova K, Jirsova K. Organ culture, but not hypothermic storage, facilitates the
repair of the corneal endothelium following mechanical damage. Acta Ophthalmol.2010;88:413–19.
10. EEBA Directory. European Eye Bank Association, Directory, 24th ed. Denmark: Aarhus;2016.
11. Stocker FW, King EH, Lucas DO, Georgiade N. A comparison of two different stainingmethods for evaluating corneal endothelial viability. Arch Ophthalmol. 1966;76:833–5.
12. Pels E, Beekhuis WH, Völker-Dieben HJ. Long-term tissue storage for keratoplasty. In:Brightbill FS, editor. Corneal surgery: Theory, technique, and tissue. 3rd edition. St. Louis:CV Mosby; 1999. pp 897–906.
13. van Dooren BT, Beekhuis WH, Pels E. Biocompatibility of trypan blue with human cornealcells. Arch Ophthalmol. 2004;122:736–42.
14. Pels E, Schuchard Y. Tissue storage. E: Organ culture and endothelial evaluation as apreservation method for human corneas. In: Brightbill FS, editor. Corneal surgery. Theory,technique, and tissue. St. Louis: CV Mosby; 1986. pp 93–102.
15. Gain P, Thuret G, Chiquet C, Dumollard JM, Mosnier JF, Burillon C, et al. Value of twomortality assessment techniques for organ cultured corneal endothelium: trypan blue versusTUNEL technique. Br J Ophthalmol. 2002;86:306–10.
16. Rao GN, Aquavella JV, Goldberg SH, Berk SL. Pseudophakic bullous keratopathy.Relationship to preoperative corneal endothelial status. Ophthalmology. 1984;91:1135–40.
17. Acquart S, Gain P, Zhao M, Gavet Y, Defreyn A, Piselli S, et al. Endothelial morphometry byimage analysis of corneas organ cultured at 31 degrees C. Invest Ophthalmol Vis Sci.2010;51:1356–64.
18. Schimmelpfennig BH. Direct and indirect determination of nonuniform cell densitydistribution in human corneal endothelium. Invest Ophthalmol Vis Sci. 1984;25:223–9.
19. Amann J, Holley GP, Lee SB, Edelhauser HF. Increased endothelial cell density in theparacentral and peripheral regions of the human cornea. Am J Ophthalmol. 2003;135:584–90.
20. Sperling S. Combined staining of corneal endothelium by alizarine red and trypane blue. ActaOphthalmol (Copenh). 1977;55:573–80.
21. Taylor MJ, Hunt CJ. Dual staining of corneal endothelium with trypan blue and alizarin red S:importance of pH for the dye-like reaction. Br J Ophthalmol. 1981;65:815–19.
22. Jhanji V, Pollock GA, Mackey AL, Beltz J, Vajpayee RB. Histopathological evaluation ofanterior lamellar corneal tissue-on/-off storage conditions on DSAEK donor tissue afterstorage in organ culture. Curr Eye Res. 2012;37:155–8.
23. Yang CS, Chen KH, Hsu WM, Li YS. Cytotoxicity of silicone oil on cultivated humancorneal endothelium. Eye (Lond). 2008;22:282–8.
24. Pipparelli A, Thuret G, Toubeau D, He Z, Piselli S, Lefevre S, et al. Pan-corneal endothelialviability assessment: application to endothelial grafts predissected by eye banks. InvestOphthalmol Vis Sci. 2011;52:6018–25.
25. Deb-Joardar N, Thuret G, Zhao M, Acquart S, Peoc’h M, Garraud O, Gain P. Comparison oftwo semiautomated methods for evaluating endothelial cells of eye bank corneas. InvestOphthalmol Vis Sci. 2007;48:3077–82.
72 K. Jirsova et al.

26. Thuret G, Manissolle C, Acquart S, Le Petit JC, Maugery J, Campos-Guyotat L, et al. Ismanual counting of corneal endothelial cell density in eye banks still acceptable? The Frenchexperience. Br J Ophthalmol. 2003;87:1481–6.
27. Maurice DM. Cellular membrane activity in the corneal endothelium of the intact eye.Experientia. 1968;24:1094–5.
28. McCarey BE, Edelhauser HF, Lynn MJ. Review of corneal endothelial specular microscopyfor FDA clinical trials of refractive procedures, surgical devices, and new intraocular drugsand solutions. Cornea. 2008;27:1–6.
29. Laing RA, Sandstrom MM, Leibowitz HM. Clinical specular microscopy. I. Opticalprinciples. Arch Ophthalmol. 1979;97:1714–19.
30. Bourne WM, Kaufman HE. Cataract extraction and the corneal endothelium. Am JOphthalmol. 1976;82:44–7.
31. Saad H, Stoeger C. Specular microscopic imaging results may be deceiving, as demonstratedby vital dye staining. Int J Eye Banking. 2013;1:1–4.
32. Lass JH, Gal RL, Ruedy KJ, Benetz BA, Beck RW, Baratz KH, et al. An evaluation of imagequality and accuracy of eye bank measurement of donor cornea endothelial cell density in theSpecular Microscopy Ancillary Study. Ophthalmology. 2005;112:431–40.
33. Brooks AM, Grant G, Gillies WE. A comparison of corneal endothelial morphology in corneaguttata, Fuchs’ dystrophy and bullous keratopathy. Aust N Z J Ophthalmol. 1988;16 :93–100.
34. Wilhelmus KR, Stulting RD, Sugar J, Khan MM. Primary corneal graft failure. A nationalreporting system. Medical Advisory Board of the Eye Bank Association of America. ArchOphthalmol. 1995;113:1497–1502.
35. Lester JM, McFarland JL, Bursell SE, Laing RA, Brenner JF. Automated morphometricanalysis of corneal endothelial cells. Invest Ophthalmol Vis Sci. 1981;20:407–10.
36. Delbosc B, Cantenot L, Fellmann D, Blum D, Montard M. [In vitro semi-automatedmorphometry of preserved human corneal endothelium]. J Fr Ophthalmol. 1986;9:445–54.
37. Hirneiss C, Schumann RG, Gruterich M, Welge-Luessen UC, Kampik A, Neubauer AS.Endothelial cell density in donor corneas: a comparison of automatic software programs withmanual counting. Cornea. 2007;26:80–3.
38. Jonuscheit S, Doughty MJ, Ramaesh K. Assessment of a variable frame (polygonal) methodto estimate corneal endothelial cell counts after corneal transplantation. Eye (Lond).2012;26:803–09.
39. Deb-Joardar N, Thuret G, Gavet Y, Acquart S, Garraud O, Egelhoffer H,Gain P. Reproducibility of endothelial assessment during corneal organ culture: comparisonof a computer-assisted analyzer with manual methods. Invest Ophthalmol Vis Sci.2007;48:2062 –67.
40. Benetz BA, Gal RL, Ruedy KJ, Rice C, Beck RW, Kalajian AD, et al. Specular microscopyancillary study methods for donor endothelial cell density determination of Cornea DonorStudy images. Curr Eye Res. 2006;31:319–327.
41. Barisani-Asenbauer T, Kaminski S, Schuster E, Dietrich A, Biowski R, Lukas J,Gosch-Baumgartner I. Impact of growth factors on morphometric corneal endothelial cellparameters and cell density in culture-preserved human corneas. Cornea. 1997;16:537–40.
42. Gain P, Thuret G, Kodjikian L, Gavet Y, Turc PH, Theillere C, et al. Automated tri-imageanalysis of stored corneal endothelium. Br J Ophthalmol. 2002;86:801–8.
43. Benetz BA, Diaconu E, Bowlin SJ, Oak SS, Laing RA, Lass JH. Comparison of cornealendothelial image analysis by Konan SP8000 noncontact and Bio-Optics Bambi systems.Cornea 1999;18:67–72.
44. de Sanctis U, Machetta F, Razzano L, Dalmasso P, Grignolo FM. Corneal endotheliumevaluation with 2 noncontact specular microscopes and their semiautomated methods ofanalysis. Cornea. 2006;25:501–6.
45. Szalai E, Nemeth G, Berta A, Modis L Jr. Evaluation of the corneal endothelium usingnoncontact and contact specular microscopy. Cornea. 2011;30:567–70.
4 Various Approaches to the Microscopic Assessment … 73

46. Ohno K, Nelson LR, McLaren JW, Hodge DO, Bourne WM. Comparison of recordingsystems and analysis methods in specular microscopy. Cornea. 1999;18:416–23.
47. Flury M, He Z, Campolmi N, Gain P, Kress B, Thuret G. Fabrication of optical mosaicsmimicking human corneal endothelium for the training and assessment of eye banktechnicians. Opt Lett. 2012;37:22–4.
74 K. Jirsova et al.

Chapter 5Light and Specular MicroscopyAssessment of the Cornea for Grafting
Katerina Jirsova, Jameson Clover, Christopher G. Stoegerand W. John Armitage
Abstract A detailed microscopic assessment of corneal quality is a crucial step indetermining the suitability of a cornea for grafting. This chapter describes in detailthe assessment of quantitative and qualitative corneal/endothelial parameters andtheir irregularities as observed by light and specular microscopy, together with linksto images presented in the atlas (see Chap. 6). Endothelial cell density, the mostimportant quantitative parameter of corneas intended for grafting, should generallybe at least 2000 cells/mm2. In this regard, the detection of dead endothelial cells isimportant for preventing the overestimation of endothelial cell density.Polymegethism (variation in cell size) and pleomorphism (variation in cell shape),two basic qualitative morphologic parameters of the endothelium, together with thepresence of Descemet membrane folds, cornea guttata, intracellular changes, andforeign bodies or precipitates are also assessed. The tissue should also be checkedfor the presence of severe epithelial defects or stromal opacities as signs of variousstromal pathologies. In addition to initial cornea quality, changes affecting storedcorneas or alterations arising as a consequence of the preparation of various types ofendothelial lamellae may influence the quality and survival of a graft. Cornealalterations characteristic of certain corneal pathologies (endothelial dystrophies)that may be seen during the microscopic assessment of a donor cornea are described
K. Jirsova (&)Laboratory of the Biology and Pathology of the Eye, Institute of Biology and MedicalGenetics, First Faculty of Medicine, Charles University, Prague, Czech Republice-mail: [email protected]
J. Clover � C.G. StoegerLions VisionGift, 2201 SE 11th Ave, Portland, OR 97214, USAe-mail: [email protected]
C.G. Stoegere-mail: [email protected]
W.J. ArmitageBristol Eye Bank, NHS Blood and Transplant, and School of Clinical Sciences, University ofBristol, Bristol Eye Hospital, Lower Maudlin Street, Bristol BS1 2LX, UKe-mail: [email protected]
© Springer International Publishing AG 2017K. Jirsova, Light and Specular Microscopy of the Cornea,DOI 10.1007/978-3-319-48845-5_5
75

and linked to images of corneal explants (light microscopy) or patients’ corneas(specular microscopy) in the atlas.
Keywords Light microscopy � Specular microscopy � Endothelial cell density �Cell vitality � Polymegethism and pleomorphism � Corneal lamellae
5.1 Assessment of the Corneal Endothelium
The microscopic assessment of the cornea, and particularly of the endothelium, bylight or specular microscopy is a crucial process to judge if the tissue is suitable forgrafting. As light microscopy is preferentially used for assessing corneas stored inorgan culture (OC), and specular microscopy is mostly used for corneas stored inhypothermia, the particular parameters that are assessed are generally describedwith respect to the corresponding microscopic approach.
A knowledge of the morphology of the healthy cornea, particularly of theendothelium (see Figs. 6.1–6.13 for light and Figs. 6.131 and 6.132 for specularmicroscopy), is a prerequisite for recognizing various pathologic alterations.
Light microscopy is usually carried out twice during OC. The aim of the firstassessment, performed before storage of the cornea or during the very first days ofstorage, is to quickly discard corneas unsuitable for grafting. When the initialquality cannot be determined with certainty that all of the essential parameters areacceptable, or if all parameters cannot be assessed (e.g., if the cornea is edematousor shows numerous Descemet membrane (DM) folds or epithelial or stromalcloudiness), the tissue can be stored and subsequently assessed again. Knowledgeof the cornea’s condition (particularly the endothelial parameters) before storageenables the evaluation of any changes occurring during the culture period [1].
The assessment at the end of storage is performed shortly before the cornea isprovided for grafting according to the practices of the individual bank and the typeof storage and deswelling media used. The cornea can be evaluated just before itstransfer from storage to deswelling medium or after 8 to 48 h in a deswellingmedium [2, 3]. The latter procedure exploits a dehydrating effect that leads to anefflux of excess water from the cornea, thus thinning the tissue and allowing betterfocus on the individual layers.
The assessment of corneas stored in hypothermia using specular microscopy todetermine their initial surgical suitability is usually performed once (particularlywhen slit lamp examination is performed twice), at the beginning of storage, ortwice, at the beginning and end of storage. Tissue processed for endothelial ker-atoplasty by an eye bank is reassessed after processing.
An assessment at the end of OC storage should be mandatory because the statusof the endothelium is critical for deciding whether the tissue possesses the qualityrequired for grafting. The final assessment enables the eye banker: (1) to acceptcorneas categorized as acceptable for grafting during a previous assessment withoutsignificant quality deterioration during storage; (2) to accept or exclude corneas that
76 K. Jirsova et al.

were not initially assessable, for instance because of the presence of edema or theabsence of proper intercellular space dilatation after osmotic preparation; (3) toaccept or exclude corneas whose quality was not conclusively determined during aprevious assessment; (4) to exclude corneas of initial good quality but whoseparameters deteriorated during storage.
Reassessment carried out shortly before transplantation results in a decrease inthe occurrence of primary graft failure, and its importance has been repeatedlydemonstrated [4–6].
5.1.1 Endothelial Cell Density (ECD)
The corneal endothelium, which is directly involved in maintaining the constantthickness and metabolic homeostasis of the cornea, is the most important layer forthe long-term survival and functionality of a corneal graft. The ECD represents thenumber of cells per mm2. Usually, 50–300 neighboring cells are assessed usingboth light and specular microscopy [7–9]. During the assessment, it is necessary toconsider that the ECD increases from the central to the peripheral zones of theendothelium [10].
Most eye banks release corneas for penetrating keratoplasty with an ECD above2000 cells/mm2, although some banks require a density higher than 2300 or even2500 cells/mm2 [11–14]. By modeling changes in the ECD, it was shown thatcorneas with 2200 cells/mm2 should retain a sufficient ECD to maintain cornealtransparency for at least 25 years [12]. OC corneas with an ECD at the lower limitof accepted values are often used as emergency corneas, i.e., for clinically urgenttransplantation in cases when other tissue is not available [15]. Corneas with a lowECD or impaired endothelium can also be used for grafts that do not require afunctional endothelium (e.g., tectonic transplantation, Boston keratoprosthesis) orfor the preparation of lamellae for deep anterior lamellar keratoplasty [16].
The average ECD of corneas provided for transplantation is about 2500–2700cells/mm2 (Fig. 5.1). In some cases, corneas provided for grafting are subdividedbased on their ECD into four or five categories, e.g.: excellent (ECD > 3000cells/mm2), very good (2500–3000 cells/mm2), good (2200–2500 cells/mm2), andemergency corneas (2000–2200 cells/mm2) [17]. Due to increased numbers oflamellar techniques, corneas may be rated as suitable for various types of surgery,such as penetrating keratoplasty, endothelial keratoplasty, anterior lamellar ker-atoplasty, or tectonic keratoplasty [18, 19]. Research using paired donor corneashas shown that in 98 % of cases, the ECD of the two corneas are very similar ornearly identical [13, 20]. On the other hand, paired corneas from a donor with acranial trauma may exhibit completely different ECD.
The ECD decreases with age [21–23]. The mean ECD is lower in contact lenswearers as well as in patients suffering from systemic or corneal diseases, especiallyendothelial dystrophies [24, 25]. Endothelial mosaic integrity after cell loss ismaintained by the migration and spreading of the remaining cells to cover the
5 Light and Specular Microscopy Assessment of the Cornea … 77

Fig. 5.1 Various endothelial cell densities (about 1000, 2000, 3000, 4000 cells/mm2) are shownin specular (left) and light microscopy (right), respectively
78 K. Jirsova et al.

denuded area. In patients between 20 and 80 years old, the average endothelial cellarea typically doubles [26]. The ECD of corneas after grafting have been monitoredusing noncontact specular endothelial microscopy, which has shown that the resultscorrelated with the ECD measured using image analysis performed on lightmicroscopy photographs [27].
The comparison of ECD between individual eye banks preparing OC corneas isdifficult because of differences in the cultivation methods used and the varioussystems employed to determine the ECD. Differences in ECD may arise as aconsequence of manual counting errors, errors in microscope calibration, or dif-ferences in counting strategies (Fig. 5.1) [7, 28].
5.1.2 Endothelial Cell Vitality and the Presenceof Dead Cells
The precise determination of endothelial quality and vitality, and thus the quality ofthe cornea as a whole for transplantation purposes, is not possible without assessingthe number of dead cells/mm2 or the percentage of dead endothelial cells (% DECs)present in the assessed cornea. Endothelial cell death is caused by many factorsrelated to the status of the cornea or donor as well as to factors affecting the corneaduring its preparation and processing. Aging, hypoxia, mechanical stress, metabolicchanges, and degeneration of the corneal endothelium are the main factors leadingto endothelial cell loss. It has been shown in both hypothermic and OC storage thatnot only endothelial but also epithelial cells and keratocytes may die throughapoptosis or necrosis [29–31]. Endothelial cell loss during storage may be causedby the manipulation of the cornea during processing and/or by nutrient deficienciesor other nonphysiologic storage conditions [1, 32, 33].
5.1.2.1 Light Microscopy
After staining the endothelium using trypan blue (for details, see Sect. 4.2.1), thenumber of dead endothelial cells (DECs) can be calculated and expressed as adensity or percentage. The blue nuclei of DECs are less visible using phase contrastcompared to bright field microscopy (see Figs. 6.23 and 6.24). Sometimes a fewDECs may be visible close together with no dead cells elsewhere on the endothelialsurface (see Fig. 6.13). Nonetheless, even a very low number of solitary DECsshould serve as a warning flag and encourage increased attention during the nextassessment. Dead cells may also be present as neighboring cell groups of varioussizes or scattered over the entire endothelial surface (see Figs. 6.14–6.16). Thepresence of isolated DECs distributed over the endothelial surface (tens of suchcells per cornea) may be physiologic or may be induced by minor damage duringprocessing. Dead cells may also arise owing to ongoing pathologic processes in thecornea, e.g., infection, endothelial dystrophies, keratitis, or diabetes [34, 35].
5 Light and Specular Microscopy Assessment of the Cornea … 79

Dead cells are commonly found on folds of the DM (see Fig. 6.17), which mayarise during the preparation of the corneoscleral disc. The endothelial cells (ECs) inDM folds are subjected to mechanical damage and may die as a result. DECs mayslough off the endothelial surface, causing lesions (see Figs. 6.18 and 6.49). Celldeath may be induced by mechanical stress during preparation, i.e., if theendothelium is touched by a surgical instrument, or it may also be related to thecause of death of the donor. A high percentage of DECs is often associated withcranial trauma [36]. When DECs are detached from the DM, they assume a roundshape and may resemble cornea guttata (see Figs. 6.45 and 6.48). Compensation forisolated DECs by the adjacent vital ECs is connected by a morphologically distinctformation, a rosette (see Fig. 6.53). If a larger lesion occurs, the cells migrate intothe vacant area, change their shape due to spreading, and enlarge their surface [37].In the human cornea it has been shown that shortly after lesion induction, elongatedECs are present, oriented directly toward the damage (see Fig. 6.54). As a result,repair of the corneal endothelium is associated with a high degree of poly-megethism and pleomorphism [13, 38]. During the assessment, large endotheliallesions (see Fig. 6.18) should be considered as areas of DECs or as areas with nocells to preclude overestimating the ECD. The first assessment (before storage) mayreveal whether the presence of DECs indicates an ongoing disease (in this caseexclusion of the tissue should be considered) or rather reflects mechanical damagethat may be repaired under OC (see Figs. 6.53 and 6.54). Corneas with more than5 % DECs at the first assessment should be reassessed; reassessed corneas stillshowing more than 5 % DECs should be excluded from grafting [4].
Bluish areas of various sizes can be observed over the endothelial mosaic with notrypan blue-stained nuclei but with the presence of ECs (see Figs. 6.19 and 6.20).These regions probably arise as a consequence of an injured, leaky endothelium,which allows trypan blue to penetrate and stain the underlying DM.
5.1.2.2 Specular Microscopy
Using specular microscopy, a healthy endothelium has distinct borders and displaysmostly hexagonal cells of consistent size (see Figs. 6.131–6.133). The evaluation ofcell death using specular microscopy is more difficult compared to with lightmicroscopy because the corneal endothelium is not stained for the presence ofDECs. Using specular microscopy, solitary dark spots (see Fig. 6.139), dark roundareas (see Figs. 6.140–6.142), or dark linear strips or areas (see Figs. 6.151–6.154)may be seen in donor corneas. Subsequent examination using trypan blue stainingand light microscopy has confirmed that these areas are composed of severelydamaged or dead endothelial cells (cell “drop out” is often used in Americanterminology). Thus, the linear strips may reflect the presence of DM folds withpotential DECs or stress lines from mechanical trauma [37, 39].
Dark circular spots on the corneal endothelium may indicate an increase of localendothelial permeability and the presence of water between the endothelium andDM as a result of an increased influx of water through the apical part of the cells.
80 K. Jirsova et al.

This situation may be induced by the accumulation of hypoxic metabolites in theanterior chamber, by hyperosmolarity of the storage medium, or as a consequenceof cold storage (see Figs. 6.157 and 6.158). It has been suggested that dark spots orareas on the endothelium are caused by disturbances of the specular reflection fromthe endothelium-aqueous humor/medium interface. These disturbances may arise asa consequence of various protuberances on the endothelium such as cellular debris,DECs, guttae, or extraneous cells, e.g., erythrocytes [40].
5.1.3 Dilatation of the Intercellular Spaces betweenEndothelial Cells
5.1.3.1 Light Microscopy
The borders between live ECs can be visualized by treatment with iso- or hypotonicsolution to dilate the intercellular spaces (for details, see Sect. 4.2.1). The fact thatthe endothelium is able to react to osmotic changes (see Fig. 6.25) indicates itsfunctionality, i.e., its ability to respond to physiologic stimulation [1, 41]. During theevaluation, the area where the dilatation of the intercellular spaces between the ECsoccurs may be assessed, and the regularity of the dilatation can be monitored.Dilatation can be evaluated, for example, in three degrees: degree 1: it occurs within2 min after exposure to 0.9 % sucrose and is visible across 80–100 % of theendothelial surface; degree 2: it occurs within 4 min after exposure to 0.9 % sucroseand is visible across greater than or equal to 30 % of the endothelial surface; degree3: it is minimal (<30 % of the endothelial surface area) or cannot be induced at all. Ifdilatation does not occur (see Figs. 6.26 and 6.27), is weak (see Fig. 6.28), irregular,or abnormal, or if areas without dilatation are observed (see Figs. 6.29–6.31), it isnecessary to reassess the cornea at a later time. In some cases, even a morpholog-ically very regular endothelium with a relatively high ECD does not react to osmoticstimulation by dilatation of the intercellular spaces. Conversely, abnormallyprominent dilatation (see Fig. 6.32) may occur, particularly with younger donors,and may prevent appropriate evaluation. In these cases it is usually sufficient to delaythe assessment for a short time (several seconds), during which the dilatation con-tinuously decreases. In most corneas dilatation disappears gradually after 2–5 min.
Unsatisfactory dilatation is often improved during cultivation, in which condi-tions close to physiologic (the composition and temperature of the storage solution)allow the endothelium to metabolize. Usually the dilatation of the intercellularspaces at the second assessment is clearly visible and allows the endothelial cellshape to be determined (see Figs. 6.101–6.106). However, in some cases just theopposite situation, a decrease or loss of dilatation, may occur. During OC storage,dilatation irregularities are often associated with other abnormalities of endothelialcell morphology. Therefore, in making the final decision concerning of use of acornea for grafting, it is necessary to consider the degree of dilatation in connectionwith other qualitative and quantitative parameters (see Figs. 6.109 and 6.110).
5 Light and Specular Microscopy Assessment of the Cornea … 81

5.1.3.2 Specular Microscopy
In a closed system in which the cornea is not manipulated in order to evaluate thetissue, dilatation cannot be induced or assessed. This makes it impossible todetermine if the endothelium is able to react physiologically to external stimuli suchas osmotic conditions. On the other hand, it is possible to observe an endotheliumwith visible nuclei and an inverted appearance, which may indicate problems withendothelial barrier function (see Figs. 6.157 and 6.158).
5.1.4 Polymegethism and Pleomorphism
The functional capacity of the corneal endothelium can be correlated with itsmorphologic appearance.
Polymegethism and pleomorphism (P&P) are two basic endothelial morpho-metric parameters determining its quality. Increased polymegethism (variation inthe cell area) and pleomorphism (deviation from hexagonality) are considerednegative indicators of the quality of the endothelial surface, and together with a lowECD they can have a direct impact on the quality of a posterior graft and itsfunctionality. The extent of changes in P&P that have a clear negative effect ongraft survival has not yet been precisely determined [42]. Both parameers can beevaluated by light and specular microscopy (see Fig. 4.10).
Polymegethism refers to differences in the size of individual ECs (see Figs. 6.33and 6.34 for light and Figs. 6.135–6.138 for specular microscopy). The coefficientof variation (CV) is calculated as the standard deviation of mean cell area/meancell area. It is generally accepted that the CV of a cornea for posterior graftingshould be 0.20–0.30 [22, 38]. The CV is usually expressed as a percentage. Thepercentage of cells with polymegethism can be calculated as CV � 100. Corneaswith a CV of less than 20 %, i.e., with ECs of similar size, are more stable andresistant to stress, which occurs even during transplantation [43]. Based onextensive studies evaluating risk parameters and graft outcome, donor corneas witha high degree of polymegethism should not be used for transplantation [44].
It was found that a high CV does not interfere with the permeability of theendothelium or its ability to maintain stromal transparency [45]. In studies usinghuman and rabbit corneas, it was demonstrated that ECs with abnormally arrangedF-actin show a greater degree of polymegethism. F-actin may be one of the keymolecules involved in maintaining the shape of a cell and protecting it againstincreased osmotic pressure and possible rupture of the cell membrane [46].Increased polymegethism may also occur in the ECs of a graft after its transplan-tation [43]. Severe polymegethism has been found in the corneas of donors usingcontact lenses, donors with diabetes, keratoconus, inflammation or infection, anddonors with a previous history of anterior chamber surgery [47].
Pleomorphism refers to the shape of individual ECs and can be expressed interms of polygonality (calculated as the number of adjacent cells) or hexagonality
82 K. Jirsova et al.

(percentage of hexagonal endothelial cells) (see Fig. 6.34 for light and Figs. 6.136–6.138 for specular microscopy). Pleomorphism is calculated as (4p x cell area)/perimeter [43].
Using specular microscopy, it was shown that under normal circumstances48–90 % of ECs are hexagonal, 25–38 % are heptagonal and 15–35 % are pen-tagonal. Three-, four-, and eight-sided cells constitute less than 5 % of the totalnumber of ECs [48]. Shapes other than hexagonal are more frequently found inolder corneas, corneas with trauma and pathologic processes, and during repair ofthe endothelium, in which DECs are replaced by their neighbors [26, 49–51].
P&P (see Figs. 6.35–6.40) often go hand in hand and affect the same cells.A high degree of P&P is frequently present, particularly in an endothelium with alower ECD (see Figs. 6.36–6.38). P&P is frequent in OC corneas, which normallyshow higher levels of metabolic activity, repair, and the replacement of DECs. Theendothelial metabolism of corneas stored under hypothermic conditions is inhibited,and DECs that may potentially appear are not removed and the endothelial surfaceis not repaired [13]. Increased P&P has been observed in patients with decom-pensated pseudophakic bullous keratopathy and with endothelial corneal dystro-phies [48, 52]. In addition to the primary pathology of the eye, both parameterssignificantly worsen in patients suffering from chronic renal failure. The mechanismresponsible probably consists in the decreased production of the reduced form ofnicotinamide adenine dinucleotide phosphate by higher levels of urea and a con-sequent decrease of the protection of cells against the toxicity of reactive oxygenspecies [53]. Worsening P&P is also seen in diabetes mellitus, particularly type I, inwhich it is accompanied by a significant decrease of ECD [34, 54].
5.1.5 Descemet Membrane Folds
DM folds may arise as a consequence of mechanical stress of the endothelium(during the preparation of a corneoscleral disc) or of changes in corneal hydration(caused by changes in osmotic conditions) [55]. DM folds vary in severity, but theymay be long, deep, and wide trenches that can extend over the whole surface of theendothelium.
5.1.5.1 Light Microscopy
With light microscopy, DM folds are visible using phase contrast; they extendeither parallel to or intersecting each other (see Figs. 6.21–6.23). Because of themechanical stresses on the ridges of DM folds, the ECs may die (see Figs. 6.17,6.23 and 6.24). The presence of DM folds itself is not a reason for the exclusion ofthe tissue from grafting, but the combination of numerous folds (more than 10) witha relatively low ECD or other endothelial pathologies (such as dead cells or P&P)may be a reason for its exclusion.
5 Light and Specular Microscopy Assessment of the Cornea … 83

5.1.5.2 Specular Microscopy
Using specular microscopy, DM folds are seen as a change in cell reflectivity and asa wavy appearance of the monolayer. Since good specular reflection is reliant on asmooth endothelial surface, which is not the case when folds are present, the imageshows inconsistent cell reflection. The severity or depth of a fold can be gauged bythe contrast between the ridge, which is more reflective, and the trench, which canbe so dark that cells are not observable (see Fig. 6.148). Often cells within thetrench are alive and can be seen by slit lamp examination; however, severe foldingcan make it difficult to observe cells with both specular microscopy and slit lampevaluation. Some DM folds are graded as trace, appearing only as a shadow (seeFig. 6.143), whereas other folds are more pronounced: mild (see Fig. 6.144), mildto moderate (see Fig. 6.145), moderate (see Figs. 6.146 and 6.147), moderate tosevere (see Fig. 6.149), or severe (see Fig. 6.148); in the last example cited specularreflection is minimal, and the cells appear edematous. DM folds can also distort thecell size and shape, making it difficult to distinguish from pleomorphism andpolymegethism (see Fig. 6.146). Depending on the cause of edema, DM folds oftendecrease over storage time as a result of constituents such as dextran and chon-droitin sulfate in hypothermic storage solution.
Endothelial stress lines (see Figs. 6.151 and 6.152) or stress areas (see Figs. 6.153and 6.154) are linear areas of cell death often extending from the limbus inward orradiating around the cornea, depending on the mechanism of stress (stress inflictedduring in situ excision versus the result of postmortem anterior chamber collapse).Stress lines can be distinguished from cell death (drop out) or guttae, as there is anabrupt edge over an elongated area as opposed to singular or clustered cell loss. Thisabruptness also identifies the difference between stress lines and folds, which arewavy. These corridors of cell death can change surgical suitability depending on theirquantity, severity, and location, which is best evaluated by slit lamp.
5.1.6 Cornea Guttata and Other Pathologic Changes
Cornea guttata (guttae) are teardrop-shaped prominences of DM penetratingthrough the endothelium into the anterior chamber. They are one of the mostcommon pathologies of the corneal endothelium, closely associated with Fuchsendothelial corneal dystrophy (FECD). The ingrowth of DM through theendothelium leads to the death of individual ECs [25, 56]. Three types of cornealguttae are known: primary central corneal guttae, a common condition of the agingcornea with no edema throughout life; FECD, in which corneal edema occurs; andsecondary corneal guttae [57]. In FECD, the guttae are typically more confluent andmore centrally located than the guttae seen with aging, which characteristicallyinvolve predominantly the peripheral cornea. Guttae are not specific for FECD andmay also arise as a feature of macular corneal dystrophy or as a response tointerstitial keratitis [25].
84 K. Jirsova et al.

In light microscopy, guttae are mostly round, highly reflective excrescences ofdifferent size, and are relatively clearly discernible (Fig. 5.2). They may be visibleas solitary or sparse structures of the size of one endothelial cell (see Figs. 6.41 and6.42). Frequently the guttae are located close together, and they can also form roundor cloverleaf-shaped structures [57]. Morphologically, solitary guttae may resembledying ECs before being sloughed off (see Figs. 6.45–6.47). The presence of guttaeis often associated with lower ECD, a worsening of P&P, and other endothelialabnormalities (see Figs. 6.43 and 6.44). Prolonged OC allows guttae to be moreeasily visualized because the ECs covering the guttae (making the guttae difficult tovisualize before storage) can detach during culturing [57]. Guttae can be clearlyidentified histologically on cross-section (Fig. 5.2c).
The number of guttae varies from none to tens per endothelial surface [20]. It hasbeen shown that guttae are present in up to 26 % of donor corneas: scattered guttaein 21 % and grouped guttae in about 5 %. It was suggested that guttae can bedifferentiated from dying sloughing cells by gently moving the container in whichthe cornea is assessed while observing the corneal endothelium. Sloughing cellsmove independently of the cornea, while guttae appear to be attached to the cornea[57].
Guttae can be readily detected by specular microscopy in corneas stored inhypothermia as dark areas where no ECs are visible (see Figs. 6.159 and 6.160).Thus specular microscopy has been recommended for assessing the donor cornealendothelium before transplantation for the presence of cornea guttata [52].
It has been suggested that guttae arise as a consequence of insufficient orinsufficiently fast repair. This hypothesis is supported by the fact that the number ofguttae is dependent on age: they are virtually absent below 50 years of age, presentin 7 % of donors between 51 and 70 years, and present in 31 % of donors between71 and 90 years [20]. With the increasing incidence of guttae with age in those over50, the age of many eye donors, it is unlikely that all corneas with guttae areexcluded from grafting. However, it has been shown that corneal grafts containingonly sparse guttae have a lower ECD but that this has no significant influence ongraft survival, postoperative visual acuity, or graft thickness during the second year
Fig. 5.2 Cornea guttata (guttae) in donor corneas. a A few sparse guttae. b Guttae coveringalmost the whole endothelial surface. c Cross section of a corneal endothelium, guttae with dyingendothelial cells (stained with hematoxylin)
5 Light and Specular Microscopy Assessment of the Cornea … 85

after grafting [57]. Similarly, it has been shown that guttae found in 4.4 % of almost1000 penetrating or endothelial keratoplasties did not negatively affect vision, ECD,or graft survival after at least two postoperative years [58].
On the other hand, the presence of grouped guttae is associated with poorer graftsurvival, and the development of guttae in grafted tissue can be a cause of severeendothelial defects leading to corneal failure in the long term [57, 59]. The use ofcorneas with only a few solitary guttae but with a high ECD and no deterioration ofP&P may be considered; however, the long-term survival of such corneas may be atgreater risk because of the normal increase in the number of guttae with advancingage.
Beside cornea guttata, pseudoguttae may be found in corneas with infiltratingcells, inflammation (keratitis, iritis), epithelial defects, or the presence of foreignbodies. Pseudoguttae are reversible and resolve completely without any damage tothe corneal endothelium as shown clinically by specular microscopy [60]. Similarstructures resembling ordinary guttae have been observed after acute anterioruveitis [61]. In specular microscopy, pseudoguttae look like guttae when the corneais stored at or near 4 °C but disappear at room temperature. Their origin is thoughtto be from ECs swelling [55]. These structures have not yet been described in OCcorneas.
Besides guttae, other morphologic abnormalities resembling the endothelialchanges occurring during FECD or posterior polymorphous corneal dystrophy canaffect the endothelial surface of donor corneas (see Figs. 6.57–6.64). The suspectedpresence of a corneal dystrophy must be treated as an indication for excluding suchcorneas from grafting.
5.1.7 Intracellular Changes
Several nuclear or cytoplasmic changes affecting the corneal endothelium can beobserved during microscopic evaluation. In ECs that react physiologically tohypotonic solution by dilatation of the intercellular spaces, the nuclei are eitherpoorly visible or not visible at all (see Figs. 6.6 and 6.25). In some cases, thenuclear morphology can be observed in an endothelium with no or only minimaldilatation (see Fig. 6.28), while in other cases, prominent, condensed, or shrunkennuclei may be seen (see Figs. 6.50 and 6.52). Vacuoles or cytoplasmic inclusionshave been observed, particularly in donors with liver diseases [20]. Vacuoles canalso be induced by osmotic stimulation, e.g., by 1.8 % sucrose [1].
Although the endothelium does not proliferate after birth, nuclear changes mayoccur, depending on age. As the cornea matures, the nuclei become more spherical,and with increasing age, the cells spread out and the cytoplasm occupies a greaterproportion of the total cell area [20]. Other changes include the formation ofmultinucleated cells, which arise by the coalescence or fusion of several ECs (seeFig. 6.51). Commonly two to four nuclei may by present in one large endothelialcell [62]. It is rare to observe the presence of micronuclei (see Fig. 6.52), which
86 K. Jirsova et al.

probably do not arise during cell division but rather by budding or the fragmen-tation of the nucleus. If multinucleated cells are regularly present over the entiresurface of the endothelium, it is necessary to judge the overall status of theendothelium and to carefully consider the use of the cornea for grafting.
Generally, endothelial nuclei are not visible using specular microscopy. On theother hand, cytoplasmic vacuolation, another morphologic alteration affectingendothelial cells, can be observed using both light and specular microscopy [63]. Ina small study of two corneas confirmed by light and electron microscopy, it wasshown that the dark, round to oval areas observed on the endothelium of donatedcorneas by specular microscopy actually represent endothelial vacuolation (seeFig. 6.156). Similar dark structures have been observed by specular microscopy inhuman and rabbit endothelium after hyperosmotic treatment. Using electronmicroscopy, it was shown that these structures represent enlarged intercellular fluidchannels, which may also act as pathways for the formation of intercellular andsubendothelial vacuoles [40].
5.1.8 Presence of Vessels, Foreign Bodies, and Precipitates
Sometimes the presence of vessels in the central or peripheral part of the cornea canbe observed (see Figs. 6.77 and 6.78); such tissue must be excluded from grafting.
Depending on their size, foreign bodies may be more easily detected using lightmicroscopy than by slit lamp microscopy. In most cases, foreign bodies contami-nate the tissue during procurement (enucleation or in situ corneal excision) orduring the processing and assessment of the cornea in the eye bank. Occasionally, aforeign body (see Figs. 6.65 and 6.66) can be carefully rinsed off or removed understerile conditions, and if there is no damage to the endothelial surface, the corneacan subsequently be used for transplantation with the condition that all otherquantitative and qualitative parameters are acceptable.
Precipitates of inflammatory cells that infiltrate the cornea because of uveitis orsecondary to sarcoidosis, tuberculosis, or toxoplasmosis are observed [64]. As ECsdisplay phagocytic activity [65], precipitates may be present not only at theendothelial surface but also intracellularly. In current practice, the remnants ofepithelial cells, erythrocytes, protein deposits, or pigment precipitates may beobserved by light microscopy (see Figs. 6.55 and 6.56). Iris pigment releasedduring the preparation of a corneoscleral disc may be attracted to the cornealendothelium. This is not a problem when it is an isolated occurrence. However,numerous pigmented precipitates over the endothelium as a result of primary (de-generative) or secondary (inflammatory, traumatic) pigment dispersion representone of the most frequent findings potentially associated with an impairedendothelium [65]. The size of this pigment may be similar to the size of bacteria andthus mimic contamination. Cell debris accumulated on the endothelial surface,particularly arising from sloughed epithelial cells, may potentially lead toendothelial damage.
5 Light and Specular Microscopy Assessment of the Cornea … 87

In specular microscopy, erythrocytes (red blood cells, RBCs) present frombleeding at the time of corneoscleral disc excision can be discernible as dark roundspots smaller than ECs (see Fig. 6.155) [55]. This is more frequently observedduring in situ corneal excision than from eye bank excision of a corneoscleral discfrom a whole enucleated eye; however, RBCs may be rinsed off during processingof the cornea (see Figs. 6.167 and 6.168). Precipitates of white blood cells, pigmentdebris and particulate contaminants may all be seen on the endothelial surface [55].Most often debris (usually small fragments of iris, scleral spur, or conjunctiva fromthe preservation of the cornea) is too small in size to warrant removal. Surgeons areadvised to rinse the tissue.
5.2 Assessment of the Corneal Epithelium
Assessment of the epithelium can be performed readily by light microscopy.Generally, if a functional limbus is present in the recipient cornea, the presence of acompletely preserved corneal epithelium is not necessary in terms of graft survivalbecause the epithelial cells are renewed from the limbal area very quickly (fordetails, see Sect. 1.2). Using a mouse model, it has been shown that the donorepithelium is totally replaced by recipient epithelial cells within two weeks [66].Moreover, corneas with an intact epithelium exhibit more rapid wound healingcompared to corneas with a damaged epithelium (for details, see Sect. 3.6). Corneaswith extensive erosions (the local absence of several or all epithelial layers) orcorneas in which the epithelium is absent (see Figs. 6.73–6.75) should not betransplanted into patients with severe damage of the ocular surface or into patientswith impaired healing of the ocular surface [67, 68].
The microscopic evaluation of the corneal epithelium consists of determining thepresence of foreign bodies (see Fig. 6.76), visible dendritic cells (see Fig. 6.71),which may be a sign of ongoing inflammation or signs of vascularization (seeFigs. 6.77 and 6.78).
Compared to the clearly visible epithelial surface of a healthy cornea(see Fig. 6.1), drying of the ocular surface as a consequence of exposure ker-atopathy or band exposure keratopathy causes increased light reflection (seeFig. 6.72) [55]. The irregular reflection of light indicates an inadequate tear film anda breakdown in the integrity of the corneal epithelium [69]. This places the corneaat risk for infection and prevents focusing throughout the entire thickness of thecornea; it is therefore necessary to reassess the cornea after OC storage. Thesechanges may worsen with time if the tissue is stored hypothermically.
The microscopic assessment of the epithelium by means of specular microscopyis not routinely done in eye bank practice (see Fig. 6.134). Epithelial defects can bedetected because of their increased cellular reflection, although the most superficialcorneal epithelium layer is seen with difficulty as the cells lack sufficient contrast.Subepithelial deposits can be recognized, but the assessment is performed mostlyunder experimental conditions [8, 70].
88 K. Jirsova et al.

5.3 Assessment of the Corneal Stroma
For penetrating and anterior lamellar keratoplasty, the corneal stroma should beclear, with no signs of pathologic processes or abnormalities. Using phase contrastmicroscopy, a healthy stroma has more or less an amorphous character, occa-sionally with the presence of fibrous structures or individual keratocytes (seeFigs. 6.4 and 6.5).
Stromal opacities may be a sign of various stromal dystrophies. Stromalpathologies that are apparent microscopically include opacities that are present as aresult of corneal scars. Nebulae are slight, diffuse, cloudlike opacities with indistinctborders; the accompanying scars are present preferentially in the superficial stroma.Maculae are well-circumscribed, moderately dense opacities whose scars are den-sely present throughout the stroma (see Figs. 6.67 and 6.68) [71, 72]. The presenceof maculae is relatively common. They occur in more than 10 % of donors, aquarter of them bilaterally. Corneas with scars localized in the anterior stroma areeither excluded from transplantation or used for the preparation of posteriorlamellae [19, 73]. Corneas with opacities are acceptable for use in anterior andpenetrating keratoplasty as long as they are located outside the field of vision,which is generally accepted as the central 6 mm of the cornea.
In the stroma of donor corneas, deposits that are typical of stromal dystrophiesmaybe observed (see Figs. 6.69 and 6.70). Characteristic crystalline infiltrates that areclearly visible in the stroma accompany relatively rare crystalline keratopathy, aslowly spreading infectious disease, graft rejection, or keratolysis (see Fig. 6.198)[74]. Besides these characteristic stromal changes, alterations in the corneal epithe-lium (see Fig. 6.197) and the degeneration of endothelial cells may be seen in cornealexplants from patients suffering from keratolysis (see Figs. 6.199 and 6.200).
In specular microscopy, hyper-reflective stromal particles as a consequence ofprevious laser-assisted in situ keratomileusis (LASIK) of the donor may be visible(see Fig. 6.161) [75].
5.4 Changes of the Cornea Occurring During Storage
5.4.1 Light Microscopy
During OC, various parameters of a cornea may improve or deteriorate. The ECDdecreases depending on storage time: less than 10 % during the first days of OC,then up to 16 % by the end of the third week of cultivation (see Figs. 6.79 and 6.80)[44, 76, 77]. The number of DECs may decrease because of their detachment fromthe endothelial mosaic and subsequent degradation (see Figs. 6.81 and 6.82).
5 Light and Specular Microscopy Assessment of the Cornea … 89

The conditions of OC being close to physiologic conditions allow the replacementof dead ECs by adjacent cells and even the repair of larger endothelial lesions,whose former location may be indicated after storage by the presence of cell debris(see Figs. 6.83–6.86).
In a study of almost 2000 OC corneas stored between 11 and 31 days,endothelial cell loss of more than 50 % occurred in 0.4–3 % of corneas [5].A greater reduction in ECD was observed in younger donors, i.e., donors with arelatively high ECD [17, 78, 79]. A pronounced decrease in the number of DECs atthe second assessment (more than 20 % compared to the first assessment duringthree to four weeks storage) may be a signal to exclude the cornea from grafting[76]. This decrease is indicative of excessive cell death during storage, for whichthe endothelium itself is unable to compensate. This situation may reflect inap-propriate culture conditions or the presence of pathologic processes in the corneaitself, such as viral infections (see Figs. 6.87 and 6.88) [5, 80]. In contrast to viralinfection, the occurrence of bacteria or fungi may be indicated by turbidity or acolor change of the culture medium; alternatively/in addition, the presence of fungi(see Figs. 6.89 and 6.90) or bacteria (see Figs. 6.91–6.94) may be detected bymicroscopy on the corneal surface or in the culture medium. Nevertheless, appro-priate microbiologic testing is required to reliably detect bacterial or fungal con-tamination (for details, see Sect. 3.5).
Very rarely some deterioration in terms of corneal edema or endothelial cellvisualization may occur during OC storage (see Figs. 6.95 and 6.96). However,more often the use of deswelling media allows for better visualization of endothelialmorphology than at the first assessment, particularly if the cornea was edematous(see Figs. 6.97–6.100). Moreover, in many cases absent, inappropriate or irregulardilatation of the intercellular spaces between ECs is improved during cultivation(see Figs. 6.101–6.108), and in such cases pathologic structures can be bettercharacterized (see Figs. 6.109 and 6.110).
Epithelial cells, from both intact and damaged epithelium, gradually slough offduring storage in OC (see Figs. 6.111 and 6.112) or hypothermia. After four toseven days in OC, the epithelium is reduced to about three layers, but the lowerlayers are retained after 40 days [11, 31]. If a corneoscleral disc of sufficientdiameter (more than 11 to 12 mm) is prepared and thus a functional limbus ispreserved, the corneal epithelium is renewed during storage in OC. The cellsmigrating centripetally from the periphery to the center of the cornea [81] form thereticular bundles of the new epithelial layer (see Figs. 6.113 and 6.114).
When the donor cornea is edematous or if exposure keratopathy affects theepithelium, stromal opacities or scars can be more difficult to detect either by slitlamp or even by light microscopy owing to the difficulty of focusing on internalstructures; following cultivation, when epithelial cells are spontaneously sloughingoff the cornea, focusing becomes easier and such opacities can be clearly seen (seeFigs. 6.115 and 6.116).
90 K. Jirsova et al.

5.4.2 Specular Microscopy
The specular microscopic appearance of the endothelium preserved underhypothermic conditions depends upon the temperature of the tissue, the preserva-tion time, and the media used for storage. Newly stored tissue at room temperatureis the easiest to evaluate, while storage at or near 4 °C results in a temporarydeterioration of endothelial morphology. After cooling, the cell borders becomeincreasingly indistinct, and dark spots of the same size as individual ECs, large darkareas, and an inverted appearance of ECs (dark cell bodies and light cell borders)can be observed (see Fig. 6.157) [39]. Refrigerated tissue must therefore be allowedto warm up to room temperature in order to allow the ECs to resume their normalshape (see Figs. 6.149, 6.150, 6.162–6.164); the warming process should not berushed. Most of the morphologic distortions of the endothelium related tohypothermia are reversible, disappearing with increasing time at room temperature.However, persistent black spots or dark areas are composed of damaged or DECs,as shown by trypan blue staining [39]. The specular microscopy examinationshould usually be performed 2–2.5 h after the removal of the tissue from therefrigerator [55, 82].
5.5 The Preparation and Assessment of EndothelialLamellae
The eye bank preparation of tissue for lamellar grafts increases the utilization ofavailable tissue and allows standardization of the method, tissue storage, andquality control, particularly the measurement of graft thickness and ECD [83–85].Various techniques can be used for preparing lamellae (for details, see Sect. 2.7)from corneas stored in OC or under hypothermic conditions.
The lamellae (lenticules) for Descemet stripping automated endothelial kerato-plasty (DSAEK) are usually prepared by an automated microkeratome or a fem-tosecond laser [85–87]. The endothelial quality is checked by light (see Figs. 6.117and 6.118) or specular microscopy (see Figs. 6.165–6.168) before and after lamelladissection and storage. Beside the endothelium and DM the lamellae contain a thinlayer of the stroma that somewhat protects the fragile endothelium againstmechanical stress during manipulation. Attention must be paid to standardizing thedissection technique and the tissue storage conditions with the aim of preparingDSAEK grafts of consistent thickness. Such standardization can be achieved bycontrolled stromal dehydration utilizing new types of storage media, by intervals ofsterile airflow, or by customizing lamellae preparation by personalizing the cuttingparameters for the preparers [88–90].
Various manual techniques for DM endothelial keratoplasty (DMEK) lamellapreparation have been introduced [91–96]. Usually DM is peeled from the under-lying stroma over 80–90 % of its surface area leaving an area of residual attachment
5 Light and Specular Microscopy Assessment of the Cornea … 91

either in the center or at the periphery. The graft is then laid back against the stromato facilitate storage and transportation (see Figs. 6.119, 6.120 for light, and 6.169–6.172 for specular microscopy, respectively) [97]. Various improvements of DMEKprocessing techniques have been introduced by eye banks with the aim ofdecreasing endothelial cell loss during preparation and quality assessment (seeFigs. 6.121–6.124) [98]. During the pneumatic dissection of lamellae for DMEK,air or, as demonstrated recently, liquid can be successfully used to yield lamellae oflarger diameter and higher ECD (see Figs. 6.125 and 6.126) [99].
As DMEK lamellae exhibit a natural tendency to curl up into a scroll with theendothelial layer facing outward, increased attention must be paid when manipu-lating (assessment, transport) this delicate and easily damaged tissue. As an alter-native to laying the partially attached graft back down on the stroma, lamellae canbe stored and thus protected from external damage, then transported in variousinsertion devices (mostly glass injectors or injector cartridges), allowing the sur-geon to introduce the graft into the anterior chamber without further manipulation(see Figs. 6.127 and 6.128) [96, 100–103]. Another important point for successfulendothelial lamella grafting is proper orientation of the graft. In some eye banks amark in the sclera is made to denote the area of attachment of the DM for easycommunication to the surgeon. This mark or scleral resection guides the surgeon asto which way the tissue should be lifted from the cornea before implantation.Additionally, an orientation mark, such as an S stamp or peripheral markings, isvery important to the surgeon in the operating room to ensure proper orientation ofthe graft [101, 102, 104].
DMEK with a stromal rim (DMEK-S or DMAEK if lamellar dissection is madewith microkeratome) and other hybrid endothelial lamellae with stromal support areless fragile compared to DMEK lamellae and thus allow for easier manipulation[105–107]. The stromal rim also simplifies the orientation of the tissue in theanterior chamber, thus reducing the likelihood of inserting the lamellae upsidedown (see Figs. 6.129 and 6.130). The preparation of lamellae for DMEK orDMEK-S usually leads to an average endothelial cell loss of approximately 4–7 %,depending on the method used, the tissue quality, and the experience of the preparer[73, 93, 108]. It has been suggested that tissues from donors with diabetes mellitus,hyperlipidemia, or obesity are associated with higher failure rates in DMEKpreparation [97], but there is no universal agreement concerning the influence ofthese factors.
The storage of dissected lamellae in OC close to physiologic conditions is aprerequisite for the subsequent repair of potential endothelial damage occurringduring preparation [73, 93]. However, no differences in best-corrected visual acuity,postoperative ECD, or central corneal thickness have been observed between cor-neas stored in OC or hypothermia [109]. The donor age and the length of storageprior to tissue dissection may influence the successful preparation of lamellae forDMEK or DMEK-S [73, 110].
92 K. Jirsova et al.

5.6 The Changes Characterizing Corneal PathologiesObserved in Corneal Explants and Patients
During the long-term practice of evaluating the suitability of donor corneas forgrafting, eye bank staff may find themselves assessing corneas from patients suf-fering from various corneal diseases. In order to clarify and better understand theendothelial alterations that can be met in the course of normal eye banking practice,the changes characteristic of frequently encountered corneal diseases, as reflectedby changes in the morphology of the endothelium, are described here. Additionally,links to light microscopy images of the endothelium of corneal explants obtainedduring penetrating keratoplasty and specular microscopy images of the endotheliumof diseased patients are presented.
Abnormalities of the corneal endothelium and DM are characteristic of a groupof posterior corneal dystrophies. In particular, these include Fuchs endothelialcorneal dystrophy (FECD), posterior polymorphous corneal dystrophy (PPCD), andcongenital hereditary endothelial dystrophy (CHED) [25].
Explants from patients suffering from FECD show DM protrusions through theendothelial layer, guttae. Solitary, grouped, or coalesced guttae are clearly dis-cernible using both light (see Figs. 6.173–6.176, 6.179 and 6.180) and specularmicroscopy (see Figs. 6.203 and 6.204), similarly to corneal edema (see Fig. 6.174).Apoptotic endothelial cells are frequently observed in FECD, probably as a con-sequence of oxidative stress to which FECD endothelial cells are more susceptiblethan normal ECs [111]. Melanosomes (granules containing melanin) within theendothelial cells and cellular debris (see Fig. 6.175) or a degenerated endotheliumcan be observed using both bright field and phase contrast of light microscopy (seeFigs. 6.177, 6.178 and 6.180) [25]. A decreased ECD, polymegethism, and pleo-morphism are other, less specific changes that can be seen in FECD endothelium.Compared with the normal endothelial mosaic (see Figs. 6.201 and 6.202), abnormalendothelial cells and stromal edema can be observed by specular microscopy inadvanced FECD (see Figs. 6.205 and 6.206).
PPCD is genetically heterogeneous: PPCD1 is caused by mutations in theOVOL2 promoter, PPCD2 has been associated with mutations in COL8A2, andPPCD3 with mutations in ZEB1 [112]. In PPCD, local foci of the original cells losetheir endothelial characteristics and acquire an epithelial-like phenotype with thestrong expression of a wide spectrum of keratins, predominantly keratins 7, 19,3/12, 4, 5/6, 14, and 16 [113, 114]. PPCD explants show prominent P&P (seeFigs. 6.181 and 6.182); in particular the enlargement of endothelial cells (seeFigs. 6.181 and 6.183) is typical in cases for which grafting is necessary. Areas ofendothelial cells are often localized in the vicinity of epithelial-like cells (seeFigs. 6.183–6.185). Other morphologic abnormalities such as the presence offibroblast-like spindle-shaped cells (see Fig. 6.186), cells showing abnormalintracellular (nuclear) morphology (see Fig. 6.187), or other unusual changes havebeen observed in both endothelial (see Figs. 6.188 and 6.189) as well as epithelialcells (see Fig. 6.190). In specular microscopy, lesions are present at the level of the
5 Light and Specular Microscopy Assessment of the Cornea … 93

endothelium and DM, appearing as vesicular lesions, bands, or geographic opaci-ties; the enlargement of abnormal endothelial cells, P&P, and corneal edema is alsofound (see Figs. 6.207–6.212).
Epithelialization also occurs in CHED and iridocorneal endothelial syndrome(ICE), which is not a hereditary disorder [115]. In ICE explants a very low ECD,abnormal dilatation of the intercellular spaces, and prominent pleomorphism havebeen observed (see Figs. 6.191 and 6.192). With specular microscopy, abnormalendothelial cells, probably arising as a consequence of corneal edema, appear as thenegative image of normal endothelium: the cell borders appear light and the cellbodies appear dark (see Figs. 6.213 and 6.214) [35].
Detailed scanning of the stroma may reveal abnormal structures such asbranching filaments typical of lattice corneal dystrophy (see Figs. 6.193 and 6.194)or deposits of various size as can be observed in macular corneal dystrophy (seeFigs. 6.195 and 6.196). Characteristic star-like structures present in the stroma aretypical of crystalline keratopathy or keratolysis, in which degenerated dyingendothelium or the enlargement of epithelial cells may also be found (seeFigs. 6.197–6.200).
References
1. Schroeter J, Rieck P. Endothelial evaluation in the cornea bank. Dev Ophthalmol.2009;43:47–62.
2. Pels E, Schuchard Y. The effects of high molecular weight dextran on the preservation ofhuman corneas. Cornea. 1984;3:219–27.
3. Borderie VM, Baudrimont M, Lopez M, Carvajal S, Laroche L. Evaluation of the deswellingperiod in dextran-containing medium after corneal organ culture. Cornea. 1997;16:215–23.
4. Pels E, Beekhuis WH, Völker-Dieben HJ. Long-term tissue storage for keratoplasty. In:Brightbill FS, editor. Corneal surgery: theory, technique, and tissue. 3rd ed. St. Louis, MO:Mosby Co; 1999. pp 897–906.
5. Builles N, Kodjikian L, Burillon C, Damour O. Major endothelial loss from corneas in organculture: importance of second endothelial count. Cornea. 2006;25:815–20.
6. Pels E, Beele H, Claerhout I. Eye bank issues: II. Preservation techniques: warm versus coldstorage. Int Ophthalmol. 2008;28:155–63.
7. Gain P, Thuret G, Kodjikian L, Gavet Y, Turc PH, Theillere C, et al. Automated tri-imageanalysis of stored corneal endothelium. Br J Ophthalmol. 2002;86:801–8.
8. Lass JH, Gal RL, Ruedy KJ, Benetz BA, Beck RW, Baratz KH, et al. Cornea Donor StudyG: an evaluation of image quality and accuracy of eye bank measurement of donor corneaendothelial cell density in the Specular Microscopy Ancillary Study. Ophthalmology.2005;112:431–40.
9. Benetz BA, Gal RL, Ruedy KJ, Rice C, Beck RW, Kalajian AD, Lass JH, Cornea DonorStudy G (2006). Specular microscopy ancillary study methods for donor endothelial celldensity determination of Cornea Donor Study images. Curr Eye Res. 2006;31:319–27.
10. Schimmelpfennig BH. Direct and indirect determination of nonuniform cell densitydistribution in human corneal endothelium. Invest Ophthalmol Vis Sci. 1984;25:223–9.
11. Pels E, Schuchard Y. Tissue storage. E: Organ culture and endothelial evaluation as apreservation method for human corneas. In: Brightbill FS, editor. Corneal surgery. theory,technique, and tissue. St. Louis, MO: CV Mosby; 1986. pp 93–102.
94 K. Jirsova et al.

12. Armitage WJ, Dick AD, Bourne WM. Predicting endothelial cell loss and long-term cornealgraft survival. Invest Ophthalmol Vis Sci. 2003;44:3326–31.
13. Nejepinska J, Juklova K, Jirsova K. Organ culture, but not hypothermic storage, facilitatesthe repair of the corneal endothelium following mechanical damage. Acta Ophthalmol.2010;88:413–9.
14. EEBA Directory. European Eye Bank Association, Directory, 23rd edition. Venice, Italy;2015.
15. Rijneveld WJ, Wolff R, Volker-Dieben HJ, Pels E. Validation of tissue quality parametersfor donor corneas, designated for emergency cases: corneal graft survival. Acta Ophthalmol.2011;89:734–40.
16. Muraine M, Toubeau D, Gueudry J, Brasseur G. Impact of new lamellar techniques ofkeratoplasty on eye bank activity. Graefes Arch Clin Exp Ophthalmol. 2007;245:32–8.
17. Armitage WJ, Easty DL. Factors influencing the suitability of organ-cultured corneas fortransplantation. Invest Ophthalmol Vis Sci. 1997;38:16–24.
18. Armour RL, Ousley PJ, Wall J, Hoar K, Stoeger C, Terry MA. Endothelial keratoplastyusing donor tissue not suitable for full-thickness penetrating keratoplasty. Cornea.2007;26:515–9.
19. Phillips PM, Terry MA, Shamie N, Chen ES, Hoar KL, Stoeger C, et al. Descemet’sstripping automated endothelial keratoplasty (DSAEK) using corneal donor tissue notacceptable for use in penetrating keratoplasty as a result of anterior stromal scars, pterygia,and previous corneal refractive surgical procedures. Cornea. 2009;28:871–6.
20. Kaufman HE, Capella JA, Robbins JE. The human corneal endothelium. Am J Ophthalmol.1996;61 (5 Pt 1):835–41.
21. Murphy C, Alvarado J, Juster R, Maglio M. Prenatal and postnatal cellularity of the humancorneal endothelium. A quantitative histologic study. Invest Ophthalmol Vis Sci. 1984;25:312–22.
22. Yee RW, Matsuda M, Schultz RO, Edelhauser HF. Changes in the normal cornealendothelial cellular pattern as a function of age. Curr Eye Res. 1985;4:671–8.
23. Bourne WM, Nelson LR, Hodge DO. Central corneal endothelial cell changes over aten-year period. Invest Ophthalmol Vis Sci. 1997;38:779–82.
24. Sheng H, Bullimore MA. Factors affecting corneal endothelial morphology. Cornea.2007;26:520–5.
25. Klintworth GK. Corneal dystrophies. Orphanet J Rare Dis. 2009;4:7.26. Laing RA, Sanstrom MM, Berrospi AR, Leibowitz HM. Changes in the corneal endothelium
as a function of age. Exp Eye Res. 1976;22:587–94.27. Thuret G, Deb-Joardar N, Manissolle C, Zhao M, Peoch M, Gain P, Gavet Y. Assessment of
the human corneal endothelium: in vivo Topcon SP2000P specular microscope versusex vivo sambacornea eye bank analyser. Br J Ophthalmol. 2007;91:265–6.
28. Hirneiss C, Schumann RG, Gruterich M, Welge-Luessen UC, Kampik A, Neubauer AS.Endothelial cell density in donor corneas: a comparison of automatic software programs withmanual counting. Cornea. 2007;26:80–83.
29. Komuro A, Hodge DO, Gores GJ, Bourne WM. Cell death during corneal storage at 4degrees C. Invest Ophthalmol Vis Sci. 1999;40:2827–32.
30. Albon J, Tullo AB, Aktar S, Boulton ME. Apoptosis in the endothelium of human corneasfor transplantation. Invest Ophthalmol Vis Sci. 2000;41:2887–93.
31. Crewe JM, Armitage WJ. Integrity of epithelium and endothelium in organ-cultured humancorneas. Invest Ophthalmol Vis Sci. 2001;42:1757–61.
32. Engelmann K, Sobottka Ventura A, Drexler D, Staude HJ. A sensitive method for testing thequality of organ culture media and of individual medium components in a cornea bank.Graefes Arch Clin Exp Ophthalmol. 1998;236:312–9.
33. Moller-Pedersen T, Hartmann U, Moller HJ, Ehlers N, Engelmann K. Evaluation of potentialorgan culture media for eye banking using human donor corneas. Br J Ophthalmol.2001;85:1075–9.
5 Light and Specular Microscopy Assessment of the Cornea … 95

34. Schultz RO, Matsuda M, Yee RW, Edelhauser HF, Schultz KJ. Corneal endothelial changesin type I and type II diabetes mellitus. Am J Ophthalmol. 1984;98:401–10.
35. Bourne WM. Biology of the corneal endothelium in health and disease. Eye (Lond).2003;17:912–8.
36. Grabska-Liberek I, Szaflik J, Brix-Warzecha M. The importance of various factors relatingto the morphological quality of corneas used for PKP by the Warsaw Eye Bank from 1996 to2002. Ann Transplant. 2003;8:26–31.
37. Sperling S. Early morphological changes in organ cultured human corneal endothelium.Acta Ophthalmol (Copenh). 1978;56:785–92.
38. McCarey BE, Edelhauser HF, Lynn MJ. Review of corneal endothelial specular microscopyfor FDA clinical trials of refractive procedures, surgical devices, and new intraocular drugsand solutions. Cornea. 2008;27:1–16.
39. Neubauer L, Laing RA, Leibowitz HM. Specular microscopic appearance of damaged anddead endothelial cells in corneas following short-term storage. Arch Ophthalmol.1984;102:439–44.
40. Nartey IN, Cavanagh HD, Jester JV, Andrews P, Petroll WM. Characterization of specular“dark events” in human donor corneal endothelium by scanning and transmission electronmicroscopy. Cornea. 1998;17:544–49.
41. Sperling S. Evaluation of the endothelium of human donor corneas by induced dilation ofintercellular spaces and trypan blue. Graefes Arch Clin Exp Ophthalmol. 1986;224:428–34.
42. Acquart S, Gain P, Zhao M, Gavet Y, Defreyn A, Piselli S, et al. Endothelial morphometryby image analysis of corneas organ cultured at 31 degrees C. Invest Ophthalmol Vis Sci.2010;51:1356–64.
43. Harper CL, Boulton ME, Marcyniuk B, Tullo AB, Ridgway AE. Endothelial viability oforgan-cultured corneas following penetrating keratoplasty. Eye (Lond). 1998;12(Pt 5):834–8.
44. Borderie VM, Scheer S, Touzeau O, Vedie F, Carvajal-Gonzalez S, Laroche L. Donor organcultured corneal tissue selection before penetrating keratoplasty. Br J Ophthalmol. 1998;82(4):382–8.
45. Bourne WM, Hodge DO, McLaren JW. Estimation of corneal endothelial pump function inlong-term contact lens wearers. Invest Ophthalmol Vis Sci.1999;40:603–11.
46. Kim EK, Geroski DH, Holley GP, Urken SI, Edelhauser HF. Corneal endothelialcytoskeletal changes in F-actin with aging, diabetes, and after cytochalasin exposure.Am J Ophthalmol. 1992;114:329–35.
47. Bourne WM, Kaufman HE. Cataract extraction and the corneal endothelium. Am JOphthalmol. 1976;82:44–7.
48. Rao GN, Aquavella JV, Goldberg SH, Berk SL. Pseudophakic bullous keratopathy.Relationship to preoperative corneal endothelial status. Ophthalmology. 1984;91:1135–40.
49. Doughman DJ, Van Horn D, Rodman WP, Byrnes P, Lindstrom RL. Human cornealendothelial layer repair during organ culture. Arch Ophthalmol. 1976;94:1791–6.
50. Mishima S. Clinical investigations on the corneal endothelium-XXXVIII. Edward JacksonMemorial Lecture. Am J Ophthalmol. 1982;93:1–29.
51. Treffers WF. Human corneal endothelial wound repair. In vitro and in vivo. Ophthalmology.1982;89:605–13.
52. Brooks AM, Grant G, Gillies WE. A comparison of corneal endothelial morphology incornea guttata, Fuchs’ dystrophy and bullous keratopathy. Aust N Z J Ophthalmol. 1988;16:93–100.
53. Ohguro N, Matsuda M, Fukuda M. Corneal endothelial changes in patients with chronicrenal failure. Am J Ophthalmol. 1999;128:234–6.
54. Modis L Jr, Szalai E, Kertesz K, Kemeny-Beke A, Kettesy B, Berta A. Evaluation of thecorneal endothelium in patients with diabetes mellitus type I and II. Histol Histopathol.2010;25:1531–7.
55. Rosenwasser GOD, Nicholson WJ. Introduction to Eye Banking: A Handbook and Atlas: AGuide to Eye Bank Techniques, Corneal Evaluation, and Grading. Cybersight; 2013. http://www.cybersight.org/bins/content_page.asp?cid=1-1581.
96 K. Jirsova et al.

56. Zhang J, Patel DV. The pathophysiology of Fuchs’ endothelial dystrophy–a review ofmolecular and cellular insights. Exp Eye Res. 2015;130:97–105.
57. Borderie VM, Sabolic V, Touzeau O, Scheer S, Carvajal-Gonzalez S, Laroche L. Screeninghuman donor corneas during organ culture for the presence of guttae. Br J Ophthalmol.2001;85:272–6.
58. Nahum Y, Canton V, Ponzin D, Busin M. Prevalence of guttae in the graft following cornealtransplantation. Br J Ophthalmol. 2015;99:1660–3.
59. Christopoulos V, Garner A. Emergence of cornea guttata in donor tissue: a cause of late graftfailure. Eye (Lond). 1993;7:772–4.
60. Nakashima Y, Yoshitomi F, Oshika T. Clinical evaluation of cornea pseudoguttata. Br JOphthalmol. 2007;91:22–5.
61. Olsen T. Transient changes in specular appearance of the corneal endothelium and in cornealthickness during anterior uveitis. Acta Ophthalmol (Copenh). 1981;59:100–9.
62. Faure JP, Kim YZ, Graf B. Formation of giant cells in the corneal endothelium during itsregeneration after destruction by freezing. Exp Eye Res. 1971;12:6–12.
63. Kanavi MR, Javadi MA, Chamani T. Specular microscopic features of corneal endothelialvacuolation. J Ophthalmic Vis Res. 2011;6:5–7.
64. Trinh L, Brignole-Baudouin F, Labbe A, Raphael M, Bourges JL, Baudouin C. The cornealendothelium in an endotoxin-induced uveitis model: correlation between in vivo confocalmicroscopy and immunohistochemistry. Mol Vis. 2008;14:1149–56.
65. Hartmann C. Studies on the development of extra-endothelial and intra-endothelial pigmentdeposits by means of direct and indirect contact specular microscopy of the cornea. GraefesArch Clin Exp Ophthalmol. 1982;218:75–82.
66. Hori J, Streilein JW. Dynamics of donor cell persistence and recipient cell replacement inorthotopic corneal allografts in mice. Invest Ophthalmol Vis Sci. 2001;42:1820–8.
67. Maguire MG, Stark WJ, Gottsch JD, Stulting RD, Sugar A, Fink NE, Schwartz A. Riskfactors for corneal graft failure and rejection in the collaborative corneal transplantationstudies. Collaborative Corneal Transplantation Studies Research Group. Ophthalmology.1994;101:1536–47.
68. Jeng BH. Preserving the cornea: corneal storage media. Curr Opin Ophthalmol.2006;17:332–7.
69. Gregory DG. Nursing interventions. Rocky Mountains Lions Eye Bank. http://www.corneas.org/index.cfm/ID/153#intervene.
70. Marechal-Courtois C, Delcourt JC. [Examination of the corneal epithelium using thespecular microscope.] J Fr Ophtalmol. 1983;6:639–46.
71. Agrawal PK. The pathology of cornea (a histopathological study). Indian J Ophthalmol.1993;31:662–5.
72. Yanoff MD, Sassani JW. Ocular Pathology. 6th edition. Philadelphia, PA: Mosby Elsevier;2009.
73. Krabcova I, Studeny P, Jirsova K. Endothelial quality of pre-cut posterior corneal lamellaefor Descemet membrane endothelial keratoplasty with a stromal rim (DMEK-S): two-yearoutcome of manual preparation in an ocular tissue bank. Cell Tissue Bank. 2013;14:325–31.
74. Mesiwala NK, Chu CT, Raju LV. Infectious crystalline keratopathy predominantly affectingthe posterior cornea. Int J Clin Exp Pathol. 2014;7:5250–3.
75. Mootha VV, Dawson D, Kumar A, Gleiser J, Qualls C, Albert DM. Slitlamp, specular, andlight microscopic findings of human donor corneas after laser-assisted in situ keratomileusis.Arch Ophthalmol. 2004;122:686–92.
76. Pels E, Schuchard Y. Organ-culture preservation of human corneas. Doc Ophthalmol.1983;56:147–153.
77. Frueh BE, Bohnke M. Corneal grafting of donor tissue preserved for longer than 4 weeks inorgan-culture medium. Cornea. 1995;14:463–6.
78. Bourne WM. Chronic endothelial cell loss in transplanted corneas. Cornea. 1983;2:289–94.
5 Light and Specular Microscopy Assessment of the Cornea … 97

79. Gain P, Thuret G, Chiquet C, Rizzi P, Pugniet JL, Acquart S, et al. Cornea procurement fromvery old donors: post organ culture cornea outcome and recipient graft outcome. Br JOphthalmol. 2002;86:404–11.
80. Biswas S, Suresh P, Bonshek RE, Corbitt G, Tullo AB, Ridgway AE. Graft failure in humandonor corneas due to transmission of herpes simplex virus. Br J Ophthalmol. 2000;84:701–5.
81. Slettedal JK, Lyberg T, Ramstad H, Beraki K, Nicolaissen B. Regeneration of the epitheliumin organ-cultured donor corneas with extended post-mortem time. Acta Ophthalmol Scand.2007;85:371–6.
82. Cornea Donor Study Investigator G, gal RL, Dontchev M, Beck RW, Mannis MJ,Holland EJ, et al. The effect of donor age on corneal transplantation outcome results of thecornea donor study. Ophthalmology. 2008;115:620–26:e626.
83. Terry MA. Endothelial keratoplasty: a comparison of complication rates and endothelialsurvival between precut tissue and surgeon-cut tissue by a single DSAEK surgeon. TransAm Ophthalmol Soc. 2009;107:184–91.
84. Parekh M, Salvalaio G, Ruzza A, Camposampiero D, Griffoni C, Zampini A, et al. Posteriorlamellar graft preparation: a prospective review from an eye bank on current and futureaspects. J Ophthalmol. 2013:769–860.
85. Boynton GE, Woodward MA. Eye-bank preparation of endothelial tissue. Curr OpinOphthalmol. 2014;25:319–24.
86. Chen ES, Terry MA, Shamie N, Hoar KL, Friend DJ. Precut tissue in Descemet’s strippingautomated endothelial keratoplasty donor characteristics and early postoperative complica-tions. Ophthalmology. 2008;115:497–02.
87. Fuest M, Salla S, Walter P, Plange N, Kuerten D, Flammersfeld A, Hermel M. Comparisonof Gebauer SLc and Moria CBm Carriazo-Barraquer ALK Microkeratomes for Descemet’sstripping automated endothelial keratoplasty preparation. Curr Eye Res. 2016;41:343–9.
88. Rossi M, Misto R, Gatto C, Garimoldi P, Campanelli M, D’Amato Tothova J. Protectiveeffects of deswelling on stromal collagen denaturation after a corneal femtosecond laser cut.Invest Ophthalmol Vis Sci. 2013;54:4148–57.
89. Thomas PB, Mukherjee AN, O’Donovan D, Rajan MS. Preconditioned donor cornealthickness for microthin endothelial keratoplasty. Cornea. 2013;32:173–8.
90. Locke G, Perez O. Processed tissue customization: development of an operator-specificnomogram for eye bank pre-cut tissue for DSAEK. 2016;IJEB:4:1–4.
91. Melles GR, Wijdh RH, Nieuwendaal CP. A technique to excise the Descemet membranefrom a recipient cornea (descemetorhexis). Cornea. 2004;23:286–8.
92. Ignacio TS, Nguyen TT, Sarayba MA, Sweet PM, Piovanetti O, Chuck RS, Behrens A.A technique to harvest Descemet’s membrane with viable endothelial cells for selectivetransplantation. Am J Ophthalmol. 2005;139:325–30.
93. Lie JT, Birbal R, Ham L, van der Wees J, Melles GR. Donor tissue preparation for Descemetmembrane endothelial keratoplasty. J Cataract Refract Surg. 2008;34:1578–83.
94. Price MO, Giebel AW, Fairchild KM, Price FW, Jr. Descemet’s membrane endothelialkeratoplasty: prospective multicenter study of visual and refractive outcomes and endothelialsurvival. Ophthalmology. 2009;116:2361–8.
95. Groeneveld-van Beek EA, Lie JT, van der Wees J, Bruinsma M, Melles GR. Standardized‘no-touch’ donor tissue preparation for DALK and DMEK: harvesting undamaged anteriorand posterior transplants from the same donor cornea. Acta Ophthalmol. 2013;91:145–50.
96. Muraine M, Gueudry J, He Z, Piselli S, Lefevre S, Toubeau D. Novel technique for thepreparation of corneal grafts for descemet membrane endothelial keratoplasty. Am JOphthalmol. 2013;156:851–9.
97. Vianna LM, Stoeger CG, Galloway JD, Terry M, Cope L, Belfort R, Jr., Jun AS. Riskfactors for eye bank preparation failure of Descemet membrane endothelial keratoplastytissue. Am J Ophthalmol. 2015;159:829–34.
98. Menzel-Severing J, Salla S, Plum WJ, Tourtas T, Fuchsluger T, Schlotzer-Schrehardt U,Kruse FE. Instrument to enhance visualization of Descemet membrane during graftpreparation for DMEK surgery. Cornea. 2016;35:904–7.
98 K. Jirsova et al.

99. Ruzza A, Parekh M, Salvalaio G, Ferrari S, Camposampiero D, Amoureux MC, et al. Bubbletechnique for Descemet membrane endothelial keratoplasty tissue preparation in an eyebank: air or liquid? Acta Ophthalmol. 2015;93:e129–34.
100. Macaluso C. Closed-chamber pulling-injection system for donor graft insertion inendothelial keratoplasty. J Cataract Refract Surg. 2008;34:353–6.
101. Kruse FE, Laaser K, Cursiefen C, Heindl LM, Schlotzer-Schrehardt U, Riss S, et al.A stepwise approach to donor preparation and insertion increases safety and outcome ofDescemet membrane endothelial keratoplasty. Cornea. 2011;30:580–7.
102. Terry MA, Straiko MD, Veldman PB, Talajic JC, VanZyl C, Sales CS, Mayko ZM.Standardized DMEK technique: Reducing complications using prestripped tissue, novelglass injector, and sulfur hexafluoride (SF6) gas. Cornea. 2015;34:845–52.
103. Parekh M, Ruzza A, Ferrari S, Busin M, Ponzin D. Preloaded tissues for Descemetmembrane endothelial keratoplasty. Am J Ophthalmol. 2016;166:120–5.
104. Veldman PB, Dye PK, Holiman JD, Mayko ZM, Sales CS, Straiko MD, et al. Stamping an Son DMEK donor tissue to prevent upside-down grafts: laboratory validation and detailedpreparation technique description. Cornea. 2015;34:1175–8.
105. Studeny P, Farkas A, Vokrojova M, Liskova P, Jirsova K. Descemet membrane endothelialkeratoplasty with a stromal rim (DMEK-S). Br J Ophthalmol. 2010;94:909–14.
106. Busin M, Patel AK, Scorcia V, Galan A, Ponzin D. Stromal support for Descemet’smembrane endothelial keratoplasty. Ophthalmology. 2010;117:2273–7.
107. Pereira Cda R, Guerra FP, Price FW, Jr, Price MO. Descemet’s membrane automatedendothelial keratoplasty (DMAEK): visual outcomes and visual quality. Br J Ophthalmol.2011;95:951–4.
108. Busin M, Scorcia V, Patel AK, Salvalaio G, Ponzin D. Pneumatic dissection and storage ofdonor endothelial tissue for Descemet’s membrane endothelial keratoplasty: a noveltechnique. Ophthalmology. 2010;117:1517–20.
109. Laaser K, Bachmann BO, Horn FK, Schlotzer-Schrehardt U, Cursiefen C, Kruse FE. Donortissue culture conditions and outcome after descemet membrane endothelial keratoplasty.Am J Ophthalmol. 2011;151:1007–18.
110. Rodriguez-Calvo de Mora M, Groeneveld-van Beek EA, Frank LE, van der Wees J,Oellerich S, Bruinsma M, Melles GR. Association between graft storage time and donor agewith endothelial cell density and graft adherence after Descemet membrane. Endothelialkeratoplasty. JAMA Ophthalmol. 2016;134:91–4.
111. Azizi B, Ziaei A, Fuchsluger T, Schmedt T, Chen Y, Jurkunas UV. p 53-regulated increasein oxidative-stress–induced apoptosis in Fuchs endothelial corneal dystrophy: a native tissuemodel. Invest Ophthalmol Vis Sci. 2011;52:9291–7.
112. Davidson AE, Liskova P, Evans CJ, Dudakova L, Noskova L, Pontikos N, et al.Autosomal-dominant corneal endothelial dystrophies CHED1 and PPCD1 are allelicdisorders caused by non-coding mutations in the promoter of OVOL2. Am J Hum Genet.2016;98:75–89.
113. Krachmer JH. Posterior polymorphous corneal dystrophy: a disease characterized byepithelial-like endothelial cells which influence management and prognosis. Trans AmOphthalmol Soc. 1985;83:413–75.
114. Jirsova K, Merjava S, Martincova R, Gwilliam R, Ebenezer ND, Liskova P, Filipec M.Immunohistochemical characterization of cytokeratins in the abnormal corneal endotheliumof posterior polymorphous corneal dystrophy patients. Exp Eye Res. 2007;84:680–6.
115. Hirst LW, Bancroft J, Yamauchi K, Green WR. Immunohistochemical pathology of thecorneal endothelium in iridocorneal endothelial syndrome. Invest Ophthalmol Vis Sci.1995;36:820–7.
5 Light and Specular Microscopy Assessment of the Cornea … 99

Chapter 6Atlas of Light and Specular Microscopyof the Cornea
Katerina Jirsova
Abstract This chapter consists of a photographic atlas containing more than 200images of the cornea (particularly of the corneal endothelium), taken during theassessment of both donor and patient corneas. The atlas is divided into four parts.
Keywords Light microscopy � Specular microscopy � Cornea � Endothelial cellimages � Healthy and pathological endothelium � Dead endothelial cells �Polymegethism and pleomorphism � Corneal lamellae
Part 6.1 presents photographs of the individual layers of the healthy cornea andlimbus (Figs. 6.1–6.12).Part 6.2 features photographs of corneas and lamellae processed for grafting. Thispart is divided into three sections:
• Section 6.2.1 contains images of the corneal endothelium at the time of firstassessment (that is, before storage). Included are photographs of corneas thatwere used for grafting, as well as corneas that were excluded from use intransplantation because of a low endothelial cell density, abnormal endothelialmorphology, or various endothelial pathologies or irregularities. The imagesshow the presence of dead endothelial cells, endothelial lesions, various degreesof polymegethism and pleomorphism, the presence of Descemet membranefolds, regular and abnormal dilatation of the intercellular spaces betweenendothelial cells, cornea guttata, the presence of foreign bodies and precipitates,and intracellular changes (Figs.6.13–6.78).
• Section 6.2.2 contains images of the endothelium taken before and after storagein organ culture, showing the changes that can occur during such storage. Shownare examples of both improved and worsened tissue quality (Figs. 6.79–6.116).
K. Jirsova (&)Laboratory of the Biology and Pathology of the Eye, Institute of Biology and MedicalGenetics, First Faculty of Medicine, Charles University, Prague, Czech Republice-mail: [email protected]
© Springer International Publishing AG 2017K. Jirsova, Light and Specular Microscopy of the Cornea,DOI 10.1007/978-3-319-48845-5_6
101

• Section 6.2.3 shows corneas before and after the preparation of lamellae fordifferent types of endothelial keratoplasty (Figs. 6.117–6.130).
All photographs in parts 6.1 and 6.2 were taken using bright field or phasecontrast light microscopy after treating the endothelium with trypan blue and ahypotonic solution.
Part 6.3 includes specular microscopy photographs of corneas and endotheliallamellae processed for grafting and stored under hypothermic conditions(Figs. 6.131–6.172). Photographs show healthy endothelium as well as the endothe-lium showing cell death, polymegethism and pleomorphism, cornea guttata (guttae),and other abnormalities.Part 6.4 presents images of patients’ corneal explants (obtained as a consequenceof penetrating keratoplasty) and the native corneas of patients suffering fromvarious endothelial pathologies, taken using light or specular microscopy. Shownare the characteristic features of various endothelial dystrophies, including Fuchsendothelial corneal dystrophy, posterior polymorphous corneal dystrophy, andother corneal pathologies (Figs. 6.173–6.214).
102 K. Jirsova

6.1 Light Microscopy of the Normal Cornea and Limbus
Part 6.1 of the atlas presents photographs of the individual layers of the healthycornea and limbus. The layers are shown from the outside in, i.e., from theepithelium to the endothelium. Nerve fibres, peripheral vessels, and Vogt palisadesin the limbal area are also shown. If not otherwise indicated, the photographs weretaken from the endothelial side of normal corneas using bright field (BF) or phasecontrast (PC) inverted light microscopy after treating the endothelial layer withtrypan blue (0.12 %, incubated for 90 s) and sucrose hypotonic solution (0.9 or1.8 %). Scale bars and magnifications are included in the images and Fig. legends,respectively (Figs. 6.1–6.12).
6 Atlas of Light and Specular Microscopy of the Cornea 103

Fig. 6.2 Epithelium: layer of basal cells (PC, 200�). Scale bar = 10 µm
Fig. 6.1 Epithelium: superficial layer of polygonal, terminally differentiated epithelial cells withprominent nuclei (phase contrast [PC], original magnification 200�). Scale bar = 10 µm
104 K. Jirsova

Fig. 6.3 Nerve fibres forming the subbasal terminal epithelial plexus in the basal epithelium(PC, 200�). Scale bar = 10 µm
Fig. 6.4 Extracellular matrix with fibrous structures in the posterior part of the stroma. The imagewas taken from the posterior side of corneal lamellae prepared for Descemet stripping automatedendothelial keratoplasty (DSAEK) (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 105

Fig. 6.6 Monolayer of regular, mostly hexagonal endothelial cells with clearly visible nuclei(PC, 200�). Scale bar = 10 µm
Fig. 6.5 Spindle-shaped keratocytes scattered among the stromal lamellae, connected toneighbouring cells by the tips of long processes, forming a dense network. The image wastaken from the posterior side of corneal lamellae prepared for DSAEK (PC, 200�). Scalebar = 10 µm
106 K. Jirsova

Fig. 6.8 Extreme periphery of the endothelium showing Hassall-Henle bodies surrounded byendothelial cells. Melanin pigment is present and physiological. Dead endothelial cells (trypanblue positive) are also present (BF, 100�). Scale bar = 10 µm (Courtesy of G. Thuret and Z. He,Jean Monnet University, St-Etienne, France)
Fig. 6.7 Regular hexagonal arrangement of the endothelial monolayer (bright field [BF], 100�).Scale bar = 100 µm
6 Atlas of Light and Specular Microscopy of the Cornea 107

Fig. 6.10 Peripheral part of the cornea and limbus. The palisades of Vogt are clearly visible in thelimbal area (BF, 40�). Scale bar = 100 µm
Fig. 6.9 Avascular cornea (left) and vessel endings in the limbus. Blood remains in the vesselloops (BF, 40�). Scale bar = 100 µm
108 K. Jirsova

Fig. 6.11 The palisades of Vogt in the limbal area are visible, owing to the presence of melaningranules (PC, 100�). Scale bar = 100 µm
Fig. 6.12 The palisades of Vogt in the limbal area are visible, owing to the presence ofmelanocytes containing melanin granules (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 109


6.2 Light Microscopy of Donor Corneas
6.2.1 Corneas Before Storage in Organ Culture
This section features photographs of corneas processed for grafting. Included arephotographs of corneas that were ultimately used for grafting, as well as corneasthat were excluded from use in transplantation because of a low endothelial celldensity (ECD), abnormal endothelial morphology, or endothelial pathology. In eachcase, we see the cornea at the time of first assessment, before storage. If nototherwise indicated, the photographs were taken from the endothelial side of thecorneas using bright field (BF) or phase contrast (PC) inverted light microscopyafter treating the endothelial layer with trypan blue (0.12 %, 90 s) and sucrosehypotonic solution (0.9 or 1.8 %). Scale bars and magnifications are included(Figs. 6.13–6.78).
6 Atlas of Light and Specular Microscopy of the Cornea 111

Fig. 6.13 Rare, isolated, dead endothelial cells (trypan blue positive) (BF, 100�). Scalebar = 100 µm
Fig. 6.14 Dead endothelial cells (trypan blue positive) are present in small clusters (BF, 100�).Scale bar = 100 µm
112 K. Jirsova

Fig. 6.15 Dead endothelial cells (trypan blue positive) are present in groups of different size (BF,100�). Scale bar = 100 µm
Fig. 6.16 Dead endothelial cells (trypan blue positive) are present over the entire endothelialsurface (BF, 100�). Scale bar = 100 µm
6 Atlas of Light and Specular Microscopy of the Cornea 113

Fig. 6.17 Dead endothelial cells (trypan blue positive) are present in the folds of Descemetmembrane (BF, 100�). Scale bar = 100 µm
Fig. 6.18 Dead endothelial cells (trypan blue positive) are present at the borders of an endotheliallesion with pale staining of the denuded Descemet membrane. A direct trauma can be suspected(BF, 100�). Scale bar = 100 µm
114 K. Jirsova

Fig. 6.19 Disseminated bluish areas present in the corneal endothelium, likely as a consequenceof an injured, leaky endothelium that allows trypan blue penetration and the staining of Descemetmembrane. Scale bar = 100 µm
Fig. 6.20 Dead endothelial cells (trypan blue positive) and disseminated blue areas (partiallytrypan blue positive), probably as a consequence of a leaky endothelium that allows trypan blue topenetrate and stain Descemet membrane. Scale bar = 100 µm
6 Atlas of Light and Specular Microscopy of the Cornea 115

Fig. 6.22 Intersecting Descemet membrane folds in which the intercellular spaces of theendothelial cells exhibit minimal dilatation (PC, 40�). Scale bar = 100 µm
Fig. 6.21 Parallel folds of Descemet membrane in which the intercellular spaces of theendothelial cells exhibit minimal dilatation (PC, 40�). Scale bar = 100 µm
116 K. Jirsova

Fig. 6.23 Descemet membrane folds exhibiting dead endothelial cells (trypan blue positive)(BF, 40�). Scale bar = 100 µm
Fig. 6.24 Dead endothelial cells (arrows) in a Descemet membrane fold are clearly visible athigher magnification (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 117

Fig. 6.25 Regular dilatation of the intercellular spaces between endothelial cells (PC, 200�).Scale bar = 10 µm
Fig. 6.26 Almost no dilatation of the intercellular spaces of the endothelium. The cornea is notsuitable for grafting (PC, 200�). Scale bar = 10 µm
118 K. Jirsova

Fig. 6.27 Almost no dilatation of the intercellular spaces of the endothelium. With the exceptionof several isolated areas, it was impossible to induce normal intercellular dilatation. The cornea isnot suitable for grafting (PC, 200�). Scale bar = 10 µm
Fig. 6.28 Weak dilatation of the intercellular spaces of the endothelium is often accompanied bythe presence of clearly visible condensed nuclei (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 119

Fig. 6.29 Irregular dilatation of the intercellular spaces of the endothelium (PC, 200�). Scalebar = 10 µm
Fig. 6.30 Partial irregular dilatation of the intercellular spaces of the endothelium. The corneaneeds to be assessed again to determine if it is suitable for grafting (PC, 200�). Scale bar = 10 µm
120 K. Jirsova

Fig. 6.32 Very strong dilatation of the intercellular spaces of the endothelium (PC, 200�). Scalebar = 10 µm
Fig. 6.31 A larger sporadic gap in the intercellular dilatation of the endothelium. (PC, 200�).Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 121

Fig. 6.33 Polymegethism of the endothelium: a huge cell surrounded by cells of normal size withprominent nuclei and minimal dilatation of the intercellular spaces. The cornea is not suitable forgrafting (PC, 200�). Scale bar = 10 µm
Fig. 6.34 Polymegethism and pleomorphism (P&P) of the endothelium: cells with variousnumbers of neighbouring cells, suggesting large size differences. The cornea is not suitable forgrafting (PC, 200�). Scale bar = 10 µm
122 K. Jirsova

Fig. 6.35 P&P of the endothelium: tiny cells in the close vicinity of significantly enlarged cells ofmostly nonhexagonal shape. The cornea is not suitable for grafting (PC, 200�). Scalebar = 10 µm
Fig. 6.36 P&P of the corneal endothelium: significantly enlarged cells and very low endothelialcell density (ECD). The cornea is not suitable for grafting (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 123

Fig. 6.37 P&P of the corneal endothelium: significantly enlarged cells adjacent to an area of cellsof normal size. The cornea is not suitable for grafting (PC, 200�). Scale bar = 10 µm
Fig. 6.38 P&P of the corneal endothelium: the presence of significantly enlarged cells andstromal edema. The cornea is not suitable for grafting (PC, 200�). Scale bar = 10 µm
124 K. Jirsova

Fig. 6.39 P&P of the corneal endothelium: the presence of significantly enlarged cells, abnormalmorphology, and dilatation of the intercellular spaces. The cornea is not suitable for grafting (PC,200�). Scale bar = 10 µm
Fig. 6.40 Abnormal endothelium expressing a high degree of P&P and irregular dilatation of theintercellular spaces. The cornea is not suitable for grafting (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 125

Fig. 6.41 Cornea guttata (guttae) (arrow). Guttae are about the same size as normal endothelialcells (PC, 200�). Scale bar = 10 µm
Fig. 6.42 Guttae. A regular endothelial mosaic with the presence of guttae (arrows). The corneais not suitable for grafting (PC, 200�). Scale bar = 10 µm
126 K. Jirsova

Fig. 6.43 Guttae, a high degree of P&P, and irregular dilatation of the intercellular spaces. Thecornea is not suitable for grafting (PC, 200�). Scale bar = 10 µm
Fig. 6.44 Guttae and dying cells are abundant. The endothelium exhibits a high degree of P&Pand irregular dilatation of the intercellular spaces. The cornea is not suitable for grafting(PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 127

Fig. 6.45 Guttae (arrows) and dying cells (asterisks). The endothelium exhibits abnormal cellmorphology. Dilatation of the intercellular spaces is absent. The cornea is not suitable for grafting(PC, 200�). Scale bar = 10 µm
Fig. 6.46 Guttae. A group of guttae, with the presence of dying endothelial cells and cell debris(arrows). The cornea is not suitable for grafting (PC, 200�). Scale bar = 10 µm
128 K. Jirsova

Fig. 6.47 Guttae. A group of guttae of various sizes. The cornea is not suitable for grafting(PC, 200�). Scale bar = 10 µm
Fig. 6.48 A grape-like structure likely to be a cluster of dead endothelial cells. It is also possiblethat dead epithelial cells were shifted to the endothelium from the ocular surface during handlingof the cornea. The cornea is not suitable for grafting (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 129

Fig. 6.49 An endothelial lesion surrounded by dead cells (PC, 200�). Scale bar = 10 µm
Fig. 6.50 Prominent nuclei, weak intracellular dilatation of the intercellular spaces, and a clearlyvisible binucleated cell probably arising from coalescence. The cornea is not suitable for grafting(PC, 200�). Scale bar = 10 µm
130 K. Jirsova

Fig. 6.51 Abnormal endothelium exhibiting multinucleated cells (including a huge cell with atleast three nuclei) and P&P. The cornea is not suitable for grafting (PC, 200�). Scale bar = 10 µm
Fig. 6.52 Prominent nuclei and clearly visible micronuclei (arrow) indicating nuclear materialinstability (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 131

Fig. 6.53 Repair of the corneal endothelium. After releasing dead cells, the area is repopulated byneighbouring enlarged cells, and a typical rosette structure is formed (PC, 200�). Scalebar = 10 µm
Fig. 6.54 Repair of the corneal endothelium. Elongated endothelial cells are present, orienteddirectly towards the area of damage (not shown) (PC, 200�). Scale bar = 10 µm
132 K. Jirsova

Fig. 6.55 A small, isolated, pigmented precipitate on the corneal endothelium usually does notimpair endothelial quality (PC, 200�). Scale bar = 10 µm
Fig. 6.56 A large, pigmented precipitate (arrow), together with the presence of guttae, dead cells,and cell debris indicate an impaired endothelium (PC, 100�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 133

Fig. 6.57 Abnormal endothelial morphology with a loss of polygonality (arrow), suspectedactivation of proliferation, and endothelial dystrophy. The cornea is not suitable for grafting (PC,200�). Scale bar = 10 µm
Fig. 6.58 Abnormal endothelium exhibiting probable dying cells, suspected endothelial prolif-eration, and endothelial transformation or endothelial dystrophy. The findings are morphologicallyconsistent with those seen in posterior polymorphous corneal dystrophy (PPCD) (see Fig. 6.184).The cornea is not suitable for grafting (PC, 200�). Scale bar = 10 µm
134 K. Jirsova

Fig. 6.59 An endothelial lesion, probably resulting from an endothelial dystrophy. Fibrousstructures can be seen bridging the endothelium around the lesion, a suspected attempt at repair.The cornea is not suitable for grafting (PC, 200�). Scale bar = 10 µm
Fig. 6.60 Abnormal degenerative endothelium and suspected endothelial dystrophy. The corneais not suitable for grafting (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 135

Fig. 6.61 Star-like branching structure visible at the level of the corneal endothelium. It could bea retrodescemetic precipitate resulting from uveitis such as Fuchs’ heterochromic cyclitis, or aformation that arose as a consequence of endothelial dystrophy. The cornea is not suitable forgrafting (PC, 200�). Scale bar = 10 µm
Fig. 6.62 A nest of abnormal, likely dead cells (trypan blue positive) with no dilatation of theintercellular spaces in an otherwise relatively well-arranged endothelium. The finding ismorphologically consistent with those observed in PPCD, see Fig. 6.184. The cornea is notsuitable for grafting (PC, 200�). Scale bar = 10 µm
136 K. Jirsova

Fig. 6.63 Endothelial lesions seen as opacities in the posterior part of the stroma projecting to theendothelial layer. The cornea is not suitable for grafting (PC, 200�). Scale bar = 10 µm
Fig. 6.64 Abnormal structures seen in the posterior part of the stroma projecting to theendothelial layer. Elongated endothelial cells are oriented directly towards the endothelial lesion(as typical for endothelial repair; see Figs. 6.53 and 6.54) between the rounded structures. Thecornea is not suitable for grafting (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 137

Fig. 6.65 The presence of a foreign body (fibrillar structure) on the endothelium (PC, 100�).Scale bar = 100 µm
Fig. 6.66 The presence of a foreign body (glass-like structure) and a developing lesion on theendothelium. The cornea is not suitable for grafting without removal of the foreign body and asecond assessment after storage (PC, 100�). Scale bar = 100 µm
138 K. Jirsova

Fig. 6.67 Clearly visible maculae in the corneal stroma. (A normal endothelial mosaic waspresent.) The diameter of the maculae is 0.25 mm. The cornea is not suitable for penetratingkeratoplasty (PC, 100�). Scale bar = 100 µm
Fig. 6.68 Inconspicuous maculae in the corneal stroma. The cornea is not suitable for penetratingkeratoplasty (PC, 100�). The diameter of the maculae is 0.68 mm (PC, 100�). Scalebar = 100 µm
6 Atlas of Light and Specular Microscopy of the Cornea 139

Fig. 6.69 Stromal deposits or precipitates of unknown origin. The cornea is not suitable forgrafting (PC, 200�). Scale bar = 100 µm
Fig. 6.70 Stromal deposits or precipitates of unknown, possibly post-traumatic origin. The corneais not suitable for grafting (PC, 200�). Scale bar = 10 µm
140 K. Jirsova

Fig. 6.71 The presence of dendritic (Langerhans) cells in the central part of the epithelium(arrows) may indicate inflammation (PC, 400�). Scale bar = 10 µm
Fig. 6.72 Exposure keratopathy of corneal epithelium characterized by increased reflexion(PC, 100�). Scale bar = 100 µm
6 Atlas of Light and Specular Microscopy of the Cornea 141

Fig. 6.73 A small lesion of the corneal epithelium (PC, 100�). Scale bar = 100 µm
Fig. 6.74 A lesion of the corneal epithelium (PC, 100�). Scale bar = 100 µm
142 K. Jirsova

Fig. 6.75 A lesion of the corneal epithelium (PC, 100�). Scale bar = 100 µm
Fig. 6.76 A foreign body on the surface of the corneal epithelium (PC, 100�). Scalebar = 100 µm
6 Atlas of Light and Specular Microscopy of the Cornea 143

Fig. 6.77 Abnormal neovascularisation of the central cornea (arrows). Blood remains in thevessels (PC, 100�). Scale bar = 100 µm
Fig. 6.78 Vascularisation of the peripheral cornea (arrows). The border between the limbus andthe cornea is marked by the dashed line (PC, 100�). Scale bar = 100 µm
144 K. Jirsova

6.2.2 Corneas Before and After Storage in Organ Culture:A Comparison
Part 6.2.2 shows corneas before and after storage in organ culture (OC), that is,corneas before and after storage and after transfer into a deswelling medium for 8–48 h. If not otherwise indicated, the photographs were taken from the endothelialside of the corneas using bright field (BF) or phase contrast (PC) inverted lightmicroscopy after treating the endothelial layer with trypan blue (0.12 %, 90 s) andsucrose hypotonic solution (0.9 or 1.8 %). Scale bars and magnifications areincluded (Figs. 6.79–6.116).
6 Atlas of Light and Specular Microscopy of the Cornea 145

Fig. 6.80 A regular endothelial mosaic after 14 days in OC and 24 h in deswelling medium. Thesame cornea as in Fig. 6.79. ECD about 2500 cells/mm2 (PC, 200�). Scale bar = 10 µm
Fig. 6.79 Aregular endothelialmosaic before organ culture (OC) storage;ECDabout 3000cells/mm2
(PC, 200�). Scale bar = 10 µm
146 K. Jirsova

Fig. 6.82 The same cornea as in Fig. 6.81 after 7 days in storage medium and 24 h in deswellingmedium. The endothelium is repaired, and no dead cells are present (BF, 100�). Scalebar = 100 µm
Fig. 6.81 The presence of dead endothelial cells and cell debris before storage in OC (BF, 100�).Scale bar = 100 µm
6 Atlas of Light and Specular Microscopy of the Cornea 147

Fig. 6.84 Cell debris after 5 days in OC and 24 h in deswelling medium. The same cornea as inFig. 6.83. (BF, 100�). Scale bar = 100 µm
Fig. 6.83 A regular endothelial mosaic before OC; some dead cells are present over theendothelial surface (BF, 100�). Scale bar = 100 µm
148 K. Jirsova

Fig. 6.86 The same cornea as in Fig. 6.85 after 5 days in storage medium and 24 h in deswellingmedium. The endothelium is repaired, with cell debris visible at the former lesion site (BF, 100�).Scale bar = 100 µm
Fig. 6.85 The presence of an endothelial lesion and dead endothelial cells before storage in OC.Descemet membrane at the site of the lesion (large blue area) is stained by trypan blue. Similarly,circular areas around the dead cells appear blue from the leakage of trypan blue through thedamaged endothelium (BF, 100�). Scale bar = 100 µm
6 Atlas of Light and Specular Microscopy of the Cornea 149

Fig. 6.88 The same cornea as in Fig. 6.87 after 9 days in OC. Dead endothelial cells are presentover the entire endothelial surface. Viral contamination (Herpes simplex virus type 1) was laterconfirmed (BF, 100�). Scale bar = 10 µm (Courtesy of S. Acquart, Eye Bank, Saint-Etienne,France)
Fig. 6.87 Endothelium after 2 days in OC, showing a regular mosaic with no visible alterations(BF, 100�). Scale bar = 10 µm. Figures 6.87–6.89 were taken by upright transmitted lightmicroscopy after treatment of the endothelium with trypan blue and 0.9 % NaCl for 4 min(Courtesy of S. Acquart, Eye Bank, Saint-Etienne, France)
150 K. Jirsova

Fig. 6.89 Fungal contamination of the corneal endothelium (Aspergillus fumigatus). Theendothelial cells are dying (BF, 100�). Scale bar = 10 µm (Courtesy of S. Acquart, Eye Bank,Saint-Etienne, France)
Fig. 6.90 Fungal contamination of the corneal endothelium during OC. Fibrous structuresovergrow the corneal endothelium. Scale bar = 100 µm
6 Atlas of Light and Specular Microscopy of the Cornea 151

Fig. 6.91 Bacterial contamination of the corneal endothelium during OC (BF, 100�). Scalebar = 100 µm
Fig. 6.92 Bacterial contamination of the corneal endothelium during OC (PC, 200�). Scalebar = 10 µm
152 K. Jirsova

Fig. 6.93 Bacterial contamination of the corneal endothelium (arrow). The endothelial cells aredying (PC, 400�). Scale bar = 10 µm
Fig. 6.94 Bacterial contamination of the corneal endothelium (asterisks). The endothelium isdegenerating and cells are dying (PC, 400�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 153

Fig. 6.95 A regular endothelial mosaic before OC; the cornea is not edematous (PC, 200�). Scalebar = 10 µm
Fig. 6.96 The same cornea as in Fig. 6.95 after 11 days in OC. Mild corneal edema preventsfocusing on the corneal endothelium, even from the endothelial side of the cornea. The cornea isnot suitable for grafting (PC, 200�). Scale bar = 10 µm
154 K. Jirsova

Fig. 6.97 Before storage, edema of the corneal stroma prevents focusing on the cornealendothelium (PC, 200�). Scale bar = 10 µm
Fig. 6.98 The same cornea as in Fig. 6.97 after 7 days in storage medium and 24 h in deswellingmedium. The endothelial mosaic is easily visible (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 155

Fig. 6.99 Endothelium barely visible because of mild edema of the stroma (PC, 200�). Scalebar = 10 µm
Fig. 6.100 The same cornea as in Fig. 6.99 after 4 days in OC and 24 h in deswelling medium.As a consequence of the dehydration of the stroma, the endothelial mosaic is clearly visible(PC, 200�). Scale bar = 10 µm
156 K. Jirsova

Fig. 6.101 Prior to storage, it was not possible to induce dilatation of the intercellular spaces inthe central part of the corneal endothelium; shrunken nuclei are easily visible (PC, 200�). Scalebar = 10 µm
Fig. 6.102 The same cornea as in Fig. 6.101 after 6 days in OC. Regular dilatation of theintercellular spaces (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 157

Fig. 6.103 No endothelial morphology is apparent before storage, and no dilatation of theintercellular spaces can be seen (PC, 200�). Scale bar = 10 µm
Fig. 6.104 Regular dilatation in the same cornea as in Fig. 6.103 after 5 days in OC and 24 h indeswelling medium (PC, 200�). Scale bar = 10 µm
158 K. Jirsova

Fig. 6.105 Irregular dilatation of the intercellular spaces before OC (PC, 200�). Scalebar = 10 µm
Fig. 6.106 Regular dilatation in the same cornea as in Fig. 6.105 after 5 days in OC and 24 h indeswelling medium (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 159

Fig. 6.107 Very strong dilatation of the intercellular spaces before OC (PC, 200�). Scalebar = 10 µm
Fig. 6.108 Regular dilatation in the same cornea as in Fig. 6.107 after 5 days in OC and 24 h indeswelling medium (PC, 200�). Scale bar = 10 µm
160 K. Jirsova

Fig. 6.109 Very strong dilatation of the intercellular spaces before OC; guttae are not visible(PC, 200�). Scale bar = 10 µm
Fig. 6.110 Irregular dilatation of the intercellular spaces in the same cornea as in Fig. 6.109 after5 days in OC. Guttae are abundant. The cornea is not suitable for grafting (PC, 200�). Scalebar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 161

Fig. 6.111 During OC, the epithelial cells are sloughed off (PC, 100�). Scale bar = 100 µm
Fig. 6.112 During OC, the epithelial cells are sloughed off (PC, 400�). Scale bar = 10 µm
162 K. Jirsova

Fig. 6.113 The epithelial cells are replaced during OC. A network of newly formed epithelialcells migrating from the limbus to the corneal centre is clearly visible (PC, 100�). Scalebar = 100 µm
Fig. 6.114 The epithelial cells are replaced during OC. A network of newly formed epithelialcells can be seen on the right; nerve fibres are visible on the left (PC, 400�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 163

Fig. 6.115 Exposure keratopathy of corneal epithelium characterized by increased reflexion isseen before OC (PC, 100�). Scale bar = 100 µm
Fig. 6.116 During OC, the superficial epithelial layers are sloughed off from the same cornea asin Fig. 6.115. The macula, hidden by epithelial cells before OC, appears after cultivation(PC, 100�). Scale bar = 100 µm
164 K. Jirsova

6.2.3 Corneas Before and After Lamellae Preparation
This part shows corneas and the corneal endothelium before lamellae preparation,as well as the endothelial layer immediately after dissection or after the storage oflamellae in organ culture. Images representing various preparation techniques,including Descemet stripping automated endothelial keratoplasty (DSAEK),Descemet membrane endothelial keratoplasty (DMEK), and Descemet membraneendothelial keratoplasty with a stromal rim (DMEK-S), are presented. The pho-tographs were taken using bright field (BF) or phase contrast (PC) inverted lightmicroscopy (Figs. 6.117–6.130).
6 Atlas of Light and Specular Microscopy of the Cornea 165

Fig. 6.117 Cornea prior to the preparation of Descemet’s stripping automated endothelialkeratoplasty (DSAEK) lamella. Corneal endothelium after 3 weeks cultivation in storage mediumand 1 day storage in deswelling medium. The endothelium was treated with trypan blue (0.3 %)and hypotonic balanced salt solution (the same in Figs. 6.118, 6.122–6.124). Scale bar = 100 µm(Courtesy of S. Salla, M. Hermel, and W. Plum, RWTH Aachen University, Germany)
Fig. 6.118 DSAEK. Lamella (the same tissue as in Fig. 6.117) prepared with a fully automaticmicrokeratome, 5 days after dissection and after 6 days of storage overall in deswelling medium.No dead endothelial cells are present. Scale bar = 100 µm (Courtesy of S. Salla, M. Hermel, andW. Plum, RWTH Aachen University, Germany)
166 K. Jirsova

Fig. 6.119 Cornea prior to the preparation of DMEK. Corneal endothelium before lamellastripping (PC, 200�). Scale bar = 100 µm. Figures 6.119, 6.120 and 6.125–6.128 were takenusing PC inverted light microscopy after treatment with trypan blue (0.2 %, 20–30 s) and sucrosehypotonic solution (1.8 %) (Courtesy of M. Parekh, A. Ruzza, and D. Camposampiero, VenetoEye Bank Foundation, Italy)
Fig. 6.120 DMEK lamella immediately after mechanical stripping (the same tissue as inFig. 6.119). Only a few dead cells are present over the entire endothelial surface (PC, 200�). Scalebar = 100 µm (Courtesy of M. Parekh, A. Ruzza, and D. Camposampiero, Veneto Eye BankFoundation, Italy)
6 Atlas of Light and Specular Microscopy of the Cornea 167

Fig. 6.122 DMEK. Lamella (the same tissue as in Fig. 6.121) 1 day after preparation bystripping. Slight damage to the endothelial layer and some dead cells are visible. Scalebar = 100 µm (Courtesy of S. Salla, M. Hermel, and W. Plum, RWTH Aachen University,Germany)
Fig. 6.121 Cornea prior to the preparation of Descemet membrane endothelial keratoplasty(DMEK) lamella. Corneal endothelium after 3 weeks in OC and 1 day storage in deswellingmedium. Scale bar = 100 µm (Courtesy of S. Salla, M. Hermel, and W. Plum, RWTH AachenUniversity, Germany)
168 K. Jirsova

Fig. 6.123 Cornea prior to the preparation of DMEK lamella. Corneal endothelium after 25 daysin OC and 1 day storage in deswelling medium. Scale bar = 100 µm (Courtesy of S. Salla, M.Hermel, and W. Plum, RWTH Aachen University, Germany)
Fig. 6.124 DMEK. Lamella (the same tissue as in Fig. 6.123) 3 days after preparation. No deadendothelial cells are present. Scale bar = 100 µm (Courtesy of S. Salla, M. Hermel, and W. Plum,RWTH Aachen University, Germany)
6 Atlas of Light and Specular Microscopy of the Cornea 169

Fig. 6.125 Cornea prior to the preparation of DMEK lamella, submerged hydro-separationtechnique. The endothelium of an OC cornea after bubble induction with culture medium. A fewdead endothelial cells are present (asterisk) (PC, 200�). Scale bar = 100 µm (Courtesy ofM. Parekh, A. Ruzza, and D. Camposampiero, Veneto Eye Bank Foundation, Italy)
Fig. 6.126 DMEK lamella prepared by submerged hydro-separation technique. The same tissueas in Fig. 6.125 after 7 days in OC (PC, 200�). Scale bar = 100 µm (Courtesy of M. Parekh,A. Ruzza, and D. Camposampiero, Veneto Eye Bank Foundation, Italy)
170 K. Jirsova

Fig. 6.127 Cornea prior to the preparation of pre-loaded DMEK lamella. The stripping of alamella for DMEK was performed after 4 days of OC in deswelling medium. The endothelium wasflapped inwards manually, and the DMEK tissue was preserved in an intra-ocular lens cartridge for4 days at room temperature (PC, 200�). Scale bar = 100 µm (Courtesy of M. Parekh, A. Ruzza,and D. Camposampiero, Veneto Eye Bank Foundation, Italy)
Fig. 6.128 Pre-loaded DMEK lamella. Post-preservation of a pre-loaded DMEK lamella (thesame as in Fig. 6.127) in the funnel of an intra-ocular lens cartridge after 4 days storage indeswelling medium at room temperature (PC, 200�). Scale bar = 100 µm (Courtesy ofM. Parekh,A. Ruzza, and D. Camposampiero, Veneto Eye Bank Foundation, Italy)
6 Atlas of Light and Specular Microscopy of the Cornea 171

Fig. 6.129 Cornea suggested for Descemet membrane endothelial keratoplasty with a stromal rim(DMEK-S). Peripheral part of a lamella immediately after preparation. Only a few dead cells arepresent over the entire endothelial surface (upper panel, BF; lower panel, PC, 100�). Scalebar = 100 µm (Courtesy of P. Studeny, Kralovske Vinohrady University Hospital, andI. Rybickova, Charles University, Prague, Czech Republic)
Fig. 6.130 DMEK-S. Central part of a lamella immediately after preparation. Only a few deadcells are present over the entire endothelial surface (upper panel, BF; lower panel, PC, 100�).Scale bar = 100 µm (Courtesy of P. Studeny, Kralovske Vinohrady University Hospital, andI. Rybickova, Charles University, Prague, Czech Republic)
172 K. Jirsova

6.3 Donor Corneas Assessed by Specular Microscopy
Part 6.3 includes specular microscopy photographs of corneas processed for graftingand stored under hypothermic conditions. This section was prepared by KaterinaJirsova, Jameson Clover, Andrea Gareiss-Lok, and Christopher G. Stoeger.This section includes photographs of corneas that were ultimately used for grafting,as well as corneas that were excluded from use in transplantation owing to a lowendothelial cell density (ECD), abnormal endothelial morphology, or endothelialpathology. Additionally, corneas and corneal lamellae prepared by various types oftechniques for DSAEK and DMEK are shown before and after processing(Figs. 6.131–6.172). All images were taken of corneas stored in Optisol-GS andanalysed using a Konan CellChek EB10 Eye Bank System specular microscope,unless otherwise indicated. The reported endothelial cell density, coefficient ofvariation (CV), and percentage of hexagonal endothelial cells (HEX) are the averagevalues calculated from three images of the same cornea; only one image is shown.The severity of various endothelial parameters (Descemet membrane folds, celldeath, stress lines, and pleomorphism/polymegethism) is indicated using a scaleranging from none < trace < mild < mild to moderate < moderate < moderate tosevere < severe. Descemet membrane folds, edema, stress lines, and cell death alsowere assessed during slit lamp evaluation.
6 Atlas of Light and Specular Microscopy of the Cornea 173

Fig. 6.132 Endothelium, regularly arranged cell mosaic: distinct borders between cells(2755 cells/mm2) coefficient of variation (CV) 26, percentage of hexagonal cells (HEX) 63.Scale bar = 10 µm
Fig. 6.131 Endothelium, regularly arranged cell mosaic: distinct borders, hexagon-shaped cells,and a consistent cell size (4082 cells/mm2). Scale bar = 10 µm
174 K. Jirsova

Fig. 6.134 Epithelium photographed under the standard conditions of an eye bank (not routinelyassessed in eye bank practice). Scale bar = 10 µm
Fig. 6.133 Endothelium: relatively mild corneal edema (3448 cells/mm2). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 175

Fig. 6.136 Mild to moderate polymegethism and pleomorphism (P&P) (ECD 2747 cells/mm2,CV 38, HEX 56). Scale bar = 10 µm
Fig. 6.135 Mild polymegethism (2907 cells/mm2, CV 31, HEX 61). Scale bar = 10 µm
176 K. Jirsova

Fig. 6.138 Severe P&P (998 cells/mm2, CV 66, HEX 40). Scale bar = 10 µm
Fig. 6.137 Moderate P&P (2217 cells/mm2, CV 41, HEX 52). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 177

Fig. 6.140 Endothelium showing mild to moderate cell death (drop out), and mild to moderateP&P (3040 cells/mm2). Scale bar = 10 µm
Fig. 6.139 Endothelium showing mild cell death (drop out) (arrows) and mild P&P(2358 cells/mm2). Scale bar = 10 µm
178 K. Jirsova

Fig. 6.142 Endothelium showing moderate to severe cell death (drop out) (black arrows) and aDescemet membrane fold (white arrows) (2283 cells/mm2). Scale bar = 10 µm
Fig. 6.141 Endothelium showing moderate cell death (drop out) (2066 cells/mm2). Scalebar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 179

Fig. 6.144 Mild Descemet membrane fold (arrows) (2506 cells/mm2). Scale bar = 10 µm
Fig. 6.143 A trace Descemet membrane fold (arrows) (3311 cells/mm2). Scale bar = 10 µm
180 K. Jirsova

Fig. 6.146 Moderate Descemet membrane fold, mild to moderate edema; dead cells are visible asdark areas (arrows). Some polymegethism (asterisks) may arise as a result of distortion due to theDescemet membrane folds (2639 cells/mm2). Scale bar = 10 µm
Fig. 6.145 Mild to moderate Descemet membrane fold, mild edema (2463 cells/mm2). Scalebar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 181

Fig. 6.148 Severe Descemet membrane fold with moderately edematous cells. The endothelialcell density could not be assessed because of the severity of the edema and the Descemetmembrane fold. Scale bar = 10 µm
Fig. 6.147 Moderate Descemet membrane fold (2532 cells/mm2). Scale bar = 10 µm
182 K. Jirsova

Fig. 6.150 Trace Descemet membrane fold. The same cornea as in Fig. 6.149 has been removedfrom the refrigerator after 10 h of storage and allowed to warm to ambient temperature forreassessment. Scale bar = 10 µm
Fig. 6.149 Moderate to severe Descemet membrane fold. The image was taken shortly afterin situ excision and storage under hypothermic conditions. Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 183

Fig. 6.152 Endothelium showing moderate stress line with the presence of dead cells (dark area).Scale bar = 10 µm
Fig. 6.151 Endothelium showing a stress line with the presence of dead cells (dark area). Scalebar = 10 µm
184 K. Jirsova

Fig. 6.154 Endothelium displaying stress areas with the presence of dead cells (dark areas), mildto moderate P&P. Scale bar = 10 µm
Fig. 6.153 Endothelium showing a stress area with the presence of dead cells (dark area). Scalebar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 185

Fig. 6.156 Endothelial vacuolation: dark, round to oval areas representing endothelial vacuola-tion as confirmed by histology and electron microscopy. The image was analysed with a KonanEye Bank keratoanalyser (Hyogo, Japan) (Courtesy ofM.R. Kanavi, Shahid Beheshti University ofMedical Sciences, Tehran, Iran.) Scale bar = 10 µm
Fig. 6.155 Red blood cells. Endothelium showing distinct cell borders with a hexagonal shapeand slight polymegethism. Black spots represent red blood cells (RBCs, erythrocytes) (confirmedon slit lamp examination) resulting from bleeding in the anterior chamber during in situ cornealexcision (2252 cells/mm2). Scale bar = 10 µm
186 K. Jirsova

Fig. 6.158 Partial cell inversion, possibly representing edematous cells (darker cell centre andwhite borders, arrows); endothelial cells displaying indistinct cell borders and polymegethism(2096 cells/mm2). Scale bar = 10 µm
Fig. 6.157 Dark cells may represent edematous cells (e.g., as a consequence of cold storage).Endothelium is consistent in size and shape without any apparent cell death. Endothelial cells havean inverted appearance with dark cell bodies and light cell borders (2899 cells/mm2). Scalebar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 187

Fig. 6.160 Guttae. Dark areas represent guttae (confirmed by slit lamp examination); the singulardark spot in the centre is an RBC (2469 cells/mm2). Scale bar = 10 µm
Fig. 6.159 Cornea guttata (guttae). Dark areas represent guttae (confirmed by slit lampexamination); high degree of P&P (2755 cells/mm2). Scale bar = 10 µm
188 K. Jirsova

Fig. 6.162 The influence of temperature on endothelial assessment. The corneal endotheliumimmediately after removal from the refrigerator is not a good representation of actual cell health.Cells can be identified, but they are edematous, with indistinct borders. Scale bar = 10 µm
Fig. 6.161 Stroma of a donor cornea that underwent laser-assisted in situ keratomileusis9 months before the donor’s death. Two hyperreflective stromal particles are present. The imagewas analysed with the Konan Eye Bank keratoanalyser (Konan Medical, Tokyo, Japan). Scalebar = 10 µm (Courtesy of V.V. Mootha, University of Texas Southwestern Medical Center,Dallas, TX, USA.)
6 Atlas of Light and Specular Microscopy of the Cornea 189

Fig. 6.164 The influence of temperature on endothelial assessment. The same tissue as inFigs. 6.162 and 6.163; image captured 2 h and 40 min after removal from the refrigerator(3096 cells/mm2). Scale bar = 10 µm
Fig. 6.163 The influence of temperature on endothelial assessment. The same tissue as inFig. 6.162, imaged 1 h and 15 min after removal from the refrigerator. The endothelial mosaic ismore clearly visible but is still indistinct because of decreased metabolic activity, a consequence ofhypothermic storage (2577 cells/mm2). Scale bar = 10 µm
190 K. Jirsova

Fig. 6.166 DSAEK, lamella after precutting. Specular image of the same tissue as in Fig. 6.165,taken approximately 1 h after processing. The endothelium exhibits a regular cell mosaic(2571 cells/mm2). Scale bar = 10 µm
Fig. 6.165 Cornea intended for Descemet stripping automated endothelial keratoplasty(DSAEK). Regularly arranged corneal endothelium, distinct borders between cells(2545 cells/mm2). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 191

Fig. 6.168 DSAEK, lamella after precutting. Image of the same tissue as in Fig. 6.167, capturedapproximately 1 h after processing. RBCs seen prior to precutting are no longer present, as theywere washed off during the procedure; some P&P is present (2890 cells/mm2). Scale bar = 10 µm
Fig. 6.167 Cornea intended for DSAEK. Dark spots represent RBCs as confirmed by slit lampexamination. Image captured 4 days prior to precutting (2882 cells/mm2). Scale bar = 10 µm
192 K. Jirsova

Fig. 6.170 DMEK, lamella after Descemet membrane peeling. This image of the same tissue as inFig. 6.169 is of lesser quality owing to the nature of the free-floating Descemet membrane, butcells can be identified. Image captured approximately 30 min after processing. Scale bar = 10 µm
Fig. 6.169 Cornea intended for Descemet membrane endothelial keratoplasty (DMEK).Endothelium presents uniformly and without any dead cells (3096 cells/mm2). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 193

Fig. 6.172 DMEK, lamella after Descemet membrane peeling. In the same tissue as in Fig. 6.171,RBCs are no longer present. Trace Descemet membrane folds can be seen as trenches or darklinear areas. It is difficult to obtain a good specular reflection because of the free-floating nature ofthe membrane post-peel (3067 cells/mm2). Image captured approximately 30 min after processing.Scale bar = 10 µm
Fig. 6.171 Cornea intended for DMEK. The endothelium prior to peeling Descemet membrane.Distinct, hexagonal cells with mild P&P. Dark spots represent RBCs, as confirmed by slit lampexamination (3003 cells/mm2). Scale bar = 10 µm
194 K. Jirsova

6.4 Pathological Corneal Explants (Light Microscopy)and Patients’ Corneas (Specular Microscopy)
Part 6.4 includes light microscopy photographs of pathological corneal explantsobtained during perforating keratoplasty of patients with a clinically confirmeddiagnosis (Figs. 6.173–6.200). If not otherwise indicated, the photographs weretaken from the endothelial side of the corneas after treating the endothelial layerwith trypan blue (0.12 %, 90 s) and sucrose hypotonic solution (0.9 or 1.8 %).Scale bars and magnifications are included. Additionally, images of the corneas ofpatients suffering from corneal endothelial dystrophies are presented (Figs. 6.201–6.214), photographed and analysed using a Konan NONCON ROBO SP-9000specular microscope. Part 6.4 presents images showing changes that are particularlycharacteristic of different endothelial pathologies, particularly endothelial dystro-phies, including Fuchs endothelial corneal dystrophy, posterior polymorphouscorneal dystrophy, and iridocorneal endothelial syndrome.
6 Atlas of Light and Specular Microscopy of the Cornea 195

Fig. 6.173 Fuchs endothelial corneal dystrophy (FECD). Almost the entire endothelial surface iscovered by guttae of various sizes; the endothelial cells are hardly visible between them(PC, 200�). Scale bar = 10 µm
Fig. 6.174 FECD. Corneal edema; the endothelial surface is covered by guttae (PC, 200�). Scalebar = 10 µm
196 K. Jirsova

Fig. 6.175 FECD. Besides guttae, cellular fragments probably arising as a consequence ofapoptosis (arrow) are visible (PC, 200�). Scale bar = 10 µm
Fig. 6.176 FECD. Guttae, no dilatation of the intercellular spaces between endothelial cells, andabnormally enlarged cells (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 197

Fig. 6.178 FECD. Degenerated, dying endothelium with abnormal fibrillar structures (PC, 200�).Scale bar = 10 µm
Fig. 6.177 FECD. Degenerated, dying endothelium with abnormal fibrillar structures (PC, 200�).Scale bar = 10 µm
198 K. Jirsova

Fig. 6.180 FECD. The whole endothelial surface is covered by guttae of different sizes and bydead endothelial cells (PC, 200�). Scale bar = 10 µm
Fig. 6.179 FECD. Abnormal endothelium displaying spiral structures and covered by guttae andreleased dying cells (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 199

Fig. 6.182 PPCD. Abnormal cell enlargement and prominent polymegethism, as well asendothelial lesions (PC, 200�). Scale bar = 10 µm
Fig. 6.181 Posterior polymorphous corneal dystrophy (PPCD). Prominent pleomorphism. Cellarrangement forms a whirl (PC, 200�). Scale bar = 10 µm
200 K. Jirsova

Fig. 6.184 PPCD. Prominent pleomorphism; small, round, epithelialized cells; and probablyactivated proliferation (PC, 200�). Scale bar = 10 µm
Fig. 6.183 PPCD. Enlarged endothelial cells (short arrows), round epithelialized cells withpycnotic nuclei (long arrows), and a lesion in the middle (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 201

Fig. 6.186 PPCD. An endothelial lesion, abnormal endothelial cells morphologically resemblingfibroblasts, and probably degenerating and dying cells (PC, 200�). Scale bar = 10 µm
Fig. 6.185 PPCD. Partially or fully epithelialized cells of an abnormal endothelium. No swellingwas induced (PC, 200�). Scale bar = 10 µm
202 K. Jirsova

Fig. 6.188 PPCD. Endothelium showing abnormal structures, with the presence of only a fewlive cells (PC, 200�). Scale bar = 10 µm
Fig. 6.187 PPCD. Abnormally large cells undergoing apoptosis or nuclear fragmentation(PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 203

Fig. 6.190 PPCD. Abnormally enlarged epithelial cells and an irregular morphology, which mayarise as a consequence of corneal edema (PC, 200�). Scale bar = 10 µm
Fig. 6.189 PPCD. Abnormal branching structure on the endothelium (PC, 200�). Scalebar = 10 µm
204 K. Jirsova

Fig. 6.192 Iridocorneal endothelial syndrome. Low ECD (1890/mm2), prominent pleomorphism(PC, 200�). Scale bar = 10 µm
Fig. 6.191 Iridocorneal endothelial syndrome. Very low ECD (700/mm2), abnormal dilatation ofthe intercellular spaces (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 205

Fig. 6.194 Lattice corneal dystrophy. Branching filaments in the corneal stroma (BF, 200�). Thisimage and image at Fig. 6.193 were taken using upright transmitted light microscopy aftertreatment of the endothelium with trypan blue and 0.9 % NaCl for 4 min. Scale bar = 100 µm(Courtesy of G. Thuret and Z. He, Jean Monnet University, St-Etienne, France)
Fig. 6.193 Lattice corneal dystrophy. Branching filaments in the corneal stroma. Slightopacification in the central part of the cornea (BF, 200�). Scale bar = 1 mm (Courtesy ofG. Thuret and Z. He, Jean Monnet University, St-Etienne, France)
206 K. Jirsova

Fig. 6.196 Macular corneal dystrophy. Deposits of various sizes (arrows) in the anterior part ofthe corneal stroma (PC, 200�). Scale bar = 10 µm
Fig. 6.195 Macular corneal dystrophy. Abnormal epithelium (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 207

Fig. 6.198 Keratolysis. Starlike structures in the corneal stroma (PC, 200�). Crystallinekeratopathy is potentially present in this cornea. Scale bar = 10 µm
Fig. 6.197 Keratolysis. Epithelium with enlarged cells of abnormal shape (PC, 200�). Scalebar = 10 µm
208 K. Jirsova

Fig. 6.200 Keratolysis. Released dead cells above degenerated endothelium with almost nodilatation of intercellular spaces (arrow) (PC, 200�). Scale bar = 10 µm
Fig. 6.199 Keratolysis. Dying, degenerated endothelium with an endothelial lesion in the lowerpart of the photograph (PC, 200�). Scale bar = 10 µm
6 Atlas of Light and Specular Microscopy of the Cornea 209

Fig. 6.202 Control endothelium. Regularly arranged cell mosaic; distinct borders between cells(about 2500 cells/mm2). Scale bar = 10 µm (Courtesy of P. Liskova, General University Hospitalin Prague, Czech Republic)
Fig. 6.201 Control endothelium. Compact, uniform, hexagonal appearance of the endothelialcells (about 3600 cells/mm2). Scale bar = 10 µm (Courtesy of P. Liskova, General UniversityHospital in Prague, Czech Republic)
210 K. Jirsova

Fig. 6.203 Fuchs endothelial corneal dystrophy (FECD). Early changes in the paracentral part ofthe cornea. Solitary or grouped guttae and some degree of polymegethism (about 1220 cells/mm2).Scale bar = 10 µm (Courtesy of P. Liskova, General University Hospital in Prague, CzechRepublic)
Fig. 6.204 FECD. The same eye as in Fig. 6.203, central area. A moderate form of the disease isapparent, with coalesced corneal guttae in the form of dark structures. The colour of the endothelialcells is reversed, with black surrounded by a white border (right panel) (about 600 cells/mm2).Scale bar = 10 µm (Courtesy of P. Liskova, General University Hospital in Prague, CzechRepublic)
6 Atlas of Light and Specular Microscopy of the Cornea 211

Fig. 6.205 FECD. Patient with an advanced form of the disease, with abnormal enlargement ofthe endothelial cells in the paracentral area (left panel) and stromal edema in the central area (rightpanel), right eye. Scale bar = 10 µm (Courtesy of P. Liskova, General University Hospital inPrague, Czech Republic)
Fig. 6.206 FECD. The same patient as in Fig. 6.205, advanced form, stromal edema in theparacentral area (left panel) and the central area (right panel), left eye. Scale bar = 10 µm(Courtesy of P. Liskova, General University Hospital in Prague, Czech Republic)
212 K. Jirsova

Fig. 6.207 Posterior polymorphous corneal dystrophy (PPCD). Patient with PPCD1, right eye(about 1090 cells/mm2). Scale bar = 10 µm (Courtesy of P. Liskova, General University Hospitalin Prague, Czech Republic)
Fig. 6.208 PPCD. Patient with PPCD1 (the same as in Fig. 6.207), right eye. Clinically, thepatient did not exhibit stromal edema; the changes are probably related to the presence of amultilayered, abnormal endothelium and irregularities of the posterior corneal surface. Scalebar = 10 µm (Courtesy of P. Liskova, General University Hospital in Prague, Czech Republic)
6 Atlas of Light and Specular Microscopy of the Cornea 213

Fig. 6.210 PPCD. Patient with PPCD3, right eye. Some degree of polymegethism andpleomorphism (P&P). Small focal excrescence with well-circumscribed borders (about 1400cells/mm2). Scale bar = 10 µm (Courtesy of P. Liskova, General University Hospital in Prague,Czech Republic)
Fig. 6.209 PPCD. Patient with PPCD3, right eye. Focal excrescence of Descemet membrane withwell-circumscribed borders, low ECD (about 1100 cells/mm2). Scale bar = 10 µm (Courtesy ofP. Liskova, General University Hospital in Prague, Czech Republic)
214 K. Jirsova

Fig. 6.212 PPCD. The same patient as in Fig. 6.211. P&P, abnormally enlarged endothelial cells(left panel); dark areas probably represent irregularities of the endothelial surface (right panel),right eye. Scale bar = 10 µm (Courtesy of P. Liskova, General University Hospital in Prague,Czech Republic)
Fig. 6.211 PPCD. Patient with PPCD (molecular genetic cause not identified), right eye. P&P;abnormally enlarged endothelial cells are especially present. Scale bar = 10 µm (Courtesy ofP. Liskova, General University Hospital in Prague, Czech Republic)
6 Atlas of Light and Specular Microscopy of the Cornea 215

Fig. 6.214 Iridocorneal endothelial syndrome. The same patient as in Fig. 6.213, right eye.Severe edema; only parts of the endothelial cell borders are discernible. Scale bar = 10 µm(Courtesy of P. Liskova, General University Hospital in Prague, Czech Republic)
Fig. 6.213 Iridocorneal endothelial syndrome. Relatively normal appearance of the endothelialmosaic (left); the colour of the cells is reversed, with black surrounded by a white border (appearsas a negative image of the normal endothelium), right eye (about 2400 cells/mm2). Scalebar = 10 µm (Courtesy of P. Liskova, General University Hospital in Prague, Czech Republic)
216 K. Jirsova

Acknowledgments Author thanks for critical reading of parts 6.1, 6.2 and 6.4 Prof. Gilles Thuret,Jean Monnet University, St-Etienne, France, and part 6.3 Andrea Gareiss-Lok, CBAT,Hornhautbank, Munich, Germany.
Image Contributors
Katerina Jirsova, Charles University, Prague, Czech Republic.If not otherwise indicated, all Figs. in Parts 6.1, 6.2, and 6.4. Most of the pho-tographs were taken in the Ocular Tissue Bank, General University Hospital inPrague between 2000 and 2011.
Gilles Thuret and Zhiguo He; Biology, Engineering and Imaging of Corneal Grafts,Jean Monnet University, St-Etienne, France.Figures 6.8, 6.193 and 6.194.
Ivana Rybickova, Charles University, Prague, Czech Republic.Figures 6.129 and 6.130.
Jameson Clover and Christopher G. Stoeger.If not otherwise indicated, all Figs. in Part 6.3.
Mohit Parekh, Alessandro Ruzza, and Davide Camposampiero; Veneto Eye BankFoundation, Venice, Italy.Figures 6.116, 6.120 and 6.125–6.128.
Mozhgan Rezaei Kanavi, Ocular Tissue Engineering Research Center; ShahidBeheshti, University of Medical Sciences, Tehran, Iran.Figure 6.156.
Pavel Studeny, Kralovske Vinohrady, University Hospital, Prague, Czech Republic.Figures 6.129 and 6.130.
Petra Liskova, General University Hospital in Prague, Prague, Czech Republic.Figures 6.201–6.214.
Sabine Salla, Martin Hermel, and Wolfgang Plum; RWTH Aachen University,Germany.Figures 6.117, 6.118 and 6.121–6.124.
Sophie Acquart, Eye Bank, French Blood Center, Saint-Etienne, France.Figures 6.87–6.89.
V. Vinod Mootha, University of Texas Southwestern Medical Center, Dallas, TX,USA.Figure 6.161.
6 Atlas of Light and Specular Microscopy of the Cornea 217





![Analysis of RPE morphometry in human eyes · 2016. 8. 1. · pathology using specular microscopy [15]. We hypothesize that with increasing distance from the optic nerve and with increasing](https://img.pdfslide.net/doc/110x75/5fe19a2793245564573089a6/analysis-of-rpe-morphometry-in-human-2016-8-1-pathology-using-specular-microscopy.jpg)