Embed Size (px)
Citation preview

L’impiego del Viscum in oncologia : dalla medicina antroposofica alla medicina
integrata del XXI secolo
Dr Alessandra Longhi
Medico Oncologo
Ist Ortopedico Rizzoli Bologna

Medicina antroposofica
Novita della m antroposofica rispetto alla medicina dei primi del 900’ dominata dal positivismo
Consapevolezza della dimensione spirituale (anima, spirito)
Importanza della biografia x comprendere la malattia (malattia come linguaggio nel proprio destino)
auto regolazione x la propia guarigione.
Altre forme di terapie non farmacologiche: euritmia , musicoterapia, pittura e scultura

Medicina antroposofica integrata a medicina convenzionale
Terapia multimodale:
-farmaci omeopatici
-farmaci convenzionali
-fitoterapici
-farmaci antroposofici (es.vischio)
Altre terapie: arteterapia, ginnastica euritmica, massaggi, counseling biografico, psicoterapia antroposofica.
La malattia va vista all’interno della propria biografia e puo’ essere un’occasione di trasformazione.

Self regulation :6 esercizi base R Steiner
1) Controllo del pensiero:concentrarsi su oggetto x 5’/d 2) Controllo della volonta’ 3) Controllo dell’espressione dei sentimenti 4) Positivita, verita , bonta 5) Mente aperta ricettiva a nuove esprienze 6) Armonizzare

Vol 40, Oct 2018

Integrative cancer care in a certified Cancer Centre of a German
Anthroposophic hospital. Thronicke A, Oei SL, Merkle A, Herbstreit C, Lemmens HP, Grah C, Kröz M, Matthes H, Schad
F.Complement Ther Med. 2018 Oct;40:151-157
2011-2016: 2382 Pazienti oncologici (ca.mammario. Ca colon, ca polmone) eta mediana 66 aa, 25% metastatici 64% chirurgia, 53% Chemioterapia, 30% Viscum 87% interventi non farmacologici

Viscum
Mistletoe (Viscum) pianta semiparasitica cresce su alberi nei paesi del Nord Europa (bacche bianche) ed e’ uno dei farmaci piu’ prescritti nella medicina Integrata fra I pazienti oncologici in Europa , nel 60% nei paesi di lingua tedesca.
Over 1200 articoli pubblicati col nome mistletoe/Viscum molti in lingua tedesca. Una revsione Cochrane ne ha evidenziato il beneficio su Qualita di vita Gli studi su efficacia come antitumorale ancora pochi e con debolezze metodologiche
vari studi sui composti del Viscum ne hanno dimostrato attivita citotossica in vitro su varie cell tumorali (LECTINE) e attivita immunostimolante (VISCOTOSSINE e POLISACCARIDI)
Iscador e’ Viscum Album Fermentatum fermentazione batterica (bacche e foglie) secondo le procedure descritte da Steiner R .Iscador M=Mali, P=Pini, Q=Quercus , U=Ulmus ecc

Registrato come “biologic response modifier”
Utilizzato per lo piu sottocute 2o 3 volte alla settimana
Altri tipi Helixor, Viscum Abnova, Iscucin, Plenosol
Alcuni studi anche via orale, intratumorale, intrapleurica e ev
Per via sc pochi effetti collaterali (reazione locale, febbricola ) anafilassi (raro)

Ten year follow up of a randomized study of Viscum
album Fermentatum Pini vs Etoposide in osteosarcoma
in complete surgical remission after second relapse Alessandra Longhi MD
Chemotherapy Div
Istituto Ortopedico Rizzoli IRCCS
Bologna Italy [email protected]
Soc Integrative Oncology 29 October 2018 Scottsdale AZ,USA

Incidence of primitive bone sarcoma: 2 - 3 / 1 M people
Proportion of osteosarcoma: 45 %
Median age at first diagnosis: 15 years
5-year Overall Survival (OS):
without antineoplastic therapy: 10 %
after surgery / chemotherapy : 70 – 80 %
• Doxorubicine, Methotrexate, Cisplatin, Ifosfamide
5-year Post Relapse Disease Free Survival (PRDFS)6-27%
Osteosarcoma rare tumor
patient age [years]
Age at first diagnosis of osteosarcoma
perc
enta
ge o
f patients

1) 620 patients with localized osteosarcoma of an extremity treated between 1985-1998 (Bacci G., Acta Oncol 2005, 44(7) 748-55)
235 of 620 patients relapsed
Average time interval between diagnosis and 1° relapse: 25.4 months
1° and 2° relapse: 12.7 months
2° and 3° relapse: 11.8 months
3° and 4° relapse: 15.2 months
4° and 5° relapse : 4.0 months
Only 14/120 (11,6%) pts who had a second relapse had a prolonged survival
Istituto Orthopedico Rizzoli (IOR) experience

2) Survival after second and subsequent recurrences in osteosarcoma: a
retrospective multicenter analysis Tirtei E et al 2017 Tumori May1 tj:5000636
60 patients with osteosarcoma after second relapse (2003-2013) 5 yrs Overall survival 22% 5 years Overall Survival after Complete Surgical Remission after 2° relapse was 33,4% Lungs metatastases vs other metastatic site : 5 yrs OS 33,6% vs 5%
84% dei pazienti ha una seconda ricaduta dopo <12 ms. Solo il 16%ha un post relapse Disease free > 12 ms dopo la 2 ricaduta

Early first relapse ( 24 months from diagnosis)
Surgery (when feasible plus chemotherapy HDIFO,Gem-docetaxel)
Late first relapse (> 24 months from diagnosis)
Limited disease: only surgery
Extended disease: HDIFO,Gem-docetaxel from 2012
Second relapse
Surgery whenever possible
Chemotherapy (HDIFO,Gem-Docetaxel from 2012)
Further experimental drugs
2007 : in high-risk patients free from disease after surgery: w/s or oral etoposide,Interferon.
Actual treatment of relapsed patients

Topoisomerase II inhibitor
Employed in several tumors, p.o. or i.v.
lymphomas, lung cancer, ovarian cancer, Ewing's sarcoma
Off-label as "adjuvant" post relapse in bone sarcoma
Well tolerated
Only one trial published (Kebudi et al., Pediatr Blood Cancer 2004; 42:320-4)
Remissions in 14% of 21 pediatric sarcoma patients (age 3-16 years)
Rationale for oral etoposide in osteosarcoma

Immunotherapy in Osteosarcoma:the past
1) Interferon Alfa: utilized in ‘60 at Karolinka Institute in pre Chemotherapy era.
2) EURAMOS 1: MAP+/•Pegilated Interferon in HG osteosarcoma Gresponder

Immunomodulating activity
Increase of NK cells, T-lymphocytes, macrophages
Apoptotic activity (in vitro)
Lukasklinik Arlesheim/Switzerland
Positive outcomes after surgery in 13 patients with bone sarcoma
IOR: Individual therapy attempts
5 osteosarcoma pts. after 2° relapse
V.album fermentatum Pini treatment over 12 months
Average DFS 18 months
Very well tolerated
Rationale for Viscum album fermentatum Pini
PILOT :Post relapse disease free survival
0 10 20 30 40 50 60

Study Design
PROTOCOL DESIGN
Pts Disease Free after
Second relapse
RANDOMIZATION
18 Patients:
Etoposide 50 mg/m2/d po
for 21 d every 28 d for 6 cycles
18 Patients:
Viscum album ferm. Pini
1 vial/sc x 3/wk for 12 months
Study visits at baseline and months 3, 6, 9
Exit visit at month 12
Inclusion Criteria 1. Osteosarcoma / spindle cell sarcoma of bone after second relapse,
histologically confirmed
2. Actually free from metastases or local relapse
3. Age ≥10 years
4. ECOG Performance Status 0-2
5. Adequate bone marrow function, bilirubin, creatinine
6. No other malignancy prior study entry and during follow up
7. Last antineoplastic treatment received ≥ 30 days prior to study entry
Exclusion Criteria
1. Missing staging criteria showing disease-free condition
2. Concomitant treatment with immunomodulating drugs
3. Treatment with etoposide or Viscum album prior to study entry
Study Patients

Post Relapse Disease free Survival (PRDFS)
Primary efficacy parameter: 12-months PRDFS rate
Clinical hypothesis: increase from 12% to 40%
Treatment arms are independently from each other compared to expected value of 12%
Quality of Life (QoL)
EORTC QLQ-C30 (adults) or PedsQL (juveniles – not shown here)
Safety / tolerability of etoposide and Viscum album
Adverse events, adverse drug reactions
Immune response to treatment
Clinical Endpoints

Etoposide
Alkaloid derived from Juniperus virginia or Podophyllum peltatum
6 cycles of 50 mg/m²/day p.o. for 21 days every 28 days
Viscum album fermentatum Pini (Iscador P)
Fermented aqueous extract of Viscum album ssp. austriacum grown on pine trees (Iscador® P)
1 vial injected s.c., 3/week for 12 months
Dose escalation from 0.01 to 20mg or best tolerated dose
Treatment Regimes
Initial phase:
week 1 2 3 4 5
e.g. weekday mon wed fri mon wed fri mon wed fri mon wed fri mon wed fri
Iscador P Series 0 Series 0 Series 1
mg / injection 0,01 0,01 0,1 0,1 1 1 1 0,01 0,01 0,1 0,1 1 1 1 0,1
week 6 7 8 9 10
e.g. weekday mon wed fri mon wed fri mon wed fri mon wed fri mon wed fri
Iscador P Serie 1 Series 1 Series 2
mg / injection 0,1 1 1 10 10 10 0,1 0,1 1 1 10 10 10 1 1
Maintenance phase:
week 11 12 13 14 15
e.g. weekday mon wed fri mon wed fri mon wed fri mon wed fri mon wed fri
Iscador P Series 2 Series 2 Series 2 (etc.)
mg / injection 10 10 20 20 20 1 1 10 10 20 20 20 1 1 10
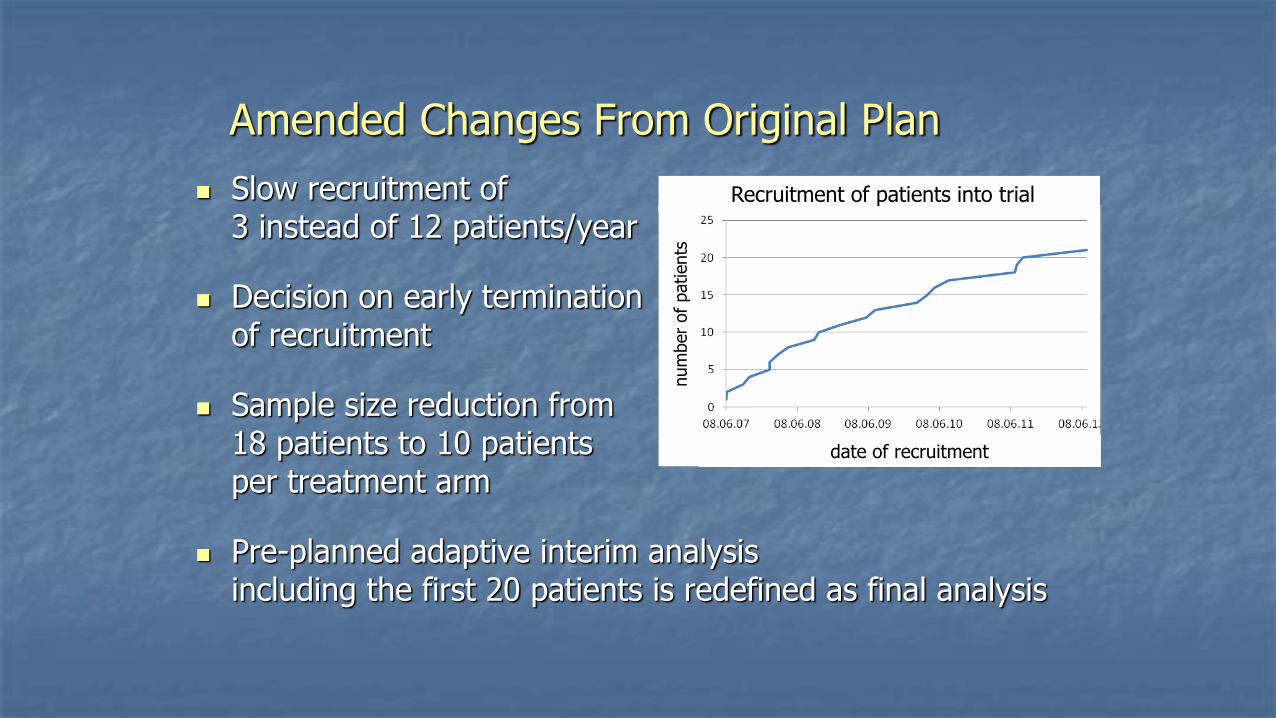
Slow recruitment of 3 instead of 12 patients/year
Decision on early termination of recruitment
Sample size reduction from 18 patients to 10 patients per treatment arm
Pre-planned adaptive interim analysis including the first 20 patients is redefined as final analysis
Amended Changes From Original Plan
date of recruitment
Recruitment of patients into trial
num
ber
of
patients

Patient Characteristics frequency (percentage) or mean (range)
Viscum n=9
Etoposide n=11
Male:Female 4:5 7 :4
Age [years] 28 (18-48) 39 (11-66)
Interval from primary disease [years] 4.0 (1.5-10.5) 3.7 (1.4-7.2)
median DFS 1° interval [months] 19,1 (2-40) 26.9 (14.5-39.4)
DFS 2° interval [months] 21.1 (3-82) 15.6 (2-47.4)
Time from 2° relapse to baseline
[weeks]
13.9 (0.9-76.6) 7.6 (1.9-24.6)

PTS start TX age SEX ARM site relpse 1st Interval2°interv last FUPDFS Dec17 ms OS Sept 2018 OUTCOME Status
GMF 39241 48 F Viscum P lung 27 5 21.01.17 115 115 NED NED
RG 39328 18 F Viscum P lung 13 13 13.11.2017 122 122 NED NED
TS 39357 28 M Viscum P lung 40 82 23.06.2017 116 116 NED NED
GG 39559 29 M ViscumP lung 25 3 3 17 Relapsed dead
VB 39710 30 F Viscum P lung 24 16 05.10.2017 108 108 NED NED
DCJ 39714 21 F viscum P lung 12 8 08.05.17 104 104 Relapsed NED
RMG 40270 20 F ViscumP bone 10 42 08.05.17 85 85 NED NED
DOD 40382 41 M Viscum P lung 2 8 2 24 Relapsed dead
UA 40724 22 M Viscum P lung 19 13 27.3.15 11 46 Relapsed dead
DSA 39245 28 M Etoposide bone 24 11 3 5 Relapsed dead
AA 39464 62 F Etoposide lung 27 33 22.9.2017 12 92 Relapsed NED
SM 39464 48 M Etoposide lung 24 34 23.3.17 6 110 Relapsed NED
AG 39524 16 F Etoposide lung 36 6 3 5 Relapsed dead
PM 39820 11 M Etoposide lung 14 3 1 3 Relapsed dead
FS 40004 35 F Etoposide lung 21 11 5.5.17 9 94 Relapsed NED
GP 39961 65 M Etoposide lung 37 40 5.10.2017 84 102 Relapsed NED
UF 40220 17 M Etoposide lung 33 3 4 25 Relapsed dead
PS 40309 63 M Etoposide lung 18 3 42 60 Relapsed dead
CM 40732 17 F Etoposide lung 35 12 8 23 Relapsed dead
PM 08/08/11 65 M Etop never started lung 6 dead dead

Quality of Life – EORTC QLQ-C30 Selected Scales – Mean Change from Baseline
Global Health Status / QoL
Insomnia Fatigue
Pain

Quality of Life – EORTC QLQ-C30
Physical Functioning Role Functioning Emotional Functioning Cognitive Functioning Social Functioning
Global Health Status / QoL Fatigue Nausea / Vomiting Pain Dyspnea
Insomnia Appetite loss Constipation Diarrhea Financial Problems
All Scales – Change from Baseline
RESULTS 31.12.2017 From 2007 to 2011: pts enrolled ITT 20
Evaluable for response 19
9 patients enrolled in Viscum Arm
11 patients enrolled in Etoposide arm
Median follow up 84 months (1-122)
Median age 33.9(11-65)
F:M=11:9
1 year Post Relapse DFS of Viscum 55,6%compared to
historical12%rate: (𝑃 = 0.0041)
1 year PRDFS of Etoposide 27,6%.

Post Relapse Disease Free Survival
PRDFS Rate after 12 months
Binomial estimate [percentage ± 95% confidence interval]
0
20
40
60
80
100
Intention to treat analysis
Viscum Etoposide
0
20
40
60
80
100
Complete case analysis
Viscum Etoposide
5 of 9 patients
p≠12% = 0.00412
3 of 11 patients
p≠12% = 0.27239
5 of 9 patients
p≠12% = 0.00412
2 of 10 patients
(1 drop-out)
p≠12% = 0.68345

Post-Trial Follow Up
VISCUM ALBUM IN RELAPSING OSTEOSARCOMA
Post Relapse Disease Free Survival
Hazard Ratio HR=0.287 CI=(0.087-0.944) p=0.0399
Follow up
10 year PRDFS
years since randomisation
PRDFS – Kaplan-Meier curve
pro
babili
ty o
f PRD
FS
Trial
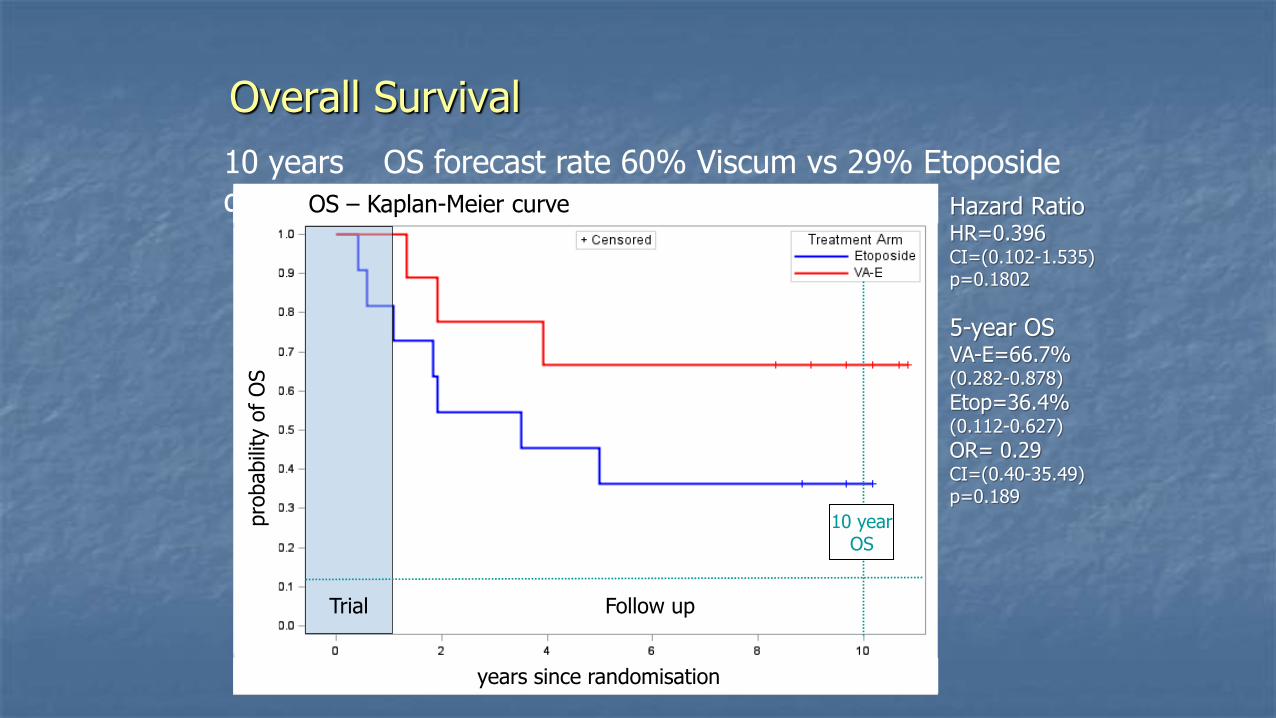
10 years OS forecast rate 60% Viscum vs 29% Etoposide de (p=0.087)
Overall Survival
pro
babili
ty o
f O
S
years since randomisation
OS – Kaplan-Meier curve
Follow up
10 year OS
Trial
Hazard Ratio HR=0.396 CI=(0.102-1.535) p=0.1802
5-year OS VA-E=66.7% (0.282-0.878)
Etop=36.4% (0.112-0.627)
OR= 0.29 CI=(0.40-35.49) p=0.189
Median PRDFS: Viscum 104 ms(2-122) vs Etoposide 7 ms(1-84) Median OS: Viscum 104 (17-122 vs Etoposide 42,5ms (3-110) 10 years OS forecast rate 60% (viscum) vs 29% Etoposide (p=0.087)

Immune response to Viscum
Lymphocytes count (CD3,CD4,CD8,CD16)
at T0,T3,T6,T9 T12 months in
both Viscum arm and Etoposide arm


Conclusions (1)
Limiti di uno studio con pochi pazienti(rare disease)
Etoposide :non ha dato benefici in termini di Post relapse DFS a 1 aa ,piu tossico
Viscum migliore PRDFS
Overall Survival dopo la terza ricaduta non e’ statisticamente significativo dovuto alla terapia di salvataggio (chirurgia) dopo la terza ricaduta

Conclusioni (2)
Valutare l’efficacia del Viscum come terapia di mantenimento in pazienti ad alto rischio di ricaduta dopo Remissione Completa
Comparare il Vischio con farmaci piu costosi gia impiegati nell’osteosarcoma x efficacia e costi
Interferone (in adiuvante in EURAMOS1)
Mifamurtide (in adiuvante in ISG-OS2)

Grazie Erminia Mariani, PHD Immunology res. Dept, Rizzoli Inst, Bologna, Italy
Marcus Reif , Inst Klinical reaserch ,Berlin, Germany
Silvana Becker PHD Pharmacist , Weleda,Italy.














![KÜLÖNBÖZÔ SZISZTÉMIKUS HERBICIDEK FEHÉR FAGYÖNGY … · A fehér fagyöngy (Viscum album L.) a fa-gyöngyfélék (Viscaceae [synonym: Santalaceae sensu lato]) családjába](https://img.pdfslide.net/doc/110x75/60677fc08110456b01575ffa/koelnbz-szisztmikus-herbicidek-fehr-fagyngy-a-fehr-fagyngy-viscum.jpg)


![lexique homeopathique SN 2012 ver02 · [carbo vegetabilis, podophyllum]. Réveil fréquent Podophyllum Le premier remède de diarrhées transpiration pendant les douleurs à l'estomac](https://img.pdfslide.net/doc/110x75/5e7449ec2bbc257b9533bdf0/lexique-homeopathique-sn-2012-ver02-carbo-vegetabilis-podophyllum-rveil-frquent.jpg)











