Embed Size (px)
Citation preview

Dipartimento di CardioScienzeUnità Operativa Complessa
Cardiologia Interventistica e UTIC
Marino Scherillo
LINEE GUIDA PER L’IMPIANTO
CORONARICO DI STENT E CORRETTA TERAPIA ANTIAGGREGANTE
Napoli 12-15 ottobre 2008 Mostra d’Oltremare
Cardiologia Interventistica ed UTIC – A.O. G.Rummo - BENEVENTO
G.F. , 52 y / male, Diabetes ,Tn I+NSTEMIStrategia Farmaco-Interventistica Precoce
ASA CLOPIDOGREL
LMWHSTATINA
PCI - STENT

Recommendations for Oral Antiplatelet Drugs
I IIaIIb • Aspirin• Loading dose (160 - 325 mg)
• Maintenance (75 - 100 mg)
• Clopidogrel• Loading dose 300 mg + 75 mg
• 12 months maintenance
• Contraindication for Aspirin
• 600 mg LD for PCI
• Postpone CABG 5 days after withdrawal
III
A
AA
BA
BC
ESC 2007

LG come Bussola per Medici e Pazienti
Linee Guida : Verso una Definizione Linee Guida : Verso una Definizione Operativa per la ComunitOperativa per la Comunitàà
“ Le LG indicano genericamente la Direzione e non lo
specifico Percorso per Migliorare la Quantitàe la Qualità della Vita
dei Pazienti ”
Le Linee Guida non sono il TomTom
La Conoscenza non èSapere Certo
“Episteme” ma Sapere Congetturale
“Doxa”e Noi tutti siamo
Ricercatori non Possessori della Verità
Karl Popper
La Grappa diLa Grappa di PopperPopperLinee Guida come Distillato della VeritLinee Guida come Distillato della Veritàà ScientificaScientifica
Osservazioni Trial
Ragionamenti Studi Fisiopatologici
Linee Guida
Trombosi Tardiva IntrastentSTEMI 9 mesi dopoPCI - DES 3.5x15 mm Durante ASA - CLO
PCI - BMS3.5x18 mmABCXMAB
….. e se fosse un paziente CLOPIDOGREL Non Responder
9
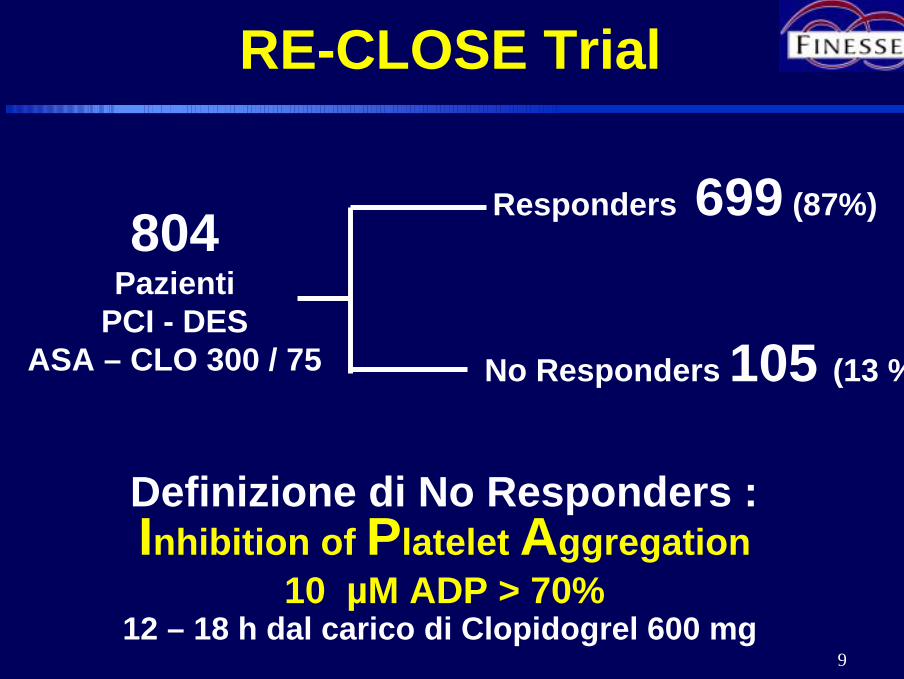
804Pazienti
PCI - DESASA – CLO 300 / 75
Responders 699 (87%)
No Responders 105 (13 %)
Inhibition of Platelet Aggregation10 µM ADP > 70%
RE-CLOSE Trial
Definizione di No Responders :
12 – 18 h dal carico di Clopidogrel 600 mg

10
STENT THROMBOSIS
Non - Responders Responders9 / 105 (8.6 %) 16 / 699 (2.3 %)
AMI 3 (33%) 7 (44%)
Bifurcation 5 (55%) 10 (62%)
Multivessel PCI 5 (55%) 10 (62%)
Stent length > 30mm 8 (89%) 8 (50%)
LVEF < 30% 5 (55%) 8 (55%)
11
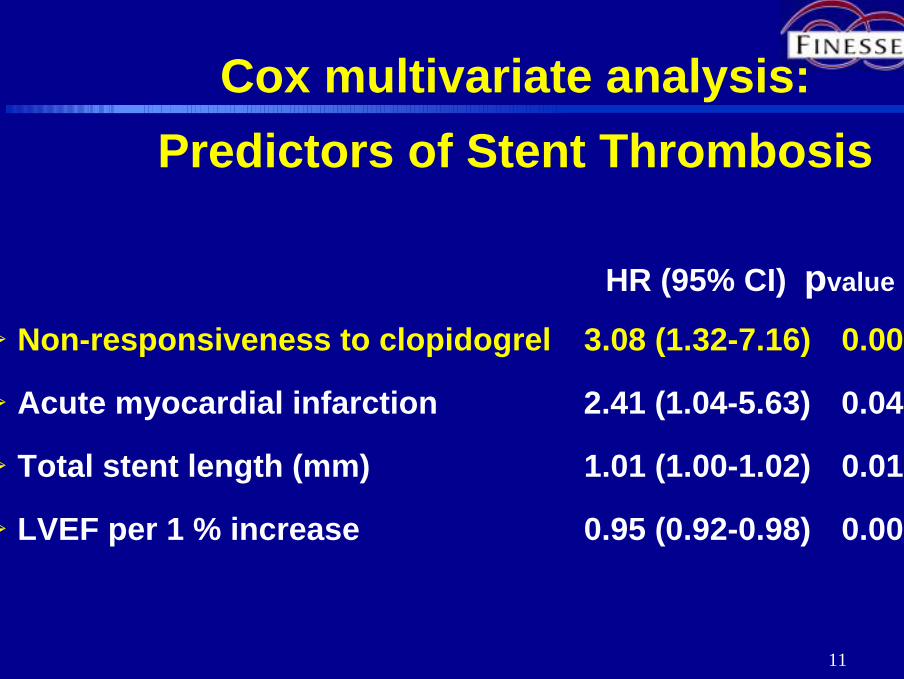
Cox multivariate analysis:Predictors of Stent Thrombosis
HR (95% CI) pvalue
! Non-responsiveness to clopidogrel 3.08 (1.32-7.16) 0.009
! Acute myocardial infarction 2.41 (1.04-5.63) 0.041
! Total stent length (mm) 1.01 (1.00-1.02) 0.010
! LVEF per 1 % increase 0.95 (0.92-0.98) 0.001
12
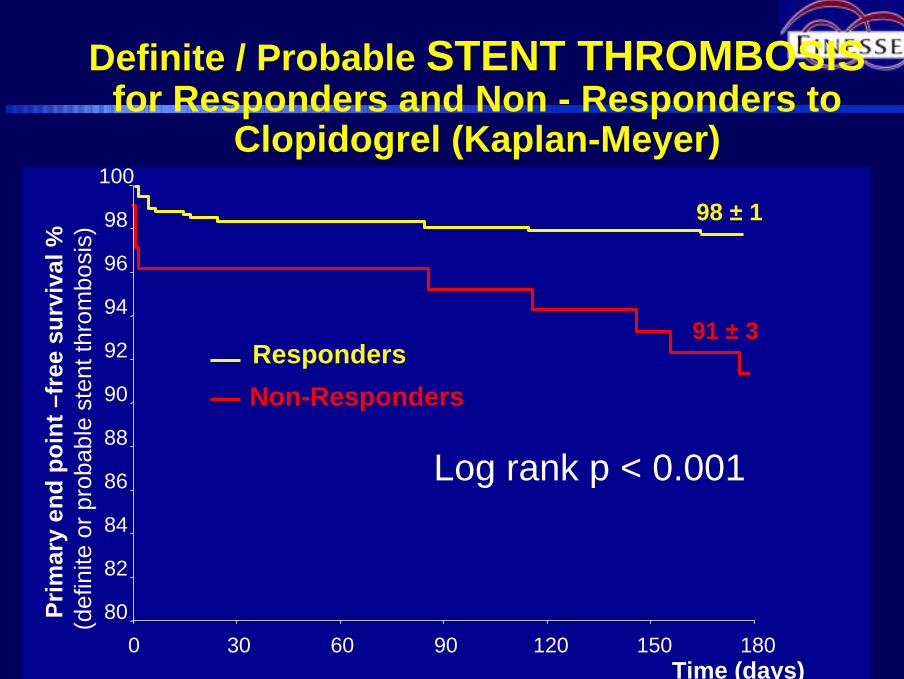
Definite / Probable STENT THROMBOSISfor Responders and Non - Responders to
Clopidogrel (Kaplan-Meyer)
91 ± 3
98 ± 1
Prim
ary
end
poin
t–fr
ee s
urvi
val%
(def
inite
or p
roba
ble
sten
tthr
ombo
sis)
80
82
84
86
88
90
92
94
96
98
100
Time (days)0 30 60 90 120 150 180
Log rank p < 0.001
Non-RespondersResponders
13
Time (days)
80
85
90
95
100
0 60 120 180 240 300 360 420 480 540 600 660 720
Even
t-fre
e su
rviv
al%
(def
inite
orp
roba
ble
sten
t thr
ombo
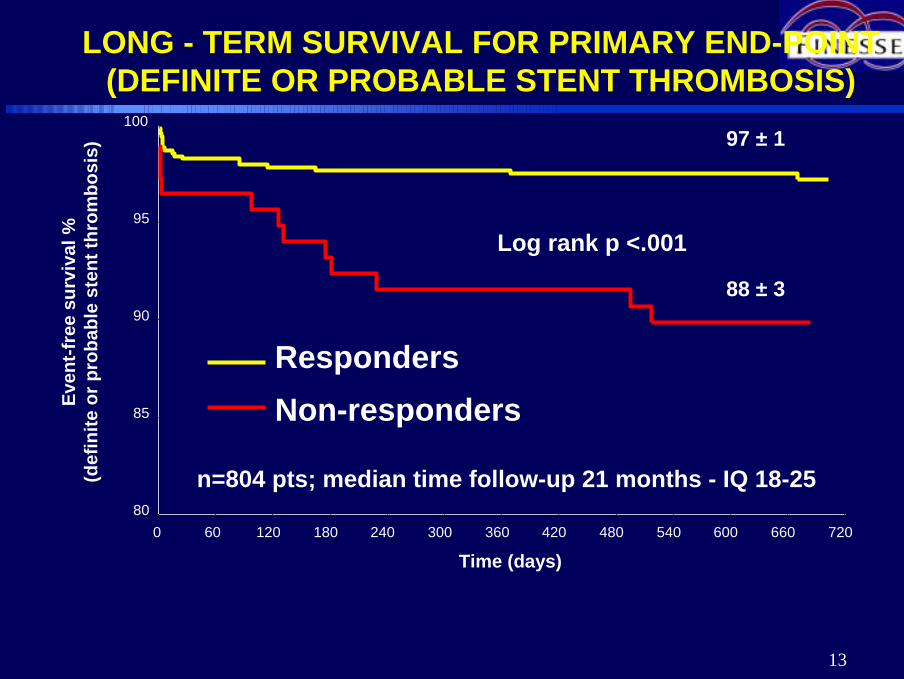
sis) 97 ± 1
88 ± 3
Log rank p <.001
RespondersNon-responders
LONG - TERM SURVIVAL FOR PRIMARY END-POINT(DEFINITE OR PROBABLE STENT THROMBOSIS)
n=804 pts; median time follow-up 21 months - IQ 18-25
14
Non-responsiveness to CLOPIDOGREL is a strong
independent predictor of stent thrombosis and
mortality in patients receiving DES. Alternative
revascularization strategies (BMS or CABG), or
pharmacologic strategies using increasing dose of
clopidogrel or other antiplatelet agents should be
considered to reduce the risk of thrombotic
events.
Conclusion

Possible Causes / Mechanisms of Variability Platelet Response With
Antiplatelet Agents• Genetic1
– Receptors: P2Y12 H2 haplotype (clopidogrel), GPIIb/IIIa, collagen,thromboxane
– Enzymes: COX-1, COX-2, thromboxane A2 synthetase, etc. (aspirin)
• Pharmacokinetic / Bioavailability1
– Non-compliance– Underdosing– Poor absorption (e.g., enteric coated aspirin)– Interference: NSAIDs coadministration (aspirin); atorvastatin (clopidogrel)
• Pharmacodynamic1
– Incomplete suppression of thromboxane A2 generation (aspirin)– Accelerated platelet turnover, with introduction into the blood stream of newly
formed, drug-unaffected platelets– Stress-induced COX-2 in platelets (aspirin)– Increased platelet sensitivity to ADP and collagen
• Environment / Concomitant disease– Diabetes mellitus (aspirin)2
1 Michelson A. Circulation 2004;110:e489-932 Albert SG et al. Diabetes Res Clin Pract 2005;70:195-9
16
Follow-up Time (Months)N
Follow-up Time (Months)N
80859095
100
80859095
100
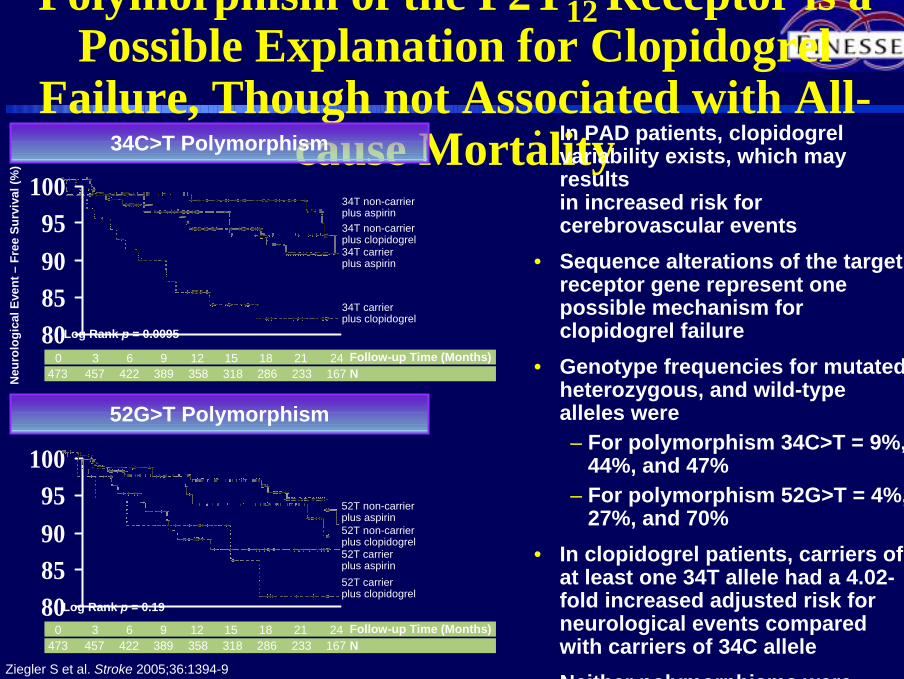
Polymorphism of the P2Y12 Receptor is a Possible Explanation for Clopidogrel
Failure, Though not Associated with All-cause Mortality• In PAD patients, clopidogrel
variability exists, which may results in increased risk forcerebrovascular events
• Sequence alterations of the target receptor gene represent one possible mechanism forclopidogrel failure
• Genotype frequencies for mutated, heterozygous, and wild-type alleles were– For polymorphism 34C>T = 9%,
44%, and 47% – For polymorphism 52G>T = 4%,
27%, and 70%• In clopidogrel patients, carriers of
at least one 34T allele had a 4.02-fold increased adjusted risk for neurological events compared with carriers of 34C allele
• Neither polymorphisms were i t d ith ll t lit
Ziegler S et al. Stroke 2005;36:1394-9
34C>T Polymorphism
Neu
rolo
gica
l Eve
nt –
Free
Sur
viva
l (%
)
0 3 6 9 12 15 18 21 24
34T non-carrierplus aspirin34T non-carrierplus clopidogrel
34T carrierplus clopidogrel
34T carrierplus aspirin
473 457 422 389 358 318 286 233 167
Log Rank p = 0.0095
0 3 6 9 12 15 18 21 24
52T non-carrierplus aspirin52T non-carrierplus clopidogrel
52T carrierplus clopidogrel
52T carrierplus aspirin
473 457 422 389 358 318 286 233 167
Log Rank p = 0.19
52G>T Polymorphism

Novel ADP P2YNovel ADP P2Y1212Receptor AntagonistReceptor Antagonist
PrasugrelPrasugrel
AZD 6140AZD 6140
CangrelorCangrelor
18
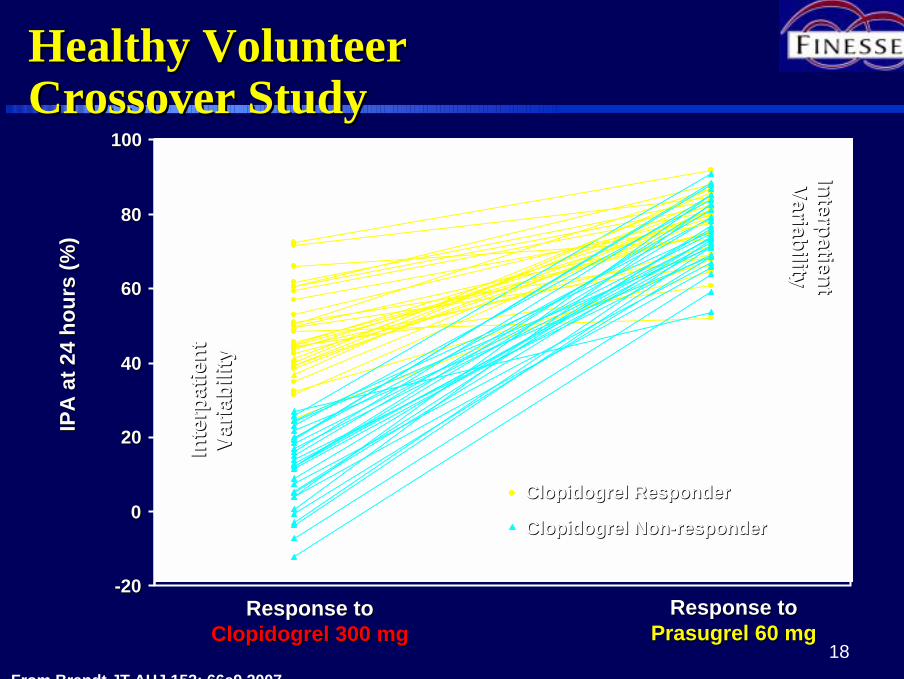
Healthy VolunteerHealthy VolunteerCrossover StudyCrossover Study
--2020
00
2020
4040
6060
8080
100100
IPA
at 2
4 ho
urs
(%)
IPA
at 2
4 ho
urs
(%)
Response toResponse toPrasugrelPrasugrel 60 mg60 mg
Response toResponse toClopidogrelClopidogrel 300 mg300 mg
ClopidogrelClopidogrel ResponderResponder
ClopidogrelClopidogrel NonNon--responderresponder
Inte
rpat
ient
Inte
rpat
ient
Varia
bilit
yVa
riabi
lity
InterpatientInterpatientVariabilityVariability
From Brandt JT AHJ 153: 66e9,2007
N=66
elevato non ènecessariamente migliore perché ècorrelato al Rischio Emorragico
20
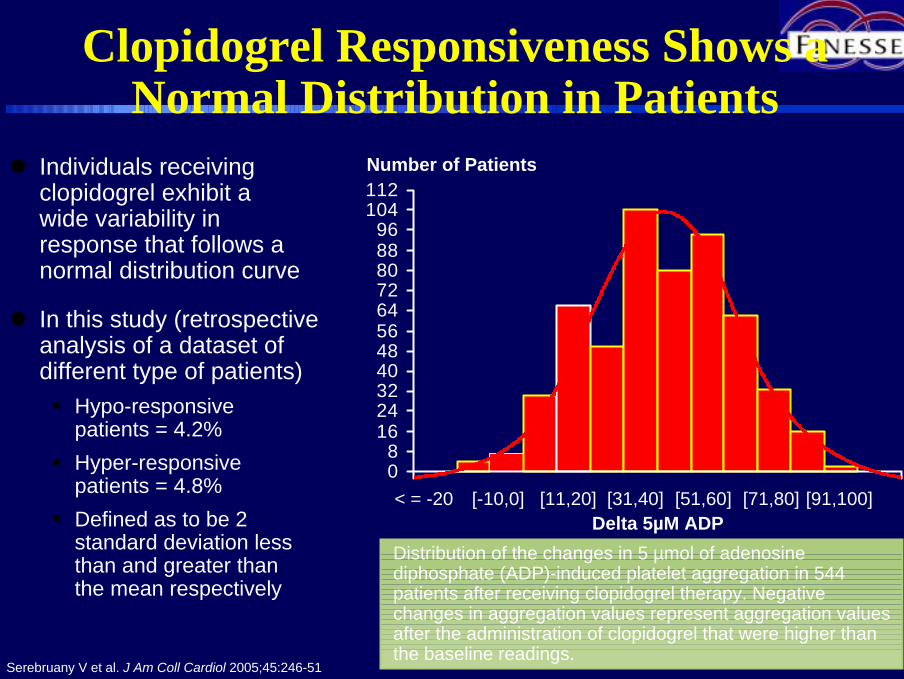
Clopidogrel Responsiveness Shows a Normal Distribution in Patients
" Individuals receivingclopidogrel exhibit awide variability in response that follows a normal distribution curve
" In this study (retrospective analysis of a dataset of different type of patients)# Hypo-responsive
patients = 4.2%# Hyper-responsive
patients = 4.8%# Defined as to be 2
standard deviation lessthan and greater thanthe mean respectively
Serebruany V et al. J Am Coll Cardiol 2005;45:246-51
08
1624324048566472808896
104112
< = -20Delta 5µM ADP
[-10,0] [11,20] [31,40] [51,60] [71,80] [91,100]
Number of Patients
Distribution of the changes in 5 µmol of adenosinediphosphate (ADP)-induced platelet aggregation in 544 patients after receiving clopidogrel therapy. Negative changes in aggregation values represent aggregation values after the administration of clopidogrel that were higher than the baseline readings.

21
Change in Aggregation to 5µM ADP
What Are the Clinical Implications?
0
16
32
48
64
80
96
112
< = -20 [-10,0] [11,20] [31,40] [51,60] [71,80] [91,100]
Num
ber o
f Pat
ient
s
Adapted from: Serebrauny V et al. J Am Coll Cardiol 2005;45:246-51
Are hypo-responders at risk for thrombotic
events?
Are hyper-responders at risk for bleeding
events?
22
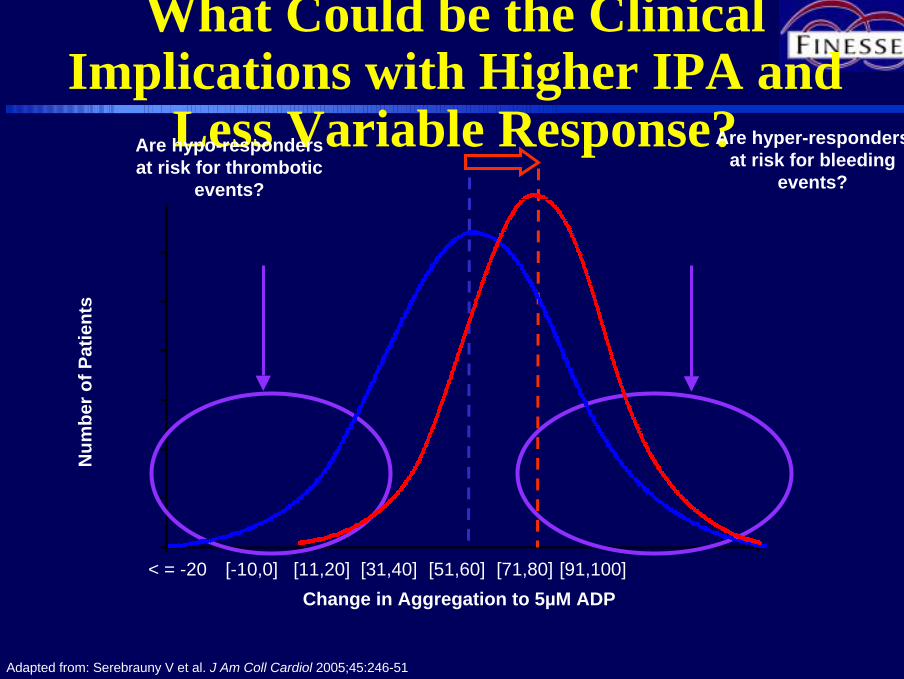
Change in Aggregation to 5µM ADP
What Could be the Clinical Implications with Higher IPA and
Less Variable Response?
< = -20 [-10,0] [11,20] [31,40] [51,60] [71,80] [91,100]
Num
ber o
f Pat
ient
s
Adapted from: Serebrauny V et al. J Am Coll Cardiol 2005;45:246-51
Are hyper-responders at risk for bleeding
events?
Are hypo-responders at risk for thrombotic
events?

Il Bravo Cardiologo Tra Scilla e Cariddi
ScillaTrombosi
CariddiEmorragia

24
TRial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet InhibitioN with Prasugrel
TRITONTRITON--TIMI 38TIMI 38AHA 2007AHA 2007
Orlando, FloridaOrlando, Florida
Disclosure StatementDisclosure Statement: : The TRITONThe TRITON--TIMI 38 trial was supported by a research grant to the TIMI 38 trial was supported by a research grant to the
Brigham and WomenBrigham and Women’’s Hospital from Daiichi Sankyo Co. Ltd and Eli Lilly & Co.s Hospital from Daiichi Sankyo Co. Ltd and Eli Lilly & Co.
25
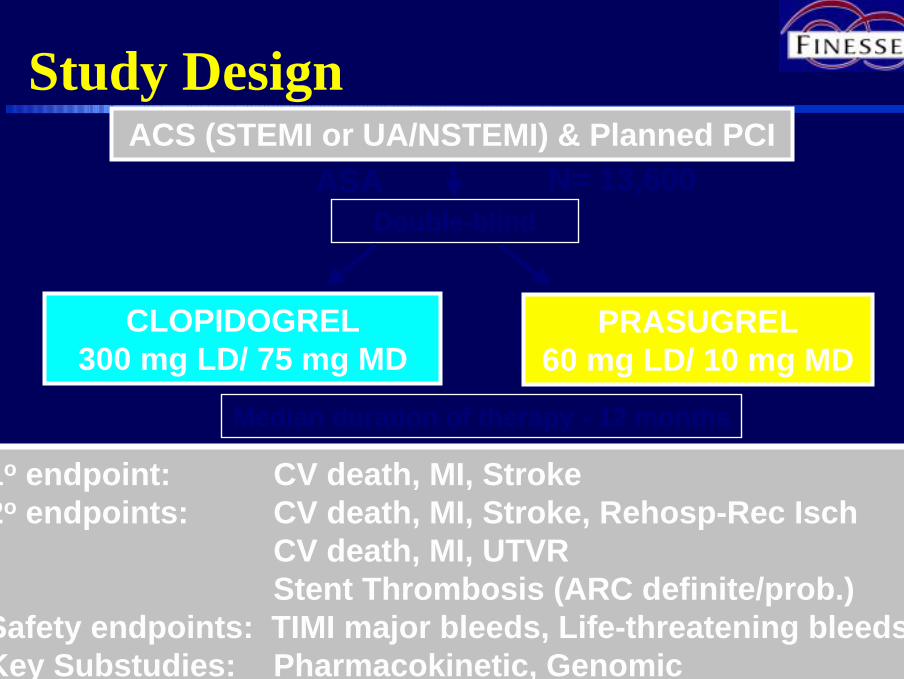
Study Design
Double-blind
ACS (STEMI or UA/NSTEMI) & Planned PCIASA
PRASUGREL60 mg LD/ 10 mg MD
CLOPIDOGREL300 mg LD/ 75 mg MD
1o endpoint: CV death, MI, Stroke2o endpoints: CV death, MI, Stroke, Rehosp-Rec Isch
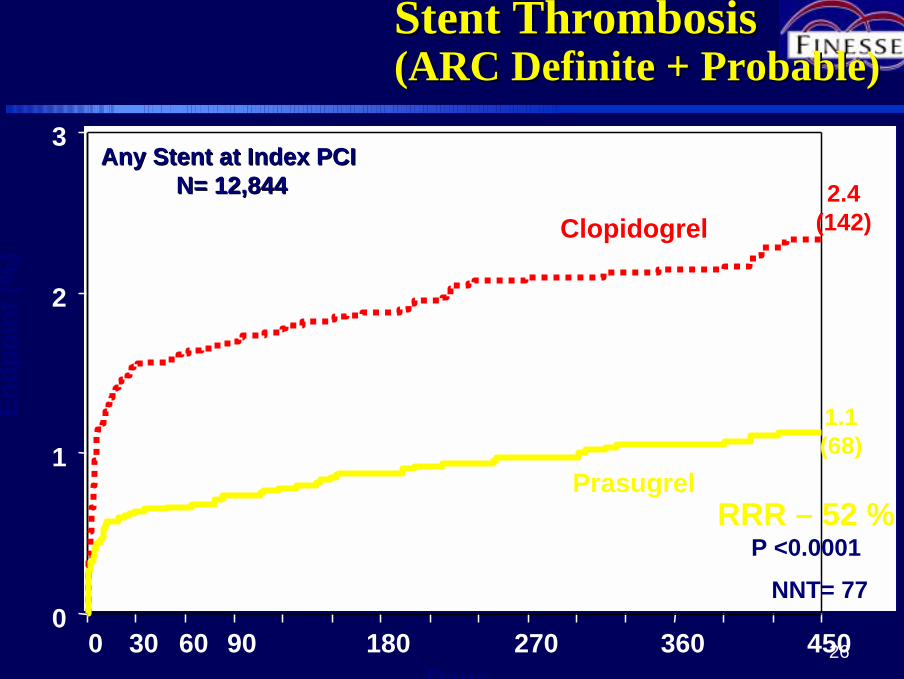
CV death, MI, UTVRStent Thrombosis (ARC definite/prob.)
Safety endpoints: TIMI major bleeds, Life-threatening bleedsKey Substudies: Pharmacokinetic, Genomic
Median duration of therapy - 12 months
N= 13,600
26
StentStent ThrombosisThrombosis(ARC Definite + Probable)(ARC Definite + Probable)
0
1
2
3
0 30 60 90 180 270 360 450
RRR – 52 %P <0.0001
Prasugrel
Clopidogrel2.4
(142)
NNT= 77
1.1 (68)
Days
Endp
oint
(%)
AnyAny StentStent at Index PCIat Index PCIN= 12,844N= 12,844
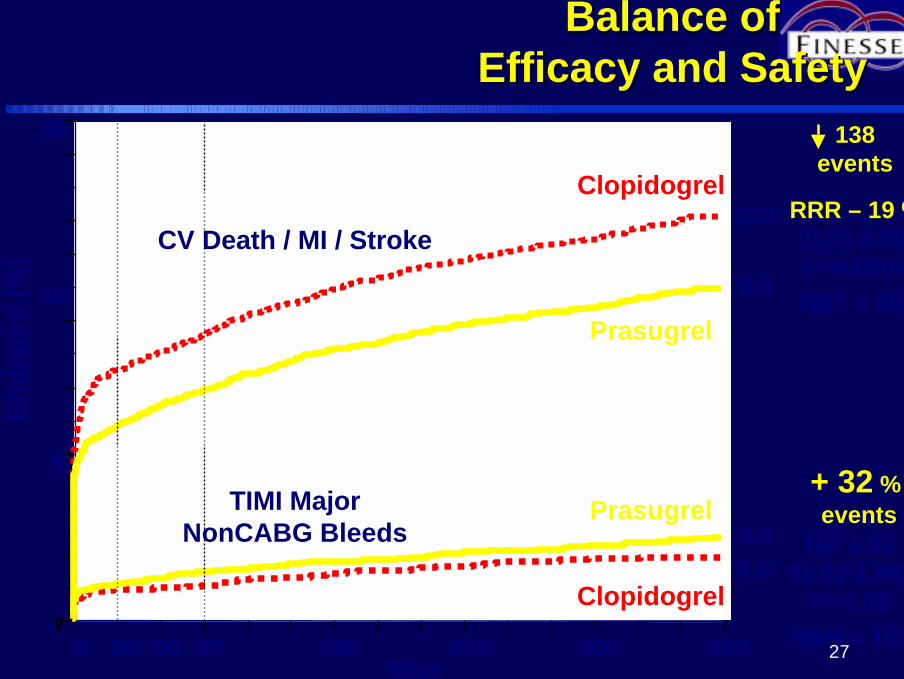
270
5
10
15
0 30 60 90 180 270 360 450
RRR – 19 % (0.73-0.90)P=0.0004
Prasugrel
Clopidogrel
Days
Endp
oint
(%)
12.1
9.9
HR 1.32(1.03-1.68)
P=0.03
Prasugrel
Clopidogrel1.82.4
138events
+ 32 %events
Balance of Balance of Efficacy and SafetyEfficacy and Safety
CV Death / MI / Stroke
TIMI MajorNonCABG Bleeds
NNT = 46
NNH = 167
28
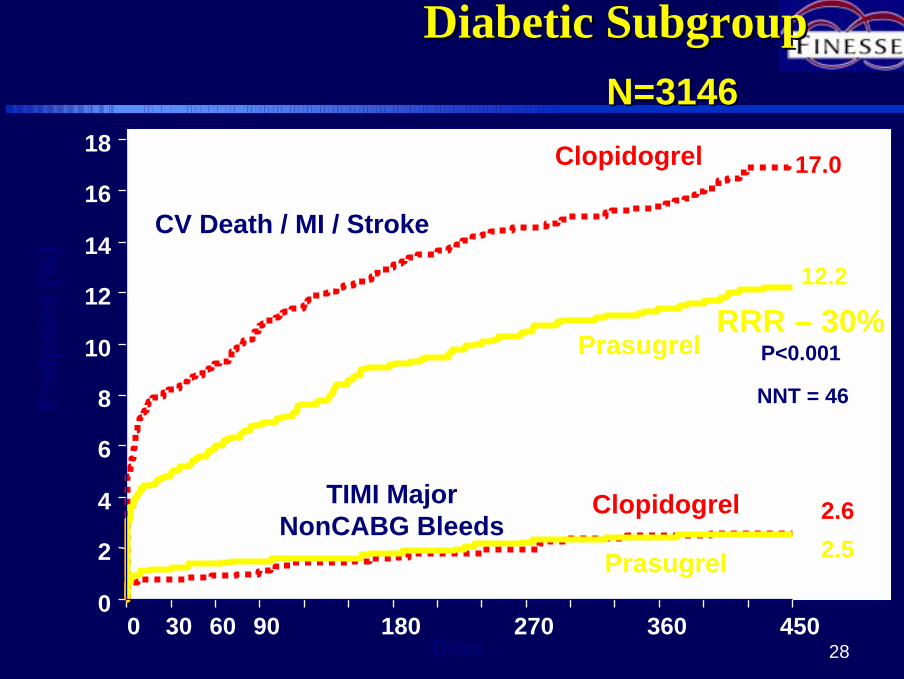
Diabetic SubgroupDiabetic Subgroup
0
2
4
6
8
10
12
14
16
18
0 30 60 90 180 270 360 450
RRR – 30%P<0.001
Days
Endp
oint
(%)
CV Death / MI / Stroke
TIMI MajorNonCABG Bleeds
NNT = 46
N=3146N=3146
17.0
12.2
Prasugrel
Clopidogrel
Prasugrel
Clopidogrel 2.62.5
29
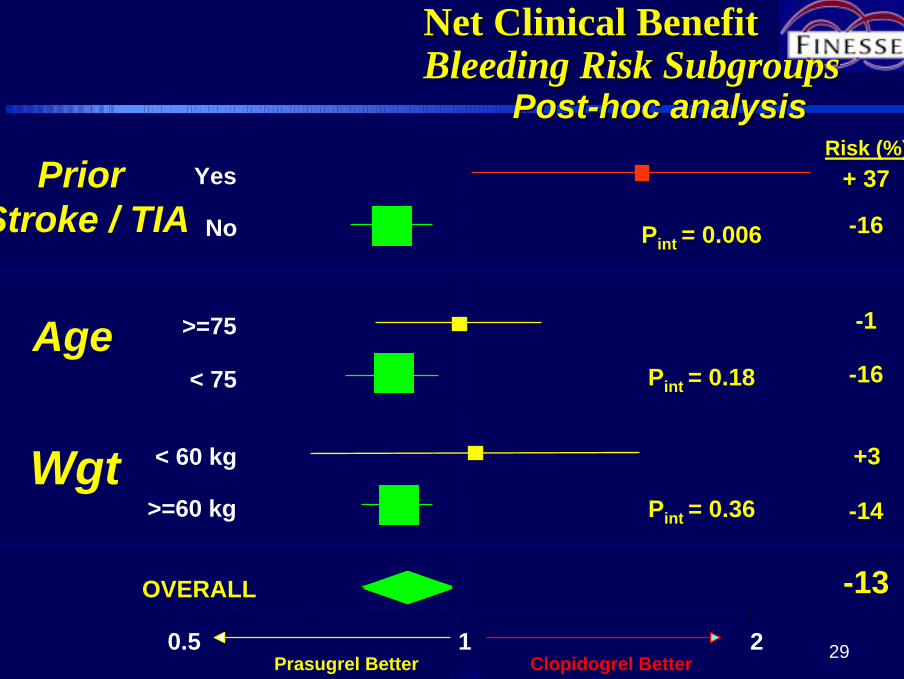
Net Clinical BenefitNet Clinical BenefitBleeding Risk SubgroupsBleeding Risk Subgroups
OVERALL
>=60 kg
< 60 kg
< 75
>=75
No
Yes
0.5 1 2
PriorStroke / TIA
Age
Wgt
Risk (%)+ 37
-16
-1
-16
+3
-14
-13
Prasugrel Better Clopidogrel BetterHR
Pint = 0.006
Pint = 0.18
Pint = 0.36
PostPost--hoc analysishoc analysis

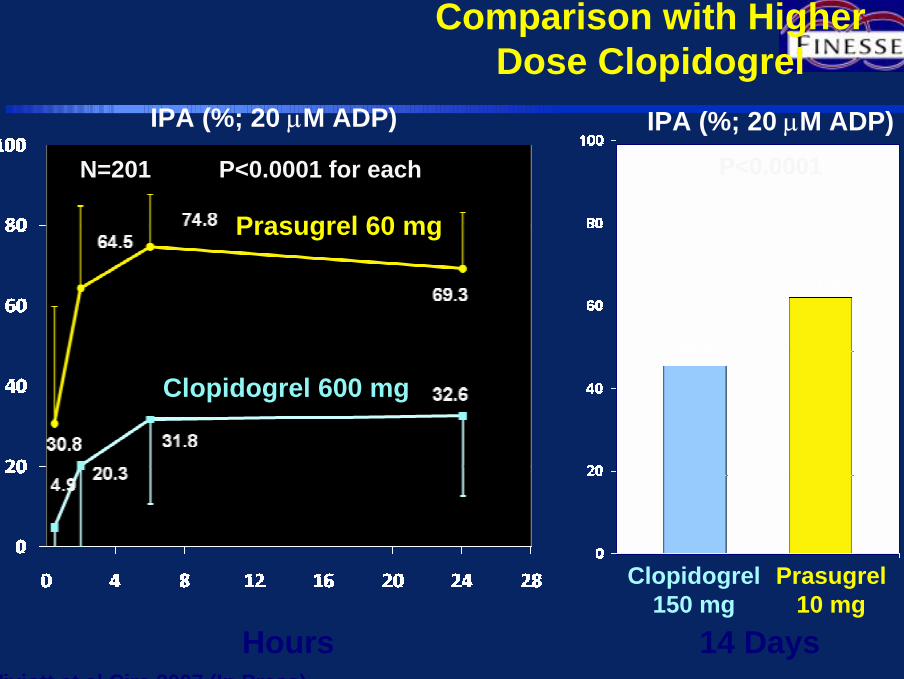
……. e se utilizzoClopidogrel ad alte dosi (600 / 150 mg) aumento IPA senza incrementare il rischio emorragico ?
31
Comparison with Higher Dose Clopidogrel
P<0.0001 for each
IPA (%; 20 µM ADP)
Hours 14 Days
IPA (%; 20 µM ADP)P<0.0001
Prasugrel10 mg
Clopidogrel150 mg
Wiviott et al Circ 2007 (In Press)
N=201
Prasugrel 60 mg
Clopidogrel 600 mg
32
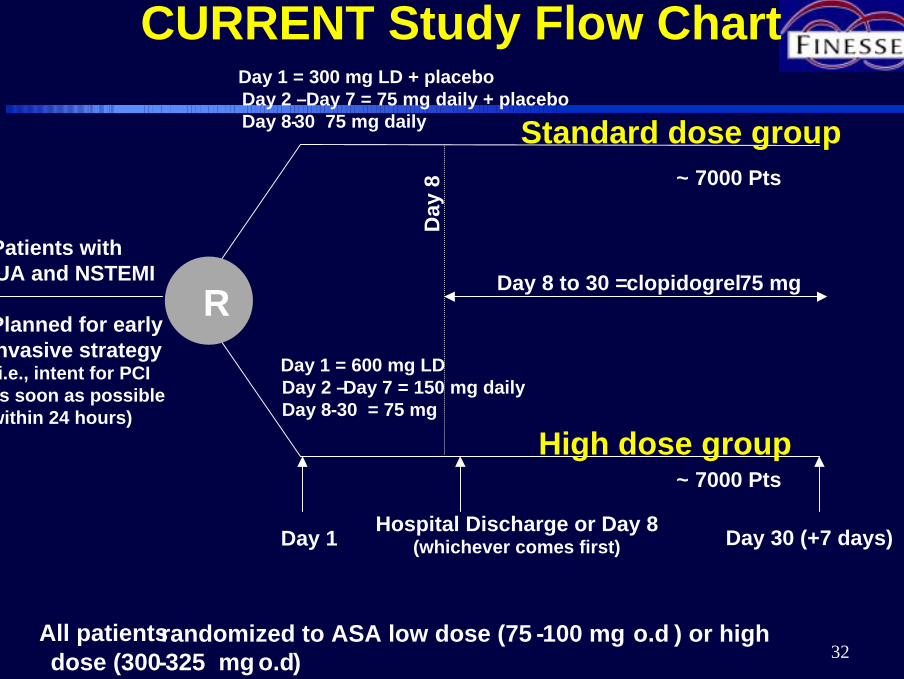
CURRENT Study Flow Chart
All patientsrandomized to ASA low dose (75 -100 mg o.d ) or high dose (300-325 mg o.d)
RPatients with UA and NSTEMI
Planned for early invasive strategy (i.e., intent for PCI as soon as possible within 24 hours)
Day 1 Hospital Discharge or Day 8 (whichever comes first) Day 30 (+7 days)
Day 1 = 600 mg LDDay 2 –Day 7 = 150 mg dailyDay 8-30 = 75 mg
Day 1 = 300 mg LD + placeboDay 2 –Day 7 = 75 mg daily + placebo Day 8-30 75 mg daily
Day
8
Day 8 to 30 = clopidogrel75 mg
High dose group
Standard dose group~ 7000 Pts
~ 7000 Pts
Scienziato non é colui che sa
dare le vere Risposte,
ma colui che sa porre le giuste
Domande
Claude Levi Strauss





























