Embed Size (px)
Citation preview
Cumming School of MEDICINE
Division of Rheumatology
CALGARY AND AREA
Specialist LINKLinking Physicians
|September,2017-1
CONFIRMATION: ReferralReceived
TRIAGECATEGORY: EnhancedPrimaryCarePathway:GoutREFERRALSTATUS: ACCEPTEDconsideractionsinthemedicalhomeasoutlinedbelowDearColleague,Theclinicalanddiagnosticinformationyouhaveprovidedfortheabove-namedpatientisconsistentwithadiagnosisofgout.ManypatientswithgoutcanbemanagedsuccessfullywithinthemedicalhomewithouttheneedforspecialistconsultationusingtheattachedEnhancedPrimaryCarePathway.Pleasefeelcomfortableinstartingthispatientonstandardtherapywhiletheywaittobeseen.Ifyoufeelthatconsultationisnolongerrequired,pleasecancelthereferral.Adefinitivediagnosisandlongtermtreatmentplanshouldbesoughtwhenevergoutissuspected.Somepatientsdorequirespecialistcare,particularlyiftheirpresentationisatypical,theyarenotrespondingtostandardtherapyortheyhavesignificantcomorbiditiessuchaschronicrenalfailure.ThisclinicalpathwayhasbeendevelopedbytheCalgaryZonePrimaryCareNetworksinpartnershipwiththeSectionofRheumatologyandAlbertaHealthServices.Theselocalguidelinesarebasedonbestavailableevidence,currentlocalresourcesandarepracticalintheprimarycaresetting.Thispackageincludes:
1. Focusedsummaryofgoutrelevanttoprimarycare2. Checklisttoguideyourin-clinicpatientreview3. Linkstoadditionalresourcesforthisspecificcondition4. Clinicalflowdiagramwithexpandeddetail
ThisreferralisACCEPTEDandanappointmenttimeispending.Thepatientwillbecontacteddirectlywithappointmentinformationonceavailable.Fornon-urgentrheumatologyadvicecallSpecialistLINKat403.910.2551ortoll-freeat1.844.962.5465available08:00-17:00weekdays.Thankyou,DivisionofRheumatology
PatientName: DateofReferral:
DateofBirth: ReferringMD:
CalgaryRHRN: Fax:
PHN/ULI: Today’sDate:
September,2017-2
EnhancedPrimaryCarePathway:Gout
1.FocusedsummaryofgoutrelevanttoprimarycareSignificance:Goutisachronic,progressive,inflammatorydiseaserequiringappropriatelong-termmanagement.Goutisincreasinginincidenceandprevalenceandisthemostcommoncauseofinflammatoryarthritisinmenover40yearsofage.Itisveryrareinpremenopausalwomen.Goutisacurablediseasethatisvastlyundertreatedworldwide,mainlyduetomisconceptionsregardingurateloweringtherapy,resultinginpermanentjointdamageanddisability.Pooradherencetotherapyiscommon,andpatientsrequireongoingeducationandmonitoring.Hyperuricemiaandgoutarestronglyassociatedwithhypertension,themetabolicsyndrome,renalimpairmentandcardiovasculardisease.ClinicalFeatures:Classicacutegouttypicallyaffectsonejointbutseveraljointscanalsobeinvolved.Themostcommonlyinvolvedareas(indecreasingfrequency)are:thefirstMTP(“podagra”),instep,ankle,heel,knee,wrist,fingersandelbow.Goutcanalsoaffectbursae,especiallyovertheelbows,kneesorAchillestendon.Theaffectedjointandsurroundingsofttissuesareexquisitelypainful,warm,redandswollen,andcanresemblecellulitis.Patientsmaynotbeabletotolerateevenabedsheettouchingtheaffectedjointandmaybeunabletowalk.Theattacksusuallylast3to10days,andpeelingoftheskinoverthejointmayoccurastheattackresolves.Withouturateloweringtherapy,theattacksmayincreaseinfrequency,involvemultiplejoints,persistlongeranddepositsofuricacidinthesofttissues(tophi)willoccur.Tophiarestronglyassociatedwithdestructiveanddeformingjointdisease.PotentialTriggersofGoutAttacks:
Diagnosis:Althoughthegoldstandardtestisidentificationofuricacidcrystalsinfreshsynovialfluidonpolarizedmicroscopy,thismaynotbefeasibleinsomepatients,orinaprimarycaresetting.Serumuricacidlevelscanbenormalduringanacutegoutattack,butwillbeelevatedatsomepointinalmostallgoutpatients.Althoughnotallhyperuricemicpatientshavegout,theriskofgoutishighwithpersistentserumuratelevels>580umol/L.X-raysareNOTusefulformakinganearlydiagnosisbeforepermanentdamageoccurs.DiagnosticdilemmasshouldbereferredtoRheumatology.Ifsynovialfluidanalysisisnotpossible,diagnosticalgorithmsmayhelptodeterminewhethertheprobabilityofgoutislow,intermediateorhigh.The“GoutDiagnosisCalculator”wasdevelopedforthispurpose(seeLinksbelowforfreeapp).Iftheprobabilityisintermediate,thepatientshouldbefollowedcloselyandsynovialfluidanalysisperformedwhenpossible.TheACR-EULARGoutClassificationCriteriaCalculator(seeLinksbelowforURL)isanotherhelpfuldiagnostictoolforgout.
Dietary Excessalcohol,purines(meat,seafood),fructose(soda,juice,energydrinks)Drugs/iatrogenic Diuretics,lowdoseASA,chemotherapy,radiationAcutemedicalillness Hemorrhage,infection,renalinsufficiency,dehydration,surgeryTrauma Injurytojoint(maybeminor)Endocrine Hypothyroidism,hyperparathyroidism
September,2017-3
2.Checklisttoguideyourin-clinicreviewofthispatientwithgoutsymptoms
o Isthehistoryconsistentwithtypicalgoutattacks?Considerusingdiagnostictool(seelinkbelow)
o Arethereanyredflagstosuggestinfection?
o Doesthepatienthaveahistoryofkidneystones,ortophionexamination?
o Arethereanypotentialgouttriggers,includinglifestylefactors?
o Reviewandtreatmodifiablecardiacriskfactors.
3.Linkstoadditionalresources
Forphysicians:
Diagnosticruleforgoutwithoutjointfluidanalysis: Download“GoutDiagnosisCalculator”freefromtheAppStoreorusetheonlinetoolat:https://www.mdcalc.com/acute-gout-diagnosis-rule
ClassificationCriteriaforGout(onlinetool)http://goutclassificationcalculator.auckland.ac.nz/
http://rheuminfo.com/diseases/gout(hasinformationforphysiciansandpatients)
www.goutinstitute.ca
https://www.niams.nih.gov/health_Info/Gout/default.asp
Forpatients:
www.rheuminfo.com/diseases/gout
www.gouteducation.org
http://www.albertahealthservices.ca/assets/info/nutrition/if-nfs-healthy-eating-for-managing-gout.pdf
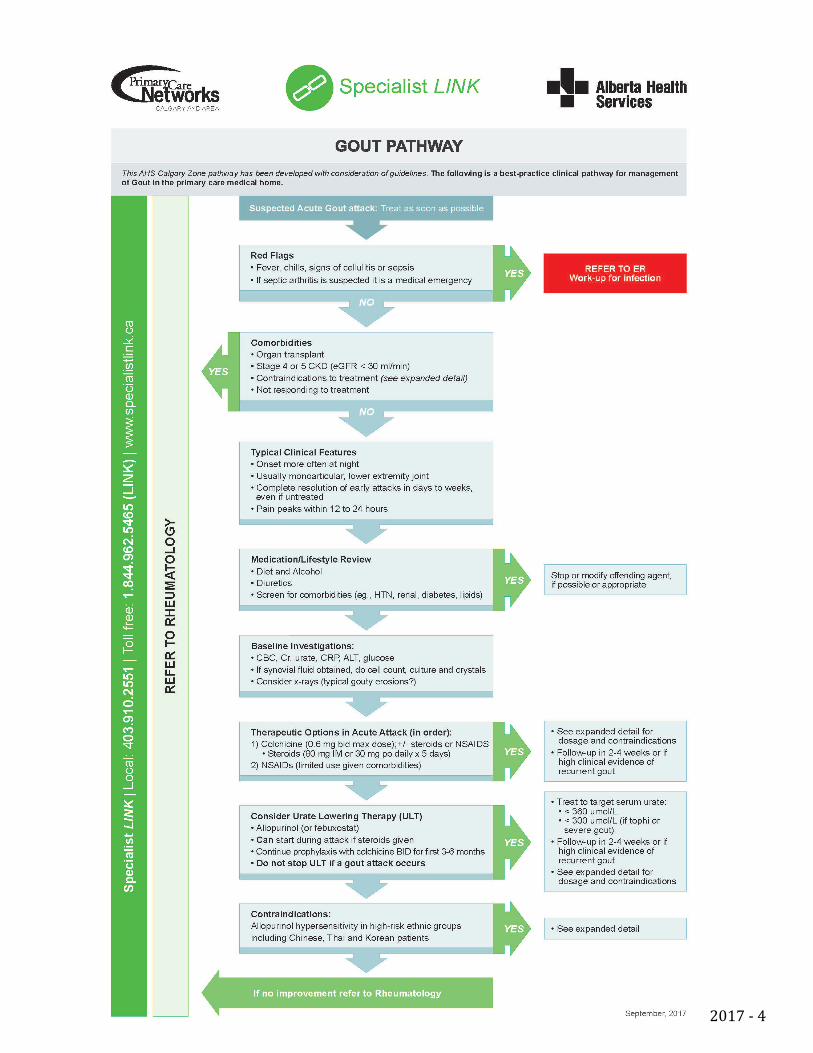
ThisAHSCalgaryZonepathwayhasbeendevelopedwithconsiderationofguidelines.Thefollowingisabest-practiceclinicalpathwayformanagementofGoutintheprimarycaremedicalhome.
4.SuspectedGoutPathway
September,2017-4
September,2017-5
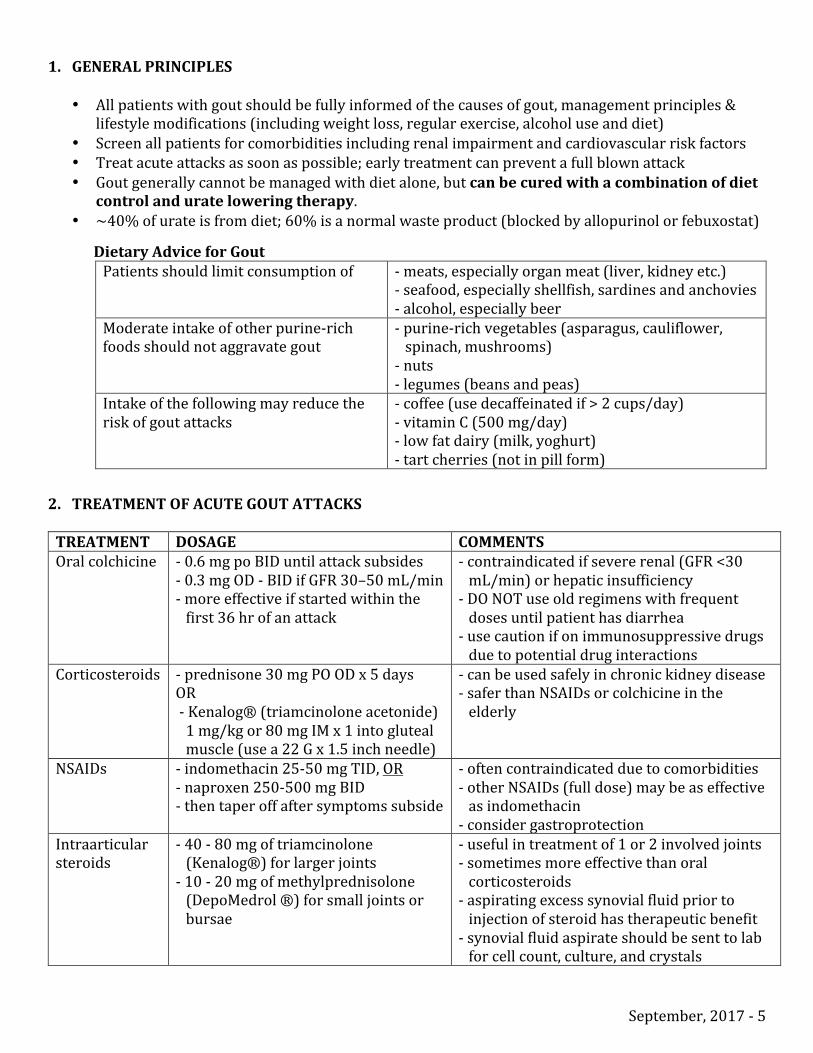
1. GENERALPRINCIPLES• Allpatientswithgoutshouldbefullyinformedofthecausesofgout,managementprinciples&
lifestylemodifications(includingweightloss,regularexercise,alcoholuseanddiet)• Screenallpatientsforcomorbiditiesincludingrenalimpairmentandcardiovascularriskfactors• Treatacuteattacksassoonaspossible;earlytreatmentcanpreventafullblownattack• Goutgenerallycannotbemanagedwithdietalone,butcanbecuredwithacombinationofdiet
controlandurateloweringtherapy.• ~40%ofurateisfromdiet;60%isanormalwasteproduct(blockedbyallopurinolorfebuxostat)
DietaryAdviceforGout
Patientsshouldlimitconsumptionof -meats,especiallyorganmeat(liver,kidneyetc.)-seafood,especiallyshellfish,sardinesandanchovies-alcohol,especiallybeer
Moderateintakeofotherpurine-richfoodsshouldnotaggravategout
-purine-richvegetables(asparagus,cauliflower,spinach,mushrooms)-nuts-legumes(beansandpeas)
Intakeofthefollowingmayreducetheriskofgoutattacks
-coffee(usedecaffeinatedif>2cups/day)-vitaminC(500mg/day)-lowfatdairy(milk,yoghurt)-tartcherries(notinpillform)
2. TREATMENTOFACUTEGOUTATTACKSTREATMENT DOSAGE COMMENTSOralcolchicine -0.6mgpoBIDuntilattacksubsides
-0.3mgOD-BIDifGFR30–50mL/min-moreeffectiveifstartedwithinthefirst36hrofanattack
-contraindicatedifsevererenal(GFR<30mL/min)orhepaticinsufficiency-DONOTuseoldregimenswithfrequentdosesuntilpatienthasdiarrhea-usecautionifonimmunosuppressivedrugsduetopotentialdruginteractions
Corticosteroids -prednisone30mgPOODx5daysOR-Kenalog®(triamcinoloneacetonide)1mg/kgor80mgIMx1intoglutealmuscle(usea22Gx1.5inchneedle)
-canbeusedsafelyinchronickidneydisease-saferthanNSAIDsorcolchicineintheelderly
NSAIDs -indomethacin25-50mgTID,OR-naproxen250-500mgBID-thentaperoffaftersymptomssubside
-oftencontraindicatedduetocomorbidities-otherNSAIDs(fulldose)maybeaseffectiveasindomethacin-considergastroprotection
Intraarticularsteroids
-40-80mgoftriamcinolone(Kenalog®)forlargerjoints-10-20mgofmethylprednisolone(DepoMedrol®)forsmalljointsorbursae
-usefulintreatmentof1or2involvedjoints-sometimesmoreeffectivethanoralcorticosteroids-aspiratingexcesssynovialfluidpriortoinjectionofsteroidhastherapeuticbenefit-synovialfluidaspirateshouldbesenttolabforcellcount,culture,andcrystals
September,2017-6
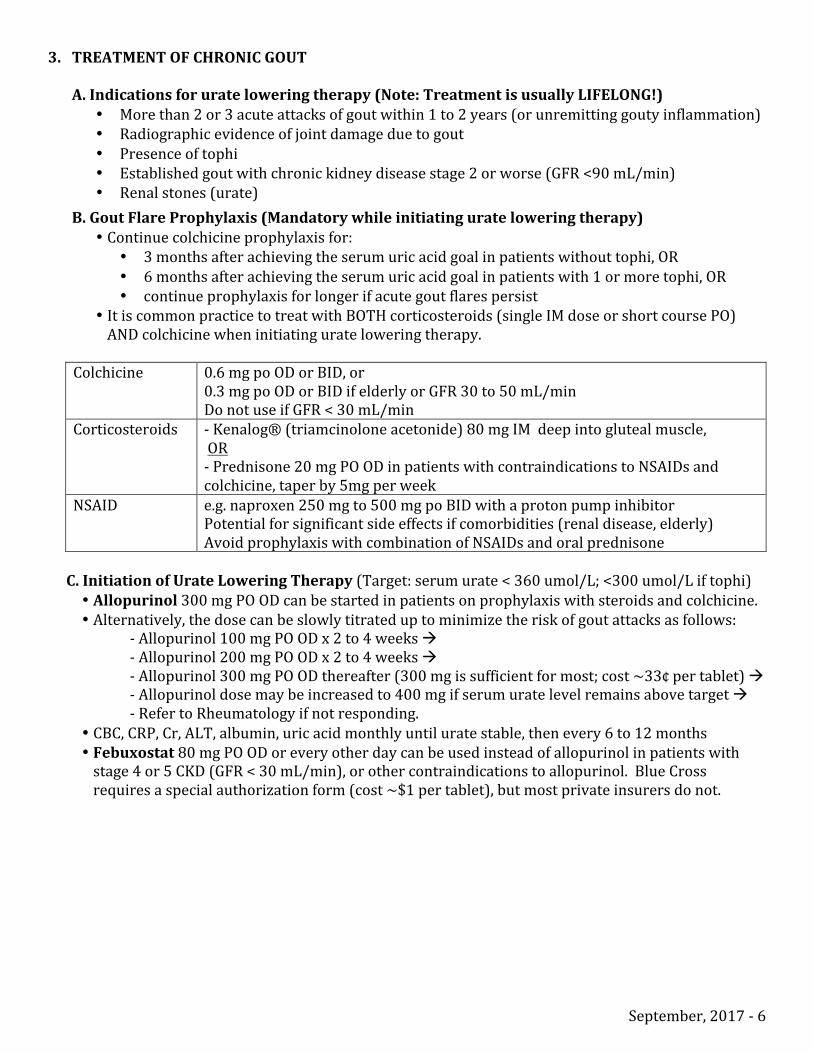
3. TREATMENTOFCHRONICGOUTA.Indicationsforurateloweringtherapy(Note:TreatmentisusuallyLIFELONG!)
• Morethan2or3acuteattacksofgoutwithin1to2years(orunremittinggoutyinflammation)• Radiographicevidenceofjointdamageduetogout• Presenceoftophi• Establishedgoutwithchronickidneydiseasestage2orworse(GFR<90mL/min)• Renalstones(urate)
B.GoutFlareProphylaxis(Mandatorywhileinitiatingurateloweringtherapy)• Continuecolchicineprophylaxisfor:
• 3monthsafterachievingtheserumuricacidgoalinpatientswithouttophi,OR• 6monthsafterachievingtheserumuricacidgoalinpatientswith1ormoretophi,OR• continueprophylaxisforlongerifacutegoutflarespersist
• ItiscommonpracticetotreatwithBOTHcorticosteroids(singleIMdoseorshortcoursePO)ANDcolchicinewheninitiatingurateloweringtherapy.
Colchicine 0.6mgpoODorBID,or
0.3mgpoODorBIDifelderlyorGFR30to50mL/minDonotuseifGFR<30mL/min
Corticosteroids -Kenalog®(triamcinoloneacetonide)80mgIMdeepintoglutealmuscle,OR-Prednisone20mgPOODinpatientswithcontraindicationstoNSAIDsandcolchicine,taperby5mgperweek
NSAID e.g.naproxen250mgto500mgpoBIDwithaprotonpumpinhibitorPotentialforsignificantsideeffectsifcomorbidities(renaldisease,elderly)AvoidprophylaxiswithcombinationofNSAIDsandoralprednisone
C.InitiationofUrateLoweringTherapy(Target:serumurate<360umol/L;<300umol/Liftophi)
• Allopurinol300mgPOODcanbestartedinpatientsonprophylaxiswithsteroidsandcolchicine.• Alternatively,thedosecanbeslowlytitrateduptominimizetheriskofgoutattacksasfollows:
-Allopurinol100mgPOODx2to4weeksà-Allopurinol200mgPOODx2to4weeksà-Allopurinol300mgPOODthereafter(300mgissufficientformost;cost~33¢pertablet)à-Allopurinoldosemaybeincreasedto400mgifserumuratelevelremainsabovetargetà-RefertoRheumatologyifnotresponding.
• CBC,CRP,Cr,ALT,albumin,uricacidmonthlyuntiluratestable,thenevery6to12months• Febuxostat80mgPOODoreveryotherdaycanbeusedinsteadofallopurinolinpatientswithstage4or5CKD(GFR<30mL/min),orothercontraindicationstoallopurinol.BlueCrossrequiresaspecialauthorizationform(cost~$1pertablet),butmostprivateinsurersdonot.

September,2017-7
4. CONTRAINDICATIONS/REASONSTOSTOPURATELOWERINGTHERAPYThevastmajoritywilltolerateallopurinolwell.Themostcommonconcernisan↑ingoutattacksduringinitiationoftreatment,suchthatgoutprophylaxisismandatory.DONOTstopallopurinolforagoutattack.Allopurinolandfebuxostatshouldnotbeusedinpatientsonazathioprine(Imuran®)duetotheriskofbonemarrowfailure(refertorheumatology).Patientswithallopurinolhypersensitivity(rash,fever,↓platelets,↑liverenzymes)shouldstopimmediatelyandnevertakethisdrugagain.
HLA-B*58:01TESTINGFORETHNICGROUPSATRISKFORHYPERSENSITIVITYREACTIONSChinese,ThaiandKoreanpatientsareatriskforlife-threateningallopurinolhypersensitivityreactions.HLA-B*5801screeningshouldbeconsideredinthesepatientsbeforestartingallopurinol,andifpositiveallopurinolshouldnotbeused.ThisgenetictestcanbeorderedthroughCLS.High-riskindividualsshouldbetreatedwithfebuxostatinstead.
TheGoutEnhancedPrimaryCarePathwaywasdevelopedbythefollowingindividualsincollaborationwiththeCalgaryZonePrimaryCareNetworks,theDivisionofRheumatology,andAlbertaHealthServices:
SusanBarrMD,MSc,FRCPCAssociateProfessorofMedicineSectionofRheumatology
PaulMacMullanMD,MBBChBAO,MRCPIClinicalAssociateProfessorSectionofRheumatology
MonicaSargiousMD,CCFP,FCFPSectionChiefCommunityPrimaryCareDepartmentofFamilyMedicineAlbertaHealthServices–CalgaryZone
OliverDavidMD,CCFPMedicalDirector,MosaicPrimaryCareNetwork