-
8/4/2019 Lip Piercing
1/5
JCDAwww.cda-adc.ca/jcda May 2007, Vol. 73, No. 4 327
Clinicalp r a c t i c E
ContactAuthor
Body piercing is a cultural practice ortradition in various
civilizations dating
back to antiquity. In recent years, body
piercing has become increasingly ashionable
or purely esthetic reasons, and the practice
cuts across all sectors o society. Te emer-gence o oral
piercing, especial ly among young
adults, is o concern to dental and medical
proessionals because o the risks and com-
plications or oral, dental and general health.
Intraoral piercings involve the tongue, whileperioral piercings
involve the lips, the cheeks
and, to a lesser extent, the uvula and therenum. Among those
with non-traditional
body piercings, the tongue is the most preva-
lent site ollowed by the lips.1 Since the rst
warnings by Chen and Scully in 19922 o therisks and
complications associated with oral
piercings, an increasing number o studies on
this issue have been published. Risks and com-
plications (Box 1) are diverse and range rom
temporary inconveniences related to the pres-ence o the
jewellery in the mouth, to gingival
recession and severe systemic inections.
In this article, we present a brie reviewo the current
literature on potential compli-cations and adverse consequences o
tongueand lip piercings. Our objective is to provide
a general overview o possible problems thatmay be encountered by
dentists. In addition,we highlight the urgent need or dentists
and
doctors to inorm target patients o the risksassociated with oral
piercings.
OralPiercingProcedures
Te tongue is usually pierced at the mid-
line, typically in the median lingual sulcus,although piercings
may also be perormed onthe dorsolateral lingual surace anterior to
the
lingual renum. Te principal type o jewelleryused in tongue
piercings is barbells, whichconsist o a bar with a ball screwed
onto each
end. Lip piercings are mainly perormed onthe middle portion o
the lower lip, but mayalso be near the commissura and on the
lower
lip near the canines. Labrets, with the fatend on the mucosal
side o the lip, as well asrings and barbells, are commonly used or
lip
Dr. Grenier
Email:[email protected]
Overview of Complications Secondaryto Tongue and Lip
Piercings
Lo-Franois Maheu-Robert, DMD; Elisoa Andrian, PhD; Daniel
Grenier, PhD
ABSTRACT
In recent years, intraoral and perioral piercings have grown in
popularity among teen-
agers and young adults. This is of concern to dental and medical
professionals because
of the risks and complications for oral, dental and general
health. The risks and compli-
cations associated with tongue and lip piercings range from
abnormal tooth wear and
cracked tooth syndrome to gingival recession and systemic
infections. In this report, we
provide an overview of possible problems associated with oral
piercings that may beencountered by dentists.
For citation purposes, the electronic version is the definitive
version of this article:
www.cda-adc.ca/jcda/vol-73/issue-4/327.html
mailto:[email protected]:[email protected]:[email protected]:[email protected]:[email protected]
-
8/4/2019 Lip Piercing
2/5
328 JCDAwww.cda-adc.ca/jcda May 2007, Vol. 73, No. 4
Grenier
piercings. Aer the piercing procedure, regular rinsing
with warm salt water or antiseptic mouthwash is sug-
gested, and smoking and alcoholic beverages should be
avoided. It is generally recommended that the jewellery
not be removed or a long period to prevent the piercing
site rom closing spontaneously. However, once healing
is complete, the jewellery should be removed daily andcleaned
and brushed thoroughly to maintain good oral
hygiene and avoid plaque and calculus build-up. In a
recent survey, De Moor and others3 reported that most
patients never remove their jewellery or cleaning.
Piercing procedures are usually perormed without
anesthesia by unlicensed, non-medical people, who
are oen sel-trained and have little knowledge o the
anatomy o the intraoral and perioral area; serious med-
ical conditions, such as heart valve disease and bleeding
disorders; sterilization procedures; or prevention o com-
plications ollowing piercing.4
MucosalInjury
Because o its extreme vascularity and its location in
the upper airway, the tongue is particularly vulnerable to
complications, which are diverse and range rom minor
to potentially lie-threatening. Oral and dental complica-
tions associated with tongue piercings are categorized
as acute (early) or chronic (late).5 Acute complications
typically arise within 24 hours ollowing insertion o
the jewellery into the tongue and are usually conned to
injuries o weak tissues.3 Te most common immediate
acute symptoms include pain, swelling, bleeding and
localized inection.4,6 Potential complications that occur
within weeks o the piercing include unctional prob-lems, such as
dysphonia, dysphagia, intererence with
mastication and the generation o galvanic currents
between the barbell and metallic dental
restorations.3,7Hypersensitivity reactions, known as allergic
contact
dermatitis, to the metal when jewellery is not o thebest quality
or contains nickel have been reported. 8 Lesscommon acute symptoms
include increased salivary fow
rates. Irritation o the skin around the jewellery inserted
into the lower lip has been shown to be related to
contactallergy and to saliva fowing through the pierced site.9
In
most cases, these complications have not been detrimental
and tend to disappear with time. However, more seriousand
potentially lie-threatening complications have been
reported, including prolonged bleeding,1012 inections,
disease transmission and airway problems secondary toswelling o
the tongue.10,13,14 Finally, the potential risk o
aspiration or inhalation o parts o the jewellery i theycome
loose should not be overlooked.1,3,4
RiskofHemorrhage
Although in 1977 Boardman and Smith1 stated thatbleeding is not
the most requent complication o tongue
piercings, prolonged bleeding is o great concern in med-
ically compromised patients. During the piercing process,blood
vessels may be torn and vascular nerves damaged.
Hardee and others11 reported a signicant loss o blood
rom hemorrhage ollowing a tongue piercing, whichresulted in
hypotensive collapse. Prolonged bleeding,
hematomas and disturbed wound healing have also beenreported
ollowing lip piercings.3 Because o the signi-cant complications
that may arise when hemorrhage oc-
curs, intraoral and perioral piercings should be regulated
by licensing piercing establishments. Hardee and others11have
suggested that all establishments should be given
documentation on potential problems and the manage-
ment o bleeding. Furthermore, a systematic review othe customers
medical history beore the piercing pro-
cedure should be recommended to rule out a history o a
bleeding disorder.12
LocalizedTissueOvergrowthAmong later complications ollowing oral
piercings,
traumatic injuries to the mucosal suraces at the pier-
cing site have been documented. Tese include enlarge-
ment o the piercing hole,4 chemical burns associatedwith
excessive aercare,15 paresthesia,6 sialadenitis,16
lymphadenitis,1719 sarcoid-like oreign-body reactions,20
granulomas and scar tissue ormation at the piercingsite aer the
removal o a labret or barbell. 3,9 Moreover,
barbell shanks that are too short may lead to localized
tissue overgrowth, with the mucosal surace o the tonguehealing
over the barbell.21 Lingual piercings that become
Airway compromise
Allergic reaction to metal
Bleeding and risk o hemorrhage
Galvanism
Gingival recession
Hyperplasic and scar tissue ormation
Increased salivary fow
Inhalation o the jewellery
Intererence with radiographic images
Intererence with speech, chewing and swallowing
Localized and systemic inections
Nerve damage and paresthesia
Pain
Swellingooth racture or chipping
Box1 Risks and complications associated with oralpiercings
-
8/4/2019 Lip Piercing
3/5
JCDAwww.cda-adc.ca/jcda May 2007, Vol. 73, No. 4 329
Oral Piercings
embedded (buried) in the ventral5 or dorsal surace o thetongue
have been reported.21,22 In contrast, an excessivelylong shank
(long-stem barbell) may allow the barbell tomove in the tissue,
which may lead to an infammatoryhyperplastic tissue reaction1 and
the accumulation odental plaque and calculus on the
shank.1,3,4,23
Intraoral piercings have also been implicated in theormation o
hypertrophic keloid tissue.23,24 Keloid lesionsare ormed when
unaected tissue inltrates the piercing;they are characterized by
the production o an interstitialmucinous material on the collagen o
connective tissue.In the episodic case o keloid or hypertrophic
tissuewithout any signs o inection reported by Neiburger,23an
improvement in the patients oral hygiene and a re-duction in the
size o the barbell shank resulted in asignicant improvement, but
did not completely resolvethe lesion. In most reported cases o
tissue prolierationollowing tongue piercings, surgical
interventions were
not required and complete healing occurred ollowingremoval o the
jewellery.23,24
DentalTrauma
raumatic injuries to the hard dental tissue have beendirectly
associated with jewellery. ongue piercings arethe most commonly
reported cause o damage to thedentition. In 1997, DiAngelis25 rst
suggested that tonguepiercings may result in abnormal tooth wear
(abrasion)that may lead to cold sensitivity in the lower rst
molarteeth caused by cracked-tooth syndrome.
eeth may be injured during speaking or masticatingor by biting
the barbell or hitting it against the teeth.Injuries to the teeth
are usually limited to the enamel orthe dentin but may also involve
the pulp. 7,26,27 Based onpublished case reports, Campbell and
others5 reportedthat ractures o the posterior teeth, including
molarsand premolars, are requently caused by tongue
jewellery.Physical damage to the dentition may occur within therst
year o use o the device, especially i the long-shankbarbell used or
initial placement is not replaced aer 2weeks.27,28 A positive
correlation between the duration owear and the occurrence o trauma
to posterior teeth hasbeen demonstrated.5 Other actors contributing
to toothractures ollowing tongue piercing include habitual
biting or chewing o the device, barbell stem length, thesize o
the ornament attached to the barbell and the typeo material used in
it.
Te restorative method used or a tooth traumatizedby tongue
jewellery depends on the individual case.Restorative approaches
compatible with the existingtongue jewellery must be considered to
increase theirclinical longevity.29 Porcelain onlays, or example,
are notsuitable in the presence o barbell tongue ornaments be-cause
o the brittle nature o porcelain and its low resist-ance to
impact.30 Porcelain crowns may also be chippedby tongue jewellery.
Tus, patients should be advised to
remove the oral jewellery permanently or to replace metal
balls with non-metallic ones. Recently, so rubber ends
and acrylic screw caps have become available and are
considered less likely to cause tooth chipping.
GingivalTrauma
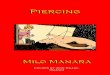
Increasing numbers o case reports have pointed to
oral piercings as a signicant actor in gingival trauma
(Fig. 1). Te nature, extent and severity o mucogingival
deects are usually categorized using Millers classica-
tion o marginal tissue recession.31 Gingival recession has
been especially correlated with lip studs or labrets1,3,7,17
and requently occurs on the labial aspect o the lower
central incisors.3,5,9,17,28,32,33 Gingival recession,
particularly
on the lingual aspect o the mandibular anterior teeth,
has also been associated with tongue
jewellery.3,5,7,16,32,34
A positive correlation has been demonstrated between
the prevalence o gingival recession due to tongue and lip
piercing and duration o wear.5,33 According to Campbell
and others,5 lingual recession o gingiva is observed aer
2 years o wear. Long-stem barbells signicantly increase
the prevalence o lingual recession. Recently, Leichter
and Monteith33 reported an increased incidence and se-
verity o buccal recession with lip piercing and duration
o wear.
Jewellery-associated recession requently develops
as a narrow, cle-like deect on the lingual and buccal
aspects o the mandibular incisors, 32 with recession
depths o 23 mm or more oen extending to or beyond
the level o the mucogingival junction.5 Patients with
oral jewellery may also be at risk o developing signi-
cant loss o periodontal attachment that may lead to
tooth loss.32 Severe attachment loss can develop even
when gingival recession is minimal.5 Because attach-
ment loss may escape detection,5,32,35 regular checks o
the periodontium and examinations or gingival reces-
sion, especially on the lingual aspect o the anterior teeth,
are recommended or patients with oral piercings or a
history o oral piercings.5,35
Figure1: Localized gingival recession due tothe presence of lip
piercing.
-
8/4/2019 Lip Piercing
4/5
330 JCDAwww.cda-adc.ca/jcda May 2007, Vol. 73, No. 4
Grenier
LocalizedInfections
Because piercings invade the subcutaneous tissues,
they have an inherently high potential or inectious
complications. During piercing procedures, inection
control standards, which include the use o disposable
gloves, sterile or disposable instruments and sterilized
jewellery, should be ollowed. However, as body pier-
cing remains largely unregulated, it is oen perormed
without adequate cross-inection protection and hygiene
measures. Tus, oral piercing customers are at high risk
o developing localized and generalized systemic
inections.
Inections are the most common generalized compli-
cation o tongue piercings.6,13 One recent report estimated
a 20% inection rate with intraoral piercing.36 Te ac-
cumulation o dental biolm and calculus at pierced sites
may promote the development o inections.10 reatment
includes improving oral hygiene with the use o antiseptic
oral cleanser, the administration o adequate antibiotic
therapy and surgical drainage and incision o abscess.
SystemicInfections
Te open wound at the pierced site may also be a
source o systemic inectious complications as it may
allow microorganisms to enter the bloodstream. Tis may
lead to subsequent inection o other organs by microor-
ganisms inhabiting the oral cavity. Recurrent bacteremias
may constitute a threat long aer tongue piercing, espe-
cially in immunocompromised people.37
Rheumatic heart disease, congenital deormities,hypertrophic
cardiomyopathy, mitral valve prolapse as-
sociated with murmur and mitral calcication have been
cited as predisposing actors. Inective endocarditis may
be caused by metastatic oral bacteria. Once bacteria have
entered the bloodstream, the subsequent colonization o
the endocardium typically aects valves with congenital
or acquired dysunction. Inective bacterial endocard-
itis ollowing body piercing is relatively rare. However,
over the past ew years, an increasing number o case
reports have described episodes o inective endocarditis
ollowing tongue piercings.3740 A recent survey investi-
gating the practice o tongue piercing revealed that ewpiercers
are aware o the risk o bacterial endocarditis in
certain categories o people.4
o avoid the serious sequelae o these inections, pa-
tients at risk o endocarditis should receive preventive
antibiotics beore the piercing procedure just as those
at high risk o complications receive antibiotic treat-
ment beore invasive dental procedures.41 Although rela-
tively rare, other serious lie-threatening complications,
such as the development o cerebral brain abscesses 42
and Ludwigs angina,43 as a result o inections ollowing
tongue piercings have been described.
Inadequate aseptic surgical techniques and inappro-priate
instrument sterilization during piercing proced-ures may
signicantly increase the incidence o inectiousdisease
transmission.Although no statistical studies as-sessing the
potential risks o inectious disease trans-mission ollowing oral
piercing have been reported, the
National Institutes o Health identied piercing proced-ures as a
possible means o transmission o bloodborne viruses, such as
hepatitis and human immunodeciencyvirus.44 Hepatitis B and C are
the most common virusestransmitted by body piercing.45 Many have
suggested thatoral piercing may allow transmission o human
immuno-deciency virus, although no reports have appeared inthe
literature.
Conclusion
ongue and lip piercings represent a signicant riskor direct and
indirect damage to so and hard oral tis-
sues. Although much less prevalent, lethal systemic inec-tions
may also occur. Considering the growing popularityo intraoral and
perioral piercings, dental proessionalsshould be aware o the
potential complications associatedwith this practice and be able to
identiy those at highrisk or adverse outcomes. ogether with parents
andeducators, dental proessionals should play an active rolein
warning patients o the serious consequences o oralpiercing and
should provide appropriate guidance. a
THE AUTHORS
Dr. Maheu-Robertis a dentist at the Basse-Cte-Nord HealthCentre,
Lourdes-de-Blanc-Sablon, Quebec.
Dr. Andrian is a ormer PhD student in the Oral EcologyResearch
Group, aculty o dentistry, Laval University,Quebec City,
Quebec.
Dr. Grenier is proessor in the aculty o dentistry and dir-ector
o the Oral Ecology Research Group, Laval University,Quebec City,
Quebec.
Correspondence to: Dr. Daniel Grenier, Oral Ecology Research
Group,Faculty o Dentistry, Laval University, Quebec City, QC G1K
7P4.
Te authors have no declared fnancial interests.
Tis article has been peer reviewed.
References1. Boardman R, Smith RA. Dental implications of oral
piercing. J Calif Dent
Assoc1997; 25(3):2007.
2. Chen M, Scully C. Tongue piercing: a new fad in body ar t. Br
Dent J1992;172(3):87.
3. De Moor RJ, De Witte AM, Delme KI, De Bruyne MA, Hommez
GM,Goyvaerts D. Dental and oral complications of lip and tongue
piercings.Br Dent J2005; 199(8):5069.
-
8/4/2019 Lip Piercing
5/5
JCDAwww.cda-adc.ca/jcda May 2007, Vol. 73, No. 4 331
Oral Piercings
4. Stead LR, Williams JV, Williams AC, Robinson CM. An
investigation intothe practice of tongue piercing in the South West
of England. Br Dent J2006; 200(2):1037.
5. Campbell A, Moore A, Williams E, Stephens J, Tatakis DN.
Tongue pier-cing: impact of time and barbell stem length on lingual
gingival recessionand tooth chipping.J Periodontol2002;
73(3):28997.
6. Farah CS, Harmon DM. Tongue piercing: case report and review
of currentpractice. Aust Dent J1998; 43(6):3879.
7. De Moor RJ, De Witte AM, De Bruyne MA. Tongue piercing and
associatedoral and dental complications. Endod Dent Traumatol2000;
16(5):2327.
8. Abramovits W, Stevenson LC. Hand eczema in a 22-year-old
woman withpiercings. Proc (Bayl Univ Med Cent) 2004;
17(2):2113.
9. Venta I, Lakoma A, Haahtela S, Peltola J, Ylipaavalniemi P,
Turtola L. Oralpiercings among first-year university students. Oral
Surg Oral Med OralPathol Oral Radiol Endod2005; 99(5):5469.
10. Shacham R, Zaguri A, Librus HZ, Bar T, Eliav E, Nahlieli O.
Tongue piercingand its adverse effects. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod2003; 95(3):2746.
11. Hardee PS, Mallya LR, Hutchison IL. Tongue piercing
resulting in hypoten-sive collapse. Br Dent J2000;
188(12):6578.
12. Rosivack RG, Kao JY. Prolonged bleeding following tongue
piercing: acase report and review of complications. Pediatr
Dent2003; 25(2):1546.
13. Keogh IJ, OLeary G. Serious complication of tongue
piercing.J LaryngolOtol2001; 115(3):2334.
14. Trachsel D, Hammer J. A vote for inhaled adrenaline in the
treatment ofsevere upper airway obstruction caused by piercing of
the tongue in heredi-tary angioedema. Intensive Care Med1999;
25(11):13356.
15. Knevel RJ, Kuijkens A. Tongue piercing: part I. Int J Dent
Hyg 2004;2(2):98100.
16. Soileau KM. Treatment of a mucogingival defect associated
with intra-oral piercing.J Am Dent Assoc2005; 136(4):4904.
17. Kieser JA, Thomson WM, Koopu P, Quick AN. Oral piercing and
oraltrauma in a New Zealand sample. Dent Traumatol2005;
21(5):2547.
18. Zaharopoulos P. Fine-needle aspiration cy tology in lesions
related to orna-mental body procedures (skin tattooing, intraoral
piercing) and recreationaluse of drugs (intranasal route). Diagn
Cytopathol2003; 28(5):25863.
19. Dyce O, Bruno JR, Hong D, Silverstein K, Brown MJ, Mirza N.
Tonguepiercing. The new rusty nail? Head Neck2000; 22(7):72832.
20. Ng KH, Siar CH, Ganesapillai T. Sarcoid-like foreign body
reaction inbody piercing: a report of two cases. Oral Surg Oral Med
Oral Pathol Oral
Radiol Endod1997; 84(1):2831.21. Theodossy T. A complication of
tongue piercing. A case report and re-view of the literature. Br
Dent J2003; 194 (10):5512.
22. Lopez-Jornet P, Camacho-Alonso F, Pons-Fuster JM. A
complication oflingual piercing: a case report. Oral Surg Oral Med
Oral Pathol Oral RadiolEndod2005; 99(2):E1819.
23. Neiburger E. A large hypertrophic-keloid lesion associated
with tonguepiercing: case report. Gen Dent2006; 54(1):467.
24. Dunn WJ, Reeves TE. Tongue piercing: case report and ethical
overview.Gen Dent2004; 52(3):2447.
25. DiAngelis AJ. The lingual barbell: a new etiology for the
cracked-toothsyndrome. J Am Dent Assoc1997; 128(10):14389.
26. Brennan M, OConnell B, OSullivan M. Multiple dental
fractures fol-lowing tongue barbell placement: a case report. Dent
Traumatol 2006;22(1):413.
27. Ram D, Peretz B. Tongue piercing and insertion of metal
studs: threecases of dental and oral consequences.ASDC J Dent
Child2000; 67(5):3269, 302.
28. Chambrone L, Chambrone LA. Gingival recessions caused by lip
piercing:case report. Dent Assist2004; 73(5):14, 167, 19.
29. Bassiouny MA, Deem LP, Deem TE. Tongue piercing: a
restorative per-spective. Quintessence Int2001; 32(6):47781.
30. Lesser R. Tongue piercing: a restorative perspective? Todays
FDA 2003;15(11):178.
31. Miller PD Jr. A classification of marginal tissue recession.
Int J PeriodonticsRestorative Dent1985; 5(2):813.
32. Brooks JK, Hooper KA, Reynolds MA. Formation of mucogingival
defectsassociated with intraoral and perioral piercing: case
reports. J Am Dent
Assoc2003; 134(7):83743.
33. Leichter JW, Monteith BD. Prevalence and risk of traumatic
gingival re-cession following elective lip piercing. Dent
Traumatol2006; 22(1):713.
34. Kretchmer MC, Moriarty JD. Metal piercing through the tongue
and local-ized loss of attachment: a case report. J
Periodontol2001; 72(6):8313.
35. Knevel RJ. Tongue piercing: part II. Int J Dent Hyg 2004;
2(3):1456.
36. McGeary SP, Studen-Pavlovich D, Ranalli DN. Oral piercing in
athletes:implications for general dentists. Gen Dent2002;
50(2):16872.
37. Lick SD, Edozie SN, Woodside KJ, Conti VR. Streptococcus
viridans endo-carditis from tongue piercing.J Emerg Med2005;
29(1):579.
38. Tronel H, Chaudemanche H, Pechier N, Doutrelant L, Hoen B.
Endocarditis
due to Neisseria mucosaafter tongue piercing. Clin Microbiol
Infect2001;7(5):2756.
39. Akhondi H, Rahimi AR. Haemophilus aphrophilus endocarditis
aftertongue piercing. Emerg Infect Dis 2002; 8(8):8501.
40. Friedel JM, Stehlik J, Desai M, Granato JE. Infective
endocarditis afteroral body piercing. Cardiol Rev2003;
11(5):2525.
41. Dajani AS, Taubert KA, Wilson W, Bolger AF, Bayer A,
Ferrieri P,and others. Prevention of bacterial endocarditis.
Recommendations by theAmerican Heart Association. JAMA 1997;
277(22):1794801.
42. Martinello RA, Cooney EL. Cerebellar brain abscess
associated withtongue piercing. Clin Infect Dis 2003;
36(2):e324.
43. Perkins CS, Meisner J, Harrison JM. A complication of tongue
piercing.Br Dent J1997; 182(4):1478.
44. Management of Hepatitis C. National Institutes of Health.
ConsensusDevelopment Conference Statement, March 2426, 1997.
Available fromURL:
www.consensus.nih.gov/1997/1997HepatitisC105html.htm (accessed
March 12, 2007).45. Tweeten SS, Rickman LS. Infectious
complications of body piercing. ClinInfect Dis 1998;
26(3):73540.