Embed Size (px)
Citation preview

Lipid Peroxidation in Bronchial Asthma
Anita Sharma, Satish Bansal and R.K. NagpaP
Departments of Pediatrics and IBiochemistry, Pt. B.D. Sharma Postgraduate Institute of Medical Sciences, Rohtak, Haryana, India.
Abstract. Objective : To study the levels of free oxygen radicals in children with bronchial asthma during an attack and symptom free interval. Methods : Serum Malondiadehyde (MDA) levels were studied in 25 children between the age of 6 years-14 years who presented with an acute attack of bronchial asthma. In each patient, serum MDA levels were measured at the time of admission, 24-48 hours after good response to treatment and after a symptom free interval of 3 weeks. Results were compared with control group. Results : In study group serum MDA levels were highest at the time of admission, which decreased significantly at 24-48 hours with treatment. After a 3 weeks symptom free interval serum MDA levels had decreased further but were still higher than healthy control group. Conclusion : Lipid peroxidation is increased in bronchial asthma dudng an acute attack and symptom free period. [Indian J Pedlatr 2003; 70 (9) : 715-717] E-mail: [email protected]
Kay words : Free oxygen radicals; MDA; Bronchial asthma
Free oxygen radicals have been incriminated as the causative agent in a number of diseases including bronchial asthma. TM Although all the tissues in the body are vulnerable, by virtue of its location, anatomy and functions the epithelial tissue of the lung is the most vulnerable,5~because lung is exposed to oxidants of ambient air 7 and also to those which are generated by inflammatory cells on the epithelial surface. 14~
Bronchial asthma is defined as a chronic inflammatory disorder of airways in which bronchial mucosa is infilterated by a number of inflammatory cells. 8 These cells secrete a number of chemicals including free oxygen radicals which are responsible for chronic inflammation and increased hyper-responsiveness of airways. 14~
Free oxygen radicals can cause widespread damage of all biological membranes by attacking their proteins, lipids, nucleic acids and glycoconjugates. Lipid peroxidation is the oxidation process of polyunsaturated fatty acids present in the cell membrane which yields peroxide radicals-lipid hydroperoxides and aldehyde products such as Malondialdehyde (MDA). These products in turn enhance the vascular permeability and leucocyte chemotaxis and alter the prostaglandin synthesis and histamine release thus perpetuat ing inflammation2 -1~ Lipid peroxidation and degradation products formed by free radicals are an important measures of a ongoing oxidative damage. Serum MDA estimation is an important method to determine this ongoing lipid peroxidation and therefore oxidative damage. H
In view of the scanty literature on the status of lipid
Reprint requests : Dr. Anita Sharma, 39/9J Medical Campus, Rohtak-124 001, Haryana.
peroxidation by measuring serum MDA during an acute attack and in symptom free period of bronchial asthma this study was planned.
MATERIALS AND METHODS
Twenty five children (Group I) of either sex between the age group of 7-14 years, who presented in acute attack of bronchial asthma as per classification of International Pediatric Asthma Consensus group were taken. For each patient, serum MDA levels were measured thrice : (la) at the time of presentation, (lb) after 24--48 hours, when the acute attack was well controlled by standard treatment and (lc) lastly after a symptom free intervals of 3 weeks and ensuring that patient was off bronchodilators and steroids for at least 7 days prior to estimation of serum MDA levels.
Guidelines of International Pediatric Asthma Consensus groups were followed for the diagnosis, treatment and assessing the response of treatment. 8
Exclusion Cr i t e r i a : Children who had received any bronchodilator therapy six hours before reporting to hospital, smokers, suspected foreign body inhalation and ~tildren with associated pneumonia were exluded from study.
Control group (Group ]I) comprised of 25 age matched children, who had been hospitalized for elective surgery and had no symptoms suggestive of bronchial asthma presently or in the past. Only one serum MDA level estimation was done in them.
All the children who fulfilled the inclusion criteria were enrolled after a written consent from parents. A detailed history and physical examination were carried out. In the s tudy group, laboratory test including
Indian Joumal of Pediatrics, Volume 70--September, 2003 715
Anita Sharma et al
complete hemogram, total eosinophil count, X-ray chest PA, Mantoux test, stool and ur ine examina t ion was carded out and was approved by the Postgraduate Board of Studies of the Institution.
Method of MDA Estimation : 5 ml venous blood was taken for estimation. Malondialdehyde (MDA) level was estimated by the method of Placer et at22 The test is based on the principle that Thiobarbituric acid (TBA) reacts with MDA to form a stable p ink co lour wh ich has an absorp t ion ma x im um at 535 nm and 548 nm, and is estimated by calorimeter. Because of its simplicity and sensitivity the TBA method is the most widely used test for lipid peroxidation.
RESULTS
S
U M ,4
M D A 3 . . . ~ J '
1
0 I , I I i I I 0 2 4 6 8 10 12 14
Duration of disease (in years)
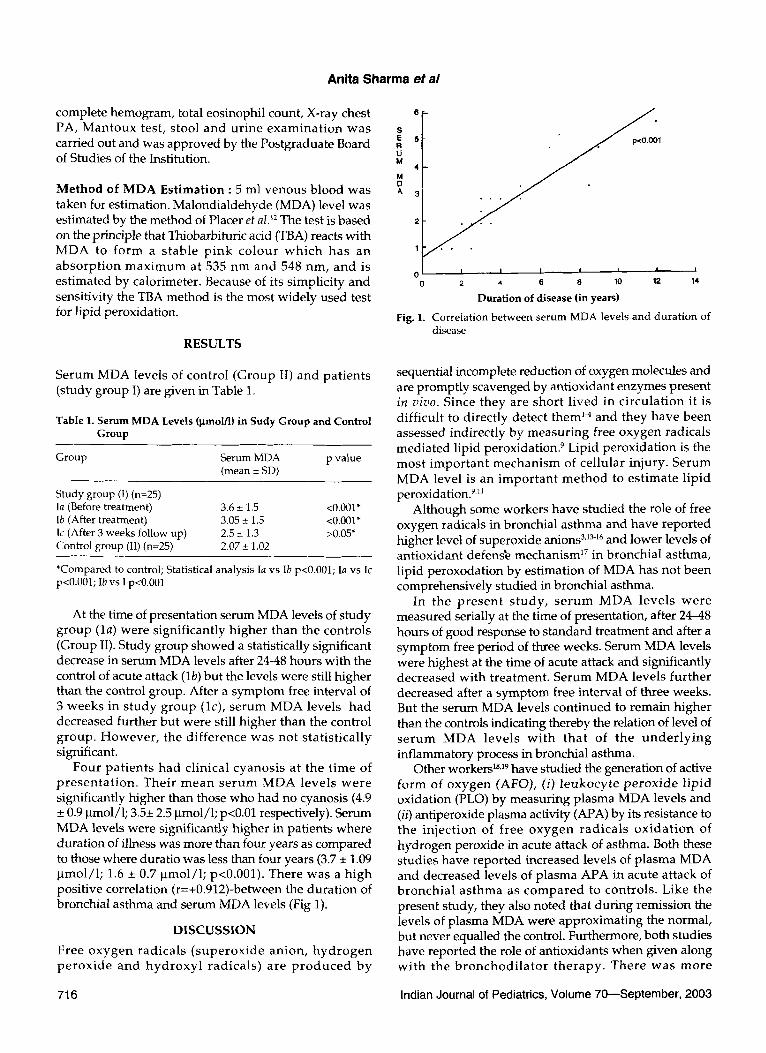
Fig. 1. Correlation between serum MDA levels and dura t ion of disease
Serum MDA levels of control (Group II) and patients (study group I) are given in Table 1.
Table 1. Serum MDA Levels (lamolFl) in Sudy Group and Control Group
Group Serum MDA p value (mean _+ SD)
Study group (I) (n=25) la (Before treatment) 3.6 _+ 1.5 <0.001" lb (After treatment) 3.05 -+ 1.5 <0.001" lc (After 3 weeks follow up) 2.5 _+ 1.3 >0.05* Control group (II) (n=25) 2.07 + 1.02
*Compared to control; Statistical analysis I avs Ib p<0.001; Ia vs Ic p<0.001; Ib vs I p<0.001
At the time of presentation serum MDA levels of study group (la) were significantly higher than the controls (Group II). Study group showed a statistically significant decrease in serum MDA levels after 24-48 hours with the control of acute attack (lb) but the levels were still higher than the control group. After a symptom free interval of 3 weeks in s tudy group (lc), serum MDA levels had decreased further but were still higher than the control group. However , the difference was not statistically significant.
Four pat ients had clinical cyanosis at the t ime of p re sen ta t ion . Their mean se rum MDA levels were significantly higher than those who had no cyanosis (4.9 + 0.9 Bmol/l; 3.5_+ 2.5 Bmol/1; p<0.01 respectively). Serum MDA levels were significantly higher in patients where duration of illness was more than four years as compared to those where duratio was less than four years (3.7 _+ 1.09 pmol/1; 1.6 -+ 0.7 ~tmol/1; p<0.001). There was a high positive correlation (r=+0.912)-between the duration of bronchial asthma and serum MDA levels (Fig 1).
DISCUSSION
Free oxygen radicals ( supe rox ide anion, h y d r o g e n p e r o x i d e and h y d r o x y l radicals) are p r o d u c e d by
sequential incomplete reduction of oxygen molecules and are promptly scavenged by antioxidant enzymes present in vivo. Since they are short l ived in circulat ion it is difficult to directly detect them 14 and they have been assessed indirectly by measuring free oxygen radicals mediated lipid peroxidation. 9 Lipid peroxidation is the most impor tant mechanism of cellular injury. Serum MDA level is an impor tant me thod to est imate lipid peroxidation? ,~
Although some workers have studied the role of free oxygen radicals in bronchial asthma and have reported higher level of superoxide anions 3,1~16 and lower levels of antioxidant defens~ mechanism ~7 in bronchial asthma, lipid peroxodation by estimation of MDA has not been comprehensively studied in bronchial asthma.
In the p re sen t s tudy , s e rum MDA levels were measured serially at the time of presentation, after 24-48 hours of good response to standard treatment and after a symptom free period of three weeks. Serum MDA levels were highest at the time of acute attack and significantly decreased with treatment. Serum MDA levels further decreased after a symptom free interval of three weeks. But the serum MDA levels continued to remain higher than the controls indicating thereby the relation of level of s e rum MDA levels wi th that of the u n d e r l y i n g inflammatory process in bronchial asthma.
Other workers ]s,19 have studied the generation of active form of oxygen (AFO), (i) l eukocy te p e ro x id e l ipid oxidation (PLO) by measuring plasma MDA levels and (iI~ antiperoxide plasma activity (APA) by its resistance to the inject ion of free oxygen radicals ox ida t i on of hydrogen peroxide in acute attack of asthma. Both these studies have reported increased levels of plasma MDA and decreased levels of plasma APA in acute attack of bronchia l as thma as compared to controls. Like the present study, they also noted that during remission the levels of plasma MDA were approximating the normal, but never equalled the control. Furthermore, both studies have reported the role of antioxidants when given along wi th the b r o n c h o d i l a t o r the rapy . There was more
716 Indian Journal of Pediatrics, Volume 70--September, 2003
Lipid Peroxidation in Bronchial Asthma
pronounced lowering of p lasma M D A levels in the g roup given antioxidants along wi th bronchodilators compared to those b ronch ia l a s t h m a pa t ien ts w h o rece ived on ly s tandard therapy bu t wi thou t antioxidants.
Like o the r s tud i e s 16,18 w e a lso o b s e r v e d a pos i t i ve corre la t ion b e t w e e n the du ra t i on of illness a nd s e r u m M D A levels. This c o u l d be p r o b a b l y d u e to c o n s t a n t p r o d u c t i o n o f f r ee o x y g e n r a d i c a l s b y u n d e r l y i n g inflammation.
In t he p r e s e n t s t u d y , s e r u m M D A leve l s w e r e significantly higher in 4 patients who had clinical cyanosis at t he t i m e of p r e s e n t a t i o n . T he e x t e n t o f l ip id p e r o x i d a t i o n (cell m e m b r a n e d a m a g e ) d e n o t e s the amoun t of free oxygen radicals generated which have not been probably scavengered by defense mechanism. Lipid pe rox ida t ion m a y no t be re la ted to the p r i m a r y t issue injury, bu t m a y ampl i fy the original injury.
C O N C L U S I O N
C h i l d r e n o f b r o n c h i a l a s t h m a h a d i n c r e a s e d l ip id peroxidat ion as indicated by se rum M D A levels. Serum M D A levels are correlated with the severity and durat ion of illness. Their diagnostic and prognostic role needs to be evaluated further.
REFERENCES
1. Sedgwick JB, Geiger KM, Busse WW. Superoxide generation by hypodense eosinophils from patients with asthma. Am Rev Resp/r D/s 1990; 142 : 120-125.
2. Zakharian AK, Amatuni VG. The interconnection of changes in the levels of prostaglandins, catecholamines and lipid peroxidation of membrane lipids in patients with bronchial asthma. Vopr Med Khim 1991; 37(3) : 45-47.
3. Neijens HJ, Raatgeep RE, Dejenhart HJ, Duiverman EJ, Kerrebijan KF. Altered leukocyte response in relation to the basic abnormality in children with asthma and bronchial hyper responsiveness. Am Rev Respir D/s1984; 130 : 744-747.
4. Chanez P, Dent G, Yukawa T, Barnes PJ, Chung KF. Generatio of oxygen free radicals from blood eosinophils from asthma patients after stimulation with PAF or phorbol ester. Eur Respir J 1990; 3 : 1002-1007.
5. Cross CE, Halliwell B. Biological consequences of general environmental contaminants. In Crystal RG, West JB, eds. The Lung Scientific Foundations. New York; Raven Press, 1991; 1875- 1980.
6. Parson PE, Warthen GS, Henson PM. Injury from inflammatory cells. In Crystals RG, West JB, eds. The Lung Scientific Foundation. New York; Raven Press, 1991; 1981-1992.
7. Crystal RG. Oxidant and respiratory tract epithelial injury : Pathogenesis and strategies for therapeutic intervention. Am J Med 1991; 91 (Supp136) : 39-44.
8. The International Study of Asthma - Allerges in childhood (ISAAC) Steering Committee. World wide variatio in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema; ISAAC. Lancet 1998; 351 : 1225-1232.
9. Chesseman KH. Mechanism and effects of lipid peroxidatiom Molec Aspects Med 1993; 14 : 191-197.
10. Babior BM. The respiratory burst of phagocytes. J Clin Invest 1984; 73 : 599-601.
11. Meneely GR, Renzetti AD, Steek JD, Wyatt JP, Harsis HW. American Thoracic Society. Thorax 1960; 15 (132) : 762-768.
12. Placer ZA, Cushmann LL, Johnson BC. Estimation of production of lipid peroxidation (malondialdehyde) in biochemical assay. Anal Biochemistry 1966; 16 : 359-364.
13. Vachier I, Damon M, Doucen CL et al. Increased oxygen species generation in blood monocytes of asthmatic patients. Am Rev Respir Dis 1992; 146 : 1161-1166.
14. Cluzel M, Damon M, Chanez Pet al. Enhanced alveolar cell luminol - dependent Chemiluminescence in asthma. J Allergy Clin Immuno11987; 80 : 195-201.
15. Chanez P, Dent G, Yukawa T, Barnes PJ, Chung KF. Generation of oxygen free radicals from blood eosinophils from asthma patients after stimullation with PAF or phorbol ester. Eur Respir J 1990; 3 : 1002-1007.
16. Kanazawa H, Kurihara N, Hirata K, Takeda T. The role of free radicals in airways obstruction in asthmatic children. Chest 1991; 100 : 1319-1322.
17. Novak Z, Nemeth I, Gyurkovits K, Varga SL Matkovics B. Examination of the role of oxygen free radicals in bronchial asthma in childhood. Clinical Chemica Acta 1991; 201 : 247-252.
18. Boljevic S, Daniljak IG, Kogan AH. Changes in free radicals and possibility of their correction in patients with bronchial asthma. Vojnosanit Preg11993; 50(1) : 3-18.
19. Daniliak IG, Koagan AH, Bolevich S. The generation of active forms of oxygen by the blood leukocytes, lipid peroxidation and antiperoxide protection in bronchial asthma patients. Ter Arkh 1992; 64 : 54-57.
Indian Journal of Pediatrics, Volume 70--September, 2003 717