Embed Size (px)
Citation preview

http://informahealthcare.com/lprISSN: 0898-2104 (print), 1532-2394 (electronic)
J Liposome Res, Early Online: 1–9! 2014 Informa Healthcare USA, Inc. DOI: 10.3109/08982104.2014.911315
RESEARCH ARTICLE
Liposomal lidocaine gel for topical use at the oral mucosa:characterization, in vitro assays and in vivo anesthetic efficacyin humans
Michelle Franz-Montan1, Daniela Baroni1, Giovana Brunetto2, Viviane Roberta Vieira Sobral2,Camila Morais Goncalves da Silva2, Paulo Venancio1, Patricia Wiziack Zago1, Cintia Maria Saia Cereda2,Maria Cristina Volpato1, Daniele Ribeiro de Araujo3, Eneida de Paula2, and Francisco Carlos Groppo1
1Department of Physiological Sciences, Piracicaba Dental School, University of Campinas – UNICAMP, Piracicaba, Sao Paulo, Brazil, 2Department of
Biochemistry, Institute of Biology, University of Campinas – UNICAMP, Campinas, Sao Paulo, Brazil, and 3Human and Natural Sciences Centre,
Federal University of ABC, Sao Paulo, Brazil
Abstract
Objective: To characterize liposomal-lidocaine formulations for topical use on oral mucosa andto compare their in vitro permeation and in vivo anesthetic efficacy with commercially availablelidocaine formulations.Materials and methods: Large unilamellar liposomes (400 nm) containing lidocaine wereprepared using phosphatidylcholine, cholesterol, and a-tocoferol (4:3:0.07, w:w:w) and werecharacterized in terms of membrane/water partition coefficient, encapsulation efficiency, size,polydispersity, zeta potential, and in vitro release. In vitro permeation across pig palatal mucosaand in vivo topical anesthetic efficacy on the palatal mucosa in healthy volunteers (double-blinded cross-over, placebo controlled study) were performed. The following formulations weretested: liposome-encapsulated 5% lidocaine (Liposome-Lido5); liposome-encapsulated 2.5%lidocaine (Liposome-Lido2.5); 5% lidocaine ointment (Xylocaina�), and eutectic mixture oflidocaine and prilocaine 2.5% (EMLA�).Results: The Liposome-Lido5 and EMLA showed the best in vitro permeation parameters(flux and permeability coefficient) in comparison with Xylocaina and placebo groups, as well asthe best in vivo topical anesthetic efficacy.Conclusion: We successfully developed and characterized a liposome encapsulated 5%lidocaine gel. It could be considered an option to other topical anesthetic agents for oralmucosa.
Keywords
Lidocaine, liposome, oral mucosa, topicalanesthesia
History
Received 14 January 2014Revised 27 March 2014Accepted 30 March 2014Published online 7 May 2014
Introduction
Anxiety and fear induced by pain are still associated with
dental treatment, and one of the most feared procedures is
local anesthesia (Armfield & Milgrom, 2011). The pain
during this procedure leads to the lack of cooperation by
patients, prolonged dental attendance time, unsuccessful/
repeated attempts, and additional pain (Taddio et al., 2005).
In long term, repeated painful procedures contribute to
conditioned anxiety responses and increased pain perception
(Meechan, 2002). In order to alleviate pain from needle
insertion and anesthetic injection, and reduce anxiety, topical
anesthesia is recommended in dental practice (Meechan,
2000, 2002).
Lidocaine (LDC) is an amine–amide local anesthetic with
moderate action and fast onset widely used in topical and
local anesthesia in Dentistry (Meechan, 2000, 2002).
Nevertheless, its efficacy in topical anesthesia is questionable
and the results are conflicting. It was demonstrated a high
incidence of inefficacy in reducing pain during: anesthetic
injection in the palatal mucosa (Bhalla et al., 2009; Hutchins
et al., 1997), intraligamentary injection (Meechan &
Thomason, 1999), and gingival probing (Donaldson &
Meechan, 1995).
The palatal mucosa is known for its difficulty in acquiring
adequate topical anesthesia (Meechan et al., 2005). This site
has a firmly attached keratinized tissue (which reduces tissue
distension), poor drug penetration through this highly
keratinized tissue, and a decreased tissue buffering capacity
(Primosch & Robinson, 1996). Therefore, a topical anes-
thetic able to eliminate pain from needle insertion and
Address for correspondence: Michelle Franz-Montan, Faculdade deOdontologia de Piracicaba, Universidade Estadual de Campinas, Av.Limeira, 901, Bairro Areiao, CEP 13414-903, Piracicaba – SP – Brazil.Tel/Fax: +55 19 2106 5306. E-mail: [email protected]
Jour
nal o
f L
ipos
ome
Res
earc
h D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Que
ensl
and
on 0
6/01
/14
For
pers
onal
use
onl
y.

anesthetic injection in the palatal mucosa would be a benefit
in dentistry.
The encapsulation of drugs into liposomes represents an
alternative method of drug delivery system for local anes-
thetics because it increases the duration of analgesia, and
decreases both central nervous and cardiac toxicity
(Boogaerts et al., 1993, 1994). Several studies have demon-
strated that local anesthetics, including lidocaine, provide
efficient topical anesthesia of the skin when encapsulated into
these lipid vesicles (Eidelman et al., 2005; Taddio et al.,
2005).
Regarding the oral mucosa, significant topical anesthesia
was induced by liposome-encapsulated local anesthetics
(Franz-Montan et al., 2007, 2010; Paphangkorakit et al.,
2012). However, it was recently demonstrated that liposome
encapsulated ropivacaine at 1 or 2% was not different than a
placebo gel in reducing pain during needle insertion in the
palatal mucosa when compared with the eutectic mixture of
2.5% lidocaine/2.5% prilocaine (EMLA�) (Franz-Montan
et al., 2012).
The aim of the present study was to characterize a
liposomal-lidocaine formulation aimed for topical use at the
oral mucosa, to evaluate its in vitro permeation across pig
palatal mucosa, and to measure its in vivo topical anesthetic
efficacy in reducing the pain caused by needle insertion and
local anesthetic injection in the palatal mucosa of healthy
volunteers.
Materials and methods
Materials
Lidocaine hydrochloride was donated by Cristalia Prod.
Quim. Farm. Ltda (Itapira, SP, Brazil). Egg phosphatidylcho-
line (EPC), cholesterol (Ch), and a-tocopherol (a-T) were
purchased from Sigma Chemical Company (St Louis, MO).
All other reagents used were analytical grade.
The commercial topical formulations used in this study
were eutectic mixture of 2.5% lidocaine and 2.5% prilocaine
(EMLA�, Astra-Zeneca, Cotia, SP, Brazil – batch no. 26099)
and 5% lidocaine ointment (Xylocaina� ointment –
AstraZeneca, Cotia, SP, Brazil – batch no. 26438).
Liposome preparation
The liposomes (large unilamellar vesicles with 400 nm
diameters) were prepared according to previously described
methodology (Cereda et al., 2008; de Araujo et al., 2008).
EPC-Ch-a-T (4:3:0.07, molar ratio) films were obtained by
evaporating stock chloroform solutions under a stream of wet
nitrogen, followed by vacuum for 2 h. Films were suspended
in 20 mM HEPES buffer (pH 7.4, containing 154 mM NaCl),
and multilamellar vesicles were obtained after vortexing at
ambient temperature (5 min, 25 �C). Large unilamellar ves-
icles were prepared by extrusion (15 cycles) of the multi-
lamellar vesicles within 400 nm membrane filters (25 �C),
using a Lipex Biomembranes Inc. (Vancouver, Canada)
extruder.
Lidocaine encapsulation was performed by adding the
local anesthetic directly to the liposomes after extrusion at the
final concentration of 2.5% or 5%. The suspensions were then
sterilized by autoclaving (121 �C, 1 atm during 15 min)
(Cereda et al., 2008).
Liposome characterization
Determination of encapsulation efficiency (EE%) and
partition coefficient (P)
The encapsulation efficiency (EE%) and partition coefficient
(P) values of lidocaine into the liposomes was optically
determined, in triplicates. The liposomal suspension (4 mM)
containing LDC (2 mM) was submitted to ultracentrifugation
(120 000 g for 2 h at 10 �C) (de Araujo et al., 2008) and the
supernatant was analyzed at 260 nm for LDC concentration.
The EE% was calculated by subtracting the supernatant
concentration from the total LDC concentration, measured
previously to phase mixing. The partition coefficient (P) was
calculated by using equation 1 (de Paula & Schreier, 1995).
P ¼ ðnm=VmÞðnm=VwÞ ð1Þ
where n is the number of moles of lidocaine, V denotes the
volume (L), m and w refer to the membrane and aqueous
phase, respectively.
Determination of liposome size and polydispersity
The average particle size (hydrodynamic diameter in nm) and
polydispersity index (PDI) of the extruded liposomes (diluted
to 1 mM) were determined by dynamic light scattering, in a
ZS-90 particle analyzer (Zetasizer, Malvern Instruments,
Malvern, UK). All parameters were analyzed 24 h after
liposomal preparation, in triplicate, in three different days, at
a fixed angle (90�) and at 25 �C.
Determination of liposomes morphology by transmission
electron microscopy (TEM)
Morphology of liposomes containing LDC was performed by
TEM (EM-900; Carl Zeiss, Jena, Germany) according to a
previously described method (Franz-Montan et al., 2013).
A drop of the liposomal suspension was placed on copper
grids of 200 meshes for 15 min. Excess of the formulation was
removed with a filter paper. A 2% uranyl acetate solution was
dropped onto the grid, and the excess of this staining solution
was removed with a filter paper. The grid was examined 2 min
after staining under TEM at 80 kV.
In vitro release study
The release of LDC from liposome vesicles was evaluated
using a two-compartment system consisting of a donor
compartment (2 mL) and an acceptor compartment (250 mL
HEPES buffer, pH 7.4) separated by a cellulose membrane
with 14 000 Da molecular exclusion pores, kept under light
magnetic stirring at 37 �C (Paavola et al., 1995). Aliquots of
2 mL were withdrawn from the acceptor compartment at
intervals of 15, 30, and 60 min, during a total period of
300 min, and quantified by UV spectroscopy (260 nm).
The acceptor compartment was refilled with buffer after
removal of each aliquot to maintain a constant volume of
liquid. Absorbance measures obtained were converted into
2 M. Franz-Montan et al. J Liposome Res, Early Online: 1–9
Jour
nal o
f L
ipos
ome
Res
earc
h D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Que
ensl
and
on 0
6/01
/14
For
pers
onal
use
onl
y.

percentages of released drug, using a standard solution of free
lidocaine.
Higuchi and zero-order theoretical models were used to
analyze the release profiles of lidocaine from plain and
liposomal formulation. Zero-order kinetics describes that drug
release rate is independent of the concentration of the drug.
In contrast, the Higuchi model follows Fick’s law and
determines that the mechanism of drug release is dependent
on to the square root time, as described by the following
equations, respectively:
Qt ¼ Q0 þ K0 � t ð2Þ
where Qt is the cumulative amount of drug released at time t,
Q0 is the initial amount of drug, K0 is the zero-order release
constant, and t is the time
Q ¼ K � t12 ð3Þ
where Q is the amount of drug released at a time t and K is the
release kinetics constant.
Topical formulations
The liposome and placebo gel formulations were prepared by
the same operator (not involved in the application or
anesthetic efficacy evaluation) and consisted of identical
color, taste, smell and fluidity, based on a patented
method (Silva et al., 2008), using the components according
to Table 1.
The resulting gel (placebo gel) was stored in the dark in
capped glass containers at 4 �C, until the preparation of
liposomal based gels, which were obtained by mixing
carbopol base gel with liposome suspension with or without
the local anesthetic (50:50, v/v) at the final desired drug
concentration (2.5% w/w or 5% w/w). The following gels
were prepared: liposome-encapsulated 5% lidocaine
(Liposome-Lido5), liposome-encapsulated 2.5% lidocaine
(Liposome-Lido2.5), liposomal placebo gel, and plain pla-
cebo gel.
The gel formulations were placed into coded flasks to
ensure blindness of the volunteers and the investigator
involved in the application and evaluation of the topical
anesthetics.
In vitro permeation of lidocaine through pig palatalmucosa
Lidocaine analysis
Lidocaine was quantified by high performance liquid
chromatography (HPLC – Varian ProStar HPLC,
Biodirect Inc, Taunton, MA, a PS 325 UV–Vis detector, a
PS 210 solvent delivery module, and an automatic injector).
The local anesthetic lidocaine was separated on a C18
reversed-phase column (5 mm, 150� 4.60 mm, Phenomenex)
at 40 �C. The mobile phase consisted of the mixture
methanol:buffer (4.35 mM NH4H2PO4, pH 7.0, adjusted
with triethylamine) at the volume ratio 60:40, pumped at
1.5 mL/min and an injection volume of 40 mL. Lidocaine
detection was monitored at 220 nm.
A calibration curve was constructed from a stock solution,
prepared by dissolving lidocaine in 0.9% NaCl (0.2 mg/mL)
followed by dilution into six working solutions by using 0.9%
NaCl (from 0.2 to 0.04 mg/mL). For each concentration, three
samples were injected in order to obtain calibration curves,
which were analyzed by linear regression analysis of the peak
area versus the concentration (r2¼ 0.9991). The limit of
detection was 0.34 mg/mL, and the limit of quantification was
1.13 mg/mL.
This method was validated according to the ‘‘International
Conference on the Harmonization of Technical Requirements
for the Registration of Pharmaceuticals for Human Use’’
and Resolution 899/2003 of the Brazilian National
Agency for Health Monitoring (Agencia Nacional de
Vigilancia Sanitaria or ANVISA) (ANVISA, 2003; ICH,
1996).
Tissue preparation for permeation study
Pig maxilla was obtained from a local slaughterhouse and
transported to the laboratory in isotonic phosphate buffer pH
7.4. The tissue preparation was adapted from a previous
described methodology (Franz-Montan et al., 2013). Briefly,
the palatal mucosa was removed from the palatal bone and
rinsed with saline. Pieces of palatal tissue were cut out and
immersed into deionized water at 65 �C for 60 s, to allow
separation of the epithelia from the connective tissue.
Samples were quickly rinsed in deionized water, drained on
a cellulose filter, and frozen at �20 �C until use. All
experiments were conducted using tissue from at least two
animals, with eight replicates.
Permeation experiments
Permeation studies were carried out in Franz diffusion cells
(Disa, Magenta Milano, Italy), with 0.6 cm2 of permeation
area and a receiver compartment of 4.2 mL in volume. The
mucosa was placed over a 0.45 mm cellulose filter (connect-
ive side of tissue facing the membrane filter) due to its
fragility, avoiding any damage that could alter permeation
parameters without altering lidocaine transport. Gel formula-
tions were applied in infinite dose conditions (1.66 g/cm2) in
the donor compartment. The receptor chambers were filled
with degassed isotonic saline solution magnetically stirred at
37 �C. Permeation experiments were performed in non-
occlusive conditions during 5 h. Samples (300 mL) were
periodically withdrawn from the receptor phase and analyzed
by HPLC, being replaced with fresh receptor solution in equal
volumes.
The flux of drug was calculated from the slope of the linear
portion of the curve (cumulative amounts of lidocaine
transported across the mucosa per unit of area� time). The
lag time was obtained from the interception to the time axis.
Table 1. Components of the base gel, according to Silva et al. (2008)(Patent # WO/2008/138089).
Component Function
Carbopol (2%) Used as a gelling agentPropylene glycol (5%) Acts as a solvent and wettingMethylparaben (0.2%) PreservativeGlycerin (8%) Wetting and emollient agentDeionized water SolventTriethanolamine Alkalinizing agent pH¼ 7.0
DOI: 10.3109/08982104.2014.911315 Liposomal lidocaine gel for topical use 3
Jour
nal o
f L
ipos
ome
Res
earc
h D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Que
ensl
and
on 0
6/01
/14
For
pers
onal
use
onl
y.

The permeability coefficient was calculated according to the
following equation (de Araujo et al., 2010):
J ¼ P� Cd ð4Þ
where J (mg cm�2 h�1) is the lidocaine flux across the skin,
P (cm h�1) is the permeability coefficient and Cd is the LDC
concentration in the donor compartment (mg cm�3).
In vivo anesthetic efficacy evaluation in healthyvolunteers
Subjects
The Ethical Committee of Piracicaba Dental School,
University of Campinas Piracicaba, Brazil, approved this
research (Protocol # 112/2007), according to the requirements
of the International Conference on Harmonization Guidelines
for Good Clinical Practice and the Declaration of Helsinki.
The ClinicalTrials.gov trial registration number of this study
is NCT01425840.
A power calculation indicated that a sample size of 40
subjects would provide 95% power to detect a difference of
10 mm in VAS scores between two groups, assuming a
significance level of 5% (two-tailed).
Forty volunteers (20 women) aging 18–29 years-old
(20.3 ± 2.3 years) were selected based on a satisfactory
medical history evaluation and their agreement to provide
informed consent. All the subjects were undergraduate or
graduate students at Piracicaba Dental School and were in
good health. Exclusion criteria included history of allergy to
any of the local anesthetics used, intake of drugs that would
alter pain perception, pregnancy, and presence of lesion in the
site of topical application.
The study was conducted at Piracicaba Dental School/
University of Campinas, Sao Paulo, Brazil, at the ambulatory
office of the Pharmacology, Anesthesiology and Therapeutics
Area.
Anesthetic procedure
The volunteers randomly received six different topical
formulations in a double-blinded, placebo-controlled, cross-
over, three-period treatment design. Each volunteer received
bilaterally 100 mg of two of the following topical anesthetics
applied by the same operator: liposome-encapsulated 5%
lidocaine (Liposome-Lido5), liposome-encapsulated 2.5%
lidocaine (Liposome-Lido2.5), commercial 5% lidocaine
ointment (Xylocaina�), eutectic mixture of 2.5% lidocaine
and 2.5% prilocaine (EMLA�), placebo gel, and liposomal
placebo gel, in three different appointments spaced at least
1 week apart. The subjects served as their own controls.
A researcher not involved in anesthetic application or
anesthetic parameters evaluation selected the volunteers and
performed the randomization. Site (right or left side) and
order of application were predetermined by a random number
table, with no restriction. To allow blindness of the experi-
ment, neither the dentist nor the patient knew which
formulation was applied.
Before topical application, the palatal mucosa of both
right- and left-upper canines was dried using the sterile gauze.
The topical anesthetic agents were previously weighed and
applied on the dried sites, approximately 1.0 cm away from
the canines’ gingival margin, by using a cotton swab. Each
topical anesthetic was kept on the mucosal surface for 2 min.
After topical application, the mucosa was gently wiped with
sterile gauze followed by a water rinse.
According to a previous described procedure (Franz-
Montan et al., 2012), after the removal of the topical
formulations, a second operator inserted a 30-gauge dental
needle attached to an aspirating syringe in the same region of
topical application, until periosteum contact. Immediately
after, the volunteer was informed that the anesthetic solution
would be injected, and 0.3 mL of 2% lidocaine with 1:100.000
epinephrine cartridge (Alphacaine� – DFL Ind. Com. Ltd,
Rio de Janeiro, RJ, Brazil) was injected at a rate of 1 mL/min.
Pain perception was accessed in two different moments,
after needle insertion and after local anesthetic injection, on
two separated visual analogue scales (VAS). VAS consisted of
a 10-cm non-graded line showing ‘‘no pain’’ and ‘‘unbearable
pain’’ at the left and right ends, respectively. Subjects were
asked to mark a point on the line according to their level of
perceived pain. A ruler was used to measure the distance from
the left end-point to the mark made by the volunteer.
In addition, at the end of all sessions, the volunteers were
asked to choose the most efficient topical anesthetic for the
palatal mucosa.
Statistical analysis
Characterization and in vitro permeation data were expressed
as percentage or mean (±SD) and analyzed by a one-way
analysis of variance (ANOVA) and Tukey–Kramer’s post-hoc
test or unpaired t-test. In vivo anesthetic efficacy data were
compared by the Friedman test. Correlation between in vivo
efficacy and in vitro studies was performed by Pearson’s
correlation test. All tests were performed by using GraphPad
Instat (GraphPad Software, Inc., La Jolla, CA) with signifi-
cance level set at 5%.
Results and discussion
Characterization of liposomes containing lidocaine
Table 2 shows particle size, polydispersity index (PDI),
encapsulation efficiency (EE%), and partition coefficient (P)
of liposomal LDC. The encapsulation of LDC did not affect
vesicles size and homogeneity of the system, since there was
no statistically significant difference in size and polydisper-
sity index between empty and lidocaine-containing liposomes
(p40.05). The low polydispersity values indicate a good
stability of the system (Ntimenou et al., 2012).
Few studies were reported in the literature regarding the
development of a liposomal lidocaine formulation for oral
mucosa use. Paphangkorakit et al. observed an improved
Table 2. Encapsulation efficiency (EE%), partition coefficient (P),particle size, and polydispersity index (PI) of empty liposomes andliposome-encapsulated LDC.
Samples EE% ± SD P ± SD Size (nm ± SD) PI ± SD
Liposomes – – 376.9 ± 48.1 0.16 ± 0.01Liposomes
with LDC21.63 ± 2.6 114.5 ± 16.8 392.8 ± 39.3 0.20 ± 0.03
4 M. Franz-Montan et al. J Liposome Res, Early Online: 1–9
Jour
nal o
f L
ipos
ome
Res
earc
h D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Que
ensl
and
on 0
6/01
/14
For
pers
onal
use
onl
y.

topical anesthetic efficacy in the palatal mucosa of a
liposome-encapsulated 2% lidocaine with epinephrine
1:100 000. The liposomes consisted of cholesterol and egg
phospholipid (1:1, w:w, prepared by the sonication method –
ultrasonic dental scaler). The authors did not study particle
size or encapsulation efficiency (Paphangkorakit et al., 2012).
In the present study, the partition coefficient and encap-
sulation efficiency were similar to the results obtained by
others with different local anesthetics encapsulated into
liposomes with the same composition (Cereda et al., 2006;
de Araujo et al., 2008).
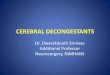
TEM images confirmed the particle size and vesicles
morphology (Franz-Montan et al., 2013). The morphological
analysis of liposomes images demonstrated the existence of
spherical-shaped vesicles (Figure 1) around 400 nm in
diameter, which is in accordance to the DLS results in
Table 2.
The LDC release profile was significantly reduced after
encapsulation in liposomes (1.5–1.2 times, p50.001, after 15
and 60 min, respectively) when compared with the free drug
(Figure 2). The time required for total release (100%) of
LDC+liposome formulation was achieved after 180 min.
Theoretical model analysis revealed that the release rate
from liposomes follows the Higuchi model, as observed by
high correlation coefficient value when compared with zero-
order kinetics analysis (Table 3), suggesting that the release of
LDC from liposomes is a process dependent on diffusion.
In vitro permeation of lidocaine through pig palatalmucosa
Lidocaine permeation profiles across pig palatal mucosa from
different topical formulations and in infinite dose condition
are observed in Figure 3. Permeation parameters are
described in Table 4.
Porcine buccal or esophageal mucosae are frequently used
for in vitro drug permeation studies due to their similar
structure and permeability with human tissues (Diaz Del
Consuelo et al., 2005a,b). In the present study, palatal mucosa
was chosen due to its keratinized layer, allowing a more
efficient permeability barrier characteristic (Ganem-
Quintanar et al., 1998) and it represents the same application
site used in clinical studies.
The Liposome-Lido5 formulation presented the highest
flux when compared with the other formulations (Table 3;
p50.001). This result was unexpected, since in this formu-
lation, 21.6% of lidocaine was encapsulated into the lipo-
somes and, therefore, less free drug was available to cross the
barrier in comparison with the commercial 5% lidocaine
formulation (Xylocaina�). The results observed in the present
study differ from others that demonstrated free drug present-
ing higher flux when compared with drug encapsulated into
Figure 1. Transmission electron micrographs of a typical EPC-Ch-a-T (4:3:0.07, mole%) liposome without (a) and with (b) lidocaine. Magnification100 000�.
0 40 80 120 160 200 240 280 3200
20
40
60
80
100
LDCLUV
LDC
Time (min)
LD
C r
elea
se (
%)
Figure 2. In vitro release profile of lidocaine (plain and encapsulated inliposomes) (mean values ± SD).
DOI: 10.3109/08982104.2014.911315 Liposomal lidocaine gel for topical use 5
Jour
nal o
f L
ipos
ome
Res
earc
h D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Que
ensl
and
on 0
6/01
/14
For
pers
onal
use
onl
y.

lipid carriers or liposomes (Maestrelli et al., 2009; Puglia
et al., 2011).
Beyond the use of propylene glycol as a solvent in topical
formulations (Herkenne et al., 2008; Kang et al., 2007), the
literature also demonstrated its ability to increase drug
absorption after topical application (Bailey, 1992; Gee
et al., 2014; Herkenne et al., 2008; Melero et al., 2008;
Merino et al., 2008). The presence of propylene glycol at the
liposomal gel could explain why this formulation presented
the highest flux. Curiously, despite having the lowest
lidocaine concentration, EMLA� presented a higher flux
(p50.001) when compared with Xylocaina�. A possible
explanation for its higher flux could be the well-known
physical–chemical properties. Since EMLA is a eutectic
mixture, its melting point is lower than that of the isolated
compounds (EMLA¼ 18 �C; lidocaine¼ 67 �C). Therefore, at
the body temperature (37 �C), the same condition used in the
in vitro experiment, lidocaine was in the liquid form and
could present a faster permeation.
In addition, such altered fluxes could be possibly
associated to the diverse composition and nature of the
formulations, influencing drug solubility and partitioning,
leading to different drug transports across the barrier
(de Araujo et al., 2010). It is worth notice that both
commercial formulations, EMLA� and Xylocaina�, are not
gel-based formulations, but a cream and an ointment,
respectively.
The lidocaine concentration also varies: EMLA� contains
2.5% and Xylocaina� contains 5%. In the present study,
these two different lidocaine concentrations were used in
the liposomal formulations in order to compare them
with the same concentrations of the two commercial
formulations.
In relation to permeability coefficient Xylocaina� pre-
sented the lowest value (p50.001); Liposome-Lido5 did not
differ from EMLA� and Liposome-Lido2.5 (p40.05) and
EMLA� present higher permeability coefficient than
Liposome-Lido2.5 (p50.05). These differences could also
be explained based on the factors previously discussed,
formulation composition, concentration of local anesthetic,
and physical–chemical properties.
In vivo anesthetic efficacy evaluation in healthyvolunteers
Table 5 shows formulation preference considering the anes-
thetic effect and VAS concerning pain during needle insertion
and anesthetic injection. Liposome-Lido5 was equivalent to
EMLA� (positive control) in reducing pain during needle
insertion and anesthetic injection (p40.05). However,
EMLA� was preferred by most of the volunteers, followed
by Liposome-Lido5. Both formulations showed superior
anesthetic efficacy (p50.05) when compared with
Xylocaina� and placebo groups, and probably this result has
influenced the preference reported by the volunteers.
In the present study, the non-encapsulated lidocaine was
not excluded from the formulation. Moreover, the 79% of non-
encapsulated lidocaine also contribute for its efficacy.
Similarly, our research group has previously demonstrated
an increase of 26.1% in the intensity of total anesthetic effect
induced by 2% liposomal lidocaine after infra-orbital nerve
block in rats, when compared with plain lidocaine formulation
(Cereda et al., 2006). In addition, the formulation good
performance can also be attributed to the presence of
propylene glycol, which can act as a permeation enhancer
(Bailey, 1992; Gee et al., 2014; Herkenne et al., 2008; Melero
et al., 2008; Merino et al., 2008), increasing lidocaine
solubility in the palatal mucosa, and leading to a better
efficacy.
Topical anesthesia is widely used in dentistry to reduce
pain from both needle insertion and injection of a local
anesthetic solution. However, an efficient topical anesthetic is
not yet available, especially concerning the palatal mucosa,
and even after topical anesthesia, most patients still feel pain
(Meechan, 2000, 2002).
Adequate topical anesthesia on palatal mucosa is usually
not achieved, especially in the anterior region (Meechan,
2000). Harker (1997) attributed the pain during injection to
the dislocation of the palatine muco-periosteum during local
anesthetic administration. However, in most of the studies
involving topical anesthetics efficacy, pain is evaluated solely
by the needle insertion, with no local anesthetic injection into
the tissues (Meechan, 2000, 2002). In the present study, the
efficacy of the liposomal topical anesthetics was evaluated
considering their ability to reduce pain during injection of an
anesthetic solution in the anterior portion of the palatal
mucosa.
Since 1985, several authors have been evaluating the
anesthetic efficacy of EMLA� on oral mucosa, and most of
them demonstrated its superiority when compared with
other commercial available formulations in dentistry
00,2
5 0,5 0,75 1 1,5 2 2,5 3 4 5
0.0
0.5
1.0
1.5
2.0
2.5 Liposome-Lido5
Liposome-Lido2.5
EMLA®Xylocaína®
Time (h)
Lid
ocai
ne p
erm
eate
d (m
g/cm
²)
Figure 3. Permeation profiles of lidocaine from liposomal andcommercial formulations applied in infinite dose condition (meanvalues ± SD).
Table 3. In vitro release kinetics of lidocaine (free or encapsulated inliposomes) according to Higuchi and zero-order theoretical models.
Release kinetics
FormulationZero-order
modelHiguchimodel
R2
(zero-ordermodel)
R2
(Higuchimodel)
LDC 0.70 ± 0.15% h�1 72.1 ± 5.1% h�1/2 0.8525 0.955LDCLUV 0.65 ± 0.16% h�1 66.8 ± 0.16% h�1 0.8724 0.988
6 M. Franz-Montan et al. J Liposome Res, Early Online: 1–9
Jour
nal o
f L
ipos
ome
Res
earc
h D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Que
ensl
and
on 0
6/01
/14
For
pers
onal
use
onl
y.

(Al-Melh & Andersson, 2007; Holst & Evers, 1985). The
reported efficacy of EMLA� in inducing local anesthesia in
the palatal mucosa (Al-Melh & Andersson, 2007; Holst &
Evers, 1985) was the main reason to its choice as a positive
control in the present study.
The efficacy of lidocaine formulations on the oral mucosa
was previously compared with EMLA�. It was concluded that
a 2-min application of EMLA� was better than 2% lidocaine
gel on tongue mucosa and anterior buccal gingiva (Svensson
et al., 1992), and better than 5% lidocaine on the buccal
mucosa (McMillan et al., 2000). However, EMLA� was not
previously compared with a liposome encapsulated-lidocaine
in topical anesthesia in dentistry.
The potential of liposomal local anesthetic formulations to
provide topical anesthesia was demonstrated in the literature
as 4% and 5% lidocaine liposomal formulations provided the
same anesthetic efficacy as EMLA� on intact skin (Friedman
et al., 1999). Similarly, in the present study, the liposomal
encapsulated 5% lidocaine gel was equivalent to EMLA� in
reducing pain from needle insertion and anesthetic injection
at palatal mucosa.
Concerning oral mucosa, another local anesthetic encap-
sulated into liposomes (1% ropivacaine) was equivalent
to EMLA� in reducing pain during needle insertion
(no anesthetic solution was injected) in the maxillary buccal
fold after a 2-min application. Even in a different application
site, the present study also concluded that liposome
encapsulated 5% lidocaine gel was equivalent to EMLA� in
reducing pain during needle insertion.
Nevertheless, Franz-Montan et al. (2012) were not able to
show the effectiveness of a liposomal formulation on the
palatal mucosa, considering pain during needle insertion
using the same methodology of the present study.
These authors also evaluated pain during anesthetic injection
and even the positive control (EMLA�) was not able to
reduce pain during anesthetic injection. Contrary to those
results, in the present study, both liposomal lidocaine (5%)
and EMLA� were effective in reducing pain during injection.
In agreement to the present study, Paphangkorakit et al.
demonstrated that the liposomal lidocaine encapsulation was
able to improve topical anesthetic efficacy in reducing pain
during anesthetic injection in the palatal mucosa, in com-
parison with a commercial formulation. In such study, a
different liposomal formulation (cholesterol and egg phospho-
lipid 1:1, w:w, prepared by the sonication method – ultrasonic
dental scaler) was used (Paphangkorakit et al., 2012).
Correlation between in vitro permeation and in vivoanesthetic efficacy
Figure 4 shows the relationship between flux of lidocaine
across pig palatal mucosa (in vitro) and in vivo efficacy of
lidocaine formulations in reducing pain during needle inser-
tion (Figure 4a) and local anesthetic injection (Figure 4b) in
volunteers. A moderate (rPearson40.3, p40.05) correlation
was found between flux and VAS-Insertion.
Even though a high permeation rate and flux were not
expected for Liposome-Lido5 (Maestrelli et al., 2009; Puglia
et al., 2011), the moderate correlation between flux and
VAS-insertion indicates that the highest in vitro flux deter-
mines a better performance in oral topical anesthesia in vivo.
Similarly, a high correlation between flux of benzocaine
across pig esophageal mucosa and pain scores during needle
insertion in the canine’s maxillary buccal fold was recently
demonstrated (Franz-Montan et al., 2013). Therefore, the
anesthetic flux seems to be a valuable parameter to predict
Table 4. Permeation parameters (mean ± SD) of lidocaine through pig palatal mucosa from liposomal and commercialformulations applied in infinite dose condition (n¼ 6–7).
Lidocaine formulation Flux (mg cm�2 h�1) Permeability coefficient (cm h�1)�10�3 Lag time (h)
Liposome-Lido5 (0.5–5 h) 0.44 ± 0.04a,b,c*** 8.80 ± 0.85c*** –Liposome-Lido2.5 (0.5–4 h) 0.16 ± 0.04 6.51 ± 1.58f*** –EMLA� (0.5–5 h) 0.24 ± 0.05d*** 9.44 ± 2.14d***,e* –Xylocaına� (2–5 h) 0.09 ± 0.05 1.73 ± 1.21 1.46 ± 0.14c,d,f***
aLiposome-Lido5 versus Liposome-Lido2.5.bLiposome-Lido5 versus EMLA�.cLiposome-Lido5 versus Xylocaına�.dEMLA� versus Xylocaına�.eEMLA� versus Liposome-Lido2.5.fLiposome-Lido2.5 versus Xylocaına�.***p50.001 and *p50.05.
Table 5. VAS median (first and third quartiles) and preference considering the anesthetic effect rated by volunteers after needle insertion and anestheticinjection.
Anesthetic agentNeedle insertion VAS median
(first and third quartiles)Anesthetic injection VAS median
(first and third quartiles)Preference reported by
the volunteers in %
Liposome-Lido5 0.70 (0.34–2.75) 0.90 (0.34–2.43) 25.6Liposome-Lido2.5 1.25 (0.60–2.45) 1.60 (0.78–3.79) 7.7EMLA� 0.60 (0.10–1.20) 0.73 (0.24–1.70) 41.0Xylocaina� 2.00 (0.89–2.45) 2.10 (0.90–3.00) 20.5Placebo 2.10 (1.08–3.98) 2.48 (1.10–3.53) 2.6Liposomal placebo 1.40 (1.10–3.45) 2.30 (1.20–3.83) 2.6
DOI: 10.3109/08982104.2014.911315 Liposomal lidocaine gel for topical use 7
Jour
nal o
f L
ipos
ome
Res
earc
h D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Que
ensl
and
on 0
6/01
/14
For
pers
onal
use
onl
y.

anesthetic efficacy during the preclinical phase, as previously
observed by Mura et al. (2008).
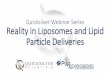
Figure 5 shows the correlation between permeability
coefficient of lidocaine across pig palatal mucosa (in vitro)
and in vivo efficacy of lidocaine formulations in reducing
pain during needle insertion (Figure 5a) and local anesthetic
injection (Figure 5b) in volunteers. A high (rPearson40.7,
p40.05) correlation was verified between P and
VAS-injection; and a moderate (rPearson40.3, p40.05)
correlation between P and VAS-insertion.
The permeability coefficient demonstrated to be another
worthy in vitro permeation parameter to predict topical
anesthetic efficacy in the oral mucosa as a high correlation
was found between P and VAS-injection; and a moderate
between P and VAS-insertion.
The correlation between in vitro parameters and in vivo
topical anesthetic efficacy can be explained by the hypothesis
previously suggested: a drug with a higher flux and perme-
ability coefficient presents a greater penetration into the
epithelium, resulting in a more-intense superficial analgesia
(Franz-Montan et al., 2013).
Conclusion
In conclusion, we successfully developed and characterized a
liposomal lidocaine formulation. The liposome encapsulated
5% lidocaine gel presented both in vitro and in vivo
performances similar to the gold standard commercial
formulation EMLA� in terms of permeation profile and in
reducing pain during needle insertion and anesthetic injection.
Therefore, it should be considered an efficient topical
anesthetic in dentistry.
In addition, the correlation between in vitro and in vivo
parameters suggests that in vitro studies could be helpful to
predict the effect of topical anesthetic agents.
Declaration of interest
No external funding and no competing interests declared. The
authors alone are responsible for the content and writing of
this paper. This study was financially supported by Sao Paulo
Research Foundation – FAPESP (grant # 2006/00121-9).
Daniela Belisario Baroni and Michelle Franz-Montan
acknowledge the scholarship provided by FAPESP (Grants #
2007/05734-1 and # 2009/08860-3, respectively).
References
Al-Melh MA, Andersson L. (2007). Comparison of topical anesthetics(EMLA/Oraqix vs. benzocaine) on pain experienced during palatalneedle injection. Oral Surg Oral Med Oral Pathol Oral Radiol Endod103:e16–20.
0 5 10 150
1
2
3
P(cm.h-1).103
VA
S I
nse
rtio
n (
in c
m)
0 5 10 150
1
2
3
4
P(cm.h-1).103
VA
S In
ject
ion
(in
cm)
(a) (b)
Figure 5. Relationship (mean ± SD) between permeability coefficient of lidocaine across pig palatal mucosa (in vitro) and pain scores duringneedle insertion (a) and anesthetic injection (b) in volunteers. Square: Xilocaına�; Circle: EMLA�; Triangle: LipoLido 5%; Lozenge: LipoLido 5%.(a) rPearson ¼ �0.2657 and (b) rPearson ¼ �0.6725.
0.0 0.2 0.4 0.60
1
2
3
Flux (mg.cm-2.h-1)
VA
S I
nse
rtio
n (
in c
m)
0.0 0.2 0.4 0.60
1
2
3
4
Flux (mg.cm-2.h-1)
VA
S In
ject
ion
(in
cm)
(a) (b)
Figure 4. Relationship (mean ± SD) between flux of lidocaine across pig palatal mucosa (in vitro) and pain scores during needle insertion (a) andanesthetic injection (b) in volunteers. (a) rPearson ¼ 0.3955 and (b): rPearson ¼ �0.0094.
8 M. Franz-Montan et al. J Liposome Res, Early Online: 1–9
Jour
nal o
f L
ipos
ome
Res
earc
h D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Que
ensl
and
on 0
6/01
/14
For
pers
onal
use
onl
y.

Agencia Nacional de Vigilancia Sanitaria – ANVISA. (2003). ResolutionRE no. 899; May 29, 2003; Brazil.
Armfield JM, Milgrom P. (2011). A clinician guide to patients afraid ofdental injections and numbness. SAAD Dig 27:33–9.
Bailey DN. (1992). Propylene glycol as a vehicle for percutaneousabsorption of therapeutic agents. J Anal Toxicol 16:97–8.
Bhalla J, Meechan JG, Lawrence HP, et al. (2009). Effect of time onclinical efficacy of topical anesthesia. Anesth Prog 56:36–41.
Boogaerts J, Declercq A, Lafont N, et al. (1993). Toxicity of bupivacaineencapsulated into liposomes and injected intravenously: comparisonwith plain solutions. Anesth Analg 76:553–5.
Boogaerts JG, Lafont ND, Declercq AG, et al. (1994). Epiduraladministration of liposome-associated bupivacaine for the manage-ment of postsurgical pain: a first study. J Clin Anesth 6:315–20.
Cereda CM, Brunetto GB, de Araujo DR, de Paula E. (2006). Liposomalformulations of prilocaine, lidocaine and mepivacaine prolonganalgesic duration. Can J Anaesth 53:1092–7.
Cereda CM, Tofoli GR, de Brito Junior RB, et al. (2008). Stabilityand local toxicity evaluation of a liposomal prilocaine formulation.J Liposome Res 18:329–39.
de Araujo DR, Cereda CM, Brunetto GB, et al. (2008). Pharmacologicaland local toxicity studies of a liposomal formulation for the novellocal anaesthetic ropivacaine. J Pharm Pharmacol 60:1449–57.
de Araujo DR, Padula C, Cereda CM, et al. (2010). Bioadhesive filmscontaining benzocaine: correlation between in vitro permeation andin vivo local anesthetic effect. Pharm Res 27:1677–86.
de Paula E, Schreier S. (1995). Use of a novel method for determinationof partition coefficients to compare the effect of local anesthetics onmembrane structure. Biochim Biophys Acta 1240:25–33.
Diaz Del Consuelo I, Pizzolato GP, Falson F, et al. (2005a). Evaluationof pig esophageal mucosa as a permeability barrier model for buccaltissue. J Pharm Sci 94:2777–88.
Diaz-Del Consuelo I, Jacques Y, Pizzolato GP, et al. (2005b).Comparison of the lipid composition of porcine buccal and esopha-geal permeability barriers. Arch Oral Biol 50:981–7.
Donaldson D, Meechan JG. (1995). A comparison of the effects ofEMLA cream and topical 5% lidocaine on discomfort during gingivalprobing. Anesth Prog 42:7–10.
Eidelman A, Weiss JM, Lau J, Carr DB. (2005). Topical anesthetics fordermal instrumentation: a systematic review of randomized, con-trolled trials. Ann Emerg Med 46:343–51.
Franz-Montan M, Cereda CM, Gaspari A, et al. (2013). Liposomal-benzocaine gel formulation: correlation between in vitro assays andin vivo topical anesthesia in volunteers. J Liposome Res 23:54–60.
Franz-Montan M, de Paula E, Groppo F, et al. (2010). Liposome-encapsulated ropivacaine for intraoral topical anesthesia. Oral SurgOral Med Oral Pathol Oral Radiol Endod 110:800–4.
Franz-Montan M, de Paula E, Groppo FC, et al. (2012). Liposomaldelivery system for topical anaesthesia of the palatal mucosa.Br J Oral Maxillofac Surg 50:60–4.
Franz-Montan M, Silva ALR, Cogo K, et al. (2007). Liposome-encapsulated ropivacaine for topical anesthesia of human oralmucosa. Anesth Analg 104:1528–31.
Friedman PM, Fogelman JP, Nouri K, et al. (1999). Comparative studyof the efficacy of four topical anesthetics. Dermatol Surg 25:950–4.
Ganem-Quintanar A, Quintanar-Guerrero D, Falson-Rieg F, Buri P.(1998). Ex vivo oral mucosal permeation of lidocaine hydrochloridewith sucrose fatty acid esters as absorption enhancers. Int J Pharm173:203–10.
Gee CM, Watkinson AC, Nicolazzo JA, Finnin BC. (2014). The effect offormulation excipients on the penetration and lateral diffusion ofibuprofen on and within the stratum corneum following topicalapplication to humans. J Pharm Sci 103:909–19.
Harker T. (1997). What injection? Br Dent J 182:50.
Herkenne C, Naik A, Kalia YN, et al. (2008). Effect of propylene glycolon ibuprofen absorption into human skin in vivo. J Pharm Sci 97:185–97.
Holst A, Evers H. (1985). Experimental studies of new topicalanaesthetics on the oral mucosa. Swed Dent J 9:185–91.
Hutchins HS, Young FA, Lackland DT, Fishburne CP. (1997). Theeffectiveness of topical anesthesia and vibration in alleviating the painof oral injections. Anesth Prog 44:87–9.
ICH. (1996). International conference on harmonisation of technicalrequirements for registration of pharmaceuticals for human use.Q2B. Validation of analytical procedures: methodology.
Kang L, Poh AL, Fan SK, et al. (2007). Reversible effects of permeationenhancers on human skin. Eur J Pharm Biopharm 67:149–55.
Maestrelli F, Capasso G, Gonzalez-Rodrıguez ML, et al. (2009). Effectof preparation technique on the properties and in vivo efficacy ofbenzocaine-loaded ethosomes. J Liposome Res 19:253–60.
McMillan AS, Walshaw D, Meechan JG. (2000). The efficacy ofEmla and 5% lignocaine gel for anaesthesia of human gingivalmucosa. Br J Oral Maxillofac Surg 38:58–61.
Meechan JG. (2000). Intra-oral topical anaesthetics: a review. J Dent 28:3–14.
Meechan JG. (2002). Effective topical anesthetic agents and techniques.Dent Clin North Am 46:759–66.
Meechan JG, Howlett PC, Smith BD. (2005). Factors influencing thediscomfort of intraoral needle penetration. Anesth Prog 52:91–4.
Meechan JG, Thomason JM. (1999). A comparison of 2 topicalanesthetics on the discomfort of intraligamentary injections: adouble-blind, split-mouth volunteer clinical trial. Oral Surg OralMed Oral Pathol Oral Radiol Endod 87:362–5.
Melero A, Garrigues TM, Almudever P, et al. (2008). Nortriptylinehydrochloride skin absorption: development of a transdermal patch.Eur J Pharm Biopharm 69:588–96.
Merino V, Mico-Albinana T, Nacher A, et al. (2008). Enhancement ofnortriptyline penetration through human epidermis: influence ofchemical enhancers and iontophoresis. J Pharm Pharmacol 60:415–20.
Mura P, Capasso G, Maestrelli F, Furlanetto S. (2008). Optimization offormulation variables of benzocaine liposomes using experimentaldesign. J Liposome Res 18:113–25.
Ntimenou V, Fahr A, Antimisiaris SG. (2012). Elastic vesicles fortransdermal drug delivery of hydrophilic drugs: a comparison ofimportant physicochemical characteristics of different vesicle types.J Biomed Nanotechnol 8:613–23.
Paavola A, Yliruusi J, Kajimoto Y, et al. (1995). Controlled release oflidocaine from injectable gels and efficacy in rat sciatic nerve block.Pharm Res 12:1997–2002.
Paphangkorakit J, Sangsirinakagul C, Priprem A. (2012). Relief ofpalatal injection pain by liposome-encapsulated 2% lignocaineprepared by ultrasonic dental scaler. Br J Oral Maxillofac Surg 50:784–7.
Primosch RE, Robinson L. (1996). Pain elicited during intraoralinfiltration with buffered lidocaine. Am J Dent 9:5–10.
Puglia C, Sarpietro MG, Bonina F, et al. (2011). Development,characterization, and in vitro and in vivo evaluation of benzocaine-and lidocaine-loaded nanostructrured lipid carriers. J Pharm Sci 100:1892–9.
Silva ALR, Franz-Montan M, Groppo FC, et al. (2008). Pharmaceuticalcomposition comprising a local anaesthetic and a carboxyvinylpolymer. International Patent Number # WO/2008/1380892008.
Svensson P, Bjerring P, Arendt-Nielsen L, Kaaber S. (1992).Hypoalgesic effect of EMLA and lidocaine gel applied on humanoral mucosa: quantitative evaluation by sensory and pain thresholds toargon laser stimulation. Anesth Prog 39:4–8.
Taddio A, Soin HK, Schuh S, et al. (2005). Liposomal lidocaine toimprove procedural success rates and reduce procedural pain amongchildren: a randomized controlled trial. CMAJ 172:1691–5.
DOI: 10.3109/08982104.2014.911315 Liposomal lidocaine gel for topical use 9
Jour
nal o
f L
ipos
ome
Res
earc
h D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Que
ensl
and
on 0
6/01
/14
For
pers
onal
use
onl
y.