Embed Size (px)
Citation preview

Gut, 1982, 23, 465-474
Liver disease after bone marrow transplantationM J G FARTHING*, M L CLARK, J P SLOANE,R L POWLES, and T J McELWAIN
From the Department of Gastroenterology, St Bartholomew's Hospital, London, and the Leukaemia Unit,The Royal Marsden Hospital, Sutton, Surrey
SUMMARY Liver dysfunction occurs after bone marrow transplantation but the relativeimportance of graft versus host disease and other factors, such as infection, radiation, and drugs,has not been clearly established. We have studied liver status before and after bone marrowtransplantation in 43 consecutive patients and have related this to survival and factors that arerecognised to cause liver injury. Minor abnormalities of liver tests occurred in 21% of patientsbefore grafting but this did not influence survival or the development of liver disease aftertransplantation. During the first 50 days after grafting, 83% of patients had abnormal liver testswhich were more severe in patients who subsequently died. Alanine transaminase was
significantly higher in non-survivors and appeared to predict survival early after transplantation.Only non-survivors developed clinical signs of liver disease. Severe liver disease was alwaysassociated with graft versus host disease and atypia of the small bile ducts was the most usefulhistological marker of hepatic involvement with this disease. Two of the patients with hepaticgraft versus host disease also had hepatic veno-occlusive disease and three fatalities hadopportunistic infection of the liver, although, in the latter, death was not due primarily to liverdysfunction. Previous hepatitis and androgen therapy could not be implicated as importantcauses of hepatic damage but chemotherapy for acute leukaemia and conditioning regimens forbone marrow transplanatation appear to be the most important factors in the development ofhepatic veno-occlusive disease.
Hepatic dysfunction is a well-recognised feature ofgraft versus host disease (GVHD) complicatingbone marrow transplantationl13 and usually occurswhen there is already skin or gut involvement.GVHD can occur in up to 70% of successfulallogeneic grafts2 4 5 and now accounts for many ofthe deaths after grafts for acute leukaemia. Thedevelopment of severe liver disease has beenreported6 7 but its prevalence and effect on survivalremain uncertain. Hepatic dysfunction after bonemarrow grafting is often attributed to GVHD butmany other factors, such as previous hepatitis,chemotherapy, radiation, opportunistic infection,and drugs used to treat GVHD, are also likely to beimportant. Severe distrubance of liver function hascommonly been associated with death after bonemarrow transplantation at the Royal Marsden Unitand we have therefore made a retrospective study of
* Address for correspondence: Dr M J G Farthing, Division of GeographicMedicine, Tufts University School of Medicine, Box 22, 136 Harrison Avenue,Boston, MA 02111, USA.Received for publication 28 August 1981
liver function before and after bone marrowgrafting. We have examined the relationshipbetween GVHD and other possible aetiologicalfactors and searched for markers that might predictsurvival and the development of liver disease.
Methods
PATIENTSForty consecutive patients, 14 with aplasticanaemia, 21 with acute leukaemia and two withdisseminated malignancy received allogeneic bonemarrow transplants from HLA identical and mixed-lymphocyte-culture compatible siblings, and threepatients with acute leukaemia (nos. 31, 32, and 41)received syngeneic marrow from an identical twin.Bone marrow transplantation was performed
according to the Seattle schedule.8 Five days beforegrafting the donor buffy coat was given, followed inpatients with leukaemia and other neoplastic diseaseby cyclophosphamide, 65 mg/kg for the next twodays. Thirty-six hours later these patients were given1000 rads total body irradiation as a single fraction
465
on October 1, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.23.6.465 on 1 June 1982. D
ownloaded from

Farthing, Clark, Sloane, Powles, and McElwain
from a cobalt source at 2.5 rad/min, after whichbone marrow was infused intravenously. Patientsgrafted for aplastic anaemia were treated similarly,except that cyclophosphamide was given at 60 mg/kgfor four days and they did not receive total bodyirradiation. On the day after transplantation oralmethotrexate2 9 or cyclosporin Al0 or both weregiven as a prophylaxis against GVHD. After trans-plantation patients were nursed in reverse barrierisolation, ate sterile food, and received oral non-
adsorbable antibiotics.'1 All transfused bloodproducts were irradiated to 1500 rads. Clinicaldetails with respect to age, initial diagnosis, previouschemotherapy and total body irradiation, GVHD,and liver histopathology are outlined in Tables 1 and2.
CLINICAL AND BIOCHEMICAL ASSESSMENT OFLIVER STATUSA clinical history was taken with particular emphasison drugs and previous hepatic disorders, particularlyhepatitis. Overall liver status was assessed by a
combined clinical and biochemical grading system,the details of which are shown in Table 3. This was
used to assess liver status before grafting and duringan early (<50 days) and a late (>50 days) periodafter grafting. Alanine transaminase (ALT 'opti-mised' UV system, Boehringer Corporation,
London), alkaline phosphatase (Technicon auto-analyser II technique), and bilirubin (by auto-analyser using a standard alkaline diazo-couplingmethod) were measured regularly before trans-plantation, daily for at least three weeks aftertransplantation, and then at least weekly thereafter.Serum was tested for the presence of HbsAg(Hepatest, Burroughs Wellcome) and also, whenappropriate, for antibodies to a variety ofpathogens.
HISTOPATHOLOGICAL ASSESSMENT OF LIVER
Post mortem examinations were carried out in 17 ofthe 23 patients who died, which provided materialfor histological examination by conventional lightmicroscopy. In addition, liver obtained by percuta-neous biopsy was available in three survivors. Gramstains were used for the identification of bacteriaand Grocott methanamine silver for fungi in theliver sections.
DEFINITION OF GVHDGraft versus host disease was considered present ifthe characteristic erythematous and desquamativeskin rash was accompanied by at least grade 2histological changes in the skin.12 Diarrhoea andtypical histological abnormalities in the rectalmucosa13 were taken as evidence of GVHD
Table 1 Survivors ofbone marrow transplantation
GVHD TreatmentPatient Sex-age Daysno. Diagnosis (yr) post-graft Skin Gut Liver Androgens TBI Chemotherapy
1 AA F16 750 - - + - CY,MX2 AA M6 900 - - - - CY,MX3 AA F10 690 - - - - CY, MX, PR4 AA M5 540 - - + - CY,MX5 AA F24 690 - - + - CY,MX6 AA M40 300 - - + -7 ALL M17 270 + - -* - + CY, CA, MX, ARAC, 6MP, VI, PR, AS8 ALL M3 480 - - - + CY, MX, ARAC, PR, VI9 ALL M18 150 + - - + CY, CA, ARAC, DA, 6MP, PR, VI10 ALL F14 77 - - - + CY, CA, ARAC, DA, 6MP PR, VI11 AML F17 210 - - - + CY, MX, ARAC, 6MP, RU 6TG12 AML M12- 210 - - - + CY, MX, ARAC, 6MP, 6TG, VI13 AML M25 540 - - - + CY, MX, ARAC, AD, DA, 6MP14 AML F15 270 - - - + CY, MX, ARAC, AD, 6MP, 6TG15 AML F27 180 + - - + CY, CA, ARAC, AD, 6MP, RU, 6TG16 AML M34 210 + + +* - + CY, CA, ARAC, DA, 6MP, 6TG17 AML F8 140 - - - + CY, CA, ARAC, DA, 6MP, 6TG18 AML F23 90 - - -* + CY, CA, ARAC, AD, DA, 6MP, 6TG19 AML M45 70 + - - + CY, CA, MX, 6MP, PR, VI, AS20 AML F14 56 - - - + CY,CA, ARAC, RU,6TG,VI
AA: aplastic anaemia. ALL: acute lymphoblastic leukaemia. AML: acute myeloid leukaemia. TBI: total body irradiation. CY:cyclophosphamide. MX: methotrexate. PR: prednisolone. CA: cyclosporin A. ARAC: cytosine arabinoside. VI: vincristine. 6MP:6-mercaptopurine. DA: daunorubicin. AD: adriamycin. 6TG: 6-thioguanine. RU: rubidomycin. AS: asparaginase.* Liver tissue obtained by needle biopsy available for histological examination. Patient 16 had the bile duct lesions of GVHD, but theothers had no abnormality.
466
on October 1, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.23.6.465 on 1 June 1982. D
ownloaded from

Liver disease after bone marrow transplantation
:2 6 6 ¢, 66::6< < <
< < < ~ <<
Ii 1 <5<(,,;< < <5< <X < < < < <t~~~~~~~~~~ 04<>pp^pXF>^>^Fs>>UUUUU
< > < > <~ < < <
~~~~~~~~ ~~ ~ ~ ~ ~ ~ .0 ~ c,U~~~~~~~ UU U U U Uo~> ~ W U ut)uto
II 1 1 1 1 11 +
++
EI
A
+1
+ 1
+ 1
+ +
Z um
a
Zr
-9 IS
+ + + + + + + +
I
+
+ +
+1+
+ +
+ + ++
_9 _
«<t-C4 m I*-
oo o Na o-
< < <n < oo
+
+ +
+ +
+
+ +
1-1
_- 0%
"ICc Z
0-
m m
1 )U U
z W W W
C1 m n tnm m m m.X -X
+ + + + ++
I
.6 .2m
-
U >
I
+ +
+ +
+ + +
+ 1
1 +
1 +
++
+ +
0 -
N Cz
00
r-
0
,c 1- 000
N} tZ Zz W
X X
00 028 0
m~ m~ c~
0
k }
-0
0
0n
.U
0?Q
CO
0
0Y
CO
0
467
cuE0
cu
zD
2
0
c
0
*.00C.Q~>
..
00
oCU>Cu0
0 .UWC
0
EI0U:
CO
0:0
I"
M.
I-,E0kZ
I".0
0h0
U.00
,+ + +
1
on October 1, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.23.6.465 on 1 June 1982. D
ownloaded from

Farthing, Clark, Sloane, Powles, and McElwain
Table 3 Biochemical and clinical grading of liver status
Alanine Alkalinetransaminase phosphatase Bilirubin Clinical
Grade (IUll) (IUlI) (,umolll) signs
0 Normal Normal Normal NoneI 21-100 100-300 Normal NoneII >100 >300 Normal NoneIII >100 >300 13-30 NoneIV >100 >300 >30 Jaundice,
ascites,Liver failure
Normalrange <21 <100 <13
involvement of the gastrointestinal tract. Thediagnosis of hepatic GVHD was based solely on thehistological findings of bile duct atypia with orwithout hepatocelhllar necrosis.
Results
SURVIVAL, GVHD, AND LIVER DISEASE AFTERBONE MARROW TRANSPLANTATIONOf the first 43 patients grafted, 20 are alive withmedian survival times of 21 months, eight months,and six months for patients grafted for aplasticanaemia, acute myeloid leukaemia, and acutelymphoblastic leukaemia respectively. These samediagnostic groups have plateaux of survival extend-ing to longer than three years, two years, and 1.5years respectively. GVHD was observed in 19 of the40 patients who received allogeneic grafts and in 14of the 20 patients who died (70%). The occurrenceof the clinical signs of liver disease and GVHD andtheir relationship to survival in individual patientsare shown in Tables 1 and 2.
LIVER STATUS BEFORE BONE MARROWTRANSPLANTATIONPrevious hepatitisAplastic anaemia followed acute hepatitis in three ofthe patients who subsequently received bonemarrow transplants (nos. 1, 21, and 28), one ofwhom was HbsAg positive (no. 28). Otherserological markers of acute hepatitis were notdetermined. Two of these patients (including theone who was HbsAg positive) died with severeGVHD with obvious hepatic involvement (nos. 21and 28); the third is alive after a successful,uncomplicated graft. Another patient with acutemyeloid leukaemia (no. 40) had HbsAg negativehepatitis during remission on maintenance chemo-therapy one year before grafting. Liver tests at thetime of grafting were normal but he died 47 dayslater with severe GVHD with liver involvement.
Liver testsA rise in ALT (always less than 100 IUll) occurredin only nine of the 43 patients grafted, and was notassociated with any abnormality of bilirubin oralkaline phosphatase. Abnormalities of ALT couldnot be related to any particular chemotherapeuticregimen and bore no relationship to survival or tothe development of liver disease after bone marrowtransplantation.
LIVER STATUS AFTER BONE MARROWTRANSPLANTATIONLiver status during the early and late post-transplantation periods is shown for both survivorsand non-survivors in Fig. 1. During the first 50 daysafter grafting, disturbance of liver tests occurred in83% of patients. During this early period, dif-ferences were apparent between survivors andnon-survivors. Forty per cent of the non-survivorshad moderate to severe (grade II-IV) liverdysfunction compared with 18% of the survivors,none of whom had developed clinical signs of liverdisease (grade IV).
In the later period (>50 days) after bone marrowtransplantation this pattern persisted: 56% of thenon-survivors had grade II-IV hepatic dysfunctioncompared with 12% of the survivors (grade II andIII only). To examine the relationship betweenabnormalities of liver tests and survival aftergrafting we analysed serial estimations of bilirubin,ALT, and alkaline phosphatase during the first 100days. Hyperbilirubinaemia above 30 iimol/l occur-red only in non-survivors. Median alkaline phospha-tase tended to rise throughout this period (Fig. 2)but differences between survivors and non-survivorsat 10, 20, 50, and 100 days were not significant.Median values' for ALT were greater in non-survivors at 20 days after grafting and by 50 days thisdifference was significant (survivors, median 24IU/l, range 9-130; non-survivors, median 69 IU/1,range 16-550; Mann Whitney U test, p<0-02).Additional examination of these data showed that, ifthe ALT was abnormal at 20 days after grafting, thechance of long-term survival was only 25%.
PREVIOUS DRUG THERAPYWe found no relation between previous androgen/anabolic steroid therapy and survival or thelikelihood of developing liver disease after trans-plantation. In addition, there was no correlationbetween the intensity of pre-graft chemotherapy andthe development of liver disease after grafting.
OPPORTUNISTIC INFECTION AND LIVER DISEASEAFTER BONE MARROW TRANSPLANTATIONThree of the 23 patients who died (13%) had
468
on October 1, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.23.6.465 on 1 June 1982. D
ownloaded from

Liver disease after bone marrow transplantation
Survivors Non-survivors
<50 days82% 18%
80 r
60% 4mPatients 40
20 r0 1 11 Ill lV
> 50 days88% 12%
80
60 [
Patients 40j-
20
60% 40%.5
0 1 11 Ill lV
42% 58%9 &
Fig. 1 Combined biochemicaland clinical assessment ofliverfunction in survivors and non-survivors during early (<50days) and late (>50 days)periods after bone marrowtransplantation.
0 1 11 Ill lV
unequivocal histological evidence of opportunisticinfection involving the liver (Table 2). One hadvaricella hepatitis, a second was found to havehepatic micro-abscesses containing Candida species,and the third had unspecified Gram-positive bacilliwithin the liver sinusoids. Despite these necropsyfindings in the liver, all of these patients haddisseminated disease and were thought to have diedfrom the effects of overwhelming sepsis rather thanliver failure. A fourth patient (no. 27) with mild skinGVHD, became jaundiced, developed clinical signsof liver failure, and had a rising titre to Toxoplasmagondii. However, the organism was not culturedbefore or after death, nor was it detected histo-logically in the liver. The significance of this risingtitre remains uncertain, although the specific IgMtitre also increased suggesting that there was recentinfection.
HISTOPATHOLOGICAL ASSESSMENT OF LIVERAFTER BONE MARROW TRANSPLANTATIONThe histopathological features of the 17 liversobtained at necropsy, together with percutaneousliver biopsies in three survivors have already beendescribed in detaillo but are summarised in Tables 1and 2.
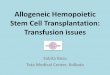
Atypia of the bile duct epithelium (Fig. 3) was
0 1 11 Ill lV
present in eight patients and involved only small bileducts. All of these patients had histological evidenceof moderate to severe GVHD in the skin or gut, orboth. In all but the mildest case, this bile duct lesionwas associated with histological evidence ofcholestasis, a mild lymphocytic infiltration, and arise in serum alkaline phosphatase, although thelatter was not significantly higher than in thosepatients without bile duct atypia. Four of thesepatients with bile duct atypia also had evidence ofportal fibrosis. Focal hepatocyte necrosis was foundin only four patients and in all cases the lesion wasminor. In only one patient did it occur in associationwith the bile duct lesion. All the livers examined hadevidence of moderate to severe siderosis.Evidence of veno-occlusive disease (Fig. 4) was
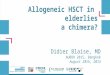
found in two patients (nos. 36 and 40), both ofwhom were jaundiced by the 20th day after trans-plantation and had other liver test abnormalities. Atthis time one had evidence of skin GVHD, as didthe other within a further five days. Both subse-quently developed oedema, ascites, and hypo-albuminaemia, and died in hepatic failure. Both ofthese patients had received a variety of chemothera-peutic agents including cytosine arabinoside, 6-thioguanine, and adriamycin, both had severeGVHD, and both had had total body irradiation.
469
.L-
on October 1, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.23.6.465 on 1 June 1982. D
ownloaded from

Farthing, Clark, Sloane, Powles, and McElwain
AlanineTransaminuwu/I80
70
60
50 /
40
30
20
10
0 20 50
Days
AlkalinePhos*patsu/I160 r
140
120
100
80
60
40
20
* Non survivors
o Survivors
a a
100 0 20 50 100
Days
Fig. 2 Median alanine transaminase and alkaline phosphatase in survivors and non-survivors during thefirstl100days afterbone marrow transplantation.
Fig. 3 Bile duct atypia. Smallbile ducts showing epithelial
Aq atypia surrounded byafewj ~~~~~chronic inflammatory cells and~~~~~~~~~ ~~~~~~~~several large irregular clumps
\ 4,~~~~~~~~.. ofhaemosiderin. Haematoxylinand eosin stain, X500 (original
" A.~~~~~~~4 ~~~~ ~magnification).
470
on October 1, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.23.6.465 on 1 June 1982. D
ownloaded from

Liver disease after bone marrow transplantation
Fig. 4 Veno-occlusive disease.Central vein partially occludedby afine meshwork of reticulinfibres. Reticulin stain, x300(original magnification).
Minor abnormalities in reticulin pattern were
observed in 16 patients and in six (nos. 21, 23, 28,38, 42, and 43) it was particularly evident around thecentral veins.
Discussion
In the present study severe liver dysfunctionoccurred in seven of the 23 patients who died (30%)and in all of these the disturbance of liver functionwas thought to be either the cause or a majorcontributor to death. The prevalence is similar tothat reported previously when nine of the 29 (31%)patients who died after bone marrow trans-plantation for aplastic anaemia had evidence of liverdysfunction,'5 one of whom was thought to havechronic aggressive hepatitis and the remainderGVHD involvement of the liver. The clinical stateof these patients and the histological criteria formaking the diagnosis of hepatic GVHD were notreported. Our retrospective study demonstratesthat, during the first 50 days after grafting, milddisturbances of liver tests occur in the majority ofpatients but in survivors were limited to rises in ALTand alkaline phosphatase, whereas significant hyper-bilirubinaemia above 30 ,umol/l was seen only in thenon-survivors. During the later period after grafting(>50 days), liver tests tended to improve insurvivors, whereas in non-survivors they deterio-rated: 58% had moderate to severe liver dysfunc-tion. Although we are reluctant to place undueemphasis on these liver tests, the proposal arising
from this study-that abnormalities of the ALT maypredict survival after bone marrow transplantationas early as 20 days after grafting-requiresprospective evaluation.While the aetiology of this abnormality is likely to
be multifactorial, it does suggest that factors otherthan the bile duct disturbance of GVHD contributeto transplantation liver injury.
PRE-GRAFT DRUG THERAPY AND ACUTE HEPATITISAlthough many of the drugs used to treat acuteleukaemia have been shown to be hepatotoxic,16 wewere unable to find a relationship between the typeor the extent of pre-graft chemotherapy and post-transplantation liver dysfunction. It is now appa-rent, however, that survival has been improved bygrafting patients with acute myeloid leukaemiaduring their first remission.5 17 The reduced amountof chemotherapy that these patients have receivedmay be an important factor in survival. Although 17a-alkylated androgenic and anabolic steroids areknown to cause hepatic damage,18 19 we found nocorrelation between previous androgen therapy andeither survival or the propensity to develop liverdysfunction after grafting.The effect of previous hepatitis on survival in the
present study cannot be evaluated satisfactorilybecause of inadequate numbers of patients. How-ever, it may be worth commenting that two of ourthree patients with post-hepatic aplastic anaemiadied after grafting with severe hepatic GVHD andfour of six patients with the same initial diagnosis inSeattle died, two of whom had liver complications.15
471
on October 1, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.23.6.465 on 1 June 1982. D
ownloaded from

Farthing, Clark, Sloane, Powles, and McElwain
CONDITIONING REGIMEN FOR BONE MARROWAlthough high-dose cyclophosphamide causeshepatic damage in animals,20 2 there is littleevidence of severe hepatotoxicity in man.22 Ionisingradiation, however, is known to cause hepatitis,hepatic fibrosis,23 24 and hepatic veno-occlusivedisease.25 In addition, hepatic tolerance to radiationis reduced when combined with certain drugs,particularly adriamycin,26 antinomycin D, and 5-fluoro-uracil.27 However, our patients withleukaemia received the same conditioning regimenso the specific effects of chemotherapy and radiationcannot be determined, but a recent study6 hasdemonstrated increased hepatotoxicity of condition-ing regimens which included carmustine andbusulfan. In our study, the prevalence of clinicalliver disease was not significantly reduced in patientsgrafted for aplastic anaemia (conditioned withouttotal body irradiation), although a direct compari-son cannot be made, as these patients received moreprolonged conditioning with cyclophosphamide.
GVHD
GVHD occurred in 48% of the 40 patients whoreceived allogeneic grafts and in 70% of thefatalities. Although there was a strong associationbetween the occurrence of severe clinical liverdisease and the presence of GVHD elsewhere,biochemical abnormalities were more common andoccurred in 83% of the patients, suggesting thatfactors other than GVHD are responsible forhepatic dysfunction after bone marrow trans-plantation. The most striking histological feature inthe liver associated with skin and gut GVHD wascellular atypia of small bile ducts which was almostinvariably associated with cholestasis. This featurehas been reported previously in man,3 13 28 and hasbeen shown recently to be a reliable indicator ofhepatic involvement by GVHD in the dog.29 Thesefindings suggest that bile duct atypia is probably themost important single feature of hepatic GVHDand may also be a guide to its severity.13 Thereare previous reports both in animals29 30 andman' 6 31 32 of focal necrosis occurring in the liver inGVHD but, in this study, it was seen infrequentlyand was always minor. Using the criterion of bileduct atypia, only seven of the 14 patients who diedwith GVHD were regarded as having hepaticGVHD, although all of the remainder had moderateto severe abnormalities of liver tests. We did notobserve bile duct atypia in patients who did not haveGVHD in another organ.
10
Methotrexate and cyclosporin A' were used inprophylaxis and treatment of GVHD. Althoughmethotrexate can cause liver damage33 34 we did notdiscover any obvious toxic effects in our patients
which we could definitely attribute to the drug,although it may have contributed to the abnormal-ities of hepatic reticulin pattern seen in somepatients.6 7Cyclosporin A causes reversible abnor-malities of liver tests in man'0 35 and animals andliver cell necrosis in the dog.36 Cyclosporin A wasgiven to 12 patients in this study and the six whoreceived it prophylactically are all alive. It appearsto be effective in controlling skin GVHD'0 but itseffect on the liver and hepatic GVHD requiresclarification.
VENO-OCCLUSIVE DISEASEHistological evidence of hepatic veno-occlusivedisease accompanied by the clinical syndrome ofjaundice, ascites, and hepatic failure was found intwo patients in the present study. Several recentstudies have reported similar findings.6 7 32 37 38Although Berk et al.32 found a striking associationbetween hepatic VOD and the presence of GVHDin other organs, the absence of small bile ductabnormalities in their patients-a feature whichwe14 and others13 29 now regard as indicative ofhepatic GVHD-makes it difficult to be certainwhether there was hepatic GVHD involvement intheir patients. Both of our patients received totalbody irradiation which itself can cause veno-occlusive disease,25 but hepatic veno-occlusivedisease has now been described in patientsconditioned without total body irradiation.32Radiation, however, may be a contributory factor inthe production of veno-occlusive disease in somerecipients of bone marrow transplants. Thedevelopment of veno-occlusive disease can clearlybe independent of the presence of hepatic GVHD,as the former has occurred in patients grafted withautologous marrow.7 38 Current evidence indicatesthat veno-occlusive disease occurs more commonlyin patients grafted for acute leukaemia,7 38suggesting that chemotherapeutic agents have animportant place in its pathogenesis. Shulman et al.7have also shown a significantly increased prevalenceof veno-occlusive disease in patients who receivedmore intensive chemotherapy and in those whoseconditioning included dimethyl busulfan. Analysisof the current literature on veno-occlusive diseaseafter bone marrow transplantation suggests thatthe antimetabolites cytosine arabinoside and6-thioguanine are the drugs most commonlyassociated with this disease,3 both of which wereamong the drugs received by our patients.
Liver dysfunction after bone marrow transplanta-tion is common and clearly a complex matter and itis unlikely that any single factor is responsible.Severe liver disease after bone marrow trans-plantation, however, was always associated with
472
on October 1, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.23.6.465 on 1 June 1982. D
ownloaded from

Liver disease after bone marrow transplantation 473
GVHD alone or in combination with veno-occlusivedisease. It would seem important that histologicaldiagnostic criteria are established for hepaticGVHD and current evidence would favour bile ductatypia as the most useful. Liver test abnormalityalone is insufficient to make a diagnosis of hepaticGVHD.
Drugs, radiation, or opportunistic infection canbe important in some patients either alone or incombination. The cause of hepatic veno-occlusivedisease and the abnormalities of hepatic reticulinremains uncertain, although chemotherapy for acuteleukaemia and pre-graft conditioning regimensappear at present to be the most important factors.
References
1 Kruger GRF, Berard CW, DeLellis RA et al. Graft-versus-host disease. Am J Pathol 1971; 63: 179-201.
2 Thomas ED, Storb R, Clift RA et al. Bone marrowtransplantation (second of two parts). N Engl J Med1975; 292: 895-902.
3 Woodruff JM, Hansen JA, Good RA et al. Thepathology of graft-versus-host reaction (GVHR) inadults receiving bone marrow transplants. TransplantProc 1976; 8: 675-84.
4 Storb R, Prentice RL, Thomas ED. Treatment ofaplastic anaemia by marrow transplantation from HLAidentical siblings. Prognostic factors associated withgraft versus host disease and survival. J Clin Invest1977; 59: 625-32.
5 Thomas ED, Buckner CD, Clift RA et al. Marrowtransplantation for acute nonlymphoblastic leukaemiain first remission. N Engl J Med 1979; 301: 597-9.
6 Beschorner WE, Pino J, Boitnott JK, Tutschka PJ,Santos G. Pathology of the liver with bone marrowtransplantation. Effects of busulfan, carmustine, acutegraft-versus-host disease and cytomegalovirus infec-tion. Am J Pathol 1980; 99: 369-85.
7 Shulman HM, McDonald GB, Matthews D, DoneyKC, Kopecky KJ, Gauvreau JM, Thomas ED. Ananalysis of hepatic venocclusive disease and centri-lobular hepatic degeneration following bone marrowtransplantation. Gastroenterology 1980; 79: 1178-91.
8 Thomas ED, Buckner CD, Banaji M et al. Onehundred patients with acute leukaemia treated bychemotherapy, total body irradiation and allogeneicbone marrow transplantation. Blood 1977; 49: 511-33.
9 Storb R, Epstein RB, Graham TC, Thomas ED.Methotrexate regimens for control of graft-versus-hostdisease in dogs with allogeneic marrow grafts. Trans-plantation 1970; 9: 240-6.
10 Powles RL, Clink H, Sloane J, Barrett AJ, Kay HEM,McElwain TJ. Cyclosporin A for the treatment ofgraft-versus-host disease in man. Lancet 1978; 2:1327-31.
11 Storring RA, Jameson B, McElwain TJ, Wiltshaw E,Spiers ASD, Gaya H. Oral non-absorbed antibioticsprevent infection in acute non-lymphoblastic
leukaemia. Lancet 1977; 2: 837-40.12 Sale GE, Lerner KG, Barker EA, Shulman HM,
Thomas ED. The skin biopsy in the diagnosis of acutegraft-versus-host disease in man. Am J Pathol 1977; 89:621-36.
13 Slavin RE, Santos GW. The graft versus host reactionin man after bone marrow transplantation: pathology,pathogenesis, clinical features and implication. ClinImmunol Immunopathol 1973; 1: 472-98.
14 Sloane JP, Farthing MJG, Powles RL. Histopatho-logical changes in the liver following allogeneic bonemarrow transplantation. J Clin Pathol 1980; 33: 344-50.
15 Storb R, Thomas ED, Weiden PL et al. Aplasticanaemia treated by allogeneic bone marrow trans-plantation: A report on 49 new cases from Seattle.Blood 1976; 48: 817-41.
16 Ludwig J. Drug effects on the liver. A tabularcompilation of drugs and drug-related hepatic diseases.Dig Dis Sci 1979; 24: 785-96.
17 Powles RL, Clink HM, Bandini G et al. Bone marrowtransplantation in acute myelogenous leukaemia.Lancet 1980; 1: 1047-50.
18 Bagheri SA, Boyer JL. Peliosis hepatitis associatedwith androgenic anabolic steroid therapy. A severeform of hepatic injury. Ann Intern Med 1974; 81:610-8.
19 Westaby D, Paradinas FJ, Ogles J et al. Liver damagefrom long-term methyltestosterone. Lancet 1977; 2:261-3.
20 Lee C, Castles TR, Kintner LD. Single dose toxicity ofcyclophosphamide (NSC-26271) in dogs and monkeys.Cancer Chemother Rep 1973; Pt 3, 4: 51-76.
21 Celle G, Dodero M, Bogliolo G et al. Chronictreatment with azathioprine and cyclophosphamide inrats: Structural and functional effects on small intestineand liver. GEN 1977; 31: 179-84.
22 Aubrey DA. Massive hepatic necrosis after cyclo-phosphamide. Br Med J 1970; 2: 588.
23 Lansing AM, Davis WM, Brizel HE. Radiationhepatitis. Arch Surg 1968; 96: 878-82.
24 Lewin K, Millis RR. Human radiation hepatitis. ArchPathol 1973; 96: 21-6.
25 Reed GB, Cox AJ. The human liver after radiationinjury. Am J Pathol 1966; 48: 597-611.
26 Kun LE, Camitta BM. Hepatopathy following irradia-tion and adriamycin. Cancer 1978; 42: 81-4.
27 Tefft M, Mitus A, Jaffe N. Irradiation of the liver inchildren: acute effects enhanced by concomitantchemotherapeutic administration. AJR 1971; 111: 165-73.
28 Lerner KG, Kao GF, Storb R et al. Histopathology ofgraft versus host reaction (GVHR) in human recipientsof marrow from HL-A matched sibling donors. Trans-plant Proc 1974; 6: 367-71.
29 Sale GE, Storb R, Kolb H. Histopathology of acutegraft-versus-host disease in the dog. Transplantation1978; 26: 103-6.
30 Van Bekkum DW, De Vries MJ. Radiation chimeras.New York: Academic Press, 1967.
31 Slavin RE, Woodruff JM. Pathology of bone marrowtransplantation. Pathol Ann 1974; 9: 291-344.
32 Berk PD, Popper H, Kruger GRF, Decter J, Herzig G,
on October 1, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.23.6.465 on 1 June 1982. D
ownloaded from

474 Farthing, Clark, Sloane, Powles, and McElwain
Graw RG. Veno-occlusive disease of the liver afterallogeneic bone marrow transplantation. Ann InternMed 1979; 90: 158-64.
33 Dahl MGC, Gregory MM, Scheuer PJ. Liver damagedue to methotrexate in patients with psoriasis. Br MedJ 1971; 1: 625-30.
34 Dahl MGC, Gregory MM, Scheuer PJ. Methotrexatehepatotoxicity in psoriasis - comparison of differentdose regimens. Br Med J 1972; 1: 654.
35 Calne RY, Thiru S, McMaster P et al. Cyclosporin A inpatients receiving renal allografts from cadaver donors.Lancet 1978; 2: 1324-7.
36 Calne RY. White JG, Pentlow BD et al. Cyclosporin
A: Preliminary observations in dogs with pancreaticduodenal allografts and patients with cadaveric renaltransplants. Transplant Proc 1979; 11: 860-4.
37 Jacobs P, Miller JL, Uys CJ, Dietrich BE. Fatalveno-occlusive disease of the liver after chemotherapy,whole body irradiation and bone marrow transplanta-tion for refractory acute leukaemia. S Afr Med J 1979;55: 5-10.
38 Woods WG, Dehner LP, Nesbit ME, Krivit W, CocciaPF, Ramsay NKC, Kim TH, Kersey JH. Fatal veno-occlusive disease of the liver following high dosechemotherapy, irradiation and bone marrow trans-plantation. Am J Med 1980; 68: 285-90.
on October 1, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.23.6.465 on 1 June 1982. D
ownloaded from