Embed Size (px)
DESCRIPTION
Liver disease and how to manage it!. Dr Allister J Grant Consultant Hepatologist Leicester Liver Unit University Hospitals Leicester NHS Trust. IVC. Portal Vein. Hepatic Artery. Splenic Vein. CBD. Gallbladder. SMV. Anatomy &Physiology. Anatomy &Physiology. Liver Functions. - PowerPoint PPT Presentation
Citation preview
Liver disease and how Liver disease and how to manage it!to manage it!
Dr Allister J GrantDr Allister J GrantConsultant HepatologistConsultant Hepatologist
Leicester Liver UnitLeicester Liver UnitUniversity Hospitals Leicester NHS TrustUniversity Hospitals Leicester NHS Trust

Anatomy &PhysiologyAnatomy &Physiology
Hepatic Artery
IVC
Splenic Vein
SMVGallbladder
Portal Vein
CBD

Anatomy &PhysiologyAnatomy &Physiology

Liver FunctionsLiver Functions
Nutrition/MetabolicNutrition/Metabolic– – stores glycogen (glucose chains)stores glycogen (glucose chains)– – releases glucosereleases glucose– – absorbs fats, fat soluble vitaminsabsorbs fats, fat soluble vitamins– – manufactures cholesterolmanufactures cholesterol
Bile SaltsBile Salts– – lipids derived from cholesterollipids derived from cholesterol– – dissolves dietary fats (detergent)dissolves dietary fats (detergent)
BilirubinBilirubin– – breakdown product of haemoglobinbreakdown product of haemoglobin

Liver FunctionsLiver Functions
Clotting FactorsClotting Factors– – manufactures most clotting factorsmanufactures most clotting factors
Immune functionImmune function– – Kupfer cells engulf antigens (bacteria)Kupfer cells engulf antigens (bacteria)
DetoxificationDetoxification– – drug excretion (sometimes activation)drug excretion (sometimes activation)– – alcohol breakdownalcohol breakdown
Manufactures ProteinsManufactures Proteins– – albuminalbumin– – binding proteinsbinding proteins

Liver Function TestsLiver Function Tests
Different cells have different enzymes inside them, Different cells have different enzymes inside them, depending on the function of the cell.depending on the function of the cell.
AST and ALT are associated with AST and ALT are associated with hepatocytehepatocyte damage damage
GGT and ALP are associated with GGT and ALP are associated with cholangiocytecholangiocyte damage ie biliary diseasedamage ie biliary disease

AminotransferasesAminotransferases
1. Alanine aminotransferase (ALT) and 1. Alanine aminotransferase (ALT) and
Aspartate aminotransferase (AST) Aspartate aminotransferase (AST)
These are enzymes that help to process These are enzymes that help to process proteins.proteins.
ALT is more specific for liver disease than AST ALT is more specific for liver disease than AST as AST is found in more types of cell (e.g. heart, as AST is found in more types of cell (e.g. heart, intestine, muscle). intestine, muscle).

Alkaline PhosphataseAlkaline Phosphatase This enzyme level is elevated in a large number of disorders that affect the This enzyme level is elevated in a large number of disorders that affect the
drainage of bile e.g.drainage of bile e.g.
• Gallstones damaging the bile ductGallstones damaging the bile duct• Tumor blocking the common bile ductTumor blocking the common bile duct• Drug-induced cholestatic hepatitis, blocking the flow of bile in smaller bile Drug-induced cholestatic hepatitis, blocking the flow of bile in smaller bile
channels within the liverchannels within the liver
The alkaline phosphatase is also released from damagedThe alkaline phosphatase is also released from damaged
• bone, bone, • placenta, andplacenta, and• intestine (isoenzymes)intestine (isoenzymes)
For this reason, the GGT is utilized as a supplementary test to be sure that For this reason, the GGT is utilized as a supplementary test to be sure that the elevation of alkaline phosphatase is indeed coming from the liver or the the elevation of alkaline phosphatase is indeed coming from the liver or the biliary tractbiliary tract


Other Liver “Enzymes”Other Liver “Enzymes”
3) 3) AlbuminAlbumin is a major protein which is produced by the liver is a major protein which is produced by the liver
In more advanced liver disease, the level of the serum albumin is In more advanced liver disease, the level of the serum albumin is reduced.reduced.
4)4) Bilirubin Bilirubin is the main bile pigment in humans. is the main bile pigment in humans.
Bilirubin is formed primarily from the breakdown of called "haem” Bilirubin is formed primarily from the breakdown of called "haem” from red blood cells from red blood cells
When elevated, bilirubin causes the yellow discoloration of the skin When elevated, bilirubin causes the yellow discoloration of the skin and eyes- jaundice and maybe associated with dark urine.and eyes- jaundice and maybe associated with dark urine.
The bilirubin may be elevated in many forms of liver or biliary tract The bilirubin may be elevated in many forms of liver or biliary tract disease, and thus it is also relatively nonspecific.disease, and thus it is also relatively nonspecific.

Other Liver EnzymesOther Liver Enzymes
5) 5) Gamma Glutamyl Transpeptidase Gamma Glutamyl Transpeptidase is often elevated in liver is often elevated in liver disorders but disorders but notnot in diseases of bone, placenta, or intestine. in diseases of bone, placenta, or intestine.
HoweverHowever the high sensitivity and very low specificity of this test the high sensitivity and very low specificity of this test seriously hampers its usefulness.seriously hampers its usefulness.
GGT is elevated in a whole host of liver diseases GGT is elevated in a whole host of liver diseases
BUT also in BUT also in
• obesityobesity• hyperlipidaemiahyperlipidaemia• diabetesdiabetes• congestive cardiac failurecongestive cardiac failure• diseases of the kidney, pancreas and prostate.diseases of the kidney, pancreas and prostate.

ALT elevated? (>53)ALT elevated? (>53)
Hepatitic illnessHepatitic illness
AcuteAcute AgeAge SexSex DrugsDrugs AlcoholAlcohol TravelTravel ContactsContacts Risky behaviourRisky behaviour AutoimmunityAutoimmunity FeverFever AF/BP/CCFAF/BP/CCF Pregnant?Pregnant?
ChronicChronic Age/sexAge/sex EthnicityEthnicity BMIBMI LipidsLipids DiabetesDiabetes AlcoholAlcohol TravelTravel Risky behaviourRisky behaviour FHxFHx
• AutoimmunityAutoimmunity• Unexplained CirrhosisUnexplained Cirrhosis

The majority of abnormal LFTs in The majority of abnormal LFTs in asymptomatic people occur in those with:asymptomatic people occur in those with:
Diabetes or metabolic syndrome Diabetes or metabolic syndrome (increased risk of NAFLD) (increased risk of NAFLD)
Excessive alcohol intake Excessive alcohol intake Chronic hepatitis B or CChronic hepatitis B or C DrugsDrugs


ALT elevatedALT elevated
Hepatitic illnessHepatitic illness
AcuteAcute Hep A,B,C,EHep A,B,C,E EBV, CMV, TOXOEBV, CMV, TOXO Drugs screen?Drugs screen? ImmunoglobulinsImmunoglobulins Autoimmune profileAutoimmune profile Caeruloplasmin (<50)Caeruloplasmin (<50)
ChronicChronic TFTTFT Diabetic screenDiabetic screen Hep B, CHep B, C LipidsLipids ImmunoglobulinsImmunoglobulins Autoimmune profileAutoimmune profile FerritinFerritin Caeruloplasmin (<50)Caeruloplasmin (<50) αα-1 antitrypsin-1 antitrypsin TTGTTG (ACE)(ACE)
ALP Elevated? (>130)ALP Elevated? (>130)
Cholestatic IllnessCholestatic Illness((With or without jaundice)With or without jaundice)
AcuteAcute
Age/SexAge/Sex Drugs/AntibioticsDrugs/Antibiotics FHx gallstonesFHx gallstones Abdo PainAbdo Pain Red flag symptomsRed flag symptoms Jaundice?Jaundice?
Differentiate from bonyDifferentiate from bony
ChronicChronic
Family HxFamily Hx Metabolic syndromeMetabolic syndrome Recurrent FeverRecurrent Fever Itch/lethargyItch/lethargy Dry eyes/mouthDry eyes/mouth ColitisColitis PainPain SOB/Resp symptomsSOB/Resp symptoms CCFCCF

Liver ALP ElevatedLiver ALP Elevated Cholestatic IllnessCholestatic Illness
AcuteAcute
CBD stones/GallstonesCBD stones/Gallstones Tumours 1Tumours 1ºº or 2 or 2ºº Pancreatic pathologyPancreatic pathology DrugsDrugs InfiltrationInfiltration SODSOD
ChronicChronic
PBCPBC Sclerosing CholangitisSclerosing Cholangitis
• 11ºº or 2 or 2ºº NASHNASH αα-1 antitrypsin-1 antitrypsin SarcoidSarcoid AmyloidAmyloid HIVHIV
Drug Induced CholestasisDrug Induced Cholestasis Intrahepatic Hepatocellular Intrahepatic Hepatocellular
Cholestasis Cholestasis
Intrahepatic Ductular cholestasisIntrahepatic Ductular cholestasis
DuctopenicDuctopenic
GranulomatousGranulomatous
AllopurinolAllopurinolAntithyroid agentsAntithyroid agents
AugmentinAugmentinAzathioprineAzathioprineBarbituratesBarbituratesCaptoprilCaptoprilCarbamezepineCarbamezepineChlorpromazineChlorpromazineChlorpropamideChlorpropamideClindamycinClindamycin
ClofibrateClofibrateDiltiazemDiltiazem
Erythromycin estolateErythromycin estolateFlucloxacillinFlucloxacillin
IsoniazidIsoniazid
LisinoprilLisinoprilMethyltestosteroneMethyltestosterone
Oral contraceptives (containing estrogens)Oral contraceptives (containing estrogens)Oral hypoglycemics Oral hypoglycemics PhenytoinPhenytoinTrimethoprim-sulfamethoxazole Trimethoprim-sulfamethoxazole
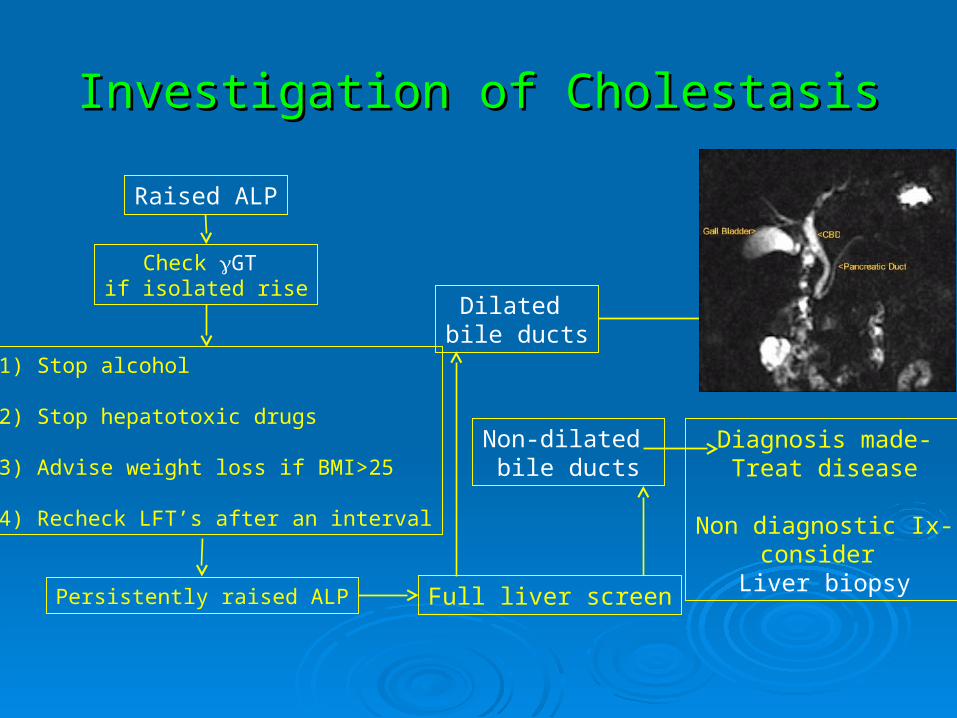
Investigation of CholestasisInvestigation of Cholestasis
Dilated bile ducts
Non-dilated bile ducts
Full liver screen
Raised ALP
Check GT if isolated rise
1) Stop alcohol
2) Stop hepatotoxic drugs
3) Advise weight loss if BMI>25
4) Recheck LFT’s after an interval
Persistently raised ALP
ConsiderMRCPERCP
Other imaging
Diagnosis made-Treat disease
Non diagnostic Ix-consider
Liver biopsy
Isolated raise in Bilirubin (>22)Isolated raise in Bilirubin (>22)
DifferentialDifferential Gilberts vs HaemolysisGilberts vs Haemolysis
Gilberts- Gilberts- Unconjugated hyperbilirubinaemiaUnconjugated hyperbilirubinaemia
Haemolysis-Haemolysis-Unconjugated hyperbilirubinaemiaUnconjugated hyperbilirubinaemia
splenomegaly, anaemia , splenomegaly, anaemia , DCT, haptoglobin, reticulocyte count, filmDCT, haptoglobin, reticulocyte count, film

Disease ProgressionDisease ProgressionL
iver
fu
nct
ion
100%
Cirrhosis
Liver Failure
Years
A
B
CD
Mrs WMrs W 48 year old 48 year old ♀ admitted from a surgical clinic with ♀ admitted from a surgical clinic with
jaundice and unwelljaundice and unwell
Unwell for 6 wks after holiday in MexicoUnwell for 6 wks after holiday in Mexico
Hx of xs alcohol 30u/wkHx of xs alcohol 30u/wk
No previous jaundiceNo previous jaundice
USS normal size liver and spleen – biliary tree normalUSS normal size liver and spleen – biliary tree normal

OEOE
JaundiceJaundice DrowsyDrowsy Agitated/IrritableAgitated/Irritable Doesn’t obey Doesn’t obey
commandscommands No stigmata of CLDNo stigmata of CLD Asterixis (Liver Flap)Asterixis (Liver Flap)
No spleenNo ascites

Mrs WMrs W
U&EU&E normalnormal
ALPALP 107107 ALTALT 736736 Bili Bili 363363 Alb Alb 2424
FBC FBC NormalNormal
INRINR 3.73.7

Causes of Acute Liver FailureCauses of Acute Liver Failure
DrugsDrugs• Paracetamol (UK)Paracetamol (UK)• INHINH• HalothaneHalothane• EcstacyEcstacy
ViralViral• Hepatitis AHepatitis A• Hepatitis BHepatitis B• Hepatitis EHepatitis E• Non-A Non-BNon-A Non-B
Wilsons DiseaseWilsons Disease
Autoimmune HepatitisAutoimmune Hepatitis
Reye’s SyndromeReye’s Syndrome
CardiovascularCardiovascular• Ischaemic hepatitisIschaemic hepatitis• Budd ChiariBudd Chiari
Acute Fatty Liver of PregnancyAcute Fatty Liver of Pregnancy

Cirrhosis
Expanded Portal Tracts(Blue)
Signs of Chronic Liver DiseaseSigns of Chronic Liver Disease
NoneNone Asterixis/FlapAsterixis/Flap Relative hypotensionRelative hypotension OedemaOedema Jaundice/No jaundiceJaundice/No jaundice Large/Small liverLarge/Small liver SplenomegalySplenomegaly GynecomastiaGynecomastia Testicular atrophy-loss of secondary sexual Testicular atrophy-loss of secondary sexual
characteristicscharacteristics ImpotenceImpotence

Decompensation in CirrhosisDecompensation in Cirrhosis
Means the development of-Means the development of-
AscitesAscites
Hepatic EncephalopathyHepatic Encephalopathy
Portal hypertension (variceal haemorrhage)Portal hypertension (variceal haemorrhage)
The Development of AscitesThe Development of Ascites
50% of compensated cirrhotics develop ascites over 10yrs
50% of cirrhotics with ascites will die within 2 yrs

EncephalopathyEncephalopathy
Grade 1Grade 1• Constructional apraxiaConstructional apraxia• Poor memory – number connection testPoor memory – number connection test• Agitation/ irritabilityAgitation/ irritability• Reversed sleep patternReversed sleep pattern
Grade 2Grade 2• Lethargy, disorientationLethargy, disorientation• AsterixisAsterixis
Grade 3Grade 3• Drowsy, reduced conscious levelDrowsy, reduced conscious level
Grade 4Grade 4• ComaComa


Decompensation in CirrhosisDecompensation in Cirrhosis
Means the development of-Means the development of-
AscitesAscites
Hepatic EncephalopathyHepatic Encephalopathy
Portal hypertension (variceal haemorrhage)Portal hypertension (variceal haemorrhage)

Portal Portal CirculationCirculation

Oesophageal varicesOesophageal varices

Management of Bleeding VaricesManagement of Bleeding Varices
PreventionPrevention
Prophylactic AntibioticsProphylactic Antibiotics
ResuscitationResuscitation
Endoscopy -Endoscopy - Band LigationBand LigationSclerotherapySclerotherapy
Pharmacotherapy- TerlipressinPharmacotherapy- Terlipressin
Balloon TamponadeBalloon Tamponade
TIPSTIPS

Management of Bleeding VaricesManagement of Bleeding Varices
PreventionPrevention
Prophylactic AntibioticsProphylactic Antibiotics
ResuscitationResuscitation
Endoscopy -Endoscopy - Band LigationBand LigationSclerotherapySclerotherapy
Pharmacotherapy- TerlipressinPharmacotherapy- Terlipressin
Balloon TamponadeBalloon Tamponade
TIPSTIPS

Oesophageal varicesOesophageal varices

Bleeding Gastric VaricesBleeding Gastric Varices
Variceal BanderVariceal Bander

Variceal Band LigationVariceal Band Ligation
Management of Bleeding VaricesManagement of Bleeding Varices
ResuscitationResuscitation
Endoscopy -Endoscopy - Band LigationBand LigationSclerotherapySclerotherapy
Pharmacotherapy- Pharmacotherapy- Terlipressin 2mg qds i.vTerlipressin 2mg qds i.v
Balloon TamponadeBalloon Tamponade
TIPSTIPS

Management of Bleeding VaricesManagement of Bleeding Varices
ResuscitationResuscitation
Endoscopy -Endoscopy - Band LigationBand LigationSclerotherapySclerotherapy
Pharmacotherapy- TerlipressinPharmacotherapy- Terlipressin
Balloon TamponadeBalloon Tamponade
TIPSTIPS






























