Embed Size (px)
DESCRIPTION
Ashfaq ul Hassan, Rohul Afza Kaloo, Shifan, Obaid, Nisar Chaudhary, Muneeb ul Hassan. Liver lacerations in abdominal trauma - Management based on anatomical Knowledge: Case series. IAIM, 2014; 1(3): 27-30.
Citation preview
Liver lacerations in abdominal trauma
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
Case Series
Liver lacerations in abdominal trauma
Management based on anatomical
Knowledge: Case series
Ashfaq ul Hassan
Nisar Chaudhary
1Lecturer, Clinical Anatomy, Sher2Tutor, Clinical Anatomy, Sher
3Assistant Professor, Dubai Girls Medical College, Dubai
4Department of Radiology, Sher
5Professor, Surgery, Sher-I
6Physician, Directorate of Health Services, Kashmir, India
*Corresponding author’s email:
How to cite this article: Ashfaq ul Hassan, Rohul
Muneeb ul Hassan. Liver lacerations in abdominal trauma
Knowledge: Case series. IAIM, 2014; 1(3):
Available online at
Received on: 21-10-2014
Abstract
The Liver is commonly injured following penetrating trauma and the second most commonly injured
organ following blunt trauma. Due to the soft consistency of the liver parenchyma
often minor and can be easily managed. The article p
characteristics and how they relate to
cases of abdominal trauma where both the patients had
bleeding within the substance of liver.
road traffic accident and was brought to the casualty in a state of shock. The se
fall from bike and fell on the road by his side.
Key words
Trauma, Couinad, Liver, Portal vein, Hepatic artery, Segments.
Introduction
Liver lacerations in abdominal trauma
International Archives of Integrated Medicine, Vol. 1, Issue. 3, November, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
Liver lacerations in abdominal trauma
Management based on anatomical
Knowledge: Case series
Ashfaq ul Hassan1*
, Rohul Afza Kaloo2, Shifan
3, Obaid
Nisar Chaudhary5, Muneeb ul Hassan
6
Lecturer, Clinical Anatomy, Sher-I-Kashmir Institute of Medical Sciences, Srinagar, Kashmir, India
Tutor, Clinical Anatomy, Sher-I-Kashmir Institute of Medical Sciences, Srinagar, Kashmir, India
Assistant Professor, Dubai Girls Medical College, Dubai
Sher-I-Kashmir Institute of Medical Sciences, Srinagar, Kashmir
I-Kashmir Institute of Medical Sciences, Srinagar, Kashmir
Physician, Directorate of Health Services, Kashmir, India
*Corresponding author’s email: [email protected]
Ashfaq ul Hassan, Rohul Afza Kaloo, Shifan, Obaid, Nisar Chaudhary,
Liver lacerations in abdominal trauma - Management based on anatomical
IAIM, 2014; 1(3): 27-30.
Available online at www.iaimjournal.com
2014 Accepted on:
is commonly injured following penetrating trauma and the second most commonly injured
organ following blunt trauma. Due to the soft consistency of the liver parenchyma
often minor and can be easily managed. The article pinpoints the various anatomical and
eristics and how they relate to liver injuries and trauma management. We report
cases of abdominal trauma where both the patients had liver injuries in the form of l
of liver. The first case was of a young patient who had a high velocity
ccident and was brought to the casualty in a state of shock. The se
bike and fell on the road by his side.
vein, Hepatic artery, Segments.
Trauma to abdomen is common and the liver is
commonly injured. The large size of this largest
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 27
Liver lacerations in abdominal trauma -
Management based on anatomical
, Obaid4,
, Srinagar, Kashmir, India
Srinagar, Kashmir, India
Srinagar, Kashmir, India
Srinagar, Kashmir, India
[email protected] , Shifan, Obaid, Nisar Chaudhary,
Management based on anatomical
Accepted on: 28-10-2014
is commonly injured following penetrating trauma and the second most commonly injured
organ following blunt trauma. Due to the soft consistency of the liver parenchyma, the injuries are
ous anatomical and surgical
management. We reported here two
liver injuries in the form of lacerations and
atient who had a high velocity
ccident and was brought to the casualty in a state of shock. The second patient had a
Trauma to abdomen is common and the liver is
arge size of this largest
Liver lacerations in abdominal trauma
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
gland, soft consistency of the liver
of liver in upper three quadrants
and high vascularity makes it vulnerable and
injuries of liver can well managed by
good understanding of anatomico
knowledge of liver.
Case series
The first case of trauma was of a young p
who had a high velocity road traffic a
was brought to the casualty in a state of shock.
The second case was also a trauma case of a
patient who had a fall from bike and fell on the
road by his side. The second p
developing pain on upper right abdomen.
Investigations of case - 1
� Temperature: 98.7 0F
� Blood pressure (BP): 126/78
� Respiratory rate (RR): 12/m
� Pulse: 82/min
� Hemoglobin (Hb): 13.7 gm/dl
� White blood cell count (
11,200/microlitre
� Platelet count: 2,30,000/microlitre (n
150000-400,000)
� Sodium: 144 meq/L (n 135
� Potassium: 4 meq/L (n 3.5
� Chest X-ray (CXR): Normal
� USG Abdomen: Initially normal
� CT scan: Liver laceration
Investigations of case - 2
� Temperature: 98.6 0F
� Blood pressure (BP): 120/72
� Respiratory rate (RR): 14
� Pulse: 88/min
� Hemoglobin (Hb): 12.7 gm/dl
� White cell count (WBC): 7000
� Platelet count: 2,38,000/microlitre (n
150000-400,000)
� Sodium: 140 meq/L (n 135
� Potassium: 4.2 meq/L (n 3.5
Liver lacerations in abdominal trauma
International Archives of Integrated Medicine, Vol. 1, Issue. 3, November, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
soft consistency of the liver, the location
of liver in upper three quadrants of abdomen
makes it vulnerable and
injuries of liver can well managed by having a
good understanding of anatomico-surgical
of a young patient
who had a high velocity road traffic accident and
was brought to the casualty in a state of shock.
The second case was also a trauma case of a
bike and fell on the
. The second patient had slow
developing pain on upper right abdomen.
: 126/78 mmHg
Respiratory rate (RR): 12/min
: 13.7 gm/dl
White blood cell count (WBC):
: 2,30,000/microlitre (n
meq/L (n 135-145)
(n 3.5-5)
: Normal
USG Abdomen: Initially normal
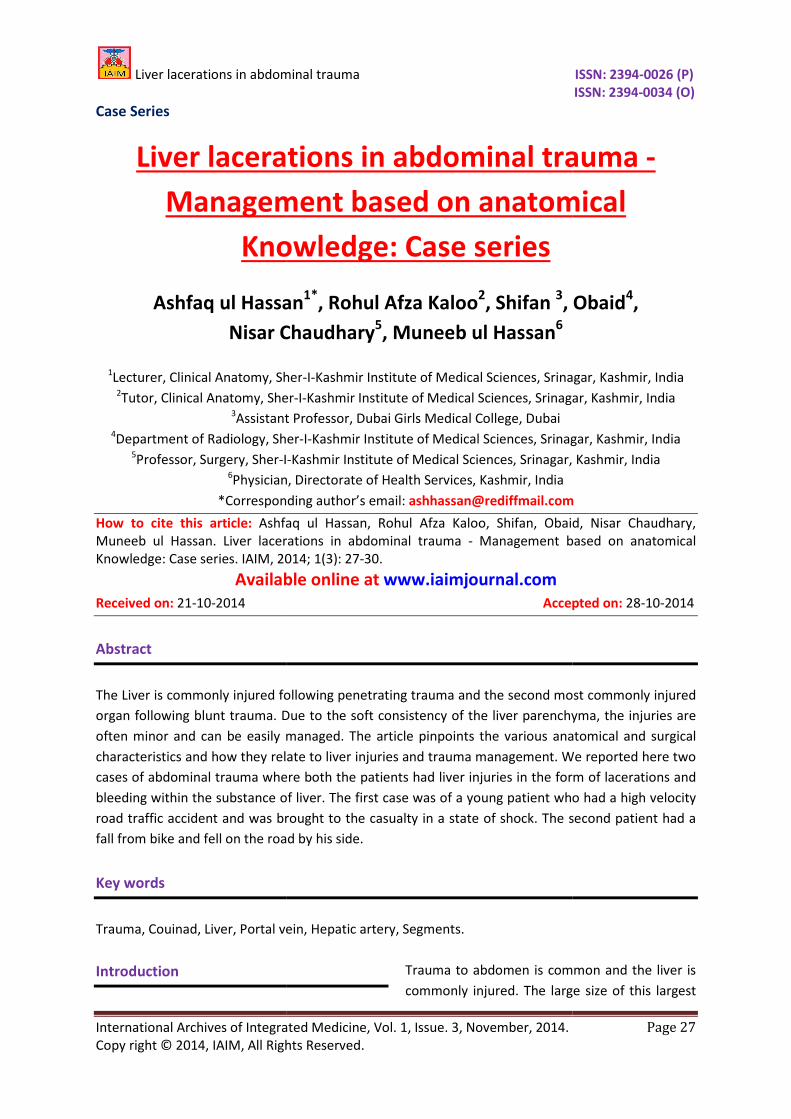
aceration (Photo – 1)
: 120/72 mmHg
: 14/min
: 12.7 gm/dl
: 7000/microlitre
: 2,38,000/microlitre (n
(n 135-145)
(n 3.5-5)
� Chest X-ray (CXR): Normal
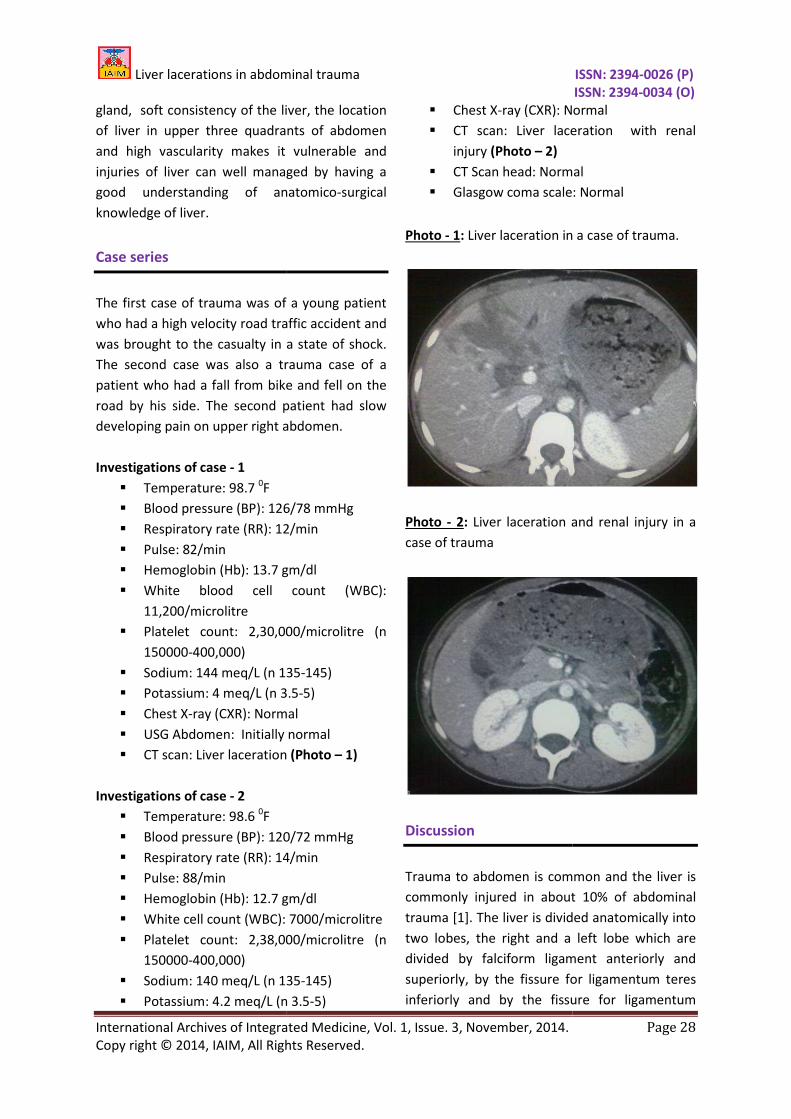
� CT scan: Liver laceration with renal
injury (Photo – 2)
� CT Scan head: Normal
� Glasgow coma scale: Normal
Photo - 1: Liver laceration in a case of trauma.
Photo - 2: Liver laceration and renal injury in a
case of trauma
Discussion
Trauma to abdomen is common and
commonly injured in about
trauma [1]. The liver is divided anatomically into
two lobes, the right and a left
divided by falciform ligament anteriorly and
superiorly, by the fissure for ligamentum teres
inferiorly and by the fissure for ligamentum
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 28
: Normal
CT scan: Liver laceration with renal
ead: Normal
cale: Normal
Liver laceration in a case of trauma.
Liver laceration and renal injury in a
Trauma to abdomen is common and the liver is
commonly injured in about 10% of abdominal
The liver is divided anatomically into
right and a left lobe which are
falciform ligament anteriorly and
superiorly, by the fissure for ligamentum teres
inferiorly and by the fissure for ligamentum

Liver lacerations in abdominal trauma
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
venosum posteriorly. The blood supply of the
liver is unique in the fact that it receives most of
its blood from a vein (Portal Vein)
receives 20% of its blood from the hepatic artery
and 80% from portal vein. Before entry, these
divide into right and left branches. Within liver
they divide to form segmental vessels and re
divide into interlobular vessels w
portal canals. Further divisions open into the
hepatic sinusoids. Thus in the hepatic sinusoids
both arterial and venous blood mix. In isol
cases of abdominal trauma, when liver is the
only organ injured, most of the
non-bleeding and do not require any surgical
intervention [2, 3].
The trauma can be from blunt mechanisms as in
the result of vehicular collisions, fall from height
direct blow in abdomen or penetrating
from stab injury or gunshot wound or can be in
the form of lacerations, hematoma, active
hemorrhage, major hepatic vei
fistulas. The association can be with injuries like
renal injuries of right side, rib fractures on right
side, right lower lobe pulmonary contusion.
Patients may present with a wide range of
symptoms and the astute clinician must always
have a high index of suspicion for internal injury.
The trauma patient may range from entirely
asymptomatic or may present
hypochondriac pain, and even hypotension or
shock. In more severe injury,
bleeding and the source is within the substance
of the liver, and control can be obtained by
direct ligation of the vessel torn or area of liver
severed. This is followed by obtaining adequate
exposure and assessing the depth
and taking notice of any significant va
biliary damage. In case of severe and deeper
lacerations, bleeding may initially be so
significant as to prevent adequate exposure.
Under these conditions, the next maneuver is
that of inflow occlusion also termed as the
Liver lacerations in abdominal trauma
International Archives of Integrated Medicine, Vol. 1, Issue. 3, November, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
. The blood supply of the
is unique in the fact that it receives most of
vein (Portal Vein). The liver
the hepatic artery
and 80% from portal vein. Before entry, these
divide into right and left branches. Within liver
they divide to form segmental vessels and re-
divide into interlobular vessels which run in
portal canals. Further divisions open into the
hepatic sinusoids. Thus in the hepatic sinusoids
both arterial and venous blood mix. In isolated
when liver is the
organ injured, most of the lacerations are
eding and do not require any surgical
from blunt mechanisms as in
the result of vehicular collisions, fall from height,
direct blow in abdomen or penetrating trauma
shot wound or can be in
form of lacerations, hematoma, active
hemorrhage, major hepatic vein injury or
. The association can be with injuries like
renal injuries of right side, rib fractures on right
side, right lower lobe pulmonary contusion.
a wide range of
symptoms and the astute clinician must always
have a high index of suspicion for internal injury.
The trauma patient may range from entirely
asymptomatic or may present with right
and even hypotension or
severe injury, where there is
source is within the substance
of the liver, and control can be obtained by
he vessel torn or area of liver
obtaining adequate
exposure and assessing the depth of the wound
any significant vascular or
. In case of severe and deeper
lacerations, bleeding may initially be so
significant as to prevent adequate exposure.
Under these conditions, the next maneuver is
cclusion also termed as the
Pringle [4] maneuver, where a
across the hepato-duodenal ligament, which
occludes the common hepatic artery and the
portal vein. It is an effective method that often
controls and slows bleeding enough to provide
adequate exposure and to allow visualization
and direct ligation of vessels and biliary radicals.
In underdeveloped countries Pringles maneuver
is still practiced. But in case of more severe
degrees of liver trauma additional requirements
are needed. Surgeons often notice that deep
liver lacerations should not simply be sutured
closed as this predisposes to liver abscesses and
hemobilia [5].
In most of the trivial cases,
observed without any procedure
severe cases may require extensive procedures.
The role of examination as well as the emerging
role of ultrasound in diagnosis of liver trauma
cannot be underestimated as in developing
countries the more sophisticated diagnostic
modalities do not always exist.
The advocation of the procedure of selective
ligation of the right or left hepatic artery was
done in most cases initially but it is nowadays
reserved for selected stab wound or the gunshot
wound involving one lobe where exposure of
the wound will require extensive incis
liver. The proper hepatic artery must never be
ligated. Injudicious hepatic artery ligation may
result in liver infarction, particularly if asso
with portal vein injury. Res
parenchyma is not a common procedure. In
most circumstances, resection is performed to
debride a segment or lobe that has been
completely fractured or devitalized. The liver is
divided into two functional (physiological) ri
and left lobe, based on the
distribution of the hepatic artery
and biliary ducts. These lobes do not correspond
to the anatomical lobes of the liver. The
physiological lobers are separated by a plane
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 29
where a clamp is placed
duodenal ligament, which
occludes the common hepatic artery and the
portal vein. It is an effective method that often
controls and slows bleeding enough to provide
adequate exposure and to allow visualization
and direct ligation of vessels and biliary radicals.
In underdeveloped countries Pringles maneuver
is still practiced. But in case of more severe
degrees of liver trauma additional requirements
eons often notice that deep
liver lacerations should not simply be sutured
closed as this predisposes to liver abscesses and
, the injuries can be
observed without any procedure [6, 7] but
re extensive procedures.
well as the emerging
ltrasound in diagnosis of liver trauma
cannot be underestimated as in developing
countries the more sophisticated diagnostic
modalities do not always exist.
of the procedure of selective
ligation of the right or left hepatic artery was
done in most cases initially but it is nowadays
reserved for selected stab wound or the gunshot
wound involving one lobe where exposure of
the wound will require extensive incision of the
liver. The proper hepatic artery must never be
ligated. Injudicious hepatic artery ligation may
result in liver infarction, particularly if associated
Resection of hepatic
not a common procedure. In
rcumstances, resection is performed to
debride a segment or lobe that has been
completely fractured or devitalized. The liver is
divided into two functional (physiological) right
and left lobe, based on the intra-hepatic
hepatic artery, portal vein
and biliary ducts. These lobes do not correspond
to the anatomical lobes of the liver. The
physiological lobers are separated by a plane

Liver lacerations in abdominal trauma
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
passing on the antero-superior surface along a
line joining the cystic notch to the groove for
inferior vena cava, on the inferior surface the
plane passes through gall bladder fossa and on
the posterior surface through the middle of
caudate lobe. But the more effective way of
determining liver lobes is by classification of
Couinads segments and resection should be
followed on basis of this classification.
Conclusion
The knowledge of anatomy of the liver and the
distribution of injuries permit separation of the
role of each of these approaches. Hepatic
trauma management remains a significant
challenge for emergency surgeons
cases mentioned the repair was done and the
knowledge of the anatomy of liver was given
due consideration.
References
1 Romano L, Giovine S, Guidi G
Hepatic trauma: CT findings and
considerations based on our experience
in emergency diagnostic imaging. Eur J
Radiol., 2004; 50(1): 59-66.
2 Levin A, Gover P, Nance FC. Surgical
restraint in the management of hepatic
Liver lacerations in abdominal trauma
International Archives of Integrated Medicine, Vol. 1, Issue. 3, November, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
superior surface along a
line joining the cystic notch to the groove for
inferior vena cava, on the inferior surface the
plane passes through gall bladder fossa and on
the posterior surface through the middle of
caudate lobe. But the more effective way of
determining liver lobes is by classification of
Couinads segments and resection should be
followed on basis of this classification.
The knowledge of anatomy of the liver and the
distribution of injuries permit separation of the
of these approaches. Hepatic
trauma management remains a significant
emergency surgeons. In both the
cases mentioned the repair was done and the
knowledge of the anatomy of liver was given
S, Guidi G, et al.
Hepatic trauma: CT findings and
considerations based on our experience
in emergency diagnostic imaging. Eur J
66.
Levin A, Gover P, Nance FC. Surgical
management of hepatic
injury: A review of C
Experience. J Trauma.
404.
3 Moore FA, Moore EE, Seagraves A.
Nonresectional management of major
hepatic trauma. An evolving concept.
Am J Surg., 1985; 150:
4 Pringle JH. Notes on the Arrest of
Hepatic Hemorrhage Due
Ann Surg., 1908; 48(4):
5 Gur S, Orsel A, Atahan K, Hokmez A,
Tarcan E. Surgical treatment of liver
trauma (analysis of 244 p
Hepatogastroenterology,
2109–11.
6 Croce MA, Fabian TC, Menke PG,
Waddle-Smith L, Minard G,
al. Non-operative management of blunt
hepatic trauma is the treatment of
choice for hemodynamically stable
patients. Results of a prospective trial.
Ann Surg., 1995; 221:
7 Pachter HL, Hofstetter SR. The current
status of non-operative
adult blunt hepatic injuries. Am J Surg.
1995; 169: 442–54.
Source of support: Nil
Conflict of interest: None declared.
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 30
review of Charity Hospital
Experience. J Trauma., 1978; 18(6): 399–
Moore FA, Moore EE, Seagraves A.
Nonresectional management of major
hepatic trauma. An evolving concept.
150: 725–956.
Notes on the Arrest of
Hepatic Hemorrhage Due to Trauma.
48(4): 541–549.
Gur S, Orsel A, Atahan K, Hokmez A,
Tarcan E. Surgical treatment of liver
trauma (analysis of 244 patients)
Hepatogastroenterology, 2003; 50:
Croce MA, Fabian TC, Menke PG,
Smith L, Minard G, Kudsk KA, et
operative management of blunt
hepatic trauma is the treatment of
choice for hemodynamically stable
patients. Results of a prospective trial.
221: 744–53.
Pachter HL, Hofstetter SR. The current
operative management of
adult blunt hepatic injuries. Am J Surg.,
None declared.





























