Embed Size (px)
Citation preview

Liver Transplantation for AdvancedHepatocellular Carcinoma after Downstaging
Without Up-Front Stage RestrictionsWilliam C Chapman, MD, FACS, Sandra Garcia-Aroz, MD, Neeta Vachharajani, BS, Kathryn Fowler, MD,Nael Saad, MD, Yiing Lin, MD, PhD, Jason Wellen, MD, FACS, Benjamin Tan, MD,Adeel S Khan, MD, FACS, MB Majella Doyle, MD, FACS
BACKGROUND: The incidence of hepatocellular carcinoma (HCC) continues to increase dramatically world-wide. Liver transplantation (LT) is now the standard and optimal treatment for patients withHCC in the setting of cirrhosis, but only for tumors within Milan criteria. In patients pre-senting beyond Milan criteria, locoregional therapy (LRT) can downstage to within Milancriteria for consideration for LT. Although controversial, the current study aims to evaluatethe outcomes of LT in patients presenting with advanced-stage HCC who underwentdownstaging and compare these outcomes with those of patients who met Milan criteria atpresentation.
STUDY DESIGN: Our protocol does not set a priori limitations as long as HCC is confined to the liver. In thisretrospective study between January 1, 2002 and December 31, 2014, we reviewed outcomesassociated with 284 patients who presented within Milan criteria and patients who presentedwith more-advanced stage tumor who were potential transplantation candidates. The patientswith advanced disease were then subdivided into those who were within or beyond Universityof California San Francisco criteria. Imaging, details of LRT, recurrence, and survival werecompared between the groups.
RESULTS: Sixty-three of 210 (30%) eligible patients were downstaged and underwent transplantation;14 additional downstaged and listed patients were withdrawn for the following reasons: deathwhile waiting (n ¼ 4), disease progression (n ¼ 8), development of other malignancy (n ¼ 1),and declined LT (n ¼ 1). Twelve patients underwent resection after downstaging and did notrequire LT. Survival for patients who were downstaged was similar to those who were withinMilan criteria initially. Recurrence of HCC at 5 years was similar between groups (10.9% vs10.8%; p ¼ 0.84).
CONCLUSIONS: Patients with beyondeMilan criteria HCC who are otherwise candidates for LT shouldundergo aggressive attempts at downstaging without a priori exclusion. This highly selectiveapproach allows for excellent long-term results, similar to patients presenting with earlier-stage disease. (J Am Coll Surg 2017;224:610e621. Published by Elsevier Inc. on behalf ofthe American College of Surgeons.)
Hepatocellular carcinoma (HCC) is the fifth most com-mon malignancy worldwide and the second leading causeof cancer-related mortality in the world, responsible forabout 1 million deaths per year.1-4 In the US, HCC
Disclosure Information: Nothing to disclose.
Presented at the Southern Surgical Association 128th Annual Meeting,Palm Beach, FL, December 2016.
Received December 19, 2016; Accepted December 19, 2016.From the Departments of Surgery (Chapman, Garcia-Aroz, Vachharajani,Lin, Wellen, Khan, Doyle), Radiology (Fowler, Saad), and Medical
610Published by Elsevier Inc. on behalf of the American College of Surgeons.
is predicted to become one of the leading causes ofcancer-related mortality by 2030. Noninvasive criteriafor HCC diagnosis are based on imaging techniques ob-tained by 4-phase multidetector CT scan or dynamic
Oncology (Tan), Washington University School of Medicine, St Louis,MO.Correspondence address: William C Chapman, MD, FACS, Department ofSurgery, Washington University School of Medicine, 660 S Euclid Ave,Campus Box 8109, St Louis, MO 63110. email: [email protected]
http://dx.doi.org/10.1016/j.jamcollsurg.2016.12.020
ISSN 1072-7515/16

Abbreviations and Acronyms
AFP ¼ a-fetoproteinALTSG ¼ American Liver Tumor Study GroupB-UCSF
¼ beyond University of California San Franciscocriteria
HCC ¼ hepatocellular carcinomaLRT ¼ locoregional therapyLT ¼ liver transplantationMELD ¼ Model for End-Stage Liver DiseaseRFA ¼ radiofrequency ablationTACE ¼ transarterial chemoembolizationUCSF ¼ University of California San FranciscoW-UCSF
¼ within University of California San Franciscocriteria
Y-90 ¼ yttrium-90 radioembolization
Vol. 224, No. 4, April 2017 Chapman et al Hepatocellular Carcinoma Downstaging 611
contrast-enhanced MRI. This diagnosis is usually based onidentification of a hypervascular lesion in the arterial phasewith washout in the portal venous or delayed phases.5,6
Treatment for HCC depends on the number of tumors,tumor size, and overall liver function. Liver function isassessed according to Child-Turcotte-Pugh class andModel for End-Stage Liver Disease (MELD) criteria.7-10
Liver transplantation (LT) represents the first-line treat-ment option for selected patients with HCC in the settingof cirrhosis. In 1996, Mazzaferro and colleagues11 pro-vided sentinel work showing that patients with early-stage HCC could undergo LT with excellent results.The criteria as defined by the authorsdsolitary tumor�5 cm or �3 tumors each <3 cmdare now referred toas the Milan criteria, and have been applied worldwidein the selection of patients with HCC for LT. When theseselection criteria are applied, excellent overall 4-year actu-arial (75%) and recurrence-free survival rates (83%) canbe achieved.6,12-14 Although the Milan criteria remainthe standard for the selection of patients with HCC, inrecent years, specialized centers have proposed the expan-sion of these criteria. A few sites have reported survivalrates in appropriately downstaged patients that are similarto patients who present within Milan criteria.15,16
Some authors consider the Milan criteria too restrictiveand can exclude patients who would benefit from LT.The University of California San Francisco (UCSF)criteriada single HCC nodule up to 6.5 cm, or up to3 lesions, the largest of which is �4.5 cm and the sumof the diameters (cumulative tumor size) no larger than8 cmdhave shown outcomes comparable with those ofpatients meeting the Milan criteria.17 Other centersbelieve that patients who present with advanced-stage dis-ease might become reasonable candidates for transplanta-tion after downstaging with locoregional therapy (LRT).
Locoregional therapy includes transarterial chemoemboli-zation (TACE), selective yttrium-90 radioembolization(Y-90), and/or radiofrequency ablation (RFA). Thesetechniques, when used in the setting of multidisciplinarycare and in properly selected patients, can be used todownstage tumor burden to within an acceptable range,that is, within Milan criteria.18 The consideration ofmore-advanced stage patients, especially those who aredownstaged using LRT, for LT remains controversialand additional validation of good outcomes is necessary,given the limited pool of transplantable organs. In thisstudy, we present 63 patients with HCC beyond Milancriteria who underwent LT after successful downstagingto within Milan criteria. We compared the results withpatients, initially within Milan criteria, who receivedtransplants in the same time period.
METHODSApproval was obtained from the Washington UniversityIRB for this retrospective study. Our prospective livertransplant database was queried to identify HCC patientswho received transplants between January 1, 2002 andDecember 31, 2014. Their original HCC disease extentwas analyzed based on Milan criteria and the AmericanLiver Tumor Study Group (ALTSG) staging. Variablespotentially impacting survival and disease recurrence afterLT were identified and compared.Throughout the majority of the study timeline,
HCC tumors were diagnosed by cross-sectional imagingaccording to the diagnostic criteria defined in the AmericanAssociation for the Study of Liver Diseases guidelines,which require a contrast-enhancing mass >1 cm in sizein the arterial phase with venous or delayed phase washoutin the setting of cirrhosis. After implementation of a newnational policy on October 31, 2013, the more stringentOrgan Procurement and Transplantation Network criteriafor imaging diagnosis were used.19 Liver biopsies were notperformed unless atypical features were present.Inclusion criteria for the study were age older than 18
years atHCC diagnosis; a single nodule>5 cm, 2 to 3 nod-ules at least 1 >3 cm, corresponding to stage III of theALTSG Classification, or �4 nodules of any size (stageIVA1 of the ALTSG classification), or HCC with any tu-mor stage plus intrahepatic portal or hepatic vein involve-ment (stage IVA2 of the ALTSG classification); possibletransplantation candidate; and able to undergo LRT forpossible downstaging. a-Fetoprotein (AFP) level was notincluded as an inclusion or exclusion criteria. Patientswith regional lymph nodes or metastatic disease (includingextrahepatic main portal or hepatic vein involvement),

612 Chapman et al Hepatocellular Carcinoma Downstaging J Am Coll Surg
stage IVB of ALTSG classification, were excluded from thisstudy. Two hundred and ten patients met the inclusioncriteria and followed the downstaging protocol.16
Locoregional therapy and evaluation of response
Each patient was evaluated by a multidisciplinary team,and TACE, Y-90, RFA, or a combination of these thera-pies, were applied according to case-by-case discussion. Ingeneral, patients with unilobar disease were treated with asingle TACE session. The technique and procedure havebeen described previously.14 Patients with bilobar diseasewere treated at 4- to 6-week intervals with serial TACEuntil all nodules were treated or treatment failureoccurred due to progression of underlying liver diseaseprecluding additional therapy. When the treatment wascompleted, a new imaging study (contrasted CT orMRI) was performed to evaluate the liver 4 to 6 weeks af-ter the last LRT. Viability of tumor on follow-up imagingstudies was determined by the presence of arterial phasehyper-enhancement within the nodule, as described bymodified Response Evaluation Criteria in Solid Tumors.Assessment of tumor response took into account treatedlesions, untreated lesions, and any new observations onfollow-up imaging. Consideration for transplantationwas made when residual tumor burden after treatmentmet ALTSG stage II criteria (1 nodule <5 cm or 2 to 3nodules, all <3 cm). The presence of extrahepatic disease,progression of intrahepatic disease, or failure to achievestage II criteria resulted in exclusion from considerationfor LT. All patients were submitted to the UnitedNetwork for Organ Sharing Regional Review Board forRegion 8 after downstaging was completed and MELDexception points were granted, similar to patients initiallywithin Milan criteria.The number of LRTs and time needed for downstaging
were recorded. Tumor progression, other malignancies,and death were also noted. Tumor burden at baselinewas described using Milan criteria and UCSF criteria.11,17
Patients were classified as beyond Milan criteria/withinUCSF (W-UCSF), or beyond UCSF (B-UCSF) at base-line. Success of downstaging and LT rate was assessedfor each group. LT outcomes (overall survival, graft sur-vival, disease-specific survival, disease-free survival, andrecurrence rate) were also analyzed.
Control group
To compare results of our study group (patients beyondMilan criteria), we also collected data of all patientswith HCC who met Milan criteria at the outset and un-derwent LT between January 2002 and December 2014.Demographic, clinical, and tumor characteristics werestudied. Outcomes after LT (overall survival, graft
survival, disease-specific survival, disease-free survival,and recurrence rate) were also analyzed for this group.
Statistical analysis
Statistical analyses were done using GraphPad Prism,version 5.0 (GraphPad Software). Categorical variables,presented as n (%), were compared using Fisher’s exacttest or chi-square test, as applicable. Continuous variablespresented as median (range) or mean (SD) were comparedusing one-way ANOVA (for 3-group comparison) orMann-Whitney test (for intention-to-treat analysis). Sur-vival graphs were plotted using Kaplan-Meier curves andsurvival rates were compared using log-rank test. Multi-variate analysis was run using SPSS, version 23 (IBMCorp). For every comparison, differences with a p value<0.05 were considered statistically significant.
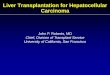
RESULTSBetween January 1, 2002 and December 31, 2014, fourhundred and fifty-six new patients presenting withbeyond-Milan criteria HCC without metastatic diseasereceived LRT at our center. Of these, 246 patients werenot considered future transplantation candidates from pre-sentation; 28 were aged older than 80 years, 28 were notsurgical candidates, 27 had social contraindications, and47 had major comorbidities. Within 3 months from theirlast LRT, 78 patients died and 38 were lost to follow-up.The remaining 210 patients with beyondeMilan criteriaHCC were considered possible future LT candidates atthe time, initiating the downstaging LRT protocol.Sixty-three of 210 (30%) eligible patients were down-
staged and received transplants; 14 (6.7%) additional down-staged and listed patients were withdrawn for the followingreasons: death while waiting (n ¼ 4), disease progression(n ¼ 8), development of other malignancy (n ¼ 1), anddeclined LT (n¼ 1). Twelve (5.7%) underwent resection af-ter downstaging and did not require LT. One hundred andtwenty-one patients began LRT with an intention to down-stage to within Milan criteria, but failed to reach it (Fig. 1).
Demographics and tumor characteristics
Demographics, clinical parameters, and tumor character-istics of the study population are listed in Table 1. Mean� SD age at first LRT was 61.5 � 10.4 years. Mean �SD AFP level at the time of first LRT was 5,788 �21,728 ng/mL. The most frequent underlying liverdisease was hepatitis C virus (44.3%), followed by alco-holic liver disease (9.5%). Thirty-five patients (16.7%)were W-UCSF and 175 patients (83.3%) were B-UCSF. The most commonly used LRT was TACE, eitheralone (n ¼ 171 [81.4%]) or in combination with Y-90

Figure 1. Patient population of the study. Distribution of hepatocellular carcinoma (HCC) patientsbeyond Milan criteria who underwent locoregional therapy (LRT).
Vol. 224, No. 4, April 2017 Chapman et al Hepatocellular Carcinoma Downstaging 613
(n ¼ 16 [7.6%]). The remaining 23 (11.0%) patientsreceived Y-90 alone. Eleven patients (5.2%) receivedRFA in addition to either TACE (n ¼ 10) or Y-90(n ¼ 1). The number of LRTs received was also recorded.Patients received a median of 2 (range 1 to 6) LRTs.Of these patients, 89 were successfully downstaged.
Demographic and tumor characteristics were comparedto assess the differences between groups (downstaged vsnot downstaged after LRT). Results are also describedin Table 1. Significant differences were found when wecompared age at first LRT, 58 vs 63 years old, respectively(p ¼ 0.004). Presence of hepatitis C virus cirrhosis wassignificantly higher in the downstaged group (56.2% vs35.3%; p ¼ 0.003). The size of the largest tumor wassignificantly greater in the patients who did not achievedownstaging (6.5 vs 5.0 cm; p ¼ 0.002). Numerical dif-ferences were present for the ALTSG tumor stage andnumber of tumors at presentation, with a higher percent-age of patients with more advanced stage and greaternumber of tumors not achieving downstaging, althoughthese differences did not achieve statistical significance.
Locoregional therapy response
Downstaged group
Thirty-five patients showed a complete response by modi-fied Response Evaluation Criteria in Solid Tumors, and52 patients presented a partial response with viable tumordemonstrated in the CT/MRI pretransplantation. Twopatients showed stable disease.Fourteen patients were listed but were later withdrawn;
3 patients had complete response and 11 had partialresponse. Of the 12 patients that received resection, 2demonstrated pathologic complete response, 8 had path-ologic partial response, and 2 showed stable disease.For the 63 patients that underwent LT after downstag-
ing, a comparison between the radiologic description andthe pathology results was performed. Thirty of these 63
patients achieved complete response to LRT based oncross-sectional imaging before transplantation. Fourteenof these did not show viable tumor on explant, 8 showed<20% tumor viability, and 8 showed >20% viability. Atotal of 9 patients showed beyondeMilan criteria diseasein the explant. Seven of these 9 cases were beyond Milancriteria because of the multiple sub-centimeter tumors.The remaining 2 explants showed vascular thrombus,which was not seen on pre-LT imaging.
Failure to achieve downstaging group
Of the 121 patients that failed to achieve downstagingto Milan criteria, most patients showed partial response(n ¼ 58 [47.9%]), but disease progressed in 28 of these58 patients in short-term follow-up. Of these 28 patientsthat showed partial response followed by disease progres-sion, 4 patients received follow-up LRT (RFA [n ¼ 3]and TACE [n ¼ 1]) as palliative care, 4 patients receivedsorafenib therapy, 7 died within 3 months from that im-aging, 7 were lost to follow-up after that imaging, and 6patients chose the no-treatment option. Of the 6 that didnot accept the offered treatment options, 2 died 4 and 23months later, 3 were lost to follow-up with extensive dis-ease 13, 14, and 46 months later, and 1 still follows withus (24 months) and disease has not progressed. Of theremaining 30 patients in whom disease progression wasnot documented, 21 additional patients died (14 within3 months after showing partial response, 4 within 3 to6 months, and 3 within 6 to 12 months). Of the remain-ing 9 of these patients, 3 were lost to follow-up 3 monthsafter last imaging, 2 received additional LRTs as palliativecare, and the others were not eligible or not interested inany definitive treatment.
Factors affecting downstaging success
Binary logistic regression analysis was performed toassess the effect of age at first LRT (age older than 70years), presence of cirrhosis, hepatitis C virus liver disease,

Table 1. Demographics and Tumor Characteristics in Downstaged Group vs Not Downstaged Group
CharacteristicOverall
(n ¼ 210)Downstaged(n ¼ 89)
Not downstaged(n ¼ 121) p Value
Age at first LRT, y, median(IQR) 61.5 (18e89) 58 (41e89) 63 (18e80) 0.004*
a-Fetoprotein before LRT,ng/mL, median (IQR) 22.1 (3.0e151,806) 16.7 (3.0e113,727) 45.7 (3.0e151,806) 0.0636
Sex, n (%) 0.473
Male 171 (81.4) 75 (84.3) 96 (79.3)
Female 39 (18.6) 14 (15.7) 25 (20.7)
Cause of cirrhosis, n (%)
Hepatitis C virus 93 (44.3) 50 (56.2) 43 (35.3) 0.003*
Alcohol 20 (9.5) 12 (13.5) 8 (6.6) 0.102
Nonalcoholicsteatohepatitis 13 (6.2) 9 (10.1) 4 (3.3) 0.078
Cryptogenic 9 (4.3) 5 (5.6) 4 (3.3) 0.132
Criteria, n (%) 0.042*
Beyond Milan criteria/within UCSF criteria 35 (16.7) 21 (23.6) 15 (12.4)
Beyond UCSF criteria 175 (83.3) 68 (76.4) 106 (87.6)
No. of tumors at baseline,n (%) 0.202
1 69 (32.9) 28 (31.5) 41 (33.9)
2 49 (23.3) 25 (28.1) 24 (19.8)
3 20 (9.5) 11 (12.3) 9 (7.4)
>3 72 (34.3) 25 (28.1) 47 (38.8)
Initial largest tumordiameter, median (IQR) 5.8 (1.2e27.0) 5.0 (1.7e27.0) 6.5 (1.2e17.8) 0.002*
Initial total tumor burden>8 cm, n (%) 99 (47.1) 36 (40.4) 63 (52.1) 0.096
Tumor thrombus, n (%) 36 (17.1) 11 (12.4) 25 (20.7) 0.139
LRTs, n (%) 0.031*
TACE only 171 (81.4) 78 (87.6) 93 (76.9)
Y-90 only 23 (11.0) 6 (6.7) 17 (14.0)
Combination 16 (7.6) 5 (5.7) 11 (9.1)
Associated radiofrequencyablation 11 (5.2) 5 (5.7) 6 (5.0)
No. of LRTsy 0.831
1, n (%) 63 (30.0) 25 (28.1) 38 (31.4)
2, n (%) 78 (37.1) 33 (37.1) 45 (37.2)
�3, n (%) 69 (32.9) 31 (34.8) 38 (31.4)
Mean (SD) 2.2 (1.2) 2.2 (1.1) 2.3 (1.3)
*Significant.yExcludes radiofrequency ablation.IQR, interquartile range; LRT, locoregional therapy; UCSF, University of California San Francisco; Y-90, yttrium-90 radioembolization.
614 Chapman et al Hepatocellular Carcinoma Downstaging J Am Coll Surg
Y-90 therapy,>3 LRTs given,>3 tumors at presentation,largest tumor diameter >8 cm at presentation, and AFPlevel >1,000 ng/mL at first LRT on the downstaging out-comes. The analysis showed that younger (70 years oryounger at first LRT) patients with cirrhosis, with �3tumors, and no tumor thrombus at the time of diseaseidentification were more likely to downstage. Contrary
to our expectation, AFP >1,000 ng/mL at presentationdid not predict failure of successful downstaging.
Long-term outcomes in hepatocellular carcinomapatients
As described previously, between January 2002 andDecember 2014, 63 patients with HCC were beyond

Vol. 224, No. 4, April 2017 Chapman et al Hepatocellular Carcinoma Downstaging 615
Milan criteria at diagnosis and, after successful downstag-ing, underwent LT. Of these 63 patients, 18 were W-UCSF, and 45 patients were beyond Milan criteria andB-UCSF criteria.During the same period, 289 transplantations were per-
formed at our center in patients that presented HCCwithin Milan criteria when the disease was identified.Fifty of these 289 patients were identified incidentallyin the liver explant after LT, and were excluded fromthis analysis. Therefore, 239 cases of HCC patients withinMilan criteria at diagnosis represent our control group(within Milan criteria) for this study.
Demographics
Results of univariate analysis comparing the withinMilan criteria, W-UCSF, and B-UCSF groups are
Table 2. Univariate Analysis Between Within Milan Criteria,Beyond University of California San Francisco Groups
VariableWithin MC(n ¼ 239)
Male sex, n (%) 182 (76.2)
Caucasian, n (%) 198 (82.8)
Age, y, mean (SD) 58.3 (7.3)
Cirrhosis, n (%)
Hepatitis C virus 162 (67.8)
Alcoholic 33 (13.8)
Nonalcoholic steatohepatitis 20 (8.4)
Cholestatic 5 (2.1)
Calculated Model for End-stageLiver Disease, median (range) 12 (6e41)
Last AFP before LT, ng/mL,median (IQR) 9.8 (5e9,458)
AFP peak level, ng/mL, median(IQR) 15.2 (6.5e9,729)
Child-Turcotte-Pugh class, n (%)
A 120 (50.2)
B 82 (34.3)
C 37 (15.5)
Time on waiting list, median(IQR) 100 (1e2,749)
Last locoregional therapy to LTinterval, median (IQR) 90 (3e597)
Tumors, n (%)
1 180 (75.3)
2 37 (15.5)
3 22 (9.2)
>3 0 (0)
No. of tumors, mean (SD) 1.3 (0.6)
Largest tumor diameter, mean(SD) 2.7 (0.9)
*Significant.AFP, a-fetoprotein; LT, liver transplantation; MC, Milan criteria; UCSF, Univ
presented in Table 2. A higher proportion of male pa-tients was found in the B-UCSF group (76.2% vs83.3% vs 93.3%, respectively; p ¼ 0.031). Causes ofcirrhosis were comparable between the groups. Themost common cause of HCC and cirrhosis for the 3groups was hepatitis C virus (67.8%, 61.1%, and66.7%, respectively), followed by a history of alcoholabuse. Patients in the B-UCSF group had more-advanced underlying liver disease, with a median calcu-lated MELD of 14 vs 12 (within Milan criteria) and 11(W-UCSF) (p ¼ 0.023). Although the last pre-LT AFPlevels were comparable between groups, significant dif-ferences were found when the peak AFP levels beforetransplantation were compared; 15.2, 10.2, and 57.2ng/dL, respectively, reporting the highest levels in B-UCSF group (p < 0.0001). Patients in the B-UCSF
Within University of California San Francisco Criteria, and
Within UCSFcriteria (n ¼ 18)
Beyond UCSFcriteria (n ¼ 45) p Value
15 (83.3) 42 (93.3) 0.031*
14 (77.8) 35 (77.8) 0.860
56.4 (5.5) 59.1 (7.0) 0.427
11 (61.1) 30 (66.7) 0.841
3 (16.7) 9 (20.0) 0.551
3 (16.7) 4 (8.9) 0.493
0 (0) 0 (0)
11 (6e22) 14 (6e49) 0.023*
5.5 (5e140) 10.6 (5e1,909) 0.778
10.2 (5.5e1,999) 57.2 (10.7e39,660) <0.0001*
11 (61.1) 23 (51.1) 0.762
4 (22.2) 13 (28.9)
3 (16.7) 9 (20.0)
92 (12e345) 113 (2e2,934) 0.433
120 (22e303) 135 (11e610) 0.0003*
6 (33.3) 13 (28.9) <0.0001*
9 (50.0) 13 (28.9)
3 (16.7) 5 (11.1)
0 (0) 14 (31.1)
1.8 (0.7) 2.9 (2.3) <0.0001*
4.5 (1.2) 5.1 (2.5) <0.0001*
ersity of California San Francisco.

616 Chapman et al Hepatocellular Carcinoma Downstaging J Am Coll Surg
group also waited the longest after their last LRT (135days) compared with within Milan criteria (90 days)and W-UCSF (120) groups (p ¼ 0.0003). Wait timeafter listing was comparable among the groups. Patientsin the within Milan criteria group had solitary tumorsmore frequently (75.3%) compared with W-UCSF(33.3%) and B-UCSF (28.9%) groups. As expected,the largest tumor diameter was also smaller in withinMilan criteria group (2.7 cm) compared with the other2 groups (4.5 and 5.1 cm, respectively) (p < 0.0001).In the B-UCSF group, 31.1% patients had >3 tumors.
On average, these patients had 2.9 (�2.3) tumors withmean � SD largest diameter of 5.1 � 2.5 cm. Nineteen(42.2%) patients in this group started with a total tumorburden of >8 cm. Of these 19 patients, 5 had a singletumor >8 cm, 7 had 2 to 3 tumors, and 7 had >3tumors.
Overall survival
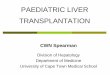
Thirty day, 1-, 3-, 5-, and 10-year overall survival rates inthe full cohort of 302 transplanted HCC cases were97.7%, 92.7%, 82.3%, 73.7%, and 60.4%, respectively.Median follow-up was 51.4 months. Overall 1-, 3-, 5-,and 10-year survival rates in the B-UCSF group(88.9%, 73.2%, 66.2%, and 49.7%, respectively) werecomparable with those in the W-UCSF and within Milancriteria groups (94.4%, 94.4%, 85.8%, and 62.6%;and 93.2%, 83.0%, 74.1%, and 61.9%, respectively)(p ¼ 0.29) (Fig. 2).
Figure 2. Overall survival in hepatocellular carcinoma patients afterliver transplantation by meeting Milan criteria or University of Cali-fornia San Francisco (UCSF) criteria; p ¼ 0.29. B-UCSF, beyondUCSF criteria; W-MC, within Milan criteria; W-UCSF, within UCSFcriteria.
Disease-specific survival
Thirty day, 1-, 3-, 5-, and 10-year disease-specific survivalrates in the full cohort of 302 transplanted HCC caseswere 100.0%, 99.3%, 94.8%, 92.6%, and 90.6%, respec-tively. One-, 3-, 5-, and 10-year disease-specific survivalrates in the B-UCSF group (97.7%, 92.3%, 92.3%, and92.3%, respectively) were also comparable with those inW-UCSF and within Milan criteria groups (100%,100%, 90.9%, and 90.9%; and 99.6%, 94.8%, 92.9%,and 90.5%, respectively) (p ¼ 0.95) (Fig. 3).
Deaths and hepatocellular carcinoma-relateddeaths
Ninety-two (30.5%) patients died during the observationperiod. In the B-UCSF group, 16 (35.6%) patients havedied. Causes of death were recurrent HCC (n ¼ 3) at 0.6,1.1, and 2.2 years from transplantation, cancer other thanHCC (n ¼ 2), multisystem failure and sepsis (n ¼ 4), car-diac (n ¼ 1), gastrointestinal bleeding (n ¼ 1), respiratoryfailure (n ¼ 1), and miscellaneous (n ¼ 4).In the W-UCSF group, 4 (22.2%) patients have died.
Causes of death were recurrent HCC (n ¼ 1) at 3.9 yearsfrom the transplantation, liver graft failure (n ¼ 2), andcardiac (n ¼ 1).In the within Milan criteria group, 72 (30.1%) patients
have died. Causes of death were recurrent HCC (n ¼ 16)at a median interval of 1.9 (range 1.0 to 6.4) years fromtransplantation, intraoperative bleeding (n ¼ 2), cancerother than HCC (n ¼ 6), multisystem failure and
Figure 3. Disease-specific survival in hepatocellular carcinomapatients after liver transplantation by meeting Milan criteria orUniversity of California San Francisco (UCSF) criteria; p ¼ 0.95.B-UCSF, beyond UCSF criteria; W-MC, within Milan criteria; W-UCSF,within UCSF criteria.

Figure 5. Disease recurrence in hepatocellular carcinoma patientsafter liver transplantation by meeting Milan criteria or University ofCalifornia San Francisco (UCSF) criteria; p ¼ 0.85. B-UCSF, beyondUCSF criteria; W-MC, within Milan criteria; W-UCSF, within UCSFcriteria.
Vol. 224, No. 4, April 2017 Chapman et al Hepatocellular Carcinoma Downstaging 617
sepsis (n ¼ 6), cardiac (n ¼ 5), gastrointestinal bleeding(n ¼ 2), respiratory failure (n ¼ 5), liver graftfailure (n ¼ 8), renal failure (n ¼ 6), hepatorenal failure(n ¼ 3), and miscellaneous (n ¼ 13).
Disease-free survival
Thirty day, 1-, 3-, 5-, and 10-year disease-free survivalrates in the full cohort of 302 transplanted HCC caseswere 97.7%, 89.0%, 80.3%, 70.6%, and 58.1%, respec-tively. One-, 3-, 5-, and 10-year disease-free survival ratesin the B-UCSF group (84.4%, 73.5%, 62.8%, and44.9%, respectively) were also comparable with those inW-UCSF and within Milan criteria groups (94.4%,87.2%, 87.2%, and 63.6%; and 89.5%, 80.9%, 70.7%,and 59.6%, respectively) (p ¼ 0.28) (Fig. 4).
Hepatocellular carcinoma recurrence
Thirty day, 1-, 3-, 5-, and 10-year disease recurrence ratesin the full cohort of 302 transplanted HCC cases were0.0%, 4.5%, 7.3%, 10.9%, and 11.6%, respectively.One-, 3-, 5-, and 10-year HCC recurrence rates in theB-UCSF group (6.9%, 6.9%, 12.1%, and 12.1%, respec-tively) were also comparable with those in W-UCSF andwithin Milan criteria groups (0.0%, 7.7%, 7.7%, and7.7%; and 4.4%, 7.2%, 10.9%, and 11.9%, respectively)(p ¼ 0.85) (Fig. 5).
Disease recurrence
Hepatocellular carcinoma developed in 27 patients. Four(8.9%) were B-UCSF patients, 1 (5.6%) was a W-UCSFpatient, and 22 (9.2%) were withinMilan criteria patients.
Figure 4. Disease-free survival in hepatocellular carcinoma pa-tients after liver transplantation by meeting Milan criteria orUniversity of California San Francisco (UCSF) criteria; p ¼ 0.28.B-UCSF, beyond UCSF criteria; W-MC, within Milan criteria; W-UCSF,within UCSF criteria.
In the 4 B-UCSF patients with disease recurrence, 2recurrences were in the lungs, 0.6 and 2.2 years afterthe transplantation. One patient had more widespreadrecurrent disease in the lumbar vertebrae, lungs, andbilateral 12th ribs, 0.5 years after the transplant. Hepato-cellular carcinoma developed in the transplanted liver ofthe other patient after 4.2 years.Recurrent disease in the soft tissue over the left scapular
region developed in 1 W-UCSF patient 3 years aftertransplantation. Of the 22 within Milan criteria patientswith recurrent disease, recurrence was restricted to thetransplanted liver in 4 cases. These recurrences wereobserved 0.5, 1.1, 4.0, and 5.4 years after transplantation.Of the remaining 18, 9 recurrences occurred during thefirst year after the transplantation (4 in lymph nodes, 2in bone, 1 in lung þ liver, 1 in lung þ both adrenals,and 1 with widespread disease).Five recurrences occurred after the first year, but before
completing 3 years post-orthotopic liver transplantation(2 liver þ vertebrae, 1 omentum, 1 lymph nodes, 1 wide-spread). The last 4 recurrences occurred between 3 and5.4 years post-orthotopic liver transplantation (2 in lungs,1 on the chest wall, and 1 in the mediastinum).
Graft survival
Thirty-day, 1-, 3-, 5-, and 10-year graft survival rates in thefull cohort of 302 transplanted HCC patients were 96.0%,90.3%, 80.0%, 72.2%, and 59.6%, respectively. One-, 3-,5-, and 10-year graft survival rates in the B-UCSF group(86.7%, 73.7%, 66.7%, and 50.0%%, respectively) werealso comparable with those in W-UCSF and within Milan

Figure 6. Graft survival in hepatocellular carcinoma patients afterliver transplantation by meeting Milan criteria or University of Cali-fornia San Francisco (UCSF) criteria; p ¼ 0.39. B-UCSF, beyondUCSF criteria; W-MC, within Milan criteria; W-UCSF, within UCSFcriteria.
618 Chapman et al Hepatocellular Carcinoma Downstaging J Am Coll Surg
criteria groups (94.4%, 94.4%, 85.9%, and 62.6%;and 90.7%, 80.0%, 72.2%, and 60.9%, respectively)(p ¼ 0.39) (Fig. 6).
a-Fetoprotein levels
Historical AFP levels before transplantation were analyzedin our cohort. Sixteen (5.3%) patients presented withAFP levels >1,000 ng/mL at some point during the eval-uation for LT. Seven of 239 (2.9%) of these were in thewithin Milan criteria group, 1 of 18 (5.6%) was from theW-UCSF group, and 8 of 45 (17.8%) patients were fromthe B-UCSF group. Nine of these 16 LTs occurred before2009. All 16 received LRT between this >1,000 ng/mLpeak AFP report and LT.After LRT, AFP level came down to <500 ng/mL
before LT in 6 patients (2 from the within Milan criteriagroup, 1 W-UCSF case, and 3 from the B-UCSF group).In 1 of these patients (from within Milan criteria group),metastatic disease developed in the lymph nodes within 5months post-LT; the patient received radiation therapyand had post-LT survival of 4 years. Median overall sur-vival of these 6 patients was 5.6 years.Four patients from the B-UCSF group had partial
response as their AFP level came down to <1,000 ng/mL,but could not be brought down to <500 ng/mL. Therewas no recurrence in these 4 patients. Their median post-LT survival is 5.1 years.Despite LRT, 6 patients’ AFP levels remained >1,000
ng/mL. One of these was in the B-UCSF group and theother 5 were in within Milan criteria group. Five of the6 cases were performed before 2009. Recurrent HCC
developed in 1 of these patients (within Milan criteriacase) 10 months after transplantation in his transplantedliver as well as in the left lung and he died 20 monthslater, despite receiving cryoablation of the liver lesionand resection of the lung lesions. Median overall survivalof these patients was 8.1 years.Of the 286 patients who never had their AFP level
>1,000 ng/mL, 10 had their last pre-LT AFP >500ng/mL. Four of them were in B-UCSF group and 6were in the within Milan criteria group. No LRT wasgiven in the interval between this AFP report and LT.Recurrence developed in 2 of these patients from thewithin Milan criteria group. One of the 2 patients showedrecurrent disease in bone 4 months post-LT, was advisedchemoradiation but chose not to pursue additional treat-ment and died with post-LT survival of 1 year. The otherpatient’s recurrent disease was restricted to the liver,discovered 14 months post-LT. He received RFA and isalive and disease-free 12þ years after LT.
Cox regression analysis
As an independent factor, beyondeMilan criteria diseasewas not found to significantly affect survival (overall,disease-specific, disease-free, and graft survival) or diseaserecurrence. There were no differences in these outcomesbetween B-UCSF and W-UCSF groups. The variablesthat significantly affected overall survival were hepatitisC virus cirrhosis (p ¼ 0.031; hazard ratio ¼ 1.689; 95%CI 1.049 to 2.725) and alcohol-associated cirrhosis (p ¼0.018; hazard ratio ¼ 1.869; 95% CI 1.114 to 3.135).Longer interval between last LRT and transplantation(>3 months) was independently associated with improveddisease-free survival (p¼ 0.038; hazard ratio¼ 1.529; 95%CI 1.022 to 2.283). Waiting on the list for longer than 6months showed a trend to affect the time to disease recur-rence, but with a p value of 0.054, failed to reach the level ofsignificance.
DISCUSSIONTreatment of patients with cirrhosis and HCC withinMilan criteria is well established in Western countries.After the introduction of these criteria by Mazzaferro andcolleagues11 in 1996, liver transplantation has become thestandard treatment for patients with early-stage HCC.Patients within Milan criteria receive MELD prioritypoints, allowing for prioritization for transplantation,usually within 6 to 12 months. However, patients whoexceed these criteria do not receive automatic priority onthe waiting list, which can lead to dropout and deathfrom progression of disease. The application of LRTto achieve reduction of the tumor stage allows patients

Vol. 224, No. 4, April 2017 Chapman et al Hepatocellular Carcinoma Downstaging 619
outside these criteria to potentially access transplantation.In the current report, we demonstrate that patients beyondMilan criteria can be successfully downstaged to withinMilan criteria, with post-transplantation survival resultsthat mirror those for patients initially presenting withinMilan criteria. In addition, a priori restriction of candidatesfor possible downstaging was not required, as long as HCCwas confined to the liver, and this included patientswith AFP >1,000 ng/mL and patients with evidence ofintrahepatic portal and hepatic venous tumor thrombus.In the current report, we analyzed a total of 210
patients with HCC beyond Milan criteria who receivedLRT with the goal of downstaging to within Milancriteria; 89 (42%) of these patients underwent successfuldownstaging and 63 (30%) subsequently underwent LT.We performed an analysis of factors that could havepredisposed to a greater probability of downstaging,comparing these 89 patients with the 121 patients thatwere not successfully downstaged. Based on our results,younger patients appear to have a greater probability ofdownstaging. Interestingly, meeting UCSF criteria atinitial presentation was not a limiting factor to achievedownstaging in our study and did not impact post-transplantation survival results. In a related study investi-gating the effect of LRT on long-term outcomes in 501patients (both within and outside of Milan criteria), Ago-pian and colleagues20 analyzed the response to LRT onoutcomes after LT. Patients achieving complete responsewith LRT had post-transplantation recurrence risk of 2%compared with 18% for those who did not achieve com-plete response. They found that tumor size was not pre-dictive of achieving complete response after LRT, andincreasing tumor number did lower the likelihood ofachieving complete response. In our series, tumor sizedid not have a significant effect on downstaging success,although patients who did not achieve downstagingtended to have larger tumor sizes compared with thosewho were successfully downstaged.We did not find differences when we compared the
number of LRTs received in each group based on the like-lihood of achieving downstaging. Of note, we did notfollow a single protocol for downstaging, but instead,each case was individually evaluated by a multidisciplinaryteam and the type of LRT and number of sessions wasdecided on a case-by-case basis. Despite the desirabilityof a single standardized approach for LRT, no methodhas yet been proven superior based on studies to date,and our limited use of Y-90 and RFA do not allow usto comment on this aspect of LRT.21-24 Agopian and col-leagues20 described lower HCC recurrence rates afterobtaining complete response with direct ablation thera-pies (eg RFA), although they found that the combination
therapy with TACE and ablation was the strongesttreatment-specific factor in predicting complete response.In our study, the most commonly used LRT was TACE(81.4%), 23 (11%) patients received Y-90 as uniqueLRT, and 16 patients (7.6%) received combination ther-apy with TACE þ Y-90. Ten patients receiving TACEand 1 patient receiving Y-90 also received RFA as a com-bination therapy. There is a high variability of LRT tech-niques, and so far there is insufficient evidence to suggestsuperiority of any single or combination technique.Patients with HCC within Milan criteria at initial pre-
sentation who underwent LT were used as our controlgroup to compare the outcomes obtained after transplanta-tion in patients W-UCSF and B-UCSF who underwentdownstaging LRT. All groups represented a homogeneousdistribution of age, race, cause of cirrhosis, MELD score,and Child-Turcotte-Pugh class. As expected, patients inthe B-UCSF group initially presented with a greater num-ber of tumors and larger tumor size than other groups(within Milan criteria and B-UCSF). We found that thetime between LRT and LT was greater in the B-UCSFgroup. Several studies have described a minimum observa-tion period of 3months after downstaging and before LT asa tool to monitor tumor biology and to select tumors withmore favorable prognosis.13,20,25We found that the time in-terval between the last LRT and transplantation (�3 vs>3months) independently affected disease-free survival andpatients with longer waiting times had greater disease-free survival (p ¼ 0.04). In our practice, an imaging study(CT/MRI) was usually performed 4 to 6 weeks after LRTand, if downstaging was achieved, patients were able toundergo listing for LT. With the recently enacted UnitedNetwork for Organ Sharing policy of a mandatory6-month delay between listing for LT for HCC andgranting of priority points, this will result in a more than6-month delay in all patients between last LRT and trans-plantation for downstaged and within Milan criteriapatients.The AFP levels have been suggested to play an important
role when selecting patients as candidates for downstagingand as a predictor of treatment response. Most studies thathave compared patients that achieved downstaging withpatients that were unsuccessful, showed higher levels ofAFP in the nondownstaged group.21,26,27 Barakat andcolleagues21 found that the mean AFP level at the time ofpresentation was significantly higher in the nondownstagedgroup. On the other hand, De Luna and colleagues26 foundno significant predictors for successful downstaging toMilan criteria, including AFP levels. Our data demonstratehigher levels of AFP in the nondownstaged group and AFPlevels before the first LRT showed a trend to be a predictorof downstaging failure, but did not reach the level of

620 Chapman et al Hepatocellular Carcinoma Downstaging J Am Coll Surg
significance (45.7 vs 16.7 ng/mL; p ¼ 0.06). Yao andcolleagues28 reported that an AFP level >1,000 ng/mLwas a predictor of treatment failure in the UCSF study,and an AFP level >1,000 ng/mL was included as anadditional exclusion criterion (unless the AFP leveldecreased to <500 ng/mL with LRT) at the US nationalconference.29 Other groups have suggested that an AFPlevel >400 ng/mL should be used as an exclusion criterionfor LT.22 Although the best AFP cutoff in predicting prog-nosis after LT is still unclear, an AFP >1,000 ng/mL hasbeen associated with worse outcomes after LT for HCCwithin Milan criteria.30 We did not use AFP levels as exclu-sion criteria in the current study. Other reports havecompared patients beyond Milan criteria and patientswithin Milan criteria and describe significantly higherAFP levels at the time of diagnosis and pretransplantationin patients beyond Milan criteria.31 When the last AFPlevels pretransplantation were analyzed in our cohort, wedid not find significant differences among the groups(within Milan criteria, W-UCSF, and B-UCSF), althoughsignificant differences were found when the AFP peak levelswere compared, with higher levels in the B-UCSF group(p < 0.0001). This can be explained by a decrease inAFP levels after successful downstaging and before LTin this group. A higher proportion of patients in theB-UCSF group had AFP levels >1,000 ng/mL at leastonce compared with those in W-UCSF and within Milancriteria groups; 17.9% vs 5.6% vs 2.9%, respectively.Despite these findings, none of the patients who presentedwith AFP levels >1,000 ng/mL in the B-UCSF group hadrecurrence of disease. Of the 6 patients (1 within Milancriteria, 5 B-UCSF) whose last AFP was >1,000 ng/mLbefore transplantation, recurrent HCC developed in 1,and this patient was in the within Milan criteria category.Of the 6 patients (2 within Milan criteria, 1 W-UCSF,and 3 B-UCSF) who initially had AFP >1,000 ng/mLbut eventually decreased to <500 ng/mL, there was1 patient with recurrence in the within Milan criteria cate-gory. Of the patients with initial AFP level >1,000 ng/mL,but subsequently had AFP between 500 and 1,000 ng/mL(who would be excluded from LT under the currentUnited Network for Organ Sharing proposal), 4 (allB-UCSF) received transplants with no recurrence observedto date. We question the United Network for OrganSharing proposal that allows for LT exception pointsfor AFP up to 1,000 ng/mL, but requires those >1,000ng/mL to fall (and remain) <500 ng/mL, based onlack of sufficient evidence to exclude this group fromconsideration of transplantation.There are several limitations to the current study,
including the lack of a uniform protocol for LRT in usefor all patients with HCC. However, all patients
underwent a similar prospective multidisciplinary team re-view to determine the LRT approach and this was true forpatients withinMilan criteria and beyondMilan criteria. Inaddition, like all retrospective studies, there exists a possi-bility of unmeasured selection bias that might have affectedpatient selection for LT, however, data were obtained fromour prospective transplant database and patient follow-upafter LT is thorough and stringent, making determinationsof HCC recurrence highly accurate.Several proposals have arisen in an attempt to extend
the Milan criteria to offer the option of LT to a greaternumber of patients with advanced HCC. In 2001, theUCSF group first proposed the UCSF criteria and showedresults comparable with those obtained in patients withstage II HCC. Since that time, other centers have evalu-ated the extension of these criteria and have evaluated re-sults in patients with higher tumor burden.22,32 Our studycompares survival obtained in patients beyond Milancriteria but W-UCSF criteria, as well as patients B-UCSF criteria who underwent LRT until successfuldownstaging was achieved before LT. Both groups, W-UCSF and B-UCSF, demonstrated an overall survivalcomparable with the survival obtained in patients withinMilan criteria and an approximately 10% HCC recur-rence risk at 5 years of follow-up. After comparing graft,disease-free, and disease-specific survival, in addition torecurrence rates, our results support the concept thatregardless of tumor size and number of tumors at presen-tation, HCC patients can undergo LRT as an attempt ofdownstaging. Once patients show downstaging to withinMilan criteria based on cross-sectional imaging, patientswho initially exceed Milan criteria can undergo LT withoutcomes comparable with those obtained in stage II pa-tients. Based on these results, our belief is that thereshould be no limits for the access of these patients toLRT a priori and, regardless of the number and size of tu-mors, attempting downstaging with LRT with a goal ofachieving Milan criteria status and listing for transplanta-tion is reasonable.
CONCLUSIONSPatients with beyondeMilan criteria HCC who are other-wise candidates for LT should undergo aggressive attemptsat downstaging, without a priori exclusion. This highly se-lective approach allows for excellent long-term results,similar to patients presenting with earlier-stage disease.
Author Contributions
Study conception and design: Chapman, Garcia-Aroz,Vachharajani, Fowler, Saad, Lin, Wellen, Tan, Khan,Doyle

Vol. 224, No. 4, April 2017 Chapman et al Hepatocellular Carcinoma Downstaging 621
Acquisition of data: Chapman, Garcia-Aroz, Vachhar-ajani, Fowler, Saad, Lin, Wellen, Tan, Khan, Doyle
Analysis and interpretation of data: Chapman, Garcia-Aroz, Vachharajani, Fowler, Saad, Lin, Wellen, Tan,Khan, Doyle
Drafting of manuscript: Chapman, Garcia-Aroz, Vach-harajani, Fowler, Saad, Lin, Wellen, Tan, Khan, Doyle
Critical revision: Chapman, Garcia-Aroz, Vachharajani,Fowler, Saad, Lin, Wellen, Tan, Khan, Doyle
REFERENCES
1. Jemal A, Bray F, Center MM, et al. Global cancer statistics.CA Cancer J Clin 2011;61:69e90.
2. Bosch FX, Munoz N. Hepatocellular carcinoma in the world:epidemiologic questions. In: Tabor E, DiBisceglie AM,Purcell RH, eds. Etiology, Pathology and Treatment of Hepa-tocellular Carcinoma in America. Advances in Applied Tech-nology Series. Houston, TX: Gulf Publishing; 1991:35.
3. Okuda K. Epidemiology of primary liver cancer. In: Tobe T, ed.Primary LiverCancer in Japan.Tokyo: Springer-Verlag; 1992:3.
4. El-Serag HB, Kanwal F. Epidemiology of hepatocellular carci-noma in the United States: Where are we? Where do we go?Hepatology 2014;60:1767e1775.
5. Bruix J, Sherman M. American Association for the Study ofLiver Disease. Management of hepatocellular carcinoma: anupdate. Hepatology 2011;53:1020e1022.
6. Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lan-cet 2012;379:1245e1255.
7. Child CG, Turcotte JG. Surgery and portal hypertension. Ma-jor Probl Clin Surg 1964;1:1e85.
8. Pugh RN, Murray-Lyon IM, Dawson JL, et al. Transection ofthe oesophagus for bleeding oesophageal varices. Br J Surg1973;60:646e649.
9. Kamath PS, Wiesner RH, Malinchoc M, et al. A model to pre-dict survival in patients with end-stage liver disease. Hepatol-ogy 2001;33:464e470.
10. Kamath PS, Kim WR, Advanced Liver Disease Study Group.The model for end-stage liver disease (MELD). Hepatology2007;45:797e805.
11. Mazzaferro V, Regalia E, Doci R, et al. Liver transplantationfor the treatment of small hepatocellular carcinomas in patientswith cirrhosis. N Engl J Med 1996;334:693e699.
12. UpToDate. Liver transplantation for hepatocellular carci-noma. Available at: https://www.uptodate.com/contents/liver-transplantation-for-hepatocellular-carcinoma. AccessedNovember 16, 2016.
13. Clavien PA, Lesurtel M, Bossuyt PM, et al. Recommendations forliver transplantation for hepatocellular carcinoma: an internationalconsensus conference report. Lancet Oncol 2012;13:e11ee22.
14. Mazzaferro V, Bhoori S, Sposito C, et al. Milan criteria in livertransplantation for hepatocellular carcinoma: an evidence-based analysis of 15 years of experience. Liver Transpl 2011;17[Suppl 2]:S44eS57.
15. Yao FY, Xiao L, Bass NM, et al. Liver transplantation forhepatocellular carcinoma: validation of the UCSF-expandedcriteria based on preoperative imaging. Am J Transplant2007;7:2587e2596.
16. Chapman WC, Majella Doyle MB, Stuart JE, et al. Outcomesof neoadjuvant transarterial chemoembolization to downstage
hepatocellular carcinoma before liver transplantation. AnnSurg 2008;248:617e625.
17. Yao FY, Ferrell L, Bass NM, et al. Liver transplantation for hepa-tocellular carcinoma: expansion of the tumor size limits does notadversely impact survival. Hepatology 2001;33:1394e1403.
18. Lo C. Downstaging of hepatocellular carcinoma before trans-plantation: an advance in therapy or just another selection cri-terion. Am J Transplant 2008;8:2485e2486.
19. Wald C, Russo MW, Heimbach JK, et al. New OPTN/UNOSpolicy for liver transplant allocation: standardization of liverimaging, diagnosis, classification, and reporting of hepatocellu-lar carcinoma. Radiology 2013;266:376e382.
20. Agopian VG, Morshedi MM, McWilliams J, et al. Completepathologic response to pretransplant locoregional therapy forhepatocellular carcinoma defines cancer cure after liver trans-plantation: analysis of 501 consecutively treated patients.Ann Surg 2015;262:536e545; discussion 543e545.
21. Barakat O, Wood RP, Ozaki CF, et al. Morphological featuresof advanced hepatocellular carcinoma as a predictor of down-staging and liver transplantation: an intention-to-treat analysis.Liver Transpl 2010;16:289e299.
22. Ravaioli M, Grazi GL, Piscaglia F, et al. Liver transplantationfor hepatocellular carcinoma: results of down-staging inpatients initially outside the Milan selection criteria. AmJ Transplant 2008;8:2547e2557.
23. Yao FY, Breitenstein S, Broelsch CE, et al. Does a patient qualifyfor liver transplantation after the down-staging of hepatocellularcarcinoma? Liver Transpl 2011;17[Suppl 2]:S109eS116.
24. Bonadio I, Colle I, Geerts A, et al. Liver transplantation for he-patocellular carcinoma comparing the Milan, UCSF, and Asancriteria: long-term follow-up of a Western single institutionalexperience. Clin Transplant 2015;29:425e433.
25. Yao FY, Mehta N, Flemming J, et al. Downstaging of hepato-cellular cancer before liver transplant: long-term outcomecompared to tumors within Milan criteria. Hepatology2015;61:1968e1977.
26. De Luna W, Sze DY, Ahmed A, et al. Transarterial chemoin-fusion for hepatocellular carcinoma as downstaging therapyand a bridge toward liver transplantation. Am J Transplant2009;9:1158e1168.
27. Green TJ, Rochon PJ, Chang S, et al. Downstaging disease inpatients with hepatocellular carcinoma outside of Milancriteria: strategies using drug-eluting bead chemoembolization.J Vasc Interv Radiol 2013;24:1613e1622.
28. Yao FY, Kerlan RK Jr, Hirose R, et al. Excellent outcomefollowing down-staging of hepatocellular carcinoma prior toliver transplantation: an intention-to-treat analysis. Hepatol-ogy 2008;48:819e827.
29. Pomfret EA, Washburn K, Wald C, et al. Report of a nationalconference on liver allocation in patients with hepatocellular car-cinoma in the United States. Liver Transpl 2010;16:262e278.
30. Hameed B, Mehta N, Sapisochin G, et al. Alpha-fetoproteinlevel> 1000 ng/mL as an exclusion criterion for liver transplan-tation in patients with hepatocellular carcinoma meeting theMilan criteria. Liver Transpl 2014;20:945e951.
31. Cillo U, Vitale A, Bassanello M, et al. Liver transplantation forthe treatment of moderately or well-differentiated hepatocellu-lar carcinoma. Ann Surg 2004;239:150e159.
32. Lee SG, Hwang S, Moon DB, et al. Expanded indicationcriteria of living donor liver transplantation for hepatocellularcarcinoma at one large-volume center. Liver Transpl 2008;14:935e945.