Embed Size (px)
Citation preview

Liver Transplantation in a Patient With Clinical Manifestations ofCryptogenic Cirrhosis: A Case Report of Hepar Lobatum as a PrimaryLiver Condition
J.F.L. Bonfittoa,*, T.J.A.P. Mattosinhob, I. Nevesb, E.C. Ataideb, I.F.S.F. Boinb, R.S.B. Stucchid,D.L. Martinsc, and C.A.F. Escanhoelaa
aDepartment of Pathology, bUnit of Liver Transplantation, cDepartment of Radiology and dDepartment of Internal Medicine, Faculty ofMedical Sciences, State University of Campinas, Sao Paulo, Brazil
ª 2014 by E360 Park Av
Transplantat
ABSTRACT
Background. This article reports a case of hepar lobatum, a peculiar and rare type ofliver deformity, originally described in association with infectious or parasitic diseases andwith malignancies.Case Report. We have described a 42-year-old woman with this disorder, which wasunrelated to the known conditions and referred for liver transplantation for havingclinical manifestations of cirrhosis, portal hypertension, and impaired hepatic function.Conclusions. The observed histologic pattern suggests that hepar lobatum could be, insome patients, the effect of a primary process of hamartomatous origin involving the organvascular supply.
*Address correspondence to Joao Felipe Leite Bonfitto, Ruado Oratorio, 11, 13075-140, Campinas, Sao Paulo, Brazil. E-mail:[email protected]
THE SHRINKAGE OF LIVER PARENCHYMAinvolving �1 lobes occurs in about 13% of cirrhotic
organs, in 50% of those with noncirrhotic portal hyperten-sion, and rarely in other conditions [1]. Hepar lobatum, arare cause of chronic liver disease, was originally describedin patients with tertiary syphilis as a morphologic manifes-tation of healing gummas [2,3]. These can be single ormultiple and are tuberculoid giant cell granulomas withamorphous pale necrotic centers accompanied by plasmacells and areas of endarteritis obliterans. The subsequenthealing process is by fibrosis with broad bands of scarringwhich may distort the liver [4].In the 1990s, another infectoparasitary diseaseda case of
advanced hepatic schistosomiasis with similar morphologydwas reported; the obliteration of portal vein branchesand its consequent focal parenchymal atrophy andcollapse and the liver lymphatic plexus involvement bythe ova were suggested as the possible pathophysiologicpathways [5].As more data became available, several studies have re-
ported an association between hepar lobatum and somecases of diffuse metastatic involvement of the organ, usuallyby breast carcinoma, a situation coined as hepar lobatumcarcinomatosum [2,6e11]. The disease was also related tometastatic rectal [12] and gastric [13] carcinomas, and to
lsevier Inc. All rights reserved.enue South, New York, NY 10010-1710
ion Proceedings, 46, 2433e2436 (2014)
Hodgkin lymphoma [1,14]. The histologic picture, accordingto the main theory, is owing to vascular injury by directneoplastic invasion and its consequent ischemic damage orto the intrahepatic veins involvement by the progression ofthe stromal reaction associated with the tumor cells [7e9].Finally, many cases have been observed after chemo-
therapy [7,9,10,12,13,15], and the morphology has beenattributed to regression of the tumor nodules with subse-quent tissue collapse, fibrosis, and scar contraction [4,10,13].
CASE REPORT
A 42-year-old woman had a 17-year history of mental confusion andweakness associated with the development of telangiectasias on theface and the presternal region and with upper digestive bleedingepisodes. Previously, she had had 2 pregnancies and a personalhistory of depression, hypothyroidism, and a smoking habit. Therewas no evidence of regular alcohol intake or drug consumption. Thepatient was taking citalopram, lorazepam, and levothyroxine, andhas used oral contraceptives in the past. No known chemothera-peutic agent was mentioned. Physical examination showed jaundice,palmar erythema, spider angiomas on the trunk, ascites, and anonpalpable liver.
0041-1345/14/$esee front matterhttp://dx.doi.org/10.1016/j.transproceed.2013.09.057
2433

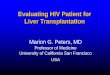
Fig 1. Axial (A) and coronal reformatted (B) portal venous phase computed tomography exhibiting a shrunken dysmorphic liver, withgrossly lobulated contours and widened fissures. Note also ascites, splenomegaly, and paraesophageal, perigastric, and periesplenicvarices (arrows).
2434 BONFITTO, MATTOSINHO, NEVES ET AL
Initial blood tests revealed increased serum levels of aspartateaminotransferase (57 U/L; normal, <27), normal levels of alanineaminotransferase (31 U/L; normal, <34), increased bilirubinemia(8.42 mg/dL; normal, <1), with 4.11 mg/dL for the conjugated form(normal, �0.3) and elevated alkaline phosphatase (254 U/L;normal, <104) and g-glutamyl-transpeptidase (216 U/L; normal,<42). They also showed thrombocytopenia, with a platelet count of62,000/mm3 (150,000 < normal < 400,000) and an InternationalNormalized Ratio of 1.60 (normal, �1.25). The patient had noevidence of chronic infection by hepatotropic viruses or by Trepo-nema pallidum (the search results for the hepatitis B surface anti-gen, hepatitis B core antibody, hepatitis B surface antibody,hepatitis C virus antibody, and for the chemiluminescent micro-particle immunoassay treponemic test were negative), the serumceruloplasmin level was 0.23 g/L (0.2 � normal � 0.6), the gammafraction in the serum protein electrophoresis was normal(1.80 g/dL), and she had a negative test for antinuclear factor.Helical multislice computed tomography showed a reduced sizeliver with lobulated contour and a significant architectural distor-tion without hypervascular lesions (Fig 1).
The patient underwent orthotopic liver transplantation (Modelfor End-stage Liver Disease score, 24; Child-Pugh score, category
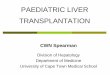
Fig 2. (AeC) Gross appearance of theliver revealing the deep fissures and thelobated smooth surface. The dilated gall-bladder can be observed near the hepat-ic hilum. (D) Cut surface showing thecrevices and the parenchyma lobatedappearance.
C) with removal of apparent appendage tissue at the splenogastricligament and the precaval region. The explant liver weighed 630 g,measured 19.5 � 12.5 � 8.8 cm, and had a gross appearance of acoarsely lobated organ, with a smooth surface and multiple crevicesand depressions sharply mingled with variously sized lobular areas,sometimes linked to the organ by a delicate strand of parenchyma.The light brown liver’s cut surface revealed sparse interconnectedthin to moderately thick dark bands, but devoid of suspected focallesions on gross examination (Fig 2). Samples were taken from 8different regions according to the conventional sampling method inwhich all of the liver segments are analyzed under gross interpre-tation and histologic examination. The gallbladder was located in itsnormal site and did not have calculi.
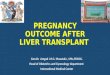
Histologic examination showed a mixed pattern of liver lesions(Fig 3), resulting in a pseudocirrhotic appearance with moderatedegree of fibrosis in some portal tracts and occasional bands ofconnective tissue in a vaguely nodular fashion, which also exhibiteddilated and tortuous vessels and proliferated bile ductules with aneutrophilic and lymphocytic infiltrate. Moreover, there was focalductopenia and mild periportal and periseptal interface activity.Lobular changes included areas of macrogoticular steatosis, hepa-tocyte ballooning, peliosis, and a moderate degree of hepatocellular

Fig 3. (A) Portal tracts enlargement withfocal parenchymal nodularity (stain:Masson trichrome; original magnifica-tion, �100). (BeE) Anomalous portalvessels exhibited in detail. (B) Portalproliferated bile ductules. (C, E) Areasof macrogoticular steatosis. (D) Enlargedportal tract with septa (stain: hematoxylinand eosin; original magnification, �200[BeD] and �100 [E]). (F) Field exhibitingfocal peliosis (stain: hematoxylin andeosin; original magnification, �200).
OLT FOR CRYPTOGENIC CIRRHOSIS 2435
siderosis, evidenced by Prussian blue staining. There was no evi-dence of neoplasia in the sampled material.
DISCUSSION
The present case showed the gross morphology of heparlobatum in a patient with portal hypertension and impairedliver function initially treated as a cryptogenic cirrhosiscarrier. Indeed, all of the known putative markers, includingthose for autoimmune liver disorders, were negative andcomputed tomography showed diffuse parenchymal archi-tectural distortion. Histologic examination, however,revealed a pseudocirrhotic appearance with a mixed patternof liver lesions; however, it was neither related to securemorphologic evidence of any infectoparasitary disease norto neoplasia. In fact, the real cause of the disease remainedinitially unclear.Nevertheless, a few important observations could be
made according to morphologic studies of other situa-tions that show some similarity to parts of the presentcase. It is true that severe tissue shrinkage and paren-chymal extinction occur when there is hepatic vein
obstruction [1]. On the other hand, focal enlargement ofthe liver, in response to a regenerative stimulus or arte-riovenous shunts, may cause tumor-like nodules such asthose seen in patients with massive hepatic necrosis,cirrhosis, Budd-Chiari syndrome, hereditary hemorrhagictelangiectasia, portal vein absence, and portal veinthrombosis [14]. Indeed, hepar lobatum shows the unionof areas of parenchymal atrophy and compensatory hy-perplasia and has been usually associated with vascularabnormalities [14].In our case, the proliferated bile ductules with a neutro-
philic and lymphocytic infiltrate, the focal ductopenia, themild periportal and periseptal interface activity, and theareas of macrogoticular steatosis, hepatocyte ballooning,and hepatocellular siderosis could be explained as lessspecific histologic signs of chronic liver damage. However,considering the peculiar morphology and way of distributionobserved in many portal vessels as well as the absence ofother clear etiologic agents, it would be reasonable to sug-gest that hepar lobatum could be, in some patients, the ef-fect of a hamartomatous process in which the primaryanomalous vascular supply would cause the same final

2436 BONFITTO, MATTOSINHO, NEVES ET AL
picture as those seen in the other described causes of thisrare type of liver deformity.
REFERENCES
[1] Wanless IR. Vascular disorders. In: Burt AD, Portmann BC,Ferrell LD, editors. McSween’s Pathology of the Liver. 5th ed.Philadelphia: Churchill Livingstone Elsevier; 2007. p. 637.
[2] Gravel DH, Bégin LR, Brisson ML, Lamoureux E. Meta-static carcinoma resulting in hepar lobatum. Am J Clin Pathol1996;105(5):621e7.
[3] Tiliakos N, Shamma’a JM, Nasrallah SM. Syphilitic hepatitis.Am J Gastroenterol 1980;73(1):60e1.
[4] Lucas SB. Other viral and infectious diseases and HIV-related liver disease. In: Burt AD, Portmann BC, Ferrell LD, edi-tors. McSween’s Pathology of the Liver. 5th ed. Philadelphia:Churchill Livingstone Elsevier; 2007. p. 452.
[5] Tsui WM, Chow LT. Advanced schistosomiasis as a cause ofhepar lobatum. Histopathology 1993;23(5):495e7.
[6] Cervoni JP, Dobrin A, Sailley N, Chaigneau L, Thevenot T,Richou C, et al. Hepar lobatum carcinomatosum: a rare cause ofportal hypertension complicating hepatic metastases in breast can-cer. Gastroenterol Clin Biol 2008;32(8-9):740e4.
[7] Graber I, Dumortier J, Poncet G, Queneau PE, Mathevet P,Scoazec JY. Hepar lobatum carcinomatosum revealing an occultmetastatic lobular carcinoma of the breast. Ann Diagn Pathol2010;14(6):438e42.
[8] Honma K. Hepar lobatum carcinomatosum due to metastaticbreast carcinoma. Virchows Arch A Pathol Anat Histopathol1987;410(6):465e9.
[9] Nakajima T, Sekoguchi S, Nishikawa T, et al. Multifocalintraportal invasion of breast carcinoma diagnosed bylaparoscopy-assisted liver biopsy. World J Gastroenterol2005;11(15):2360e3.
[10] Qizilbash A, Kontozoglou T, Sianos J, Takashima H,Watanabe T, Minami M, et al. Hepar lobatum associated withchemotherapy and metastatic breast cancer. Arch Pathol Lab Med1987;111(1):58e61.
[11] Uhlmann F, Martin H, Ringk H, Krocker J. Hepar lobatumcarcinomatosum due to chemotherapy of a metastatic breast car-cinoma. Gen Diagn Pathol 1996;141(3-4):279e84.
[12] Teke Z, Nessar G, Kiremitci S, Aksoy E, Elbir OH. Heparlobatum carcinomatosum associated with metastatic rectal carci-noma: an unusual cause of liver dysmorphy. Med Princ Pract2011;20(1):93e6.
[13] Kleiner DE, Lewis JH. Hepatic injury due to drugs, chem-icals and toxins. In: Burt AD, Portmann BC, Ferrell LD, editors.McSween’s Pathology of the Liver. 5th ed. Philadelphia: ChurchillLivingstone Elsevier; 2007. p. 684.
[14] Wanless IR. Vascular disorders of the liver. In: Saxena R,editor. Practical Hepatic Pathology, A Diagnostic Approach. Phil-adelphia: Elsevier Saunders; 2011. p. 452.
[15] Chin NW, Chapman I, Jimenez FA. Complete chemother-apeutic regression of hepatic metastases with resultant heparlobatum. Am J Gastroenterol 1987;82(2):149e51.