Embed Size (px)
Citation preview
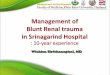
Alastair J W Millar
Red Cross War Memorial Childrenrsquos Hospital
Cape Town South Africa
Liver Trauma
J Pediatr Surg 2011985 14-18
Pediatr Surg Int 19905392-396
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71
Injury 1991 Jul22(4)310-4
Blunt liver trauma in children
Cywes S Bass DH Rode H Millar AJ
Department of Paediatric Surgery University of Cape Town South Africa
Blunt liver trauma The liver is the most frequently injured solid organ
following blunt abdominal injury in children
Selective non-operative management of blunt liver trauma
in haemodynamically stable patients is well established
and accepted by most paediatric surgical centres
Surgical intervention in paediatric liver trauma is based on
haemodynamic instability that persists despite ongoing
resuscitation
Biliary injuries are often missed until clinically manifest
Major liver trauma is still associated with a significant
mortality
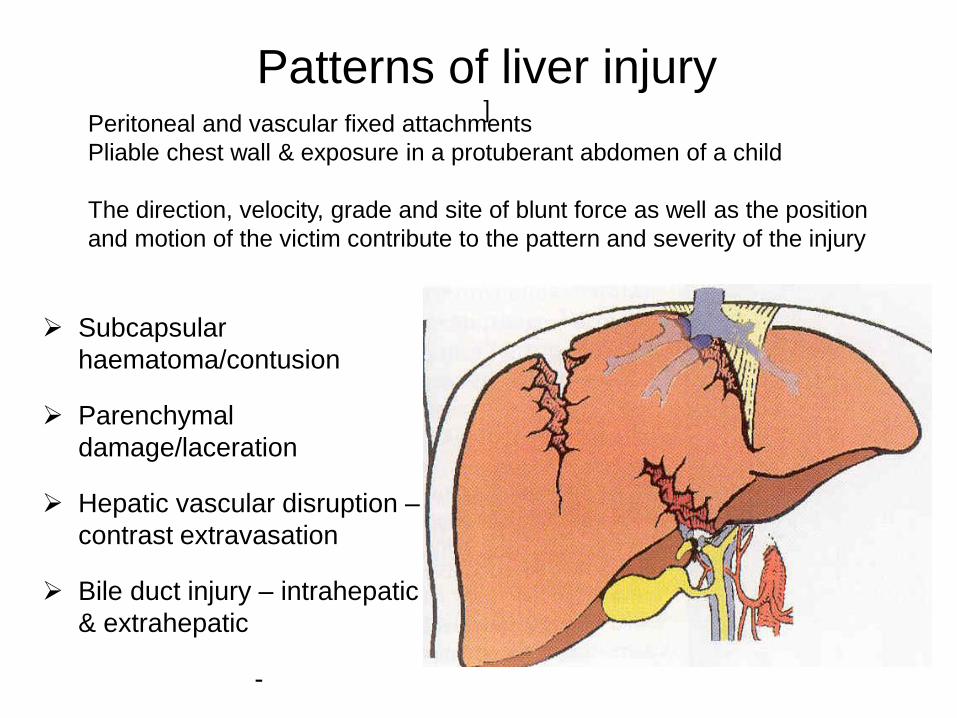
Patterns of liver injury ]
Peritoneal and vascular fixed attachments
Pliable chest wall amp exposure in a protuberant abdomen of a child
The direction velocity grade and site of blunt force as well as the position
and motion of the victim contribute to the pattern and severity of the injury
Subcapsular
haematomacontusion
Parenchymal
damagelaceration
Hepatic vascular disruption ndash
contrast extravasation
Bile duct injury ndash intrahepatic
amp extrahepatic
-
Schematic diagram of the liver
noting the structures at each
potential site of injury
Patterns of injury Oblique right chest [pedestrian traffic]
Anterior acceleration injury - laceration to the L or R of the Falciform ligament
Patterns of injury Deceleration injury [falls from a height pedestrian traffic]
Compression injury [roll over]
Natural History of different types of injury
Retroperitoneal area ndash tamponade but hepatic vein may bleed ++
Glissonrsquos capsule intact + bleeding ndash expanding subcapsular haematoma
Haematoma contained within the liver parenchyma - expansion amp liquefaction
- absorption 2 to 3 months
- infection ndash abscess
- encysted
Arterial rupture ndash expansion on-going bleeding
- pseudoaneurysm amp delayed bleed or haemobilia
- arterio-portal fistula - peripheral most close
- central may lead to portal hypertension
Bile duct - partial will heal if distal duct intact
but may require intra-ductal pressure reduction for this to occur
- larger - on-going leak and bile ascites
- stricture
- biliary fistula if duct from a segment disrupted but otherwise viable
Diagnosis History + Physical examination
plusmntachycardia plusmnhypotension peritoneal irritation
FAST
better for unstable patients not stable enough for CT
or as a screen for CT
CT with contrast
determine grade and look for active extravasation
Coley et al J Trauma 2000
AAST Liver Injury Grading [American Association for the Surgery of Trauma]
Grade I
Grade IV
CT-based Injury Severity of Blunt Hepatic Trauma
CT-based Grade Criteria
1 Capsular avulsion superficial laceration(s) less than
1 cm deep subcapsular hematoma less than 1 cm in
maximum thickness periportal blood tracking only
2 Laceration(s) 1ndash3 cm deep central-subcapsular
hematoma(s) 1ndash3 cm in diameter
3 Laceration greater than 3 cm deep central-subcapsular
hematoma(s) greater than 3 cm in diameter
4 Massive central-subcapsular hematoma greater than 10
cm lobar tissue destruction (maceration) or
devascularization
5 Bilobar tissue destruction (maceration) or
devascularization
CT Criteria for Management of Blunt Liver Trauma Correlation with Angiographic and Surgical Findings
Pierre A Poletti et al 2000 Radiology 216 418 - 427
Liver injuries at Red Cross Childrenrsquos
Hospital n=409 [32yrs] end 2013
163
246
0
50
100
150
200
250
Isolated Associated
[40]
[60]
Cause of Injury
[n=409]
350 (86) RTAs Pedestrian 303 (87) Passenger 47 (13)
Cyclist 3 (040
17 (4)
Child abuseassault
26 (6)
Falls from on top of
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
J Pediatr Surg 2011985 14-18
Pediatr Surg Int 19905392-396
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71
Injury 1991 Jul22(4)310-4
Blunt liver trauma in children
Cywes S Bass DH Rode H Millar AJ
Department of Paediatric Surgery University of Cape Town South Africa
Blunt liver trauma The liver is the most frequently injured solid organ
following blunt abdominal injury in children
Selective non-operative management of blunt liver trauma
in haemodynamically stable patients is well established
and accepted by most paediatric surgical centres
Surgical intervention in paediatric liver trauma is based on
haemodynamic instability that persists despite ongoing
resuscitation
Biliary injuries are often missed until clinically manifest
Major liver trauma is still associated with a significant
mortality
Patterns of liver injury ]
Peritoneal and vascular fixed attachments
Pliable chest wall amp exposure in a protuberant abdomen of a child
The direction velocity grade and site of blunt force as well as the position
and motion of the victim contribute to the pattern and severity of the injury
Subcapsular
haematomacontusion
Parenchymal
damagelaceration
Hepatic vascular disruption ndash
contrast extravasation
Bile duct injury ndash intrahepatic
amp extrahepatic
-
Schematic diagram of the liver
noting the structures at each
potential site of injury
Patterns of injury Oblique right chest [pedestrian traffic]
Anterior acceleration injury - laceration to the L or R of the Falciform ligament
Patterns of injury Deceleration injury [falls from a height pedestrian traffic]
Compression injury [roll over]
Natural History of different types of injury
Retroperitoneal area ndash tamponade but hepatic vein may bleed ++
Glissonrsquos capsule intact + bleeding ndash expanding subcapsular haematoma
Haematoma contained within the liver parenchyma - expansion amp liquefaction
- absorption 2 to 3 months
- infection ndash abscess
- encysted
Arterial rupture ndash expansion on-going bleeding
- pseudoaneurysm amp delayed bleed or haemobilia
- arterio-portal fistula - peripheral most close
- central may lead to portal hypertension
Bile duct - partial will heal if distal duct intact
but may require intra-ductal pressure reduction for this to occur
- larger - on-going leak and bile ascites
- stricture
- biliary fistula if duct from a segment disrupted but otherwise viable
Diagnosis History + Physical examination
plusmntachycardia plusmnhypotension peritoneal irritation
FAST
better for unstable patients not stable enough for CT
or as a screen for CT
CT with contrast
determine grade and look for active extravasation
Coley et al J Trauma 2000
AAST Liver Injury Grading [American Association for the Surgery of Trauma]
Grade I
Grade IV
CT-based Injury Severity of Blunt Hepatic Trauma
CT-based Grade Criteria
1 Capsular avulsion superficial laceration(s) less than
1 cm deep subcapsular hematoma less than 1 cm in
maximum thickness periportal blood tracking only
2 Laceration(s) 1ndash3 cm deep central-subcapsular
hematoma(s) 1ndash3 cm in diameter
3 Laceration greater than 3 cm deep central-subcapsular
hematoma(s) greater than 3 cm in diameter
4 Massive central-subcapsular hematoma greater than 10
cm lobar tissue destruction (maceration) or
devascularization
5 Bilobar tissue destruction (maceration) or
devascularization
CT Criteria for Management of Blunt Liver Trauma Correlation with Angiographic and Surgical Findings
Pierre A Poletti et al 2000 Radiology 216 418 - 427
Liver injuries at Red Cross Childrenrsquos
Hospital n=409 [32yrs] end 2013
163
246
0
50
100
150
200
250
Isolated Associated
[40]
[60]
Cause of Injury
[n=409]
350 (86) RTAs Pedestrian 303 (87) Passenger 47 (13)
Cyclist 3 (040
17 (4)
Child abuseassault
26 (6)
Falls from on top of
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
Blunt liver trauma The liver is the most frequently injured solid organ
following blunt abdominal injury in children
Selective non-operative management of blunt liver trauma
in haemodynamically stable patients is well established
and accepted by most paediatric surgical centres
Surgical intervention in paediatric liver trauma is based on
haemodynamic instability that persists despite ongoing
resuscitation
Biliary injuries are often missed until clinically manifest
Major liver trauma is still associated with a significant
mortality
Patterns of liver injury ]
Peritoneal and vascular fixed attachments
Pliable chest wall amp exposure in a protuberant abdomen of a child
The direction velocity grade and site of blunt force as well as the position
and motion of the victim contribute to the pattern and severity of the injury
Subcapsular
haematomacontusion
Parenchymal
damagelaceration
Hepatic vascular disruption ndash
contrast extravasation
Bile duct injury ndash intrahepatic
amp extrahepatic
-
Schematic diagram of the liver
noting the structures at each
potential site of injury
Patterns of injury Oblique right chest [pedestrian traffic]
Anterior acceleration injury - laceration to the L or R of the Falciform ligament
Patterns of injury Deceleration injury [falls from a height pedestrian traffic]
Compression injury [roll over]
Natural History of different types of injury
Retroperitoneal area ndash tamponade but hepatic vein may bleed ++
Glissonrsquos capsule intact + bleeding ndash expanding subcapsular haematoma
Haematoma contained within the liver parenchyma - expansion amp liquefaction
- absorption 2 to 3 months
- infection ndash abscess
- encysted
Arterial rupture ndash expansion on-going bleeding
- pseudoaneurysm amp delayed bleed or haemobilia
- arterio-portal fistula - peripheral most close
- central may lead to portal hypertension
Bile duct - partial will heal if distal duct intact
but may require intra-ductal pressure reduction for this to occur
- larger - on-going leak and bile ascites
- stricture
- biliary fistula if duct from a segment disrupted but otherwise viable
Diagnosis History + Physical examination
plusmntachycardia plusmnhypotension peritoneal irritation
FAST
better for unstable patients not stable enough for CT
or as a screen for CT
CT with contrast
determine grade and look for active extravasation
Coley et al J Trauma 2000
AAST Liver Injury Grading [American Association for the Surgery of Trauma]
Grade I
Grade IV
CT-based Injury Severity of Blunt Hepatic Trauma
CT-based Grade Criteria
1 Capsular avulsion superficial laceration(s) less than
1 cm deep subcapsular hematoma less than 1 cm in
maximum thickness periportal blood tracking only
2 Laceration(s) 1ndash3 cm deep central-subcapsular
hematoma(s) 1ndash3 cm in diameter
3 Laceration greater than 3 cm deep central-subcapsular
hematoma(s) greater than 3 cm in diameter
4 Massive central-subcapsular hematoma greater than 10
cm lobar tissue destruction (maceration) or
devascularization
5 Bilobar tissue destruction (maceration) or
devascularization
CT Criteria for Management of Blunt Liver Trauma Correlation with Angiographic and Surgical Findings
Pierre A Poletti et al 2000 Radiology 216 418 - 427
Liver injuries at Red Cross Childrenrsquos
Hospital n=409 [32yrs] end 2013
163
246
0
50
100
150
200
250
Isolated Associated
[40]
[60]
Cause of Injury
[n=409]
350 (86) RTAs Pedestrian 303 (87) Passenger 47 (13)
Cyclist 3 (040
17 (4)
Child abuseassault
26 (6)
Falls from on top of
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
Patterns of liver injury ]
Peritoneal and vascular fixed attachments
Pliable chest wall amp exposure in a protuberant abdomen of a child
The direction velocity grade and site of blunt force as well as the position
and motion of the victim contribute to the pattern and severity of the injury
Subcapsular
haematomacontusion
Parenchymal
damagelaceration
Hepatic vascular disruption ndash
contrast extravasation
Bile duct injury ndash intrahepatic
amp extrahepatic
-
Schematic diagram of the liver
noting the structures at each
potential site of injury
Patterns of injury Oblique right chest [pedestrian traffic]
Anterior acceleration injury - laceration to the L or R of the Falciform ligament
Patterns of injury Deceleration injury [falls from a height pedestrian traffic]
Compression injury [roll over]
Natural History of different types of injury
Retroperitoneal area ndash tamponade but hepatic vein may bleed ++
Glissonrsquos capsule intact + bleeding ndash expanding subcapsular haematoma
Haematoma contained within the liver parenchyma - expansion amp liquefaction
- absorption 2 to 3 months
- infection ndash abscess
- encysted
Arterial rupture ndash expansion on-going bleeding
- pseudoaneurysm amp delayed bleed or haemobilia
- arterio-portal fistula - peripheral most close
- central may lead to portal hypertension
Bile duct - partial will heal if distal duct intact
but may require intra-ductal pressure reduction for this to occur
- larger - on-going leak and bile ascites
- stricture
- biliary fistula if duct from a segment disrupted but otherwise viable
Diagnosis History + Physical examination
plusmntachycardia plusmnhypotension peritoneal irritation
FAST
better for unstable patients not stable enough for CT
or as a screen for CT
CT with contrast
determine grade and look for active extravasation
Coley et al J Trauma 2000
AAST Liver Injury Grading [American Association for the Surgery of Trauma]
Grade I
Grade IV
CT-based Injury Severity of Blunt Hepatic Trauma
CT-based Grade Criteria
1 Capsular avulsion superficial laceration(s) less than
1 cm deep subcapsular hematoma less than 1 cm in
maximum thickness periportal blood tracking only
2 Laceration(s) 1ndash3 cm deep central-subcapsular
hematoma(s) 1ndash3 cm in diameter
3 Laceration greater than 3 cm deep central-subcapsular
hematoma(s) greater than 3 cm in diameter
4 Massive central-subcapsular hematoma greater than 10
cm lobar tissue destruction (maceration) or
devascularization
5 Bilobar tissue destruction (maceration) or
devascularization
CT Criteria for Management of Blunt Liver Trauma Correlation with Angiographic and Surgical Findings
Pierre A Poletti et al 2000 Radiology 216 418 - 427
Liver injuries at Red Cross Childrenrsquos
Hospital n=409 [32yrs] end 2013
163
246
0
50
100
150
200
250
Isolated Associated
[40]
[60]
Cause of Injury
[n=409]
350 (86) RTAs Pedestrian 303 (87) Passenger 47 (13)
Cyclist 3 (040
17 (4)
Child abuseassault
26 (6)
Falls from on top of
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
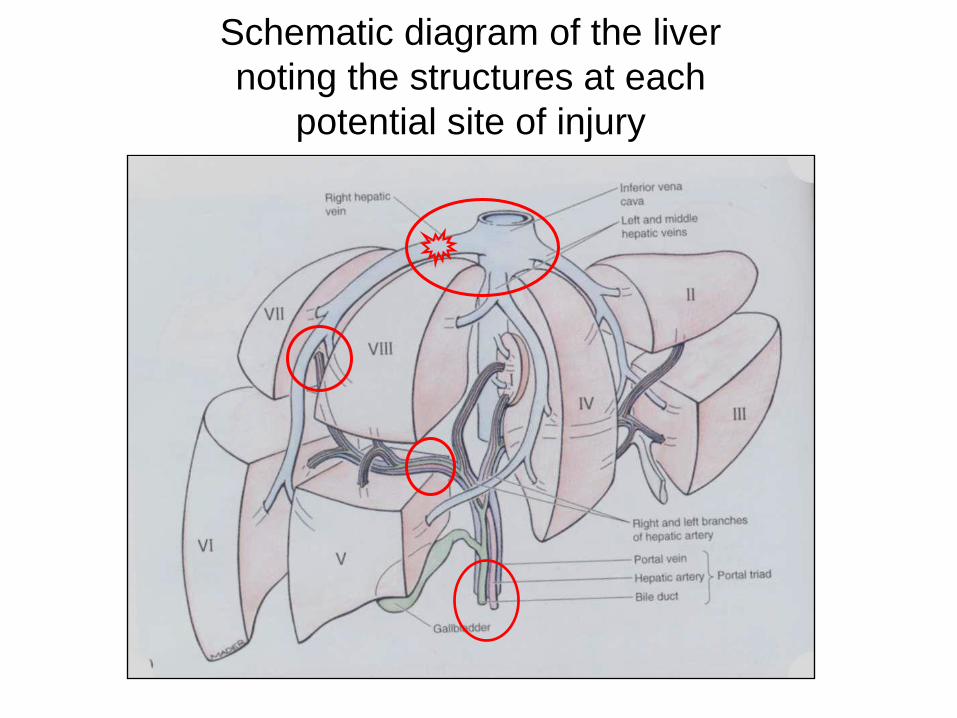
Schematic diagram of the liver
noting the structures at each
potential site of injury
Patterns of injury Oblique right chest [pedestrian traffic]
Anterior acceleration injury - laceration to the L or R of the Falciform ligament
Patterns of injury Deceleration injury [falls from a height pedestrian traffic]
Compression injury [roll over]
Natural History of different types of injury
Retroperitoneal area ndash tamponade but hepatic vein may bleed ++
Glissonrsquos capsule intact + bleeding ndash expanding subcapsular haematoma
Haematoma contained within the liver parenchyma - expansion amp liquefaction
- absorption 2 to 3 months
- infection ndash abscess
- encysted
Arterial rupture ndash expansion on-going bleeding
- pseudoaneurysm amp delayed bleed or haemobilia
- arterio-portal fistula - peripheral most close
- central may lead to portal hypertension
Bile duct - partial will heal if distal duct intact
but may require intra-ductal pressure reduction for this to occur
- larger - on-going leak and bile ascites
- stricture
- biliary fistula if duct from a segment disrupted but otherwise viable
Diagnosis History + Physical examination
plusmntachycardia plusmnhypotension peritoneal irritation
FAST
better for unstable patients not stable enough for CT
or as a screen for CT
CT with contrast
determine grade and look for active extravasation
Coley et al J Trauma 2000
AAST Liver Injury Grading [American Association for the Surgery of Trauma]
Grade I
Grade IV
CT-based Injury Severity of Blunt Hepatic Trauma
CT-based Grade Criteria
1 Capsular avulsion superficial laceration(s) less than
1 cm deep subcapsular hematoma less than 1 cm in
maximum thickness periportal blood tracking only
2 Laceration(s) 1ndash3 cm deep central-subcapsular
hematoma(s) 1ndash3 cm in diameter
3 Laceration greater than 3 cm deep central-subcapsular
hematoma(s) greater than 3 cm in diameter
4 Massive central-subcapsular hematoma greater than 10
cm lobar tissue destruction (maceration) or
devascularization
5 Bilobar tissue destruction (maceration) or
devascularization
CT Criteria for Management of Blunt Liver Trauma Correlation with Angiographic and Surgical Findings
Pierre A Poletti et al 2000 Radiology 216 418 - 427
Liver injuries at Red Cross Childrenrsquos
Hospital n=409 [32yrs] end 2013
163
246
0
50
100
150
200
250
Isolated Associated
[40]
[60]
Cause of Injury
[n=409]
350 (86) RTAs Pedestrian 303 (87) Passenger 47 (13)
Cyclist 3 (040
17 (4)
Child abuseassault
26 (6)
Falls from on top of
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
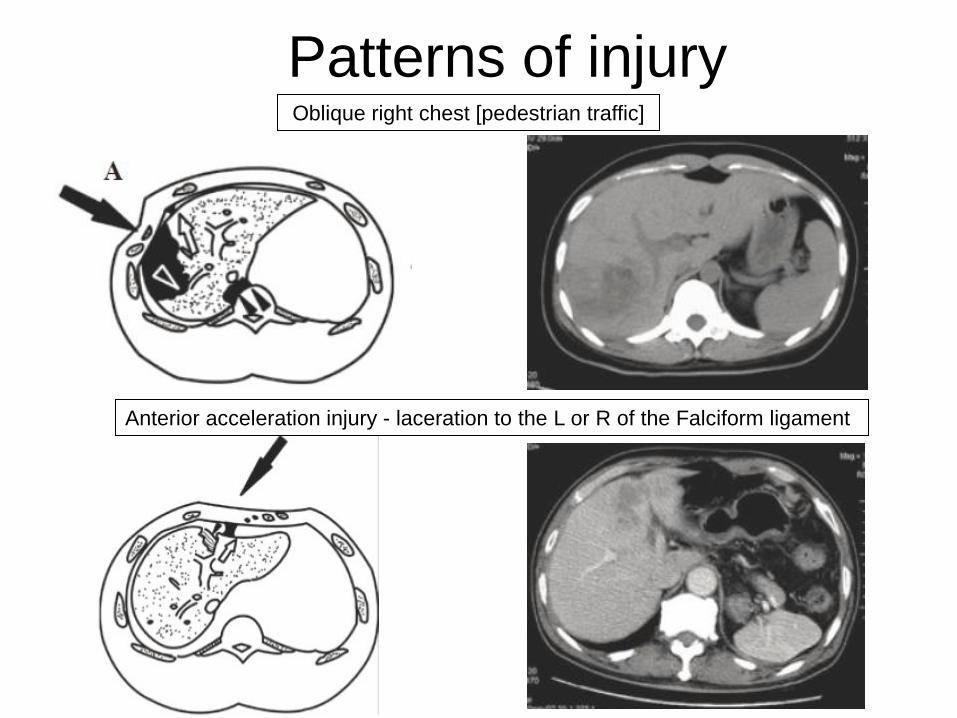
Patterns of injury Oblique right chest [pedestrian traffic]
Anterior acceleration injury - laceration to the L or R of the Falciform ligament
Patterns of injury Deceleration injury [falls from a height pedestrian traffic]
Compression injury [roll over]
Natural History of different types of injury
Retroperitoneal area ndash tamponade but hepatic vein may bleed ++
Glissonrsquos capsule intact + bleeding ndash expanding subcapsular haematoma
Haematoma contained within the liver parenchyma - expansion amp liquefaction
- absorption 2 to 3 months
- infection ndash abscess
- encysted
Arterial rupture ndash expansion on-going bleeding
- pseudoaneurysm amp delayed bleed or haemobilia
- arterio-portal fistula - peripheral most close
- central may lead to portal hypertension
Bile duct - partial will heal if distal duct intact
but may require intra-ductal pressure reduction for this to occur
- larger - on-going leak and bile ascites
- stricture
- biliary fistula if duct from a segment disrupted but otherwise viable
Diagnosis History + Physical examination
plusmntachycardia plusmnhypotension peritoneal irritation
FAST
better for unstable patients not stable enough for CT
or as a screen for CT
CT with contrast
determine grade and look for active extravasation
Coley et al J Trauma 2000
AAST Liver Injury Grading [American Association for the Surgery of Trauma]
Grade I
Grade IV
CT-based Injury Severity of Blunt Hepatic Trauma
CT-based Grade Criteria
1 Capsular avulsion superficial laceration(s) less than
1 cm deep subcapsular hematoma less than 1 cm in
maximum thickness periportal blood tracking only
2 Laceration(s) 1ndash3 cm deep central-subcapsular
hematoma(s) 1ndash3 cm in diameter
3 Laceration greater than 3 cm deep central-subcapsular
hematoma(s) greater than 3 cm in diameter
4 Massive central-subcapsular hematoma greater than 10
cm lobar tissue destruction (maceration) or
devascularization
5 Bilobar tissue destruction (maceration) or
devascularization
CT Criteria for Management of Blunt Liver Trauma Correlation with Angiographic and Surgical Findings
Pierre A Poletti et al 2000 Radiology 216 418 - 427
Liver injuries at Red Cross Childrenrsquos
Hospital n=409 [32yrs] end 2013
163
246
0
50
100
150
200
250
Isolated Associated
[40]
[60]
Cause of Injury
[n=409]
350 (86) RTAs Pedestrian 303 (87) Passenger 47 (13)
Cyclist 3 (040
17 (4)
Child abuseassault
26 (6)
Falls from on top of
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
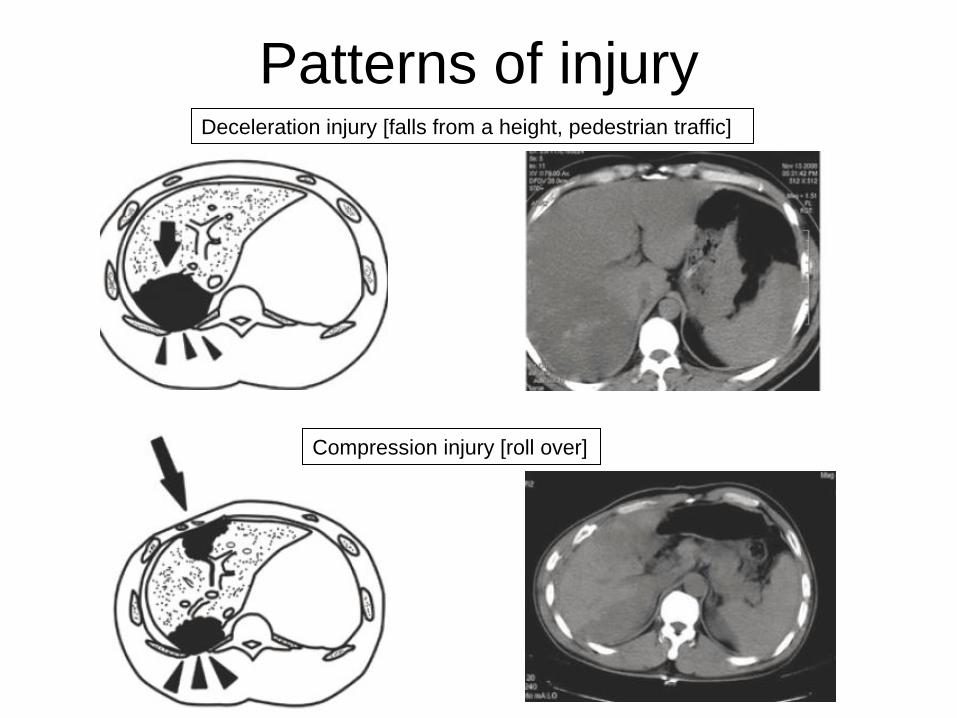
Patterns of injury Deceleration injury [falls from a height pedestrian traffic]
Compression injury [roll over]
Natural History of different types of injury
Retroperitoneal area ndash tamponade but hepatic vein may bleed ++
Glissonrsquos capsule intact + bleeding ndash expanding subcapsular haematoma
Haematoma contained within the liver parenchyma - expansion amp liquefaction
- absorption 2 to 3 months
- infection ndash abscess
- encysted
Arterial rupture ndash expansion on-going bleeding
- pseudoaneurysm amp delayed bleed or haemobilia
- arterio-portal fistula - peripheral most close
- central may lead to portal hypertension
Bile duct - partial will heal if distal duct intact
but may require intra-ductal pressure reduction for this to occur
- larger - on-going leak and bile ascites
- stricture
- biliary fistula if duct from a segment disrupted but otherwise viable
Diagnosis History + Physical examination
plusmntachycardia plusmnhypotension peritoneal irritation
FAST
better for unstable patients not stable enough for CT
or as a screen for CT
CT with contrast
determine grade and look for active extravasation
Coley et al J Trauma 2000
AAST Liver Injury Grading [American Association for the Surgery of Trauma]
Grade I
Grade IV
CT-based Injury Severity of Blunt Hepatic Trauma
CT-based Grade Criteria
1 Capsular avulsion superficial laceration(s) less than
1 cm deep subcapsular hematoma less than 1 cm in
maximum thickness periportal blood tracking only
2 Laceration(s) 1ndash3 cm deep central-subcapsular
hematoma(s) 1ndash3 cm in diameter
3 Laceration greater than 3 cm deep central-subcapsular
hematoma(s) greater than 3 cm in diameter
4 Massive central-subcapsular hematoma greater than 10
cm lobar tissue destruction (maceration) or
devascularization
5 Bilobar tissue destruction (maceration) or
devascularization
CT Criteria for Management of Blunt Liver Trauma Correlation with Angiographic and Surgical Findings
Pierre A Poletti et al 2000 Radiology 216 418 - 427
Liver injuries at Red Cross Childrenrsquos
Hospital n=409 [32yrs] end 2013
163
246
0
50
100
150
200
250
Isolated Associated
[40]
[60]
Cause of Injury
[n=409]
350 (86) RTAs Pedestrian 303 (87) Passenger 47 (13)
Cyclist 3 (040
17 (4)
Child abuseassault
26 (6)
Falls from on top of
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
Natural History of different types of injury
Retroperitoneal area ndash tamponade but hepatic vein may bleed ++
Glissonrsquos capsule intact + bleeding ndash expanding subcapsular haematoma
Haematoma contained within the liver parenchyma - expansion amp liquefaction
- absorption 2 to 3 months
- infection ndash abscess
- encysted
Arterial rupture ndash expansion on-going bleeding
- pseudoaneurysm amp delayed bleed or haemobilia
- arterio-portal fistula - peripheral most close
- central may lead to portal hypertension
Bile duct - partial will heal if distal duct intact
but may require intra-ductal pressure reduction for this to occur
- larger - on-going leak and bile ascites
- stricture
- biliary fistula if duct from a segment disrupted but otherwise viable
Diagnosis History + Physical examination
plusmntachycardia plusmnhypotension peritoneal irritation
FAST
better for unstable patients not stable enough for CT
or as a screen for CT
CT with contrast
determine grade and look for active extravasation
Coley et al J Trauma 2000
AAST Liver Injury Grading [American Association for the Surgery of Trauma]
Grade I
Grade IV
CT-based Injury Severity of Blunt Hepatic Trauma
CT-based Grade Criteria
1 Capsular avulsion superficial laceration(s) less than
1 cm deep subcapsular hematoma less than 1 cm in
maximum thickness periportal blood tracking only
2 Laceration(s) 1ndash3 cm deep central-subcapsular
hematoma(s) 1ndash3 cm in diameter
3 Laceration greater than 3 cm deep central-subcapsular
hematoma(s) greater than 3 cm in diameter
4 Massive central-subcapsular hematoma greater than 10
cm lobar tissue destruction (maceration) or
devascularization
5 Bilobar tissue destruction (maceration) or
devascularization
CT Criteria for Management of Blunt Liver Trauma Correlation with Angiographic and Surgical Findings
Pierre A Poletti et al 2000 Radiology 216 418 - 427
Liver injuries at Red Cross Childrenrsquos
Hospital n=409 [32yrs] end 2013
163
246
0
50
100
150
200
250
Isolated Associated
[40]
[60]
Cause of Injury
[n=409]
350 (86) RTAs Pedestrian 303 (87) Passenger 47 (13)
Cyclist 3 (040
17 (4)
Child abuseassault
26 (6)
Falls from on top of
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
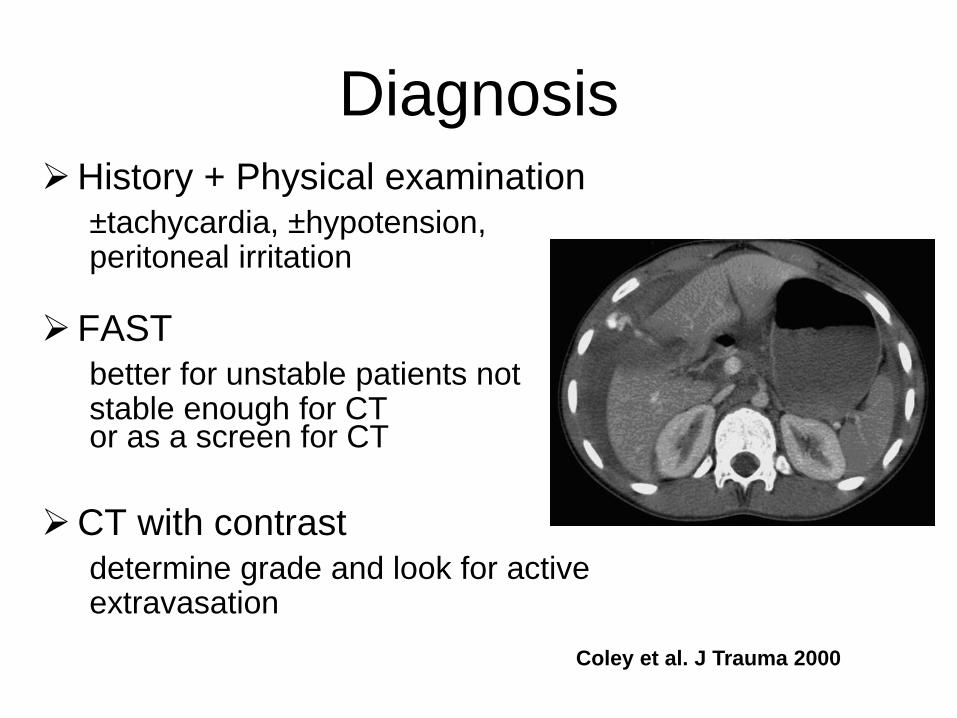
Diagnosis History + Physical examination
plusmntachycardia plusmnhypotension peritoneal irritation
FAST
better for unstable patients not stable enough for CT
or as a screen for CT
CT with contrast
determine grade and look for active extravasation
Coley et al J Trauma 2000
AAST Liver Injury Grading [American Association for the Surgery of Trauma]
Grade I
Grade IV
CT-based Injury Severity of Blunt Hepatic Trauma
CT-based Grade Criteria
1 Capsular avulsion superficial laceration(s) less than
1 cm deep subcapsular hematoma less than 1 cm in
maximum thickness periportal blood tracking only
2 Laceration(s) 1ndash3 cm deep central-subcapsular
hematoma(s) 1ndash3 cm in diameter
3 Laceration greater than 3 cm deep central-subcapsular
hematoma(s) greater than 3 cm in diameter
4 Massive central-subcapsular hematoma greater than 10
cm lobar tissue destruction (maceration) or
devascularization
5 Bilobar tissue destruction (maceration) or
devascularization
CT Criteria for Management of Blunt Liver Trauma Correlation with Angiographic and Surgical Findings
Pierre A Poletti et al 2000 Radiology 216 418 - 427
Liver injuries at Red Cross Childrenrsquos
Hospital n=409 [32yrs] end 2013
163
246
0
50
100
150
200
250
Isolated Associated
[40]
[60]
Cause of Injury
[n=409]
350 (86) RTAs Pedestrian 303 (87) Passenger 47 (13)
Cyclist 3 (040
17 (4)
Child abuseassault
26 (6)
Falls from on top of
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
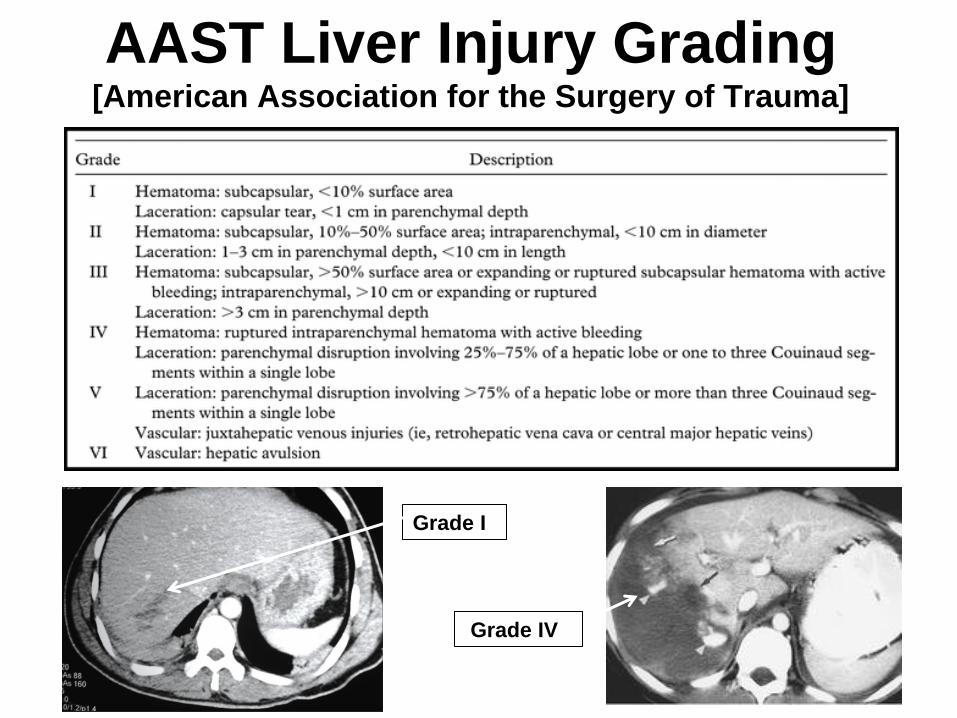
AAST Liver Injury Grading [American Association for the Surgery of Trauma]
Grade I
Grade IV
CT-based Injury Severity of Blunt Hepatic Trauma
CT-based Grade Criteria
1 Capsular avulsion superficial laceration(s) less than
1 cm deep subcapsular hematoma less than 1 cm in
maximum thickness periportal blood tracking only
2 Laceration(s) 1ndash3 cm deep central-subcapsular
hematoma(s) 1ndash3 cm in diameter
3 Laceration greater than 3 cm deep central-subcapsular
hematoma(s) greater than 3 cm in diameter
4 Massive central-subcapsular hematoma greater than 10
cm lobar tissue destruction (maceration) or
devascularization
5 Bilobar tissue destruction (maceration) or
devascularization
CT Criteria for Management of Blunt Liver Trauma Correlation with Angiographic and Surgical Findings
Pierre A Poletti et al 2000 Radiology 216 418 - 427
Liver injuries at Red Cross Childrenrsquos
Hospital n=409 [32yrs] end 2013
163
246
0
50
100
150
200
250
Isolated Associated
[40]
[60]
Cause of Injury
[n=409]
350 (86) RTAs Pedestrian 303 (87) Passenger 47 (13)
Cyclist 3 (040
17 (4)
Child abuseassault
26 (6)
Falls from on top of
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
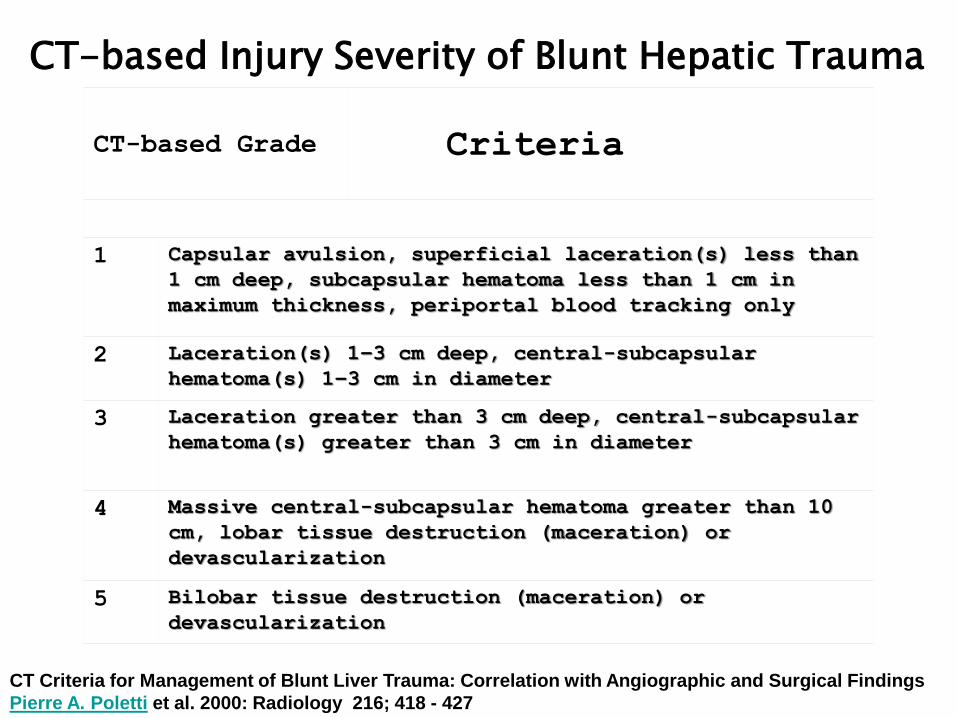
CT-based Injury Severity of Blunt Hepatic Trauma
CT-based Grade Criteria
1 Capsular avulsion superficial laceration(s) less than
1 cm deep subcapsular hematoma less than 1 cm in
maximum thickness periportal blood tracking only
2 Laceration(s) 1ndash3 cm deep central-subcapsular
hematoma(s) 1ndash3 cm in diameter
3 Laceration greater than 3 cm deep central-subcapsular
hematoma(s) greater than 3 cm in diameter
4 Massive central-subcapsular hematoma greater than 10
cm lobar tissue destruction (maceration) or
devascularization
5 Bilobar tissue destruction (maceration) or
devascularization
CT Criteria for Management of Blunt Liver Trauma Correlation with Angiographic and Surgical Findings
Pierre A Poletti et al 2000 Radiology 216 418 - 427
Liver injuries at Red Cross Childrenrsquos
Hospital n=409 [32yrs] end 2013
163
246
0
50
100
150
200
250
Isolated Associated
[40]
[60]
Cause of Injury
[n=409]
350 (86) RTAs Pedestrian 303 (87) Passenger 47 (13)
Cyclist 3 (040
17 (4)
Child abuseassault
26 (6)
Falls from on top of
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
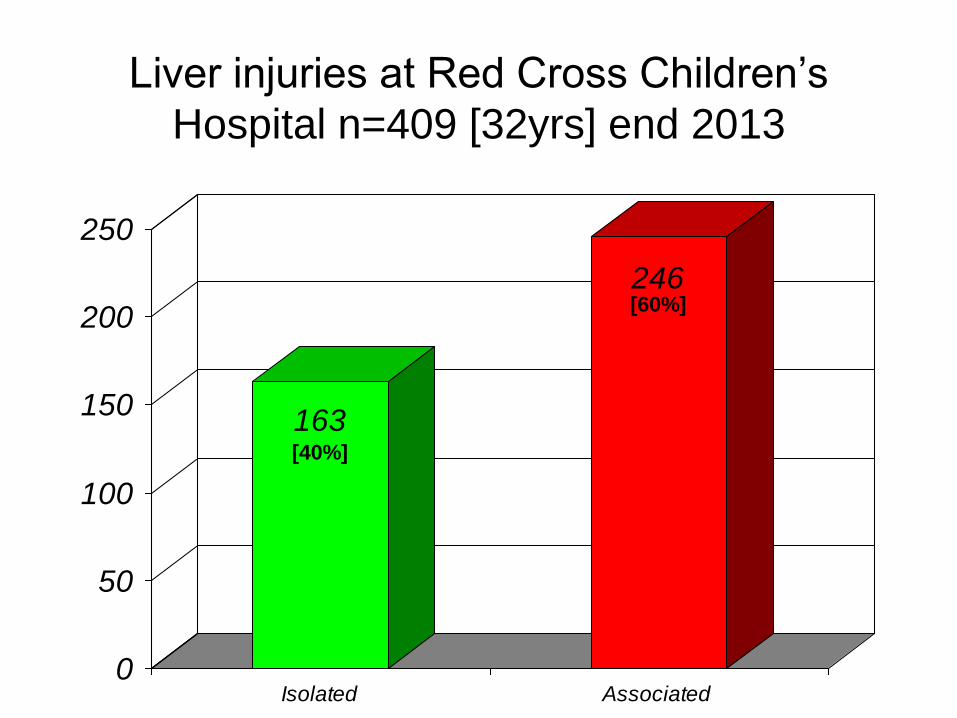
Liver injuries at Red Cross Childrenrsquos
Hospital n=409 [32yrs] end 2013
163
246
0
50
100
150
200
250
Isolated Associated
[40]
[60]
Cause of Injury
[n=409]
350 (86) RTAs Pedestrian 303 (87) Passenger 47 (13)
Cyclist 3 (040
17 (4)
Child abuseassault
26 (6)
Falls from on top of
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
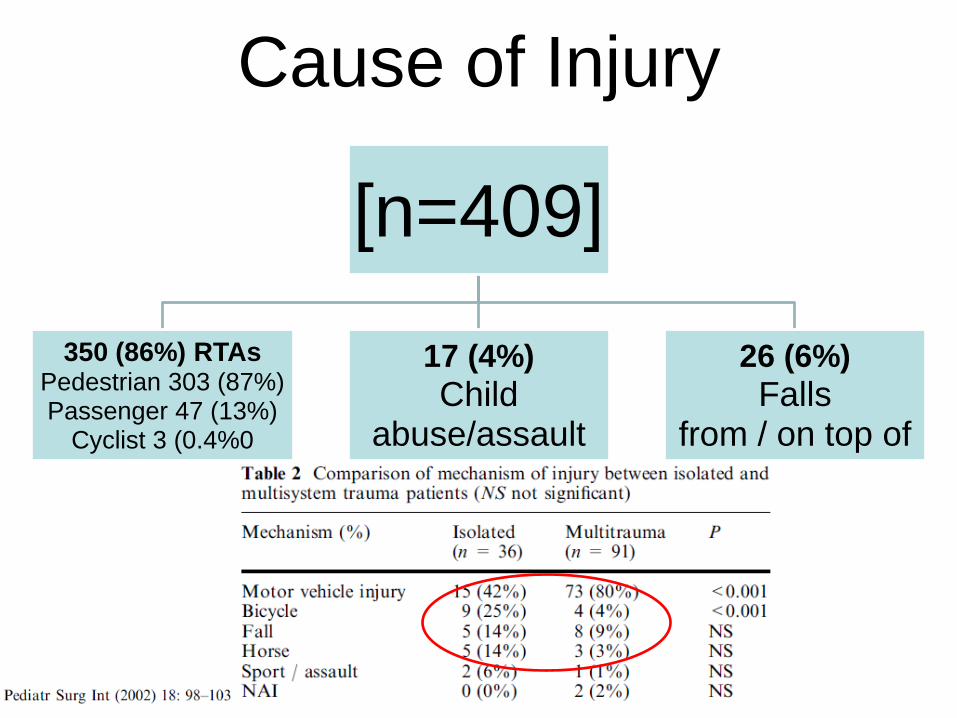
Cause of Injury
[n=409]
350 (86) RTAs Pedestrian 303 (87) Passenger 47 (13)
Cyclist 3 (040
17 (4)
Child abuseassault
26 (6)
Falls from on top of
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
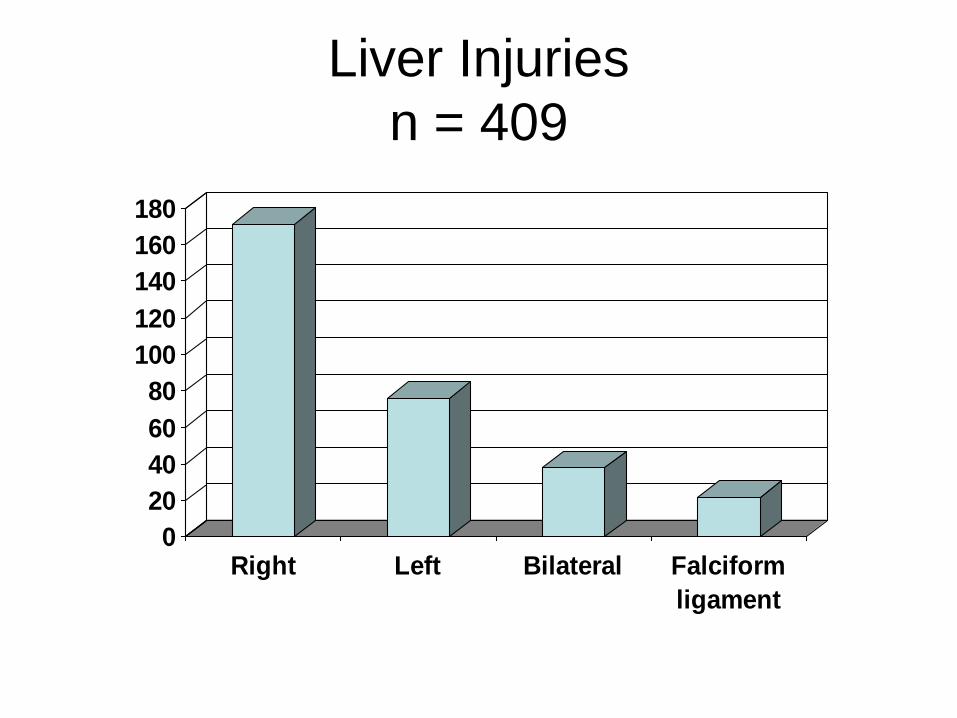
Liver Injuries
n = 409
0
20
40
60
80
100
120
140
160
180
Right Left Bilateral Falciform
ligament
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
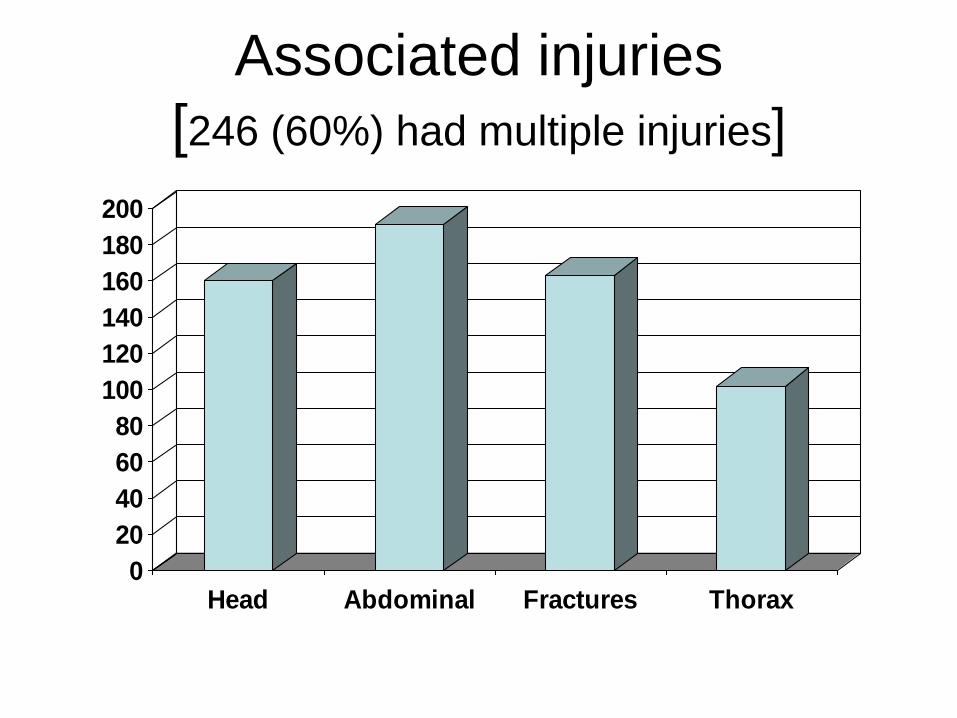
Associated injuries
[246 (60) had multiple injuries]
0
20
40
60
80
100
120
140
160
180
200
Head Abdominal Fractures Thorax
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
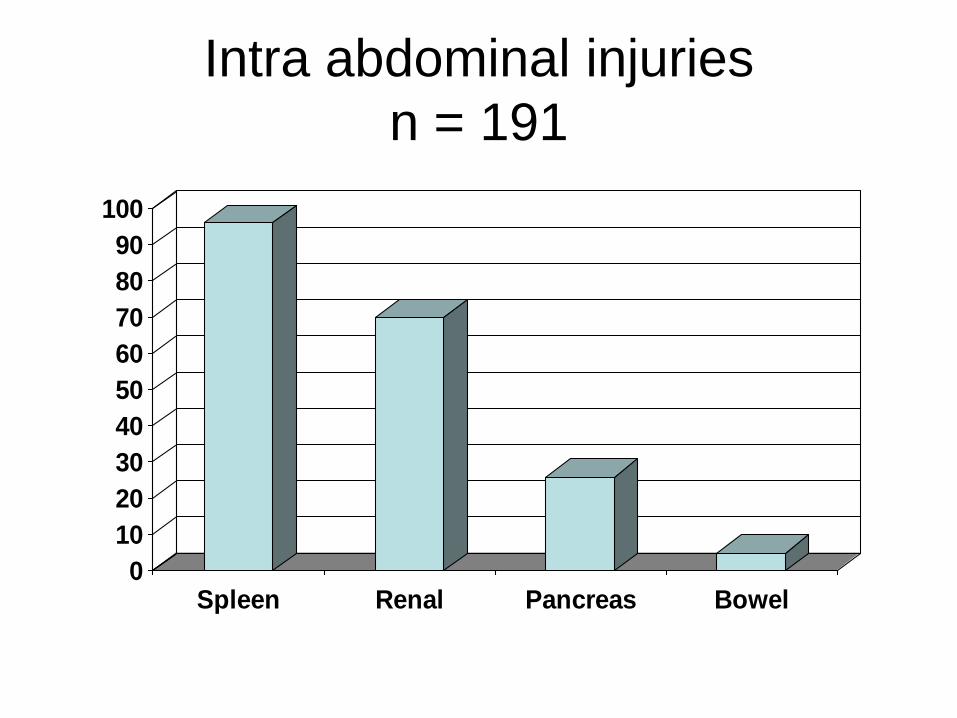
Intra abdominal injuries
n = 191
0
10
20
30
40
50
60
70
80
90
100
Spleen Renal Pancreas Bowel
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
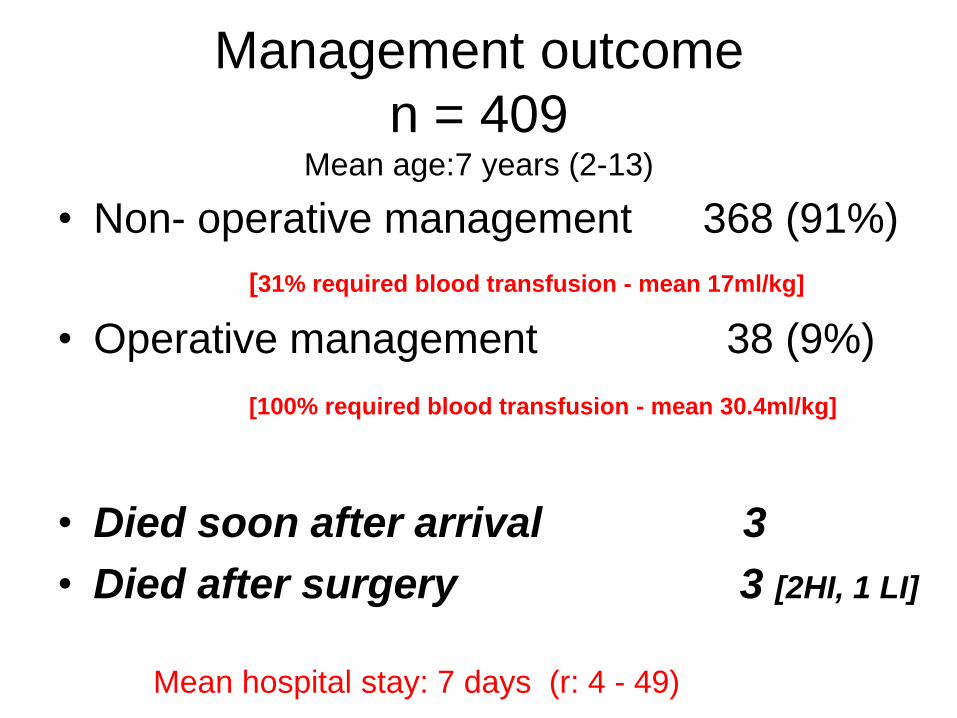
Management outcome
n = 409 Mean age7 years (2-13)
bull Non- operative management 368 (91)
[31 required blood transfusion - mean 17mlkg]
bull Operative management 38 (9)
[100 required blood transfusion - mean 304mlkg]
bull Died soon after arrival 3
bull Died after surgery 3 [2HI 1 LI]
Mean hospital stay 7 days (r 4 - 49)
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
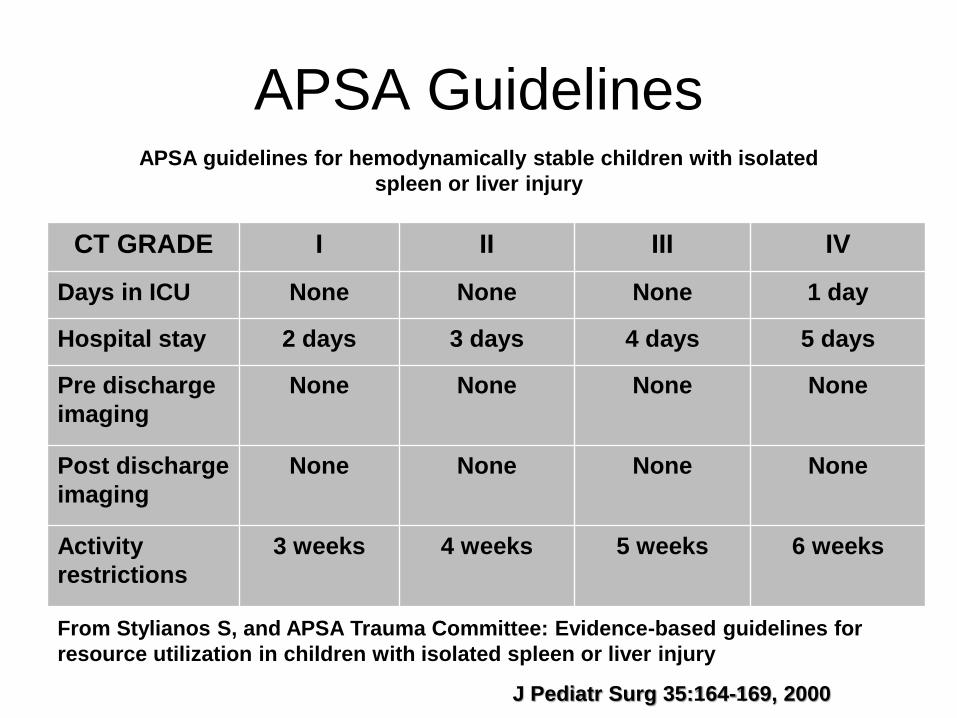
APSA Guidelines
CT GRADE I II III IV
Days in ICU None None None 1 day
Hospital stay 2 days 3 days 4 days 5 days
Pre discharge
imaging
None None None None
Post discharge
imaging
None None None None
Activity
restrictions
3 weeks 4 weeks 5 weeks 6 weeks
APSA guidelines for hemodynamically stable children with isolated
spleen or liver injury
J Pediatr Surg 35164-169 2000
From Stylianos S and APSA Trauma Committee Evidence-based guidelines for
resource utilization in children with isolated spleen or liver injury
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
Non-Operative Group (n=368)
ndash CT or liver scintigraphy [prior to 1984]
ndash NOM not ldquoconservativerdquo management
ndash High care or ICU
ndash Close monitoring of haemodynamic status
ndash Serial hemoglobin electrolytes LFTrsquos
ndash Blood pressure serum lactate base excess
ndash Transfusion requirements [lt20mlkg]
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
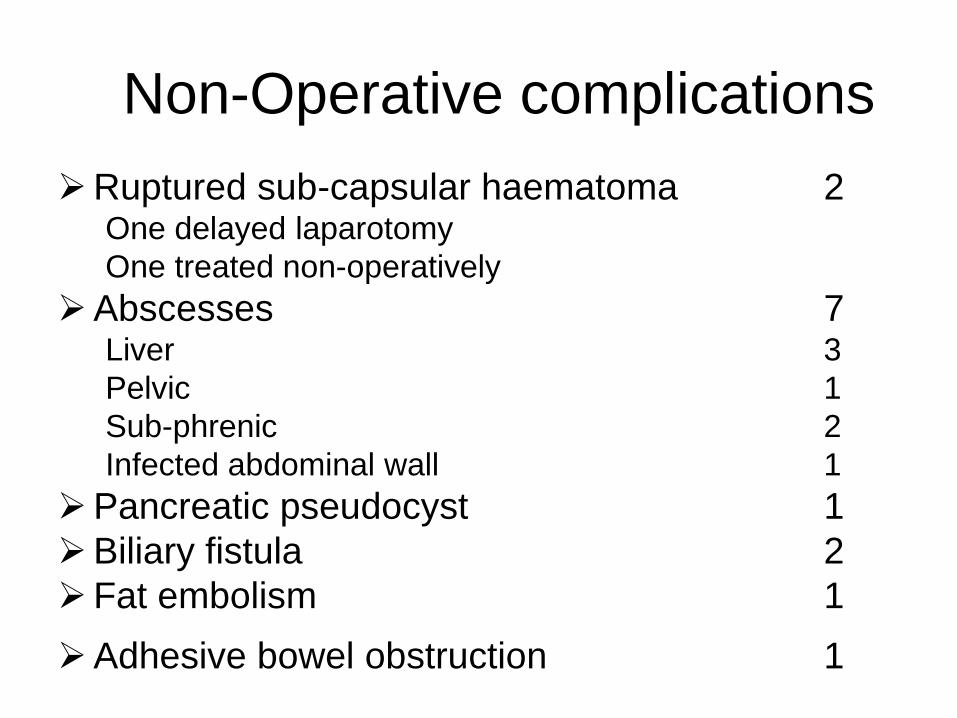
Non-Operative complications
Ruptured sub-capsular haematoma 2 One delayed laparotomy
One treated non-operatively
Abscesses 7 Liver 3
Pelvic 1
Sub-phrenic 2
Infected abdominal wall 1
Pancreatic pseudocyst 1
Biliary fistula 2
Fat embolism 1
Adhesive bowel obstruction 1
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
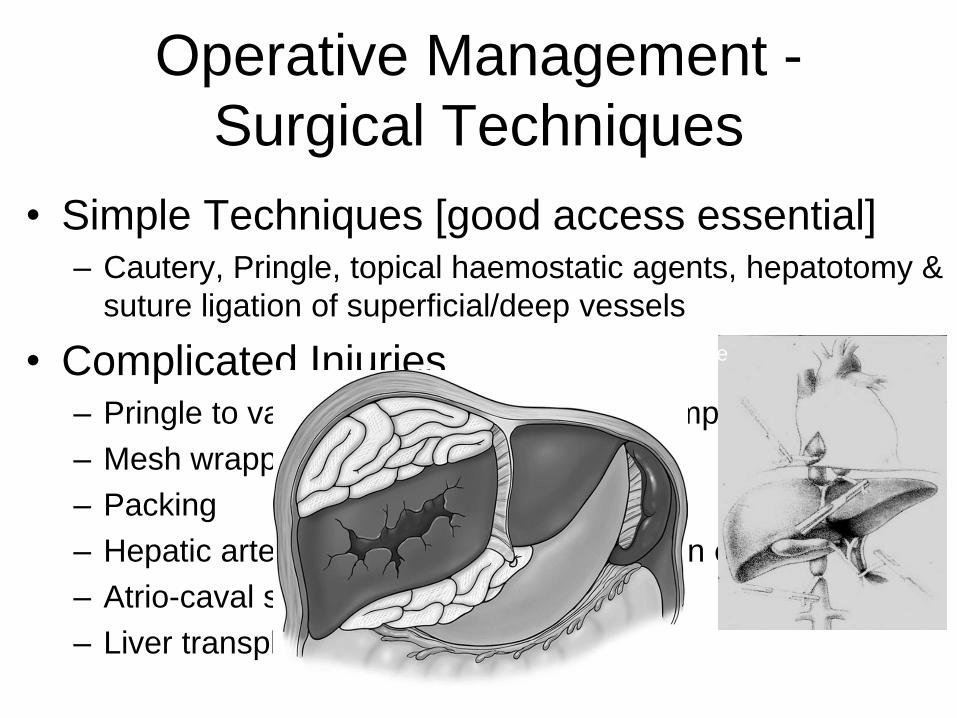
Operative Management -
Surgical Techniques
bull Simple Techniques [good access essential] ndash Cautery Pringle topical haemostatic agents hepatotomy amp
suture ligation of superficialdeep vessels
bull Complicated Injuries ndash Pringle to vascular exclusion amp aortic clamping
ndash Mesh wrapping [not used]
ndash Packing
ndash Hepatic artery ligation [used on 1 occasion only]
ndash Atrio-caval shunting [not used]
ndash Liver transplant [rare but life saving]
Pringle
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
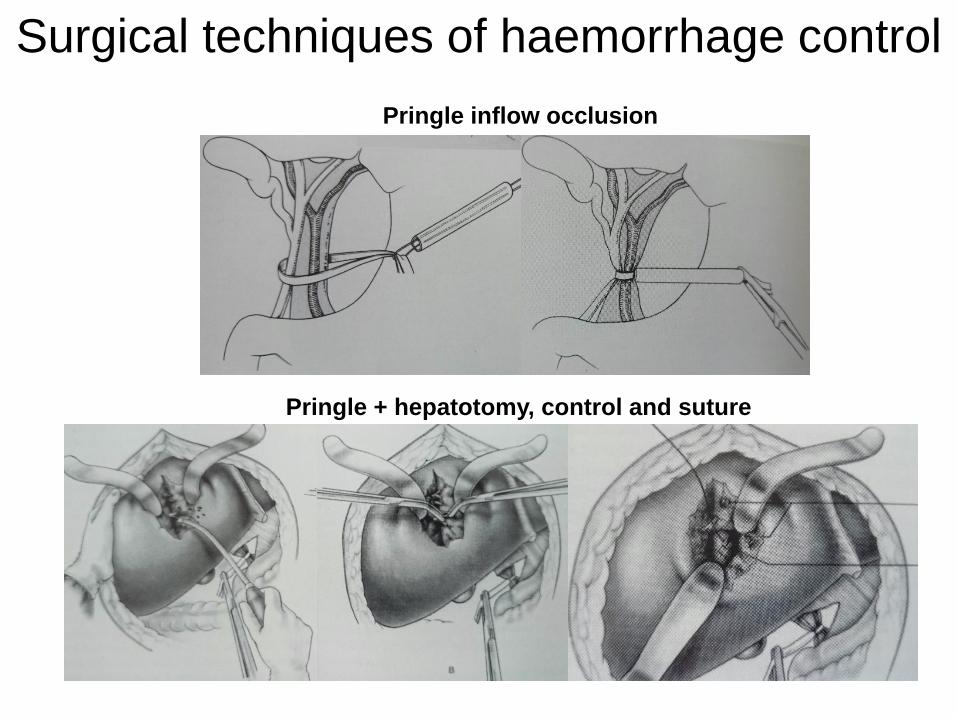
Surgical techniques of haemorrhage control
Pringle inflow occlusion
Pringle + hepatotomy control and suture
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
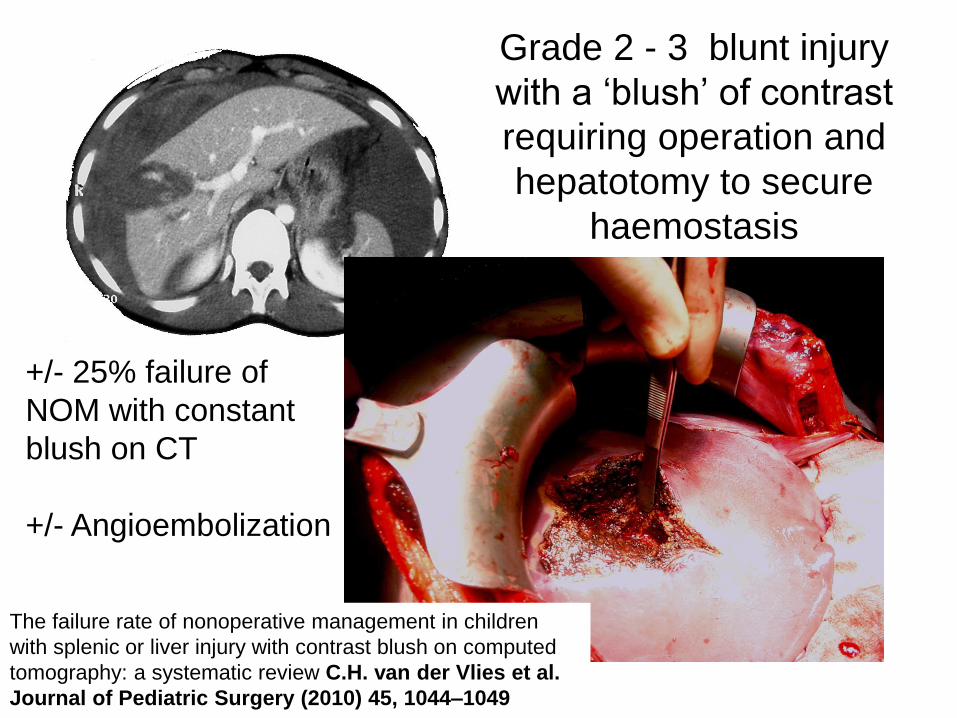
Grade 2 - 3 blunt injury
with a lsquoblushrsquo of contrast
requiring operation and
hepatotomy to secure
haemostasis
The failure rate of nonoperative management in children
with splenic or liver injury with contrast blush on computed
tomography a systematic review CH van der Vlies et al
Journal of Pediatric Surgery (2010) 45 1044ndash1049
+- 25 failure of
NOM with constant
blush on CT
+- Angioembolization
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
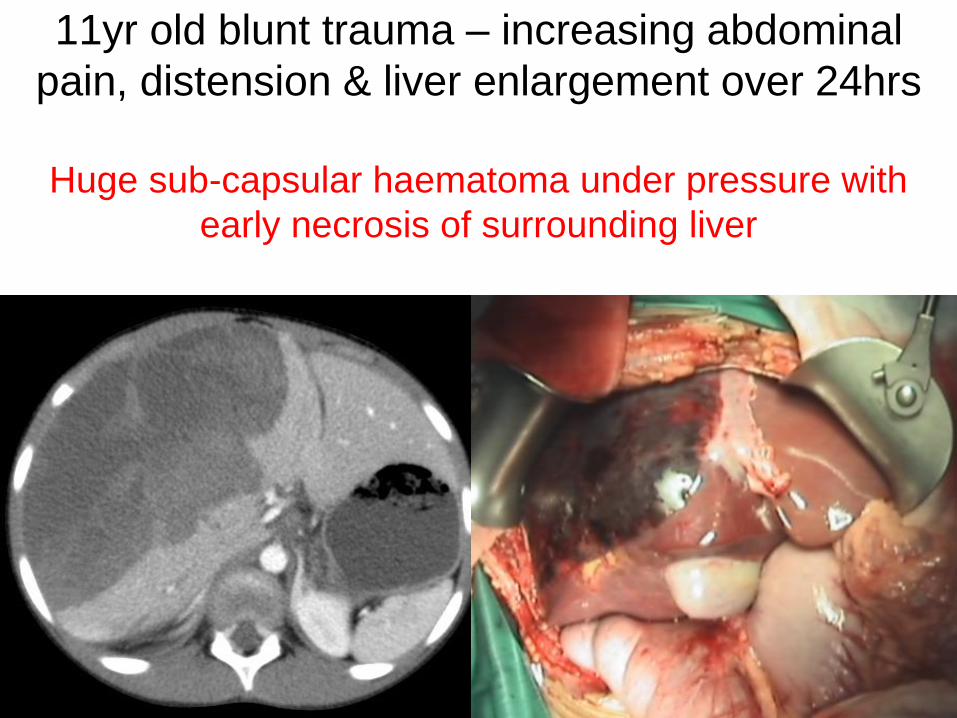
11yr old blunt trauma ndash increasing abdominal
pain distension amp liver enlargement over 24hrs
Huge sub-capsular haematoma under pressure with
early necrosis of surrounding liver
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
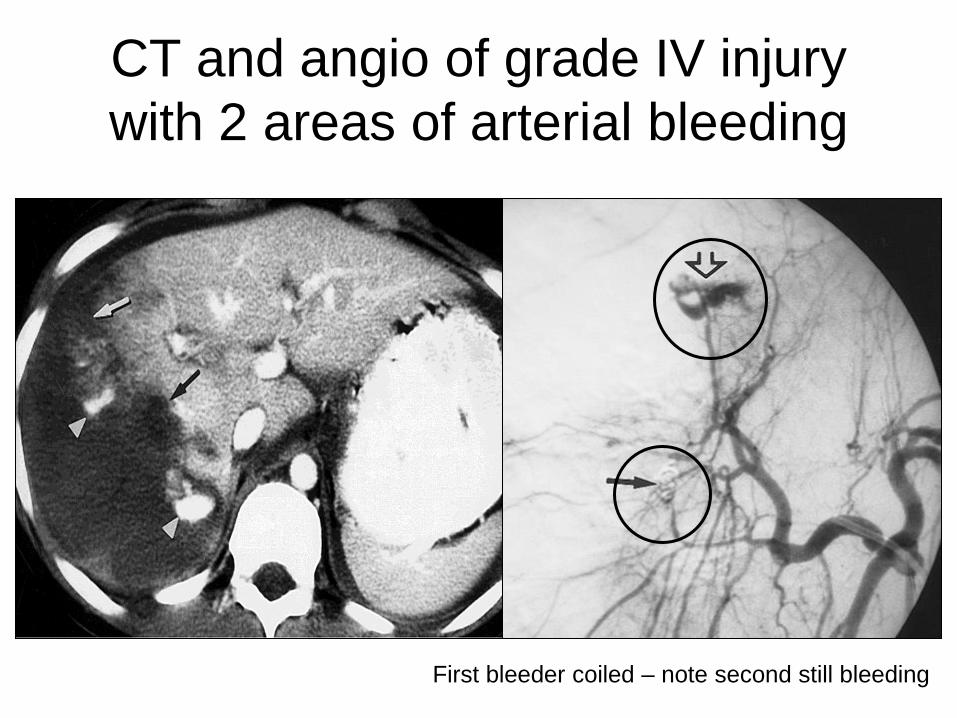
CT and angio of grade IV injury
with 2 areas of arterial bleeding
First bleeder coiled ndash note second still bleeding
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
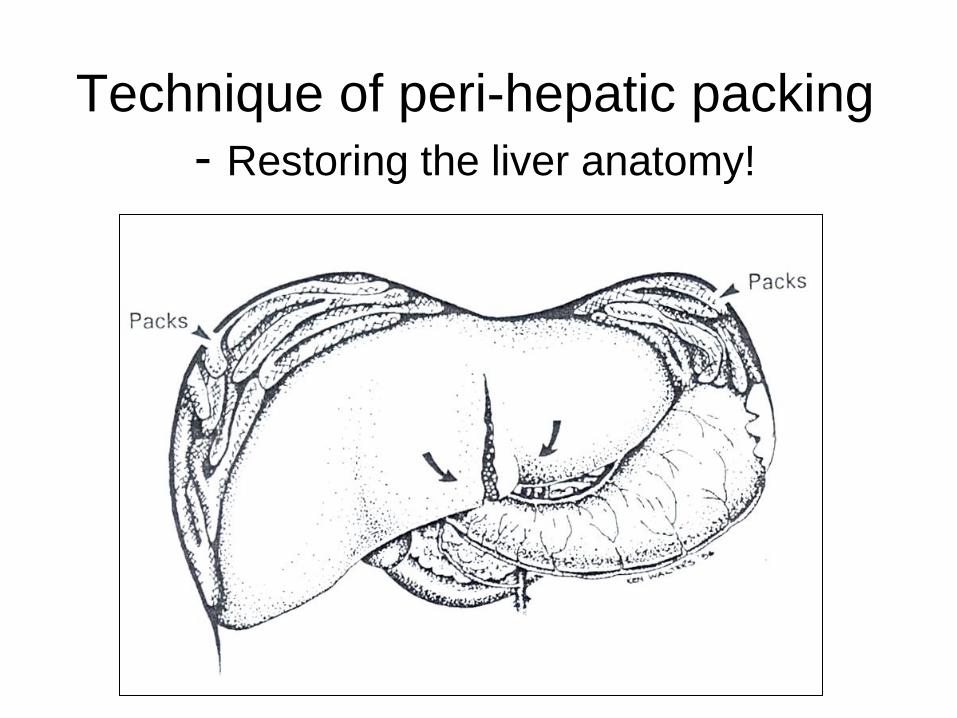
Technique of peri-hepatic packing
- Restoring the liver anatomy
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
Follow-up
bull Imaging used for follow-up
ndash Serial Ultrasound scan [long term]
ndash Serial Computer Tomography [clinical need]
ndash HIDA scan for suspected bile duct leak
bull Of those who returned for follow-up
ndash all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury
ndash Intrahepatic vascular pedicle injury may be associated segmental atrophy
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
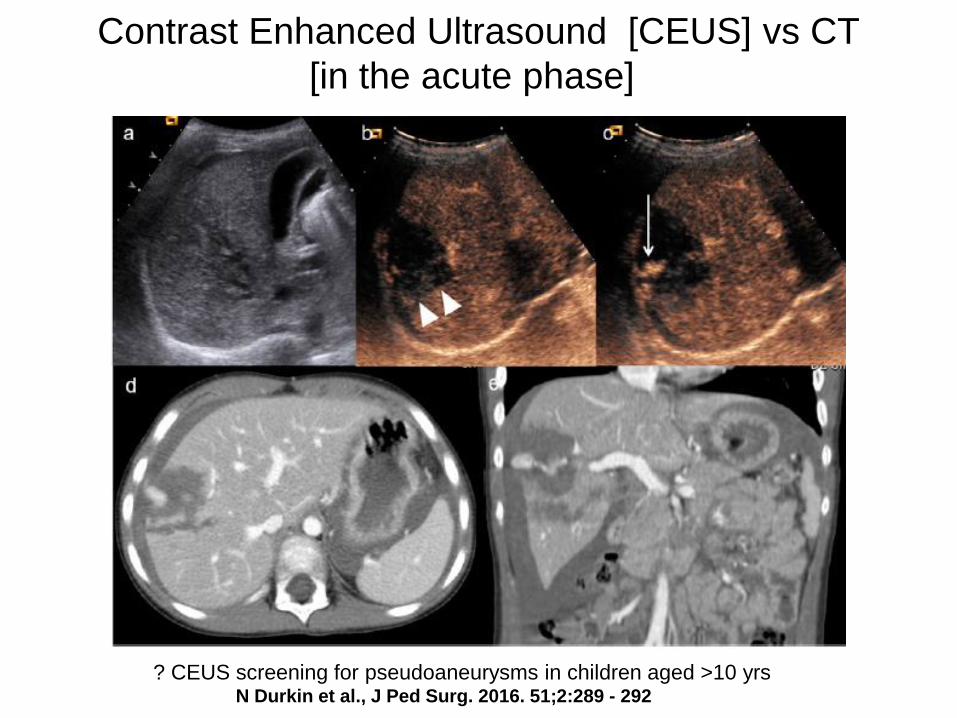
Contrast Enhanced Ultrasound [CEUS] vs CT
[in the acute phase]
CEUS screening for pseudoaneurysms in children aged gt10 yrs N Durkin et al J Ped Surg 2016 512289 - 292
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
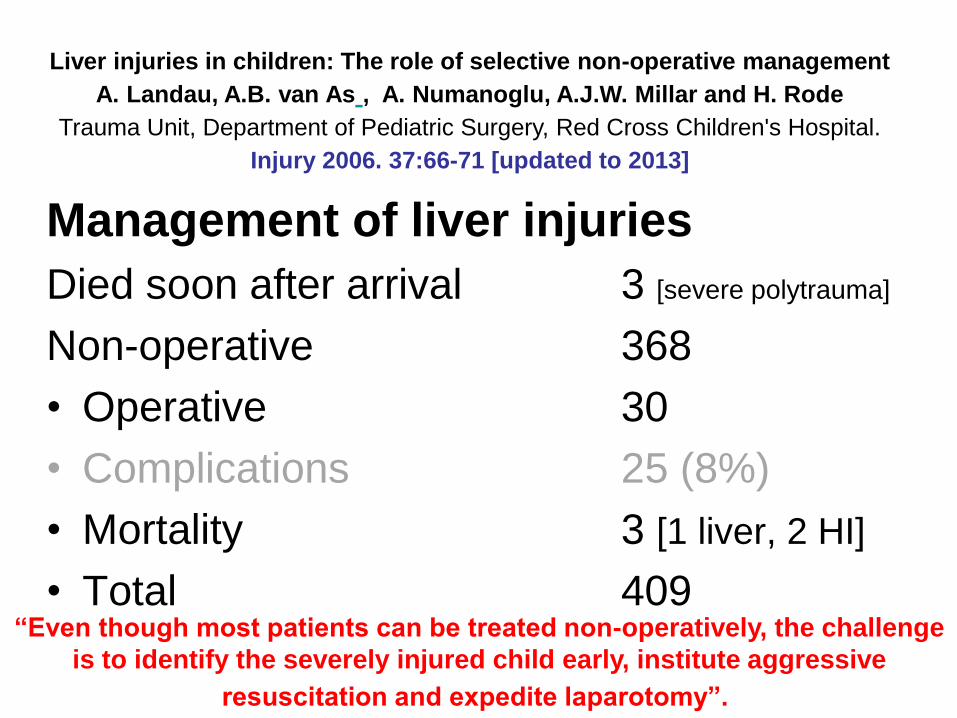
Management of liver injuries
Died soon after arrival 3 [severe polytrauma]
Non-operative 368
bull Operative 30
bull Complications 25 (8)
bull Mortality 3 [1 liver 2 HI]
bull Total 409
Liver injuries in children The role of selective non-operative management
A Landau AB van As A Numanoglu AJW Millar and H Rode
Trauma Unit Department of Pediatric Surgery Red Cross Childrens Hospital
Injury 2006 3766-71 [updated to 2013]
ldquoEven though most patients can be treated non-operatively the challenge
is to identify the severely injured child early institute aggressive
resuscitation and expedite laparotomyrdquo
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
Birmingham Childrenrsquos Hospital West Midlands UK
bull Tertiary Quaternary Hepato-biliary and Transplant Centre
bull Different spectrum of severity of injury + age up to 16yrs
bull Fewer pedestrian injuries
bull Bicycle - handle bar +
bull High speed RTA with seat belt +
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
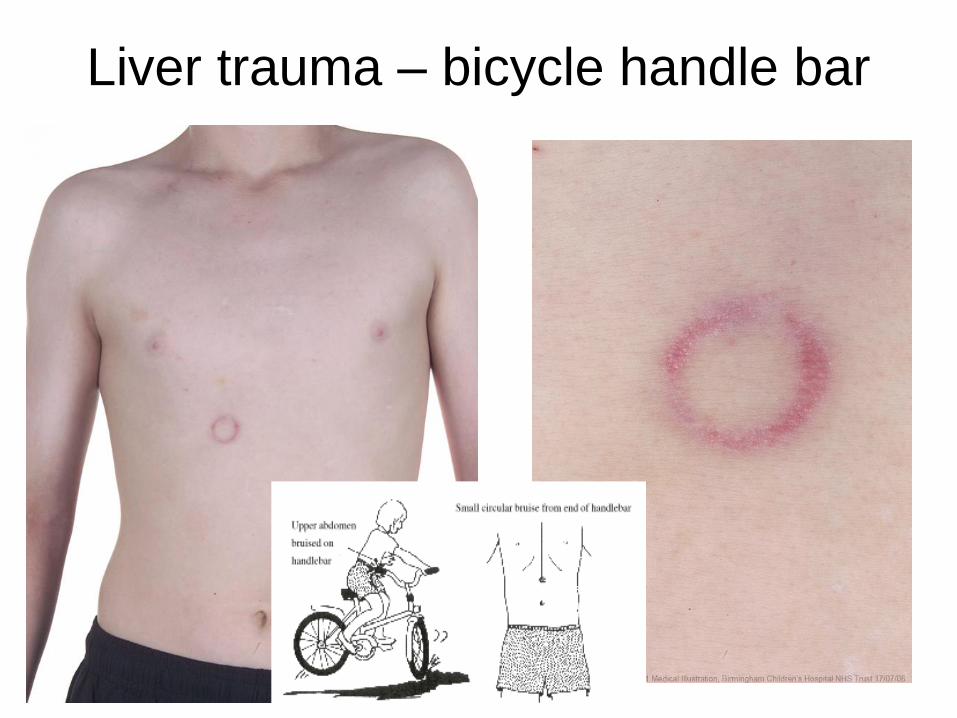
Liver trauma ndash bicycle handle bar
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
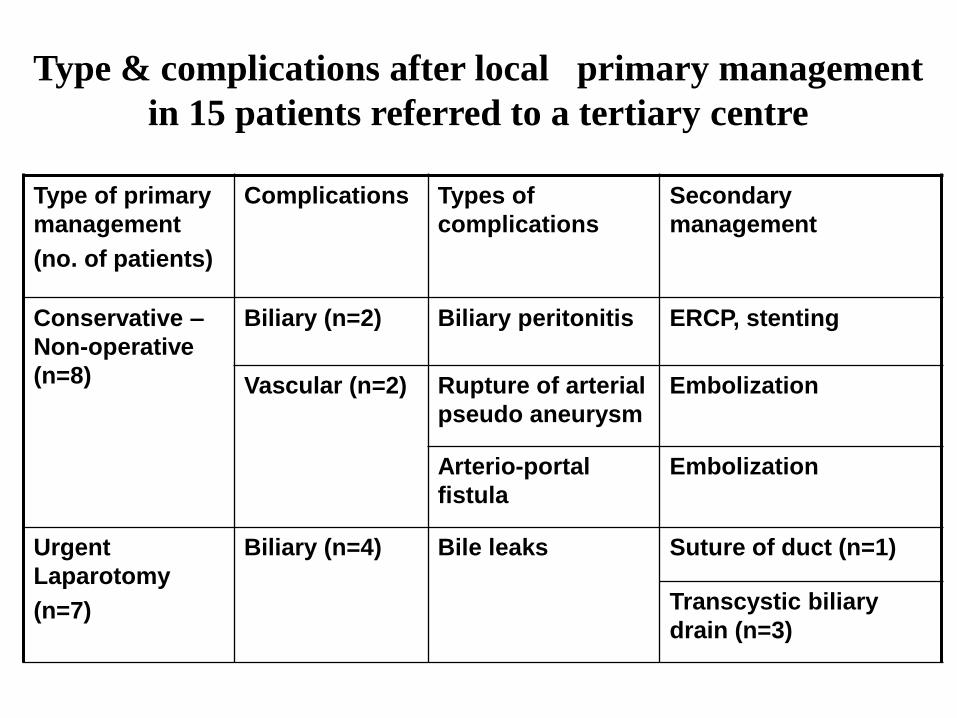
Type of primary
management
(no of patients)
Complications Types of
complications
Secondary
management
Conservative ndash
Non-operative
(n=8)
Biliary (n=2) Biliary peritonitis ERCP stenting
Vascular (n=2) Rupture of arterial
pseudo aneurysm
Embolization
Arterio-portal
fistula
Embolization
Urgent
Laparotomy
(n=7)
Biliary (n=4) Bile leaks Suture of duct (n=1)
Transcystic biliary
drain (n=3)
Type amp complications after local primary management
in 15 patients referred to a tertiary centre
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
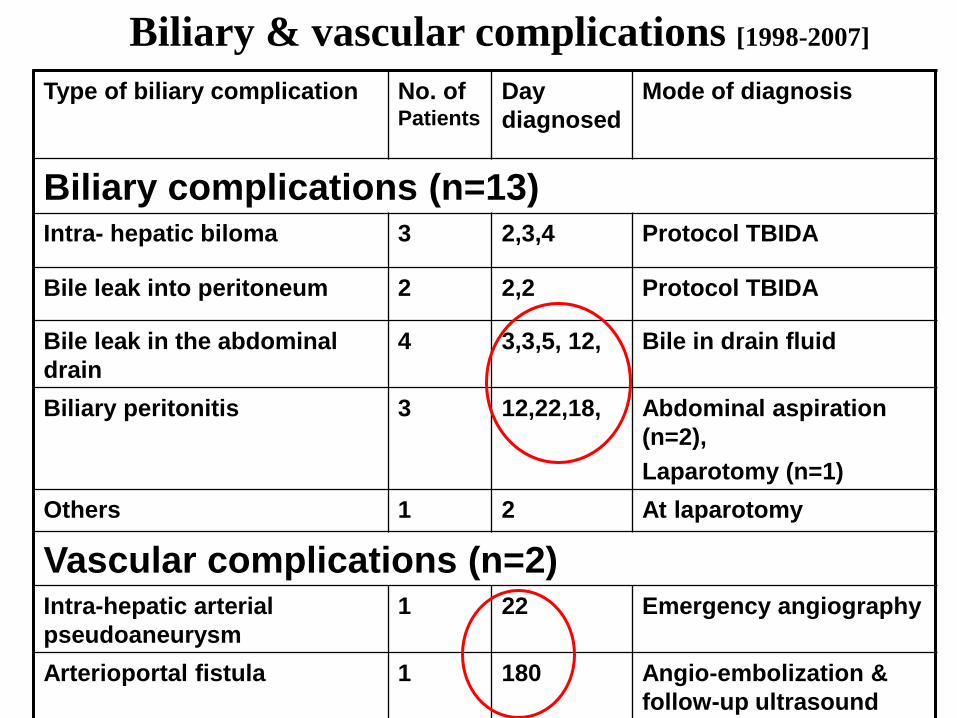
Biliary amp vascular complications [1998-2007]
Type of biliary complication No of Patients
Day
diagnosed
Mode of diagnosis
Biliary complications (n=13) Intra- hepatic biloma 3 234 Protocol TBIDA
Bile leak into peritoneum 2 22 Protocol TBIDA
Bile leak in the abdominal
drain
4 335 12 Bile in drain fluid
Biliary peritonitis 3 122218 Abdominal aspiration
(n=2)
Laparotomy (n=1)
Others 1 2 At laparotomy
Vascular complications (n=2) Intra-hepatic arterial
pseudoaneurysm
1 22 Emergency angiography
Arterioportal fistula 1 180 Angio-embolization amp
follow-up ultrasound
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
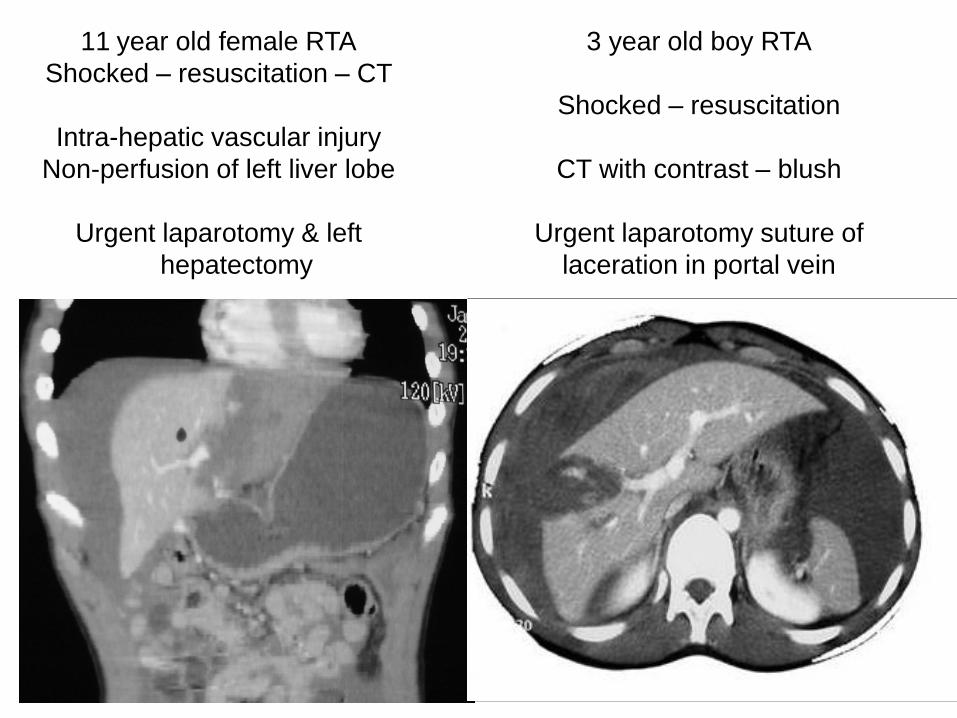
11 year old female RTA
Shocked ndash resuscitation ndash CT
Intra-hepatic vascular injury
Non-perfusion of left liver lobe
Urgent laparotomy amp left
hepatectomy
3 year old boy RTA
Shocked ndash resuscitation
CT with contrast ndash blush
Urgent laparotomy suture of
laceration in portal vein
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
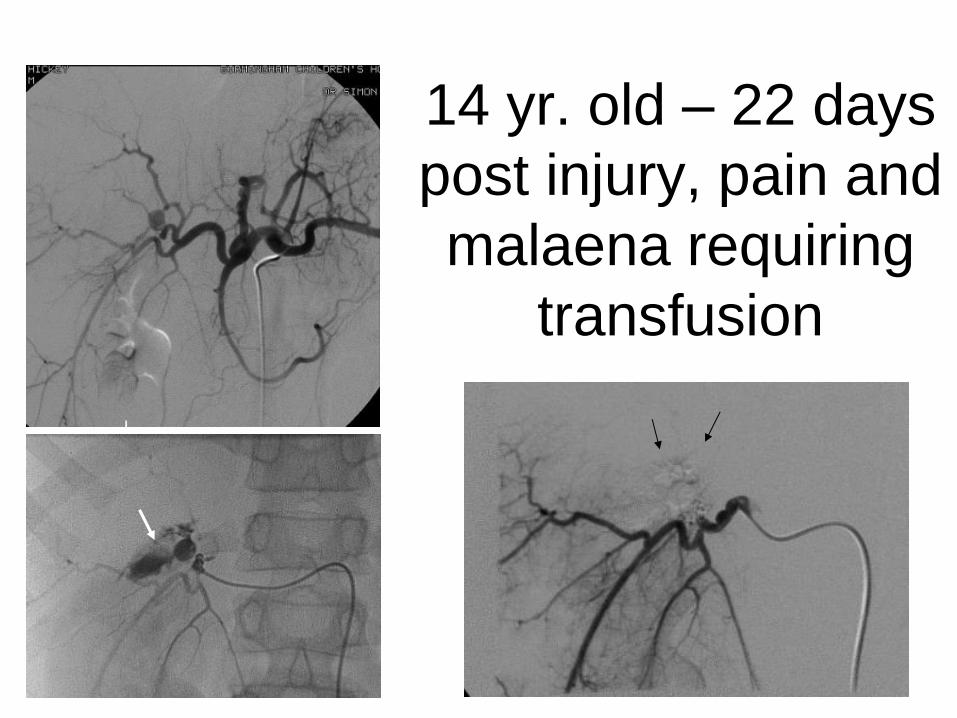
14 yr old ndash 22 days
post injury pain and
malaena requiring
transfusion
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
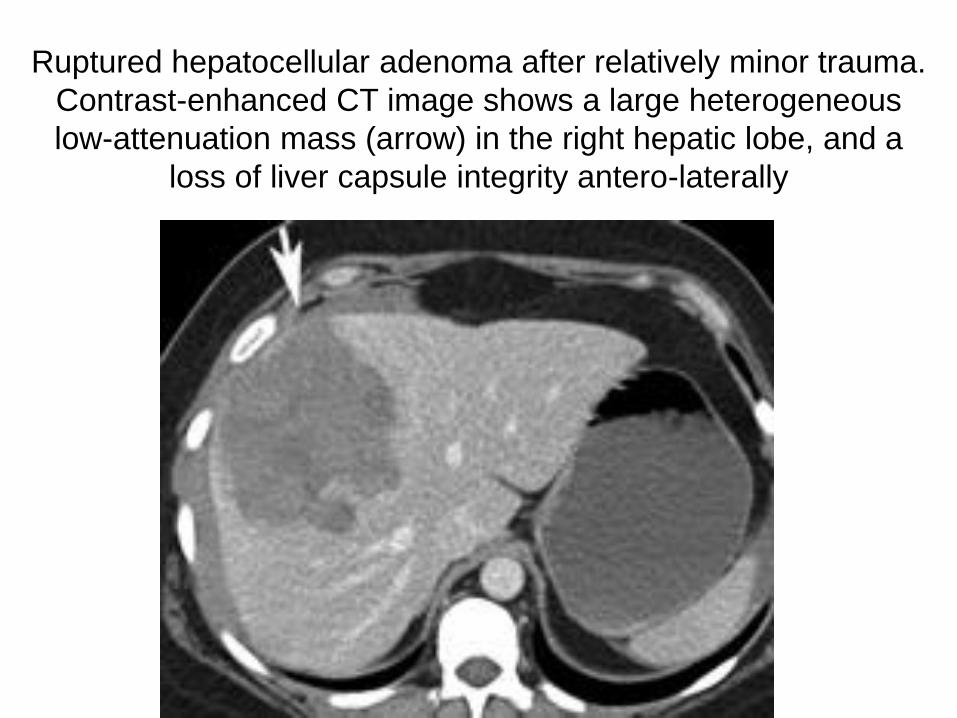
Ruptured hepatocellular adenoma after relatively minor trauma
Contrast-enhanced CT image shows a large heterogeneous
low-attenuation mass (arrow) in the right hepatic lobe and a
loss of liver capsule integrity antero-laterally
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
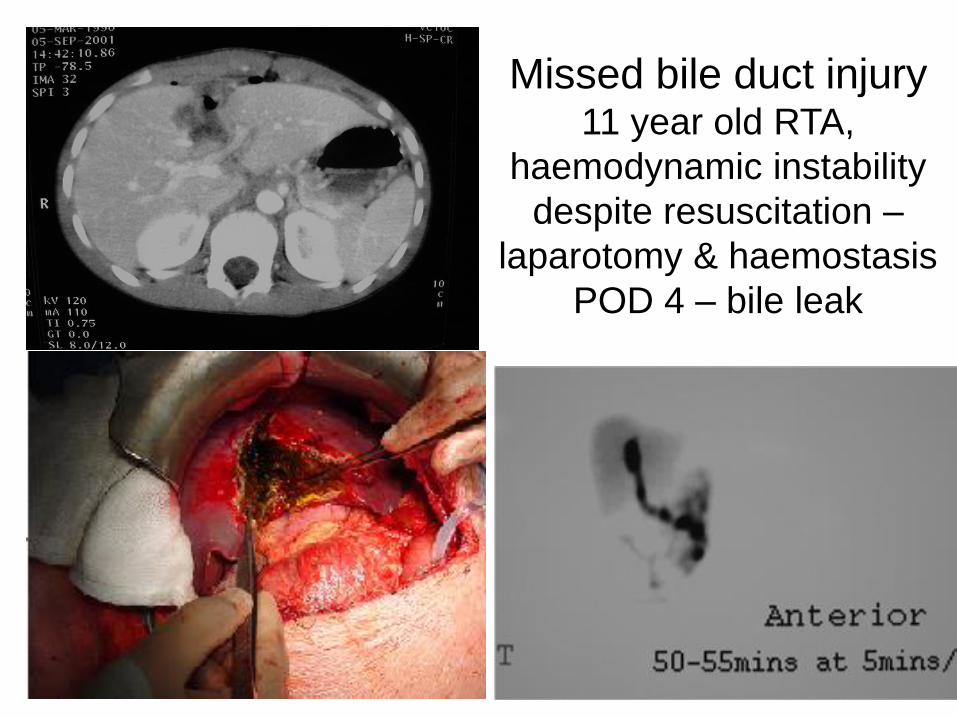
Missed bile duct injury 11 year old RTA
haemodynamic instability
despite resuscitation ndash
laparotomy amp haemostasis
POD 4 ndash bile leak
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
Bile leaks ndash what options
bull Drain (percutaneous) and wait
bull ERCP and stent +- sphincterotomy
[biodegarable stents BOTOX inj]
bull Operative repair [op cholangiogram]
bull Cholecystectomy amp trans-cystic duct
tube decompression
bull Roux-en-Y drain for persistant fistula
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
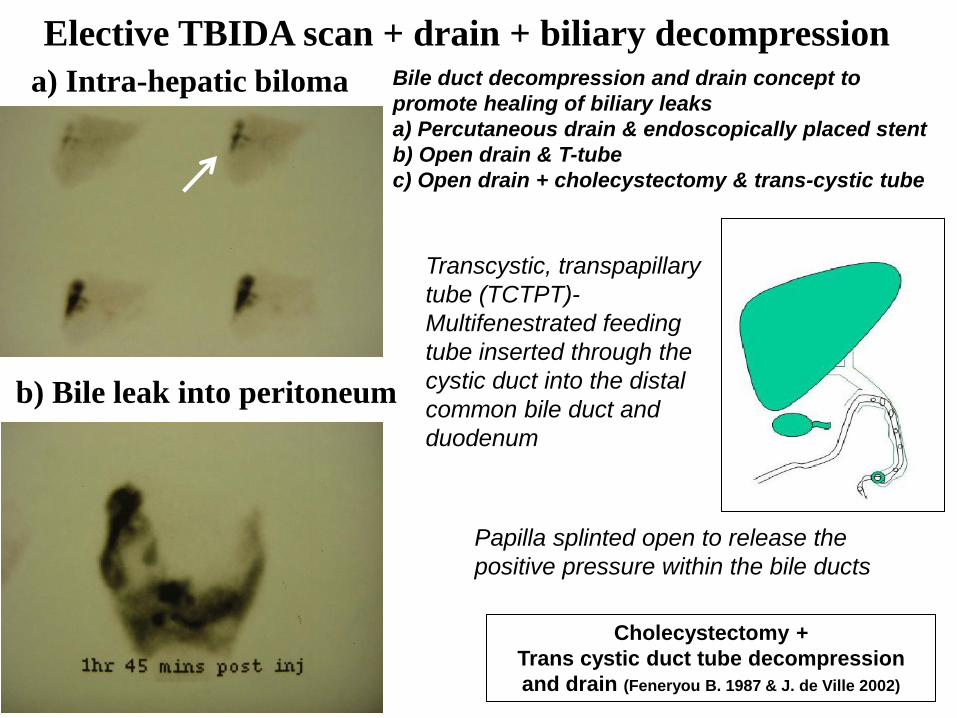
a) Intra-hepatic biloma
b) Bile leak into peritoneum
Elective TBIDA scan + drain + biliary decompression
Cholecystectomy +
Trans cystic duct tube decompression
and drain (Feneryou B 1987 amp J de Ville 2002)
Bile duct decompression and drain concept to
promote healing of biliary leaks
a) Percutaneous drain amp endoscopically placed stent
b) Open drain amp T-tube
c) Open drain + cholecystectomy amp trans-cystic tube
Transcystic transpapillary
tube (TCTPT)-
Multifenestrated feeding
tube inserted through the
cystic duct into the distal
common bile duct and
duodenum
Papilla splinted open to release the
positive pressure within the bile ducts
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
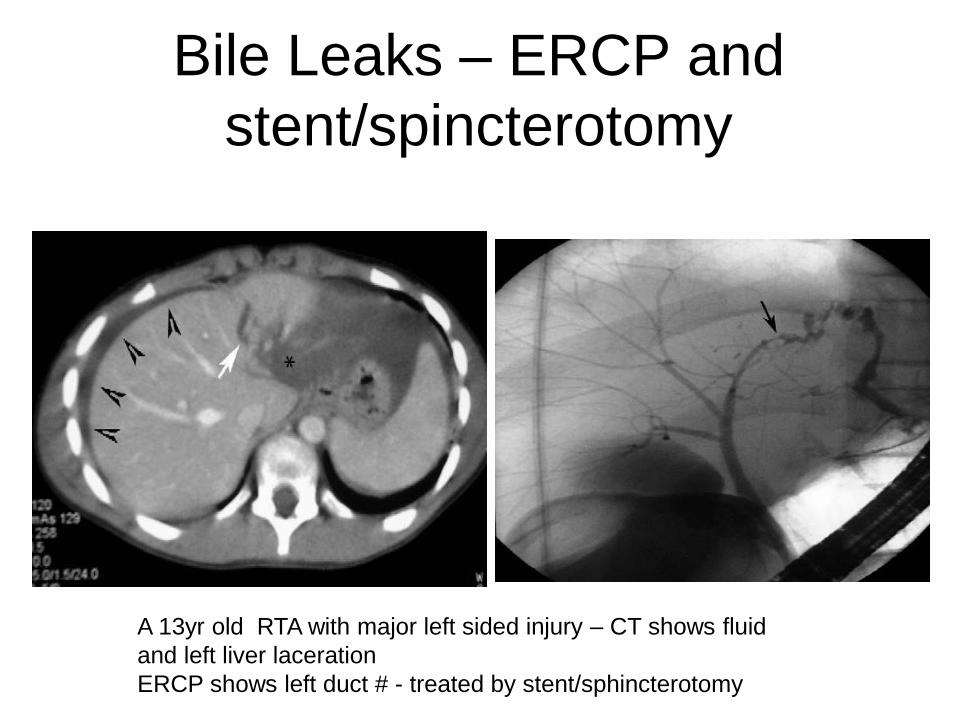
Bile Leaks ndash ERCP and
stentspincterotomy
A 13yr old RTA with major left sided injury ndash CT shows fluid
and left liver laceration
ERCP shows left duct - treated by stentsphincterotomy
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
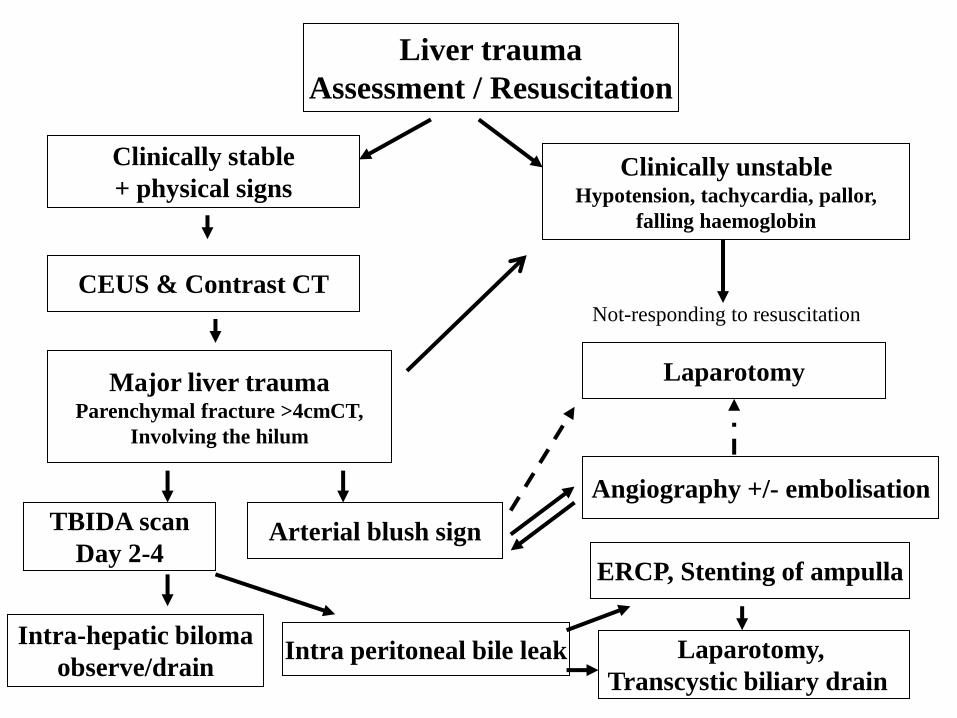
Liver trauma
Assessment Resuscitation
Clinically stable
+ physical signs Clinically unstable
Hypotension tachycardia pallor
falling haemoglobin
CEUS amp Contrast CT
Laparotomy Major liver trauma Parenchymal fracture gt4cmCT
Involving the hilum
Arterial blush sign
Angiography +- embolisation
TBIDA scan
Day 2-4
Intra peritoneal bile leak Intra-hepatic biloma
observedrain
ERCP Stenting of ampulla
Laparotomy
Transcystic biliary drain
Not-responding to resuscitation
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma
RJ Wood CJ Westgarth-Taylor H van Niekerk O Hodges J Thomas AJW Millar Department of Paediatric Surgery and Anaesthesia Red Cross War Memorial Childrenrsquos Hospital
University of Cape Town
Introduction
Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with
inhibitors against FVIIIFIX (1) It has subsequently been used successfully in treating massive haemorrhage
following cardiac surgery in non-haemophilia patients (2 3) Few studies have looked at the use of rFVIIa in
paediatric non-haemophiliac patients We present 2 cases in which it has been used in conjunction with damage
control surgery in the treatment of unresponsive Haemorrhagic shock following blunt and penetrating abdominal
trauma in paediatric patients at the Red Cross War Memorial Childrenrsquos Hospital
Mechanism of action
Discussion
Case A Patient A a 20kg seven year old male presented to the trauma unit in June 2009 following a motor vehicle
accident He had sustained blunt abdominal trauma as well as a fractured right femur He had unresponsive
Grade 4 Haemorrhagic shock mandating an emergency laparotomy At laparotomy he was found to have a grade
4 laceration to the Right Hepatic lobe Intra-operative resuscitation with 45mlkg of packed red cells and damage
control surgical techniques in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were
instituted rFVIIa (120 KIU) was administered in order to secure adequate haemostasis The patient made a
successful recovery after relook laparotomy in 48hrs to remove abdominal packs
Case B Patient B a 40kg nine year old female presented to the trauma unit in July 2009 after sustaining 2 abdominal
gunshot wounds She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy At
laparotomy extensive intra-abdominal vascular injuries were found She had sustained a through and through
injury of the inferior vena cava and left iliac vein Damage control techniques were employed and both vessels
were ligated Intra-operative resuscitation included 100mlkg packed red cell transfusion as well as 15mlkg of
fresh frozen plasma and 15mlkg of platelets rFVIIa was administered intra-operatively and satisfactory
hemostasis was secured The patient made a successful recovery after a prolonged ICU stay
The management of unresponsive and transiently responsive Grade 3 amp 4 Haemorrhagic shock usually requires
surgical haemorrhage control Abbreviated Laparotomy and Damage control techniques are well established in
adult and paediatric practice(7) Major haemorrhage and extensive fluid resuscitation leads to dilution of
coagulation factors platelet dysfunction and impaired production of clotting factors because of tissue hypoxia
caused by hypotension Acidosis and hypothermia further aggravates coagulopathy The use of rFVIIa in adult
patients undergoing surgery has been extensively reported but large randomized controlled trials are lacking (3)
Fewer reports are available on its use in the paediatric patient group but reports indicate that rFVIIa could
significantly decrease blood-product administration (2 4) Although expensive the cost must be balanced against
the potential risk of transmission of blood-borne pathogens the cost of surgery and the cost of blood and plasma
products (4) While rFVIIa may be extremely useful it can only be used in conjunction with timely surgery and
resuscitation after correction of Acidosis and Hypothermia (1 5) Recommended target blood levels before
administration are hematocrit gt24 fibrinogen gt05 to 1 gL platelets gt50 to 100000 times 109L and pH ge72 (5)
Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above)
several protocols advocating specific transfusion ratiorsquos (RBCFFPPlt) have been published (6) The role of
rFVIIa in resuscitation protocols needs to be clarified and large trials are needed to elucidate this
References 1 Mechanism of action development and clinical experience of recombinant FVIIa U Hedner Journal of
Biotechnology issue 124 March 2006 p747-75
2 Paediatric off-label use of Recombinant Factor VIIa JA Alten et al Pediatrics vol 3 number 123 March
2009 p1066-1071
3 Recombinant Activated Factor VII in Cardiac Surgery a Meta Analysis A Zangrillo et al Journal of
Cardiothoracic and Vascular Anaesthesia Vol 23 issue 1 Feb 2009 p34-40
4 Use of rFVIIa in Traumatic Liver Injuries in Children R Kulkarni et al The Journal of Trauma number 56
June 2004 p1348-1352
5 Monitoring Recombinant Factor VIIa Treatment Efficacy Depends on High Levels of Fibrinogen in a Model of
Severe Dilutional Coagulopathy MTGanter et al Journal of Cardiothoracic and Vascular Anaesthesia Vol
22 issue 5 October 2008 p675-680
6 Massive Transfusion Protocols The Role of Aggressive Resuscitation Versus Product Ratio in Mortality
Reduction DJ Riskin et al Journal of American College of Surgeons volume 209 issue 2 Aug 2009 p198-
205
7 Damage control Surgery in Children J Hamil Injury July 2004 35(7) p708-712
Novo Nordisk
Patient A a 20kg seven year old male presented to the trauma
unit in June 2009 following a motor vehicle accident He had
sustained blunt abdominal trauma as well as a fractured right
femur He had unresponsive Grade 4 Haemorrhagic shock
mandating an emergency laparotomy At laparotomy he was
found to have a grade 45 laceration to the Right Hepatic lobe
Intra-operative resuscitation with 45mlkg of packed red cells
FFP and damage control surgical techniques in-flow control
(Pringle manoeuvre) and liver packing with abdominal
swabs were instituted rFVIIa (120 KIU) was administered in
order to secure adequate haemostasis The patient made a
successful recovery after re-look laparotomy in 48hrs to remove
abdominal packs
Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving

Retro-hepatic IVC haemorrhage
1 Transverse incision with midline cranial extension
2 Packing of the liver and volume resuscitation with
Rapid Infusion System prior to vascular isolation
3 Isolation of the intra-pericardial vena cava through a
trans-diaphragmatic pericardial window
4 Control the suprarenal vena cava and porta hepatis
5 Repair of vein lacerations with vascular occlusion amp
continuous saline irrigation for improved visualization
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving
Conclusions Contrast blush on initial CT scan is a useful indicator of
ongoing haemorrhage and the need for urgent
laparotomy or angiographic intervention
Bile duct injuries are more frequently seen in the select
group of children suffering severe liver trauma
TBIDA scan is a sensitive investigation for bile duct
injury in severe liver trauma in children
Adjunctive procedures such as angiography and
embolization play an essential role in treating vascular
injuries
The challenge is to identify early the severe injury
requiring immediate life saving surgical intervention
Factor VII and packing can be life saving