Embed Size (px)
Citation preview

DOI: 10.1111/j.1540-8175.2009.01129.xC© 2010, Wiley Periodicals, Inc.
RESEARCH FROM THE UNIVERSITY OF ALABAMA AT BIRMINGHAM
Live/Real Time Three-Dimensional TransthoracicEchocardiographic Findings in an Adult withComplete Atrioventricular Septal Defect
Preeti Singh, M.D., Anjlee Mehta, M.D., and Navin C. Nanda, M.D.
Division of Cardiovascular Disease, University of Alabama at Birmingham, Birmingham, Alabama
Live/real time three-dimensional transthoracic echocardiography provided incremental value over two-dimensional transthoracic echocardiography in an adult patient with complete atrioventricular (AV) septaldefect by (1) making a confident diagnosis of Rastelli type A defect, (2) providing en face view of all the fiveleaflets of the common AV valve, (3) diagnosing left ventricle to right atrial shunt, and (4) permitting moreaccurate quantitative assessment of regurgitant lesions. (Echocardiography 2010;27:87-90)
Key words: two-dimensional echocardiography, three-dimensional echocardiography, live/real time three-dimensional echocardiography, atrioventricular septal defect in adults, complete atrioventricular septal defect
Several methods of classification and nomen-clature for atrioventricular (AV) septal defects havebeen described but most commonly, these defectsare classified into complete or incomplete (par-tial) form. In the former, there is a large defectwith an atrial component, ventricular component,as well as a common AV valve, and a common AVring. The common AV valve has a single annulusand five leaflets (superior bridging, inferior bridg-ing, mural lateral, anterosuperior, and mural infe-rior). It is important to note the attachment of supe-rior bridging leaflet to further classify complete AVseptal defects using the Rastelli classification system.Rastelli, based largely on considerations for potentialsurgical corrections, had classified them into typesA, B, and C. In most advanced form of develop-ment (Rastelli type A), the superior bridging leafletis attached to the crest of the ventricular septum.In type B, the superior bridging leaflet extends overthe ventricular septum and attaches to an anoma-lous papillary muscle of the right ventricle and in themost primitive form (Rastelli type C), the superiorbridging leaflet is free-floating, not attached to theventricular septum with the lateral margins attachedto an anterior papillary muscle in each ventricle.1,2
The partial form has two distinct AV orifices withan atrial component but the ventricular componentis filled in and closed by tissue either from the AVvalves or from the endocardial cushion tissue it-self. During development, the superior and infe-
Address for correspondence and reprint requests: Navin C.Nanda, M.D., F.A.C.C., University of Alabama at Birmingham,Heart Station SWB/S102, 619 19th Street South, Birmingham,Alabama 35249. Fax: 205-934-6747; E-mail: [email protected]
rior bridging leaflets combine to form the anteriorleaflet of the mitral valve and the septal leaflet ofthe tricuspid valve. But incomplete fusion of the su-perior and inferior bridging leaflets of the AV valveresults in a cleft in the left-sided AV valve leaflet.3
Regurgitation can occur through the cleft and/orcommissures.
In the present study, we demonstrate the in-cremental value of live/real time three-dimensionaltransthoracic echocardiography (3DTTE) overtwo-dimensional transthoracic echocardiography(2DTTE) in an adult patient with a complete AVseptal defect. For purposes of comparison, we alsopresent a second case of an adult patient with apartial (incomplete) AV septal defect. Both of ourpatients were evaluated by 2DTTE using a 3.5 MHzadult probe in a standard manner and by 3DTTEusing a 4 MHz matrix array probe (Phillips iE33ultrasound system, Bothell, WA, USA).4 Both 2DTTEand 3DTTE findings, including the incrementalvalue of 3DTTE over 2DTTE are described in Table I.
In our patient with a complete AV septal defect,2DTTE was unable to adequately visualize all theAV leaflets or their attachments. But with sequen-tial cropping of the 3D data sets, it was possibleto accurately assess all five leaflets of the commonAV valve by visualizing them en face. Also, unlike2DTTE the atrial and ventricular components of thedefects could be well visualized en face and theirextent comprehensively delineated by 3DTTE. Fur-thermore, 3DTTE clearly identified the site of attach-ment of the superior bridging leaflet to the crest ofthe ventricular septum thereby providing a moreconfident diagnosis of Rastelli type A defect as com-pared to 2DTTE. The deficiency of the AV septum
87
Singh, Mehta, and Nanda
TABLE I
Two-Dimensional and Live/Real time Three-Dimensional Transthoracic Echocardiographic Findings in Two Adult Patients with Atrioventricular Septal Defects
Clinical Findings 2DTTE Findings Additional 3DTTE Findings Incremental Value
Case 1. 67-year-old female.Shortness of breath andhypoxia. Congestive heartfailure. Severe pulmonaryhypertension with Eisenmengerphysiology. Not a surgicalcandidate (Figs. 1 and 2).
Complete atrioventricular (AV)septal defect of common AVvalve. Possible attachment ofcommon AV valve to theventricular septum. Type ARastelli defect. Severe AV valveregurgitation into LA from LVand into RA from RV by colorDoppler.
Both atrial and ventricular components of the defectseen en face. All five leaflets of common AV valvevisualized en face. Clear-cut attachment of thesuperior bridging leaflet to the ventricular septum.Extent of superior bridging leaflet into RV well seen.Unwedging of the aorta. Three AV valveregurgitation jets visualized: one moving into RAfrom RV (VC = 0.4 cm2, reg V = 43.6 mL) c/wmoderate reg, another from LV to RA (VC = 1.11cm2, reg V = 184 mL) c/w severe reg/shunt andthe third from LV to LA (VC = 0.98 cm2, reg V =164 mL) c/w severe reg.
Assessment of size, site, andnumber of common AV valveleaflets. Definitive diagnosis ofRastelli type A defect. Diagnosisof LV–RA regurgitation/shunt.Quantification of AV valveregurgitations.
Case 2. 26-year-old female.Palpitations and shortness ofbreath on exertion.Supraventricular tachycardia.Surgery: Repair of AV defectwith autologous pericardialpatch and repair of left-sidedAV valve cleft (Fig. 3).
Partial AV septal defect. Cleft inleft-sided AV valve not seen.Severe left-sided AV valveregurgitation into LA.
En face view of partial AV septal defect. Two separateAV rings clearly seen en face. Site and size of cleft inleft-sided AV valve well seen and measured 1.01 ×0.54 cm, area = 0.59 cm2. Medial direction of thecleft clearly seen. Left-sided AV valve regurgitation(VC = 1.07 cm2) c/w severe reg.
Definite identification of two AVrings. Identification of site, size,and direction of cleft in theleft-sided AV valve anddifferentiation from isolatedmitral valve cleft.Quantification of left-sided AVvalve regurgitation.
c/w = consistent with; LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle; reg = regurgitation; V = volume; VC = vena contracta.
also results in an elongated and narrow left ven-tricular outflow tract and an “unwedging” of theaorta.2 This was well appreciated by 3DTTE butnot with 2DTTE. Meticulous cropping of the color
Doppler data sets demonstrated in our patient, ashunt from the left ventricle to the right atriumand regurgitant jets from the left ventricle to leftatrium, and right ventricle to right atrium. Shunt
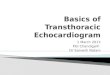
Figure 1. Live/real time three-dimensional transthoracic echocardiographic assessment of complete atrioventricular septal defect in a 67-year-old female. Case 1. A. Apicalfour-chamber view. Upper arrow points to the ventricular component and lower arrow to the much larger atrial component of the defect. B. Arrowhead shows the discreteattachment of the common atrioventricular (AV) valve to the crest of the ventricular septum indicative of Rastelli type A defect. C. En face view of the atrial component(arrowhead) of the defect. D. En face view of the common AV valve showing all five leaflets. 1 = superior bridging leaflet extending into RV; 2 = mural lateral leaflet; 3 =inferior bridging leaflet; 4 = mural inferior leaflet; 5 = anterosuperior leaflet. AO = aorta; LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle.
88
3D TTE in Complete AV Septal Defect
Figure 2.
Figure 3.
89

Singh, Mehta, and Nanda
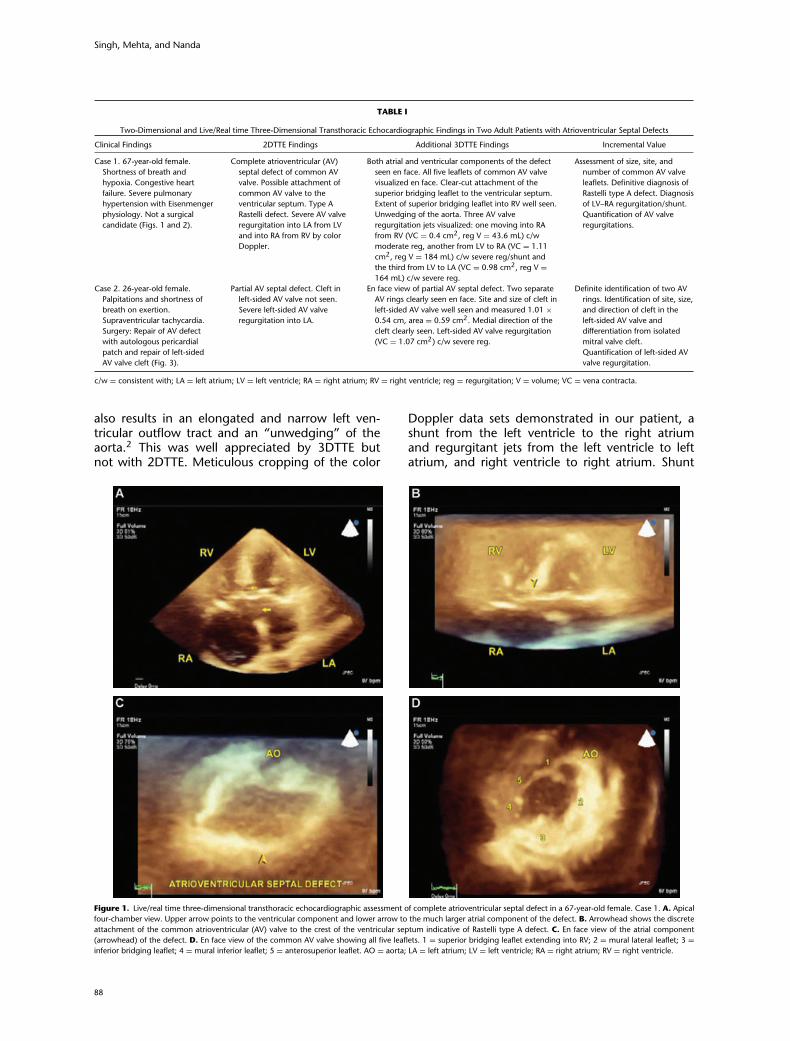
←−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−Figure 2. Live/real time three-dimensional transthoracic color Doppler echocar-diographic assessment of complete atrioventricular septal defect. Case 1. A. Crop-ping of the three-dimensional data set displays three AV valve regurgitation jets:one moving into right atrium (RA) from right ventricle (RV) (No. 1), another fromleft ventricle (LV) to RA (LV-RA shunt, No. 2) and the third from LV to right atrium(LA) (No. 3). B. Notation 1 represents en face view of the vena contracta (VC)of RV–RA jet. It measured 0.4 cm2 consistent with moderate regurgitation. Nos.2 and 3 represent other regurgitant jets cropped below the level of the VC andtherefore they appear larger. C. Notation 2 points to en face view of the VC ofLV–RA regurgitation/shunt. It measured 1.11 cm2 consistent with a severe regur-gitation (large shunt). D. Notation 3 represents en face view of the VC of LV-LAregurgitant jet. It measured 0.98 cm2, indicative of severe regurgitation. IAS =interatrial septum. Other abbreviations as in Figure 1.
regurgitation from left ventricle into right atriumwas not diagnosed by 2DTTE. In addition, 3DTTEpermitted direct visualization of the vena con-tracta (VC) of these jets en face facilitating accu-rate measurement of its area by planimetry, andcalculation of regurgitant volumes.5,6 This alloweda more precise quantitative evaluation of AV valveregurgitation as compared to 2DTTE that utilizesmostly incorrect assumptions in the assessment ofregurgitation and shunt volumes. Thus, 3DTTE ledto an enhanced level of confidence in the quantita-tive assessment of valvular regurgitation and shunt.This is important to assess as the natural history ofthe disease process is directly related to severity ofregurgitation.7
In the second patient with partial AV septal de-fect, 3DTTE unlike 2DTTE permitted a definitiveidentification of two AV valve rings as well as acomprehensive assessment of the cleft in the left-sided AV valve leaflet through cropping, and tilt-ing the plane at any desired angulation. The length,width, and extent of the cleft could be accuratelyassessed using 3DTTE. This information was valu-able to the surgeon when the patient underwentsurgical repair. In addition, 3DTTE detected the di-rection of the cleft that was seen pointing medi-ally toward the right ventricle, thus differentiatingit from isolated mitral valve clefts that are directedanterosuperiorly toward the left ventricular outflowtract.2,8 More quantitative assessment of left-sidedAV valve regurgitation was also provided by 3DTTEthat obviates some of the assumptions inherent in2DTTE quantification of regurgitant shunts.
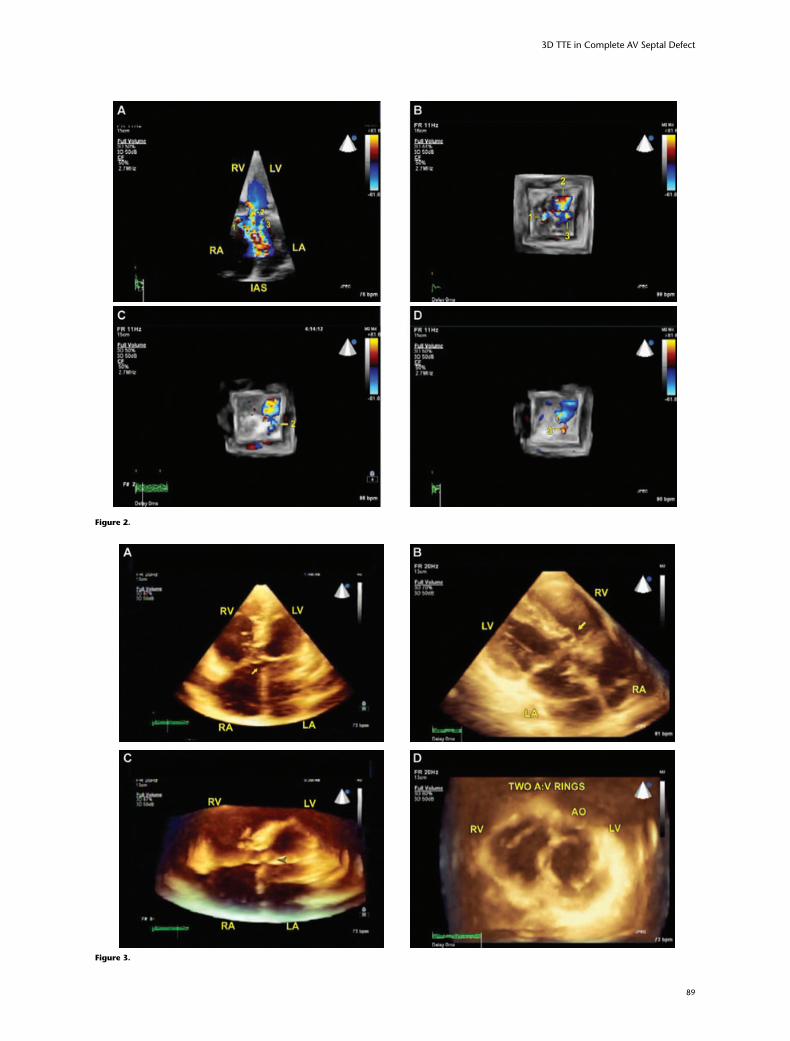
←−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−Figure 3. Live/real time three-dimensional transthoracic echocardiographic as-sessment of partial atrioventricular septal defect in a 26-year-old female. Case 2. A.Apical four-chamber view. Arrow points to atrial component of the defect. B. Arrowshows right-sided AV valve leaflet tissue closing the ventricular component of thedefect. C. Arrow points to a cleft in the left-sided AV valve. The cleft is directed me-dially and away from the LV outflow tract. D. En face view of two separate AV rings.Arrow points to a cleft in the left-sided AV valve. Other abbreviations as in Figures 1and 2.
A previous study has shown the usefulness of3DTTE in adult patients with AV septal defect aftersurgical repair.9 But ours is the first description of3DTTE assessment of this lesion in an unoperatedadult patient.
AV septal defects have many variable compo-nents and the ability to visualize these componentsis imperative for making surgical and medical man-agement decisions. As these two cases demonstrate,3DTTE provided an incremental value over 2DTTEby giving a more comprehensive and accurate as-sessment of the morphological features of AV septaldefects and the associated AV valve abnormalitiesand regurgitant jets. Thus, 3DTTE has the potentialto substantially increase the level of diagnostic con-fidence when used in conjunction with 2DTTE, inthe evaluation of AV septal defects.
References1. Rastelli G, Kirklin JW, Titus JL: Anatomic observations on complete form of per-
sistent common atrioventricular canal with special reference to atrioventricular
valves. Mayo Clin Proc 1996;41:296–308.
2. Ebels T, Anderson RH: Atrioventricular septal defects. In Anderson HA, Baker EJ,
Macartney FJ, et al. (eds): Paediatric Cardiology. London, UK, Harcourt Publishers
Limited, 2002. pp. 939–981.
3. Smallhorn JF: Cross-sectional echocardiographic assessment of atrioventricular
septal defect: Basic morphology and preoperative risk factors. Echocardiography
2001;18:415–432.
4. Sinha A, Nanda NC, Khanna D, et al: Morphological assessment of left throm-
bus by live three-dimensional transthoracic echocardiography. Echocardiogra-
phy 2004;21(7):649–655.
5. Khanna D, Vengal S, Miller AP, et al: Quantification of mitral regurgitation
by live three-dimensional transthoracic echocardiographic measurements of
vencontracta area. Echocardiography 2004 Nov;21(8):707–713.
6. Velayudhan DE, Brown TM, Nanda NC, et al: Quantification of tricuspid regurgi-
tation by live three-dimensional transthoracic echocardiographic measurements
of vena contracta area. Echocardiography 2006 Oct;23(9):793–800.
7. Warnes CA, Deanfield JA: Congenital heart disease in adults. In Fuster V, Alexan-
der RW, Hurst JW, et al. (eds): Hurst’s The Heart. New York: McGraw-Hill Pub-
lishers, 2004, pp. 1862–1863.
8. Singh A, Romp RL, Nanda NC, et al: Usefulness of live/real time three-
dimensional transthoracic echocardiography in the assessment of atrioventric-
ular septal defects. Echocardiography 2006;23:598–608.
9. Van Den Bosch AE, Van Dijk VF, McGhie JS, et al: Real-time transthoracic three-
dimensional echocardiography provides additional information of left-sided AV
valve morphology after AVSD repair. Int J Cardiol 2006;106(3):360–364.
Supporting InformationAdditional Supporting Information may be found inthe online version of this article:
The following movie clips are available online:Figure 1A–D, Figure 2A, Figure 3A–D.
Please note: Wiley-Blackwell are not responsiblefor the content or functionality of any supportingmaterials supplied by the authors. Any queries (otherthan missing material) should be directed to the cor-responding author for the article.
90