Embed Size (px)
Citation preview

ALLEGHENY COUNTY MEDICAL SOCIETY
BulletinDECEMBER 2020
Gratitude
A review of IV acetaminophen

Download Headspace for free with your membership to the Pennsylvania Medical Society and Allegheny County Medical Society ($65 value).
Learn the life-changing skills of meditation and mindfulness with hundreds of guided exercises for any mood.
855-PAMED4U (855-726-3348) • [email protected] • www.pamedsoc.org/Join
Visit our Member $avings Page: www.pamedsoc.org/MemberSavings.

BulletinDECEMBER 2020 / VOL. 110 NO. 12
ALLEGHENY COUNTY MEDICAL SOCIETY
ArticlesOpinion Departments
Materia Medica .....................383A potential spin on pain control: A review of IV acetaminophenMarissa Rees, PharmD
Materia Medica .....................388Pitolisant (WAKIX®) Cassidy Williams, PharmD Sehrish Panjwani, PharmD, BCPS
Legal Report ........................391Physician cybersecurity vigilance and resourcesMichael A. Cassidy, Esq.
Special Report .....................394An adventure in understanding: A history of the C.F. Reynolds Medical History SocietyKristen Ann Ehrenberger, MD, PhD
Special Report .....................396ACMS Election report
Feature .................................398A look back at 713 Ridge Avenue
Editorial ............................... 369GratitudeDeval (Reshma) Paranjpe, MD, MBA, FACS
Editorial ................................370Finding my niche: A kind, well-shaven face Anthony L. Kovatch, MD
Editorial ................................373Rightly forgotten Richard H. Daffner, MD, FACR
Perspective ..........................376Reducing disparities in musculoskeletal care: Focusing on bone and joint health Anthony M. DiGioia III, MD Gina Edwards Angela DeVanney Gigi Crowley
Perspective ..........................378A physician’s reflection on Roberto Clemente and his leadership legacy Johanna Vidal-Phelan, MD, MBA, FAAP
Society News .......................380• Fit with Your Physician walk held • ACMS Foundation awards medical student scholarship• ACMS member assists with removal of prior auth code• Pennsylvania Geriatrics Society – Western Division
Classifieds ...........................381
Activities & Accolades.........382
Membership Benefits...........384
Editorial Index......................402
Advertising Index.................403
On the coverBridges on MonAndrew W. Eller, MD
Dr. Eller specializes in ophthalmology.
For up-to-date resources on COVID-19,
visit: www.acms.org/covid-19-resources

2020 Executive Committee
and Board of Directors
PresidentWilliam K. Johnjulio
President-electPatricia L. Bononi
Vice PresidentPeter G. Ellis
SecretaryMatthew B. Straka
TreasurerDavid L. BlinnBoard Chair
Adele L. Towers
DIRECTORS 2020
Wendy E. BraundBruce A. MacLeod
Amelia A. ParéAngela M. Stupi John P. Williams
2021William F. CoppulaDavid J. Deitrick Kevin O. Garrett
Marcy L. Jackovic Raymond E. Pontzer
2022Ragunath AppasamyMark A. Goodman
Keith T. Kanel Maria J. Sunseri G. Alan Yeasted
PEER REVIEW BOARD2020
James W. Boyle Matthew A. Vasil
2021Marcela BÖhm-VélezThomas P. Campbell
2022Kimberly A. Hennon
Jan W. Madison
PAMED DISTRICT TRUSTEEAmelia A. Paré
COMMITTEESAwards
Keith T. KanelBylaws
Peter G. EllisFinance
Raymond E. PontzerGala
Patricia L. Bononi Maria J. Sunseri
MembershipPatricia L. Bononi
Nominating Matthew B. Straka
COPYRIGHT 2020:ALLEGHENY COUNTY MEDICAL SOCIETYPOSTMASTER—Send address changes to: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212.
ADMINISTRATIVE STAFF
Chief Executive OfficerJeremy T. Bonfini
Manager, Medical Community Engagement and Society
Governance Michelle Besanceney
Director of PublicationsMeagan K. Sable
Vice President of Physician Engagement and Digital Strategy
James D. Ireland ([email protected])
Director, Medical Community Engagement
Nadine M. Popovich ([email protected])
EDITORIAL/ADVERTISING OFFICES: Bulletin of the Allegheny County Medical Society, 850 Ridge Avenue, Pittsburgh, PA 15212; (412) 321-5030; fax (412) 321-5323. USPS #072920. PUBLISHER: Allegheny County Medical Society at above address.
The Bulletin of the Allegheny County Medical Society is presented as a report in accordance with ACMS Bylaws, Articles 6, 8, and 11.
The Bulletin of the Allegheny County Medical Society welcomes contributions from readers, physicians, medical students, members of allied professions, spouses, etc. Items may be letters, informal clinical reports, editorials, or articles. Contributions are received with the understanding that they are not under simultaneous consideration by another publication.
Issued the third Saturday of each month. Deadline for submission of copy is the SECOND Monday preceding publication date. Periodical postage paid at Pittsburgh, PA.
Bulletin of the Allegheny County Medical Society reserves the right to edit all reader contributions for brevity, clarity and length as well as to reject any subject material submitted.
The opinions expressed in the Editorials and other opinion pieces are those of the writer and do not necessarily reflect the official policy of the Allegheny County Medical Society, the institution with which the author is affiliated, or the opinion of the Editorial Board. Advertisements do not imply sponsorship by or endorsement of the ACMS, except where noted.Publisher reserves the right to exclude any advertisement which in its opinion does not conform to the standards of the publication. The acceptance of advertising in this publication in no way constitutes approval or endorse-ment of products or services by the Allegheny County Medical Society of any company or its products.
Annual subscriptions: $60
Advertising rates and information available by calling (412) 321-5030 or online at www.acms.org.
ISSN: 0098-3772
Improving Healthcare through Education, Service, and Physician Well-Being.
www.acms.org
ACMS ALLIANCECo-PresidentsPatty Barnett
Barbara WibleRecording Secretary
Justina Purpura Corresponding Secretary
Doris DelseroneTreasurer
Sandra Da CostaAssistant Treasurers
Liz BlumeKate Fitting
Bulletin Medical Editor
Deval (Reshma) Paranjpe([email protected])
Associate EditorsRichard H. Daffner
([email protected])Charles Horton
([email protected])Anthony L. Kovatch
([email protected])Scott Miller
([email protected])Amelia A. Paré
([email protected])Joseph C. Paviglianiti
([email protected])Anna Evans Phillips
([email protected])Andrea G. Witlin
Managing EditorMeagan K. Sable
Editorial
369ACMS Bulletin / December 2020
GratitudeDEVAL (RESHMA) PARANJPE, MD, MBA, FACS
As I write this, COVID-19 cases in our area are soaring; as you
read this, they will undoubtedly have reached record-setting peaks. Vaccines loom on the horizon, but approval, roll-out and distribution are still challenges which remain to be overcome.
In this cocktail called December 2020, we have equal parts terror and hope, dread and resolve, resignation and revelation. Add a sugar cube of faith and the bitters of loss, and muddle together.
Allow me to suggest a garnish which might make this cocktail slightly more palatable: gratitude.
Let us be grateful for our lives and the lives of our loved ones and friends.
Let us be grateful for the joy and good that existed in the lives of those we have lost this year.
Let us be grateful for our good memories.
Let us be grateful for the roof over our heads, food on the table, and warm clothes to wear.
Let us be grateful for the ability to
share our comforts with others less fortunate – and do so.
Let us be grateful for our medical education and training, by which we can help our fellow man.
Let us be grateful that our calling – though it tethers us to pain, illness and death – gives us insights denied to others and allows us to keenly appreci-ate what is truly important in life.
Let us be grateful for the wisdom we have crystallized from our traumas.
Let us be grateful for the wisdom of our mentors, the comradery of our col-leagues and the support of our families.
Let us be grateful – and humbled – by the trust of our patients.
Let us be grateful for every person – scientist, physician, nurse, health care worker, EMT, janitor, administrator, essential service worker and all others – who by their work and dedication keep our nation afloat in the face of daily challenges.
Let us be grateful for every busi-ness that chooses humanity over profit at this time, and let us actively support
small businesses and people in need that they may survive.
Let us be grateful for every person who believes in the idea of a civil, decent and kind society and behaves accordingly.
Let us be grateful for every person who wears a mask properly, who puts the safety and well-being of his fellow humans ahead of his own self-interest, and who truly loves his neighbor as himself.
Let us be grateful for the chance to believe in a higher power and a greater good.
Let us be grateful for the unselfish.Let us be grateful for hope.Amen.
Dr. Paranjpe is an ophthalmologist and medical editor of the ACMS Bul-letin. She can be reached at [email protected].
The opinion expressed in this column is that of the writer and does not necessarily reflect the
opinion of the Editorial Board, the Bulletin, or the Allegheny County Medical Society.
Happy Holidays from all of us at ACMS!

Every night, although I wish to cast off the anxiety of falling and staying
asleep, I am reluctant to retire because there may be someone who needs the reviving compassion of a “kind, well-shaven face.”
Now that I am in the “sudden death overtime” of my 40-plus years as a pedi-atrician and more interested in commen-tary than in productivity, I often ask myself in times of reverie what got the ball rolling in this “blood sport” of medicine and how did I get where I find myself today. Whence came the seeds of a career dedicated to compassion at its inception, faltering through the vicissitudes of life’s considerations, and hopefully ending in some degree of enlightenment without the torment of regret.
I believe I was programmed for kindness and meekness at conception; my parents were anxious, unassuming folks by nature with humble upbring-ings in coal mining villages in north-eastern Pennsylvania. My mother and her 12 siblings had great reverence for my uncle who was the local small town general practitioner, sacrificing every-thing but his own family for his gracious patients. However, it was his diagnosis of my mother’s progressive neurolog-ical and psychiatric deterioration that I will remember most; the diagnosis is still only mentioned in a whisper: Huntington’s Chorea.
My mother, Virginia, was the index case; as geneticists would inexorably predict, six of her 12 siblings would suffer the same. The “coin toss” of the Fates recognizes no favorites. Over the years, the funerals were resonant with the gnashing of teeth and with the same question: Who will be the next to succumb? The pathos reached its peak when one young aunt – the kindest of women and the most beloved by her nephews and nieces – became pregnant well into the course of her disease in an attempt to reverse the progression; she suffered inordinately but was able to take care of her child for several years.
Although I was witness to much of the suffering, I am not one of the phys-
ically afflicted. However, I remained one of the very worried well for much of my life – not so much for myself as for my loved ones. For me now, the worry is extinct. The aftermath of the psy-chological suffering is controlled. But as American author William Faulkner taught in his writings: “The past is nev-er dead; it’s never even past!”
As a naïve yearling in the medical field, I resolved that I would find a cure, especially after the horror of spec-tating a “parade” of institutionalized victims of various neurological mala-dies around a gymnasium floor during my second year of medical school; if justice could not be granted to all by the Higher Powers, then mankind must supersede. I promised to follow in the
Editorial
370 www.acms.org
Finding my niche: A kind, well-shaven face
ANTHONY L. KOVATCH, MD
“I am of those who like to stay late at the café,” the older waiter said. “With all those who do not want to go to bed. With all those who need a light for the night.”
“I want to go home and into bed,” said the younger waiter.“We are of two different kinds,” the older waiter said. He was now dressed
to go home. “It is not only a question of youth and confidence although those things are very beautiful. Each night I am reluctant to close up because there may be someone who needs the café…..
This is a clean and pleasant café. It is well lighted. The light is very good and also, now, there are shadows of the leaves.”
– From “A Clean, Well-Lighted Place” by American Lost Generation author Ernest Hemingway

Editorial
371ACMS Bulletin / December 2020
footsteps of Andrew Manson, the pro-tagonist in Dr. A.J. Cronin’s landmark novel “The Citadel,” (noteworthy for its indictment of the medical profession for its “bumbug” in the way of bureaucracy, pretension and lack of integrity), but to avoid the pitfalls to which the idealistic fledgling physician succumbs.
By the end of elementary school, it had become apparent to myself and others that, in spite of a dullness of wit and a rather clownesque face, I had inherited the strength of memory of the Italian ancestors and the persevering work ethic of the Hungarians (“if you want to dance, you have to play the fiddle” – to the day you die, I might add!). There was a joint inheritance, a double-edged sword – an obses-sive-compulsive disposition – indeed, an excessive compulsive disposition, manifested personally by my conviction that “you are never fully dressed with-out an excessively clean, well-shaven face.” I blame this practice for the de-velopment of so many “old age spots” in my later years.
If nothing gradually inflates the ego like the comfort of being at the top of the heap in high school and college and a consequent acceptance into medical school, nothing rapidly deflates it like the subsequent stark realization in medical school and residency that one is just another “brick in the wall” – a struggling “face in the crowd” of the many players competing in the “blood sport.” The angst and “imposter complex” I suffered through as a result of my OCD and perfectionism (and wayward conviction that I was rather ugly) during those formative years I perceived to be a prerequisite for some divine mission entrusted upon me by “the gods of Huntington’s.” If I
were to be spared by winning the coin toss at conception, the gods and fates must eventually be appeased. In the meantime, I coped by undertaking discipleship with Austrian philosopher/psychiatrist Viktor Frankl, Holocaust survivor and author of “Man’s Search of Meaning.” I quote: “In some ways suffering ceases to be suffering at the moment it finds a meaning, such as the meaning of a sacrifice.”
So, I was to be a specialist. How-ever, fate likes to play its little pranks on all of us. I moved from the East Coast to the inland city of Pittsburgh to jump start an academic career with a fellowship in pediatric infectious diseases that I argued would last for no more than two lonely years. Despite the glamour of research publications, poster sessions and presentations at national meetings, I learned that academic medicine has no place for a meek, kind, well-shaven face – I precipitously fell off the ladder after climbing only the bottom rungs. Again, fate eminently knows what is best for us, what we most yearn for in our heart of hearts.
I met the love of my life in the lab where I worked as an ID fellow at Children’s Hospital performing clinical research on the respiratory pathogen Branhamella catarrhalis (like all things in medicine, the name was changed to Moraxella catarrhalis the last time I looked it up). And the last time I looked it up I had been married for 38 years to the beautiful, meek woman who had prepared the cultures for my research, bore me four wonderful children (and subsequent bonnie grandchildren), en-gineered most of the family’s domestic affairs, and made me a card-carrying member of her own large (12 children)
family. My in-laws invited me into their family like I was some “dude of honor,” becoming surrogates for the parents I had lost by chronic disease when I was merely in my early 20s.
However, excessive compulsive being that I am, it was essential that I take on a second family. I spent the next 36 years in clinical pediatric prac-tice hoping to do justice caring for the children of the North Hills of Pittsburgh as if they were my own. I shaved my aging face vigorously every morning. I often confused service and employ-ment with devotion and compassion. I sometimes stole time from my family, as the poet-pediatrician William Carlos Williams accused himself of. I learned that trying to be everybody’s every-thing and being a people-pleaser can produce compassion fatigue, alienation from co-workers, and, in spite of finan-cial success and the adulation of the community, a longing for redemption and an ultimate appeasement to the aforementioned “gods.”
Throughout my career in pediatric practice, I would entertain special focuses. It started as expected with infectious diseases, transferred to orthopedics when my children were regularly injured playing sports, and finally settled on psychiatry when I personally admitted to myself amid tribulations that the brain controls the “whole enchilada!” To the displeasure of my colleagues, I accepted the challenge of managing more and more psychiatric conundrums in my practice – an involvement which interfaced inev-itably with those suffering from Autism Spectrum Disorders, Attention Deficit Hyperactivity Disorder, and related neurodevelopmental disabilities.
Continued on Page 372

372 www.acms.org
I accepted the reality that I was becoming a psychiatrist who just hap-pened to be a pediatrician. Moreover, I had to ratchet up the intensity of my compassion.
A pivotal phone call occurred around the time of entry into the au-tumn of my career. A nurse with whom I had collaborated in the spring years implored for my caretaking of special needs children fostered in the residen-tial treatment facilities of an established pediatric psychiatry network. Most of the inmates had Autism or complex disorders requiring institutionalization, the orphans of society who had lost the coin toss; many of them were reminis-cent of the neurological victims I had witnessed parading around the gym-nasium floor in medical school. Some brought back heartbreaking memories of my afflicted ancestors with Hunting-ton’s. “The past is never even past.”
So, I took on a third family quite distinct from the first two; I became “Thursday’s Pap,” the kind, well-shaven face who holds back no fondness and no compassion for the dispossessed. All the children were wayward “have nots,” were needy of the most funda-mental of human emotion and disci-pline. I gifted those engendering the deepest pathos (My “David Copper-field” favorites) with perks such as old running shirts – realizing that “you can’t take them with you” – worn-out wrist bands, and, if they were literate, read-ing material ranging from comic books to treatises on the deepest-thinking philosophers.
Rarely, if ever, was a “thank you” heard from any of them – never was there requited affection. It was es-sentially “good solely for the sake of
good.” The staff were the surrogate guardian angels, and I was merely one of them; it was all part of some inscru-table divine plan calculated to liberate an old man from the cynicism which befalls those in the seventh decade of life. I argued that it lead to the final destination that would take me back to my roots and grant me the redemption awarded to Andrew Manson in Cronin’s semi-autobiographical novel.
“All children start out loving their parents; next they judge them; rarely, if ever, do they forgive them,” wrote the cynical, nihilistic British playwright Oscar Wilde. All physicians start out loving their high ideals and ambitions; next, they question their validity and plausibility; but in the end, they circle back to where they started, revisit those high ideals, and become worthy of their ordination as a healer. We bear the professional weight of living up to the ideals of our revered profession and of striving to reverse all suffering, or, at least, of being compassionate always.
As the sun sets and dusk beckons retirement, I find comfort in that I have finally found the niche – the “sweet spot” – that I had long been searching for, that I had appeased the ancestors and the Huntington gods, and that I had played the “blood sport” of med-icine with fairness and courage. And, ultimately, that I had kept open the café for those in need of it.
In short time, I would no longer have to daily shave the clownesque, but kind, face which I had inherited and could transfer the effort into praying to someday enter the Clean, Well-Lighted Place that we all long for.
Dr. Kovatch is a pediatrician and associate editor of the ACMS Bulletin. He can be reached at [email protected].
Editorial
The opinion expressed in this column is that of the writer and does not necessarily reflect the
opinion of the Editorial Board, the Bulletin, or the Allegheny County Medical Society.
From Page 371
Photo Provided by dr. Kovatch
My favorite of the three blended families. Note the clownesque face in the middle of the photo!

373ACMS Bulletin / December 2020
Editorial
Rightly forgottenRICHARD H. DAFFNER, MD, FACR
Many of the men and women of science and medicine have been
honored by having their names asso-ciated with the fruits of their labors. We have Paget disease of bone and breast (Sir James Paget 1814 – 1899), Pasteurization (Louis Pasteur 1822 – 1895), Koch’s postulates (Robert Koch 1843 – 1910), and the Curie, a unit of radiation (Marie Curie 1867 – 1934). And then we have Phillipp Lenard, Hans Reiter, Eduard Pernkopf and Hans Asperger, all of whom made significant contributions to science and/or medicine, but whose names are all but forgotten. Lenard was awarded the Nobel Prize; Reiter and Asperger had syndromes named for them; and Pernkopf produced the most realistic anatomy atlas. Why then, have their memories been relegated to the dung heap of history? At one time in their careers, they all embraced an evil phi-losophy, Nazism, and its false messiah, Adolf Hitler.
I have long had an interest in medical history. I teach a course on the history of medical imaging for the Osh-er program at CMU and I have written an editorial on Roentgen’s discovery of x-rays for the Bulletin to commemorate the 125th anniversary of this event. I hope to write future historic vignettes for the Bulletin. While doing research for my course, I came across an
interesting footnote to medical history in the work of Phillipp Lenard. So, what did Lenard and the others contribute to medical science, and when did they turn toward “the dark side?” 2020 is the 75th anniversary of the end of World War II (WWII), in which Lenard and the others participated in their own ways in one way or another.
Lenard (1862 – 1947) was a Hun-garian-born German physicist, who, like many other European physicists, became fascinated with cathode ray tubes. (In the mid-19th century to the mid-20th centuries, Germany led the world in scientific and medical tech-nology.) Lenard created a thin metal window in his Crookes cathode ray tubes to allow him to study the rays the tubes produced, and he duly reported his findings of their characteristics. He concluded that cathode rays were streams of negatively charged energy particles (electrons). He also found that photographic plates in his laboratory were fogged when he was operating his apparatus and concluded that the fogging was the result of cathode rays. He reported this in a scientific paper in 1894. Wilhelm Conrad Roentgen (1845 – 1923), a colleague of Lenard, and using cathode ray tubes lent by Lenard, made the same observations and proved that the fogging was due to “a new type of ray,” which we now
recognize as x-rays. Roentgen proved that x-rays were a distinct entity that had different characteristics than did cathode rays. Roentgen asked why his findings occurred; Lenard did not. Roentgen was awarded the first Nobel Prize in physics in 1901. Lenard, who felt he should have shared the prize, became Roentgen’s enemy and aired his anti-Semitic feelings by publicly saying that Roentgen behaved like a typical Jew in not acknowledging the help received. (Roentgen was not Jewish.) Lenard was awarded his own Nobel Prize in 1905 in recognition of his other scientific contributions.
Lenard was a strong German nationalist and joined the National Socialist (Nazi) Party in the 1920s. He was an outspoken promoter of “Deutsche Physik,” as opposed to “English physics,” which he believed to have stolen its ideas from Germany, as well as “Jewish physics” – pri-marily the theories of Albert Einstein. He became an advisor to Hitler, who named him Chief of Aryan Physics. In 1933, he published a book, “Great Men in Science, a History of Scientific Progress,” and omitted listing Einstein and Roentgen. Lenard held the post of emeritus professor of theoretical physics at the University of Heidelberg
Continued on Page 374

374 www.acms.org
until he was expelled, in 1945, by the Allied occupation forces as part of their denazification campaign. He died in obscurity in 1947.
Hans Conrad Reiter (1881 – 1969) was a German physician who de-spite impeccable medical credentials became a Nazi war criminal for con-ducting medical experiments at the Buchenwald concentration camp. His claim to medical fame owes to his having served as a physician in the German army in World War I (WWI), where he described a soldier with non-gonococcal urethritis, arthritis and uveitis. This triad became known as Reiter syndrome. Reiter was interested in politics after WWI and became an early supporter of Hitler and the Nazis. He joined the party officially in 1932 and was named director of the Kai-ser Wilhelm Institute of Experimental Therapy in 1933. He also was a strong supporter of the Nazi’s racial policies and eugenics, and an enthusiastic supporter of Hitler’s anti-smoking campaign.
During WWII, Reiter became a member of the SS and was the chief medical officer at the Buchenwald con-centration camp. There, he conducted medical experiments on the inmates. He claimed to “know” of sterilization, euthanasia and the murder of mental hospital patients, but denied direct par-ticipation. He, like many other “good” Nazis were “only following orders.” Following the war, he was arrested by the Soviet Red Army and was tried at Nuremberg. Although he was convicted as a war criminal and sentenced to prison, he received an early release for assisting the Allies with his knowledge of germ warfare. After his release, he
conducted research in rheumatology. He died in 1969. In 1977, a campaign was launched to replace the term “Re-iter syndrome” with “reactive arthritis,” the term that is in common use today.
Eduard Pernkopf (1888 – 1955) was an Austrian anatomist who was rector (the highest academic official) of the University of Vienna. He is best known for his seven-volume “Atlas of Topographical and Applied Human Anatomy.” The “Pernkopf atlas,” as it is commonly called, was the result of 20 years of work by Pernkopf and four additional medical artists. Despite its tainted provenance, it is still considered an artistic and scientific masterpiece for its lifelike and accurate display of human anatomy. Why tainted? Most anatomy atlases are based on dissections performed on embalmed cadavers. The full color drawings in the Pernkopf atlas appeared so realistic because they were created from fresh corpses, the bodies of executed politi-cal prisoners and concentration camp internees.
Pernkopf began his medical studies at the University of Vienna in 1907 and it was there that he became a member of the German nationalistic Student Academic Fraternity of Germany. Following WWI, where he served as a military physician, Pernkopf returned to Vienna, where he quickly rose through the ranks on the faculty of his alma mater to become the director of the medical school’s anatomical institute. In 1933, he joined the foreign orga-nization of the Nazi party, and a year later became a member of the SA, the Storm Troopers (“brownshirts”). Following the Anschluss (Germany’s annexation of Austria into the Third Reich) in 1938, he was named dean of
the medical school. It was here that he put his Nazi beliefs into action, purging all Jewish faculty and preaching Nazi racial theories and policies.
Pernkopf hired four artists to collab-orate on his atlas. All were members of the Nazi Party and were committed to its principles and goals. Interestingly, these artists cleverly incorporated Nazi symbols into their work. One of them, Erich Lepier, inserted a swastika at the end of his signature; another, Karl Endtresser used the SS lightning bolt runes for the “ss” in his name. The first volume of the anatomy atlas was completed in 1937 and the second in 1941. At the end of the war, Pernkopf was arrested by American authorities and spent three years as a POW. Upon his release, he returned to Vienna to take up his work on his atlas when he was reunited with his four artists, all of whom also had been interned in POW camps. Pernkopf died in 1955 while working on a new volume to the set.
A two-volume edition of the atlas was published in five languages, with the first American edition published in 1963. In 1995, Pernkopf and his atlas became the focus of an ethics investigation following the publication of a paper that described the Nazi takeover of the University of Vienna and Pernkopf’s role in the human experimentation that followed. In 1996, it was revealed that the subject bodies portrayed in the atlas may have been those of executed political prisoners, LGBT men and women, Romani (Gyp-sies) and Jews. (Interestingly, similar issues have been raised about the “Bodies … The Exhibit” from China). Later editions of the atlas had the Nazi symbols removed. There is still a debate whether it is ethical to use the
Editorial
From Page 373
375ACMS Bulletin / December 2020
atlas, which, although out of print, is still available on eBay.
Johann (Hans) Friedrich Karl Asperger (1906 – 1980) was an Austrian pediatrician who also dabbled in medical theories and eugenics. After earning his medical degree in 1931 from the University of Vienna, he became director of the special educa-tion section of the university’s pediatric clinic the next year. Asperger was fascinated with psychologic disorders in children and wrote more than 300 scientific papers, mostly concerning a condition he termed “autistic psy-chopathy.” Interestingly, his work went generally unnoticed outside of Vienna during his lifetime. It was only after his death in 1980 that his contributions to psychiatry were recognized. These contributions included autism spectrum disorders and Asperger syndrome that was named after him following his pub-lishing a paper in the German literature in 1944.
Asperger’s work, however, was considered controversial in two areas. The first was disagreement with the scientific merits of his studies, that were published in German and rare-ly translated into English. Despite a
resurgence of interest in his work in the 1990s, the diagnosis of Asperger syndrome remains controversial due to an unclear relationship to the autism spectrum. This is based on the inability of contemporary researchers to repli-cate his results.
The second controversy arose more recently (2018) with the publication by Edith Scheffer of “Asperger’s Children: The Origins of Autism in Nazi Vien-na.”1 Asperger joined the Austrofascist Fatherland Front in 1934 and later accommodated himself to the Nazi re-gime, although never actually becom-ing a member of the Nazi Party. He is alleged to have publicly promoted the Nazi racial hygiene policies, including forced sterilizations and active coop-eration with the euthanasia program for children (and adults) with mental disorders. It is mainly for these reasons that the “syndrome” is now referred to as autism spectrum disorder.
Four men of science, who were lured into following a false god and accepting that god’s pseudoscientific rantings about racial purity and eu-genics, made significant contributions to medicine. However, those contri-butions and the memories of the men
who made them were forever lost in the dung heap of history. Interestingly, these men were not alone. A more complete list of medical eponyms with Nazi associations is available.2,3
Dr. Daffner, associate editor of the ACMS Bulletin, is a retired radiologist, who practiced at Allegheny General Hospital for more than 30 years. He is emeritus clinical professor of Radiology at Temple University School of Med-icine and is the author of nine text-books. He can be reached at [email protected].
Editorial
The opinion expressed in this column is that of the writer and does not necessarily reflect the
opinion of the Editorial Board, the Bulletin, or the Allegheny County Medical Society.
References1. Scheffer E. Asperger’s Children: The
origins of Autism in Nazi Vienna. New York, W.W. Norton and Company, 2018.
2. Strous RD, Edelman MC. Eponyms and the Nazi era: time to remember and time for change. Israel Med Assn J 2007; 9:207 – 214.
3. Kondziella D. Thirty neurologic eponyms associated with the Nazi era. European Neurology 2009; 62: 56 – 64.
Where-to-Turn cards give important information and phone numbers for victims of domestic violence. The cards are the size of a business card
and are discreet enough to carry in a wallet or purse.Call ACMS at (412) 321-5030 for more information.
Where to turn…Domestic Abuse Palm Cards Available at ACMS

376 www.acms.org
PerspectivePerspectivePerspective
Reducing disparities in musculoskeletal care: Focusing on bone and joint healthLiving an active life requires bone
and joint health. Musculoskeletal conditions like osteoarthritis, a de-generative joint disease, inflammatory arthritis and osteoporosis lessen a person’s quality of life, cause pain and disability, and significantly increase healthcare costs. The threat of limited mobility and disability from chronic pain and weakened bones is concerning for increasingly large portions of the aging U.S. population.
Did you know? Estimates suggest that by 2040, the
number of adults affected by arthritis will grow from the current 54 million Americans to more than 78.4 million. In addition, 12 million people (80% of whom are women) suffer from osteopo-rosis, a condition that weakens bones, and can cause harmful fractures that may lead to surgery or disabilities with chronic pain.
Gender-based disparities in bone and joint health also present a sig-nificant challenge to meet patients’ needs. A “disparity” is defined as when there is a discrepancy, inconsistency, or imbalance of care and outcomes. For example, women are more likely to develop hip and knee arthritis than men, suffer worse severity of pain, and are more likely to delay seeking evaluation and treatment. Women also are four times more likely to suffer from osteoporosis than men.
Disparities also exist around treat-ment and interventions. Although 26%
of women have arthritis (as opposed to 18% of men), women are three times less likely than men to undergo total joint replacement surgery (TJR), de-spite both having end-stage degener-ation. Even when women elect to have surgery, they are typically older and frailer, report worse arthritis pain and have worse pre-op and post-op func-tion scores. Unfortunately, these bone and joint health disparities only worsen when factoring in social determinants of health like race, ethnicity, culture, sexual orientation and others.
However, there also are opportu-nities to better understand and meet patients’ needs for non-operative interventions long before surgery is indicated. The progression of arthritis and degeneration can be slowed if diagnosed early and appropriately addressed. In addition, by learning to manage pain and symptoms at earlier stages, arthritis and osteoporosis suf-ferers can decelerate the disease pro-gression while prolonging their mobility. Establishing this approach requires us
to develop unique interdisciplinary care teams that focus on global bone and joint health.
Co-designing personalized patient care to address disparities
At the core of patient-centered care is individualizing treatment to best meet their specific needs. By viewing the experience through the eyes of pa-tients and families and engaging them in co-designing their own care around what matters most, we can develop more personalized programs. Jointly creating improved care programs with patients and families as co-designers can guide these efforts by putting the needs of the end user as the highest priority.
At the Bone and Joint Center in UPMC Magee-Womens Hospital, we sought to first better understand the issues facing our patients and then start to address disparities. Instead of asking patients and families “What’s the matter with you?” we changed the conversation and asked, “What matters to you?” In
ANTHONY M. DIGIOIA III, MD
ANGELA DEVANNEY
GINA EDWARDS GIGICROWLEY

377ACMS Bulletin / December 2020
PerspectivePerspectivePerspective
this way, the simple yet revolutionary What Matters to You (WMTY) con-cept makes healthcare conversations more meaningful and patient centered. Through the “What Matters to You?” surveys, distributed at several clinical services at UPMC Magee-Womens Hospital, we uncovered priority areas.
These collaborative efforts have resulted in several pilot projects, including the creation of the 90% female patient community, Arthritis Together (facebook.com/groups/arthrit-istogether), a woman-specific exer-cise program, gender specific patient educational materials, updated pain management education, and virtual bone and joint health presentations and multimedia content. We also are developing educational programs for patients, community members and providers to address disparities on the provider side. As an example, analysis of provider disparities revealed that only 6% of orthopaedic surgeons are women, with even fewer in the adult reconstruction subspecialty (<<1%).
Next steps: An interdisciplinary approach to bone and joint health
Patient and community feedback have pointed us to three areas of op-portunity to improve care and popula-tion health: coordinated care, compre-hensive pain management strategies using complementary, alternative and integrative medicine (CAIM), and en-hanced education for patients, commu-nity members, and providers.
Through this emerging effort, along
with related service lines at UPMC Magee-Womens Hospital, including the Midlife Health and Osteoporosis Care Center, Bariatric and Nutritional Services, and Pain Management, we hope to transform care by coordinating services based around what matters most to patients rather than along sub-specialty lines. To that end, our mission and goals are as follows:
• Identify and reduce gender and cultural disparities related to muscu-loskeletal care by developing unique teams and care programs in the areas of bone and joint health.
• Co-design clinical programs with patients and providers that address patients’ needs.
• Develop educational and train-ing programs for patients, community, and providers to accelerate awareness of these disparities within the patient and provider communities.
Ultimately, we hope to develop and support system-wide changes that better address patients’ priorities, implement coordinated treatment plans and identify opportunities for improve-ments. Expanded pain management offerings that include complementary and alternative approaches will provide options and access to combinations of treatment modalities that work best for particular patients. Customized educa-tion will ensure patients are informed and prepared to take charge of their wellness journey.
We believe our shared goal of reducing disparities in bone and joint health can unite us in developing
immediate and long-term changes and improvements for patients. We are continuing to co-design and refine pro-grams by listening to patients’ needs, leading to unique clinical collaborations that we expect to have high impact in patient experiences and care.
Dr. DiGioia is medical director of the Bone and Joint Center at UPMC Magee-Womens Hospital and UPMC Innovation Center as well as co-med-ical director of Operation Walk Pitts-burgh.
Ms. Edwards is a project analyst at the UPMC Innovation Center, where she coordinates the Center for Bone and Joint Health.
Ms. Crowley is the director of Out-
patient Orthopaedics at the Bone and Joint Center at UPMC Magee-Womens Hospital.
Ms. DeVanney is the founder of go-
Shadow, a technology startup focused on end-user engagement, experien-tial redesign, process mapping and improvement.
The authors can be reached at
The opinion expressed in this column is that of the writer and does not necessarily reflect the
opinion of the Editorial Board, the Bulletin, or the Allegheny County Medical Society.
Allegheny County Medical Society www.acms.org • (412) 321-5030
378 www.acms.org
PerspectivePerspectivePerspective
A physician’s reflection on Roberto Clemente and his leadership legacy
JOHANNA VIDAL-PHELAN, MD, MBA, FAAP
I am a physician who was born and raised in Puerto Rico. I confess that
since I was a child, I have always want-ed to visit Roberto Clemente’s statue in Pittsburgh, Pennsylvania. Recently, my dream came true when a meeting I attended in the city allowed me to see it for the first time. I was overjoyed to personally witness how Pittsburgh had honored Roberto’s memory. There I was, standing in front of such a power-ful statue of my childhood hero. They had placed the statue next to a bright yellow-colored bridge leading to PNC Park, the current home of the Pitts-burgh Pirates professional baseball team. When I arrived at the site, I was not the only one struck by the moment, gasping in awe. I was just one of many fans from all over the country taking pictures with his statue and enjoying a wonderful memorial to an extraordinary human being.
I was beaming, of course, while telling complete strangers how I had grown up in Carolina and Puerto Rico – the very same town that Roberto and his family are from. Experiencing with others the grandeur of such an amazing role model was very special to me. Others beside me recognized his legacy just as vividly, even 47 years after his death. Many of us took a moment to celebrate Roberto’s ac-complishments, recalling how Roberto
played a major part in two Pittsburgh Pirates World Series championship teams – first in 1960 and then in 1971. Roberto Clemente was a 15-time all-star, a 12-time Gold Glove winner, the 1966 National League MVP, a four-time batting champion and the first Latin-American baseball player in the National Baseball Hall of Fame!
On my drive home, I couldn’t stop thinking how astounding it was to meet with and witness fans from all over the country sharing the same admiration for my Puerto Rican hero. When I first arrived at the site, I totally expected to be the most excited person to see Roberto’s statue, especially since I had heard so many first-hand stories about him while growing up on our Isla del Encanto. It was pleasantly surprising to see entire families and so many non-Latino fans there paying respect to Roberto. This was all so very moving to me that it made me ponder, “Just what had Roberto done to deserve such reverence and admiration? How is it that his legacy continues? What personal character traits made him such an extraordinary person besides his tremendous athletic abilities? What leadership lessons can be learned from my childhood hero?”
As I began to recall my childhood memories of people talking about Roberto in Puerto Rico, I remembered
him being described as a humble and simple man. I can still see in my mem-ories how he was admired by so many for his hard work and perseverance. Roberto was a superstar who never forgot his humble beginnings and the critical importance of family.
I also recall listening to stories of Roberto’s compassion towards those in need, especially for children. Near our hometown in Puerto Rico, “Cuidad Deportiva” (Sports City), was created to provide a safe place for children of all socio-economic backgrounds to learn and to play sports. As a child, I was very fortunate to have lived so close to this park. Above all, I remem-bered that no matter whether he was in or out of the spotlight, Roberto was a man of integrity who proudly represent-ed Puerto Rico, as well as the entire Latin-American community, with dignity. Roberto was proud of his heritage and was a fearless advocate for social and economic justice, openly speaking out against racism and repression.
After much reflection, I truly believe that Roberto Clemente’s legacy contin-ues because of his leadership, com-passion, and perseverance. Roberto was a trailblazer who was passionate and focused enough to become the best in his profession. Roberto’s dedi-cation and perseverance against all the odds makes him a genuine example to
379ACMS Bulletin / December 2020
others, including his teammates, family, and friends. Roberto demonstrated a tireless commitment to serving others, especially those in situations of great need. Leading by example and by en-thusiastically engaging others to do the same, Roberto transcended cultures, languages, and ethnic differences. And above all, Roberto knew that when he was faced with challenging times, his family and his faith would carry him through.
On the 24th of July in 1970, the Pittsburgh Pirates held “Roberto Clemente Night” at Three Rivers Stadium. There in a packed stadium, Roberto, next to his wife and three sons, with his mother and father in attendance, was recognized for his
lifetime of achievements. I was told how Roberto became overwhelmed when he looked towards right field and saw hundreds of spectators wearing “Pavas,” the traditional straw hats worn by his father and countless sugarcane workers in Puerto Rico. Roberto didn’t shy away from his roots or the people who helped him to get where he was. As a result of his deep connection with and honor for his past, Roberto was adored by his fans for his authenticity. I can only hope that those of us who have been given the opportunity to work and serve as Latino professionals in the United States will follow Roberto Clemente’s example. We should all strive to honor his legacy and culture with the utmost
dedication, compassion, and profound commitment to the communities which we have been chosen to serve.
Dr. Vidal-Phelan is senior medical director of pediatrics at UPMC Health Plan. She can be reached at [email protected].
This article was originally pub-lished on KevinMD.com: https://www.kevinmd.com/blog/2019/07/a-phy-sicians-reflection-on-roberto-clem-ente-and-his-leadership-legacy.html.
PerspectivePerspectivePerspective
The opinion expressed in this column is that of the writer and does not necessarily reflect the
opinion of the Editorial Board, the Bulletin, or the Allegheny County Medical Society.
SURPLUS MEDICAL OR OFFICE ITEMS? DONATE THEM TO GLOBAL LINKS!
SUPPLIES, EXAM TABLES,CHAIRS, F ILE CABINETS,
DESKS AND MORE!
WE CAN ACCEPT:
CONTACT US:[email protected]
412.361.3424
TIMEfor a
Physician Billing Audit?If you’re working harder, but your revenue
isn’t keeping up, maybe it is time.
To learn more, please contact John Fenner at 412-638-1846 or [email protected].
3 PENN CENTER WEST
PITTSBURGH, PA 15276412-788-8007
fennercorp.com
A LEADER IN PHYSICIAN BILLINGAND CONSULTING SINCE 1991

PerspectivePerspectiveSociety News
380 www.acms.org
Fit with Your Physician walk heldA Fit with Your Physician
Walk was held Nov. 20 on Mt. Washington.
The walk was led by Terence W. Starz, MD;
Jessie VanSwearingen, PhD, PT, FAPTA, PhD; and Anne Wuenschel, PT. The
walks are live-streamed via the Jewish Health-
care Foundation’s Senior Connection Program on the
Virtual Senior Academy, virtualsenioracademy.org.
Photo Provided by dr. Starz
ACMS Foundation awards medical student scholarship
The Allegheny County Medical Society (ACMS) Foundation awarded a $4,000 scholarship to Stephen Canton, a 4th-year student attending the Universi-ty of Pittsburgh School of Medicine.
In a letter to the ACMS Foundation and the Foundation of PAMED, Mr. Canton expressed his gratitude:
“I am humbled by this recognition and graciously accept the Foundation Education Award Scholarship and ACMS Medical Student Scholarship. While medical school is a tough jour-ney in general, it is particularly difficult
to navigate as an underrepresented student. I can honestly say that in addition to my family and friends, the University of Pittsburgh School of Med-icine has been unbelievably supportive during this tough yet rewarding jour-ney,” Mr. Canton wrote.
“When I received the good news from your foundation, it evoked many feelings. Of course, these awards help to alleviate some of the financial burden of medical school, but for me, it represents much more than that – it represents belief and affirmation. I am at a very pivotal point in my medical career as I prepare to matriculate into Orthopaedic Surgery residency, and this recognition from your committees reinforces my belief that I am ready for the next step. I am honored to be a recipient of these awards and a representation of the Pennsylvania Med-
ical Society, as I continue to strive to be the change that medicine needs to see. Thank you so much!”
In 2004, the ACMS Foundation established this annual scholarship with $10,000 in seed money, which has grown to maturity thanks to generous contri-butions from the ACMS Foundation and local physicians. Eligibility includes status as a third- or fourth-year Pennsylvania medical student from Allegheny County; U.S. citizenship; and full-time enrollment in a Pennsylvania medical school.
The Foundation of the Pennsylvania Medical Society (PAMED) is pleased to administer the fund for the ACMS Foundation. For information about this scholarship, call the PAMED Foun-dation’s Student Financial Services office at (717) 558-7854, or visit www.foundationpamedsoc.org.
Mr. Canton

381ACMS Bulletin / December 2020
ACMS member assists with removal of prior auth code
Effective Jan. 1, 2021, CPT code 67840, for removal of benign eyelid le-sions, will be eliminated from the prior authorization list at Highmark.
David. S. Webster, MD, MBA, ACMS member and vice president and executive medical director of Highmark, was helpful in removing the code with feedback from ophthalmol-ogists and leadership at Pennsylvania Medical Society and the Pennsylvania Academy of Ophthalmology (PAO), who advocated for the removal.
PAGS-WD holds virtual 2020 Fall Program
The Pennsylvania Geriatrics Society – Western Division (PAGS-WD) hosted the 2020 Fall Program virtually on Nov. 10.
More than 64 internists, family prac-titioners, geriatricians, pharmacists, nurses, nursing home administrators and social workers participated in the evening program
Due to crowd restrictions imposed by the CDC to avoid the spread of COVID-19, this was the first virtual program using the Zoom platform, organized by the Society in collaboration with the Jewish Healthcare Foundation (JHF). The trailer for the JHF’s upcom-ing documentary “What COVID-19 Ex-posed in Long-term Care,” was viewed by program participants. The documen-tary, scheduled to be released at the end of 2020, provides expert insight into the current state of long-term care and how COVID-19 exacerbated existing issues. A link to the documentary will be provided to members of the Society.
Thanks to program sponsors includ-ing AHN Healthcare@Home, Commu-
nity LIFE, Optum, Grane Hospice Care, Inc., Presbyterian SeniorCare Network, and Oasis Senior Advisors, educational program costs were minimal for the Society to host.
The program, which began in 2003, is popular with members, attracts dis-tinguished guest speakers comprised of both national and local faculty. This year was no exception, with an expert panel comprised of ER, Critical Care and Long-term Care physicians and a Clinical Pharmacy Specialist in Infec-tious Diseases exploring: “COVID-19 Across the Healthcare Spectrum.”
Leading the panel presentation and serving as moderator was David Nace, MD, MPH, clinical chief of Geriatric Medicine, director, Long-Term Care Division of Geriatric Medicine at the University of Pittsburgh, chief of Medical Affairs, UPMC Senior Communities. The remaining panel members included: Eitan Dickman, MD, MMM, FACEP, FAI-UM, executive vice chairman and med-ical director, Department of Emergency Medicine at Maimonides Medical Center in Brooklyn, N.Y.; Aaron Pickering, PharmD, BCPS, clinical pharmacy spe-cialist – Infectious Diseases at UPMC St. Margaret; and Douglas White, MD, MAS, vice chair and professor of Critical Care Medicine, UPMC Endowed Chair for Ethics in Critical Care Medicine, di-rector, Program on Ethics and Decision Making in Critical Illness at the Universi-ty of Pittsburgh School of Medicine.
Presenters explored the impact of the COVID-19 pandemic in detail, each providing their expertise and expe-riences with patient care on several levels and the effect of this crisis on physicians and frontline caregivers. The presentations were followed by a lively question-and-answer session.
Per-Classifieds
FOR SALESolo ophthalmology turnkey
opportunity for sale/successor near airport. Suitable satellite for established group. Three lanes, minor surgery suite, IOL Mas-ter, Spectralis, Humphrey AVF, DIopsys, topography, cosmetic lasers. EHR with seamless practice management and billing team. Real estate option with additional office suite, off-street parking for 22 cars. Willing to stay on during transition.
Contact [email protected].
HELP AVAILABLEOverwhelmed, Burned Out,
Not in Control? Non-reportable, Confidential and Highly Profession-al Physician Stress Coaching.
Call Winning Focus, 724-875-4111, www.winfordoc.com, [email protected].
For classi�ed advertising
information, including special
member rates, email
[email protected], call
(412) 321-5030, or visit
www.acms.org.
Perspec-PerspectiveSociety News

ACMS member elected to ACEP Board of Directors
Arvind Venkat, MD, FACEP, an emergency medicine physician and vice chair for research and faculty academic affairs in the Depart-ment of Emergency Medicine at Allegheny Health Network (AHN), has been elect-ed to the national board of directors of the American College of Emergency Physicians (ACEP).
Dr. Venkat has practiced emer-gency medicine at AHN since 2007. He has held a variety of leadership positions at AHN including ethics con-sultant and director of research in the Department of Emergency Medicine at Allegheny General Hospital. He is also national director of research for US Acute Care Solutions and professor of medicine at Drexel University College of Medicine.
He is a past president of the Penn-sylvania chapter of ACEP and past chair of the ACEP Ethics Committee. He earned his medical degree from the Yale University School of Medicine and completed his residency in emergency medicine at the University of Cincinnati College of Medicine/University Hospital.
As the immediate past president of the Pennsylvania College of Emer-gency Physicians, Dr. Venkat repre-sented both that organization and AHN as a spokesperson to media outlets throughout the greater Pittsburgh area and beyond to educate the public about the COVID-19 pandemic.
“I am truly honored to be elected to the ACEP Board of Directors,” Dr. Ven-
kat said. “In these extraordinary times, when our nearly 40,000-member emer-gency physicians are on the frontlines of the pandemic, I will try to be worthy of their everyday heroism and an effective voice for our members and patients.”
ACMS member honored by Commission on Cancer
James McCor-mick, DO, FACS, FASCRS, Allegheny Health Network’s system chief of colon and rectal surgery and medical director of the Rectal Cancer Center of Excellence at AHN Cancer Institute, was named recipient of the Commission on Cancer’s (CoC) State Chair Outstanding Performance Award.
Dr. McCormick is board certified by the American Board of Colon and Rectal Surgery and the American Board of Surgery.
The award is given to physicians who have exhibited outstanding leadership and innovation, and have made significant contributions to the improvement of cancer care in their state. CoC State Chairs represent the CoC by providing leadership and support to programs and physicians in their region. As collaborators, innova-tors and experts, they work alongside other cancer professionals to improve the quality of cancer care.
The CoC is a consortium of pro-fessional organizations dedicated to improving survival and quality of life for cancer patients through standard setting, which promotes cancer preven-tion, research, education and monitor-ing of comprehensive quality care.
ACMS member has second book published
Maria J. Sunseri, MD, FAASM, recently had her second book published: “Sleep After Menopause, 2nd Edition.”
Dr. Sunseri is a board-certified neu-rologist specializing in sleep disorders, including women’s sleep disorders, and their connection to other conditions and illnesses.
The book focuses on how your body sleeps: that is, your circadian rhythm, changes to your body temperature, and attention to your surroundings. Dr. Sunseri gives you the insight of over 25 years of experience in neurology and sleep medicine. The book includes a bonus chapter, Sex After Menopause, by Marcia Klein-Patel, MD, PhD, chief of the Women’s Institute of Allegheny Health Network. It is available on Ama-zon at https://amzn.to/3r1eEc8.
The first edition of Sleep After Menopause was published in 2015 and was an international success and rec-ognized as a valuable resource by the North American Menopause Society. This second edition is filled with more valuable insights and the latest scientif-ic and medical information.
Dr. Sunseri is certified by the Ameri-can Board of Psychiatry and Neurology with an additional subspecialty certifi-cation in Clinical Neurophysiology. She also is certified by the American Board of Medical Specialties subspecializing in Sleep Medicine. Other certifications include the American Board of Sleep Medicine and the American Board of Clinical Neurophysiology.
382 www.acms.org
PerspectivePerspectiveActivities & Accolades
Dr. McCormick
Dr. SunseriDr. Venkat

383ACMS Bulletin / December 2020
Acetaminophen, better known by its brand name Tylenol®, is widely
used in the inpatient and outpatient settings for pain management and fever relief. It is favorable in many pop-ulations because of its opioid sparing properties and relatively favorable side effect profile. Acetaminophen is most commonly used in oral formulations including tablets, capsules and oral solutions, and also is available as a suppository. In 2010, intravenous acet-aminophen, also known as Ofirmev®, was approved by the FDA. However, the place in therapy of intravenous acetaminophen has not yet been well established.
The FDA-approved uses of intrave-nous acetaminophen include manage-ment of mild to moderate pain, man-agement of moderate to severe pain with adjunctive opioid analgesics, and reduction of fever, which are identical to that of oral acetaminophen.1,2 The mechanism of action of acetaminophen has not exactly been identified, but is known to inhibit cyclooxygenase (COX) pathways.3 The adverse effects of acetaminophen include nausea, vom-iting, headache and insomnia. Among its side effects, the most serious is risk for hepatic injury, which may be reduced in IV administration due to avoidance of first-pass hepatic expo-sure.1,2 Acetaminophen is contraindi-cated in patients with severe hepatic
impairment or liver disease due to the risk of hepatotoxicity.1,2 The dosing is typically weight-based for children, but for adults, there is a more standard-ized dosing regimen. Oral Tylenol® is available in regular strength 325 mg tablets, 500 mg extra strength tablets, and 650 mg extended-release tablets. In pediatrics, it is recommended not to exceed five doses in 24 hours regard-less of weight. For adult patients, the maximum daily recommended dose is 3000 mg, though this was lowered from 4000 mg per day to encourage safer use of acetaminophen and reduce risk of hepatotoxicity.1
In terms of pharmacokinetics, the main differences between oral
Materia Medica
A potential spin on pain control: A review of IV acetaminophen
MARISSA REES, PHARMD
Continued on Page 386

Get the support your practice needs.
EDUCATION. ADVOCACY. SAVINGS.
PROSURANT INCLUDES:
|
Professional Liability, Patient Acquisition
Population Health Management
Revenue Cycle Management
Payer Relations, Health Insurance
Medical and Office Suppplies
Personal Benefits (Home, Auto,
Life Insurance, Physician Wellness)
And More!
HIPAA Compliance, OSHA Compliance
Legal, PA State Required Training
Staffing, Recruiting, IT Services
Hardware/Software Solutions
Your Allegheny County Medical Society Membership is enhanced with a $624 credit that can be applied to an annual subscription to our Group Purchasing Organization, Prosurant. We empower independents to deliver exceptional care.
NEW!
FOR O
UR
INDEP
ENDEN
T
PRACTIC
ES
Advocacy. Education. Resources.Allegheny County Medical Society.
Membership benefi ts ($1792 value)
ACMS Bulletin• Free annual subscription, 12 monthly issues.
• $60 valuePhysician Wellness Program• Confi dential assistance
• $800 value
Liberty Mutual Auto & Homeowners Insurance• Up to 20% savings• $782 value
Educational Programming• State-mandated training programs for
license renewal• $150 value
Legal Advice from Tucker Arsenberg• Resident/Fellow contract review
• Flat rate — even with multiple contracts • Salary negotiation. Save over $150
Insurance Programs: term, whole, long-term care, and disability • Personal coverage
• Group discounts not available on the public market
2020
EMPL
OYED
PHYSIC
IAN M
EMBE
R
BENEF
ITS
2020 ACMS Membership Benefits
For information, contact James Ireland at [email protected], or (412) 321-5030, ext. 101.
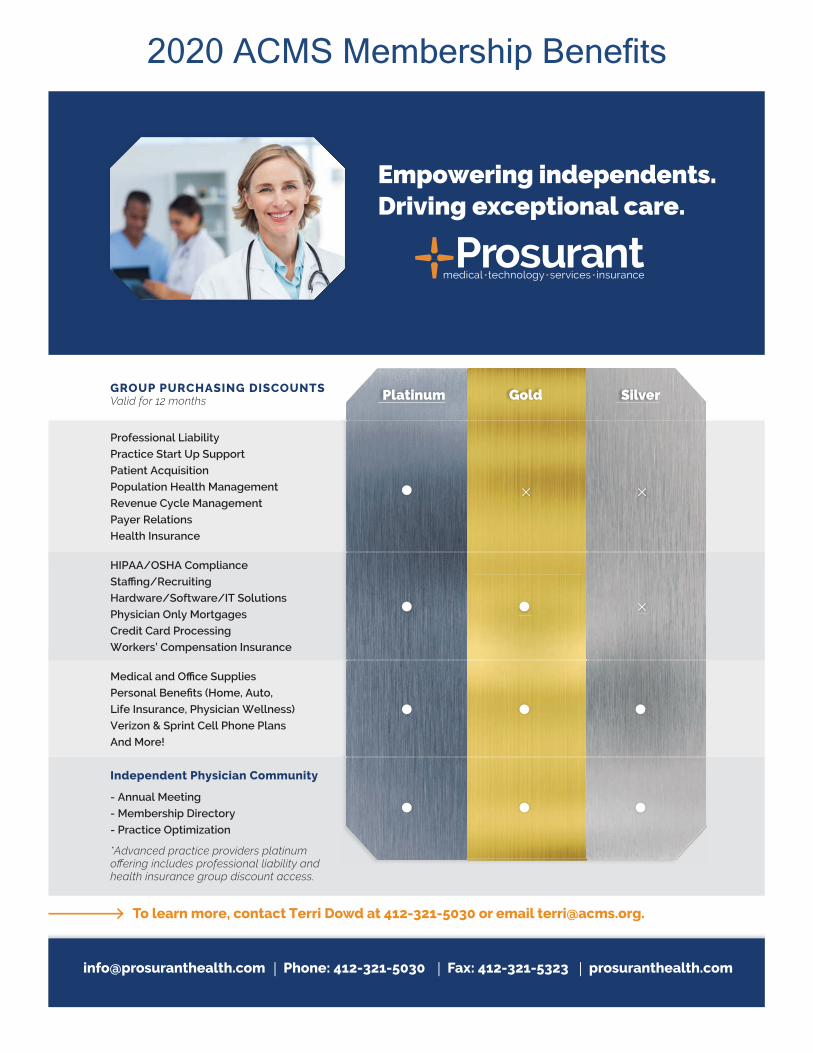
GROUP PURCHASING DISCOUNTSValid for 12 months
To learn more, contact Terri Dowd at 412-321-5030 or email [email protected].
Empowering independents. Driving exceptional care.
[email protected] | Phone: 412-321-5030 | Fax: 412-321-5323 | prosuranthealth.com
Platinum Gold Silver
Professional Liability
Practice Start Up Support
Patient Acquisition
Population Health Management
Revenue Cycle Management
Payer Relations
Health Insurance
HIPAA/OSHA Compliance
Staffing/Recruiting
Hardware/Software/IT Solutions
Physician Only Mortgages
Credit Card Processing
Workers’ Compensation Insurance
Medical and Office Supplies
Personal Benefits (Home, Auto,
Life Insurance, Physician Wellness)
Verizon & Sprint Cell Phone Plans
And More!
- Annual Meeting
- Membership Directory
- Practice Optimization
Independent Physician Community
*Advanced practice providers platinum offering includes professional liability and health insurance group discount access.
2020 ACMS Membership Benefits

386 www.acms.org
Materia Medica
and intravenous acetaminophen are the time of onset and duration of action. Oral acetaminophen has an onset of action of less than an hour, but intravenous acetaminophen has an onset of five to 10 minutes. In addition, oral acetaminophen has a duration of action of four to six hours, whereas intravenous acetaminophen has a duration exceeding six hours.4 Intravenous acetaminophen also has more predictable pharmacokinetic and pharmacodynamic properties due to the formulation itself. Van der Westhuizen, et al., found that 96% of patients receiving intravenous acet-aminophen reached target concen-tration, whereas only 67% in the oral group reached target concentration.5 More reliable absorption rates are a possible advantage compared to oral preparations.
Though these pharmacokinetic properties may make intravenous acetaminophen appear more favorable, it has several disadvantages. Intravenous acetaminophen is much more costly than oral acetaminophen. The average cost of a dose of intravenous acetamin-ophen is $29.26, which is considerably more expensive than the average cost of $0.04 for an oral tablet dose.4 Additionally, it must be infused over 15 minutes which may be inconvenient for some patients.2 When reconstituted, intravenous acetaminophen is prepared as 1000 mg in 100 mL of solution, which should be considered in patients who require fluid restriction, as this may be an issue. Acetaminophen for injection also is packaged in a glass vial, which is not ideal for storage purposes and can lead to increased wasting since each vial must be used within six hours of opening.6
Many studies have been performed to assess the differences between oral and intravenous acetaminophen, but mixed evidence has been reported. A systematic review by Jibil and others comparing the literature of analgesic efficacy, safety and pharmacokinetics between intravenous and oral acet-aminophen identified no clear indica-tion for intravenous over oral dosage forms in the majority of patients.7 Six randomized studies met inclusion criteria for this study with data on com-parison of outcomes between patients receiving intravenous acetaminophen and patients receiving oral acetamino-phen. Of the studies reviewed, efficacy, safety and pharmacokinetic outcomes between intravenous and oral acet-aminophen were analyzed. Pettersson, et al., which was included in this study, found that the use of opioids was lower in patients receiving intravenous acetaminophen compared to the group receiving oral therapy in the post-op-erative setting. However, they did not report any differences in postoperative nausea and vomiting or difference in pain scores. This was likely due to the quicker onset of action of the intravenous formulation.7,8 In studies analyzing pharmacokinetic outcomes, Van der Westhuizen, et al., for exam-ple, found no evidence suggesting intravenous acetaminophen is superior to oral administration.5 The statistically significant findings of the article were not considered clinically significant and would not change current practic-es. However, this study did suggest intravenous acetaminophen may have a place in therapy for patients who can-not take oral formulations and concur-rently require an adjunctive agent for pain control to avoid the use of opioids.
In consideration of the findings of these studies, this systematic review con-cluded that intravenous formulations of acetaminophen are not needed, except, perhaps, for patients without a functional gastrointestinal tract.7
In terms of more population-spe-cific acetaminophen use, oral versus intravenous acetaminophen use has been analyzed in several studies focusing on patients receiving total joint arthroplasties. Brett and others, for example, found oral acetaminophen to be non-inferior to IV acetaminophen.9 This study compared postoperative pain scores, length of stay in recovery, and opioid-sparing effects of oral and intravenous acetaminophen in patients who had undergone knee arthroplasty. Among the results of the study, there was one significant difference in visual analog scale (VAS) pain scores in favor of intravenous acetaminophen over oral (p = 0.025) at 50 minutes after arrival in recovery.9 This significant finding can likely be attributed to the quicker onset of action of intravenous acetaminophen. In a similar study, Fill-ingham, et al., performed a systematic review of the use of intravenous acet-aminophen in patients following total joint arthoplasty.10 This study reviewed a total of 17 publications, including five randomized clinical trials analyzing these outcomes in patients receiving intravenous and oral acetaminophen, none of which reported significant dif-ferences in postoperative pain or opioid consumption between the two dosage forms. Additionally, no post-operative complications were observed across these studies. Consequently, this study concluded that there is an absence of evidence favoring intravenous acet-aminophen use. The author also noted
From Page 383

387ACMS Bulletin / December 2020
Materia Medica
the concern for cost, and that further studies are warranted to determine differences in efficacy between oral and intravenous acetaminophen.
Another study performed by Politi, et al., also analyzed intravenous ac-etaminophen use in total joint arthro-plasty and found similar outcomes.11 In this prospective study, the average VAS used to assess pain was more statistically favorable in the intravenous acetaminophen group, but only in the zero- to four-hour post-operative inter-val. Otherwise, there were no differenc-es between the groups. Though there was a significant difference in pain with intravenous acetaminophen in this ini-tial time window after operative proce-dures, this is not regarded as clinically significant. Thus, this study determined similar outcomes to the aforemen-tioned studies, and suggested using oral acetaminophen over intravenous acetaminophen as an adjunct to a multimodal pain regimen.
As determined from these large-scale studies and others, the place in therapy of intravenous acetaminophen remains unclear. However, intravenous acetaminophen may have a role as an
adjunct agent in patients requiring pain control when opioids are to be avoided. Due to the nature of its formulation, it has a much quicker onset of action compared to the oral products, which make it seem like a desirable additional agent for multimodal pain control. De-spite these benefits, there is a paucity of evidence recommending the use of intravenous acetaminophen when directly compared with oral acetamin-ophen, with the exception of patients who are unable to use their gastroin-testinal tract. Additionally, the increased cost of intravenous acetaminophen alone is a deterrent of many hospitals including the drug in their formularies. No significant study findings have been suggestive of using intravenous acet-aminophen over oral formulations in the studied patient populations. Thus, the differences between the formula-tions in pharmacokinetics and phar-macodynamics are likely insignificant in terms clinical applicability. Further studies could help in formulating a clearer conclusion and role in therapy, but at this time, there is no compelling indication for the use of intravenous acetaminophen.
However, the drug manufacturing company Perrigo has been granted rights to market a generic intravenous acetaminophen product starting in De-cember 2020 by Cadence, the manufac-turer of Ofirmev®. Pending the emer-gence of this generic formulation, there is great potential for increased utilization of intravenous acetaminophen. Though there is no overwhelming evidence supporting the use of intravenous acet-aminophen over oral, hospitals may be more inclined to add this to formulary if it is less costly. Still, the place in therapy of intravenous acetaminophen would not be well established and it may only offer an alternative to opioids in patients requiring pain control who are unable to receive enteral therapy.
Dr. Rees is a PGY-1 acute care pharmacy practice resident at Alleghe-ny General Hospital. For any questions concerning this article, please contact Dr. Rees at the Allegheny Health Network, Allegheny General Hospital, Center for Pharmaceutical Care, Pitts-burgh, Pa., (412) 359-3192 or [email protected].
References1. TYLENOL for Healthcare Professionals. TY-
LENOL Professional. https://www.tylenolprofessional.com/adult-dosage. 2020
2. Ofirmev. Package Insert. Cadence Pharma-ceuticals; 2010
3. Gerriets V, Anderson J, Nappe TM. Acetamin-ophen. In: StatPearls. StatPearls Publishing; 2020.
4. Acetaminophen. Lexi-Drugs. Lexicomp. Wolt-ers Kluwer Health, Inc. Riverwoods, IL. Available at: http://online.lexi.com. Accessed November 2, 2020.
5. van der Westhuizen J, Kuo PY, Reed PW, Holder K. Randomised controlled trial comparing oral and intravenous paracetamol (acetaminophen) plasma levels when given as preoperative analge-sia. Anaesth Intensive Care. 2011;39(2):242-246.
doi:10.1177/0310057X11039002146. Yeh YC, Reddy P. Clinical and economic
evidence for intravenous acetaminophen. Phar-macotherapy. 2012;32(6):559-579. doi:10.1002/j.1875-9114.2011.01085.
7. Jibril F, Sharaby S, Mohamed A, Wilby KJ. Intravenous versus Oral Acetaminophen for Pain: Systematic Review of Current Evidence to Support Clinical Decision-Making. Can J Hosp Pharm. 2015;68(3):238-247. doi:10.4212/cjhp.v68i3.1458
8. Pettersson PH, Jakobsson J, Owall A. Intra-venous acetaminophen reduced the use of opioids compared with oral administration after coronary artery bypass grafting. J Cardiothorac Vasc Anesth. 2005;19(3):306-309. doi:10.1053/j.jvca.2005.03.006
9. Brett CN, Barnett SG, Pearson J. Post-
operative plasma paracetamol levels following oral or intravenous paracetamol administration: a double-blind randomised controlled trial. An-aesth Intensive Care. 2012;40(1):166-171. doi:10.1177/0310057X1204000121
10. Fillingham YA, Hannon CP, Erens GA, et al. The Efficacy and Safety of Acetaminophen in Total Joint Arthroplasty: Systematic Review and Direct Meta-Analysis. J Arthroplasty. 2020;35(10):2715-2729. doi:10.1016/j.arth.2020.05.037
11. Politi JR, Davis RL 2nd, Matrka AK. Randomized Prospective Trial Comparing the Use of Intravenous versus Oral Acetaminophen in Total Joint Arthroplasty. J Arthroplasty. 2017;32(4):1125-1127. doi:10.1016/j.arth.2016.10.018

388 www.acms.org
Materia Medica
Pitolisant (WAKIX®) is the first and only FDA-approved selective hista-
mine 3 (H3) antagonist/inverse agonist for the treatment of excessive daytime sleepiness in narcolepsy. 1,2 Excessive daytime sleepiness in narcolepsy is de-fined as the inability to remain awake and alert throughout the day. It can in-clude unintentional sleep at inappropri-ate times and interfere with day-to-day activities and functions.3 Other agents that treat excessive daytime sleepiness in narcolepsy are stimulants, modafinil and sodium oxybate. These treatments have something in common – they all are controlled substances and pri-marily affect the release/reuptake of dopamine, norepinephrine or function similarly to gamma aminobutyric acid. Pitolisant has a unique place in thera-py, as it decreases excessive daytime sleepiness by increasing the synthesis and release of histamine in the brain to promote wakefulness and is not a controlled substance.1
Safety Pitolisant is contraindicated in pa-
tients with severe hepatic impairment, and not recommended in patients with end stage renal disease. It has warn-ings for QTc prolongation, use with agents that cause QTc prolongation, patients with cardiac arrythmias, or patient with high risk for developing torsades de pointes.2 A randomized, double-blind, 4-period, crossover
study evaluated the effect pitolisant had on ventricular repolarization and if it caused QTc prolongation. Sin-gle dose administration of pitolisant 40mg, pitolisant 120mg, moxifloxacin 400mg, and placebo were all com-pared. Moxifloxacin was included in the study to establish the assay sensitivity, acting as a positive control. The 40mg of pitolisant did not increase the QTc significantly, with a mean change of 3.69 millisecond (ms) (CI 90%, 1.43 to 5.94). The 120mg dose of pitolisant did increase the QTc significantly, with a mean change of9.91 ms (CI 90%, 7.63 to 12.18).4,5 In a phase I study, pitolisant 160mg, 200mg, and 240mg were evaluated for their effect on changes in the Fridericia-corrected QTc interval (QTcF) in comparison to moxifloxacin. It was concluded that the QTcF increased significantly for the 160mg, 200mg and 240mg doses. The increase was 11.9, 13.3, and 9.9 ms (CI 95%, 6.7 to 17.1, 8.1 to 18.5, and 4.7 to 15.1) respectively. The 160mg and 200mg doses caused increases greater than moxifloxacin’s effect on QTcF which is 10.7 ms.4,5 Serious adverse effects found included one case of severe nausea, one case of a spontaneous abortion, and one case of severe abdominal discomfort.6-8
Tolerability Pitolisant is well tolerated. The Har-
mony III trial studied the effects of long-term use of pitolisant over 12 months. The side effects experienced by the pitolisant monotherapy group and com-bined therapies experienced mainly
psychiatric (38.4% of the reported side effects) and nervous system effect (20.5% of the reported side effects) in the first three months of treatment. After three months, the most common side effect was headache (11.8%). The other common side effects were in-somnia (8.8%), anxiety (6.9%), nausea (4.9%), depressive symptoms (4.9%), and weight gain (7.8%). The side ef-fects were mild to moderate and more common during the first three months of treatment at 37.8% (92/168) and declined during the last three months to 12.5% (21/168).6 Similar effects also were found in the Harmony I and Harmony-CTP trials.7,8
Effectiveness The effectiveness of pitolisant was
studied in three clinical trials. The first trial, Harmony I, was a multi-country, randomized, double-blind, parallel group-controlled trial. Ninety-five patients were divided into three groups: placebo, pitolisant, or modafinil, and received eight weeks of treatment. The pitolisant doses were titrated up over three weeks using 10mg, 20mg, or 40mg daily, and the modafinil doses were titrated using 100mg, 200mg, or 400mg daily. At week three, the doses were adjusted for each patient based on their symptoms and efficacy. After the initial titration at week three, the doses in each group were consistent for five weeks and treatment was stopped at eight weeks. The subjects were studied for an additional week to note any withdrawal symptoms. None was found in the pitolisant group. The
Pitolisant (WAKIX®)CASSIDY WILLIAMS, PHARMD SEHRISH PANJWANI, PHARMD, BCPS

efficacy was evaluated by the Epworth Sleepiness Scale (ESS). This scale has high specificity and sensitivity for the diagnosis of narcolepsy. The ESS ranges from 0 to 24. The lowest score of 0 corresponds to the lower normal daytime sleepiness and the highest score of 24 corresponds to severe ex-cessive daytime sleepiness.2 After eight weeks of treatment, the pitolisant group had a decreased ESS by 5.8 (SD 6.2), placebo group had a decreased ESS by 3.4 (SD 4.2) and the modafinil group had a decreased ESS by 6.9 (SD 6.2). Pitolisant was shown to be superior to placebo with a difference of -3.0 (95% CI, -5.6 to -0.4; p=0.024), but non-in-ferior to modafinil with a difference of 0.12 (95% CI, -2.5 to 2.7; p=0.250).7
The Harmony-CTP trial was a randomized, double-blind, place-bo-controlled study that included 106 patients. The patients were divided into two groups: pitolisant or placebo. The primary outcome was weekly cataplexy rate (WCR) and safety. The patients received 5mg to 40mg of pitolisant or placebo that were titrated for three weeks and four weeks of stable doses for a total of seven weeks of treat-ment. WCR decreased by 75% in the pitolisant group (WCRfinal/baseline=0.25) and 38% in the placebo group (WCR final/baseline=0.62 (rate ratio 0.512, 95% CI 0.43-0.60, p<0.0001)).8
The Harmony III trial was an open-label, single arm, pragmatic study that involved 102 patients with narco-lepsy. Within the 102 patients, 75 also had cataplexy. The 102 patients were divided into pitolisant monotherapy (n=48) and in combination with other therapies such as modafinil, sodium oxybate, and methylphenidate (n=54). The goal of this study was to evaluate
the long-term efficacy and safety of pitolisant, determined at twelve months of treatment. The primary endpoint was safety and the secondary endpoints were ESS, cataplexy and side effects. The patients were titrated up from 5mg to 20mg of pitolisant over one month. After one month, the patients received 40mg of pitolisant. Only 68 patients finished the 12 months of treatment. The total ESS score decreased by 4.6±0.6 (95% CI, -5.82 to -3.44; p-val-ue=0.001). The mean of daily gener-alized cataplexy episodes decreased by 76% which is a -0.25 change from baseline (95% CI, -0.67 to 0.17) and the mean daily partial cataplexy episodes decreased by 65% which is a -0.49 change from baseline (95% CI -1.09 to 0.10).6 All three trials supported the safety and efficacy of pitolisant. The Harmony-CTP and Harmony III trials showed evidence that pitolisant is not only effective in decreasing EDS, but also cataplexy. Pitolisant also was shown to not induce withdrawal effects after cessation.6-8
Price The cash price for the 4.45mg dose
is $113.70 per each tablet, and the 17.8mg dose is $227.40 per each tab-let. It is set to be available in the fourth quarter of 2019.9
Simplicity Pitolisant is a tablet that is available
in a 4.45mg dose and 17.8mg dose.9 The 4.45mg and 17.8mg doses are equivalent to 5mg and 20mg of pi-tolisant hydrochloride, respectively.10 The initial dose is 8.9mg by mouth dai-ly upon awakening for one week, then 17.8mg daily for one week. Pitolisant can be increased to a maximum dose
of 35.6mg daily after two weeks of titra-tion. It may take up to eight weeks for the full effect to be achieved. If a dose is missed, skip the missed dose and resume usual dosing schedule. It is not recommended to take double doses.9 Dosage adjustments are required for CYP2D6 poor metabolizers, strong CYP3A4 inducers, and strong CYP2D6 inhibitors. Pitolisant use in patients that are poor CYP2D6 metabolizers are limited to a maximum of 17.8mg daily. Patients that are on pitolisant and start a strong CYP3A4 inducer should have their pitolisant dose doubled, unless already at the maximum dose of 35.6mg. The patient should be assessed for efficacy at the new dose. If a strong CYP3A4 inducer is stopped, pitolisant should be decreased by 50%. If a strong CYP2D6 inhibitor is being initiated when a patient is stable on pitolisant, the pitolisant dose will need to be reduced by 50%. If the patient is already on a CYP2D6 inhibitor and pitolisant is being initiated, the pa-tient’s maximum daily dose should be 17.8mg. In hepatic and renal impair-ment, pitolisant’s maximum daily dose is 17.8mg. It is contraindicated in hepatic failure and not recommended in end stage renal disease. The effect of hormonal contraceptives can be reduced by pitolisant. It is recommend-ed to use a non-hormonal form of birth control during treatment and up to 21 days after ceasing treatment. Use of histamine 1 receptor antagonists should be avoided because these will decrease the effect of pitolisant.11 Histamine 1 receptor antagonists are commonly used over the counter prod-ucts, and patients should be counseled not to use them while taking pitolisant.
389ACMS Bulletin / December 2020
Continued on Page 390
Materia Medica

390 www.acms.org
Materia Medica
Bottom line Pitolisant is the first and only FDA
approved H3 antagonist/inverse agonist and only non-narcotic treatment for ex-cessive daytime sleepiness in patients with narcolepsy.1 It is well tolerated with the most common side effects being headache, insomnia and weight gain.6 Significant drug interactions are
present with pitolisant and should be considered before initiation. Pitolisant has shown to be safe and effective in patients suffering from excessive daytime sleepiness and cataplexy in narcolepsy. 6-8
Dr. Williams is a PGY1 pharmacy practice resident at UPMC St. Margaret and can be reached at williamscb2@
upmc.edu. Dr. Panjwani is a PGY2 geriatric pharmacy resident at UPMC St. Margaret and can be reached at [email protected]. Heather Sakely, PharmD, BCPS, BCGP, the director of Geriatric Pharmacotherapy and director of the PGY2 Geriatric Pharmacy Residency, served as editor and mentor for this work and can be reached at [email protected].
References1. Leone N, Baker S. Harmony Biosci-
ences Announces FDA Approval of WAKIX (pitolisant), A First-In-Class Medication for The Treatment of Excessive Daytime Sleepiness in Adult Patients with Narcolepsy. https://www.harmonybiosciences.com/newsroom/harmony-biosciences-announces-fda-approv-al-of-wakix-r-pitolisant-a-first-in/. Accessed October 12, 2019.
2. Narcolepsy. In DynaMed [database online]. EBSCO Information Services. https://www.dynamed.com/condition/narcolepsy#GUID-E457C-1CF-716D-46B9-8D6A-8F8E2BBF64E7. Updated April 22, 2019. Accessed October 9, 2019.
3. Chervin RD. Approach to the patient with excessive daytime sleepiness - UpTo-Date. UpToDate, Inc. and/or its affiliates. https://www.uptodate.com/contents/ap-proach-to-the-patient-with-excessive-day-time-sleepiness?search=excessive daytime sleepiness&source=search_result&selectedTi-tle=1~150&usage_type=default&display_rank=1. Published 2019. Accessed October 12, 2019.
4. Shah RR, Maison-Blanche P, Robert P, Denis E, Duvauchelle T. Can an early phase clinical pharmacology study replace a thorough QT study? Experience with a novel H3-re-ceptor antagonist/inverse agonist. Eur J Clin Pharmacol. 2016;72(5):533-543. doi:10.1007/s00228-016-2023-3
5. CHMP. Committee for Medicinal Products for Human Use (CHMP) Assessment Report: Wakix. www.ema.europa.eu/contact. Accessed October 12, 2019.
6. Dauvilliers Y, Arnulf I, Szakacs Z, et al. Long-term use of pitolisant to treat patients with narcolepsy: Harmony III Study. Sleep. July 2019. doi:10.1093/sleep/zsz174
7. Dauvilliers Y, Bassetti C, Lammers GJ, et al. Pitolisant versus placebo or modafinil in patients with narcolepsy: a double-blind, ran-domized trial. www.thelancet.com/neurology. 2013;12. doi:10.1016/S1474-4422(13)70225-4
8. Szakacs Z, Dauvilliers Y, Mikhaylov V, et al. Safety and efficacy of pitolisant on cataplexy in patients with narcolepsy: a randomised, double-blind, placebo-controlled trial. Lancet
Neurol. 2017;16(3):200-207. doi:10.1016/S1474-4422(16)30333-7
9. Pitolisant: Drug Information - Up-ToDate. UpToDate, Inc. and/or its affili-ates. https://www.uptodate.com/contents/pitolisant-drug-information?search=pi-tolisant&source=panel_search_result&select-edTitle=1~9&usage_type=panel&kp_tab=drug_general&display_rank=1#F53638506. Published 2019. Accessed November 19, 2019.
10. Shah, Dhara. CENTER FOR DRUG EVALUATION AND RESEARCH: 211150Orig1s000 Other Reviews. Food and Drug Administration; Published 2019. Accessed November 20, 2019.
11. Hart L, Auth D. CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 211150Orig1s000 RISK ASSESS-MENT and RISK MITIGATION REVIEW(S) 1 Division of Risk Management (DRISK) Office of Medication Error Prevention and Risk Manage-ment (OMEPRM) Office of Surveillance and E. Food and Drug Administration; Published 2019. Accessed October 12, 2019.
From Page 389
ACMS Members:Professional announcement advertisements
are available to ACMS members at our lowest prices.
Contact Meagan Sable, managing editor, at [email protected].
Congratulatory message?
Retiring? New Partner?
New Address?
391ACMS Bulletin / December 2020
Legal Report
Physician cybersecurity vigilance and resources
MICHAEL A. CASSIDY, ESQ.
The COVID-19 pandemic has exac-erbated the already too prevalent
public health information (PHI) hacks, providing a target rich environment of both businesses and individuals, and therefore medical practices, who are more susceptible to phishing attempts linked to providing test kits, PPE, pan-
demic information, etc. The data avail-able through the hacking and other cy-ber crimes is highly valuable because it can contain significant PHI, i.e., name, birth date, account numbers, insurance numbers, phone numbers, addresses, social security numbers.
This threat is irrevocably intertwined
with the increasing reliance on tele-health, because much of this information is being exchanged and stored via non-secure or less protected networks and through medical devices that do not have robust or effective cybersecurity protection, culminating in the following:
Continued on Page 392
For additional information contact any of the following attorneys at (412) 566-1212:
Tucker Arensberg lawyers have experience in all major healthcare law issues including:
• Compliance • Cybersecurity • Reimbursement • Mergers & Acquisitions • Credentialing & Licensing for Individuals & Healthcare Facilities •
Employment Contracts and Restrictive Covenants • Tax & Employment Benefits
medlawblog.com
Pittsburgh, PA Harrisburg, PA New York, NY
Mike Cassidy - Compliance; Contracts, Peer Review, Stark/AKS Ryan Siney - Cybersecurity, Compliance
Paul Welk - Mergers & Acquisitions Jerry Russo - Investigations
Danielle Dietrich - HIPAA, Collections & Litigation
Rebecca Moran - Mergers & Acquisitions and Physician Contracts

392 www.acms.org
Legal Report
• Increased remote telehealth inter-actions without appropriate additional security,
• Individual and institutional fears re-garding pandemic issues have created more, susceptible targets, and
• A fragmented and outdated IT infrastructure, especially with individual physicians, small medical practices, and financially challenged hospitals.
Last month’s article in the Bulletin entitled “Cybersecurity: Hackers Raise Stacks with Patient Safety and Provid-er Operations” by Beth Ann Jackson, Esq., was a timely prescient clarion call to physicians and medical practices to increase their cybersecurity vigilance. Recently, IT security publications have reported a majority of hospitals and more than 70% of all businesses have been victims of cybersecurity and ran-somware attacks within the last twelve months.
This article is intended to provide physicians a basic understanding of the improved resources being made available to physicians in this area.
AMA: Working from Home White Paper
The American Medical Association (AMA) has published a short white paper entitled “Working from Home During COVID-19 Pandemic,” which you can reach through the follow-ing link: https://www.ama-assn.org/system/files/2020-04/cybersecuri-ty-work-from-home-covid-19.pdf.
AMA makes a number of recom-mendations, which are described in greater detail in the white paper, but include the following:
• Consider using a virtual private
network (VPN) and/or a cloud-based service for your home connection, because they provide the ability to se-curely connect back to EHR/IT systems using a range of different devices.
• Inventory the devices you use to connect, i.e., home computer, smart-phone, tablet, etc., and determine whether those connections are secure to your home network and whether your home network is secure.
• If you are using an EHR app as part of your home practice, you must verify that the app you are using is the most current version of that app for connection to the system’s medical records.
The AMA white paper provides detailed recommendations regarding the following:
• Steps to improve your cybersecuri-ty practices
• Cybersecurity checklists for your computers
• Advice on protecting your medical practice from cyber threats
HHS launches physician cybersecurity website
The Department of Health and Human Services (HHS) Health Sector Cybersecurity Coordination (HC3) has recently launched a new website to help physicians and their medical prac-tices be better informed about potential cyber threats at this link: https://www.hhs.gov/about/agencies/asa/ocio/hc3/index.html.
One of the extremely useful re-sources accessible through this web-site is a series of “Threat Briefs,” which HHS is publishing on a regular basis to provide detailed information regarding cybersecurity threats to physicians and their medical practices.
Although there are several dozen Threat Briefs existing on the website now, four of the most informative, in my opinion, are the following:
• Securely Teleworking in Healthcare: https://www.hhs.gov/sites/default/files/securely-teleworking-healthcare.pdf
• COVID-19 Cyber Threats (Update):
From Page 391
Resources to reinforce cybersecurity• AMA –“Working from Home
During COVID-19 Pandemic,” https://www.ama-assn.org/sys-tem/files/2020-04/cybersecuri-ty-work-from-home-covid-19.pdf
• HHS – Potential cyber threats, https://www.hhs.gov/about/agencies/asa/ocio/hc3/index.html
HHS Threat Briefs• Securely Teleworking in
Healthcare: https://www.hhs.gov/sites/default/files/securely-telework-ing-healthcare.pdf. NOTE: Section on
multifactor authentication and virtual private networks (VPNs) in relation to password strength.
• COVID-19 Cyber Threats (Update): https://www.hhs.gov/sites/default/files/covid-19-cyber-threats-update.pdf
• Social Media Attacks: https://www.hhs.gov/sites/default/files/so-cial-media-attacks.pdf
• 5G Security for Healthcare: https://www.hhs.gov/sites/default/files/5g-security-for-healthcare.pdf
393ACMS Bulletin / December 2020
https://www.hhs.gov/sites/default/files/covid-19-cyber-threats-update.pdf
• Social Media Attacks: https://www.hhs.gov/sites/default/files/social-media-attacks.pdf
• 5G Security for Healthcare: https://www.hhs.gov/sites/default/files/5g-security-for-healthcare.pdf
The threat brief entitled “Securely Teleworking in Health Care” is very similar to the AMA website, and emphasizes critical cybersecurity defense such as multifactor authentica-tion and virtual private networks (VPNs) that are structurally and inherently more secure than the “wifi” typically available from the commercial carriers.
The importance of multifactor authentication is gramma-tized recently by a report by Irongate Technology providing a visual graph of the time it would take a hacker to “brute force” your password.
• With passwords of four to six characters using numbers only, lower case letters only, upper case and lower case letters, any combination of all of those or any combination
of numbers, upper and lower case letters, and symbols, the access time goes from “instantly to all of 5 seconds.”
• Conversely, a 10-word password with numbers, upper- and lowercase letters, and symbols would take an estimated five years; an 11-character password would take 400 years; and a 12-character password would take 34,000 years. The time increases are exponential; a 15-character password with all of those combinations would take 15 billion years – considerably longer than any of our life spans!
ConclusionHIPAA requires you to take reasonable steps to protect
the privacy and security of your PHI data. Consulting these resources would be an appropriate next step.
Mr. Cassidy is a shareholder at Tucker Arensberg and is chair of the firm’s Healthcare Practice Group; he also serves as legal counsel to ACMS. He can be reached at (412) 594-5515 or [email protected].
Legal Report
Thank you for your membership in the Allegheny County Medical Society
The ACMS Membership Committee
appreciates your support. Your membership
strengthens the society and helps protect
our patients.Please make your medical society stronger by encouraging your colleagues to become members of the
ACMS. For information, call the membership department at (412) 321-5030, ext. 109, or email [email protected].
In the spring of 1940, a history of medicine society had its stuttering
beginnings at the University of Pitts-burgh. A year later, on April 28, 1941, the Pittsburgh Society of the History of Medicine held the area’s first such symposium, presumably in the Med-ical School Library of the Old Mellon Institute building. Surgeon Thomas S. Arbuthnot (1871-1956) spoke to the 16 attendees about “primitive medicine” in Canada; pharmacologist Paul L. McLain (1908-1981) talked of William Harvey; and hematologist George J. Kastlin (1900-1948) displayed portraits of important medical figures that had ap-peared in Vanity Fair from 1872 to 1907. According to notes from cardiologist George G. Burkley (1902-1991), the group planned to meet again in October – but we have no records of further meetings. Burkley was called up to serve with the Navy before taking his most famous position as President John F. Kennedy’s physician, and Kastlin died prematurely. The idea languished for two decades.
In the spring of 1961, a new group formed as The Western Pennsylvania Society for Medical History under the guidance of rheumatologist Gerald P. Rodnan (1927-1983) and historian of public health John Duffy (1915-1996). When they met in Lecture Room #1 of Scaife Hall on November 15, 1961, Dr. McLain showed a film about William Harvey, and Dr. Rodnan gave a lecture on “The Golden Age of Gout,” illustrated with original texts from the 18th and early 19th century that his children later donated to the University. The cover page of the Society’s constitution declared, “Realizing the cultural, humanistic, and scientific values inherent in the study of history and recognizing that the area of medicine, broadly conceived, is especially rich in historical significance, a group of interested persons of rather diverse backgrounds and professional commitments … decided to organize a society to ‘promote interest in and
study of the history of medicine and its allied arts, scienc-es, and professions.’”
Rheumatologist Thomas G. Benedek, MD (1926- ) and anthropologist David Landy (1917-2007) stepped into lead-ership roles, but this second iteration folded in 1966, a year after Duffy departed for Tulane University.
The third time was indeed the charm, but not without a trag-edy at its center. When the Rare Books and Special Collections were organized in 1974-5, interest in the history of medicine redounded. A “Group for the History of the Health Professions” offered its first guest lecture in March 1975, “Physicians and Books,” by internist William B. Bean (1909-1989), director of the Institute for the Humanities in Medicine at the University of Tex-as Medical Branch in Galveston and a charter member of the American Osler Society. Just six months later, beloved librarian Carroll Foster Reynolds (1910-1975) died one month before his scheduled retirement. The latest – and current – iteration of the society was named for him.
After earning a BS from West Virginia University, MA and PhD degrees from University of Pittsburgh, and a library degree from Columbia University, Reynolds joined the Pitt faculty in 1947. He became the first director of the Maurice and Laura Falk Library of the Health Professions in 1957. Interestingly, Reynolds was instrumental not just in local collections but in establishing medical libraries in Ibadan, Nigeria; Bangkok, Thailand; and Dacca, Bangla-desh, through the Rockefeller Foundation.
394 www.acms.org
If anyone has memories, photographs, newsletters, lecture posters, or other ephemera from any of these medical
history societies, we invite you to contact us at [email protected].
Links to the free public lectures and a schedule can be found at
Special Report
KRISTEN ANN EHRENBERGER, MD, PHD
A history of the C.F. Reynolds Medical History SocietyAn adventure in understanding:
395ACMS Bulletin / December 2020
Special Report
Before his untimely passing, Reynolds had sent col-leagues questionnaires, asking about their interest in a society “with History of the Health Professions as its focus.” Some responses have been preserved, and their handwrit-ten marginalia make for interesting reading.
Neuropathologist John Y. Moossy (1925-2012) circled the word “Health Professions” and wrote, “This amorphous term needs discussion & clarification. My enthusiasm would be diluted if Medicine were not the major ‘Health Profession’ referred to.”
By contrast, Virginia Burk replied, “I would be interested only if the definition of Health Professions is broadened to in-clude Nursing, Dentistry, Pharmacy, etc.” As it was, the topics covered in the Society’s first decade included early modern botany, famous surgeons and anesthesiologists, histories of hematology and histology, clean-water infrastructure in Pitts-burgh, and the invention of the bronchoscope and the micro-scope. A two-day symposium at Children’s Hospital in 1983 focused on the history of prematurity and of “infant” cholera.
The definition of “health professions” has been broad ever since. This year’s lecture series ranges from the pioneers of open-heart surgery to public health in colonial East Africa, and from an illegal abortion clinic in Philadelphia to the gleaming hospital towers of Pittsburgh. Even as the past recedes from our view, there is always more to learn about it. If anyone has memories, photographs, newsletters, lecture posters, or other ephemera from any of these med-ical history societies, we invite you to contact us at [email protected]. Links to the free public lectures and a schedule can be found at [email protected].
Dr. Ehrenberger, MD, PhD (History), is assistant profes-sor of Internal Medicine and director of the Progressive Eval-uation & Referral Center (PERC) at UPMC. She is secretary of the C.F. Reynolds Medical History Society and can be reached at [email protected].
Colour lithograph of Rudolf Ludwig Karl Virchow by Sir L. Ward [Spy], 1893. Credit: Wellcome Collection. Attribution 4.0 International (CC BY 4.0)
For advertising information, visit www.acms.org,call (412) 321-5030,
or email [email protected].
396 www.acms.org
Special Report ALLEGHENY COUNTY MEDICAL SOCIETY 850 RIDGE AVENUE • PITTSBURGH, PA 15212-6098 P: 412-321-5030 • f: 412-321-5323 • www.acms.org
Election Report
for Officers and Delegates December 8, 2020
The following physicians have been elected to office in 2021, as certified by AssociationVoting. President Patricia L. Bononi, MD President-elect Peter G. Ellis, MD Vice President Matthew B. Straka, MD Secretary David L. Blinn, MD Treasurer Raymond E. Pontzer, MD Term Expires 2023 Steven Evans, MD Bruce A. MacLeod, MD Amelia A. Paré, MD Maritsa Scoulos-Hanson, DO Adele L. Towers, MD
Other Directors currently serving:
William K. Johnjulio, MD, Chair 2021 Term Expires 2021 Term Expires 2022 William F. Coppula, MD Ragunath Appasamy, MD David J. Deitrick, DO Mark A. Goodman, MD Kevin O. Garrett, MD Keith T. Kanel, MD Marcy L. Jackovic, DO G. Alan Yeasted, MD Fulfilling unexpired term of Raymond E. Pontzer, MD
Douglas F. Clough, MD Maria J. Sunseri, MD
Peer Review Board Term Expires in 2023 Lauren C. Rossman, DO Angela M. Stupi, MD
Other members currently serving: Term Expires in 2021 Term Expires in 2022 Thomas P. Campbell, MD Kimberly Hennon, MD Marcia Bohm-Velez, MD Jan W. Madison, MD

397ACMS Bulletin / December 2020
Special Report Delegates (Term 2021-2022) Ragunuth Appasamy, MD Douglas F. Clough, MD Amber L. Elway, DO Deborah A. Gentile, MD Scott L. Heyl, MD Barbara S. Nightingale, MD Joseph C. Paviglianiti, MD Angela M. Stupi, MD Rajiv R. Varma, MD David S. Webster, MD David L. Blinn, MD (Secretary)
Other members currently serving:
William F. Coppula, MD Keith T. Kanel, MD Adele L. Towers, MD David J. Deitrick, DO Bruce A. MacLeod, MD Matthew Vasil, DO Kevin O. Garrett, MD Jan W. Madison, MD G. Alan Yeasted, MD
Mark A. Goodman, MD William Simmons, MD
Alternate Delegates Weston F. Bettner, MD (Term Expires 2021) Vint R. Blackburn, MD Hui Wei Chen, MD Richard A. Fortunato, DO Richard B. Hoffmaster, MD Michael S. Hu, MD Micah A. Jacobs, MD James T. McCormick, DO Derek M. McQuade, MD Nadia K. Sundlass, MD Respectfully submitted, Matthew B. Straka, MD Chair, Nominating Committee 2020 NOMINATING COMMITTEE Ragunath Appasamy, MD Mark A. Goodman,MD Angela M. Stupi, MD James W. Boyle, MD Jan W. Madison, MD Matthew A. Vasil, DO David J. Deitrick, DO Bruce A. MacLeod, MD G. Alan Yeasted, MD Amber L. Elway, MD Michael M. McDowell, MD

398 www.acms.org
Feature
A look back at 713 Ridge AvenueMore than 50 years ago, the Allegh-
eny County Medical Society found its new home at 713 Ridge Avenue.
Built in 1895 as a carriage house and driver’s quarters for the wealthy Denny family, the building eventually was converted into a place of business.
In the large meeting room, many physicians, nurses, practice managers, emergency medical staff and health-care professionals would gather over the years, learning and growing togeth-er at ACMS, while sharing a meal and establishing professional relationships – and friendships.
The second floor changed many times, with upgrades to include sepa-rate offices for ACMS staff members and a large conference area. To look straight down the hallway, though, one could always find the beautiful fireplace with white crown molding accenting its appeal.
In the bountiful front lawn, with land-scaping kept immaculate by our faithful groundskeeper and maintenance guru Chuck, bread was broken, discussions were held and ACMS Board photos were taken.
It would be remiss not to mention the tailgates held in the ACMS parking lot, where many Pittsburgh sports fans (ACMS members included, of course) gathered to cheer on their team.
A place for gathering, a place for learning, a place to improve healthcare in Allegheny County by working and growing together; it’s not just a build-ing, but part of our ACMS history, and we will be forever grateful for our time at 713 Ridge Avenue.
Above, a view of the front of 713 Ridge Avenue, with the Allegheny County Medical Society sign visible at front. Below, a view from inside the building looking out the familiar windows and doors at the manicured lawn.

399ACMS Bulletin / December 2020
Feature
Board of Directors meeting, 2014 Practice Managers meeting, 2014
Pittsburgh Ophthalmology
Society meeting, 2016
2015 ACMS Board of Directors
Board of Directors meeting, 2016

400 www.acms.org
Feature
Greater Pittsburgh Diabetes Club, 2015 Board of Directors meeting, 2018
Practice Managers
‘Speed- dating’
event, 2015
Practice Managers meeting, 2014
PAMED and ACMS event, 2015

401ACMS Bulletin / December 2020
Feature
Pittsburgh Ophthalmology Society meeting, 2015
Board of Directors meeting, 2015
Practice Managers HIPAA event, 2013
2017 ACMS Board of Directors
Social Determinants of Health meeting, 2019 ACMS PPE distribution, 2020

402 www.acms.org
Volume 110 No. 7 July 2020 Pages 197-228Volume 110 No. 8 August 2020 Pages 229-260Volume 110 No. 9 September 2020 Pages 261-292Volume 110 No. 10 October 2020 Pages 293-324Volume 110 No. 11 November 2020 Pages 325-364Volume 110 No. 12 December 2020 Pages 365-404
PerspectivePerspectiveEditorial Index
AACMS Alliance News.................................349Activities & Accolades ......220, 253, 348, 382B, CClassifieds .................................282, 361, 381Community Notes......................................220D, EEditorial:Nourishment: Pandemic edition.....................201 Deval (Reshma) Paranjpe, MD, MBA, FACSGateway Medical Society celebrates new star – A history of supporting African American youth...203Amelia A. Paré, MD, FACS12 essential leadership skills......................207Richard H. Daffner, MD, FACRFinding my niche: Residency and beyond...214Andrea G. Witlin, DO, PhDThe malady lingers on..................................234 Deval (Reshma) Paranjpe, MD, MBA, FACSScientific misconduct...................................238Richard H. Daffner, MD, FACRReconnecting during COVID........................241Andrea G. Witlin, DO, PhD The splendor of autumn................................266 Deval (Reshma) Paranjpe, MD, MBA, FACSPandemic lemonade.....................................267 Joseph C. Paviglianiti, MD Finding my niche – fellowship and beyond...269 Andrea G. Witlin, DO, PhD Curmudgeons..............................................271Richard H. Daffner, MD, FACR Reclaiming autonomy....................................297 Deval (Reshma) Paranjpe, MD, MBA, FACS The lost year and stuff..................................299Andrea G. Witlin, DO, PhD Tests.............................................................304Richard H. Daffner, MD, FACRFall nourishment..........................................329Deval (Reshma) Paranjpe, MD, MBA, FACSRoentgen and the discovery that changed medicine.......................................................331Richard H. Daffner, MD, FACRPhysicians in mourning: Greiving with purpose....336Anna Evans Phillips, MD, MSGone too soon: An ode to Micah Man..........338Andrea G. Witlin, DO, PhD Gratitude.......................................................369
Deval (Reshma) Paranjpe, MD, MBA, FACSFinding my niche: A kind, well-shaven face...370Anthony L. Kovatch, MDRightly forgotten...........................................373 Richard H. Daffner, MD, FACRFFeature:Improving the ‘health’ of health care prescription: Mentorship and diversity..........354Natalia Ortiz-Torrent, MD, DFAPA, FACLP, FPCPJohanna Vidal-Phelan, MD, MBA, FAAPA look back at 713 Ridge Avenue................398 G, H, IIn Memoriam:George F. Buerger Jr., MD ..........................219Eugene W. Delserone, MD..........................307Robert Love Baker, MD...............................424John Emboaba Da Costa, MD.....................282 J, K, LLegal Report:Avoid employment law violations when dealing with COVID-19.............................................225 William M. Maruca, Esq. Future of telehealth: Boom, or back to business as usual?......................................................287 Michael A. Cassidy, Esq. Physician recruitment: A cautionary tale......318 William M. Maruca, Esq. Wheeling Hospital settles $50M False Claims case with OIG: enters long-term agreement with WVU.....................................................320Michael A. Cassidy, Esq. Jerry J. Russo, Esq.Physician cybersecurity vigilance and resources......................................................391Michael A. Cassidy, Esq. Legal Summary: Beth Anne Jackson, Esq. .............61, 256, 352Letter to the Editor.....................................282MMateria Medica:Innovations in postmenopausal osteoporosis: Romosozumab (Evenity®)............................222Karen M. Fancher, PharmD, BCOPIstradefylline (Nourianz®)................. ..........254Samantha DeMarco, PharmD Rachael Cardinal, PharmD, BCPS
TauvidTM (flortaucipir F 18 injection: The first FDA-approved imaging drug for detecing tau in patients with suspected Alzheimer’s Disease.....283Kelly Slipak, PharmDAssisting statins: Current roles of non-statin therapies and upcoming agents...................313Erin L. Cole Kristina Jacoway Matthew C. Davis Rebecca Schoen, PharmD, BCACP Esketamine nasal spray (Spravato®)...........350Nolan R. Schmitz, PharmD Kevin Wissman, PharmDA potential spin on pain control: A review of IV acetaminophen.............................................383Marissa Rees, PharmDPitolisant (WAKIX®).....................................388Cassidy Williams, PharmD, Sehrish Panjwani, PharmD, BCPSMembership Benefits:.......212, 244, 276, 308, 344, 384Miller Time:A Viral Ode...................................................335 Scott Miller, MD, MA, FAAHPMN, O, PPerspective:COVID-19 masquerade...............................215Wendy Palastro, MDTelepsychiatry appointment adherence and productivity during COVID-19............. . . ......246Timothy Lesaca, MD Pamela Pyle, AASReflections after 52 years..........................249Richard L. Green, MD Pandemicology: Lessons learned (or not)....305Bruce L. Wilder, MD, MPH, JD OPTIMISM ... did you lose it?.....................310Jorge Lindenbaum, MDThe Donora Smog....................................340Kristen Ann Ehrenberger, MDReflections on physician wellness and the challenges of COVID.......................342Lawrence R. John, MDReducing disparities in musculoskeletal care: Focusing on bone and joint health...............376 Anthony M. DiGioia III, MD Gina Edwards
The Bulletin depends on its advertisers. Be sure to tell them you saw their ad here.
ACMS members: We want to hear your
opinions on important topics a�ecting healthcare. Email [email protected]
to learn more about submitting a Perspective column to the Bulletin.
ACMS Bulletin 2021 Copy DeadlinesIssue DeadlineFebruary 2021 Monday, Jan. 11March 2021 Monday, Feb. 15April 2021 Monday, March 15May 2021 Monday, April 12June 2021 Monday, May 10July 2021 Monday, June 14August 2021 Monday, July 12September 2021 Monday, Aug. 16October 2021 Monday, Sept. 13November 2021 Monday, Oct. 11December 2021 Monday, Nov. 15January 2022 Monday, Dec. 13
403ACMS Bulletin / December 2020
PerspectivePerspectiveAdvertising Index
2020 Bulletin Advertising Index: July-DecemberAccountingKline Keppel & Koryak PC (412) 281-1901
Billing/Claims/CollectionsFenner Consulting (412) 788-8007ClinicalAllegheny Health Network (724) 933-1445 Encompass Health(877) 937-7342
ComplianceHIPAA One (801) 770-1199Financial InstitutionsPNC Bank (800) PNC-7908
InsuranceLiberty Mutual (412) 334-1480
LegalHouston Harbaugh PC (412) 281-5060Tucker Arensberg PC (412) 566-1212
MiscellaneousUPMC Health Services Division (412) 514-0120
Real Estate/DevelopmentBerkshire Hathaway: Julie Wolff Rost (412) 521-5500
Angela DeVanney Gigi CrowleyA physician’s reflection on Roberto Clemente and his leadership legacy.............................378Johanna Vidal-Phelan, MD, MBA, FAAPQ, RReportable Diseases.............93, 191, 290, 360SSociety News .....218, 251, 278, 310, 346, 380Special Report:Pilot of new perinatal Hepatitis C Surveillance Program coming to Allegheny County..........257Rachael Bieltz, MPH, CHES Bethany (Hallam) Reynolds, MPH Nominating Committee report......................3222020 House of Delegates report..................358New program brings a fresh approach to supporting parents....................................361Nakia GranbergAn adventure in understanding: A history of the C.F. Reynolds Medical History Society.........394Kristen Ann Ehrenberger, MD PhDACMS Election report...................................396
Editorial Index
Allegheny County Medical Society • www.acms.org

Adding more specialized care for your patients.When your patients need the best possible
specialty care, AHN has physicians with
the right expertise — like our new
plastic surgeon.
Dr. Moreira o�ers some of the most advanced
treatments and techniques, so your patients
can have the best possible outcomes.
To refer your patient, call1-844-MD-REFER (1-844-637-3337).Most major insurance plans are accepted.
Andrea Moreira, MDAHN Plastic Surgery
Co-Director, AHN Reconstructive Breast Surgery
Locations:Allegheny General Hospital
West Penn Hospital
Wexford Health + Wellness Pavilion
Specialties:Breast reconstruction and microsurgery
Liposuction, fat grafting, and cosmetic surgery
MX145129 • ACMS December 2020 Bulletin• 11/20 • 7.5”w x 9.75”h