Embed Size (px)
Citation preview


Local Application of Heat and Cold
• Applied for short periods to produce desired results (15 to 30 minutes)– Repeat at intervals specified by physician– Prolonged application not recommended:
• Results in adverse secondary effectsResults in adverse secondary effects

• Patient’s heat/cold receptors adjust to changes in temperature
– Results in decreased heat/cold sensation
– Temperature actually remains the same• Still provides therapeutic effects

Factors Affecting the Application of Heat and Cold
• Age of the patient: young children and elderly patients more sensitive to heat and cold

Location of the application
• certain areas of the body more sensitive
– Chest, back, and abdomen
– Broken skin USE CAUTION

Factors Affecting the Application of Heat and Cold
• Impaired circulation: patients are more sensitive to heat and cold
Peripheral vascular disease
Diabetes
Congestive heart failure

• Impaired sensation: these patients must be watched carefully– Tissue damage may occur without the patient's
awareness• Example: diabetic patient
• Individual tolerance to change in temperature: some patients cannot tolerate temperature change as easily as others

Application of Heat and Cold• Observe application area: before, during, and
after treatment– Look for signs indicating that a modification of
temperature needed:• Erythema• Paleness• Pain• Swelling• Blisters
– Ask patient how application feels

PALLOR
ER
YT
HE
MA
BLISTERING/CELLULITISSWELLING

Local Effects of Heat• Local Effects of Heat (15 to 30 minutes)
– Dilation of blood vessels at the site of the application
• Blood vessels increase in diameter• Results in increased blood supply to area:
– Tissue metabolism increases– Nutrients and oxygen provided to cells at faster rate– Waste and toxins carried away faster


– These changes promote healing– Skin in area becomes warm and exhibits
erythema
• Erythema: reddening of the skin caused by dilation of superficial blood vessels

Local Effects of Heat
– Prolonged application (>1 hour) produces secondary effects that reverse healing process
• Blood vessels constrict• Blood supply to the area decreases
– Apply heat for proper length of time ordered by physician

Purpose of Applying Heat
– Relieves:• Pain• Congestion• Muscle spasms• Inflammation

Heat often prescribed for
• Low back pain
• Arthritis
• Menstrual cramps

Heat Works by:
– Promoting muscle relaxation• Relieves pain caused by excessive contraction of
muscle fibers (muscle spasms)
– Decreasing edema• Edema: The retention of fluid in the tissues,
resulting in swelling -Increased blood supply: increases absorption of
fluid from tissues

– Softening exudates (using moist compress)• Exudate: discharge produced by the body's
tissues–Exudate may form a hard crust and require
removal
– Increasing suppuration• Suppuration: process of pus formation
–Helps in the relief of inflammation by breaking down infected tissue

Heat- Not recommended for
•Acute inflammation
•Trauma

Hot Compress
• Soft, moist absorbent cloth - Immersed in a warm solution - Applied to a body part


Cold
• Local Effects of Cold (15 to 30 minutes)– Constriction of blood vessels
• Results in decreased blood supply to area– Tissue metabolism decreases– Less oxygen used– Fewer wastes
accumulate
•Skin in area becomes cool and pale


– Prolonged application (>1 hour) produces reverse secondary effects•Blood vessels dilate• Increase in tissue metabolism
– Apply cold for proper length of time ordered by physician

Purpose of Applying Cold
– Prevents edema if applied immediately after patient has suffered direct trauma:
– Relieves discomfort

• Bruise
• Minor burn
• Joint injury
• Fracture
• Sprain: trauma to a joint that causes injury to the ligaments
• Strain: an overstretching of a muscle caused by trauma

– Limits accumulation of fluid in tissues by:• Constricting blood vessels• Reducing leakage of fluid into tissues
– Controls bleeding: by constricting peripheral blood vessels

– Relieves pain: due to numbing effect• Reduces stimulation of pain receptors
– Reduces inflammation:
– decreases suppuration in early stages of infection by inhibiting activity of microorganisms

•Always place cold application in a protective covering
• Applying cold directly to skin
–Could result in a skin burn

-Prevent swelling -Control bleeding -Relieve pain -Relieve inflammation


Casts
• Stiff cylindrical synthetic or plaster casing
–Used to immobilize a body part• Purpose of applying a cast
– Immobilize a fracture: most frequent use• Keeps fractured bones aligned until proper
healing takes place

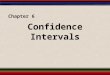
Fracture of TibiaFracture of Tibia
From McRae R, Esser M: Practical fracture treatment, ed 4, Philadelphia, 2002, Churchill Livingstone.From McRae R, Esser M: Practical fracture treatment, ed 4, Philadelphia, 2002, Churchill Livingstone.

Casts
– Support and stabilize weak or dislocated joints
– Promote healing after surgical correction– Nonsurgical correction of deformities
(congenital dislocation of hip)
• Casts are applied by an orthopedist

Pressure area: occurs when cast presses or rubs against patient's skin– Most apt to occur over bony prominence– Prevents adequate circulation to area– Causes painful rubbing, burning, or stinging
sensation under cast
– If permitted to continue: pressure ulcer can develop

Pressure ulcer: skin breaks down
– Begins with a red patch of skin– Erodes into subcutaneous tissue– Eventually erodes into muscle and bone– Deep pressure ulcers often become
infected by microorganisms• Develop gangrene
Important to detect pressure area early
• Prompt treatment: to prevent serious complications



Cast Application
– Apply the cast padding• Soft cotton material• Available in widths of 2 to 4 inches
• Purpose– Prevents pressure
areas– Shields patient’s
skin
when cast is removed
Courtesy 3M Health Care, St. Paul, Minn

Cast Application
• 2 to 3 layers applied over stockinette using spiral turn
– Each turn: overlaps by one-half width of roll
• Extra layers applied over bony prominences
–To prevent pressure areas
Courtesy 3M Health Care, St. Paul, Minn

– Apply the cast bandage or tape•Applied over cast padding•Number of rolls depends on desired
strength of cast–Synthetic cast: usually 3 to 5 layers–Plaster cast: usually 4 to 6 layers

Cast Application
•Cast must be completely dry–Becomes hard and inflexible–Is then able to bear weight
•Supportive device usually prescribed (e.g., sling, crutches)–Prevents strain–Minimizes swelling

Cast Application
– Instruct patient that warmth may be felt during application
• Usually has a soothing effect
– Instruct patient not to put weight on cast until dry (24 hours)
• Wet cast may break down

Cast Application Precautions,
– Take precautions to prevent indentions: can cause pressure areas
•Indentations may be caused by:–Cast coming in contact with hard surfaces while drying
–Handling wet cast with palm of hands (rather than fingertips)

• Plaster Cast and Synthetic Cast:– Remove excess casting particles
• If not removed: can get under cast: causes irritation and infection
– Plaster cast: remove plaster crumbs from skin with damp, warm cloth
– Synthetic cast: remove synthetic material with alcohol swab or acetone

– Physician makes sure cast is not too tight by checking:•Circulation•Sensation•Movement of extremity
– Physician makes sure joints excluded from cast are free to move

Guidelines for Cast Care
• YOU are responsible for explaining cast care to patient
• Often presented on an instruction sheet– Signed by patient– Copy filed in patient's chart

Cast Care Guidelines
• Wait before putting pressure or weight on a cast– Plaster cast: wait 24 hours
• Allows plaster to dry completely• Prevents cast from breaking down
– Synthetic cast: can bear weight 30 minutes to 1 hour after application

• Elevate cast above heart level for 24 to 48 hours:– Prop up on pillows– Decreases swelling and pain

• Gently move toes or fingers frequently– Prevents swelling and joint stiffness
• Ice can be applied to casted extremity: reduces swelling– Ice chips in ice bag: loosely wrapped around
cast at injury site
• Prevent foreign particles from being trapped under cast (dirt, sand, powder)– Can irritate skin and lead to infection

• Do not use any object to scratch skin under cast (e.g., coat hanger, pencil)
– May cause break in skin• Could become infected
– Object could be lost in cast
• Do not engage in activities that could cause injury due to physical disability (e.g., driving a car)

•Keep cast dry– Bath or shower: cover with plastic bag and
secure with tape– Hang limb over side of tub or outside shower– Wet plaster cast: loses shape and may break
down– Synthetic cast
• Outside of cast is moisture resistant, but cast padding is not
• If becomes wet: dry ASAP to prevent maceration
–Maceration: softening and breaking down of the skin, which can lead to infection

• To dry a wet cast:– Blot outside with towel– Blow dry on low setting (high setting can
burn skin) NOT DURING INTIAL CAST APPLICATION
– Use a sweeping motion until completely dry
• Inspect skin around cast at regular intervals for:– Redness– Sores– Swelling

• Do not trim cast or break off rough edges: may weaken or break cast– If rough edge occurs: file with emery board– Notify physician if cast becomes:
• Loose• Broken• Cracked
• Synthetic casts: can be signed with permanent markers

Report immediately
Increased swelling or pain that does not go away with meds, elevation, or rest– Tingling or numbness of fingers or toes– Coldness, paleness, or blueness of fingers or
toes
– May indicate cast is too
tight or infection is developing

– Painful rubbing, burning, or stinging under cast– Foul odor or drainage coming from cast– Sore areas around edge of cast– Chills, fever, nausea, or vomiting

Cast Removal
• Bivalve cast: cut cast in half
• Entire length of cast cut on two opposite sides: down to level of cast padding
• Cast cutter: electric hand-held saw with a circular blade that oscillates (saw vibrates but does not rotate)

Cast Removal
• Reassure patient: saw is noisy but only a tickling sensation and some heat will be felt
• Cast pried apart with cast spreader

•Bandage scissors: used to cut through cast padding and stockinette

Cast is removed
– Skin: typically appears yellow and scaly– Extremity: thinner with flabby muscles
• Explain to patient: is normal and results from lack of use
• Physician may recommend exercises and physical therapy– To regain strength and function

Splints and Braces
•Splint– Rigid removable device used to:
• Support and immobilize displaced or fractured part of the body
• Protect areas that are sprained or strained

SplintSplint
COCKUP SPLINT

Splints and Braces
– Molded to fit specific part of the body– Well padded: provides comfort and
prevents pressure areas– Can be made by orthopedist or commercially
available

Splints and Braces
– May be applied initially to fracture• Can be adjusted to accommodate swelling• After swelling subsides: cast is usually applied
– When fracture is almost healed• Cast may be removed• Another splint applied -Allows for bathing of extremity -Easy removal for therapy
– After fracture heals completely: splint no longer needed

Brace:
– Supports a part of the body and holds in correct position
• Allow for functioning of body part while healing takes place

Splints and Braces
– Short leg walker: rigid frame with removable padded liner
• Type of brace aka- CAM WALKER• Used (instead of a cast) to heal a stable fracture of
lower leg– Example: stress fracture
• Extends from just below knee to toes• Permits walking and standing, which encourage
healing• Can be removed to permit bathing of leg

Short Leg Walker/ Cam WalkerShort Leg Walker/ Cam Walker

Ambulatory Aids
• Used by individuals who require aid in ambulation– Ambulation: walking or moving from one place to
another
– Ambulatory: Able to walk as opposed to being confined to a wheelchair or a bed

Ambulatory Aids
• Includes:– Crutches– Canes– Walkers

Ambulatory Aids
• Device used depends on:– Type and severity of
disability– Amount of support required– Patient's age and degree of
muscular coordination

Ambulatory Aids
• May be prescribed for:– Temporary condition:
• Fracture• Sprain to lower extremity• Disability following orthopedic surgery

Crutches
• Artificial support made of wood or aluminum
• Provide assistance in walking for patients with problems of lower extremities:– Disease– Injury– Birth defects
• Remove weight from legs and transfer it to arms

Crutches
• Axillary crutch: used most frequently– Consists of shoulder rest and handgrips– Extends from ground almost to patient's axilla– Rubber tips prevent crutches from slipping on
the floor– Made of wood or tubular aluminum

Axillary CrutchAxillary Crutch

Crutches, cont.
• Forearm crutch (Lofstrand)– Tube of aluminum that extends to forearm– Metal cuff attached to crutch: fits around
forearm– Handgrip extends from crutch for weight
bearing– Advantage: individual can release handgrip
• Enables use of hand; metal cuff holds crutch in place
– Used by patients who are paraplegic or have cerebral palsy

Forearm CrutchForearm Crutch

Axillary Crutch Measurement
• Purpose– To ensure correct crutch length– Proper placement of handgrip

Axillary Crutch Measurement,
• Crutches that are too long– Shoulder rest exerts pressure on axilla
•Can injure radial nerve leading to crutch palsy:–Crutch palsy: muscular weakness in the forearm, wrist, and hand
– Forces patient's shoulders forward• Prevents patient from pushing body off ground

NO NO NO !!!! YES YES YES!!!

Axillary Crutch Measurement
• Crutches that are too short– Patient is bent over and uncomfortable– Crutches are awkward to use

Axillary Crutch Measurement
• Handgrips that are too low– Pressure exerted on axilla
• Handgrips that are too high– Crutches are awkward to use

Axillary Crutch Measurement, cont.
• Wooden crutches: bolts and wing nuts used to adjust– Adjusted with bolts and wing nuts
• Aluminum crutches: spring-loaded push buttons used to adjust– Adjusted with spring-loaded push buttons on
an inner tube• Pop into holes on an outer tube

Crutch Guidelines
• MA is responsible for instructing patient of the following:– Wear well-fitting shoes with nonskid soles
• Provide good traction• Provides stability

Use correct posture to:
• Prevent strain on muscles and joints• Maintain balance
– Support weight with hands on the handgrips
• Axillary pads should press against side of rib cage
• Do not support weight on axilla: may cause crutch palsy

• Look ahead when walking rather than down at feet– Be aware of the surface walking on
• Should be clean, flat, and dry• Remove throw rugs and obstacles to prevents falls
– Keep crutches 4 to 6 inches out from the side of feet
• Prevents obstruction of pathway for feet

Crutch Guidelines
– Take steps by:• Moving crutches forward a safe and comfortable
distance (6 inches)• Take small steps when first learning• Do not move forward more than 12 to 15 inches
with each step– Greater distance: crutches could slide
»Patient could lose balance

Crutch Guidelines
– Report tingling or numbness in the upper body
• May be using crutches incorrectly• Crutches may be wrong size

Crutch Guidelines
– Extra padding can be added to the shoulder rests for more comfort
• Make sure padding does not press against axilla• Handgrips can also be padded
– Keep crutch tips dry• Prevents slipping

Crutch Gaits
• Type of gait used depends on:– Amount of weight patient able to support– Patient's physical condition– Patient's muscular coordination

Crutch Guidelines
• Patient should learn a fast and a slow gait– Fast gait: for speed in open areas– Slow gait: for crowded areas
• More than one gait reduces patient's fatigue (different combination of muscles used for each)

Crutch Gaits, cont.
• Four-Point Gait– Very basic and slow gait– Patient must be able to bear considerable
weight on both legs– Most stable and safest gait– Used by patients with:
• Leg muscle weakness or spasticity• Poor muscular coordination or balance• Degenerative leg joint disease

Crutch Gaits, cont.
• Two-Point Gait– Similar to, but faster than four-point gait– Only two points support body at one time– Patient must have partial weight bearing on
each foot– Patient must have good muscular
coordination

Crutch Guidelines
• Three-Point Gait– Patients who cannot bear weight on one
leg– Patient must be able to support full weight
on unaffected leg
– Patient must have good muscular coordination and arm strength

Crutch Guidelines, cont.
– Used by patients:• Who are amputees without a prosthesis• With musculoskeletal or soft tissue trauma to a
lower extremity– Fracture– Sprain
• With acute leg inflammation• With recent leg surgery

Crutch Gaits, cont.
• Swing Gaits– Includes:
• Swing-to • Swing-through
– Used by patients:• With severe lower extremity disabilities
– Example: paralysis
• Who wear leg braces

STAIR WALKING
• GOING UP-GOING UP-• Place strong leg on first step
• Pull weak leg up to step and move crutches up to first step
• repeat

Going Down Stairs
• Place weight on strong leg
• Move crutches down to next lower step
• Place partial weight on hands on crutches
• Move weak leg down to the step with crutches
• Move strong leg to same step as weak leg and crutches
• Lather rinse repeat

Memory booster…
•Good angels go to heaven
•Bad devils go to……

Now, for the final 5 Now, for the final 5

Canes
• Lightweight, easily moveable device
• Made of wood or aluminum with a rubber tip(s)
• Provides balance
and support
Courtesy 3M Health Care, St. Paul, Minn.

Canes.
• Used by patients who have weakness on one side of body– Hemiparesis– Joint disabilities– Defects of neuromuscular system

Canes
• Types of canes– Standard cane: provide least amount of support
• Used by patients who require only slight assistance
– Tripod and quad canes: three or four legs• Easier to hold and provide greater stability• Cane can stand alone; frees patient's arms when getting
up• Disadvantage: bulkier and more difficult to move

Courtesy of 3M Health Care, St. Paul, MN.

Canes
• Hold cane on side of body opposite to the side that needs support
• Properly adjust cane length– Cane handle should be level with greater
trochanter– Elbow flexed at 25- to 30-degree angle
• Instruct patient to stand erect and not lean on cane– Ensures good balance

Walkers
• Aluminum frame with handgrips and four widely placed legs; open on one side
• Lightweight and easily movable

Walkers
• Should extend from the ground to the level of patient's hip joint
• Used by patients who need more help with balance and walking than can be provided by crutches or cane:– Geriatric patients with weakness or
balance problems– During healing process for knee or hip joint
replacement surgery

Walkers
• Provides the greatest amount of stability
• Disadvantages– Slow pace– Difficulty maneuvering
in small room


• Typically used for fx fingers and toes
• prevents movement of the injured finger during the healing stage of rehabilitation.

What is Required?
• 2.5 cm (1 inch) non stretch white tape.
• for small fingers a narrower tape can be used or the tape can be torn along it's length to make thinner strips.
• thin strip of padding foam to place between the fingers for comfort and protection.

Step 1
• Apply two strips of 1.25 cm (half inch) white non stretch tape - one above the injured joint and one below.
• These will provide an anchor from which to attach the supporting strips.

Step 2
• Place the strip of padded foam between the fingers to be taped.

Step 3
• Apply two supporting strips from the two anchors above and below the joint around the 'buddy' finger.
• This taping should allow the fingers to bend together but sideways movement should be limited.



• Used for sprains• Compression reduces swelling.
• Reduced swelling, greatly minimizes amount of time required to heal sprains.

Ankle wraps
• Loop the bandage around the ball of the foot twice. pull on the end lightly to make sure there's tension.
• Don't wrap it too tightly or you can risk constraining blood circulation.
• Hold the bandage up vertically.• wrap it around the foot twice diagonally creating a
criss-cross (figure 8) pattern until you reach the ankle.
• Wrap the ankle until completely bandaged. Remember that compression is the goal. Make sure that the ankle is sufficiently covered and supported.
• Tuck the end of the wrap in a part of the bandage • Secure with fasteners

• cover the entire ankle and foot except the toes and the heel.
• wrap should reach about four inches to the calf.
• Make sure that the bandage is neither too loose or too tight.
• Remove at bedtime



Things You'll Need:
• 2- 3 inch elastic compression bandage
• 2 metal clasps

Turn the injured wrist over so that the palm is facing you.
Place one end of the 2-inch elastic bandage underneath the wrist approximately 1 inch below the wrist joint
Wrap the bandage twice around the wrist. The piece of the bandage should now be in the same place where you first started the wrap.

• Pull the bandage up and across the open face of the palm.
• Pull through the space between your thumb and forefinger and down the backside of your hand back to your wrist
• Wrap the bandage once around the wrist. Stagger the bandage so it does not line up exactly with the previous wrap.
• Approximately one-third of the previous wrap should show.

• Draw the bandage up and across the open palm and down the backside to the wrist once.
• Stagger the bandage so it does not line up exactly with the previous wrap.
• Wrap along the wrist until you have come to the end of the bandage. Stagger the bandage so that you overlap two-thirds of the previous wrap.
• Fasten using the two metal clasps.• Be sure to hold the end firmly in place so that the
entire wrap does not loosen






















![7KH 6PDUW $] DQ &ORFN · "Set intervals for Azkar" is heard. One of the following intervals (15-30-45-00) is selected by pressing (+) or (-) Press ( ) to browse and select the desired](https://img.pdfslide.net/doc/110x75/61238a8139d0a36fc1314892/7kh-6pduw-dq-set-intervals-for-azkar-is-heard-one-of-the-following.jpg)