Embed Size (px)
Citation preview

BRIEF COMMUNICATIONS
Several kindreds have been described with presenile au- tosomal dominant frontotemporal dementia that maps to chromosome 17q2 1 [ 1 - 41. Similarities in clinical and pathological manifestations, in addition to consis- tent linkage to chromosome 17q21, has led to the sug- gestion that the disease in each family is caused by mu- tations in the same gene [2-51. The disease in these kindreds was recently named frontotemporal dementia with parkinsonism linked to chromosome 17 (FTDP-
We studied an Australian family with autosomal dominant nonspecific dementia [6] in which 28 af- fected cases (16 men, 12 women) have been identified. The age of onset was 39 to 66 years (mean, 53 2 8.9 years) and the age at death was 49 to 72 years (mean, 62 years). Disease duration ranged from 4 to 15 years. Clinical symptoms included early personality change, most frequently manifested as disinhibition, although 1 case became “depressed and withdrawn.” Parkinsonism was observed in 1 patient. Early in the disease course, memory was relatively preserved, although loss of exec- utive functions was apparent; in the latter stages pa- tients became progressively demented with deteriora- tion of memory and speech. At autopsy, all 4 cases examined displayed neuronal loss, gray matter gliosis, and neuropil vacuolation in both frontal and temporal lobes. Balloon neurons were present in the cortex, and degeneration of the substantia nigra zona compacta was observed with neuronal loss, gliosis, and free melanin. a-Crystallin and tau immunostaining was apparent in balloon neurons and in some small neurons. Specific lesions associated with Alzheimer’s disease, L e y body disease, and Picks disease were absent.
We examined this kindred for linkage to chromo- some 17q, the results of which demonstrate that this is another example of a frontotemporal dementia linked to this region. Sequence analysis of five candidate genes in the critical region (D 17S800 -D 1 7S79 1) for FTDP-17 was performed to examine each gene for pathogenic mutations.
17) [51.
Localization of Frontotemporal Dementia with Parkinsonism in an Australian Kindred to Chromosome 17q2 1-22 Matt Baker, BSc,* John B. J. Kwok, PhD,I. Steve Kucera, PhD,$ Richard Crook, BSc,* Matthew Farrer, PhD,* Henry Houlden, MD,* Adrian Isaacs,* Sarah Lincoln, BSc,* Luisa Onstead, BSc,* John Hardy, PhD,* Leonie Wittenber
Nick Hayward, PhD)’ Tony Tannenberg, MB, BS, FRCPA,S Athena Andreadis, PhD,“ Marianne Hallupp, BSc,t Peter Schofield, PhD,? Frances Dark, MD,** and Michael Hutton, PhD*
BSc,§ Peter Dodd, PhD,$ Sonja Webb, BSc, 5/
An Australian family with autosomal dominant presenile nonspecific dementia was recently described. The disease results in behavioral changes, usually disinhibition, fol- lowed by the onset of dementia accompanied occasionally by parkinsonism. Twenty-eight affected individuals were identified with an age of onset of 39 to 66 years (mean, 53 f 8.9 years). We mapped the disease locus to an ap- proximately 26-cM region of chromosome 17q21-22 with a maximum two-point LOD score of 2.87. Affected individuals share a common haplotype between markers D17S783 and D17S808. This region of chromosome 17 contains the loci for several neurodegenerative diseases that lack distinctive pathological features, suggesting that these dementias, collectively referred to as frontotemporal dementia with parkinsonism linked to chromosome 17 (FTDP-17), are caused by mutations in the same gene. The entire coding region of five genes, mapped to the FTDP-17 candidate region, were also sequenced. This analysis included the microtubule-associated protein tau that is the major component of the paired helical fila- ments observed in Alzheimer’s disease. No pathogenic mutations were identified in either the tau gene or in any of the other genes analyzed.
Baker M, Kwok JBJ, Kucera S, Crook R, Farrer M, Houlden H , Isaacs A, Lincoln S, Onstead L, Hardy J,
Wittenberg L, Dodd P, Webb S, Hayward N, Tannenberg T, Andreadis A, Hallupp M, Schofield P,
Dark F, Hutton M. Localization of frontotemporal dementia with parkinsonism in an Australian kindred to chromosome 17q21-22. Ann Neurol 1997;42:794-798
~ ~ ~ ~ ~~ ~ ~ ~~
From the *Mayo Clinic Jacksonville, Jacksonville; and *University of Tampa, Tampa, FI.; ?Garvan Institute of Medical Research, Syd- ney; SCRC, Royal Brisbane Hospital Research Foundation, and SDepartment of Anatomical Pathology, Mater Misericordiae Hospi- tal, Brisbane; “Human Genetics Laboratory, Queensland Institiice of Medical Research, Herston, and **Department of Psychiatry, Prin- cess Alexandra Hospital, Woolloongaba, Australia; and ”Department of Biomedical Sciences, E. K. Shriver Center, Waltham, and
Materials and Methods Family Ascertainment Thirty-three family members from the 4th (17) and 5th (16) generations (see Fig) were evaluated by F.D. Standardized clinical information was obtained by using the Cambridge Mental Disorders of the Elderly Examination (CAMDEX),
~
794 Copyright 0 1997 by the American Neurological Association
Departments of Neurology, Massachusetts General Hospital and Harvard Medical School, Boston, MA.
Received Mar 26, 1997, and in revised form Apr 25 and May 15. Accepted for publication May 17, 1997.
Address correspondence to Dr Hutton, Birdsall Building, Mayo Clinic Jacksonville, 4500 San Pablo Road, Jacksonville, FL 32224.

the National Adult Reading Test (NART), and vocabulary and digit subscales of the Wechsler Adult Intelligence Scale, revised edition (WAIS-R). Blood was drawn for DNA extrac- tion and establishment of lymphoblastoid cell lines. Genetic analysis was performed on samples from 4 patients with de- mentia and 8 unaffected individuals.
Genotype Analysis Microsatellite repeat polymorphisms from chromosome 3pl l -ql1 and chromosome 17q21-22 were amplified from patient genomic DNA. Polymerase chain reaction (PCR) was performed with one unlabeled primer and one primer 5‘ end-labeled with fluorescein using standard conditions. Prod- ucts were analyzed on A.L.F. automated sequencers running fragment manager software version 1.1 (Pharmacia). Apoli- poprotein E (ApoE) genoryping was performed by using PCR-restriction fragment length polymorphism (PCR- RFLP) analysis with primers and restriction enzymes de- scribed by Crook and colleagues [7].
Linkage Analysis Painvise LOD scores were calculated using FASTLINK and LINK version 5.1. The dementia was assumed autosomal dominant with 95% penetrance at age 65. Three liability classes were assigned (<45 years, 0.01; 45-65 years, 0.5; >65 years, 0.95). Analysis was also performed using a low- penetrance model with liability set at 1% for all ages. Gene frequency was set at 0.0001. Marker allele frequencies were from the Genome Database. Simulations were performed us- ing SIMLINK, version 4.12, the disease was treated as a di- chotomous trait, and “affecteds-only” analysis was per- formed. Allele frequency for disease was set at 0.0001, marker frequencies were set at 0.25, and 500 replicates were performed. The estimated mean maximum LOD scores for both linked and unlinked markers were calculated (at 8 = 0 - 0.4).
Candidate Gene Sequencing Exonic and flanking intron sequences were used to design primers to amplify the coding regions of genes, ie, tau [8], VAT-1 [9], and exons 4 to 12 of DLG-2 [lo] from family genomic D N A . The coding regions of VHR [ 1 I], y-tubulin [12], and exons 1 to 3 of DLG-2 [lo] were amplified from cDNA from lymphoblastoid lines. Specific primers and con- ditions for each PCR are available from the authors. Se- quencing of PCR products was performed manually, using [y-33PP]ATP-labeled primers and the fmol Cycle sequencing system (Promega), or on A.L.F. automated sequencers (Phar- macia), using fluorescein-tagged primers and the Thermose- quenase cycle sequencing kit (Amersham). Each gene was se- quenced in 2 affected family members on both strands. DLG-2, VAT-1, and VHR were also sequenced in an unaf- fected member who did not share the disease haplotype.
Allele frequencies of polymorphisms were determined by PCR-RFLP analysis in about 50 unrelated controls.
Results Linkage Analysis DNA samples were analyzed from 4 affected individu- als, with ages of onset of 49 to 58 years (mean, 51.5 -t-
4.9 years), and from 8 unaffecteds. Although only four samples from affected individuals were available, there was no evidence of association between particular ApoE genotypes and age of onset (data not shown).
Linkage studies focused on chromosome 3pl1-3ql1 and chromosome 17q21-22 for which loci for FTDP had been reported [l-4, 131. Negative LOD scores and haplotype nonsegregation were observed between chromosome 3 markers (D3S1595,Z = -4.90 at 0 = 0; and D3S1603, Z = -4.32 at 8 = 0) and disease. However, positive LOD scores were obtained with markers on chromosome 175. Twenty-three markers from chromosome 17q12-22 were typed; LOD scores are shown in the Table (Z,,,, = 2.87 at D17S250 with 8 = 0). LOD scores were calculated by using both age- adjusted and low-penetrance models. Low-penetrance analysis was used due to the variable age-dependent penetrance reported in FTDP-17 families [3, 51.
Simulations predict the mean maximum LOD score (ELOD) for a linked marker in this kindred would be 1.357 ? 0.036, Emax 3.057 (at 8 = 0). For unlinked markers, SIMLINK predicted an ELOD of -1.749 ?
LOD score of greater than 2.5 for an unlinked marker was predicted, with p < 0.001. The peak LOD score (Zma = 2.87) obtained with affected only analysis in the Australian family is thus predicted to be highly sug- gestive of linkage by SIMLINK calculations.
Haplotype analysis (Fig) revealed that all affecteds share a common allele for markers benveen D17S783 and D17S808, indicating that the disease locus lies in this interval, a distance of approximately 26 cM.
One unaffected individual (IV.10) who is currently above the age of onset range (39-66 years) also shares the affected haplotype (see Fig). This individual may subsequently develop FTDP- 17; however, incomplete penetrance of the disease mutation, in this family, is also possible. Elderly unaffected individuals with af- fected haplotypes were also observed in a Dutch family (HFTDIII) [3] and in a large American family (HDDD2, Corinne Lendon personal communication) with chromosome 17-linked dementia.
0.067, (e = o.oi), E,~, = -4.884, E,, = 2.141. A
Candidate Gene Analysis MICROTUBULE-BINDING PROTEIN TAU. The micro- tubule-binding protein tau is the major component of neurofibrillary tangles found in the brains of Alz- heimer’s patients. Tau-positive neuronal and glial in- clusions have also been reported in families with FTDP-17 [l, 2, 51. The localization of tau to 17q21 [ 141, therefore, identified tau as a strong candidate gene.
No sequence variants were detected in the tau cod- ing region in affected family members. However, our analysis does not exclude the possibility that a muta- tion within intronic sequences that affects splicing may
Brief Communication: Baker et al: Localization of FTDP 795

Table. Two-Point LOD Scores Between Disease and Chromosome 17 Markers
Recombination Fraction
Marker 0 = 0 0 = 0.1 e = 0.2 0 = 0.3 0 = 0.4
Age adjusted 783 798 250 579 951 950 79 1 Thral 920 PYg 93 1 806 958 943 94 1 787 808 795
Low penetrance 783 798 250 579 95 1 950 79 1 Thral 920 PYg 93 1 806 958 943 94 1 787 808 795
-4.110 -0.049
2.415 0.800 0.024 1.716 2.064 2.200 0.801 1.293
-0.023 0.760 2.188 1.065
-0.647 0.531
- 1.654 -3.472
-2.802 0.647 2.865 1.216 0.896 2.177 2.816 2.075 0.989 1.671 0.528 1.365 2.605 1.490
-0.214 0.963
- 1.028 -2.81
-0.939 0.204 2.217 0.744 0.174 1.572 1.816 1.740 0.543 0.965 0.197 0.766 1.985 1.041
-0.271 0.741 1.003
-1.011
-0.527 0.476 2.323 0.819 0.581 1.690 2.259 1.583 0.669 1.232 0.344 0.953 2.052 1.121
-0.124 0.858 0.974
-0.874
-0.402 0.213 1.729 0.476 0.121 1.167 1.398 1.234 0.3 14 0.648 0.160 0.546 1.500 0.757
-0.165 0.587 0.812
-0.446
-0.228 0.323 1.731 0.460 0.322 1.178 1.660 I .089 0.388 0.815 0.182 0.562 1.465 0.743
-0.107 0.608 0.776
-0.373
-0.149 0.159 1.124 0.213 0.058 0.690 0.890 0.724 0.135 0.362 0.082 0.289 0.920 0.423
-0.106 0.328 0.497
-0.184
-0.092 0.196 1.094 0.184 0.141 0.667 1.028 0.618 0.171 0.447 0.067 0.24 1 0.862 0.395
-0.082 0.3 18 0.469
-0.152
-0.036 0.084 0.485 0.049 0.021 0.250 0.374 0.278 0.304 0.139 0.023 0.084 0.350 0.147
-0.051 0.096 0.200
-0.057
-0.027 0.090 0.460 0.036 0.042 0.232 0.423 0.231 0.042 0.167 0.121 0.053 0.317 0.137
-0.044 0.087 0.187
-0.047
LOD scores were calculated by using both an age-adjusted and a low-penetrance analysis. Only markers (18 of 23) that were informative for linkage (LOD score > +0.5 or < -0.5), in either analysis, were included.
be pathogenic. Indeed tau proteins generated from al- ternate splice variants form paired helical filaments (PHFs) with different efficiencies in vitro [15]. This suggests that aberrant splicing of the tau gene is a pos- sible mechanism in the pathogenesis of neurodegenera- tive disease.
hDLG-2 (DISKS-LARGE GENE-2). The DLG-2 gene is a member of the disks-large family of proteins [16] that include Drosophila dlg-A, the lin-2A and lin-2B C. el- egans vulva1 induction proteins, and the PSD95 rat synaptic proteins.
Sequence analysis of DLG-2 exons 1 to 3, amplified from lymphoblast cDNA, revealed that most tran-
scripts lacked exon 2 [lo]. Similar results were also ob- tained from cDNA derived from several different tis- sues (brain, lung, heart, and skeletal muscle) from an unrelated individual (Clontech). This indicates the presence of possible alternate splicing in this gene.
Two additional sequence variants were identified in family DNAs in the DLG-2 gene, the first, in exon 4 (+453 G-+A), was observed in affected individuals (4 affected and 2 unaffected tested) who were heterozy- gous at this position. However, the polymorphism does not alter an encoded amino acid, suggesting that it is unlikely to be pathogenic. The frequency of the A al- lele in 50 unrelated individuals was 0.13. The second variant occurs in exon 5 (+725 A-G) and alters the
796 Annals of Neurology Vol 42 No 5 November 1997

w
4 3 7 3 9 4 2 2 1 8 1 6 4 3 5 4 4 2 2 3 4 12 6 2 4 6 2 1
4 5 . . . . 25 .....
Deceased individual
1 4 110 2 4 3 2
11 11 6 1 6 5 5 4 2 2 1 2
1313 52 5 6 3 2 3 1 . . . . 1 4
I 1
1 1 1 4 2 3 3 2
11 6 6 12 6 6 5 2 2 3 1 3
13 3 5 7 5 2 2 2 3 5
IV.13 IV.14
1 1 1 2 2 4 3 2
11 12 6 4 6 6 5 1 2 4 1 4
13 13 5 6 5 4 3 2 . I t . . .
6 3 5 5 2 9 4 1 2 5 4 2 4 1
13 15 4 2 6 6 2 1 6 9 1 1 6 6
.I.?. . . . . . . 3 4 9 10 3 3 3 2 5 7 6 10 2 1 2 5 4 2 7 5
12 3 4 4 6 6 1 2
. 2 3 . ...-.
v1 IV.5 .1.1.. .. . 2 5 . . . 1 4 1 1 1 7 9 9 2 3 3 3 3 3 3 4
117 5 5 6 5 6 7 6 6 2 2 5 1 2 2 2 4 4 2 1 1 7 1
1311 126 5 2 4 8 5 6 6 6 3 1 1 1 1 3 . ... .23.. . . . ._
7 7 1 1
2 2 3 6
11 6 6 7 6 4
4 2 2 3
1310 1312 412 !! 5 6 I 11 4 6 6 2
3 1 2 1 .<.I. . . . I 1 . . . . . 23. .
. . IV.9 IV.10 IV.11 . . . 22 . . . 9 3 . . . . .2.2.. .
4 5 1.:: 1 i: 7 3 9 4 2 2
6 1 1 6 6 4 4 3 5 4 5 4
v.3 v.4 . 2 2 . ;5783-
1 5 -5796-
4 3 -THRAl- 2 4 -s920- 4 4 -PYQ- 3 1 -5931-
12 14 -5606- 6 2 -5956- 3 6 -5943-
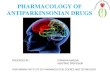
Fig. Family pedigree and haplo type analysis. The Australian FTDP (fontotemporal dementia with parkinsonism) family that has been simplified and disguised to prevent recognition. The genotypes of each marker analyzed in each individual are shown and the disease haplotype marked by a filled vertical bar. Note that I individual (IV 10) who has the disease haplo type is currently unaf- fected despite being older than the known age of onjet range for this fdmily [6] (see Results). A second individual ( X I ) shares part of the disease haploype (D17S798-DI7S943); however, this person is currently within the age o f onset range f o r this family. The minimal candidate region (D17S800-Dl7S791) dejned by analysis o f other families is indicated [5]. All five candidate genes se- quenced in this study, hdve been mapped within this region (D17S8OO-D17S791),
codon Asp242Ser. All individuals sequenced from the family and 50 unrelated coimols were homozygous for the G allele.
VHR DUAL-SPECIFICITY PHOSPHATASE. VHR dephos- phorylates a variety of proteins at both tyrosine and serine residues [I 11. The gene was previously localized to human chromosome 17q21 near BRCAl [ I l l . In addition, the abnormal phosphorylation of tau ob- served in PHFs, in Alzheimer's disease patients, sug- gests that abnormal activity of a protein serine phos- phatase may lead to neurodegenerative disease [ 171.
Sequence analysis of VHR in the Australian family revealed two polymorphisms in the 3' UTR of the gene. At $571 there is a G-+A transversion (allele fre- quency = 0.04) in a single unaffected who is heterozy- gous at this position. The second polymorphism at +606 (G+C) was observed in all family members se- quenced and all unrelated controls (50) who were ho- mozygous for the C allele.
hV4T-1. hVAT-1 is the human homologue of an abundant synaptic vesicle protein from the electric lobe of T. califarnica [18]. Synaptic vesicles are responsible for the storage and release of neurotransmitters; thus, proteins, such as VAT-I, that may perform a role in vesicle function ate obvious candidates for involvement in neuropsychiatric disease.
Sequence analysis of the VAT-1 gene in the Austra- lian family revealed a single change from database se- quence, $895 (C+G), which alters the codon Gln299Glu. However, all family members sequenced (affected and unaffected) and all unrelated controls (50) were homozygous for the G allele.
y-TUBULIN. The y-tubulin was previously mapped to 17q21 and is thought to be involved in the assembly of microtubules [ 121. Sequence analysis of the coding re- gion of the y-tubulin gene, in a panel of 2 affected and 2 unaffected family members, revealed no deviation from the published y-tubulin sequence.
Brief Communication: Baker et al: Localization of FTDP 797

Discussion We report here linkage of FTDP to chromosome 17q in an Australian family [6]. Haplotype analysis indi- cates the disease locus lies between D17S783 and D17S808, an interval of more than 20 cM (-26 cM) on the CEPH/Genethon linkage map. This region is consistent with the mapping of several variants of FTDP, in multiple kindreds, suggesting that mutations in the same gene are responsible for the disease in each family. Examination of the critical region in each fam- ily [1-41 reveals that the gene should lie in an ap- proximately 2-cM interval between D17S800 and D I7S79 I . However, given the clinical and pathologic variability between FTDP- 17 kindreds, it remains pos- sible that multiple genes localized closely on chromo- some 17q cause dementia in these families.
One unaffected member of the Australian family who is older than the age of disease onset range (39 - 66 years) shares the entire disease haplotype. This individual may subsequently develop disease, given the already wide range in onset age in this kindred. How- ever, this demonstrates the variability in the age- dependent penetrance observed both within and be- tween families with FTDP-17 [ l , 3, 51. Despite this individual, positive two-point LOD scores, strongly suggestive of linkage, were obtained with chromosome 17q markers by using both age-adjusted (Z,,, = 2.42 at D17S250, 0 = 0) and low-penetrance (Zmn = 2.87 at D17S250, 0 = 0) analyses. The peak LOD score obtained from low-penetrance linkage studies (2 = 2.87) was very close to the maximum (Z = 3.057) pre- dicted for a linked marker by simulation studies. This further strengthens the evidence for linkage to 17q in this family, because the actual LOD scores were close to the maximum that the power of the family to detect linkage was expected to allow.
The critical region on chromosome 17 for FTDP-17 (D17S800-DI7S791) contains many potential candi- date genes, most identified during the search for BRCAl. We selected five genes for initial analysis as candidates for FTDP- 17, ie, tau, VAT- 1, DLG-2, VHR, and y-tubulin. Sequence analysis of the coding region in each gene revealed no pathogenic mutations; however, several polymorphisms were observed.
The identification of the gene(s) responsible for FTDP-17 in the Australian family and other similar kindreds will allow assessment of the prevalence of these conditions in patients with dementia. This infor- mation may prove crucial in determining which pa- tients are best managed with particular treatments, be- cause the cause of FTDP-17 is likely to differ from that of other dementias such as Alzheimer’s disease.
Supported in part by National Health and Medical Research Coun- cil (NHMRC) grants to the Garvan Institute and the NHMRC
Network of Brain Research into Mental Disorder and the Vincent Fairfax Family foundation.
We acknowledge Prof C. Kidson for his tole in the initial collection of samples from this family and M. Walters and Dr W. Relf for establishing the lymphoblastoid cell lines. Unpublished sequence from the VAT-1 gene was provided by Mary-Claire King.
References 1.
2.
3.
4.
5 .
6.
7.
8.
9.
10.
11
12
13
14
15
16
1-
Wilhelmson KC, Lynch T, Pavlou E, Nygaard TG. Localiza- tion of disinhibition-dementia-parkinsonism-amyotrophy com- plex to 17q21-22. Am J Hum Genet 1994;55:1159-1165 Wijker M, Wszokk ZK, Wolters ECH, et al. Localization of the gene for rapidly progressive autosomal dominant parkinson- ism and dementia with pallido-ponto-nigral degeneration to chromosome 17q21. Hum Mol Genet 1996;5:151-154 Heutink P, Stevens M, Rizzu P, et al. Hereditary frontotempo- ral dementia is linked to chromosome 17q21-22: a genetic and clinicopathological study of three Dutch families. Ann Neurol 1996;41: 150-159 Yamaoka LH, Welshhohmer KA, Huiette CM, et al. Linkage of frontotemporal dementia to chromosome 17-clinical and neu- ropathological characterization of phenotype. Am J Hum Genet
Foster NL, Wilhelmsen KC, Sima AAF, et al. Frontotemporal dementia and parkinsonism linked to chromosome 17: a con- sensus conference. Ann Neurol 1997;41:706-715 Dark F. A family with autosomal dominant, non-Azheimer’s presenile dementia. Aust N Z J Psychiatry 1997;3 1 : 130-144 Crook R, Hardy J, Duff K. Single day ApoE genotyping. J Neurosci Methods 1994;53:125-127 Andreadis A, Brown WM, Kosik KS. Structure and novel exons of the human tau gene. Biochemistry 1992;31:10626-10633 Friedman LS, Ostermeyer EA, Lynch ED, et al. 22 genes from chromosome 17q21: cloning, sequencing and characterization of mutations in breast caner families and tumors. Genomics
Mazoyer S, Gayther SA, Nagai MA, et al. A gene (DLG2) lo- cated at 17q12-q21 encodes a new homologue of the Dvoso- phila tumor suppressor dlg-A. Genomics 1995;28:25-3 1 Kamb A, Futreal PA, Rosenthal J , et al. Localization of die VHR phosphatase gene and its analysis as a candidate for BRCAl. Genomics 1994;23:163-167 Zheng Y, Jung MK, Oakley BR. y-Tubulin is present in Dro- sophila melanogaster and Homo sapiens and is associated with the centrosome. Cell 199 1;65:8 17- 823 Brown J, Ashworth A, Gydesen S, et al. Familial non-specific dementia maps to chromosome 3. Hum Mol Genet 1995;4: 1625-1628 Donlon TA, Harris P, Neve RL. Localization of microtubuk- associated protein tau (MTBT1) to chromosome 17q21. Cyto- genet Cell Genet 1987;46:607 (Abstract) Goedert M, Jakes R, Spillantini MG, et al. Assembly of microtubule-associated protein tau into Alzheimer-like filaments induced by sulphated glycosaminoglycans. Nature 1996;383:
Sheng M. PDZs and receptorlchannrl clustering: rounding up the latest suspects. Cell 1996; 17:575-578
1996;59: 1306-1 31 2
1995;25:256-263
550 -553
I / . Bramblett GT, Goedert M, Jakes R, et al. Abnormal tau phos- phorylation at Ser396 in Alzheimer’s disease recapitulates devel- opment and contributes to reduced microtubule binding. NKU- ron 1993;lO: 1083-1 099
18. Linial M, Miller K, Schekr RH. VAT-1: an abundant mem- brane protein from Torpedo chohnergic synaptic vesicles. Neu- ron 1989;2:1265-1273
798 Annals of Neurology Vol 42 No 5 November 1997




![Vascular parkinsonism · Vascular parkinsonism – REVIEW future science groupfuture science group 239 20%) suffered from parkinsonism with strong evidence of CVD [23]](https://img.pdfslide.net/doc/110x75/5c12e69c09d3f208438bb500/vascular-parkinsonism-vascular-parkinsonism-review-future-science-groupfuture.jpg)