Embed Size (px)
Citation preview
Acta path. microbiol. scand. Sect. A, 82, 559-563, 1974
LOCALIZATION OF IMMUNOGLOBULINS IN URINARY BLADDER TUMOURS
BENCT JOIIANSSON and ARNE LJUNGQVIST
The Departments of Urology and Pathology, Karolinska sjukhuset, Stockholm Sweden
Biopsy specimens from primary tumours of the urinary bladder in 36 patients were examined for the presence of immunoglobulins, using a direct immunofluorescence technique. The tumours were also studied by normal histological methods to determine the malignancy grade and degree of invasive growth as well as the presence of lymphocytes and plasma cells. An immunoglobulin estimation in urine and serum from the patients was performed by immunodiffusion. The IgM demonstrated in lymphocytes and plasma cells of the tumoun’ connective tissue stroma was found to be directly related to the malignancy grading. There was even a correlation to the urinary output of zgM, but not to its serum concentration. These results further support the view that an immune reaction occurs in epithelial tumours of the urinary bladder, and that an estimation of the urinary output of IgM can be of diagnostic value in these cases.
Patients with transitional cell tumours show a high urinary excretion of immunoglobulins, particularly of IgM, and a low excretion of a-l-globulin and transferrin compared with patients with proteinuria due to glomerulo- nephritis and pyelonephritis (Iohansson et al. 1971). Moreover, the amount of IgM in the urine is directly related to the size of the tumour, as judged from a cystoscopical ex- amination (Iohansson & Kir tner) . It there- fore appears that IgM passes into the urine from the tumour, but the actual presence of IgM in these tumours has never been de- monstrated. In the present study, the presence of IgM in bladder tumours is investigated by immunofluorescence and the concentration of IgM in serum and urine is examined by im- munodiffusion.
Received 2 l.iii.74 Requests for reprints should be addressed to:
Dr. Bengt Johansson, Department of Urology, Ka- rolinska sjukhuset, S-104 01 Stockholm, Sweden.
36*
Accepted 2 1 K . 7 4
M A T E R I A L A N D M E T H O D S
Investigations were performed on 36 consecutive patients who were admitted to the department of Urology on account of a primary tumour of the urinary bladder. Although most of these patients had microscopical haematuria, patients with gross macroscopical haematuria were not included in the study. Samples of urine and serum as well as a tumour biopsy from each patients were examined.
Serum creatinine was less than 1.3 mg/100 ml in 27 patients, 1.3-1.5mg/100ml in 5 and 1.5-1.8mg/ 100 ml in the remaining 4. Twenty-eight of the patients had negative urine cultures, growth of enterococci was seen in 5, of E. coli in 2, and of staphylococcus albus in 1. Patients with positive urine cultures, however, showed no other signs of urinary tract infection. In all patients, the serum concentration and the 24 hours’ urinary excretion of immunoglobulins was determined (Johansson & Kistner) .
Biopsy specimens from the tumour and from the intact bladder wall as far removed from the tumour as possible were taken during a cytoscopical exam- ination. Cryostat sections were prepared, for im- munofluorescence reactions, from the biopsies, after which the frozen blocks were fixed in a 10 per cent neutral solution of formalin and embedded in par-
559
affin for the production of routine histological sections.
Inmunofluorescence The cryostat sections for direct immunofluorcs-
ccnce were prepared as follows: I g M . As regards the entire series of 36 patients,
three sections were cut from each block and in- cubated with fluorescein conjugated sheep-anti- human IgM serum (SBL, Stockholm).
ZgC. As regards 30 out of the 36 patients, threc sections were cut from each block and incubated with fluorescein conjugated sheep-anti-human IgG scrum (SBL, Stockholm).
I g A . As regards 10 out of the 36 patients, three scctions were cut from each block and incubated with fluorescein conjugated sheep-anti-human IgA serum (SBI,, Stockholm).
The reaction with fluorescein conjugated anti- immunoglobulin serum was inhibited in three sec- tions from each block by pretreatment with the corresponding, non-conjugated anti-immunoglobulin serum.
All sections were studied by fluorescence micro- scopy with UV light.
Histology The histological sections were stained with
haematoxylin-eosin and van Gieson’s connective tissue stain. Particular attention was paid to the malignancy of the tumour as judged from its cellu- lar characteristics (Bergkvist et al. 1965), its de- gree of invasion, and the infiltration of lympho- cytes and plasma cells in the stroma and bladder wall. Only slight cellular infiltration was denoted +, a moderate amount + + and a massive in- filtration + + +.
R E S U L T S
Immuno fluorescence ZgM. Test sections from 15 of the 36
tumours showed positive immunofluorescence reaction for IgM, whereas all control sections were negative, as were the sections from the non-tumourous bladder wall. Positive reac- tion were judged by the occurrence of in- tensely fluorescent cells in the connective tis- sue stroma of the tumour (Fig. 1 a) . Most of these were classified as plasma cells because of the eccentric location of their nuclei (Fig. 1 b) , but some others were probably lympho- cytes. The tumour cells were not fluorescent.
ZgG. A positive reaction was observed in 6 of the 30 tumours examined, whereas the
560
Fig. 1 . A. Fluorescence microphotograph of section from urinary bladder tumour incubated with fluo- rescein conjugated anti-human IgM serum. Groups of fluorescent cells are seen and these are located in the Connective tissue stroma. Non-fluorescent areas correspond to tumour cells. x 100.
B. Fluorescence microphotograph of section from urinary bladder tumour incubated with fluorescein conjugated anti-human IgM serum. In many fluo- rescent cells dark arcas ( = nuclei) are excen- trically located (arrows). Left and bottom right, non-fluorescent tumour cell areas. x 360.
control sections were negative with the ex- ception of one bladder wall biopsy. Fluores- cence was again located in plasma cells and lymphocytes, but in three cases even in a more diffuse fashion in the stroma (Fig. 2 ) . The tumour cells were not fluorescent.
ZgA. A positive reaction was observed in 2 of the 10 tumours examined whereas all the control sections, including those from the non-tumourous bladder wall, were negative. Fluorescence was located in cells in the con- nective tissue stroma but not in the tumour cells. Diffuse fluorescence in the stroma was absent.
Both patients who were positive for IgA were also positive for IgG and IgM. Among the remaining 13 patients who were positive for IgM, only one showed a positive reaction for IgG, whereas the remaining 3 patients with a positive reaction for IgG were negative for IgM.
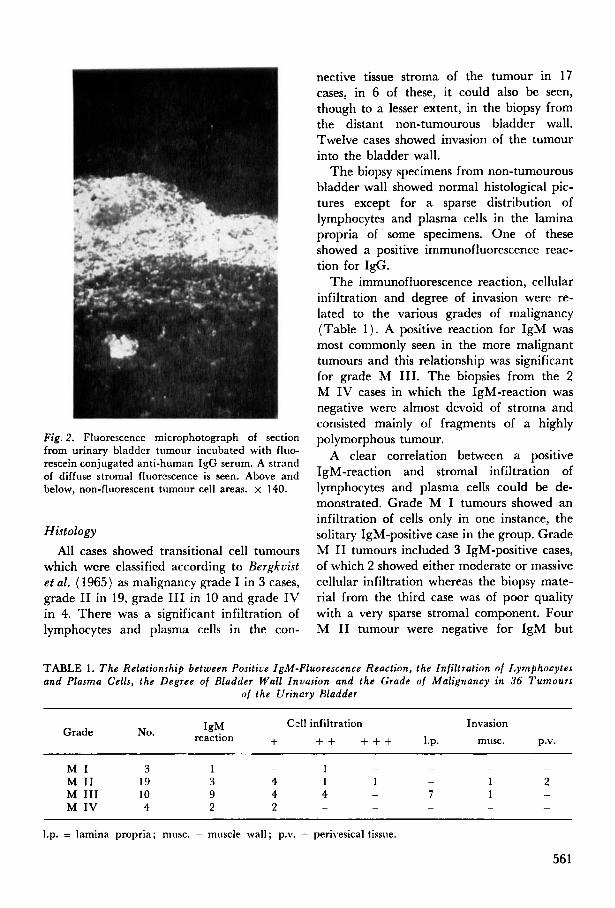
Fig. 2 . Fluorescence microphotograph of section from urinary bladder tumour incubated with fluo- rescein conjugated anti-human IgG serum. A strand of diffuse stromal fluorescence is seen. Above and below, non-fluorescent tumour cell areas. x 140.
Histology All cases showed transitional cell tumours
which were classified according to Bergkvist e t al. ( 1965) as malignancy grade I in 3 cases, grade I1 in 19, grade I11 in 10 and grade IV in 4. There was a significant infiltration of lymphocytes and plasma cells in the con-
nective tissue stroma of the tumour in 17 cases, in 6 of these, it could also be seen, though to a lesser extent, in the biopsy from the distant non-tumourous bladder wall. Twelve cases showed invasion of the tumour into the bladder wall.
The biopsy specimens from non-tumourous bladder wall showed normal histological pic- tures except for a sparse distribution of lymphocytes and plasma cells in the lamina propria of some specimens. One of these showed a positive immunofluorescence reac- tion for IgG.
The immunofluorescence reaction, cellular infiltration and degree of invasion were re- lated to the various grades of malignancy (Table 1 ) . A positive reaction for IgM was most commonly seen in the more malignant tumours and this relationship was significant for grade M 111. The biopsies from the 2 M IV cases in which the IgM-reaction was negative were almost devoid of stroma and consisted mainly of fragments of a highly polymorphous tumour.
A clear correlation between a positive IgM-reaction and stromal infiltration of lymphocytes and plasma cells could be de- monstrated. Grade M I tumours showed an infiltration of cells only in one instance, the solitary IgM-positive case in the group. Grade M I1 tumours included 3 IgM-positive cases, of which 2 showed either moderate or massive cellular infiltration whereas the biopsy mate- rial from the third case was of poor quality with a very sparse stromal component. Four M I1 tumour were negative for IgM but
TABLE 1 . T h e Relationship between Positive IgM-Fluorescence Reaction, the Infiltration of Lymphocytes and Plasma Cells, the Degree of Bladder Wall Invasion and the Grade of Malignancy in 36 Tumours
of the Urinary Bladder
Cell infiltration Invasion IgM reaction + + + + + + 1.p. musc. p.v.
Grade No.
- - - - 1 - M I 3 1 M I1 19 3 4 1 1 1 2 M I11 10 9 4 4 7 1 M IV 4 2 2
-
- -
- - - - -
1.p. = lamina propria; musc. = muscle wall; p.v. = perivesical tissue.
56 1
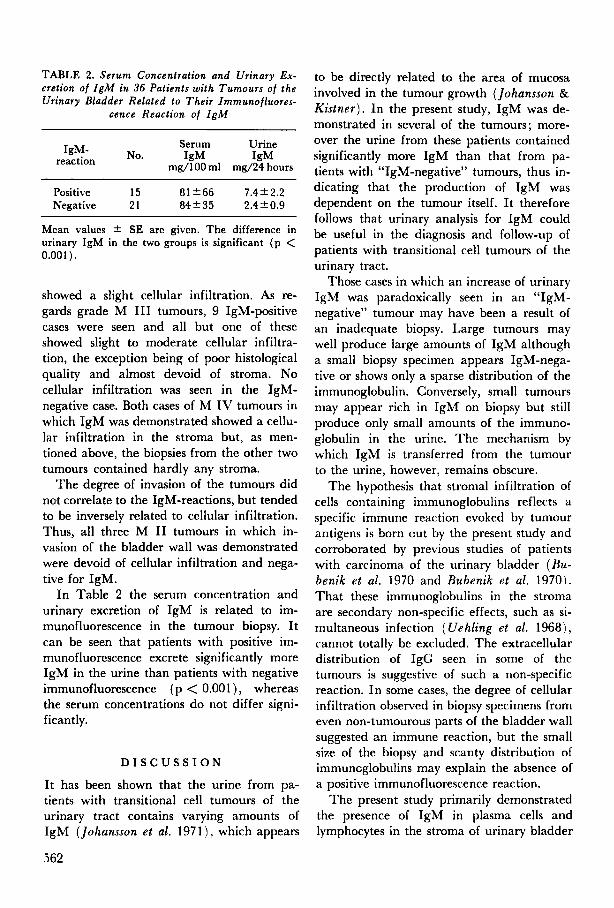
TABLE 2. Serum Concentration and Urinary Ex- cretion o f IgM in 36 Patients wi th Turnours of the Urinary Bladder Related to Their Immunofluores-
cence Reaction of IgM
Serum Urine
mg/100 ml m d 2 4 hours No. IgM IgM ‘gM-
reaction
Positive 15 81 +66 7.4k2.2 Negative 21 84+35 2.4k0.9
Mean values + SE are given. The difference in urinary IgM in the two groups is significant (p < 0.001 ).
showed a slight cellular infiltration. As re- gards grade M I11 tumours, 9 IgM-positive cases were seen and all but one of these showed slight to moderate cellular infiltra- tion, the exception being of poor histological quality and almost devoid of stroma. No cellular infiltration was seen in the IgM- negative case. Both cases of M IV tumours in which IgM was demonstrated showed a cellu- lar infiltration in the stroma but, as men- tioned above, the biopsies from the other two tumours contained hardly any stroma.
The degree of invasion of the tumours did not correlate to the IgM-reactions, but tended to be inversely related to cellular infiltration. Thus, all three M I1 tumours in which in- vasion of the bladder wall was demonstrated were devoid of cellular infiltration and nega- tive for IgM.
In Table 2 the serum concentration and urinary excretion of IgM is related to im- munofluorescence in the tumour biopsy. It can be seen that patients with positive im- munofluorescence excrete significantly more IgM in the urine than patients with negative immunofluorescence ( p < 0.001 ) , whereas the serum concentrations do not differ signi- ficantly.
D I S C U S S I O N
It has been shown that the urine from pa- tients with transitional cell tumours of the urinary tract contains varying amounts of IgM (Johansson et al. 1971), which appears
to be directly related to the area of mucosa involved in the tumour growth (Johansson & Kis tner) . In the present study, IgM was de- monstrated in several of the tumours; more- over the urine from these patients contained significantly more IgM than that from pa- tients with “IgM-negative” tumours, thus in- dicating that the production of IgM was dependent on the tumour itself. I t therefore follows that urinary analysis for IgM could be useful in the diagnosis and follow-up of patients with transitional cell tumours of the urinary tract.
Those cases in which an increase of urinary IgM was paradoxically seen in an “IgM- negative’’ tumour may have been a result of an inadequate biopsy. Large tumours may well produce large amounts of IgM although a small biopsy specimen appears IgM-nega- tive or shows only a sparse distribution of the immunoglobulin. Conversely, small tumours may appear rich in IgM on biopsy but still produce only small amounts of the immuno- globulin in the urine. The mechanism by which IgM is transferred from the tumour to the urine, however, remains obscure.
The hypothesis that stromal infiltration of cells containing immunoglobulins reflects a specific immune reaction evoked by tumour antigens is born cut by the present study and corroborated by previous studies of patients with carcinoma of the urinary bladder (Bu- benik et al. 1970 and Bubenik et al. 1970). That these immunoglobulins in the stroma are secondary non-specific effects, such as si- multaneous infection ( Uehling et al. 1968), cannot totally be excluded. The extracellular distribution of IgC seen in some of the tumours is suggestive of such a non-specific reaction. In some cases, the degree of cellular infiltration observed in biopsy specimens from even non-tumourous parts of the bladder wall suggested an immune reaction, but the small size of the biopsy and scanty distribution of immuncglobulins may explain the absence of a positive immunofluorescence reaction.
The present study primarily demonstrated the presence of IgM in plasma cells and lymphocytes in the stroma of urinary bladder
562
tumours, with a concurrent increase of IgM excretion in the urine. These observations cannot evaluate the effect of an immunolo- gical reaction as a limiting factor in tumour growth, nor can they ascertain whether the immune reaction appears early or only when the tumour becomes increasingly aggressive. Whereas Sarma (1970) found a heavy cellu- lar infiltration to be a good prognostic sign, others deny this correlation (Tanaka et al. 1970). The absence of cellular infiltration and IgM in three M I1 tumours which showed marked invasive tendencies, suggests that an immunological reaction may be of some importance in limiting tumour growth. On the other hand, the remaining nine M I1 tumours also were devoid of cellular infiltra- tion and did not display any invasion. An analysis of the more malignant tumours ( M I11 and M IV) does not elucidate this problem any further, the only constant fea- ture being a stromal infiltration of IgM-posi- tive cells, quite independent of the invasive characteristics of the tumour.
This study was supported by the Swedish Cancer Society (Project No. 523-71-OIX).
R E F E R E N C E S
1. Bergkvist, A., Ljungqvist, A . & Moberger, G.: Classification of bladder tumours based on the cellular pattern. Preliminary report of a clini- cal-pathological study of 300 cases with a minimum follow-up of eight years. Acta Chir. Scand. 130: 371-378, 1965.
2. Bubenik, J . , Perlmann, P. , Helmstein, K . & Moberger, G.: Immune response to urinary bladder tumours in man. Int. J. Cancer 5: 39-46, 1970.
3. Bubenik, J . , Perlmann, P. , Helmstein, K . & Moberger, G.: Cellular and humoral immune responses to human urinary bladder carcino- mas. Int. J. Cancer 5: 310-319, 1970.
4. Johansson, B., Kistner, S . & Norberg, R.: Pro- teinuria in patients with urinary tract tumours. Scand. J. Urol. Nephrol. 5: 229-233, 1971.
5. Johansson, B. & Kistner, S . : Proteinuria in patients with urinary tract tumour with refer- ence to tumour size, clinical stage, and degree of malignancy. In press.
6 . Sarma, K . P.: The role of lymphoid reaction in bladder cancer. J. Urol. 104: 843-849, 1970.
7. Tanaka, T . , Cooper, E . H . & Anderson, C . K . : Lymphocyte infiltration in bladder carcinoma. Rev. Europ. Etudes Clin. Biol. 15: 1084-1089, 1970. Uehling, D. T., Barnhart, D . D . & Seastone, C . V . : Antibody production in urinary bladder infection. Invest. Urol. 6: 21 1-222, 1968.
8.
563





























