Embed Size (px)
Citation preview
1
Executive MeetingOctober 29, 2010
Long-Term Care Pharmacy 101Growing Your Business in the Long-Term Care and Alternate Site Markets
Welcome to Long-Term Care Pharmacy 101, the first of two long-term care training courses sponsored by McKesson. This presentation will provide an overview of long-term care and alternate site pharmacy and discuss the opportunities for your pharmacy in these markets.
You can print a copy of these slides to assist in your viewing. Please go to the “print slides” link to do this.
Before You Begin
Before we begin the course, let’s review the various screen components and control features available. •Use the Next button to go the next slide. •Use the Back button to return to the previous slide. •Audio for the course is enabled by default. You can control the volume by using the Audio Volume Slider.
•If you wish to view the captions for the audio, click the Notes tab to the left of your screen.
•To move back and forth within each slide, click and drag the Timeline Slider. •To replay a page after the timeline slider reaches the end, click and drag the slider back to the beginning or anywhere along the timeline. •You can pause the current slide at any time by clicking the Play-Pause toggle button. Please note that if you are at the end of a slide, you can click the Play-Pause toggle button to go to the next slide.
•You can change the way the slides and slide components are displayed by using the View Mode button at the bottom right of the screen.
•The default view for this course is the Standard view. In this view, the left sidebar listing all the slides is displayed. •Click the View Mode button to change the default Standard view to the No Sidebar view where the left sidebar is collapsed, and the audio transcript can be activated by using the Slide Notes button.•You can also use the View Mode button to change to the Slide Only view, where only the slide is visible on screen. However, the buttons on the lower right can be used to view the slide notes, play or pause the slide, and to go to
LTC Pharmacy 101 Overview and Objectives– This Web-based program is divided into three short modules.
– Your progress can be saved at any time. Go at your own pace.
– The overall objectives of LTC Pharmacy 101 are to:
– Provide an overview of long-term care (LTC) and medicationusage across the LTC continuum
– Provide an overview of alternate site pharmacy and highlightkey trends in this segment
– Define the service required within long-term care andalternate site pharmacy
– Describe the reimbursement process and howlong-term care is profitable
3
Long-Term Care Pharmacy 101 is a web-based program that consists of three short, easy-to-follow, modules. These modules are designed so that you can stop, review the materials at any time, and pick up where you left off. This will allow you to go through the modules at your own pace. The modules will:• Provide an overview of long-term care (LTC) and medication usage across the
LTC continuum• Provide an overview of alternate site pharmacy and highlight key trends in this
segment• Define the service required in long-term care and alternate site pharmacy • Describe the reimbursement process and how long-term care pharmacy is
profitable.
This program is intended for retail pharmacies that may be interested in expanding into long-term care pharmacy.
We hope this program provides useful guidance to help you decide whether LTC is a good fit for your business.
Long-Term Care Pharmacy 101 is a web-based program that consists of three short, easy-to-follow, modules. These modules are designed so that you can stop, review the materials at any time, and pick up where you left off. This will allow you to go through the modules at your own pace. The modules will:• Provide an overview of long-term care (LTC) and medication usage across the
LTC continuum• Provide an overview of alternate site pharmacy and highlight key trends in this
segment• Define the service required in long-term care and alternate site pharmacy • Describe the reimbursement process and how long-term care pharmacy is
profitable.
This program is intended for retail pharmacies that may be interested in expanding into long-term care pharmacy.
We hope this program provides useful guidance to help you decide whether LTC is a good fit for your business.
4
An Overview of Long-Term Care and Alternate Site Pharmacy
Long-Term Care Pharmacy 101Module #1
Let’s get started with Long-Term Care Pharmacy 101. We’ll begin with Module #1—What is long-term care and alternate site pharmacy?
What Is Long-Term Care?– Range of medical and/or social services designed to help
people who have disabilities or chronic care needs. Servicesmay be short- or long-term and may be provided in a person’s home, in the community or in residential facilities (e.g., nursing homes or assisted-living facilities).
– Approximately 11 million people age 18 years andolder require these services in the U.S. A majority (57%)are over age 65.
– Short-term stay payor is Medicare, long-term stay payor isprimarily Medicaid, except prescription medications reimbursed through Medicare.
Long-Term Care: Consumers, Services, and Financing. National Health Policy Forum. November 28, 2008.
5
What is long-term care?
Long-term care is a range of medical and/or social services for people with chronic care needs. These services may be required for a long or short duration, with care being provided in various settings, including a person’s home, in the community, or in a residential setting, such as a nursing facility.
Long-term care is a large market, with approximately 11 million people over the age of 18 requiring some type of care. Not all long-term care is for the elderly—only 57% of those served are over the age of 65.
Medicare is the primary payor for a short-stay in a long-term care facility. Medicaid is the primary payor for healthcare services for long-term stays, with Medicare being the primary payor for medications.
Reimbursement, including the role of Medicare, will be discussed in greater detail later in this program.
Long-Term Care: Consumers, Services, and Financing. National Health Policy Forum. November 28, 2008.
Data on file. MatureHealth Communications.The Alliance for Quality Nursing Home Care. Trends in Post-Acute and Long-Term Care. September 2009.
The Long-Term Care ContinuumHospital
Subacute Care
Skilled Nursing
Assisted Living
Independent Living
Active Adult Living
Senior’s Home
Closed SystemClosed System
Home Health Care-Skilled Home Care-Physicians-Rehabilitation
Home Health Care-Skilled Home Care-Physicians-Rehabilitation
Home Support-Home Health Aides-Home Maker-Home Maintenance
Home Support-Home Health Aides-Home Maker-Home Maintenance
Special Care-Dementia-Alzheimer’s-Hospice
Special Care-Dementia-Alzheimer’s-Hospice
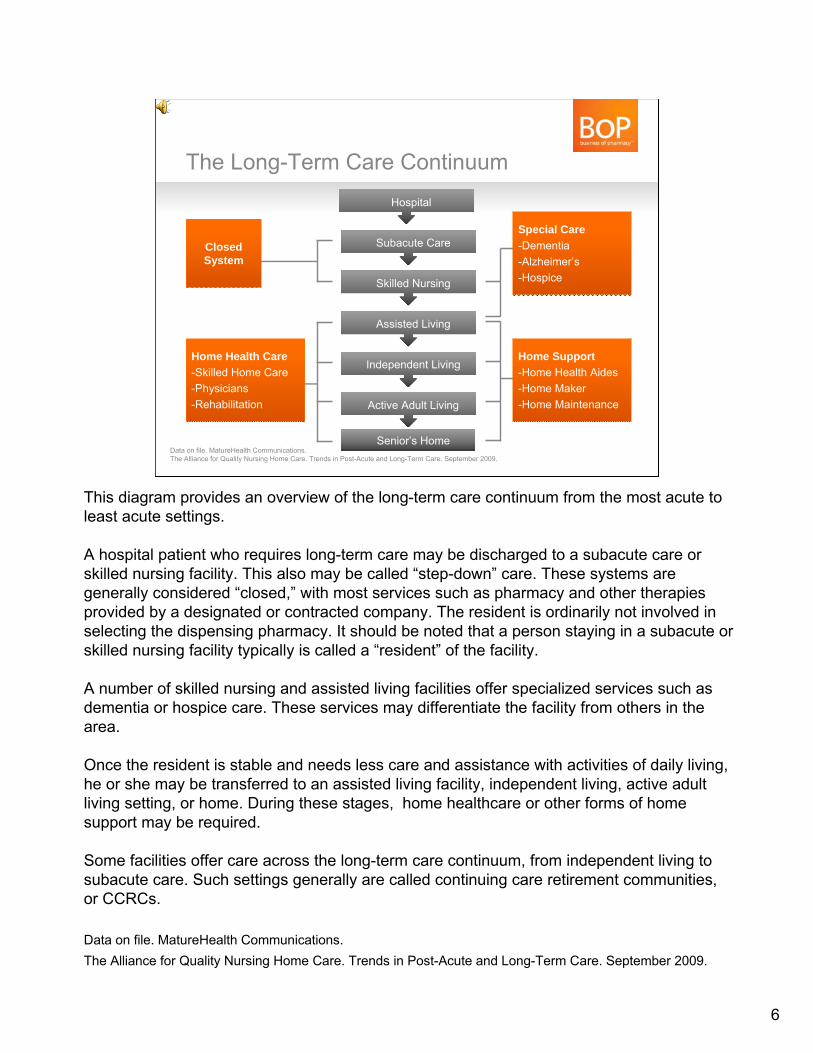
This diagram provides an overview of the long-term care continuum from the most acute to least acute settings.
A hospital patient who requires long-term care may be discharged to a subacute care or skilled nursing facility. This also may be called “step-down” care. These systems are generally considered “closed,” with most services such as pharmacy and other therapies provided by a designated or contracted company. The resident is ordinarily not involved in selecting the dispensing pharmacy. It should be noted that a person staying in a subacute or skilled nursing facility typically is called a “resident” of the facility.
A number of skilled nursing and assisted living facilities offer specialized services such as dementia or hospice care. These services may differentiate the facility from others in the area.
Once the resident is stable and needs less care and assistance with activities of daily living, he or she may be transferred to an assisted living facility, independent living, active adult living setting, or home. During these stages, home healthcare or other forms of home support may be required.
Some facilities offer care across the long-term care continuum, from independent living to subacute care. Such settings generally are called continuing care retirement communities, or CCRCs.
Data on file. MatureHealth Communications.The Alliance for Quality Nursing Home Care. Trends in Post-Acute and Long-Term Care. September 2009.
6
Number of LTC Facilities and Beds (2009)
The American Health Care Association. The State of Long-Term Care Sector. November 23, 2010.
# of
Fac
ilitie
s/Be
ds
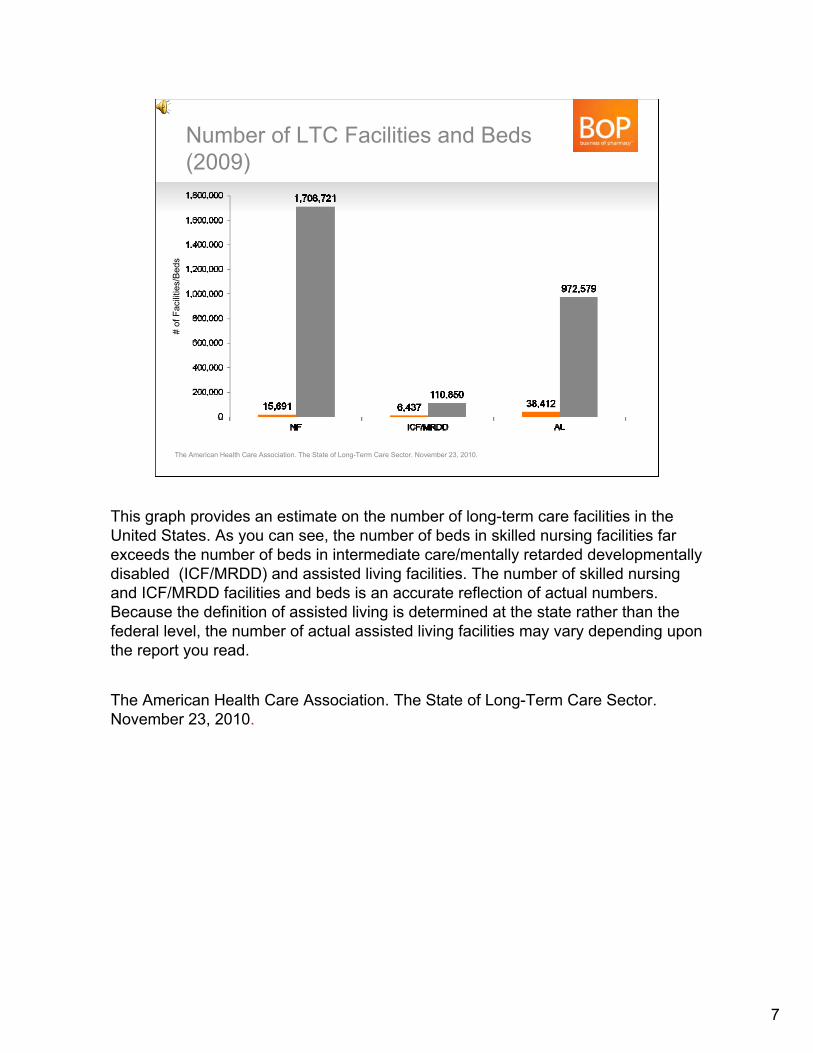
This graph provides an estimate on the number of long-term care facilities in the United States. As you can see, the number of beds in skilled nursing facilities far exceeds the number of beds in intermediate care/mentally retarded developmentally disabled (ICF/MRDD) and assisted living facilities. The number of skilled nursing and ICF/MRDD facilities and beds is an accurate reflection of actual numbers. Because the definition of assisted living is determined at the state rather than the federal level, the number of actual assisted living facilities may vary depending upon the report you read.
The American Health Care Association. The State of Long-Term Care Sector. November 23, 2010.
7
LTC Accounts for Larger Proportion of Scripts and Spending per Pharmacy
MedPac. A Data Book: Healthcare Spending and the Medicare Program. June 2010.
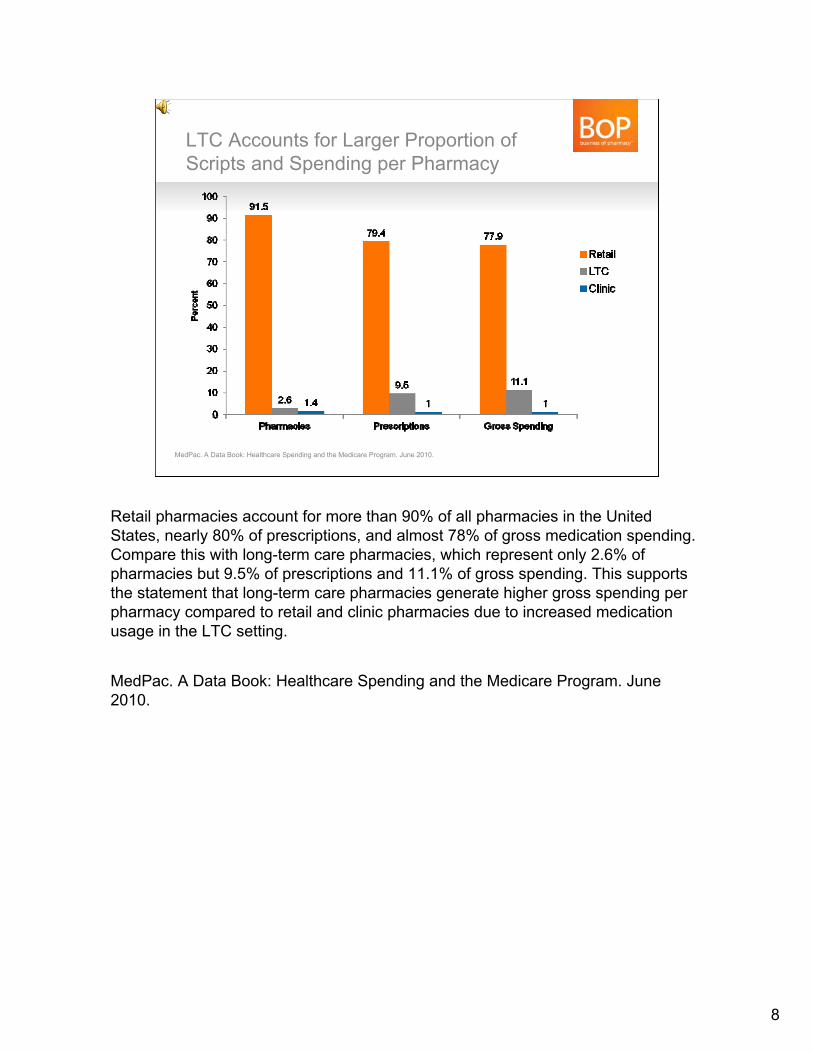
Retail pharmacies account for more than 90% of all pharmacies in the United States, nearly 80% of prescriptions, and almost 78% of gross medication spending. Compare this with long-term care pharmacies, which represent only 2.6% of pharmacies but 9.5% of prescriptions and 11.1% of gross spending. This supports the statement that long-term care pharmacies generate higher gross spending per pharmacy compared to retail and clinic pharmacies due to increased medication usage in the LTC setting.
MedPac. A Data Book: Healthcare Spending and the Medicare Program. June 2010.
8
Medication Use Is Much Higher in Facilities Compared to the Community
Henry J. Kaiser Family Foundation. Medicare Spending and Use of Medical Services or Beneficiaries in Nursing Homes and Other LTC Facilities. October 2010.
Average Spending
$7,552
2006
Dol
lars
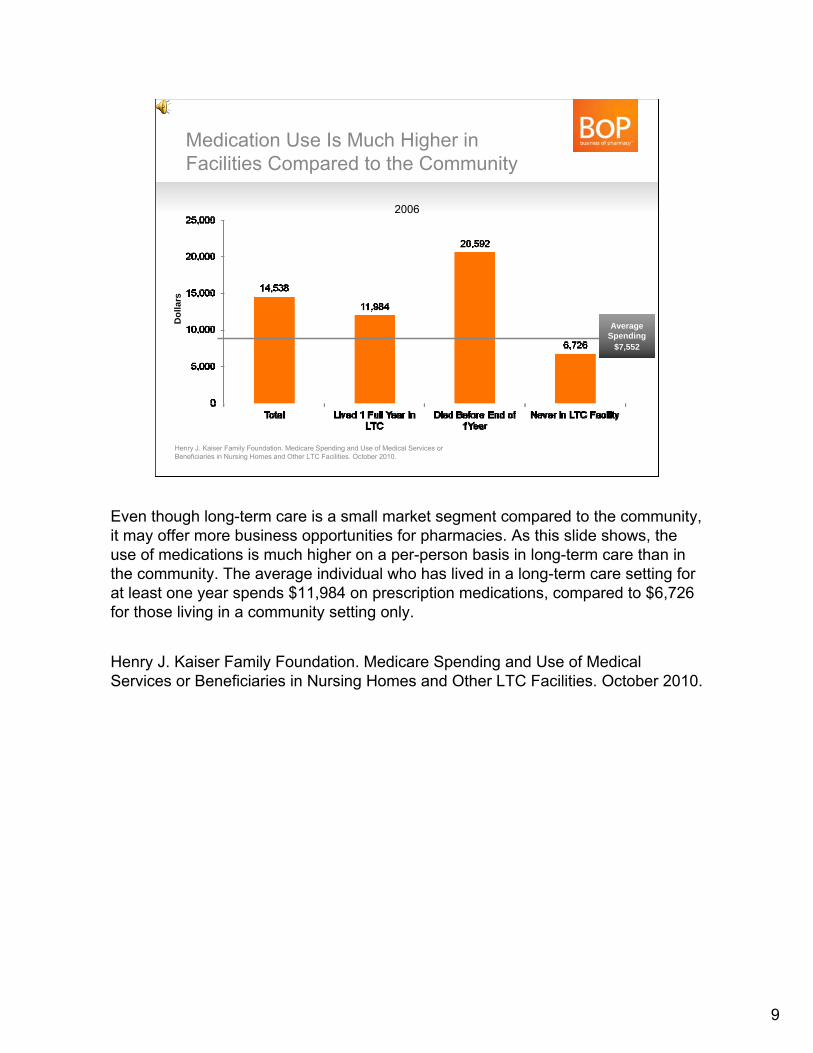
Even though long-term care is a small market segment compared to the community, it may offer more business opportunities for pharmacies. As this slide shows, the use of medications is much higher on a per-person basis in long-term care than in the community. The average individual who has lived in a long-term care setting for at least one year spends $11,984 on prescription medications, compared to $6,726 for those living in a community setting only.
Henry J. Kaiser Family Foundation. Medicare Spending and Use of Medical Services or Beneficiaries in Nursing Homes and Other LTC Facilities. October 2010.
9
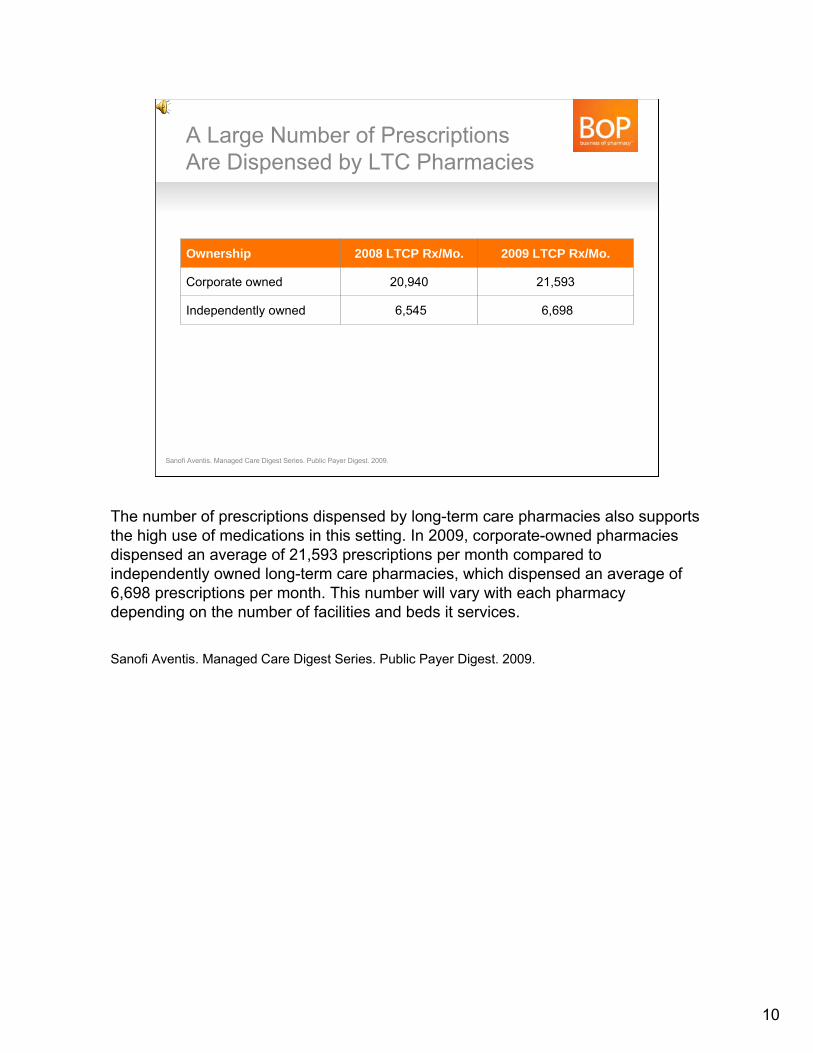
A Large Number of Prescriptions Are Dispensed by LTC Pharmacies
Ownership 2008 LTCP Rx/Mo. 2009 LTCP Rx/Mo.
Corporate owned 20,940 21,593
Independently owned 6,545 6,698
Sanofi Aventis. Managed Care Digest Series. Public Payer Digest. 2009.
10
The number of prescriptions dispensed by long-term care pharmacies also supports the high use of medications in this setting. In 2009, corporate-owned pharmacies dispensed an average of 21,593 prescriptions per month compared to independently owned long-term care pharmacies, which dispensed an average of 6,698 prescriptions per month. This number will vary with each pharmacy depending on the number of facilities and beds it services.
Sanofi Aventis. Managed Care Digest Series. Public Payer Digest. 2009.
Definition of an SNF– A skilled nursing service is a service that must be provided by a registered nurse, or a
licensed practical (vocational) nurse under the supervision of a registered nurse.
– In determining whether a service requires the skills of a nurse, consider both the inherent complexity of the service, the condition of the patient, and accepted standards of medical and nursing practice.
– Some services may be classified as a skilled-nursing service on the basis of complexity alone, e.g., intravenous and intramuscular injections or insertion of catheters, and if reasonable and necessary to the treatment of the patient’s illness or injury, would be covered on that basis.
– However, in some cases the condition of the patient may cause a service that would ordinarily be considered unskilled to be considered a skilled-nursing service. This would occur when the patient’s condition is such that the service can be safely and effectively provided only by a nurse.
Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual. Sections 205.1 and 205.2.Centers for Medicare and Medicaid Services. Glossary of Medicare.gov. Available at http://www.medicare.gov/glossary/search.asp?SelectAlphabet=S&Language=English#Content. Accessed April 1, 2011.
11
The federal government provides a definition of a skilled nursing facility.A skilled nursing facility must provide services by a registered nurse, or a licensed practical (vocational) nurse under the supervision of a registered nurse. The level and/or extent of nursing care will depend upon the complexity and type of services required. Some of these services may be based on the complexity of care required, such as the need for pulmonary therapy, or the condition of the resident receiving the care. An example would be medication administration for a resident with dementia.
Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual. Sections 205.1 and 205.2.Centers for Medicare and Medicaid Services. Glossary of Medicare.gov. Available at http://www.medicare.gov/glossary/search.asp?SelectAlphabet=S&Language=English#Content. Accessed April 1, 2011.
The “Typical” SNF – 89 residents– 109 beds– 114 employees
– Approx. 60% of employees are nurses, nurse aides– Direct care by a staff member averages approximately
3.5 hours/day
– Profit margins average 16%, with some facilities having greater than 20% profit margin
The American Health Care Association. The State of Long-Term Care Sector. November 23, 2010.
12
Skilled nursing facilities vary widely in type and size. The typical facility will have:• 89 residents with various types of healthcare coverage.• 109 beds, though this number can range from 10 beds up to several hundred.• 114 employees, including healthcare professional and nonprofessional staff.
For healthcare professional staff, the average direct care time with residents is 3.5 hours per day.
Profit margins vary widely among skilled nursing facilities, but data from 2008 indicate an overall average profit margin of 16% in the average facility.
The American Health Care Association. The State of Long-Term Care Sector. November 23, 2010.
The “Typical” SNF Resident– >85 years old, white female
– Length of stay will vary widely
– Average length of stay is over 450 days, but approximately 15% of population covered byshort-stay Medicare Part A
– Most have multiple comorbidities, with approximately 50% of residents receiving nine or more medications
U.S. Department of Health and Human Services. Centers for Disease Control and Prevention. National Center for Health Statistics. The National Nursing Home Survey 2004. Available at http://www.cdc.gov/nchs/nnhs.htm. Accessed January 10, 2011.Stevenson DG, Huskamp HA, Newhouse JP. Medicare Part D, Nursing Homes, and Long-Term Care Pharmacies. June 2007. No 07-2.
13
The typical resident of a skilled nursing facility may be different from the one who comes into your pharmacy.
The most common residents in a facility are white women over the age of 85.
Their length of stay in the facility will vary depending upon the reason for admission. The average length of stay is over 450 days, but a large percentage (approximately 15%) will be in the facility for a short time―less than 30 days. The percentage of short-stay residents varies by facility, so this is an important question to ask when evaluating a facility.
Most residents will have multiple comorbidities, and approximately half are on 9 or more medications at any one time.
US Department of Health and Human Services. Centers for Disease Control and Prevention. National Center for Health Statistics. The National Nursing Home Survey 2004. Available at http://www.cdc.gov/nchs/nnhs.htm. Accessed January 10,2011.Stevenson DG, Huskamp HA, Newhouse JP. Medicare Part D, Nursing Homes, and Long-Term Care Pharmacies. June 2007. No 07-2.
Most SNF Residents Are Receiving at Least Five Medications
U.S. Department of Health and Human Services. Centers for Disease Control and Prevention. National Center for Health Statistics. The National Nursing Home Survey 2004. Available at http://www.cdc.gov/nchs/nnhs.htm.Accessed January 10, 2011
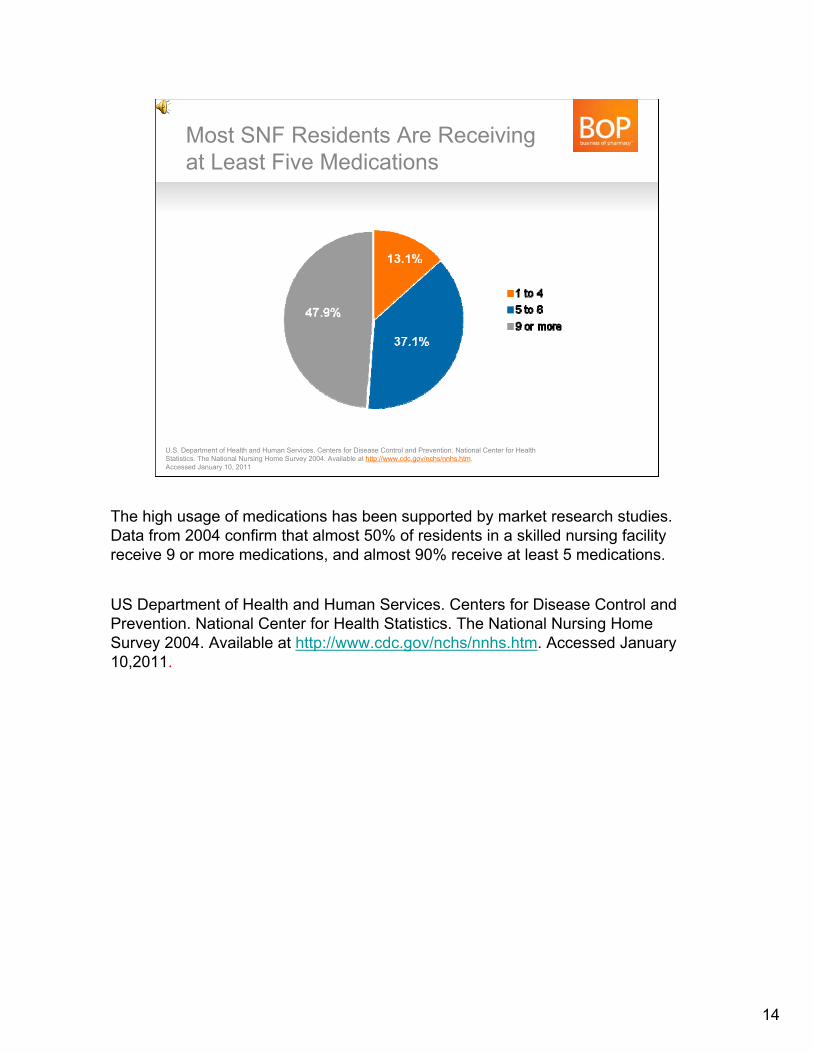
The high usage of medications has been supported by market research studies. Data from 2004 confirm that almost 50% of residents in a skilled nursing facility receive 9 or more medications, and almost 90% receive at least 5 medications.
US Department of Health and Human Services. Centers for Disease Control and Prevention. National Center for Health Statistics. The National Nursing Home Survey 2004. Available at http://www.cdc.gov/nchs/nnhs.htm. Accessed January 10,2011.
14
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
1,600,000
1,800,000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Certified Beds
SNF: Largest Long-Term Care Segment, but Limited Growth
Bed
s an
d R
esid
ents
15,000
15,500
16,000
16,500
17,000
Certified Facilities Certified Residents
American Health Care Association. Trend in Certified Nursing Facilities, Beds and Residents. Available at www.ahca.org. Accessed January 2011.
15
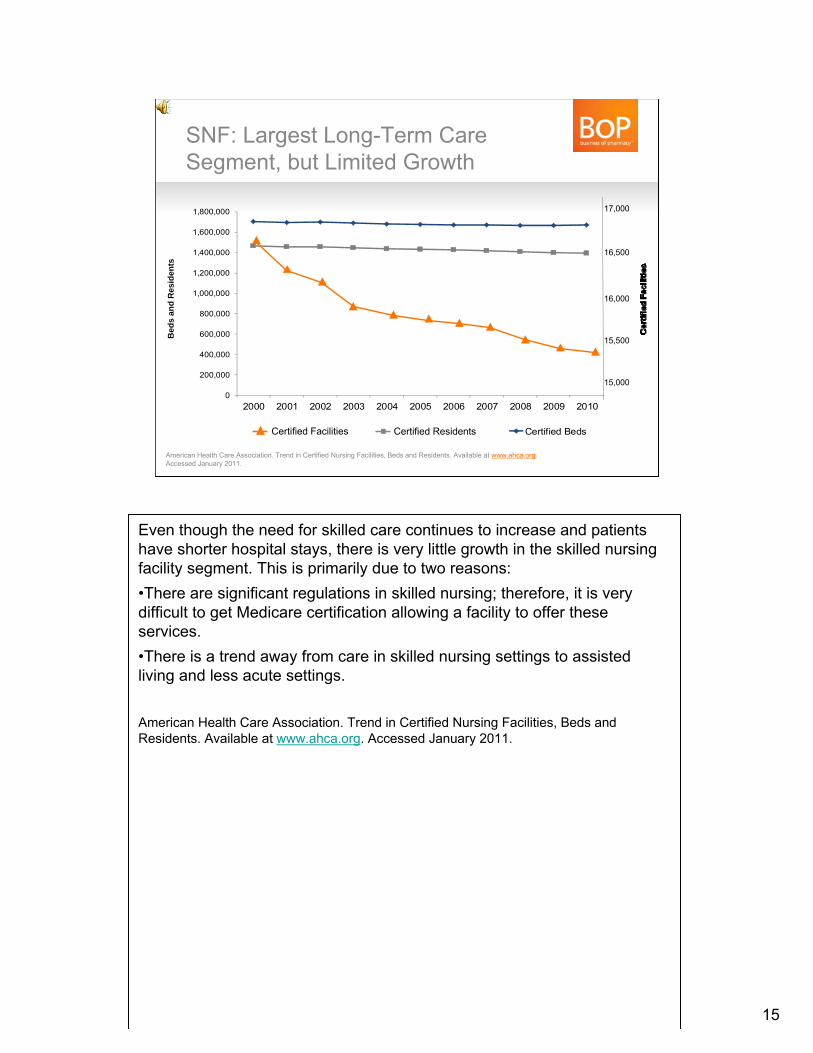
Even though the need for skilled care continues to increase and patients have shorter hospital stays, there is very little growth in the skilled nursing facility segment. This is primarily due to two reasons:•There are significant regulations in skilled nursing; therefore, it is very difficult to get Medicare certification allowing a facility to offer these services. •There is a trend away from care in skilled nursing settings to assisted living and less acute settings.
American Health Care Association. Trend in Certified Nursing Facilities, Beds and Residents. Available at www.ahca.org. Accessed January 2011.
A Definition of Assisted LivingAssisted-Living Workgroup–Assisted living is a state-regulated and monitored residential long-term care option. Assisted living provides or coordinates oversight and services to meet the residents’ individualized scheduled needs, based on the residents’ assessments and service plans, and their unscheduled needs as they arise.
–Services that are required by state law and regulation to be provided or coordinatedmust include but are not limited to:
– 24-hour awake staff to provide oversight and meet scheduled and unscheduled needs– Provision and oversight of personal care and supportive services– Health-related services (e.g., medication management services)– Meals, housekeeping and laundry– Recreational activities– Transportation and social services
–A cash model for most living and healthcare– Federal government does not generally provide reimbursement, except medications
under Medicare Part D– Medicaid waiver programs are the exception
Overview of Residential Care and Assisted Living Policy 2007. Available at: http://aspe.hhs.gov/daltcp/reports/2007/07alcom1.pdf. Accessed February 2011.
16
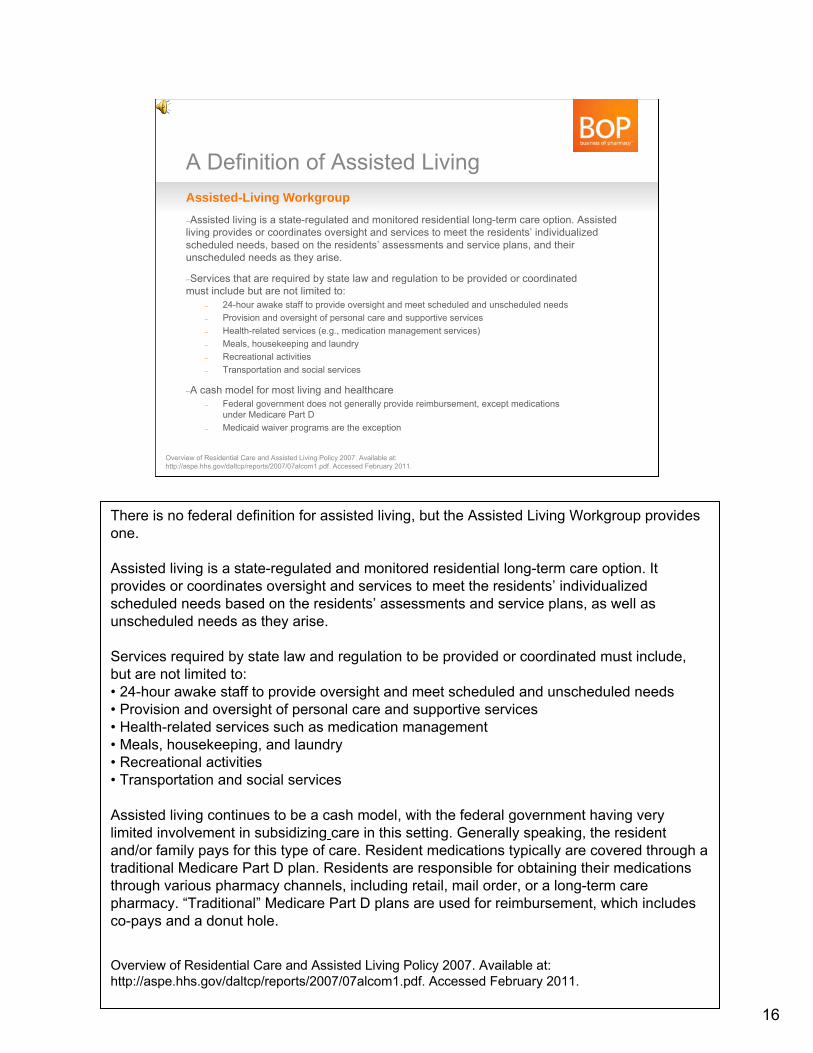
There is no federal definition for assisted living, but the Assisted Living Workgroup provides one.
Assisted living is a state-regulated and monitored residential long-term care option. It provides or coordinates oversight and services to meet the residents’ individualized scheduled needs based on the residents’ assessments and service plans, as well as unscheduled needs as they arise.
Services required by state law and regulation to be provided or coordinated must include, but are not limited to:• 24-hour awake staff to provide oversight and meet scheduled and unscheduled needs• Provision and oversight of personal care and supportive services• Health-related services such as medication management• Meals, housekeeping, and laundry• Recreational activities• Transportation and social services
Assisted living continues to be a cash model, with the federal government having very limited involvement in subsidizing care in this setting. Generally speaking, the resident and/or family pays for this type of care. Resident medications typically are covered through a traditional Medicare Part D plan. Residents are responsible for obtaining their medications through various pharmacy channels, including retail, mail order, or a long-term care pharmacy. “Traditional” Medicare Part D plans are used for reimbursement, which includes co-pays and a donut hole.
Overview of Residential Care and Assisted Living Policy 2007. Available at: http://aspe.hhs.gov/daltcp/reports/2007/07alcom1.pdf. Accessed February 2011.
Typical Assisted Living Resident– Average age 83–85 years old, female
– Requires assistance with two activities of daily living (ADLs)
– Largest growth is the population with cognitive dysfunction
– High prevalence of:– Hypertension– Arthritis– Depression– Osteoporosis– Heart disease– Diabetes
National Center for Assisted Living. The 2006 Overview of Assisted Living: Facts and Trends.Available at www.ncal.org.Overview of Residential Care and Assisted Living Policy 2007. Available at www.aspe.hhs.gov.
17
The demographics of a typical assisted living resident are similar to those of the typical skilled nursing facility resident.
Most require assistance with two activities of daily living, or “ADLs,” such as meals and transportation.
The largest area of growth in this setting is in residents with cognitive dysfunction. This disease state makes it difficult for individuals to reside at home. With progression of cognitive dysfunction, residents may enter a living setting in which there is greater monitoring and assistance with ADLs.
In addition to cognitive dysfunction in this population, there is a high prevalence of diseases that are common in the elderly, including cardiovascular disease and diabetes.
National Center for Assisted Living. The 2006 Overview of Assisted Living: Facts and Trends. Available at www.ncal.org.Overview of residential care and assisted living policy 2007. Available at www.aspe.hhs.gov.
Assisted Living:Let’s Look at the Numbers– Approximately 1 million people residing in AL
– State licensed; therefore, rules and regulations will vary
– This will result in services required/provided varying from facility to facility
– AL may be called various names– Assisted living– Residential care– Basic-care facility
– Reimbursement for medications– Primarily a cash business– Private insurance for some residents– Medicare Part B for some supplies
– Some state Medicaid models
– Very fragmented industry, with 10 largest companiesresponsible for less than 15% of beds
National Center for Assisted Living. Assisted Living State Regulatory Review 2009. March 2009.Available at www.ncal.org. Provider. 50 Largest Nursing Home Chains 2010. June 2010.
18
Let’s now look at some statistics on assisted living.
About one million Americans make their home in assisted living settings.
These settings are state licensed, so the rules and regulations will vary from state to state.
Assisted living may be called by various names, including residential care and basic care facilities, so it is important to do research in your area.
As already noted, medications generally are reimbursed through a “traditional”Medicare Part D plan that includes copays and a donut hole. Medications administered in a physician’s office or requiring special administration techniques may be covered through Medicare Part B.
Most care is reimbursed through a cash model, but there are some Medicaid state pilot programs being implemented, so be on the lookout for these in your area. They may affect reimbursement for medications.
Similar to skilled nursing, assisted living is a very fragmented industry, with the 10 largest companies responsible for less that 15% of beds.
National Center for Assisted Living. Assisted Living State Regulatory Review 2009. March 2009. Available at www.ncal.orgProvider. 50 Largest Nursing Home Chains 2010. June 2010.
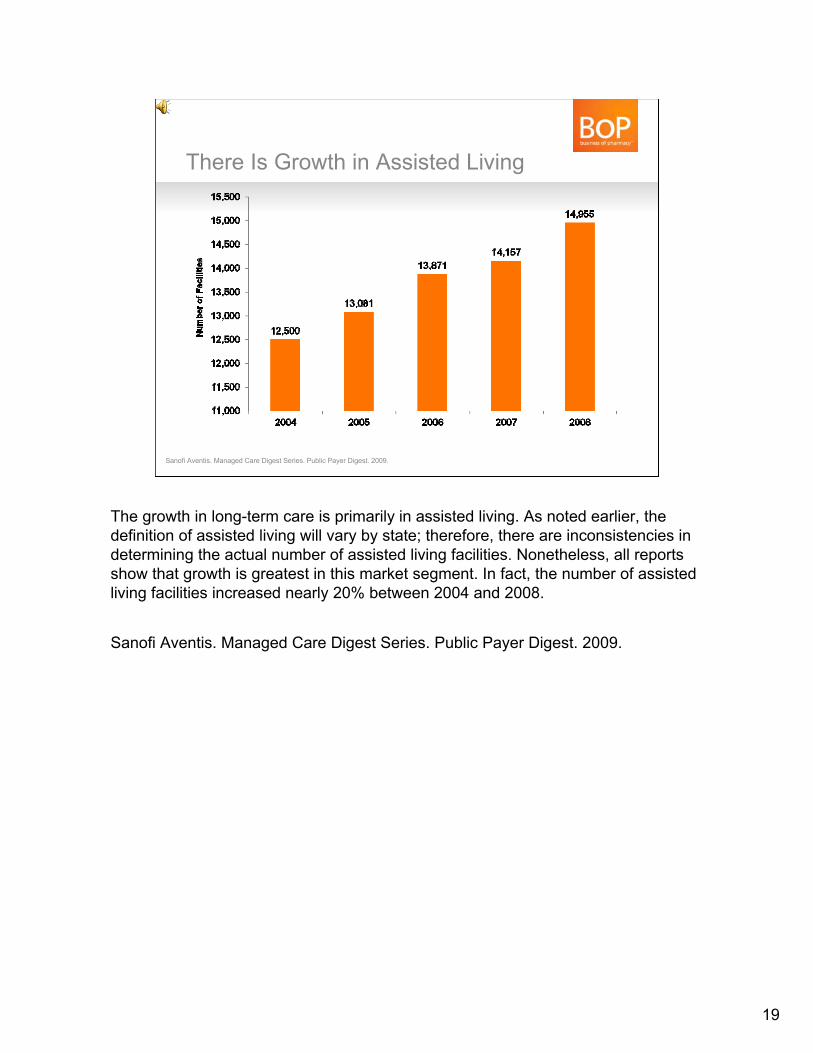
There Is Growth in Assisted Living
Sanofi Aventis. Managed Care Digest Series. Public Payer Digest. 2009.
The growth in long-term care is primarily in assisted living. As noted earlier, thedefinition of assisted living will vary by state; therefore, there are inconsistencies in determining the actual number of assisted living facilities. Nonetheless, all reports show that growth is greatest in this market segment. In fact, the number of assisted living facilities increased nearly 20% between 2004 and 2008.
Sanofi Aventis. Managed Care Digest Series. Public Payer Digest. 2009.
19
20
Pharmacies Driven to Seek New Growth Areas– Historically, LTC closed-door pharmacies focused on
services for SNFs and AL
– Significant brand-to-generic shift and reduced reimbursements strained the margins forLTC pharmacies
– Significant growth in home infusion and specialty markets presents additional revenue opportunities
– Result: Independent LTC pharmacies began taking lead to serve patients in alternate sites of care
Date on file. MatureHealth Communications. 2011.
With the lack of growth in skilled nursing facilities and significant shift from branded pharmaceuticals to generics, long-term care pharmacies’ profit margins have been reduced in this marketplace. Pharmacies have been looking for alternative areas to grow their business, with a key area being alternate sites of care.
Date on file. MatureHealth Communications. 2011.
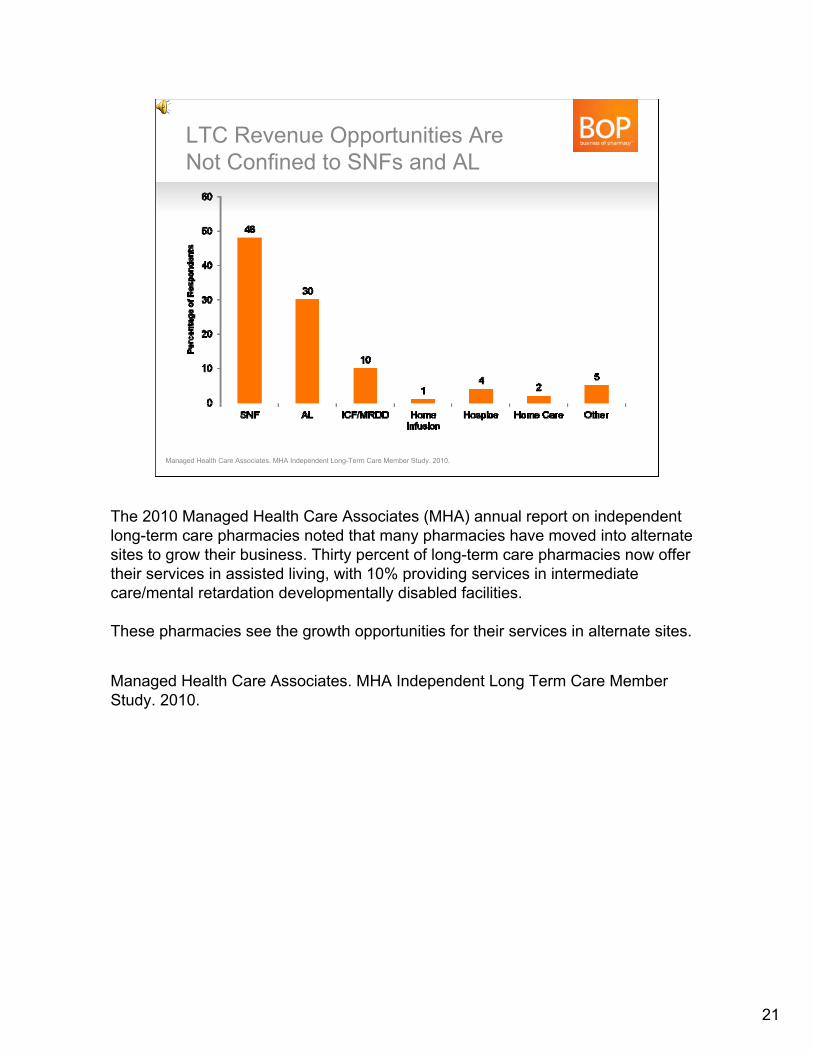
LTC Revenue Opportunities Are Not Confined to SNFs and AL
Managed Health Care Associates. MHA Independent Long-Term Care Member Study. 2010.
The 2010 Managed Health Care Associates (MHA) annual report on independent long-term care pharmacies noted that many pharmacies have moved into alternate sites to grow their business. Thirty percent of long-term care pharmacies now offer their services in assisted living, with 10% providing services in intermediate care/mental retardation developmentally disabled facilities.
These pharmacies see the growth opportunities for their services in alternate sites.
Managed Health Care Associates. MHA Independent Long Term Care Member Study. 2010.
21
LTC Pharmacy: A Segment within Alternate Site Pharmacy
AlternateSite Pharmacy
Long-Term Care Pharmacy
Behavioral Health
Home Infusion
Hospice
Correctional
Specialty
Non-chain Mail Order
Data on file. McKesson. 2011.
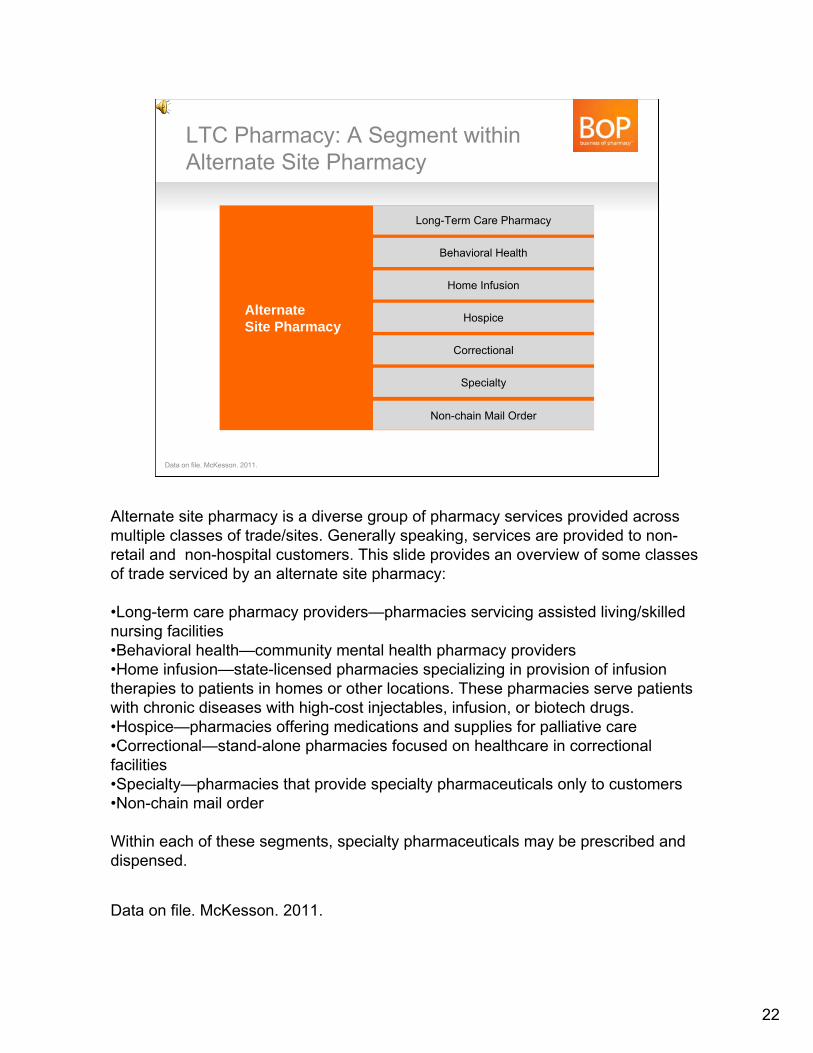
Alternate site pharmacy is a diverse group of pharmacy services provided across multiple classes of trade/sites. Generally speaking, services are provided to non-retail and non-hospital customers. This slide provides an overview of some classes of trade serviced by an alternate site pharmacy:
•Long-term care pharmacy providers—pharmacies servicing assisted living/skilled nursing facilities•Behavioral health—community mental health pharmacy providers•Home infusion—state-licensed pharmacies specializing in provision of infusion therapies to patients in homes or other locations. These pharmacies serve patients with chronic diseases with high-cost injectables, infusion, or biotech drugs.•Hospice—pharmacies offering medications and supplies for palliative care•Correctional—stand-alone pharmacies focused on healthcare in correctional facilities•Specialty—pharmacies that provide specialty pharmaceuticals only to customers•Non-chain mail order
Within each of these segments, specialty pharmaceuticals may be prescribed and dispensed.
Data on file. McKesson. 2011.
22
Main Drivers for Use of Specialty Pharmaceuticals in Alternate SiteSpecialty therapy prevalence increase
– Improving diagnostic tools – Earlier use of medication in treatment regimen – Expanded indications within a disease state
Specialty pharmaceutical cost/unit (inflation) increase– Limited generic pressure– Limited clinical competition
New drug entrants– Research/development resulting in robust specialty pipeline– New treatments for rare diseases expanding
orphan drug class
Express Scripts 2009 Drug Trend ReportMurray LA. 2011 MHA Business Summit Presentation. March 17, 2011.
23
There are several reasons for the growth of specialty pharmaceuticals in alternate site pharmacy.
One factor is an increased prevalence of management options to treat diseases that require these types of medications. Often these medications are used early in therapy.
Many specialty pharmaceuticals have a high cost due to limited brand and generic competition.
Most important is the growth in the number of new drugs in this marketplace. There are currently more than 280 medications in phase III development; most of these are oncology agents. Many of these agents are new treatments for rare diseases in the orphan drug class.
Express Scripts 2009 Drug Trend Report.Murray LA. 2011 MHA Business Summit Presentation. March 17, 2011
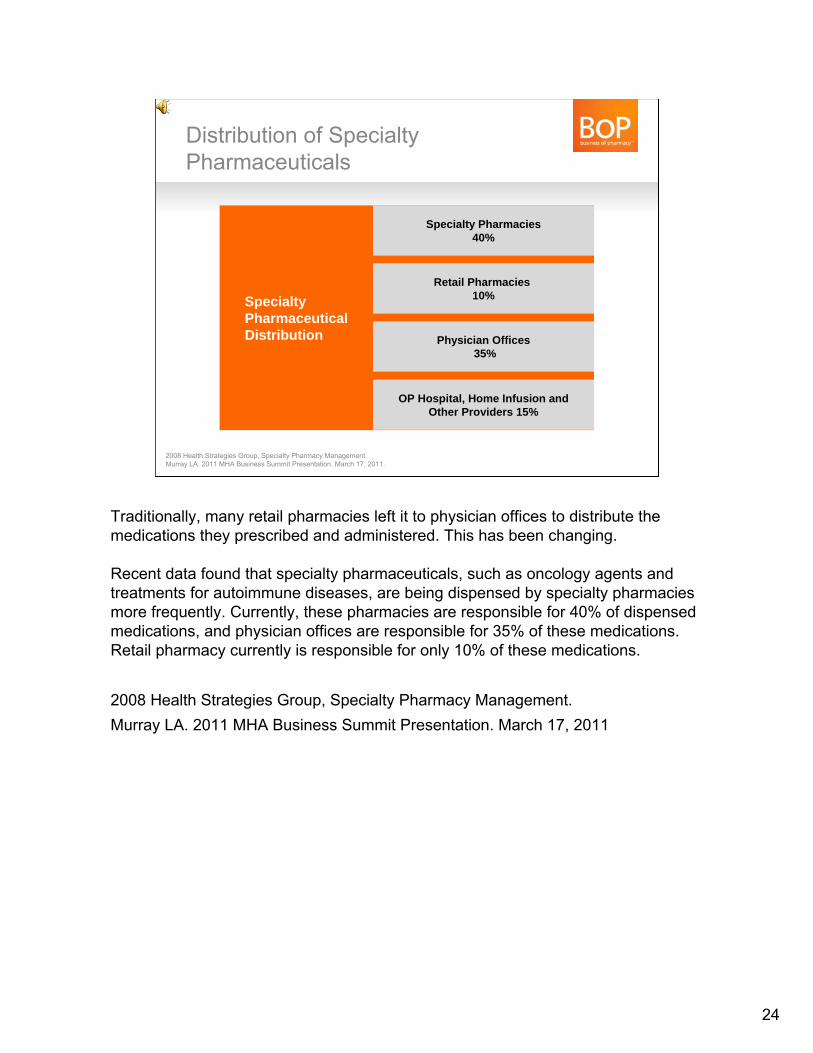
Distribution of Specialty Pharmaceuticals
SpecialtyPharmaceuticalDistribution
Specialty Pharmacies40%
Retail Pharmacies 10%
Physician Offices35%
OP Hospital, Home Infusion andOther Providers 15%
2008 Health Strategies Group, Specialty Pharmacy Management.Murray LA. 2011 MHA Business Summit Presentation. March 17, 2011.
Traditionally, many retail pharmacies left it to physician offices to distribute the medications they prescribed and administered. This has been changing.
Recent data found that specialty pharmaceuticals, such as oncology agents and treatments for autoimmune diseases, are being dispensed by specialty pharmacies more frequently. Currently, these pharmacies are responsible for 40% of dispensed medications, and physician offices are responsible for 35% of these medications. Retail pharmacy currently is responsible for only 10% of these medications.
2008 Health Strategies Group, Specialty Pharmacy Management.Murray LA. 2011 MHA Business Summit Presentation. March 17, 2011
24
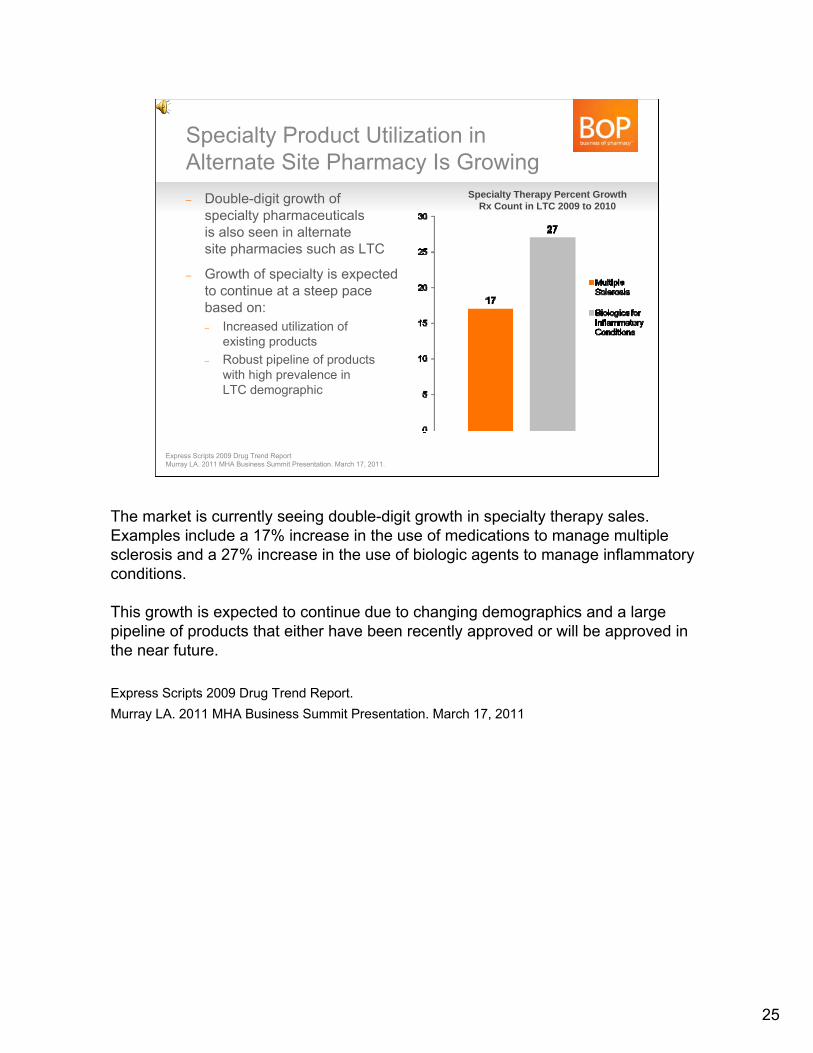
Specialty Product Utilization in Alternate Site Pharmacy Is Growing– Double-digit growth of
specialty pharmaceuticalsis also seen in alternatesite pharmacies such as LTC
– Growth of specialty is expectedto continue at a steep pacebased on:– Increased utilization of
existing products– Robust pipeline of products
with high prevalence inLTC demographic
Specialty Therapy Percent Growth Rx Count in LTC 2009 to 2010
Express Scripts 2009 Drug Trend ReportMurray LA. 2011 MHA Business Summit Presentation. March 17, 2011.
25
The market is currently seeing double-digit growth in specialty therapy sales. Examples include a 17% increase in the use of medications to manage multiple sclerosis and a 27% increase in the use of biologic agents to manage inflammatory conditions.
This growth is expected to continue due to changing demographics and a large pipeline of products that either have been recently approved or will be approved in the near future.
Express Scripts 2009 Drug Trend Report.Murray LA. 2011 MHA Business Summit Presentation. March 17, 2011
Home infusion therapy was an$11 billion market in 2009,with projected growth toapproach $16 billion by 2012
Home infusion therapy was an$11 billion market in 2009,with projected growth toapproach $16 billion by 2012
Home Infusion Segment Growth = Opportunity
Beyond an aging population, growth caused by:–Increased awareness and acceptance of home health–Patient preference for home-based care–Ability to provide broader scope of home-based services due to technology and clinical advances–Lower-cost setting relative to other institutional settings–A changing reimbursement environment
McClinton D. The Right Dose. HomeCare. Available at http://homecaremag.com/mag/home-infusion-therapy-market-200910/. Accessed April 28, 2011.
26
Home infusion therapy was an $11 billion market in 2009, with a projected growth to approach $16 billion by 2012. The growth in this market is due to several factors, primarily an aging population. Other causes include an increased awareness and acceptance of home healthcare as a treatment option and patient preference for management at home.
McClinton D. The Right Dose. HomeCare. Available at http://homecaremag.com/mag/home-infusion-therapy-market-200910/. Accessed April 28, 2011.
27
Services Provided in Long-Term Care and Alternate Site Pharmacy
Long-Term Care Pharmacy 101Module #2
Let’s move on to Long-Term Care Pharmacy 101, Module #2. This section will provide an overview of the services provided in long-term care and alternate site pharmacy.
Types of LTC Pharmacy Will Vary– Currently over 1,000 LTC pharmacies and an estimated
200,000 pharmacists are involved in providing services in LTC settings
– Concentrated within two large pharmacy corporations, plus many independents– Omnicare — approximately 500,000 SNF beds (2008)– PharMerica — approximately 300,000 SNF beds (2008)
– Margins vary from 7% to 30%, depending upon population served and product mix– Branded vs. generic, orals vs. injectables
Stevenson DG, Huskamp HA, Newhouse JP. Medicare Part D, Nursing Homes, and Long-Term Care Pharmacies. June 2007. No 07-2.
28
The types of pharmacies servicing long-term care facilities will vary.
Currently there are more than 1,000 long-term care pharmacies servicing this segment, with more than 200,000 pharmacists providing some type of care. These pharmacies can range from a local retail pharmacy near a facility to a large long-term care pharmacy corporation.
Services currently are concentrated among two large long-term care pharmacy corporations, Omnicare and PharMerica. Many smaller independent long-term care pharmacies also provide services across the country.
Many of these pharmacies started out providing services only in skilled nursing facilities. Over the last several years these pharmacies have expanded their scope of business to include alternate sites of care, including assisted living, intermediate care facilities, mental retardation/developmentally disabled, and specialty pharmacy.
Margins among these pharmacies vary greatly but average 7% to 30%, depending upon the contracts and medications dispensed.
Stevenson DG, Huskamp HA, Newhouse JP. Medicare Part D, Nursing Homes, and Long-Term Care Pharmacies. June 2007. No 07-2.
Advantages and Challenges of Smaller LTC PharmaciesAdvantages–Successes in retail pharmacy can translate to success in LTC pharmacy–Established relationships in the community–Ability to personalize services to facility–Ability to purchase through GPO or network
Challenges–Ability to hold receivables for Part D charges–Lack of economies of scale
Crawford P, Burton, R, Eldridge G, Belcher M. Introduction to Long-Term Care Pharmacy-Profitable Opportunities for Independents. Presented October 14, 2007. National Community Pharmacists Association.
29
As the owner of a retail pharmacy, you should be aware of the advantages and challenges of expanding your business base into long-term care. This slide provides an overview of these factors.
From an advantage perspective, the business methods you have used in retail pharmacy can translate to long-term care. A first step would be to establish relationships in your community to determine who may be in need of your services. As a local business owner, you have this advantage over larger corporate long-term care pharmacies.
A key would be to personalize your service to the needs of the facility. As a business owner, you have the ability to be flexible and meet the needs of the facility.
Similar to retail pharmacy, joining a group purchasing organization or long-term care pharmacy network can result in medication pricing that is competitive with that of larger organizations.
A challenge for retail pharmacies is the ability to hold receivables that occur with dispensing of medications. Retail prescriptions are paid at the time of dispensing; skilled nursing prescriptions generally are not. Your pharmacy may not be paid for 30 to 90 days after the prescription is dispensed. This will be discussed in greater detail later in this presentation.
In addition, your pharmacy may not have the economies of scale that a pharmacy specifically focused on long-term care may have.
Crawford P, Burton, R, Eldridge G, Belcher M. Introduction to Long-Term Care Pharmacy-Profitable Opportunities for Independents. Presented October 14, 2007. National Community Pharmacists Association.
There Are Differences Between LTC and Other Settings Serviced by Pharmacies
– Regulatory environment with an emphasis on survey and certification
– Importance and need for interdisciplinary care planning– Very labor-intensive, with fewer professionals managing
a large number of direct-care staff– Integration of care across the healthcare continuum– The technology differences between settings
Consultant Pharmacist Handbook. A Guide for Consulting to Nursing Facilities. American Society of Consultant Pharmacists. 2004.
30
Let’s now compare long-term care with other healthcare settings being serviced by retail pharmacies.
There is a much greater emphasis on the regulatory environment in long-term care than in other settings.
The LTC setting focuses on interdisciplinary care planning. Nurses, pharmacists, physicians, nurse practitioners, social workers, and other healthcare providers all have important roles.
Long-term care is very labor-intensive. Compared to staff in the hospital setting, a nurse or other healthcare provider in long-term care generally is responsible for managing a larger number of direct-care staff such as nurse aides.
We have already mentioned CCRCs and the integration of care across the continuum. A challenge in this setting is the need for appropriate care to move with a resident who transfers from one setting to another.
At this time, technology such as electronic medical records has had a limited impact in this setting. But as new technologies are shown to improve care and efficiency in these systems, acceptance will occur.
Consultant Pharmacist Handbook. A Guide for Consulting to Nursing Facilities. American Society of Consultant Pharmacists. 2004.
Pharmacy Services Mandated by Federal Government
Omnibus Budget Reconciliation Act of 1987 (OBRA ‘87)
Residents – Must be free from unnecessary medications, those given in excessive doses, in
excessive duration, or without adequate monitoring– May self-administer medications if deemed appropriate
Facility– Medication error rate must not be higher than 5%– Must provide routine and emergency drugs and biologicals– Must employ a licensed pharmacist
– Provides consulting services– Record-keeping for controlled substances– Determines medication records are in order
Thorough drug regimen review, proper labeling and storage of medication and biologicals
The Lewin Group. CMS Review of Current Standards of Practice for Long-Term Care Pharmacy Services. Long-Term Care Primer. Dec 30, 2004 .
31
Pharmacy services in skilled nursing facilities are mandated by the federal government—these services must be provided by a registered pharmacy.
The regulations in place for pharmacy services were passed in the 1987 Omnibus Budget Reconciliation Act. This act provided guidance on how medications must be monitored and administered to residents in skilled nursing facilities.
The facilities also must meet certain criteria to avoid being considered deficient in care. These criteria include:• A medication error rate no higher than 5%• The ability to provide routine and emergency drugs and biologicals• The use of a licensed pharmacist to provide required services, including consulting and dispensing
In addition, long-term care pharmacies must provide drug regimen review (called “DRR”) and proper labeling and storage of medications used in the facility.
The Lewin Group. CMS Review of Current Standards of Practice for Long-Term Care Pharmacy Services Long Term Care Primer. Dec 30, 2004 .
Mapping the Pharmacy Process: Nursing Facility/Closed-Door Pharmacy
Receive MedicationsReceive Medications
LTC Pharmacy Processes NF PrescriptionLTC Pharmacy Processes NF Prescription
Patient-SpecificRecord Update
Patient-SpecificSafety Check
Formulary Check
If Unused: Dispose at NFSite or Return to LTCP
If Unused: Dispose at NFSite or Return to LTCP
Nursing Facility or Other Closed-Door Pharmacy
Physician, Nursing FacilityStaff, and Pharmacist
DetermineTherapeutic Need
Physician, Nursing FacilityStaff, and Pharmacist
DetermineTherapeutic Need
New Order, Refill, orChange Request
New Order, Refill, orChange Request LTC Pharmacy Dispenses MedicationLTC Pharmacy Dispenses Medication
Specialized Packaging Labeling
Delivery 2-3x Day, 7 Days a Week,2-4 Hours in Emergency
Delivery 2-3x Day, 7 Days a Week,2-4 Hours in Emergency
The Lewin Group. CMS Review of Current Standards of Practice for Long-Term Care PharmacyServices. Long-Term Care Primer. Dec 30, 2004 .
32
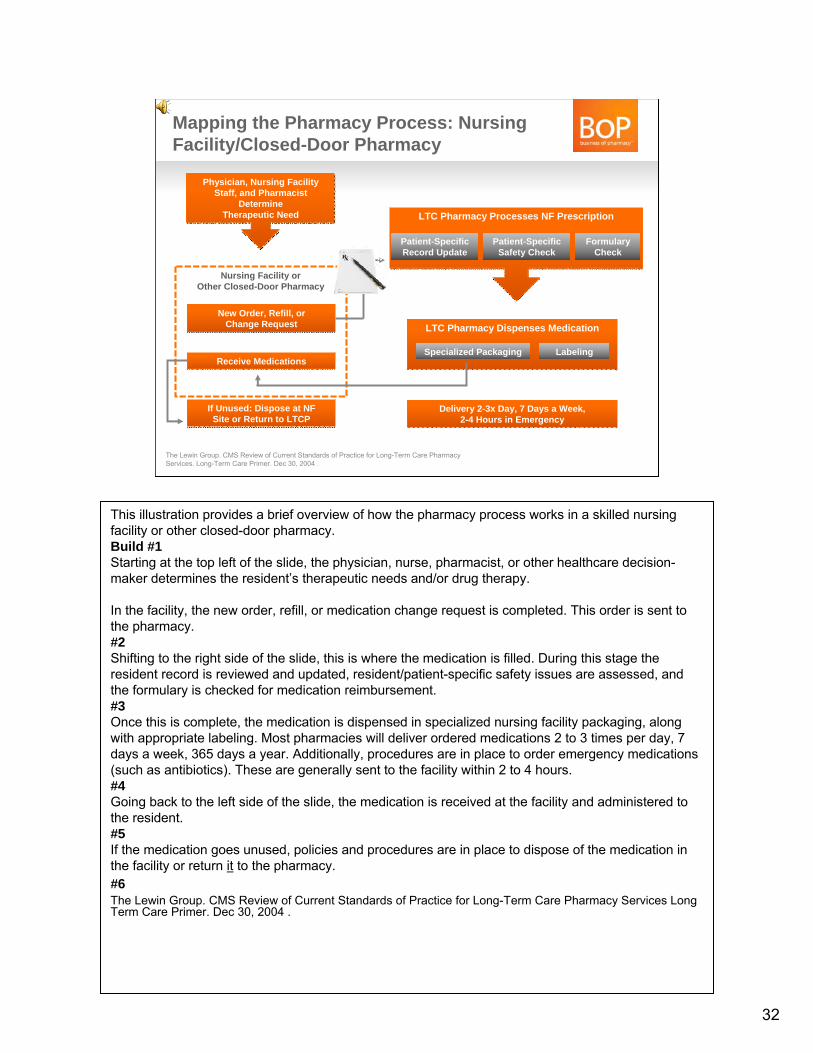
This illustration provides a brief overview of how the pharmacy process works in a skilled nursing facility or other closed-door pharmacy.Build #1Starting at the top left of the slide, the physician, nurse, pharmacist, or other healthcare decision-maker determines the resident’s therapeutic needs and/or drug therapy.
In the facility, the new order, refill, or medication change request is completed. This order is sent to the pharmacy. #2Shifting to the right side of the slide, this is where the medication is filled. During this stage the resident record is reviewed and updated, resident/patient-specific safety issues are assessed, and the formulary is checked for medication reimbursement. #3Once this is complete, the medication is dispensed in specialized nursing facility packaging, along with appropriate labeling. Most pharmacies will deliver ordered medications 2 to 3 times per day, 7 days a week, 365 days a year. Additionally, procedures are in place to order emergency medications (such as antibiotics). These are generally sent to the facility within 2 to 4 hours. #4Going back to the left side of the slide, the medication is received at the facility and administered to the resident.#5If the medication goes unused, policies and procedures are in place to dispose of the medication in the facility or return it to the pharmacy. #6The Lewin Group. CMS Review of Current Standards of Practice for Long-Term Care Pharmacy Services Long Term Care Primer. Dec 30, 2004 .
Pharmacy Services That Can Be Provided to LTC Facilities
Prescription Processing
Dispensing and Delivery
Medication Administration and Management
Return/Reuseand Disposal
Create medication record
Package medications in preferred packaging
Perform QA checks Accept return of unused medications
Clarify med orders Ensure proper labeling
Supply medication carts
Assist in disposal of medications (including controlled substances)
Respond to emergency med orders
Provide timely delivery
Perform consultant pharmacy services
Perform DRR Maintain Urgent Kit, floor stock
Apply formulary
The Lewin Group. CMS Review of Current Standards of Practice for Long-Term Care Pharmacy Services. Long-Term Care Pharmacy Primer. Dec 30, 2004.
33
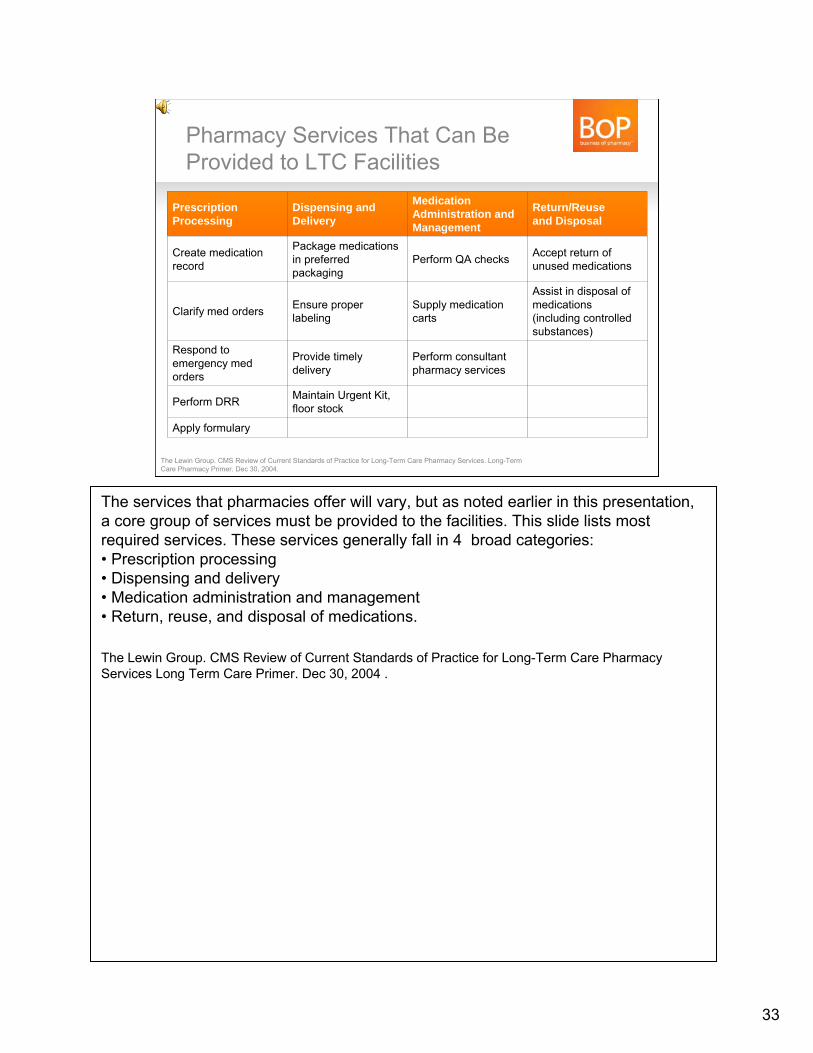
The services that pharmacies offer will vary, but as noted earlier in this presentation, a core group of services must be provided to the facilities. This slide lists most required services. These services generally fall in 4 broad categories:• Prescription processing• Dispensing and delivery• Medication administration and management• Return, reuse, and disposal of medications.
The Lewin Group. CMS Review of Current Standards of Practice for Long-Term Care Pharmacy Services Long Term Care Primer. Dec 30, 2004 .
What Is a Consultant Pharmacist?– A provider of pharmacy systems and medications– An educator– A drug information resource– A clinical practitioner– A patient/resident care advocate– A member of the healthcare team
Consultant Pharmacist Handbook. A Guide for Consulting to Nursing Facilities. American Society of Consultant Pharmacists. 2004.
34
What is a consultant pharmacist? The consultant pharmacist has several important roles. These include functioning as:•A provider of pharmacy systems and medications•A source for medication education and drug information•A clinical practitioner assisting in resident care; and advocating for residents•An important member of the healthcare team.
Consultant Pharmacist Handbook. A Guide for Consulting to Nursing Facilities. American Society of Consultant Pharmacists. 2004.
Selected Services Provided by a Consultant PharmacistPrimary Care Services–Drug regimen review–Medication dosing services–Diabetes management education and training–Patient/resident counseling–IV therapy services–Therapeutic drug monitoring
Information/Education Services–Medication delivery systems–QA programs–Drug information–In-service education–Outpatient compliance packaging–Medical/surgical supplies–Financial management support
Consultant Pharmacist Handbook. A Guide for Consulting to Nursing Facilities. American Society of Consultant Pharmacists. 2004.
35
Consultant pharmacist services can be organized into 2 categories:•Primary care services—These are services that all consultant pharmacists generally provide to a facility and are mandated in the Centers for Medicare and Medicaid Services State Operations Manual.•Information and education services—Most of these services are provided by a consultant pharmacist, but the level of involvement may vary from one facility to another. Discussions with your facilities will determine the level of services they require.
Consultant Pharmacist Handbook. A Guide for Consulting to Nursing Facilities. American Society of Consultant Pharmacists. 2004.
Consulting Services Working with the Interdisciplinary Team– Pharmacy and Therapeutic Committee
– Staff education
– Care-planning meetings
– Chart audit
– Survey review meetings
– Medication “brown bags” in AL settings
Consultant Pharmacist Handbook. A Guide for Consulting to Nursing Facilities. American Society of Consultant Pharmacists. 2004.
36
Providing consulting services is an important component of LTC pharmacy.
The pharmacy may be involved in various committees and/or have responsibility for diverse services in the facility, including: •The Pharmacy and Therapeutics Committee. This generally is chaired by the medical director, but the pharmacist has an integral role in evaluating medication usage within the facility.•Staff education, including training nurses and nurse aides•Care planning meetings with all members of the resident care team•Chart audit to evaluate trends in medication usage •Survey review meetings to minimize survey issues and keep the facility compliant•Medication “brown bags” in AL settings to minimize medication problems.
Consultant Pharmacist Handbook. A Guide for Consulting to Nursing Facilities. American Society of Consultant Pharmacists. 2004.
Computer SoftwareSystem must have the ability to:
–Maintain patient demographic info
–Monitor for drug interactions
–Adjudicate third-party payors– Generally not in real time but after medication is dispensed
–Print drug dispensing materials
–Maximize workflow efficiencies
Introduction to Long-Term Care Pharmacy Services. A Certificate Training Program. Monograph 3: Setting up Your Operations. American Society of Consultant Pharmacists. 2007.
37
Computer software is used in all facilities and all pharmacies.
These computer systems will vary, but all must have the ability to:•Maintain patient demographic information, including all important clinical data related to medication usage, such as laboratory results•Monitor for drug interactions. This would be similar to the system used within your pharmacy, but it must include records of all medications, bit prescription, and over-the-counter•Adjudicate third-party payors. This would include prescription drug plans and other insurers•Print drug dispensing materials for use by the nursing staff, caregivers, and residents within the facilities •Maximize workflow efficiencies to minimize errors and wastage, improve care, and maximize profitability.
Introduction to Long-Term Care Pharmacy Services. A Certificate Training Program. Monograph 3: Setting up Your Operations. American Society of Consultant Pharmacists. 2007.
Moving to a Paperless System– Maximize efficiencies by moving from a paper to a
digital system– Faxed prescription link to prescription number for retrieval
and review– Links order to inventory control and reordering– Verify accuracy of dispensed product– Assists in tracking pharmacy workflow
– Must address medication returns and credits
Introduction to Long-Term Care Pharmacy Services. A Certificate Training Program. Monograph 3: Setting up Your Operations. American Society of Consultant Pharmacists. 2007.
38
Long-term care pharmacies are following retail pharmacies’ lead by moving from a paper process to electronic management. Long-term care is not fully electronic, but it is moving in that direction through the use of fax and electronic systems to transmit prescriptions from the nursing facility to the pharmacy. At the pharmacy the order is reviewed and linked to other orders to monitor inventory control and reordering.
All medications are verified for accuracy and compared with the clinical information in the pharmacy database. Only after all aspects of medication dispensing have been evaluated will the prescription be provided.
During this process, the pharmacy monitors pharmacy workflow for accuracy and consistency.
In addition to the dispensing process, pharmacies must address medication returns and credits.
Introduction to Long-Term Care Pharmacy Services. A Certificate Training Program. Monograph 3: Setting up Your Operations. American Society of Consultant Pharmacists. 2007.
Must Have the Ability to Generate and Track Using Facility Forms– Physician order sheet
– Medication administration record (MAR)
– Treatment administration record
– Pain management forms
– Nutritional forms
– Infusion therapy forms
– Control substance forms
Introduction to Long-Term Care Pharmacy Services. A Certificate Training Program. Monograph 3: Setting up Your Operations. American Society of Consultant Pharmacists. 2007.
39
All pharmacy systems must have the ability to generate and track using forms that are consistent with the facility’s forms. This generally is one of the first discussions you willhave with a facility, either before or after you are contracted by the facility.
Forms that your pharmacy may be required to provide include:• Physician order sheet• Medication administration record (MAR)• Treatment administration record• Pain management forms• Nutritional forms• Infusion therapy forms• Control substance forms
Introduction to Long-Term Care Pharmacy Services. A Certificate Training Program. Monograph 3: Setting up Your Operations. American Society of Consultant Pharmacists. 2007.
Medication Dispensing Customizedfor LTC24/7 pharmacy availability7- to 30-day packaging
– Currently at 30-day, but will be moving to 14-day by 2013 for branded medications
Bingo or punch cards– Most commonly used system
Box system– Up to 30-day supply for a resident
“Opus” system– More common in AL settings
Automated dispensing system– Medication packaged based on medication pass time– Generally 1–2 week supply at one time, delivered to the facility
Introduction to Long-Term Care Pharmacy Services. A Certificate Training Program. Monograph 3: Setting up Your Operations. American Society of Consultant Pharmacists. 2007.
40
The type of medication dispensing system that will be required also will be an initial discussion topic when you are contracted to provide services to a facility.
Most facilities will require pharmacy services 24 hours a day, 7 days a week. Systems must be in place to provide services at night, on weekends, and during holidays.
Most packaging currently used in facilities is for 7 to 30 days of medications. Recent federal legislation has dictated that pharmacies move to “short cycle dispensing” of 14 days for branded medications. This will be discussed in greater detail in Long-Term Care Pharmacy 102.
The most common system in current use is bingo or punch cards for 30 days. These are similar to unit dose packaging used in hospitals. Other systems that may be used include a box system and the “Opus” system used in assisted living settings.
The use of automated dispensing systems is increasing and generally includes delivering a 1- to 2-week supply of medication to the automated delivery system. These medications are then dispensed through the system to nurses in the facility.
Introduction to Long-Term Care Pharmacy Services. A Certificate Training Program. Monograph 3: Setting up Your Operations. American Society of Consultant Pharmacists. 2007.
The Urgent/Emergency Box– Regulated by state
– LTC pharmacy responsible for stocking
– Used for emergency doses and first doses
– Sealed box usually secured in a locked area
– Policies and procedures for use developed bypharmacy and facility
Introduction to Long-Term Care Pharmacy Services. A Certificate Training Program. Monograph 3: Setting up Your Operations. American Society of Consultant Pharmacists. 2007.
41
One pharmacy delivery system that is unique to long-term care is the urgent or emergency box. This includes medications that may be needed right away and cannot wait for a pharmacy delivery, such as antibiotics and acute pain medications.
What is included in the urgent/emergency box will be dictated by the state board of pharmacy. The facility can determine which of these medications should be kept in the box.
The pharmacy is responsible for providing and stocking this box.
The urgent/emergency box is typically sealed and stored in a locked area, especially if controlled substances are included.
How the urgent/emergency box is used will be defined by policies and procedures developed by the pharmacy and approved and implemented within the facility.
Introduction to Long-Term Care Pharmacy Services. A Certificate Training Program. Monograph 3: Setting up Your Operations. American Society of Consultant Pharmacists. 2007.
Medication Returns– Returned-medication policies dictated by state and board
of pharmacy– Must develop a policy and procedure for each facility– Must track unused medications within the facility– Generally two-part form — one to facility, the other to the pharmacy– Must have verification in place throughout process from facility back
to the pharmacy– Credit for unused medications will vary from state to state– Disposal of medications — flush/burn/bury — will also vary from
state to state http://www.ncsl.org/default.aspx?tabid=14425– This is an ongoing issue that is currently under
discussion with CMS and the DEA– Education of all personnel involved is essential
Introduction to Long-Term Care Pharmacy Services. A Certificate Training Program. Monograph 3: Setting up Your Operations. American Society of Consultant Pharmacists. 2007.National Conference of State Legislatures. State Prescription Drug Return, Reuse and Recycling Laws. Available at http://www.ncsl.org/default.aspx?tabid=14425.
42
Medication returns are a unique issue in nursing facilities. In a community setting, a person may just discard the medications; in the nursing facility this is not an option, and disposal is governed by state and federal regulations, as well as state boards of pharmacy.
Each facility must have a policy and procedure in place to account for all unused medications.
All unused medications must be tracked very closely, even if they stay in the facility and then are disposed of or returned to the pharmacy.
How medications can or should be disposed of will vary from state to state. This slide provides a website that has current information on how to handle these medications. Medication disposal continues to be an issue in facilities and should be closely monitored.
It is important for the pharmacy to educate all facility staff on how to handle unused medications and those that need to be returned.
Introduction to Long-Term Care Pharmacy Services. A Certificate Training Program. Monograph 3: Setting up Your Operations. American Society of Consultant Pharmacists. 2007.National Conference of State Legislatures. State Prescription Drug Return, Reuse and Recycling Laws. Available at http://www.ncsl.org/default.aspx?tabid=14425.
What Do Facilities Want?– Lowest cost for medications, including Medicare Part A
and stock supplies
– Comprehensive services
– Reliability and confidence with services
– Ability to track product usage and monitor closely
– Being proactive and aware that the market iscontinually changing
Crawford P, Burton, R, Eldridge G, Belcher M. Introduction to Long-Term Care Pharmacy — Profitable Opportunities for Independents. Presented October 14, 2007. National Community Pharmacists Association.
43
What are nursing facilities—both skilled nursing and assisted living—looking for from a pharmacy provider? The same characteristics needed to run a successful retail pharmacy are required for success in long-term care pharmacy.
First and foremost is low cost. The pharmacy’s costs don’t necessarily need to be the lowest, but they need to be competitive. This includes all costs associated with consulting and dispensing fees. In addition to prescription?? medications, also ask about other supplies the facility may need, such as over-the-counter medications and medical supplies. If you can provide these, their costs must be competitive.
Comprehensive consulting and dispensing services may require additional pharmacy resources and time, including the ability to get medications to the facility during nighttime hours, providing additional delivery services, and offering educational programming to the facility staff.
Services to facilities must be reliable, with a minimal error rate for dispensed medications. The facility must be confident in your ability to provide effective services.
Your pharmacy must have the ability to closely monitor and track product usage. The administrator and/or director of nursing will require you to monitor all expenses to the facility.
Above all, your service must be dependable and available when the facility needs it.
As a pharmacy owner, you must be proactive with respect to changes in your customer requests and also those mandated by the marketplace. Change is a constant. You need to be aware of changes and adapt your pharmacy when they occur.
Crawford P, Burton, R, Eldridge G, Belcher M. Introduction to Long-Term Care Pharmacy-Profitable Opportunities for Independents. Presented October 14, 2007 National Community Pharmacists Association.
Estimated Cost of LTCPharmacy Services
The Lewin Group. CMS Review of Current Standards of Practice for Long-Term Care Pharmacy Services. Long-Term Care Pharmacy Primer. Dec 30, 2004.
Service Fee Charged to Facility Cost for Pharmacy toProvide the Service
Specialized packaging
Medication delivery
Medication and treatment carts
Emergency backup systems
Medical records
Fax machines
Drug regimen review
Facility-specific reports
Counsel residents
Attend/participate in meetings, in-services
Med pass training /observation
On-call, 24-hour pharmacy dispensing
Controlled/dispose of medications
Manage controlled substances
Estimated Total
44
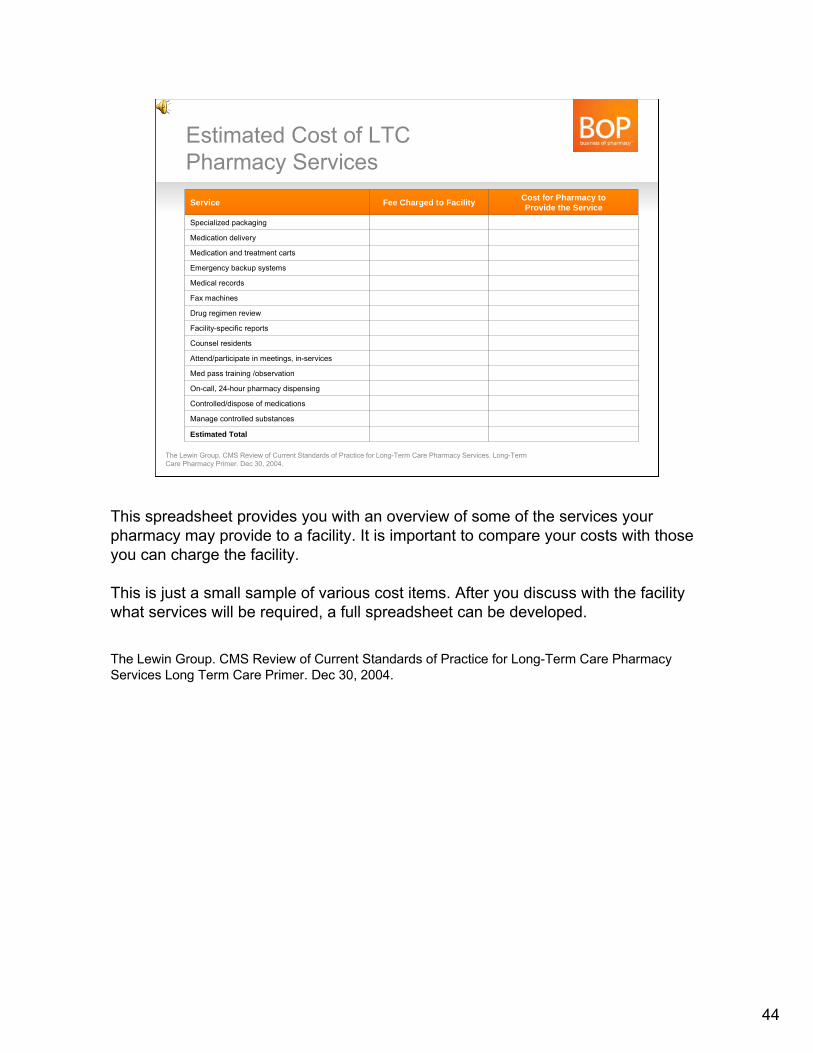
This spreadsheet provides you with an overview of some of the services your pharmacy may provide to a facility. It is important to compare your costs with those you can charge the facility.
This is just a small sample of various cost items. After you discuss with the facility what services will be required, a full spreadsheet can be developed.
The Lewin Group. CMS Review of Current Standards of Practice for Long-Term Care Pharmacy Services Long Term Care Primer. Dec 30, 2004.
Some Requirements for an Alternate Site Pharmacy– A pharmacy that maintains inventory and dispenses high-cost
medications to patients undergoing intensive therapies for illnessesthat are chronic or complex acute
– Have sufficient staff with training and expertise in: – Reimbursement– Patient education – Clinical monitoring– Inventory/packaging/shipping
– The pharmacy collects and reports medication usage andpurchasing activities
– Home-infusion pharmacies must meet sterile criteria andpackaging requirements
– Specialty pharmacies must meet packaging, shipping, andstorage requirements
Data on file. McKesson.National Home Infusion Association. Sterile Compounding: Issues and Resources.Available at http://www.nhia.org/about/sterilecompounding.cfm#topic6.National Home Infusion Association. Infusion FAQs. Available at http://www.nhia.org/faqs.cfm#faq13.
45
Federal, state, and prescription drug plans (PDPs) all have requirements for alternate site pharmacies.
A first step is to define an alternate site pharmacy. Most plans define this type of pharmacy as one that maintains an inventory and dispenses high-cost medications to patients undergoing therapies for chronic illnesses.
These pharmacies must offer and provide sufficient training for their staff in all areas associated with dispensing, storage, and usage of these medications. Pharmacies also must market and sell their services to key customers, such as hospitals, physicians, and other payors in alternate site pharmacy.
The pharmacy also must collect and report information that is required by federal or state organizations and PDPs. These reports must be available at any time for analysis, audits, and confirmation of reconciliation.
Data on file. McKesson.National Home Infusion Association. Sterile Compounding: Issues and Resources.Available at http://www.nhia.org/about/sterilecompounding.cfm#topic6.National Home Infusion Association. Infusion FAQs. Available at http://www.nhia.org/faqs.cfm#faq13.
46
Reimbursement for Product and Services in Long-Term Care and Alternate Site Pharmacy
Long-Term Care Pharmacy 101Module #3
The third and final module in this presentation will discuss the reimbursement process for long-term care and alternate site pharmacy. It will also provide an overview of how your pharmacy makes money providing services to these customers.

Medicare CoverageMedicare Part A
– Inpatient hospital– Skilled nursing facility – Home health– Hospice
Medicare Part B– Physician services, including medication administered in office– Services in ER, outpatient clinic– Home health not covered by Part A– Labs, x-rays, other diagnostics– Physical therapy – Ambulance services
Medicare Part D– Medications
The Henry J Kaiser Family Foundation. Medicaid: a primer 2009. Available at www.kff.org.The Henry J Kaiser Family Foundation. A primer on Medicare Financing. Available at www.kff.org.The Henry J Kaiser Family Foundation. Medicare 101: The Basics. Available at www.kff.org.
47
Let’s first discuss the major payors in healthcare and how this relates to long-term care and alternate site pharmacy.
Medicare is a healthcare entitlement program for people over age 65. This program is administered federally—all funds come from the federal government.
Medicare Part A covers short stays (up to 100 days) in a skilled nursing facility after a resident has been transferred from a hospital following a minimum 3-day stay. Medicare Part A also covers inpatient hospital stays, home healthcare, and Medicare-certified hospice care. In the hospice setting, a resident must be considered hospice-eligible by his or her attending physician. Hospice will then cover the patient’s costs for up to 6 months. After 6 months, the patient must reapply for Medicare hospice eligibility.
Medicare Part B covers physician and physician extender (such as a nurse practitioner) services, emergency room visits, home health services not covered by Medicare Part A, lab work, diagnostic tests, physical therapy, and ambulance services. This last covered service is important for skilled nursing facility residents who may require transport to or from a hospital.
Medicare Part D covers prescription medications. This coverage is offered through a medication-only prescription drug plan or Medicare Advantage plan.
The Henry J Kaiser Family Foundation. Medicaid: a primer 2009. Available at www.kff.org.The Henry J Kaiser Family Foundation. A primer on Medicare Financing. Available at www.kff.org.The Henry J Kaiser Family Foundation. Medicare 101: The Basics. Available at www.kff.org.
Medicare Part DPrescription Drug Plans (PDPs)– In 2011, 1,109 PDPs will be offered
– 332 plans will be available to low-income subsidy (LIS) enrollees — “Benchmark Plans”
– Total 8 million LIS enrollees — these include thoseresiding in LTC settings such as SNF
– Major plans include:– Humana– CVS Caremark– UnitedHealthcare– Wellcare– Universal American
The Henry J Kaiser Family Foundation. Medicare Part D Spotlight: Part D Plan Availability In 2011 And Key Changes Since 2006. Available at www.kff.org/medicare/8107.cfm.
48
Medicare Part D has impacted your pharmacy’s business and also has an impact on long-term care pharmacy. This will be discussed in greater detail in Long-Term Care Pharmacy 102.
In general, most long-term care low-income subsidy (or “LIS”) Medicare beneficiaries are placed in low-income plans called “Benchmark Plans.” Many residents in skilled nursing facilities are auto-enrolled into or assigned to one of these Benchmark Plans. For 2011, there are a total of 1,109 PDPs and 332 Benchmark Plans with approximately 8 million enrollees.
PDPs that offer Benchmark Plans include Humana, CVS Caremark, and UnitedHealthcare.
The Henry J Kaiser Family Foundation. Medicare Part D Spotlight: Part D Plan Availability In 2011 And Key Changes Since 2006. Available at www.kff.org/medicare/8107.cfm.
Long-Term Care Pharmacy
Nursing Facility and Residents
Stevenson DG, Huskamp HA, Newhouse JP. Medicare Part D, Nursing Homes, and Long-Term Care Pharmacies. June 2007. No 07-2.
Facility and Pharmacy Have Exclusive Contract, but Many PDPs
49
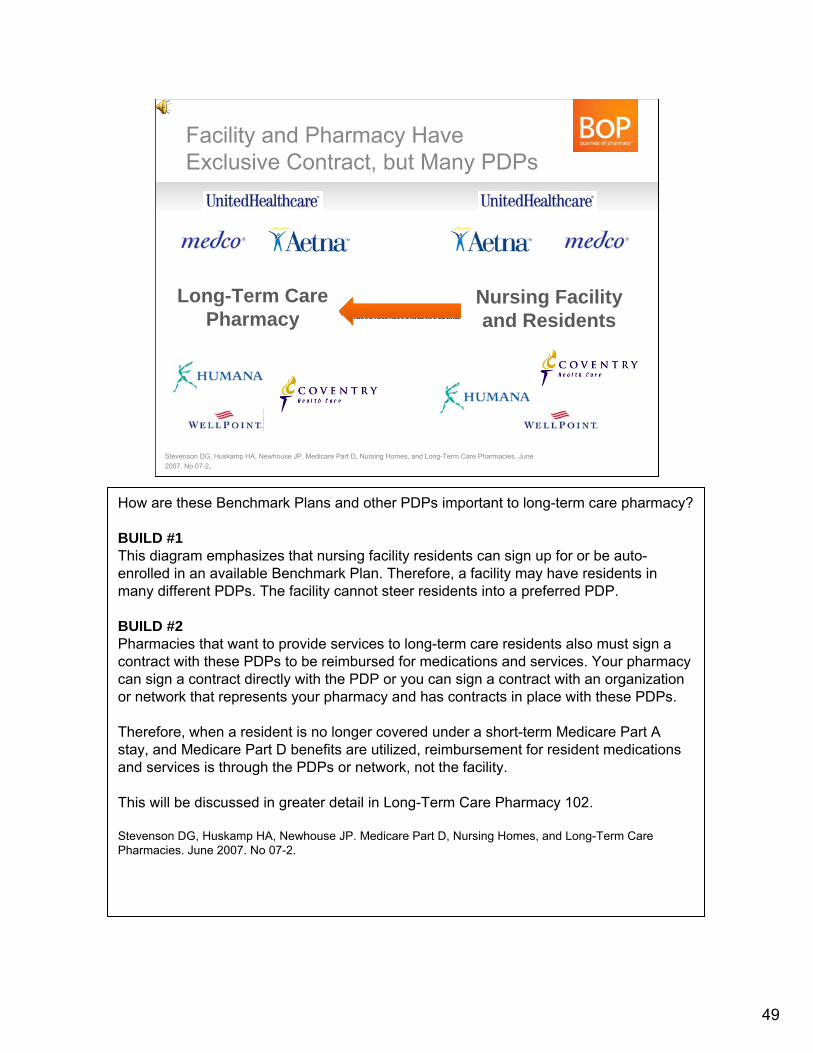
How are these Benchmark Plans and other PDPs important to long-term care pharmacy?
BUILD #1This diagram emphasizes that nursing facility residents can sign up for or be auto-enrolled in an available Benchmark Plan. Therefore, a facility may have residents in many different PDPs. The facility cannot steer residents into a preferred PDP.
BUILD #2Pharmacies that want to provide services to long-term care residents also must sign a contract with these PDPs to be reimbursed for medications and services. Your pharmacy can sign a contract directly with the PDP or you can sign a contract with an organization or network that represents your pharmacy and has contracts in place with these PDPs.
Therefore, when a resident is no longer covered under a short-term Medicare Part A stay, and Medicare Part D benefits are utilized, reimbursement for resident medications and services is through the PDPs or network, not the facility.
This will be discussed in greater detail in Long-Term Care Pharmacy 102.
Stevenson DG, Huskamp HA, Newhouse JP. Medicare Part D, Nursing Homes, and Long-Term Care Pharmacies. June 2007. No 07-2.
Medicaid– Entitlement program funded by federal and state governments.
Managed by state. Coverage includes:
– Hospitalization– Outpatient services– Labs– Nursing home services after Medicare– Home and community health programs– Limited medication coverage in LTC
– Coverage and rules/regulations will vary from state to state– After day 100 Medicaid will cover most services,
except medications– LTC accounts for a significant portion of
Medicaid payments
The Henry J Kaiser Family Foundation. Medicaid: a primer 2009. Available at www.kff.org.
50
Medicaid is a federal and state program, with funding coming from both sources. The federal government provides monies, but the program is managed through guidelines set by each state.
Medicaid is a program for the indigent—those below a certain income level.
It covers most healthcare services for those eligible for this program. In those over age 65, medications are covered through Medicare Part D rather than Medicaid. For most people under age 65, Medicaid covers medications.
In skilled nursing facilities, Medicare will cover the short-term costs up to the first 100 days. Medicaid then picks up most costs after day 100. Pharmacy services is the exception, which after 100 days is covered through Medicare Part D.
With most costs being covered through Medicaid, this program continues to be the biggest payor of all long-term care services.
The Henry J Kaiser Family Foundation. Medicaid: a primer 2009. Available at www.kff.org.
Let’s Follow Medication Reimbursement in a Skilled-Nursing Facility
Up to Day 100Medicare Part A Prospective Payment System (PPS)
The Henry J Kaiser Family Foundation. The Role of Medicare for the People Dually Eligible for Medicare and Medicaid. Available at www.kff.org/medicare/upload/8138.pdf
After Day 100–Housing and healthcare
Medicaid/cash/insurance–Medications through
Medicare Part D
51
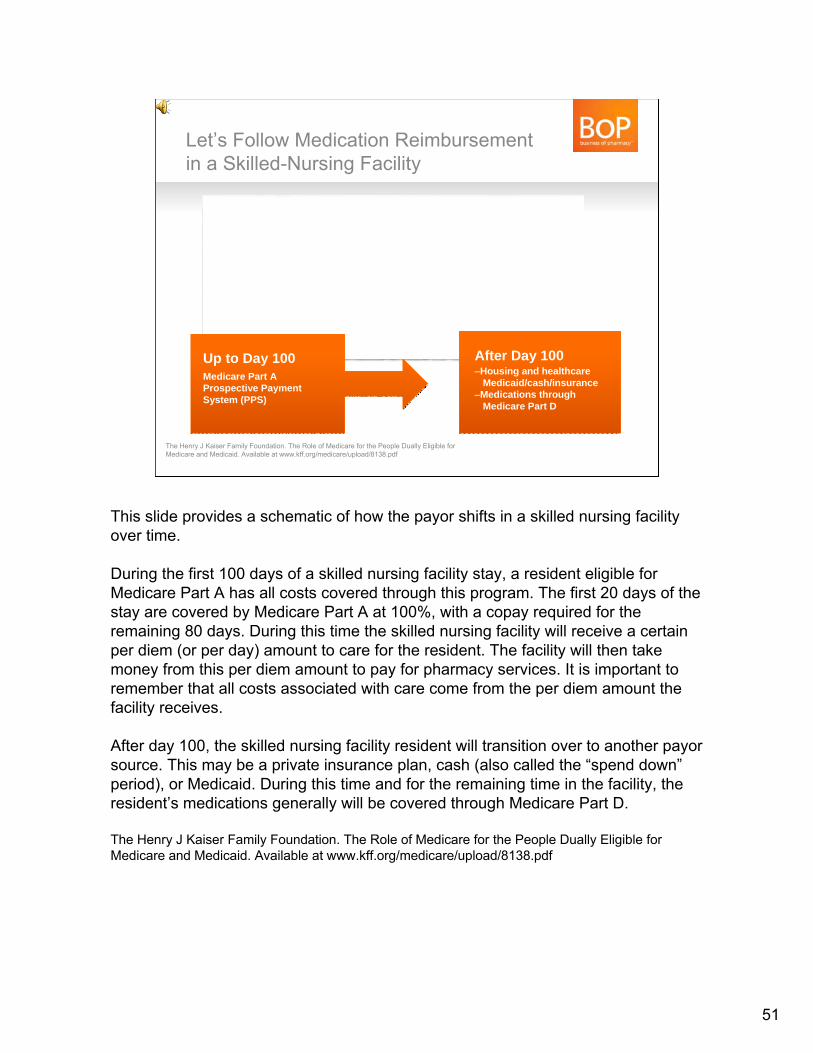
This slide provides a schematic of how the payor shifts in a skilled nursing facility over time.
During the first 100 days of a skilled nursing facility stay, a resident eligible for Medicare Part A has all costs covered through this program. The first 20 days of the stay are covered by Medicare Part A at 100%, with a copay required for the remaining 80 days. During this time the skilled nursing facility will receive a certain per diem (or per day) amount to care for the resident. The facility will then take money from this per diem amount to pay for pharmacy services. It is important to remember that all costs associated with care come from the per diem amount the facility receives.
After day 100, the skilled nursing facility resident will transition over to another payorsource. This may be a private insurance plan, cash (also called the “spend down”period), or Medicaid. During this time and for the remaining time in the facility, the resident’s medications generally will be covered through Medicare Part D.
The Henry J Kaiser Family Foundation. The Role of Medicare for the People Dually Eligible for Medicare and Medicaid. Available at www.kff.org/medicare/upload/8138.pdf
There Are an Estimated 9 Million Dual Eligibles (2007)
Medicare34 million
Medicaid49 million
DualEligibles9 million
21% of the Medicare and 15% of the Medicaid Populations
The Henry J Kaiser Family Foundation. The Role of Medicare for the People Dually Eligible for Medicare and Medicaid. Available at www.kff.org/medicare/upload/8138.pdf
This population is placed in “Benchmark” PDPs
and is not required to pay co-pays
This population is placed in “Benchmark” PDPs
and is not required to pay co-pays
52
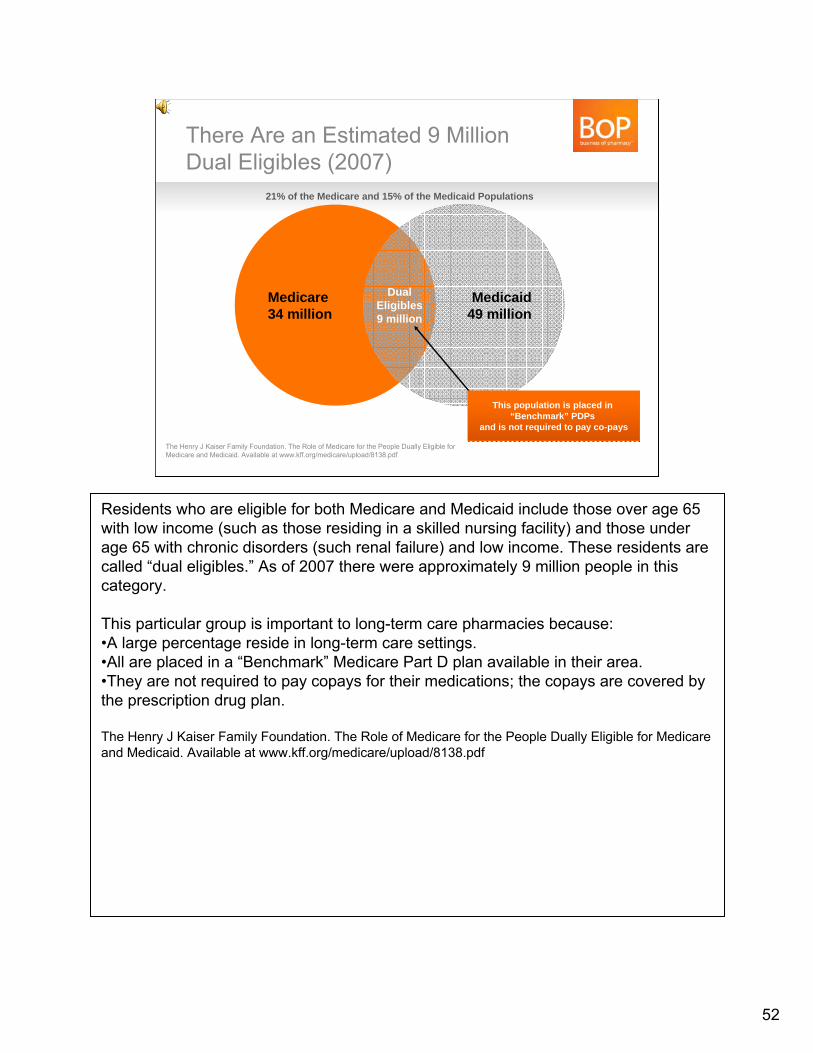
Residents who are eligible for both Medicare and Medicaid include those over age 65 with low income (such as those residing in a skilled nursing facility) and those under age 65 with chronic disorders (such renal failure) and low income. These residents are called “dual eligibles.” As of 2007 there were approximately 9 million people in this category.
This particular group is important to long-term care pharmacies because:•A large percentage reside in long-term care settings.•All are placed in a “Benchmark” Medicare Part D plan available in their area.•They are not required to pay copays for their medications; the copays are covered by the prescription drug plan.
The Henry J Kaiser Family Foundation. The Role of Medicare for the People Dually Eligible for Medicare and Medicaid. Available at www.kff.org/medicare/upload/8138.pdf
Reimbursement Process for Medications in LTC
MedicareMedicare
Data on file. MatureHealth Communications.Stevenson DG, Huskamp HA, Newhouse JP. Medicare Part D, Nursing Homes, and Long-Term Care Pharmacies. June 2007. No 07-2.
WholesalerWholesalerGPOGPO
MedicaidMedicaid Private PayPrivate Pay
Out-of-Pocket Co-Pay and “Spend Down”
PDPPDP
FacilityFacility
Medicare Part D (After Day 100)
LTCPLTCP
Medicare Part D
Medicare Part A
Medicare Part A (Short Stay)
Comm/Private Insurance
Comm/Private Insurance
53
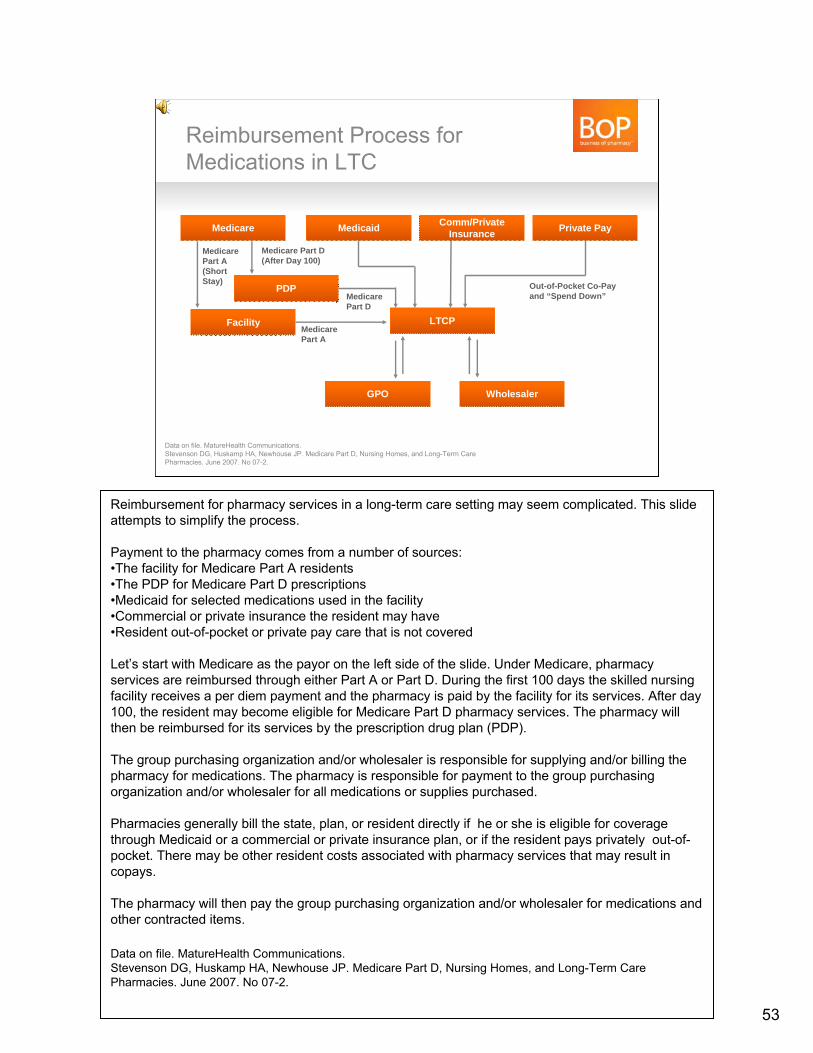
Reimbursement for pharmacy services in a long-term care setting may seem complicated. This slide attempts to simplify the process.
Payment to the pharmacy comes from a number of sources:•The facility for Medicare Part A residents •The PDP for Medicare Part D prescriptions•Medicaid for selected medications used in the facility•Commercial or private insurance the resident may have•Resident out-of-pocket or private pay care that is not covered
Let’s start with Medicare as the payor on the left side of the slide. Under Medicare, pharmacy services are reimbursed through either Part A or Part D. During the first 100 days the skilled nursing facility receives a per diem payment and the pharmacy is paid by the facility for its services. After day 100, the resident may become eligible for Medicare Part D pharmacy services. The pharmacy will then be reimbursed for its services by the prescription drug plan (PDP).
The group purchasing organization and/or wholesaler is responsible for supplying and/or billing the pharmacy for medications. The pharmacy is responsible for payment to the group purchasing organization and/or wholesaler for all medications or supplies purchased.
Pharmacies generally bill the state, plan, or resident directly if he or she is eligible for coverage through Medicaid or a commercial or private insurance plan, or if the resident pays privately out-of-pocket. There may be other resident costs associated with pharmacy services that may result in copays.
The pharmacy will then pay the group purchasing organization and/or wholesaler for medications and other contracted items.
Data on file. MatureHealth Communications.Stevenson DG, Huskamp HA, Newhouse JP. Medicare Part D, Nursing Homes, and Long-Term Care Pharmacies. June 2007. No 07-2.
How Does an LTC PharmacyMake Money?– The medication cost
– The dispensing fee
– Profit based on facility charge minusthe acquisition cost
– Rebates
Stevenson DG, Huskamp HA, Newhouse JP. Medicare Part D, Nursing Homes, and Long-Term Care Pharmacies. June 2007. No 07-2.The Lewin Group. CMS Review of Current Standards of Practice for Long-Term Care Pharmacy Services. Long Term Care Primer. Dec 30, 2004.
54
Now let’s switch our focus to the pharmacy and ask the important question of how a long-term care pharmacy makes money.
Currently, there are four ways a pharmacy can make money on a long-term care prescription:•The medication cost—This is similar to how you would make money on a retail prescription.•The dispensing fee—This is similar to how you would make money on a retail prescription.•A profit from the facility cost minus the acquisition cost—This is similar to a retail prescription, but these costs may be much different than those of a retail pharmacy.•A rebate that has been determined through contracting—This is determined by the contract the pharmacy may have with a group purchasing organization, pharmacy network, wholesaler, or manufacturer.
Stevenson DG, Huskamp HA, Newhouse JP. Medicare Part D, Nursing Homes, and Long-Term Care Pharmacies. June 2007. No 07-2.The Lewin Group. CMS Review of Current Standards of Practice for Long-Term Care Pharmacy Services Long Term Care Primer. Dec 30, 2004 .
Pricing of LTC Pharmacy Services
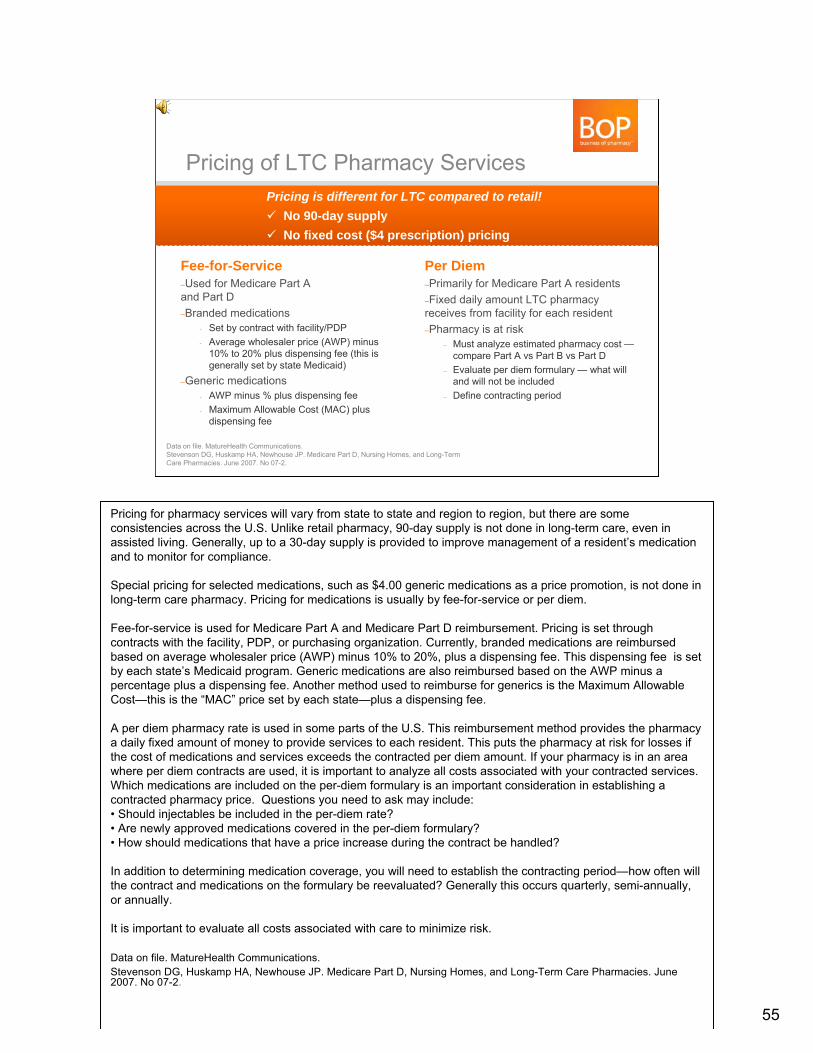
Fee-for-Service–Used for Medicare Part Aand Part D–Branded medications
- Set by contract with facility/PDP- Average wholesaler price (AWP) minus
10% to 20% plus dispensing fee (this is generally set by state Medicaid)
–Generic medications- AWP minus % plus dispensing fee- Maximum Allowable Cost (MAC) plus
dispensing fee
Per Diem–Primarily for Medicare Part A residents–Fixed daily amount LTC pharmacy receives from facility for each resident –Pharmacy is at risk
– Must analyze estimated pharmacy cost —compare Part A vs Part B vs Part D
– Evaluate per diem formulary — what will and will not be included
– Define contracting period
Pricing is different for LTC compared to retail!No 90-day supplyNo fixed cost ($4 prescription) pricing
Pricing is different for LTC compared to retail!No 90-day supplyNo fixed cost ($4 prescription) pricing
Data on file. MatureHealth Communications. Stevenson DG, Huskamp HA, Newhouse JP. Medicare Part D, Nursing Homes, and Long-Term Care Pharmacies. June 2007. No 07-2.
55
Pricing for pharmacy services will vary from state to state and region to region, but there are some consistencies across the U.S. Unlike retail pharmacy, 90-day supply is not done in long-term care, even in assisted living. Generally, up to a 30-day supply is provided to improve management of a resident’s medication and to monitor for compliance.
Special pricing for selected medications, such as $4.00 generic medications as a price promotion, is not done in long-term care pharmacy. Pricing for medications is usually by fee-for-service or per diem.
Fee-for-service is used for Medicare Part A and Medicare Part D reimbursement. Pricing is set through contracts with the facility, PDP, or purchasing organization. Currently, branded medications are reimbursed based on average wholesaler price (AWP) minus 10% to 20%, plus a dispensing fee. This dispensing fee is set by each state’s Medicaid program. Generic medications are also reimbursed based on the AWP minus a percentage plus a dispensing fee. Another method used to reimburse for generics is the Maximum Allowable Cost—this is the “MAC” price set by each state—plus a dispensing fee.
A per diem pharmacy rate is used in some parts of the U.S. This reimbursement method provides the pharmacy a daily fixed amount of money to provide services to each resident. This puts the pharmacy at risk for losses if the cost of medications and services exceeds the contracted per diem amount. If your pharmacy is in an area where per diem contracts are used, it is important to analyze all costs associated with your contracted services. Which medications are included on the per-diem formulary is an important consideration in establishing a contracted pharmacy price. Questions you need to ask may include:• Should injectables be included in the per-diem rate?• Are newly approved medications covered in the per-diem formulary?• How should medications that have a price increase during the contract be handled?
In addition to determining medication coverage, you will need to establish the contracting period—how often will the contract and medications on the formulary be reevaluated? Generally this occurs quarterly, semi-annually, or annually.
It is important to evaluate all costs associated with care to minimize risk.
Data on file. MatureHealth Communications. Stevenson DG, Huskamp HA, Newhouse JP. Medicare Part D, Nursing Homes, and Long-Term Care Pharmacies. June 2007. No 07-2.
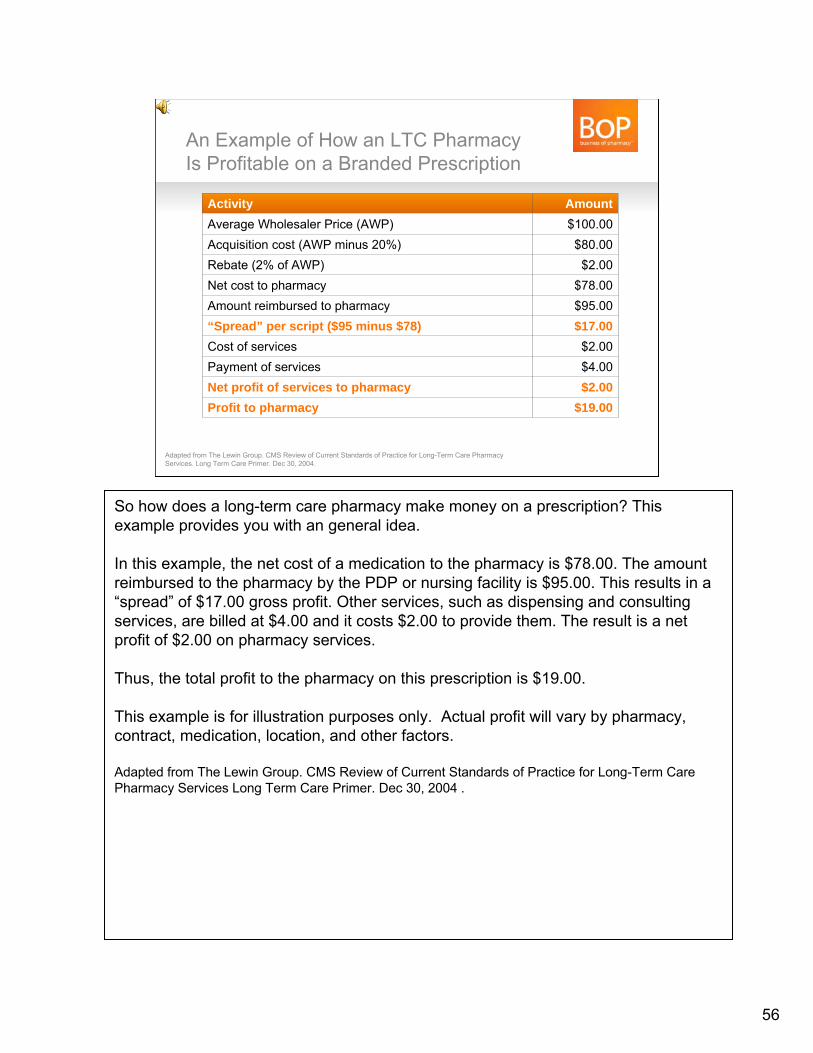
An Example of How an LTC Pharmacy Is Profitable on a Branded Prescription
Activity AmountAverage Wholesaler Price (AWP) $100.00Acquisition cost (AWP minus 20%) $80.00Rebate (2% of AWP) $2.00Net cost to pharmacy $78.00Amount reimbursed to pharmacy $95.00“Spread” per script ($95 minus $78) $17.00Cost of services $2.00Payment of services $4.00Net profit of services to pharmacy $2.00Profit to pharmacy $19.00
Adapted from The Lewin Group. CMS Review of Current Standards of Practice for Long-Term Care Pharmacy Services. Long Term Care Primer. Dec 30, 2004.
56
So how does a long-term care pharmacy make money on a prescription? This example provides you with an general idea.
In this example, the net cost of a medication to the pharmacy is $78.00. The amount reimbursed to the pharmacy by the PDP or nursing facility is $95.00. This results in a “spread” of $17.00 gross profit. Other services, such as dispensing and consulting services, are billed at $4.00 and it costs $2.00 to provide them. The result is a net profit of $2.00 on pharmacy services.
Thus, the total profit to the pharmacy on this prescription is $19.00.
This example is for illustration purposes only. Actual profit will vary by pharmacy, contract, medication, location, and other factors.
Adapted from The Lewin Group. CMS Review of Current Standards of Practice for Long-Term Care Pharmacy Services Long Term Care Primer. Dec 30, 2004 .
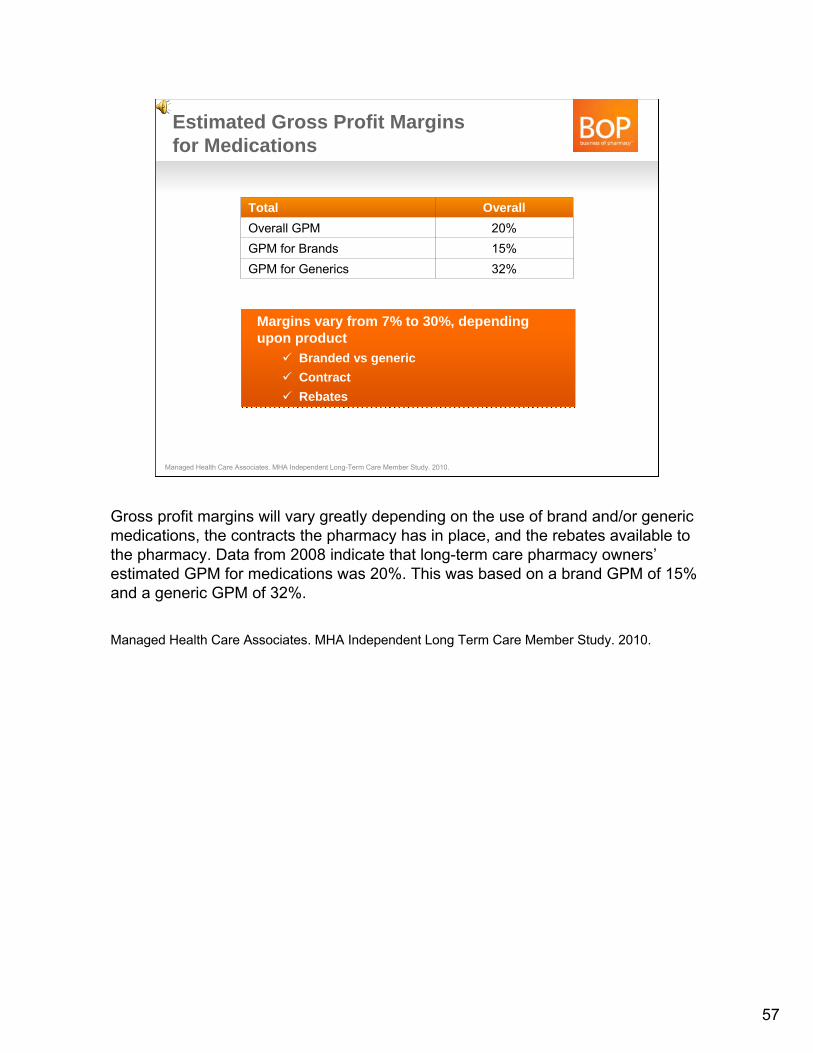
Total OverallOverall GPM 20%GPM for Brands 15%GPM for Generics 32%
Estimated Gross Profit Margins for Medications
Managed Health Care Associates. MHA Independent Long-Term Care Member Study. 2010.
Margins vary from 7% to 30%, dependingupon product
Branded vs genericContractRebates
Margins vary from 7% to 30%, dependingupon product
Branded vs genericContractRebates
57
Gross profit margins will vary greatly depending on the use of brand and/or generic medications, the contracts the pharmacy has in place, and the rebates available to the pharmacy. Data from 2008 indicate that long-term care pharmacy owners’estimated GPM for medications was 20%. This was based on a brand GPM of 15% and a generic GPM of 32%.
Managed Health Care Associates. MHA Independent Long Term Care Member Study. 2010.
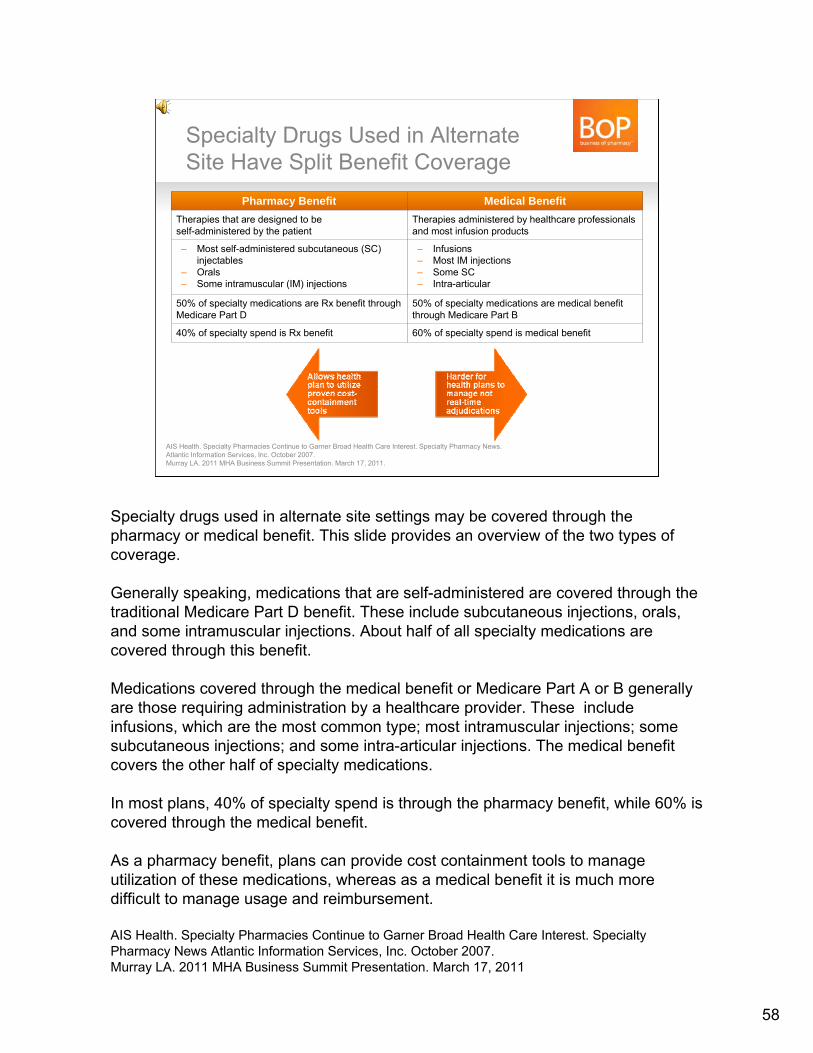
Specialty Drugs Used in Alternate Site Have Split Benefit Coverage
Pharmacy Benefit Medical BenefitTherapies that are designed to be self-administered by the patient
Therapies administered by healthcare professionals and most infusion products
– Most self-administered subcutaneous (SC) injectables
– Orals– Some intramuscular (IM) injections
– Infusions – Most IM injections– Some SC– Intra-articular
50% of specialty medications are Rx benefit through Medicare Part D
50% of specialty medications are medical benefit through Medicare Part B
40% of specialty spend is Rx benefit 60% of specialty spend is medical benefit
AIS Health. Specialty Pharmacies Continue to Garner Broad Health Care Interest. Specialty Pharmacy News. Atlantic Information Services, Inc. October 2007.Murray LA. 2011 MHA Business Summit Presentation. March 17, 2011.
58
Specialty drugs used in alternate site settings may be covered through the pharmacy or medical benefit. This slide provides an overview of the two types of coverage.
Generally speaking, medications that are self-administered are covered through the traditional Medicare Part D benefit. These include subcutaneous injections, orals, and some intramuscular injections. About half of all specialty medications are covered through this benefit.
Medications covered through the medical benefit or Medicare Part A or B generally are those requiring administration by a healthcare provider. These include infusions, which are the most common type; most intramuscular injections; some subcutaneous injections; and some intra-articular injections. The medical benefit covers the other half of specialty medications.
In most plans, 40% of specialty spend is through the pharmacy benefit, while 60% is covered through the medical benefit.
As a pharmacy benefit, plans can provide cost containment tools to manage utilization of these medications, whereas as a medical benefit it is much more difficult to manage usage and reimbursement.
AIS Health. Specialty Pharmacies Continue to Garner Broad Health Care Interest. Specialty Pharmacy News Atlantic Information Services, Inc. October 2007.Murray LA. 2011 MHA Business Summit Presentation. March 17, 2011
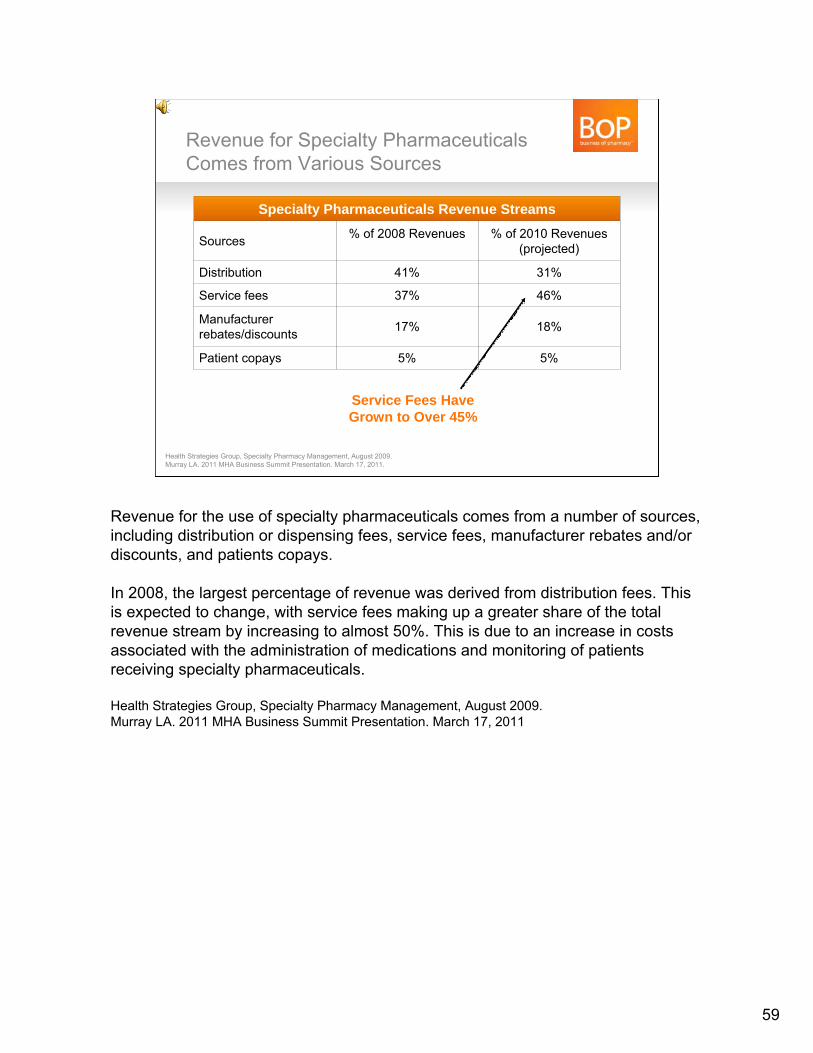
Revenue for Specialty Pharmaceuticals Comes from Various Sources
Health Strategies Group, Specialty Pharmacy Management, August 2009.Murray LA. 2011 MHA Business Summit Presentation. March 17, 2011.
Specialty Pharmaceuticals Revenue Streams
Sources % of 2008 Revenues % of 2010 Revenues (projected)
Distribution 41% 31%
Service fees 37% 46%
Manufacturer rebates/discounts 17% 18%
Patient copays 5% 5%
Service Fees Have Grown to Over 45%
59
Revenue for the use of specialty pharmaceuticals comes from a number of sources, including distribution or dispensing fees, service fees, manufacturer rebates and/or discounts, and patients copays.
In 2008, the largest percentage of revenue was derived from distribution fees. This is expected to change, with service fees making up a greater share of the total revenue stream by increasing to almost 50%. This is due to an increase in costs associated with the administration of medications and monitoring of patients receiving specialty pharmaceuticals.
Health Strategies Group, Specialty Pharmacy Management, August 2009.Murray LA. 2011 MHA Business Summit Presentation. March 17, 2011
Action Steps– Identify LTC facilities and alternate site pharmacy opportunities in
your area
– Define and understand the types of services pharmacies are providing to long-term care and alternate site customers
– Determine the needs of potential customers
– Learn the reimbursement process used when providing pharmacy services in LTC and alternate sites and determine how these services can be profitable
– Define the steps required for your pharmacy to have the ability to contract with these potential customers
60
This completes the three modules of Long-Term Care Pharmacy 101.
Action steps your pharmacy should take if you are interested in expanding into long-term care and/or alternate site pharmacy include:•Identify LTC facilities and alternate site pharmacy opportunities in your area•Define and understand the types of services pharmacies are providing to long-term care and alternate site customers•Determine the needs of potential customers•Learn the reimbursement process used when providing pharmacy services in LTC and alternate sites and determine how these services can be profitable•Define the steps required for your pharmacy to have the ability to contract with these potential customers.

Selected References for More Information– Long-Term Care: Consumers, Services, and Financing. National Health Policy Forum.
November 28, 2008– The Henry J Kaiser Family Foundation. The Role of Medicare for the People Dually Eligible for Medicare
and Medicaid. Available at www.kff.org/medicare/upload/8138.pdf– The Lewin Group. CMS Review of Current Standards of Practice for Long-Term Care Pharmacy Services
Long-Term Care Primer. Dec 30, 2004. – Stevenson DG, Huskamp HA, Newhouse JP. Medicare Part D, Nursing Homes, and Long-Term Care
Pharmacies. June 2007. No 07-2.
– National Conference of State Legislatures. State Prescription Drug Return, Reuse and Recycling Laws. Available at http://www.ncsl.org/default.aspx?tabid=14425.
– NABP/ASCP Joint Report: Model Rules for Long-Term Care Pharmacy Practice. Available at http://www.nabp.net/assets/NABP%20ASCP%20Report%20on%20Long%20Term%20Care.pdfAccessed April 10, 2011.
– Introduction to Long-Term Care Pharmacy Services. A Certificate Training Program. Monograph 3: Setting up Your Operations. American Society of Consultant Pharmacists. 2007.
– AIS Health. Specialty Pharmacies Continue to Garner Broad Health Care Interest. Specialty Pharmacy News Atlantic Information Services, Inc. October 2007.
– Consultant Pharmacist Handbook. A Guide for Consulting to Nursing Facilities. American Society of Consultant Pharmacists. 2004.
– McKesson Alternate Site Pharmacy: www.mckessonbop.com/alternatesite
61
This slide provides you with selected references for more information.
How to Exit and Resume the Course
Click the button at the bottom right corner of the screen.
The view of the screen will change, and you will see the Exit button at the top right corner of the screen, use this Exit button to exit the course.
When you resume the course, the “Resume presentation” pop-up will be displayed. You can click “Yes” if you wish to resume the course from where you left it, or click “No” if you want to start the course from the beginning and
reset your Course History.
To exit the course, you may need to change the view mode.
To exit the course, click the button at the bottom right corner of the screen. The view of the screen will change, and you will see the Exit button at the top right corner of the screen, use this Exit button to exit the course.
When you resume the course, the “Resume presentation” pop-up will be displayed. You can click “Yes” if you wish to resume the course from where you left it, or click “No” if you want to start the course from the beginning and reset your Course History.
62