Embed Size (px)
Citation preview
—
National Lung Health Education Programwww.NLHEP.org
Long Term OxygenTherapy (LTOT)
History, Scientific Foundations, andEmerging Technologies
Thomas L. Petty, M.D.Robert W. McCoy, B.S., RRT
Dennis E. Doherty, M.D.
6th Oxygen Consensus Conference Recommendations
Historical Highlights Page 2
Physiologic Responses to LTOT Page 3
Two Major Randomized Clinical Trials Page 5
The British Medical Research Council Clinical Trial
The Nocturnal Oxygen Therapy Trial (NOTT)
Other Benefits from Oxygen Page 7
Oxygen “Dosing” (Liter Flow) Page 7
Prescribing Criteria Page 8
Oxygen Toxicity Page 9
Oxygen Safety Page 10
A Re-Examination of the Nocturnal Oxygen Therapy Trials (NOTT) Page 10
Oxygen Technologies Page 15
Cost Effectiveness of LTOT Page 21
The National Lung Health Education Program (NLHEP) Page 22
Appendix: Recommendations of the Six Oxygen Consensus Conferences
(2006, 1999, 1993, 1990, 1987, 1986) Page 24
References Page 34
www.nlhep.org
Contents
Long term oxygen therapy (LTOT) is well established as the standard of care for manypatients with chronic stable hypoxemia. Most studies have been done in ChronicObstructive Pulmonary Disease (COPD), but patients with other causes of chronichypoxemia and its consequences are also likely to benefit. Both the length and qualityof life are improved with LTOT used inside and outside the home. It is believed thatincreased blood flow to central organs, made possible by increasing exercise withambulatory oxygen, is the main reason for those benefits.
Industry has continued to produce new ultra-light weight oxygen systems, which cantruly be called “ambulatory.” Low weight oxygen concentrators are making oxygentravel more practical and realistic for patients who require oxygen around the clock. Atthe very time that these advances are occurring, third party payors, mainly Medicare, arecontinuing to plan reductions in reimbursement for newer systems. A realisticreimbursement system is critical to the future of LTOT, which, involves the lives ofapproximately 1.2 million Americans.
The original purpose of this monograph was to provide background for participants inthe Sixth Oxygen Conference held in Denver, Colorado in August 2005. (2006 RespCare51(5):519-525) The purpose of this booklet is to provide the important historical andscientific highlights for LTOT and to present a better understanding of the new life thatoccurs with LTOT.
This booklet briefly presents the history of LTOT and the state of our knowledgeabout the scientific basis for LTOT. Emerging technologies promise to make LTOT moreavailable and effective for the growing number of patients with a medical necessity forLTOT. Increased mobility is key to improving quality of life.
Preface
1www.nlhep.org
History records that oxygen was firstdiscovered by Joseph Priestley on August 1,1774, when he obtained a colorless gas byheating red mercuric oxide. He recognized thatthe candle flame would burn brighter in whathe had termed “dephlogisticated air.” Hecaptured the gas in an inverted bell, and he andtwo mice were the first to breathe this “pureair.” He noted a “light and easy feeling” andremarked, “who can tell but that in time thispure air may become a fashionable article inluxury.”1,2 Carl Wilhelm Scheele, a Swedishchemist, also discovered oxygen, maybe asearly as 1773.3 Priestley’s friend, AntoineLavoisier, successfully repeated Priestley’soriginal experiment and named the newlydiscovered gas oxygen. Oxygen was first usedclinically in dental anesthesia as early as 1868.
The first recorded use of oxygen, during thetreatment of acute bacterial pneumonia, was inYork, Pennsylvania, on March 6, 1885. Dr.George Holtzapple produced oxygen fromchlorate of potassium and black oxide ofmanganese by heating the chemicals in a largeglass cylinder with a flame from a lamp. Theresultant oxygen was delivered via rubbertubing to the face of a young man who wasdying from pneumonia (presumably secondaryto the consequences of his hypoxemia). Afterseveral hours the crisis passed and the youngman recovered.4
The nasal catheter first came to be used asa conduit for oxygen therapy at around theturn of the century. Other oxygen deliverydevices were soon to follow.5
Following John S. Haldane’s expedition toPike’s Peak in 1913, he concluded in his landmarkarticle in the British Medical Journal in 1919 that“partial anoxia means not a mere slowing downof life, but progressive, and perhaps irreparabledamage to human structure.”6 Haldane predictedthat oxygen would soon be used in hospitals.
Alvan Barach was the first to systematicallyemploy oxygen for the treatment of bacterialpneumonia.7 Barach modified an oxygen tent,originally invented by Leonard Hill.7,8 Barachwas also interested in the role of oxygen andrelief of dyspnea during exercise. In 1958 hedeveloped a small transfillable oxygen cylindersuitable for use during exercise (Figure 1).Cotes and Gilson also gave oxygen toambulatory patients from small portable high-pressure cylinders in the United Kingdom (UK).Cotes reported on increased walking time andimproved arterial oxygen saturation with theuse of supplemental oxygen during exercise.9
By 1955 approximately 30% of all “chemists”in Wales and Monmouthshire (population 2.6million) were supplying oxygen by prescription,at that time, to an astonishing 860 patients.Oxygen cylinders were the only modalityutilized for the delivery of oxygen therapy inthat era. Apparently this practice did notcontinue in the UK, or else it is not recorded inthe literature. Barach died in 1976, and hadbeen an inspiration to many who began tolearn the values of LTOT and developinnovative new oxygen systems.
2www.nlhep.org
1. Historical Highlights
Figure 1. Cartoon diagram by Dr. Barach emphasizingthe importance of walking with ambulatory oxygen.
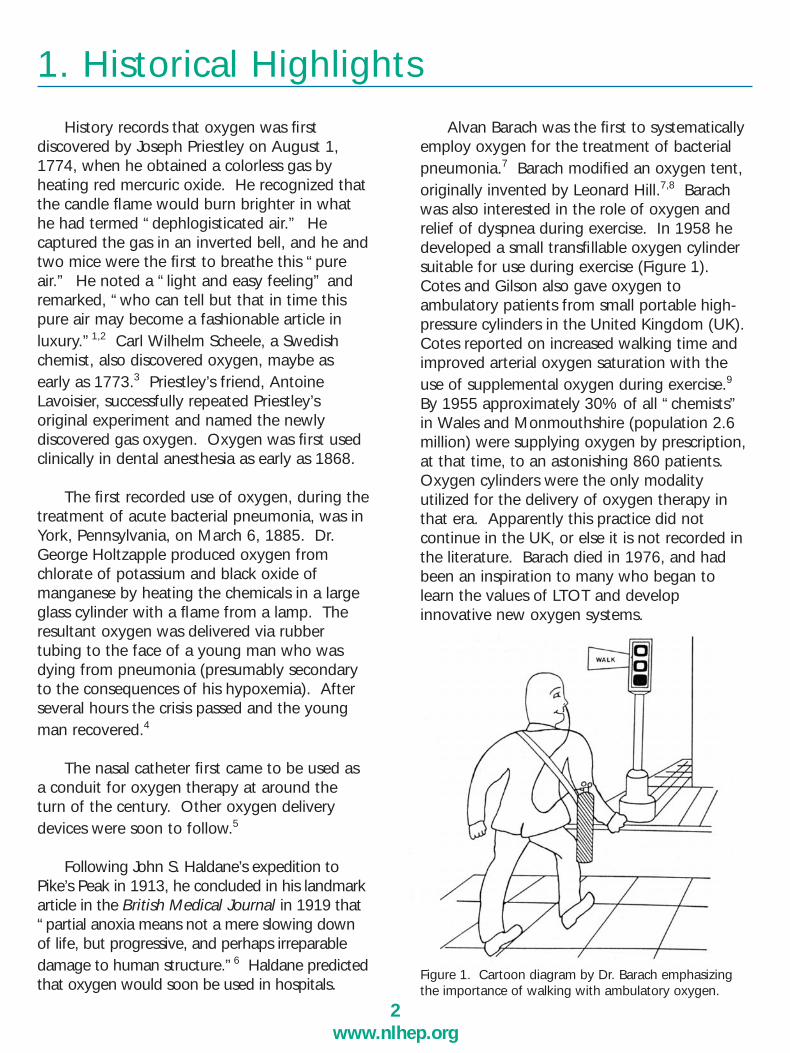
The first liquid transfillable systems becameavailable commercially from the LindeCorporation in 1965. The Denver Groupenrolled 6 patients in a study to investigate theutility of supplemental oxygen on the basis ofclinical evidence of severe pulmonaryhypertension, erythrocytosis, hematocrit >55%, and markedly reduced exercisetolerance.10 These six patients were admittedto a clinical research unit for the purpose ofstabilization for one month, when no oxygenwas used. During stabilization, theadministration of bronchodilators, diuretics,cardiac glycosides when indicated, andtreatment of any evidence of infection wasinstituted and provided for clinical stabilization.Patients were encouraged to eat a high-caloriediet and exercised systematically each day toimprove physical conditioning and to increaseexercise capability. At the end of this controlmonth, cardiac catheterization was done tomeasure pulmonary artery pressure, cardiacoutput, and pulmonary vascular resistance.Chromium-51-tagged red cell massdeterminations were also made.10 During thesecond month, the patients were maintained onthe same diet and maintenance medications,and oxygen was administered by nasal canulaat a flow sufficient to bring oxygen saturationabove 90% during rest and exercise. In allpatients, this required 1-3 L/min, averaging 2L/min. At the end of one month, cardiaccatheterization and red cell mass studies wererepeated. Marked reductions in pulmonaryartery pressure and pulmonary vascular resistance were observed in 4 of the 6 patients.The red cell mass improved in 4 of the sixpatients in whom both determinations could beaccomplished. The most dramatic outcome wasthe markedly increased exercise tolerance inthese patients (Figure 2).
The first of these oxygen study patientsbecame our first home care patient in Denver.Pictures of his quality of life and homefunctioning have been reported on numerousoccasions in previous writing by one of us(TLP).11
At approximately the same time, an almostidentical study was done in Birmingham,England, which resulted in exactly the sameconclusions about hemodynamic improvementsand red cell mass in response to supplementaloxygen therapy.12 Formal exercise studies werenot conducted by the Birmingham group,largely because cumbersome high-pressure
3www.nlhep.org
2. Physiologic Responses to LTOT
Figure 2. Improvement in exercise tolerance in twopatients trained at level walk. Note the slow changeduring the control month, and the marked rapid risein tolerance during the oxygen month. W.M. and H.S.are the patients’ initials. Temporary decrease in H.S.’sexercise tolerance during the oxygen month was dueto an episode of acute bronchitis.

cylinders were used. However, these were usedwith a “trolley,” so some degree of ambulationwas possible while pushing the oxygencylinders. Although no accounts of exercisetolerance are reported, the authors remark,“Exercise tolerance increased remarkably . . .even though there was no specific program oftraining.”
In 1968 we reported on 20 patients withadvanced chronic obstructive pulmonary disease(COPD) who received continuous ambulatoryoxygen therapy from a liquid oxygen portablesystem for up to 18 months.13 In that article weshowed crude anecdotal evidence ofimprovement in cor pulmonale, with evidenceof improvement in electro-cardiograph tracingsand in the cardiac silhouette, with resolution inright ventricular size as a result of 6 months ofoxygen administration. This report also documented a progressive reduction in hematocrit and an increase in dry body weightover one year, which suggested some nutritional or metabolic benefit from LTOT. Inthis paper, we demonstrated a reduction in hospitalizations visually documented in one dramatic illustration showing the size of apatient’s hospital record before and after oxygen, during an equal 18-month period(Figure 3).13
Following these original observations, otherinvestigators in the UK focused on the dailyrequirements of oxygen required to reverse pulmonary hypertension in patients withCOPD.14,15 These studies gave evidence thatoxygen delivered from a stationary source for aslittle as 15 hours per day resulted in animprovement in pulmonary hypertension insome, but not all, patients. There was even asuggestion that 12 hours of oxygen could beeffective.14,15
In a later report, the Denver Group was ableto show an improvement in survival in patientsbefore and following oxygen administrationwith clinical evidence of cor pulmonale beforeand following response to supplemental oxygenadministration, compared with historical controls from the Veterans Administration-Armed Forces study on course and prognosis inCOPD.16 A similar survival benefit was notfound in patients who did not have clinical evidence of cor pulmonale.16 It must beemphasized that all of these early studies werein small groups of patients without a contemporary cohort comparison group.
2. Physiologic Responses to LTOT (Cont.)
Figure 3. Size of a patient’s hospital record before andafter oxygen, during an equal 18-month period. (From
4www.nlhep.org
THE BRITISH MEDICAL RESEARCH COUNCILCLINICAL TRIAL
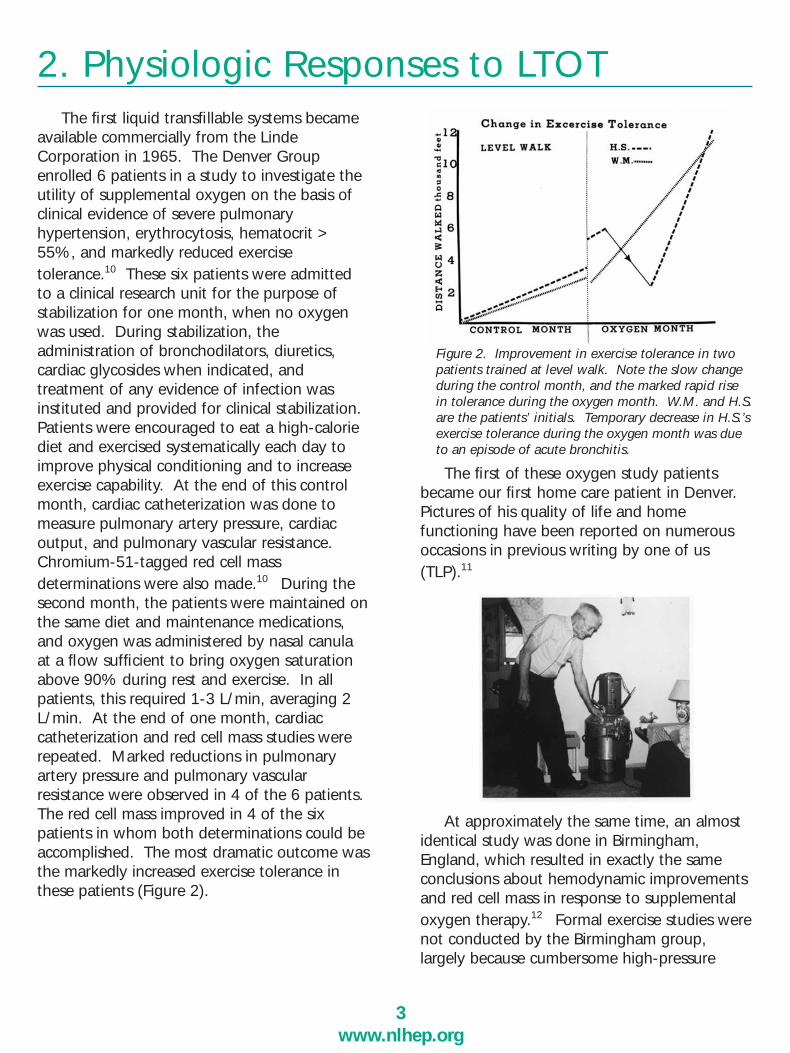
Clinical investigators in the UK, led by thelate David Flenley, asked an important questionabout the treatment of patients with COPD andchronic stable hypoxemia (arterial oxygen tension [PaO2] ≤ 55 mm Hg) and the effect ofLTOT on survival. In a multicenter trial in theUK, the patients were randomized to receiveeither 15 hours of oxygen (including the hoursof sleep) from a stationary system or no supplemental oxygen.17 Figure 4 shows a survival curve from this study. It is interestingthat improvement in survival in thesupplemental oxygen group does not appearuntil after 500 days.
THE NOCTURNAL OXYGEN THERAPY TRIAL(NOTT)
The NOTT enrolled 203 patients in 6 centers.The requirements for entry included PaO2 of≤ 55 mm Hg in the 3-week stabilization period,during which bronchodilators and antimicrobialswere used as indicated. Patients were exercised on a daily basis to improve physicalconditioning during the stabilization period. Atthe end of this stabilization phase, the oxygentension in 45 subjects improved while breathingroom air to the extent that they no longer qualified for the study, (i.e., the oxygen tensionhad improved to 55 mm Hg during the stabilization period.18) A few patients with anoxygen tension of 55-59 mm Hg were alsoentered into the study because of clinical evidence of cor pulmonale based on electrocardiograph criteria and/or a hematocritvalue of 55 or higher. In the NOTT only 4patients were considered too ill to enter the stabilization period without oxygen.19 Otherexclusion criteria were the presence of seriouscomorbidity, refusal by the patient to follow acomplex protocol that required two cardiaccatheterizations, and residence too far from thetesting center for the necessary close observations required by this study.19
Patients were randomized to receive eithernocturnal oxygen therapy (NOT) using a stationary source or continuous oxygen therapy(COT). The randomization process resulted inpatients who were excellently matched by age,gender, ethnic background, years of formaleducation, physiologic tests during rest andexercise, pulmonary pressure, and pulmonaryvascular resistance. The survival outcome ispresented in Figure 5. Significant survival differences between the groups were observedat 12, 24, and 36 months (p < 0.01).
5www.nlhep.org
3. Two Major Randomized Clinical Trials
Figure 4. Survival in the British Medical Research Councilstudy comparing oxygen for 15 hours a day from astationary source, compared with no oxygen. (Fromreference 17, with permission)
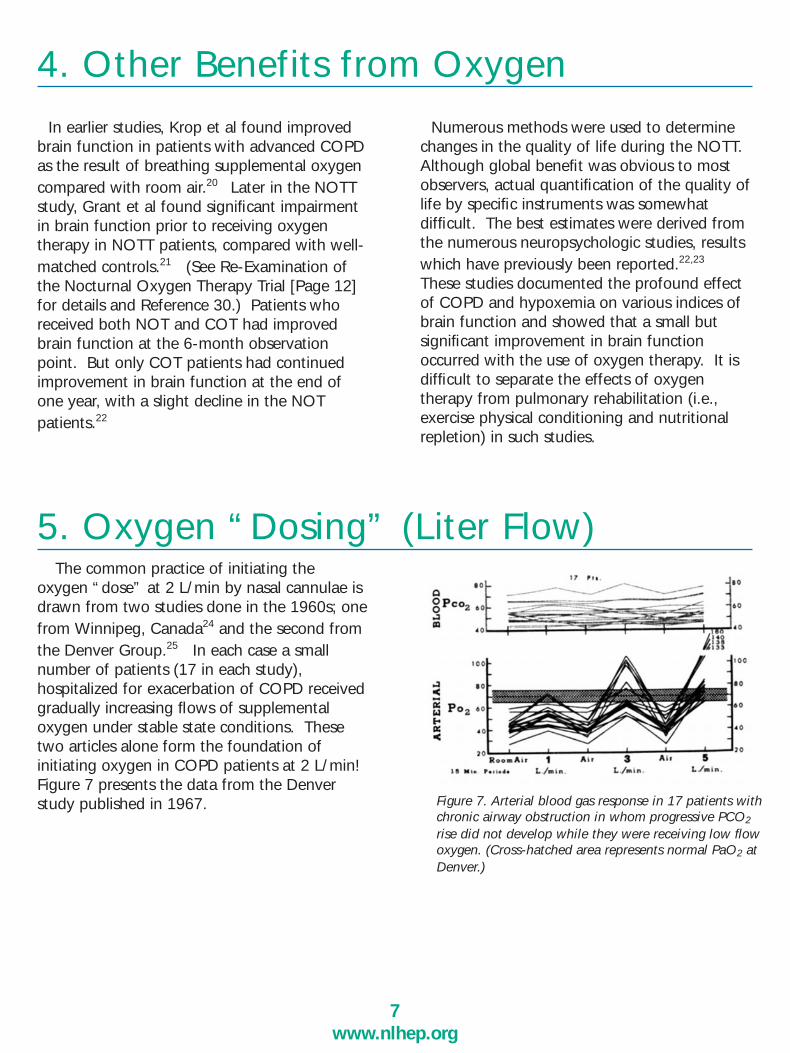
Since the demographics and disease severityof COPD patients in the MRC and the NOTTstudies were quite similar, it is reasonable tocompare the survival curves. This is done inFigure 6. In brief, this figure shows that survivalin COPD with chronic stable hypoxemia is poorwhen supplemental oxygen is not given.Survival is better in patients who received 12 to15 hours of oxygen therapy a day. Survival wasbest in patients who received nearly continuousoxygen from an ambulatory system. These differences in survival could have been related tothe duration of oxygen therapy, the method, orboth.
6www.nlhep.org
Two Clinical Trials (cont.)
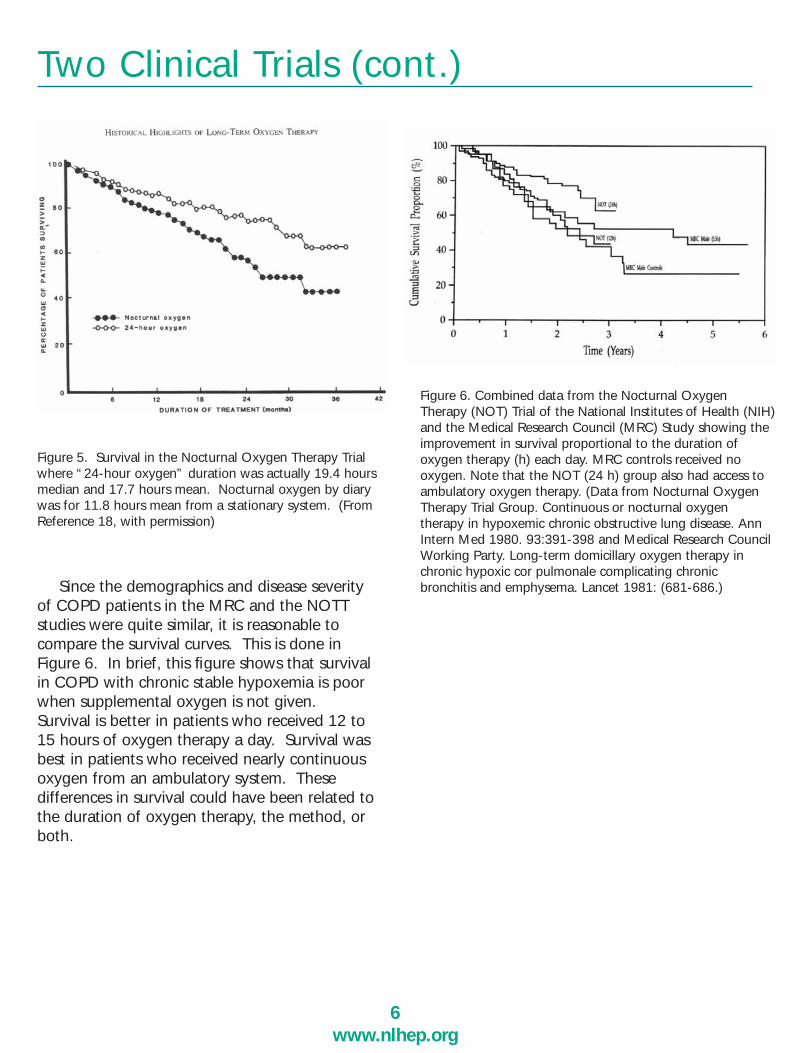
Figure 5. Survival in the Nocturnal Oxygen Therapy Trialwhere “24-hour oxygen” duration was actually 19.4 hoursmedian and 17.7 hours mean. Nocturnal oxygen by diarywas for 11.8 hours mean from a stationary system. (FromReference 18, with permission)
Figure 6. Combined data from the Nocturnal OxygenTherapy (NOT) Trial of the National Institutes of Health (NIH)and the Medical Research Council (MRC) Study showing theimprovement in survival proportional to the duration of oxygen therapy (h) each day. MRC controls received no oxygen. Note that the NOT (24 h) group also had access toambulatory oxygen therapy. (Data from Nocturnal OxygenTherapy Trial Group. Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease. AnnIntern Med 1980. 93:391-398 and Medical Research CouncilWorking Party. Long-term domicillary oxygen therapy inchronic hypoxic cor pulmonale complicating chronic bronchitis and emphysema. Lancet 1981: (681-686.)
In earlier studies, Krop et al found improvedbrain function in patients with advanced COPDas the result of breathing supplemental oxygencompared with room air.20 Later in the NOTTstudy, Grant et al found significant impairmentin brain function prior to receiving oxygen therapy in NOTT patients, compared with well-matched controls.21 (See Re-Examination ofthe Nocturnal Oxygen Therapy Trial [Page 12]for details and Reference 30.) Patients whoreceived both NOT and COT had improvedbrain function at the 6-month observationpoint. But only COT patients had continuedimprovement in brain function at the end ofone year, with a slight decline in the NOTpatients.22
Numerous methods were used to determinechanges in the quality of life during the NOTT.Although global benefit was obvious to mostobservers, actual quantification of the quality oflife by specific instruments was somewhat difficult. The best estimates were derived fromthe numerous neuropsychologic studies, resultswhich have previously been reported.22,23
These studies documented the profound effectof COPD and hypoxemia on various indices ofbrain function and showed that a small but significant improvement in brain functionoccurred with the use of oxygen therapy. It isdifficult to separate the effects of oxygen therapy from pulmonary rehabilitation (i.e.,exercise physical conditioning and nutritionalrepletion) in such studies.
7www.nlhep.org
4. Other Benefits from Oxygen
5. Oxygen “Dosing” (Liter Flow)The common practice of initiating the
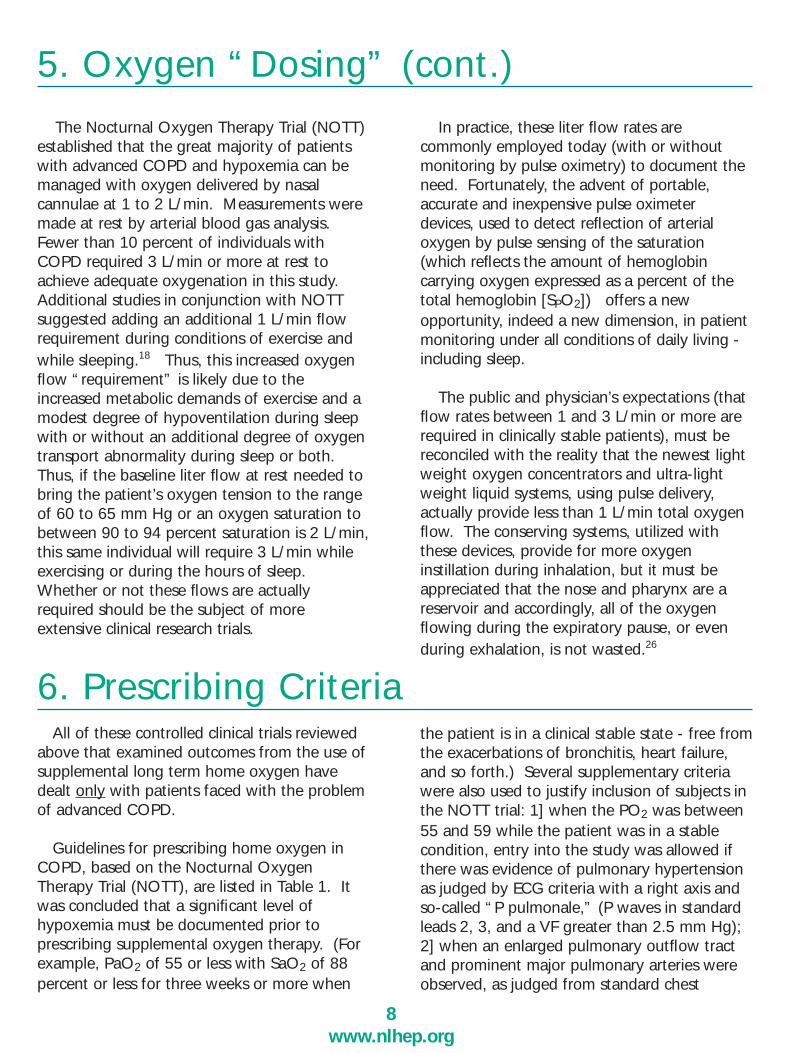
oxygen “dose” at 2 L/min by nasal cannulae isdrawn from two studies done in the 1960s; onefrom Winnipeg, Canada24 and the second fromthe Denver Group.25 In each case a smallnumber of patients (17 in each study), hospitalized for exacerbation of COPD receivedgradually increasing flows of supplemental oxygen under stable state conditions. Thesetwo articles alone form the foundation of initiating oxygen in COPD patients at 2 L/min!Figure 7 presents the data from the Denverstudy published in 1967. Figure 7. Arterial blood gas response in 17 patients with
chronic airway obstruction in whom progressive PCO2
rise did not develop while they were receiving low flowoxygen. (Cross-hatched area represents normal PaO2 atDenver.)
The Nocturnal Oxygen Therapy Trial (NOTT)established that the great majority of patientswith advanced COPD and hypoxemia can bemanaged with oxygen delivered by nasal cannulae at 1 to 2 L/min. Measurements weremade at rest by arterial blood gas analysis.Fewer than 10 percent of individuals withCOPD required 3 L/min or more at rest toachieve adequate oxygenation in this study.Additional studies in conjunction with NOTTsuggested adding an additional 1 L/min flowrequirement during conditions of exercise andwhile sleeping.18 Thus, this increased oxygenflow “requirement” is likely due to theincreased metabolic demands of exercise and amodest degree of hypoventilation during sleepwith or without an additional degree of oxygentransport abnormality during sleep or both.Thus, if the baseline liter flow at rest needed tobring the patient’s oxygen tension to the rangeof 60 to 65 mm Hg or an oxygen saturation tobetween 90 to 94 percent saturation is 2 L/min,this same individual will require 3 L/min whileexercising or during the hours of sleep.Whether or not these flows are actuallyrequired should be the subject of more extensive clinical research trials.
In practice, these liter flow rates are commonly employed today (with or withoutmonitoring by pulse oximetry) to document theneed. Fortunately, the advent of portable, accurate and inexpensive pulse oximeterdevices, used to detect reflection of arterial oxygen by pulse sensing of the saturation(which reflects the amount of hemoglobin carrying oxygen expressed as a percent of thetotal hemoglobin [SPO2]) offers a new opportunity, indeed a new dimension, in patientmonitoring under all conditions of daily living -including sleep.
The public and physician’s expectations (thatflow rates between 1 and 3 L/min or more arerequired in clinically stable patients), must bereconciled with the reality that the newest lightweight oxygen concentrators and ultra-lightweight liquid systems, using pulse delivery,actually provide less than 1 L/min total oxygenflow. The conserving systems, utilized withthese devices, provide for more oxygen instillation during inhalation, but it must beappreciated that the nose and pharynx are areservoir and accordingly, all of the oxygenflowing during the expiratory pause, or evenduring exhalation, is not wasted.26
All of these controlled clinical trials reviewedabove that examined outcomes from the use ofsupplemental long term home oxygen havedealt only with patients faced with the problemof advanced COPD.
Guidelines for prescribing home oxygen inCOPD, based on the Nocturnal OxygenTherapy Trial (NOTT), are listed in Table 1. Itwas concluded that a significant level of hypoxemia must be documented prior to prescribing supplemental oxygen therapy. (Forexample, PaO2 of 55 or less with SaO2 of 88percent or less for three weeks or more when
the patient is in a clinical stable state - free fromthe exacerbations of bronchitis, heart failure,and so forth.) Several supplementary criteriawere also used to justify inclusion of subjects inthe NOTT trial: 1] when the PO2 was between55 and 59 while the patient was in a stablecondition, entry into the study was allowed ifthere was evidence of pulmonary hypertensionas judged by ECG criteria with a right axis andso-called “P pulmonale,” (P waves in standardleads 2, 3, and a VF greater than 2.5 mm Hg);2] when an enlarged pulmonary outflow tractand prominent major pulmonary arteries wereobserved, as judged from standard chest
8www.nlhep.org
5. Oxygen “Dosing” (cont.)
6. Prescribing Criteria
6. Prescribing Criteria (cont.)
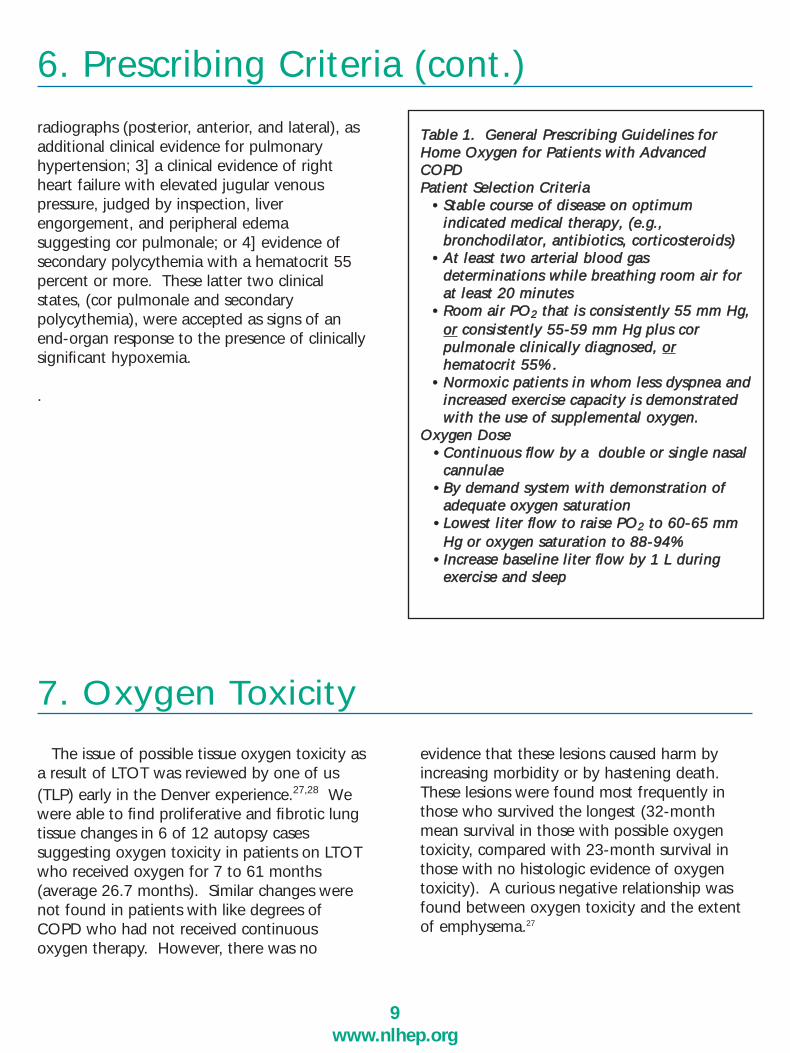
TTaabbllee 11.. GGeenneerraall PPrreessccrriibbiinngg GGuuiiddeelliinneess ffoorrHHoommee OOxxyyggeenn ffoorr PPaattiieennttss wwiitthh AAddvvaanncceeddCCOOPPDDPPaattiieenntt SSeelleeccttiioonn CCrriitteerriiaa
•• SSttaabbllee ccoouurrssee ooff ddiisseeaassee oonn ooppttiimmuummiinnddiiccaatteedd mmeeddiiccaall tthheerraappyy,, ((ee..gg..,,bbrroonncchhooddiillaattoorr,, aannttiibbiioottiiccss,, ccoorrttiiccoosstteerrooiiddss))
•• AAtt lleeaasstt ttwwoo aarrtteerriiaall bblloooodd ggaassddeetteerrmmiinnaattiioonnss wwhhiillee bbrreeaatthhiinngg rroooomm aaiirr ffoorraatt lleeaasstt 2200 mmiinnuutteess
•• RRoooomm aaiirr PPOO22 tthhaatt iiss ccoonnssiisstteennttllyy 5555 mmmm HHgg,,oorr ccoonnssiisstteennttllyy 5555--5599 mmmm HHgg pplluuss ccoorrppuullmmoonnaallee cclliinniiccaallllyy ddiiaaggnnoosseedd,, oorrhheemmaattooccrriitt 5555%%..
•• NNoorrmmooxxiicc ppaattiieennttss iinn wwhhoomm lleessss ddyyssppnneeaa aannddiinnccrreeaasseedd eexxeerrcciissee ccaappaacciittyy iiss ddeemmoonnssttrraatteeddwwiitthh tthhee uussee ooff ssuupppplleemmeennttaall ooxxyyggeenn..
OOxxyyggeenn DDoossee•• CCoonnttiinnuuoouuss flflooww bbyy aa ddoouubbllee oorr ssiinnggllee nnaassaall
ccaannnnuullaaee•• BByy ddeemmaanndd ssyysstteemm wwiitthh ddeemmoonnssttrraattiioonn ooff
aaddeeqquuaattee ooxxyyggeenn ssaattuurraattiioonn•• LLoowweesstt lliitteerr flflooww ttoo rraaiissee PPOO22 ttoo 6600--6655 mmmm
HHgg oorr ooxxyyggeenn ssaattuurraattiioonn ttoo 8888--9944%% •• IInnccrreeaassee bbaasseelliinnee lliitteerr flflooww bbyy 11 LL dduurriinngg
eexxeerrcciissee aanndd sslleeeepp
9www.nlhep.org
radiographs (posterior, anterior, and lateral), as additional clinical evidence for pulmonaryhypertension; 3] a clinical evidence of rightheart failure with elevated jugular venous pressure, judged by inspection, liver engorgement, and peripheral edema suggesting cor pulmonale; or 4] evidence ofsecondary polycythemia with a hematocrit 55percent or more. These latter two clinicalstates, (cor pulmonale and secondary polycythemia), were accepted as signs of anend-organ response to the presence of clinicallysignificant hypoxemia.
.
7. Oxygen Toxicity
The issue of possible tissue oxygen toxicity asa result of LTOT was reviewed by one of us(TLP) early in the Denver experience.27,28 Wewere able to find proliferative and fibrotic lungtissue changes in 6 of 12 autopsy cases suggesting oxygen toxicity in patients on LTOTwho received oxygen for 7 to 61 months (average 26.7 months). Similar changes werenot found in patients with like degrees ofCOPD who had not received continuous oxygen therapy. However, there was no
evidence that these lesions caused harm byincreasing morbidity or by hastening death.These lesions were found most frequently inthose who survived the longest (32-monthmean survival in those with possible oxygentoxicity, compared with 23-month survival inthose with no histologic evidence of oxygentoxicity). A curious negative relationship wasfound between oxygen toxicity and the extentof emphysema.27
8. Oxygen Safety
cannulae whether by accident or purposefully!More recently a burn unit has reported on aretrospective analysis of burns related to oxygen use. Only twenty-three patients, mostly with COPD, average age of 70, weretreated for burns associated with supplementaloxygen use over a 12-year period, whichrequired admission to a burn unit! Averageburn size was 3.9% of total body size.29
However, amended reports of some burns continue to be mentioned in reviews about LTOT.A central registry for the recording of oxygenburns and other accidents is badly needed.
A myth needs to be dispelled: Oxygen willnot explode, and it in itself is not combustible.Oxygen does vigorously support and acceleratethe combustion of flammable materials in adose-dependent fashion.
10www.nlhep.org
9. A Re-Examination of the NocturnalOxygen Therapy Trial (NOTT)
Early in our experience with the use of LTOT,the Center on Pulmonary Rehabilitation of theAmerican College of Chest Physicians conducted a nationwide survey to seek anyinformation about the occurrence of major fires,facial burns, etc. as a result of oxygen use inthe home. This survey did not show a significant number of severe fires related tooxygen and the Center issued a statement that“Home oxygen is a safe form of therapy.”Decades of home oxygen use in patients withchronic obstructive pulmonary disease andother respiratory and cardiovascular diseaseshas proved this concept. This is largely attributable to the dedication of medical staffand home oxygen suppliers who spend timeproviding oxygen patients with proper instruction in safety measures to avoid hazards.During the early years of LTOT, a few burnswere reported when patients ignited their nasal
The main purpose of this section on ambulatoryoxygen is to offer a new analysis of the NocturnalOxygen Therapy Trial (NOTT) data in order toexplore why continuous oxygen therapy (COT)was superior to nocturnal oxygen therapy (NOT).We aimed to determine if survival was related tothe exercise capacities of the patients at the timeof randomization to oxygen or if it was a functionof the duration of oxygen administration.
In the brief review, the NOTT study collectedextensive data from a well-defined populationof patients with advanced chronic obstructivepulmonary disease (COPD), who were randomlyassigned to receive either NOT for approximately 12 hours per day from a stationary source or ambulatory oxygen (i.e.,COT that was intended to be used as close to24 hours per day as possible). In the NOTT,extensive outcome data was obtained that can
answer important questions about oxygen therapy and its effects on the outcomes ofexercise capacity, survival, and hospitalizationrequirements in this well-defined population.
The details of the original NOTT study havebeen reported elsewhere.18 Patients with chronicstable hypoxemia with partial pressure of oxygenPO2 of ≤ 55 mm Hg (who had no significant co-morbidities and were willing to participate inan exercise-oriented rehabilitation program utilizing oxygen) were randomized to receiveeither NOT from a stationary oxygen system orCOT from an ambulatory system.18,19 Therandomization process resulted in the enrollmentof patients who were well-matched by age,gender, and indices of disease severity. After theNOTT report, the magnetic data tapes wereplaced in the public domain in hopes that furtheranalyses would be made by other investigators.
The original NOTT data set was obtainedfrom the National Heart, Lung, and BloodInstitute in its original format and convertedinto an Access (Microsoft Corporation,Redmond, Washington) database. From thisdatabase, information was imported into Excelspreadsheets (Microsoft Corporation, Redmond,Washington) for matching and analysis.30
WALKING ABILITYIn the NOTT, each candidate for the study
participated in a comprehensive pulmonaryrehabilitation program, with exercise performedon a daily basis for 3 weeks prior torandomization to NOT or COT. Each patientwas urged to walk as much as possible each dayduring the 3-week stabilization period, and eachwas given a pedometer to monitor the distancewalked each day. The distance was recorded bya research nurse or technician. This 3-weekperiod was intended to bring each patient to afunctional optimum before randomization toNOT or COT. The average number of feet thateach patient walked per day was calculatedduring the third week of the stabilization period.We called this factor “walking level.”Pedometer data for the 3-week stabilization andoptimization period was available for 157 of the203 total patients. We had maximum oxygenconsumption measurements for 106 of the 203total patients enrolled in the NOTT. In ourmatched group of 80 subjects, we had maximumoxygen consumption measurements for 18subjects with a low walking level (39 mL/min),and 24 subjects with a high walking level (59mL/min (p= 0.007). Thus, the walking level canbe taken as a surrogate indicator of themaximum oxygen consumption measurement inthis analysis. Patient demographics are in Table 2.
We divided the patients into a low walkingand a high walking group by separating thembased on the median walking distance achievedat the end of 3 weeks.
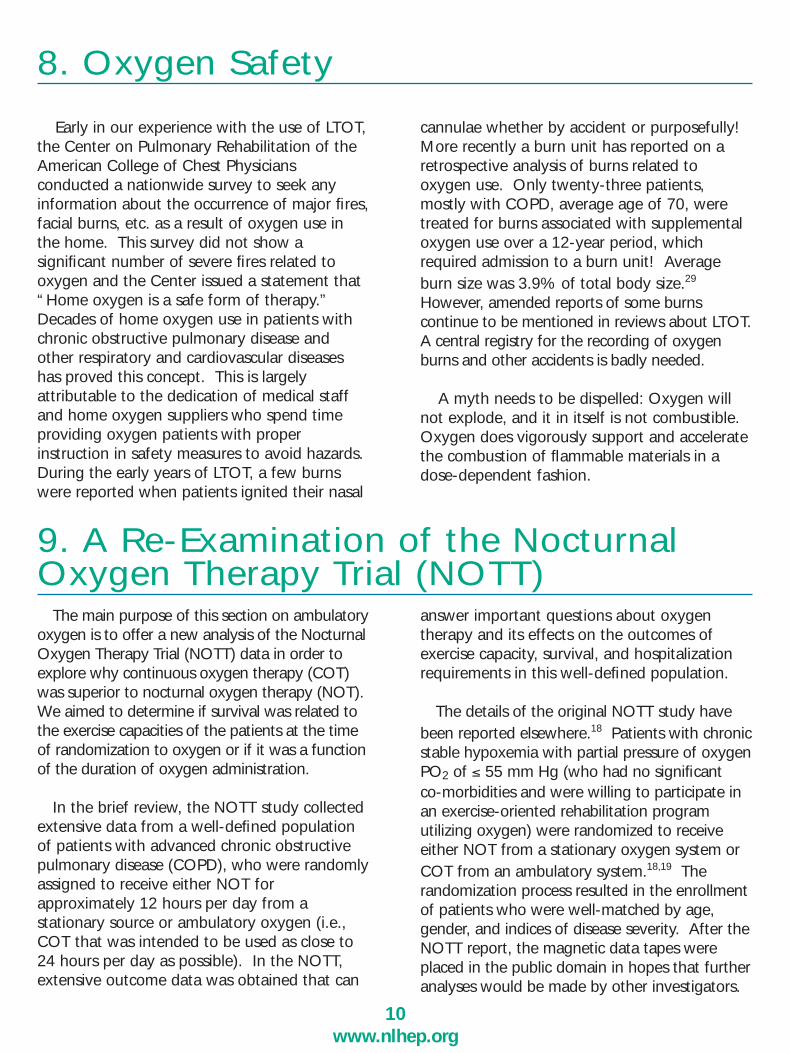
Figure 8 presents the origins of the 80matched patients. The initial division of thepatients by walking level at the median (3,590ft/d) yielded groups that were not well matchedby age. The low walking group wasapproximately 6 years older than the high walkinggroup. To overcome this weakness, each lowwalking patient was manually matched with ahigh walking patient of similar age, treatmentgroup (COT vs NOT), and percent of predictedforced expiratory volume in the first second(FEV1). The resulting groups were 40 patientseach in the low and high walking groups. These80 patients were then further divided into COTand NOT groups. Table 2 shows that the resultsof this method lead to good matching of allparameters listed.
DATA ANALYSISThe methods of Kaplan and Meier31 were
used to produce the survival function, using theproduct-limit estimate model. Statisticalsignificance was tested using the methoddescribed by Cox.32 Hospitalization data wereanalyzed by analysis of variance.
11www.nlhep.org
A Re-Examination of the NOTT (Cont.)
Figure 8. Re-Examiniation of the Nocturnal OxygenTherapy Trial by pretreatment ambulation status. Origins ofthe 80 matched patients.
A Re-Examination of the NOTT (cont.)
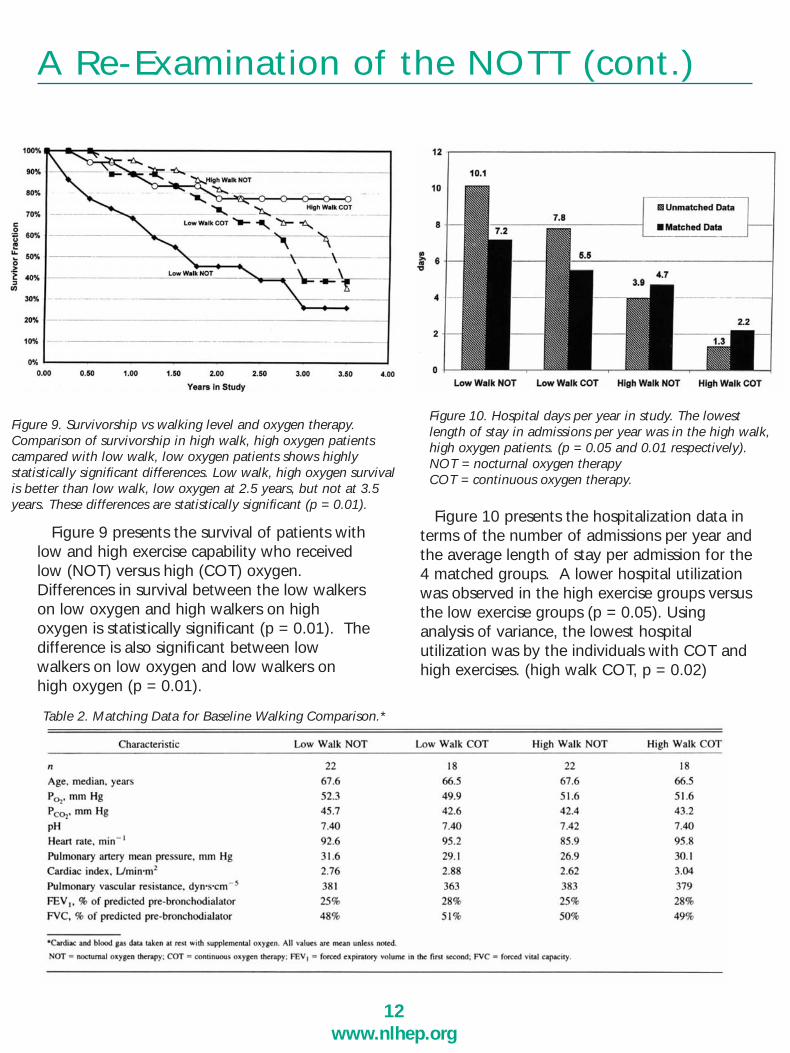
Figure 10 presents the hospitalization data interms of the number of admissions per year andthe average length of stay per admission for the4 matched groups. A lower hospital utilizationwas observed in the high exercise groups versusthe low exercise groups (p = 0.05). Usinganalysis of variance, the lowest hospitalutilization was by the individuals with COT andhigh exercises. (high walk COT, p = 0.02)
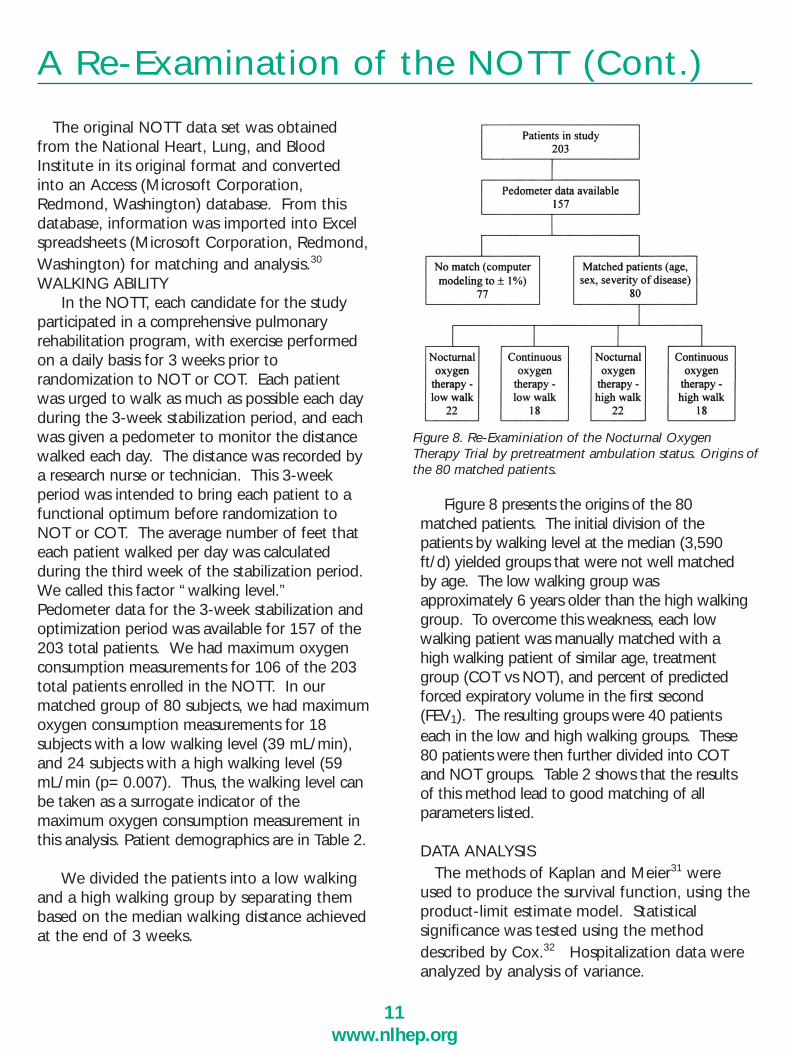
Figure 9 presents the survival of patients withlow and high exercise capability who receivedlow (NOT) versus high (COT) oxygen.Differences in survival between the low walkerson low oxygen and high walkers on highoxygen is statistically significant (p = 0.01). Thedifference is also significant between lowwalkers on low oxygen and low walkers onhigh oxygen (p = 0.01).
Figure 10. Hospital days per year in study. The lowestlength of stay in admissions per year was in the high walk,high oxygen patients. (p = 0.05 and 0.01 respectively).NOT = nocturnal oxygen therapy COT = continuous oxygen therapy.
Figure 9. Survivorship vs walking level and oxygen therapy.Comparison of survivorship in high walk, high oxygen patientscampared with low walk, low oxygen patients shows highlystatistically significant differences. Low walk, high oxygen survivalis better than low walk, low oxygen at 2.5 years, but not at 3.5years. These differences are statistically significant (p = 0.01).
Table 2. Matching Data for Baseline Walking Comparison.*
12www.nlhep.org

COMMENTImproved survival in the NOTT study was in
part related to reversibility of pulmonaryhypertension.33 Similar conclusions have beendrawn by other investigators.34-36 It is difficultto understand, however, how a modestreduction in mean pulmonary artery pressure(only 3-5 mm Hg), which causes only a slightdecrease in the afterload of the right ventricle,could be the sole reason for the improvedsurvival. In one study, improved survival wasrelated to both a reduction in pulmonarypressure and an increase in maximum oxygenconsumption.34 In some patients who had areduction in pulmonary artery pressure, therewas an increase of left ventricular ejectionfraction, which may be a reflection of improvedglobal cardiac function because of relief ofhypoxemia.34
Extensive exercise studies evaluating rightventricular function during exercise in COPDhave shown that an increase in exercisetolerance is related to an increase in rightventricular function and increased oxygenconsumption.37,38 Increased exercise capacity inhypoxemic COPD patients often results fromlong term supplemental oxygen administrationand is related to an improvement in rightventricular function.37-39 Increased rightventricular function and oxygen consumptionmay occur in spite of increases in pulmonaryartery pressure and pulmonary vascularresistance. The elevated pulmonary pressureand resistance are most likely due to fixedvascular changes in the pulmonary vascularbed, which are not reversible, even with long-term oxygen therapy (LTOT).40 One studyfound a relationship between mixed venousoxygen tension and survival in patients whowere candidates for LTOT.39 The 5-yearsurvival was better in patients with the highestmixed venous PO2 and higher coefficient ofoxygen extraction.41 This study suggested that
13www.nlhep.org
A Re-Examination of the NOTT (cont.)
measures designed to increase cardiac outputwould be appropriate to improve tissue oxygendelivery.41,42
In other studies, patients who exhibited little orno ability to increase their cardiac output andsystemic oxygen transport did not have increasedexercise capacity.37-39 These observations led tothe conceptualization of the “right ventricularhypothesis.”41,43 The right ventricular hypothesisis based on the concept that limitation of rightventricular function limits systemic tissue organtransport. Before oxygen is given, ventricularfunction and oxygen transport may be limited bypoor oxygenation of the myocardium. Afteroxygen is administered, right ventricular functioncan still be limited by structural damage of theright ventricle or by elevated right ventricularafterload from fixed pulmonary vascular changes.In any event, failure to improve right ventricularsystolic function may limit tissue oxygentransport. By improving oxygen to the rightventricular myocardium, and by reducing rightventricular afterload, right ventricular functionmay improve. This, in turn, results in improvedglobal cardiac function, increased tissue oxygentransport, and increased tissue energy production.
It is likely that tissue metabolic phenomenaare responsible for improved survival. In theBritish Medical Research Council Study of LTOTin COPD, men who received oxygen versusmen who did not receive oxygen, had animprovement in survival but this difference didnot become apparent until after 500 days onLTOT.17 In the NOTT study, improved survivaldid not become statistically significant until 18months into LTOT.18 These data suggest thatthe survival benefit from oxygen was a functionof restorative metabolic changes in multipleorgans, which occurred over months of LTOT.
The restorative value of oxygen on brainfunction has been previously reported.22
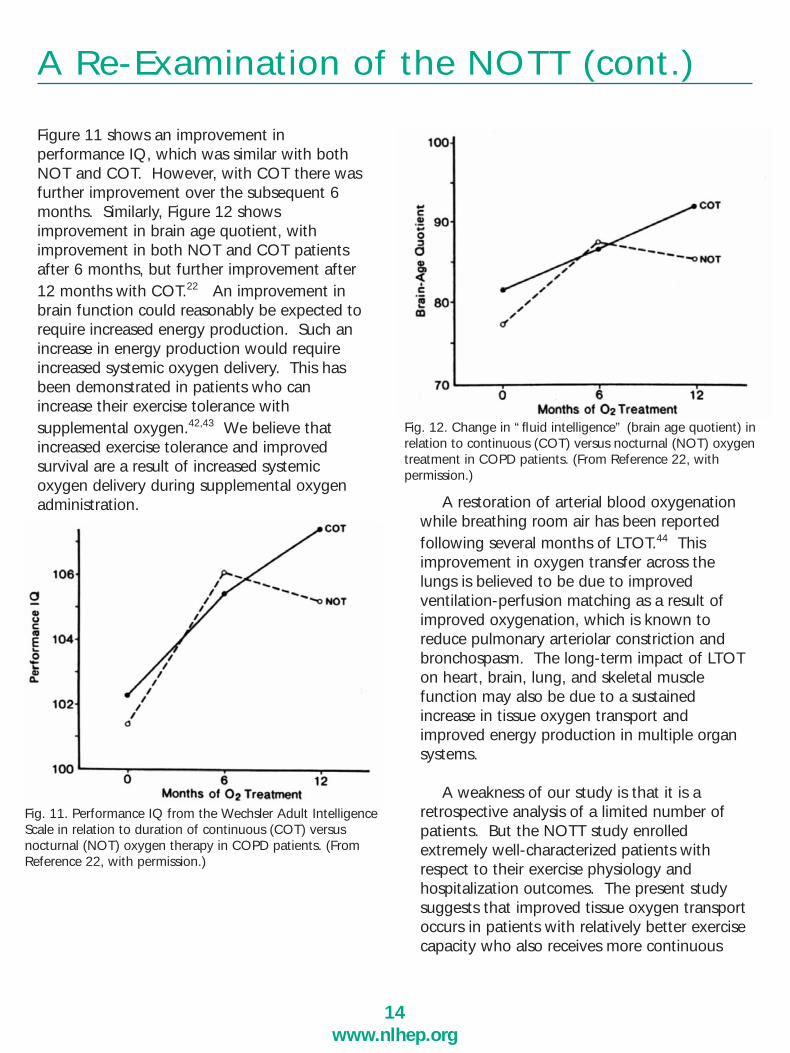
Figure 11 shows an improvement inperformance IQ, which was similar with bothNOT and COT. However, with COT there wasfurther improvement over the subsequent 6months. Similarly, Figure 12 showsimprovement in brain age quotient, withimprovement in both NOT and COT patientsafter 6 months, but further improvement after12 months with COT.22 An improvement inbrain function could reasonably be expected torequire increased energy production. Such anincrease in energy production would requireincreased systemic oxygen delivery. This hasbeen demonstrated in patients who canincrease their exercise tolerance withsupplemental oxygen.42,43 We believe thatincreased exercise tolerance and improvedsurvival are a result of increased systemicoxygen delivery during supplemental oxygenadministration. A restoration of arterial blood oxygenation
while breathing room air has been reportedfollowing several months of LTOT.44 Thisimprovement in oxygen transfer across thelungs is believed to be due to improvedventilation-perfusion matching as a result ofimproved oxygenation, which is known toreduce pulmonary arteriolar constriction andbronchospasm. The long-term impact of LTOTon heart, brain, lung, and skeletal musclefunction may also be due to a sustainedincrease in tissue oxygen transport andimproved energy production in multiple organsystems.
A weakness of our study is that it is aretrospective analysis of a limited number ofpatients. But the NOTT study enrolledextremely well-characterized patients withrespect to their exercise physiology andhospitalization outcomes. The present studysuggests that improved tissue oxygen transportoccurs in patients with relatively better exercisecapacity who also receives more continuous
14www.nlhep.org
A Re-Examination of the NOTT (cont.)
Fig. 11. Performance IQ from the Wechsler Adult IntelligenceScale in relation to duration of continuous (COT) versus nocturnal (NOT) oxygen therapy in COPD patients. (FromReference 22, with permission.)
Fig. 12. Change in “fluid intelligence” (brain age quotient) inrelation to continuous (COT) versus nocturnal (NOT) oxygentreatment in COPD patients. (From Reference 22, with permission.)
ambulatory oxygen. Patients with lower levelsof exercise capacity had better survival withoxygen delivered for a longer period of time.
This study suggests that new clinical trialsare needed to compare outcomes in patientswho utilize ambulatory oxygen for as manyhours per day as possible, compared withstationary oxygen for an equivalent length oftime. Such studies could answer the criticalquestion about survival in relation to anambulatory or stationary oxygen deliverysources, and address the question: doescontinuous ambulatory LTOT reducehospitalizations?
COMMENTThe NOTT study showed improved survival in
COT patients who received LTOT for longerperiods (mean 17.7 h/d, median 19.4 h/d) froman ambulatory oxygen system, compared withthe survival of NOT patients who receivedoxygen for a mean of 11.8 h/d from astationary system. The differences in survivalcould have been due to the method or theduration of oxygen therapy, or both. Anincrease in cardiac output and increasedoxygenation of the arterial blood (oxygencontent) results in increased tissue oxygentransport. In addition, COT was associated withbetter survival and reduced hospitalizations,compared with NOT patients who were unableto increase their walking level.
15www.nlhep.org
A Re-Examination of the NOTT (cont.)
10. Oxygen TechnologiesOxygen Therapy Devices
Long Term Oxygen Therapy (LTOT) devicesare evolving to a new level of sophistication.Equipment used for home oxygen therapy is beingdeveloped with the patients’ needs in mind, plusan appreciation for the costs associated with theservice of LTOT equipment. This new breed ofoxygen therapy equipment is arriving on themarket at an opportune time, since a large numberof “Baby Boomers” needing LTOT are just startingto receive prescriptions for home oxygen therapy.Historical perspective
Not more than thirty years ago, aprescription for home oxygen therapy wouldrequire an industrial gas supplier to deliverseveral large (H size) cylinders to a patient’shome. A large brass regulator would be put onthe cylinder and a permanent humidifierattached for patient comfort. No portablesystems were provided since oxygen therapywas prescribed at the end stage of the disease,and the patients were typically bed-bound.This therapy would most often be provided forless than a year and in many cases only a fewweeks.
The late 1970’s brought a new concept tohome oxygen therapy. A device was developedthat could generate oxygen in the home andnever need to be refilled. Oxygenconcentrators became popular since theyprovided a convenience to the provider andunlimited oxygen to the patient – barringmechanistic problems such as a loss of theenergy source (i.e. electrical power failure) torun the concentrator. Portable oxygen wasavailable as an emergency backup for theconcentrator and could be used for short visitsto the doctor or hospital. Patients were still notvery ambulatory due to the progression of theirdisease and the lack of emphasis for activity.Liquid oxygen (LOX) for home application wasavailable and popular for patients that wantedto be active, since the portable system waslighter in weight (compared to cylinders) andlonger lasting (compared to cylinders). LOXcontinued to grow in popularity as patients, andphysicians realized the advantages of thesesystems for optimizing use of LTOT duringroutine activities of daily living, exercise, andpulmonary rehabilitation.

16www.nlhep.org
Oxygen Technologies (cont.)
Two major changes have occurred over thepast twenty years: 1) Patients are beingprescribed oxygen earlier in their disease, oftenwhen they are younger and require LTOT tobecome more active. 2) Younger, active patientsrequire an oxygen system that meets their needsfor regular daily activity inside and outside theirplace of residence. Steel cylinders have evolvedto aluminum, and sizes have been shrinking fromE cylinders holding 680 liters to M cylindersholding 140 liters of gas. Oxygen conservingdevices (OCD) have made the smaller cylindersmore practical since the average 3:1 savings ratioallows for approximately 4 hours of mobility at a2 L/min prescription.
OCDs have also helped LOX systems reducesize and last longer. The new 3 to 4 poundliquid oxygen portables can last from 6-8 hoursat a 2 L/min setting. These new LOX portableshave rejuvenated the home LOX industry, withseveral manufacturers introducing new small,lightweight portable systems.
Evolution of the technologyCylinders are still being used during certain
circumstances as portable oxygen systems.Patients may prefer an E cylinder as their portablesince there is a safety factor of having enoughoxygen available if the OCD should fail. Andthere is the option of using a wheeled cart tokeep the weight of the portable off the patients’shoulders. Other patients like the M6 cylinderdue to the small size and light weight. Thesesystems can be placed in a case that hides thefact that the patient is using oxygen. Aconserving device makes the small cylinders morepractical, since there is a minimal operating timefrom these units versus using continuous flow.
LOX is the most efficient method of storingoxygen. With an 860:1 ratio of gas to liquid, avery small amount of liquid oxygen can expandto a large amount of gas. Early LOX portablesheld 1 liter of liquid. Expanding to 860 liters of
gas, a 9-pound LOX portable could provide moregas than an E cylinder at less weight. OCD on aLOX portable can reduce the amount of oxygenneeded to provide the desired operating time,which is why the new generation of LOXportables are smaller, lighter and longer lasting.45
LOX base units have improved to reduce thenormal evaporation rate (NER), and severalsystems have telemetry to allow for monitoringof content and schedule delivery.
Concentrators have improved significantly inrecent years. Systems currently on the marketare more reliable at a lower cost and are thebasis of most home oxygen therapy programs.
Concentrators that fill portable cylinders arenew to the market. The ability to fill a cylinderin the patient’s home gives patients freedom torefill the cylinders as often as their lifestylepermits, plus the provider does not need todeliver cylinders to patients’ homes on a regularbasis. Delivery of products to the home is oneof the most expensive portions of a provider’scost of LTOT services. The continuedreductions in reimbursement from CMS havedriven manufacturers and providers to focus onways to reduce delivery expenses.
The purchase price of the home-fillingconcentrator has been the barrier to providersto generally accept the system. A home-fillingsystem can cost up to three times the purchaseprice of a standard concentrator. Theeconomics of eliminating the delivery ofcylinders, and the reduced inventory ofcylinders and accessories to support LTOT hasnot been clearly documented by independentresearch. Other issues of concern related to thehome filling concentrators are the additionalcost of electricity that is the responsibility of thepatient, plus the issue of 93% oxygen from acylinder filled by a concentrator. Cylinders aretypically used during exercise, and an OCD is

utilized to extend operating time. The use of acombination of 93% oxygen, an OCD, andincreased respiratory rate has not been provenby research studies to improve specificoutcomes, but this approach might still have apositive impact on the patient’s oxygensaturation.
Portable oxygen concentrators (POC) are new tothe market. Featuring 9 pound weight, 1-8 hoursof battery operating time and 93% oxygen purity,these devices utilize an OCD and have doseselection options. These units will have the samechallenges to market entry as the home fillingsystems — higher cost and the issue of 93%oxygen delivered with an OCD to a patient with anincreased respiratory rate. Clinicians have requesteda portable oxygen concentrator for years and thesenew entries will start the process of refinement andimprovement. Allowing one system to be both thebase unit and portable will further reduce the costof LTOT and provide the independence patients arelooking for from their oxygen system.
Oxygen conserving devices are one of thefastest growing areas of LTOT. Frost and Sullivanhave estimated that the total number of OCDsold in 2001 was 129,971, and sales werepredicted to grow 15% annually.46 In 1984 thefirst intermittent flow oxygen delivery device wasintroduced to the home care market.Appreciating the fact that oxygen deliveredwhen the patient was exhaling was wasteful, thisproduct sensed the patient’s inspiratory effortand delivered a dose of oxygen only at thebeginning of inhalation. This system eliminatedthe 2/3 of wasted oxygen that was beingdelivered during the patient’s exhalation andpause between breaths. Eliminating wasteimproved operating times and has been the basisfor most new oxygen systems used in the home.An OCD can reduce the scheduled delivery ofoxygen via LOX and high pressure cylindersystems, and reduce associated costs. Newerportable concentrators and those developed inthe future will depend on OCD technology to
improve efficiency and minimize weight, makinglightweight portable concentrators a moreattractive and practical option for the delivery ofLTOT possible.
Not all OCDs operate the same. The methodof delivery for different systems has beendescribed as a pulse delivery, demand deliveryand hybrid.46 The method of delivery impactsthe volume of oxygen that is provided to thepatient. The volume per breath determines thefraction of inspired oxygen (FIO2) the patient isreceiving at each setting. The settings on eachOCD are reference points and should not beconsidered the same FIO2 as continuous flow orother OCDs at the same setting. Thismisconception by patients, prescribers, andothers involved in the care of LTOT patients wasone of the reasons OCDs were not fullyunderstood nor used optimally in the past – dueto poor patient oxygenation at a certain settings.Most patients can be oxygenated with an OCDif the setting is changed to meet their oxygendose requirement. This essentially equates to theneed for oxygen titration at rest and during usualactivities of daily living on an individualized basis– using the device(s) that the LTOT patient willbe utilizing in the home and during ambulationand activity.
“Saving ratio” has been a claim of severalmanufacturers that feel their device performsbetter than others. The goal of oxygen therapyis to correct the patient’s hypoxemia. Oncethat goal is reached, the amount of oxygensaving can be a value. Withholding neededoxygen from a patient to improve saving ratio isillogical and dangerous. Most consensusconferences on LTOT recommend that a patientis tested on an OCD at each activity level andthe appropriate setting selected to maintainoxygenation. This concept applies to all oxygentherapy not just for conserving devices.
17www.nlhep.org
Oxygen Technologies (cont.)
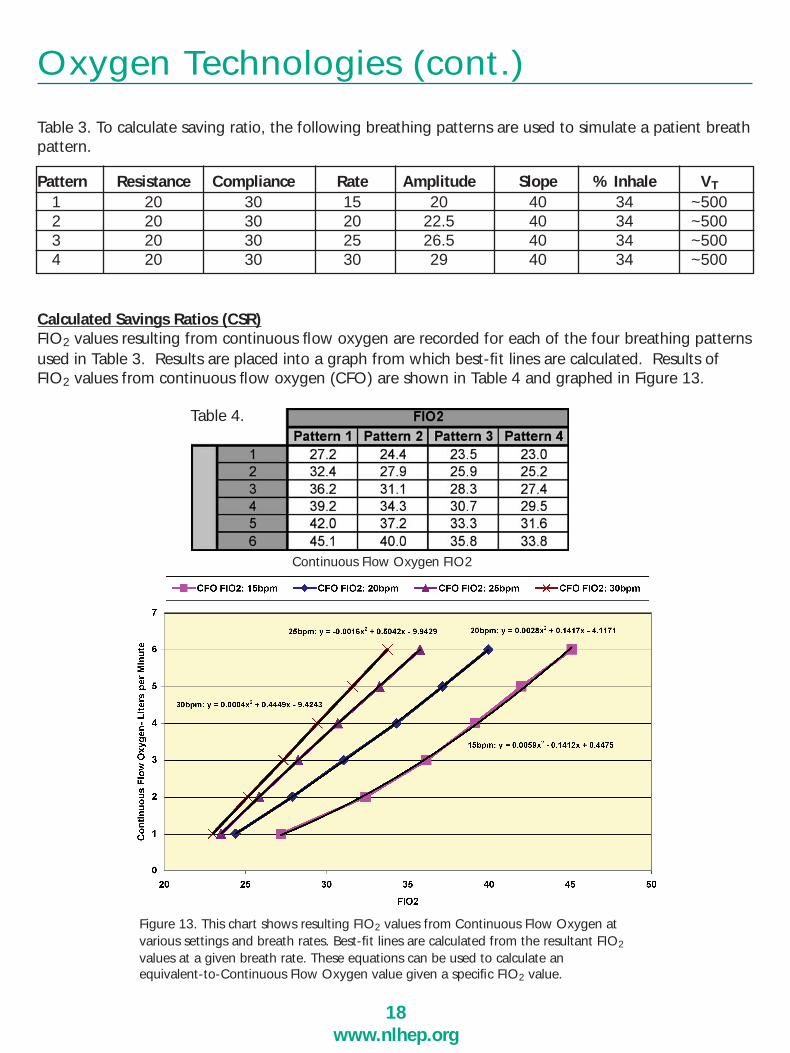
Table 3. To calculate saving ratio, the following breathing patterns are used to simulate a patient breathpattern.
Calculated Savings Ratios (CSR)FIO2 values resulting from continuous flow oxygen are recorded for each of the four breathing patternsused in Table 3. Results are placed into a graph from which best-fit lines are calculated. Results ofFIO2 values from continuous flow oxygen (CFO) are shown in Table 4 and graphed in Figure 13.
18www.nlhep.org
Oxygen Technologies (cont.)
Pattern Resistance Compliance Rate Amplitude Slope % Inhale VT
1 20 30 15 20 40 34 ~5002 20 30 20 22.5 40 34 ~5003 20 30 25 26.5 40 34 ~5004 20 30 30 29 40 34 ~500
Table 4.
Continuous Flow Oxygen FIO2
Figure 13. This chart shows resulting FIO2 values from Continuous Flow Oxygen at various settings and breath rates. Best-fit lines are calculated from the resultant FIO2
values at a given breath rate. These equations can be used to calculate an equivalent-to-Continuous Flow Oxygen value given a specific FIO2 value.
Using the FIO2 values found when testing agiven device and substituting those values intothe best fit line equation, an ‘Equivalent CFO’value is calculated.
Below is an example taken from the FIO2
values recorded from an OCD device on Pattern2, along with the resulting calculated equivalentto CFO.
To determine the Calculated Savings Ratio for agiven device setting and breath rate, take theEquivalent CFO value and divide by the totaloxygen volume delivered (in liters) multiplied bythe breath rate. Below is an example of theresulting CSR values from the same OCDdevice tested on Pattern 2.
Thus, at Setting 1 and a breath rate of 20bpm,the total volume delivered was 16.4mL, or.0164L. The CSR calculation is 1.1 / (.0164 x20), which results in a CSR value of 3.4.
There are several methods of oxygenconservation. The most popular is intermittentoxygen delivery systems. Early generations ofOCDs offered the conserving unit separatefrom the oxygen regulator. The first majorbreakthrough in the technology was a systemthat integrated the regulator with theconserving unit. This “donut” style system hasa cleaner presentation and convenience for thepatient and requires changing the regulatorwhen a cylinder is empty. The nextbreakthrough was the introduction of apneumatic OCD. This simplified the system by
19www.nlhep.org
Oxygen Technologies (cont.)
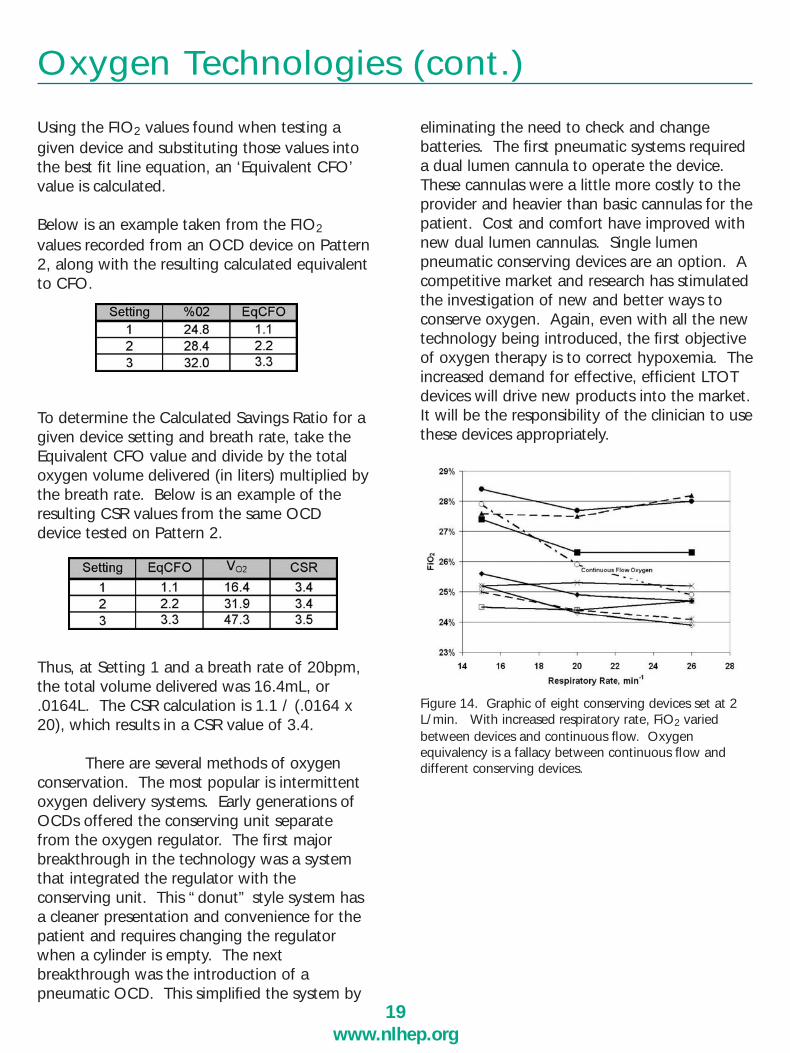
eliminating the need to check and changebatteries. The first pneumatic systems requireda dual lumen cannula to operate the device.These cannulas were a little more costly to theprovider and heavier than basic cannulas for thepatient. Cost and comfort have improved withnew dual lumen cannulas. Single lumenpneumatic conserving devices are an option. Acompetitive market and research has stimulatedthe investigation of new and better ways toconserve oxygen. Again, even with all the newtechnology being introduced, the first objectiveof oxygen therapy is to correct hypoxemia. Theincreased demand for effective, efficient LTOTdevices will drive new products into the market.It will be the responsibility of the clinician to usethese devices appropriately.
Figure 14. Graphic of eight conserving devices set at 2L/min. With increased respiratory rate, FiO2 variedbetween devices and continuous flow. Oxygenequivalency is a fallacy between continuous flow anddifferent conserving devices.
ConclusionThere are new lightweight oxygen systemsenteringthe market and new oxygen conservingdevicesintroduced almost every year. Optionsfor reducing delivery costs associated withpackaged oxygen are being developed whichinclude:
• Portable Oxygen Concentrators (POC)• Concentrators that fill cylinders in the home• Concentrators that fill LOX portables in thehome • LOX base units with conserving devices
“Baby boomers” are hitting the age and healthstatus where there will be the largest number ofpatients in that age bracket then has ever beenexperienced in the past. This group of patientswill have specific healthcare needs and a largenumber will be prescribed LTOT. A new breedof ‘healthcare savvy’ patients is emerging –ones that know what they want and seeksolutions to their health care needs – includingoptimal LTOT devices and accessories. Theoxygen device market is primed for growth andthe quality of care for LTOT patients should bethe best it has ever been with innovativetechnology and appropriate services.
Oxygen Technologies (cont.)
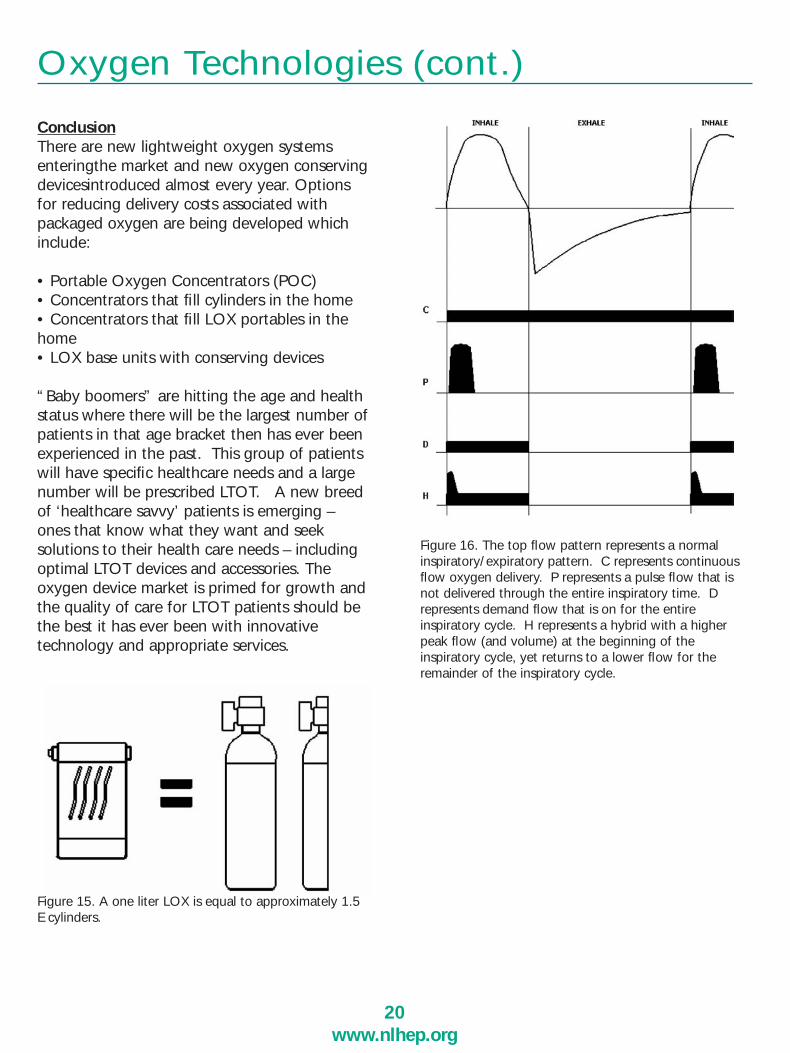
Figure 15. A one liter LOX is equal to approximately 1.5 E cylinders.
Figure 16. The top flow pattern represents a normalinspiratory/expiratory pattern. C represents continuousflow oxygen delivery. P represents a pulse flow that isnot delivered through the entire inspiratory time. Drepresents demand flow that is on for the entireinspiratory cycle. H represents a hybrid with a higherpeak flow (and volume) at the beginning of theinspiratory cycle, yet returns to a lower flow for theremainder of the inspiratory cycle.
20www.nlhep.org

When the original NOTT Study waspublished, a theoretic consideration of LTOTcost effectiveness was published in anaccompanying editorial.47 The NOTTconcluded that survival was improved by nearlycontinuous ambulatory oxygen, compared withnocturnal oxygen from a stationary source. Thecost of increased life was also a consideration,as well as the cost of the associated morbiditydue to increased longevity (i.e., drugs, doctors’visits, hospitalizations). In our re-analysis of theoriginal NOTT data and the finding of reducedhospitalizations in ambulatory patients withpreserved walk tolerance, it can be argued thatambulatory oxygen in functional patients canactually reduce costs even more than initiallythought by reducing hospitalizations.
LTOT is not expensive when compared withother treatments for serious and life threateningillness. In 2006 ambulatory systems are reimbursedat approximately $225 per month, or $2700 peryear. Stationary systems are reimbursed at a slightlylower level of $200 per month, or $2400 per year.This is far less than the annual cost for outpatienthome hemodialysis (which costs $51,252 [USD] peryear) or for home peritoneal dialysis ($29,96548
[USD] per year). The reimbursement structure forthe costs associated with the chronic managementof end stage kidney dialysis has been mandated byCongress since 1972!
Based on data generated from the recentlycompleted National Emphysema Treatment Trial(NETT), direct medical costs for lung volumereduction surgery (LVRS) are $71,515 comparedwith $23,271 for medical therapy for COPDpatients in the first 12 months followingrandomization.49 Direct medical costs in thefollowing two years for patients havingundergone LVRS and medical therapy were notsignificantly different.49 Today LVRS is approvedby Medicare. Quality of life improvement isconsidered a reasonable outcome by Medicare.Cancer chemotherapy and AIDS medications
often cost $10,000 to $15,000 per month, or$120,000 to $180,000 per year.
Today LTOT is reimbursed at a flat rate, nomatter what modality is prescribed or necessaryfor the patient. This is the so called “modalityneutral” principle, which does not make sense.This policy also invites abuse, since some suppliersmay choose to provide the least expensivetechnology, in spite of what is appropriate for thepatient. Also, some who prescribe LTOT are notaware of all the devices available to deliveroxygen. This policy must change. If prospectivecontrolled clinical trials prove the medicalsuperiority of ambulatory oxygen worn by thepatient (to allow for increased activities of dailyliving and restoration of organ system functions),and if the use of ambulatory oxygen also reduceshospitalizations, (as suggested in Figure 10),ambulatory oxygen may prove to be the mostcost-effective modality. With emergingtechnologies, it is possible for suppliers to providea wearable system for all appropriate patients.Both refillable low weight cylinders and homegeneration of liquid oxygen to fill ultra lightweight wearable devices, are now approved bythe FDA and are becoming more generallyavailable. Oxygen reimbursement should beapproved by Medicare to provide an appropriateambulatory system for all patients who have theability to benefit from these “wearable” systems(i.e. a device(s) and accessories that adequatelyoxygenate the patient in need of LTOT at rest andduring usual activities of daily living inside andoutside their place of residence). It is self-evidentthat current policies for LTOT reimbursementmust be re-evaluated to be consistent with otherreimbursement precedents already existing in theU.S. healthcare system to insure the principle ofdistributive justice.
LTOT is a bargain when compared with othertechnologies and surgeries used to extend life orto improve the quality of life. This fact should berespected: LTOT needs appropriatereimbursement!
21www.nlhep.org
11. Cost Effectiveness of LTOT

Many organizations – professional societies,device and pharmaceutical companies, LTOTpatients, their caregivers and payers, patientadvocacy groups, physicians, nurses, respiratorytherapists and other respiratory care professionals,governmental and other regulatory agencies, aswell as LTOT manufacturers, and providers – haveworked laboriously over the years on the issuessurrounding optimal and cost-effective use ofLTOT by patients in need. Representatives frommost of these organizations participated in the 6th
Oxygen Consensus Conference held in Denver,CO, August 25-28, 2005. One of theseorganizations, the NLHEP, has been active foryears in these pursuits. The NLHEP celebrates its10th anniversary in 2006. The rich history of theNLHEP has been previously recorded.50 Themission of the NLHEP is to reduce the impact andenhance the earlier detection of COPD, andinitiate appropriate therapies for COPD andrelated disorders. Ensuring optimal and cost-effective use of LTOT is a high priority of theNLHEP.
The National Lung Health Education Program(NLHEP) is designed to identify and treat those inthe early stages of COPD (emphysema and relatedchronic bronchitis). The NLHEP was actually‘conceived’ at the 37th Aspen Lung Conferencewhich led to: 1) a planning conference in 1994;2)a second and more comprehensive workshop inBethesda, MD, on August 29-31, 1995, chaired byone of us (TLP); 3)the launch of a new initiative“Building a National Strategy for the Preventionand Management of and Research in COPD”(JAMA 1997; 277:246-253)51; and 4) the ‘birth’ in1996 of the NLHEP. The NLHEP executivecommittee meets semi-annually and is comprisedof representatives from numerous collaboratingprofessional, patient, and government groups.Members include the ACCP, ATS, ACP, AACVPR,AARC, ACAAI, AAPA, SIGM, NEF, andgovernmental liaisons from NCI, NHLBI, andNIOSH. NLHEP is supportive of andcomplementary to the Global Initiative for ChronicObstructive Lung Disease (GOLD), the US COPD
Coalition, and the International COPD Coalition.The NLHEP’s missions are: 1) to reduce the impactof COPD and related disorders by raisingawareness of these diseases by the public, primarycare clinicians, healthcare agencies, and policymakers, and 2) to establish that COPD is a majorhealth problem and that the earlier detection andtreatment of COPD will improve quality of life,minimize premature deaths, and reduce the cost ofthis disease and its related disorders. It is knownthat at least 50% (12 to 15 million) of people withCOPD are not diagnosed or treated, despite theirbeing symptomatic, and during the later stages ofCOPD, LTOT is required by some.52
The original NLHEP logo, and its recentlymodified logo which retains its originalmessage, symbolize the lungs and the need forearlier identification of lung diseases.
A DECADE OF DEDICATION (1996 – 2006)
NLHEP Celebrates Its 10TH Birthday
“Test Your Lungs–Know Your Numbers.” Thisbecame the NLHEP motto, and indeed our call toarms. We have had some major successes,including an often quoted consensusrecommendation supporting the use of simpleoffice spirometry as an early detection method todetermine the presence of airflow obstruction in allsmokers age 45 and older, and recent formersmokers, and in anyone of any age with chroniccough, dyspnea on exertion, mucus hypersecretionand/or wheeze.53 The NLHEP has encouragedindustry to develop new, accurate, but inexpensive
22www.nlhep.org
12. The National Lung Health EducationProgram (NLHEP)
spirometers, suitable for office and clinic use in theprimary care setting.54 Only the FEV1 and FVC, orFEV6 (as a surrogate for FVC), and the ratio ofthese two values are advised for use by primarycare physicians for an earlier detection of COPD.
In 2000, a NLHEP spirometry sub-committeepublished a widely referenced consensusstatement that reinforces the importance and needfor earlier diagnosis and monitoring of COPD viathe use of spirometry in primary care offices (Chest117:1146-61).53 This report established criteria foridentifying those at risk for COPD and led to the‘Spirometry Review Process’ that evaluates theutility and quality of commercial ‘officespirometers’ (see Resource section ofwww.nlhep.org).
NLHEP has awarded seed grants to supportresearch efforts in COPD, and has sponsoredCOPD demonstration projects in communityhospitals, These pilot projects, based on theNLHEP concept, have been established (for earlyidentification and treatment of COPD) in variouscommunities such as in Hanover, PA. These andother NLHEP-sponsored programs have mademajor progress to raise awareness and promoteearlier detection of this disease- the first steps incontrolling the increased morbidity and mortalityassociated with COPD.52
The Saturday AM CME symposia educationalmaterials for primary care COPD education weredeveloped, and following a successfully updatedseminar, the first one in the modern series waslaunched in Tulsa, OK in February, 2002. JamesSeebass, Dennis E. Doherty and Thomas Petty ledthis seminar. This model proved successful andhas been repeated on many occasions. A “Trainthe Trainer” workshop for young pulmonologistswas held in Dallas, TX, to provide them withCOPD information and educational instrumentsfor future regional CME programs. “Trainers” arethe “Disciples” of the NLHEP who can also carrythe message to the grass roots of the nation.
In 2000, the NLHEP developed a strategicpartnership with the AARC for COPD educationalprograms. Educational materials developed by theNLHEP include an informational brochure thatestablished the NHLEP motto “Test YourLungs–Know Your Numbers” (and containinganswers to 20 commonly asked questions byCOPD patients); the development of a user-friendly educational web site for patients andclinicians (www.nlhep.org), publication ofnumerous articles on COPD, COPD andspirometry education booklets, and a 6 yearnational media campaign to raise publicawareness of COPD. We (TLP, DED) authoredthree booklets: “Prevent COPD Now” and “TheEarly Recognition and Management of COPD”for primary care physicians to encourage theirsearch for asymptomatic COPD patients in theirpractices, and a booklet “Save Your BreathAmerica! Prevent Emphysema Now,” whichcontains information written in lay language forpatients who may have or be developing COPD.Many thousands of these booklets have beendistributed by the NLHEP and the AARC.
In 2004, the administrative functions of theNLHEP were transferred to Irving, Texas, whereoffice space is being graciously provided by theAARC. Dennis E. Doherty assumed the role ofChairman, following his yeoman service as co-chairman for three previous years. Tom Petty andhis associate, Louise Nett RN, RRT, remainemeritus members and consultants.
It is hoped that the current and futuresuccess of the NLHEP will ultimately lead to theearlier diagnosis, treatment, stabilization, andrehabilitation of patients in early symptomaticor incipient stages of disease in the future.
23www.nlhep.org
The NLHEP (cont.)
Recommendations of the Sixth OxygenConsensus Conference. 22000066 55
Recommendation 1: In order to assure quality LTOT patient care, werecommend comprehensive education for patients,prescribing primary-care and specialist physicians,respiratory therapists (RTs) and other respiratoryprofessionals, regulatory agencies, payers, families,caregivers, and the public. Easy-to-use,understandable, and readily available educationalresources should be further developed to meetthese needs, including printed and audiovisualmaterials, as well as Internet resources. LTOTeducation should also be incorporated into thecurriculum of health-professional trainingprograms for those who will provide care to LTOTpatients. Consensus was not reached with regardto the practicality and requirement for credentialededucators to initiate and follow LTOT delivery topatients. However, it was agreed that suchprograms of education and/or certification shouldbe developed and implemented to meet thesepotential needs in the future.
Recommendation 2: Clinical educational materials should be developedand provided to the patient and LTOTcaregiver/provider, including but not limited to:
• Details of competitive bidding with qualitystandards (supplier selection process)
• Self-monitoring (e.g., spirometry, oxygen literflow, and oxygen saturation)
• Reimbursement (understand the criteria of theCenters for Medicare and Medicaid Services(CMS) and other 3rd-party payers, includingmanaged-care organizations)
• Compliance and adherence to the LTOTprescription
• Benefits and availability of pulmonary rehabilitation
• What to do in emergency situations (e.g., loss ofelectrical power or malfunction of stationary/portable delivery device such as liquid-oxygensource equipment)
Recommendation 3: All patients of all groups should have access to theappropriate LTOT delivery systems and accessoriesto optimize maximal medical compliance, activitiesof daily living inside and outside the home, andtravel (planes, trains, automobiles, and cruiseships). Patients should have access to respiratorycare professionals, including RTs, adequatelytrained in LTOT, on an intermittent basis in thehome/place-of-residence or the clinic, dependingon the patient’s degree of mobility, as deemedappropriate by the physician or physician-designated respiratory care professional, includingRTs, following that patient’s LTOT.
Recommendation 4: Standards for LTOT should be further developedthat would provide clinical practice guidelines that,whenever possible, are evidence-based and/orsupplemented by expert opinion. These standardsshould be interdisciplinary and address the role ofnot only physicians, but also of RTs and other alliedhealth and respiratory professionals providing LTOTcare. The pediatric patient should also be consideredin the development of these standards. Thesestandards, for example, could include, but not belimited to, indications for LTOT, patient education,matching the proper LTOT delivery device andaccessories to patient needs and abilities, appropriatemonitoring, the role of pulmonary rehabilitation, andcurrent policies and procedures for travel withsupplemental oxygen therapy. Performancemeasures should be established to evaluate qualityof care.
Recommendation 5:All patients who are provided an intermittent-flowdevice (which is one category of oxygen-conservingdevice) must be clinically evaluated and titrated to theintermittent flow required by the specific device beingemployed, in order to ensure optimal oxygen delivery
24www.nlhep.org
Appendix
for that individual patient during rest and duringroutine activities of daily living.
Recommendation 6: Consideration should be encouraged for improvingall of the processes involved in the delivery ofLTOT. This would include education for physicians,case managers, discharge planners, home-medical-equipment providers, RTs, and other professionalsinvolved in the management of LTOT patients.
Recommendation 7: Evidence-based criteria are needed to defineambulatory/portable/wearable oxygentechnologies, as they apply to each specificpatient’s clinical and lifestyle needs, on anindividualized basis. Until such evidence exists, thephysician, patient, and home-medical-equipmentprovider must effectively collaborate, using theirbest efforts and state-of-the-art knowledge in thattime frame to ensure that all LTOT users haveaccess to the best and most appropriatetechnologies that fit their clinical and lifestyleneeds.
Recommendation 8: LTOT should be reimbursed adequately for theLTOT delivery device, accessories, and associatedLTOT services provided, linked to approvedstandards of care when available, and whereverpossible based on clinical outcomes research.Reimbursement obstacles to providing quality LTOTin the patient’s home or other place of residence byRTs or other respiratory care professionals involved inthe care of the LTOT patient should be resolved, aswell as obstacles to providing comprehensivepulmonary rehabilitation. Reimbursement should bebased on the LTOT device that is “best for thepatient” as prescribed by an M.D. or D.O.
Recommendation 9: CMS and other payer organizations should beencouraged to support appropriate reimbursementthat will ensure access to innovative technologiesthat are appropriate for the individual patient’sclinical and daily lifestyle needs.
Recommendation 10: LTOT should be incorporated into the disease-management/health-maintenance approach to thecomprehensive care of patients with chronic lungand/or cardiac disease. This recognizes theimportance of providing an interdisciplinarycontinuum of care across all sites, including, butnot limited to, facilitating access to pulmonaryrehabilitation by adequate reimbursement. Thebenefits of such disease management should beevaluated on an ongoing basis by appropriateoutcome evaluations and performance-improvement measures.
Recommendation 11: Funding should be provided for research thatevaluates the outcome and cost-effectiveness ofLTOT, including, but not limited to, research onthe safety and efficacy of established, as well asnew, oxygen-delivery devices, and research onother indications for LTOT, such as enhancingquality of life and reduction of symptoms. Thismight be accomplished by joint projects with CMSand other payers and research organizations, andby helping to recruit patients needed for ongoingand future research studies.
Recommendation 12: All professional and lay organizations and societiesshould incorporate LTOT patients into theiradvocacy efforts for LTOT.
Recommendation 13: We recommend development of a demonstrationproject(s) to evaluate the utilization of resourcesfor LTOT and incorporate compliance data into are-certification process(es) when oxygen isprescribed in acute situations. An example mightbe establishment of a regional facility for conductof re-certification examinations. Such a centerwould be capable of evaluating LTOT prescriptionat rest, during exercise, and during sleep. Studiesshould utilize the equipment modality that thepatient is currently using or will be using in thenear future. Recommendations might also bemade as to the LTOT modality that would provide
25www.nlhep.org
greatest benefit for the patient, based on his orher individualized activities of daily living andlifestyle (at rest and during usual daily activity).This would relieve the prescribing primary-carephysician, pulmonologist, RT, or home-medical-equipment provider from the responsibility toconduct these examinations. Feedback should beprovided to the physician/clinician and home-medical-equipment provider. A study to evaluatethe need for an initial LTOT prescription followingan exacerbation of COPD and for the need tocontinue LTOT after recovery and stabilization isrecommended.
Recommendations of the Fifth OxygenConsensus Conference. 11999999 56
Recommendation 1:Respiratory Home Care Services are endorsed asessential in LTOT. We recommend that LTOTshould be viewed as a compendium oftherapeutic services including educatingpatients, assessing patients, monitoringtherapeutic benefits, evaluating patientcompliance, communicating with primary carephysicians, and providing and maintaining thenecessary technology. Establish minimumservice standards with respect to supplyingoxygen services for homecare providers. (e.g.respiratory srofessionals, fafety, 24-hr access….)
Recommendation 2:The NIH should fund a scientific study todetermine the benefits of truly portable O2
therapy in terms of survival, quality of life,healthcare utilization and physiologicaloutcomes.
Recommendation 3:The evolution of our healthcare system hasresulted in the discharge of patients fromhospital based care into the home setting at ahigher acuity level and the management ofmore acutely ill patients in the outpatientsetting. It is recommended that patients beingdiagnosed with unstable respiratory disease
with prescribed oxygen therapy be re-certifiedafter the initial 90 days of therapy for long-termoxygen therapy. Once the need for long-termoxygen therapy is established, repeatmeasurement of arterial blood gases orsaturation is not necessary or justifiable for re-certification. These measurements are medicallynecessary and justifiable for the physician toevaluate the course of the disease and to makeadjustments in oxygen flow rate.
Recommendation 4:Standardized education of patients, caregiversand medical professionals is of primeimportance, utilizing existing materials. AnEducation Consensus Conference isrecommended for the evaluation of currentliterature and to define tools to be used toeducate patients, caregivers and others.Enhance education with a national oxygenawareness and lobbying effort. Employ nationalgroups such as NHOPA, ACCP, ATS, AARC,NAMES, AACVPR, NAMDRC, PERF, VA and amanufacturer’s coalition.
Recommendation 5:Provision for ambulation oxygen portable mustbe defined and reimbursed accordingly.“Ambulatory” to mean availability for daily use,carried by the patient, weighing less than 10pounds, minimum oxygen duration of at least4-6 hours at 2 L/min continuous flow orequivalent. Redefine portable O2 as equipmentthat can be carried by most patients on theirperson during ADL, weighing 10 pounds orless, 2 L/min. System must be selected for theneeds of a specific patient. Consider portability(weight), duration, and frequency of use. Werecommend that technology development focuson technologies that are more compatible withpatients’ lifestyles such as lightweight, portableoxygen systems.
Recommendation 6:To assure patients rights and an informedchoice of LTOT that meets their medical needs,
26www.nlhep.org
an accepted definition of access must bedeveloped by clinicians, which addresses issuessuch as access to medical care, pulmonaryrehabilitation, service, equipment, and supplies.Once the definition is established, it must bepresented to HCFA and other third partypayers. Re-define “access to care” to facilitateprovision of truly portable oxygen.
Recommendation 7:Support O2 patients in their need for airlinetravel. DOT / Coast Guard criteria to beadapted by FAA/ Airlines. Patients have a rightto medically necessary oxygen therapy duringall phases of air travel. Acceptable airline servicemust include the establishment of consistentpolicies and the provision of appropriate andsufficient oxygen, equipment and supplies (e.g.adjustable flow meters) that will meet thepatient’s prescribed oxygen order.
Recommendation 8:It is recommended that upon initial setup andperiodically thereafter, that all O2 therapydevices, particularly OCD, that patients betitrated to the proper flow rate at rest, exercise,and sleep, to achieve maximum benefit. TheAARC and/or AACVPR should create clinicalpractice guidelines for the evaluation andmonitoring of LTOT. This should include bothshort and long term plans.
Recommendation 9:Patient compliance is essential to the efficiencyof LTOT and can be improved though initialand on-going patient education andintervention with access to appropriate servicesand oxygen systems. Compliance will beenhanced by optimized reimbursement andempowering the patient with choices to bestmeet their medical needs. Health careprofessionals should continue efforts to assurecompliance to M.D. prescription.
Recommendation 10:An oxygen patients Bill of Rights should bedeveloped to assure a standardized andappropriate level of patient care that will beused by all patients and health care providers.Supporting documents should include educationchecklists, defined patient responsibilities, and adefined role of the RCP in the care of LTOTpatients.
Recommendation 11:A system of patient advocacy should bedeveloped to represent LTOT users andproviders. The system should include amechanism to resolve complaints and concerns,which would improve patient compliance andsatisfaction. Tell HCFA about it.
Recommendation 12:Encourage scientific investigations to explorefurther indications for oxygen therapy. e.g.exercise, sleep with daytime normoxia.
Recommendation 13:Acknowledge the electrical power costs of O2
equipment device usage, as well as otherhidden costs.
Recommendation 14:Adequate reimbursement for medicallynecessary and technology appropriate oxygendelivery systems (e.g. ambulatory oxygen,conserving devices and transtracheal oxygen)will improve patient compliance and optimizeclinical outcomes.
Further Recommendations forPrescribing, Reimbursement,Technology Development, and Researchin Long-term Oxygen Therapy. 11999933 57
Recommendation 1:The Certification of Medical Necessity (CMN)for prescribing LTOT, HCFA From 484 isacceptable but still complex and difficult for
27www.nlhep.org

primary care physicians to complete. Furthersimplification is needed. There is no need forany additional treatment form or orders by thephysicians in prescribing LTOT.
Recommendation 2:Continued efforts are essential to educatephysicians, particularly primary care physicians,on the indications for LTOT and how it shouldbe prescribed. Major organizations such as theAmerican College of Physicians (ACP), theAmerican Academy of Family Practice (AAFP),and the American College of Family Physicians –Osteopathic (ACFP) should provide regulareducation workshops for primary care physicianson prescribing LTOT. Principles of prescribingLTOT should be taught in all medical schools,both for M.D. and Osteopathic degrees.
Recommendation 3:To improve communications and “standardize”LTOT terminology, especially for use in theCMN and for medical reimbursement policy, thefollowing definitions are suggested: (1)Stationary oxygen equipment – a large reservoirof oxygen or oxygen producing device thatcannot be easily moved or carried by thepatient. Examples: H or K cylinder withcompressed oxygen; stationary home oxygenconcentrator; or liquid oxygen reservoir. (2)Portable oxygen equipment that can be movedor transported by patients, but not “on theirperson” during daily activities. This equipmentusually weighs more than 10 lbs. Examples: Ecylinder and regulator mounted on a cart orstroller or suitcase-sized battery operatedoxygen concentrator. (3) Ambulatory oxygen –any oxygen equipment that can be carried bymost adults “on their person” during activitiesof daily living, weighing 10 lbs or less.Additionally, the oxygen supply must last atleast 4-6 hr at 2 L/min or the physiologicequivalent. Examples: small liquid oxygencanister or small lightweight high-pressurecylinder and regulator.
Recommendation 4:New or revised LTOT orders should include theoxygen flow necessary to correct hypoxemia,both at rest and during usual exercise. Thephysician or qualified laboratory personnelunder medical supervision are responsible formaking or supervising these measurements,utilizing arterial oxygen saturation or tensionmonitoring.
Recommendation 5:Because supplying ambulatory oxygen has ahigher cost than portable oxygen for bothequipment and service, it is recommended thatthese facts be taken into consideration insetting oxygen reimbursement policy.Specifically a higher reimbursement category isrecommended for ambulatory oxygen in excessof that currently allowed for portable systems.
Recommendation 6:A prospective longitudinal multicenter study isneeded to evaluate the medical efficiency ofambulatory oxygen systems versus stationaryoxygen delivery systems in hypoxemic patientswith COPD. Some objectives of the studywould include (1) patient compliance, (2)quality of life, (3) exercise tolerance, and (4)survival. The Veterans Administration MedicalCenters would appear to be ideal sites for sucha study. Since many of these centers currentlyhave contacts with home oxygen suppliers thatprovide only stationary oxygen systems withportable, but not ambulatory, capability; theprovision of ambulatory equipment for a groupof study patients would not compromise thecare that currently exists. The VA MedicalCenters also serve a large population of patientswith COPD.
Recommendation 7:A prospective study in patients with COPDwithout daytime hypoxemia should beundertaken with the primary goal of examiningthe effect of oxygen therapy during sleep onmortality. Additional goals should be to follow a
28www.nlhep.org
noninvasive measure of cardiopulmonary functionand to determine a cost outcome in terms of thenumber of hospitalization days, clinic visits, etc.This investigation should be prospective,multicentered, double-blind, and includeappropriate sham-treated desaturators andnondesaturator controls. It could be carried outbest in centers with broad populations of COPDpatients and with existing sleep laboratories toidentify potential subjects. The final design couldbe similar to, and incorporate many of thetechniques used in, the NOT study (4).
Recommendation 8:It is recognized that current scientific dataappear insufficient to make solid conclusionsabout the efficiency of nocturnal supplementaloxygen in patients who are not hypoxemic(PaO2 > 60mmHG) while awake. Thecommittee recommends that current prescribingpractices in this setting be determined byindividual practitioners within the framework ofHCFA guidelines, based upon their experienceand the facilities available for detecting NOD. Atthe same time, it should be realized that futureprescribing practices may need to be modified asscientific data becomes available to support orrefute them.
New Problems in Supply,Reimbursement, and Certification ofMedical Necessity for Long-TermOxygen Therapy. 11999900 58
Recommendation 1:A new policy for oxygen reimbursement isnecessary. It is illogical and detrimental topatient care to base reimbursement of homeoxygen therapy on flow rate and ignore thesource of oxygen and the variable costsinvolved in providing oxygen from differentdevices and in different forms (liquid vs.gaseous). Reimbursement should be based onthe DME provider’s reasonable costs forsupplying these different modalities of oxygen
therapy. The geographic discrepancies inreimbursement for oxygen therapy must also beaddressed. Rural areas should be considered ashigh cost areas when liquid oxygen systems arebeing provided because of the low populationdensity and the greater distances involved inproviding systems. It should also be recognizedby HCFA that portable oxygen and ambulatoryoxygen are not synonymous. Portable systems,such as cylinders or strollers, are cumbersomeand impede full activity. Ambulatory systemscan be carried easily by patients and aredesigned to allow and encourage full mobility.Ambulatory systems, e.g., liquid ambulatoryunits, allow daily exercise, which is key topulmonary rehabilitation.
Recommendation 2:In redesigning the reimbursement system, thedevelopment and use of oxygen-conservingdevices and techniques should be encouragedand not discouraged by reimbursement policy.Cost savings that can be achieved throughoxygen conservation must be viewed in thecontext that oxygen is the least expensivecomponent in oxygen therapy. The real benefitfrom oxygen-conserving technology isimproved patient care and better compliancewith therapy because of smaller, lightweightambulatory oxygen units that allow greatermobility and improved quality of life. Theincreased costs of new oxygen deliveryequipment and technology can be balanced tosome degree by the modest reduction in thecost of supplying oxygen, but the cost savingsfor the DME provider are likely to be small.
Recommendation 3:Until reimbursement policy can be changed, it isrecommended that all oxygen be reimbursed atthe flow rate necessary to achieve correction ofhypoxemia using flow through a nasal cannulaas a uniform standard and that the “dualreporting” of flow rate and amount of oxygendelivered be eliminated.
29www.nlhep.org
Recommendation 4:It is recommended that patients with unstablerespiratory disease, such as those leaving anacute care hospital, who have not previouslyqualified for long-term oxygen therapy andwho at the time of discharge qualify for homeoxygen therapy under currently establishedcriteria, be issued a CMN for short-term oxygentherapy. Recertification for long-term oxygentherapy would be necessary in 30 to 90 dayswhen the patient is judged by the physician tobe clinically stable and receiving optimaltherapy. Once the need for long-term oxygentherapy is established, repeat measurement ofarterial blood gases or oxygen saturation is notmedically necessary or justifiable for thephysician to evaluate the course of the diseaseand to make adjustments in oxygen flow rates.
Recommendation 5:The previous recommendation has a greatpotential for cost savings and can improvequality of care by eliminating unnecessaryoxygen therapy. Some of the cost savingsachieved in this area should be applied tocorrection of the inequalities that exist in thecurrent reimbursement system. Considerationshould also be given to reimbursement of short-term oxygen therapy at a higher rate becausethe initial delivery, setup, and educational costsmust be amortized over a shorter time periodand the maintenance and storage costs willincrease.
Recommendation 6:It is recommended that the CMN form be aone-page document with the informationnecessary for certification on one side andinstructions for completion on the reverse side.The physician should continue to provide thedocumentation of medical necessity andprescribe the oxygen delivery system that ismedically indicated for the patient as well as theappropriate oxygen flow rates that may varybetween rest, activities of daily living, andsleep. Many items can be more quickly and
efficiently completed by a check list format. TheDME provider should be able to fill in portionsof the certificate that do not change theprescription.
Recommendation 7:It is recommended that when home oxygen isprescribed in the hospital, the CMN formshould be completed before discharge and theDME supplier notified in ample time to providethe equipment and instructions necessary forappropriate therapy. Physicians recognize thatother medications cannot be dispensed until thedischarge prescription is completed. Eachhospital should be responsible for compliancewith this policy and this should become an areaof review by the Joint Commission onAccreditation of Healthcare Organizations. TheCMN forms must be readily available in allacute medical facilities where patients are likelyto be discharged with home oxygen therapy.
Recommendation 8:A program must be established to educateprimary care physicians who are responsible forordering home oxygen therapy. The CMN formis now and will continue to be one of the mostcomplex prescriptions that physicians arerequired to complete. The prescribing physiciannot only must understand the indications forshort-term and long-term oxygen therapy butalso must be familiar with the various systemsfor supply and delivery of oxygen and knowwhich best meets the needs of each patient. Atthe present time, there are striking variations inMedicare carrier policies for documentation,certification and reimbursement of homeoxygen therapy. Education of carrier medicaldirectors, who usually are not specialists inrespiratory disease, would help alleviate most ofthese discrepancies. Other health care providerswho are involved in home oxygen therapywould also benefit from a comprehensiveeducation program.
30www.nlhep.org
Further Recommendations forPrescribing and Supplying Long-TermOxygen Therapy. 11998877 59
Recommendation 1:For the purposes of LTOT, the definition of theterm “ambulation” should be expanded toinclude all activities requiring mobility beyondthe delivery range of a stationary oxygensource (up to 50 feet of oxygen tubing).
Recommendation 2:The medical standard for LTOT should becontinuous administration (24 h/day) withambulatory capability.
Recommendation 3:Exceptions to continuous administration withambulatory capability (e.g. a portable oxygensource) should be specified and would beexpected to include (1) patients who are notcapable or desirous of activity beyond thedelivery range of a stationary oxygen source;(2) patients requiring oxygen only during sleep;(3) patients requiring oxygen only duringambulation; (4) patients who prove to benoncompliant with prescribed therapy and inwhom it is demonstrated repeatedly that theportable oxygen source is not being used.
Recommendation 4:Initial documentation of the medical necessityfor LTOT should consist of an arterial blood gasmeasurement performed when the patient isstable and receiving optimal medicalmanagement and analyzed by a duly approvedlaboratory (e.g. American Thoracic Society,College of American Pathologists, JointCommittee on Accreditation of HealthcareOrganizations, etc). Oximetry is recognized asan appropriate and acceptable methodology fordocumenting hypoxemia during activity andsleep. It is also an acceptable follow-upmethodology for evaluating and monitoringLTOT. The need for continued use of LTOT
should be verified on an annual basis by thepatient’s physician.
Recommendation 5:The physician should prescribe the oxygensource (such as compressed gas, liquid oxygen,or concentrators) and must also prescribe thedelivery device (such as continuous nasalcannula, transtracheal administration, reservoirnasal cannulas, pulse-dose oxygenadministration and demand valve) based on themost appropriate therapeutic regimen for eachindividual patient. The liter flow to correcthypoxemia must be specified by the physician.
Recommendation 6:Once a hospitalized patient is identified asneeding home oxygen therapy, transfer to thehome setting should include, but not be limitedto (1) whether the patient should be givenoxygen en route from hospital to home (to bedetermined by the physician), and (2) adequateinstruction and familiarization of the patient(and his/her family) with the oxygen equipmentprior to discharge and upon arrival home.
Recommendation 7:Equipment maintenance is best handled byclose adherence to the manufacturer’srecommendations for each specific item ofequipment. Therefore, it is important that (1)manufacturers always provide, coincident withthe market introduction of any new equipment,comprehensive maintenance and repairinstructions appropriate to the nature andanticipated level of field service of theequipment, and (2) such instructions are to bekept up to date as design modifications aremade.
Recommendation 8:Clinical evaluation should include regularassessments of patient compliance withprescribed therapy, potential complications,potential hazards, and the need for continuededucation. Patients receiving LTOT share
31www.nlhep.org

responsibility with the prescribing physicians forremaining in communication with theirphysician or designate in order to assurecontinued appropriate care for their condition.
Recommendation 9:For patients receiving LTOT, routinemeasurement of their arterial blood gases oroxygen saturation in the home environment isnot necessary; however, such measurementsmay be useful in patients found to be clinicallyunstable. Furthermore, the physician continuesto have the responsibility of documenting theefficiency and safety of the LTOT in correctingthe patient’s hypoxemia and its clinicalconsequences after the initiation of homeoxygen therapy.
Recommendation 10:The development of quality assurance standardsfor continuing medical management of thehome oxygen patient is beyond the scope ofthe current committee. It is recommended,however, that a conference of appropriatehealthcare providers (physicians, respiratorycare practitioners, respiratory nurses, durablemedical equipment (DME) providers, etc.)should develop a set of guidelines forappropriate medical followup.
Recommendation 11:In view of the need for education of physiciansconcerning the indications, means ofadministration and complications of LTOT, it isrecommended that the appropriate professionalsocieties set up continuing medical educationcourses leading to certification in long-termoxygen treatment. The certification should onlybe awarded after competence is shown by anobjective evaluation and should be for adefined period of time. The necessarycontinuing medical education and certificationshould be made available to all practicingphysicians who seek certification of competencein LTOT.
Recommendation 12:Reimbursement must be based on: (1) patient’scontinuous oxygen flow requirementsregardless of the oxygen source or deliverydevice employed; (2) whether or not thepatient is ambulatory in accordance withrecommendations 1 through 3; (3) thetechnological and professional componentsnecessary to meet the therapeutic requirements.
Problems in Prescribing and SupplyingOxygen for Medicare Patients. 11998866 60
Recommendation 1:There is no substitute for oxygen therapy. It isappropriate that each patient should receiveoptimum therapy before long term oxygentherapy is ordered. The term “optimumtherapy” will depend on the overall conditionof the patient as viewed by the prescribingphysician. Furthermore, “optimum therapy” willremain a part of the patient’s total treatmenteven while receiving oxygen therapy.
Recommendation 2:In patients with arterial PO2’s of 55 at rest, it isdeemed medically necessary that a portablesystem be provided to facilitate ambulation inaddition to a stationary oxygen delivery system.Similarly, in patients demonstrated to develophypoxemia (PaO2 = 55 mmHg) only duringexertion, a portable system should be approvedfor ambulation.
Recommendation 3:The requirement to demonstrate “clinicalimprovement” in the patient’s condition, asevidenced by an increase in the patient’s abilityto exercise or perform various activities shouldbe removed. That exertion induced hypoxemiaoccurs is sufficient evidence of the need foroxygen therapy during exercise. Data fromcarefully conducted clinical trials clearlydocuments the long-term benefits of oxygen
32www.nlhep.org
therapy in hypoxemic chronic lung diseasepatients.
Recommendation 4:It should be recognized that the cost of varioussystems and accompanying support servicesmay vary considerably. The physicians’considered judgement regarding the type ofsystem to be provided is based on physical,psychological, social, and regional factors aswell as cost. Therefore, cost considerationsshould not be used to overrule the medicalnecessity of a particular method of providingoxygen.
Recommendation 5:When ambulation in and outside of the home isjudged to be part of the therapeutic regimen, aportable system will be necessary. Whenoxygen concentrators are provided as the solemeans of oxygen delivery, a supplementaloxygen system is medically necessary becauseof unpredictable power failures or electricalmalfunctions. The current regulations requirethat the physician indicate the concentration ofoxygen to be used. If the delivery systemprovides greater than 85% oxygen at the literflow prescribed, then the requirement for astatement of the concentration is unnecessary.For purposes of these regulations, oxygen levelsof 85% percent or greater are therapeuticallyequivalent to 100% oxygen.
Recommendation 6:Consideration should be given to developing astandardized prescription form for use bysuppliers and carriers. Such a form wouldfacilitate compliance by physicians in providingthe data required by the regulations.
Recommendation 7:HCFA should urge carriers to obtain consultantswho are experts in the nuances of oxygentherapy to advise them on unusual prescriptionsfor home oxygen therapy, as set forth inregulations 4 and 5, Page 13746, Federal
Register. In addition, HCFA itself should solicitthe comments of experts in the field as part ofthe policy-making process.
Recommendation 8:It is not possible to offer a recommendation atpresent concerning the clinical use of oxygenconserving devices. Long-term studies aresorely needed.
Recommendation 9:An educational effort needs to be mounted tobetter educate the profession in the principlesand practice of home and ambulatory oxygentherapy. The appropriate professional bodiesshould be contacted to begin planning such aneffort.
Recommendation 10:A small workshop of 20-30 persons should beconvened to explore areas of concern betweensuppliers and carriers, with representatives ofHCFA and the medical profession serving asresource personnel. The emphasis in thisworkshop should be on makingrecommendations for resolving differences andestablishing open lines of communicationbetween carriers and suppliers. Ideally, thisworkshop should be convened under theauspices of the Department of Health andHuman Services, and with co-sponsorship byprofessional organizations such as the AmericanThoracic Society, the American Association forRespiratory Care and other interestedorganizations.
33www.nlhep.org
1. Barach AL: Historical background. Symposium oninhalation therapy. Anesthesiology 1962;23:407-421.
2. Petty TL, Burtis BB, Bigelow DB: Oxygen, animportant pharmacologic agent (review). Rocky MtnMed J 1967;64:66-71.
3. Encyclopedia Britannica. Joseph Priestley.1997;9:696-697.
4. Foreword: a new kind of special issue. Respir Care1986;31:761-763.
5. Sackner MA: A history of oxygen usage in chronicobstructive pulmonary disease. Am Rev Respir Dis1974;110:25-34.
6. Haldane JS: Symptoms, causes, and prevention ofanoxemia. British Med J 1919:65-72.
7. Hill L: A simple oxygen bed tent and its use in a caseof edema and chronic ulcer of the lung. Proceedingsof the Physiological Society. J Physiol 1921;55:20-21.
8. Barach AL: The therapeutic use of oxygen. JAMA1922;79:693-699.
9. Cotes JE, Gilson JC: Effect of oxygen in exerciseability in chronic respiratory insufficiency: use of aportable apparatus. Lancet 1956;1:822-826.
10. Levine BE, Bigelow DB, Hamstra RD, et al: The roleof long-term continuous oxygen administration inpatients with chronic airway obstruction withhypoxemia. Ann Intern Med 1967;66(4):639-650.
11. Petty TL: Historical highlights of long term oxygen.Resp Care 2000;45:29-36.
12. Abraham AS, Cole RB, Bishop JM: Reversal ofpulmonary hypertension by prolonged oxygenadministration to patients with chronic bronchitis.Circ Res 1968;23:147-157.
13. Petty TL, Finigan MM: Clinical evaluation ofprolonged ambulatory oxygen therapy in chronicairway obstruction. Am J Med 1968;45:242-252.
14. Stark RD, Finnegan P, Bishop JM: Daily requirementof oxygen to reverse pulmonary hypertension inpatients with chronic bronchitis. Br Med J1972;3:724-728.
15. Stark RD, Finnegan P, Bishop JM: Long-termdomiciliary oxygen in chronic bronchitis withpulmonary hypertension. Br Med J 1973;3:467-470.
16. Neff TA, Petty TL: Long-term continuous oxygentherapy in chronic airway obstruction: mortality inrelationship to cor pulmonale, hypoxia, andhypercapnia. Ann Intern Med 1970;72:621-626.
17. Long term domiciliary oxygen therapy in chronichypoxic cor pulmonale complicating chronicbronchitis and emphysema. Report of the MedicalResearch Council Working Party. Lancet1981;1(8222):681-686.
18. Continuous or nocturnal oxygen therapy inhypoxemic chronic obstructive lung disease: a clinicaltrial. Nocturnal Oxygen Therapy Trial Group. AnnIntern Med 1980;93:391-398.
19. Timms RM, Kvale PA, Anthonisen NR, et al: Selectionof patients with chronic obstructive pulmonarydisease for long-term oxygen therapy. JAMA1981;245:2514-2515.
20. Krop HD, Block AJ, Cohen E: Neuropsychologiceffects of continuous oxygen therapy in chronicobstructive pulmonary disease. Chest 1973;64:317-322.
21. Grant I, Heaton RK, McSweeny AJ, et al:Neuropsychologic findings in hypoxemic chronicobstructive pulmonary disease. Arch Intern Med1982;142:1470-1476.
22. Heaton RK, Grant I, McSweeny AJ, et al: Psychologiceffects of continuous and nocturnal oxygen therapyin hypoxemic chronic obstructive pulmonary disease.Arch Intern Med 1983;143:1941-1947.
23. Petty TL: Home oxygen – a revolution in the care ofadvanced COPD. Med Clin North Am 1990;74:715-729.
24. Cherniack RM, Hakimpour K: The rational use ofoxygen in respiratory insufficiency. JAMA1967;199:178-182.
25. Bigelow DB, Petty TL, Levine BE, et al: The effect ofoxygen breathing on arterial blood gases in patientswith chronic airflow obstruction living at 5, 200 feet.Am Rev Respir Dis 1967;96:28-34.
26. Petty TL: (unpublished observations)27. Petty TL, Stanford RE, Neff TA: Continuous oxygen
in chronic airway obstruction. Observations onpossible oxygen toxicity and survival. Ann InternMed 1971;75:361-307.
28. Petty TL, Neff TA, Creagh CE, et al: Outpatientoxygen therapy in chronic obstructive pulmonarydisease: A review of 13 years’ experience and anevaluation of modes of therapy. Arch Intern Med1979;139:28-32.
29. Chang TT, Lipinski CA, Sherman HF: A hazard ofhome oxygen therapy. J Burn Care Rehabil2001;22:71-74.
30. Petty TL, Bliss PL: Ambulatory oxygen therapy,exercise and survival with advanced chronicobstructive pulmonary disease. (The NocturnalOxygen Therapy Trial Revisited.) Resp Care2000;45:204-213.
31. Kaplan EL, Meier P: Non-parametric estimation fromincomplete observation. J Am Statist Assoc1958;53:457-481.
32. Cox DR: Regression models and life tables. J R StatSoc (Series B) 1972;35:187-220.
33. Timms RM, Khaja FU, Williams GW: Hemodynamicresponse to oxygen therapy in chronic obstructivepulmonary disease. Ann Intern Med 1985;102:29-36.
34. Ashutosh K, Mead G, Dunsky M: Early effects ofoxygen administration and prognosis in chronicobstructive pulmonary disease and cor pulmonale.
34www.nlhep.org
References
Am Rev Respir Dis 1983;127:399-404.35. Weitzenblum E, Hirth C, Ducolone A, et al:
Prognostic value of pulmonary artery pressure inchronic obstructive pulmonary disease. Thorax1981;36:752-758.
36. Weitzenblum E, Sautegeau A, Ehrhart M, et al: Longterm oxygen therapy can reverse the progression ofpulmonary hypertension in patients with chronicobstructive pulmonary disease. Am Rev Respir Dis1985;131:493-498.
37. Morrison DA, Adcock K, Collins CM, et al: Rightventricular dysfunction and exercise limitation ofchronic obstructive pulmonary disease. J Am CollCardiol 1987;9:1219-1229.
38. Morrison DA, Stovall JR: Increased exercise capacityin hypoxemic patients after long term oxygentherapy. Chest 1992;102:542-550.
39. Morrison DA, Zuckerman BD, Laskey WK:Cardiovascular effects of oxygen therapy in patientswith chronic hypoxemia. In: Donohue WJ Jr. Long-term oxygen therapy: scientific basis and clinicalapplication. New York: Marcel Dekker; 1995: pp 69-85.
40. Wright JL, Petty TL, Thurlbeck WM: Analysis of thestructure of the muscular pulmonary arteries inpatients with pulmonary hyper tension and COPD:National Institutes of Health Nocturnal OxygenTherapy Trial. Lung 1992;170:109-124.
41. Kawakami Y, Kishi F, Yamamoto H, et al: Relation ofoxygen delivery, mixed venous oxygenation, andpulmonary hemodynamics to prognosis in chronicobstructive pulmonary disease. N Engl J Med1983;308:1045-1049.
42. Bergofsky EH: Tissue oxygen delivery and corpulmonale in chronic obstructive pulmonary disease.N Engl J Med 1983;308:1092-1094.
43. Morrison DA: Pulmonary hypertension in chronicobstructive pulmonary disease: the right ventricularhypothesis. (editorial). Chest 1987;92:387-389.
44. O’Donohue WJ Jr: Effect of oxygen therapy onincreasing arterial oxygen tension in hypoxemicpatients with stable chronic obstructive pulmonarydisease while breathing ambient air. Chest1991;100:968-972.
45. Frost and Sullivan: U.S. Oxygen Therapy DeviceMarkets. 1999
46. McCoy R: Oxygen-conserving techniques anddevices. Respir Care 2000;45:95-103.
47. Roberts SD: Cost-effective Oxygen Therapy. AnnIntern Med 1980;93:499-500.
48. Lee H, Manns B, Taub K, et al: Cost analysis ofongoing care of patients with end-stage renaldisease: the impact of dialysis modality and dialysisaccess. Am J Kidney Dis 2002;40:611-622.
49. Ramsey SD, Berry K, Etzioni, et al: NationalEmphysema Treatment Trial Research Group. Costeffectiveness of lung volume-reduction surgery forpatients with severe emphysema. N Engl J Med2003;348:2092-2102.
50. Petty TL, Doherty DE: The National Lung HealthEducation Program: Roots, Mission, FutureDirections. Resp Care 2004; 49:678-683.
51. Petty TL, Weinmann GG, Building a NationalStrategy for the Prevention and Management of andResearch in Chronic Obstructive Pulmonary Disease.National Heart, Lung and Blood Institute, WorkshopSummary. Bethesda, MD, August 29-32, 1995.JAMA 1997; 277:246-253.
52. Petty TL (Guest editor). The National Lung HealthEducation Program (NLHEP). Strategies in preservinglung health and preventing COPD and associateddiseases. Chest 1998; 113 (2 Suppl):123s-163s.
53. Ferguson GT, Enright PL, Buist AS, Higgins MW.Office Spirometry for Lung Health Assessment inAdults: A consensus statement from The NationalLung Health Education Program. Chest 2000;117:1146-1161; Resp Care 2000;45:513-530.
54. Schoh RJ, Fero LJ, Shapiro H, Aslor JP, Kaelin OJ,Rollins DR. Performance of a New ScreeningSpirometer at a Community Health Fair. Respir Care2002; 47:1150-1157.
55. Recommendations of the Sixth Oxygen Consensus Conference. Resp Care 2006(5):51-55.
56. Petty TL, Casaburi R. Recommendations of the 5thOxygen Consensus Conference. Writing andOrganizing Committees. Respir Care2000;45(8):957–961
57. Petty TL, O’Donohue WJ Jr. Further recommendationsfor prescribing, reimbursement, technologydevelopment, and research in long-term oxygentherapy. Summary of the Fourth Oxygen ConsensusConference, Washington DC, October 15–16, 1993.Am J Respir Crit Care Med 1994;150(3):875–877.
58 New problems in supply, reimbursement, andcertification of medical necessity for long-termoxygen therapy. Summary of the Third ConsensusConference held in Washington, DC, March 15–16,1990. Am Rev Respir Dis 1990;142(3):721–724.
59. Further recommendations for prescribing andsupplying long-term oxygen therapy. Summary of theSecond Conference on Long-Term Oxygen Therapyheld in Denver, Colorado, December 11–12, 1987.Am Rev Respir Dis 1988;138(3):745–747.
60. Problems in prescribing and supplying oxygen forMedicare patients. Summary of a Conference onHome Oxygen Therapy held in Denver, February 28and March 1, 1986. Am Rev Respir Dis 1986;134(2):340–341.
35www.nlhep.org

36www.nlhep.org
Notes:
Put’m Out!
Keep’m Out!
The New Era
The prevention of lung disease and the promotion of lung health is the goal of theNational Lung Health Education Program(NLHEP), conducted in collaboration with government, medical and other health professional organizations. Chronic ObstructivePulmonary Disease (COPD) is the fourthleading cause of death in the United States.Because of this, the NLHEP was implementedto develop and promote a nationwideeducation program designed to identify COPDin its early stages. One objective is to promotea program of intervention to slow theprogression of COPD before development ofclinical symptoms of chronic cough, excessmucus and shortness of breath, which are earlysigns of risk leading to disabling forms of thischronic lung disease. The spirometer can beused to identify early stages of COPD and canalso identify people at risk of death from lungcancer, heart attack, and stroke. Indeed,preservation of lung health is the key to goodhealth in general.
—
National Lung Health EducationProgram (NLHEP)
9425 N. MacArthur Blvd Suite 100
Irving, TX 75063
Phone: 972-910-8555
Fax: 972-484-2720
Web Site: nlhep.org
The National Lung Health
Education Program would like
to thank the 6th Long Term
Oxygen Therapy Consensus
Conference for funding the
first printing of this booklet.
—
8/05 F