-
a report by
D r A l a n N G o r d on
Clinical Professor of Obstetrical Gynecology, University of
Arizona School of Medicine
Long- term Sur v iva l Advantage for Recurrent Ovar ian Cancer
Pat ient sRece iv ing Pegy la ted L iposomal Doxorub ic in
B U S I N E S S B R I E F I N G : E U R O P E A N O N C O L O G
Y R E V I E W 2 0 0 5
83
Pharmacological Therapy OVARIAN CANCER
Ovarian cancer remains the leading cause of deathfrom
gynaecologic malignancies. Althoughendometrial cancer occurs more
frequently, thevast majority of patients who develop this
diseasepresent with post-menopausal or other irregularbleeding
problems and are usually diagnosed withearly-stage disease and
experience long survival. Incontrast, the presenting signs and
symptoms ofovarian cancer are non-specific and almost 75%
ofpatients already have extensive abdominal disease atthe time of
diagnosis (stage IIIC and IV). Thefailure to be able to detect
ovarian cancer at earlierstages has led to it being labelled ‘the
silent killer’.
The use of extensive debulking procedures, whichmay include
resections of the gastrointestinal (GI)or urinary tracts, can
decrease the tumour burdenfor cytotoxic chemotherapy and help to
prolongsurvival. The addition of taxanes to platinum-basedtherapy
have led to significant improvement inboth progression-free and
overall survival inpatients with either optimally reduced or
sub-optimally reduced advanced-stage disease.
Currently, ovarian cancer patients are living longerand as the
disease tends to remain within theperitoneal cavity without
affecting vital organs,patients may maintain a good performance
statusfor a long time. Unfortunately, disease usuallyrelapses.
Relapse may be heralded by elevation ofCA-125 and eventually
symptoms and evidence ofdisease will appear, leading to treatment
ofrecurrent disease. With patients living longer andreceiving
therapy for longer periods of time, thereis a need for agents that
are well tolerated, lackingof cumulative toxicity and able to
maintain qualityof life rather than worsen it due to unintended
side effects.
Treatment at time of relapse has been guided bythe interval from
the patients’ prior platinumexposure. Those patients who had
demonstratedprogression of disease while on platinum-basedtherapy,
or relapsed within six months from theirlast platinum therapy, were
thought to beplatinum-resistant and should be treated with
othernon-cross-resistant agents. Patients who had
initially responded and demonstrated clinicalprogression more
than six months after their lastplatinum therapy were thought to
have potentiallyplatinum-sensitive disease and would be
re-treatedwith platinum agents.
The probability of responding to re-treatmentincreases with time
from the last platinumexposure. After a platinum-free interval of
twoyears, response rates may approach 60%, which issimilar to
initial response rates in untreated disease.Although response rates
at earlier intervals werelower, prior to the late 1990s there were
no agentsthat were thought to have significant activity inrelapsed
ovarian cancer and platinum-based therapywas the standard.
Paclitaxel did exhibit activity in recurrent ovariancancer but,
based on several studies, quickly movedinto first-line therapy as
part of a taxane andplatinum-based combination. Then, several
agentsin phase II trials showed promising activity inrelapsed
ovarian cancer. A phase III trial,comparing topotecan with
paclitaxel, showedstatistically equivalent response rates and
survivaldata in paclitaxel naïve patients. Based largely onthis
data, topotecan was approved for use inrelapsed ovarian cancer by
the US Food and DrugAdministration (FDA). Phase II trials
withpegylated liposomal doxorubicin (PLD) that hadbeen underway had
shown activity for PLD inplatinum refractory ovarian cancer. It was
thendecided to proceed with a phase III trial comparingPLD with
topotecan.
The results of this phase III trial were initiallyreported in
2001. There were 474 patients enrolledfrom 104 sites from around
the world. Patientswere stratified upon enrollment based on
platinumsensitivity or resistance and on the presence orabsence of
bulky disease. There was no differencein response rates in the
overall or any subgroupanalysis. In the survival data that were
available,there was no difference in progression-free oroverall
survival for the entire group. However,there was a significant
improvement inprogression-free survival and an even greater
Gordon.qxp 21/7/05 4:32 pm Page 83
DOI: 10.17925/OHR.2005.00.00.83
-
84
Pharmacological Therapy OVARIAN CANCER
B U S I N E S S B R I E F I N G : E U R O P E A N O N C O L O G
Y R E V I E W 2 0 0 5
improvement in overall survival for the platinum-sensitive
patients initially treated with PLD. Therewas a large number of
censored events as many ofthe patients had not progressed or died
at the timeof the report. After more than 90% of the patientshad
recurred or died, a planned updated analysiswas performed to
re-evaluate the survival data.
With long-term follow-up, overall survival for allpatients now
showed a statistically significantimprovement for initial therapy
with PLD.Although the median survivals were similar at 63weeks for
PLD versus 60 weeks for topotecan,there was an 18% risk reduction
in death for allpatients that was significant, with p=0.032.
Therewere still no significant differences in the patientswith
platinum-resistant disease. However, in theplatinum-sensitive
group, patients initially treatedwith PLD did significantly better.
The mediansurvival was 27 months for initial treatment withPLD
versus 17.5 months for initial treatment withtopotecan. Overall,
there was a 30% risk reduction
in death for initial treatment with PLD that wassignificant at
p=0.017.
What does this mean for patients with platinumrefractory
disease? Currently, there are threerandomised phase III trials of
single agents inplatinum-resistant disease. All agents have
shownsimilar activity whether measured by response orsurvival data.
No single agent has been shown to besuperior to another; therefore,
in patients withplatinum-refractory disease, the choice of
agentshould be based on toxicity and quality of lifecriteria. The
lack of alopecia, minimal nausea/vomiting, minimal myelosuppression
and ease ofadministration, with a lack of cumulative toxicity,would
favour PLD as an initial choice for manypatients with
platinum-refractory disease. Someauthors have shown activity for
the combination of gemcitabene and cisplatinum in patients
withresistant disease; however, there is significanttoxicity with
this regimen and a randomisedcomparison has not been performed.
In patients with platinum-sensitive disease, severalphase III
trials have compared non-platinumagents; however, there are no
available datacomparing platinum with a non-platinum agent
inplatinum-sensitive disease. Response rates for allagents in all
the randomised trials are about 30%,which is similar to the
response rates reported forplatinum re-treatment in the 12- to
24-monthplatinum-free interval. In view of the
prolongedprogression-free and overall survival seen withPLD
relative to topotecan, response rates may not
be the best measure of activity in this group ofpatients. It is
still not possible to compare a non-platinum agent with a platinum
analogue;however, based on the improved progression-freeand overall
survival with PLD, this should be thefirst choice of the
non-platinum agents.
Recently, two randomised trials have comparedsingle-agent
carboplatin with carboplatincombination in platinum-sensitive
patients. ICON4 used paclitaxel as the second agent anddemonstrated
significantly improved response rates,progression-free survival and
overall survival in thepatients receiving the combination. The
AGO-
Table 1: Patient Demographics
ICON 4 30–49 AGO
>12 75% 44% 60%
months
No Prior 58% 26% 32%
Taxane
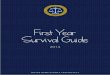
Figure 1: PLD Relative to ICON 4
1-year survival (%) 2-year survival (%) Median survival (months)
Response (months)
PLD
Carbo
T+C79 78
83
5550
57
2824
29 29
54
66
100
75
50
25
0
With long-term follow-up, overall survival for all patients
now showed a statistically significant improvement for
initial
therapy with PLD.
Gordon.qxp 21/7/05 4:32 pm Page 84
-
ABBREVIATED PRESCRIBING INFORMATION
Caelyx 10ml contains doxorubicin hydrochloride 2mg/ml in a
liposome formulation for intravenous infusion.Uses: Caelyx is
indicated as monotherapy for patients withmetastatic breast cancer,
where there is an increased cardiac risk; for treatment of advanced
ovarian cancer in women who have failed a first-line
platinum-basedchemotherapy regimen; for treatment of
AIDS-relatedKaposi’s sarcoma (KS) in patients with low CD4 counts
< 200 CD4 lymphocytes/mm3) and extensive muco-cutaneous or
visceral disease, as first-line or second linechemotherapy of
disease that has progressed with, or inpatients intolerant to,
prior combination systemicchemotherapy comprising at least two of
the followingagents: a vinca alkaloid, bleomycin and standard
doxoru-bicin (or other anthracycline).Dosage: Breast Cancer/Ovarian
cancer: Caelyx is adminis-tered intravenously at a dose of 50mg/m2
once every 4weeks for as long as the disease does not progress and
thepatient continues to tolerate treatment.For doses < 90mg:
dilute Caelyx in 250ml 5% (50mg/ml)glucose solution for
infusion.For doses ≥ 90mg: dilute Caelyx in 500ml 5%
(50mg/ml)glucose solution for infusion.To minimize the risk of
infusion reactions, the initial dose isadministered at a rate no
greater than 1mg/minute. If noinfusion reaction is observed,
subsequent Caelyx infusionsmay be administered over a 60 minute
period.AIDS-related KS: Caelyx should be administered
intra-venously at 20mg/m2 every two-three weeks. Intervalsshorter
than 10 days should be avoided to prevent drugaccumulations and
possible increased toxicity. Treatmentshould last for 2-3 months to
achieve a therapeuticresponse and continued as needed to maintain
response.
Contra-indications: Patients with history of hypersensitiv-ity
to doxorubicin or other components, or who arebreast-feeding.
Caelyx should not be used in AIDS-KS thatmay be effectively treated
with local therapy or systemicalfa-interferon.Precautions and
Warnings: As with all doxorubicin treat-ment, patients should
undergo frequent ECG monitoringfor reduction of QRS which may
indicate cardiac toxicityand monitoring of cardiac function (eg
echocardiographyor MUGA). Patients with history of cardiovascular
diseaseshould only receive Caelyx if the benefits outweigh
poten-tial risk. Infusion-associated reactions may occur—see SPCfor
details.Caution is needed in patients who have received
prioranthracycline therapy and dosage adjustment may be need-ed.
Myelosuppression should be monitored by periodicblood counts during
treatment with Caelyx. Caelyx is not recommended for use in
pregnant women. Women ofchild-bearing potential should avoid
pregnancy whilst theyor their male partners are receiving
Caelyx.The most common undesirable effect reported inbreast/ovarian
clinical trials palmar-plantar erythrodyses-thesia (PPE),
characterised by painful, macular reddeningskin eruptions, mostly
mild. PPE infrequently resulted inpermanent treatment
discontinuation. Stomatitis/mucositisand nausea were also commonly
reported in breast/ovari-an cancer patient populations, whereas
myelosuppression(mostly leukopaenia) was the most common side
effect inAIDS-KS patients.Clinically significant laboratory
abnormalities were infre-quent, with elevated total bilirubin, AST
and ALT reportedin 2.4%, 1.6% and < 1% of patients respectively.
No clinical-ly significant increases in serum creatinine were
reported.Most frequent side-effects are myelosuppression,
leukopae-nia, anaemia, neutropaenia and thrombocytopaenia.
Adjustment of Caelyx dosing interval may be needed insuch
cases.Other effects are nausea, asthenia, alopecia,
fever,diarrhoea, infusion associated reactions, stomatitis,
palmar-plantar syndrome, oral candidiasis, nausea and
vomiting,weight loss, rash, mouth ulceration, dyspnoea,
abdominalpain, allergic reaction, vasodilation, anorexia,
glossitis, con-stipation, paresthesia, pain, skin decolouration,
dry skin,pharyngitis, dyspepsia, somnolence and retinitis.
Bullouseruption has been reported rarely in AIDS-KS
patients.Undesirable effects reported for Caelyx-treated
breastcancer patients, were breast pain, leg cramps, oedema,
legoedema, peripheral neuropathy, oral pain, ventriculararrhythmia,
folliculitis, bone pain, musculo-skeletal pain,thrombocythemia,
cold sores (non-herpetic), fungal infec-tion, epistaxis, upper
respiratory tract infection, bullouseruption, dermatitis,
erythematous rash, nail disorder, scalyskin, lacrimation, and
blurred vision.Overdosage worsens myelosuppression and
patientsshould be hospitalised for symptomatic treatment of
toxiceffects. Summary of Product Characteristics (SmPC) shouldbe
consulted for further details.Presentations: 10ml vial containing
2mg/ml doxorubicinhydrochloride; 25ml vial containing 2mg/ml
doxorubicinhydrochlorideLegal Category: Prescription Only
Medicine;Marketing Authorisation Numbers: 10ml
vial:EU/1/96/011/001; 25ml vial: EU/1/96/011/002.Marketing
Authorisation Holder: S-P Europe, Rue deStalle 73, Brussels,
Belgium.Date of Revision of text: February 2003
Schering-Plough
In platinum-sensitive recurrent ovarian cancerConfirmed:
CAELYXTMsignificantly prolongs survival compared with
topotecan1
*National Institute for Health and Clinical Excellence.
CAELYX™ is indicated as monotherapy for patients with metastatic
breast cancer, wherethere is an increased cardiac risk; for
treatment of advanced ovarian cancer in women whohave failed a
first-line platinum-based chemotherapy regimen; and for treatment
of AIDS-relatedKaposi’s sarcoma.
References: 1. Long-term survival advantage for recurrent
ovarian cancer patients receivingpegylated liposomal doxorubicin.
US Oncology Review 2004 (Business Briefing) 24-26.2. Overall
survival advantage for pegylated liposomal doxorubicin compared to
topotecanin recurrent epithelial ovarian cancer. Eur J Cancer (ECCO
12, Copenhagen, Denmark,Sept 21-25, 2003);1(5):Abstr 157. 3.
NationaI Institute for Clinical Excellence, FinalAppraisal
Determination, March 2005.
LONG - TERM ANALYSIS REINFORCES CAELYX™ SUPERIORITY1, 2
• 18% risk reduction in death for all patients withCAELYX™ vs
topotecan: P=0.032 (N=474)
UPDATED NICE* GUIDELINES RECOMMEND EARLIER USE OF CAELYX™3
• The only single agent option for the newly recognized category
of partial platinum sensitivity3– Tumor recurrence at 6 to 12
months following initial
platinum-based treatment
• Also recommended for platinum-resistant or platinum-refractory
advanced disease
“…the only non-platinum agent to demonstrate a progression-free
and overall survival advantagein platinum-sensitive disease…”1
Schering_p_ad.qxp 19/7/05 9:35 am Page 85
-
GCIC trial used gemcitabene as the second agent inthe
combination. While the combination againshowed a significantly
better response rate andprogression-free survival, there was no
difference inoverall survival.
Does this mean that all patients with platinum-sensitive disease
should be retreated withcombination platinum-based therapy?
Although allof these trials were randomised, there aresignificant
demographic differences that mayexplain some of the apparent
differences in thestudy results (see Table 1).
The ICON 4 study had a greater number ofpatients who relapsed
after 12 months relative tothe AGO-GCIC trial, which in turn was
greaterthan that in the trial of PLD versus topotecan. Asimilar
pattern was seen when looking at thenumber of patients who had not
received prior
taxane in each study. A single agent wouldcertainly be expected
to have a lower response ratethan a combination; however, the
two-yearsurvival with single agent PLD was similar to thatof the
platinum–taxane combination in ICON 4and the median survival was
equivalent to thecombination (see Figure 1). The response rate
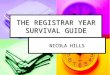
ofsingle-agent PLD was equivalent to that of single-agent
carboplatin in the AGO trial (see Figure 2).The progression-free
survival was superior tosingle-agent carboplatin and similar to
thegemcitabene combination and the median overallsurvival of
single-agent PLD was superior to eitherarm of the AGO trial.
Those patients who have a prolonged platinum-free interval, will
probably have a betterprogression-free and possibly overall
survival withcombination therapy; however, for those patientswith
early platinum-sensitive relapse, i.e. six to 12months, the data
does not clearly indicate anadvantage for platinum-based therapy at
this time.
In summary, no agent or combination has shownany significant
improvement by any measure inplatinum-resistant disease. The ease
ofadministration and low toxicity profile wouldfavour the use of
PLD as the agent of choice inplatinum-resistant disease. PLD is the
only non-platinum agent to demonstrate a progression-freeand
overall survival advantage in platinum-sensitivedisease and should
be the first choice wheneverresorting to a non-platinum agent.
Although combination therapy has shownimprovement on response
rates and progression-free survival in platinum-sensitive patients,
it is notclear at this time that equivalent results might notbe
achieved with sequential single-agent therapy,without the added
toxicity. ■
0
10
20
30
40
50
Response (%) PFS (%) Median Survival (months)
PLD
Carbo
G+C
2931
47
7.25.8
8.6
28
17.3 18
Figure 2: PLD Relative to GCIG
Table 2: Randomised Trials in Platinum-resistant Ovarian
Cancer
Study Author/year N Conclusion
Paclitaxel versus Topotecan* ten Bokkel Huinink; 226 Equivalent
activity
J. Clin. Oncol. 1997, Annals 2004
PLD versus Topotecan Gordon; J. Clin. Oncol. 2001, 255
Equivalent activity; less
Gynecol. Oncol. 2004 serious toxicity
PLD versus Paclitaxel O’Byrne; ASCO 2002 131 Equivalent
activity;
alternative without alopecia,
neuropathy
Topotecan qd X 5 versus Hoskins; J. Clin. Oncol. 1998 63
Improved activity with daily
q wk* administration
Paclitaxel q 3 week versus Andersson; ASCO 2000 208 Equivalent
activity; q wk
q wk* regimen has less toxicity
Paclitaxel/epirubicin Bolis; Gynecol. Oncol. 1999 81 Equivalent
activity
versus paclitaxel
*Includes patients with platinum-sensitive disease.
B U S I N E S S B R I E F I N G : E U R O P E A N O N C O L O G
Y R E V I E W 2 0 0 5
Pharmacological Therapy OVARIAN CANCER
86
Gordon.qxp 22/7/05 1:03 pm Page 86
-
E S G O 1 4 I S T A N B U L 2 0 0 5
www.esgo.org/esgo14
Meeting Secretariat - ESGO1417 rue du Cendrier, P.O. Box 1726,
CH-1211 Geneva 1, SwitzerlandTel: +41 22 908 0488; Fax: +41 22 732
2850; E-mail: [email protected]
Please visit the website forupdates, online abstractsubmission
and registration
Chairman, ESGO 14Uzi Beller
Co - Chairman, ESGO 14Ali Ayhan
ESGO PresidentIgnace Vergote
European Society ofGynaecological Oncology
ESGO
ISTANBUL, TURKEY, SEPTEMBER 25-29, 2005
14th INTERNATIONAL MEETINGOF THE
EUROPEAN SOCIETY OFGYNAECOLOGICAL ONCOLOGY (ESGO)
ESGO_ad.qxp 20/7/05 2:06 pm Page 87