Embed Size (px)
Citation preview

Journal of Surgical Oncology 23:99-103 (1983)
Long-Term Survivors After Adjuvant Pelvic Irradiation in Rectal and Sigmoid Carcinoma:
An Assessment of Late Results
GENE KOPELSON, MD
From the Tufts-New hngland Medical Center and Tufts University School of Medicine, Boston
Twenty-six patients with adenocarcinomas of the rectum, rectosigmoid, or sigmoid colon given adjuvant pre- or postoperative pelvic radiation therapy followed at least 5 years were retrospectively reviewed to evaluate late tumor control and complication rates. The overall 7-year survival rate was 80 & 8% with B2,3 patients faring better than C2.3 (94 -t 6% versus 43 & 19%, p < 0.005). Local pelvic tumor control was achieved in 23/ 26 patients (88 %); patients with high-stage (C2J or poorly-differentiated adenocarcinomas had a higher postirradiation pelvic relapse rate (3/ 11) versus low stage, well or moderately-well differentiated tumors (0/ 15). A major complication (none fatal) occurred in 2 of 26 patients (8 %) and was not correlated with either irradiation dose nor volume.
Long-term follow-up is now available on patients who received adjuvant pelvic irradiation for rectal or sigmoid carcinomas and indicates a high pelvic tumor control rate. The 8% major complication rate may be de- creased in the future by more sophisticated irradiation treatment planning.
KEY WORDS: colon neoplasms, rectal neoplasms, radiotherapy
INTRODUCTION Several prospective randomized trials in cancer of the
rectum have demonstrated improved survival when ad- juvant pelvic irradiation is used preoperatively [ 1-31, and multiinstitutional cooperative groups are prospectively testing adjuvant pelvic irradiation when used postopera- tively. Similarly in carcinoma of the sigmoid (above the peritoneal reflection), a nonrandomized retrospective analysis from this institution has found an improvement in survival for postoperative adjuvant pelvic irradiation
However, most of the above studies have analyzed relatively short-term survival results (ie, usually less than 5 years), and thus there is little available data on ultimate tumor control and potential long-term morbidity of adju- vant pre- or postoperative pelvic irradiation when used in this clinical setting.
The present retrospective analysis is a long-term fol- low-up (minimum 5 years) study of patients receiving adjuvant pre- or postoperative Delvic irradiation in carci-
~41.
noma of the rectum and sigmoid colon emphasizing late tumor control rates and complications.
MATERIALS AND METHODS The Tumor Registry records at the Tufts-New England
Medical Center were reviewed for all patients with the diagnosis of carcinoma of the rectum, rectosigmoid, and sigmoid colon from 1974- 1976 inclusive. All patients who received adjuvant pelvic radiation therapy at the Department of Therapeutic Radiology at this center were reviewed. Included were 12 patients who had initial cu- rative surgery followed by elective postoperative pelvic irradiation as well as 14 who had preoperative pelvic irradiation with subsequent definitive surgery. Excluded from this analysis were most of the patients with carci- noma of the rectum, rectosigmoid, or sigmoid colon who were irradiated in this department over this time period
Accepted for publication October 22, 1982. Address reprint requests to G. Kopelson, MD, Department Radiation Oncology, Salem Hospital, 81 Highland Avenue, Salem, MA 01970.
0 1983 Alan R. Liss, Inc.
100 Kopelson
(those who had preoperative irradiation in whom later radical curative surgery was not carried out, those given primary radical irradiation usually because of medical contraindications or refusal for curative surgery, those given palliative irradiation alone, and those treated post- operatively with gross residual or microscopic residual disease). Long-term follow-up of patients irradiated pre- operatively because of initially unresectable disease is provided elsewhere IS]. The time period 1974-1976 was used because during this time the radiation technique was fairly well standardized, all records were available for review, and a minimum 5-year follow-up was attainable.
PATIENT AND TUMOR CHARACTERISTICS There were 11 men and 15 women with their age at
diagnosis ranging from 33-86 years with a median of 65 years. Anatomic location of the primary tumor was rec- tum (15 patients), rectosigmoid (5 patients), and sigmoid (6 patients). All tumors were adenocarcinomas with his- tologic grades of well-differentiated (6 patients), moder- ately-well differentiated (13 patients), poorly differ- entiated (3 patients). (In 4 cases, the histologic grade of the patient’s adenocarcinoma was unavailable for re- view .)
TREATMENT METHODS Postoperative Irradiation
For the 12 patients receiving elective postoperative pelvic irradiation, 8 had an anterior or sigmoid resection and 4 had a combined abdominoperineal resection (CAPR) . Pathologic stage (Gunderson-Sosin modifica- tion of the Astler-Coller Dukes’ stage [6]) was B2 (6 patients), B3 (1 patient), and C2 (5 patients). Patients usually began irradiation 4-6 weeks postoperatively, al- though in one patient 2.5 months were required for proper healing of the perineal incision. Supervoltage (60Co or 45-MeV Brown-Boveri Betatron depending upon patient thickness) was used for each patient. Treatment volume was to the pelvis (usually L5 to the obturator foramen) alone in eight patients; in four others an extended field was used to electively irradiate the lower paraaortic nodes (superiorly to b-L3). Parallel-opposed anterior-poste- rior unshaped fields were used in all cases to treat the pelvis to 4500-4600 rad in 175-200 rad fractions 5 days a week. In nine cases (including the one B3 case), a boost (500 rad, 8 cases; lo00 rad, 1 case) was delivered via small fields to the areas considered to be at highest risk. The decision whether to boost was by personal choice of the physician. For the four patients who had CAPR, the entire perineal scar was covered in the initial pelvic field in each case but was given such an additional boost in only two of the four cases (each with a separate perineal electron field). For the four cases having extended field
irradiation, the paraaortic dose ranged between 4000- 4500 rad.
Preoperative Irradiation For these 14 patients, similar supervoltage equipment
was used to deliver similar pelvic fields and doses (ie, 4500-4600 rad) as in the prior group; 4 of 14 had a 500- rad boost; in addition 2 patients had extended irradiation fields as above. Curative surgery (anterior or sigmoid resection, 6 patients, CAPR-8) was performed 5-8 weeks later in each case. The tumor stages (utilizing the more advanced of preoperative or postoperative stage were): B1 (2 patients), B2 (6 patients), B3 (4 patients), C2 (1 patient), and C3 ( 1 patient).
FOLLOW-UP Each patient has had follow-up for a minimum of 5
years and was evaluated for late recurrences and any gastrointestinal, genitourinary, or other chronic compli- cations attributable directly or indirectly to the adjuvant pelvic irradiation. No patients had elective chemotherapy in this series.
RESULTS survival
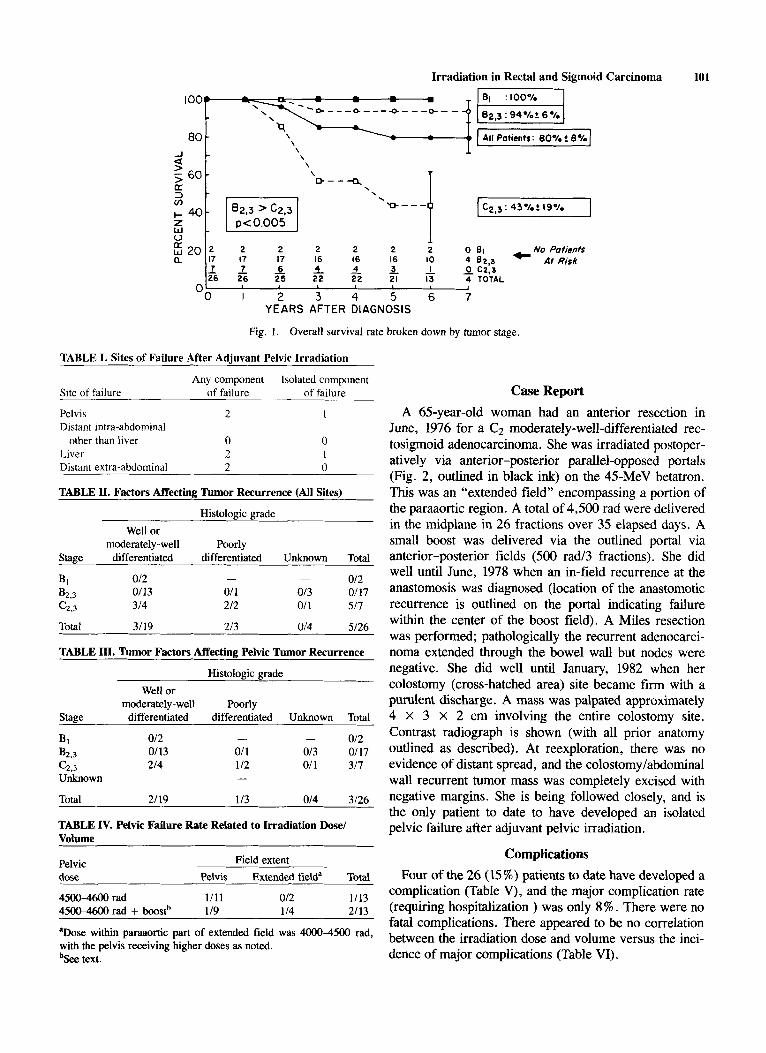
The overall 7-year survival rate was 80% (Fig. 1) and was better for B2,3 compared with C2,3.
Tumor Control Five of 26 (19%) patients had recurrences at 1 year
and 6 months, 2 years (2 patients), 2 years and 6 months, and 2 years and 8 months after diagnosis, respectively (Table I). One patient developed a second primary can- cer; she had a CAPR after preoperative pelvic irradiation for a moderately-well differentiated rectal adenocarci- noma of stage B1, and 5 years and 2 months later had a right hemicolectomy for a hepatic flexure C2 adenocar- cinoma felt to be a metachronous primary. Tumor recur- rence appeared to relate to both stage and tumor grade although numbers in each group are small (Table 11).
Pelvic Tumor Control
Adjuvant irradiation controlled the tumor in the pelvis in 23 of 26 cases (88%, Table I). Pelvic failure after irradiation appeared to relate to histologic grade and stage although numbers in each group are small (Table III). Neither the extent of irradiated volume nor whether a boost was added appeared to correlate with pelvic tumor control although there were few numbers of pa- tients in each category for proper comparison (Table IV). The interesting course of the one patient who has devel- oped isolated postirradiation pelvic relapse is illustrated here.
Irradiation in Rectal and Sigmoid Carcinoma 101
U 60-
E 3 - cn
z w - + 40- 0
2 2 2 2 2 o 131 No Potienh 17 16 16 16 10 4 6 2 3 At Risk
- - 7 7 - 6 - 4 - 4 - 3 - ' _ 0 c2:3 26 26 25 22 22 21 I3 4 TOTAL
n I ~
" 0 I 2 3 4 5 6 7 YEARS AFTER DIAGNOSIS
Fig. 1. Overall survival rate broken down by tumor stage.
TABLE I. Sites of Failure After Adjuvant Pelvic Irradiation
Any component Isolated component Site of failure of failure of failure
Pelvis 2 Distant intra-abdominal
other than liver 0 Liver 2 Distant extra-abdominal 2
TABLE II. Factors Affecting Tumor Recurrence (A11 Sites)
Histologic grade Well or
moderately -well Poorly Stage differentiated differentiated Unknown Total
012 B2,3 0113 01 1 013 0117 c2.3 314 212 01 1 517
- - BI 012
Total 3/19 213 0/4 5126
TABLE III. Tumor Factors Affecting Pelvic Tumor Recurrence
Histologic grade Well or
moderately-well Poorly Stage differentiated differentiated Unknown Total
012 B2.3 0113 01 1 013 0117 c2,3 214 112 011 317 Unknown -
Total 21 19 113 014 3/26
- - Bl 012
TABLE IV. Pelvic Failure Rate Related to Irradiation Dose1 Volume
Pelvic Field extent dose Pelvis Extended fielda Total
4500-4600 rad 1111 012 1/13 4500-4600 rad + boostb 119 114 2/13
aDose within paraaortic part of extended field was 4000-4500 rad, with the pelvis receiving higher doses as noted. b ~ e e text.
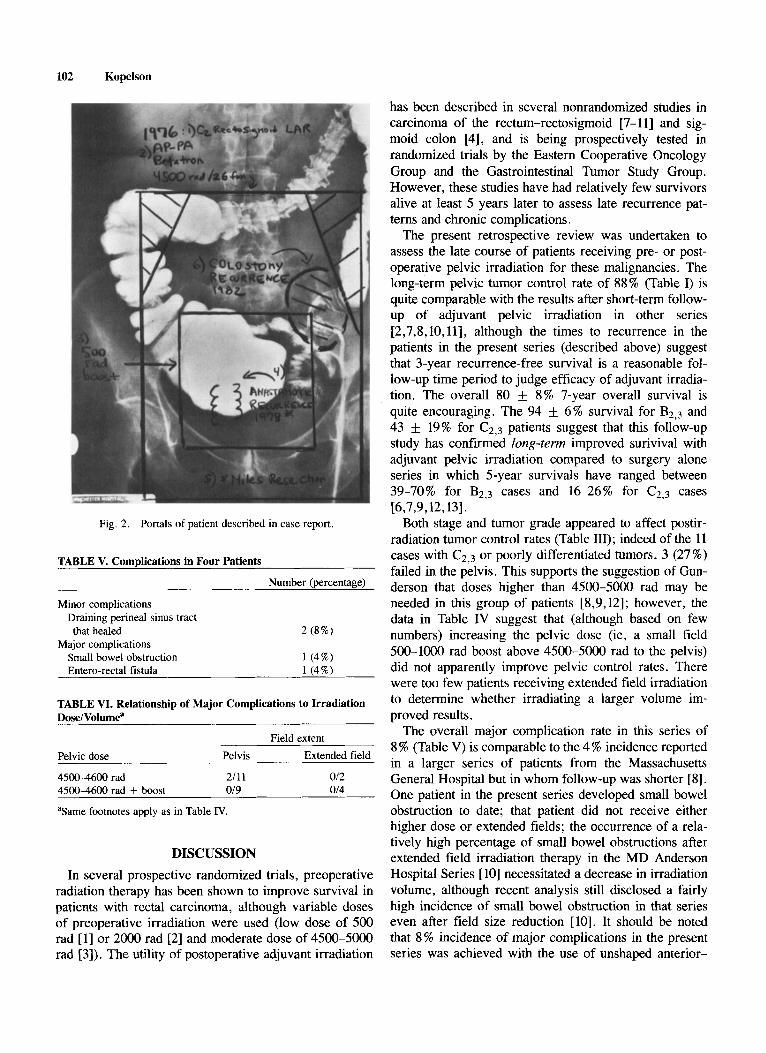
Case Report A 65-year-old woman had an anterior resection in
June, 1976 for a Cz moderately-well-differentiated rec- tosigmoid adenocarcinoma. She was irradiated postoper- atively via anterior-posterior parallel-opposed portals (Fig. 2, outlined in black ink) on the 45-MeV betatron. This was an "extended field" encompassing a portion of the paraaortic region. A total of 4,500 rad were delivered in the midplane in 26 fractions over 35 elapsed days. A small boost was delivered via the outlined portal via anterior-posterior fields (500 rad/3 fractions). She did well until June, 1978 when an in-field recurrence at the anastomosis was diagnosed (location of the anastomotic recurrence is outlined on the portal indicating failure within the center of the boost field). A Miles resection was performed; pathologically the recurrent adenocarci- noma extended through the bowel wall but nodes were negative. She did well until January, 1982 when her colostomy (cross-hatched area) site became firm with a purulent discharge. A mass was palpated approximately 4 x 3 x 2 cm involving the entire colostomy site. Contrast radiograph is shown (with all prior anatomy outlined as described). At reexploration, there was no evidence of distant spread, and the colostomy/abdominal wall recurrent tumor mass was completely excised with negative margins. She is being followed closely, and is the only patient to date to have developed an isolated pelvic failure after adjuvant pelvic irradiation.
Complications Four of the 26 (15 %) patients to date have developed a
complication (Table V), and the major complication rate (requiring hospitalization ) was only 8%. There were no fatal complications. There appeared to be no correlation between the irradiation dose and volume versus the inci- dence of major complications (Table VI) .
102 Kopelson
Fig. 2. Portals of patient described in case report.
TABLE V. Complications in Four Patients
Number (percentage)
Minor complications Draining perineal sinus tract that healed 2 (8%)
Small bowel obstruction 1 (4%) Entero-rectal fistula 1 (4%)
Major complications
TABLE VI. Relationship of Major Complications to Irradiation Dose/Volumea
Field extent Pelvic dose Pelvis Extended field
4500-4600 rad 2111 012 4500-4600 rad + boost 019 014
aSame footnotes apply as in Table IV.
DISCUSSION In several prospective randomized trials, preoperative
radiation therapy has been shown to improve survival in patients with rectal carcinoma, although variable doses of preoperative irradiation were used (low dose of 500 rad [l] or 2000 rad [2] and moderate dose of 4500-5000 rad [3]). The utility of postoperative adjuvant irradiation
has been described in several nonrandomized studies in carcinoma of the rectum-rectosigmoid [7-111 and sig- moid colon [4], and is being prospectively tested in randomized trials by the Eastern Cooperative Oncology Group and the Gastrointestinal Tumor Study Group. However, these studies have had relatively few survivors alive at least 5 years later to assess late recurrence pat- terns and chronic complications.
The present retrospective review was undertaken to assess the late course of patients receiving pre- or post- operative pelvic irradiation for these malignancies. The long-term pelvic tumor control rate of 88% (Table I) is quite comparable with the results after short-term follow- up of adjuvant pelvic irradiation in other series [2,7,8,10,11], although the times to recurrence in the patients in the present series (described above) suggest that 3-year recurrence-free survival is a reasonable fol- low-up time period to judge efficacy of adjuvant irradia- tion. The overall 80 k 8% 7-year overall survival is quite encouraging. The 94 k 6% survival for B z , ~ and 43 & 19% for C2,3 patients suggest that this follow-up study has confirmed long-term improved surivival with adjuvant pelvic irradiation compared to surgery alone series in which 5-year survivals have ranged between 39-70% for B2,3 cases and 16-26% for C2,3 cases [6,7,9,12,13].
Both stage and tumor grade appeared to affect postir- radiation tumor control rates (Table 111); indeed of the 11 cases with C2,3 or poorly differentiated tumors, 3 (27%) failed in the pelvis. This supports the suggestion of Gun- derson that doses higher than 4500-5000 rad may be needed in this group of patients [8,9,12]; however, the data in Table IV suggest that (although based on few numbers) increasing the pelvic dose (ie, a small field 500-1000 rad boost above 4500-5000 rad to the pelvis) did not apparently improve pelvic control rates. There were too few patients receiving extended field irradiation to determine whether irradiating a larger volume im- proved results.
The overall major complication rate in this series of 8 % (Table V) is comparable to the 4 % incidence reported in a larger series of patients from the Massachusetts General Hospital but in whom follow-up was shorter [8]. One patient in the present series developed small bowel obstruction to date; that patient did not receive either higher dose or extended fields; the occurrence of a rela- tively high percentage of small bowel obstructions after extended field irradiation therapy in the MD Anderson Hospital Series [ 101 necessitated a decrease in irradiation volume, although recent analysis still disclosed a fairly high incidence of small bowel obstruction in that series even after field size reduction [lo]. It should be noted that 8% incidence of major complications in the present series was achieved with the use of unshaped anterior-
Irradiation in Rectal and Sigmoid Carcinoma 103
ronto trial. Can J Surg 20:335-338, 1977. 2. Higgins GA, et al: Adjuvant therapy for large bowel cancer-
update of Veterans Administration Surgical Oncology Group trials. Surg Clin North Am 61:1311-1318, 1981.
3. Kligennan MM: Preoperative radiation therapy in rectal cancer. Cancer 36:691-695, 1975.
4. Kopelson G: Adjuvant postoperative radiation therapy for colo- rectal carcinoma above the peritoneal reflection: 1. Sigmoid co- lon. Cancer (in press).
5. Kopelson G: Long-term survivors after preoperative pelvic radia- tion therapy for locally unresectable rectal and sigmoid carci- noma: An assessment of late results. Dis Colon Rectum 25:644- 647, 1982.
6. Gunderson LL, Sosin H: Areas of failure found at reoperation (second or symptomatic look) following “curative surgery” for adenocarcinoma of the rectum. Cancer 34: 1278-1292, 1974.
7. Gunderson LL: Combined irradiation and surgery for rectal and sigmoid cancer. Curr Probl Cancer 1 5 9 , 1976.
8. Hoskins B, Gunderson L, Dosoretz D, Galdabini J: Adjuvant postoperative radiotherapy in carcinoma of the rectum and rec- tosigmoid (abstr). Int J Radiat Oncol Biol Phys 6: 1379, 1980.
9. Sugarbaker P, MacDonald JS, Gunderson LL: Colorectal cancer. In DeVita VT, Hellman S, Rosenber SA (eds): “Principles and Practices of Oncology.” Philadelphia: JB Lippincott, 1982, pp
10. Withers HR, Romsdahl MM, Saxton JP: Postoperative radiother- apy for cancer of the rectum and rectosigmoid (abstr). Int J Radiat Oncol Biol Phys 6: 1380, 1980.
11. Ghossein NA, et al: Elective postoperative radiotherapy after incomplete resection of colorectal cancer. Dis Colon Rectum
12. Gunderson LL: Radiation therapy of gastrointestinal cancer- Primary and adjuvant. In Sherlock P, Winawir SJ (eds): “Practi- cal Gastroenterology Symposium on Gastrointestinal Cancer. ” in press.
13. Gunderson LL: Radiation oncology: Pathways of tumor spread; Radiation therapy-Current state of the art. In Margolis AR, Burhenne HJ (eds): “Alimentary Tract Radiology,” vol. 111. St. Louis: CV Mosby, 1979, pp 593-619.
14. Gunderson LL, Doppke KP, Llewellyn HJ, Russell AH: Use of small bowel films in treatment planning for colorectal carcinoma 11. Residual, inoperable or recurrent disease (abstr). Int J Radiat Oncol Biol Phys 4:115, 1978.
15. Freund H, Gunderson LL, Krause R, Fisher JE: Prevention of radiation enteritis after abdominoperineal resection and radiother- apy. Surg Gynecol Obstet 149:206-208, 1979.
16. Gunderson LL, Cohen AM, Welch CE: Residual, inoperable or recurrent colorectal cancer. Am J Surg 139:518-525, 1980.
17. Green N, Ira G , Smith WR: Measures to minimize small intestine injury in the irradiated pelvis. Cancer 35: 1633-1640, 1975.
643-723.
24:252-256, 1981.
posterior parallel, opposed portals with or without small field boost treatment. Because of continuing concern for small bowel tolerance as emphasized in various publica- tions by Gunderson [13-161 and others [17], it is advo- cated to exclude as much small bowel as possible from the radiation field especially when going above 4500 rad; this may be done via shaped fields, multiple shaped fields, bladder distension, reperitonealization, etc [ 13- 161. In fact, although the data in Table VI suggests that higher dose, larger volume treatments may in fact be well tolerated, the small numbers in each subgroup sug- gests that continued care to exclude as much small bowel as possible should continue to be emphasized.
CONCLUSION AND SUMMARY Twenty-six patients with adenocarcinoma of the rec-
tum, rectosigmoid, or sigmoid colon receiving adjuvant pre- or postoperative pelvic radiation therapy were ana- lyzed for long-term tumor control and chronic complica- tion rates. With a minimum 5-year follow-up, pelvic tumor control was achieved in 23/26 cases (88%). Four of 26 cases (15%) developed a complication, although the major complication rate (that requring hospitaliza- tion) was only 8%. There was no apparent correlation between the incidence of complications and the irradia- tion dose or volume. Although these patients were not treated with specific attention to minimizing the volume of irradiated small bowel, the refinement in radiation techniques described by Gunderson [ 13-16] is strongly advocated.
Adjuvant pre- or post-operative pelvic irradiation ther- apy can ultimately provide long-term tumor control with a reasonably low level of major complications for high risk patients with carcinoma of the rectum, rectosigmoid, or sigmoid colon.
REFERENCES 1 . Rider WD, Paler JA, Mahoney LJ, Robertson CT: Preoperative
irradiation in operable cancer of the rectum: Report of the To-





























