Embed Size (px)
Citation preview

Long-term Survivors after Preoperative Pelvic Radiation Therapy for Locally Unresectable Rectal and Sigmoid Carcinoma An Assessment o f Late Results*
GENE KOPELSON, M.D.
Kopelson G. Long-term survivors after preoperative pelvic radia- tion therapy for locally unresectable rectal and sigmoid car- c inoma: as a s s e s s m e n t o f late results . Dis Co lon R e c t u m 1982;25:644-647.
From 1972 to 1976, 11 patients received moderate.dose pelvic preoperative radiation therapy (4500-4600 lad • 500 tad boost) for initially unresectable rectal or sigmoid carcinoma. Of six pa- tients subsequently explored, five had radical surgery and are alive without disease at least five years later. Comparison of the present long- term f o l l o w - u p ser ies wi th prior (short- term follow-up) series suggests that moderate-dose preoperative pelvic radiation therapy can convert many of these lesions to being re- sectable ones for which long-term survival-without-disease can be achieved. Attention to irradiation dose and field size is stressed, and a suggestion is made that patients whose tumors at final pathology still demonstrate exlrarectal extension receive p o s t o p e r a t i v e s m a l l - f i e l d boos t i rrad ia t ion . [Key words: Neoplasma, colonic, rectal; Colon; Rectum; Radiotherapy]
APPROXIMATELY 15 per cent of colorectal-cancer patients have locally unresectable tumors due to adja- cent organ involvement. 1,2 In patients with adherence to the pelvic side wall, sacrum, prostate, bladder base, etc., initial complete tumor resection with adequate margins is usually precluded. Several series using preoperative irradiation in this setting have been re- ported, ~-7 although follow-up time has been short. The present series is a five-year minimum follow-up study on the use of preoperative irradiation for loc- ally unresectable rectal-sigmoid carcinoma which up- dates a prior preliminary report from the Depart- ment of Therapeutic Radiology at Tufts-New Eng- land Medical Center Hospital. 3
* Received for publication January 22, 1982.
Address reprint request to Dr. Kopelson: Department of Radia- tion Oncology, Salem Hospital, 81 Highland Avenue, Salem, Mas- sachusetts 01970.
From the Department of Therapeutic Radiology, Tufts-New England Medical Center Hospital,
Boston, Massachusetts
M e t h o d s and Material
From 1972 to 1976, 11 patients with unresectable carcinoma of the rectum, rectosigmoid, or sigmoid were accepted for preoperative moderate-dose pelvic irradiation in an attempt to increase resectability.
There were six women and five men, ranging in age from 50 to 86 years, with a median of 65 years. Anatomic locations of the tumors were: rec tum-- eight patients, rectosigmoid--one, s igmoid--two. Two patients had anastomotic recurrent cancers pre- viously t rea ted surgically, in whom combined preoperative irradiation and possible surgery were offered as potentially curative treatment for the re- cu r ren t disease. T u m o r s were g r aded as well- differentiated (one case), moderately well-differ- entiated (two cases), or poorly di f ferent ia ted (2 cases) adenocarcinoma; in six patients, the original histologic slides did not grade the adenocarcinoma.
No patients included in this series had medical con- traindications to major surgery at the time preopera- tive irradiation was begun.
Criteria of unresectability for each patient were ag- reed upon between the surgeon and radia t ion therapist (Table 1). For six patients, the assessment of initial unresectability was made clinically, and in five it was made at initial exploration prior to irradiation, at which time a diverting colostomy was performed.
Supervoltage irradiation (8~ or 45-MV x-rays from a Brown-Boveri Betatron) was used in each case
0012-3706/82/1000/0644/$01.00 �9 American Society of Colon and Rectal Surgeons
644
Volume 25 Number 7 P R E O P E R A T I V E PELVIC R A D I A T I O N 645
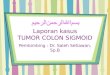
TABLE 1. Causes of Unresectability
N u m b e r o f
Patients
Fixed to s a c r u m Fixed to b ladder base Fixed to vessels* and pelvic wall Extens ion to anus and pelvic wall
* Adventi t ia o f iliac vessels.
in an a t tempt to convert these lesions to being resect- able. Parallel-opposed an te r io r -pos t e r io r unshaped ports were used to treat the pelvis at 175- to 200-rad dai/y fractions five times a week. In seven patients, the pelvis initially received 4500 to 4600 rads, and in three of the seven, a 500-rad boost was given to the highest risk area via reduced fields. In two patients, the pelvis initially received 5000 rads. In two patients,
the initial pelvic dose was less, i.e., 4000 rads in one pat ient and 3600 rads to the pelvis and a 500-rad boost in the other .
T h e present repor t is not an update of all patients included in the pr ior prel iminary r epor t f rom this depa r tmen t a because that r epor t included patients f rom several affiliated hospitals; the smaller numbers o f patients in the present repor t were selected be- cause, du r ing the t ime per iod studied, i r radia t ion t echn ique was fairly s t andard ized , and f ive-year min imum analysis was possible.
Resul t s
After complet ion of the initial course of irradiation, there was marked clinical improvemen t in 7 patients and minimal change in four (Table 2). Of the latter group, one had metastases diagnosed, and the o ther had a myocardial infarction and died; each had re- ceived no fu r the r irradiation. T h e third patient de-
TABLE 2. Tumor Status After Irradiation
Marked Regress ion
No C h a n g e T o or Minimal Potentially
C h a n g e Resectable
Initial pelvic dose < 4500 rad 2 0
4500 rad 2 7
Final t u m o r dose < 4500 rad 1 0 4 5 0 0 - 5 5 0 0 rad 1 7
5500 rad 2 0
TABLE 3. Ultimate Five-Year Cure Rates
Number Per Cent
O f all pat ients beg inn ing mode ra t e - dose preopera t ive i r radiat ion 6/11
O f all pat ients reexplored 5/7
O f all pat ients given radical curat ive surgery 5/5
55
71
100
veloped cardiac contraindicat ion to surgery and pro- ceeded to radical irradiation to 6000 rads. T h e four th patient cont inued, af ter 4000 rads to the pelvis, with a r educed field to 5000 rads; the t u m o r remained unresectable, and this pateint p roceeded to have radi- cal i rradiat ion to 6000 rads. T h e correlat ion between initial pelvic dose and clinical t u m o r response as well as between final t u m o r dose and clinical t u m o r re- sponse appears in Table 2.
O f the four patients who had no change or minimal change initially or even af ter addit ional pelvic irradia- tion, all died with locally persistent t u m o r and two with distant metastases also.
O f the seven patients who demons t ra t ed marked t u m o r regression, one refused radical surgery. This patient had only a local t u m o r excision, failed locally three months later, had local t u m o r reexcision, and has been alive with no evidence o f disease for six years since.
O f the six pat ients who were r e e x p l o r e d , one had p e r i t o n e a l s eed in g ; a l t h o u g h c o m b i n e d a b d o m i n o p e r i n e a l r e s e c t i o n (CAPR) was pe r - f o r m e d , the pa t ien t d ied o f disease at one year postoperatively.
O f the remaining five patients who were explored, all had radical curative surgery (four CAPR, one an- ter ior resection), and all were alive with no evidence o f disease at least five years later.
A summary of the clinical course o f the patients appears in Figure 1, with the final cure rates in
Table 3. Complications developed in three of 11 patients (27
per cent) and have occur red in two of o u r six five- year survivors (33 per cent) (Table 4). No complica- tion requ i red hospitalization, and in one case the symptomatology, which is scored as a radiat ion com- plication, was present pr ior to irradiation.
TABLr 4. Complications in Three Cases
Dra in ing per ineal s inus tract which healed Decubi tus ulcer within por t which healed Persis tent d i a r rhea and incont inence*
* Each p re sen t pr ior to irradiat ion.

646 G. KOPELSON Dis C,,I. & Rect. ()ctobez 1982
lMinimal or No Change (4 Cases) 1
5 Radical Surgery
! AllDOD ] 5A, NED < 5 Years ] >~ 5 Years
Initial Preoperative Irradiation 1 (11 Cases)
Marked Improvement j (7 Cases)
~ 1,, I 1 CAPR with
Peritoneal Seeding
1
1 Refused Radical Surgery ]
FIG. 1. Course of patients. A, NED Local Excision = alive, no evidence of disease. DOD =
dead of disease. Local Failure
Local Reexcision
I Salvaged A, NED by 6 months
D i s c u s s i o n
Local ly u n r e s e c t a b l e r e c t o s i g m o i d c a r c i n o m a lS o f ten de f ined at the t ime o f e xp l o r a t i on fo r lesions above 8 to 10 cm, bu t fo r low rectal lesions, f ixat ion can be d e t e r m i n e d clinically.
Data f r o m five series on the utility o f p r e ope ra t i ve i r rad ia t ion fo r such technical ly initially unresec tab le cancers a p p e a r in T a b l e 5. T h e i r r ad ia ted vo lume, as well as dose, was quite variable; escalat ing doses were used in the p r e sen t series and in the series f r o m B e r g e n 6 fo r those pa t i en t s in w h o m , a f t e r init ial p r e o p e r a t i v e i r radia t ion, only min imal sh r inkage had occu r red . T h a t h i g h e r doses o f i r rad ia t ion m a y be r e q u i r e d in this g r o u p o f pat ients is sugges ted by the data in Tab le 2 in which m a r k e d regress ion o c c u r r e d in seven o f n ine pat ients who received at least 4500
rads o f initial pelvic i r rad ia t ion vs. 0 o f two who re- ceived less t h a n 4500 rads. W h e t h e r even h i g h e r ir- rad ia t ion doses are n e e d e d p reope ra t ive ly is unclear . In the p resen t series, o f the seven pat ients who ex- p e r i e n c e d m a r k e d t u m o r r eg re s s ion a f t e r at least 4500 rads, all received 4500 to 4600 rads -+ a 500- rad boost i r radia t ion, and five o f seven were d isease- f ree at least five years later. I n each case (none o f which h a d e x t e n d e d o r g a n resect ion) , at final p a t h o l o g y there was no gross o r microscopic ex t ra rec ta l disease, conf i rming the data o f Dosoretz et al. 7 showing that, f o r p r e o p e r a t i v e i r r ad ia t ion fo r unresec tab le disease
in which e x t e n d e d o r g a n resect ion is no t done , the inc idence o f local fai lure co r re la t ed with the ex ten t o f disease f o u n d at final su rgery . Howeve r , a l t h o u g h G u n d e r s o n 8 has sugges ted that, pe rhaps , dose levels h i g h e r t han 4500 to 4600 rads migh t be n e e d e d fo r
TABLE 5. Preoperative Irradiation for Unresectable Colorectal Adenocarcinoma*
Overall Five-Year Total Survival
Total Number Rad Number of Subsequently No Radical All Radically
Series Field Size Dose Patients Explored Resection Patients Resected
Yale 4 Pelvis (_+ extended field -+ tumor bed boost) 3500-5800 15 13 9 2/15 2/9
Oregon 5 Tumor Bed 3800-7000 35 19 18 3/35 2/18 Bergen n Pelvis + extended
field to L1 3150 or 6150 27 22 16 0/27 0/16 Massachusetts Pelvis (-+ intraopera-
General 7 tive irradiation) 4500-5500 25 18 17 5/25 5/17 Tufts update Pelvis _+ tumor
(present report) bed boost 4500-6000 11 6 5 6/11 5/5
* Total overall cure rate = 11/113 (10 per cent), total of those radically resected = 14/64 (22 per cent).

Volume 25 Number 7 PREOPERATIVE PELVIC R A D I A T I O N 647
pat ients f o r w h o m e x t e n d e d o r g a n resect ion is no t c o n t e m p l a t e d (because viable t u m o r cells are p roba - bly be ing left at the marg ins o f areas o f initial a d h e r -
ence), the f ive-year survival with no ev idence o f dis- ease o f the pat ients in this series suggests tha t an a l t e rna te a p p r o a c h wou ld be 4500 to 4600 rads fol- lowed by defini t ive su rge ry with an addi t iona l post- opera t ive boos t be ing de l ivered to the h ighes t risk a rea o f p r i o r a d h e r e n c e only for those pat ients who have ex t ra rec ta l t u m o r extens ion. P re l imina ry results o f this s t ra tegy utilizing in t r aopera t ive i r rad ia t ion as the boos t moda l i ty are e n c o u r a g i n g . 9"~~
T h e f ive-year overal l survival rate o f 55 p e r cen t in the p re sen t series (Table 2) c o m p a r e d with tha t o f 10 per cent in the poo l ed da ta in the l i te ra ture (Table 5) suggests tha t pa t ients s tud ied re t rospect ive ly in this p a p e r are p robab ly no t r ep resen ta t ive o f all pat ients with locally unresec tab le rectal ca rc inoma; i.e., favor- able cases m i g h t have b e e n prese lec ted a n d consu l t ed fo r the c o m b i n e d a p p r o a c h . In addi t ion , because the dis t inct ion be tween f ixat ion due to i n f l a m m a t i o n ver- sus f ixat ion due to t u m o r invasion c a n n o t always be accura te ly assessed e i the r clinically o r gross ly at an initial exp lora t ion , ~'2 p e r h a p s some o f o u r l o n g - t e r m survivors in fact may not have had initial f ixat ion due to t u m o r (especially because n o n e o f the pat ients who had curat ive resect ion [wi thou t e x t e n d e d o r g a n resec- tion] had ex t ra rec ta l t u m o r extens ion, c o m p a r e d with n ine o f 12 in the series o f Dosore tz et al.). 7
A l t h o u g h the compl ica t ion rate was 27 pe r cent (Table 4) (one pa t i en t who is scored as a compl ica t ion in fact had s y m p t o m s p r io r to i r radia t ion) , fo r no pa- t ient was hospi ta l iza t ion requ i red . A l t h o u g h no pa- t ient has d e v e l o p e d smal l -bowel obs t ruc t ion to date, the i r rad ia t ion t echn iques e m p l o y e d in the p resen t series d id no t emphas i ze the i m p o r t a n c e o f a t t e m p t - ing to exc lude as m u c h small bowel as possible f r o m the i r r ad i a t i on fields, especial ly w h e n us ing m o r e t h a n 4 5 0 0 rads~~ such t e c h n i q u e is e n d o r s e d enthusiast ically.
In addi t ion , at present , c o m p u t e r i z e d t o m o g r a p h y is be ing ut i l ized in this clinical se t t ing p r i o r to i r rad ia- t ion in o r d e r to be t t e r assess the ent i re vo lume to be e n c o m p a s s e d wi th in the p r e o p e r a t i v e i r r a d i a t i o n field.12-15
Conclusion
T h e use o f m o d e r a t e - d o s e p r e ope ra t i ve i r rad ia t ion fo r initially unresec tab le rec ta l -s igmoid c a r c i n o m a has
resu l ted in f ive-year r e c u r r e n c e - f r e e survival in five o f l 1 (45 pe r cent) cases. A n a p p r o a c h is sugges t ed fo r those pa t ien ts o f us ing 4 5 0 0 to 5000 rads o f p r eope ra t i ve i r rad ia t ion to the pelvis fo l lowed by re- exp lo ra t i on and a t t e m p t e d radical s u r g e r y if the le- s ion b e c o m e s resec tab le ; a p o s t o p e r a t i v e b o o s t is sugges ted fo r those pat ients d e m o n s t r a t i n g ex t ra rec- tal t u m o r extens ion .
References
1. Allen CV, Fletcher WS. A pilot study on preoperative irradia- tion of rectosigmoid carcinoma. A JR 1972; 114: 504-8.
2. de Peyster FA, Gilchrist RK. Pathology and manifestations of cancer of the colon and rectum. In: Turell R, ed. Diseases of the colon and anorectum. 2rid ed. Philadelphia: WB Saun- ders, 1969;2:428-52.
3. Pilepich MV, MunzenriderJE, Tak WK, Miller HH. Preopera- tive irradiation of primarily unresectable colorectal car- cinoma. Cancer 1978;42:1077-81.
4. Kligerman MM, Urdaneta-Lafee N. Observations on fifteen inoperable/nonresectable cases of rectal cancer given preoperative irradiation. AJR 1974; 120: 624-6.
5. Stevens KR Jr, Allen CV, Fletcher WS. Preoperative radiotherapy for adenocarcinoma of the rectosigmoid. Cancer 1976;37:2866-74.
6. Bjerkeset T, Dahl O. Irradiation and surgery for primarily inoperable rectal adenocarcinoma. Dis Colon Rectum 1980;23:298-303.
7. Dosoretz D, Gunderson LL, Hoskins B, et al. Pre-operative irradiation for localized carcinoma of the rectum and rec- tosigmoid: patterns of failure, survival and future treat- ment strategies (abstr). Int J Radiat Oncol Biol Phys 1980;6:1380-1.
8. Gunderson LL. Colorectal cancer. In: Brady LW, Perez CA, eds. Basis and clinical practice of radiation oncology. New York: John Wiley & Sons. {In pr'ess.)
9. Gunderson LL, Shipley WU, Cohen AC, et al. Residual, unre- sectable or recurrent colorectal cancer: external beam ir- radiation and intraoperative electron beam boost _.+ resec- tion (abstr). Int J Radiat Oncol Biol Phys 1981 ;7:1205.
10. Gunderson LL, Cohen AM, Welch CE. Residual, inoperable or recurrent colorectal cancer: interaction of surgery and radiotherapy. Am J Surg 1980; 139:518-25.
l 1. Gunderson LL, Doppke KP, Llewellyn H J, Russell AH. Use of small bowel films in treatment planning for colorectal ca> cinoma. II. Residual, inoperable or recurrent disease (abstr). IntJ Radiat Oncol Biol Phys 1978;4:115.
12. Gunderson LL. Radiation oncology and new modalities. In: Margolis AR, Burkenne H J, eds. Alimentary tract radiology. St. Louis: CV Mosby, 1979;3:593-619.
13. Goitein M, WittenberyJ, Mendiondo M, et al. The value of CT scanning in radiation therapy treatment planning: a pro- spective study. Int J Radiat Oncol Biol Phys 1979;5:1787- 98.
14. Brizel HE, Livingston PA, Grayson EV. Radiotherapeutic ap- plications of pelvic computed tomography. J Comput Assist Tomogr 1979;3:453-66.
15. Dixon AK, Fry IK, Morson BC, Nicholls RJ, Mason AY. Pre- operative computed tomography of carcinoma of the rec- tum. Br J Radiol 1981;54:655-9.