Embed Size (px)
Citation preview

L O O S E CONNECTIONS
The Magazine About Living With EDS Spring 2012
Conference Information ...................................................................................................................... 2
My Pain BobbieSue Leonard Milbank ............................................................................................. 5
Snowboarding Joel & Molly Troumbly .............................................................................................. 5
Our Search for Help Dawn Rowley ..................................................................................................... 7
Book Review The Calling (Blair Grubb, MD) reviewed by Amy Bianco ........................................... 8
Fundraisers & Support Group Meetings ................................................................................................ 9
Mayo Clinic Offers Newly Approved Treatment for Acid Reflux Disease .............................................. 10
From the Editor’s Desk Pain & Managing Pain from an EDS Patient’s View Mark C. Martino ............................................................................................................................ 11
Book Review The Forever Fix: Gene Therapy & the Boy Who Saved It (Ricki Lewis) reviewed by Amy Bianco .................................................................................................................................... 26
Publisher's Index ............................................................................................................................ 30

SPRING 2012PAGE 2
2012 Learning Conference Living with EDSNorthern Kentucky Convention CenterCincinnati, Ohio § August 9-11
THE EDNF 2012 National Learning Conference is coming up fast! This year’s
event is centered around “Living with EDS” and provides an opportunity to hear the leading experts, to ask questions, to see old friends and make new ones, to be surrounded by people who understand, and to have an amazing weekend filled with learning and fun. Don’t miss it!
The speakers
Our speaker list includes favorites from years past and some outstanding newcomers. We are so grateful to all who come to meet with our EDS community to share their knowledge and caring with us. Click here for the Speaker List Web page. Click here for the Speaker Biographies Web page.
The consultations
Several of our physicians have volunteered to see patients for brief consultations on Thursday
afternoon. This is an incredible opportunity to ask questions you have been unable to get answered elsewhere. If you would like to speak with one of the doctors, please fill out an application. There are limited spots available, so don’t delay! Click here for an application.
The venues
This year we will be at the Northern Kentucky Convention Center. Along the banks of the Ohio River, the convention center is situated at the heart of a rapidly expanding business and entertainment district just across a picturesque 19th-century suspension bridge from downtown Cincinnati. The center is fully wheelchair accessible, as are the two main conference hotels, The Cincinnati Marriott at RiverCenter and the Embassy Suites Cincinnati - RiverCenter.
The activities
The conference officially kicks off on Thursday
SPRING 2012PAGE 3
with the Welcome Reception, a chance to have a drink, get a nibble, catch up with those friends you haven’t seen since last year, and meet some great new people.
We will once again hold a silent auction on Saturday. A large portion of the proceeds from the auction will go to fund scholarships for future conferences, so we are hoping to raise a lot of money! Please consider donating items to be auctioned. Anything “zebra” is always a hit, but there are many great ideas—think gift baskets, jewelry, artwork, etc. It is also very
easy to ask merchants you know for goods, and gives you the opportunity to educate someone about EDS in the process.
The closing banquet on Saturday evening is when we all gather to wrap up the amazing weekend. (Many people like to dress up a bit for this event.) Hope to see you all in August!
Sandra A. ChackConference Director
Silent Call for Silent Auction Items!A portion of the funds raised through our silent auction will be used for the Conference Scholarship fund. We are seeking new items from near and far, and we request members ask businesses, friends, neighbors to provide gift items, gift certificates, etc. Our auction is only as much fun as the items for bidding so help us create the best auction yet. To contribute items for the silent auction, please visit this web page.
2012 Conference web page LinksFrequently Asked Questions
General Information
Handouts
Physician Consultations
Silent Auction
Speaker Biographies
Speaker List
Sponsor Prospectus
Sponsors
Things to Do in Cincinnati
Travel to and in Cincinnati
SPRING 2012PAGE 4
Conference registration is open!
After you’ve registered, you’ll receive a confirmation email that will include this link to reserve your hotel room.
This year there are two conference hotels. A block of rooms has been reserved for your convenience at the Headquarter Hotel, Embassy Suites Cincinnati - RiverCenter and the Cincinnati Marriott at RiverCenter. Both are adjacent to the Northern Kentucky Convention Center. A limited number of ADA-accessible rooms as well as Pure Allergy friendly suites are available. The two hotels are fully wheelchair accessible, as is the convention center.
Headquarter Hotel: Embassy Suites Cincinnati – RiverCenter 10 East RiverCenter Boulevard
• Complimentary Internet in guest rooms• Mini refrigerators in each guest room• Hotel pool• Complimentary hot breakfast in hotel lobby• Manager’s Reception with complimentary
beverages each day from 5:30 – 7:30 p.m.• Onsite restaurants• Reduced self-parking rates of $8/day (you can
come and go as you please).
Cincinnati Marriott at RiverCenter 10 West RiverCenter Boulevard
• Reduced Internet in guest rooms for $5.95/day• Self-parking $10/day (note: must pay to
leave and park again) or $28 Valet/day with availability to come and go as you please
• Hotel pool• Refrigerator by special request (limited
availability)• Onsite restaurants• Located on Southbank Trolley Route to
transport you to area attractions and restaurants.
EDNFKids & Teens
Another fabulous programMore information to come!
Early registration ends on 06/04/2012.
Type EDNF Member Registration Non-Member Registration
Full $259 $309
Full Kids & Teens (ages 6-14) $159 $159
Friday one-day $104 $129
Saturday one-day $154 $179
Children (age 5 and younger) $0 $0
Prices go up when regular registration starts on 06/05/2012.Late registration starts on 07/30/2012.

SPRING 2012PAGE 5
MY PAIN
SNOWBOARDING
YOU are there every morning,you are there for every move.
You are there when I’m resting,and there for every mood.You are with me every step,you are present when I’m still.You slip into every moment,you are immune to every pill.You are visible at times,but stay hidden most.You are burned into my mind,and haunt me like a ghost.You are never really gone,yet you never really stay.You are in a different place,almost every single day.You are silent like a villain,you slowly drive me insane.You are apart of me,you are my pain.
BobbieSue Leonard MilbankI wrote this before I had my EDS Classical diagnosis. It was a time that no one believed that I was in pain, no one (except my mother) believed me when I was telling them my joints were dislocating, and all I got from doctors was that I was making it up to get medication. I am 26, and at times I feel like I’m 86. I get to go to the conference in August, it’s the first time I will get to meet anyone with EDS. I am excited and scared at the same time. I have lived so long with people who don’t understand what it is like in this body, and to be able to reach out to get a gentle hug from someone who means it when they say “I understand” is all I am wanting in life. know there are others who feel this way, and who are living with pain as their mistress in life.
OUR son, JC Troumbly, snowboarding. He was diagnosed with EDS in October of
2010. He fights hard to stay active. He has had to give up some sports and physical activities, but keeps snowboarding. With therapy and bracing he as been able to reduce pain and dislocations. He recently competed in a snowboarding competition. He didn’t place but we couldn’t be more proud of him for fighting hard to do what he loves. This picture was taken at the snowboarding competition by Steve Diamond Elements Photography.
Joel & Molly Troumbly
SPRING 2012PAGE 6
I AM the mother of a 24-year-old woman who was diagnosed with Ehlers-Danlos
syndrome, Hypermobility type, this past summer. I believe that this came from my side of the family through my mother. However, like so many out there with this disorder, my daughter Kara was the first to exhibit extreme symptoms. I now realize that I have some hypermobile joints and subluxate a lot, I just did not realize that this was not normal.
When Kara began having worsening pain and symptoms that were beyond what the doctors felt that she should be experiencing ,even for someone diagnosed with fibromyalgia syndrome, I continued researching. After about two years I had acquired all the puzzle pieces needed to get her to a geneticist to get this diagnosis of EDS. So here we are with this lifelong genetic condition that means she will never be pain-free as long as she lives; we need to find away to treat her pain so that she can have some kind of a life. Add the complications of Von Willebrand disease and absorption issues. How do we manage pain when there is very little medication that she can take, because some does not work at all and others work only for acute pain and inflammation.
Kara has not been able to attend physical therapy (PT) as often as she should or do it at home. The pain is sometimes so bad that just moving makes it worse, but she needs physical therapy to strengthen the muscles that must support her joints.
We needed help and I decided to make a leap of fait. In our area of Salt Lake City, Utah, we have a chiropractic spine and disc clinic that boasts pain relief using multiple modalities that include chiropractic treatmentsif you need or
OUR SEARCH FOR HELP
can have them), spine decompression (traction), and laser therapy. I know chiropractors have a place in the world of medicine because my parents swear by them, but I myself had never felt a need for the treatments — probably a good thing, since I did not know that I had EDS. Choosing to place my trust in this particular science was difficult, but too many physicians simply told us, “I have nothing to offer you,” meaning I think in most cases,“I do not want to take the time to learn.”
We have this clinic — there are others that use some or all of the treatments mentioned above — but this clinic is so sure of itself that they offer your first two treatments for free. What could we lose? So I made an appointment.
Kara never leaves the house because there is no way to know if the seating at other homes, church, movie theatres, and so on will offer enough support for her lower back or have high enough head rests. The Saturday before her appointment, she made plans to hang out with friends, and ended up having to support her own head and putting pressure on her lower back for the entire day. The rest of the week she was bed-ridden. She could not go to PT. She had headaches, neck aches and back aches. I was beginning to realize that a lot of her pains are probably soft tissue injury on top of soft tissue injuries that are not healing. She had injuries beginning on the high school swim team and multiple falls since, and a day supporting her own head and body caused all of those injuries to really flair up.
Appointment time arrived and Kara wore her neck brace; she was going to the appointment, but hoped it would not last long because she just wanted to get back home and lie on the couch.
SPRING 2012PAGE 7
We met with a chiropractor who took her history and understood that she is not a candidate for manual manipulation. We decided that for the free treatments we wanted to treat her neck, since it was the most painful and caused blinding headaches. He laid out what the treatment would entail. First, they would use the activator to align the spine. Then they would use decompression therapy (traction) to allow blood to flow into the injured areas. Next would be the laser therapy, ending with a massage across the upper back. Kara was in extreme pain, barely lifting her head, waiting to just get the treatments over with.
After the activator treatment, we went into the room that has the traction table set up for the cervical spine. Although he weight was very small, I was concerned that she might have a reaction such as dizziness or nausea. But when the eight minutes were done, she sat up; her first reaction was she wanted to continue the treatment longer. Next came the laser therapy. The aide set the laser to the doctor’s specifications and held the wand just above the skin, moving it all around the neck area and even up into the lower part of the head. The treatment lasted about ten minutes. After the massage she was done; her pain levels had dropped from ten to below five, where she no longer considers the pain to be a problem because she is so used to pain.
We came back for the second treatment and signed up for the prescribed 25 treatments. This is very expensive; if you choose to try this route you should shop around. We really did not expect such good results or we would have searched for lower prices beforehand. But it has been worth it for us, and I will fight hard to get some of the money back from the insurance; laser therapy is still considered to be experimental because there are so many types and uses, and not enough studies have been done on each type of injury to showing one treatment plan works best.
The lasers are FDA-approved for soft tissue injuries, sports injuries, and chronic pain. We really had no other place to turn, and are now about a third of the way through the treatment plan. Kara is still relatively pain-free in her neck head and lower back. As they have increased the weight on the traction, she sometimes has resulting neck/back pain or muscle spasms; they stop increasing the weight until those symptoms resolve. The weight that they will ultimately reach is not very heavy.
Since she is feeling so much better, we are making sure that she does all of her physical therapy, both at the office and at home. We are using this period of reduced pain to get her stronger, with the hope that the combination of healing treatments from the chiropractor and the physical therapy strengthening will get her long-lasting relief.
Dawn Rowley
EDNF welcomesto the
Board of Directors
Sandy ChackDeb Makowski

SPRING 2012PAGE 8
The Calling Blair Grubb, MD University of Toledo Press, 2011 ISBN 978-0-932259-12-7, $15.00
I HAVE heard that it takes a year to get an appointment with Dr. Blair Grubb,
a cardiologist at the University of Toledo Medical Center. No doubt Dr. Grubb is a highly skilled physician, but I suspect that it is his humanity — his interest in his patients as people — that makes him worth waiting for. As is clear in this wise and moving collection of essays, Dr. Grubb practices medicine through the eyes of a storyteller. In fact, the pieces that comprise this book are more like little fables than essays, carefully told in straightforward language, and none more than a few pages long. Each is centered around a difficult moment in the author’s life or in one of his patient’s, and in each Dr. Grubb manages to find meaning and solace. In the standard paradigm of modern medicine, the patient is seeking something from the doctor; and Dr. Grubb acknowledges that the demands of practicing in a busy medical center can back physicians into a harried, defensive posture. But Dr. Grubb is that rare physician who is seeking something from his patients — a story, yes, but more than that, a connection, a glimpse into the mysteries of the human soul.
In one of the most lighthearted moments in the book, Dr. Grubb is urged to stop a while and share a glass of wine with a patient on whom he is making a house call. If you hurry through life, she tells him, you will miss its subtle pleasures; you will also fail to appreciate suffering. For “it is the stresses of life,” she says, “that give us our unique characteristics.” Dr. Grubb takes this lesson to heart: in order to treat the whole
BOOK REVIEW THE CALLING
patient you must understand his suffering — not just his symptoms, but the sorrows of his life. Again and again, Dr. Grubb probes for the stories of his patients’ lives, transforming what would normally be grimly routine medical encounters into inspirational — in some cases even extraordinary — experiences. One morning during rounds, an old “gomer” with pneumonia and congestive heart failure, who never speaks up but to complain he is cold, is prompted by Dr. Grubb to relate a horrific tale from his service in the Pacific in WWII when he had to kill an enemy soldier. From that moment the attitude of the medical staff toward the patient changes dramatically. In another story, Dr. Grubb encourages an intern to take her time with an elderly Cambodian woman as she describes how her entire family was murdered by the Khmer Rouge. Yet another tale of war emerges from an unkempt, cantankerous Vietnam veteran who suddenly begins to speak of his experiences: how he was captured and tortured and eventually escaped, but most vividly of all, how overwhelmed he was by the beauty of the Angkor Wat temple when he stumbled upon it during a jungle patrol. Thereupon Dr. Grubb’s image of this patient “slowly changed from a street drunk to a person whose life had been ravaged by war, and I realized that his broken body still held a decent man inside.” Several months later the patient dies in his sleep, and lying next to him is a book of photos of Angkor Wat that Dr. Grubb had given him.
Many of the lessons learned in these tales come from beyond the grave. In fact, death makes an appearance in almost every one of the short pieces that make up this collection. From its opening pages, where Dr. Grubb loses his composure and literally calls a young boy — his

SPRING 2012PAGE 9
patient and his “little buddy” — back from the brink of death, to its conclusion with the placing of the headstone on his father’s grave, Dr. Grubb is continually grappling with the meaning of death. Most medical professionals regard death as a failure; but as a kind and thoughtful man who must deal with gravely ill patients every day, Dr. Grubb chooses to approach his work with creative passion. He sees how suffering can bring redemption, and he believes that there is much about death that we do not understand. Several of his patients are transformed by illness or near-death experiences from selfish actors into loving and generous people who go forth to do good in the world. Dr. Grubb wonders about the legend from the Cabala that tells of the “Lamedvovnik,” or “The Just,” 36 righteous people whose goodness sustains our world. When one dies, her soul passes to another, who takes up the job of “Tikkun,” restoring and redeeming the world.
EDSers reading this book will not find any information on POTS or other medical issues specific to our condition; what we find is a deeply spiritual — though tastefully understated — exploration into what Dr. Grubb calls the nobility of the human spirit, a nobility that is powerfully expressed by those who must deal with illness, disability, and death. It is a great comfort to know that there are doctors like Dr. Grubb who appreciate their patients’ suffering and are working to restore and redeem the healing arts.
Amy BiancoEditor, Medical Section
Hoofing It for a Cause, Gluing Zebras Together
Sunday, May 20, 2012, join our fund-raising fun: 2 to 6 p.m. in Davis Park, Sapulpa OK. Click here for more information!
Front Range Ehlers-Danlos Support Group
Join the Front Range Ehlers-Danlos Support Group on Meetup for details about our next meeting: Saturday, May 12th in Lone Tree, Colorado. We already have ten members in just six weeks — considering how isolated most folks affected by EDS feel, that's pretty awesome! Plan to bring a list of the healthcare providers you have found helpful so we can share resources.
Fundraisers & Support Group MeetingsEDS Houston Group
Third Saturday each month: May 19, 2–4 p.m. at the McGovern-Stella Link Neighborhood Library, 7405 Stella Link, Houston TX 77025. Visit the EDS Houston Facebook group for more information.
To publicize your group meeting or fundraising event
Send the details you want mentioned in an email to [email protected].
Loose Connections deadlines are first week in April for the Spring issue; the last week of July for the Summer/Autumn issue; and the middle of November for the Winter issue.
The Hinge is published every two months, starting the end of January; deadline is the second week of that month.
SPRING 2012PAGE 10
MAYO CLINIC OFFERS NEWLY APPROVED TREATMENT FOR ACID REFLUX DISEASE
A NOVEL device, a ring of tiny magnetic titanium beads, acts to keep stomach acid
from leaking into the esophagus. Mayo Clinic in Florida helped test the device in patients and will be one of the first health care institutions in the United States to offer this newly approved device to treat gastroesophageal reflux disease (GERD). The U.S. Food and Drug Administration (FDA) approved the device and treatment procedure on March 22 for patients with GERD who continue to have chronic reflux symptoms despite taking medication.
Mayo Clinic in Florida expects to offer the new treatment immediately, says C. Daniel Smith, M.D., chair of the Surgery Department at Mayo Clinic in Florida, and an internationally recognized expert on the treatment of GERD.
Dr. Smith is experienced in using the system because Mayo Clinic in Florida was one of only 14 centers nationally that participated in a clinical trial that led to the FDA’s approval of the device.
GERD is a condition in which liquid, or food, in the stomach flows back up into the esophagus due to the inability of a ring of muscle between the lower esophagus and the top of the stomach to close properly.
If drugs aimed at neutralizing the acid in the stomach fail to prevent GERD, an operation designed to correct the mechanical defect is considered. But between 1.5 million and 2 million patients of those patients could benefit from treatment that is much less complex than current surgical options, Dr. Smith says.
“The new system will offer a long-needed treatment option for a large group of underserved patients,” he says.
The results of the clinical study that led to approval of the device have not yet been published. But “the data presented to the FDA revealed striking results when compared to other GERD treatments that have been investigated over the past 20 years,” Dr. Smith says. “The system offers effective control of GERD with limited side effects and thus far an excellent safety record.”
The implanted device is a ring of tiny magnetic titanium beads that is wrapped around the junction between the stomach and esophagus, serving as a mechanical augmentation of the lower esophageal sphincter (the ring of muscle). The magnetic attraction between the beads is strong enough to keep the sphincter closed to refluxing acid, but weak enough so that food can pass through it into the stomach, Dr. Smith says. The device can be implanted using minimally invasive surgery methods.
Dr. Smith performs about 200 GERD-related surgeries a year. “I expect this device to be a game changer for the treatment of GERD in select patients who have failed management with drugs,” says Dr. Smith.
Mayo Clinic physicians and scientists collaborated with Torax Medical in the development of the LINX Reflux Management System, and Mayo Clinic licensed related technology to the company in exchange for equity. Drs. DeVault and Smith are paid consultants to Torax Medical.
To schedule an appointment, please call 904-953-2228 or 904-953-2272 between 8:30 a.m. and 5 p.m. EDT. http://www.newswise.com/articles/mayo-clinic-offers-newly-approved-treatment-for-acid-reflux-disease
SPRING 2012PAGE 11
FROM THE EDITOR’S DESK: PAIN & MANAGING PAIN FROM AN EDS PATIENT’S VIEW
I HAVE been studying Ehlers-Danlos syndrome since I was diagnosed more than ten years ago, but I still find it helpful at times to think through from the fundamentals. EDS is a collection of genetic collagen defects. Each type of EDS is defined as a distinct
problem in making or using one of the types of collagen. Collagen is the most abundant protein in the body, so effects can be wide-ranging in both location and severity. Collagen is what the body uses to provide strength and elasticity to tissue; normal collagen is a strong protein that allows tissue to be stretched, but not beyond its limit, and then safely returned to normal. In most EDS types, the affected collagen is badly structured, which means that any tissue using the mutated collagen can be pulled beyond its normal limits, causing damage.
What can still surprise me is how widespread the effects of having a mutated type of collagen can be. There are five main collagen types that are affected by EDS, as far as is known to date; not all the genetic causes of EDS are known, and in particular, EDS Hypermobility Type is still largely undetermined (although a tenascin-X mutation accounts for a small percentage). One of the fundamental keys we are missing is why EDS expresses in such a wide range of severities; even in the same generation of a family with the same mutation, it can be mild in one person and severe in another. EDS was not named until 1936, so it is still a young disorder; we have learned most of what we know about EDS since the last dianogstic and nosology conference in 1997, but there is still so much we do not understand. There will be new information after the next nosology, to be formulated at the First International EDS Symposium in Belgium, September, 2012.
EDS pain can be severe and widespread. Built with collagen, the fascia is the sort of “Saran Wrap” that holds our bodies together, a connective tissue that surrounds muscles, groups of muscles, blood vessels, and nerves. The result of an overly-stretchable fascia can be literally body-wide because it is wrapped around nearly everything.
Chronic pain is a well-established and cardinal manifestation of EDS and it is common for pain to be out of proportion to physical and radiological findings. The etiology of EDS pain is not clearly understood, but some of the likely causes include muscle spasm (tender points are sometimes present) and degenerative arthritis; neuropathic pain is also common. (EDNF’s Pain Management Medical Resource Guide http://www.ednf.org/index.php?option=com_content&task=view&id=2123&Itemid=88889247)
Chronic frequently debilitating pain of early onset and diverse distribution is a constant feature in most individuals affected with different types of EDS.
90% of EDS population has chronic pain for more than 6 months84% feel it worsened over their lifetime89% had chronic pain before adulthood88% have taken pain medication51% have taken narcotics
Chronic Pain is a Manifestation of the Ehlers-Danlos Syndrome [Sacheti et al, 1997] http://www.ednf.org/index.php?option=com_content&task=view&id=1331&Itemid=88889208
SOU
RCES
& R
ESO
URC
ES

SPRING 2012PAGE 12
Chronic pain, distinct from that associated with acute dislocations or advanced osteoarthritis, is a serious complication of the condition and can be both physically and psychologically disabling. (Ehlers-Danlos Syndrome: Hypermobility Type [Levy] http://www.ncbi.nlm.nih.gov/books/NBK1279/)
Pain in Ehlers-Danlos syndrome is common, severe, and associated with functional impairment [Voermans et al] available in full http://www.ednf.org/images/stories/pdfs_medical/2010/2010_Voermans_JPainSympMgmt.pdf
“Muscle fatigue and pain” are symptoms of EDS. (http://www.mayoclinic.com/health/ehlers-danlos-syndrome/DS00706/DSECTION=symptoms)
The loose joints are unstable and prone to dislocation, chronic pain, and early-onset arthritis (in the third paragraph in the NIH overview of EDS http://ghr.nlm.nih.gov/condition/ehlers-danlos-syndrome)
Joint Hypermobility Syndrome Pain [Grahame] http://www.ednf.org/images/stories/pdfs_medical/2010/2009_Grahame_CPHR_hypermobility.pdf
Types of pain in EDS: headache, musculoskeletal pain — acute and chronic, gastrointestinal/abdominal pain
Headache in EDS and other Hypermobility syndromes: migraine, ‘low pressure’ headaches, ‘high pressure’ headaches, myofascial pain, sinus pain, temporo-mandibular joint problems, dental pain
Musculoskeletal Pain in EDS and other Joint Hypermobility Syndromes: joint laxity predisposes to acute injury, muscle spasm in response to acute injury or as a means to stabilize unstable joints, myofascial trigger points develop in response to joint laxity, nerve impingement may result from disc disease or joint laxity causing muscle spasm as well as neuropathic pain
Gastrointestinal Pain in EDS: dysmotility, constipation, irritable bowel syndrome [and food allergies], sphincter of Odi dysfunction
Comprehensive Pain Management in Ehlers-Danlos Syndrome [Francomano] http://www.ednf.org/images/2010conference/Handouts/Francomano_ppt_2_slides_per_page.pdf
Of course, there is an element of the traditional view of chronic pain, synaptic plasticity, in which the body learns pain and increases pathways for pain, setting up a cycle that remodels the nervous system. “A cardinal feature of EDS is pain. At first there are just small pains; but acute pains may accumulate, then become continual and chronic. There may be a major dislocation of injury to start the cycle; but without adequate treatment, persistent pain can change the nervous system in a process that is difficult to reverse. By lowering the threshold for pain signals, chronic pain becomes harder to treat.” (EDNF’s Pain Management Medical Resource Guide http://www.ednf.org/index.php?option=com_content&task=view&id=2123&Itemid=88889247)
But there is an added element to EDS pain that we have started recognizing these past few years: we suffer what might be called chronic acute pain. Some of us suffer frequent dislocations, and most of us endure at least joint subluxations. We do not injure a joint once and then recover. We injure a joint over and over, because if we are in motion, our joints are moving out of alignment. As a personal example, my shoulders separate with about four pounds of force, so my arms are continually, literally, falling out of the socket, even at the computer. I once kept a journal for a week of how often joints slipped or dislocated; when I was sitting still, I still managed ten or so an hour, and there were many more when I was up and moving about doing things.
Every time a joint slips or dislocates, the soft tissue connected to that joint — tendons, ligaments, muscle, fascia, blood vessels — all stretches. Because of the structural defect
SPRING 2012PAGE 13
in collagen, all that connected tissue is stretched beyond what normal should be; high-resolution MRIs reveal microtrauma, microscopic tears that start up the inflammation and coagulation cascades. But because each joint can subluxate over and over in just a single day, these microtraumas happen over and over in the same tissue without healing successfully. This was first pointed out as an EDS problem in July 2011 by Dr. Clair Francomano in her comments while presenting at the EDNF Conference: “Microtears are not visible with ordinary MRIs but are experienced by EDSers, causing pain and instability.” (From my own notes, verified by notes at http://edsers.com/2011_Conference_Notes.html; Dr. Francomano’s presentation is a great summary, Ehlers-Danlos Syndrome Update 2011: What We Know — And What We Don’t Know, available from http://bit.ly/HQDNwk.)
Tissue damage has the potential to elicit mechanisms that can create disabling, refractory, chronic situations that may prolong and even outlast the period of healing. (Hedderich & Ness, 1999)
Shoulder instability is a relatively common occurrence, reported in 2% to 8% of the population. The condition may arise from a single traumatic event (ie, subluxation or dislocation), repeated microtrauma, or constitutional ligamentous laxity, resulting in deformation and/or damage in the glenohumeral capsule and ligaments. (http://blue.regence.com/trgmedpol/surgery/sur100.html)
We postulate that the propensity for tendon degeneration in Ehlers-Danlos syndrome coupled with repetitive microtrauma might lead to fraying of the tendon fibers and, consequently, triggering. (http://www.mendeley.com/research/multiple-triggering-girl-ehlersdanlos-syndrome-case-report/)
When a joint has more movement than is ideal, stress and strain are placed on the joint, causing micro-trauma to the joint, and this can result in pain. (http://www.hypermobilot.com.au/uploads/7/0/8/7/7087979/pregnancy_a4.pdf)
No one really knows why this happens, but one theory is that every-day overuse or misuse of hypermobile joints causes “microtrauma” to the joint tissues. Eventually this “microtrauma” can build up and cause pain — a sort of “the straw that broke the camel’s back” situation.” (http://hypermobilityhope.blogspot.com/p/what-is-hms.html)
It has been speculated that when tendon is overused it becomes fatigued and loses its basal reparative ability, the repetitive microtraumatic processes thus overwhelming the ability of the tendon cells to repair the fiber damage. The intensive repetitive activity, which often is eccentric by nature, may lead to cumulative microtrauma which further weakens the collagen cross-linking, non-collagenous matrix, and vascular elements of the tendon. Overuse has also been speculated to cause chronic tendon problems, by disturbing the micro- and macrovasculature of the tendon and resulting in insufficiency in the local blood circulation. Decreased blood flow simultaneous with an increased activity may result in local tissue hypoxia, impaired nutrition and energy metabolism, and together these factors are likely to play an important role in the sequence of events leading to tendon degeneration. (Histopathological findings in chronic tendon disorders [Järvinen et al] http://www.ncbi.nlm.nih.gov/pubmed/9211609)
It is thus reasonable to postulate that excessive laxity of ligaments may predispose an individual to repeated microtrauma during even normal activity. A possible reason for recurrent joint trauma in hypermobile persons may be the recently demonstrated impairment of proprioception noted in both small and large joints. It therefore follows that recurrent microtrauma to ligamentous structures in some hypermobile individuals will lead to repeated pain experience and may trigger disordered pain responses. …A more immediate question might be the association of hypermobility and soft tissue complaints. It seems reasonable to hypothesize that loose ligaments may lead to skeletal structural instability, and predispose the body to repeated minor or more serious traumatic episodes. (Is Hypermobility a Factor in Fibromyalgia? [Fitzcharles] http://www.jrheum.com/abstracts/editorials/200106.html)
Within the physiological range, particularly towards the higher range, microscopic degeneration within the tendon may start to occur, especially with repeated and/or prolonged stressing. This can eventually lead to a symptomatic tendon with altered mechanical properties as a result of repeated microtrauma.
SOU
RCES
& R
ESO
URC
ES
SPRING 2012PAGE 14
(Current concepts in the management of tendon disorders [Rees et al] http://rheumatology.oxfordjournals.org/content/45/5/508.long)
An added problem, suggested by one of my doctors, may be that axons do not stretch; with each dislocation or subluxation, neural pathways may be pulled apart and then reconnected, adding a neuropathic pain to the mix.
Because of the constant reinjury from joint laxity to tissue and neural pathways, I have been using the term “chronic acute pain,” acute pain that is recurring chronically. From these recurring problems comes much of EDS fatigue, I would suspect, although orthostatic intolerance and dysautonomia can account for much of the fatigue as well.
Symptoms Of Orthostatic Intolerance: Lightheadedness, Dyspnea, Syncope, Chest Discomfort, Diminished concentration, Palpitations, Headache, Tremulousness, Blurred vision, Anxiety, Fatigue, Nausea, Exercise intolerance, Nocturia
Working hypothesis: Connective tissue laxity in blood vessels allows increased vascular compliance, promotes excessive pooling during upright posture, leading to diminished blood return to the heart, and thus to OI symptoms (Rowe PC, et al. J Pediatr 1999;135:494-9)
Chronic Fatigue in EDS [Rowe] (http://bit.ly/HQDNwk)
• 273 patients with EDS• 77% severe fatigue• 57% reported fatigue as 1 of their 3 most important symptoms• Severe fatigue was more common in hypermobile than classical EDS (84% vs. 69%; P=.032)• Fatigue had a greater impact on daily function than did pain
Fatigue is a frequent and clinically relevant problem in EDS (Voermans et al. Semin Arth Rheum 2010; 40:267-74)
Chronic Fatigue Often Paired With Ehlers-Danlos Syndrome [Jancin] (http://www.ednf.org/index.php?option=com_content&task=view&id=1245&Itemid=88889208)
Orthostatic intolerance and chronic fatigue syndrome associated with Ehlers-Danlos syndrome [Rowe et al.] (http://www.ncbi.nlm.nih.gov/pubmed/10518084)
Ehlers-Danlos syndrome, diffuse pain and chronic fatigue http://doctorstevesbanjo.com/ehlersdanlos-syndrome-diffuse-pain-chronic-fatigue/
Severe fatigue afflicts 75% of those with EDS http://doctorstevesbanjo.com/severe-fatigue-afflicts-those-ehlersdanlos-syndrome/
One other major contributing factor to EDS pain is the spine. The spine is, of course, a series of joints, and like any joint in the body of someone with EDS, the vertebrae are potentially hypermobile, as is the junction where the skull sits on the spine. The effects can range, like everything in EDS, widely: Chiari Type I malformation, tethered cord, syrinxes, cerebrospinal fluid abnormalities, syrinxes, and craniocervical settling.
Hereditary disorders of connective tissue may present with Chiari I malformation, occipitoatlantoaxial hypermobility, and functional cranial settling [Francomano et al.] http://www.ednf.org/index.php?option=com_content&task=view&id=1618&Itemid=88889208
Syndrome of occipitoatlantoaxial hypermobility, cranial settling, and Chiari malformation Type I in patients with hereditary disorders of connective tissue [Milhorat et al.] full PDF http://bit.ly/xesPlJ
I have EDS and was just diagnosed with Chiari, is this related to EDS? http://www.ednf.org/index.php?option=com_content&task=view&id=1580&Itemid=88889064
SOU
RCES
& R
ESO
URC
ESSO
URC
ES &
RES
OU
RCES
SPRING 2012PAGE 15
Deformation of the Nervous System in EDS Patients [Henderson] and Temporomandibular Joint & Cervicocranial Dysfunction in the EDS Patient [Mitakides] in the 2011 EDNF Conference Handouts section http://bit.ly/HQDNwk
Spine abnormalities are correlated with back pain in young persons with Ehlers-Danlos syndromes [Bangura et al.] http://www.ednf.org/index.php?option=com_content&task=view&id=1623&Itemid=88889208
Urologic Manifestations of Tethered Cord Syndrome: Clinical and Urodynamic Findings [Murdock] http://bit.ly/HQDNwk
Physical therapy
Physical therapy can be an important part of EDS pain management, with the goal of reducing muscle spasm and toning muscles around joints. There are some important factors to physical therapy for people with connective tissue disorders, and EDS specifically. In many ways, this approach is the opposite of traditional physical therapy. Instead of aggressive, short-term building of muscle mass through rapidly increasing weight or resistance, physical therapy for EDS has to be focused on long-term, gentle building of muscle tone. Special attention has to be paid to ensure that physical therapy does not continue to injure the person with EDS, that motion does not exceed normal range of motion and that joints are not ever hyperextended or slipping in place. While some degree of muscle ache is part of building muscle, one has to be aware with EDS and connective tissue disorder patients that any pain during physical therapy is probably signaling joint instability and subsequent tissue damage.
A physical therapist who is highly knowledgeable and deeply understanding about connective tissue and joint dysfunction can be useful to long-term health:• use low resistance exercise to gradually increase muscle tone and to help stabilize loose joints;• minimize joint trauma by avoiding joint hyperextension and any high resistance or impact activities;• just as it often takes years for joint laxity to cause significant pain and instability, it can take at least
months and usually years to gradually reverse the process via muscle toning exercise.Ehlers-Danlos Medical Resource Guide (http://www.ednf.org/index.php?option=com_content&task=view&id=2120&Itemid=88889244)
Physical therapy:• Myofascial release (any physical therapy modality that reduces spasm) provides short-term relief of
pain, lasting hours to days. While the duration of benefit is short and it must be repeated frequently, this pain relief may be critical to facilitate participation in toning exercise for stabilization of the joints. Modalities must be tailored to the individual; a partial list includes heat, cold, massage, ultrasound, electrical stimulation, acupuncture, acupressure, biofeedback, and conscious relaxation.
• Low resistance muscle toning exercise can improve joint stability and reduce future subluxations, dislocations, and pain.
…Improved joint stability may be achieved by low-resistance exercise to increase muscle tone (subconscious resting muscle contraction, as opposed to voluntarily recruited muscle strength). Examples include walking, bicycling, low-impact aerobics, swimming or water exercise, and simple range-of-motion exercise without added resistance. Progress should be made by increasing repetitions, frequency, or duration, not resistance. It may take months or years for significant progress to be recognized.
Ehlers-Danlos Syndrome, Hypermobility Type [Levy] at http://www.ncbi.nlm.nih.gov/books/NBK1279/)
Manual Techniques• Slow non-thrust manipulations
» Sustained stretching
SOU
RCES
& R
ESO
URC
ES
SPRING 2012PAGE 16
» Passive oscillatory movements (neural mobs) » Muscle energy techniques
• Gentle indirect techniques » Myofascial release » Strain and counter-strain » Cranio-sacral therapy
Chronic Fatigue in EDS [Rowe] http://bit.ly/HQDNwk
Physical Therapy Management of the Hypermobile Patient [Olson] http://www.ednf.org/index.php?option=com_content&task=view&id=1330&Itemid=88888988
Achieving Successful Outcomes in Physical Therapy [Zonarich] http://www.ednf.org/images/2010conference/Handouts/Zonarich_3_slides_per_page.pdf
Some of the neurological features associated with this type is; primary muscular hypotonia may occur and may cause delayed motor development, problems with ambulation, and mild motor disturbance. Fatigue and muscle cramps are relatively frequent. Physical therapy can teach certain exercise techniques that can strengthen muscles around joints and may help to prevent or limit damage. Hydrotherapy (taking place in water) may be less damaging to joints.
Is there anything that would help strengthen low muscle tone? http://www.ednf.org/index.php?option=com_content&task=view&id=1556&Itemid=88889064
Water Training and Ehlers-Danlos Syndrome http://www.ednf.org/index.php?option=com_content&task=view&id=1503&Itemid=88889208
Massage for Ehlers-Danlos Syndrome http://www.massage-therapy-benefits.net/ehlers-danlos-syndrome.html
Loose Connections Spring 2008 — “Ask the Doctor,” page 4-5 [McDonnell] about PT and exercise http://bit.ly/w7aHxc
Presently physical therapy management of patients diagnosed with Ehlers-Danlos syndrome focuses upon a compensatory/prevention approach to address the presence of specific signs and symptoms of the condition that vary specifically to each affected individual. Unfortunately, no protocol of physical therapy interventions exists to address the impairments and functional limitations associated with EDS, due largely in part to the varied presentation of the condition for each affected individual. Therefore, each physical therapy plan of care must be specially created for the patient depending upon the subtype of EDS and the signs and symptoms of that patient. In general, physical therapy intervention focuses on increasing joint stability through a low resistance, high repetition resistance training program, preventing excessive loading through weightbearing joints, avoiding excessive use of involved joints for heavy lifting, adaptive equipment to accomplish ADLs without accentuation of symptoms, and pain relief/pain management.
Resistance training• Low resistance, high repetition activities • Goal is to improve static and dynamic muscle tone to promote increased joint stability during
weightbearing and functional activities• Avoidance of recurrent joint subluxations/dislocations due to increased muscle tone to counteract
presence of excessive joint, ligament, tendon, and muscle laxityAerobic training
• Walking• Bicycling• Low-impact aerobics and/or water aerobics• Swimming• ROM exercises• Goal is to promote increased static and dynamic muscle tone to prevent acute joint subluxations/
dislocations by minor trauma or stimulus• May function as pain relief mechanism for individuals experiencing chronic joint and muscle pain
associated with EDSMyofascial release techniques
SPRING 2012PAGE 17
• Pain relief (immediate - several hours) • Allows pain free participation in resistance training or daily activities• Goal is to reduce the presence of muscle spasms that result in intense pain in muscles and surrounding
ligaments, tendon, and jointsModalities
• Hot/cold pack• Massage• Ultrasound• Electrical stimulation• Acupunture• Acupressure• Goal is to provide pain relief to the patient, who may/may not be experiencing chronic muscle
and joint pain from frequent joint subluxations/dislocations, myofascial spasms, and trigger points associated with EDS
• Selection of proper modality is dependent upon patient preferenceAdaptive Equipment
• Wheelchair/scooter• Walker/Crutches/Cane (should be used with caution and discretion due to increased weightbearing
through upper extremities with use)• Modified eating utensils (prevents excessive strain placed on small joints of hands and fingers)• Modified writing utensils (prevents excessive strain placed on small joints of hands and fingers)• Modified sleeping surface (air mattress, viscoelastic foam mattress, pillow mattress)• Goal is to allow daily functioning and promote increased quality of life by decreasing pain or chance
of joint subluxation/dislocationDespite diagnostic differences between Hypermobility Syndrome and genetic disorders (characterized by
generalized joint hypermobility), such as Ehlers-Danlos Syndrome, similar treatment approaches and interventions remain relevant and appropriate between the two diagnostic categories. Russek advocates the use of education and exercise as potential interventions for Hypermobility Syndrome. Education on ergonomics and body mechanics may result in decreases in musculoskeletal pain as well as assist in joint protection strategies. Splints, braces, and taping may also function as viable options to protect vulnerable joints. Russek suggests that therapeutic exercises, such as strengthening, proprioceptive activities, balance, and coordination to affected and surrounding joints as a means for treatment of Hypermobility Syndrome.
Physical Therapy Management (current best evidence) http://www.physio-pedia.com/index.php?title=Ehlers-Danlos_Syndrome:
Pain treatment and management
There are many solid reasons to treat and reduce pain, not least of which is simple quality of life: if someone is in pain constantly, how long before it becomes unbearable? There are known effects on cardiovascular and respiratory systems that can be more serious in someone with EDS, who might have inherent problems in these areas to which the effects of pain are added:
• adrenergic stimulation (sympathetic nervous system);• hypercoagulation, leading to blood clots;• increased heart rate;• increased cardiac output;• increased myocardial oxygen consumption;• reduced pulmonary vital capacity;• reduced alveolar ventilation;
SPRING 2012PAGE 18
• reduced functional residual capacity;• arterial hypoxemia;• suppression of immune functions, predisposing patients to wound infections
and sepsis.
There are a multitude of approaches to treating pain in EDS. As addressed in Dr. Francomano’s Comprehensive Pain Management in Ehlers-Danlos Syndrome (http://www.ednf.org/images/2010conference/Handouts/Francomano_ppt_2_slides_per_page.pdf), the approaches are generally:
• reduce muscle spasm;• myofascial trigger point release;• integrative medicine approaches;• pharmacologic therapy;• surgical approaches.
Realize that pain-free is not possible for almost anyone, whether or not they have EDS. But it is possible to reach lower levels that allow someone with EDS to enjoy life. Try each as needed, and keep what works. Each technique that works is a step closer to pain-free.
The best thing is to find a multi-modal pain doctor, one who uses all the available tools including pharmaceutical to help you. These are outlined in EDNF’s Pain Management Medical Resource Guide available from http://www.ednf.org/index.php?option=com_content&task=view&id=2123&Itemid=88889247; the Multi-Modal Pain Management chart is reprinted at the end of the article (page 26).
There are TENS units. There is massage, specifically myofascial release. Without well-built collagen to minimize the effects of movement, the fascia (and muscle, and anything attached to each joint that hyperextends) can stretch too far and suffer innumerable micro-tears, part of the chronic acute pain that keeps happening over and over. Releasing the tension held in the fascia can allow joints to realign into their natural position. Trigger points are particularly a problem in EDS, like they are in fibromyalgia, and anything that can break up the trigger points to get blood and oxygen flowing through them will help your muscular pain and fatigue. It is possible to get trigger point injections, which may or may not be helpful depending on your own resistance to anesthetic; dry needling can be helpful, too, but not to everyone. Acupuncture helps many.
Gentle chiropractic might work, using activators rather than manipulation. Chiropractic manipulation can be dangerous to hypermobile people; neck manipulation is completely out-of-bounds according to the World Health Organization (World Health Organization, 2005, Guidelines on basic training and safety in chiropractic, Geneva), and should certainly be avoided for joints that are dislocated or prone to subluxation.
SPRING 2012PAGE 19
There is little evidence that spinal manipulation is an effective treatment for headaches, according to the authors of a new study. … The authors are concerned about the potential complications associated with spinal manipulation. A 1996 RAND study found that the rate of severe complications—including strokes—was just three for every two million neck manipulations. However, in another study Dr. Ernst found more than 700 unreported severe complications, suggesting that the rate is potentially much higher. …given the lack of quality evidence supporting spinal manipulation for headaches due to neck strain, “patients should be advised to use other therapies,” Dr. Ernst said.
Can Spinal Manipulation Help People With Headaches? http://www.ednf.org/index.php?option=com_content&task=view&id=2113&Itemid=88889064
Spinal Manipulations for Cervicogenic Headaches: A Systematic Review of Randomized Clinical Trials http://onlinelibrary.wiley.com/doi/10.1111/j.1526-4610.2011.01932.x/abstract
Chiropractic manipulation of the neck carries the risk of tearing the vertebral artery that leads to the brain, thereby causing stroke or transient ischemic attack. Although the risk is low, it does happen, and physicians and patients should be aware of spinal manipulation therapy as a rare but potential risk factor for stroke. …
A 2003 study in the American Academy of Neurology's journal Neurology confirmed the connection between cervical manipulation and stroke. Wade S. Smith, M.D., Ph.D., director of the Neurovascular Service at the University of California at San Francisco and an AAN member, found that patients under age 60 who had strokes from tears in the vertebral artery were six times more likely to have had spinal manipulative therapy in the 30 days prior to their stroke than patients who had strokes from other causes … patients and physicians need to realize that a significant increase in neck pain or neurologic symptoms within 30 days following spinal manipulative therapy warrants immediate medical evaluation. Dr. Smith recommends that …chiropractic practitioners performing spinal manipulative therapy should warn patients of the risk of tearing the vertebral artery. “I encourage patients to discuss with their chiropractor the types of spinal manipulations that are practiced and whether they pose a risk of stroke,” Dr. Smith says.
Hidden Hercules: Actor Kevin Sorbo reveals his secret battle with stroke [Childers] http://journals.lww.com/neurologynow/Fulltext/2011/07050/Hidden_Hercules__Actor_Kevin_Sorbo_reveals_his.15.aspx
Distraction works: find enjoyable activities and focus on them. Meditation is helpful; I personally find Zen and other Buddhist practices particularly effective.
There are also binaural apps and programs that use sound waves to synchronize your brain into particular states similar to meditation; they can induce relaxation, help with pain relief and sleep. One I find successful is Brainwave, which allows you to combine binaural beats with environmental sounds in a wide range of tailored programs (http://itunes.apple.com/us/app/brain-wave-25-advanced-binaural/id307219387?mt=8); there are others. Brain machines add lights to sound and can help change your brain waves more dramatically and faster than the sound programs alone — some can be found at http://www.iproducts.ws/mind-machines.htm and http://www.mindplace.com/Light-and-Sound.
There are biofeedback and hypnosis techniques that also produce similar results.
My doctor suggested psychological counseling because he felt EDS would not be an easy disorder to manage, which proved very helpful to me as a way of discovering it was not all in my head and there were ways of handling my own reactions and my life that made EDS easier to endure.
SOU
RCES
& R
ESO
URC
ES
SPRING 2012PAGE 20
There are the usual pharmacologic approaches to pain, codified in the WHO escalating therapy for chronic non-cancer pain, starting with non-steroidal anti-inflammatory drugs, then adjuvants and integrative approaches, topical therapies, and tramadol or other opioid angonists. For much more information about these established treatments, see Dr. Howard Levy’s A Primer on Pain Medications (http://bit.ly/HQDNwk). These drugs work variably in EDS. Some of us have reactions to NSAIDs that range from ineffectiveness to bleeding. Local anesthetics can produce unexpected results; normal doses may not work, but once an effective dose is reached, the results may last longer than usual.
• Anesthetic/corticosteroid injections for localized areas of pain and inflammation are often helpful, but cannot be repeated indefinitely; "dry needling" without injection of any material sometimes provides similar benefit.
• Anesthetic nerve blocks can provide temporary relief of neuropathic pain. These are sometimes followed by surgical nerve root destruction and/or implantable stimulators (sensory or motor), with variable results.
Patients suffering from Ehlers-Danlos syndrome type III do not respond to local anaesthetics http://www.ednf.org/index.php?option=com_content&task=view&id=1337&Itemid=88889208
Local anaesthetic failure in joint hypermobility syndrome [p. 84, Hakim, Grahame et al.] http://www.ednf.org/images/stories/pdfs_medical/Local_anaesthetic_failure_in_joint_hypermobility_syndrome.pdf (second page)
There have been studies showing that subcutaneous infiltration of lidocaine has a reduced time of action and that transcutaneous application of a eutectic mixture of lidocaine 2.5% and prilocaine 2.5% (EMLA, AstraZeneca, Södertälje, Sweden) did not produce sufficient analgesia.
Effective plexus anaesthesia in a patient with Ehlers-Danlos syndrome type III http://www.ednf.org/images /stories/pdfs_medical/2009 _09/2009_Wegener_EJAnaeth. pdf
Ehlers-Danlos Syndrome: Complications and Solutions Concerning Anesthetic Management [Johnston et al.] http://www.ednf.org/images/stories/pdfs_medical/EHLERS-DANLOS_SYNDROME_COMPLICATIONS_AND_
SOLUTIONS_CONCERNING_ANESTHETIC_MANAGEMENT.pdf
“Do local/dental anesthetics fail for you…patients with EDS are resistant to lidocaine... http://www.mdjunction.com/forums/ehlers-danlos-syndrome-discussions/general-support/2299144-do-localdental-anesthetics-fail-for-you
Opioids can also have surprising results in EDS patients; what works may be different with each EDS patient, and effective doses may vary as widely in EDS as pain does. When dealing with opioids, it may become important to remember a few distinctions.
Tolerance is not addiction. Tolerance is: “The capacity to endure continued subjection to something, esp. a drug; diminution in the body’s response to a drug after continued use” (New Oxford American Dictionary 2007).
Physical dependence is not addiction. Physical dependence is: “A state of adaptation that often includes tolerance and is manifested by a drug class specific withdrawal syndrome that can be produced by abrupt cessation…. Physical dependence on and tolerance to prescribed drugs do not constitute sufficient evidence of psychoactive substance use disorder or addiction. They are normal responses that often occur with the persistent use of certain medications” (Definitions related to the medical use of opioids: Evolution towards universal agreement [Savage et al.] I, 2003, 26:655-67).
SOU
RCES
& R
ESO
URC
ES

SPRING 2012PAGE 21
Addiction is: “When a person has lost control over and continues use even when such use is doing them or others harm. (New Oxford American Dictionary 2007).
The choice in EDS may be as simple as dependence on drugs or dependence on pain.
Pharmacologically, there are alternatives in Lyrica (pregabalin, http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0000327/) and Cymbalta (duloxetine, http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0000274/), both approved by the FDA for musculoskeletal pain, and used successfully by some of us. Lyrica is the frontline for fibromyalgia, and is not an anti-depressant; Cymbalta is an anti-depressant, which can be an added benefit in dealing with the perception of pain. Please read up on these (and any drug) before beginning them; they can cause some serious side effects, and knowing what to look for is a major advantage to minimizing them.
Judicious use of muscle relaxers can help, too, like Flexeril (cyclobenzaprine, http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0000699/ — be particularly cautious, overuse can facilitate joint dislocations instead of just aiding in muscle spasm relief) — or Zanaflex (tizanidine, http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0000106/).
Ensure your vitamin D levels are good by having the blood test done fairly regularly; low vitamin D can make our pain worse, and restoring it to a strong, healthy level may reduce pain. Read more about vitamin D in the Winter 2010 issue of Loose Connections, which you can get free from the archives http://bit.ly/w7aHxc.
American diets are largely deficient in magnesium (http://ods.od.nih.gov/factsheets/magnesium-HealthProfessional/, which lists the Recommended Daily Allowance). Magnesium can be increased through diet or through Epsom salts, which are the best approaches because it is difficult to get too much magnesium in those ways. Usually the kidneys take care of any excess, but if you take supplements for magnesium, it is possible to take too much and get into toxic levels. Magnesium is the fourth most abundant mineral in the human body; a deficiency can result from low blood levels of calcium, which is why the two are frequently recommended together, and malabsorption, which seems to be a fairly common EDS problem (http://www.nlm.nih.gov/medlineplus/ency/article/002423.htm). Magnesium deficiency is implicated in a lot of problems: fatigue, insomnia, muscle spasms, poor memory, and heart/cardiovascular problems including rapid heartbeat. The mineral is particularly recommended with EDS for muscle pain: people who do Epsom salts baths reported their rheumatic pain disappeared. Baths are good for us because magnesium absorbs easily through the skin, and gets directly into the blood and muscles. The hot baths feel good, too. Maximum benefit seems to be two or three times a week with 500-600g Epsom salts each time (http://george-eby-research.com/html/absorption_of_magnesium_sulfate.pdf).
There are other food sources of relief, particularly white tea, rose, and witch hazel (Antioxidant and potential anti-inflammatory activity of extracts and formulations of white tea,

SPRING 2012PAGE 22
rose, and witch hazel on primary human dermal fibroblast cells [Thring et al.] http://www.journal-inflammation.com/content/8/1/27.)
Nerve blocks are another possibility. “Temporary nerve blocks are achieved by combining a local anesthetic (such as lidocaine) with epinephrine, a steroid (corticosteroid), and/or opioids. Epinephrine produces constriction of the blood vessels which delays the diffusion of the anesthetic. Steroids can help to reduce inflammation. Opioids are painkillers. Injection nerve blocks can be either single treatments, multiple injections over a period of time, or continuous infusions. A continuous peripheral nerve block can be introduced into a limb undergoing surgery, for example, a femoral nerve block to prevent pain in knee replacement. Permanent nerve block can be effected using other drugs or methods including alcohol or phenol to selectively destroy nerve tissue, cryoanalgesia to freeze nerves, and radio frequency ablation to destroy nerve tissue using heat. Nerve blocks are sterile procedures that are usually performed in an outpatient facility or hospital. The procedure can be performed with the help of ultrasound, fluoroscopy (a live X-ray) or CT. Use of any one of these imaging modalities enables the physician to view the placement of the needle. A probe positioning system can be used to hold the ultrasound transducer steady. In addition, electrical stimulation can provide feedback on the proximity of the needle to the target nerve.” (http://en.wikipedia.org/wiki/Nerve_block)
As a last resort, nerve endings can be severed surgically (http://seniorhealth.about.com/library/conditions/blchronicpain7.htm).
A new area that might prove helpful is low-level laser therapy (LLLT), a medical treatment using low-level lasers or light-emitting diodes to reportedly affect cellular function. “LLLT is controversial in mainstream medicine with ongoing research to determine the ideal location of treatment (specifically whether LLLT is more appropriately used over nerves versus joints), dose, wavelength, timing, pulsing and duration. The effects of LLLT appear to be limited to a specified set of wavelengths of laser, and administering LLLT below the dose range does not appear to be effective. Despite a lack of consensus over its ideal use, specific test and protocols for LLLT suggest it is effective in relieving short-term pain for rheumatoid arthritis, osteoarthritis, acute and chronic neck pain, tendinopathy, and possibly chronic joint disorders. The evidence for LLLT being useful in the treatment of low back pain, dentistry and wound healing is equivocal.” (http://en.wikipedia.org/wiki/Low_level_laser_therapy, also Efficacy of low-level laser therapy in the management of neck pain: a systematic review and meta-analysis of randomised placebo or active-treatment controlled trials http://www.ncbi.nlm.nih.gov/pubmed/19913903 and A systematic review of low level laser therapy with location-specific doses for pain from chronic joint disorders http://www.ncbi.nlm.nih.gov/pubmed/12775206).
Do not ignore the role of sleep; good sleep should be restorative and help reduce pain levels, but in EDS, that frequently is not what happens. Read Sleep Disorders in the Hypermobility Syndromes [Pocinki] available from http://bit.ly/HQDNwk.
SPRING 2012PAGE 23
A particularly useful resource in general is The Intractable Pain Patient’s Handbook for Survival [Tennant] (http://pain-topics.org/pdf/IntractablePainSurvival.pdf).
It still surprises me to hear of doctors claiming EDS has no associated pain. In fact, chronic pain is a minor diagnostic criterion for EDS Hypermobile Type. How could the effects of hypermobility not be painful? EDS is a collagen disorder, not a nervous system disorder; it does not have some neurological effect that negates pain.
Pain treatment may be the single most important assistance that can be offered to someone living with EDS, and no one technique will work. But each one that works adds to the total reduction in pain. If one can find small reductions here and there, the combined effect can be significant reduction in overall pain levels. A life of out-of-control pain that seemed daunting and insufferable can become one filled with joy and accomplishment. It simply takes someone willing to listen and help.
Mark C. MartinoEditor-in-Chief
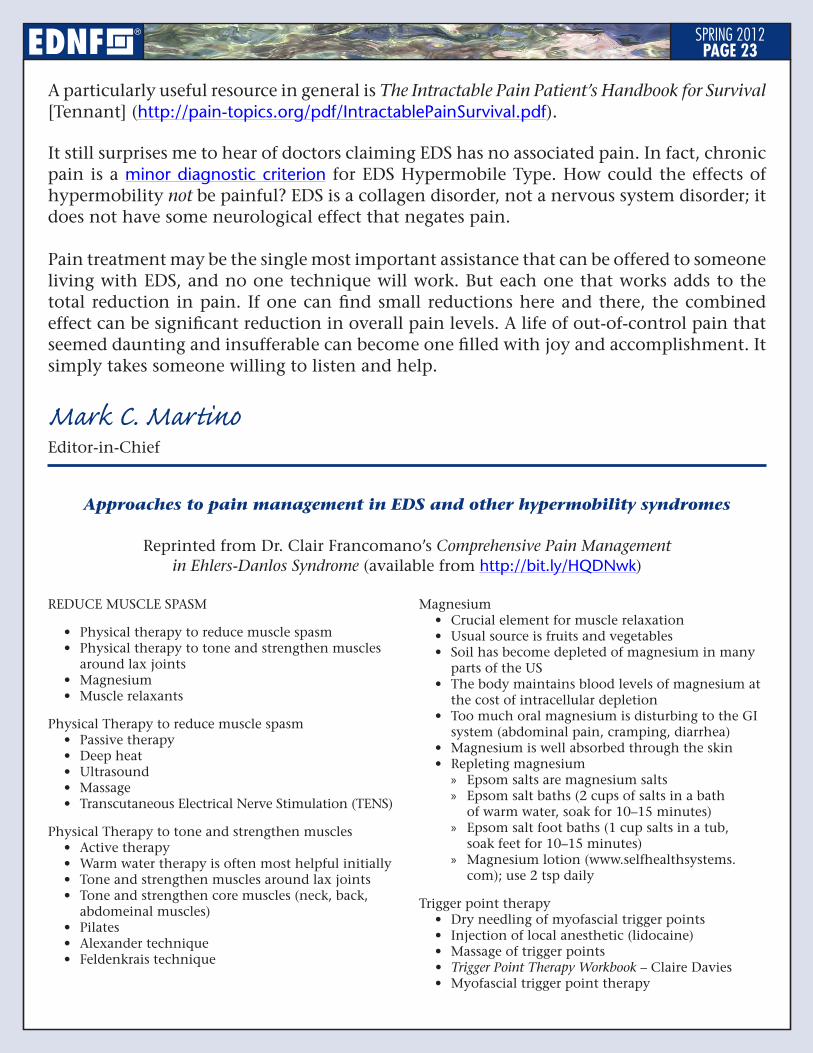
Approaches to pain management in EDS and other hypermobility syndromes
Reprinted from Dr. Clair Francomano’s Comprehensive Pain Management in Ehlers-Danlos Syndrome (available from http://bit.ly/HQDNwk)
REDUCE MUSCLE SPASM
• Physical therapy to reduce muscle spasm• Physical therapy to tone and strengthen muscles
around lax joints• Magnesium • Muscle relaxants
Physical Therapy to reduce muscle spasm• Passive therapy• Deep heat• Ultrasound• Massage• Transcutaneous Electrical Nerve Stimulation (TENS)
Physical Therapy to tone and strengthen muscles• Active therapy• Warm water therapy is often most helpful initially• Tone and strengthen muscles around lax joints• Tone and strengthen core muscles (neck, back,
abdomeinal muscles) • Pilates• Alexander technique• Feldenkrais technique
Magnesium• Crucial element for muscle relaxation• Usual source is fruits and vegetables• Soil has become depleted of magnesium in many
parts of the US• The body maintains blood levels of magnesium at
the cost of intracellular depletion• Too much oral magnesium is disturbing to the GI
system (abdominal pain, cramping, diarrhea)• Magnesium is well absorbed through the skin• Repleting magnesium
» Epsom salts are magnesium salts » Epsom salt baths (2 cups of salts in a bath
of warm water, soak for 10–15 minutes) » Epsom salt foot baths (1 cup salts in a tub,
soak feet for 10–15 minutes) » Magnesium lotion (www.selfhealthsystems.
com); use 2 tsp daily
Trigger point therapy• Dry needling of myofascial trigger points• Injection of local anesthetic (lidocaine)• Massage of trigger points• Trigger Point Therapy Workbook – Claire Davies• Myofascial trigger point therapy
SPRING 2012PAGE 24
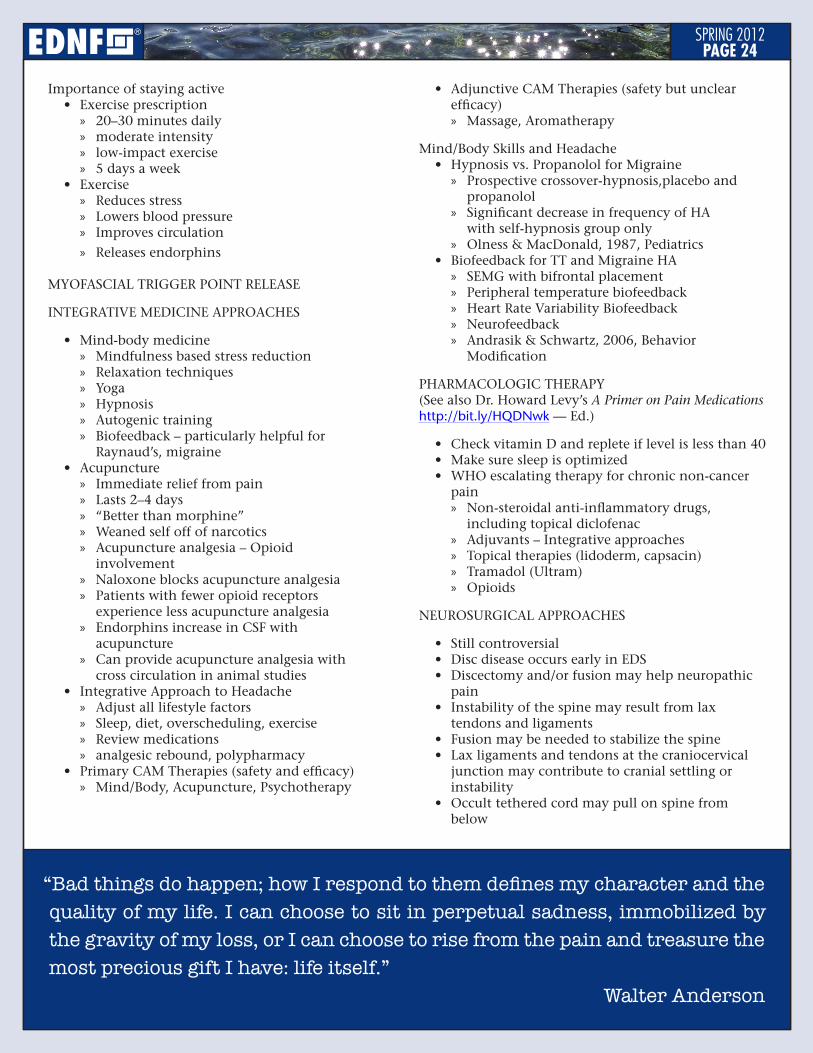
Importance of staying active• Exercise prescription
» 20–30 minutes daily » moderate intensity » low-impact exercise » 5 days a week
• Exercise » Reduces stress » Lowers blood pressure » Improves circulation
» Releases endorphins
MYOFASCIAL TRIGGER POINT RELEASE
INTEGRATIVE MEDICINE APPROACHES
• Mind-body medicine » Mindfulness based stress reduction » Relaxation techniques » Yoga » Hypnosis » Autogenic training » Biofeedback – particularly helpful for
Raynaud’s, migraine• Acupuncture
» Immediate relief from pain » Lasts 2–4 days » “Better than morphine” » Weaned self off of narcotics » Acupuncture analgesia – Opioid
involvement » Naloxone blocks acupuncture analgesia » Patients with fewer opioid receptors
experience less acupuncture analgesia » Endorphins increase in CSF with
acupuncture » Can provide acupuncture analgesia with
cross circulation in animal studies• Integrative Approach to Headache
» Adjust all lifestyle factors » Sleep, diet, overscheduling, exercise » Review medications » analgesic rebound, polypharmacy
• Primary CAM Therapies (safety and efficacy) » Mind/Body, Acupuncture, Psychotherapy
• Adjunctive CAM Therapies (safety but unclear efficacy) » Massage, Aromatherapy
Mind/Body Skills and Headache• Hypnosis vs. Propanolol for Migraine
» Prospective crossover-hypnosis,placebo and propanolol
» Significant decrease in frequency of HA with self-hypnosis group only
» Olness & MacDonald, 1987, Pediatrics• Biofeedback for TT and Migraine HA
» SEMG with bifrontal placement » Peripheral temperature biofeedback » Heart Rate Variability Biofeedback » Neurofeedback » Andrasik & Schwartz, 2006, Behavior
Modification
PHARMACOLOGIC THERAPY (See also Dr. Howard Levy’s A Primer on Pain Medications http://bit.ly/HQDNwk — Ed.)
• Check vitamin D and replete if level is less than 40• Make sure sleep is optimized• WHO escalating therapy for chronic non-cancer
pain » Non-steroidal anti-inflammatory drugs,
including topical diclofenac » Adjuvants – Integrative approaches » Topical therapies (lidoderm, capsacin) » Tramadol (Ultram) » Opioids
NEUROSURGICAL APPROACHES
• Still controversial• Disc disease occurs early in EDS• Discectomy and/or fusion may help neuropathic
pain• Instability of the spine may result from lax
tendons and ligaments• Fusion may be needed to stabilize the spine• Lax ligaments and tendons at the craniocervical
junction may contribute to cranial settling or instability
• Occult tethered cord may pull on spine from below
“Bad things do happen; how I respond to them defines my character and the quality of my life. I can choose to sit in perpetual sadness, immobilized by the gravity of my loss, or I can choose to rise from the pain and treasure the most precious gift I have: life itself.”
Walter Anderson

SPRING 2012PAGE 25
CHRONIC PAIN(constant & disturbing pain)
INFREQUENT PAIN EVENTS(less than four days per week)
ANALGESICS
PSYCHOLOGICAL THERAPY
PSYCHIATRIC THERAPY
SLEEP THERAPY
COMPLEMENTARY/ALTERNATIVE
MANAGE ACUTE EVENTSTreat acute events quickly and aggressively to defend against
central neuronal plasticity (“learned” chronic pain)
PHYSICAL THERAPY
CO
NT
RIB
UT
ING
PR
OB
LEM
S
NEUROPATHIC PAINCommon in EDS, also called neuralgia (different from usual
nociceptive pain); described as numbness, tingling, burning, electrical, hot/cold
Incl. disease/dysfunction of peripheral nerves (numbness, weakness), nerve injury, axonal loss
Antidepressants (TCAs/SNRIs)Antiseizure medicationsTopicals (capsaicin)
NON-PAIN PATHOPHYSIOLOGYAdditional genetic factors/disabilitiesSide effects from treatments, incl. overuse
or ineffectiveness of analgesics or short-acting opioids
LONG-ACTING OPIOIDS (methadone, morphine, oxycodone, fentanyl; oral/transdermal/pump)
Tolerance for pain-killing builds up readily, but not to side effects incl. GI dysmotility & reduced consciousness
PREVENT RECURRING INJURYHypermobile joints and fragile connective tissues endure chronic
acute injuryBracing may be helpful (maintain toning exercise)Orthopedic surgery should be avoided
Almost never provides long-term improvementAdded risk of soft tissue fragility and poor wound healing, esp.
Classical & Vascular EDS OCCUPATIONAL THERAPY
Delay disability and encourage activity as long as possibleBody mechanics/ergonomicsIntervention in workplace and work simplificationPacing skills
Use combinations of medicines on a schedule to keep pain under control
SURGICAL PAIN INTERVENTIONInjection (trigger point, nerve root)Implantable nerve stimulatorsMedication pumps (subarachnoid cavity)
Short-acting opioidsMuscle relaxants
if needed
May be ineffective as single agents or require excessive doses
ANALGESICS FOR CHRONIC PAIN
Short-acting opioids (breakthrough pain)Long-acting opioids (baseline pain; see at bottom)
if needed
RelaxationStress management
(incl. Mindfullness-Based Stress Reduction)Group therapyCognitive restructuring (incl. hypnosis)
Medication for mood/painIndividual counseling
Sleep disturbance is common in EDS (contributes to poor pain recovery; incl. apnea)
Tricyclic antidepressants (TCAs)
MeditationAcupunctureMassageYoga
ReconditioningExercise (gradual toning for stability, not strength1)Flare-up management by:
Distraction techniquesTrigger-point/myofascial therapyHeat/cold applicationUltrasonic/electrical stimulation
MAINTAIN GENERAL HEALTHAvoid weight extremes & smoking2
Multi-Modal Pain Management for EDS reprinted from Pain Management Medical Resource Guide
http://www.ednf.org/index.php?option=com_content&task=view&id=2123&Itemid=88889247
1The key is slow improvement in muscle tone, not strength. Tone is the degree of muscle contraction at rest; strength is voluntary force that can be invoked at will. Build tone with non-resistance exercise that gradually increases repetitions. Avoid hyperextension, resistance and impact. Elastic bands may make things worse because they combine increased resistance with joint hyperextension. Toning is a life-long strategy; if exercises are stopped, pain usually recurs. (Howard Levy, MD, PhD)
2Quit smoking (pain, depression and addiction are all modulated by the same nicotinic and muscarinic receptors). Maintain normal weight; obesity or thinness seem to present problems. (Mark Lavallee, MD, CSCS, FACSM)

SPRING 2012PAGE 26
The Forever Fix: Gene Therapy and the Boy Who Saved ItRicki LewisSt. Martin’s Press, 2012ISBN 978-0-312-68190-6, $25.99
WHAT person saddled with a genetic disorder wouldn’t be interested in an
optimistic book about gene therapy written for a lay audience? Gene therapy was officially begun with great fanfare in 1990 when two girls with ADA deficiency, a metabolic disorder that compromises immune function, were infused by Dr. French Anderson with their own T cells that had been removed from their blood and bone marrow and genetically corrected. In the months that followed the girls showed improved immunity, and it appeared that the treated cells in their bloodstreams were outliving the ADA-deficient ones. The therapy was considered a success, gene therapy research was racing ahead, and in the excitement Dr. Anderson “envisioned one day injecting gene-loaded vectors as easily as a person with diabetes injects insulin.”
Less than a decade later, however, the gene therapy train would be derailed by tragedy. European researchers at first appeared to have succeeded in curing children with SCID-X1, another immunodeficiency, with a similar ex vivo approach, this time using a retrovirus to carry the gene into T cells. But over the next two years five of the twenty boys treated developed leukemia. This came right on the heels of the best-known gene-therapy debacle, the death in Philadelphia in 1999 of 18-year-old Jesse Gelsinger four days after receiving an infusion into his liver of an ounce of viral vector carrying a gene to correct his OTC deficiency, another inborn error of metabolism. Following
BOOK REVIEW THE FOREVER FIX: GENE THERAPY & THE BOY WHO SAVED IT
Gelsinger’s death the FDA ordered a “clinical hold” on gene therapy trials until the protection of human subjects could be improved.
Dr. Lewis, a geneticist and genetic counselor as well as a journalist, chooses to focus on the successful treatment of an eight-year-old boy named Corey Haas. From Gelsinger’s death in 1999 to Corey’s treatment in 2008, gene therapy had dropped out of the public eye, though steady progress was being made in animal research. Corey’s case presented exactly the right opportunity to make an inspiring human-interest story of gene therapy again. It was a slam dunk for a number of important reasons.
Corey Haas was born with a form of Leber congential amaurosis type 2 (LCA2), a genetic defect that prevented his eyes from making a protein called RPE65, which activates vitamin A. Although it took some time and the work of highly specialized researchers and physicians to make his precise diagnosis — and Dr. Lewis tells this story well — Corey was lucky to have a disorder that was known and that followed the standard dogma of gene therapy: a gene (DNA) is copied into messenger RNA (mRNA), which then directs the synthesis of a specific protein essential to some bodily function. If the gene is defective, the protein is missing. In Corey’s case, as with most of the cases in this book, the missing protein was an enzyme, a catalyst to an essential chemical reaction in his cells.
Furthermore, Corey’s errant gene was active only in the eyes; other than his impending blindness, Corey’s health was unaffected. Neither did he look funny, which was more important than you might think, since it allowed him to become a media darling. Lewis tells a wrenching story about two baby girls

SPRING 2012PAGE 27
who received gene therapy for Canavan’s disease, a neurodegenerative disorder that quickly reduces children to a vegetative state. The TV news program 60 Minutes broadcast an uplifting segment at the time of their therapy. A few years later, it seemed the girls were doing comparatively well, and their parents considered the therapy to be a qualified success, but the girls were still severely disabled. 60 Minutes shot additional footage for a follow-up story but in the end decided not to run it because it was visually too depressing.
Another thing Corey had going for him was that there was no other treatment for his condition. All gene therapy trials in humans must be approved by an Institutional Review Board as well as various government agencies. If there is another way to treat the disorder in question — even if the treatment is expensive or difficult to administer — such entities are loath to approve a gene therapy trial, because the other treatment would have to be withheld to make the trial scientifically valid. Lewis does describe some cases where gene therapy was done concomitant with conventional therapy, but they are of minor importance to the field because the conventional therapy was a confounding factor.
Perhaps most importantly for Corey, the eye is the easiest organ to treat with gene therapy. This is because it is a closed system. The central scientific challenge in gene therapy is finding a safe way to deliver the corrected gene or gene product to the affected tissues. Usually a virus is used as a vector, or delivery vehicle, but first it must be stripped of its disease-causing potential. It took a great deal of trial and error for scientists to figure out how to do this. One of those errors was the European SCID-X1 trial, where it appears the adenovirus that was used as a vector zeroed in on a cancer-causing gene. Dr. Lewis tells of another error, in which a rheumatoid arthritis patient was given gene therapy designed to suppress her overactive
inflammatory response, and it killed her by fanning the flame of a latent fungal infection. Such unintended consequences are much less likely to occur within the confines of the eye.
The Holy Grail of gene therapy is gene transfer, where the patient’s cells take the corrected genes that are delivered to them by the vector and incorporate them into their chromosomes so that they can go on to produce the needed protein indefinitely. When it works, the therapy should have to be done only once. This is what happened with Corey. Four days after his therapy he became uncomfortable in bright sunlight, when previously his eyes could never get enough light. From there his vision improved dramatically, and as of the writing of this book it appears that he is not in danger of losing it. This is the “forever fix” of the book’s title.
Dr. Lewis does a great service in this book in humanizing some very rare disorders. She shows how science is done by following the dedicated researchers and physicians who take an idea from the lab, through animal trials, over regulatory hurdles, to the clinic. She obviously is very taken with the children she comes to know in this process, of which there are many. And she makes it clear that if it weren’t for some very persistent and energetic parents — who raise money and awareness, cultivate researchers, and badger officials — nothing would be done for these kids. But even while she touts Corey as the boy who saved gene therapy, her own account reveals him to be an outlier.
The factors that made Corey’s case so elegant rarely come together. The goal of the forever fix is an elusive one. Because she chooses to tell this story through Corey, Dr. Lewis can’t help but present the other cases in the book as somehow falling short, no matter how cheerily she recounts them. Her natural audience for this book would seem to be those of us with heritable disorders, but where does this leave us?

SPRING 2012PAGE 28
Toward the end of the book, Dr. Lewis briefly makes the case that research on rare disorders can lead to treatments for common disorders, and this is true. But that doesn’t mean that multi-factorial diseases like heart disease, cancer, or diabetes will ever be curable by gene transfer. What it really means is that all this effort directed toward understanding how molecular defects cause illness is yielding important insights into molecular pathways — all the way from the evolution of whole genomes, to the myriad forms of mutation, to the various species of RNA and what they do, to the many epigenetic factors through which environment affects gene function, to the delicate dance between expressive and inhibitory agents in the cell, and so on, and so on. Compared to a forever fix, it seems a muddle; but it is in this muddle that true hope lies for most of us.
Take Ehlers-Danlos syndrome, for example. We understand its pattern of inheritance, but for the most common forms we do not have a definitive molecular test. A gene has been identified for the vascular type, but it can mutate in more than 200 ways. We know that the protein involved is procollagen type III, but the problem is not a straightforward deficiency. The tissues affected are found throughout the body, mainly in the blood vessels and the hollow organs. It is difficult to imagine how this devastating disorder would ever be amenable to gene transfer; but by studying the molecular processes that go awry in Vascular Type EDS (vEDS), researchers are getting close to finding effective treatments. And in some cases they are pointing toward drugs that are affordable and already available.
At last summer’s EDNF conference, Dr. Nazli McDonnell presented some exciting work that is being done on vEDS in her lab and others. A small European study1 published in 2010 showed a reduced incidence of vascular events in vEDS patients taking the beta blocker celiprolol. Though the study had some
important limitations, it suggested that the effect might come from an upregulation of collagen synthesis in the blood vessel walls by increasing expression of transforming growth factor β (TGFβ) [see “Hope for vEDS Treatment?”, Loose Connections, Spring 2011]. Doctors already have several drugs in their arsenal that can dial TGFβ up or down.
Researchers are also studying the therapeutic effects of doxyclycine, an antibiotic, on collagen expression. A group led by Dr. McDonnell and Dr. Mark Talan reported that the administration of doxyclycline prevented the development of stress-induced blood vessel pathology in a mouse model of vEDS.2 These mice were bred to be haploinsufficient for the COL3A1 gene, meaning that they had only one working copy of it (we have two copies of each gene, one from each parent); this is also known as a null mutation. In people, most mutations in the COL3A1 gene are single-nucleotide substitutions, which result in a regular quantity of collagen, but the collagen is abnormal. With a null mutation, the quantity of collagen is reduced, but it is of normal quality. (Incidentally, most of the diseases Dr. Lewis discusses in her book are inherited in a recessive pattern, so a child must receive an abnormal gene from each parent to be affected. Individuals carrying one defective gene would not be ill because they would also have a good copy, which can function on its own. EDS is inherited in a dominant pattern, so it takes only one defective gene to cause a problem; it follows that there must be two healthy copies of the gene present to ensure normal functioning.) Doxyclycine is a known inhibitor of matrix metalloproteinase (MMP), a protease that degrades extracellular matrix proteins; it appears that it strengthened the abdominal aortas in the vEDS mice by reducing the destruction of collagen. The authors of the study suggest that doxycycline therapy be tried in vEDS patients with haploinsufficiency for COL3A1.

SPRING 2012PAGE 29
A group led by Dr. Peter Byers has shown that vEDS patients with a haploinsufficiency experience milder symptoms.3 So what if the more severely affected vEDS patients, those with a substitution mutation (meaning that they inherited a gene that is not a silent dud, but is actively mucking things up), could be converted to the null mutation phenotype? We’d have a halfway-to-forever fix. It appears it can be done. Dr. McDonnell described a study in which she and some colleagues used targeted small-interfering RNAs to silence the dominant-mutant gene by eliminating the mRNA that transcribes it.4 Skin fibroblasts taken from a vEDS patient were treated with a specific siRNA, and afterwards they formed networks of collagen fibrils more regular in shape. The next step is to develop a way of delivering individualized siRNAs to patients. Drugs might be developed with synthetic siRNAs, or if a suitable vector can be found, vEDS might be partially treated with gene therapy. Either way, we’ll take it.
Amy BiancoEditor, Medical Section
Footnotes
1 Ong et al: Effect of celiprolol on prevention of cardiovascular events in vascular Ehlers-Danlos syndrome: a prospective randomised, open, blinded-endpoints trial, Lancet 376:1476–84, 2010.
2 Briest et al: Doxycycline ameliorates the susceptibility to aortic lesions in a mouse model for the vascular type of Ehlers-Danlos syndrome, JPET 337(3):621-627, 2011.
3 Leistritz et al: COL3A1 haploinsufficiency results in a variety of Ehlers-Danlos syndrome type IV with delayed onset of complications and longer life expectancy, Genetics in Medicine 13(8):717-722, 2011.
4 Müller et al: Allele-specific siRNA knockdown as a personalized treatment strategy for vascular Ehlers-Danlos syndrome in human fibroblasts, FASEB J. 26:668–677, 2012.
Our Facebook community has crossed 6,200 friends and is now the largest EDS group in the world, with a weekly reach of over 20,000 people and a potential reach of nearly 1,770,000.
Our EDNF Inspire Online Community has more than 2,000 members.
EDNF is part of the RareConnect Community and is now on Google+.
Ehlers-Danlos Syndrome Awareness Month
May 2012
SPRING 2012PAGE 30
The Magazine About Living With EDSPUBLISHED BY
FOUNDERNancy Hanna Rogowski1957–1995
Executive DirectorShane Robinson
Board of DirectorsElliot H. Clark, ChairJudge Richard P. Goldenhersh, Vice ChairRichie Taffet, BS MPH, SecretarySandra Aiken ChackDeb MakowskiLinda Neumann-Potash, RN, MNRichard Riemenschneider, Director of OutreachJanine SabalBrad Tinkle, MD, PhD
To contact EDNF, email [email protected]; write to Ehlers-Danlos National Foundation, 1760 Old Meadow Road, Suite 500, McLean, Virginia 22102; or call (703) 506-2892.
GUIDELINES FOR SUBMISSIONS TO LOOSE CONNECTIONS
1. For text documents, use Arial, Helvetica or Times of at least 10 points (preferably 12 to 16) in size, so our editors can easily read your document and prepare it for publication. Attach the text document in either Word (.doc) or Rich Text Format (.rtf) to an email sent to [email protected] or [email protected] that also tells us how to reach you for more information.
2. For photographs, attach them to an email to [email protected] or [email protected]; please identify the event or cause for the photographs, including any relevant identification (persons involved, date, photographer’s name if needed) and how to reach you for more information.
3. Text articles, photographs, or any other submissions to Loose Connections are accepted only on condition that publication of that material is not under copyright or other restrictions on its publication. Ehlers-Danlos National Foundation reserves all and final editorial privileges, including the right to choose not to print a submitted story; submissions may be edited at the discretion of the editorial staff.
Copyright 2012 Ehlers-Danlos National Foundation. The opinions expressed in Loose Connections are those of the contributors, authors, or advertisers, and do not necessarily reflect the views of Ehlers-Danlos National Foundation, Inc., the editorial staff, Professional Advisory Network, or the Board of Directors. EDNF does not endorse any products.
Professional Advisory NetworkPatrick Agnew, DPMPeter Byers, MDEdith Cheng, MDHeidi Collins, MDJoseph Coselli, MD, FACCJoseph Ernest III, MDClair Francomano, MDTamison Jewett, MDMark Lavallee, MDHoward Levy, MD, PhDNazli McDonnell, MD, PhDDianna Milewicz, MD, PhDAnna Mitchell, MD, PhDJohn Mitakides, DDS, FAACPRaman Mitra, MD, PhDLinda Neumann-Potash, RN, MNTerry Olson, PTMary F. Otterson, MD, MSMelanie Pepin, MS, CSGAlan Pocinki, MD, FACPElizabeth Russell, MDUlrike Schwarze, MDKaren Sparrow, PhDBrad Tinkle, MD, PhDMike Yergler, MD
L O O S E CONNECTIONS
SPRING 2012PAGE 31
Editor/Graphics & TypeMark C. Martino
Editor, Medical SectionAmy Bianco
Copy EditorElise Makhoul
Front Cover & Page 2 Public Domain
Page HeadersCopyright © Mayang Murni Adnin, 2001-2010
BelowCopyright © 2012 Senga2




























