-
ABC ofRheumatology
LOW BACK PAIN
J R Jenner, M Barry
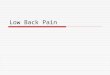
Radiation of pain after injection of 0.1-0.3 ml 6%hypertronic
saline into sacrospinal muscle (yellow)and multifidus muscle (red).
Note similarity todistribution of sciatic pain.
Low back pain is a major and increasing cause of disability in
theUnited Kingdom. In 1993, 1 1% of the population reported that
theiractivities had been restricted by back pain within the past
four weeks.Satisfactory treatment of low back pain depends on an
accuratediagnosis, but finding the cause for low back pain is often
not possiblebecause of difficulties in localising the source of the
pain.
In 1938 it was shown that many structures in the lumbar
spine,when irritated, give rise to pain with very similar
distributions. Despitetechnological advances the identification of
an exact source of pain oran exact pathological diagnosis often
remains elusive. It is importantfor doctors and patients to
understand that the diagnosis of low backpain therefore depends on
identifying some clinical syndromes on thebasis of a patient's
history and examination, with appropriateinvestigations to exclude
serious pathology and support the clinicaldiagnosis. If this
principle is misunderstood the result can be amisleading diagnosis
and inappropriate treatment.
Back pain syndromes
Clinical feature of back pain due to mechanicalcauseHistory
ofpain ExaminationSudden onset Asymmetrical lumbar
movementsPrevious recurrent episodes Asymmetrical straight leg
raise orUnilateral symptoms Femoral stretch testEased by rest
Uniradicular neurological signs
Functional distribution of lumbar nerve rootsNerve root Muscle
weakness Reflex changes SensationL2 Hip flexion Front of thigh
Hip adductionL3 Knee extension Knee Inner kneeL4 Knee extension
Knee Inner shin
Foot dorsiflexionL5 Foot inversion Outer shin
Great toe dorsiflexion Dorsum of footKnee flexion
Si Foot plantar flexion Ankle Lateral border ofKnee flexion foot
and sole
Mechanical back pain or prolapsed lumbar discIt is vital to
distinguish mechanical causes
of back pain from other causes as patientswith mechanical causes
are likely to respondto physical forms of treatment. The
symptomsand signs of mechanical back pain differconsiderably from
those associated with backpain caused by underlying systemic
disease.Most acute episodes of low back pain arise
in the triad of joints that allow one vertebra toarticulate with
another (that is, theintervertebral disc anteriorly and the two
facetjoints posteriorly). The commonest primarypathology is
degeneration of the nucleuspulposus in the lumbar disc. The disc
itself isoften not the source of pain; this may arise inother
structures, such as the facet joints or themany surrounding
ligaments, that come understress as a result of the disc pathology.
It isimportant that doctors explain this to patientsso that they
understand why just removingtheir disc will not always cure the
pain.True sciatica, with pain and numbness in
the distribution of a single lumbar nerve root,may be
accompanied by sensory, motor, orreflex changes and is most
commonly causedby a posterolateral protrusion of a discimpinging on
the nerve root.
BMJ VOLUME 310 8 APRIL 1995 929
-
Clinical feature of back pain due to systemic causeHistory
ofpainGradual onset and progressiveSymmetrical or alternating
distributionWorse with restDisturbs sleepMorning stiffness for over
30 minutes
ExaminationStiff or rigid spineSymmetrical restriction of
lumbarmovements
Symmetrical restriction of straightleg raising
Multiradicular neurological signs
Common predisposing factors for postural back painPostural
faultFlat lordosis
Exaggerated lordosisScoliosis
CauseSeating-car seats, low sofas and armchairsBeds-old, soft
bedsHousehold tasks-ironing, vacuuming, low work
surfacesBending-gardening, poor lifting techniqueFootwear-high
heeled shoesUnequal leg length-congenital, old leg fracture,
running on cambered roads
Systemic back painAs well as back pain, there may be
associated systemic features such as weightloss, pyrexia, and
general malaise.Examination should include the testicles
andprostate in male patients and the breasts infemale patients as
tumours in the sex organsmetastasise preferentially to the
skeleton.
Ankylosing spondylitisThis can be difficult to distinguish
from
mechanical pain, especially in the early stages.However, morning
stiffness for more than 30minutes, pain that alternates from side
to sideof the lumbar spine (a symptom rarelyreported in any other
cause of back pain),sternocostal pain, and chest expansion of
lessthan 5 cm suggest ankylosing spondylitis.Education,
anti-inflammatory drugs, andexercise are the mainstays of
treatment.
Special and lateral recess stenosisSpinal stenosis is common in
people aged
over 60 and is often not considered in thediagnosis of back and
leg pain. It is caused bya narrowing of the spinal canal
orintervertebral foramen resulting fromdegenerative disease. The
symptoms shouldbe compared with those of peripheral vasculardisease
(in this condition the pain eases whena patient stands still and
upright). Computedtomography is the investigation of choice.
Insevere cases surgery may be required todecompress the stenotic
area.
Postural painBad posture is probably the commonest
cause of persistent back pain. The spinedepends for its strength
on maintaining aseries of arches. Sitting and leaning forwardtend
to flatten the arch or lordosis, whilewearing high heels tends to
exaggerate thearch (hydcerlordosis or sway back).
Ideal posture for working at a computer terminal.
Unequal leg length is easily overlooked; 2% of the normal
adultpopulation have differences in leg length of at least 2 cm,
and suchpeople are more prone to back pain. This can be diagnosed
in thesurgery by placing wooden blocks of different thicknesses
under theshort leg and checking the pelvic level visually. Up to a
third of patientswith back pain and differences in leg length of
more than 2 cm willgain relief with a heel raise.
Advice on correcting bad postural habits may be difficult for
apatient to accept and may need to be reinforced through
programmessuch as a back school.
Referred painPathology in organs in the posterior part of the
abdominal cavity
may refer pain to the back-for example, aortic aneurysm or
enlargedlymph nodes. Examination of the abdomen is vital for
exclusion ofthese diagnoses.
BMJ VOLUME 310 8 APRIL 1995
Clinical feature of back pain due to spinal stenosisHistory
ofpain ExaminationLeg pain on walking Stiff spineNeurogenic
claudication Normal straight leg raisingEased by leaning forward or
sitting Normal peripheral pulses
but not standing still Nerve root signs appear lateAt ages over
60
930
-
Psychological aspects
TendernessAxial loadingSimulated rotationStraight leg
raising
Loss of sensationLoss of powerGeneral response
Physical diseaseLocalisedNo lumbar painNo lumbar painLimited
despite
distractionDermatomalMyotomalAppropriate pain
Abnormal illness behaviourSuperficial, widespread,
non-anatomicalLumbar painLumbar painImproves with distraction
RegionalRegional, jerky, giving wayOvert pain response
Some patients' symptoms seem to beexaggerated and
disproportionate to thephysical signs. A history of involvement
inmedicolegal proceedings may be obtained.While the possibility of
missed pathologymust always be borne in mind, examinationmay reveal
inappropriate physical signs.
because of back pain.
Investigations
Radiographic evidence of disc infectionor vertebral collapse
occurs late in thecourse of a disease, and blood tests areprobably
a better initial screen forsystemic disease
Computed tomogram showing malignantinfiltration of lower
thoracic vertebra.
If a patient has been offwork for many months the prognosis
ispoor; the longer people are off work with low back pain the less
likelythey are to work again. The reasons for this are unclear but
have asmuch to do with psychological processes as organic
pathology. Theconcept of learned illness behaviour is popular and
may explain thepersistence of symptoms of chronic unremitting back
pain in patientsin whom an organic cause cannot be found. This
syndrome probablyhas links with other syndromes such as
fibromyalgia and chronicfatigue syndrome.
Blood testsA blood count, erythrocyte, sedimentation rate, and
biochemical
screen (calcium, phosphate, and alkaline phosphate) should
beperformed when a systemic cause for back pain is suspected.
Testingfor prostate specific antigen is useful if prostatic
malignancy issuspected.
Radiological investigationPlain radiographs of the lumbar spine
are rarely helpful, particularly
when taken early in the course of an episode of back pain, and
shouldbe performed only if systemic disease is suspected.
Bone scans are helpful in cases of suspected malignancy and may
beabnormal in metabolic bone disease and ankylosing
spondylitis.
Other imaging techniquesThese should be performed only when
initial conservative treatment
has failed and surgery is being considered.Computed tomography
is the method of choice for showing bony
abnormalities such as bone destruction due to malignancy,
infection,or spinal canal stenosis. It can also help in revealing
lesions of discsand other soft tissue.
Magnetic resonance imaging is still not widely available but is
theinvestigation of choice for showing lesions of soft tissues,
includinglumbar disc lesions and tumours.
Radiculography was until recently the standard method
forinvestigating lumbar disc lesions. It is now used only when the
level ofthe lesion is uncertain and magnetic resonance imaging is
not available.
Discography is a specialist investigation and may help to
identifypatients who would benefit from surgical fusion of the
spine.
ElectromyographyA segmental electromyograph may help to confirm
the presence of
nerve root degeneration if radiological evidence of abnormal
anatomyis not conclusive.
BMJ VOLUME 3 1 0 8 APRIL 1995
Symptoms and signs of chronic low back pain inpatients with
physical disease and abnormal illnessbehaviour
931
-
TreatmentTreatment should be given early, with the aim of
stopping the
problem from becoming chronic.
Bed rest should be kept to a minimum,and early mobilisation
should beencouraged
pain.
The sources of the data presented in illustrations are
asfollows: J H Kellgren, Clin Sci 1939;4:35-46 for the diagramof
radiation of pain; G Wadell et al, Spine 1983;9:209-13 forthe box
of symptoms and signs of physical illness andabnormal illness
behaviour; G Wadell Spine 1987;12:632-44for the graph of return to
work after time off because of backpain; and J A Mathews et al, BrJ
Rheumatol 1987;26:416-23for the graph of effect of manipulation on
acute back pain.
J R Jenner is consultant in rheumatology andrehabilitation at
Department of Rheumatology,Addenbrooke's NHS Trust, Cambridge, andM
Barry isconsultant rheumatologist at Department ofRheumatology,
James Connolly Memorial Hospital,Dublin, Republic of Ireland.The
ABC of Rheumatology is edited by Michael L
Snaith, senior lecturer in rheumatology at Nether EdgeHospital,
Sheffield.
Bed restBed rest has been the main treatment for all forms of
acute back
pain for many years, with recommendations varying from a few
days toover six weeks. The few satisfactory trials that have been
publishedsuggest that bed rest for two or three days has the same
or greaterbenefit than longer periods of rest and that shorter bed
rest leads to anearlier return to work. Slightly longer periods of
rest may be justifiedfor sciatica.
Treatment of low back painPatient education and
exercise-Reassuring patients, giving them
appropriate information, and advising them on posture and
exerciseprogrammes are important. These measures are most effective
whengiven as part of a structured programme such as a back
school.
Back schools are effective for treating acute back pain. The
conceptof back schools was developed in Sweden and is based on a
series offour sessions, each lasting an hour. Treatment is in
groups so thatseveral patients may be treated in one session by a
single therapist withno need for specialist facilities. Patients
can also benefit from talkingwith fellow sufferers.
Manipulation has been the subject of many studies, with
conflictingresults. Manipulation seems to be effective in the first
three weeks afterthe start of acute back pain and gives quicker
relief of pain, but afterthree weeks it may have little advantage
over natural recovery. Themost effective method is unknown, but
physiotherapists, chiropractors,and osteopaths, who use a variety
of techniques, all seem effective.Manipulation should not be used
with patients with sciatica andevidence of nerve root entrapment as
it may make the root lesionworse.
Treatment of sciaticaTraction-Continuous or intermittent
traction remains a popular
treatment for patients suffering from sciatica, though recent
studieshave not consistently confirmed its benefit.
Epidural injections of local anaesthetic and depot preparations
ofcorticosteroid may speed recovery from sciatica. Both the caudal
andlumbar routes ae used. Depot corticosteroid preparations are
notlicensed for use in the epidural space, but serious adverse
reactions arerare.
Interventional treatments-For patients with symptoms of
sciaticalasting more than six weeks despite conservative treatment
and inwhom the prescence of a disc protrusion is confirmed,
surgical orchemical removal of the nucleus of the disc should be
considered. Thesuccess rates for these techniques are 70-80% at one
year aftertreatment, but the rates tend to fall with time,
particularly for somesurgical techniques.
Chronic low back painOnce back pain has been established for
more than a year the
prognosis is poor. Lesions that might be amenable to surgery,
such asdisc protrusion or spondylolysis, must be excluded. Patients
may bereferred to a pain clinic for local injections of
corticosteroid orcryotherapy to facet joints or sclerosant
injections into ligaments, butthe success of these procedures for
chronic pain is low.The main aim of treatment should be to help
patients to come to
terms with their pain and to accept that they can do much
themselvesto relieve their symptoms. This can be achieved with help
fromintensive rehabilitation programmes or "schools for bravery,"
whichare available in specialist centres. Treatment, carried out
either on aday case basis or as an intensive three to four week
inpatientprogramme, combined physical and psychological approaches
tomanaging back pain.
BMJ VOLUME 310 8 APRIL 1995
Elements of a back schoolSession 1-Principles of anatomy of the
spineSession 2-Applied body mechanics and
postureSession 3-ErgonomicsSession 4-Relaxation techniques
and
exercises
Interventional techniques fortreating
sciaticaChemonucleolysis-intradiscal injection of
proteolytic enzymePercutaneous discectomy-by automated
nucleotome or laserMicrodiscectomyConventional discectomy
932