Embed Size (px)
Citation preview

Lower Limb, part II
Barbara Kraszpulska, Ph.D.
Neuroscience, Cell Biology,
and Physiology

Popliteal fossa
Small saphenous vein
Popliteal artery and vein
Superior medial genicular a.
Superior lateral genicular a.
Gastrocnemius m.
Biceps femorisSemimembranosus m.
Semitendinosus m.
Gracilis m.
Sartorius m.
Plantaris m.
Tibial nerve
Common fibular nerve
Lateral sural cutaneous n.
Medial sural cutaneous n.
Common fibular gives rise to lateral sural
Tibial nerve gives rise to medial sural cutaneous n.
Superior genicular artery (one on lateral and one on medial side)-Superior lateral genicular a.- Superior medial genicular a.

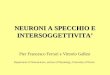
Popliteal Fossa
The popliteal fossa is a space or shallow depression locatedat the back of the knee joint.
The boundaries of the fossa are:* superior and medial: the semimembranosus m., lateral to
which is the semitendinosus m.
* superior and lateral: the biceps femoris m.
* inferior and medial: the medial head of the gastrocnemius m.
* inferior and lateral: the lateral head of the gastrocnemius m.
The contents of the politeal fossa include the:* termination of the small saphenous vein
* popliteal arteries and veins and their branches and tributaries
* tibial and common fibular nerves
* popliteal lymph nodes and lymphatic vessels
Vein lies more anteriorlyArtery lies deeper in popliteal fossa

Knee joint
This is condylar type of synovial joint (between two condyles of the femour and tibia), in addition it includes a saddle joint between the femur and the patella!Functionally this a hinge type of synovial joint – the main movement is flexion and extension, but there is also rotation when the knee is flexed !
The fibula is NOT involved in the knee joint!!!!!!!!!!!
Extracapsular ligaments( external ligaments):* patellar lig.* tibial collateral lig.* fibular collateral lig.* oblique popliteal lig. * popliteus tendon
Intracapsular ligaments:* anterior cruciate lig.* posterior cruciate lig.* medial meniscus* lateral meniscus
Bursae – there are at least about 12 bursae around knee joint!
Quadriceps tendon becomes the patellar ligament
Tibial and fibular collateral ligaments are like the ulnar and radial collateral ligaments.

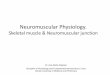
Right Knee – Cruciate and Collateral Ligaments
Anterior view
Posterior view1 – medial condyle2 – lateral condyle
3 – medial meniscus4 – lateral meniscus
5 – anterior cruciate lig.6 – posterior cruciate lig.
7 – tibial collateral lig.8 –fibular collateral lig.
11
22
7 78 8
5
6
6
54
43
39
9 – tendon of popliteus m.

Function of the Cruciate ligaments
Anterior cruciate ligamentPrevents anterior displacement of the tibia relative to the femur
Posterior cruciate ligamentPrevents posterior displacement of the tibia relative to the femur

Medial meniscusLateral meniscus
Anterior cruciate lig.
Posterior cruciate lig.
Infrapatellar fat pad
Menisci of the knee joint
Which meniscus is more frequently torn in injures and why???

1.“Unhappy triad "
2. Bursitis in the knee region
a. Tibial collateral lig.b. Medial meniscusc. Anterior cruciate lig.

Genicular anastomoses around the knee
Four genicular branches
1 & 2. Superior medial and lateral loop over respective femoral condyles
3. Inferior medial parallels superior edge ofpopliteus
4. Inferior lateral crosses popliteus

4 branches of genicular arteries – which are derived from the Popliteal artery:-Superior lateral genicular arteries
- loops over lateral femoral condyle- Superior medial genicular arteries
- loops over medial femoral condyle- Inferior medial genicular artery
- parallels superior edge of popliteus- Inferior lateral genicular artery
- crosses popliteus

Right knee
Pesanserinus
Vastus medialisVastus lateralis
Quadriceps femoris tendon
Patellar ligament
Iliotibial tract
Medial patellar retinaculum
Lateral patellar retinaculum
SemitendinosusGracilisSartorius }

Anterior (extensor) compartment
Action:1. they all extend (dorsiflex) the foot (ankle joint)
2. Tibialis anterior- inverts the foot3. Extensor. digit. long. – extend digits (toes), everts foot4. Extensor hallucis long. – extend great toe, inverts foot
Innervation: Deep fibular nerve (L5,S1)
Blood supply:Anterior tibial artery(terminal branch of popliteal a.)
Tibialis anterior M.
1
2
Tibia
Extensor hallucislongus m.
Extensor digit.longus m.
1
21. Sup. extensor retinaculum2. Inf. extensor retinaculum

Actions of the anterior extensor compartment:
-Tibialis anterior:-Extend (dorsiflexion) of foot at ankle joint- inverts foot
- Extensor digitorum longus-Extends the foot at the ankle joint-Everts foot -extend digits
“Odd man out is ED”
• Extensor hallucis longus•Extends the foot at ankle joint•Inverts foot•Extend great toe
Innervation:-Deep fibular nerve (L5, S1)
Blood supply:-Anterior tibial artery(Terminal branch of popliteal a.)

Lateral (eversion) compartment
Action:1. They both evert the foot (elevate the lateral margin of the foot)2. They weakly flex (plantarflex) the foot (because they pass posterior to the transverse axis of the ankle)
Innervation: Superficial fibular nerve (L5-S2)
Blood supply:Perforating branches ofthe anterior tibialand fibular artery (posterior tibial artery
Tendon of fibularis longus(1)
Fibularis Longus (1)
Fibularis Brevis (2)
(1)(2)

The lateral compartment is supplied by both the anterior and posterior tibial arteries (the fibular artery, in this case). However, they are perforating branches.
Unlike the anterior compartment (deep branch, L5-S1), the lateral compartment is innervated by the superficial branch (L5-S2)
Fibularis longis (lateral compartment, supplied by perforating branches of anterior tibial and fibular arteries) wraps under the flexor digitorum brevis

Common fibular N
Superficial fibular N
Deep fibular N
Deep fibular N
Lateral suralcutaneous n.
Superficialfibular n.
Deep fibular n.
Sural n.(lat. dorsal cutaneous branch)

Causes include:*Compressed nerve root, usually in the lower spine, due to a ruptured lumbar disk *Pressure or injury to the peroneal nerve in your lower leg, such as from sitting with your legs crossed for long periods *Peripheral nerve disorder (neuropathy) *Muscle disorders (myopathies) *Tumor or stroke affecting the areas of the brain that control movement of the legs *Disorders of the spinal cord such as tumors or multiple sclerosis
Injury to the common fibular nerve
Footdrop is due to weakness or paralysis of the muscles involved in lifting the front part of your foot. This can cause inability to stand on heels and walk with a foot slap. Footdrop isn't a disease but a sign of an underlying problem.
Depending on the cause, footdrop can be temporary or permanent. Treatment depends on the underlying cause but may include a brace (orthotic) worn on the ankle and foot to hold the foot in the normal position.

Footdrop is a sign of injury to the common fibular nerve (also known as the peroneal nerve)-Result of compression of nerve root, injury to nerve itself, peripheral nerve disorder, muscle disorder, tumor or stroke, disorder of spinal cord
-(Basically, damage to nerve, damage to brain, damage to spinal cord or muscle itself)

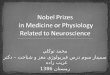
Tibialis posterior
Flexor Digitorum longus
Posterior tibial artery and vein
Tibial nerve
Flexor Hallucis longus
Flexor retinaculum
Achilles tendon(calcaneal tendon)
Posterior (plantarflexion) compartmentSuperficial group:GastrocnemiusSoleus flex the footplantaris
Deep group:TOMDICK HARRY
Soleus
Lateral to medial:Tom Dick VAN Halen
Calcaneal tendon is also known as the Achilles tendon

Tibialis posterior tendon Flexor digitorum longus
Posterior tibial A and Tibial nerve
Flexor hallucis longus
TOM – Tibialis posterior
DICK- Fl. Digitorum longus
HARRY- Fl. Hallucis longus
The tarsal tunnel is a narrow space that lies on the inside of the ankle next to the ankle bones. Tarsal tunnel syndrome is a compression, or squeezing, on the posterior tibial nerve that produces symptoms anywhere along the path of the nerve. The posterior tibial nerve runs along the inside of the ankle into the foot.
Tarsal tunnelTarsal tunnel syndrome
Flexor retinaculum

Tarsal tunnel syndrome (TTS), also known as posterior tibial neuralgia, is a painful foot condition in which the tibial nerve is impinged and compressed as it travels through the tarsal tunnel.

Tibial nerve
Popliteus muscle
Flexor digitorum longus M.
Flexor hallucis longus M.
Tibialis posterior M.
Sural nerve
Common fibular (peroneal) nerve
Soleus Muscle (cut)
Gastrocnemius muscle (cut)
Innervation: Tibial nerve (L4-S3)
Blood supply:Posterior tibial arteryand also fibular artery(branch of posterior tibial a.)

Tibial nerve innervates the posterior plantarflexion compartment
Roots?L4- S3
Muscles:-Popliteal- Gastrocnemius- Soleus- Tibial posterior- Flexor digitorum longus- Flexor hallucis longus
Tarsal bones"Tall Cocky Navy Medical Interns Lay Cuties":· In order (right foot, superior to inferior, medial to lateral): Talus Calcanous Navicular Medial cuneiform Intermediate cuneiform Lateral cuneifrom Cuboid

Foot Bones:Tarsals (7): talus, calcaneus, navicular, cuboid, and cuneiforms (3)Metatarsal – 5, Phalanges - 14
calcaneus
talus
cuboid navicular
cuneiformbones
Transversetarsal joint
Tarsometatarsal joint
Function of the foot:*Provide a stable platform*Generate propulsion*Absorb shock
calcaneus
talus
tibia
Subtalar joint
Ankle joint

Foot joints:1. Ankle joint – between the distal end of the tibia and
fibula and the superior part of talus. This is a hinge type joint!
Movements: dorsiflexion ( extension) of the foot, plantarflexion (flexion) of the foot.
2. Subtalar jointarticulation between talus and calcaneus
3. Transverse tarsal jointarticulation between talus, navicular, calcaneus and cuboid bonesMovements: inversion and eversion.
Eversion- elevation of the lateral margin of the footInversion – elevation of the medial margin of the foot.
extension
Flexion

Posterior talofibular ligament
Calcaneofibular ligament
Anterior talofibular ligament (most commonly injured in ankle sprains)
Lateral (collateral) ligament
Fibularis longus tendon
Fibularis brevis tendon
Lateral collateral ligament-Contains 3 parts
- torn under inversion

Inversion and eversion of the foot
Inversion injury- Ankle sprains!
Tibialis anterior AND tibialis posterior control inversion of the foot.-What else controls it?- Flexor hallucis longus
Fibular

1. Posterior tibiotalar part
2. Tibiocalcaneal part
3. TIbionavicular part
4. Anterior tibiotalar part
DELTOID (medial) ligament
SPRING LIGAMENT (Plantar calcaneonavicular)
Short plantar ligament
Long plantar ligament
Deltoid lig. stabilizes the ankle joint during eversion and prevents sublocation of the joint!
1
2
3
4

Although the lateral side (fibular side) is composed of 3 different ligaments, the medial side is considered one giant ligament.
This ligament is known as the deltoid ligament.-Its components are similar to the lateral compartment, with the addition of the tibionavicular ligament.
-Function?- Stabilizes the ankle joint during eversion and prevents sublocation of the jiont.
-Also laterally, we have the spring ligament (plantar calcaneonvaciular

Ankle injuries
A Pott fracture–dislocation of the ankle

Sole of foot
Superficial dissection
Plantar aponeurosis
Medial plantarfasciaLateral plantar
fascia
First layer
Abductor hallucis
Flexor digitorumbrevis
Abductor digitiminimiLateral plantarnerve(S2, S3)
Medial plantarnerve(S2, S3)
Medial plantarnerve(S2, S3)

Sole of foot
Second layer
Quadratusplantae
Lateral plantarnerve(S2, S3)
Lumbrical
Lateral and medial plantar nerve(S2, S3)
Third layer
AdductorhallucisLateral plantarnerve(S2, S3)
Flexor digiti minimi brevis
Lateral plantarnerve(S2, S3)
Flexor hallucisbrevis
Medial plantarnerve(S2, S3)

First layer of the foot• Flexor digitorum brevis
• Medial plantar nerve (S2, S3)
• Abductor hallucis• Medial plantar nerve (S2, S3)
• Abductor digiti minimi• Lateral plantar nerve (S2, S3)
The lateral and medial plantar nerves are branches of the tibial nerve, which is itself a branch of the sciatic nerve
Sole of foot:-First layer
- Flexor digitorum brevis- Medial plantar n
- Abductor hallucis- Medial plantar
- Abductor digiti minimi- lateral plantar n.
-Second layer- Quadratus plantae
- lateral plantar n.- Lumbrical
- lateral and medial plantar nerves
-Third layer- Adductor hallucis
- lateral plantar nerves
- Flexor digit minimi brevis-Lateral plantar nerves
- flexor hallucis brevis- medial plantar nerves

Muscles of the foot
Plantar muscles function primarily as a group during the support phase of stance, maintaining the arches of the foot.The muscles of the foot are of a little importance individually because fine control of the individual toe is not important for most people. Rather than producingactual movement, they are most active in fixing the foot or in increasingthe pressure applied against the ground by various aspects of the sole or toesto maintain balance.
Nerves of the foot:Medial plantar nerve (S2, S3)Lateral plantar nerve (S2, S3)Both terminal branches of tibial nerve!Deep fibular- dorsum of the foot
Arteries of the foot:Dorsalis pedis artery- terminal branch of the anterior tibial Medial plantar and lateral plantar-terminal branches of the posterior tibial

Arteries of the foot

Nerves of the Leg and Foot
Sciatic nerve (L4-S3)
Tibial nerve (L4-S3)
Medial plantar nerveLateral plantar nerve
Superficial branch Deep branch
Common fibular nerve (L4-S2)
Superficialfibular nerve Deep fibular nerve
Medial branch
Lateral branch

Medial plantar nerve: flexor digitorum brevis
abductor hallucisflexor hallucis brevis
first lumbrical
Lateral plantar nerve:abductor digiti minimi
quadratus plantaelumbricals 2, 3 and 4
adductor hallucisflexor digiti minimi brevis
dorsal and plantar interossei

Cutaneous nerves of Lower Extremity

Major ligaments of the foot (plantar aspect)
Supports thelongitudinal arch(Long plantar calcenocuboid ligament)
Calcaneocuboid lig.Supports the Longitudinal arch
Spring ligament!!1.Supports the head of the talus2. Transfers weight from the talus3. Supports thelongitudinal arch

Flexor hallucis longus supports the..
Dynamic support--Major muscles that invert foot-Major muscles that evert foot-Intrinsic plantar muscles
Passive support-On bottom of foot and ligaments
- plantar aponeurosis- plantar calcaneonavicular lig- long plantar lig- short plantar lig

Arches of the foot
Medial longitudinal arch – higher and more importantIs composed of: calcaneus, talus, navicular, three cuneiforms, three medial metatrasal bones.This is arch is supported by:tendon of the flexor hallucis longus muscle and spring ligament

Arches of the foot
Lateral longitudinal arch – much flatter.Is composed of: calcaneus, cuboid and lateral two metatarsalas.Supported by:Fibular (peroneus) longus tendon and long and short plantar ligaments.

Transverse arch of the foot – runs from side to side.Is composed of: cuboid, cuneiforms and bases of the metatarsals.Support by tendons of two muscles:Fibularis longus (FL) and tibialis posterior (TP), crossing under the sole of the foot.
Arches of the foot
FLFL TP

Factors involved in forming and maintaining the arches of the foot
Passive factors:1. the shape of the united bones
2. plantar aponeurosis
3. long plantar ligament
4. short plantar ligament
5. spring plantar ligament
Dynamic factors:1. Active action of the intrinsic muscles of foot
2. Active and tonic contraction of muscles with long tendons
extending into foot:
a. flexor hallucis longus and digitorum longus (longitudinal arch)
b. fibularis longus and tibialis posterior (transverse arch)

Questions of the day!
1. What are the primary muscles that control eversion of the foot?
1. fibularis longis and brevis
2. If a patient cannot stand on his heel, which nerve is not functioning?
1. Common fibular (more specifically, that means we cannot extend, meaning deep fibular
nerve… because extension is dorsiflexion
3. Nerves can frequently be compressed against bony structures in the lower limb. What nerve rests
against the head and neck of the fibula?
1. Common fibular
2. Foot drop is a result