Embed Size (px)
Citation preview
INVESTIGATIONS
Lumbar punctures and cerebrospinal fluid analysisJustin Pearson
Geraint Fuller
AbstractLumbar puncture is an essential neurological investigation. The anatomy
of the spinal canal allows cerebrospinal fluid (CSF) to be sampled from
the lumbar region. We describe how, with adequate preparation and cor-
rect positioning of the patient, the procedure can be performed quickly
and safely. The range of investigations that can be performed on the CSF
and their interpretation will be discussed.
Keywords cerebrospinal fluid; diagnostic techniques; lumbar puncture
Lumbar puncture and analysis of cerebrospinal fluid (CSF) are a routine part of clinical practice both in the setting of acute medi-cal admissions and in the routine investigation of neurological diseases. It is a safe procedure as long as you are aware of the risks and contraindications (see below). In the majority of cases it is performed to aid the diagnosis of central nervous system infections, subarachnoid haemorrhage, multiple sclerosis and malignancy.
Anatomy and physiology
Three layers of meninges cover the brain and spinal cord: the dura, arachnoid and pia. The CSF is contained within the sub-arachnoid space. The CSF is mostly produced by the choroid plexuses in the ventricles and flows from the lateral ventricles through the third and fourth ventricles into the subarachnoid cis-tern around the medulla and on over the surface of the brain and spinal cord where it is reabsorbed by the arachnoid villi.
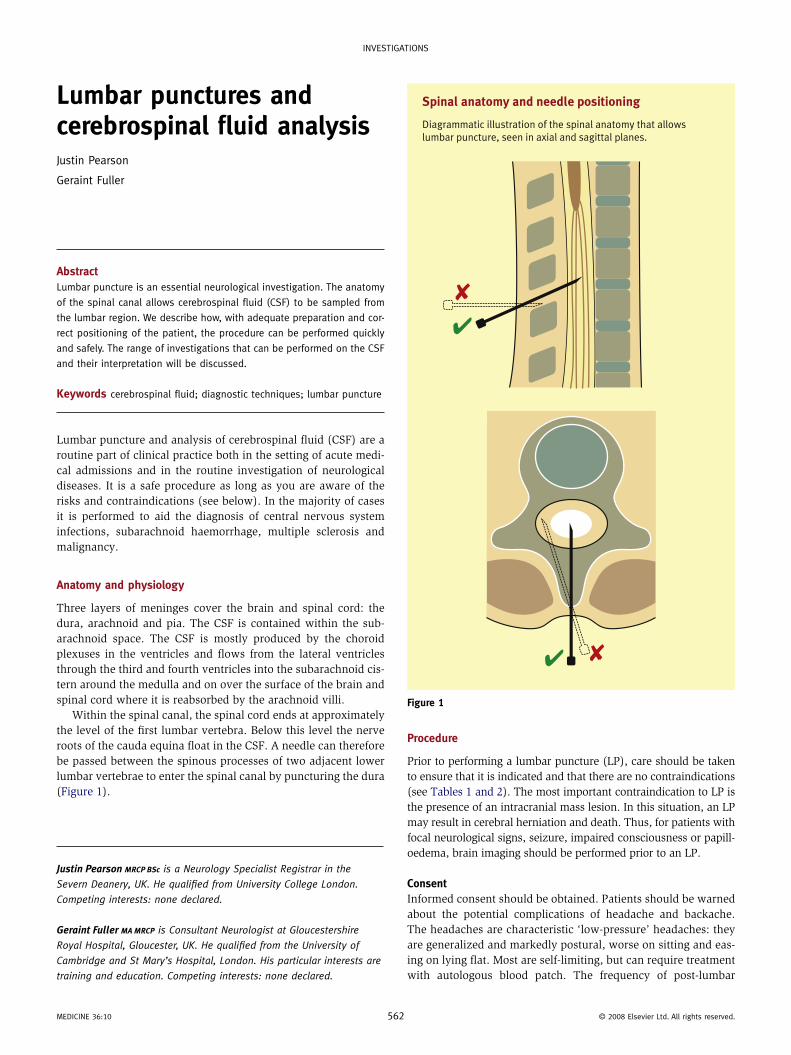
Within the spinal canal, the spinal cord ends at approximately the level of the first lumbar vertebra. Below this level the nerve roots of the cauda equina float in the CSF. A needle can therefore be passed between the spinous processes of two adjacent lower lumbar vertebrae to enter the spinal canal by puncturing the dura (Figure 1).
Justin Pearson MRCP BSc is a Neurology Specialist Registrar in the
Severn Deanery, UK. He qualified from University College London.
Competing interests: none declared.
Geraint Fuller MA MRCP is Consultant Neurologist at Gloucestershire
Royal Hospital, Gloucester, UK. He qualified from the University of
Cambridge and St Mary’s Hospital, London. His particular interests are
training and education. Competing interests: none declared.
MEDICINE 36:10 562
Procedure
Prior to performing a lumbar puncture (LP), care should be taken to ensure that it is indicated and that there are no contraindications (see Tables 1 and 2). The most important contraindication to LP is the presence of an intracranial mass lesion. In this situation, an LP may result in cerebral herniation and death. Thus, for patients with focal neurological signs, seizure, impaired consciousness or papill-oedema, brain imaging should be performed prior to an LP.
ConsentInformed consent should be obtained. Patients should be warned about the potential complications of headache and backache. The headaches are characteristic ‘low-pressure’ headaches: they are generalized and markedly postural, worse on sitting and eas-ing on lying flat. Most are self-limiting, but can require treatment with autologous blood patch. The frequency of post-lumbar
Spinal anatomy and needle positioning
Diagrammatic illustration of the spinal anatomy that allows lumbar puncture, seen in axial and sagittal planes.
Figure 1
© 2008 Elsevier Ltd. All rights reserved.
INVESTIGATIONS
puncture headache has been reduced from 32% to 6% by using a 22G pencil-point needle compared to the traditional 20G bevelled needle.1 More serious, though very rare, complications include epidural haematoma or infection.
PreparationPreparation prior to performing a lumbar puncture is essential. A well-lit room with a firm, height-adjustable couch and an assistant should be arranged. The equipment required should be prepared on a sterile field. This will include an appropriate lumbar puncture needle. As detailed above, pencil-point needles are preferred to the traditional bevelled needle. However, when the lumbar puncture is being performed to reduce CSF pressure, for example in idio-pathic intracranial hypertension, a bevelled needle can be used.
Correct patient positioning is the key to successful lumbar puncture. The patient should be asked to lie in the left lateral position (for the right-handed operator) with their back along the edge of the couch. They should be asked to adopt the foetal position with their neck, hips and knees flexed. A single pillow should be placed under the patient’s head and one between their knees. Care should be taken to ensure that their hips lie vertically above each other and likewise the shoulders.
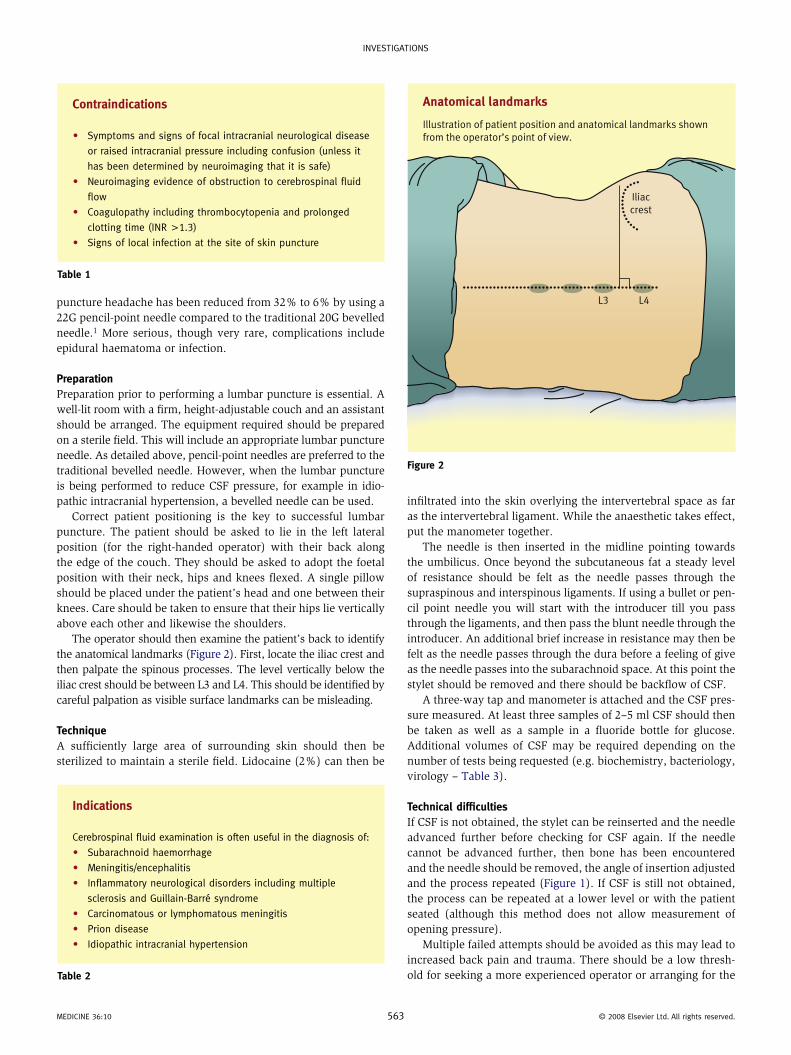
The operator should then examine the patient’s back to identify the anatomical landmarks (Figure 2). First, locate the iliac crest and then palpate the spinous processes. The level vertically below the iliac crest should be between L3 and L4. This should be identified by careful palpation as visible surface landmarks can be misleading.
TechniqueA sufficiently large area of surrounding skin should then be sterilized to maintain a sterile field. Lidocaine (2%) can then be
Contraindications
• Symptoms and signs of focal intracranial neurological disease
or raised intracranial pressure including confusion (unless it
has been determined by neuroimaging that it is safe)
• Neuroimaging evidence of obstruction to cerebrospinal fluid
flow
• Coagulopathy including thrombocytopenia and prolonged
clotting time (INR >1.3)
• Signs of local infection at the site of skin puncture
Table 1
Indications
Cerebrospinal fluid examination is often useful in the diagnosis of:
• Subarachnoid haemorrhage
• Meningitis/encephalitis
• Inflammatory neurological disorders including multiple
sclerosis and Guillain-Barré syndrome
• Carcinomatous or lymphomatous meningitis
• Prion disease
• Idiopathic intracranial hypertension
Table 2
MEDICINE 36:10 563
infiltrated into the skin overlying the intervertebral space as far as the intervertebral ligament. While the anaesthetic takes effect, put the manometer together.
The needle is then inserted in the midline pointing towards the umbilicus. Once beyond the subcutaneous fat a steady level of resistance should be felt as the needle passes through the supraspinous and interspinous ligaments. If using a bullet or pen-cil point needle you will start with the introducer till you pass through the ligaments, and then pass the blunt needle through the introducer. An additional brief increase in resistance may then be felt as the needle passes through the dura before a feeling of give as the needle passes into the subarachnoid space. At this point the stylet should be removed and there should be backflow of CSF.
A three-way tap and manometer is attached and the CSF pres-sure measured. At least three samples of 2–5 ml CSF should then be taken as well as a sample in a fluoride bottle for glucose. Additional volumes of CSF may be required depending on the number of tests being requested (e.g. biochemistry, bacteriology, virology – Table 3).
Technical difficultiesIf CSF is not obtained, the stylet can be reinserted and the needle advanced further before checking for CSF again. If the needle cannot be advanced further, then bone has been encountered and the needle should be removed, the angle of insertion adjusted and the process repeated (Figure 1). If CSF is still not obtained, the process can be repeated at a lower level or with the patient seated (although this method does not allow measurement of opening pressure).
Multiple failed attempts should be avoided as this may lead to increased back pain and trauma. There should be a low thresh-old for seeking a more experienced operator or arranging for the
Anatomical landmarks
Illustration of patient position and anatomical landmarks shown from the operator’s point of view.
L3 L4
Iliaccrest
Figure 2
© 2008 Elsevier Ltd. All rights reserved.
INVESTIGATIONS
procedure to be performed under fluoroscopy. Very rarely CSF will not be obtained because of an infiltrating intraspinal lesion.
Interpretation
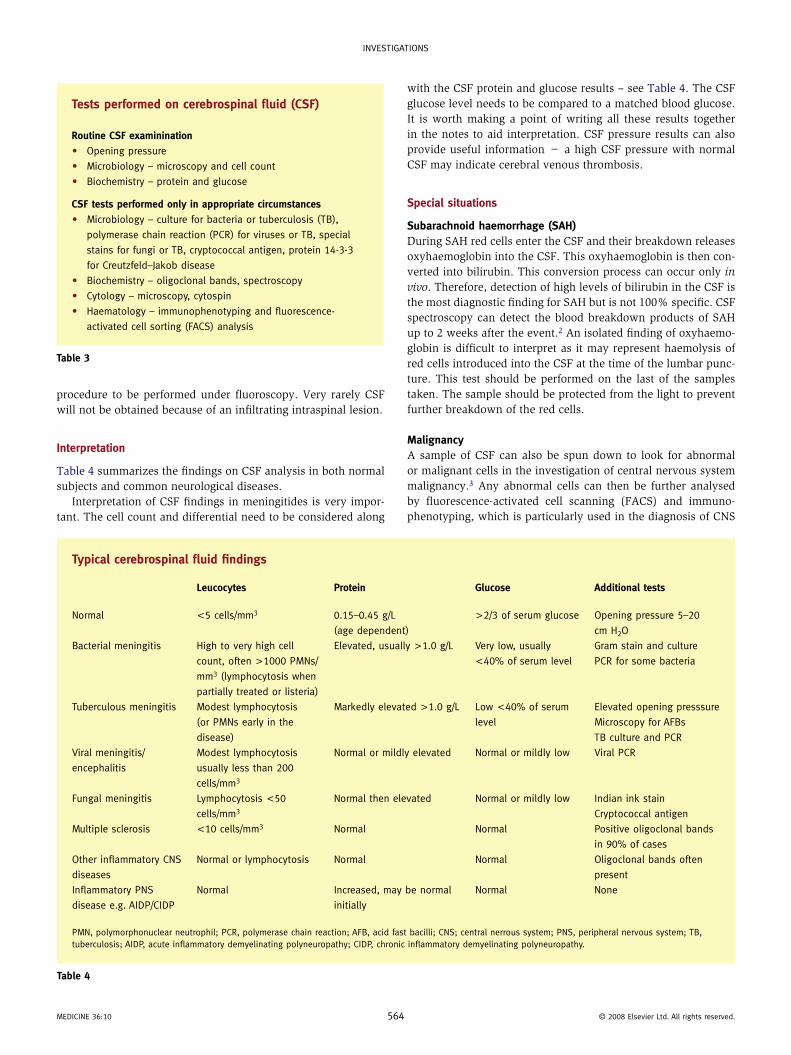
Table 4 summarizes the findings on CSF analysis in both normal subjects and common neurological diseases.
Interpretation of CSF findings in meningitides is very impor-tant. The cell count and differential need to be considered along
Tests performed on cerebrospinal fluid (CSF)
Routine CSF examinination
• Opening pressure
• Microbiology – microscopy and cell count
• Biochemistry – protein and glucose
CSF tests performed only in appropriate circumstances
• Microbiology – culture for bacteria or tuberculosis (TB),
polymerase chain reaction (PCR) for viruses or TB, special
stains for fungi or TB, cryptococcal antigen, protein 14-3-3
for Creutzfeld–Jakob disease
• Biochemistry – oligoclonal bands, spectroscopy
• Cytology – microscopy, cytospin
• Haematology – immunophenotyping and fluorescence-
activated cell sorting (FACS) analysis
Table 3
MEDICINE 36:10 56
with the CSF protein and glucose results – see Table 4. The CSF glucose level needs to be compared to a matched blood glucose. It is worth making a point of writing all these results together in the notes to aid interpretation. CSF pressure results can also provide useful information − a high CSF pressure with normal CSF may indicate cerebral venous thrombosis.
Special situations
Subarachnoid haemorrhage (SAH)During SAH red cells enter the CSF and their breakdown releases oxyhaemoglobin into the CSF. This oxyhaemoglobin is then con-verted into bilirubin. This conversion process can occur only in vivo. Therefore, detection of high levels of bilirubin in the CSF is the most diagnostic finding for SAH but is not 100% specific. CSF spectroscopy can detect the blood breakdown products of SAH up to 2 weeks after the event.2 An isolated finding of oxyhaemo-globin is difficult to interpret as it may represent haemolysis of red cells introduced into the CSF at the time of the lumbar punc-ture. This test should be performed on the last of the samples taken. The sample should be protected from the light to prevent further breakdown of the red cells.
MalignancyA sample of CSF can also be spun down to look for abnormal or malignant cells in the investigation of central nervous system malignancy.3 Any abnormal cells can then be further analysed by fluorescence-activated cell scanning (FACS) and immuno-phenotyping, which is particularly used in the diagnosis of CNS
Typical cerebrospinal fluid findings
Leucocytes Protein Glucose Additional tests
Normal <5 cells/mm3 0.15–0.45 g/L
(age dependent)
>2/3 of serum glucose Opening pressure 5–20
cm H2O
Bacterial meningitis High to very high cell
count, often >1000 PMNs/
mm3 (lymphocytosis when
partially treated or listeria)
Elevated, usually >1.0 g/L Very low, usually
<40% of serum level
Gram stain and culture
PCR for some bacteria
Tuberculous meningitis Modest lymphocytosis
(or PMNs early in the
disease)
Markedly elevated >1.0 g/L Low <40% of serum
level
Elevated opening presssure
Microscopy for AFBs
TB culture and PCR
Viral meningitis/
encephalitis
Modest lymphocytosis
usually less than 200
cells/mm3
Normal or mildly elevated Normal or mildly low Viral PCR
Fungal meningitis Lymphocytosis <50
cells/mm3
Normal then elevated Normal or mildly low Indian ink stain
Cryptococcal antigen
Multiple sclerosis <10 cells/mm3 Normal Normal Positive oligoclonal bands
in 90% of cases
Other inflammatory CNS
diseases
Normal or lymphocytosis Normal Normal Oligoclonal bands often
present
Inflammatory PNS
disease e.g. AIDP/CIDP
Normal Increased, may be normal
initially
Normal None
PMN, polymorphonuclear neutrophil; PCR, polymerase chain reaction; AFB, acid fast bacilli; CNS; central nerrous system; PNS, peripheral nervous system; TB, tuberculosis; AIDP, acute inflammatory demyelinating polyneuropathy; CIDP, chronic inflammatory demyelinating polyneuropathy.
Table 4
4 © 2008 Elsevier Ltd. All rights reserved.
INVESTIGATIONS
lymphoma.4 Repeated lumbar punctures are often required to identify malignant cells.
DementiaMeasurement of the brain-specific protein 14-3-3 in CSF is used in the diagnosis of rapidly progressive dementia.5 In the appro-priate clinical scenario, an elevated level is very suggestive of Creutzfeld–Jakob disease (CJD), but is not entirely specific as it can be elevated in other rapidly progressive dementias and fol-lowing prolonged seizures. Other potential CSF biomarkers for dementia are also being studied including CSF tau and amyloid, but these are not currently used in routine clinical practice. ◆
ReFeRenCeS
1 Kleyweg RP, Hertzberger LI, Carbaat PA. Significant reduction in
post-lumbar puncture headache using an atraumatic needle.
A double-blind, controlled clinical trial. Cephalalgia 1998; 18: 635–37.
2 UK National External Quality Assessment Scheme for
Immunochemistry Working Group. National guidelines for analysis
of cerebrospinal fluid for bilirubin in suspected subarachnoid
haemorrhage. Ann Clin Biochem 2003; 40: 48–88.
MEDICINE 36:10 565
3 Gleissner B, Chamberlain MC. Neoplastic meningitis. Lancet Neurol
2006; 5: 443–52.
4 Urbanits S, Griesmacher A, Hopfinger G, et al. FACS analysis – a new
and accurate tool in the diagnosis of lymphoma in the cerebrospinal
fluid. Clin Chim Acta 2002; 317: 101–07.
5 Van Everbroeck B, Boons J, Cras P. Cerebrospinal fluid biomarkers
in Creutzfeldt-Jakob disease. Clin Neurol Neurosurg 2005; 107:
355–60.
Practice points
• CSF analysis is an essential part of investigation of
neurological disease
• Lumbar puncture is a safe routine procedure
• Adequate preparation and correct patient positioning are
essential for successful completion of a lumbar puncture
• Accurate diagnosis depends on requesting the appropriate
CSF tests and interpreting the results in the clinical context
© 2008 Elsevier Ltd. All rights reserved.