Embed Size (px)
Citation preview

LUTforum Highlights 2015Christian Gratzke
LMU Munich

What is LUTforum?
• Web-based platform to provide specialists with highlights
in functional urology presented at major urological
congresses
– PowerPoint slide sets
– Freely available at www.lutforum.org
– Downloadable

Approach LUTforum programme
Abstract presentations at congresses
Selection of abstracts by reporter team
Slides rated for impact on clinical practice & commented by reviewers
Publication of slides on website within 2 mo after congress
Information spread at national/regional meetings

LUTforum slide libraries


EVALUATION

Gratzke et al, Eur Urol 2015www.uroweb.org
EAU Assessment Guidelines

www.uroweb.org
Medical History

Evaluation of risk factors for BPH
• #PD39-02: Pooled analysis of men with ≥6 mo BPH/LUTS history and IPSS
≥13 enrolled in 1 of 3 tadalafil RCTs: N=1,129
• Baseline oestrogen (E2):
– Inverse correlation with total IPSS (P<0.05) and IPSS-storage (P<0.05)
– Associated with improvements in IPSS-storage scores after tadalafil treatment
• #PD39-09: Prospective study in placebo arm of Prostate Cancer Prevention
Trial; N=4,969 men without BPH; statin use at baseline and every 3 mo
• Ever using statins: 27.1%
• Statin use was associated with an increased BPH risk (multivariate model):
Oestrogen and statin drug use seem to be associated with LUTS/BPH
Miner M. J Urol 2015;193(4 Suppl):e830-e831(abs.PD39-02);
Patel D. J Urol 2015;193(4 Suppl):e833(abs.PD39-09)

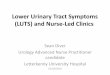
Association between cardiovascular risk and severity of
LUTS
• Cross-sectional study: 336 pts with BPH related LUTS
• LUTS classified as mild (IPSS 0-7) or moderate-severe (IPSS 8-35)
• 10-year cardiovascular disease Framingham risk score (F-score; %); low
<10%, intermediate 10-20%, high >20%)
Increased Framingham risk seems to be associated with LUTS severity
Russo GI. J Urol 2015;193(4 Suppl):e916(abs.MP71-12)
14.5
7.5
23.5
17.0
8.0
23.0
19.0
8.5
16.0
0
5
10
15
20
25
IPSS IPPS storage IIEF
Low F-score Intermediate F-score High F-score
*
*
*
* *
* P<0.05
Mean s
core

MEDICAL THERAPY

MEDICAL THERAPY -
MIRABEGRON

Persistence with mirabegron vs antimuscarinics in OAB
• Analysis of prescription data from a UK longitudinal database: pts starting a new
course of OAB therapy (2012-2013) and followed for 12 mo
– N=10,238 pts receiving antimuscarinics; N=141 pts receiving mirabegron
• Treatment cessation = discontinuation of treatment >1.5 times the expected duration
of the previous prescription, including switching to other drug
• Mirabegron had a higher persistence than antimuscarinics at 12 mo:
Mirabegron seems to have a higher persistence rate at 12 mo than
antimuscarinics in pts starting a new course of OAB treatment
Wagg A. Eur Urol Suppl 2015;14(2):e267

Efficacy and safety of mirabegron add-on treatment to
solifenacin for OAB: phase IIIb study
• Phase IIIb RCT, N=2,174 adult pts with OAB ≥3 mo, who still report ≥1
incontinence episode/3d after single-blind solifenacin (SOLI) treatment (5
mg od for 4 wk)
• Pts randomised to daily, double-blind treatment COMBN (SOLI 5 mg +
mirabegron 50 mg; N=727), SOLI 5 mg (N=728) or SOLI 10 mg (N=719) for
12 wk
• Primary endpoint:
Drake M. J Urol 2015;193(4 Suppl):e498-e499(abs.PII-LBA9)
-1.80
-1.53
-1.67
-1.9
-1.8
-1.7
-1.6
-1.5
-1.4
-1.3
Adju
ste
d m
ean c
hange
from
baselin
e
Incontinence episodes/24h
COMBN (N=707)
SOLI 5 mg (N=705)
SOLI 10 mg (N=698)
1 of 2
Adjusted mean difference: -0.26;
P=0.001

Efficacy and safety of mirabegron add-on treatment to
solifenacin for OAB: phase IIIb study
• Secondary endpoints:
– Significant greater reductions in COMBN vs SOLI 5 mg group:
– COMBN superior to SOLI 10 mg for * and non-inferior to SOLI 10 mg for **
• Safety: well tolerated in all treatment arms
– AE profile in COMBN consistent with known SOLI and mirabegron profiles
– No new AEs
Add-on mirabegron treatment seems to be an efficient and safe
treatment option for incontinent OAB patients with an insufficient
response to SOLI 5 mg
Drake M. J Urol 2015;193(4 Suppl):e498-e499(abs.PII-LBA9)
2 of 2
COMBN
(N=707)
SOLI 5 mg
(N=705)
SOLI 10 mg
(N=698)
P (COMBN vs
SOLI 5 mg)
Mean # micturitions/24h• Mean change from baseline -1.59 -1.14 -1.12* <0.001
# incontinence episodes during 3d diary• Mean baseline
• Mean end of treatment9.60
4.25
9.33
4.87
9.86**
4.72**
0.014

Mirabegron in pts with mixed urinary incontinence (MUI)
• Pooled analysis of 3, 12-wk, phase III RCTs in pts with OAB symptoms;
retrospective, subgroup analysis of pts with MUI
• MUI: stress urinary incontinence (positive cough provocation test) +
urgency urinary incontinence (UUI) with urgency being predominant
Mirabegron 25 mg and 50 mg seem to improve OAB symptoms also in
pts with MUI with urgency being predominant
Cruz F. Eur Urol Suppl 2015;14(2):e265

MEDICAL THERAPY –
UNDERACTIVE BLADDER


Safety and pharmacokinetics of ONO-8055, a prostanoid
EP2/EP3 receptor dual agonist
• Single-centre study in healthy subjects (N=145);
• Administration of single and multiple oral ascending doses of ONO-8055
– Solutes: 0.5, 2 and 8 μg; Tablets: 25, 100, 300, 500, 700 and 1000 μg
– Single/multiple dose; effect of food (fasting/high fat diet), gender and age
• Safety findings:
– Gastrointestinal treatment-emergent adverse events (GI TEAE) most common
– GI TEAE: mainly diarrhoea (26.1% vs 17.6% in controls)
possible dose relationship
women more susceptible
– No serious adverse events; 56% reported ≥1 TEAE
• Pharmacokinetic (PK) findings:
– Multiple doses of ONO-8055 led to steady state plasma concentrations on day 5
– In a fed state, plasma Tmax of ONO-8055 was significantly later (3.5h) compared
with fasted state
Chapple C. J Urol 2015;193(4 Suppl):e235(abs.MP21-07)
In healthy subjects, ONO-8055 was generally well tolerated and there
were no PK concerns Data from poster

SURGICAL THERAPY

SURGICAL THERAPY –
VAPORISATION TECHNIQUES

Comparison of photoselective vaporisation of the prostate
(PVP) and transurethral resection of the prostate (TURP);
24-month outcomes of the Goliath study
• Prospective, non-inferiority study in N=269 men with BPO randomised to
180W GreenLight-XPS or TURP
• At 24 mo FU:
• No significant differences in IIEF-5, IPSS-QoL, PVR, prostate volume and
PSA between groups
At 24 mo, PVP seems to show comparable efficacy and safety to TURP
in men with BPO
Thomas JA. Eur Urol Suppl 2015;14(2):e572

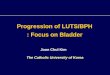
Effect of photoselective vaporisation of the prostate (PVP)
and transurethral resection of the prostate (TURP) on
erectile function: results of the Goliath study
• Goliath: Prospective, multi-centre study in 291 men with BPH randomised to
180W GreenLight-XPS (N=136) or TURP (N=133); 24 mo FU
• IIEF-5 questionnaire: no change from baseline at 2-yr FU and no difference
between groups
• Quality of life: no differences between PVP and TURP (EQ-5D-3L, SF-36)
Neither PVP, nor TURP seem to be associated with worsening of
erectile function due to surgery
Thomas JA. J Urol 2015;193(4 Suppl):e96(abs.PD5-10)
13.2 13.712.9
13.9
0
2
4
6
8
10
12
14
16
PVP TURP
Mean I
IEF
-5 s
core
Baseline
24 mo FU
N132 129124 119

SURGICAL THERAPY –
ENUCLEATION TECHNIQUES

Assessment of symptom improvement after HoLEP in
patients with BPH-related LUTS
• #MP3-16: prospective; holmium laser enucleation of the prostate (HoLEP); N=144
– IPSS: pre- and postop (1,2,3,4,6,8,12,16,20,24 and 52 wk)
– IIEF: pre- and postop (8, 12, 16, 20, 24, 52 wk)
* All postoperative IPSS scores are significantly lower compared to baseline, with
significant effect of time. Rebound at 6-8 wk
– Pts with severe symptoms: postop IPSS scores: 3.8 (vs mild) and 2.3 (vs
moderate)
– Significant decrease in IIEF at wk 8, 12 16, 20,14 with complete recovery at 52 wk
Ahyai S. J Urol 2015;193(4 Suppl):e24-e25(abs.MP3-16);
Group stratification Mild Moderate Severe
IPSS 0-7 8-19 20-35
1 wk 2 wk 3 wk 4 wk 6 wk 8 wk 12 wk 16 wk 20 wk 24 wk 52 wk
IPSS* ↓ ↓ ↓ ↓ ↑ ↑ ↓ ↓ ↓ ↓ ↓
LUTS and erectile function seem to improve after laser surgery in
patients suffering from BPH-related LUTS

Learning curve and the impact of training for laser
enucleation of prostate
• #MP13-19: Single-centre, prospective pilot study
– Pts undergoing ThuLEP or HoLEP; N=513; 10 surgeons
– Learning threshold (LT) defined as
• Operative speed of 0.35 g/min considering pathological specimen weight
• Hospital stay of 2 days
– # operated cases = significant predictive factor to achieve LTs (P<0.0001)
Learning time appears to be based on the amount of procedures
performed
Lopater J. J Urol 2015;193(4 Suppl):e144-e145(abs.MP13-19)
Operative speed Hospital stay 2d
Achievement LT After 30 cases After 29 cases
Variable Value
Median operative time 80 min
Median pathological prostate volume 39 g
Median hospital stay 2 d

Thulium vapo-enucleation of the prostate (ThuVEP) in
patients with BPH-related LUTS: single-centre long-term
retrospective results
• #MP13-10: N=500
– Low reintervention and complication rate at 72 mo FU
• #MP13-11: N=90; with PV ≥80 ml
– Low incidence of complications at 72 mo FU
ThuVEP appears to be effective and safe for the treatment of BPH-
related LUTS, also in pts with PV >80 ml and regardless of age
Netsch C. J Urol 2015;193(4 Suppl):e140(abs.MP13-10); Netsch C. J Urol 2015;193(4 Suppl):e140(abs.MP13-11);
Improvement from
baseline
Qmax (ml/s) PVR (ml) IPSS QoL
12 mo (N=340) (all P<0.001) 10.2 97 16 4
72 mo (N=20) (all P≤0.015) 6.1 67 19 4
Improvement from baseline Qmax (ml/s) PVR (ml) IPSS QoL
12 mo (N=64) (all P≤0.001) 14.25 249 20 4
72 mo (N=20) (all P≤0.001) 13.35 235 20 4
Data from poster

SURGICAL THERAPY – ROBOT-
ASSISTED PROSTATECTOMY

Robot-assisted simple prostatectomy (RASP) in the
treatment of BPH-related LUTS
• #MP3-05: multi-centre; N=100; retropubic/suprapubic/posterior-transvesical
RASP; mean removed prostate volume: 92.0 g
• #MP3-06: single-centre; N=15, RASP; 1:1 matched to control patients
undergoing open simple prostatectomy (OSP); mean prostate size: 156 ml
RASP might be a safe and effective procedure to improve BPH-related
LUTS with possible shorter length of stay than OSP
Harbin A. J Urol 2015;193(4 Suppl):e20-e21(abs.MP3-05);
Zhao P. J Urol 2015;193(4 Suppl):e21(abs.MP3-06)
Preoperative Postoperative P value
AUA-SI 19.4 5.6 <0.0001
SHIM* 12.2 11.5 0.18
Haemoglobin (g/dl) 13.5 12.3 <0.0001
PVR (ml) 411.1 45.9 <0.0001
RASP OSP P value
Resected tissue volume (cc) 104.7 112.6 0.42
Length of stay (d) 2.4 6.0 <0.05
Postoperative haemoglobin decrease 1.13 1.69 0.07
Foley duration (d) 8.7 9.5 0.54
IPSS change -12.0 -16.1 /

Cost-benefit comparison of robotic-assisted simple
prostatectomy (RASP), transurethral resection of the
prostate (TURP) and photovaporisation (PVP) for BPH
• Single-centre, retrospective study in 231 pts treated for BPH (2012-2014)
• Grouped by procedure: RASP (N=43), TURP (N=126) PVP (N=62)
• Perioperative comparison:
RASP seems to be associated with greater operative costs, estimated
blood loss, operative time and catheter duration than TURP and PVP
Eschenroeder A. J Urol 2015;193(4 Suppl):e94(abs.PD5-07)
Mean values RASP (N=43) TURP (N=126) PVP (N=62)
Operation time (min) 200.8** 80.2 82.2
Estimated blood loss (ml) 332.2** 25.3* 7.7
Length of stay (d) 1.7 1.3 1.3
Catheter duration (d) 8.1** 4.5* 1.5
Operative costs (USD) 60,626.7** 23,488.2 22,944.0
*P<0.05 compared with PVP
**P<0.05 compared with TURP and PVP

SURGICAL THERAPY -
UROLIFT

Minimally-invasive treatment options - Urolift
PRE POST


QMAX (ml/sec)
SHIM
MSHQ-EjD
Efficacy

Sexual Side Effects

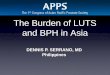
Multi-centre studies on prostatic urethral lift (PUL) as
treatment for BPH-related LUTS
PUL may offer a meaningful improvement in BPH-related LUTS both in
the short and in the long term
• #PD5-01: N=140; PUL; age ≥50, AUA-SI ≥13, PV 30-80ml
– Primary endpoint: AUA-SI at FU 1 mo, 3 mo, 1 yr, 2 yr and 3 yr
22.3
12.3 11.2 11.5 12.6 12
0
5
10
15
20
25
Baseline(N=140)
1mo(N=135)
3 mo(N=136)
1 yr(N=123)
2 yr(N=104)
3 yr(N=62)
AU
A-S
I score
* * * **
* P<0.0001 vs baseline
Roehrborn C. J Urol 2015;193(4 Suppl):e92(abs.PD5-01)

SURGICAL THERAPY - BOTOX

The effect of long-term onabotulinumtoxinA (onabotA)
treatment on UI in patients with OAB: final results of a 3.5
year study
• Multi-centre 3.5 yr extension study after 2 24 wk randomised, phase III trials;
N=543
• OAB pts treated ‘as needed’: 1 – 6 onabotA 100U injections
• 51.2% (N=278) completed the study
• Reasons for discontinuation: – Adverse events (5.3%)
– Lack of efficacy (2.8%)
– Other (91.9%)
• Duration of effect:– Longer if fewer injections
– Overall median 7.6 mo
Long-term treatment with onabotA (100U) seems to result in consistent
reductions in daily UI episodes
Nitti V. J Urol 2015;193(4 Suppl):e719-e720(abs.PI-04)
# injections 1 2 3 4 5 6
Baseline mean UI episodes/day
4.5 5.0 5.8 5.9 5.2 5.7
Mean reduction UI episodes/day at 12 wk FU
3.1 2.9-3.2 4.1-4.5 3.4-3.8 3.0-3.6 3.1-4.1
34%
37%
29% < 6 mo
6 - 12 mo
>12 mo
Median time to request re-treatment

Long-term outcomes of onabotulinumtoxinA (onabotA)
treatment for neurogenic detrusor overactivity (NDO)
• 3-yr extension study of a 1-yr phase III study; N=122 pts with NDO treated
with ‘as needed’ onabotA 200U
• Median time to next treatment: 9.2 mo
• Efficacy outcomes:
– UI reduction:
• ≥50% reduction in UI episodes/day in each yr: 88-90%
• 100% reduction in UI episodes/day in each yr: 44-52%
• Safety:
– Most common AE: UTI, no increased incidence over time
OnabotA treatment for NDO seems to have a good long-term efficacy
without new safety signals appearing over time
Rovner E. J Urol 2015;193(4 Suppl):e35(abs.PD1-01)
Yr 1 Yr 2 Yr 3 Yr 4
Mean injections/yr 1.5 1.4 1.5 1.5
↓ in mean UI episodes/d -3.4 -3.6 -3.8 -3.7
De novo CIC (% pts) 39 11 8 0

INFECTIONS/INFLAMMATION

Effect of cranberry supplementation on bacterial
colonisation and UTIs in females with neurogenic bladder
dysfunction dependent on self-catheterisation
• Prospective, randomised, double-blind, placebo-controlled study
• Female pts (>18 yr) with neurogenic bladder who performed CIC >3x/d
(N=24); FU=16 wk
• Daily oral 36 mg cranberry supplementation PACBL-DMAC (N=14) or placebo
(N=10)
• Causes of neurogenic bladder dysfunction: multiple sclerosis (N=15),
myelomeningocele, transverse myelitis and spinal cord injury
• No significant difference between beginning and end of study for
– Mean colony counts in treatment (P=0.1) and control (P=0.84) group
• No significant difference between treatment and control group for
– Urine colony counts (P=0.947)
– Symptomatic UTI (P=0.665)
– Time to developing symptomatic UTI (P=0.490)
Cranberry supplementation may not reduce colony counts or prolong
the time to symptomatic UTI in women with neurogenic bladder
dysfunction dependent on self-catheterisation
Scovell J. J Urol 2015;193(4 Suppl):e192-e193(abs.PD8-07)

The effect of blood transfusion (BT) on the incidence of
infectious complications after urologic surgery
• Pts undergoing 1 of the 30 most common urologic operations (N=30,651)
• Pts requiring BT*: preoperative 0.5%, peri/postoperative 3.7%
• Odds ratio (95% CI) for complications after BT based on multivariate logistic
regression controlling for confounding factors:
BT might be associated with a significantly increased risk of
postoperative infectious complications
Matulewicz R. J Urol 2015;193(4 Suppl):e192(abs.PD8-06)
Preoperative BT
Peri/
Postoperative BT
-5 -4 -3 -2 -1 0 1 2 3 4 5 6 7 8 9 1 0 1 1 1 2 1 3 1 4 1 5
O d d s ra t io (9 5 % C I)Odds ratio (95% CI)
Pneumonia
UTIPostop sepsis
Superficial surgical site infection
Deep surgical site infection
Organ space infection
Pneumonia
UTI
Postop sepsis
Postop septic shock

SURGICAL THERAPY – MALE
INCONTINENCE

Efficacy and safety of the AdVance XP male sling: long-
term results
• #MP88-09: multi-centre, prospective study in 83 pts with SUI after RP
treated with AdVance XP male sling
• Efficacy:
– % pts cured (0-5 g in pad test): 63.9 and 66.7 at 3 and 24 mo
– % pts improved (>50%↓ urine loss): 31.3 and 13.3 at 3 and 24 mo
– Pad test results:
• QoL: Significant improvement (P<0.001)
• Safety:
– No intraoperative complications, no erosion or explantation
– Persistent urinary retention: 9.2% at 12 mo due to overtensioning
The AdVance XP male sling seems to be an effective and safe
treatment for men with SUI
Bauer R. J Urol 2015;193(4 Suppl):e1095-e1096(abs.MP88-09)
349
43 19 18.5 6.80
100
200
300
400
Pre-operative 3 mo 6 mo 12 mo 24 moMean u
rine
loss (
g)
All P<0.001

SURGICAL THERAPY –
FEMALE INCONTINENCE

MiniArc™ vs Monarc™ for female SUI: long-term outcomes
• Retrospective, single-centre study in N=381 women with SUI
• Mean FU: 65 mo; N=195 pts (51%) had FU ≥5 yr
• No significant differences in surgical failure rate, erosion-free rate and
objective cure rate
MiniArc and Monarc seem to have comparable outcomes for female
SUI at long-term FU
Tutolo M. Eur Urol Suppl 2015;14(2):e74
Continence: patient reported absence of SUI

Long-term outcomes of tension-free vaginal tapes (TVT) for
female SUI
• Analysis of single-centre, prospective database; N=139 women with 10 yr
FU after placement of TVT for SUI (63%) or MUI (25%)
• % highly satisfied pts decreased: 2 yr: 82%; 5 yr: 76%; 10 yr: 66%
• Predictors for unsatisfactory outcome:
– MUI, nocturia and urgency at baseline
– Development of OAB symptoms after TVT placement
TVT seems to have a good long-term efficacy for treatment of SUI.
Development of OAB symptoms may lead to less satisfaction
Bock H. Eur Urol Suppl 2015;14(2):e65

Thank you!