Embed Size (px)
Citation preview

LV Dssynchrony and Cardiac Resynchronization Therapy
in Heart Failure
Nisha I. Parikh MD MPH
August 13th 2008

Summary of Talk Background CRT Rational and Evidence for Benefit LV Dssynchrony by Echocardiography Evidence for Ability of Echo to Predict CRT
Response

Hospital discharges for HF from 1979-2004
0
100
200
300
400
500
600
700
79 80 85 90 95 00 04
Years
Dis
ch
arg
es i
n T
ho
usa
nd
s
Male Female
399,000
1,099,000
American Heart Association. Heart Disease and Stroke Statistics — 2007 Update
1,099,000

HF Total Expenditures: $27.9 Billion
American Heart Association. Heart Disease and Stroke Statistics — 2007 Update

Percent Change in United States Crude Death Rates
from 1972 to 2000 by cause
NHLBI Morbidity and Mortality Chart Book. 2004

HF Therapy
Jessup M, Brozena S. Medical Progress--Heart Failure. N Eng J Med 2003; 348: 2007-2018. Copyright 2002 Massachusetts Medical Society. All rights reserved.

Electrical dyssynchrony Abnormal ventricular depolarization,
causing increased QRSd generates early and delayed ventricular contraction
QRSd directly associated with EF BBB present in 20% of HF patients and
35% of patients with severely impaired EF BBB is an independent predictor of
mortality especially QRSd > 120 ms

Mechanical dyssynchrony Intraventricular- refers to delayed activation
of one LV region to another Interventricular- refers to delayed activation
of LV relative to RV CRT aims to correct both

Achieving Cardiac ResynchronizationGoal: Atrial synchronous biventricular pacing
Transvenous approach for left ventricular lead via coronary sinus
Back-up epicardial approach
Right AtrialLead
Right VentricularLead
Left VentricularLead
From Dr. A. Goldman’s CRT Talk 2007

Cumulative Enrollment in Cardiac Resynchronization Randomized Trials
0
1000
2000
3000
4000
1999 2000 2001 2002 2003 2004 2005
Results Presented
Cum
ulat
ive
Pat
ient
s
PATH CHF
MUSTIC SR
MUSTIC AF
MIRACLE
CONTAK CD
MIRACLE ICD
PATH CHF II
COMPANION
MIRACLE ICD II
CARE HF

CRT benefits Reduced mitral regurgitation Increased 6-minute hall walk distance Improved NYHA functional class ranking Increased peak VO2 and treadmill exercise time Reduced QRS duration Reversal of maladaptive remodeling Fewer days in hospital over 6 months Improved clinical composite response Reduced morbidity and mortality

Improvement with CRT - MR

Regional Wall Motion With CRT: Improved LVEF
Septum
Lateral
Pacing OffPacing On
Reg
ion
al F
ract
ion
al A
rea
Ch
ang
e
Seconds 0.40
Seconds 0.40
Adapted from Kass DA. Rev Cardiovasc Med. 2003;4(suppl 2):S3-S13.
Adapted from Kawaguchi M, et al. J Am Coll Cardiol. 2002;39:2052-2058.

CRT Promotes Reverse Remodeling in Class II CHF
Left Ventricular End Diastolic Diameter
200
250
300
350
400cm3
Base 6 Mo
Left Ventricular End Systolic Diameter
200
250
300
350
400cm3
Base 6 Mo
Left Ventricular Ejection Fraction
20
22
24
26
28
30%
Base 6 Mo
Control (n=85) CRT (n=69)
Abraham et al., Circulation 2004; 110:2864-2868
P=0.04 P=0.01 P=0.02

CRT Improves Quality of Life and NYHA Functional Class
Average Change in Score
-20
-15
-10
-5
0
MIR
ACLE
MUS
TIC
SRCO
NTAK
CD
MIR
ACLE
ICD
Control CRT
* * * *
* P < 0.05
NYHA: Proportion Improving 1 or More Class
0%
20%
40%
60%
80%
MIRACLE CONTAKCD
MIRACLEICD
Control CRT
**
*
Abraham et al., 2003

CRT Improves Exercise Capacity
Average Change in 6 Minute Walk Distance
-40
-20
0
20
40
60
MIR
ACLE
MUS
TIC
SRCO
NTAK
CD
MIR
ACLE
ICD
m
Control CRT
**
*
* P < 0.05
Average Change in Peak VO2
00
1
2
3
mL/
kg/m
in
Control CRT
*
*
*
*
Abraham et al., 2003

Progressive Heart Failure Mortality51% Relative Reduction with CRT
0.1 1.0 10.0Odds Ratio (95% CI)0.5
Favors CRT Favors No CRT
CONTAK CD (n=490)
MIRACLE ICD (n=554)
MIRACLE (n=532)
MUSTIC (n=58)
Overall (n=1634)
Bradley DJ, et al. JAMA 2003;289:730-740
Overall odds ratio (95% CI) of 0.49 (0.25 - 0.93)

Summary of Major Trials Significant clinical benefit of CRT in patients with class III-IV
HF, low EF, and QRS > 120 Improvement in symptoms Improvement in objective standards of HF
Meta-analysis 29% decrease in HF hospitalization (13% vs. 17.4%) 51% decrease in deaths from HF (1.7% vs. 3.5%) Trend toward decrease in overall mortality (4.9% vs 6.3%)
BUT: >30% non-responders consistent through most trials
Bradley et al. JAMA 2003;289:730

How to best predict who will respond to CRT?
?Use of Echo/ imaging parameters

Intraventricular Dyssynchrony M-Mode Echo Tissue Velocity Strain Imaging Three Dimensional Echo

M-Mode Septal to posterior wall delay Measures time between maximal
displacement of septum and posterior wall (SPWMD)
≥ 130 ms considered significant Easy to perform No specific equipment needed

Copyright ©2008 American Heart Association Anderson, L. J. et al. Circulation 2008;117:2009-2023
M-mode echocardiography with color-coded tissue velocity. a, Timing of ventricular septal (VS) wall motion is difficult to define because of
its severe hypokinesis and the lack of distinct peaks. b, Color coding of tissue velocity helps to identify the exact wall motion timing as
transition point of blue to red color for septal wall (arrows) and red to blue color for posterior wall (arrowheads) (right)

M-Mode- SPWMD Disadvantages Can only be quantified in regions
perpendicular to U/S beam Only feasible in half of patients studied In several reports, septal-posterior wall
delay didn’t predict outcome after CRT Only assesses motion of septal and
posterior walls

Tissue Velocity Measurement of either longitudinal tissue velocity
or deformation (strain)- Opposing wall peak delay of > 60-65 ms1-2
- Yu index: global 12 segment Asynchrony Index ≥ 33 ms3
High temporal resolution Color-coded TDI- allows simultaneous processing
of multiple samples from the same image Susceptible to translational motion or tethering
effect
Bax et al, Am J Card 2003Bax et al, Am J Card 2004

Copyright ©2008 American Heart Association
Anderson, L. J. et al. Circulation 2008;117:2009-2023
Tissue velocity waveforms in a normal subject from 4-chamber (left), apical long-axis (middle), and 2-chamber views (right)

Copyright ©2008 American Heart Association
Anderson, L. J. et al. Circulation 2008;117:2009-2023
Color-coded tissue velocity recordings from 12 LV segments before (a) and after (b) CRT in 65-year-old patient with
nonischemic cardiomyopathy whose LVEF improved by 17% at 6 months after CRT
Before CRT
After CRT
Apical 4 Ch Long axis 2 Chamber

Tissue Velocity- Disadvantages Susceptible to translational motion or
tethering effect Color coding can vary with time window
setting Requires specific equipment

Strain Imaging TDI-derived and Speckle tracking Abnormal strain pattern- premature early
systolic shortening of septum accompanied by lateral prestretch and followed by postsystolic lateral wall shortening
Less affected by tethering / translational motion

Copyright ©2008 American Heart Association
Anderson, L. J. et al. Circulation 2008;117:2009-2023
Radial strain curves from short-axis view of speckle tracking Echocardiography: Significant timing difference was found among
time to peak radial strain before CRT (a), and it was reduced after CRT (b).

Strain imaging Dependent on image quality; not feasible in
all patients Mixed results with respects to predicting
success after CRT

3-D Echo Only one image allows entire assessment Short-term improvements in 3-D
dyssynchrony index noted after CRT

Three Dimensional Echocardiography

3-D Echo No study to date shows 3D Echo predicts
response to CRT Highly dependent on image quality Incomplete inclusion of the apex Can’t perform in a-fib or rhythm with several
ectopic beats

Interventricular Dyssynchrony Difference in preejection period between PW
doppler in Ao and PA- Correlates with QRSd- Exceeds 40s in patients with QRDs>150 ms- Shown to be predictive of response post-CRT in
SCART and CARE-HF trials TV delay between RV and LV free wall not
predictive of effect of CRT

Evidence for echo in predicting CRT outcomes
Limited echo-CRT studies with hard endpoints
Thus far, trials have enrolled 4000 patients based on ECG versus ~500 by echocardiogram
PROSPECT Study- largest study

Copyright ©2008 American Heart Association
Chung, E. S. et al. Circulation 2008;117:2608-2616
Enrollment and follow-up of patients in PROSPECT

PROSPECT patient population
Mean age 68 years
Male 71%
NYHA class III 96%
Mean LVEF 23%
Prior MI 48%
Beta-blockers 85%
Ace-I 92%

Endpoints- Composite clinical score Worsened (died, hospitalized, worsened heart failure,
demonstrated worsening in NYHA class at last observation carried forward, moderate or marked worsening of patient global assessment score at last observation carried forward, or permanently discontinued CRT because of or associated with worsening heart failure
Improved (not worsened as defined above and demonstrated improvement in NYHA class at last observation carried forward or had moderate or marked improvement in patient global assessment score at last observation carried forward)
Unchanged (the patient was neither improved nor worsened)

Copyright ©2008 American Heart Association
Chung, E. S. et al. Circulation 2008;117:2608-2616
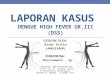
PROSPECT RESULTS: CCS and LVESV response rates

Table 5. Sensitivity, Specificity, and Area Under the Curve for Primary End Points
CCS
LVESV
Echocardiography
Type
Dyssynchrony Measure
Evaluable Echocardiograms,
(yield) %
Sensitivity, %
Specificity, %
AUC
P for AUC
Sensitivity, %
Specificity, %
AUC
P for AUC
M mode SPWMD 71.7 55.4 (48.3–
62.3) 50.0 (39.1–
60.9) 0.54 0.27 63.6 (54.8–
71.8) 52.1 (41.6–
62.4) 0.62 0.003
IVMD 92.4 55.2 (48.9–61.4)
56.4 (46.9–65.6)
0.58 0.013 59.7 (51.5–67.6)
54.1 (44.8–63.2)
0.59 0.009
LVFT/RR 85.3 36.3 (30.2–42.7)
76.6 (67.5–84.3)
0.57 0.032 41.0 (32.9–49.5)
74.1 (65.0–81.9)
0.60 0.007
Pulsed Doppler
LPEI 94.6 66.3 (60.2–72.0)
47.1 (38.0–56.4)
0.60 0.001 72.0 (64.3–78.8)
42.4 (33.6–51.6)
0.59 0.014
M mode+ Doppler LLWC 60.7 6.3 (3.2–11.0)
91.7 (82.7–96.9)
0.52 0.63 9.5 (4.7–16.8)
92.9 (85.3–97.4)
0.50 0.98
Ts (Lat-Sep) 66.8 42.4 (34.4–50.7)
56.9 (44.7–68.6)
0.50 0.85 52.6 (42.1–63.0)
69.2 (57.8–79.2)
0.61 0.012
Ts-SD 50.0 74.1 (65.2–81.8)
35.3 (22.4–49.9)
0.60 0.034 77.5 (66.0–86.5)
30.6 (19.6–43.7)
0.55 0.35
TDI, published
PVD 81.4 67.6 (60.3–74.3)
37.8 (27.8–48.6)
0.51 0.89 67.8 (58.6–76.1)
34.4 (25.0–44.8)
0.55 0.30
TDI+SRI DLC 81.1 41.7 (34.4–49.2)
60.4 (49.6–70.5)
0.51 0.75 43.6 (34.4–53.1)
59.4 (48.9–69.3)
0.51 0.75
Ts-peak displacement
37.4 54.8 (43.5–65.7)
56.1 (39.7–71.5)
0.56 0.32 58.0 (43.2–71.8)
54.5 (38.8–69.6)
0.57 0.25 TDI, median value used as cutoff
Ts-peak basal 82.0 51.9 (44.4– 53.8 (43.1– 0.55 0.19 52.1 (42.8– 55.7 (45.2– 0.57 0.10

Area Under the Curve
Sen
sitiv
ity
1-Specificity
Sen
sitiv
ity
1-Specificity
Odds ratios fora binary markerOdds ratios fora binary marker

PROSPECT Conclusions Echocardiographic measures of dyssynchrony
aimed at improving patient selection criteria for CRT did not have a clinically relevant impact on improving response rates
Echocardiographic parameters assessing dyssynchrony do not have enough predictive value to be recommended as selection criteria for CRT beyond current indications

Current ACC/AHA/NASPE 2005 Guideline Update Patients with LVEF 35%, sinus rhythm,
and New York Heart Association functional class III or ambulatory class IV symptoms despite recommended optimal medical therapy and who have cardiac dyssynchrony, which is currently defined as a QRS duration >120 ms, should receive CRT unless contraindicated (Class: I, Level of Evidence: A).

Other roles for Echo in CRT Assess LVEF Assess pre- and post-valvular regurgitation Assess best location of lead placement

Future directions >30% non-responders consistent through most
trials Studies should aim to characterize the non-
responders