Embed Size (px)
Citation preview

J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 9 , N O . 1 9 , 2 0 1 7
ª 2 0 1 7 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 7 . 0 3 . 5 5 9
EDITORIAL VIEWPOINT
Lymphodynamics inCongenital Heart DiseaseThe Forgotten Circulation*
Jacqueline Kreutzer, MD,a Christian Kreutzer, MDb
I n this issue of the Journal, the paper by Savlaet al. (1) opens a new door into a relatively poorlyunderstood subject in our field: lymphatic dy-
namic disorders after congenital heart surgery. Usingdynamic contrast-enhanced magnetic resonancelymphangiography and intranodal lymphangiographyin 25 patients, these investigators undertake a uniqueapproach and provide further insight into the under-standing of lymphatic disorders after cardiac surgery.
SEE PAGE 2410
Although the morbidity and mortality related tothese conditions is well-known (2), the lymphaticcirculation continues to be a relatively undiscoveredterritory for the pediatric cardiologist and cardiotho-racic surgeon. Still, the scientific background to thiswork is quite extensive and not new.
In the last decade of the 19th century, Ernest Star-ling at University College of London described theretention of plasma in the interstitial space as a “safetyvalve” to the circulation defending the failing heartfrom volume load (3,4). Thereafter, research inlymphatic circulation in heart failure flourished (4–7).Over the past decades, a series of discoveries haverevealed new knowledge in the vascular andmolecularaspects of the lymphatic system (8). However, theseconcepts are not commonly considered when
*Editorials published in the Journal of the American College of Cardiology
reflect the views of the authors and do not necessarily represent the
views of JACC or the American College of Cardiology.
From the aDivision of Cardiology, Department of Pediatrics, University of
Pittsburgh, School of Medicine, Children’s Hospital of Pittsburgh of
UPMC, Pittsburgh, Pennsylvania; and the bCardiac Surgery Department,
Austral University Hospital, Pilar, Provincia de Buenos Aires, Argentina.
Both authors have reported that they have no relationships relevant to
the contents of this paper to disclose.
evaluating cardiac physiology in patients withcongenital heart disease. It is common knowledge thatthe majority of vascularized tissues contain alymphatic capillary network. The lymphatic systemhas numerous crucial physiological functions inmammals, including fluid balance between the plasmaand interstitial compartments of the extracellularspace by returning protein and fluid filtered out ofthe capillaries to the vascular system and absorptionof fat from the small intestines. It also maintainsimportant immune functions; various antigens andactivated antigen-presenting cells are transported intothe lymph nodes and export immune effector cells andhumoral response factors into the blood circulation.
The lymphatic vascular system consists of 2 typesof vessels, the noncontractile initial lymphaticnetwork and the collecting vessels. Lymphatic endo-thelial cells are strongly attached at the anchoringfilaments to the surrounding collagen and elastin fi-bers. These cells show tight, single contact, andinterdigitated junctions. During expansion of theinitial lymphatic vessels, these junctions can beopened, allowing fluid to flow from the interstitiuminto the lymphatic vessels, whereas during compres-sion, overlapping junctions can be closed, therebyattenuating the return of lymph flow into the inter-stitium, and acting as “flap valves” (8). If thelymphatic pressure increases, the safety function isactivated and the system responds by increasing theamount of lymph contained within and transportedby the system. In this way, the system functions as areservoir, “protecting the failing heart” from volumeoverload (the Starling resistor effect).
The lymphatic capillaries drain into precollectingvessels, followed by larger collecting lymphatic ves-sels. The lymphatic drainage shows an extremelyefficient centripetal flow of lymph augmented by

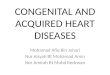
FIGURE 1 Anatomy of the Thoracic Lymphatic Circulation
DiaphragmDiaphragm
Internal jugular vein
Subclavian vein
Aorta
Thoracic duct
Azygos vein
Cisterna chyli
Right lumbar trunk
IVC Esophagus
Anatomy of the thoracic lymphatic circulation as seen from a posterior view (9).
Kreutzer and Kreutzer J A C C V O L . 6 9 , N O . 1 9 , 2 0 1 7
Lymphodynamics in Congenital Heart Disease M A Y 1 6 , 2 0 1 7 : 2 4 2 3 – 7
2424
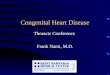
rhythmic contractions (8). In humans, the thoracicduct (TD) originates in the cisterna chyle (Figure 1)and ascends anterior to the vertebrae, with the aortaon its left and the azygous vein to its right (9). Belowthe fifth thoracic vertebra, the duct is usually doubleor plexiform; above fifth thoracic vertebra, it is usu-ally singular. At the level of the fifth thoracicvertebra, the TD inclines toward the left side to enterthe superior mediastinum and ascends behind theaortic arch and the thoracic part of the left subclavianartery, between the left side of the esophagus and theleft pleura, to the thoracic inlet (Figure 2). It ends byopening into the angle of junction of the left subcla-vian vein with the left internal jugular vein. Here, thedrainage can be single (in nearly 50% of the cases) or
multiple (10). At the most proximal end of the TD, avalve prevents blood from entering the duct, becausecontact with blood produces thrombosis or occlusionof the lymphatic vessels.
Given the proximity of lymphatic vessels to cardiacstructures manipulated during surgical repair ofcongenital heart defects trauma of TD can occur. Inaddition, after congenital heart surgery, abnormallyincreased venous pressure is common. The effects ofthe abnormal physiological states prevalent incongenital heart disease on the lymphatic circulationare now being discovered (11). The long oblivion forthe lymphatic circulation in pediatric cardiology iscoming to an end. Several contributions havedemonstrated its relevance and effect on devastatingcomplications after surgery, such as effusions, chy-lothorax, plastic bronchitis, and protein-losing en-teropathy (12,13). Lymphatic imaging and selectivecatheterization as reported by Dori et al. (1,12,13) nowallow understanding lymphodynamics and identifi-cation of 3 modes of lymphatic failure: leak from a TDbranch (traumatic leak); pulmonary lymphaticperfusion syndrome, when retrograde flow from theTD to the lung or mediastinum; and central lymphaticflow disorder, a newly characterized condition withabnormally low or absent central lymphatic flow, ef-fusions in more than 1 compartment, and dermalbackflow through abdominal lymphatic collaterals.
It is not surprising that in this most recent contri-bution from Dori’s group (1), the vast majority of pa-tients who suffered either from TD leak or pulmonarylymphatic perfusion syndrome had conditions typi-cally associated with increased central venous pres-sure and secondary impaired lymphatic drainage. Inpure right heart failure, as seen in the Glenn and theFontan circulations, the lung is exposed to a paradoxin which lymph from the lung is required to drain at ahigher pressure than it is created. In the normal lung,both the pulmonary arteriolar pressure and pulmo-nary capillary wedge pressures are higher than thecentral venous pressure, resulting in normal reab-sorption of fluid. After the superior cavopulmonaryanastomosis, the lung interstitium is subjected to anormal hydrostatic pressure, because more than 80%of the total lung arterial flow returns to the heart viapulmonary veins. However, there is a constant pro-pensity toward fluid accumulation in the lung,because the lymphatic circulation drains to a higherpressure compared with normal. The increase inresistance to lymphatic drainage results in lymphaticendothelial cells adherence and lymph cannot beeffectively removed from the interstitium. In contrastwith pulmonary edema resulting from increasedpulmonary capillary wedge pressure as a result

FIGURE 2 Anatomy of Central Lymphatic Circulation
Jugular lymph trunk
Internal jugular vein
Subclavian lymph trunk
Subclavian artery
Bronchomediastinal lymph trunk
Azygos vein
Thoracic duct
Esophagus
Left jugular lymph trunk
Subclavian lymph trunk
Subclavian artery
Subclavian vein
Left bronchomediastinal lymph trunk
Aortic arch
Left pulmonary artery
Left pulmonary veins
Intercostal lymph trunks
Left ventricle
Aorta
Pulmonary artery
Pulmonary veins
Intercostal lymph trunks
Superior vena cava
Right lymphatic duct
Anatomy of central lymphatic circulation view (9).
J A C C V O L . 6 9 , N O . 1 9 , 2 0 1 7 Kreutzer and KreutzerM A Y 1 6 , 2 0 1 7 : 2 4 2 3 – 7 Lymphodynamics in Congenital Heart Disease
2425
left heart pump failure or left-sided obstruction,the congested lung commonly seen in the earlyGlenn/Fontan patient is often related to lymph for-mation and accumulation, with pleural effusions as amanifestation of this imbalance (11).
This represents another paradox of the Fontancirculation and a challenge to Starling’s forces: pul-monary lymph is required to drain at a higher or verysimilar pressure as it is produced (Figures 3A and 3B).As a consequence, it is not surprising that lymphaticdisorders, such as chylous effusions, plastic
bronchitis, and protein-losing enteropathy, are seenin this patient population, and that most of the pa-tients reported in the study from Savla et al. (1) had aform of single ventricle variant.
The morbidity and mortality from post-operativechylothorax continues to be high (2). Historically,there have been limited diagnostic or therapeuticstrategies available to treat these patients. Standardtherapies are frequently ineffective (e.g., surgical TDligation) and/or have significant unwanted side ef-fects (e.g., eliminating fat from the diet during key

FIGURE 3 Mean Pressures in the Biventricular Circulation and Single Ventricle Circulation
Typical mean pressures in millimeters of mercury in the biventricular circulation (A) and single ventricle circulation (B). Lymph formed at the pulmonary capillary level
in the single ventricle circulation (B) is at a lower pressure at the capillary level than the pressure it is expected to drain at. *Thoracic duct.
Kreutzer and Kreutzer J A C C V O L . 6 9 , N O . 1 9 , 2 0 1 7
Lymphodynamics in Congenital Heart Disease M A Y 1 6 , 2 0 1 7 : 2 4 2 3 – 7
2426
growing stages of childhood, use of total parenteralnutrition, chemical pleuridesis often leading tomassive formation of aortopulmonary chest wallcollaterals, medical therapy with octreotide, pleuro-peritoneal shunts) (1,2). Thus, the use of dynamiccontrast-enhanced magnetic resonance lymphangi-ography to understand the pathophysiology of theselymphatic disorders after congenital heart surgeryand allow directed effective therapy reported bySavla et al. (1) is a breakthrough in our field. Inaddition to the diagnostic value, the technique pro-vides an opportunity for a therapeutic benefit basedon the particular diagnosis; 23 of the 25 patientsstudied underwent directed lymphatic intervention.Among the 25 patients, there were 16 with either atraumatic leak from the TD or pulmonary lymphaticperfusion syndrome, and in this group lymphatic in-terventions performed had 100% success. The pro-cedures were, however, mostly unsuccessful for thegroup with central lymphatic flow disorder (only 1 of7 benefited), for whom there seem to be no reliably
successful therapies known to date. All patients re-ported had previously failed standard therapies.Specific lymphatic interventions applied in this studyincluded a variety of procedures with or withoutclosure of the TD. These interventions aimed to closethe leaking sites. Direct leak of contrast into thepleural space due to trauma was indeed rare (2 pa-tients), and lymphatic intervention for these patientswas highly successful.
Further studies to understand the physiopathologyof lymphatic disorders after congenital heart surgeryand testing of potential new modalities of directedtherapy, such as lymphovenous anastomosis (14,15),may eventually reduce these patients’ morbidity.Indeed, promising surgical procedures are nowadaysbeing reintroduced (14,15) with early success to divertthe lymph flow to the lower pressure side of theFontan circulation, primarily for treatment of bothprotein-losing enteropathy and plastic bronchitis,and secondarily to reduce the chronic end organlymphedema.

J A C C V O L . 6 9 , N O . 1 9 , 2 0 1 7 Kreutzer and KreutzerM A Y 1 6 , 2 0 1 7 : 2 4 2 3 – 7 Lymphodynamics in Congenital Heart Disease
2427
CONCLUSIONS
This study enlightens a path to therapy of a poorlyunderstood serious problem after congenital heartsurgery, and one that has been largely mis-managed. As further pointed out in the discussionsection by Savla et al. (1), many of the assumptionsfrequently used to base treatment plans in thispatient population are proven to be wrong. Theauthors demonstrate how essential it is to under-stand the underlying physiopathology of thelymphatic system disorder to provide a directedtherapy to the problem, as indeed simple surgicalligation of the TD may possibly worsen the leak insome cases.
Dori et al. (1) should be congratulated for reporting aninnovative diagnostic and therapeutic tool with adefined relevant application in our field, which can bringa solution to a serious life-threatening postoperativecondition. We recommend increased use of the pro-posed diagnostic approach to further discover ways toachieve a lasting positive impact on the outcome oflymphatic flow disorders after congenital heart surgery.
ADDRESS FOR CORRESPONDENCE: Dr. JacquelineKreutzer, University of Pittsburgh School of Medicine,Cardiac Catheterization Laboratory, Children’s Hospitalof Pittsburgh of UPMC, One Children’s Hospital Drive,4401 Penn Avenue, Pittsburgh, Pennsylvania 15224.E-mail: [email protected].
RE F E RENCE S
1. Savla JJ, Itkin M, Rossano JW, Dori Y. Post-operative chylothorax in patients with congen-ital heart disease. J Am Coll Cardiol 2017;69:2410–22.
2. MeryCM,MoffettBS,KhanMS, etal. Incidence andtreatment of chylothorax after cardiac surgery inchildren: Analysis of a large multi-institution data-base. J Thorac Cardiovasc Surg 2014;147:678–86.
3. Starling EH. On the absorption of fluid from theconnective tissue spaces. J Physiol 1896;19:312–32.
4. Foldi M, Papp N. The role of lymph circulationin congestive heart failure. Jap Circ J 1961;25:703.
5. Wegria R, Zekert H, Walter KE, et al. Effect ofsystemic venous pressure on drainage of lymphfrom the thoracic duct. AmJPhysiol 1963;204:284.
6. Dumont AE, Clauss RH, Reed GE, Tice D. Ob-servations on lymph drainage in patients withcongestive heart failure: comparison with
findings in hepatic cirrhosis. N Engl J Med 1963;269:949.
7. Zotti E, Lesage A, Bradham RR, et al. Preventionand treatment of experimentally induced ascites indogs by thoracic duct to vein shunt. Surgery 1966;60:28–34.
8. Choi I, Lee S, Hong Y-K. The new era of thelymphatic system: No longer secondary to theblood vascular system. Cold Spring Harb PerspectMed 2012;2:a006445.
9. Brotons ML, Bolca C, Fréchette E, Deslauriers J.Anatomy and physiology of the thoracic lymphaticsystem. Thorac Surg Clin 2012;22:139–53.
10. Chen JM. The thoracic duct: predictably unpre-dictable? J Thorac Cardiovasc Surg 2015;150:497.
11. Menon S, Chennapragada M, Ugaki S, et al. Thelymphatic circulation in adaptations to the Fontancirculation. Pediatr Cardiol 2017 Feb 16 [E-pubahead of print].
12. Dori Y, Keller MS, Fogel MA, et al. MRIof lymphatic abnormalities after functionalsingle-ventricle palliation surgery. Am J Roent-genol 2014;203:426–31.
13. Dori Y, Keller MS, Rome JJ, et al. Percutaneouslymphatic embolization of abnormal pulmonarylymphatic flow as treatment of plastic bronchitisin patients with congenital heart disease. Circula-tion 2016;22:1160–70.
14. Cole WR, Witte MH, Kash SL, Rodger M,Bleisch WR, Muelheims GH. Thoracic duct-to-pulmonary vein shunt in the treatment of experi-mental right heart failure. Circulation 1967;36:539–43.
15. Hra�ska V. Decompression of thoracic duct: newapproach for the treatment of failing Fontan. AnnThorac Surg 2013;96:709–11.
KEY WORDS chylothorax, congenital heartdisease, lymphatics