-
8/2/2019 Lymphoma Discussion
1/23
Your Answer is CORRECT presented byEdward G. Weir, M.D.
You answered:Marginal zone lymphoma
The correct diagnosis is:Marginal zone lymphoma
Review the Slides
Histology: Lymph node histology is notable for an atypical
nodular lymphoidproliferation and a paracortex that is largely
replaced by fibrosis andadipocytes. Patent and occasionally
distended lymph node sinuses can beappreciated. Some of the
lymphoid nodules demonstrate germinal centers.Cytologically, the
nodules are composed of a monomorphous population ofsmall, slightly
irregular lymphocytes with mature chromatin. In addition,
thelymphocytes have moderately abundant clear cytoplasm, rendering
them amonocytoid appearance. There is no evidence of
plasmacytoiddifferentiation. The germinal centers comprise a
polymorphous populationof centrocytes, centroblasts and tingible
body macrophages.
By immunohistochemistry, the monomorphous lymphocytes are
positive forCD20 and negative for both CD5 and CD10. The stain for
CD5 highlightsonly the few paracortical T cells present, and the
stain for CD10 highlightsonly the germinal center cells. Also, an
immunostain for bcl-2 (not shown) ispositive on the monomorphous
population of lymphocytes and is negative
in the germinal centers.
Discussion: The monocytoid morphology of the malignant cells is
a classic histologicmanifestation of a low-grade marginal zone B
cell lymphoma. The nodulargrowth pattern and apparent follicular
colonization of the lymphomaunderscores the marginal zone origin of
the infiltrate. Furthermore, the lackof a prominent interfollicular
expansion suggests an early stage oflymphoma development.
The immunohistochemical studies clearly confirm that the
lymphoma is ofmarginal zone and not mantle or follicular
derivation. The lack of aberrantCD5 expression essentially excludes
a diagnosis of mantle cell lymphomaas well as small lymphocytic
lymphoma. A follicular lymphoma of low-grade
histology should be positive for CD10 and should show germinal
centerreactivity for bcl-2.
Most patients present with localized or generalized
peripherallymphadenopathy and a good performance status. Occasional
bonemarrow involvement is observed. The clinical course of nodal
marginalzone lymphomas has not been well studied. Recent series
suggest thatpatients respond to chemotherapy, but show a high early
relapse rate.Nonetheless, the relatively long median survival in
these patients is
http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047
-
8/2/2019 Lymphoma Discussion
2/23
consistent with an indolent biology.
Next Case
Case prepared by: Bahram R. Oliai, M.D.
[email protected]
Your Answer is CORRECT presented byEdward G. Weir, M.D.
You answered:Small lymphocytic lymphoma The correct diagnosis
is:Small lymphocytic lymphoma
Review the Slides
Histology: The nodal architecture is diffusely effaced by an
abnormal lymphoidinfiltrate. Lymph node sinuses are inapparent and
cortical follicles areessentially absent. Numerous pale zones
render the infiltrate a vaguenodular appearance on low power
examination. Cytologically, theinfiltrate is predominantly
comprised of a monomorphous population ofsmall, mature lymphocytes.
The pale zones are comprised of slightlylarger lymphocytes with
moderately abundant cytoplasm andprominent central nucleoli.
Mitoses are few and there is no evidence of
necrosis. By immunohistochemistry, the infiltrate is positive
for CD20and CD5, and negative for CD3 and CD10.
Discussion: Small lymphocytic lymphoma (SLL) is generally a
disease of theelderly, and is the lymph node manifestation of
chronic lymphocyticleukemia. Though occasional patients present
with aleukemic nodalinvolvement at diagnosis, most patients will
ultimately develop bonemarrow and peripheral blood infiltration.
Moreover, generalizedlymphadenopathy and hepatosplenomegaly are not
uncommon clinicalmanifestations. Furthermore, advanced stages of
the disease aretypically characterized by hypogammaglobulinemia and
autoimmunephenomenon, often resulting in infectious complications,
hemolyticanemia and thrombocytopenia. Like most indolent lymphomas,
SLL is
not considered to be curable with currently available therapy.
However,treatment with alkylating agents, prednisone, and more
recently, purineanalogs has been found to be remarkably effective
in producing long-term remissions. The extent of the disease at the
time of diagnosis isthe best predictor of survival. Lymph nodes
involved by SLL usuallydemonstrate diffuse architectural effacement
by a monomorphousproliferation of small, mature lymphocytes with
sparse cytoplasm. Thelymphocyte nuclei typically are round and have
a condensed chromatinpattern. A very specific histomorphologic
feature of SLL is the
mailto:[email protected]:[email protected]:[email protected]:[email protected]://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047mailto:[email protected]:[email protected]
-
8/2/2019 Lymphoma Discussion
3/23
presence of pseudofollicular growth centers, which renders the
infiltratea vaguely nodular appearance on low power examination.
Unlike the Bcell follicles of follicular hyperplasia and follicular
lymphoma, growthcenters have ill-defined margins and are
cytologically comprised ofpredominantly prolymphocytes.
Prolymphocytes are characterized aslarger lymphoid cells with more
abundant, slightly basophilic cytoplasm
and a prominent central nucleolus. Immunophenotypically, the
tumorcells demonstrate expression of B cell markers (CD20 and
CD79a) andaberrant expression of the T-related markers, CD5 and
CD43. Theyare negative for the T cell marker CD3 and the follicle
center cellmarker CD10. Among CD5-positive B cell lymphomas, the
presence ofCD23 reactivity distinguishes SLL from mantle cell
lymphoma. Mantlecell lymphoma, which is not characterized by growth
centers, isnegative for CD23 but positive for the PRAD1 oncogene
proteinproduct CyclinD1. SLL is a low-grade lymphoma with few
mitoses anda low proliferation index. Alternatively, Burkitts
lymphoma is a veryaggressive tumor characterized by numerous
mitoses, macrophagesengulfing apoptotic bodies, and necrosis.
Next Case
Case prepared by:Carol Allan, M.D.
[email protected]
Contact Us| Johns Hopkins Medical Laboratories| Pathology
Consultation| Pathology Homepage | Conference Home
Copyright 2000-2006 The Johns Hopkins UniversityAll rights
reserved. No part of this website may be reproduced in any form or
by any means or
incorporated into any information retrievel system, electronic
or mechanical, without the written permission of JHU.
Contact Us| Johns Hopkins Medical Laboratories| Pathology
Consultation | Pathology Homepage | Conference Home
Copyright 2000-2006 The Johns Hopkins UniversityAll rights
reserved. No part of this website may be reproduced in any form or
by any means orincorporated into any information retrievel system,
electronic or mechanical, without the written permission of
JHU.
mailto:[email protected]:[email protected]:[email protected]://pathology2.jhu.edu/sp/mailform.cfmhttp://pathology2.jhu.edu/sp/mailform.cfmhttp://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology.jhu.edu/http://pathology.jhu.edu/http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/mailform.cfmhttp://pathology2.jhu.edu/sp/mailform.cfmhttp://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology.jhu.edu/http://pathology.jhu.edu/http://pathology.jhu.edu/http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology.jhu.edu/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology2.jhu.edu/sp/mailform.cfmhttp://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology.jhu.edu/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology2.jhu.edu/sp/mailform.cfmmailto:[email protected]
-
8/2/2019 Lymphoma Discussion
4/23
Your Answer is CORRECT presented byEdward G. Weir, M.D.
You answered:T cell-rich B cell lymphoma
The correct diagnosis is:T cell-rich B cell lymphoma
Review the Slides
Histology: Histologic sections of the lymph node demonstrate
complete architecturaleffacement by a diffuse lymphoid infiltrate.
Both lymph node sinuses andcortical follicles are absent. The
infiltrate is comprised of numerous large,atypical cells surrounded
by a background population of small, maturelymphocytes. Few plasma
cells and granulocytes are identified. The atypicalcells have
abundant cytoplasm and complex nuclei; some cells appear to
bebinucleated. Many of the atypical cells are mitotically active.
Byimmunohistochemistry, the large cells are positive for CD20, and
negative forCD3, CD15 and CD30. Moreover, several of these large
cells demonstratekappa Ig light chain expression and none of them
demonstrate lambda lightchain expression. The vast majority of
small lymphocytes in the backgroundare positive for CD3, and
negative for CD20 and CD57.
Discussion: Diffuse effacement of lymph node architecture by a
dual population of largeatypical cells and small mature lymphocytes
is characteristic of manylymphoma types, including those listed
above. Though these lymphomas mayhave unique but often subtle
morphologic features, immunophenotypicstudies are frequently
necessary to establish a definitive diagnosis. A T cell-rich large
B cell lymphoma (TCRBCL) is cytologically notable for
numerouslarge, atypical cells that typically have an unequivocally
malignantappearance. These cells are very polymorphous, may have
bizarrely-shapednuclei, and are mitotically active. The small cells
in the background, whichusually predominate in number, are round
and regular and represent hostreactive T cells. This pattern is in
contrast to a peripheral T cell lymphoma,which characteristically
demonstrates a spectrum of atypicality from small-to-
intermediate-to-large lymphocytes. Also, unlike both mixed
cellularityHodgkins lymphoma and peripheral T cell lymphoma, there
is a generalpaucity of plasma cells and granulocytes. Moreover, the
large atypical cells inTCRBCL are immunophenotypically positive for
the B cell marker CD20, andnegative for the T cell marker CD3 and
the Hodgkins markers CD15 andCD30. In addition, the lack of
reactivity for CD30 differentiates TCRBCL fromanaplastic large cell
lymphoma, often referred to as Ki-1(CD30) lymphoma. Itshould be
noted that TCRBCL may be difficult to distinguish from a
diffusevariant of lymphocyte predominant Hodgkin lymphoma (LPHL),
bothmorphologically and immunophenotypically. Like TCRBCL, LPHL
isconsidered to be a B cell neoplasm. However, the malignant cells
of TCRBCLlack the popcorn cytology of the L&H cells of LPHL.
Furthermore, animmunostain for CD57 may be helpful since increased
numbers of CD57-positive T cells are commonly found in LPHL and are
usually distributed inrings around the L&H cells. TCRBCL is
considered to be a morphologicvariant of diffuse large B cell
lymphoma. It is an aggressive lymphoma but isamenable to cure with
multiagent chemotherapy.
Next Case
Case prepared by: Carol Allan, M.D.
http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047mailto:[email protected]:[email protected]:[email protected]://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047
-
8/2/2019 Lymphoma Discussion
5/23
[email protected]
Your Answer is CORRECT presented byRisa Mann, M.D.
You answered:Burkitts lymphoma
The correct diagnosis is:Burkitts lymphoma
Review the Slides
Histology: A large abdominal mass is composed of a monotonous
cellular
proliferation infiltrating diffusely through adipose tissue. The
neoplasticcells have a high mitotic rate and this is associated
with the so-calledstarry sky pattern, which is due to the presence
of benign appearinghistiocytes scattered throughout the tumor mass.
The neoplastic cellshave relatively round nuclei with multiple
medium sized nucleoli. Thetumor has an extremely high proliferation
rate with many mitoticfigures. The nuclei of the tumor cells are
approximately the same sizeas the nuclei of the benign starry sky
histiocytes. The neoplastic cellshave a small amount of basophilic
cytoplasm. Although not visible onH&E stained slides, a touch
prep of these tumor cells woulddemonstrate deep basophilic
cytoplasm with numerous cytoplasmiclipid vacuoles.
Discussion: The dense infiltrate in the abdominal adipose tissue
is easilyrecognized as a neoplastic lymphomatous process. The
differentialdiagnosis involves the subclassification of this
lymphoma. The starrysky pattern which is characteristic of any
lymphoma with a highproliferation rate is commonly seen in Burkitt
lymphoma but it may alsobe seen in other high grade lymphomas such
as lymphoblasticlymphoma as well as large cell lymphomas. The size
of the nuclei ishelpful in further subclassifying this tumor. In
Burkitt lymphoma theneoplastic cells have nuclei, which are about
the same size of thenuclei of starry sky histiocytes. In contrast,
the nuclei of lymphoblasticlymphoma cells are usually smaller than
the nuclei of the benignhistiocytes and the nuclei of large cell
lymphomas are usually largerthan the nuclei of the starry sky
histiocytes. Lastly, most helpful in this
differential diagnosis is the immunophenotype. The neoplastic
cells ofBurkitt lymphoma usually demonstrate membranous IgM with
lightchain restriction and B cell associated antigens such as CD19,
CD20,CD22, CD10 and BCL6. The cells are negative for CD23, CD5
andTdT. Burkitt lymphoma has one of the highest proliferation rates
of alllymphomas and nearly 100% of the cells are positive for Ki-67
staining.
The tumor cells show clonal rearrangement of the
immunoglobulinheavy and light chains and most cases have a
translocation of MYC
http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047
-
8/2/2019 Lymphoma Discussion
6/23
from chromosome 8 to the IgG heavy chain region on chromosome
14or less commonly to the light chain loci on chromosomes 11 or
22.Epstein Barr Virus (EBV) is identified in the majority of the
neoplasticcells in endemic cases, however, the frequency of EBV
association insporadic Burkitt lymphoma is low. Sporadic Burkitt
lymphoma occursmainly in children and young adults but it can occur
at any age.
Patients usually present with bulky disease often presenting
inextranodal sites.
Next Case
Case prepared by:Bahram R. Oliai, M.D.
[email protected]
Contact Us| Johns Hopkins Medical Laboratories| Pathology
Consultation| Pathology Homepage | Conference Home
Copyright 2000-2006 The Johns Hopkins UniversityAll rights
reserved. No part of this website may be reproduced in any form or
by any means orincorporated into any information retrievel system,
electronic or mechanical, without the written permission of
JHU.
Your Answer is CORRECT presented byEdward G. Weir, M.D.
You answered:Follicular lymphoma
The correct diagnosis is:Follicular lymphoma
Review the Slides
Histology: Histologic sections of lymph node demonstrate
significant fattyreplacement and an abnormal nodular proliferation
of lymphocytes.
The lymphoid nodules, which are round, discrete and
fairlyhomogeneous in size, resemble B cell follicles. However,
unlike normalB cell follicles, they lack well-defined mantle zones
and polarizedgerminal centers. Furthermore, the abnormal lymphoid
nodules arelargely comprised of a monomorphous population of small,
mature,cleaved lymphocytes and are notable for a conspicuous
absence oftingible body macrophages. By immunohistochemistry,
theselymphocytes are positive for CD20, CD10 and Bcl-2, and are
negativefor CD3, CD43 and CD5. The Ki-67 proliferation marker
demonstrates
mailto:[email protected]:[email protected]:[email protected]://pathology2.jhu.edu/sp/mailform.cfmhttp://pathology2.jhu.edu/sp/mailform.cfmhttp://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology.jhu.edu/http://pathology.jhu.edu/http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology.jhu.edu/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology2.jhu.edu/sp/mailform.cfmmailto:[email protected]
-
8/2/2019 Lymphoma Discussion
7/23
a low level of expression.
Discussion: Follicular lymphoma is morphologically defined as a
tumor comprisedof follicle center cells, usually a mixture of
small, cleaved centrocytesand larger, noncleaved centroblasts.
Low-grade follicular lymphomastypically demonstrate a nodular
growth pattern and a predominance of
centrocytes, whereas more aggressive follicular lymphomas tend
to bearchitecturally diffuse and show a greater proportion of
centroblasts.Molecularly, follicular lymphomas are characterized by
thet(14;18)(q32;q21) chromosomal translocation that has been
identifiedin approximately 80% of cases using routine karyotyping
methods. Thet(14;18) is a reciprocal translocation that juxtaposes
the bcl-2oncogene on chromosome 18q21 with the IgH gene on 14q32.
As aresult, transcription of the bcl-2 gene is brought under the
control of theIgH gene regulatory elements, most likely an enhancer
region, leadingto constitutive overexpression of the bcl-2 gene.
The bcl-2 protein,which is localized to subcellular membranes such
as the outermitochondrial membrane, endoplasmic reticulum and
nuclearenvelope, plays a prominent role in protecting the cell from
apoptotic
death. Cells, which overexpress the bcl-2 protein, have a
prolongedhalf-life, rendering these cells more susceptible to
secondary geneticevents that may result in transformation to a more
aggressivephenotype. By immunohistochemistry, the neoplastic
follicular cells arepositive for the B cell markers CD20 and CD79a,
as well as thegerminal center cell marker CD10. Other low-grade B
cell lymphomaslack CD10 expression. Also, unlike small lymphocytic
lymphoma andmantle cell lymphoma, follicular lymphoma cells lack
expression ofCD5 and CD43. Lastly, the immunohistochemical
expression of thebcl-2 protein is useful in distinguishing
follicular lymphoma fromfollicular hyperplasia, since bcl-2 is
absent from reactive processes.
Next Case
Case prepared by:Carol Allan, M.D.
[email protected]
Contact Us| Johns Hopkins Medical Laboratories| Pathology
Consultation| Pathology Homepage | Conference Home
Copyright 2000-2006 The Johns Hopkins UniversityAll rights
reserved. No part of this website may be reproduced in any form or
by any means orincorporated into any information retrievel system,
electronic or mechanical, without the written permission of
JHU.
mailto:[email protected]:[email protected]:[email protected]://pathology2.jhu.edu/sp/mailform.cfmhttp://pathology2.jhu.edu/sp/mailform.cfmhttp://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology.jhu.edu/http://pathology.jhu.edu/http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology.jhu.edu/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology2.jhu.edu/sp/mailform.cfmmailto:[email protected]
-
8/2/2019 Lymphoma Discussion
8/23
Your Answer is CORRECT presented byRisa Mann, M.D.
You answered:Follicular lymphoma, mixed smallcleaved and large
cell type (WHOgrade 2)
The correct diagnosis is:Follicular lymphoma, mixed smallcleaved
and large cell type (WHOgrade 2)
Review the Slides
Histology: This lymph node shows replacement of the normal nodal
architectureby prominent nodular proliferation of lymphoid cells.
The normalsinuses have been obliterated by this process. The
germinal center-likestructures proliferate within the lymph node in
a back-to-back patternwith little intervening paracortical areas.
The germinal center-like
structures lack tingible body macrophages and lack obvious areas
ofpolarization. At high power, the cellular proliferation within
the germinalcenters demonstrates a mixed cell population comprised
predominantlyof small cleaved lymphocytes admixed with larger
centroblasts whichdemonstrate more cytoplasm and prominent
nucleoli, sometimesopposed to the nuclear membrane.
Discussion: The major differential diagnosis in this case is
between that of a floridreactive follicular hyperplasia and
follicular lymphoma. A mantle celllymphoma may grow in a vaguely
nodular pattern, but rarelydemonstrates this prominent follicular
growth pattern. The germinalcenters in this case proliferate in a
back-to-back pattern within thelymph nodes, leaving very little
intervening paracortical areas. This
pattern is more typical of a neoplastic rather than a reactive
process.Other features that morphologically favor a neoplastic
follicular processinclude the lack of tingible body macrophages and
the lack ofpolarization within the germinal centers. On closer
examination theneoplastic proliferation within the germinal centers
is composedpredominantly of small cleaved lymphocytes admixed with
largeratypical lymphocytes (centroblasts). The number of large
cells seen athigh power within the nodules is within the range
accepted for a mixedsmall cleaved and follicular lymphoma (greater
than 5 and less than 15large cells per high powered field).
Although the morphologic features described above are helpful
inarriving at a diagnosis of follicular lymphoma, flow cytometry
and/or
immunoperoxidase stains may be helpful in further documenting
thediagnosis. Flow cytometry in this case showed the phenotype
typical offollicular lymphoma. The cells are CD10 positive B cells,
whichdemonstrated light chain restriction. In addition, BCL2 stains
could beperformed on the paraffin embedded tissue, documenting the
BCL2positivity of the proliferating B cells within the neoplastic
nodules. Thisobservation correlates with the characteristic 14/18
translocationassociated with follicular lymphomas.
http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047
-
8/2/2019 Lymphoma Discussion
9/23
Next Case
Case prepared by:Greg Seidel, M.D.
[email protected]
Contact Us| Johns Hopkins Medical Laboratories| Pathology
Consultation| Pathology Homepage | Conference Home
Copyright 2000-2006 The Johns Hopkins UniversityAll rights
reserved. No part of this website may be reproduced in any form or
by any means orincorporated into any information retrievel system,
electronic or mechanical, without the written permission of
JHU.
Your Answer is CORRECT presented byMichael Borowitz, M.D.,
Ph.D.
You answered:Small lymphocytic lymphoma/chroniclymphocytic
leukemia transforming todiffuse large B cell lymphoma(Richter
syndrome)
The correct diagnosis is:Small lymphocytic
lymphoma/chroniclymphocytic leukemia transforming todiffuse large B
cell lymphoma(Richter syndrome)
Review the Slides
Histology: Much of the node shows characteristic changes of
SLL/CLL, witharchitecture effacement by a pseudofollicular
proliferation. Cells are roundand outside the pseudofollicles the
cells are mostly small. Cells in thepseudofollicles have more
abundant cytoplasm and include manyprolymphocytes and
paraimmunoblasts with larger nuclei and moreprominent nucleoli.
Other parts of the node, however, show a very differentpattern,
with diffuse architectural effacement by a more
monotonouspopulation of large cells. Immunophentoypically these two
areas are alsodifferent; both express CD20,
mailto:[email protected]:[email protected]:[email protected]://pathology2.jhu.edu/sp/mailform.cfmhttp://pathology2.jhu.edu/sp/mailform.cfmhttp://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology.jhu.edu/http://pathology.jhu.edu/http://pathology.jhu.edu/http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology.jhu.edu/researchbrochure/division.cfm?id=9Borowitzhttp://pathology.jhu.edu/researchbrochure/division.cfm?id=9Borowitzhttp://pathology.jhu.edu/researchbrochure/division.cfm?id=9Borowitzhttp://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology.jhu.edu/researchbrochure/division.cfm?id=9Borowitzhttp://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology.jhu.edu/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology2.jhu.edu/sp/mailform.cfmmailto:[email protected]
-
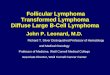
8/2/2019 Lymphoma Discussion
10/23
but there is loss of CD23 on the larger cells,
-
8/2/2019 Lymphoma Discussion
11/23
and a much higher expression of the proliferation marker
Ki-67.
-
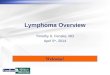
8/2/2019 Lymphoma Discussion
12/23
Flow cytometry plots also show this; while all cells are CD5+ B
cells withclonal expression of kappa light chain, there is a
distinct population of largercells with much brighter CD20, FMC7,
and loss of CD23.
-
8/2/2019 Lymphoma Discussion
13/23
Discussion: The number of large cells can vary greatly in
SLL/CLL, and their numberalone is not sufficient to establish a
diagnosis of transformation. It isparticularly important not to
over-interpret cases with unusually prominentpseudofollicles, some
of which can even coalesce. True Richtertransformation is
invariably associated with a distinctly different
architecturalappearance from the background SLL/CLL.
-
8/2/2019 Lymphoma Discussion
14/23
Next Case
Case prepared by:Amy Duffield, M.D., Ph.D.
[email protected]
Contact Us| Johns Hopkins Medical Laboratories | Pathology
Consultation| Pathology Homepage | Conference Home
Copyright 2000-2006 The Johns Hopkins UniversityAll rights
reserved. No part of this website may be reproduced in any form or
by any means or
Your Answer is CORRECT presented byAndrea Subhawong, M.D.
You answered:Anaplastic large cell lymphoma
The correct diagnosis is:Anaplastic large cell lymphoma
Review the Slides
Histology: The biopsy is notable for large lymphoid cells which
infiltrate in a cohesivepattern with a predilection for the nodal
sinuses. Cytologically the nuclei areenlarged, often
multinucleated, and have prominent nucleoli, which tend tobe
smaller and less eosinophilic than those observe in Hodgkin
lymphoma.Some cells have nuclei which are eccentric and indented by
a cytoplasmiclight zone (hoff), and are thus defined as hallmark
cells
Discussion: The morphologic findings are highly suggestive of
ALCL.Immunohistochemical confirmation is made by intense and
diffusemembranous and golgi staining with CD30 in the absence of
B-cell markers.
mailto:[email protected]:[email protected]:[email protected]://pathology2.jhu.edu/sp/mailform.cfmhttp://pathology2.jhu.edu/sp/mailform.cfmhttp://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology.jhu.edu/http://pathology.jhu.edu/http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology.jhu.edu/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology2.jhu.edu/sp/mailform.cfmmailto:[email protected]
-
8/2/2019 Lymphoma Discussion
15/23
In this context, ALK positivity confirms the diagnosis but is
not positive in allcases and in fact becomes less frequent as a
function of patient age.
In ALK negative cases, staining with CD4, CD2 and/or TIA-1 can
beconfirmatory in conjunction with appropriate morphology, however
thereappears to be no uniform criteria for separating ALK negative
ALCL fromperipheral T-cell lymphoma, NOS. The distinction is
prognostically relevantas the survival decreases from ALCL ALK+
(best), ALCL ALK-(intermediate), to PTCL NOS (worst). Isolated
cutaneous ALCL has the best
-
8/2/2019 Lymphoma Discussion
16/23
prognosis of all.
This is the last case for Week 470.
Return to List of Conferences
Contact Us| Johns Hopkins Medical Laboratories| Pathology
Consultation| Pathology Homepage
Copyright 2000-2006 The Johns Hopkins UniversityAll rights
reserved. No part of this website may be reproduced in any form or
by any means orincorporated into any information retrievel system,
electronic or mechanical, without the written permission of
JHU.
Your Answer is CORRECT presented byAndrea Subhawong, M.D.
You answered:
T cell/ histiocyte rich large B-celllymphoma
The correct diagnosis is:
T cell/ histiocyte rich large B-celllymphoma
Review the Slides
Histology: The architecture is effaced by a diffuse lymphoid
infiltrate. Most of theinfiltrate is composed of small lymphocytes
and histiocytes, but thereare scattered large, atypical cells with
abundant cytoplasm andcomplex nuclei; some cells appear to be
binucleated. Byimmunohistochemistry, the large cells are positive
for CD20, andnegative for CD3, CD15 and CD30 (not shown). There is
no residualnodularity in the background of the node.
Discussion: TCRBCL may be difficult to distinguish from a
diffuse variant of nodularlymphocyte predominant Hodgkin lymphoma
(NLPHL), bothmorphologically and immunophenotypically. Like TCRBCL,
NLPHL isconsidered to be a B cell neoplasm. However, the malignant
cells ofTCRBCL lack the popcorn cytology of the atypical cells of
NLPHL.Furthermore, an immunostain for CD57 may be helpful since
increasednumbers of CD57-positive T cells are commonly found in
NLPHL andare usually distributed in rings around the popcorn cells.
TCRBCL is
http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/mailform.cfmhttp://pathology2.jhu.edu/sp/mailform.cfmhttp://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology.jhu.edu/http://pathology.jhu.edu/http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology.jhu.edu/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology2.jhu.edu/sp/mailform.cfmhttp://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047
-
8/2/2019 Lymphoma Discussion
17/23
considered to be a morphologic variant of diffuse large B
celllymphoma. It is an aggressive lymphoma but is amenable to cure
withmulti-agent chemotherapy.
This is the last case for Week 471.
Return to List of Conferences
Contact Us| Johns Hopkins Medical Laboratories| Pathology
Consultation| Pathology Homepage
Copyright 2000-2006 The Johns Hopkins UniversityAll rights
reserved. No part of this website may be reproduced in any form or
by any means orincorporated into any information retrievel system,
electronic or mechanical, without the written permission of
JHU.
incorporated into any information retrievel system, electronic
or mechanical, without the written permission of JHU.
Contact Us| Johns Hopkins Medical Laboratories| Pathology
Consultation| Pathology Homepage | Conference Home
Copyright 2000-2006 The Johns Hopkins UniversityAll rights
reserved. No part of this website may be reproduced in any form or
by any
means or
incorporated into any information retrievel system, electronic
or mechanical, without the
written permission of JHU. Discussion:
MALT lymphoma is characterized by a dense, monotonous
population of centrocyte-like cells, lymphoepithelial
lesions
(infiltration of glandular epithelium by lymphocytes) and
frequent follicular colonization. The tumor cells may also
have plasmacytoid differentiation. Tumor cells are
immunoreactive for B cell markers, including CD19, CD20,
and CD79a, as well as bcl-10, with variable CD43 staining.
They exhibit monoclonal light chain staining. This case
demonstrated monoclonal heavy chain rearrangement by
molecular studies.
http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/mailform.cfmhttp://pathology2.jhu.edu/sp/mailform.cfmhttp://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology.jhu.edu/http://pathology.jhu.edu/http://pathology2.jhu.edu/sp/mailform.cfmhttp://pathology2.jhu.edu/sp/mailform.cfmhttp://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology.jhu.edu/http://pathology.jhu.edu/http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/result.cfm?CFID=6417107&CFTOKEN=32851047http://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047http://pathology.jhu.edu/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology2.jhu.edu/sp/mailform.cfmhttp://pathology.jhu.edu/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pds17.pathology.jhmi.edu/N/n.web?EP=N&URL=/MCGI/DICLKUP%5EWEBDICT%28304,1%29/http://pathology2.jhu.edu/sp/mailform.cfmhttp://pathology2.jhu.edu/sp/continue.cfm?grp=0&CFID=6417107&CFTOKEN=32851047
-
8/2/2019 Lymphoma Discussion
18/23
Gastric MALT lymphomas are closely linked to Helicobacter
pyloriinfection, and H. pylorieradication therapy produces
a long term favorable outcome (Tohoku J Exp Med
2008;214:79)
Celiac disease, or gluten-sensitive enteropathy, is a T-cell
mediated disease of genetically susceptible individuals,
induced by ingesting proteins in wheat (gliadins), barley
(hordeins) or rye (secalinin). Symptoms include episodic
diarrhea, abdominal pain and distention and weight loss
(Clin Med Res 2004;2:71), with clinical and microscopic
improvement after dietary withdrawal. Microscopic changes
include an increase in intraepithelial lymphocytes of
40+lymphocytes/100 surface or upper crypt enterocytes, or early
clustering of 12+ lymphocytes at the tip of villi and
extending
evenly down the sides of the villus (Mod Path
2003;16:342). There is also diffuse enteritis with marked
atrophy or total loss of villi and elongated crypts.
Definitive
diagnosis requires these histologic findings plus positive
serology and favorable clinical and serologic responses
after
dietary change. The differential diagnosis includes duodenal
intraepithelial lymphocytosis with normal villous
architecture,
associated with H. pyloriinfection, but without any other
features of celiac disease (Mod Path 2005;18:1134).
In this case, the presence of celiac sprue appears to be
incidental. Celiac sprue is associated with an increased
risk
of malignant intestinal disease, but this is usually T cell
intestinal lymphoma of the small bowel, not MALT lymphoma
of the stomach. Celiac sprue does not appear to be
associated with H. pylorigastritis (Am J Gastroenterol
2006;101:1880).
Additional references: PathologyOutlines.com chapters
-small bowel,Lymphoma: B cell,Stomach
http://www.ncbi.nlm.nih.gov/pubmed/18212490http://www.ncbi.nlm.nih.gov/pubmed/18212490http://www.ncbi.nlm.nih.gov/pubmed/18212490http://www.ncbi.nlm.nih.gov/pubmed/18212490http://www.ncbi.nlm.nih.gov/pubmed/15931338http://www.ncbi.nlm.nih.gov/pubmed/15931338http://www.ncbi.nlm.nih.gov/pubmed/15931338http://www.ncbi.nlm.nih.gov/pubmed/12692199http://www.ncbi.nlm.nih.gov/pubmed/12692199http://www.ncbi.nlm.nih.gov/pubmed/12692199http://www.ncbi.nlm.nih.gov/pubmed/12692199http://www.ncbi.nlm.nih.gov/pubmed/15803187http://www.ncbi.nlm.nih.gov/pubmed/15803187http://www.ncbi.nlm.nih.gov/pubmed/15803187http://www.ncbi.nlm.nih.gov/pubmed/16780559http://www.ncbi.nlm.nih.gov/pubmed/16780559http://www.ncbi.nlm.nih.gov/pubmed/16780559http://www.ncbi.nlm.nih.gov/pubmed/16780559http://www.pathologyoutlines.com/smallbowel.html#celiacspruehttp://www.pathologyoutlines.com/smallbowel.html#celiacspruehttp://www.pathologyoutlines.com/smallbowel.html#celiacspruehttp://www.pathologyoutlines.com/lymphoma.html#MALThttp://www.pathologyoutlines.com/lymphoma.html#MALThttp://www.pathologyoutlines.com/lymphoma.html#MALThttp://pathologyoutlines.com/stomach.html#MALThttp://pathologyoutlines.com/stomach.html#MALThttp://pathologyoutlines.com/stomach.html#MALThttp://pathologyoutlines.com/stomach.html#MALThttp://www.pathologyoutlines.com/lymphoma.html#MALThttp://www.pathologyoutlines.com/smallbowel.html#celiacspruehttp://www.ncbi.nlm.nih.gov/pubmed/16780559http://www.ncbi.nlm.nih.gov/pubmed/16780559http://www.ncbi.nlm.nih.gov/pubmed/15803187http://www.ncbi.nlm.nih.gov/pubmed/12692199http://www.ncbi.nlm.nih.gov/pubmed/12692199http://www.ncbi.nlm.nih.gov/pubmed/15931338http://www.ncbi.nlm.nih.gov/pubmed/18212490http://www.ncbi.nlm.nih.gov/pubmed/18212490
-
8/2/2019 Lymphoma Discussion
19/23
-
8/2/2019 Lymphoma Discussion
20/23
Grossly, most central lymphomas are solid, grey,
ill-defined,
and usually deep-seated. Some travel along white matter
tracts and transcend the corpus callosum, like infiltrating
gliomas. Histologically, they are widely infiltrating with
aperivascular predilection. Most are discohesive, but may
occur in a glial meshwork within the CNS. Primary brain
lymphomas have scant cytoplasm, high grade nuclei and
multiple nucleoli, but less pleomorphism than other high
grade CNS tumors. Most primary CNS lymphomas are
diffuse large B cell subtype, and are immunoreactive for
CD20, CD79a and CD22, but negative for CD3. However,
nearly all tumors have a background of reactive T cells that
may lead to an erroneous diagnosis of T cell lymphoma.
The mitotic index is often > 50%.
Smears show single cells with discrete cell borders,
vesicular nuclei, prominent nucleoli and frequent apoptosis.
Treatment includes high-dose methotrexate therapy with or
without radiation. Chemotherapy has extended median
survival in immunocompetent patients to 44 months
(eMedicine). Although tumors can be classified by
immunohistochemistry into germinal center and non-
germinal center phenotypes, this does not appear to
influence prognosis (Neuropathology 2009 Nov 18 [Epub
ahead of print],J Ne
Discussion
Intravascular lymphoma is a rare subtype of diffuse large B
cell lymphoma, with intravascular growth in the skin, CNS,
and other sites. The presenting signs and symptoms are
often complex, and include mental status changes, as in this
case, and rapidly progressive dementia. Patients may
present with a mass lesion (Pathol Int 2004;54:231), a skin
http://emedicine.medscape.com/article/1157638-overviewhttp://emedicine.medscape.com/article/1157638-overviewhttp://emedicine.medscape.com/article/1157638-overviewhttp://www.ncbi.nlm.nih.gov/pubmed/19925562http://www.ncbi.nlm.nih.gov/pubmed/19925562http://www.ncbi.nlm.nih.gov/pubmed/19925562http://www.ncbi.nlm.nih.gov/pubmed/19925562http://www.ncbi.nlm.nih.gov/pubmed/20012911http://www.ncbi.nlm.nih.gov/pubmed/20012911http://www.ncbi.nlm.nih.gov/pubmed/20012911http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=15028023&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=15028023&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=15028023&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=15028023&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/pubmed/20012911http://www.ncbi.nlm.nih.gov/pubmed/19925562http://www.ncbi.nlm.nih.gov/pubmed/19925562http://emedicine.medscape.com/article/1157638-overview
-
8/2/2019 Lymphoma Discussion
21/23
rash or fever of unknown origin.
Patients are typically elderly, with a median age of 71
years.
Although chemotherapy may be effective (Ann Oncol
2004;15:1215), these tumors are often not diagnosed until
autopsy, which typically shows involvement of most organs.
In this case, the patient was 72 years old, and expired two
weeks after the brain biopsy. A post-mortem examination
revealed widespread disease, with involvement of the heart,
lung, kidneys, adrenals, stomach, pancreas and spleen. No
skin lesions were found.
Histologically, the tumor is composed of large centroblast-
like lymphoid cells with prominent nucleoli within small
vessel lumina, often capillaries. Mitotic figures are
frequent,
and there are often fibrin thrombi. Immunohistochemistry
results are similar to diffuse large B cell lymphoma, with
immunoreactivity for CD19, CD20, CD22 and CD79a.
Tumors are usually bcl2 positive. Rarely, these tumors are T
cell lymphomas with corresponding immunoreactivity.
Discussion
The initial flow cytometry showed CD20 and CD5 co-
expression without CD23 expression, generating a
differential diagnosis of atypical CLL (atypical since CD23
was not expressed), prolymphocytic leukemia (either de
novo or secondary to CLL) and mantle cell lymphoma. A
diagnosis of atypical CLL was favored based on the lack of
organomegaly / lymphadenopathy, only moderately
increased and stable WBC counts, prolymphocytes < 55%
and lack of t(11;14). The subsequent lymph node biopsyhad the
characteristic CLL/SLL immunophenotype of CD5+,
CD23+ B cells.
The paraimmunoblastic variant of SLL/CLL is a rare
morphologic variant characterized by a diffuse to nodular
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=15277261&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=15277261&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=15277261&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=15277261&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=15277261&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=15277261&query_hl=1&itool=pubmed_docsum
-
8/2/2019 Lymphoma Discussion
22/23
proliferation of paraimmunoblasts, the cells usually seen in
pseudoproliferation centers of SLL. In classic SLL, the
predominant population is small lymphocytes with scant
cytoplasm, coarsely clumped chromatin and inconspicuous
nucleoli. In the paraimmunoblastic variant, the predominant
cells are slightly larger, with moderately abundant
cytoplasm,more open/vesicular chromatin and a single prominent,
central nucleolus. The paraimmunoblasts have the same
staining pattern as classic CLL/SLL (i.e. expression of
CD19,
CD20, CD5 and CD23, negative for CD10 and FMC7). It is
considered the tissue counterpart of a prolymphocytic
transformation of CLL.
The paraimmunoblastic variant was first described by Pugh
as an aggressive variant that presents with
generalizedlymphadenopathy, and occasionally splenomegaly (Am J
Surg Pathol 1988;12:907). The term paraimmunoblast
was first used by Lennert (Malignant Lymphomas other than
Hodgkins disease. Berlin/Heidelberg: Springer-Verlag,
1978:111-36) to describe a mitotically active, medium-sized
cell with weakly staining eosinophilic cytoplasm, irregular
nuclear borders, vesicular chromatin and a single,
prominent, central nucleolus. In contrast, immunoblasts are
larger cells with moderate basophilic cytoplasm, large round
nuclei and a similar prominent, central nucleolus.
Centroblasts are larger cells with multiple basophilic,
peripherally-placed nucleoli.
The differential diagnosis in this case includes a Richters
transformation and blastoid variant of mantle cell lymphoma.
Richters transformation of CLL/SLL usually presents with a
single area of marked nodal growth, unlike the diffuse,
symmetrical lymphadenopathy in this and other
paraimmunoblast variant cases. The Richters node may
show complete or partial involvement by sheets of
centroblasts or immunoblasts with a proliferation fraction
in
transformed areas greater than 40% (Cancer J
2005;11:161).
Blastoid variant of mantle cell lymphoma also has a vaguely
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=3059831&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=3059831&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=3059831&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=3059831&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=16053658&query_hl=7&itool=pubmed_DocSumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=16053658&query_hl=7&itool=pubmed_DocSumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=16053658&query_hl=7&itool=pubmed_DocSumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=16053658&query_hl=7&itool=pubmed_DocSumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=16053658&query_hl=7&itool=pubmed_DocSumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=16053658&query_hl=7&itool=pubmed_DocSumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=3059831&query_hl=1&itool=pubmed_docsumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=3059831&query_hl=1&itool=pubmed_docsum
-
8/2/2019 Lymphoma Discussion
23/23
nodular architecture and slightly larger cells with less
clumped chromatin. However, cyclin D1 is overexpressed
and t(11;14) is detected by FISH analysis.
The original flow cytometric examination demonstrated
several features associated with a poor prognosis, including
CD38 expression, a complex karyotype and p53 mutation
(Jaffe: WHO Classification of Tumors, Pathology and
Genetics of Tumours of the Haematopoietic and
Lymphoid System,Blood 1998;91:4342, Blood
2001;98:181). In addition, patients with the
paraimmunoblastic variant of CLL/SLL have an aggressive
clinical course (Hum Path 2002;33:1145).
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.30100 Telegraph Road, Suite
404Bingham Farms, Michigan (USA) 48025Telephone: 248/646-0325
Fax: 248/646-1736
http://www.amazon.com/exec/obidos/ASIN/9283224116/pathologyoutl-20http://www.amazon.com/exec/obidos/ASIN/9283224116/pathologyoutl-20http://www.amazon.com/exec/obidos/ASIN/9283224116/pathologyoutl-20http://www.amazon.com/exec/obidos/ASIN/9283224116/pathologyoutl-20http://www.amazon.com/exec/obidos/ASIN/9283224116/pathologyoutl-20http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?orig_db=PubMed&db=PubMed&cmd=Search&term=blood%5BJour%5D+AND+91%5Bvolume%5D+AND+4342%5Bpage%5Dhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?orig_db=PubMed&db=PubMed&cmd=Search&term=blood%5BJour%5D+AND+91%5Bvolume%5D+AND+4342%5Bpage%5Dhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?orig_db=PubMed&db=PubMed&cmd=Search&term=blood%5BJour%5D+AND+98%5Bvolume%5D+AND+181%5Bpage%5Dhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?orig_db=PubMed&db=PubMed&cmd=Search&term=blood%5BJour%5D+AND+98%5Bvolume%5D+AND+181%5Bpage%5Dhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?orig_db=PubMed&db=PubMed&cmd=Search&term=blood%5BJour%5D+AND+98%5Bvolume%5D+AND+181%5Bpage%5Dhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?orig_db=PubMed&db=PubMed&cmd=Search&term=%22Human+pathology%22%5BJour%5D+AND+33%5Bvolume%5D+AND+1145%5Bpage%5Dhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?orig_db=PubMed&db=PubMed&cmd=Search&term=%22Human+pathology%22%5BJour%5D+AND+33%5Bvolume%5D+AND+1145%5Bpage%5Dhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?orig_db=PubMed&db=PubMed&cmd=Search&term=%22Human+pathology%22%5BJour%5D+AND+33%5Bvolume%5D+AND+1145%5Bpage%5Dhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?orig_db=PubMed&db=PubMed&cmd=Search&term=%22Human+pathology%22%5BJour%5D+AND+33%5Bvolume%5D+AND+1145%5Bpage%5Dhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?orig_db=PubMed&db=PubMed&cmd=Search&term=blood%5BJour%5D+AND+98%5Bvolume%5D+AND+181%5Bpage%5Dhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?orig_db=PubMed&db=PubMed&cmd=Search&term=blood%5BJour%5D+AND+98%5Bvolume%5D+AND+181%5Bpage%5Dhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?orig_db=PubMed&db=PubMed&cmd=Search&term=blood%5BJour%5D+AND+91%5Bvolume%5D+AND+4342%5Bpage%5Dhttp://www.amazon.com/exec/obidos/ASIN/9283224116/pathologyoutl-20http://www.amazon.com/exec/obidos/ASIN/9283224116/pathologyoutl-20http://www.amazon.com/exec/obidos/ASIN/9283224116/pathologyoutl-20
![𝛾𝛿T-Cell Acute Lymphoblastic Leukemia/Lymphoma: Discussion of … · 2019. 7. 30. · [7]E.D.Merrill,R.Agbay,R.N.Mirandaetal.,“Primarycutaneous T-celllymphomasshowinggamma-delta(𝛾𝛿)phenotypeand](https://img.pdfslide.net/doc/110x75/60aa64bf856b015a425f2e48/t-cell-acute-lymphoblastic-leukemialymphoma-discussion-of-2019-7-30.jpg)