Embed Size (px)
Citation preview

Lymphomasaffecting the CNS
Michele Ghielmini
Oncology Institute of Southern SwitzerlandOspedale San Giovanni - 6500 Bellinzona, Switzerland
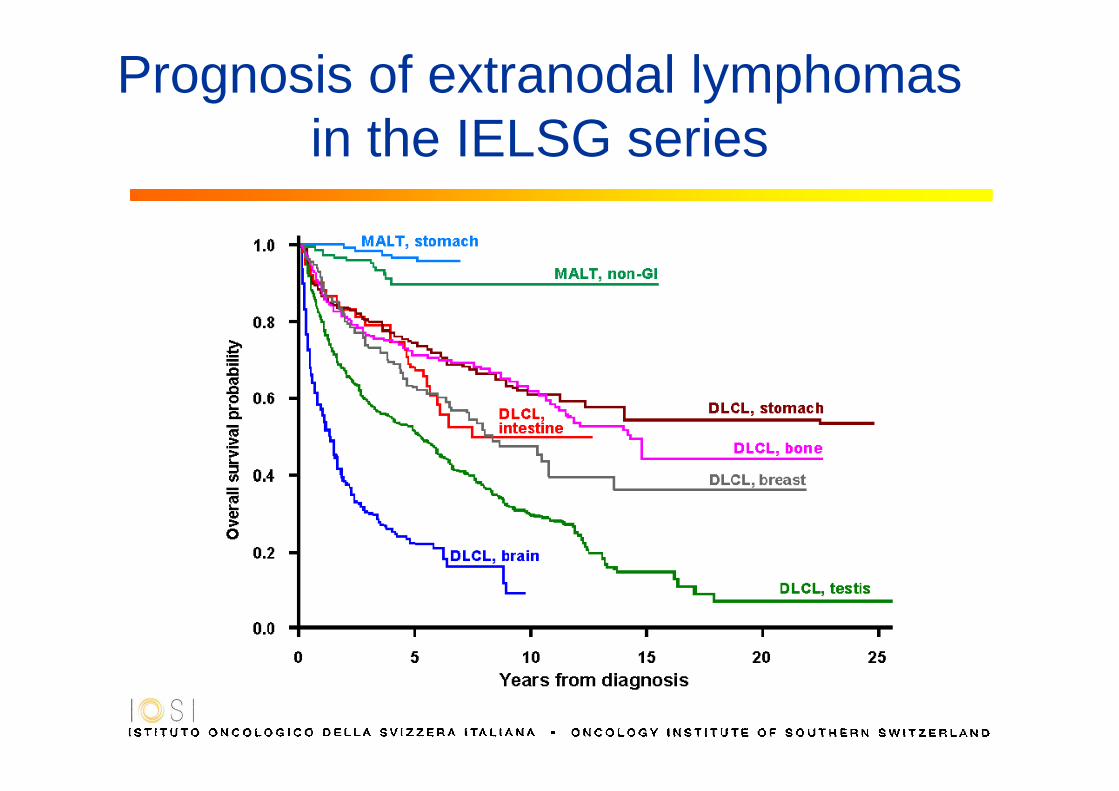
Prognosis of extranodal lymphomasin the IELSG series

The clinical peculiarities of CNS lymphomas
• Radiotherapy to CNS is particularly toxic
• CNS is a drug sanctuary

Neurotoxicity
• As disabling as lymphoma itself (dementia,ataxia, incontinence in 40% and relatedmortality of 30%).
• More common in elderly pts treated withHD-MTX + WBRT.

Chemotherapy and CNS
BBB: Blood-Brain Barrier
BBB penetration
Doses CNS availability
Examples
Good conventional good steroids, alkylating ag.
Low to moderate
high good MTX, araC
Poor conventional(-limiting tox)
low anthracyclines, vinca-alkaloids
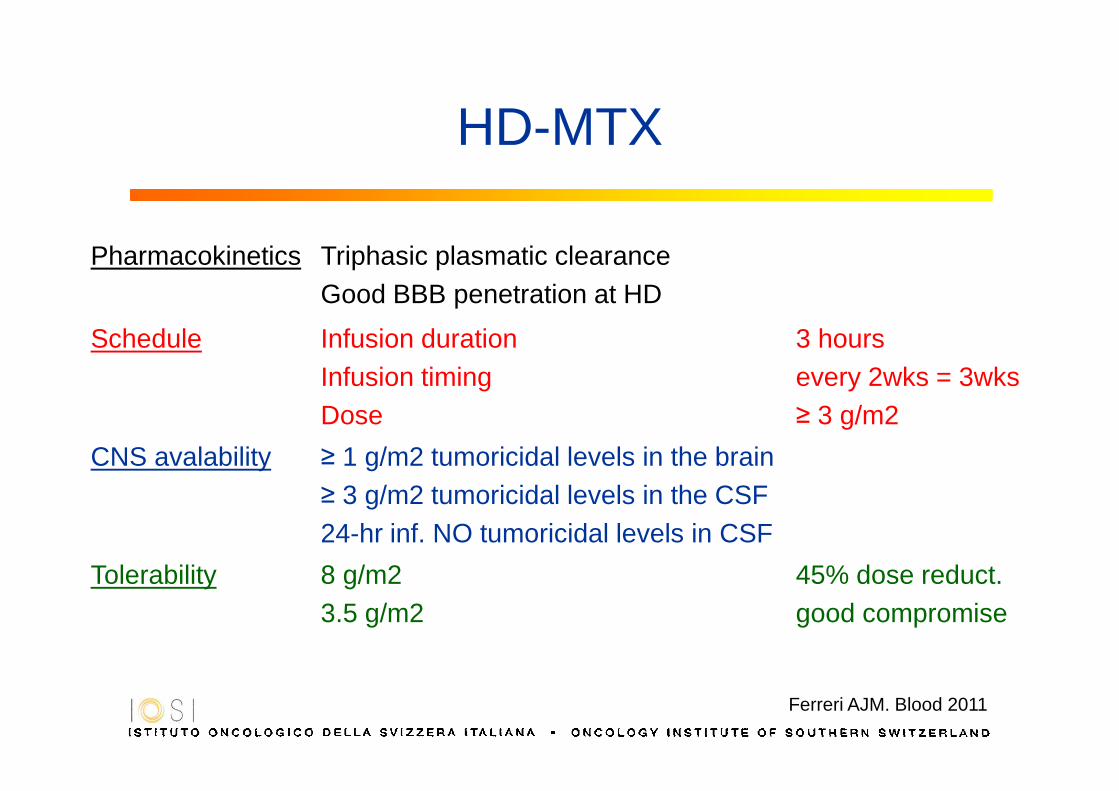
HD-MTX
Pharmacokinetics Triphasic plasmatic clearanceGood BBB penetration at HD
Schedule Infusion durationInfusion timingDose
3 hoursevery 2wks = 3wks≥ 3 g/m2
CNS avalability ≥ 1 g/m2 tumoricidal levels in the brain≥ 3 g/m2 tumoricidal levels in the CSF24-hr inf. NO tumoricidal levels in CSF
Tolerability 8 g/m23.5 g/m2
45% dose reduct.good compromise
Ferreri AJM. Blood 2011

Alkylating Agents
BCNU, CCNU, Ifosfamide, Temozolomide, Thiotepa
- are largely used to treat aggressive lymphomas
- are able to cross BBB
- increase antimetabolites cytotoxicity
- hit quiescent (G0 phase) cells
- increase overall toxicity
0.9 mg/Kg = 33 – 35 mg/m 2
Strong JM, et al. Cancer Res 1986
Thiotepa

New DrugsRegimen N ORR m OR
durationG3-4 neutro G3-4 thrombo
RituximabBatchelor T, et al. Neurology 2011
12 5 (42%) 8 0% 0%
RituximabRaizer JJ, et al. Pro ASCO 2000
3 2 N/A
TemozolomideReni M, et al. Br J Cancer 2007
36 11 (31%) 7+ 6% 3%
Temozolomide (Upfront - old)Kurzwelly D, et al. JNO 2010
17 9 (53%) 21+ 12% 12%
Temozolomide + RituximabEnting RH, et al. Neurology 2004
15 8 (53%) 14 20% 27%
Temozolomide + RituximabWong ET, et al. Cancer 2004
7 7 6
TopotecanVoloschin A, et al. JNO 2008
15 6 (40%) 3 30% 5%
TopotecanFischer L, et al. Ann Oncol 2006
27 9 (33%) 9 26% 11%
PemetrexedAltman JK, et al. ASCO 2008
8 4 (50%) 5+ 63% 50%
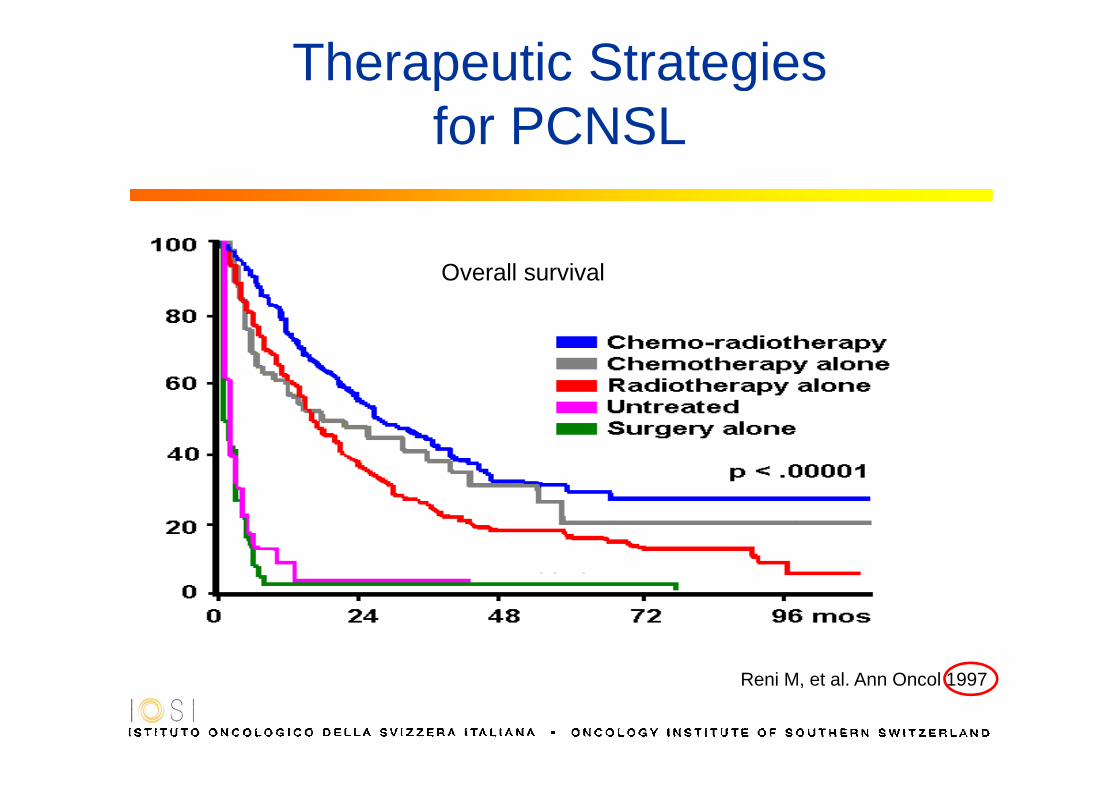
Therapeutic Strategies for PCNSL
Reni M, et al. Ann Oncol 1997
Overall survival

History: the MSKCC schemeYear 2000: «The next step»
Cases: n=5723<60y34>60y
Schedule:
MTX 3.5g/m2 qd 2wks x 5+ VCR and procarbazine+ it MTX
+ RT 45 Gy (only if age<60)
+ HD-AraC x 2
10 years follow-up
Gavrilovic at al, JCO 2006

MTX 3.5 g/m 2 , d1(x 4 c., every 3 weeks)
Histological or cytological diagnosis of NHLDisease exclusively localized in the CNS
At least one measurable lesionAge 18 - 75 ys - ECOG-PS ≤ 3
MTX 3.5 g/m 2 , d1araC 2 g/m 2 x 2/d, d2-3(x 4 c., every 3 weeks)
Followed by WBRT

IELSG #20: Survival Curvesn = 80
Median f-up: 30 months
0
20
40
60
80
100
0 12 24 36 48 60 72
months
Pro
babi
lity
OS
Median f-up: 46 months
MTX
MTX-araC
24 ± 8%
45 ± 8%
p= 0.05
Ferreri AJM, et al. The Lancet 2009
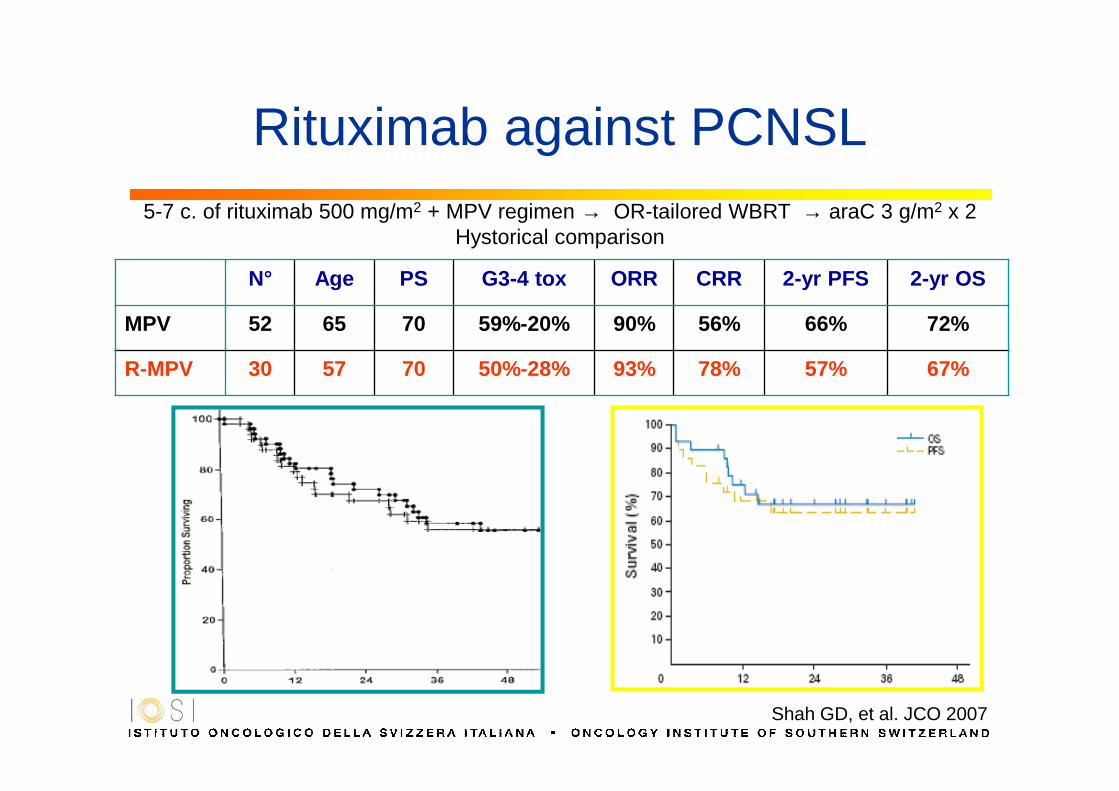
Rituximab against PCNSL5-7 c. of rituximab 500 mg/m2 + MPV regimen → OR-tailored WBRT → araC 3 g/m2 x 2
Hystorical comparison
N° Age PS G3-4 tox ORR CRR 2-yr PFS 2-yr OS
MPV 52 65 70 59%-20% 90% 56% 66% 72%
R-MPV 30 57 70 50%-28% 93% 78% 57% 67%
Shah GD, et al. JCO 2007

The role of RT: PCNSL-G1 trial
MTX 4 g/m 2 d 1 (max. 6x) (+ IFO 1.5 g/m 2 d 3-5)
CR
WBI WBI at relapse WBI AraC 3 g/m2 x 2/dd 1-2 (max. 4x)
RandomWBI or no WBI
437 pts
Thiel et al, lancet Oncol. 2010
No CR

G-PCNSL-SG-1 trial: results
Thiel et al, lancet Oncol. 2010

PCNSL [≤ 65 ys. + PS 0-3] or [65-70 ys. + PS ≤2]
®
®WBRT 36 Gy± boost 9 Gy
BCNU 400 mg/m 2 d.1 Thiotepa 5 mg/Kg x 2/d; d.2-3
+ APBSCT
4 c. MTX 3.5 g/m 2 d.1araC 2 g/m 2 x 2/d, d. 2-3every 3 weeks
4 c. rituximab 375 mg/m 2 d-5 & 0MTX 3.5 g/m 2 d.1araC 2 g/m 2 x 2/d, d. 2-3every 3 weeks
4 c. rituximab 375 mg/m 2 d-5 & 0MTX 3.5 g/m 2 d.1araC 2 g/m 2 x 2/d, d. 2-3Thiotepa 30 mg/m 2 d.4every 3 weeks
Response assessment
CR – PR - SD PD – tox� SC harvest
WBRT 40 Gy± boost 9 Gy

Randomised study of HD MTX/AraC+/- Thiotepa +/- Rituximab
PFS OS
A vs. B= 0,01
A vs. C= 0,00005
B vs. C= 0,13
A vs. B= 0,01
A vs. C= 0,0005
B vs. C= 0,24
Ferreri et al, Abstract ICML Lugano, 2015
IELSG 32 trialRitux d -5 and 0 of each cycle
Conclusions PCNSL
• Main component of treatment is HD-MTX
• Give 3.5 g/m2 every 2-3 weeks for 4-8 times
• If possible, add HD-araC (2g/m2 x4)
• Consolidation with RT is still standard if age<60
• Consider temozolomide instead of AraC in elderly
• Consider HDCT instead of RT in younger
Frequency of lymphomatous meningitis in NHL subtypes
van Besien et al. Blood 1998Zinzani et al. Leuk Lymphoma 1999Herrlinger et al. Semin Oncol 2009
Ferreri et al. Hemato Oncol 2009
• indolent lymphomas <3%
• DLBCL & PTCL ~5%
• lymphoblastic and Burkitt’s ~30%

Risk Factors : sites
• Particular organs • testis (breast, ovary, skin, soft tissue, bone marrow ?)
• Localisations in the anatomical regions near to the base of the skull or spinal canal• oral cavity, tongue, salivary glands, orbita, paranasal sinuses • retroperitoneal mass > 10 cm
Feugier P et al. Ann Oncol 2004 Avilés A e al. Oncology 2005Boehme V et al Ann Oncol 2007 Laskin JJ et al. Leuk Lymphoma 2005Zucca E et al. J Clin Oncol 2003 Savage K et al JCO 2009

Months
Pro
port
ion
0 10 20 30 40 50 60 70 80 90 1000.00
0.05
0.10
0.15
0.20
0.25
0.30
Kidney/adrenal not involved(n=2074)
Kidney/adrenal involved
(n=90)
p<0.001
Impact of kidney/adrenal involvement on CNS relapse treated with R- CHO(E)P (n=2164)
Factor (adjusting forthe IPI)
Relative risk
p-value 95% CI
Kidney and/or adrenal gland
2.8 0.006 (1.3; 5.8)

DLBCL – Risk of CNS relapse
Risk of CNS relapse according to the CNS International Prognostic Index. BCCA, British Columbia Cancer Agency; DSHNHL, German High-Grade Non- HodgkinLymphoma Study Group.
/
Schmitz N, JCO 2016
DLBCL – which kind of prophylaxis?
• Before 2008 : no CNS prophylaxis• After 2007 CNS prophylaxis was indicated in DLBCL
pts with high CNS recurrence risk, defined by:– Involvement of testis, spine, skull, paranasal sinuses, orbit,
nasopharynx, kidney/adrenal and/or breast– Simultaneous presence of advanced stage and high LDH
• CNS prophylaxis consisted of 3-4 courses of methotrexate 3 g/m2 with or without four doses of IT liposomal cytarabine
Ferreri A, BJH 2014

DLBCL – which kind of prophylaxis?
* Pts managed with IT only due to concomitant renal insufficiency
Ferreri A, BJH 2014
• CNS relapse : 12% without prophylaxis 2.5% with prophylaxis (P=.08)

DLBCL – which kind of prophylaxis?
Cheah CY, BJC 2014
• Retrospective multicenter study
• 217 DLBCL high risk for CNS involvement

Double hit lymphoma
Oki Y, BJH 2014
• 129 cases of DHL
• the cumulative incidence of CNS involvement was 13% at 3 years
• incidence of CNS involvement was lower in patients receiving prophylactic intrathecal che-motherapy (5% at 3 years) than in those who did not (15% at 3 years, P = 0017)
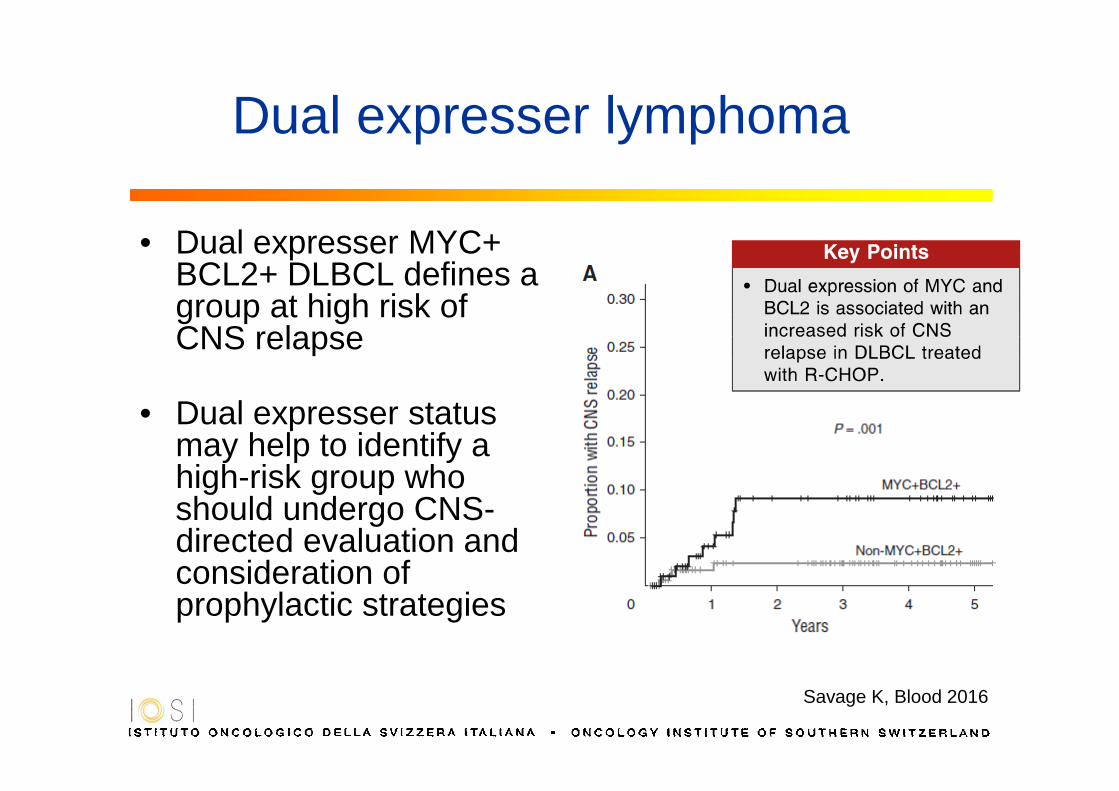
Dual expresser lymphoma
Savage K, Blood 2016
• Dual expresser MYC+ BCL2+ DLBCL defines a group at high risk of CNS relapse
• Dual expresser status may help to identify a high-risk group who should undergo CNS-directed evaluation and consideration of prophylactic strategies

Conclusions CNS prophylaxis
• CNS prophylaxis for DLBCL is controversial
• Usually CNS relapse is associated with systemic relapse
• Modern (+R) and aggressive first line regimens might reduce
the risk for CNS relapse
• If prophylaxis is to be done, HD-MTX may be preferred