Embed Size (px)
Citation preview

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
Influences on the quality of practice learning
Chapter 9

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
Learning objectives
• Understand how issues, such as high patient caseloads and service improvement initiatives, can have an impact on learning through practice
• Appreciate how multidisciplinary working can facilitate or hinder learning through practice
• Acknowledge the role of emotional labour within healthcare
• Recognize effective strategies to minimise the effect of constraints within varying contexts of practice
Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
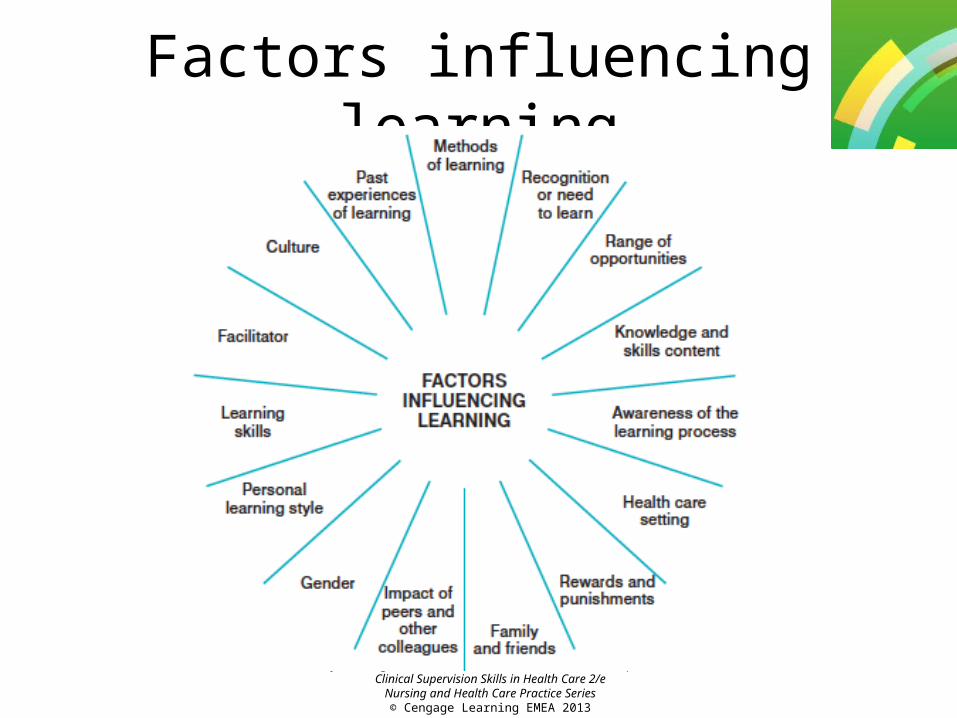
Factors influencing learning

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
Resource issues
• Staff shortages can hamper learning, as existing practitioners need to manage high workloads and there is an increased reliance on temporary staff.
• With part-time working on the increase, a single student may work with a number of registered practitioners during their placement.
• Recruitment and retention is important as the loss of experienced staff affects the continuity of care and the overall learning environment in the clinical area.
Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
• Shortages of placement opportunities in certain specialties can be compounded by the lack of adequately prepared clinical educators.
• Circumstances affect learning, because of the opportunities offered (or withheld) by the context.
• The time available and the complexity of the situation are important variables, and shortages of time force people to adopt a more intuitive approach, and intuitive routines help experienced staff to do things more quickly (Eraut, 2000b).
• Professionals may be reluctant to talk about routines if they feel that these differ from those espoused in theories (such as individualized care) as they think that doing so will highlight inadequacies.

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
• There are a number of strategies for coping with time pressure and information overload, including speeding up (acceleration), selecting the input of information (filtering), prioritizing, using ‘decision rules’, omitting or avoiding, and locking on to one approach.
• Learning to cope with (or even override) stress is part of ‘situated learning’ (Wigens, 2004).
• Being able to constantly prioritise at speed and handle uncertainty whilst appearing calm and in control of the situation is the sign of an experienced nurse and something to which new staff nurses aspire.
• Changes in skill mix that increase the level of non-registered staff may also affect learning through practice.

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
Specialities• Health care students have to learn to adapt to
each placement, its characteristics and associated reputations by getting to know staff, and this is helped by having placements of a reasonable length).
• Students have been found to go through three phases whilst on placement: 1. adaptation (becoming part of the community) 2. stabilization (increased knowledge and skills) 3. consolidation (requiring reduced supervision)
(Crawford and Kiger, 1998).

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
Emotional labour• You may, perhaps, take the view that emotions just
happen to you and that you are not fully responsible for them; however, they involve a degree of cognition and are also ‘socioculturally constituted’.
• A clinical team’s belief systems and values affect the capacity and characteristics of emotional expression.
• When the management of nursing care results in a requirement to speed-up ‘the human assembly line’, this makes ‘genuine’ personal service harder to deliver and it becomes virtually impossible to deliver emotional labour and individualised psychological care (Wigens, 1997).

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
• From an emotional labour approach, emotions are brought in line with feeling rules by two means: • Surface acting – in this case, the nurse puts on the expressive visage or body
stance of the emotion in the hope of stimulating the authentic feeling, changing feeling from the outside in.
• Deep acting – here, more profound strategies, such as imaging and verbal and physical prompting are used, modifying bodily or mental states, changing the feeling from the inside out (Hochschild, 1983). An example of prompts to deep acting might be the way the nurses talk to each other during a handover when they are discussing the care of a dying patient and his or her relatives.
• The concept of emotional labour helps in understanding how emotions have become a commodity in the work environment, just like technical skills, such as prescribing
• Students learn to ‘tune into’ the emerging priorities within a placement and to calls for situated understanding of the emotional labour requirements.

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
Service improvement
• A fundamental change in thinking, practice and delivery of healthcare has been called for to build a health service around the needs of the patient alongside ambitious plans to make the health service a better place to work.
• Modernization and transformation of care pathways have become a key driver, workforce issues focus on a steady improvement in productivity and quality, and good systematic management and organizational development.
• Transformation of health services requires a breaking down of traditional barriers to find new and flexible ways of thinking and doing, calling for creative responses.
Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
• The changes required to implement evidence-based practice can sometimes tip the fine balance of everyday coping, where much of this practice is based on tacit knowledge, sometimes made explicit through reflection.
• Change, even when acknowledged as improving patient care, can overload and stretch clinical staff who have ‘learnt to manage’.
• Clinical teams who feel a sense of ‘change overload’ more easily accept change if patient care is improved as an outcome.
• Service improvements can be a route for career diversity for nurses and other health care professions, such as specialist, advanced practitioner and consultant roles that add to the highly differentiated careers.

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
The PDSA cycle

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
Responding to the challenges of service assurance• Services and organizations, whether they are healthcare
providers or higher education institutions at some point need to demonstrate either compliance or adherence to mandatory standards set by their governing bodies.
• Local governance processes therefore should be robust and transparent, inclusive of the need for clear and open communication channels.
• Practitioners play a major role in all aspects of quality patient care management, however the frequency with which new policies and directives are being published can be overwhelming (Glasper, 2010).

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
The learning organization
• The quality of education is now being judged on its impact on practitioners’ ability to deliver health services as part of a flexible competent workforce.
• The importance of getting health professional education ‘right’ is an area of continuing debate.
• Increasing access to education and development is important, and guidelines for determining individual, team and Trust access to study leave should be transparent.

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
Education cycle

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
Factors driving an education strategyThe identification and analysis of training needs: •Finance available – (scarce resources can be targeted, e.g. replacement finance for staff) •New developments in the service •The costs of study programmes (travel) •Identification of available education (off the job) or the need for the creation of new education programmes based on learning objectives •Format for the education, e.g. on the job – demonstration, coaching, rotation (planned experience), assignments or projects •Improvements in staff knowledge and skills that are required•The identification of key people who will be able to attend (can the education be interprofessional?)•What benefits will be gained from the experience/education? l How will staff pass on their knowledge and skills?• Realistic timescales for completion
Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
Training needs analysis
• Training needs analysis can be undertaken for an organization as a whole, for departments or teams, or for individuals (sometimes the latter is called learning needs assessment)
• Learning needs assessment is a part of TNA that assesses and understands an individual’s needs through personal development planning
• Skilled contracting practices by Trusts, using best available data, assist organizations and their local education providers in ensuring that appropriate spending on education is targeted towards local priorities and staff needs.

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
Evaluating educationIt is important that education is evaluated not only by seeing whether the objectives for the individual and the service area have been met but also whether the overall purpose has been achieved. 1.Reaction – how the participants felt about the education; can be obtained through discussion, an evaluation sheet or questionnaire 2.Learning – determining what skills and knowledge have been learnt 3.Through assessment 4.Behaviour – observing the application of learning within the workplace 5.Results–determining the effect on the organization or the department of the educationHealthcare provider organizations should be lifelong learning organizations, making use of every opportunity to develop their staff, strengthening the image of the organization as a ‘good’ employer.

Lynne Wigens & Rachel Heathershaw, Mentorship and Clinical Supervision Skills in Health Care 2/e
Nursing and Health Care Practice Series© Cengage Learning EMEA 2013
Rapid recap1. What strategies may nurses use to cope with high
workloads, time pressures and information overload? 2. What three phases do Crawford and Kiger (1998) suggest
students progress through whilst on clinical placement? 3. Outline the main aspects of the four models of
practitioner–patient relationship. 4. What is meant by the term ‘emotional labour’? 5. What do the letters PDSA stand for in the service
improvement cycle? 6. How might a multidisciplinary team that could be
described as ‘committed’ (Bruce, 1980) show that they are working interprofessionally?