Embed Size (px)
Citation preview

12/5/2011
1
M 6Practical Tools to Spread
Improvements and Achieve Results at Scale
December 5, 2011
Orlando, FL
Session Objectives
• Describe different spread models and how
to apply them
• Acknowledge the unique needs of the
culture in each local department or setting
• Assess both site readiness and an
improvement’s readiness to spread
• Apply lessons to your own practice and
care delivery situation
Agenda - AM
• Overview of Spread and Scale-up
─Concepts and Strategies
─ Introduction to Case Studies
• Readiness
─Start with the End in Mind (Step 1)
─Link to Strategic Objectives (Step 2)
─Assess Readiness (Steps 3 and 4)
• Lunch
3

12/5/2011
2
Agenda - PM
• Recap/Reflections from AM Session
• Develop a Spread/Scale-up Plan
─Choose a Spread Approach (Step 5)
─Key Elements of a Plan (Step 6)
• Execute the Plan
─Prepare for Testing and Implementation (Step 7)
─Gather Information; Make Adjustments (Step 8)
─ Identify Sites in Need of Support (Step 9)
4
Faculty
• Marie Schall, MA, Institute for Healthcare Improvement
• Gail Nielsen, BSHCA, Iowa Health System
• Jim Bellows, PhD, KP Care Management
Institute
• Lisa Schilling, RN, MPH, Kaiser Permanente
• Kristene Cristobal, MS, Kaiser Permanente
• Denise Myers, RN, MPH, Kaiser Permanente
5
Meet Your Colleagues
• At your tables – in 5 minutes:
1. Introduce yourselves
2. Examples of successful spread?
3. Current/planned spread effort? What topic?
4. Challenges and/or questions you have for today?
• Be prepared to share the experience from
your table
6
12/5/2011
3
Overview of Spread and
Scale-up
Marie W. Schall, MA, IHI
Lisa Schilling, RN, MPH, Kaiser
Permanente
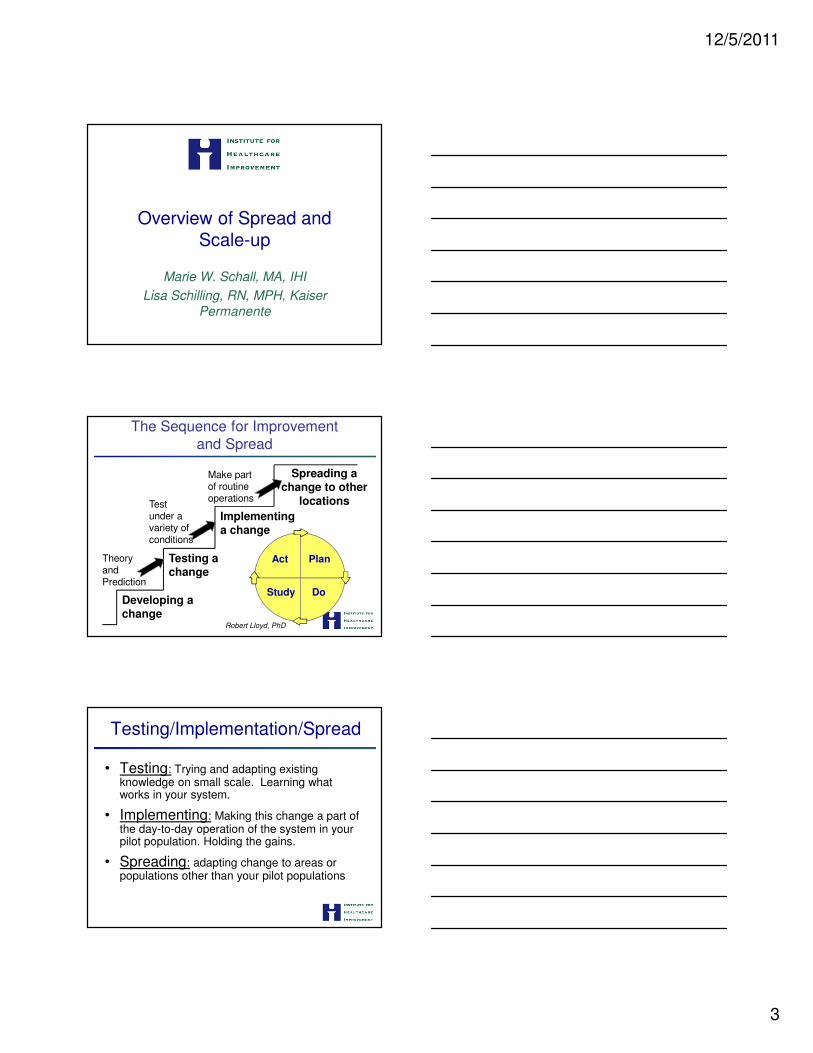
The Sequence for Improvement
and Spread
Spreading a change to other
locations
Developing a change
Implementing a change
Testing a change
Act Plan
Study Do
Theory and Prediction
Test under a variety of conditions
Make part of routine operations
Robert Lloyd, PhD
Testing/Implementation/Spread
• Testing: Trying and adapting existing knowledge on small scale. Learning what works in your system.
• Implementing: Making this change a part of the day-to-day operation of the system in your pilot population. Holding the gains.
• Spreading: adapting change to areas or populations other than your pilot populations

12/5/2011
4
Implementation: Key Components of Strategy
• Communication
─ Publicize benefits, document improvement, keep contact w/
team
• Infrastructure
─ Job descriptions, policies, hiring, orientation, supply stream, etc.
─ Assign ownership for improvement and maintenance work of the new process
─ Senior leaders held responsible for efforts to sustain
• Design Effective Control System
─ Use your internal quality assurance or improvement resources
─ Plan to standardize new process and verify conformance to the
standard
─ Graphically monitor measures for performance/outcomes from
the collaborative.
Spreading Improvements
IHI Breakthrough Series(6 to 18 Months Time Frame)
Select Topic
(Develop Mission)
Planning
Group
Develop
Framework & Changes
Participants (10-100 Teams)
Prework
LS 1
P
S
A D
P
S
A D
LS 3LS 2
Supports
Email (listserv) Phone Conferences
Visits Assessments
Monthly Team Reports
Dissemination
Publications,
Congress. etc.A D
P
SExpert
Meeting
AP1 AP2 AP3*
LS – Learning Session
AP – Action Period
*AP3 –continue
reporting data as
needed to
document success
Holding
the Gains

12/5/2011
5
Set-up-Target population
-Adopter audiences
-Successful sites
-Key partners
-Initial spread strategy
A Framework for Spread
Social System-Key messengers
-Communities
-Technical support
-Transition issues
Knowledge Management
Measurement and Feedback
Leadership-Topic is a key strategic initiative
-Goals and incentives aligned-Executive sponsor assigned
-Day-to-day managers identified
Better Ideas-Develop the case
-Describe the ideas
Nolan K, Schall M, Erb F, Nolan T. Jt Comm J Qual Saf 31(6):339-347, June 2005
Scale up vs. Spread
• Scale-up: The progressive design of a system of interrelated parts;
moving from one setting to a larger setting and then an even larger setting within an interrelated system.
─ Expect new learning and structural changes to achieve results at scale.
─ Ex: A pilot unit at MGH successfully implements electronic medical records (EMR). The hospital decides to implement EMR in all units in the hospital.
• Spread: Taking a system or intervention and replicating it in an
independent site.
─ Active adaptation and replication by adopter sites but without significant new learning (about the system or intervention) or structural changes.
─ Ex: A pilot unit at MGH successfully implements EMR. A hospital in an unrelated setting, such as Chicago or St. Louis, is interested in their work and decides to
implement EMR in a pilot unit in this new, unrelated hospital.

12/5/2011
6
Scale-up of New System for Improving
Transitions in Care
Entire Hospital
All Surgical Units
All Medical Units
Pilot Unit(s)
….redesigning care processes to improve transitions for all patients (e.g., enhanced assessment, handover communications between settings, etc.)
From Pilot Units to Clinical Departments (multiple units) to Entire Hospital….
Spread: Pilot Sites to Similar Sites in other Systems
P
S
S
P
P
S
S
S
S S
P
S
Spreading Effective Practices
December 5, 2011
Lisa Schilling RN MPH
VP, Healthcare Performance Improvement

12/5/2011
7
19
KP/IHI CFO Dialog
• Practices are hard to transfer
• We don’t know the best infrastructure to spread
• We don’t have the will to spread
• We don’t make great decisions about what to spread (few return what’s promised)
20Source: Institute for Healthcare Improvement, 2006.
Mental Model for Spread
21
What you need to know about effectiveness…
A x Q = E
A= strategies to build acceptance and commitment (culture, accountability)
Q= quality of technical solution (both the
change and the reliable application of change)
Source: Jack Welch

12/5/2011
8
22
Applying this in Operations
Org
an
iza
tio
na
l A
lig
nm
en
t
High
TransferabilityHigh Low
Low
Source: Stacey 2002
23
A Tool to Lead Spread in 9 Steps
Determine organizational readiness for spread1. Start with the end in mind2. Determine whether linked to strategic objectives of
organization3. Assess readiness to spread (using tool)4. Assess readiness to receive (using tool)
Develop a plan:5. Choose spread approach. 6. Develop a plan for spread
Execute on the plan:7. Prepare for testing and implementation8. Gather information over time to allow adjustment of
spread plan9. Identify sites in need of support
Case Studies: Overview
• Iowa Health System
─ Gail Nielsen, BSHCA
• Kaiser Permanente
─ Kristene Cristobal, MS
─ Denise Myers, RN MPH
24

12/5/2011
9
Spread Project
• What: Medication Safety
• Where: 10 IHS hospitals
• AIM: Reduce Adverse Drug Events
50% in two consecutive years
• Time Frame: 2 years (2002-2003)
Iowa Health System
Medication Safety Components
─Culture of Safety
�Unit Briefings
�Executive WalkRounds ©
─FMEA
─Medication Reconciliation
─Hazard Drugs
Iowa Health Spread Project
Iowa Health Spread Project
• Full Scale Plan at Outset:
─ System Strategic Aim
─ System-wide Patient Safety Implementation Team
─Hospitals’ VPMAs, Pharmacy Directors, Quality Leaders, Educators, and front-line representation
• Prototypes
─ Pilots 1 and 2 then
─ System-wide collaborative for 10 hospitals

12/5/2011
10
Iowa Health System
Aim: 50% Reduction in ADEs System-wide in 2002 & 2003
Iowa Health System Adverse Drug Events: % of Sampled Charts with Harm Levels ADEs E-I
Targets: 2002 = 10%, 2003 = 4%
20%
14%
9% 9%10%
6%
4%
6%5% 5%
3%
6% 6%
10%11%
2%
10%
6%
3%4%
0%
10%
20%
30%
N-01 D-01 J-02 F-02 M -02 A-02 M -02 J-02 J-02 A-02 S-02 O-02 N-02 D-02 J-03 F-03 M -03 A-03 M -03 J-04
% o
f C
ha
rts
'03 Target 4%
Reduced Sample Size
Sepsis Case study
Spreading Effective Practices
Why Sepsis ?
205,000 Adult Hospital Admissions
5,500 Sepsis Admissions
200,000 Other Admissions
1,400 Deaths from Sepsis
4,300 Deaths from Everything Else
24% of All Deaths
2.7% of All Admissions
Mortality Rate 2.2%Mortality Rate 25%
2007 KPNC Adult Hospital Stays, includes OB
1 in 4 deaths11 times the mortality rate

12/5/2011
11
Step 1.
Start with the End in Mind
Marie Schall, MA, IHI
Start with the End in Mind
• Determine what is being spread
• Define target population and end
state
• Establish timeframe to achieve scale
• Identify system level metrics and
outcome
• Define “sites” participating in effort
32
Why it Matters
• Because WHAT you are trying to do
is going to effect HOW you will do it─What methods you will use, i.e., spread
versus scale up
─ If spread, then which spread methods
─ If scale-up, then what structures to pay attention to
─ If both, how to develop an integrated plan
33

12/5/2011
12
Things to Consider in Selecting a Spread Approach
• Nature of the Intervention(s)
• Organizational Structure
• Social System
• Ability to reach target sites all at once
• Constraints
Scale-up Planning
• Define targeted scale at project setup
• Use the system issues in discussions with executives of the participating organizations. What structures need to change to accommodate scale-up?─ Administration structures ─Responsibility, accountability control structures ─ Physical structures─Human resource requirements─ Information systems
• Being aware of constraint changes as you expand
Case Studies and Exercises
• Iowa Health System
─ Gail Nielsen, BSHCA
• Kaiser Permanente
─ Kristene Cristobal, MS
─ Denise Myers, RN MPH
36

12/5/2011
13
Step 2.
Link to Strategic Objectives
Gail Nielsen, BSHCA, Iowa Health
System
Link to Strategic Objectives
• Determine whether linking to a strategic
goal aligns with initiatives
• Craft a compelling message and cascade
• Charter the team
38
Strategic Alignment
• System AIM adopted by all 10 hospitals:
─ Reduce Adverse Drug Events 50% in two consecutive years 2002-2003
• A compelling message cascaded system-wide
─ 1 in 5 patients are experiencing serious medication events in our hospitals, and we
now know how to improve. We need help from everyone!
39Iowa Health System

12/5/2011
14
Cascade Compelling Message
• Provide visible senior leader commitment to communities being engaged
• Coach Senior Leaders to show up at meetings and ask questions about progress
• Focus on possibilities rather than always on barriers
Iowa Health System
Cascade Compelling Message
• Help Senior Leaders keep the initiative
alive through “sense-making”
─explaining the criticality, relating it to everyone’s role
• Coach Senior Leaders to ask illustrative
questions and coach during WalkRounds©
─signaling priority of the work
Iowa Health System
Establishing the Charter
• AIM, boundaries, scope, measures, timeline
• Recommended changes
• Team members:
- Vice Presidents of Medical Affairs
- Pharmacy Directors
- Quality Improvement Directors
- Educators
- Front-line representation
- Improvement coaches
42
Iowa Health System

12/5/2011
15
KP Case Study and Exercise
• Kaiser Permanente
─ Kristene Cristobal, MS
─ Denise Myers, RN MPH
43
Step 3.
Assess Practice and Readiness
Jim Bellows, PhD, KP Care
Management Institute
45
IHI Minicourse:
Practical Tools to Spread Improvements and Achieve Results at Scale
Readiness for Spread
Jim Bellows, PhD December 5, 2011Senior DirectorKP Care Management Institute

12/5/2011
16
46
In this segment
� Understand what makes a practice ready for successful spread
� Understand what makes a site ready to import a practice
� Know how to use readiness assessment tools
� Apply the readiness tools to your project
47
Why assess Readiness?
Have you ever…
… tried to import a practice that was successful for the
innovator, but you just couldn’t make it work?
… tried unsuccessfully to interest others in a practice that
seemed great to you?
… had a senior leader ask you to spread a practice that was too complicated? Gave little return?
The solution? Due diligence
• Don’t assume every promising pilot produces a ready-to-
spread practice
48
Is the site
ready to receive?
Yes
Site frustration –
Practice may be imported, but without
anticipated value
Success!
NoDon’t even try it
:-(
Leadership frustration –
The practice won’t take root
No Yes
Is the practice ready for spread?

12/5/2011
17
49
Assess Readiness to Spread
50
Sources for Readiness tools in KP’s Spreading Effective Practices Toolkit
Sources
� Diffusion of Innovations, E Rogers. 1962.
� Diffusion of Innovations in Service Organizations: Systematic
Review and Recommendations. Greenhalgh T, et al. 2004.
� Sustainability – Ensuring Continuity in Improvement. UK NHS Institute for Innovation and Improvement. 2006.
� Options for Large-scale Spread of Simple, High-impact
Interventions. Massoud R et al. 2010.
51
Some innovations are destined to spread
� Trialability
� Advantage
� Compatibility
� Observability
� Simplicityper Everett Rogers
Plus…
� Task relevance
� Task usefulness
� Feasibility
� Implementation complexity
� Divisibility
� Explicit knowledge base
per Trisha Greenhalgh 2004

12/5/2011
18
52
Impact on Other
Aspects of Care
� Implementation Sustainability and Reliability
� Implementation Support
� Observability
� Simplicity
� Adaptability
� Cultural Fit
� Goal Alignment
Dimensions of practice readiness
� Cost
� Savings
� Revenue
� Return on Investment
� Certainty and Timing
� Harvestability
Impact on
Primary ObjectiveBusiness Case
� Magnitude
� Confidence
� Patient Safety
� Effectiveness
� Patient Experience
� Physician & Staff Work Experience
Maturity &
Transferability
53
Effectiveness –
Primary Objective
Other Impacts(Unintended Consequences)
Business Case
Maturity &
Transferability
Readiness Bingo –Is the practice ready for spread?
54
How ready for spread was the sepsis bundle?
� Early pilot reduced sepsis mortality to 13% compared with a 34% among sepsis patients in whom the protocol was not completed (p = 0.008).
� Some physicians felt that early central line placement created unneeded risk of complications, and discounted their ability to make accurate, timely diagnoses.
� Length of stay averaged 8 days compared with 12 days for patients in whom the bundle was not completed, so the return on investment must have been excellent.
� Results had been replicated or exceeded at other hospitals, and training materials and protocols were available to smooth implementation.
This scenario is provided for discussion only.

12/5/2011
19
55
Effectiveness –
Primary Objective �
Other Impacts(Unintended Consequences) �
Business Case �
Maturity &
Transferability �
Could readiness for spread be improved by refinement or better data?
This scenario is provided for discussion only.
Step 4.
Assess Site Readiness
Jim Bellows, PhD, KP Care
Management Institute
57
Assess site readiness to receive

12/5/2011
20
58
Organizational
Culture
� Project Management & Championship
� Training
� Measurement and Monitoring
Dimensions of site readiness
� Staff Capacity & Competency
� Space
� Technology
Leadership
Alignment
Operational
Resources
� Strategic Alignment with Goals and Priorities
� Sponsorship & Leadership
� Oversight Infrastructure
� Cultural Readiness for Change
� Operational Infrastructure (# of units involved, relationships)
Implementation
Infrastructure
59
Leadership
Alignment
Organizational
Culture
Operational
Resources
Spread
Infrastructure
Readiness Bingo –Is the site ready to receive?
60
How ready is Blossomville?
� Blossomville Medical Center serves 150,000 KP members, with
a 300 bed hospital + primary and specialty care facilities.
� Senior leadership didn’t expect ROI, but want to improve
hospital mortality so the initiative was well aligned with goals.
� The leadership and staff often felt stretched by having many
initiatives underway.
� The Improvement Director reports to the COO, and gets 3-5
minutes at monthly executive meetings to report on initiatives.
� Blossomville’s top leadership supported the initial launch by sending three emails to the ED staff.
� Blossomville had participated in IHI’s Transforming Care at the Bedside, which built a culture of openness to trying new things.
� The initiative required the ED physicians and nurses to
coordinate closely with the lab, Admissions process, and others.
This scenario is provided for discussion only.

12/5/2011
21
61
How ready is Blossomville? Part 2
� The Blossomville ED found that the intervention was causing
operational wrinkles that had not been reported at pilot sites.
� The PI director heard that central line placement often didn’t
happen on time because the supply kits were in short supply.
� The PI Director had secured a capable project manager for the
spread effort. Her “day job” as administrative services director
allowed her to spend 30% of her time for 2 months.
� Because the intervention was a collection of many separate
practices, the project manager wasn’t sure what the real priorities were.
� The initiative promised to decrease hospital mortality, but
physicians and nurses couldn’t see any gains after several weeks of effort.
This scenario is provided for discussion only.
62
Leadership
Alignment �
Organizational
Culture �
Operational
Resources �
Spread
Infrastructure �
Where should effort be devoted to increase site readiness?
This scenario is provided for discussion only.
63
Using the Readiness tools
Invest the time
• How much time will you spend trying to drive spread?
Be a hard grader
• Be realistic about challenges – recognition will help you prepare for resistance
• A low Readiness score is just information, not a sign of failure
Complete the tools as a team

12/5/2011
22
64
Summary: The Readiness tools can help address…
� Is this spread project positioned for success?What’s missing?
� How could gaps be addressed in the spread plan?
� Do sponsors and other key stakeholders have a shared understanding of strengths and barriers?
Iowa Health System
• Revisiting scale, scope, and speed
─Reducing Readmissions, Year 1
�Most team leads were novice improvers – doing most of the testing work
�Senior leaders partially engaged – some new to sponsoring improvement
�Changed scope and speed mid year to help teams dig deeper, learn implementation and reliability skills and build larger teams
65
Scale, Scope, and Speed
• Create monitoring
and review plan
66
STAAR Recommended Changes
for Transitioning Patients from
Hospital to Home
# of Teams currently
testing, implementing,
or spreading
recommended changes
Enhanced Assessment
•Include Patients, Families and Community
•Reconcile Medications
•Identify Initial Risk
•Customize Discharge Plan
624
5
Teaching and Learning
•Customize Education and Print Materials
•Identifying Learners and Teaching Them
•Teach Back
546
Follow up
•Identify Risk for Readmission
•Schedule Follow up Appointments
32
Handover
•Medication Reconciliation at Discharge
•Critical Information to Next Site of Care
•Patient Friendly Discharge Plan
•Clinician-to-Clinician Handover
332
2
Iowa Health System
12/5/2011
23
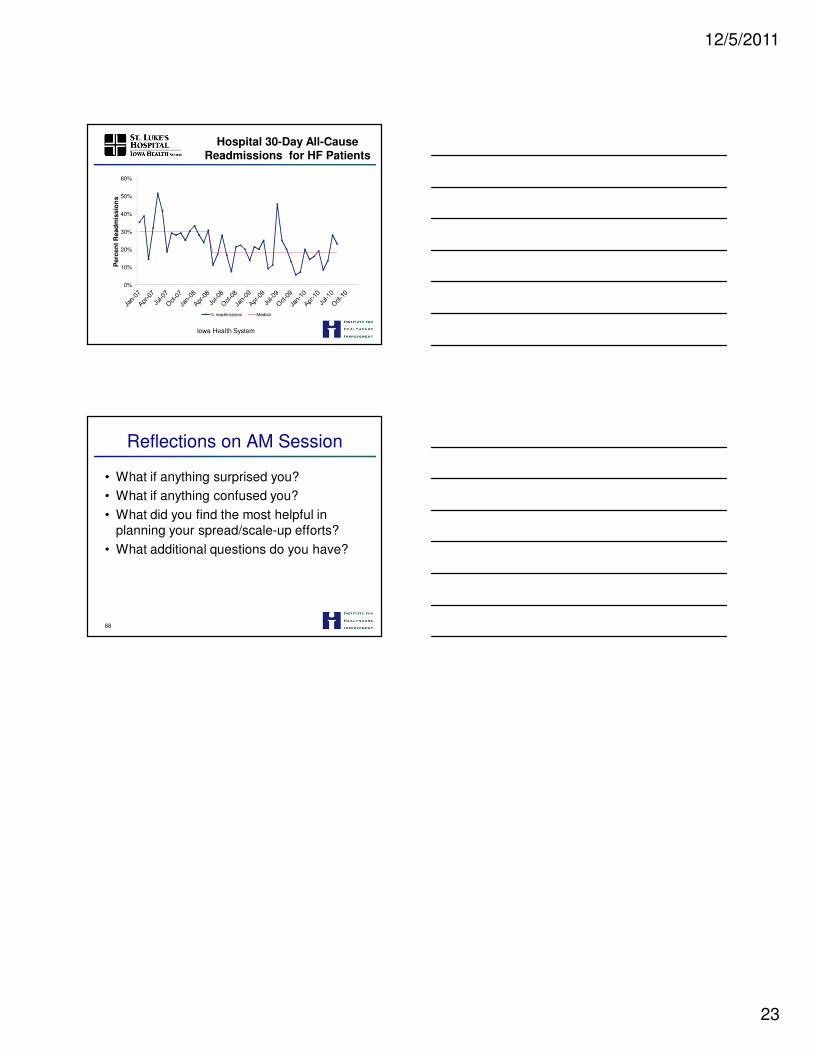
Hospital 30-Day All-Cause Readmissions for HF Patients
0%
10%
20%
30%
40%
50%
60%
Pe
rce
nt
Re
ad
mis
sio
ns
% readmissions Median
Iowa Health System
Reflections on AM Session
• What if anything surprised you?
• What if anything confused you?
• What did you find the most helpful in planning your spread/scale-up efforts?
• What additional questions do you have?
68


















![Achieve About Introducing iLase™ - Henry Schein … · FOLDRite™ Template Master: B-1 4-page Standard [Side B] Inside Spread Left Inside Spread Right. iLase™ Diode Dental Laser](https://img.pdfslide.net/doc/110x75/5b3db7557f8b9a5e1f8e3077/achieve-about-introducing-ilase-henry-schein-foldrite-template-master.jpg)










