Embed Size (px)
Citation preview

No. 44 / February 2019
M Pro-, Pre-, and Synbiotics: Myths and FactsGut Microbiota and Probiotics, Prebiotics, and SynbioticsHania Szajewska (Poland)
Human Milk Oligosaccharides versus Prebiotic Oligosaccharides Clemens Kunz (Germany)
Do Probiotics Really Need to Be "Alive"?Yvan Vandenplas (Belgium)
©2019, Nestlé Nutrition Institute CH–1800 Vevey Switzerland

thenest
2 3
Gut Microbiota Is Not a Forgotten
Organ Any More
Gut microbiota refers to organisms (bacteria, viruses, or eukaryotes) that are present in the gut. It has a profound impact on immunological, nutritional, physiological, and protective processes [1], it has been linked to health, and it is considered by some to represent a new organ in the human body. While it is often called “the forgotten organ” [2], the gut microbiota is no longer forgot-ten. On the contrary, it is a hot topic for research, as documented by the rapidly increasing number of scientific papers on this subject as well as coverage in the lay press, TV and radio programs, and social media.
Dysbiosis
Dysbiosis refers to altered gut microbi-ota composition and/or activity. A low diversity of gut microbiota may be con-sidered a marker of dysbiosis. At least in part, dysbiosis contributes to the de-velopment and progression of diseases such as allergy, obesity, irritable bowel syndrome, necrotizing enterocolitis, type 1 diabetes, and autism (in addition to other factors such as genes or envi-ronmental factors) [3]. However, the exact underlying mechanisms remain unclear. It remains to be determined whether the gut microbiota alterations
are a cause or a consequence of these
disorders. For none of the diseases has a specific “microbiota signature” been identified. The lack of standard-ized methods for microbiota evaluation may be responsible for inconsistencies among studies. Still, the association between low diversity of gut microbi-ota, which may be considered a marker of dysbiosis, and disease has been documented in a number of studies. From a functional point of view, low gut microbiota diversity is associated with reduced butyrate-producing bacteria, increased mucus degradation poten-tial, reduced hydrogen and methane production potential combined with in-creased hydrogen sulfide formation potential, and an increased potential to manage oxidative stress [4].
Modulating the Gut Microbiota
Targeting the gut microbiome with pro-biotics, prebiotics, or synbiotics could potentially benefit human health and reduce the risk of diseases. Other meth-ods, not discussed here, include antibi-otics and fecal microbiota transplants.
Probiotics
Probiotics are “live microorganisms that, when administered in adequate amounts, confer a health benefit on the host” [5]. The most commonly
used probiotics are Bifidobacterium and Lactobacillus species, and a spe cies of yeast (Saccharomyces boulardii). Possible main mechanisms of probi-otic action include:R production of metabolites such as
short-chain fatty acids, the majority of which are acetate, propionate, and butyrate;
R modulation of the composition and/or activity of the host microbiota (e.g., through colonization);
R enhancement of epithelial barrier in-tegrity;
R modulation of the host immune system;
R adherence to the mucosa and epithe-lium with inhibition of pathogen adhe-sion and/or growth;
R production of enzymes (e.g., lactase to promote lactose digestion);
R production of bacteriocins.
For a summary of the clinical ef-fects of probiotics in children [6], see Table 1. Considering that probiotics have many strain-specific effects, the focus should be on individual probiotic strains not on probiotics in general. The clinical effects and safety of any single probiotic or combination of pro-biotics should not be extrapolated to other probiotics. For a guide on how to choose a probiotic, see Table 2.
Key Messages
• A balanced gut microbiota is crucial for health. Conversely, an altered gut microbiota composition and/or activ-ity (dysbiosis) contributes to diseases
• Targeting gut microbiota using probi-otics and/or prebiotics has the poten-tial to treat or even prevent diseases
• Not all probiotics and/or prebiotics are equal. The clinical effects and safety of any of them used alone or in combination should be evaluated separately
• The use of probiotics or prebiotics with no documented health benefits should be discouraged
Gut Microbiota and Probiotics, Prebiotics, and Synbiotics
H a n i a S z a j e w s k a , M D
Department of Paediatrics, The Medical University of Warsaw, Warsaw, Poland
[email protected] Table 1. Effects of probiotics in children (based on ref. [6])
Condition Examples of probiotics with documented efficacy
Treatment of acute gastroenteritis ESPGHAN, WGO LGG*; S. boulardii (strong recommendation)L. reuteri DSM 17938 (weak recommendation)
Prevention of antibiotic-associated diarrhea
ESPGHANLGG; S. boulardii (strong recommendation)
Prevention of nosocomial diarrhea ESPGHAN LGG (strong recommendation)
Prevention of respiratory tract infections LGG
Prevention of eczema WAO suggests the use of probiotics in select high-risk populations; however, there is no clear indication regarding which strain(s) to use (conditional recommendation)
Development of tolerance in infants with cow’s milk allergy
LGG
Prevention of necrotizing enterocolitis No clear indications regarding which strain(s) to use
H. pylori infection ESPGHAN: not recommended
Infantile colic (management) L. reuteri DSM 17938 (well-documented in breast-fed infants)
Infantile colic (prevention) L. reuteri DSM 17938
Abdominal functional pain LGG
Maintenance of remission in ulcerative colitis
E. coli Nissle 1917; VSL#3
Induction of remission in Crohn’s disease
ECCO/ESPGHAN: not recommended
Functional constipation ESPGHAN/NASPGHAN: not recommended
ECCO, European Crohn’s and Colitis Organization; ESPGHAN, European Society for Paediatric Gastroenterology, Hepatology and Nutrition; LGG, Lactobacillus rhamnosus GG; NASPGHAN, North American Society for Pediatric Gastroenterology, Hepatology and Nutrition; WAO, World Allergy Organization; WGO, World Gastroenterology Organization * New data question the efficacy of LGG [16]
www.nestlenutrition-institute.org

Table 2. How to choose a probiotic [based on ref. 15]
Genus, species, strain
• Only probiotic strains for which identity and genetic stability have been demonstrated should be used.
• Example of an identification: Lactobacillus (genus) rhamnosus (species) GG (strain) ATCC 53103 (microbiological culture deposition)
Multi-strain versus single-strain products
• A multi-strain probiotic per se does not guarantee more benefit. For each product, the effect has to be documented in well-designed RCTs.
Expiration date • The manufacturer should guarantee: • the minimum number of live cells throughout the
shelf-life of the product or • the maximum number of live cells at the time
of manufacturing (no guarantee on the viability by the end of shelf-life).
Storage needs • Storage needs recommended by the manufacturers have to be followed.
Dose • One dose cannot be assumed to be effective for all strains.
• A larger dose is not always better. • It is prudent to use the treatment regimen proven to be effective in well-designed and executed RCTs for the same indication.
Formulation • Can be added to infant formulas, foods, dietary supplements, or drugs.
Quality • Each formulation is subject to different quality control processes.
Evidence • See Table 1. • Regulations may limit the nature of claims allowed on food and dietary supplement products.
thenest
4 5
ATCC, American Type Culture Collection; RCTs, randomized controlled trials.
8 Puccio G, Alliet P, Cajozzo C, Janssens E, Corsello G, Sprenger N, et al. Effects of infant formula with human milk oligosac-charides on growth and morbidity: a randomized multicenter trial. J Pediatr Gastroenterol Nutr. 2017 Apr;64(4):624–31.
9 Marriage BJ, Buck RH, Goehring KC, Oliver JS, Williams JA. Infants fed a lower calorie formula with 2 FL show growth and 2 FL uptake like breast-fed infants. J Pediatr Gastroenterol Nutr. 2015 Dec;61(6):649–58.
10 Skórka A, Piescik-Lech M, Kołodziej M, Szajewska H. Infant formulae supplemented with prebiotics: are they better than unsupplemented formulae? An updated systematic review. Br J Nutr. 2018 Apr;119(7):810–25.
11 Lohner S, Küllenberg D, Antes G, Decsi T, Meerpohl JJ. Prebiotics in healthy infants and children for prevention of acute infectious diseases: a systematic review and meta-analysis. Nutr Rev. 2014 Aug;72(8):523–31.
12 Cuello-Garcia CA, Fiocchi A, Pawankar R, Yepes-Nuñez JJ, Morgano GP, Zhang Y, et al. World Allergy Organization-McMaster University Guidelines for Allergic Disease Prevention (GLAD-P): Prebiotics. World Allergy Organ J. 2016 Mar 1;9:10.
13 Panigrahi P, Parida S, Nanda NC, Satpathy R, Pradhan L, Chandel DS, et al. A randomized synbiotic trial to prevent sepsis among infants in rural India. Nature. 2017 Aug 24;548(7668):407–12. Erratum in: Nature. 2017 Nov 29.
14 Chang YS, Trivedi MK, Jha A, Lin YF, Dimaano L, García-Romero MT. Synbiotics for prevention and treatment of atopic dermatitis: a meta-analysis of randomized clinical trials. JAMA Pediatr. 2016 Mar;170(3):236–42.
15 https://isappscience.org16 Schnadower D, Tarr PI, Casper TC,
Gorelick MH, Dean JM, O'Connell KJ, et al. Lactobacillus rhamnosus GG versus placebo for acute gastroenteritis in children. N Engl J Med. 2018 Nov 22;379(21):2002–2014.
be evaluated in well-designed and executed randomized controlled trials with clinically important outcome mea-sures. In pediatrics, these out comes relate to the risk of allergy, gastrointes-tinal and respiratory tract infections, overweight/obesity, and neurodevel-opment. For now, it is best to recom-mend the use of only those probiotics and/or prebiotics with documented ef-ficacy and safety and to use a regimen (dose and formulation, duration of treatment) proven to be effective in well-designed trials for the same indication.
Prebiotics
A prebiotic is “a substrate that is selec-tively utilized by host microorganisms conferring a health benefit” [7]. One example of naturally occurring prebiot-ics are human milk oligosaccharides. Selected human milk oligosaccharides, such as 2-fucosylactose and lacto- N-neo-tetraose, are currently being added to some infant formulas [8, 9]. Inulin, oligofructose, fructooligosac-charides, galactofructose, and galac-tooligosaccharides are other examples of commonly used and studied prebi-otics, as they increase the fecal counts of bifidobacteria or certain butyrate producers.
In the pediatric population, selec ted prebiotics have the potential to:R soften stool, which may be beneficial
in some infants and has been consis-tently documented with the admi-nistration of prebiotic-supplemented infant formulas (primarily with a mix-ture of short-chain galactooligosac-charides and long-chain fructooligo-saccharides) [10];
R reduce rates of gastrointestinal or re-spiratory infections (documented in some trials only) [11];
R reduce allergy (the World Allergy Or-ganization recommends the use of prebiotics in non-exclusively breast-fed infants; however, no specific rec-ommendations with regard to the choice of prebiotics were given) [12].
Synbiotics
Probiotics and prebiotics combined to act synergistically are called “synbiot-
ics.” Potentially, synbiotics have stron-ger effects on gut microbiota than either probiotics or prebiotics alone. Com-pared to probiotics or prebiotics, data on the efficacy of synbiotics are scarce.
In the pediatric population, synbiot-ics have the potential to:R reduce the risk of sepsis (L. plantarum ATCC 202195 plus frucotooligosac-charides reduced the risk of neonatal sepsis in a developing country) [13];
References1 Lynch SV, Pedersen O. The human intestinal
microbiome in health and disease. N Engl J Med. 2016 Dec 15;375(24):2369–79.
2 Marchesi JR, Adams DH, Fava F, et al. The gut microbiota and host health: a new clinical frontier. Gut. 2016;65:330–9.
3 Gilbert JA, Blaser MJ, Caporaso JG, Jansson JK, Lynch SV, Knight R. Current understanding of the human microbiome. Nat Med. 2018 Apr 10;24(4):392–400.
4 WGO Handbook on Gut Microbes. http://www.worldgastroenterology.org.
5 Hill C, Guarner F, Reid G, Gibson GR, Merenstein DJ, Pot B, et al. Expert consensus document. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol. 2014 Aug;11(8):506–14.
6 Szajewska H. What are the indications for using probiotics in children? Arch Dis Child. 2016 Apr;101(4):398–403.
7 Gibson GR, Hutkins R, Sanders ME, Prescott SL, Reimer RA, Salminen SJ, et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat Rev Gastroenterol Hepatol. 2017 Aug;14(8):491–502.
R contribute to the management of atopic dermatitis in children aged ≥1 year with mixed strains of probiotic bacteria (but they cannot be used as prevention) [14].
What Is Next?
Gaining a better understanding of how microbiota is linked to health and dis-ease is needed to develop next-gener-ation modulators of the gut microbiota. The latter, once developed, need to
www.nestlenutrition-institute.org

thenest
6 7
Key Messages
• Both human milk oligosaccharides (HMOs) and prebiotic oligosaccha-rides (PBOs) belong to the large class of carbohydrates, but they have com-pletely different structures
• HMOs and PBOs have a high poten-tial for various functions
• However, to date, there has been no human study showing similar or com-parable functions
Background
The concept of prebiotics has received much attention during the last decade. Prebiotic oligosaccharides (PBOs) are discussed to have various health ben-efits mainly due to an influence on the colonic microbial composition or activ-ity [1–3].
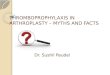
During the last 5 years, research on human milk oligosaccharides (HMOs) has developed into one of the “hottest” topics in infant nutrition, especially due to the enormous progress in producing some of these components on a large scale (Fig. 1). Today, some HMOs can be added to infant formula or used for other purposes. Therefore, we are at the beginning of a new era in infant nu-trition [4].
In the following, a few basic ques-tions will be addressed.
What Are “Prebiotics”?
The first definition was published in 1995 by Gibson and Roberfroid [5]: “Prebiotics are nondigestible food in-gredients that beneficially affect the host by selectively stimulating the growth and/or activity of one or a lim-ited number of bacteria in the colon that
can improve host health.” Although this definition has been modified over the years, it has not been possible to phrase a more specific description [2]. This, however, would help to clearly describe “a prebiotic effect in infants.” A most re-cent consensus statement states that a prebiotic is “a substrate that is selec-tively utilized by host microorganisms conferring a health benefit” [3].
What Does a “Prebiotic Effect in
Infants” Mean?
In studies involving human infants, there are different opinions about what a “prebiotic effect” is. Often, studies concentrate on various goals:a. Determination of the total number of
Bifidobacteria is reported; however, today we know that not all Bifidobacteria can utilize HMOs or gala-tooligosaccharides (GOS)/fructooli-gosaccharides (FOS). It is important to investigate not only Bifidobacteria subspecies but also the interaction between the different microorgan-isms in infants.
b. If no effect on the microbiota can be found, authors will focus on the pro-duction of short-chain fatty acids such as butyrate, acetate, or propio-nate, and others.
C l e m e n s K u n z
Institute of Nutritional Sciences, Justus Liebig University, Giessen, Germany
c. If no effect can be found on such metabolites either, investigators will concentrate on the effect on fecal consistency to compare, e.g., the ef-fects of galactosylated oligosaccha-rides with those of breast-feeding.
As there is no clear definition of what is meant by “a prebiotic effect has been found,” the question “how can it be concluded that GOS, FOS, and other PBOs have the same prebi-otic effect as HMOs” arises.
Human Milk Oligosaccharides versus Prebiotic Oligosaccharides
HMOs in human milk
Lactose
• extremely high structural diversity
• about 150 different HMOs identified
• Total amount an infant receives per day: 5–15 g/L
3’SL
6’FL
TS-LNH DS-LNFP I
LNDFHLNFP III3FL
2’FLLNFP I
LNFP II
LNTLnNT
β1–4
β1–3
β1–3
β1–4
β1–3β1–4
β1–4
β1–4
β1–4
β1–4
β1–4
β1–3
β1–3
β1–4β1–4
β1–4
β1–4
β1–3
β1–3
β1–3
β1–3
β1–4
β1–4
β1–4
β1–3
β1–3
β1–3
β1–3
β1–3α1–2
α1–3
α2–6
α2–6
α2–3
α2–6
α2–3
α1–3
α1–2
α1–4
α1–4
α1–3
α1–2
α2–6
α2–3
GlcNAc Glucose Galactose Sialic acid Fucose
Monosaccharides
β 4
Figure 1: Examples of the complexity of single HMOs with a high potential for specific functions due to their different linkages between monosaccharides. No other biological fluid contains such a high variety and structures as human milk [6].
Is There a Similarity between
PBOs and HMOs?
In most scientific publications, PBOs are compared and considered to be similar to or even identical with HMOs, including reviews on their functional
www.nestlenutrition-institute.org

thenest
8 9
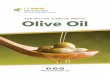
Figure 2: Monosaccharide composition of human milk oligosaccharides (HMOs) and prebiotics (PBOs) (a) and examples of specific linkages (b)
a HMOs PBOs
Glucose traces +
Galactose + +
N-Acetylglucosamine + –
Fucose + –
Sialic Acid (Neu5Ac) + –
Fructose – +
Xylose – +
Arabinose – +
Galactooligosaccharides (GOS)
R
Fructooligosaccharides (FOS)
HMOs
HMOs versus GOS/FOS
LNFP III
3‘SL2‘FL
LNnT
β1–3
α1–2 α2–3
α1–3
β1–4
β1–4β1–4
β1–4β1–4
β1–3
β1–4
Linear structures:unbranched, simple linkages
Complex structures:branched side chains, specific linkages
b
aspects. Some infant formula-produc-ing companies go as far as to claim in consumer information that both groups of carbohydrates share similarities re-garding structure and function.
However, although PBOs and HMOs belong to the same chemical class of carbohydrates, they do not share structural similarities that would be necessary to speculate about sim-ilar biological functions. If there were structural similarities, human studies would be needed to definitely show (i) what a “prebiotic effect” specifically means and (ii) that PBOs such as GOS and FOS show the same effects as HMOs in infants?
To demonstrate the difference be-tween GOS/FOS and HMOs, two ma-jor aspects have to be considered: (i) the monosaccharide composition and (ii) the linkage between them. The lat-ter is of particular importance, since specific functions including defence mechanisms, immune functions, or anti-inflammatory effects strongly de-pend on those linkages.
References1 Hill C, Guarner F, Reid G, Gibson GR,
Merenstein DJ, Pot B, et al. Expert consensus document. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol. 2014 Aug;11(8):506–14.
2 Hutkins RW, Krumbeck JA, Bindels LB, Cani PD, Fahey G Jr, Goh YJ, et al. Prebiotics: why definitions matter. Curr Opi Biotechnol. 2016 Feb;37:1–7.
3 Gibson GR, Hutkins R, Sanders ME, Prescott SL, Reimer RA, Salminen SJ, et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat Rev Gastroenterol Hepatol. 2017 Aug;14(8):491–502.
In prebiotics added to infant for-mula, the main monosaccharides are, e.g., galactose, glucose, fructose, xy-lose, and arabinose. Except for glucose and galactose, these monosaccharides are not present in human milk (Fig. 2). In HMOs, specific monosac charides are N-acetyl-glucosamine, fucose, and N-acetyl-neuraminic acid (sialic acid), which cannot be found in PBOs.
Where Do HMOs Come from?
Naturally, HMOs are solely produced in the lactating mammary glands. Only re-cently it has become possible to pro-duce some of them on a large scale by various means. To differentiate be-tween HMOs from the mammary gland and technically produced HMOs, I sug-gest to called the latter “identical HMOs” (iHMOs), since they are the same as those produced in lactating mothers.
Are GOSs and FOSs Present in
Human Milk?
GOS and FOS are not present in hu-man milk. For commercial reasons, some companies conclude that the addition of GOS and FOS to infant for-
mula will bring them closer to human milk. However, there is no structural similarity between PBOs and HMOs. This is even the case for “galacto-sylated oligosaccharides from milk” (a term that can be found on the label of commercial products). Those GOS from milk are synthesized by lactose, either cleaving off glucose and galac-tose or using lactose itself, to elongate it by the attachment of galactose moi-eties in various numbers. These linear short or longer GOS still share no structural similarity with HMOs either. So far, no study has been carried out proving that the effects of GOS/FOS on, e.g., the immune system are com-parable to those of HMOs.
What Is Needed?
In recent years, major advances have been made in the field of prebiotics, mainly influenced by the progress made in understanding the role of the micro-biota in health and disease. Effective strategies to achieve a healthy micro-biota are certainly needed. In this con-text, the appropriate use of the term “prebiotics” would be helpful, but this also requires a more specific definition.
4 Kunz C, Kuntz S, Rudloff S. Bioactivity of human milk oligosaccharides. In Moreno FJ, Sanz ML (eds). Food Oligosaccharides: Production, Analysis, and Bioactivity. Chichester; John Wiley & Sons, Inc. 2014. p 5–17. ISBN: 978–1–118–42649–4.
5 Gibson GR, Roberfroid MB. Dietary modulation of the human colonic microbiota: introducing the concept of prebiotics. J Nutr. 1995 Jun;125(6):1401–12.
6 Morozov V, Hansmann G, Hanisch FG, Schroten H, Kunz C. Human milk oligosaccharides as promising antivirals. Mol Nutr Food Res. 2018 Mar;62(6): e1700679.
www.nestlenutrition-institute.org

thenest
10 11
Key Messages
• The potential beneficial health effects of “not live” microorganisms deserve to be better studied as their produc-tion and preservation are much easier than for living organisms
• Some data suggest that particles of microorganisms and/or their metabo-lites may be sufficient to induce im-munological effects
• More evidence is needed regarding the potential benefits of non-viable microorganisms
What does “probiotic” mean? Some researchers give the word a full Greek etymology, but it appears to be a com-posite of the Latin preposition pro (“for”) and the Greek adjective βιωτικός (biōtikos, “fit for life, lively”), the latter deriving from the noun βίος (bios, “life”). A probiotic is defined as living microor-ganisms that, when consumed in ade-quate amounts, has a health benefit for the host. Although the definition of a probiotic requires that the micro-organisms ingested are “alive,” the question arises if dead microorgan-isms cannot also have a health benefit. It is beyond any doubt that the evi-dence for beneficial health effects of “living” bacteria is much larger and stronger than for “dead” bacteria. A major reason for this difference is due to the simple fact that living bacteria have been studied much more than dead bacteria. What do we know about “not living bacteria”?
Literature on the efficacy of heat-killed probiotic microorganisms is booming. Lactobacillus LB, for exam-ple, are used in the treatment of acute gastroenteritis [1]. Other products have been shown to be effective in the treat-ment of infantile colic [2]. Spore-based
probiotics, or sporebiotics consist of the cell wall of bacillus microorgan-isms. The lay-publicity and claims for sporebiotics are impressive: “Because of the sporebiotics’ unique abilities, scientists believe they may benefit people with health problems such as autism, neurological disorders, and im-mune-related diseases. In addition, spore-based probiotics may help for-tify the body against environmental ag-gressors such as electromagnetic fields (EMFs), pesticides, and airborne pollutants.” However, there is hardly any information in the scientific litera-ture. The term postbiotic was intro-duced to describe a product containing dead microorganisms and their metab-olites: soluble factors (products or metabolic by-products), secreted by live bacteria, or released after bacterial lysis, such as enzymes, peptides, te-ichoic acids, peptidoglycan-derived muropeptides, polysaccharides, cell surface proteins, and organic acids. Some dead probiotics have been shown to modulate the immune sys-tem (compounds of the cell wall might boost the immunological system) and to have increased adhesion to intesti-nal cells which further results in inhi-bition of pathogens (Table 1).
Y v a n V a n d e n p l a s
Department of Pediatrics, Vrije Universiteit Brussel, Brussels, Belgium
Fermented infant formula has been widely available in many countries for a few decades. It contains bacteria that were “killed” during the production/fer-mentation process, resulting in the presence of dead bacteria and metab-olites in the final product [3]. Five ran-domized controlled trials involving 1,326 infants compared the use of fer-mented formula with non-fermented routine formula and showed that weight and length gain during the study pe-riod were similar. Fermented infant for-mula also has the potential to reduce some digestive symptoms. Current evidence does not support the use of fermented formula for preventing cow’s milk allergy [3].
In conclusion, potential beneficial health effects of dead microorganisms deserve to be better studied as the pro-duction and preservation of dead micro-organisms are much easier than for liv-ing organisms. Although it seems likely that living microorganisms are needed to restore or influence the intestinal mi-crobiome composition, it seems also likely that particles of microorganisms and/or their metabolites may be suffi-cient to induce immunological effects. However, more evidence is needed re-garding the potential benefits of non- viable microorganisms. Legislation and claims are running far behind the imag-ination of marketeers.
Do Probiotics Really Need to Be “Alive”?
References1 Salazar-Lindo E, Figueroa-Quintanilla D,
Caciano MI, Reto-Valiente V, Chauviere G, Colin P; Lacteol Study Group. Effectiveness and safety of Lactobacillus LB in the treatment of mild acute diarrhea in children. J Pediatr Gastroenterol Nutr. 2007 May;44(5):571–6.
2 Vandenplas Y, Bacarea A, Marusteri M, Bacarea V, Constantin M, Manolache M. Efficacy and safety of APT198K for the treatment of infantile colic: a pilot study. J Comp Eff Res. 2017 Mar;6(2):137–44.
3 Szajewska H, Skórka A, Piescik-Lech M. Fermented infant formulas without live bacteria: a systematic review. Eur J Pediatr. 2015 Nov;174(11):1413–20.
Table 1: Main characteristics of probiotics and postbiotics
Probiotics Postbiotics
Definition Living microorganism that, when consumed in adequate amounts, has a health benefit for the host
Dead microorganisms and their metabolites: soluble factors secreted by live bacteria or released after bacterial lysis
Examples Bifidobacterium and Lactobacillus speciesSaccaromyces boulardii (a species of yeast)
Enzymes, peptides, teichoic acids, pepti doglycan-derived muropeptides, poly saccharides, cell surface proteins, and organic acids
Additional comments: • Some health benefits of specific strains are well documented (see also Table 1, article by H. Szajewska in this publication)
• Not all probiotics are the same, health bene fits are strain-specific
• Some potential benefits may be attributed to postbiotics, but more evidence is still needed
• The impact of different metabolites produced by specific bacteria needs to be better understood
www.nestlenutrition-institute.org

To learn more about the Nestlé Nutrition Institute and Wyeth Nutrition Science Center resources, visit:
www.nestlenutrition-institute.orgwww.wyethnutritionsc.org
This booklet is protected by copyright.
However, it may be reproduced without
the prior written permission of Nestlé
Nutrition Institute or S. Karger AG, but is
subject to acknowledgement of the
original publication.
The material contained in this booklet
was submitted as previously unpublished
material, except in the instances in
which credit has been given to the source
from which some of the illustrative
material was derived.
Great care has been taken to maintain
the accuracy of the information contained
in this booklet. However, neither Nestlé
Nutrition Institute nor S. Karger AG can be
held responsible for errors or for any
consequences arising from the use of the
information contained herein.
Published by S. Karger AG, Switzerland
© Copyright 2019 by
Nestlé Nutrition Institute, Switzerland
ISSN 1270–9743
No. 44 / February 2019
M Pro-, Pre-, and Synbiotics:
Myths and Facts
Gut Microbiota and Probiotics,
Prebiotics, and Synbiotics
Hania Szajewska (Poland)
Human Milk Oligosaccharides
versus Prebiotic Oligosaccharides
Clemens Kunz (Germany)
Do Probiotics Really Need
to Be "Alive"?
Yvan Vandenplas (Belgium)
©2019, Nestlé Nutrition Institute
CH–1800 Vevey
Switzerland