Embed Size (px)
Citation preview
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 20191
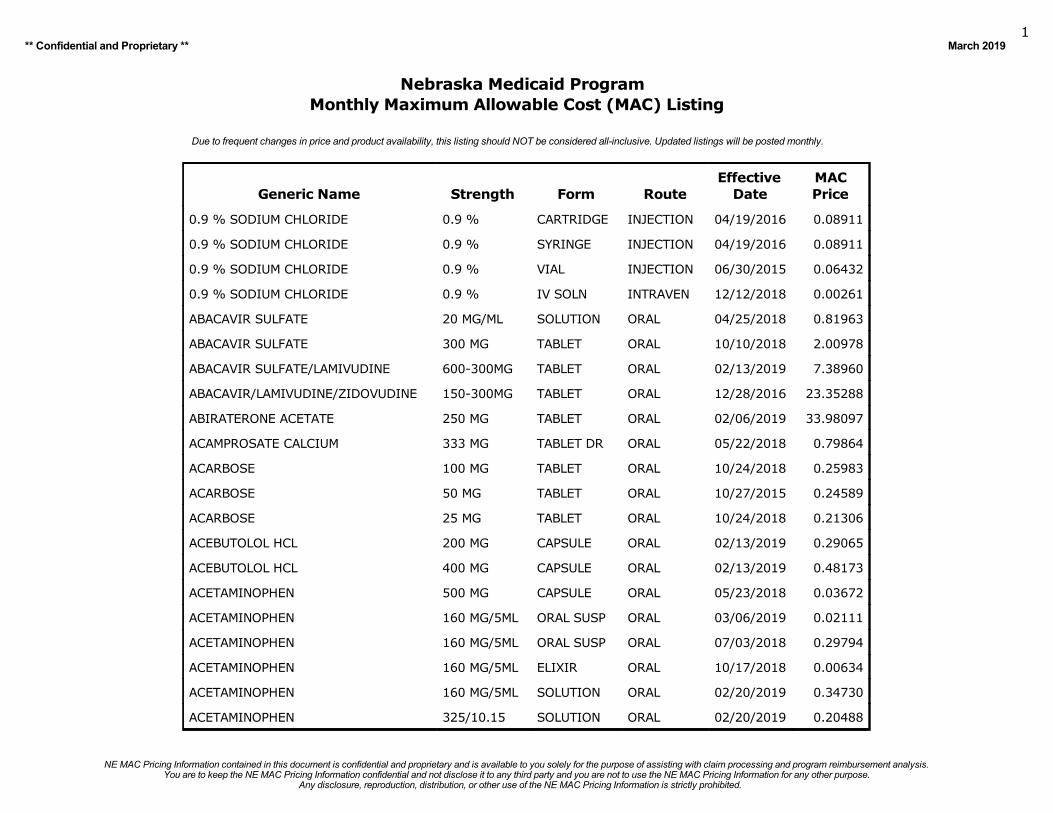
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 20191
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
0.9 % SODIUM CHLORIDE 0.9 % CARTRIDGE INJECTION 04/19/2016 0.08911
0.9 % SODIUM CHLORIDE 0.9 % SYRINGE INJECTION 04/19/2016 0.08911
0.9 % SODIUM CHLORIDE 0.9 % VIAL INJECTION 06/30/2015 0.06432
0.9 % SODIUM CHLORIDE 0.9 % IV SOLN INTRAVEN 12/12/2018 0.00261
ABACAVIR SULFATE 20 MG/ML SOLUTION ORAL 04/25/2018 0.81963
ABACAVIR SULFATE 300 MG TABLET ORAL 10/10/2018 2.00978
ABACAVIR SULFATE/LAMIVUDINE 600-300MG TABLET ORAL 02/13/2019 7.38960
ABACAVIR/LAMIVUDINE/ZIDOVUDINE 150-300MG TABLET ORAL 12/28/2016 23.35288
ABIRATERONE ACETATE 250 MG TABLET ORAL 02/06/2019 33.98097
ACAMPROSATE CALCIUM 333 MG TABLET DR ORAL 05/22/2018 0.79864
ACARBOSE 100 MG TABLET ORAL 10/24/2018 0.25983
ACARBOSE 50 MG TABLET ORAL 10/27/2015 0.24589
ACARBOSE 25 MG TABLET ORAL 10/24/2018 0.21306
ACEBUTOLOL HCL 200 MG CAPSULE ORAL 02/13/2019 0.29065
ACEBUTOLOL HCL 400 MG CAPSULE ORAL 02/13/2019 0.48173
ACETAMINOPHEN 500 MG CAPSULE ORAL 05/23/2018 0.03672
ACETAMINOPHEN 160 MG/5ML ORAL SUSP ORAL 03/06/2019 0.02111
ACETAMINOPHEN 160 MG/5ML ORAL SUSP ORAL 07/03/2018 0.29794
ACETAMINOPHEN 160 MG/5ML ELIXIR ORAL 10/17/2018 0.00634
ACETAMINOPHEN 160 MG/5ML SOLUTION ORAL 02/20/2019 0.34730
ACETAMINOPHEN 325/10.15 SOLUTION ORAL 02/20/2019 0.20488
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 20192
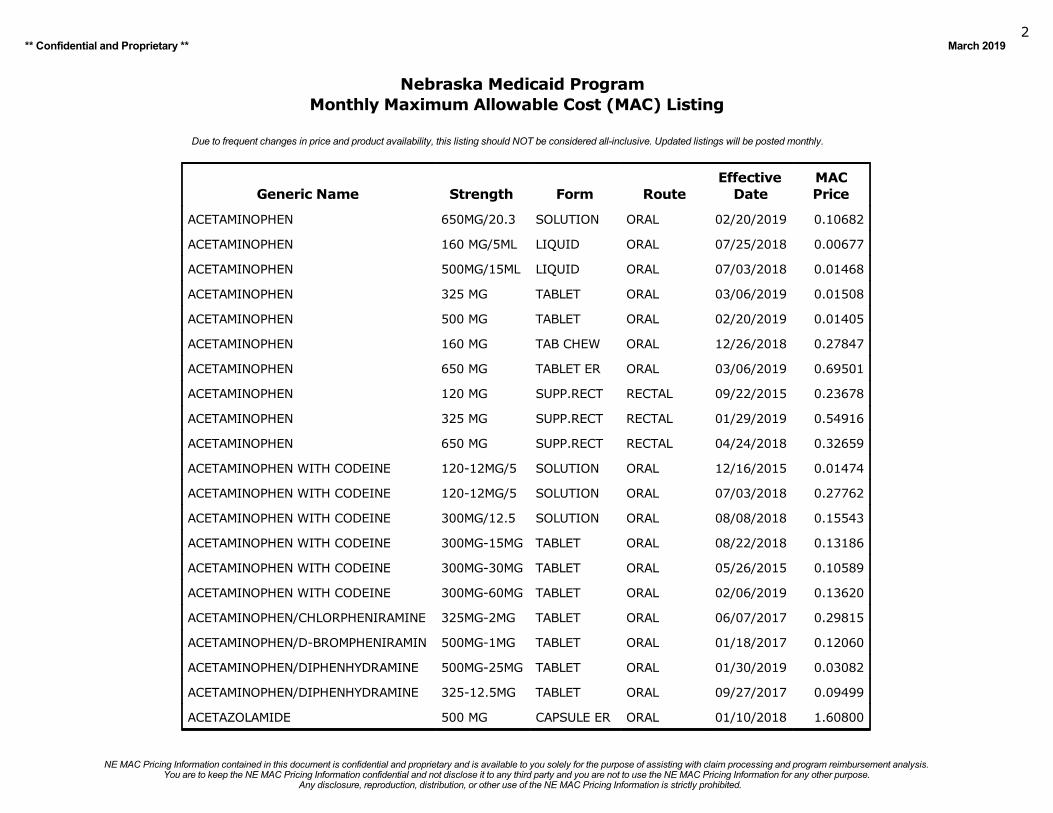
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ACETAMINOPHEN 650MG/20.3 SOLUTION ORAL 02/20/2019 0.10682
ACETAMINOPHEN 160 MG/5ML LIQUID ORAL 07/25/2018 0.00677
ACETAMINOPHEN 500MG/15ML LIQUID ORAL 07/03/2018 0.01468
ACETAMINOPHEN 325 MG TABLET ORAL 03/06/2019 0.01508
ACETAMINOPHEN 500 MG TABLET ORAL 02/20/2019 0.01405
ACETAMINOPHEN 160 MG TAB CHEW ORAL 12/26/2018 0.27847
ACETAMINOPHEN 650 MG TABLET ER ORAL 03/06/2019 0.69501
ACETAMINOPHEN 120 MG SUPP.RECT RECTAL 09/22/2015 0.23678
ACETAMINOPHEN 325 MG SUPP.RECT RECTAL 01/29/2019 0.54916
ACETAMINOPHEN 650 MG SUPP.RECT RECTAL 04/24/2018 0.32659
ACETAMINOPHEN WITH CODEINE 120-12MG/5 SOLUTION ORAL 12/16/2015 0.01474
ACETAMINOPHEN WITH CODEINE 120-12MG/5 SOLUTION ORAL 07/03/2018 0.27762
ACETAMINOPHEN WITH CODEINE 300MG/12.5 SOLUTION ORAL 08/08/2018 0.15543
ACETAMINOPHEN WITH CODEINE 300MG-15MG TABLET ORAL 08/22/2018 0.13186
ACETAMINOPHEN WITH CODEINE 300MG-30MG TABLET ORAL 05/26/2015 0.10589
ACETAMINOPHEN WITH CODEINE 300MG-60MG TABLET ORAL 02/06/2019 0.13620
ACETAMINOPHEN/CHLORPHENIRAMINE 325MG-2MG TABLET ORAL 06/07/2017 0.29815
ACETAMINOPHEN/D-BROMPHENIRAMIN 500MG-1MG TABLET ORAL 01/18/2017 0.12060
ACETAMINOPHEN/DIPHENHYDRAMINE 500MG-25MG TABLET ORAL 01/30/2019 0.03082
ACETAMINOPHEN/DIPHENHYDRAMINE 325-12.5MG TABLET ORAL 09/27/2017 0.09499
ACETAZOLAMIDE 500 MG CAPSULE ER ORAL 01/10/2018 1.60800
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 20193
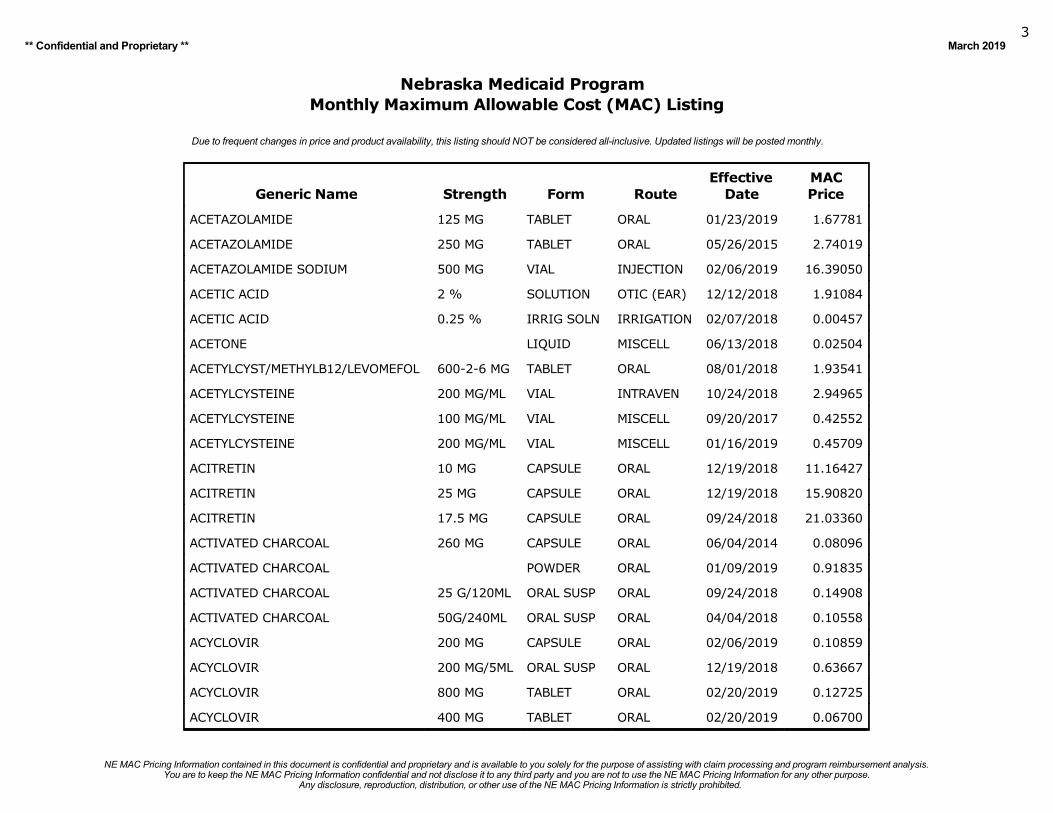
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ACETAZOLAMIDE 125 MG TABLET ORAL 01/23/2019 1.67781
ACETAZOLAMIDE 250 MG TABLET ORAL 05/26/2015 2.74019
ACETAZOLAMIDE SODIUM 500 MG VIAL INJECTION 02/06/2019 16.39050
ACETIC ACID 2 % SOLUTION OTIC (EAR) 12/12/2018 1.91084
ACETIC ACID 0.25 % IRRIG SOLN IRRIGATION 02/07/2018 0.00457
ACETONE LIQUID MISCELL 06/13/2018 0.02504
ACETYLCYST/METHYLB12/LEVOMEFOL 600-2-6 MG TABLET ORAL 08/01/2018 1.93541
ACETYLCYSTEINE 200 MG/ML VIAL INTRAVEN 10/24/2018 2.94965
ACETYLCYSTEINE 100 MG/ML VIAL MISCELL 09/20/2017 0.42552
ACETYLCYSTEINE 200 MG/ML VIAL MISCELL 01/16/2019 0.45709
ACITRETIN 10 MG CAPSULE ORAL 12/19/2018 11.16427
ACITRETIN 25 MG CAPSULE ORAL 12/19/2018 15.90820
ACITRETIN 17.5 MG CAPSULE ORAL 09/24/2018 21.03360
ACTIVATED CHARCOAL 260 MG CAPSULE ORAL 06/04/2014 0.08096
ACTIVATED CHARCOAL POWDER ORAL 01/09/2019 0.91835
ACTIVATED CHARCOAL 25 G/120ML ORAL SUSP ORAL 09/24/2018 0.14908
ACTIVATED CHARCOAL 50G/240ML ORAL SUSP ORAL 04/04/2018 0.10558
ACYCLOVIR 200 MG CAPSULE ORAL 02/06/2019 0.10859
ACYCLOVIR 200 MG/5ML ORAL SUSP ORAL 12/19/2018 0.63667
ACYCLOVIR 800 MG TABLET ORAL 02/20/2019 0.12725
ACYCLOVIR 400 MG TABLET ORAL 02/20/2019 0.06700
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 20194
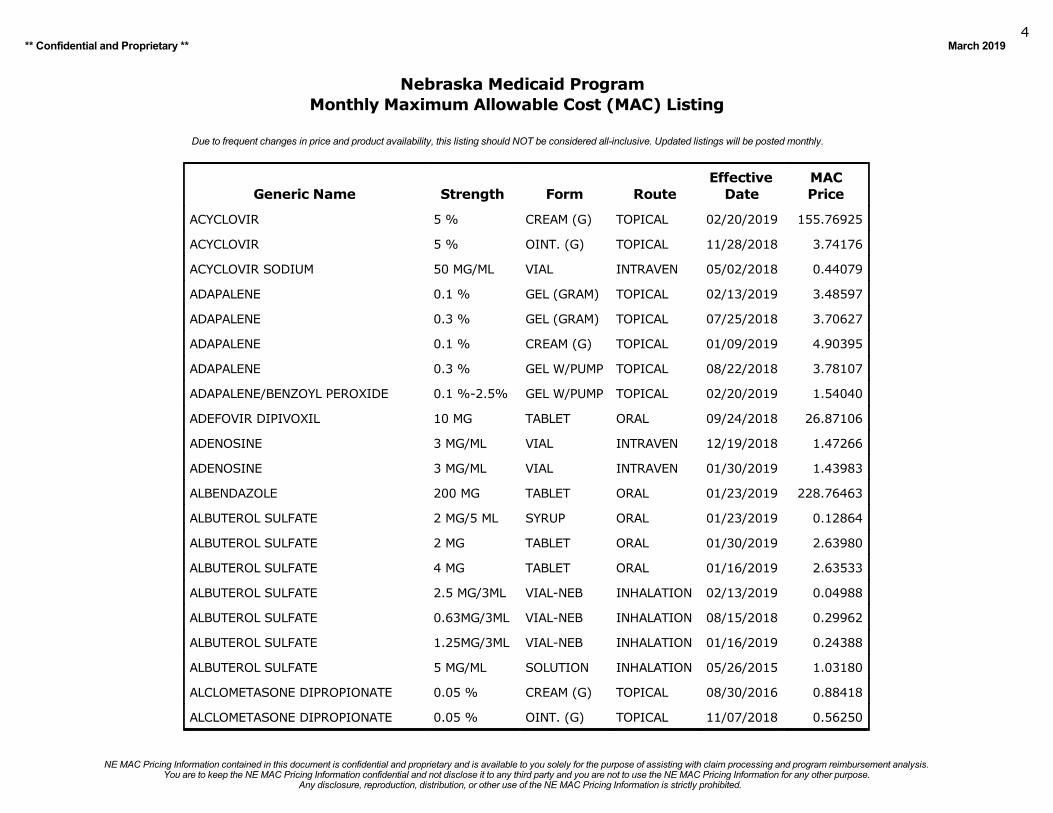
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ACYCLOVIR 5 % CREAM (G) TOPICAL 02/20/2019 155.76925
ACYCLOVIR 5 % OINT. (G) TOPICAL 11/28/2018 3.74176
ACYCLOVIR SODIUM 50 MG/ML VIAL INTRAVEN 05/02/2018 0.44079
ADAPALENE 0.1 % GEL (GRAM) TOPICAL 02/13/2019 3.48597
ADAPALENE 0.3 % GEL (GRAM) TOPICAL 07/25/2018 3.70627
ADAPALENE 0.1 % CREAM (G) TOPICAL 01/09/2019 4.90395
ADAPALENE 0.3 % GEL W/PUMP TOPICAL 08/22/2018 3.78107
ADAPALENE/BENZOYL PEROXIDE 0.1 %-2.5% GEL W/PUMP TOPICAL 02/20/2019 1.54040
ADEFOVIR DIPIVOXIL 10 MG TABLET ORAL 09/24/2018 26.87106
ADENOSINE 3 MG/ML VIAL INTRAVEN 12/19/2018 1.47266
ADENOSINE 3 MG/ML VIAL INTRAVEN 01/30/2019 1.43983
ALBENDAZOLE 200 MG TABLET ORAL 01/23/2019 228.76463
ALBUTEROL SULFATE 2 MG/5 ML SYRUP ORAL 01/23/2019 0.12864
ALBUTEROL SULFATE 2 MG TABLET ORAL 01/30/2019 2.63980
ALBUTEROL SULFATE 4 MG TABLET ORAL 01/16/2019 2.63533
ALBUTEROL SULFATE 2.5 MG/3ML VIAL-NEB INHALATION 02/13/2019 0.04988
ALBUTEROL SULFATE 0.63MG/3ML VIAL-NEB INHALATION 08/15/2018 0.29962
ALBUTEROL SULFATE 1.25MG/3ML VIAL-NEB INHALATION 01/16/2019 0.24388
ALBUTEROL SULFATE 5 MG/ML SOLUTION INHALATION 05/26/2015 1.03180
ALCLOMETASONE DIPROPIONATE 0.05 % CREAM (G) TOPICAL 08/30/2016 0.88418
ALCLOMETASONE DIPROPIONATE 0.05 % OINT. (G) TOPICAL 11/07/2018 0.56250
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 20195
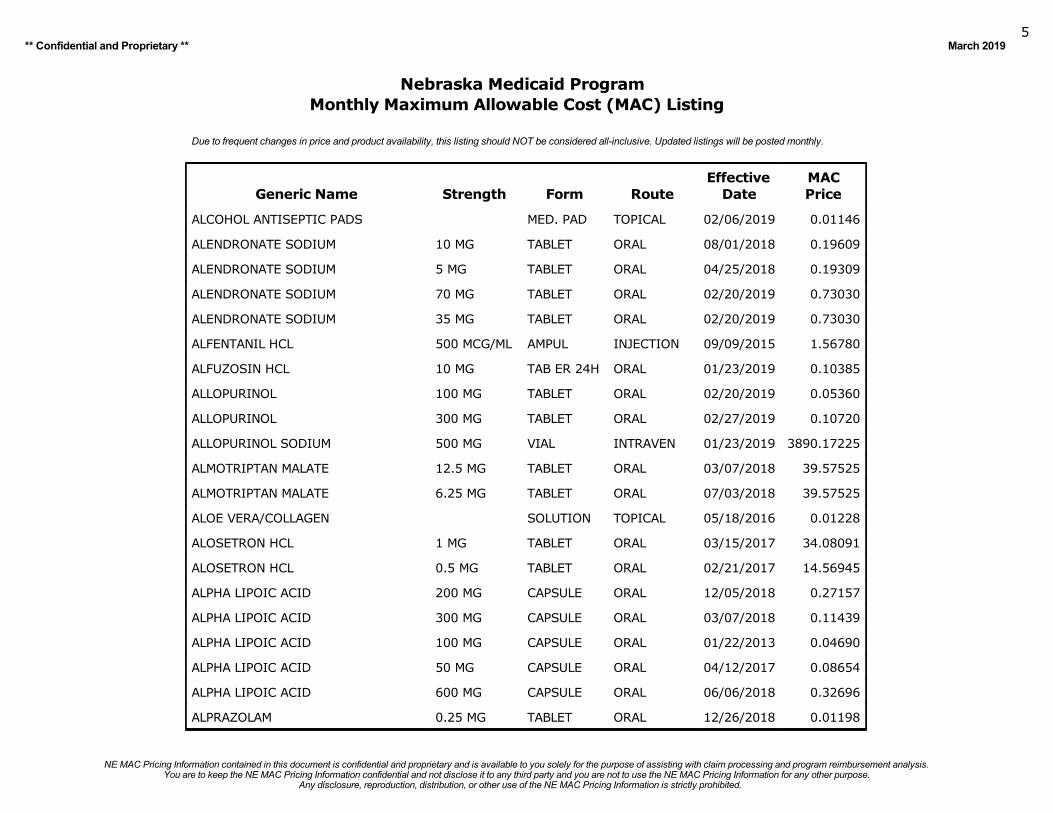
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ALCOHOL ANTISEPTIC PADS MED. PAD TOPICAL 02/06/2019 0.01146
ALENDRONATE SODIUM 10 MG TABLET ORAL 08/01/2018 0.19609
ALENDRONATE SODIUM 5 MG TABLET ORAL 04/25/2018 0.19309
ALENDRONATE SODIUM 70 MG TABLET ORAL 02/20/2019 0.73030
ALENDRONATE SODIUM 35 MG TABLET ORAL 02/20/2019 0.73030
ALFENTANIL HCL 500 MCG/ML AMPUL INJECTION 09/09/2015 1.56780
ALFUZOSIN HCL 10 MG TAB ER 24H ORAL 01/23/2019 0.10385
ALLOPURINOL 100 MG TABLET ORAL 02/20/2019 0.05360
ALLOPURINOL 300 MG TABLET ORAL 02/27/2019 0.10720
ALLOPURINOL SODIUM 500 MG VIAL INTRAVEN 01/23/2019 3890.17225
ALMOTRIPTAN MALATE 12.5 MG TABLET ORAL 03/07/2018 39.57525
ALMOTRIPTAN MALATE 6.25 MG TABLET ORAL 07/03/2018 39.57525
ALOE VERA/COLLAGEN SOLUTION TOPICAL 05/18/2016 0.01228
ALOSETRON HCL 1 MG TABLET ORAL 03/15/2017 34.08091
ALOSETRON HCL 0.5 MG TABLET ORAL 02/21/2017 14.56945
ALPHA LIPOIC ACID 200 MG CAPSULE ORAL 12/05/2018 0.27157
ALPHA LIPOIC ACID 300 MG CAPSULE ORAL 03/07/2018 0.11439
ALPHA LIPOIC ACID 100 MG CAPSULE ORAL 01/22/2013 0.04690
ALPHA LIPOIC ACID 50 MG CAPSULE ORAL 04/12/2017 0.08654
ALPHA LIPOIC ACID 600 MG CAPSULE ORAL 06/06/2018 0.32696
ALPRAZOLAM 0.25 MG TABLET ORAL 12/26/2018 0.01198
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 20196
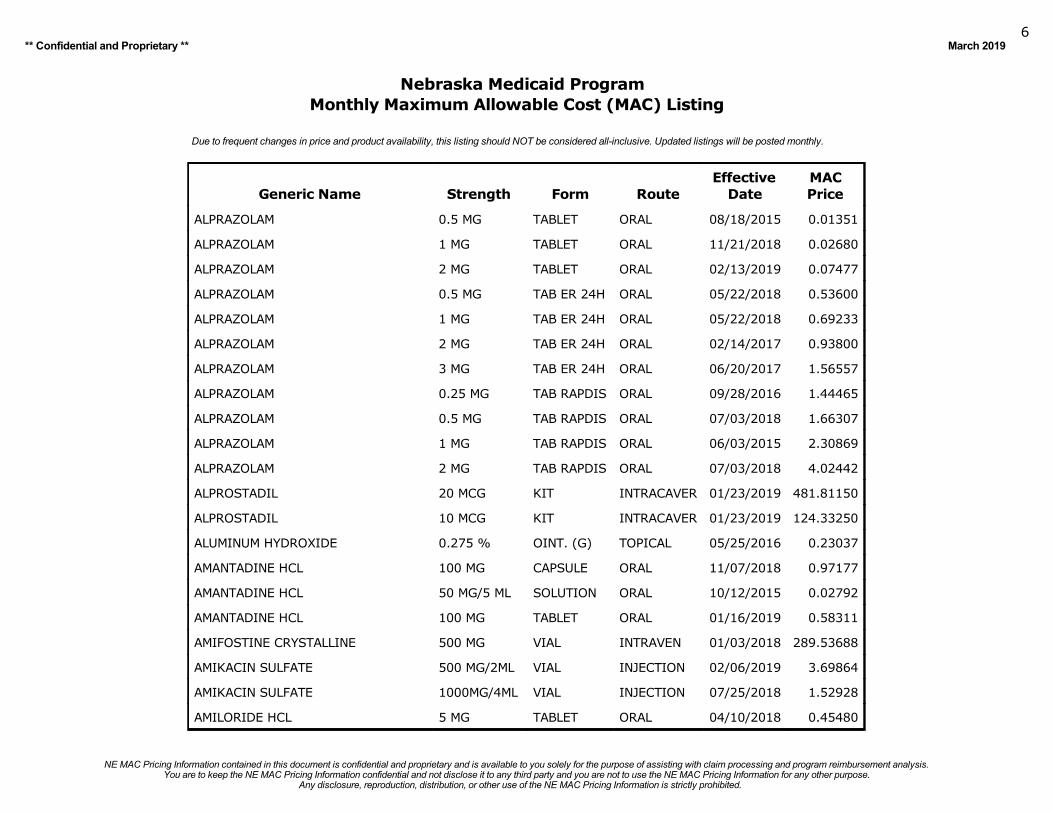
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ALPRAZOLAM 0.5 MG TABLET ORAL 08/18/2015 0.01351
ALPRAZOLAM 1 MG TABLET ORAL 11/21/2018 0.02680
ALPRAZOLAM 2 MG TABLET ORAL 02/13/2019 0.07477
ALPRAZOLAM 0.5 MG TAB ER 24H ORAL 05/22/2018 0.53600
ALPRAZOLAM 1 MG TAB ER 24H ORAL 05/22/2018 0.69233
ALPRAZOLAM 2 MG TAB ER 24H ORAL 02/14/2017 0.93800
ALPRAZOLAM 3 MG TAB ER 24H ORAL 06/20/2017 1.56557
ALPRAZOLAM 0.25 MG TAB RAPDIS ORAL 09/28/2016 1.44465
ALPRAZOLAM 0.5 MG TAB RAPDIS ORAL 07/03/2018 1.66307
ALPRAZOLAM 1 MG TAB RAPDIS ORAL 06/03/2015 2.30869
ALPRAZOLAM 2 MG TAB RAPDIS ORAL 07/03/2018 4.02442
ALPROSTADIL 20 MCG KIT INTRACAVER 01/23/2019 481.81150
ALPROSTADIL 10 MCG KIT INTRACAVER 01/23/2019 124.33250
ALUMINUM HYDROXIDE 0.275 % OINT. (G) TOPICAL 05/25/2016 0.23037
AMANTADINE HCL 100 MG CAPSULE ORAL 11/07/2018 0.97177
AMANTADINE HCL 50 MG/5 ML SOLUTION ORAL 10/12/2015 0.02792
AMANTADINE HCL 100 MG TABLET ORAL 01/16/2019 0.58311
AMIFOSTINE CRYSTALLINE 500 MG VIAL INTRAVEN 01/03/2018 289.53688
AMIKACIN SULFATE 500 MG/2ML VIAL INJECTION 02/06/2019 3.69864
AMIKACIN SULFATE 1000MG/4ML VIAL INJECTION 07/25/2018 1.52928
AMILORIDE HCL 5 MG TABLET ORAL 04/10/2018 0.45480
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 20197
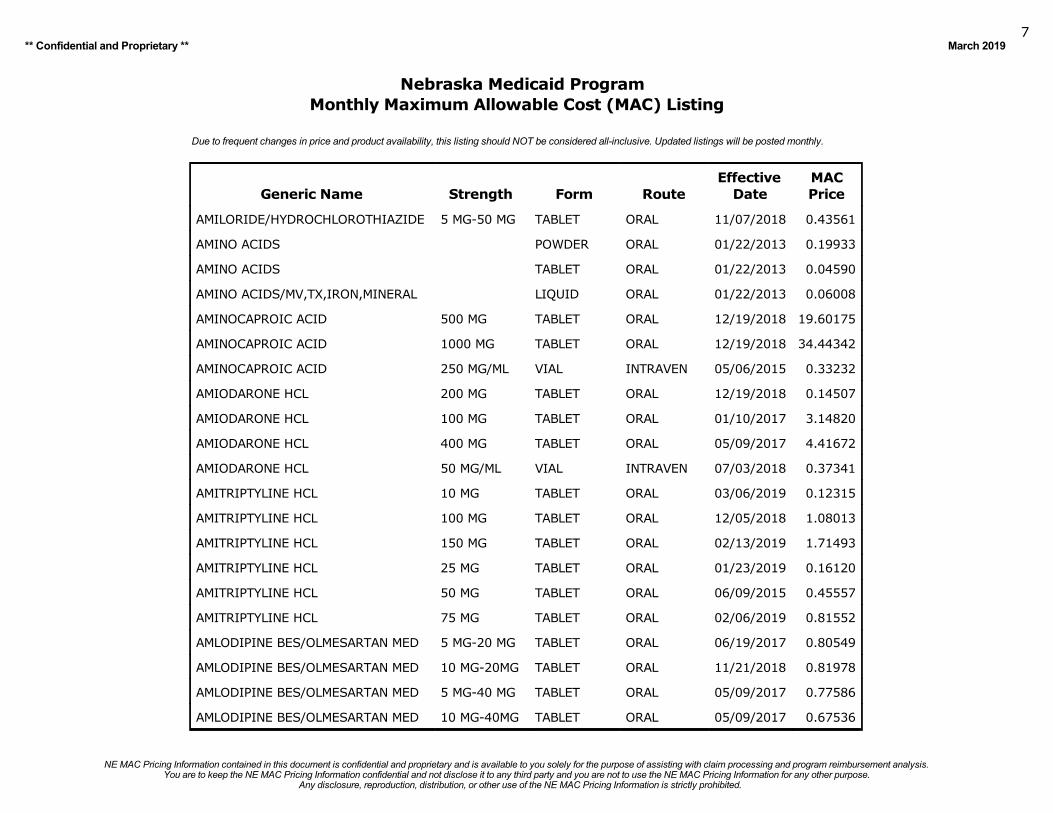
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
AMILORIDE/HYDROCHLOROTHIAZIDE 5 MG-50 MG TABLET ORAL 11/07/2018 0.43561
AMINO ACIDS POWDER ORAL 01/22/2013 0.19933
AMINO ACIDS TABLET ORAL 01/22/2013 0.04590
AMINO ACIDS/MV,TX,IRON,MINERAL LIQUID ORAL 01/22/2013 0.06008
AMINOCAPROIC ACID 500 MG TABLET ORAL 12/19/2018 19.60175
AMINOCAPROIC ACID 1000 MG TABLET ORAL 12/19/2018 34.44342
AMINOCAPROIC ACID 250 MG/ML VIAL INTRAVEN 05/06/2015 0.33232
AMIODARONE HCL 200 MG TABLET ORAL 12/19/2018 0.14507
AMIODARONE HCL 100 MG TABLET ORAL 01/10/2017 3.14820
AMIODARONE HCL 400 MG TABLET ORAL 05/09/2017 4.41672
AMIODARONE HCL 50 MG/ML VIAL INTRAVEN 07/03/2018 0.37341
AMITRIPTYLINE HCL 10 MG TABLET ORAL 03/06/2019 0.12315
AMITRIPTYLINE HCL 100 MG TABLET ORAL 12/05/2018 1.08013
AMITRIPTYLINE HCL 150 MG TABLET ORAL 02/13/2019 1.71493
AMITRIPTYLINE HCL 25 MG TABLET ORAL 01/23/2019 0.16120
AMITRIPTYLINE HCL 50 MG TABLET ORAL 06/09/2015 0.45557
AMITRIPTYLINE HCL 75 MG TABLET ORAL 02/06/2019 0.81552
AMLODIPINE BES/OLMESARTAN MED 5 MG-20 MG TABLET ORAL 06/19/2017 0.80549
AMLODIPINE BES/OLMESARTAN MED 10 MG-20MG TABLET ORAL 11/21/2018 0.81978
AMLODIPINE BES/OLMESARTAN MED 5 MG-40 MG TABLET ORAL 05/09/2017 0.77586
AMLODIPINE BES/OLMESARTAN MED 10 MG-40MG TABLET ORAL 05/09/2017 0.67536
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 20198
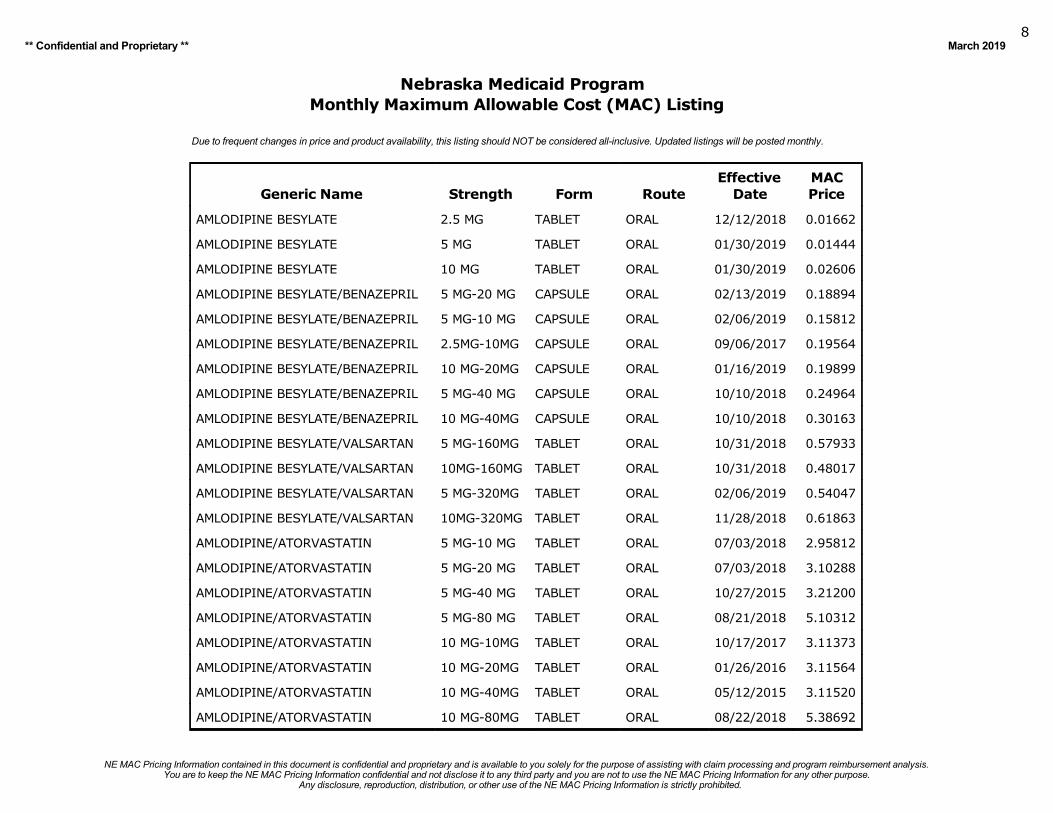
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
AMLODIPINE BESYLATE 2.5 MG TABLET ORAL 12/12/2018 0.01662
AMLODIPINE BESYLATE 5 MG TABLET ORAL 01/30/2019 0.01444
AMLODIPINE BESYLATE 10 MG TABLET ORAL 01/30/2019 0.02606
AMLODIPINE BESYLATE/BENAZEPRIL 5 MG-20 MG CAPSULE ORAL 02/13/2019 0.18894
AMLODIPINE BESYLATE/BENAZEPRIL 5 MG-10 MG CAPSULE ORAL 02/06/2019 0.15812
AMLODIPINE BESYLATE/BENAZEPRIL 2.5MG-10MG CAPSULE ORAL 09/06/2017 0.19564
AMLODIPINE BESYLATE/BENAZEPRIL 10 MG-20MG CAPSULE ORAL 01/16/2019 0.19899
AMLODIPINE BESYLATE/BENAZEPRIL 5 MG-40 MG CAPSULE ORAL 10/10/2018 0.24964
AMLODIPINE BESYLATE/BENAZEPRIL 10 MG-40MG CAPSULE ORAL 10/10/2018 0.30163
AMLODIPINE BESYLATE/VALSARTAN 5 MG-160MG TABLET ORAL 10/31/2018 0.57933
AMLODIPINE BESYLATE/VALSARTAN 10MG-160MG TABLET ORAL 10/31/2018 0.48017
AMLODIPINE BESYLATE/VALSARTAN 5 MG-320MG TABLET ORAL 02/06/2019 0.54047
AMLODIPINE BESYLATE/VALSARTAN 10MG-320MG TABLET ORAL 11/28/2018 0.61863
AMLODIPINE/ATORVASTATIN 5 MG-10 MG TABLET ORAL 07/03/2018 2.95812
AMLODIPINE/ATORVASTATIN 5 MG-20 MG TABLET ORAL 07/03/2018 3.10288
AMLODIPINE/ATORVASTATIN 5 MG-40 MG TABLET ORAL 10/27/2015 3.21200
AMLODIPINE/ATORVASTATIN 5 MG-80 MG TABLET ORAL 08/21/2018 5.10312
AMLODIPINE/ATORVASTATIN 10 MG-10MG TABLET ORAL 10/17/2017 3.11373
AMLODIPINE/ATORVASTATIN 10 MG-20MG TABLET ORAL 01/26/2016 3.11564
AMLODIPINE/ATORVASTATIN 10 MG-40MG TABLET ORAL 05/12/2015 3.11520
AMLODIPINE/ATORVASTATIN 10 MG-80MG TABLET ORAL 08/22/2018 5.38692
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 20199
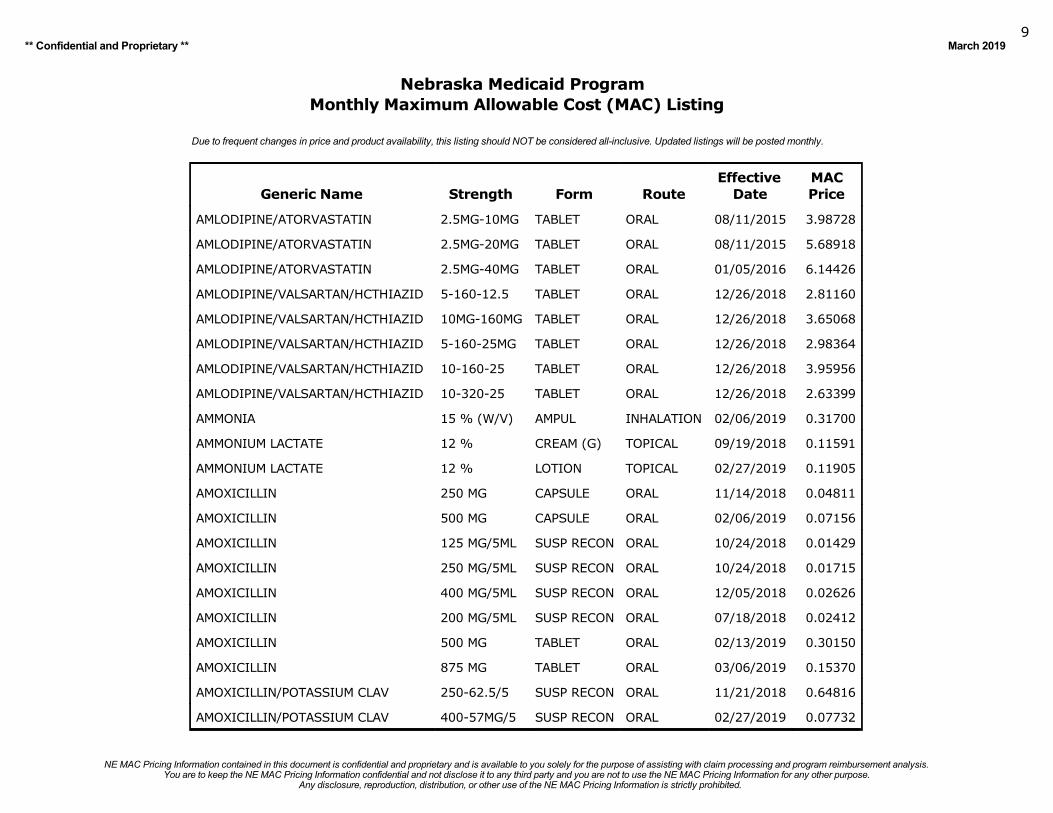
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
AMLODIPINE/ATORVASTATIN 2.5MG-10MG TABLET ORAL 08/11/2015 3.98728
AMLODIPINE/ATORVASTATIN 2.5MG-20MG TABLET ORAL 08/11/2015 5.68918
AMLODIPINE/ATORVASTATIN 2.5MG-40MG TABLET ORAL 01/05/2016 6.14426
AMLODIPINE/VALSARTAN/HCTHIAZID 5-160-12.5 TABLET ORAL 12/26/2018 2.81160
AMLODIPINE/VALSARTAN/HCTHIAZID 10MG-160MG TABLET ORAL 12/26/2018 3.65068
AMLODIPINE/VALSARTAN/HCTHIAZID 5-160-25MG TABLET ORAL 12/26/2018 2.98364
AMLODIPINE/VALSARTAN/HCTHIAZID 10-160-25 TABLET ORAL 12/26/2018 3.95956
AMLODIPINE/VALSARTAN/HCTHIAZID 10-320-25 TABLET ORAL 12/26/2018 2.63399
AMMONIA 15 % (W/V) AMPUL INHALATION 02/06/2019 0.31700
AMMONIUM LACTATE 12 % CREAM (G) TOPICAL 09/19/2018 0.11591
AMMONIUM LACTATE 12 % LOTION TOPICAL 02/27/2019 0.11905
AMOXICILLIN 250 MG CAPSULE ORAL 11/14/2018 0.04811
AMOXICILLIN 500 MG CAPSULE ORAL 02/06/2019 0.07156
AMOXICILLIN 125 MG/5ML SUSP RECON ORAL 10/24/2018 0.01429
AMOXICILLIN 250 MG/5ML SUSP RECON ORAL 10/24/2018 0.01715
AMOXICILLIN 400 MG/5ML SUSP RECON ORAL 12/05/2018 0.02626
AMOXICILLIN 200 MG/5ML SUSP RECON ORAL 07/18/2018 0.02412
AMOXICILLIN 500 MG TABLET ORAL 02/13/2019 0.30150
AMOXICILLIN 875 MG TABLET ORAL 03/06/2019 0.15370
AMOXICILLIN/POTASSIUM CLAV 250-62.5/5 SUSP RECON ORAL 11/21/2018 0.64816
AMOXICILLIN/POTASSIUM CLAV 400-57MG/5 SUSP RECON ORAL 02/27/2019 0.07732
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201910
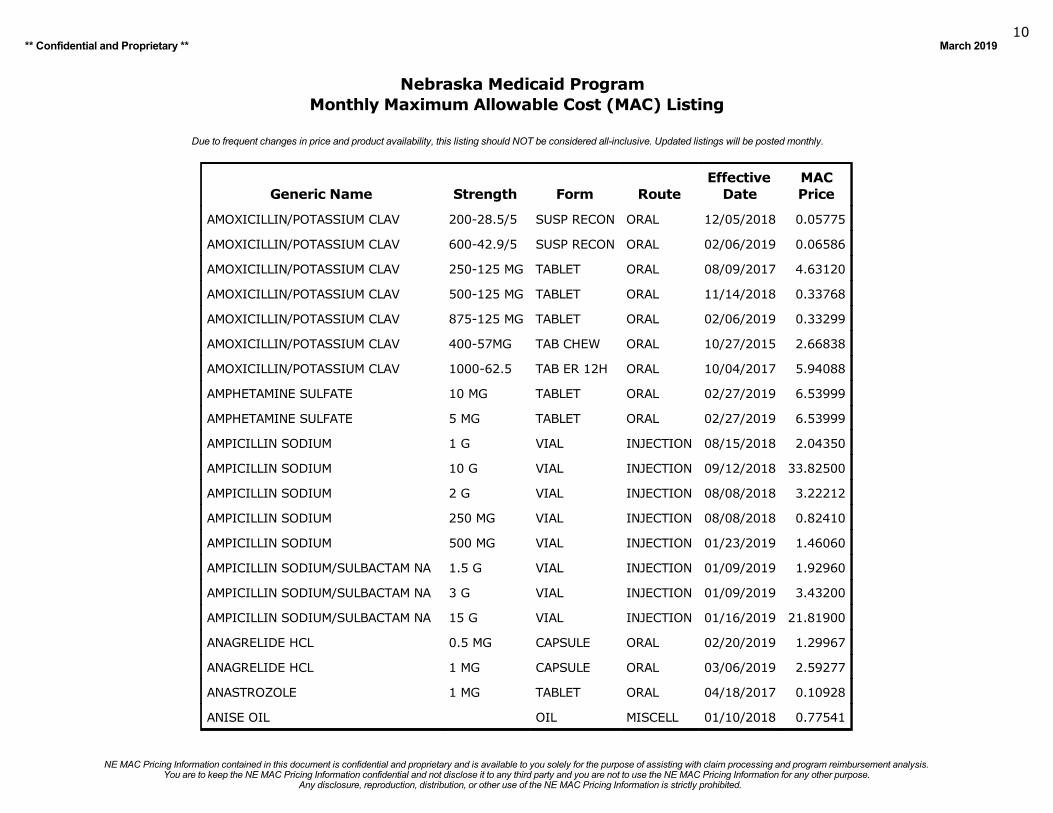
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
AMOXICILLIN/POTASSIUM CLAV 200-28.5/5 SUSP RECON ORAL 12/05/2018 0.05775
AMOXICILLIN/POTASSIUM CLAV 600-42.9/5 SUSP RECON ORAL 02/06/2019 0.06586
AMOXICILLIN/POTASSIUM CLAV 250-125 MG TABLET ORAL 08/09/2017 4.63120
AMOXICILLIN/POTASSIUM CLAV 500-125 MG TABLET ORAL 11/14/2018 0.33768
AMOXICILLIN/POTASSIUM CLAV 875-125 MG TABLET ORAL 02/06/2019 0.33299
AMOXICILLIN/POTASSIUM CLAV 400-57MG TAB CHEW ORAL 10/27/2015 2.66838
AMOXICILLIN/POTASSIUM CLAV 1000-62.5 TAB ER 12H ORAL 10/04/2017 5.94088
AMPHETAMINE SULFATE 10 MG TABLET ORAL 02/27/2019 6.53999
AMPHETAMINE SULFATE 5 MG TABLET ORAL 02/27/2019 6.53999
AMPICILLIN SODIUM 1 G VIAL INJECTION 08/15/2018 2.04350
AMPICILLIN SODIUM 10 G VIAL INJECTION 09/12/2018 33.82500
AMPICILLIN SODIUM 2 G VIAL INJECTION 08/08/2018 3.22212
AMPICILLIN SODIUM 250 MG VIAL INJECTION 08/08/2018 0.82410
AMPICILLIN SODIUM 500 MG VIAL INJECTION 01/23/2019 1.46060
AMPICILLIN SODIUM/SULBACTAM NA 1.5 G VIAL INJECTION 01/09/2019 1.92960
AMPICILLIN SODIUM/SULBACTAM NA 3 G VIAL INJECTION 01/09/2019 3.43200
AMPICILLIN SODIUM/SULBACTAM NA 15 G VIAL INJECTION 01/16/2019 21.81900
ANAGRELIDE HCL 0.5 MG CAPSULE ORAL 02/20/2019 1.29967
ANAGRELIDE HCL 1 MG CAPSULE ORAL 03/06/2019 2.59277
ANASTROZOLE 1 MG TABLET ORAL 04/18/2017 0.10928
ANISE OIL OIL MISCELL 01/10/2018 0.77541
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201911
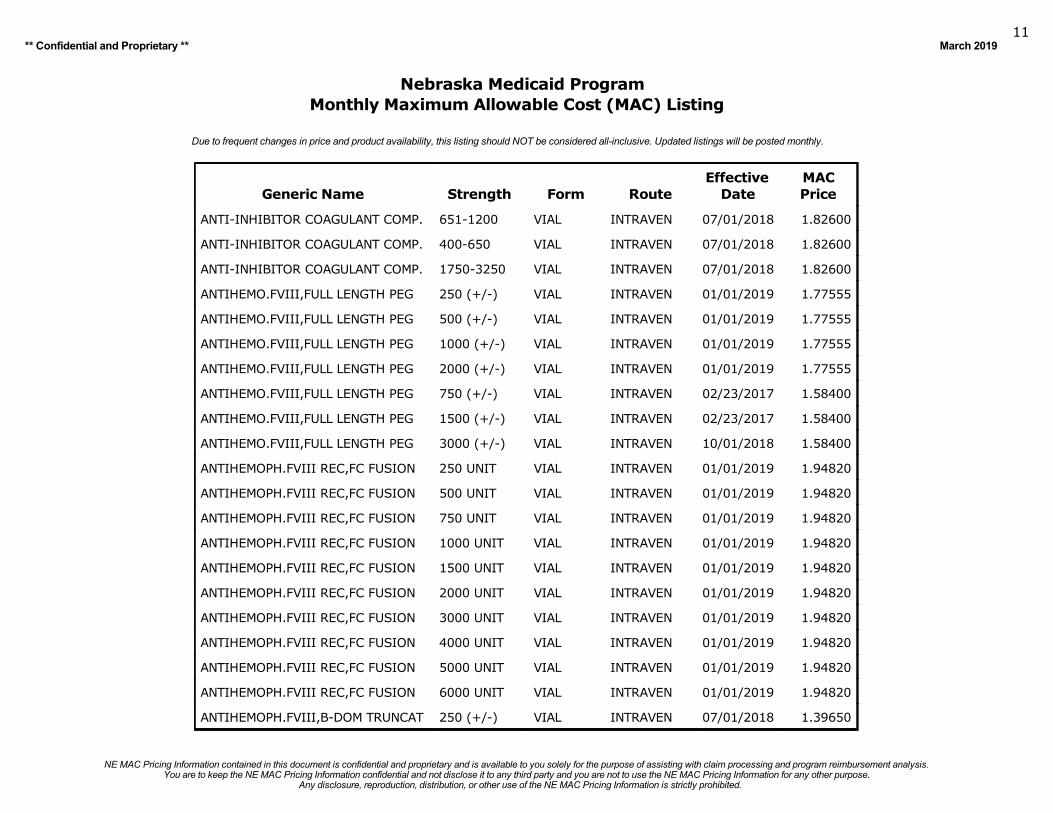
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ANTI-INHIBITOR COAGULANT COMP. 651-1200 VIAL INTRAVEN 07/01/2018 1.82600
ANTI-INHIBITOR COAGULANT COMP. 400-650 VIAL INTRAVEN 07/01/2018 1.82600
ANTI-INHIBITOR COAGULANT COMP. 1750-3250 VIAL INTRAVEN 07/01/2018 1.82600
ANTIHEMO.FVIII,FULL LENGTH PEG 250 (+/-) VIAL INTRAVEN 01/01/2019 1.77555
ANTIHEMO.FVIII,FULL LENGTH PEG 500 (+/-) VIAL INTRAVEN 01/01/2019 1.77555
ANTIHEMO.FVIII,FULL LENGTH PEG 1000 (+/-) VIAL INTRAVEN 01/01/2019 1.77555
ANTIHEMO.FVIII,FULL LENGTH PEG 2000 (+/-) VIAL INTRAVEN 01/01/2019 1.77555
ANTIHEMO.FVIII,FULL LENGTH PEG 750 (+/-) VIAL INTRAVEN 02/23/2017 1.58400
ANTIHEMO.FVIII,FULL LENGTH PEG 1500 (+/-) VIAL INTRAVEN 02/23/2017 1.58400
ANTIHEMO.FVIII,FULL LENGTH PEG 3000 (+/-) VIAL INTRAVEN 10/01/2018 1.58400
ANTIHEMOPH.FVIII REC,FC FUSION 250 UNIT VIAL INTRAVEN 01/01/2019 1.94820
ANTIHEMOPH.FVIII REC,FC FUSION 500 UNIT VIAL INTRAVEN 01/01/2019 1.94820
ANTIHEMOPH.FVIII REC,FC FUSION 750 UNIT VIAL INTRAVEN 01/01/2019 1.94820
ANTIHEMOPH.FVIII REC,FC FUSION 1000 UNIT VIAL INTRAVEN 01/01/2019 1.94820
ANTIHEMOPH.FVIII REC,FC FUSION 1500 UNIT VIAL INTRAVEN 01/01/2019 1.94820
ANTIHEMOPH.FVIII REC,FC FUSION 2000 UNIT VIAL INTRAVEN 01/01/2019 1.94820
ANTIHEMOPH.FVIII REC,FC FUSION 3000 UNIT VIAL INTRAVEN 01/01/2019 1.94820
ANTIHEMOPH.FVIII REC,FC FUSION 4000 UNIT VIAL INTRAVEN 01/01/2019 1.94820
ANTIHEMOPH.FVIII REC,FC FUSION 5000 UNIT VIAL INTRAVEN 01/01/2019 1.94820
ANTIHEMOPH.FVIII REC,FC FUSION 6000 UNIT VIAL INTRAVEN 01/01/2019 1.94820
ANTIHEMOPH.FVIII,B-DOM TRUNCAT 250 (+/-) VIAL INTRAVEN 07/01/2018 1.39650
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201912
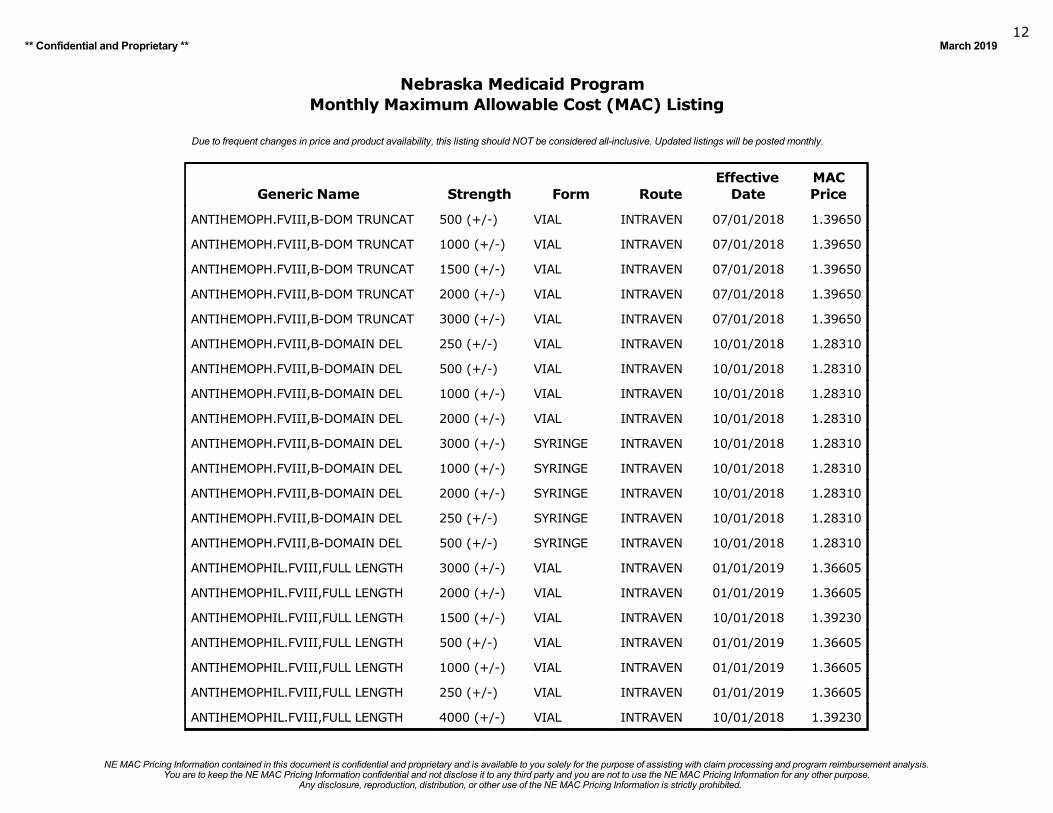
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ANTIHEMOPH.FVIII,B-DOM TRUNCAT 500 (+/-) VIAL INTRAVEN 07/01/2018 1.39650
ANTIHEMOPH.FVIII,B-DOM TRUNCAT 1000 (+/-) VIAL INTRAVEN 07/01/2018 1.39650
ANTIHEMOPH.FVIII,B-DOM TRUNCAT 1500 (+/-) VIAL INTRAVEN 07/01/2018 1.39650
ANTIHEMOPH.FVIII,B-DOM TRUNCAT 2000 (+/-) VIAL INTRAVEN 07/01/2018 1.39650
ANTIHEMOPH.FVIII,B-DOM TRUNCAT 3000 (+/-) VIAL INTRAVEN 07/01/2018 1.39650
ANTIHEMOPH.FVIII,B-DOMAIN DEL 250 (+/-) VIAL INTRAVEN 10/01/2018 1.28310
ANTIHEMOPH.FVIII,B-DOMAIN DEL 500 (+/-) VIAL INTRAVEN 10/01/2018 1.28310
ANTIHEMOPH.FVIII,B-DOMAIN DEL 1000 (+/-) VIAL INTRAVEN 10/01/2018 1.28310
ANTIHEMOPH.FVIII,B-DOMAIN DEL 2000 (+/-) VIAL INTRAVEN 10/01/2018 1.28310
ANTIHEMOPH.FVIII,B-DOMAIN DEL 3000 (+/-) SYRINGE INTRAVEN 10/01/2018 1.28310
ANTIHEMOPH.FVIII,B-DOMAIN DEL 1000 (+/-) SYRINGE INTRAVEN 10/01/2018 1.28310
ANTIHEMOPH.FVIII,B-DOMAIN DEL 2000 (+/-) SYRINGE INTRAVEN 10/01/2018 1.28310
ANTIHEMOPH.FVIII,B-DOMAIN DEL 250 (+/-) SYRINGE INTRAVEN 10/01/2018 1.28310
ANTIHEMOPH.FVIII,B-DOMAIN DEL 500 (+/-) SYRINGE INTRAVEN 10/01/2018 1.28310
ANTIHEMOPHIL.FVIII,FULL LENGTH 3000 (+/-) VIAL INTRAVEN 01/01/2019 1.36605
ANTIHEMOPHIL.FVIII,FULL LENGTH 2000 (+/-) VIAL INTRAVEN 01/01/2019 1.36605
ANTIHEMOPHIL.FVIII,FULL LENGTH 1500 (+/-) VIAL INTRAVEN 10/01/2018 1.39230
ANTIHEMOPHIL.FVIII,FULL LENGTH 500 (+/-) VIAL INTRAVEN 01/01/2019 1.36605
ANTIHEMOPHIL.FVIII,FULL LENGTH 1000 (+/-) VIAL INTRAVEN 01/01/2019 1.36605
ANTIHEMOPHIL.FVIII,FULL LENGTH 250 (+/-) VIAL INTRAVEN 01/01/2019 1.36605
ANTIHEMOPHIL.FVIII,FULL LENGTH 4000 (+/-) VIAL INTRAVEN 10/01/2018 1.39230
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201913
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
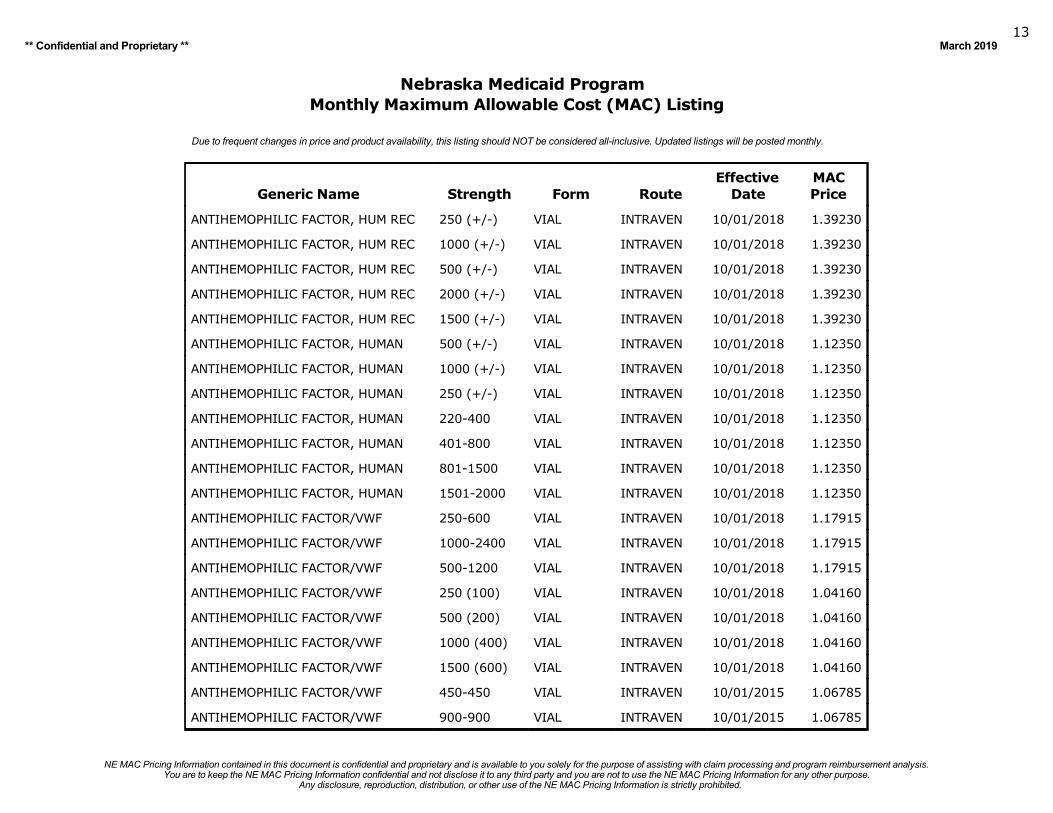
ANTIHEMOPHILIC FACTOR, HUM REC 250 (+/-) VIAL INTRAVEN 10/01/2018 1.39230
ANTIHEMOPHILIC FACTOR, HUM REC 1000 (+/-) VIAL INTRAVEN 10/01/2018 1.39230
ANTIHEMOPHILIC FACTOR, HUM REC 500 (+/-) VIAL INTRAVEN 10/01/2018 1.39230
ANTIHEMOPHILIC FACTOR, HUM REC 2000 (+/-) VIAL INTRAVEN 10/01/2018 1.39230
ANTIHEMOPHILIC FACTOR, HUM REC 1500 (+/-) VIAL INTRAVEN 10/01/2018 1.39230
ANTIHEMOPHILIC FACTOR, HUMAN 500 (+/-) VIAL INTRAVEN 10/01/2018 1.12350
ANTIHEMOPHILIC FACTOR, HUMAN 1000 (+/-) VIAL INTRAVEN 10/01/2018 1.12350
ANTIHEMOPHILIC FACTOR, HUMAN 250 (+/-) VIAL INTRAVEN 10/01/2018 1.12350
ANTIHEMOPHILIC FACTOR, HUMAN 220-400 VIAL INTRAVEN 10/01/2018 1.12350
ANTIHEMOPHILIC FACTOR, HUMAN 401-800 VIAL INTRAVEN 10/01/2018 1.12350
ANTIHEMOPHILIC FACTOR, HUMAN 801-1500 VIAL INTRAVEN 10/01/2018 1.12350
ANTIHEMOPHILIC FACTOR, HUMAN 1501-2000 VIAL INTRAVEN 10/01/2018 1.12350
ANTIHEMOPHILIC FACTOR/VWF 250-600 VIAL INTRAVEN 10/01/2018 1.17915
ANTIHEMOPHILIC FACTOR/VWF 1000-2400 VIAL INTRAVEN 10/01/2018 1.17915
ANTIHEMOPHILIC FACTOR/VWF 500-1200 VIAL INTRAVEN 10/01/2018 1.17915
ANTIHEMOPHILIC FACTOR/VWF 250 (100) VIAL INTRAVEN 10/01/2018 1.04160
ANTIHEMOPHILIC FACTOR/VWF 500 (200) VIAL INTRAVEN 10/01/2018 1.04160
ANTIHEMOPHILIC FACTOR/VWF 1000 (400) VIAL INTRAVEN 10/01/2018 1.04160
ANTIHEMOPHILIC FACTOR/VWF 1500 (600) VIAL INTRAVEN 10/01/2018 1.04160
ANTIHEMOPHILIC FACTOR/VWF 450-450 VIAL INTRAVEN 10/01/2015 1.06785
ANTIHEMOPHILIC FACTOR/VWF 900-900 VIAL INTRAVEN 10/01/2015 1.06785
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201914
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
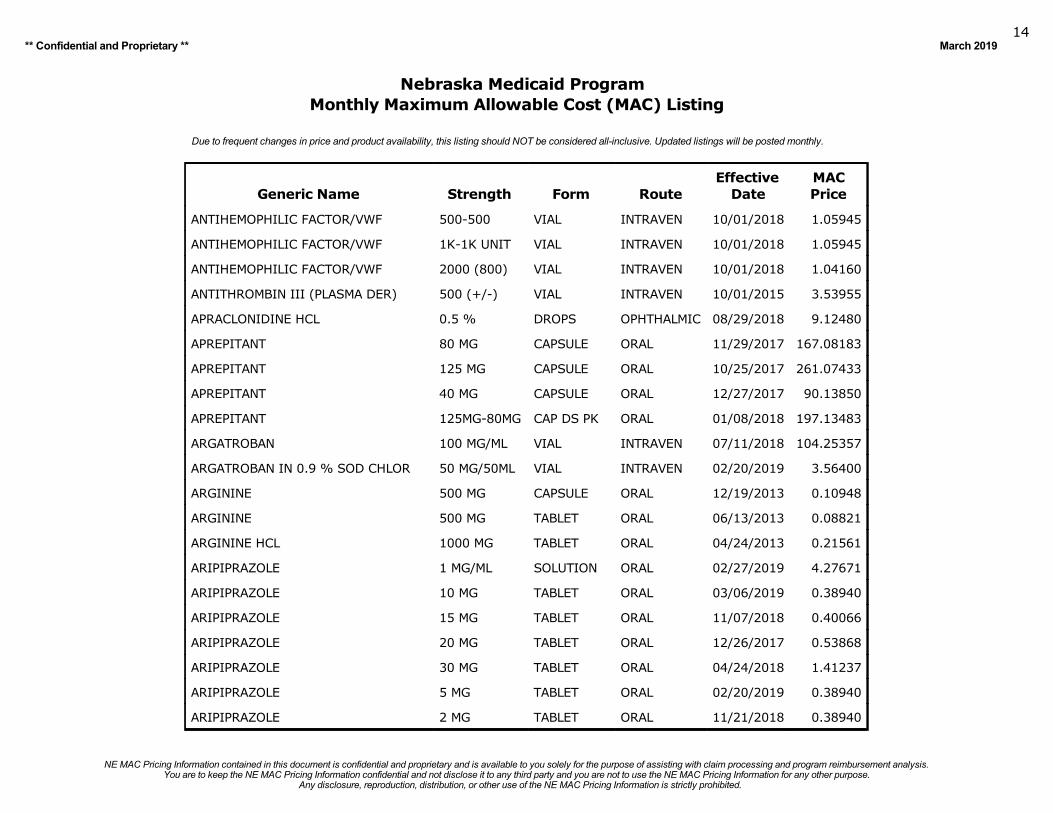
ANTIHEMOPHILIC FACTOR/VWF 500-500 VIAL INTRAVEN 10/01/2018 1.05945
ANTIHEMOPHILIC FACTOR/VWF 1K-1K UNIT VIAL INTRAVEN 10/01/2018 1.05945
ANTIHEMOPHILIC FACTOR/VWF 2000 (800) VIAL INTRAVEN 10/01/2018 1.04160
ANTITHROMBIN III (PLASMA DER) 500 (+/-) VIAL INTRAVEN 10/01/2015 3.53955
APRACLONIDINE HCL 0.5 % DROPS OPHTHALMIC 08/29/2018 9.12480
APREPITANT 80 MG CAPSULE ORAL 11/29/2017 167.08183
APREPITANT 125 MG CAPSULE ORAL 10/25/2017 261.07433
APREPITANT 40 MG CAPSULE ORAL 12/27/2017 90.13850
APREPITANT 125MG-80MG CAP DS PK ORAL 01/08/2018 197.13483
ARGATROBAN 100 MG/ML VIAL INTRAVEN 07/11/2018 104.25357
ARGATROBAN IN 0.9 % SOD CHLOR 50 MG/50ML VIAL INTRAVEN 02/20/2019 3.56400
ARGININE 500 MG CAPSULE ORAL 12/19/2013 0.10948
ARGININE 500 MG TABLET ORAL 06/13/2013 0.08821
ARGININE HCL 1000 MG TABLET ORAL 04/24/2013 0.21561
ARIPIPRAZOLE 1 MG/ML SOLUTION ORAL 02/27/2019 4.27671
ARIPIPRAZOLE 10 MG TABLET ORAL 03/06/2019 0.38940
ARIPIPRAZOLE 15 MG TABLET ORAL 11/07/2018 0.40066
ARIPIPRAZOLE 20 MG TABLET ORAL 12/26/2017 0.53868
ARIPIPRAZOLE 30 MG TABLET ORAL 04/24/2018 1.41237
ARIPIPRAZOLE 5 MG TABLET ORAL 02/20/2019 0.38940
ARIPIPRAZOLE 2 MG TABLET ORAL 11/21/2018 0.38940
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201915
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
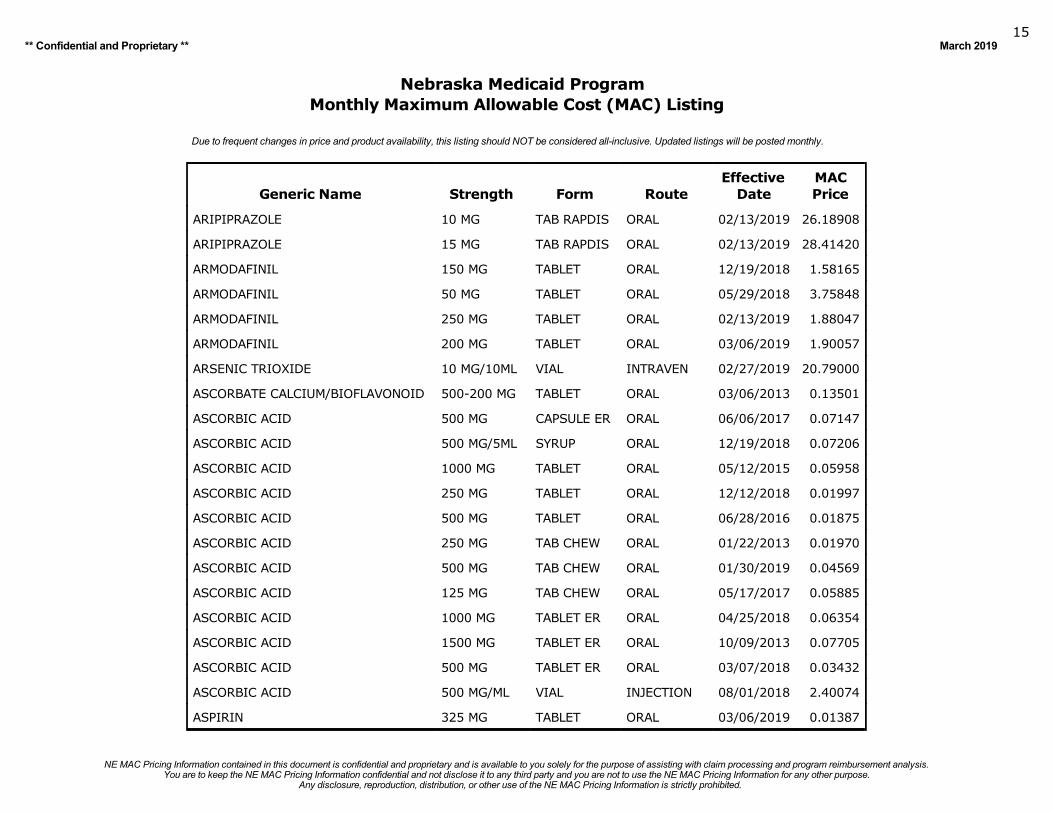
ARIPIPRAZOLE 10 MG TAB RAPDIS ORAL 02/13/2019 26.18908
ARIPIPRAZOLE 15 MG TAB RAPDIS ORAL 02/13/2019 28.41420
ARMODAFINIL 150 MG TABLET ORAL 12/19/2018 1.58165
ARMODAFINIL 50 MG TABLET ORAL 05/29/2018 3.75848
ARMODAFINIL 250 MG TABLET ORAL 02/13/2019 1.88047
ARMODAFINIL 200 MG TABLET ORAL 03/06/2019 1.90057
ARSENIC TRIOXIDE 10 MG/10ML VIAL INTRAVEN 02/27/2019 20.79000
ASCORBATE CALCIUM/BIOFLAVONOID 500-200 MG TABLET ORAL 03/06/2013 0.13501
ASCORBIC ACID 500 MG CAPSULE ER ORAL 06/06/2017 0.07147
ASCORBIC ACID 500 MG/5ML SYRUP ORAL 12/19/2018 0.07206
ASCORBIC ACID 1000 MG TABLET ORAL 05/12/2015 0.05958
ASCORBIC ACID 250 MG TABLET ORAL 12/12/2018 0.01997
ASCORBIC ACID 500 MG TABLET ORAL 06/28/2016 0.01875
ASCORBIC ACID 250 MG TAB CHEW ORAL 01/22/2013 0.01970
ASCORBIC ACID 500 MG TAB CHEW ORAL 01/30/2019 0.04569
ASCORBIC ACID 125 MG TAB CHEW ORAL 05/17/2017 0.05885
ASCORBIC ACID 1000 MG TABLET ER ORAL 04/25/2018 0.06354
ASCORBIC ACID 1500 MG TABLET ER ORAL 10/09/2013 0.07705
ASCORBIC ACID 500 MG TABLET ER ORAL 03/07/2018 0.03432
ASCORBIC ACID 500 MG/ML VIAL INJECTION 08/01/2018 2.40074
ASPIRIN 325 MG TABLET ORAL 03/06/2019 0.01387
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201916
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
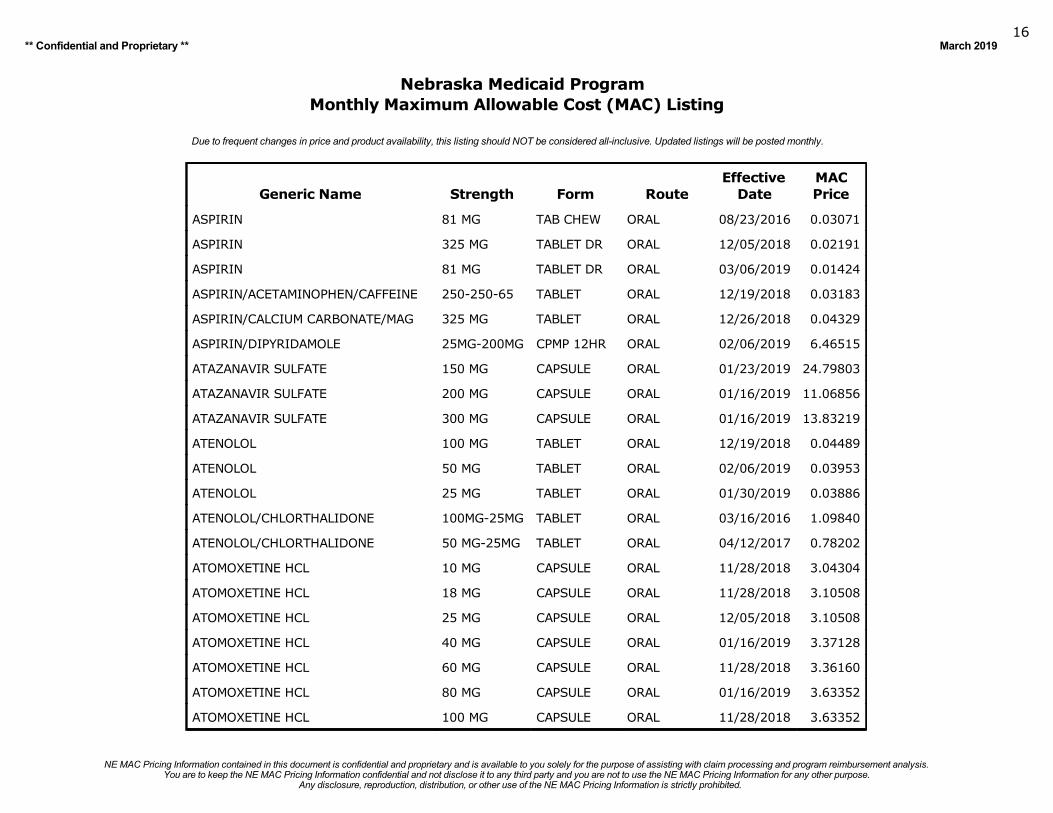
ASPIRIN 81 MG TAB CHEW ORAL 08/23/2016 0.03071
ASPIRIN 325 MG TABLET DR ORAL 12/05/2018 0.02191
ASPIRIN 81 MG TABLET DR ORAL 03/06/2019 0.01424
ASPIRIN/ACETAMINOPHEN/CAFFEINE 250-250-65 TABLET ORAL 12/19/2018 0.03183
ASPIRIN/CALCIUM CARBONATE/MAG 325 MG TABLET ORAL 12/26/2018 0.04329
ASPIRIN/DIPYRIDAMOLE 25MG-200MG CPMP 12HR ORAL 02/06/2019 6.46515
ATAZANAVIR SULFATE 150 MG CAPSULE ORAL 01/23/2019 24.79803
ATAZANAVIR SULFATE 200 MG CAPSULE ORAL 01/16/2019 11.06856
ATAZANAVIR SULFATE 300 MG CAPSULE ORAL 01/16/2019 13.83219
ATENOLOL 100 MG TABLET ORAL 12/19/2018 0.04489
ATENOLOL 50 MG TABLET ORAL 02/06/2019 0.03953
ATENOLOL 25 MG TABLET ORAL 01/30/2019 0.03886
ATENOLOL/CHLORTHALIDONE 100MG-25MG TABLET ORAL 03/16/2016 1.09840
ATENOLOL/CHLORTHALIDONE 50 MG-25MG TABLET ORAL 04/12/2017 0.78202
ATOMOXETINE HCL 10 MG CAPSULE ORAL 11/28/2018 3.04304
ATOMOXETINE HCL 18 MG CAPSULE ORAL 11/28/2018 3.10508
ATOMOXETINE HCL 25 MG CAPSULE ORAL 12/05/2018 3.10508
ATOMOXETINE HCL 40 MG CAPSULE ORAL 01/16/2019 3.37128
ATOMOXETINE HCL 60 MG CAPSULE ORAL 11/28/2018 3.36160
ATOMOXETINE HCL 80 MG CAPSULE ORAL 01/16/2019 3.63352
ATOMOXETINE HCL 100 MG CAPSULE ORAL 11/28/2018 3.63352
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201917
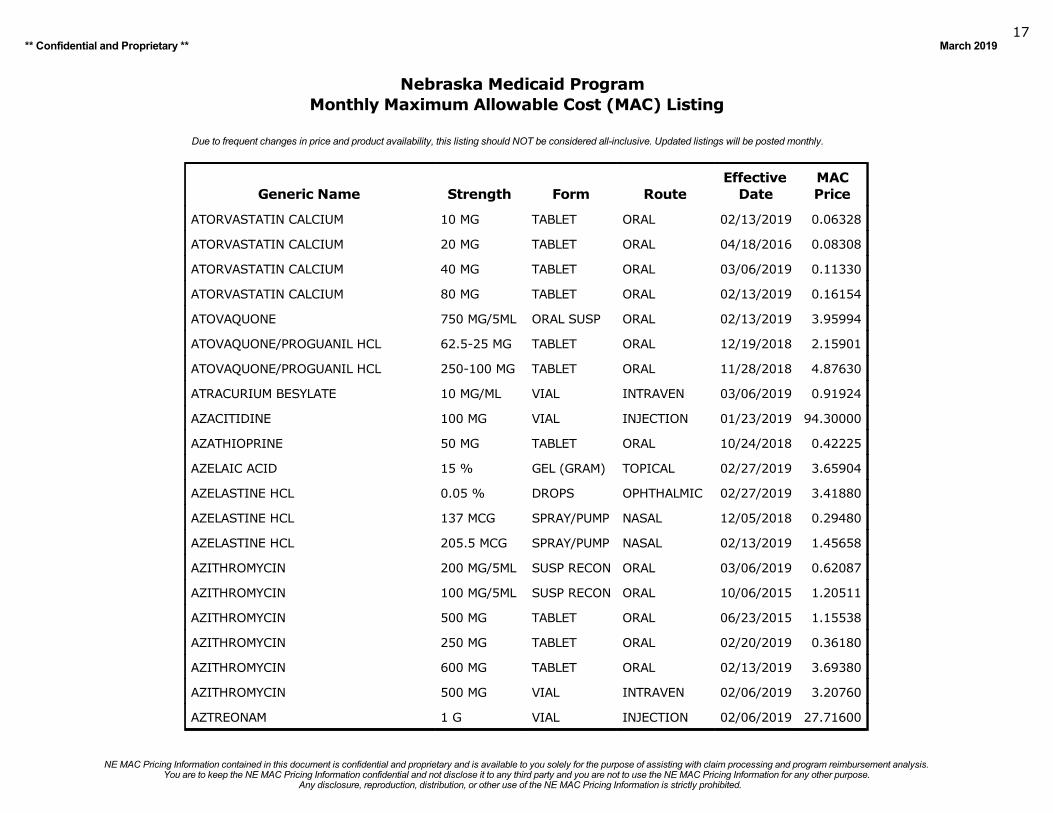
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ATORVASTATIN CALCIUM 10 MG TABLET ORAL 02/13/2019 0.06328
ATORVASTATIN CALCIUM 20 MG TABLET ORAL 04/18/2016 0.08308
ATORVASTATIN CALCIUM 40 MG TABLET ORAL 03/06/2019 0.11330
ATORVASTATIN CALCIUM 80 MG TABLET ORAL 02/13/2019 0.16154
ATOVAQUONE 750 MG/5ML ORAL SUSP ORAL 02/13/2019 3.95994
ATOVAQUONE/PROGUANIL HCL 62.5-25 MG TABLET ORAL 12/19/2018 2.15901
ATOVAQUONE/PROGUANIL HCL 250-100 MG TABLET ORAL 11/28/2018 4.87630
ATRACURIUM BESYLATE 10 MG/ML VIAL INTRAVEN 03/06/2019 0.91924
AZACITIDINE 100 MG VIAL INJECTION 01/23/2019 94.30000
AZATHIOPRINE 50 MG TABLET ORAL 10/24/2018 0.42225
AZELAIC ACID 15 % GEL (GRAM) TOPICAL 02/27/2019 3.65904
AZELASTINE HCL 0.05 % DROPS OPHTHALMIC 02/27/2019 3.41880
AZELASTINE HCL 137 MCG SPRAY/PUMP NASAL 12/05/2018 0.29480
AZELASTINE HCL 205.5 MCG SPRAY/PUMP NASAL 02/13/2019 1.45658
AZITHROMYCIN 200 MG/5ML SUSP RECON ORAL 03/06/2019 0.62087
AZITHROMYCIN 100 MG/5ML SUSP RECON ORAL 10/06/2015 1.20511
AZITHROMYCIN 500 MG TABLET ORAL 06/23/2015 1.15538
AZITHROMYCIN 250 MG TABLET ORAL 02/20/2019 0.36180
AZITHROMYCIN 600 MG TABLET ORAL 02/13/2019 3.69380
AZITHROMYCIN 500 MG VIAL INTRAVEN 02/06/2019 3.20760
AZTREONAM 1 G VIAL INJECTION 02/06/2019 27.71600
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201918
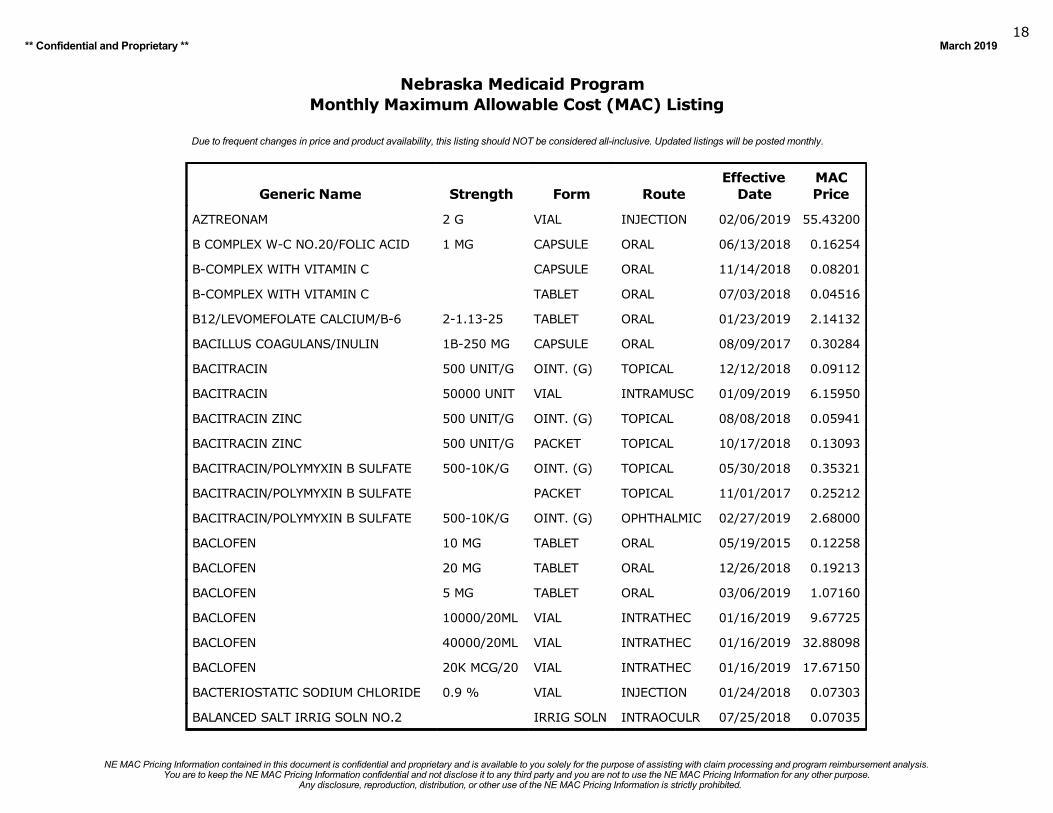
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
AZTREONAM 2 G VIAL INJECTION 02/06/2019 55.43200
B COMPLEX W-C NO.20/FOLIC ACID 1 MG CAPSULE ORAL 06/13/2018 0.16254
B-COMPLEX WITH VITAMIN C CAPSULE ORAL 11/14/2018 0.08201
B-COMPLEX WITH VITAMIN C TABLET ORAL 07/03/2018 0.04516
B12/LEVOMEFOLATE CALCIUM/B-6 2-1.13-25 TABLET ORAL 01/23/2019 2.14132
BACILLUS COAGULANS/INULIN 1B-250 MG CAPSULE ORAL 08/09/2017 0.30284
BACITRACIN 500 UNIT/G OINT. (G) TOPICAL 12/12/2018 0.09112
BACITRACIN 50000 UNIT VIAL INTRAMUSC 01/09/2019 6.15950
BACITRACIN ZINC 500 UNIT/G OINT. (G) TOPICAL 08/08/2018 0.05941
BACITRACIN ZINC 500 UNIT/G PACKET TOPICAL 10/17/2018 0.13093
BACITRACIN/POLYMYXIN B SULFATE 500-10K/G OINT. (G) TOPICAL 05/30/2018 0.35321
BACITRACIN/POLYMYXIN B SULFATE PACKET TOPICAL 11/01/2017 0.25212
BACITRACIN/POLYMYXIN B SULFATE 500-10K/G OINT. (G) OPHTHALMIC 02/27/2019 2.68000
BACLOFEN 10 MG TABLET ORAL 05/19/2015 0.12258
BACLOFEN 20 MG TABLET ORAL 12/26/2018 0.19213
BACLOFEN 5 MG TABLET ORAL 03/06/2019 1.07160
BACLOFEN 10000/20ML VIAL INTRATHEC 01/16/2019 9.67725
BACLOFEN 40000/20ML VIAL INTRATHEC 01/16/2019 32.88098
BACLOFEN 20K MCG/20 VIAL INTRATHEC 01/16/2019 17.67150
BACTERIOSTATIC SODIUM CHLORIDE 0.9 % VIAL INJECTION 01/24/2018 0.07303
BALANCED SALT IRRIG SOLN NO.2 IRRIG SOLN INTRAOCULR 07/25/2018 0.07035
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201919
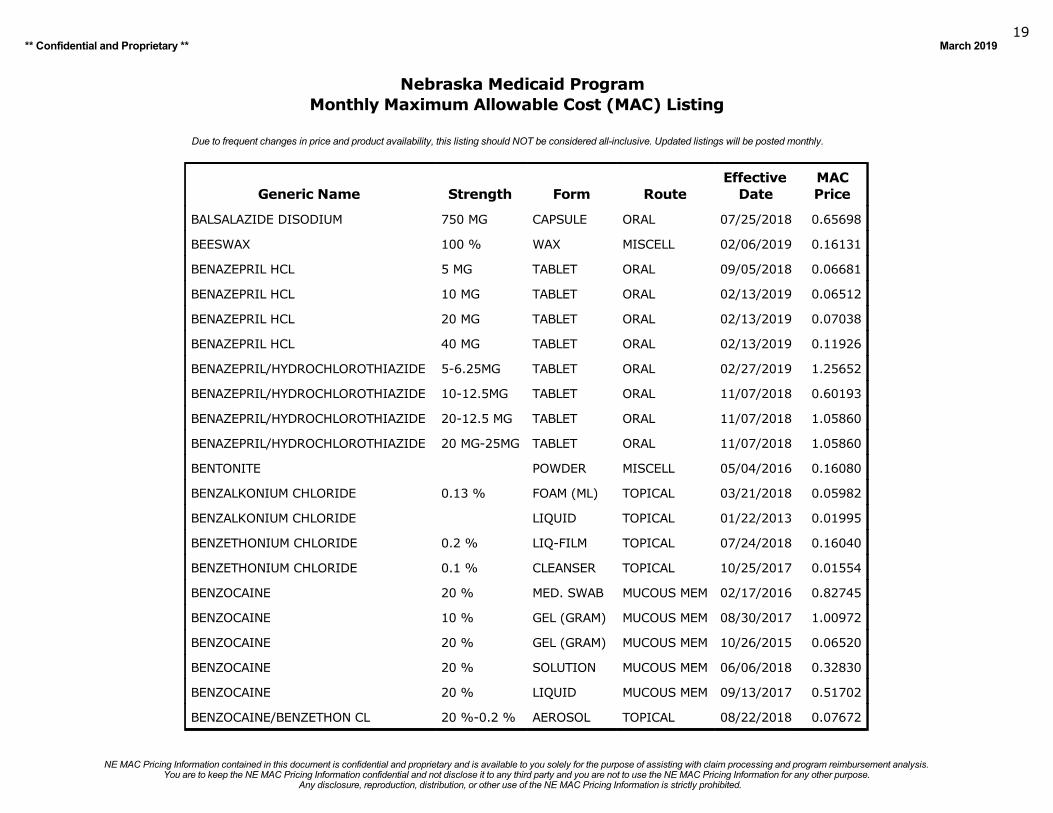
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
BALSALAZIDE DISODIUM 750 MG CAPSULE ORAL 07/25/2018 0.65698
BEESWAX 100 % WAX MISCELL 02/06/2019 0.16131
BENAZEPRIL HCL 5 MG TABLET ORAL 09/05/2018 0.06681
BENAZEPRIL HCL 10 MG TABLET ORAL 02/13/2019 0.06512
BENAZEPRIL HCL 20 MG TABLET ORAL 02/13/2019 0.07038
BENAZEPRIL HCL 40 MG TABLET ORAL 02/13/2019 0.11926
BENAZEPRIL/HYDROCHLOROTHIAZIDE 5-6.25MG TABLET ORAL 02/27/2019 1.25652
BENAZEPRIL/HYDROCHLOROTHIAZIDE 10-12.5MG TABLET ORAL 11/07/2018 0.60193
BENAZEPRIL/HYDROCHLOROTHIAZIDE 20-12.5 MG TABLET ORAL 11/07/2018 1.05860
BENAZEPRIL/HYDROCHLOROTHIAZIDE 20 MG-25MG TABLET ORAL 11/07/2018 1.05860
BENTONITE POWDER MISCELL 05/04/2016 0.16080
BENZALKONIUM CHLORIDE 0.13 % FOAM (ML) TOPICAL 03/21/2018 0.05982
BENZALKONIUM CHLORIDE LIQUID TOPICAL 01/22/2013 0.01995
BENZETHONIUM CHLORIDE 0.2 % LIQ-FILM TOPICAL 07/24/2018 0.16040
BENZETHONIUM CHLORIDE 0.1 % CLEANSER TOPICAL 10/25/2017 0.01554
BENZOCAINE 20 % MED. SWAB MUCOUS MEM 02/17/2016 0.82745
BENZOCAINE 10 % GEL (GRAM) MUCOUS MEM 08/30/2017 1.00972
BENZOCAINE 20 % GEL (GRAM) MUCOUS MEM 10/26/2015 0.06520
BENZOCAINE 20 % SOLUTION MUCOUS MEM 06/06/2018 0.32830
BENZOCAINE 20 % LIQUID MUCOUS MEM 09/13/2017 0.51702
BENZOCAINE/BENZETHON CL 20 %-0.2 % AEROSOL TOPICAL 08/22/2018 0.07672
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201920
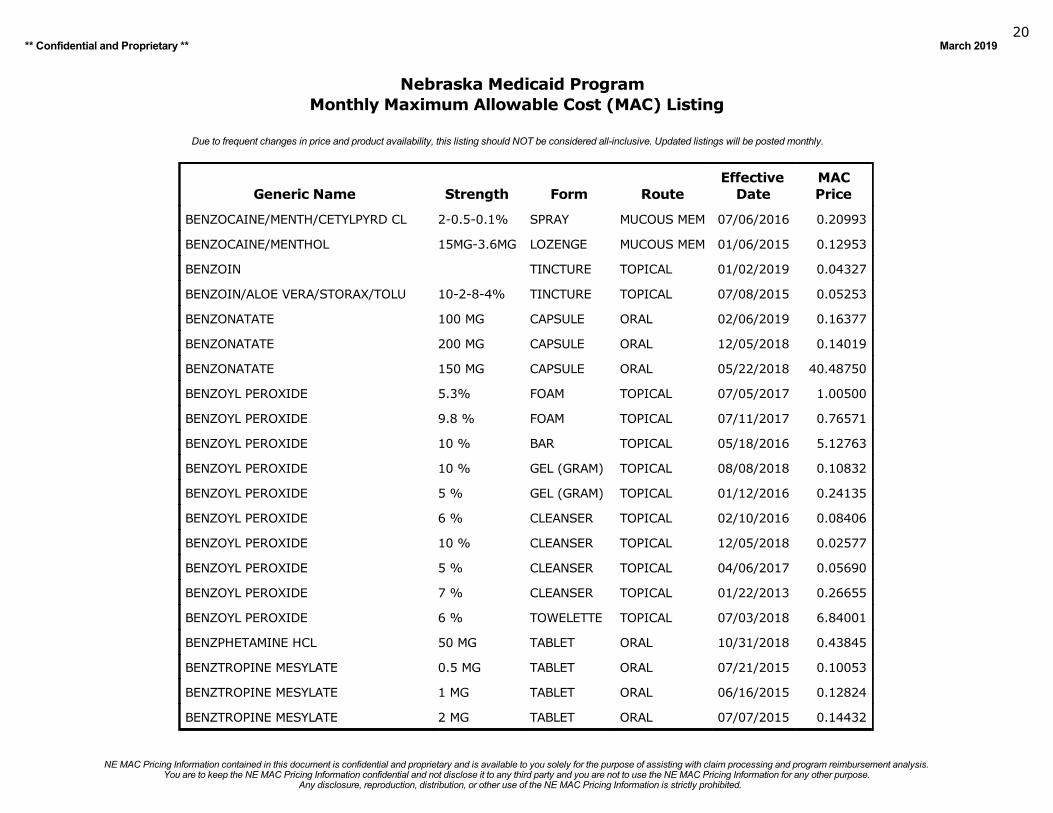
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
BENZOCAINE/MENTH/CETYLPYRD CL 2-0.5-0.1% SPRAY MUCOUS MEM 07/06/2016 0.20993
BENZOCAINE/MENTHOL 15MG-3.6MG LOZENGE MUCOUS MEM 01/06/2015 0.12953
BENZOIN TINCTURE TOPICAL 01/02/2019 0.04327
BENZOIN/ALOE VERA/STORAX/TOLU 10-2-8-4% TINCTURE TOPICAL 07/08/2015 0.05253
BENZONATATE 100 MG CAPSULE ORAL 02/06/2019 0.16377
BENZONATATE 200 MG CAPSULE ORAL 12/05/2018 0.14019
BENZONATATE 150 MG CAPSULE ORAL 05/22/2018 40.48750
BENZOYL PEROXIDE 5.3% FOAM TOPICAL 07/05/2017 1.00500
BENZOYL PEROXIDE 9.8 % FOAM TOPICAL 07/11/2017 0.76571
BENZOYL PEROXIDE 10 % BAR TOPICAL 05/18/2016 5.12763
BENZOYL PEROXIDE 10 % GEL (GRAM) TOPICAL 08/08/2018 0.10832
BENZOYL PEROXIDE 5 % GEL (GRAM) TOPICAL 01/12/2016 0.24135
BENZOYL PEROXIDE 6 % CLEANSER TOPICAL 02/10/2016 0.08406
BENZOYL PEROXIDE 10 % CLEANSER TOPICAL 12/05/2018 0.02577
BENZOYL PEROXIDE 5 % CLEANSER TOPICAL 04/06/2017 0.05690
BENZOYL PEROXIDE 7 % CLEANSER TOPICAL 01/22/2013 0.26655
BENZOYL PEROXIDE 6 % TOWELETTE TOPICAL 07/03/2018 6.84001
BENZPHETAMINE HCL 50 MG TABLET ORAL 10/31/2018 0.43845
BENZTROPINE MESYLATE 0.5 MG TABLET ORAL 07/21/2015 0.10053
BENZTROPINE MESYLATE 1 MG TABLET ORAL 06/16/2015 0.12824
BENZTROPINE MESYLATE 2 MG TABLET ORAL 07/07/2015 0.14432
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201921
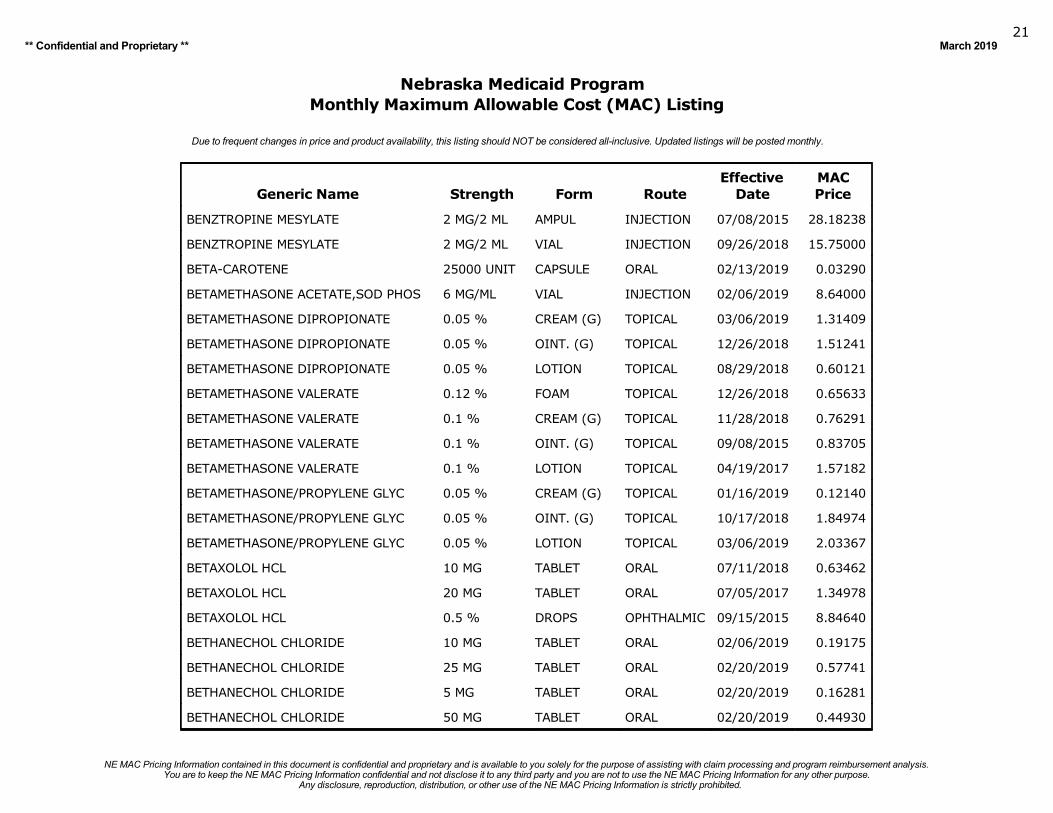
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
BENZTROPINE MESYLATE 2 MG/2 ML AMPUL INJECTION 07/08/2015 28.18238
BENZTROPINE MESYLATE 2 MG/2 ML VIAL INJECTION 09/26/2018 15.75000
BETA-CAROTENE 25000 UNIT CAPSULE ORAL 02/13/2019 0.03290
BETAMETHASONE ACETATE,SOD PHOS 6 MG/ML VIAL INJECTION 02/06/2019 8.64000
BETAMETHASONE DIPROPIONATE 0.05 % CREAM (G) TOPICAL 03/06/2019 1.31409
BETAMETHASONE DIPROPIONATE 0.05 % OINT. (G) TOPICAL 12/26/2018 1.51241
BETAMETHASONE DIPROPIONATE 0.05 % LOTION TOPICAL 08/29/2018 0.60121
BETAMETHASONE VALERATE 0.12 % FOAM TOPICAL 12/26/2018 0.65633
BETAMETHASONE VALERATE 0.1 % CREAM (G) TOPICAL 11/28/2018 0.76291
BETAMETHASONE VALERATE 0.1 % OINT. (G) TOPICAL 09/08/2015 0.83705
BETAMETHASONE VALERATE 0.1 % LOTION TOPICAL 04/19/2017 1.57182
BETAMETHASONE/PROPYLENE GLYC 0.05 % CREAM (G) TOPICAL 01/16/2019 0.12140
BETAMETHASONE/PROPYLENE GLYC 0.05 % OINT. (G) TOPICAL 10/17/2018 1.84974
BETAMETHASONE/PROPYLENE GLYC 0.05 % LOTION TOPICAL 03/06/2019 2.03367
BETAXOLOL HCL 10 MG TABLET ORAL 07/11/2018 0.63462
BETAXOLOL HCL 20 MG TABLET ORAL 07/05/2017 1.34978
BETAXOLOL HCL 0.5 % DROPS OPHTHALMIC 09/15/2015 8.84640
BETHANECHOL CHLORIDE 10 MG TABLET ORAL 02/06/2019 0.19175
BETHANECHOL CHLORIDE 25 MG TABLET ORAL 02/20/2019 0.57741
BETHANECHOL CHLORIDE 5 MG TABLET ORAL 02/20/2019 0.16281
BETHANECHOL CHLORIDE 50 MG TABLET ORAL 02/20/2019 0.44930
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201922
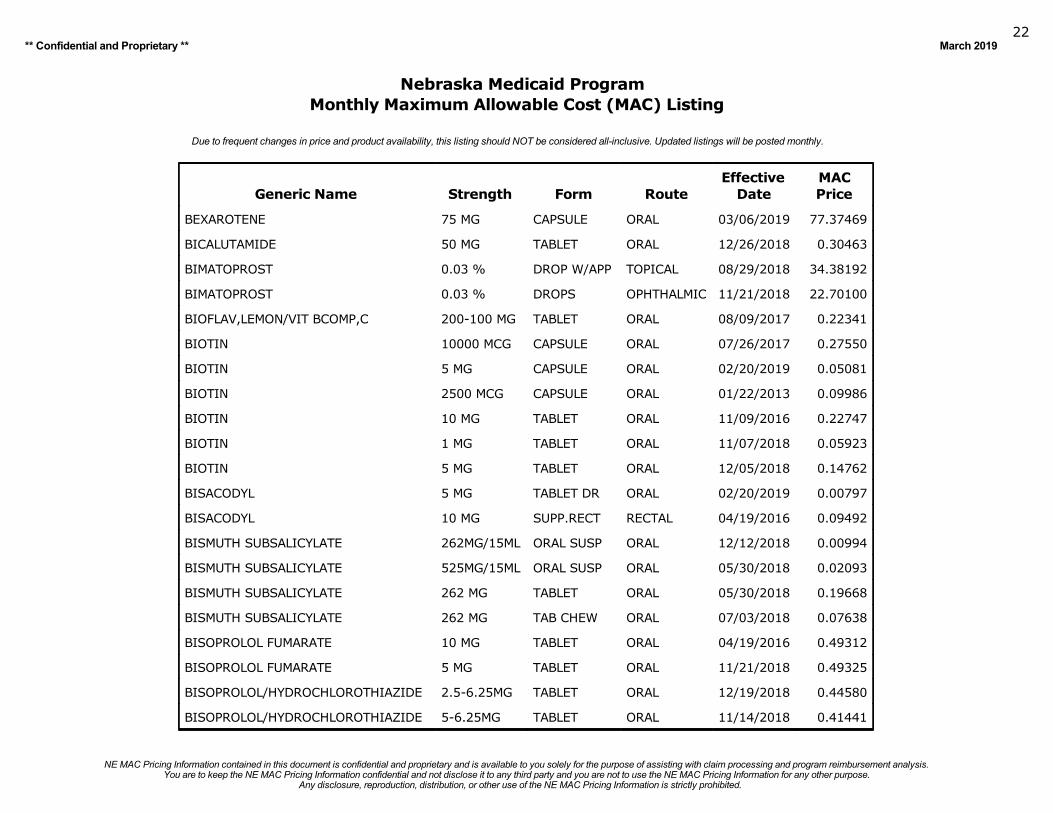
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
BEXAROTENE 75 MG CAPSULE ORAL 03/06/2019 77.37469
BICALUTAMIDE 50 MG TABLET ORAL 12/26/2018 0.30463
BIMATOPROST 0.03 % DROP W/APP TOPICAL 08/29/2018 34.38192
BIMATOPROST 0.03 % DROPS OPHTHALMIC 11/21/2018 22.70100
BIOFLAV,LEMON/VIT BCOMP,C 200-100 MG TABLET ORAL 08/09/2017 0.22341
BIOTIN 10000 MCG CAPSULE ORAL 07/26/2017 0.27550
BIOTIN 5 MG CAPSULE ORAL 02/20/2019 0.05081
BIOTIN 2500 MCG CAPSULE ORAL 01/22/2013 0.09986
BIOTIN 10 MG TABLET ORAL 11/09/2016 0.22747
BIOTIN 1 MG TABLET ORAL 11/07/2018 0.05923
BIOTIN 5 MG TABLET ORAL 12/05/2018 0.14762
BISACODYL 5 MG TABLET DR ORAL 02/20/2019 0.00797
BISACODYL 10 MG SUPP.RECT RECTAL 04/19/2016 0.09492
BISMUTH SUBSALICYLATE 262MG/15ML ORAL SUSP ORAL 12/12/2018 0.00994
BISMUTH SUBSALICYLATE 525MG/15ML ORAL SUSP ORAL 05/30/2018 0.02093
BISMUTH SUBSALICYLATE 262 MG TABLET ORAL 05/30/2018 0.19668
BISMUTH SUBSALICYLATE 262 MG TAB CHEW ORAL 07/03/2018 0.07638
BISOPROLOL FUMARATE 10 MG TABLET ORAL 04/19/2016 0.49312
BISOPROLOL FUMARATE 5 MG TABLET ORAL 11/21/2018 0.49325
BISOPROLOL/HYDROCHLOROTHIAZIDE 2.5-6.25MG TABLET ORAL 12/19/2018 0.44580
BISOPROLOL/HYDROCHLOROTHIAZIDE 5-6.25MG TABLET ORAL 11/14/2018 0.41441
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201923
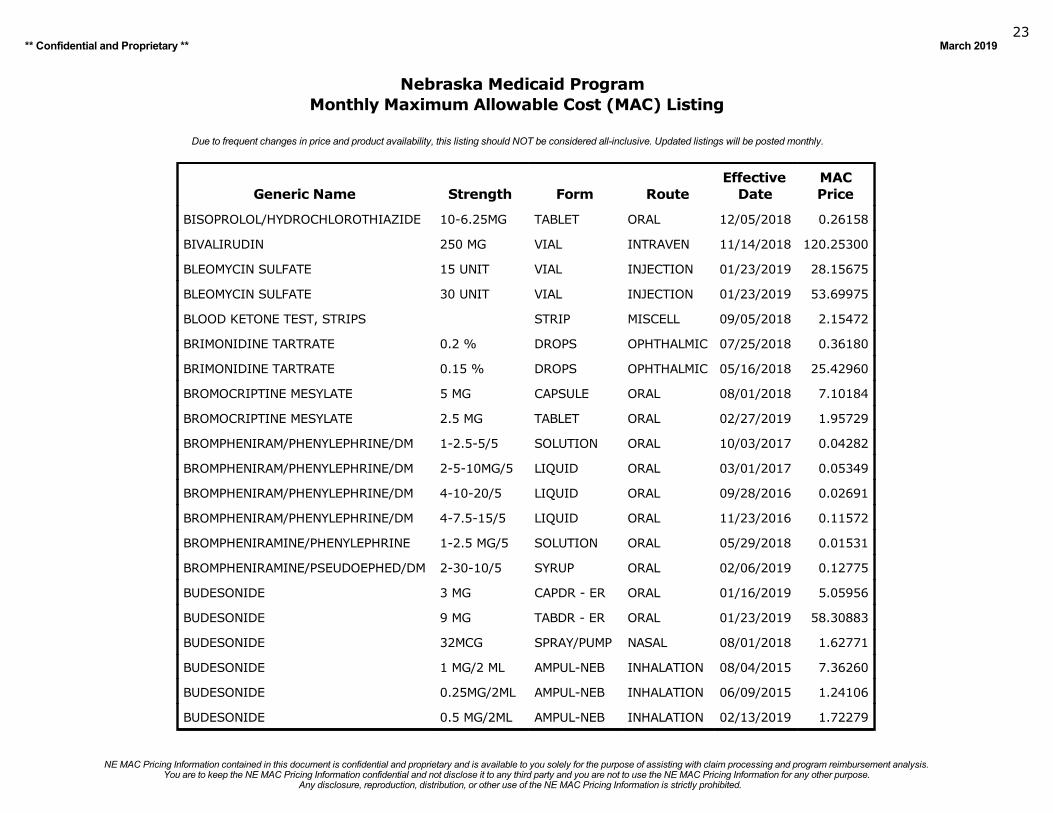
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
BISOPROLOL/HYDROCHLOROTHIAZIDE 10-6.25MG TABLET ORAL 12/05/2018 0.26158
BIVALIRUDIN 250 MG VIAL INTRAVEN 11/14/2018 120.25300
BLEOMYCIN SULFATE 15 UNIT VIAL INJECTION 01/23/2019 28.15675
BLEOMYCIN SULFATE 30 UNIT VIAL INJECTION 01/23/2019 53.69975
BLOOD KETONE TEST, STRIPS STRIP MISCELL 09/05/2018 2.15472
BRIMONIDINE TARTRATE 0.2 % DROPS OPHTHALMIC 07/25/2018 0.36180
BRIMONIDINE TARTRATE 0.15 % DROPS OPHTHALMIC 05/16/2018 25.42960
BROMOCRIPTINE MESYLATE 5 MG CAPSULE ORAL 08/01/2018 7.10184
BROMOCRIPTINE MESYLATE 2.5 MG TABLET ORAL 02/27/2019 1.95729
BROMPHENIRAM/PHENYLEPHRINE/DM 1-2.5-5/5 SOLUTION ORAL 10/03/2017 0.04282
BROMPHENIRAM/PHENYLEPHRINE/DM 2-5-10MG/5 LIQUID ORAL 03/01/2017 0.05349
BROMPHENIRAM/PHENYLEPHRINE/DM 4-10-20/5 LIQUID ORAL 09/28/2016 0.02691
BROMPHENIRAM/PHENYLEPHRINE/DM 4-7.5-15/5 LIQUID ORAL 11/23/2016 0.11572
BROMPHENIRAMINE/PHENYLEPHRINE 1-2.5 MG/5 SOLUTION ORAL 05/29/2018 0.01531
BROMPHENIRAMINE/PSEUDOEPHED/DM 2-30-10/5 SYRUP ORAL 02/06/2019 0.12775
BUDESONIDE 3 MG CAPDR - ER ORAL 01/16/2019 5.05956
BUDESONIDE 9 MG TABDR - ER ORAL 01/23/2019 58.30883
BUDESONIDE 32MCG SPRAY/PUMP NASAL 08/01/2018 1.62771
BUDESONIDE 1 MG/2 ML AMPUL-NEB INHALATION 08/04/2015 7.36260
BUDESONIDE 0.25MG/2ML AMPUL-NEB INHALATION 06/09/2015 1.24106
BUDESONIDE 0.5 MG/2ML AMPUL-NEB INHALATION 02/13/2019 1.72279
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201924
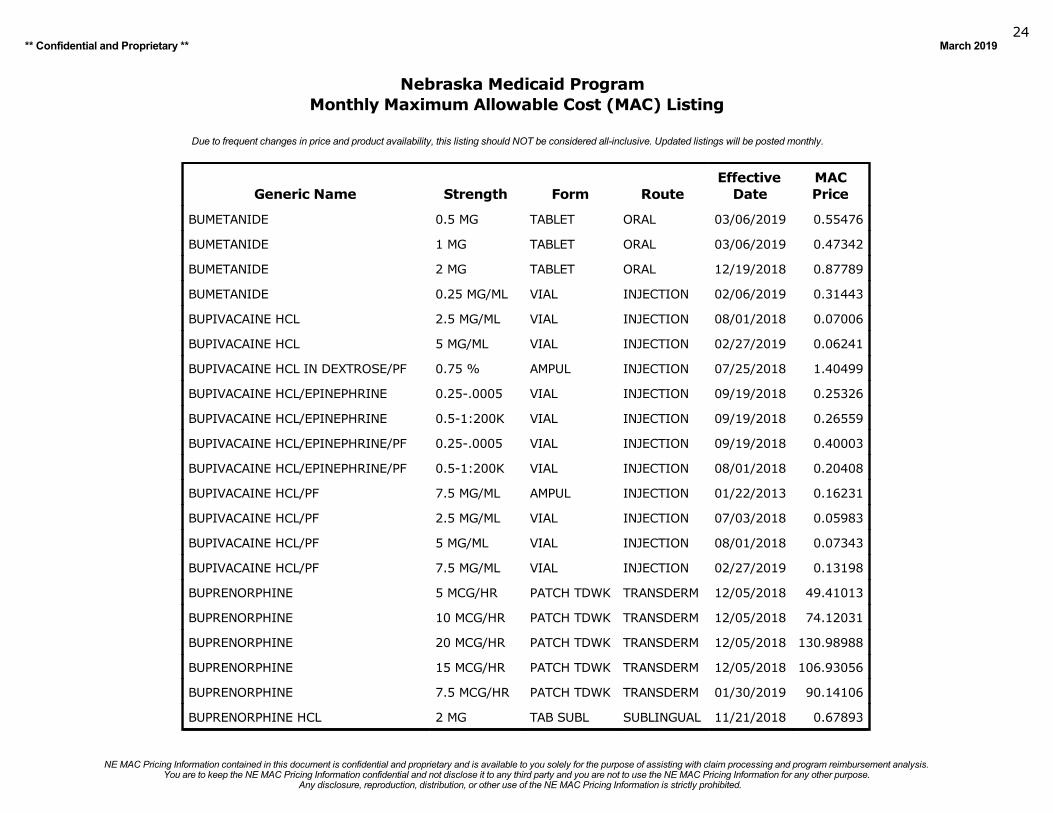
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
BUMETANIDE 0.5 MG TABLET ORAL 03/06/2019 0.55476
BUMETANIDE 1 MG TABLET ORAL 03/06/2019 0.47342
BUMETANIDE 2 MG TABLET ORAL 12/19/2018 0.87789
BUMETANIDE 0.25 MG/ML VIAL INJECTION 02/06/2019 0.31443
BUPIVACAINE HCL 2.5 MG/ML VIAL INJECTION 08/01/2018 0.07006
BUPIVACAINE HCL 5 MG/ML VIAL INJECTION 02/27/2019 0.06241
BUPIVACAINE HCL IN DEXTROSE/PF 0.75 % AMPUL INJECTION 07/25/2018 1.40499
BUPIVACAINE HCL/EPINEPHRINE 0.25-.0005 VIAL INJECTION 09/19/2018 0.25326
BUPIVACAINE HCL/EPINEPHRINE 0.5-1:200K VIAL INJECTION 09/19/2018 0.26559
BUPIVACAINE HCL/EPINEPHRINE/PF 0.25-.0005 VIAL INJECTION 09/19/2018 0.40003
BUPIVACAINE HCL/EPINEPHRINE/PF 0.5-1:200K VIAL INJECTION 08/01/2018 0.20408
BUPIVACAINE HCL/PF 7.5 MG/ML AMPUL INJECTION 01/22/2013 0.16231
BUPIVACAINE HCL/PF 2.5 MG/ML VIAL INJECTION 07/03/2018 0.05983
BUPIVACAINE HCL/PF 5 MG/ML VIAL INJECTION 08/01/2018 0.07343
BUPIVACAINE HCL/PF 7.5 MG/ML VIAL INJECTION 02/27/2019 0.13198
BUPRENORPHINE 5 MCG/HR PATCH TDWK TRANSDERM 12/05/2018 49.41013
BUPRENORPHINE 10 MCG/HR PATCH TDWK TRANSDERM 12/05/2018 74.12031
BUPRENORPHINE 20 MCG/HR PATCH TDWK TRANSDERM 12/05/2018 130.98988
BUPRENORPHINE 15 MCG/HR PATCH TDWK TRANSDERM 12/05/2018 106.93056
BUPRENORPHINE 7.5 MCG/HR PATCH TDWK TRANSDERM 01/30/2019 90.14106
BUPRENORPHINE HCL 2 MG TAB SUBL SUBLINGUAL 11/21/2018 0.67893
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201925
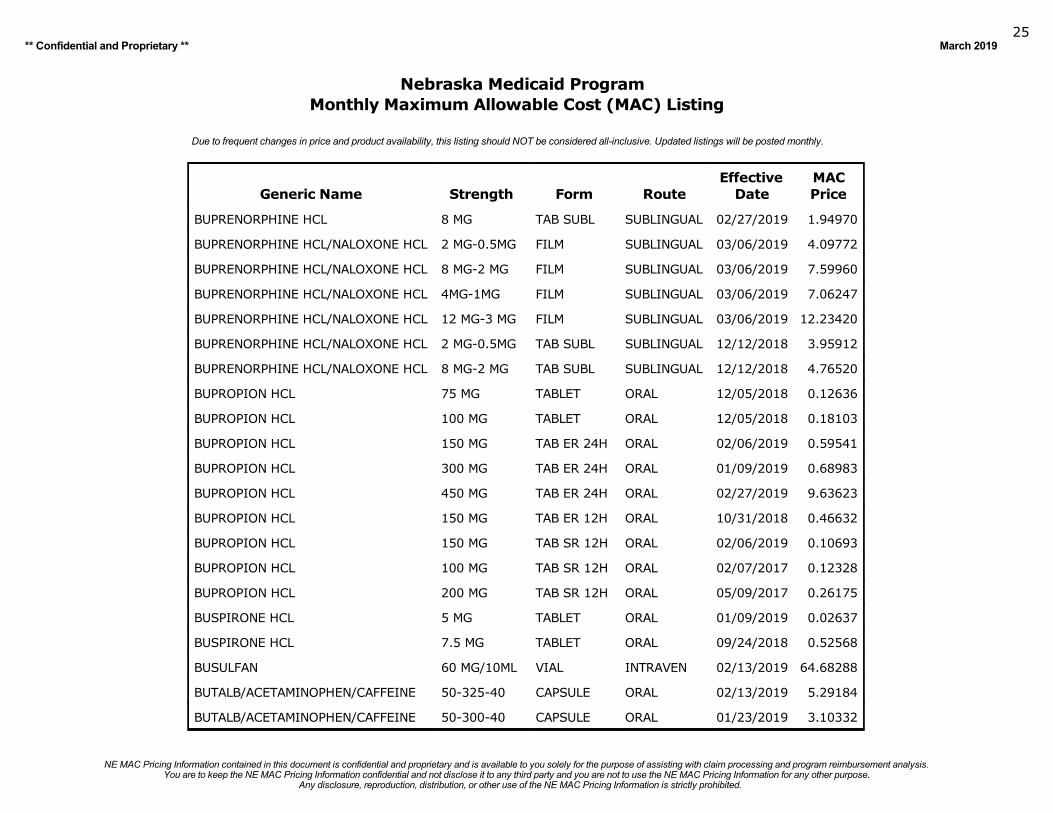
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
BUPRENORPHINE HCL 8 MG TAB SUBL SUBLINGUAL 02/27/2019 1.94970
BUPRENORPHINE HCL/NALOXONE HCL 2 MG-0.5MG FILM SUBLINGUAL 03/06/2019 4.09772
BUPRENORPHINE HCL/NALOXONE HCL 8 MG-2 MG FILM SUBLINGUAL 03/06/2019 7.59960
BUPRENORPHINE HCL/NALOXONE HCL 4MG-1MG FILM SUBLINGUAL 03/06/2019 7.06247
BUPRENORPHINE HCL/NALOXONE HCL 12 MG-3 MG FILM SUBLINGUAL 03/06/2019 12.23420
BUPRENORPHINE HCL/NALOXONE HCL 2 MG-0.5MG TAB SUBL SUBLINGUAL 12/12/2018 3.95912
BUPRENORPHINE HCL/NALOXONE HCL 8 MG-2 MG TAB SUBL SUBLINGUAL 12/12/2018 4.76520
BUPROPION HCL 75 MG TABLET ORAL 12/05/2018 0.12636
BUPROPION HCL 100 MG TABLET ORAL 12/05/2018 0.18103
BUPROPION HCL 150 MG TAB ER 24H ORAL 02/06/2019 0.59541
BUPROPION HCL 300 MG TAB ER 24H ORAL 01/09/2019 0.68983
BUPROPION HCL 450 MG TAB ER 24H ORAL 02/27/2019 9.63623
BUPROPION HCL 150 MG TAB ER 12H ORAL 10/31/2018 0.46632
BUPROPION HCL 150 MG TAB SR 12H ORAL 02/06/2019 0.10693
BUPROPION HCL 100 MG TAB SR 12H ORAL 02/07/2017 0.12328
BUPROPION HCL 200 MG TAB SR 12H ORAL 05/09/2017 0.26175
BUSPIRONE HCL 5 MG TABLET ORAL 01/09/2019 0.02637
BUSPIRONE HCL 7.5 MG TABLET ORAL 09/24/2018 0.52568
BUSULFAN 60 MG/10ML VIAL INTRAVEN 02/13/2019 64.68288
BUTALB/ACETAMINOPHEN/CAFFEINE 50-325-40 CAPSULE ORAL 02/13/2019 5.29184
BUTALB/ACETAMINOPHEN/CAFFEINE 50-300-40 CAPSULE ORAL 01/23/2019 3.10332
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201926
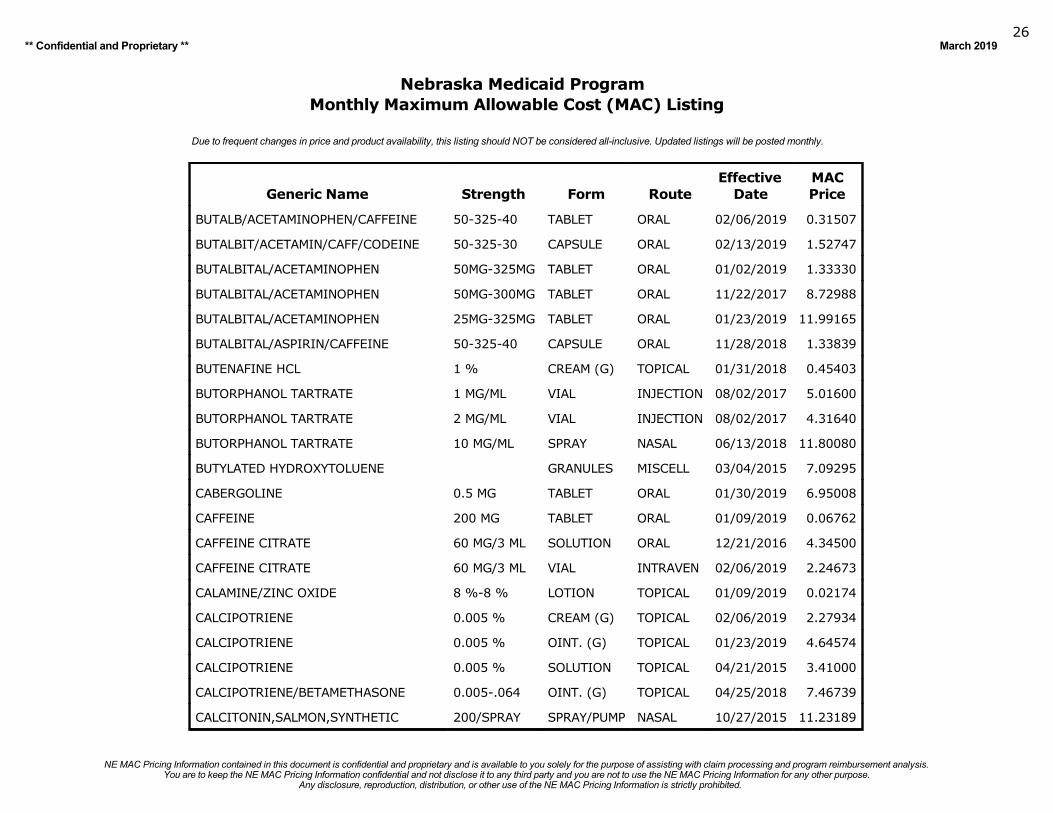
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
BUTALB/ACETAMINOPHEN/CAFFEINE 50-325-40 TABLET ORAL 02/06/2019 0.31507
BUTALBIT/ACETAMIN/CAFF/CODEINE 50-325-30 CAPSULE ORAL 02/13/2019 1.52747
BUTALBITAL/ACETAMINOPHEN 50MG-325MG TABLET ORAL 01/02/2019 1.33330
BUTALBITAL/ACETAMINOPHEN 50MG-300MG TABLET ORAL 11/22/2017 8.72988
BUTALBITAL/ACETAMINOPHEN 25MG-325MG TABLET ORAL 01/23/2019 11.99165
BUTALBITAL/ASPIRIN/CAFFEINE 50-325-40 CAPSULE ORAL 11/28/2018 1.33839
BUTENAFINE HCL 1 % CREAM (G) TOPICAL 01/31/2018 0.45403
BUTORPHANOL TARTRATE 1 MG/ML VIAL INJECTION 08/02/2017 5.01600
BUTORPHANOL TARTRATE 2 MG/ML VIAL INJECTION 08/02/2017 4.31640
BUTORPHANOL TARTRATE 10 MG/ML SPRAY NASAL 06/13/2018 11.80080
BUTYLATED HYDROXYTOLUENE GRANULES MISCELL 03/04/2015 7.09295
CABERGOLINE 0.5 MG TABLET ORAL 01/30/2019 6.95008
CAFFEINE 200 MG TABLET ORAL 01/09/2019 0.06762
CAFFEINE CITRATE 60 MG/3 ML SOLUTION ORAL 12/21/2016 4.34500
CAFFEINE CITRATE 60 MG/3 ML VIAL INTRAVEN 02/06/2019 2.24673
CALAMINE/ZINC OXIDE 8 %-8 % LOTION TOPICAL 01/09/2019 0.02174
CALCIPOTRIENE 0.005 % CREAM (G) TOPICAL 02/06/2019 2.27934
CALCIPOTRIENE 0.005 % OINT. (G) TOPICAL 01/23/2019 4.64574
CALCIPOTRIENE 0.005 % SOLUTION TOPICAL 04/21/2015 3.41000
CALCIPOTRIENE/BETAMETHASONE 0.005-.064 OINT. (G) TOPICAL 04/25/2018 7.46739
CALCITONIN,SALMON,SYNTHETIC 200/SPRAY SPRAY/PUMP NASAL 10/27/2015 11.23189
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201927
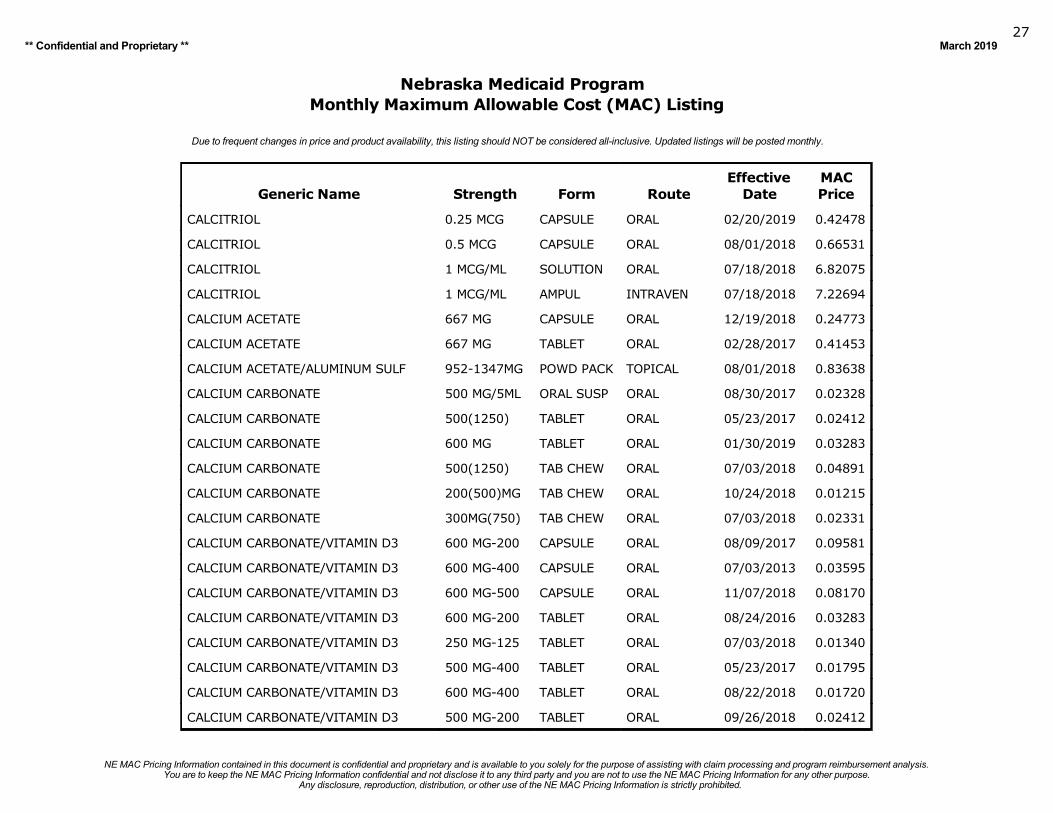
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CALCITRIOL 0.25 MCG CAPSULE ORAL 02/20/2019 0.42478
CALCITRIOL 0.5 MCG CAPSULE ORAL 08/01/2018 0.66531
CALCITRIOL 1 MCG/ML SOLUTION ORAL 07/18/2018 6.82075
CALCITRIOL 1 MCG/ML AMPUL INTRAVEN 07/18/2018 7.22694
CALCIUM ACETATE 667 MG CAPSULE ORAL 12/19/2018 0.24773
CALCIUM ACETATE 667 MG TABLET ORAL 02/28/2017 0.41453
CALCIUM ACETATE/ALUMINUM SULF 952-1347MG POWD PACK TOPICAL 08/01/2018 0.83638
CALCIUM CARBONATE 500 MG/5ML ORAL SUSP ORAL 08/30/2017 0.02328
CALCIUM CARBONATE 500(1250) TABLET ORAL 05/23/2017 0.02412
CALCIUM CARBONATE 600 MG TABLET ORAL 01/30/2019 0.03283
CALCIUM CARBONATE 500(1250) TAB CHEW ORAL 07/03/2018 0.04891
CALCIUM CARBONATE 200(500)MG TAB CHEW ORAL 10/24/2018 0.01215
CALCIUM CARBONATE 300MG(750) TAB CHEW ORAL 07/03/2018 0.02331
CALCIUM CARBONATE/VITAMIN D3 600 MG-200 CAPSULE ORAL 08/09/2017 0.09581
CALCIUM CARBONATE/VITAMIN D3 600 MG-400 CAPSULE ORAL 07/03/2013 0.03595
CALCIUM CARBONATE/VITAMIN D3 600 MG-500 CAPSULE ORAL 11/07/2018 0.08170
CALCIUM CARBONATE/VITAMIN D3 600 MG-200 TABLET ORAL 08/24/2016 0.03283
CALCIUM CARBONATE/VITAMIN D3 250 MG-125 TABLET ORAL 07/03/2018 0.01340
CALCIUM CARBONATE/VITAMIN D3 500 MG-400 TABLET ORAL 05/23/2017 0.01795
CALCIUM CARBONATE/VITAMIN D3 600 MG-400 TABLET ORAL 08/22/2018 0.01720
CALCIUM CARBONATE/VITAMIN D3 500 MG-200 TABLET ORAL 09/26/2018 0.02412
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201928
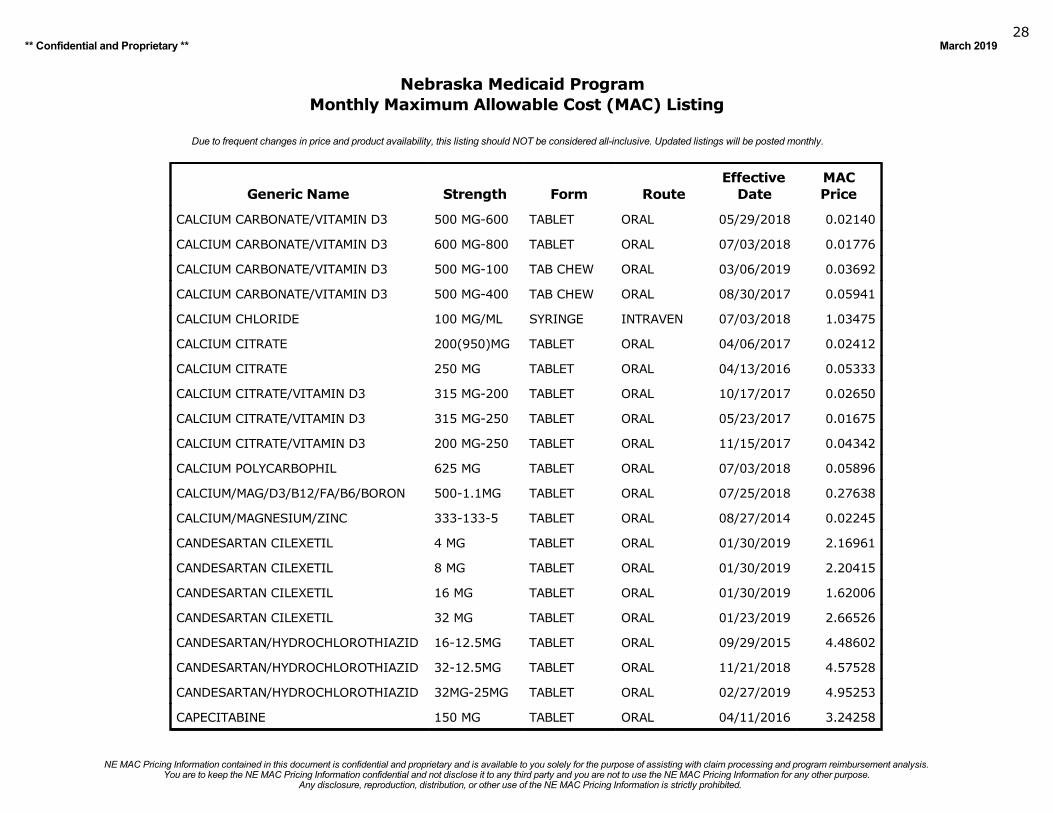
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CALCIUM CARBONATE/VITAMIN D3 500 MG-600 TABLET ORAL 05/29/2018 0.02140
CALCIUM CARBONATE/VITAMIN D3 600 MG-800 TABLET ORAL 07/03/2018 0.01776
CALCIUM CARBONATE/VITAMIN D3 500 MG-100 TAB CHEW ORAL 03/06/2019 0.03692
CALCIUM CARBONATE/VITAMIN D3 500 MG-400 TAB CHEW ORAL 08/30/2017 0.05941
CALCIUM CHLORIDE 100 MG/ML SYRINGE INTRAVEN 07/03/2018 1.03475
CALCIUM CITRATE 200(950)MG TABLET ORAL 04/06/2017 0.02412
CALCIUM CITRATE 250 MG TABLET ORAL 04/13/2016 0.05333
CALCIUM CITRATE/VITAMIN D3 315 MG-200 TABLET ORAL 10/17/2017 0.02650
CALCIUM CITRATE/VITAMIN D3 315 MG-250 TABLET ORAL 05/23/2017 0.01675
CALCIUM CITRATE/VITAMIN D3 200 MG-250 TABLET ORAL 11/15/2017 0.04342
CALCIUM POLYCARBOPHIL 625 MG TABLET ORAL 07/03/2018 0.05896
CALCIUM/MAG/D3/B12/FA/B6/BORON 500-1.1MG TABLET ORAL 07/25/2018 0.27638
CALCIUM/MAGNESIUM/ZINC 333-133-5 TABLET ORAL 08/27/2014 0.02245
CANDESARTAN CILEXETIL 4 MG TABLET ORAL 01/30/2019 2.16961
CANDESARTAN CILEXETIL 8 MG TABLET ORAL 01/30/2019 2.20415
CANDESARTAN CILEXETIL 16 MG TABLET ORAL 01/30/2019 1.62006
CANDESARTAN CILEXETIL 32 MG TABLET ORAL 01/23/2019 2.66526
CANDESARTAN/HYDROCHLOROTHIAZID 16-12.5MG TABLET ORAL 09/29/2015 4.48602
CANDESARTAN/HYDROCHLOROTHIAZID 32-12.5MG TABLET ORAL 11/21/2018 4.57528
CANDESARTAN/HYDROCHLOROTHIAZID 32MG-25MG TABLET ORAL 02/27/2019 4.95253
CAPECITABINE 150 MG TABLET ORAL 04/11/2016 3.24258
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201929
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
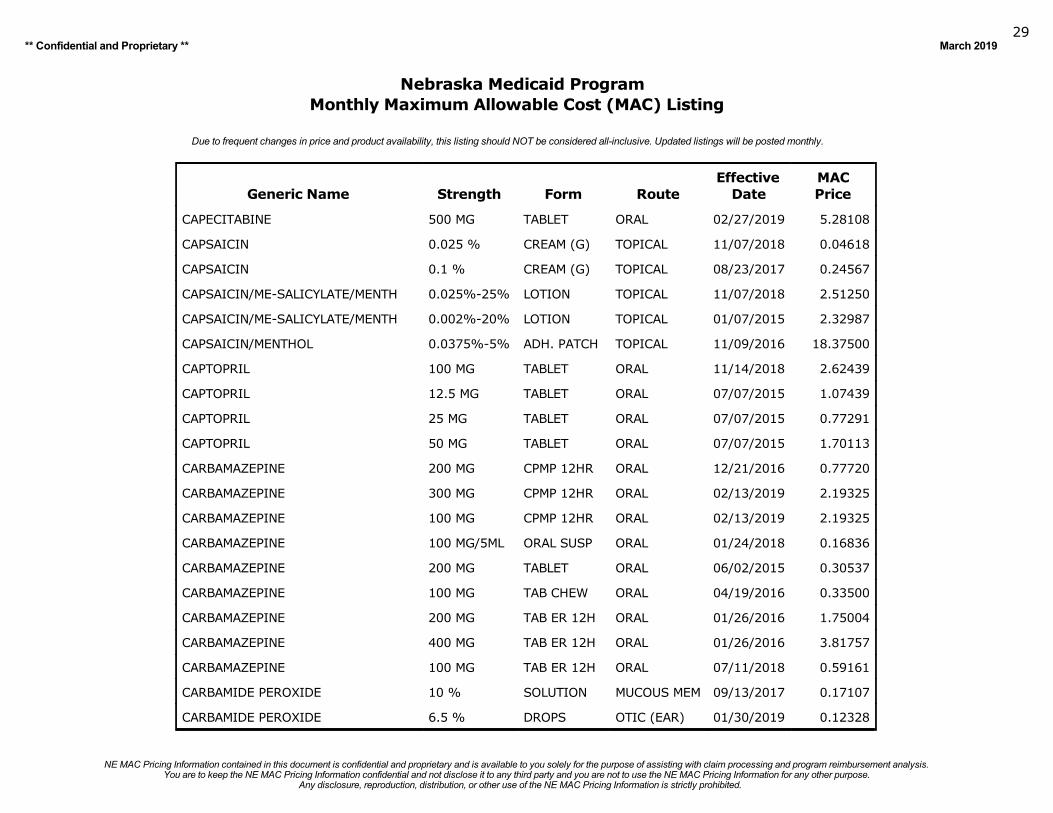
CAPECITABINE 500 MG TABLET ORAL 02/27/2019 5.28108
CAPSAICIN 0.025 % CREAM (G) TOPICAL 11/07/2018 0.04618
CAPSAICIN 0.1 % CREAM (G) TOPICAL 08/23/2017 0.24567
CAPSAICIN/ME-SALICYLATE/MENTH 0.025%-25% LOTION TOPICAL 11/07/2018 2.51250
CAPSAICIN/ME-SALICYLATE/MENTH 0.002%-20% LOTION TOPICAL 01/07/2015 2.32987
CAPSAICIN/MENTHOL 0.0375%-5% ADH. PATCH TOPICAL 11/09/2016 18.37500
CAPTOPRIL 100 MG TABLET ORAL 11/14/2018 2.62439
CAPTOPRIL 12.5 MG TABLET ORAL 07/07/2015 1.07439
CAPTOPRIL 25 MG TABLET ORAL 07/07/2015 0.77291
CAPTOPRIL 50 MG TABLET ORAL 07/07/2015 1.70113
CARBAMAZEPINE 200 MG CPMP 12HR ORAL 12/21/2016 0.77720
CARBAMAZEPINE 300 MG CPMP 12HR ORAL 02/13/2019 2.19325
CARBAMAZEPINE 100 MG CPMP 12HR ORAL 02/13/2019 2.19325
CARBAMAZEPINE 100 MG/5ML ORAL SUSP ORAL 01/24/2018 0.16836
CARBAMAZEPINE 200 MG TABLET ORAL 06/02/2015 0.30537
CARBAMAZEPINE 100 MG TAB CHEW ORAL 04/19/2016 0.33500
CARBAMAZEPINE 200 MG TAB ER 12H ORAL 01/26/2016 1.75004
CARBAMAZEPINE 400 MG TAB ER 12H ORAL 01/26/2016 3.81757
CARBAMAZEPINE 100 MG TAB ER 12H ORAL 07/11/2018 0.59161
CARBAMIDE PEROXIDE 10 % SOLUTION MUCOUS MEM 09/13/2017 0.17107
CARBAMIDE PEROXIDE 6.5 % DROPS OTIC (EAR) 01/30/2019 0.12328
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201930
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
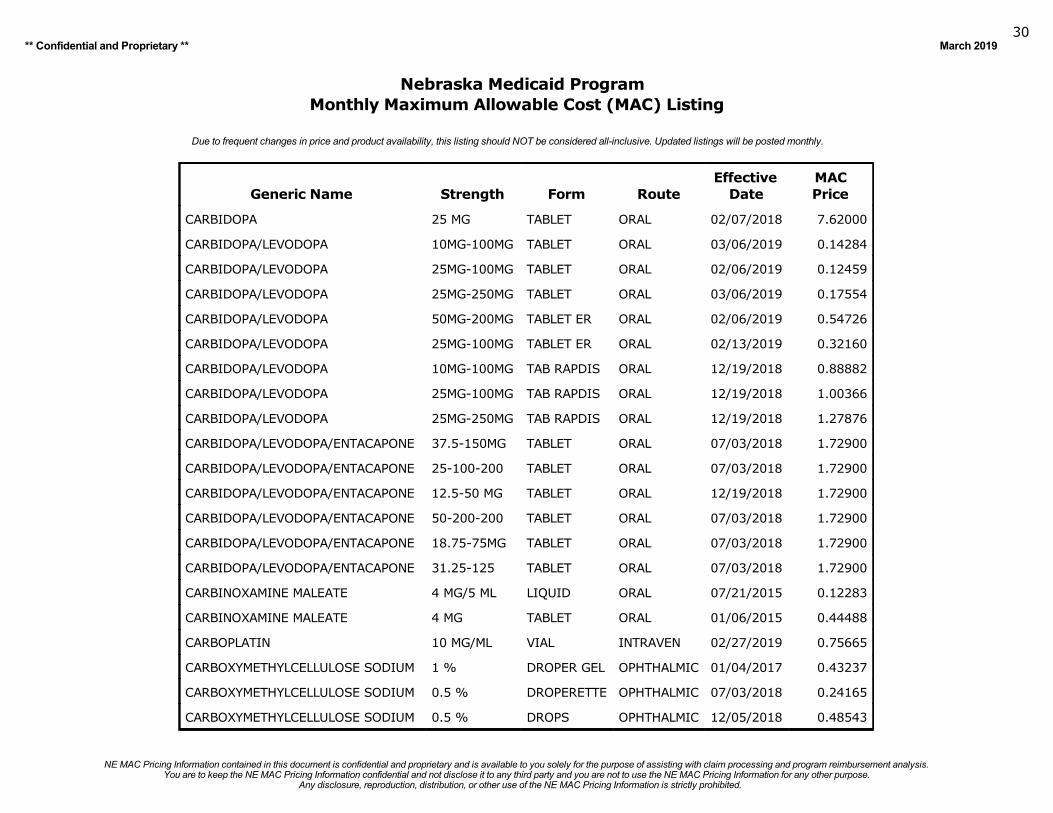
CARBIDOPA 25 MG TABLET ORAL 02/07/2018 7.62000
CARBIDOPA/LEVODOPA 10MG-100MG TABLET ORAL 03/06/2019 0.14284
CARBIDOPA/LEVODOPA 25MG-100MG TABLET ORAL 02/06/2019 0.12459
CARBIDOPA/LEVODOPA 25MG-250MG TABLET ORAL 03/06/2019 0.17554
CARBIDOPA/LEVODOPA 50MG-200MG TABLET ER ORAL 02/06/2019 0.54726
CARBIDOPA/LEVODOPA 25MG-100MG TABLET ER ORAL 02/13/2019 0.32160
CARBIDOPA/LEVODOPA 10MG-100MG TAB RAPDIS ORAL 12/19/2018 0.88882
CARBIDOPA/LEVODOPA 25MG-100MG TAB RAPDIS ORAL 12/19/2018 1.00366
CARBIDOPA/LEVODOPA 25MG-250MG TAB RAPDIS ORAL 12/19/2018 1.27876
CARBIDOPA/LEVODOPA/ENTACAPONE 37.5-150MG TABLET ORAL 07/03/2018 1.72900
CARBIDOPA/LEVODOPA/ENTACAPONE 25-100-200 TABLET ORAL 07/03/2018 1.72900
CARBIDOPA/LEVODOPA/ENTACAPONE 12.5-50 MG TABLET ORAL 12/19/2018 1.72900
CARBIDOPA/LEVODOPA/ENTACAPONE 50-200-200 TABLET ORAL 07/03/2018 1.72900
CARBIDOPA/LEVODOPA/ENTACAPONE 18.75-75MG TABLET ORAL 07/03/2018 1.72900
CARBIDOPA/LEVODOPA/ENTACAPONE 31.25-125 TABLET ORAL 07/03/2018 1.72900
CARBINOXAMINE MALEATE 4 MG/5 ML LIQUID ORAL 07/21/2015 0.12283
CARBINOXAMINE MALEATE 4 MG TABLET ORAL 01/06/2015 0.44488
CARBOPLATIN 10 MG/ML VIAL INTRAVEN 02/27/2019 0.75665
CARBOXYMETHYLCELLULOSE SODIUM 1 % DROPER GEL OPHTHALMIC 01/04/2017 0.43237
CARBOXYMETHYLCELLULOSE SODIUM 0.5 % DROPERETTE OPHTHALMIC 07/03/2018 0.24165
CARBOXYMETHYLCELLULOSE SODIUM 0.5 % DROPS OPHTHALMIC 12/05/2018 0.48543
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201931
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
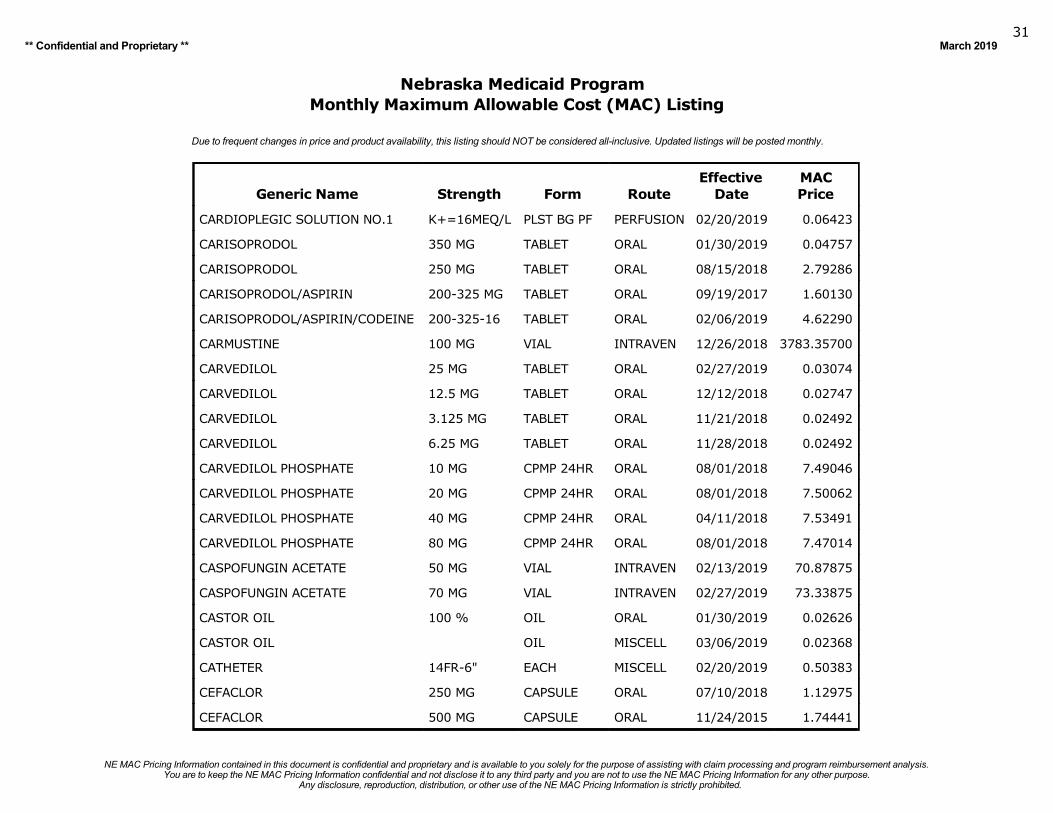
CARDIOPLEGIC SOLUTION NO.1 K+=16MEQ/L PLST BG PF PERFUSION 02/20/2019 0.06423
CARISOPRODOL 350 MG TABLET ORAL 01/30/2019 0.04757
CARISOPRODOL 250 MG TABLET ORAL 08/15/2018 2.79286
CARISOPRODOL/ASPIRIN 200-325 MG TABLET ORAL 09/19/2017 1.60130
CARISOPRODOL/ASPIRIN/CODEINE 200-325-16 TABLET ORAL 02/06/2019 4.62290
CARMUSTINE 100 MG VIAL INTRAVEN 12/26/2018 3783.35700
CARVEDILOL 25 MG TABLET ORAL 02/27/2019 0.03074
CARVEDILOL 12.5 MG TABLET ORAL 12/12/2018 0.02747
CARVEDILOL 3.125 MG TABLET ORAL 11/21/2018 0.02492
CARVEDILOL 6.25 MG TABLET ORAL 11/28/2018 0.02492
CARVEDILOL PHOSPHATE 10 MG CPMP 24HR ORAL 08/01/2018 7.49046
CARVEDILOL PHOSPHATE 20 MG CPMP 24HR ORAL 08/01/2018 7.50062
CARVEDILOL PHOSPHATE 40 MG CPMP 24HR ORAL 04/11/2018 7.53491
CARVEDILOL PHOSPHATE 80 MG CPMP 24HR ORAL 08/01/2018 7.47014
CASPOFUNGIN ACETATE 50 MG VIAL INTRAVEN 02/13/2019 70.87875
CASPOFUNGIN ACETATE 70 MG VIAL INTRAVEN 02/27/2019 73.33875
CASTOR OIL 100 % OIL ORAL 01/30/2019 0.02626
CASTOR OIL OIL MISCELL 03/06/2019 0.02368
CATHETER 14FR-6" EACH MISCELL 02/20/2019 0.50383
CEFACLOR 250 MG CAPSULE ORAL 07/10/2018 1.12975
CEFACLOR 500 MG CAPSULE ORAL 11/24/2015 1.74441
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201932
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
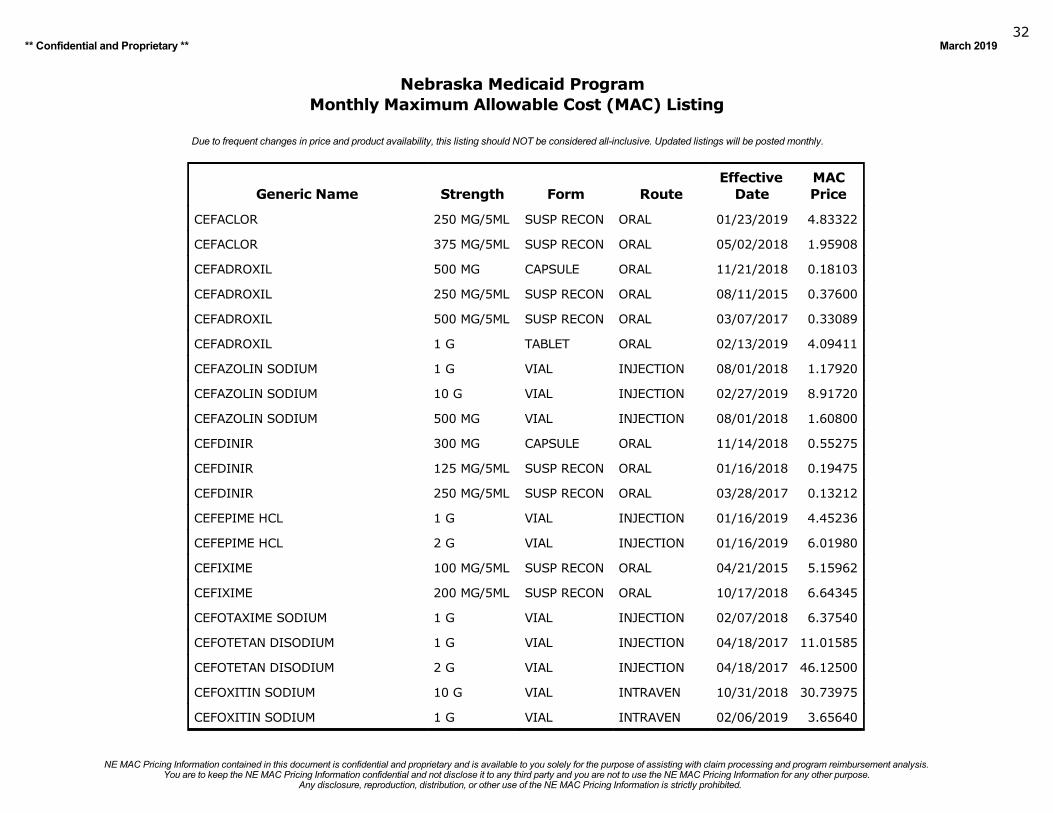
CEFACLOR 250 MG/5ML SUSP RECON ORAL 01/23/2019 4.83322
CEFACLOR 375 MG/5ML SUSP RECON ORAL 05/02/2018 1.95908
CEFADROXIL 500 MG CAPSULE ORAL 11/21/2018 0.18103
CEFADROXIL 250 MG/5ML SUSP RECON ORAL 08/11/2015 0.37600
CEFADROXIL 500 MG/5ML SUSP RECON ORAL 03/07/2017 0.33089
CEFADROXIL 1 G TABLET ORAL 02/13/2019 4.09411
CEFAZOLIN SODIUM 1 G VIAL INJECTION 08/01/2018 1.17920
CEFAZOLIN SODIUM 10 G VIAL INJECTION 02/27/2019 8.91720
CEFAZOLIN SODIUM 500 MG VIAL INJECTION 08/01/2018 1.60800
CEFDINIR 300 MG CAPSULE ORAL 11/14/2018 0.55275
CEFDINIR 125 MG/5ML SUSP RECON ORAL 01/16/2018 0.19475
CEFDINIR 250 MG/5ML SUSP RECON ORAL 03/28/2017 0.13212
CEFEPIME HCL 1 G VIAL INJECTION 01/16/2019 4.45236
CEFEPIME HCL 2 G VIAL INJECTION 01/16/2019 6.01980
CEFIXIME 100 MG/5ML SUSP RECON ORAL 04/21/2015 5.15962
CEFIXIME 200 MG/5ML SUSP RECON ORAL 10/17/2018 6.64345
CEFOTAXIME SODIUM 1 G VIAL INJECTION 02/07/2018 6.37540
CEFOTETAN DISODIUM 1 G VIAL INJECTION 04/18/2017 11.01585
CEFOTETAN DISODIUM 2 G VIAL INJECTION 04/18/2017 46.12500
CEFOXITIN SODIUM 10 G VIAL INTRAVEN 10/31/2018 30.73975
CEFOXITIN SODIUM 1 G VIAL INTRAVEN 02/06/2019 3.65640
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
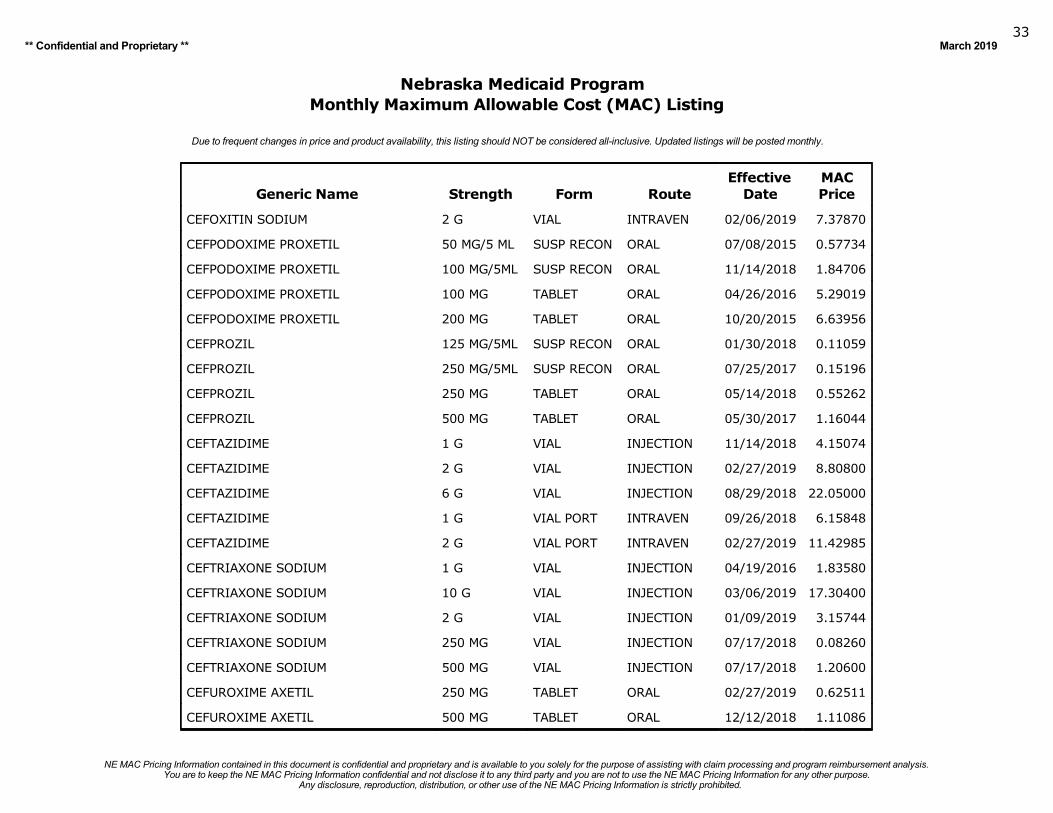
** Confidential and Proprietary ** March 201933
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CEFOXITIN SODIUM 2 G VIAL INTRAVEN 02/06/2019 7.37870
CEFPODOXIME PROXETIL 50 MG/5 ML SUSP RECON ORAL 07/08/2015 0.57734
CEFPODOXIME PROXETIL 100 MG/5ML SUSP RECON ORAL 11/14/2018 1.84706
CEFPODOXIME PROXETIL 100 MG TABLET ORAL 04/26/2016 5.29019
CEFPODOXIME PROXETIL 200 MG TABLET ORAL 10/20/2015 6.63956
CEFPROZIL 125 MG/5ML SUSP RECON ORAL 01/30/2018 0.11059
CEFPROZIL 250 MG/5ML SUSP RECON ORAL 07/25/2017 0.15196
CEFPROZIL 250 MG TABLET ORAL 05/14/2018 0.55262
CEFPROZIL 500 MG TABLET ORAL 05/30/2017 1.16044
CEFTAZIDIME 1 G VIAL INJECTION 11/14/2018 4.15074
CEFTAZIDIME 2 G VIAL INJECTION 02/27/2019 8.80800
CEFTAZIDIME 6 G VIAL INJECTION 08/29/2018 22.05000
CEFTAZIDIME 1 G VIAL PORT INTRAVEN 09/26/2018 6.15848
CEFTAZIDIME 2 G VIAL PORT INTRAVEN 02/27/2019 11.42985
CEFTRIAXONE SODIUM 1 G VIAL INJECTION 04/19/2016 1.83580
CEFTRIAXONE SODIUM 10 G VIAL INJECTION 03/06/2019 17.30400
CEFTRIAXONE SODIUM 2 G VIAL INJECTION 01/09/2019 3.15744
CEFTRIAXONE SODIUM 250 MG VIAL INJECTION 07/17/2018 0.08260
CEFTRIAXONE SODIUM 500 MG VIAL INJECTION 07/17/2018 1.20600
CEFUROXIME AXETIL 250 MG TABLET ORAL 02/27/2019 0.62511
CEFUROXIME AXETIL 500 MG TABLET ORAL 12/12/2018 1.11086
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
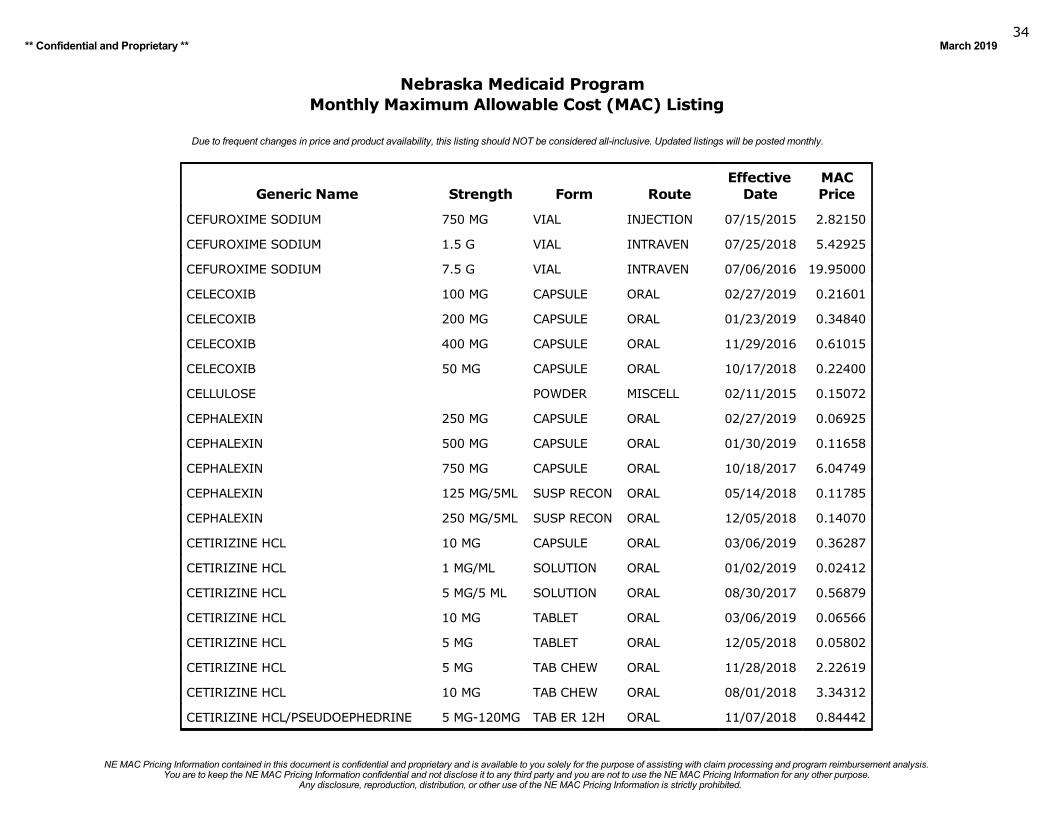
** Confidential and Proprietary ** March 201934
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CEFUROXIME SODIUM 750 MG VIAL INJECTION 07/15/2015 2.82150
CEFUROXIME SODIUM 1.5 G VIAL INTRAVEN 07/25/2018 5.42925
CEFUROXIME SODIUM 7.5 G VIAL INTRAVEN 07/06/2016 19.95000
CELECOXIB 100 MG CAPSULE ORAL 02/27/2019 0.21601
CELECOXIB 200 MG CAPSULE ORAL 01/23/2019 0.34840
CELECOXIB 400 MG CAPSULE ORAL 11/29/2016 0.61015
CELECOXIB 50 MG CAPSULE ORAL 10/17/2018 0.22400
CELLULOSE POWDER MISCELL 02/11/2015 0.15072
CEPHALEXIN 250 MG CAPSULE ORAL 02/27/2019 0.06925
CEPHALEXIN 500 MG CAPSULE ORAL 01/30/2019 0.11658
CEPHALEXIN 750 MG CAPSULE ORAL 10/18/2017 6.04749
CEPHALEXIN 125 MG/5ML SUSP RECON ORAL 05/14/2018 0.11785
CEPHALEXIN 250 MG/5ML SUSP RECON ORAL 12/05/2018 0.14070
CETIRIZINE HCL 10 MG CAPSULE ORAL 03/06/2019 0.36287
CETIRIZINE HCL 1 MG/ML SOLUTION ORAL 01/02/2019 0.02412
CETIRIZINE HCL 5 MG/5 ML SOLUTION ORAL 08/30/2017 0.56879
CETIRIZINE HCL 10 MG TABLET ORAL 03/06/2019 0.06566
CETIRIZINE HCL 5 MG TABLET ORAL 12/05/2018 0.05802
CETIRIZINE HCL 5 MG TAB CHEW ORAL 11/28/2018 2.22619
CETIRIZINE HCL 10 MG TAB CHEW ORAL 08/01/2018 3.34312
CETIRIZINE HCL/PSEUDOEPHEDRINE 5 MG-120MG TAB ER 12H ORAL 11/07/2018 0.84442
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
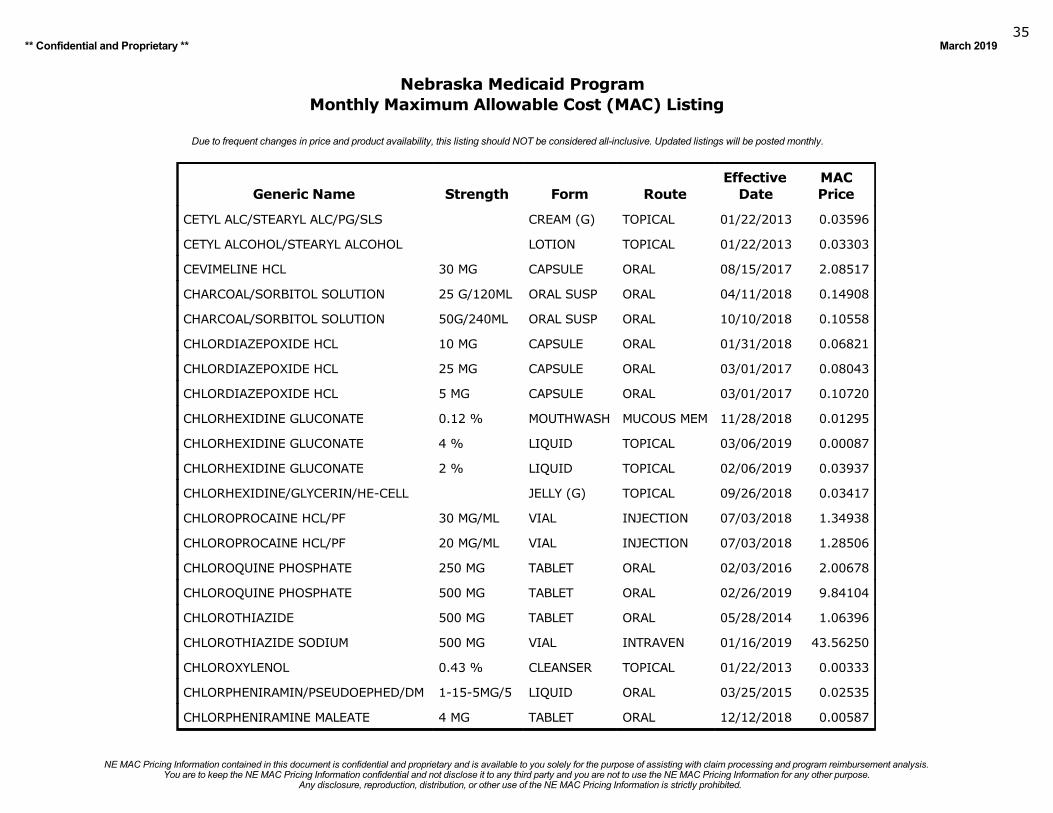
** Confidential and Proprietary ** March 201935
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CETYL ALC/STEARYL ALC/PG/SLS CREAM (G) TOPICAL 01/22/2013 0.03596
CETYL ALCOHOL/STEARYL ALCOHOL LOTION TOPICAL 01/22/2013 0.03303
CEVIMELINE HCL 30 MG CAPSULE ORAL 08/15/2017 2.08517
CHARCOAL/SORBITOL SOLUTION 25 G/120ML ORAL SUSP ORAL 04/11/2018 0.14908
CHARCOAL/SORBITOL SOLUTION 50G/240ML ORAL SUSP ORAL 10/10/2018 0.10558
CHLORDIAZEPOXIDE HCL 10 MG CAPSULE ORAL 01/31/2018 0.06821
CHLORDIAZEPOXIDE HCL 25 MG CAPSULE ORAL 03/01/2017 0.08043
CHLORDIAZEPOXIDE HCL 5 MG CAPSULE ORAL 03/01/2017 0.10720
CHLORHEXIDINE GLUCONATE 0.12 % MOUTHWASH MUCOUS MEM 11/28/2018 0.01295
CHLORHEXIDINE GLUCONATE 4 % LIQUID TOPICAL 03/06/2019 0.00087
CHLORHEXIDINE GLUCONATE 2 % LIQUID TOPICAL 02/06/2019 0.03937
CHLORHEXIDINE/GLYCERIN/HE-CELL JELLY (G) TOPICAL 09/26/2018 0.03417
CHLOROPROCAINE HCL/PF 30 MG/ML VIAL INJECTION 07/03/2018 1.34938
CHLOROPROCAINE HCL/PF 20 MG/ML VIAL INJECTION 07/03/2018 1.28506
CHLOROQUINE PHOSPHATE 250 MG TABLET ORAL 02/03/2016 2.00678
CHLOROQUINE PHOSPHATE 500 MG TABLET ORAL 02/26/2019 9.84104
CHLOROTHIAZIDE 500 MG TABLET ORAL 05/28/2014 1.06396
CHLOROTHIAZIDE SODIUM 500 MG VIAL INTRAVEN 01/16/2019 43.56250
CHLOROXYLENOL 0.43 % CLEANSER TOPICAL 01/22/2013 0.00333
CHLORPHENIRAMIN/PSEUDOEPHED/DM 1-15-5MG/5 LIQUID ORAL 03/25/2015 0.02535
CHLORPHENIRAMINE MALEATE 4 MG TABLET ORAL 12/12/2018 0.00587
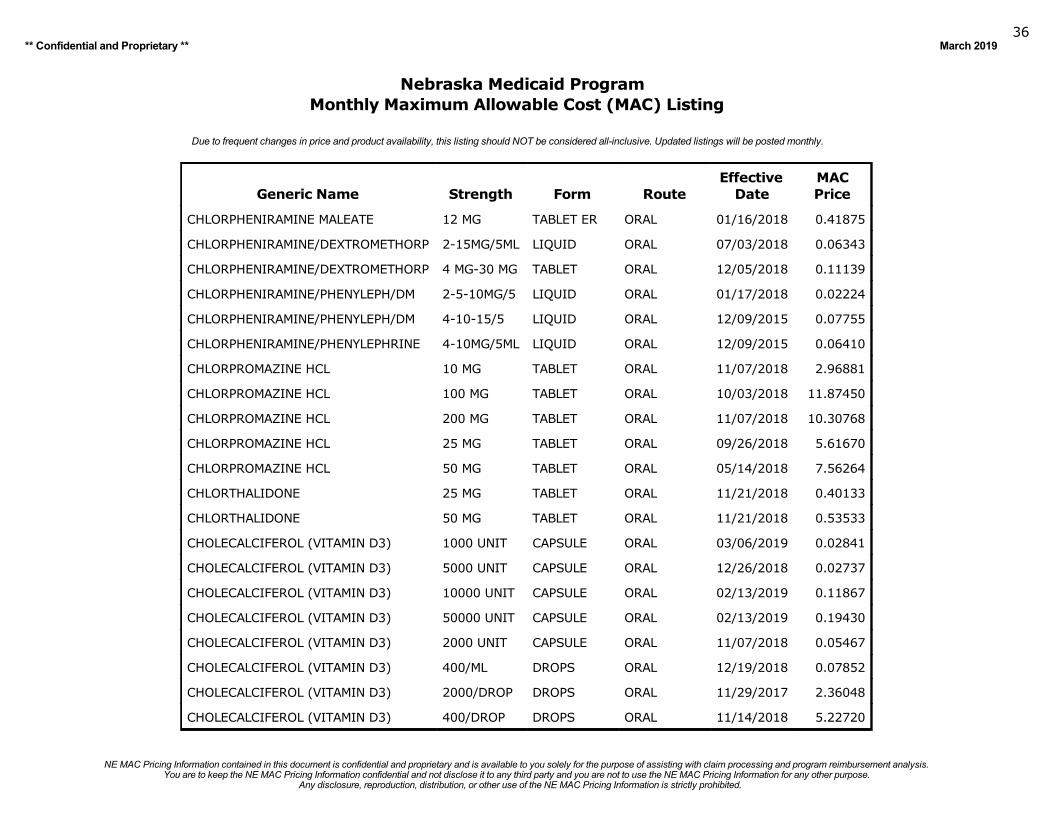
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201936
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CHLORPHENIRAMINE MALEATE 12 MG TABLET ER ORAL 01/16/2018 0.41875
CHLORPHENIRAMINE/DEXTROMETHORP 2-15MG/5ML LIQUID ORAL 07/03/2018 0.06343
CHLORPHENIRAMINE/DEXTROMETHORP 4 MG-30 MG TABLET ORAL 12/05/2018 0.11139
CHLORPHENIRAMINE/PHENYLEPH/DM 2-5-10MG/5 LIQUID ORAL 01/17/2018 0.02224
CHLORPHENIRAMINE/PHENYLEPH/DM 4-10-15/5 LIQUID ORAL 12/09/2015 0.07755
CHLORPHENIRAMINE/PHENYLEPHRINE 4-10MG/5ML LIQUID ORAL 12/09/2015 0.06410
CHLORPROMAZINE HCL 10 MG TABLET ORAL 11/07/2018 2.96881
CHLORPROMAZINE HCL 100 MG TABLET ORAL 10/03/2018 11.87450
CHLORPROMAZINE HCL 200 MG TABLET ORAL 11/07/2018 10.30768
CHLORPROMAZINE HCL 25 MG TABLET ORAL 09/26/2018 5.61670
CHLORPROMAZINE HCL 50 MG TABLET ORAL 05/14/2018 7.56264
CHLORTHALIDONE 25 MG TABLET ORAL 11/21/2018 0.40133
CHLORTHALIDONE 50 MG TABLET ORAL 11/21/2018 0.53533
CHOLECALCIFEROL (VITAMIN D3) 1000 UNIT CAPSULE ORAL 03/06/2019 0.02841
CHOLECALCIFEROL (VITAMIN D3) 5000 UNIT CAPSULE ORAL 12/26/2018 0.02737
CHOLECALCIFEROL (VITAMIN D3) 10000 UNIT CAPSULE ORAL 02/13/2019 0.11867
CHOLECALCIFEROL (VITAMIN D3) 50000 UNIT CAPSULE ORAL 02/13/2019 0.19430
CHOLECALCIFEROL (VITAMIN D3) 2000 UNIT CAPSULE ORAL 11/07/2018 0.05467
CHOLECALCIFEROL (VITAMIN D3) 400/ML DROPS ORAL 12/19/2018 0.07852
CHOLECALCIFEROL (VITAMIN D3) 2000/DROP DROPS ORAL 11/29/2017 2.36048
CHOLECALCIFEROL (VITAMIN D3) 400/DROP DROPS ORAL 11/14/2018 5.22720
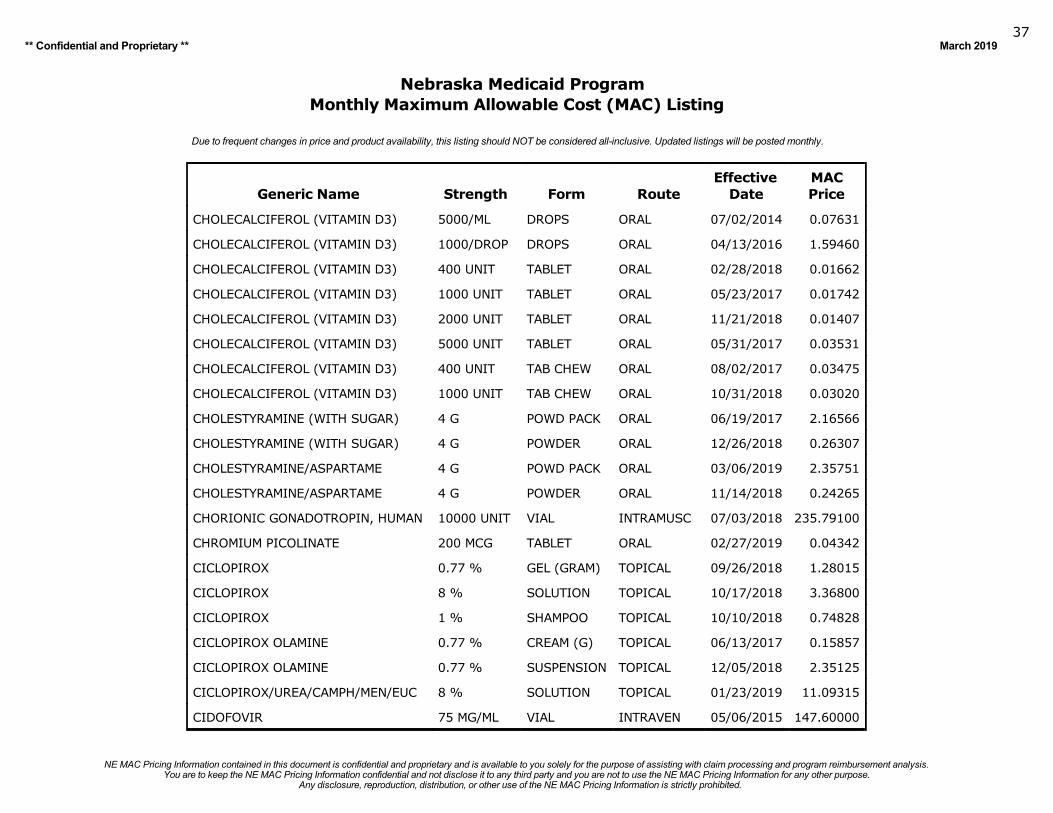
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201937
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CHOLECALCIFEROL (VITAMIN D3) 5000/ML DROPS ORAL 07/02/2014 0.07631
CHOLECALCIFEROL (VITAMIN D3) 1000/DROP DROPS ORAL 04/13/2016 1.59460
CHOLECALCIFEROL (VITAMIN D3) 400 UNIT TABLET ORAL 02/28/2018 0.01662
CHOLECALCIFEROL (VITAMIN D3) 1000 UNIT TABLET ORAL 05/23/2017 0.01742
CHOLECALCIFEROL (VITAMIN D3) 2000 UNIT TABLET ORAL 11/21/2018 0.01407
CHOLECALCIFEROL (VITAMIN D3) 5000 UNIT TABLET ORAL 05/31/2017 0.03531
CHOLECALCIFEROL (VITAMIN D3) 400 UNIT TAB CHEW ORAL 08/02/2017 0.03475
CHOLECALCIFEROL (VITAMIN D3) 1000 UNIT TAB CHEW ORAL 10/31/2018 0.03020
CHOLESTYRAMINE (WITH SUGAR) 4 G POWD PACK ORAL 06/19/2017 2.16566
CHOLESTYRAMINE (WITH SUGAR) 4 G POWDER ORAL 12/26/2018 0.26307
CHOLESTYRAMINE/ASPARTAME 4 G POWD PACK ORAL 03/06/2019 2.35751
CHOLESTYRAMINE/ASPARTAME 4 G POWDER ORAL 11/14/2018 0.24265
CHORIONIC GONADOTROPIN, HUMAN 10000 UNIT VIAL INTRAMUSC 07/03/2018 235.79100
CHROMIUM PICOLINATE 200 MCG TABLET ORAL 02/27/2019 0.04342
CICLOPIROX 0.77 % GEL (GRAM) TOPICAL 09/26/2018 1.28015
CICLOPIROX 8 % SOLUTION TOPICAL 10/17/2018 3.36800
CICLOPIROX 1 % SHAMPOO TOPICAL 10/10/2018 0.74828
CICLOPIROX OLAMINE 0.77 % CREAM (G) TOPICAL 06/13/2017 0.15857
CICLOPIROX OLAMINE 0.77 % SUSPENSION TOPICAL 12/05/2018 2.35125
CICLOPIROX/UREA/CAMPH/MEN/EUC 8 % SOLUTION TOPICAL 01/23/2019 11.09315
CIDOFOVIR 75 MG/ML VIAL INTRAVEN 05/06/2015 147.60000
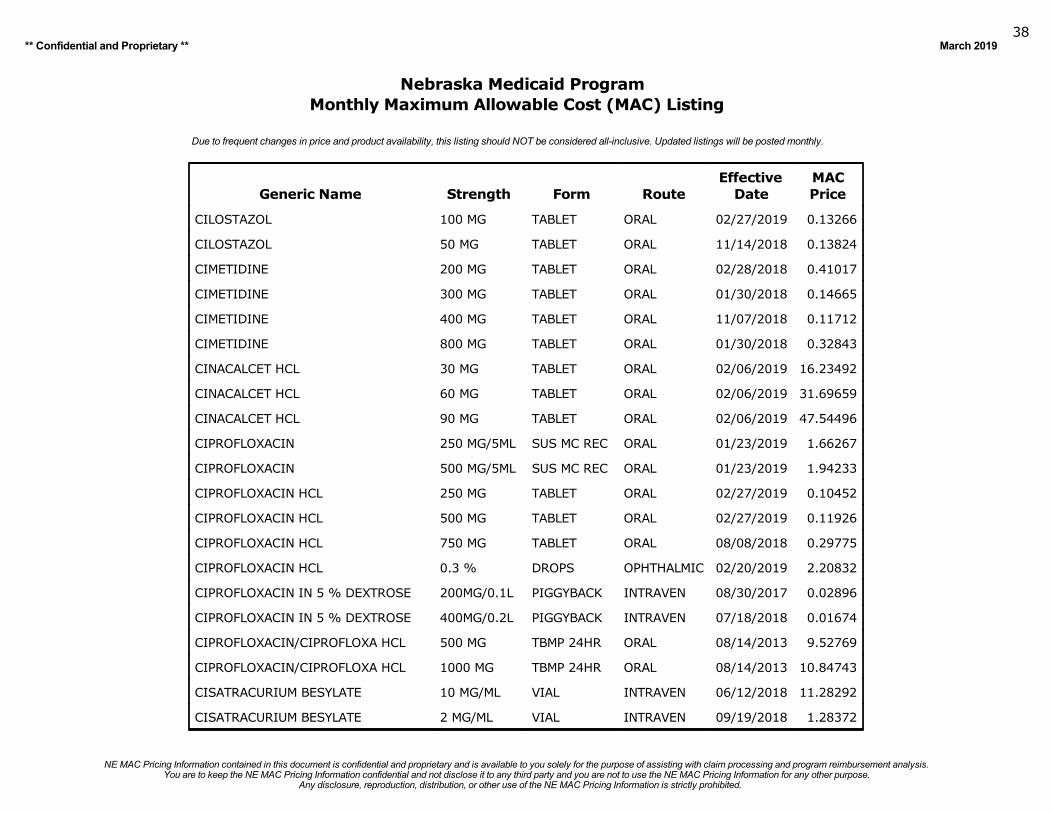
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201938
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CILOSTAZOL 100 MG TABLET ORAL 02/27/2019 0.13266
CILOSTAZOL 50 MG TABLET ORAL 11/14/2018 0.13824
CIMETIDINE 200 MG TABLET ORAL 02/28/2018 0.41017
CIMETIDINE 300 MG TABLET ORAL 01/30/2018 0.14665
CIMETIDINE 400 MG TABLET ORAL 11/07/2018 0.11712
CIMETIDINE 800 MG TABLET ORAL 01/30/2018 0.32843
CINACALCET HCL 30 MG TABLET ORAL 02/06/2019 16.23492
CINACALCET HCL 60 MG TABLET ORAL 02/06/2019 31.69659
CINACALCET HCL 90 MG TABLET ORAL 02/06/2019 47.54496
CIPROFLOXACIN 250 MG/5ML SUS MC REC ORAL 01/23/2019 1.66267
CIPROFLOXACIN 500 MG/5ML SUS MC REC ORAL 01/23/2019 1.94233
CIPROFLOXACIN HCL 250 MG TABLET ORAL 02/27/2019 0.10452
CIPROFLOXACIN HCL 500 MG TABLET ORAL 02/27/2019 0.11926
CIPROFLOXACIN HCL 750 MG TABLET ORAL 08/08/2018 0.29775
CIPROFLOXACIN HCL 0.3 % DROPS OPHTHALMIC 02/20/2019 2.20832
CIPROFLOXACIN IN 5 % DEXTROSE 200MG/0.1L PIGGYBACK INTRAVEN 08/30/2017 0.02896
CIPROFLOXACIN IN 5 % DEXTROSE 400MG/0.2L PIGGYBACK INTRAVEN 07/18/2018 0.01674
CIPROFLOXACIN/CIPROFLOXA HCL 500 MG TBMP 24HR ORAL 08/14/2013 9.52769
CIPROFLOXACIN/CIPROFLOXA HCL 1000 MG TBMP 24HR ORAL 08/14/2013 10.84743
CISATRACURIUM BESYLATE 10 MG/ML VIAL INTRAVEN 06/12/2018 11.28292
CISATRACURIUM BESYLATE 2 MG/ML VIAL INTRAVEN 09/19/2018 1.28372
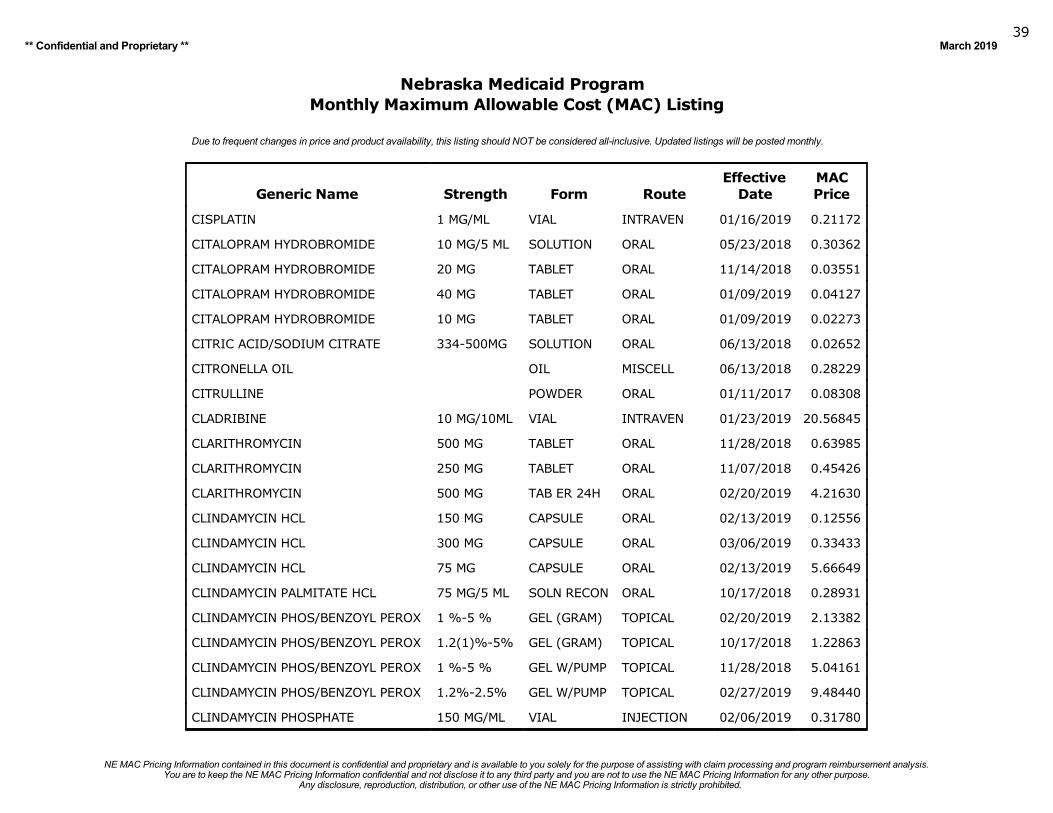
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201939
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CISPLATIN 1 MG/ML VIAL INTRAVEN 01/16/2019 0.21172
CITALOPRAM HYDROBROMIDE 10 MG/5 ML SOLUTION ORAL 05/23/2018 0.30362
CITALOPRAM HYDROBROMIDE 20 MG TABLET ORAL 11/14/2018 0.03551
CITALOPRAM HYDROBROMIDE 40 MG TABLET ORAL 01/09/2019 0.04127
CITALOPRAM HYDROBROMIDE 10 MG TABLET ORAL 01/09/2019 0.02273
CITRIC ACID/SODIUM CITRATE 334-500MG SOLUTION ORAL 06/13/2018 0.02652
CITRONELLA OIL OIL MISCELL 06/13/2018 0.28229
CITRULLINE POWDER ORAL 01/11/2017 0.08308
CLADRIBINE 10 MG/10ML VIAL INTRAVEN 01/23/2019 20.56845
CLARITHROMYCIN 500 MG TABLET ORAL 11/28/2018 0.63985
CLARITHROMYCIN 250 MG TABLET ORAL 11/07/2018 0.45426
CLARITHROMYCIN 500 MG TAB ER 24H ORAL 02/20/2019 4.21630
CLINDAMYCIN HCL 150 MG CAPSULE ORAL 02/13/2019 0.12556
CLINDAMYCIN HCL 300 MG CAPSULE ORAL 03/06/2019 0.33433
CLINDAMYCIN HCL 75 MG CAPSULE ORAL 02/13/2019 5.66649
CLINDAMYCIN PALMITATE HCL 75 MG/5 ML SOLN RECON ORAL 10/17/2018 0.28931
CLINDAMYCIN PHOS/BENZOYL PEROX 1 %-5 % GEL (GRAM) TOPICAL 02/20/2019 2.13382
CLINDAMYCIN PHOS/BENZOYL PEROX 1.2(1)%-5% GEL (GRAM) TOPICAL 10/17/2018 1.22863
CLINDAMYCIN PHOS/BENZOYL PEROX 1 %-5 % GEL W/PUMP TOPICAL 11/28/2018 5.04161
CLINDAMYCIN PHOS/BENZOYL PEROX 1.2%-2.5% GEL W/PUMP TOPICAL 02/27/2019 9.48440
CLINDAMYCIN PHOSPHATE 150 MG/ML VIAL INJECTION 02/06/2019 0.31780
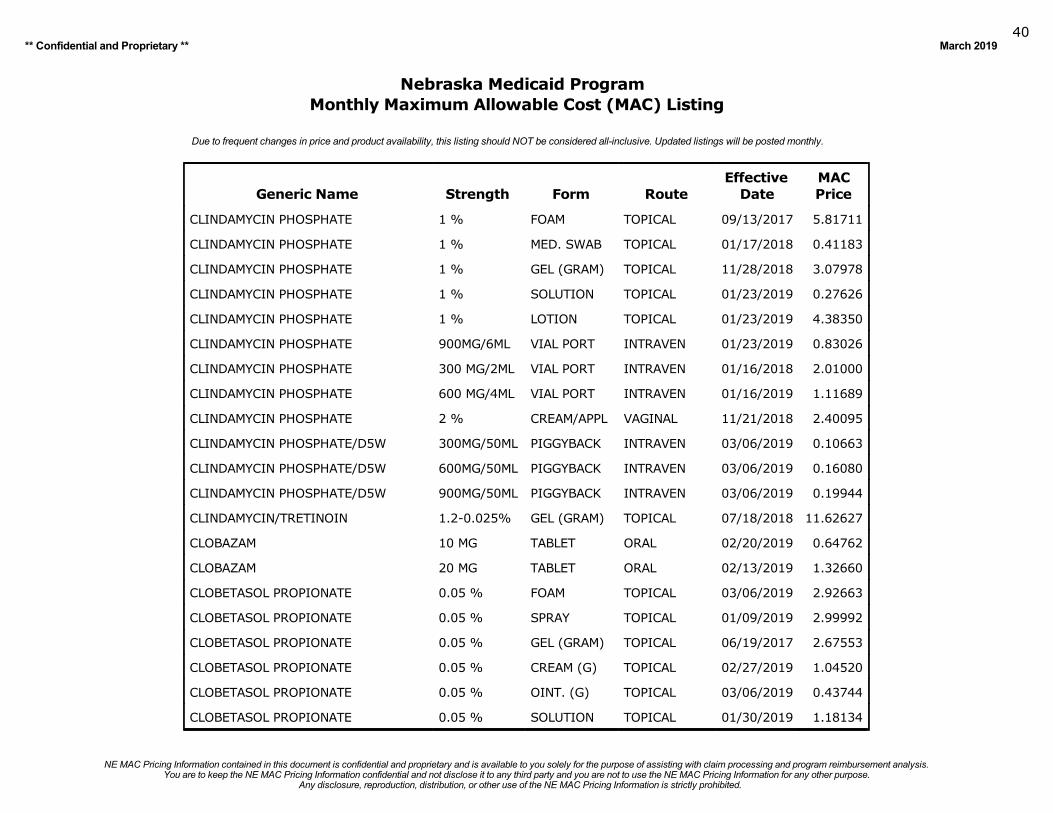
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201940
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CLINDAMYCIN PHOSPHATE 1 % FOAM TOPICAL 09/13/2017 5.81711
CLINDAMYCIN PHOSPHATE 1 % MED. SWAB TOPICAL 01/17/2018 0.41183
CLINDAMYCIN PHOSPHATE 1 % GEL (GRAM) TOPICAL 11/28/2018 3.07978
CLINDAMYCIN PHOSPHATE 1 % SOLUTION TOPICAL 01/23/2019 0.27626
CLINDAMYCIN PHOSPHATE 1 % LOTION TOPICAL 01/23/2019 4.38350
CLINDAMYCIN PHOSPHATE 900MG/6ML VIAL PORT INTRAVEN 01/23/2019 0.83026
CLINDAMYCIN PHOSPHATE 300 MG/2ML VIAL PORT INTRAVEN 01/16/2018 2.01000
CLINDAMYCIN PHOSPHATE 600 MG/4ML VIAL PORT INTRAVEN 01/16/2019 1.11689
CLINDAMYCIN PHOSPHATE 2 % CREAM/APPL VAGINAL 11/21/2018 2.40095
CLINDAMYCIN PHOSPHATE/D5W 300MG/50ML PIGGYBACK INTRAVEN 03/06/2019 0.10663
CLINDAMYCIN PHOSPHATE/D5W 600MG/50ML PIGGYBACK INTRAVEN 03/06/2019 0.16080
CLINDAMYCIN PHOSPHATE/D5W 900MG/50ML PIGGYBACK INTRAVEN 03/06/2019 0.19944
CLINDAMYCIN/TRETINOIN 1.2-0.025% GEL (GRAM) TOPICAL 07/18/2018 11.62627
CLOBAZAM 10 MG TABLET ORAL 02/20/2019 0.64762
CLOBAZAM 20 MG TABLET ORAL 02/13/2019 1.32660
CLOBETASOL PROPIONATE 0.05 % FOAM TOPICAL 03/06/2019 2.92663
CLOBETASOL PROPIONATE 0.05 % SPRAY TOPICAL 01/09/2019 2.99992
CLOBETASOL PROPIONATE 0.05 % GEL (GRAM) TOPICAL 06/19/2017 2.67553
CLOBETASOL PROPIONATE 0.05 % CREAM (G) TOPICAL 02/27/2019 1.04520
CLOBETASOL PROPIONATE 0.05 % OINT. (G) TOPICAL 03/06/2019 0.43744
CLOBETASOL PROPIONATE 0.05 % SOLUTION TOPICAL 01/30/2019 1.18134
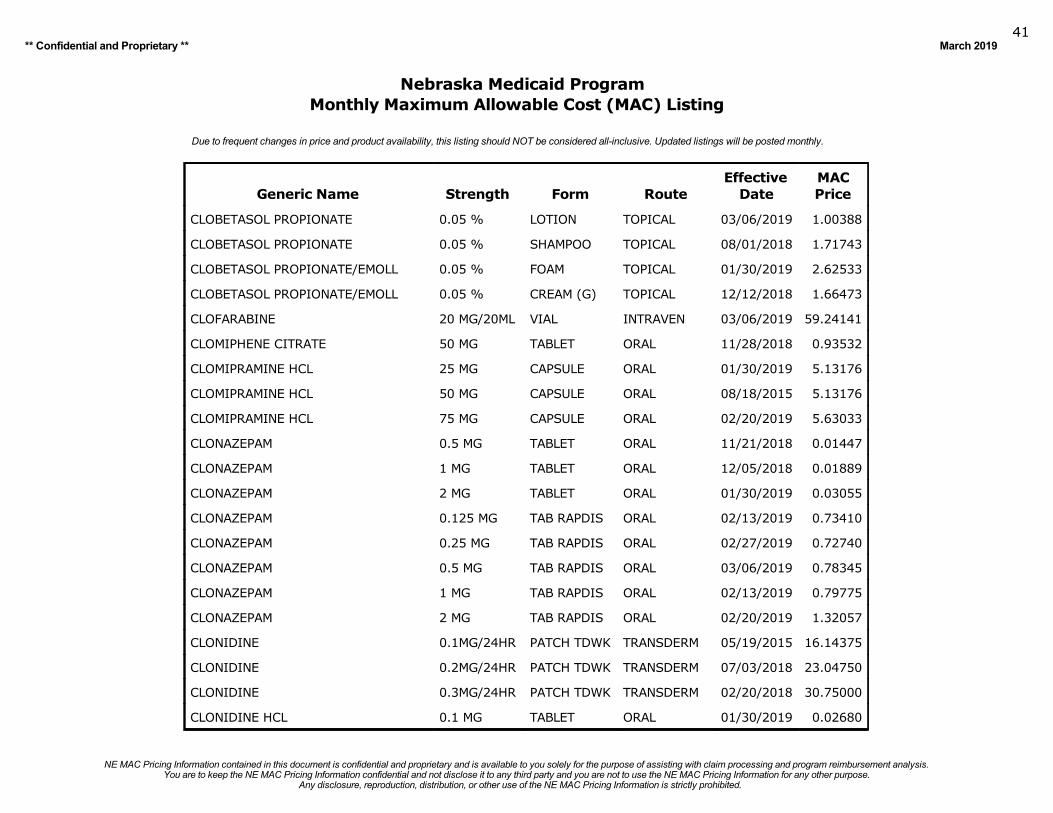
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201941
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CLOBETASOL PROPIONATE 0.05 % LOTION TOPICAL 03/06/2019 1.00388
CLOBETASOL PROPIONATE 0.05 % SHAMPOO TOPICAL 08/01/2018 1.71743
CLOBETASOL PROPIONATE/EMOLL 0.05 % FOAM TOPICAL 01/30/2019 2.62533
CLOBETASOL PROPIONATE/EMOLL 0.05 % CREAM (G) TOPICAL 12/12/2018 1.66473
CLOFARABINE 20 MG/20ML VIAL INTRAVEN 03/06/2019 59.24141
CLOMIPHENE CITRATE 50 MG TABLET ORAL 11/28/2018 0.93532
CLOMIPRAMINE HCL 25 MG CAPSULE ORAL 01/30/2019 5.13176
CLOMIPRAMINE HCL 50 MG CAPSULE ORAL 08/18/2015 5.13176
CLOMIPRAMINE HCL 75 MG CAPSULE ORAL 02/20/2019 5.63033
CLONAZEPAM 0.5 MG TABLET ORAL 11/21/2018 0.01447
CLONAZEPAM 1 MG TABLET ORAL 12/05/2018 0.01889
CLONAZEPAM 2 MG TABLET ORAL 01/30/2019 0.03055
CLONAZEPAM 0.125 MG TAB RAPDIS ORAL 02/13/2019 0.73410
CLONAZEPAM 0.25 MG TAB RAPDIS ORAL 02/27/2019 0.72740
CLONAZEPAM 0.5 MG TAB RAPDIS ORAL 03/06/2019 0.78345
CLONAZEPAM 1 MG TAB RAPDIS ORAL 02/13/2019 0.79775
CLONAZEPAM 2 MG TAB RAPDIS ORAL 02/20/2019 1.32057
CLONIDINE 0.1MG/24HR PATCH TDWK TRANSDERM 05/19/2015 16.14375
CLONIDINE 0.2MG/24HR PATCH TDWK TRANSDERM 07/03/2018 23.04750
CLONIDINE 0.3MG/24HR PATCH TDWK TRANSDERM 02/20/2018 30.75000
CLONIDINE HCL 0.1 MG TABLET ORAL 01/30/2019 0.02680
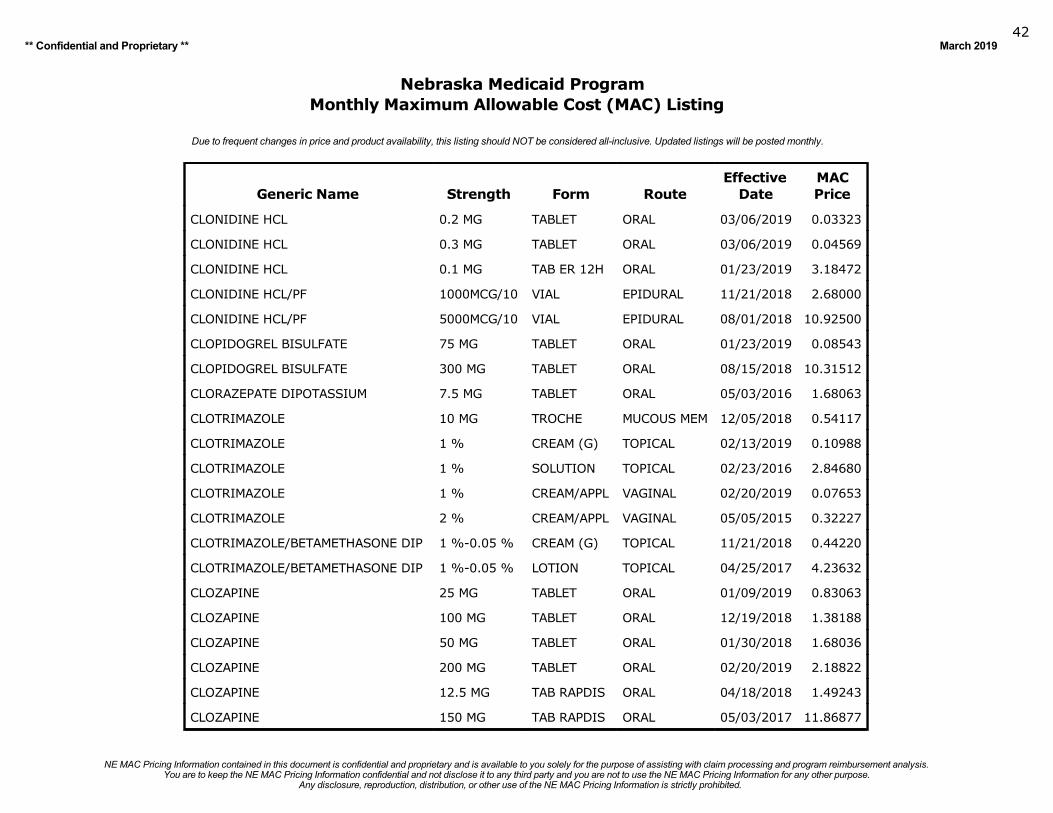
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201942
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CLONIDINE HCL 0.2 MG TABLET ORAL 03/06/2019 0.03323
CLONIDINE HCL 0.3 MG TABLET ORAL 03/06/2019 0.04569
CLONIDINE HCL 0.1 MG TAB ER 12H ORAL 01/23/2019 3.18472
CLONIDINE HCL/PF 1000MCG/10 VIAL EPIDURAL 11/21/2018 2.68000
CLONIDINE HCL/PF 5000MCG/10 VIAL EPIDURAL 08/01/2018 10.92500
CLOPIDOGREL BISULFATE 75 MG TABLET ORAL 01/23/2019 0.08543
CLOPIDOGREL BISULFATE 300 MG TABLET ORAL 08/15/2018 10.31512
CLORAZEPATE DIPOTASSIUM 7.5 MG TABLET ORAL 05/03/2016 1.68063
CLOTRIMAZOLE 10 MG TROCHE MUCOUS MEM 12/05/2018 0.54117
CLOTRIMAZOLE 1 % CREAM (G) TOPICAL 02/13/2019 0.10988
CLOTRIMAZOLE 1 % SOLUTION TOPICAL 02/23/2016 2.84680
CLOTRIMAZOLE 1 % CREAM/APPL VAGINAL 02/20/2019 0.07653
CLOTRIMAZOLE 2 % CREAM/APPL VAGINAL 05/05/2015 0.32227
CLOTRIMAZOLE/BETAMETHASONE DIP 1 %-0.05 % CREAM (G) TOPICAL 11/21/2018 0.44220
CLOTRIMAZOLE/BETAMETHASONE DIP 1 %-0.05 % LOTION TOPICAL 04/25/2017 4.23632
CLOZAPINE 25 MG TABLET ORAL 01/09/2019 0.83063
CLOZAPINE 100 MG TABLET ORAL 12/19/2018 1.38188
CLOZAPINE 50 MG TABLET ORAL 01/30/2018 1.68036
CLOZAPINE 200 MG TABLET ORAL 02/20/2019 2.18822
CLOZAPINE 12.5 MG TAB RAPDIS ORAL 04/18/2018 1.49243
CLOZAPINE 150 MG TAB RAPDIS ORAL 05/03/2017 11.86877
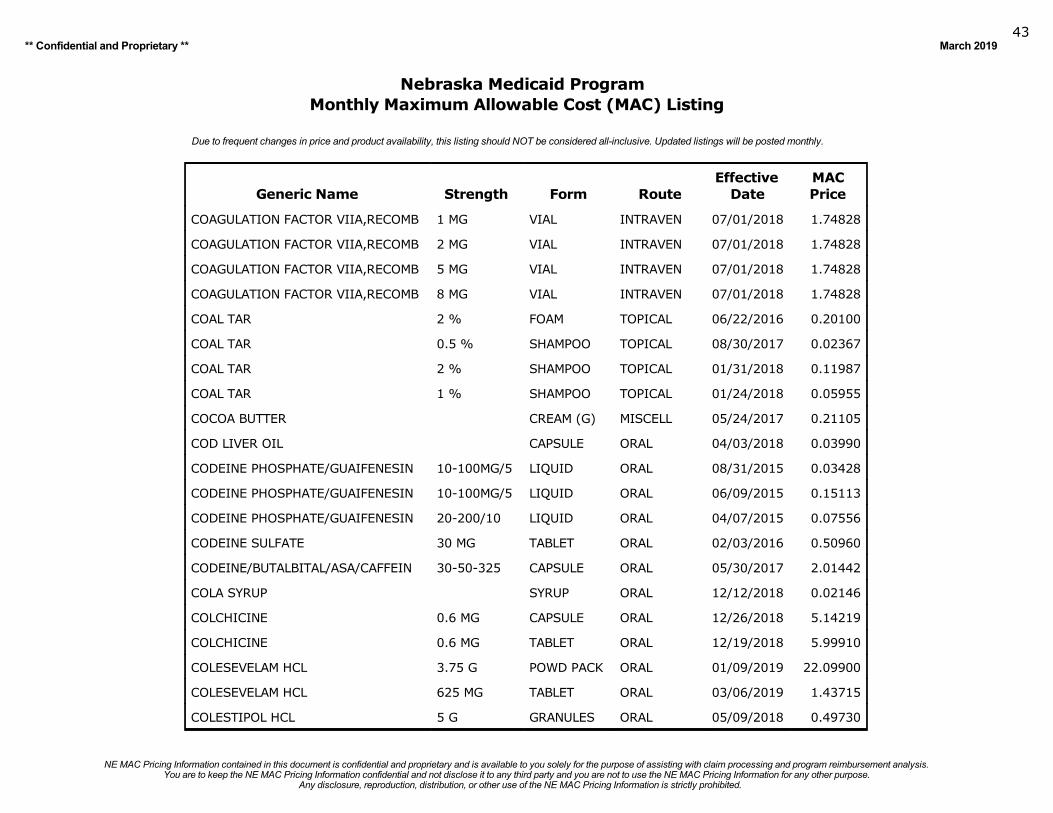
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201943
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
COAGULATION FACTOR VIIA,RECOMB 1 MG VIAL INTRAVEN 07/01/2018 1.74828
COAGULATION FACTOR VIIA,RECOMB 2 MG VIAL INTRAVEN 07/01/2018 1.74828
COAGULATION FACTOR VIIA,RECOMB 5 MG VIAL INTRAVEN 07/01/2018 1.74828
COAGULATION FACTOR VIIA,RECOMB 8 MG VIAL INTRAVEN 07/01/2018 1.74828
COAL TAR 2 % FOAM TOPICAL 06/22/2016 0.20100
COAL TAR 0.5 % SHAMPOO TOPICAL 08/30/2017 0.02367
COAL TAR 2 % SHAMPOO TOPICAL 01/31/2018 0.11987
COAL TAR 1 % SHAMPOO TOPICAL 01/24/2018 0.05955
COCOA BUTTER CREAM (G) MISCELL 05/24/2017 0.21105
COD LIVER OIL CAPSULE ORAL 04/03/2018 0.03990
CODEINE PHOSPHATE/GUAIFENESIN 10-100MG/5 LIQUID ORAL 08/31/2015 0.03428
CODEINE PHOSPHATE/GUAIFENESIN 10-100MG/5 LIQUID ORAL 06/09/2015 0.15113
CODEINE PHOSPHATE/GUAIFENESIN 20-200/10 LIQUID ORAL 04/07/2015 0.07556
CODEINE SULFATE 30 MG TABLET ORAL 02/03/2016 0.50960
CODEINE/BUTALBITAL/ASA/CAFFEIN 30-50-325 CAPSULE ORAL 05/30/2017 2.01442
COLA SYRUP SYRUP ORAL 12/12/2018 0.02146
COLCHICINE 0.6 MG CAPSULE ORAL 12/26/2018 5.14219
COLCHICINE 0.6 MG TABLET ORAL 12/19/2018 5.99910
COLESEVELAM HCL 3.75 G POWD PACK ORAL 01/09/2019 22.09900
COLESEVELAM HCL 625 MG TABLET ORAL 03/06/2019 1.43715
COLESTIPOL HCL 5 G GRANULES ORAL 05/09/2018 0.49730
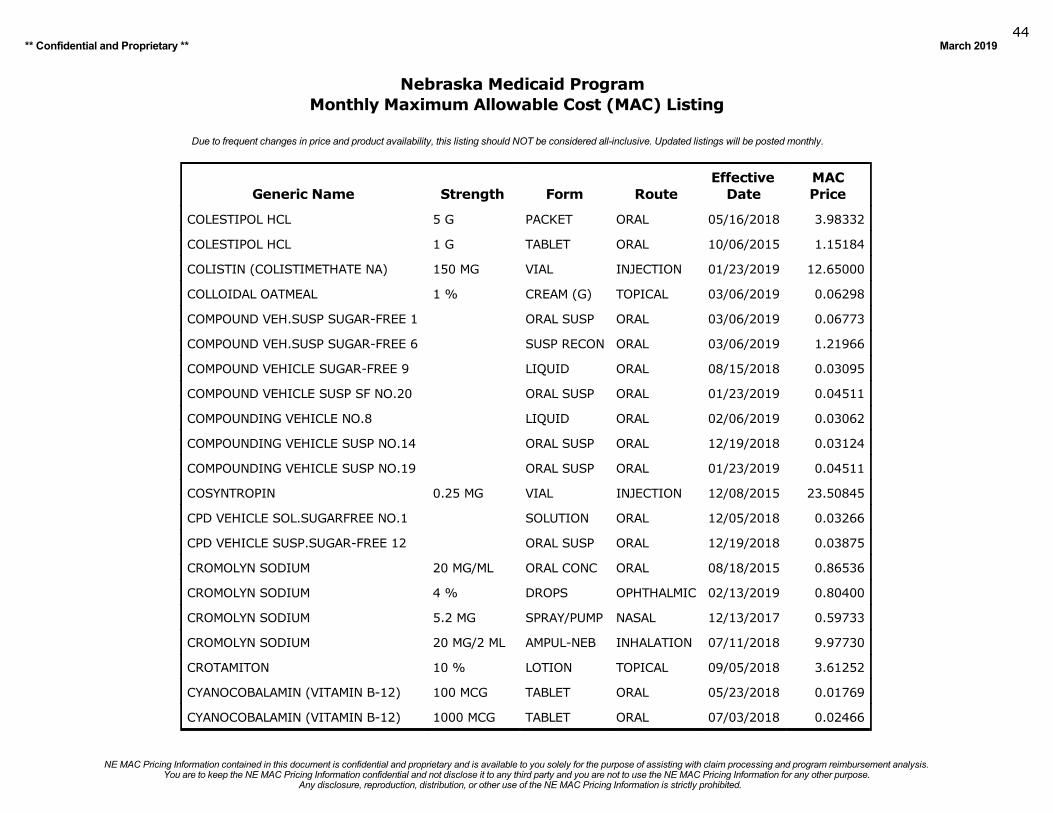
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201944
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
COLESTIPOL HCL 5 G PACKET ORAL 05/16/2018 3.98332
COLESTIPOL HCL 1 G TABLET ORAL 10/06/2015 1.15184
COLISTIN (COLISTIMETHATE NA) 150 MG VIAL INJECTION 01/23/2019 12.65000
COLLOIDAL OATMEAL 1 % CREAM (G) TOPICAL 03/06/2019 0.06298
COMPOUND VEH.SUSP SUGAR-FREE 1 ORAL SUSP ORAL 03/06/2019 0.06773
COMPOUND VEH.SUSP SUGAR-FREE 6 SUSP RECON ORAL 03/06/2019 1.21966
COMPOUND VEHICLE SUGAR-FREE 9 LIQUID ORAL 08/15/2018 0.03095
COMPOUND VEHICLE SUSP SF NO.20 ORAL SUSP ORAL 01/23/2019 0.04511
COMPOUNDING VEHICLE NO.8 LIQUID ORAL 02/06/2019 0.03062
COMPOUNDING VEHICLE SUSP NO.14 ORAL SUSP ORAL 12/19/2018 0.03124
COMPOUNDING VEHICLE SUSP NO.19 ORAL SUSP ORAL 01/23/2019 0.04511
COSYNTROPIN 0.25 MG VIAL INJECTION 12/08/2015 23.50845
CPD VEHICLE SOL.SUGARFREE NO.1 SOLUTION ORAL 12/05/2018 0.03266
CPD VEHICLE SUSP.SUGAR-FREE 12 ORAL SUSP ORAL 12/19/2018 0.03875
CROMOLYN SODIUM 20 MG/ML ORAL CONC ORAL 08/18/2015 0.86536
CROMOLYN SODIUM 4 % DROPS OPHTHALMIC 02/13/2019 0.80400
CROMOLYN SODIUM 5.2 MG SPRAY/PUMP NASAL 12/13/2017 0.59733
CROMOLYN SODIUM 20 MG/2 ML AMPUL-NEB INHALATION 07/11/2018 9.97730
CROTAMITON 10 % LOTION TOPICAL 09/05/2018 3.61252
CYANOCOBALAMIN (VITAMIN B-12) 100 MCG TABLET ORAL 05/23/2018 0.01769
CYANOCOBALAMIN (VITAMIN B-12) 1000 MCG TABLET ORAL 07/03/2018 0.02466
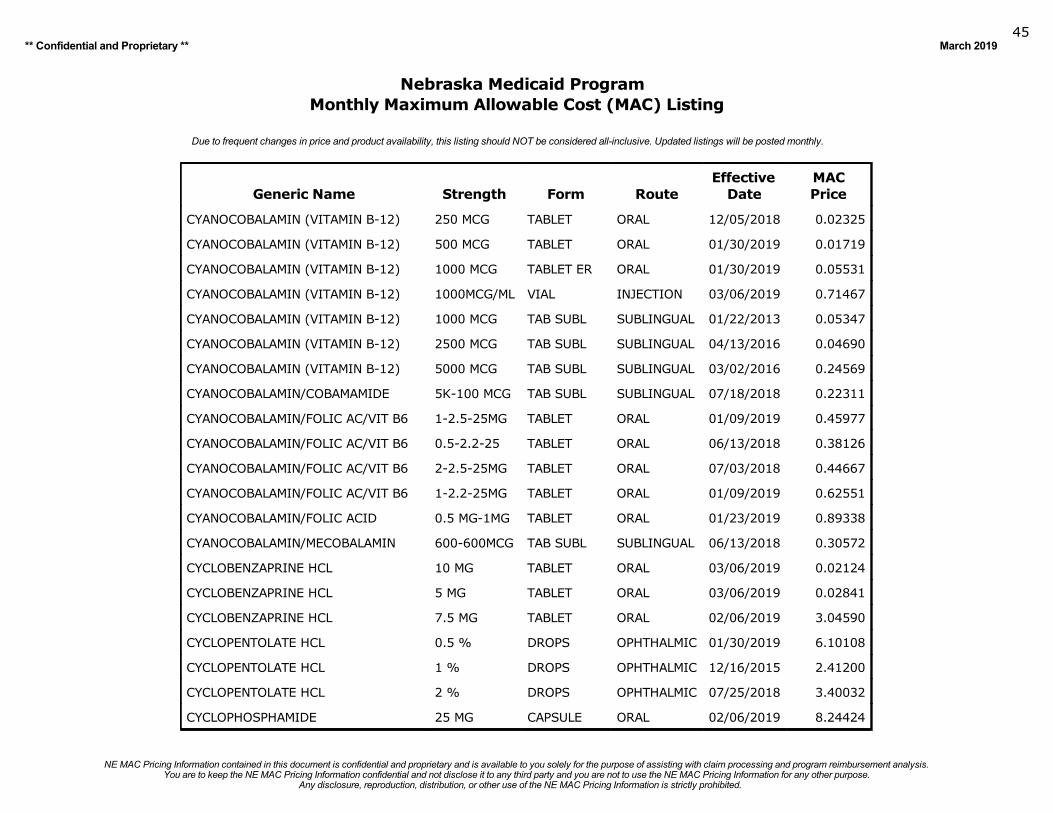
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201945
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CYANOCOBALAMIN (VITAMIN B-12) 250 MCG TABLET ORAL 12/05/2018 0.02325
CYANOCOBALAMIN (VITAMIN B-12) 500 MCG TABLET ORAL 01/30/2019 0.01719
CYANOCOBALAMIN (VITAMIN B-12) 1000 MCG TABLET ER ORAL 01/30/2019 0.05531
CYANOCOBALAMIN (VITAMIN B-12) 1000MCG/ML VIAL INJECTION 03/06/2019 0.71467
CYANOCOBALAMIN (VITAMIN B-12) 1000 MCG TAB SUBL SUBLINGUAL 01/22/2013 0.05347
CYANOCOBALAMIN (VITAMIN B-12) 2500 MCG TAB SUBL SUBLINGUAL 04/13/2016 0.04690
CYANOCOBALAMIN (VITAMIN B-12) 5000 MCG TAB SUBL SUBLINGUAL 03/02/2016 0.24569
CYANOCOBALAMIN/COBAMAMIDE 5K-100 MCG TAB SUBL SUBLINGUAL 07/18/2018 0.22311
CYANOCOBALAMIN/FOLIC AC/VIT B6 1-2.5-25MG TABLET ORAL 01/09/2019 0.45977
CYANOCOBALAMIN/FOLIC AC/VIT B6 0.5-2.2-25 TABLET ORAL 06/13/2018 0.38126
CYANOCOBALAMIN/FOLIC AC/VIT B6 2-2.5-25MG TABLET ORAL 07/03/2018 0.44667
CYANOCOBALAMIN/FOLIC AC/VIT B6 1-2.2-25MG TABLET ORAL 01/09/2019 0.62551
CYANOCOBALAMIN/FOLIC ACID 0.5 MG-1MG TABLET ORAL 01/23/2019 0.89338
CYANOCOBALAMIN/MECOBALAMIN 600-600MCG TAB SUBL SUBLINGUAL 06/13/2018 0.30572
CYCLOBENZAPRINE HCL 10 MG TABLET ORAL 03/06/2019 0.02124
CYCLOBENZAPRINE HCL 5 MG TABLET ORAL 03/06/2019 0.02841
CYCLOBENZAPRINE HCL 7.5 MG TABLET ORAL 02/06/2019 3.04590
CYCLOPENTOLATE HCL 0.5 % DROPS OPHTHALMIC 01/30/2019 6.10108
CYCLOPENTOLATE HCL 1 % DROPS OPHTHALMIC 12/16/2015 2.41200
CYCLOPENTOLATE HCL 2 % DROPS OPHTHALMIC 07/25/2018 3.40032
CYCLOPHOSPHAMIDE 25 MG CAPSULE ORAL 02/06/2019 8.24424

Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201946
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
CYCLOPHOSPHAMIDE 50 MG CAPSULE ORAL 02/27/2019 12.46520
CYCLOPHOSPHAMIDE 1 G VIAL INTRAVEN 11/07/2018 359.86725
CYCLOPHOSPHAMIDE 2 G VIAL INTRAVEN 11/07/2018 719.73450
CYCLOPHOSPHAMIDE 500 MG VIAL INTRAVEN 11/07/2018 179.93875
CYCLOSPORINE 100 MG CAPSULE ORAL 04/25/2017 9.43000
CYCLOSPORINE 25 MG CAPSULE ORAL 12/19/2018 4.01280
CYCLOSPORINE 250 MG/5ML AMPUL INTRAVEN 01/23/2019 12.02212
CYCLOSPORINE, MODIFIED 100 MG CAPSULE ORAL 11/14/2018 2.53305
CYCLOSPORINE, MODIFIED 25 MG CAPSULE ORAL 01/12/2016 0.54895
CYCLOSPORINE, MODIFIED 50 MG CAPSULE ORAL 03/07/2018 4.39234
CYCLOSPORINE, MODIFIED 100 MG/ML SOLUTION ORAL 02/04/2015 3.95380
CYPROHEPTADINE HCL 2 MG/5 ML SYRUP ORAL 08/15/2018 0.09478
CYPROHEPTADINE HCL 4 MG TABLET ORAL 11/21/2018 0.21440
CYTARABINE/PF 2 G/20 ML VIAL INJECTION 01/23/2019 1.04520
CYTARABINE/PF 100 MG/5ML VIAL INJECTION 12/28/2016 0.76380
CYTARABINE/PF 20 MG/ML VIAL INJECTION 02/27/2019 0.66276
D-METHORPHAN/PE/ACETAMINOPHEN 10-5-325MG CAPSULE ORAL 12/05/2018 0.26485
D-METHORPHAN/PE/ACETAMINOPHEN 5-325MG/15 LIQUID ORAL 12/26/2018 0.02657
D-METHORPHAN/PE/ACETAMINOPHEN 10-5-325MG TABLET ORAL 12/26/2018 0.26892
DACARBAZINE 200 MG VIAL INTRAVEN 01/23/2019 15.86235
DACTINOMYCIN 0.5 MG VIAL INTRAVEN 02/27/2019 1330.93175
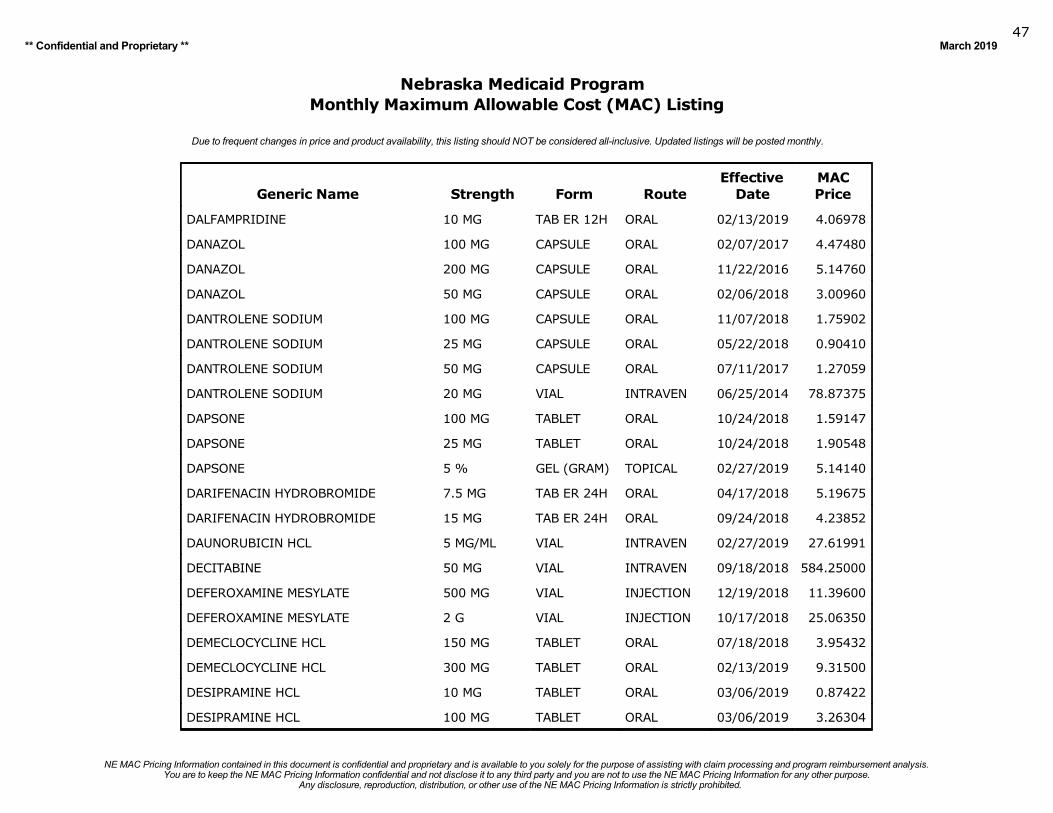
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201947
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DALFAMPRIDINE 10 MG TAB ER 12H ORAL 02/13/2019 4.06978
DANAZOL 100 MG CAPSULE ORAL 02/07/2017 4.47480
DANAZOL 200 MG CAPSULE ORAL 11/22/2016 5.14760
DANAZOL 50 MG CAPSULE ORAL 02/06/2018 3.00960
DANTROLENE SODIUM 100 MG CAPSULE ORAL 11/07/2018 1.75902
DANTROLENE SODIUM 25 MG CAPSULE ORAL 05/22/2018 0.90410
DANTROLENE SODIUM 50 MG CAPSULE ORAL 07/11/2017 1.27059
DANTROLENE SODIUM 20 MG VIAL INTRAVEN 06/25/2014 78.87375
DAPSONE 100 MG TABLET ORAL 10/24/2018 1.59147
DAPSONE 25 MG TABLET ORAL 10/24/2018 1.90548
DAPSONE 5 % GEL (GRAM) TOPICAL 02/27/2019 5.14140
DARIFENACIN HYDROBROMIDE 7.5 MG TAB ER 24H ORAL 04/17/2018 5.19675
DARIFENACIN HYDROBROMIDE 15 MG TAB ER 24H ORAL 09/24/2018 4.23852
DAUNORUBICIN HCL 5 MG/ML VIAL INTRAVEN 02/27/2019 27.61991
DECITABINE 50 MG VIAL INTRAVEN 09/18/2018 584.25000
DEFEROXAMINE MESYLATE 500 MG VIAL INJECTION 12/19/2018 11.39600
DEFEROXAMINE MESYLATE 2 G VIAL INJECTION 10/17/2018 25.06350
DEMECLOCYCLINE HCL 150 MG TABLET ORAL 07/18/2018 3.95432
DEMECLOCYCLINE HCL 300 MG TABLET ORAL 02/13/2019 9.31500
DESIPRAMINE HCL 10 MG TABLET ORAL 03/06/2019 0.87422
DESIPRAMINE HCL 100 MG TABLET ORAL 03/06/2019 3.26304
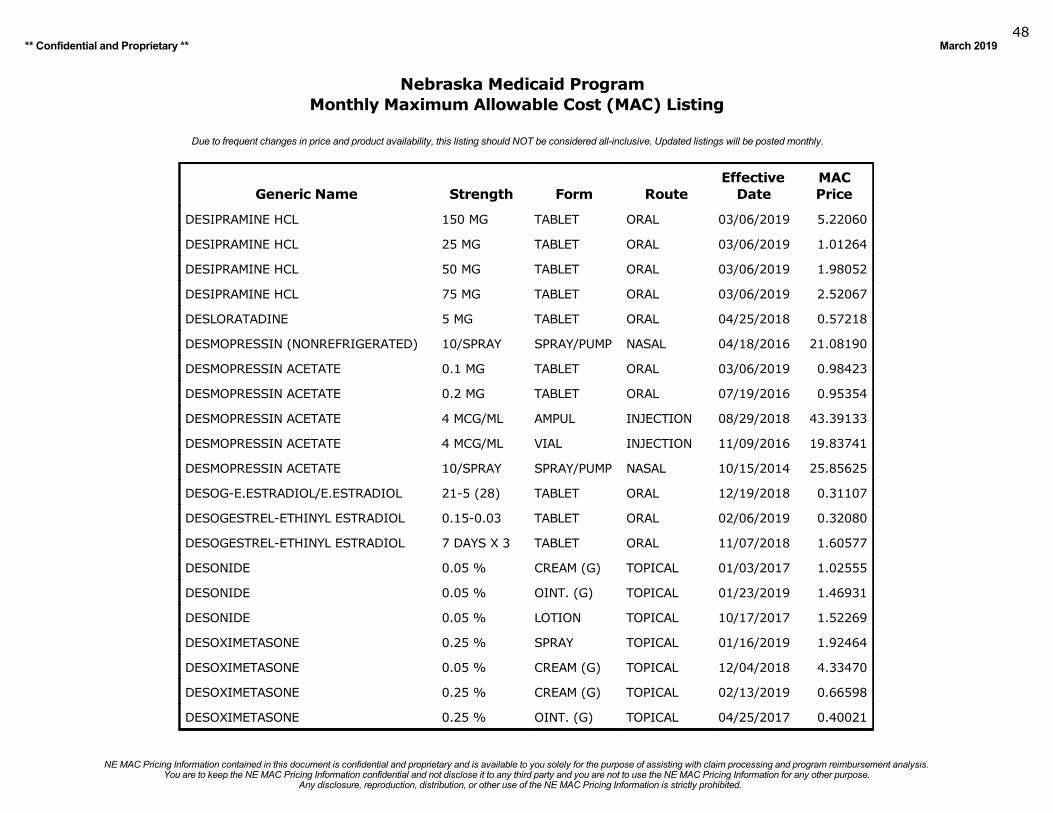
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201948
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DESIPRAMINE HCL 150 MG TABLET ORAL 03/06/2019 5.22060
DESIPRAMINE HCL 25 MG TABLET ORAL 03/06/2019 1.01264
DESIPRAMINE HCL 50 MG TABLET ORAL 03/06/2019 1.98052
DESIPRAMINE HCL 75 MG TABLET ORAL 03/06/2019 2.52067
DESLORATADINE 5 MG TABLET ORAL 04/25/2018 0.57218
DESMOPRESSIN (NONREFRIGERATED) 10/SPRAY SPRAY/PUMP NASAL 04/18/2016 21.08190
DESMOPRESSIN ACETATE 0.1 MG TABLET ORAL 03/06/2019 0.98423
DESMOPRESSIN ACETATE 0.2 MG TABLET ORAL 07/19/2016 0.95354
DESMOPRESSIN ACETATE 4 MCG/ML AMPUL INJECTION 08/29/2018 43.39133
DESMOPRESSIN ACETATE 4 MCG/ML VIAL INJECTION 11/09/2016 19.83741
DESMOPRESSIN ACETATE 10/SPRAY SPRAY/PUMP NASAL 10/15/2014 25.85625
DESOG-E.ESTRADIOL/E.ESTRADIOL 21-5 (28) TABLET ORAL 12/19/2018 0.31107
DESOGESTREL-ETHINYL ESTRADIOL 0.15-0.03 TABLET ORAL 02/06/2019 0.32080
DESOGESTREL-ETHINYL ESTRADIOL 7 DAYS X 3 TABLET ORAL 11/07/2018 1.60577
DESONIDE 0.05 % CREAM (G) TOPICAL 01/03/2017 1.02555
DESONIDE 0.05 % OINT. (G) TOPICAL 01/23/2019 1.46931
DESONIDE 0.05 % LOTION TOPICAL 10/17/2017 1.52269
DESOXIMETASONE 0.25 % SPRAY TOPICAL 01/16/2019 1.92464
DESOXIMETASONE 0.05 % CREAM (G) TOPICAL 12/04/2018 4.33470
DESOXIMETASONE 0.25 % CREAM (G) TOPICAL 02/13/2019 0.66598
DESOXIMETASONE 0.25 % OINT. (G) TOPICAL 04/25/2017 0.40021
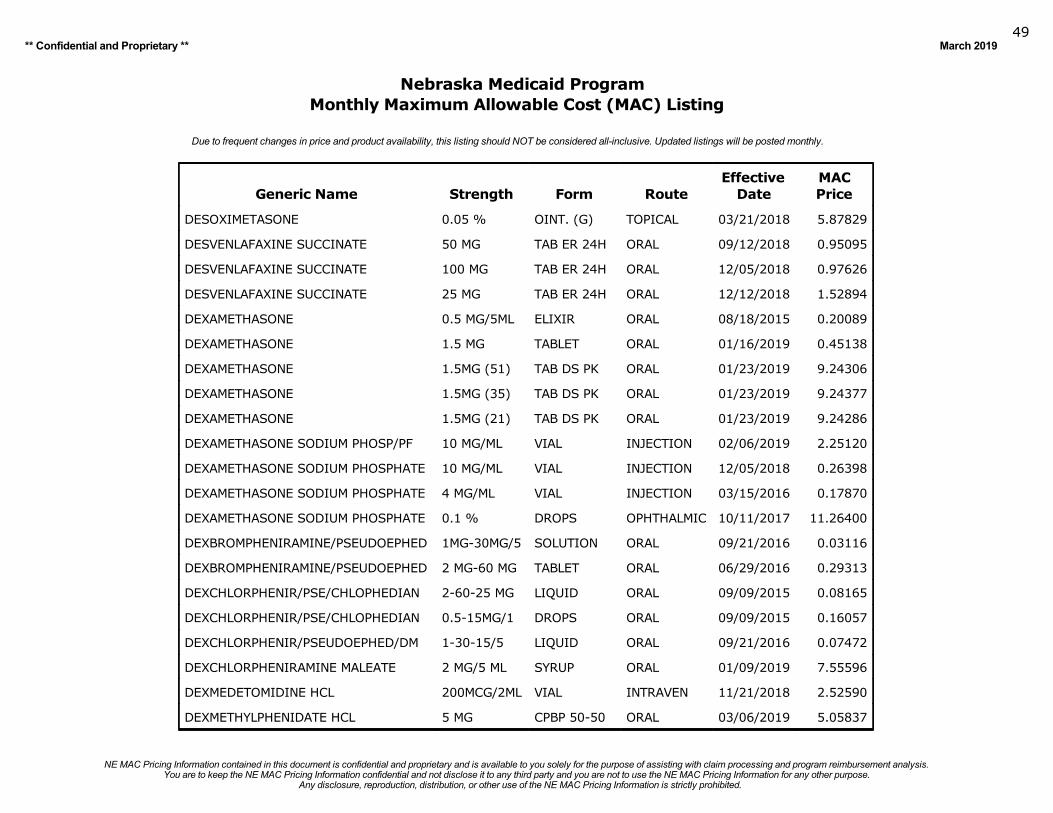
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201949
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DESOXIMETASONE 0.05 % OINT. (G) TOPICAL 03/21/2018 5.87829
DESVENLAFAXINE SUCCINATE 50 MG TAB ER 24H ORAL 09/12/2018 0.95095
DESVENLAFAXINE SUCCINATE 100 MG TAB ER 24H ORAL 12/05/2018 0.97626
DESVENLAFAXINE SUCCINATE 25 MG TAB ER 24H ORAL 12/12/2018 1.52894
DEXAMETHASONE 0.5 MG/5ML ELIXIR ORAL 08/18/2015 0.20089
DEXAMETHASONE 1.5 MG TABLET ORAL 01/16/2019 0.45138
DEXAMETHASONE 1.5MG (51) TAB DS PK ORAL 01/23/2019 9.24306
DEXAMETHASONE 1.5MG (35) TAB DS PK ORAL 01/23/2019 9.24377
DEXAMETHASONE 1.5MG (21) TAB DS PK ORAL 01/23/2019 9.24286
DEXAMETHASONE SODIUM PHOSP/PF 10 MG/ML VIAL INJECTION 02/06/2019 2.25120
DEXAMETHASONE SODIUM PHOSPHATE 10 MG/ML VIAL INJECTION 12/05/2018 0.26398
DEXAMETHASONE SODIUM PHOSPHATE 4 MG/ML VIAL INJECTION 03/15/2016 0.17870
DEXAMETHASONE SODIUM PHOSPHATE 0.1 % DROPS OPHTHALMIC 10/11/2017 11.26400
DEXBROMPHENIRAMINE/PSEUDOEPHED 1MG-30MG/5 SOLUTION ORAL 09/21/2016 0.03116
DEXBROMPHENIRAMINE/PSEUDOEPHED 2 MG-60 MG TABLET ORAL 06/29/2016 0.29313
DEXCHLORPHENIR/PSE/CHLOPHEDIAN 2-60-25 MG LIQUID ORAL 09/09/2015 0.08165
DEXCHLORPHENIR/PSE/CHLOPHEDIAN 0.5-15MG/1 DROPS ORAL 09/09/2015 0.16057
DEXCHLORPHENIR/PSEUDOEPHED/DM 1-30-15/5 LIQUID ORAL 09/21/2016 0.07472
DEXCHLORPHENIRAMINE MALEATE 2 MG/5 ML SYRUP ORAL 01/09/2019 7.55596
DEXMEDETOMIDINE HCL 200MCG/2ML VIAL INTRAVEN 11/21/2018 2.52590
DEXMETHYLPHENIDATE HCL 5 MG CPBP 50-50 ORAL 03/06/2019 5.05837
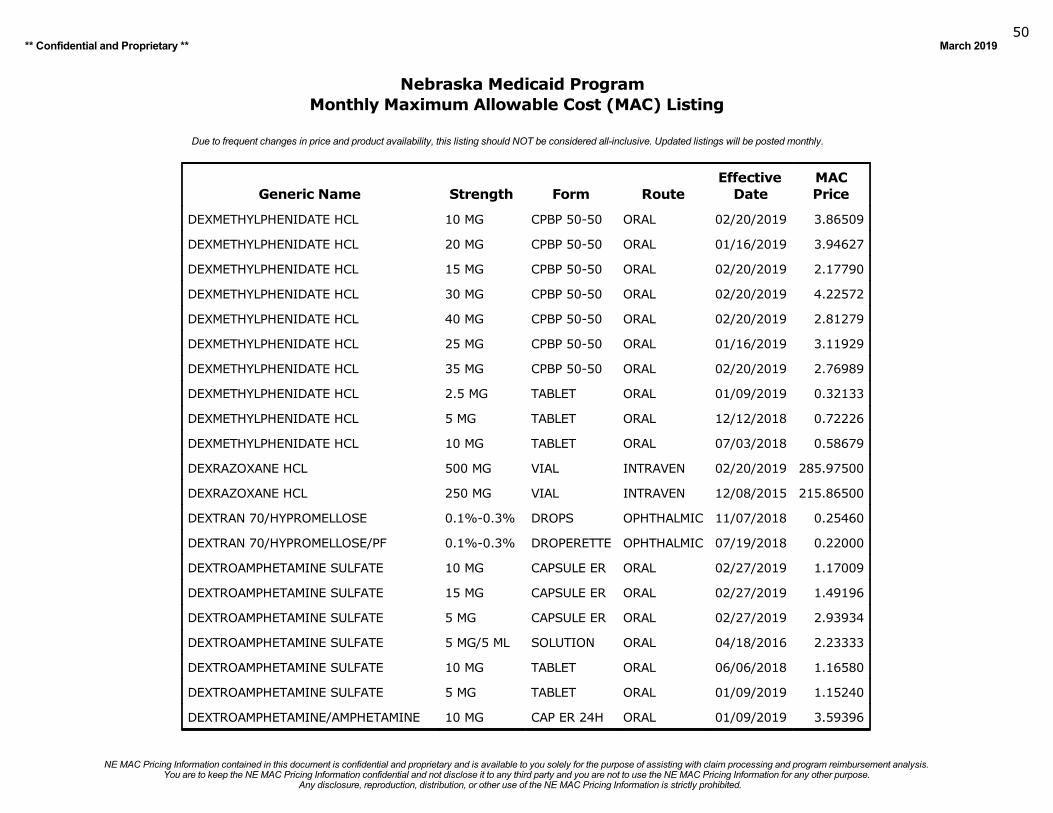
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201950
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DEXMETHYLPHENIDATE HCL 10 MG CPBP 50-50 ORAL 02/20/2019 3.86509
DEXMETHYLPHENIDATE HCL 20 MG CPBP 50-50 ORAL 01/16/2019 3.94627
DEXMETHYLPHENIDATE HCL 15 MG CPBP 50-50 ORAL 02/20/2019 2.17790
DEXMETHYLPHENIDATE HCL 30 MG CPBP 50-50 ORAL 02/20/2019 4.22572
DEXMETHYLPHENIDATE HCL 40 MG CPBP 50-50 ORAL 02/20/2019 2.81279
DEXMETHYLPHENIDATE HCL 25 MG CPBP 50-50 ORAL 01/16/2019 3.11929
DEXMETHYLPHENIDATE HCL 35 MG CPBP 50-50 ORAL 02/20/2019 2.76989
DEXMETHYLPHENIDATE HCL 2.5 MG TABLET ORAL 01/09/2019 0.32133
DEXMETHYLPHENIDATE HCL 5 MG TABLET ORAL 12/12/2018 0.72226
DEXMETHYLPHENIDATE HCL 10 MG TABLET ORAL 07/03/2018 0.58679
DEXRAZOXANE HCL 500 MG VIAL INTRAVEN 02/20/2019 285.97500
DEXRAZOXANE HCL 250 MG VIAL INTRAVEN 12/08/2015 215.86500
DEXTRAN 70/HYPROMELLOSE 0.1%-0.3% DROPS OPHTHALMIC 11/07/2018 0.25460
DEXTRAN 70/HYPROMELLOSE/PF 0.1%-0.3% DROPERETTE OPHTHALMIC 07/19/2018 0.22000
DEXTROAMPHETAMINE SULFATE 10 MG CAPSULE ER ORAL 02/27/2019 1.17009
DEXTROAMPHETAMINE SULFATE 15 MG CAPSULE ER ORAL 02/27/2019 1.49196
DEXTROAMPHETAMINE SULFATE 5 MG CAPSULE ER ORAL 02/27/2019 2.93934
DEXTROAMPHETAMINE SULFATE 5 MG/5 ML SOLUTION ORAL 04/18/2016 2.23333
DEXTROAMPHETAMINE SULFATE 10 MG TABLET ORAL 06/06/2018 1.16580
DEXTROAMPHETAMINE SULFATE 5 MG TABLET ORAL 01/09/2019 1.15240
DEXTROAMPHETAMINE/AMPHETAMINE 10 MG CAP ER 24H ORAL 01/09/2019 3.59396
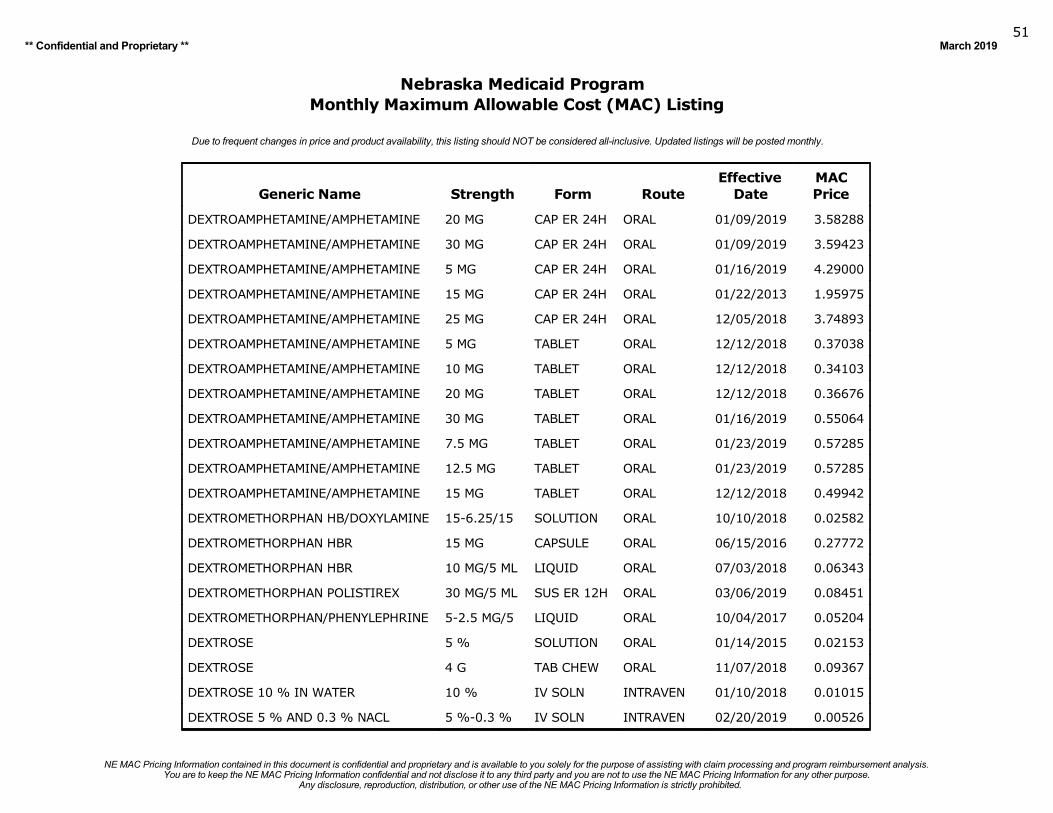
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201951
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DEXTROAMPHETAMINE/AMPHETAMINE 20 MG CAP ER 24H ORAL 01/09/2019 3.58288
DEXTROAMPHETAMINE/AMPHETAMINE 30 MG CAP ER 24H ORAL 01/09/2019 3.59423
DEXTROAMPHETAMINE/AMPHETAMINE 5 MG CAP ER 24H ORAL 01/16/2019 4.29000
DEXTROAMPHETAMINE/AMPHETAMINE 15 MG CAP ER 24H ORAL 01/22/2013 1.95975
DEXTROAMPHETAMINE/AMPHETAMINE 25 MG CAP ER 24H ORAL 12/05/2018 3.74893
DEXTROAMPHETAMINE/AMPHETAMINE 5 MG TABLET ORAL 12/12/2018 0.37038
DEXTROAMPHETAMINE/AMPHETAMINE 10 MG TABLET ORAL 12/12/2018 0.34103
DEXTROAMPHETAMINE/AMPHETAMINE 20 MG TABLET ORAL 12/12/2018 0.36676
DEXTROAMPHETAMINE/AMPHETAMINE 30 MG TABLET ORAL 01/16/2019 0.55064
DEXTROAMPHETAMINE/AMPHETAMINE 7.5 MG TABLET ORAL 01/23/2019 0.57285
DEXTROAMPHETAMINE/AMPHETAMINE 12.5 MG TABLET ORAL 01/23/2019 0.57285
DEXTROAMPHETAMINE/AMPHETAMINE 15 MG TABLET ORAL 12/12/2018 0.49942
DEXTROMETHORPHAN HB/DOXYLAMINE 15-6.25/15 SOLUTION ORAL 10/10/2018 0.02582
DEXTROMETHORPHAN HBR 15 MG CAPSULE ORAL 06/15/2016 0.27772
DEXTROMETHORPHAN HBR 10 MG/5 ML LIQUID ORAL 07/03/2018 0.06343
DEXTROMETHORPHAN POLISTIREX 30 MG/5 ML SUS ER 12H ORAL 03/06/2019 0.08451
DEXTROMETHORPHAN/PHENYLEPHRINE 5-2.5 MG/5 LIQUID ORAL 10/04/2017 0.05204
DEXTROSE 5 % SOLUTION ORAL 01/14/2015 0.02153
DEXTROSE 4 G TAB CHEW ORAL 11/07/2018 0.09367
DEXTROSE 10 % IN WATER 10 % IV SOLN INTRAVEN 01/10/2018 0.01015
DEXTROSE 5 % AND 0.3 % NACL 5 %-0.3 % IV SOLN INTRAVEN 02/20/2019 0.00526
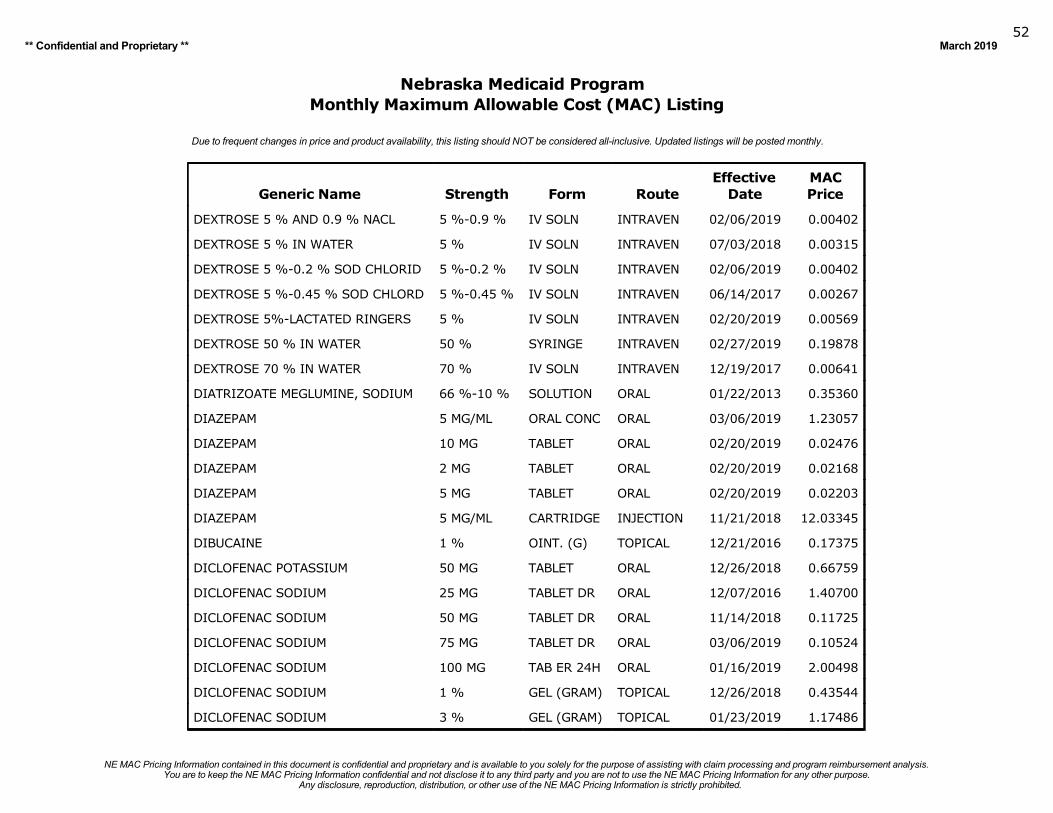
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201952
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DEXTROSE 5 % AND 0.9 % NACL 5 %-0.9 % IV SOLN INTRAVEN 02/06/2019 0.00402
DEXTROSE 5 % IN WATER 5 % IV SOLN INTRAVEN 07/03/2018 0.00315
DEXTROSE 5 %-0.2 % SOD CHLORID 5 %-0.2 % IV SOLN INTRAVEN 02/06/2019 0.00402
DEXTROSE 5 %-0.45 % SOD CHLORD 5 %-0.45 % IV SOLN INTRAVEN 06/14/2017 0.00267
DEXTROSE 5%-LACTATED RINGERS 5 % IV SOLN INTRAVEN 02/20/2019 0.00569
DEXTROSE 50 % IN WATER 50 % SYRINGE INTRAVEN 02/27/2019 0.19878
DEXTROSE 70 % IN WATER 70 % IV SOLN INTRAVEN 12/19/2017 0.00641
DIATRIZOATE MEGLUMINE, SODIUM 66 %-10 % SOLUTION ORAL 01/22/2013 0.35360
DIAZEPAM 5 MG/ML ORAL CONC ORAL 03/06/2019 1.23057
DIAZEPAM 10 MG TABLET ORAL 02/20/2019 0.02476
DIAZEPAM 2 MG TABLET ORAL 02/20/2019 0.02168
DIAZEPAM 5 MG TABLET ORAL 02/20/2019 0.02203
DIAZEPAM 5 MG/ML CARTRIDGE INJECTION 11/21/2018 12.03345
DIBUCAINE 1 % OINT. (G) TOPICAL 12/21/2016 0.17375
DICLOFENAC POTASSIUM 50 MG TABLET ORAL 12/26/2018 0.66759
DICLOFENAC SODIUM 25 MG TABLET DR ORAL 12/07/2016 1.40700
DICLOFENAC SODIUM 50 MG TABLET DR ORAL 11/14/2018 0.11725
DICLOFENAC SODIUM 75 MG TABLET DR ORAL 03/06/2019 0.10524
DICLOFENAC SODIUM 100 MG TAB ER 24H ORAL 01/16/2019 2.00498
DICLOFENAC SODIUM 1 % GEL (GRAM) TOPICAL 12/26/2018 0.43544
DICLOFENAC SODIUM 3 % GEL (GRAM) TOPICAL 01/23/2019 1.17486
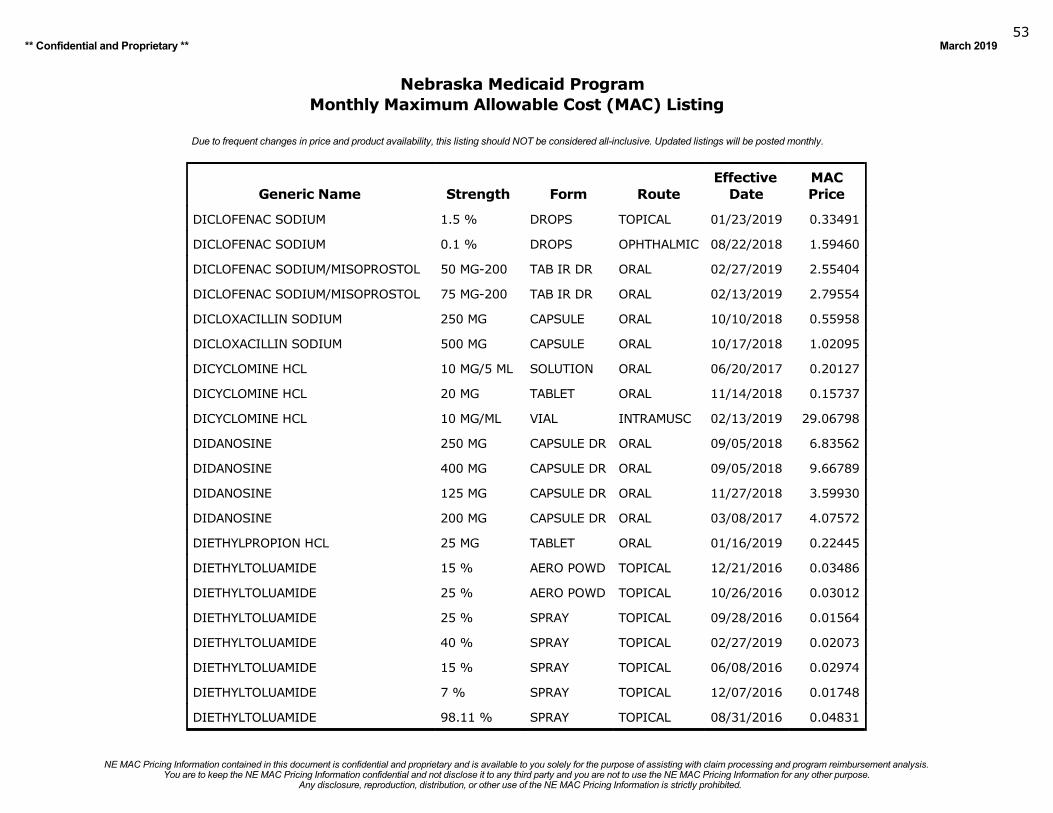
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201953
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DICLOFENAC SODIUM 1.5 % DROPS TOPICAL 01/23/2019 0.33491
DICLOFENAC SODIUM 0.1 % DROPS OPHTHALMIC 08/22/2018 1.59460
DICLOFENAC SODIUM/MISOPROSTOL 50 MG-200 TAB IR DR ORAL 02/27/2019 2.55404
DICLOFENAC SODIUM/MISOPROSTOL 75 MG-200 TAB IR DR ORAL 02/13/2019 2.79554
DICLOXACILLIN SODIUM 250 MG CAPSULE ORAL 10/10/2018 0.55958
DICLOXACILLIN SODIUM 500 MG CAPSULE ORAL 10/17/2018 1.02095
DICYCLOMINE HCL 10 MG/5 ML SOLUTION ORAL 06/20/2017 0.20127
DICYCLOMINE HCL 20 MG TABLET ORAL 11/14/2018 0.15737
DICYCLOMINE HCL 10 MG/ML VIAL INTRAMUSC 02/13/2019 29.06798
DIDANOSINE 250 MG CAPSULE DR ORAL 09/05/2018 6.83562
DIDANOSINE 400 MG CAPSULE DR ORAL 09/05/2018 9.66789
DIDANOSINE 125 MG CAPSULE DR ORAL 11/27/2018 3.59930
DIDANOSINE 200 MG CAPSULE DR ORAL 03/08/2017 4.07572
DIETHYLPROPION HCL 25 MG TABLET ORAL 01/16/2019 0.22445
DIETHYLTOLUAMIDE 15 % AERO POWD TOPICAL 12/21/2016 0.03486
DIETHYLTOLUAMIDE 25 % AERO POWD TOPICAL 10/26/2016 0.03012
DIETHYLTOLUAMIDE 25 % SPRAY TOPICAL 09/28/2016 0.01564
DIETHYLTOLUAMIDE 40 % SPRAY TOPICAL 02/27/2019 0.02073
DIETHYLTOLUAMIDE 15 % SPRAY TOPICAL 06/08/2016 0.02974
DIETHYLTOLUAMIDE 7 % SPRAY TOPICAL 12/07/2016 0.01748
DIETHYLTOLUAMIDE 98.11 % SPRAY TOPICAL 08/31/2016 0.04831
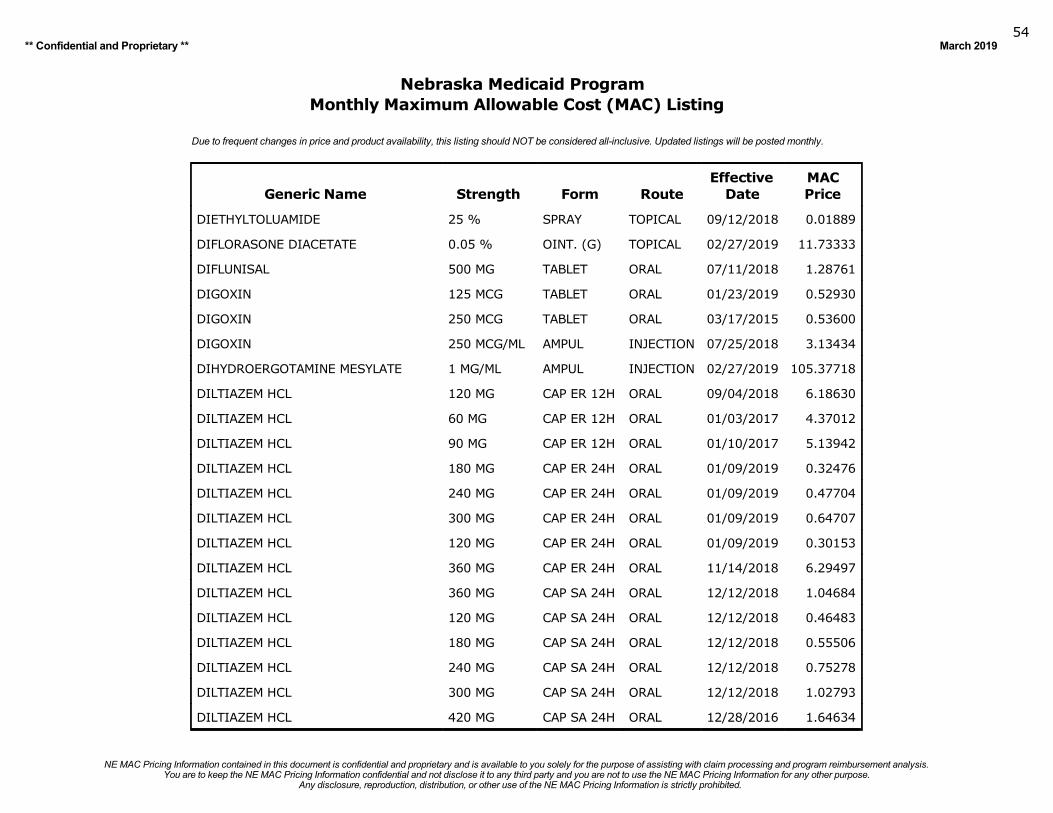
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201954
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DIETHYLTOLUAMIDE 25 % SPRAY TOPICAL 09/12/2018 0.01889
DIFLORASONE DIACETATE 0.05 % OINT. (G) TOPICAL 02/27/2019 11.73333
DIFLUNISAL 500 MG TABLET ORAL 07/11/2018 1.28761
DIGOXIN 125 MCG TABLET ORAL 01/23/2019 0.52930
DIGOXIN 250 MCG TABLET ORAL 03/17/2015 0.53600
DIGOXIN 250 MCG/ML AMPUL INJECTION 07/25/2018 3.13434
DIHYDROERGOTAMINE MESYLATE 1 MG/ML AMPUL INJECTION 02/27/2019 105.37718
DILTIAZEM HCL 120 MG CAP ER 12H ORAL 09/04/2018 6.18630
DILTIAZEM HCL 60 MG CAP ER 12H ORAL 01/03/2017 4.37012
DILTIAZEM HCL 90 MG CAP ER 12H ORAL 01/10/2017 5.13942
DILTIAZEM HCL 180 MG CAP ER 24H ORAL 01/09/2019 0.32476
DILTIAZEM HCL 240 MG CAP ER 24H ORAL 01/09/2019 0.47704
DILTIAZEM HCL 300 MG CAP ER 24H ORAL 01/09/2019 0.64707
DILTIAZEM HCL 120 MG CAP ER 24H ORAL 01/09/2019 0.30153
DILTIAZEM HCL 360 MG CAP ER 24H ORAL 11/14/2018 6.29497
DILTIAZEM HCL 360 MG CAP SA 24H ORAL 12/12/2018 1.04684
DILTIAZEM HCL 120 MG CAP SA 24H ORAL 12/12/2018 0.46483
DILTIAZEM HCL 180 MG CAP SA 24H ORAL 12/12/2018 0.55506
DILTIAZEM HCL 240 MG CAP SA 24H ORAL 12/12/2018 0.75278
DILTIAZEM HCL 300 MG CAP SA 24H ORAL 12/12/2018 1.02793
DILTIAZEM HCL 420 MG CAP SA 24H ORAL 12/28/2016 1.64634
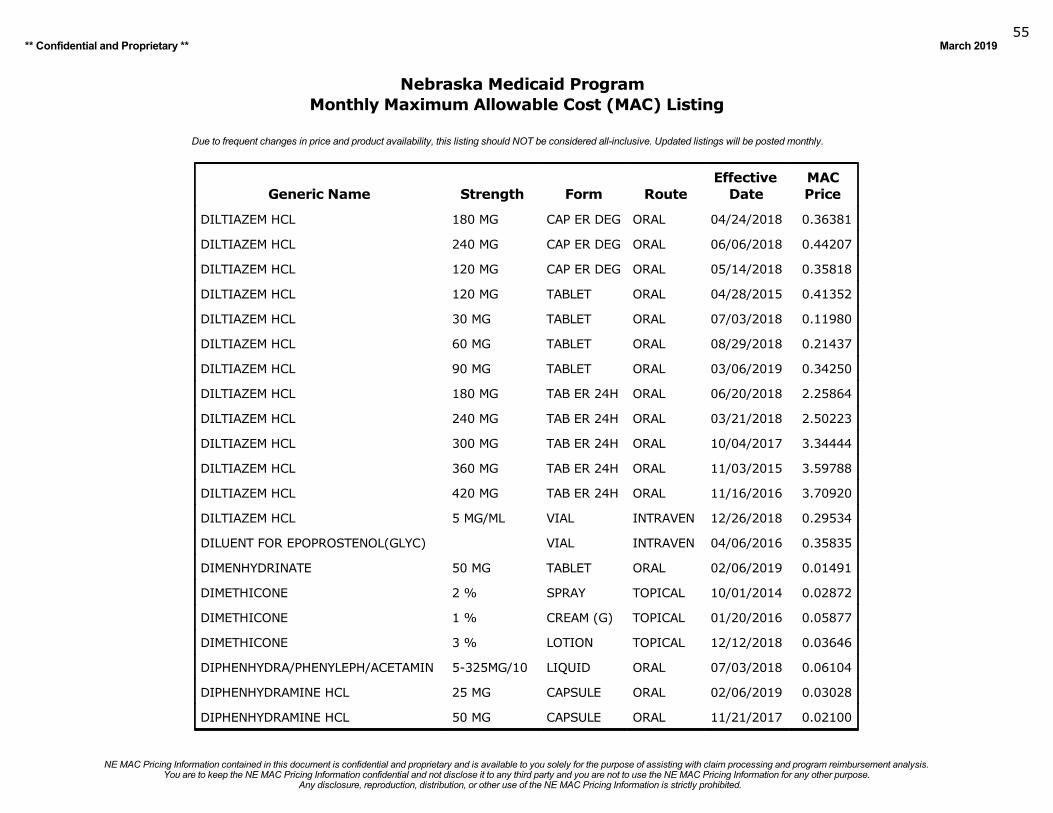
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201955
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DILTIAZEM HCL 180 MG CAP ER DEG ORAL 04/24/2018 0.36381
DILTIAZEM HCL 240 MG CAP ER DEG ORAL 06/06/2018 0.44207
DILTIAZEM HCL 120 MG CAP ER DEG ORAL 05/14/2018 0.35818
DILTIAZEM HCL 120 MG TABLET ORAL 04/28/2015 0.41352
DILTIAZEM HCL 30 MG TABLET ORAL 07/03/2018 0.11980
DILTIAZEM HCL 60 MG TABLET ORAL 08/29/2018 0.21437
DILTIAZEM HCL 90 MG TABLET ORAL 03/06/2019 0.34250
DILTIAZEM HCL 180 MG TAB ER 24H ORAL 06/20/2018 2.25864
DILTIAZEM HCL 240 MG TAB ER 24H ORAL 03/21/2018 2.50223
DILTIAZEM HCL 300 MG TAB ER 24H ORAL 10/04/2017 3.34444
DILTIAZEM HCL 360 MG TAB ER 24H ORAL 11/03/2015 3.59788
DILTIAZEM HCL 420 MG TAB ER 24H ORAL 11/16/2016 3.70920
DILTIAZEM HCL 5 MG/ML VIAL INTRAVEN 12/26/2018 0.29534
DILUENT FOR EPOPROSTENOL(GLYC) VIAL INTRAVEN 04/06/2016 0.35835
DIMENHYDRINATE 50 MG TABLET ORAL 02/06/2019 0.01491
DIMETHICONE 2 % SPRAY TOPICAL 10/01/2014 0.02872
DIMETHICONE 1 % CREAM (G) TOPICAL 01/20/2016 0.05877
DIMETHICONE 3 % LOTION TOPICAL 12/12/2018 0.03646
DIPHENHYDRA/PHENYLEPH/ACETAMIN 5-325MG/10 LIQUID ORAL 07/03/2018 0.06104
DIPHENHYDRAMINE HCL 25 MG CAPSULE ORAL 02/06/2019 0.03028
DIPHENHYDRAMINE HCL 50 MG CAPSULE ORAL 11/21/2017 0.02100
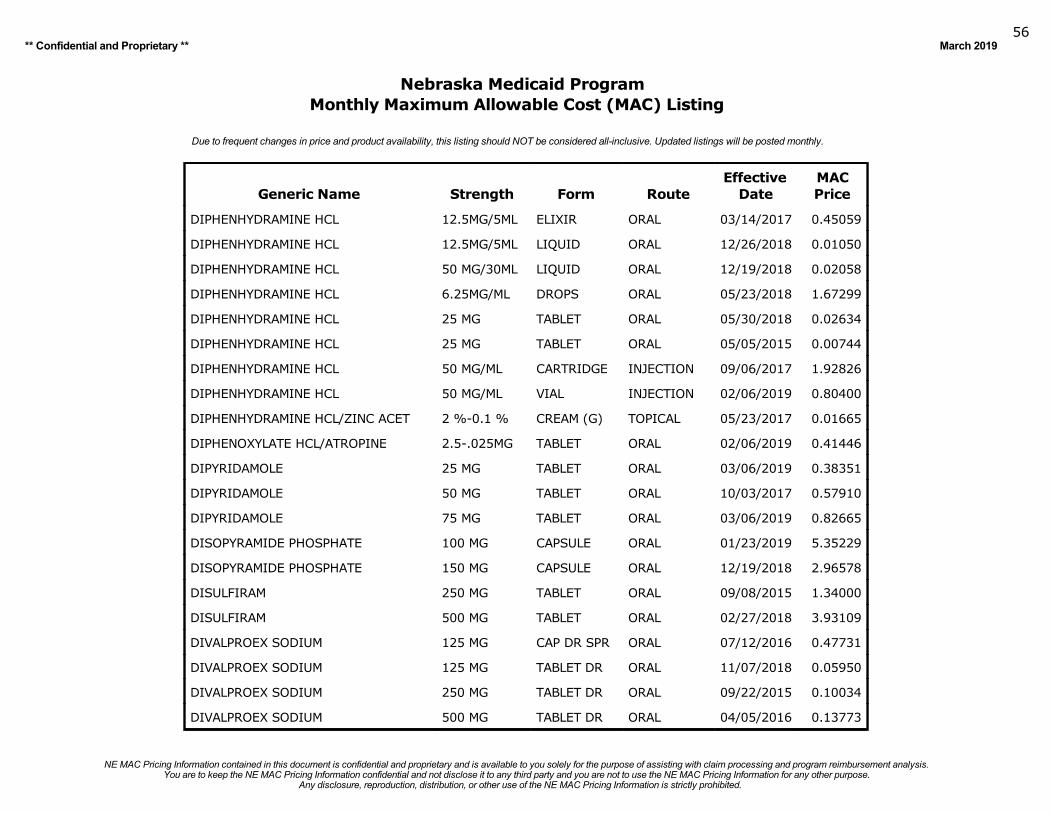
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201956
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DIPHENHYDRAMINE HCL 12.5MG/5ML ELIXIR ORAL 03/14/2017 0.45059
DIPHENHYDRAMINE HCL 12.5MG/5ML LIQUID ORAL 12/26/2018 0.01050
DIPHENHYDRAMINE HCL 50 MG/30ML LIQUID ORAL 12/19/2018 0.02058
DIPHENHYDRAMINE HCL 6.25MG/ML DROPS ORAL 05/23/2018 1.67299
DIPHENHYDRAMINE HCL 25 MG TABLET ORAL 05/30/2018 0.02634
DIPHENHYDRAMINE HCL 25 MG TABLET ORAL 05/05/2015 0.00744
DIPHENHYDRAMINE HCL 50 MG/ML CARTRIDGE INJECTION 09/06/2017 1.92826
DIPHENHYDRAMINE HCL 50 MG/ML VIAL INJECTION 02/06/2019 0.80400
DIPHENHYDRAMINE HCL/ZINC ACET 2 %-0.1 % CREAM (G) TOPICAL 05/23/2017 0.01665
DIPHENOXYLATE HCL/ATROPINE 2.5-.025MG TABLET ORAL 02/06/2019 0.41446
DIPYRIDAMOLE 25 MG TABLET ORAL 03/06/2019 0.38351
DIPYRIDAMOLE 50 MG TABLET ORAL 10/03/2017 0.57910
DIPYRIDAMOLE 75 MG TABLET ORAL 03/06/2019 0.82665
DISOPYRAMIDE PHOSPHATE 100 MG CAPSULE ORAL 01/23/2019 5.35229
DISOPYRAMIDE PHOSPHATE 150 MG CAPSULE ORAL 12/19/2018 2.96578
DISULFIRAM 250 MG TABLET ORAL 09/08/2015 1.34000
DISULFIRAM 500 MG TABLET ORAL 02/27/2018 3.93109
DIVALPROEX SODIUM 125 MG CAP DR SPR ORAL 07/12/2016 0.47731
DIVALPROEX SODIUM 125 MG TABLET DR ORAL 11/07/2018 0.05950
DIVALPROEX SODIUM 250 MG TABLET DR ORAL 09/22/2015 0.10034
DIVALPROEX SODIUM 500 MG TABLET DR ORAL 04/05/2016 0.13773
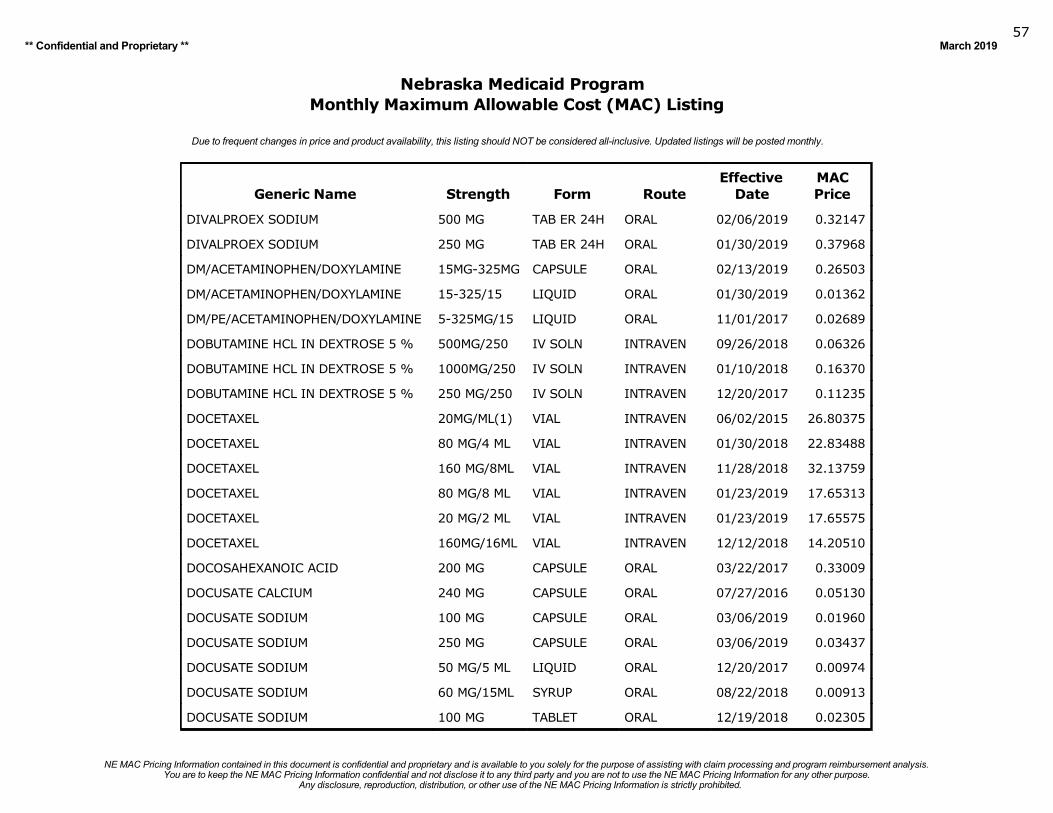
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201957
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DIVALPROEX SODIUM 500 MG TAB ER 24H ORAL 02/06/2019 0.32147
DIVALPROEX SODIUM 250 MG TAB ER 24H ORAL 01/30/2019 0.37968
DM/ACETAMINOPHEN/DOXYLAMINE 15MG-325MG CAPSULE ORAL 02/13/2019 0.26503
DM/ACETAMINOPHEN/DOXYLAMINE 15-325/15 LIQUID ORAL 01/30/2019 0.01362
DM/PE/ACETAMINOPHEN/DOXYLAMINE 5-325MG/15 LIQUID ORAL 11/01/2017 0.02689
DOBUTAMINE HCL IN DEXTROSE 5 % 500MG/250 IV SOLN INTRAVEN 09/26/2018 0.06326
DOBUTAMINE HCL IN DEXTROSE 5 % 1000MG/250 IV SOLN INTRAVEN 01/10/2018 0.16370
DOBUTAMINE HCL IN DEXTROSE 5 % 250 MG/250 IV SOLN INTRAVEN 12/20/2017 0.11235
DOCETAXEL 20MG/ML(1) VIAL INTRAVEN 06/02/2015 26.80375
DOCETAXEL 80 MG/4 ML VIAL INTRAVEN 01/30/2018 22.83488
DOCETAXEL 160 MG/8ML VIAL INTRAVEN 11/28/2018 32.13759
DOCETAXEL 80 MG/8 ML VIAL INTRAVEN 01/23/2019 17.65313
DOCETAXEL 20 MG/2 ML VIAL INTRAVEN 01/23/2019 17.65575
DOCETAXEL 160MG/16ML VIAL INTRAVEN 12/12/2018 14.20510
DOCOSAHEXANOIC ACID 200 MG CAPSULE ORAL 03/22/2017 0.33009
DOCUSATE CALCIUM 240 MG CAPSULE ORAL 07/27/2016 0.05130
DOCUSATE SODIUM 100 MG CAPSULE ORAL 03/06/2019 0.01960
DOCUSATE SODIUM 250 MG CAPSULE ORAL 03/06/2019 0.03437
DOCUSATE SODIUM 50 MG/5 ML LIQUID ORAL 12/20/2017 0.00974
DOCUSATE SODIUM 60 MG/15ML SYRUP ORAL 08/22/2018 0.00913
DOCUSATE SODIUM 100 MG TABLET ORAL 12/19/2018 0.02305
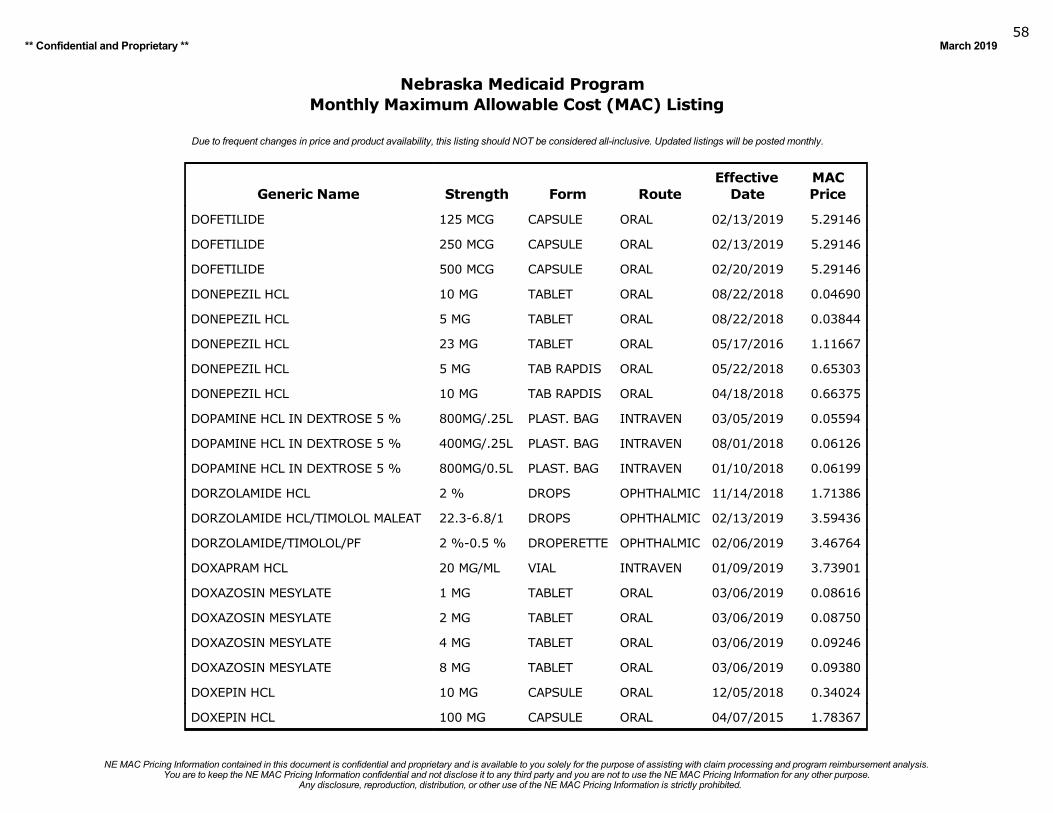
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201958
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DOFETILIDE 125 MCG CAPSULE ORAL 02/13/2019 5.29146
DOFETILIDE 250 MCG CAPSULE ORAL 02/13/2019 5.29146
DOFETILIDE 500 MCG CAPSULE ORAL 02/20/2019 5.29146
DONEPEZIL HCL 10 MG TABLET ORAL 08/22/2018 0.04690
DONEPEZIL HCL 5 MG TABLET ORAL 08/22/2018 0.03844
DONEPEZIL HCL 23 MG TABLET ORAL 05/17/2016 1.11667
DONEPEZIL HCL 5 MG TAB RAPDIS ORAL 05/22/2018 0.65303
DONEPEZIL HCL 10 MG TAB RAPDIS ORAL 04/18/2018 0.66375
DOPAMINE HCL IN DEXTROSE 5 % 800MG/.25L PLAST. BAG INTRAVEN 03/05/2019 0.05594
DOPAMINE HCL IN DEXTROSE 5 % 400MG/.25L PLAST. BAG INTRAVEN 08/01/2018 0.06126
DOPAMINE HCL IN DEXTROSE 5 % 800MG/0.5L PLAST. BAG INTRAVEN 01/10/2018 0.06199
DORZOLAMIDE HCL 2 % DROPS OPHTHALMIC 11/14/2018 1.71386
DORZOLAMIDE HCL/TIMOLOL MALEAT 22.3-6.8/1 DROPS OPHTHALMIC 02/13/2019 3.59436
DORZOLAMIDE/TIMOLOL/PF 2 %-0.5 % DROPERETTE OPHTHALMIC 02/06/2019 3.46764
DOXAPRAM HCL 20 MG/ML VIAL INTRAVEN 01/09/2019 3.73901
DOXAZOSIN MESYLATE 1 MG TABLET ORAL 03/06/2019 0.08616
DOXAZOSIN MESYLATE 2 MG TABLET ORAL 03/06/2019 0.08750
DOXAZOSIN MESYLATE 4 MG TABLET ORAL 03/06/2019 0.09246
DOXAZOSIN MESYLATE 8 MG TABLET ORAL 03/06/2019 0.09380
DOXEPIN HCL 10 MG CAPSULE ORAL 12/05/2018 0.34024
DOXEPIN HCL 100 MG CAPSULE ORAL 04/07/2015 1.78367
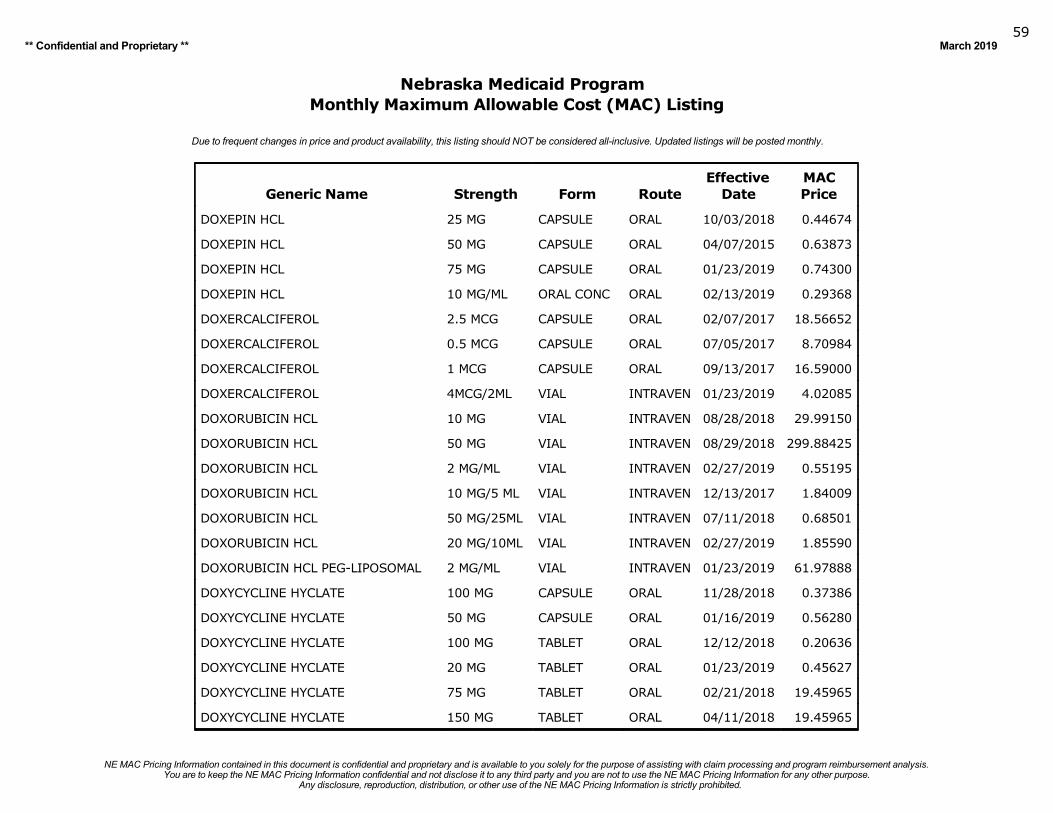
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201959
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DOXEPIN HCL 25 MG CAPSULE ORAL 10/03/2018 0.44674
DOXEPIN HCL 50 MG CAPSULE ORAL 04/07/2015 0.63873
DOXEPIN HCL 75 MG CAPSULE ORAL 01/23/2019 0.74300
DOXEPIN HCL 10 MG/ML ORAL CONC ORAL 02/13/2019 0.29368
DOXERCALCIFEROL 2.5 MCG CAPSULE ORAL 02/07/2017 18.56652
DOXERCALCIFEROL 0.5 MCG CAPSULE ORAL 07/05/2017 8.70984
DOXERCALCIFEROL 1 MCG CAPSULE ORAL 09/13/2017 16.59000
DOXERCALCIFEROL 4MCG/2ML VIAL INTRAVEN 01/23/2019 4.02085
DOXORUBICIN HCL 10 MG VIAL INTRAVEN 08/28/2018 29.99150
DOXORUBICIN HCL 50 MG VIAL INTRAVEN 08/29/2018 299.88425
DOXORUBICIN HCL 2 MG/ML VIAL INTRAVEN 02/27/2019 0.55195
DOXORUBICIN HCL 10 MG/5 ML VIAL INTRAVEN 12/13/2017 1.84009
DOXORUBICIN HCL 50 MG/25ML VIAL INTRAVEN 07/11/2018 0.68501
DOXORUBICIN HCL 20 MG/10ML VIAL INTRAVEN 02/27/2019 1.85590
DOXORUBICIN HCL PEG-LIPOSOMAL 2 MG/ML VIAL INTRAVEN 01/23/2019 61.97888
DOXYCYCLINE HYCLATE 100 MG CAPSULE ORAL 11/28/2018 0.37386
DOXYCYCLINE HYCLATE 50 MG CAPSULE ORAL 01/16/2019 0.56280
DOXYCYCLINE HYCLATE 100 MG TABLET ORAL 12/12/2018 0.20636
DOXYCYCLINE HYCLATE 20 MG TABLET ORAL 01/23/2019 0.45627
DOXYCYCLINE HYCLATE 75 MG TABLET ORAL 02/21/2018 19.45965
DOXYCYCLINE HYCLATE 150 MG TABLET ORAL 04/11/2018 19.45965
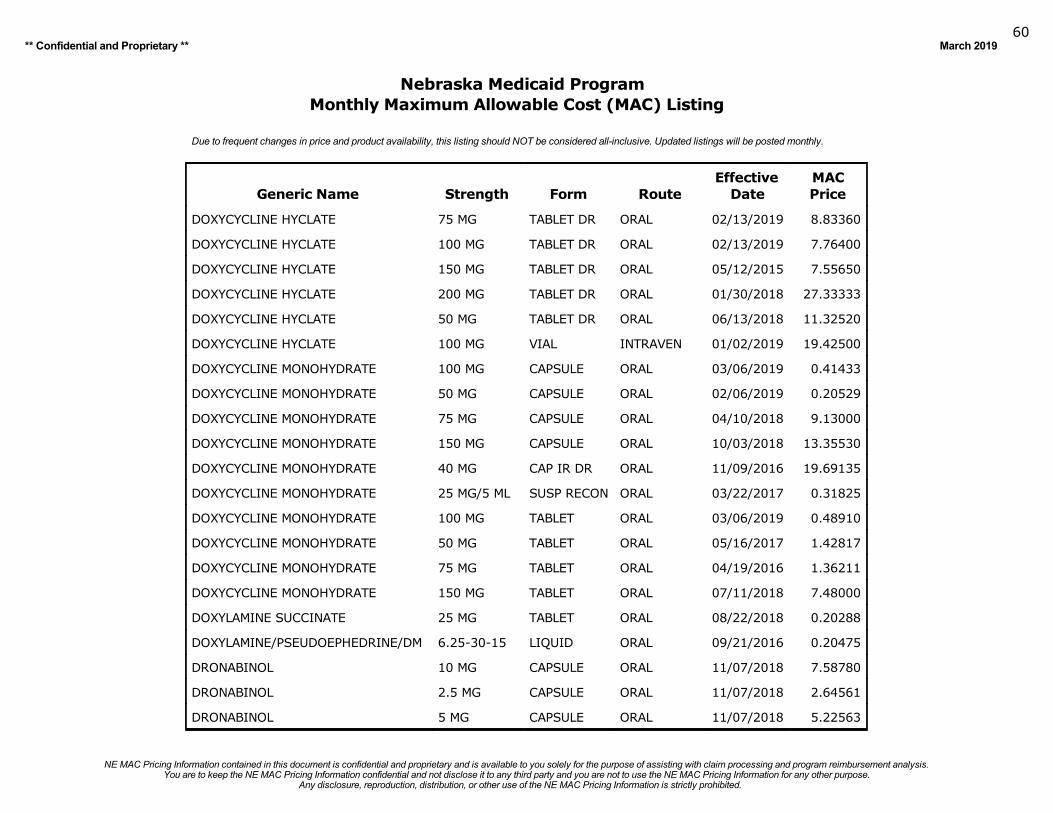
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201960
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DOXYCYCLINE HYCLATE 75 MG TABLET DR ORAL 02/13/2019 8.83360
DOXYCYCLINE HYCLATE 100 MG TABLET DR ORAL 02/13/2019 7.76400
DOXYCYCLINE HYCLATE 150 MG TABLET DR ORAL 05/12/2015 7.55650
DOXYCYCLINE HYCLATE 200 MG TABLET DR ORAL 01/30/2018 27.33333
DOXYCYCLINE HYCLATE 50 MG TABLET DR ORAL 06/13/2018 11.32520
DOXYCYCLINE HYCLATE 100 MG VIAL INTRAVEN 01/02/2019 19.42500
DOXYCYCLINE MONOHYDRATE 100 MG CAPSULE ORAL 03/06/2019 0.41433
DOXYCYCLINE MONOHYDRATE 50 MG CAPSULE ORAL 02/06/2019 0.20529
DOXYCYCLINE MONOHYDRATE 75 MG CAPSULE ORAL 04/10/2018 9.13000
DOXYCYCLINE MONOHYDRATE 150 MG CAPSULE ORAL 10/03/2018 13.35530
DOXYCYCLINE MONOHYDRATE 40 MG CAP IR DR ORAL 11/09/2016 19.69135
DOXYCYCLINE MONOHYDRATE 25 MG/5 ML SUSP RECON ORAL 03/22/2017 0.31825
DOXYCYCLINE MONOHYDRATE 100 MG TABLET ORAL 03/06/2019 0.48910
DOXYCYCLINE MONOHYDRATE 50 MG TABLET ORAL 05/16/2017 1.42817
DOXYCYCLINE MONOHYDRATE 75 MG TABLET ORAL 04/19/2016 1.36211
DOXYCYCLINE MONOHYDRATE 150 MG TABLET ORAL 07/11/2018 7.48000
DOXYLAMINE SUCCINATE 25 MG TABLET ORAL 08/22/2018 0.20288
DOXYLAMINE/PSEUDOEPHEDRINE/DM 6.25-30-15 LIQUID ORAL 09/21/2016 0.20475
DRONABINOL 10 MG CAPSULE ORAL 11/07/2018 7.58780
DRONABINOL 2.5 MG CAPSULE ORAL 11/07/2018 2.64561
DRONABINOL 5 MG CAPSULE ORAL 11/07/2018 5.22563
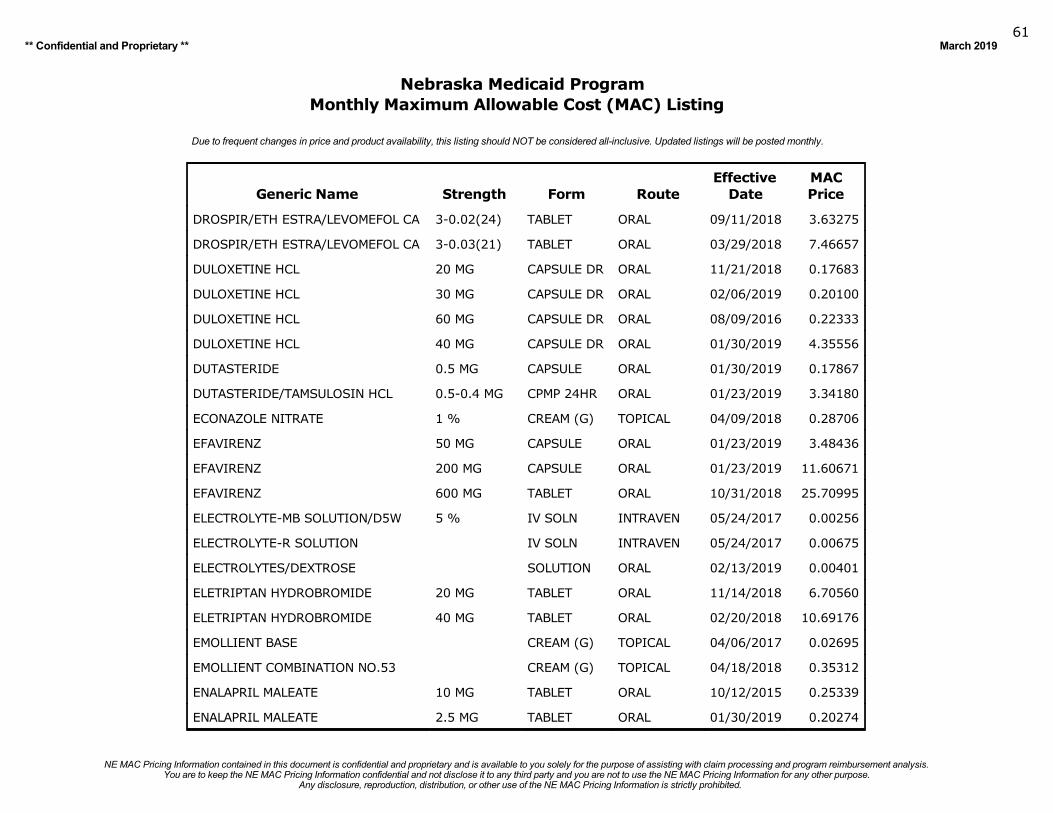
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201961
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
DROSPIR/ETH ESTRA/LEVOMEFOL CA 3-0.02(24) TABLET ORAL 09/11/2018 3.63275
DROSPIR/ETH ESTRA/LEVOMEFOL CA 3-0.03(21) TABLET ORAL 03/29/2018 7.46657
DULOXETINE HCL 20 MG CAPSULE DR ORAL 11/21/2018 0.17683
DULOXETINE HCL 30 MG CAPSULE DR ORAL 02/06/2019 0.20100
DULOXETINE HCL 60 MG CAPSULE DR ORAL 08/09/2016 0.22333
DULOXETINE HCL 40 MG CAPSULE DR ORAL 01/30/2019 4.35556
DUTASTERIDE 0.5 MG CAPSULE ORAL 01/30/2019 0.17867
DUTASTERIDE/TAMSULOSIN HCL 0.5-0.4 MG CPMP 24HR ORAL 01/23/2019 3.34180
ECONAZOLE NITRATE 1 % CREAM (G) TOPICAL 04/09/2018 0.28706
EFAVIRENZ 50 MG CAPSULE ORAL 01/23/2019 3.48436
EFAVIRENZ 200 MG CAPSULE ORAL 01/23/2019 11.60671
EFAVIRENZ 600 MG TABLET ORAL 10/31/2018 25.70995
ELECTROLYTE-MB SOLUTION/D5W 5 % IV SOLN INTRAVEN 05/24/2017 0.00256
ELECTROLYTE-R SOLUTION IV SOLN INTRAVEN 05/24/2017 0.00675
ELECTROLYTES/DEXTROSE SOLUTION ORAL 02/13/2019 0.00401
ELETRIPTAN HYDROBROMIDE 20 MG TABLET ORAL 11/14/2018 6.70560
ELETRIPTAN HYDROBROMIDE 40 MG TABLET ORAL 02/20/2018 10.69176
EMOLLIENT BASE CREAM (G) TOPICAL 04/06/2017 0.02695
EMOLLIENT COMBINATION NO.53 CREAM (G) TOPICAL 04/18/2018 0.35312
ENALAPRIL MALEATE 10 MG TABLET ORAL 10/12/2015 0.25339
ENALAPRIL MALEATE 2.5 MG TABLET ORAL 01/30/2019 0.20274
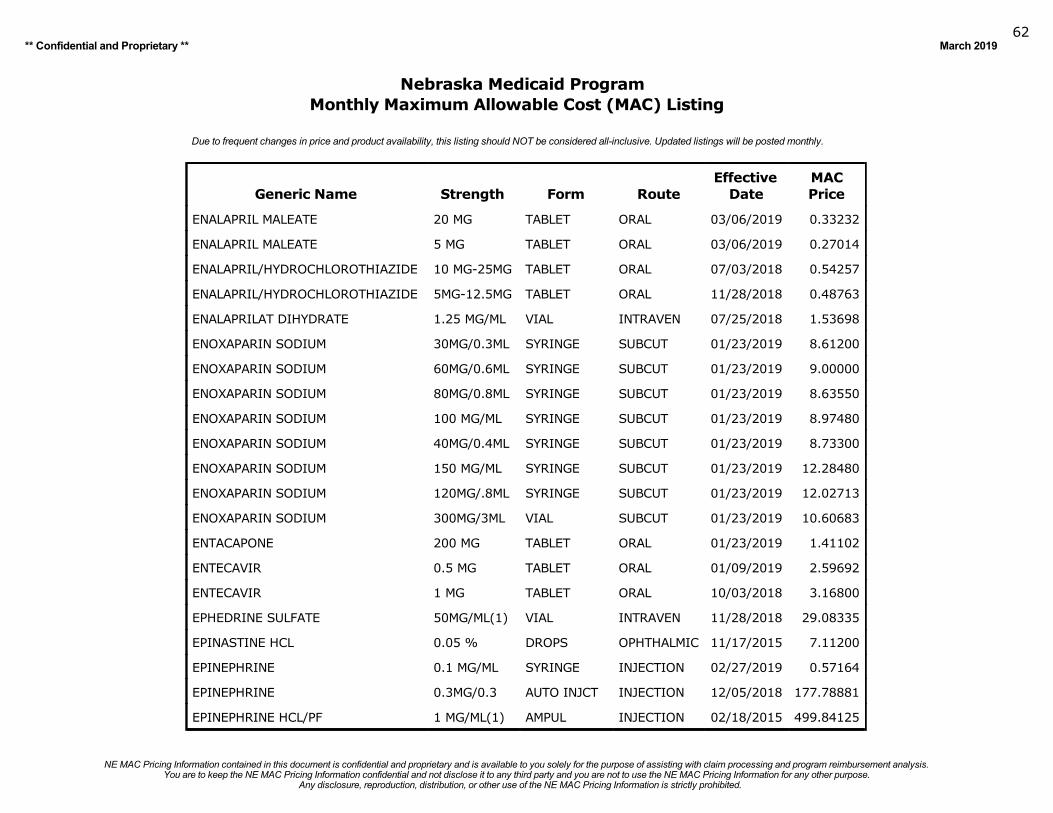
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201962
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ENALAPRIL MALEATE 20 MG TABLET ORAL 03/06/2019 0.33232
ENALAPRIL MALEATE 5 MG TABLET ORAL 03/06/2019 0.27014
ENALAPRIL/HYDROCHLOROTHIAZIDE 10 MG-25MG TABLET ORAL 07/03/2018 0.54257
ENALAPRIL/HYDROCHLOROTHIAZIDE 5MG-12.5MG TABLET ORAL 11/28/2018 0.48763
ENALAPRILAT DIHYDRATE 1.25 MG/ML VIAL INTRAVEN 07/25/2018 1.53698
ENOXAPARIN SODIUM 30MG/0.3ML SYRINGE SUBCUT 01/23/2019 8.61200
ENOXAPARIN SODIUM 60MG/0.6ML SYRINGE SUBCUT 01/23/2019 9.00000
ENOXAPARIN SODIUM 80MG/0.8ML SYRINGE SUBCUT 01/23/2019 8.63550
ENOXAPARIN SODIUM 100 MG/ML SYRINGE SUBCUT 01/23/2019 8.97480
ENOXAPARIN SODIUM 40MG/0.4ML SYRINGE SUBCUT 01/23/2019 8.73300
ENOXAPARIN SODIUM 150 MG/ML SYRINGE SUBCUT 01/23/2019 12.28480
ENOXAPARIN SODIUM 120MG/.8ML SYRINGE SUBCUT 01/23/2019 12.02713
ENOXAPARIN SODIUM 300MG/3ML VIAL SUBCUT 01/23/2019 10.60683
ENTACAPONE 200 MG TABLET ORAL 01/23/2019 1.41102
ENTECAVIR 0.5 MG TABLET ORAL 01/09/2019 2.59692
ENTECAVIR 1 MG TABLET ORAL 10/03/2018 3.16800
EPHEDRINE SULFATE 50MG/ML(1) VIAL INTRAVEN 11/28/2018 29.08335
EPINASTINE HCL 0.05 % DROPS OPHTHALMIC 11/17/2015 7.11200
EPINEPHRINE 0.1 MG/ML SYRINGE INJECTION 02/27/2019 0.57164
EPINEPHRINE 0.3MG/0.3 AUTO INJCT INJECTION 12/05/2018 177.78881
EPINEPHRINE HCL/PF 1 MG/ML(1) AMPUL INJECTION 02/18/2015 499.84125
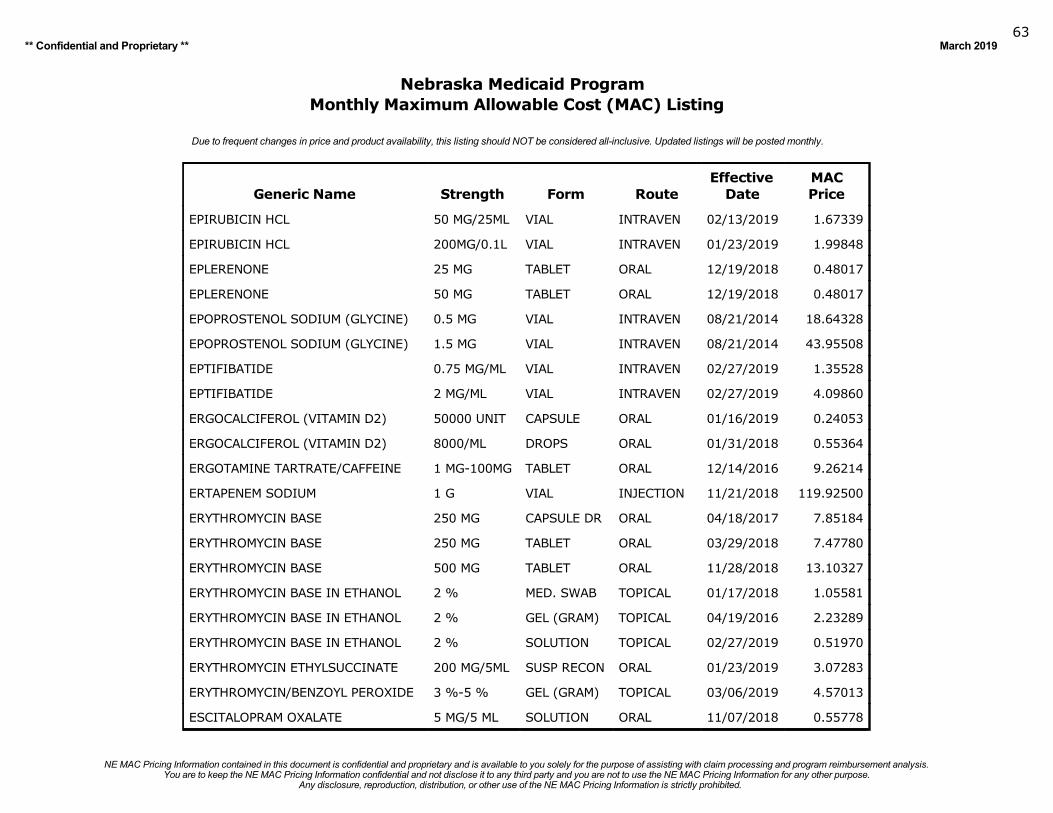
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201963
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
EPIRUBICIN HCL 50 MG/25ML VIAL INTRAVEN 02/13/2019 1.67339
EPIRUBICIN HCL 200MG/0.1L VIAL INTRAVEN 01/23/2019 1.99848
EPLERENONE 25 MG TABLET ORAL 12/19/2018 0.48017
EPLERENONE 50 MG TABLET ORAL 12/19/2018 0.48017
EPOPROSTENOL SODIUM (GLYCINE) 0.5 MG VIAL INTRAVEN 08/21/2014 18.64328
EPOPROSTENOL SODIUM (GLYCINE) 1.5 MG VIAL INTRAVEN 08/21/2014 43.95508
EPTIFIBATIDE 0.75 MG/ML VIAL INTRAVEN 02/27/2019 1.35528
EPTIFIBATIDE 2 MG/ML VIAL INTRAVEN 02/27/2019 4.09860
ERGOCALCIFEROL (VITAMIN D2) 50000 UNIT CAPSULE ORAL 01/16/2019 0.24053
ERGOCALCIFEROL (VITAMIN D2) 8000/ML DROPS ORAL 01/31/2018 0.55364
ERGOTAMINE TARTRATE/CAFFEINE 1 MG-100MG TABLET ORAL 12/14/2016 9.26214
ERTAPENEM SODIUM 1 G VIAL INJECTION 11/21/2018 119.92500
ERYTHROMYCIN BASE 250 MG CAPSULE DR ORAL 04/18/2017 7.85184
ERYTHROMYCIN BASE 250 MG TABLET ORAL 03/29/2018 7.47780
ERYTHROMYCIN BASE 500 MG TABLET ORAL 11/28/2018 13.10327
ERYTHROMYCIN BASE IN ETHANOL 2 % MED. SWAB TOPICAL 01/17/2018 1.05581
ERYTHROMYCIN BASE IN ETHANOL 2 % GEL (GRAM) TOPICAL 04/19/2016 2.23289
ERYTHROMYCIN BASE IN ETHANOL 2 % SOLUTION TOPICAL 02/27/2019 0.51970
ERYTHROMYCIN ETHYLSUCCINATE 200 MG/5ML SUSP RECON ORAL 01/23/2019 3.07283
ERYTHROMYCIN/BENZOYL PEROXIDE 3 %-5 % GEL (GRAM) TOPICAL 03/06/2019 4.57013
ESCITALOPRAM OXALATE 5 MG/5 ML SOLUTION ORAL 11/07/2018 0.55778
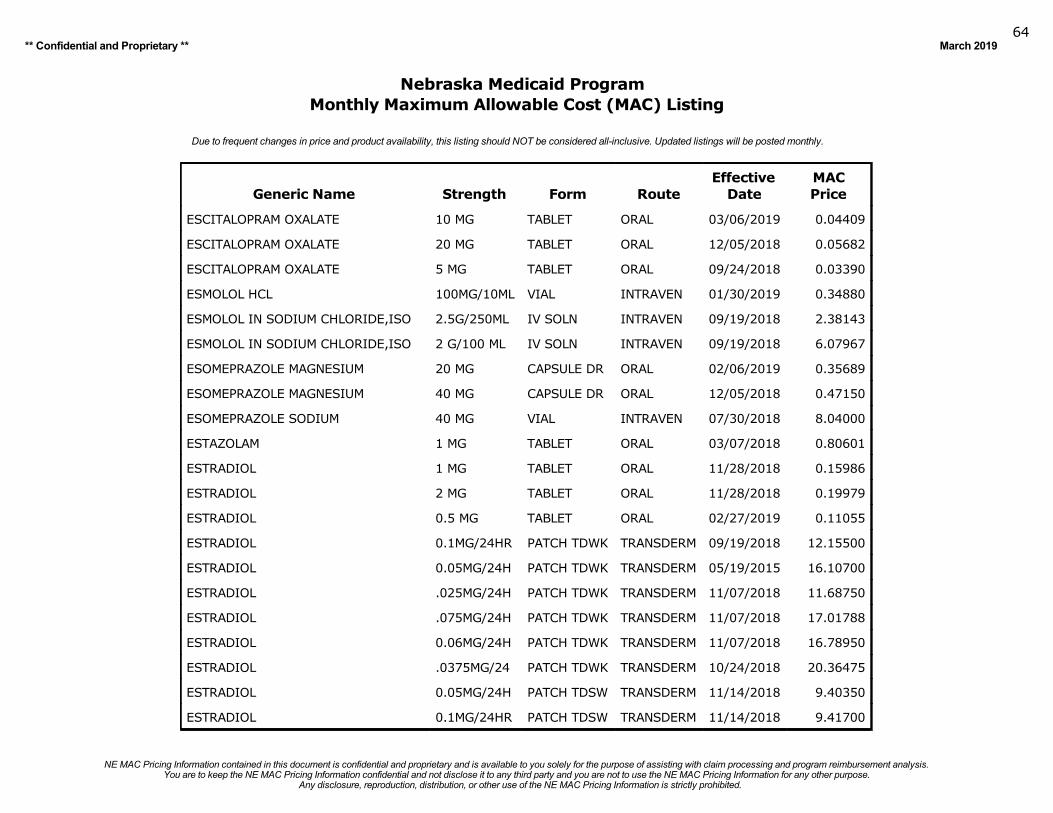
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201964
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ESCITALOPRAM OXALATE 10 MG TABLET ORAL 03/06/2019 0.04409
ESCITALOPRAM OXALATE 20 MG TABLET ORAL 12/05/2018 0.05682
ESCITALOPRAM OXALATE 5 MG TABLET ORAL 09/24/2018 0.03390
ESMOLOL HCL 100MG/10ML VIAL INTRAVEN 01/30/2019 0.34880
ESMOLOL IN SODIUM CHLORIDE,ISO 2.5G/250ML IV SOLN INTRAVEN 09/19/2018 2.38143
ESMOLOL IN SODIUM CHLORIDE,ISO 2 G/100 ML IV SOLN INTRAVEN 09/19/2018 6.07967
ESOMEPRAZOLE MAGNESIUM 20 MG CAPSULE DR ORAL 02/06/2019 0.35689
ESOMEPRAZOLE MAGNESIUM 40 MG CAPSULE DR ORAL 12/05/2018 0.47150
ESOMEPRAZOLE SODIUM 40 MG VIAL INTRAVEN 07/30/2018 8.04000
ESTAZOLAM 1 MG TABLET ORAL 03/07/2018 0.80601
ESTRADIOL 1 MG TABLET ORAL 11/28/2018 0.15986
ESTRADIOL 2 MG TABLET ORAL 11/28/2018 0.19979
ESTRADIOL 0.5 MG TABLET ORAL 02/27/2019 0.11055
ESTRADIOL 0.1MG/24HR PATCH TDWK TRANSDERM 09/19/2018 12.15500
ESTRADIOL 0.05MG/24H PATCH TDWK TRANSDERM 05/19/2015 16.10700
ESTRADIOL .025MG/24H PATCH TDWK TRANSDERM 11/07/2018 11.68750
ESTRADIOL .075MG/24H PATCH TDWK TRANSDERM 11/07/2018 17.01788
ESTRADIOL 0.06MG/24H PATCH TDWK TRANSDERM 11/07/2018 16.78950
ESTRADIOL .0375MG/24 PATCH TDWK TRANSDERM 10/24/2018 20.36475
ESTRADIOL 0.05MG/24H PATCH TDSW TRANSDERM 11/14/2018 9.40350
ESTRADIOL 0.1MG/24HR PATCH TDSW TRANSDERM 11/14/2018 9.41700
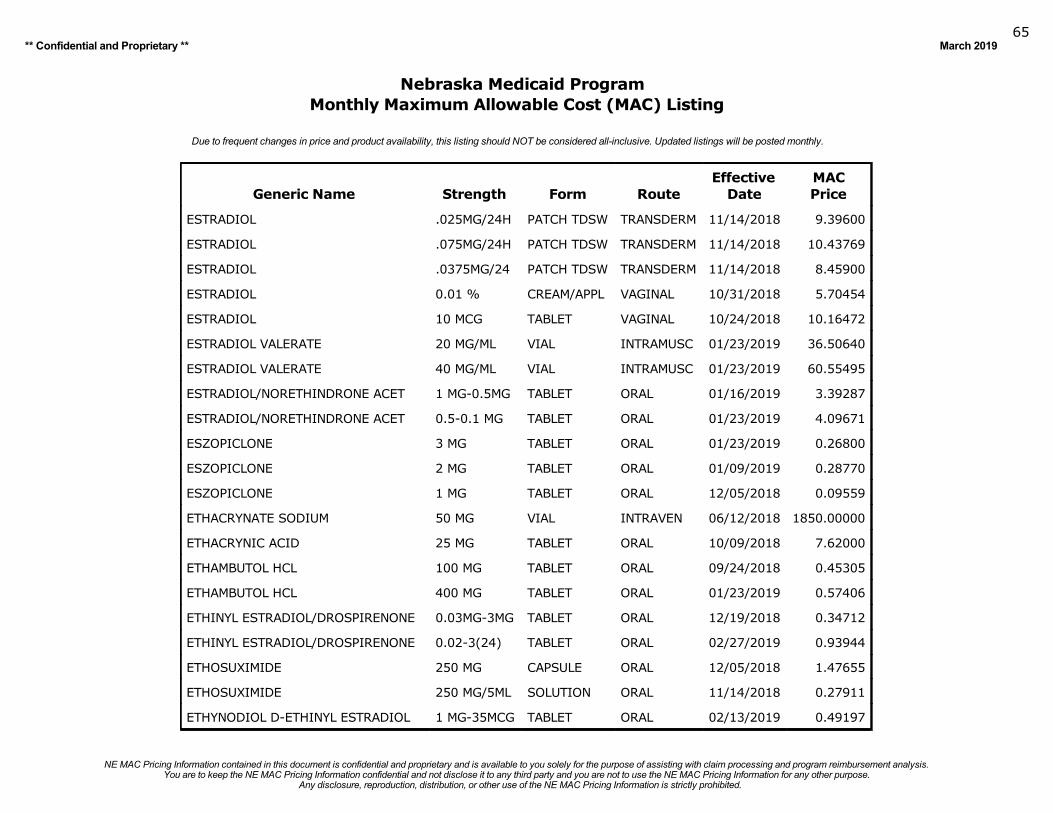
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201965
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ESTRADIOL .025MG/24H PATCH TDSW TRANSDERM 11/14/2018 9.39600
ESTRADIOL .075MG/24H PATCH TDSW TRANSDERM 11/14/2018 10.43769
ESTRADIOL .0375MG/24 PATCH TDSW TRANSDERM 11/14/2018 8.45900
ESTRADIOL 0.01 % CREAM/APPL VAGINAL 10/31/2018 5.70454
ESTRADIOL 10 MCG TABLET VAGINAL 10/24/2018 10.16472
ESTRADIOL VALERATE 20 MG/ML VIAL INTRAMUSC 01/23/2019 36.50640
ESTRADIOL VALERATE 40 MG/ML VIAL INTRAMUSC 01/23/2019 60.55495
ESTRADIOL/NORETHINDRONE ACET 1 MG-0.5MG TABLET ORAL 01/16/2019 3.39287
ESTRADIOL/NORETHINDRONE ACET 0.5-0.1 MG TABLET ORAL 01/23/2019 4.09671
ESZOPICLONE 3 MG TABLET ORAL 01/23/2019 0.26800
ESZOPICLONE 2 MG TABLET ORAL 01/09/2019 0.28770
ESZOPICLONE 1 MG TABLET ORAL 12/05/2018 0.09559
ETHACRYNATE SODIUM 50 MG VIAL INTRAVEN 06/12/2018 1850.00000
ETHACRYNIC ACID 25 MG TABLET ORAL 10/09/2018 7.62000
ETHAMBUTOL HCL 100 MG TABLET ORAL 09/24/2018 0.45305
ETHAMBUTOL HCL 400 MG TABLET ORAL 01/23/2019 0.57406
ETHINYL ESTRADIOL/DROSPIRENONE 0.03MG-3MG TABLET ORAL 12/19/2018 0.34712
ETHINYL ESTRADIOL/DROSPIRENONE 0.02-3(24) TABLET ORAL 02/27/2019 0.93944
ETHOSUXIMIDE 250 MG CAPSULE ORAL 12/05/2018 1.47655
ETHOSUXIMIDE 250 MG/5ML SOLUTION ORAL 11/14/2018 0.27911
ETHYNODIOL D-ETHINYL ESTRADIOL 1 MG-35MCG TABLET ORAL 02/13/2019 0.49197
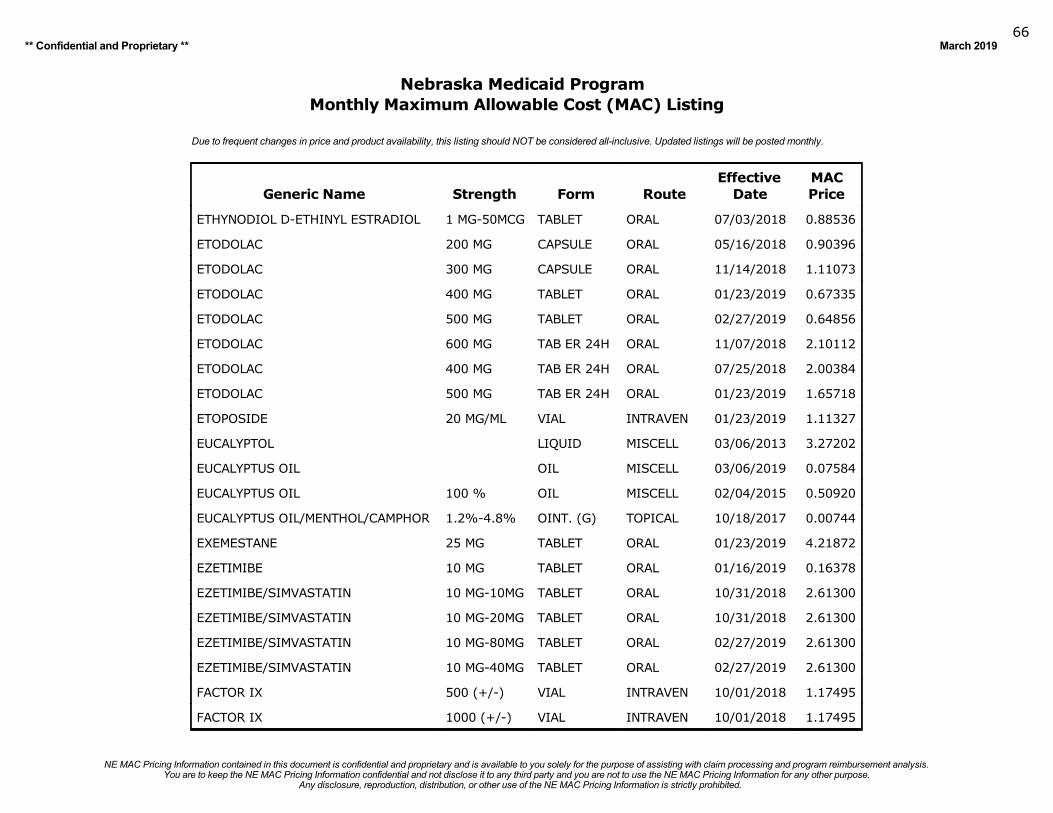
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201966
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ETHYNODIOL D-ETHINYL ESTRADIOL 1 MG-50MCG TABLET ORAL 07/03/2018 0.88536
ETODOLAC 200 MG CAPSULE ORAL 05/16/2018 0.90396
ETODOLAC 300 MG CAPSULE ORAL 11/14/2018 1.11073
ETODOLAC 400 MG TABLET ORAL 01/23/2019 0.67335
ETODOLAC 500 MG TABLET ORAL 02/27/2019 0.64856
ETODOLAC 600 MG TAB ER 24H ORAL 11/07/2018 2.10112
ETODOLAC 400 MG TAB ER 24H ORAL 07/25/2018 2.00384
ETODOLAC 500 MG TAB ER 24H ORAL 01/23/2019 1.65718
ETOPOSIDE 20 MG/ML VIAL INTRAVEN 01/23/2019 1.11327
EUCALYPTOL LIQUID MISCELL 03/06/2013 3.27202
EUCALYPTUS OIL OIL MISCELL 03/06/2019 0.07584
EUCALYPTUS OIL 100 % OIL MISCELL 02/04/2015 0.50920
EUCALYPTUS OIL/MENTHOL/CAMPHOR 1.2%-4.8% OINT. (G) TOPICAL 10/18/2017 0.00744
EXEMESTANE 25 MG TABLET ORAL 01/23/2019 4.21872
EZETIMIBE 10 MG TABLET ORAL 01/16/2019 0.16378
EZETIMIBE/SIMVASTATIN 10 MG-10MG TABLET ORAL 10/31/2018 2.61300
EZETIMIBE/SIMVASTATIN 10 MG-20MG TABLET ORAL 10/31/2018 2.61300
EZETIMIBE/SIMVASTATIN 10 MG-80MG TABLET ORAL 02/27/2019 2.61300
EZETIMIBE/SIMVASTATIN 10 MG-40MG TABLET ORAL 02/27/2019 2.61300
FACTOR IX 500 (+/-) VIAL INTRAVEN 10/01/2018 1.17495
FACTOR IX 1000 (+/-) VIAL INTRAVEN 10/01/2018 1.17495
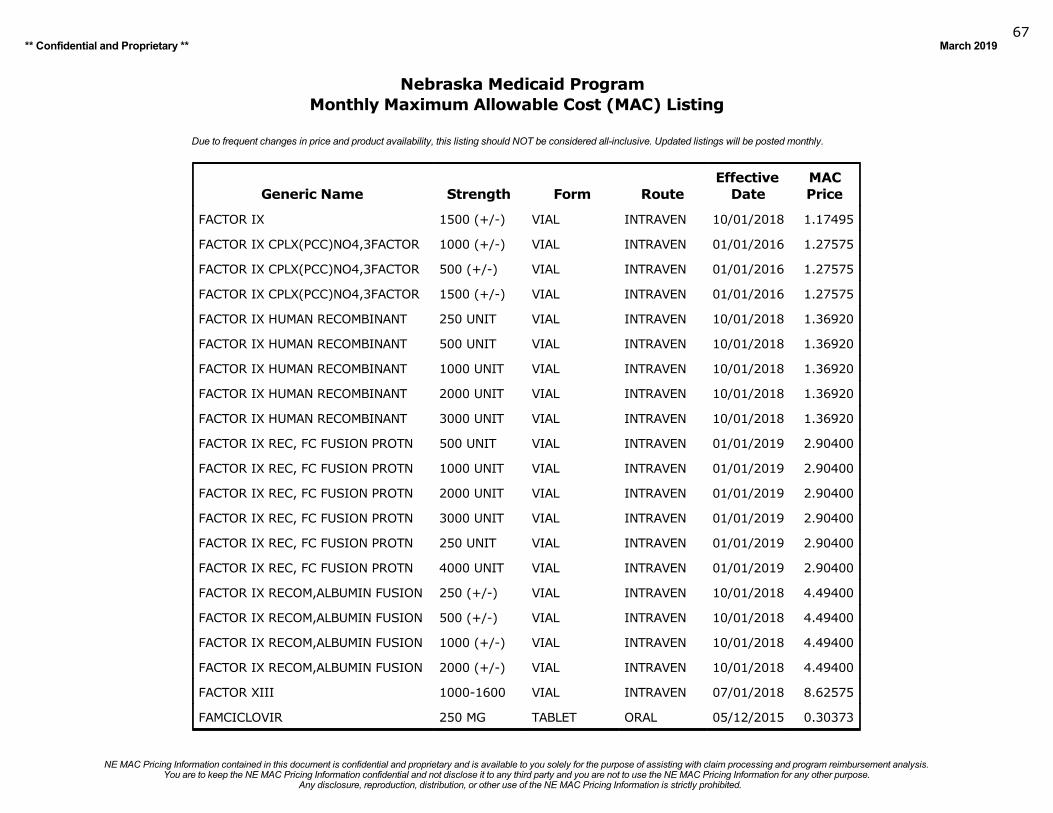
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201967
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
FACTOR IX 1500 (+/-) VIAL INTRAVEN 10/01/2018 1.17495
FACTOR IX CPLX(PCC)NO4,3FACTOR 1000 (+/-) VIAL INTRAVEN 01/01/2016 1.27575
FACTOR IX CPLX(PCC)NO4,3FACTOR 500 (+/-) VIAL INTRAVEN 01/01/2016 1.27575
FACTOR IX CPLX(PCC)NO4,3FACTOR 1500 (+/-) VIAL INTRAVEN 01/01/2016 1.27575
FACTOR IX HUMAN RECOMBINANT 250 UNIT VIAL INTRAVEN 10/01/2018 1.36920
FACTOR IX HUMAN RECOMBINANT 500 UNIT VIAL INTRAVEN 10/01/2018 1.36920
FACTOR IX HUMAN RECOMBINANT 1000 UNIT VIAL INTRAVEN 10/01/2018 1.36920
FACTOR IX HUMAN RECOMBINANT 2000 UNIT VIAL INTRAVEN 10/01/2018 1.36920
FACTOR IX HUMAN RECOMBINANT 3000 UNIT VIAL INTRAVEN 10/01/2018 1.36920
FACTOR IX REC, FC FUSION PROTN 500 UNIT VIAL INTRAVEN 01/01/2019 2.90400
FACTOR IX REC, FC FUSION PROTN 1000 UNIT VIAL INTRAVEN 01/01/2019 2.90400
FACTOR IX REC, FC FUSION PROTN 2000 UNIT VIAL INTRAVEN 01/01/2019 2.90400
FACTOR IX REC, FC FUSION PROTN 3000 UNIT VIAL INTRAVEN 01/01/2019 2.90400
FACTOR IX REC, FC FUSION PROTN 250 UNIT VIAL INTRAVEN 01/01/2019 2.90400
FACTOR IX REC, FC FUSION PROTN 4000 UNIT VIAL INTRAVEN 01/01/2019 2.90400
FACTOR IX RECOM,ALBUMIN FUSION 250 (+/-) VIAL INTRAVEN 10/01/2018 4.49400
FACTOR IX RECOM,ALBUMIN FUSION 500 (+/-) VIAL INTRAVEN 10/01/2018 4.49400
FACTOR IX RECOM,ALBUMIN FUSION 1000 (+/-) VIAL INTRAVEN 10/01/2018 4.49400
FACTOR IX RECOM,ALBUMIN FUSION 2000 (+/-) VIAL INTRAVEN 10/01/2018 4.49400
FACTOR XIII 1000-1600 VIAL INTRAVEN 07/01/2018 8.62575
FAMCICLOVIR 250 MG TABLET ORAL 05/12/2015 0.30373
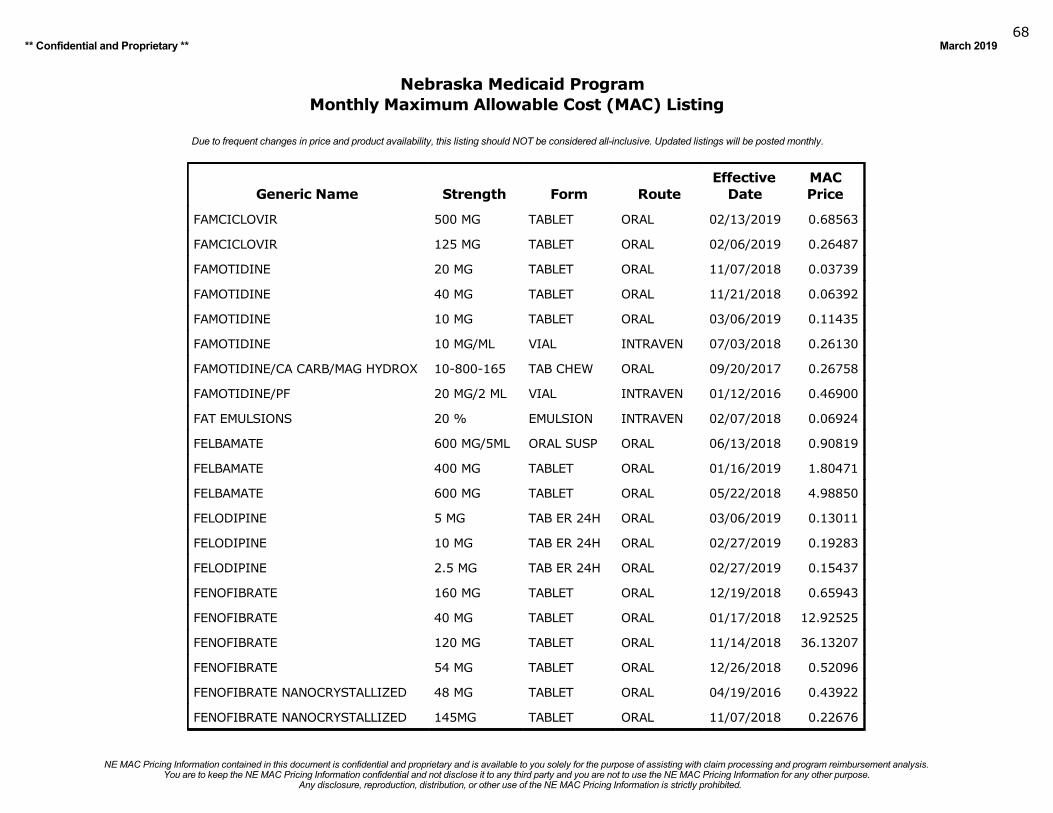
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201968
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
FAMCICLOVIR 500 MG TABLET ORAL 02/13/2019 0.68563
FAMCICLOVIR 125 MG TABLET ORAL 02/06/2019 0.26487
FAMOTIDINE 20 MG TABLET ORAL 11/07/2018 0.03739
FAMOTIDINE 40 MG TABLET ORAL 11/21/2018 0.06392
FAMOTIDINE 10 MG TABLET ORAL 03/06/2019 0.11435
FAMOTIDINE 10 MG/ML VIAL INTRAVEN 07/03/2018 0.26130
FAMOTIDINE/CA CARB/MAG HYDROX 10-800-165 TAB CHEW ORAL 09/20/2017 0.26758
FAMOTIDINE/PF 20 MG/2 ML VIAL INTRAVEN 01/12/2016 0.46900
FAT EMULSIONS 20 % EMULSION INTRAVEN 02/07/2018 0.06924
FELBAMATE 600 MG/5ML ORAL SUSP ORAL 06/13/2018 0.90819
FELBAMATE 400 MG TABLET ORAL 01/16/2019 1.80471
FELBAMATE 600 MG TABLET ORAL 05/22/2018 4.98850
FELODIPINE 5 MG TAB ER 24H ORAL 03/06/2019 0.13011
FELODIPINE 10 MG TAB ER 24H ORAL 02/27/2019 0.19283
FELODIPINE 2.5 MG TAB ER 24H ORAL 02/27/2019 0.15437
FENOFIBRATE 160 MG TABLET ORAL 12/19/2018 0.65943
FENOFIBRATE 40 MG TABLET ORAL 01/17/2018 12.92525
FENOFIBRATE 120 MG TABLET ORAL 11/14/2018 36.13207
FENOFIBRATE 54 MG TABLET ORAL 12/26/2018 0.52096
FENOFIBRATE NANOCRYSTALLIZED 48 MG TABLET ORAL 04/19/2016 0.43922
FENOFIBRATE NANOCRYSTALLIZED 145MG TABLET ORAL 11/07/2018 0.22676
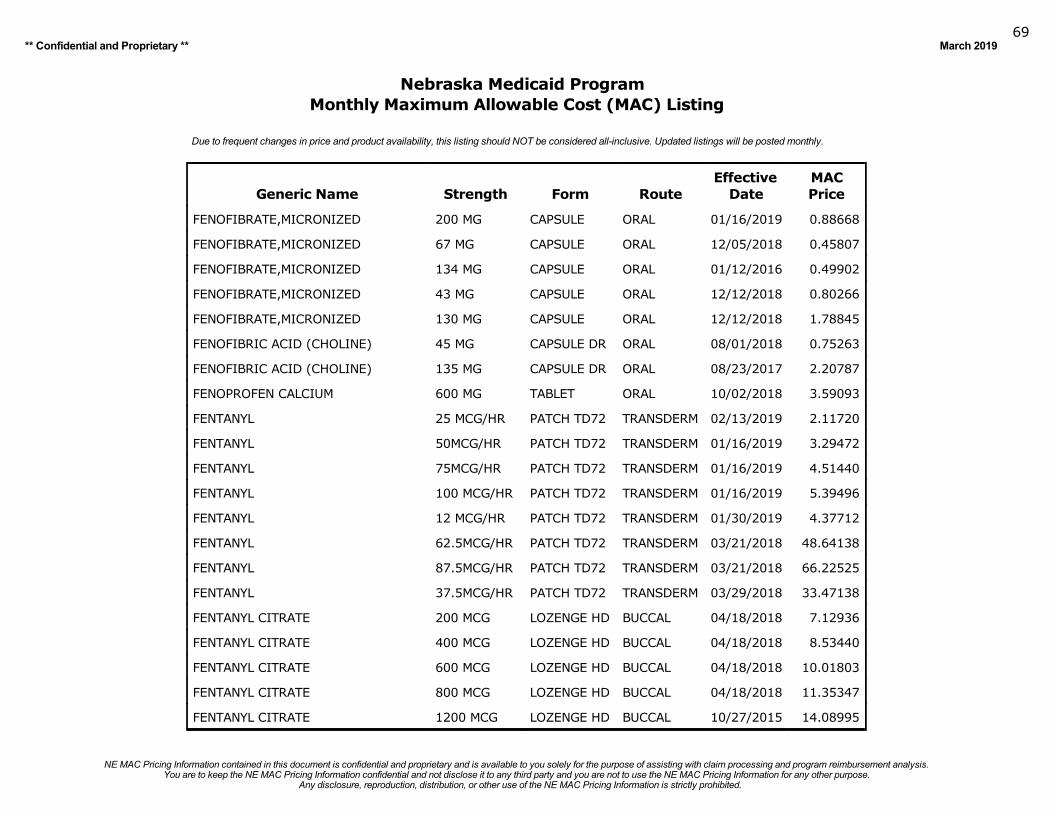
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201969
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
FENOFIBRATE,MICRONIZED 200 MG CAPSULE ORAL 01/16/2019 0.88668
FENOFIBRATE,MICRONIZED 67 MG CAPSULE ORAL 12/05/2018 0.45807
FENOFIBRATE,MICRONIZED 134 MG CAPSULE ORAL 01/12/2016 0.49902
FENOFIBRATE,MICRONIZED 43 MG CAPSULE ORAL 12/12/2018 0.80266
FENOFIBRATE,MICRONIZED 130 MG CAPSULE ORAL 12/12/2018 1.78845
FENOFIBRIC ACID (CHOLINE) 45 MG CAPSULE DR ORAL 08/01/2018 0.75263
FENOFIBRIC ACID (CHOLINE) 135 MG CAPSULE DR ORAL 08/23/2017 2.20787
FENOPROFEN CALCIUM 600 MG TABLET ORAL 10/02/2018 3.59093
FENTANYL 25 MCG/HR PATCH TD72 TRANSDERM 02/13/2019 2.11720
FENTANYL 50MCG/HR PATCH TD72 TRANSDERM 01/16/2019 3.29472
FENTANYL 75MCG/HR PATCH TD72 TRANSDERM 01/16/2019 4.51440
FENTANYL 100 MCG/HR PATCH TD72 TRANSDERM 01/16/2019 5.39496
FENTANYL 12 MCG/HR PATCH TD72 TRANSDERM 01/30/2019 4.37712
FENTANYL 62.5MCG/HR PATCH TD72 TRANSDERM 03/21/2018 48.64138
FENTANYL 87.5MCG/HR PATCH TD72 TRANSDERM 03/21/2018 66.22525
FENTANYL 37.5MCG/HR PATCH TD72 TRANSDERM 03/29/2018 33.47138
FENTANYL CITRATE 200 MCG LOZENGE HD BUCCAL 04/18/2018 7.12936
FENTANYL CITRATE 400 MCG LOZENGE HD BUCCAL 04/18/2018 8.53440
FENTANYL CITRATE 600 MCG LOZENGE HD BUCCAL 04/18/2018 10.01803
FENTANYL CITRATE 800 MCG LOZENGE HD BUCCAL 04/18/2018 11.35347
FENTANYL CITRATE 1200 MCG LOZENGE HD BUCCAL 10/27/2015 14.08995
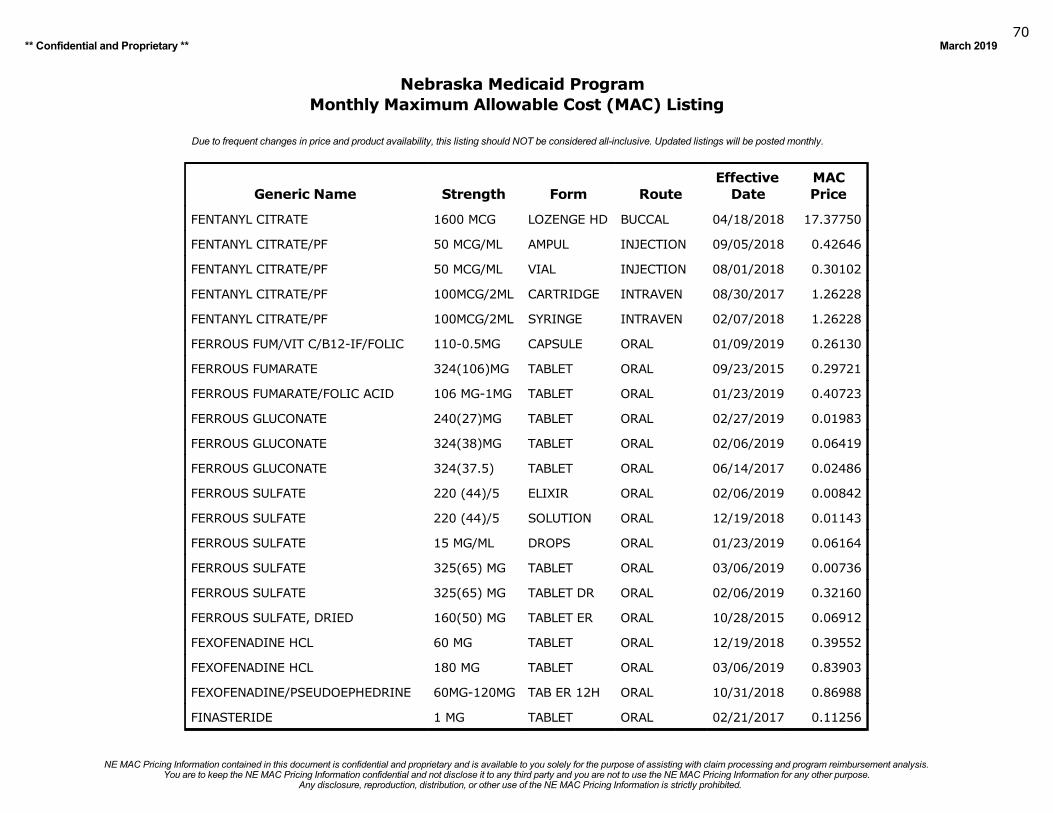
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201970
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
FENTANYL CITRATE 1600 MCG LOZENGE HD BUCCAL 04/18/2018 17.37750
FENTANYL CITRATE/PF 50 MCG/ML AMPUL INJECTION 09/05/2018 0.42646
FENTANYL CITRATE/PF 50 MCG/ML VIAL INJECTION 08/01/2018 0.30102
FENTANYL CITRATE/PF 100MCG/2ML CARTRIDGE INTRAVEN 08/30/2017 1.26228
FENTANYL CITRATE/PF 100MCG/2ML SYRINGE INTRAVEN 02/07/2018 1.26228
FERROUS FUM/VIT C/B12-IF/FOLIC 110-0.5MG CAPSULE ORAL 01/09/2019 0.26130
FERROUS FUMARATE 324(106)MG TABLET ORAL 09/23/2015 0.29721
FERROUS FUMARATE/FOLIC ACID 106 MG-1MG TABLET ORAL 01/23/2019 0.40723
FERROUS GLUCONATE 240(27)MG TABLET ORAL 02/27/2019 0.01983
FERROUS GLUCONATE 324(38)MG TABLET ORAL 02/06/2019 0.06419
FERROUS GLUCONATE 324(37.5) TABLET ORAL 06/14/2017 0.02486
FERROUS SULFATE 220 (44)/5 ELIXIR ORAL 02/06/2019 0.00842
FERROUS SULFATE 220 (44)/5 SOLUTION ORAL 12/19/2018 0.01143
FERROUS SULFATE 15 MG/ML DROPS ORAL 01/23/2019 0.06164
FERROUS SULFATE 325(65) MG TABLET ORAL 03/06/2019 0.00736
FERROUS SULFATE 325(65) MG TABLET DR ORAL 02/06/2019 0.32160
FERROUS SULFATE, DRIED 160(50) MG TABLET ER ORAL 10/28/2015 0.06912
FEXOFENADINE HCL 60 MG TABLET ORAL 12/19/2018 0.39552
FEXOFENADINE HCL 180 MG TABLET ORAL 03/06/2019 0.83903
FEXOFENADINE/PSEUDOEPHEDRINE 60MG-120MG TAB ER 12H ORAL 10/31/2018 0.86988
FINASTERIDE 1 MG TABLET ORAL 02/21/2017 0.11256
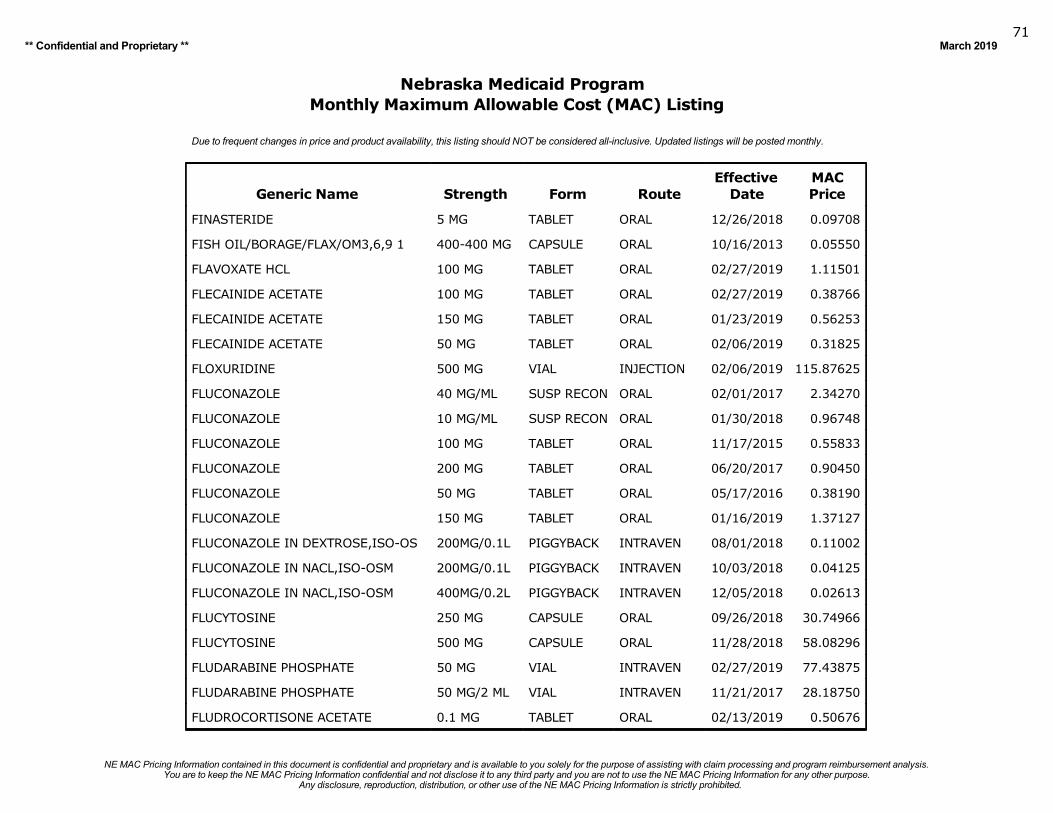
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201971
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
FINASTERIDE 5 MG TABLET ORAL 12/26/2018 0.09708
FISH OIL/BORAGE/FLAX/OM3,6,9 1 400-400 MG CAPSULE ORAL 10/16/2013 0.05550
FLAVOXATE HCL 100 MG TABLET ORAL 02/27/2019 1.11501
FLECAINIDE ACETATE 100 MG TABLET ORAL 02/27/2019 0.38766
FLECAINIDE ACETATE 150 MG TABLET ORAL 01/23/2019 0.56253
FLECAINIDE ACETATE 50 MG TABLET ORAL 02/06/2019 0.31825
FLOXURIDINE 500 MG VIAL INJECTION 02/06/2019 115.87625
FLUCONAZOLE 40 MG/ML SUSP RECON ORAL 02/01/2017 2.34270
FLUCONAZOLE 10 MG/ML SUSP RECON ORAL 01/30/2018 0.96748
FLUCONAZOLE 100 MG TABLET ORAL 11/17/2015 0.55833
FLUCONAZOLE 200 MG TABLET ORAL 06/20/2017 0.90450
FLUCONAZOLE 50 MG TABLET ORAL 05/17/2016 0.38190
FLUCONAZOLE 150 MG TABLET ORAL 01/16/2019 1.37127
FLUCONAZOLE IN DEXTROSE,ISO-OS 200MG/0.1L PIGGYBACK INTRAVEN 08/01/2018 0.11002
FLUCONAZOLE IN NACL,ISO-OSM 200MG/0.1L PIGGYBACK INTRAVEN 10/03/2018 0.04125
FLUCONAZOLE IN NACL,ISO-OSM 400MG/0.2L PIGGYBACK INTRAVEN 12/05/2018 0.02613
FLUCYTOSINE 250 MG CAPSULE ORAL 09/26/2018 30.74966
FLUCYTOSINE 500 MG CAPSULE ORAL 11/28/2018 58.08296
FLUDARABINE PHOSPHATE 50 MG VIAL INTRAVEN 02/27/2019 77.43875
FLUDARABINE PHOSPHATE 50 MG/2 ML VIAL INTRAVEN 11/21/2017 28.18750
FLUDROCORTISONE ACETATE 0.1 MG TABLET ORAL 02/13/2019 0.50676
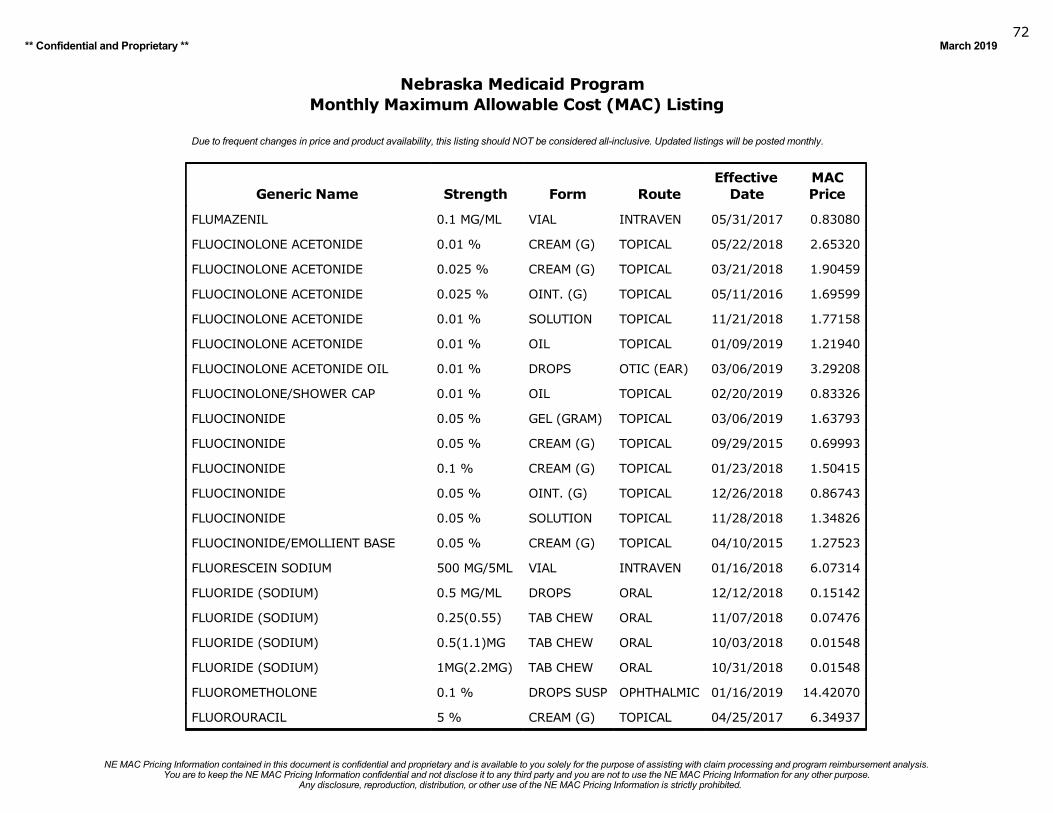
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201972
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
FLUMAZENIL 0.1 MG/ML VIAL INTRAVEN 05/31/2017 0.83080
FLUOCINOLONE ACETONIDE 0.01 % CREAM (G) TOPICAL 05/22/2018 2.65320
FLUOCINOLONE ACETONIDE 0.025 % CREAM (G) TOPICAL 03/21/2018 1.90459
FLUOCINOLONE ACETONIDE 0.025 % OINT. (G) TOPICAL 05/11/2016 1.69599
FLUOCINOLONE ACETONIDE 0.01 % SOLUTION TOPICAL 11/21/2018 1.77158
FLUOCINOLONE ACETONIDE 0.01 % OIL TOPICAL 01/09/2019 1.21940
FLUOCINOLONE ACETONIDE OIL 0.01 % DROPS OTIC (EAR) 03/06/2019 3.29208
FLUOCINOLONE/SHOWER CAP 0.01 % OIL TOPICAL 02/20/2019 0.83326
FLUOCINONIDE 0.05 % GEL (GRAM) TOPICAL 03/06/2019 1.63793
FLUOCINONIDE 0.05 % CREAM (G) TOPICAL 09/29/2015 0.69993
FLUOCINONIDE 0.1 % CREAM (G) TOPICAL 01/23/2018 1.50415
FLUOCINONIDE 0.05 % OINT. (G) TOPICAL 12/26/2018 0.86743
FLUOCINONIDE 0.05 % SOLUTION TOPICAL 11/28/2018 1.34826
FLUOCINONIDE/EMOLLIENT BASE 0.05 % CREAM (G) TOPICAL 04/10/2015 1.27523
FLUORESCEIN SODIUM 500 MG/5ML VIAL INTRAVEN 01/16/2018 6.07314
FLUORIDE (SODIUM) 0.5 MG/ML DROPS ORAL 12/12/2018 0.15142
FLUORIDE (SODIUM) 0.25(0.55) TAB CHEW ORAL 11/07/2018 0.07476
FLUORIDE (SODIUM) 0.5(1.1)MG TAB CHEW ORAL 10/03/2018 0.01548
FLUORIDE (SODIUM) 1MG(2.2MG) TAB CHEW ORAL 10/31/2018 0.01548
FLUOROMETHOLONE 0.1 % DROPS SUSP OPHTHALMIC 01/16/2019 14.42070
FLUOROURACIL 5 % CREAM (G) TOPICAL 04/25/2017 6.34937
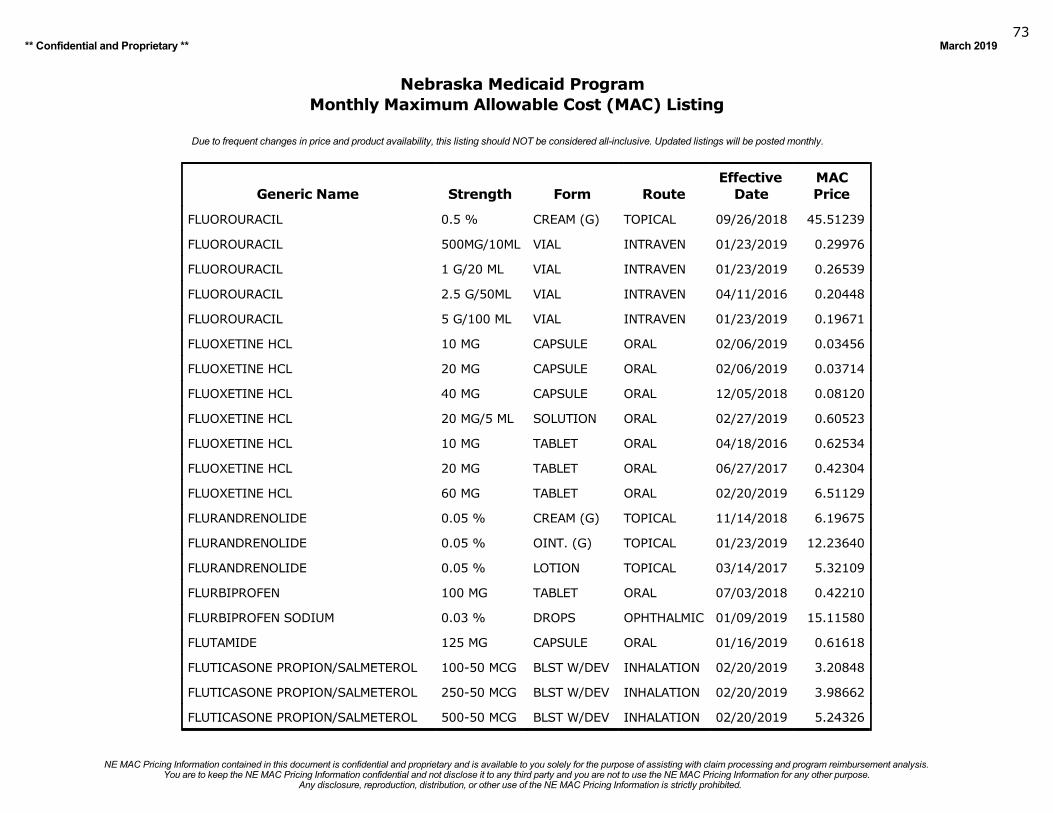
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201973
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
FLUOROURACIL 0.5 % CREAM (G) TOPICAL 09/26/2018 45.51239
FLUOROURACIL 500MG/10ML VIAL INTRAVEN 01/23/2019 0.29976
FLUOROURACIL 1 G/20 ML VIAL INTRAVEN 01/23/2019 0.26539
FLUOROURACIL 2.5 G/50ML VIAL INTRAVEN 04/11/2016 0.20448
FLUOROURACIL 5 G/100 ML VIAL INTRAVEN 01/23/2019 0.19671
FLUOXETINE HCL 10 MG CAPSULE ORAL 02/06/2019 0.03456
FLUOXETINE HCL 20 MG CAPSULE ORAL 02/06/2019 0.03714
FLUOXETINE HCL 40 MG CAPSULE ORAL 12/05/2018 0.08120
FLUOXETINE HCL 20 MG/5 ML SOLUTION ORAL 02/27/2019 0.60523
FLUOXETINE HCL 10 MG TABLET ORAL 04/18/2016 0.62534
FLUOXETINE HCL 20 MG TABLET ORAL 06/27/2017 0.42304
FLUOXETINE HCL 60 MG TABLET ORAL 02/20/2019 6.51129
FLURANDRENOLIDE 0.05 % CREAM (G) TOPICAL 11/14/2018 6.19675
FLURANDRENOLIDE 0.05 % OINT. (G) TOPICAL 01/23/2019 12.23640
FLURANDRENOLIDE 0.05 % LOTION TOPICAL 03/14/2017 5.32109
FLURBIPROFEN 100 MG TABLET ORAL 07/03/2018 0.42210
FLURBIPROFEN SODIUM 0.03 % DROPS OPHTHALMIC 01/09/2019 15.11580
FLUTAMIDE 125 MG CAPSULE ORAL 01/16/2019 0.61618
FLUTICASONE PROPION/SALMETEROL 100-50 MCG BLST W/DEV INHALATION 02/20/2019 3.20848
FLUTICASONE PROPION/SALMETEROL 250-50 MCG BLST W/DEV INHALATION 02/20/2019 3.98662
FLUTICASONE PROPION/SALMETEROL 500-50 MCG BLST W/DEV INHALATION 02/20/2019 5.24326
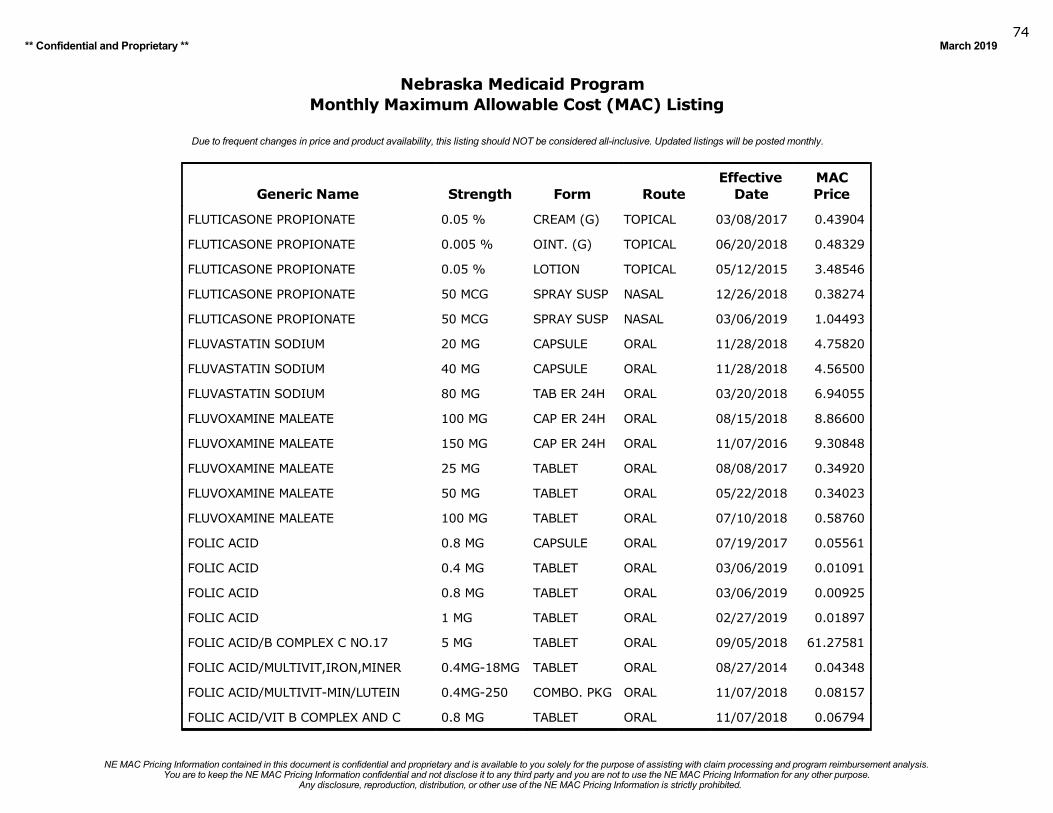
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201974
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
FLUTICASONE PROPIONATE 0.05 % CREAM (G) TOPICAL 03/08/2017 0.43904
FLUTICASONE PROPIONATE 0.005 % OINT. (G) TOPICAL 06/20/2018 0.48329
FLUTICASONE PROPIONATE 0.05 % LOTION TOPICAL 05/12/2015 3.48546
FLUTICASONE PROPIONATE 50 MCG SPRAY SUSP NASAL 12/26/2018 0.38274
FLUTICASONE PROPIONATE 50 MCG SPRAY SUSP NASAL 03/06/2019 1.04493
FLUVASTATIN SODIUM 20 MG CAPSULE ORAL 11/28/2018 4.75820
FLUVASTATIN SODIUM 40 MG CAPSULE ORAL 11/28/2018 4.56500
FLUVASTATIN SODIUM 80 MG TAB ER 24H ORAL 03/20/2018 6.94055
FLUVOXAMINE MALEATE 100 MG CAP ER 24H ORAL 08/15/2018 8.86600
FLUVOXAMINE MALEATE 150 MG CAP ER 24H ORAL 11/07/2016 9.30848
FLUVOXAMINE MALEATE 25 MG TABLET ORAL 08/08/2017 0.34920
FLUVOXAMINE MALEATE 50 MG TABLET ORAL 05/22/2018 0.34023
FLUVOXAMINE MALEATE 100 MG TABLET ORAL 07/10/2018 0.58760
FOLIC ACID 0.8 MG CAPSULE ORAL 07/19/2017 0.05561
FOLIC ACID 0.4 MG TABLET ORAL 03/06/2019 0.01091
FOLIC ACID 0.8 MG TABLET ORAL 03/06/2019 0.00925
FOLIC ACID 1 MG TABLET ORAL 02/27/2019 0.01897
FOLIC ACID/B COMPLEX C NO.17 5 MG TABLET ORAL 09/05/2018 61.27581
FOLIC ACID/MULTIVIT,IRON,MINER 0.4MG-18MG TABLET ORAL 08/27/2014 0.04348
FOLIC ACID/MULTIVIT-MIN/LUTEIN 0.4MG-250 COMBO. PKG ORAL 11/07/2018 0.08157
FOLIC ACID/VIT B COMPLEX AND C 0.8 MG TABLET ORAL 11/07/2018 0.06794
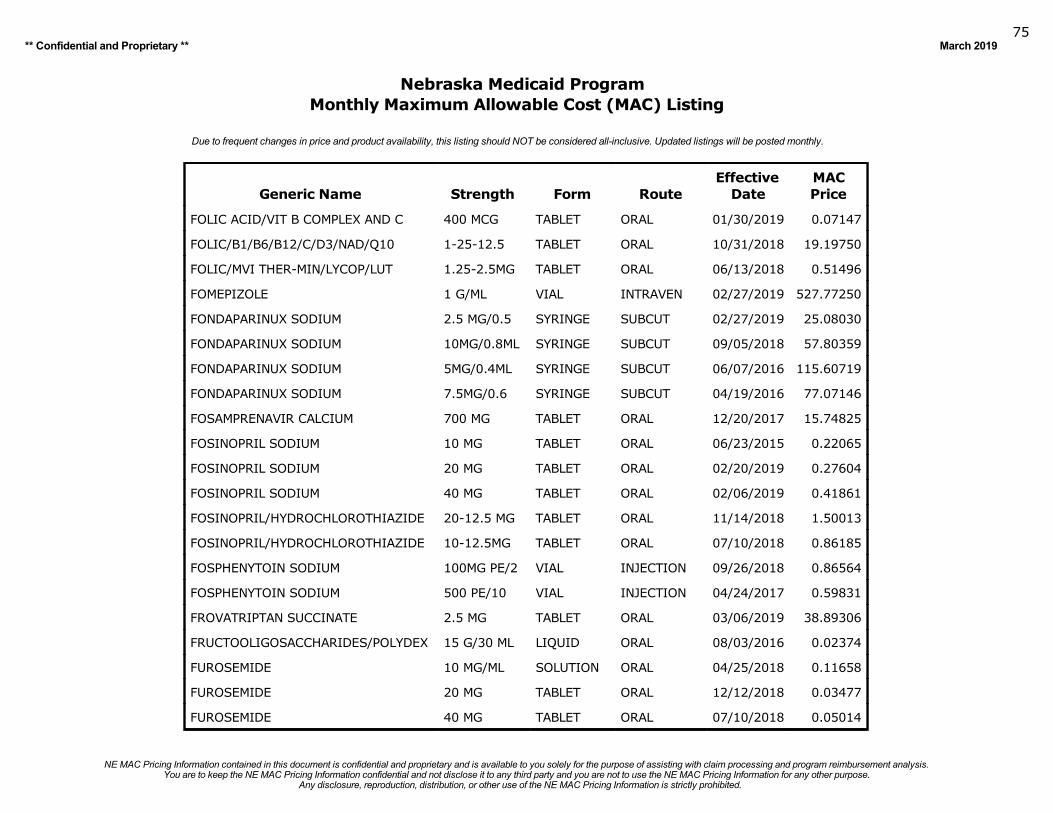
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201975
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
FOLIC ACID/VIT B COMPLEX AND C 400 MCG TABLET ORAL 01/30/2019 0.07147
FOLIC/B1/B6/B12/C/D3/NAD/Q10 1-25-12.5 TABLET ORAL 10/31/2018 19.19750
FOLIC/MVI THER-MIN/LYCOP/LUT 1.25-2.5MG TABLET ORAL 06/13/2018 0.51496
FOMEPIZOLE 1 G/ML VIAL INTRAVEN 02/27/2019 527.77250
FONDAPARINUX SODIUM 2.5 MG/0.5 SYRINGE SUBCUT 02/27/2019 25.08030
FONDAPARINUX SODIUM 10MG/0.8ML SYRINGE SUBCUT 09/05/2018 57.80359
FONDAPARINUX SODIUM 5MG/0.4ML SYRINGE SUBCUT 06/07/2016 115.60719
FONDAPARINUX SODIUM 7.5MG/0.6 SYRINGE SUBCUT 04/19/2016 77.07146
FOSAMPRENAVIR CALCIUM 700 MG TABLET ORAL 12/20/2017 15.74825
FOSINOPRIL SODIUM 10 MG TABLET ORAL 06/23/2015 0.22065
FOSINOPRIL SODIUM 20 MG TABLET ORAL 02/20/2019 0.27604
FOSINOPRIL SODIUM 40 MG TABLET ORAL 02/06/2019 0.41861
FOSINOPRIL/HYDROCHLOROTHIAZIDE 20-12.5 MG TABLET ORAL 11/14/2018 1.50013
FOSINOPRIL/HYDROCHLOROTHIAZIDE 10-12.5MG TABLET ORAL 07/10/2018 0.86185
FOSPHENYTOIN SODIUM 100MG PE/2 VIAL INJECTION 09/26/2018 0.86564
FOSPHENYTOIN SODIUM 500 PE/10 VIAL INJECTION 04/24/2017 0.59831
FROVATRIPTAN SUCCINATE 2.5 MG TABLET ORAL 03/06/2019 38.89306
FRUCTOOLIGOSACCHARIDES/POLYDEX 15 G/30 ML LIQUID ORAL 08/03/2016 0.02374
FUROSEMIDE 10 MG/ML SOLUTION ORAL 04/25/2018 0.11658
FUROSEMIDE 20 MG TABLET ORAL 12/12/2018 0.03477
FUROSEMIDE 40 MG TABLET ORAL 07/10/2018 0.05014
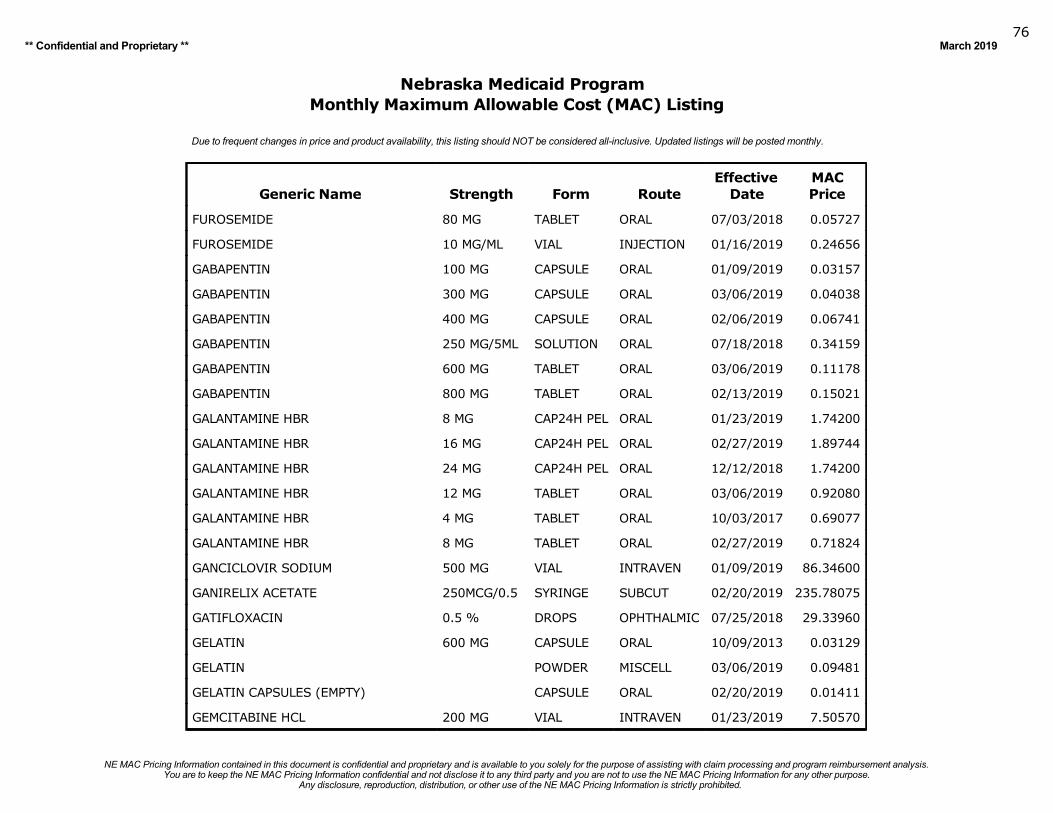
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201976
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
FUROSEMIDE 80 MG TABLET ORAL 07/03/2018 0.05727
FUROSEMIDE 10 MG/ML VIAL INJECTION 01/16/2019 0.24656
GABAPENTIN 100 MG CAPSULE ORAL 01/09/2019 0.03157
GABAPENTIN 300 MG CAPSULE ORAL 03/06/2019 0.04038
GABAPENTIN 400 MG CAPSULE ORAL 02/06/2019 0.06741
GABAPENTIN 250 MG/5ML SOLUTION ORAL 07/18/2018 0.34159
GABAPENTIN 600 MG TABLET ORAL 03/06/2019 0.11178
GABAPENTIN 800 MG TABLET ORAL 02/13/2019 0.15021
GALANTAMINE HBR 8 MG CAP24H PEL ORAL 01/23/2019 1.74200
GALANTAMINE HBR 16 MG CAP24H PEL ORAL 02/27/2019 1.89744
GALANTAMINE HBR 24 MG CAP24H PEL ORAL 12/12/2018 1.74200
GALANTAMINE HBR 12 MG TABLET ORAL 03/06/2019 0.92080
GALANTAMINE HBR 4 MG TABLET ORAL 10/03/2017 0.69077
GALANTAMINE HBR 8 MG TABLET ORAL 02/27/2019 0.71824
GANCICLOVIR SODIUM 500 MG VIAL INTRAVEN 01/09/2019 86.34600
GANIRELIX ACETATE 250MCG/0.5 SYRINGE SUBCUT 02/20/2019 235.78075
GATIFLOXACIN 0.5 % DROPS OPHTHALMIC 07/25/2018 29.33960
GELATIN 600 MG CAPSULE ORAL 10/09/2013 0.03129
GELATIN POWDER MISCELL 03/06/2019 0.09481
GELATIN CAPSULES (EMPTY) CAPSULE ORAL 02/20/2019 0.01411
GEMCITABINE HCL 200 MG VIAL INTRAVEN 01/23/2019 7.50570
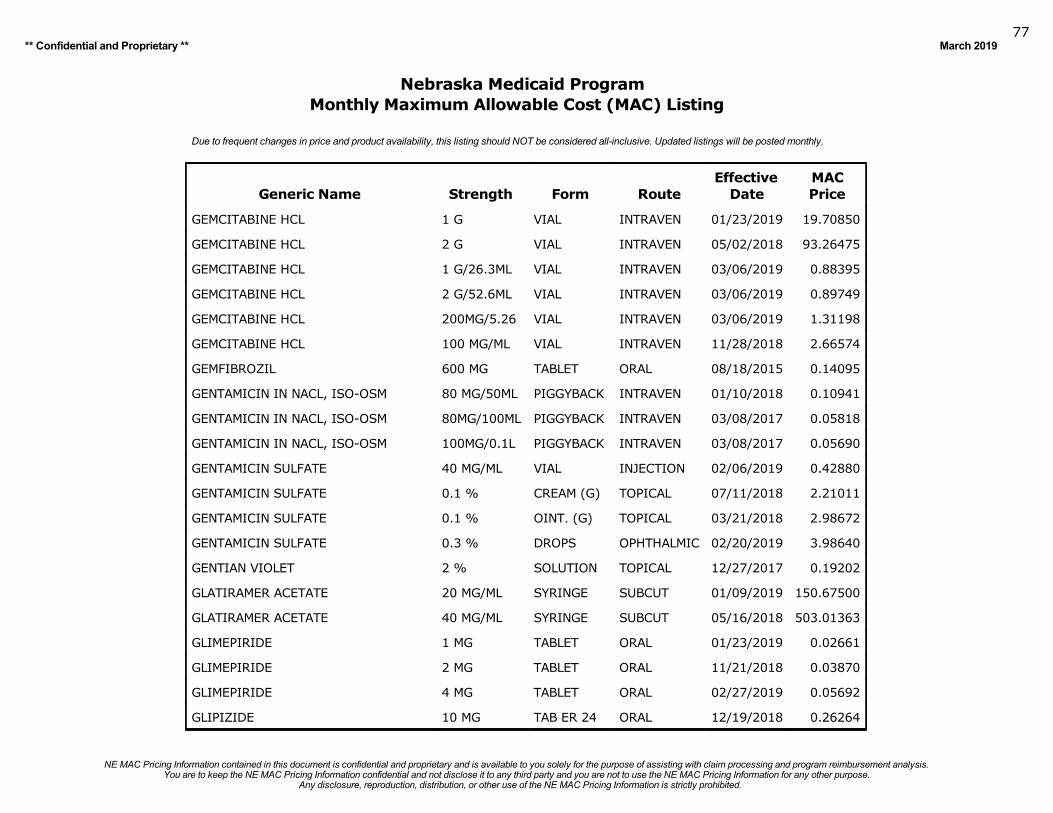
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201977
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
GEMCITABINE HCL 1 G VIAL INTRAVEN 01/23/2019 19.70850
GEMCITABINE HCL 2 G VIAL INTRAVEN 05/02/2018 93.26475
GEMCITABINE HCL 1 G/26.3ML VIAL INTRAVEN 03/06/2019 0.88395
GEMCITABINE HCL 2 G/52.6ML VIAL INTRAVEN 03/06/2019 0.89749
GEMCITABINE HCL 200MG/5.26 VIAL INTRAVEN 03/06/2019 1.31198
GEMCITABINE HCL 100 MG/ML VIAL INTRAVEN 11/28/2018 2.66574
GEMFIBROZIL 600 MG TABLET ORAL 08/18/2015 0.14095
GENTAMICIN IN NACL, ISO-OSM 80 MG/50ML PIGGYBACK INTRAVEN 01/10/2018 0.10941
GENTAMICIN IN NACL, ISO-OSM 80MG/100ML PIGGYBACK INTRAVEN 03/08/2017 0.05818
GENTAMICIN IN NACL, ISO-OSM 100MG/0.1L PIGGYBACK INTRAVEN 03/08/2017 0.05690
GENTAMICIN SULFATE 40 MG/ML VIAL INJECTION 02/06/2019 0.42880
GENTAMICIN SULFATE 0.1 % CREAM (G) TOPICAL 07/11/2018 2.21011
GENTAMICIN SULFATE 0.1 % OINT. (G) TOPICAL 03/21/2018 2.98672
GENTAMICIN SULFATE 0.3 % DROPS OPHTHALMIC 02/20/2019 3.98640
GENTIAN VIOLET 2 % SOLUTION TOPICAL 12/27/2017 0.19202
GLATIRAMER ACETATE 20 MG/ML SYRINGE SUBCUT 01/09/2019 150.67500
GLATIRAMER ACETATE 40 MG/ML SYRINGE SUBCUT 05/16/2018 503.01363
GLIMEPIRIDE 1 MG TABLET ORAL 01/23/2019 0.02661
GLIMEPIRIDE 2 MG TABLET ORAL 11/21/2018 0.03870
GLIMEPIRIDE 4 MG TABLET ORAL 02/27/2019 0.05692
GLIPIZIDE 10 MG TAB ER 24 ORAL 12/19/2018 0.26264
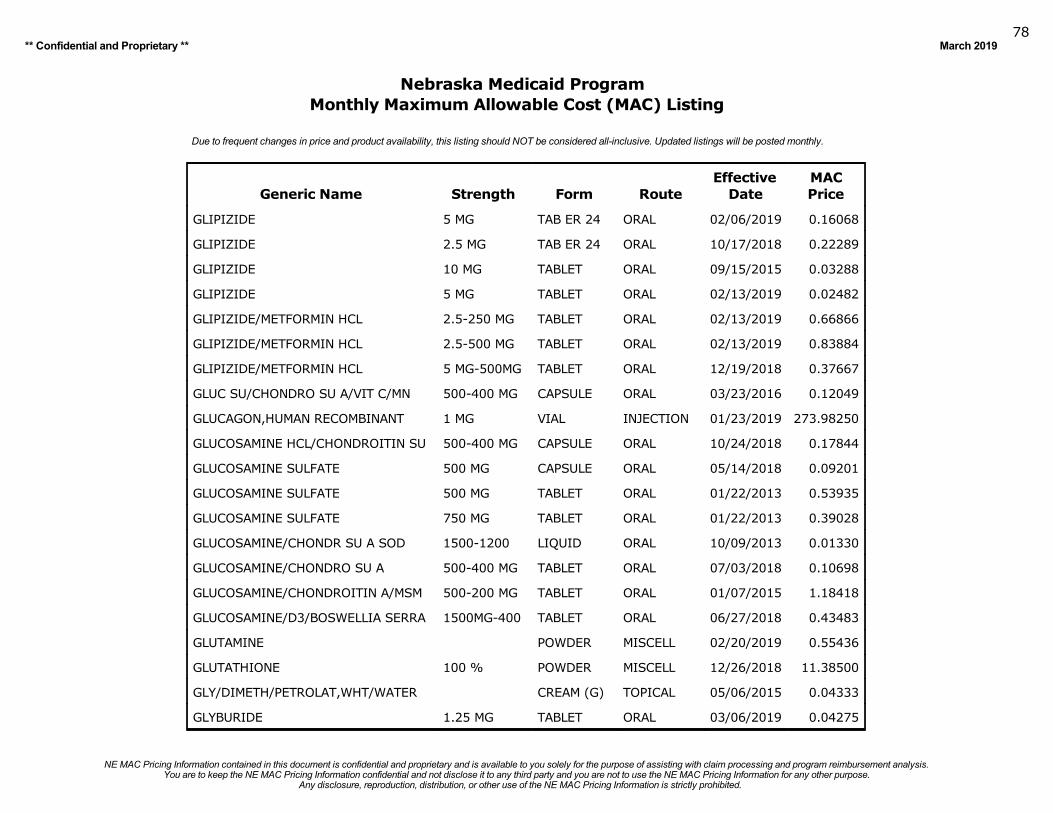
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201978
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
GLIPIZIDE 5 MG TAB ER 24 ORAL 02/06/2019 0.16068
GLIPIZIDE 2.5 MG TAB ER 24 ORAL 10/17/2018 0.22289
GLIPIZIDE 10 MG TABLET ORAL 09/15/2015 0.03288
GLIPIZIDE 5 MG TABLET ORAL 02/13/2019 0.02482
GLIPIZIDE/METFORMIN HCL 2.5-250 MG TABLET ORAL 02/13/2019 0.66866
GLIPIZIDE/METFORMIN HCL 2.5-500 MG TABLET ORAL 02/13/2019 0.83884
GLIPIZIDE/METFORMIN HCL 5 MG-500MG TABLET ORAL 12/19/2018 0.37667
GLUC SU/CHONDRO SU A/VIT C/MN 500-400 MG CAPSULE ORAL 03/23/2016 0.12049
GLUCAGON,HUMAN RECOMBINANT 1 MG VIAL INJECTION 01/23/2019 273.98250
GLUCOSAMINE HCL/CHONDROITIN SU 500-400 MG CAPSULE ORAL 10/24/2018 0.17844
GLUCOSAMINE SULFATE 500 MG CAPSULE ORAL 05/14/2018 0.09201
GLUCOSAMINE SULFATE 500 MG TABLET ORAL 01/22/2013 0.53935
GLUCOSAMINE SULFATE 750 MG TABLET ORAL 01/22/2013 0.39028
GLUCOSAMINE/CHONDR SU A SOD 1500-1200 LIQUID ORAL 10/09/2013 0.01330
GLUCOSAMINE/CHONDRO SU A 500-400 MG TABLET ORAL 07/03/2018 0.10698
GLUCOSAMINE/CHONDROITIN A/MSM 500-200 MG TABLET ORAL 01/07/2015 1.18418
GLUCOSAMINE/D3/BOSWELLIA SERRA 1500MG-400 TABLET ORAL 06/27/2018 0.43483
GLUTAMINE POWDER MISCELL 02/20/2019 0.55436
GLUTATHIONE 100 % POWDER MISCELL 12/26/2018 11.38500
GLY/DIMETH/PETROLAT,WHT/WATER CREAM (G) TOPICAL 05/06/2015 0.04333
GLYBURIDE 1.25 MG TABLET ORAL 03/06/2019 0.04275
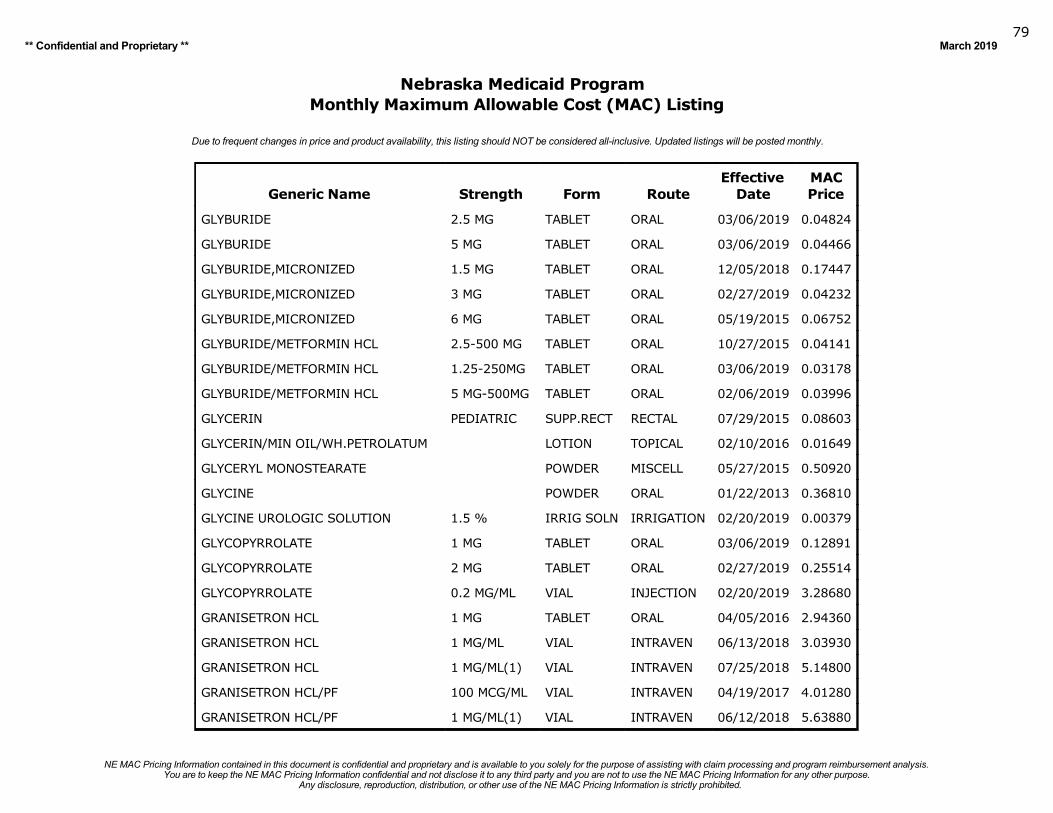
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201979
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
GLYBURIDE 2.5 MG TABLET ORAL 03/06/2019 0.04824
GLYBURIDE 5 MG TABLET ORAL 03/06/2019 0.04466
GLYBURIDE,MICRONIZED 1.5 MG TABLET ORAL 12/05/2018 0.17447
GLYBURIDE,MICRONIZED 3 MG TABLET ORAL 02/27/2019 0.04232
GLYBURIDE,MICRONIZED 6 MG TABLET ORAL 05/19/2015 0.06752
GLYBURIDE/METFORMIN HCL 2.5-500 MG TABLET ORAL 10/27/2015 0.04141
GLYBURIDE/METFORMIN HCL 1.25-250MG TABLET ORAL 03/06/2019 0.03178
GLYBURIDE/METFORMIN HCL 5 MG-500MG TABLET ORAL 02/06/2019 0.03996
GLYCERIN PEDIATRIC SUPP.RECT RECTAL 07/29/2015 0.08603
GLYCERIN/MIN OIL/WH.PETROLATUM LOTION TOPICAL 02/10/2016 0.01649
GLYCERYL MONOSTEARATE POWDER MISCELL 05/27/2015 0.50920
GLYCINE POWDER ORAL 01/22/2013 0.36810
GLYCINE UROLOGIC SOLUTION 1.5 % IRRIG SOLN IRRIGATION 02/20/2019 0.00379
GLYCOPYRROLATE 1 MG TABLET ORAL 03/06/2019 0.12891
GLYCOPYRROLATE 2 MG TABLET ORAL 02/27/2019 0.25514
GLYCOPYRROLATE 0.2 MG/ML VIAL INJECTION 02/20/2019 3.28680
GRANISETRON HCL 1 MG TABLET ORAL 04/05/2016 2.94360
GRANISETRON HCL 1 MG/ML VIAL INTRAVEN 06/13/2018 3.03930
GRANISETRON HCL 1 MG/ML(1) VIAL INTRAVEN 07/25/2018 5.14800
GRANISETRON HCL/PF 100 MCG/ML VIAL INTRAVEN 04/19/2017 4.01280
GRANISETRON HCL/PF 1 MG/ML(1) VIAL INTRAVEN 06/12/2018 5.63880
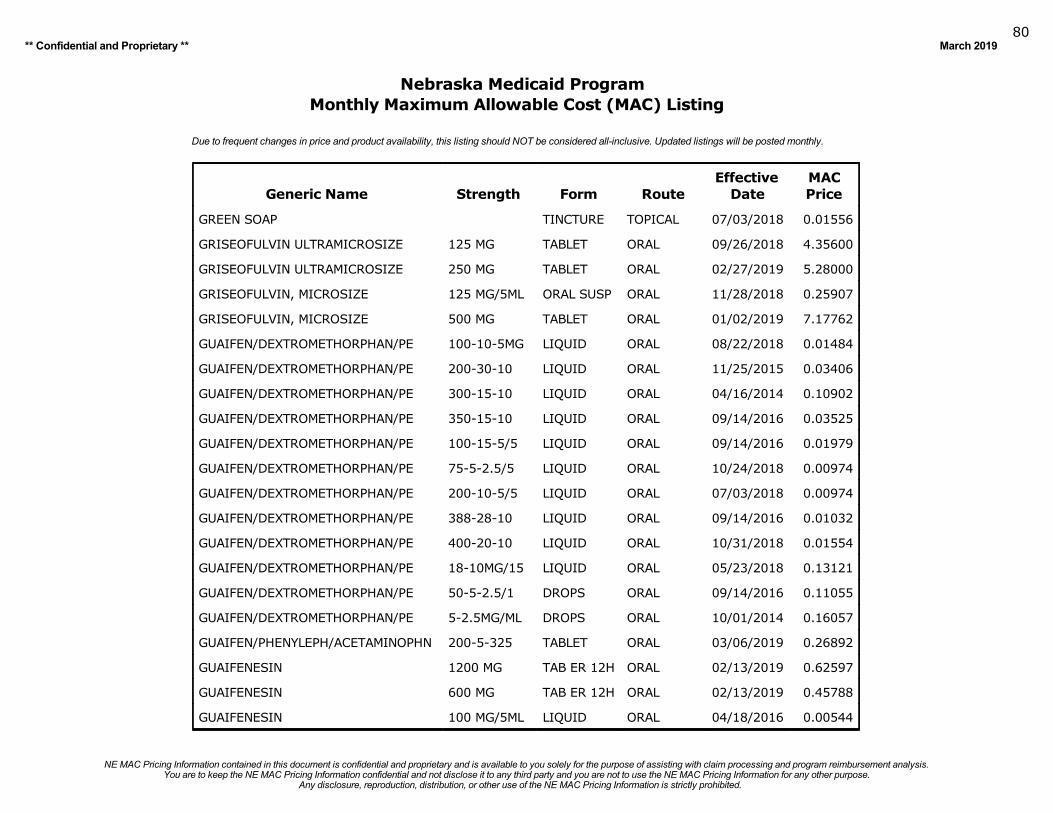
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201980
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
GREEN SOAP TINCTURE TOPICAL 07/03/2018 0.01556
GRISEOFULVIN ULTRAMICROSIZE 125 MG TABLET ORAL 09/26/2018 4.35600
GRISEOFULVIN ULTRAMICROSIZE 250 MG TABLET ORAL 02/27/2019 5.28000
GRISEOFULVIN, MICROSIZE 125 MG/5ML ORAL SUSP ORAL 11/28/2018 0.25907
GRISEOFULVIN, MICROSIZE 500 MG TABLET ORAL 01/02/2019 7.17762
GUAIFEN/DEXTROMETHORPHAN/PE 100-10-5MG LIQUID ORAL 08/22/2018 0.01484
GUAIFEN/DEXTROMETHORPHAN/PE 200-30-10 LIQUID ORAL 11/25/2015 0.03406
GUAIFEN/DEXTROMETHORPHAN/PE 300-15-10 LIQUID ORAL 04/16/2014 0.10902
GUAIFEN/DEXTROMETHORPHAN/PE 350-15-10 LIQUID ORAL 09/14/2016 0.03525
GUAIFEN/DEXTROMETHORPHAN/PE 100-15-5/5 LIQUID ORAL 09/14/2016 0.01979
GUAIFEN/DEXTROMETHORPHAN/PE 75-5-2.5/5 LIQUID ORAL 10/24/2018 0.00974
GUAIFEN/DEXTROMETHORPHAN/PE 200-10-5/5 LIQUID ORAL 07/03/2018 0.00974
GUAIFEN/DEXTROMETHORPHAN/PE 388-28-10 LIQUID ORAL 09/14/2016 0.01032
GUAIFEN/DEXTROMETHORPHAN/PE 400-20-10 LIQUID ORAL 10/31/2018 0.01554
GUAIFEN/DEXTROMETHORPHAN/PE 18-10MG/15 LIQUID ORAL 05/23/2018 0.13121
GUAIFEN/DEXTROMETHORPHAN/PE 50-5-2.5/1 DROPS ORAL 09/14/2016 0.11055
GUAIFEN/DEXTROMETHORPHAN/PE 5-2.5MG/ML DROPS ORAL 10/01/2014 0.16057
GUAIFEN/PHENYLEPH/ACETAMINOPHN 200-5-325 TABLET ORAL 03/06/2019 0.26892
GUAIFENESIN 1200 MG TAB ER 12H ORAL 02/13/2019 0.62597
GUAIFENESIN 600 MG TAB ER 12H ORAL 02/13/2019 0.45788
GUAIFENESIN 100 MG/5ML LIQUID ORAL 04/18/2016 0.00544
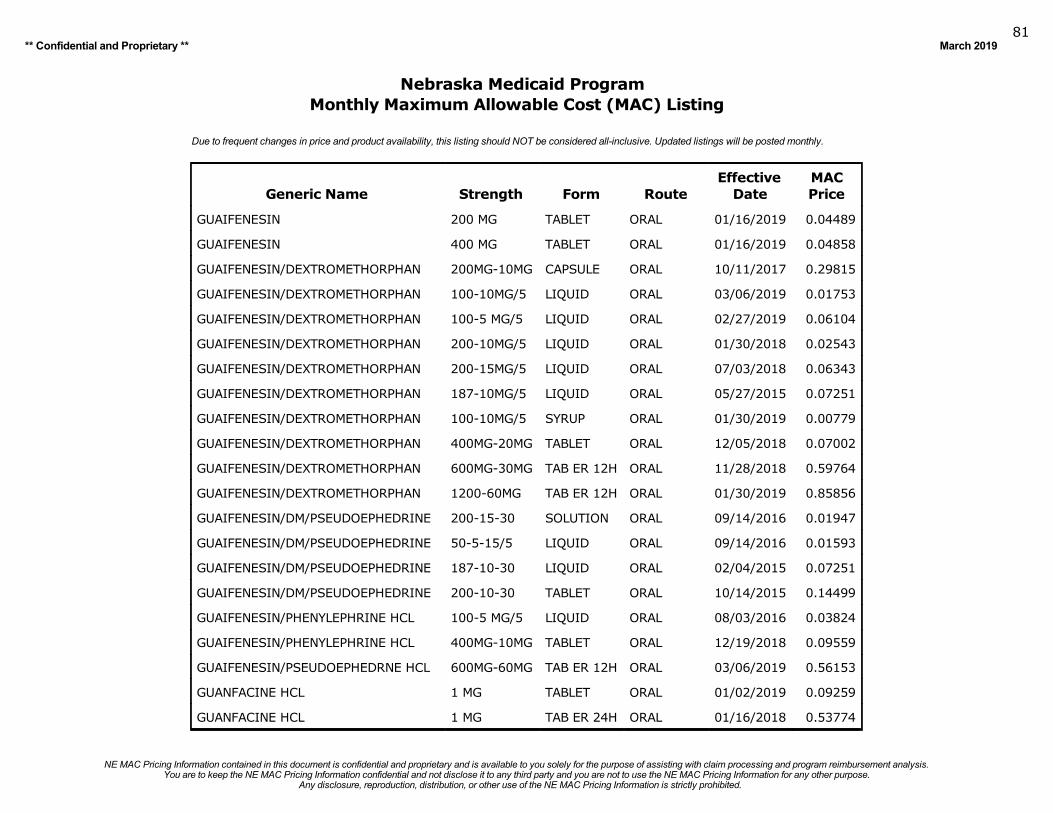
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201981
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
GUAIFENESIN 200 MG TABLET ORAL 01/16/2019 0.04489
GUAIFENESIN 400 MG TABLET ORAL 01/16/2019 0.04858
GUAIFENESIN/DEXTROMETHORPHAN 200MG-10MG CAPSULE ORAL 10/11/2017 0.29815
GUAIFENESIN/DEXTROMETHORPHAN 100-10MG/5 LIQUID ORAL 03/06/2019 0.01753
GUAIFENESIN/DEXTROMETHORPHAN 100-5 MG/5 LIQUID ORAL 02/27/2019 0.06104
GUAIFENESIN/DEXTROMETHORPHAN 200-10MG/5 LIQUID ORAL 01/30/2018 0.02543
GUAIFENESIN/DEXTROMETHORPHAN 200-15MG/5 LIQUID ORAL 07/03/2018 0.06343
GUAIFENESIN/DEXTROMETHORPHAN 187-10MG/5 LIQUID ORAL 05/27/2015 0.07251
GUAIFENESIN/DEXTROMETHORPHAN 100-10MG/5 SYRUP ORAL 01/30/2019 0.00779
GUAIFENESIN/DEXTROMETHORPHAN 400MG-20MG TABLET ORAL 12/05/2018 0.07002
GUAIFENESIN/DEXTROMETHORPHAN 600MG-30MG TAB ER 12H ORAL 11/28/2018 0.59764
GUAIFENESIN/DEXTROMETHORPHAN 1200-60MG TAB ER 12H ORAL 01/30/2019 0.85856
GUAIFENESIN/DM/PSEUDOEPHEDRINE 200-15-30 SOLUTION ORAL 09/14/2016 0.01947
GUAIFENESIN/DM/PSEUDOEPHEDRINE 50-5-15/5 LIQUID ORAL 09/14/2016 0.01593
GUAIFENESIN/DM/PSEUDOEPHEDRINE 187-10-30 LIQUID ORAL 02/04/2015 0.07251
GUAIFENESIN/DM/PSEUDOEPHEDRINE 200-10-30 TABLET ORAL 10/14/2015 0.14499
GUAIFENESIN/PHENYLEPHRINE HCL 100-5 MG/5 LIQUID ORAL 08/03/2016 0.03824
GUAIFENESIN/PHENYLEPHRINE HCL 400MG-10MG TABLET ORAL 12/19/2018 0.09559
GUAIFENESIN/PSEUDOEPHEDRNE HCL 600MG-60MG TAB ER 12H ORAL 03/06/2019 0.56153
GUANFACINE HCL 1 MG TABLET ORAL 01/02/2019 0.09259
GUANFACINE HCL 1 MG TAB ER 24H ORAL 01/16/2018 0.53774
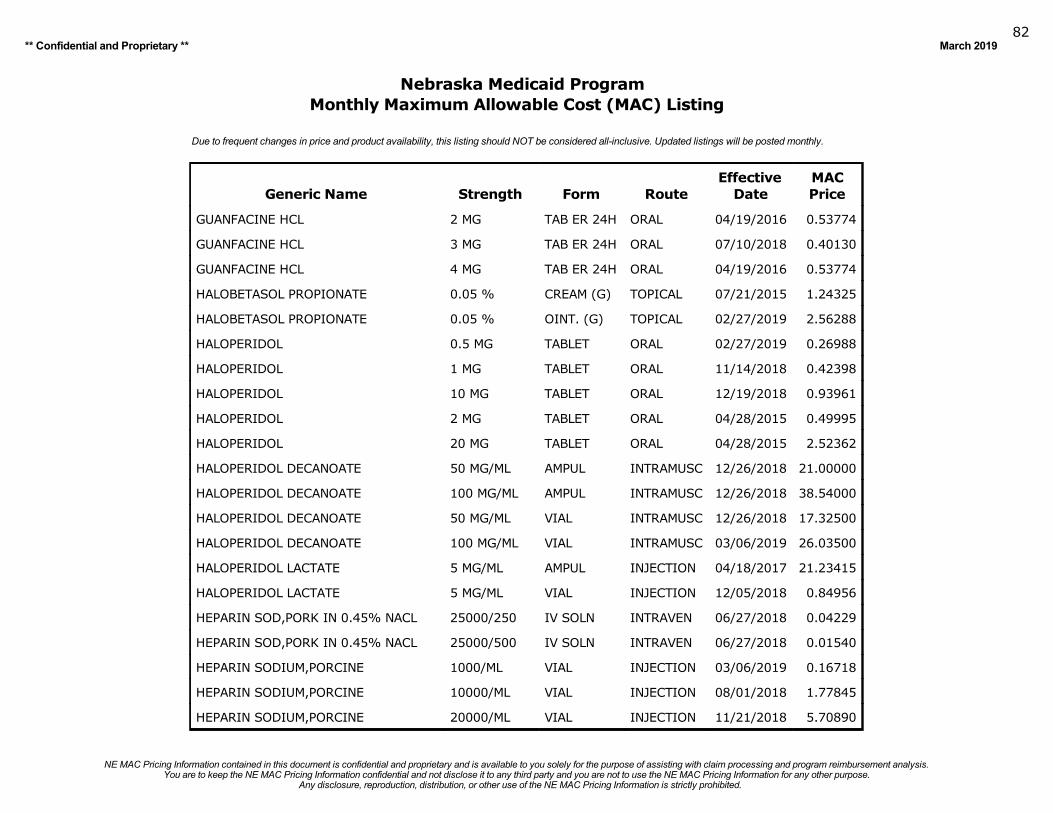
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201982
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
GUANFACINE HCL 2 MG TAB ER 24H ORAL 04/19/2016 0.53774
GUANFACINE HCL 3 MG TAB ER 24H ORAL 07/10/2018 0.40130
GUANFACINE HCL 4 MG TAB ER 24H ORAL 04/19/2016 0.53774
HALOBETASOL PROPIONATE 0.05 % CREAM (G) TOPICAL 07/21/2015 1.24325
HALOBETASOL PROPIONATE 0.05 % OINT. (G) TOPICAL 02/27/2019 2.56288
HALOPERIDOL 0.5 MG TABLET ORAL 02/27/2019 0.26988
HALOPERIDOL 1 MG TABLET ORAL 11/14/2018 0.42398
HALOPERIDOL 10 MG TABLET ORAL 12/19/2018 0.93961
HALOPERIDOL 2 MG TABLET ORAL 04/28/2015 0.49995
HALOPERIDOL 20 MG TABLET ORAL 04/28/2015 2.52362
HALOPERIDOL DECANOATE 50 MG/ML AMPUL INTRAMUSC 12/26/2018 21.00000
HALOPERIDOL DECANOATE 100 MG/ML AMPUL INTRAMUSC 12/26/2018 38.54000
HALOPERIDOL DECANOATE 50 MG/ML VIAL INTRAMUSC 12/26/2018 17.32500
HALOPERIDOL DECANOATE 100 MG/ML VIAL INTRAMUSC 03/06/2019 26.03500
HALOPERIDOL LACTATE 5 MG/ML AMPUL INJECTION 04/18/2017 21.23415
HALOPERIDOL LACTATE 5 MG/ML VIAL INJECTION 12/05/2018 0.84956
HEPARIN SOD,PORK IN 0.45% NACL 25000/250 IV SOLN INTRAVEN 06/27/2018 0.04229
HEPARIN SOD,PORK IN 0.45% NACL 25000/500 IV SOLN INTRAVEN 06/27/2018 0.01540
HEPARIN SODIUM,PORCINE 1000/ML VIAL INJECTION 03/06/2019 0.16718
HEPARIN SODIUM,PORCINE 10000/ML VIAL INJECTION 08/01/2018 1.77845
HEPARIN SODIUM,PORCINE 20000/ML VIAL INJECTION 11/21/2018 5.70890
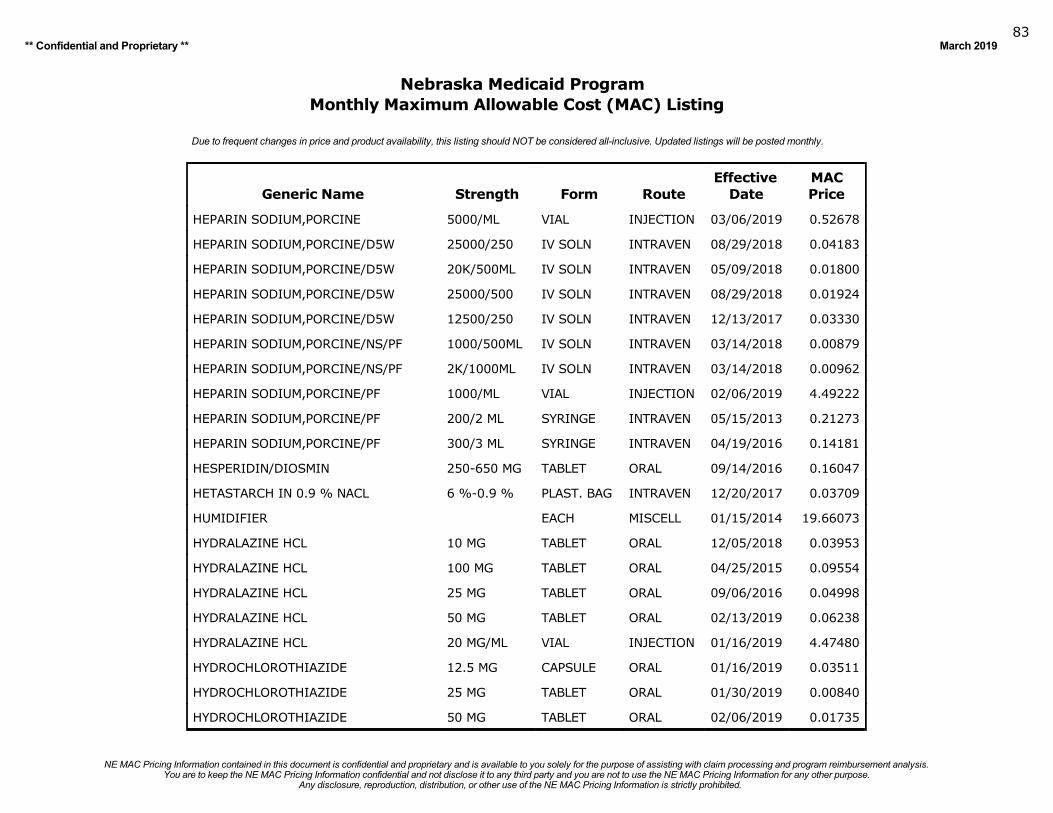
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201983
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
HEPARIN SODIUM,PORCINE 5000/ML VIAL INJECTION 03/06/2019 0.52678
HEPARIN SODIUM,PORCINE/D5W 25000/250 IV SOLN INTRAVEN 08/29/2018 0.04183
HEPARIN SODIUM,PORCINE/D5W 20K/500ML IV SOLN INTRAVEN 05/09/2018 0.01800
HEPARIN SODIUM,PORCINE/D5W 25000/500 IV SOLN INTRAVEN 08/29/2018 0.01924
HEPARIN SODIUM,PORCINE/D5W 12500/250 IV SOLN INTRAVEN 12/13/2017 0.03330
HEPARIN SODIUM,PORCINE/NS/PF 1000/500ML IV SOLN INTRAVEN 03/14/2018 0.00879
HEPARIN SODIUM,PORCINE/NS/PF 2K/1000ML IV SOLN INTRAVEN 03/14/2018 0.00962
HEPARIN SODIUM,PORCINE/PF 1000/ML VIAL INJECTION 02/06/2019 4.49222
HEPARIN SODIUM,PORCINE/PF 200/2 ML SYRINGE INTRAVEN 05/15/2013 0.21273
HEPARIN SODIUM,PORCINE/PF 300/3 ML SYRINGE INTRAVEN 04/19/2016 0.14181
HESPERIDIN/DIOSMIN 250-650 MG TABLET ORAL 09/14/2016 0.16047
HETASTARCH IN 0.9 % NACL 6 %-0.9 % PLAST. BAG INTRAVEN 12/20/2017 0.03709
HUMIDIFIER EACH MISCELL 01/15/2014 19.66073
HYDRALAZINE HCL 10 MG TABLET ORAL 12/05/2018 0.03953
HYDRALAZINE HCL 100 MG TABLET ORAL 04/25/2015 0.09554
HYDRALAZINE HCL 25 MG TABLET ORAL 09/06/2016 0.04998
HYDRALAZINE HCL 50 MG TABLET ORAL 02/13/2019 0.06238
HYDRALAZINE HCL 20 MG/ML VIAL INJECTION 01/16/2019 4.47480
HYDROCHLOROTHIAZIDE 12.5 MG CAPSULE ORAL 01/16/2019 0.03511
HYDROCHLOROTHIAZIDE 25 MG TABLET ORAL 01/30/2019 0.00840
HYDROCHLOROTHIAZIDE 50 MG TABLET ORAL 02/06/2019 0.01735
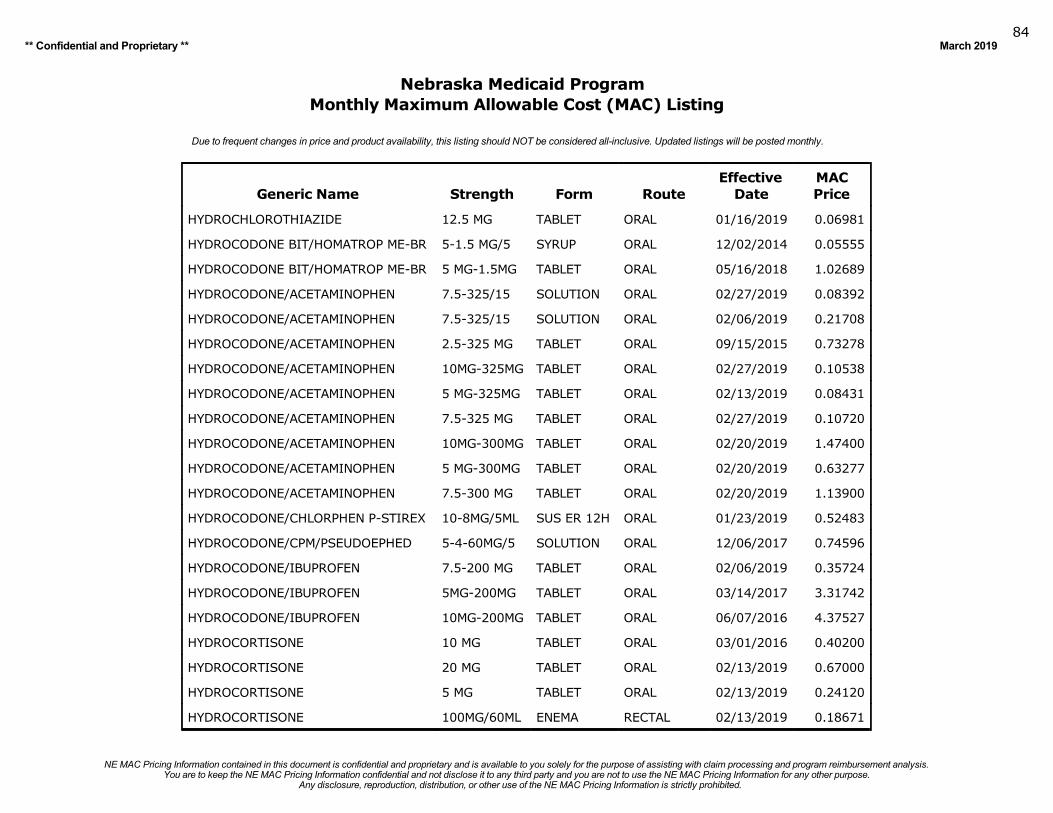
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201984
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
HYDROCHLOROTHIAZIDE 12.5 MG TABLET ORAL 01/16/2019 0.06981
HYDROCODONE BIT/HOMATROP ME-BR 5-1.5 MG/5 SYRUP ORAL 12/02/2014 0.05555
HYDROCODONE BIT/HOMATROP ME-BR 5 MG-1.5MG TABLET ORAL 05/16/2018 1.02689
HYDROCODONE/ACETAMINOPHEN 7.5-325/15 SOLUTION ORAL 02/27/2019 0.08392
HYDROCODONE/ACETAMINOPHEN 7.5-325/15 SOLUTION ORAL 02/06/2019 0.21708
HYDROCODONE/ACETAMINOPHEN 2.5-325 MG TABLET ORAL 09/15/2015 0.73278
HYDROCODONE/ACETAMINOPHEN 10MG-325MG TABLET ORAL 02/27/2019 0.10538
HYDROCODONE/ACETAMINOPHEN 5 MG-325MG TABLET ORAL 02/13/2019 0.08431
HYDROCODONE/ACETAMINOPHEN 7.5-325 MG TABLET ORAL 02/27/2019 0.10720
HYDROCODONE/ACETAMINOPHEN 10MG-300MG TABLET ORAL 02/20/2019 1.47400
HYDROCODONE/ACETAMINOPHEN 5 MG-300MG TABLET ORAL 02/20/2019 0.63277
HYDROCODONE/ACETAMINOPHEN 7.5-300 MG TABLET ORAL 02/20/2019 1.13900
HYDROCODONE/CHLORPHEN P-STIREX 10-8MG/5ML SUS ER 12H ORAL 01/23/2019 0.52483
HYDROCODONE/CPM/PSEUDOEPHED 5-4-60MG/5 SOLUTION ORAL 12/06/2017 0.74596
HYDROCODONE/IBUPROFEN 7.5-200 MG TABLET ORAL 02/06/2019 0.35724
HYDROCODONE/IBUPROFEN 5MG-200MG TABLET ORAL 03/14/2017 3.31742
HYDROCODONE/IBUPROFEN 10MG-200MG TABLET ORAL 06/07/2016 4.37527
HYDROCORTISONE 10 MG TABLET ORAL 03/01/2016 0.40200
HYDROCORTISONE 20 MG TABLET ORAL 02/13/2019 0.67000
HYDROCORTISONE 5 MG TABLET ORAL 02/13/2019 0.24120
HYDROCORTISONE 100MG/60ML ENEMA RECTAL 02/13/2019 0.18671
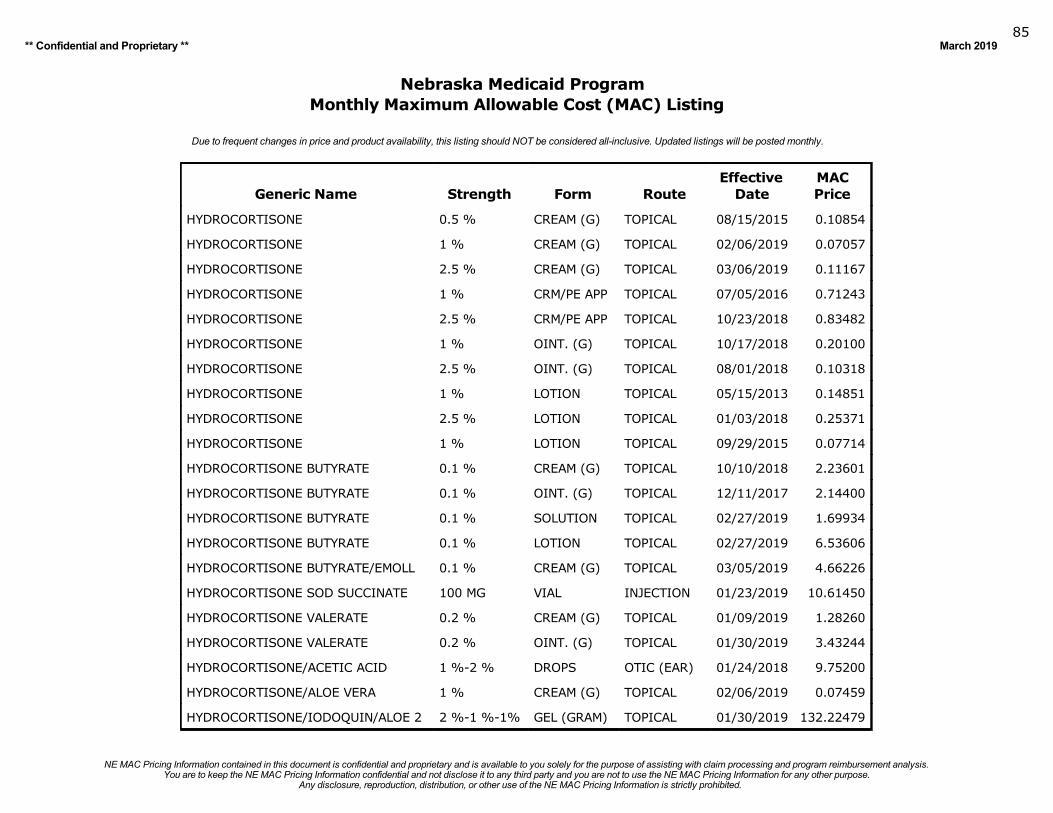
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201985
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
HYDROCORTISONE 0.5 % CREAM (G) TOPICAL 08/15/2015 0.10854
HYDROCORTISONE 1 % CREAM (G) TOPICAL 02/06/2019 0.07057
HYDROCORTISONE 2.5 % CREAM (G) TOPICAL 03/06/2019 0.11167
HYDROCORTISONE 1 % CRM/PE APP TOPICAL 07/05/2016 0.71243
HYDROCORTISONE 2.5 % CRM/PE APP TOPICAL 10/23/2018 0.83482
HYDROCORTISONE 1 % OINT. (G) TOPICAL 10/17/2018 0.20100
HYDROCORTISONE 2.5 % OINT. (G) TOPICAL 08/01/2018 0.10318
HYDROCORTISONE 1 % LOTION TOPICAL 05/15/2013 0.14851
HYDROCORTISONE 2.5 % LOTION TOPICAL 01/03/2018 0.25371
HYDROCORTISONE 1 % LOTION TOPICAL 09/29/2015 0.07714
HYDROCORTISONE BUTYRATE 0.1 % CREAM (G) TOPICAL 10/10/2018 2.23601
HYDROCORTISONE BUTYRATE 0.1 % OINT. (G) TOPICAL 12/11/2017 2.14400
HYDROCORTISONE BUTYRATE 0.1 % SOLUTION TOPICAL 02/27/2019 1.69934
HYDROCORTISONE BUTYRATE 0.1 % LOTION TOPICAL 02/27/2019 6.53606
HYDROCORTISONE BUTYRATE/EMOLL 0.1 % CREAM (G) TOPICAL 03/05/2019 4.66226
HYDROCORTISONE SOD SUCCINATE 100 MG VIAL INJECTION 01/23/2019 10.61450
HYDROCORTISONE VALERATE 0.2 % CREAM (G) TOPICAL 01/09/2019 1.28260
HYDROCORTISONE VALERATE 0.2 % OINT. (G) TOPICAL 01/30/2019 3.43244
HYDROCORTISONE/ACETIC ACID 1 %-2 % DROPS OTIC (EAR) 01/24/2018 9.75200
HYDROCORTISONE/ALOE VERA 1 % CREAM (G) TOPICAL 02/06/2019 0.07459
HYDROCORTISONE/IODOQUIN/ALOE 2 2 %-1 %-1% GEL (GRAM) TOPICAL 01/30/2019 132.22479
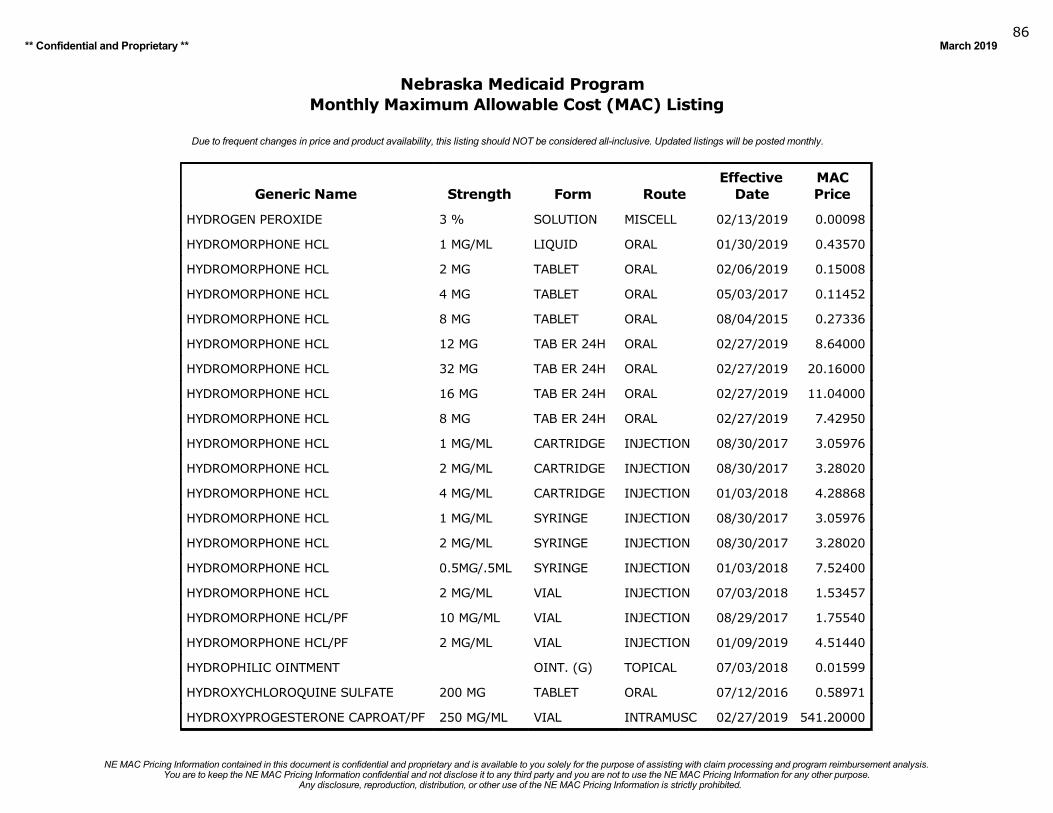
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201986
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
HYDROGEN PEROXIDE 3 % SOLUTION MISCELL 02/13/2019 0.00098
HYDROMORPHONE HCL 1 MG/ML LIQUID ORAL 01/30/2019 0.43570
HYDROMORPHONE HCL 2 MG TABLET ORAL 02/06/2019 0.15008
HYDROMORPHONE HCL 4 MG TABLET ORAL 05/03/2017 0.11452
HYDROMORPHONE HCL 8 MG TABLET ORAL 08/04/2015 0.27336
HYDROMORPHONE HCL 12 MG TAB ER 24H ORAL 02/27/2019 8.64000
HYDROMORPHONE HCL 32 MG TAB ER 24H ORAL 02/27/2019 20.16000
HYDROMORPHONE HCL 16 MG TAB ER 24H ORAL 02/27/2019 11.04000
HYDROMORPHONE HCL 8 MG TAB ER 24H ORAL 02/27/2019 7.42950
HYDROMORPHONE HCL 1 MG/ML CARTRIDGE INJECTION 08/30/2017 3.05976
HYDROMORPHONE HCL 2 MG/ML CARTRIDGE INJECTION 08/30/2017 3.28020
HYDROMORPHONE HCL 4 MG/ML CARTRIDGE INJECTION 01/03/2018 4.28868
HYDROMORPHONE HCL 1 MG/ML SYRINGE INJECTION 08/30/2017 3.05976
HYDROMORPHONE HCL 2 MG/ML SYRINGE INJECTION 08/30/2017 3.28020
HYDROMORPHONE HCL 0.5MG/.5ML SYRINGE INJECTION 01/03/2018 7.52400
HYDROMORPHONE HCL 2 MG/ML VIAL INJECTION 07/03/2018 1.53457
HYDROMORPHONE HCL/PF 10 MG/ML VIAL INJECTION 08/29/2017 1.75540
HYDROMORPHONE HCL/PF 2 MG/ML VIAL INJECTION 01/09/2019 4.51440
HYDROPHILIC OINTMENT OINT. (G) TOPICAL 07/03/2018 0.01599
HYDROXYCHLOROQUINE SULFATE 200 MG TABLET ORAL 07/12/2016 0.58971
HYDROXYPROGESTERONE CAPROAT/PF 250 MG/ML VIAL INTRAMUSC 02/27/2019 541.20000
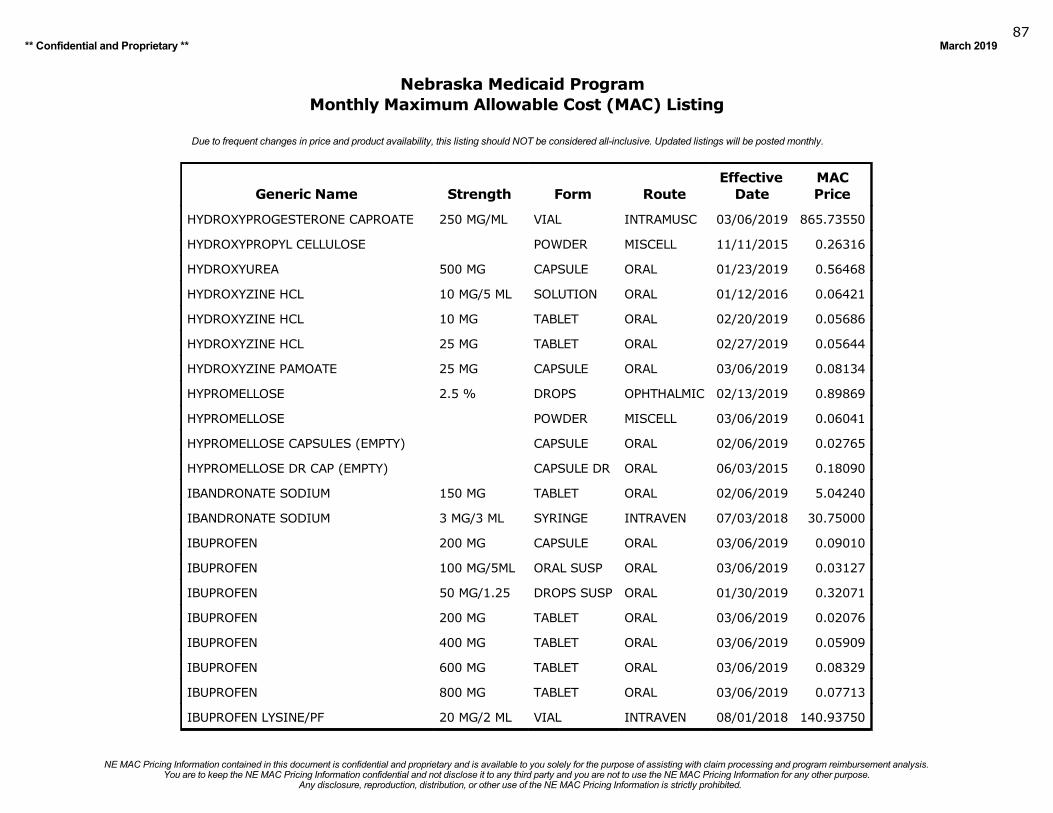
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201987
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
HYDROXYPROGESTERONE CAPROATE 250 MG/ML VIAL INTRAMUSC 03/06/2019 865.73550
HYDROXYPROPYL CELLULOSE POWDER MISCELL 11/11/2015 0.26316
HYDROXYUREA 500 MG CAPSULE ORAL 01/23/2019 0.56468
HYDROXYZINE HCL 10 MG/5 ML SOLUTION ORAL 01/12/2016 0.06421
HYDROXYZINE HCL 10 MG TABLET ORAL 02/20/2019 0.05686
HYDROXYZINE HCL 25 MG TABLET ORAL 02/27/2019 0.05644
HYDROXYZINE PAMOATE 25 MG CAPSULE ORAL 03/06/2019 0.08134
HYPROMELLOSE 2.5 % DROPS OPHTHALMIC 02/13/2019 0.89869
HYPROMELLOSE POWDER MISCELL 03/06/2019 0.06041
HYPROMELLOSE CAPSULES (EMPTY) CAPSULE ORAL 02/06/2019 0.02765
HYPROMELLOSE DR CAP (EMPTY) CAPSULE DR ORAL 06/03/2015 0.18090
IBANDRONATE SODIUM 150 MG TABLET ORAL 02/06/2019 5.04240
IBANDRONATE SODIUM 3 MG/3 ML SYRINGE INTRAVEN 07/03/2018 30.75000
IBUPROFEN 200 MG CAPSULE ORAL 03/06/2019 0.09010
IBUPROFEN 100 MG/5ML ORAL SUSP ORAL 03/06/2019 0.03127
IBUPROFEN 50 MG/1.25 DROPS SUSP ORAL 01/30/2019 0.32071
IBUPROFEN 200 MG TABLET ORAL 03/06/2019 0.02076
IBUPROFEN 400 MG TABLET ORAL 03/06/2019 0.05909
IBUPROFEN 600 MG TABLET ORAL 03/06/2019 0.08329
IBUPROFEN 800 MG TABLET ORAL 03/06/2019 0.07713
IBUPROFEN LYSINE/PF 20 MG/2 ML VIAL INTRAVEN 08/01/2018 140.93750
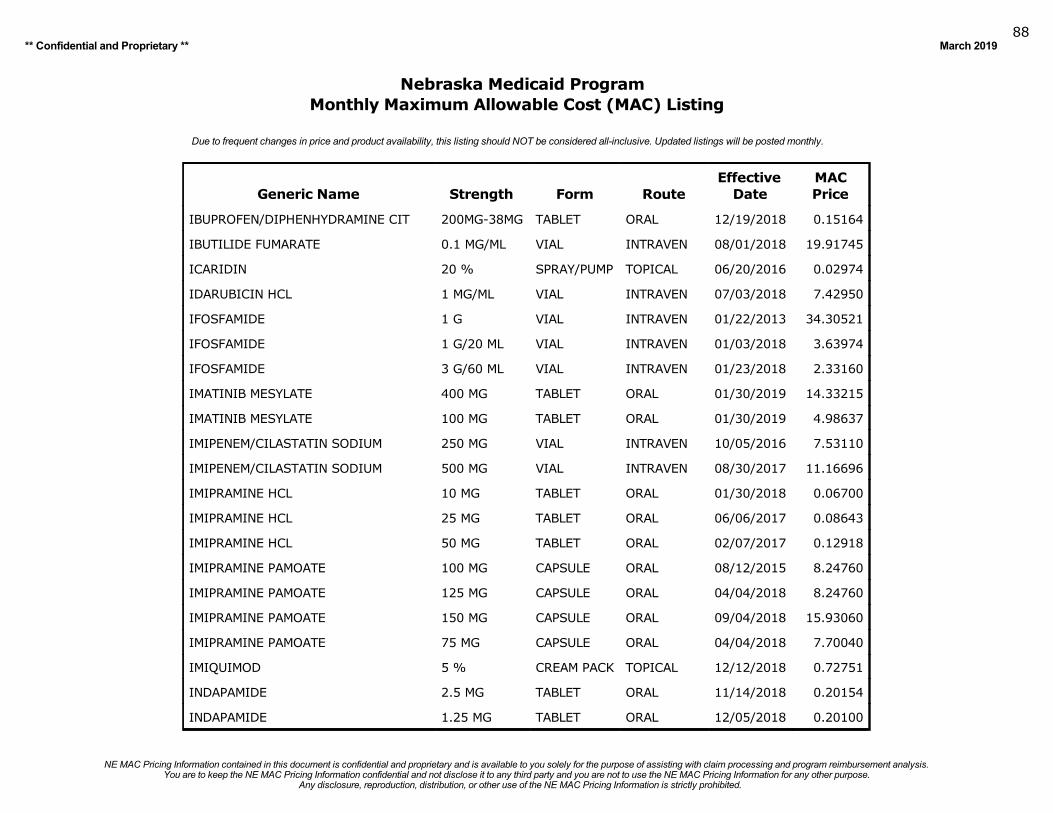
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201988
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
IBUPROFEN/DIPHENHYDRAMINE CIT 200MG-38MG TABLET ORAL 12/19/2018 0.15164
IBUTILIDE FUMARATE 0.1 MG/ML VIAL INTRAVEN 08/01/2018 19.91745
ICARIDIN 20 % SPRAY/PUMP TOPICAL 06/20/2016 0.02974
IDARUBICIN HCL 1 MG/ML VIAL INTRAVEN 07/03/2018 7.42950
IFOSFAMIDE 1 G VIAL INTRAVEN 01/22/2013 34.30521
IFOSFAMIDE 1 G/20 ML VIAL INTRAVEN 01/03/2018 3.63974
IFOSFAMIDE 3 G/60 ML VIAL INTRAVEN 01/23/2018 2.33160
IMATINIB MESYLATE 400 MG TABLET ORAL 01/30/2019 14.33215
IMATINIB MESYLATE 100 MG TABLET ORAL 01/30/2019 4.98637
IMIPENEM/CILASTATIN SODIUM 250 MG VIAL INTRAVEN 10/05/2016 7.53110
IMIPENEM/CILASTATIN SODIUM 500 MG VIAL INTRAVEN 08/30/2017 11.16696
IMIPRAMINE HCL 10 MG TABLET ORAL 01/30/2018 0.06700
IMIPRAMINE HCL 25 MG TABLET ORAL 06/06/2017 0.08643
IMIPRAMINE HCL 50 MG TABLET ORAL 02/07/2017 0.12918
IMIPRAMINE PAMOATE 100 MG CAPSULE ORAL 08/12/2015 8.24760
IMIPRAMINE PAMOATE 125 MG CAPSULE ORAL 04/04/2018 8.24760
IMIPRAMINE PAMOATE 150 MG CAPSULE ORAL 09/04/2018 15.93060
IMIPRAMINE PAMOATE 75 MG CAPSULE ORAL 04/04/2018 7.70040
IMIQUIMOD 5 % CREAM PACK TOPICAL 12/12/2018 0.72751
INDAPAMIDE 2.5 MG TABLET ORAL 11/14/2018 0.20154
INDAPAMIDE 1.25 MG TABLET ORAL 12/05/2018 0.20100
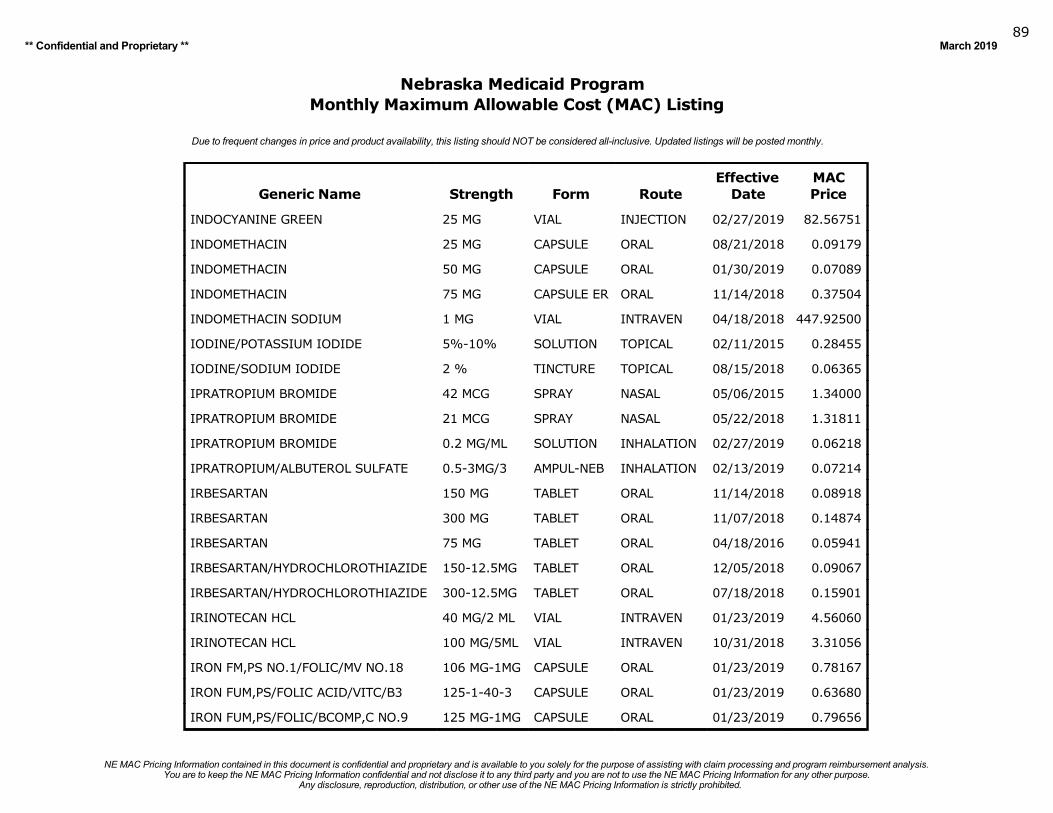
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201989
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
INDOCYANINE GREEN 25 MG VIAL INJECTION 02/27/2019 82.56751
INDOMETHACIN 25 MG CAPSULE ORAL 08/21/2018 0.09179
INDOMETHACIN 50 MG CAPSULE ORAL 01/30/2019 0.07089
INDOMETHACIN 75 MG CAPSULE ER ORAL 11/14/2018 0.37504
INDOMETHACIN SODIUM 1 MG VIAL INTRAVEN 04/18/2018 447.92500
IODINE/POTASSIUM IODIDE 5%-10% SOLUTION TOPICAL 02/11/2015 0.28455
IODINE/SODIUM IODIDE 2 % TINCTURE TOPICAL 08/15/2018 0.06365
IPRATROPIUM BROMIDE 42 MCG SPRAY NASAL 05/06/2015 1.34000
IPRATROPIUM BROMIDE 21 MCG SPRAY NASAL 05/22/2018 1.31811
IPRATROPIUM BROMIDE 0.2 MG/ML SOLUTION INHALATION 02/27/2019 0.06218
IPRATROPIUM/ALBUTEROL SULFATE 0.5-3MG/3 AMPUL-NEB INHALATION 02/13/2019 0.07214
IRBESARTAN 150 MG TABLET ORAL 11/14/2018 0.08918
IRBESARTAN 300 MG TABLET ORAL 11/07/2018 0.14874
IRBESARTAN 75 MG TABLET ORAL 04/18/2016 0.05941
IRBESARTAN/HYDROCHLOROTHIAZIDE 150-12.5MG TABLET ORAL 12/05/2018 0.09067
IRBESARTAN/HYDROCHLOROTHIAZIDE 300-12.5MG TABLET ORAL 07/18/2018 0.15901
IRINOTECAN HCL 40 MG/2 ML VIAL INTRAVEN 01/23/2019 4.56060
IRINOTECAN HCL 100 MG/5ML VIAL INTRAVEN 10/31/2018 3.31056
IRON FM,PS NO.1/FOLIC/MV NO.18 106 MG-1MG CAPSULE ORAL 01/23/2019 0.78167
IRON FUM,PS/FOLIC ACID/VITC/B3 125-1-40-3 CAPSULE ORAL 01/23/2019 0.63680
IRON FUM,PS/FOLIC/BCOMP,C NO.9 125 MG-1MG CAPSULE ORAL 01/23/2019 0.79656
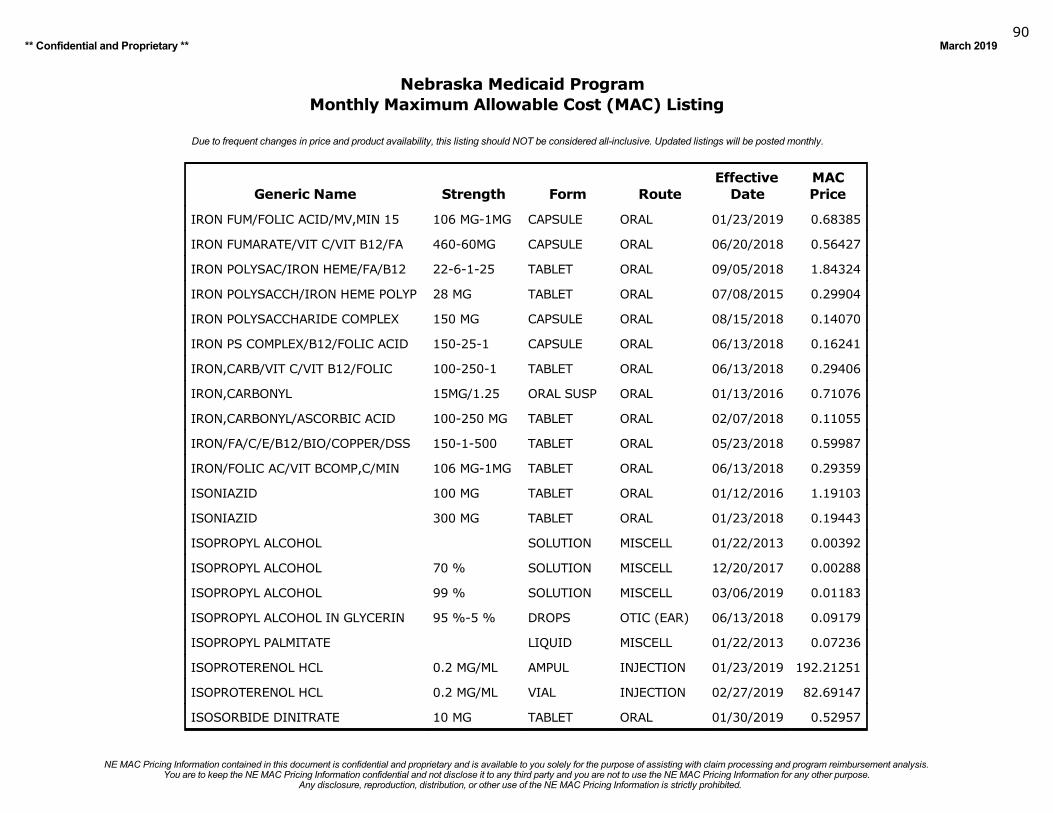
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201990
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
IRON FUM/FOLIC ACID/MV,MIN 15 106 MG-1MG CAPSULE ORAL 01/23/2019 0.68385
IRON FUMARATE/VIT C/VIT B12/FA 460-60MG CAPSULE ORAL 06/20/2018 0.56427
IRON POLYSAC/IRON HEME/FA/B12 22-6-1-25 TABLET ORAL 09/05/2018 1.84324
IRON POLYSACCH/IRON HEME POLYP 28 MG TABLET ORAL 07/08/2015 0.29904
IRON POLYSACCHARIDE COMPLEX 150 MG CAPSULE ORAL 08/15/2018 0.14070
IRON PS COMPLEX/B12/FOLIC ACID 150-25-1 CAPSULE ORAL 06/13/2018 0.16241
IRON,CARB/VIT C/VIT B12/FOLIC 100-250-1 TABLET ORAL 06/13/2018 0.29406
IRON,CARBONYL 15MG/1.25 ORAL SUSP ORAL 01/13/2016 0.71076
IRON,CARBONYL/ASCORBIC ACID 100-250 MG TABLET ORAL 02/07/2018 0.11055
IRON/FA/C/E/B12/BIO/COPPER/DSS 150-1-500 TABLET ORAL 05/23/2018 0.59987
IRON/FOLIC AC/VIT BCOMP,C/MIN 106 MG-1MG TABLET ORAL 06/13/2018 0.29359
ISONIAZID 100 MG TABLET ORAL 01/12/2016 1.19103
ISONIAZID 300 MG TABLET ORAL 01/23/2018 0.19443
ISOPROPYL ALCOHOL SOLUTION MISCELL 01/22/2013 0.00392
ISOPROPYL ALCOHOL 70 % SOLUTION MISCELL 12/20/2017 0.00288
ISOPROPYL ALCOHOL 99 % SOLUTION MISCELL 03/06/2019 0.01183
ISOPROPYL ALCOHOL IN GLYCERIN 95 %-5 % DROPS OTIC (EAR) 06/13/2018 0.09179
ISOPROPYL PALMITATE LIQUID MISCELL 01/22/2013 0.07236
ISOPROTERENOL HCL 0.2 MG/ML AMPUL INJECTION 01/23/2019 192.21251
ISOPROTERENOL HCL 0.2 MG/ML VIAL INJECTION 02/27/2019 82.69147
ISOSORBIDE DINITRATE 10 MG TABLET ORAL 01/30/2019 0.52957
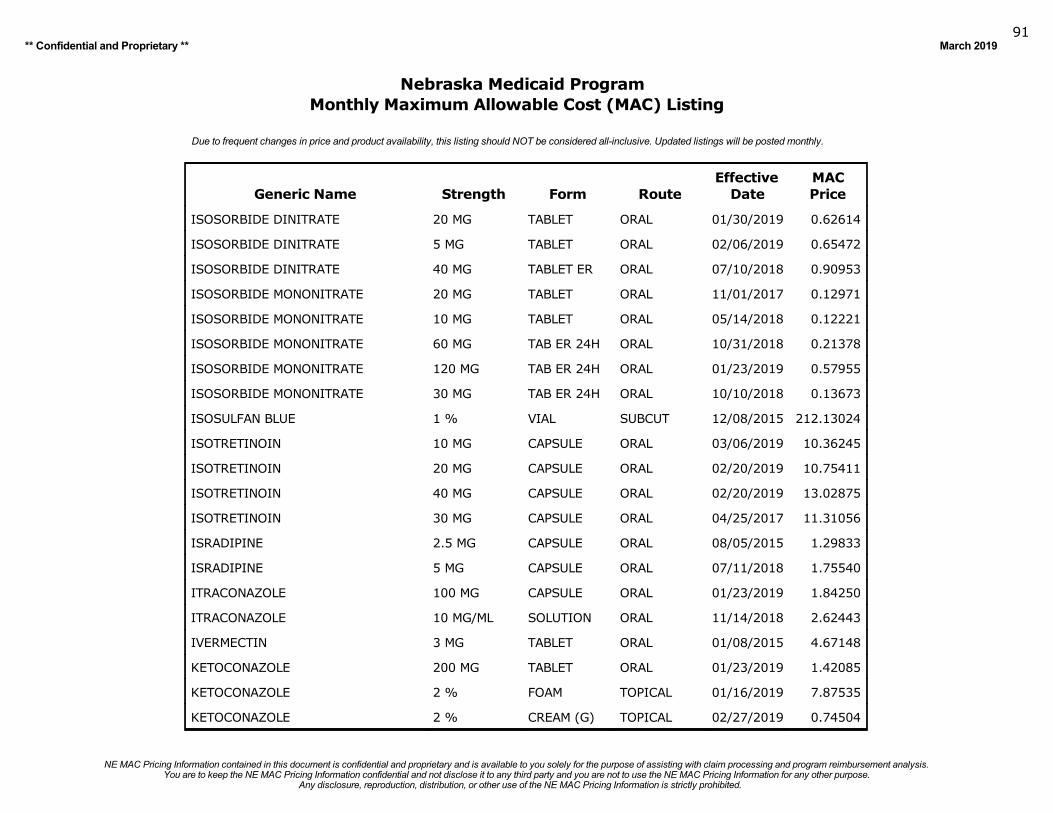
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201991
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ISOSORBIDE DINITRATE 20 MG TABLET ORAL 01/30/2019 0.62614
ISOSORBIDE DINITRATE 5 MG TABLET ORAL 02/06/2019 0.65472
ISOSORBIDE DINITRATE 40 MG TABLET ER ORAL 07/10/2018 0.90953
ISOSORBIDE MONONITRATE 20 MG TABLET ORAL 11/01/2017 0.12971
ISOSORBIDE MONONITRATE 10 MG TABLET ORAL 05/14/2018 0.12221
ISOSORBIDE MONONITRATE 60 MG TAB ER 24H ORAL 10/31/2018 0.21378
ISOSORBIDE MONONITRATE 120 MG TAB ER 24H ORAL 01/23/2019 0.57955
ISOSORBIDE MONONITRATE 30 MG TAB ER 24H ORAL 10/10/2018 0.13673
ISOSULFAN BLUE 1 % VIAL SUBCUT 12/08/2015 212.13024
ISOTRETINOIN 10 MG CAPSULE ORAL 03/06/2019 10.36245
ISOTRETINOIN 20 MG CAPSULE ORAL 02/20/2019 10.75411
ISOTRETINOIN 40 MG CAPSULE ORAL 02/20/2019 13.02875
ISOTRETINOIN 30 MG CAPSULE ORAL 04/25/2017 11.31056
ISRADIPINE 2.5 MG CAPSULE ORAL 08/05/2015 1.29833
ISRADIPINE 5 MG CAPSULE ORAL 07/11/2018 1.75540
ITRACONAZOLE 100 MG CAPSULE ORAL 01/23/2019 1.84250
ITRACONAZOLE 10 MG/ML SOLUTION ORAL 11/14/2018 2.62443
IVERMECTIN 3 MG TABLET ORAL 01/08/2015 4.67148
KETOCONAZOLE 200 MG TABLET ORAL 01/23/2019 1.42085
KETOCONAZOLE 2 % FOAM TOPICAL 01/16/2019 7.87535
KETOCONAZOLE 2 % CREAM (G) TOPICAL 02/27/2019 0.74504
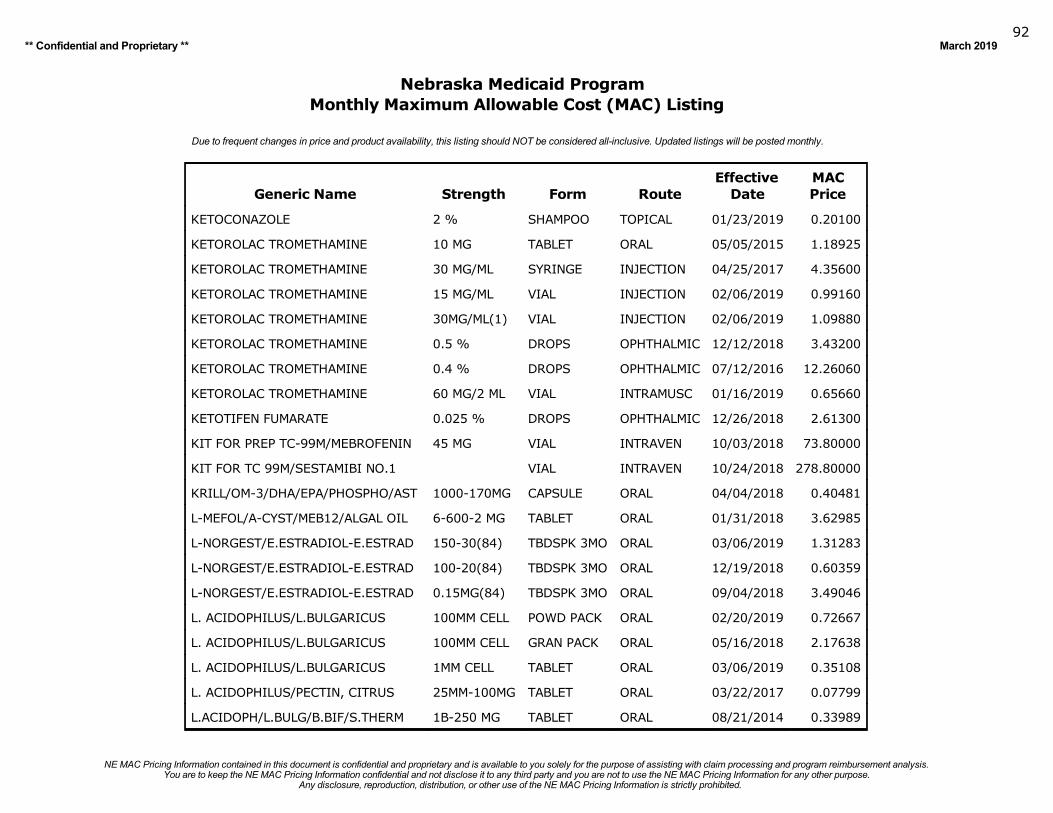
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201992
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
KETOCONAZOLE 2 % SHAMPOO TOPICAL 01/23/2019 0.20100
KETOROLAC TROMETHAMINE 10 MG TABLET ORAL 05/05/2015 1.18925
KETOROLAC TROMETHAMINE 30 MG/ML SYRINGE INJECTION 04/25/2017 4.35600
KETOROLAC TROMETHAMINE 15 MG/ML VIAL INJECTION 02/06/2019 0.99160
KETOROLAC TROMETHAMINE 30MG/ML(1) VIAL INJECTION 02/06/2019 1.09880
KETOROLAC TROMETHAMINE 0.5 % DROPS OPHTHALMIC 12/12/2018 3.43200
KETOROLAC TROMETHAMINE 0.4 % DROPS OPHTHALMIC 07/12/2016 12.26060
KETOROLAC TROMETHAMINE 60 MG/2 ML VIAL INTRAMUSC 01/16/2019 0.65660
KETOTIFEN FUMARATE 0.025 % DROPS OPHTHALMIC 12/26/2018 2.61300
KIT FOR PREP TC-99M/MEBROFENIN 45 MG VIAL INTRAVEN 10/03/2018 73.80000
KIT FOR TC 99M/SESTAMIBI NO.1 VIAL INTRAVEN 10/24/2018 278.80000
KRILL/OM-3/DHA/EPA/PHOSPHO/AST 1000-170MG CAPSULE ORAL 04/04/2018 0.40481
L-MEFOL/A-CYST/MEB12/ALGAL OIL 6-600-2 MG TABLET ORAL 01/31/2018 3.62985
L-NORGEST/E.ESTRADIOL-E.ESTRAD 150-30(84) TBDSPK 3MO ORAL 03/06/2019 1.31283
L-NORGEST/E.ESTRADIOL-E.ESTRAD 100-20(84) TBDSPK 3MO ORAL 12/19/2018 0.60359
L-NORGEST/E.ESTRADIOL-E.ESTRAD 0.15MG(84) TBDSPK 3MO ORAL 09/04/2018 3.49046
L. ACIDOPHILUS/L.BULGARICUS 100MM CELL POWD PACK ORAL 02/20/2019 0.72667
L. ACIDOPHILUS/L.BULGARICUS 100MM CELL GRAN PACK ORAL 05/16/2018 2.17638
L. ACIDOPHILUS/L.BULGARICUS 1MM CELL TABLET ORAL 03/06/2019 0.35108
L. ACIDOPHILUS/PECTIN, CITRUS 25MM-100MG TABLET ORAL 03/22/2017 0.07799
L.ACIDOPH/L.BULG/B.BIF/S.THERM 1B-250 MG TABLET ORAL 08/21/2014 0.33989
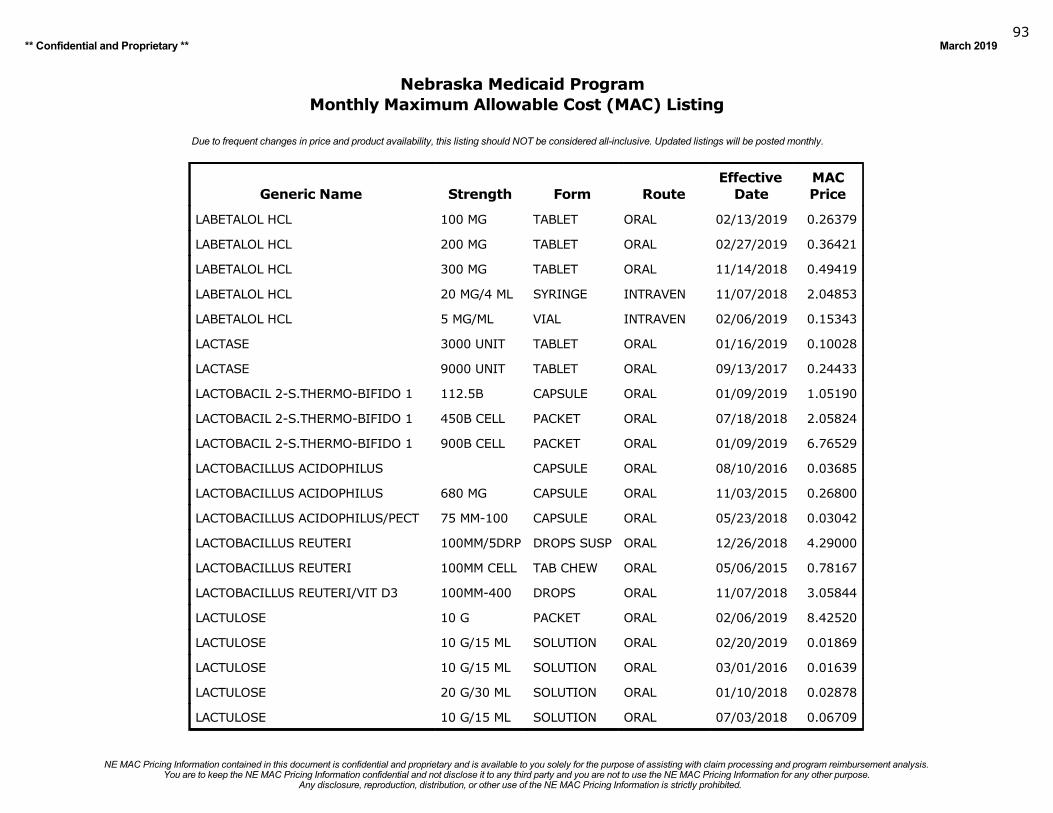
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201993
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
LABETALOL HCL 100 MG TABLET ORAL 02/13/2019 0.26379
LABETALOL HCL 200 MG TABLET ORAL 02/27/2019 0.36421
LABETALOL HCL 300 MG TABLET ORAL 11/14/2018 0.49419
LABETALOL HCL 20 MG/4 ML SYRINGE INTRAVEN 11/07/2018 2.04853
LABETALOL HCL 5 MG/ML VIAL INTRAVEN 02/06/2019 0.15343
LACTASE 3000 UNIT TABLET ORAL 01/16/2019 0.10028
LACTASE 9000 UNIT TABLET ORAL 09/13/2017 0.24433
LACTOBACIL 2-S.THERMO-BIFIDO 1 112.5B CAPSULE ORAL 01/09/2019 1.05190
LACTOBACIL 2-S.THERMO-BIFIDO 1 450B CELL PACKET ORAL 07/18/2018 2.05824
LACTOBACIL 2-S.THERMO-BIFIDO 1 900B CELL PACKET ORAL 01/09/2019 6.76529
LACTOBACILLUS ACIDOPHILUS CAPSULE ORAL 08/10/2016 0.03685
LACTOBACILLUS ACIDOPHILUS 680 MG CAPSULE ORAL 11/03/2015 0.26800
LACTOBACILLUS ACIDOPHILUS/PECT 75 MM-100 CAPSULE ORAL 05/23/2018 0.03042
LACTOBACILLUS REUTERI 100MM/5DRP DROPS SUSP ORAL 12/26/2018 4.29000
LACTOBACILLUS REUTERI 100MM CELL TAB CHEW ORAL 05/06/2015 0.78167
LACTOBACILLUS REUTERI/VIT D3 100MM-400 DROPS ORAL 11/07/2018 3.05844
LACTULOSE 10 G PACKET ORAL 02/06/2019 8.42520
LACTULOSE 10 G/15 ML SOLUTION ORAL 02/20/2019 0.01869
LACTULOSE 10 G/15 ML SOLUTION ORAL 03/01/2016 0.01639
LACTULOSE 20 G/30 ML SOLUTION ORAL 01/10/2018 0.02878
LACTULOSE 10 G/15 ML SOLUTION ORAL 07/03/2018 0.06709
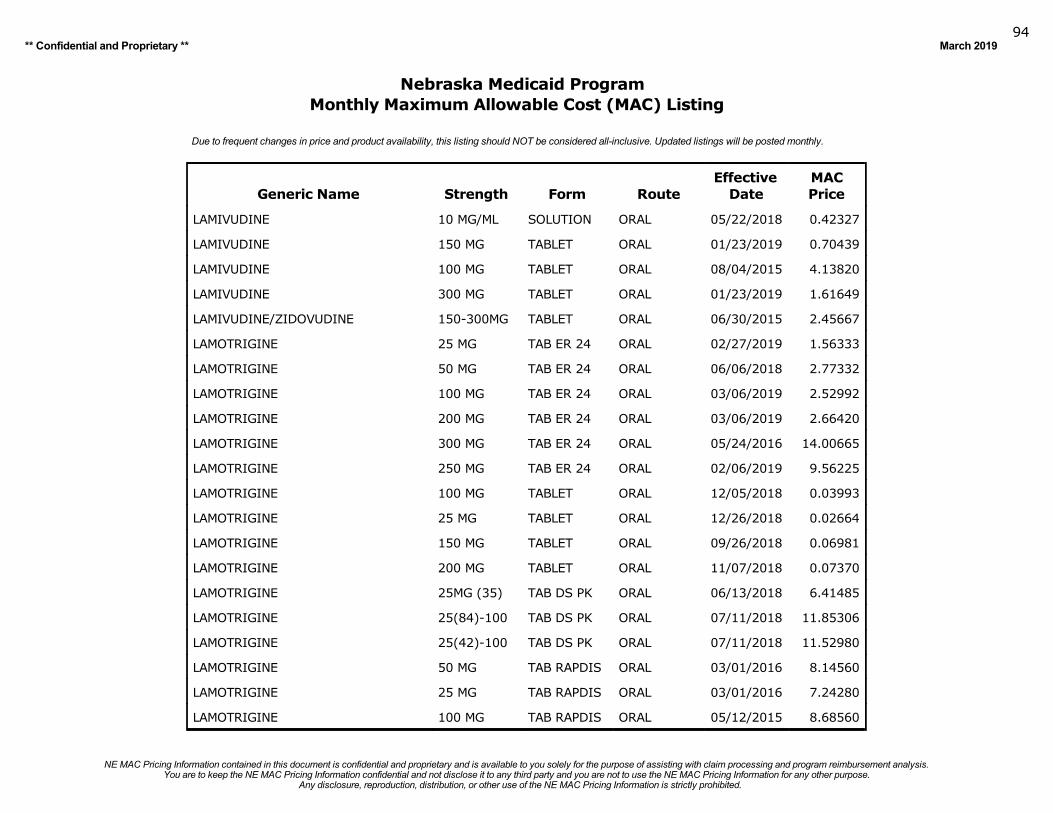
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201994
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
LAMIVUDINE 10 MG/ML SOLUTION ORAL 05/22/2018 0.42327
LAMIVUDINE 150 MG TABLET ORAL 01/23/2019 0.70439
LAMIVUDINE 100 MG TABLET ORAL 08/04/2015 4.13820
LAMIVUDINE 300 MG TABLET ORAL 01/23/2019 1.61649
LAMIVUDINE/ZIDOVUDINE 150-300MG TABLET ORAL 06/30/2015 2.45667
LAMOTRIGINE 25 MG TAB ER 24 ORAL 02/27/2019 1.56333
LAMOTRIGINE 50 MG TAB ER 24 ORAL 06/06/2018 2.77332
LAMOTRIGINE 100 MG TAB ER 24 ORAL 03/06/2019 2.52992
LAMOTRIGINE 200 MG TAB ER 24 ORAL 03/06/2019 2.66420
LAMOTRIGINE 300 MG TAB ER 24 ORAL 05/24/2016 14.00665
LAMOTRIGINE 250 MG TAB ER 24 ORAL 02/06/2019 9.56225
LAMOTRIGINE 100 MG TABLET ORAL 12/05/2018 0.03993
LAMOTRIGINE 25 MG TABLET ORAL 12/26/2018 0.02664
LAMOTRIGINE 150 MG TABLET ORAL 09/26/2018 0.06981
LAMOTRIGINE 200 MG TABLET ORAL 11/07/2018 0.07370
LAMOTRIGINE 25MG (35) TAB DS PK ORAL 06/13/2018 6.41485
LAMOTRIGINE 25(84)-100 TAB DS PK ORAL 07/11/2018 11.85306
LAMOTRIGINE 25(42)-100 TAB DS PK ORAL 07/11/2018 11.52980
LAMOTRIGINE 50 MG TAB RAPDIS ORAL 03/01/2016 8.14560
LAMOTRIGINE 25 MG TAB RAPDIS ORAL 03/01/2016 7.24280
LAMOTRIGINE 100 MG TAB RAPDIS ORAL 05/12/2015 8.68560
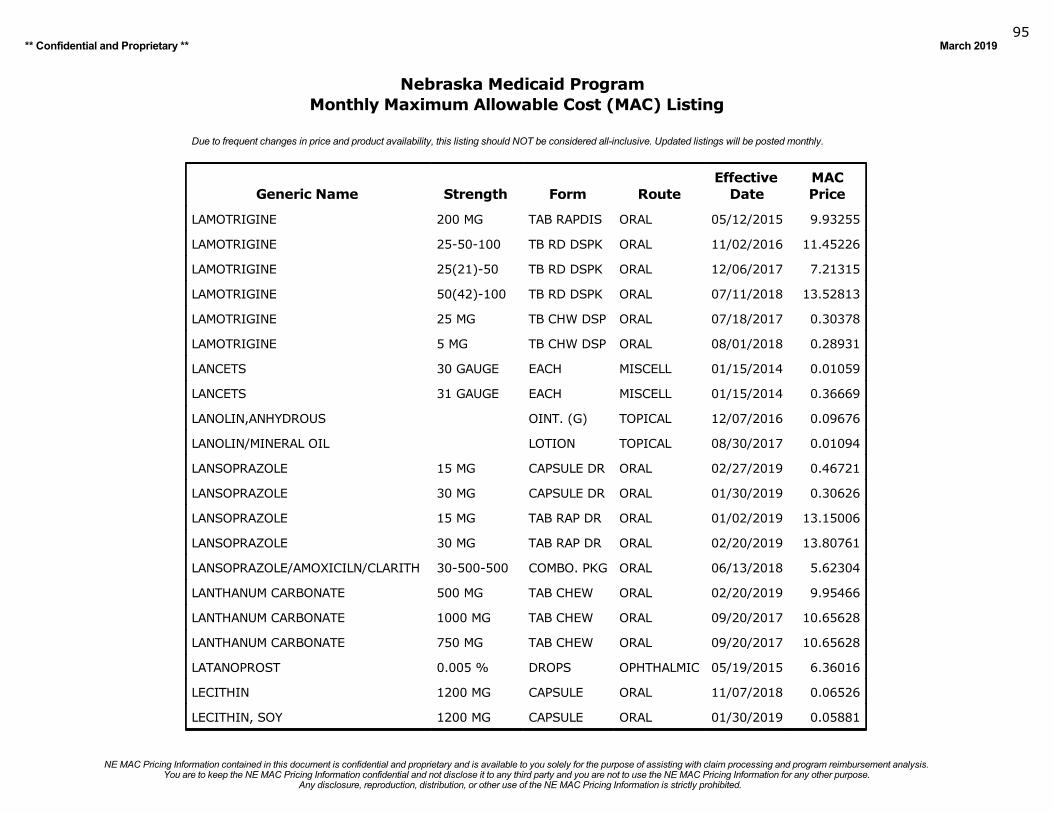
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201995
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
LAMOTRIGINE 200 MG TAB RAPDIS ORAL 05/12/2015 9.93255
LAMOTRIGINE 25-50-100 TB RD DSPK ORAL 11/02/2016 11.45226
LAMOTRIGINE 25(21)-50 TB RD DSPK ORAL 12/06/2017 7.21315
LAMOTRIGINE 50(42)-100 TB RD DSPK ORAL 07/11/2018 13.52813
LAMOTRIGINE 25 MG TB CHW DSP ORAL 07/18/2017 0.30378
LAMOTRIGINE 5 MG TB CHW DSP ORAL 08/01/2018 0.28931
LANCETS 30 GAUGE EACH MISCELL 01/15/2014 0.01059
LANCETS 31 GAUGE EACH MISCELL 01/15/2014 0.36669
LANOLIN,ANHYDROUS OINT. (G) TOPICAL 12/07/2016 0.09676
LANOLIN/MINERAL OIL LOTION TOPICAL 08/30/2017 0.01094
LANSOPRAZOLE 15 MG CAPSULE DR ORAL 02/27/2019 0.46721
LANSOPRAZOLE 30 MG CAPSULE DR ORAL 01/30/2019 0.30626
LANSOPRAZOLE 15 MG TAB RAP DR ORAL 01/02/2019 13.15006
LANSOPRAZOLE 30 MG TAB RAP DR ORAL 02/20/2019 13.80761
LANSOPRAZOLE/AMOXICILN/CLARITH 30-500-500 COMBO. PKG ORAL 06/13/2018 5.62304
LANTHANUM CARBONATE 500 MG TAB CHEW ORAL 02/20/2019 9.95466
LANTHANUM CARBONATE 1000 MG TAB CHEW ORAL 09/20/2017 10.65628
LANTHANUM CARBONATE 750 MG TAB CHEW ORAL 09/20/2017 10.65628
LATANOPROST 0.005 % DROPS OPHTHALMIC 05/19/2015 6.36016
LECITHIN 1200 MG CAPSULE ORAL 11/07/2018 0.06526
LECITHIN, SOY 1200 MG CAPSULE ORAL 01/30/2019 0.05881
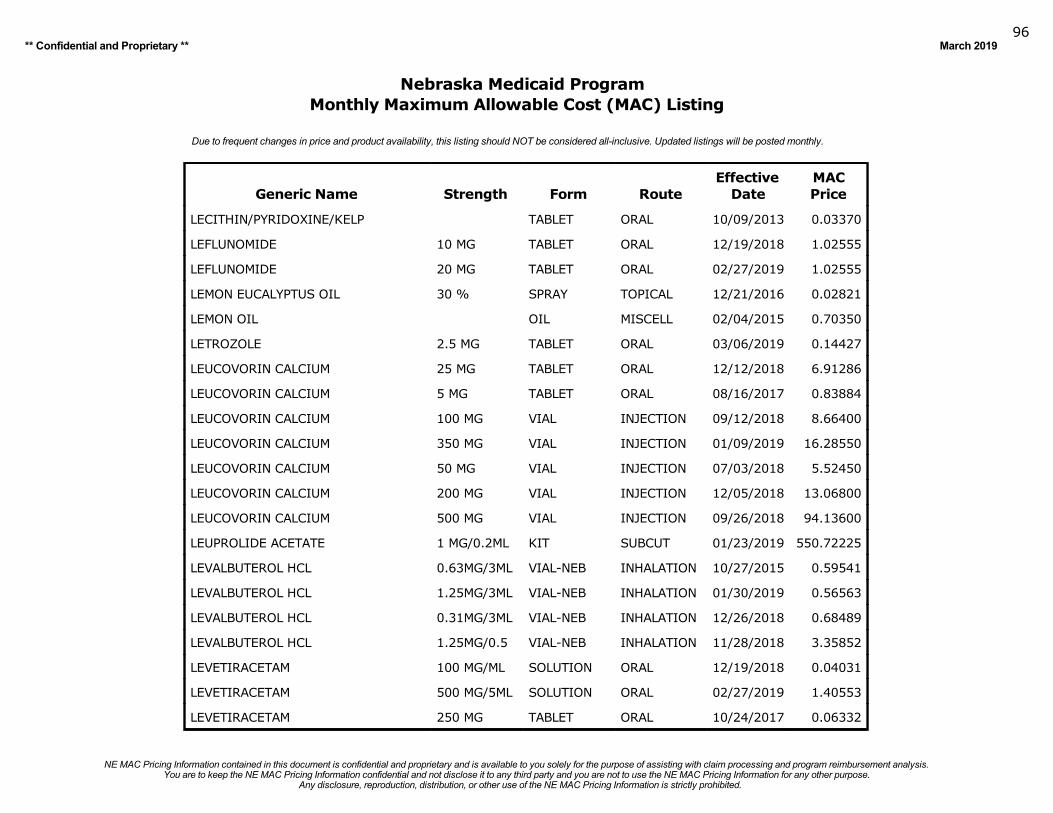
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201996
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
LECITHIN/PYRIDOXINE/KELP TABLET ORAL 10/09/2013 0.03370
LEFLUNOMIDE 10 MG TABLET ORAL 12/19/2018 1.02555
LEFLUNOMIDE 20 MG TABLET ORAL 02/27/2019 1.02555
LEMON EUCALYPTUS OIL 30 % SPRAY TOPICAL 12/21/2016 0.02821
LEMON OIL OIL MISCELL 02/04/2015 0.70350
LETROZOLE 2.5 MG TABLET ORAL 03/06/2019 0.14427
LEUCOVORIN CALCIUM 25 MG TABLET ORAL 12/12/2018 6.91286
LEUCOVORIN CALCIUM 5 MG TABLET ORAL 08/16/2017 0.83884
LEUCOVORIN CALCIUM 100 MG VIAL INJECTION 09/12/2018 8.66400
LEUCOVORIN CALCIUM 350 MG VIAL INJECTION 01/09/2019 16.28550
LEUCOVORIN CALCIUM 50 MG VIAL INJECTION 07/03/2018 5.52450
LEUCOVORIN CALCIUM 200 MG VIAL INJECTION 12/05/2018 13.06800
LEUCOVORIN CALCIUM 500 MG VIAL INJECTION 09/26/2018 94.13600
LEUPROLIDE ACETATE 1 MG/0.2ML KIT SUBCUT 01/23/2019 550.72225
LEVALBUTEROL HCL 0.63MG/3ML VIAL-NEB INHALATION 10/27/2015 0.59541
LEVALBUTEROL HCL 1.25MG/3ML VIAL-NEB INHALATION 01/30/2019 0.56563
LEVALBUTEROL HCL 0.31MG/3ML VIAL-NEB INHALATION 12/26/2018 0.68489
LEVALBUTEROL HCL 1.25MG/0.5 VIAL-NEB INHALATION 11/28/2018 3.35852
LEVETIRACETAM 100 MG/ML SOLUTION ORAL 12/19/2018 0.04031
LEVETIRACETAM 500 MG/5ML SOLUTION ORAL 02/27/2019 1.40553
LEVETIRACETAM 250 MG TABLET ORAL 10/24/2017 0.06332
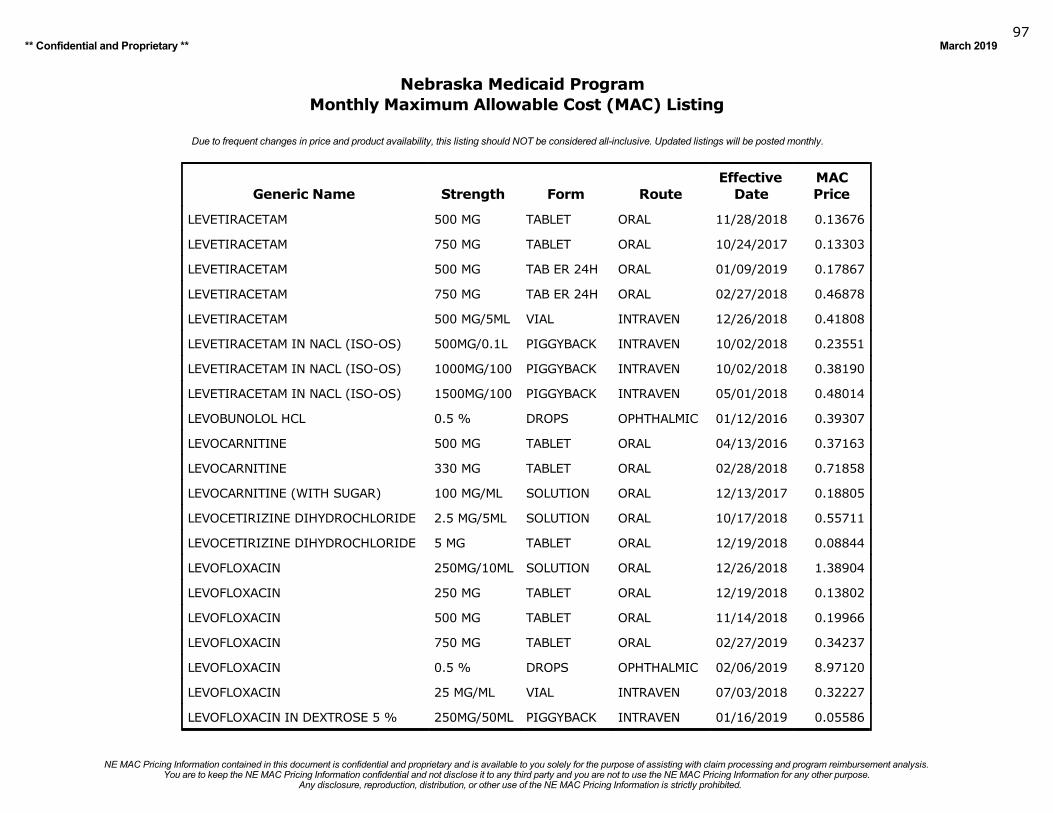
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201997
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
LEVETIRACETAM 500 MG TABLET ORAL 11/28/2018 0.13676
LEVETIRACETAM 750 MG TABLET ORAL 10/24/2017 0.13303
LEVETIRACETAM 500 MG TAB ER 24H ORAL 01/09/2019 0.17867
LEVETIRACETAM 750 MG TAB ER 24H ORAL 02/27/2018 0.46878
LEVETIRACETAM 500 MG/5ML VIAL INTRAVEN 12/26/2018 0.41808
LEVETIRACETAM IN NACL (ISO-OS) 500MG/0.1L PIGGYBACK INTRAVEN 10/02/2018 0.23551
LEVETIRACETAM IN NACL (ISO-OS) 1000MG/100 PIGGYBACK INTRAVEN 10/02/2018 0.38190
LEVETIRACETAM IN NACL (ISO-OS) 1500MG/100 PIGGYBACK INTRAVEN 05/01/2018 0.48014
LEVOBUNOLOL HCL 0.5 % DROPS OPHTHALMIC 01/12/2016 0.39307
LEVOCARNITINE 500 MG TABLET ORAL 04/13/2016 0.37163
LEVOCARNITINE 330 MG TABLET ORAL 02/28/2018 0.71858
LEVOCARNITINE (WITH SUGAR) 100 MG/ML SOLUTION ORAL 12/13/2017 0.18805
LEVOCETIRIZINE DIHYDROCHLORIDE 2.5 MG/5ML SOLUTION ORAL 10/17/2018 0.55711
LEVOCETIRIZINE DIHYDROCHLORIDE 5 MG TABLET ORAL 12/19/2018 0.08844
LEVOFLOXACIN 250MG/10ML SOLUTION ORAL 12/26/2018 1.38904
LEVOFLOXACIN 250 MG TABLET ORAL 12/19/2018 0.13802
LEVOFLOXACIN 500 MG TABLET ORAL 11/14/2018 0.19966
LEVOFLOXACIN 750 MG TABLET ORAL 02/27/2019 0.34237
LEVOFLOXACIN 0.5 % DROPS OPHTHALMIC 02/06/2019 8.97120
LEVOFLOXACIN 25 MG/ML VIAL INTRAVEN 07/03/2018 0.32227
LEVOFLOXACIN IN DEXTROSE 5 % 250MG/50ML PIGGYBACK INTRAVEN 01/16/2019 0.05586
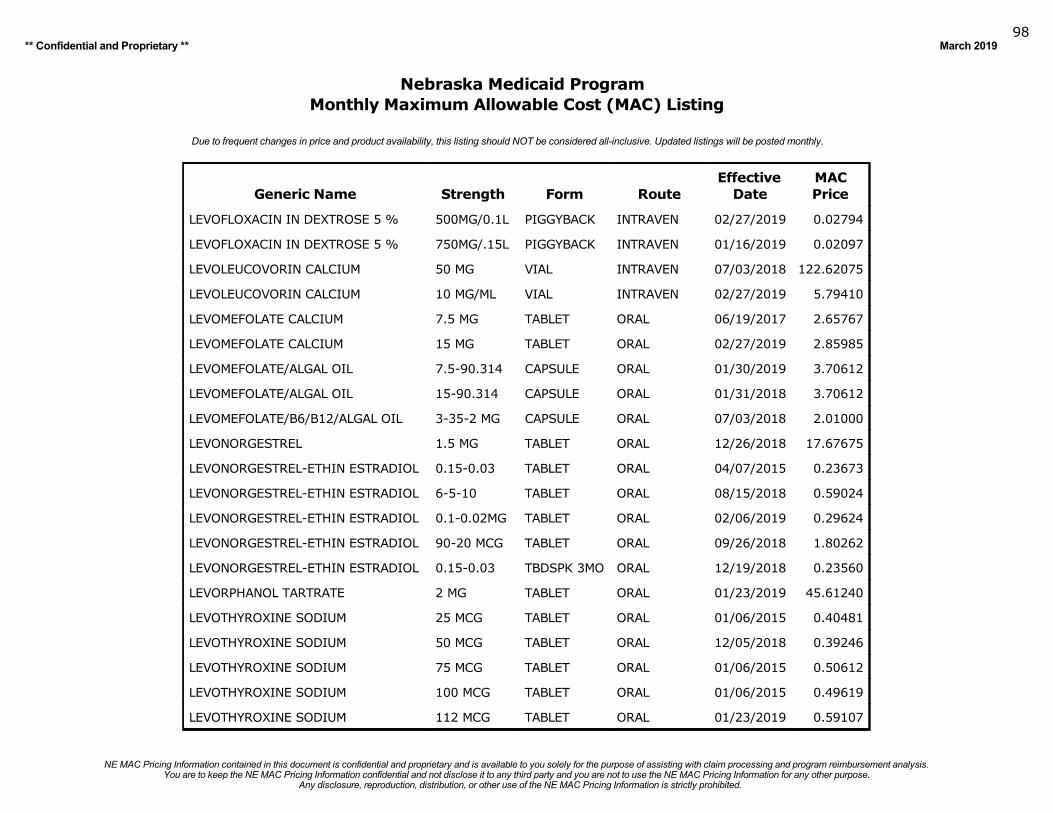
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201998
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
LEVOFLOXACIN IN DEXTROSE 5 % 500MG/0.1L PIGGYBACK INTRAVEN 02/27/2019 0.02794
LEVOFLOXACIN IN DEXTROSE 5 % 750MG/.15L PIGGYBACK INTRAVEN 01/16/2019 0.02097
LEVOLEUCOVORIN CALCIUM 50 MG VIAL INTRAVEN 07/03/2018 122.62075
LEVOLEUCOVORIN CALCIUM 10 MG/ML VIAL INTRAVEN 02/27/2019 5.79410
LEVOMEFOLATE CALCIUM 7.5 MG TABLET ORAL 06/19/2017 2.65767
LEVOMEFOLATE CALCIUM 15 MG TABLET ORAL 02/27/2019 2.85985
LEVOMEFOLATE/ALGAL OIL 7.5-90.314 CAPSULE ORAL 01/30/2019 3.70612
LEVOMEFOLATE/ALGAL OIL 15-90.314 CAPSULE ORAL 01/31/2018 3.70612
LEVOMEFOLATE/B6/B12/ALGAL OIL 3-35-2 MG CAPSULE ORAL 07/03/2018 2.01000
LEVONORGESTREL 1.5 MG TABLET ORAL 12/26/2018 17.67675
LEVONORGESTREL-ETHIN ESTRADIOL 0.15-0.03 TABLET ORAL 04/07/2015 0.23673
LEVONORGESTREL-ETHIN ESTRADIOL 6-5-10 TABLET ORAL 08/15/2018 0.59024
LEVONORGESTREL-ETHIN ESTRADIOL 0.1-0.02MG TABLET ORAL 02/06/2019 0.29624
LEVONORGESTREL-ETHIN ESTRADIOL 90-20 MCG TABLET ORAL 09/26/2018 1.80262
LEVONORGESTREL-ETHIN ESTRADIOL 0.15-0.03 TBDSPK 3MO ORAL 12/19/2018 0.23560
LEVORPHANOL TARTRATE 2 MG TABLET ORAL 01/23/2019 45.61240
LEVOTHYROXINE SODIUM 25 MCG TABLET ORAL 01/06/2015 0.40481
LEVOTHYROXINE SODIUM 50 MCG TABLET ORAL 12/05/2018 0.39246
LEVOTHYROXINE SODIUM 75 MCG TABLET ORAL 01/06/2015 0.50612
LEVOTHYROXINE SODIUM 100 MCG TABLET ORAL 01/06/2015 0.49619
LEVOTHYROXINE SODIUM 112 MCG TABLET ORAL 01/23/2019 0.59107
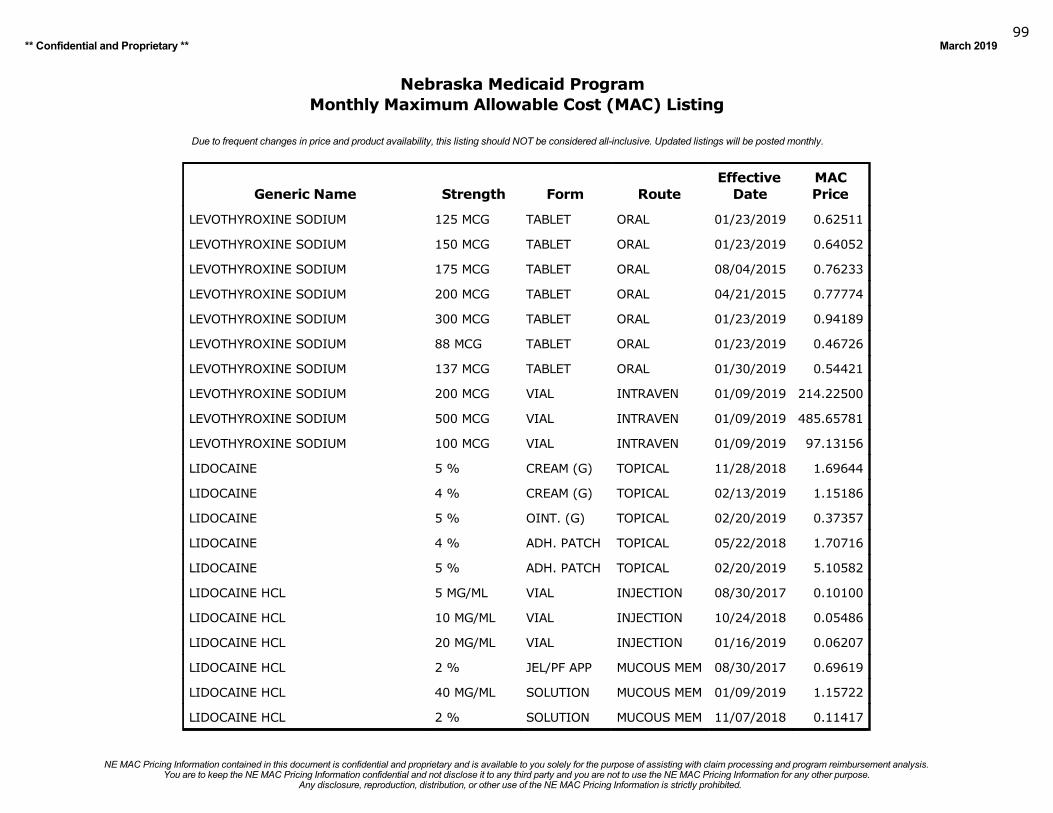
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 201999
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
LEVOTHYROXINE SODIUM 125 MCG TABLET ORAL 01/23/2019 0.62511
LEVOTHYROXINE SODIUM 150 MCG TABLET ORAL 01/23/2019 0.64052
LEVOTHYROXINE SODIUM 175 MCG TABLET ORAL 08/04/2015 0.76233
LEVOTHYROXINE SODIUM 200 MCG TABLET ORAL 04/21/2015 0.77774
LEVOTHYROXINE SODIUM 300 MCG TABLET ORAL 01/23/2019 0.94189
LEVOTHYROXINE SODIUM 88 MCG TABLET ORAL 01/23/2019 0.46726
LEVOTHYROXINE SODIUM 137 MCG TABLET ORAL 01/30/2019 0.54421
LEVOTHYROXINE SODIUM 200 MCG VIAL INTRAVEN 01/09/2019 214.22500
LEVOTHYROXINE SODIUM 500 MCG VIAL INTRAVEN 01/09/2019 485.65781
LEVOTHYROXINE SODIUM 100 MCG VIAL INTRAVEN 01/09/2019 97.13156
LIDOCAINE 5 % CREAM (G) TOPICAL 11/28/2018 1.69644
LIDOCAINE 4 % CREAM (G) TOPICAL 02/13/2019 1.15186
LIDOCAINE 5 % OINT. (G) TOPICAL 02/20/2019 0.37357
LIDOCAINE 4 % ADH. PATCH TOPICAL 05/22/2018 1.70716
LIDOCAINE 5 % ADH. PATCH TOPICAL 02/20/2019 5.10582
LIDOCAINE HCL 5 MG/ML VIAL INJECTION 08/30/2017 0.10100
LIDOCAINE HCL 10 MG/ML VIAL INJECTION 10/24/2018 0.05486
LIDOCAINE HCL 20 MG/ML VIAL INJECTION 01/16/2019 0.06207
LIDOCAINE HCL 2 % JEL/PF APP MUCOUS MEM 08/30/2017 0.69619
LIDOCAINE HCL 40 MG/ML SOLUTION MUCOUS MEM 01/09/2019 1.15722
LIDOCAINE HCL 2 % SOLUTION MUCOUS MEM 11/07/2018 0.11417
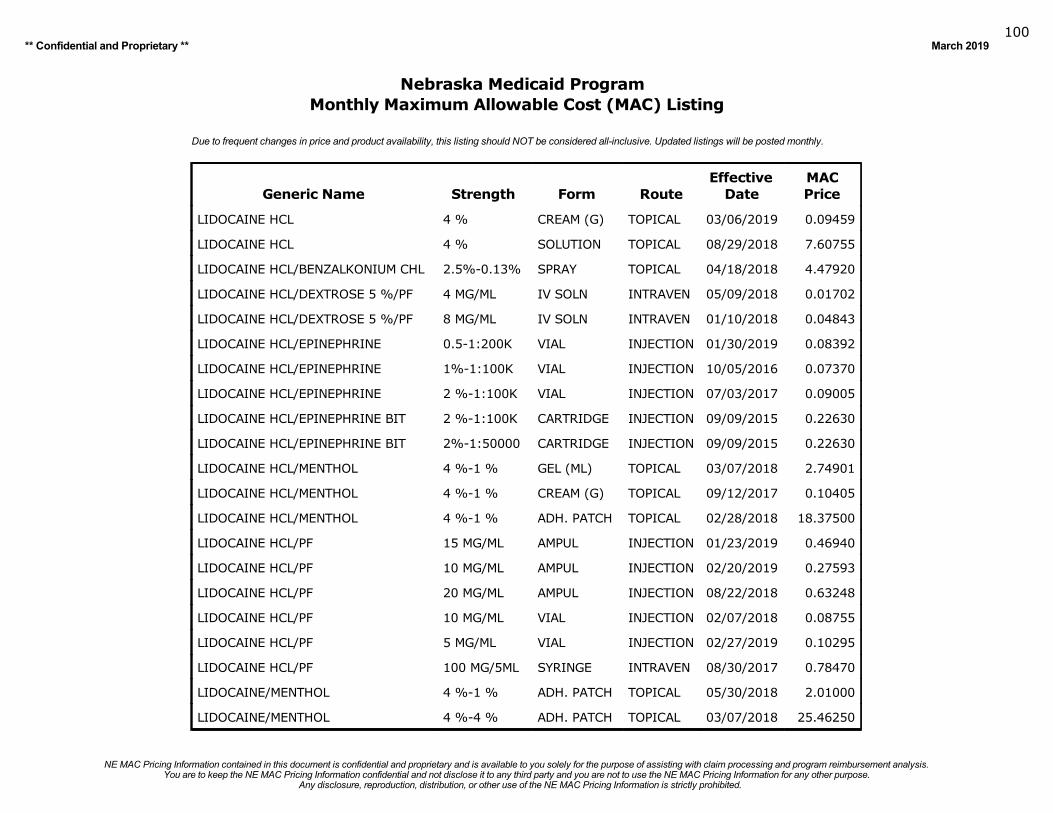
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019100
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
LIDOCAINE HCL 4 % CREAM (G) TOPICAL 03/06/2019 0.09459
LIDOCAINE HCL 4 % SOLUTION TOPICAL 08/29/2018 7.60755
LIDOCAINE HCL/BENZALKONIUM CHL 2.5%-0.13% SPRAY TOPICAL 04/18/2018 4.47920
LIDOCAINE HCL/DEXTROSE 5 %/PF 4 MG/ML IV SOLN INTRAVEN 05/09/2018 0.01702
LIDOCAINE HCL/DEXTROSE 5 %/PF 8 MG/ML IV SOLN INTRAVEN 01/10/2018 0.04843
LIDOCAINE HCL/EPINEPHRINE 0.5-1:200K VIAL INJECTION 01/30/2019 0.08392
LIDOCAINE HCL/EPINEPHRINE 1%-1:100K VIAL INJECTION 10/05/2016 0.07370
LIDOCAINE HCL/EPINEPHRINE 2 %-1:100K VIAL INJECTION 07/03/2017 0.09005
LIDOCAINE HCL/EPINEPHRINE BIT 2 %-1:100K CARTRIDGE INJECTION 09/09/2015 0.22630
LIDOCAINE HCL/EPINEPHRINE BIT 2%-1:50000 CARTRIDGE INJECTION 09/09/2015 0.22630
LIDOCAINE HCL/MENTHOL 4 %-1 % GEL (ML) TOPICAL 03/07/2018 2.74901
LIDOCAINE HCL/MENTHOL 4 %-1 % CREAM (G) TOPICAL 09/12/2017 0.10405
LIDOCAINE HCL/MENTHOL 4 %-1 % ADH. PATCH TOPICAL 02/28/2018 18.37500
LIDOCAINE HCL/PF 15 MG/ML AMPUL INJECTION 01/23/2019 0.46940
LIDOCAINE HCL/PF 10 MG/ML AMPUL INJECTION 02/20/2019 0.27593
LIDOCAINE HCL/PF 20 MG/ML AMPUL INJECTION 08/22/2018 0.63248
LIDOCAINE HCL/PF 10 MG/ML VIAL INJECTION 02/07/2018 0.08755
LIDOCAINE HCL/PF 5 MG/ML VIAL INJECTION 02/27/2019 0.10295
LIDOCAINE HCL/PF 100 MG/5ML SYRINGE INTRAVEN 08/30/2017 0.78470
LIDOCAINE/MENTHOL 4 %-1 % ADH. PATCH TOPICAL 05/30/2018 2.01000
LIDOCAINE/MENTHOL 4 %-4 % ADH. PATCH TOPICAL 03/07/2018 25.46250
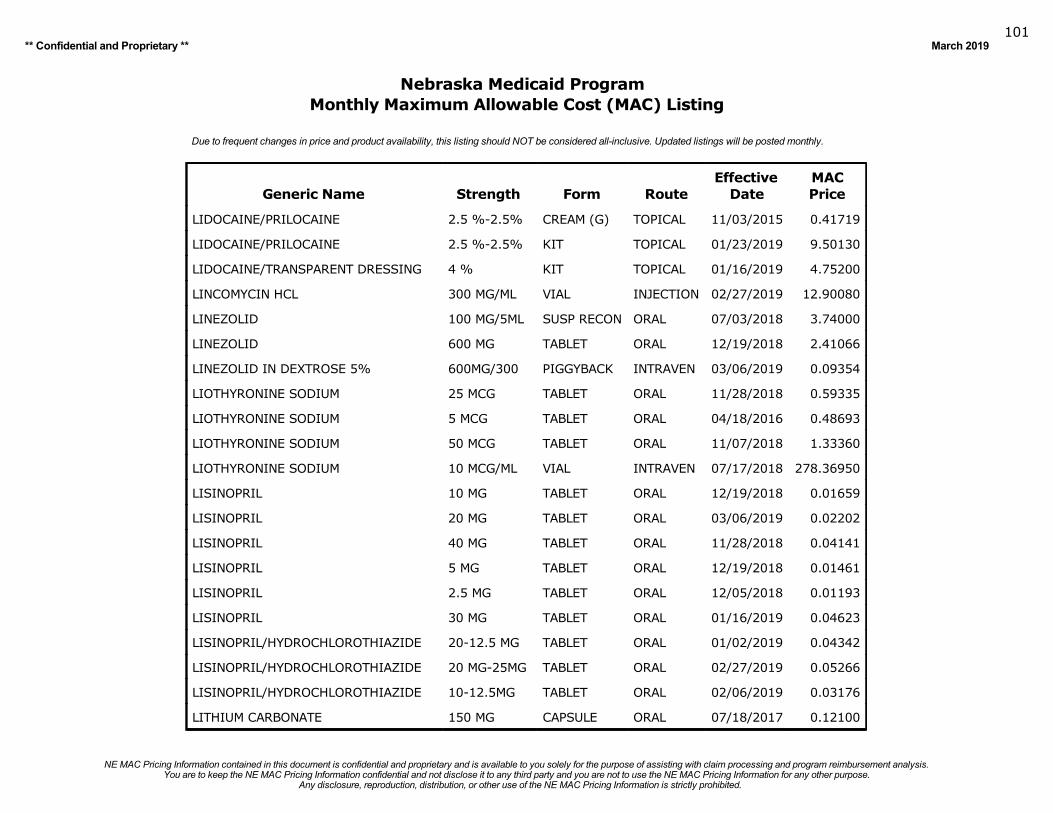
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019101
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
LIDOCAINE/PRILOCAINE 2.5 %-2.5% CREAM (G) TOPICAL 11/03/2015 0.41719
LIDOCAINE/PRILOCAINE 2.5 %-2.5% KIT TOPICAL 01/23/2019 9.50130
LIDOCAINE/TRANSPARENT DRESSING 4 % KIT TOPICAL 01/16/2019 4.75200
LINCOMYCIN HCL 300 MG/ML VIAL INJECTION 02/27/2019 12.90080
LINEZOLID 100 MG/5ML SUSP RECON ORAL 07/03/2018 3.74000
LINEZOLID 600 MG TABLET ORAL 12/19/2018 2.41066
LINEZOLID IN DEXTROSE 5% 600MG/300 PIGGYBACK INTRAVEN 03/06/2019 0.09354
LIOTHYRONINE SODIUM 25 MCG TABLET ORAL 11/28/2018 0.59335
LIOTHYRONINE SODIUM 5 MCG TABLET ORAL 04/18/2016 0.48693
LIOTHYRONINE SODIUM 50 MCG TABLET ORAL 11/07/2018 1.33360
LIOTHYRONINE SODIUM 10 MCG/ML VIAL INTRAVEN 07/17/2018 278.36950
LISINOPRIL 10 MG TABLET ORAL 12/19/2018 0.01659
LISINOPRIL 20 MG TABLET ORAL 03/06/2019 0.02202
LISINOPRIL 40 MG TABLET ORAL 11/28/2018 0.04141
LISINOPRIL 5 MG TABLET ORAL 12/19/2018 0.01461
LISINOPRIL 2.5 MG TABLET ORAL 12/05/2018 0.01193
LISINOPRIL 30 MG TABLET ORAL 01/16/2019 0.04623
LISINOPRIL/HYDROCHLOROTHIAZIDE 20-12.5 MG TABLET ORAL 01/02/2019 0.04342
LISINOPRIL/HYDROCHLOROTHIAZIDE 20 MG-25MG TABLET ORAL 02/27/2019 0.05266
LISINOPRIL/HYDROCHLOROTHIAZIDE 10-12.5MG TABLET ORAL 02/06/2019 0.03176
LITHIUM CARBONATE 150 MG CAPSULE ORAL 07/18/2017 0.12100
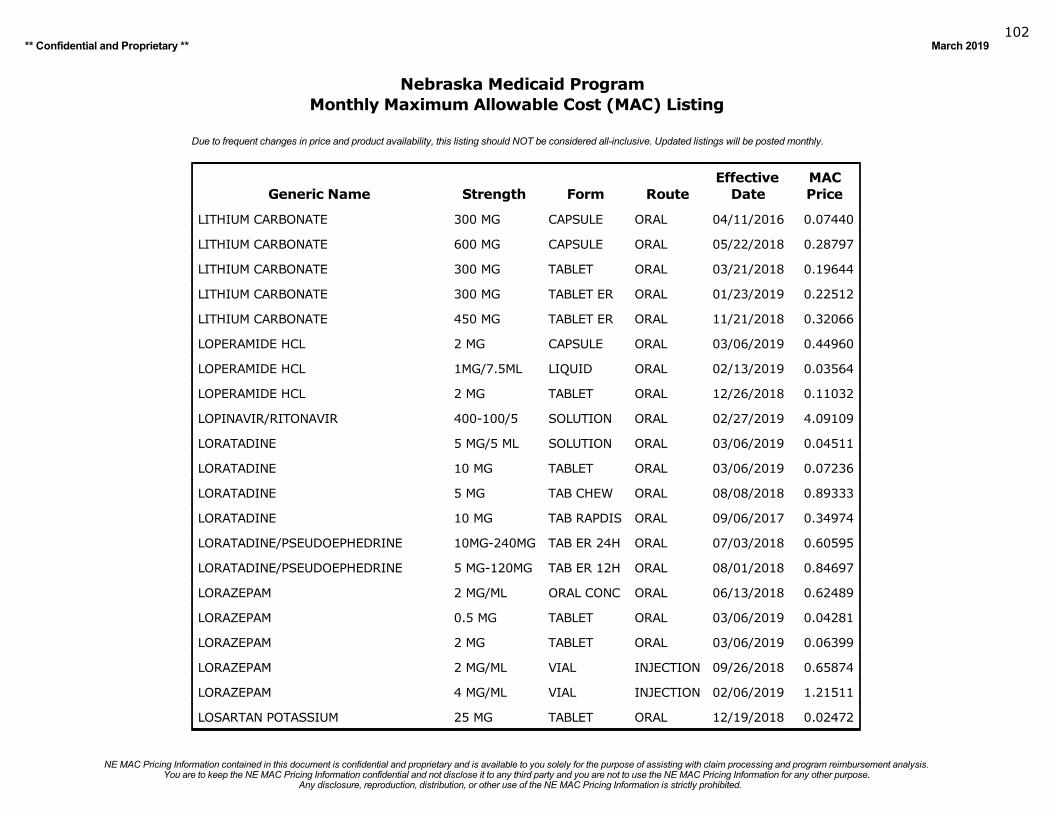
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019102
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
LITHIUM CARBONATE 300 MG CAPSULE ORAL 04/11/2016 0.07440
LITHIUM CARBONATE 600 MG CAPSULE ORAL 05/22/2018 0.28797
LITHIUM CARBONATE 300 MG TABLET ORAL 03/21/2018 0.19644
LITHIUM CARBONATE 300 MG TABLET ER ORAL 01/23/2019 0.22512
LITHIUM CARBONATE 450 MG TABLET ER ORAL 11/21/2018 0.32066
LOPERAMIDE HCL 2 MG CAPSULE ORAL 03/06/2019 0.44960
LOPERAMIDE HCL 1MG/7.5ML LIQUID ORAL 02/13/2019 0.03564
LOPERAMIDE HCL 2 MG TABLET ORAL 12/26/2018 0.11032
LOPINAVIR/RITONAVIR 400-100/5 SOLUTION ORAL 02/27/2019 4.09109
LORATADINE 5 MG/5 ML SOLUTION ORAL 03/06/2019 0.04511
LORATADINE 10 MG TABLET ORAL 03/06/2019 0.07236
LORATADINE 5 MG TAB CHEW ORAL 08/08/2018 0.89333
LORATADINE 10 MG TAB RAPDIS ORAL 09/06/2017 0.34974
LORATADINE/PSEUDOEPHEDRINE 10MG-240MG TAB ER 24H ORAL 07/03/2018 0.60595
LORATADINE/PSEUDOEPHEDRINE 5 MG-120MG TAB ER 12H ORAL 08/01/2018 0.84697
LORAZEPAM 2 MG/ML ORAL CONC ORAL 06/13/2018 0.62489
LORAZEPAM 0.5 MG TABLET ORAL 03/06/2019 0.04281
LORAZEPAM 2 MG TABLET ORAL 03/06/2019 0.06399
LORAZEPAM 2 MG/ML VIAL INJECTION 09/26/2018 0.65874
LORAZEPAM 4 MG/ML VIAL INJECTION 02/06/2019 1.21511
LOSARTAN POTASSIUM 25 MG TABLET ORAL 12/19/2018 0.02472
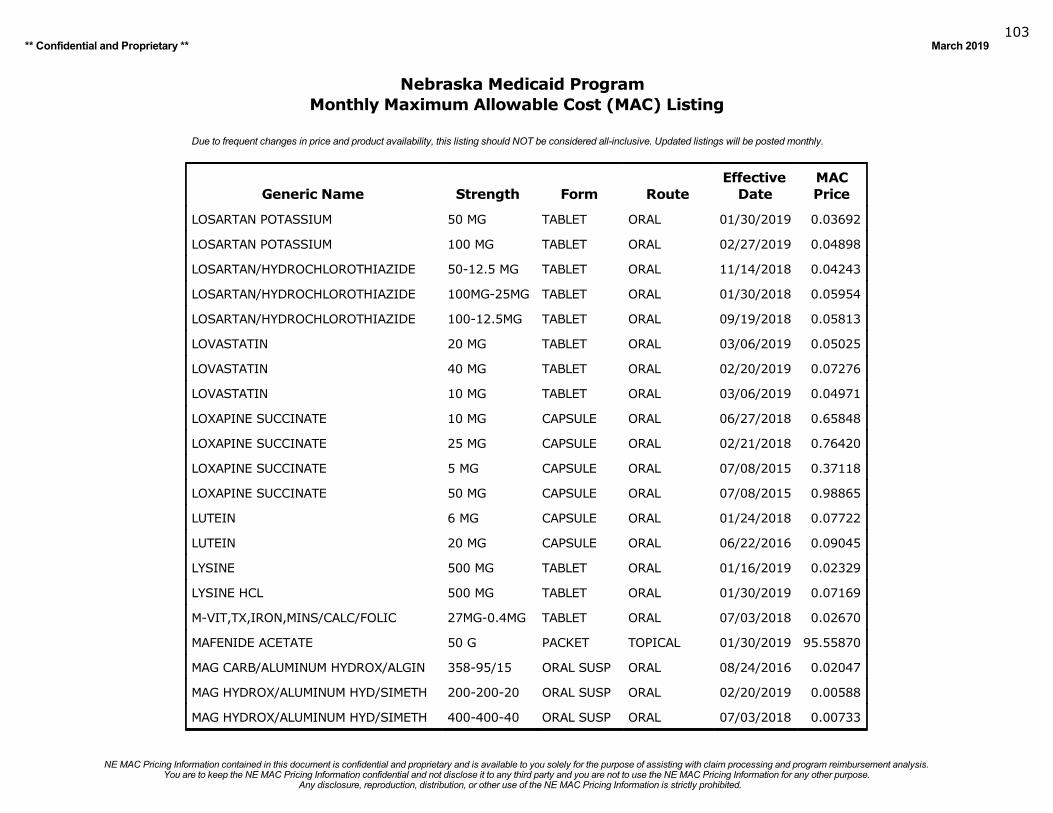
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019103
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
LOSARTAN POTASSIUM 50 MG TABLET ORAL 01/30/2019 0.03692
LOSARTAN POTASSIUM 100 MG TABLET ORAL 02/27/2019 0.04898
LOSARTAN/HYDROCHLOROTHIAZIDE 50-12.5 MG TABLET ORAL 11/14/2018 0.04243
LOSARTAN/HYDROCHLOROTHIAZIDE 100MG-25MG TABLET ORAL 01/30/2018 0.05954
LOSARTAN/HYDROCHLOROTHIAZIDE 100-12.5MG TABLET ORAL 09/19/2018 0.05813
LOVASTATIN 20 MG TABLET ORAL 03/06/2019 0.05025
LOVASTATIN 40 MG TABLET ORAL 02/20/2019 0.07276
LOVASTATIN 10 MG TABLET ORAL 03/06/2019 0.04971
LOXAPINE SUCCINATE 10 MG CAPSULE ORAL 06/27/2018 0.65848
LOXAPINE SUCCINATE 25 MG CAPSULE ORAL 02/21/2018 0.76420
LOXAPINE SUCCINATE 5 MG CAPSULE ORAL 07/08/2015 0.37118
LOXAPINE SUCCINATE 50 MG CAPSULE ORAL 07/08/2015 0.98865
LUTEIN 6 MG CAPSULE ORAL 01/24/2018 0.07722
LUTEIN 20 MG CAPSULE ORAL 06/22/2016 0.09045
LYSINE 500 MG TABLET ORAL 01/16/2019 0.02329
LYSINE HCL 500 MG TABLET ORAL 01/30/2019 0.07169
M-VIT,TX,IRON,MINS/CALC/FOLIC 27MG-0.4MG TABLET ORAL 07/03/2018 0.02670
MAFENIDE ACETATE 50 G PACKET TOPICAL 01/30/2019 95.55870
MAG CARB/ALUMINUM HYDROX/ALGIN 358-95/15 ORAL SUSP ORAL 08/24/2016 0.02047
MAG HYDROX/ALUMINUM HYD/SIMETH 200-200-20 ORAL SUSP ORAL 02/20/2019 0.00588
MAG HYDROX/ALUMINUM HYD/SIMETH 400-400-40 ORAL SUSP ORAL 07/03/2018 0.00733
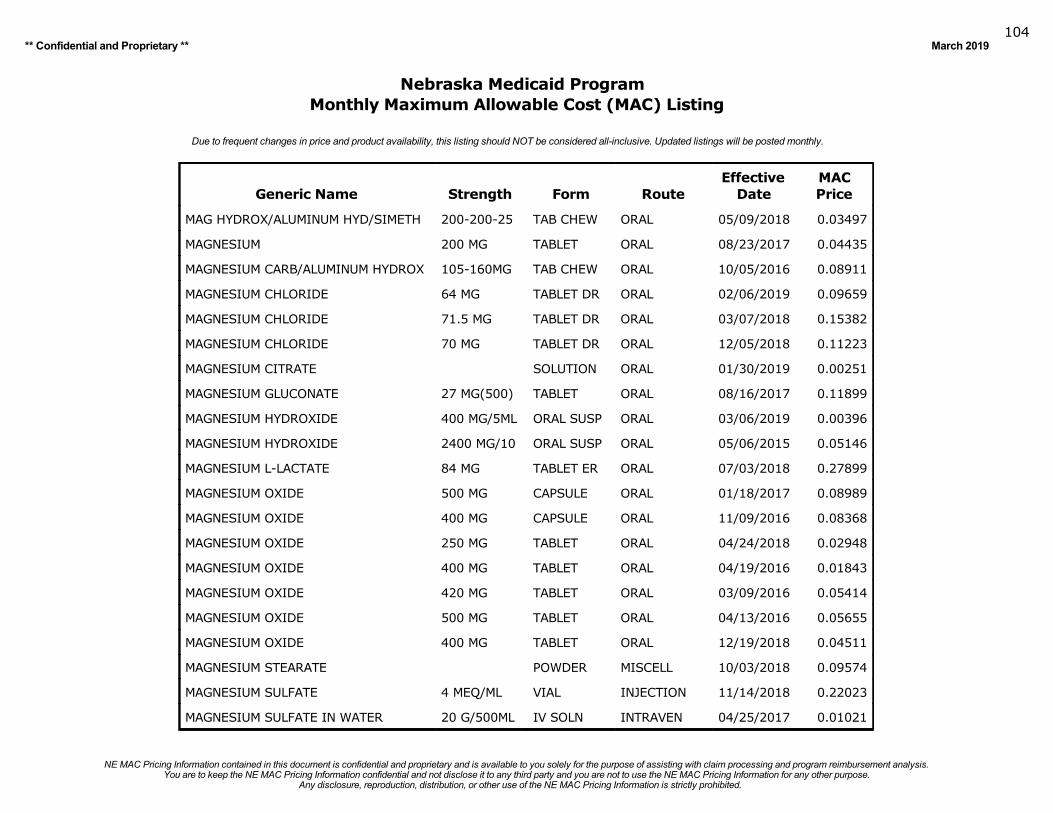
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019104
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
MAG HYDROX/ALUMINUM HYD/SIMETH 200-200-25 TAB CHEW ORAL 05/09/2018 0.03497
MAGNESIUM 200 MG TABLET ORAL 08/23/2017 0.04435
MAGNESIUM CARB/ALUMINUM HYDROX 105-160MG TAB CHEW ORAL 10/05/2016 0.08911
MAGNESIUM CHLORIDE 64 MG TABLET DR ORAL 02/06/2019 0.09659
MAGNESIUM CHLORIDE 71.5 MG TABLET DR ORAL 03/07/2018 0.15382
MAGNESIUM CHLORIDE 70 MG TABLET DR ORAL 12/05/2018 0.11223
MAGNESIUM CITRATE SOLUTION ORAL 01/30/2019 0.00251
MAGNESIUM GLUCONATE 27 MG(500) TABLET ORAL 08/16/2017 0.11899
MAGNESIUM HYDROXIDE 400 MG/5ML ORAL SUSP ORAL 03/06/2019 0.00396
MAGNESIUM HYDROXIDE 2400 MG/10 ORAL SUSP ORAL 05/06/2015 0.05146
MAGNESIUM L-LACTATE 84 MG TABLET ER ORAL 07/03/2018 0.27899
MAGNESIUM OXIDE 500 MG CAPSULE ORAL 01/18/2017 0.08989
MAGNESIUM OXIDE 400 MG CAPSULE ORAL 11/09/2016 0.08368
MAGNESIUM OXIDE 250 MG TABLET ORAL 04/24/2018 0.02948
MAGNESIUM OXIDE 400 MG TABLET ORAL 04/19/2016 0.01843
MAGNESIUM OXIDE 420 MG TABLET ORAL 03/09/2016 0.05414
MAGNESIUM OXIDE 500 MG TABLET ORAL 04/13/2016 0.05655
MAGNESIUM OXIDE 400 MG TABLET ORAL 12/19/2018 0.04511
MAGNESIUM STEARATE POWDER MISCELL 10/03/2018 0.09574
MAGNESIUM SULFATE 4 MEQ/ML VIAL INJECTION 11/14/2018 0.22023
MAGNESIUM SULFATE IN WATER 20 G/500ML IV SOLN INTRAVEN 04/25/2017 0.01021
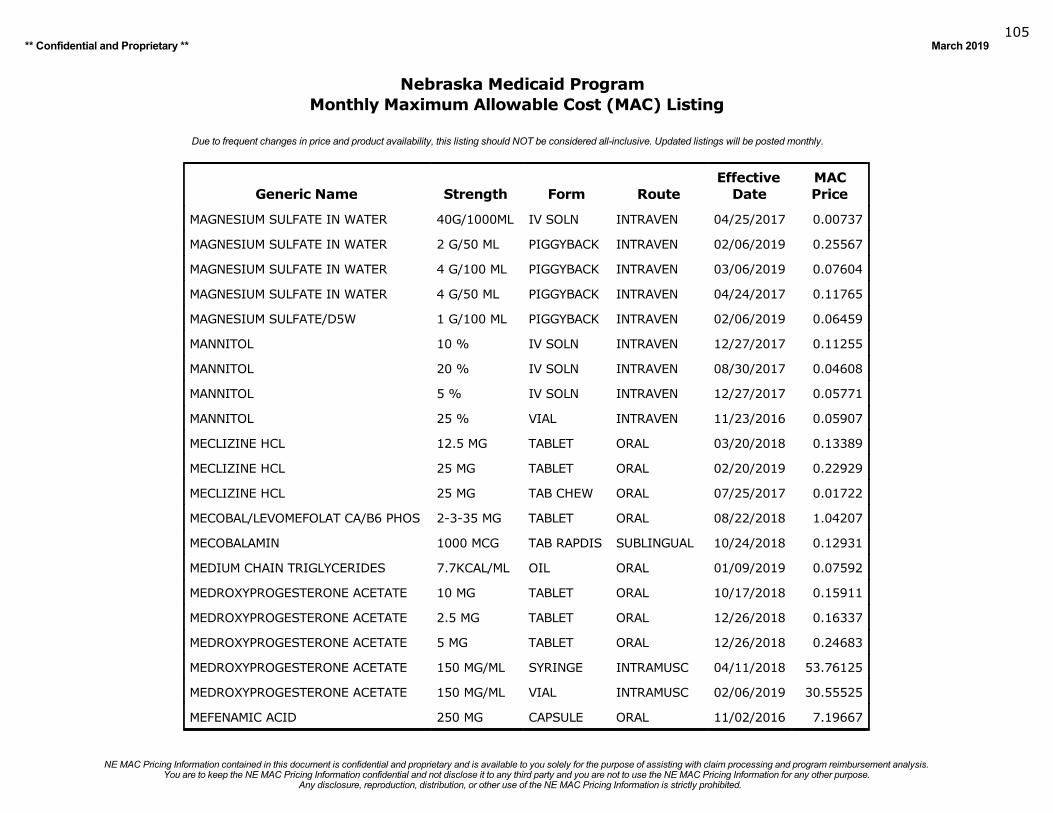
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019105
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
MAGNESIUM SULFATE IN WATER 40G/1000ML IV SOLN INTRAVEN 04/25/2017 0.00737
MAGNESIUM SULFATE IN WATER 2 G/50 ML PIGGYBACK INTRAVEN 02/06/2019 0.25567
MAGNESIUM SULFATE IN WATER 4 G/100 ML PIGGYBACK INTRAVEN 03/06/2019 0.07604
MAGNESIUM SULFATE IN WATER 4 G/50 ML PIGGYBACK INTRAVEN 04/24/2017 0.11765
MAGNESIUM SULFATE/D5W 1 G/100 ML PIGGYBACK INTRAVEN 02/06/2019 0.06459
MANNITOL 10 % IV SOLN INTRAVEN 12/27/2017 0.11255
MANNITOL 20 % IV SOLN INTRAVEN 08/30/2017 0.04608
MANNITOL 5 % IV SOLN INTRAVEN 12/27/2017 0.05771
MANNITOL 25 % VIAL INTRAVEN 11/23/2016 0.05907
MECLIZINE HCL 12.5 MG TABLET ORAL 03/20/2018 0.13389
MECLIZINE HCL 25 MG TABLET ORAL 02/20/2019 0.22929
MECLIZINE HCL 25 MG TAB CHEW ORAL 07/25/2017 0.01722
MECOBAL/LEVOMEFOLAT CA/B6 PHOS 2-3-35 MG TABLET ORAL 08/22/2018 1.04207
MECOBALAMIN 1000 MCG TAB RAPDIS SUBLINGUAL 10/24/2018 0.12931
MEDIUM CHAIN TRIGLYCERIDES 7.7KCAL/ML OIL ORAL 01/09/2019 0.07592
MEDROXYPROGESTERONE ACETATE 10 MG TABLET ORAL 10/17/2018 0.15911
MEDROXYPROGESTERONE ACETATE 2.5 MG TABLET ORAL 12/26/2018 0.16337
MEDROXYPROGESTERONE ACETATE 5 MG TABLET ORAL 12/26/2018 0.24683
MEDROXYPROGESTERONE ACETATE 150 MG/ML SYRINGE INTRAMUSC 04/11/2018 53.76125
MEDROXYPROGESTERONE ACETATE 150 MG/ML VIAL INTRAMUSC 02/06/2019 30.55525
MEFENAMIC ACID 250 MG CAPSULE ORAL 11/02/2016 7.19667
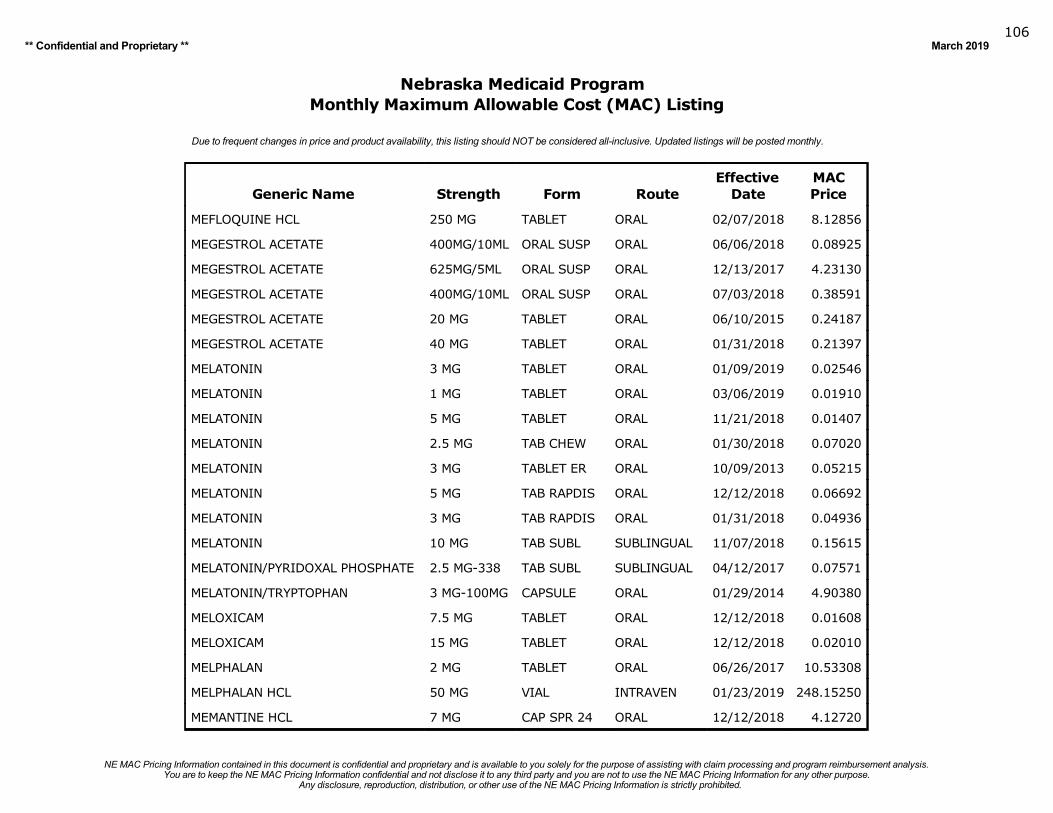
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019106
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
MEFLOQUINE HCL 250 MG TABLET ORAL 02/07/2018 8.12856
MEGESTROL ACETATE 400MG/10ML ORAL SUSP ORAL 06/06/2018 0.08925
MEGESTROL ACETATE 625MG/5ML ORAL SUSP ORAL 12/13/2017 4.23130
MEGESTROL ACETATE 400MG/10ML ORAL SUSP ORAL 07/03/2018 0.38591
MEGESTROL ACETATE 20 MG TABLET ORAL 06/10/2015 0.24187
MEGESTROL ACETATE 40 MG TABLET ORAL 01/31/2018 0.21397
MELATONIN 3 MG TABLET ORAL 01/09/2019 0.02546
MELATONIN 1 MG TABLET ORAL 03/06/2019 0.01910
MELATONIN 5 MG TABLET ORAL 11/21/2018 0.01407
MELATONIN 2.5 MG TAB CHEW ORAL 01/30/2018 0.07020
MELATONIN 3 MG TABLET ER ORAL 10/09/2013 0.05215
MELATONIN 5 MG TAB RAPDIS ORAL 12/12/2018 0.06692
MELATONIN 3 MG TAB RAPDIS ORAL 01/31/2018 0.04936
MELATONIN 10 MG TAB SUBL SUBLINGUAL 11/07/2018 0.15615
MELATONIN/PYRIDOXAL PHOSPHATE 2.5 MG-338 TAB SUBL SUBLINGUAL 04/12/2017 0.07571
MELATONIN/TRYPTOPHAN 3 MG-100MG CAPSULE ORAL 01/29/2014 4.90380
MELOXICAM 7.5 MG TABLET ORAL 12/12/2018 0.01608
MELOXICAM 15 MG TABLET ORAL 12/12/2018 0.02010
MELPHALAN 2 MG TABLET ORAL 06/26/2017 10.53308
MELPHALAN HCL 50 MG VIAL INTRAVEN 01/23/2019 248.15250
MEMANTINE HCL 7 MG CAP SPR 24 ORAL 12/12/2018 4.12720
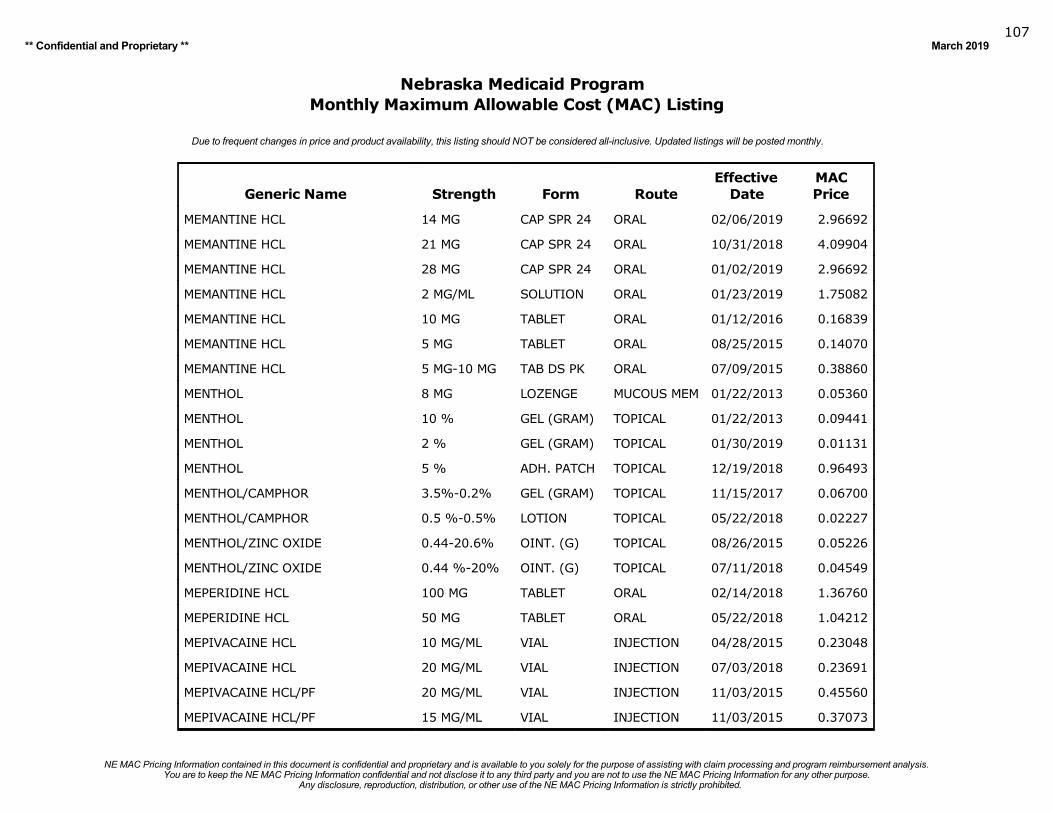
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019107
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
MEMANTINE HCL 14 MG CAP SPR 24 ORAL 02/06/2019 2.96692
MEMANTINE HCL 21 MG CAP SPR 24 ORAL 10/31/2018 4.09904
MEMANTINE HCL 28 MG CAP SPR 24 ORAL 01/02/2019 2.96692
MEMANTINE HCL 2 MG/ML SOLUTION ORAL 01/23/2019 1.75082
MEMANTINE HCL 10 MG TABLET ORAL 01/12/2016 0.16839
MEMANTINE HCL 5 MG TABLET ORAL 08/25/2015 0.14070
MEMANTINE HCL 5 MG-10 MG TAB DS PK ORAL 07/09/2015 0.38860
MENTHOL 8 MG LOZENGE MUCOUS MEM 01/22/2013 0.05360
MENTHOL 10 % GEL (GRAM) TOPICAL 01/22/2013 0.09441
MENTHOL 2 % GEL (GRAM) TOPICAL 01/30/2019 0.01131
MENTHOL 5 % ADH. PATCH TOPICAL 12/19/2018 0.96493
MENTHOL/CAMPHOR 3.5%-0.2% GEL (GRAM) TOPICAL 11/15/2017 0.06700
MENTHOL/CAMPHOR 0.5 %-0.5% LOTION TOPICAL 05/22/2018 0.02227
MENTHOL/ZINC OXIDE 0.44-20.6% OINT. (G) TOPICAL 08/26/2015 0.05226
MENTHOL/ZINC OXIDE 0.44 %-20% OINT. (G) TOPICAL 07/11/2018 0.04549
MEPERIDINE HCL 100 MG TABLET ORAL 02/14/2018 1.36760
MEPERIDINE HCL 50 MG TABLET ORAL 05/22/2018 1.04212
MEPIVACAINE HCL 10 MG/ML VIAL INJECTION 04/28/2015 0.23048
MEPIVACAINE HCL 20 MG/ML VIAL INJECTION 07/03/2018 0.23691
MEPIVACAINE HCL/PF 20 MG/ML VIAL INJECTION 11/03/2015 0.45560
MEPIVACAINE HCL/PF 15 MG/ML VIAL INJECTION 11/03/2015 0.37073
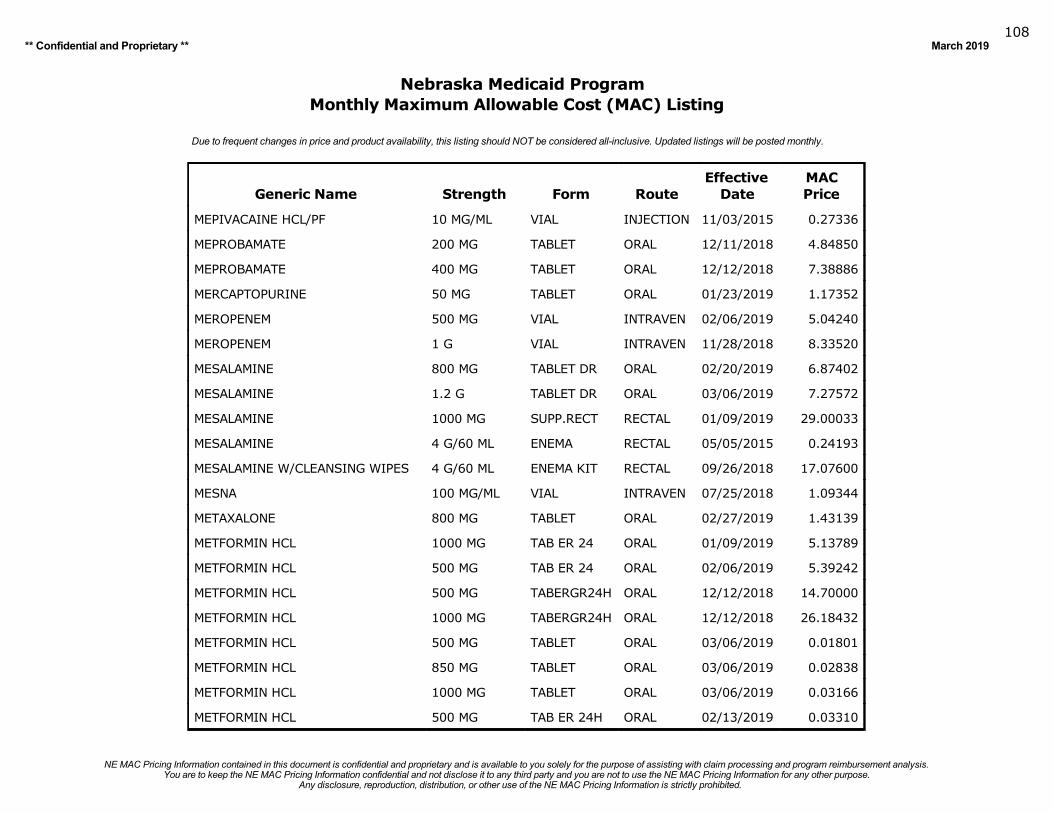
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019108
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
MEPIVACAINE HCL/PF 10 MG/ML VIAL INJECTION 11/03/2015 0.27336
MEPROBAMATE 200 MG TABLET ORAL 12/11/2018 4.84850
MEPROBAMATE 400 MG TABLET ORAL 12/12/2018 7.38886
MERCAPTOPURINE 50 MG TABLET ORAL 01/23/2019 1.17352
MEROPENEM 500 MG VIAL INTRAVEN 02/06/2019 5.04240
MEROPENEM 1 G VIAL INTRAVEN 11/28/2018 8.33520
MESALAMINE 800 MG TABLET DR ORAL 02/20/2019 6.87402
MESALAMINE 1.2 G TABLET DR ORAL 03/06/2019 7.27572
MESALAMINE 1000 MG SUPP.RECT RECTAL 01/09/2019 29.00033
MESALAMINE 4 G/60 ML ENEMA RECTAL 05/05/2015 0.24193
MESALAMINE W/CLEANSING WIPES 4 G/60 ML ENEMA KIT RECTAL 09/26/2018 17.07600
MESNA 100 MG/ML VIAL INTRAVEN 07/25/2018 1.09344
METAXALONE 800 MG TABLET ORAL 02/27/2019 1.43139
METFORMIN HCL 1000 MG TAB ER 24 ORAL 01/09/2019 5.13789
METFORMIN HCL 500 MG TAB ER 24 ORAL 02/06/2019 5.39242
METFORMIN HCL 500 MG TABERGR24H ORAL 12/12/2018 14.70000
METFORMIN HCL 1000 MG TABERGR24H ORAL 12/12/2018 26.18432
METFORMIN HCL 500 MG TABLET ORAL 03/06/2019 0.01801
METFORMIN HCL 850 MG TABLET ORAL 03/06/2019 0.02838
METFORMIN HCL 1000 MG TABLET ORAL 03/06/2019 0.03166
METFORMIN HCL 500 MG TAB ER 24H ORAL 02/13/2019 0.03310
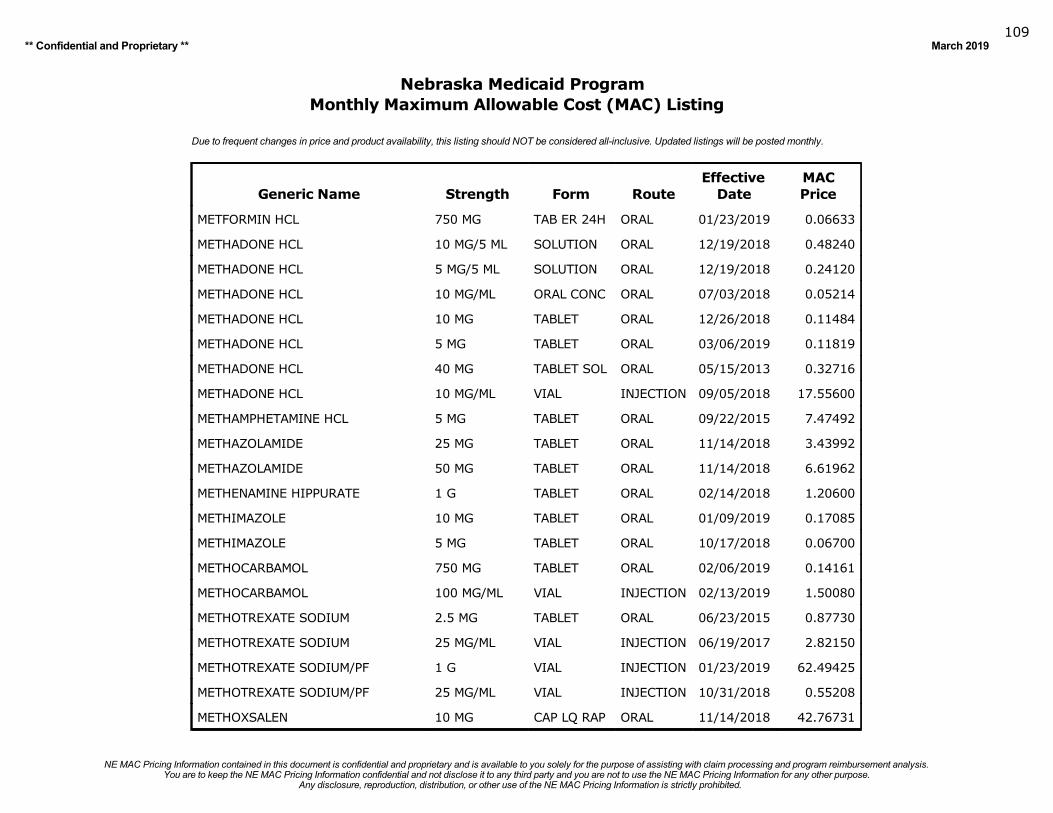
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019109
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
METFORMIN HCL 750 MG TAB ER 24H ORAL 01/23/2019 0.06633
METHADONE HCL 10 MG/5 ML SOLUTION ORAL 12/19/2018 0.48240
METHADONE HCL 5 MG/5 ML SOLUTION ORAL 12/19/2018 0.24120
METHADONE HCL 10 MG/ML ORAL CONC ORAL 07/03/2018 0.05214
METHADONE HCL 10 MG TABLET ORAL 12/26/2018 0.11484
METHADONE HCL 5 MG TABLET ORAL 03/06/2019 0.11819
METHADONE HCL 40 MG TABLET SOL ORAL 05/15/2013 0.32716
METHADONE HCL 10 MG/ML VIAL INJECTION 09/05/2018 17.55600
METHAMPHETAMINE HCL 5 MG TABLET ORAL 09/22/2015 7.47492
METHAZOLAMIDE 25 MG TABLET ORAL 11/14/2018 3.43992
METHAZOLAMIDE 50 MG TABLET ORAL 11/14/2018 6.61962
METHENAMINE HIPPURATE 1 G TABLET ORAL 02/14/2018 1.20600
METHIMAZOLE 10 MG TABLET ORAL 01/09/2019 0.17085
METHIMAZOLE 5 MG TABLET ORAL 10/17/2018 0.06700
METHOCARBAMOL 750 MG TABLET ORAL 02/06/2019 0.14161
METHOCARBAMOL 100 MG/ML VIAL INJECTION 02/13/2019 1.50080
METHOTREXATE SODIUM 2.5 MG TABLET ORAL 06/23/2015 0.87730
METHOTREXATE SODIUM 25 MG/ML VIAL INJECTION 06/19/2017 2.82150
METHOTREXATE SODIUM/PF 1 G VIAL INJECTION 01/23/2019 62.49425
METHOTREXATE SODIUM/PF 25 MG/ML VIAL INJECTION 10/31/2018 0.55208
METHOXSALEN 10 MG CAP LQ RAP ORAL 11/14/2018 42.76731
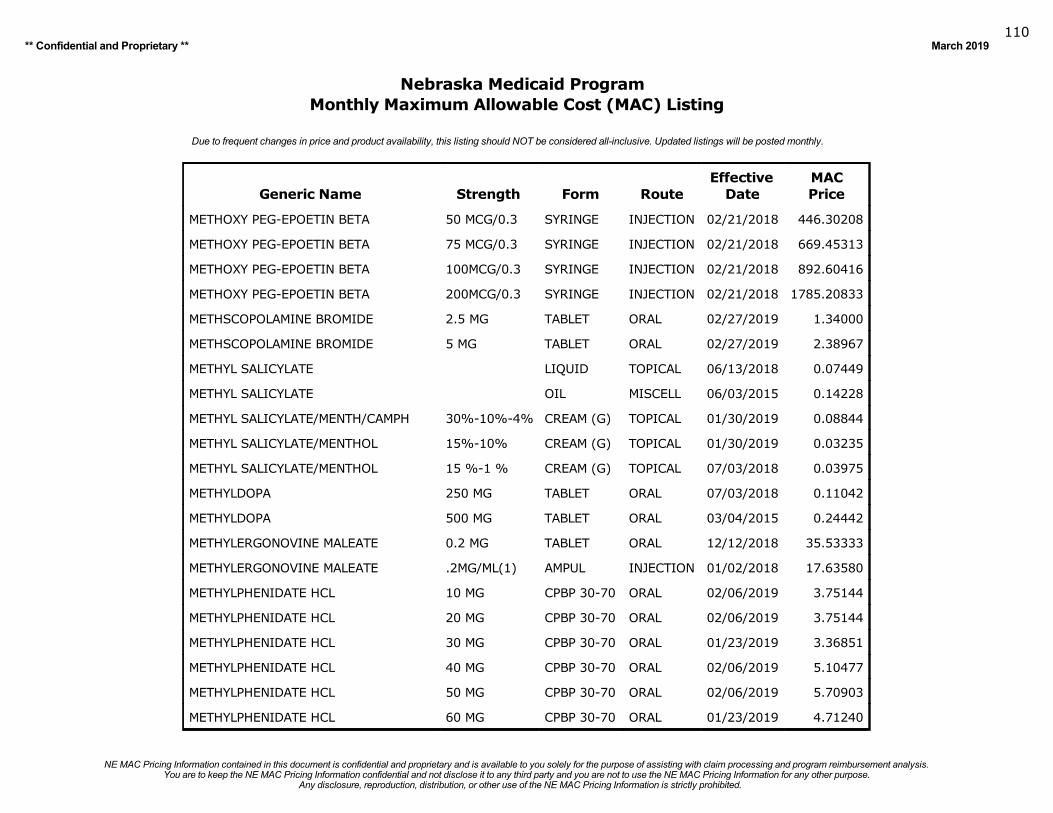
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019110
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
METHOXY PEG-EPOETIN BETA 50 MCG/0.3 SYRINGE INJECTION 02/21/2018 446.30208
METHOXY PEG-EPOETIN BETA 75 MCG/0.3 SYRINGE INJECTION 02/21/2018 669.45313
METHOXY PEG-EPOETIN BETA 100MCG/0.3 SYRINGE INJECTION 02/21/2018 892.60416
METHOXY PEG-EPOETIN BETA 200MCG/0.3 SYRINGE INJECTION 02/21/2018 1785.20833
METHSCOPOLAMINE BROMIDE 2.5 MG TABLET ORAL 02/27/2019 1.34000
METHSCOPOLAMINE BROMIDE 5 MG TABLET ORAL 02/27/2019 2.38967
METHYL SALICYLATE LIQUID TOPICAL 06/13/2018 0.07449
METHYL SALICYLATE OIL MISCELL 06/03/2015 0.14228
METHYL SALICYLATE/MENTH/CAMPH 30%-10%-4% CREAM (G) TOPICAL 01/30/2019 0.08844
METHYL SALICYLATE/MENTHOL 15%-10% CREAM (G) TOPICAL 01/30/2019 0.03235
METHYL SALICYLATE/MENTHOL 15 %-1 % CREAM (G) TOPICAL 07/03/2018 0.03975
METHYLDOPA 250 MG TABLET ORAL 07/03/2018 0.11042
METHYLDOPA 500 MG TABLET ORAL 03/04/2015 0.24442
METHYLERGONOVINE MALEATE 0.2 MG TABLET ORAL 12/12/2018 35.53333
METHYLERGONOVINE MALEATE .2MG/ML(1) AMPUL INJECTION 01/02/2018 17.63580
METHYLPHENIDATE HCL 10 MG CPBP 30-70 ORAL 02/06/2019 3.75144
METHYLPHENIDATE HCL 20 MG CPBP 30-70 ORAL 02/06/2019 3.75144
METHYLPHENIDATE HCL 30 MG CPBP 30-70 ORAL 01/23/2019 3.36851
METHYLPHENIDATE HCL 40 MG CPBP 30-70 ORAL 02/06/2019 5.10477
METHYLPHENIDATE HCL 50 MG CPBP 30-70 ORAL 02/06/2019 5.70903
METHYLPHENIDATE HCL 60 MG CPBP 30-70 ORAL 01/23/2019 4.71240
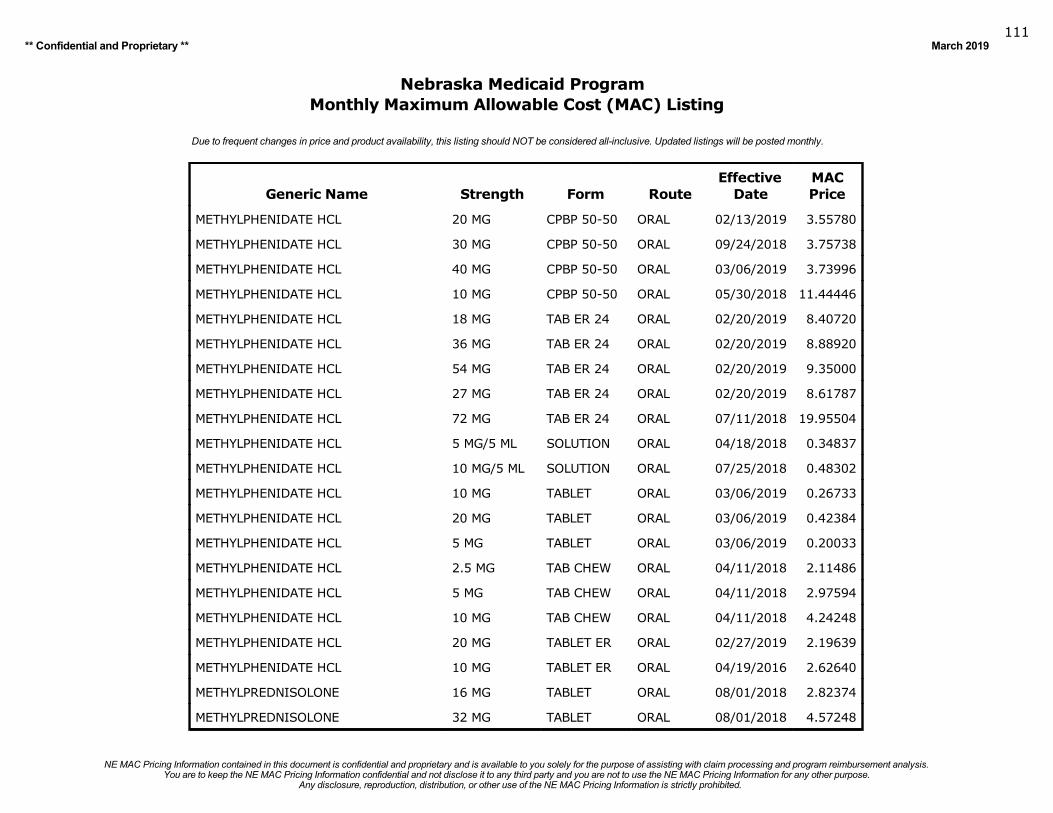
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019111
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
METHYLPHENIDATE HCL 20 MG CPBP 50-50 ORAL 02/13/2019 3.55780
METHYLPHENIDATE HCL 30 MG CPBP 50-50 ORAL 09/24/2018 3.75738
METHYLPHENIDATE HCL 40 MG CPBP 50-50 ORAL 03/06/2019 3.73996
METHYLPHENIDATE HCL 10 MG CPBP 50-50 ORAL 05/30/2018 11.44446
METHYLPHENIDATE HCL 18 MG TAB ER 24 ORAL 02/20/2019 8.40720
METHYLPHENIDATE HCL 36 MG TAB ER 24 ORAL 02/20/2019 8.88920
METHYLPHENIDATE HCL 54 MG TAB ER 24 ORAL 02/20/2019 9.35000
METHYLPHENIDATE HCL 27 MG TAB ER 24 ORAL 02/20/2019 8.61787
METHYLPHENIDATE HCL 72 MG TAB ER 24 ORAL 07/11/2018 19.95504
METHYLPHENIDATE HCL 5 MG/5 ML SOLUTION ORAL 04/18/2018 0.34837
METHYLPHENIDATE HCL 10 MG/5 ML SOLUTION ORAL 07/25/2018 0.48302
METHYLPHENIDATE HCL 10 MG TABLET ORAL 03/06/2019 0.26733
METHYLPHENIDATE HCL 20 MG TABLET ORAL 03/06/2019 0.42384
METHYLPHENIDATE HCL 5 MG TABLET ORAL 03/06/2019 0.20033
METHYLPHENIDATE HCL 2.5 MG TAB CHEW ORAL 04/11/2018 2.11486
METHYLPHENIDATE HCL 5 MG TAB CHEW ORAL 04/11/2018 2.97594
METHYLPHENIDATE HCL 10 MG TAB CHEW ORAL 04/11/2018 4.24248
METHYLPHENIDATE HCL 20 MG TABLET ER ORAL 02/27/2019 2.19639
METHYLPHENIDATE HCL 10 MG TABLET ER ORAL 04/19/2016 2.62640
METHYLPREDNISOLONE 16 MG TABLET ORAL 08/01/2018 2.82374
METHYLPREDNISOLONE 32 MG TABLET ORAL 08/01/2018 4.57248
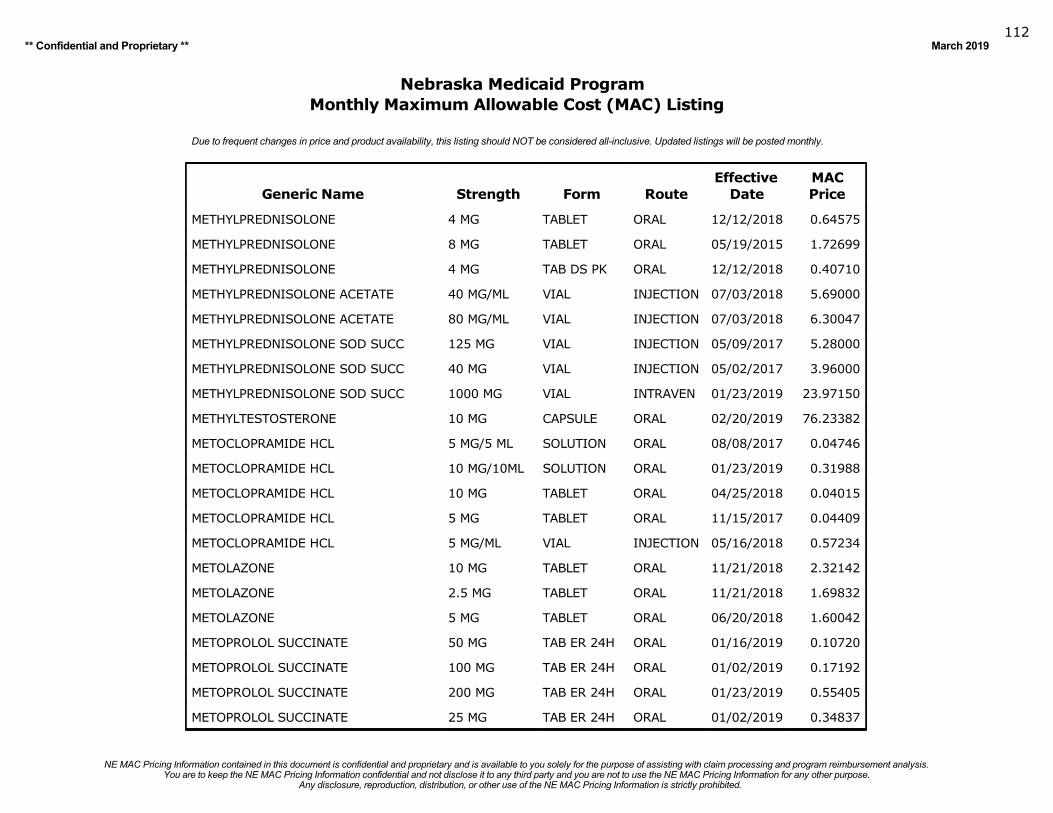
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019112
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
METHYLPREDNISOLONE 4 MG TABLET ORAL 12/12/2018 0.64575
METHYLPREDNISOLONE 8 MG TABLET ORAL 05/19/2015 1.72699
METHYLPREDNISOLONE 4 MG TAB DS PK ORAL 12/12/2018 0.40710
METHYLPREDNISOLONE ACETATE 40 MG/ML VIAL INJECTION 07/03/2018 5.69000
METHYLPREDNISOLONE ACETATE 80 MG/ML VIAL INJECTION 07/03/2018 6.30047
METHYLPREDNISOLONE SOD SUCC 125 MG VIAL INJECTION 05/09/2017 5.28000
METHYLPREDNISOLONE SOD SUCC 40 MG VIAL INJECTION 05/02/2017 3.96000
METHYLPREDNISOLONE SOD SUCC 1000 MG VIAL INTRAVEN 01/23/2019 23.97150
METHYLTESTOSTERONE 10 MG CAPSULE ORAL 02/20/2019 76.23382
METOCLOPRAMIDE HCL 5 MG/5 ML SOLUTION ORAL 08/08/2017 0.04746
METOCLOPRAMIDE HCL 10 MG/10ML SOLUTION ORAL 01/23/2019 0.31988
METOCLOPRAMIDE HCL 10 MG TABLET ORAL 04/25/2018 0.04015
METOCLOPRAMIDE HCL 5 MG TABLET ORAL 11/15/2017 0.04409
METOCLOPRAMIDE HCL 5 MG/ML VIAL INJECTION 05/16/2018 0.57234
METOLAZONE 10 MG TABLET ORAL 11/21/2018 2.32142
METOLAZONE 2.5 MG TABLET ORAL 11/21/2018 1.69832
METOLAZONE 5 MG TABLET ORAL 06/20/2018 1.60042
METOPROLOL SUCCINATE 50 MG TAB ER 24H ORAL 01/16/2019 0.10720
METOPROLOL SUCCINATE 100 MG TAB ER 24H ORAL 01/02/2019 0.17192
METOPROLOL SUCCINATE 200 MG TAB ER 24H ORAL 01/23/2019 0.55405
METOPROLOL SUCCINATE 25 MG TAB ER 24H ORAL 01/02/2019 0.34837
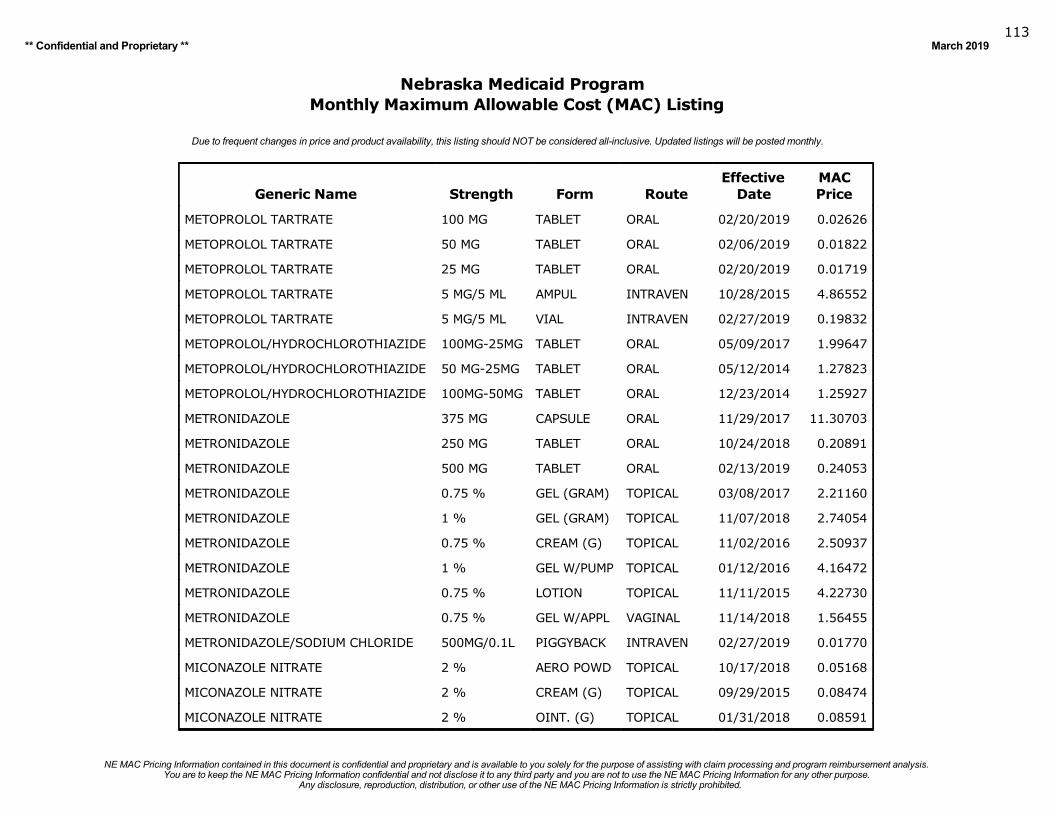
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019113
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
METOPROLOL TARTRATE 100 MG TABLET ORAL 02/20/2019 0.02626
METOPROLOL TARTRATE 50 MG TABLET ORAL 02/06/2019 0.01822
METOPROLOL TARTRATE 25 MG TABLET ORAL 02/20/2019 0.01719
METOPROLOL TARTRATE 5 MG/5 ML AMPUL INTRAVEN 10/28/2015 4.86552
METOPROLOL TARTRATE 5 MG/5 ML VIAL INTRAVEN 02/27/2019 0.19832
METOPROLOL/HYDROCHLOROTHIAZIDE 100MG-25MG TABLET ORAL 05/09/2017 1.99647
METOPROLOL/HYDROCHLOROTHIAZIDE 50 MG-25MG TABLET ORAL 05/12/2014 1.27823
METOPROLOL/HYDROCHLOROTHIAZIDE 100MG-50MG TABLET ORAL 12/23/2014 1.25927
METRONIDAZOLE 375 MG CAPSULE ORAL 11/29/2017 11.30703
METRONIDAZOLE 250 MG TABLET ORAL 10/24/2018 0.20891
METRONIDAZOLE 500 MG TABLET ORAL 02/13/2019 0.24053
METRONIDAZOLE 0.75 % GEL (GRAM) TOPICAL 03/08/2017 2.21160
METRONIDAZOLE 1 % GEL (GRAM) TOPICAL 11/07/2018 2.74054
METRONIDAZOLE 0.75 % CREAM (G) TOPICAL 11/02/2016 2.50937
METRONIDAZOLE 1 % GEL W/PUMP TOPICAL 01/12/2016 4.16472
METRONIDAZOLE 0.75 % LOTION TOPICAL 11/11/2015 4.22730
METRONIDAZOLE 0.75 % GEL W/APPL VAGINAL 11/14/2018 1.56455
METRONIDAZOLE/SODIUM CHLORIDE 500MG/0.1L PIGGYBACK INTRAVEN 02/27/2019 0.01770
MICONAZOLE NITRATE 2 % AERO POWD TOPICAL 10/17/2018 0.05168
MICONAZOLE NITRATE 2 % CREAM (G) TOPICAL 09/29/2015 0.08474
MICONAZOLE NITRATE 2 % OINT. (G) TOPICAL 01/31/2018 0.08591
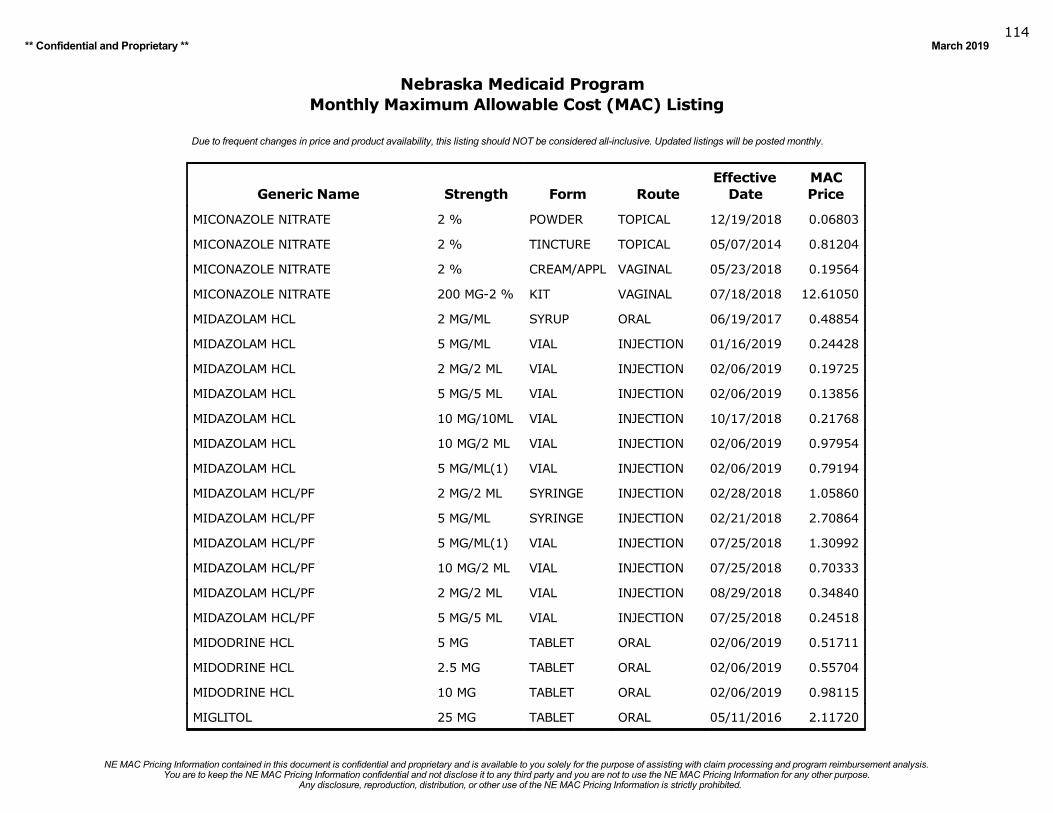
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019114
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
MICONAZOLE NITRATE 2 % POWDER TOPICAL 12/19/2018 0.06803
MICONAZOLE NITRATE 2 % TINCTURE TOPICAL 05/07/2014 0.81204
MICONAZOLE NITRATE 2 % CREAM/APPL VAGINAL 05/23/2018 0.19564
MICONAZOLE NITRATE 200 MG-2 % KIT VAGINAL 07/18/2018 12.61050
MIDAZOLAM HCL 2 MG/ML SYRUP ORAL 06/19/2017 0.48854
MIDAZOLAM HCL 5 MG/ML VIAL INJECTION 01/16/2019 0.24428
MIDAZOLAM HCL 2 MG/2 ML VIAL INJECTION 02/06/2019 0.19725
MIDAZOLAM HCL 5 MG/5 ML VIAL INJECTION 02/06/2019 0.13856
MIDAZOLAM HCL 10 MG/10ML VIAL INJECTION 10/17/2018 0.21768
MIDAZOLAM HCL 10 MG/2 ML VIAL INJECTION 02/06/2019 0.97954
MIDAZOLAM HCL 5 MG/ML(1) VIAL INJECTION 02/06/2019 0.79194
MIDAZOLAM HCL/PF 2 MG/2 ML SYRINGE INJECTION 02/28/2018 1.05860
MIDAZOLAM HCL/PF 5 MG/ML SYRINGE INJECTION 02/21/2018 2.70864
MIDAZOLAM HCL/PF 5 MG/ML(1) VIAL INJECTION 07/25/2018 1.30992
MIDAZOLAM HCL/PF 10 MG/2 ML VIAL INJECTION 07/25/2018 0.70333
MIDAZOLAM HCL/PF 2 MG/2 ML VIAL INJECTION 08/29/2018 0.34840
MIDAZOLAM HCL/PF 5 MG/5 ML VIAL INJECTION 07/25/2018 0.24518
MIDODRINE HCL 5 MG TABLET ORAL 02/06/2019 0.51711
MIDODRINE HCL 2.5 MG TABLET ORAL 02/06/2019 0.55704
MIDODRINE HCL 10 MG TABLET ORAL 02/06/2019 0.98115
MIGLITOL 25 MG TABLET ORAL 05/11/2016 2.11720
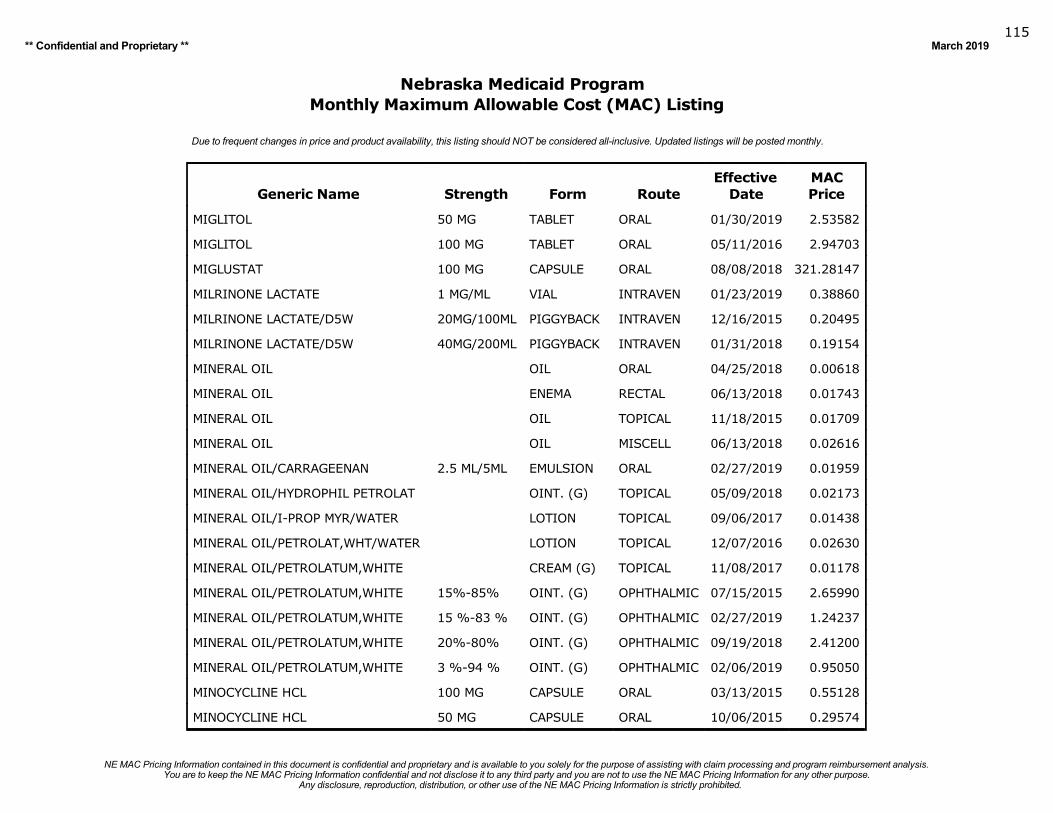
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019115
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
MIGLITOL 50 MG TABLET ORAL 01/30/2019 2.53582
MIGLITOL 100 MG TABLET ORAL 05/11/2016 2.94703
MIGLUSTAT 100 MG CAPSULE ORAL 08/08/2018 321.28147
MILRINONE LACTATE 1 MG/ML VIAL INTRAVEN 01/23/2019 0.38860
MILRINONE LACTATE/D5W 20MG/100ML PIGGYBACK INTRAVEN 12/16/2015 0.20495
MILRINONE LACTATE/D5W 40MG/200ML PIGGYBACK INTRAVEN 01/31/2018 0.19154
MINERAL OIL OIL ORAL 04/25/2018 0.00618
MINERAL OIL ENEMA RECTAL 06/13/2018 0.01743
MINERAL OIL OIL TOPICAL 11/18/2015 0.01709
MINERAL OIL OIL MISCELL 06/13/2018 0.02616
MINERAL OIL/CARRAGEENAN 2.5 ML/5ML EMULSION ORAL 02/27/2019 0.01959
MINERAL OIL/HYDROPHIL PETROLAT OINT. (G) TOPICAL 05/09/2018 0.02173
MINERAL OIL/I-PROP MYR/WATER LOTION TOPICAL 09/06/2017 0.01438
MINERAL OIL/PETROLAT,WHT/WATER LOTION TOPICAL 12/07/2016 0.02630
MINERAL OIL/PETROLATUM,WHITE CREAM (G) TOPICAL 11/08/2017 0.01178
MINERAL OIL/PETROLATUM,WHITE 15%-85% OINT. (G) OPHTHALMIC 07/15/2015 2.65990
MINERAL OIL/PETROLATUM,WHITE 15 %-83 % OINT. (G) OPHTHALMIC 02/27/2019 1.24237
MINERAL OIL/PETROLATUM,WHITE 20%-80% OINT. (G) OPHTHALMIC 09/19/2018 2.41200
MINERAL OIL/PETROLATUM,WHITE 3 %-94 % OINT. (G) OPHTHALMIC 02/06/2019 0.95050
MINOCYCLINE HCL 100 MG CAPSULE ORAL 03/13/2015 0.55128
MINOCYCLINE HCL 50 MG CAPSULE ORAL 10/06/2015 0.29574
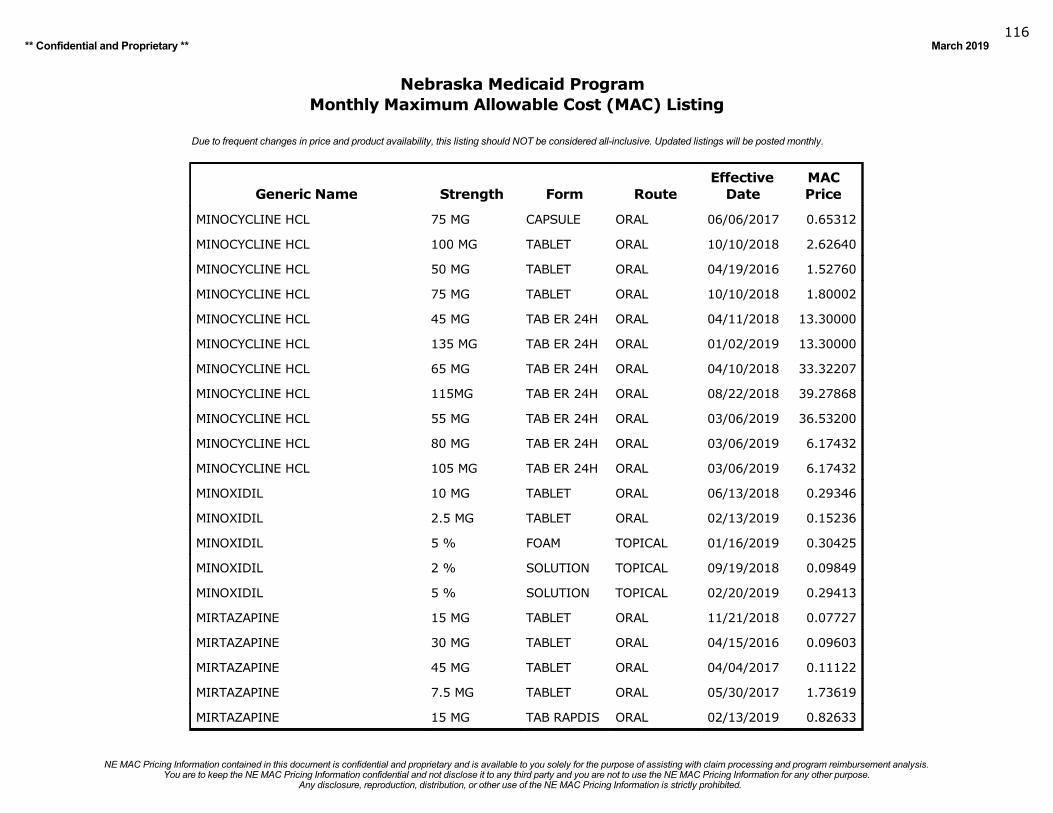
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019116
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
MINOCYCLINE HCL 75 MG CAPSULE ORAL 06/06/2017 0.65312
MINOCYCLINE HCL 100 MG TABLET ORAL 10/10/2018 2.62640
MINOCYCLINE HCL 50 MG TABLET ORAL 04/19/2016 1.52760
MINOCYCLINE HCL 75 MG TABLET ORAL 10/10/2018 1.80002
MINOCYCLINE HCL 45 MG TAB ER 24H ORAL 04/11/2018 13.30000
MINOCYCLINE HCL 135 MG TAB ER 24H ORAL 01/02/2019 13.30000
MINOCYCLINE HCL 65 MG TAB ER 24H ORAL 04/10/2018 33.32207
MINOCYCLINE HCL 115MG TAB ER 24H ORAL 08/22/2018 39.27868
MINOCYCLINE HCL 55 MG TAB ER 24H ORAL 03/06/2019 36.53200
MINOCYCLINE HCL 80 MG TAB ER 24H ORAL 03/06/2019 6.17432
MINOCYCLINE HCL 105 MG TAB ER 24H ORAL 03/06/2019 6.17432
MINOXIDIL 10 MG TABLET ORAL 06/13/2018 0.29346
MINOXIDIL 2.5 MG TABLET ORAL 02/13/2019 0.15236
MINOXIDIL 5 % FOAM TOPICAL 01/16/2019 0.30425
MINOXIDIL 2 % SOLUTION TOPICAL 09/19/2018 0.09849
MINOXIDIL 5 % SOLUTION TOPICAL 02/20/2019 0.29413
MIRTAZAPINE 15 MG TABLET ORAL 11/21/2018 0.07727
MIRTAZAPINE 30 MG TABLET ORAL 04/15/2016 0.09603
MIRTAZAPINE 45 MG TABLET ORAL 04/04/2017 0.11122
MIRTAZAPINE 7.5 MG TABLET ORAL 05/30/2017 1.73619
MIRTAZAPINE 15 MG TAB RAPDIS ORAL 02/13/2019 0.82633
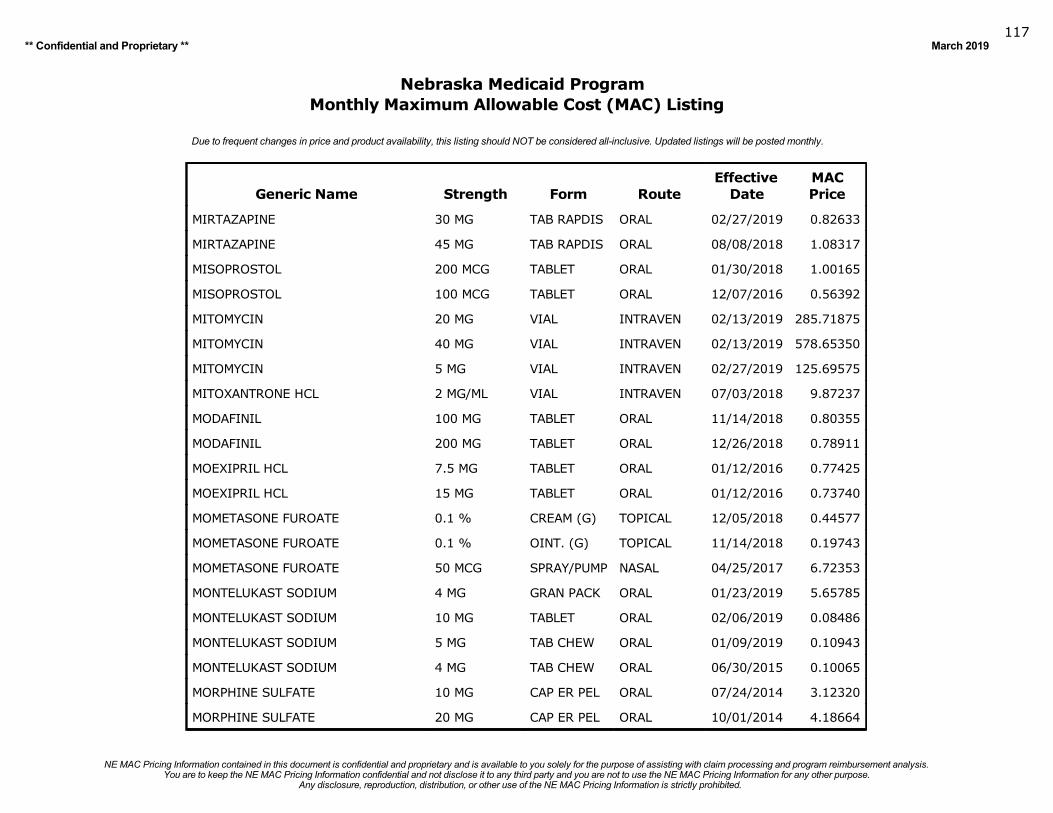
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019117
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
MIRTAZAPINE 30 MG TAB RAPDIS ORAL 02/27/2019 0.82633
MIRTAZAPINE 45 MG TAB RAPDIS ORAL 08/08/2018 1.08317
MISOPROSTOL 200 MCG TABLET ORAL 01/30/2018 1.00165
MISOPROSTOL 100 MCG TABLET ORAL 12/07/2016 0.56392
MITOMYCIN 20 MG VIAL INTRAVEN 02/13/2019 285.71875
MITOMYCIN 40 MG VIAL INTRAVEN 02/13/2019 578.65350
MITOMYCIN 5 MG VIAL INTRAVEN 02/27/2019 125.69575
MITOXANTRONE HCL 2 MG/ML VIAL INTRAVEN 07/03/2018 9.87237
MODAFINIL 100 MG TABLET ORAL 11/14/2018 0.80355
MODAFINIL 200 MG TABLET ORAL 12/26/2018 0.78911
MOEXIPRIL HCL 7.5 MG TABLET ORAL 01/12/2016 0.77425
MOEXIPRIL HCL 15 MG TABLET ORAL 01/12/2016 0.73740
MOMETASONE FUROATE 0.1 % CREAM (G) TOPICAL 12/05/2018 0.44577
MOMETASONE FUROATE 0.1 % OINT. (G) TOPICAL 11/14/2018 0.19743
MOMETASONE FUROATE 50 MCG SPRAY/PUMP NASAL 04/25/2017 6.72353
MONTELUKAST SODIUM 4 MG GRAN PACK ORAL 01/23/2019 5.65785
MONTELUKAST SODIUM 10 MG TABLET ORAL 02/06/2019 0.08486
MONTELUKAST SODIUM 5 MG TAB CHEW ORAL 01/09/2019 0.10943
MONTELUKAST SODIUM 4 MG TAB CHEW ORAL 06/30/2015 0.10065
MORPHINE SULFATE 10 MG CAP ER PEL ORAL 07/24/2014 3.12320
MORPHINE SULFATE 20 MG CAP ER PEL ORAL 10/01/2014 4.18664
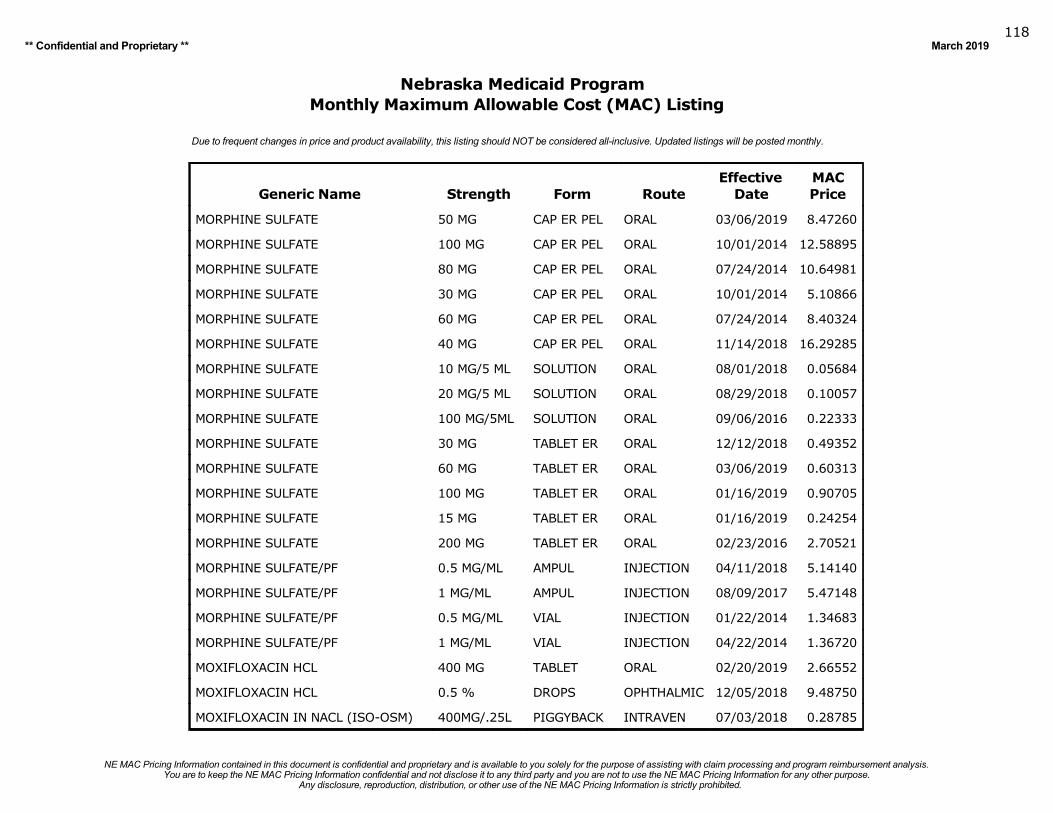
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019118
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
MORPHINE SULFATE 50 MG CAP ER PEL ORAL 03/06/2019 8.47260
MORPHINE SULFATE 100 MG CAP ER PEL ORAL 10/01/2014 12.58895
MORPHINE SULFATE 80 MG CAP ER PEL ORAL 07/24/2014 10.64981
MORPHINE SULFATE 30 MG CAP ER PEL ORAL 10/01/2014 5.10866
MORPHINE SULFATE 60 MG CAP ER PEL ORAL 07/24/2014 8.40324
MORPHINE SULFATE 40 MG CAP ER PEL ORAL 11/14/2018 16.29285
MORPHINE SULFATE 10 MG/5 ML SOLUTION ORAL 08/01/2018 0.05684
MORPHINE SULFATE 20 MG/5 ML SOLUTION ORAL 08/29/2018 0.10057
MORPHINE SULFATE 100 MG/5ML SOLUTION ORAL 09/06/2016 0.22333
MORPHINE SULFATE 30 MG TABLET ER ORAL 12/12/2018 0.49352
MORPHINE SULFATE 60 MG TABLET ER ORAL 03/06/2019 0.60313
MORPHINE SULFATE 100 MG TABLET ER ORAL 01/16/2019 0.90705
MORPHINE SULFATE 15 MG TABLET ER ORAL 01/16/2019 0.24254
MORPHINE SULFATE 200 MG TABLET ER ORAL 02/23/2016 2.70521
MORPHINE SULFATE/PF 0.5 MG/ML AMPUL INJECTION 04/11/2018 5.14140
MORPHINE SULFATE/PF 1 MG/ML AMPUL INJECTION 08/09/2017 5.47148
MORPHINE SULFATE/PF 0.5 MG/ML VIAL INJECTION 01/22/2014 1.34683
MORPHINE SULFATE/PF 1 MG/ML VIAL INJECTION 04/22/2014 1.36720
MOXIFLOXACIN HCL 400 MG TABLET ORAL 02/20/2019 2.66552
MOXIFLOXACIN HCL 0.5 % DROPS OPHTHALMIC 12/05/2018 9.48750
MOXIFLOXACIN IN NACL (ISO-OSM) 400MG/.25L PIGGYBACK INTRAVEN 07/03/2018 0.28785
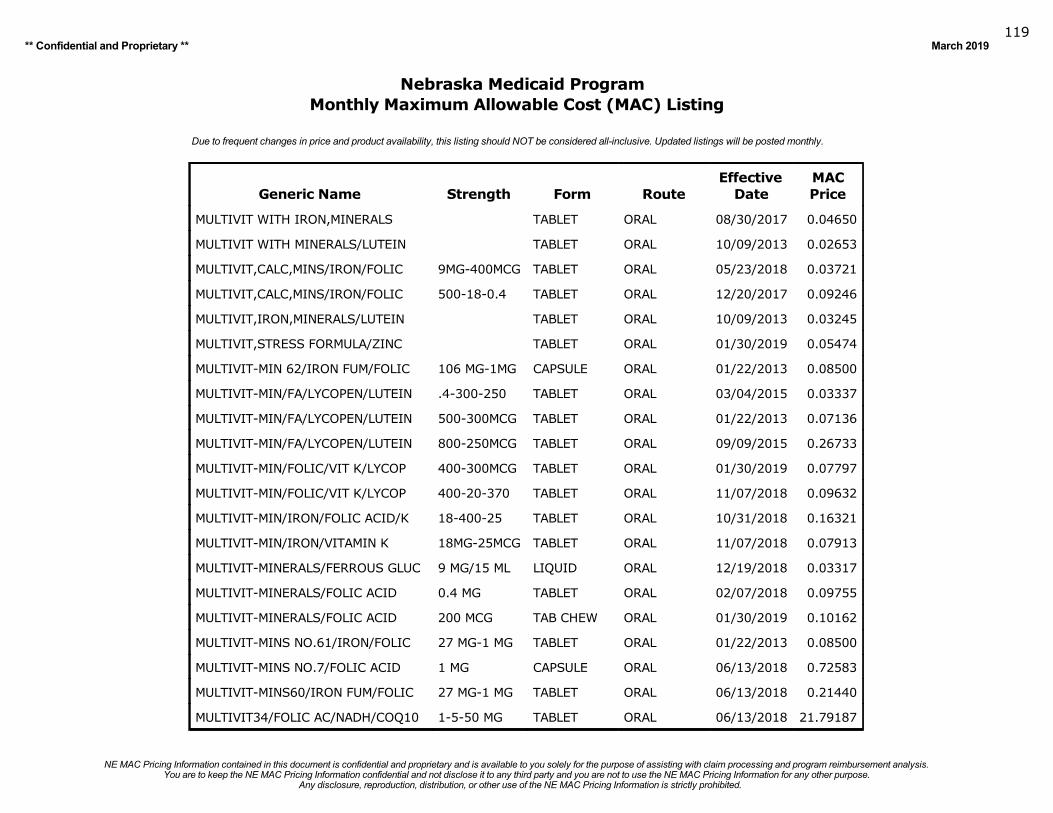
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019119
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
MULTIVIT WITH IRON,MINERALS TABLET ORAL 08/30/2017 0.04650
MULTIVIT WITH MINERALS/LUTEIN TABLET ORAL 10/09/2013 0.02653
MULTIVIT,CALC,MINS/IRON/FOLIC 9MG-400MCG TABLET ORAL 05/23/2018 0.03721
MULTIVIT,CALC,MINS/IRON/FOLIC 500-18-0.4 TABLET ORAL 12/20/2017 0.09246
MULTIVIT,IRON,MINERALS/LUTEIN TABLET ORAL 10/09/2013 0.03245
MULTIVIT,STRESS FORMULA/ZINC TABLET ORAL 01/30/2019 0.05474
MULTIVIT-MIN 62/IRON FUM/FOLIC 106 MG-1MG CAPSULE ORAL 01/22/2013 0.08500
MULTIVIT-MIN/FA/LYCOPEN/LUTEIN .4-300-250 TABLET ORAL 03/04/2015 0.03337
MULTIVIT-MIN/FA/LYCOPEN/LUTEIN 500-300MCG TABLET ORAL 01/22/2013 0.07136
MULTIVIT-MIN/FA/LYCOPEN/LUTEIN 800-250MCG TABLET ORAL 09/09/2015 0.26733
MULTIVIT-MIN/FOLIC/VIT K/LYCOP 400-300MCG TABLET ORAL 01/30/2019 0.07797
MULTIVIT-MIN/FOLIC/VIT K/LYCOP 400-20-370 TABLET ORAL 11/07/2018 0.09632
MULTIVIT-MIN/IRON/FOLIC ACID/K 18-400-25 TABLET ORAL 10/31/2018 0.16321
MULTIVIT-MIN/IRON/VITAMIN K 18MG-25MCG TABLET ORAL 11/07/2018 0.07913
MULTIVIT-MINERALS/FERROUS GLUC 9 MG/15 ML LIQUID ORAL 12/19/2018 0.03317
MULTIVIT-MINERALS/FOLIC ACID 0.4 MG TABLET ORAL 02/07/2018 0.09755
MULTIVIT-MINERALS/FOLIC ACID 200 MCG TAB CHEW ORAL 01/30/2019 0.10162
MULTIVIT-MINS NO.61/IRON/FOLIC 27 MG-1 MG TABLET ORAL 01/22/2013 0.08500
MULTIVIT-MINS NO.7/FOLIC ACID 1 MG CAPSULE ORAL 06/13/2018 0.72583
MULTIVIT-MINS60/IRON FUM/FOLIC 27 MG-1 MG TABLET ORAL 06/13/2018 0.21440
MULTIVIT34/FOLIC AC/NADH/COQ10 1-5-50 MG TABLET ORAL 06/13/2018 21.79187
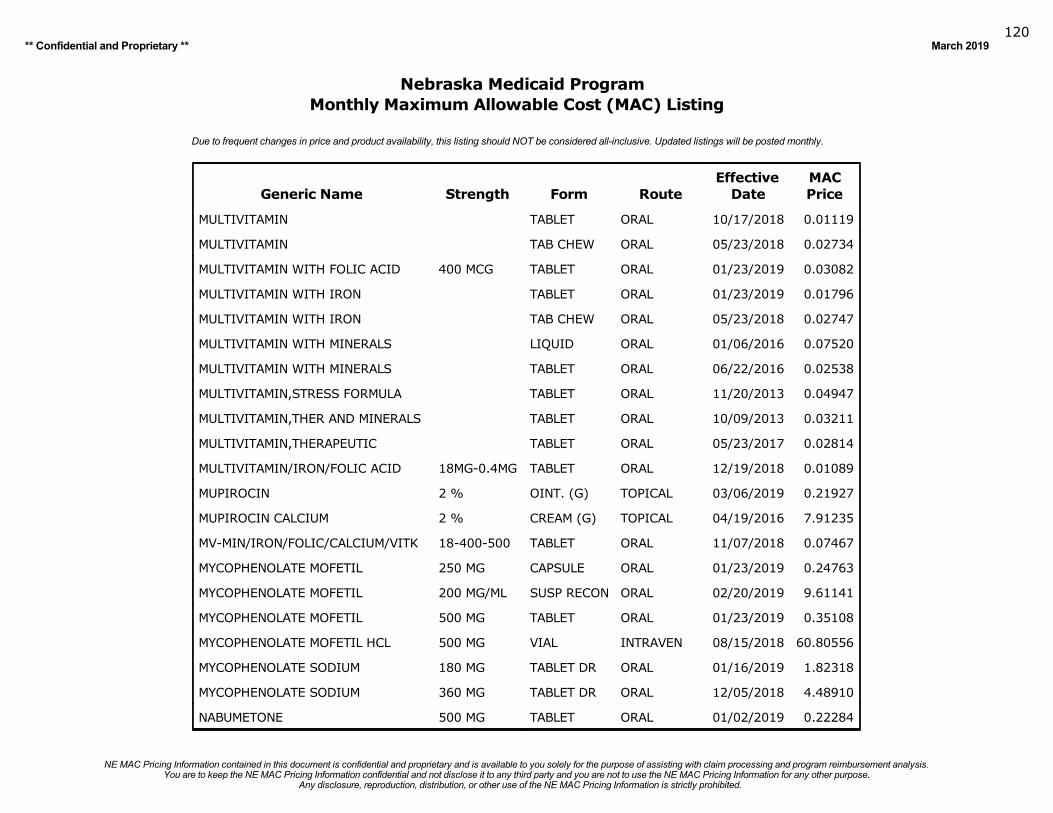
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019120
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
MULTIVITAMIN TABLET ORAL 10/17/2018 0.01119
MULTIVITAMIN TAB CHEW ORAL 05/23/2018 0.02734
MULTIVITAMIN WITH FOLIC ACID 400 MCG TABLET ORAL 01/23/2019 0.03082
MULTIVITAMIN WITH IRON TABLET ORAL 01/23/2019 0.01796
MULTIVITAMIN WITH IRON TAB CHEW ORAL 05/23/2018 0.02747
MULTIVITAMIN WITH MINERALS LIQUID ORAL 01/06/2016 0.07520
MULTIVITAMIN WITH MINERALS TABLET ORAL 06/22/2016 0.02538
MULTIVITAMIN,STRESS FORMULA TABLET ORAL 11/20/2013 0.04947
MULTIVITAMIN,THER AND MINERALS TABLET ORAL 10/09/2013 0.03211
MULTIVITAMIN,THERAPEUTIC TABLET ORAL 05/23/2017 0.02814
MULTIVITAMIN/IRON/FOLIC ACID 18MG-0.4MG TABLET ORAL 12/19/2018 0.01089
MUPIROCIN 2 % OINT. (G) TOPICAL 03/06/2019 0.21927
MUPIROCIN CALCIUM 2 % CREAM (G) TOPICAL 04/19/2016 7.91235
MV-MIN/IRON/FOLIC/CALCIUM/VITK 18-400-500 TABLET ORAL 11/07/2018 0.07467
MYCOPHENOLATE MOFETIL 250 MG CAPSULE ORAL 01/23/2019 0.24763
MYCOPHENOLATE MOFETIL 200 MG/ML SUSP RECON ORAL 02/20/2019 9.61141
MYCOPHENOLATE MOFETIL 500 MG TABLET ORAL 01/23/2019 0.35108
MYCOPHENOLATE MOFETIL HCL 500 MG VIAL INTRAVEN 08/15/2018 60.80556
MYCOPHENOLATE SODIUM 180 MG TABLET DR ORAL 01/16/2019 1.82318
MYCOPHENOLATE SODIUM 360 MG TABLET DR ORAL 12/05/2018 4.48910
NABUMETONE 500 MG TABLET ORAL 01/02/2019 0.22284
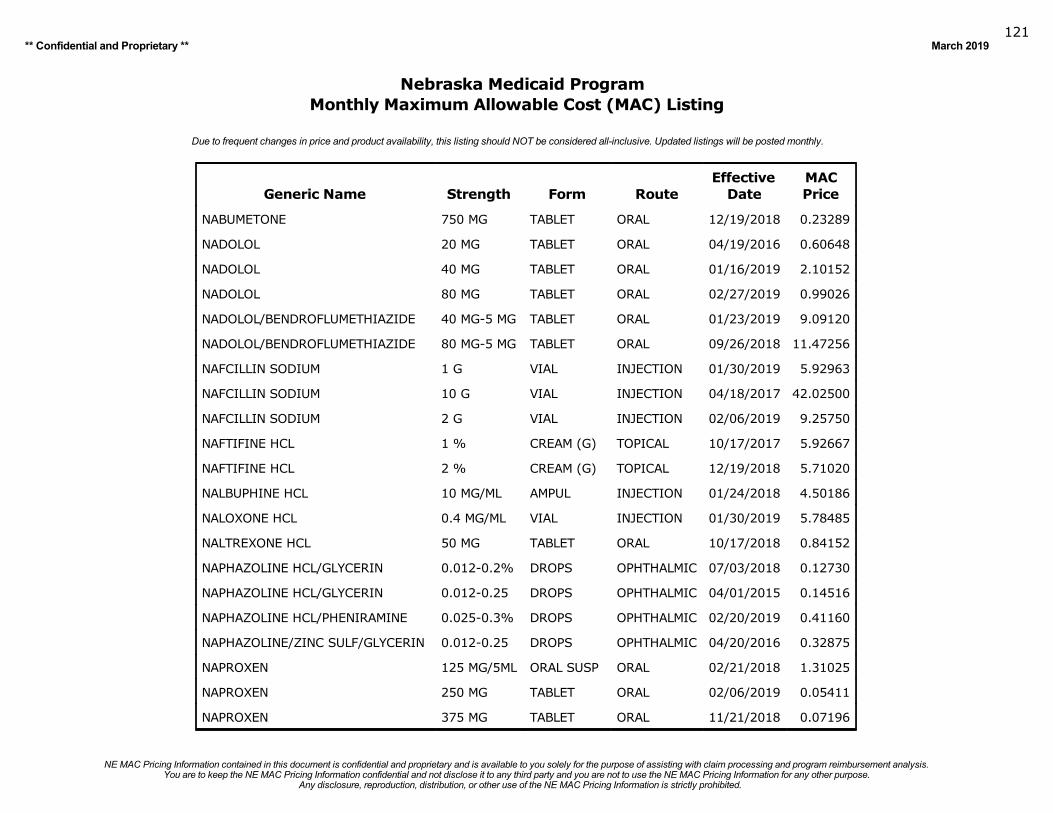
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019121
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
NABUMETONE 750 MG TABLET ORAL 12/19/2018 0.23289
NADOLOL 20 MG TABLET ORAL 04/19/2016 0.60648
NADOLOL 40 MG TABLET ORAL 01/16/2019 2.10152
NADOLOL 80 MG TABLET ORAL 02/27/2019 0.99026
NADOLOL/BENDROFLUMETHIAZIDE 40 MG-5 MG TABLET ORAL 01/23/2019 9.09120
NADOLOL/BENDROFLUMETHIAZIDE 80 MG-5 MG TABLET ORAL 09/26/2018 11.47256
NAFCILLIN SODIUM 1 G VIAL INJECTION 01/30/2019 5.92963
NAFCILLIN SODIUM 10 G VIAL INJECTION 04/18/2017 42.02500
NAFCILLIN SODIUM 2 G VIAL INJECTION 02/06/2019 9.25750
NAFTIFINE HCL 1 % CREAM (G) TOPICAL 10/17/2017 5.92667
NAFTIFINE HCL 2 % CREAM (G) TOPICAL 12/19/2018 5.71020
NALBUPHINE HCL 10 MG/ML AMPUL INJECTION 01/24/2018 4.50186
NALOXONE HCL 0.4 MG/ML VIAL INJECTION 01/30/2019 5.78485
NALTREXONE HCL 50 MG TABLET ORAL 10/17/2018 0.84152
NAPHAZOLINE HCL/GLYCERIN 0.012-0.2% DROPS OPHTHALMIC 07/03/2018 0.12730
NAPHAZOLINE HCL/GLYCERIN 0.012-0.25 DROPS OPHTHALMIC 04/01/2015 0.14516
NAPHAZOLINE HCL/PHENIRAMINE 0.025-0.3% DROPS OPHTHALMIC 02/20/2019 0.41160
NAPHAZOLINE/ZINC SULF/GLYCERIN 0.012-0.25 DROPS OPHTHALMIC 04/20/2016 0.32875
NAPROXEN 125 MG/5ML ORAL SUSP ORAL 02/21/2018 1.31025
NAPROXEN 250 MG TABLET ORAL 02/06/2019 0.05411
NAPROXEN 375 MG TABLET ORAL 11/21/2018 0.07196
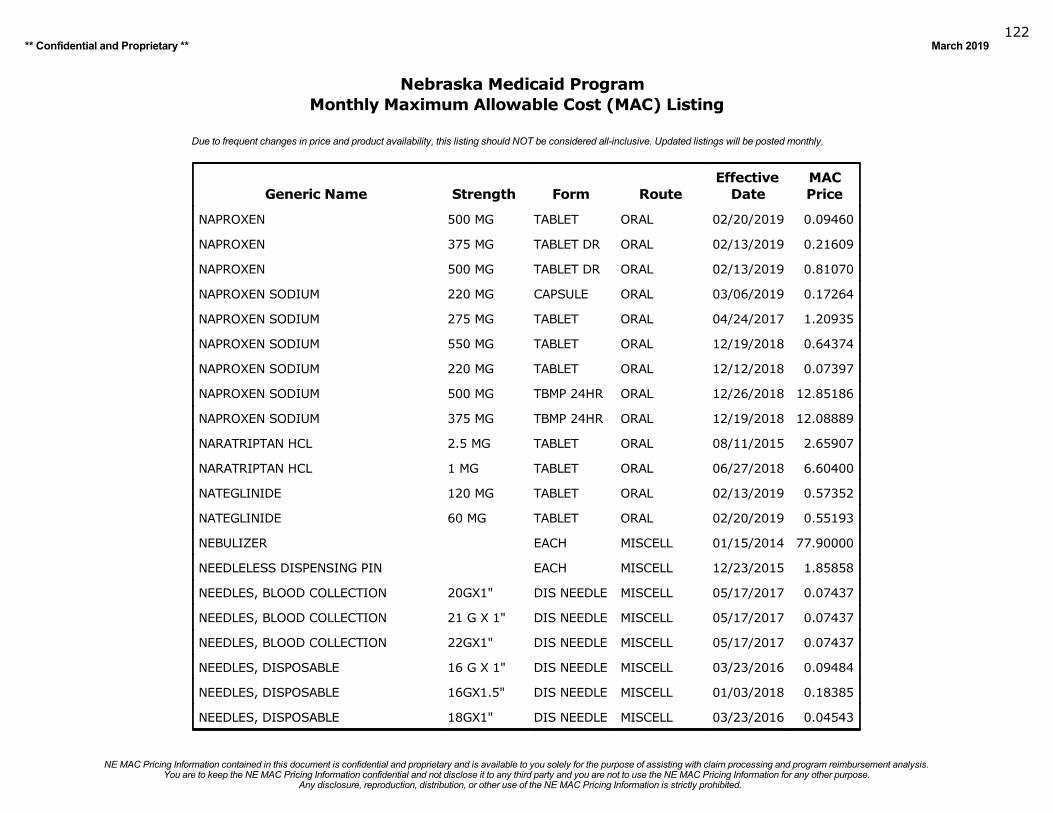
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019122
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
NAPROXEN 500 MG TABLET ORAL 02/20/2019 0.09460
NAPROXEN 375 MG TABLET DR ORAL 02/13/2019 0.21609
NAPROXEN 500 MG TABLET DR ORAL 02/13/2019 0.81070
NAPROXEN SODIUM 220 MG CAPSULE ORAL 03/06/2019 0.17264
NAPROXEN SODIUM 275 MG TABLET ORAL 04/24/2017 1.20935
NAPROXEN SODIUM 550 MG TABLET ORAL 12/19/2018 0.64374
NAPROXEN SODIUM 220 MG TABLET ORAL 12/12/2018 0.07397
NAPROXEN SODIUM 500 MG TBMP 24HR ORAL 12/26/2018 12.85186
NAPROXEN SODIUM 375 MG TBMP 24HR ORAL 12/19/2018 12.08889
NARATRIPTAN HCL 2.5 MG TABLET ORAL 08/11/2015 2.65907
NARATRIPTAN HCL 1 MG TABLET ORAL 06/27/2018 6.60400
NATEGLINIDE 120 MG TABLET ORAL 02/13/2019 0.57352
NATEGLINIDE 60 MG TABLET ORAL 02/20/2019 0.55193
NEBULIZER EACH MISCELL 01/15/2014 77.90000
NEEDLELESS DISPENSING PIN EACH MISCELL 12/23/2015 1.85858
NEEDLES, BLOOD COLLECTION 20GX1" DIS NEEDLE MISCELL 05/17/2017 0.07437
NEEDLES, BLOOD COLLECTION 21 G X 1" DIS NEEDLE MISCELL 05/17/2017 0.07437
NEEDLES, BLOOD COLLECTION 22GX1" DIS NEEDLE MISCELL 05/17/2017 0.07437
NEEDLES, DISPOSABLE 16 G X 1" DIS NEEDLE MISCELL 03/23/2016 0.09484
NEEDLES, DISPOSABLE 16GX1.5" DIS NEEDLE MISCELL 01/03/2018 0.18385
NEEDLES, DISPOSABLE 18GX1" DIS NEEDLE MISCELL 03/23/2016 0.04543
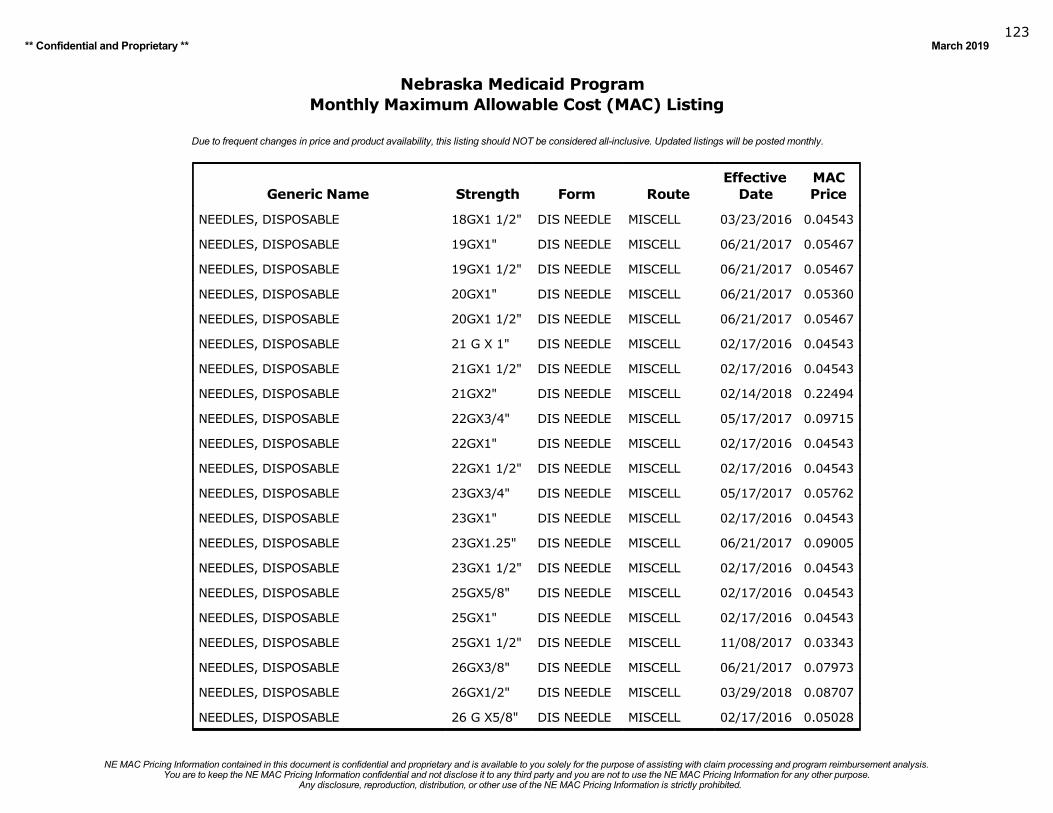
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019123
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
NEEDLES, DISPOSABLE 18GX1 1/2" DIS NEEDLE MISCELL 03/23/2016 0.04543
NEEDLES, DISPOSABLE 19GX1" DIS NEEDLE MISCELL 06/21/2017 0.05467
NEEDLES, DISPOSABLE 19GX1 1/2" DIS NEEDLE MISCELL 06/21/2017 0.05467
NEEDLES, DISPOSABLE 20GX1" DIS NEEDLE MISCELL 06/21/2017 0.05360
NEEDLES, DISPOSABLE 20GX1 1/2" DIS NEEDLE MISCELL 06/21/2017 0.05467
NEEDLES, DISPOSABLE 21 G X 1" DIS NEEDLE MISCELL 02/17/2016 0.04543
NEEDLES, DISPOSABLE 21GX1 1/2" DIS NEEDLE MISCELL 02/17/2016 0.04543
NEEDLES, DISPOSABLE 21GX2" DIS NEEDLE MISCELL 02/14/2018 0.22494
NEEDLES, DISPOSABLE 22GX3/4" DIS NEEDLE MISCELL 05/17/2017 0.09715
NEEDLES, DISPOSABLE 22GX1" DIS NEEDLE MISCELL 02/17/2016 0.04543
NEEDLES, DISPOSABLE 22GX1 1/2" DIS NEEDLE MISCELL 02/17/2016 0.04543
NEEDLES, DISPOSABLE 23GX3/4" DIS NEEDLE MISCELL 05/17/2017 0.05762
NEEDLES, DISPOSABLE 23GX1" DIS NEEDLE MISCELL 02/17/2016 0.04543
NEEDLES, DISPOSABLE 23GX1.25" DIS NEEDLE MISCELL 06/21/2017 0.09005
NEEDLES, DISPOSABLE 23GX1 1/2" DIS NEEDLE MISCELL 02/17/2016 0.04543
NEEDLES, DISPOSABLE 25GX5/8" DIS NEEDLE MISCELL 02/17/2016 0.04543
NEEDLES, DISPOSABLE 25GX1" DIS NEEDLE MISCELL 02/17/2016 0.04543
NEEDLES, DISPOSABLE 25GX1 1/2" DIS NEEDLE MISCELL 11/08/2017 0.03343
NEEDLES, DISPOSABLE 26GX3/8" DIS NEEDLE MISCELL 06/21/2017 0.07973
NEEDLES, DISPOSABLE 26GX1/2" DIS NEEDLE MISCELL 03/29/2018 0.08707
NEEDLES, DISPOSABLE 26 G X5/8" DIS NEEDLE MISCELL 02/17/2016 0.05028
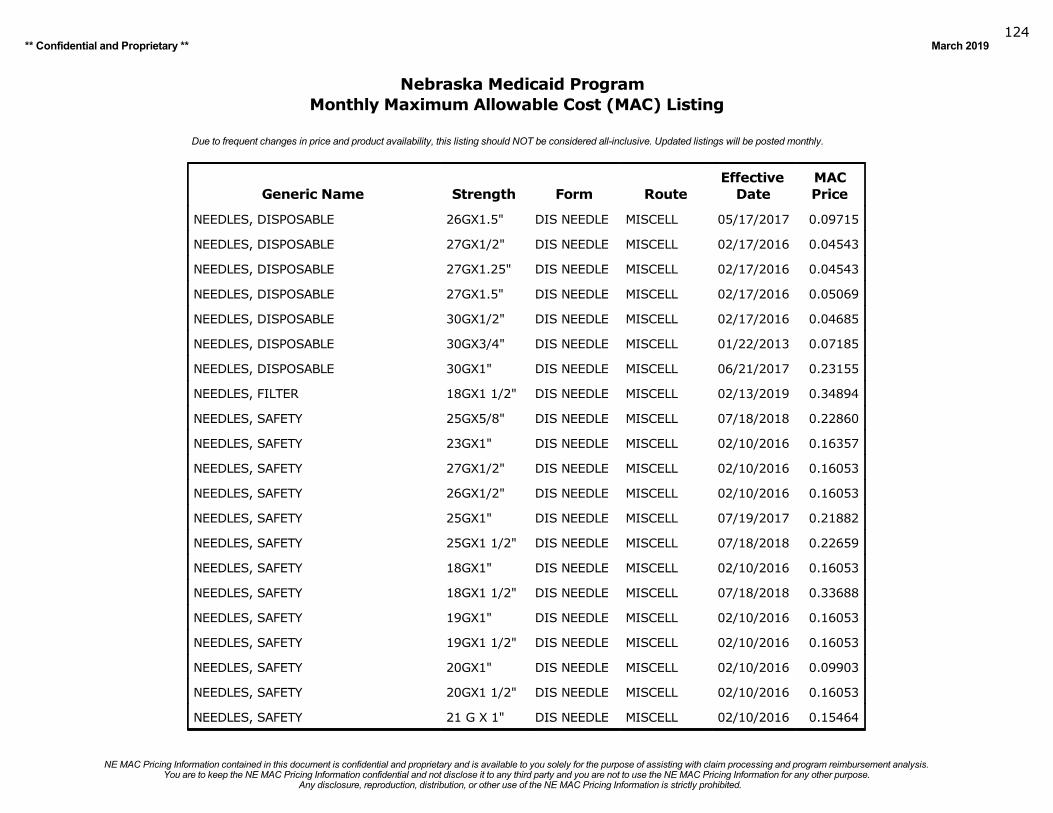
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019124
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
NEEDLES, DISPOSABLE 26GX1.5" DIS NEEDLE MISCELL 05/17/2017 0.09715
NEEDLES, DISPOSABLE 27GX1/2" DIS NEEDLE MISCELL 02/17/2016 0.04543
NEEDLES, DISPOSABLE 27GX1.25" DIS NEEDLE MISCELL 02/17/2016 0.04543
NEEDLES, DISPOSABLE 27GX1.5" DIS NEEDLE MISCELL 02/17/2016 0.05069
NEEDLES, DISPOSABLE 30GX1/2" DIS NEEDLE MISCELL 02/17/2016 0.04685
NEEDLES, DISPOSABLE 30GX3/4" DIS NEEDLE MISCELL 01/22/2013 0.07185
NEEDLES, DISPOSABLE 30GX1" DIS NEEDLE MISCELL 06/21/2017 0.23155
NEEDLES, FILTER 18GX1 1/2" DIS NEEDLE MISCELL 02/13/2019 0.34894
NEEDLES, SAFETY 25GX5/8" DIS NEEDLE MISCELL 07/18/2018 0.22860
NEEDLES, SAFETY 23GX1" DIS NEEDLE MISCELL 02/10/2016 0.16357
NEEDLES, SAFETY 27GX1/2" DIS NEEDLE MISCELL 02/10/2016 0.16053
NEEDLES, SAFETY 26GX1/2" DIS NEEDLE MISCELL 02/10/2016 0.16053
NEEDLES, SAFETY 25GX1" DIS NEEDLE MISCELL 07/19/2017 0.21882
NEEDLES, SAFETY 25GX1 1/2" DIS NEEDLE MISCELL 07/18/2018 0.22659
NEEDLES, SAFETY 18GX1" DIS NEEDLE MISCELL 02/10/2016 0.16053
NEEDLES, SAFETY 18GX1 1/2" DIS NEEDLE MISCELL 07/18/2018 0.33688
NEEDLES, SAFETY 19GX1" DIS NEEDLE MISCELL 02/10/2016 0.16053
NEEDLES, SAFETY 19GX1 1/2" DIS NEEDLE MISCELL 02/10/2016 0.16053
NEEDLES, SAFETY 20GX1" DIS NEEDLE MISCELL 02/10/2016 0.09903
NEEDLES, SAFETY 20GX1 1/2" DIS NEEDLE MISCELL 02/10/2016 0.16053
NEEDLES, SAFETY 21 G X 1" DIS NEEDLE MISCELL 02/10/2016 0.15464
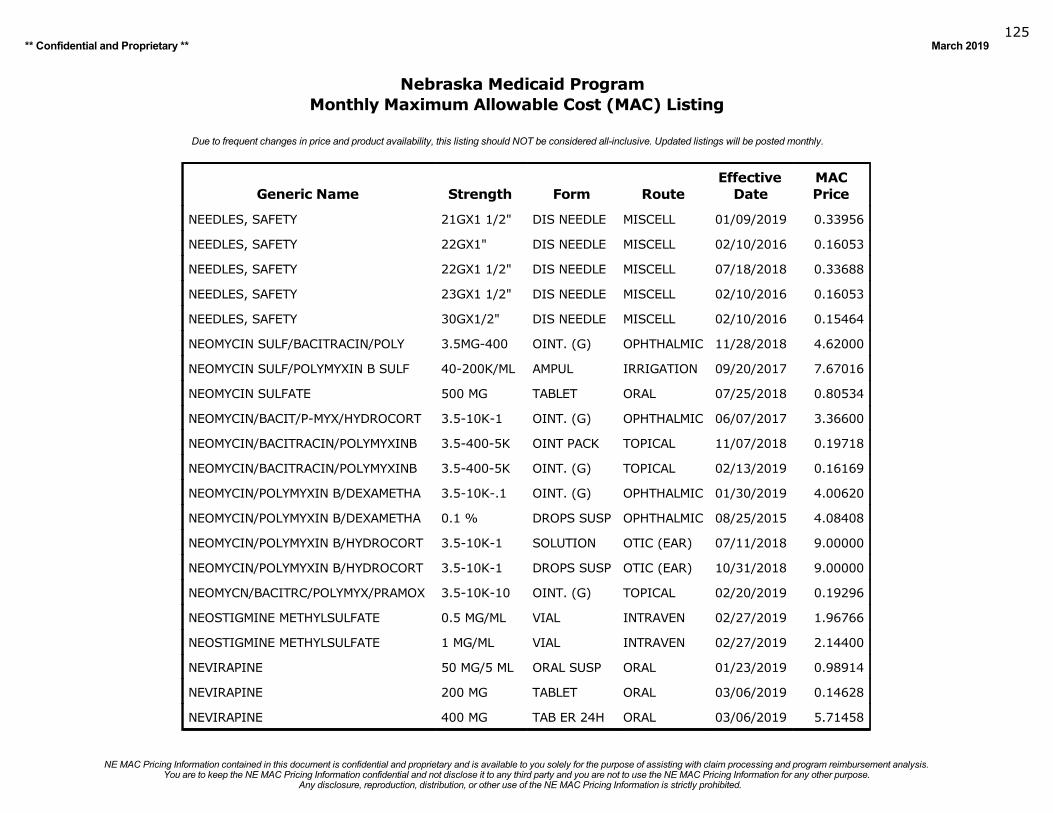
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019125
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
NEEDLES, SAFETY 21GX1 1/2" DIS NEEDLE MISCELL 01/09/2019 0.33956
NEEDLES, SAFETY 22GX1" DIS NEEDLE MISCELL 02/10/2016 0.16053
NEEDLES, SAFETY 22GX1 1/2" DIS NEEDLE MISCELL 07/18/2018 0.33688
NEEDLES, SAFETY 23GX1 1/2" DIS NEEDLE MISCELL 02/10/2016 0.16053
NEEDLES, SAFETY 30GX1/2" DIS NEEDLE MISCELL 02/10/2016 0.15464
NEOMYCIN SULF/BACITRACIN/POLY 3.5MG-400 OINT. (G) OPHTHALMIC 11/28/2018 4.62000
NEOMYCIN SULF/POLYMYXIN B SULF 40-200K/ML AMPUL IRRIGATION 09/20/2017 7.67016
NEOMYCIN SULFATE 500 MG TABLET ORAL 07/25/2018 0.80534
NEOMYCIN/BACIT/P-MYX/HYDROCORT 3.5-10K-1 OINT. (G) OPHTHALMIC 06/07/2017 3.36600
NEOMYCIN/BACITRACIN/POLYMYXINB 3.5-400-5K OINT PACK TOPICAL 11/07/2018 0.19718
NEOMYCIN/BACITRACIN/POLYMYXINB 3.5-400-5K OINT. (G) TOPICAL 02/13/2019 0.16169
NEOMYCIN/POLYMYXIN B/DEXAMETHA 3.5-10K-.1 OINT. (G) OPHTHALMIC 01/30/2019 4.00620
NEOMYCIN/POLYMYXIN B/DEXAMETHA 0.1 % DROPS SUSP OPHTHALMIC 08/25/2015 4.08408
NEOMYCIN/POLYMYXIN B/HYDROCORT 3.5-10K-1 SOLUTION OTIC (EAR) 07/11/2018 9.00000
NEOMYCIN/POLYMYXIN B/HYDROCORT 3.5-10K-1 DROPS SUSP OTIC (EAR) 10/31/2018 9.00000
NEOMYCN/BACITRC/POLYMYX/PRAMOX 3.5-10K-10 OINT. (G) TOPICAL 02/20/2019 0.19296
NEOSTIGMINE METHYLSULFATE 0.5 MG/ML VIAL INTRAVEN 02/27/2019 1.96766
NEOSTIGMINE METHYLSULFATE 1 MG/ML VIAL INTRAVEN 02/27/2019 2.14400
NEVIRAPINE 50 MG/5 ML ORAL SUSP ORAL 01/23/2019 0.98914
NEVIRAPINE 200 MG TABLET ORAL 03/06/2019 0.14628
NEVIRAPINE 400 MG TAB ER 24H ORAL 03/06/2019 5.71458
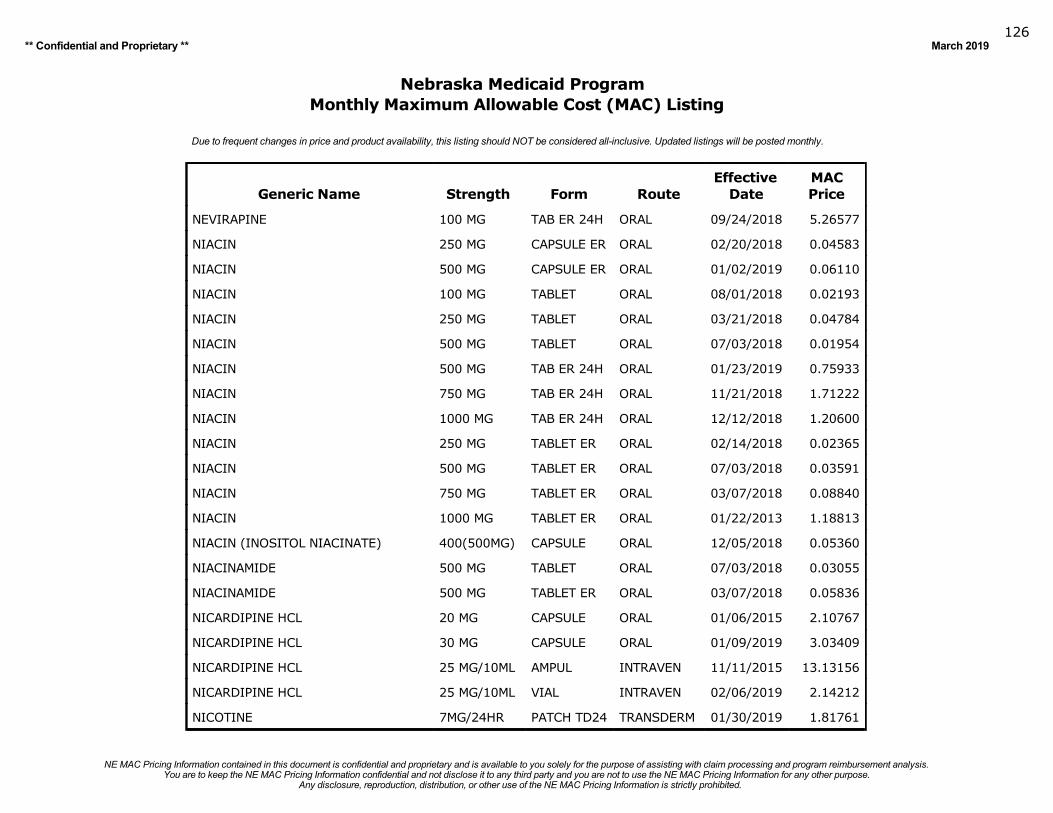
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019126
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
NEVIRAPINE 100 MG TAB ER 24H ORAL 09/24/2018 5.26577
NIACIN 250 MG CAPSULE ER ORAL 02/20/2018 0.04583
NIACIN 500 MG CAPSULE ER ORAL 01/02/2019 0.06110
NIACIN 100 MG TABLET ORAL 08/01/2018 0.02193
NIACIN 250 MG TABLET ORAL 03/21/2018 0.04784
NIACIN 500 MG TABLET ORAL 07/03/2018 0.01954
NIACIN 500 MG TAB ER 24H ORAL 01/23/2019 0.75933
NIACIN 750 MG TAB ER 24H ORAL 11/21/2018 1.71222
NIACIN 1000 MG TAB ER 24H ORAL 12/12/2018 1.20600
NIACIN 250 MG TABLET ER ORAL 02/14/2018 0.02365
NIACIN 500 MG TABLET ER ORAL 07/03/2018 0.03591
NIACIN 750 MG TABLET ER ORAL 03/07/2018 0.08840
NIACIN 1000 MG TABLET ER ORAL 01/22/2013 1.18813
NIACIN (INOSITOL NIACINATE) 400(500MG) CAPSULE ORAL 12/05/2018 0.05360
NIACINAMIDE 500 MG TABLET ORAL 07/03/2018 0.03055
NIACINAMIDE 500 MG TABLET ER ORAL 03/07/2018 0.05836
NICARDIPINE HCL 20 MG CAPSULE ORAL 01/06/2015 2.10767
NICARDIPINE HCL 30 MG CAPSULE ORAL 01/09/2019 3.03409
NICARDIPINE HCL 25 MG/10ML AMPUL INTRAVEN 11/11/2015 13.13156
NICARDIPINE HCL 25 MG/10ML VIAL INTRAVEN 02/06/2019 2.14212
NICOTINE 7MG/24HR PATCH TD24 TRANSDERM 01/30/2019 1.81761
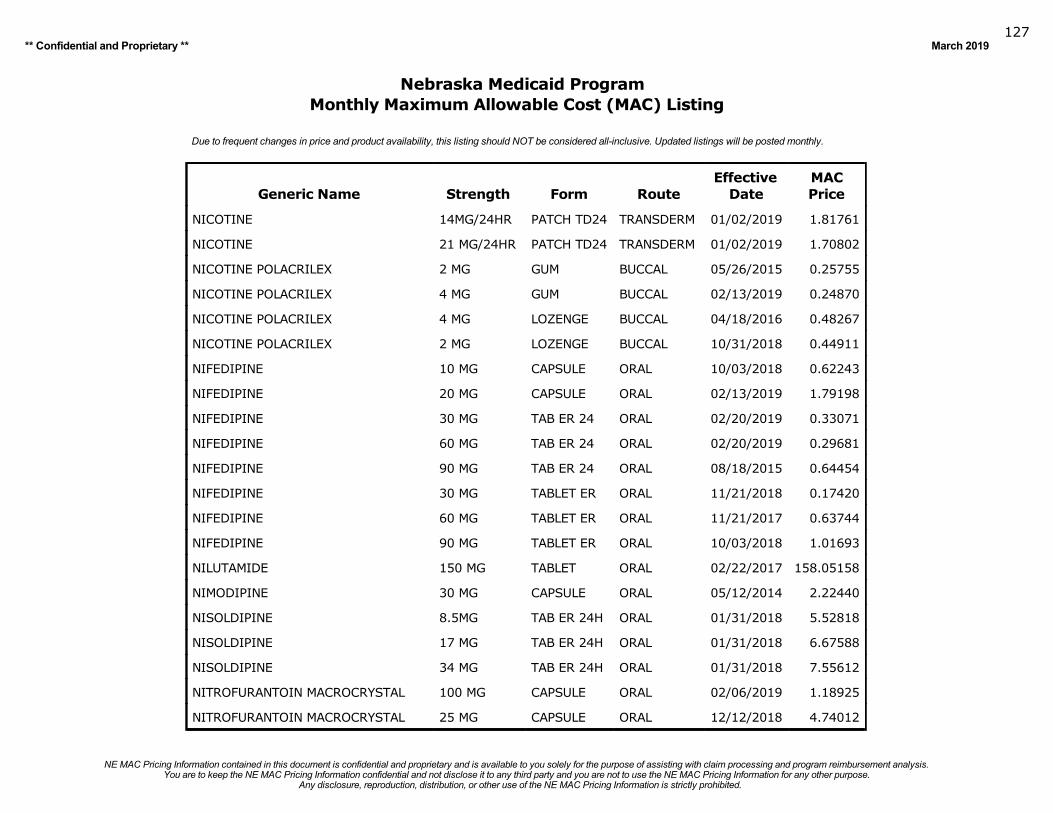
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019127
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
NICOTINE 14MG/24HR PATCH TD24 TRANSDERM 01/02/2019 1.81761
NICOTINE 21 MG/24HR PATCH TD24 TRANSDERM 01/02/2019 1.70802
NICOTINE POLACRILEX 2 MG GUM BUCCAL 05/26/2015 0.25755
NICOTINE POLACRILEX 4 MG GUM BUCCAL 02/13/2019 0.24870
NICOTINE POLACRILEX 4 MG LOZENGE BUCCAL 04/18/2016 0.48267
NICOTINE POLACRILEX 2 MG LOZENGE BUCCAL 10/31/2018 0.44911
NIFEDIPINE 10 MG CAPSULE ORAL 10/03/2018 0.62243
NIFEDIPINE 20 MG CAPSULE ORAL 02/13/2019 1.79198
NIFEDIPINE 30 MG TAB ER 24 ORAL 02/20/2019 0.33071
NIFEDIPINE 60 MG TAB ER 24 ORAL 02/20/2019 0.29681
NIFEDIPINE 90 MG TAB ER 24 ORAL 08/18/2015 0.64454
NIFEDIPINE 30 MG TABLET ER ORAL 11/21/2018 0.17420
NIFEDIPINE 60 MG TABLET ER ORAL 11/21/2017 0.63744
NIFEDIPINE 90 MG TABLET ER ORAL 10/03/2018 1.01693
NILUTAMIDE 150 MG TABLET ORAL 02/22/2017 158.05158
NIMODIPINE 30 MG CAPSULE ORAL 05/12/2014 2.22440
NISOLDIPINE 8.5MG TAB ER 24H ORAL 01/31/2018 5.52818
NISOLDIPINE 17 MG TAB ER 24H ORAL 01/31/2018 6.67588
NISOLDIPINE 34 MG TAB ER 24H ORAL 01/31/2018 7.55612
NITROFURANTOIN MACROCRYSTAL 100 MG CAPSULE ORAL 02/06/2019 1.18925
NITROFURANTOIN MACROCRYSTAL 25 MG CAPSULE ORAL 12/12/2018 4.74012
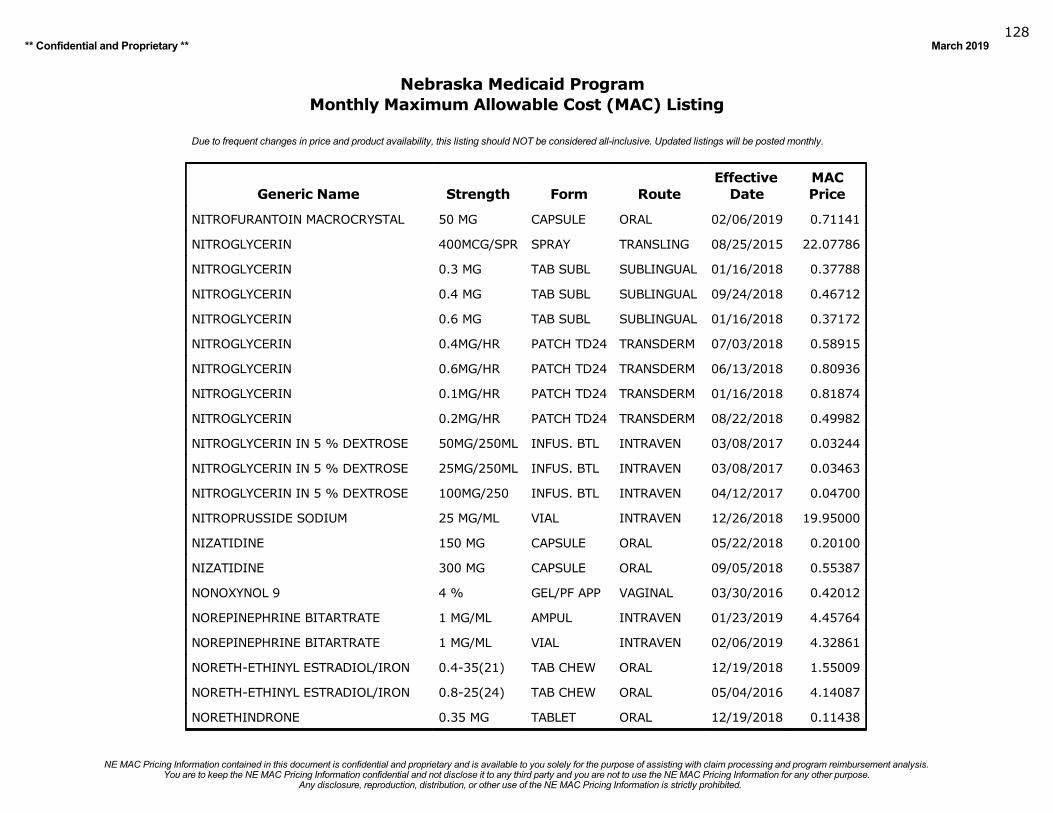
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019128
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
NITROFURANTOIN MACROCRYSTAL 50 MG CAPSULE ORAL 02/06/2019 0.71141
NITROGLYCERIN 400MCG/SPR SPRAY TRANSLING 08/25/2015 22.07786
NITROGLYCERIN 0.3 MG TAB SUBL SUBLINGUAL 01/16/2018 0.37788
NITROGLYCERIN 0.4 MG TAB SUBL SUBLINGUAL 09/24/2018 0.46712
NITROGLYCERIN 0.6 MG TAB SUBL SUBLINGUAL 01/16/2018 0.37172
NITROGLYCERIN 0.4MG/HR PATCH TD24 TRANSDERM 07/03/2018 0.58915
NITROGLYCERIN 0.6MG/HR PATCH TD24 TRANSDERM 06/13/2018 0.80936
NITROGLYCERIN 0.1MG/HR PATCH TD24 TRANSDERM 01/16/2018 0.81874
NITROGLYCERIN 0.2MG/HR PATCH TD24 TRANSDERM 08/22/2018 0.49982
NITROGLYCERIN IN 5 % DEXTROSE 50MG/250ML INFUS. BTL INTRAVEN 03/08/2017 0.03244
NITROGLYCERIN IN 5 % DEXTROSE 25MG/250ML INFUS. BTL INTRAVEN 03/08/2017 0.03463
NITROGLYCERIN IN 5 % DEXTROSE 100MG/250 INFUS. BTL INTRAVEN 04/12/2017 0.04700
NITROPRUSSIDE SODIUM 25 MG/ML VIAL INTRAVEN 12/26/2018 19.95000
NIZATIDINE 150 MG CAPSULE ORAL 05/22/2018 0.20100
NIZATIDINE 300 MG CAPSULE ORAL 09/05/2018 0.55387
NONOXYNOL 9 4 % GEL/PF APP VAGINAL 03/30/2016 0.42012
NOREPINEPHRINE BITARTRATE 1 MG/ML AMPUL INTRAVEN 01/23/2019 4.45764
NOREPINEPHRINE BITARTRATE 1 MG/ML VIAL INTRAVEN 02/06/2019 4.32861
NORETH-ETHINYL ESTRADIOL/IRON 0.4-35(21) TAB CHEW ORAL 12/19/2018 1.55009
NORETH-ETHINYL ESTRADIOL/IRON 0.8-25(24) TAB CHEW ORAL 05/04/2016 4.14087
NORETHINDRONE 0.35 MG TABLET ORAL 12/19/2018 0.11438
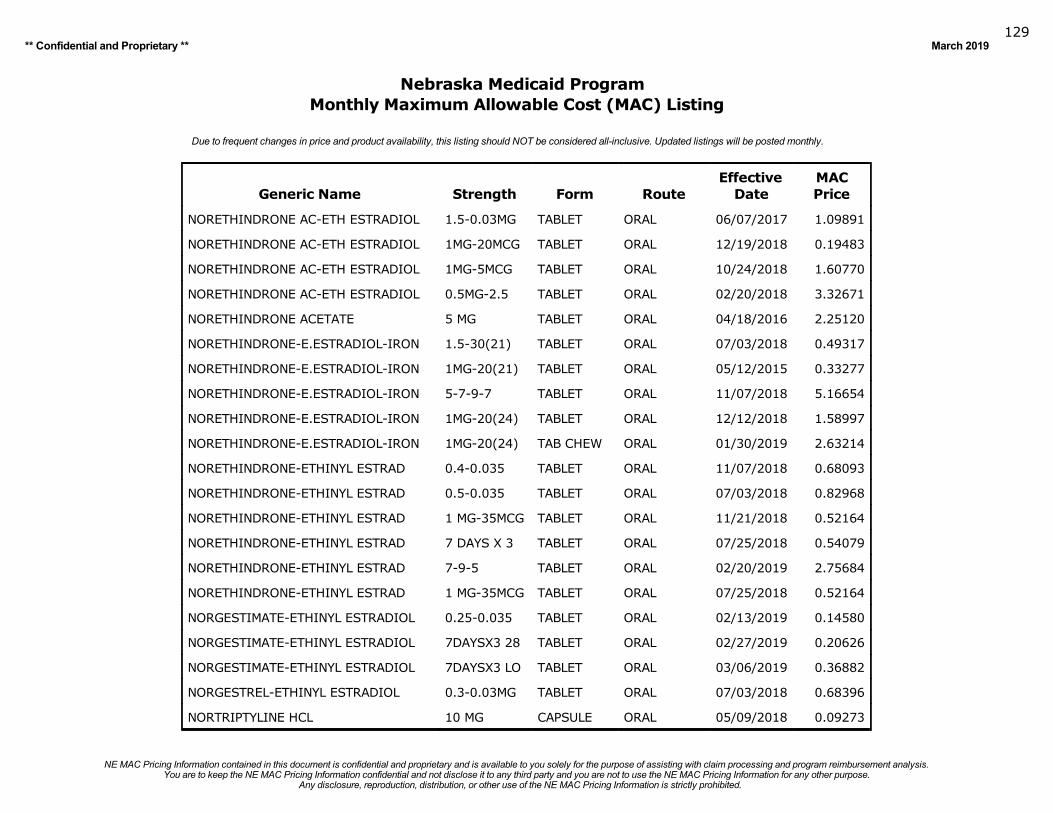
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019129
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
NORETHINDRONE AC-ETH ESTRADIOL 1.5-0.03MG TABLET ORAL 06/07/2017 1.09891
NORETHINDRONE AC-ETH ESTRADIOL 1MG-20MCG TABLET ORAL 12/19/2018 0.19483
NORETHINDRONE AC-ETH ESTRADIOL 1MG-5MCG TABLET ORAL 10/24/2018 1.60770
NORETHINDRONE AC-ETH ESTRADIOL 0.5MG-2.5 TABLET ORAL 02/20/2018 3.32671
NORETHINDRONE ACETATE 5 MG TABLET ORAL 04/18/2016 2.25120
NORETHINDRONE-E.ESTRADIOL-IRON 1.5-30(21) TABLET ORAL 07/03/2018 0.49317
NORETHINDRONE-E.ESTRADIOL-IRON 1MG-20(21) TABLET ORAL 05/12/2015 0.33277
NORETHINDRONE-E.ESTRADIOL-IRON 5-7-9-7 TABLET ORAL 11/07/2018 5.16654
NORETHINDRONE-E.ESTRADIOL-IRON 1MG-20(24) TABLET ORAL 12/12/2018 1.58997
NORETHINDRONE-E.ESTRADIOL-IRON 1MG-20(24) TAB CHEW ORAL 01/30/2019 2.63214
NORETHINDRONE-ETHINYL ESTRAD 0.4-0.035 TABLET ORAL 11/07/2018 0.68093
NORETHINDRONE-ETHINYL ESTRAD 0.5-0.035 TABLET ORAL 07/03/2018 0.82968
NORETHINDRONE-ETHINYL ESTRAD 1 MG-35MCG TABLET ORAL 11/21/2018 0.52164
NORETHINDRONE-ETHINYL ESTRAD 7 DAYS X 3 TABLET ORAL 07/25/2018 0.54079
NORETHINDRONE-ETHINYL ESTRAD 7-9-5 TABLET ORAL 02/20/2019 2.75684
NORETHINDRONE-ETHINYL ESTRAD 1 MG-35MCG TABLET ORAL 07/25/2018 0.52164
NORGESTIMATE-ETHINYL ESTRADIOL 0.25-0.035 TABLET ORAL 02/13/2019 0.14580
NORGESTIMATE-ETHINYL ESTRADIOL 7DAYSX3 28 TABLET ORAL 02/27/2019 0.20626
NORGESTIMATE-ETHINYL ESTRADIOL 7DAYSX3 LO TABLET ORAL 03/06/2019 0.36882
NORGESTREL-ETHINYL ESTRADIOL 0.3-0.03MG TABLET ORAL 07/03/2018 0.68396
NORTRIPTYLINE HCL 10 MG CAPSULE ORAL 05/09/2018 0.09273
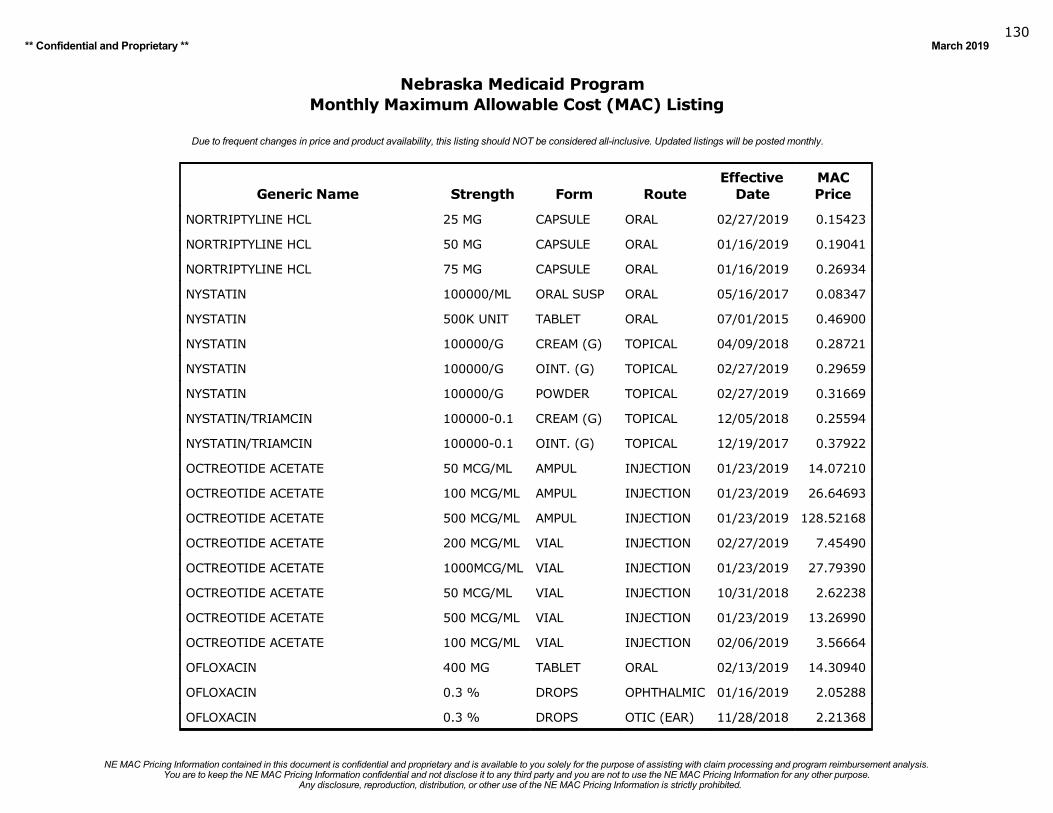
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019130
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
NORTRIPTYLINE HCL 25 MG CAPSULE ORAL 02/27/2019 0.15423
NORTRIPTYLINE HCL 50 MG CAPSULE ORAL 01/16/2019 0.19041
NORTRIPTYLINE HCL 75 MG CAPSULE ORAL 01/16/2019 0.26934
NYSTATIN 100000/ML ORAL SUSP ORAL 05/16/2017 0.08347
NYSTATIN 500K UNIT TABLET ORAL 07/01/2015 0.46900
NYSTATIN 100000/G CREAM (G) TOPICAL 04/09/2018 0.28721
NYSTATIN 100000/G OINT. (G) TOPICAL 02/27/2019 0.29659
NYSTATIN 100000/G POWDER TOPICAL 02/27/2019 0.31669
NYSTATIN/TRIAMCIN 100000-0.1 CREAM (G) TOPICAL 12/05/2018 0.25594
NYSTATIN/TRIAMCIN 100000-0.1 OINT. (G) TOPICAL 12/19/2017 0.37922
OCTREOTIDE ACETATE 50 MCG/ML AMPUL INJECTION 01/23/2019 14.07210
OCTREOTIDE ACETATE 100 MCG/ML AMPUL INJECTION 01/23/2019 26.64693
OCTREOTIDE ACETATE 500 MCG/ML AMPUL INJECTION 01/23/2019 128.52168
OCTREOTIDE ACETATE 200 MCG/ML VIAL INJECTION 02/27/2019 7.45490
OCTREOTIDE ACETATE 1000MCG/ML VIAL INJECTION 01/23/2019 27.79390
OCTREOTIDE ACETATE 50 MCG/ML VIAL INJECTION 10/31/2018 2.62238
OCTREOTIDE ACETATE 500 MCG/ML VIAL INJECTION 01/23/2019 13.26990
OCTREOTIDE ACETATE 100 MCG/ML VIAL INJECTION 02/06/2019 3.56664
OFLOXACIN 400 MG TABLET ORAL 02/13/2019 14.30940
OFLOXACIN 0.3 % DROPS OPHTHALMIC 01/16/2019 2.05288
OFLOXACIN 0.3 % DROPS OTIC (EAR) 11/28/2018 2.21368
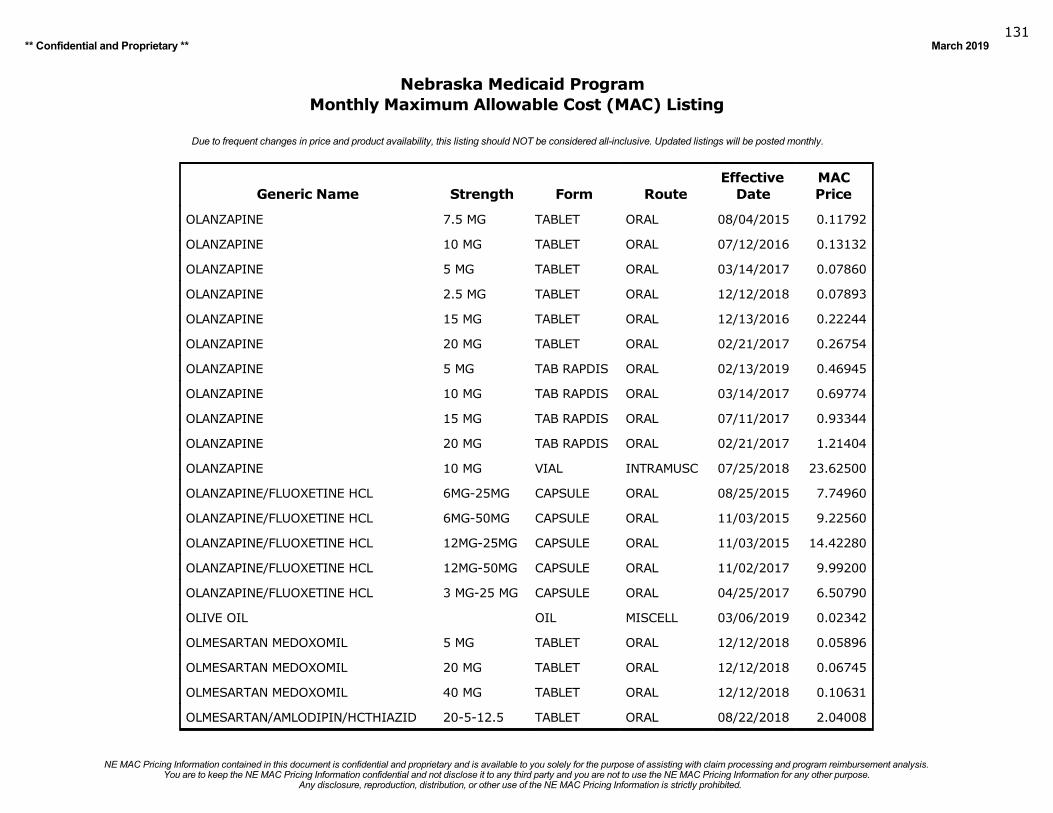
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019131
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
OLANZAPINE 7.5 MG TABLET ORAL 08/04/2015 0.11792
OLANZAPINE 10 MG TABLET ORAL 07/12/2016 0.13132
OLANZAPINE 5 MG TABLET ORAL 03/14/2017 0.07860
OLANZAPINE 2.5 MG TABLET ORAL 12/12/2018 0.07893
OLANZAPINE 15 MG TABLET ORAL 12/13/2016 0.22244
OLANZAPINE 20 MG TABLET ORAL 02/21/2017 0.26754
OLANZAPINE 5 MG TAB RAPDIS ORAL 02/13/2019 0.46945
OLANZAPINE 10 MG TAB RAPDIS ORAL 03/14/2017 0.69774
OLANZAPINE 15 MG TAB RAPDIS ORAL 07/11/2017 0.93344
OLANZAPINE 20 MG TAB RAPDIS ORAL 02/21/2017 1.21404
OLANZAPINE 10 MG VIAL INTRAMUSC 07/25/2018 23.62500
OLANZAPINE/FLUOXETINE HCL 6MG-25MG CAPSULE ORAL 08/25/2015 7.74960
OLANZAPINE/FLUOXETINE HCL 6MG-50MG CAPSULE ORAL 11/03/2015 9.22560
OLANZAPINE/FLUOXETINE HCL 12MG-25MG CAPSULE ORAL 11/03/2015 14.42280
OLANZAPINE/FLUOXETINE HCL 12MG-50MG CAPSULE ORAL 11/02/2017 9.99200
OLANZAPINE/FLUOXETINE HCL 3 MG-25 MG CAPSULE ORAL 04/25/2017 6.50790
OLIVE OIL OIL MISCELL 03/06/2019 0.02342
OLMESARTAN MEDOXOMIL 5 MG TABLET ORAL 12/12/2018 0.05896
OLMESARTAN MEDOXOMIL 20 MG TABLET ORAL 12/12/2018 0.06745
OLMESARTAN MEDOXOMIL 40 MG TABLET ORAL 12/12/2018 0.10631
OLMESARTAN/AMLODIPIN/HCTHIAZID 20-5-12.5 TABLET ORAL 08/22/2018 2.04008
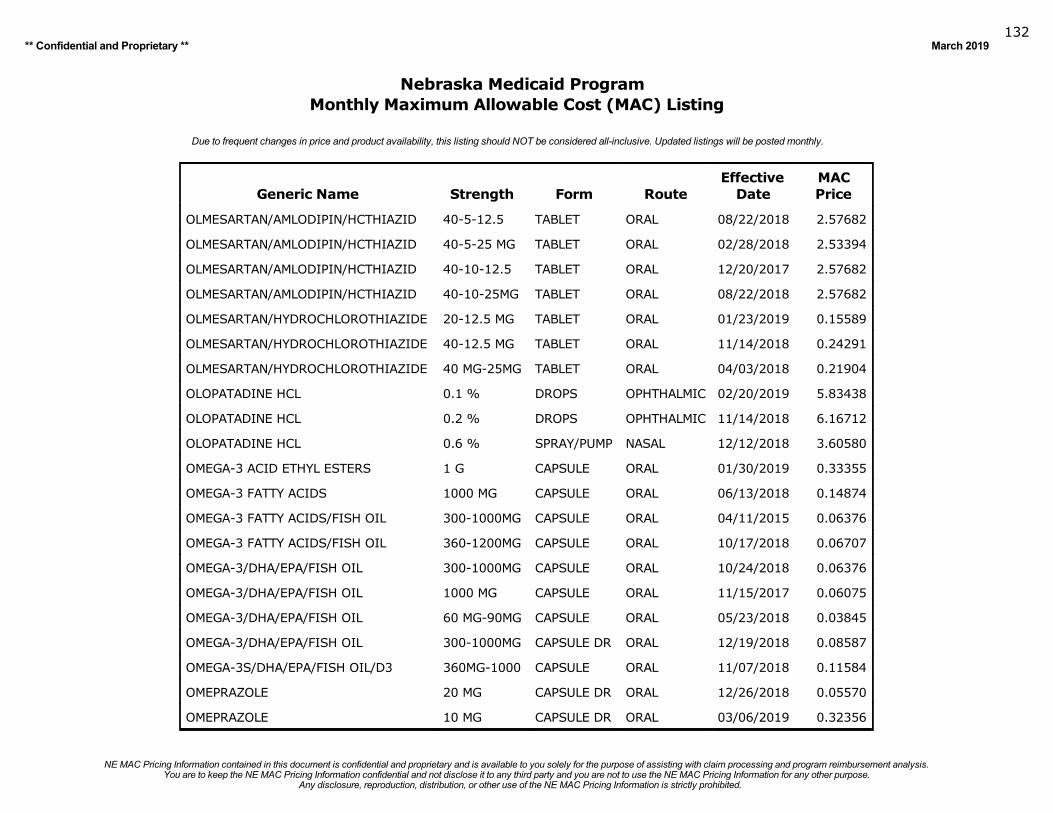
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019132
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
OLMESARTAN/AMLODIPIN/HCTHIAZID 40-5-12.5 TABLET ORAL 08/22/2018 2.57682
OLMESARTAN/AMLODIPIN/HCTHIAZID 40-5-25 MG TABLET ORAL 02/28/2018 2.53394
OLMESARTAN/AMLODIPIN/HCTHIAZID 40-10-12.5 TABLET ORAL 12/20/2017 2.57682
OLMESARTAN/AMLODIPIN/HCTHIAZID 40-10-25MG TABLET ORAL 08/22/2018 2.57682
OLMESARTAN/HYDROCHLOROTHIAZIDE 20-12.5 MG TABLET ORAL 01/23/2019 0.15589
OLMESARTAN/HYDROCHLOROTHIAZIDE 40-12.5 MG TABLET ORAL 11/14/2018 0.24291
OLMESARTAN/HYDROCHLOROTHIAZIDE 40 MG-25MG TABLET ORAL 04/03/2018 0.21904
OLOPATADINE HCL 0.1 % DROPS OPHTHALMIC 02/20/2019 5.83438
OLOPATADINE HCL 0.2 % DROPS OPHTHALMIC 11/14/2018 6.16712
OLOPATADINE HCL 0.6 % SPRAY/PUMP NASAL 12/12/2018 3.60580
OMEGA-3 ACID ETHYL ESTERS 1 G CAPSULE ORAL 01/30/2019 0.33355
OMEGA-3 FATTY ACIDS 1000 MG CAPSULE ORAL 06/13/2018 0.14874
OMEGA-3 FATTY ACIDS/FISH OIL 300-1000MG CAPSULE ORAL 04/11/2015 0.06376
OMEGA-3 FATTY ACIDS/FISH OIL 360-1200MG CAPSULE ORAL 10/17/2018 0.06707
OMEGA-3/DHA/EPA/FISH OIL 300-1000MG CAPSULE ORAL 10/24/2018 0.06376
OMEGA-3/DHA/EPA/FISH OIL 1000 MG CAPSULE ORAL 11/15/2017 0.06075
OMEGA-3/DHA/EPA/FISH OIL 60 MG-90MG CAPSULE ORAL 05/23/2018 0.03845
OMEGA-3/DHA/EPA/FISH OIL 300-1000MG CAPSULE DR ORAL 12/19/2018 0.08587
OMEGA-3S/DHA/EPA/FISH OIL/D3 360MG-1000 CAPSULE ORAL 11/07/2018 0.11584
OMEPRAZOLE 20 MG CAPSULE DR ORAL 12/26/2018 0.05570
OMEPRAZOLE 10 MG CAPSULE DR ORAL 03/06/2019 0.32356
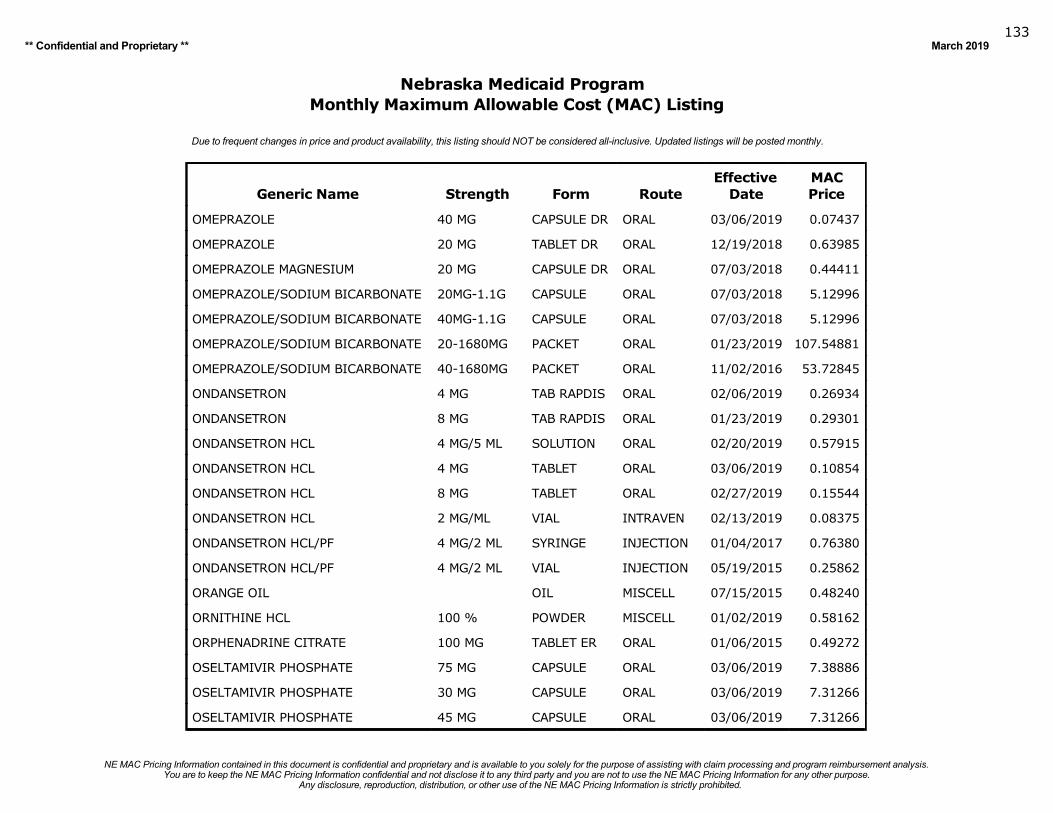
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019133
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
OMEPRAZOLE 40 MG CAPSULE DR ORAL 03/06/2019 0.07437
OMEPRAZOLE 20 MG TABLET DR ORAL 12/19/2018 0.63985
OMEPRAZOLE MAGNESIUM 20 MG CAPSULE DR ORAL 07/03/2018 0.44411
OMEPRAZOLE/SODIUM BICARBONATE 20MG-1.1G CAPSULE ORAL 07/03/2018 5.12996
OMEPRAZOLE/SODIUM BICARBONATE 40MG-1.1G CAPSULE ORAL 07/03/2018 5.12996
OMEPRAZOLE/SODIUM BICARBONATE 20-1680MG PACKET ORAL 01/23/2019 107.54881
OMEPRAZOLE/SODIUM BICARBONATE 40-1680MG PACKET ORAL 11/02/2016 53.72845
ONDANSETRON 4 MG TAB RAPDIS ORAL 02/06/2019 0.26934
ONDANSETRON 8 MG TAB RAPDIS ORAL 01/23/2019 0.29301
ONDANSETRON HCL 4 MG/5 ML SOLUTION ORAL 02/20/2019 0.57915
ONDANSETRON HCL 4 MG TABLET ORAL 03/06/2019 0.10854
ONDANSETRON HCL 8 MG TABLET ORAL 02/27/2019 0.15544
ONDANSETRON HCL 2 MG/ML VIAL INTRAVEN 02/13/2019 0.08375
ONDANSETRON HCL/PF 4 MG/2 ML SYRINGE INJECTION 01/04/2017 0.76380
ONDANSETRON HCL/PF 4 MG/2 ML VIAL INJECTION 05/19/2015 0.25862
ORANGE OIL OIL MISCELL 07/15/2015 0.48240
ORNITHINE HCL 100 % POWDER MISCELL 01/02/2019 0.58162
ORPHENADRINE CITRATE 100 MG TABLET ER ORAL 01/06/2015 0.49272
OSELTAMIVIR PHOSPHATE 75 MG CAPSULE ORAL 03/06/2019 7.38886
OSELTAMIVIR PHOSPHATE 30 MG CAPSULE ORAL 03/06/2019 7.31266
OSELTAMIVIR PHOSPHATE 45 MG CAPSULE ORAL 03/06/2019 7.31266
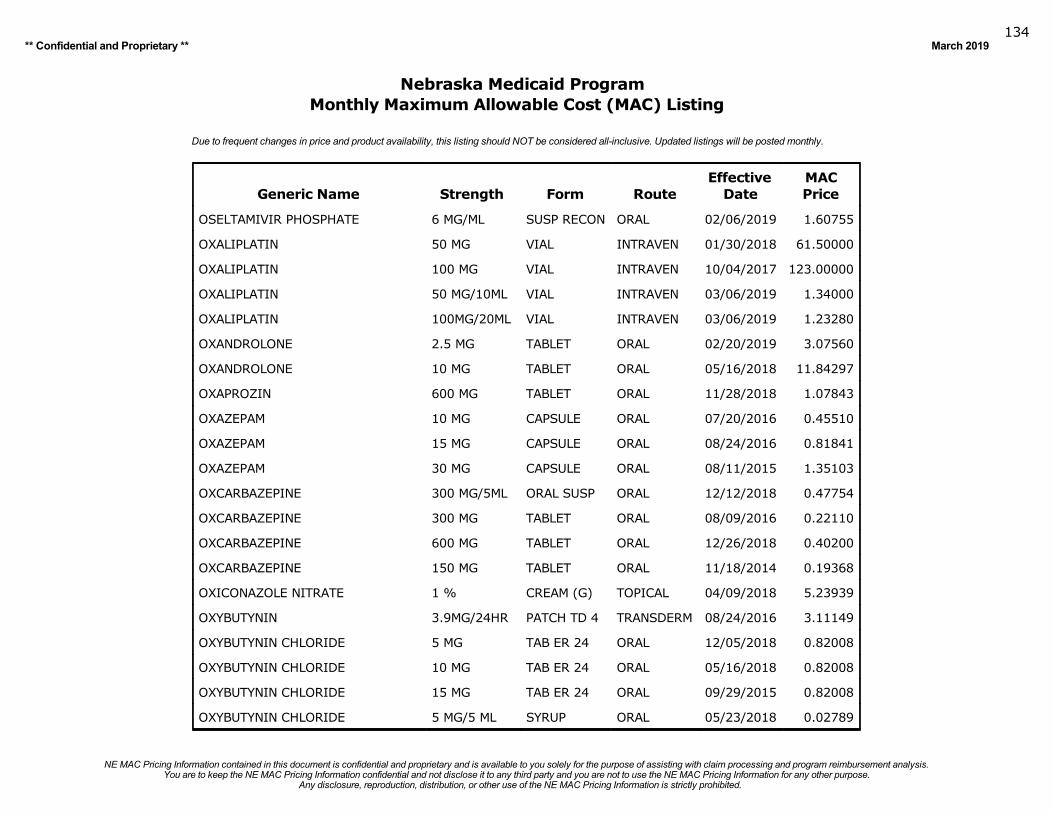
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019134
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
OSELTAMIVIR PHOSPHATE 6 MG/ML SUSP RECON ORAL 02/06/2019 1.60755
OXALIPLATIN 50 MG VIAL INTRAVEN 01/30/2018 61.50000
OXALIPLATIN 100 MG VIAL INTRAVEN 10/04/2017 123.00000
OXALIPLATIN 50 MG/10ML VIAL INTRAVEN 03/06/2019 1.34000
OXALIPLATIN 100MG/20ML VIAL INTRAVEN 03/06/2019 1.23280
OXANDROLONE 2.5 MG TABLET ORAL 02/20/2019 3.07560
OXANDROLONE 10 MG TABLET ORAL 05/16/2018 11.84297
OXAPROZIN 600 MG TABLET ORAL 11/28/2018 1.07843
OXAZEPAM 10 MG CAPSULE ORAL 07/20/2016 0.45510
OXAZEPAM 15 MG CAPSULE ORAL 08/24/2016 0.81841
OXAZEPAM 30 MG CAPSULE ORAL 08/11/2015 1.35103
OXCARBAZEPINE 300 MG/5ML ORAL SUSP ORAL 12/12/2018 0.47754
OXCARBAZEPINE 300 MG TABLET ORAL 08/09/2016 0.22110
OXCARBAZEPINE 600 MG TABLET ORAL 12/26/2018 0.40200
OXCARBAZEPINE 150 MG TABLET ORAL 11/18/2014 0.19368
OXICONAZOLE NITRATE 1 % CREAM (G) TOPICAL 04/09/2018 5.23939
OXYBUTYNIN 3.9MG/24HR PATCH TD 4 TRANSDERM 08/24/2016 3.11149
OXYBUTYNIN CHLORIDE 5 MG TAB ER 24 ORAL 12/05/2018 0.82008
OXYBUTYNIN CHLORIDE 10 MG TAB ER 24 ORAL 05/16/2018 0.82008
OXYBUTYNIN CHLORIDE 15 MG TAB ER 24 ORAL 09/29/2015 0.82008
OXYBUTYNIN CHLORIDE 5 MG/5 ML SYRUP ORAL 05/23/2018 0.02789
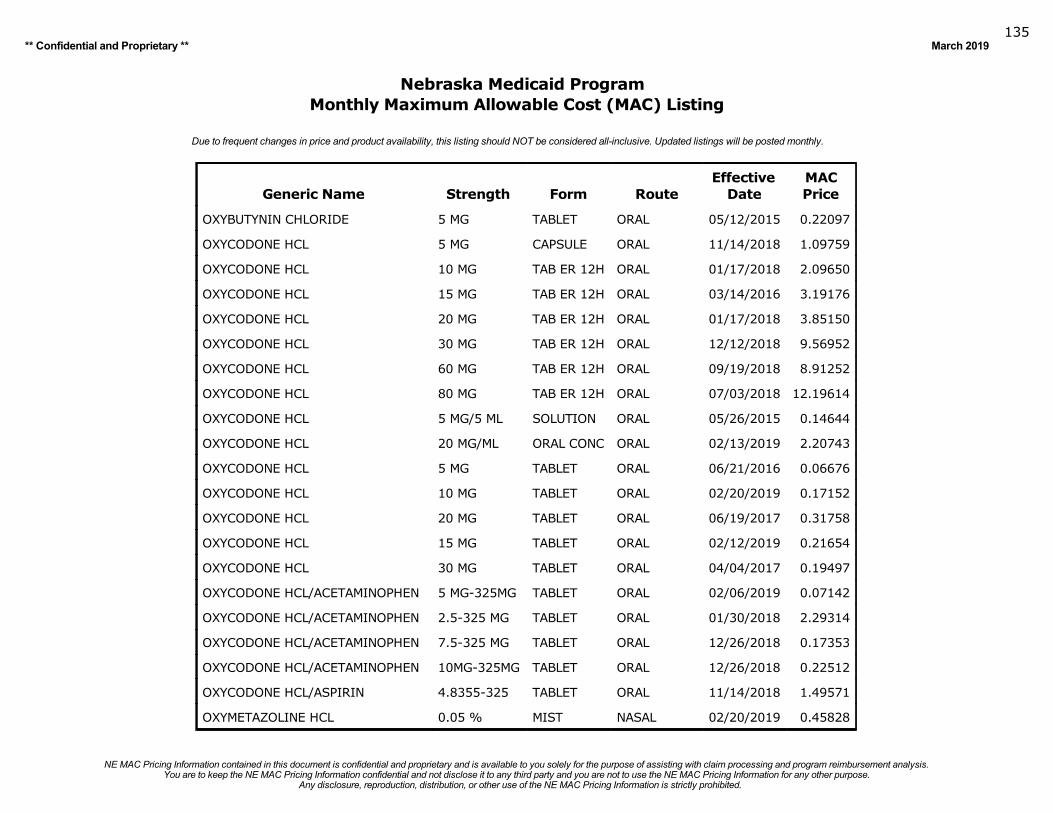
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019135
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
OXYBUTYNIN CHLORIDE 5 MG TABLET ORAL 05/12/2015 0.22097
OXYCODONE HCL 5 MG CAPSULE ORAL 11/14/2018 1.09759
OXYCODONE HCL 10 MG TAB ER 12H ORAL 01/17/2018 2.09650
OXYCODONE HCL 15 MG TAB ER 12H ORAL 03/14/2016 3.19176
OXYCODONE HCL 20 MG TAB ER 12H ORAL 01/17/2018 3.85150
OXYCODONE HCL 30 MG TAB ER 12H ORAL 12/12/2018 9.56952
OXYCODONE HCL 60 MG TAB ER 12H ORAL 09/19/2018 8.91252
OXYCODONE HCL 80 MG TAB ER 12H ORAL 07/03/2018 12.19614
OXYCODONE HCL 5 MG/5 ML SOLUTION ORAL 05/26/2015 0.14644
OXYCODONE HCL 20 MG/ML ORAL CONC ORAL 02/13/2019 2.20743
OXYCODONE HCL 5 MG TABLET ORAL 06/21/2016 0.06676
OXYCODONE HCL 10 MG TABLET ORAL 02/20/2019 0.17152
OXYCODONE HCL 20 MG TABLET ORAL 06/19/2017 0.31758
OXYCODONE HCL 15 MG TABLET ORAL 02/12/2019 0.21654
OXYCODONE HCL 30 MG TABLET ORAL 04/04/2017 0.19497
OXYCODONE HCL/ACETAMINOPHEN 5 MG-325MG TABLET ORAL 02/06/2019 0.07142
OXYCODONE HCL/ACETAMINOPHEN 2.5-325 MG TABLET ORAL 01/30/2018 2.29314
OXYCODONE HCL/ACETAMINOPHEN 7.5-325 MG TABLET ORAL 12/26/2018 0.17353
OXYCODONE HCL/ACETAMINOPHEN 10MG-325MG TABLET ORAL 12/26/2018 0.22512
OXYCODONE HCL/ASPIRIN 4.8355-325 TABLET ORAL 11/14/2018 1.49571
OXYMETAZOLINE HCL 0.05 % MIST NASAL 02/20/2019 0.45828
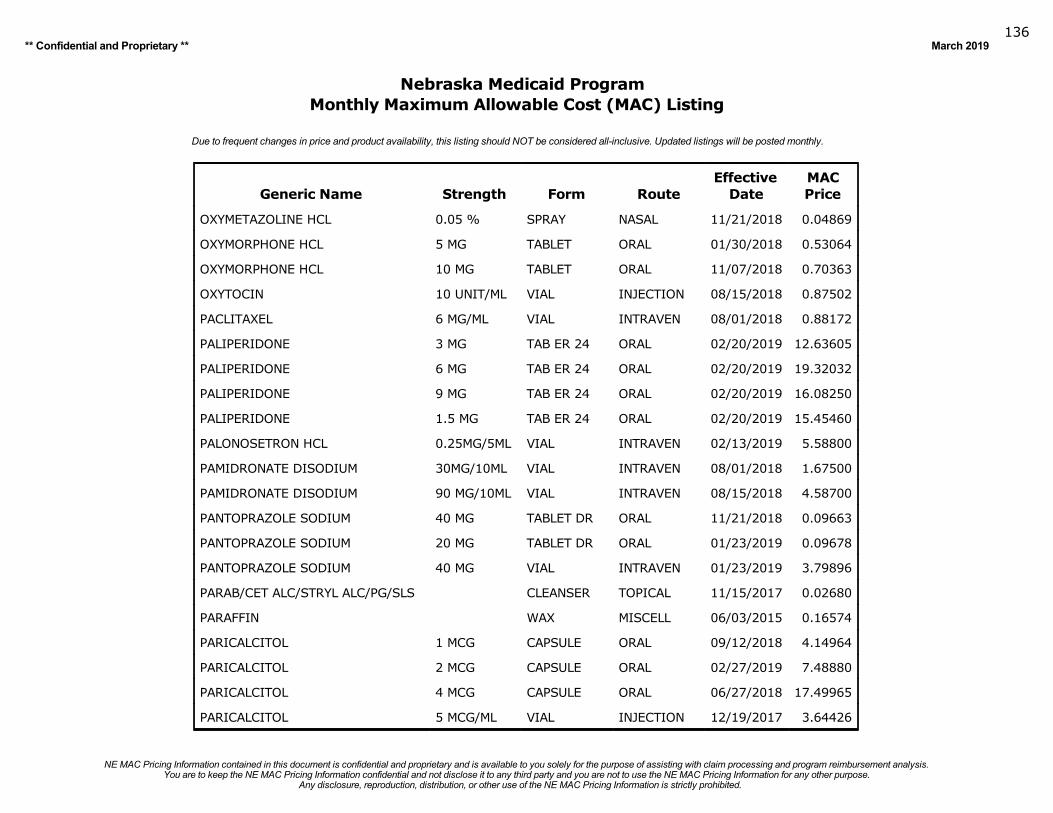
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019136
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
OXYMETAZOLINE HCL 0.05 % SPRAY NASAL 11/21/2018 0.04869
OXYMORPHONE HCL 5 MG TABLET ORAL 01/30/2018 0.53064
OXYMORPHONE HCL 10 MG TABLET ORAL 11/07/2018 0.70363
OXYTOCIN 10 UNIT/ML VIAL INJECTION 08/15/2018 0.87502
PACLITAXEL 6 MG/ML VIAL INTRAVEN 08/01/2018 0.88172
PALIPERIDONE 3 MG TAB ER 24 ORAL 02/20/2019 12.63605
PALIPERIDONE 6 MG TAB ER 24 ORAL 02/20/2019 19.32032
PALIPERIDONE 9 MG TAB ER 24 ORAL 02/20/2019 16.08250
PALIPERIDONE 1.5 MG TAB ER 24 ORAL 02/20/2019 15.45460
PALONOSETRON HCL 0.25MG/5ML VIAL INTRAVEN 02/13/2019 5.58800
PAMIDRONATE DISODIUM 30MG/10ML VIAL INTRAVEN 08/01/2018 1.67500
PAMIDRONATE DISODIUM 90 MG/10ML VIAL INTRAVEN 08/15/2018 4.58700
PANTOPRAZOLE SODIUM 40 MG TABLET DR ORAL 11/21/2018 0.09663
PANTOPRAZOLE SODIUM 20 MG TABLET DR ORAL 01/23/2019 0.09678
PANTOPRAZOLE SODIUM 40 MG VIAL INTRAVEN 01/23/2019 3.79896
PARAB/CET ALC/STRYL ALC/PG/SLS CLEANSER TOPICAL 11/15/2017 0.02680
PARAFFIN WAX MISCELL 06/03/2015 0.16574
PARICALCITOL 1 MCG CAPSULE ORAL 09/12/2018 4.14964
PARICALCITOL 2 MCG CAPSULE ORAL 02/27/2019 7.48880
PARICALCITOL 4 MCG CAPSULE ORAL 06/27/2018 17.49965
PARICALCITOL 5 MCG/ML VIAL INJECTION 12/19/2017 3.64426
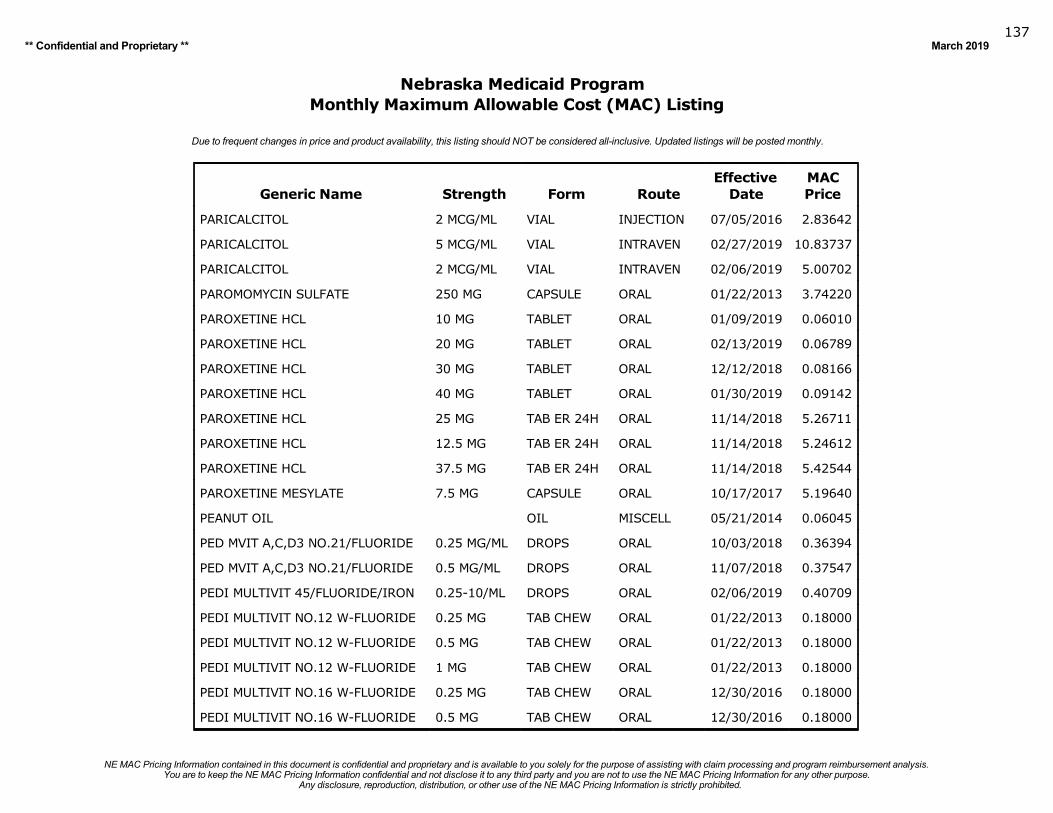
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019137
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PARICALCITOL 2 MCG/ML VIAL INJECTION 07/05/2016 2.83642
PARICALCITOL 5 MCG/ML VIAL INTRAVEN 02/27/2019 10.83737
PARICALCITOL 2 MCG/ML VIAL INTRAVEN 02/06/2019 5.00702
PAROMOMYCIN SULFATE 250 MG CAPSULE ORAL 01/22/2013 3.74220
PAROXETINE HCL 10 MG TABLET ORAL 01/09/2019 0.06010
PAROXETINE HCL 20 MG TABLET ORAL 02/13/2019 0.06789
PAROXETINE HCL 30 MG TABLET ORAL 12/12/2018 0.08166
PAROXETINE HCL 40 MG TABLET ORAL 01/30/2019 0.09142
PAROXETINE HCL 25 MG TAB ER 24H ORAL 11/14/2018 5.26711
PAROXETINE HCL 12.5 MG TAB ER 24H ORAL 11/14/2018 5.24612
PAROXETINE HCL 37.5 MG TAB ER 24H ORAL 11/14/2018 5.42544
PAROXETINE MESYLATE 7.5 MG CAPSULE ORAL 10/17/2017 5.19640
PEANUT OIL OIL MISCELL 05/21/2014 0.06045
PED MVIT A,C,D3 NO.21/FLUORIDE 0.25 MG/ML DROPS ORAL 10/03/2018 0.36394
PED MVIT A,C,D3 NO.21/FLUORIDE 0.5 MG/ML DROPS ORAL 11/07/2018 0.37547
PEDI MULTIVIT 45/FLUORIDE/IRON 0.25-10/ML DROPS ORAL 02/06/2019 0.40709
PEDI MULTIVIT NO.12 W-FLUORIDE 0.25 MG TAB CHEW ORAL 01/22/2013 0.18000
PEDI MULTIVIT NO.12 W-FLUORIDE 0.5 MG TAB CHEW ORAL 01/22/2013 0.18000
PEDI MULTIVIT NO.12 W-FLUORIDE 1 MG TAB CHEW ORAL 01/22/2013 0.18000
PEDI MULTIVIT NO.16 W-FLUORIDE 0.25 MG TAB CHEW ORAL 12/30/2016 0.18000
PEDI MULTIVIT NO.16 W-FLUORIDE 0.5 MG TAB CHEW ORAL 12/30/2016 0.18000
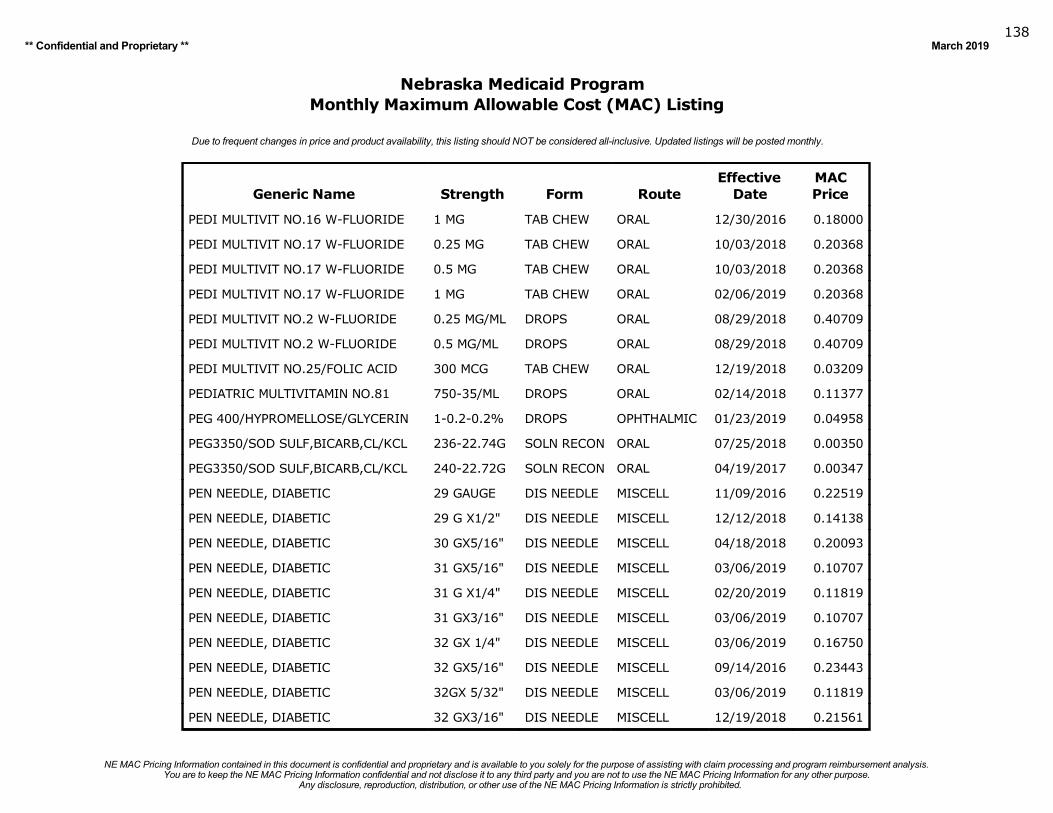
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019138
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PEDI MULTIVIT NO.16 W-FLUORIDE 1 MG TAB CHEW ORAL 12/30/2016 0.18000
PEDI MULTIVIT NO.17 W-FLUORIDE 0.25 MG TAB CHEW ORAL 10/03/2018 0.20368
PEDI MULTIVIT NO.17 W-FLUORIDE 0.5 MG TAB CHEW ORAL 10/03/2018 0.20368
PEDI MULTIVIT NO.17 W-FLUORIDE 1 MG TAB CHEW ORAL 02/06/2019 0.20368
PEDI MULTIVIT NO.2 W-FLUORIDE 0.25 MG/ML DROPS ORAL 08/29/2018 0.40709
PEDI MULTIVIT NO.2 W-FLUORIDE 0.5 MG/ML DROPS ORAL 08/29/2018 0.40709
PEDI MULTIVIT NO.25/FOLIC ACID 300 MCG TAB CHEW ORAL 12/19/2018 0.03209
PEDIATRIC MULTIVITAMIN NO.81 750-35/ML DROPS ORAL 02/14/2018 0.11377
PEG 400/HYPROMELLOSE/GLYCERIN 1-0.2-0.2% DROPS OPHTHALMIC 01/23/2019 0.04958
PEG3350/SOD SULF,BICARB,CL/KCL 236-22.74G SOLN RECON ORAL 07/25/2018 0.00350
PEG3350/SOD SULF,BICARB,CL/KCL 240-22.72G SOLN RECON ORAL 04/19/2017 0.00347
PEN NEEDLE, DIABETIC 29 GAUGE DIS NEEDLE MISCELL 11/09/2016 0.22519
PEN NEEDLE, DIABETIC 29 G X1/2" DIS NEEDLE MISCELL 12/12/2018 0.14138
PEN NEEDLE, DIABETIC 30 GX5/16" DIS NEEDLE MISCELL 04/18/2018 0.20093
PEN NEEDLE, DIABETIC 31 GX5/16" DIS NEEDLE MISCELL 03/06/2019 0.10707
PEN NEEDLE, DIABETIC 31 G X1/4" DIS NEEDLE MISCELL 02/20/2019 0.11819
PEN NEEDLE, DIABETIC 31 GX3/16" DIS NEEDLE MISCELL 03/06/2019 0.10707
PEN NEEDLE, DIABETIC 32 GX 1/4" DIS NEEDLE MISCELL 03/06/2019 0.16750
PEN NEEDLE, DIABETIC 32 GX5/16" DIS NEEDLE MISCELL 09/14/2016 0.23443
PEN NEEDLE, DIABETIC 32GX 5/32" DIS NEEDLE MISCELL 03/06/2019 0.11819
PEN NEEDLE, DIABETIC 32 GX3/16" DIS NEEDLE MISCELL 12/19/2018 0.21561
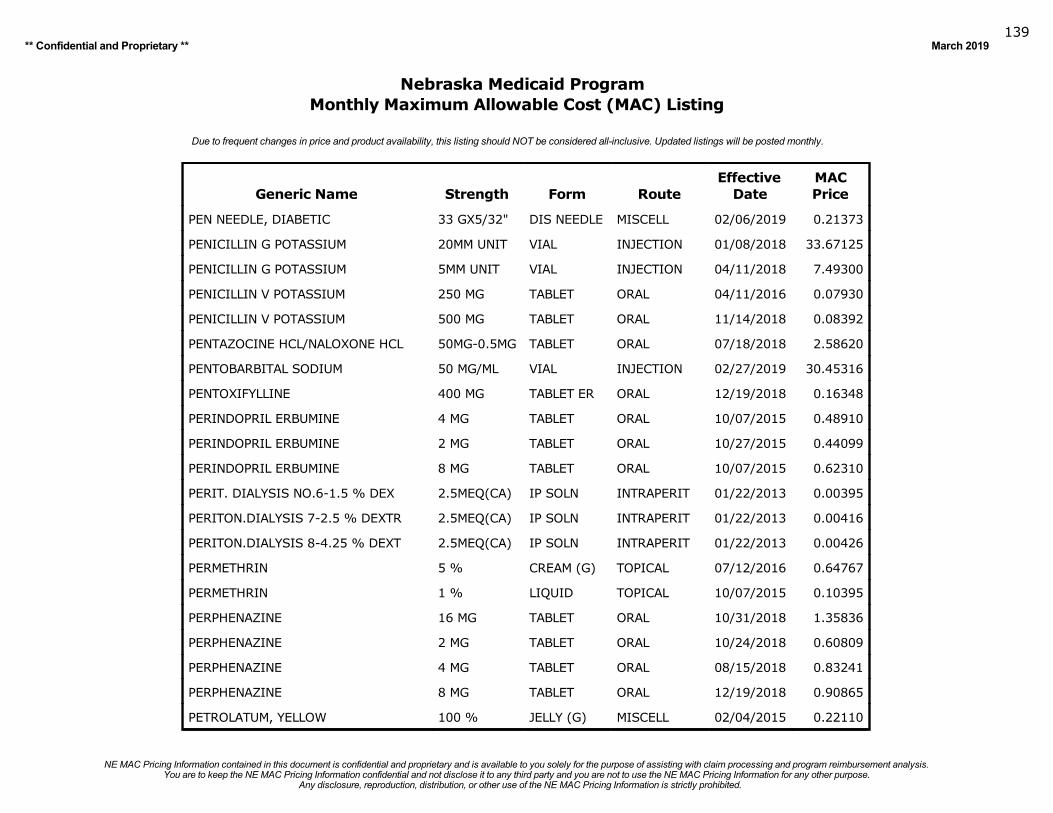
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019139
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PEN NEEDLE, DIABETIC 33 GX5/32" DIS NEEDLE MISCELL 02/06/2019 0.21373
PENICILLIN G POTASSIUM 20MM UNIT VIAL INJECTION 01/08/2018 33.67125
PENICILLIN G POTASSIUM 5MM UNIT VIAL INJECTION 04/11/2018 7.49300
PENICILLIN V POTASSIUM 250 MG TABLET ORAL 04/11/2016 0.07930
PENICILLIN V POTASSIUM 500 MG TABLET ORAL 11/14/2018 0.08392
PENTAZOCINE HCL/NALOXONE HCL 50MG-0.5MG TABLET ORAL 07/18/2018 2.58620
PENTOBARBITAL SODIUM 50 MG/ML VIAL INJECTION 02/27/2019 30.45316
PENTOXIFYLLINE 400 MG TABLET ER ORAL 12/19/2018 0.16348
PERINDOPRIL ERBUMINE 4 MG TABLET ORAL 10/07/2015 0.48910
PERINDOPRIL ERBUMINE 2 MG TABLET ORAL 10/27/2015 0.44099
PERINDOPRIL ERBUMINE 8 MG TABLET ORAL 10/07/2015 0.62310
PERIT. DIALYSIS NO.6-1.5 % DEX 2.5MEQ(CA) IP SOLN INTRAPERIT 01/22/2013 0.00395
PERITON.DIALYSIS 7-2.5 % DEXTR 2.5MEQ(CA) IP SOLN INTRAPERIT 01/22/2013 0.00416
PERITON.DIALYSIS 8-4.25 % DEXT 2.5MEQ(CA) IP SOLN INTRAPERIT 01/22/2013 0.00426
PERMETHRIN 5 % CREAM (G) TOPICAL 07/12/2016 0.64767
PERMETHRIN 1 % LIQUID TOPICAL 10/07/2015 0.10395
PERPHENAZINE 16 MG TABLET ORAL 10/31/2018 1.35836
PERPHENAZINE 2 MG TABLET ORAL 10/24/2018 0.60809
PERPHENAZINE 4 MG TABLET ORAL 08/15/2018 0.83241
PERPHENAZINE 8 MG TABLET ORAL 12/19/2018 0.90865
PETROLATUM, YELLOW 100 % JELLY (G) MISCELL 02/04/2015 0.22110
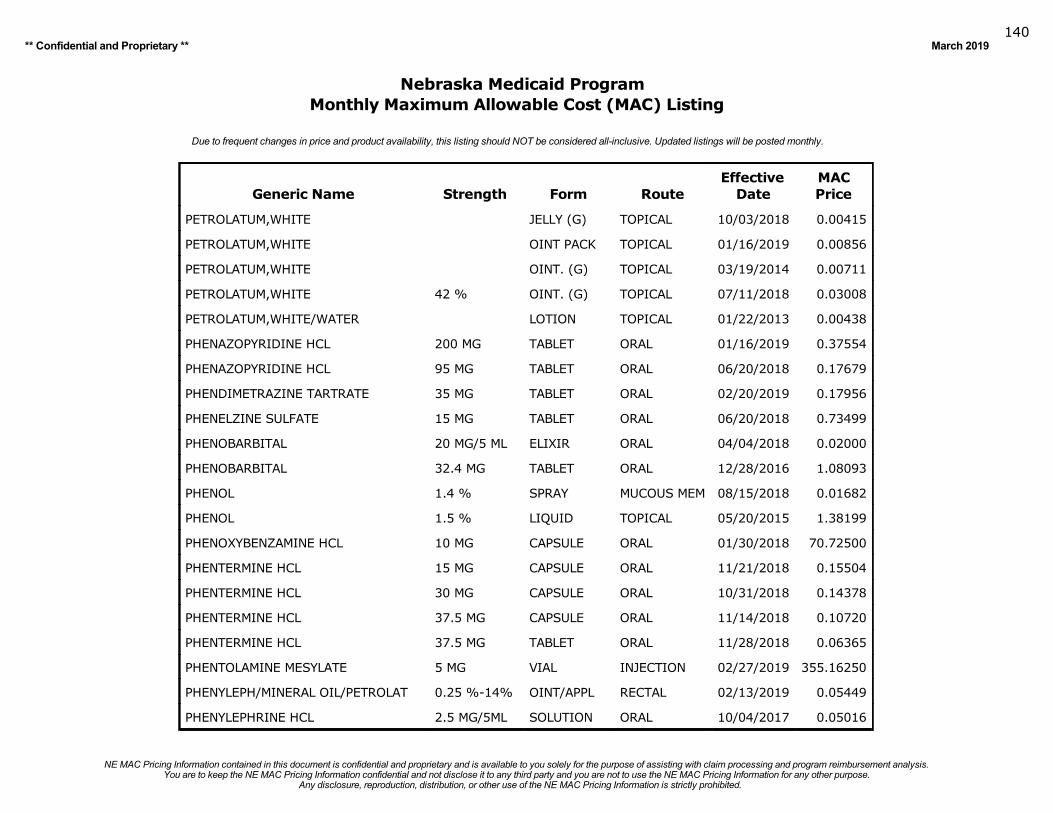
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019140
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PETROLATUM,WHITE JELLY (G) TOPICAL 10/03/2018 0.00415
PETROLATUM,WHITE OINT PACK TOPICAL 01/16/2019 0.00856
PETROLATUM,WHITE OINT. (G) TOPICAL 03/19/2014 0.00711
PETROLATUM,WHITE 42 % OINT. (G) TOPICAL 07/11/2018 0.03008
PETROLATUM,WHITE/WATER LOTION TOPICAL 01/22/2013 0.00438
PHENAZOPYRIDINE HCL 200 MG TABLET ORAL 01/16/2019 0.37554
PHENAZOPYRIDINE HCL 95 MG TABLET ORAL 06/20/2018 0.17679
PHENDIMETRAZINE TARTRATE 35 MG TABLET ORAL 02/20/2019 0.17956
PHENELZINE SULFATE 15 MG TABLET ORAL 06/20/2018 0.73499
PHENOBARBITAL 20 MG/5 ML ELIXIR ORAL 04/04/2018 0.02000
PHENOBARBITAL 32.4 MG TABLET ORAL 12/28/2016 1.08093
PHENOL 1.4 % SPRAY MUCOUS MEM 08/15/2018 0.01682
PHENOL 1.5 % LIQUID TOPICAL 05/20/2015 1.38199
PHENOXYBENZAMINE HCL 10 MG CAPSULE ORAL 01/30/2018 70.72500
PHENTERMINE HCL 15 MG CAPSULE ORAL 11/21/2018 0.15504
PHENTERMINE HCL 30 MG CAPSULE ORAL 10/31/2018 0.14378
PHENTERMINE HCL 37.5 MG CAPSULE ORAL 11/14/2018 0.10720
PHENTERMINE HCL 37.5 MG TABLET ORAL 11/28/2018 0.06365
PHENTOLAMINE MESYLATE 5 MG VIAL INJECTION 02/27/2019 355.16250
PHENYLEPH/MINERAL OIL/PETROLAT 0.25 %-14% OINT/APPL RECTAL 02/13/2019 0.05449
PHENYLEPHRINE HCL 2.5 MG/5ML SOLUTION ORAL 10/04/2017 0.05016
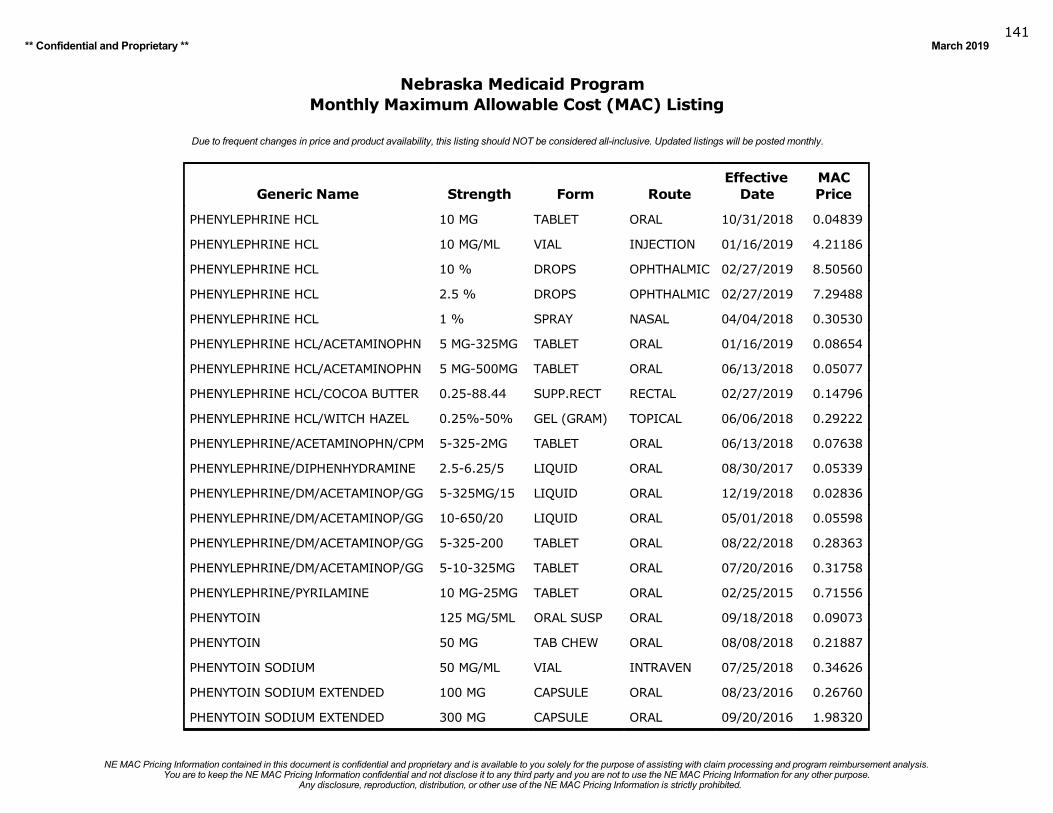
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019141
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PHENYLEPHRINE HCL 10 MG TABLET ORAL 10/31/2018 0.04839
PHENYLEPHRINE HCL 10 MG/ML VIAL INJECTION 01/16/2019 4.21186
PHENYLEPHRINE HCL 10 % DROPS OPHTHALMIC 02/27/2019 8.50560
PHENYLEPHRINE HCL 2.5 % DROPS OPHTHALMIC 02/27/2019 7.29488
PHENYLEPHRINE HCL 1 % SPRAY NASAL 04/04/2018 0.30530
PHENYLEPHRINE HCL/ACETAMINOPHN 5 MG-325MG TABLET ORAL 01/16/2019 0.08654
PHENYLEPHRINE HCL/ACETAMINOPHN 5 MG-500MG TABLET ORAL 06/13/2018 0.05077
PHENYLEPHRINE HCL/COCOA BUTTER 0.25-88.44 SUPP.RECT RECTAL 02/27/2019 0.14796
PHENYLEPHRINE HCL/WITCH HAZEL 0.25%-50% GEL (GRAM) TOPICAL 06/06/2018 0.29222
PHENYLEPHRINE/ACETAMINOPHN/CPM 5-325-2MG TABLET ORAL 06/13/2018 0.07638
PHENYLEPHRINE/DIPHENHYDRAMINE 2.5-6.25/5 LIQUID ORAL 08/30/2017 0.05339
PHENYLEPHRINE/DM/ACETAMINOP/GG 5-325MG/15 LIQUID ORAL 12/19/2018 0.02836
PHENYLEPHRINE/DM/ACETAMINOP/GG 10-650/20 LIQUID ORAL 05/01/2018 0.05598
PHENYLEPHRINE/DM/ACETAMINOP/GG 5-325-200 TABLET ORAL 08/22/2018 0.28363
PHENYLEPHRINE/DM/ACETAMINOP/GG 5-10-325MG TABLET ORAL 07/20/2016 0.31758
PHENYLEPHRINE/PYRILAMINE 10 MG-25MG TABLET ORAL 02/25/2015 0.71556
PHENYTOIN 125 MG/5ML ORAL SUSP ORAL 09/18/2018 0.09073
PHENYTOIN 50 MG TAB CHEW ORAL 08/08/2018 0.21887
PHENYTOIN SODIUM 50 MG/ML VIAL INTRAVEN 07/25/2018 0.34626
PHENYTOIN SODIUM EXTENDED 100 MG CAPSULE ORAL 08/23/2016 0.26760
PHENYTOIN SODIUM EXTENDED 300 MG CAPSULE ORAL 09/20/2016 1.98320
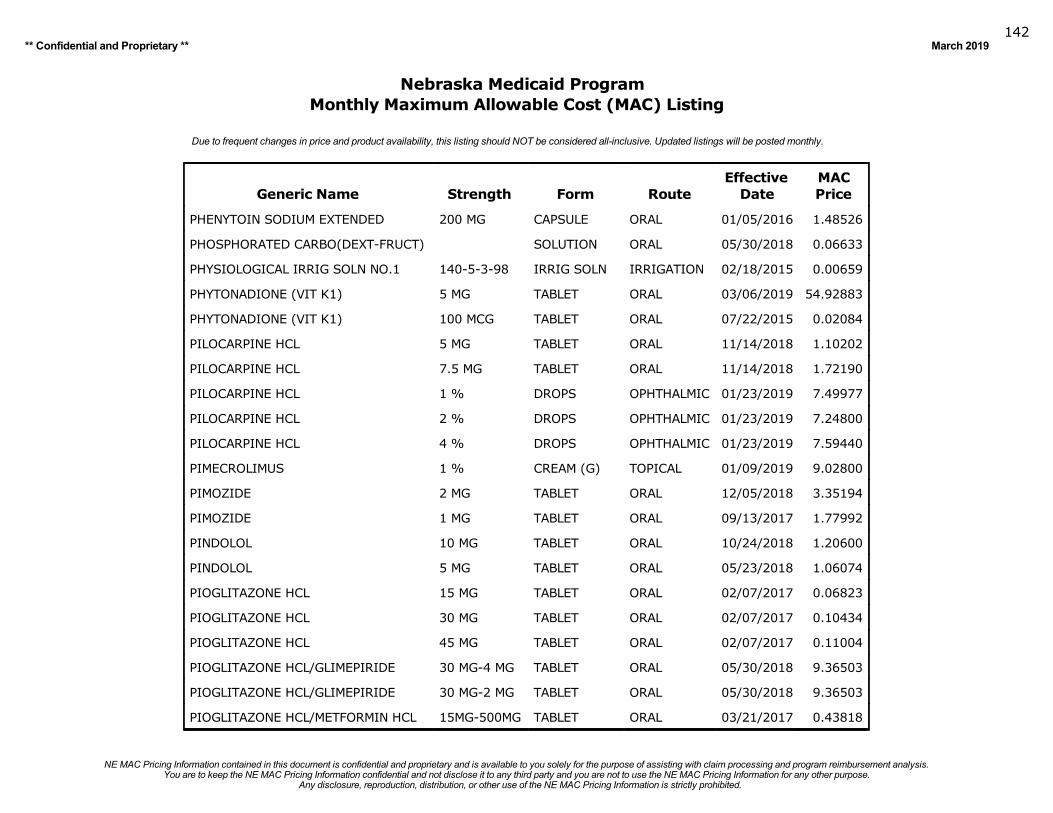
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019142
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PHENYTOIN SODIUM EXTENDED 200 MG CAPSULE ORAL 01/05/2016 1.48526
PHOSPHORATED CARBO(DEXT-FRUCT) SOLUTION ORAL 05/30/2018 0.06633
PHYSIOLOGICAL IRRIG SOLN NO.1 140-5-3-98 IRRIG SOLN IRRIGATION 02/18/2015 0.00659
PHYTONADIONE (VIT K1) 5 MG TABLET ORAL 03/06/2019 54.92883
PHYTONADIONE (VIT K1) 100 MCG TABLET ORAL 07/22/2015 0.02084
PILOCARPINE HCL 5 MG TABLET ORAL 11/14/2018 1.10202
PILOCARPINE HCL 7.5 MG TABLET ORAL 11/14/2018 1.72190
PILOCARPINE HCL 1 % DROPS OPHTHALMIC 01/23/2019 7.49977
PILOCARPINE HCL 2 % DROPS OPHTHALMIC 01/23/2019 7.24800
PILOCARPINE HCL 4 % DROPS OPHTHALMIC 01/23/2019 7.59440
PIMECROLIMUS 1 % CREAM (G) TOPICAL 01/09/2019 9.02800
PIMOZIDE 2 MG TABLET ORAL 12/05/2018 3.35194
PIMOZIDE 1 MG TABLET ORAL 09/13/2017 1.77992
PINDOLOL 10 MG TABLET ORAL 10/24/2018 1.20600
PINDOLOL 5 MG TABLET ORAL 05/23/2018 1.06074
PIOGLITAZONE HCL 15 MG TABLET ORAL 02/07/2017 0.06823
PIOGLITAZONE HCL 30 MG TABLET ORAL 02/07/2017 0.10434
PIOGLITAZONE HCL 45 MG TABLET ORAL 02/07/2017 0.11004
PIOGLITAZONE HCL/GLIMEPIRIDE 30 MG-4 MG TABLET ORAL 05/30/2018 9.36503
PIOGLITAZONE HCL/GLIMEPIRIDE 30 MG-2 MG TABLET ORAL 05/30/2018 9.36503
PIOGLITAZONE HCL/METFORMIN HCL 15MG-500MG TABLET ORAL 03/21/2017 0.43818
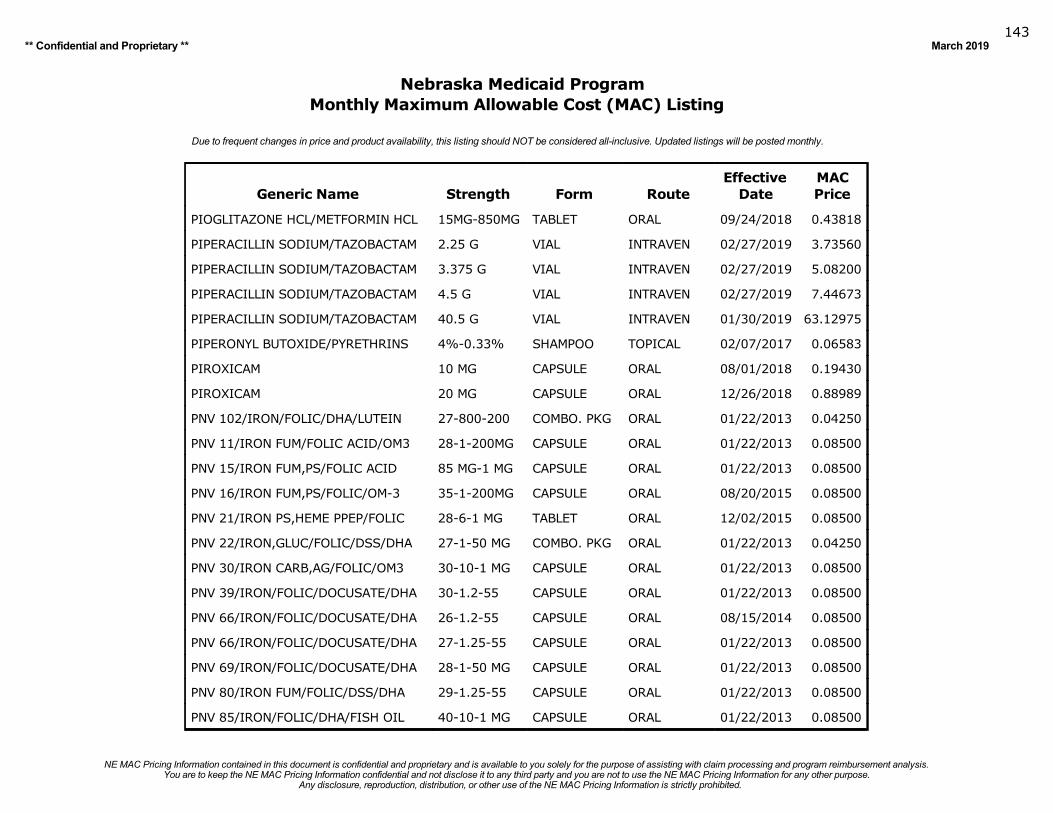
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019143
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PIOGLITAZONE HCL/METFORMIN HCL 15MG-850MG TABLET ORAL 09/24/2018 0.43818
PIPERACILLIN SODIUM/TAZOBACTAM 2.25 G VIAL INTRAVEN 02/27/2019 3.73560
PIPERACILLIN SODIUM/TAZOBACTAM 3.375 G VIAL INTRAVEN 02/27/2019 5.08200
PIPERACILLIN SODIUM/TAZOBACTAM 4.5 G VIAL INTRAVEN 02/27/2019 7.44673
PIPERACILLIN SODIUM/TAZOBACTAM 40.5 G VIAL INTRAVEN 01/30/2019 63.12975
PIPERONYL BUTOXIDE/PYRETHRINS 4%-0.33% SHAMPOO TOPICAL 02/07/2017 0.06583
PIROXICAM 10 MG CAPSULE ORAL 08/01/2018 0.19430
PIROXICAM 20 MG CAPSULE ORAL 12/26/2018 0.88989
PNV 102/IRON/FOLIC/DHA/LUTEIN 27-800-200 COMBO. PKG ORAL 01/22/2013 0.04250
PNV 11/IRON FUM/FOLIC ACID/OM3 28-1-200MG CAPSULE ORAL 01/22/2013 0.08500
PNV 15/IRON FUM,PS/FOLIC ACID 85 MG-1 MG CAPSULE ORAL 01/22/2013 0.08500
PNV 16/IRON FUM,PS/FOLIC/OM-3 35-1-200MG CAPSULE ORAL 08/20/2015 0.08500
PNV 21/IRON PS,HEME PPEP/FOLIC 28-6-1 MG TABLET ORAL 12/02/2015 0.08500
PNV 22/IRON,GLUC/FOLIC/DSS/DHA 27-1-50 MG COMBO. PKG ORAL 01/22/2013 0.04250
PNV 30/IRON CARB,AG/FOLIC/OM3 30-10-1 MG CAPSULE ORAL 01/22/2013 0.08500
PNV 39/IRON/FOLIC/DOCUSATE/DHA 30-1.2-55 CAPSULE ORAL 01/22/2013 0.08500
PNV 66/IRON/FOLIC/DOCUSATE/DHA 26-1.2-55 CAPSULE ORAL 08/15/2014 0.08500
PNV 66/IRON/FOLIC/DOCUSATE/DHA 27-1.25-55 CAPSULE ORAL 01/22/2013 0.08500
PNV 69/IRON/FOLIC/DOCUSATE/DHA 28-1-50 MG CAPSULE ORAL 01/22/2013 0.08500
PNV 80/IRON FUM/FOLIC/DSS/DHA 29-1.25-55 CAPSULE ORAL 01/22/2013 0.08500
PNV 85/IRON/FOLIC/DHA/FISH OIL 40-10-1 MG CAPSULE ORAL 01/22/2013 0.08500

Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019144
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PNV NO.118/IRON FUMARATE/FA 29 MG-1 MG TAB CHEW ORAL 12/12/2018 0.93143
PNV NO.5/FERROUS FUM/FOLIC AC 106.5-1MG CAPSULE ORAL 11/14/2014 0.08500
PNV NO.95/FERROUS FUM/FOLIC AC 28MG-0.8MG TABLET ORAL 12/05/2018 0.03628
PNV, CALCIUM 70/IRON/FOLIC/DHA 28-1-250MG CAPSULE ORAL 07/09/2014 0.08500
PNV/FERROUS FUM/DOCUSATE/FOLIC 90-50-1MG TABLET ER ORAL 01/22/2013 0.08500
PNV/IRON,CARB/DOCUSAT/FOLIC AC 90-50-1MG TABLET ORAL 01/22/2013 0.08500
PNV119/IRON FUM/FOLIC/DOCUSATE 29-1-25 MG TABLET ORAL 08/24/2016 0.49513
PNV19/IRON BG,S.P/FOLIC AC/OM3 29-1-400MG CMBPKGDRCP ORAL 01/22/2013 0.04250
PNV81/IRON EDTA,PS/FOLIC/OMEG3 27-1-430MG CMBPKGDRCP ORAL 01/22/2013 0.04250
PNV83/IRON,CARB,ASP/FOLIC ACID 30-20-1 MG TABLET ORAL 01/22/2013 0.08500
PODOFILOX 0.5 % SOLUTION TOPICAL 02/20/2019 12.80700
POLYDIMETHYLSILOXANES/SILICON GEL (GRAM) TOPICAL 03/01/2017 2.00933
POLYETHYLENE GLYCOL 1450 POWDER MISCELL 02/13/2019 0.01873
POLYETHYLENE GLYCOL 300 LIQUID MISCELL 02/13/2019 0.01729
POLYETHYLENE GLYCOL 3350 17G/DOSE POWDER ORAL 02/20/2019 0.02352
POLYMYXIN B SULF/TRIMETHOPRIM 10000-1/ML DROPS OPHTHALMIC 09/19/2018 0.67670
POLYMYXIN B SULFATE 500K UNIT VIAL INJECTION 12/19/2018 5.08762
POLYSORBATE 80 SOLUTION MISCELL 02/06/2019 0.04233
POLYVINYL ALCOHOL 1.4 % DROPS OPHTHALMIC 01/09/2019 0.36180
POTASSIUM ACETATE 2 MEQ/ML VIAL INTRAVEN 01/31/2018 0.20620
POTASSIUM BICARBONATE/CIT AC 25 MEQ TABLET EFF ORAL 05/20/2015 1.05197
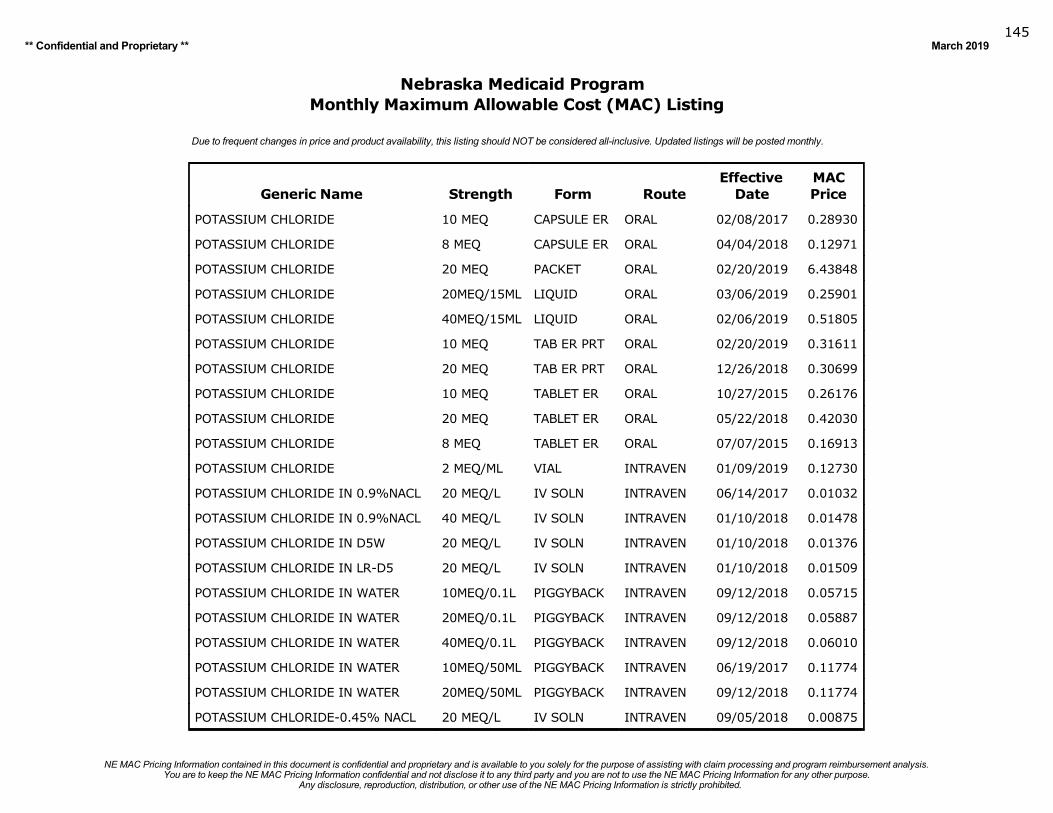
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019145
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
POTASSIUM CHLORIDE 10 MEQ CAPSULE ER ORAL 02/08/2017 0.28930
POTASSIUM CHLORIDE 8 MEQ CAPSULE ER ORAL 04/04/2018 0.12971
POTASSIUM CHLORIDE 20 MEQ PACKET ORAL 02/20/2019 6.43848
POTASSIUM CHLORIDE 20MEQ/15ML LIQUID ORAL 03/06/2019 0.25901
POTASSIUM CHLORIDE 40MEQ/15ML LIQUID ORAL 02/06/2019 0.51805
POTASSIUM CHLORIDE 10 MEQ TAB ER PRT ORAL 02/20/2019 0.31611
POTASSIUM CHLORIDE 20 MEQ TAB ER PRT ORAL 12/26/2018 0.30699
POTASSIUM CHLORIDE 10 MEQ TABLET ER ORAL 10/27/2015 0.26176
POTASSIUM CHLORIDE 20 MEQ TABLET ER ORAL 05/22/2018 0.42030
POTASSIUM CHLORIDE 8 MEQ TABLET ER ORAL 07/07/2015 0.16913
POTASSIUM CHLORIDE 2 MEQ/ML VIAL INTRAVEN 01/09/2019 0.12730
POTASSIUM CHLORIDE IN 0.9%NACL 20 MEQ/L IV SOLN INTRAVEN 06/14/2017 0.01032
POTASSIUM CHLORIDE IN 0.9%NACL 40 MEQ/L IV SOLN INTRAVEN 01/10/2018 0.01478
POTASSIUM CHLORIDE IN D5W 20 MEQ/L IV SOLN INTRAVEN 01/10/2018 0.01376
POTASSIUM CHLORIDE IN LR-D5 20 MEQ/L IV SOLN INTRAVEN 01/10/2018 0.01509
POTASSIUM CHLORIDE IN WATER 10MEQ/0.1L PIGGYBACK INTRAVEN 09/12/2018 0.05715
POTASSIUM CHLORIDE IN WATER 20MEQ/0.1L PIGGYBACK INTRAVEN 09/12/2018 0.05887
POTASSIUM CHLORIDE IN WATER 40MEQ/0.1L PIGGYBACK INTRAVEN 09/12/2018 0.06010
POTASSIUM CHLORIDE IN WATER 10MEQ/50ML PIGGYBACK INTRAVEN 06/19/2017 0.11774
POTASSIUM CHLORIDE IN WATER 20MEQ/50ML PIGGYBACK INTRAVEN 09/12/2018 0.11774
POTASSIUM CHLORIDE-0.45% NACL 20 MEQ/L IV SOLN INTRAVEN 09/05/2018 0.00875

Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019146
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
POTASSIUM CHLORIDE/D5-0.2%NACL 20 MEQ/L IV SOLN INTRAVEN 01/10/2018 0.01254
POTASSIUM CHLORIDE/D5-0.45NACL 10 MEQ/L IV SOLN INTRAVEN 09/12/2018 0.00831
POTASSIUM CHLORIDE/D5-0.45NACL 20 MEQ/L IV SOLN INTRAVEN 09/12/2018 0.00626
POTASSIUM CHLORIDE/D5-0.45NACL 30 MEQ/L IV SOLN INTRAVEN 01/10/2018 0.01278
POTASSIUM CHLORIDE/D5-0.45NACL 40 MEQ/L IV SOLN INTRAVEN 09/12/2018 0.00831
POTASSIUM CHLORIDE/D5-0.9%NACL 20 MEQ/L IV SOLN INTRAVEN 09/12/2018 0.00836
POTASSIUM CHLORIDE/D5-0.9%NACL 40 MEQ/L IV SOLN INTRAVEN 01/10/2018 0.01214
POTASSIUM CITRATE 5 MEQ TABLET ER ORAL 03/06/2019 0.70524
POTASSIUM CITRATE 10 MEQ TABLET ER ORAL 03/06/2019 0.98463
POTASSIUM CITRATE 15 MEQ TABLET ER ORAL 01/12/2016 2.28001
POTASSIUM CITRATE/CITRIC ACID 1100-334/5 SOLUTION ORAL 10/31/2018 0.07116
POTASSIUM GLUCONATE 595(99)MG TABLET ORAL 02/20/2019 0.03913
POTASSIUM GLUCONATE 550(90)MG TABLET ORAL 11/21/2018 0.02275
POTASSIUM PHOS,M-BASIC-D-BASIC 3MMOL/ML VIAL INTRAVEN 02/27/2019 1.17834
POVIDONE-IODINE 10 % MED. SWAB TOPICAL 10/17/2018 0.23977
POVIDONE-IODINE 10 % OINT. (G) TOPICAL 10/03/2017 0.15792
POVIDONE-IODINE 10 % SOLUTION TOPICAL 01/30/2019 0.00404
POVIDONE-IODINE 7.5 % SOLUTION TOPICAL 05/14/2018 0.00510
POVIDONE-IODINE 0.3 % SOLUTION VAGINAL 01/04/2017 0.01119
PRAMIPEXOLE DI-HCL 1 MG TABLET ORAL 03/22/2017 0.07042
PRAMIPEXOLE DI-HCL 1.5 MG TABLET ORAL 06/20/2018 0.08427
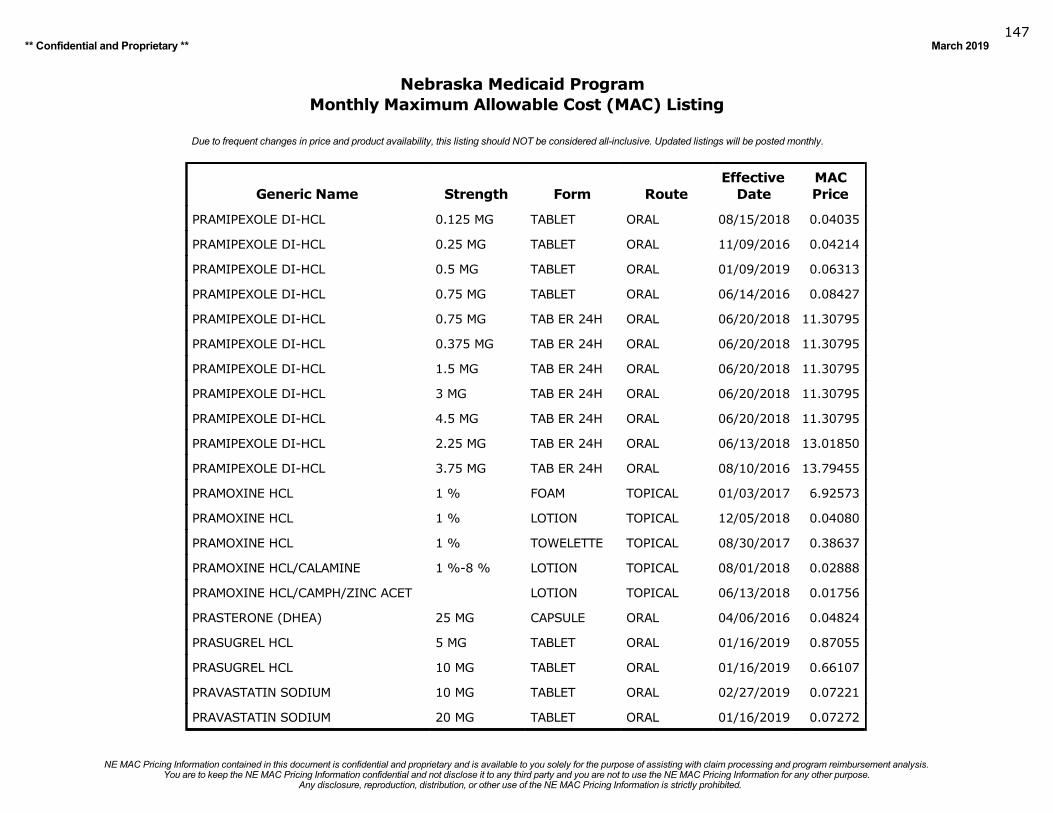
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019147
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PRAMIPEXOLE DI-HCL 0.125 MG TABLET ORAL 08/15/2018 0.04035
PRAMIPEXOLE DI-HCL 0.25 MG TABLET ORAL 11/09/2016 0.04214
PRAMIPEXOLE DI-HCL 0.5 MG TABLET ORAL 01/09/2019 0.06313
PRAMIPEXOLE DI-HCL 0.75 MG TABLET ORAL 06/14/2016 0.08427
PRAMIPEXOLE DI-HCL 0.75 MG TAB ER 24H ORAL 06/20/2018 11.30795
PRAMIPEXOLE DI-HCL 0.375 MG TAB ER 24H ORAL 06/20/2018 11.30795
PRAMIPEXOLE DI-HCL 1.5 MG TAB ER 24H ORAL 06/20/2018 11.30795
PRAMIPEXOLE DI-HCL 3 MG TAB ER 24H ORAL 06/20/2018 11.30795
PRAMIPEXOLE DI-HCL 4.5 MG TAB ER 24H ORAL 06/20/2018 11.30795
PRAMIPEXOLE DI-HCL 2.25 MG TAB ER 24H ORAL 06/13/2018 13.01850
PRAMIPEXOLE DI-HCL 3.75 MG TAB ER 24H ORAL 08/10/2016 13.79455
PRAMOXINE HCL 1 % FOAM TOPICAL 01/03/2017 6.92573
PRAMOXINE HCL 1 % LOTION TOPICAL 12/05/2018 0.04080
PRAMOXINE HCL 1 % TOWELETTE TOPICAL 08/30/2017 0.38637
PRAMOXINE HCL/CALAMINE 1 %-8 % LOTION TOPICAL 08/01/2018 0.02888
PRAMOXINE HCL/CAMPH/ZINC ACET LOTION TOPICAL 06/13/2018 0.01756
PRASTERONE (DHEA) 25 MG CAPSULE ORAL 04/06/2016 0.04824
PRASUGREL HCL 5 MG TABLET ORAL 01/16/2019 0.87055
PRASUGREL HCL 10 MG TABLET ORAL 01/16/2019 0.66107
PRAVASTATIN SODIUM 10 MG TABLET ORAL 02/27/2019 0.07221
PRAVASTATIN SODIUM 20 MG TABLET ORAL 01/16/2019 0.07272
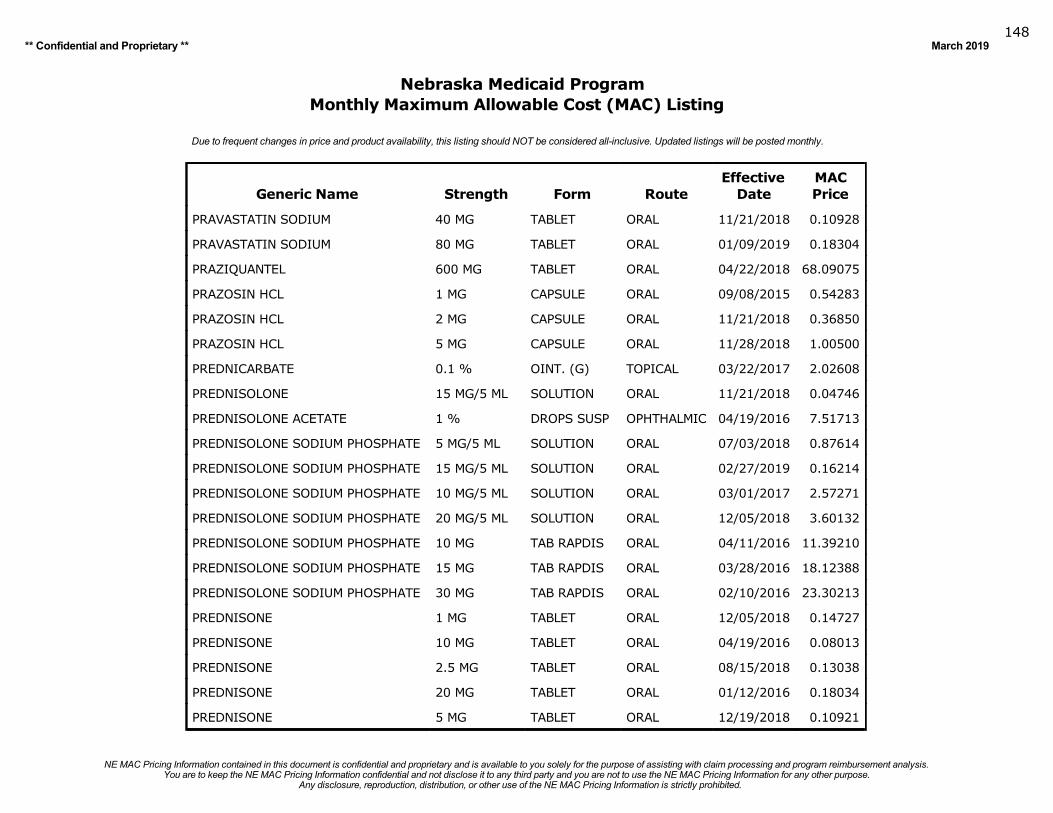
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019148
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PRAVASTATIN SODIUM 40 MG TABLET ORAL 11/21/2018 0.10928
PRAVASTATIN SODIUM 80 MG TABLET ORAL 01/09/2019 0.18304
PRAZIQUANTEL 600 MG TABLET ORAL 04/22/2018 68.09075
PRAZOSIN HCL 1 MG CAPSULE ORAL 09/08/2015 0.54283
PRAZOSIN HCL 2 MG CAPSULE ORAL 11/21/2018 0.36850
PRAZOSIN HCL 5 MG CAPSULE ORAL 11/28/2018 1.00500
PREDNICARBATE 0.1 % OINT. (G) TOPICAL 03/22/2017 2.02608
PREDNISOLONE 15 MG/5 ML SOLUTION ORAL 11/21/2018 0.04746
PREDNISOLONE ACETATE 1 % DROPS SUSP OPHTHALMIC 04/19/2016 7.51713
PREDNISOLONE SODIUM PHOSPHATE 5 MG/5 ML SOLUTION ORAL 07/03/2018 0.87614
PREDNISOLONE SODIUM PHOSPHATE 15 MG/5 ML SOLUTION ORAL 02/27/2019 0.16214
PREDNISOLONE SODIUM PHOSPHATE 10 MG/5 ML SOLUTION ORAL 03/01/2017 2.57271
PREDNISOLONE SODIUM PHOSPHATE 20 MG/5 ML SOLUTION ORAL 12/05/2018 3.60132
PREDNISOLONE SODIUM PHOSPHATE 10 MG TAB RAPDIS ORAL 04/11/2016 11.39210
PREDNISOLONE SODIUM PHOSPHATE 15 MG TAB RAPDIS ORAL 03/28/2016 18.12388
PREDNISOLONE SODIUM PHOSPHATE 30 MG TAB RAPDIS ORAL 02/10/2016 23.30213
PREDNISONE 1 MG TABLET ORAL 12/05/2018 0.14727
PREDNISONE 10 MG TABLET ORAL 04/19/2016 0.08013
PREDNISONE 2.5 MG TABLET ORAL 08/15/2018 0.13038
PREDNISONE 20 MG TABLET ORAL 01/12/2016 0.18034
PREDNISONE 5 MG TABLET ORAL 12/19/2018 0.10921
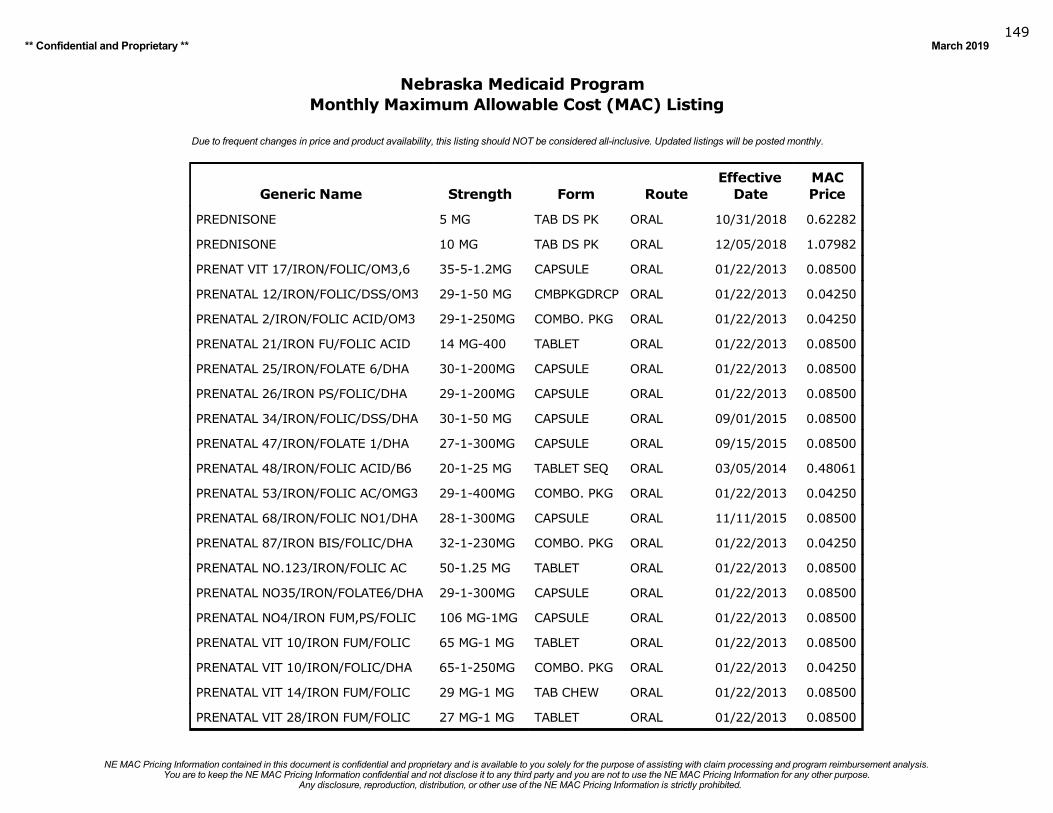
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019149
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PREDNISONE 5 MG TAB DS PK ORAL 10/31/2018 0.62282
PREDNISONE 10 MG TAB DS PK ORAL 12/05/2018 1.07982
PRENAT VIT 17/IRON/FOLIC/OM3,6 35-5-1.2MG CAPSULE ORAL 01/22/2013 0.08500
PRENATAL 12/IRON/FOLIC/DSS/OM3 29-1-50 MG CMBPKGDRCP ORAL 01/22/2013 0.04250
PRENATAL 2/IRON/FOLIC ACID/OM3 29-1-250MG COMBO. PKG ORAL 01/22/2013 0.04250
PRENATAL 21/IRON FU/FOLIC ACID 14 MG-400 TABLET ORAL 01/22/2013 0.08500
PRENATAL 25/IRON/FOLATE 6/DHA 30-1-200MG CAPSULE ORAL 01/22/2013 0.08500
PRENATAL 26/IRON PS/FOLIC/DHA 29-1-200MG CAPSULE ORAL 01/22/2013 0.08500
PRENATAL 34/IRON/FOLIC/DSS/DHA 30-1-50 MG CAPSULE ORAL 09/01/2015 0.08500
PRENATAL 47/IRON/FOLATE 1/DHA 27-1-300MG CAPSULE ORAL 09/15/2015 0.08500
PRENATAL 48/IRON/FOLIC ACID/B6 20-1-25 MG TABLET SEQ ORAL 03/05/2014 0.48061
PRENATAL 53/IRON/FOLIC AC/OMG3 29-1-400MG COMBO. PKG ORAL 01/22/2013 0.04250
PRENATAL 68/IRON/FOLIC NO1/DHA 28-1-300MG CAPSULE ORAL 11/11/2015 0.08500
PRENATAL 87/IRON BIS/FOLIC/DHA 32-1-230MG COMBO. PKG ORAL 01/22/2013 0.04250
PRENATAL NO.123/IRON/FOLIC AC 50-1.25 MG TABLET ORAL 01/22/2013 0.08500
PRENATAL NO35/IRON/FOLATE6/DHA 29-1-300MG CAPSULE ORAL 01/22/2013 0.08500
PRENATAL NO4/IRON FUM,PS/FOLIC 106 MG-1MG CAPSULE ORAL 01/22/2013 0.08500
PRENATAL VIT 10/IRON FUM/FOLIC 65 MG-1 MG TABLET ORAL 01/22/2013 0.08500
PRENATAL VIT 10/IRON/FOLIC/DHA 65-1-250MG COMBO. PKG ORAL 01/22/2013 0.04250
PRENATAL VIT 14/IRON FUM/FOLIC 29 MG-1 MG TAB CHEW ORAL 01/22/2013 0.08500
PRENATAL VIT 28/IRON FUM/FOLIC 27 MG-1 MG TABLET ORAL 01/22/2013 0.08500
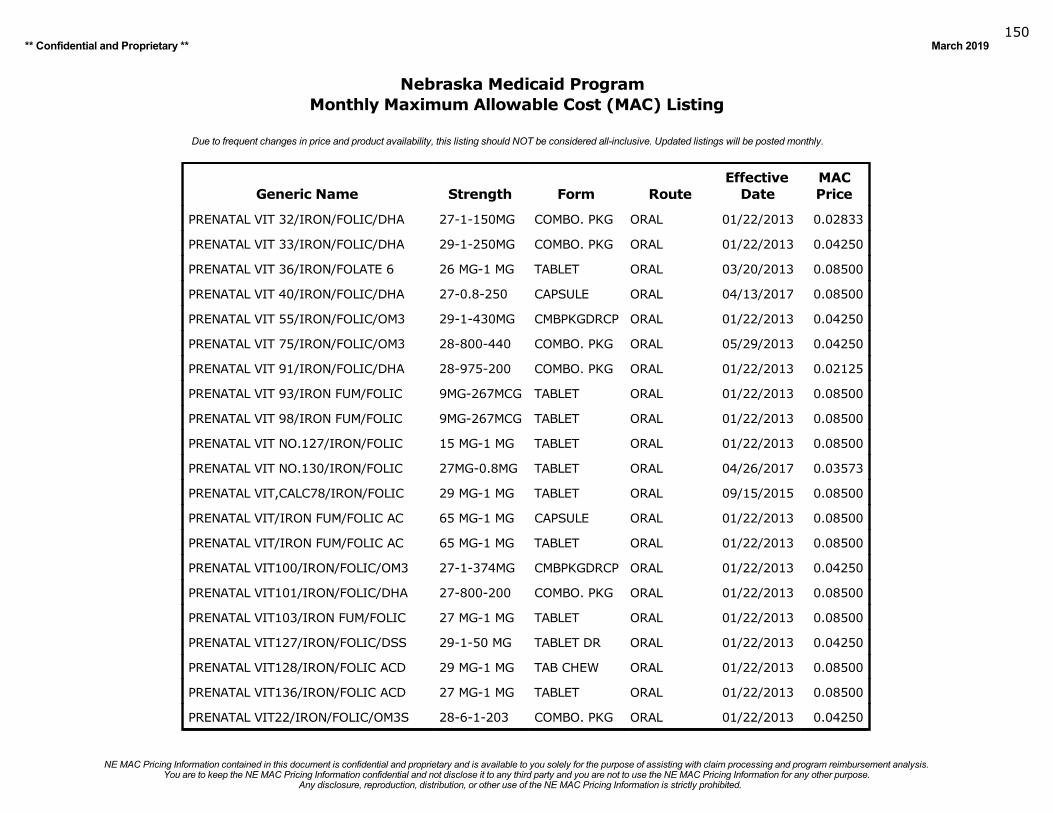
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019150
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PRENATAL VIT 32/IRON/FOLIC/DHA 27-1-150MG COMBO. PKG ORAL 01/22/2013 0.02833
PRENATAL VIT 33/IRON/FOLIC/DHA 29-1-250MG COMBO. PKG ORAL 01/22/2013 0.04250
PRENATAL VIT 36/IRON/FOLATE 6 26 MG-1 MG TABLET ORAL 03/20/2013 0.08500
PRENATAL VIT 40/IRON/FOLIC/DHA 27-0.8-250 CAPSULE ORAL 04/13/2017 0.08500
PRENATAL VIT 55/IRON/FOLIC/OM3 29-1-430MG CMBPKGDRCP ORAL 01/22/2013 0.04250
PRENATAL VIT 75/IRON/FOLIC/OM3 28-800-440 COMBO. PKG ORAL 05/29/2013 0.04250
PRENATAL VIT 91/IRON/FOLIC/DHA 28-975-200 COMBO. PKG ORAL 01/22/2013 0.02125
PRENATAL VIT 93/IRON FUM/FOLIC 9MG-267MCG TABLET ORAL 01/22/2013 0.08500
PRENATAL VIT 98/IRON FUM/FOLIC 9MG-267MCG TABLET ORAL 01/22/2013 0.08500
PRENATAL VIT NO.127/IRON/FOLIC 15 MG-1 MG TABLET ORAL 01/22/2013 0.08500
PRENATAL VIT NO.130/IRON/FOLIC 27MG-0.8MG TABLET ORAL 04/26/2017 0.03573
PRENATAL VIT,CALC78/IRON/FOLIC 29 MG-1 MG TABLET ORAL 09/15/2015 0.08500
PRENATAL VIT/IRON FUM/FOLIC AC 65 MG-1 MG CAPSULE ORAL 01/22/2013 0.08500
PRENATAL VIT/IRON FUM/FOLIC AC 65 MG-1 MG TABLET ORAL 01/22/2013 0.08500
PRENATAL VIT100/IRON/FOLIC/OM3 27-1-374MG CMBPKGDRCP ORAL 01/22/2013 0.04250
PRENATAL VIT101/IRON/FOLIC/DHA 27-800-200 COMBO. PKG ORAL 01/22/2013 0.08500
PRENATAL VIT103/IRON FUM/FOLIC 27 MG-1 MG TABLET ORAL 01/22/2013 0.08500
PRENATAL VIT127/IRON/FOLIC/DSS 29-1-50 MG TABLET DR ORAL 01/22/2013 0.04250
PRENATAL VIT128/IRON/FOLIC ACD 29 MG-1 MG TAB CHEW ORAL 01/22/2013 0.08500
PRENATAL VIT136/IRON/FOLIC ACD 27 MG-1 MG TABLET ORAL 01/22/2013 0.08500
PRENATAL VIT22/IRON/FOLIC/OM3S 28-6-1-203 COMBO. PKG ORAL 01/22/2013 0.04250
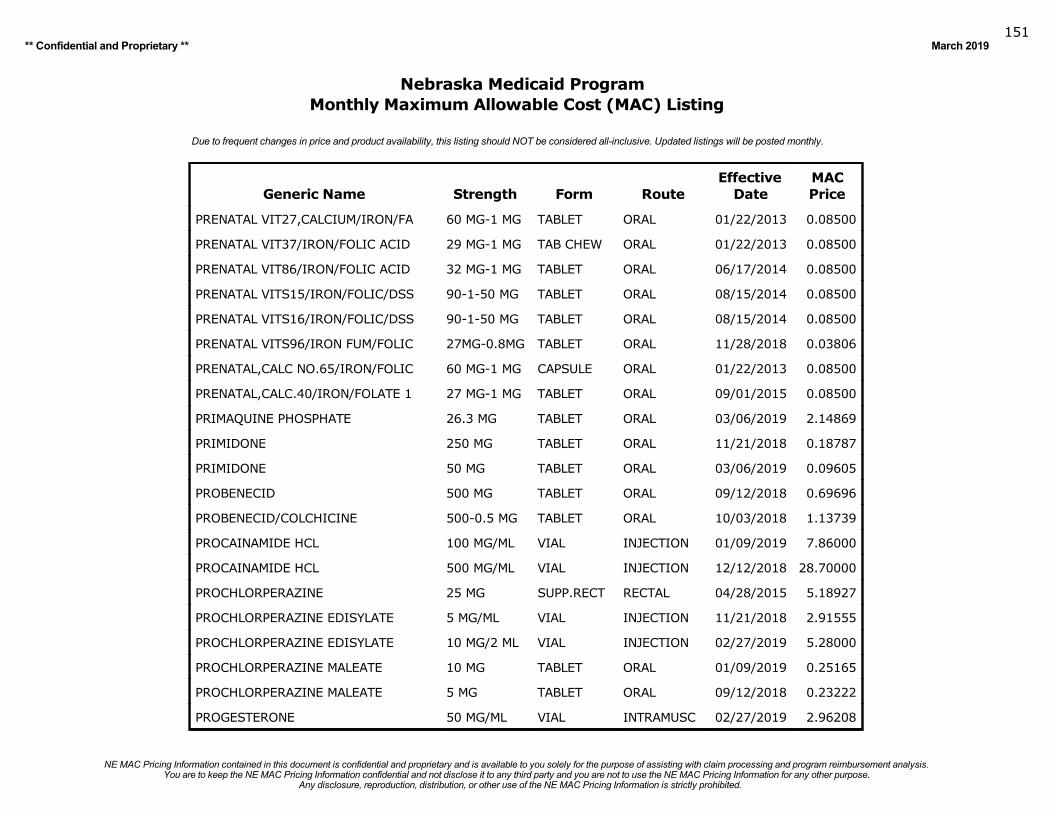
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019151
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PRENATAL VIT27,CALCIUM/IRON/FA 60 MG-1 MG TABLET ORAL 01/22/2013 0.08500
PRENATAL VIT37/IRON/FOLIC ACID 29 MG-1 MG TAB CHEW ORAL 01/22/2013 0.08500
PRENATAL VIT86/IRON/FOLIC ACID 32 MG-1 MG TABLET ORAL 06/17/2014 0.08500
PRENATAL VITS15/IRON/FOLIC/DSS 90-1-50 MG TABLET ORAL 08/15/2014 0.08500
PRENATAL VITS16/IRON/FOLIC/DSS 90-1-50 MG TABLET ORAL 08/15/2014 0.08500
PRENATAL VITS96/IRON FUM/FOLIC 27MG-0.8MG TABLET ORAL 11/28/2018 0.03806
PRENATAL,CALC NO.65/IRON/FOLIC 60 MG-1 MG CAPSULE ORAL 01/22/2013 0.08500
PRENATAL,CALC.40/IRON/FOLATE 1 27 MG-1 MG TABLET ORAL 09/01/2015 0.08500
PRIMAQUINE PHOSPHATE 26.3 MG TABLET ORAL 03/06/2019 2.14869
PRIMIDONE 250 MG TABLET ORAL 11/21/2018 0.18787
PRIMIDONE 50 MG TABLET ORAL 03/06/2019 0.09605
PROBENECID 500 MG TABLET ORAL 09/12/2018 0.69696
PROBENECID/COLCHICINE 500-0.5 MG TABLET ORAL 10/03/2018 1.13739
PROCAINAMIDE HCL 100 MG/ML VIAL INJECTION 01/09/2019 7.86000
PROCAINAMIDE HCL 500 MG/ML VIAL INJECTION 12/12/2018 28.70000
PROCHLORPERAZINE 25 MG SUPP.RECT RECTAL 04/28/2015 5.18927
PROCHLORPERAZINE EDISYLATE 5 MG/ML VIAL INJECTION 11/21/2018 2.91555
PROCHLORPERAZINE EDISYLATE 10 MG/2 ML VIAL INJECTION 02/27/2019 5.28000
PROCHLORPERAZINE MALEATE 10 MG TABLET ORAL 01/09/2019 0.25165
PROCHLORPERAZINE MALEATE 5 MG TABLET ORAL 09/12/2018 0.23222
PROGESTERONE 50 MG/ML VIAL INTRAMUSC 02/27/2019 2.96208

Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019152
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PROGESTERONE, MICRONIZED 100 MG CAPSULE ORAL 02/13/2019 0.64387
PROGESTERONE, MICRONIZED 200 MG CAPSULE ORAL 02/13/2019 1.25169
PROMETHAZINE HCL 6.25MG/5ML SYRUP ORAL 02/27/2019 0.02208
PROMETHAZINE HCL 12.5 MG TABLET ORAL 02/06/2019 0.10117
PROMETHAZINE HCL 25 MG TABLET ORAL 01/30/2019 0.04208
PROMETHAZINE HCL 50 MG TABLET ORAL 01/30/2019 0.11149
PROMETHAZINE HCL 25 MG/ML AMPUL INJECTION 08/03/2016 1.06932
PROMETHAZINE HCL 50 MG/ML AMPUL INJECTION 02/06/2019 2.38520
PROMETHAZINE HCL 25 MG/ML VIAL INJECTION 12/20/2017 1.09478
PROMETHAZINE HCL 50 MG/ML VIAL INJECTION 01/22/2013 2.35505
PROMETHAZINE HCL 12.5 MG SUPP.RECT RECTAL 03/06/2019 7.21600
PROMETHAZINE HCL 25 MG SUPP.RECT RECTAL 01/30/2019 7.55968
PROMETHAZINE HCL 50 MG SUPP.RECT RECTAL 12/06/2017 52.67419
PROMETHAZINE HCL/CODEINE 6.25-10/5 SYRUP ORAL 03/07/2018 0.01963
PROMETHAZINE/DEXTROMETHORPHAN 6.25-15/5 SYRUP ORAL 10/03/2018 0.01709
PROPAFENONE HCL 225 MG CAP ER 12H ORAL 02/06/2019 2.42406
PROPAFENONE HCL 325 MG CAP ER 12H ORAL 02/06/2019 3.40538
PROPAFENONE HCL 425 MG CAP ER 12H ORAL 02/06/2019 3.02500
PROPAFENONE HCL 150 MG TABLET ORAL 01/23/2019 0.20113
PROPAFENONE HCL 300 MG TABLET ORAL 01/23/2019 1.80887
PROPAFENONE HCL 225 MG TABLET ORAL 01/23/2019 0.38726
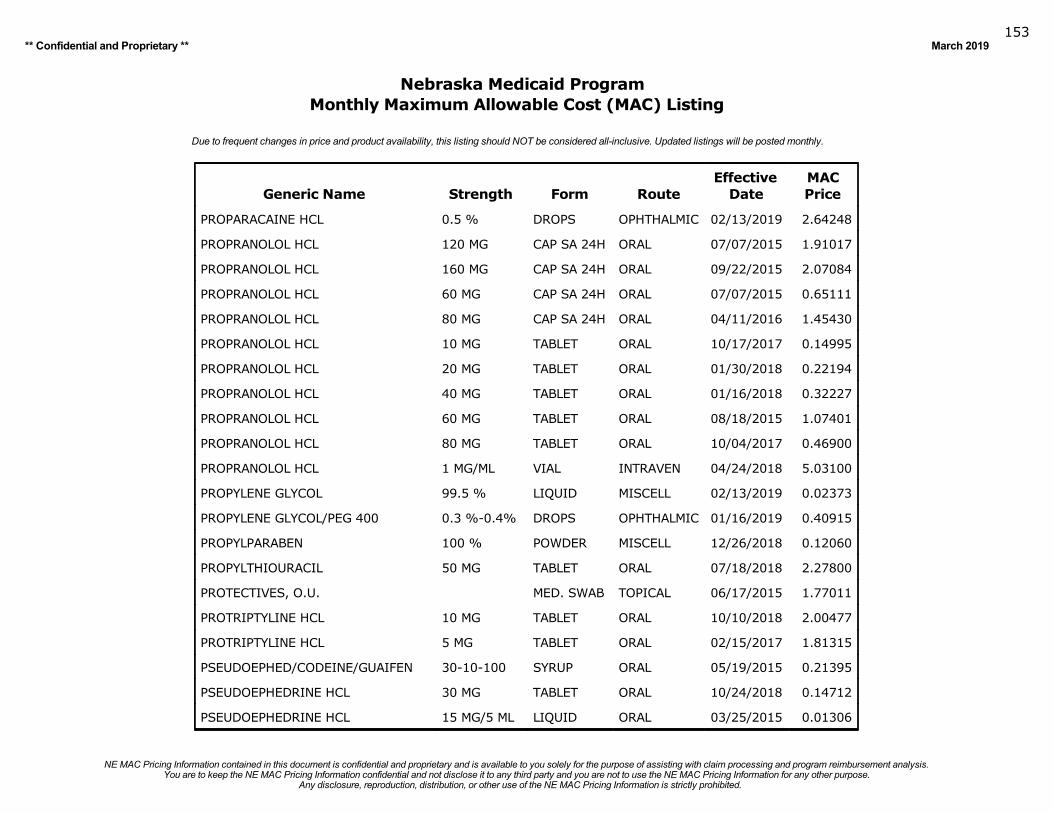
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019153
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
PROPARACAINE HCL 0.5 % DROPS OPHTHALMIC 02/13/2019 2.64248
PROPRANOLOL HCL 120 MG CAP SA 24H ORAL 07/07/2015 1.91017
PROPRANOLOL HCL 160 MG CAP SA 24H ORAL 09/22/2015 2.07084
PROPRANOLOL HCL 60 MG CAP SA 24H ORAL 07/07/2015 0.65111
PROPRANOLOL HCL 80 MG CAP SA 24H ORAL 04/11/2016 1.45430
PROPRANOLOL HCL 10 MG TABLET ORAL 10/17/2017 0.14995
PROPRANOLOL HCL 20 MG TABLET ORAL 01/30/2018 0.22194
PROPRANOLOL HCL 40 MG TABLET ORAL 01/16/2018 0.32227
PROPRANOLOL HCL 60 MG TABLET ORAL 08/18/2015 1.07401
PROPRANOLOL HCL 80 MG TABLET ORAL 10/04/2017 0.46900
PROPRANOLOL HCL 1 MG/ML VIAL INTRAVEN 04/24/2018 5.03100
PROPYLENE GLYCOL 99.5 % LIQUID MISCELL 02/13/2019 0.02373
PROPYLENE GLYCOL/PEG 400 0.3 %-0.4% DROPS OPHTHALMIC 01/16/2019 0.40915
PROPYLPARABEN 100 % POWDER MISCELL 12/26/2018 0.12060
PROPYLTHIOURACIL 50 MG TABLET ORAL 07/18/2018 2.27800
PROTECTIVES, O.U. MED. SWAB TOPICAL 06/17/2015 1.77011
PROTRIPTYLINE HCL 10 MG TABLET ORAL 10/10/2018 2.00477
PROTRIPTYLINE HCL 5 MG TABLET ORAL 02/15/2017 1.81315
PSEUDOEPHED/CODEINE/GUAIFEN 30-10-100 SYRUP ORAL 05/19/2015 0.21395
PSEUDOEPHEDRINE HCL 30 MG TABLET ORAL 10/24/2018 0.14712
PSEUDOEPHEDRINE HCL 15 MG/5 ML LIQUID ORAL 03/25/2015 0.01306
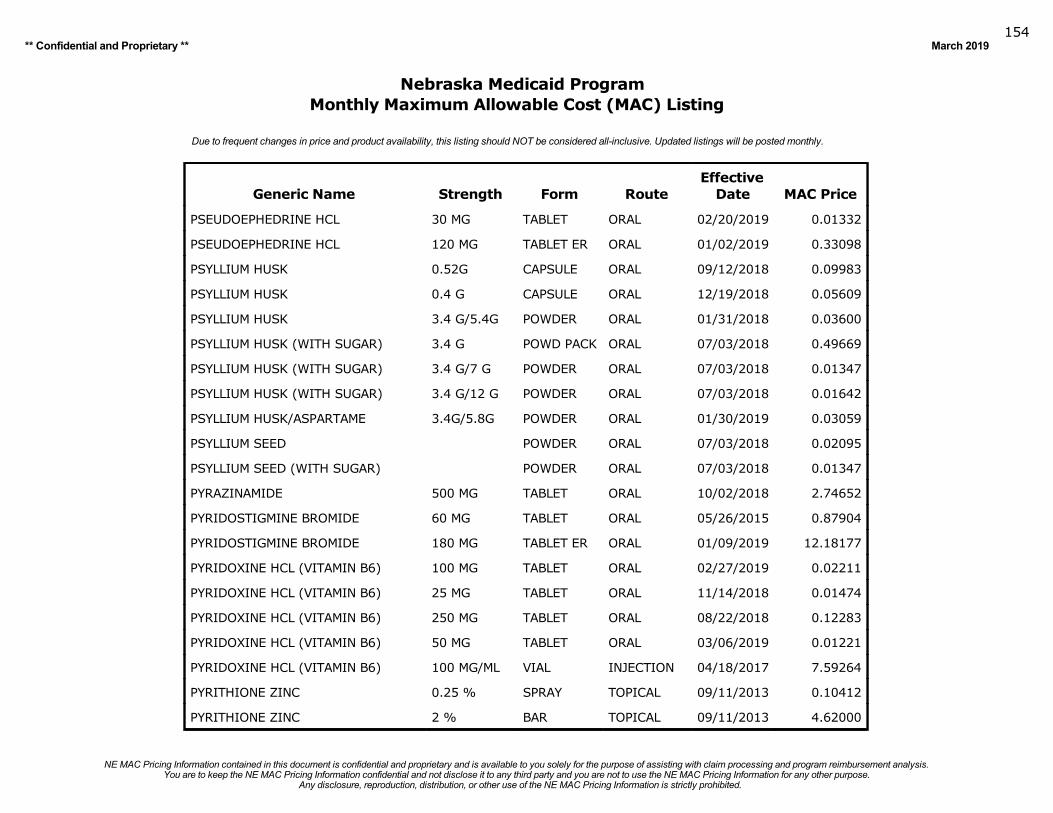
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019154
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
Date MAC Price
PSEUDOEPHEDRINE HCL 30 MG TABLET ORAL 02/20/2019 0.01332
PSEUDOEPHEDRINE HCL 120 MG TABLET ER ORAL 01/02/2019 0.33098
PSYLLIUM HUSK 0.52G CAPSULE ORAL 09/12/2018 0.09983
PSYLLIUM HUSK 0.4 G CAPSULE ORAL 12/19/2018 0.05609
PSYLLIUM HUSK 3.4 G/5.4G POWDER ORAL 01/31/2018 0.03600
PSYLLIUM HUSK (WITH SUGAR) 3.4 G POWD PACK ORAL 07/03/2018 0.49669
PSYLLIUM HUSK (WITH SUGAR) 3.4 G/7 G POWDER ORAL 07/03/2018 0.01347
PSYLLIUM HUSK (WITH SUGAR) 3.4 G/12 G POWDER ORAL 07/03/2018 0.01642
PSYLLIUM HUSK/ASPARTAME 3.4G/5.8G POWDER ORAL 01/30/2019 0.03059
PSYLLIUM SEED POWDER ORAL 07/03/2018 0.02095
PSYLLIUM SEED (WITH SUGAR) POWDER ORAL 07/03/2018 0.01347
PYRAZINAMIDE 500 MG TABLET ORAL 10/02/2018 2.74652
PYRIDOSTIGMINE BROMIDE 60 MG TABLET ORAL 05/26/2015 0.87904
PYRIDOSTIGMINE BROMIDE 180 MG TABLET ER ORAL 01/09/2019 12.18177
PYRIDOXINE HCL (VITAMIN B6) 100 MG TABLET ORAL 02/27/2019 0.02211
PYRIDOXINE HCL (VITAMIN B6) 25 MG TABLET ORAL 11/14/2018 0.01474
PYRIDOXINE HCL (VITAMIN B6) 250 MG TABLET ORAL 08/22/2018 0.12283
PYRIDOXINE HCL (VITAMIN B6) 50 MG TABLET ORAL 03/06/2019 0.01221
PYRIDOXINE HCL (VITAMIN B6) 100 MG/ML VIAL INJECTION 04/18/2017 7.59264
PYRITHIONE ZINC 0.25 % SPRAY TOPICAL 09/11/2013 0.10412
PYRITHIONE ZINC 2 % BAR TOPICAL 09/11/2013 4.62000
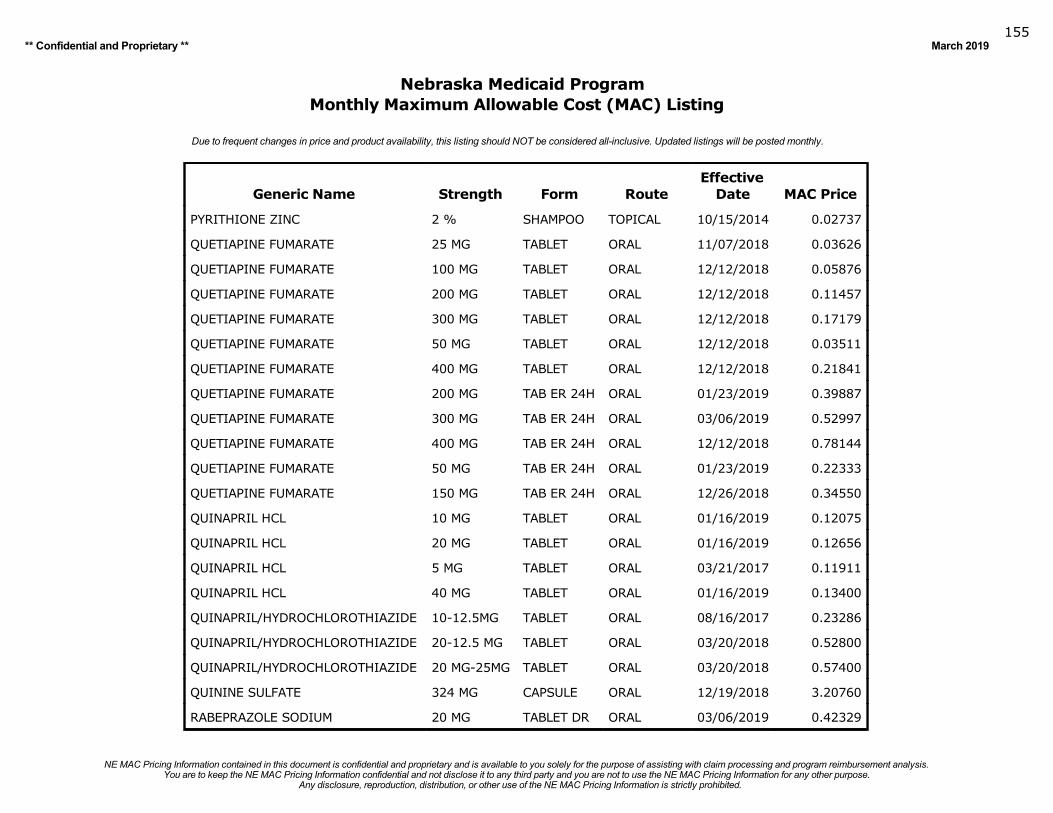
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019155
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
Date MAC Price
PYRITHIONE ZINC 2 % SHAMPOO TOPICAL 10/15/2014 0.02737
QUETIAPINE FUMARATE 25 MG TABLET ORAL 11/07/2018 0.03626
QUETIAPINE FUMARATE 100 MG TABLET ORAL 12/12/2018 0.05876
QUETIAPINE FUMARATE 200 MG TABLET ORAL 12/12/2018 0.11457
QUETIAPINE FUMARATE 300 MG TABLET ORAL 12/12/2018 0.17179
QUETIAPINE FUMARATE 50 MG TABLET ORAL 12/12/2018 0.03511
QUETIAPINE FUMARATE 400 MG TABLET ORAL 12/12/2018 0.21841
QUETIAPINE FUMARATE 200 MG TAB ER 24H ORAL 01/23/2019 0.39887
QUETIAPINE FUMARATE 300 MG TAB ER 24H ORAL 03/06/2019 0.52997
QUETIAPINE FUMARATE 400 MG TAB ER 24H ORAL 12/12/2018 0.78144
QUETIAPINE FUMARATE 50 MG TAB ER 24H ORAL 01/23/2019 0.22333
QUETIAPINE FUMARATE 150 MG TAB ER 24H ORAL 12/26/2018 0.34550
QUINAPRIL HCL 10 MG TABLET ORAL 01/16/2019 0.12075
QUINAPRIL HCL 20 MG TABLET ORAL 01/16/2019 0.12656
QUINAPRIL HCL 5 MG TABLET ORAL 03/21/2017 0.11911
QUINAPRIL HCL 40 MG TABLET ORAL 01/16/2019 0.13400
QUINAPRIL/HYDROCHLOROTHIAZIDE 10-12.5MG TABLET ORAL 08/16/2017 0.23286
QUINAPRIL/HYDROCHLOROTHIAZIDE 20-12.5 MG TABLET ORAL 03/20/2018 0.52800
QUINAPRIL/HYDROCHLOROTHIAZIDE 20 MG-25MG TABLET ORAL 03/20/2018 0.57400
QUININE SULFATE 324 MG CAPSULE ORAL 12/19/2018 3.20760
RABEPRAZOLE SODIUM 20 MG TABLET DR ORAL 03/06/2019 0.42329
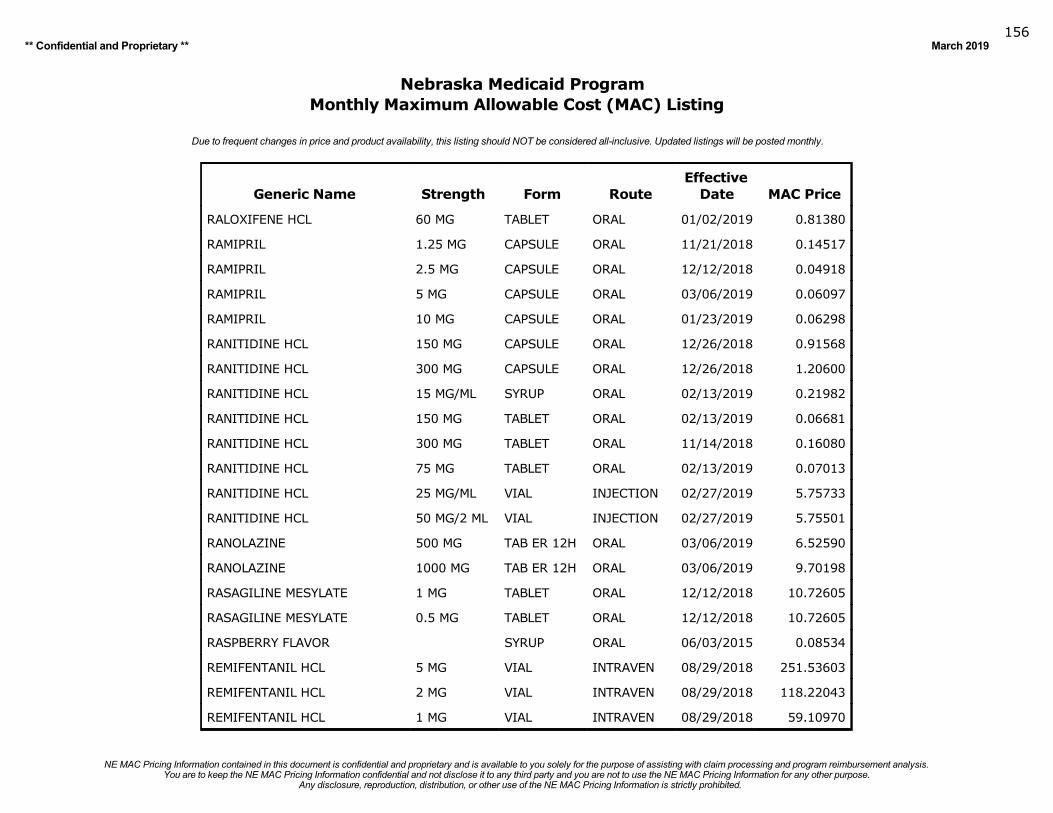
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019156
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
Date MAC Price
RALOXIFENE HCL 60 MG TABLET ORAL 01/02/2019 0.81380
RAMIPRIL 1.25 MG CAPSULE ORAL 11/21/2018 0.14517
RAMIPRIL 2.5 MG CAPSULE ORAL 12/12/2018 0.04918
RAMIPRIL 5 MG CAPSULE ORAL 03/06/2019 0.06097
RAMIPRIL 10 MG CAPSULE ORAL 01/23/2019 0.06298
RANITIDINE HCL 150 MG CAPSULE ORAL 12/26/2018 0.91568
RANITIDINE HCL 300 MG CAPSULE ORAL 12/26/2018 1.20600
RANITIDINE HCL 15 MG/ML SYRUP ORAL 02/13/2019 0.21982
RANITIDINE HCL 150 MG TABLET ORAL 02/13/2019 0.06681
RANITIDINE HCL 300 MG TABLET ORAL 11/14/2018 0.16080
RANITIDINE HCL 75 MG TABLET ORAL 02/13/2019 0.07013
RANITIDINE HCL 25 MG/ML VIAL INJECTION 02/27/2019 5.75733
RANITIDINE HCL 50 MG/2 ML VIAL INJECTION 02/27/2019 5.75501
RANOLAZINE 500 MG TAB ER 12H ORAL 03/06/2019 6.52590
RANOLAZINE 1000 MG TAB ER 12H ORAL 03/06/2019 9.70198
RASAGILINE MESYLATE 1 MG TABLET ORAL 12/12/2018 10.72605
RASAGILINE MESYLATE 0.5 MG TABLET ORAL 12/12/2018 10.72605
RASPBERRY FLAVOR SYRUP ORAL 06/03/2015 0.08534
REMIFENTANIL HCL 5 MG VIAL INTRAVEN 08/29/2018 251.53603
REMIFENTANIL HCL 2 MG VIAL INTRAVEN 08/29/2018 118.22043
REMIFENTANIL HCL 1 MG VIAL INTRAVEN 08/29/2018 59.10970
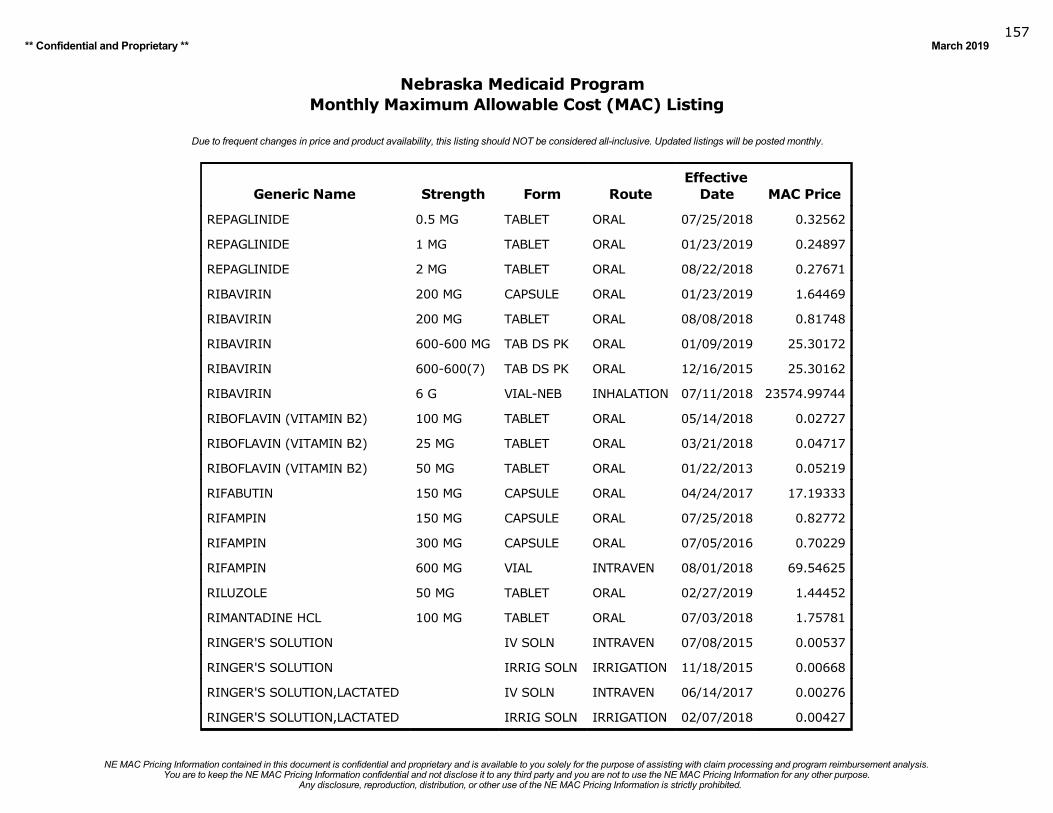
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019157
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
Date MAC Price
REPAGLINIDE 0.5 MG TABLET ORAL 07/25/2018 0.32562
REPAGLINIDE 1 MG TABLET ORAL 01/23/2019 0.24897
REPAGLINIDE 2 MG TABLET ORAL 08/22/2018 0.27671
RIBAVIRIN 200 MG CAPSULE ORAL 01/23/2019 1.64469
RIBAVIRIN 200 MG TABLET ORAL 08/08/2018 0.81748
RIBAVIRIN 600-600 MG TAB DS PK ORAL 01/09/2019 25.30172
RIBAVIRIN 600-600(7) TAB DS PK ORAL 12/16/2015 25.30162
RIBAVIRIN 6 G VIAL-NEB INHALATION 07/11/2018 23574.99744
RIBOFLAVIN (VITAMIN B2) 100 MG TABLET ORAL 05/14/2018 0.02727
RIBOFLAVIN (VITAMIN B2) 25 MG TABLET ORAL 03/21/2018 0.04717
RIBOFLAVIN (VITAMIN B2) 50 MG TABLET ORAL 01/22/2013 0.05219
RIFABUTIN 150 MG CAPSULE ORAL 04/24/2017 17.19333
RIFAMPIN 150 MG CAPSULE ORAL 07/25/2018 0.82772
RIFAMPIN 300 MG CAPSULE ORAL 07/05/2016 0.70229
RIFAMPIN 600 MG VIAL INTRAVEN 08/01/2018 69.54625
RILUZOLE 50 MG TABLET ORAL 02/27/2019 1.44452
RIMANTADINE HCL 100 MG TABLET ORAL 07/03/2018 1.75781
RINGER'S SOLUTION IV SOLN INTRAVEN 07/08/2015 0.00537
RINGER'S SOLUTION IRRIG SOLN IRRIGATION 11/18/2015 0.00668
RINGER'S SOLUTION,LACTATED IV SOLN INTRAVEN 06/14/2017 0.00276
RINGER'S SOLUTION,LACTATED IRRIG SOLN IRRIGATION 02/07/2018 0.00427
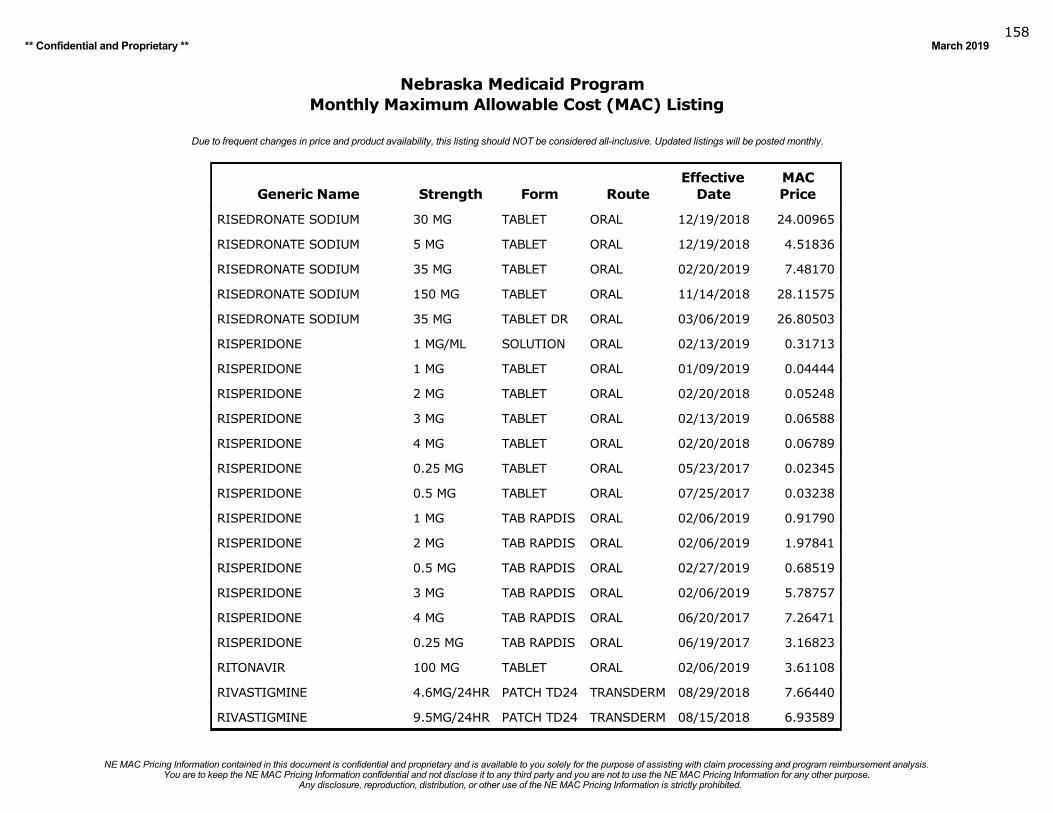
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019158
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
RISEDRONATE SODIUM 30 MG TABLET ORAL 12/19/2018 24.00965
RISEDRONATE SODIUM 5 MG TABLET ORAL 12/19/2018 4.51836
RISEDRONATE SODIUM 35 MG TABLET ORAL 02/20/2019 7.48170
RISEDRONATE SODIUM 150 MG TABLET ORAL 11/14/2018 28.11575
RISEDRONATE SODIUM 35 MG TABLET DR ORAL 03/06/2019 26.80503
RISPERIDONE 1 MG/ML SOLUTION ORAL 02/13/2019 0.31713
RISPERIDONE 1 MG TABLET ORAL 01/09/2019 0.04444
RISPERIDONE 2 MG TABLET ORAL 02/20/2018 0.05248
RISPERIDONE 3 MG TABLET ORAL 02/13/2019 0.06588
RISPERIDONE 4 MG TABLET ORAL 02/20/2018 0.06789
RISPERIDONE 0.25 MG TABLET ORAL 05/23/2017 0.02345
RISPERIDONE 0.5 MG TABLET ORAL 07/25/2017 0.03238
RISPERIDONE 1 MG TAB RAPDIS ORAL 02/06/2019 0.91790
RISPERIDONE 2 MG TAB RAPDIS ORAL 02/06/2019 1.97841
RISPERIDONE 0.5 MG TAB RAPDIS ORAL 02/27/2019 0.68519
RISPERIDONE 3 MG TAB RAPDIS ORAL 02/06/2019 5.78757
RISPERIDONE 4 MG TAB RAPDIS ORAL 06/20/2017 7.26471
RISPERIDONE 0.25 MG TAB RAPDIS ORAL 06/19/2017 3.16823
RITONAVIR 100 MG TABLET ORAL 02/06/2019 3.61108
RIVASTIGMINE 4.6MG/24HR PATCH TD24 TRANSDERM 08/29/2018 7.66440
RIVASTIGMINE 9.5MG/24HR PATCH TD24 TRANSDERM 08/15/2018 6.93589
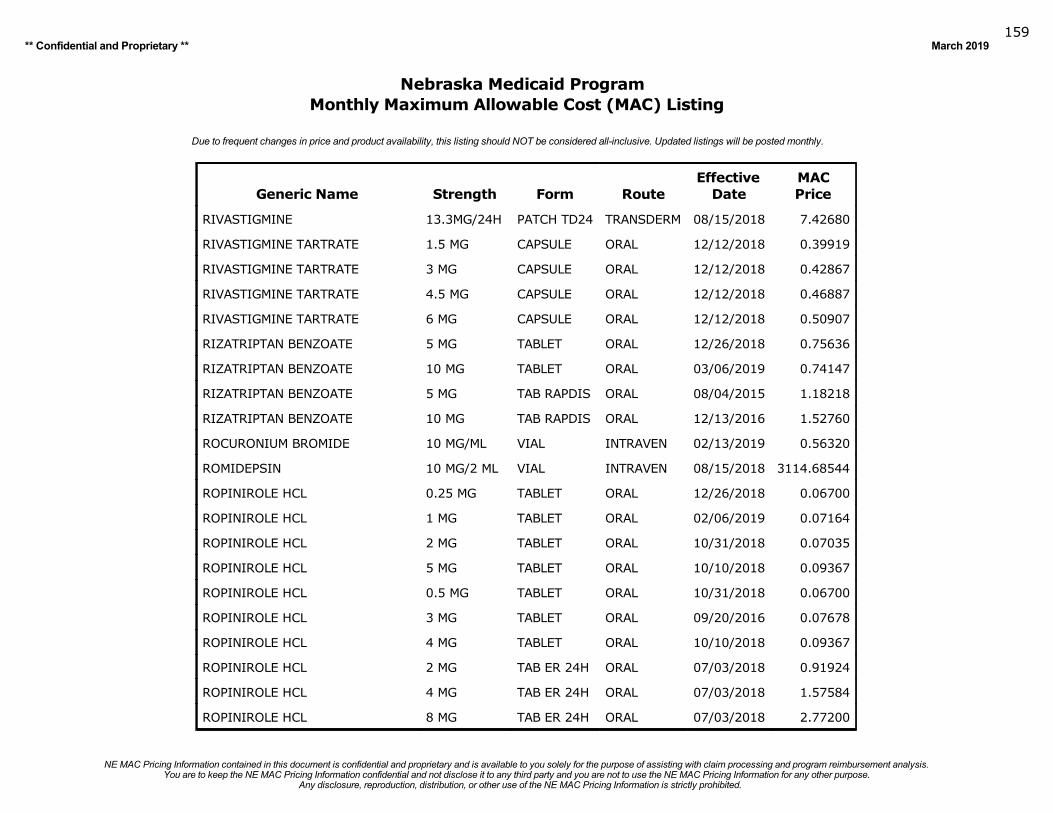
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019159
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
RIVASTIGMINE 13.3MG/24H PATCH TD24 TRANSDERM 08/15/2018 7.42680
RIVASTIGMINE TARTRATE 1.5 MG CAPSULE ORAL 12/12/2018 0.39919
RIVASTIGMINE TARTRATE 3 MG CAPSULE ORAL 12/12/2018 0.42867
RIVASTIGMINE TARTRATE 4.5 MG CAPSULE ORAL 12/12/2018 0.46887
RIVASTIGMINE TARTRATE 6 MG CAPSULE ORAL 12/12/2018 0.50907
RIZATRIPTAN BENZOATE 5 MG TABLET ORAL 12/26/2018 0.75636
RIZATRIPTAN BENZOATE 10 MG TABLET ORAL 03/06/2019 0.74147
RIZATRIPTAN BENZOATE 5 MG TAB RAPDIS ORAL 08/04/2015 1.18218
RIZATRIPTAN BENZOATE 10 MG TAB RAPDIS ORAL 12/13/2016 1.52760
ROCURONIUM BROMIDE 10 MG/ML VIAL INTRAVEN 02/13/2019 0.56320
ROMIDEPSIN 10 MG/2 ML VIAL INTRAVEN 08/15/2018 3114.68544
ROPINIROLE HCL 0.25 MG TABLET ORAL 12/26/2018 0.06700
ROPINIROLE HCL 1 MG TABLET ORAL 02/06/2019 0.07164
ROPINIROLE HCL 2 MG TABLET ORAL 10/31/2018 0.07035
ROPINIROLE HCL 5 MG TABLET ORAL 10/10/2018 0.09367
ROPINIROLE HCL 0.5 MG TABLET ORAL 10/31/2018 0.06700
ROPINIROLE HCL 3 MG TABLET ORAL 09/20/2016 0.07678
ROPINIROLE HCL 4 MG TABLET ORAL 10/10/2018 0.09367
ROPINIROLE HCL 2 MG TAB ER 24H ORAL 07/03/2018 0.91924
ROPINIROLE HCL 4 MG TAB ER 24H ORAL 07/03/2018 1.57584
ROPINIROLE HCL 8 MG TAB ER 24H ORAL 07/03/2018 2.77200
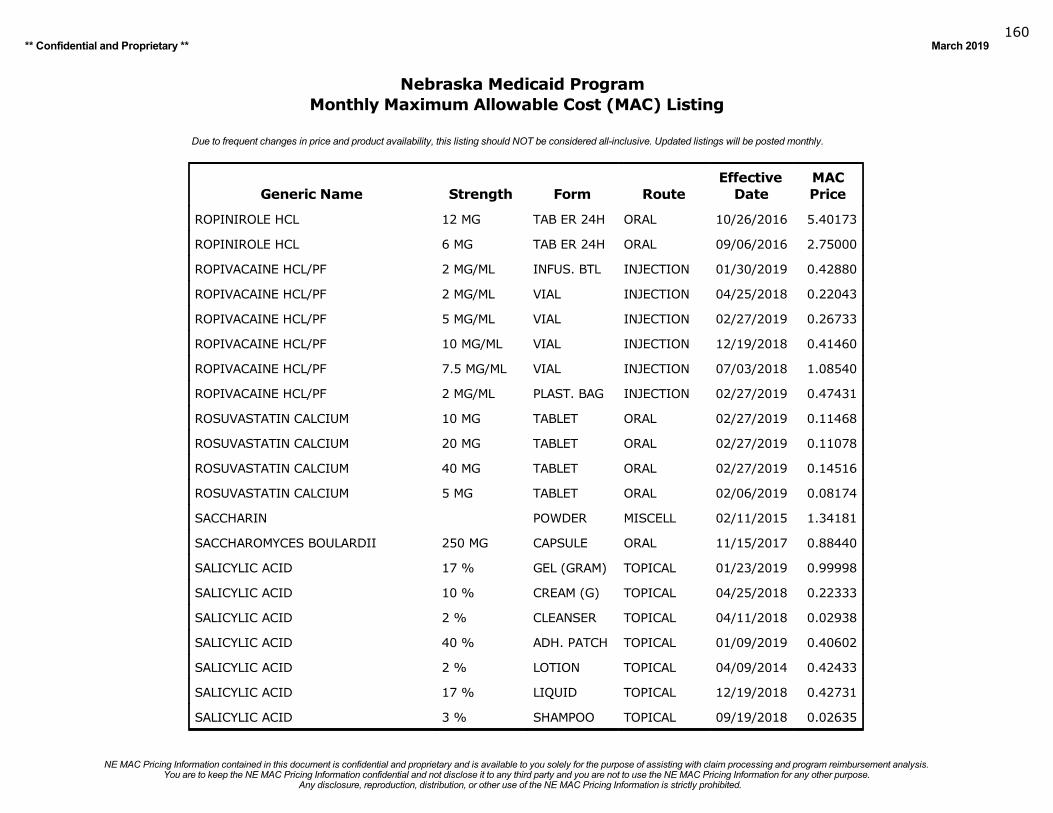
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019160
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ROPINIROLE HCL 12 MG TAB ER 24H ORAL 10/26/2016 5.40173
ROPINIROLE HCL 6 MG TAB ER 24H ORAL 09/06/2016 2.75000
ROPIVACAINE HCL/PF 2 MG/ML INFUS. BTL INJECTION 01/30/2019 0.42880
ROPIVACAINE HCL/PF 2 MG/ML VIAL INJECTION 04/25/2018 0.22043
ROPIVACAINE HCL/PF 5 MG/ML VIAL INJECTION 02/27/2019 0.26733
ROPIVACAINE HCL/PF 10 MG/ML VIAL INJECTION 12/19/2018 0.41460
ROPIVACAINE HCL/PF 7.5 MG/ML VIAL INJECTION 07/03/2018 1.08540
ROPIVACAINE HCL/PF 2 MG/ML PLAST. BAG INJECTION 02/27/2019 0.47431
ROSUVASTATIN CALCIUM 10 MG TABLET ORAL 02/27/2019 0.11468
ROSUVASTATIN CALCIUM 20 MG TABLET ORAL 02/27/2019 0.11078
ROSUVASTATIN CALCIUM 40 MG TABLET ORAL 02/27/2019 0.14516
ROSUVASTATIN CALCIUM 5 MG TABLET ORAL 02/06/2019 0.08174
SACCHARIN POWDER MISCELL 02/11/2015 1.34181
SACCHAROMYCES BOULARDII 250 MG CAPSULE ORAL 11/15/2017 0.88440
SALICYLIC ACID 17 % GEL (GRAM) TOPICAL 01/23/2019 0.99998
SALICYLIC ACID 10 % CREAM (G) TOPICAL 04/25/2018 0.22333
SALICYLIC ACID 2 % CLEANSER TOPICAL 04/11/2018 0.02938
SALICYLIC ACID 40 % ADH. PATCH TOPICAL 01/09/2019 0.40602
SALICYLIC ACID 2 % LOTION TOPICAL 04/09/2014 0.42433
SALICYLIC ACID 17 % LIQUID TOPICAL 12/19/2018 0.42731
SALICYLIC ACID 3 % SHAMPOO TOPICAL 09/19/2018 0.02635
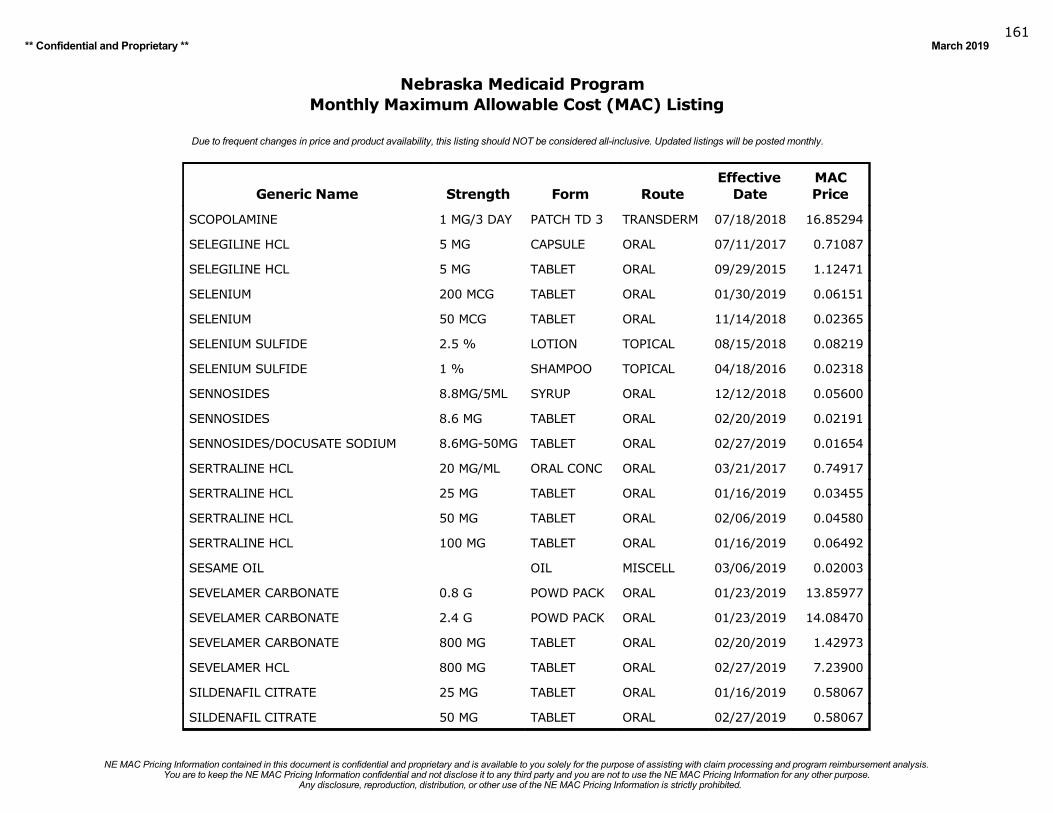
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019161
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
SCOPOLAMINE 1 MG/3 DAY PATCH TD 3 TRANSDERM 07/18/2018 16.85294
SELEGILINE HCL 5 MG CAPSULE ORAL 07/11/2017 0.71087
SELEGILINE HCL 5 MG TABLET ORAL 09/29/2015 1.12471
SELENIUM 200 MCG TABLET ORAL 01/30/2019 0.06151
SELENIUM 50 MCG TABLET ORAL 11/14/2018 0.02365
SELENIUM SULFIDE 2.5 % LOTION TOPICAL 08/15/2018 0.08219
SELENIUM SULFIDE 1 % SHAMPOO TOPICAL 04/18/2016 0.02318
SENNOSIDES 8.8MG/5ML SYRUP ORAL 12/12/2018 0.05600
SENNOSIDES 8.6 MG TABLET ORAL 02/20/2019 0.02191
SENNOSIDES/DOCUSATE SODIUM 8.6MG-50MG TABLET ORAL 02/27/2019 0.01654
SERTRALINE HCL 20 MG/ML ORAL CONC ORAL 03/21/2017 0.74917
SERTRALINE HCL 25 MG TABLET ORAL 01/16/2019 0.03455
SERTRALINE HCL 50 MG TABLET ORAL 02/06/2019 0.04580
SERTRALINE HCL 100 MG TABLET ORAL 01/16/2019 0.06492
SESAME OIL OIL MISCELL 03/06/2019 0.02003
SEVELAMER CARBONATE 0.8 G POWD PACK ORAL 01/23/2019 13.85977
SEVELAMER CARBONATE 2.4 G POWD PACK ORAL 01/23/2019 14.08470
SEVELAMER CARBONATE 800 MG TABLET ORAL 02/20/2019 1.42973
SEVELAMER HCL 800 MG TABLET ORAL 02/27/2019 7.23900
SILDENAFIL CITRATE 25 MG TABLET ORAL 01/16/2019 0.58067
SILDENAFIL CITRATE 50 MG TABLET ORAL 02/27/2019 0.58067
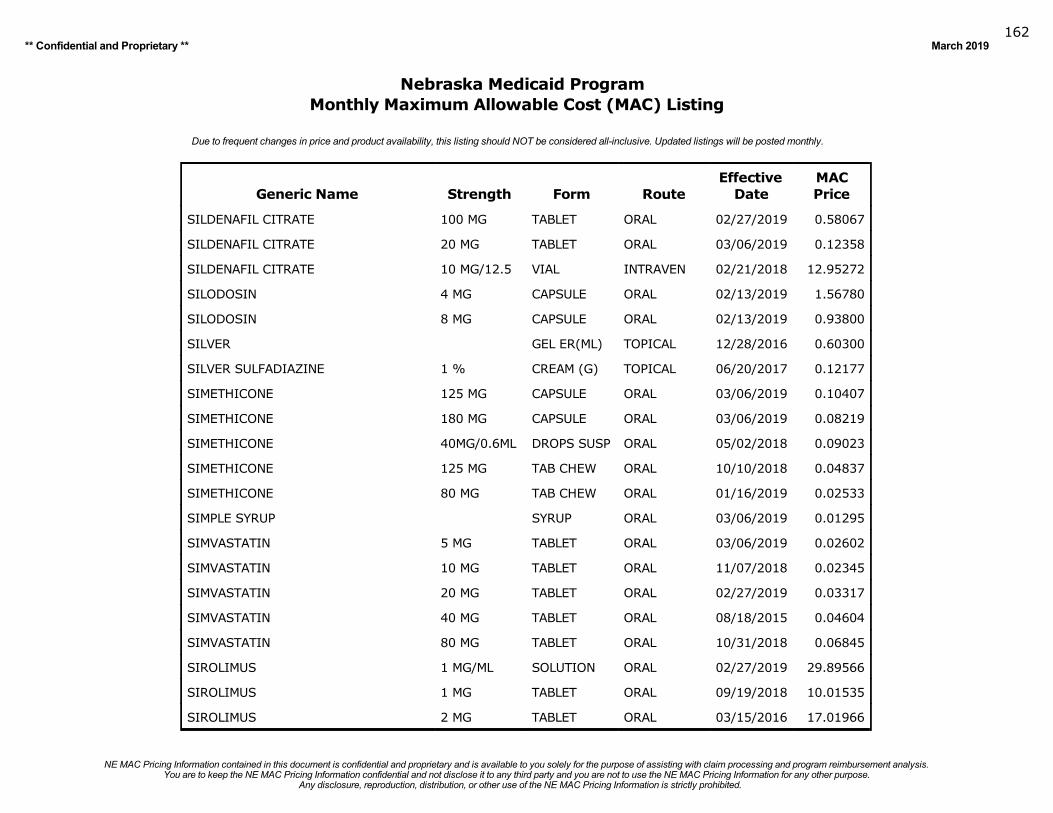
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019162
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
SILDENAFIL CITRATE 100 MG TABLET ORAL 02/27/2019 0.58067
SILDENAFIL CITRATE 20 MG TABLET ORAL 03/06/2019 0.12358
SILDENAFIL CITRATE 10 MG/12.5 VIAL INTRAVEN 02/21/2018 12.95272
SILODOSIN 4 MG CAPSULE ORAL 02/13/2019 1.56780
SILODOSIN 8 MG CAPSULE ORAL 02/13/2019 0.93800
SILVER GEL ER(ML) TOPICAL 12/28/2016 0.60300
SILVER SULFADIAZINE 1 % CREAM (G) TOPICAL 06/20/2017 0.12177
SIMETHICONE 125 MG CAPSULE ORAL 03/06/2019 0.10407
SIMETHICONE 180 MG CAPSULE ORAL 03/06/2019 0.08219
SIMETHICONE 40MG/0.6ML DROPS SUSP ORAL 05/02/2018 0.09023
SIMETHICONE 125 MG TAB CHEW ORAL 10/10/2018 0.04837
SIMETHICONE 80 MG TAB CHEW ORAL 01/16/2019 0.02533
SIMPLE SYRUP SYRUP ORAL 03/06/2019 0.01295
SIMVASTATIN 5 MG TABLET ORAL 03/06/2019 0.02602
SIMVASTATIN 10 MG TABLET ORAL 11/07/2018 0.02345
SIMVASTATIN 20 MG TABLET ORAL 02/27/2019 0.03317
SIMVASTATIN 40 MG TABLET ORAL 08/18/2015 0.04604
SIMVASTATIN 80 MG TABLET ORAL 10/31/2018 0.06845
SIROLIMUS 1 MG/ML SOLUTION ORAL 02/27/2019 29.89566
SIROLIMUS 1 MG TABLET ORAL 09/19/2018 10.01535
SIROLIMUS 2 MG TABLET ORAL 03/15/2016 17.01966
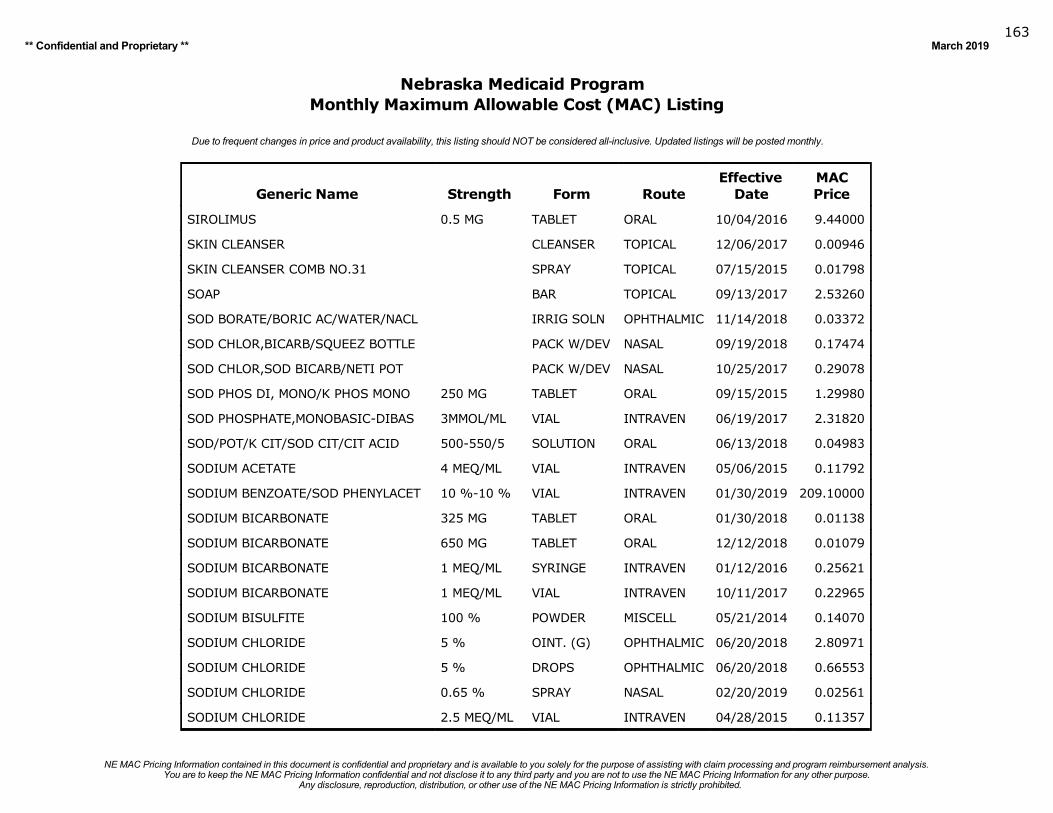
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019163
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
SIROLIMUS 0.5 MG TABLET ORAL 10/04/2016 9.44000
SKIN CLEANSER CLEANSER TOPICAL 12/06/2017 0.00946
SKIN CLEANSER COMB NO.31 SPRAY TOPICAL 07/15/2015 0.01798
SOAP BAR TOPICAL 09/13/2017 2.53260
SOD BORATE/BORIC AC/WATER/NACL IRRIG SOLN OPHTHALMIC 11/14/2018 0.03372
SOD CHLOR,BICARB/SQUEEZ BOTTLE PACK W/DEV NASAL 09/19/2018 0.17474
SOD CHLOR,SOD BICARB/NETI POT PACK W/DEV NASAL 10/25/2017 0.29078
SOD PHOS DI, MONO/K PHOS MONO 250 MG TABLET ORAL 09/15/2015 1.29980
SOD PHOSPHATE,MONOBASIC-DIBAS 3MMOL/ML VIAL INTRAVEN 06/19/2017 2.31820
SOD/POT/K CIT/SOD CIT/CIT ACID 500-550/5 SOLUTION ORAL 06/13/2018 0.04983
SODIUM ACETATE 4 MEQ/ML VIAL INTRAVEN 05/06/2015 0.11792
SODIUM BENZOATE/SOD PHENYLACET 10 %-10 % VIAL INTRAVEN 01/30/2019 209.10000
SODIUM BICARBONATE 325 MG TABLET ORAL 01/30/2018 0.01138
SODIUM BICARBONATE 650 MG TABLET ORAL 12/12/2018 0.01079
SODIUM BICARBONATE 1 MEQ/ML SYRINGE INTRAVEN 01/12/2016 0.25621
SODIUM BICARBONATE 1 MEQ/ML VIAL INTRAVEN 10/11/2017 0.22965
SODIUM BISULFITE 100 % POWDER MISCELL 05/21/2014 0.14070
SODIUM CHLORIDE 5 % OINT. (G) OPHTHALMIC 06/20/2018 2.80971
SODIUM CHLORIDE 5 % DROPS OPHTHALMIC 06/20/2018 0.66553
SODIUM CHLORIDE 0.65 % SPRAY NASAL 02/20/2019 0.02561
SODIUM CHLORIDE 2.5 MEQ/ML VIAL INTRAVEN 04/28/2015 0.11357
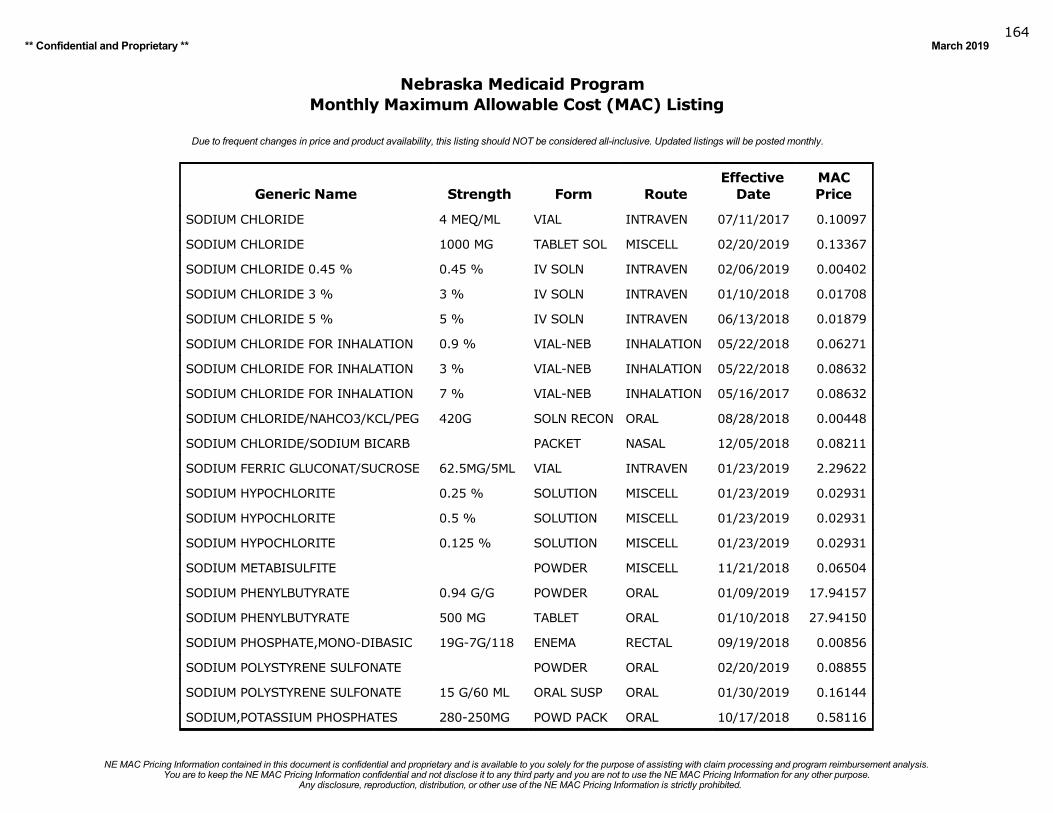
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019164
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
SODIUM CHLORIDE 4 MEQ/ML VIAL INTRAVEN 07/11/2017 0.10097
SODIUM CHLORIDE 1000 MG TABLET SOL MISCELL 02/20/2019 0.13367
SODIUM CHLORIDE 0.45 % 0.45 % IV SOLN INTRAVEN 02/06/2019 0.00402
SODIUM CHLORIDE 3 % 3 % IV SOLN INTRAVEN 01/10/2018 0.01708
SODIUM CHLORIDE 5 % 5 % IV SOLN INTRAVEN 06/13/2018 0.01879
SODIUM CHLORIDE FOR INHALATION 0.9 % VIAL-NEB INHALATION 05/22/2018 0.06271
SODIUM CHLORIDE FOR INHALATION 3 % VIAL-NEB INHALATION 05/22/2018 0.08632
SODIUM CHLORIDE FOR INHALATION 7 % VIAL-NEB INHALATION 05/16/2017 0.08632
SODIUM CHLORIDE/NAHCO3/KCL/PEG 420G SOLN RECON ORAL 08/28/2018 0.00448
SODIUM CHLORIDE/SODIUM BICARB PACKET NASAL 12/05/2018 0.08211
SODIUM FERRIC GLUCONAT/SUCROSE 62.5MG/5ML VIAL INTRAVEN 01/23/2019 2.29622
SODIUM HYPOCHLORITE 0.25 % SOLUTION MISCELL 01/23/2019 0.02931
SODIUM HYPOCHLORITE 0.5 % SOLUTION MISCELL 01/23/2019 0.02931
SODIUM HYPOCHLORITE 0.125 % SOLUTION MISCELL 01/23/2019 0.02931
SODIUM METABISULFITE POWDER MISCELL 11/21/2018 0.06504
SODIUM PHENYLBUTYRATE 0.94 G/G POWDER ORAL 01/09/2019 17.94157
SODIUM PHENYLBUTYRATE 500 MG TABLET ORAL 01/10/2018 27.94150
SODIUM PHOSPHATE,MONO-DIBASIC 19G-7G/118 ENEMA RECTAL 09/19/2018 0.00856
SODIUM POLYSTYRENE SULFONATE POWDER ORAL 02/20/2019 0.08855
SODIUM POLYSTYRENE SULFONATE 15 G/60 ML ORAL SUSP ORAL 01/30/2019 0.16144
SODIUM,POTASSIUM PHOSPHATES 280-250MG POWD PACK ORAL 10/17/2018 0.58116
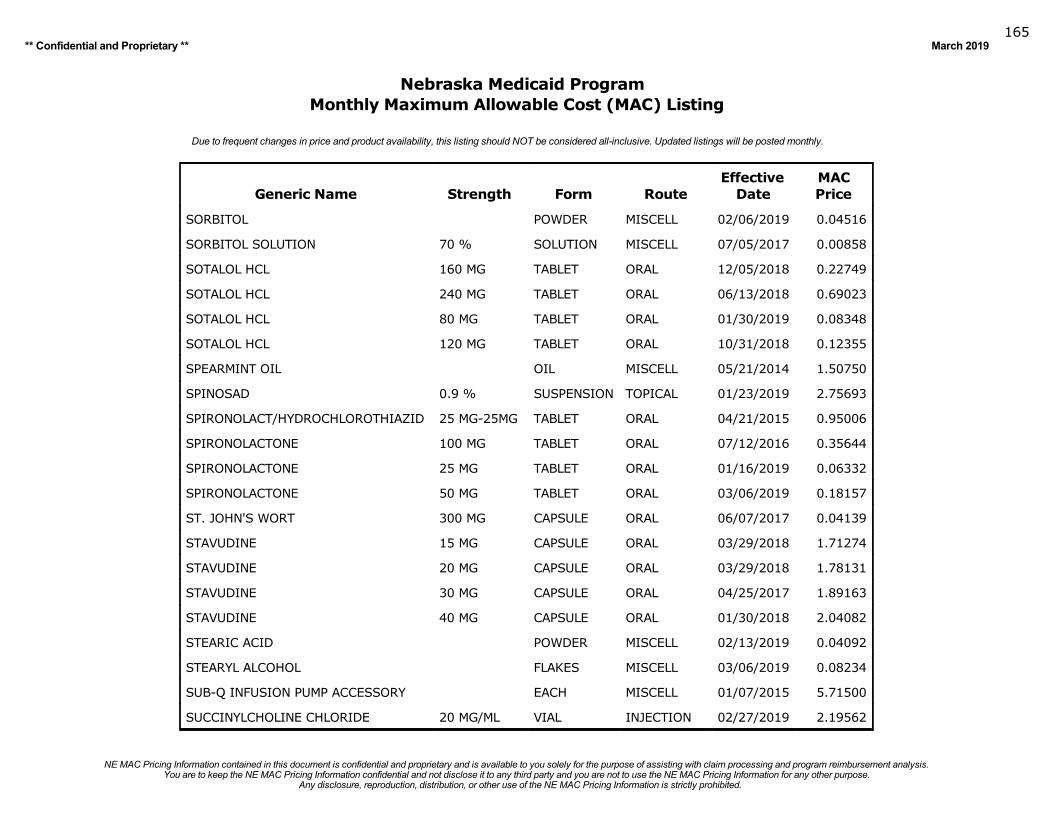
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019165
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
SORBITOL POWDER MISCELL 02/06/2019 0.04516
SORBITOL SOLUTION 70 % SOLUTION MISCELL 07/05/2017 0.00858
SOTALOL HCL 160 MG TABLET ORAL 12/05/2018 0.22749
SOTALOL HCL 240 MG TABLET ORAL 06/13/2018 0.69023
SOTALOL HCL 80 MG TABLET ORAL 01/30/2019 0.08348
SOTALOL HCL 120 MG TABLET ORAL 10/31/2018 0.12355
SPEARMINT OIL OIL MISCELL 05/21/2014 1.50750
SPINOSAD 0.9 % SUSPENSION TOPICAL 01/23/2019 2.75693
SPIRONOLACT/HYDROCHLOROTHIAZID 25 MG-25MG TABLET ORAL 04/21/2015 0.95006
SPIRONOLACTONE 100 MG TABLET ORAL 07/12/2016 0.35644
SPIRONOLACTONE 25 MG TABLET ORAL 01/16/2019 0.06332
SPIRONOLACTONE 50 MG TABLET ORAL 03/06/2019 0.18157
ST. JOHN'S WORT 300 MG CAPSULE ORAL 06/07/2017 0.04139
STAVUDINE 15 MG CAPSULE ORAL 03/29/2018 1.71274
STAVUDINE 20 MG CAPSULE ORAL 03/29/2018 1.78131
STAVUDINE 30 MG CAPSULE ORAL 04/25/2017 1.89163
STAVUDINE 40 MG CAPSULE ORAL 01/30/2018 2.04082
STEARIC ACID POWDER MISCELL 02/13/2019 0.04092
STEARYL ALCOHOL FLAKES MISCELL 03/06/2019 0.08234
SUB-Q INFUSION PUMP ACCESSORY EACH MISCELL 01/07/2015 5.71500
SUCCINYLCHOLINE CHLORIDE 20 MG/ML VIAL INJECTION 02/27/2019 2.19562
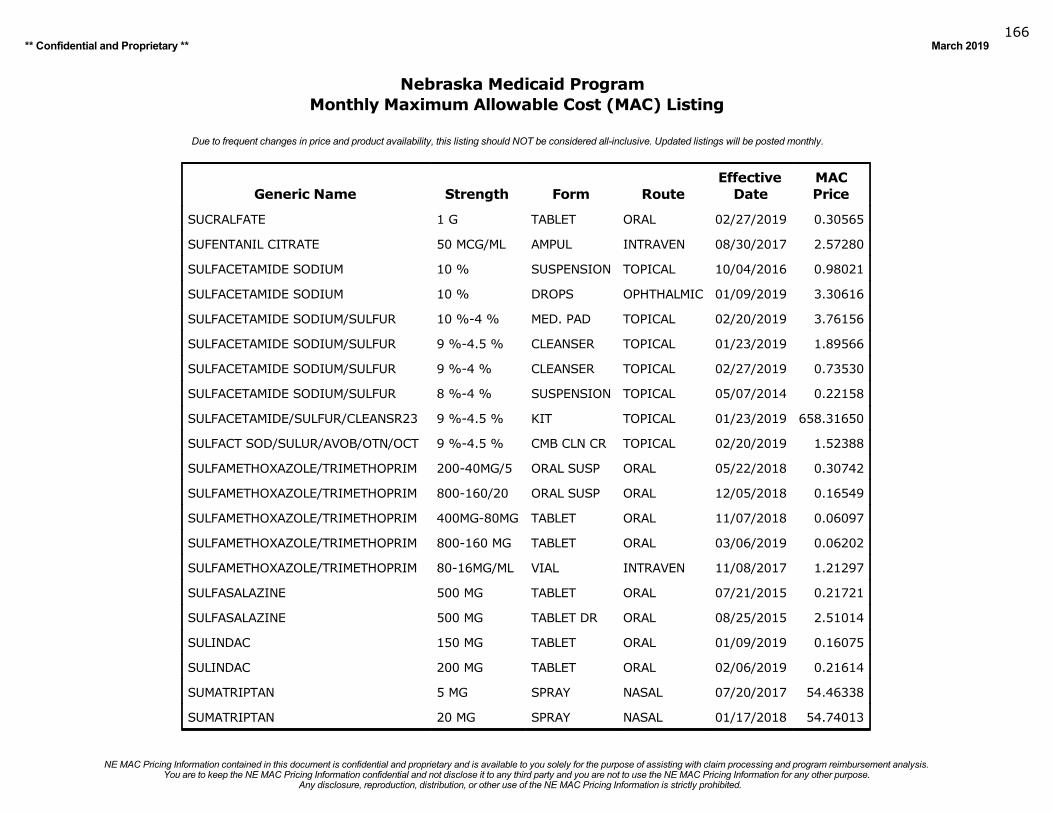
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019166
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
SUCRALFATE 1 G TABLET ORAL 02/27/2019 0.30565
SUFENTANIL CITRATE 50 MCG/ML AMPUL INTRAVEN 08/30/2017 2.57280
SULFACETAMIDE SODIUM 10 % SUSPENSION TOPICAL 10/04/2016 0.98021
SULFACETAMIDE SODIUM 10 % DROPS OPHTHALMIC 01/09/2019 3.30616
SULFACETAMIDE SODIUM/SULFUR 10 %-4 % MED. PAD TOPICAL 02/20/2019 3.76156
SULFACETAMIDE SODIUM/SULFUR 9 %-4.5 % CLEANSER TOPICAL 01/23/2019 1.89566
SULFACETAMIDE SODIUM/SULFUR 9 %-4 % CLEANSER TOPICAL 02/27/2019 0.73530
SULFACETAMIDE SODIUM/SULFUR 8 %-4 % SUSPENSION TOPICAL 05/07/2014 0.22158
SULFACETAMIDE/SULFUR/CLEANSR23 9 %-4.5 % KIT TOPICAL 01/23/2019 658.31650
SULFACT SOD/SULUR/AVOB/OTN/OCT 9 %-4.5 % CMB CLN CR TOPICAL 02/20/2019 1.52388
SULFAMETHOXAZOLE/TRIMETHOPRIM 200-40MG/5 ORAL SUSP ORAL 05/22/2018 0.30742
SULFAMETHOXAZOLE/TRIMETHOPRIM 800-160/20 ORAL SUSP ORAL 12/05/2018 0.16549
SULFAMETHOXAZOLE/TRIMETHOPRIM 400MG-80MG TABLET ORAL 11/07/2018 0.06097
SULFAMETHOXAZOLE/TRIMETHOPRIM 800-160 MG TABLET ORAL 03/06/2019 0.06202
SULFAMETHOXAZOLE/TRIMETHOPRIM 80-16MG/ML VIAL INTRAVEN 11/08/2017 1.21297
SULFASALAZINE 500 MG TABLET ORAL 07/21/2015 0.21721
SULFASALAZINE 500 MG TABLET DR ORAL 08/25/2015 2.51014
SULINDAC 150 MG TABLET ORAL 01/09/2019 0.16075
SULINDAC 200 MG TABLET ORAL 02/06/2019 0.21614
SUMATRIPTAN 5 MG SPRAY NASAL 07/20/2017 54.46338
SUMATRIPTAN 20 MG SPRAY NASAL 01/17/2018 54.74013
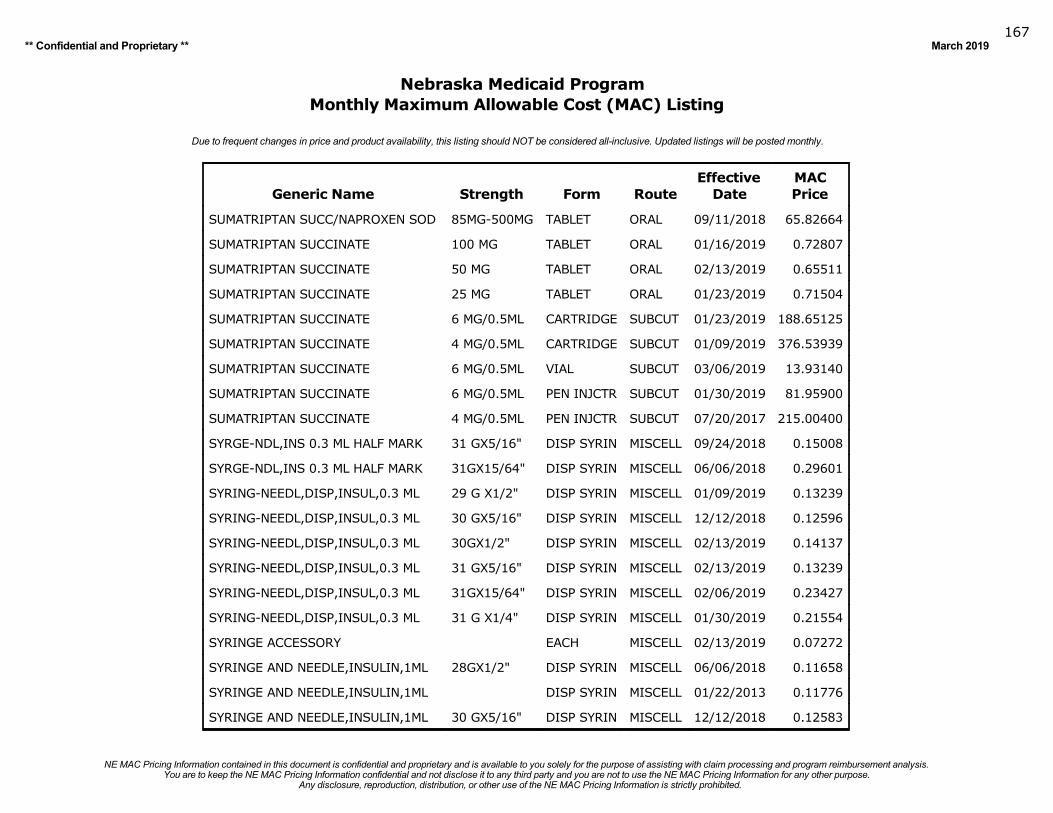
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019167
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
SUMATRIPTAN SUCC/NAPROXEN SOD 85MG-500MG TABLET ORAL 09/11/2018 65.82664
SUMATRIPTAN SUCCINATE 100 MG TABLET ORAL 01/16/2019 0.72807
SUMATRIPTAN SUCCINATE 50 MG TABLET ORAL 02/13/2019 0.65511
SUMATRIPTAN SUCCINATE 25 MG TABLET ORAL 01/23/2019 0.71504
SUMATRIPTAN SUCCINATE 6 MG/0.5ML CARTRIDGE SUBCUT 01/23/2019 188.65125
SUMATRIPTAN SUCCINATE 4 MG/0.5ML CARTRIDGE SUBCUT 01/09/2019 376.53939
SUMATRIPTAN SUCCINATE 6 MG/0.5ML VIAL SUBCUT 03/06/2019 13.93140
SUMATRIPTAN SUCCINATE 6 MG/0.5ML PEN INJCTR SUBCUT 01/30/2019 81.95900
SUMATRIPTAN SUCCINATE 4 MG/0.5ML PEN INJCTR SUBCUT 07/20/2017 215.00400
SYRGE-NDL,INS 0.3 ML HALF MARK 31 GX5/16" DISP SYRIN MISCELL 09/24/2018 0.15008
SYRGE-NDL,INS 0.3 ML HALF MARK 31GX15/64" DISP SYRIN MISCELL 06/06/2018 0.29601
SYRING-NEEDL,DISP,INSUL,0.3 ML 29 G X1/2" DISP SYRIN MISCELL 01/09/2019 0.13239
SYRING-NEEDL,DISP,INSUL,0.3 ML 30 GX5/16" DISP SYRIN MISCELL 12/12/2018 0.12596
SYRING-NEEDL,DISP,INSUL,0.3 ML 30GX1/2" DISP SYRIN MISCELL 02/13/2019 0.14137
SYRING-NEEDL,DISP,INSUL,0.3 ML 31 GX5/16" DISP SYRIN MISCELL 02/13/2019 0.13239
SYRING-NEEDL,DISP,INSUL,0.3 ML 31GX15/64" DISP SYRIN MISCELL 02/06/2019 0.23427
SYRING-NEEDL,DISP,INSUL,0.3 ML 31 G X1/4" DISP SYRIN MISCELL 01/30/2019 0.21554
SYRINGE ACCESSORY EACH MISCELL 02/13/2019 0.07272
SYRINGE AND NEEDLE,INSULIN,1ML 28GX1/2" DISP SYRIN MISCELL 06/06/2018 0.11658
SYRINGE AND NEEDLE,INSULIN,1ML DISP SYRIN MISCELL 01/22/2013 0.11776
SYRINGE AND NEEDLE,INSULIN,1ML 30 GX5/16" DISP SYRIN MISCELL 12/12/2018 0.12583
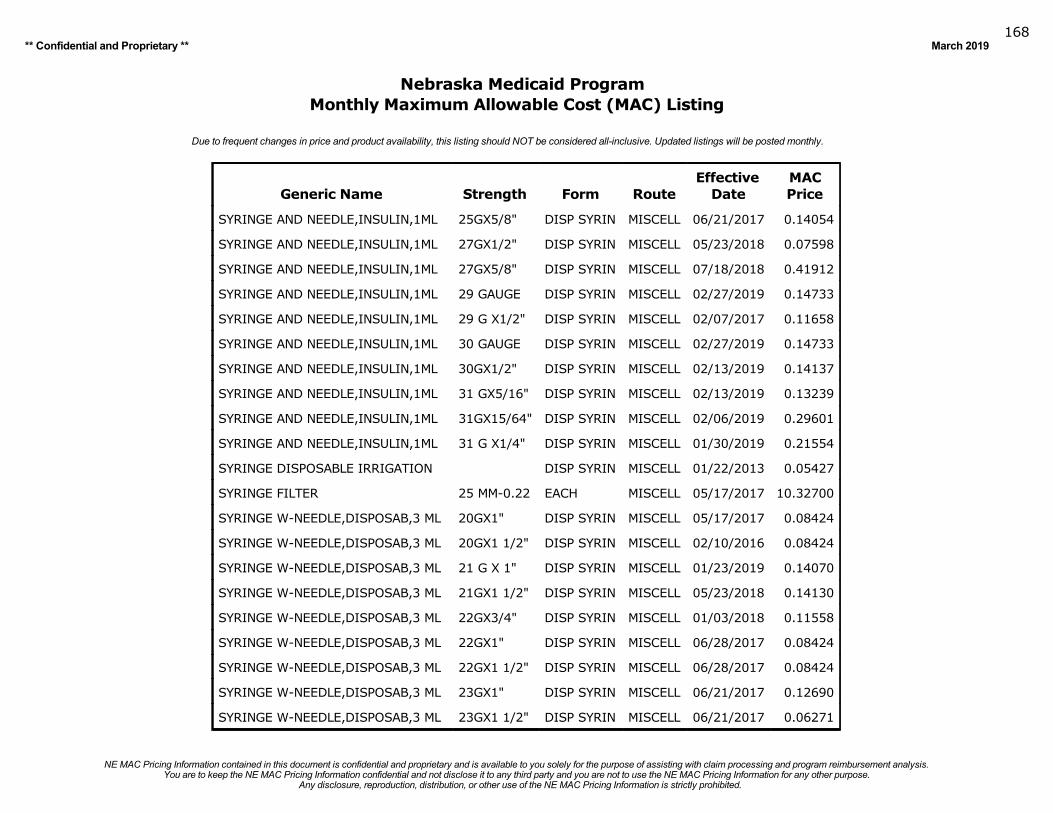
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019168
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
SYRINGE AND NEEDLE,INSULIN,1ML 25GX5/8" DISP SYRIN MISCELL 06/21/2017 0.14054
SYRINGE AND NEEDLE,INSULIN,1ML 27GX1/2" DISP SYRIN MISCELL 05/23/2018 0.07598
SYRINGE AND NEEDLE,INSULIN,1ML 27GX5/8" DISP SYRIN MISCELL 07/18/2018 0.41912
SYRINGE AND NEEDLE,INSULIN,1ML 29 GAUGE DISP SYRIN MISCELL 02/27/2019 0.14733
SYRINGE AND NEEDLE,INSULIN,1ML 29 G X1/2" DISP SYRIN MISCELL 02/07/2017 0.11658
SYRINGE AND NEEDLE,INSULIN,1ML 30 GAUGE DISP SYRIN MISCELL 02/27/2019 0.14733
SYRINGE AND NEEDLE,INSULIN,1ML 30GX1/2" DISP SYRIN MISCELL 02/13/2019 0.14137
SYRINGE AND NEEDLE,INSULIN,1ML 31 GX5/16" DISP SYRIN MISCELL 02/13/2019 0.13239
SYRINGE AND NEEDLE,INSULIN,1ML 31GX15/64" DISP SYRIN MISCELL 02/06/2019 0.29601
SYRINGE AND NEEDLE,INSULIN,1ML 31 G X1/4" DISP SYRIN MISCELL 01/30/2019 0.21554
SYRINGE DISPOSABLE IRRIGATION DISP SYRIN MISCELL 01/22/2013 0.05427
SYRINGE FILTER 25 MM-0.22 EACH MISCELL 05/17/2017 10.32700
SYRINGE W-NEEDLE,DISPOSAB,3 ML 20GX1" DISP SYRIN MISCELL 05/17/2017 0.08424
SYRINGE W-NEEDLE,DISPOSAB,3 ML 20GX1 1/2" DISP SYRIN MISCELL 02/10/2016 0.08424
SYRINGE W-NEEDLE,DISPOSAB,3 ML 21 G X 1" DISP SYRIN MISCELL 01/23/2019 0.14070
SYRINGE W-NEEDLE,DISPOSAB,3 ML 21GX1 1/2" DISP SYRIN MISCELL 05/23/2018 0.14130
SYRINGE W-NEEDLE,DISPOSAB,3 ML 22GX3/4" DISP SYRIN MISCELL 01/03/2018 0.11558
SYRINGE W-NEEDLE,DISPOSAB,3 ML 22GX1" DISP SYRIN MISCELL 06/28/2017 0.08424
SYRINGE W-NEEDLE,DISPOSAB,3 ML 22GX1 1/2" DISP SYRIN MISCELL 06/28/2017 0.08424
SYRINGE W-NEEDLE,DISPOSAB,3 ML 23GX1" DISP SYRIN MISCELL 06/21/2017 0.12690
SYRINGE W-NEEDLE,DISPOSAB,3 ML 23GX1 1/2" DISP SYRIN MISCELL 06/21/2017 0.06271
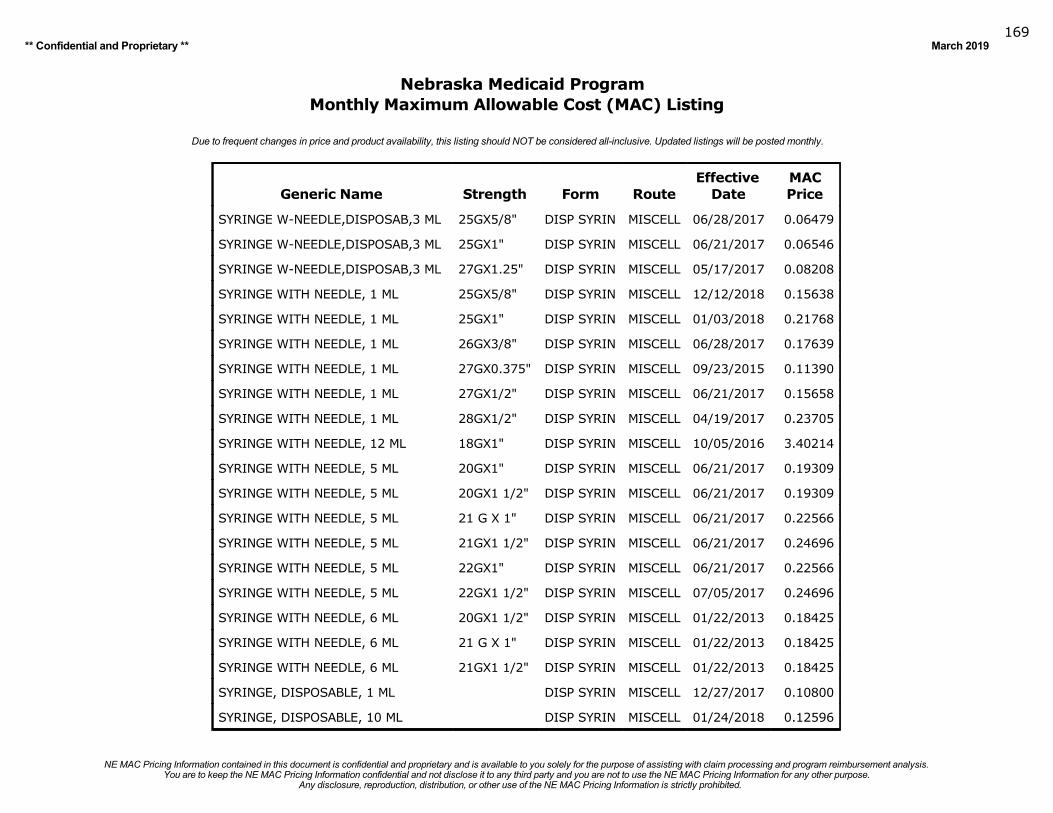
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019169
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
SYRINGE W-NEEDLE,DISPOSAB,3 ML 25GX5/8" DISP SYRIN MISCELL 06/28/2017 0.06479
SYRINGE W-NEEDLE,DISPOSAB,3 ML 25GX1" DISP SYRIN MISCELL 06/21/2017 0.06546
SYRINGE W-NEEDLE,DISPOSAB,3 ML 27GX1.25" DISP SYRIN MISCELL 05/17/2017 0.08208
SYRINGE WITH NEEDLE, 1 ML 25GX5/8" DISP SYRIN MISCELL 12/12/2018 0.15638
SYRINGE WITH NEEDLE, 1 ML 25GX1" DISP SYRIN MISCELL 01/03/2018 0.21768
SYRINGE WITH NEEDLE, 1 ML 26GX3/8" DISP SYRIN MISCELL 06/28/2017 0.17639
SYRINGE WITH NEEDLE, 1 ML 27GX0.375" DISP SYRIN MISCELL 09/23/2015 0.11390
SYRINGE WITH NEEDLE, 1 ML 27GX1/2" DISP SYRIN MISCELL 06/21/2017 0.15658
SYRINGE WITH NEEDLE, 1 ML 28GX1/2" DISP SYRIN MISCELL 04/19/2017 0.23705
SYRINGE WITH NEEDLE, 12 ML 18GX1" DISP SYRIN MISCELL 10/05/2016 3.40214
SYRINGE WITH NEEDLE, 5 ML 20GX1" DISP SYRIN MISCELL 06/21/2017 0.19309
SYRINGE WITH NEEDLE, 5 ML 20GX1 1/2" DISP SYRIN MISCELL 06/21/2017 0.19309
SYRINGE WITH NEEDLE, 5 ML 21 G X 1" DISP SYRIN MISCELL 06/21/2017 0.22566
SYRINGE WITH NEEDLE, 5 ML 21GX1 1/2" DISP SYRIN MISCELL 06/21/2017 0.24696
SYRINGE WITH NEEDLE, 5 ML 22GX1" DISP SYRIN MISCELL 06/21/2017 0.22566
SYRINGE WITH NEEDLE, 5 ML 22GX1 1/2" DISP SYRIN MISCELL 07/05/2017 0.24696
SYRINGE WITH NEEDLE, 6 ML 20GX1 1/2" DISP SYRIN MISCELL 01/22/2013 0.18425
SYRINGE WITH NEEDLE, 6 ML 21 G X 1" DISP SYRIN MISCELL 01/22/2013 0.18425
SYRINGE WITH NEEDLE, 6 ML 21GX1 1/2" DISP SYRIN MISCELL 01/22/2013 0.18425
SYRINGE, DISPOSABLE, 1 ML DISP SYRIN MISCELL 12/27/2017 0.10800
SYRINGE, DISPOSABLE, 10 ML DISP SYRIN MISCELL 01/24/2018 0.12596
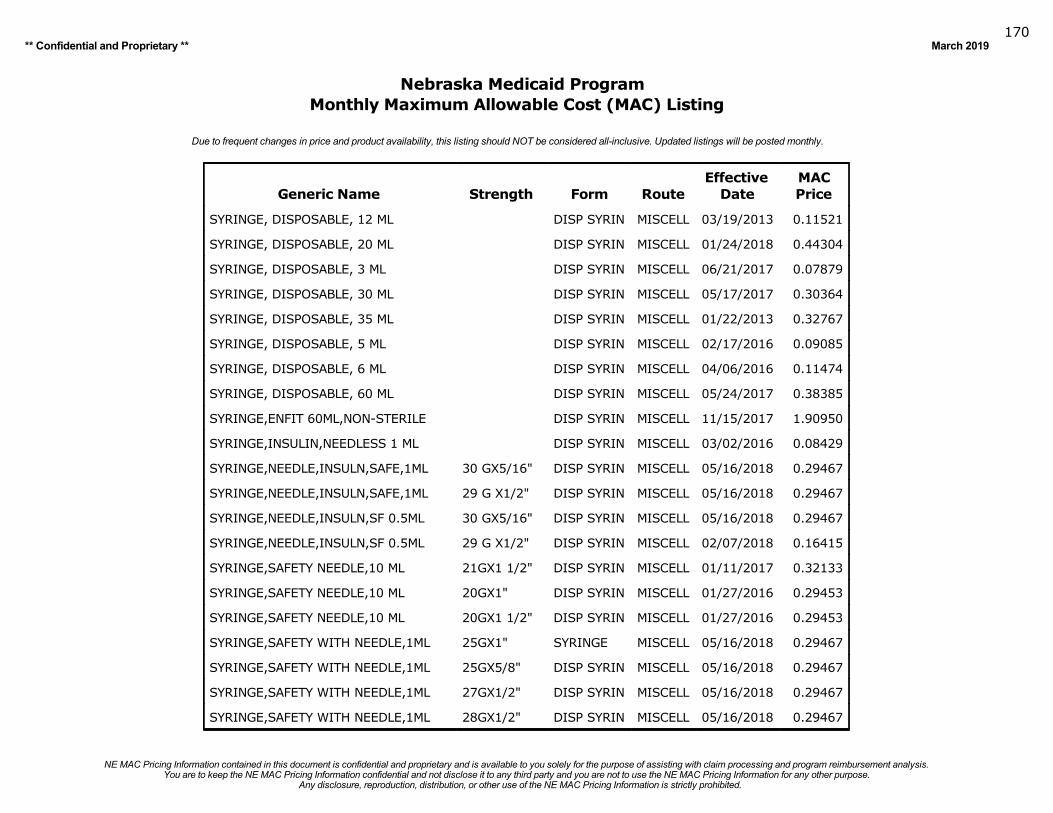
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019170
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
SYRINGE, DISPOSABLE, 12 ML DISP SYRIN MISCELL 03/19/2013 0.11521
SYRINGE, DISPOSABLE, 20 ML DISP SYRIN MISCELL 01/24/2018 0.44304
SYRINGE, DISPOSABLE, 3 ML DISP SYRIN MISCELL 06/21/2017 0.07879
SYRINGE, DISPOSABLE, 30 ML DISP SYRIN MISCELL 05/17/2017 0.30364
SYRINGE, DISPOSABLE, 35 ML DISP SYRIN MISCELL 01/22/2013 0.32767
SYRINGE, DISPOSABLE, 5 ML DISP SYRIN MISCELL 02/17/2016 0.09085
SYRINGE, DISPOSABLE, 6 ML DISP SYRIN MISCELL 04/06/2016 0.11474
SYRINGE, DISPOSABLE, 60 ML DISP SYRIN MISCELL 05/24/2017 0.38385
SYRINGE,ENFIT 60ML,NON-STERILE DISP SYRIN MISCELL 11/15/2017 1.90950
SYRINGE,INSULIN,NEEDLESS 1 ML DISP SYRIN MISCELL 03/02/2016 0.08429
SYRINGE,NEEDLE,INSULN,SAFE,1ML 30 GX5/16" DISP SYRIN MISCELL 05/16/2018 0.29467
SYRINGE,NEEDLE,INSULN,SAFE,1ML 29 G X1/2" DISP SYRIN MISCELL 05/16/2018 0.29467
SYRINGE,NEEDLE,INSULN,SF 0.5ML 30 GX5/16" DISP SYRIN MISCELL 05/16/2018 0.29467
SYRINGE,NEEDLE,INSULN,SF 0.5ML 29 G X1/2" DISP SYRIN MISCELL 02/07/2018 0.16415
SYRINGE,SAFETY NEEDLE,10 ML 21GX1 1/2" DISP SYRIN MISCELL 01/11/2017 0.32133
SYRINGE,SAFETY NEEDLE,10 ML 20GX1" DISP SYRIN MISCELL 01/27/2016 0.29453
SYRINGE,SAFETY NEEDLE,10 ML 20GX1 1/2" DISP SYRIN MISCELL 01/27/2016 0.29453
SYRINGE,SAFETY WITH NEEDLE,1ML 25GX1" SYRINGE MISCELL 05/16/2018 0.29467
SYRINGE,SAFETY WITH NEEDLE,1ML 25GX5/8" DISP SYRIN MISCELL 05/16/2018 0.29467
SYRINGE,SAFETY WITH NEEDLE,1ML 27GX1/2" DISP SYRIN MISCELL 05/16/2018 0.29467
SYRINGE,SAFETY WITH NEEDLE,1ML 28GX1/2" DISP SYRIN MISCELL 05/16/2018 0.29467
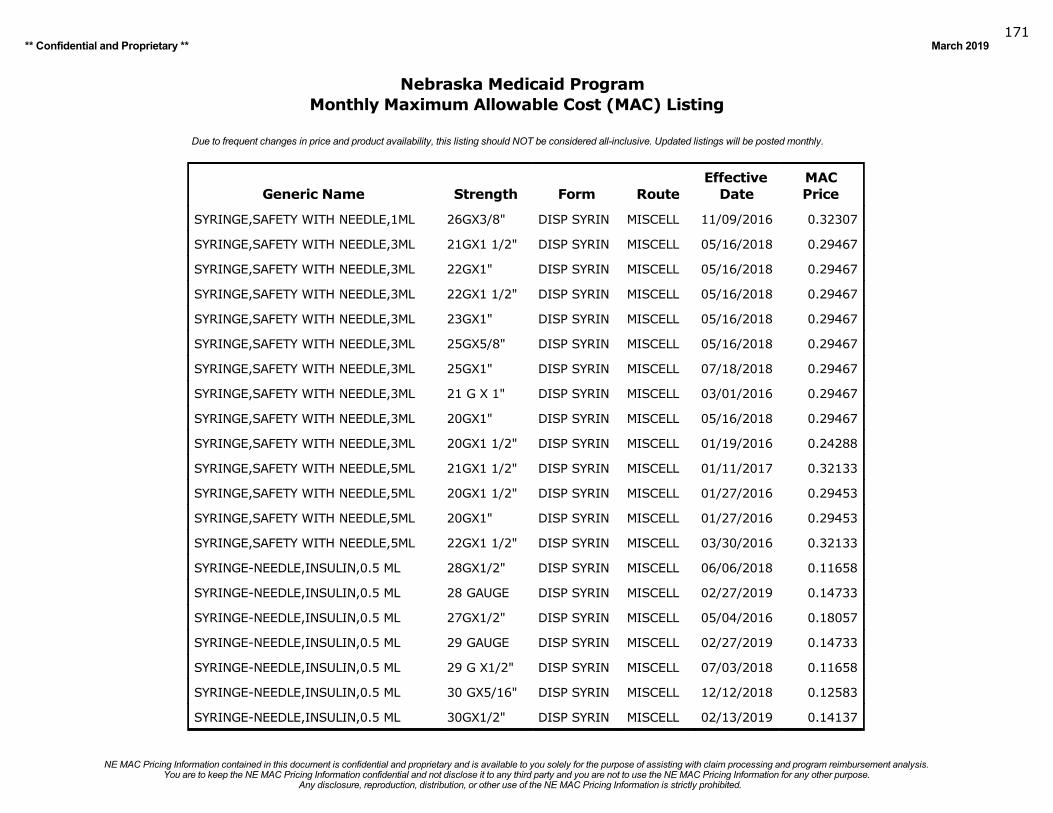
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019171
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
SYRINGE,SAFETY WITH NEEDLE,1ML 26GX3/8" DISP SYRIN MISCELL 11/09/2016 0.32307
SYRINGE,SAFETY WITH NEEDLE,3ML 21GX1 1/2" DISP SYRIN MISCELL 05/16/2018 0.29467
SYRINGE,SAFETY WITH NEEDLE,3ML 22GX1" DISP SYRIN MISCELL 05/16/2018 0.29467
SYRINGE,SAFETY WITH NEEDLE,3ML 22GX1 1/2" DISP SYRIN MISCELL 05/16/2018 0.29467
SYRINGE,SAFETY WITH NEEDLE,3ML 23GX1" DISP SYRIN MISCELL 05/16/2018 0.29467
SYRINGE,SAFETY WITH NEEDLE,3ML 25GX5/8" DISP SYRIN MISCELL 05/16/2018 0.29467
SYRINGE,SAFETY WITH NEEDLE,3ML 25GX1" DISP SYRIN MISCELL 07/18/2018 0.29467
SYRINGE,SAFETY WITH NEEDLE,3ML 21 G X 1" DISP SYRIN MISCELL 03/01/2016 0.29467
SYRINGE,SAFETY WITH NEEDLE,3ML 20GX1" DISP SYRIN MISCELL 05/16/2018 0.29467
SYRINGE,SAFETY WITH NEEDLE,3ML 20GX1 1/2" DISP SYRIN MISCELL 01/19/2016 0.24288
SYRINGE,SAFETY WITH NEEDLE,5ML 21GX1 1/2" DISP SYRIN MISCELL 01/11/2017 0.32133
SYRINGE,SAFETY WITH NEEDLE,5ML 20GX1 1/2" DISP SYRIN MISCELL 01/27/2016 0.29453
SYRINGE,SAFETY WITH NEEDLE,5ML 20GX1" DISP SYRIN MISCELL 01/27/2016 0.29453
SYRINGE,SAFETY WITH NEEDLE,5ML 22GX1 1/2" DISP SYRIN MISCELL 03/30/2016 0.32133
SYRINGE-NEEDLE,INSULIN,0.5 ML 28GX1/2" DISP SYRIN MISCELL 06/06/2018 0.11658
SYRINGE-NEEDLE,INSULIN,0.5 ML 28 GAUGE DISP SYRIN MISCELL 02/27/2019 0.14733
SYRINGE-NEEDLE,INSULIN,0.5 ML 27GX1/2" DISP SYRIN MISCELL 05/04/2016 0.18057
SYRINGE-NEEDLE,INSULIN,0.5 ML 29 GAUGE DISP SYRIN MISCELL 02/27/2019 0.14733
SYRINGE-NEEDLE,INSULIN,0.5 ML 29 G X1/2" DISP SYRIN MISCELL 07/03/2018 0.11658
SYRINGE-NEEDLE,INSULIN,0.5 ML 30 GX5/16" DISP SYRIN MISCELL 12/12/2018 0.12583
SYRINGE-NEEDLE,INSULIN,0.5 ML 30GX1/2" DISP SYRIN MISCELL 02/13/2019 0.14137
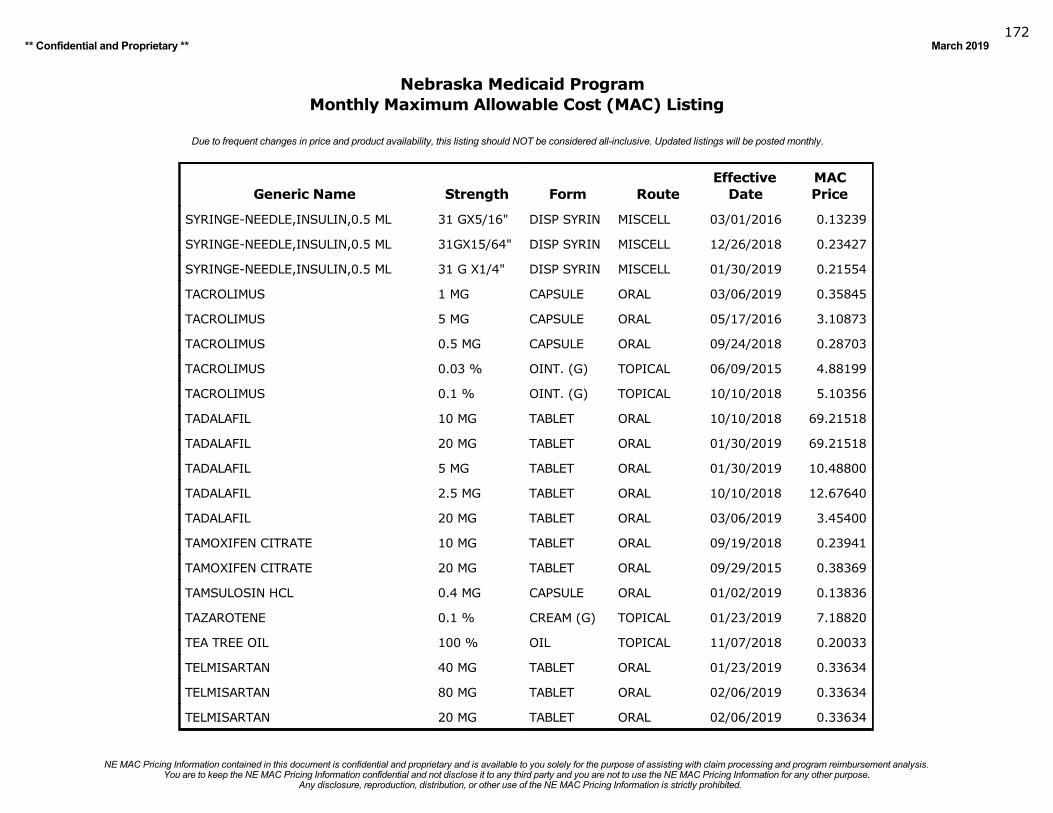
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019172
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
SYRINGE-NEEDLE,INSULIN,0.5 ML 31 GX5/16" DISP SYRIN MISCELL 03/01/2016 0.13239
SYRINGE-NEEDLE,INSULIN,0.5 ML 31GX15/64" DISP SYRIN MISCELL 12/26/2018 0.23427
SYRINGE-NEEDLE,INSULIN,0.5 ML 31 G X1/4" DISP SYRIN MISCELL 01/30/2019 0.21554
TACROLIMUS 1 MG CAPSULE ORAL 03/06/2019 0.35845
TACROLIMUS 5 MG CAPSULE ORAL 05/17/2016 3.10873
TACROLIMUS 0.5 MG CAPSULE ORAL 09/24/2018 0.28703
TACROLIMUS 0.03 % OINT. (G) TOPICAL 06/09/2015 4.88199
TACROLIMUS 0.1 % OINT. (G) TOPICAL 10/10/2018 5.10356
TADALAFIL 10 MG TABLET ORAL 10/10/2018 69.21518
TADALAFIL 20 MG TABLET ORAL 01/30/2019 69.21518
TADALAFIL 5 MG TABLET ORAL 01/30/2019 10.48800
TADALAFIL 2.5 MG TABLET ORAL 10/10/2018 12.67640
TADALAFIL 20 MG TABLET ORAL 03/06/2019 3.45400
TAMOXIFEN CITRATE 10 MG TABLET ORAL 09/19/2018 0.23941
TAMOXIFEN CITRATE 20 MG TABLET ORAL 09/29/2015 0.38369
TAMSULOSIN HCL 0.4 MG CAPSULE ORAL 01/02/2019 0.13836
TAZAROTENE 0.1 % CREAM (G) TOPICAL 01/23/2019 7.18820
TEA TREE OIL 100 % OIL TOPICAL 11/07/2018 0.20033
TELMISARTAN 40 MG TABLET ORAL 01/23/2019 0.33634
TELMISARTAN 80 MG TABLET ORAL 02/06/2019 0.33634
TELMISARTAN 20 MG TABLET ORAL 02/06/2019 0.33634
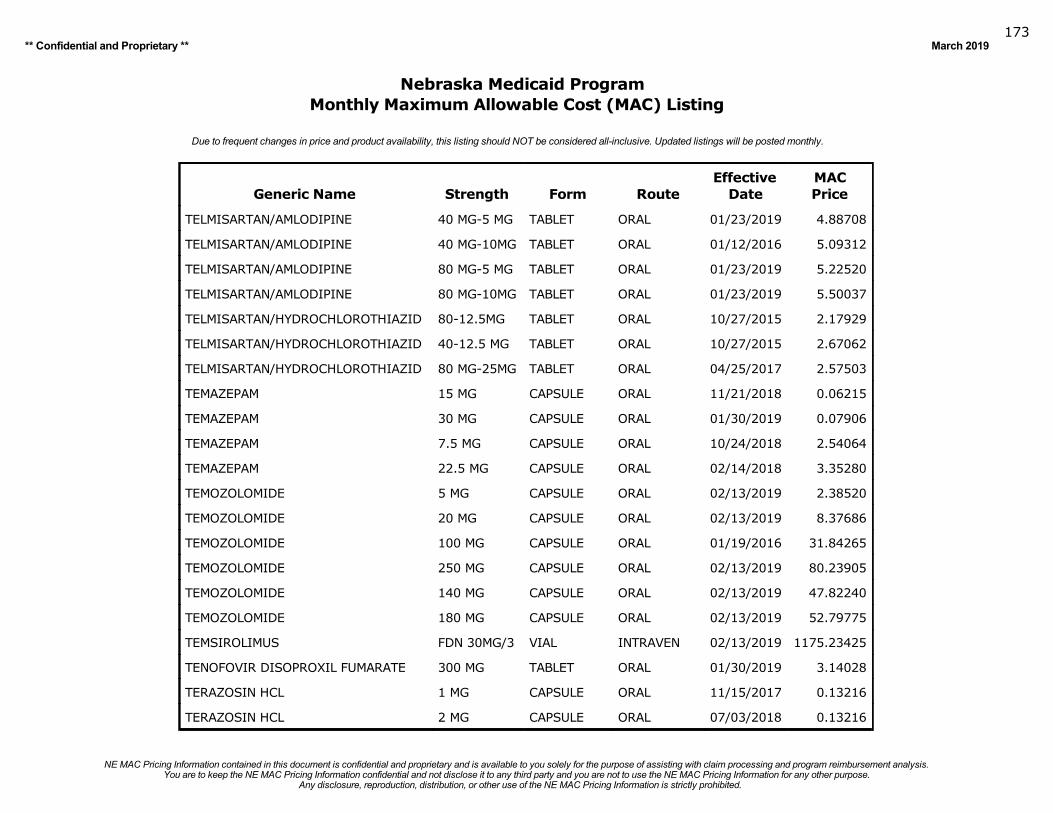
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019173
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
TELMISARTAN/AMLODIPINE 40 MG-5 MG TABLET ORAL 01/23/2019 4.88708
TELMISARTAN/AMLODIPINE 40 MG-10MG TABLET ORAL 01/12/2016 5.09312
TELMISARTAN/AMLODIPINE 80 MG-5 MG TABLET ORAL 01/23/2019 5.22520
TELMISARTAN/AMLODIPINE 80 MG-10MG TABLET ORAL 01/23/2019 5.50037
TELMISARTAN/HYDROCHLOROTHIAZID 80-12.5MG TABLET ORAL 10/27/2015 2.17929
TELMISARTAN/HYDROCHLOROTHIAZID 40-12.5 MG TABLET ORAL 10/27/2015 2.67062
TELMISARTAN/HYDROCHLOROTHIAZID 80 MG-25MG TABLET ORAL 04/25/2017 2.57503
TEMAZEPAM 15 MG CAPSULE ORAL 11/21/2018 0.06215
TEMAZEPAM 30 MG CAPSULE ORAL 01/30/2019 0.07906
TEMAZEPAM 7.5 MG CAPSULE ORAL 10/24/2018 2.54064
TEMAZEPAM 22.5 MG CAPSULE ORAL 02/14/2018 3.35280
TEMOZOLOMIDE 5 MG CAPSULE ORAL 02/13/2019 2.38520
TEMOZOLOMIDE 20 MG CAPSULE ORAL 02/13/2019 8.37686
TEMOZOLOMIDE 100 MG CAPSULE ORAL 01/19/2016 31.84265
TEMOZOLOMIDE 250 MG CAPSULE ORAL 02/13/2019 80.23905
TEMOZOLOMIDE 140 MG CAPSULE ORAL 02/13/2019 47.82240
TEMOZOLOMIDE 180 MG CAPSULE ORAL 02/13/2019 52.79775
TEMSIROLIMUS FDN 30MG/3 VIAL INTRAVEN 02/13/2019 1175.23425
TENOFOVIR DISOPROXIL FUMARATE 300 MG TABLET ORAL 01/30/2019 3.14028
TERAZOSIN HCL 1 MG CAPSULE ORAL 11/15/2017 0.13216
TERAZOSIN HCL 2 MG CAPSULE ORAL 07/03/2018 0.13216
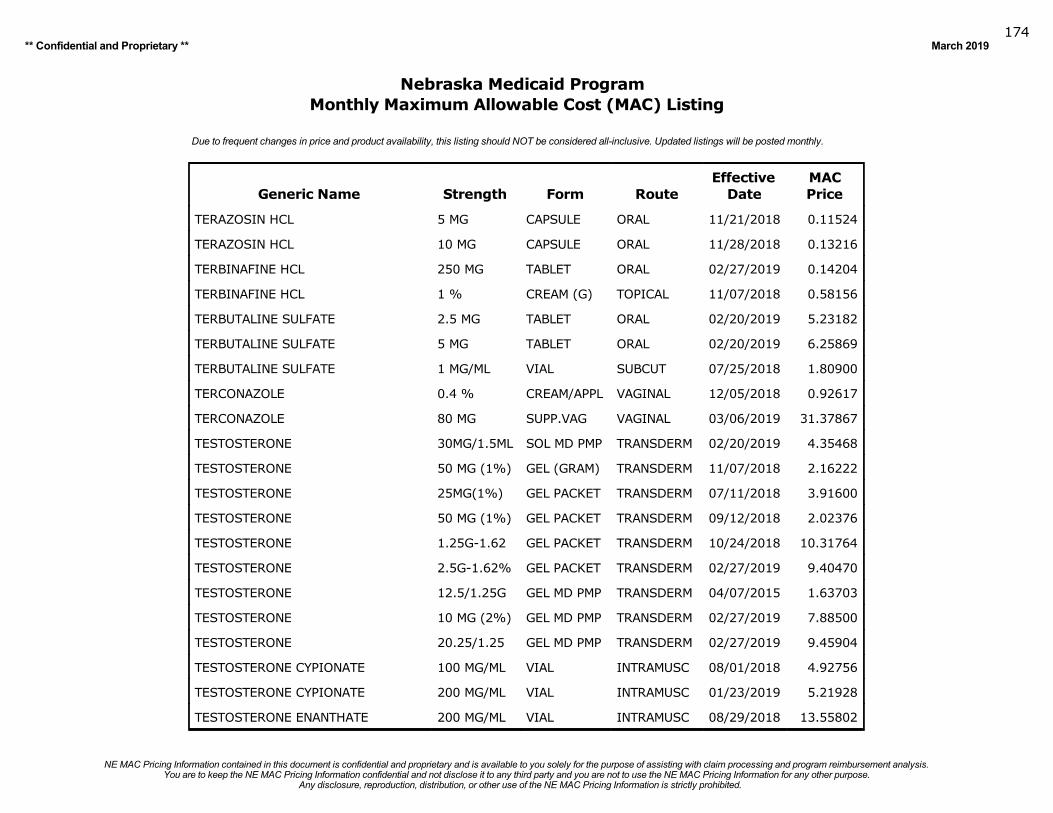
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019174
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
TERAZOSIN HCL 5 MG CAPSULE ORAL 11/21/2018 0.11524
TERAZOSIN HCL 10 MG CAPSULE ORAL 11/28/2018 0.13216
TERBINAFINE HCL 250 MG TABLET ORAL 02/27/2019 0.14204
TERBINAFINE HCL 1 % CREAM (G) TOPICAL 11/07/2018 0.58156
TERBUTALINE SULFATE 2.5 MG TABLET ORAL 02/20/2019 5.23182
TERBUTALINE SULFATE 5 MG TABLET ORAL 02/20/2019 6.25869
TERBUTALINE SULFATE 1 MG/ML VIAL SUBCUT 07/25/2018 1.80900
TERCONAZOLE 0.4 % CREAM/APPL VAGINAL 12/05/2018 0.92617
TERCONAZOLE 80 MG SUPP.VAG VAGINAL 03/06/2019 31.37867
TESTOSTERONE 30MG/1.5ML SOL MD PMP TRANSDERM 02/20/2019 4.35468
TESTOSTERONE 50 MG (1%) GEL (GRAM) TRANSDERM 11/07/2018 2.16222
TESTOSTERONE 25MG(1%) GEL PACKET TRANSDERM 07/11/2018 3.91600
TESTOSTERONE 50 MG (1%) GEL PACKET TRANSDERM 09/12/2018 2.02376
TESTOSTERONE 1.25G-1.62 GEL PACKET TRANSDERM 10/24/2018 10.31764
TESTOSTERONE 2.5G-1.62% GEL PACKET TRANSDERM 02/27/2019 9.40470
TESTOSTERONE 12.5/1.25G GEL MD PMP TRANSDERM 04/07/2015 1.63703
TESTOSTERONE 10 MG (2%) GEL MD PMP TRANSDERM 02/27/2019 7.88500
TESTOSTERONE 20.25/1.25 GEL MD PMP TRANSDERM 02/27/2019 9.45904
TESTOSTERONE CYPIONATE 100 MG/ML VIAL INTRAMUSC 08/01/2018 4.92756
TESTOSTERONE CYPIONATE 200 MG/ML VIAL INTRAMUSC 01/23/2019 5.21928
TESTOSTERONE ENANTHATE 200 MG/ML VIAL INTRAMUSC 08/29/2018 13.55802
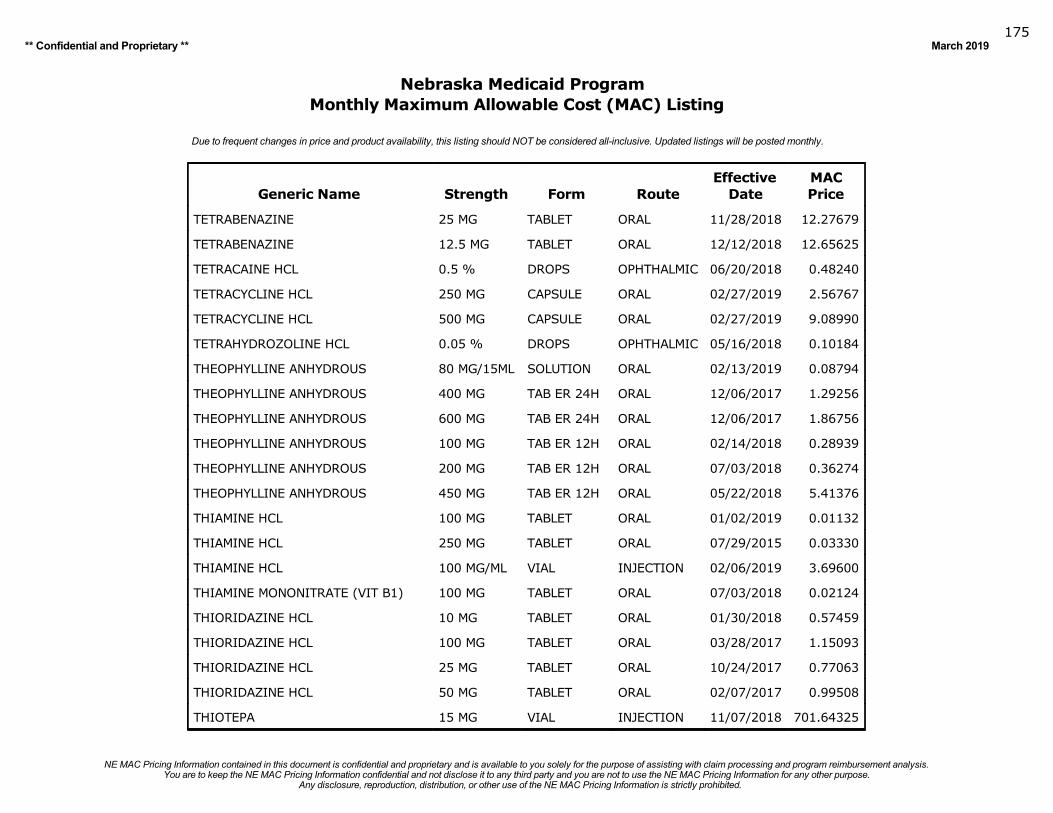
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019175
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
TETRABENAZINE 25 MG TABLET ORAL 11/28/2018 12.27679
TETRABENAZINE 12.5 MG TABLET ORAL 12/12/2018 12.65625
TETRACAINE HCL 0.5 % DROPS OPHTHALMIC 06/20/2018 0.48240
TETRACYCLINE HCL 250 MG CAPSULE ORAL 02/27/2019 2.56767
TETRACYCLINE HCL 500 MG CAPSULE ORAL 02/27/2019 9.08990
TETRAHYDROZOLINE HCL 0.05 % DROPS OPHTHALMIC 05/16/2018 0.10184
THEOPHYLLINE ANHYDROUS 80 MG/15ML SOLUTION ORAL 02/13/2019 0.08794
THEOPHYLLINE ANHYDROUS 400 MG TAB ER 24H ORAL 12/06/2017 1.29256
THEOPHYLLINE ANHYDROUS 600 MG TAB ER 24H ORAL 12/06/2017 1.86756
THEOPHYLLINE ANHYDROUS 100 MG TAB ER 12H ORAL 02/14/2018 0.28939
THEOPHYLLINE ANHYDROUS 200 MG TAB ER 12H ORAL 07/03/2018 0.36274
THEOPHYLLINE ANHYDROUS 450 MG TAB ER 12H ORAL 05/22/2018 5.41376
THIAMINE HCL 100 MG TABLET ORAL 01/02/2019 0.01132
THIAMINE HCL 250 MG TABLET ORAL 07/29/2015 0.03330
THIAMINE HCL 100 MG/ML VIAL INJECTION 02/06/2019 3.69600
THIAMINE MONONITRATE (VIT B1) 100 MG TABLET ORAL 07/03/2018 0.02124
THIORIDAZINE HCL 10 MG TABLET ORAL 01/30/2018 0.57459
THIORIDAZINE HCL 100 MG TABLET ORAL 03/28/2017 1.15093
THIORIDAZINE HCL 25 MG TABLET ORAL 10/24/2017 0.77063
THIORIDAZINE HCL 50 MG TABLET ORAL 02/07/2017 0.99508
THIOTEPA 15 MG VIAL INJECTION 11/07/2018 701.64325
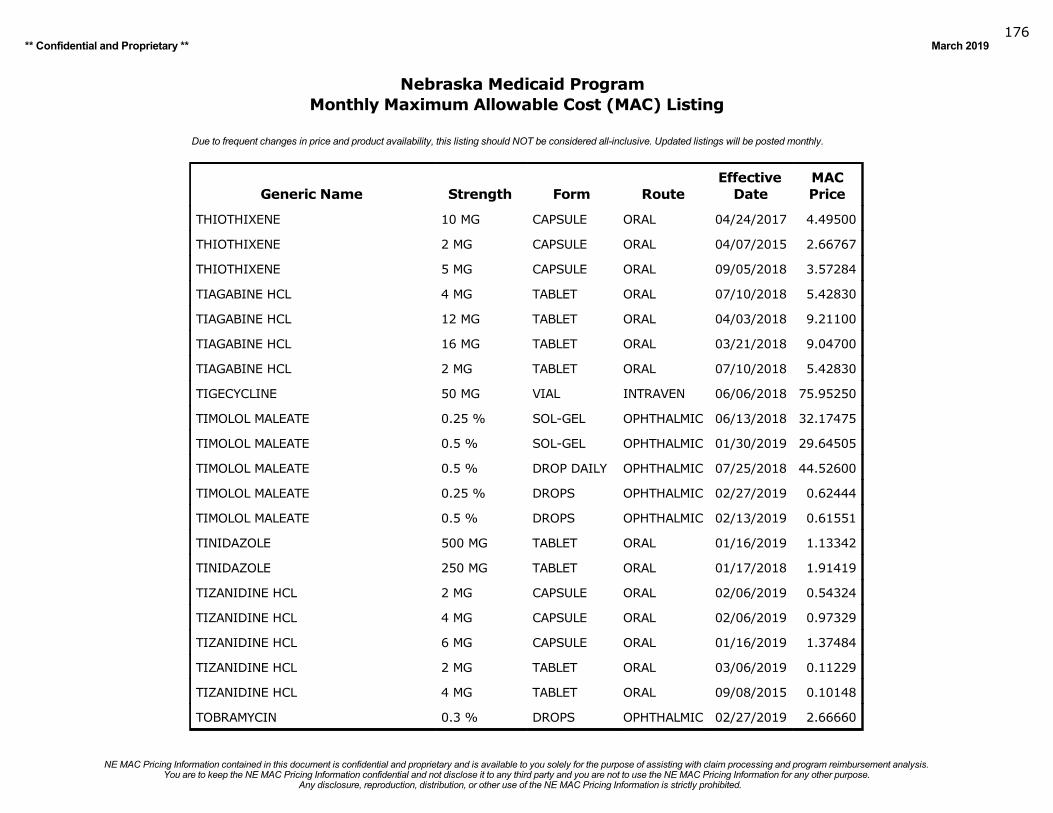
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019176
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
THIOTHIXENE 10 MG CAPSULE ORAL 04/24/2017 4.49500
THIOTHIXENE 2 MG CAPSULE ORAL 04/07/2015 2.66767
THIOTHIXENE 5 MG CAPSULE ORAL 09/05/2018 3.57284
TIAGABINE HCL 4 MG TABLET ORAL 07/10/2018 5.42830
TIAGABINE HCL 12 MG TABLET ORAL 04/03/2018 9.21100
TIAGABINE HCL 16 MG TABLET ORAL 03/21/2018 9.04700
TIAGABINE HCL 2 MG TABLET ORAL 07/10/2018 5.42830
TIGECYCLINE 50 MG VIAL INTRAVEN 06/06/2018 75.95250
TIMOLOL MALEATE 0.25 % SOL-GEL OPHTHALMIC 06/13/2018 32.17475
TIMOLOL MALEATE 0.5 % SOL-GEL OPHTHALMIC 01/30/2019 29.64505
TIMOLOL MALEATE 0.5 % DROP DAILY OPHTHALMIC 07/25/2018 44.52600
TIMOLOL MALEATE 0.25 % DROPS OPHTHALMIC 02/27/2019 0.62444
TIMOLOL MALEATE 0.5 % DROPS OPHTHALMIC 02/13/2019 0.61551
TINIDAZOLE 500 MG TABLET ORAL 01/16/2019 1.13342
TINIDAZOLE 250 MG TABLET ORAL 01/17/2018 1.91419
TIZANIDINE HCL 2 MG CAPSULE ORAL 02/06/2019 0.54324
TIZANIDINE HCL 4 MG CAPSULE ORAL 02/06/2019 0.97329
TIZANIDINE HCL 6 MG CAPSULE ORAL 01/16/2019 1.37484
TIZANIDINE HCL 2 MG TABLET ORAL 03/06/2019 0.11229
TIZANIDINE HCL 4 MG TABLET ORAL 09/08/2015 0.10148
TOBRAMYCIN 0.3 % DROPS OPHTHALMIC 02/27/2019 2.66660
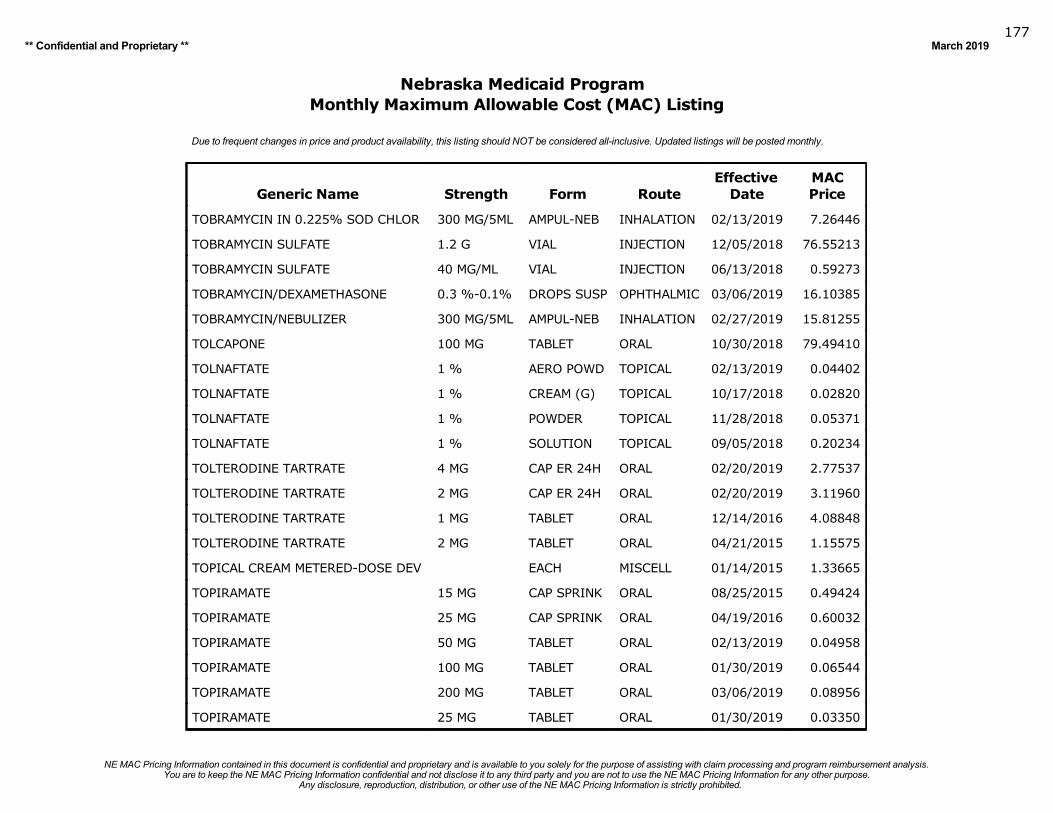
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019177
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
TOBRAMYCIN IN 0.225% SOD CHLOR 300 MG/5ML AMPUL-NEB INHALATION 02/13/2019 7.26446
TOBRAMYCIN SULFATE 1.2 G VIAL INJECTION 12/05/2018 76.55213
TOBRAMYCIN SULFATE 40 MG/ML VIAL INJECTION 06/13/2018 0.59273
TOBRAMYCIN/DEXAMETHASONE 0.3 %-0.1% DROPS SUSP OPHTHALMIC 03/06/2019 16.10385
TOBRAMYCIN/NEBULIZER 300 MG/5ML AMPUL-NEB INHALATION 02/27/2019 15.81255
TOLCAPONE 100 MG TABLET ORAL 10/30/2018 79.49410
TOLNAFTATE 1 % AERO POWD TOPICAL 02/13/2019 0.04402
TOLNAFTATE 1 % CREAM (G) TOPICAL 10/17/2018 0.02820
TOLNAFTATE 1 % POWDER TOPICAL 11/28/2018 0.05371
TOLNAFTATE 1 % SOLUTION TOPICAL 09/05/2018 0.20234
TOLTERODINE TARTRATE 4 MG CAP ER 24H ORAL 02/20/2019 2.77537
TOLTERODINE TARTRATE 2 MG CAP ER 24H ORAL 02/20/2019 3.11960
TOLTERODINE TARTRATE 1 MG TABLET ORAL 12/14/2016 4.08848
TOLTERODINE TARTRATE 2 MG TABLET ORAL 04/21/2015 1.15575
TOPICAL CREAM METERED-DOSE DEV EACH MISCELL 01/14/2015 1.33665
TOPIRAMATE 15 MG CAP SPRINK ORAL 08/25/2015 0.49424
TOPIRAMATE 25 MG CAP SPRINK ORAL 04/19/2016 0.60032
TOPIRAMATE 50 MG TABLET ORAL 02/13/2019 0.04958
TOPIRAMATE 100 MG TABLET ORAL 01/30/2019 0.06544
TOPIRAMATE 200 MG TABLET ORAL 03/06/2019 0.08956
TOPIRAMATE 25 MG TABLET ORAL 01/30/2019 0.03350
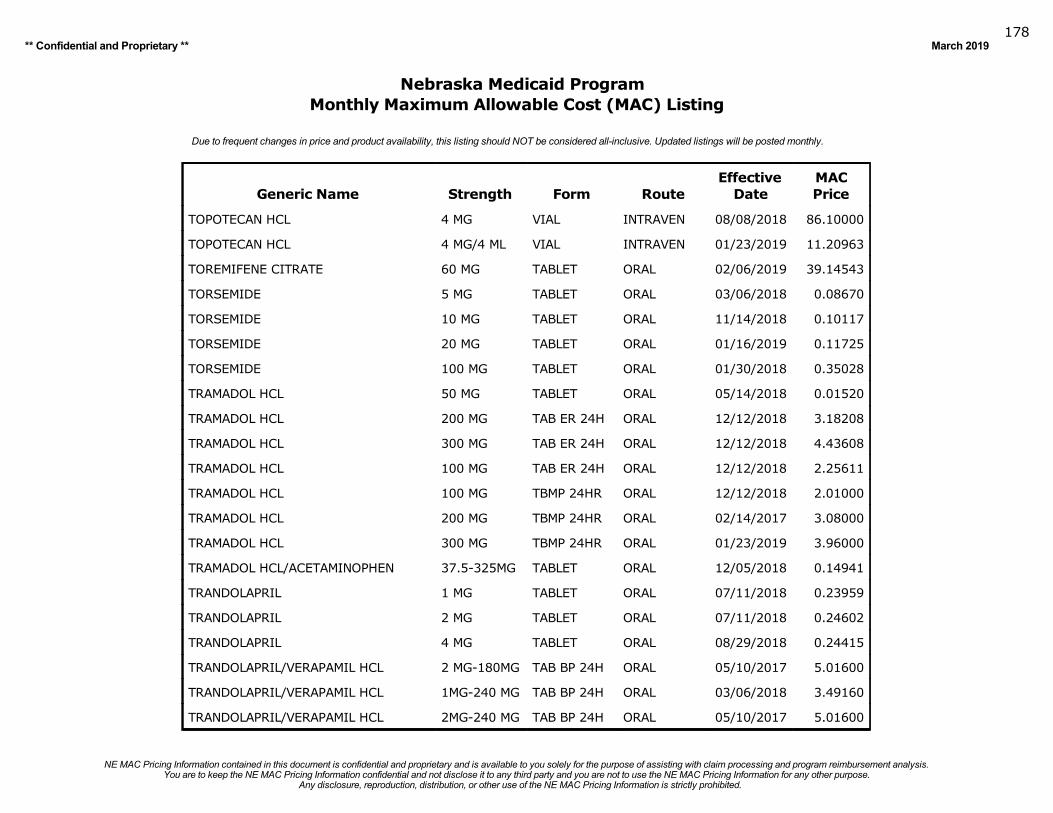
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019178
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
TOPOTECAN HCL 4 MG VIAL INTRAVEN 08/08/2018 86.10000
TOPOTECAN HCL 4 MG/4 ML VIAL INTRAVEN 01/23/2019 11.20963
TOREMIFENE CITRATE 60 MG TABLET ORAL 02/06/2019 39.14543
TORSEMIDE 5 MG TABLET ORAL 03/06/2018 0.08670
TORSEMIDE 10 MG TABLET ORAL 11/14/2018 0.10117
TORSEMIDE 20 MG TABLET ORAL 01/16/2019 0.11725
TORSEMIDE 100 MG TABLET ORAL 01/30/2018 0.35028
TRAMADOL HCL 50 MG TABLET ORAL 05/14/2018 0.01520
TRAMADOL HCL 200 MG TAB ER 24H ORAL 12/12/2018 3.18208
TRAMADOL HCL 300 MG TAB ER 24H ORAL 12/12/2018 4.43608
TRAMADOL HCL 100 MG TAB ER 24H ORAL 12/12/2018 2.25611
TRAMADOL HCL 100 MG TBMP 24HR ORAL 12/12/2018 2.01000
TRAMADOL HCL 200 MG TBMP 24HR ORAL 02/14/2017 3.08000
TRAMADOL HCL 300 MG TBMP 24HR ORAL 01/23/2019 3.96000
TRAMADOL HCL/ACETAMINOPHEN 37.5-325MG TABLET ORAL 12/05/2018 0.14941
TRANDOLAPRIL 1 MG TABLET ORAL 07/11/2018 0.23959
TRANDOLAPRIL 2 MG TABLET ORAL 07/11/2018 0.24602
TRANDOLAPRIL 4 MG TABLET ORAL 08/29/2018 0.24415
TRANDOLAPRIL/VERAPAMIL HCL 2 MG-180MG TAB BP 24H ORAL 05/10/2017 5.01600
TRANDOLAPRIL/VERAPAMIL HCL 1MG-240 MG TAB BP 24H ORAL 03/06/2018 3.49160
TRANDOLAPRIL/VERAPAMIL HCL 2MG-240 MG TAB BP 24H ORAL 05/10/2017 5.01600
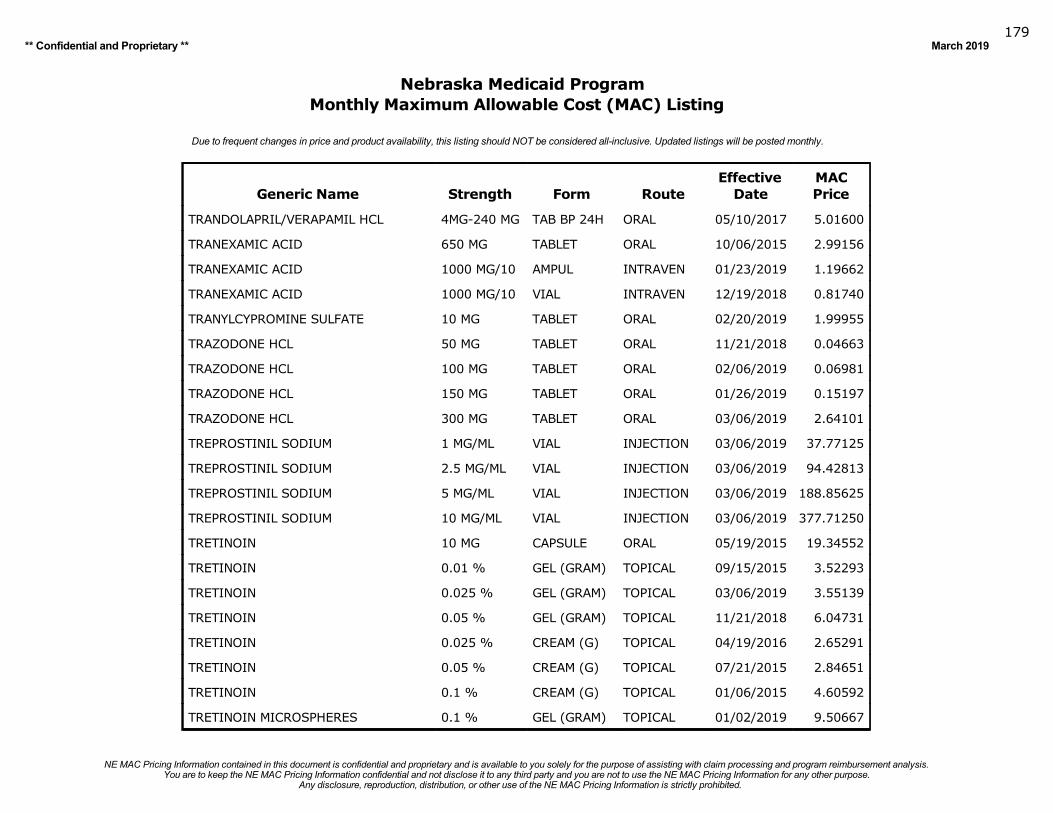
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019179
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
TRANDOLAPRIL/VERAPAMIL HCL 4MG-240 MG TAB BP 24H ORAL 05/10/2017 5.01600
TRANEXAMIC ACID 650 MG TABLET ORAL 10/06/2015 2.99156
TRANEXAMIC ACID 1000 MG/10 AMPUL INTRAVEN 01/23/2019 1.19662
TRANEXAMIC ACID 1000 MG/10 VIAL INTRAVEN 12/19/2018 0.81740
TRANYLCYPROMINE SULFATE 10 MG TABLET ORAL 02/20/2019 1.99955
TRAZODONE HCL 50 MG TABLET ORAL 11/21/2018 0.04663
TRAZODONE HCL 100 MG TABLET ORAL 02/06/2019 0.06981
TRAZODONE HCL 150 MG TABLET ORAL 01/26/2019 0.15197
TRAZODONE HCL 300 MG TABLET ORAL 03/06/2019 2.64101
TREPROSTINIL SODIUM 1 MG/ML VIAL INJECTION 03/06/2019 37.77125
TREPROSTINIL SODIUM 2.5 MG/ML VIAL INJECTION 03/06/2019 94.42813
TREPROSTINIL SODIUM 5 MG/ML VIAL INJECTION 03/06/2019 188.85625
TREPROSTINIL SODIUM 10 MG/ML VIAL INJECTION 03/06/2019 377.71250
TRETINOIN 10 MG CAPSULE ORAL 05/19/2015 19.34552
TRETINOIN 0.01 % GEL (GRAM) TOPICAL 09/15/2015 3.52293
TRETINOIN 0.025 % GEL (GRAM) TOPICAL 03/06/2019 3.55139
TRETINOIN 0.05 % GEL (GRAM) TOPICAL 11/21/2018 6.04731
TRETINOIN 0.025 % CREAM (G) TOPICAL 04/19/2016 2.65291
TRETINOIN 0.05 % CREAM (G) TOPICAL 07/21/2015 2.84651
TRETINOIN 0.1 % CREAM (G) TOPICAL 01/06/2015 4.60592
TRETINOIN MICROSPHERES 0.1 % GEL (GRAM) TOPICAL 01/02/2019 9.50667
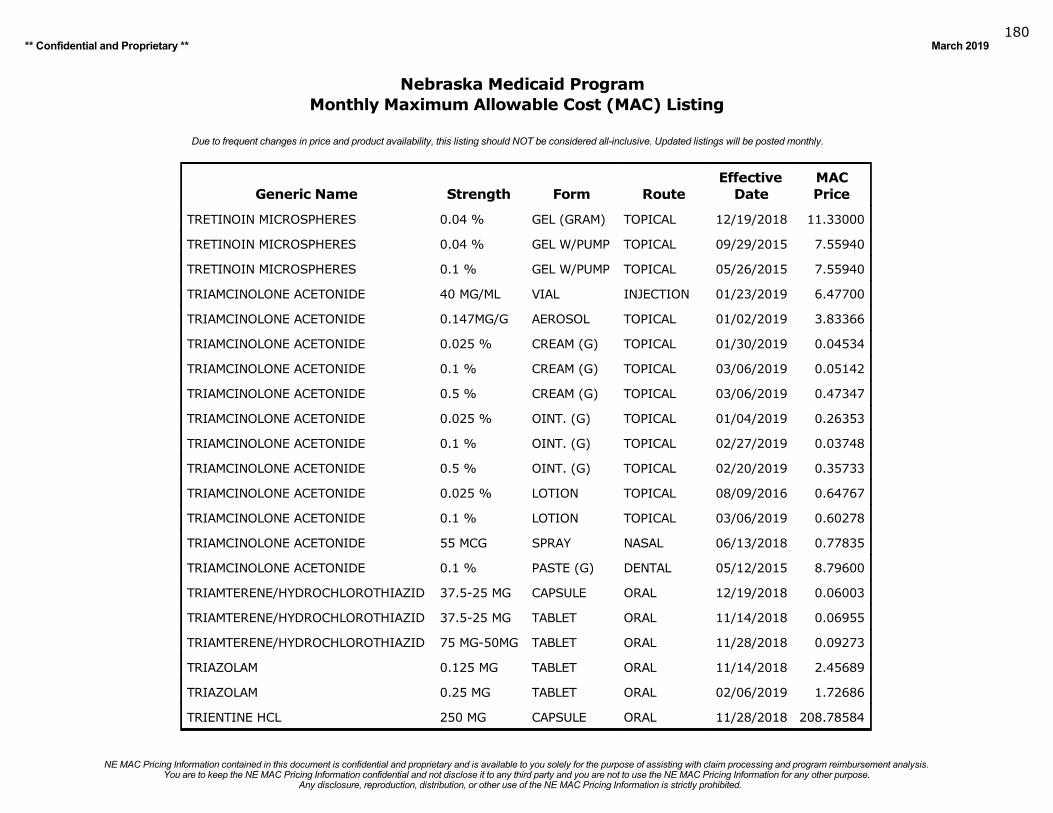
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019180
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
TRETINOIN MICROSPHERES 0.04 % GEL (GRAM) TOPICAL 12/19/2018 11.33000
TRETINOIN MICROSPHERES 0.04 % GEL W/PUMP TOPICAL 09/29/2015 7.55940
TRETINOIN MICROSPHERES 0.1 % GEL W/PUMP TOPICAL 05/26/2015 7.55940
TRIAMCINOLONE ACETONIDE 40 MG/ML VIAL INJECTION 01/23/2019 6.47700
TRIAMCINOLONE ACETONIDE 0.147MG/G AEROSOL TOPICAL 01/02/2019 3.83366
TRIAMCINOLONE ACETONIDE 0.025 % CREAM (G) TOPICAL 01/30/2019 0.04534
TRIAMCINOLONE ACETONIDE 0.1 % CREAM (G) TOPICAL 03/06/2019 0.05142
TRIAMCINOLONE ACETONIDE 0.5 % CREAM (G) TOPICAL 03/06/2019 0.47347
TRIAMCINOLONE ACETONIDE 0.025 % OINT. (G) TOPICAL 01/04/2019 0.26353
TRIAMCINOLONE ACETONIDE 0.1 % OINT. (G) TOPICAL 02/27/2019 0.03748
TRIAMCINOLONE ACETONIDE 0.5 % OINT. (G) TOPICAL 02/20/2019 0.35733
TRIAMCINOLONE ACETONIDE 0.025 % LOTION TOPICAL 08/09/2016 0.64767
TRIAMCINOLONE ACETONIDE 0.1 % LOTION TOPICAL 03/06/2019 0.60278
TRIAMCINOLONE ACETONIDE 55 MCG SPRAY NASAL 06/13/2018 0.77835
TRIAMCINOLONE ACETONIDE 0.1 % PASTE (G) DENTAL 05/12/2015 8.79600
TRIAMTERENE/HYDROCHLOROTHIAZID 37.5-25 MG CAPSULE ORAL 12/19/2018 0.06003
TRIAMTERENE/HYDROCHLOROTHIAZID 37.5-25 MG TABLET ORAL 11/14/2018 0.06955
TRIAMTERENE/HYDROCHLOROTHIAZID 75 MG-50MG TABLET ORAL 11/28/2018 0.09273
TRIAZOLAM 0.125 MG TABLET ORAL 11/14/2018 2.45689
TRIAZOLAM 0.25 MG TABLET ORAL 02/06/2019 1.72686
TRIENTINE HCL 250 MG CAPSULE ORAL 11/28/2018 208.78584
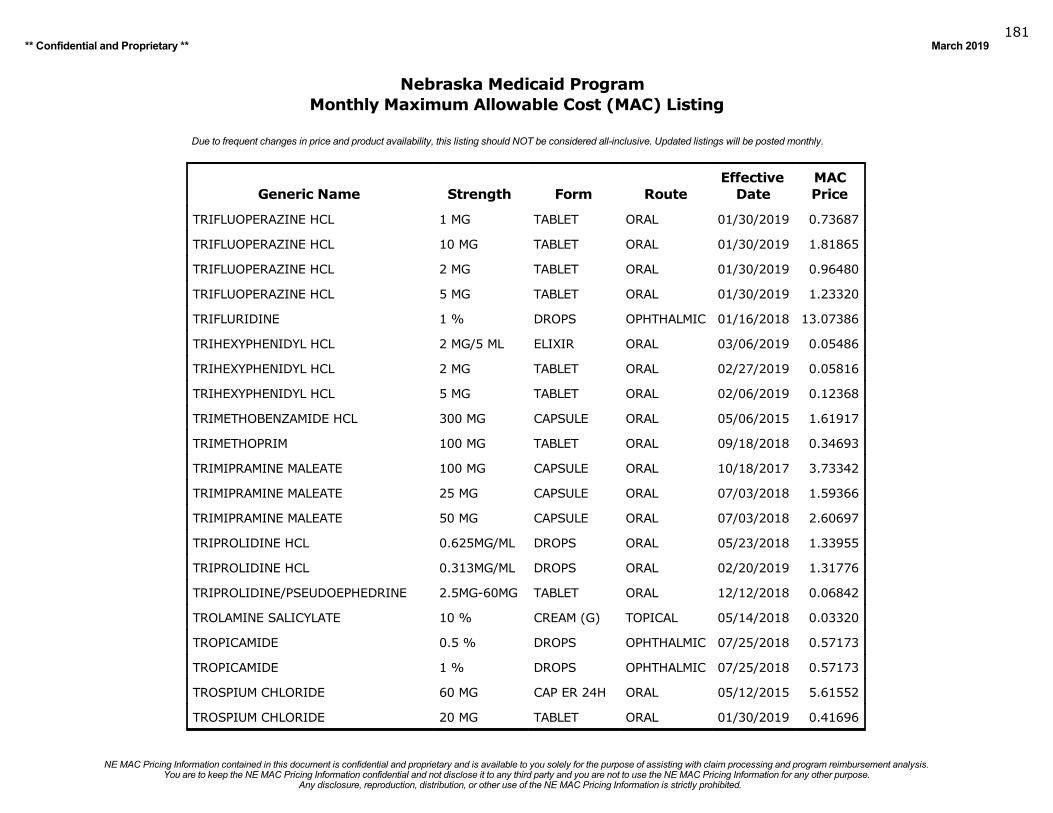
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019181
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
TRIFLUOPERAZINE HCL 1 MG TABLET ORAL 01/30/2019 0.73687
TRIFLUOPERAZINE HCL 10 MG TABLET ORAL 01/30/2019 1.81865
TRIFLUOPERAZINE HCL 2 MG TABLET ORAL 01/30/2019 0.96480
TRIFLUOPERAZINE HCL 5 MG TABLET ORAL 01/30/2019 1.23320
TRIFLURIDINE 1 % DROPS OPHTHALMIC 01/16/2018 13.07386
TRIHEXYPHENIDYL HCL 2 MG/5 ML ELIXIR ORAL 03/06/2019 0.05486
TRIHEXYPHENIDYL HCL 2 MG TABLET ORAL 02/27/2019 0.05816
TRIHEXYPHENIDYL HCL 5 MG TABLET ORAL 02/06/2019 0.12368
TRIMETHOBENZAMIDE HCL 300 MG CAPSULE ORAL 05/06/2015 1.61917
TRIMETHOPRIM 100 MG TABLET ORAL 09/18/2018 0.34693
TRIMIPRAMINE MALEATE 100 MG CAPSULE ORAL 10/18/2017 3.73342
TRIMIPRAMINE MALEATE 25 MG CAPSULE ORAL 07/03/2018 1.59366
TRIMIPRAMINE MALEATE 50 MG CAPSULE ORAL 07/03/2018 2.60697
TRIPROLIDINE HCL 0.625MG/ML DROPS ORAL 05/23/2018 1.33955
TRIPROLIDINE HCL 0.313MG/ML DROPS ORAL 02/20/2019 1.31776
TRIPROLIDINE/PSEUDOEPHEDRINE 2.5MG-60MG TABLET ORAL 12/12/2018 0.06842
TROLAMINE SALICYLATE 10 % CREAM (G) TOPICAL 05/14/2018 0.03320
TROPICAMIDE 0.5 % DROPS OPHTHALMIC 07/25/2018 0.57173
TROPICAMIDE 1 % DROPS OPHTHALMIC 07/25/2018 0.57173
TROSPIUM CHLORIDE 60 MG CAP ER 24H ORAL 05/12/2015 5.61552
TROSPIUM CHLORIDE 20 MG TABLET ORAL 01/30/2019 0.41696
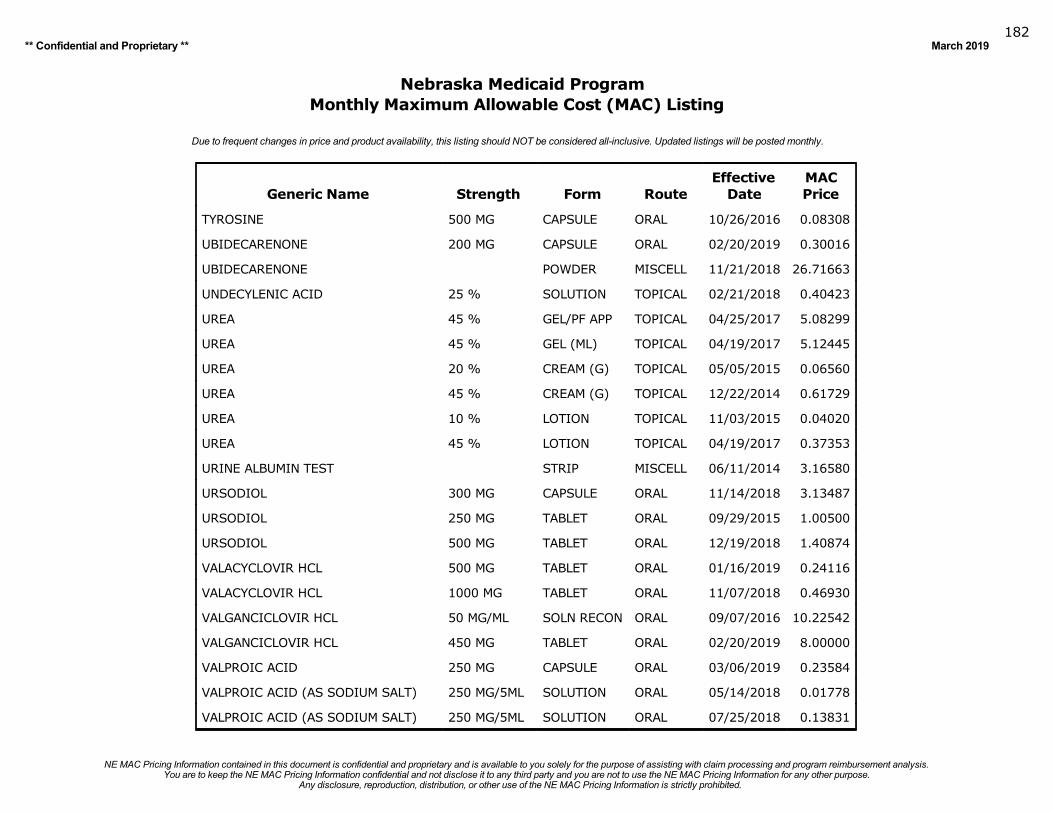
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019182
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
TYROSINE 500 MG CAPSULE ORAL 10/26/2016 0.08308
UBIDECARENONE 200 MG CAPSULE ORAL 02/20/2019 0.30016
UBIDECARENONE POWDER MISCELL 11/21/2018 26.71663
UNDECYLENIC ACID 25 % SOLUTION TOPICAL 02/21/2018 0.40423
UREA 45 % GEL/PF APP TOPICAL 04/25/2017 5.08299
UREA 45 % GEL (ML) TOPICAL 04/19/2017 5.12445
UREA 20 % CREAM (G) TOPICAL 05/05/2015 0.06560
UREA 45 % CREAM (G) TOPICAL 12/22/2014 0.61729
UREA 10 % LOTION TOPICAL 11/03/2015 0.04020
UREA 45 % LOTION TOPICAL 04/19/2017 0.37353
URINE ALBUMIN TEST STRIP MISCELL 06/11/2014 3.16580
URSODIOL 300 MG CAPSULE ORAL 11/14/2018 3.13487
URSODIOL 250 MG TABLET ORAL 09/29/2015 1.00500
URSODIOL 500 MG TABLET ORAL 12/19/2018 1.40874
VALACYCLOVIR HCL 500 MG TABLET ORAL 01/16/2019 0.24116
VALACYCLOVIR HCL 1000 MG TABLET ORAL 11/07/2018 0.46930
VALGANCICLOVIR HCL 50 MG/ML SOLN RECON ORAL 09/07/2016 10.22542
VALGANCICLOVIR HCL 450 MG TABLET ORAL 02/20/2019 8.00000
VALPROIC ACID 250 MG CAPSULE ORAL 03/06/2019 0.23584
VALPROIC ACID (AS SODIUM SALT) 250 MG/5ML SOLUTION ORAL 05/14/2018 0.01778
VALPROIC ACID (AS SODIUM SALT) 250 MG/5ML SOLUTION ORAL 07/25/2018 0.13831
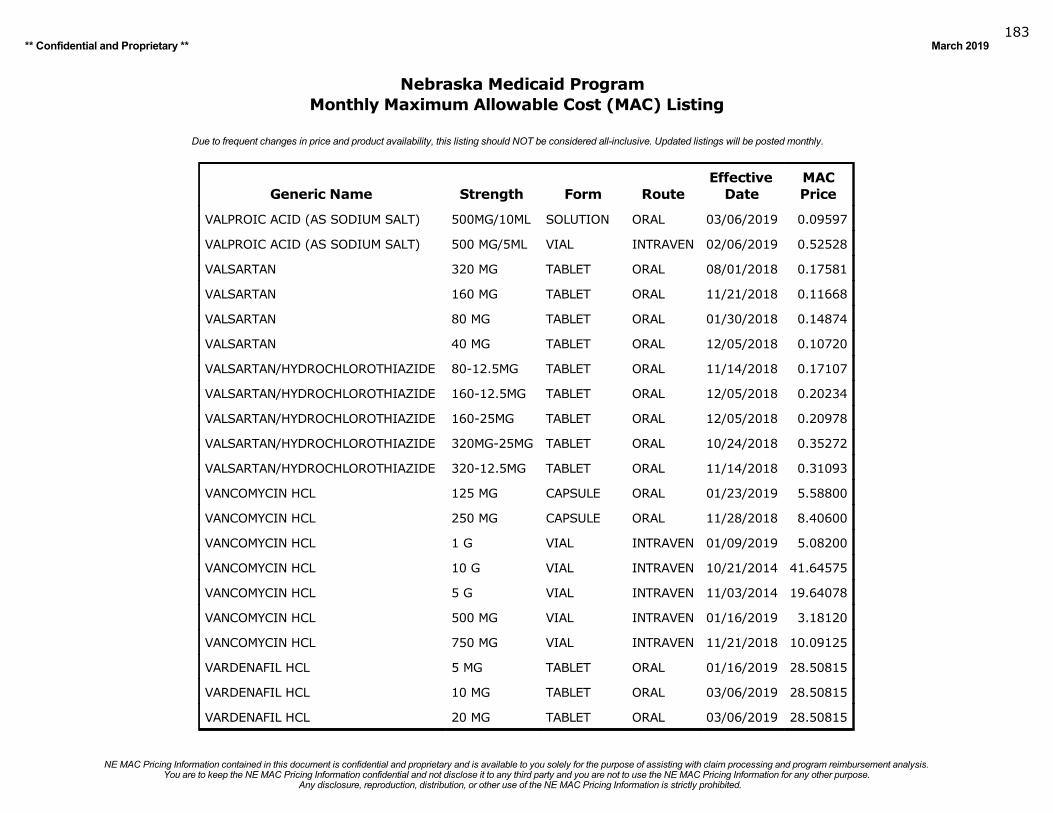
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019183
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
VALPROIC ACID (AS SODIUM SALT) 500MG/10ML SOLUTION ORAL 03/06/2019 0.09597
VALPROIC ACID (AS SODIUM SALT) 500 MG/5ML VIAL INTRAVEN 02/06/2019 0.52528
VALSARTAN 320 MG TABLET ORAL 08/01/2018 0.17581
VALSARTAN 160 MG TABLET ORAL 11/21/2018 0.11668
VALSARTAN 80 MG TABLET ORAL 01/30/2018 0.14874
VALSARTAN 40 MG TABLET ORAL 12/05/2018 0.10720
VALSARTAN/HYDROCHLOROTHIAZIDE 80-12.5MG TABLET ORAL 11/14/2018 0.17107
VALSARTAN/HYDROCHLOROTHIAZIDE 160-12.5MG TABLET ORAL 12/05/2018 0.20234
VALSARTAN/HYDROCHLOROTHIAZIDE 160-25MG TABLET ORAL 12/05/2018 0.20978
VALSARTAN/HYDROCHLOROTHIAZIDE 320MG-25MG TABLET ORAL 10/24/2018 0.35272
VALSARTAN/HYDROCHLOROTHIAZIDE 320-12.5MG TABLET ORAL 11/14/2018 0.31093
VANCOMYCIN HCL 125 MG CAPSULE ORAL 01/23/2019 5.58800
VANCOMYCIN HCL 250 MG CAPSULE ORAL 11/28/2018 8.40600
VANCOMYCIN HCL 1 G VIAL INTRAVEN 01/09/2019 5.08200
VANCOMYCIN HCL 10 G VIAL INTRAVEN 10/21/2014 41.64575
VANCOMYCIN HCL 5 G VIAL INTRAVEN 11/03/2014 19.64078
VANCOMYCIN HCL 500 MG VIAL INTRAVEN 01/16/2019 3.18120
VANCOMYCIN HCL 750 MG VIAL INTRAVEN 11/21/2018 10.09125
VARDENAFIL HCL 5 MG TABLET ORAL 01/16/2019 28.50815
VARDENAFIL HCL 10 MG TABLET ORAL 03/06/2019 28.50815
VARDENAFIL HCL 20 MG TABLET ORAL 03/06/2019 28.50815
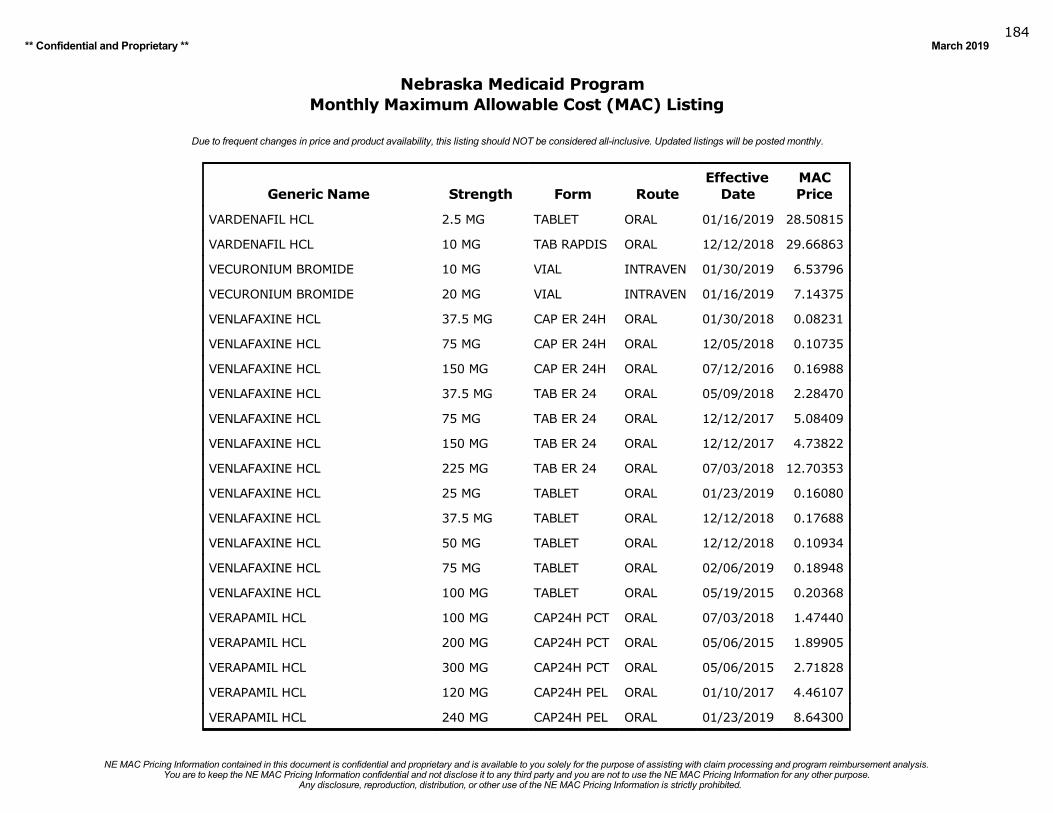
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019184
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
VARDENAFIL HCL 2.5 MG TABLET ORAL 01/16/2019 28.50815
VARDENAFIL HCL 10 MG TAB RAPDIS ORAL 12/12/2018 29.66863
VECURONIUM BROMIDE 10 MG VIAL INTRAVEN 01/30/2019 6.53796
VECURONIUM BROMIDE 20 MG VIAL INTRAVEN 01/16/2019 7.14375
VENLAFAXINE HCL 37.5 MG CAP ER 24H ORAL 01/30/2018 0.08231
VENLAFAXINE HCL 75 MG CAP ER 24H ORAL 12/05/2018 0.10735
VENLAFAXINE HCL 150 MG CAP ER 24H ORAL 07/12/2016 0.16988
VENLAFAXINE HCL 37.5 MG TAB ER 24 ORAL 05/09/2018 2.28470
VENLAFAXINE HCL 75 MG TAB ER 24 ORAL 12/12/2017 5.08409
VENLAFAXINE HCL 150 MG TAB ER 24 ORAL 12/12/2017 4.73822
VENLAFAXINE HCL 225 MG TAB ER 24 ORAL 07/03/2018 12.70353
VENLAFAXINE HCL 25 MG TABLET ORAL 01/23/2019 0.16080
VENLAFAXINE HCL 37.5 MG TABLET ORAL 12/12/2018 0.17688
VENLAFAXINE HCL 50 MG TABLET ORAL 12/12/2018 0.10934
VENLAFAXINE HCL 75 MG TABLET ORAL 02/06/2019 0.18948
VENLAFAXINE HCL 100 MG TABLET ORAL 05/19/2015 0.20368
VERAPAMIL HCL 100 MG CAP24H PCT ORAL 07/03/2018 1.47440
VERAPAMIL HCL 200 MG CAP24H PCT ORAL 05/06/2015 1.89905
VERAPAMIL HCL 300 MG CAP24H PCT ORAL 05/06/2015 2.71828
VERAPAMIL HCL 120 MG CAP24H PEL ORAL 01/10/2017 4.46107
VERAPAMIL HCL 240 MG CAP24H PEL ORAL 01/23/2019 8.64300
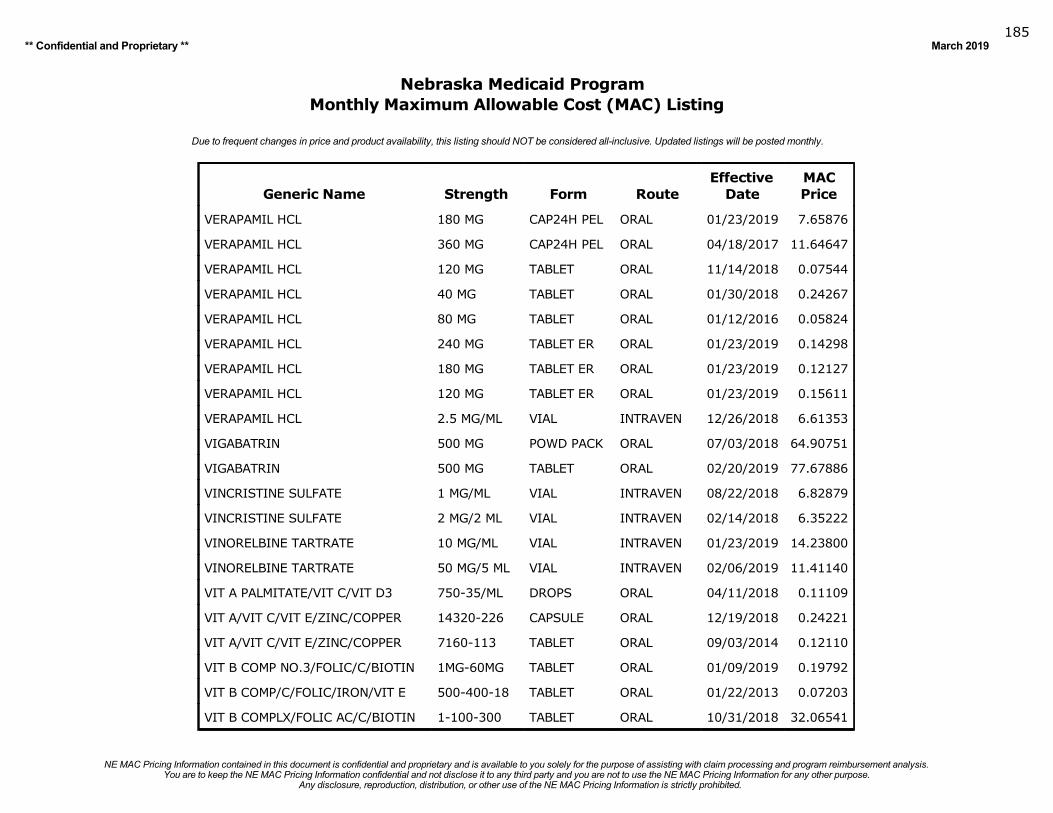
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019185
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
VERAPAMIL HCL 180 MG CAP24H PEL ORAL 01/23/2019 7.65876
VERAPAMIL HCL 360 MG CAP24H PEL ORAL 04/18/2017 11.64647
VERAPAMIL HCL 120 MG TABLET ORAL 11/14/2018 0.07544
VERAPAMIL HCL 40 MG TABLET ORAL 01/30/2018 0.24267
VERAPAMIL HCL 80 MG TABLET ORAL 01/12/2016 0.05824
VERAPAMIL HCL 240 MG TABLET ER ORAL 01/23/2019 0.14298
VERAPAMIL HCL 180 MG TABLET ER ORAL 01/23/2019 0.12127
VERAPAMIL HCL 120 MG TABLET ER ORAL 01/23/2019 0.15611
VERAPAMIL HCL 2.5 MG/ML VIAL INTRAVEN 12/26/2018 6.61353
VIGABATRIN 500 MG POWD PACK ORAL 07/03/2018 64.90751
VIGABATRIN 500 MG TABLET ORAL 02/20/2019 77.67886
VINCRISTINE SULFATE 1 MG/ML VIAL INTRAVEN 08/22/2018 6.82879
VINCRISTINE SULFATE 2 MG/2 ML VIAL INTRAVEN 02/14/2018 6.35222
VINORELBINE TARTRATE 10 MG/ML VIAL INTRAVEN 01/23/2019 14.23800
VINORELBINE TARTRATE 50 MG/5 ML VIAL INTRAVEN 02/06/2019 11.41140
VIT A PALMITATE/VIT C/VIT D3 750-35/ML DROPS ORAL 04/11/2018 0.11109
VIT A/VIT C/VIT E/ZINC/COPPER 14320-226 CAPSULE ORAL 12/19/2018 0.24221
VIT A/VIT C/VIT E/ZINC/COPPER 7160-113 TABLET ORAL 09/03/2014 0.12110
VIT B COMP NO.3/FOLIC/C/BIOTIN 1MG-60MG TABLET ORAL 01/09/2019 0.19792
VIT B COMP/C/FOLIC/IRON/VIT E 500-400-18 TABLET ORAL 01/22/2013 0.07203
VIT B COMPLX/FOLIC AC/C/BIOTIN 1-100-300 TABLET ORAL 10/31/2018 32.06541
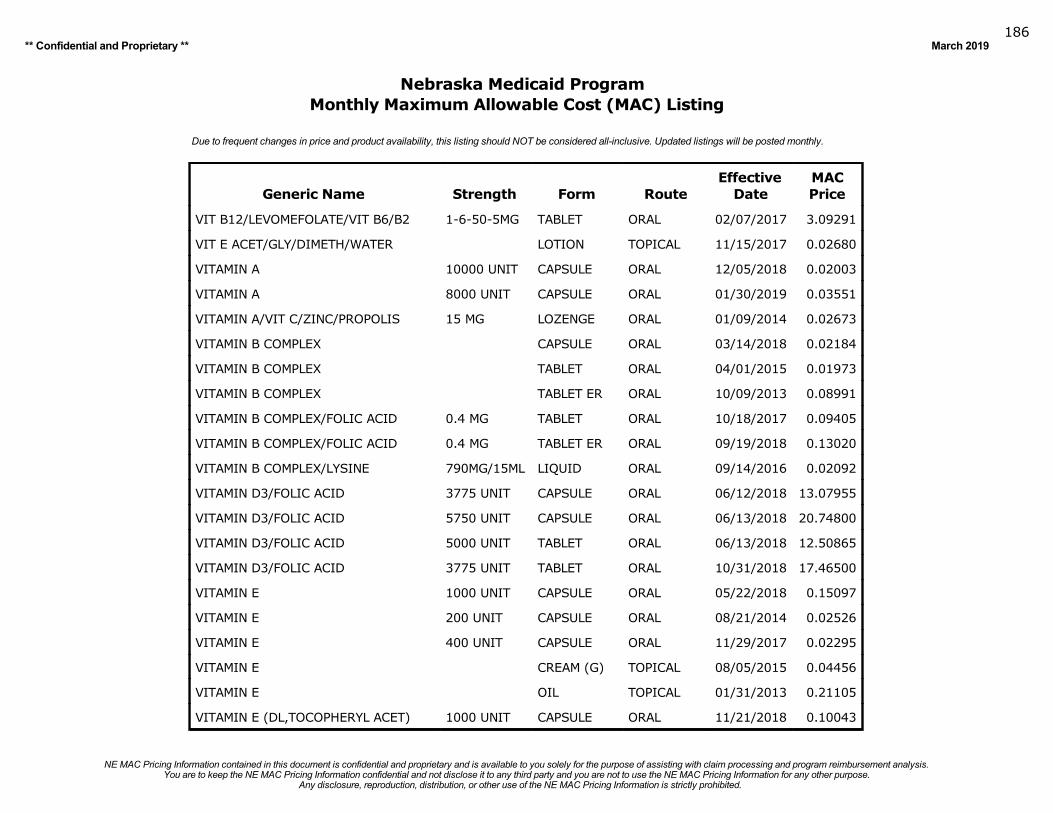
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019186
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
VIT B12/LEVOMEFOLATE/VIT B6/B2 1-6-50-5MG TABLET ORAL 02/07/2017 3.09291
VIT E ACET/GLY/DIMETH/WATER LOTION TOPICAL 11/15/2017 0.02680
VITAMIN A 10000 UNIT CAPSULE ORAL 12/05/2018 0.02003
VITAMIN A 8000 UNIT CAPSULE ORAL 01/30/2019 0.03551
VITAMIN A/VIT C/ZINC/PROPOLIS 15 MG LOZENGE ORAL 01/09/2014 0.02673
VITAMIN B COMPLEX CAPSULE ORAL 03/14/2018 0.02184
VITAMIN B COMPLEX TABLET ORAL 04/01/2015 0.01973
VITAMIN B COMPLEX TABLET ER ORAL 10/09/2013 0.08991
VITAMIN B COMPLEX/FOLIC ACID 0.4 MG TABLET ORAL 10/18/2017 0.09405
VITAMIN B COMPLEX/FOLIC ACID 0.4 MG TABLET ER ORAL 09/19/2018 0.13020
VITAMIN B COMPLEX/LYSINE 790MG/15ML LIQUID ORAL 09/14/2016 0.02092
VITAMIN D3/FOLIC ACID 3775 UNIT CAPSULE ORAL 06/12/2018 13.07955
VITAMIN D3/FOLIC ACID 5750 UNIT CAPSULE ORAL 06/13/2018 20.74800
VITAMIN D3/FOLIC ACID 5000 UNIT TABLET ORAL 06/13/2018 12.50865
VITAMIN D3/FOLIC ACID 3775 UNIT TABLET ORAL 10/31/2018 17.46500
VITAMIN E 1000 UNIT CAPSULE ORAL 05/22/2018 0.15097
VITAMIN E 200 UNIT CAPSULE ORAL 08/21/2014 0.02526
VITAMIN E 400 UNIT CAPSULE ORAL 11/29/2017 0.02295
VITAMIN E CREAM (G) TOPICAL 08/05/2015 0.04456
VITAMIN E OIL TOPICAL 01/31/2013 0.21105
VITAMIN E (DL,TOCOPHERYL ACET) 1000 UNIT CAPSULE ORAL 11/21/2018 0.10043
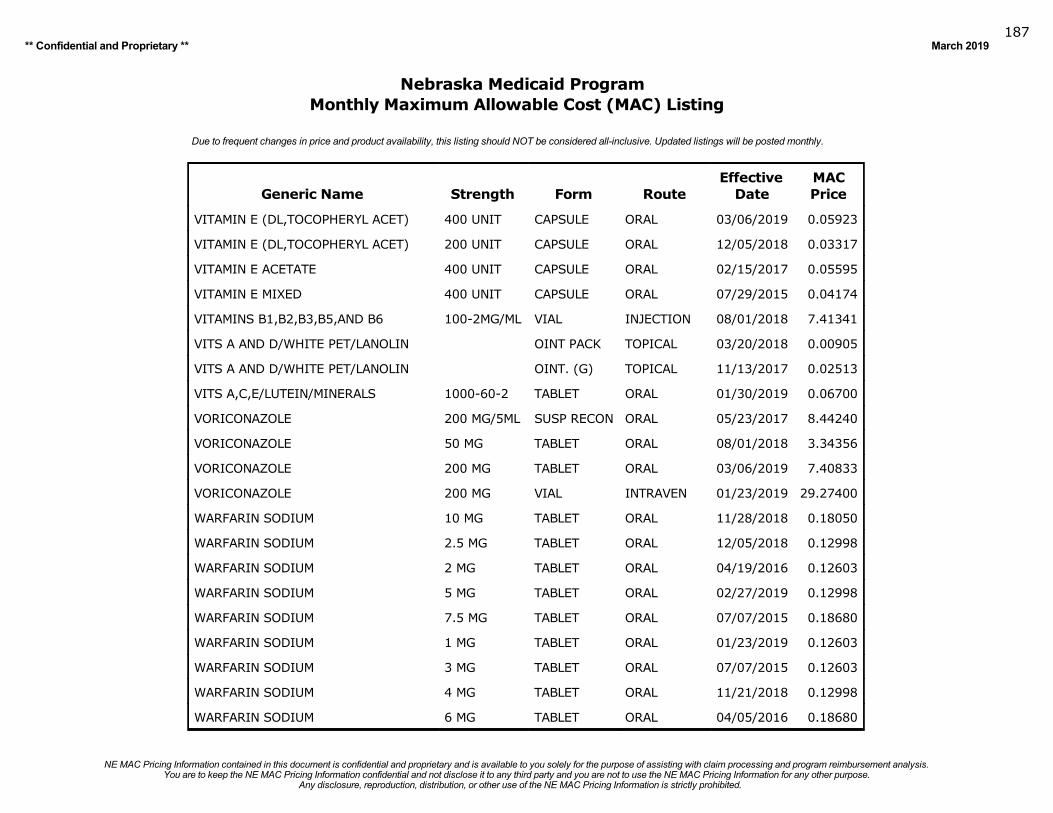
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019187
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
VITAMIN E (DL,TOCOPHERYL ACET) 400 UNIT CAPSULE ORAL 03/06/2019 0.05923
VITAMIN E (DL,TOCOPHERYL ACET) 200 UNIT CAPSULE ORAL 12/05/2018 0.03317
VITAMIN E ACETATE 400 UNIT CAPSULE ORAL 02/15/2017 0.05595
VITAMIN E MIXED 400 UNIT CAPSULE ORAL 07/29/2015 0.04174
VITAMINS B1,B2,B3,B5,AND B6 100-2MG/ML VIAL INJECTION 08/01/2018 7.41341
VITS A AND D/WHITE PET/LANOLIN OINT PACK TOPICAL 03/20/2018 0.00905
VITS A AND D/WHITE PET/LANOLIN OINT. (G) TOPICAL 11/13/2017 0.02513
VITS A,C,E/LUTEIN/MINERALS 1000-60-2 TABLET ORAL 01/30/2019 0.06700
VORICONAZOLE 200 MG/5ML SUSP RECON ORAL 05/23/2017 8.44240
VORICONAZOLE 50 MG TABLET ORAL 08/01/2018 3.34356
VORICONAZOLE 200 MG TABLET ORAL 03/06/2019 7.40833
VORICONAZOLE 200 MG VIAL INTRAVEN 01/23/2019 29.27400
WARFARIN SODIUM 10 MG TABLET ORAL 11/28/2018 0.18050
WARFARIN SODIUM 2.5 MG TABLET ORAL 12/05/2018 0.12998
WARFARIN SODIUM 2 MG TABLET ORAL 04/19/2016 0.12603
WARFARIN SODIUM 5 MG TABLET ORAL 02/27/2019 0.12998
WARFARIN SODIUM 7.5 MG TABLET ORAL 07/07/2015 0.18680
WARFARIN SODIUM 1 MG TABLET ORAL 01/23/2019 0.12603
WARFARIN SODIUM 3 MG TABLET ORAL 07/07/2015 0.12603
WARFARIN SODIUM 4 MG TABLET ORAL 11/21/2018 0.12998
WARFARIN SODIUM 6 MG TABLET ORAL 04/05/2016 0.18680
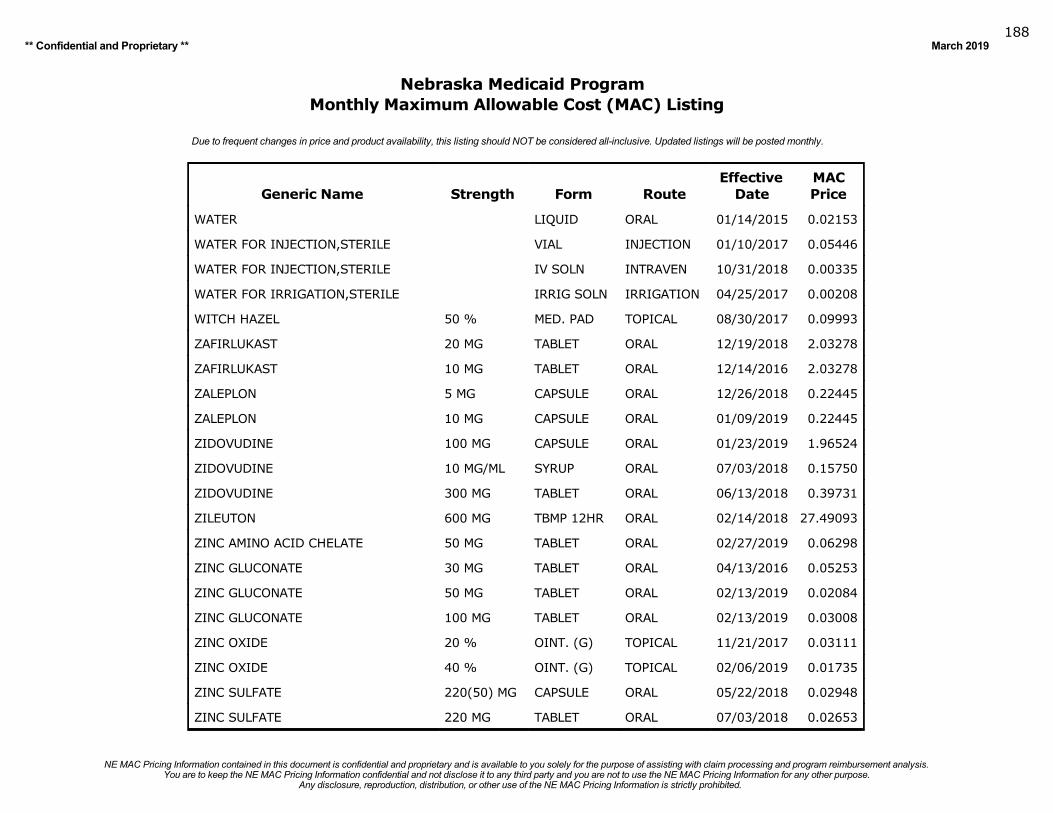
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019188
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
WATER LIQUID ORAL 01/14/2015 0.02153
WATER FOR INJECTION,STERILE VIAL INJECTION 01/10/2017 0.05446
WATER FOR INJECTION,STERILE IV SOLN INTRAVEN 10/31/2018 0.00335
WATER FOR IRRIGATION,STERILE IRRIG SOLN IRRIGATION 04/25/2017 0.00208
WITCH HAZEL 50 % MED. PAD TOPICAL 08/30/2017 0.09993
ZAFIRLUKAST 20 MG TABLET ORAL 12/19/2018 2.03278
ZAFIRLUKAST 10 MG TABLET ORAL 12/14/2016 2.03278
ZALEPLON 5 MG CAPSULE ORAL 12/26/2018 0.22445
ZALEPLON 10 MG CAPSULE ORAL 01/09/2019 0.22445
ZIDOVUDINE 100 MG CAPSULE ORAL 01/23/2019 1.96524
ZIDOVUDINE 10 MG/ML SYRUP ORAL 07/03/2018 0.15750
ZIDOVUDINE 300 MG TABLET ORAL 06/13/2018 0.39731
ZILEUTON 600 MG TBMP 12HR ORAL 02/14/2018 27.49093
ZINC AMINO ACID CHELATE 50 MG TABLET ORAL 02/27/2019 0.06298
ZINC GLUCONATE 30 MG TABLET ORAL 04/13/2016 0.05253
ZINC GLUCONATE 50 MG TABLET ORAL 02/13/2019 0.02084
ZINC GLUCONATE 100 MG TABLET ORAL 02/13/2019 0.03008
ZINC OXIDE 20 % OINT. (G) TOPICAL 11/21/2017 0.03111
ZINC OXIDE 40 % OINT. (G) TOPICAL 02/06/2019 0.01735
ZINC SULFATE 220(50) MG CAPSULE ORAL 05/22/2018 0.02948
ZINC SULFATE 220 MG TABLET ORAL 07/03/2018 0.02653
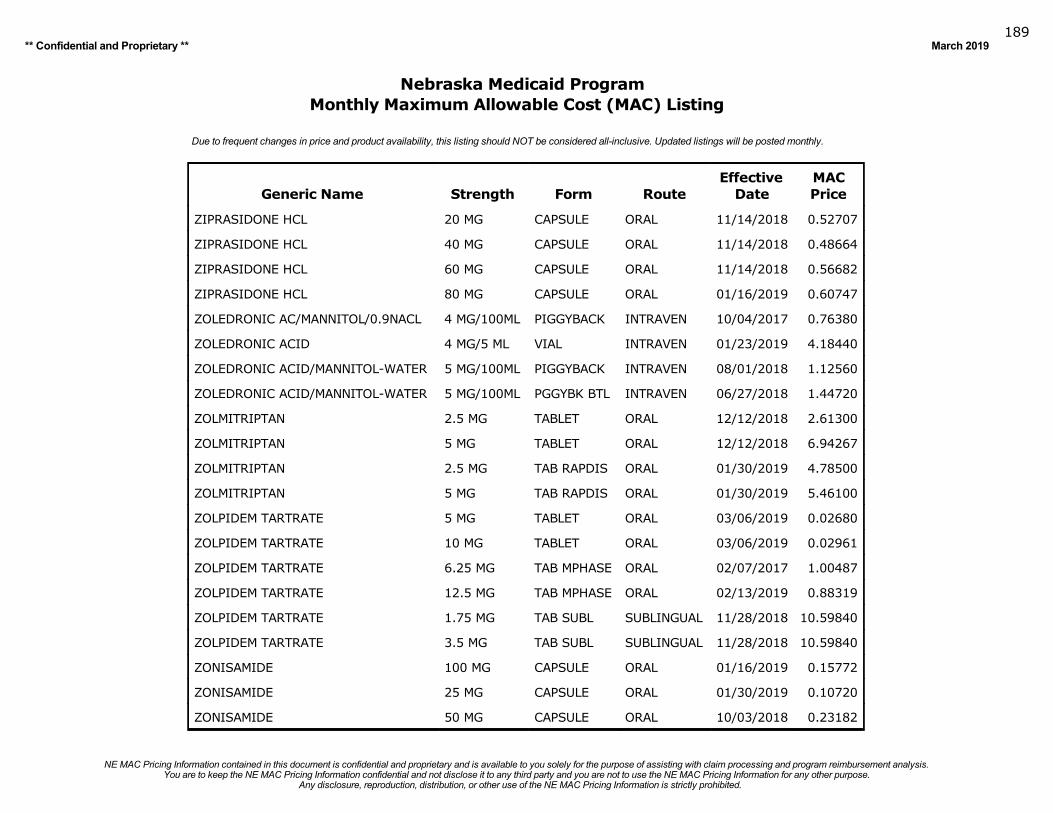
Any disclosure, reproduction, distribution, or other use of the NE MAC Pricing Information is strictly prohibited.You are to keep the NE MAC Pricing Information confidential and not disclose it to any third party and you are not to use the NE MAC Pricing Information for any other purpose.
NE MAC Pricing Information contained in this document is confidential and proprietary and is available to you solely for the purpose of assisting with claim processing and program reimbursement analysis.
** Confidential and Proprietary ** March 2019189
Nebraska Medicaid ProgramMonthly Maximum Allowable Cost (MAC) Listing
Due to frequent changes in price and product availability, this listing should NOT be considered all-inclusive. Updated listings will be posted monthly.
Generic Name Strength Form RouteEffective
DateMACPrice
ZIPRASIDONE HCL 20 MG CAPSULE ORAL 11/14/2018 0.52707
ZIPRASIDONE HCL 40 MG CAPSULE ORAL 11/14/2018 0.48664
ZIPRASIDONE HCL 60 MG CAPSULE ORAL 11/14/2018 0.56682
ZIPRASIDONE HCL 80 MG CAPSULE ORAL 01/16/2019 0.60747
ZOLEDRONIC AC/MANNITOL/0.9NACL 4 MG/100ML PIGGYBACK INTRAVEN 10/04/2017 0.76380
ZOLEDRONIC ACID 4 MG/5 ML VIAL INTRAVEN 01/23/2019 4.18440
ZOLEDRONIC ACID/MANNITOL-WATER 5 MG/100ML PIGGYBACK INTRAVEN 08/01/2018 1.12560
ZOLEDRONIC ACID/MANNITOL-WATER 5 MG/100ML PGGYBK BTL INTRAVEN 06/27/2018 1.44720
ZOLMITRIPTAN 2.5 MG TABLET ORAL 12/12/2018 2.61300
ZOLMITRIPTAN 5 MG TABLET ORAL 12/12/2018 6.94267
ZOLMITRIPTAN 2.5 MG TAB RAPDIS ORAL 01/30/2019 4.78500
ZOLMITRIPTAN 5 MG TAB RAPDIS ORAL 01/30/2019 5.46100
ZOLPIDEM TARTRATE 5 MG TABLET ORAL 03/06/2019 0.02680
ZOLPIDEM TARTRATE 10 MG TABLET ORAL 03/06/2019 0.02961
ZOLPIDEM TARTRATE 6.25 MG TAB MPHASE ORAL 02/07/2017 1.00487
ZOLPIDEM TARTRATE 12.5 MG TAB MPHASE ORAL 02/13/2019 0.88319
ZOLPIDEM TARTRATE 1.75 MG TAB SUBL SUBLINGUAL 11/28/2018 10.59840
ZOLPIDEM TARTRATE 3.5 MG TAB SUBL SUBLINGUAL 11/28/2018 10.59840
ZONISAMIDE 100 MG CAPSULE ORAL 01/16/2019 0.15772
ZONISAMIDE 25 MG CAPSULE ORAL 01/30/2019 0.10720
ZONISAMIDE 50 MG CAPSULE ORAL 10/03/2018 0.23182





























