Embed Size (px)
Citation preview
1
Click to edit Master title style
9/23/2016 1
MACRA, MIPS and APMs:Exploring the new
Quality Payment Program
Bruce Maki, MAM-CEITA / Altarum Institute
Regulatory & Incentive Program Analyst
September 27, 2016
2
Disclaimer
▲ This presentation was current at the time it was broadcast,published or uploaded to the web. Medicare and Medicaid policychanges frequently, so links to source documents and resourceshave been provided for your reference.
▲ This presentation was prepared as a service to the public and isnot intended to grant rights or impose obligations. Thispresentation may contain references or links to statutes,regulations, or other policy materials. The information provided isonly intended to be a general summary. It is not intended to takethe place of either the written law or regulations. We encourageparticipants to review the specific statutes, regulations, and otherinterpretive materials for a full and accurate statement of theircontents.
3
Agenda
▲Overview of M-CEITA
▲High-level Overview of MACRA
▲Quality Payment Program
– Merit-based Incentive Payment System (MIPS)
– Alternative Payment Models (APMs)
– Program Scoring / Incentives and Penalties
– Timeline
▲Questions & Answers
4
Who is M-CEITA?
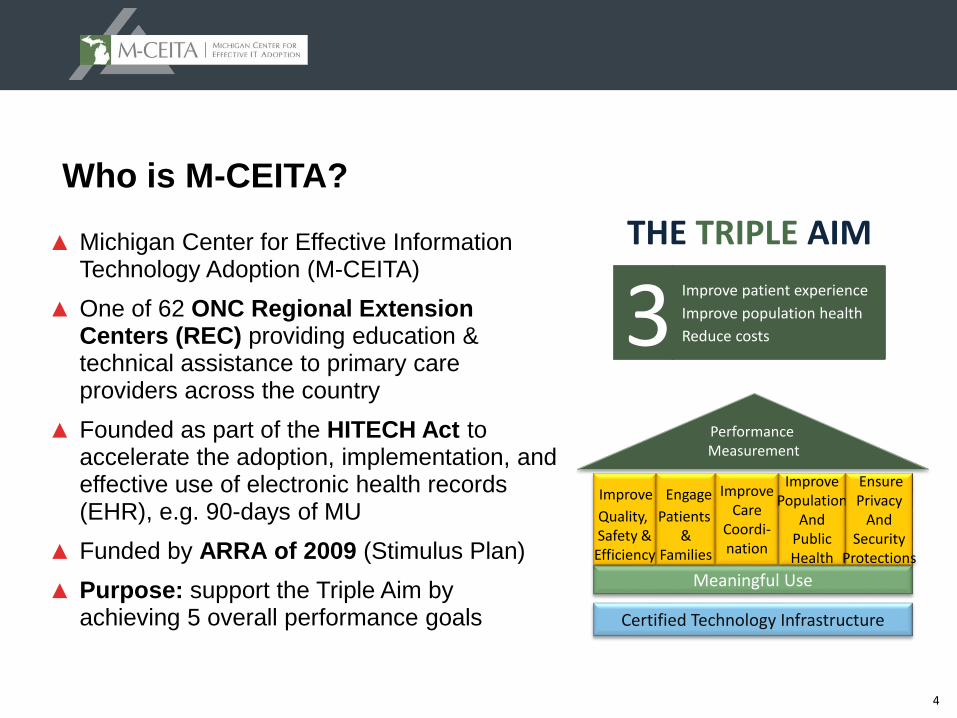
▲ Michigan Center for Effective Information Technology Adoption (M-CEITA)
▲ One of 62 ONC Regional Extension Centers (REC) providing education & technical assistance to primary care providers across the country
▲ Founded as part of the HITECH Act to accelerate the adoption, implementation, and effective use of electronic health records (EHR), e.g. 90-days of MU
▲ Funded by ARRA of 2009 (Stimulus Plan)
▲ Purpose: support the Triple Aim by achieving 5 overall performance goals
Meaningful Use
Improve
Quality, Safety &
Efficiency
Performance Measurement
Certified Technology Infrastructure
Engage
Patients &
Families
ImproveCare
Coordi-nation
ImprovePopulation
AndPublicHealth
EnsurePrivacy
AndSecurity
Protections
Improve patient experience
Improve population health
Reduce costs3THE TRIPLE AIM
5
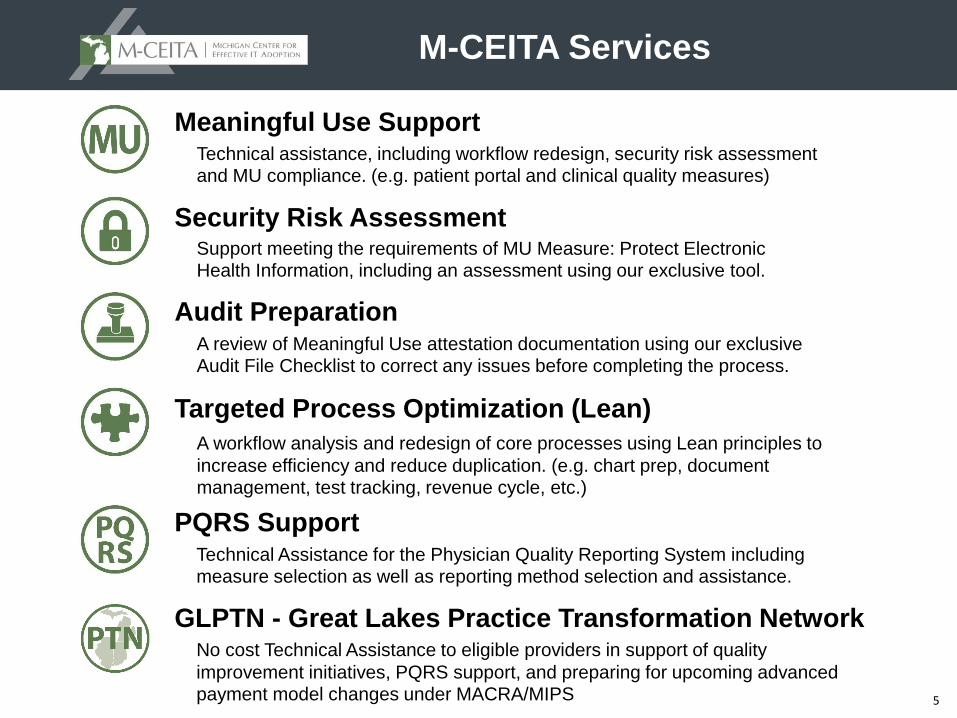
Meaningful Use Support
Security Risk Assessment
Targeted Process Optimization (Lean)
Audit Preparation
M-CEITA Services
Technical assistance, including workflow redesign, security risk assessment and MU compliance. (e.g. patient portal and clinical quality measures)
Support meeting the requirements of MU Measure: Protect Electronic Health Information, including an assessment using our exclusive tool.
A workflow analysis and redesign of core processes using Lean principles to
increase efficiency and reduce duplication. (e.g. chart prep, document management, test tracking, revenue cycle, etc.)
A review of Meaningful Use attestation documentation using our exclusive Audit File Checklist to correct any issues before completing the process.
PQRS SupportTechnical Assistance for the Physician Quality Reporting System including measure selection as well as reporting method selection and assistance.
GLPTN - Great Lakes Practice Transformation NetworkNo cost Technical Assistance to eligible providers in support of quality
improvement initiatives, PQRS support, and preparing for upcoming advanced payment model changes under MACRA/MIPS
6
MACRA:
Paying for Value and Quality
7
MACRA: What is it?
▲ Medicare Access and CHIP Reauthorization Act of 2015 (MACRA). AKA “Doc Fix” bill
▲ Bipartisan legislation (yes, really) that replaced the flawed Sustainable Growth Rate (SGR) formula by paying clinicians for the value and quality of care they provide
▲ MACRA is more predictable than SGR. It will increase the number of physicians participating in alternative payment models (APMs), with those in high quality, efficient practices benefiting financially
▲ Extends funding for Children’s Health Insurance Program (CHIP) for two years
▲ MANY of the details have yet to be determined, and there were several areas where feedback was sought from the health care community
▲ And introduces…
8
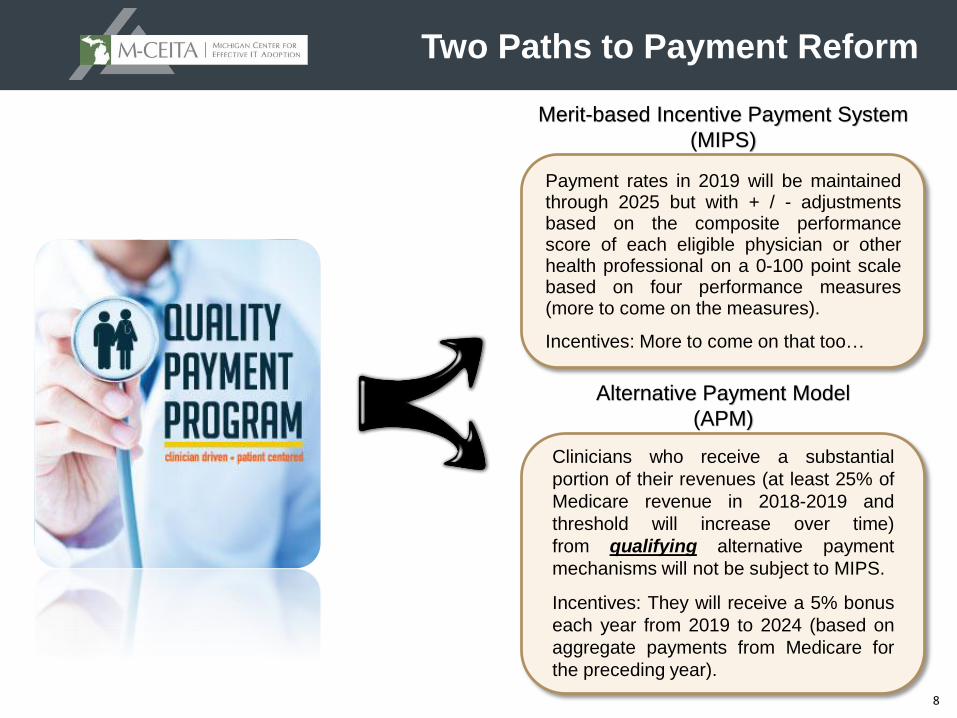
Clinicians who receive a substantial
portion of their revenues (at least 25% of
Medicare revenue in 2018-2019 and
threshold will increase over time)
from qualifying alternative payment
mechanisms will not be subject to MIPS.
Incentives: They will receive a 5% bonus
each year from 2019 to 2024 (based on
aggregate payments from Medicare for
the preceding year).
Payment rates in 2019 will be maintainedthrough 2025 but with + / - adjustmentsbased on the composite performancescore of each eligible physician or otherhealth professional on a 0-100 point scalebased on four performance measures(more to come on the measures).
Incentives: More to come on that too…
Merit-based Incentive Payment System
(MIPS)
Alternative Payment Model
(APM)
Two Paths to Payment Reform
9
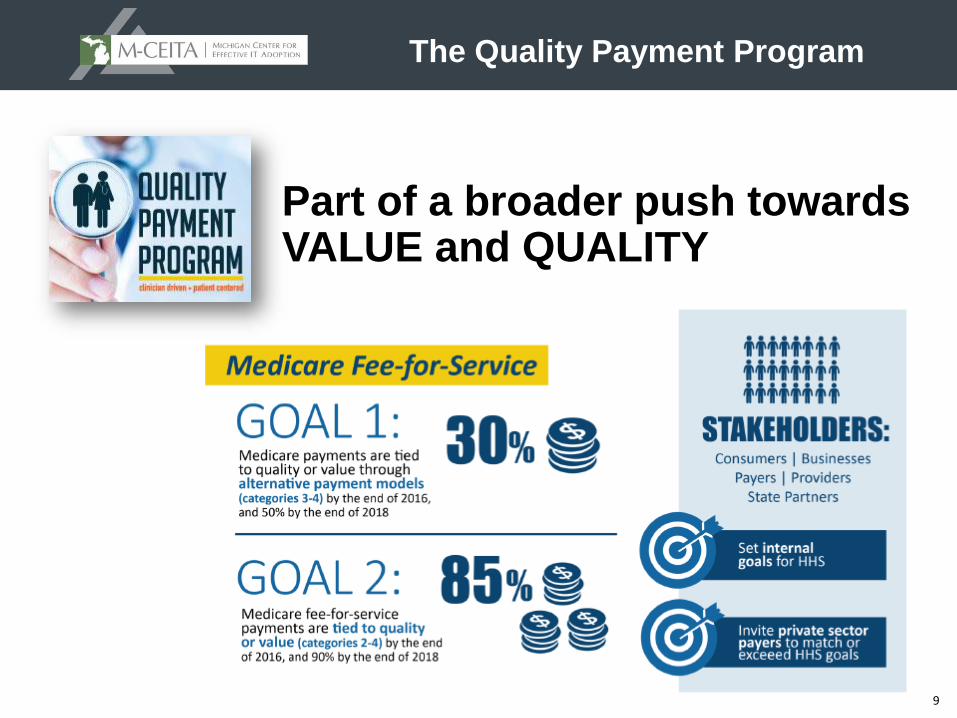
Part of a broader push towards VALUE and QUALITY
The Quality Payment Program
10
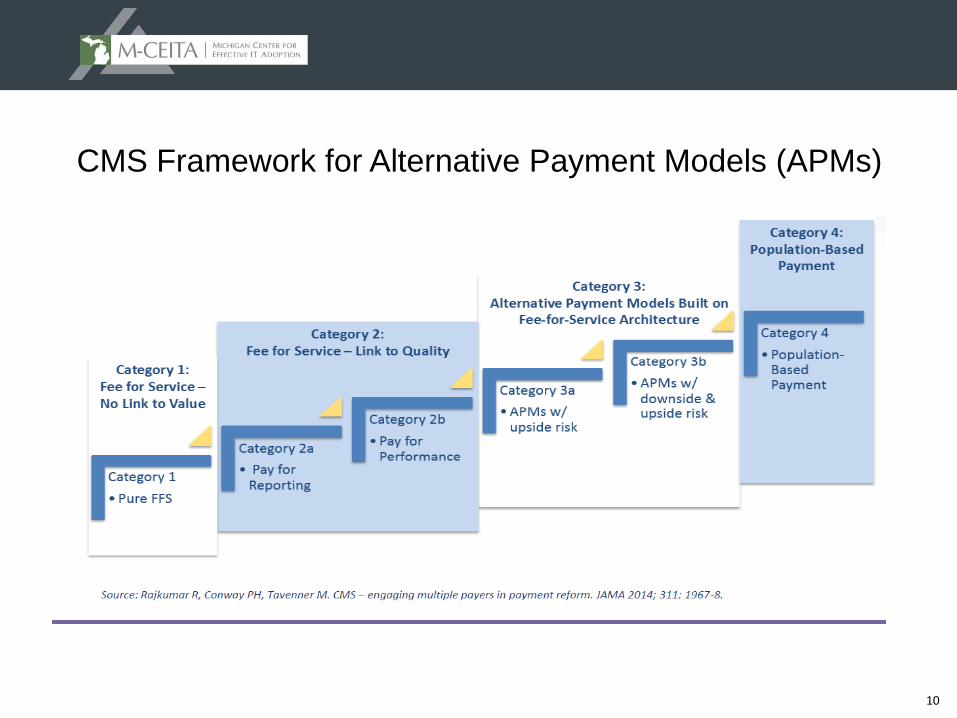
CMS Framework for Alternative Payment Models (APMs)
11
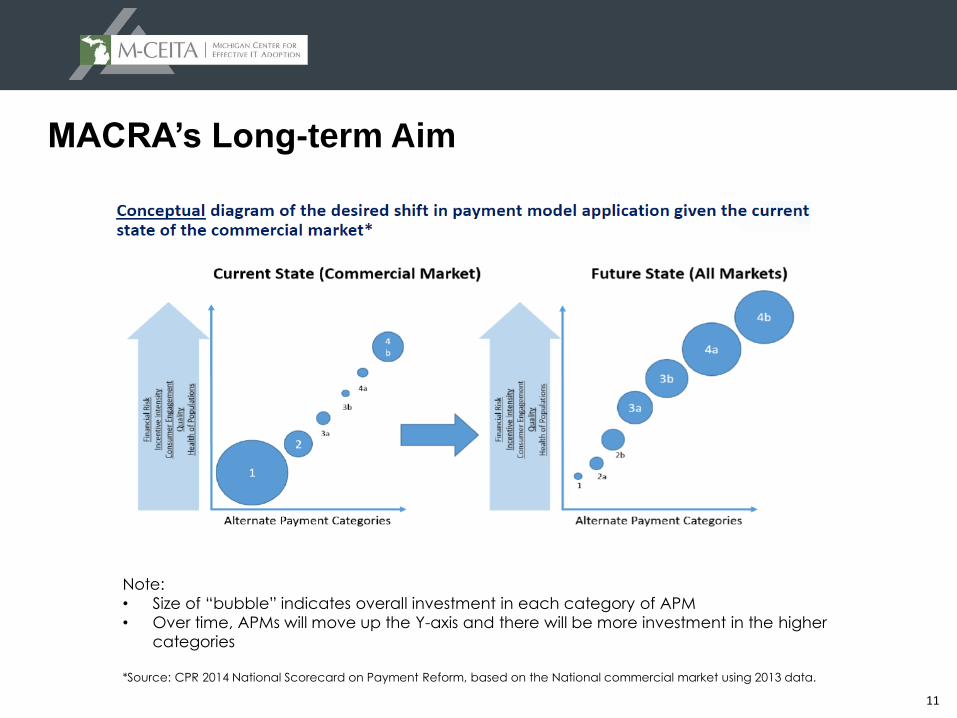
MACRA’s Long-term Aim
Note:
• Size of “bubble” indicates overall investment in each category of APM
• Over time, APMs will move up the Y-axis and there will be more investment in the higher
categories
*Source: CPR 2014 National Scorecard on Payment Reform, based on the National commercial market using 2013 data.
12
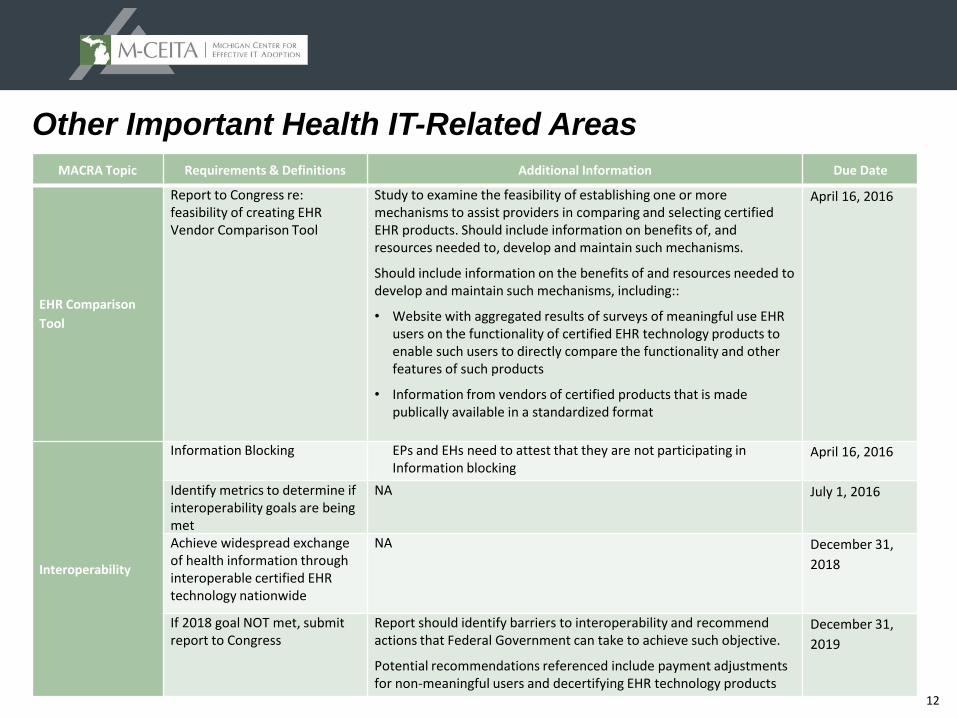
Other Important Health IT-Related Areas
MACRA Topic Requirements & Definitions Additional Information Due Date
EHR Comparison
Tool
Report to Congress re: feasibility of creating EHR Vendor Comparison Tool
Study to examine the feasibility of establishing one or more mechanisms to assist providers in comparing and selecting certified EHR products. Should include information on benefits of, and resources needed to, develop and maintain such mechanisms.
Should include information on the benefits of and resources needed to develop and maintain such mechanisms, including::
• Website with aggregated results of surveys of meaningful use EHR users on the functionality of certified EHR technology products to enable such users to directly compare the functionality and other features of such products
• Information from vendors of certified products that is made publically available in a standardized format
April 16, 2016
Interoperability
Information Blocking EPs and EHs need to attest that they are not participating inInformation blocking
April 16, 2016
Identify metrics to determine if interoperability goals are being met
NA July 1, 2016
Achieve widespread exchange of health information through interoperable certified EHR technology nationwide
NA December 31,
2018
If 2018 goal NOT met, submit report to Congress
Report should identify barriers to interoperability and recommend actions that Federal Government can take to achieve such objective.
Potential recommendations referenced include payment adjustments for non-meaningful users and decertifying EHR technology products
December 31,
2019
13
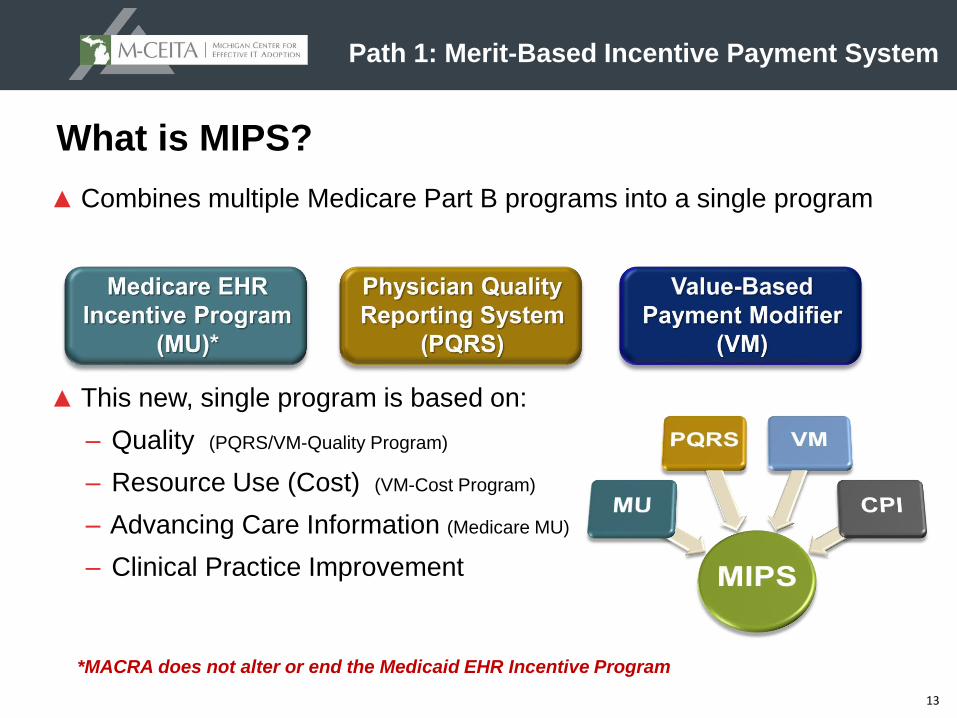
Path 1: Merit-Based Incentive Payment System
▲ Combines multiple Medicare Part B programs into a single program
▲ This new, single program is based on:
– Quality (PQRS/VM-Quality Program)
– Resource Use (Cost) (VM-Cost Program)
– Advancing Care Information (Medicare MU)
– Clinical Practice Improvement
What is MIPS?
*MACRA does not alter or end the Medicaid EHR Incentive Program
14
Merit-Based Incentive Payment System
▲ MIPS payment adjustments based on Composite Performance Score (CPS) increasing from +/- 4% in 2019 to +/- 9% in 2022 and later*
▲ Budget neutral unless an exception applies
▲ Additional funding for positive adjustments for exceptional performance (2019 – 2024)
▲ Incentive payments for certain eligible professionals (EPs) who participate in Alternative Payment Models (APMs)
▲ Higher update rate for “qualifying APM participants” (QPs) beginning in 2026
*Note: The upward adjustment may differ somewhat since it is scaled to achieve budget neutrality
15
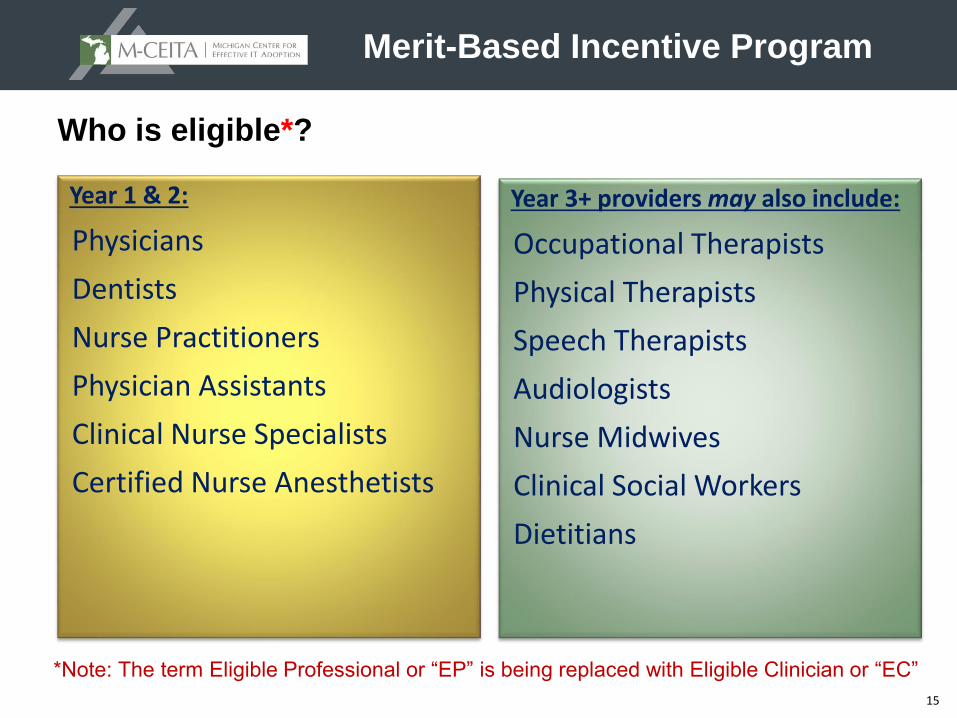
Who is eligible*?
Year 1 & 2:
Physicians
Dentists
Nurse Practitioners
Physician Assistants
Clinical Nurse Specialists
Certified Nurse Anesthetists
Merit-Based Incentive Program
Year 3+ providers may also include:
Occupational Therapists
Physical Therapists
Speech Therapists
Audiologists
Nurse Midwives
Clinical Social Workers
Dietitians
*Note: The term Eligible Professional or “EP” is being replaced with Eligible Clinician or “EC”
16
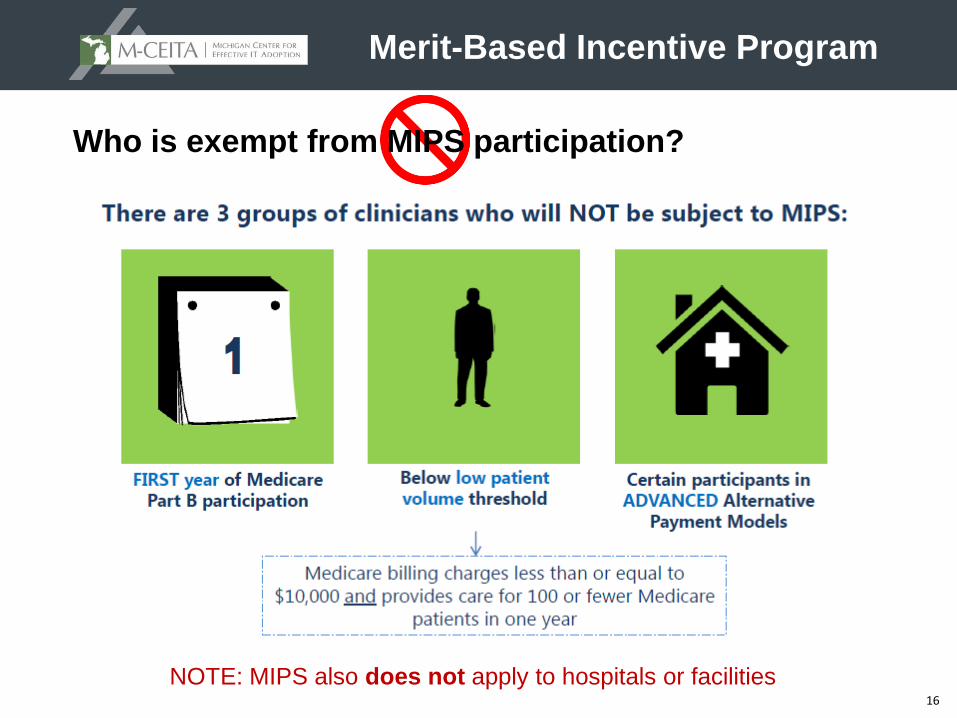
Merit-Based Incentive Program
Who is exempt from MIPS participation?
NOTE: MIPS also does not apply to hospitals or facilities
17
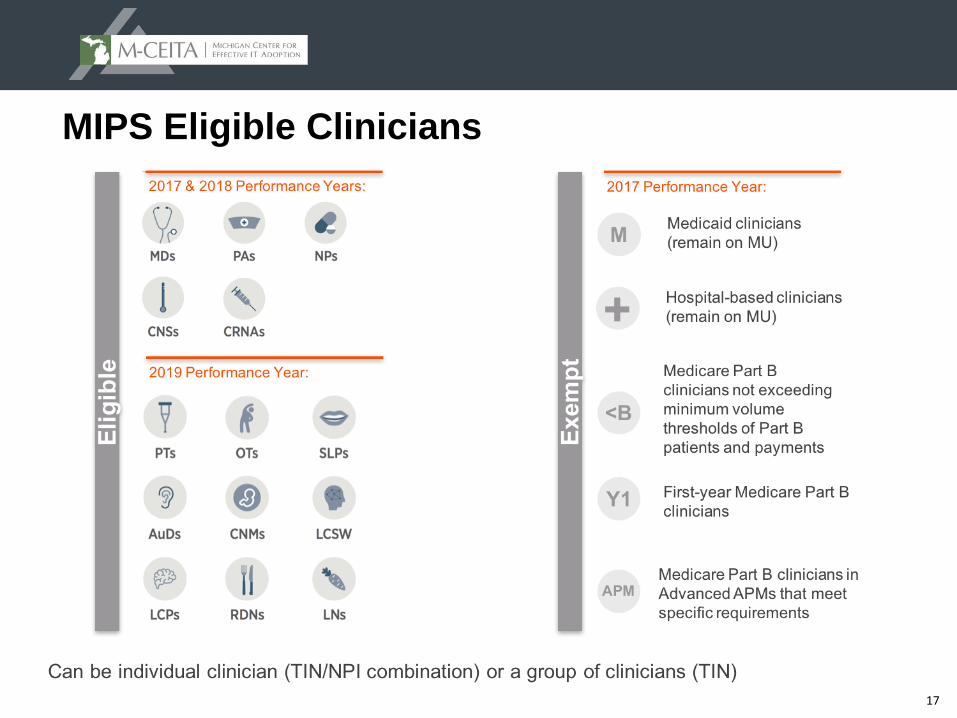
MIPS Eligible Clinicians
18
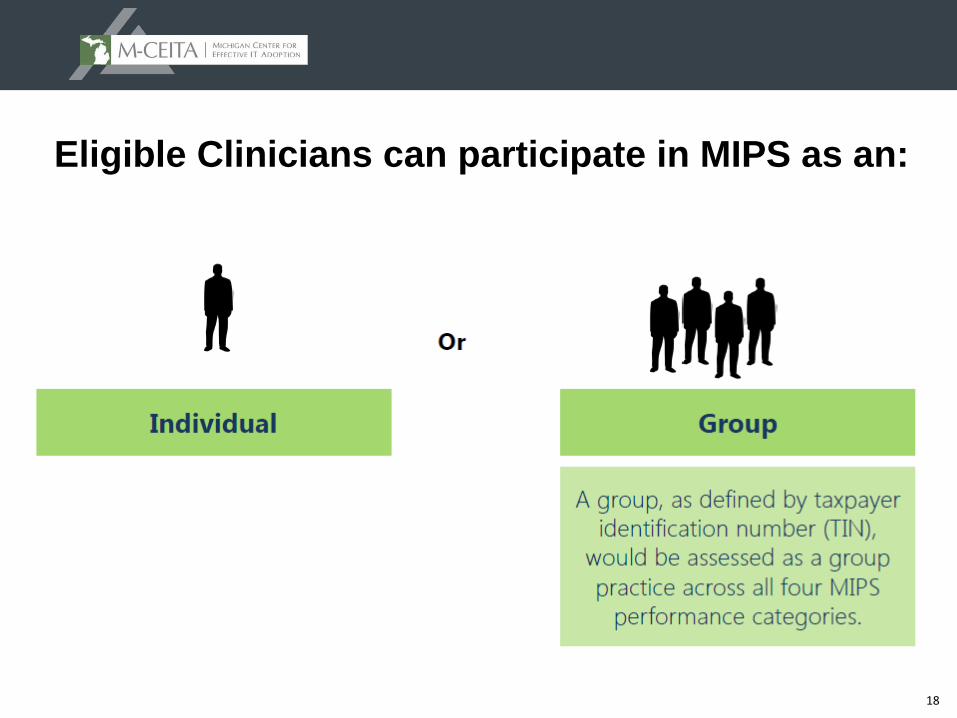
Eligible Clinicians can participate in MIPS as an:
19
Group Reporting
▲ Providers can opt to be assessed as a group of ECs
▲ Performance is measured as a combined score of all the eligible professionals in the group
▲ Clinics with 10 or fewer ECs can join with others to form a “virtual group” (option beginning in year 2)
▲ Virtual groups can be based on geography or specialty
▲ Must have a written agreement
▲ Must stay in the group for the entire performance year
▲ “All or nothing”- Individual small practice providers can not “opt out” of virtual group participation (similar to group proxy calculations for Medicaid MU program eligibility)
20
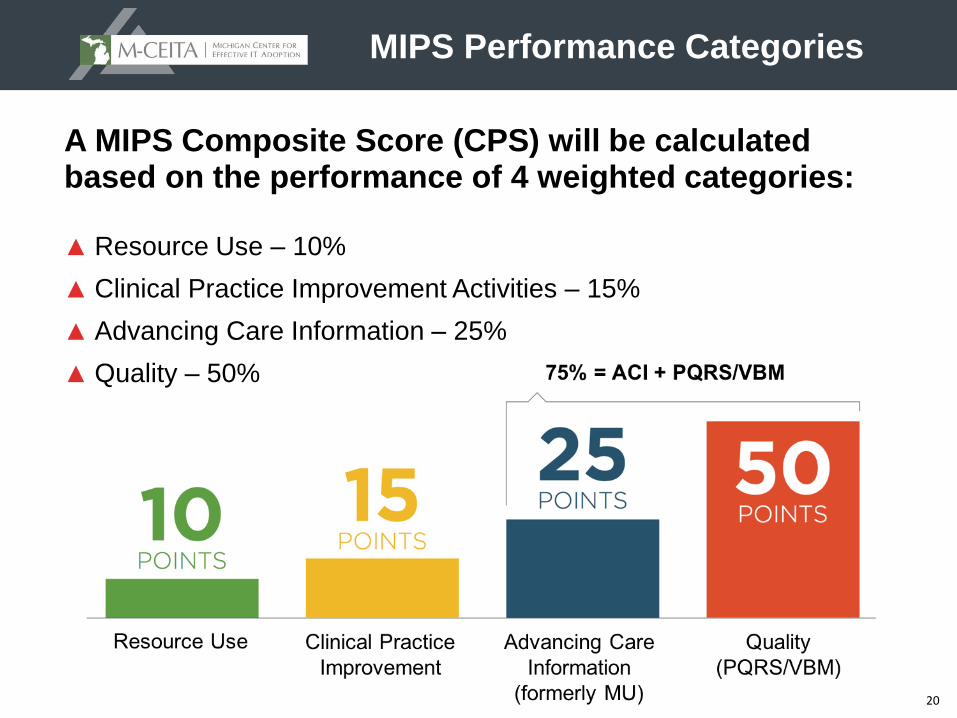
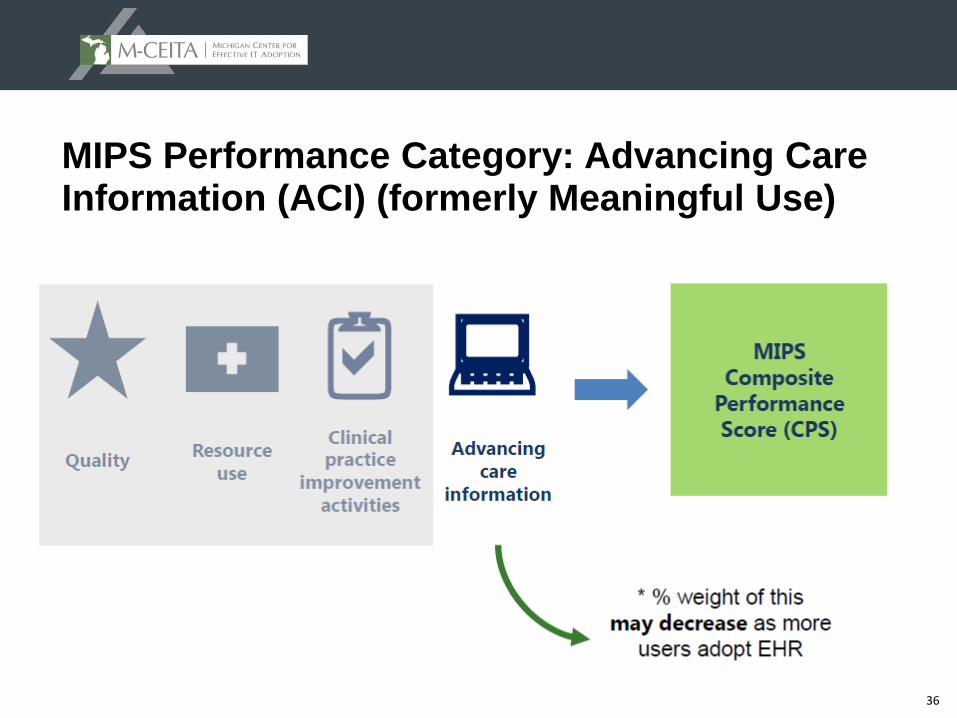
MIPS Performance Categories
A MIPS Composite Score (CPS) will be calculated based on the performance of 4 weighted categories:
▲ Resource Use – 10%
▲ Clinical Practice Improvement Activities – 15%
▲ Advancing Care Information – 25%
▲ Quality – 50%
21
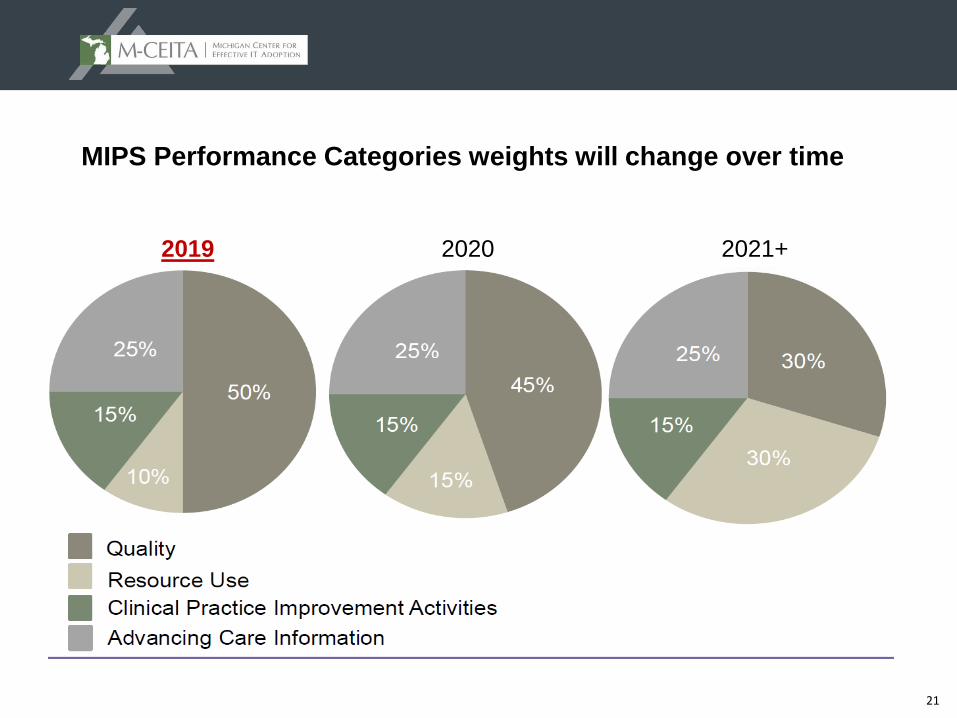
MIPS Performance Categories weights will change over time
2019 2020 2021+
22
MIPS Composite Performance Score
MIPS Performance Categories
A single MIPS composite performance score will factor
in performance in 4 weighted performance categories
on a 0-100 point scale:
23
MIPS Composite Performance Score:
▲ Weights may be adjusted if there are not sufficient measures and activities applicable for each type of EC, including assigning a scoring weight of 0 for a performance category
▲ ACI (aka MU) weighting can be decreased and shifted to other categories if Secretary estimates the proportion of physicians who are meaningful EHR users is 75% or greater (statutory floor for ACI weight is 15%)
▲ Performance threshold will be established based on the mean or median of the composite performance scores during a prior period (Yrs 1 and 2 HHS Secretary will establish threshold)
▲ The composite performance score will range from 0 – 100
▲ Those who score below the threshold will see negative payment adjustments, those who score above it will see positive adjustments
▲ Any providers who score in the bottom quartile will have their payments immediately reduced to the maximum penalty for that year
24
MIPS Performance Category: Quality
25
Quality
▲ Summary:
– Selection of 6 measures relevant to scope of practice
– 1 cross-cutting measure and 1 outcome measure, or another high priority measure if outcome is unavailable
– Select from individual measures or a specialty measure set
– Population measures automatically calculated
– Several data submission options which alter reporting requirements
– Key Changes from Current Program (PQRS):
Reduced from 9 measures to 6 measures with no domain requirement
Emphasis on outcome measurement
Year 1 Weight: 50%
What is the requirement?
26
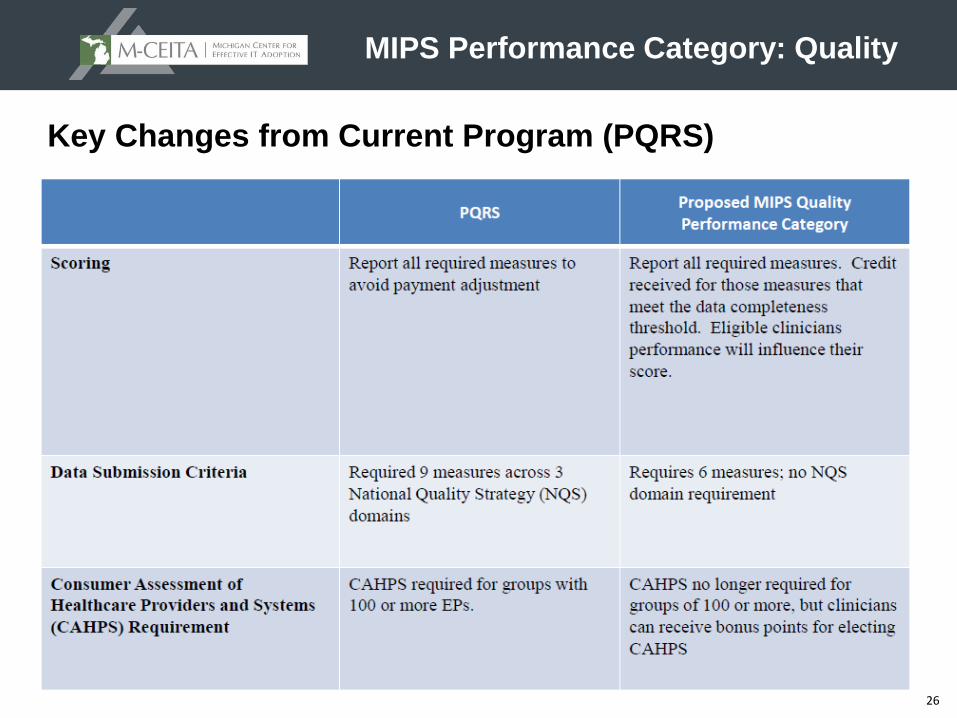
Key Changes from Current Program (PQRS)
MIPS Performance Category: Quality
27
MIPS Performance Category: Resource Use (aka Cost)
28
Resource Use (Cost)
▲ Summary:
– Assessment under all available resource use measures, as applicable to the clinician
– CMS calculates based on claims so there are no reporting requirements for clinicians
– Key Changes from Current Program (Value Modifier):
Adding up to 41 episode specific measures to address specialty concerns
Others on next slide
Year 1 Weight: 10%
What is the Requirement?
29
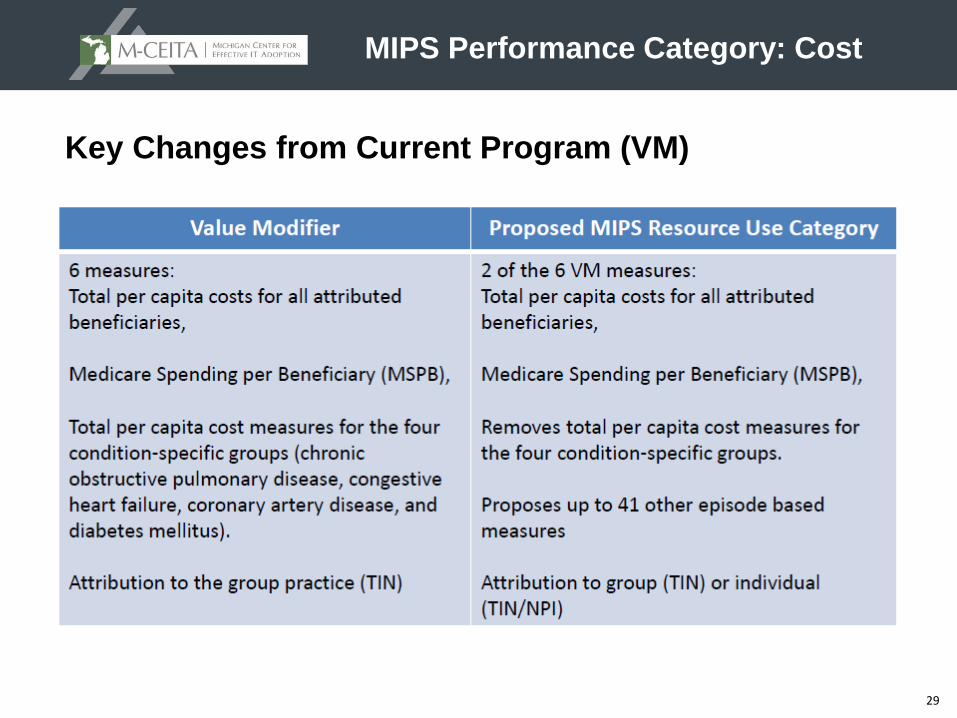
Key Changes from Current Program (VM)
MIPS Performance Category: Cost
30
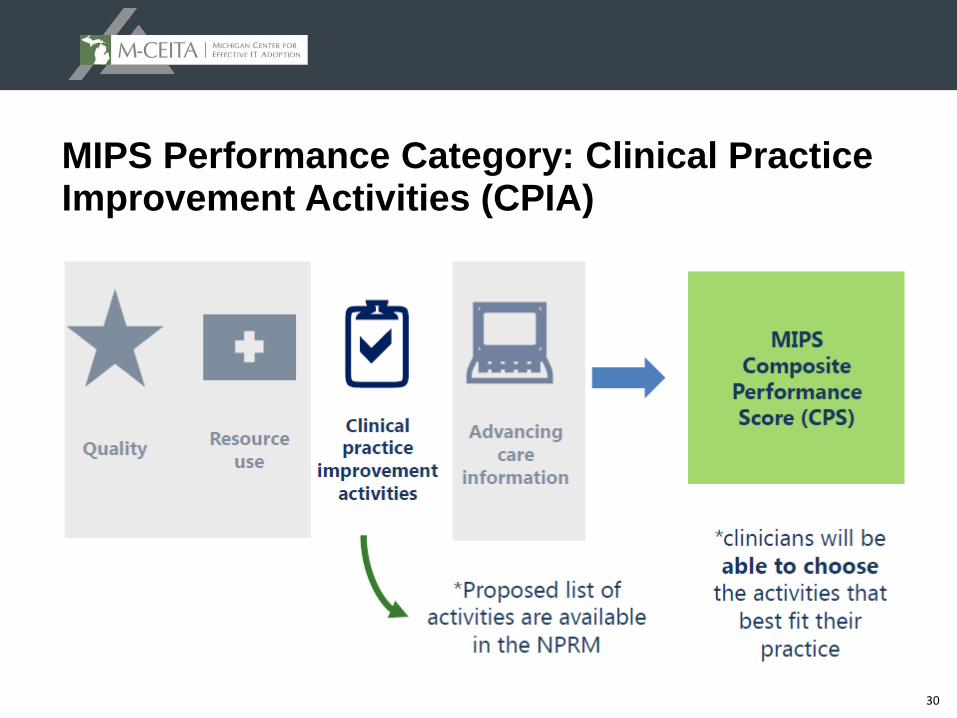
MIPS Performance Category: Clinical Practice Improvement Activities (CPIA)
31
Clinical Practice Improvement Activities
▲Summary:
–Minimum selection of one CPIA activity (from 90+ proposed activities) for a partial score, with additional scoring for more activities
–Activities categorized as “high” or “medium” weight, earning 20 or 10 points each, respectively
–Full credit is achievement of 60 points
–Full credit for patient-centered medical home, Medical Home, or comparable specialty practice
–Minimum of half credit for APM participation, with opportunity to select additional activities for full credit
–Year 1 Weight: 15%
What is the requirement?
32
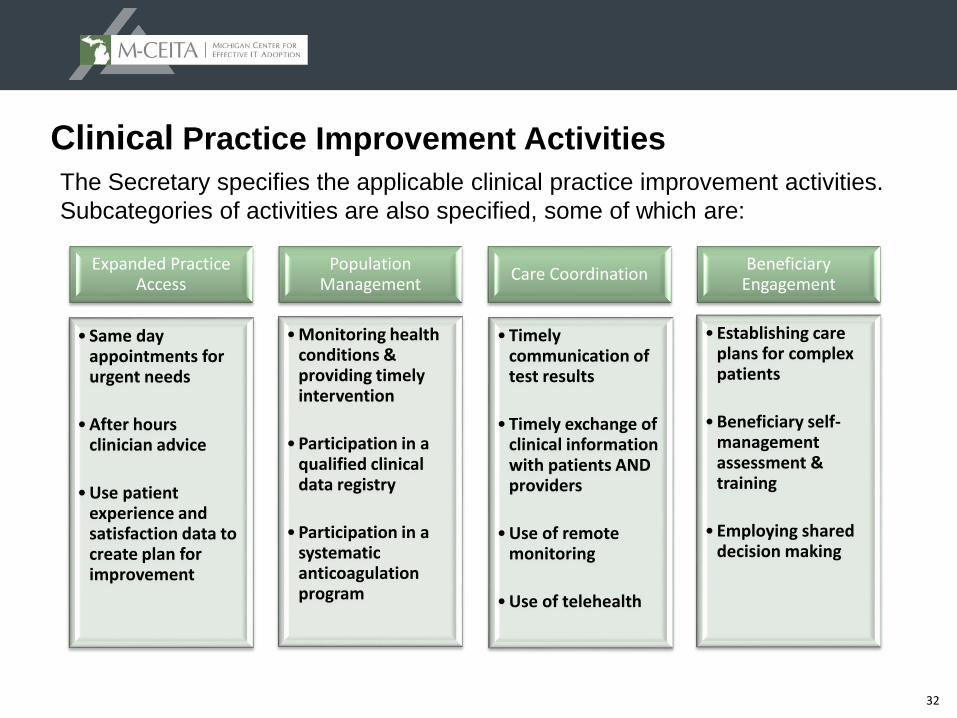
Clinical Practice Improvement Activities
Expanded Practice Access
• Same day appointments for urgent needs
•After hours clinician advice
•Use patient experience and satisfaction data to create plan for improvement
Population Management
•Monitoring health conditions & providing timely intervention
•Participation in a qualified clinical data registry
•Participation in a systematic anticoagulation program
Care Coordination
•Timely communication of test results
•Timely exchange of clinical information with patients AND providers
•Use of remote monitoring
•Use of telehealth
Beneficiary Engagement
•Establishing care plans for complex patients
•Beneficiary self-management assessment & training
•Employing shared decision making
The Secretary specifies the applicable clinical practice improvement activities.
Subcategories of activities are also specified, some of which are:
33
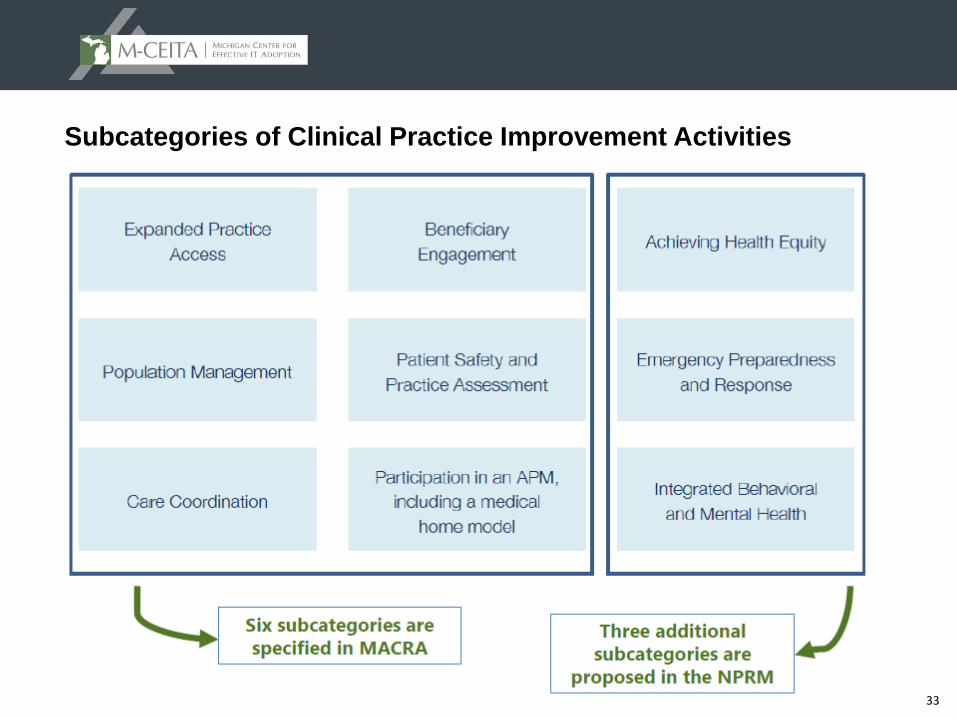
Subcategories of Clinical Practice Improvement Activities
34
CPIA Scoring Overview
In general:
▲ Each activity in the CPIA activity list is worth a certain number of points
– Most are worth 10 points (medium weight)
– Some activities are high weight and worth 20 points
▲ To get maximum credit, must achieve 60 points
– Can be achieved by selecting any combination of activities:
High- and medium-weight
All high-weight
All medium-weight activities
▲ Special scoring considerations for specific types of eligible clinicians and groups are discussed on next slide
35
CPIA: Special Scoring Considerations
▲ For non-patient facing eligible clinicians and groups, small practices (15 or fewer professionals), practices located in rural areas and geographic health professional shortage areas:
– First activity gets 50% of the 60 points
– Second activity gets 100% of the 60 points
▲ For APMs reporting in the CPIA performance category: APM participation is automatically half of highest potential score, with opportunity to select additional activities for full credit
▲ Certified patient-centered medical homes, comparable specialty practices, or Medical Homes receive highest potential score
36
MIPS Performance Category: Advancing Care Information (ACI) (formerly Meaningful Use)
37
Advancing Care Information
▲ Summary:
– Scoring based on key measures of health IT interoperability promoting patient engagement and electronic information exchange
– Flexible scoring for all measures to promote care coordination for better patient outcomes
– Key Changes from Current Program (Medicare Meaningful Use):
Dropped “all or nothing” threshold for measurement
Eliminated Computerized Provider Order Entry (CPOE) and Clinical Decision Support (CDS) objectives
Reduced the number of required public health registries reported
Year 1 Weight: 25%
– Two scores calculated
Base Score and Performance Score
What is the requirement?
38
Advancing Care Information
BASE SCORE
▲ The Advancing Care Information base score is based on the reporting of 6 measures:
– Protect Patient Health Information
– Electronic Prescribing
– Patient Electronic Access
– Coordination of Care Through Patient Engagement
– Health Information Exchange
– Public Health and Clinical Data
PERFORMANCE SCORE
▲ Physicians will select the measures that best fit their practice from the following measures:
– Patient Electronic Access
– Coordination of Care Through Patient Engagement
– Health Information Exchange
39
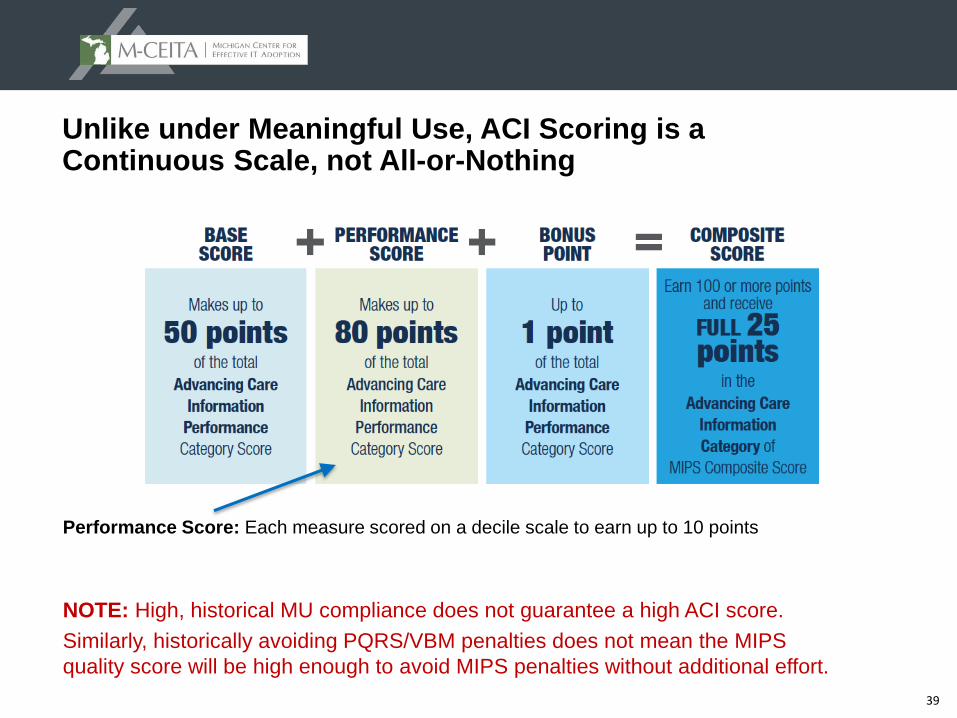
Unlike under Meaningful Use, ACI Scoring is a Continuous Scale, not All-or-Nothing
Performance Score: Each measure scored on a decile scale to earn up to 10 points
NOTE: High, historical MU compliance does not guarantee a high ACI score.
Similarly, historically avoiding PQRS/VBM penalties does not mean the MIPS
quality score will be high enough to avoid MIPS penalties without additional effort.
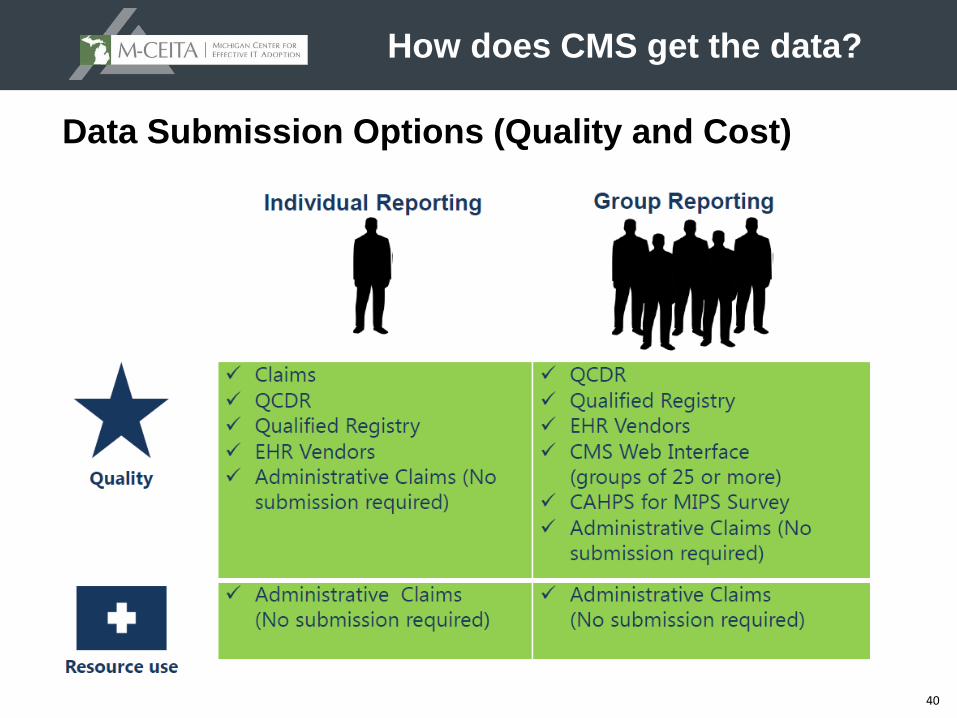
40
Data Submission Options (Quality and Cost)
How does CMS get the data?
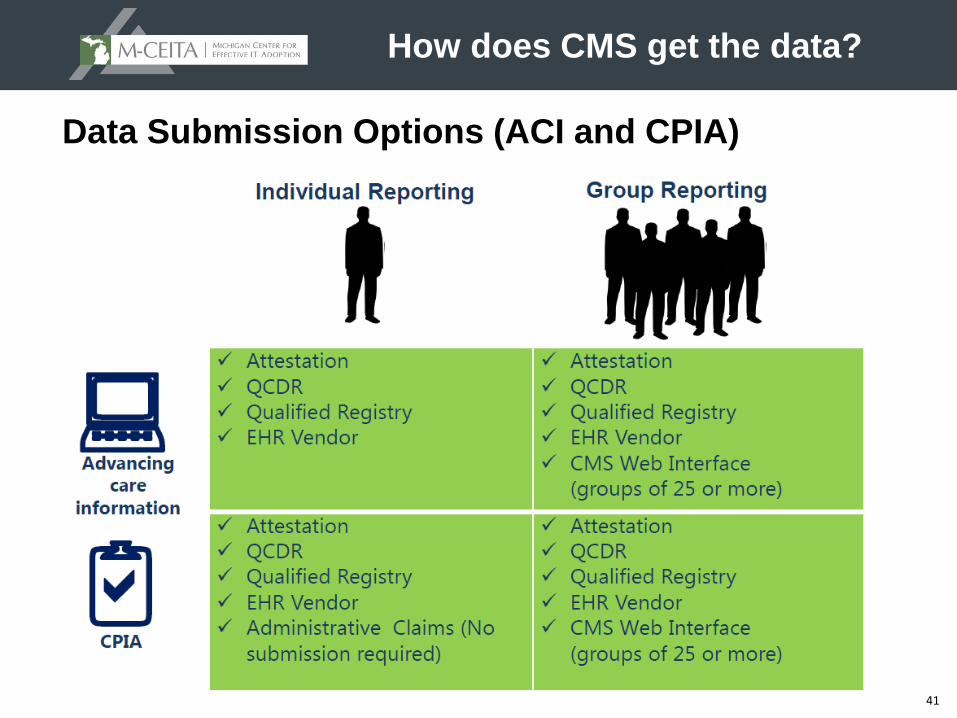
41
Data Submission Options (ACI and CPIA)
How does CMS get the data?
42
Feedback and Review
Are there checks and balances?
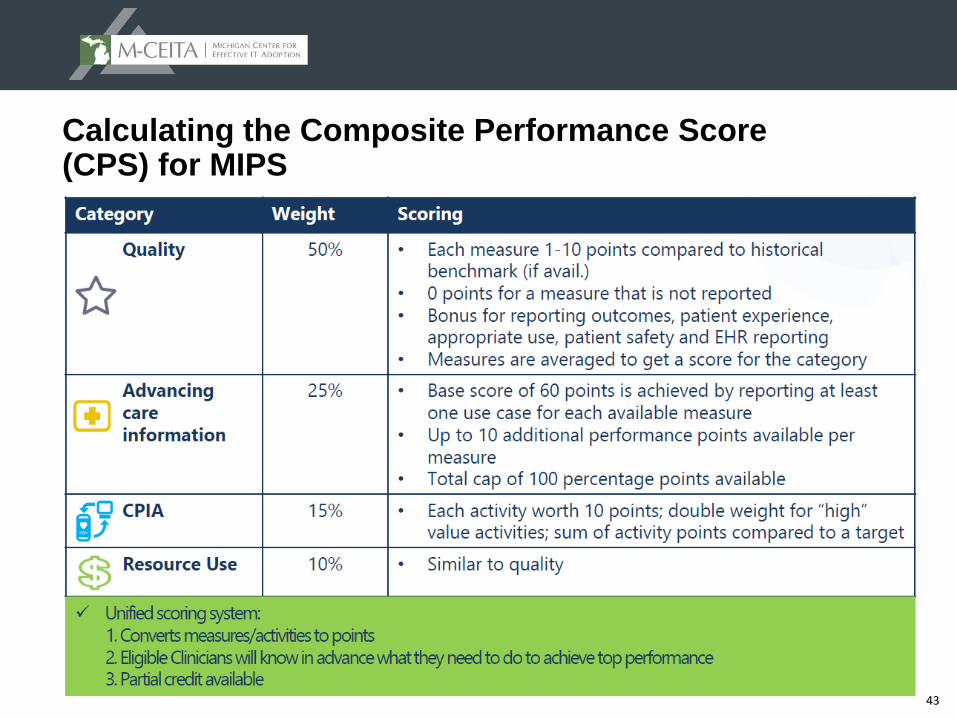
43
Calculating the Composite Performance Score (CPS) for MIPS
44
MIPS - Incentives and Penalties
▲ Adjustments applied 2 years after performance year (e.g. 2019 adjustment is based on 2017 performance year)
▲ The program is budget neutral, so ECs receiving negative adjustments pay for those receiving positive adjustments
▲ Performance threshold is mean or median of the composite score for all MIPS providers (except in first 2 years where Secretary will set)
▲ Linear adjustment based on composite score, as compared to performance threshold (positive, negative, or zero/neutral)
▲ If you score in the bottom 25% of providers, you will automatically be adjusted down to the maximum penalty for that program/payment year
▲ Higher scores receive proportionally larger incentive payments, up to three times the maximum positive adjustment for the year (4% x 3 = 12% in 2019)
▲ Highest performers eligible for “Exceptional Performance Bonus”
– Additional payment adjustment of +10% for ECs in the top 25%
– ECs have the potential to receive a 22% increase in 2019 (and 37% in 2024!)
Payment Adjustments
45
MIPS – Incentives and Penalties
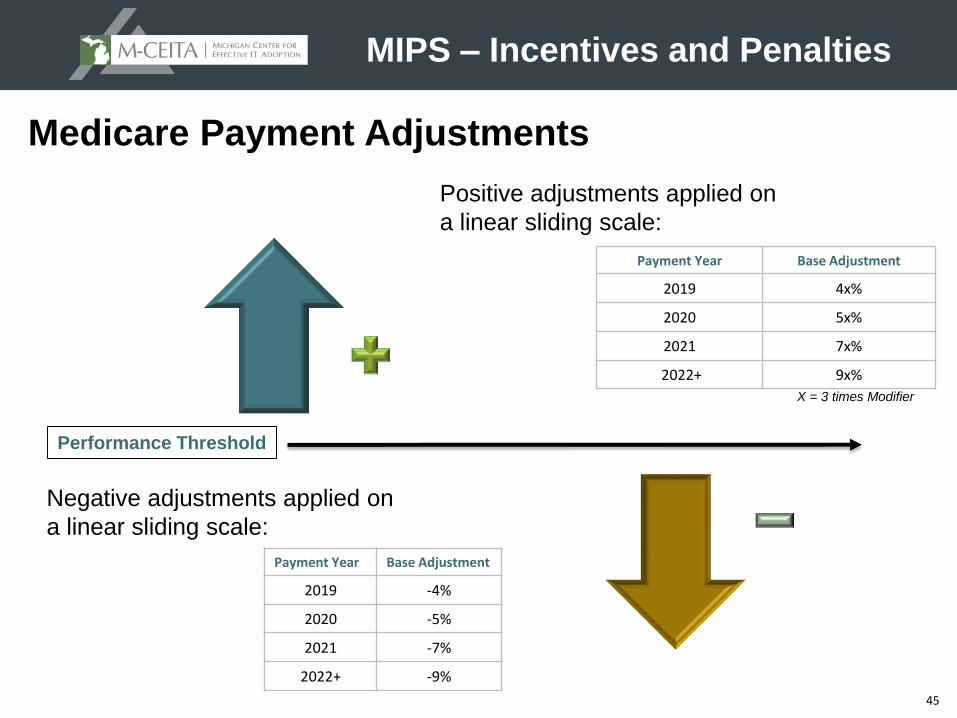
Payment Year Base Adjustment
2019 4x%
2020 5x%
2021 7x%
2022+ 9x%
Medicare Payment Adjustments
Performance Threshold
Positive adjustments applied on
a linear sliding scale:
X = 3 times Modifier
Negative adjustments applied on
a linear sliding scale:
Payment Year Base Adjustment
2019 -4%
2020 -5%
2021 -7%
2022+ -9%
46
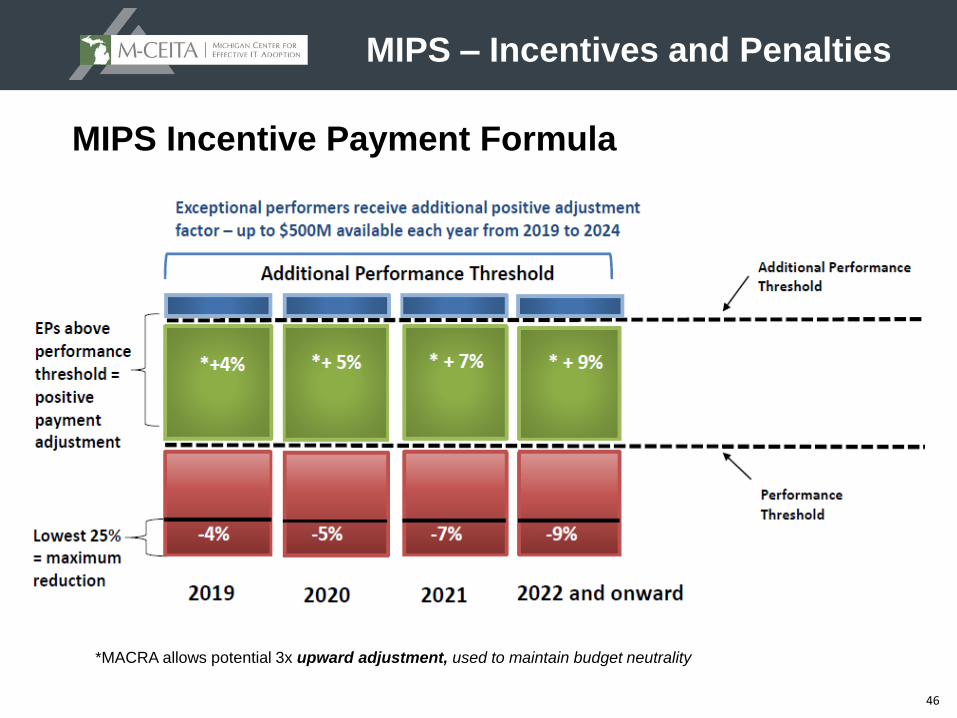
MIPS Incentive Payment Formula
*MACRA allows potential 3x upward adjustment, used to maintain budget neutrality
MIPS – Incentives and Penalties
47
The other fork in
the path to
Quality
Payments
Alternative Payment Models
48
Alternative Payment Models (APMs)What are they?
▲ Alternative Payment Model or APM is a generic term describing a payment model in which providers take responsibility for cost and quality performance and receive payments to support the services and activities designed to achieve high value
▲ According to MACRA, APMs include:
– Medicare Shared Savings Program (MSSP) ACOs
– Demonstration under the Health Care Quality Demonstration Program
– CMS Innovation Center Models
– Demonstrations required by Federal Law
▲ MACRA does not change how any particular APM pays for medical care and rewards value
▲ APM participants may receive favorable scoring under certain MIPS performance categories
▲ Only some of these APMs will be advanced APMs
49
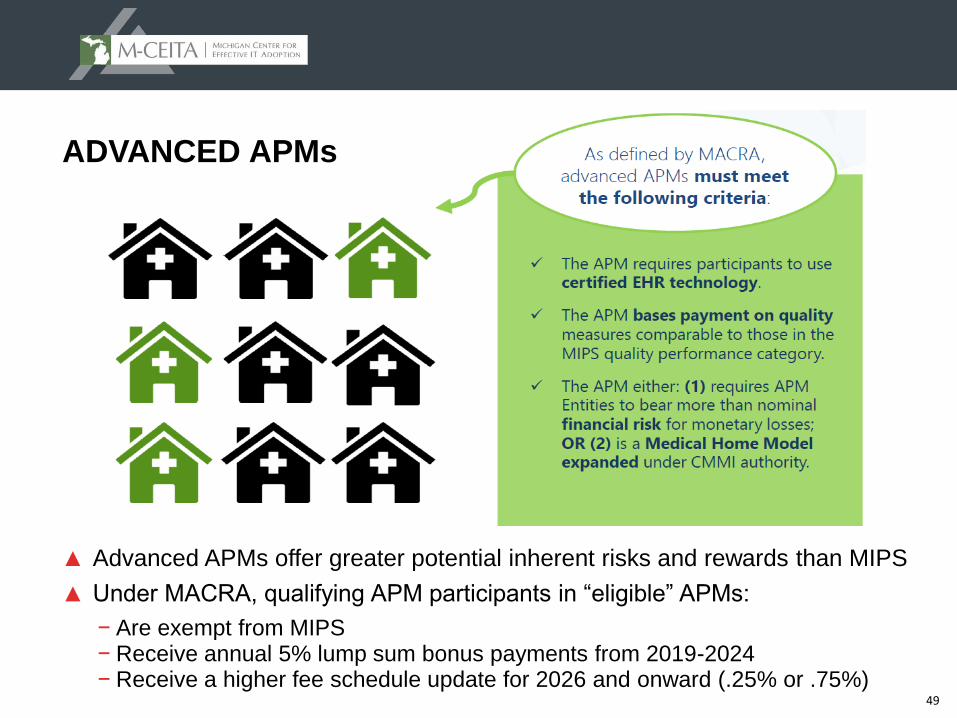
▲ Advanced APMs offer greater potential inherent risks and rewards than MIPS
▲ Under MACRA, qualifying APM participants in “eligible” APMs:
− Are exempt from MIPS− Receive annual 5% lump sum bonus payments from 2019-2024− Receive a higher fee schedule update for 2026 and onward (.25% or .75%)
ADVANCED APMs
50
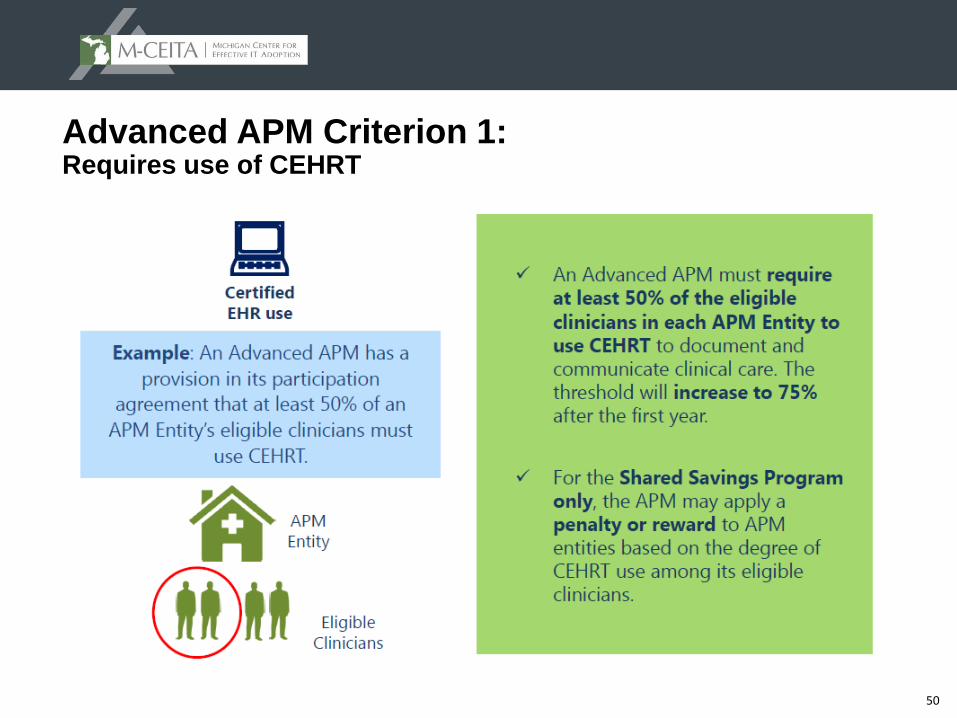
Advanced APM Criterion 1: Requires use of CEHRT
51
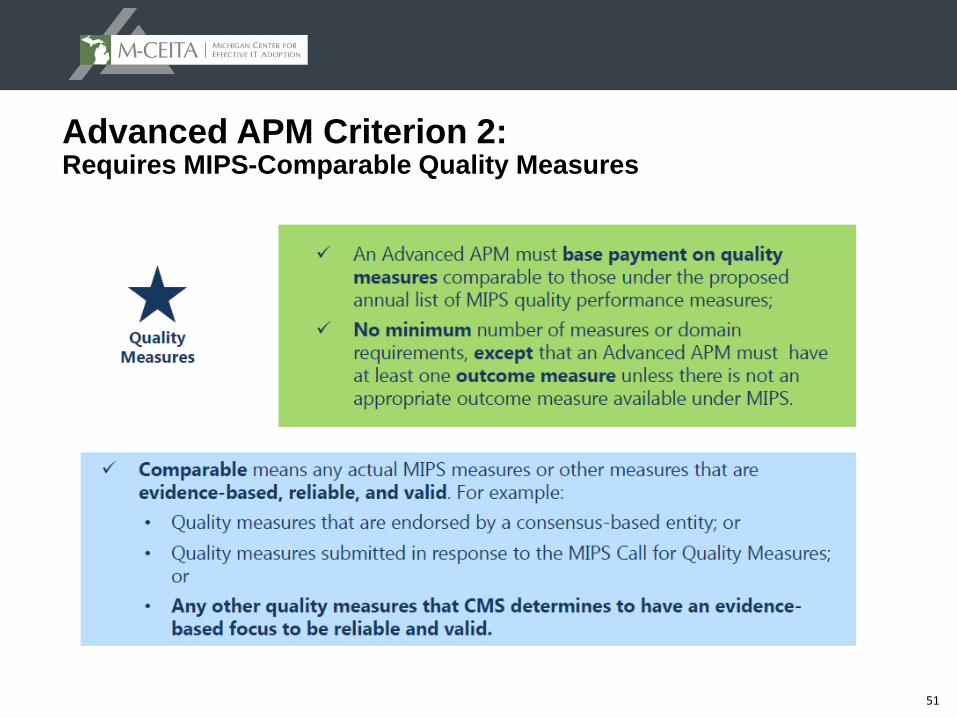
Advanced APM Criterion 2: Requires MIPS-Comparable Quality Measures
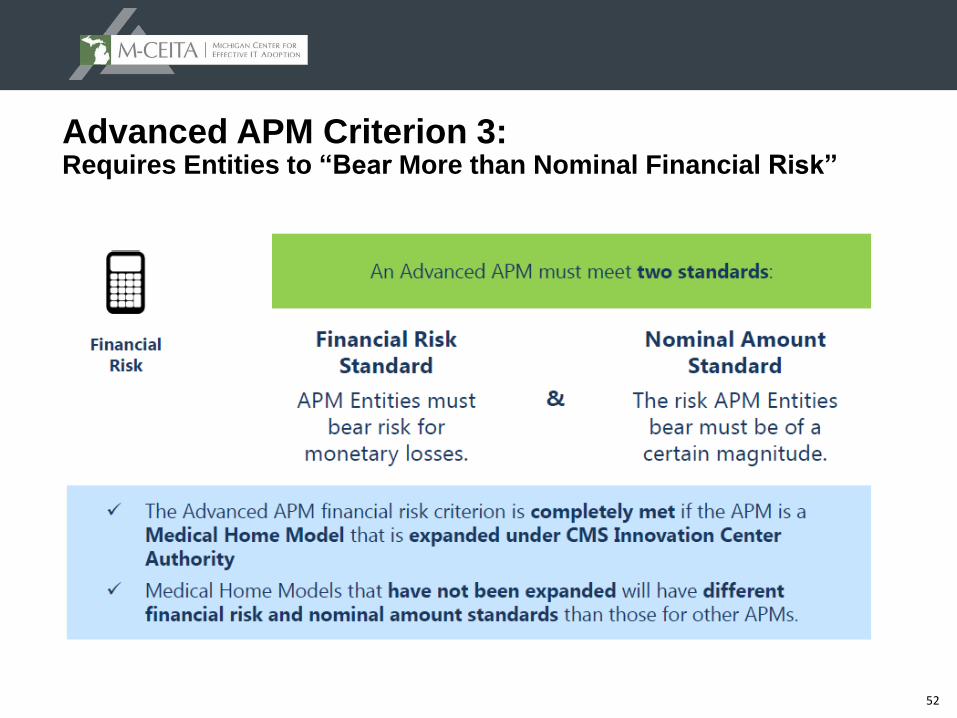
52
Advanced APM Criterion 3: Requires Entities to “Bear More than Nominal Financial Risk”
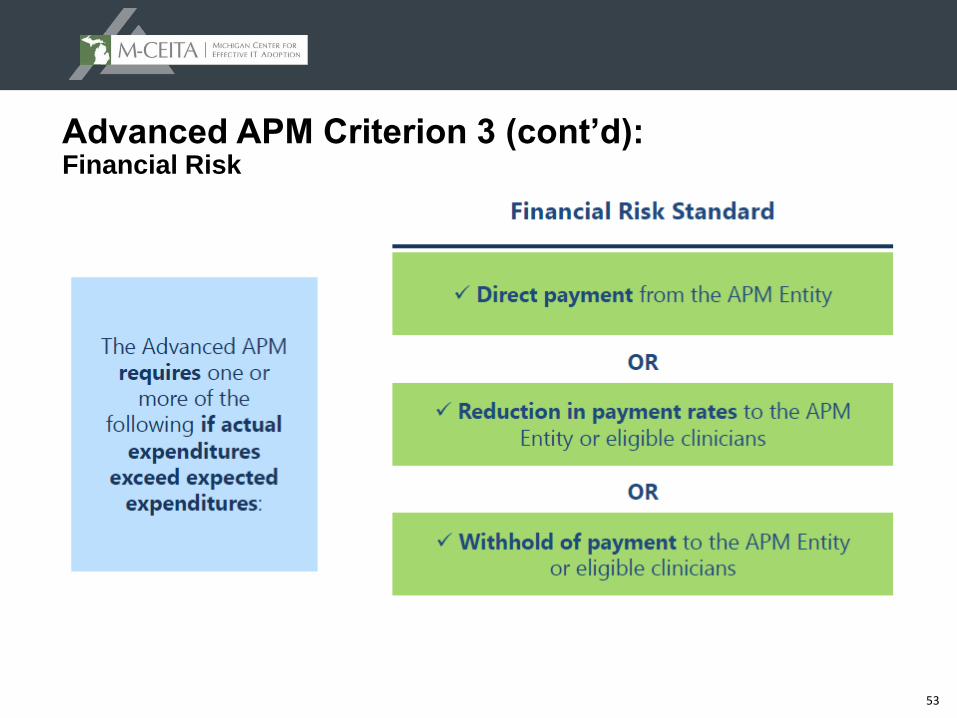
53
Advanced APM Criterion 3 (cont’d): Financial Risk
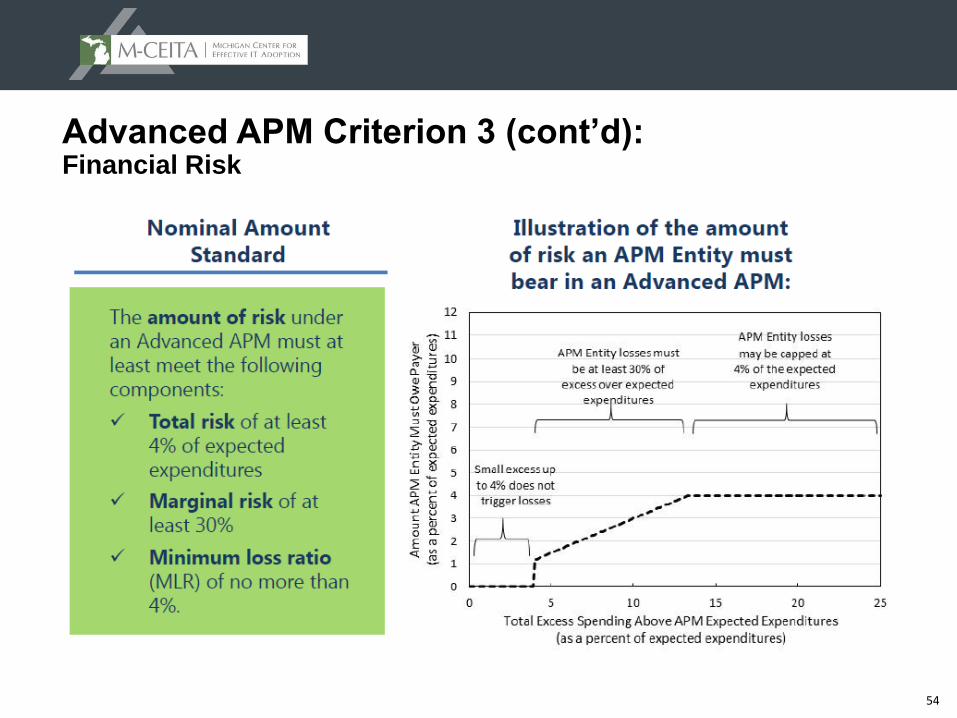
54
Advanced APM Criterion 3 (cont’d): Financial Risk
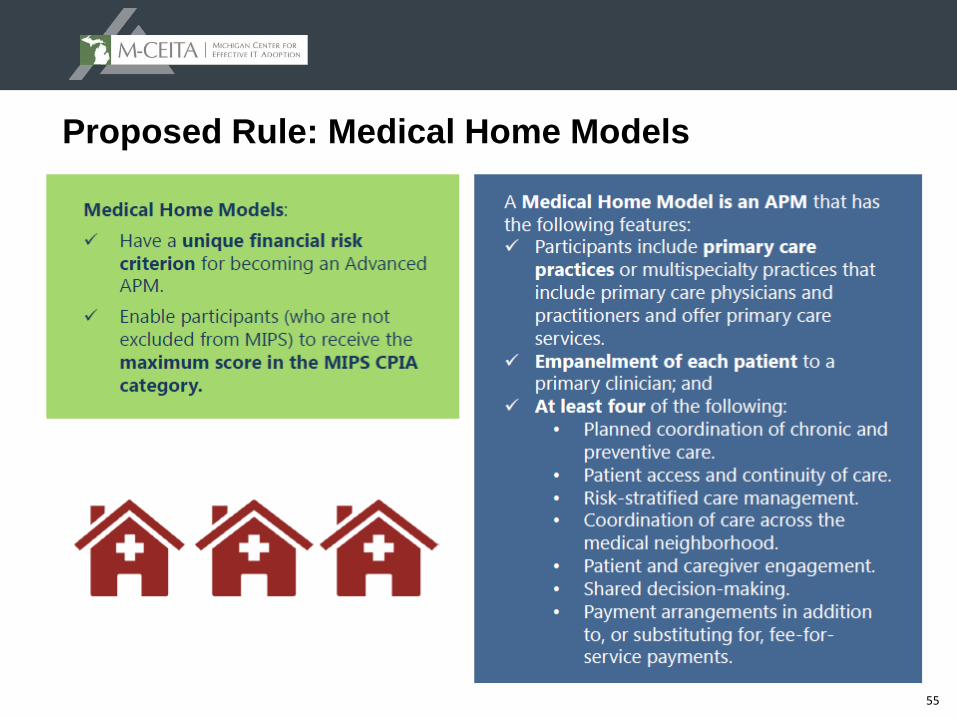
55
Proposed Rule: Medical Home Models
56
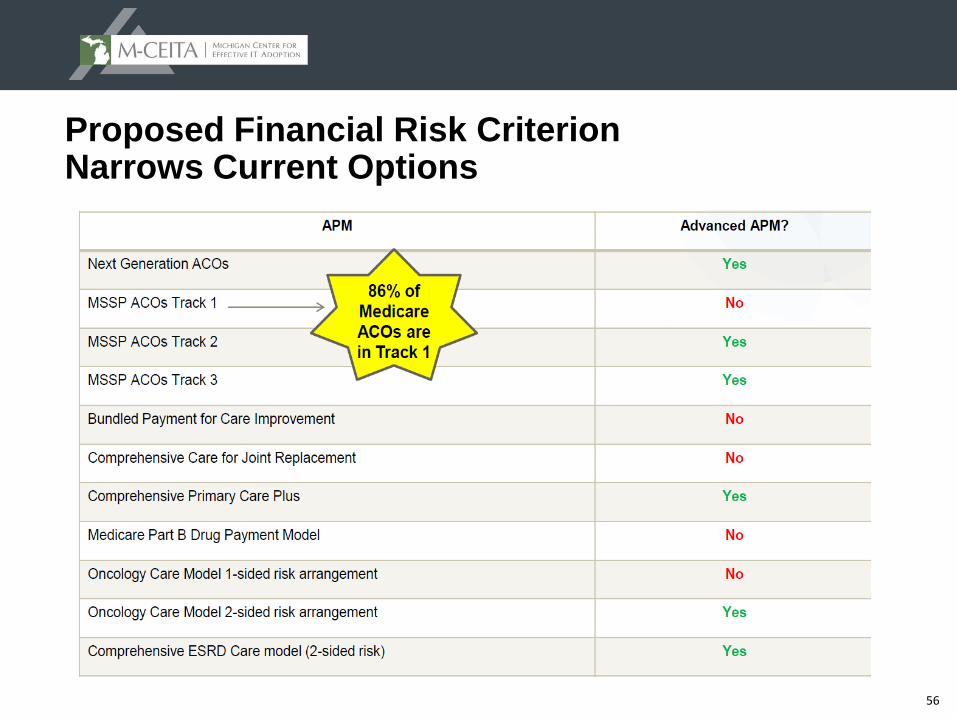
Proposed Financial Risk Criterion Narrows Current Options
57
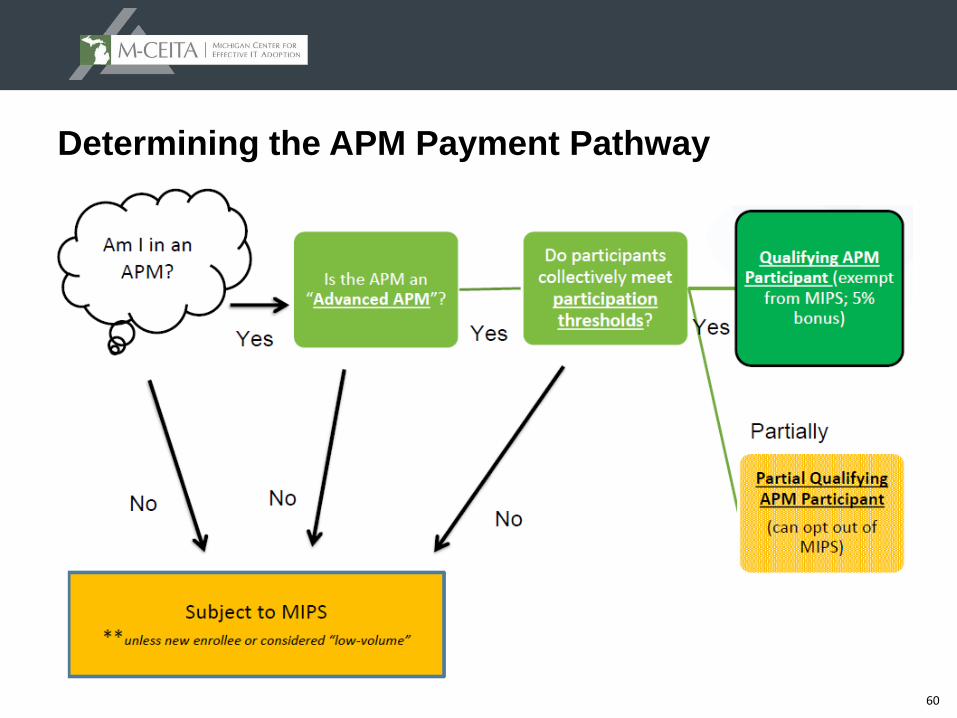
Volume Thresholds for APMs
▲ A “Qualifying APM” is one that meets increasing thresholds for the percentage of charges that pass through the APMs methodology
▲ An individual Eligible Clinician (EC) in a qualifying APM is a “Qualified APM Participant” or “QP”
▲ QP status is awarded to all advanced APM participants collectively (or to none as the case may be)
What if the threshold for QP status is not met?
▲ If ECs advanced APM does not meet the volume threshold to qualify it’s members for QP status, members are considered “Partially Qualifying”
▲ If an individual EC chooses to stay in the APM track, s/he will not receive the 5% bonus, but also will not be subject to MIPS
▲ If EC chooses, s/he can report MIPS measures and participate in the MIPS incentive track
58
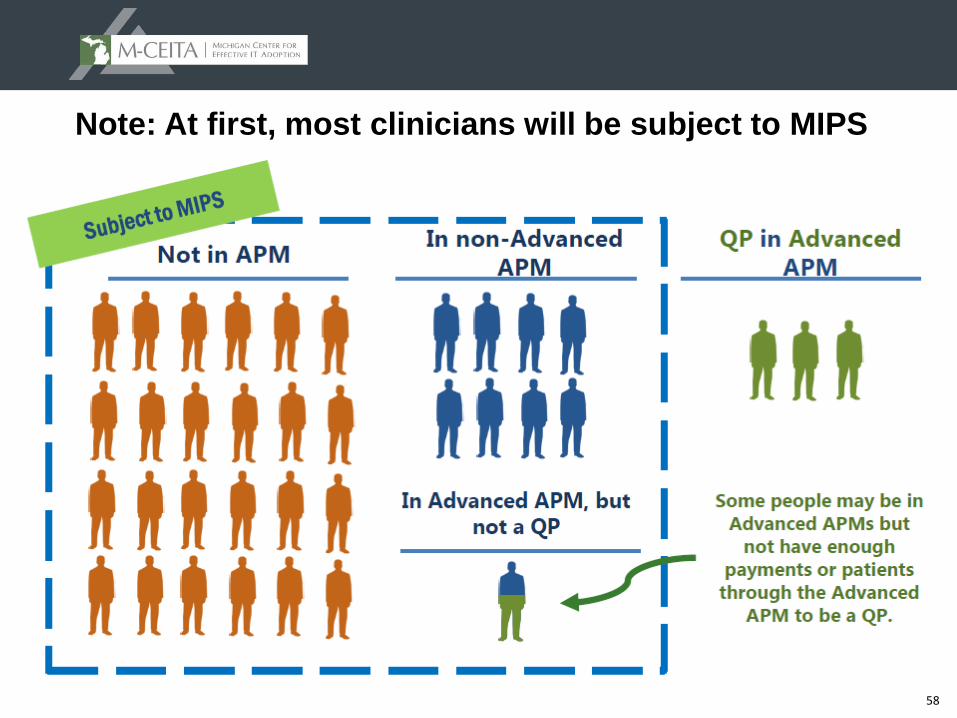
Note: At first, most clinicians will be subject to MIPS
59
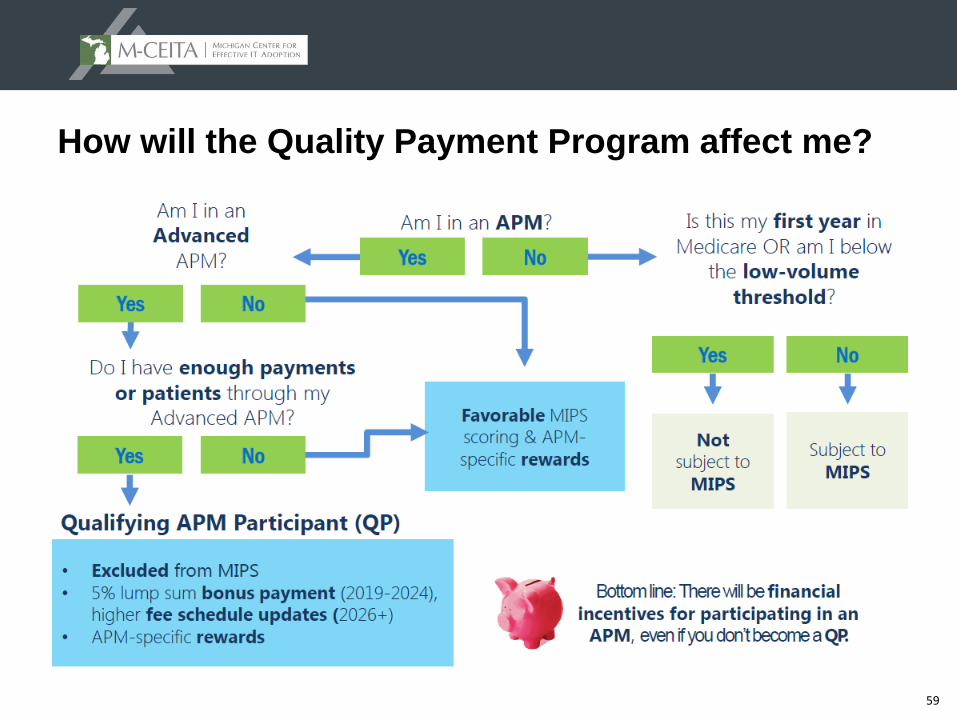
How will the Quality Payment Program affect me?
60
Determining the APM Payment Pathway
61
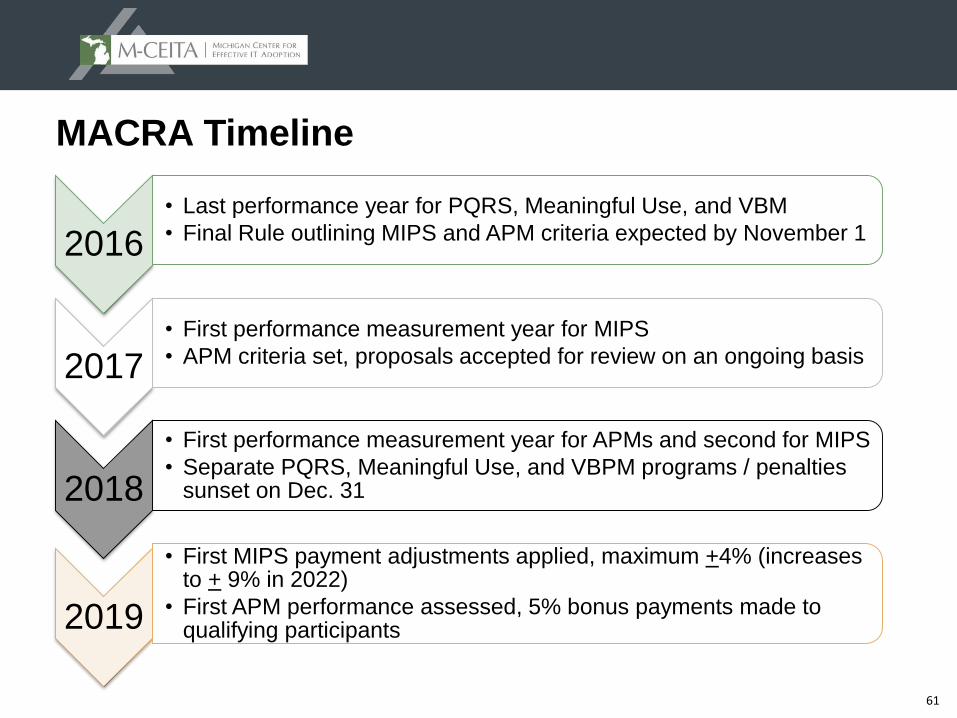
MACRA Timeline
2016
• Last performance year for PQRS, Meaningful Use, and VBM
• Final Rule outlining MIPS and APM criteria expected by November 1
2017• First performance measurement year for MIPS
• APM criteria set, proposals accepted for review on an ongoing basis
2018
• First performance measurement year for APMs and second for MIPS
• Separate PQRS, Meaningful Use, and VBPM programs / penalties sunset on Dec. 31
2019
• First MIPS payment adjustments applied, maximum +4% (increases to + 9% in 2022)
• First APM performance assessed, 5% bonus payments made to qualifying participants
62
TIMELINE
63
MACRA Timeline…proposed changes for 2017
▲ Recognizing concerns over being ready on 1/1/17, CMS has proposed some options for the first performance year
– Option 1: Test the Quality Payment Program
Submit “some” (as yet undefined) data and EC will avoid a negative payment adjustment
This first option is designed to ensure that your system is working and that you are prepared for broader participation in subsequent years
– Option 2: Participate for part of the calendar year
Submit information for a reduced number of days (# also currently undefined)
The first performance period could begin later than 1/1/17 and the EC could still qualify for a small positive payment adjustment
– Option 3: Participate for the full calendar year
For ECs ready to go on 1/1/17, fully participate in the first performance year
– Option 4: Participate in an Advanced APM in 2017
If EC achieves QP status in the Advanced APM, s/he can avoid MIPS
64
Summary of the new Schedule and Paths for EPs
▲ EPs can participate in MIPS or meet requirements to be a qualifying APM participant (QP)
▲ EPs in MIPS can receive a positive, negative or neutral payment adjustment
▲ EPs who are determined to be QPs for a year will be excluded from MIPS and receive a 5% lump sum incentive payment for that year
▲ MIPS payment adjustments and APM incentive payments will begin in 2019
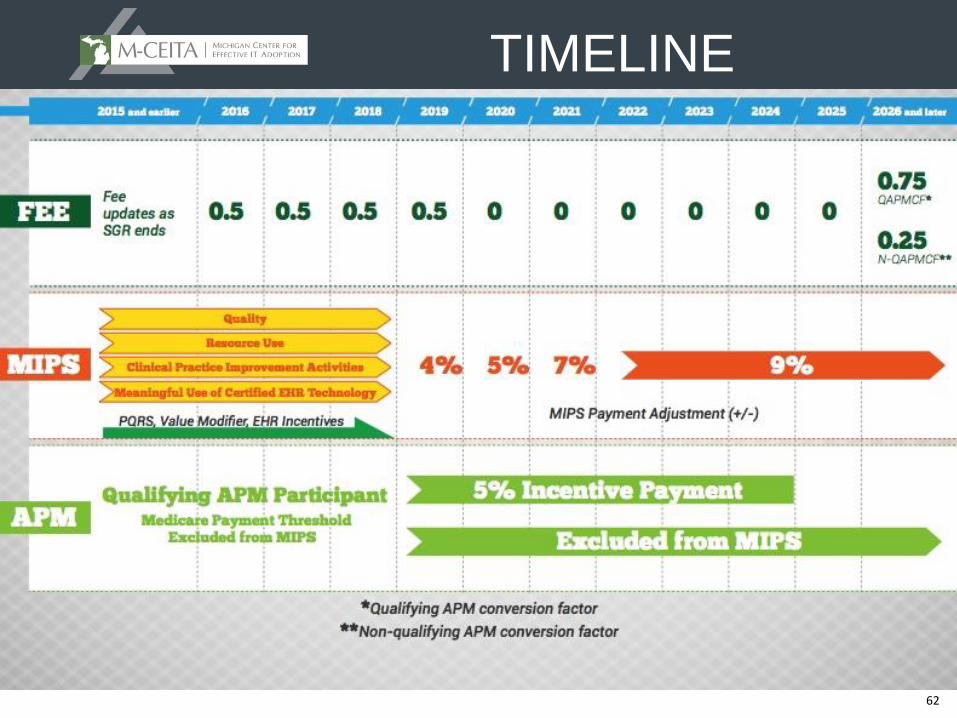
▲ The APM incentive payment will be available from 2019 through 2024. Beginning in 2026, services furnished by QPs will receive a 0.75% fee schedule update, and all other services will receive a 0.25% fee schedule update
65
Concluding Thoughts
▲ We are in the beginning stages of long overdue payment reform
▲ There is substantial work still to be done to define the rules
– There were 298 “the Secretary shall” statements in the NPRM
▲ MIPS consolidates and replaces existing quality reporting programs for Medicare Part B providers
▲ MIPS bonuses are potentially significant for high performers (37%)
▲ There is a risk for significant financial penalty (-9%) 46% gap!
▲ Don’t forget about the current rules that are still in place as we work our way to 2019
– Until Dec 2018 providers still subject to penalties/bonuses of Value Based Payment Modifier (VBPM), Meaningful Use (MU) and Physician Quality Reporting System (PQRS) assessed from the 2016 performance year
66
Resources
▲ MACRA Proposed Rule: https://s3.amazonaws.com/public-inspection.federalregister.gov/2016-10032.pdf
▲ CMS Quality Payment Program Resources: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/MACRA-MIPS-and-APMs/Quality-Payment-Program.html?v=qualitypaymentprogram
▲ CMS MACRA Webinar Archive: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/MACRA-MIPS-and-APMs/Quality-Payment-Program-Events.html