Embed Size (px)
Citation preview

Ciinicai Communication
Macrodontia of maxillary central incisors: case reportsEsther Gazit* / Myroti A. Liebertnati* *
Two cases of maxillary anterior macrodontia, resulting from fusion and gemination,were treated orthodontically. Problems of esthetics and overjet were solved in the firstpatient by sectioning and extraction of a fused mesiodem, and in the second patientby treating toward an Angle Class 111 buccal occlusion.{Quintessence Int ¡991,22:883-887.)
Introduction
Macrodontia of anterior teeth may result from ftjsionor gemination and can occur in the primary or perma-nent dentition or both. Fusion is believed to be aunion between dentin and/or enamel of two separatelydeveloping teeth, leading to a rednced total nnmber ofteeth. Fnsion may bc total or partial and may alsooccur between a normal and a supernumerary tooth.Prevalence varies between 0.5% and 2.5% and ap-pears to be a dominant trait in some families.'"^ Gemi-nation is an aborted attempt by a tooth bud to divide.As with fusion, gemination occurs mainly in the incisorarea, but, unlike fusion, the root and root canalremain undivided. A notch or groove on the coronalsurface gives evidence of the attempted division, andthe total number of teeth remains normal.'-^ Concres-cence is the union of two root surfaces by cementumonly."
Fusion or gemination may be associated with otherdental anomalies, such as dens en dente, macrodontia.hypodontia. and supemumerary teeth, and nondentalanomalies, such as syndactyly and nail disorders.' Anassociation between fused teeth in the primary detiti-tion and subsequent fusing and macrodontia in thepermanent dentition has been described."
frofessor and Chairman, Department of Occlusion. Tel AvivUniversity, The Maurice and Gabriela Goldschleger School ofDental Medicine, Ramat Aviv, ö9978Tel Aviv, Israel,Professor and Chairman, Department of Orthodontics, TelAviv University.
Macrodontia of anterior teeth, whether caused byfusion or gemination, creates problems of crowding,esthetics, and piaque accumulation because of surfacenotching.' For the orthodontist, additional problemsof tooth interdigitation and overjet reduction requirespecial treatment planning. Two case reports involvingfusion and gemination are presented.
Case 1
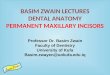
An Il-year-old boy presented with a mild Class II,division I, malocclusion and a severe bilateral spaceshortage for maxillary canines. Contributing to thisspace shortage was an oversized maxillary right centralincisor (12 mm mesiodistal) and an even larger maxil-lary left centra] incisor (15 mm) (Fig 1). The remainingprimary and permanent teeth were of normal size andshape. The overbite was 3 mm and overjet 5.5 mm.The maxillary left central incisor had a deep, verticalgroove on the labial and lingual surfaces, that dividedthe crown into a one-third mesial segment and a two-thirds distal segment. The maxillary right centralincisor had an incisai notch in the central part of theincisai edge (Figs 1 and 2). Radiographs revealed twodistinct roots of the left incisor that were probablyunited by cementum (Figs 3 and 4). The diagnosis waslate fusion of the left central incisor with a mesiodensand an early gemination of the right centrai incisor.Family and medical history were noncontributory.
Surgical exposure of the left fused incisor confirmedthe clinical diagnosis, and the smaller mesial segmentwas sectioned and extracted (Fig 5). The root surface
Quintessence International Volume 22, Number 11/1991 883
Clinical Communication
Figs 1 and 2 Oversized maxillary right and left central incisors and their grooves.
Figs 3 and 4 Radiographs reveai one large root and root canai in the right centrai and a divided rDot and root canal in theleft central.
Fig 5 Postsurgicai view of the extracted mesial segmentof the left central incisor.
884 Quintessence International Volume 22, Number 11/iggi

Clinical Communication
Figs 6 to 9 Posttreatment views. Fig 7
Fig 8 Fig 9
and enamel of the remaining segment were polished,and healing was uneventful. Orthodontic treatmentwas instituted and completed on a nonextraction basisbecause the patient diligently wore his cervicalheadgear. Final facial photographs demonstrate es-thetically pleasing dental and facial results (Figs 6 to9). Dental esthetics will be further enhanced by repairof the fractured incisai edge of the maxillary rightcentra] incisor with composite resin.
Case 2
A 12-year-old boy presented for orthodontic consul-
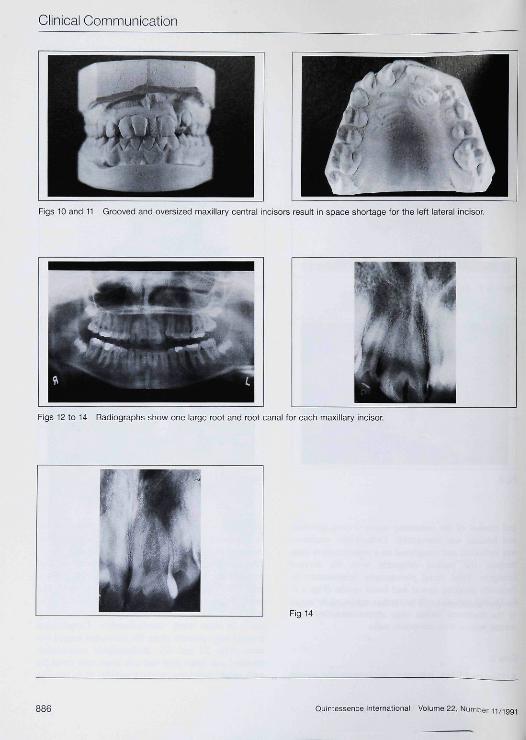
tation with a basic Class i maloeclusion. characterizedby a lingually blockcd-out maxillary left lateral incisor,excessive overjet (5 mm), and an overbite of 3 mm.The mandibular arch, aside from a slipped contactbetween the right central and lateral incisors, was nor-mal and required no orthodontic intervention. Themaxillary space shortage and excessive overjet werehoth due to the oversized central incisors, which meas-ured 14 mm each (mesiodistally). Longitudinalgrooves weie present along the labial and lingual sur-faces (Figs 10 and 11). Radiographie examinationrevealed one large root and one large root canal foreach tooth, indicating gemination (Figs 12 to 14), The
Ouintessence international Volume 22, Number 11/1991 885
Clinieal Communioation
Figs 10 and 11 Grooved and oversized maxillary central incisors result in space shortage for the left lateral incisor.
Figs 12 to 14 Radiographs show one large root and root canal for each maxillary incisor.
Fig 14
Quintessence Intemationai Volume 22, Number 11/1991
Clinical Communication
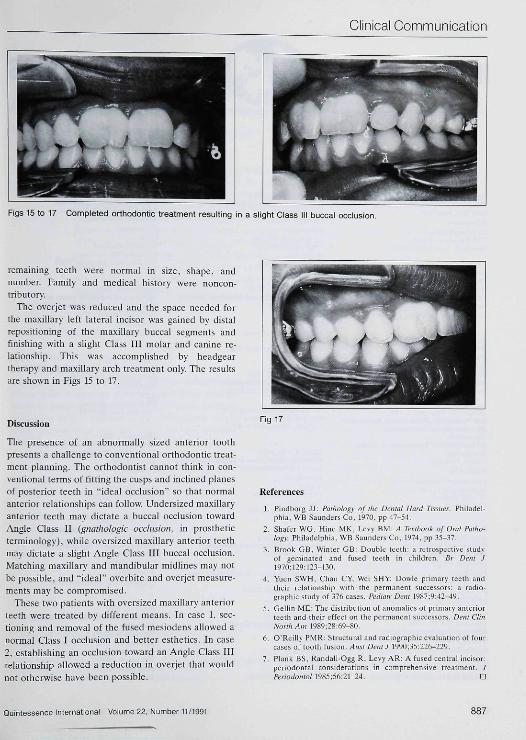
Figs 15 to 17 Completed orthodontic treatment resulting in a slight Class III buccal occlusion.
retnaining teetb were normal in size, shape, andnumber. Family and medical history were noncon-tributory,
Tbe overjet was reduced and tbe space needed forthe maxiliary left lateral ineisor was gained by distalrepositioning of ibe maxillary bueeal segments andfinishing with a sligbt Class ffl molar and eanine re-lationship, Tbis was aceomplisbed by bead geartherapy and maxillary arcb treatment only. The resultsare shown in Figs f5 to 17,
Discussion
The presence of an abnormally sized anterior tootbpresents a challenge to eonventional orthodontic treat-ment planning, Tbe orthodontist cannot tbink in con-ventional terms of fitting tbe cusps and inclined planesof posterior teetb in "ideal occlusion" so that normalanterior relationships can follow. Undersized maxillaryanterior teetb may dictate a bticcal occlusion towardAngle Class II (gnathologic occlusion, in prostbeticterminology), wbile oversized maxillary anterior teetbmay dictate a slight Angle Class III buccal occlusion.Matching maxillary and mandibular midlines may notbe possible, and "ideal" overbite and overjet measure-ments may be compromised,
Tbese two patients witb oversized maxillary anteriorteetb were treated by different means. In case f. sec-tioning and removal of tbe fused mesiodens allowed anormal Class I occlusion and better esthetics. In case2, establishing an occlusion toward an Angle Class fllrelationsbip allowed a reduction in overjet that wouldnot otherwise have been possible.
Fig 17
References1, Pindborg JJ: Paihology of the Dental Hard Tissues. Philadel-
phia, WB Saunders Co, 197Ü. pp 47-54,
2, Shafer WG, Hine MK, Levy BM: A Ti^xibook of OmI Patho-logy. Philadelphia, WB Saunders Co, 1974, pp 35-37,
3, Brook GB, Winter GB: Double teeth: a retrospective studyof geminated and fused teeth in children. Br Dent J1970;129:12.-i-]3n,
4, Yuen SWH, Chan CY. Wei SHY: Dowie primary teeth andtheir relationship with the permanent successors: a radio-graphic study of 376 cases Pediatr Dent 1^87:9:42-49.
5, Gellin ME: The distribution of anomalies of primary anteriorteeth and their effect on the permanent suecessors. Dent ClinNorlhAm 19 89; 28:69-80,
6, O'Reilly PMK: Structural and radiographie evaluation of fourcases of tooth fusion. Aiisi Dent J 1990;35:226-229,
7, Plank BS, Randall-Ogg R, Levy AR: A fused eentral incisor:periodontal considerations in comprehensive treatment. JPeriodontoi I985;56:21-24. D
Quintessence International Volume 22, Number 11/1991 887