Embed Size (px)
DESCRIPTION
EVALUATION OF THE EFFICACY OF BHUMYAMALAKYADI CHURNA IN MADHUMEHA ,SHASHIDHAR. T. HOMBAL , Post Graduate Studies & Research Center, D.G. MELMALAGI AYURVEDIC MEDICAL COLLEGE, GADAG
Citation preview
EVALUATION OF THE EFFICACY OF BHUMYAMALAKYADI CHURNA IN
MADHUMEHA
(WITH SPECIAL REFERENCE TO ITS HYPOGLYCEMIC EFFECT)
Thesis submitted to the Rajiv Gandhi University of Health Sciences Karnataka,Bangalore
In partial fulfillment of regulations for the Award of the degree of
DOCTOR OF MEDICINE (AYURVEDA)
By
SHASHIDHAR. T. HOMBAL.
Guide Dr. Ch. Ranga Rao. M . D . (Ay u )
Professor and Head of the Department Post Graduate and Research Centre D.G.M.Ay.Medical College, Gadag.
Co-Guide
Dr. Siva Rama Prasad Ketamakka. M.D. (Ayu) Reader
Post Graduate and Research Centre D.G.M.Ay.Medical College, Gadag.
POST GRADUATE AND RESEARCH CENTRE DEPARTMENT OF KAYACHIKITSA
D.G.M.AY.MEDICAL COLLEGE GADAG.
LIST OF ILLUSTRATIONS
Sl. No. Figure Name Page No. 1. Photograph of Haritaki 56 2. Photograph of Bibhitaki 58 3. Photograph of Amalaki 60 4. Photograph of Pippali 62 5. Photograph of Guggulu 64 6. Photograph of Madhu 66 7. Photograph of Gomutra 68
List of Master Charts
Sl No Master Charts Page No
1. Demographic data 79
2. Data related to Personal history 80
3. Data related to Complaints 81
4. Data related to Associated Complaints 82
5. Data related to Upadravas 83
6 A. Data related to Objective Parameters 84
6 B. Data related to Objective Parameters 85
7 A. Data related to Lab Investigations 86
7 B. Data related to Lab Investigations 87
List of Figures
Sl No Figures Page No
1. Showing Age and Sex ratio 89
2. Showing the Religion incidence 90
3. Showing the Occupation incidence 91
4. Showing the Economical status incidence 92
5. Showing the Diet incidence 93
6. Showing the Family history incidence 94
7. Showing the Chronicity 95
8 Showing the body weight of Group A 103
9. Showing the body weight of Group B 103 10. Circumference of Udara of Group A 104 11. Circumference of Udara of Group B 104 12. Circumference of Spik of Group A 105 13. Circumference of Spik of Group B 105 14. Circumference of Sthana of Group A 106 15. Circumference of Sthana of Group B 106 16. Serum Cholesterol of Group A 107
17. Serum Cholesterol of Group B 107 18. Serum Triglyceride of Group A 108
19. Serum Triglyceride of Group B 108 20. Serum HDL Cholesterol of Group A 109 21. Serum HDL Cholesterol of Group B 109 22. Serum LDL Cholesterol of Group A 110 23. Serum HDL Cholesterol of Group B 110 24. Serum VLDL Cholesterol of Group A 111 25. Serum VLDL Cholesterol of Group B 111 26. Random Blood Sugar of Group A 112 27. Random Blood Sugar of Group B 112 28. Showing the Result 114
CONTENTS Page No.
1) INTRODUCTION 1
2) SHAREERA 9
3) NIDANA Hetu 19 Samprapti 25 Poorvarupa 30 Rupa 31 Bedha 40 Sadhyasadhyata 43
Upadrava 44
4) CHIKITSA 47 5) DRUG REVIEW 54 6) MATERIAL AND METHODS 71 7) OBSERVATION, ANALYSIS AND INTERPRETATION 79
8) CONCLUSION 115 9) SUMMERY 118
BIBLIOGRAPHY APPENDIX
Acknowledgement
ACKNOWLEDGEMENT
I am highly indebted to my guide, Dr Ch. Ranga Rao, H.O.D.
Department of Post Graduate and Research centre, sri D.G.M.Ayurvedic
Medical Col lege, Gadag for his valuable suggestions and guidance in
completing this work successful ly.
I am heart i ly thankful to Dr V.V.S.Shastr i . Under whose guidance
my work was started and he was the teacher who inspired me to take the
combinat ion of the drug mentioned in this thesis.
I am ever grateful to my Co-guide Dr. Siva Ram Prasad Ketamakka
who was a helping hand throughout the work and supported me in
completing the work in st ipulated t ime.
I am thankful to our Principal Dr G.B.Pati l for his support in
completing this work successful ly.
I am very much thankful to Mr. Nandakumar for his valuable help in
stat ist ical calculations.
I am thankful to Dr A.K.Panda and al l other staff of DGM col lege for
their help.
Acknowledgement
I acknowledge to our col lage l ibrar ian Mr V.M.Mundanamani and
his assistant Mr Sureban for support ing me by providing lot of books for
the study.
I am thankful to Mr Gir iachar Off icer National Information Centre
(NIC) Gadag, for giving me information about the work going on in
di f ferent parts of the world regarding this subject.
My personal thanks to Mr.N.N.Bhat and Mr C.S.Bhat who helped
me in understanding the Sanskri t versions.
I am thankful to Dr.(Mrs) M.D.Gojanur for support ing me by
referring the cases for tr ial.
I am thankful to my col leagues and fr iends who supported me in
cl inical tr ials and made the tr ial successful.
I am thankful to al l the pat ients who agreed to undergo the
treatment with the tr ial drug.
I am highly indebted to my beloved parents, who framed a proper
path for my carr ier.
Acknowledgement
I express my heartfel t grat i tude to al l my family members for their
constant help, love and care rendered during my study.
I am thankful to al l my teachers, from primary education to post
graduate education for helping me in bui lding up my carrier.
This l ist is incomplete without remembering my small sunny Kiran
(18 months) whose smile inspired and kept me cheerful throughout my
work.
I wish to thank al l the persons who have helped me directly and
indirect ly with apologies for my inabi l i ty to identi fy them individual ly.
Acknowledgement
ACKNOWLEDGEMENT
I am highly indebted to my guide, Dr Ch. Ranga Rao, H.O.D.
Department of Post Graduate and Research centre, sri D.G.M.Ayurvedic
Medical Col lege, Gadag for his valuable suggestions and guidance in
completing this work successful ly.
I am heart i ly thankful to Dr V.V.S.Shastr i . Under whose guidance
my work was started and he was the teacher who inspired me to take the
combinat ion of the drug mentioned in this thesis.
I am ever grateful to my Co-guide Dr. Siva Ram Prasad Ketamakka
who was a helping hand throughout the work and supported me in
completing the work in st ipulated t ime.
I am thankful to our Principal Dr G.B.Pati l for his support in
completing this work successful ly.
I am very much thankful to Mr. Nandakumar for his valuable help in
stat ist ical calculations.
I am thankful to Dr A.K.Panda and al l other staff of DGM col lege for
their help.

Acknowledgement
I acknowledge to our col lage l ibrar ian Mr V.M.Mundanamani and
his assistant Mr Sureban for support ing me by providing lot of books for
the study.
I am thankful to Mr Gir iachar Off icer National Information Centre
(NIC) Gadag, for giving me information about the work going on in
di f ferent parts of the world regarding this subject.
My personal thanks to Mr.N.N.Bhat and Mr C.S.Bhat who helped
me in understanding the Sanskri t versions.
I am thankful to Dr.(Mrs) M.D.Gojanur for support ing me by
referring the cases for tr ial.
I am thankful to my col leagues and fr iends who supported me in
cl inical tr ials and made the tr ial successful.
I am thankful to al l the pat ients who agreed to undergo the
treatment with the tr ial drug.
I am highly indebted to my beloved parents, who framed a proper
path for my carr ier.
Acknowledgement
I express my heartfel t grat i tude to al l my family members for their
constant help, love and care rendered during my study.
I am thankful to al l my teachers, from primary education to post
graduate education for helping me in bui lding up my carrier.
This l ist is incomplete without remembering my small sunny Kiran
(18 months) whose smile inspired and kept me cheerful throughout my
work.
I wish to thank al l the persons who have helped me directly and
indirect ly with apologies for my inabi l i ty to identi fy them individual ly.
Introduction 1
Madhumeha is emerging as the chronic non-communicable disease
of concern in developing countr ies. With changing environment,
urbanisat ion and al tered l i fe-style giving more comforts and sedentary l i fe
to human, simultaneously offer ing metabol ic diseases l ike Madhumeha.
Madhumeha is a disease in which certain pathological changes are
noticed in ur ine, the most important being the presence of sugar. Since
this disease is connected with the urinary system with the presence of
sugar in the urine, the comparison of Madhumeha with Diabetes Mell i tus
is just i f iable.
Madhumeha is also one of the identi f ied major cause of morbidi ty
and mortal i ty in India1. In further, Indians have high ethnic susceptibi l i ty
for developing Madhumeha at a younger age group. The disease usual ly
occurs after 30 years of age, seen more in male than in female.
Being a slow onset and often relat ively asymptomatic disease,
remains undiagnosed at onset, or even i f diagnosed is often ignored by
persons aff l icted with i t . In addit ion lack of awareness amongst health
professionals and inadequate health care faci l i t ies compound the problem
of Madhumeha related complications in our country2.

Introduction 2
The alarming rise in non – communicable diseases l ike Madhumeha
warrants immediate attent ion of the experts to develop and propose,
formulate, establ ish, not only effective treatment schedules, but also to
plan preventive measures against Madhumeha and control the morbidi ty
rate due to this disease. Ayurveda proposes a comfortable remedy as
pal l iat ive therapy.
ITHIHASA
There is precious information given by our Acharyas about al l the
aspects of the disease, which reveal the pathological aspects of disease
and make them easy to understand. They had a thorough knowledge of
the entire disease that can be observed in their l i terature. We can
observe the classical references which indicate the disease as one of the
dreadful and chronic. Our ancestors have tr ied to know about the
disease from various angles, which made them to think in many aspects
of the disease. By observat ion alone they have classif ied the disease
elaborately. Thus to understand the disease we have to know the subject
already exist ing since the days of Vedas which give valuable information
about the disease.
VEDIC PERIOD
Vedas are the oldest l i terature of civi l ization. Ayurveda is the
Upanga of Atharvan Veda. In Vedas we f ind two words “Asrava” and

Introduction 3
“Prameha”. In Atharvana Veda Asrava vyadhis are mentioned in which
Nasasrava, At imootra and Atisara are included3. The term Asrava i f
formed from “A – srava” means to f low.
In Atharvana Veda 6 / 44 / 3 “Visanaka” drug is indicated in vata
vyadhi. Kesava commenting on this, explained “Vatikruta nasani” as “
Vatikruta asravasya nasani”, means i t is indicated in Asrava vyadhis. In
the Manthra 2-3-1-3 of Atharvana Veda, the drugs emerged from valmika
are indicated in At isara, Atimootra and Nadivranam4.
This clearly indicates the prevalence of this disease with i ts
remedy in the Vedic period.
SAMHITA PERIOD
After Vedic period facts about Madhumeha were further explored by
Atreya which are recorded in “ Charaka Samhita” a complete treat ise of
medical sciences of i ts era. He explains various factors pertaining to
et iology, pathogenesis, complications and methods of treatment in detai l
in his treat ise. I t is a point of histor ical importance that the book
mentions the loss of sweet substance from urine5.
Charaka also mentioned in sutra sthana that the Madhumeha
occurs due to avri ta of Vayu6, and explains the mythological origin of
Introduction 4
Madhumeha in Nidana sthana7. During the destruction of Daksha’s as
sacri f ice, Gulma f i rst manifested in human being who f led in al l direct ions
due to the agitat ions in their body. Because of f leeing, swimming,
running, f ly ing, jumping etc. Pramehas and Kustas manifested themselves
in addit ion to the intake of Ghee.
Bhela samhita which is contemporary to Charaka samhita describes
the two types of Madhumeha i .e. prakruta prabhava (congenital) and
Swakruta (acquired)Prabhava8.
The most notable contribution of Sushruta was to devote a
separate chapter for the management of Madhumeha and he has tr ied
some specif ic preparations of minerals and vegitat ions. Further he has
also described in a separate chapter for the management of Carbuncles
which are the Upadravas of Madhumeha9.
After Sushruta, Vagbhata made great contribut ion to Indian
medicine. He simpl i f ied the exist ing knowledge and gave some new
preparat ions and ideas in the text. He classif ied two types of Madhumeha
on the basis of pathogenesis are Dhatukshayaja and Avaranaja10.
Artha shastra of kout i lya (321 – 296 BC) mentions a method to
induce Prameha in Human deal ing with the sense to injure the enemy.
Introduction 5
The spot obtained from burning chancl ion (krukalaka) and house l izard
(Gruha goul ika) together with the intestines of mott led frog (chitra bheka)
and honey, i f administered causes Prameha. This evidently points the
existence of Diabetogenic technique in the ancient t imes11.
MEDIEVAL PERIOD
This period of history of Indian medicine is known as a period of
commentators. Hence most of the books of this period are of col lections
and thoughts of previous authors, commentaries of previous books.
Madhavakara (9t h century A.D.) in his book Madhava nidana
compiled the thoughts of his earl ier authors without adding any thing new
to the knowledge on Madhumeha.
Gayadasa (11t h Century A.D.) commentator of Sushruta Samhita
elucidated that avi lata of urine in Prameha was due to the presence of
some components of dooshyas i .e. meda, mamsa etc12 .
Chakrapani, the commentator of Charaka samhita and the author of
Chakradatta, in the same period contr ibuted nothing signif icant with
reference to etiology of Prameha but recommended medicines and
regimen prescribed by Charaka and Sushruta and some of his own.
Introduction 6
Dalhana, another commentator of Sushruta samhita (12t h century)
contributed a myth that females do not suffer from Madhumeha13.
Sharangadara ( 13t h century AD) prescribed some new recipes for
the management of Prameha but did not contr ibute any thing in the f ield
of et iopathogenesis.
Bhavamishra (16t h century AD) contributed to the history of
Prameha by adding some new herbal and metal l ic preparat ions for the
management of Prameha14.
After Bhavamisra the development of Ayurveda is not so optimist ic
and had been stagnated. The concepts of ancient India regarding
Madhumeha are quite al ike with modern concepts. Descript ions of
Charaka, Sushruta show that even in that ancient t ime, Indian scholars
were famil iar with etiology, pathogenesis, symptomology and
complicat ions of Prameha, out standing being the knowledge of genetic
role in the etiopathogenesis. The regimen prescribed by them are useful
even in present era also, and these texts and their concepts do not
remain mearly as the histor ical mi le stones but have become the hope
of the Madhumeha cure at present sinerio.

Introduction 7
HISTORICAL MILESTONES.15
- Atharvana Veda is the oldest l i terature, which explains Madhumeha.
- In 2500 BC Eabers Papyrus ( Egypt ) wrote the f i rst cl inical
descript ion as “the disease without pain and melts the body” was
documented.
- In 600 BC Charaka (India) cl inical ly described Madhumeha and noted
role of heredity and Sweetness in ur ine.
- In 400 BC Sushruta (India) described same as that of Charaka.
- In 30 BC – 38 AD Celsus (Greece) gave some cl inical descript ion.
- In 1s t AD Aretaus (Greece) introduced the name as diabetes meaning
“to run through a pipe” .
- In 2nd AD Claudius Galenus proved that by consuming the drinks
which weakens the kidney wi l l al low the l iquids without change.
- In the same century Tchang Tchong king proved this as the disease of
thrust.
Introduction 8
- In 600 AD Aetius (Amida) treated this disease by using sedatives.
- In 980 – 1037 AD Avicenna ( Arab ) explained about Diabetic
Gangrene and put forward the question as “ is there any relat ion
between pancreas”
- In 1727 Brunner.J.C. ( Swiss ) removed the pancreas from the dogs
and found that they developed thirst and polyurea.
- In 1770 Thomas wi l l is ( England ) proved the di f ference between
Diabetes Mallets and Diabetes Insipidus.
- In 1775 Matheu Dobson Evaporated the specimen of ur ine of a
Diabetic patient and discovered a residue which was almost glucose.
- In 1782 Thomas Cawley recorded the disease.
- In 1788 Cawley (Engl ish) described pathology of pancreas.
- In 1815 M. Chevreul found out the presence of glucose in the urine.
Introduction 9
- In 1839 Bernard Naunyn studied the relat ion between the metabol ic
disturbance and pancreas.
- In 1841 Trommer found the test for urine glucose.
- In 1848 Claude Bernard proposed that the production of sugar in the
l iver is the reason for the r ise in the blood glucose Laval. He injured
the base of the fourth ventr ic le and proved the increase of blood sugar
level, he also proved when the blood sugar level is raised the sugar
starts f lowing out through urine. Even after the lowering of the blood
glucose level the urine contains glucose was the major discovery by
Claude Bernard.
- In 1845 Boucardet establ ished the relat ion between the Diabetes and
Pancreas.
- In 1850 Fehl ing found the test for testing the urine sugar.
- In 1867 Paul Langerhans (Germany) found islets of langerhans.
- In 1874 kusmal found the symptoms caused by increase in acitone in
the body.
Introduction 10
- In 1874 Oacar Minkowski found the acidosis.
- In 1886 Joshaf wan maring and Oscar Minkowski proved the
induct ion of diabetes by removing the Pancreas.
- In 1870 Clande Bernard ( France ) Noted sugar storage in l iver as
glucogon and elevated blood sugar in diabetes.
- In 1901 E.L.O.Pie proved the increase and decrease in the blood
glucose level is due to langerhans.
- In 1907 M.L Lane di f ferent iated and named the langerhans as two
types “alpha and beta“.
- In 1921 J.J.R.Macleod, Frederick . G . Banting and Charles.H. Best
(Toronto )discovered Insul in
- In 1926 H.C.Hagedorn mixed protimine to insul in and made i t to defuse
s lowly so that i t can act for longer t ime.
- In 1944 Von Noorden ( Vienna ) Bel ieved that l iver play a role in
diabetes.
Introduction 11
- In 1952 Sanger found the structure of the insul in.
- In 1954 A. Shef found Carbutamide was working as a hypoglycemic
agent. This was the f i rst oral hypoglycemic agent, but as i t had many
side effects i t was drown back from the market and a new drug similar
in the function of Carbutamide was introduced as Tobutamide which has
less side effects.
- In 1970 On words Merwin Gl iedman and other transplanted pancreas
culture of Is lets of cel ls of pancreas transplant of beta cel ls.
Even in 1999 also the research is going on throughout the world.
St i l l we are fai l ing to put ful l point to these milestones and newer aspects
of the disease are emerging out day by day.
Some of the latest research going throughout the country and abroad is given
below16,17.
- Toxicological Evaluat ion of Fenugreek seeds in Diabetic patients.
By Sharma R.D. at PG Dept, SN Medical col lege, Agra. –1996
- Consti tut ional study of pat ients of Diabetes Mell i tus vis-Avis
Madhumeha by R H Singh at Dept of Kayachiki tsa, B.H.U. 1996
Introduction 12
- Prognosis of Prameha on the Basis of Insul in level.
By Upadhyay at Dept of KC, I.M.S, B.H.U, Varnasi. 1996
- Diabetic foot ulcers treated the Ayurvedic way
By Ojha J K. at Dept of DG, B.H.U, Varnasi. – 1997
- Scope and use of Indigenous Herbal drugs in Madhumeha an Indian
Scenario. By Mukherjee.S K at C.D.R.I, Lucknow.- 1997
- Potential antidiabetic agents form plant sources. By R K Goyal at Dept
of Pharmacology, L M Col lege of Pharmacy, Ahmedabad.- 1997
-
- Evaluat ion of hypoglycemic act ivity of Tradit ional Herbal preparat ion
By Negam S A at Department of Pharmacology, NRC, Egypt. 1997.
- Ant i diabet ic property of neem seed By Kannan J at Pharmacy Dept,
Faculty of tech and Engg, MS Universi ty of Boroda. Baroda 1997
- Hypoglycemic effect of Trigonel la foenum Leaf in Diabetic By A. Barry
at Dept of pathology and forensic Medicine, Universi ty of Basrah 1997.
Introduction 13
References
1 API Text book of Medicine pp 205
2 Diagnoses of Diabetes pp 2
3 Ayurveda I thisa pp 26
4 Ayurveda I thisa pp 29
5 Charaka Nidana 4 / 37
6 Charaka Sutra 17 / 78.
7 Charaka Nidana 8 / 11
8 Bhela Samhita Nidana sthana 6 / 1 – 4.
9 Sushruta Chiki tsa 12 / 16
10 Astanga .Hridaya.Nidana 10 / 8
11 Ardha Sastra of Kouti lya 16 / 179 / 1.
12 Su NI Naya Chandrika Commentory.6 / 6.
13 Nibandha sangraha on Su Ni 6 / 33
14 Bhava prakasha Madyama kanda 38 / 45 15 Sihimootra roga by A. Narayanappa.pp 4 16 Al l ied Ayurvedic Medical Research Abstracts (AAMRA) 17 Researches in Ayurveda 1997

Shareera 13
Charaka explained that the persons who take excess and heavy
food or food with sour and salty taste, new r ice, fresh wine and enjoy
long sleep wi l l increase, the kapha, pi t ta, meda and mamsa and obstructs
the Vata together with the ojus come down to the vast i and causes
Madhumeha1. By this i t can be seen that the vast i is involved in the
product ion of Madhumeha. In Madhumeha, Prabhoota mootrata is the
main lakshana. I t is a symptom of mootravaha srotodusti also2. Hence in
Madhumeha mootravaha srotodust i is present.
Charaka mentioned that Prameha occur whenever the Medas
(srotas) is vi t iated3. vr ikka and vapa are the moolas of Medovaha
Srotas4. So the involvement of vr ikkas is present in Madhumeha.
Thrishna is an important lakshana. The cause for tr ishna is Udakavaha
Srotodusti5. Talu and kloma are the moolas for Udakavaha srotas6.
Hence the involvement of Talu and Kloma are present in the product ion of
Madhumeha. Liver plays an important role in dhatuparinama. In
Madhumeha dhatuparinama alters because of the involvement of most of
the dhatus present in the pathogenesis. Hence the l iver is responsible in
the production of Madhumeha.
Thus i t can be said that the organs responsible for the product ion
of Madhumeha are -
Shareera 14
1. Taalu
2. Kloma
3. Vrikka
4. Vasti
5. Yakri t
But in ayurveda the knowledge of rachana and kriya of Madhumeha
are st i l l in controversy, but with the help of modern science the
Kriyatmaka vivechana can be discussed.
TALU
The classical texts in Ayurveda have given the brief descript ion
about Talu. I t is located above the kanta and becomes the base of the
siras as i t is evident from the del iberations in Bhela samhita. I t is the
moola for the Udakavaha srotas7. Charaka mentioned Talushosha and
pipasa wi l l exist i f Udakavaha Srotas is vi t iated8. Sushruta mentioned
nine Talugatha vyadhis9 . Charaka and Kashyapa stated that the union of
two bones forms Talu10.
KLOMA
Ayurveda acharyas stated that Kloma is the moola for Udakavaha
Srotas11. Al l acharyas mentioned this as one among the Kostangas12.
Shareera 15
Though there are many schools of thoughts regarding the anatomical
identi f ication, In Sushruta samhita i t is said that kloma is explained with
Yakri t which is located in the r ight side of the body13. Dalhana whi le
commenting on this said that i t is in the r ight side of body which is laying
down below the Yakri t and i t is also cal led as Ti lakam. Vagbhata says
that Kloma is located along with Yakri t in the r ight side of the body. I ts
combinat ion according to Sharangadhara samhita in Pit ta which is
agniroopa14. He has mentioned Agnashaya as i ts synonym. Adhamalla
whi le commenting on this says that i ts formation is with the sonitha ki t ta.
I t is in the r ight side and in contact with the l iver. He has also given
Ti lam as a synonym to Kloma15.
Charaka says that Talumoola and Kloma are the seats of
Udakavaha srotas. I f these srotases are vi t iated the pathological
changes i .e. shosha of above organs and thirst develops16. Chakrapani
whi le commenting on Kloma said that i t is a Pipasa sthana (thirst centre).
Sushruta also said as above and on injury to these srotases the
immediate death occurs besides polydipsia.
Based on the above descript ions i t is clear that Kloma in one
among the Kostangas and located adjacent to the Yakri t . The nearest
organs to the l iver are Gal lbladder and Pancreas. I t is also clear that

Shareera 16
only Pancreactomy causes the polydipsia and death so i t can be
considered as Kloma.
VRIKKAS
Vrikkas are two in number and are si tuated in Kosta. Al l acharyas
included vr ikkas in kostangas. In Dalhana commentary on Sushruta the
vr ikkas are described as two f leshy bodies, each si tuated on ei ther side
of spine and their shape as being l ike rounded bodies17. These are said
to be composed of the essence of the Rakta and Medas18. Sharangadara
whi le describing their function says that vr ikkas are said to be the
nourishers of the abdominal fat19. Adamalla whi le commenting on the
above states that vr ikkas are two rounded bodies in the abdomen which
are derived form the essence of the blood and fat and they originate form
fat. They are stated to be concerned with the nutr i t ion of the abdominal
fat. Ayruvedacharyas Charak, Dalhana, Chakrapani says vrikkas are two
in number and they are si tuated below the chest20.
VASTI
Embryological ly, Vasti is stated to be maternal contribut ion. I t is
stated to be derived form the essence of Rakta and kapha supported by
Pit ta in to which Vayu also enters21. Vast i has been included under
kostangas and Ashayas by al l acharyas. I t is stated to be one in
Shareera 17
number22. The term Vasti , Mutravasti , Vastipudaka, Mutrashaya and
Mutradhara seem to have been used as synonyms in Ayurvedic texts23.
Charaka whi le describing the locat ion of Vasti has stated that vasti
is si tuated in between the Sthoolaguda, Sevani, Sukravaha naadies and
Motravaha naadies24. According to Sushruta, Vast i is near to Nabhi, Kat i ,
Guda, Vankshana and Shepha. He further stated that vasti , Pourusha,
Vrushana and Guda are al l interrelated and si tuated in the pelvic cavity25.
According to Bhavamishra and Sharangadara, Vasti is located below the
Pakwashaya. Vagbhata says that i t is located inside the kat i26. Sushruta
states that i t is s ituated near the Garbhashaya in females27.
Regarding the shape and structure of the Vast i , Sushruta has
stated that i ts shape looks l ike that of “Alabu” and ful l of Siras and
Sanyus al l around. I t is stated to be Tanu twak i .e. a thin volved organ or
i ts coverings are thin and membranous. I t has one exit and l ies with i ts
mouth downwards28. Vagbhata has described i ts shape as Dhanur Vakra
i .e. bent l ike bow having one opening downwards and composed of l i t t le
muscles and blood. Adamalla described i ts shape as “Charmaka
Latwakara” that is l ike bag of leather. The Acharyas described i t to be
the storehouse of Mootra and seat of “Prana” being one of the important
marmas. Charaka says that i t is reservoir of mootra where al l the
Ambhuvaha Srotases ends. He also explained vasti as the moola of
Shareera 18
Mootravaha srotas. Sushruta stated that Mootraghata, Prameha, Sukra
doshas, Ashmari develops from Vasti only29.
YAKRIT
Since the Vedic period, the traces of gross anatomical knowledge
of Yakri t are avai lable. Sayana the commentator of Vedas whi le
commenting on the word Yakan coined in atharvana veda described that
Yakan is si tuated near the heart. The ward Yakan in his view means
Yakri t . Yakri t is described as one of the Matruja angas due to i ts
softness30 and i t is included in Kostangas. Yakri t in i ts embryonic stage
is formed by the shonitha. Yakri t is si tuated on the r ight side, below the
Hridaya31 and i t is the moola for the Raktavaha srotas32. Sushruta
mentioned Raktadharakala is present in Yakri t33.
SHAREERA KRIYA
Agni plays an important role in manifestation of Madhumeha hence
concept of Agni carr ies importance in the study of Madhumeha. Agni or
Jataragni is the main cause for every parinamas, or changes in the body.
Dahana (burning) and Paka (Chemical act ion) are the chief actions of
agni. I t spl i ts the Vi jateeya dravyas into sajateeya dravyas for easy
absorpt ion. The ingested food after reaching Amashaya enters the
digest ion by Antaragni. (Pachaka pit ta) in the presence of samana vayu
Shareera 19
and Kledaka kapha which effects the digest ion. The Ahara parinamakara
bhavas are Ushma, Vayu, Kleda, Sneha, and kala which are essential for
normal ahara pachana. The digestion and other metabol ism in the body
can be done only in presence of Agni.
The synonyms of Agni are kayagni, antaragni, kostagni,
audaryagni. There is no Agni other than Pitta, as i ts actions perform in
the l iving body is Paka or pachana. Acharyas mentioned 13 types of
agnis in the body. They are one Jataragni, f ive bhootagnis and seven
dhathwagnis. Samana vayu, which is located nearer to Jataragni moves
al l over the kosta, col lects the ingested food. Then separates prasada
and ki t ta bhagas of Ahara into Ahara rasa and mootra, pureesha
respectively.
According to the Ayurvedic physiology Bhutagnipaka fol lows
Jataragnipaka and i t completes the process of internal digestion, i t is
only after the complet ion of Bhootagnipaka the formation of ahara rasa is
possible. Dhatwagnipaka does not start t i l l the Bhootagnis completes i ts
process of digestion and supply the Sajaat iya nutrients to the
Dhatwagnis. But i t can be said that the si te of action of Bhootagnis starts
from the intestines t i l l the cel l membrane, the l iver being in between the
Bhutagnipaka that wi l l be predominant in i t . In the event of the fai lure of
the funct ion of Bhootagnis, the Dhatwagni wi l l not be in a posit ion to bui ld
Shareera 20
the respective dhatus. That is how the def icient function of Bhootagnis is
to be understood.
Agni assumes names of Vishamagni, Teekshnagni, Mandagni, and
Samagni according to doshic inf luence on i t .
Charaka says mandagni by i ts qual i t ies causes ajeerna and mala
sanchaya, thereby i t leads to several diseases. Mandagni vi t iates kapha,
kapha in turn vi t iates the other dhatus part icularly medo dhatu, and this
leads to Prameha. Hence the role of agni is to be considerable in the
study of Madhumeha.
Ayurveda has mentioned about the formation of Mootra and i ts
excret ion. Mootra has been described as the Drava Bhaga of the Kit ta
and i t is produced in Amapakvashaya, The l iquid port ion is said to
separated form the sol id fraction in the pakvashaya by the pureeshadhara
kala under the inf luence of Samana vayu, brought in to vasti and from
there i t is excreted by the Apanavata. Mootra is said to be an out come
of the digest ion of ingested food, and the seat of i ts production is
pakvashaya. Mootra is stated to be a mala derived form the food
ingested in four-fold manner. The l iquid port ion of ki t ta bhaga after
absorpt ion circulates in the body and i t is f inal ly carr ied to vrikkas by two
mutravaha dhamanis which divide in to innumerable branches forming the
mutravaha srotamsi through which i t oozes and there i t is named Mutra.
Shareera 21
From vrikkas, two Gavinis carry i t to vasti . Even though Vrikkas have
been mentioned in Ayurveda their relat ion with the formation of mootra
has not been clearly described. A deep study of Ayurveda classics
enl ightens to certain extent about mootropatt i . I f Vrikka, Gavini and
Medhra are considered as one system of srotas for the purpose of the
product ion and excretion of ur ine, I t remains stored in vast i t i l l is
excreted during mutra pravrutt i . I f so, there can be no di fference between
the views of Ayurveda and modern medicine.
MODERN ASPECT
Diabetes mell i tus is a chronic disease. I t results due to disturbance
in carbohydrate metabol ism and deficiency of Insul in34 secreted by the
Beta cel ls of Is lets of langerhans of pancreas, but hormones of pi tui tary
and adrenal glands are also int imately related to the development of
Diabetes State. Liver plays an important role in the metabol ism for
carbohydrate. I t stores glucose in the form of glycogen under the
inf luence of Insul in. Any alterat ion in this function leads to diabetes35.
So the involvement of organs in diabetes mell i tus are
- pi tui tary gland
- Pancreas.
- Adrenal gland
- Liver.
Shareera 22
PITUTARY GLAND36
This is a exceedingly important endocrine gland with a wide range
of functions including the control of the other endocrine glands and of
body growth.
This gland measures 1.5 cm in the coronal plane, 1 cm in the
sagital plane and 0.75 cm in vert ical form. I t l ies within the sel la Tarsica
of the sphenoid bone and posterio superior to the sphenoid air sinuses
below the optic chiasma. I t is f lattened ovoid lying in the hypophyseal
fossa (sel la Tarasica) and connected to the inferior surface of the
hypothalamic part of the brain by the infundibulum. Structural ly the gland
can be divided into two main parts
a) Anterior lobe which is composed of Adeno hypophyseas t issue.
b) Posterior lobe which is Neurohypophuyseas.
Posterior lobe of the hypophysis is the expanded inferior end of the
infundibulum and is developed from the brain. The anterior lobe is much
larger than the posterior lobe and consists of three parts, which part ly
surround that lobe and the infundibulum. The distal part forms most of
the anterior lobe. I t is separated form the posterior lobe by the thin sheet
of glandular t issues ( intermediate part) appl ied to the posterior lobe. The
infudibular part is a narrow upward projection of the distal part. The
Shareera 23
anterior lobe develops from the ectoderm and has only vascular
connection with the brain.
Anterior lobe is the master gland of endocrine system, because i t
produces proteotrophic hormones which effects the other ductless glands.
In these secretions two hormones are having direct action on
carbohydrate metabol ism. If any disturbance occurs i t leads to
Hyperglycemia or Hypoglycemia.
The hormones secreted are Growth hormone or somatotrophic
hormone (GH of STH ) and Adreno Cort ico Trophic Hormone (ACTH).
The pitui tary effect of STH on carbohydrate metabol ism is to st imulate i ts
storage. Administrat ion of growth hormone in animal or in man produces
hyperglycemia and glycosuria. So the growth hormone is diabetogenic
effect especial ly in man. The hormone is however increases the
glycogen content of cardiac muscle. Administrat ion of ACTH produces
simi lar effects as induced by growth hormone. Both STH and ACTH
increase gluconeogenesis and diminish the rate of oxidat ion of glucose.
Thus the anterior pi tui tary has a diabetogenic role.
GH (growth hormone) is also known as somatotropin, i ts pr incipal
function is to act on the skeleton and skeletal muscles, in part icular to
Shareera 24
increase their rate of growth and maintain their size once growth is
attained. GH causes cel ls to grow and mult iply by direct ly increasing the
rate at which amino acids enter cel ls and are bui l t up into proteins. GH is
considered to be a hormone of protein anabol ism since i t increases the
rate of protein synthesis. GH also promotes fat catabol ism that is i t
causes cel ls to switch from burning carbohydrates to burning fats for
energy released. At the same t ime GH accelerates the rate at which
glycogen stored in the l iver is converted into glucose and released in the
blood. Since the cel ls loosing fats for energy however they do not
consume as much glucose, the result is the increase in the blood sugar
level. A condit ion cal led hyperglycemia. This process is cal led
diabetogenic effect because it masks the elevated blood glucose level of
diabetes mell i tus. GH seems to produce many of i ts effects by convert ing
other factors in to growth promoting substance cal led soerto medians and
insul in l ike growth factors (IGF).
Other hormones can indirectly affect insul in production however for
instance GH raises blood glucose level and the r ise in glucose level
tr iggers insul in secret ion. ACTH by st imulat ing the secret ion of
glucocort icoids brings about hyperglycemia and also directly st imulates
the release of insul in GHIF (romatostatin) inhibi ts the secret ion of insul in.
One stimulus that inhibi ts GH secret ion is hyperglycemia high blood
sugar level. An abnormally high blood sugar level st imulates the
Shareera 25
hypothalamus to secrete the regulat ing factor GHIF (somatisat ion) GHIF
inhibi ts the release of GHAF and thus the secretion of GH. As a result
blood sugar level decreases.
PANCREAS37
The pancreas is a compound alveolar gland. I t has got both
endocrine and exocrine funct ions. I t l ies against the posterior abdominal
wal l behind peri toneum. The adult pancreas consists of a Head, Neck,
Body and Tai l . The whole organ is about 15 cm long with the r ight margin
of the head in contact with the descending part of the duodenum and the
tai l is in contact with the spleen. The disease diabetes mell i tus is
considered only to i ts endocrine secretion that is Insul in, so i t is more
important to go through i ts endocrine part.
ISLETS OF LANGERHANS
The islets of Langerhans are composed of various components that
are organized to form micro-organs. The mass of is lets within a pancreas
is dynamic and changes both with growth and development and with
functional chal lenges. As we learn more about the regulat ion of
di f ferent iat ion of is let cel l types, we also may learn how to enhance the
growth of is let cel ls, part icularly the beta cel ls.
Shareera 26
Is lets function both singly and in concert. Recent work has
revealed grater diversi ty in is lets than that previously recognized. There
is funct ional heterogeneity between islets and beta cel ls within the same
islet. Numerous peptides other than the four main is let hormones
( insul in, glucagon, somatostat in, and pancreat ic polypeptide) have been
immuno-local ized in is lets.
The islets of Langerhans are clusters of endocrine t issue scattered
throughout the exocrine pancreas. In the adult mammal, the is lets are 1
to 2% of the pancreat ic mass and thus comprise around 1gm of t issue in
the adult human. Islets are a complex mixture of cel ls and function both
separately as micro-organs and in concert as the endocrine pancreas.
Although the direct secret ion of insul in and glucagon form islets into the
portal vein has obvious advantages with respect to inf luence on hepatic
function. The islet mass is dynamic, adjusting to meet the changing
needs of the individual, whose size and level of activ i ty vary at di f ferent
stages of l i fe. When the islet mass cannot adjust to meet the demand,
diabetes results.
The pancreas of the adult human contains about 200 units, or 8mg,
of insul in. The size of an islet can range from only a few cel ls and less
than 40 micrometer in diameter to about 5000 cel ls and 400 micrometer
in diameter.
Shareera 27
GROWTH OF ISLET
The growth capacity of the beta cel l depends on the st imulus and
the abi l i ty of the cel l to recognize the st imulus as wel l as on the number
of beta cel ls that can enter the cel l cycle and undergo mitosis. There is
an increased incidence of polyploid beta cel ls in the diabetic human.
Although there may be numerous st imul i for beta-cel l growth, three major
st imul i are known. Glucose has been shown to st imulate modest growth
of ei ther neonatal or adult pancreat ic beta-cel ls in culture. Pregnancy
has been shown to cause both increased repl icat ion and mass of beta-
cel ls. As a paral lel f inding, in vi tro studies have shown that prolact in,
placental lactogen and growth hormone can st imulate repl icat ion of beta-
cel ls. Diabetes results only i f increased cel l loss or functional demands
cannot be met.
COMPONENTS OF THE ISLETS OF LANGERHANS
There are three major endocrine cel l types in is lets : the insul in
producing beta-cel l , the glucagon producing alpha-cel l , the somatostat in
producing delta-cel l .
Alpha-cell
The alpha cel ls are usual ly smaller and more columnar than the
beta cel ls and wel l granulated with granules 200 to 250 nm in diameter.
The granules are electron dense with narrow halo of less-dense material
Shareera 28
and a t ight ly f i t t ing granule-l imit ing membrane. There is l i t t le species of
variat ion.
Beta-cell
The beta cel ls are polyhedral, being trancated pyramids, and are
usual ly wel l granulated with secretary granules 250 to 350 nm in
diameter.
Delta-cell
The delta-cel ls are usual ly smaller than either alpha or beta cel ls,
are wel l granulated, and are often dendri t ic in shape. Within a delta cel l
the electron density of granules varies great ly. Each granule, 200 to 250
nm in diameter, contains material of homogenous moderate density that
f i l ls the granule-l imit ing membrane.
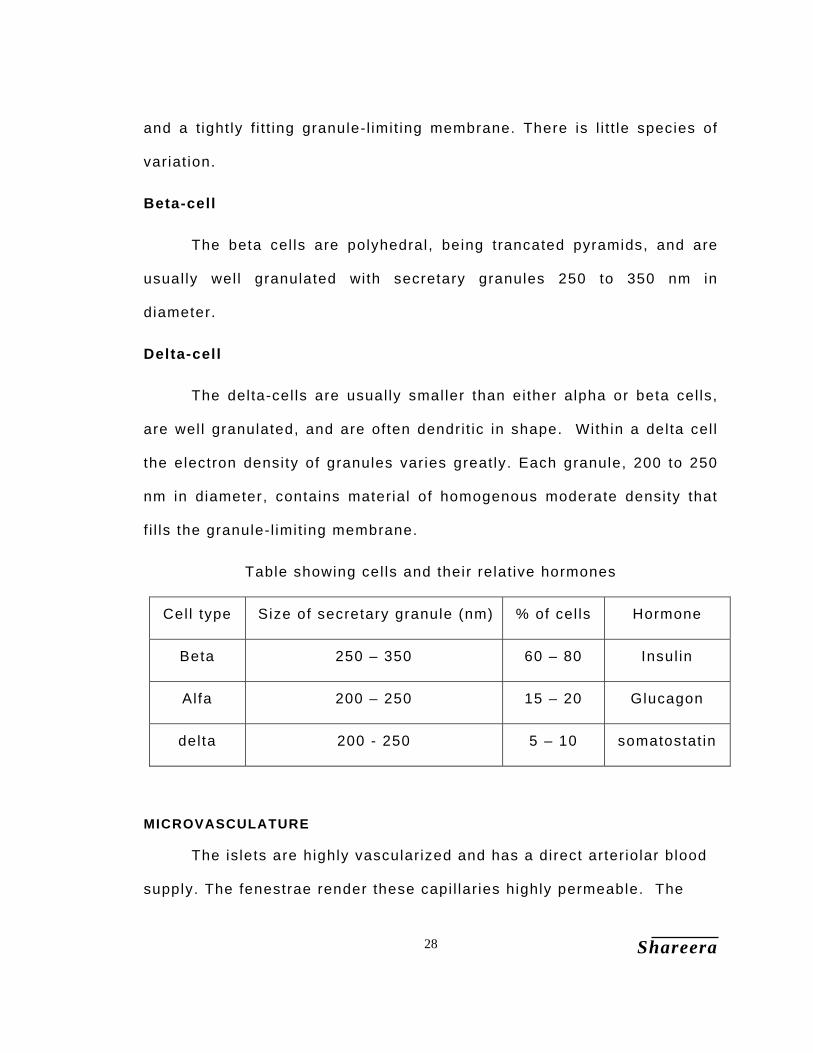
Table showing cel ls and their relat ive hormones
Cel l type Size of secretary granule (nm) % of cel ls Hormone
Beta 250 – 350 60 – 80 Insul in
Alfa 200 – 250 15 – 20 Glucagon
delta 200 - 250 5 – 10 somatostat in
MICROVASCULATURE
The islets are highly vascularized and has a direct arter iolar blood
supply. The fenestrae render these capi l laries highly permeable. The
Shareera 29
blood f low to the islets has been found to be disproport ionately large (10
to 20% of the pancreatic blood f low) for the 1 – 2% of pancreatic volume
. Factors regulat ing islet blood f low may effect is let hormone secretion.
High concentrations of glucose have been shown to enhance pancreat ic
blood f low and to preferent ial ly increase islet blood f low.
NERVES
The pancreas is innervated by sympathetic f ibers from the cel iac
gangl ion and by parasympathetic f ibers form the vagus nerve. These
parasympathetic f ibers synapse in small gangl ia dispersed in the
pancreas. They may act as pacemakers for the osci l lat ions in hormone
levels that occur without extr insic nervous connections, as in the isolated
perfused canine pancreas. Within the pancreas, nerve f ibers terminate in
perivascular, periacinar, and perinsular areas. Within the is lets the
nerves fol low the blood vessels and terminate within the pericapi l lary
space, within the capi l lary basement membrane, or closely apposed to
the endocrine cel ls38
Functions of these hormones :
INSULIN:
The insul in is hypoglycemic, ant i diabetic factor and the protein
bound hormone that regulates the blood glucose. I t also increases the
Shareera 30
oxidat ion of glucose to CO2 in the t issues and depresses
gluconeogenesis i .e. formation of glucose from the sources other than
carbohydrates.
Insul in increases combustion of sugar in the t issue and also helps
in the treatment of glucose in the cel ls. I t increases synthesis of
glycogen from sugar and lactate both in the l iver and muscle. This is
cal led the directive effect of insul in. Insul in promotes the uptake of
glucose inside the cel ls and the intercel lular phosphorylat ion of glucose
to glucose–6–phosphate. Glucose–6–phosphate i tsel f also appears to be
a specif ic activator of glycogen synthesis.
Insulin effect on protein metabolism:
I t prevents gluconeogenesis Glucose is normally formed from
proteins and l ipids in the l iver. In diabetes this process is enhanced.
High blood sugar level in diabetes is due to over product ion of glucose.
In the starving diabetes dextrose ni trogen ratio is fair ly constant. This
shows that both sugar and ni trogen are coming form the same source i .e.
proteins. When insul in is given both sugar and nitrogen excretion fai ls,
showing that formation of new glucose from proteins has been interfered.
Shareera 31
Insulin effect on fat metabolism:
I t prevents formation of ketone bodies (anti ketogenic). In advance
diabetes, excess ketone bodies are formed in l iver, due to incomplete
combustion of fatty acids. After the administrat ion of Insul in more sugars
burn and l iver glycogen increases displacing the l ipids. Hence l ipid
combustion is discouraged and ketosis disappears.
Insul in decreases the cholesteremia and l ipademia. I t also prevents
accumulation of excess l ipid in the l iver and breakdown of l ipid in
Adipose t issue.
GLUCOGON :-
The Alpha cel ls of the islets of Langerhans secrete Glucogon. I t is
a polypeptide hormone with 29 aminoacids having molecular weight of
3,485. This polypeptide has been completely synthesized. Glucogon
causes glycogenolysis in the l iver and antagonist to l iver by depriving the
action of Insul in.
The blood sugar level chief ly controls the secretary activi ty of
Alpha and Beta cel ls. Hyperglycemia st imulates the release of Insul in
where as, hypoglycemia wi l l release the glycogen. There is no good
evidence that a tropic hormone secreted by the pitui tary, directly
inf luences the secretary act ivi ty of the pancreatic is lets, through
secret ions derived form other endocrine glands for example, the adrenal
Shareera 32
gland have some effects. I f the is lets are completely removed or
extensively damaged, the lack of or reduced Insul in formation results in
hyperglycemia and the condit ion of diabetes mell i tus (Madhumeha).
Relat ively normal carbohydrates metabol ism can then be restored by
supplementat ion of insul in.
I t is necessary to point out however that though a def iciency of
insul in production and release may result in Diabetes, not al l cases of
Diabetes are due to a deficiency in Insul in product ion. Even pi tui tary,
Liver and Adrenals are also involved in this process. Cl inical syndromes
involving abnormal carbohydrate metabol ism and abnormal blood sugar
levels may result f rom either deficiency or excess product ion of Insul in
and Glycogen. The latter when injected result in an increase in blood
sugar. Excess production of insul in as in cases of Islet tumors results in
hypoglycemic and attains neurological changes, excess product ion of
Gastrin, acidi ty and peptic ulceration.
ADRENAL (SUPRA RENAL) GLANDS
The adrenal glands are si tuated on the upper poles of the kidneys.
Each gland weighs about 4 gm.
Microscopic structure - A dist inct connect ive t issue capsule surrounds
the parenchyma of the gland. Beneath the capsule the cortex is arranged
in 3 layers. They are -
Shareera 33
Zona Glomerulosa.
Zona Fasculata
Zona Reticularis
Zona Glomerulosa : - The outer layer which varies in thickness form
almost total absence to clusters of a dozen or more smal l cel ls is known
as Zona Glomerulosa. Zona Glomerulosa secretes mainly aldosterone
that is concerned with the salt and water balance and acts on the distal
convoluted tubule and col lecting ducts of the kidney. I t also secrets a
small amount of glucocort icoids and sex hormones.
Zona Fasculata : - inside the f i rst layer the cel ls are larger and form
more or less paral lel radial columns. They commonly contain fat droplets
which give them a spongy appearance. This region is known as a Zona
Fasculata. This layer secretes predominantly Glucocort icoide.
Zona Reticularis . : - Centre of the gland the regular arrangement of cel ls
of the Zona fasciculata is replaced by one of anastomosing cel l cords
forming the Zona Reticular is, which secretes sex hormones and a small
amount of Glucocort icoids but no Aldosterone.
The adrenal Medul la is chief ly composed of chromaff in cel ls
(phaeochromocytes) which ei ther secrete Adrenal ine or Nor- adrenal ine.
Shareera 34
LIVER :-
The l iver is the largest gland in the body. The greater part of the
Liver l ies under the covering of the r ibs and coastal cart i lage. The l iver
is a dark brown, highly vascular and soft organ that is commonly ruptured
or torn in abdominal injur ies. I t is approximately one f i f teenth of the body
weight in adult.
The l iver is determined by the surrounding organs i t retains the
shape of a blunt edge i t has two surfaces. Diaphragmatic surface
divisible into Superior, Anterio, posterior and right parts according to the
direct ion in which i f faces and visceral (posterior) surface faces
posterior ly and Inferiorly. Liver is divided into four lobes Right,
Quadrate, Caudate and Left lobes.
Functions of l iver in carbohydrate metabol ism are:-
1. Storage of Glycogen.
2. Conversion of Galactose and fructose into glucose.
3. Gluconeogenesis
4. Formation of many important chemical compounds from the
intermediate products of Carbohydrate Metabol ism.
Shareera 35
Liver is especial ly important for maintaining a normal blood glucose
concentration. For instance storage of glycogen al lows the l iver to
remove excess glucose from blood, store i t and then return i t in to the
blood when the blood glucose concentrat ion begins to fal l too low. This
is cal led the glucose buffer function of the l iver. As an example,
immediately after a meal containing large amounts of carbohydrates the
blood glucose concentrat ion raises about three t imes as much in the
person with a non functional l iver as in a person with a normal l iver.
Gluconeogenesis in the l iver is also concerned with maintaining a
normal blood glucose concentration for glucose neogenesis occurs to a
signif icant extent only when the glucose concentration begins to fal l
below normal. In such case large amounts of amino acids are converted
into glucose, there by helping to maintain a relat ively normal blood
glucose concentrat ion.
Shareera 36
SHAREERA
References
1 Charaka Nidana 4 / 4
2 Charaka Vimana 5 / 7
3 Ibid 5 / 7
4 Ibid 5 / 7
5 Ibid 5 / 7
6 Ibid 5 / 7
7 Sushruta Shareera 9 / 15
8 Charaka Vimana 5 / 7
9 Sushruta Nidana 16 / 42
10 Ibid 16 /45
11 Charaka Vimana 5 / 8
12 Charaka Shareera 7 /15
13 Sushruta Shareera 4 / 23
14 Sharangadara Poorva khanda 5 / 63
15 Adamalla on Sharngadhara 5 / 83
16 Charaka Vimana 5 / 8
17 Sushruta Nidana 7 / 18
18 Sushruta Shareera 4 / 30
19 Sharangadhara poorva khanda 5 / 40
20 Charaka Shareera 7 / 7

Shareera 37
21 Sushruta Shreera 4 / 26
22 Ibid 4 / 47
23 Charaka Shareera 9 / 4
24 Ibid 9 / 4
25 Sushruta Nidana 3 / 17,29
26 Astanga Hridaya Shareera 4 / 10
27 Sushruta Chikitsa 7 / 33
28 Sushruta Nidana 3 / 18
29 Ibid 3 /15
30 Sushruta Nidana 3 / 15
31 Dalhana on Su Sh 4 /23
32 Charaka Vimana 5 / 7
33 Sushruta Shareera 4 / 10
34 API Text of Medicine by Sanani pp 205
35 Ibid pp 204
36 Principles of Anatomy and Physiology by Gregfard Tortara
37 Joslin’s diabetes Mellitus. pp15
38 Ibid pp 216
Nidana 36
HETU
I t is bel ieved that Prameha is a hereditary disease and many
factors play an important in the product ion of the disease as a cl inical
enti ty. They are age, sex, diet, body weight, Infect ion, pregnancy, etc.
Emotional stress and trauma have also been considered as etiological
factors of Prameha. Charaka considers Madhumeha as one out of the four
veri t ies of vataja Pramehas1. He has also stated that al l factors that
increase Kapha are the causative factors of the Pramehas2. The general
et iological factors of Prameha as stated by Charaka are3 – “Addict ion to
the pleasures of lounging and sleeping, excessive use of curds, meat
juice of domestic, aquatic and wet land animals, mi lk or diary products,
newly harvested grains and drinks and products of jaggery".
The et iological factors as stated by Sushruta are simi lar to Charaka
and capable of vi t iat ing mainly the Kapha dosha. Sushruta states that al l
variet ies of Prameha, i f not properly treated and attended to at the onset,
may ult imately develop into Madhumeha4. Based on the etiology,
Sushruta has classif ied Prameha into two variet ies as sahaja and
apathya nimittaja. Apathya nimit taja is subdivided into two as Ahara
nimit taja and vihara nimit taja.
Nidana 37
1. Sahaja or Genetic origin.
Charaka4 and Susrata5 have evaluated that beeja dosha is also a
cause for Prameha. Further Sushruta has included Madhumeha in the
Adibala pravri t taja category of disease.
The term beeja has been considered as a sukra and shonitha5,
which correlates with the sperm and ovum of modern concepts. Beejas
are vi t iated with dosha (Vata especial ly responsible for division of cel ls
makes certain abnormali t ies in chromosomal galaxy of sperm or ovum)
are responsible for genesis of Prameha, In gross the organs which are
responsible for producing Prameha are ambuvaha srotas, mamsa, kleda,
kloma, mootravaha srotas. They are deformed since bir th and susceptible
to get Prameha, aggravated by nimit ta karana. This may be because of
the selective discriminative of these organs to develop Prameha. As a
result of defective beeja when Prameha is developed, then the person is
cal led as a Jatha Pramehi pat ient. Jata Pramehi6 has been considered as
a Kulaja vikara7. Few diseases included under this category are Kusta,
Arsha, Meha, Kshaya etc. Kulaja vikaras means the diseases, which are
carr ied from the former generat ion to the successive generat ion, and they
are of the defects in the genetic code.
Nidana 38
2. Apatya nimittaja
Apathya is the main cause for the disease. Apathya includes both
ahara and vihara. Al l acharyas have stressed the indulgence of
unwholesome food and vihara in the production of Prameha. Ahara and
vihara that increases kapha, medas and mootra lead to the genesis of
Prameha.
Charaka explains the Nidana8 as Amla, Lavana, Madhura Rasa and
Guru, Snigdha guna dravyas, Curd, Milk, Mamsa rasa of aquatic animals,
Fresh cereals. Guda and Guda vikara.aharas and Sitt ing idle, Excessive
sleep, Disl ike for walking, act ivi t ies and to take bath are the viharas for
Madhumeha.
Sushruta explains the Nidana9 as Madhura Rasa, Medhya, Snigdha,
Sheeta guna dravyas. Nava anna, Wine, Meat of animals l iv ing in marshy
lands and Guda as aaharaj hetus. Laziness, Day sleep, inactiveness as
viharaja hetus of Madhumeha.
Vagbhata explains the Nidana10 as Madhura, Amla, Lavana Rasa,
Guru, Snigdha, Sheeta, Picchi la Guna dravyas, Nava anna, Madhya,
Anupa Mamsa, Ikshu rasa, Guda and Guda vikara, Dadhi, Paya as ahara
Nidana 39
and Sit t ing for long t ime, Sexual intercourse, Sleeping excessively as
viharaja Nidana for Madhumeha.
Charaka has explained the vishista nidanas, of Prameha according
to their doshas, they are as fol low.
Kaphaja prameha nidana11.
Aharaja.
The frequent and excessive use of newly harvested rice
(Hayanaka), Yavaka, Chanaka, Uddalaka, Naisadha, Itkata,
Mukundaka, Mahavrihi , Promodaka and Sugandhaka grains.
The use of new blackgram and other pulses
The f lesh of domestic, land and aquatic animals.
Sugarcane juice, or the abundant use of mi lk, curds, ghee or sweet
and unripe art ic les.
Viharaja:
Avoidance of cleanl iness and exercise, excess indulgence in
sleeping, ly ing or sedentary habits, and al l factors which are l ikely
to increase kapha, Medas and mootra
The special morbid factor of the humor is excessive f luidi ty of
kapha.

Nidana 40
Pittaja prameha nidana12.
Aharaja:
The habitual use of ushna, amla, lavana, kshara and katu art ic les.
Adhyashana, Vishama ahara.
Viharaja:
Teekshna santapa sevana, Sharma , Krodha, Anxiety.
Vataja prameha nidana13.
Aharaja
The habitual use of rooksha, kashaya, katu, t ikta, laghu and sheeta
art ic les.
Viharaja:
Adhika Vyavaya and Vyayama, Excessive use of panchakarmas.
Vegadharana, Exessive indulgence in fasting, Atapa, Udvega,
Shoka, Abighata.
Nidana 41
Aetiology according to Modern concept
The cause of hyperglycemia can be divided into Heredity and
Acquired14,15.
Heredity
Posit ive family history may be obtained in around 40 % of patients
with NIDDM (Non Insul in Dependent Diabetes Mell i tus). Genes
responsible for this heret ic carriage of the disease are one for insul in
(Chromosome 11) insul in receptor (Chromosome 19) and glucose
transporter (Chromosome 1). But a defini te association of any of these
genes with cl inical NIDDM is yet to be establ ished.
Acquired and environmental factors.
Analysis of epidemiological data leads to identi f ication of aging,
obesity, composit ion of diet, physical inact ivi ty, stress and urbanisation
as environmental predisposing factors for NIDDM.
Nidana 42
SAMPRAPTI
The suppress ion or the inc idence of the d isease is dependent
upon the resul t o f the var ia t ions in the et io log ica l factors (n idana) .
In tens i ty o f the morb id factors (doshas) and suscept ib i l i ty o f the body–
elements (dushyas) . I f these three factors , main ly the et io log ica l
factors etc . , do not mutual ly assoc iate or suppor t , or i f do so af ter a
long lapse of t ime, or in a very mi ld form, e i ther there occurs no
mani festat ion of the d isease at a l l or the d isease takes a long per iod to
evolve, or appears ambulatory form. Under the contrary condi t ions, i t
g ives cont rary resul ts . Thus the d i f ferent causes of the modes of
inc idence la id down are suppressed in a l l d iseases16.
The samprapt i o f a d isease expla ins the method or process by
which the v i t ia ted doshas reach wi th the dushyas and produce the
anatomica l and phys io log ical changes in the target organs leading to
the express ion as a d isease. In terms of Kr iyakalas, the samprapt i
deals wi th the chaya, prakopa, prasara and Sthana samsraya of the
d isease-causing doshas, which leads to the dosha-dushya
sammurchana i .e . , the in teract ion between d is turbed funct ional factors
wi th the bas ic s t ructura l ent i t ies of the body.
Nidana 43
Charaka had c lear ly expla ined the samprapt i o f the Kaphaja
Prameha in the Prameha Nidana. Even though the d isease Prameha is
s ta ted to be due to the v i t ia t ion of the t r i -doshas, the spec i f ic morbi f ic
factors of the humor is excess ive f lu id i ty o f Kapha. The specia l
features of the suscept ib le body e lements(dushyas) are excess iveness
and demin ished v iscousness of Medas, Mamsa, Body f lu id (sareera
k leda) , Sukra, Rakta, Vasa, Maj ja , Las ika, Rasa and Ojus17.
When there is the s imul taneous congress of these three
patholog ica l condi t ions, the kapha is suddenly provoked s ince i t is
a l ready in chaya s tage. The v i t ia ted kapha quick ly spreads throughout
the body which is a l ready in degenerated condi t ion. In the path of i ts
c i rcu la t ion the kapha f i rs t encounters and mixes wi th the medas, owing
to the patholog ica l changes in the medas, v iz . , excess iveness and
d imin ished v iscousness and a lso owing to the great s imi lar i ty o f the
qual i t ies between the kapha and medas. Due to th is combinat ion of
v i t ia ted kapha and medas, the la t ter is v i t ia ted. The v i t ia ted kapha
coupled wi th the v i t ia ted medas now comes in contact wi th the sareera
k leda and mamsa which are in excess ive increase in the body. The
v i t ia ted body f lu id is changed in to ur ine. The or i f ices or pores of the
mootravahasrotas, represented by the k idneys and b ladder are in a
s ta te of d i la ta t ion due to the act ions of v i t ia ted medas and sareera

Nidana 44
kleda. The v i t ia ted kapha, upon reaching the mootravahasrotasas,
gets local ised there and thus develops the d isease ca l led Prameha 18.
The sareera- k leda combined wi th the kapha and the medas whi le
be ing conver ted in to ur ine on i ts ent rance in to the mootrasaya,
acqui res the fo l lowing ten patholog ica l character is t ics of Kapha. They
are unctuousness, heav iness, sweetness, denseness and s lowness.
Then i t acqui res a spec ia l name accompanied wi th the qual i t ies of one
or more of the other condi t ions by which i t has been main ly modi f ied19.
The vit iated pitta produces Prameha by the same process as
described above20.
V i t ia ted Vata br ings about the mani festat ion of Vata ja Prameha
by the same process as descr ibed above. I f Vata by i ts rooksha qual i ty
changes the o jus which is natura l ly o f sweet taste, in to one of
ast r ingent taste and carr ies i t to the mootrasaya, then i t causes the
condi t ion ca l led Madhumeha21.
Charaka in Prameha Chik i tsa has expla ined the samprapt i in
br ie f 22. “ the Kapha, hav ing v i t ia ted the medas and mamsa dhatus and
the body f lu id , becomes loca l ised in the geni to-ur inary system and
causes Pramehas7 . The p i t ta, too, which is provoked by ushna dravyas
v i t ia t ing those very t issues, causes in the same manner o ther var ie t ies
Nidana 45
of Prameha. On the d iminut ion of the other two humors, the morb id
Vata draws in to the geni to – ur inary system the essent ia l dhatus, and
g ive r ise to the th i rd group of Pramehas. In every case the morb id
humor, hav ing reached the geni to-ur inary system, v i t ia tes the ur ine and
generates Pramehas corresponding to i ts spec i f ic nature” .
Sushruta has g iven more deta i ls about pathogenesis o f
Prameha 23. “ In a person who indulges in the mi thya ahara v ihara the
three doshas which are v i t ia ted and in an immature s tate jo in the
medas and t ravel to the mootrava srotas, gets loca l ised at the ent rance
of the vast i , when they are emi t ted through the urethra the d isease is
known as Prameha.
“The deranged kapha, in conjunct ion wi th the (morb id) p i t ta , vayu
and medas, g ives r ise to a l l kaphaja types of Prameha. The deranged
p i t ta , in conjunct ion wi th the deranged vayu, kapha, rakta and medas
produced the p i t ta ja ones; whi le the deranged vayu, in un ion wi th the
deranged kapha, p i t ta , medas, maj ja and vasa, engenders the types of
Vata ja Prameha” 24.
From the references c i ted above, the fo l lowing facts can be
e l ic i ted:
1 . The main dosha v i t ia ted in Prameha is kapha.
Nidana 46
2. But the other two doshas are a lso af fected and depending upon the
predominance of the s igns and symptoms of one par t icu lar
dosha, the d isease is named accord ing ly .
3 . The af fected dushyas are rasa, rakta, mamsa, medas, maj ja and
shukra. I t should be not iced that the asth i dhatu is not ment ioned
in the dushyas of th is d isease.
4 . In addi t ion shareera k leda, o jus, vasa and laseka are a lso af fected.
5 . Therefore i t is c lear ly understood that the dhatu par inama in
genera l is d is turbed.
6 . The v i t ia ted doshas get local ised in mootravaha srotas and d is turb
i ts normal funct ions, by d i la t ing i ts or f ices.
7 . The main s igns and symptoms v iz . Polyur ia and turb id i ty expresses
i tse l f the patholog ica l changes in the ur ine.v iz Mootravaha srotas
and vast i .
8 . The body- f lu id or shareera k leda is t ransformed in to a l iqu id mala
which is excreted as ur ine. S ince a l l the nut r ient e lements and
malas c i rcu la te a long wi th the rasarakta complex, i t is c lear that
there is a change in the composi t ion of the rasarakta complex.
9 . Because of th is change in the composi t ion of the rasarakta
complex, the d is turbance in the dhatu par inama can be eas i ly
understood.
Nidana 47
Charaka and vagbhata have descr ibed the pathogenesis of
Madhumeha as separate f rom Prameha. Vagbhata s tates that the
pathogenesis o f Madhumeha is o f two var ie t ies 25.
1 . The deplet ion of the dhatu leading to the v i t ia t ion of Vata
2. Obstruct ion to the normal c i rcu la t ion of Vata by the other doshas
leading to the v i t ia t ion of the former.
Th is par t icu lar in format ion leads us to inc lude that Madhumeha is
main ly due to the v i t ia t ion of Vata. Even accord ing to Charaka,
Madhumeha is enumerated as one of the Vata ja Pramehas. Vagbhata
has a lso s ta ted that any Prameha, i f not t reated and at tended to at the
outset , wi l l u l t imate ly develop in to Madhumeha. He has a lso c lear ly
s ta ted that there is an increase in the sweetness or sweet substances
in the body, which is expressed through the phys ica l qual i t ies of ur ine,
be ing the co lour and taste resembles honey 26.
A l l organs and par ts o f the body are made o f the i r u l t imate un i ts
or jeevaparamanus27. These innumerable jeevaparamanus or ce l ls o f
d i f ferent shareera avayavas are held together cemented to form
d i f ferent s t ructures and organs of the body. The substance that un i tes
and cements a ce l l w i th another for the format ion of var ious s t ructures
and organs is the in ter -ce l lu lar substance. By v i r tue of i ts v iscos i ty ,
smoothness, s l iminess and lubr icabi l i tuy, the in ter – ce l lu lar substance
Nidana 48
is cons idered s la ishmic in nature. Through th is in ter -ce l lu lar
substance pass the nut r ient mater ia l f rom capi l lar ies to ce l ls and the
metabol i tes pass in the reverse d i rect ion. In ter ference wi th i ts funct ion
leads u l t imate ly to the degenerat ion and decay of the ce l l and
consequent ly o f the s t ructures or dhatus of the body.
The physical and chemical characteristics of cell protoplasm in
general are parallel to those of the Kapha and the functions
ascribed to both are l ikewise. Therefore it can be seen that the
body structure including all the dhatus are completely made up of
kapha. Therefore kapha is that factor of the dosha-triad which not
only imparts strength to all dhatus but also prevents their decay and
degeneration28.
I f there is a disturbance in the nourishment of the cel ls, a
disturbance in the general dhatuparinama is surmised. Accordingly, there
can be a defic iency in the functions of kapha and also the sleshmika ojus
that is responsible for general immunity of the body.
The term kapha has been defined as “kapha the product of jala”29
and therefore there is no surprise to not ice that the body’s major
component is water. Since there is the vi t iat ion of kapha in Prameha, i t
can be easi ly understood the functions of shareera kleda or body-f luid.
Nidana 49
In the process of Ahara pachana the waste materials are separated
in two forms, one is l iquid and the another is sol id. The l iquid part is
absorbed from the kostha through the purishadharakala to be transformed
into urine and excreted through the mootrashaya30. The sara bhaga of
the food is ut i l ised by the respective dhatwagnis and the nutrients are
ut i l ised in the construct ion of the dhatus. This dhatwagni paka of
dhatuparinama also produces di f ferent ki t tas31. The ki t tas of the
dhatwagni paka which are ejected by cel ls wi l l natural ly enter into the
circulat ing rasa dhatu to be transported to their respect ive out lets. Since
i t has been stated that the shareera kleda, which is affected due to the
vi t iat ion of kapha, is changed into mootra32, i t is to be understood that
there is increased production of ki t ta bhaga in dhatwagni paka. I f there
is an increased product ion of ki t ta bhaga, i t can be easi ly summarised
that there is a decreased product ion of the prasadabhaga which is meant
for the construction of the dhatus or the organs of the body, leading to a
deficient repair and so degeneration of the body. The same thing has
been explained by the ancient scholars that in a Prameha patient, as
shareera saithi lyata.
The major port ion of the ki t ta bhaga, which is in a l iquid state, is
excreted by the mootravaha srotas. The normal function of mootravaha
srotas is to al low the ki t ta bhaga to pass through i ts pores and to prevent
the nutrient material from escaping out of the body. The vit iated kapha
upon reaching the mootravaha srotas gets local ised there and along with

Nidana 50
the vi t iated medas produces di latat ion of the pores of the mootravaha
srotas. Therefore, not only the substances that are to be excreted but
also some of the nutrient materials are also al lowed to pass through
these di lated pores.
According to Vagbhata, there is an increase in the sweetness or
sweet substances in the body of a Madhumeha pat ient33. This part icular
fact is noticed by the sweetness of the ur ine that can be observed and
recognised by attraction and assemblage of ants near the urine34. The
urine of a normal or healthy person is not sweet in taste. This sweetness
of the urine of a Madhumeha patient is due to the madhuradravya, which
is f i l tered by the mootravaha srotas from the rasarakta complex but could
not be reabsorbed completely during the paka or maturat ion of urine.
The madhuradravya is a natural component of the rasarakta
complex. Even though the ayurveda laid down that a person should
partake a food containing the six tastes, the major component of the
regular food is madhuradravya. Charaka considered cereals
(shukadhanya varga) as main source of food and the others l ike pulses,
legumes, meat, f ishes, frui ts, spices etc,. As support ing diet art ic les35.
The main const i tuent of al l cereals is carbohydrate, which are
madhuradravyas. Therefore the main product of the al imentary digestion
of these cereals to be absorbed into the blood is also a madhuradravya.
Nidana 51
Charaka also states that the madhurarasa confers bala or strength
on the Dhatus and ojus and that madhurarasa is compatible to the body36.
The madhurarasa therefore produces an increase in the body bulk i .e. i t
is the best in brimhanadravyas37. A substance which is having the
physiochemical qual i t ies / propert ies of Pridvhi and Ap is stated to be
Brimhana dravya38. I t should also be noted that substance of
madhurarasa is also having the qual i t ies of Pridhvi and Ap39. The Sharira
Bala is of two variet ies :
1) Vyayamashakti – the strength required to perform vigorous
physical work and
2) Vyadhikshamatwa shakti – the power to resist and overcome
forces or factors which bring about disease.
Vyayamashakti is dependent of wel l formed and i t confers the
Karmasadhana shakti on body. Vyadhikshamatwa is bestowed in the
normal functioning of Ojus, which is the essence of healthy Dhatus. Ojus
is also a madhuradravya. From the above the importance of the
madhuradravya for the nourishment and also strength of the body can be
clearly understood.
Nidana 52
Since i t is stated that the madhuradravya is excreted in the urine,
there can be only two causes for this excretion:
1) Excess of madhuradravya in the circulat ing rasarakta complex,
more than the amount required for the nourishment and strength
of the Dhatus and consequent overf lowing through mootravaha
srotases.
2) The increased release by the ori f ices of the mootravaha
srotases. I t has already been stated earl ier that these ori f ices of
the mootravaha srotases have been di lated due to the vi t iated
Tridoshas.
The dhatus of a Madhumeha pat ient are in a state of Saidhi lya40.
These indicate that the Dhatus are not being nourished in a proper
manner. But the madhuradravya, which is the main source of
nourishment and strength, is stated to be in excess in the Rasarakta
complex. I t is also a fact that al l the organs and parts of the body are
made up of their ul t imate units or Jeevaparamanus or cel ls. The
nourishment of these cel ls, which const i tute the Dhatus of the body, is
dependent upon the nutrients derived from the food freely entering into
them for their ut i l isation. I f there is an obstruction to the path or
entrance of these madhuradravyas into the cel ls, the Dhatus do not get
suff ic ient nutr i t ion and they’re by degenerate and decay. Because of this
obstruct ion entrance of the madhuradravyas into the cel l of the body
Nidana 53
interfered. There is an excess of such substances in the Rasarakta
complex developed in the body. The nourishment of the cel ls of the
dhatus is maintained by the ut i l isation of the respective nutrients by the
Dhatwagni. This dhatwagnipaka is possible only after the nutrients-
madhuradravya in this respect-enter the dhatus. Since there is an
obstruct ion to the entrance of the madhuradravya, the product of the
al imentary digest ion, into the Dhatus, we have to presume that there is a
deficiency in the function of the Bhutagnis.
Since the Dhatus are def iciently nourished due to the obstruction to
the entrance of the madhuradravya into the Dhatus, there wil l be deficient
formation and defect ive funct ioning of the Ojus, the essence of Dhatus.
Sushruta has already stated that Ojokshaya develops due to excessive
hunger41 – the hunger of the Dhatus for the madhuradravya in
Madhumeha patient. As stated earl ier, the vyadhikshamatwa of a person
is dependent on the normal functioning of the Ojus. Therefore in a
Madhumeha patient whose ojus is deficient ly formed, or vyadhikshamatwa
shakti is substandard. Therefore his body / dhatus are not capable of
resist ing the virulence of diseases especial ly of the Vaikarika krimi origin.
The Vaikarika krimi also thr ive to grow powerful in the presence of the
excessive madhuradravya. Not only the disease Madhumeha but also the
diseases due to vaikarika kr imis cause a hastening of the degeneration
and decay of the body.
Nidana 54
The important and ul t imate aim of a human being is to maintain the
l i fe as long as possible. Therefore when the madhuradravyas essential
for the maintenance of the l i fe are not al lowed to enter the Dhatus, the
body tr ies to deplete the store-houses of the madhuradravyas to be
ut i l ised by the body. In a healthy person, i f madhuradravyas are
consumed in excess of the requirement of the body, they are converted
into medas42,43.and stored for future use. Therefore, once the store-
house of the madhuradravyas are completely depleted, the medas and
other important dhatus (which contain protein mainly) are slowly
disintegrated for maintenance of l i fe. During this disintegrat ion of the
Dhatus which are mainly effected by the pachakamshas, the
products/metabol i tes, which are not capable of nourishing the body, some
t imes prove to be noxious producing several complicat ions l ike moorcha,
hr idgraha etc. One of the important condit ion due to this disintegrat ion of
medas is the dhatuja medovyapat with consequent development of
dhamaniprat ichaya44. Thus the knowledge of samprapti is important to
handle the Madhumeha patients.

Nidana 55
POORVARUPA
The prodormal symptomology of a disease has been described as
poorvaroopa. The knowledge of poorvaroopa has importance in early
management of patient and also in di f ferent ial diagnosis of disease so
that the disease is control led easi ly. The state of prodroma or poorvarupa
is expressed as when vi t iated doshas become local ised due to
srotovaigunya leading to the dosha-dushya-sammurchana. Kapha
predominant tr idoshas and dhatus along with ojus are chief ly effected in
Prameha. Thus poorvaroopa are very much varied in nature.
The fol lowing are the prodroma of Prameha.
1. Burning sensation of the palms of hands and the soles of the feet45,46,47.
2. Dryness in the mouth, palate and throat and thirst48.
3. Heaviness of the body49.
4. Coldness or sl iminess of the skin and l imbs, thermalgia and
numbness in the body50.
5. Smell l ike raw-meet in the body51.
6. Somnolence and continuous torpor and lassitude52.
7. Sweet taste in the mouth53,54.
8. Sl imy mucous deposit on the tongue, palate, pharynx and teeth55.
9. Increased excrement in the body, increased discharge from the
ori f ices in the body56,57.
Nidana 56
10. Sweetness and whiteness of urine58.
11. Attract ion of insects and ants to the body and urine59.
12. Matt ing of the hair and inordinate growth of the f inger and toe
nai ls60,61.
13. A bad smell ing breath and shortness of breath62.
Vagbhata has mentioned some more addit ional prodroma for Prameha.
1. Excessive perspirat ion63.
2. Laziness64.
3. Liking of cold comforts65.
From the above prodroma i t can be clearly seen that there is an
increased production of ki t ta bhaga in dhatu parinama as explained
earl ier.
Nidana 57
ROOPA
In the Roopa or actual manifestation of the disease, dosha dushya
sammurchana completes, and the onset of the disease wi l l be
commenced. The roopas may change from time to t ime and certain
symptoms may newly appear or some may disappear. Roopa is the
prominent diagnostic key, hence the knowledge of the various lakshanas
disease is essential for the benefi t of prognosis.
Cl inical features of the present disease Madhumeha are divided
into two groups
1. General features of Prameha
2. Special features of the Madhumeha.
Charaka has not described the general features of Prameha where
as Sushruta66 and Vagbhata67 have described the general features as
a. Avi la mootrata
b. Prabhoota mootrata.
Nidana 58
Specif ic Lakshanas of Madhumeha.
I t is one of the four Vataja Pramehas. The person with Madhumeha
passes urine which is astr ingent and sweet in taste, yel lowish or whit ish
in colour. The urine contains simi lar propert ies of Honey68,69,70.
Apart from the above lakshanas, Sushruta described typical lakshanas
for Madhumeha rogi71, that he desires –
1. To stay whi le walking.
2. To si t whi le staying
3. To take rest on bed whi le si t t ing
4. To go to sleep whi le taking rest.
Nidana 59
BHEDHA
Though Prameha is stated to be developed due to the vi t iat ion of
al l three doshas, the disease is mainly divided into three groups.
1. kaphaja Pramehas - which are again subdivided into 10 types72.
2. Pit taja Pramehas - which are again subdivided into 6 types73.
3. Vataja Pramehas - which are again subdivided into 4 types74.
Even though the three Ayurveda authori t ies Charaka, Sushruta and
Vagbhata agree the same number of Prameha in each group, there seems
to be di f ference in the nomenclature used by them. Increased quanti ty of
ur ine and increased turbidi ty in the urine are the main symptom in al l
Pramehas.
The name of each variety of Prameha is decided according to the
combinat ion of dosha and dushya, and the physical character
resemblance to the urine.
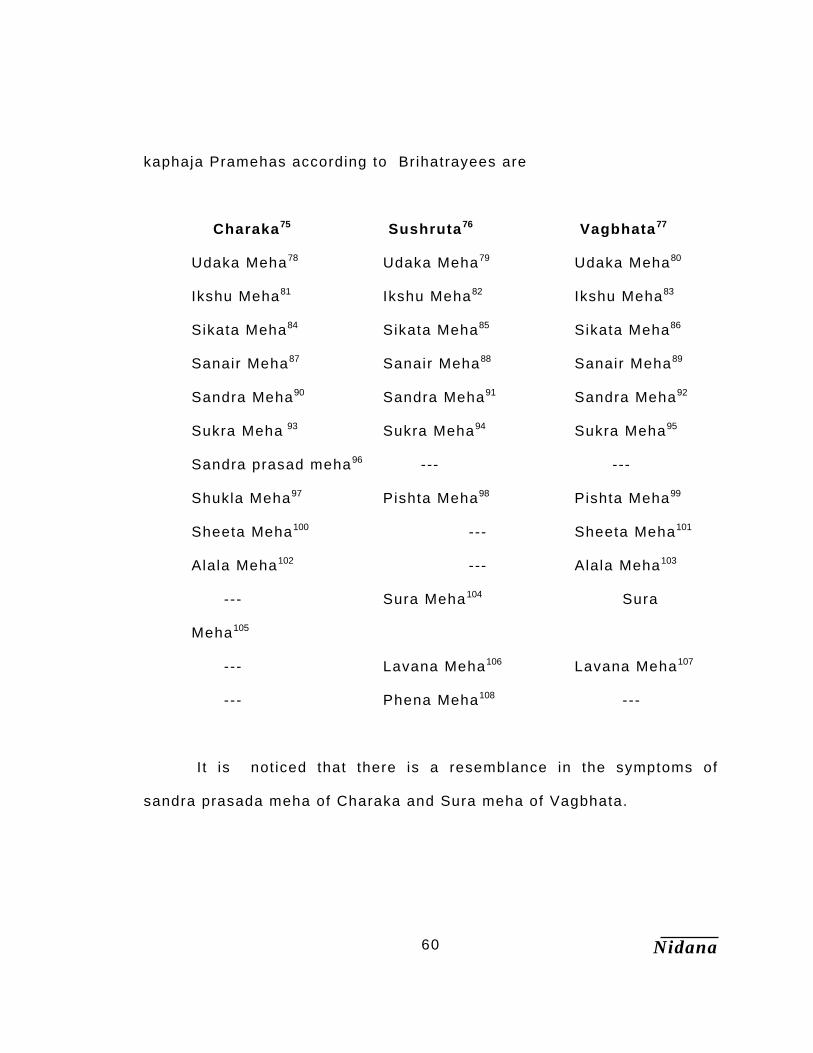
Nidana 60
kaphaja Pramehas according to Brihatrayees are
Charaka75 Sushruta76 Vagbhata77
Udaka Meha78 Udaka Meha79 Udaka Meha80
Ikshu Meha81 Ikshu Meha82 Ikshu Meha83
Sikata Meha84 Sikata Meha85 Sikata Meha86
Sanair Meha87 Sanair Meha88 Sanair Meha89
Sandra Meha90 Sandra Meha91 Sandra Meha92
Sukra Meha 93 Sukra Meha94 Sukra Meha95
Sandra prasad meha96 --- ---
Shukla Meha97 Pishta Meha98 Pishta Meha99
Sheeta Meha100 --- Sheeta Meha101
Alala Meha102 --- Alala Meha103
--- Sura Meha104 Sura
Meha105
--- Lavana Meha106 Lavana Meha107
--- Phena Meha108 ---
I t is not iced that there is a resemblance in the symptoms of
sandra prasada meha of Charaka and Sura meha of Vagbhata.
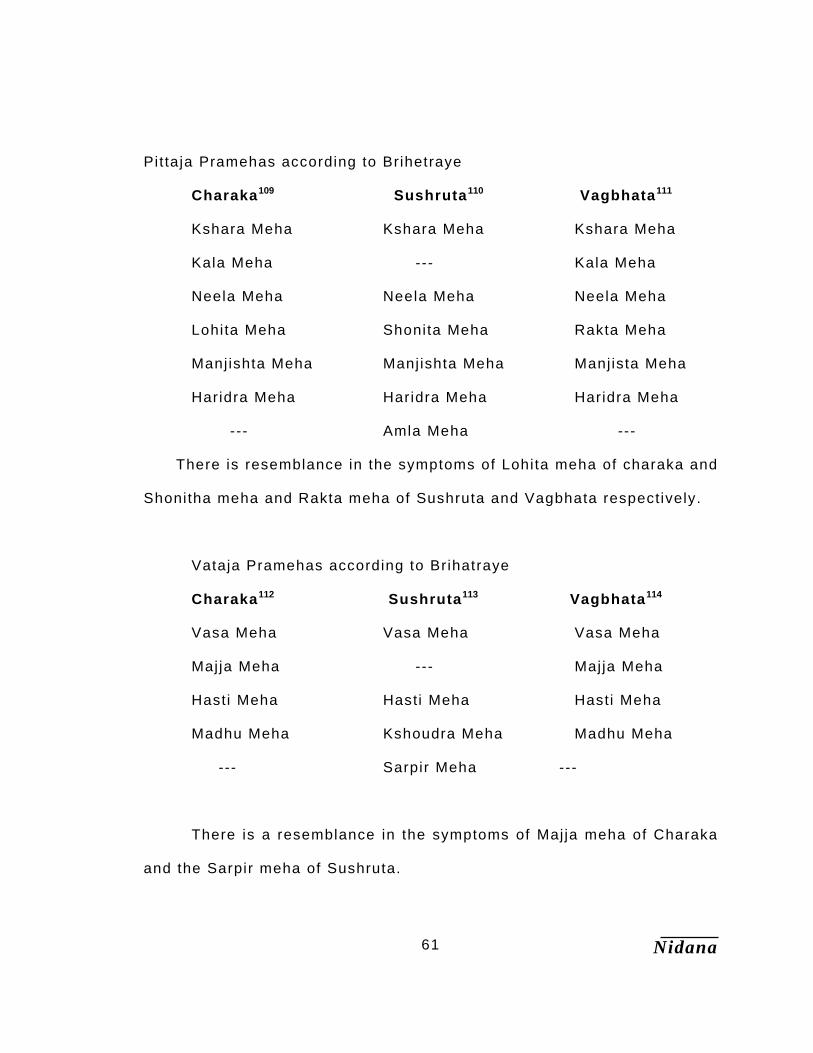
Nidana 61
Pit taja Pramehas according to Brihetraye
Charaka109 Sushruta110 Vagbhata111
Kshara Meha Kshara Meha Kshara Meha
Kala Meha --- Kala Meha
Neela Meha Neela Meha Neela Meha
Lohita Meha Shonita Meha Rakta Meha
Manj ishta Meha Manj ishta Meha Manj ista Meha
Haridra Meha Haridra Meha Haridra Meha
--- Amla Meha ---
There is resemblance in the symptoms of Lohita meha of charaka and
Shonitha meha and Rakta meha of Sushruta and Vagbhata respectively.
Vataja Pramehas according to Brihatraye
Charaka112 Sushruta113 Vagbhata114
Vasa Meha Vasa Meha Vasa Meha
Majja Meha --- Maj ja Meha
Hasti Meha Hasti Meha Hasti Meha
Madhu Meha Kshoudra Meha Madhu Meha
--- Sarpir Meha ---
There is a resemblance in the symptoms of Maj ja meha of Charaka
and the Sarpir meha of Sushruta.
Nidana 62
It is evident form the above table that Vagbhata closely fol lows
Charaka whi le Sushruta had a sl ight di f ferences.
MADHUMEHA:
Madhumeha can be sub classif ied mainly into two types.
Type one a) Kulaja or Sahaja (Hereditary)
b) Doshaja or Apathya nimit taja ( acquired)
Type two a) Dhatu kshaya janya Madhumeha115
b) Doshavruta janya Madhumeha
Charaka has divided the Madhumeha pat ients into two veri t ies basing
on the l ine of treatment aspect116.
1. Sthoola (stout or strong)
2. Krisha (emaciated or week)
Sushruta accepts Sahaja rogi as krisha and the Apathya nimitaaja rogi
as sthoola rogi in his classif icat ion.
.
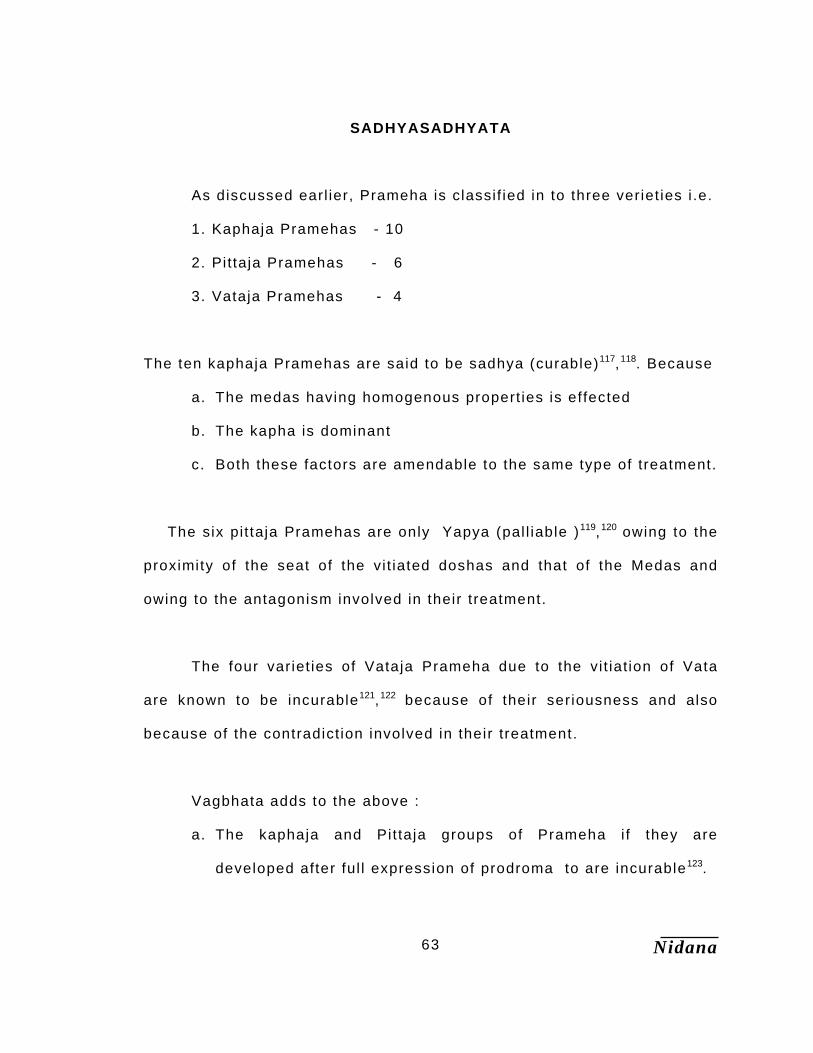
Nidana 63
SADHYASADHYATA
As discussed earl ier, Prameha is classif ied in to three veriet ies i .e.
1. Kaphaja Pramehas - 10
2. Pittaja Pramehas - 6
3. Vataja Pramehas - 4
The ten kaphaja Pramehas are said to be sadhya (curable)117,118. Because
a. The medas having homogenous propert ies is effected
b. The kapha is dominant
c. Both these factors are amendable to the same type of treatment.
The six pit taja Pramehas are only Yapya (pal l iable )119,120 owing to the
proximity of the seat of the vi t iated doshas and that of the Medas and
owing to the antagonism involved in their treatment.
The four variet ies of Vataja Prameha due to the vi t iat ion of Vata
are known to be incurable121,122 because of their seriousness and also
because of the contradict ion involved in their treatment.
Vagbhata adds to the above :
a. The kaphaja and Pit taja groups of Prameha i f they are
developed after ful l expression of prodroma to are incurable123.
Nidana 64
b. Kaphaja Pramehas gradual ly develops into pi t taja Pramehas and
they both transforms into Vataja Pramehas that are incurable.
c. I f kaphaja Pramehas gradual ly turns into pi t taja Pramehas these
are yapya.
d. Even the pit taja Pramehas are curable i f there is no severe
vi t iat ion of medas124, even this is appl icable for Vataja mehas.
Charaka has stated that this disease is relapsing in nature.
Though certain varieties are stated to be curable they appear to be
so only for certain period and relapse is definite.
Madhumeha, which is a veri ty of Vataja Prameha, is also to be
considered, as incurable but with specif ic l ine of treatment these can be
pal l iable.
Jata pramehi or Beeja doshaja are incurable due to leenata of dosha
and as they themselves makes inf luence of prakrit i of pat ient.
Sushruta stated that i f Prameha patient suffering with pidikas and
complicat ions l ike Hridgraha, then he should be considered as
incurable125.
Interestingly Basavrajeeyum 16t h century Ayurvedic text from Andra
pradesh, has mentioned a test for urine to know the prognosis of each
dosha group. The urine of a Prameha patient has to be col lected in a
wide mouthed vessel and boi led on a mild f lame t i l l evaporat ion. The
incurabi l i ty of the disease depends upon the amount of residue. A Vataja
Nidana 65
Prameha is considered incurable i f the residue is 1/5t h of the volume of
ur ine taken for the test. Pittaja Prameha is incurable i f the residue is
1/7t h and kaphaja Prameha is incurable i f the residue is 1/9t h of the
volume of ur ine in the test126.
Nidana 66
VYAVACHEDAKA NIDANA
I t was stated that cordinal signs of Madhumeha are
Bahumootrata and Avilamootrata127. The bahumootrata is noticed as
a symptom in many diseases. But the combination of bahumootrata
and Avilamootrata is noticed in Prameha only.
Urine is stated to be Madhura in the fol lowing variet ies of
Pramehas.
Ikshumeha128 – Due to kapha the patients pass the urine which is
sweet, cold, st icky and l ike a sugarcane juice.
Sheetha meha129 - Due to kapha the patient passes the urine which is
cold, sweet and frequency of the urination is increased.
Madhumeha130 - Due to Vata prokopa urine of the patient wi l l be
kashya, madhura, pandu and ruksha.
The chief physical qual i t ies of the urine of Madhumeha patient are
the colour and the taste resembling honey. Sushruta stated that a pat ient
who is suffer ing from pidikas, hridgraha, and other complicat ions in
addit ion to the other characterist ics of ur ine should be considered as
Madhumeha patient.
Nidana 67
Vagbhata stated that mootra madhuryata is not diagnost ic lakshana
of Madhumeha, but i f the patient is having shareera madhuryata, then i t
is considered as Madhumeha131. I t is observed that the urine and body are
attracted by the ants. No specif ic test for the Madhumeha patient has not
been ascribed in any Ayurvedic classics. Here the attract ion of ants to
the body is an indicat ion of the presence of the madhuryata in the body
i .e. Rasa and Rakta. Since these two dhatus exist in the superf ic ial parts
of the body in abundance as such the ants are natural ly attracted towards
twak. The madhuryata corresponds to the raised blood sugar levels in
Madhumeha (diabetes mell i tus).
Nidana 68
UPADRAVA
Upadrava is a disease produced after the manifestation of the
original disease and depends on this disease irrespective of whether
upadrava is major or minor132. After the occurrence of the original
disease the dosha or doshas are further vi t iated owing to abnormal
ahara, vihar etc., thus leading to a secondary disease or complicat ion
which is known as an upadrava.
If al l the Pramehas are not treated properly and attended, they
may ult imately develop into Madhumeha. Madhumeha is considered
to be one of the 20 Pramehas by Charaka. Apart form this Charaka
has described the upadravas of Prameha in general. Where as
Sushruta and Vagbhata have mentioned upadravas separately for
each doshic group.
The general upadravas of Pramehas according to Charaka are
as fol lows133. Trishna, Atisara, Jwara, Daha, Dourabalya,
Arochaka, Avipaka, Puti mamsa, Pidika , Alaji, Vidradhi.
Charaka mentioned the upadravas (complications) of
Madhumeha as134 Trishna, Shwasa, Mamsa kotha, Moha, Hikka,
Mada, Jwara, Visarpa among them many of upadravas are seen in
patients, they have been explained under the heading of
observation.
Nidana 69
References 1 Charaka Nidana 4 / 44
2 Ibid 4 / 5
3 Ibid 4 / 5
4 Sushruta Nidana 6 / 30
5 Chakrapani on Ch su 3 / 17
6 Charaka Chiki tsa 6 / 57
7 Ibid 6 / 57
8 Charaka Nidana 4 / 5
9 Sushruta Nidana 6 / 3
10 Astanga Sangraha Nidana 10 / 3
11 Charaka Nidana 4 / 5
12 Ibid 4 / 23
13 Ibid 4 / 36
14 API Text Book of Medicine. pp 205
15 Josl in’s Diabetes Mell i tus pp 240 16 Charaka Nidana 4 / 4
17 Ibid 4 / 7
18 Ibid 4 / 8
19 Ibid 4 / 9
20 Ibid 4 / 5
21 Ibid 4 / 37
Nidana 70
22 Charaka Chiki tsa 6 / 5,6
23 Sushruta Nidana 6 / 4
24 Ibid 6 / 4
25 Astanga hridhya Nidana 10 / 8
26 Ibid 10 / 8
27 Chharaka Shareera 7 / 17
28 Diabetes and treatment by VVS Sastri pp18
29 Sabdastoma Mahanidhi
30 Astanga hridhya sutra 3 / 61
31 Chakrapani on Ch Chi 15 / 15
32 Charaka Nidana 4 / 8
33 Astanga hridhya Nidana 10 / 20,21
34 Charaka Nidana 4 / 47
35 Charaka sutra 27 / 28
36 Ibid 26 / 43
37 Asthanga hridhaya sutra 10 / 7,8
38 Hemadri on Ah su 14 / 3
39 Astanga Hridhaya sutra 10 / 1
40 Charaka Nidana 4 / 8
41 Sushruta Sutra 15 / 23
42 Charaka sutra 26 / 43

Nidana 71
43 Astanga Hridhya sutra 10 / 9
44 Dhamanipratichaya by VVS Sastr i .pp 69
45 Sushruta Nidana 6 / 5
46 Charaka Nidana 4 / 47 47 Astanga Sangraha Nidana 10 / 7 48 Sushruta Nidana 6 / 5
49 Ibid 6 / 5
50 Charaka Nidana 4 / 47
51 Ibid 4 / 47
52 Ibid 4 / 47
53 Ibid 4 / 47
54 Astanga Sangraha Nidana 10 / 7 55 Sushruta Nidana 6 / 5
56 Charaka Nidana 4 / 47
57 Astanga Sangraha Nidana 10 / 7 58 Sushruta Nidana 6 / 5
59 Charaka Nidana 4 / 47
60 Sushruta Nidana 6 / 5
61 Charaka Nidana 4 / 47 62 Sushruta Nidana 6 / 5
63 Astanga Sangraha Nidana 10 / 7
64 Ibid 10 / 7
65 Ibid 10 / 7
Nidana 72
66 Sushruta Nidana 6 / 6
67 Astanga Hridhya Nidana 10 / 7
68 Astanga Sangraha Nidana 10 / 8
69 Charaka Nidana 4 / 44 70 Sushruta Nidana 6 / 14 71 Sushruta Nidana 6 / 28
72 Charaka Nidana 4 / 11
73 Ibid 4 / 24
74 Ibid 4 / 38
75 Ibid 4 / 4
76 Sushruta Nidana 6 / 5
77 Astanga Sangraha Nidana 10 / 8
78 Charaka Nidana 4 / 13
79 Sushruta Nidana 6 / 12
80 Astanga Sangraha Nidana 10 / 8
81 Charaka Nidana 4 / 14
82 Sushruta Nidana 6 / 12
83 Astanga Sangraha Nidana 10 / 8
84 Charaka Nidana 4 / 20
85 Sushruta Nidana 6 / 12
86 Astanga Sangraha Nidana 10 / 8
87 Charaka Nidana 4 / 21
88 Sushruta Nidana 6 / 12
Nidana 73
89 Astanga Sangraha Nidana 10 / 8
90 Charaka Nidana 4 / 15
91 Sushruta Nidana 6 / 12
92 Astanga Sangraha Nidana 10 / 8
93 Charaka Nidana 4 / 18
94 Sushruta Nidana 6 / 12
95 Astanga Sangraha Nidana 10 / 8
96 Charaka Nidana 4 / 16
97 Ibid 4 / 17
98 Sushruta Nidana 6 / 12
99 Astanga Sangraha Nidana 10 / 8
100 Charaka Nidana 4 / 19
101 Astanga Sangraha Nidana 10 / 8
102 Charaka Nidana 4 / 22
103 Astanga Sangraha Nidana 10 / 8
104 Sushruta Nidana 6 / 12
105 Astanga Sangraha Nidana 10 / 8
106 Sushruta Nidana 6 / 12
107 Astanga Sangraha Nidana 10 / 8
108 Sushruta Nidana 6 / 12
109 Charaka Nidana 4 / 18
110 Sushruta Nidana 6 / 13
111 Astanga Sangraha Nidana 10 / 8
Nidana 74
112 Charaka Nidana 4 / 28
113 Sushruta Nidana 6 / 41
114 Astanga Sangraha 10 / 8
115 Astanga hridhya Nidana 10 / 18
116 Charaka Chikitsa 6 / 15
117 Ibid 6 / 7
118 Sangraha Nidana 10 / 5 119 Astanga Sangraha Nidana 10 / 5
120 Charaka Nidana 4 / 27 121 Astanga Sangraha Nidana 10 / 5
122 Charaka Nidana 4 / 38 123 Astanga Sangraha Nidana 10 / 41
124 Astanga Sangraha Nidana 10 / 17
125 Sushruta Nidana 6 / 27
126 Basavarajeeyam 9 / 30
127 Astanga hridhya Nidana 10 / 7
128 Charaka Nidana 4 / 14
129 Ibid 4 / 19
130 Ibid 4 / 44
131 Astanga hridhya Nidana 10 / 21
132 Charaka Chikitsa 21 / 40 133 Charaka Nidana 4 / 42 134 Charaka sutra 17 / 109
Drug Review 72
The treatment of Madhumeha with herbal drugs is wel l known
since the t ime of Charaka and Sushruta. Even today the herbal drugs
carry equal importance because of their effect ive and safe action. The
fol lowing drugs are selected for the tr ial after keenly observing the
pathophysiology of the disease according to Modern and Ayurvedic
science. Propert ies and act ions of Madhunashini , Bringaraj,
Bhumyamalaki and Eranda when combined, are found very much
suitable for treat ing Madhumeha. Al l these drugs are abundantly
avai lable and very effect ive. As Madhumeha is asadhya i t can be made
yapya with proper and continues treatment, patients have to consume
the drug for long periods, thus an economical and effective remedy
can be offered for the patients suffering from Madhumeha.
Individual drug used in Bhumyamalakyadi churna is explained
below.
Drug Review 73
MADHUNASANI1,2,3
Sanskri t - Madhunasani
Hindi - Gudamar
Kannada - kadachigana bal l i
Engl ish - Smal l Indian Ipecacuanha
Latin - Gymnema sylvestre
Family - Asclepiadaceae
Synonyms4 - Anyada, Chakrashreni, Meshashrangi, Meshaval l i ,
Sarpadanshtr ika.
Distribution5 -
A cl imbing plant common in Central and Southern India, on the
Western Ghats and in the Goa terri tory.
Parts used -
Dr ied panchanga of the plant is used.
Brief description6 -
A large woody much-branched cl imber running over the tops of
high trees. Leaves 3.2–5 by 1.3–3.2 cm., ovate, el l ipt ic. Base
rounded, petioles 6–13 mm. Long, pubescent. Flowers in pedunculate,
densely pubescent, shorter than the petioles, pedicels 3 – 13 mm long,
corol la yel low, 4 –5 mm.. fol l ic les 6.3 – 7.5 by 0.8 cm., trerete, r igid.
Seeds 1.3cm long, narrowly ovoid, f lat with a thin broad marginal wing,
brown, glabrous.
Drug Review 74
Pharmacological properties7 –
Guna – Laghu, Ruksha.
Rasa – Kashaya, t ikta.
Vipaka – Katu.
Veerya – Ushna.
Doshaghnata – Kapha vata hara.
Chemical composition –
Gymnemic acid, Quercitol , calcium oxalate, carbonic acid,
Phosphoric acid, Ferr ic oxide, Manganese, some tartar ic acid etc.
The sweetness - suppressing polypeptide gurmarin isolated
form the leaves consists of 35 amino acid residues including three
intramolecular disulf ide bonds. Herein, the total chemical synthesis of
grumarin was done and gurmarin being 1.9% based on the start ing
amino acid resin8.
The sweetness - suppressing polypeptide gurmarin has been
isolated form the leaves of Gymnema sylvestre and consists of 35
amino acid residues including three intramolecular disulf ide bonds.
The primary structure has already been determined. The posi t ions of
the disulf ide bonds were located, by a combinat ion of mass
spectrometr ic analysis and swquencing of cystine-containing peptides
obtained bythermolysin – catalyzed hydrolysis of grumarin to be cys3-
cys18, cys10-cts23, and cys17- csy339.
Drug Review 75
Actions concerned to disease –
The powdered leaves were found to have an oxidise act ion on
glucose solut ion and glycolysis occurred which reduced the strength of
the glucose solut ion from 2.3 to 0.66 % in 29 hours10. Drug acts
indirect ly through stimulation in insul in secretion of the pancreas, as i t
has no direct action on the carbohydrate metabol ism11.
Destroys glycosuria and other urinary disorders12.
The leaves cause hypoglycemia which sets in soon after the
administrat ion of the drug whether by mouth or by inject ion, lasts for a
variable t ime, is not necessari ly proport ionate to the dose and in never
excessive. They do not contain any water soluble or alcohol soluble
substance which destroys glucose in vi tro; nor do they yield any
chemical body resembling insul in. The drug has no direct act ion in
carbohydrate metabol ism, and acts indirect ly through st imulation of
insul in secret ion of the pancreas.
Kapha medo hara, Meha hara, sarva Meha hara13,
Extracts of gymnemic acids, which wre taken form gymnema
sylverstre ware tested for their act ion on blood glucose. The
conclusion of the study was gymnemic acids suppress the elevat ion of
blood glucose level by inhibi t ing glucose uptake in the intestine14.
Drug Review 76
Gymnemic acid inhibi tes smooth muscle from uptaking the
glucose, which is the energy source of the muscle15.
Intravenous injection of gurmarin did not cause any signif icant
effect on taste responses at al l . These results suggest that gurmarin
acts on the apical side of the taste cel l . Possibly by binding to the
sweet taste receptor protein16.
Drug Review 77
BHRINGARAJ17, 18,19
Sanskri t - BRINGARAJ
Hindi - Bringra
Kannada - kadiggaraga
Latin - Ecl ipta alba Hassk.
Family - Compositae20
Synonyms - Angaraka, Bhringa, Ekaraja, Ni lapushpa, Shyamala.
Distribtuion21 -
Bangal, Burma, Malay peninsula, Central India, Punjab,
W.Rajputana, Peninsular India, Ceylon. (IMP 1361)
Parts used - Dried panchanga of the plant is used.
Brief discription22 -
I t is annual, erect or prostrate, branched. Oftern rooting at the
nodes; stem and branches str igose with appressed white hairs.
Leaves are sessile, 2.5 – 7.5 cm. Long, variable in breadth, usual ly
oblong – lanceolate, subentire, acute or sub acute, sparsely str igose
with appressed hairs on both sides, base tapering. Flower Heads are 6
– 8 mm. Diam., soli tary or two together on unequal axi l lary peduncles.
Ray f lowers are l igulate, l igule smal l, spreading, white. Disk f lowers
are tubular, corol las often 4 toothed. Achenes cuneate, compressed
and with a narrow wing.
Drug Review 78
Pharmacological properties23 –
Guna – Laghu, Ruksha.
Rasa – katu, t ikta.
Vipaka – katu.
Veerya – ushna.
Doshaghnata – kapha vata shamak.
Chemical composition24 –
Alkaloid ecl ipt ine, Resin, Ecl ipt ine, Wedelolactone,
Actions concerned to disease –
Pr incipal ly used in Liver enlargements, used in jaundice,
scalding of urine25,Used in derangement’s of the l iver26
Drug Review 79
BHUMYAMALAKI27,28,29
Sanskrit - BHUMYAMALAKI
Hindhi - Bhuie amla
Kannada - Guggri kasa
Latin - Phyl lanthus urinaria Linn.
Family - Euphorbiaceae.
Synonyms30 - Hajata, Bahupatra, Bahuphala, Charat i
Dalasparshini .
Distribtuion31 -
Tropics general ly, al l over India.
Parts used -
Dried panchanga of the plant is used.
Brief discription32 -
Annual, 30 – 60 cm high, glabrous, Stems erect, s l ightly
branched; leaf bearing branchlets short, f lat tened or sl ight ly winged.
Leaves closely placed, sessi le, 6 – 13 by 2.5 – 6 mm, oblong,
rounded, apiculate at the apex, pale beneath, glabrous, base rounded,
st ipules pelate, very acute,. Flowers minute, axi l lary, sol i tary,
yel lowish. Sepals 0.8 – 1 mm. Long, oblong. Rounded, not enlarged in
frui t . Capsules 3 mm. Diam., globose, scarcely lobed, echinate.
Seeds 1.5 mm. Long, 3 – gonous, rounded on the back, transversely
furrowed. ( imp 2223)
Drug Review 80
Pharmacological properties33 –
Guna – Laghu, Ruksha.
Rasa – kashaya, t ikta, Madhura.
Vipaka –. Madhura.
Veerya – Sheeta.
Doshaghnata – Kapha Pit ta shamak. (DGV 640)
Chemical composition34 –
Acrid, sour, cooling, bit ter, sweetish; alexipharmic components
are present
Actions concerned to disease –
Useful in thirst, urinary discharges35. in jaundice36,and i t is l iver
st imulant, thrust control ler37, i t is best for urinary disorders especial ly
Prameha, controls Daha38
Drug Review 81
ERANDA39,40,41
Sanskri t - ERANDA
Hindhi - Endi
Kannada - Audala
Latin - Ricinus communis Linn.
Family - Euphorbiaceae.
Synonyms42 - Gandharva hasthah, Panchangulam, Vatari ,
Eranda.
Distribution43 -
This plant is common and quite wi ld in the jungles in India, I t is
cult ivated throughout India, chiefly in the Tamil nadu, Bengal and
Maharastra Presidencies. And also widely cult ivated in tropical
countries.
Part used -
Leaves.
Brief description44 -
Eranda is eka varshika or bahuvarshayu gulma or vr ikshaka
which grows up to 17feet. Leaves are green 30 – 60 cm in diameter
with 5 – 10 projections. leaf stem wil l be 4 – 12 inch long and tublar.
Flowers are unisexual, male f lowers are above and the females are
Drug Review 82
below in the plant. Frui t is thorny and 1 – 3 cms in diameter. Seeds
are oval, shiny, mult icolored and hard, which yields oi l .
Pharmacological properties45 –
Guna – Snigdha, Tikshna, Sukshma.
Rasa – kashaya, Madhura.
Vipaka –. Madhura.
Veerya – Ushna.
Doshaghnata – Kapha vata shamak.
Chemical composition46 –
Fixed oi l 45 to 52 %, Ricinine, proteins 20 pc., starch, mucilage,
and ash 10pc.,
Actions concerned to disease –
Leaves are useful in “vata” and “kapha” diseases, used in l iver
troubles47, especial ly enlarged Liver and Mutravishodaka48,

Drug Review 83
REFERENCE
1 The Indian Materia medica pp 596 2 Indian Medicinal Plants pp 1625 3 Bhava prakasha Guduchadi verga pp 443 4 Indian Medicinal Plants pp 1627 5 Indian Medicinal Plants pp 1625 6 Indian Medicinal Plants pp 1625 7 Bhava prakasha pp 444 8 by Tonosaki K at Central Reseach Laborator ies, Aj inomoto Co., Inc.
Kawasaki, Japan. In 1996 9 by Ota M at Central Research Laboratories Aj inomoto Co , Inc,
Kawasaki, Japan in 1995 10 The Indian Materia medica pp 598 11 The Indian Materia medica pp 598 12 The Indian Materia medica pp 598 13 Sushruta Sutrasthana 38 / 13, 74 14 by Tanaka K at Division of veterinary pharmacology, Nippon veterinary and
animal science university, Tokyo. Japan. In 1997 15 by Nakajyo S at Division of veterinary pharmacology, Nippon veterinary and
animal science university, Tokyo. Japan. In 1996 16 by Imoto T at Department of physiology, Faculty of Medicine, Tottor i
University, Yonago, Japan. In 1995 17 The Indian Materica Medica pp 469 18 Indian Medicinal Plants pp 1361 19 Bhava Prakasha, Gudchadi varga – pp 429 20 Indian Medicinal Plants pp 1363 21 Indian Medicinal Plants pp 1361 22 Indian Medicinal Plants pp 1361 23 Bhava Prakasha, Gudchadi varga – pp 430 24 The Indian Materica Medica pp 469 25 Indian Medicinal Plants pp 1361 26 The Indian Materica Medica pp 469 27 Indian Medicinal Plants pp 2223
Drug Review 84
28 The Indian Materica Medica pp 949 29 Bhava Prakasha, Gudchadi varga – pp 460 30 Indian Medicinal Plants pp 2223 31 Indian Medicinal Plants pp 2223 32 Indian Medicinal Plants pp 2223 33 Bhava Prakasha, Gudchadi varga – pp 460 34 Indian Medicinal Plants pp 2223 35 Indian Medicinal Plants pp 2223 36 The Indian Materica Medica pp 949 37 Bhava Prakasha, Gudchadi varga – pp 460 38 Raja Niguntu pp 263 39 Bhava Prakasha, Gudchadi varga – pp 299 40 The Indian Materica Medica pp1065 41 Indian Medicinal Plants pp 2275 42 The Indian Materica Medica pp1065 43 The Indian Materica Medica pp1065 44 The Indian Materica Medica pp1065 45 Bhava Prakasha, Gudchadi varga – pp 299 46 The Indian Materica Medica pp1065 47 Indian Medicinal Plants pp 2275 48 Bhava Prakasha, Gudchadi varga – pp 299
Chikitsa 69
The term Chiki tsa is derived form the root “KIT ROGAPANAYANE”1.
According to Amaarkosha Chikitsa is Ruk Pratikr iya. Chikitsa is the
process by which the doshas and dhatus are brought into normalcy.
Madhumeha is a chronic relapsing disease and may also develop as a
hereditary disease. Madhumeha patients are divided in two variet ies.
1. Sthula and 2. Krisa
Sthula patients are capable of withstanding the shodhana karma and
the krisa patients are incapable of withstanding i t . Therefore a sthula
patient has to be treated with the sodhana chiki tsa and drisha with
pal iat ive treatment.
For every Shodhana chiki tsa the pat ient should undergo poorva
karma. But the Madhumeha patient is prohibi ted from undergoing sweda
karma 3. In sthula patient after complet ion of sneha karma the doshas
should be el iminated by urdhava and adhosodhana as Vamana and
Virechana respect ively.
After the completion of the Sodhana karma the pat ient has to be
subjected for samsarjana krama. Even though the madhumeha is
santarpana janya roga, the pat ient should not be subjected to Apatarpana
kriya, because i t may result in to Gulma, Kshaya, Mehana shoola, vasti
Chikitsa 70
shoola and Mootra graha. The Brimhana chiki tsa should be carried out
considering the strength of the jataragni of the individual pat ient4. A krisa
or emaciated, and Durbala or weak pat ient who is not capable of
withstanding the shodhana karma requires Bhrimhana chiki tsa5.
Even though the vataja Pramehas are stated to be incurable the duty
of physician is to treat the pat ient and prevent the future complicat ions.
Therefore vataja Prameha should be treated.
SHAMSAMANA CHIKITSA
Shamana chiki tsa is indicated for a Prameha patient who is not
el igible for shodhana chiki tsa, and also the patient who has completed the
shodana karma.
Many variet ies of decoctions, choornas and lehyas have been
described for the treatment of the twenty variet ies of Pramehas by al l
Ayurvedic authori t ies. Vyayam, udvarthana, snana, jala sechana and the
lepas with Twak, Ela, Agar and chandana are useful in Prameha patient6.
Avoiding the causative factors (Nidana) is also a treatment7. In our
tr ial we have used only shamana therapy, which has yield a very
signif icant result.
Chikitsa 71
The pat ient of prameha who is not f i t for evacuation should be
subjected to pacif icatory management for al leviat ion of the disease such
as mantha (churned drink), extracts, l inctus made of barley powder and
l ight edibles. He should eat rough food art ic les such as boi led barley,
barley cakes, f lour of parched grains and apupa with palatable meat -
soup of wi ld birds part icularly gal l inaceous and peckers. He should take
old shal i r ice with soup of mudga etc. and bit ter vegetables added with oi l
of dant i and ingudi or l inseed and mustard. In cereals, he should use
shashtika and wi ld r ice. The diet of the patient of prameha should consist
mainly of barley. One suffering form kaphaja prameha should eat various
preparat ions of barley added with honey. Barley grain dipped in decoction
of tr iphala for the whole night make a saturat ing food taken with honey.
The patient may also take them regularly mixed with vinegar for al leviat ion
of Prameha. He should use f lour of parched grains, bolus, parched grains
and other various edibles made of barley impregnated with deccoctions of
durgs prescribed in kaphaja prameha. Various preparat ions of barley
mixed with the meat of ass, horse, bul l , swan and spotted deer should be
prescribed. The seeds of bamboo and wheat may also be used in forms
simi lar to those of barley8.
Chikitsa 72
REFERENCE
1 Shabda Sthoma Mahanidhi
3 Charaka Sutra 14 / 16
4 Charaka Chikitsa 6 / 16,17
5 Ibid 6 / 15
6 Ibid 6 / 48
7 Ibid 6 / 51
8 Ibid 6 / 18 – 24.
Materials & Methods 83
MATERIAL AND METHODS
Materials -
a. Materials for literary search.
Literary search is done from classical Ayurvedic texts, Modern
texts, Medlar search and updated through journals.
b. Materials for clinical study.
Bhumyamalakyadi churna, composed of
Madhunashini
Eranda
Bhumyamalaki
Bhringaraj
is taken for the cl inical tr ial .
Collection of Drugs: -
Al l the drugs were personally col lected from Kapat hi l ls, and were
conf irmed their identi ty by the Botanist.
Method of Preparation: -
Panchangas of above said drugs were cleaned thoroughly by
running water to take out physical impuri t ies and dried in the shade. The
dried herbs were powdered separately in the pulval iser to get a f ine
powder.
Materials & Methods 84
Again the wet drugs are col lected, to extract swarasa, which is
ut i l ised for giving bhavana to the corresponding herb powders to increase
their potency. These powders are mixed in proport ions and f i l led in
500mg capsules for easy palatabi l i ty for the patient.
CLINICAL TRIAL
Methods :
Selection of Sample
Pat ients suffer ing from Madhumeha are selected from the
Post Graduate And Research Centre OPD/IPD of D.G.M. Ayurvedic
Col lege Hospital and medical camp organised exclusively for
Madhumeha patients at Post Graduate And Research Centre of
D.G.M. Ayurvedic col lege Hospital , Gadag.
Inclusive criteria -
- Pat ients between the age of 25 to 65 years
- Irrespective of sex
- Less than 5 years chronici ty.
Exclusive criteria -
- Pat ients having known organic lesions.
- Insul in dependent

Materials & Methods 85
Laboratory Investigations
The selected pat ients were subjected to fol lowing laboratory
investigat ions
Fast ing blood sugar
Post partal blood sugar
Urine sugar
Serum cholesterol
Diagnostic Criteria
Diagnosis was made on the basis of subject ive parameters
mentioned in the classics and object ive ( lab invest igations) parameters.
Table showing the normal values of objective parameters.
Lab investigat ions Normal values
Fasting blood sugar 80 –120 mg%
Post partal blood sugar 110 – 140 mg%
Serum Cholesterol 120 – 250 mg%
Urine sugar Ni l
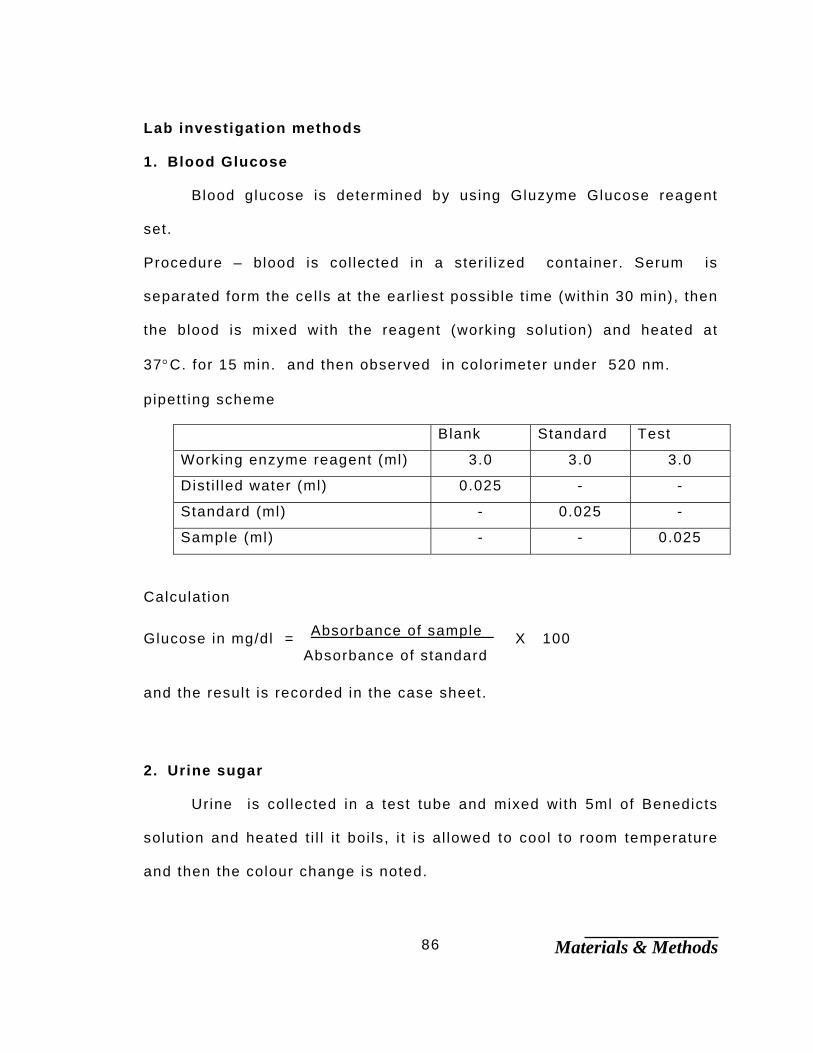
Materials & Methods 86
Lab investigation methods
1. Blood Glucose
Blood glucose is determined by using Gluzyme Glucose reagent
set.
Procedure – blood is col lected in a ster i l ized container. Serum is
separated form the cel ls at the earl iest possible t ime (within 30 min), then
the blood is mixed with the reagent (working solution) and heated at
37°C. for 15 min. and then observed in colorimeter under 520 nm.
pipett ing scheme
Blank Standard Test
Working enzyme reagent (ml) 3.0 3.0 3.0
Dist i l led water (ml) 0.025 - -
Standard (ml) - 0.025 -
Sample (ml) - - 0.025
Calculation
Glucose in mg/dl = Absorbance of sample X 100 Absorbance of standard
and the result is recorded in the case sheet.
2. Urine sugar
Urine is col lected in a test tube and mixed with 5ml of Benedicts
solution and heated t i l l i t boi ls, i t is al lowed to cool to room temperature
and then the colour change is noted.
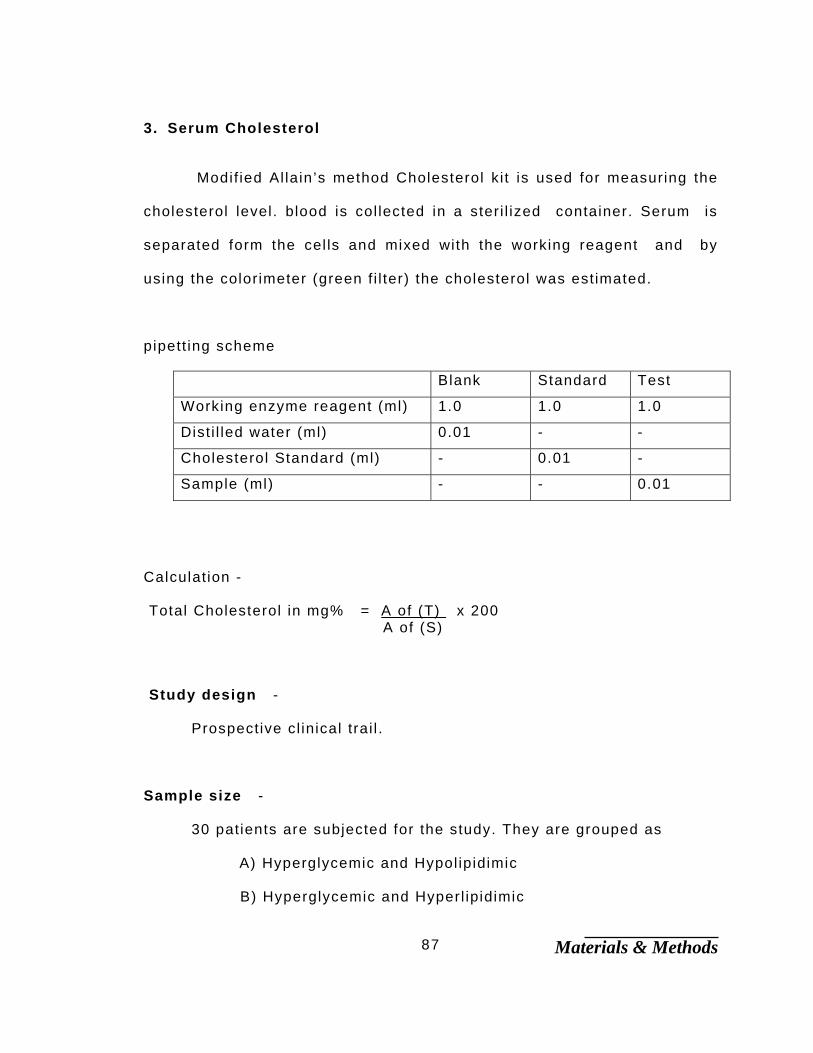
Materials & Methods 87
3. Serum Cholesterol
Modif ied Al lain’s method Cholesterol ki t is used for measuring the
cholesterol level. blood is col lected in a ster i l ized container. Serum is
separated form the cel ls and mixed with the working reagent and by
using the colorimeter (green f i l ter) the cholesterol was estimated.
pipett ing scheme
Blank Standard Test
Working enzyme reagent (ml) 1.0 1.0 1.0
Dist i l led water (ml) 0.01 - -
Cholesterol Standard (ml) - 0.01 -
Sample (ml) - - 0.01
Calculation -
Total Cholesterol in mg% = A of (T) x 200 A of (S)
Study design -
Prospective cl inical trai l .
Sample size -
30 patients are subjected for the study. They are grouped as
A) Hyperglycemic and Hypol ipidimic
B) Hyperglycemic and Hyperl ipidimic
Materials & Methods 88
In each group 15 patients are included on the bases of lab
investigat ions.
Posology - 3gms / 24 hours in divided dose
Duration of treatment -
Durat ion of the study was 30 days from the day of ini t iat ion of
“Bhumyamalakyadi Churna”.
Follow up –
Al l the patients were asked to report every Partnight fol lowup.
Diet -
Pat ients were asked to take regular bl ind diet as far as possible.
-
Criteria for assessment of treatment –
Results of the treatment were assessed on the bases of di f ferences
between the base l ine data and assessment data. The lab investigat ion
variables were subjected for stat ist ical analysis by applying student ‘ t ’
test and paired ‘ t ’ test.
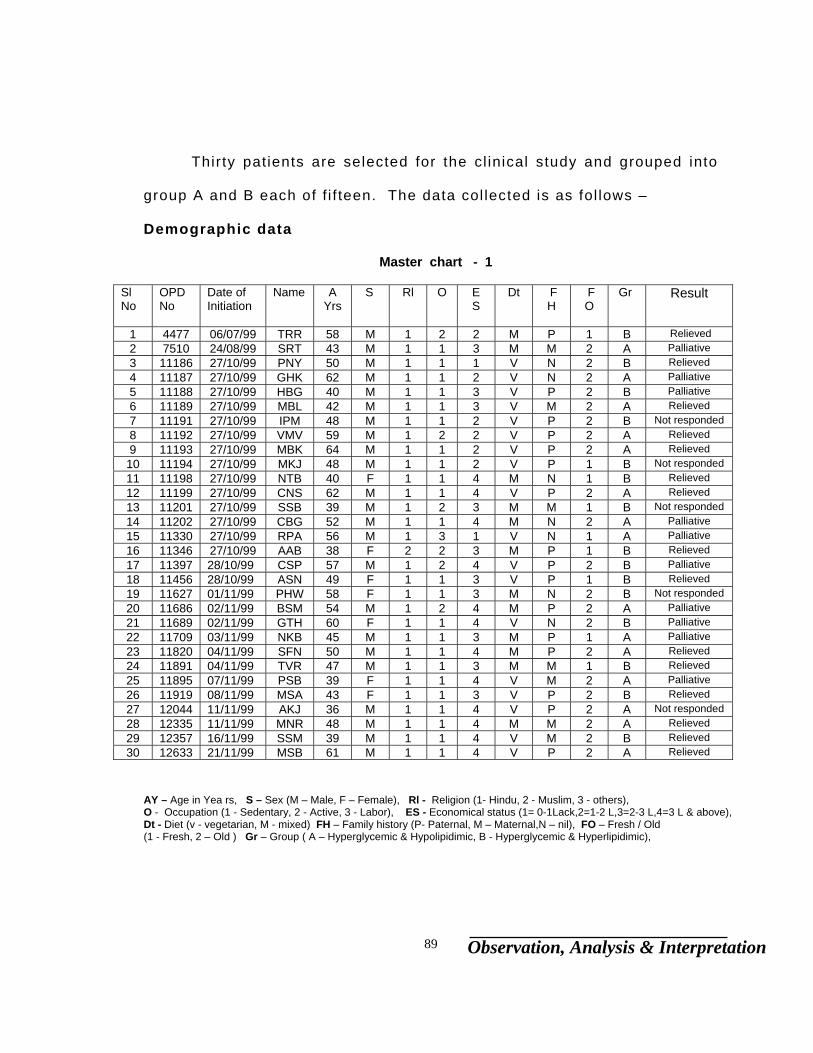
Observation, Analysis & Interpretation 89
Thirty patients are selected for the cl inical study and grouped into
group A and B each of f i f teen. The data col lected is as fol lows –
Demographic data
Master chart - 1
Sl No
OPD No
Date of Initiation
Name A Yrs
S Rl
O E S
Dt F H
F O
Gr Result
1 4477 06/07/99 TRR 58 M 1 2 2 M P 1 B Relieved 2 7510 24/08/99 SRT 43 M 1 1 3 M M 2 A Palliative 3 11186 27/10/99 PNY 50 M 1 1 1 V N 2 B Relieved 4 11187 27/10/99 GHK 62 M 1 1 2 V N 2 A Palliative 5 11188 27/10/99 HBG 40 M 1 1 3 V P 2 B Palliative 6 11189 27/10/99 MBL 42 M 1 1 3 V M 2 A Relieved 7 11191 27/10/99 IPM 48 M 1 1 2 V P 2 B Not responded 8 11192 27/10/99 VMV 59 M 1 2 2 V P 2 A Relieved 9 11193 27/10/99 MBK 64 M 1 1 2 V P 2 A Relieved 10 11194 27/10/99 MKJ 48 M 1 1 2 V P 1 B Not responded 11 11198 27/10/99 NTB 40 F 1 1 4 M N 1 B Relieved 12 11199 27/10/99 CNS 62 M 1 1 4 V P 2 A Relieved 13 11201 27/10/99 SSB 39 M 1 2 3 M M 1 B Not responded 14 11202 27/10/99 CBG 52 M 1 1 4 M N 2 A Palliative 15 11330 27/10/99 RPA 56 M 1 3 1 V N 1 A Palliative 16 11346 27/10/99 AAB 38 F 2 2 3 M P 1 B Relieved 17 11397 28/10/99 CSP 57 M 1 2 4 V P 2 B Palliative 18 11456 28/10/99 ASN 49 F 1 1 3 V P 1 B Relieved 19 11627 01/11/99 PHW 58 F 1 1 3 M N 2 B Not responded 20 11686 02/11/99 BSM 54 M 1 2 4 M P 2 A Palliative 21 11689 02/11/99 GTH 60 F 1 1 4 V N 2 B Palliative 22 11709 03/11/99 NKB 45 M 1 1 3 M P 1 A Palliative 23 11820 04/11/99 SFN 50 M 1 1 4 M P 2 A Relieved 24 11891 04/11/99 TVR 47 M 1 1 3 M M 1 B Relieved 25 11895 07/11/99 PSB 39 F 1 1 4 V M 2 A Palliative 26 11919 08/11/99 MSA 43 F 1 1 3 V P 2 B Relieved 27 12044 11/11/99 AKJ 36 M 1 1 4 V P 2 A Not responded 28 12335 11/11/99 MNR 48 M 1 1 4 M M 2 A Relieved 29 12357 16/11/99 SSM 39 M 1 1 4 V M 2 B Relieved 30 12633 21/11/99 MSB 61 M 1 1 4 V P 2 A Relieved
AY – Age in Yea rs, S – Sex (M – Male, F – Female), Rl - Religion (1- Hindu, 2 - Muslim, 3 - others), O - Occupation (1 - Sedentary, 2 - Active, 3 - Labor), ES - Economical status (1= 0-1Lack,2=1-2 L,3=2-3 L,4=3 L & above), Dt - Diet (v - vegetarian, M - mixed) FH – Family history (P- Paternal, M – Maternal,N – nil), FO – Fresh / Old (1 - Fresh, 2 – Old ) Gr – Group ( A – Hyperglycemic & Hypolipidimic, B - Hyperglycemic & Hyperlipidimic),
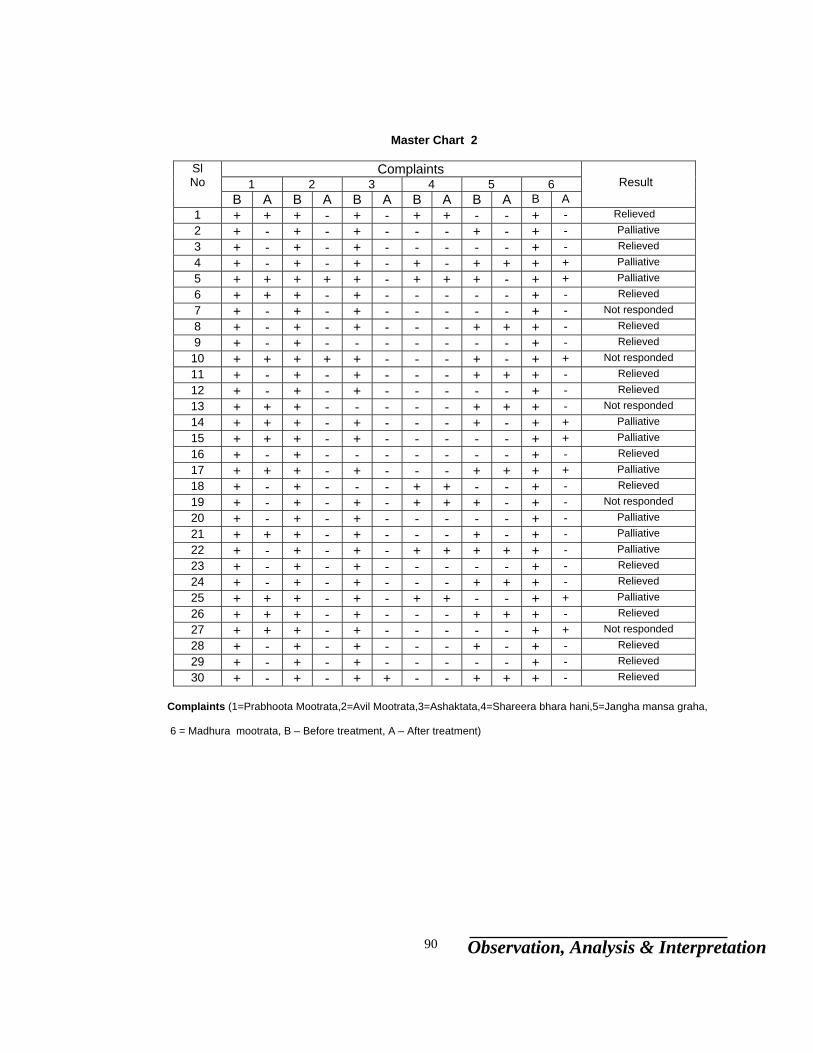
Observation, Analysis & Interpretation 90
Master Chart 2
Complaints
1 2 3 4 5 6 Sl No
B A B A B A B A B A B A
Result
1 + + + - + - + + - - + - Relieved 2 + - + - + - - - + - + - Palliative 3 + - + - + - - - - - + - Relieved 4 + - + - + - + - + + + + Palliative 5 + + + + + - + + + - + + Palliative 6 + + + - + - - - - - + - Relieved 7 + - + - + - - - - - + - Not responded 8 + - + - + - - - + + + - Relieved 9 + - + - - - - - - - + - Relieved 10 + + + + + - - - + - + + Not responded 11 + - + - + - - - + + + - Relieved 12 + - + - + - - - - - + - Relieved 13 + + + - - - - - + + + - Not responded 14 + + + - + - - - + - + + Palliative 15 + + + - + - - - - - + + Palliative 16 + - + - - - - - - - + - Relieved 17 + + + - + - - - + + + + Palliative 18 + - + - - - + + - - + - Relieved 19 + - + - + - + + + - + - Not responded 20 + - + - + - - - - - + - Palliative 21 + + + - + - - - + - + - Palliative 22 + - + - + - + + + + + - Palliative 23 + - + - + - - - - - + - Relieved 24 + - + - + - - - + + + - Relieved 25 + + + - + - + + - - + + Palliative 26 + + + - + - - - + + + - Relieved 27 + + + - + - - - - - + + Not responded 28 + - + - + - - - + - + - Relieved
29 + - + - + - - - - - + - Relieved 30 + - + - + + - - + + + - Relieved
Complaints (1=Prabhoota Mootrata,2=Avil Mootrata,3=Ashaktata,4=Shareera bhara hani,5=Jangha mansa graha,
6 = Madhura mootrata, B – Before treatment, A – After treatment)
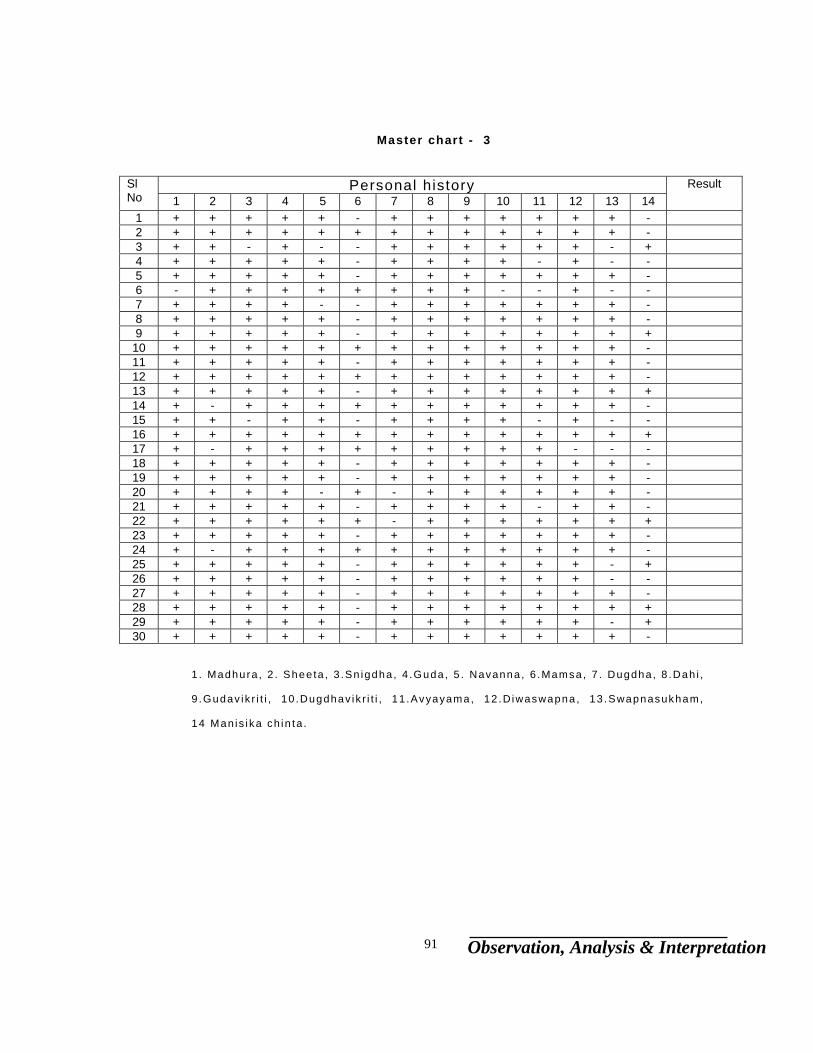
Observation, Analysis & Interpretation 91
Master chart - 3
Personal history Sl No 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Result
1 + + + + + - + + + + + + + - 2 + + + + + + + + + + + + + - 3 + + - + - - + + + + + + - + 4 + + + + + - + + + + - + - - 5 + + + + + - + + + + + + + - 6 - + + + + + + + + - - + - - 7 + + + + - - + + + + + + + - 8 + + + + + - + + + + + + + - 9 + + + + + - + + + + + + + + 10 + + + + + + + + + + + + + - 11 + + + + + - + + + + + + + - 12 + + + + + + + + + + + + + - 13 + + + + + - + + + + + + + + 14 + - + + + + + + + + + + + - 15 + + - + + - + + + + - + - - 16 + + + + + + + + + + + + + + 17 + - + + + + + + + + + - - - 18 + + + + + - + + + + + + + - 19 + + + + + - + + + + + + + - 20 + + + + - + - + + + + + + - 21 + + + + + - + + + + - + + - 22 + + + + + + - + + + + + + + 23 + + + + + - + + + + + + + - 24 + - + + + + + + + + + + + - 25 + + + + + - + + + + + + - + 26 + + + + + - + + + + + + - - 27 + + + + + - + + + + + + + - 28 + + + + + - + + + + + + + + 29 + + + + + - + + + + + + - + 30 + + + + + - + + + + + + + -
1 . Madhura , 2 . Shee ta , 3 .Sn igdha , 4 .Guda , 5 . Navanna , 6 .Mamsa, 7 . Dugdha, 8 .Dah i ,
9 .Gudav ik r i t i , 10 .Dugdhav ik r i t i , 11 .Avyayama, 12 .D iwaswapna , 13 .Swapnasukham,
14 Man is ika ch in ta .
Observation, Analysis & Interpretation 92
Master Chart – 4 POORVAROOPA poorvaroopa
B – Before treatment, A – After treatment. 1 – Dantadeenam malatavam, 2 – Pada daha, 3 – Panidaha, 4 – Deha chikkanata, 5 – Shareera durgandha, 6 – Mukha madhurata, 7 – Talu klomashosha, 8 – Kesha jatilata, 9 – Nakha vriddhi, 10 – Alasya, 11 – Trishna, 12 – Maldhikyata in bahya chidra, 13 – Swedadhikya, 14 – Shitaiccha, 15 – Swasa, 16 – Mutramadhurata, 17 – Mutrashuklata.
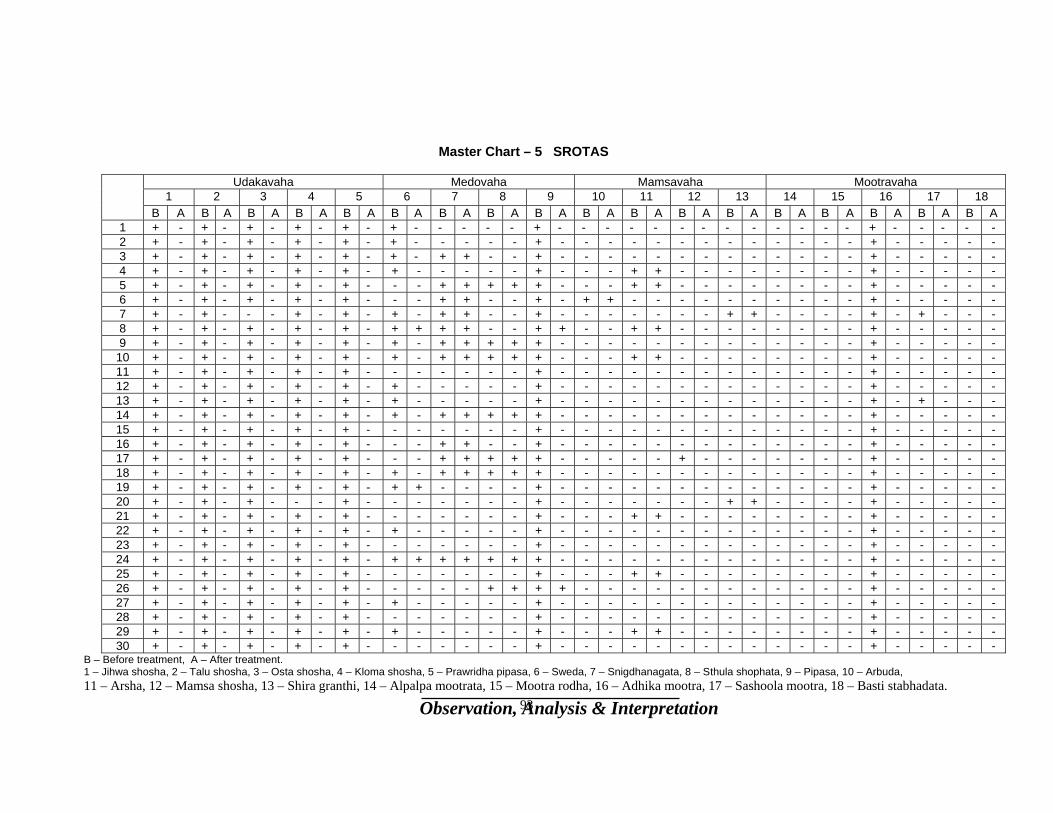
Observation, Analysis & Interpretation 93
Master Chart – 5 SROTAS
Udakavaha Medovaha Mamsavaha Mootravaha 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
B A B A B A B A B A B A B A B A B A B A B A B A B A B A B A B A B A B A 1 + - + - + - + - + - + - - - - - + - - - - - - - - - - - - - + - - - - - 2 + - + - + - + - + - + - - - - - + - - - - - - - - - - - - - + - - - - - 3 + - + - + - + - + - + - + + - - + - - - - - - - - - - - - - + - - - - - 4 + - + - + - + - + - + - - - - - + - - - + + - - - - - - - - + - - - - - 5 + - + - + - + - + - - - + + + + + - - - + + - - - - - - - - + - - - - - 6 + - + - + - + - + - - - + + - - + - + + - - - - - - - - - - + - - - - - 7 + - + - - - + - + - + - + + - - + - - - - - - - + + - - - - + - + - - - 8 + - + - + - + - + - + + + + - - + + - - + + - - - - - - - - + - - - - - 9 + - + - + - + - + - + - + + + + + - - - - - - - - - - - - - + - - - - -
10 + - + - + - + - + - + - + + + + + - - - + + - - - - - - - - + - - - - - 11 + - + - + - + - + - - - - - - - + - - - - - - - - - - - - - + - - - - - 12 + - + - + - + - + - + - - - - - + - - - - - - - - - - - - - + - - - - - 13 + - + - + - + - + - + - - - - - + - - - - - - - - - - - - - + - + - - - 14 + - + - + - + - + - + - + + + + + - - - - - - - - - - - - - + - - - - - 15 + - + - + - + - + - - - - - - - + - - - - - - - - - - - - - + - - - - - 16 + - + - + - + - + - - - + + - - + - - - - - - - - - - - - - + - - - - - 17 + - + - + - + - + - - - + + + + + - - - - - + - - - - - - - + - - - - - 18 + - + - + - + - + - + - + + + + + - - - - - - - - - - - - - + - - - - - 19 + - + - + - + - + - + + - - - - + - - - - - - - - - - - - - + - - - - - 20 + - + - + - - - + - - - - - - - + - - - - - - - + + - - - - + - - - - - 21 + - + - + - + - + - - - - - - - + - - - + + - - - - - - - - + - - - - - 22 + - + - + - + - + - + - - - - - + - - - - - - - - - - - - - + - - - - - 23 + - + - + - + - + - - - - - - - + - - - - - - - - - - - - - + - - - - - 24 + - + - + - + - + - + + + + + + + - - - - - - - - - - - - - + - - - - - 25 + - + - + - + - + - - - - - - - + - - - + + - - - - - - - - + - - - - - 26 + - + - + - + - + - - - - - + + + + - - - - - - - - - - - - + - - - - - 27 + - + - + - + - + - + - - - - - + - - - - - - - - - - - - - + - - - - - 28 + - + - + - + - + - - - - - - - + - - - - - - - - - - - - - + - - - - - 29 + - + - + - + - + - + - - - - - + - - - + + - - - - - - - - + - - - - - 30 + - + - + - + - + - - - - - - - + - - - - - - - - - - - - - + - - - - -
B – Before treatment, A – After treatment. 1 – Jihwa shosha, 2 – Talu shosha, 3 – Osta shosha, 4 – Kloma shosha, 5 – Prawridha pipasa, 6 – Sweda, 7 – Snigdhanagata, 8 – Sthula shophata, 9 – Pipasa, 10 – Arbuda, 11 – Arsha, 12 – Mamsa shosha, 13 – Shira granthi, 14 – Alpalpa mootrata, 15 – Mootra rodha, 16 – Adhika mootra, 17 – Sashoola mootra, 18 – Basti stabhadata.

Observation, Analysis & Interpretation 94
Master Chart – 6 Upadravas
Upadravas 1 2 3 4 5 6 7 8 9
Sl N B A B A B A B A B A B A B A B A B A
1 - - - - - - + - - - - - + - - - - - 2 - - - - - - + - - - + - - - + - - - 3 - - - - - - + - + - - - - - - - - - 4 + - - - - - + - - - + - - - - - - - 5 + - - - - - + - + - - - - - - - + - 6 - - - - - - + - + - - - - - - - - - 7 - - - - - - + - + - - - - - - - - - 8 - - - - - - + - + - + - - - - - - - 9 - - - - - - - - - - - - - - - - - - 10 - - - - - - + - + - - - - - - - - - 11 - - - - + - - - - - - - - - - - + - 12 - - - - - - + - + - + - - - - - - - 13 - - - - - - - - - - - - - - - - - - 14 - - - - - - + - - - + - - - - - - - 15 + - + - - - - - - - - - - - + - + - 16 - - - - - - - - + - - - - - - - - - 17 - - - - + - + - + - - - - - - - - - 18 - - + - - - - - - - - - + - - - - - 19 - - - - - - + - + - - - - - - - - - 20 - - - - - - + - + - - - - - - - - - 21 - - - - - - - - + - - - - - - - - - 22 - - - - - - + - + - + - + - - - - - 23 - - - - - - - - - - - - - - - - - - 24 - - - - - - + - + - - - - - - - - - 25 - - - - - - - - - - - - - - - - - - 26 - - - - - - + - - - - - - - - - - - 27 - - - - - - - - - - - - - - - - - - 28 + - - - - - + - - - - - - - - - - - 29 - - - - - - - - - - - - - - - - - - 30 - - - - - - + - - - - - - - - - + -
1 – Prameha pidika, 2 – Atisara, 3 – Jwara, 4 – Daha, 5 – Arochaka, 6 – avipaka
7 – Chardi, 8 – Kasa, 9 – Pratishyaya
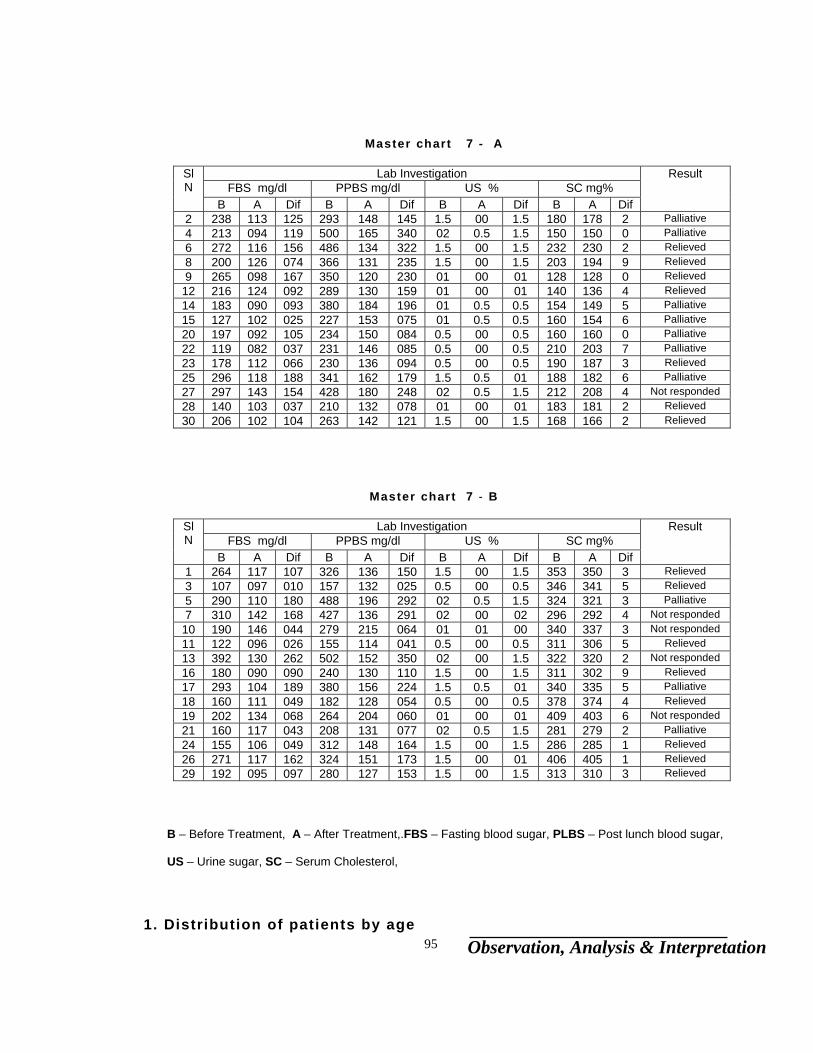
Observation, Analysis & Interpretation 95
Master chart 7 - A
Lab Investigation FBS mg/dl PPBS mg/dl US % SC mg%
Sl N B A Dif B A Dif B A Dif B A Dif
Result
2 238 113 125 293 148 145 1.5 00 1.5 180 178 2 Palliative 4 213 094 119 500 165 340 02 0.5 1.5 150 150 0 Palliative 6 272 116 156 486 134 322 1.5 00 1.5 232 230 2 Relieved 8 200 126 074 366 131 235 1.5 00 1.5 203 194 9 Relieved 9 265 098 167 350 120 230 01 00 01 128 128 0 Relieved
12 216 124 092 289 130 159 01 00 01 140 136 4 Relieved 14 183 090 093 380 184 196 01 0.5 0.5 154 149 5 Palliative 15 127 102 025 227 153 075 01 0.5 0.5 160 154 6 Palliative 20 197 092 105 234 150 084 0.5 00 0.5 160 160 0 Palliative 22 119 082 037 231 146 085 0.5 00 0.5 210 203 7 Palliative 23 178 112 066 230 136 094 0.5 00 0.5 190 187 3 Relieved 25 296 118 188 341 162 179 1.5 0.5 01 188 182 6 Palliative 27 297 143 154 428 180 248 02 0.5 1.5 212 208 4 Not responded 28 140 103 037 210 132 078 01 00 01 183 181 2 Relieved 30 206 102 104 263 142 121 1.5 00 1.5 168 166 2 Relieved
Master chart 7 - B
Lab Investigation FBS mg/dl PPBS mg/dl US % SC mg%
Sl N B A Dif B A Dif B A Dif B A Dif
Result
1 264 117 107 326 136 150 1.5 00 1.5 353 350 3 Relieved 3 107 097 010 157 132 025 0.5 00 0.5 346 341 5 Relieved 5 290 110 180 488 196 292 02 0.5 1.5 324 321 3 Palliative 7 310 142 168 427 136 291 02 00 02 296 292 4 Not responded
10 190 146 044 279 215 064 01 01 00 340 337 3 Not responded 11 122 096 026 155 114 041 0.5 00 0.5 311 306 5 Relieved 13 392 130 262 502 152 350 02 00 1.5 322 320 2 Not responded 16 180 090 090 240 130 110 1.5 00 1.5 311 302 9 Relieved 17 293 104 189 380 156 224 1.5 0.5 01 340 335 5 Palliative 18 160 111 049 182 128 054 0.5 00 0.5 378 374 4 Relieved 19 202 134 068 264 204 060 01 00 01 409 403 6 Not responded 21 160 117 043 208 131 077 02 0.5 1.5 281 279 2 Palliative 24 155 106 049 312 148 164 1.5 00 1.5 286 285 1 Relieved 26 271 117 162 324 151 173 1.5 00 01 406 405 1 Relieved 29 192 095 097 280 127 153 1.5 00 1.5 313 310 3 Relieved
B – Before Treatment, A – After Treatment,.FBS – Fasting blood sugar, PLBS – Post lunch blood sugar, US – Urine sugar, SC – Serum Cholesterol,
1. Distribution of patients by age
Observation, Analysis & Interpretation 96
Age No of patients Percentage Responded Percentage
36 – 45 11 37% 10 91%
46 – 55 9 30% 6 67%
56 - 65 10 33% 9 90%
Largest incidences are found in the age group of 36 – 45. I t
shows middle-aged people are more prone to get into this
condit ion.
3. Distribution of patients by sex
sex No of patients Percentage Responded Percentage
Male 23 77% 20 87%
Female 7 23% 5 71%
This data shows among 30 pat ients 23 (77%) are male and
only 7 (23%) are female. This indicates the incidence of
Madhumeha is more in male.
Graphic representat ion of age and sex is shown in f igure 1
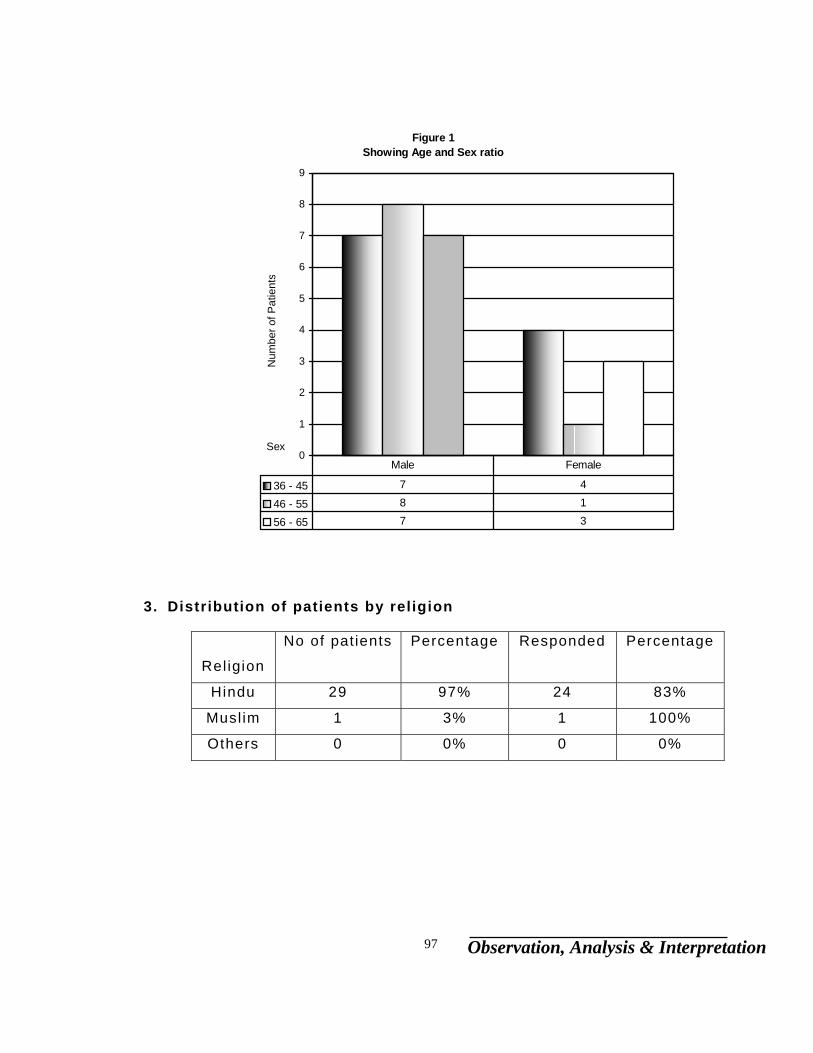
Observation, Analysis & Interpretation 97
3. Distribution of patients by religion
Rel igion
No of patients Percentage Responded Percentage
Hindu 29 97% 24 83%
Musl im 1 3% 1 100%
Others 0 0% 0 0%
Figure 1 Showing Age and Sex ratio
0
1
2
3
4
5
6
7
8
9
Sex
Num
ber o
f Pat
ient
s
36 - 45 7 4
46 - 55 8 1
56 - 65 7 3
Male Female
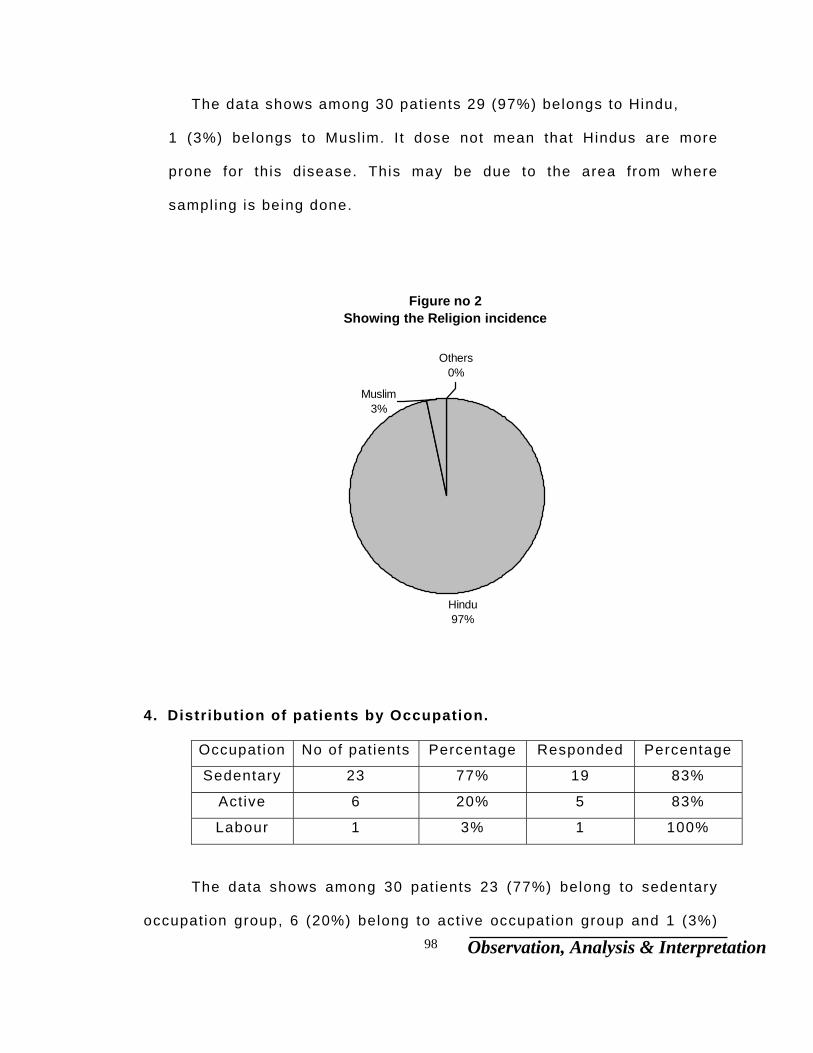
Observation, Analysis & Interpretation 98
The data shows among 30 pat ients 29 (97%) belongs to Hindu,
1 (3%) belongs to Musl im. I t dose not mean that Hindus are more
prone for this disease. This may be due to the area from where
sampling is being done.
4. Distribution of patients by Occupation.
Occupation No of patients Percentage Responded Percentage
Sedentary 23 77% 19 83%
Active 6 20% 5 83%
Labour 1 3% 1 100%
The data shows among 30 pat ients 23 (77%) belong to sedentary
occupation group, 6 (20%) belong to act ive occupation group and 1 (3%)
Figure no 2 Showing the Religion incidence
Hindu97%
Others0%
Muslim3%
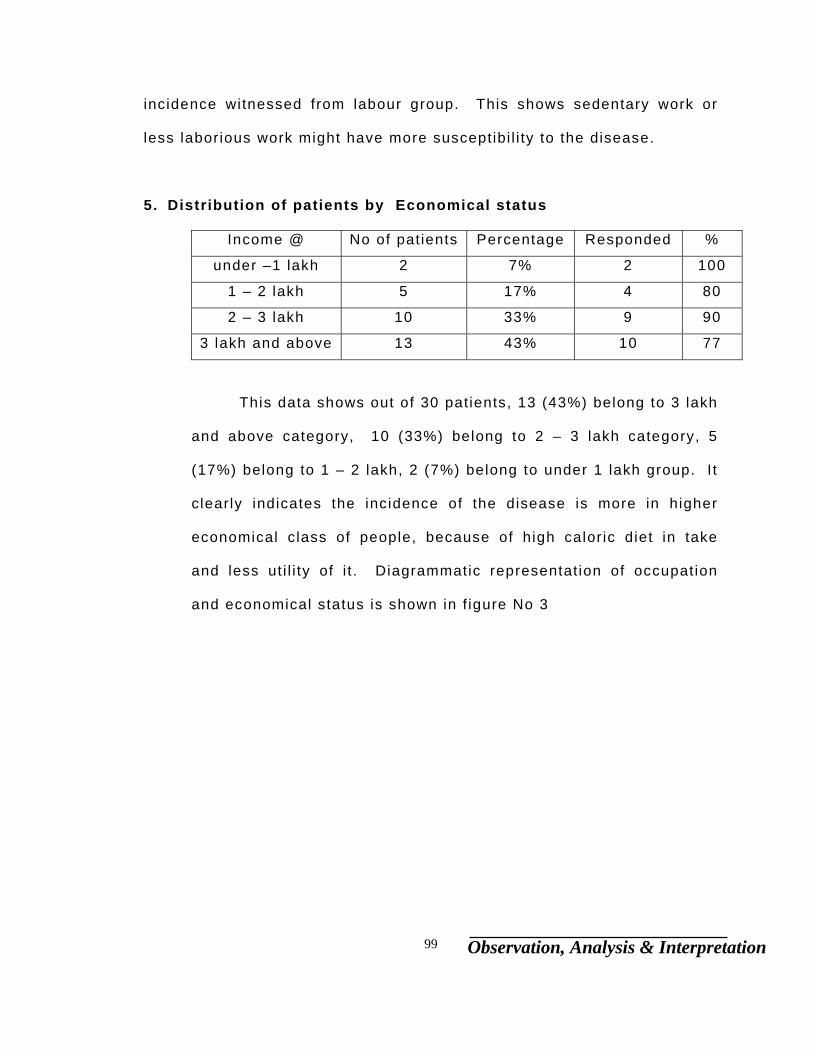
Observation, Analysis & Interpretation 99
incidence witnessed from labour group. This shows sedentary work or
less laborious work might have more susceptibi l i ty to the disease.
5. Distribution of patients by Economical status
Income @ No of patients Percentage Responded %
under –1 lakh 2 7% 2 100
1 – 2 lakh 5 17% 4 80
2 – 3 lakh 10 33% 9 90
3 lakh and above 13 43% 10 77
This data shows out of 30 patients, 13 (43%) belong to 3 lakh
and above category, 10 (33%) belong to 2 – 3 lakh category, 5
(17%) belong to 1 – 2 lakh, 2 (7%) belong to under 1 lakh group. I t
c learly indicates the incidence of the disease is more in higher
economical class of people, because of high calor ic diet in take
and less ut i l i ty of i t . Diagrammatic representat ion of occupation
and economical status is shown in f igure No 3
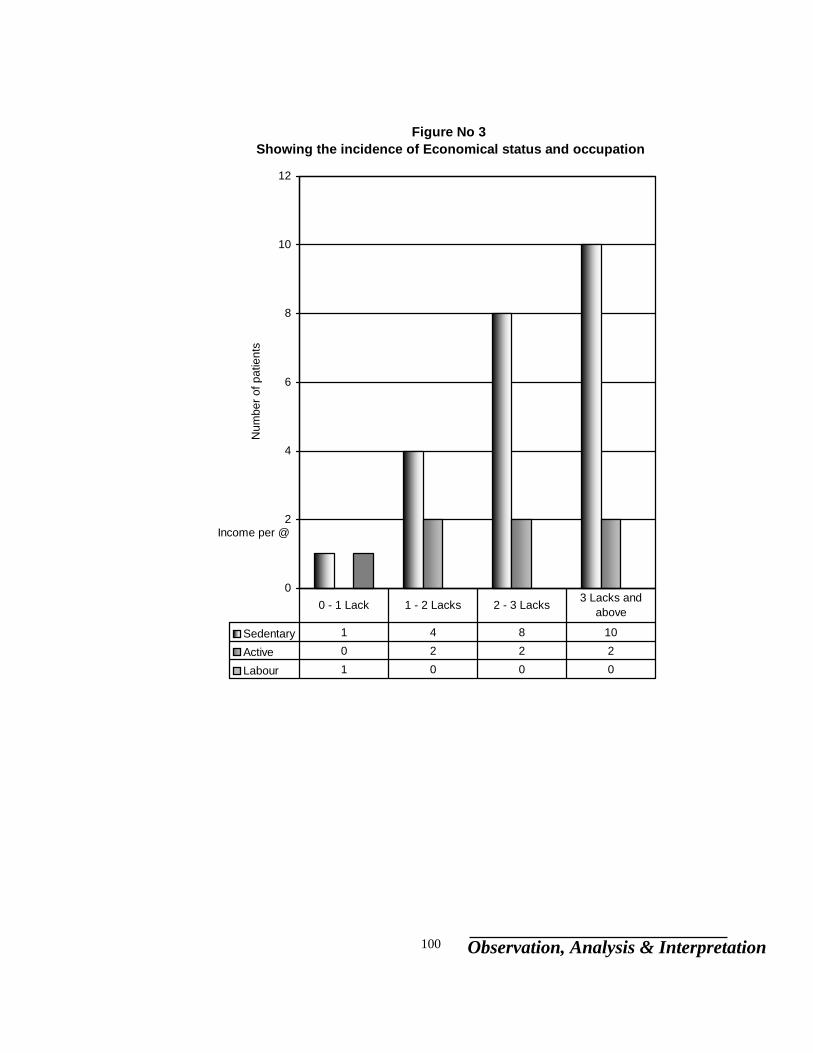
Observation, Analysis & Interpretation 100
Figure No 3 Showing the incidence of Economical status and occupation
0
2
4
6
8
10
12
Income per @
Num
ber o
f pat
ient
s
Sedentary 1 4 8 10
Active 0 2 2 2
Labour 1 0 0 0
0 - 1 Lack 1 - 2 Lacks 2 - 3 Lacks 3 Lacks and above
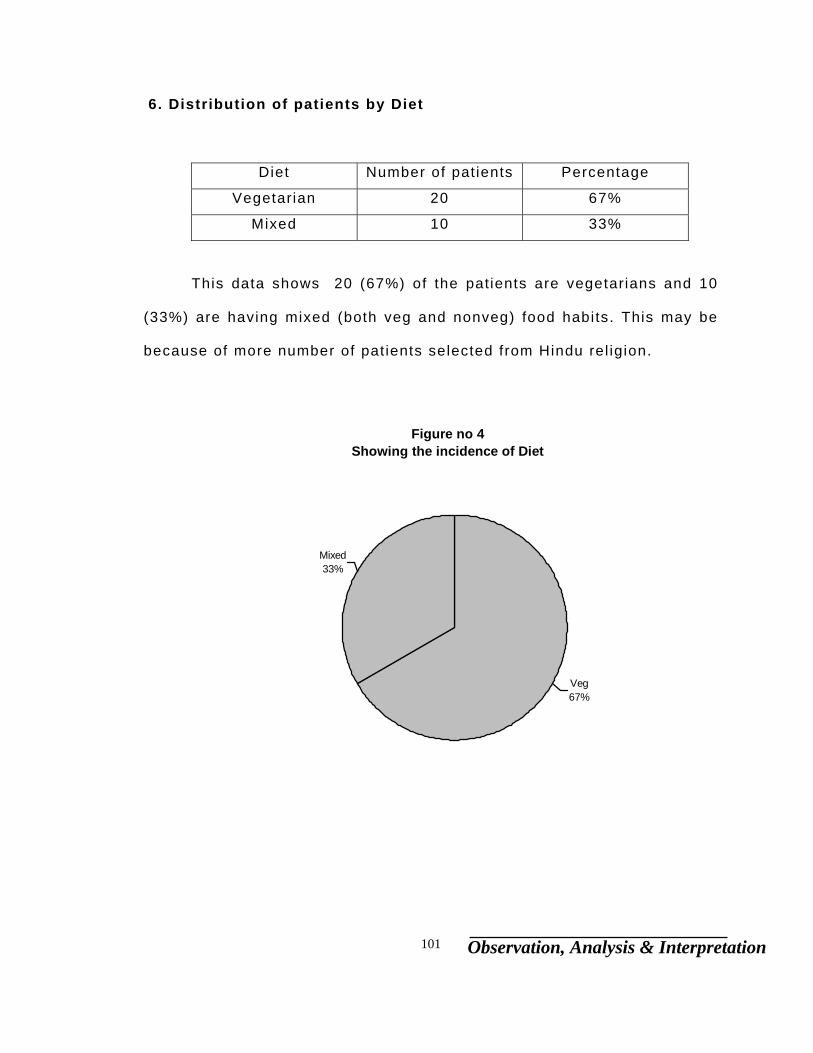
Observation, Analysis & Interpretation 101
6. Distribution of patients by Diet
Diet Number of pat ients Percentage
Vegetarian 20 67%
Mixed 10 33%
This data shows 20 (67%) of the patients are vegetarians and 10
(33%) are having mixed (both veg and nonveg) food habits. This may be
because of more number of pat ients selected from Hindu rel igion.
Figure no 4 Showing the incidence of Diet
Veg67%
Mixed33%
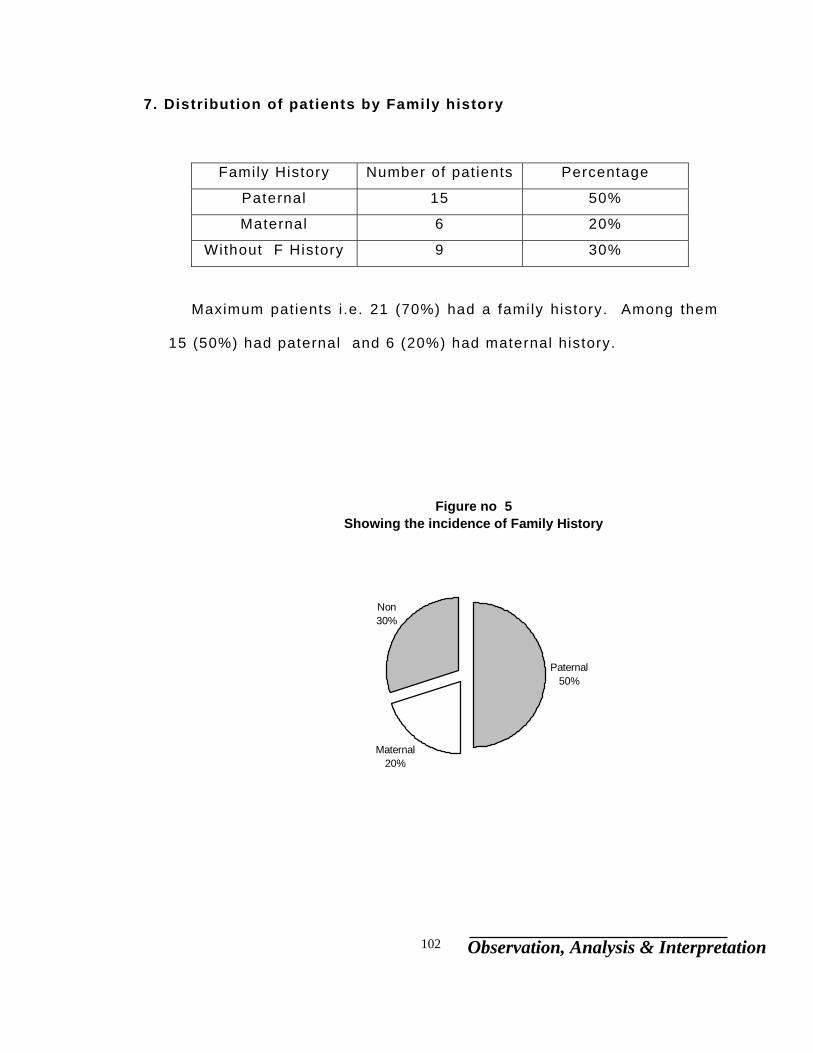
Observation, Analysis & Interpretation 102
7. Distribution of patients by Family history
Family History Number of pat ients Percentage
Paternal 15 50%
Maternal 6 20%
Without F History 9 30%
Maximum patients i .e. 21 (70%) had a family history. Among them
15 (50%) had paternal and 6 (20%) had maternal history.
Figure no 5Showing the incidence of Family History
Maternal20%
Non30%
Paternal50%

Observation, Analysis & Interpretation 103
Data related to Result
Total
Result No of patients Percentage
Rel ieved 15 50%
pal l iat ive 10 33%
Not responded 5 17%
Group A
Result No of patients Percentage
Rel ieved 7 46%
pal l iat ive 7 46%
Not responded 1 6%
Group B
Result No of patients Percentage
Rel ieved 3 20%
pal l iat ive 8 53%
Not responded 4 26%
By the above data we can observe the effect of the medicine is
signif icant, and is working better on group A pat ients than in Group B.
Graphical representat ion of i t is given in f ig No 6.
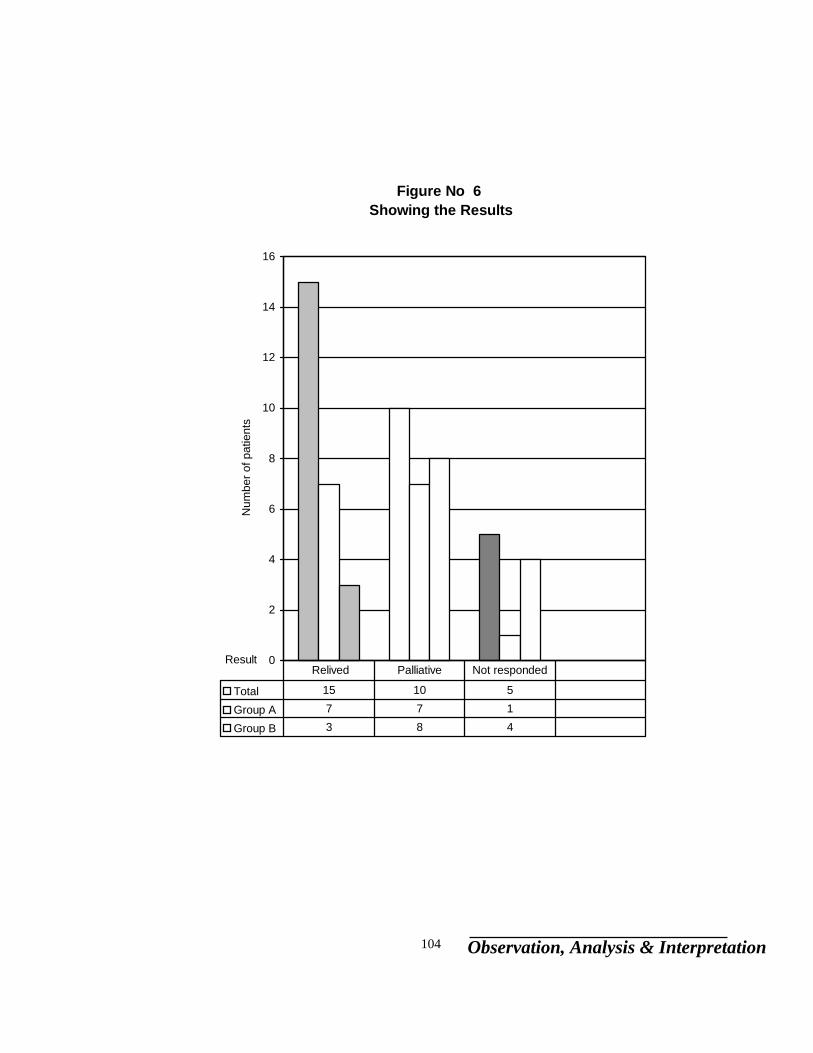
Observation, Analysis & Interpretation 104
Figure No 6 Showing the Results
0
2
4
6
8
10
12
14
16
Result
Num
ber o
f pat
ient
s
Total 15 10 5
Group A 7 7 1
Group B 3 8 4
Relived Palliative Not responded
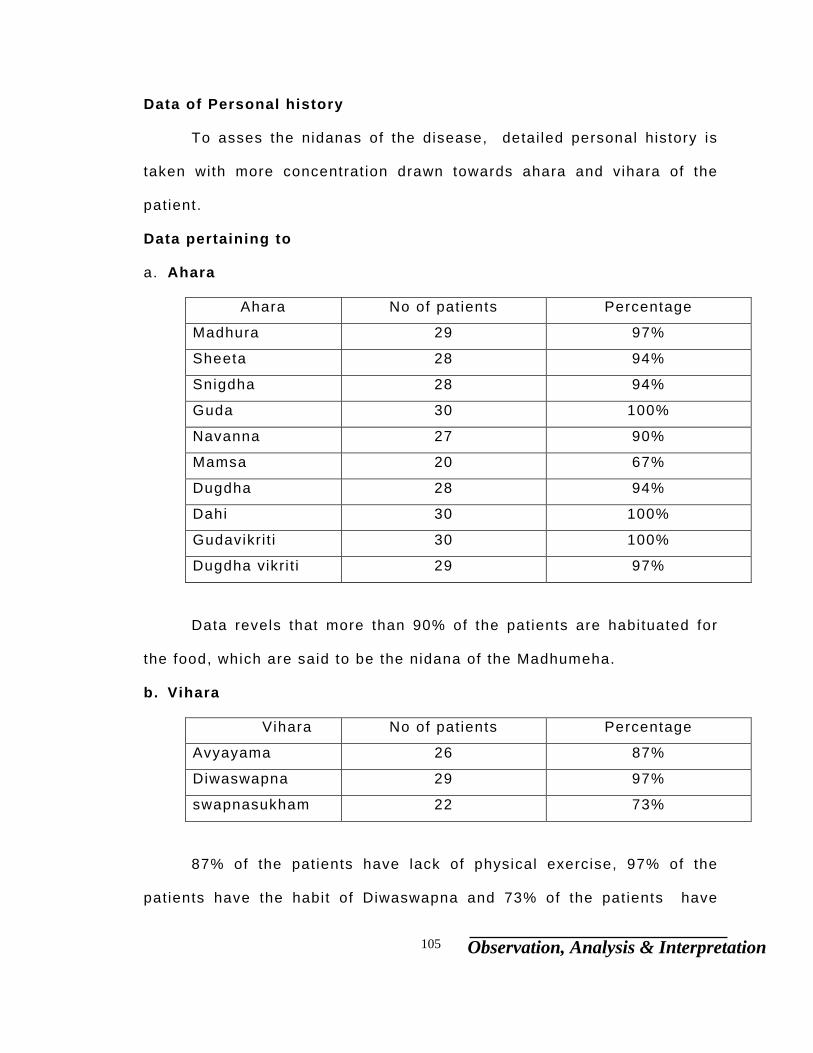
Observation, Analysis & Interpretation 105
Data of Personal history
To asses the nidanas of the disease, detai led personal history is
taken with more concentrat ion drawn towards ahara and vihara of the
patient.
Data pertaining to
a. Ahara
Ahara No of patients Percentage
Madhura 29 97%
Sheeta 28 94%
Snigdha 28 94%
Guda 30 100%
Navanna 27 90%
Mamsa 20 67%
Dugdha 28 94%
Dahi 30 100%
Gudavikri t i 30 100%
Dugdha vikri t i 29 97%
Data revels that more than 90% of the patients are habituated for
the food, which are said to be the nidana of the Madhumeha.
b. Vihara
Vihara No of patients Percentage
Avyayama 26 87%
Diwaswapna 29 97%
swapnasukham 22 73%
87% of the pat ients have lack of physical exercise, 97% of the
patients have the habit of Diwaswapna and 73% of the pat ients have

Observation, Analysis & Interpretation 106
swapnasukham , these factors intensif ies the disease along with aharaja
karana.
c. Manasika
Chinta No of patients Percentage
Present 8 27%
Absent 22 73%
73% of the pat ients are leading happy l i fe without much worr ies,
which is one of the causative factor for Madhumeha.
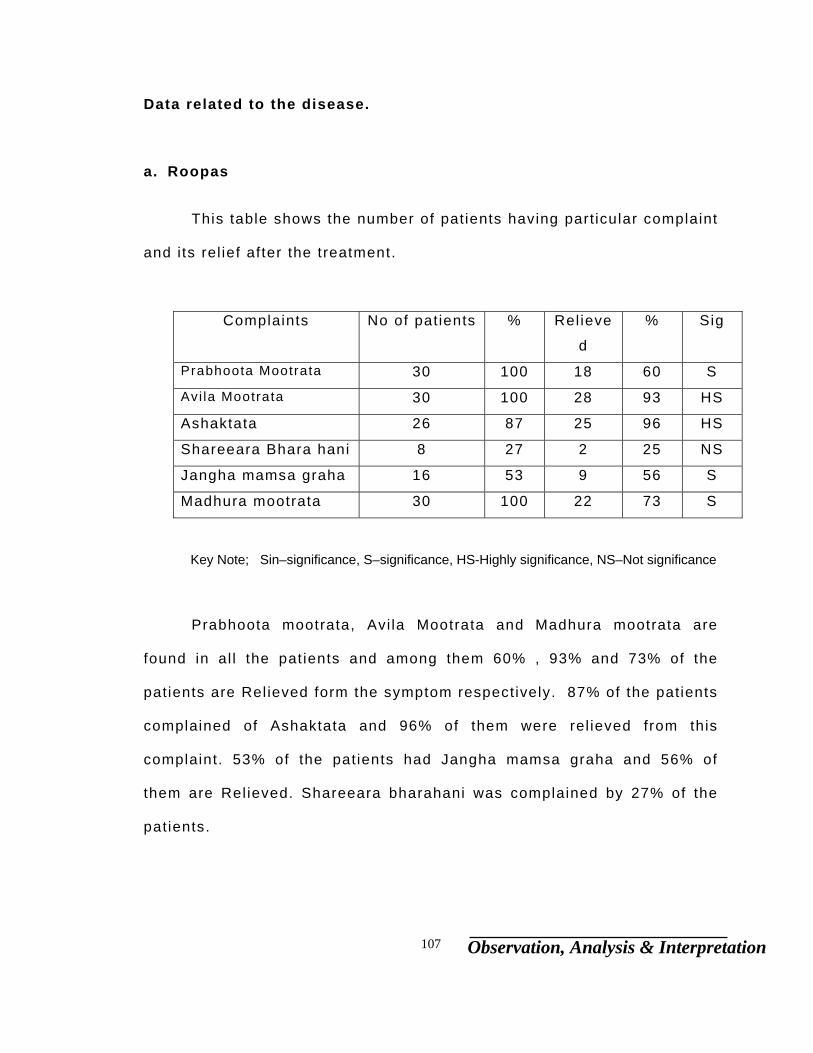
Observation, Analysis & Interpretation 107
Data related to the disease.
a. Roopas
This table shows the number of patients having part icular complaint
and i ts rel ief after the treatment.
Complaints No of patients % Rel ieve
d
% Sig
Prabhoota Mootrata 30 100 18 60 S
Avi la Mootrata 30 100 28 93 HS
Ashaktata 26 87 25 96 HS
Shareeara Bhara hani 8 27 2 25 NS
Jangha mamsa graha 16 53 9 56 S
Madhura mootrata 30 100 22 73 S
Key Note; Sin–significance, S–significance, HS-Highly significance, NS–Not significance
Prabhoota mootrata, Avi la Mootrata and Madhura mootrata are
found in al l the pat ients and among them 60% , 93% and 73% of the
patients are Rel ieved form the symptom respectively. 87% of the patients
complained of Ashaktata and 96% of them were rel ieved from this
complaint. 53% of the patients had Jangha mamsa graha and 56% of
them are Rel ieved. Shareeara bharahani was complained by 27% of the
patients.
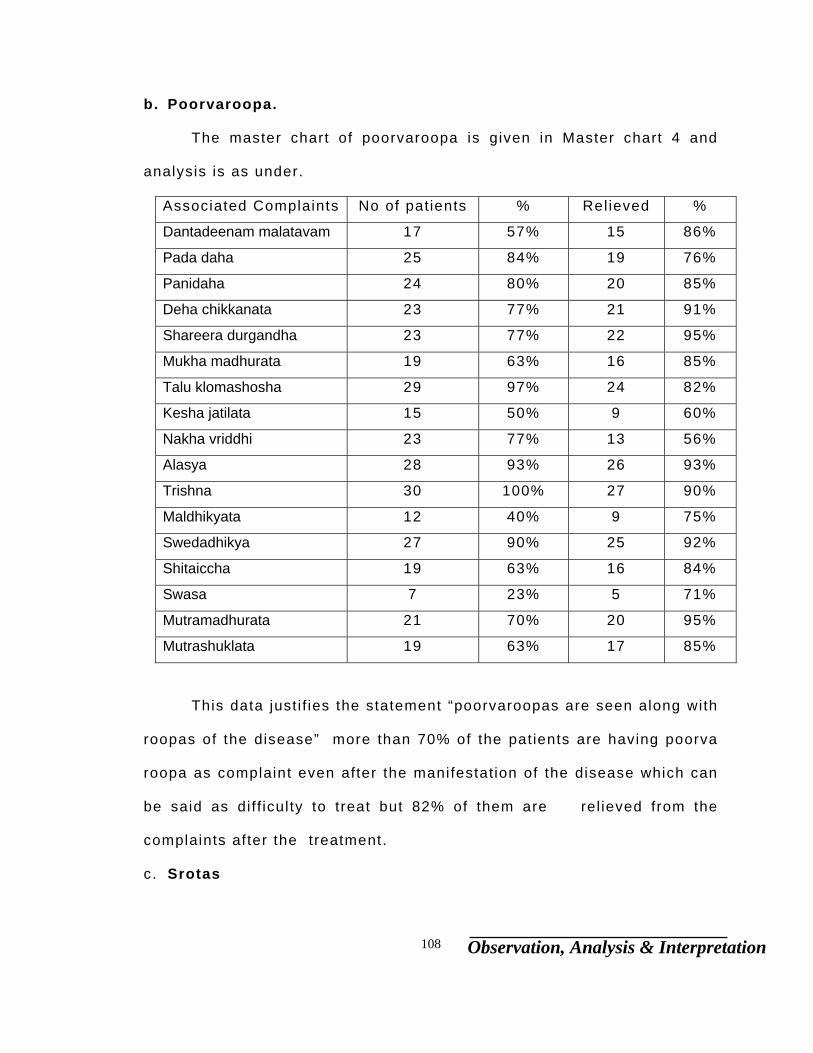
Observation, Analysis & Interpretation 108
b. Poorvaroopa.
The master chart of poorvaroopa is given in Master chart 4 and
analysis is as under.
Associated Complaints No of patients % Rel ieved %
Dantadeenam malatavam 17 57% 15 86%
Pada daha 25 84% 19 76%
Panidaha 24 80% 20 85%
Deha chikkanata 23 77% 21 91%
Shareera durgandha 23 77% 22 95%
Mukha madhurata 19 63% 16 85%
Talu klomashosha 29 97% 24 82%
Kesha jatilata 15 50% 9 60%
Nakha vriddhi 23 77% 13 56%
Alasya 28 93% 26 93%
Trishna 30 100% 27 90%
Maldhikyata 12 40% 9 75%
Swedadhikya 27 90% 25 92%
Shitaiccha 19 63% 16 84%
Swasa 7 23% 5 71%
Mutramadhurata 21 70% 20 95%
Mutrashuklata 19 63% 17 85%
This data justi f ies the statement “poorvaroopas are seen along with
roopas of the disease” more than 70% of the patients are having poorva
roopa as complaint even after the manifestation of the disease which can
be said as di f f icul ty to treat but 82% of them are rel ieved from the
complaints after the treatment.
c. Srotas
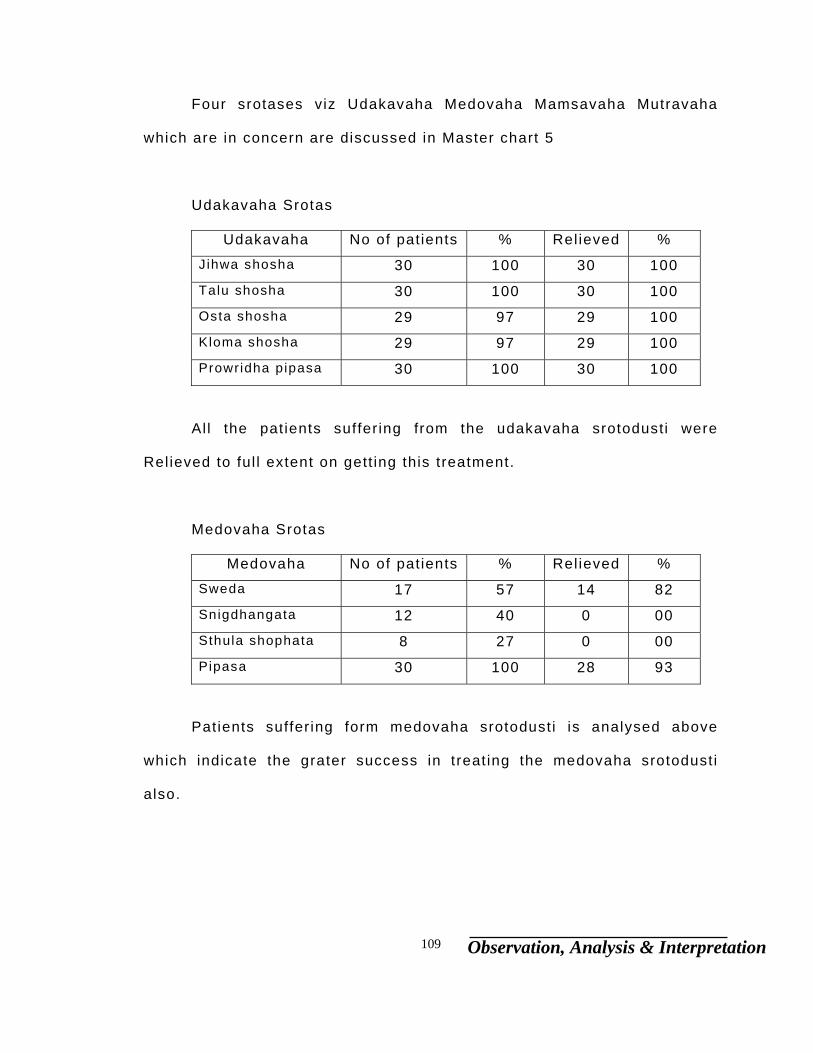
Observation, Analysis & Interpretation 109
Four srotases viz Udakavaha Medovaha Mamsavaha Mutravaha
which are in concern are discussed in Master chart 5
Udakavaha Srotas
Udakavaha No of patients % Rel ieved %
Jihwa shosha 30 100 30 100
Talu shosha 30 100 30 100
Osta shosha 29 97 29 100
Kloma shosha 29 97 29 100
Prowridha pipasa 30 100 30 100
Al l the pat ients suffer ing from the udakavaha srotodusti were
Rel ieved to ful l extent on gett ing this treatment.
Medovaha Srotas
Medovaha No of patients % Rel ieved %
Sweda 17 57 14 82
Snigdhangata 12 40 0 00
Sthula shophata 8 27 0 00
Pipasa 30 100 28 93
Pat ients suffer ing form medovaha srotodust i is analysed above
which indicate the grater success in treat ing the medovaha srotodust i
also.
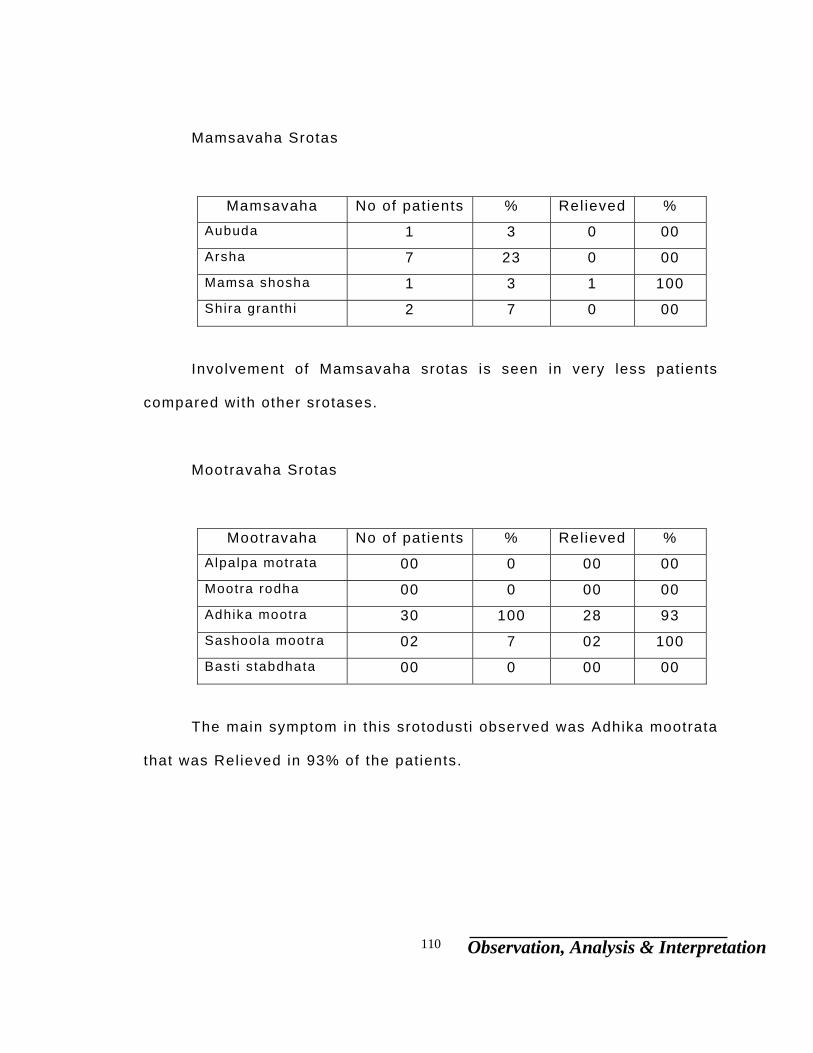
Observation, Analysis & Interpretation 110
Mamsavaha Srotas
Mamsavaha No of patients % Rel ieved %
Aubuda 1 3 0 00
Arsha 7 23 0 00
Mamsa shosha 1 3 1 100
Shira granthi 2 7 0 00
Involvement of Mamsavaha srotas is seen in very less patients
compared with other srotases.
Mootravaha Srotas
Mootravaha No of patients % Rel ieved %
Alpalpa motrata 00 0 00 00
Mootra rodha 00 0 00 00
Adhika mootra 30 100 28 93
Sashoola mootra 02 7 02 100
Bast i s tabdhata 00 0 00 00
The main symptom in this srotodusti observed was Adhika mootrata
that was Rel ieved in 93% of the patients.

Observation, Analysis & Interpretation 111
d. Upadravas
Detai led Master chart of upadravas is given in master chart 6
Complaints No of patients % Rel ieved %
Prameha pidika 4 13 3 75
At isara 2 7 2 100
Jwara 2 7 2 100
Daha 19 63 16 84
Arochaka 14 47 12 86
Avipaka 6 20 6 100
Chardi 3 10 3 100
Kasa 2 7 1 50
pratishyaya 4 13 4 100
Data revi les 63% of the pat ients were suffer ing from Daha, 84% of
them were Rel ieved among them. 47% of the pat ients were complaining
of Arochaka, among them 86% of the patients were Rel ieved from this
complicat ion after the treatment of madhumeha.13% of the pat ients had
prameha pidika which is Rel ieved in 75% . Other minor complicat ions
were also reported and Rel ieved to a grater extent as shown in the table.

Observation, Analysis & Interpretation 112
e. Laboratory investigations.
The f igures of lab investigat ions are shown below.
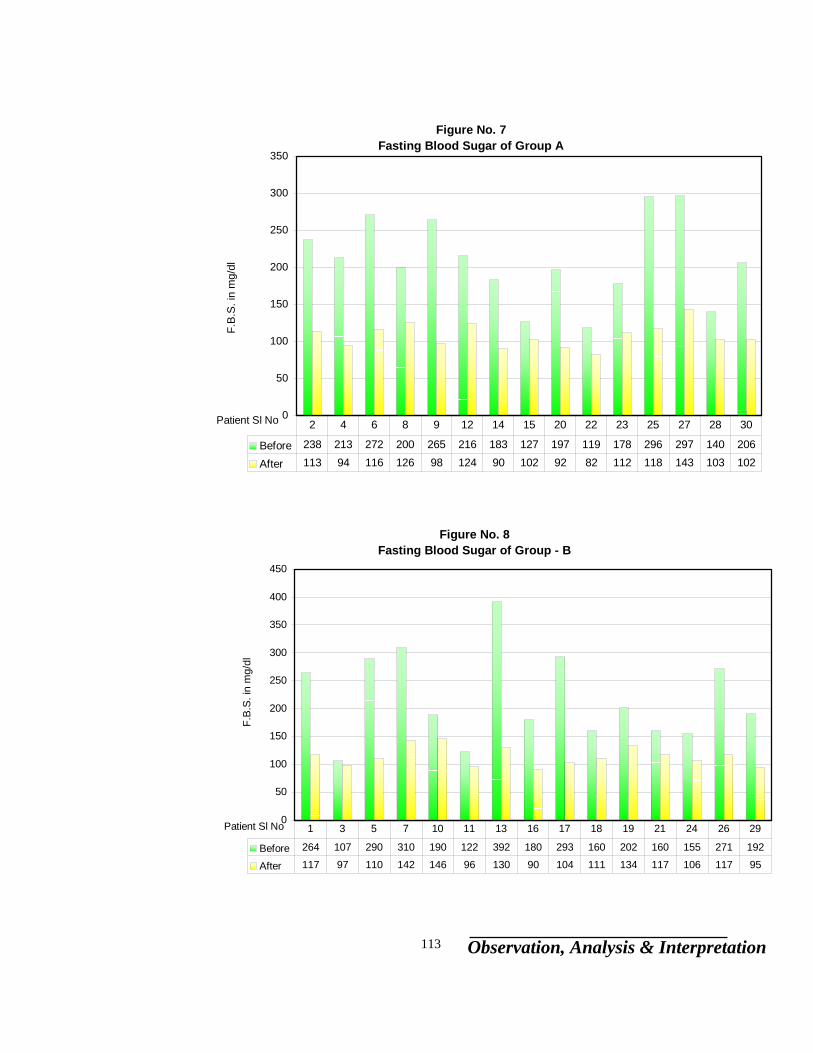
Observation, Analysis & Interpretation 113
Figure No. 8Fasting Blood Sugar of Group - B
0
50
100
150
200
250
300
350
400
450
Patient Sl No
F.B
.S. i
n m
g/dl
Before 264 107 290 310 190 122 392 180 293 160 202 160 155 271 192
After 117 97 110 142 146 96 130 90 104 111 134 117 106 117 95
1 3 5 7 10 11 13 16 17 18 19 21 24 26 29
Figure No. 7Fasting Blood Sugar of Group A
0
50
100
150
200
250
300
350
Patient Sl No
F.B
.S. i
n m
g/dl
Before 238 213 272 200 265 216 183 127 197 119 178 296 297 140 206
After 113 94 116 126 98 124 90 102 92 82 112 118 143 103 102
2 4 6 8 9 12 14 15 20 22 23 25 27 28 30
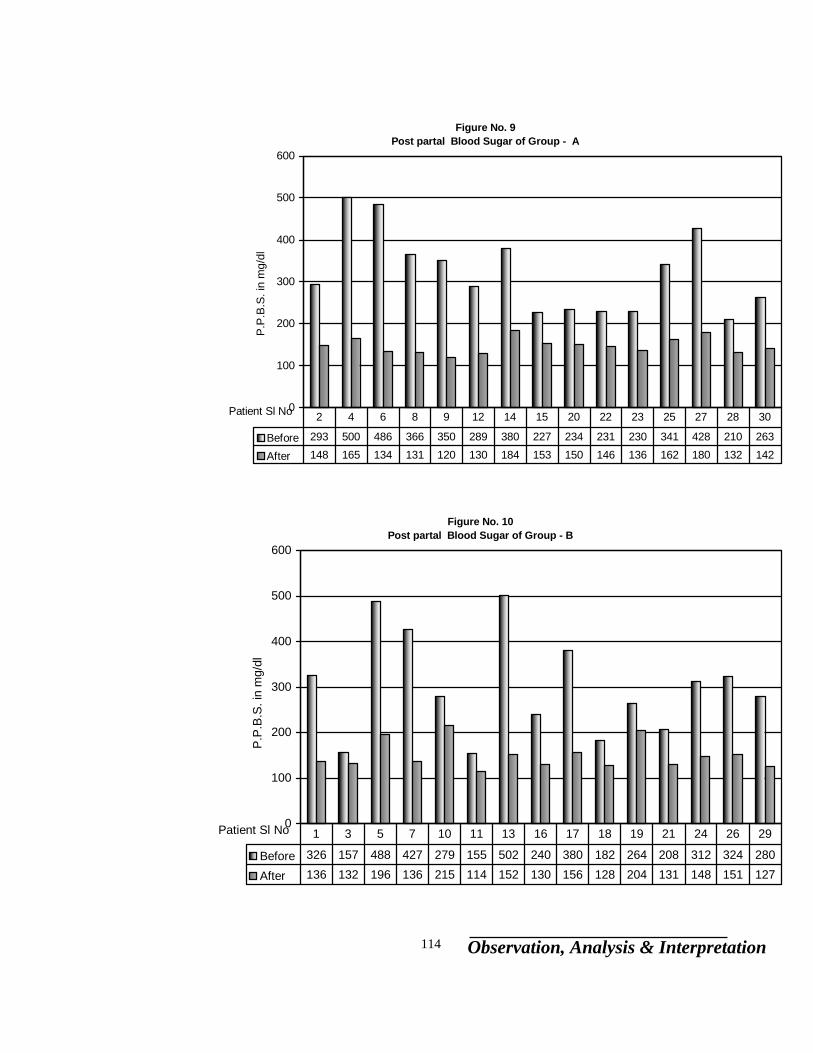
Observation, Analysis & Interpretation 114
Figure No. 9Post partal Blood Sugar of Group - A
0
100
200
300
400
500
600
Patient Sl No
P.P
.B.S
. in
mg/
dl
Before 293 500 486 366 350 289 380 227 234 231 230 341 428 210 263
After 148 165 134 131 120 130 184 153 150 146 136 162 180 132 142
2 4 6 8 9 12 14 15 20 22 23 25 27 28 30
Figure No. 10Post partal Blood Sugar of Group - B
0
100
200
300
400
500
600
Patient Sl No
P.P
.B.S
. in
mg/
dl
Before 326 157 488 427 279 155 502 240 380 182 264 208 312 324 280
After 136 132 196 136 215 114 152 130 156 128 204 131 148 151 127
1 3 5 7 10 11 13 16 17 18 19 21 24 26 29
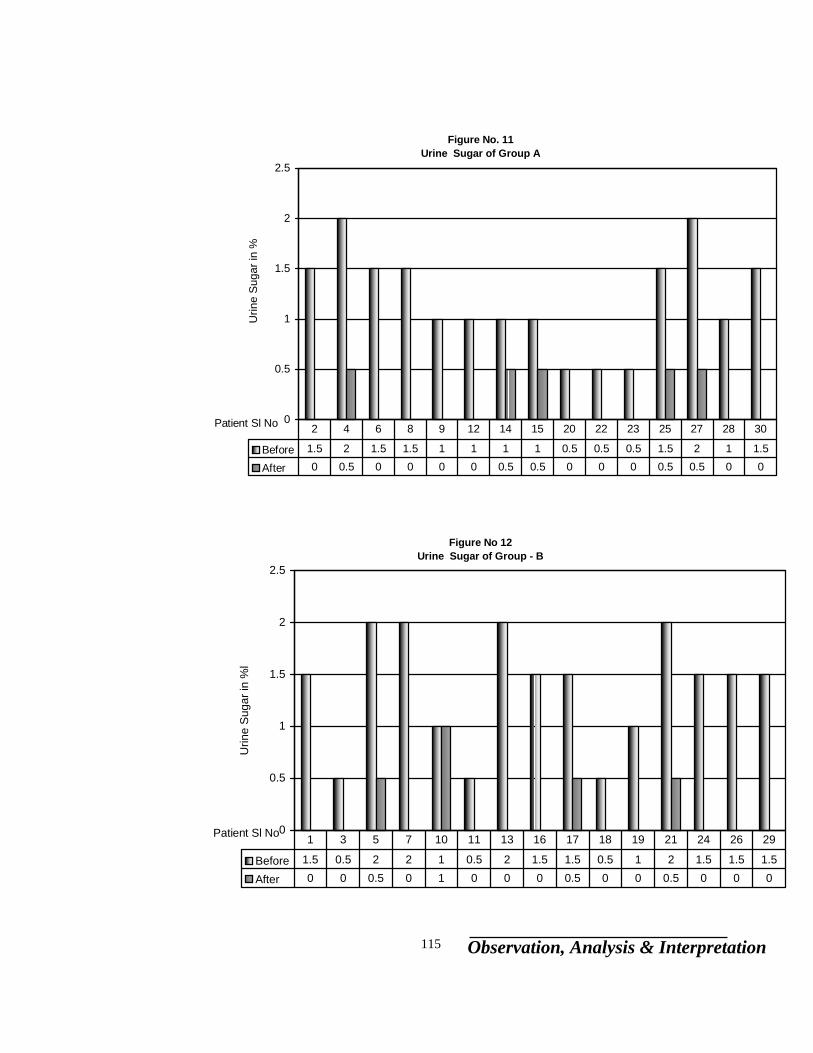
Observation, Analysis & Interpretation 115
Figure No. 11Urine Sugar of Group A
0
0.5
1
1.5
2
2.5
Patient Sl No
Urin
e S
ugar
in %
Before 1.5 2 1.5 1.5 1 1 1 1 0.5 0.5 0.5 1.5 2 1 1.5
After 0 0.5 0 0 0 0 0.5 0.5 0 0 0 0.5 0.5 0 0
2 4 6 8 9 12 14 15 20 22 23 25 27 28 30
Figure No 12Urine Sugar of Group - B
0
0.5
1
1.5
2
2.5
Patient Sl No
Urin
e S
ugar
in %
l
Before 1.5 0.5 2 2 1 0.5 2 1.5 1.5 0.5 1 2 1.5 1.5 1.5
After 0 0 0.5 0 1 0 0 0 0.5 0 0 0.5 0 0 0
1 3 5 7 10 11 13 16 17 18 19 21 24 26 29
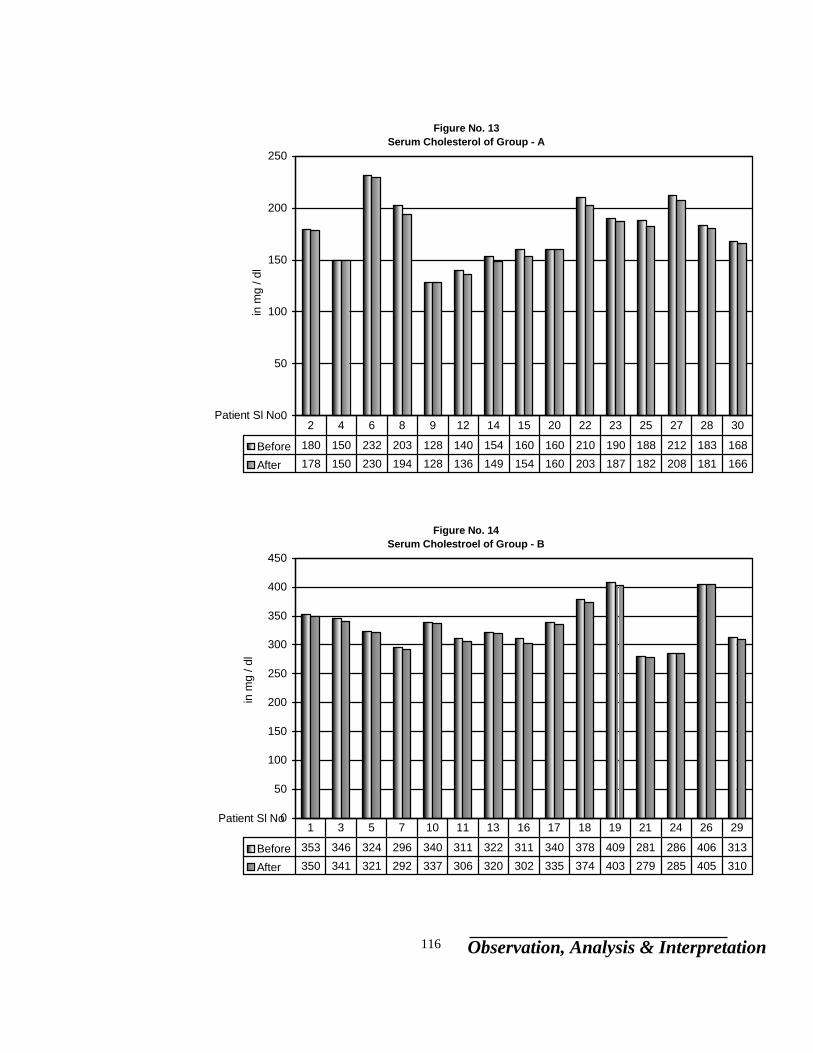
Observation, Analysis & Interpretation 116
Figure No. 13Serum Cholesterol of Group - A
0
50
100
150
200
250
Patient Sl No
in m
g / d
l
Before 180 150 232 203 128 140 154 160 160 210 190 188 212 183 168
After 178 150 230 194 128 136 149 154 160 203 187 182 208 181 166
2 4 6 8 9 12 14 15 20 22 23 25 27 28 30
Figure No. 14Serum Cholestroel of Group - B
0
50
100
150
200
250
300
350
400
450
Patient Sl No
in m
g / d
l
Before 353 346 324 296 340 311 322 311 340 378 409 281 286 406 313
After 350 341 321 292 337 306 320 302 335 374 403 279 285 405 310
1 3 5 7 10 11 13 16 17 18 19 21 24 26 29
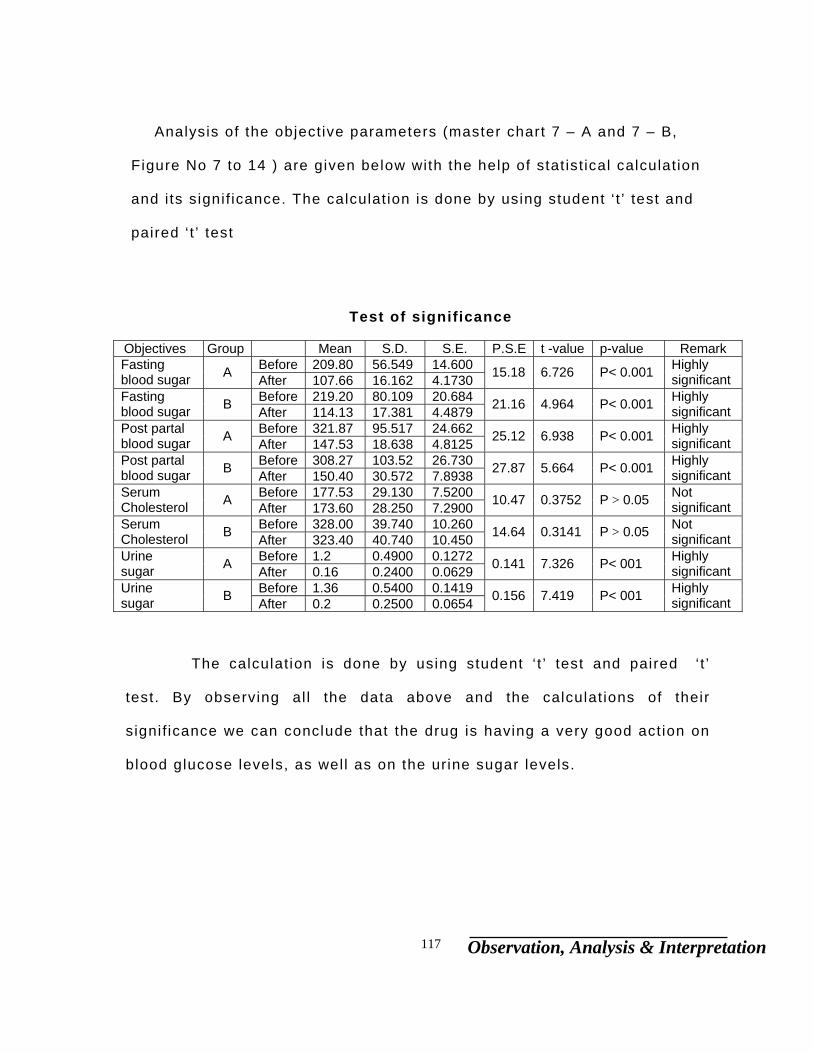
Observation, Analysis & Interpretation 117
Analysis of the objective parameters (master chart 7 – A and 7 – B,
Figure No 7 to 14 ) are given below with the help of stat ist ical calculation
and i ts signif icance. The calculat ion is done by using student ‘ t ’ test and
paired ‘ t ’ test
Test of significance
Objectives Group Mean S.D. S.E. P.S.E t -value p-value Remark
Before 209.80 56.549 14.600 Fasting blood sugar A After 107.66 16.162 4.1730 15.18 6.726 P< 0.001 Highly
significant Before 219.20 80.109 20.684 Fasting
blood sugar B After 114.13 17.381 4.4879 21.16 4.964 P< 0.001 Highly significant
Before 321.87 95.517 24.662 Post partal blood sugar A After 147.53 18.638 4.8125 25.12 6.938 P< 0.001 Highly
significant Before 308.27 103.52 26.730 Post partal
blood sugar B After 150.40 30.572 7.8938 27.87 5.664 P< 0.001 Highly significant
Before 177.53 29.130 7.5200 Serum Cholesterol A After 173.60 28.250 7.2900 10.47 0.3752 P > 0.05 Not
significant Before 328.00 39.740 10.260 Serum
Cholesterol B After 323.40 40.740 10.450 14.64 0.3141 P > 0.05 Not significant
Before 1.2 0.4900 0.1272 Urine sugar A After 0.16 0.2400 0.0629 0.141 7.326 P< 001 Highly
significant Before 1.36 0.5400 0.1419 Urine
sugar B After 0.2 0.2500 0.0654 0.156 7.419 P< 001 Highly significant
The calculation is done by using student ‘ t ’ test and paired ‘ t ’
test. By observing al l the data above and the calculat ions of their
s ignif icance we can conclude that the drug is having a very good act ion on
blood glucose levels, as well as on the urine sugar levels.
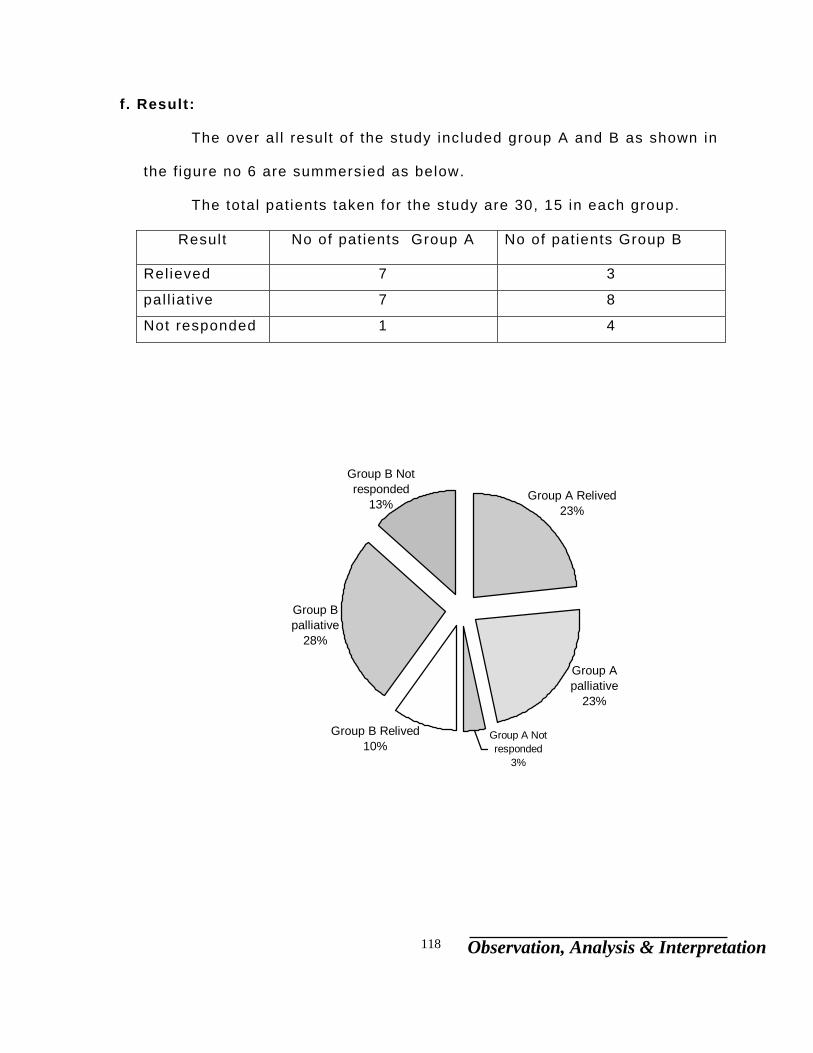
Observation, Analysis & Interpretation 118
f . Result:
The over al l result of the study included group A and B as shown in
the f igure no 6 are summersied as below.
The total patients taken for the study are 30, 15 in each group.
Result No of patients Group A No of patients Group B
Rel ieved 7 3
pal l iat ive 7 8
Not responded 1 4
Group A Not responded
3%
Group B Relived10%
Group A palliative
23%
Group B Not responded
13%
Group B palliative
28%
Group A Relived23%
Conclusion 118
In the present tr ial 30 cases were taken for the study. The tr ial
drug, “Bhumamalakidi churna” had a very good effect on al l the pat ients,
not only by regulat ing their blood glucose levels down but also by
rel ieving them from the signs and symptoms. Especial ly al l the patients
were sat isf ied because of reduced frequency of mituration and burning
sensation of hands and feet.
Even though the combinat ion of t r ial drug is not mentioned in the
classics of Ayurveda, we have combined i t by observing the
pathophysiology of the disease and the actions of the individual drugs,
viz Madhu nasani as an establ ished hypoglycemic agent, Bhumamalaki
and Bhranjraja are good l iver correctors as the l iver is the main organ
involved in glucose metabol ism. Eranda is included in the combination
because of i ts establ ished vata hara effect, as Madhumeha is a vataja
prameha,. After col lecting the herbs personal ly identi f ied by Botanist and,
they were processed as the tr ial drug.
One pat ient (Sl No 1, OPD No 4477 ) approached our PG Hospital
for chronic (one and half month duration) non heal ing ulcers, he was
detected as a diabetic, he was the f i rst patient for our tr ial , even though
the ulcers were big enough (as shown in the photo graph 5 ) we took
bold steps to treat him with our tr ial drug (without any al lopathic drug),
When the patient reported at regular intervals of 15 days, the changes in
the ulcers are noted as (photograph 6 ), and after 31 days the ulcer was

Conclusion 119
ful ly disappeared (photograph 7 ). A camp was set up on 25 – 10 – 99 to
screen the pat ients for the tr ial . We screened 46 pat ients and 18
patients were selected among them.
By the observat ion of the laboratory reports of the pat ients we can
assume the tr ial drug “Bhumamalakadi churna” is highly effect ive on
the NIDDM (Non Insul in Dependent Diabetes Mell i tus ) pat ients. Two
patients other than that of the tr ial patients who were on insul in therapy
were also given the tr ial drug out of interest to know the effect on the
insul in dependent pat ients, even these two patients responded wel l . The
task for these two patients was dif f icult and r isky so i t was done under
close observation and even though the insul in was slowly reduced (2
units per day) the blood sugar level were reduced. This tr ial of these two
patients out of st ipulated inclusive cri ter ia has shown signif icance of
result .
By the assesment of parameters, i t is confirmed that the eff icacy of
tr ial drug “Bhumamalakadi churna´is one of the best al ternate therapy for
the patients of NIDDM. I t has shown remarkable results over the patients
within 30 days. Prolonged use of the medicine doesn’t have any side
effects and further at an economical price the pal l iat ion is possible.

Summary 120
This thesis enti t led “EVALUATION OF THE EFFECT OF
BHUMYAMALAKYADI CHURNA IN MADHUMEHA (With special reference to
i ts hypoglycemic effect)” is summarised as fol lows.
- Madhumeha is one out of the 20 variet ies of Pramehas. I t is Vata
predominant there by considered under vataja mehas. Madhumeha is a
yapya vyadhi.
- I ts treatment is to be a vatahara, kaphahara, and dusta medohara
along with i ts action over mootravaha srotas.
- The present drug selected is having i ts effect over Vata, kapha and
medas. Moreover i ts pharmacological action is over the l iver, in the
process of neoglucogenises as a part of glucose metabol ism in the
body. Secondly i t acts over the Vata, specif ical ly pacifying Vata and
i ts involvement in the disease. Hypoglycemic act ion of
“BHUMYAMALAKYADI CHURNA” is remarkable.
- The classical aff i rmed pathogenesis, as the involvement of medas with
i ts classical signs and symptoms in Madhumeha are stand st i l l even in
21s t century. The pratyatmaniyata lakshana of Madhumeha are
Prabhutamootrata and Avi la mootrata along with ashaktata.
Summary 121
- The cl inical study of the ent i t led thesis “ EVALUATION OF THE EFFECT
OF BHUMYAMALAKYADI CHURNA IN MADHUMEHA (With special
reference to i ts hypoglycemic effect)” have studied over 30 patients in
two groups A ) Hyperglycemic and Hypolipidimic
B ) Hyperglycemic and Hyperl ipidimic.
- Observation of the signs and symptoms, sex, age, incidence, and
results are explained in tubular and graphic forms.
- Results of the treatment were assessed on the bases of di f ferences
between the base l ine data and assessment data . The lab
investigat ion variables were subjected for stat ist ical analysis by
applying student ‘ t ’ test and paired ‘ t ’ test.
- The subjective and objective parameters under stat ist ical viabi l i ty
have shown high signif icance rate with respect to both groups. In
Hyperglycemic and Hypol ipidimic group, 46% of the patient are
rel ieved, 46% are in pal l iat ive group and only 6% of the patients are
not responded. Similarly in Hyperglycemic and Hyperl ipidimic group,
20% of the patients are rel ieved, 53% pal l iat ive and 26% are not
responded. This data reveals the effect of Bhumyamalakyadi churna
highly signif icant. Not responded dosent mean their blood sugar did
not decrease but i t was not up to the mark.
Bibliography
BIBLIOGRAPHY
Charak Samhita Poorvardha
By Vaidya Satyanaryana Shastri . 1s t edit ion 1962
Publ ished by Chowkhamba Vidya Bhavan. Varanasi.
Charak Samhita Uttarardha
By Vaidya Satyanaryana Shastr i . 1s t edit ion 1962
Publ ished by Chowkhamba Vidya Bhavan. Varanasi.
Sushruta Samhita Poorvardha
By Kaviraja Ambikadutta shastr i . 8t h edit ion
Publ ished by Chowkhamba Sanskri t Sansthan, Varanasi.
Sushruta Samhita Uttarardha
By Kaviraja Ambikadutta shastr i . 8t h edit ion
Publ ished by Chowkhamba Sanskri t Sansthan, Varanasi
Astanga Samgraha of Vagbhata
By Prof K.R.Srikantha Murthy. 1s t edit ion 1996
Published by Chowkhamba Oriental ia, Varanasi.
Astanga Hridaya with commentaries of Arunadatta and Hemadri
By Harisastry paradakar Vaidya, 1939
Published by Nirnaya sagar press Bombay.
Bhavaprakasa
By Sri Brahmasankara Misra. 4t h edit ion 1984
Published by Chowkhamba Sanskri t Sansthan, Varanasi.
Bibliography
Madhava Nidana with Madhukosha sanskri t vyakarna.
By Acharya Sri Narindranath shastr i . 1s t edit ion 1989
Publ ished by Moti lal Banarasidas, Varnasi.
Rajanighantu
By Pandit Narahari . 2nd edit ion 1998
Publ ished by Krishnadas Academy, Varansai.
Bhela Samhita
By Gir i ja Dayal Shukla, 1959
Publ ished by Chowkhamba publ ication, Varnasi.
Essentials of Basic Ayurveda Concepts.
By Prof Dr. V.V.S.Sastri . 1999
Publ ished by Publ ication Division, PGARC,
DGM Ay Medical Col lege, Gadag
Josl in’s Diabetes Mell i tus.
By C. Ronald Kahn. 13t h edit ion 1994
Published by Lea and Febiger, A Waverly company, London.
API Text book of Medicine.
By G.S.Sainani 5t h edit ion 1992
Published by Associat ion of Physicians of India, Bombay.
Indian Materia Medica
by K.M.Nadkarni. Vol 1 - 2 2nd edit ion 1982
Publ ished by Popular Prakashan Bombay
Bibliography
Indian Medicinal Plants
by Kirt ikar & Basu Vol 1 - 3 2n d edit ion 1975
Shareera kriya vi jnanam
By M. Ramasundar Rao 2n d edit ion 1994
Publ ished by M. Madhava, Metro Printers, Vi jayawada.
Chakradatta
By Priyavrat Sharma. 2n d edit ion 1998
Publ ished by Chowkhamba Oriental ia, Varanasi.
Researches in Ayurveda
By Dr. M.S.Baghel. 1s t edit ion 1997
Published by Mridu Ayruvedic Publ icat ion and Sales. Jamnagar.
Cunninghama Manual of Pratactical Anatomy Vol 1 to 3
Publ ished at Great Bri tain, Oxford Universi ty Press.
Dorland’s Pocket Medical Dict ionary.
By Douglas M. Anderson. 24t h edit ion 1989
Publ ished by Oxford & IBH publ ishing Co. Pvt. Ltd. Bombay.
Human Physiology
By Dr C.C.Chatter jee 11t h edit ion 1992
Publ ished by Medical Al l ide Agency. Calcutta.
Digestion and Metabol ism in Ayurveda,
By C.Dwarkanath,
Published by Baidyanath Publ ications, Calcutta.
Bibliography
Davidsons Principles and Practice of medicine,
by John Maclod 1992
Publ ished by Pitman press, Great Bri tain.
Gray’s Anatomy
by Henry Gray 1973
Publ ished by Longman group Ltd.
Introduct ion to Kayachiktsa,
by C. Dwarkanath,
Publ ished by Chowkamba offest press, Varanasi.
Kashyapa Samhita,
by Vridha Jeevaka, 1953
Publ ished by Chowkhamba Vidya Bhavan. Varanasi
Principles of Internal Medicine
by T.R. Harr ison and Co. 1962
A Hand book on Endocrine disorders
by Natoobhai. J. Shah 2n d edit ion 1962
publ ished by Unichem Laboratories, Bombay.
Review of medical Physiology
by Wil lam. F. Ganong, 11t h edit ion 1983
Publ ished by Lange Medical publ icat ions, Maruzen.
The Ayurveda Encyclopedia
by Swami Sada shiva Tirtha. 1s t edit ion 1998
Publ ished by Indian books centre, Delhi. Your Guide to Health
Bibliography
By Cl i f ford R. Anderson. 10t h edit ion 1999
Publ ished by G.S.Robert Cl ive, Pune.
Yogaratnakara with Vaidyaprabha hindi commentary
By Dr Indradev Tripathi 1s t edit ion 1998
Publ ished by krishnadas Academy, Varanasi.
Nidana Chiki tsa Hastamalaka
By Ranaji t Roy Desai. 1s t edit ion 1978
Publ ished by Baidyanath Ayurveda bhavan, Nagapur.
Cl inical Methods in Ayurveda
By K.R. Srikantamurthy. 2n d edit ion 1996
Publ ished by Chaukhambha Oriental ia, Varanasi.
From Fat to Fi t
By Dr D.R.Gala. 1s t edit ion 1998
Publ ished by Navneet Publ icat ions Ltd, Gujarat.
Schafer’s essentials of Histology
By Schafers 16t h edit ion 1954
Publ ished by Orient longmans l td.
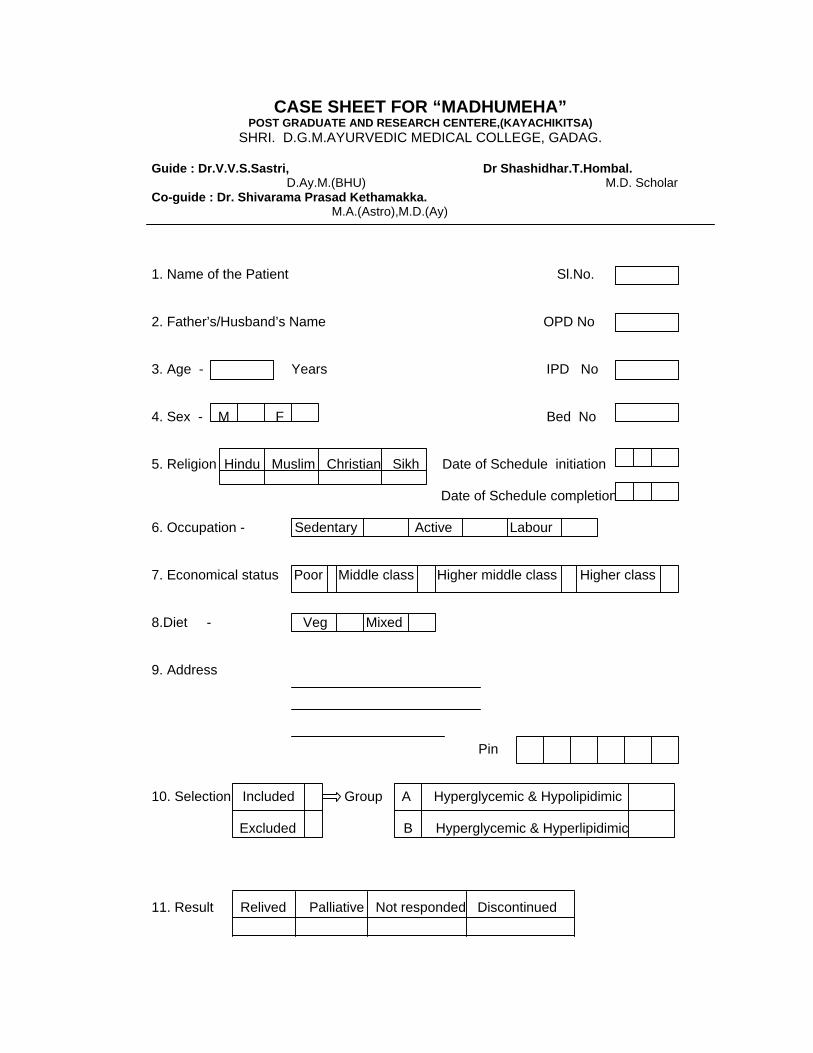
CASE SHEET FOR “MADHUMEHA”
POST GRADUATE AND RESEARCH CENTERE,(KAYACHIKITSA) SHRI. D.G.M.AYURVEDIC MEDICAL COLLEGE, GADAG.
Guide : Dr.V.V.S.Sastri, Dr Shashidhar.T.Hombal. D.Ay.M.(BHU) M.D. Scholar Co-guide : Dr. Shivarama Prasad Kethamakka. M.A.(Astro),M.D.(Ay) 1. Name of the Patient Sl.No. 2. Father’s/Husband’s Name OPD No 3. Age - Years IPD No 4. Sex - M F Bed No 5. Religion Hindu Muslim Christian Sikh Date of Schedule initiation Date of Schedule completion 6. Occupation - Sedentary Active Labour 7. Economical status Poor Middle class Higher middle class Higher class 8.Diet - Veg Mixed 9. Address Pin 10. Selection Included Group A Hyperglycemic & Hypolipidimic
Excluded B Hyperglycemic & Hyperlipidimic 11. Result Relived Palliative Not responded Discontinued
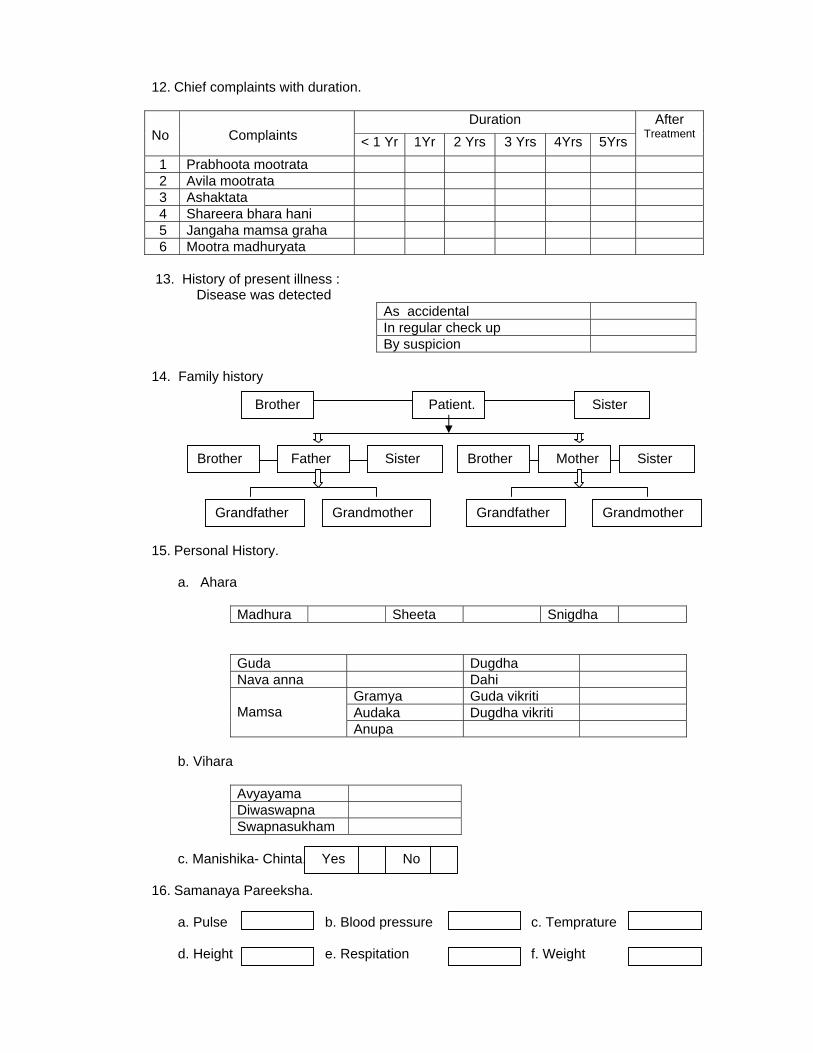
12. Chief complaints with duration.
Duration No
Complaints < 1 Yr 1Yr 2 Yrs 3 Yrs 4Yrs 5Yrs
After Treatment
1 Prabhoota mootrata 2 Avila mootrata 3 Ashaktata 4 Shareera bhara hani 5 Jangaha mamsa graha 6 Mootra madhuryata 13. History of present illness : Disease was detected
As accidental In regular check up By suspicion
14. Family history 15. Personal History.
a. Ahara
Madhura Sheeta Snigdha
Guda Dugdha Nava anna Dahi
Gramya Guda vikriti Audaka Dugdha vikriti
Mamsa
Anupa b. Vihara
Avyayama Diwaswapna Swapnasukham
c. Manishika- Chinta. Yes No
16. Samanaya Pareeksha.
a. Pulse b. Blood pressure c. Temprature d. Height e. Respitation f. Weight
Patient. Brother Sister
Brother Father Mother
Grandfather Grandmother
Sister Sister Brother
Grandfather Grandmother
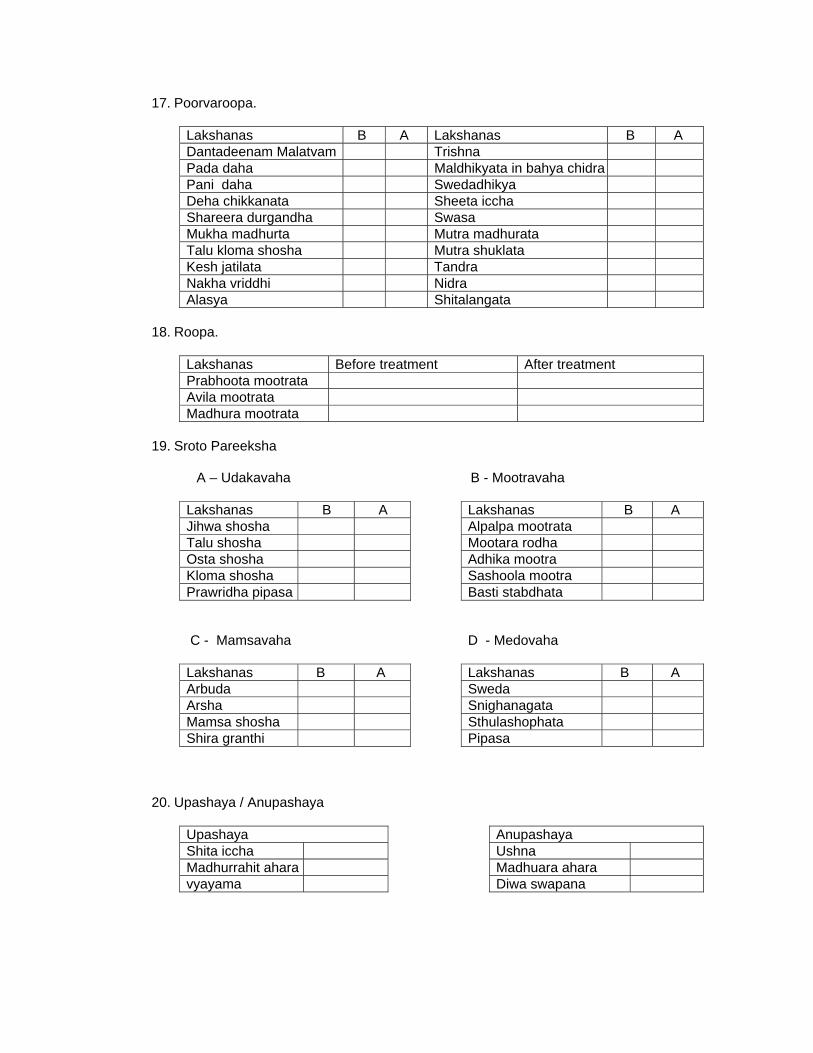
17. Poorvaroopa.
Lakshanas B A Lakshanas B A Dantadeenam Malatvam Trishna Pada daha Maldhikyata in bahya chidra Pani daha Swedadhikya Deha chikkanata Sheeta iccha Shareera durgandha Swasa Mukha madhurta Mutra madhurata Talu kloma shosha Mutra shuklata Kesh jatilata Tandra Nakha vriddhi Nidra Alasya Shitalangata
18. Roopa.
Lakshanas Before treatment After treatment Prabhoota mootrata Avila mootrata Madhura mootrata
19. Sroto Pareeksha
A – Udakavaha B - Mootravaha
Lakshanas B A Lakshanas B A Jihwa shosha Alpalpa mootrata Talu shosha Mootara rodha Osta shosha Adhika mootra Kloma shosha Sashoola mootra Prawridha pipasa Basti stabdhata C - Mamsavaha
D - Medovaha
Lakshanas B A Lakshanas B A Arbuda Sweda Arsha Snighanagata Mamsa shosha Sthulashophata Shira granthi
Pipasa
20. Upashaya / Anupashaya
Upashaya Anupashaya Shita iccha Ushna Madhurrahit ahara Madhuara ahara vyayama
Diwa swapana
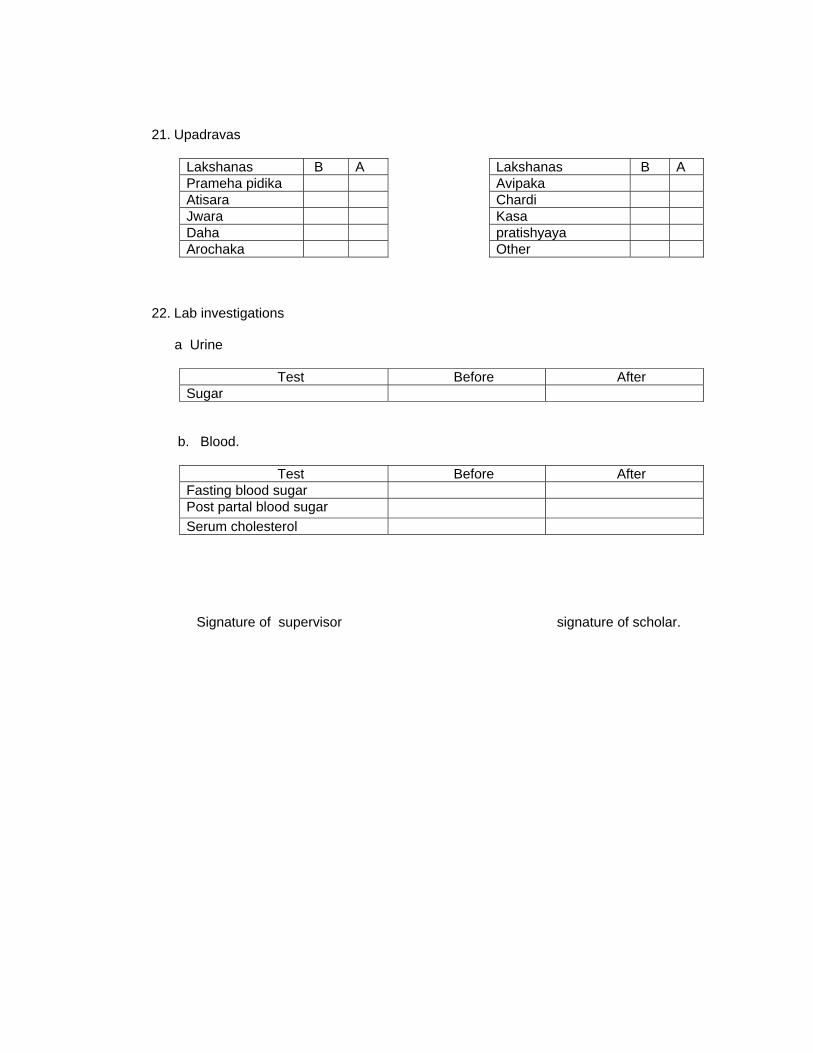
21. Upadravas
Lakshanas B A Lakshanas B A Prameha pidika Avipaka Atisara Chardi Jwara Kasa Daha pratishyaya Arochaka
Other
22. Lab investigations a Urine
Test Before After Sugar
b. Blood.
Test Before After Fasting blood sugar Post partal blood sugar Serum cholesterol
Signature of supervisor signature of scholar.

WEL COME

““Evaluation of the efficacy ofEvaluation of the efficacy ofBhumyamalakyadi churnaBhumyamalakyadi churna inin
madhumehamadhumeha””(with special reference to its hypoglycemic effect)(with special reference to its hypoglycemic effect)
NIRUKTI
“ prachuram varamvaram va mehati mootratyagam karoti yasmin roge sa prameha”
Madhumeha = Madhu + Meha
Madhu = Honey
Meha = Urination
NIDANA
Asya sukham Swapna sukham dadhini gramyodakanuparasa payamsi |
Navanna panam gudavaikratam cha prameha hetu kaphakrut survam ||
Cha Chi 6/4M.N. 33/1
DOSHA DUSHYA
Kapha sapitta pawanascha dosha medhoassrasukrambhuvasalasika |Majja rasouja pishitum cha dushya pramehinam vimshathireva meha||
Cha Chi 6/8M.N. 33/41
SAMPRAPTI
Medascha mamsacha shareerajam cha kledam kaphovastigatam pradushya |
Karoti mehan samoodernamusnisthaneva pittam paridushya chapi ||
Kshineshu dosheshwavakrushya vasthou dathun pramehananila karoti |
Cha Chi 6/5

SAMPRAPTI TALIKA
Favorable combination of Nidana, Dosha & Dushya.
Kapha immediately aggravates.
Aggravated kapha spreads all over the body.
First mixes with medas.

Vitiated kapha with vitiated medas mixes with mamsa and shareera kleda
Vitiation of mamsa provides manifestation of putrified carbuncles = pidika.
The liquefied dhatus further vitiate and transfer into urine.
Prabhoota mutrata & avila mutrata.
PRAMEHA

PURVA RUPA
Dhanthadinam maladythwam pragrupam panipadhayoho |
Daha chikkanatha dehe trut swadyasyam cha jayate ||
M.N. 33/5
LAKSHANA
Samanyam lakshanam tesham prabootavilamootrata |
M.N. 33/6
BHEDA
Doshadushyavisheshapi tatsamyoga visheshatha |
Mutravarnadi bhedena bhedo meheshu kalpyate ||
M.N.33/6
KAPHAJA = 10PITTAJA = 06VATAJA = 04TOTAL = 20 Types
CHIKITSA
Madhunashini (Gymnema sylvestre)Eranda (Ricinus communis Linn.)Bhumyamalaki (Phyllanthus urinaria Linn)Bhringaraj (Eclipta alba)
SADYASADHYATA
Sadhya kaphota dasha pittaja shat yapya na sadhya pavanachatuska |
Samakriyatwathdwishamakriyathwath mahatyatwacha yathakramam ||
Chi Chi 6/7.
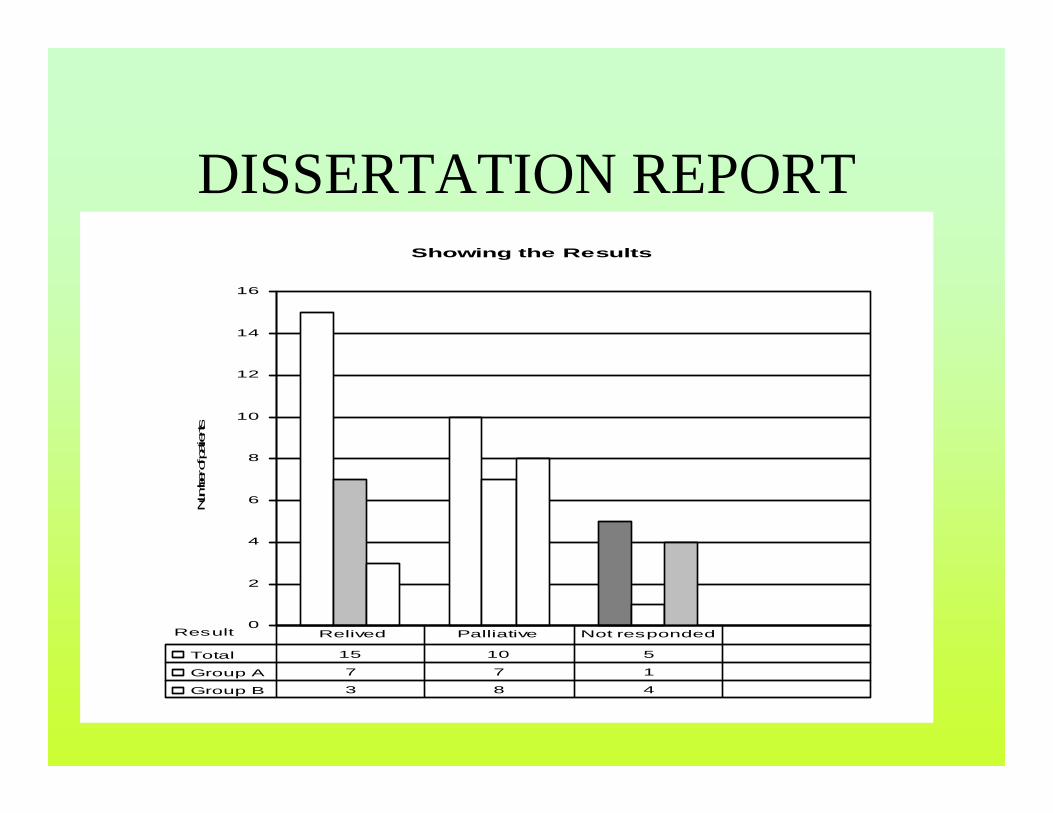
Showing the Results
0
2
4
6
8
10
12
14
16
Result
Num
ber o
f patients
Total 15 10 5
Group A 7 7 1
Group B 3 8 4
Relived Palliative Not responded
DISSERTATION REPORT
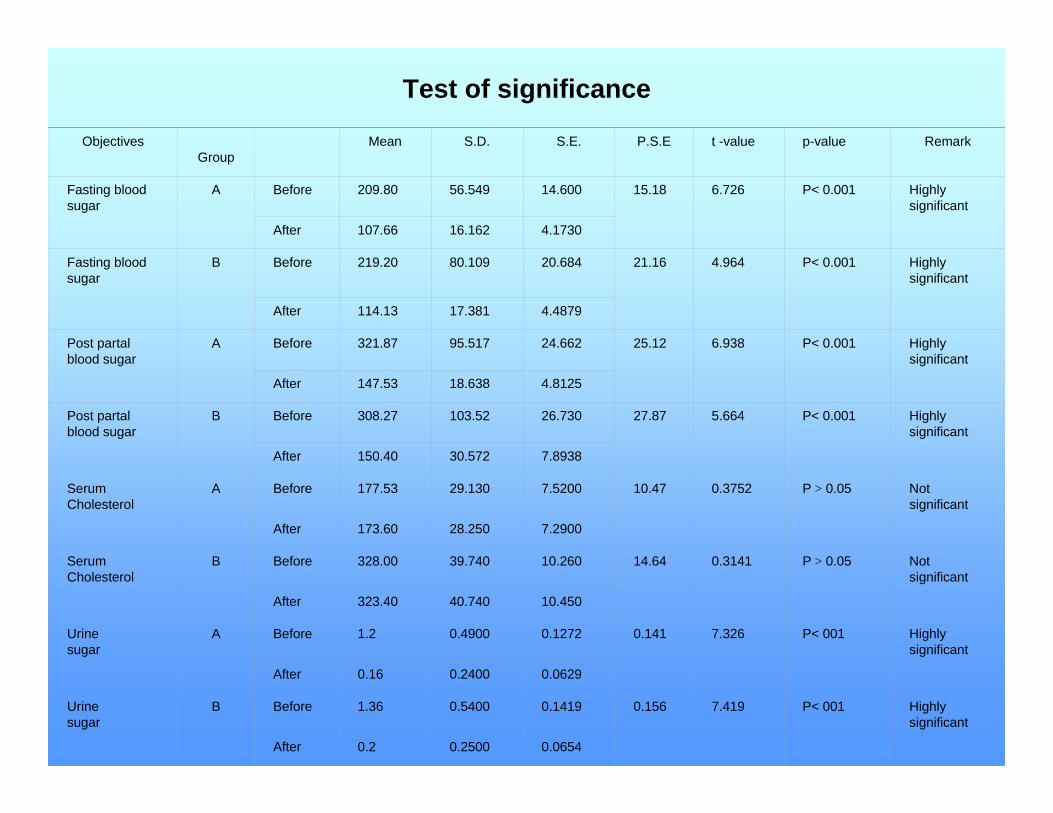
Test of significance
ObjectivesGroup
Mean S.D. S.E. P.S.E t -value p-value Remark
Fasting blood sugar
A Before 209.80 56.549 14.600 15.18 6.726 P< 0.001 Highly significant
After 107.66 16.162 4.1730
Fasting blood sugar
B Before 219.20 80.109 20.684 21.16 4.964 P< 0.001 Highly significant
After 114.13 17.381 4.4879
Post partalblood sugar
A Before 321.87 95.517 24.662 25.12 6.938 P< 0.001 Highly significant
After 147.53 18.638 4.8125
Post partalblood sugar
B Before 308.27 103.52 26.730 27.87 5.664 P< 0.001 Highly significant
After 150.40 30.572 7.8938
Serum Cholesterol
A Before 177.53 29.130 7.5200 10.47 0.3752 P > 0.05 Notsignificant
After 173.60 28.250 7.2900
Serum Cholesterol
B Before 328.00 39.740 10.260 14.64 0.3141 P > 0.05 Not significant
After 323.40 40.740 10.450
Urine sugar
A Before 1.2 0.4900 0.1272 0.141 7.326 P< 001 Highly significant
After 0.16 0.2400 0.0629
Urine sugar
B Before 1.36 0.5400 0.1419 0.156 7.419 P< 001 Highly significant
After 0.2 0.2500 0.0654
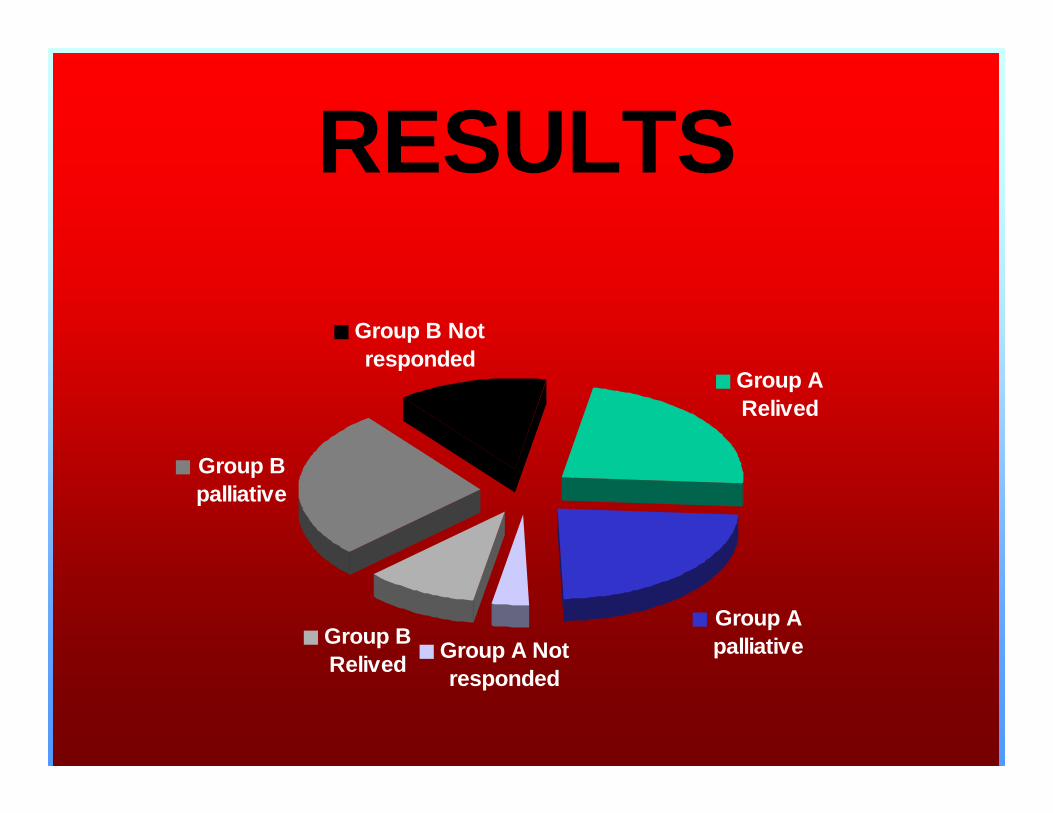
RESULTS
Group A Relived
Group A palliative Group A Not
responded
Group B Relived
Group B palliative
Group B Not responded
CONCLUSION
The trial drug, “Bhumymalakyadi churna” had a very good effect on all the patients, not only by regulating their blood glucose levels but also by relieving them from the signs and symptoms.

Thank you